User login
Evaluation of Health Professions Trainee Experiences Transitioning to New VHA Electronic Health Record
Evaluation of Health Professions Trainee Experiences Transitioning to New VHA Electronic Health Record
The Veterans Health Administration (VHA) is transitioning from its native electronic health record (EHR) Vista/Computerized Patient Record System to the commercial Cerner/Oracle Health EHR. Though this process was temporarily discontinued in April 2023 due to patient safety, usability, and reliability concerns, it resumed in April 2026. It was originally projected to cost $50 billion to implement. 1-3 As of March 9, 2024, 6 sites had transitioned to the new EHR.2 The transition is the largest of its kind in the US, offering an unparalleled opportunity to examine the effects of EHR transitions on an often overlooked part of the workforce: health professions trainees (HPTs).
HPTs serve a central role in VHA. About one-third of patients receive care directly from HPTs who make up about one-third of the VHA workforce. VHA trains > 60 clinical disciplines, comprising > 122,000 trainees annually.4,5 A paucity of literature exists exploring the experiences of HPTs during EHR transitions, and many studies are often limited to single-site or small populations. HPTs face distinct challenges and needs during EHR transitions and are particularly vulnerable to their negative impacts on retention, clinical training, and efficiency and confidence in EHR use.6-10 HPTs at VHA sites that have already transitioned to the Cerner/Oracle Health EHR identified many challenges, including significant delays in gaining EHR access, pervasive perceptions of poor training, concerns that EHR functionality issues limited patient care, and decreased ability to track clinical skill acquisition.6 These challenges may impact some HPTs more than others (eg, students on short rotations are affected more acutely by delayed EHR access and usage).
This quality improvement project evaluated HPT EHR transition experiences at the Captain James A. Lovell Federal Health Care Center (FHCC). This article contributes to the limited literature on HPT transition experiences, identifies opportunities to support HPTs, and informs broader efforts in teaching HPTs new technologies.
Methods
FHCC is jointly operated by the US Department of Defense and US Department of Veterans Affairs (VA). It treats 80,000 inpatient and outpatients annually. FHCC was the sixth VA facility to transition to the new EHR, which went live on March 9, 2024.2,11 About 700 HPTs rotate through FHCC annually. HPTs were eligible for inclusion if they were present during the March 9 transition according to a VA Office of Academic Affiliations database. A total of 216 HPTs were identified for inclusion.
Preparations for the transition included scaling down operations (ie, blocking clinician schedules, not scheduling future appointments that may conflict with the transition, making decisions on new facility- and service-line workflows, required EHR training, and speaking with support staff, including VHA National EHR Modernization Supplemental Staffing Unit [NESSU]). This evaluation was designated nonresearch/quality improvement by the VA Bedford Healthcare System Institutional Review Board.
Surveys
Forty-seven interviews were conducted with HPTs, site leaders, and supervisors from January 2024 to June 2024 (Table 1). Participants were identified by service leads and recruited via email; snowball sampling identified additional participants.
The evaluation team developed semistructured interview guides using grounded probes based on a pilot evaluation and existing research on EHR transitions.12 Questions focused on participant experiences preparing for the EHR transition, learning and using the site’s EHR, and the impact the transition had on clinical training experiences. Interviews were conducted at different times to capture the range of user experiences: 1 month prelaunch, 2 to 6 weeks postlaunch, and 2 months postlaunch. Interviewees were informed of participant rights and provided verbal consent.
HPTs present at FHCC at each survey’s release were emailed invitations and 2 reminders. The anonymous surveys took about 10 minutes to complete. Survey items queried HPTs about their experiences preparing to use the new EHR, perceptions of the current EHR (adapted from the System Usability Scale), satisfaction with VHA training, impact on clinical training, ability to work with preceptors and patients, and experiences with the VHA clinical learning environment (adapted from the VHA Learners Preceptor Survey).13-15 Survey questions used a 5-point Likert response scale.
Analysis
Interviewers completed postinterview summaries for team debriefing and consensus building. Interviews were coded using a priori (from piloting evaluations and relevant literature) and emergent (refined and developed from data) codes. Deductive and inductive content analyses were conducted. 16 Deductive analysis used a priori categories (eg, care coordination, EHR training). Inductive content analysis consisted of open and unstructured coding, capturing data outside a priori categories. Emergent codes captured unidentified categories. Qualitative researchers met weekly to discuss data and reach consensus on interpretation.
Descriptive analysis was conducted using top-2 box scoring (proportion responding within the 2 most favorable responses [agree/ strongly agree]). Survey data were analyzed in SAS.17 The analysis used a merging approach on simultaneously collected qualitative and quantitative data to reach findings consensus.18
Researcher and research team decisions may shape the data collected due to prior assumptions and experience.19 This analysis attempted to integrate reflexivity practices to enhance awareness of the researchers’ assumptions and positionality, including by integrating intent collaborative conversing and memorandum writing into the processes.20,21
Results
This analysis created a survey and fielded responses from HPTs present at FHCC across 3 time points (6 months prelaunch, 1 month prelaunch, and 2 months postlaunch), resulting in a total of 103 responses and an average response rate of 19.0% (Table 2). Six key findings were identified in analysis of responses: (1) critiques of transition management; (2) concerns with training; (3) hope about the EHR; (4) at-the-elbow support was essential; (5) HPTs adjusted to, and later preferred, the new EHR; and (6) transition impacted clinical training, but not overall career plans for HPTs. Findings are presented in this section, with illustrative quantitative data and qualitative data quotes available in the eAppendix.
Critiques of the Transition’s Management
While participants were aware of the transition to the new EHR, most felt they did not have enough information or time to prepare for it, indicating it was “too little, too late.” HPTs felt necessary workflow processes for Cerner/Oracle Health were not determined with enough time to learn them prior to transition. Supervisors shared that important workflow and onboarding decisions remained undecided mere weeks before the transition. Some service lines did not decrease patient loads until right before the transition, making it difficult to manage their schedules and resulting in insufficient time to learn the new EHR.
EHR Training Concerns
Overall, HPTs expressed low satisfaction with computer-based Training Management System (TMS) EHR training, believing it did not prepare them for the new EHR. The percentage of HPTs satisfied or very satisfied with the quality of TMS training was lower than that of instructor-based training pre- and posttransition, with 50% of 36 prelaunch respondents, and 43% of 29 postlaunch respondents expressing satisfaction with computer-based trainings (Figure 1). HPTs were dissatisfied with the training content. They felt it was too general and failed to teach basic tasks in the workflow for their service areas and roles, such as writing a note or order. Furthermore, poor content was exacerbated by poor and unengaging instruction, and HPTs were dissatisfied with the practice EHR used in training, which glitched frequently.
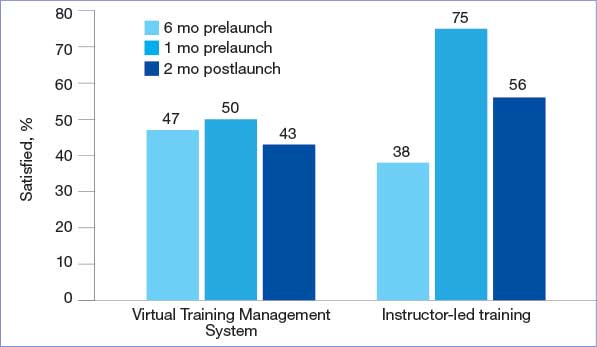
quality of electronic health record training.
EHR Transition Optimism
Even though the transition was stressful, most HPTs hoped it would be a temporary disruption and that they would quickly adjust to the new EHR. Many participants expected that once they switched to the new EHR, they would pick it up quickly. In addition, many anticipated Cerner/Oracle Health would be better and easier to use in the long run.
At-The-Elbow Support Essential
VHA peer support with NESSU was highly valued among HPTs. NESSU staff were highly knowledgeable and could provide both broad and service-line-specific support. NESSU provided prompt answers to EHR questions. This was particularly critical as other forms of in-person support were often inaccessible or absent during the transition.
HPTs found facility support helpful: 85% of 36 respondents reported being satisfied/ very satisfied with support from supervisors and preceptors, and 84% of 36 respondents were satisfied/very satisfied with technical support from facility informatics staff pretransition (n = 36) (Figure 2). NESSU and supervisor support with daily workflows were particularly helpful, as pretransition training only provided a general introduction to the EHR.
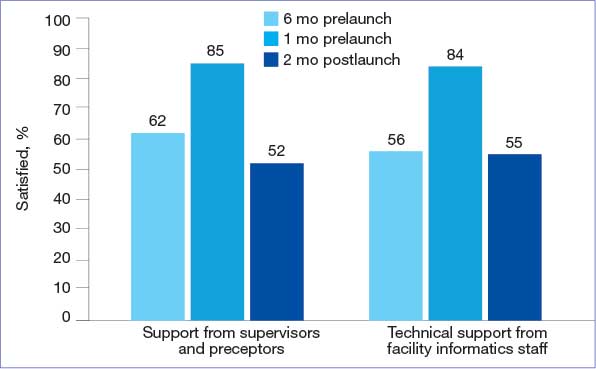
health record training.
HPTs Adjusted to and Later Preferred the New EHR
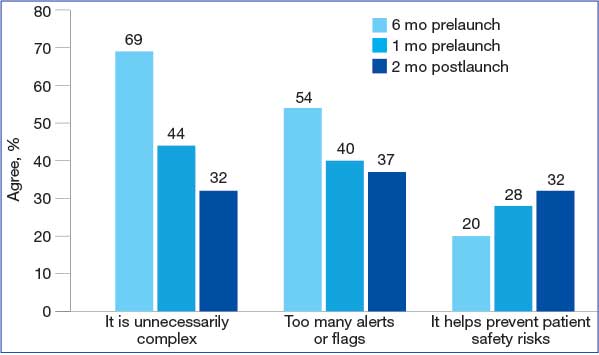
The EHR learning experience was intense but short, with many HPTs feeling able to use it only 2 to 4 weeks posttransition. Confidence grew as HPTs came to view Cerner/Oracle Health as a more integrated and intuitive system than the previous EHR. Most participants preferred the new EHR, even if they criticized some features (eg, no group documentation capabilities). Survey participants frequently rated Cerner/Oracle Health usability higher than the original. A total of 32% of 29 posttransition respondents agreed or strongly agreed that Cerner/Oracle Health helps prevent situations that can lead to patient safety risks—higher than pretransition rates. Additionally, fewer respondents found the new EHR unnecessarily complex or thought it contained too many alerts and flags compared to the original EHR (Figure 3).
health record usability.
Impact on Clinical Training, Not Career Plans
The extensive time and energy the transition demanded of HPTs caused stress and affected their clinical training. Many believed they would have learned more if their training had happened outside the transition.
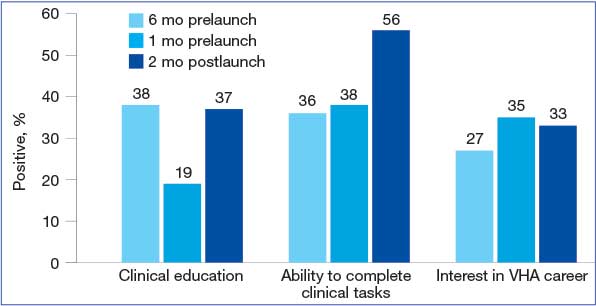
Concerns that the transition affected learning were most acutely felt pretransition. HPTs reporting that EHR implementation positively affected their clinical education fell from 38% of 36 respondents 6 months pretransition to 19% of 29 respondents 1 month pretransition, but returned to 37% posttransition (Figure 4). However, some HPTs believed there was a silver lining: it provided a learning experience they otherwise would not have had.
new Veterans Health Administration (VHA) electronic health record.
HPTs who believed the transition positively impacted their likelihood of pursuing future career opportunities within the VHA rose to 33% of 29 respondents posttransition. Overall, Cerner/Oracle Health was characterized as a tool: something used in training, but not something that precluded wanting VHA careers or having meaningful experiences, such as caring for patients.
Discussion
This evaluation addressed an underexplored aspect of EHR transitions: their impact on HPTs. It identified HPT challenges, including dissatisfaction with poor transition preparation and EHR training experiences. Promising findings include positive experiences with transition support, EHR uptake, and overall positive educational experiences despite the transition’s disruption.
When EHR users, including HPTs, are dissatisfied with transition preparations, consequent stress can lead to undesired effects, including increased burnout, inappropriate EHR use, and low work satisfaction.22-24 Negative EHR transition experiences shape HPTs’ subsequent EHR adoption, user satisfaction, as well as confidence and career intent.3,25,26 Health systems have strong incentives to implement effective transition change management.
HPTs at previous VHA EHR transition sites reported significantly more disruption to their clinical training compared with HPTs at FHCC. Academic programs were shut down at the first transition site, and HPTs expressed decreased interest in VHA careers at another, even a year posttransition.6,27 These findings are consistent with the limited literature on the adverse impacts that EHR transitions have on HPTs.7,28
HPT retention is critical. VA is mandated to prepare the next generation of HPTs for its needs, and those of the nation. The VA relies heavily on HPT retention to recruit clinicians: > 65% of VHA physicians nationwide participated in VHA training programs prior to recruitment into staff positions.5,29
VHA should invest in transition change management with demonstrated, positive impacts on HPTs, such as in-house support from clinicians. Previous research found that lack of support was a major source of stress and negative outcomes.6,27 Consequently, supporting HPTs through EHR transitions directly contributes to the VHA’s ability to attract high-quality staff from its HPTs. The challenges and promising practices described in this analysis underscore the necessity of understanding how all EHR users are affected by transitions. What happens to them has direct implications for the VA mission to provide safe, efficient care, and its mandate to provide quality clinical training to HPTs.
These findings hold hopeful implications for supporting HPT EHR use, both during and outside EHR transitions. HPTs expressing that an EHR is only 1 part of their clinical training experience suggests that change management can improve EHR transitions. HPT learning can enhance known factors that are important for HPTs in clinical training, including the health care organization’s mission, caring for patients, and personal development.
Further investigations may engage HPTs at future VHA sites making the transition to the new EHR. One focus would involve applying a learning health systems framework to examine the nature of change management efforts—and their effects on HPT transition experiences—iteratively across transition sites to evaluate the effect of the efforts. Another focus may be longitudinal engagement with HPTs at health care systems and sites transitioning to new EHRs. Research has found that disruptions to EHR usability, satisfaction, and care provision can persist for 2 years and beyond following an EHR transition.30 Evaluating the long-term effects of transitions on HPTs is of interest, given their distinct characteristics and differences from employees.
Limitations
Study data came from voluntary participants at 1 highly engaged site, raising the possibility of self-selection bias. HPT experiences at other VA and non-VA sites may differ. Employees and HPTs were engaged during a high-stress event; snowballing recruitment reach was limited by high workloads and limited time for engagement. Statistical data were descriptive and should not be interpreted as causal. Results may reflect, in part, temporal effects, and respondents include HPTs at different stages of training and with different levels of VA experience. Survey sample sizes may limit generalizability; however, merging data streams strengthened the reliability of findings.
Conclusions
The results of this analysis of FHCC HPTs were notably more positive than those of HPTs at previous VHA EHR transition sites. VHA is one of many health care systems that provide clinical training for HPTs and relies on this population to provide patient care. By highlighting challenges and positive experiences of HPTs during an EHR transition, this evaluation produces actionable insights that can inform the actions of health care systems seeking to support HPTs during disruptive EHR transitions.
- US Department of Veterans Affairs Office of the Inspector General. VA needs to strengthen controls to address electronic health record system major performance incidents. September 23, 2024. Accessed February 3, 2026. https://www.vaoig.gov/sites/default/files /reports/2024-09/vaoig-22-03591-231.pdf
- EHR deployment schedule. VA EHR Modernization. Updated February 2, 2026. Accessed February 3, 2026. https://digital.va.gov/ehr-modernization/ehr-deployment -schedule/
- Heckman J. VA in 2026 looks to get EHR rollout back on track, embark on health care reorganization. Federal News Network. December 24, 2025. Accessed February 3, 2026. https://federalnewsnetwork.com/veterans-affairs/2025/12 /va-in-2026-looks-to-get-ehr-rollout-back-on-track -embark-on-health-care-reorganization/
- US Department of Veterans Affairs Office of Academic Affiliations. Medical and dental education. Updated September 12, 2025. Accessed February 3, 2026. https://department.va.gov/academic-affiliations /medical-and-dental/
- Functions of Veterans Health Administration: health-care personnel education and training programs. 38 U.S.C. § 7302 (2026). Accessed February 3, 2026. https://uscode.house.gov/view.xhtml ?req=(title:38%20section:7302%20edition:prelim)
- Ahlness EA, Molloy-Paolillo BK, Brunner J, et al. Impacts of an electronic health record transition on Veterans Health Administration health professions trainee experience. J Gen Intern Med. 2023;38:1031-1039. doi:10.1007/s11606-023-08283-4
- Roberts DL, Mishark KJ, Alessandro STD, et al. Impact of electronic medical record transitions on the educational experiences of medical students. J Health Care Finance. 2014;41:1-5.
- Varpio L, Day K, Elliot‐Miller P, et al. The impact of adopting EHRs: how losing connectivity affects clinical reasoning. Med Educ. 2015;49:476-486. doi:10.1111/medu.12665
- Gali HE, Baxter SL, Lander L, et al. Impact of electronic health record implementation on ophthalmology trainee time expenditures. J Acad Ophthalmol (2017). 2019;11:e65-e72. doi:10.1055/s-0039-3401986
- Humphrey‐Murto S, Makus D, Moore S, et al. Training physicians and residents for the use of electronic health records— a comparative case study between two hospitals. Med Educ. 2023;57:337-348. doi:10.1111/medu.14944
- US Department of Defense. Captain James A. Lovell Federal Health Care Center: readying warriors & caring for heroes. Presentation August 10, 2022.
- Sayre G, Young J. Beyond openended questions: purposeful interview guide development to elicit rich, trustworthy data. Patient Aligned Care Teams (PACT) Demonstration Labs cyber seminar. March 21, 2018. Accessed February 3, 2026. https://www.hsrd.research.va.gov/for _researchers/cyber_seminars/catalog/transcripts/2439.doc
- Jordan PW, Thomas B, McClelland IL, Weerdmeester B, eds. Usability Evaluation In Industry. CRC Press; 1996.
- Keitz SA, Holland GJ, Melander EH, et al. The Veterans Affairs Learners’ Perceptions Survey: the foundation for educational quality improvement. Acad Med. 2003;78:910- 917. doi:10.1097/00001888-200309000-00016
- Byrne JM, Chang BK, Gilman SC, et al. The learners’ perceptions survey—primary care: assessing resident perceptions of internal medicine continuity clinics and patient- centered care. J Grad Med Educ. 2013;5:587-593. doi:10.4300/JGME-D-12-00233.1
- Elo S, Kyngäs H. The qualitative content analysis process. J Adv Nurs. 2008;62:107-115. doi:10.1111/j.1365-2648.2007.04569.x
- Siller AB, Tompkins L. The big four: analyzing complex sample survey data using SAS, SPSS, STATA, and SUDAAN. Poster presented at: 31st Annual SAS Users Group International Conference; March 27, 2006; San Francisco, CA. Accessed February 3, 2026. https://support.sas.com /resources/papers/proceedings/proceedings/sugi31/172 -31.pdf
- Tashakkori A, Johnson RB, Teddlie C. Foundations of Mixed Methods Research: Integrating Quantitative and Qualitative Approaches in the Social and Behavioral Sciences. 2nd ed. SAGE Publications, Inc.; 2020.
- Olmos-Vega FM, Stalmeijer RE, Varpio L, et al. A practical guide to reflexivity in qualitative research: AMEE Guide No. 149. Med Teach. 2023;45:241-251. doi:10.1080/0142159X.2022.2057287
- Mezirow J. Fostering Critical Reflection in Adulthood: A Guide to Transformative and Emancipatory Learning. JosseyBass; 1991.
- Probst B, Berenson L. The double arrow: how qualitative social work researchers use reflexivity. Qual Soc Work. 2014;13:813-827. doi:10.1177/1473325013506248
- Huang C, Koppel R, McGreevey JD 3rd, et al. Transitions from one electronic health record to another: challenges, pitfalls, and recommendations. Appl Clin Infor. 2020;11:742-754. doi:10.1055/s-0040-1718535
- Zheng K, Abraham J, Novak LL, et al. A survey of the literature on unintended consequences associated with health information technology: 2014–2015. Yearb Med Inform. 2016;25:13-29. doi:10.15265/IY-2016-036
- Campbell EM, Sittig DF, Ash JS, et al. Types of unintended consequences related to computerized provider order entry. J Am Med Inform Assoc. 2006;13:547-556. doi:10.1197/jamia.M2042
- Sittig DF, Lakhani P, Singh H. Applying requisite imagination to safeguard electronic health record transitions. JAMA. 2022;29:1014-1018. doi:10.1093/jamia/ocab291
- Ko HH, Lee TK, Leung Y, et al. Factors influencing career choices made by medical students, residents, and practising physicians. B C Med J. 2007;49:482-489.
