User login
Time for transparency in skin cancer treatment
I heard Marty Makary, MD, speak at the annual meeting of the American College of Mohs Surgery (ACMS) a few months ago, and got to meet with him there. He is the author of the book “Unaccountable: What Hospitals Won’t Tell You and How Transparency Can Revolutionize Health Care,” published in 2013, and is a potent advocate for physicians, patients, and effective, safe, and efficient medical care.
His personal epiphany centered around the stubborn, continued use of open colonic resection of polyps by one of his professors, despite the availability of much safer and less expensive endoscopic removal. He is a powerful advocate for abandoning obsolete treatment techniques for safer and more effective ones. He insists on transparency in selecting the best treatments for patients.

In his writings, Dr. Makary points out that when looking for areas to improve, it is most productive to focus on treatments that have wide variations in treatment settings and modalities. Sometimes, this is due to a lack of data to support a consensus, a lack of information about a superior treatment modality – or more disturbing, stubbornness and ingrained patterns of behavior. This is the familiar, “This is the way we have always done it” syndrome that was behind his personal epiphany.
This is exactly the situation we face in the United States with the continued treatment of skin cancer in the hospital operating room. At least 40% of all skin cancers are excised in the hospital setting, in the face of overwhelming evidence that excision or destruction in the office setting is safer, yields higher cure rates, and is much less expensive.
It is time to speak up, and admit that 99% of all skin cancers should be treated in the office setting, under local anesthesia. Currently, this is most commonly done by a dermatologist, or a primary care physician, who is not operating room dependent. Those specialists who have been trained exclusively in hospital operating rooms need to become more knowledgeable about local anesthesia, and how to operate in their offices. This should be fertile ground for the government, insurers, patient advocates, and accountable care organizations looking to cut costs and improve quality of care. Moreover, the percentage of these conditions being treated in the office setting by a provider should be a quality indicator.
Maybe it is time for Dr. Makary, a surgical oncologist, to issue a shout out to physicians to stop treating thin melanomas (80% of those diagnosed), nonmelanoma skin cancer, and “lumps and bumps” in the operating room.
We need to publicly expound on the benefits of office-based surgery, and take this message to national patient advocacy groups and the public. New “bedless” hospitals are being built to perform outpatient surgery, and avoid the serious infections (think methicillin-resistant Staphylococcus aureus and Clostridium difficile) that are prevalent in hospitals. It is time to realize a properly equipped physician’s office is as good as a bedless hospital operating room for the treatment of skin cancer, with additional benefits of already being built and staffed.
Dr. Makary, this is a great opportunity to improve the health care of the United States, and at reduced cost.
Dr. Coldiron is past president of the American Academy of Dermatology. He is currently in private practice, but maintains a clinical assistant professorship at the University of Cincinnati. He cares for patients, teaches medical students and residents, and has several active clinical research projects. Dr. Coldiron is the author of more than 80 scientific letters, papers, and several book chapters, and he speaks frequently on a variety of topics.
I heard Marty Makary, MD, speak at the annual meeting of the American College of Mohs Surgery (ACMS) a few months ago, and got to meet with him there. He is the author of the book “Unaccountable: What Hospitals Won’t Tell You and How Transparency Can Revolutionize Health Care,” published in 2013, and is a potent advocate for physicians, patients, and effective, safe, and efficient medical care.
His personal epiphany centered around the stubborn, continued use of open colonic resection of polyps by one of his professors, despite the availability of much safer and less expensive endoscopic removal. He is a powerful advocate for abandoning obsolete treatment techniques for safer and more effective ones. He insists on transparency in selecting the best treatments for patients.
In his writings, Dr. Makary points out that when looking for areas to improve, it is most productive to focus on treatments that have wide variations in treatment settings and modalities. Sometimes, this is due to a lack of data to support a consensus, a lack of information about a superior treatment modality – or more disturbing, stubbornness and ingrained patterns of behavior. This is the familiar, “This is the way we have always done it” syndrome that was behind his personal epiphany.
This is exactly the situation we face in the United States with the continued treatment of skin cancer in the hospital operating room. At least 40% of all skin cancers are excised in the hospital setting, in the face of overwhelming evidence that excision or destruction in the office setting is safer, yields higher cure rates, and is much less expensive.
It is time to speak up, and admit that 99% of all skin cancers should be treated in the office setting, under local anesthesia. Currently, this is most commonly done by a dermatologist, or a primary care physician, who is not operating room dependent. Those specialists who have been trained exclusively in hospital operating rooms need to become more knowledgeable about local anesthesia, and how to operate in their offices. This should be fertile ground for the government, insurers, patient advocates, and accountable care organizations looking to cut costs and improve quality of care. Moreover, the percentage of these conditions being treated in the office setting by a provider should be a quality indicator.
Maybe it is time for Dr. Makary, a surgical oncologist, to issue a shout out to physicians to stop treating thin melanomas (80% of those diagnosed), nonmelanoma skin cancer, and “lumps and bumps” in the operating room.
We need to publicly expound on the benefits of office-based surgery, and take this message to national patient advocacy groups and the public. New “bedless” hospitals are being built to perform outpatient surgery, and avoid the serious infections (think methicillin-resistant Staphylococcus aureus and Clostridium difficile) that are prevalent in hospitals. It is time to realize a properly equipped physician’s office is as good as a bedless hospital operating room for the treatment of skin cancer, with additional benefits of already being built and staffed.
Dr. Makary, this is a great opportunity to improve the health care of the United States, and at reduced cost.
Dr. Coldiron is past president of the American Academy of Dermatology. He is currently in private practice, but maintains a clinical assistant professorship at the University of Cincinnati. He cares for patients, teaches medical students and residents, and has several active clinical research projects. Dr. Coldiron is the author of more than 80 scientific letters, papers, and several book chapters, and he speaks frequently on a variety of topics.
I heard Marty Makary, MD, speak at the annual meeting of the American College of Mohs Surgery (ACMS) a few months ago, and got to meet with him there. He is the author of the book “Unaccountable: What Hospitals Won’t Tell You and How Transparency Can Revolutionize Health Care,” published in 2013, and is a potent advocate for physicians, patients, and effective, safe, and efficient medical care.
His personal epiphany centered around the stubborn, continued use of open colonic resection of polyps by one of his professors, despite the availability of much safer and less expensive endoscopic removal. He is a powerful advocate for abandoning obsolete treatment techniques for safer and more effective ones. He insists on transparency in selecting the best treatments for patients.
In his writings, Dr. Makary points out that when looking for areas to improve, it is most productive to focus on treatments that have wide variations in treatment settings and modalities. Sometimes, this is due to a lack of data to support a consensus, a lack of information about a superior treatment modality – or more disturbing, stubbornness and ingrained patterns of behavior. This is the familiar, “This is the way we have always done it” syndrome that was behind his personal epiphany.
This is exactly the situation we face in the United States with the continued treatment of skin cancer in the hospital operating room. At least 40% of all skin cancers are excised in the hospital setting, in the face of overwhelming evidence that excision or destruction in the office setting is safer, yields higher cure rates, and is much less expensive.
It is time to speak up, and admit that 99% of all skin cancers should be treated in the office setting, under local anesthesia. Currently, this is most commonly done by a dermatologist, or a primary care physician, who is not operating room dependent. Those specialists who have been trained exclusively in hospital operating rooms need to become more knowledgeable about local anesthesia, and how to operate in their offices. This should be fertile ground for the government, insurers, patient advocates, and accountable care organizations looking to cut costs and improve quality of care. Moreover, the percentage of these conditions being treated in the office setting by a provider should be a quality indicator.
Maybe it is time for Dr. Makary, a surgical oncologist, to issue a shout out to physicians to stop treating thin melanomas (80% of those diagnosed), nonmelanoma skin cancer, and “lumps and bumps” in the operating room.
We need to publicly expound on the benefits of office-based surgery, and take this message to national patient advocacy groups and the public. New “bedless” hospitals are being built to perform outpatient surgery, and avoid the serious infections (think methicillin-resistant Staphylococcus aureus and Clostridium difficile) that are prevalent in hospitals. It is time to realize a properly equipped physician’s office is as good as a bedless hospital operating room for the treatment of skin cancer, with additional benefits of already being built and staffed.
Dr. Makary, this is a great opportunity to improve the health care of the United States, and at reduced cost.
Dr. Coldiron is past president of the American Academy of Dermatology. He is currently in private practice, but maintains a clinical assistant professorship at the University of Cincinnati. He cares for patients, teaches medical students and residents, and has several active clinical research projects. Dr. Coldiron is the author of more than 80 scientific letters, papers, and several book chapters, and he speaks frequently on a variety of topics.
Coding: Things often forgotten
First, I want to correct a misstatement I made in a recent column regarding incident to billing by an extender (Dermatology News, July 2016, p. 1) When an extender sees a patient for an established problem, they can bill at 100% if there is a supervising physician in the house, AND it should be under that supervising physician’s number – NOT necessarily by the physician who saw the original problem. This change was promulgated by the Centers for Medicare & Medicaid Services in the proposed rule, and everyone thought it was a done deal, but the billing remained unchanged in the final rule. Apologies for any confusion.
Coding
As all of you know, in 2010, the Centers for Medicare & Medicaid Services stopped recognizing the Current Procedural Terminology (CPT) consultation codes for Medicare Part B payment CMS decided (after an Office of Inspector General study) that consultations were really just new patient visits and stopped paying for consultations. Visits are now coded with new or follow-up patient evaluation and management codes. This is unfortunate, because a consultation pays more, and importantly, does not establish the patient as a patient in your practice for the next three years. If originally billed as a consultation, the patient can be seen back for another problem in the next three years, and be billed for a consultation, or a new patient as appropriate. Therefore, it is a big advantage to be able to bill for a consultation, assuming another doctor has asked your opinion and you call with or send them a report of your findings.
Just because Medicare says you cannot bill for consultations does not mean that all insurers are the same. The consultation codes are still in the CPT code book and your contracts with private insurers probably stipulate that the insurers must comply with CPT convention. In this case, you can bill your private insurers (including Medicare Advantage Plans, which are private insurers) for consultations when your documentation supports it. Be aware, that some of the more popular electronic health records that perform billing automatically default to a new patient visit, when a new patient consultation might be more appropriate.
While discussing evaluation and management coding, you should be aware that 97% of visits billed by dermatologists are level 3 or lower. This means that, even if your EHR can propel you to heights unimagined before, that it could become a problem. You cannot bill a higher level beyond what is medically appropriate. For example, you don’t usually need to do a full-body skin exam during an acne follow-up.
I’ll never forget the poor soul who explained to me that she was being audited “because all my visits were level 4 or 5, and the software agreed with it.” The software company (or the consultant) will not be sharing the joys of an audit with you. You can do a quick and easy check of your evaluation and management patterns, compared with others by checking either of the online Medicare databases, the Wall Street Journal’s “Medicare Unmasked” site or the “Treatment Tracker” for Doctors and Services in Medicare Part B, on the ProPublica website.
While you are there, check your procedure numbers against others. Are you a freeze-y king? Are you the shave master? There are often valid and justifiable reasons for unusual billing patterns. If you are an outlier, make sure you have a good reason to be there. For example, I am in the top 10% paid per patient visit in the state of Ohio. The reason is that I treat only skin cancer, and it usually involves surgery. The world is looking at these data. So should you.
Dr. Coldiron is a past president of the American Academy of Dermatology. He is currently in private practice, but maintains a clinical assistant professorship at the University of Cincinnati. He cares for patients, teaches medical students and residents, and has several active clinical research projects. Dr. Coldiron is the author of more than 80 scientific letters, papers, and several book chapters, and he speaks frequently on a variety of topics. Write to him at [email protected].
First, I want to correct a misstatement I made in a recent column regarding incident to billing by an extender (Dermatology News, July 2016, p. 1) When an extender sees a patient for an established problem, they can bill at 100% if there is a supervising physician in the house, AND it should be under that supervising physician’s number – NOT necessarily by the physician who saw the original problem. This change was promulgated by the Centers for Medicare & Medicaid Services in the proposed rule, and everyone thought it was a done deal, but the billing remained unchanged in the final rule. Apologies for any confusion.
Coding
As all of you know, in 2010, the Centers for Medicare & Medicaid Services stopped recognizing the Current Procedural Terminology (CPT) consultation codes for Medicare Part B payment CMS decided (after an Office of Inspector General study) that consultations were really just new patient visits and stopped paying for consultations. Visits are now coded with new or follow-up patient evaluation and management codes. This is unfortunate, because a consultation pays more, and importantly, does not establish the patient as a patient in your practice for the next three years. If originally billed as a consultation, the patient can be seen back for another problem in the next three years, and be billed for a consultation, or a new patient as appropriate. Therefore, it is a big advantage to be able to bill for a consultation, assuming another doctor has asked your opinion and you call with or send them a report of your findings.
Just because Medicare says you cannot bill for consultations does not mean that all insurers are the same. The consultation codes are still in the CPT code book and your contracts with private insurers probably stipulate that the insurers must comply with CPT convention. In this case, you can bill your private insurers (including Medicare Advantage Plans, which are private insurers) for consultations when your documentation supports it. Be aware, that some of the more popular electronic health records that perform billing automatically default to a new patient visit, when a new patient consultation might be more appropriate.
While discussing evaluation and management coding, you should be aware that 97% of visits billed by dermatologists are level 3 or lower. This means that, even if your EHR can propel you to heights unimagined before, that it could become a problem. You cannot bill a higher level beyond what is medically appropriate. For example, you don’t usually need to do a full-body skin exam during an acne follow-up.
I’ll never forget the poor soul who explained to me that she was being audited “because all my visits were level 4 or 5, and the software agreed with it.” The software company (or the consultant) will not be sharing the joys of an audit with you. You can do a quick and easy check of your evaluation and management patterns, compared with others by checking either of the online Medicare databases, the Wall Street Journal’s “Medicare Unmasked” site or the “Treatment Tracker” for Doctors and Services in Medicare Part B, on the ProPublica website.
While you are there, check your procedure numbers against others. Are you a freeze-y king? Are you the shave master? There are often valid and justifiable reasons for unusual billing patterns. If you are an outlier, make sure you have a good reason to be there. For example, I am in the top 10% paid per patient visit in the state of Ohio. The reason is that I treat only skin cancer, and it usually involves surgery. The world is looking at these data. So should you.
