User login
Doug Brunk is a San Diego-based award-winning reporter who began covering health care in 1991. Before joining the company, he wrote for the health sciences division of Columbia University and was an associate editor at Contemporary Long Term Care magazine when it won a Jesse H. Neal Award. His work has been syndicated by the Los Angeles Times and he is the author of two books related to the University of Kentucky Wildcats men's basketball program. Doug has a master’s degree in magazine journalism from the S.I. Newhouse School of Public Communications at Syracuse University. Follow him on Twitter @dougbrunk.
Identifying AK Variants Is Key to Management
The ability to distinguish between the two key variants of actinic keratosis is key to effective management, according to Dr. Theodore Rosen.
Pigmented actinic keratosis (AK) that spreads typically occurs in patients older than age 60 years and affects more women than men. The lesions are larger than 1.5 cm and have a history of lateral spread. "The lesions are flat, with a smooth, scaly surface, and they occur on sun-exposed skin, mostly the face, and near other manifestations of photodamage," noted Dr. Rosen at the annual Hawaii Dermatology Seminar sponsored by Skin Disease Education Foundation (SDEF).

Differential diagnosis includes solar lentigo, lentigo maligna, lentigo maligna melanoma, seborrheic keratosis, and pigmented squamous cell carcinoma in situ. "The presence of dots, globules, and asymmetry on dermatoscopy can help you distinguish spreading pigmented AKs from other lesions," said Dr. Rosen, professor of dermatology at Baylor College of Medicine, Houston.
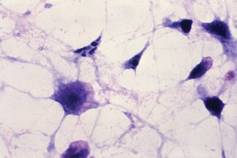
The other main variant, proliferating AK, also tends to affect patients older than age 60 but it occurs more commonly in men than in women. This variant is greater than 1.5 cm in size with a history of rapid lateral spread, and it is marked by a confluent scaly surface with some palpability. Affected areas include sun-exposed skin, mostly the face, and areas near other manifestations of photodamage. "This variant is resistant to usual topical therapy, and the differential diagnosis may include eczema, psoriasis, squamous cell carcinoma in situ, and superficial basal cell carcinoma," said Dr. Rosen, who is also chief of the dermatology clinic at the Houston-based Michael E. DeBakey VA Medical Center. Histology reveals fingerlike invasive projections into the dermis of atypical squamous cells.
The appearance of multiple AKs in a cosmetic unit indicates that the clinician should consider the entire photodamaged area to be diseased. This concept, known as field-directed therapy, "not only addresses apparent clinical lesions, but also reveals and may treat subclinical lesions," he said. "Field therapy may also offer the advantage of reversing basic cellular aberrations leading to transition into invasive cutaneous malignancy."

Another trend in the treatment of AKs is the development of new imiquimod formulations. Results from two placebo-controlled studies of daily application of 2.5% and 3.75% imiquimod creams to the face and balding scalp for two 3-week cycles revealed that both formulations were more effective than placebo and had an acceptable safety profile (J. Am. Acad. Dermatol. 2010;62:573-81). The final evaluation occurred 8 weeks after the final treatment, said Dr. Rosen, who was one of the study investigators. Results from this and other studies led to Food and Drug Administration approval of imiquimod 2.5% (Zyclara) for AKs on July 19, 2011, but the formulation is not yet commercially available.
In a more recent analysis, investigators assessed complete clearance rates in AK patients from four phase III trials of imiquimod who were followed for 1 year (J. Drugs Dermatol. 2011;10:165-70). For imiquimod 3.75% and 2.5% cream, respectively, complete clearance was sustained for 1 year in 40.5% and 33.3% of patients from the 2-week cycle studies, and in 47.9% and 43.2% of patients from the 3-week cycle studies.
Combination therapies for AKs have become increasingly popular. Treatments include cryosurgery followed by diclofenac, 5-fluorouracil followed by cryosurgery, cryosurgery followed by imiquimod 5% or 3.75%, photodynamic therapy (PTD) followed by imiquimod 5%, and tazarotene followed by PDT. "For all studies where field therapy is combined with lesion-directed therapy or with another field therapy, the combination proved superior to monotherapy," Dr. Rosen said.
He went on to note that there is considerable user variation – such as time, the distance the device is held from the skin, and the type of unit used – in the delivery of cryosurgery to treat AKs. The variation "may have more to do with skin temperature than any other variable," said Dr. Rosen. In one study, investigators used an infrared detector in a liquid nitrogen container to deliver cryotherapy to a temperature of –5° C in 36 patients with 180 thin AKs (Dermatol. Surg. 2010;36:1956-61). The clearance rates were 67% at 1 week and 100% at 6 weeks.

Treatment of AKs with radiation is another area of study. In one recent trial, 12 patients with refractory AK and 4 patients with AKs near a nonmelanoma skin cancer underwent external beam radiation therapy five times a week for 4-6 weeks. The total dose of radiation ranged from 4 to 60 Gy (J. Clin. Aesthet. Dermatol. 2011;4:47-50). Of the 16 patients, 13 had complete resolution of AKs, 1 noted a prompt recurrence, and 90% said they were "very satisfied" with the treatment results.
Treating AKs with methyl aminolevulinate photodynamic therapy (MAL-PDT) is also being investigated. In a multicenter study conducted in Scandinavia, 120 patients with 1,572 AKs underwent MAL-PDT followed by immediate exposure to the sun for 1.5-2.5 hours (Br. J. Dermatol. 2011;164:1083-90). At 3 months, 75%-77% of the lesions had cleared. This approach "has an advantage for the health care provider in that no equipment is needed," Dr. Rosen said. "The advantage for the patient is that the therapy is nearly pain free."
Dr. Rosen disclosed that he is a consultant and a member of the speakers bureau for Medicis, which makes imiquimod. He is also a consultant for LEO Pharma.
SDEF and this news organization are owned by Elsevier.
The ability to distinguish between the two key variants of actinic keratosis is key to effective management, according to Dr. Theodore Rosen.
Pigmented actinic keratosis (AK) that spreads typically occurs in patients older than age 60 years and affects more women than men. The lesions are larger than 1.5 cm and have a history of lateral spread. "The lesions are flat, with a smooth, scaly surface, and they occur on sun-exposed skin, mostly the face, and near other manifestations of photodamage," noted Dr. Rosen at the annual Hawaii Dermatology Seminar sponsored by Skin Disease Education Foundation (SDEF).
Differential diagnosis includes solar lentigo, lentigo maligna, lentigo maligna melanoma, seborrheic keratosis, and pigmented squamous cell carcinoma in situ. "The presence of dots, globules, and asymmetry on dermatoscopy can help you distinguish spreading pigmented AKs from other lesions," said Dr. Rosen, professor of dermatology at Baylor College of Medicine, Houston.
The other main variant, proliferating AK, also tends to affect patients older than age 60 but it occurs more commonly in men than in women. This variant is greater than 1.5 cm in size with a history of rapid lateral spread, and it is marked by a confluent scaly surface with some palpability. Affected areas include sun-exposed skin, mostly the face, and areas near other manifestations of photodamage. "This variant is resistant to usual topical therapy, and the differential diagnosis may include eczema, psoriasis, squamous cell carcinoma in situ, and superficial basal cell carcinoma," said Dr. Rosen, who is also chief of the dermatology clinic at the Houston-based Michael E. DeBakey VA Medical Center. Histology reveals fingerlike invasive projections into the dermis of atypical squamous cells.
The appearance of multiple AKs in a cosmetic unit indicates that the clinician should consider the entire photodamaged area to be diseased. This concept, known as field-directed therapy, "not only addresses apparent clinical lesions, but also reveals and may treat subclinical lesions," he said. "Field therapy may also offer the advantage of reversing basic cellular aberrations leading to transition into invasive cutaneous malignancy."
Another trend in the treatment of AKs is the development of new imiquimod formulations. Results from two placebo-controlled studies of daily application of 2.5% and 3.75% imiquimod creams to the face and balding scalp for two 3-week cycles revealed that both formulations were more effective than placebo and had an acceptable safety profile (J. Am. Acad. Dermatol. 2010;62:573-81). The final evaluation occurred 8 weeks after the final treatment, said Dr. Rosen, who was one of the study investigators. Results from this and other studies led to Food and Drug Administration approval of imiquimod 2.5% (Zyclara) for AKs on July 19, 2011, but the formulation is not yet commercially available.
In a more recent analysis, investigators assessed complete clearance rates in AK patients from four phase III trials of imiquimod who were followed for 1 year (J. Drugs Dermatol. 2011;10:165-70). For imiquimod 3.75% and 2.5% cream, respectively, complete clearance was sustained for 1 year in 40.5% and 33.3% of patients from the 2-week cycle studies, and in 47.9% and 43.2% of patients from the 3-week cycle studies.
Combination therapies for AKs have become increasingly popular. Treatments include cryosurgery followed by diclofenac, 5-fluorouracil followed by cryosurgery, cryosurgery followed by imiquimod 5% or 3.75%, photodynamic therapy (PTD) followed by imiquimod 5%, and tazarotene followed by PDT. "For all studies where field therapy is combined with lesion-directed therapy or with another field therapy, the combination proved superior to monotherapy," Dr. Rosen said.
He went on to note that there is considerable user variation – such as time, the distance the device is held from the skin, and the type of unit used – in the delivery of cryosurgery to treat AKs. The variation "may have more to do with skin temperature than any other variable," said Dr. Rosen. In one study, investigators used an infrared detector in a liquid nitrogen container to deliver cryotherapy to a temperature of –5° C in 36 patients with 180 thin AKs (Dermatol. Surg. 2010;36:1956-61). The clearance rates were 67% at 1 week and 100% at 6 weeks.
Treatment of AKs with radiation is another area of study. In one recent trial, 12 patients with refractory AK and 4 patients with AKs near a nonmelanoma skin cancer underwent external beam radiation therapy five times a week for 4-6 weeks. The total dose of radiation ranged from 4 to 60 Gy (J. Clin. Aesthet. Dermatol. 2011;4:47-50). Of the 16 patients, 13 had complete resolution of AKs, 1 noted a prompt recurrence, and 90% said they were "very satisfied" with the treatment results.
Treating AKs with methyl aminolevulinate photodynamic therapy (MAL-PDT) is also being investigated. In a multicenter study conducted in Scandinavia, 120 patients with 1,572 AKs underwent MAL-PDT followed by immediate exposure to the sun for 1.5-2.5 hours (Br. J. Dermatol. 2011;164:1083-90). At 3 months, 75%-77% of the lesions had cleared. This approach "has an advantage for the health care provider in that no equipment is needed," Dr. Rosen said. "The advantage for the patient is that the therapy is nearly pain free."
Dr. Rosen disclosed that he is a consultant and a member of the speakers bureau for Medicis, which makes imiquimod. He is also a consultant for LEO Pharma.
SDEF and this news organization are owned by Elsevier.
The ability to distinguish between the two key variants of actinic keratosis is key to effective management, according to Dr. Theodore Rosen.
Pigmented actinic keratosis (AK) that spreads typically occurs in patients older than age 60 years and affects more women than men. The lesions are larger than 1.5 cm and have a history of lateral spread. "The lesions are flat, with a smooth, scaly surface, and they occur on sun-exposed skin, mostly the face, and near other manifestations of photodamage," noted Dr. Rosen at the annual Hawaii Dermatology Seminar sponsored by Skin Disease Education Foundation (SDEF).
Differential diagnosis includes solar lentigo, lentigo maligna, lentigo maligna melanoma, seborrheic keratosis, and pigmented squamous cell carcinoma in situ. "The presence of dots, globules, and asymmetry on dermatoscopy can help you distinguish spreading pigmented AKs from other lesions," said Dr. Rosen, professor of dermatology at Baylor College of Medicine, Houston.
The other main variant, proliferating AK, also tends to affect patients older than age 60 but it occurs more commonly in men than in women. This variant is greater than 1.5 cm in size with a history of rapid lateral spread, and it is marked by a confluent scaly surface with some palpability. Affected areas include sun-exposed skin, mostly the face, and areas near other manifestations of photodamage. "This variant is resistant to usual topical therapy, and the differential diagnosis may include eczema, psoriasis, squamous cell carcinoma in situ, and superficial basal cell carcinoma," said Dr. Rosen, who is also chief of the dermatology clinic at the Houston-based Michael E. DeBakey VA Medical Center. Histology reveals fingerlike invasive projections into the dermis of atypical squamous cells.
The appearance of multiple AKs in a cosmetic unit indicates that the clinician should consider the entire photodamaged area to be diseased. This concept, known as field-directed therapy, "not only addresses apparent clinical lesions, but also reveals and may treat subclinical lesions," he said. "Field therapy may also offer the advantage of reversing basic cellular aberrations leading to transition into invasive cutaneous malignancy."