- Brunner J, Ahlness EA, Anderson E, et al. VA’s EHR transition and health professions trainee programs: findings and impacts of a multistakeholder learning community. Learn Health Sys. 2024;9:e10460. doi:10.1002/lrh2.10460
- Rosdahl JA, Rudd M, Benjamin R, et al. Effect of the adoption of a comprehensive electronic health record on graduate medical education: perceptions of faculty and trainees. South Med J. 2018;111:476-483. doi:10.14423/SMJ.0000000000000847
- Hill C. U.S. Medical education at VA: it’s all about the veterans. VA News. August 18, 2021. Accessed February 3, 2026. https://news.va.gov/93370/medical-education-at-va -its-all-about-the-veterans
- Hanauer DA, Branford GL, Greenberg G, et al. Twoyear longitudinal assessment of physicians’ perceptions after replacement of a longstanding homegrown electronic health record: does a J-curve of satisfaction really exist? J Am Med Inform Assoc. 2017;24:e157-e165. doi:10.1093/jamia/ocw077
The Veterans Health Administration (VHA) is transitioning from its native electronic health record (EHR) Vista/Computerized Patient Record System to the commercial Cerner/Oracle Health EHR. Though this process was temporarily discontinued in April 2023 due to patient safety, usability, and reliability concerns, it resumed in April 2026. It was originally projected to cost $50 billion to implement. 1-3 As of March 9, 2024, 6 sites had transitioned to the new EHR.2 The transition is the largest of its kind in the US, offering an unparalleled opportunity to examine the effects of EHR transitions on an often overlooked part of the workforce: health professions trainees (HPTs).
HPTs serve a central role in VHA. About one-third of patients receive care directly from HPTs who make up about one-third of the VHA workforce. VHA trains > 60 clinical disciplines, comprising > 122,000 trainees annually.4,5 A paucity of literature exists exploring the experiences of HPTs during EHR transitions, and many studies are often limited to single-site or small populations. HPTs face distinct challenges and needs during EHR transitions and are particularly vulnerable to their negative impacts on retention, clinical training, and efficiency and confidence in EHR use.6-10 HPTs at VHA sites that have already transitioned to the Cerner/Oracle Health EHR identified many challenges, including significant delays in gaining EHR access, pervasive perceptions of poor training, concerns that EHR functionality issues limited patient care, and decreased ability to track clinical skill acquisition.6 These challenges may impact some HPTs more than others (eg, students on short rotations are affected more acutely by delayed EHR access and usage).
This quality improvement project evaluated HPT EHR transition experiences at the Captain James A. Lovell Federal Health Care Center (FHCC). This article contributes to the limited literature on HPT transition experiences, identifies opportunities to support HPTs, and informs broader efforts in teaching HPTs new technologies.
Methods
FHCC is jointly operated by the US Department of Defense and US Department of Veterans Affairs (VA). It treats 80,000 inpatient and outpatients annually. FHCC was the sixth VA facility to transition to the new EHR, which went live on March 9, 2024.2,11 About 700 HPTs rotate through FHCC annually. HPTs were eligible for inclusion if they were present during the March 9 transition according to a VA Office of Academic Affiliations database. A total of 216 HPTs were identified for inclusion.
Preparations for the transition included scaling down operations (ie, blocking clinician schedules, not scheduling future appointments that may conflict with the transition, making decisions on new facility- and service-line workflows, required EHR training, and speaking with support staff, including VHA National EHR Modernization Supplemental Staffing Unit [NESSU]). This evaluation was designated nonresearch/quality improvement by the VA Bedford Healthcare System Institutional Review Board.
Surveys
Forty-seven interviews were conducted with HPTs, site leaders, and supervisors from January 2024 to June 2024 (Table 1). Participants were identified by service leads and recruited via email; snowball sampling identified additional participants.
The evaluation team developed semistructured interview guides using grounded probes based on a pilot evaluation and existing research on EHR transitions.12 Questions focused on participant experiences preparing for the EHR transition, learning and using the site’s EHR, and the impact the transition had on clinical training experiences. Interviews were conducted at different times to capture the range of user experiences: 1 month prelaunch, 2 to 6 weeks postlaunch, and 2 months postlaunch. Interviewees were informed of participant rights and provided verbal consent.
HPTs present at FHCC at each survey’s release were emailed invitations and 2 reminders. The anonymous surveys took about 10 minutes to complete. Survey items queried HPTs about their experiences preparing to use the new EHR, perceptions of the current EHR (adapted from the System Usability Scale), satisfaction with VHA training, impact on clinical training, ability to work with preceptors and patients, and experiences with the VHA clinical learning environment (adapted from the VHA Learners Preceptor Survey).13-15 Survey questions used a 5-point Likert response scale.
Analysis
Interviewers completed postinterview summaries for team debriefing and consensus building. Interviews were coded using a priori (from piloting evaluations and relevant literature) and emergent (refined and developed from data) codes. Deductive and inductive content analyses were conducted. 16 Deductive analysis used a priori categories (eg, care coordination, EHR training). Inductive content analysis consisted of open and unstructured coding, capturing data outside a priori categories. Emergent codes captured unidentified categories. Qualitative researchers met weekly to discuss data and reach consensus on interpretation.
Descriptive analysis was conducted using top-2 box scoring (proportion responding within the 2 most favorable responses [agree/ strongly agree]). Survey data were analyzed in SAS.17 The analysis used a merging approach on simultaneously collected qualitative and quantitative data to reach findings consensus.18
Researcher and research team decisions may shape the data collected due to prior assumptions and experience.19 This analysis attempted to integrate reflexivity practices to enhance awareness of the researchers’ assumptions and positionality, including by integrating intent collaborative conversing and memorandum writing into the processes.20,21
Results
This analysis created a survey and fielded responses from HPTs present at FHCC across 3 time points (6 months prelaunch, 1 month prelaunch, and 2 months postlaunch), resulting in a total of 103 responses and an average response rate of 19.0% (Table 2). Six key findings were identified in analysis of responses: (1) critiques of transition management; (2) concerns with training; (3) hope about the EHR; (4) at-the-elbow support was essential; (5) HPTs adjusted to, and later preferred, the new EHR; and (6) transition impacted clinical training, but not overall career plans for HPTs. Findings are presented in this section, with illustrative quantitative data and qualitative data quotes available in the eAppendix.
Critiques of the Transition’s Management
While participants were aware of the transition to the new EHR, most felt they did not have enough information or time to prepare for it, indicating it was “too little, too late.” HPTs felt necessary workflow processes for Cerner/Oracle Health were not determined with enough time to learn them prior to transition. Supervisors shared that important workflow and onboarding decisions remained undecided mere weeks before the transition. Some service lines did not decrease patient loads until right before the transition, making it difficult to manage their schedules and resulting in insufficient time to learn the new EHR.
EHR Training Concerns
Overall, HPTs expressed low satisfaction with computer-based Training Management System (TMS) EHR training, believing it did not prepare them for the new EHR. The percentage of HPTs satisfied or very satisfied with the quality of TMS training was lower than that of instructor-based training pre- and posttransition, with 50% of 36 prelaunch respondents, and 43% of 29 postlaunch respondents expressing satisfaction with computer-based trainings (Figure 1). HPTs were dissatisfied with the training content. They felt it was too general and failed to teach basic tasks in the workflow for their service areas and roles, such as writing a note or order. Furthermore, poor content was exacerbated by poor and unengaging instruction, and HPTs were dissatisfied with the practice EHR used in training, which glitched frequently.
quality of electronic health record training.
EHR Transition Optimism
Even though the transition was stressful, most HPTs hoped it would be a temporary disruption and that they would quickly adjust to the new EHR. Many participants expected that once they switched to the new EHR, they would pick it up quickly. In addition, many anticipated Cerner/Oracle Health would be better and easier to use in the long run.
At-The-Elbow Support Essential
VHA peer support with NESSU was highly valued among HPTs. NESSU staff were highly knowledgeable and could provide both broad and service-line-specific support. NESSU provided prompt answers to EHR questions. This was particularly critical as other forms of in-person support were often inaccessible or absent during the transition.
HPTs found facility support helpful: 85% of 36 respondents reported being satisfied/ very satisfied with support from supervisors and preceptors, and 84% of 36 respondents were satisfied/very satisfied with technical support from facility informatics staff pretransition (n = 36) (Figure 2). NESSU and supervisor support with daily workflows were particularly helpful, as pretransition training only provided a general introduction to the EHR.
health record training.
HPTs Adjusted to and Later Preferred the New EHR
The EHR learning experience was intense but short, with many HPTs feeling able to use it only 2 to 4 weeks posttransition. Confidence grew as HPTs came to view Cerner/Oracle Health as a more integrated and intuitive system than the previous EHR. Most participants preferred the new EHR, even if they criticized some features (eg, no group documentation capabilities). Survey participants frequently rated Cerner/Oracle Health usability higher than the original. A total of 32% of 29 posttransition respondents agreed or strongly agreed that Cerner/Oracle Health helps prevent situations that can lead to patient safety risks—higher than pretransition rates. Additionally, fewer respondents found the new EHR unnecessarily complex or thought it contained too many alerts and flags compared to the original EHR (Figure 3).
health record usability.
Impact on Clinical Training, Not Career Plans
The extensive time and energy the transition demanded of HPTs caused stress and affected their clinical training. Many believed they would have learned more if their training had happened outside the transition.
Concerns that the transition affected learning were most acutely felt pretransition. HPTs reporting that EHR implementation positively affected their clinical education fell from 38% of 36 respondents 6 months pretransition to 19% of 29 respondents 1 month pretransition, but returned to 37% posttransition (Figure 4). However, some HPTs believed there was a silver lining: it provided a learning experience they otherwise would not have had.
new Veterans Health Administration (VHA) electronic health record.
HPTs who believed the transition positively impacted their likelihood of pursuing future career opportunities within the VHA rose to 33% of 29 respondents posttransition. Overall, Cerner/Oracle Health was characterized as a tool: something used in training, but not something that precluded wanting VHA careers or having meaningful experiences, such as caring for patients.
Discussion
This evaluation addressed an underexplored aspect of EHR transitions: their impact on HPTs. It identified HPT challenges, including dissatisfaction with poor transition preparation and EHR training experiences. Promising findings include positive experiences with transition support, EHR uptake, and overall positive educational experiences despite the transition’s disruption.
When EHR users, including HPTs, are dissatisfied with transition preparations, consequent stress can lead to undesired effects, including increased burnout, inappropriate EHR use, and low work satisfaction.22-24 Negative EHR transition experiences shape HPTs’ subsequent EHR adoption, user satisfaction, as well as confidence and career intent.3,25,26 Health systems have strong incentives to implement effective transition change management.
HPTs at previous VHA EHR transition sites reported significantly more disruption to their clinical training compared with HPTs at FHCC. Academic programs were shut down at the first transition site, and HPTs expressed decreased interest in VHA careers at another, even a year posttransition.6,27 These findings are consistent with the limited literature on the adverse impacts that EHR transitions have on HPTs.7,28
HPT retention is critical. VA is mandated to prepare the next generation of HPTs for its needs, and those of the nation. The VA relies heavily on HPT retention to recruit clinicians: > 65% of VHA physicians nationwide participated in VHA training programs prior to recruitment into staff positions.5,29
VHA should invest in transition change management with demonstrated, positive impacts on HPTs, such as in-house support from clinicians. Previous research found that lack of support was a major source of stress and negative outcomes.6,27 Consequently, supporting HPTs through EHR transitions directly contributes to the VHA’s ability to attract high-quality staff from its HPTs. The challenges and promising practices described in this analysis underscore the necessity of understanding how all EHR users are affected by transitions. What happens to them has direct implications for the VA mission to provide safe, efficient care, and its mandate to provide quality clinical training to HPTs.
These findings hold hopeful implications for supporting HPT EHR use, both during and outside EHR transitions. HPTs expressing that an EHR is only 1 part of their clinical training experience suggests that change management can improve EHR transitions. HPT learning can enhance known factors that are important for HPTs in clinical training, including the health care organization’s mission, caring for patients, and personal development.
Further investigations may engage HPTs at future VHA sites making the transition to the new EHR. One focus would involve applying a learning health systems framework to examine the nature of change management efforts—and their effects on HPT transition experiences—iteratively across transition sites to evaluate the effect of the efforts. Another focus may be longitudinal engagement with HPTs at health care systems and sites transitioning to new EHRs. Research has found that disruptions to EHR usability, satisfaction, and care provision can persist for 2 years and beyond following an EHR transition.30 Evaluating the long-term effects of transitions on HPTs is of interest, given their distinct characteristics and differences from employees.
Limitations
Study data came from voluntary participants at 1 highly engaged site, raising the possibility of self-selection bias. HPT experiences at other VA and non-VA sites may differ. Employees and HPTs were engaged during a high-stress event; snowballing recruitment reach was limited by high workloads and limited time for engagement. Statistical data were descriptive and should not be interpreted as causal. Results may reflect, in part, temporal effects, and respondents include HPTs at different stages of training and with different levels of VA experience. Survey sample sizes may limit generalizability; however, merging data streams strengthened the reliability of findings.
Conclusions
The results of this analysis of FHCC HPTs were notably more positive than those of HPTs at previous VHA EHR transition sites. VHA is one of many health care systems that provide clinical training for HPTs and relies on this population to provide patient care. By highlighting challenges and positive experiences of HPTs during an EHR transition, this evaluation produces actionable insights that can inform the actions of health care systems seeking to support HPTs during disruptive EHR transitions.
The Veterans Health Administration (VHA) is transitioning from its native electronic health record (EHR) Vista/Computerized Patient Record System to the commercial Cerner/Oracle Health EHR. Though this process was temporarily discontinued in April 2023 due to patient safety, usability, and reliability concerns, it resumed in April 2026. It was originally projected to cost $50 billion to implement. 1-3 As of March 9, 2024, 6 sites had transitioned to the new EHR.2 The transition is the largest of its kind in the US, offering an unparalleled opportunity to examine the effects of EHR transitions on an often overlooked part of the workforce: health professions trainees (HPTs).
HPTs serve a central role in VHA. About one-third of patients receive care directly from HPTs who make up about one-third of the VHA workforce. VHA trains > 60 clinical disciplines, comprising > 122,000 trainees annually.4,5 A paucity of literature exists exploring the experiences of HPTs during EHR transitions, and many studies are often limited to single-site or small populations. HPTs face distinct challenges and needs during EHR transitions and are particularly vulnerable to their negative impacts on retention, clinical training, and efficiency and confidence in EHR use.6-10 HPTs at VHA sites that have already transitioned to the Cerner/Oracle Health EHR identified many challenges, including significant delays in gaining EHR access, pervasive perceptions of poor training, concerns that EHR functionality issues limited patient care, and decreased ability to track clinical skill acquisition.6 These challenges may impact some HPTs more than others (eg, students on short rotations are affected more acutely by delayed EHR access and usage).
This quality improvement project evaluated HPT EHR transition experiences at the Captain James A. Lovell Federal Health Care Center (FHCC). This article contributes to the limited literature on HPT transition experiences, identifies opportunities to support HPTs, and informs broader efforts in teaching HPTs new technologies.
Methods
FHCC is jointly operated by the US Department of Defense and US Department of Veterans Affairs (VA). It treats 80,000 inpatient and outpatients annually. FHCC was the sixth VA facility to transition to the new EHR, which went live on March 9, 2024.2,11 About 700 HPTs rotate through FHCC annually. HPTs were eligible for inclusion if they were present during the March 9 transition according to a VA Office of Academic Affiliations database. A total of 216 HPTs were identified for inclusion.
Preparations for the transition included scaling down operations (ie, blocking clinician schedules, not scheduling future appointments that may conflict with the transition, making decisions on new facility- and service-line workflows, required EHR training, and speaking with support staff, including VHA National EHR Modernization Supplemental Staffing Unit [NESSU]). This evaluation was designated nonresearch/quality improvement by the VA Bedford Healthcare System Institutional Review Board.
Surveys
Forty-seven interviews were conducted with HPTs, site leaders, and supervisors from January 2024 to June 2024 (Table 1). Participants were identified by service leads and recruited via email; snowball sampling identified additional participants.
The evaluation team developed semistructured interview guides using grounded probes based on a pilot evaluation and existing research on EHR transitions.12 Questions focused on participant experiences preparing for the EHR transition, learning and using the site’s EHR, and the impact the transition had on clinical training experiences. Interviews were conducted at different times to capture the range of user experiences: 1 month prelaunch, 2 to 6 weeks postlaunch, and 2 months postlaunch. Interviewees were informed of participant rights and provided verbal consent.
HPTs present at FHCC at each survey’s release were emailed invitations and 2 reminders. The anonymous surveys took about 10 minutes to complete. Survey items queried HPTs about their experiences preparing to use the new EHR, perceptions of the current EHR (adapted from the System Usability Scale), satisfaction with VHA training, impact on clinical training, ability to work with preceptors and patients, and experiences with the VHA clinical learning environment (adapted from the VHA Learners Preceptor Survey).13-15 Survey questions used a 5-point Likert response scale.
Analysis
Interviewers completed postinterview summaries for team debriefing and consensus building. Interviews were coded using a priori (from piloting evaluations and relevant literature) and emergent (refined and developed from data) codes. Deductive and inductive content analyses were conducted. 16 Deductive analysis used a priori categories (eg, care coordination, EHR training). Inductive content analysis consisted of open and unstructured coding, capturing data outside a priori categories. Emergent codes captured unidentified categories. Qualitative researchers met weekly to discuss data and reach consensus on interpretation.
Descriptive analysis was conducted using top-2 box scoring (proportion responding within the 2 most favorable responses [agree/ strongly agree]). Survey data were analyzed in SAS.17 The analysis used a merging approach on simultaneously collected qualitative and quantitative data to reach findings consensus.18
Researcher and research team decisions may shape the data collected due to prior assumptions and experience.19 This analysis attempted to integrate reflexivity practices to enhance awareness of the researchers’ assumptions and positionality, including by integrating intent collaborative conversing and memorandum writing into the processes.20,21
Results
This analysis created a survey and fielded responses from HPTs present at FHCC across 3 time points (6 months prelaunch, 1 month prelaunch, and 2 months postlaunch), resulting in a total of 103 responses and an average response rate of 19.0% (Table 2). Six key findings were identified in analysis of responses: (1) critiques of transition management; (2) concerns with training; (3) hope about the EHR; (4) at-the-elbow support was essential; (5) HPTs adjusted to, and later preferred, the new EHR; and (6) transition impacted clinical training, but not overall career plans for HPTs. Findings are presented in this section, with illustrative quantitative data and qualitative data quotes available in the eAppendix.
Critiques of the Transition’s Management
While participants were aware of the transition to the new EHR, most felt they did not have enough information or time to prepare for it, indicating it was “too little, too late.” HPTs felt necessary workflow processes for Cerner/Oracle Health were not determined with enough time to learn them prior to transition. Supervisors shared that important workflow and onboarding decisions remained undecided mere weeks before the transition. Some service lines did not decrease patient loads until right before the transition, making it difficult to manage their schedules and resulting in insufficient time to learn the new EHR.
EHR Training Concerns
Overall, HPTs expressed low satisfaction with computer-based Training Management System (TMS) EHR training, believing it did not prepare them for the new EHR. The percentage of HPTs satisfied or very satisfied with the quality of TMS training was lower than that of instructor-based training pre- and posttransition, with 50% of 36 prelaunch respondents, and 43% of 29 postlaunch respondents expressing satisfaction with computer-based trainings (Figure 1). HPTs were dissatisfied with the training content. They felt it was too general and failed to teach basic tasks in the workflow for their service areas and roles, such as writing a note or order. Furthermore, poor content was exacerbated by poor and unengaging instruction, and HPTs were dissatisfied with the practice EHR used in training, which glitched frequently.
quality of electronic health record training.
EHR Transition Optimism
Even though the transition was stressful, most HPTs hoped it would be a temporary disruption and that they would quickly adjust to the new EHR. Many participants expected that once they switched to the new EHR, they would pick it up quickly. In addition, many anticipated Cerner/Oracle Health would be better and easier to use in the long run.
At-The-Elbow Support Essential
VHA peer support with NESSU was highly valued among HPTs. NESSU staff were highly knowledgeable and could provide both broad and service-line-specific support. NESSU provided prompt answers to EHR questions. This was particularly critical as other forms of in-person support were often inaccessible or absent during the transition.
HPTs found facility support helpful: 85% of 36 respondents reported being satisfied/ very satisfied with support from supervisors and preceptors, and 84% of 36 respondents were satisfied/very satisfied with technical support from facility informatics staff pretransition (n = 36) (Figure 2). NESSU and supervisor support with daily workflows were particularly helpful, as pretransition training only provided a general introduction to the EHR.
health record training.