Dr. Coldiron is a past president of the American Academy of Dermatology. He is currently in private practice, but maintains a clinical assistant professorship at the University of Cincinnati. He cares for patients, teaches medical students and residents, and has several active clinical research projects. Dr. Coldiron is the author of more than 80 scientific letters, papers, and several book chapters, and he speaks frequently on a variety of topics. Write to him at [email protected].
First, I want to correct a misstatement I made in a recent column regarding incident to billing by an extender (Dermatology News, July 2016, p. 1) When an extender sees a patient for an established problem, they can bill at 100% if there is a supervising physician in the house, AND it should be under that supervising physician’s number – NOT necessarily by the physician who saw the original problem. This change was promulgated by the Centers for Medicare & Medicaid Services in the proposed rule, and everyone thought it was a done deal, but the billing remained unchanged in the final rule. Apologies for any confusion.
Coding
As all of you know, in 2010, the Centers for Medicare & Medicaid Services stopped recognizing the Current Procedural Terminology (CPT) consultation codes for Medicare Part B payment CMS decided (after an Office of Inspector General study) that consultations were really just new patient visits and stopped paying for consultations. Visits are now coded with new or follow-up patient evaluation and management codes. This is unfortunate, because a consultation pays more, and importantly, does not establish the patient as a patient in your practice for the next three years. If originally billed as a consultation, the patient can be seen back for another problem in the next three years, and be billed for a consultation, or a new patient as appropriate. Therefore, it is a big advantage to be able to bill for a consultation, assuming another doctor has asked your opinion and you call with or send them a report of your findings.
Just because Medicare says you cannot bill for consultations does not mean that all insurers are the same. The consultation codes are still in the CPT code book and your contracts with private insurers probably stipulate that the insurers must comply with CPT convention. In this case, you can bill your private insurers (including Medicare Advantage Plans, which are private insurers) for consultations when your documentation supports it. Be aware, that some of the more popular electronic health records that perform billing automatically default to a new patient visit, when a new patient consultation might be more appropriate.
While discussing evaluation and management coding, you should be aware that 97% of visits billed by dermatologists are level 3 or lower. This means that, even if your EHR can propel you to heights unimagined before, that it could become a problem. You cannot bill a higher level beyond what is medically appropriate. For example, you don’t usually need to do a full-body skin exam during an acne follow-up.
I’ll never forget the poor soul who explained to me that she was being audited “because all my visits were level 4 or 5, and the software agreed with it.” The software company (or the consultant) will not be sharing the joys of an audit with you. You can do a quick and easy check of your evaluation and management patterns, compared with others by checking either of the online Medicare databases, the Wall Street Journal’s “Medicare Unmasked” site or the “Treatment Tracker” for Doctors and Services in Medicare Part B, on the ProPublica website.
While you are there, check your procedure numbers against others. Are you a freeze-y king? Are you the shave master? There are often valid and justifiable reasons for unusual billing patterns. If you are an outlier, make sure you have a good reason to be there. For example, I am in the top 10% paid per patient visit in the state of Ohio. The reason is that I treat only skin cancer, and it usually involves surgery. The world is looking at these data. So should you.
Dr. Coldiron is a past president of the American Academy of Dermatology. He is currently in private practice, but maintains a clinical assistant professorship at the University of Cincinnati. He cares for patients, teaches medical students and residents, and has several active clinical research projects. Dr. Coldiron is the author of more than 80 scientific letters, papers, and several book chapters, and he speaks frequently on a variety of topics. Write to him at [email protected].
Should we pursue board certification in Mohs micrographic surgery?
The medical director was direct and blunt: “You’ve got a problem with two very different levels of training in Mohs surgery. This is a big problem for your specialty.”
The remarks came at a medical director summit that I was attending to speak on the value of dermatology. I was explaining to medical directors how including small dermatology practices in their plans would realize cost savings when treating skin cancer in the office setting. An awkward silence followed the medical director’s remarks. Then I uttered a lame “we may have a board certification someday.”

My interview with the New York Times reporter before the meeting quickly became adversarial. “What about these guys who do Mohs after a 3-day course?” I explained that there is more involved than just the 3-day course, that there is a preceptorship and case reviews. Plus, some of “those guys” wrote some of the best Mohs textbooks. The reporter wasn’t buying it, and the rest of the interview went downhill.
And the training issues surrounding Mohs surgery are playing out in practice. One dermatologist wrote me complaining that an insurer will no longer let him bill for Mohs because “he can’t document his residency training in Mohs and did not do a fellowship.” Another wrote me saying he can no longer teach Mohs surgery at the VA or the medical school “because he didn’t do a formal Mohs fellowship.”
The issue of who is qualified to perform Mohs surgery is coming to a head. There are more than 2,500 dermatologists billing Medicare for Mohs, and insurers are groaning at the expense. They are looking for any possible reason to exclude dermatologists from billing for Mohs surgery.
A possible solution is a board certification in Mohs surgery. Osteopathic dermatologists have had this option for 20 years. Unfortunately, allopathic dermatologists cannot sit for the osteopathic exam. A new certification exam for allopathic dermatologists who have successfully completed a dermatology residency accredited by the Accreditation Council for Graduate Medical Education (ACGME) seems worthy of a discussion.
Downsides of certification include the likely $1,000 or more cost of a test, the costs of preparing for the test, and the risk of failing a test. A new certification would give the Maintenance of Certification (MOC) haters another reason to complain, since about 600 lifetime certified, board-exempt dermatologists would be dragged back into MOC to maintain a Mohs surgery subspecialty certification. Some of the current fellowship-trained Mohs surgeons will not like being grouped with the nonfellowship-trained surgeons, whom they consider their inferiors and who will now have the opportunity to be board certified.
The name of the fellowship, which is “micrographic surgery and dermatologic oncology,” also has some paranoid types fearing that they will lose the right to treat skin cancer if such a subspecialty is created. That shouldn’t be an issue, since all dermatologists are trained in residency to treat skin cancer. The formal fellowships already exist. There are already 1,600 fellowship-trained Mohs surgeons out there, and they have not cornered the market on skin cancer. The situation should not change since general dermatologists remain the gatekeepers – and entry point – for most skin cancer patients. Certification exams in dermatopathology and pediatric dermatology have not had a negative impact on general dermatologists, who still read their own slides and see kids for skin disease. In fact, having dermatopathology as a certified part of dermatology has been a huge benefit in our struggle to maintain the right to read our own slides.
Developing a certification exam would take at least 2 years if the American Board of Dermatology decided to do it. There would be no “grandfathering” automatic certification. Everyone would have to take the same exam – young, old, formally trained, or not.
Members of the American Board of Dermatology explained the qualifiers to sit for an exam (if there was an exam) at a summit I held in Cincinnati in 2015. They are interested in including all ABD dermatologists who currently practice Mohs surgery, fellowship trained or not. Suggested parameters included any ABD fellow whose practice is 20% Mohs and reconstructive surgery (by volume or income), or anyone who performs Mohs once a week. Fellowship-trained micrographic surgeons could be eligible, and this would be a self-attestation! There would be no case log reviews, no visits by inspectors, no secret questions or passwords. This pathway would remain open for 5 years as were the exams for dermatopathology and pediatric dermatology. After that point, only ACGME fellowship–trained Mohs surgeons would be eligible to take the exam.
Upsides to this approach include decreasing divisiveness in the specialty, creating a better brand, and elevating the specialty. A board certification will help in obtaining a Medicare specialty designation, which will help stop the delisting of Mohs surgeons from insurance networks based on their average charges compared with general dermatologists. This action would particularly help small practices.
The American Academy of Dermatology board of directors sent this issue to the education committee to inform and poll the membership. You should expect to hear more about the proposed process. As an AAD member, you will get to express your opinion so make sure you are well informed. The AAD membership opinion will be important in whether or not the American Board of Dermatology decides to pursue this. Remember, this is an American Board of Dermatology decision, not an AAD decision.
More reasons for a board certification include that the ACGME expects its fellowships to develop a board exam at some point (although not all have). The 1,000 ACGME fellowship–trained micrographic surgeons deserve a chance to be board certified, which is the medical profession’s way to demonstrate competence to the public.
Having all Mohs surgeons board certified would heal a huge rift in the house of dermatology, and give us a united, consistent face to present to other specialties, the Congress, and the media. Physicians are judged by their training and credentials. Love them or hate them, the ACGME is the gold standard. Perhaps the greatest beneficiaries would be those practicing Mohs who did not complete a formal fellowship. I think a board exam is overdue, and will be a boon to all of dermatology.
Dr. Coldiron is a past president of the American Academy of Dermatology. He is currently in private practice, but maintains a clinical assistant professorship at the University of Cincinnati. He cares for patients, teaches medical students and residents, and has several active clinical research projects. Dr. Coldiron is the author of more than 80 scientific letters, papers, and several book chapters, and he speaks frequently on a variety of topics.
The medical director was direct and blunt: “You’ve got a problem with two very different levels of training in Mohs surgery. This is a big problem for your specialty.”
The remarks came at a medical director summit that I was attending to speak on the value of dermatology. I was explaining to medical directors how including small dermatology practices in their plans would realize cost savings when treating skin cancer in the office setting. An awkward silence followed the medical director’s remarks. Then I uttered a lame “we may have a board certification someday.”
My interview with the New York Times reporter before the meeting quickly became adversarial. “What about these guys who do Mohs after a 3-day course?” I explained that there is more involved than just the 3-day course, that there is a preceptorship and case reviews. Plus, some of “those guys” wrote some of the best Mohs textbooks. The reporter wasn’t buying it, and the rest of the interview went downhill.
And the training issues surrounding Mohs surgery are playing out in practice. One dermatologist wrote me complaining that an insurer will no longer let him bill for Mohs because “he can’t document his residency training in Mohs and did not do a fellowship.” Another wrote me saying he can no longer teach Mohs surgery at the VA or the medical school “because he didn’t do a formal Mohs fellowship.”
The issue of who is qualified to perform Mohs surgery is coming to a head. There are more than 2,500 dermatologists billing Medicare for Mohs, and insurers are groaning at the expense. They are looking for any possible reason to exclude dermatologists from billing for Mohs surgery.
A possible solution is a board certification in Mohs surgery. Osteopathic dermatologists have had this option for 20 years. Unfortunately, allopathic dermatologists cannot sit for the osteopathic exam. A new certification exam for allopathic dermatologists who have successfully completed a dermatology residency accredited by the Accreditation Council for Graduate Medical Education (ACGME) seems worthy of a discussion.
Downsides of certification include the likely $1,000 or more cost of a test, the costs of preparing for the test, and the risk of failing a test. A new certification would give the Maintenance of Certification (MOC) haters another reason to complain, since about 600 lifetime certified, board-exempt dermatologists would be dragged back into MOC to maintain a Mohs surgery subspecialty certification. Some of the current fellowship-trained Mohs surgeons will not like being grouped with the nonfellowship-trained surgeons, whom they consider their inferiors and who will now have the opportunity to be board certified.
The name of the fellowship, which is “micrographic surgery and dermatologic oncology,” also has some paranoid types fearing that they will lose the right to treat skin cancer if such a subspecialty is created. That shouldn’t be an issue, since all dermatologists are trained in residency to treat skin cancer. The formal fellowships already exist. There are already 1,600 fellowship-trained Mohs surgeons out there, and they have not cornered the market on skin cancer. The situation should not change since general dermatologists remain the gatekeepers – and entry point – for most skin cancer patients. Certification exams in dermatopathology and pediatric dermatology have not had a negative impact on general dermatologists, who still read their own slides and see kids for skin disease. In fact, having dermatopathology as a certified part of dermatology has been a huge benefit in our struggle to maintain the right to read our own slides.
Developing a certification exam would take at least 2 years if the American Board of Dermatology decided to do it. There would be no “grandfathering” automatic certification. Everyone would have to take the same exam – young, old, formally trained, or not.
Members of the American Board of Dermatology explained the qualifiers to sit for an exam (if there was an exam) at a summit I held in Cincinnati in 2015. They are interested in including all ABD dermatologists who currently practice Mohs surgery, fellowship trained or not. Suggested parameters included any ABD fellow whose practice is 20% Mohs and reconstructive surgery (by volume or income), or anyone who performs Mohs once a week. Fellowship-trained micrographic surgeons could be eligible, and this would be a self-attestation! There would be no case log reviews, no visits by inspectors, no secret questions or passwords. This pathway would remain open for 5 years as were the exams for dermatopathology and pediatric dermatology. After that point, only ACGME fellowship–trained Mohs surgeons would be eligible to take the exam.
Upsides to this approach include decreasing divisiveness in the specialty, creating a better brand, and elevating the specialty. A board certification will help in obtaining a Medicare specialty designation, which will help stop the delisting of Mohs surgeons from insurance networks based on their average charges compared with general dermatologists. This action would particularly help small practices.
The American Academy of Dermatology board of directors sent this issue to the education committee to inform and poll the membership. You should expect to hear more about the proposed process. As an AAD member, you will get to express your opinion so make sure you are well informed. The AAD membership opinion will be important in whether or not the American Board of Dermatology decides to pursue this. Remember, this is an American Board of Dermatology decision, not an AAD decision.
More reasons for a board certification include that the ACGME expects its fellowships to develop a board exam at some point (although not all have). The 1,000 ACGME fellowship–trained micrographic surgeons deserve a chance to be board certified, which is the medical profession’s way to demonstrate competence to the public.
Having all Mohs surgeons board certified would heal a huge rift in the house of dermatology, and give us a united, consistent face to present to other specialties, the Congress, and the media. Physicians are judged by their training and credentials. Love them or hate them, the ACGME is the gold standard. Perhaps the greatest beneficiaries would be those practicing Mohs who did not complete a formal fellowship. I think a board exam is overdue, and will be a boon to all of dermatology.
Dr. Coldiron is a past president of the American Academy of Dermatology. He is currently in private practice, but maintains a clinical assistant professorship at the University of Cincinnati. He cares for patients, teaches medical students and residents, and has several active clinical research projects. Dr. Coldiron is the author of more than 80 scientific letters, papers, and several book chapters, and he speaks frequently on a variety of topics.
The medical director was direct and blunt: “You’ve got a problem with two very different levels of training in Mohs surgery. This is a big problem for your specialty.”
The remarks came at a medical director summit that I was attending to speak on the value of dermatology. I was explaining to medical directors how including small dermatology practices in their plans would realize cost savings when treating skin cancer in the office setting. An awkward silence followed the medical director’s remarks. Then I uttered a lame “we may have a board certification someday.”
