User login
How Common Is Hip Pain Among Older Adults?
OBJECTIVE: To determine the incidence of self-reported significant hip pain using a nationally representative sample of older adults in the United States.
STUDY DESIGN: Subjects were interviewed to determine their leisure time physical activity levels and whether they experienced severe hip pain. Sampling weights were calculated to account for unequal selection probabilities. The impact of race, age, and physical activity status was examined as influential factors affecting hip pain.
POPULATION: We interviewed 6596 adults aged 60 years and older as part of the third National Health and Nutrition Examination Survey (NHANES III).
OUTCOME MEASURED: We measured the prevalence of hip pain.
RESULTS: A total of 14.3% of participants aged 60 years and older reported significant hip pain on most days over the past 6 weeks. Men reported hip pain less frequently than women. Age did not influence self-reported hip pain in men. The lowest prevalence of hip pain was found in women aged 60 to 70 years. Sixteen percent of non-Hispanic white women reported hip pain, compared with 14.8% of black women and 19.3% of Mexican American women. Among non-Hispanic white men, 12.4% reported hip pain, a proportion no different from that of their black and Mexican American male counterparts. Among older US adults, 18.4% of those who had not participated in leisure time physical activity during the previous month reported severe hip pain; 12.6% of those who did engage in physical activity reported hip pain.
CONCLUSIONS: Self-reported hip pain has increased since NHANES I (1971-1975). Further studies are needed to identify individuals at highest risk for severe hip pain and to identify optimal treatment of hip pain.
- Self-reported hip pain has increased in older adults since surveys conducted from 1971 to 1975.
- A total of 14.3% of older adults report significant hip pain; men report hip pain less frequently than women.
- Sex, age, and race are important determinants of hip pain in older adults.
According to a report by the National Arthritis Data Workgroup based on data from the first National Health and Nutrition Examination Survey (NHANES I), the prevalence of symptomatic hip osteoarthritis (OA) is 0.7% in both adult women and men; 0.5% have moderate or severe symptoms.1 The incidence of symptomatic hip OA was higher in women than in men, and increased with age in both sexes until age 80 years, with a slight decline beyond that age.2 In a study of patients in a health maintenance organization, the incidence of symptomatic hip OA in elderly women was 239 per 100,000 person-years at ages 60 to 69 years, 583 per 100,000 person-years at ages 70 to 79 years, and 441 per 100,000 person-years for women older than 80 years. The corresponding rates for elderly men per 100,000 person-years were 158, 445, and 264, respectively.
In contrast, the prevalence of radiographic hip OA is 3.1%; risk factors for the development of radiographic changes appear different in women and men.3 As has been demonstrated in the knee, radiographic hip OA is more prevalent than symptomatic disease. Only 61% of older individuals with confirmed radiologic hip OA reported pain at the hip, while 11% without radiologic changes of OA had significant hip pain, presumably of nonarticular etiology. Factors that affect patients’ reporting of symptoms of hip pain, both from OA and from nonarticular sources, have not yet been fully elucidated.
We are not aware of any current nationally representative reports on the sex-specific and race-specific prevalence of hip pain in older adults. Therefore, the purpose of our investigation was to examine the age-specific prevalence of hip pain using a current nationally representative sample of older US adults. We will also describe the prevalence of self-reported hip pain among older adults from 2 of the largest minority groups in the United States: non-Hispanic blacks and Mexican Americans.
Methods
Sample design
The Third National Health and Nutrition Examination Survey (NHANES III) was conducted by the Centers for Disease Control and Prevention, National Center for Health Statistics. The plan and operation of NHANES III have been described elsewhere.5,6 Briefly, the survey was designed to produce a nationally representative sample of the civilian noninstitutionalized US population. One of the main goals of this survey was to estimate the national prevalence of selected health conditions and risk factors.
The NHANES III represents a 6-year study that was conducted from 1988 through 1994 consisting of 2 phases lasting 3 years each: phase I, 1988 through 1992, and phase II, 1991 through 1994. The survey was designed so that each phase was a nationally representative sample. Information presented in this report reflect data from phases I and II combined. The NHANES III oversampled Mexican Americans, non-Hispanic blacks, and older adults to ensure weighted, reliable estimates from these groups.
Each interview was conducted in the participant’s home. In addition, a detailed clinical examination was conducted in a mobile examination center. For the purposes of this investigation, we examined the data from the 6596 adults 60 years and older. The interviewing staff consisted of experienced persons, many of Hispanic origin or fluent in both English and Spanish. All staff members attended annual training sessions to ensure maintenance of effective interviewing skills.
Information on self-reported race and ethnicity was used to classify persons as non-Hispanic white, non-Hispanic blacks, or Mexican American (persons of Mexican origin living in the United States). Age was defined as the age, in years, at the time of the household interview, which preceded the medical examination by 2 to 3 weeks.
Hip pain
Participating adults 60 years and older were asked to report “whether they had experienced significant hip pain on most days over the preceding 6 weeks.”