HPTs Adjusted to and Later Preferred the New EHR
The EHR learning experience was intense but short, with many HPTs feeling able to use it only 2 to 4 weeks posttransition. Confidence grew as HPTs came to view Cerner/Oracle Health as a more integrated and intuitive system than the previous EHR. Most participants preferred the new EHR, even if they criticized some features (eg, no group documentation capabilities). Survey participants frequently rated Cerner/Oracle Health usability higher than the original. A total of 32% of 29 posttransition respondents agreed or strongly agreed that Cerner/Oracle Health helps prevent situations that can lead to patient safety risks—higher than pretransition rates. Additionally, fewer respondents found the new EHR unnecessarily complex or thought it contained too many alerts and flags compared to the original EHR (Figure 3).
health record usability.
Impact on Clinical Training, Not Career Plans
The extensive time and energy the transition demanded of HPTs caused stress and affected their clinical training. Many believed they would have learned more if their training had happened outside the transition.
Concerns that the transition affected learning were most acutely felt pretransition. HPTs reporting that EHR implementation positively affected their clinical education fell from 38% of 36 respondents 6 months pretransition to 19% of 29 respondents 1 month pretransition, but returned to 37% posttransition (Figure 4). However, some HPTs believed there was a silver lining: it provided a learning experience they otherwise would not have had.
new Veterans Health Administration (VHA) electronic health record.
HPTs who believed the transition positively impacted their likelihood of pursuing future career opportunities within the VHA rose to 33% of 29 respondents posttransition. Overall, Cerner/Oracle Health was characterized as a tool: something used in training, but not something that precluded wanting VHA careers or having meaningful experiences, such as caring for patients.
Discussion
This evaluation addressed an underexplored aspect of EHR transitions: their impact on HPTs. It identified HPT challenges, including dissatisfaction with poor transition preparation and EHR training experiences. Promising findings include positive experiences with transition support, EHR uptake, and overall positive educational experiences despite the transition’s disruption.
When EHR users, including HPTs, are dissatisfied with transition preparations, consequent stress can lead to undesired effects, including increased burnout, inappropriate EHR use, and low work satisfaction.22-24 Negative EHR transition experiences shape HPTs’ subsequent EHR adoption, user satisfaction, as well as confidence and career intent.3,25,26 Health systems have strong incentives to implement effective transition change management.
HPTs at previous VHA EHR transition sites reported significantly more disruption to their clinical training compared with HPTs at FHCC. Academic programs were shut down at the first transition site, and HPTs expressed decreased interest in VHA careers at another, even a year posttransition.6,27 These findings are consistent with the limited literature on the adverse impacts that EHR transitions have on HPTs.7,28
HPT retention is critical. VA is mandated to prepare the next generation of HPTs for its needs, and those of the nation. The VA relies heavily on HPT retention to recruit clinicians: > 65% of VHA physicians nationwide participated in VHA training programs prior to recruitment into staff positions.5,29
VHA should invest in transition change management with demonstrated, positive impacts on HPTs, such as in-house support from clinicians. Previous research found that lack of support was a major source of stress and negative outcomes.6,27 Consequently, supporting HPTs through EHR transitions directly contributes to the VHA’s ability to attract high-quality staff from its HPTs. The challenges and promising practices described in this analysis underscore the necessity of understanding how all EHR users are affected by transitions. What happens to them has direct implications for the VA mission to provide safe, efficient care, and its mandate to provide quality clinical training to HPTs.
These findings hold hopeful implications for supporting HPT EHR use, both during and outside EHR transitions. HPTs expressing that an EHR is only 1 part of their clinical training experience suggests that change management can improve EHR transitions. HPT learning can enhance known factors that are important for HPTs in clinical training, including the health care organization’s mission, caring for patients, and personal development.
Further investigations may engage HPTs at future VHA sites making the transition to the new EHR. One focus would involve applying a learning health systems framework to examine the nature of change management efforts—and their effects on HPT transition experiences—iteratively across transition sites to evaluate the effect of the efforts. Another focus may be longitudinal engagement with HPTs at health care systems and sites transitioning to new EHRs. Research has found that disruptions to EHR usability, satisfaction, and care provision can persist for 2 years and beyond following an EHR transition.30 Evaluating the long-term effects of transitions on HPTs is of interest, given their distinct characteristics and differences from employees.
Limitations
Study data came from voluntary participants at 1 highly engaged site, raising the possibility of self-selection bias. HPT experiences at other VA and non-VA sites may differ. Employees and HPTs were engaged during a high-stress event; snowballing recruitment reach was limited by high workloads and limited time for engagement. Statistical data were descriptive and should not be interpreted as causal. Results may reflect, in part, temporal effects, and respondents include HPTs at different stages of training and with different levels of VA experience. Survey sample sizes may limit generalizability; however, merging data streams strengthened the reliability of findings.
Conclusions
The results of this analysis of FHCC HPTs were notably more positive than those of HPTs at previous VHA EHR transition sites. VHA is one of many health care systems that provide clinical training for HPTs and relies on this population to provide patient care. By highlighting challenges and positive experiences of HPTs during an EHR transition, this evaluation produces actionable insights that can inform the actions of health care systems seeking to support HPTs during disruptive EHR transitions.
- US Department of Veterans Affairs Office of the Inspector General. VA needs to strengthen controls to address electronic health record system major performance incidents. September 23, 2024. Accessed February 3, 2026. https://www.vaoig.gov/sites/default/files /reports/2024-09/vaoig-22-03591-231.pdf
- EHR deployment schedule. VA EHR Modernization. Updated February 2, 2026. Accessed February 3, 2026. https://digital.va.gov/ehr-modernization/ehr-deployment -schedule/
- Heckman J. VA in 2026 looks to get EHR rollout back on track, embark on health care reorganization. Federal News Network. December 24, 2025. Accessed February 3, 2026. https://federalnewsnetwork.com/veterans-affairs/2025/12 /va-in-2026-looks-to-get-ehr-rollout-back-on-track -embark-on-health-care-reorganization/
- US Department of Veterans Affairs Office of Academic Affiliations. Medical and dental education. Updated September 12, 2025. Accessed February 3, 2026. https://department.va.gov/academic-affiliations /medical-and-dental/
- Functions of Veterans Health Administration: health-care personnel education and training programs. 38 U.S.C. § 7302 (2026). Accessed February 3, 2026. https://uscode.house.gov/view.xhtml ?req=(title:38%20section:7302%20edition:prelim)
- Ahlness EA, Molloy-Paolillo BK, Brunner J, et al. Impacts of an electronic health record transition on Veterans Health Administration health professions trainee experience. J Gen Intern Med. 2023;38:1031-1039. doi:10.1007/s11606-023-08283-4
- Roberts DL, Mishark KJ, Alessandro STD, et al. Impact of electronic medical record transitions on the educational experiences of medical students. J Health Care Finance. 2014;41:1-5.
- Varpio L, Day K, Elliot‐Miller P, et al. The impact of adopting EHRs: how losing connectivity affects clinical reasoning. Med Educ. 2015;49:476-486. doi:10.1111/medu.12665
- Gali HE, Baxter SL, Lander L, et al. Impact of electronic health record implementation on ophthalmology trainee time expenditures. J Acad Ophthalmol (2017). 2019;11:e65-e72. doi:10.1055/s-0039-3401986
- Humphrey‐Murto S, Makus D, Moore S, et al. Training physicians and residents for the use of electronic health records— a comparative case study between two hospitals. Med Educ. 2023;57:337-348. doi:10.1111/medu.14944
- US Department of Defense. Captain James A. Lovell Federal Health Care Center: readying warriors & caring for heroes. Presentation August 10, 2022.
- Sayre G, Young J. Beyond openended questions: purposeful interview guide development to elicit rich, trustworthy data. Patient Aligned Care Teams (PACT) Demonstration Labs cyber seminar. March 21, 2018. Accessed February 3, 2026. https://www.hsrd.research.va.gov/for _researchers/cyber_seminars/catalog/transcripts/2439.doc
- Jordan PW, Thomas B, McClelland IL, Weerdmeester B, eds. Usability Evaluation In Industry. CRC Press; 1996.
- Keitz SA, Holland GJ, Melander EH, et al. The Veterans Affairs Learners’ Perceptions Survey: the foundation for educational quality improvement. Acad Med. 2003;78:910- 917. doi:10.1097/00001888-200309000-00016
- Byrne JM, Chang BK, Gilman SC, et al. The learners’ perceptions survey—primary care: assessing resident perceptions of internal medicine continuity clinics and patient- centered care. J Grad Med Educ. 2013;5:587-593. doi:10.4300/JGME-D-12-00233.1
- Elo S, Kyngäs H. The qualitative content analysis process. J Adv Nurs. 2008;62:107-115. doi:10.1111/j.1365-2648.2007.04569.x
- Siller AB, Tompkins L. The big four: analyzing complex sample survey data using SAS, SPSS, STATA, and SUDAAN. Poster presented at: 31st Annual SAS Users Group International Conference; March 27, 2006; San Francisco, CA. Accessed February 3, 2026. https://support.sas.com /resources/papers/proceedings/proceedings/sugi31/172 -31.pdf
- Tashakkori A, Johnson RB, Teddlie C. Foundations of Mixed Methods Research: Integrating Quantitative and Qualitative Approaches in the Social and Behavioral Sciences. 2nd ed. SAGE Publications, Inc.; 2020.
- Olmos-Vega FM, Stalmeijer RE, Varpio L, et al. A practical guide to reflexivity in qualitative research: AMEE Guide No. 149. Med Teach. 2023;45:241-251. doi:10.1080/0142159X.2022.2057287
- Mezirow J. Fostering Critical Reflection in Adulthood: A Guide to Transformative and Emancipatory Learning. JosseyBass; 1991.
- Probst B, Berenson L. The double arrow: how qualitative social work researchers use reflexivity. Qual Soc Work. 2014;13:813-827. doi:10.1177/1473325013506248
- Huang C, Koppel R, McGreevey JD 3rd, et al. Transitions from one electronic health record to another: challenges, pitfalls, and recommendations. Appl Clin Infor. 2020;11:742-754. doi:10.1055/s-0040-1718535
- Zheng K, Abraham J, Novak LL, et al. A survey of the literature on unintended consequences associated with health information technology: 2014–2015. Yearb Med Inform. 2016;25:13-29. doi:10.15265/IY-2016-036
- Campbell EM, Sittig DF, Ash JS, et al. Types of unintended consequences related to computerized provider order entry. J Am Med Inform Assoc. 2006;13:547-556. doi:10.1197/jamia.M2042
- Sittig DF, Lakhani P, Singh H. Applying requisite imagination to safeguard electronic health record transitions. JAMA. 2022;29:1014-1018. doi:10.1093/jamia/ocab291
- Ko HH, Lee TK, Leung Y, et al. Factors influencing career choices made by medical students, residents, and practising physicians. B C Med J. 2007;49:482-489.
- Brunner J, Ahlness EA, Anderson E, et al. VA’s EHR transition and health professions trainee programs: findings and impacts of a multistakeholder learning community. Learn Health Sys. 2024;9:e10460. doi:10.1002/lrh2.10460
- Rosdahl JA, Rudd M, Benjamin R, et al. Effect of the adoption of a comprehensive electronic health record on graduate medical education: perceptions of faculty and trainees. South Med J. 2018;111:476-483. doi:10.14423/SMJ.0000000000000847
- Hill C. U.S. Medical education at VA: it’s all about the veterans. VA News. August 18, 2021. Accessed February 3, 2026. https://news.va.gov/93370/medical-education-at-va -its-all-about-the-veterans
- Hanauer DA, Branford GL, Greenberg G, et al. Twoyear longitudinal assessment of physicians’ perceptions after replacement of a longstanding homegrown electronic health record: does a J-curve of satisfaction really exist? J Am Med Inform Assoc. 2017;24:e157-e165. doi:10.1093/jamia/ocw077
- US Department of Veterans Affairs Office of the Inspector General. VA needs to strengthen controls to address electronic health record system major performance incidents. September 23, 2024. Accessed February 3, 2026. https://www.vaoig.gov/sites/default/files /reports/2024-09/vaoig-22-03591-231.pdf
- EHR deployment schedule. VA EHR Modernization. Updated February 2, 2026. Accessed February 3, 2026. https://digital.va.gov/ehr-modernization/ehr-deployment -schedule/
- Heckman J. VA in 2026 looks to get EHR rollout back on track, embark on health care reorganization. Federal News Network. December 24, 2025. Accessed February 3, 2026. https://federalnewsnetwork.com/veterans-affairs/2025/12 /va-in-2026-looks-to-get-ehr-rollout-back-on-track -embark-on-health-care-reorganization/
- US Department of Veterans Affairs Office of Academic Affiliations. Medical and dental education. Updated September 12, 2025. Accessed February 3, 2026. https://department.va.gov/academic-affiliations /medical-and-dental/
- Functions of Veterans Health Administration: health-care personnel education and training programs. 38 U.S.C. § 7302 (2026). Accessed February 3, 2026. https://uscode.house.gov/view.xhtml ?req=(title:38%20section:7302%20edition:prelim)
- Ahlness EA, Molloy-Paolillo BK, Brunner J, et al. Impacts of an electronic health record transition on Veterans Health Administration health professions trainee experience. J Gen Intern Med. 2023;38:1031-1039. doi:10.1007/s11606-023-08283-4
- Roberts DL, Mishark KJ, Alessandro STD, et al. Impact of electronic medical record transitions on the educational experiences of medical students. J Health Care Finance. 2014;41:1-5.
- Varpio L, Day K, Elliot‐Miller P, et al. The impact of adopting EHRs: how losing connectivity affects clinical reasoning. Med Educ. 2015;49:476-486. doi:10.1111/medu.12665
- Gali HE, Baxter SL, Lander L, et al. Impact of electronic health record implementation on ophthalmology trainee time expenditures. J Acad Ophthalmol (2017). 2019;11:e65-e72. doi:10.1055/s-0039-3401986
- Humphrey‐Murto S, Makus D, Moore S, et al. Training physicians and residents for the use of electronic health records— a comparative case study between two hospitals. Med Educ. 2023;57:337-348. doi:10.1111/medu.14944
- US Department of Defense. Captain James A. Lovell Federal Health Care Center: readying warriors & caring for heroes. Presentation August 10, 2022.
- Sayre G, Young J. Beyond openended questions: purposeful interview guide development to elicit rich, trustworthy data. Patient Aligned Care Teams (PACT) Demonstration Labs cyber seminar. March 21, 2018. Accessed February 3, 2026. https://www.hsrd.research.va.gov/for _researchers/cyber_seminars/catalog/transcripts/2439.doc
- Jordan PW, Thomas B, McClelland IL, Weerdmeester B, eds. Usability Evaluation In Industry. CRC Press; 1996.
- Keitz SA, Holland GJ, Melander EH, et al. The Veterans Affairs Learners’ Perceptions Survey: the foundation for educational quality improvement. Acad Med. 2003;78:910- 917. doi:10.1097/00001888-200309000-00016
- Byrne JM, Chang BK, Gilman SC, et al. The learners’ perceptions survey—primary care: assessing resident perceptions of internal medicine continuity clinics and patient- centered care. J Grad Med Educ. 2013;5:587-593. doi:10.4300/JGME-D-12-00233.1
- Elo S, Kyngäs H. The qualitative content analysis process. J Adv Nurs. 2008;62:107-115. doi:10.1111/j.1365-2648.2007.04569.x
- Siller AB, Tompkins L. The big four: analyzing complex sample survey data using SAS, SPSS, STATA, and SUDAAN. Poster presented at: 31st Annual SAS Users Group International Conference; March 27, 2006; San Francisco, CA. Accessed February 3, 2026. https://support.sas.com /resources/papers/proceedings/proceedings/sugi31/172 -31.pdf
- Tashakkori A, Johnson RB, Teddlie C. Foundations of Mixed Methods Research: Integrating Quantitative and Qualitative Approaches in the Social and Behavioral Sciences. 2nd ed. SAGE Publications, Inc.; 2020.
- Olmos-Vega FM, Stalmeijer RE, Varpio L, et al. A practical guide to reflexivity in qualitative research: AMEE Guide No. 149. Med Teach. 2023;45:241-251. doi:10.1080/0142159X.2022.2057287
- Mezirow J. Fostering Critical Reflection in Adulthood: A Guide to Transformative and Emancipatory Learning. JosseyBass; 1991.
- Probst B, Berenson L. The double arrow: how qualitative social work researchers use reflexivity. Qual Soc Work. 2014;13:813-827. doi:10.1177/1473325013506248
- Huang C, Koppel R, McGreevey JD 3rd, et al. Transitions from one electronic health record to another: challenges, pitfalls, and recommendations. Appl Clin Infor. 2020;11:742-754. doi:10.1055/s-0040-1718535
- Zheng K, Abraham J, Novak LL, et al. A survey of the literature on unintended consequences associated with health information technology: 2014–2015. Yearb Med Inform. 2016;25:13-29. doi:10.15265/IY-2016-036
- Campbell EM, Sittig DF, Ash JS, et al. Types of unintended consequences related to computerized provider order entry. J Am Med Inform Assoc. 2006;13:547-556. doi:10.1197/jamia.M2042
- Sittig DF, Lakhani P, Singh H. Applying requisite imagination to safeguard electronic health record transitions. JAMA. 2022;29:1014-1018. doi:10.1093/jamia/ocab291
- Ko HH, Lee TK, Leung Y, et al. Factors influencing career choices made by medical students, residents, and practising physicians. B C Med J. 2007;49:482-489.
- Brunner J, Ahlness EA, Anderson E, et al. VA’s EHR transition and health professions trainee programs: findings and impacts of a multistakeholder learning community. Learn Health Sys. 2024;9:e10460. doi:10.1002/lrh2.10460
- Rosdahl JA, Rudd M, Benjamin R, et al. Effect of the adoption of a comprehensive electronic health record on graduate medical education: perceptions of faculty and trainees. South Med J. 2018;111:476-483. doi:10.14423/SMJ.0000000000000847
- Hill C. U.S. Medical education at VA: it’s all about the veterans. VA News. August 18, 2021. Accessed February 3, 2026. https://news.va.gov/93370/medical-education-at-va -its-all-about-the-veterans
- Hanauer DA, Branford GL, Greenberg G, et al. Twoyear longitudinal assessment of physicians’ perceptions after replacement of a longstanding homegrown electronic health record: does a J-curve of satisfaction really exist? J Am Med Inform Assoc. 2017;24:e157-e165. doi:10.1093/jamia/ocw077
Evaluation of Health Professions Trainee Experiences Transitioning to New VHA Electronic Health Record
Evaluation of Health Professions Trainee Experiences Transitioning to New VHA Electronic Health Record

Common Ground: Primary Care and Specialty Clinicians’ Perceptions of E-Consults in the Veterans Health Administration
Electronic consultation (e-consult) is designed to increase access to specialty care by facilitating communication between primary care and specialty clinicians without the need for outpatient face-to-face encounters.1–4 In 2011, the US Department of Veterans Affairs (VA) implemented an e-consult program as a component of its overall strategy to increase access to specialty services, reduce costs of care, and reduce appointment travel burden on patients.
E-consult has substantially increased within the VA since its implementation.5,6 Consistent with limited evaluations from other health care systems, evaluations of the VA e-consult program demonstrated reduced costs, reduced travel time for patients, and improved access to specialty care.2,5–11 However, there is wide variation in e-consult use across VA specialties, facilities, and regions.5,6,12,13 For example, hematology, preoperative evaluation, neurosurgery, endocrinology, and infectious diseases use e-consults more frequently when compared with in-person consults in the VA.6 Reasons for this variation or specific barriers and facilitators of using e-consults have not been described.
Prior qualitative studies report that primary care practitioners (PCPs) describe e-consults as convenient, educational, beneficial for patient care, and useful for improving patient access to specialty care.8,14,15 One study identified limited PCP knowledge of e-consults as a barrier to use.16 Specialists have reported that e-consult improves clinical communication, but increases their workload.1,14,17,18 These studies did not assess perspectives from both clinicians who initiate e-consults and those who respond to them. This is the first qualitative study to assess e-consult perceptions from perspectives of both PCPs and specialists among a large, national sample of VA clinicians who use e-consults. The objective of this study was to understand perspectives of e-consults between PCPs and specialists that may be relevant to increasing adoption in the VA.
Methods
The team (CL, ML, PG, 2 analysts under the guidance of GS and JS and support from RRK, and a biostatistician) conducted semistructured interviews with PCPs, specialists, and specialty division leaders who were employed by VA in 2016 and 2017. Specialties of interest were identified by the VA Office of Specialty Care and included cardiology, endocrinology, gastroenterology, and hematology.