My interview with the New York Times reporter before the meeting quickly became adversarial. “What about these guys who do Mohs after a 3-day course?” I explained that there is more involved than just the 3-day course, that there is a preceptorship and case reviews. Plus, some of “those guys” wrote some of the best Mohs textbooks. The reporter wasn’t buying it, and the rest of the interview went downhill.
And the training issues surrounding Mohs surgery are playing out in practice. One dermatologist wrote me complaining that an insurer will no longer let him bill for Mohs because “he can’t document his residency training in Mohs and did not do a fellowship.” Another wrote me saying he can no longer teach Mohs surgery at the VA or the medical school “because he didn’t do a formal Mohs fellowship.”
The issue of who is qualified to perform Mohs surgery is coming to a head. There are more than 2,500 dermatologists billing Medicare for Mohs, and insurers are groaning at the expense. They are looking for any possible reason to exclude dermatologists from billing for Mohs surgery.
A possible solution is a board certification in Mohs surgery. Osteopathic dermatologists have had this option for 20 years. Unfortunately, allopathic dermatologists cannot sit for the osteopathic exam. A new certification exam for allopathic dermatologists who have successfully completed a dermatology residency accredited by the Accreditation Council for Graduate Medical Education (ACGME) seems worthy of a discussion.
Downsides of certification include the likely $1,000 or more cost of a test, the costs of preparing for the test, and the risk of failing a test. A new certification would give the Maintenance of Certification (MOC) haters another reason to complain, since about 600 lifetime certified, board-exempt dermatologists would be dragged back into MOC to maintain a Mohs surgery subspecialty certification. Some of the current fellowship-trained Mohs surgeons will not like being grouped with the nonfellowship-trained surgeons, whom they consider their inferiors and who will now have the opportunity to be board certified.
The name of the fellowship, which is “micrographic surgery and dermatologic oncology,” also has some paranoid types fearing that they will lose the right to treat skin cancer if such a subspecialty is created. That shouldn’t be an issue, since all dermatologists are trained in residency to treat skin cancer. The formal fellowships already exist. There are already 1,600 fellowship-trained Mohs surgeons out there, and they have not cornered the market on skin cancer. The situation should not change since general dermatologists remain the gatekeepers – and entry point – for most skin cancer patients. Certification exams in dermatopathology and pediatric dermatology have not had a negative impact on general dermatologists, who still read their own slides and see kids for skin disease. In fact, having dermatopathology as a certified part of dermatology has been a huge benefit in our struggle to maintain the right to read our own slides.
Developing a certification exam would take at least 2 years if the American Board of Dermatology decided to do it. There would be no “grandfathering” automatic certification. Everyone would have to take the same exam – young, old, formally trained, or not.
Members of the American Board of Dermatology explained the qualifiers to sit for an exam (if there was an exam) at a summit I held in Cincinnati in 2015. They are interested in including all ABD dermatologists who currently practice Mohs surgery, fellowship trained or not. Suggested parameters included any ABD fellow whose practice is 20% Mohs and reconstructive surgery (by volume or income), or anyone who performs Mohs once a week. Fellowship-trained micrographic surgeons could be eligible, and this would be a self-attestation! There would be no case log reviews, no visits by inspectors, no secret questions or passwords. This pathway would remain open for 5 years as were the exams for dermatopathology and pediatric dermatology. After that point, only ACGME fellowship–trained Mohs surgeons would be eligible to take the exam.
Upsides to this approach include decreasing divisiveness in the specialty, creating a better brand, and elevating the specialty. A board certification will help in obtaining a Medicare specialty designation, which will help stop the delisting of Mohs surgeons from insurance networks based on their average charges compared with general dermatologists. This action would particularly help small practices.
The American Academy of Dermatology board of directors sent this issue to the education committee to inform and poll the membership. You should expect to hear more about the proposed process. As an AAD member, you will get to express your opinion so make sure you are well informed. The AAD membership opinion will be important in whether or not the American Board of Dermatology decides to pursue this. Remember, this is an American Board of Dermatology decision, not an AAD decision.
More reasons for a board certification include that the ACGME expects its fellowships to develop a board exam at some point (although not all have). The 1,000 ACGME fellowship–trained micrographic surgeons deserve a chance to be board certified, which is the medical profession’s way to demonstrate competence to the public.
Having all Mohs surgeons board certified would heal a huge rift in the house of dermatology, and give us a united, consistent face to present to other specialties, the Congress, and the media. Physicians are judged by their training and credentials. Love them or hate them, the ACGME is the gold standard. Perhaps the greatest beneficiaries would be those practicing Mohs who did not complete a formal fellowship. I think a board exam is overdue, and will be a boon to all of dermatology.
Dr. Coldiron is a past president of the American Academy of Dermatology. He is currently in private practice, but maintains a clinical assistant professorship at the University of Cincinnati. He cares for patients, teaches medical students and residents, and has several active clinical research projects. Dr. Coldiron is the author of more than 80 scientific letters, papers, and several book chapters, and he speaks frequently on a variety of topics.

Pharmacy board redux
The struggles with the State of Ohio Board of Pharmacy continue. The pharmacy board reopened its comment period for 2 weeks and received many comments from multiple physicians, organizations, and patients who would be adversely affected by the Board’s move to hold physicians’ offices to the same standard as compounding pharmacies. This was the topic of my recent column, in which I pointed out that as a result, “any practitioners who reconstitute any drug in their offices is considered to be a compounding pharmacy, ordered to pay compounding pharmacy registration fees ($112 yearly), and to undergo the same inspections as compounding pharmacies”.
At their last meeting, the pharmacy board members made a few minor changes, but practitioners will still have to throw out their neurotoxins after 1-6 hours (the exact time is still under debate). Incidentally, I have spoken to all three neurotoxin manufacturers, and they have no interest in adding preservative to their products or in bringing out smaller unit dose packaging. These regulations will have broad impact across the house of medicine because many specialties use neurotoxin.

You should know the back story behind all of this, and how the house of medicine came to this sad place.
About 20 years ago, pain control became a cause célèbre in medicine championed by no less than the World Health Organization. Numerous publications, thought leaders, and policy wonks decried the inadequacy of pain control both in and out of the hospital. It was explained loud and long that patients should have their pain controlled and that physicians fell short if they did not do so, never mind that there is no quantifiable way to measure pain. Further, it was explained that patients in severe pain did not become addicted to narcotics. And the Joint Commission heralded pain control as “the fifth vital sign.”
Where are these thought leaders now?
Graded on responsiveness to patients’ pain and the results of patient surveys on pain control, physicians grudgingly opened the narcotic floodgates and large quantities of prescription narcotics hit the streets. Admittedly, some were written by bad doctors running “pill mills,” but other supplies were diverted by producers, pharmacists, pharmacies, and pharmacy technicians. Hundreds of thousands of Americans became addicted to prescription narcotics, but overdoses were infrequent because there was a unit dose on the street.
Then the medical pendulum swung back, and it was decided that there was too much pain medicine on the streets. The narcotic supply spigots were tightened sharply by the Drug Enforcement Administration, medical boards, and legislatures. It became hard for drug-seeking patients to fill multiple prescriptions, pill mills were shut down, doctors were encouraged to prescribe minimum dosages of narcotic pain relievers, and the price of the unit dose shot up on the street. The patterns of abuse and addiction shifted as heroin became cheaper and more readily available, but hard to dose, particularly when Mexican fentanyl was being sold as “heroin.” Unable to judge the dose of illicitly obtained drugs, addicts began overdosing and dying all over America.
Angry, bereaved family members demanded an accounting for the addiction and deaths of their relatives. Heat was applied to politicians, and a “culprit” was found, physicians! Physicians had made these drugs available and caused all of these people to be addicted!
And thus began the political ascendancy of the pharmacy board, whose members claimed clean hands in this affair. Keen to expand their scope of practice, pharmacists have been trying to find a way into clinical medicine for years. The pharmacy board offered their expertise, and politicians angry at doctors were willing to give the pharmacists’ recommendations a try.
Last year in Ohio, the legislature passed a huge budget reconciliation bill with language tucked in it that authorized the pharmacy board to regulate buprenorphine and other dangerous drugs. The obvious reading of this authority would be that pharmacists were supposed to regulate compounding pharmacies, like the one that produced tainted steroid injections that resulted in 64 deaths in 2012.The regulation is so vague, however, that it could be construed that pharmacists were supposed to regulate everyone in the state, especially since the pharmacy board unilaterally moved to define “dangerous” as any prescription drug. This puts all of medicine in play. The board then declared that it would apply U.S. Pharmacopeial Convention standards (those used for compounding pharmacies) to all physician offices and declared that reconstitution of any drug is considered to be compounding.
To consider physician’s offices as compounding pharmacies is absurd and will degrade patient care by increasing expense and denying access to treatments. Physicians have made and applied individual customized medications to their patients since Galen. It is an integral part of the practice of medicine and has not suddenly become the practice of pharmacy. Using this logic, pharmacists, who have recently won the right to administer vaccinations, should obtain special licenses from the state medical board, since injecting medications is clearly in the purview of medical practice. Physicians have not been killing patients by running dirty compounding pharmacies, pharmacists have. Good, clean up the compounding pharmacies! But applying these compounding rules to physicians’ offices will not save any lives.
This battle has just been joined. The American Medical Association recently passed a resolution declaring that physician compounding should be regulated by state medical boards. This action is most helpful, and another reason for you to join and support the AMA. If you practice in Ohio, you should join the Ohio State Medical Association post haste. They are a big dog in the Ohio legislature, and your membership will influence their efforts.
I hope the Ohio governor’s Common Sense Initiative Office will convene a joint meeting that allows physicians, especially dermatologists, to demonstrate the absurdity of these rules, and their potentially destructive effects on patient care. However, I do not expect the pharmacy board to readily give up this power. Ultimately, the language in the legislative code must add two words after the word “compounding.” The words to be added are “by pharmacists.”
These rules may have to be stayed by a legal injunction. If the legislation is not clarified, a lawsuit against the pharmacy board based on restraint of trade should be successful.
Be vigilant, and watch your state legislatures. Just recently, the pharmacy board of North Dakota has made the same power grab. Stay tuned, as this struggle has national implications.
Dr. Coldiron is past president of the American Academy of Dermatology. He is currently in private practice, but maintains a clinical assistant professorship at the University of Cincinnati. He cares for patients, teaches medical students and residents, and has several active clinical research projects. Dr. Coldiron is the author of more than 80 scientific letters, papers, and several book chapters, and he speaks frequently on a variety of topics. Write to him at [email protected].
The struggles with the State of Ohio Board of Pharmacy continue. The pharmacy board reopened its comment period for 2 weeks and received many comments from multiple physicians, organizations, and patients who would be adversely affected by the Board’s move to hold physicians’ offices to the same standard as compounding pharmacies. This was the topic of my recent column, in which I pointed out that as a result, “any practitioners who reconstitute any drug in their offices is considered to be a compounding pharmacy, ordered to pay compounding pharmacy registration fees ($112 yearly), and to undergo the same inspections as compounding pharmacies”.
At their last meeting, the pharmacy board members made a few minor changes, but practitioners will still have to throw out their neurotoxins after 1-6 hours (the exact time is still under debate). Incidentally, I have spoken to all three neurotoxin manufacturers, and they have no interest in adding preservative to their products or in bringing out smaller unit dose packaging. These regulations will have broad impact across the house of medicine because many specialties use neurotoxin.
You should know the back story behind all of this, and how the house of medicine came to this sad place.
About 20 years ago, pain control became a cause célèbre in medicine championed by no less than the World Health Organization. Numerous publications, thought leaders, and policy wonks decried the inadequacy of pain control both in and out of the hospital. It was explained loud and long that patients should have their pain controlled and that physicians fell short if they did not do so, never mind that there is no quantifiable way to measure pain. Further, it was explained that patients in severe pain did not become addicted to narcotics. And the Joint Commission heralded pain control as “the fifth vital sign.”
Where are these thought leaders now?
Graded on responsiveness to patients’ pain and the results of patient surveys on pain control, physicians grudgingly opened the narcotic floodgates and large quantities of prescription narcotics hit the streets. Admittedly, some were written by bad doctors running “pill mills,” but other supplies were diverted by producers, pharmacists, pharmacies, and pharmacy technicians. Hundreds of thousands of Americans became addicted to prescription narcotics, but overdoses were infrequent because there was a unit dose on the street.
Then the medical pendulum swung back, and it was decided that there was too much pain medicine on the streets. The narcotic supply spigots were tightened sharply by the Drug Enforcement Administration, medical boards, and legislatures. It became hard for drug-seeking patients to fill multiple prescriptions, pill mills were shut down, doctors were encouraged to prescribe minimum dosages of narcotic pain relievers, and the price of the unit dose shot up on the street. The patterns of abuse and addiction shifted as heroin became cheaper and more readily available, but hard to dose, particularly when Mexican fentanyl was being sold as “heroin.” Unable to judge the dose of illicitly obtained drugs, addicts began overdosing and dying all over America.
Angry, bereaved family members demanded an accounting for the addiction and deaths of their relatives. Heat was applied to politicians, and a “culprit” was found, physicians! Physicians had made these drugs available and caused all of these people to be addicted!
And thus began the political ascendancy of the pharmacy board, whose members claimed clean hands in this affair. Keen to expand their scope of practice, pharmacists have been trying to find a way into clinical medicine for years. The pharmacy board offered their expertise, and politicians angry at doctors were willing to give the pharmacists’ recommendations a try.
Last year in Ohio, the legislature passed a huge budget reconciliation bill with language tucked in it that authorized the pharmacy board to regulate buprenorphine and other dangerous drugs. The obvious reading of this authority would be that pharmacists were supposed to regulate compounding pharmacies, like the one that produced tainted steroid injections that resulted in 64 deaths in 2012.The regulation is so vague, however, that it could be construed that pharmacists were supposed to regulate everyone in the state, especially since the pharmacy board unilaterally moved to define “dangerous” as any prescription drug. This puts all of medicine in play. The board then declared that it would apply U.S. Pharmacopeial Convention standards (those used for compounding pharmacies) to all physician offices and declared that reconstitution of any drug is considered to be compounding.
To consider physician’s offices as compounding pharmacies is absurd and will degrade patient care by increasing expense and denying access to treatments. Physicians have made and applied individual customized medications to their patients since Galen. It is an integral part of the practice of medicine and has not suddenly become the practice of pharmacy. Using this logic, pharmacists, who have recently won the right to administer vaccinations, should obtain special licenses from the state medical board, since injecting medications is clearly in the purview of medical practice. Physicians have not been killing patients by running dirty compounding pharmacies, pharmacists have. Good, clean up the compounding pharmacies! But applying these compounding rules to physicians’ offices will not save any lives.