Another trend in the treatment of AKs is the development of new imiquimod formulations. Results from two placebo-controlled studies of daily application of 2.5% and 3.75% imiquimod creams to the face and balding scalp for two 3-week cycles revealed that both formulations were more effective than placebo and had an acceptable safety profile (J. Am. Acad. Dermatol. 2010;62:573-81). The final evaluation occurred 8 weeks after the final treatment, said Dr. Rosen, who was one of the study investigators. Results from this and other studies led to Food and Drug Administration approval of imiquimod 2.5% (Zyclara) for AKs on July 19, 2011, but the formulation is not yet commercially available.
In a more recent analysis, investigators assessed complete clearance rates in AK patients from four phase III trials of imiquimod who were followed for 1 year (J. Drugs Dermatol. 2011;10:165-70). For imiquimod 3.75% and 2.5% cream, respectively, complete clearance was sustained for 1 year in 40.5% and 33.3% of patients from the 2-week cycle studies, and in 47.9% and 43.2% of patients from the 3-week cycle studies.
Combination therapies for AKs have become increasingly popular. Treatments include cryosurgery followed by diclofenac, 5-fluorouracil followed by cryosurgery, cryosurgery followed by imiquimod 5% or 3.75%, photodynamic therapy (PTD) followed by imiquimod 5%, and tazarotene followed by PDT. "For all studies where field therapy is combined with lesion-directed therapy or with another field therapy, the combination proved superior to monotherapy," Dr. Rosen said.
He went on to note that there is considerable user variation – such as time, the distance the device is held from the skin, and the type of unit used – in the delivery of cryosurgery to treat AKs. The variation "may have more to do with skin temperature than any other variable," said Dr. Rosen. In one study, investigators used an infrared detector in a liquid nitrogen container to deliver cryotherapy to a temperature of –5° C in 36 patients with 180 thin AKs (Dermatol. Surg. 2010;36:1956-61). The clearance rates were 67% at 1 week and 100% at 6 weeks.
Treatment of AKs with radiation is another area of study. In one recent trial, 12 patients with refractory AK and 4 patients with AKs near a nonmelanoma skin cancer underwent external beam radiation therapy five times a week for 4-6 weeks. The total dose of radiation ranged from 4 to 60 Gy (J. Clin. Aesthet. Dermatol. 2011;4:47-50). Of the 16 patients, 13 had complete resolution of AKs, 1 noted a prompt recurrence, and 90% said they were "very satisfied" with the treatment results.
Treating AKs with methyl aminolevulinate photodynamic therapy (MAL-PDT) is also being investigated. In a multicenter study conducted in Scandinavia, 120 patients with 1,572 AKs underwent MAL-PDT followed by immediate exposure to the sun for 1.5-2.5 hours (Br. J. Dermatol. 2011;164:1083-90). At 3 months, 75%-77% of the lesions had cleared. This approach "has an advantage for the health care provider in that no equipment is needed," Dr. Rosen said. "The advantage for the patient is that the therapy is nearly pain free."
Dr. Rosen disclosed that he is a consultant and a member of the speakers bureau for Medicis, which makes imiquimod. He is also a consultant for LEO Pharma.
SDEF and this news organization are owned by Elsevier.
EXPERT ANALYSIS FROM THE SDEF HAWAII DERMATOLOGY SEMINAR
Social Media Impacting Plastic Surgery Choices
Social media are changing the way patients obtain advice and information about cosmetic surgery before choosing a procedure, a survey has shown.
The 2011 American Academy of Facial Plastic and Reconstructive Surgery (AAFPRS) membership study, released on Feb. 9, found that 42% of patients obtained plastic surgery information from social networking sites, up from 29% in 2010, while 48% reported receiving information from friends, down from 63% in 2010.
"We are encouraged by the possibilities that Facebook, Twitter, and other social channels offer for prospective patients, but urge all patients to exercise caution in researching facial plastic procedures to ensure information is from a reliable source," AAFPRS President Tom D. Wang said in a press release about the survey. "There’s a great deal of misinformation out there."
In response to the survey results, social media expert Dr. Jeffrey Benabio said, "The whole social networking phenomenon has changed the position of patients to some extent. In many ways it makes them more empowered than they were before. They’re actually coming to us with information that previously they didn’t have access to. Oftentimes it’s very good information. Sometimes it’s not."
However, added Dr. Benabio, a dermatologist at Kaiser Permanente in San Diego, "it’s important for physicians to acknowledge that your patient [who brings you information from the Internet] is engaged; your patient is trying to learn. ... Look at what they [bring to you], and don’t dismiss it out of hand because it’s going to be the norm of the future that patients will either supplement what we provide them as physicians or else bypass us altogether to get information about their health."
The survey results also found that 63% of procedures performed by facial plastic surgeons were cosmetic versus reconstructive in nature, with Botox (onabotulinumtoxinA) and hyaluronic acid injections leading the way.
Survey respondents reported rhinoplasty as the most common surgical procedure in 2011, followed by blepharoplasty, face-lift, ablative skin resurfacing, and lip augmentation. The majority of surgical and nonsurgical procedures were performed on patients aged 35-60 years, with the exception of rhinoplasty, which was mostly performed on patients aged 22-34 years. The majority of all surgical and nonsurgical procedures (82%) were performed on women.
The 2011 survey revealed certain differences, compared with AAFPRS membership surveys conducted in previous years. For example, the overall number of procedures performed in 2011 was down 6% from 2010, yet was up 36% from 2008. This was driven by an 11% rise in cosmetic nonsurgical procedures. In addition, the average costs of most surgical and nonsurgical procedures decreased in 2011, with the exception of otoplasty, implants, and chemical peels.
One-quarter or more of respondents reported an increase in the proportion of procedures performed among ethnic populations in 2011. White patients topped the list, increasing 37% compared with 2010, followed by a corresponding 14% increase in Hispanic patients, an 11% increase in Asian American patients, and a 9% increase in black patients.
Black and Hispanic patients were most likely to have received rhinoplasty in 2011 (88% and 67%, respectively). Asian Americans were most likely to have received blepharoplasty (56%) or rhinoplasty (35%), while white patients were more likely to have received rhinoplasty (41%), followed by face-lifts (34%).
The full survey can be downloaded at www.aafprs.org.
Social media are changing the way patients obtain advice and information about cosmetic surgery before choosing a procedure, a survey has shown.
The 2011 American Academy of Facial Plastic and Reconstructive Surgery (AAFPRS) membership study, released on Feb. 9, found that 42% of patients obtained plastic surgery information from social networking sites, up from 29% in 2010, while 48% reported receiving information from friends, down from 63% in 2010.
"We are encouraged by the possibilities that Facebook, Twitter, and other social channels offer for prospective patients, but urge all patients to exercise caution in researching facial plastic procedures to ensure information is from a reliable source," AAFPRS President Tom D. Wang said in a press release about the survey. "There’s a great deal of misinformation out there."
In response to the survey results, social media expert Dr. Jeffrey Benabio said, "The whole social networking phenomenon has changed the position of patients to some extent. In many ways it makes them more empowered than they were before. They’re actually coming to us with information that previously they didn’t have access to. Oftentimes it’s very good information. Sometimes it’s not."
However, added Dr. Benabio, a dermatologist at Kaiser Permanente in San Diego, "it’s important for physicians to acknowledge that your patient [who brings you information from the Internet] is engaged; your patient is trying to learn. ... Look at what they [bring to you], and don’t dismiss it out of hand because it’s going to be the norm of the future that patients will either supplement what we provide them as physicians or else bypass us altogether to get information about their health."
The survey results also found that 63% of procedures performed by facial plastic surgeons were cosmetic versus reconstructive in nature, with Botox (onabotulinumtoxinA) and hyaluronic acid injections leading the way.
Survey respondents reported rhinoplasty as the most common surgical procedure in 2011, followed by blepharoplasty, face-lift, ablative skin resurfacing, and lip augmentation. The majority of surgical and nonsurgical procedures were performed on patients aged 35-60 years, with the exception of rhinoplasty, which was mostly performed on patients aged 22-34 years. The majority of all surgical and nonsurgical procedures (82%) were performed on women.
The 2011 survey revealed certain differences, compared with AAFPRS membership surveys conducted in previous years. For example, the overall number of procedures performed in 2011 was down 6% from 2010, yet was up 36% from 2008. This was driven by an 11% rise in cosmetic nonsurgical procedures. In addition, the average costs of most surgical and nonsurgical procedures decreased in 2011, with the exception of otoplasty, implants, and chemical peels.
One-quarter or more of respondents reported an increase in the proportion of procedures performed among ethnic populations in 2011. White patients topped the list, increasing 37% compared with 2010, followed by a corresponding 14% increase in Hispanic patients, an 11% increase in Asian American patients, and a 9% increase in black patients.
Black and Hispanic patients were most likely to have received rhinoplasty in 2011 (88% and 67%, respectively). Asian Americans were most likely to have received blepharoplasty (56%) or rhinoplasty (35%), while white patients were more likely to have received rhinoplasty (41%), followed by face-lifts (34%).
The full survey can be downloaded at www.aafprs.org.
Social media are changing the way patients obtain advice and information about cosmetic surgery before choosing a procedure, a survey has shown.
The 2011 American Academy of Facial Plastic and Reconstructive Surgery (AAFPRS) membership study, released on Feb. 9, found that 42% of patients obtained plastic surgery information from social networking sites, up from 29% in 2010, while 48% reported receiving information from friends, down from 63% in 2010.
"We are encouraged by the possibilities that Facebook, Twitter, and other social channels offer for prospective patients, but urge all patients to exercise caution in researching facial plastic procedures to ensure information is from a reliable source," AAFPRS President Tom D. Wang said in a press release about the survey. "There’s a great deal of misinformation out there."
In response to the survey results, social media expert Dr. Jeffrey Benabio said, "The whole social networking phenomenon has changed the position of patients to some extent. In many ways it makes them more empowered than they were before. They’re actually coming to us with information that previously they didn’t have access to. Oftentimes it’s very good information. Sometimes it’s not."
However, added Dr. Benabio, a dermatologist at Kaiser Permanente in San Diego, "it’s important for physicians to acknowledge that your patient [who brings you information from the Internet] is engaged; your patient is trying to learn. ... Look at what they [bring to you], and don’t dismiss it out of hand because it’s going to be the norm of the future that patients will either supplement what we provide them as physicians or else bypass us altogether to get information about their health."
The survey results also found that 63% of procedures performed by facial plastic surgeons were cosmetic versus reconstructive in nature, with Botox (onabotulinumtoxinA) and hyaluronic acid injections leading the way.
Survey respondents reported rhinoplasty as the most common surgical procedure in 2011, followed by blepharoplasty, face-lift, ablative skin resurfacing, and lip augmentation. The majority of surgical and nonsurgical procedures were performed on patients aged 35-60 years, with the exception of rhinoplasty, which was mostly performed on patients aged 22-34 years. The majority of all surgical and nonsurgical procedures (82%) were performed on women.
The 2011 survey revealed certain differences, compared with AAFPRS membership surveys conducted in previous years. For example, the overall number of procedures performed in 2011 was down 6% from 2010, yet was up 36% from 2008. This was driven by an 11% rise in cosmetic nonsurgical procedures. In addition, the average costs of most surgical and nonsurgical procedures decreased in 2011, with the exception of otoplasty, implants, and chemical peels.
One-quarter or more of respondents reported an increase in the proportion of procedures performed among ethnic populations in 2011. White patients topped the list, increasing 37% compared with 2010, followed by a corresponding 14% increase in Hispanic patients, an 11% increase in Asian American patients, and a 9% increase in black patients.
Black and Hispanic patients were most likely to have received rhinoplasty in 2011 (88% and 67%, respectively). Asian Americans were most likely to have received blepharoplasty (56%) or rhinoplasty (35%), while white patients were more likely to have received rhinoplasty (41%), followed by face-lifts (34%).
The full survey can be downloaded at www.aafprs.org.
Report Spotlights National IVF Trends
Fewer embryos per cycle are being transferred in favor of increased use of single cell embryo transfer, leading to further reductions in the percentage of twins and high-order multiple births, according to the latest data on the use of assisted reproductive technologies in the United States.
The data come from the Society for Assisted Reproductive Technology’s 2010 IVF Success Rate National Summary, a yearly report that has been generated since 2003.