E-Consult Procedures
Within the VA, the specific procedures used to initiate, triage and manage e-consults are coordinated at VA medical centers (VAMCs) and at the Veterans Integrated Service Network (VISN) regional level. E-consult can be requested by any clinician. Generally, e-consults are initiated by PCPs through standardized, specialty-specific templates. Recipients, typically specialists, respond by answering questions, suggesting additional testing and evaluation, or requesting an in-person visit. Communication is documented in the patient’s electronic health record (EHR). Specialists receive different levels of workload credit for responding to e-consults similar to a relative value unit reimbursement model. Training in the use of e-consults is available to practitioners but may vary at local and regional levels.
Recruitment
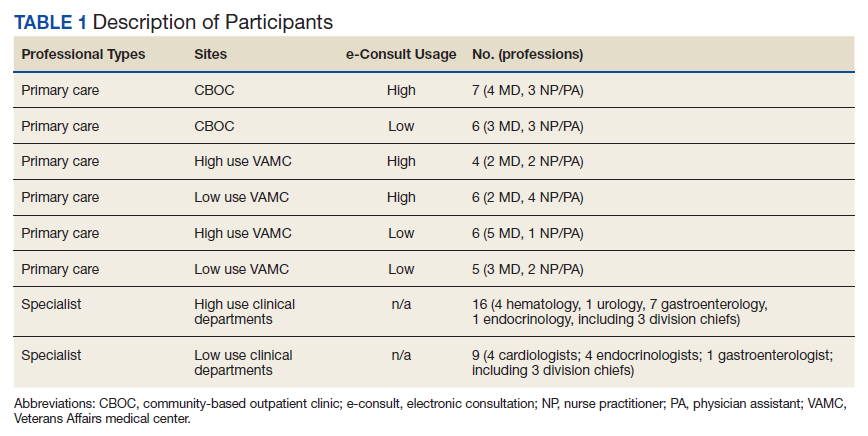
Our sample included PCPs, specialists, and specialty care division leaders. We first quantified e-consult rates (e-consults per 100 patient visits) between July 2016 and June 2017 at VA facilities within primary care and the 4 priority specialties and identified the 30 sites with the highest e-consult rates and 30 sites with the lowest e-consult rates. Sites with < 500 total visits, < 3 specialties, or without any e-consult visit during the study period were excluded. E-consult rates at community-based outpatient clinics were included with associated VAMCs. We then stratified PCPs by whether they were high or low users of e-consults (determined by the top and bottom users within each site) and credentials (MD vs nurse practitioner [NP] or physician assistant [PA]). Specialists were sampled based on their rate of use relative to colleagues within their site and the use rate of their division. We sampled division chiefs and individuals who had > 300 total visits and 1 e-consult during the study period. To recruit participants, the primary investigator sent an initial email and 2 reminder emails. The team followed up with respondents to schedule an interview.
Interview guides were designed to elicit rich descriptions of barriers and facilitators to e-consult use (eAppendix available at doi:10.12788/fp.0214). The team used the Practical Robust Implementation and Sustainability Model (PRISM), which considers factors along 6 domains for intervention planning, implementation, and sustainment.19 Telephone interviews lasted about 20 minutes and were conducted between September 2017 and March 2018. Interviews were recorded and transcribed verbatim.
Analysis
The team used an iterative, team-based, inductive/deductive approach to conventional content analysis.20,21 Initial code categories were created so that we could identify e-consult best practices—facilitators of e-consult that were recommended by both PCPs and specialists. Inductive codes or labels applied to identify meaningful quotations, phrases, or key terms were used to identify emergent ideas and were added throughout coding after discussion among team members. Consensus was reached using a team-based approach.21 Four analysts independently coded the same 3 transcripts and met to discuss points of divergence and convergence. Analyses continued with emergent themes, categories, and conclusions. Atlas.ti. v.7 was used for coding and data management.22
Results
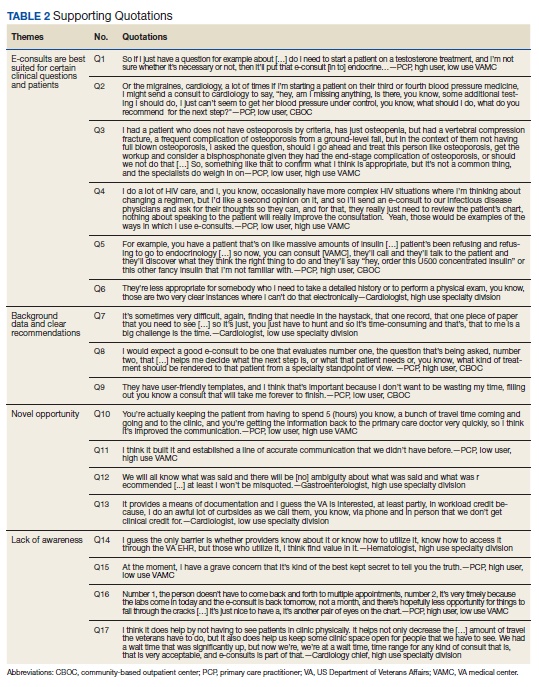
We conducted 34 interviews with clinicians (Table 1) from 13 VISNs. Four best-practice themes emerged among both PCPs and specialists, including that e-consults (1) are best suited for certain clinical questions and patients; (2) require relevant background information from requesting clinicians and clear recommendations from responding clinicians; (3) are a novel opportunity to provide efficient, transparent care; and (4) may not be fully adopted due to low awareness. Supporting quotations for the following findings are provided in Table 2.
Specific Clinical Questions and Patients
PCPs described specific patients and questions for which they most frequently used e-consults, such as for medication changes (Q1), determining treatment steps (Q2,3), and or clarifying laboratory or imaging findings. PCPs frequently used e-consults for patients who did not require a physical examination or when specialists could make recommendations without seeing patients face-to-face (Q3). An important use of e-consults described by PCPs was for treating conditions they could manage within primary care if additional guidance were available (Q4). Several PCPs and specialists also noted that e-consults were particularly useful for patients who were unable to travel or did not want face-to-face appointments (Q5). Notably, PCPs and specialists mentioned situations for which e-consults were inappropriate, including when a detailed history or physical examination was needed, or if a complex condition was suspected (Q6).
Background Data and Clear Recommendations
Participants described necessary data that should be included in high-quality e-consults. Specialists voiced frustration in time-consuming chart reviews that were often necessary when these data were not provided by the requestor. In some cases, specialists were unable to access necessary EHR data, which delayed responses (Q7). PCPs noted that the most useful responses carefully considered the question, used current patient information to determine treatments, provided clear recommendations, and defined who was responsible for next steps (Q8). PCPs and specialists stated that e-consult templates that required relevant information facilitated high-quality e-consults. Neither wanted to waste the other clinician's time (Q8).
A Novel Opportunity
Many PCPs felt that e-consults improved communication (eg, efficiency, response time), established new communication between clinicians, and reduced patients’ appointment burden (Q10, Q11). Many specialists felt that e-consults improved documentation of communication between clinicians and increased transparency of clinical decisions (Q12). Additionally, many specialists mentioned that e-consults capture previously informal curbside consults, enabling them to receive workload credit (Q13).
Lack of Awareness
Some noted that the biggest barrier to e-consults was not being aware of them generally, or which specialties offer e-consults (Q14). One PCP described e-consults as the best kept secret and found value in sharing the utility of e-consults with colleagues (Q15). All participants, including those who did not frequently use e-consults, felt that e-consults improved the quality of care by providing more timely care or better answers to clinical questions (Q16). Several practitioners also felt that e-consults increased access to specialty care. For example, specialists reported that e-consults enabled them to better manage patient load by using e-consults to answer relatively simple questions, reserving face-to-face consults for more complex patients (Q17).
Discussion
The objective of this study was to identify potential best practices for e-consults that may help increase their quality and use within the VA. We built on prior studies that offered insights on PCP and specialists’ overall satisfaction with e-consult by identifying several themes relevant to the further adoption of e-consults in the VA and elsewhere without a face-to-face visit.8,13,14,16–18 Future work may be beneficial in identifying whether the study themes identified can explain variation in e-consult use or whether addressing these factors might lead to increased or higher quality e-consult use. We are unaware of any qualitative study of comparable scale in a different health care system. Further, this is the first study to assess perspectives on e-consults among those who initiate and respond to them within the same health care system. Perhaps the most important finding from this study is that e-consults are generally viewed favorably, which is a necessary leverage point to increase their adoption within the system.
Clinicians reported several benefits to e-consults, including timely responses to clinical questions, efficient communication, allow for documentation of specialist recommendations, and help capture workload. These benefits are consistent with prior literature that indicates both PCPs and specialists in the VA and other health care systems feel that e-consults improves communication, decreases unnecessary visits, and improves quality of care.1,14,17,18 In particular, clinicians reported that e-consults improve their practice efficiency and efficacy. This is of critical importance given the pressures of providing timely access to primary and specialty care within the VA. Interestingly, many VA practitioners were unaware which specialties offered e-consults within their facilities, reflecting previous work showing that PCPs are often unaware of e-consult options.16 This may partially explain variation in e-consult use. Increasing awareness and educating clinicians on the benefits of e-consults may help promote use among non- and low users.
A common theme reported by both groups was the importance of providing necessary information within e-consult questions and responses. Specialists felt there was a need to ensure that PCPs provide relevant and patient-specific information that would enable them to efficiently and accurately answer questions without the need for extensive EHR review. This reflects previous work showing that specialists are often unable to respond to e-consult requests because they do not contain sufficient information.22 PCPs described a need to ensure that specialists’ responses included information that was detailed enough to make clinical decisions without the need for a reconsult. This highlights a common challenge to medical consultation, in that necessary or relevant information may not be apparent to all clinicians. To address this, there may be a role in developing enhanced, flexible templating that elicits necessary patient-specific information. Such a template may automatically pull relevant data from the EHR and prompt clinicians to provide important information. We did not assess how perspectives of templates varied, and further work could help define precisely what constitutes an effective template, including how it should capture appropriate patient data and how this impacts acceptability or use of e-consults generally. Collaboratively developed service agreements and e-consult templates could help guide PCPs and specialists to engage in efficient communication.
Another theme among both groups was that e-consult is most appropriate within specific clinical scenarios. Examples included review of laboratory results, questions about medication changes, or for patients who were reluctant to travel to appointments. Identifying and promoting specific opportunities for e-consults may help increase their use and align e-consult practices with scenarios that are likely to provide the most benefit to patients. For example, it could be helpful to understand the distance patients must travel for specialty care. Providing that information during clinical encounters could trigger clinicians to consider e-consults as an option. Future work might aim to identify clinical scenarios that clinicians feel are not well suited for e-consults and determine how to adapt them for those scenarios.
Limitations
Generalizability of these findings is limited given the qualitative study design. Participants’ descriptions of experiences with e-consults reflect the experiences of clinicians in the VA and may not reflect clinicians in other settings. We also interviewed a sample of clinicians who were already using e-consults. Important information could be learned from future work with those who have not yet adopted e-consult procedures or adopted and abandoned them.
Conclusions
E-consult is perceived as beneficial by VA PCPs and specialists. Participants suggested using e-consults for appropriate questions or patients and including necessary information and next steps in both the initial e-consult and response. Finding ways to facilitate e-consults with these suggestions in mind may increase delivery of high-quality e-consults. Future work could compare the findings of this work to similar work assessing clinicians perceptions of e-consults outside of the VA.
1. Battaglia C, Lambert-Kerzner A, Aron DC, et al. Evaluation of e-consults in the VHA: provider perspectives. Fed Pract. 2015;32(7):42-48.
2. Haverhals LM, Sayre G, Helfrich CD, et al. E-consult implementation: lessons learned using consolidated framework for implementation research. Am J Manag Care. 2015;21(12):e640-e647. Published 2015 Dec 1.
3. Sewell JL, Telischak KS, Day LW, Kirschner N, Weissman A. Preconsultation exchange in the United States: use, awareness, and attitudes. Am J Manag Care. 2014;20(12):e556-e564. Published 2014 Dec 1.
4. Horner K, Wagner E, Tufano J. Electronic consultations between primary and specialty care clinicians: early insights. Issue Brief (Commonw Fund). 2011;23:1-14.
5. Kirsh S, Carey E, Aron DC, et al. Impact of a national specialty e-consultation implementation project on access. Am J Manag Care. 2015;21(12):e648-654. Published 2015 Dec 1.
6. Saxon DR, Kaboli PJ, Haraldsson B, Wilson C, Ohl M, Augustine MR. Growth of electronic consultations in the Veterans Health Administration. Am J Manag Care. 2021;27(1):12-19. doi:10.37765/ajmc.2021.88572
7. Olayiwola JN, Anderson D, Jepeal N, et al. Electronic consultations to improve the primary care-specialty care interface for cardiology in the medically underserved: a cluster-randomized controlled trial. Ann Fam Med. 2016;14(2):133-140. doi:10.1370/afm.1869
8. Schettini P, Shah KP, O’Leary CP, et al. Keeping care connected: e-Consultation program improves access to nephrology care. J Telemed Telecare. 2019;25(3):142-150. doi:10.1177/1357633X17748350
9. Whittington MD, Ho PM, Kirsh SR, et al. Cost savings associated with electronic specialty consultations. Am J Manag Care. 2021;27(1):e16-e23. Published 2021 Jan 1. doi:10.37765/ajmc.2021.88579
10. Shipherd JC, Kauth MR, Matza A. Nationwide interdisciplinary e-consultation on transgender care in the Veterans Health Administration. Telemed J E Health. 2016;22(12):1008-1012. doi:10.1089/tmj.2016.0013
11. Strymish J, Gupte G, Afable MK, et al. Electronic consultations (E-consults): advancing infectious disease care in a large Veterans Affairs Healthcare System. Clin Infect Dis. 2017;64(8):1123-1125. doi:10.1093/cid/cix058
12. Williams KM, Kirsh S, Aron D, et al. Evaluation of the Veterans Health Administration’s Specialty Care Transformational Initiatives to promote patient-centered delivery of specialty care: a mixed-methods approach. Telemed J E-Health. 2017;23(7):577-589. doi:10.1089/tmj.2016.0166
13. US Department of Veterans Affairs, Veterans Health Administration, Specialty Care Transformational Initiative Evaluation Center. Evaluation of specialty care initiatives. Published 2013.
14. Vimalananda VG, Gupte G, Seraj SM, et al. Electronic consultations (e-consults) to improve access to specialty care: a systematic review and narrative synthesis. J Telemed Telecare. 2015;21(6):323-330. doi:10.1177/1357633X15582108
15. Lee M, Leonard C, Greene P, et al. Perspectives of VA primary care clinicians toward electronic consultation-related workload burden. JAMA Netw Open. 2020;3(10):e2018104. Published 2020 Oct 1. doi:10.1001/jamanetworkopen.2020.18104
16. Deeds SA, Dowdell KJ, Chew LD, Ackerman SL. Implementing an opt-in eConsult program at seven academic medical centers: a qualitative analysis of primary care provider experiences. J Gen Intern Med. 2019;34(8):1427-1433. doi:10.1007/s11606-019-05067-7
17. Rodriguez KL, Burkitt KH, Bayliss NK, et al. Veteran, primary care provider, and specialist satisfaction with electronic consultation. JMIR Med Inform. 2015;3(1):e5. Published 2015 Jan 14. doi:10.2196/medinform.3725
18. Gupte G, Vimalananda V, Simon SR, DeVito K, Clark J, Orlander JD. Disruptive innovation: implementation of electronic consultations in a Veterans Affairs Health Care System. JMIR Med Inform. 2016;4(1):e6. Published 2016 Feb 12. doi:10.2196/medinform.4801
19. Feldstein AC, Glasgow RE. A practical, robust implementation and sustainability model (PRISM) for integrating research findings into practice. Jt Comm J Qual Patient Saf. 2008;34(4):228-243. doi:10.1016/s1553-7250(08)34030-6
20. Patton MQ. Qualitative Research and Evaluation Methods. 3rd ed. Sage Publications; 2002.
21. Bradley EH, Curry LA, Devers KJ. Qualitative data analysis for health services research: developing taxonomy, themes, and theory. Health Serv Res. 2007;42(4):1758-1772. doi:10.1111/j.1475-6773.2006.00684.x
22. Kim EJ, Orlander JD, Afable M, et al. Cardiology electronic consultation (e-consult) use by primary care providers at VA medical centres in New England. J Telemed Telecare. 2019;25(6):370-377. doi:10.1177/1357633X18774468
Electronic consultation (e-consult) is designed to increase access to specialty care by facilitating communication between primary care and specialty clinicians without the need for outpatient face-to-face encounters.1–4 In 2011, the US Department of Veterans Affairs (VA) implemented an e-consult program as a component of its overall strategy to increase access to specialty services, reduce costs of care, and reduce appointment travel burden on patients.
E-consult has substantially increased within the VA since its implementation.5,6 Consistent with limited evaluations from other health care systems, evaluations of the VA e-consult program demonstrated reduced costs, reduced travel time for patients, and improved access to specialty care.2,5–11 However, there is wide variation in e-consult use across VA specialties, facilities, and regions.5,6,12,13 For example, hematology, preoperative evaluation, neurosurgery, endocrinology, and infectious diseases use e-consults more frequently when compared with in-person consults in the VA.6 Reasons for this variation or specific barriers and facilitators of using e-consults have not been described.
Prior qualitative studies report that primary care practitioners (PCPs) describe e-consults as convenient, educational, beneficial for patient care, and useful for improving patient access to specialty care.8,14,15 One study identified limited PCP knowledge of e-consults as a barrier to use.16 Specialists have reported that e-consult improves clinical communication, but increases their workload.1,14,17,18 These studies did not assess perspectives from both clinicians who initiate e-consults and those who respond to them. This is the first qualitative study to assess e-consult perceptions from perspectives of both PCPs and specialists among a large, national sample of VA clinicians who use e-consults. The objective of this study was to understand perspectives of e-consults between PCPs and specialists that may be relevant to increasing adoption in the VA.
Methods
The team (CL, ML, PG, 2 analysts under the guidance of GS and JS and support from RRK, and a biostatistician) conducted semistructured interviews with PCPs, specialists, and specialty division leaders who were employed by VA in 2016 and 2017. Specialties of interest were identified by the VA Office of Specialty Care and included cardiology, endocrinology, gastroenterology, and hematology.
E-Consult Procedures
Within the VA, the specific procedures used to initiate, triage and manage e-consults are coordinated at VA medical centers (VAMCs) and at the Veterans Integrated Service Network (VISN) regional level. E-consult can be requested by any clinician. Generally, e-consults are initiated by PCPs through standardized, specialty-specific templates. Recipients, typically specialists, respond by answering questions, suggesting additional testing and evaluation, or requesting an in-person visit. Communication is documented in the patient’s electronic health record (EHR). Specialists receive different levels of workload credit for responding to e-consults similar to a relative value unit reimbursement model. Training in the use of e-consults is available to practitioners but may vary at local and regional levels.
Recruitment
Our sample included PCPs, specialists, and specialty care division leaders. We first quantified e-consult rates (e-consults per 100 patient visits) between July 2016 and June 2017 at VA facilities within primary care and the 4 priority specialties and identified the 30 sites with the highest e-consult rates and 30 sites with the lowest e-consult rates. Sites with < 500 total visits, < 3 specialties, or without any e-consult visit during the study period were excluded. E-consult rates at community-based outpatient clinics were included with associated VAMCs. We then stratified PCPs by whether they were high or low users of e-consults (determined by the top and bottom users within each site) and credentials (MD vs nurse practitioner [NP] or physician assistant [PA]). Specialists were sampled based on their rate of use relative to colleagues within their site and the use rate of their division. We sampled division chiefs and individuals who had > 300 total visits and 1 e-consult during the study period. To recruit participants, the primary investigator sent an initial email and 2 reminder emails. The team followed up with respondents to schedule an interview.
Interview guides were designed to elicit rich descriptions of barriers and facilitators to e-consult use (eAppendix available at doi:10.12788/fp.0214). The team used the Practical Robust Implementation and Sustainability Model (PRISM), which considers factors along 6 domains for intervention planning, implementation, and sustainment.19 Telephone interviews lasted about 20 minutes and were conducted between September 2017 and March 2018. Interviews were recorded and transcribed verbatim.
Analysis
The team used an iterative, team-based, inductive/deductive approach to conventional content analysis.20,21 Initial code categories were created so that we could identify e-consult best practices—facilitators of e-consult that were recommended by both PCPs and specialists. Inductive codes or labels applied to identify meaningful quotations, phrases, or key terms were used to identify emergent ideas and were added throughout coding after discussion among team members. Consensus was reached using a team-based approach.21 Four analysts independently coded the same 3 transcripts and met to discuss points of divergence and convergence. Analyses continued with emergent themes, categories, and conclusions. Atlas.ti. v.7 was used for coding and data management.22
Results
We conducted 34 interviews with clinicians (Table 1) from 13 VISNs. Four best-practice themes emerged among both PCPs and specialists, including that e-consults (1) are best suited for certain clinical questions and patients; (2) require relevant background information from requesting clinicians and clear recommendations from responding clinicians; (3) are a novel opportunity to provide efficient, transparent care; and (4) may not be fully adopted due to low awareness. Supporting quotations for the following findings are provided in Table 2.