This battle has just been joined. The American Medical Association recently passed a resolution declaring that physician compounding should be regulated by state medical boards. This action is most helpful, and another reason for you to join and support the AMA. If you practice in Ohio, you should join the Ohio State Medical Association post haste. They are a big dog in the Ohio legislature, and your membership will influence their efforts.
I hope the Ohio governor’s Common Sense Initiative Office will convene a joint meeting that allows physicians, especially dermatologists, to demonstrate the absurdity of these rules, and their potentially destructive effects on patient care. However, I do not expect the pharmacy board to readily give up this power. Ultimately, the language in the legislative code must add two words after the word “compounding.” The words to be added are “by pharmacists.”
These rules may have to be stayed by a legal injunction. If the legislation is not clarified, a lawsuit against the pharmacy board based on restraint of trade should be successful.
Be vigilant, and watch your state legislatures. Just recently, the pharmacy board of North Dakota has made the same power grab. Stay tuned, as this struggle has national implications.
Dr. Coldiron is past president of the American Academy of Dermatology. He is currently in private practice, but maintains a clinical assistant professorship at the University of Cincinnati. He cares for patients, teaches medical students and residents, and has several active clinical research projects. Dr. Coldiron is the author of more than 80 scientific letters, papers, and several book chapters, and he speaks frequently on a variety of topics. Write to him at [email protected].
The struggles with the State of Ohio Board of Pharmacy continue. The pharmacy board reopened its comment period for 2 weeks and received many comments from multiple physicians, organizations, and patients who would be adversely affected by the Board’s move to hold physicians’ offices to the same standard as compounding pharmacies. This was the topic of my recent column, in which I pointed out that as a result, “any practitioners who reconstitute any drug in their offices is considered to be a compounding pharmacy, ordered to pay compounding pharmacy registration fees ($112 yearly), and to undergo the same inspections as compounding pharmacies”.
At their last meeting, the pharmacy board members made a few minor changes, but practitioners will still have to throw out their neurotoxins after 1-6 hours (the exact time is still under debate). Incidentally, I have spoken to all three neurotoxin manufacturers, and they have no interest in adding preservative to their products or in bringing out smaller unit dose packaging. These regulations will have broad impact across the house of medicine because many specialties use neurotoxin.
You should know the back story behind all of this, and how the house of medicine came to this sad place.
About 20 years ago, pain control became a cause célèbre in medicine championed by no less than the World Health Organization. Numerous publications, thought leaders, and policy wonks decried the inadequacy of pain control both in and out of the hospital. It was explained loud and long that patients should have their pain controlled and that physicians fell short if they did not do so, never mind that there is no quantifiable way to measure pain. Further, it was explained that patients in severe pain did not become addicted to narcotics. And the Joint Commission heralded pain control as “the fifth vital sign.”
Where are these thought leaders now?
Graded on responsiveness to patients’ pain and the results of patient surveys on pain control, physicians grudgingly opened the narcotic floodgates and large quantities of prescription narcotics hit the streets. Admittedly, some were written by bad doctors running “pill mills,” but other supplies were diverted by producers, pharmacists, pharmacies, and pharmacy technicians. Hundreds of thousands of Americans became addicted to prescription narcotics, but overdoses were infrequent because there was a unit dose on the street.
Then the medical pendulum swung back, and it was decided that there was too much pain medicine on the streets. The narcotic supply spigots were tightened sharply by the Drug Enforcement Administration, medical boards, and legislatures. It became hard for drug-seeking patients to fill multiple prescriptions, pill mills were shut down, doctors were encouraged to prescribe minimum dosages of narcotic pain relievers, and the price of the unit dose shot up on the street. The patterns of abuse and addiction shifted as heroin became cheaper and more readily available, but hard to dose, particularly when Mexican fentanyl was being sold as “heroin.” Unable to judge the dose of illicitly obtained drugs, addicts began overdosing and dying all over America.
Angry, bereaved family members demanded an accounting for the addiction and deaths of their relatives. Heat was applied to politicians, and a “culprit” was found, physicians! Physicians had made these drugs available and caused all of these people to be addicted!
And thus began the political ascendancy of the pharmacy board, whose members claimed clean hands in this affair. Keen to expand their scope of practice, pharmacists have been trying to find a way into clinical medicine for years. The pharmacy board offered their expertise, and politicians angry at doctors were willing to give the pharmacists’ recommendations a try.
Last year in Ohio, the legislature passed a huge budget reconciliation bill with language tucked in it that authorized the pharmacy board to regulate buprenorphine and other dangerous drugs. The obvious reading of this authority would be that pharmacists were supposed to regulate compounding pharmacies, like the one that produced tainted steroid injections that resulted in 64 deaths in 2012.The regulation is so vague, however, that it could be construed that pharmacists were supposed to regulate everyone in the state, especially since the pharmacy board unilaterally moved to define “dangerous” as any prescription drug. This puts all of medicine in play. The board then declared that it would apply U.S. Pharmacopeial Convention standards (those used for compounding pharmacies) to all physician offices and declared that reconstitution of any drug is considered to be compounding.
To consider physician’s offices as compounding pharmacies is absurd and will degrade patient care by increasing expense and denying access to treatments. Physicians have made and applied individual customized medications to their patients since Galen. It is an integral part of the practice of medicine and has not suddenly become the practice of pharmacy. Using this logic, pharmacists, who have recently won the right to administer vaccinations, should obtain special licenses from the state medical board, since injecting medications is clearly in the purview of medical practice. Physicians have not been killing patients by running dirty compounding pharmacies, pharmacists have. Good, clean up the compounding pharmacies! But applying these compounding rules to physicians’ offices will not save any lives.
This battle has just been joined. The American Medical Association recently passed a resolution declaring that physician compounding should be regulated by state medical boards. This action is most helpful, and another reason for you to join and support the AMA. If you practice in Ohio, you should join the Ohio State Medical Association post haste. They are a big dog in the Ohio legislature, and your membership will influence their efforts.
I hope the Ohio governor’s Common Sense Initiative Office will convene a joint meeting that allows physicians, especially dermatologists, to demonstrate the absurdity of these rules, and their potentially destructive effects on patient care. However, I do not expect the pharmacy board to readily give up this power. Ultimately, the language in the legislative code must add two words after the word “compounding.” The words to be added are “by pharmacists.”
These rules may have to be stayed by a legal injunction. If the legislation is not clarified, a lawsuit against the pharmacy board based on restraint of trade should be successful.
Be vigilant, and watch your state legislatures. Just recently, the pharmacy board of North Dakota has made the same power grab. Stay tuned, as this struggle has national implications.
Dr. Coldiron is past president of the American Academy of Dermatology. He is currently in private practice, but maintains a clinical assistant professorship at the University of Cincinnati. He cares for patients, teaches medical students and residents, and has several active clinical research projects. Dr. Coldiron is the author of more than 80 scientific letters, papers, and several book chapters, and he speaks frequently on a variety of topics. Write to him at [email protected].

Incident to billing
There is apparently confusion about incident to billing of Medicare when employing nurse practitioners and physician assistants. Letters have been published in Dermatology News and other venues that confuse what is straightforward (JAMA Dermatol. 2014;150[11]:1153-9). I will, in my usual blunt fashion, explain incident to billing in dermatology.
First, private insurers may have different standards, but for Medicare, the most succinct government explanation is the introduction of the Office of Inspector General’s audit of incident to billing in the office. More recently, the rules have changed just a little, requiring the incident to biller to bill under the original supervising physician’s billing number, instead of whichever doctor is in the house. When a licensed extender bills under the supervising physician’s NPI number, the extender gets paid at 100% of the Medicare rates. If billing independently, the extender earns only 85%, so it behooves the employing dermatologist to make sure they are billing incident to, whenever possible.

The following examples should cover 95% of dermatologic encounters.
Example No. 1
A new patient is seen by the extender and supervising physician and is diagnosed with a chronic condition such as acne, warts, rosacea, psoriasis, eczema, or benign moles. A care plan is arrived at by the supervising physician, and the treatment is initiated by the extender. This and all subsequent visits can be billed at 100% under the physician’s billing number as long as the problems remain the same and there is a supervising physician in the building. Note that the supervising physician does not have to see the patient on the subsequent visits for the extender to continue to bill incident to. The extender can also bill under the original physician’s number at 100% if there is another physician in the house; the extender doesn’t have to change who they bill under depending on who is available (unless that physician sees the patient). The extender can change medications and change treatments as long as the original problems remain the same.
If the patient develops a new problem – say a growth that may need biopsy – the supervising physician must see the patient in order to bill at 100%. If the patient is not seen by the supervising physician, the extender must bill under their own number and collect only 85%.
Example No. 2
Let’s say a new patient comes in with extensive actinic damage, and is seen by the supervising physician, multiple skin lesions are identified, then the extender freezes multiple actinic keratoses (AKs), and does multiple skin biopsies. These can all be billed under the supervising physician’s number and paid at 100%.
When the same patient returns 6 months later with new AKs and suspicious growths, and the supervising physician does not see the patient, or is not in the house, the extender freezes AKs and does skin biopsies per their best judgment. These procedures must be billed under the extender’s NPI number because they are new problems.
Thus, you can see that for the great majority of diseases that dermatologists treat, you should be collecting the full amount from Medicare, for use of your extenders.
Either physicians are giving away a lot of income (not correctly billing incident to) or there are a lot of unsupervised extenders identifying suspicious lesions and performing surgery without formal training and direct supervision.
What makes me anxious is when I see in the Medicare database that the percentage of skin biopsies billed independently by extenders has increased from 0% to 14% over 10 years (2004-2014). I believe these lesions are being selected for biopsy by the extenders, and the supervising physician never sees them, and these are being billed correctly. This supports my concern about dermatologists setting up extenders in satellite biopsy clinics.
I get even more anxious when I see text from video outreach efforts from the president of the dermatology physician assistants society , stating, “I have my own patient schedule, my own medical assistant, my own rooms, I see new patients, I do my own surgeries, and see my own return patients,” apparently having become a dermatologist by shadowing and working for one.
I believe this is magical thinking. Either the many years of medical school and residency dermatologists went through were unnecessary (possible, but unlikely) or the extenders are overextended. Patients may never know they have not seen a dermatologist after scheduling an appointment with a dermatology group. At least one study has shown that unsupervised extenders may take up to twice as many skin biopsies to make a malignant diagnosis. This suggests that patients are being operated on unnecessarily and costs are being added to the health care system.
In addition, the Medicare data show that the number of skin biopsies has risen 34% over the past 10 years, while the number of skin cancer procedures has increased only 14%. No, these skin biopsies are not being done by extenders working for primary care doctors. Primary care docs perform only 3% of skin biopsies.
Perhaps these extenders are supervised, and their dermatologist employers just don’t want the possibility of a Medicare audit. Let me see: Dermatologists, the most accurate of all coding specialties, are willing to give up 15% of their income because they are confused by these simple rules? What do you think?
Dr. Coldiron is a past president of the American Academy of Dermatology. He is currently in private practice, but maintains a clinical assistant professorship at the University of Cincinnati. He cares for patients, teaches medical students and residents, and has several active clinical research projects. Dr. Coldiron is the author of more than 80 scientific letters, papers, and several book chapters, and he speaks frequently on a variety of topics.
There is apparently confusion about incident to billing of Medicare when employing nurse practitioners and physician assistants. Letters have been published in Dermatology News and other venues that confuse what is straightforward (JAMA Dermatol. 2014;150[11]:1153-9). I will, in my usual blunt fashion, explain incident to billing in dermatology.
First, private insurers may have different standards, but for Medicare, the most succinct government explanation is the introduction of the Office of Inspector General’s audit of incident to billing in the office. More recently, the rules have changed just a little, requiring the incident to biller to bill under the original supervising physician’s billing number, instead of whichever doctor is in the house. When a licensed extender bills under the supervising physician’s NPI number, the extender gets paid at 100% of the Medicare rates. If billing independently, the extender earns only 85%, so it behooves the employing dermatologist to make sure they are billing incident to, whenever possible.
The following examples should cover 95% of dermatologic encounters.
Example No. 1
A new patient is seen by the extender and supervising physician and is diagnosed with a chronic condition such as acne, warts, rosacea, psoriasis, eczema, or benign moles. A care plan is arrived at by the supervising physician, and the treatment is initiated by the extender. This and all subsequent visits can be billed at 100% under the physician’s billing number as long as the problems remain the same and there is a supervising physician in the building. Note that the supervising physician does not have to see the patient on the subsequent visits for the extender to continue to bill incident to. The extender can also bill under the original physician’s number at 100% if there is another physician in the house; the extender doesn’t have to change who they bill under depending on who is available (unless that physician sees the patient). The extender can change medications and change treatments as long as the original problems remain the same.
If the patient develops a new problem – say a growth that may need biopsy – the supervising physician must see the patient in order to bill at 100%. If the patient is not seen by the supervising physician, the extender must bill under their own number and collect only 85%.
Example No. 2
Let’s say a new patient comes in with extensive actinic damage, and is seen by the supervising physician, multiple skin lesions are identified, then the extender freezes multiple actinic keratoses (AKs), and does multiple skin biopsies. These can all be billed under the supervising physician’s number and paid at 100%.
When the same patient returns 6 months later with new AKs and suspicious growths, and the supervising physician does not see the patient, or is not in the house, the extender freezes AKs and does skin biopsies per their best judgment. These procedures must be billed under the extender’s NPI number because they are new problems.
Thus, you can see that for the great majority of diseases that dermatologists treat, you should be collecting the full amount from Medicare, for use of your extenders.
Either physicians are giving away a lot of income (not correctly billing incident to) or there are a lot of unsupervised extenders identifying suspicious lesions and performing surgery without formal training and direct supervision.
What makes me anxious is when I see in the Medicare database that the percentage of skin biopsies billed independently by extenders has increased from 0% to 14% over 10 years (2004-2014). I believe these lesions are being selected for biopsy by the extenders, and the supervising physician never sees them, and these are being billed correctly. This supports my concern about dermatologists setting up extenders in satellite biopsy clinics.
I get even more anxious when I see text from video outreach efforts from the president of the dermatology physician assistants society , stating, “I have my own patient schedule, my own medical assistant, my own rooms, I see new patients, I do my own surgeries, and see my own return patients,” apparently having become a dermatologist by shadowing and working for one.