Physical activity assessment
Trained interviewers used a questionnaire to obtain information on leisure time physical activity (LTPA) during the previous month. The questionnaire was adapted from the 1985 National Health Interview Survey (NHIS), which was used to establish baseline estimates for several Healthy People 2000 physical activity objectives. Participants were asked to specify the frequency of participation in LTPA during the previous month for the following activities: jogging or running, riding a bicycle outdoors or an indoor stationary bicycle, swimming, aerobic dancing, other dancing, calisthenics or floor exercises, gardening or yard work, and weight lifting. Four open-ended questions assessed information on physical activities not previously listed. Participants who responded negatively to all LTPA questions, including the 4 open-ended questions, were classified as persons who participate in no LTPA.
Statistical analysis
Statistical analyses were carried out using the SAS7 and WesVar PC8 software packages. For each survey, sampling weights were calculated that took into account the unequal selection probabilities resulting from the cluster design and from planned oversampling of certain subgroups. All analyses have incorporated sampling weights.
Results
Overall, 14.3% (95% CI, 13.1-15.5) of older US adults reported significant hip pain on most days over the previous 6 weeks. The age-specific and sex-specific prevalence estimates of US adults reporting severe hip pain on most days are shown in Figure 1 Men reported hip pain less frequently (11.9.1%; 95% CI, 10.2-13.7) than women (16.2%; 95% CI, 14.5-17.8). Reports of hip pain are similar in men aged 60 to 70 years, 70 to 80 years, or older than 80 years. The lowest prevalence of hip pain was reported by women aged 60 to 70 years.
The race-specific prevalence of severe hip pain on most days during the previous 6 weeks is shown in Figure 2. Among non-Hispanic white adults aged 60 years and older, 12.4% of men (95% CI, 10.2-14.1) and 16.0% of women (95% CI, 14.0-17.9) reported hip pain. In contrast, 14.8% (95% CI, 11.7-17.9) of non-Hispanic black women reported hip pain, as did 19.3% (95% CI, 14.9-23.7) of Mexican American women. Reports of hip pain among non-Hispanic black men and Mexican American men were similar to those of their non-Hispanic white male counterparts.
Among adults aged 60 years or older, 18.4% (95% CI, 16.5-20.7) of those who participated in no leisure time physical activity reported severe hip pain, while 12.6% (95% CI, 11.7-14.1) of those who did participate in some activity reported such pain.
FIGURE 1
PREVALENCE OF SIGNIFICANT HIP PAIN ON MOST DAYS IN OLDER ADULTS, STRATIFIED BY AGE AND SEX
FIGURE 2
PREVALENCE OF SIGNIFICANT HIP PAIN ON MOST DAYS IN OLDER ADULTS, STRATIFIED BY RACE AND SEX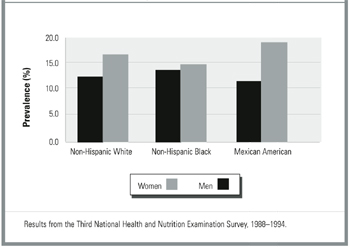
Discussion
This study offers a current report of the prevalence estimates of significant hip pain among US adults aged 60 years or older. We found that hip pain affects a higher number of older Americans than would be expected from previous studies. For instance, data from NHANES I demonstrated that from 1971 through 1975, 0.7% of patients reported hip pain secondary to OA.1 NHANES I, however, did not include any subjects older than 74 years. Our study found that 14.3% of US adults aged 60 years or older report hip pain on most days of previous 6 weeks, but we cannot yet determine the etiology of this pain.
There are 2 possible explanations of this apparent increase in hip pain between the time of NHANES I and that of NHANES III. First, the source of most hip pain in the elderly may be nonarticular in nature. Once radiographic data become available for NHANES III, this possibility can be further analyzed. A second explanation may be that the incidence of hip OA is increasing over time. This explanation is plausible, considering both the aging of the population in the United States and the increasing rates of obesity and sedentary lifestyle. Here, too, radiographic data will be useful.
We recently reported that sex, age, and race have a strong impact on knee pain.9 In our current study, we found that these are also important determinants of hip pain, but the findings were less striking than with knee pain. Men reported hip pain less often than women (11.9% versus 16.2%, respectively), but men aged 60 to 69 years were as likely to report hip pain as the men 80 years and older. There was no difference between the women in the 70- to 79-year group and those 80 years and older, but the women in both groups reported pain more often than did those aged 60 to 69 years. These findings are similar to those of Frankel and colleagues,10 who found that hip pain in a United Kingdom population was higher for women (overall prevalence 173 per 1000) than for men (overall prevalence 107 per 1000) at every age group; for both sexes it increased with age. This result is surprising, given that the prevalence of radiographic OA of the hip is more common in men than women aged 55 to 74 years, and in both sexes the prevalence of radiographic OA increases with age.1 The effects of sex and age on nonarticular hip pain (eg, bursitis) may partially explain the discrepancy. Additionally, there may be a reporting bias because women are more likely to report pain at any joint than are men.11 In one report, women had a higher rate of elective total hip replacement, but men tended to be younger at the time of surgery.12
We found no previous reports of the effect of race on the reporting of hip pain. In our study, Mexican American women were more likely to report hip pain (19.3%) than were non-Hispanic black (14.8%) or non-Hispanic white (15.9%) women. Race did not significantly affect reports of hip pain in men. In addition, people who report no leisure time activity were more likely to report hip pain. A sedentary lifestyle is more common among non-Hispanic blacks and Mexican Americans than among whites13-15 and may partially explain some of the difference in reporting by racial groups.