For 2010, 370 clinics reported data to SART on 146,693 treatment cycles leading to the birth of 58,727 babies. The percentage of cycles resulting in live births among women younger than age 35 years was 41.7%, compared with 31.9% for those aged 35-37 years, 22.1% for those aged 38-40, 12.5% for those aged 41-42, and 4.1% for those older than age 42. Corresponding live birth rates from the 2003 IVF Success Rate National Summary were 37.5% for women younger than age 35, 30.4% for those aged 35-37, 20.2% for those aged 38-40, 11.2% for those aged 41-42, and 4.5% for those older than age 42.
According to the 2010 report, the average number of embryos transferred per cycle was 2.0 for women younger than age 35 years, 2.2 for those aged 35-37, 2.6 for those aged 38-40, 3.0 for those aged 41-42, and 3.1 for those older than age 42. In 2003, the corresponding average number of embryos transferred per cycle was 2.6 for women younger than age 35 years, 2.9 for those aged 35-37, 3.2 for those aged 38-40, 3.5 for those aged 41-42, and 3.5 for those older than age 42.
A striking increase in the use of elective single cell embryo transfer (eSET) has occurred since 2003. In that year, the percentage of cycles with elective single embryo transfer was only 0.7% for women younger than age 35 years, 0.4% for those aged 35-37 years, 0.2% for those aged 38-40, 0.1% for those aged 41-42, and 0.0% for those older than age 42. In 2010, percentage of cycles with elective single embryo transfer was 9.6% for women younger than age 35 years, 5.3% for those aged 35-37 years, 1.7% for those aged 38-40, 0.6% for those aged 41-42, and 0.5% for those older than age 42.
The percentage of live births with twins has decreased only slightly over time, but only in the three youngest age categories. In 2003, those rates were 33.5% for women younger than age 35 years, 27.9% for those aged 35-37 years, 22.7% for those aged 38-40, 14.8% for those aged 41-42, and 7.3% for those older than age 42. By 2010 the percentage of live births with twins was 32.4% for women younger than age 35, 27.2% for those aged 35-37, and 22.1% for those aged 38-40, yet had increased to 16.9% for those aged 41-42 and 9.6% for those older than age 42.
In the meantime, the percentage of live births with triplets or more has decreased sharply. In 2003, those rates were 6.4% for women younger than age 35 years, 6.1 % for those aged 35-37 years, 5.6% for those aged 38-40, 2.8% for those aged 41-42, and 0.6% for those older than age 42. By 2010 the percentage of live births with triplets or more had fallen to 1.5% for women younger than age 35 years, 1.5% for those aged 35-37 years, 1.1% for those aged 38-40, 1.1% for those aged 41-42, and 0.9% for those older than age 42.
SART sponsored the national study.
Fewer embryos per cycle are being transferred in favor of increased use of single cell embryo transfer, leading to further reductions in the percentage of twins and high-order multiple births, according to the latest data on the use of assisted reproductive technologies in the United States.
The data come from the Society for Assisted Reproductive Technology’s 2010 IVF Success Rate National Summary, a yearly report that has been generated since 2003.
For 2010, 370 clinics reported data to SART on 146,693 treatment cycles leading to the birth of 58,727 babies. The percentage of cycles resulting in live births among women younger than age 35 years was 41.7%, compared with 31.9% for those aged 35-37 years, 22.1% for those aged 38-40, 12.5% for those aged 41-42, and 4.1% for those older than age 42. Corresponding live birth rates from the 2003 IVF Success Rate National Summary were 37.5% for women younger than age 35, 30.4% for those aged 35-37, 20.2% for those aged 38-40, 11.2% for those aged 41-42, and 4.5% for those older than age 42.
According to the 2010 report, the average number of embryos transferred per cycle was 2.0 for women younger than age 35 years, 2.2 for those aged 35-37, 2.6 for those aged 38-40, 3.0 for those aged 41-42, and 3.1 for those older than age 42. In 2003, the corresponding average number of embryos transferred per cycle was 2.6 for women younger than age 35 years, 2.9 for those aged 35-37, 3.2 for those aged 38-40, 3.5 for those aged 41-42, and 3.5 for those older than age 42.
A striking increase in the use of elective single cell embryo transfer (eSET) has occurred since 2003. In that year, the percentage of cycles with elective single embryo transfer was only 0.7% for women younger than age 35 years, 0.4% for those aged 35-37 years, 0.2% for those aged 38-40, 0.1% for those aged 41-42, and 0.0% for those older than age 42. In 2010, percentage of cycles with elective single embryo transfer was 9.6% for women younger than age 35 years, 5.3% for those aged 35-37 years, 1.7% for those aged 38-40, 0.6% for those aged 41-42, and 0.5% for those older than age 42.
The percentage of live births with twins has decreased only slightly over time, but only in the three youngest age categories. In 2003, those rates were 33.5% for women younger than age 35 years, 27.9% for those aged 35-37 years, 22.7% for those aged 38-40, 14.8% for those aged 41-42, and 7.3% for those older than age 42. By 2010 the percentage of live births with twins was 32.4% for women younger than age 35, 27.2% for those aged 35-37, and 22.1% for those aged 38-40, yet had increased to 16.9% for those aged 41-42 and 9.6% for those older than age 42.
In the meantime, the percentage of live births with triplets or more has decreased sharply. In 2003, those rates were 6.4% for women younger than age 35 years, 6.1 % for those aged 35-37 years, 5.6% for those aged 38-40, 2.8% for those aged 41-42, and 0.6% for those older than age 42. By 2010 the percentage of live births with triplets or more had fallen to 1.5% for women younger than age 35 years, 1.5% for those aged 35-37 years, 1.1% for those aged 38-40, 1.1% for those aged 41-42, and 0.9% for those older than age 42.
SART sponsored the national study.
Fewer embryos per cycle are being transferred in favor of increased use of single cell embryo transfer, leading to further reductions in the percentage of twins and high-order multiple births, according to the latest data on the use of assisted reproductive technologies in the United States.
The data come from the Society for Assisted Reproductive Technology’s 2010 IVF Success Rate National Summary, a yearly report that has been generated since 2003.
For 2010, 370 clinics reported data to SART on 146,693 treatment cycles leading to the birth of 58,727 babies. The percentage of cycles resulting in live births among women younger than age 35 years was 41.7%, compared with 31.9% for those aged 35-37 years, 22.1% for those aged 38-40, 12.5% for those aged 41-42, and 4.1% for those older than age 42. Corresponding live birth rates from the 2003 IVF Success Rate National Summary were 37.5% for women younger than age 35, 30.4% for those aged 35-37, 20.2% for those aged 38-40, 11.2% for those aged 41-42, and 4.5% for those older than age 42.
According to the 2010 report, the average number of embryos transferred per cycle was 2.0 for women younger than age 35 years, 2.2 for those aged 35-37, 2.6 for those aged 38-40, 3.0 for those aged 41-42, and 3.1 for those older than age 42. In 2003, the corresponding average number of embryos transferred per cycle was 2.6 for women younger than age 35 years, 2.9 for those aged 35-37, 3.2 for those aged 38-40, 3.5 for those aged 41-42, and 3.5 for those older than age 42.
A striking increase in the use of elective single cell embryo transfer (eSET) has occurred since 2003. In that year, the percentage of cycles with elective single embryo transfer was only 0.7% for women younger than age 35 years, 0.4% for those aged 35-37 years, 0.2% for those aged 38-40, 0.1% for those aged 41-42, and 0.0% for those older than age 42. In 2010, percentage of cycles with elective single embryo transfer was 9.6% for women younger than age 35 years, 5.3% for those aged 35-37 years, 1.7% for those aged 38-40, 0.6% for those aged 41-42, and 0.5% for those older than age 42.
The percentage of live births with twins has decreased only slightly over time, but only in the three youngest age categories. In 2003, those rates were 33.5% for women younger than age 35 years, 27.9% for those aged 35-37 years, 22.7% for those aged 38-40, 14.8% for those aged 41-42, and 7.3% for those older than age 42. By 2010 the percentage of live births with twins was 32.4% for women younger than age 35, 27.2% for those aged 35-37, and 22.1% for those aged 38-40, yet had increased to 16.9% for those aged 41-42 and 9.6% for those older than age 42.
In the meantime, the percentage of live births with triplets or more has decreased sharply. In 2003, those rates were 6.4% for women younger than age 35 years, 6.1 % for those aged 35-37 years, 5.6% for those aged 38-40, 2.8% for those aged 41-42, and 0.6% for those older than age 42. By 2010 the percentage of live births with triplets or more had fallen to 1.5% for women younger than age 35 years, 1.5% for those aged 35-37 years, 1.1% for those aged 38-40, 1.1% for those aged 41-42, and 0.9% for those older than age 42.
SART sponsored the national study.
Major Finding: In 2010, the percentage of treatment cycles resulting in live births among women younger than age 35 was 41.7%, compared with 31.9% for those aged 35-37, 22.1% for those aged 38-40, 12.5% for those aged 41-42, and 4.1% for those older than age 42.
Data Source: : This is a summary of findings from 370 IVF clinics in the United States reporting data to the Society for Assisted Reproductive Technology on 146,693 treatment cycles leading to the birth of 58,727 babies.
Disclosures: SART sponsored the national study.
Medical Website Expert Shares Design Tips
LAS VEGAS – There are two audiences to consider when creating an effective website design for a cosmetic dermatology practice: consumers and search engine robots, said Merrill Whatley.
"People and search engine robots want the same things from your design," Mr. Whatley, chief technical officer at Culver City, Calif.–based NKP Medical Marketing, said at the annual meeting of the American Academy of Cosmetic Surgery. "Both audiences like well-written, clean code using modern programming languages. This means that users are going to have the same experience across different browsers. So you want to make sure your website is operational on Internet Explorer, Firefox, Google Chrome, Safari, or however else they may be coming to you. They want it to be fast loading, and they want the content to be readable."

Consider the following when developing a website:
• Set a tone and spark interest. "You want to talk about what makes you special," Mr. Whatley said. "Do you have any special deals on procedures that you’re offering? And how are the aesthetics of your website design? Is the website pretty?"
• Answer questions at a glance. A homepage should include information about who the physicians at the practice are, contact information, and testimonials from patients and other physicians. "The first thing [users] look for is your phone number in the upper right part of the screen," he said. "They’re also going to be looking for Facebook, Twitter, and YouTube icons. What this represents to people is that you’re out there: You’re not just broadcasting to them, but you’re interacting with them; you’re listening to them. Search engines are also figuring in your social media efforts by returning results from social media sites much more than they used to."
• Consider user experience. This involves anticipating the questions and concerns of visitors to a website, such as physician training, qualifications, and memberships and other affiliations; financing options; and access to before and after clinical photos.
"If you don’t have a photo gallery yet, or permission from patients to use their photos, still include a photo gallery link on your website," Mr. Whatley advised. "When users click there, you could have a message that reads, ‘due to patient confidentiality, we are not featuring photos at this time,’ and that message could go on to invite patients in for a consultation. You’d be surprised at the number of contacts some of our clients have received from a contact form like this."

Increasingly, website designers are creating device-specific displays for smartphones and other mobile devices. Mr. Whatley recommended not only device-specific displays but a device-specific experience for users. "You have to consider that the user’s needs are going to be different and more action oriented when they are visiting your site from a mobile device," he explained. "Both people and search engines recognize these efforts at improving the user experience."
A mobile-specific interface "helps bring people into your office and makes them feel like you are accessible," Mr. Whatley said. "They get an app-like experience without having to download an app." The site page should resemble an app, with a prominent call button, an e-mail button, and a way for users to send a text message. "This is going to get you better results when people are searching from a mobile device," he said of device-specific displays. "Up to 50% of visits to some of our clients’ websites come from mobile devices."
His list of features to avoid on a website includes autoplaying video and audio, splash pages, and bad navigation choices. "For example, alphabetic ordering of the procedures offered in your practice may seem elementary, but it’s important from the user’s standpoint," he said.
Mr. Whatley said he had no relevant financial disclosures.
LAS VEGAS – There are two audiences to consider when creating an effective website design for a cosmetic dermatology practice: consumers and search engine robots, said Merrill Whatley.
"People and search engine robots want the same things from your design," Mr. Whatley, chief technical officer at Culver City, Calif.–based NKP Medical Marketing, said at the annual meeting of the American Academy of Cosmetic Surgery. "Both audiences like well-written, clean code using modern programming languages. This means that users are going to have the same experience across different browsers. So you want to make sure your website is operational on Internet Explorer, Firefox, Google Chrome, Safari, or however else they may be coming to you. They want it to be fast loading, and they want the content to be readable."
Consider the following when developing a website:
• Set a tone and spark interest. "You want to talk about what makes you special," Mr. Whatley said. "Do you have any special deals on procedures that you’re offering? And how are the aesthetics of your website design? Is the website pretty?"