I believe this is magical thinking. Either the many years of medical school and residency dermatologists went through were unnecessary (possible, but unlikely) or the extenders are overextended. Patients may never know they have not seen a dermatologist after scheduling an appointment with a dermatology group. At least one study has shown that unsupervised extenders may take up to twice as many skin biopsies to make a malignant diagnosis. This suggests that patients are being operated on unnecessarily and costs are being added to the health care system.
In addition, the Medicare data show that the number of skin biopsies has risen 34% over the past 10 years, while the number of skin cancer procedures has increased only 14%. No, these skin biopsies are not being done by extenders working for primary care doctors. Primary care docs perform only 3% of skin biopsies.
Perhaps these extenders are supervised, and their dermatologist employers just don’t want the possibility of a Medicare audit. Let me see: Dermatologists, the most accurate of all coding specialties, are willing to give up 15% of their income because they are confused by these simple rules? What do you think?
Dr. Coldiron is a past president of the American Academy of Dermatology. He is currently in private practice, but maintains a clinical assistant professorship at the University of Cincinnati. He cares for patients, teaches medical students and residents, and has several active clinical research projects. Dr. Coldiron is the author of more than 80 scientific letters, papers, and several book chapters, and he speaks frequently on a variety of topics.
There is apparently confusion about incident to billing of Medicare when employing nurse practitioners and physician assistants. Letters have been published in Dermatology News and other venues that confuse what is straightforward (JAMA Dermatol. 2014;150[11]:1153-9). I will, in my usual blunt fashion, explain incident to billing in dermatology.
First, private insurers may have different standards, but for Medicare, the most succinct government explanation is the introduction of the Office of Inspector General’s audit of incident to billing in the office. More recently, the rules have changed just a little, requiring the incident to biller to bill under the original supervising physician’s billing number, instead of whichever doctor is in the house. When a licensed extender bills under the supervising physician’s NPI number, the extender gets paid at 100% of the Medicare rates. If billing independently, the extender earns only 85%, so it behooves the employing dermatologist to make sure they are billing incident to, whenever possible.
The following examples should cover 95% of dermatologic encounters.
Example No. 1
A new patient is seen by the extender and supervising physician and is diagnosed with a chronic condition such as acne, warts, rosacea, psoriasis, eczema, or benign moles. A care plan is arrived at by the supervising physician, and the treatment is initiated by the extender. This and all subsequent visits can be billed at 100% under the physician’s billing number as long as the problems remain the same and there is a supervising physician in the building. Note that the supervising physician does not have to see the patient on the subsequent visits for the extender to continue to bill incident to. The extender can also bill under the original physician’s number at 100% if there is another physician in the house; the extender doesn’t have to change who they bill under depending on who is available (unless that physician sees the patient). The extender can change medications and change treatments as long as the original problems remain the same.
If the patient develops a new problem – say a growth that may need biopsy – the supervising physician must see the patient in order to bill at 100%. If the patient is not seen by the supervising physician, the extender must bill under their own number and collect only 85%.
Example No. 2
Let’s say a new patient comes in with extensive actinic damage, and is seen by the supervising physician, multiple skin lesions are identified, then the extender freezes multiple actinic keratoses (AKs), and does multiple skin biopsies. These can all be billed under the supervising physician’s number and paid at 100%.
When the same patient returns 6 months later with new AKs and suspicious growths, and the supervising physician does not see the patient, or is not in the house, the extender freezes AKs and does skin biopsies per their best judgment. These procedures must be billed under the extender’s NPI number because they are new problems.
Thus, you can see that for the great majority of diseases that dermatologists treat, you should be collecting the full amount from Medicare, for use of your extenders.
Either physicians are giving away a lot of income (not correctly billing incident to) or there are a lot of unsupervised extenders identifying suspicious lesions and performing surgery without formal training and direct supervision.
What makes me anxious is when I see in the Medicare database that the percentage of skin biopsies billed independently by extenders has increased from 0% to 14% over 10 years (2004-2014). I believe these lesions are being selected for biopsy by the extenders, and the supervising physician never sees them, and these are being billed correctly. This supports my concern about dermatologists setting up extenders in satellite biopsy clinics.
I get even more anxious when I see text from video outreach efforts from the president of the dermatology physician assistants society , stating, “I have my own patient schedule, my own medical assistant, my own rooms, I see new patients, I do my own surgeries, and see my own return patients,” apparently having become a dermatologist by shadowing and working for one.
I believe this is magical thinking. Either the many years of medical school and residency dermatologists went through were unnecessary (possible, but unlikely) or the extenders are overextended. Patients may never know they have not seen a dermatologist after scheduling an appointment with a dermatology group. At least one study has shown that unsupervised extenders may take up to twice as many skin biopsies to make a malignant diagnosis. This suggests that patients are being operated on unnecessarily and costs are being added to the health care system.
In addition, the Medicare data show that the number of skin biopsies has risen 34% over the past 10 years, while the number of skin cancer procedures has increased only 14%. No, these skin biopsies are not being done by extenders working for primary care doctors. Primary care docs perform only 3% of skin biopsies.
Perhaps these extenders are supervised, and their dermatologist employers just don’t want the possibility of a Medicare audit. Let me see: Dermatologists, the most accurate of all coding specialties, are willing to give up 15% of their income because they are confused by these simple rules? What do you think?
Dr. Coldiron is a past president of the American Academy of Dermatology. He is currently in private practice, but maintains a clinical assistant professorship at the University of Cincinnati. He cares for patients, teaches medical students and residents, and has several active clinical research projects. Dr. Coldiron is the author of more than 80 scientific letters, papers, and several book chapters, and he speaks frequently on a variety of topics.

Coldiron Truth: Beware the state pharmacy board
What does the pharmacy board have to do with me? I’m a physician, regulated by the state medical board. Well heads up. If regulations coming your way are adopted, you will have the additional privilege of being licensed, inspected by, and financially supporting your state pharmacy board.
How did all this happen? In 2012, a compounding pharmacy inadequately sterilized multiple lots of methylprednisolone, which were sold around the country and used for intrathecal injections. As a result, 753 patients developed fungal infections, including 386 cases of meningitis, and 64 of them died. The owner of the pharmacy and the head pharmacist are up on second degree murder charges.

But what does this have to do with you?
After a media bonfire, a congressional hearing complete with the taking of the fifth amendment, and a major rewrite of pharmacy regulations with increased scrutiny and oversight, the State of Ohio Board of Pharmacy rushed to adopt rules before reasonable regulations could be worked out by the Food and Drug Administration, the American Medical Association, and the Federation of State Medical Boards. The Ohio board of pharmacy adopted the U.S. Pharmacopeial Convention (USP) regulations, written for compounding pharmacies, and applied them to physicians’ offices.
In an overreaching bureaucratic coup de grace, any practitioners who reconstitute any drug in their offices is considered to be a compounding pharmacy, ordered to pay compounding pharmacy registration fees ($112 yearly), and to undergo the same inspections as compounding pharmacies. You can’t be too safe, you know, and all those registration fees (totaling about $2 million per year in Ohio alone) will decrease what would have been an onerous registration and inspection expense for true compounding pharmacies.
This is the reality we are facing in Ohio, and this situation may soon be “coming to a theater near you.” I understand that several pharmacy boards in other states are preparing to roll out similar regulations.
As a kicker, if the product you reconstitute is preservative free (botulinum toxin anyone?), you must use it or dispose of it within one hour. Yes, one hour. If you dilute bleomycin or 5-fluorouracil (5-FU), you must install an outside vented laminar flow hood, and wear level 5 hazmat gear while drawing it up.
Is this situation insane or what? As the result of a pharmacy in Massachusetts that skirted existing regulations and sold contaminated drugs that killed patients, doctors now need more regulations, licensing, inspections, and fees?
The real problem here, of course, is not the $112 fee. It will be the loss of many drugs and therapies that can be used inexpensively in the office, but will now either be unavailable to patients or available at a greatly increased cost. I pointed this situation out at a pharmacy board meeting, and they helpfully responded that I can have my friendly local pharmacist compound any drug I need in a specific strength and unit dose. Who is going to pay for this? I can make diclofenac or 5-FU cream in my office for less than $20. Instead, it will cost over $700 at the pharmacy! Further, making something fiscally impossible, like installing a laminar flow hood, is not different that denying it outright. I consider this to be restraint of trade.
Don’t allow yourselves to be compromised as Ohio physicians have been. You must be vigilant. Attend the public hearings and testify. In Ohio, the hearings were held over the Christmas holidays. Guess what? No one came to the hearings! You must show up and complain. Loudly. You must point out how patients are going to be hurt, not helped, by these rules. You must point out the superb safety record of physicians when using in-office pharmaceuticals. You must alert your neurology, ophthalmology, gynecology, and urology colleagues to the problem since they all use neurotoxins, too. The primary care doctors all reconstitute drugs (think antibiotics) for office use, too.
These efforts are also part of a larger campaign to give pharmacists a larger clinical role in patient care. If pharmacists license you, if they inspect your office, how can you oppose them when they want clinical privileges?
The fix is to enact a moratorium on regulations until the FDA rules come out. These will be more reasonable than the rules issued by the USP. Another fix is a legislative change that instructs that physicians, not pharmacists, will define what is considered to be a dangerous drug.
It is time to be alert, vigilant, and outspoken. You must do this to preserve your ability to do what is best for patients, to be able to deliver care in an expeditious, efficient, and cost-effective manner. This is what being physician is all about! Keep your state board of pharmacy off your license and out of your office.
Dr. Coldiron is a past president of the American Academy of Dermatology. He is currently in private practice, but maintains a clinical assistant professorship at the University of Cincinnati. He cares for patients, teaches medical students and residents, and has several active clinical research projects. Dr. Coldiron is the author of more than 80 scientific letters, papers, and several book chapters, and he speaks frequently on a variety of topics. Reach him at [email protected].
What does the pharmacy board have to do with me? I’m a physician, regulated by the state medical board. Well heads up. If regulations coming your way are adopted, you will have the additional privilege of being licensed, inspected by, and financially supporting your state pharmacy board.
How did all this happen? In 2012, a compounding pharmacy inadequately sterilized multiple lots of methylprednisolone, which were sold around the country and used for intrathecal injections. As a result, 753 patients developed fungal infections, including 386 cases of meningitis, and 64 of them died. The owner of the pharmacy and the head pharmacist are up on second degree murder charges.
But what does this have to do with you?
After a media bonfire, a congressional hearing complete with the taking of the fifth amendment, and a major rewrite of pharmacy regulations with increased scrutiny and oversight, the State of Ohio Board of Pharmacy rushed to adopt rules before reasonable regulations could be worked out by the Food and Drug Administration, the American Medical Association, and the Federation of State Medical Boards. The Ohio board of pharmacy adopted the U.S. Pharmacopeial Convention (USP) regulations, written for compounding pharmacies, and applied them to physicians’ offices.
In an overreaching bureaucratic coup de grace, any practitioners who reconstitute any drug in their offices is considered to be a compounding pharmacy, ordered to pay compounding pharmacy registration fees ($112 yearly), and to undergo the same inspections as compounding pharmacies. You can’t be too safe, you know, and all those registration fees (totaling about $2 million per year in Ohio alone) will decrease what would have been an onerous registration and inspection expense for true compounding pharmacies.
This is the reality we are facing in Ohio, and this situation may soon be “coming to a theater near you.” I understand that several pharmacy boards in other states are preparing to roll out similar regulations.
As a kicker, if the product you reconstitute is preservative free (botulinum toxin anyone?), you must use it or dispose of it within one hour. Yes, one hour. If you dilute bleomycin or 5-fluorouracil (5-FU), you must install an outside vented laminar flow hood, and wear level 5 hazmat gear while drawing it up.
Is this situation insane or what? As the result of a pharmacy in Massachusetts that skirted existing regulations and sold contaminated drugs that killed patients, doctors now need more regulations, licensing, inspections, and fees?
The real problem here, of course, is not the $112 fee. It will be the loss of many drugs and therapies that can be used inexpensively in the office, but will now either be unavailable to patients or available at a greatly increased cost. I pointed this situation out at a pharmacy board meeting, and they helpfully responded that I can have my friendly local pharmacist compound any drug I need in a specific strength and unit dose. Who is going to pay for this? I can make diclofenac or 5-FU cream in my office for less than $20. Instead, it will cost over $700 at the pharmacy! Further, making something fiscally impossible, like installing a laminar flow hood, is not different that denying it outright. I consider this to be restraint of trade.
Don’t allow yourselves to be compromised as Ohio physicians have been. You must be vigilant. Attend the public hearings and testify. In Ohio, the hearings were held over the Christmas holidays. Guess what? No one came to the hearings! You must show up and complain. Loudly. You must point out how patients are going to be hurt, not helped, by these rules. You must point out the superb safety record of physicians when using in-office pharmaceuticals. You must alert your neurology, ophthalmology, gynecology, and urology colleagues to the problem since they all use neurotoxins, too. The primary care doctors all reconstitute drugs (think antibiotics) for office use, too.
These efforts are also part of a larger campaign to give pharmacists a larger clinical role in patient care. If pharmacists license you, if they inspect your office, how can you oppose them when they want clinical privileges?
The fix is to enact a moratorium on regulations until the FDA rules come out. These will be more reasonable than the rules issued by the USP. Another fix is a legislative change that instructs that physicians, not pharmacists, will define what is considered to be a dangerous drug.
It is time to be alert, vigilant, and outspoken. You must do this to preserve your ability to do what is best for patients, to be able to deliver care in an expeditious, efficient, and cost-effective manner. This is what being physician is all about! Keep your state board of pharmacy off your license and out of your office.
Dr. Coldiron is a past president of the American Academy of Dermatology. He is currently in private practice, but maintains a clinical assistant professorship at the University of Cincinnati. He cares for patients, teaches medical students and residents, and has several active clinical research projects. Dr. Coldiron is the author of more than 80 scientific letters, papers, and several book chapters, and he speaks frequently on a variety of topics. Reach him at [email protected].
What does the pharmacy board have to do with me? I’m a physician, regulated by the state medical board. Well heads up. If regulations coming your way are adopted, you will have the additional privilege of being licensed, inspected by, and financially supporting your state pharmacy board.
How did all this happen? In 2012, a compounding pharmacy inadequately sterilized multiple lots of methylprednisolone, which were sold around the country and used for intrathecal injections. As a result, 753 patients developed fungal infections, including 386 cases of meningitis, and 64 of them died. The owner of the pharmacy and the head pharmacist are up on second degree murder charges.
But what does this have to do with you?