We acknowledge the limitations of self-report and the cross-sectional nature of this study. Given the cross-sectional nature of this study, we cannot determine the direction of causality; however, it is of concern that significant hip pain may contribute to a more sedentary lifestyle (and its attendant risks). As such, significant hip pain deserves a thorough investigation.
Conclusions
Our study reports on the most current nationally representative data that provide estimates of the prevalence of hip pain in older adults in the United States. Future studies are needed to further identify those at highest risk for hip pain and resultant debility and to determine optimal treatment of hip pain, particularly in Mexican American women.
Acknowledgments
Dr Andersen’s work is supported by Grant No. 97214-G from The John A. Hartford Foundation and by Grant No. DK 53907 from the National Institute of Digestive, Diabetes, and Kidney Diseases.
1. Lawrence RC, Hochberg MC, Kelsey JL, et al. Estimates of the prevalence of selected arthritic and musculoskeletal diseases in the United States. J Rheumatol 1989;16:427-41.
2. Oliveria SA, Felson DT, Reed JI, Cirillo PA, Walker AM. Incidence of symptomatic hand, hip, and knee osteoarthritis among patients in a health maintenance organization. Arthritis Rheum 1995;38:1134-141.
3. Tepper S, Hochberg MC. Factors associated with hip osteoarthritis: data from the First National Health and Nutrition Examination Survey (NHANES I). Am J Epidemiol 1993;137:1081-8.
4. Lawrence JS, Bremner JM, Bier F. Osteoarthrosis. Ann Rheum Dis 1966;25:1-24.
5. National Center for Health Statistics. Plan and operation of the Third National Health and Nutrition Examination Survey, 1988-94. Hyattsville, Md: US Department of Health and Human Services, Public Health Service, Centers for Disease Control and Prevention, National Center for Health Statistics; 1994.
6. Ezzati TM, Massey JT, Waksberg J, Chu A, Maurer KR. Sample design: Third National Health and Nutrition Examination Survey. Vital Health Stat 1992;2:1-35.
7. SAS Institute Inc. SASå/STAT User’s Guide, Version 6. Cary, NC: SAS Institute; 1989.
8. Brick JM, Broene P, James P, Severynse J. A user’s guide to WesVar PC. Rockville, Md: Westat Inc.; 1997.
9. Andersen RE, Crespo CJ, Ling SM, Bathon JM, Bartlett SJ. Prevalence of significant knee pain among older Americans: results from the Third National Health and Nutrition Examination Survey. J Am Geriatr Soc 1999;1435-8.
10. Frankel S, Eachus J, Pearson N, et al. Population requirement for primary hip-replacement surgery: a cross sectional study. Lancet 1999;353:1304-9.
11. Ling SM, Bathon JM. Osteoarthritis in older adults. J Am Geriatr Soc 1998;46:216-25.
12. Madhok R, Lewallen DG, Wallrichs SL, Ilstrup DM, Kurland RL, Melton LJ. Trends in the utilization of primary total hip arthroplasty, 1969 through 1990: a population-based study in Olmsted County, Minnesota. Mayo Clin Proc 1993;68:11-18.
13. Crespo CJ, Keteyian SJ, Heath GW, Sempos CT. Leisure-time physical activity among US adults: results from the third National Health and Nutrition Examination Survey. Arch Intern Med 1996;156:93-8.
14. US Department of Health and Human Services. Physical activity and health: a report of the surgeon general. Atlanta, Ga: US Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion; 1996.
15. Crespo CJ, Keteyian SJ, Snelling A, Smit E, Andersen RE. Prevalence of no leisure time physical activity in persons with chronic disease. Clin Exerc Physiol 2000;1:68-73.
OBJECTIVE: To determine the incidence of self-reported significant hip pain using a nationally representative sample of older adults in the United States.
STUDY DESIGN: Subjects were interviewed to determine their leisure time physical activity levels and whether they experienced severe hip pain. Sampling weights were calculated to account for unequal selection probabilities. The impact of race, age, and physical activity status was examined as influential factors affecting hip pain.
POPULATION: We interviewed 6596 adults aged 60 years and older as part of the third National Health and Nutrition Examination Survey (NHANES III).
OUTCOME MEASURED: We measured the prevalence of hip pain.
RESULTS: A total of 14.3% of participants aged 60 years and older reported significant hip pain on most days over the past 6 weeks. Men reported hip pain less frequently than women. Age did not influence self-reported hip pain in men. The lowest prevalence of hip pain was found in women aged 60 to 70 years. Sixteen percent of non-Hispanic white women reported hip pain, compared with 14.8% of black women and 19.3% of Mexican American women. Among non-Hispanic white men, 12.4% reported hip pain, a proportion no different from that of their black and Mexican American male counterparts. Among older US adults, 18.4% of those who had not participated in leisure time physical activity during the previous month reported severe hip pain; 12.6% of those who did engage in physical activity reported hip pain.
CONCLUSIONS: Self-reported hip pain has increased since NHANES I (1971-1975). Further studies are needed to identify individuals at highest risk for severe hip pain and to identify optimal treatment of hip pain.
- Self-reported hip pain has increased in older adults since surveys conducted from 1971 to 1975.