• Answer questions at a glance. A homepage should include information about who the physicians at the practice are, contact information, and testimonials from patients and other physicians. "The first thing [users] look for is your phone number in the upper right part of the screen," he said. "They’re also going to be looking for Facebook, Twitter, and YouTube icons. What this represents to people is that you’re out there: You’re not just broadcasting to them, but you’re interacting with them; you’re listening to them. Search engines are also figuring in your social media efforts by returning results from social media sites much more than they used to."
• Consider user experience. This involves anticipating the questions and concerns of visitors to a website, such as physician training, qualifications, and memberships and other affiliations; financing options; and access to before and after clinical photos.
"If you don’t have a photo gallery yet, or permission from patients to use their photos, still include a photo gallery link on your website," Mr. Whatley advised. "When users click there, you could have a message that reads, ‘due to patient confidentiality, we are not featuring photos at this time,’ and that message could go on to invite patients in for a consultation. You’d be surprised at the number of contacts some of our clients have received from a contact form like this."
Increasingly, website designers are creating device-specific displays for smartphones and other mobile devices. Mr. Whatley recommended not only device-specific displays but a device-specific experience for users. "You have to consider that the user’s needs are going to be different and more action oriented when they are visiting your site from a mobile device," he explained. "Both people and search engines recognize these efforts at improving the user experience."
A mobile-specific interface "helps bring people into your office and makes them feel like you are accessible," Mr. Whatley said. "They get an app-like experience without having to download an app." The site page should resemble an app, with a prominent call button, an e-mail button, and a way for users to send a text message. "This is going to get you better results when people are searching from a mobile device," he said of device-specific displays. "Up to 50% of visits to some of our clients’ websites come from mobile devices."
His list of features to avoid on a website includes autoplaying video and audio, splash pages, and bad navigation choices. "For example, alphabetic ordering of the procedures offered in your practice may seem elementary, but it’s important from the user’s standpoint," he said.
Mr. Whatley said he had no relevant financial disclosures.
LAS VEGAS – There are two audiences to consider when creating an effective website design for a cosmetic dermatology practice: consumers and search engine robots, said Merrill Whatley.
"People and search engine robots want the same things from your design," Mr. Whatley, chief technical officer at Culver City, Calif.–based NKP Medical Marketing, said at the annual meeting of the American Academy of Cosmetic Surgery. "Both audiences like well-written, clean code using modern programming languages. This means that users are going to have the same experience across different browsers. So you want to make sure your website is operational on Internet Explorer, Firefox, Google Chrome, Safari, or however else they may be coming to you. They want it to be fast loading, and they want the content to be readable."
Consider the following when developing a website:
• Set a tone and spark interest. "You want to talk about what makes you special," Mr. Whatley said. "Do you have any special deals on procedures that you’re offering? And how are the aesthetics of your website design? Is the website pretty?"
• Answer questions at a glance. A homepage should include information about who the physicians at the practice are, contact information, and testimonials from patients and other physicians. "The first thing [users] look for is your phone number in the upper right part of the screen," he said. "They’re also going to be looking for Facebook, Twitter, and YouTube icons. What this represents to people is that you’re out there: You’re not just broadcasting to them, but you’re interacting with them; you’re listening to them. Search engines are also figuring in your social media efforts by returning results from social media sites much more than they used to."
• Consider user experience. This involves anticipating the questions and concerns of visitors to a website, such as physician training, qualifications, and memberships and other affiliations; financing options; and access to before and after clinical photos.
"If you don’t have a photo gallery yet, or permission from patients to use their photos, still include a photo gallery link on your website," Mr. Whatley advised. "When users click there, you could have a message that reads, ‘due to patient confidentiality, we are not featuring photos at this time,’ and that message could go on to invite patients in for a consultation. You’d be surprised at the number of contacts some of our clients have received from a contact form like this."
Increasingly, website designers are creating device-specific displays for smartphones and other mobile devices. Mr. Whatley recommended not only device-specific displays but a device-specific experience for users. "You have to consider that the user’s needs are going to be different and more action oriented when they are visiting your site from a mobile device," he explained. "Both people and search engines recognize these efforts at improving the user experience."
A mobile-specific interface "helps bring people into your office and makes them feel like you are accessible," Mr. Whatley said. "They get an app-like experience without having to download an app." The site page should resemble an app, with a prominent call button, an e-mail button, and a way for users to send a text message. "This is going to get you better results when people are searching from a mobile device," he said of device-specific displays. "Up to 50% of visits to some of our clients’ websites come from mobile devices."
His list of features to avoid on a website includes autoplaying video and audio, splash pages, and bad navigation choices. "For example, alphabetic ordering of the procedures offered in your practice may seem elementary, but it’s important from the user’s standpoint," he said.
Mr. Whatley said he had no relevant financial disclosures.
EXPERT ANALYSIS FROM THE ANNUAL MEETING OF THE AMERICAN ACADEMY OF COSMETIC SURGERY
Facial Affect Recognition's Role in Aggression Explored
Deficits in facial affect recognition – the ability to identify and discriminate emotion in the faces of others – might significantly contribute to aggressive behavior in psychotic illness, according to a literature review on the topic.
Reporting in the January-February 2012 issue of Aggression and Violent Behavior, researchers led by Aisling Malone used the General Aggression Model (GAM), to explore the theory that facial affect recognition (FAR) deficits may contribute to increased aggression in psychosis. The GAM "suggests that an aggressive response is determined by specific features of the person and the situation interacting with cognitions, affect and arousal to produce a particular outcome," wrote Ms. Malone of the School of Psychology and Psychiatry at Monash University, Clayton, Australia, and her colleagues. "In other words, it is not only what an individual brings to the situation but how they process social information that decides the likelihood of an aggressive response."
The GAM model was applied in the review because many published studies examining the relationship between FAR deficits in individuals with psychosis "have been inconclusive and hampered by small sample sizes and other methodological problems," the researchers explained (Aggress. Violent Behav. 2012;17:27-35). "They failed to consistently measure history of violence or to control for relevant confounding variables such as psychopathy, childhood trauma, and substance abuse." When these three potential confounding variables are taken into account, they continued, it spotlights socioemotional processing deficits such as impaired FAR as "a fruitful area for research aimed at understanding, and hence reducing the risk of violence in psychosis."
"It is not only what an individual brings to the situation but how they process social information that decides the likelihood of an aggressive response."
According to the review, any relationship between FAR deficits and aggression in psychosis might be attributable to a subgroup with comorbid psychopathy. For example, in one study, psychopathic inmates demonstrated difficulty in identifying emotions generally and less intense facial expressions, as well as deficits in identifying happy and sad expressions (Pers. Individ. Dif. 2008;44:1474-83). Another study found that males with schizophrenia and high psychopathy scores demonstrated deficits in recognizing sadness, with a marked impairment for lower intensity expressions (Psychiatry Res. 2006;141:29-37).
While the effects of childhood trauma on FAR deficits in psychosis remain unexplored, "what is known is that such childhood trauma is both a significant risk factor for later violence and highly prevalent in psychosis," the researchers wrote. "Child abuse appears to result in hypersensitivity to threat, which may facilitate the development of a hostile attribution bias that primes them to perceive threat in neutral social interactions. These biases may persist into adult life, increasing the likelihood of engaging in violence."
Substance abuse also might negatively affect FAR abilities. One study found that compared with controls, individuals with alcohol dependence tended to mislabel facial expressions as angry or disgusted (Psychiatry Res. 2002;113:161-71). However, the review notes, "it is unclear whether alcohol causes a hostile attrition bias or whether it is attributable to an aggressive response pattern learned early in life as all subjects had at least one alcoholic parent." Another study found that regular cocaine users had difficulty recognizing fearful facial expressions, compared with occasional users or nonusers (Psychopharmacol. 2007;194:151-9).
Socioemotional processing deficits and FAR deficits are a promising avenue to future research in this area, the researchers wrote.
Neither Ms. Malone nor her colleagues disclosed relevant financial conflicts of interest.
Deficits in facial affect recognition – the ability to identify and discriminate emotion in the faces of others – might significantly contribute to aggressive behavior in psychotic illness, according to a literature review on the topic.
Reporting in the January-February 2012 issue of Aggression and Violent Behavior, researchers led by Aisling Malone used the General Aggression Model (GAM), to explore the theory that facial affect recognition (FAR) deficits may contribute to increased aggression in psychosis. The GAM "suggests that an aggressive response is determined by specific features of the person and the situation interacting with cognitions, affect and arousal to produce a particular outcome," wrote Ms. Malone of the School of Psychology and Psychiatry at Monash University, Clayton, Australia, and her colleagues. "In other words, it is not only what an individual brings to the situation but how they process social information that decides the likelihood of an aggressive response."
The GAM model was applied in the review because many published studies examining the relationship between FAR deficits in individuals with psychosis "have been inconclusive and hampered by small sample sizes and other methodological problems," the researchers explained (Aggress. Violent Behav. 2012;17:27-35). "They failed to consistently measure history of violence or to control for relevant confounding variables such as psychopathy, childhood trauma, and substance abuse." When these three potential confounding variables are taken into account, they continued, it spotlights socioemotional processing deficits such as impaired FAR as "a fruitful area for research aimed at understanding, and hence reducing the risk of violence in psychosis."
"It is not only what an individual brings to the situation but how they process social information that decides the likelihood of an aggressive response."
According to the review, any relationship between FAR deficits and aggression in psychosis might be attributable to a subgroup with comorbid psychopathy. For example, in one study, psychopathic inmates demonstrated difficulty in identifying emotions generally and less intense facial expressions, as well as deficits in identifying happy and sad expressions (Pers. Individ. Dif. 2008;44:1474-83). Another study found that males with schizophrenia and high psychopathy scores demonstrated deficits in recognizing sadness, with a marked impairment for lower intensity expressions (Psychiatry Res. 2006;141:29-37).
While the effects of childhood trauma on FAR deficits in psychosis remain unexplored, "what is known is that such childhood trauma is both a significant risk factor for later violence and highly prevalent in psychosis," the researchers wrote. "Child abuse appears to result in hypersensitivity to threat, which may facilitate the development of a hostile attribution bias that primes them to perceive threat in neutral social interactions. These biases may persist into adult life, increasing the likelihood of engaging in violence."
Substance abuse also might negatively affect FAR abilities. One study found that compared with controls, individuals with alcohol dependence tended to mislabel facial expressions as angry or disgusted (Psychiatry Res. 2002;113:161-71). However, the review notes, "it is unclear whether alcohol causes a hostile attrition bias or whether it is attributable to an aggressive response pattern learned early in life as all subjects had at least one alcoholic parent." Another study found that regular cocaine users had difficulty recognizing fearful facial expressions, compared with occasional users or nonusers (Psychopharmacol. 2007;194:151-9).
Socioemotional processing deficits and FAR deficits are a promising avenue to future research in this area, the researchers wrote.
Neither Ms. Malone nor her colleagues disclosed relevant financial conflicts of interest.
Deficits in facial affect recognition – the ability to identify and discriminate emotion in the faces of others – might significantly contribute to aggressive behavior in psychotic illness, according to a literature review on the topic.
Reporting in the January-February 2012 issue of Aggression and Violent Behavior, researchers led by Aisling Malone used the General Aggression Model (GAM), to explore the theory that facial affect recognition (FAR) deficits may contribute to increased aggression in psychosis. The GAM "suggests that an aggressive response is determined by specific features of the person and the situation interacting with cognitions, affect and arousal to produce a particular outcome," wrote Ms. Malone of the School of Psychology and Psychiatry at Monash University, Clayton, Australia, and her colleagues. "In other words, it is not only what an individual brings to the situation but how they process social information that decides the likelihood of an aggressive response."
The GAM model was applied in the review because many published studies examining the relationship between FAR deficits in individuals with psychosis "have been inconclusive and hampered by small sample sizes and other methodological problems," the researchers explained (Aggress. Violent Behav. 2012;17:27-35). "They failed to consistently measure history of violence or to control for relevant confounding variables such as psychopathy, childhood trauma, and substance abuse." When these three potential confounding variables are taken into account, they continued, it spotlights socioemotional processing deficits such as impaired FAR as "a fruitful area for research aimed at understanding, and hence reducing the risk of violence in psychosis."
"It is not only what an individual brings to the situation but how they process social information that decides the likelihood of an aggressive response."