After a media bonfire, a congressional hearing complete with the taking of the fifth amendment, and a major rewrite of pharmacy regulations with increased scrutiny and oversight, the State of Ohio Board of Pharmacy rushed to adopt rules before reasonable regulations could be worked out by the Food and Drug Administration, the American Medical Association, and the Federation of State Medical Boards. The Ohio board of pharmacy adopted the U.S. Pharmacopeial Convention (USP) regulations, written for compounding pharmacies, and applied them to physicians’ offices.
In an overreaching bureaucratic coup de grace, any practitioners who reconstitute any drug in their offices is considered to be a compounding pharmacy, ordered to pay compounding pharmacy registration fees ($112 yearly), and to undergo the same inspections as compounding pharmacies. You can’t be too safe, you know, and all those registration fees (totaling about $2 million per year in Ohio alone) will decrease what would have been an onerous registration and inspection expense for true compounding pharmacies.
This is the reality we are facing in Ohio, and this situation may soon be “coming to a theater near you.” I understand that several pharmacy boards in other states are preparing to roll out similar regulations.
As a kicker, if the product you reconstitute is preservative free (botulinum toxin anyone?), you must use it or dispose of it within one hour. Yes, one hour. If you dilute bleomycin or 5-fluorouracil (5-FU), you must install an outside vented laminar flow hood, and wear level 5 hazmat gear while drawing it up.
Is this situation insane or what? As the result of a pharmacy in Massachusetts that skirted existing regulations and sold contaminated drugs that killed patients, doctors now need more regulations, licensing, inspections, and fees?
The real problem here, of course, is not the $112 fee. It will be the loss of many drugs and therapies that can be used inexpensively in the office, but will now either be unavailable to patients or available at a greatly increased cost. I pointed this situation out at a pharmacy board meeting, and they helpfully responded that I can have my friendly local pharmacist compound any drug I need in a specific strength and unit dose. Who is going to pay for this? I can make diclofenac or 5-FU cream in my office for less than $20. Instead, it will cost over $700 at the pharmacy! Further, making something fiscally impossible, like installing a laminar flow hood, is not different that denying it outright. I consider this to be restraint of trade.
Don’t allow yourselves to be compromised as Ohio physicians have been. You must be vigilant. Attend the public hearings and testify. In Ohio, the hearings were held over the Christmas holidays. Guess what? No one came to the hearings! You must show up and complain. Loudly. You must point out how patients are going to be hurt, not helped, by these rules. You must point out the superb safety record of physicians when using in-office pharmaceuticals. You must alert your neurology, ophthalmology, gynecology, and urology colleagues to the problem since they all use neurotoxins, too. The primary care doctors all reconstitute drugs (think antibiotics) for office use, too.
These efforts are also part of a larger campaign to give pharmacists a larger clinical role in patient care. If pharmacists license you, if they inspect your office, how can you oppose them when they want clinical privileges?
The fix is to enact a moratorium on regulations until the FDA rules come out. These will be more reasonable than the rules issued by the USP. Another fix is a legislative change that instructs that physicians, not pharmacists, will define what is considered to be a dangerous drug.
It is time to be alert, vigilant, and outspoken. You must do this to preserve your ability to do what is best for patients, to be able to deliver care in an expeditious, efficient, and cost-effective manner. This is what being physician is all about! Keep your state board of pharmacy off your license and out of your office.
Dr. Coldiron is a past president of the American Academy of Dermatology. He is currently in private practice, but maintains a clinical assistant professorship at the University of Cincinnati. He cares for patients, teaches medical students and residents, and has several active clinical research projects. Dr. Coldiron is the author of more than 80 scientific letters, papers, and several book chapters, and he speaks frequently on a variety of topics. Reach him at [email protected].

Health care reform 6 years out
Well, UnitedHealthcare has announced that it’s pulling out of the health insurance exchanges because of huge losses. This may be the mortal wound. It is apparent that health care reform is undergoing a slow-motion implosion. Most of the Affordable Care Act has been delayed or canceled, including the individual and employer mandates, the independent payment advisory board (thank goodness), Medicare Advantage payment cuts, the Cadillac health insurance tax, and auto enrollment. Half the insurance co-ops have failed, and the remainder are running at a deficit. The exchange-plan premiums are increasing dramatically. In fact, with 71 cancellations and delays, health care reform has already effectively been repealed.
Insurance coverage has increased by about 8% (10 million more into Medicaid, 80% of all new insureds), particularly of the poor. On the flip side, millions have lost their old insurance, now have very high deductibles, and have lost their doctors. High-deductible insurance means that patients really aren’t going to be able to use their insurance, unless they have a catastrophic event and are hospitalized.
High-deductible insurance that pays at Medicaid rates, and Medicaid, are a particularly bad mix for dermatologists. Medicaid does not even cover the cost of overhead in the office setting, and many patients cannot afford their high deductibles. Almost all of the cost-efficient in-office curative procedures we offer cost less than the deductible. We are all seeing patients delay and delay treatment until the end of the year, hoping they won’t have to meet their deductible.
Many patients, excited that they finally have health insurance, are bitterly disappointed to find that they really don’t, except for their annual physical exam and the emergency room. The doctor is put in the poisonous position of explaining insurance policy limitations, and being collection agent. Poor Medicaid patients, who get free care at the hospital, go to the emergency room for minor complaints that would be much more efficiently handled in the office setting. This clogs emergency rooms, and is ferociously expensive. This is the opposite of what health care reform was supposed to do.
Insurance premiums are rising rapidly because somebody has to pay for coverage of the millions who could not formerly qualify for health insurance because of preexisting conditions. The current exchanges allow dropping in and out of insurance coverage and, with the elimination of preexisting conditions, this allows patients to game the system and wait until they fall ill to buy insurance. Historically, almost all were in the pool of insureds and the risk was predictable.
There is no way for politicians to go back and remove millions of chronically ill from the coverage rolls. Imagine the nightly news. As a physician, it is impossible not to feel compassion for these chronically ill patients, but it would have cost a lot less to just make them eligible for Medicaid to begin with.
OK, it is easy to complain, but what are possible solutions? Patients need health care savings accounts for a sizable portion of their deductibles. Physician rosters need to be real time and accurate. Networks need to be adequate (another column, another day). Medicaid rates need to increase to Medicare levels, as they did for the initial 2-year teaser period for primary care physicians. Exchange plan payment rates need to match their commercial insurance wrappers, instead of Medicaid rates, so physicians can afford to accept them. Stricter enrollment periods are needed, so patients cannot game the system, signing up only when they get sick or want a joint replaced. If you are going to provide health insurance for all, then make sure the health insurance is real, not hollow.
Dr. Coldiron is a past president of the American Academy of Dermatology. He is currently in private practice, but maintains a clinical assistant professorship at the University of Cincinnati. He cares for patients, teaches medical students and residents, and has several active clinical research projects. Dr. Coldiron is the author of more than 80 scientific letters, papers, and several book chapters, and he speaks frequently on a variety of topics. Write to him at [email protected].
Well, UnitedHealthcare has announced that it’s pulling out of the health insurance exchanges because of huge losses. This may be the mortal wound. It is apparent that health care reform is undergoing a slow-motion implosion. Most of the Affordable Care Act has been delayed or canceled, including the individual and employer mandates, the independent payment advisory board (thank goodness), Medicare Advantage payment cuts, the Cadillac health insurance tax, and auto enrollment. Half the insurance co-ops have failed, and the remainder are running at a deficit. The exchange-plan premiums are increasing dramatically. In fact, with 71 cancellations and delays, health care reform has already effectively been repealed.
Insurance coverage has increased by about 8% (10 million more into Medicaid, 80% of all new insureds), particularly of the poor. On the flip side, millions have lost their old insurance, now have very high deductibles, and have lost their doctors. High-deductible insurance means that patients really aren’t going to be able to use their insurance, unless they have a catastrophic event and are hospitalized.
High-deductible insurance that pays at Medicaid rates, and Medicaid, are a particularly bad mix for dermatologists. Medicaid does not even cover the cost of overhead in the office setting, and many patients cannot afford their high deductibles. Almost all of the cost-efficient in-office curative procedures we offer cost less than the deductible. We are all seeing patients delay and delay treatment until the end of the year, hoping they won’t have to meet their deductible.
Many patients, excited that they finally have health insurance, are bitterly disappointed to find that they really don’t, except for their annual physical exam and the emergency room. The doctor is put in the poisonous position of explaining insurance policy limitations, and being collection agent. Poor Medicaid patients, who get free care at the hospital, go to the emergency room for minor complaints that would be much more efficiently handled in the office setting. This clogs emergency rooms, and is ferociously expensive. This is the opposite of what health care reform was supposed to do.
Insurance premiums are rising rapidly because somebody has to pay for coverage of the millions who could not formerly qualify for health insurance because of preexisting conditions. The current exchanges allow dropping in and out of insurance coverage and, with the elimination of preexisting conditions, this allows patients to game the system and wait until they fall ill to buy insurance. Historically, almost all were in the pool of insureds and the risk was predictable.
There is no way for politicians to go back and remove millions of chronically ill from the coverage rolls. Imagine the nightly news. As a physician, it is impossible not to feel compassion for these chronically ill patients, but it would have cost a lot less to just make them eligible for Medicaid to begin with.
OK, it is easy to complain, but what are possible solutions? Patients need health care savings accounts for a sizable portion of their deductibles. Physician rosters need to be real time and accurate. Networks need to be adequate (another column, another day). Medicaid rates need to increase to Medicare levels, as they did for the initial 2-year teaser period for primary care physicians. Exchange plan payment rates need to match their commercial insurance wrappers, instead of Medicaid rates, so physicians can afford to accept them. Stricter enrollment periods are needed, so patients cannot game the system, signing up only when they get sick or want a joint replaced. If you are going to provide health insurance for all, then make sure the health insurance is real, not hollow.
Dr. Coldiron is a past president of the American Academy of Dermatology. He is currently in private practice, but maintains a clinical assistant professorship at the University of Cincinnati. He cares for patients, teaches medical students and residents, and has several active clinical research projects. Dr. Coldiron is the author of more than 80 scientific letters, papers, and several book chapters, and he speaks frequently on a variety of topics. Write to him at [email protected].
Well, UnitedHealthcare has announced that it’s pulling out of the health insurance exchanges because of huge losses. This may be the mortal wound. It is apparent that health care reform is undergoing a slow-motion implosion. Most of the Affordable Care Act has been delayed or canceled, including the individual and employer mandates, the independent payment advisory board (thank goodness), Medicare Advantage payment cuts, the Cadillac health insurance tax, and auto enrollment. Half the insurance co-ops have failed, and the remainder are running at a deficit. The exchange-plan premiums are increasing dramatically. In fact, with 71 cancellations and delays, health care reform has already effectively been repealed.
Insurance coverage has increased by about 8% (10 million more into Medicaid, 80% of all new insureds), particularly of the poor. On the flip side, millions have lost their old insurance, now have very high deductibles, and have lost their doctors. High-deductible insurance means that patients really aren’t going to be able to use their insurance, unless they have a catastrophic event and are hospitalized.
High-deductible insurance that pays at Medicaid rates, and Medicaid, are a particularly bad mix for dermatologists. Medicaid does not even cover the cost of overhead in the office setting, and many patients cannot afford their high deductibles. Almost all of the cost-efficient in-office curative procedures we offer cost less than the deductible. We are all seeing patients delay and delay treatment until the end of the year, hoping they won’t have to meet their deductible.
Many patients, excited that they finally have health insurance, are bitterly disappointed to find that they really don’t, except for their annual physical exam and the emergency room. The doctor is put in the poisonous position of explaining insurance policy limitations, and being collection agent. Poor Medicaid patients, who get free care at the hospital, go to the emergency room for minor complaints that would be much more efficiently handled in the office setting. This clogs emergency rooms, and is ferociously expensive. This is the opposite of what health care reform was supposed to do.
Insurance premiums are rising rapidly because somebody has to pay for coverage of the millions who could not formerly qualify for health insurance because of preexisting conditions. The current exchanges allow dropping in and out of insurance coverage and, with the elimination of preexisting conditions, this allows patients to game the system and wait until they fall ill to buy insurance. Historically, almost all were in the pool of insureds and the risk was predictable.
There is no way for politicians to go back and remove millions of chronically ill from the coverage rolls. Imagine the nightly news. As a physician, it is impossible not to feel compassion for these chronically ill patients, but it would have cost a lot less to just make them eligible for Medicaid to begin with.
OK, it is easy to complain, but what are possible solutions? Patients need health care savings accounts for a sizable portion of their deductibles. Physician rosters need to be real time and accurate. Networks need to be adequate (another column, another day). Medicaid rates need to increase to Medicare levels, as they did for the initial 2-year teaser period for primary care physicians. Exchange plan payment rates need to match their commercial insurance wrappers, instead of Medicaid rates, so physicians can afford to accept them. Stricter enrollment periods are needed, so patients cannot game the system, signing up only when they get sick or want a joint replaced. If you are going to provide health insurance for all, then make sure the health insurance is real, not hollow.
Dr. Coldiron is a past president of the American Academy of Dermatology. He is currently in private practice, but maintains a clinical assistant professorship at the University of Cincinnati. He cares for patients, teaches medical students and residents, and has several active clinical research projects. Dr. Coldiron is the author of more than 80 scientific letters, papers, and several book chapters, and he speaks frequently on a variety of topics. Write to him at [email protected].
Coldiron Truth: Office safety
Wait, I know what you’re thinking, boring, dry, and don’t scold me. I am not going to do any of that today, and instead am going to tell you how to easily improve patient care, save money, and improve staff morale.
The easiest things to do to improve safety in the office include better communications, infection control, correct patient/site identification, dealing with emergencies, and staff safety.

Staff communication is often surprisingly poor, and physicians often assume staff can read our minds (and if they have worked for you for many years, maybe they can!). Always make sure staff – and patients – repeat back complicated instructions (better to start by making them less complicated). Never assume your patients are literate, 14% of adults cannot read, so make sure your staff goes over printed materials with the patients.
Something easy you can do is eliminate abbreviations from your prescription pad and your medical record.
Failure to follow up on path reports and lost biopsies is a frequent cause for lawsuits. You need to make sure you have a redundant system for tracking and reporting pathology results. In addition to the old reliable pathology log book, you need a sequential system ensuring that the specimen made it to the lab, that the result was generated and received, that the patient was notified, and that further action was taken if needed. If this is integrated into your electronic medical record, so much the better, but you still need a paper backup log book, “just in case.”