Specific Clinical Questions and Patients
PCPs described specific patients and questions for which they most frequently used e-consults, such as for medication changes (Q1), determining treatment steps (Q2,3), and or clarifying laboratory or imaging findings. PCPs frequently used e-consults for patients who did not require a physical examination or when specialists could make recommendations without seeing patients face-to-face (Q3). An important use of e-consults described by PCPs was for treating conditions they could manage within primary care if additional guidance were available (Q4). Several PCPs and specialists also noted that e-consults were particularly useful for patients who were unable to travel or did not want face-to-face appointments (Q5). Notably, PCPs and specialists mentioned situations for which e-consults were inappropriate, including when a detailed history or physical examination was needed, or if a complex condition was suspected (Q6).
Background Data and Clear Recommendations
Participants described necessary data that should be included in high-quality e-consults. Specialists voiced frustration in time-consuming chart reviews that were often necessary when these data were not provided by the requestor. In some cases, specialists were unable to access necessary EHR data, which delayed responses (Q7). PCPs noted that the most useful responses carefully considered the question, used current patient information to determine treatments, provided clear recommendations, and defined who was responsible for next steps (Q8). PCPs and specialists stated that e-consult templates that required relevant information facilitated high-quality e-consults. Neither wanted to waste the other clinician's time (Q8).
A Novel Opportunity
Many PCPs felt that e-consults improved communication (eg, efficiency, response time), established new communication between clinicians, and reduced patients’ appointment burden (Q10, Q11). Many specialists felt that e-consults improved documentation of communication between clinicians and increased transparency of clinical decisions (Q12). Additionally, many specialists mentioned that e-consults capture previously informal curbside consults, enabling them to receive workload credit (Q13).
Lack of Awareness
Some noted that the biggest barrier to e-consults was not being aware of them generally, or which specialties offer e-consults (Q14). One PCP described e-consults as the best kept secret and found value in sharing the utility of e-consults with colleagues (Q15). All participants, including those who did not frequently use e-consults, felt that e-consults improved the quality of care by providing more timely care or better answers to clinical questions (Q16). Several practitioners also felt that e-consults increased access to specialty care. For example, specialists reported that e-consults enabled them to better manage patient load by using e-consults to answer relatively simple questions, reserving face-to-face consults for more complex patients (Q17).
Discussion
The objective of this study was to identify potential best practices for e-consults that may help increase their quality and use within the VA. We built on prior studies that offered insights on PCP and specialists’ overall satisfaction with e-consult by identifying several themes relevant to the further adoption of e-consults in the VA and elsewhere without a face-to-face visit.8,13,14,16–18 Future work may be beneficial in identifying whether the study themes identified can explain variation in e-consult use or whether addressing these factors might lead to increased or higher quality e-consult use. We are unaware of any qualitative study of comparable scale in a different health care system. Further, this is the first study to assess perspectives on e-consults among those who initiate and respond to them within the same health care system. Perhaps the most important finding from this study is that e-consults are generally viewed favorably, which is a necessary leverage point to increase their adoption within the system.
Clinicians reported several benefits to e-consults, including timely responses to clinical questions, efficient communication, allow for documentation of specialist recommendations, and help capture workload. These benefits are consistent with prior literature that indicates both PCPs and specialists in the VA and other health care systems feel that e-consults improves communication, decreases unnecessary visits, and improves quality of care.1,14,17,18 In particular, clinicians reported that e-consults improve their practice efficiency and efficacy. This is of critical importance given the pressures of providing timely access to primary and specialty care within the VA. Interestingly, many VA practitioners were unaware which specialties offered e-consults within their facilities, reflecting previous work showing that PCPs are often unaware of e-consult options.16 This may partially explain variation in e-consult use. Increasing awareness and educating clinicians on the benefits of e-consults may help promote use among non- and low users.
A common theme reported by both groups was the importance of providing necessary information within e-consult questions and responses. Specialists felt there was a need to ensure that PCPs provide relevant and patient-specific information that would enable them to efficiently and accurately answer questions without the need for extensive EHR review. This reflects previous work showing that specialists are often unable to respond to e-consult requests because they do not contain sufficient information.22 PCPs described a need to ensure that specialists’ responses included information that was detailed enough to make clinical decisions without the need for a reconsult. This highlights a common challenge to medical consultation, in that necessary or relevant information may not be apparent to all clinicians. To address this, there may be a role in developing enhanced, flexible templating that elicits necessary patient-specific information. Such a template may automatically pull relevant data from the EHR and prompt clinicians to provide important information. We did not assess how perspectives of templates varied, and further work could help define precisely what constitutes an effective template, including how it should capture appropriate patient data and how this impacts acceptability or use of e-consults generally. Collaboratively developed service agreements and e-consult templates could help guide PCPs and specialists to engage in efficient communication.
Another theme among both groups was that e-consult is most appropriate within specific clinical scenarios. Examples included review of laboratory results, questions about medication changes, or for patients who were reluctant to travel to appointments. Identifying and promoting specific opportunities for e-consults may help increase their use and align e-consult practices with scenarios that are likely to provide the most benefit to patients. For example, it could be helpful to understand the distance patients must travel for specialty care. Providing that information during clinical encounters could trigger clinicians to consider e-consults as an option. Future work might aim to identify clinical scenarios that clinicians feel are not well suited for e-consults and determine how to adapt them for those scenarios.
Limitations
Generalizability of these findings is limited given the qualitative study design. Participants’ descriptions of experiences with e-consults reflect the experiences of clinicians in the VA and may not reflect clinicians in other settings. We also interviewed a sample of clinicians who were already using e-consults. Important information could be learned from future work with those who have not yet adopted e-consult procedures or adopted and abandoned them.
Conclusions
E-consult is perceived as beneficial by VA PCPs and specialists. Participants suggested using e-consults for appropriate questions or patients and including necessary information and next steps in both the initial e-consult and response. Finding ways to facilitate e-consults with these suggestions in mind may increase delivery of high-quality e-consults. Future work could compare the findings of this work to similar work assessing clinicians perceptions of e-consults outside of the VA.
Electronic consultation (e-consult) is designed to increase access to specialty care by facilitating communication between primary care and specialty clinicians without the need for outpatient face-to-face encounters.1–4 In 2011, the US Department of Veterans Affairs (VA) implemented an e-consult program as a component of its overall strategy to increase access to specialty services, reduce costs of care, and reduce appointment travel burden on patients.
E-consult has substantially increased within the VA since its implementation.5,6 Consistent with limited evaluations from other health care systems, evaluations of the VA e-consult program demonstrated reduced costs, reduced travel time for patients, and improved access to specialty care.2,5–11 However, there is wide variation in e-consult use across VA specialties, facilities, and regions.5,6,12,13 For example, hematology, preoperative evaluation, neurosurgery, endocrinology, and infectious diseases use e-consults more frequently when compared with in-person consults in the VA.6 Reasons for this variation or specific barriers and facilitators of using e-consults have not been described.
Prior qualitative studies report that primary care practitioners (PCPs) describe e-consults as convenient, educational, beneficial for patient care, and useful for improving patient access to specialty care.8,14,15 One study identified limited PCP knowledge of e-consults as a barrier to use.16 Specialists have reported that e-consult improves clinical communication, but increases their workload.1,14,17,18 These studies did not assess perspectives from both clinicians who initiate e-consults and those who respond to them. This is the first qualitative study to assess e-consult perceptions from perspectives of both PCPs and specialists among a large, national sample of VA clinicians who use e-consults. The objective of this study was to understand perspectives of e-consults between PCPs and specialists that may be relevant to increasing adoption in the VA.
Methods
The team (CL, ML, PG, 2 analysts under the guidance of GS and JS and support from RRK, and a biostatistician) conducted semistructured interviews with PCPs, specialists, and specialty division leaders who were employed by VA in 2016 and 2017. Specialties of interest were identified by the VA Office of Specialty Care and included cardiology, endocrinology, gastroenterology, and hematology.
E-Consult Procedures
Within the VA, the specific procedures used to initiate, triage and manage e-consults are coordinated at VA medical centers (VAMCs) and at the Veterans Integrated Service Network (VISN) regional level. E-consult can be requested by any clinician. Generally, e-consults are initiated by PCPs through standardized, specialty-specific templates. Recipients, typically specialists, respond by answering questions, suggesting additional testing and evaluation, or requesting an in-person visit. Communication is documented in the patient’s electronic health record (EHR). Specialists receive different levels of workload credit for responding to e-consults similar to a relative value unit reimbursement model. Training in the use of e-consults is available to practitioners but may vary at local and regional levels.
Recruitment
Our sample included PCPs, specialists, and specialty care division leaders. We first quantified e-consult rates (e-consults per 100 patient visits) between July 2016 and June 2017 at VA facilities within primary care and the 4 priority specialties and identified the 30 sites with the highest e-consult rates and 30 sites with the lowest e-consult rates. Sites with < 500 total visits, < 3 specialties, or without any e-consult visit during the study period were excluded. E-consult rates at community-based outpatient clinics were included with associated VAMCs. We then stratified PCPs by whether they were high or low users of e-consults (determined by the top and bottom users within each site) and credentials (MD vs nurse practitioner [NP] or physician assistant [PA]). Specialists were sampled based on their rate of use relative to colleagues within their site and the use rate of their division. We sampled division chiefs and individuals who had > 300 total visits and 1 e-consult during the study period. To recruit participants, the primary investigator sent an initial email and 2 reminder emails. The team followed up with respondents to schedule an interview.
Interview guides were designed to elicit rich descriptions of barriers and facilitators to e-consult use (eAppendix available at doi:10.12788/fp.0214). The team used the Practical Robust Implementation and Sustainability Model (PRISM), which considers factors along 6 domains for intervention planning, implementation, and sustainment.19 Telephone interviews lasted about 20 minutes and were conducted between September 2017 and March 2018. Interviews were recorded and transcribed verbatim.
Analysis
The team used an iterative, team-based, inductive/deductive approach to conventional content analysis.20,21 Initial code categories were created so that we could identify e-consult best practices—facilitators of e-consult that were recommended by both PCPs and specialists. Inductive codes or labels applied to identify meaningful quotations, phrases, or key terms were used to identify emergent ideas and were added throughout coding after discussion among team members. Consensus was reached using a team-based approach.21 Four analysts independently coded the same 3 transcripts and met to discuss points of divergence and convergence. Analyses continued with emergent themes, categories, and conclusions. Atlas.ti. v.7 was used for coding and data management.22
Results
We conducted 34 interviews with clinicians (Table 1) from 13 VISNs. Four best-practice themes emerged among both PCPs and specialists, including that e-consults (1) are best suited for certain clinical questions and patients; (2) require relevant background information from requesting clinicians and clear recommendations from responding clinicians; (3) are a novel opportunity to provide efficient, transparent care; and (4) may not be fully adopted due to low awareness. Supporting quotations for the following findings are provided in Table 2.
Specific Clinical Questions and Patients
PCPs described specific patients and questions for which they most frequently used e-consults, such as for medication changes (Q1), determining treatment steps (Q2,3), and or clarifying laboratory or imaging findings. PCPs frequently used e-consults for patients who did not require a physical examination or when specialists could make recommendations without seeing patients face-to-face (Q3). An important use of e-consults described by PCPs was for treating conditions they could manage within primary care if additional guidance were available (Q4). Several PCPs and specialists also noted that e-consults were particularly useful for patients who were unable to travel or did not want face-to-face appointments (Q5). Notably, PCPs and specialists mentioned situations for which e-consults were inappropriate, including when a detailed history or physical examination was needed, or if a complex condition was suspected (Q6).
Background Data and Clear Recommendations
Participants described necessary data that should be included in high-quality e-consults. Specialists voiced frustration in time-consuming chart reviews that were often necessary when these data were not provided by the requestor. In some cases, specialists were unable to access necessary EHR data, which delayed responses (Q7). PCPs noted that the most useful responses carefully considered the question, used current patient information to determine treatments, provided clear recommendations, and defined who was responsible for next steps (Q8). PCPs and specialists stated that e-consult templates that required relevant information facilitated high-quality e-consults. Neither wanted to waste the other clinician's time (Q8).
A Novel Opportunity
Many PCPs felt that e-consults improved communication (eg, efficiency, response time), established new communication between clinicians, and reduced patients’ appointment burden (Q10, Q11). Many specialists felt that e-consults improved documentation of communication between clinicians and increased transparency of clinical decisions (Q12). Additionally, many specialists mentioned that e-consults capture previously informal curbside consults, enabling them to receive workload credit (Q13).
Lack of Awareness
Some noted that the biggest barrier to e-consults was not being aware of them generally, or which specialties offer e-consults (Q14). One PCP described e-consults as the best kept secret and found value in sharing the utility of e-consults with colleagues (Q15). All participants, including those who did not frequently use e-consults, felt that e-consults improved the quality of care by providing more timely care or better answers to clinical questions (Q16). Several practitioners also felt that e-consults increased access to specialty care. For example, specialists reported that e-consults enabled them to better manage patient load by using e-consults to answer relatively simple questions, reserving face-to-face consults for more complex patients (Q17).
Discussion
The objective of this study was to identify potential best practices for e-consults that may help increase their quality and use within the VA. We built on prior studies that offered insights on PCP and specialists’ overall satisfaction with e-consult by identifying several themes relevant to the further adoption of e-consults in the VA and elsewhere without a face-to-face visit.8,13,14,16–18 Future work may be beneficial in identifying whether the study themes identified can explain variation in e-consult use or whether addressing these factors might lead to increased or higher quality e-consult use. We are unaware of any qualitative study of comparable scale in a different health care system. Further, this is the first study to assess perspectives on e-consults among those who initiate and respond to them within the same health care system. Perhaps the most important finding from this study is that e-consults are generally viewed favorably, which is a necessary leverage point to increase their adoption within the system.
Clinicians reported several benefits to e-consults, including timely responses to clinical questions, efficient communication, allow for documentation of specialist recommendations, and help capture workload. These benefits are consistent with prior literature that indicates both PCPs and specialists in the VA and other health care systems feel that e-consults improves communication, decreases unnecessary visits, and improves quality of care.1,14,17,18 In particular, clinicians reported that e-consults improve their practice efficiency and efficacy. This is of critical importance given the pressures of providing timely access to primary and specialty care within the VA. Interestingly, many VA practitioners were unaware which specialties offered e-consults within their facilities, reflecting previous work showing that PCPs are often unaware of e-consult options.16 This may partially explain variation in e-consult use. Increasing awareness and educating clinicians on the benefits of e-consults may help promote use among non- and low users.
A common theme reported by both groups was the importance of providing necessary information within e-consult questions and responses. Specialists felt there was a need to ensure that PCPs provide relevant and patient-specific information that would enable them to efficiently and accurately answer questions without the need for extensive EHR review. This reflects previous work showing that specialists are often unable to respond to e-consult requests because they do not contain sufficient information.22 PCPs described a need to ensure that specialists’ responses included information that was detailed enough to make clinical decisions without the need for a reconsult. This highlights a common challenge to medical consultation, in that necessary or relevant information may not be apparent to all clinicians. To address this, there may be a role in developing enhanced, flexible templating that elicits necessary patient-specific information. Such a template may automatically pull relevant data from the EHR and prompt clinicians to provide important information. We did not assess how perspectives of templates varied, and further work could help define precisely what constitutes an effective template, including how it should capture appropriate patient data and how this impacts acceptability or use of e-consults generally. Collaboratively developed service agreements and e-consult templates could help guide PCPs and specialists to engage in efficient communication.
Another theme among both groups was that e-consult is most appropriate within specific clinical scenarios. Examples included review of laboratory results, questions about medication changes, or for patients who were reluctant to travel to appointments. Identifying and promoting specific opportunities for e-consults may help increase their use and align e-consult practices with scenarios that are likely to provide the most benefit to patients. For example, it could be helpful to understand the distance patients must travel for specialty care. Providing that information during clinical encounters could trigger clinicians to consider e-consults as an option. Future work might aim to identify clinical scenarios that clinicians feel are not well suited for e-consults and determine how to adapt them for those scenarios.
Limitations
Generalizability of these findings is limited given the qualitative study design. Participants’ descriptions of experiences with e-consults reflect the experiences of clinicians in the VA and may not reflect clinicians in other settings. We also interviewed a sample of clinicians who were already using e-consults. Important information could be learned from future work with those who have not yet adopted e-consult procedures or adopted and abandoned them.
Conclusions
E-consult is perceived as beneficial by VA PCPs and specialists. Participants suggested using e-consults for appropriate questions or patients and including necessary information and next steps in both the initial e-consult and response. Finding ways to facilitate e-consults with these suggestions in mind may increase delivery of high-quality e-consults. Future work could compare the findings of this work to similar work assessing clinicians perceptions of e-consults outside of the VA.
1. Battaglia C, Lambert-Kerzner A, Aron DC, et al. Evaluation of e-consults in the VHA: provider perspectives. Fed Pract. 2015;32(7):42-48.
2. Haverhals LM, Sayre G, Helfrich CD, et al. E-consult implementation: lessons learned using consolidated framework for implementation research. Am J Manag Care. 2015;21(12):e640-e647. Published 2015 Dec 1.
3. Sewell JL, Telischak KS, Day LW, Kirschner N, Weissman A. Preconsultation exchange in the United States: use, awareness, and attitudes. Am J Manag Care. 2014;20(12):e556-e564. Published 2014 Dec 1.
4. Horner K, Wagner E, Tufano J. Electronic consultations between primary and specialty care clinicians: early insights. Issue Brief (Commonw Fund). 2011;23:1-14.
5. Kirsh S, Carey E, Aron DC, et al. Impact of a national specialty e-consultation implementation project on access. Am J Manag Care. 2015;21(12):e648-654. Published 2015 Dec 1.
6. Saxon DR, Kaboli PJ, Haraldsson B, Wilson C, Ohl M, Augustine MR. Growth of electronic consultations in the Veterans Health Administration. Am J Manag Care. 2021;27(1):12-19. doi:10.37765/ajmc.2021.88572
7. Olayiwola JN, Anderson D, Jepeal N, et al. Electronic consultations to improve the primary care-specialty care interface for cardiology in the medically underserved: a cluster-randomized controlled trial. Ann Fam Med. 2016;14(2):133-140. doi:10.1370/afm.1869
8. Schettini P, Shah KP, O’Leary CP, et al. Keeping care connected: e-Consultation program improves access to nephrology care. J Telemed Telecare. 2019;25(3):142-150. doi:10.1177/1357633X17748350
9. Whittington MD, Ho PM, Kirsh SR, et al. Cost savings associated with electronic specialty consultations. Am J Manag Care. 2021;27(1):e16-e23. Published 2021 Jan 1. doi:10.37765/ajmc.2021.88579
10. Shipherd JC, Kauth MR, Matza A. Nationwide interdisciplinary e-consultation on transgender care in the Veterans Health Administration. Telemed J E Health. 2016;22(12):1008-1012. doi:10.1089/tmj.2016.0013
11. Strymish J, Gupte G, Afable MK, et al. Electronic consultations (E-consults): advancing infectious disease care in a large Veterans Affairs Healthcare System. Clin Infect Dis. 2017;64(8):1123-1125. doi:10.1093/cid/cix058
12. Williams KM, Kirsh S, Aron D, et al. Evaluation of the Veterans Health Administration’s Specialty Care Transformational Initiatives to promote patient-centered delivery of specialty care: a mixed-methods approach. Telemed J E-Health. 2017;23(7):577-589. doi:10.1089/tmj.2016.0166
13. US Department of Veterans Affairs, Veterans Health Administration, Specialty Care Transformational Initiative Evaluation Center. Evaluation of specialty care initiatives. Published 2013.