According to the review, any relationship between FAR deficits and aggression in psychosis might be attributable to a subgroup with comorbid psychopathy. For example, in one study, psychopathic inmates demonstrated difficulty in identifying emotions generally and less intense facial expressions, as well as deficits in identifying happy and sad expressions (Pers. Individ. Dif. 2008;44:1474-83). Another study found that males with schizophrenia and high psychopathy scores demonstrated deficits in recognizing sadness, with a marked impairment for lower intensity expressions (Psychiatry Res. 2006;141:29-37).
While the effects of childhood trauma on FAR deficits in psychosis remain unexplored, "what is known is that such childhood trauma is both a significant risk factor for later violence and highly prevalent in psychosis," the researchers wrote. "Child abuse appears to result in hypersensitivity to threat, which may facilitate the development of a hostile attribution bias that primes them to perceive threat in neutral social interactions. These biases may persist into adult life, increasing the likelihood of engaging in violence."
Substance abuse also might negatively affect FAR abilities. One study found that compared with controls, individuals with alcohol dependence tended to mislabel facial expressions as angry or disgusted (Psychiatry Res. 2002;113:161-71). However, the review notes, "it is unclear whether alcohol causes a hostile attrition bias or whether it is attributable to an aggressive response pattern learned early in life as all subjects had at least one alcoholic parent." Another study found that regular cocaine users had difficulty recognizing fearful facial expressions, compared with occasional users or nonusers (Psychopharmacol. 2007;194:151-9).
Socioemotional processing deficits and FAR deficits are a promising avenue to future research in this area, the researchers wrote.
Neither Ms. Malone nor her colleagues disclosed relevant financial conflicts of interest.
FROM AGGRESSION AND VIOLENT BEHAVIOR
C. difficile Diarrhea Can Be Linked to PPIs, FDA Says
The Food and Drug Administration today released a drug safety communication about proton pump inhibitors (PPIs) through its MedWatch Safety Information and Adverse Reporting Program, telling the public that Clostridium difficile–associated diarrhea can be associated with use of PPIs.
The PPI products listed in the communication are AcipHex (rabeprazole sodium); Dexilant (dexlansoprazole); Nexium (esomeprazole magnesium); omeprazole over-the-counter (OTC), Prevacid (lansoprazole) and OTC Prevacid 24hr; Prilosec (omeprazole) and its OTC product, Protonix (pantoprazole sodium), Vimovo (esomeprazole magnesium and naproxen); and Zegerid (omeprazole and sodium bicarbonate) and its OTC product.
"Patients should immediately contact their healthcare professional and seek care if they take PPIs and develop diarrhea that does not improve," according to the communication.
It also recommends that clinicians consider a diagnosis of Clostridium difficile–associated diarrhea in PPI users with diarrhea that does not improve. "Advise patients to seek immediate care from a healthcare professional if they experience watery stool that does not go away, abdominal pain, and fever while taking PPIs," the communication reads. "Patients should use the lowest dose and shortest duration of PPI therapy appropriate to the condition being treated."
In an interview, Dr. David Abend, who practices family medicine and osteopathic manipulative treatment in Oradell, N.J., said that the FDA notice surprised him. "Quite frankly, it’s pretty distressing, because usually you think upper GI issues with these medications, not lower GI issues," he said. "These are really good medications when they’re used correctly. It’s good we have an alert like this, but it doesn’t mean people should freak out and stop using these medications."
To listen to a podcast concerning Clostridium dificile-associated diarrhea and PPI's, click on the "Listen" button below. Podcast courtesy of the FDA.

"Many of the purported adverse properties attributed to PPIs have not been confirmed, and some are questionable," Dr. M. Michael Wolfe, a gastroenterologist, told this news organization. "For example, it is difficult to mechanistically attribute an increase in Clostridium difficile infection to the suppression of acid secretion by PPIs when the organism is transmitted by acid-resistant spores. Rather, this purported adverse property may be [an artifact] and potentially attributable to the use of PPIs in individuals with more serious systemic diseases," said Dr. Wolfe, who chairs the Case Western Reserve University department of medicine at MetroHealth Medical Center, Cleveland.
Serious adverse events associated with these and other drugs should be reported to the FDA’s MedWatch program at 800-332-1088.
The Food and Drug Administration today released a drug safety communication about proton pump inhibitors (PPIs) through its MedWatch Safety Information and Adverse Reporting Program, telling the public that Clostridium difficile–associated diarrhea can be associated with use of PPIs.
The PPI products listed in the communication are AcipHex (rabeprazole sodium); Dexilant (dexlansoprazole); Nexium (esomeprazole magnesium); omeprazole over-the-counter (OTC), Prevacid (lansoprazole) and OTC Prevacid 24hr; Prilosec (omeprazole) and its OTC product, Protonix (pantoprazole sodium), Vimovo (esomeprazole magnesium and naproxen); and Zegerid (omeprazole and sodium bicarbonate) and its OTC product.
"Patients should immediately contact their healthcare professional and seek care if they take PPIs and develop diarrhea that does not improve," according to the communication.
It also recommends that clinicians consider a diagnosis of Clostridium difficile–associated diarrhea in PPI users with diarrhea that does not improve. "Advise patients to seek immediate care from a healthcare professional if they experience watery stool that does not go away, abdominal pain, and fever while taking PPIs," the communication reads. "Patients should use the lowest dose and shortest duration of PPI therapy appropriate to the condition being treated."
In an interview, Dr. David Abend, who practices family medicine and osteopathic manipulative treatment in Oradell, N.J., said that the FDA notice surprised him. "Quite frankly, it’s pretty distressing, because usually you think upper GI issues with these medications, not lower GI issues," he said. "These are really good medications when they’re used correctly. It’s good we have an alert like this, but it doesn’t mean people should freak out and stop using these medications."
To listen to a podcast concerning Clostridium dificile-associated diarrhea and PPI's, click on the "Listen" button below. Podcast courtesy of the FDA.
"Many of the purported adverse properties attributed to PPIs have not been confirmed, and some are questionable," Dr. M. Michael Wolfe, a gastroenterologist, told this news organization. "For example, it is difficult to mechanistically attribute an increase in Clostridium difficile infection to the suppression of acid secretion by PPIs when the organism is transmitted by acid-resistant spores. Rather, this purported adverse property may be [an artifact] and potentially attributable to the use of PPIs in individuals with more serious systemic diseases," said Dr. Wolfe, who chairs the Case Western Reserve University department of medicine at MetroHealth Medical Center, Cleveland.
Serious adverse events associated with these and other drugs should be reported to the FDA’s MedWatch program at 800-332-1088.
The Food and Drug Administration today released a drug safety communication about proton pump inhibitors (PPIs) through its MedWatch Safety Information and Adverse Reporting Program, telling the public that Clostridium difficile–associated diarrhea can be associated with use of PPIs.
The PPI products listed in the communication are AcipHex (rabeprazole sodium); Dexilant (dexlansoprazole); Nexium (esomeprazole magnesium); omeprazole over-the-counter (OTC), Prevacid (lansoprazole) and OTC Prevacid 24hr; Prilosec (omeprazole) and its OTC product, Protonix (pantoprazole sodium), Vimovo (esomeprazole magnesium and naproxen); and Zegerid (omeprazole and sodium bicarbonate) and its OTC product.
"Patients should immediately contact their healthcare professional and seek care if they take PPIs and develop diarrhea that does not improve," according to the communication.
It also recommends that clinicians consider a diagnosis of Clostridium difficile–associated diarrhea in PPI users with diarrhea that does not improve. "Advise patients to seek immediate care from a healthcare professional if they experience watery stool that does not go away, abdominal pain, and fever while taking PPIs," the communication reads. "Patients should use the lowest dose and shortest duration of PPI therapy appropriate to the condition being treated."
In an interview, Dr. David Abend, who practices family medicine and osteopathic manipulative treatment in Oradell, N.J., said that the FDA notice surprised him. "Quite frankly, it’s pretty distressing, because usually you think upper GI issues with these medications, not lower GI issues," he said. "These are really good medications when they’re used correctly. It’s good we have an alert like this, but it doesn’t mean people should freak out and stop using these medications."
To listen to a podcast concerning Clostridium dificile-associated diarrhea and PPI's, click on the "Listen" button below. Podcast courtesy of the FDA.
"Many of the purported adverse properties attributed to PPIs have not been confirmed, and some are questionable," Dr. M. Michael Wolfe, a gastroenterologist, told this news organization. "For example, it is difficult to mechanistically attribute an increase in Clostridium difficile infection to the suppression of acid secretion by PPIs when the organism is transmitted by acid-resistant spores. Rather, this purported adverse property may be [an artifact] and potentially attributable to the use of PPIs in individuals with more serious systemic diseases," said Dr. Wolfe, who chairs the Case Western Reserve University department of medicine at MetroHealth Medical Center, Cleveland.
Serious adverse events associated with these and other drugs should be reported to the FDA’s MedWatch program at 800-332-1088.
Don't Delegate Cosmetic Procedures, Expert Says
LAS VEGAS – Soon after completing a cosmetic dermatologic surgery fellowship at the University of Pittsburgh Medical Center in 2001, Dr. Suzan Obagi stayed on to help launch one of the first academically based cosmetic surgery practices.
There was no previous business plan, no model at another university," Dr. Obagi said at the annual meeting of the American Academy of Cosmetic Surgery.

Today, toxin and filler treatments at the UPMC cosmetic surgery and skin health center are booked 4 months out, and Dr. Obagi said she treats about 1,200 patients with botulinum toxin type A each year and another 600-700 patients with dermal fillers. "If I’ve managed to build a successful cosmetic surgery practice in an academic setting, all of you can certainly do so in a noncampus setting," said Dr. Obagi, who directs the center.
Botulinum toxin type A and dermal fillers are the mainstays of any cosmetic surgery practice because patients strive for the instant results that come from using them. "Instant gratification: That’s what it’s all about," said Dr. Obagi. "Patients don’t want the prolonged down time or the stigma of looking like they’ve had something done. They love the natural look you can give them with injectables. For me, it’s a fun part of my practice. ... I get to be artistic."
Demand for injectables persists during times of economic uncertainty, she added. "When we had the downturn in the economy in 2008, we saw that the number of large [cosmetic surgery] cases dropped off, but the number of small procedures like injections of botulinum toxin type A and other fillers remained the same. What we did to get through some of that downturn was to open up more slots and get more patients in for these procedures."
She offered the following tips on how to enhance an injectables practice:
• Stand out from the competition. "Part of this is how your practice handles patients when they come in, but a bigger part of your practice is, how good are you with the needle?" Dr. Obagi said. "Your artistry is what’s going to speak volumes, so you have to differentiate yourself with your skill, and you have to make sure patients are able to come in every 3-4 months. If your schedule does not allow that to be booked, then you’re going to miss out."
• Set up rooms for efficiency. She said she equips each exam room with a wire basket full of needles, syringes, gauze, anesthetic, and other supplies she’ll need to treat every botulinum toxin type A and dermal filler patient who comes in. "I walk into a room and I can do two to three different things on that patient without having to step out of that room again," Dr. Obagi explained. "I don’t have to go fumbling for anything. I can spend all of that time talking to the patient, inquiring about their family, their adventures, learning about them. It diffuses the situation because patients know you’re going to come at them with a needle. They know they’re going to be feeling some pain shortly. Whatever you can do to calm them before you come at them with that needle really makes a difference."
To optimize the patient experience, she purchased powered procedure chairs for each exam room. "They’re about $10,000 per chair, but they have foot pedals for adjustment so you don’t have to touch anything with your hands," she said. "It’s all about comfort for you and the patient."
She also stocks the waiting room and each exam room with brochures that describe each procedure offered at the center.
• Evaluate each patient at every visit. If a patient has been treated with botulinum toxin type A for the last 5 years, she or he "may need it in other areas now that you’ve taken care of areas they were initially bothered by," Dr. Obagi said. "You need to keep reassessing the patient every time she or he comes in."
• Inject patients quickly and comfortably. Dr. Obagi said she uses the smallest needle possible and stabilizes the fingers on her nondominating hand "so my hand is steady; it’s not going to shake [during injection]," she said. "I have been on the receiving end of good and bad botulinum toxin type A treatments. What makes the difference is being quick with the injection. Make sure your hand is stabilized, and don’t go deeper than you need to. Botulinum toxin type A is not meant to be injected into the periosteum. Don’t go there; it hurts."
• Do the procedures yourself. This allows you to see the patient every 3-4 months to recommend ancillary treatments and surgery.
Dr. Obagi said she charges patients by the amount of toxin or filler used, not by the specific anatomic area she treats. That works well, she said, "because some patients may require 12 U in an area of the face while another patient may require 50 U in that same area."