- A total of 14.3% of older adults report significant hip pain; men report hip pain less frequently than women.
- Sex, age, and race are important determinants of hip pain in older adults.
According to a report by the National Arthritis Data Workgroup based on data from the first National Health and Nutrition Examination Survey (NHANES I), the prevalence of symptomatic hip osteoarthritis (OA) is 0.7% in both adult women and men; 0.5% have moderate or severe symptoms.1 The incidence of symptomatic hip OA was higher in women than in men, and increased with age in both sexes until age 80 years, with a slight decline beyond that age.2 In a study of patients in a health maintenance organization, the incidence of symptomatic hip OA in elderly women was 239 per 100,000 person-years at ages 60 to 69 years, 583 per 100,000 person-years at ages 70 to 79 years, and 441 per 100,000 person-years for women older than 80 years. The corresponding rates for elderly men per 100,000 person-years were 158, 445, and 264, respectively.
In contrast, the prevalence of radiographic hip OA is 3.1%; risk factors for the development of radiographic changes appear different in women and men.3 As has been demonstrated in the knee, radiographic hip OA is more prevalent than symptomatic disease. Only 61% of older individuals with confirmed radiologic hip OA reported pain at the hip, while 11% without radiologic changes of OA had significant hip pain, presumably of nonarticular etiology. Factors that affect patients’ reporting of symptoms of hip pain, both from OA and from nonarticular sources, have not yet been fully elucidated.
We are not aware of any current nationally representative reports on the sex-specific and race-specific prevalence of hip pain in older adults. Therefore, the purpose of our investigation was to examine the age-specific prevalence of hip pain using a current nationally representative sample of older US adults. We will also describe the prevalence of self-reported hip pain among older adults from 2 of the largest minority groups in the United States: non-Hispanic blacks and Mexican Americans.
Methods
Sample design
The Third National Health and Nutrition Examination Survey (NHANES III) was conducted by the Centers for Disease Control and Prevention, National Center for Health Statistics. The plan and operation of NHANES III have been described elsewhere.5,6 Briefly, the survey was designed to produce a nationally representative sample of the civilian noninstitutionalized US population. One of the main goals of this survey was to estimate the national prevalence of selected health conditions and risk factors.
The NHANES III represents a 6-year study that was conducted from 1988 through 1994 consisting of 2 phases lasting 3 years each: phase I, 1988 through 1992, and phase II, 1991 through 1994. The survey was designed so that each phase was a nationally representative sample. Information presented in this report reflect data from phases I and II combined. The NHANES III oversampled Mexican Americans, non-Hispanic blacks, and older adults to ensure weighted, reliable estimates from these groups.
Each interview was conducted in the participant’s home. In addition, a detailed clinical examination was conducted in a mobile examination center. For the purposes of this investigation, we examined the data from the 6596 adults 60 years and older. The interviewing staff consisted of experienced persons, many of Hispanic origin or fluent in both English and Spanish. All staff members attended annual training sessions to ensure maintenance of effective interviewing skills.
Information on self-reported race and ethnicity was used to classify persons as non-Hispanic white, non-Hispanic blacks, or Mexican American (persons of Mexican origin living in the United States). Age was defined as the age, in years, at the time of the household interview, which preceded the medical examination by 2 to 3 weeks.
Hip pain
Participating adults 60 years and older were asked to report “whether they had experienced significant hip pain on most days over the preceding 6 weeks.”
Physical activity assessment
Trained interviewers used a questionnaire to obtain information on leisure time physical activity (LTPA) during the previous month. The questionnaire was adapted from the 1985 National Health Interview Survey (NHIS), which was used to establish baseline estimates for several Healthy People 2000 physical activity objectives. Participants were asked to specify the frequency of participation in LTPA during the previous month for the following activities: jogging or running, riding a bicycle outdoors or an indoor stationary bicycle, swimming, aerobic dancing, other dancing, calisthenics or floor exercises, gardening or yard work, and weight lifting. Four open-ended questions assessed information on physical activities not previously listed. Participants who responded negatively to all LTPA questions, including the 4 open-ended questions, were classified as persons who participate in no LTPA.
Statistical analysis
Statistical analyses were carried out using the SAS7 and WesVar PC8 software packages. For each survey, sampling weights were calculated that took into account the unequal selection probabilities resulting from the cluster design and from planned oversampling of certain subgroups. All analyses have incorporated sampling weights.
Results
Overall, 14.3% (95% CI, 13.1-15.5) of older US adults reported significant hip pain on most days over the previous 6 weeks. The age-specific and sex-specific prevalence estimates of US adults reporting severe hip pain on most days are shown in Figure 1 Men reported hip pain less frequently (11.9.1%; 95% CI, 10.2-13.7) than women (16.2%; 95% CI, 14.5-17.8). Reports of hip pain are similar in men aged 60 to 70 years, 70 to 80 years, or older than 80 years. The lowest prevalence of hip pain was reported by women aged 60 to 70 years.