14. Vimalananda VG, Gupte G, Seraj SM, et al. Electronic consultations (e-consults) to improve access to specialty care: a systematic review and narrative synthesis. J Telemed Telecare. 2015;21(6):323-330. doi:10.1177/1357633X15582108
15. Lee M, Leonard C, Greene P, et al. Perspectives of VA primary care clinicians toward electronic consultation-related workload burden. JAMA Netw Open. 2020;3(10):e2018104. Published 2020 Oct 1. doi:10.1001/jamanetworkopen.2020.18104
16. Deeds SA, Dowdell KJ, Chew LD, Ackerman SL. Implementing an opt-in eConsult program at seven academic medical centers: a qualitative analysis of primary care provider experiences. J Gen Intern Med. 2019;34(8):1427-1433. doi:10.1007/s11606-019-05067-7
17. Rodriguez KL, Burkitt KH, Bayliss NK, et al. Veteran, primary care provider, and specialist satisfaction with electronic consultation. JMIR Med Inform. 2015;3(1):e5. Published 2015 Jan 14. doi:10.2196/medinform.3725
18. Gupte G, Vimalananda V, Simon SR, DeVito K, Clark J, Orlander JD. Disruptive innovation: implementation of electronic consultations in a Veterans Affairs Health Care System. JMIR Med Inform. 2016;4(1):e6. Published 2016 Feb 12. doi:10.2196/medinform.4801
19. Feldstein AC, Glasgow RE. A practical, robust implementation and sustainability model (PRISM) for integrating research findings into practice. Jt Comm J Qual Patient Saf. 2008;34(4):228-243. doi:10.1016/s1553-7250(08)34030-6
20. Patton MQ. Qualitative Research and Evaluation Methods. 3rd ed. Sage Publications; 2002.
21. Bradley EH, Curry LA, Devers KJ. Qualitative data analysis for health services research: developing taxonomy, themes, and theory. Health Serv Res. 2007;42(4):1758-1772. doi:10.1111/j.1475-6773.2006.00684.x
22. Kim EJ, Orlander JD, Afable M, et al. Cardiology electronic consultation (e-consult) use by primary care providers at VA medical centres in New England. J Telemed Telecare. 2019;25(6):370-377. doi:10.1177/1357633X18774468
1. Battaglia C, Lambert-Kerzner A, Aron DC, et al. Evaluation of e-consults in the VHA: provider perspectives. Fed Pract. 2015;32(7):42-48.
2. Haverhals LM, Sayre G, Helfrich CD, et al. E-consult implementation: lessons learned using consolidated framework for implementation research. Am J Manag Care. 2015;21(12):e640-e647. Published 2015 Dec 1.
3. Sewell JL, Telischak KS, Day LW, Kirschner N, Weissman A. Preconsultation exchange in the United States: use, awareness, and attitudes. Am J Manag Care. 2014;20(12):e556-e564. Published 2014 Dec 1.
4. Horner K, Wagner E, Tufano J. Electronic consultations between primary and specialty care clinicians: early insights. Issue Brief (Commonw Fund). 2011;23:1-14.
5. Kirsh S, Carey E, Aron DC, et al. Impact of a national specialty e-consultation implementation project on access. Am J Manag Care. 2015;21(12):e648-654. Published 2015 Dec 1.
6. Saxon DR, Kaboli PJ, Haraldsson B, Wilson C, Ohl M, Augustine MR. Growth of electronic consultations in the Veterans Health Administration. Am J Manag Care. 2021;27(1):12-19. doi:10.37765/ajmc.2021.88572
7. Olayiwola JN, Anderson D, Jepeal N, et al. Electronic consultations to improve the primary care-specialty care interface for cardiology in the medically underserved: a cluster-randomized controlled trial. Ann Fam Med. 2016;14(2):133-140. doi:10.1370/afm.1869
8. Schettini P, Shah KP, O’Leary CP, et al. Keeping care connected: e-Consultation program improves access to nephrology care. J Telemed Telecare. 2019;25(3):142-150. doi:10.1177/1357633X17748350
9. Whittington MD, Ho PM, Kirsh SR, et al. Cost savings associated with electronic specialty consultations. Am J Manag Care. 2021;27(1):e16-e23. Published 2021 Jan 1. doi:10.37765/ajmc.2021.88579
10. Shipherd JC, Kauth MR, Matza A. Nationwide interdisciplinary e-consultation on transgender care in the Veterans Health Administration. Telemed J E Health. 2016;22(12):1008-1012. doi:10.1089/tmj.2016.0013
11. Strymish J, Gupte G, Afable MK, et al. Electronic consultations (E-consults): advancing infectious disease care in a large Veterans Affairs Healthcare System. Clin Infect Dis. 2017;64(8):1123-1125. doi:10.1093/cid/cix058
12. Williams KM, Kirsh S, Aron D, et al. Evaluation of the Veterans Health Administration’s Specialty Care Transformational Initiatives to promote patient-centered delivery of specialty care: a mixed-methods approach. Telemed J E-Health. 2017;23(7):577-589. doi:10.1089/tmj.2016.0166
13. US Department of Veterans Affairs, Veterans Health Administration, Specialty Care Transformational Initiative Evaluation Center. Evaluation of specialty care initiatives. Published 2013.
14. Vimalananda VG, Gupte G, Seraj SM, et al. Electronic consultations (e-consults) to improve access to specialty care: a systematic review and narrative synthesis. J Telemed Telecare. 2015;21(6):323-330. doi:10.1177/1357633X15582108
15. Lee M, Leonard C, Greene P, et al. Perspectives of VA primary care clinicians toward electronic consultation-related workload burden. JAMA Netw Open. 2020;3(10):e2018104. Published 2020 Oct 1. doi:10.1001/jamanetworkopen.2020.18104
16. Deeds SA, Dowdell KJ, Chew LD, Ackerman SL. Implementing an opt-in eConsult program at seven academic medical centers: a qualitative analysis of primary care provider experiences. J Gen Intern Med. 2019;34(8):1427-1433. doi:10.1007/s11606-019-05067-7
17. Rodriguez KL, Burkitt KH, Bayliss NK, et al. Veteran, primary care provider, and specialist satisfaction with electronic consultation. JMIR Med Inform. 2015;3(1):e5. Published 2015 Jan 14. doi:10.2196/medinform.3725
18. Gupte G, Vimalananda V, Simon SR, DeVito K, Clark J, Orlander JD. Disruptive innovation: implementation of electronic consultations in a Veterans Affairs Health Care System. JMIR Med Inform. 2016;4(1):e6. Published 2016 Feb 12. doi:10.2196/medinform.4801
19. Feldstein AC, Glasgow RE. A practical, robust implementation and sustainability model (PRISM) for integrating research findings into practice. Jt Comm J Qual Patient Saf. 2008;34(4):228-243. doi:10.1016/s1553-7250(08)34030-6
20. Patton MQ. Qualitative Research and Evaluation Methods. 3rd ed. Sage Publications; 2002.
21. Bradley EH, Curry LA, Devers KJ. Qualitative data analysis for health services research: developing taxonomy, themes, and theory. Health Serv Res. 2007;42(4):1758-1772. doi:10.1111/j.1475-6773.2006.00684.x
22. Kim EJ, Orlander JD, Afable M, et al. Cardiology electronic consultation (e-consult) use by primary care providers at VA medical centres in New England. J Telemed Telecare. 2019;25(6):370-377. doi:10.1177/1357633X18774468
The Group Practice Manager in the VHA: A View From the Field
The Veterans Health Administration (VHA) provides care for 9 million veterans at 1,255 health care sites linked to one of 170 local medical systems.1 Recognizing that providing timely care requires effective access management, the US Congress mandated training of VHA staff to manage and improve access to care but did not provide additional local funds for new positions.2 In response, the VHA created the group practice manager (GPM), a new position responsible for improving clinical practice management and unifying access improvement across leadership levels, professions, and services within each local medical system.
In May 2015, the VHA began hiring and training GPMs to spearhead management of access to services. The US Department of Veterans Affairs (VA) Office of Veteran Access to Care spearheaded GPM training, including face-to-face sessions, national calls, webinars, and educational materials. Five local medical systems were selected by the VA Office of Veteran Access to Care to implement the GPM role to allow for an early evaluation of the program that would inform a subsequent nationwide rollout. Implementation of the GPM role remained in the hands of local medical systems.
Longer wait times are shown to impact patient health.3,4 Open access scheduling and other patient-centered access management interventions have been shown to improve availability of primary care appointments.5 However, little empirical evidence exists regarding the managers who focus on clinic access interventions. While the nonpeer-reviewed literature includes references to such roles, including GPMs, the empirical literature has focused on external practice faciliators,6-8 “mid-level managers,”9 and clinic staff.10 We found no peer-reviewed articles on the needs and experiences of practice managers who are focused on improving access. The purpose of this study was to examine GPM prototype sites to both enhance subsequent nationwide implementation and to advance empirical literature on managing patient access within health care.
Methods
In 2015, the VA identified 5 prototype sites representing diverse geographic locations, size, and complexity for the implementation of the GPM role (Table 1). These sites self-identified as having clinical practice management experience. GPMs attended 4 training sessions between February and August 2015.
Data Collection
Participants from each prototype site included GPMs, national trainers, clinic leaders, and frontline staff. Table 2 includes the roles and sample size. Participants were recruited through purposive sampling followed by snowball sampling until thematic saturation was reached (the point at which subsequent data fail to produce new findings across sites and roles of interest).
Guided by the Consolidated Framework for Implementation Research (CFIR), the research team developed semistructured interview guides tailored to participants’ roles to elicit rich descriptions regarding overall impressions, practice management strategies, goals, activities, relationship to clinic roles, data analytics usage, challenges, barriers, and facilitators.11 These guides included open-ended questions and structured prompts utilizing participant language for follow-up probes to minimize interviewing bias (eAppendix:
Data Analysis
Data were analyzed using iterative deductive and inductive content analysis.12 Deductive content analysis consisted of identifying quotes that fit within preidentified categories (ie, perceptions of national effort, organizational structure for GPM, challenges, facilitators, metrics and tools, and mobilizing access culture) developed by the interdisciplinary research team. Further content analysis entailed open-coding and iteratively revisiting and reconciling codes associated within each preidentified category as new codes emerged. The team analyzed the resulting codes to inductively and iteratively identify and stabilize themes regarding the GPM role: roles and tasks, GPM characteristics, issues, and challenges. Through this process we moved coded data to reconciled descriptions suited to addressing the purposes of this study. Dedoose 7.0.23 software was used for qualitative data management and analysis.
Results
The study identified participants’ overall impressions of the GPM initiative and key themes within 4 major domains regarding implementing the GPM role: roles and tasks (implementing clinic practice management, leading patient access, supporting data analytics, and enabling self and staff); GPM characteristics (familiarity with clinical services, knowledge of VHA systems, ability to analyze patient data, communication skills, and the ability to work with others); and issues, and challenges (technical, social, and structural).
Overall Impressions
Interviewees perceived the GPM initiative as a consolidation of existing distributed responsibilities into one role that directly reported to local top-level management with indirect reporting to national leaders. Many of the sites reported that they had designated or planned to designate a role resembling the GPM prior to the initiative. “There are staff who’ve been doing some of this work all along,” a GPM noted. “We just didn’t have them grouped together. They weren’t necessarily all working in the same type of service under the same type of structure.”
Whether the GPM position was new or not, participants referenced the importance and challenges of engaging the local facility in recognizing the agency associated with the GPM position. According to national support, the staff are trying to get the facility to understand “why the group practice manager is so important… we’ve got to embed that standard position in the system.”
While the GPM was recognized as the hub of access management, respondents recognized that transformation regarding access involved many players. “We have to create [an] orchestrated team inside each facility,” an advisor argued.
Respondents discussed how the initiative allows local facilities to appoint a specific person with a specific title and role who helps facilitate, organize, and legitimize an access focus at their sites. One GPM interviewee noted how the initiative helped refocus some of their previously less centralized efforts. “We’ve always looked at productivity; we’ve always looked at access; we’ve always looked at efficiency. I think the bigger difference is now there are individuals identified in the clinics, as practice managers as well…I interact with them. They interact with individual clinic staff, and it’s more of a group process than a single individual.”
The value of having tools available and being able to track and manage patient care as a specific example of the positive impact of this new role was noted by participants. A GPM noted that many health care providers will be happy to have tools to better manage their services and a process “that flows from a service level all the way up to executive management, where there is a common interest in making those things happen—I think that’s going to be a tremendous help.”
Participants expressed concern that the national GPM rollout would be a one-size-fits-all approach. These respondents emphasized the need to have the flexibility to customize their activities to meet their unique site and patient needs.
GPM Roles and Tasks
Participants described 4 primary roles that the GPM was expected to fill: implementing clinic practice management, leading patient access, supporting data analytics, and enabling self and staff. Some activities overlapped in that they served to support multiple role areas (Figure 1).
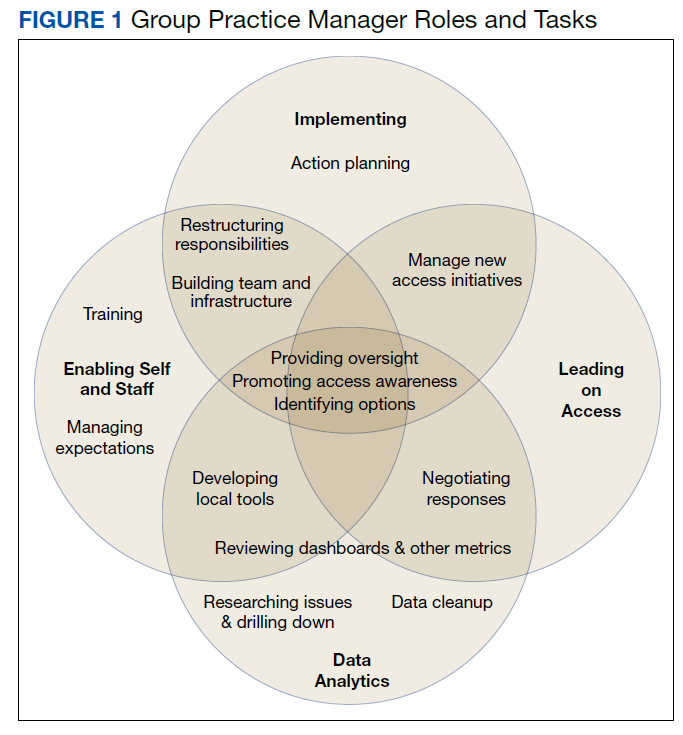
Implementing clinic practice management. In the early stages of the initiative, the GPM’s primary role was to prepare the facility to implement a standardized set of clinic practice management (CPM) team processes. Part of standardizing the CPM process was defining the scope and tasks of the GPM, which requires significant planning for the implementation. “My big job is to finalize what we think group practice management is going to look [like] here,” a GPM reported.
Each prototype site had latitude to interpret the GPM initiative in a way that would work in their context within given VHA boundaries and ongoing initiatives. To achieve the high-level vision and purpose, the GPM first had to develop action plans that accounted for the operating environment of the facility. According to one GPM, VA national officials are “constantly” asking for action plans, which required significant time by specific deadlines. “They want an action plan [and to] clean up all your consults, [and to] clean up all your recall reminders.”
Leading on improving access efforts. Participants saw the GPM as the central staff member responsible for providing oversight of any activities and people involved in improving access. “I ensure everybody is doing what they’re supposed to do,” one GPM reported. When the GPM sees areas that are not being addressed, the individual tries to develop a process or training to “close those gaps.”
GPMs promoted an awareness of their goals, changes in process, and new tools accompanying the initiative. However, other access initiatives were occurring simultaneously creating confusion for health care providers and patients; thus GPMs found they were managing a wide array of related initiatives.
GPMs have to negotiate with leaders across the VHA facility, many of whom operated at a higher leadership level and had different priorities, to address access problems.
“I’m a lieutenant as a GPM in a clinic, a GPM noted. “How is the lieutenant going to talk to a major or a colonel in the clinic and say your clinic has problems. How[‘s] that lieutenant...going to do that? With people skills!”
Managing expectations about the speed and to what extent a problem could be resolved was an important part of the GPM leadership role. “I see myself as managing expectations both up to the leadership and down to the frontline,” a GPM explained. “I find myself talking to leadership [about] our progress. But at the same time, we have to say, ‘not everything can be fixed overnight.’”
Providing leadership on access-related issues included developing a range of options for addressing patient access problems. One analytics manager recounted how the GPM role led to evaluating how physical space limited efficiency in clinic flow. The first step was identifying possible additional rooms to improve clinic flow. This required working with the space committee to “get someone to look at our overarching space and find someplace else for them to sit” to avoid adding to congestion in the clinic area.
Supporting data analytics.
GPMs routinely immersed themselves in the data to understand access issues. GPMs worked with clinic leaders to identify the underlying causes and various solutions. The GPMs maintained access through administrative scrubbing of the data and finding “smart ways to get patients scheduled,” a GPM explained. “I don’t think our facility would have taken care of as many veterans in the time frame as we did....We’ve cleared over 4,000 consults that were older than 90 days. We have cleared thousands and thousands of weekly reminders.”
GPMs expressed the need for aggregated (ie, dashboard) and standardized information to efficiently address access issues. “I would like to have some more standardization on what’s being reviewed; it seems to change frequently, and so [to] be able to track and trend and have something given to me to review,” one health care provider requested. On the other hand, participants also described a need for decision support tools that would lead to action aligned with best practices. “Instead of a dashboard or something that’s just measuring their performance, it’s more something that they can look at and take action” a national support staff advisor suggested.
Enabling self and staff. GPMs felt they were most effective if they enabled themselves and stakeholders through training and by cultivating relationships and team building. Figure 2 illustrates the various stakeholders GPMs reported engaging with. The GPMS should be building relationships, bridging relationships, developing trust, and then providing a higher level of hands-on management. However, “that doesn’t really happen right now, day to day,” one member of leadership reported.
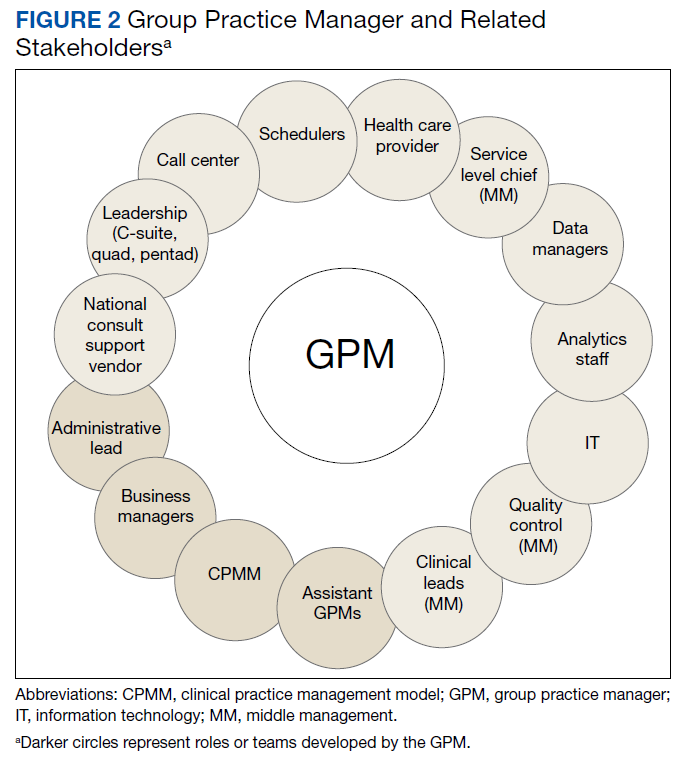
Key topics in GPM leadership training included both soft skills (change management, culture change, and negotiation skills) and crucial analytic/technical training (understanding each metric and dashboard available, data analytics, and supply/demand balancing techniques). The GPMs not only wanted to understand metrics as part of their training, but also want to know what to do about them.
An “operationalization” training approach (discerning the meaning of data, data-based decision making, and determining action from multiple options) inspired by real-life situations was preferred by participants. Other effective learning structures included job aids in the form of templated Gantt charts, process maps to guide GPMs through implementation of new processes, formalized peer learning (accumulated field insights shared during training courses), and informal peer sharing of direct experiences during calls.
GPMs also emphasized training for frontline clinical and support staff, including schedulers. VHA schedulers typically have less education and experience higher turnover rates than do other clinic staff, yet they carry out complex and critical tasks. Providing training and ensuring that any materials developed for training and education were appropriate to the level of education of schedulers was an important task for GPMs. “If they don’t understand all of the scheduling principles and potential,” one GPM explained, “we will not be maximizing the utilization of our parts.”
GPMs also provided informal education to clinicians. Participants noted GPMs have to avoid appearing to overstep their positions or presuming more knowledge and expertise than clinicians. They “have to be able to teach a physician without being overbearing, in a way a physician will accept it as advisement,” one program leader reported.
GPM knowledge, skills, and abilities. GPMs presented a complex range of knowledge, skills, and abilities, including clinical, administrative, analytics, and people skills. All interviewees reported that their prior education and experience did not sufficiently train them for the GPM role. GPMs identified a willingness to learn quickly as a critical characteristic. Many GPMs tended to have a formal education in health administration or business (eg, MBAs); others had administrative experience (eg, administrative assistance to executive leadership) or clinical training (eg, physician assistant). Detailed clinical knowledge was not expected, but clinical familiarity was helpful.