She said she runs two parallel schedules to optimize efficiency. For example, her afternoon consultation times are at 1 p.m., 1:30 p.m., 2 p.m., 2:30 p.m., 3 p.m., 3:30 p.m., and 4 p.m., while her treatment times for botulinum toxin type A and filler patients are at 1:45 p.m., 2:15 p.m., 2:45 p.m., 3:15 p.m., and 3:45 p.m. "So after I finish a consult in one room, I go into another room and do a quick treatment," she said. "I come back out and go to the next consult."
Dr. Obagi said she had no relevant financial disclosures.
LAS VEGAS – Soon after completing a cosmetic dermatologic surgery fellowship at the University of Pittsburgh Medical Center in 2001, Dr. Suzan Obagi stayed on to help launch one of the first academically based cosmetic surgery practices.
There was no previous business plan, no model at another university," Dr. Obagi said at the annual meeting of the American Academy of Cosmetic Surgery.
Today, toxin and filler treatments at the UPMC cosmetic surgery and skin health center are booked 4 months out, and Dr. Obagi said she treats about 1,200 patients with botulinum toxin type A each year and another 600-700 patients with dermal fillers. "If I’ve managed to build a successful cosmetic surgery practice in an academic setting, all of you can certainly do so in a noncampus setting," said Dr. Obagi, who directs the center.
Botulinum toxin type A and dermal fillers are the mainstays of any cosmetic surgery practice because patients strive for the instant results that come from using them. "Instant gratification: That’s what it’s all about," said Dr. Obagi. "Patients don’t want the prolonged down time or the stigma of looking like they’ve had something done. They love the natural look you can give them with injectables. For me, it’s a fun part of my practice. ... I get to be artistic."
Demand for injectables persists during times of economic uncertainty, she added. "When we had the downturn in the economy in 2008, we saw that the number of large [cosmetic surgery] cases dropped off, but the number of small procedures like injections of botulinum toxin type A and other fillers remained the same. What we did to get through some of that downturn was to open up more slots and get more patients in for these procedures."
She offered the following tips on how to enhance an injectables practice:
• Stand out from the competition. "Part of this is how your practice handles patients when they come in, but a bigger part of your practice is, how good are you with the needle?" Dr. Obagi said. "Your artistry is what’s going to speak volumes, so you have to differentiate yourself with your skill, and you have to make sure patients are able to come in every 3-4 months. If your schedule does not allow that to be booked, then you’re going to miss out."
• Set up rooms for efficiency. She said she equips each exam room with a wire basket full of needles, syringes, gauze, anesthetic, and other supplies she’ll need to treat every botulinum toxin type A and dermal filler patient who comes in. "I walk into a room and I can do two to three different things on that patient without having to step out of that room again," Dr. Obagi explained. "I don’t have to go fumbling for anything. I can spend all of that time talking to the patient, inquiring about their family, their adventures, learning about them. It diffuses the situation because patients know you’re going to come at them with a needle. They know they’re going to be feeling some pain shortly. Whatever you can do to calm them before you come at them with that needle really makes a difference."
To optimize the patient experience, she purchased powered procedure chairs for each exam room. "They’re about $10,000 per chair, but they have foot pedals for adjustment so you don’t have to touch anything with your hands," she said. "It’s all about comfort for you and the patient."
She also stocks the waiting room and each exam room with brochures that describe each procedure offered at the center.
• Evaluate each patient at every visit. If a patient has been treated with botulinum toxin type A for the last 5 years, she or he "may need it in other areas now that you’ve taken care of areas they were initially bothered by," Dr. Obagi said. "You need to keep reassessing the patient every time she or he comes in."
• Inject patients quickly and comfortably. Dr. Obagi said she uses the smallest needle possible and stabilizes the fingers on her nondominating hand "so my hand is steady; it’s not going to shake [during injection]," she said. "I have been on the receiving end of good and bad botulinum toxin type A treatments. What makes the difference is being quick with the injection. Make sure your hand is stabilized, and don’t go deeper than you need to. Botulinum toxin type A is not meant to be injected into the periosteum. Don’t go there; it hurts."
• Do the procedures yourself. This allows you to see the patient every 3-4 months to recommend ancillary treatments and surgery.
Dr. Obagi said she charges patients by the amount of toxin or filler used, not by the specific anatomic area she treats. That works well, she said, "because some patients may require 12 U in an area of the face while another patient may require 50 U in that same area."
She said she runs two parallel schedules to optimize efficiency. For example, her afternoon consultation times are at 1 p.m., 1:30 p.m., 2 p.m., 2:30 p.m., 3 p.m., 3:30 p.m., and 4 p.m., while her treatment times for botulinum toxin type A and filler patients are at 1:45 p.m., 2:15 p.m., 2:45 p.m., 3:15 p.m., and 3:45 p.m. "So after I finish a consult in one room, I go into another room and do a quick treatment," she said. "I come back out and go to the next consult."
Dr. Obagi said she had no relevant financial disclosures.
LAS VEGAS – Soon after completing a cosmetic dermatologic surgery fellowship at the University of Pittsburgh Medical Center in 2001, Dr. Suzan Obagi stayed on to help launch one of the first academically based cosmetic surgery practices.
There was no previous business plan, no model at another university," Dr. Obagi said at the annual meeting of the American Academy of Cosmetic Surgery.
Today, toxin and filler treatments at the UPMC cosmetic surgery and skin health center are booked 4 months out, and Dr. Obagi said she treats about 1,200 patients with botulinum toxin type A each year and another 600-700 patients with dermal fillers. "If I’ve managed to build a successful cosmetic surgery practice in an academic setting, all of you can certainly do so in a noncampus setting," said Dr. Obagi, who directs the center.
Botulinum toxin type A and dermal fillers are the mainstays of any cosmetic surgery practice because patients strive for the instant results that come from using them. "Instant gratification: That’s what it’s all about," said Dr. Obagi. "Patients don’t want the prolonged down time or the stigma of looking like they’ve had something done. They love the natural look you can give them with injectables. For me, it’s a fun part of my practice. ... I get to be artistic."
Demand for injectables persists during times of economic uncertainty, she added. "When we had the downturn in the economy in 2008, we saw that the number of large [cosmetic surgery] cases dropped off, but the number of small procedures like injections of botulinum toxin type A and other fillers remained the same. What we did to get through some of that downturn was to open up more slots and get more patients in for these procedures."
She offered the following tips on how to enhance an injectables practice:
• Stand out from the competition. "Part of this is how your practice handles patients when they come in, but a bigger part of your practice is, how good are you with the needle?" Dr. Obagi said. "Your artistry is what’s going to speak volumes, so you have to differentiate yourself with your skill, and you have to make sure patients are able to come in every 3-4 months. If your schedule does not allow that to be booked, then you’re going to miss out."
• Set up rooms for efficiency. She said she equips each exam room with a wire basket full of needles, syringes, gauze, anesthetic, and other supplies she’ll need to treat every botulinum toxin type A and dermal filler patient who comes in. "I walk into a room and I can do two to three different things on that patient without having to step out of that room again," Dr. Obagi explained. "I don’t have to go fumbling for anything. I can spend all of that time talking to the patient, inquiring about their family, their adventures, learning about them. It diffuses the situation because patients know you’re going to come at them with a needle. They know they’re going to be feeling some pain shortly. Whatever you can do to calm them before you come at them with that needle really makes a difference."
To optimize the patient experience, she purchased powered procedure chairs for each exam room. "They’re about $10,000 per chair, but they have foot pedals for adjustment so you don’t have to touch anything with your hands," she said. "It’s all about comfort for you and the patient."
She also stocks the waiting room and each exam room with brochures that describe each procedure offered at the center.
• Evaluate each patient at every visit. If a patient has been treated with botulinum toxin type A for the last 5 years, she or he "may need it in other areas now that you’ve taken care of areas they were initially bothered by," Dr. Obagi said. "You need to keep reassessing the patient every time she or he comes in."
• Inject patients quickly and comfortably. Dr. Obagi said she uses the smallest needle possible and stabilizes the fingers on her nondominating hand "so my hand is steady; it’s not going to shake [during injection]," she said. "I have been on the receiving end of good and bad botulinum toxin type A treatments. What makes the difference is being quick with the injection. Make sure your hand is stabilized, and don’t go deeper than you need to. Botulinum toxin type A is not meant to be injected into the periosteum. Don’t go there; it hurts."
• Do the procedures yourself. This allows you to see the patient every 3-4 months to recommend ancillary treatments and surgery.
Dr. Obagi said she charges patients by the amount of toxin or filler used, not by the specific anatomic area she treats. That works well, she said, "because some patients may require 12 U in an area of the face while another patient may require 50 U in that same area."
She said she runs two parallel schedules to optimize efficiency. For example, her afternoon consultation times are at 1 p.m., 1:30 p.m., 2 p.m., 2:30 p.m., 3 p.m., 3:30 p.m., and 4 p.m., while her treatment times for botulinum toxin type A and filler patients are at 1:45 p.m., 2:15 p.m., 2:45 p.m., 3:15 p.m., and 3:45 p.m. "So after I finish a consult in one room, I go into another room and do a quick treatment," she said. "I come back out and go to the next consult."
Dr. Obagi said she had no relevant financial disclosures.
EXPERT ANALYSIS FROM THE ANNUAL MEETING OF THE AMERICAN ACADEMY OF COSMETIC SURGERY
Stem Cell Fat Grafting Dynamically Restores Volume
LAS VEGAS – When using fat and stem cell transfer for facial volume enhancement, it's disingenuous to tell patients a stem cell face-lift is being performed, said Dr. Mark Berman.
The accurate description is to tell patients a stem cell fat graft is being performed. "Tell them 'we're using a fat graft, and the reason it works is because your fat is loaded with stem cells, which can turn on, proliferate, and grow new fat cells,' " Dr. Berman said at the annual meeting of the American Academy of Cosmetic Surgery. "This is a dynamic process."

In 2008, Dr. Hee Young Lee introduced Dr. Berman to a system he created, known as the Lipokit (Medi-Khan, Korea and currently distributed as the Adivive system by Palomar), a closed device approved for condensed autologous fat transfer. Dr. Berman said he began using the system at his Beverly Hills, Calif.–based cosmetic surgery practice for facial volume enhancement.
A key component of the device, he said, is the fat-processing unit, a single-use, disposable syringe with a bidirectional moving piston, a microfilter, a fluid gate, and a weighted metallic ring. "What makes this syringe unique is that it allows you to compress and filter the fat at the same time, so you actually increase the concentration of cells," said Dr. Berman. "You can also put in tumescent anesthesia in this system real easily."
Early in his clinical experience with the Adivive system, he said he would spin harvested fat in a centrifuge at 4,000 rpm for 8 minutes. Now he spins the harvested fat at 2,800 rpm for 3 minutes. "The difference is, at the lower rate, the stem cells tend to have increased viability, while at the higher rate you get increased concentration of stem cells," Dr. Berman explained.
The results of stem cell fat grafting for facial volume enhancement are generally superior to those achieved with dermal filler injections because the process restores facial volume naturally. "Most of our face-lift patients don’t want to look different; they want to look like they used to," he said. "Aging is not about sagging skin caused by gravity. Gravity does not cause aging; it just affects how you look in different positions."
Aging, he continued, is caused by "loss of facial fat, loss of skin elasticity, and loss of bone volume very late in life or related to tooth loss. Your face is basically skin, fat, muscle, and bone. You have about 60% of fat between the first layer of skin and muscle, and the rest is under the muscle."
Stem cell fat grafting can restore a three-dimensional appearance to the patient's skin, said Dr. Berman, who coined the term "space lift" to describe the concept of lifting the skin away from the facial bones by fat-grafting techniques.
"I have traveled around the world talking with people who are experts on fat grafting, and we all agree on one thing: The variable is not our technique," he said. "The big variable is the quality of the stem cells mixed in with the patient's fat. I tell the patient, 'If you're not willing to repeat the operation, don't do it at all,' because at some point noticeable losses of the transferred fat may occur. Some people find that frustrating."
Dr. Berman disclosed teaching the technique in courses sponsored by Palomar.
LAS VEGAS – When using fat and stem cell transfer for facial volume enhancement, it's disingenuous to tell patients a stem cell face-lift is being performed, said Dr. Mark Berman.
The accurate description is to tell patients a stem cell fat graft is being performed. "Tell them 'we're using a fat graft, and the reason it works is because your fat is loaded with stem cells, which can turn on, proliferate, and grow new fat cells,' " Dr. Berman said at the annual meeting of the American Academy of Cosmetic Surgery. "This is a dynamic process."