The race-specific prevalence of severe hip pain on most days during the previous 6 weeks is shown in Figure 2. Among non-Hispanic white adults aged 60 years and older, 12.4% of men (95% CI, 10.2-14.1) and 16.0% of women (95% CI, 14.0-17.9) reported hip pain. In contrast, 14.8% (95% CI, 11.7-17.9) of non-Hispanic black women reported hip pain, as did 19.3% (95% CI, 14.9-23.7) of Mexican American women. Reports of hip pain among non-Hispanic black men and Mexican American men were similar to those of their non-Hispanic white male counterparts.
Among adults aged 60 years or older, 18.4% (95% CI, 16.5-20.7) of those who participated in no leisure time physical activity reported severe hip pain, while 12.6% (95% CI, 11.7-14.1) of those who did participate in some activity reported such pain.
FIGURE 1
PREVALENCE OF SIGNIFICANT HIP PAIN ON MOST DAYS IN OLDER ADULTS, STRATIFIED BY AGE AND SEX
FIGURE 2
PREVALENCE OF SIGNIFICANT HIP PAIN ON MOST DAYS IN OLDER ADULTS, STRATIFIED BY RACE AND SEX
Discussion
This study offers a current report of the prevalence estimates of significant hip pain among US adults aged 60 years or older. We found that hip pain affects a higher number of older Americans than would be expected from previous studies. For instance, data from NHANES I demonstrated that from 1971 through 1975, 0.7% of patients reported hip pain secondary to OA.1 NHANES I, however, did not include any subjects older than 74 years. Our study found that 14.3% of US adults aged 60 years or older report hip pain on most days of previous 6 weeks, but we cannot yet determine the etiology of this pain.
There are 2 possible explanations of this apparent increase in hip pain between the time of NHANES I and that of NHANES III. First, the source of most hip pain in the elderly may be nonarticular in nature. Once radiographic data become available for NHANES III, this possibility can be further analyzed. A second explanation may be that the incidence of hip OA is increasing over time. This explanation is plausible, considering both the aging of the population in the United States and the increasing rates of obesity and sedentary lifestyle. Here, too, radiographic data will be useful.
We recently reported that sex, age, and race have a strong impact on knee pain.9 In our current study, we found that these are also important determinants of hip pain, but the findings were less striking than with knee pain. Men reported hip pain less often than women (11.9% versus 16.2%, respectively), but men aged 60 to 69 years were as likely to report hip pain as the men 80 years and older. There was no difference between the women in the 70- to 79-year group and those 80 years and older, but the women in both groups reported pain more often than did those aged 60 to 69 years. These findings are similar to those of Frankel and colleagues,10 who found that hip pain in a United Kingdom population was higher for women (overall prevalence 173 per 1000) than for men (overall prevalence 107 per 1000) at every age group; for both sexes it increased with age. This result is surprising, given that the prevalence of radiographic OA of the hip is more common in men than women aged 55 to 74 years, and in both sexes the prevalence of radiographic OA increases with age.1 The effects of sex and age on nonarticular hip pain (eg, bursitis) may partially explain the discrepancy. Additionally, there may be a reporting bias because women are more likely to report pain at any joint than are men.11 In one report, women had a higher rate of elective total hip replacement, but men tended to be younger at the time of surgery.12
We found no previous reports of the effect of race on the reporting of hip pain. In our study, Mexican American women were more likely to report hip pain (19.3%) than were non-Hispanic black (14.8%) or non-Hispanic white (15.9%) women. Race did not significantly affect reports of hip pain in men. In addition, people who report no leisure time activity were more likely to report hip pain. A sedentary lifestyle is more common among non-Hispanic blacks and Mexican Americans than among whites13-15 and may partially explain some of the difference in reporting by racial groups.
We acknowledge the limitations of self-report and the cross-sectional nature of this study. Given the cross-sectional nature of this study, we cannot determine the direction of causality; however, it is of concern that significant hip pain may contribute to a more sedentary lifestyle (and its attendant risks). As such, significant hip pain deserves a thorough investigation.
Conclusions
Our study reports on the most current nationally representative data that provide estimates of the prevalence of hip pain in older adults in the United States. Future studies are needed to further identify those at highest risk for hip pain and resultant debility and to determine optimal treatment of hip pain, particularly in Mexican American women.
Acknowledgments
Dr Andersen’s work is supported by Grant No. 97214-G from The John A. Hartford Foundation and by Grant No. DK 53907 from the National Institute of Digestive, Diabetes, and Kidney Diseases.
OBJECTIVE: To determine the incidence of self-reported significant hip pain using a nationally representative sample of older adults in the United States.
STUDY DESIGN: Subjects were interviewed to determine their leisure time physical activity levels and whether they experienced severe hip pain. Sampling weights were calculated to account for unequal selection probabilities. The impact of race, age, and physical activity status was examined as influential factors affecting hip pain.
POPULATION: We interviewed 6596 adults aged 60 years and older as part of the third National Health and Nutrition Examination Survey (NHANES III).
OUTCOME MEASURED: We measured the prevalence of hip pain.
RESULTS: A total of 14.3% of participants aged 60 years and older reported significant hip pain on most days over the past 6 weeks. Men reported hip pain less frequently than women. Age did not influence self-reported hip pain in men. The lowest prevalence of hip pain was found in women aged 60 to 70 years. Sixteen percent of non-Hispanic white women reported hip pain, compared with 14.8% of black women and 19.3% of Mexican American women. Among non-Hispanic white men, 12.4% reported hip pain, a proportion no different from that of their black and Mexican American male counterparts. Among older US adults, 18.4% of those who had not participated in leisure time physical activity during the previous month reported severe hip pain; 12.6% of those who did engage in physical activity reported hip pain.