We all take basic infection precautions when performing procedures, including alcohol hand gel, eye protection, gloves, mask, and cleaning of surgical sites prior to excision. When there are wound infections, which should be rare, you should always culture, and if there is a cluster of infections, particularly with methicillin-resistant staphylococcus aureus (MRSA), you should consider culturing the anterior nares of the staff. Alternatively, you can preemptively treat the staff with intranasal topical mupirocin daily for 2 weeks.
Measuring the use of alcohol gel before and after staff education is an easy and beneficial quality improvement project. You and your staff are, of course, vaccinated for hepatitis B, and yearly for influenza, and you should consider PPD testing every 2 years for everyone. My asymptomatic receptionist converted, and needed prophylactic tuberculosis treatment and contact tracing.
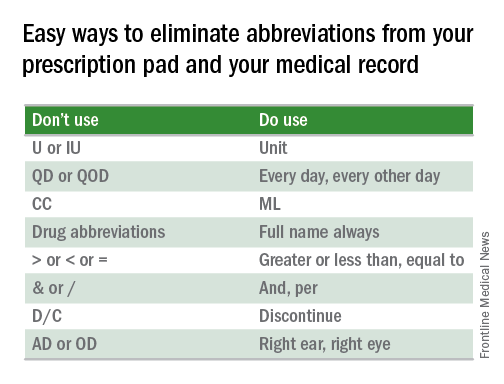
Wrong-site surgery is a frequent problem for dermatologists. Many of our biopsies are tangential, heal almost invisibly, without marking sutures, and patients have battle-scarred skin, and are elderly. The patients may have trouble remembering or seeing where the biopsy was, so good charts and family members are helpful. Photographs of the biopsy sites can be priceless. If the site still cannot be identified, then rebiopsy, or close follow-up is indicated.
Emergencies are rare, but it is prudent to have an automatic external defibrillator in the office. These are automated, so Advanced Cardiovascular Life Support (ACLS), or even basic CPR is not required to operate them, and the survival rate after cardiac arrest increases from 2% to 50%. When it has to be replaced after 5 years, take the old one home and teach your spouse how to use it, and maybe they will.
If you do a lot of surgery you may want to get the ACLS training and buy the crash cart drug kit, but many of the drugs have become ferociously expensive, despite being generic.
Staff safety is a crucial consideration and showing concern boosts staff morale. You should dispose of sharps directly into a sharps container and remove the sharps from the tray at the end of the case. You should have a written protocol for needle sticks. I keep the red top tubes, and the first 2 days of HIV medication on site. Sometimes a patient is HIV positive, the sharp exposure is unknown (a cryostat tissue tease for example), or the patient refuses to have their blood drawn. Less obvious, but important to staff, are locks on doors, alarm systems, good parking lot lighting, and security cameras.
Office safety may seem mundane but a few simple measures can save you a fortune, boost employee morale, and most important of all, improve patient care.
Dr. Coldiron is a past president of the American Academy of Dermatology. He is currently in private practice, but maintains a clinical assistant professorship at the University of Cincinnati. He cares for patients, teaches medical students and residents, and has several active clinical research projects. Dr. Coldiron is the author of more than 80 scientific letters, papers, and several book chapters, and he speaks frequently on a variety of topics.
Wait, I know what you’re thinking, boring, dry, and don’t scold me. I am not going to do any of that today, and instead am going to tell you how to easily improve patient care, save money, and improve staff morale.
The easiest things to do to improve safety in the office include better communications, infection control, correct patient/site identification, dealing with emergencies, and staff safety.
Staff communication is often surprisingly poor, and physicians often assume staff can read our minds (and if they have worked for you for many years, maybe they can!). Always make sure staff – and patients – repeat back complicated instructions (better to start by making them less complicated). Never assume your patients are literate, 14% of adults cannot read, so make sure your staff goes over printed materials with the patients.
Something easy you can do is eliminate abbreviations from your prescription pad and your medical record.
Failure to follow up on path reports and lost biopsies is a frequent cause for lawsuits. You need to make sure you have a redundant system for tracking and reporting pathology results. In addition to the old reliable pathology log book, you need a sequential system ensuring that the specimen made it to the lab, that the result was generated and received, that the patient was notified, and that further action was taken if needed. If this is integrated into your electronic medical record, so much the better, but you still need a paper backup log book, “just in case.”
We all take basic infection precautions when performing procedures, including alcohol hand gel, eye protection, gloves, mask, and cleaning of surgical sites prior to excision. When there are wound infections, which should be rare, you should always culture, and if there is a cluster of infections, particularly with methicillin-resistant staphylococcus aureus (MRSA), you should consider culturing the anterior nares of the staff. Alternatively, you can preemptively treat the staff with intranasal topical mupirocin daily for 2 weeks.
Measuring the use of alcohol gel before and after staff education is an easy and beneficial quality improvement project. You and your staff are, of course, vaccinated for hepatitis B, and yearly for influenza, and you should consider PPD testing every 2 years for everyone. My asymptomatic receptionist converted, and needed prophylactic tuberculosis treatment and contact tracing.
Wrong-site surgery is a frequent problem for dermatologists. Many of our biopsies are tangential, heal almost invisibly, without marking sutures, and patients have battle-scarred skin, and are elderly. The patients may have trouble remembering or seeing where the biopsy was, so good charts and family members are helpful. Photographs of the biopsy sites can be priceless. If the site still cannot be identified, then rebiopsy, or close follow-up is indicated.
Emergencies are rare, but it is prudent to have an automatic external defibrillator in the office. These are automated, so Advanced Cardiovascular Life Support (ACLS), or even basic CPR is not required to operate them, and the survival rate after cardiac arrest increases from 2% to 50%. When it has to be replaced after 5 years, take the old one home and teach your spouse how to use it, and maybe they will.
If you do a lot of surgery you may want to get the ACLS training and buy the crash cart drug kit, but many of the drugs have become ferociously expensive, despite being generic.
Staff safety is a crucial consideration and showing concern boosts staff morale. You should dispose of sharps directly into a sharps container and remove the sharps from the tray at the end of the case. You should have a written protocol for needle sticks. I keep the red top tubes, and the first 2 days of HIV medication on site. Sometimes a patient is HIV positive, the sharp exposure is unknown (a cryostat tissue tease for example), or the patient refuses to have their blood drawn. Less obvious, but important to staff, are locks on doors, alarm systems, good parking lot lighting, and security cameras.
Office safety may seem mundane but a few simple measures can save you a fortune, boost employee morale, and most important of all, improve patient care.
Dr. Coldiron is a past president of the American Academy of Dermatology. He is currently in private practice, but maintains a clinical assistant professorship at the University of Cincinnati. He cares for patients, teaches medical students and residents, and has several active clinical research projects. Dr. Coldiron is the author of more than 80 scientific letters, papers, and several book chapters, and he speaks frequently on a variety of topics.
Wait, I know what you’re thinking, boring, dry, and don’t scold me. I am not going to do any of that today, and instead am going to tell you how to easily improve patient care, save money, and improve staff morale.
The easiest things to do to improve safety in the office include better communications, infection control, correct patient/site identification, dealing with emergencies, and staff safety.
Staff communication is often surprisingly poor, and physicians often assume staff can read our minds (and if they have worked for you for many years, maybe they can!). Always make sure staff – and patients – repeat back complicated instructions (better to start by making them less complicated). Never assume your patients are literate, 14% of adults cannot read, so make sure your staff goes over printed materials with the patients.
Something easy you can do is eliminate abbreviations from your prescription pad and your medical record.
Failure to follow up on path reports and lost biopsies is a frequent cause for lawsuits. You need to make sure you have a redundant system for tracking and reporting pathology results. In addition to the old reliable pathology log book, you need a sequential system ensuring that the specimen made it to the lab, that the result was generated and received, that the patient was notified, and that further action was taken if needed. If this is integrated into your electronic medical record, so much the better, but you still need a paper backup log book, “just in case.”
We all take basic infection precautions when performing procedures, including alcohol hand gel, eye protection, gloves, mask, and cleaning of surgical sites prior to excision. When there are wound infections, which should be rare, you should always culture, and if there is a cluster of infections, particularly with methicillin-resistant staphylococcus aureus (MRSA), you should consider culturing the anterior nares of the staff. Alternatively, you can preemptively treat the staff with intranasal topical mupirocin daily for 2 weeks.
Measuring the use of alcohol gel before and after staff education is an easy and beneficial quality improvement project. You and your staff are, of course, vaccinated for hepatitis B, and yearly for influenza, and you should consider PPD testing every 2 years for everyone. My asymptomatic receptionist converted, and needed prophylactic tuberculosis treatment and contact tracing.
Wrong-site surgery is a frequent problem for dermatologists. Many of our biopsies are tangential, heal almost invisibly, without marking sutures, and patients have battle-scarred skin, and are elderly. The patients may have trouble remembering or seeing where the biopsy was, so good charts and family members are helpful. Photographs of the biopsy sites can be priceless. If the site still cannot be identified, then rebiopsy, or close follow-up is indicated.
Emergencies are rare, but it is prudent to have an automatic external defibrillator in the office. These are automated, so Advanced Cardiovascular Life Support (ACLS), or even basic CPR is not required to operate them, and the survival rate after cardiac arrest increases from 2% to 50%. When it has to be replaced after 5 years, take the old one home and teach your spouse how to use it, and maybe they will.
If you do a lot of surgery you may want to get the ACLS training and buy the crash cart drug kit, but many of the drugs have become ferociously expensive, despite being generic.
Staff safety is a crucial consideration and showing concern boosts staff morale. You should dispose of sharps directly into a sharps container and remove the sharps from the tray at the end of the case. You should have a written protocol for needle sticks. I keep the red top tubes, and the first 2 days of HIV medication on site. Sometimes a patient is HIV positive, the sharp exposure is unknown (a cryostat tissue tease for example), or the patient refuses to have their blood drawn. Less obvious, but important to staff, are locks on doors, alarm systems, good parking lot lighting, and security cameras.
Office safety may seem mundane but a few simple measures can save you a fortune, boost employee morale, and most important of all, improve patient care.
Dr. Coldiron is a past president of the American Academy of Dermatology. He is currently in private practice, but maintains a clinical assistant professorship at the University of Cincinnati. He cares for patients, teaches medical students and residents, and has several active clinical research projects. Dr. Coldiron is the author of more than 80 scientific letters, papers, and several book chapters, and he speaks frequently on a variety of topics.

Getting involved
I hear it at least 6 times a month: “How can I get involved? How do I get on an AAD committee?” The quick answer is to pick a committee where you have some expertise, and get others (including other organizations where you have done committee work) to write supporting letters to the American Academy of Dermatology president-elect (this year Henry Lim). In October, the president-elect fills the empty committee spots, and whoever has the most expertise and support usually gets the spot. The support of the existing committee chair is most helpful as well.
The focus of the question above, however, is too limited. AAD committee work is important, but there are many other venues in which you can develop your skills and make an impact. The best spot to start is probably your local and state dermatology or county and state medical societies. They are always looking for new enthusiastic members. You will learn about parliamentary order and how to write and defend a resolution, and you may advance quickly – perhaps right up to a state leadership position or the state American Medical Association delegation. In the state and local societies, you will also learn about challenges practitioners face outside of dermatology. The skills you will develop are useful in any physician organization, including the AAD. The state medical societies are always interested in members who will travel to testify at the state legislature. This can be a valuable experience as well.

There are many state dermatology societies that need you for advocacy, service, and leadership. These are superb places to learn leadership skills and state advocacy.
The AAD “sister” societies – including the American Society for Dermatologic Surgery (ASDS), the American College of Mohs Surgery (ACMS), the American Society for Mohs Surgery ASMS, and the Women’s Dermatologic Society (WDS) – also have multiple committees, boards, and officer positions, which do advocacy and develop policy, and are arenas in which you can learn and contribute.
You should attend a meeting of the advisory board to the AAD. This is full-throttle democracy. State and local dermatology organizations are allowed to send delegates and alternate delegates to the advisory board, and these spots often go empty. The advisory board’s resolutions go directly to the AAD board of directors to be acted on. In addition, the advisory board also appoints one of the directors to the AAD board of directors. This opportunity is underappreciated.
Involvement in SkinPAC would be most welcome (and earns you an asterisk by your name on the committee nomination roster!). The importance of legislative efforts cannot be overemphasized. Attending the legislative conference should be high on your list of things to do when you ask how to get involved.
You should also consider community involvement, regardless of your other activities. This will help your larger community in ways you could never imagine. I have served on the local health department for many years and find it rewarding and interesting. They are always keen to have more medical doctors on the board.
You can get appointed by writing the local officials (the county judge executive or mayor of the city) and expressing an interest, or to the medical director of the health department.
State medical boards are a large time commitment and a lot of work, but can be most important. We need more dermatologists on state medical boards since we are a unique specialty, and other physicians have no idea what you do in your office. Medical boards often make policy, and can have a huge impact. These positions are competitive in larger states and may require some political support from the governor in order for you to be appointed.
Charitable work is also important. Most of us volunteer to do skin cancer screenings, but there are also opportunities to provide dermatology services overseas. Dermatologists are rare in most of the world, and you will find the service most gratifying. There are opportunities closer to home in the free clinics almost anywhere.
Engagement and service by as many as possible is crucial for a specialty as small as ours, and your efforts will be noted and appreciated. There are thousands of ways to get involved, and I encourage you to get in there and do it.
Dr. Coldiron is a past president of the American Academy of Dermatology. He is currently in private practice, but maintains a clinical assistant professorship at the University of Cincinnati. He cares for patients, teaches medical students and residents, and has several active clinical research projects. Dr. Coldiron is the author of more than 80 scientific letters, papers, and several book chapters, and he speaks frequently on a variety of topics.
I hear it at least 6 times a month: “How can I get involved? How do I get on an AAD committee?” The quick answer is to pick a committee where you have some expertise, and get others (including other organizations where you have done committee work) to write supporting letters to the American Academy of Dermatology president-elect (this year Henry Lim). In October, the president-elect fills the empty committee spots, and whoever has the most expertise and support usually gets the spot. The support of the existing committee chair is most helpful as well.
The focus of the question above, however, is too limited. AAD committee work is important, but there are many other venues in which you can develop your skills and make an impact. The best spot to start is probably your local and state dermatology or county and state medical societies. They are always looking for new enthusiastic members. You will learn about parliamentary order and how to write and defend a resolution, and you may advance quickly – perhaps right up to a state leadership position or the state American Medical Association delegation. In the state and local societies, you will also learn about challenges practitioners face outside of dermatology. The skills you will develop are useful in any physician organization, including the AAD. The state medical societies are always interested in members who will travel to testify at the state legislature. This can be a valuable experience as well.