In 2008, Dr. Hee Young Lee introduced Dr. Berman to a system he created, known as the Lipokit (Medi-Khan, Korea and currently distributed as the Adivive system by Palomar), a closed device approved for condensed autologous fat transfer. Dr. Berman said he began using the system at his Beverly Hills, Calif.–based cosmetic surgery practice for facial volume enhancement.
A key component of the device, he said, is the fat-processing unit, a single-use, disposable syringe with a bidirectional moving piston, a microfilter, a fluid gate, and a weighted metallic ring. "What makes this syringe unique is that it allows you to compress and filter the fat at the same time, so you actually increase the concentration of cells," said Dr. Berman. "You can also put in tumescent anesthesia in this system real easily."
Early in his clinical experience with the Adivive system, he said he would spin harvested fat in a centrifuge at 4,000 rpm for 8 minutes. Now he spins the harvested fat at 2,800 rpm for 3 minutes. "The difference is, at the lower rate, the stem cells tend to have increased viability, while at the higher rate you get increased concentration of stem cells," Dr. Berman explained.
The results of stem cell fat grafting for facial volume enhancement are generally superior to those achieved with dermal filler injections because the process restores facial volume naturally. "Most of our face-lift patients don’t want to look different; they want to look like they used to," he said. "Aging is not about sagging skin caused by gravity. Gravity does not cause aging; it just affects how you look in different positions."
Aging, he continued, is caused by "loss of facial fat, loss of skin elasticity, and loss of bone volume very late in life or related to tooth loss. Your face is basically skin, fat, muscle, and bone. You have about 60% of fat between the first layer of skin and muscle, and the rest is under the muscle."
Stem cell fat grafting can restore a three-dimensional appearance to the patient's skin, said Dr. Berman, who coined the term "space lift" to describe the concept of lifting the skin away from the facial bones by fat-grafting techniques.
"I have traveled around the world talking with people who are experts on fat grafting, and we all agree on one thing: The variable is not our technique," he said. "The big variable is the quality of the stem cells mixed in with the patient's fat. I tell the patient, 'If you're not willing to repeat the operation, don't do it at all,' because at some point noticeable losses of the transferred fat may occur. Some people find that frustrating."
Dr. Berman disclosed teaching the technique in courses sponsored by Palomar.
LAS VEGAS – When using fat and stem cell transfer for facial volume enhancement, it's disingenuous to tell patients a stem cell face-lift is being performed, said Dr. Mark Berman.
The accurate description is to tell patients a stem cell fat graft is being performed. "Tell them 'we're using a fat graft, and the reason it works is because your fat is loaded with stem cells, which can turn on, proliferate, and grow new fat cells,' " Dr. Berman said at the annual meeting of the American Academy of Cosmetic Surgery. "This is a dynamic process."
In 2008, Dr. Hee Young Lee introduced Dr. Berman to a system he created, known as the Lipokit (Medi-Khan, Korea and currently distributed as the Adivive system by Palomar), a closed device approved for condensed autologous fat transfer. Dr. Berman said he began using the system at his Beverly Hills, Calif.–based cosmetic surgery practice for facial volume enhancement.
A key component of the device, he said, is the fat-processing unit, a single-use, disposable syringe with a bidirectional moving piston, a microfilter, a fluid gate, and a weighted metallic ring. "What makes this syringe unique is that it allows you to compress and filter the fat at the same time, so you actually increase the concentration of cells," said Dr. Berman. "You can also put in tumescent anesthesia in this system real easily."
Early in his clinical experience with the Adivive system, he said he would spin harvested fat in a centrifuge at 4,000 rpm for 8 minutes. Now he spins the harvested fat at 2,800 rpm for 3 minutes. "The difference is, at the lower rate, the stem cells tend to have increased viability, while at the higher rate you get increased concentration of stem cells," Dr. Berman explained.
The results of stem cell fat grafting for facial volume enhancement are generally superior to those achieved with dermal filler injections because the process restores facial volume naturally. "Most of our face-lift patients don’t want to look different; they want to look like they used to," he said. "Aging is not about sagging skin caused by gravity. Gravity does not cause aging; it just affects how you look in different positions."
Aging, he continued, is caused by "loss of facial fat, loss of skin elasticity, and loss of bone volume very late in life or related to tooth loss. Your face is basically skin, fat, muscle, and bone. You have about 60% of fat between the first layer of skin and muscle, and the rest is under the muscle."
Stem cell fat grafting can restore a three-dimensional appearance to the patient's skin, said Dr. Berman, who coined the term "space lift" to describe the concept of lifting the skin away from the facial bones by fat-grafting techniques.
"I have traveled around the world talking with people who are experts on fat grafting, and we all agree on one thing: The variable is not our technique," he said. "The big variable is the quality of the stem cells mixed in with the patient's fat. I tell the patient, 'If you're not willing to repeat the operation, don't do it at all,' because at some point noticeable losses of the transferred fat may occur. Some people find that frustrating."
Dr. Berman disclosed teaching the technique in courses sponsored by Palomar.
EXPERT ANALYSIS FROM THE ANNUAL MEETING OF THE AMERICAN ACADEMY OF COSMETIC SURGERY
Internal Marketing Key to Gaining New Patients
LAS VEGAS – It is not uncommon for cosmetic dermatologists to follow their competitors when it comes to external marketing efforts, according to Tracy L. Drumm, an aesthetic medical marketing expert.
"Maybe it’s print advertising, pay-per-click online advertising, or maybe it’s social media," Ms. Drumm said at the annual meeting of the American Academy of Cosmetic Surgery. "The problem is external marketing – marketing to patients who don’t already know you – is the most expensive form of marketing."

According to Ms. Drumm, vice president of Chicago-based IF Marketing, a more effective way to generate new patients is through internal marketing, which she described as "talking to people who are already coming through the door, who already know you, who come to you every 3-4 months for their Botox treatments."
The best way to do this is to provide tools to patients that "empower them to talk to their friends about you." This may be in the form of business cards that contain practice information, such as how many neurotoxin treatments or specific cosmetic surgeries were performed last year, or a list of the procedures offered with corresponding columns for before and after photos. "Highlight what makes you special and unique," advised Ms. Drumm.
Another strategy is to have a dedicated space in the waiting room for a "referral station" stocked with business cards customized for each of the procedures offered, with a corresponding sign that reads: "The greatest compliment you can give us is a referral." One practice that adopted the referral station now replenishes the cards weekly. "People take the cards," she said. "They’re portable, small, and discreet to pass on."
Creating a "patient passport" card for existing patients is another way to advertise. This is a laminated business card–size tool that contains a before and after photo of the patient, along with office contact information. This strategy "reminds patients of how they looked before their procedure and provides a visual reminder of their improvement," Ms. Drumm said. "It’s also something they can share with their friends."
Profiling patients who consent to advertise their "transformation" on postcards, brochures, handouts, posters, or in a newsletter is another effective way to promote a practice. "The nice thing is that you can send these profiles to your existing patients to help keep them coming back," she said. "But you can also purchase data and have this sent out to people who match the demographics of your current patients."
In today’s business climate, relationship building is more important than ever, Ms. Drumm said, so she recommends mailing cards to mark patient birthdays, Mother’s Day, and other special holidays. Consider inserting a $50 gift certificate for patients in each card, as well as a $50 gift certificate for a friend. In 2 years of tracking results of this tactic at one practice, 17 new patients referred from friends spent about $35,000. "A qualified referral from a friend is a very powerful source," she said. "You want to keep encouraging these referrals."
For direct mail promotions, Ms. Drumm recommended the acronym TOIB for teaser, offer, immediacy, and brand.
The teaser should consist of a catchy phrase to get people’s attention, she said, such as "four ways to look younger overnight" or "four steps to a summer bikini." The offer, paired with the teaser, should be of perceived value, such as a free consultation or free microdermabrasion.
"Then, offer immediacy to make sure you are at the top of someone’s to-do list," Ms. Drumm said. "Maybe it’s something like, ‘the first 15 people to RSVP get a complimentary swag bag.’ Offer something to make that person want to take action."
The fourth component is brand. "Everything you do should be stamped with the logo and name of your practice," she said.
Ms. Drumm said that she had no relevant financial conflicts to disclose.
LAS VEGAS – It is not uncommon for cosmetic dermatologists to follow their competitors when it comes to external marketing efforts, according to Tracy L. Drumm, an aesthetic medical marketing expert.
"Maybe it’s print advertising, pay-per-click online advertising, or maybe it’s social media," Ms. Drumm said at the annual meeting of the American Academy of Cosmetic Surgery. "The problem is external marketing – marketing to patients who don’t already know you – is the most expensive form of marketing."
According to Ms. Drumm, vice president of Chicago-based IF Marketing, a more effective way to generate new patients is through internal marketing, which she described as "talking to people who are already coming through the door, who already know you, who come to you every 3-4 months for their Botox treatments."
The best way to do this is to provide tools to patients that "empower them to talk to their friends about you." This may be in the form of business cards that contain practice information, such as how many neurotoxin treatments or specific cosmetic surgeries were performed last year, or a list of the procedures offered with corresponding columns for before and after photos. "Highlight what makes you special and unique," advised Ms. Drumm.
Another strategy is to have a dedicated space in the waiting room for a "referral station" stocked with business cards customized for each of the procedures offered, with a corresponding sign that reads: "The greatest compliment you can give us is a referral." One practice that adopted the referral station now replenishes the cards weekly. "People take the cards," she said. "They’re portable, small, and discreet to pass on."
Creating a "patient passport" card for existing patients is another way to advertise. This is a laminated business card–size tool that contains a before and after photo of the patient, along with office contact information. This strategy "reminds patients of how they looked before their procedure and provides a visual reminder of their improvement," Ms. Drumm said. "It’s also something they can share with their friends."
Profiling patients who consent to advertise their "transformation" on postcards, brochures, handouts, posters, or in a newsletter is another effective way to promote a practice. "The nice thing is that you can send these profiles to your existing patients to help keep them coming back," she said. "But you can also purchase data and have this sent out to people who match the demographics of your current patients."
In today’s business climate, relationship building is more important than ever, Ms. Drumm said, so she recommends mailing cards to mark patient birthdays, Mother’s Day, and other special holidays. Consider inserting a $50 gift certificate for patients in each card, as well as a $50 gift certificate for a friend. In 2 years of tracking results of this tactic at one practice, 17 new patients referred from friends spent about $35,000. "A qualified referral from a friend is a very powerful source," she said. "You want to keep encouraging these referrals."
For direct mail promotions, Ms. Drumm recommended the acronym TOIB for teaser, offer, immediacy, and brand.
The teaser should consist of a catchy phrase to get people’s attention, she said, such as "four ways to look younger overnight" or "four steps to a summer bikini." The offer, paired with the teaser, should be of perceived value, such as a free consultation or free microdermabrasion.
"Then, offer immediacy to make sure you are at the top of someone’s to-do list," Ms. Drumm said. "Maybe it’s something like, ‘the first 15 people to RSVP get a complimentary swag bag.’ Offer something to make that person want to take action."
The fourth component is brand. "Everything you do should be stamped with the logo and name of your practice," she said.
Ms. Drumm said that she had no relevant financial conflicts to disclose.
LAS VEGAS – It is not uncommon for cosmetic dermatologists to follow their competitors when it comes to external marketing efforts, according to Tracy L. Drumm, an aesthetic medical marketing expert.
"Maybe it’s print advertising, pay-per-click online advertising, or maybe it’s social media," Ms. Drumm said at the annual meeting of the American Academy of Cosmetic Surgery. "The problem is external marketing – marketing to patients who don’t already know you – is the most expensive form of marketing."
According to Ms. Drumm, vice president of Chicago-based IF Marketing, a more effective way to generate new patients is through internal marketing, which she described as "talking to people who are already coming through the door, who already know you, who come to you every 3-4 months for their Botox treatments."
The best way to do this is to provide tools to patients that "empower them to talk to their friends about you." This may be in the form of business cards that contain practice information, such as how many neurotoxin treatments or specific cosmetic surgeries were performed last year, or a list of the procedures offered with corresponding columns for before and after photos. "Highlight what makes you special and unique," advised Ms. Drumm.
Another strategy is to have a dedicated space in the waiting room for a "referral station" stocked with business cards customized for each of the procedures offered, with a corresponding sign that reads: "The greatest compliment you can give us is a referral." One practice that adopted the referral station now replenishes the cards weekly. "People take the cards," she said. "They’re portable, small, and discreet to pass on."
Creating a "patient passport" card for existing patients is another way to advertise. This is a laminated business card–size tool that contains a before and after photo of the patient, along with office contact information. This strategy "reminds patients of how they looked before their procedure and provides a visual reminder of their improvement," Ms. Drumm said. "It’s also something they can share with their friends."