CONCLUSIONS: Self-reported hip pain has increased since NHANES I (1971-1975). Further studies are needed to identify individuals at highest risk for severe hip pain and to identify optimal treatment of hip pain.
- Self-reported hip pain has increased in older adults since surveys conducted from 1971 to 1975.
- A total of 14.3% of older adults report significant hip pain; men report hip pain less frequently than women.
- Sex, age, and race are important determinants of hip pain in older adults.
According to a report by the National Arthritis Data Workgroup based on data from the first National Health and Nutrition Examination Survey (NHANES I), the prevalence of symptomatic hip osteoarthritis (OA) is 0.7% in both adult women and men; 0.5% have moderate or severe symptoms.1 The incidence of symptomatic hip OA was higher in women than in men, and increased with age in both sexes until age 80 years, with a slight decline beyond that age.2 In a study of patients in a health maintenance organization, the incidence of symptomatic hip OA in elderly women was 239 per 100,000 person-years at ages 60 to 69 years, 583 per 100,000 person-years at ages 70 to 79 years, and 441 per 100,000 person-years for women older than 80 years. The corresponding rates for elderly men per 100,000 person-years were 158, 445, and 264, respectively.
In contrast, the prevalence of radiographic hip OA is 3.1%; risk factors for the development of radiographic changes appear different in women and men.3 As has been demonstrated in the knee, radiographic hip OA is more prevalent than symptomatic disease. Only 61% of older individuals with confirmed radiologic hip OA reported pain at the hip, while 11% without radiologic changes of OA had significant hip pain, presumably of nonarticular etiology. Factors that affect patients’ reporting of symptoms of hip pain, both from OA and from nonarticular sources, have not yet been fully elucidated.
We are not aware of any current nationally representative reports on the sex-specific and race-specific prevalence of hip pain in older adults. Therefore, the purpose of our investigation was to examine the age-specific prevalence of hip pain using a current nationally representative sample of older US adults. We will also describe the prevalence of self-reported hip pain among older adults from 2 of the largest minority groups in the United States: non-Hispanic blacks and Mexican Americans.
Methods
Sample design
The Third National Health and Nutrition Examination Survey (NHANES III) was conducted by the Centers for Disease Control and Prevention, National Center for Health Statistics. The plan and operation of NHANES III have been described elsewhere.5,6 Briefly, the survey was designed to produce a nationally representative sample of the civilian noninstitutionalized US population. One of the main goals of this survey was to estimate the national prevalence of selected health conditions and risk factors.
The NHANES III represents a 6-year study that was conducted from 1988 through 1994 consisting of 2 phases lasting 3 years each: phase I, 1988 through 1992, and phase II, 1991 through 1994. The survey was designed so that each phase was a nationally representative sample. Information presented in this report reflect data from phases I and II combined. The NHANES III oversampled Mexican Americans, non-Hispanic blacks, and older adults to ensure weighted, reliable estimates from these groups.
Each interview was conducted in the participant’s home. In addition, a detailed clinical examination was conducted in a mobile examination center. For the purposes of this investigation, we examined the data from the 6596 adults 60 years and older. The interviewing staff consisted of experienced persons, many of Hispanic origin or fluent in both English and Spanish. All staff members attended annual training sessions to ensure maintenance of effective interviewing skills.
Information on self-reported race and ethnicity was used to classify persons as non-Hispanic white, non-Hispanic blacks, or Mexican American (persons of Mexican origin living in the United States). Age was defined as the age, in years, at the time of the household interview, which preceded the medical examination by 2 to 3 weeks.
Hip pain
Participating adults 60 years and older were asked to report “whether they had experienced significant hip pain on most days over the preceding 6 weeks.”
Physical activity assessment
Trained interviewers used a questionnaire to obtain information on leisure time physical activity (LTPA) during the previous month. The questionnaire was adapted from the 1985 National Health Interview Survey (NHIS), which was used to establish baseline estimates for several Healthy People 2000 physical activity objectives. Participants were asked to specify the frequency of participation in LTPA during the previous month for the following activities: jogging or running, riding a bicycle outdoors or an indoor stationary bicycle, swimming, aerobic dancing, other dancing, calisthenics or floor exercises, gardening or yard work, and weight lifting. Four open-ended questions assessed information on physical activities not previously listed. Participants who responded negatively to all LTPA questions, including the 4 open-ended questions, were classified as persons who participate in no LTPA.
Statistical analysis
Statistical analyses were carried out using the SAS7 and WesVar PC8 software packages. For each survey, sampling weights were calculated that took into account the unequal selection probabilities resulting from the cluster design and from planned oversampling of certain subgroups. All analyses have incorporated sampling weights.
Results
Overall, 14.3% (95% CI, 13.1-15.5) of older US adults reported significant hip pain on most days over the previous 6 weeks. The age-specific and sex-specific prevalence estimates of US adults reporting severe hip pain on most days are shown in Figure 1 Men reported hip pain less frequently (11.9.1%; 95% CI, 10.2-13.7) than women (16.2%; 95% CI, 14.5-17.8). Reports of hip pain are similar in men aged 60 to 70 years, 70 to 80 years, or older than 80 years. The lowest prevalence of hip pain was reported by women aged 60 to 70 years.