There are many state dermatology societies that need you for advocacy, service, and leadership. These are superb places to learn leadership skills and state advocacy.
The AAD “sister” societies – including the American Society for Dermatologic Surgery (ASDS), the American College of Mohs Surgery (ACMS), the American Society for Mohs Surgery ASMS, and the Women’s Dermatologic Society (WDS) – also have multiple committees, boards, and officer positions, which do advocacy and develop policy, and are arenas in which you can learn and contribute.
You should attend a meeting of the advisory board to the AAD. This is full-throttle democracy. State and local dermatology organizations are allowed to send delegates and alternate delegates to the advisory board, and these spots often go empty. The advisory board’s resolutions go directly to the AAD board of directors to be acted on. In addition, the advisory board also appoints one of the directors to the AAD board of directors. This opportunity is underappreciated.
Involvement in SkinPAC would be most welcome (and earns you an asterisk by your name on the committee nomination roster!). The importance of legislative efforts cannot be overemphasized. Attending the legislative conference should be high on your list of things to do when you ask how to get involved.
You should also consider community involvement, regardless of your other activities. This will help your larger community in ways you could never imagine. I have served on the local health department for many years and find it rewarding and interesting. They are always keen to have more medical doctors on the board.
You can get appointed by writing the local officials (the county judge executive or mayor of the city) and expressing an interest, or to the medical director of the health department.
State medical boards are a large time commitment and a lot of work, but can be most important. We need more dermatologists on state medical boards since we are a unique specialty, and other physicians have no idea what you do in your office. Medical boards often make policy, and can have a huge impact. These positions are competitive in larger states and may require some political support from the governor in order for you to be appointed.
Charitable work is also important. Most of us volunteer to do skin cancer screenings, but there are also opportunities to provide dermatology services overseas. Dermatologists are rare in most of the world, and you will find the service most gratifying. There are opportunities closer to home in the free clinics almost anywhere.
Engagement and service by as many as possible is crucial for a specialty as small as ours, and your efforts will be noted and appreciated. There are thousands of ways to get involved, and I encourage you to get in there and do it.
Dr. Coldiron is a past president of the American Academy of Dermatology. He is currently in private practice, but maintains a clinical assistant professorship at the University of Cincinnati. He cares for patients, teaches medical students and residents, and has several active clinical research projects. Dr. Coldiron is the author of more than 80 scientific letters, papers, and several book chapters, and he speaks frequently on a variety of topics.
I hear it at least 6 times a month: “How can I get involved? How do I get on an AAD committee?” The quick answer is to pick a committee where you have some expertise, and get others (including other organizations where you have done committee work) to write supporting letters to the American Academy of Dermatology president-elect (this year Henry Lim). In October, the president-elect fills the empty committee spots, and whoever has the most expertise and support usually gets the spot. The support of the existing committee chair is most helpful as well.
The focus of the question above, however, is too limited. AAD committee work is important, but there are many other venues in which you can develop your skills and make an impact. The best spot to start is probably your local and state dermatology or county and state medical societies. They are always looking for new enthusiastic members. You will learn about parliamentary order and how to write and defend a resolution, and you may advance quickly – perhaps right up to a state leadership position or the state American Medical Association delegation. In the state and local societies, you will also learn about challenges practitioners face outside of dermatology. The skills you will develop are useful in any physician organization, including the AAD. The state medical societies are always interested in members who will travel to testify at the state legislature. This can be a valuable experience as well.
There are many state dermatology societies that need you for advocacy, service, and leadership. These are superb places to learn leadership skills and state advocacy.
The AAD “sister” societies – including the American Society for Dermatologic Surgery (ASDS), the American College of Mohs Surgery (ACMS), the American Society for Mohs Surgery ASMS, and the Women’s Dermatologic Society (WDS) – also have multiple committees, boards, and officer positions, which do advocacy and develop policy, and are arenas in which you can learn and contribute.
You should attend a meeting of the advisory board to the AAD. This is full-throttle democracy. State and local dermatology organizations are allowed to send delegates and alternate delegates to the advisory board, and these spots often go empty. The advisory board’s resolutions go directly to the AAD board of directors to be acted on. In addition, the advisory board also appoints one of the directors to the AAD board of directors. This opportunity is underappreciated.
Involvement in SkinPAC would be most welcome (and earns you an asterisk by your name on the committee nomination roster!). The importance of legislative efforts cannot be overemphasized. Attending the legislative conference should be high on your list of things to do when you ask how to get involved.
You should also consider community involvement, regardless of your other activities. This will help your larger community in ways you could never imagine. I have served on the local health department for many years and find it rewarding and interesting. They are always keen to have more medical doctors on the board.
You can get appointed by writing the local officials (the county judge executive or mayor of the city) and expressing an interest, or to the medical director of the health department.
State medical boards are a large time commitment and a lot of work, but can be most important. We need more dermatologists on state medical boards since we are a unique specialty, and other physicians have no idea what you do in your office. Medical boards often make policy, and can have a huge impact. These positions are competitive in larger states and may require some political support from the governor in order for you to be appointed.
Charitable work is also important. Most of us volunteer to do skin cancer screenings, but there are also opportunities to provide dermatology services overseas. Dermatologists are rare in most of the world, and you will find the service most gratifying. There are opportunities closer to home in the free clinics almost anywhere.
Engagement and service by as many as possible is crucial for a specialty as small as ours, and your efforts will be noted and appreciated. There are thousands of ways to get involved, and I encourage you to get in there and do it.
Dr. Coldiron is a past president of the American Academy of Dermatology. He is currently in private practice, but maintains a clinical assistant professorship at the University of Cincinnati. He cares for patients, teaches medical students and residents, and has several active clinical research projects. Dr. Coldiron is the author of more than 80 scientific letters, papers, and several book chapters, and he speaks frequently on a variety of topics.

Benchmarks are coming
We have actively avoided benchmarks in medicine since time immemorial. There is a strong argument that rote, one-size-fits-all parameters for care medicine are bad for our patients, and obviously they interfere with our flexibility in dealing with complex obscure diseases. This flexibility is critical in dermatology, where we deal with over 3,000 diseases, and there truly is more art than science involved in treating some of them.
Nonetheless, here come the benchmarks. Since we have not provided them, they have been provided for us. Look no further than United Health Care’s Optum program, or Cigna’s star ratings, both of which rank on average costs, without regard to subspecialty or intensity of disease.

Benchmarks have proven useful in industry and have improved quality there. I expect they will be most annoying to practicing physicians. There are also great variations in practice patterns we must make sure are accounted for. A pediatric dermatologist, for example, does radically fewer skin biopsies than a Mohs surgeon, and diagnoses many fewer malignancies. However, some things are inexplicable, even after opening two standard deviations, and you need to be aware they may be coming.
The Medicare data release was an eye opener for many. This information is readily available on multiple web sites in numeric and graphic display. You should look yourself and your “peers” up on the Wall Street Journal or ProPublicaweb sites. For example, it is hard to fathom how every closure can be a flap, or how every Mohs case is four stages. Or even more bizarre, how you can do Mohs and never have a second stage. It is hard to understand how most dermatologists have a certain number of skin biopsies or shave excisions per patient encounter and others ten times as many. With this in mind, I encourage all of you to look at your own ratios of procedures compared to your peers. Recall that Medicare data lag two years before publication. Areas that could be under scrutiny include:
• Number of skin biopsies per encounter.
• Number of repeat patient encounters per year.
• Number of lesion destructions per patient.
• Ratio of first to additional layers of Mohs.
• Number of Mohs procedures on trunk and extremities, compared with head and neck.
• Percentage of closures done with adjacent tissue transfers.
• Number of shave excisions per patient.
• Number of complex closures, compared with layered closures, particularly on the trunk and extremities.
• Number of diagnostic frozen sections.
• Frequency of use of special stains on pathology specimens.
We need to be actively involved in the development of these so that we are not forced into a one size fits all mold. I expect this will start with the private insurers, including Medicare advantage plans, since they have real time data analysis, and a keen desire to save money. These “benchmarks” will be a work in progress and will infuriate some of you. They are, however, more credible, and better, than the current state of affairs, where insurance companies rank you by simply averaging your costs under your tax identification number.
So heads up, benchmarks are coming your way. Review your own public data, compared with your peers and see if you are an outlier, and if so, ponder the reason why. It is not too late to take corrective action.
Dr. Coldiron is a past president of the American Academy of Dermatology. He is currently in private practice, but maintains a clinical assistant professorship at the University of Cincinnati. He cares for patients, teaches medical students and residents, and has several active clinical research projects. Dr. Coldiron is the author of more than 80 scientific letters, papers, and several book chapters, and he speaks frequently on a variety of topics. Reach him at [email protected].
We have actively avoided benchmarks in medicine since time immemorial. There is a strong argument that rote, one-size-fits-all parameters for care medicine are bad for our patients, and obviously they interfere with our flexibility in dealing with complex obscure diseases. This flexibility is critical in dermatology, where we deal with over 3,000 diseases, and there truly is more art than science involved in treating some of them.
Nonetheless, here come the benchmarks. Since we have not provided them, they have been provided for us. Look no further than United Health Care’s Optum program, or Cigna’s star ratings, both of which rank on average costs, without regard to subspecialty or intensity of disease.
Benchmarks have proven useful in industry and have improved quality there. I expect they will be most annoying to practicing physicians. There are also great variations in practice patterns we must make sure are accounted for. A pediatric dermatologist, for example, does radically fewer skin biopsies than a Mohs surgeon, and diagnoses many fewer malignancies. However, some things are inexplicable, even after opening two standard deviations, and you need to be aware they may be coming.
The Medicare data release was an eye opener for many. This information is readily available on multiple web sites in numeric and graphic display. You should look yourself and your “peers” up on the Wall Street Journal or ProPublicaweb sites. For example, it is hard to fathom how every closure can be a flap, or how every Mohs case is four stages. Or even more bizarre, how you can do Mohs and never have a second stage. It is hard to understand how most dermatologists have a certain number of skin biopsies or shave excisions per patient encounter and others ten times as many. With this in mind, I encourage all of you to look at your own ratios of procedures compared to your peers. Recall that Medicare data lag two years before publication. Areas that could be under scrutiny include:
• Number of skin biopsies per encounter.
• Number of repeat patient encounters per year.
• Number of lesion destructions per patient.
• Ratio of first to additional layers of Mohs.
• Number of Mohs procedures on trunk and extremities, compared with head and neck.
• Percentage of closures done with adjacent tissue transfers.
• Number of shave excisions per patient.
• Number of complex closures, compared with layered closures, particularly on the trunk and extremities.
• Number of diagnostic frozen sections.
• Frequency of use of special stains on pathology specimens.
We need to be actively involved in the development of these so that we are not forced into a one size fits all mold. I expect this will start with the private insurers, including Medicare advantage plans, since they have real time data analysis, and a keen desire to save money. These “benchmarks” will be a work in progress and will infuriate some of you. They are, however, more credible, and better, than the current state of affairs, where insurance companies rank you by simply averaging your costs under your tax identification number.
So heads up, benchmarks are coming your way. Review your own public data, compared with your peers and see if you are an outlier, and if so, ponder the reason why. It is not too late to take corrective action.
Dr. Coldiron is a past president of the American Academy of Dermatology. He is currently in private practice, but maintains a clinical assistant professorship at the University of Cincinnati. He cares for patients, teaches medical students and residents, and has several active clinical research projects. Dr. Coldiron is the author of more than 80 scientific letters, papers, and several book chapters, and he speaks frequently on a variety of topics. Reach him at [email protected].
We have actively avoided benchmarks in medicine since time immemorial. There is a strong argument that rote, one-size-fits-all parameters for care medicine are bad for our patients, and obviously they interfere with our flexibility in dealing with complex obscure diseases. This flexibility is critical in dermatology, where we deal with over 3,000 diseases, and there truly is more art than science involved in treating some of them.
Nonetheless, here come the benchmarks. Since we have not provided them, they have been provided for us. Look no further than United Health Care’s Optum program, or Cigna’s star ratings, both of which rank on average costs, without regard to subspecialty or intensity of disease.
Benchmarks have proven useful in industry and have improved quality there. I expect they will be most annoying to practicing physicians. There are also great variations in practice patterns we must make sure are accounted for. A pediatric dermatologist, for example, does radically fewer skin biopsies than a Mohs surgeon, and diagnoses many fewer malignancies. However, some things are inexplicable, even after opening two standard deviations, and you need to be aware they may be coming.
The Medicare data release was an eye opener for many. This information is readily available on multiple web sites in numeric and graphic display. You should look yourself and your “peers” up on the Wall Street Journal or ProPublicaweb sites. For example, it is hard to fathom how every closure can be a flap, or how every Mohs case is four stages. Or even more bizarre, how you can do Mohs and never have a second stage. It is hard to understand how most dermatologists have a certain number of skin biopsies or shave excisions per patient encounter and others ten times as many. With this in mind, I encourage all of you to look at your own ratios of procedures compared to your peers. Recall that Medicare data lag two years before publication. Areas that could be under scrutiny include:
• Number of skin biopsies per encounter.
• Number of repeat patient encounters per year.
• Number of lesion destructions per patient.
• Ratio of first to additional layers of Mohs.
• Number of Mohs procedures on trunk and extremities, compared with head and neck.
• Percentage of closures done with adjacent tissue transfers.
• Number of shave excisions per patient.
• Number of complex closures, compared with layered closures, particularly on the trunk and extremities.
• Number of diagnostic frozen sections.
• Frequency of use of special stains on pathology specimens.
We need to be actively involved in the development of these so that we are not forced into a one size fits all mold. I expect this will start with the private insurers, including Medicare advantage plans, since they have real time data analysis, and a keen desire to save money. These “benchmarks” will be a work in progress and will infuriate some of you. They are, however, more credible, and better, than the current state of affairs, where insurance companies rank you by simply averaging your costs under your tax identification number.
So heads up, benchmarks are coming your way. Review your own public data, compared with your peers and see if you are an outlier, and if so, ponder the reason why. It is not too late to take corrective action.
Dr. Coldiron is a past president of the American Academy of Dermatology. He is currently in private practice, but maintains a clinical assistant professorship at the University of Cincinnati. He cares for patients, teaches medical students and residents, and has several active clinical research projects. Dr. Coldiron is the author of more than 80 scientific letters, papers, and several book chapters, and he speaks frequently on a variety of topics. Reach him at [email protected].