Some interviewees also mentioned previous experience and familiarity with the VHA system specifically as an advantage. This was especially true for VA outpatient flows, clinic flows, and understanding what an outpatient is in a VA context. Interviewees noted the importance of GPMs needing to be able to analyze patient demand metrics and underlying data in order to determine supply of providers and then to allocate adequate resources to complement providers. Forecasting skills were referenced as a key point. “They need to be able to be assured that they can recruit more providers if needed,” a national support staff advisor noted.
Given the importance of developing effective relationships, communication skills were mentioned by most participants and underscored as critical to establishing trust between GPMs and others as the initiative was being implemented. Interviewees indicated that relationship building was further enhanced when GPMs possessed the ability to “work with” rather than command clinicians and staff; navigate politics; and were respectful of other people’s knowledge, skills, abilities, and status. “They have to work with the nursing staff and teach them,” a leader described, “so that people understand that we are going to a different place to achieve our primary objectives and goals.”
Issues and Challenges
Participants identified several technical, social, and structural challenges and barriers to successfully implementing the GPM role.
Technical challenges. Recurring themes across all phases of data analytics were GPMs’ capability to challenge data use and use large volumes of information from multiple data sources (entering and accessing data; “drilling down” from summaries; generating reports; and analyzing and interpreting resulting metrics). Interviewees reported that information assessment and analytic support were not consistent. One GPM had a data analyst pulling reports needed to support clinical units while other GPMs trained staff to pull data. Even with support, some GPMs had issues due to limited information technology (IT) skills or access privileges leading to inefficiencies and delays. “Whenever I need anything from a programmer, I have to go through, you know, the IT gods in the sky,” one GPM remarked. “That usually takes a few months or more.”
Social challenges. Instituting the GPM role was a cultural change, and interviewees reported needing to address resistance to CPM model efforts. Resistance to change “is particularly hard in the VA just because it has a unique culture,” one leader noted. “There is a comfort in the legacy way of doing things.” The GPM initiative was introduced during a time when other national level initiatives were being implemented throughout the VHA. Fulfilling requests for information for these initiatives became the responsibility of the GPM and their team, which diverted attention from the mandate to improve access. Furthermore, GPMs were often considered the “change communicators” to clinics putting them in the role of “bad messenger,” which degraded trust and made it difficult to partner with clinicians.
Efforts to work through change management and build relationships included general program awareness presentation to internal stakeholders; including key stakeholders in GPM committees; pre-emptive conversations with unit chiefs; creating awareness of the GPM activities and progress through formal and informal update meetings; and identifying successes regarding access.
Structural challenges. The GPM role did not have direct supervision over clinical and administrative leaders, making it challenging to enact change. GPMs reported that “they do not always have authority over the area that they are being asked to manage,” which made their work difficult, requiring strong negotiation skills and political savvy to affect change. However, as the clinic staff and providers saw how the GPM could support and positively impact their practice, these challenges began to subside.
Discussion
This study provides empirical evidence regarding the implementation of a new access management strategy for health care systems focused on improving timeliness of care. First, the GPM position was seen as critical at each facility, as a single point person, to help local system leaders respond effectively to both national mandates and local context. Second, requiring the GPMs to report to the medical center director or chief of staff was important for integrating access perspectives across service lines and to facilitate a strong GPM role in strategic planning. Third, the intentional flexibility of the access management initiative, beyond the nationally specified aspects of the GPM role, was key for allowing individual sites to adapt to unique local challenges, resources, and population demands. Fourth, the initiative provided GPMs with opportunities to learn important skills and support the acquisition, utilization, and communication of a tremendous range of data toward responsive action.
According to our respondents, the GPM role demands functioning across a broad set of responsibilities; understanding the big picture as well as the complex underlying variables; engaging facility leaders, clinical and administrative staff; and prioritizing competing national and local demands. Consistent with previous findings, effective GPMs must possess a complex set of skills (interpersonal, analytic, and leadership) and the ability to create a supporting team.13
In practice, improving access at individual sites of care (VA medical centers and community-based outpatient clinics) poses significant challenges, especially in the early stages, even with the assistance of a GPM. For example, some respondents reported being overwhelmed by the volume of available data and dashboards, and responding to current requests for data analysis and dissemination sometimes impeded long range planning. Multiple national access-related initiatives and local pressures also generated excessive and potentially conflicting demands. Thus, while the creation of a GPM position seemed to be essential for the pilot sites to improve local access and timeliness to care, success also requires ongoing national and facility-wide communication, education, and support. Ongoing data analysis training and support will be critical to ensuring the sustainability of the position. Last, recruiting GPMs with the needed complex skill set may prove to be challenging, and it will be important to provide resources to identify, attract, and retain well-qualified GPMs.
Limitations and Future Work
This study was based on a small initial sample of pilot sites of varying sizes and, as such, may not reflect the experience of all VHA GPMs. In addition, the use of snowball sampling, while facilitating identification of key stakeholders, may introduce bias in participant sampling. Nonetheless, the results from this study provide findings that informed the national VHA GPM initiative and can inform further studies of practice management roles outside of the VA.
Further study of the VHA GPM implementation and similar roles in other health care systems is needed. As the GPM position is fully implemented across the VHA, large scale evaluation is needed to gain a more representative picture and allow for comparison of the GPM role at various types of facilities (eg, size, rurality, complexity, ranking based on access performance metrics).
Conclusion
Improving access to care is a central goal for health care systems. The incorporation of the GPM role is an innovative approach to improve access management strategies. Early study of prototype sites provided VHA leadership with valuable insights used to influence further rollout of this initiative. Based on our findings, national and local support are important to ongoing success. National access mandates, training, and resources should focus on ensuring sufficient GPM authority, enabling GPMs to use data, and ensuring GPMs engage with frontline clinical and administrative staff to improve veteran access to care.
1. US Department of Veterans Affairs. Veterans Health Administration. https://www.va.gov/health. Updated October 25, 2019. Accessed January 8, 2020.
2. Veterans Access, Choice, and Accountability Act of 2014. 38 CFR § 17.1500 (2014).
3. Fahmy N, Aprikian A, Al-Otaibi M, et al. Impact of treatment delay in patients with bladder cancer managed with partial cystectomy in Quebec: a population-based study. Can Urol Assoc J. 2009;3(2):131-135.
4. Hill CJ, Joonas K. The impact of unacceptable wait time on health care patients’ attitudes and actions. Health Mark Q. 2005;23(2):69-87.
5. Ansell D, Crispo JAG, Simard B, Bjerre LM. Interventions to reduce wait times for primary care appointments: a systematic review. BMC Health Serv Res. 2017;17(1):295.
6. Kotecha J, Han H, Green M, Russell G, Martin MI, Birtwhistle R. The role of the practice facilitators in Ontario primary healthcare quality improvement. BMC Fam Pract. 2015;16:93.
7. Taylor EF, Machta RM, Meyers DS, Genevro J, Peikes DN. Enhancing the primary care team to provide redesigned care: the roles of practice facilitators and care managers. Ann Fam Med. 2013;11(1):80-83.
8. Liddy C, Laferriere D, Baskerville B, Dahrouge S, Knox L, Hogg W. An overview of practice facilitation programs in Canada: current perspectives and future directions. Healthc Policy. 2013;8(3):58-67.
9. Birken SA, Lee SY, Weiner BJ, Chin MH, Schaefer CT. Improving the effectiveness of health care innovation implementation: middle managers as change agents. Med Care Res Rev. 2013;70(1):29-45.
10. Ahluwalia S, Offredy M. A qualitative study of the impact of the implementation of advanced access in primary healthcare on the working lives of general practice staff. BMC Fam Pract. 2005;6:39.
11. Damschroder LJ, Aron DC, Keith RE, Kirsh SR, Alexander JA, Lowery JC. Fostering implementation of health services research findings into practice: a consolidated framework for advancing implementation science. Implement Sci. 2009;4:50.
12. Elo S, Kyngäs H. The qualitative content analysis process. J Adv Nurs. 2008;62(1):107-115.
13. Stefl ME. Common competencies for all healthcare managers: the Healthcare Leadership Alliance model. J Healthc Manag. 2008;53(6):360-374.
The Veterans Health Administration (VHA) provides care for 9 million veterans at 1,255 health care sites linked to one of 170 local medical systems.1 Recognizing that providing timely care requires effective access management, the US Congress mandated training of VHA staff to manage and improve access to care but did not provide additional local funds for new positions.2 In response, the VHA created the group practice manager (GPM), a new position responsible for improving clinical practice management and unifying access improvement across leadership levels, professions, and services within each local medical system.
In May 2015, the VHA began hiring and training GPMs to spearhead management of access to services. The US Department of Veterans Affairs (VA) Office of Veteran Access to Care spearheaded GPM training, including face-to-face sessions, national calls, webinars, and educational materials. Five local medical systems were selected by the VA Office of Veteran Access to Care to implement the GPM role to allow for an early evaluation of the program that would inform a subsequent nationwide rollout. Implementation of the GPM role remained in the hands of local medical systems.
Longer wait times are shown to impact patient health.3,4 Open access scheduling and other patient-centered access management interventions have been shown to improve availability of primary care appointments.5 However, little empirical evidence exists regarding the managers who focus on clinic access interventions. While the nonpeer-reviewed literature includes references to such roles, including GPMs, the empirical literature has focused on external practice faciliators,6-8 “mid-level managers,”9 and clinic staff.10 We found no peer-reviewed articles on the needs and experiences of practice managers who are focused on improving access. The purpose of this study was to examine GPM prototype sites to both enhance subsequent nationwide implementation and to advance empirical literature on managing patient access within health care.
Methods
In 2015, the VA identified 5 prototype sites representing diverse geographic locations, size, and complexity for the implementation of the GPM role (Table 1). These sites self-identified as having clinical practice management experience. GPMs attended 4 training sessions between February and August 2015.
Data Collection
Participants from each prototype site included GPMs, national trainers, clinic leaders, and frontline staff. Table 2 includes the roles and sample size. Participants were recruited through purposive sampling followed by snowball sampling until thematic saturation was reached (the point at which subsequent data fail to produce new findings across sites and roles of interest).
Guided by the Consolidated Framework for Implementation Research (CFIR), the research team developed semistructured interview guides tailored to participants’ roles to elicit rich descriptions regarding overall impressions, practice management strategies, goals, activities, relationship to clinic roles, data analytics usage, challenges, barriers, and facilitators.11 These guides included open-ended questions and structured prompts utilizing participant language for follow-up probes to minimize interviewing bias (eAppendix:
Data Analysis
Data were analyzed using iterative deductive and inductive content analysis.12 Deductive content analysis consisted of identifying quotes that fit within preidentified categories (ie, perceptions of national effort, organizational structure for GPM, challenges, facilitators, metrics and tools, and mobilizing access culture) developed by the interdisciplinary research team. Further content analysis entailed open-coding and iteratively revisiting and reconciling codes associated within each preidentified category as new codes emerged. The team analyzed the resulting codes to inductively and iteratively identify and stabilize themes regarding the GPM role: roles and tasks, GPM characteristics, issues, and challenges. Through this process we moved coded data to reconciled descriptions suited to addressing the purposes of this study. Dedoose 7.0.23 software was used for qualitative data management and analysis.
Results
The study identified participants’ overall impressions of the GPM initiative and key themes within 4 major domains regarding implementing the GPM role: roles and tasks (implementing clinic practice management, leading patient access, supporting data analytics, and enabling self and staff); GPM characteristics (familiarity with clinical services, knowledge of VHA systems, ability to analyze patient data, communication skills, and the ability to work with others); and issues, and challenges (technical, social, and structural).
Overall Impressions
Interviewees perceived the GPM initiative as a consolidation of existing distributed responsibilities into one role that directly reported to local top-level management with indirect reporting to national leaders. Many of the sites reported that they had designated or planned to designate a role resembling the GPM prior to the initiative. “There are staff who’ve been doing some of this work all along,” a GPM noted. “We just didn’t have them grouped together. They weren’t necessarily all working in the same type of service under the same type of structure.”
Whether the GPM position was new or not, participants referenced the importance and challenges of engaging the local facility in recognizing the agency associated with the GPM position. According to national support, the staff are trying to get the facility to understand “why the group practice manager is so important… we’ve got to embed that standard position in the system.”
While the GPM was recognized as the hub of access management, respondents recognized that transformation regarding access involved many players. “We have to create [an] orchestrated team inside each facility,” an advisor argued.
Respondents discussed how the initiative allows local facilities to appoint a specific person with a specific title and role who helps facilitate, organize, and legitimize an access focus at their sites. One GPM interviewee noted how the initiative helped refocus some of their previously less centralized efforts. “We’ve always looked at productivity; we’ve always looked at access; we’ve always looked at efficiency. I think the bigger difference is now there are individuals identified in the clinics, as practice managers as well…I interact with them. They interact with individual clinic staff, and it’s more of a group process than a single individual.”
The value of having tools available and being able to track and manage patient care as a specific example of the positive impact of this new role was noted by participants. A GPM noted that many health care providers will be happy to have tools to better manage their services and a process “that flows from a service level all the way up to executive management, where there is a common interest in making those things happen—I think that’s going to be a tremendous help.”
Participants expressed concern that the national GPM rollout would be a one-size-fits-all approach. These respondents emphasized the need to have the flexibility to customize their activities to meet their unique site and patient needs.
GPM Roles and Tasks
Participants described 4 primary roles that the GPM was expected to fill: implementing clinic practice management, leading patient access, supporting data analytics, and enabling self and staff. Some activities overlapped in that they served to support multiple role areas (Figure 1).
Implementing clinic practice management. In the early stages of the initiative, the GPM’s primary role was to prepare the facility to implement a standardized set of clinic practice management (CPM) team processes. Part of standardizing the CPM process was defining the scope and tasks of the GPM, which requires significant planning for the implementation. “My big job is to finalize what we think group practice management is going to look [like] here,” a GPM reported.
Each prototype site had latitude to interpret the GPM initiative in a way that would work in their context within given VHA boundaries and ongoing initiatives. To achieve the high-level vision and purpose, the GPM first had to develop action plans that accounted for the operating environment of the facility. According to one GPM, VA national officials are “constantly” asking for action plans, which required significant time by specific deadlines. “They want an action plan [and to] clean up all your consults, [and to] clean up all your recall reminders.”
Leading on improving access efforts. Participants saw the GPM as the central staff member responsible for providing oversight of any activities and people involved in improving access. “I ensure everybody is doing what they’re supposed to do,” one GPM reported. When the GPM sees areas that are not being addressed, the individual tries to develop a process or training to “close those gaps.”
GPMs promoted an awareness of their goals, changes in process, and new tools accompanying the initiative. However, other access initiatives were occurring simultaneously creating confusion for health care providers and patients; thus GPMs found they were managing a wide array of related initiatives.
GPMs have to negotiate with leaders across the VHA facility, many of whom operated at a higher leadership level and had different priorities, to address access problems.
“I’m a lieutenant as a GPM in a clinic, a GPM noted. “How is the lieutenant going to talk to a major or a colonel in the clinic and say your clinic has problems. How[‘s] that lieutenant...going to do that? With people skills!”
Managing expectations about the speed and to what extent a problem could be resolved was an important part of the GPM leadership role. “I see myself as managing expectations both up to the leadership and down to the frontline,” a GPM explained. “I find myself talking to leadership [about] our progress. But at the same time, we have to say, ‘not everything can be fixed overnight.’”
Providing leadership on access-related issues included developing a range of options for addressing patient access problems. One analytics manager recounted how the GPM role led to evaluating how physical space limited efficiency in clinic flow. The first step was identifying possible additional rooms to improve clinic flow. This required working with the space committee to “get someone to look at our overarching space and find someplace else for them to sit” to avoid adding to congestion in the clinic area.
Supporting data analytics.
GPMs routinely immersed themselves in the data to understand access issues. GPMs worked with clinic leaders to identify the underlying causes and various solutions. The GPMs maintained access through administrative scrubbing of the data and finding “smart ways to get patients scheduled,” a GPM explained. “I don’t think our facility would have taken care of as many veterans in the time frame as we did....We’ve cleared over 4,000 consults that were older than 90 days. We have cleared thousands and thousands of weekly reminders.”
GPMs expressed the need for aggregated (ie, dashboard) and standardized information to efficiently address access issues. “I would like to have some more standardization on what’s being reviewed; it seems to change frequently, and so [to] be able to track and trend and have something given to me to review,” one health care provider requested. On the other hand, participants also described a need for decision support tools that would lead to action aligned with best practices. “Instead of a dashboard or something that’s just measuring their performance, it’s more something that they can look at and take action” a national support staff advisor suggested.
Enabling self and staff. GPMs felt they were most effective if they enabled themselves and stakeholders through training and by cultivating relationships and team building. Figure 2 illustrates the various stakeholders GPMs reported engaging with. The GPMS should be building relationships, bridging relationships, developing trust, and then providing a higher level of hands-on management. However, “that doesn’t really happen right now, day to day,” one member of leadership reported.
Key topics in GPM leadership training included both soft skills (change management, culture change, and negotiation skills) and crucial analytic/technical training (understanding each metric and dashboard available, data analytics, and supply/demand balancing techniques). The GPMs not only wanted to understand metrics as part of their training, but also want to know what to do about them.
An “operationalization” training approach (discerning the meaning of data, data-based decision making, and determining action from multiple options) inspired by real-life situations was preferred by participants. Other effective learning structures included job aids in the form of templated Gantt charts, process maps to guide GPMs through implementation of new processes, formalized peer learning (accumulated field insights shared during training courses), and informal peer sharing of direct experiences during calls.
GPMs also emphasized training for frontline clinical and support staff, including schedulers. VHA schedulers typically have less education and experience higher turnover rates than do other clinic staff, yet they carry out complex and critical tasks. Providing training and ensuring that any materials developed for training and education were appropriate to the level of education of schedulers was an important task for GPMs. “If they don’t understand all of the scheduling principles and potential,” one GPM explained, “we will not be maximizing the utilization of our parts.”
GPMs also provided informal education to clinicians. Participants noted GPMs have to avoid appearing to overstep their positions or presuming more knowledge and expertise than clinicians. They “have to be able to teach a physician without being overbearing, in a way a physician will accept it as advisement,” one program leader reported.
GPM knowledge, skills, and abilities. GPMs presented a complex range of knowledge, skills, and abilities, including clinical, administrative, analytics, and people skills. All interviewees reported that their prior education and experience did not sufficiently train them for the GPM role. GPMs identified a willingness to learn quickly as a critical characteristic. Many GPMs tended to have a formal education in health administration or business (eg, MBAs); others had administrative experience (eg, administrative assistance to executive leadership) or clinical training (eg, physician assistant). Detailed clinical knowledge was not expected, but clinical familiarity was helpful.
Some interviewees also mentioned previous experience and familiarity with the VHA system specifically as an advantage. This was especially true for VA outpatient flows, clinic flows, and understanding what an outpatient is in a VA context. Interviewees noted the importance of GPMs needing to be able to analyze patient demand metrics and underlying data in order to determine supply of providers and then to allocate adequate resources to complement providers. Forecasting skills were referenced as a key point. “They need to be able to be assured that they can recruit more providers if needed,” a national support staff advisor noted.
Given the importance of developing effective relationships, communication skills were mentioned by most participants and underscored as critical to establishing trust between GPMs and others as the initiative was being implemented. Interviewees indicated that relationship building was further enhanced when GPMs possessed the ability to “work with” rather than command clinicians and staff; navigate politics; and were respectful of other people’s knowledge, skills, abilities, and status. “They have to work with the nursing staff and teach them,” a leader described, “so that people understand that we are going to a different place to achieve our primary objectives and goals.”
Issues and Challenges
Participants identified several technical, social, and structural challenges and barriers to successfully implementing the GPM role.
Technical challenges. Recurring themes across all phases of data analytics were GPMs’ capability to challenge data use and use large volumes of information from multiple data sources (entering and accessing data; “drilling down” from summaries; generating reports; and analyzing and interpreting resulting metrics). Interviewees reported that information assessment and analytic support were not consistent. One GPM had a data analyst pulling reports needed to support clinical units while other GPMs trained staff to pull data. Even with support, some GPMs had issues due to limited information technology (IT) skills or access privileges leading to inefficiencies and delays. “Whenever I need anything from a programmer, I have to go through, you know, the IT gods in the sky,” one GPM remarked. “That usually takes a few months or more.”
Social challenges. Instituting the GPM role was a cultural change, and interviewees reported needing to address resistance to CPM model efforts. Resistance to change “is particularly hard in the VA just because it has a unique culture,” one leader noted. “There is a comfort in the legacy way of doing things.” The GPM initiative was introduced during a time when other national level initiatives were being implemented throughout the VHA. Fulfilling requests for information for these initiatives became the responsibility of the GPM and their team, which diverted attention from the mandate to improve access. Furthermore, GPMs were often considered the “change communicators” to clinics putting them in the role of “bad messenger,” which degraded trust and made it difficult to partner with clinicians.