The race-specific prevalence of severe hip pain on most days during the previous 6 weeks is shown in Figure 2. Among non-Hispanic white adults aged 60 years and older, 12.4% of men (95% CI, 10.2-14.1) and 16.0% of women (95% CI, 14.0-17.9) reported hip pain. In contrast, 14.8% (95% CI, 11.7-17.9) of non-Hispanic black women reported hip pain, as did 19.3% (95% CI, 14.9-23.7) of Mexican American women. Reports of hip pain among non-Hispanic black men and Mexican American men were similar to those of their non-Hispanic white male counterparts.
Among adults aged 60 years or older, 18.4% (95% CI, 16.5-20.7) of those who participated in no leisure time physical activity reported severe hip pain, while 12.6% (95% CI, 11.7-14.1) of those who did participate in some activity reported such pain.
FIGURE 1
PREVALENCE OF SIGNIFICANT HIP PAIN ON MOST DAYS IN OLDER ADULTS, STRATIFIED BY AGE AND SEX
FIGURE 2
PREVALENCE OF SIGNIFICANT HIP PAIN ON MOST DAYS IN OLDER ADULTS, STRATIFIED BY RACE AND SEX
Discussion
This study offers a current report of the prevalence estimates of significant hip pain among US adults aged 60 years or older. We found that hip pain affects a higher number of older Americans than would be expected from previous studies. For instance, data from NHANES I demonstrated that from 1971 through 1975, 0.7% of patients reported hip pain secondary to OA.1 NHANES I, however, did not include any subjects older than 74 years. Our study found that 14.3% of US adults aged 60 years or older report hip pain on most days of previous 6 weeks, but we cannot yet determine the etiology of this pain.
There are 2 possible explanations of this apparent increase in hip pain between the time of NHANES I and that of NHANES III. First, the source of most hip pain in the elderly may be nonarticular in nature. Once radiographic data become available for NHANES III, this possibility can be further analyzed. A second explanation may be that the incidence of hip OA is increasing over time. This explanation is plausible, considering both the aging of the population in the United States and the increasing rates of obesity and sedentary lifestyle. Here, too, radiographic data will be useful.
We recently reported that sex, age, and race have a strong impact on knee pain.9 In our current study, we found that these are also important determinants of hip pain, but the findings were less striking than with knee pain. Men reported hip pain less often than women (11.9% versus 16.2%, respectively), but men aged 60 to 69 years were as likely to report hip pain as the men 80 years and older. There was no difference between the women in the 70- to 79-year group and those 80 years and older, but the women in both groups reported pain more often than did those aged 60 to 69 years. These findings are similar to those of Frankel and colleagues,10 who found that hip pain in a United Kingdom population was higher for women (overall prevalence 173 per 1000) than for men (overall prevalence 107 per 1000) at every age group; for both sexes it increased with age. This result is surprising, given that the prevalence of radiographic OA of the hip is more common in men than women aged 55 to 74 years, and in both sexes the prevalence of radiographic OA increases with age.1 The effects of sex and age on nonarticular hip pain (eg, bursitis) may partially explain the discrepancy. Additionally, there may be a reporting bias because women are more likely to report pain at any joint than are men.11 In one report, women had a higher rate of elective total hip replacement, but men tended to be younger at the time of surgery.12
We found no previous reports of the effect of race on the reporting of hip pain. In our study, Mexican American women were more likely to report hip pain (19.3%) than were non-Hispanic black (14.8%) or non-Hispanic white (15.9%) women. Race did not significantly affect reports of hip pain in men. In addition, people who report no leisure time activity were more likely to report hip pain. A sedentary lifestyle is more common among non-Hispanic blacks and Mexican Americans than among whites13-15 and may partially explain some of the difference in reporting by racial groups.
We acknowledge the limitations of self-report and the cross-sectional nature of this study. Given the cross-sectional nature of this study, we cannot determine the direction of causality; however, it is of concern that significant hip pain may contribute to a more sedentary lifestyle (and its attendant risks). As such, significant hip pain deserves a thorough investigation.
Conclusions
Our study reports on the most current nationally representative data that provide estimates of the prevalence of hip pain in older adults in the United States. Future studies are needed to further identify those at highest risk for hip pain and resultant debility and to determine optimal treatment of hip pain, particularly in Mexican American women.
Acknowledgments
Dr Andersen’s work is supported by Grant No. 97214-G from The John A. Hartford Foundation and by Grant No. DK 53907 from the National Institute of Digestive, Diabetes, and Kidney Diseases.
1. Lawrence RC, Hochberg MC, Kelsey JL, et al. Estimates of the prevalence of selected arthritic and musculoskeletal diseases in the United States. J Rheumatol 1989;16:427-41.
2. Oliveria SA, Felson DT, Reed JI, Cirillo PA, Walker AM. Incidence of symptomatic hand, hip, and knee osteoarthritis among patients in a health maintenance organization. Arthritis Rheum 1995;38:1134-141.