Profiling patients who consent to advertise their "transformation" on postcards, brochures, handouts, posters, or in a newsletter is another effective way to promote a practice. "The nice thing is that you can send these profiles to your existing patients to help keep them coming back," she said. "But you can also purchase data and have this sent out to people who match the demographics of your current patients."
In today’s business climate, relationship building is more important than ever, Ms. Drumm said, so she recommends mailing cards to mark patient birthdays, Mother’s Day, and other special holidays. Consider inserting a $50 gift certificate for patients in each card, as well as a $50 gift certificate for a friend. In 2 years of tracking results of this tactic at one practice, 17 new patients referred from friends spent about $35,000. "A qualified referral from a friend is a very powerful source," she said. "You want to keep encouraging these referrals."
For direct mail promotions, Ms. Drumm recommended the acronym TOIB for teaser, offer, immediacy, and brand.
The teaser should consist of a catchy phrase to get people’s attention, she said, such as "four ways to look younger overnight" or "four steps to a summer bikini." The offer, paired with the teaser, should be of perceived value, such as a free consultation or free microdermabrasion.
"Then, offer immediacy to make sure you are at the top of someone’s to-do list," Ms. Drumm said. "Maybe it’s something like, ‘the first 15 people to RSVP get a complimentary swag bag.’ Offer something to make that person want to take action."
The fourth component is brand. "Everything you do should be stamped with the logo and name of your practice," she said.
Ms. Drumm said that she had no relevant financial conflicts to disclose.
EXPERT ANALYSIS FROM THE ANNUAL MEETING OF THE AMERICAN ACADEMY OF COSMETIC SURGERY
Expert Offers Insider Marketing Tips for Cosmetic Practices
LAS VEGAS – Dermatologists who provide cosmetic services are well positioned to build and maintain a steady-stream of cash-paying patients, according to marketing strategist Catherine Maley.
"You are in an enviable position," she told attendees at the annual meeting of the American Academy of Cosmetic Surgery. "Your audience is an aging baby boomer group, people with all sorts of needs and wants. ... As the years go on the needs and wants just keep piling up. You have a good target market."
Ms. Maley of Sausalito, Calif., shared "must-haves" for a successful cosmetic practice:
• Focus on targeting mature, "preferred" patients. "Go after the patient who has the income and the age," she advised. The mature patient "has more needs, more wants, and more financial wherewithal than younger people," said Ms. Maley. "Go after the ones in your own zip code; you can’t be everything to everybody. The riches are in the niches."
• Have an A team. Receptionists, patient coordinators, and other staff members "have to offer awesome customer service," Ms. Maley said. "The patient has to be happy, or they’re not going to come back, and they’re certainly not going to refer their friends." She went on to note that a receptionist "is easily worth a quarter of a million dollars to you if you have her scripted correctly and she’s the right person on the phone. She has to have a warm voice that makes it inviting for callers. You also have to have the right patient care coordinator, a buffer between the physician and the patient. That patient has to have a bond with somebody in your office."
Another key for optimizing cosmetic surgery practice is to have the checkout staff book another appointment for patients before they leave the office. "Always book a patient when they’re standing smack in front of you," Ms. Maley said. If a patient says, " ‘I don’t know what my schedule is; I’ll have to call you later,’ you can reply, ‘It’s okay. Let’s go ahead and schedule you for the same day and time 4 months from now, and if we have to change the appointment, we’ll change it later.’ You have to get them on the books. It’s too easy for people to wander off nowadays."
She advised practices to carry certain retail products such as antiaging creams to offer patients upon checkout, as well as gift certificates, since they are perfect add-ons for the day’s purchase. The goal is to ensure that "every patient leaves your office smiling," she said.
• Build ways to retain patients so they return. "What’s the only difference between you and your competitors? The relationship you have with your patients," Ms. Maley said. "Hang on to that. It’s golden. You want to retain them so they’ll return and refer."
You can nurture patient relationships with personal e-mails, greeting cards, invitations to special events or lectures, patient letters, and social media. Optimal times to reach out, she said, include birthdays, Mother’s Day, New Year’s, and during changing seasons.
One "prop" to help spread the word about a practice is a photo note card that contains a before and after photo of the patient, with a message that says, "Thank you for your trust!" she said. "Don’t forget to include your name, website, and phone number right next to those photos so when they open up the card to show their friend, there you are."
Another effective way to build retention is to offer current patients a $50 gift card good toward their next treatment or procedure for referring new patients who book an appointment. "Your No. 1 asset is not just your patient – it’s your patient’s friends, coworkers, family members, hair stylists, and business partners," she said.
• Form strong alliances with potential referrals. Strong referral sources include hair salon owners, noncompeting aestheticians, retail shops, women’s clubs, health clubs, personal trainers, and other noncompeting clinicians. Ms. Maley spoke of one hair stylist who referred 250 of his clients per year to a dermatologist and plastic surgeon right down the street. "That guy alone was a goldmine," she said.
She recommended forming a "VIP club" for customers of alliance referrals. This might include no waiting for appointments, last-minute appointments, a free monthly peel, valet parking (if applicable), 15% off retail products, and a free surprise gift each quarter. "There’s some great psychology in this, because the hair salon owner or other referral source looks like a queen, because she got a deal for her customers through you, and then you got new patients out of it."
Ms. Maley said that she had no relevant financial disclosures.
LAS VEGAS – Dermatologists who provide cosmetic services are well positioned to build and maintain a steady-stream of cash-paying patients, according to marketing strategist Catherine Maley.
"You are in an enviable position," she told attendees at the annual meeting of the American Academy of Cosmetic Surgery. "Your audience is an aging baby boomer group, people with all sorts of needs and wants. ... As the years go on the needs and wants just keep piling up. You have a good target market."
Ms. Maley of Sausalito, Calif., shared "must-haves" for a successful cosmetic practice:
• Focus on targeting mature, "preferred" patients. "Go after the patient who has the income and the age," she advised. The mature patient "has more needs, more wants, and more financial wherewithal than younger people," said Ms. Maley. "Go after the ones in your own zip code; you can’t be everything to everybody. The riches are in the niches."
• Have an A team. Receptionists, patient coordinators, and other staff members "have to offer awesome customer service," Ms. Maley said. "The patient has to be happy, or they’re not going to come back, and they’re certainly not going to refer their friends." She went on to note that a receptionist "is easily worth a quarter of a million dollars to you if you have her scripted correctly and she’s the right person on the phone. She has to have a warm voice that makes it inviting for callers. You also have to have the right patient care coordinator, a buffer between the physician and the patient. That patient has to have a bond with somebody in your office."
Another key for optimizing cosmetic surgery practice is to have the checkout staff book another appointment for patients before they leave the office. "Always book a patient when they’re standing smack in front of you," Ms. Maley said. If a patient says, " ‘I don’t know what my schedule is; I’ll have to call you later,’ you can reply, ‘It’s okay. Let’s go ahead and schedule you for the same day and time 4 months from now, and if we have to change the appointment, we’ll change it later.’ You have to get them on the books. It’s too easy for people to wander off nowadays."
She advised practices to carry certain retail products such as antiaging creams to offer patients upon checkout, as well as gift certificates, since they are perfect add-ons for the day’s purchase. The goal is to ensure that "every patient leaves your office smiling," she said.
• Build ways to retain patients so they return. "What’s the only difference between you and your competitors? The relationship you have with your patients," Ms. Maley said. "Hang on to that. It’s golden. You want to retain them so they’ll return and refer."
You can nurture patient relationships with personal e-mails, greeting cards, invitations to special events or lectures, patient letters, and social media. Optimal times to reach out, she said, include birthdays, Mother’s Day, New Year’s, and during changing seasons.
One "prop" to help spread the word about a practice is a photo note card that contains a before and after photo of the patient, with a message that says, "Thank you for your trust!" she said. "Don’t forget to include your name, website, and phone number right next to those photos so when they open up the card to show their friend, there you are."
Another effective way to build retention is to offer current patients a $50 gift card good toward their next treatment or procedure for referring new patients who book an appointment. "Your No. 1 asset is not just your patient – it’s your patient’s friends, coworkers, family members, hair stylists, and business partners," she said.
• Form strong alliances with potential referrals. Strong referral sources include hair salon owners, noncompeting aestheticians, retail shops, women’s clubs, health clubs, personal trainers, and other noncompeting clinicians. Ms. Maley spoke of one hair stylist who referred 250 of his clients per year to a dermatologist and plastic surgeon right down the street. "That guy alone was a goldmine," she said.
She recommended forming a "VIP club" for customers of alliance referrals. This might include no waiting for appointments, last-minute appointments, a free monthly peel, valet parking (if applicable), 15% off retail products, and a free surprise gift each quarter. "There’s some great psychology in this, because the hair salon owner or other referral source looks like a queen, because she got a deal for her customers through you, and then you got new patients out of it."
Ms. Maley said that she had no relevant financial disclosures.
LAS VEGAS – Dermatologists who provide cosmetic services are well positioned to build and maintain a steady-stream of cash-paying patients, according to marketing strategist Catherine Maley.
"You are in an enviable position," she told attendees at the annual meeting of the American Academy of Cosmetic Surgery. "Your audience is an aging baby boomer group, people with all sorts of needs and wants. ... As the years go on the needs and wants just keep piling up. You have a good target market."
Ms. Maley of Sausalito, Calif., shared "must-haves" for a successful cosmetic practice:
• Focus on targeting mature, "preferred" patients. "Go after the patient who has the income and the age," she advised. The mature patient "has more needs, more wants, and more financial wherewithal than younger people," said Ms. Maley. "Go after the ones in your own zip code; you can’t be everything to everybody. The riches are in the niches."
• Have an A team. Receptionists, patient coordinators, and other staff members "have to offer awesome customer service," Ms. Maley said. "The patient has to be happy, or they’re not going to come back, and they’re certainly not going to refer their friends." She went on to note that a receptionist "is easily worth a quarter of a million dollars to you if you have her scripted correctly and she’s the right person on the phone. She has to have a warm voice that makes it inviting for callers. You also have to have the right patient care coordinator, a buffer between the physician and the patient. That patient has to have a bond with somebody in your office."
Another key for optimizing cosmetic surgery practice is to have the checkout staff book another appointment for patients before they leave the office. "Always book a patient when they’re standing smack in front of you," Ms. Maley said. If a patient says, " ‘I don’t know what my schedule is; I’ll have to call you later,’ you can reply, ‘It’s okay. Let’s go ahead and schedule you for the same day and time 4 months from now, and if we have to change the appointment, we’ll change it later.’ You have to get them on the books. It’s too easy for people to wander off nowadays."
She advised practices to carry certain retail products such as antiaging creams to offer patients upon checkout, as well as gift certificates, since they are perfect add-ons for the day’s purchase. The goal is to ensure that "every patient leaves your office smiling," she said.
• Build ways to retain patients so they return. "What’s the only difference between you and your competitors? The relationship you have with your patients," Ms. Maley said. "Hang on to that. It’s golden. You want to retain them so they’ll return and refer."
You can nurture patient relationships with personal e-mails, greeting cards, invitations to special events or lectures, patient letters, and social media. Optimal times to reach out, she said, include birthdays, Mother’s Day, New Year’s, and during changing seasons.
One "prop" to help spread the word about a practice is a photo note card that contains a before and after photo of the patient, with a message that says, "Thank you for your trust!" she said. "Don’t forget to include your name, website, and phone number right next to those photos so when they open up the card to show their friend, there you are."
Another effective way to build retention is to offer current patients a $50 gift card good toward their next treatment or procedure for referring new patients who book an appointment. "Your No. 1 asset is not just your patient – it’s your patient’s friends, coworkers, family members, hair stylists, and business partners," she said.
• Form strong alliances with potential referrals. Strong referral sources include hair salon owners, noncompeting aestheticians, retail shops, women’s clubs, health clubs, personal trainers, and other noncompeting clinicians. Ms. Maley spoke of one hair stylist who referred 250 of his clients per year to a dermatologist and plastic surgeon right down the street. "That guy alone was a goldmine," she said.
She recommended forming a "VIP club" for customers of alliance referrals. This might include no waiting for appointments, last-minute appointments, a free monthly peel, valet parking (if applicable), 15% off retail products, and a free surprise gift each quarter. "There’s some great psychology in this, because the hair salon owner or other referral source looks like a queen, because she got a deal for her customers through you, and then you got new patients out of it."
Ms. Maley said that she had no relevant financial disclosures.
EXPERT ANALYSIS FROM THE ANNUAL MEETING OF THE AMERICAN ACADEMY OF COSMETIC SURGERY