3. Tepper S, Hochberg MC. Factors associated with hip osteoarthritis: data from the First National Health and Nutrition Examination Survey (NHANES I). Am J Epidemiol 1993;137:1081-8.
4. Lawrence JS, Bremner JM, Bier F. Osteoarthrosis. Ann Rheum Dis 1966;25:1-24.
5. National Center for Health Statistics. Plan and operation of the Third National Health and Nutrition Examination Survey, 1988-94. Hyattsville, Md: US Department of Health and Human Services, Public Health Service, Centers for Disease Control and Prevention, National Center for Health Statistics; 1994.
6. Ezzati TM, Massey JT, Waksberg J, Chu A, Maurer KR. Sample design: Third National Health and Nutrition Examination Survey. Vital Health Stat 1992;2:1-35.
7. SAS Institute Inc. SASå/STAT User’s Guide, Version 6. Cary, NC: SAS Institute; 1989.
8. Brick JM, Broene P, James P, Severynse J. A user’s guide to WesVar PC. Rockville, Md: Westat Inc.; 1997.
9. Andersen RE, Crespo CJ, Ling SM, Bathon JM, Bartlett SJ. Prevalence of significant knee pain among older Americans: results from the Third National Health and Nutrition Examination Survey. J Am Geriatr Soc 1999;1435-8.
10. Frankel S, Eachus J, Pearson N, et al. Population requirement for primary hip-replacement surgery: a cross sectional study. Lancet 1999;353:1304-9.
11. Ling SM, Bathon JM. Osteoarthritis in older adults. J Am Geriatr Soc 1998;46:216-25.
12. Madhok R, Lewallen DG, Wallrichs SL, Ilstrup DM, Kurland RL, Melton LJ. Trends in the utilization of primary total hip arthroplasty, 1969 through 1990: a population-based study in Olmsted County, Minnesota. Mayo Clin Proc 1993;68:11-18.
13. Crespo CJ, Keteyian SJ, Heath GW, Sempos CT. Leisure-time physical activity among US adults: results from the third National Health and Nutrition Examination Survey. Arch Intern Med 1996;156:93-8.
14. US Department of Health and Human Services. Physical activity and health: a report of the surgeon general. Atlanta, Ga: US Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion; 1996.
15. Crespo CJ, Keteyian SJ, Snelling A, Smit E, Andersen RE. Prevalence of no leisure time physical activity in persons with chronic disease. Clin Exerc Physiol 2000;1:68-73.
1. Lawrence RC, Hochberg MC, Kelsey JL, et al. Estimates of the prevalence of selected arthritic and musculoskeletal diseases in the United States. J Rheumatol 1989;16:427-41.
2. Oliveria SA, Felson DT, Reed JI, Cirillo PA, Walker AM. Incidence of symptomatic hand, hip, and knee osteoarthritis among patients in a health maintenance organization. Arthritis Rheum 1995;38:1134-141.
3. Tepper S, Hochberg MC. Factors associated with hip osteoarthritis: data from the First National Health and Nutrition Examination Survey (NHANES I). Am J Epidemiol 1993;137:1081-8.
4. Lawrence JS, Bremner JM, Bier F. Osteoarthrosis. Ann Rheum Dis 1966;25:1-24.
5. National Center for Health Statistics. Plan and operation of the Third National Health and Nutrition Examination Survey, 1988-94. Hyattsville, Md: US Department of Health and Human Services, Public Health Service, Centers for Disease Control and Prevention, National Center for Health Statistics; 1994.
6. Ezzati TM, Massey JT, Waksberg J, Chu A, Maurer KR. Sample design: Third National Health and Nutrition Examination Survey. Vital Health Stat 1992;2:1-35.
7. SAS Institute Inc. SASå/STAT User’s Guide, Version 6. Cary, NC: SAS Institute; 1989.
8. Brick JM, Broene P, James P, Severynse J. A user’s guide to WesVar PC. Rockville, Md: Westat Inc.; 1997.
9. Andersen RE, Crespo CJ, Ling SM, Bathon JM, Bartlett SJ. Prevalence of significant knee pain among older Americans: results from the Third National Health and Nutrition Examination Survey. J Am Geriatr Soc 1999;1435-8.
10. Frankel S, Eachus J, Pearson N, et al. Population requirement for primary hip-replacement surgery: a cross sectional study. Lancet 1999;353:1304-9.
11. Ling SM, Bathon JM. Osteoarthritis in older adults. J Am Geriatr Soc 1998;46:216-25.
12. Madhok R, Lewallen DG, Wallrichs SL, Ilstrup DM, Kurland RL, Melton LJ. Trends in the utilization of primary total hip arthroplasty, 1969 through 1990: a population-based study in Olmsted County, Minnesota. Mayo Clin Proc 1993;68:11-18.
13. Crespo CJ, Keteyian SJ, Heath GW, Sempos CT. Leisure-time physical activity among US adults: results from the third National Health and Nutrition Examination Survey. Arch Intern Med 1996;156:93-8.
14. US Department of Health and Human Services. Physical activity and health: a report of the surgeon general. Atlanta, Ga: US Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion; 1996.
15. Crespo CJ, Keteyian SJ, Snelling A, Smit E, Andersen RE. Prevalence of no leisure time physical activity in persons with chronic disease. Clin Exerc Physiol 2000;1:68-73.