Efforts to work through change management and build relationships included general program awareness presentation to internal stakeholders; including key stakeholders in GPM committees; pre-emptive conversations with unit chiefs; creating awareness of the GPM activities and progress through formal and informal update meetings; and identifying successes regarding access.
Structural challenges. The GPM role did not have direct supervision over clinical and administrative leaders, making it challenging to enact change. GPMs reported that “they do not always have authority over the area that they are being asked to manage,” which made their work difficult, requiring strong negotiation skills and political savvy to affect change. However, as the clinic staff and providers saw how the GPM could support and positively impact their practice, these challenges began to subside.
Discussion
This study provides empirical evidence regarding the implementation of a new access management strategy for health care systems focused on improving timeliness of care. First, the GPM position was seen as critical at each facility, as a single point person, to help local system leaders respond effectively to both national mandates and local context. Second, requiring the GPMs to report to the medical center director or chief of staff was important for integrating access perspectives across service lines and to facilitate a strong GPM role in strategic planning. Third, the intentional flexibility of the access management initiative, beyond the nationally specified aspects of the GPM role, was key for allowing individual sites to adapt to unique local challenges, resources, and population demands. Fourth, the initiative provided GPMs with opportunities to learn important skills and support the acquisition, utilization, and communication of a tremendous range of data toward responsive action.
According to our respondents, the GPM role demands functioning across a broad set of responsibilities; understanding the big picture as well as the complex underlying variables; engaging facility leaders, clinical and administrative staff; and prioritizing competing national and local demands. Consistent with previous findings, effective GPMs must possess a complex set of skills (interpersonal, analytic, and leadership) and the ability to create a supporting team.13
In practice, improving access at individual sites of care (VA medical centers and community-based outpatient clinics) poses significant challenges, especially in the early stages, even with the assistance of a GPM. For example, some respondents reported being overwhelmed by the volume of available data and dashboards, and responding to current requests for data analysis and dissemination sometimes impeded long range planning. Multiple national access-related initiatives and local pressures also generated excessive and potentially conflicting demands. Thus, while the creation of a GPM position seemed to be essential for the pilot sites to improve local access and timeliness to care, success also requires ongoing national and facility-wide communication, education, and support. Ongoing data analysis training and support will be critical to ensuring the sustainability of the position. Last, recruiting GPMs with the needed complex skill set may prove to be challenging, and it will be important to provide resources to identify, attract, and retain well-qualified GPMs.
Limitations and Future Work
This study was based on a small initial sample of pilot sites of varying sizes and, as such, may not reflect the experience of all VHA GPMs. In addition, the use of snowball sampling, while facilitating identification of key stakeholders, may introduce bias in participant sampling. Nonetheless, the results from this study provide findings that informed the national VHA GPM initiative and can inform further studies of practice management roles outside of the VA.
Further study of the VHA GPM implementation and similar roles in other health care systems is needed. As the GPM position is fully implemented across the VHA, large scale evaluation is needed to gain a more representative picture and allow for comparison of the GPM role at various types of facilities (eg, size, rurality, complexity, ranking based on access performance metrics).
Conclusion
Improving access to care is a central goal for health care systems. The incorporation of the GPM role is an innovative approach to improve access management strategies. Early study of prototype sites provided VHA leadership with valuable insights used to influence further rollout of this initiative. Based on our findings, national and local support are important to ongoing success. National access mandates, training, and resources should focus on ensuring sufficient GPM authority, enabling GPMs to use data, and ensuring GPMs engage with frontline clinical and administrative staff to improve veteran access to care.
The Veterans Health Administration (VHA) provides care for 9 million veterans at 1,255 health care sites linked to one of 170 local medical systems.1 Recognizing that providing timely care requires effective access management, the US Congress mandated training of VHA staff to manage and improve access to care but did not provide additional local funds for new positions.2 In response, the VHA created the group practice manager (GPM), a new position responsible for improving clinical practice management and unifying access improvement across leadership levels, professions, and services within each local medical system.
In May 2015, the VHA began hiring and training GPMs to spearhead management of access to services. The US Department of Veterans Affairs (VA) Office of Veteran Access to Care spearheaded GPM training, including face-to-face sessions, national calls, webinars, and educational materials. Five local medical systems were selected by the VA Office of Veteran Access to Care to implement the GPM role to allow for an early evaluation of the program that would inform a subsequent nationwide rollout. Implementation of the GPM role remained in the hands of local medical systems.
Longer wait times are shown to impact patient health.3,4 Open access scheduling and other patient-centered access management interventions have been shown to improve availability of primary care appointments.5 However, little empirical evidence exists regarding the managers who focus on clinic access interventions. While the nonpeer-reviewed literature includes references to such roles, including GPMs, the empirical literature has focused on external practice faciliators,6-8 “mid-level managers,”9 and clinic staff.10 We found no peer-reviewed articles on the needs and experiences of practice managers who are focused on improving access. The purpose of this study was to examine GPM prototype sites to both enhance subsequent nationwide implementation and to advance empirical literature on managing patient access within health care.
Methods
In 2015, the VA identified 5 prototype sites representing diverse geographic locations, size, and complexity for the implementation of the GPM role (Table 1). These sites self-identified as having clinical practice management experience. GPMs attended 4 training sessions between February and August 2015.
Data Collection
Participants from each prototype site included GPMs, national trainers, clinic leaders, and frontline staff. Table 2 includes the roles and sample size. Participants were recruited through purposive sampling followed by snowball sampling until thematic saturation was reached (the point at which subsequent data fail to produce new findings across sites and roles of interest).
Guided by the Consolidated Framework for Implementation Research (CFIR), the research team developed semistructured interview guides tailored to participants’ roles to elicit rich descriptions regarding overall impressions, practice management strategies, goals, activities, relationship to clinic roles, data analytics usage, challenges, barriers, and facilitators.11 These guides included open-ended questions and structured prompts utilizing participant language for follow-up probes to minimize interviewing bias (eAppendix:
Data Analysis
Data were analyzed using iterative deductive and inductive content analysis.12 Deductive content analysis consisted of identifying quotes that fit within preidentified categories (ie, perceptions of national effort, organizational structure for GPM, challenges, facilitators, metrics and tools, and mobilizing access culture) developed by the interdisciplinary research team. Further content analysis entailed open-coding and iteratively revisiting and reconciling codes associated within each preidentified category as new codes emerged. The team analyzed the resulting codes to inductively and iteratively identify and stabilize themes regarding the GPM role: roles and tasks, GPM characteristics, issues, and challenges. Through this process we moved coded data to reconciled descriptions suited to addressing the purposes of this study. Dedoose 7.0.23 software was used for qualitative data management and analysis.
Results
The study identified participants’ overall impressions of the GPM initiative and key themes within 4 major domains regarding implementing the GPM role: roles and tasks (implementing clinic practice management, leading patient access, supporting data analytics, and enabling self and staff); GPM characteristics (familiarity with clinical services, knowledge of VHA systems, ability to analyze patient data, communication skills, and the ability to work with others); and issues, and challenges (technical, social, and structural).
Overall Impressions
Interviewees perceived the GPM initiative as a consolidation of existing distributed responsibilities into one role that directly reported to local top-level management with indirect reporting to national leaders. Many of the sites reported that they had designated or planned to designate a role resembling the GPM prior to the initiative. “There are staff who’ve been doing some of this work all along,” a GPM noted. “We just didn’t have them grouped together. They weren’t necessarily all working in the same type of service under the same type of structure.”
Whether the GPM position was new or not, participants referenced the importance and challenges of engaging the local facility in recognizing the agency associated with the GPM position. According to national support, the staff are trying to get the facility to understand “why the group practice manager is so important… we’ve got to embed that standard position in the system.”
While the GPM was recognized as the hub of access management, respondents recognized that transformation regarding access involved many players. “We have to create [an] orchestrated team inside each facility,” an advisor argued.
Respondents discussed how the initiative allows local facilities to appoint a specific person with a specific title and role who helps facilitate, organize, and legitimize an access focus at their sites. One GPM interviewee noted how the initiative helped refocus some of their previously less centralized efforts. “We’ve always looked at productivity; we’ve always looked at access; we’ve always looked at efficiency. I think the bigger difference is now there are individuals identified in the clinics, as practice managers as well…I interact with them. They interact with individual clinic staff, and it’s more of a group process than a single individual.”
The value of having tools available and being able to track and manage patient care as a specific example of the positive impact of this new role was noted by participants. A GPM noted that many health care providers will be happy to have tools to better manage their services and a process “that flows from a service level all the way up to executive management, where there is a common interest in making those things happen—I think that’s going to be a tremendous help.”
Participants expressed concern that the national GPM rollout would be a one-size-fits-all approach. These respondents emphasized the need to have the flexibility to customize their activities to meet their unique site and patient needs.
GPM Roles and Tasks
Participants described 4 primary roles that the GPM was expected to fill: implementing clinic practice management, leading patient access, supporting data analytics, and enabling self and staff. Some activities overlapped in that they served to support multiple role areas (Figure 1).
Implementing clinic practice management. In the early stages of the initiative, the GPM’s primary role was to prepare the facility to implement a standardized set of clinic practice management (CPM) team processes. Part of standardizing the CPM process was defining the scope and tasks of the GPM, which requires significant planning for the implementation. “My big job is to finalize what we think group practice management is going to look [like] here,” a GPM reported.
Each prototype site had latitude to interpret the GPM initiative in a way that would work in their context within given VHA boundaries and ongoing initiatives. To achieve the high-level vision and purpose, the GPM first had to develop action plans that accounted for the operating environment of the facility. According to one GPM, VA national officials are “constantly” asking for action plans, which required significant time by specific deadlines. “They want an action plan [and to] clean up all your consults, [and to] clean up all your recall reminders.”
Leading on improving access efforts. Participants saw the GPM as the central staff member responsible for providing oversight of any activities and people involved in improving access. “I ensure everybody is doing what they’re supposed to do,” one GPM reported. When the GPM sees areas that are not being addressed, the individual tries to develop a process or training to “close those gaps.”
GPMs promoted an awareness of their goals, changes in process, and new tools accompanying the initiative. However, other access initiatives were occurring simultaneously creating confusion for health care providers and patients; thus GPMs found they were managing a wide array of related initiatives.
GPMs have to negotiate with leaders across the VHA facility, many of whom operated at a higher leadership level and had different priorities, to address access problems.
“I’m a lieutenant as a GPM in a clinic, a GPM noted. “How is the lieutenant going to talk to a major or a colonel in the clinic and say your clinic has problems. How[‘s] that lieutenant...going to do that? With people skills!”
Managing expectations about the speed and to what extent a problem could be resolved was an important part of the GPM leadership role. “I see myself as managing expectations both up to the leadership and down to the frontline,” a GPM explained. “I find myself talking to leadership [about] our progress. But at the same time, we have to say, ‘not everything can be fixed overnight.’”
Providing leadership on access-related issues included developing a range of options for addressing patient access problems. One analytics manager recounted how the GPM role led to evaluating how physical space limited efficiency in clinic flow. The first step was identifying possible additional rooms to improve clinic flow. This required working with the space committee to “get someone to look at our overarching space and find someplace else for them to sit” to avoid adding to congestion in the clinic area.
Supporting data analytics.
GPMs routinely immersed themselves in the data to understand access issues. GPMs worked with clinic leaders to identify the underlying causes and various solutions. The GPMs maintained access through administrative scrubbing of the data and finding “smart ways to get patients scheduled,” a GPM explained. “I don’t think our facility would have taken care of as many veterans in the time frame as we did....We’ve cleared over 4,000 consults that were older than 90 days. We have cleared thousands and thousands of weekly reminders.”
GPMs expressed the need for aggregated (ie, dashboard) and standardized information to efficiently address access issues. “I would like to have some more standardization on what’s being reviewed; it seems to change frequently, and so [to] be able to track and trend and have something given to me to review,” one health care provider requested. On the other hand, participants also described a need for decision support tools that would lead to action aligned with best practices. “Instead of a dashboard or something that’s just measuring their performance, it’s more something that they can look at and take action” a national support staff advisor suggested.
Enabling self and staff. GPMs felt they were most effective if they enabled themselves and stakeholders through training and by cultivating relationships and team building. Figure 2 illustrates the various stakeholders GPMs reported engaging with. The GPMS should be building relationships, bridging relationships, developing trust, and then providing a higher level of hands-on management. However, “that doesn’t really happen right now, day to day,” one member of leadership reported.
Key topics in GPM leadership training included both soft skills (change management, culture change, and negotiation skills) and crucial analytic/technical training (understanding each metric and dashboard available, data analytics, and supply/demand balancing techniques). The GPMs not only wanted to understand metrics as part of their training, but also want to know what to do about them.
An “operationalization” training approach (discerning the meaning of data, data-based decision making, and determining action from multiple options) inspired by real-life situations was preferred by participants. Other effective learning structures included job aids in the form of templated Gantt charts, process maps to guide GPMs through implementation of new processes, formalized peer learning (accumulated field insights shared during training courses), and informal peer sharing of direct experiences during calls.
GPMs also emphasized training for frontline clinical and support staff, including schedulers. VHA schedulers typically have less education and experience higher turnover rates than do other clinic staff, yet they carry out complex and critical tasks. Providing training and ensuring that any materials developed for training and education were appropriate to the level of education of schedulers was an important task for GPMs. “If they don’t understand all of the scheduling principles and potential,” one GPM explained, “we will not be maximizing the utilization of our parts.”
GPMs also provided informal education to clinicians. Participants noted GPMs have to avoid appearing to overstep their positions or presuming more knowledge and expertise than clinicians. They “have to be able to teach a physician without being overbearing, in a way a physician will accept it as advisement,” one program leader reported.
GPM knowledge, skills, and abilities. GPMs presented a complex range of knowledge, skills, and abilities, including clinical, administrative, analytics, and people skills. All interviewees reported that their prior education and experience did not sufficiently train them for the GPM role. GPMs identified a willingness to learn quickly as a critical characteristic. Many GPMs tended to have a formal education in health administration or business (eg, MBAs); others had administrative experience (eg, administrative assistance to executive leadership) or clinical training (eg, physician assistant). Detailed clinical knowledge was not expected, but clinical familiarity was helpful.
Some interviewees also mentioned previous experience and familiarity with the VHA system specifically as an advantage. This was especially true for VA outpatient flows, clinic flows, and understanding what an outpatient is in a VA context. Interviewees noted the importance of GPMs needing to be able to analyze patient demand metrics and underlying data in order to determine supply of providers and then to allocate adequate resources to complement providers. Forecasting skills were referenced as a key point. “They need to be able to be assured that they can recruit more providers if needed,” a national support staff advisor noted.
Given the importance of developing effective relationships, communication skills were mentioned by most participants and underscored as critical to establishing trust between GPMs and others as the initiative was being implemented. Interviewees indicated that relationship building was further enhanced when GPMs possessed the ability to “work with” rather than command clinicians and staff; navigate politics; and were respectful of other people’s knowledge, skills, abilities, and status. “They have to work with the nursing staff and teach them,” a leader described, “so that people understand that we are going to a different place to achieve our primary objectives and goals.”
Issues and Challenges
Participants identified several technical, social, and structural challenges and barriers to successfully implementing the GPM role.
Technical challenges. Recurring themes across all phases of data analytics were GPMs’ capability to challenge data use and use large volumes of information from multiple data sources (entering and accessing data; “drilling down” from summaries; generating reports; and analyzing and interpreting resulting metrics). Interviewees reported that information assessment and analytic support were not consistent. One GPM had a data analyst pulling reports needed to support clinical units while other GPMs trained staff to pull data. Even with support, some GPMs had issues due to limited information technology (IT) skills or access privileges leading to inefficiencies and delays. “Whenever I need anything from a programmer, I have to go through, you know, the IT gods in the sky,” one GPM remarked. “That usually takes a few months or more.”
Social challenges. Instituting the GPM role was a cultural change, and interviewees reported needing to address resistance to CPM model efforts. Resistance to change “is particularly hard in the VA just because it has a unique culture,” one leader noted. “There is a comfort in the legacy way of doing things.” The GPM initiative was introduced during a time when other national level initiatives were being implemented throughout the VHA. Fulfilling requests for information for these initiatives became the responsibility of the GPM and their team, which diverted attention from the mandate to improve access. Furthermore, GPMs were often considered the “change communicators” to clinics putting them in the role of “bad messenger,” which degraded trust and made it difficult to partner with clinicians.
Efforts to work through change management and build relationships included general program awareness presentation to internal stakeholders; including key stakeholders in GPM committees; pre-emptive conversations with unit chiefs; creating awareness of the GPM activities and progress through formal and informal update meetings; and identifying successes regarding access.
Structural challenges. The GPM role did not have direct supervision over clinical and administrative leaders, making it challenging to enact change. GPMs reported that “they do not always have authority over the area that they are being asked to manage,” which made their work difficult, requiring strong negotiation skills and political savvy to affect change. However, as the clinic staff and providers saw how the GPM could support and positively impact their practice, these challenges began to subside.
Discussion
This study provides empirical evidence regarding the implementation of a new access management strategy for health care systems focused on improving timeliness of care. First, the GPM position was seen as critical at each facility, as a single point person, to help local system leaders respond effectively to both national mandates and local context. Second, requiring the GPMs to report to the medical center director or chief of staff was important for integrating access perspectives across service lines and to facilitate a strong GPM role in strategic planning. Third, the intentional flexibility of the access management initiative, beyond the nationally specified aspects of the GPM role, was key for allowing individual sites to adapt to unique local challenges, resources, and population demands. Fourth, the initiative provided GPMs with opportunities to learn important skills and support the acquisition, utilization, and communication of a tremendous range of data toward responsive action.
According to our respondents, the GPM role demands functioning across a broad set of responsibilities; understanding the big picture as well as the complex underlying variables; engaging facility leaders, clinical and administrative staff; and prioritizing competing national and local demands. Consistent with previous findings, effective GPMs must possess a complex set of skills (interpersonal, analytic, and leadership) and the ability to create a supporting team.13
In practice, improving access at individual sites of care (VA medical centers and community-based outpatient clinics) poses significant challenges, especially in the early stages, even with the assistance of a GPM. For example, some respondents reported being overwhelmed by the volume of available data and dashboards, and responding to current requests for data analysis and dissemination sometimes impeded long range planning. Multiple national access-related initiatives and local pressures also generated excessive and potentially conflicting demands. Thus, while the creation of a GPM position seemed to be essential for the pilot sites to improve local access and timeliness to care, success also requires ongoing national and facility-wide communication, education, and support. Ongoing data analysis training and support will be critical to ensuring the sustainability of the position. Last, recruiting GPMs with the needed complex skill set may prove to be challenging, and it will be important to provide resources to identify, attract, and retain well-qualified GPMs.
Limitations and Future Work
This study was based on a small initial sample of pilot sites of varying sizes and, as such, may not reflect the experience of all VHA GPMs. In addition, the use of snowball sampling, while facilitating identification of key stakeholders, may introduce bias in participant sampling. Nonetheless, the results from this study provide findings that informed the national VHA GPM initiative and can inform further studies of practice management roles outside of the VA.
Further study of the VHA GPM implementation and similar roles in other health care systems is needed. As the GPM position is fully implemented across the VHA, large scale evaluation is needed to gain a more representative picture and allow for comparison of the GPM role at various types of facilities (eg, size, rurality, complexity, ranking based on access performance metrics).
Conclusion
Improving access to care is a central goal for health care systems. The incorporation of the GPM role is an innovative approach to improve access management strategies. Early study of prototype sites provided VHA leadership with valuable insights used to influence further rollout of this initiative. Based on our findings, national and local support are important to ongoing success. National access mandates, training, and resources should focus on ensuring sufficient GPM authority, enabling GPMs to use data, and ensuring GPMs engage with frontline clinical and administrative staff to improve veteran access to care.
1. US Department of Veterans Affairs. Veterans Health Administration. https://www.va.gov/health. Updated October 25, 2019. Accessed January 8, 2020.
2. Veterans Access, Choice, and Accountability Act of 2014. 38 CFR § 17.1500 (2014).
3. Fahmy N, Aprikian A, Al-Otaibi M, et al. Impact of treatment delay in patients with bladder cancer managed with partial cystectomy in Quebec: a population-based study. Can Urol Assoc J. 2009;3(2):131-135.
4. Hill CJ, Joonas K. The impact of unacceptable wait time on health care patients’ attitudes and actions. Health Mark Q. 2005;23(2):69-87.
5. Ansell D, Crispo JAG, Simard B, Bjerre LM. Interventions to reduce wait times for primary care appointments: a systematic review. BMC Health Serv Res. 2017;17(1):295.
6. Kotecha J, Han H, Green M, Russell G, Martin MI, Birtwhistle R. The role of the practice facilitators in Ontario primary healthcare quality improvement. BMC Fam Pract. 2015;16:93.
7. Taylor EF, Machta RM, Meyers DS, Genevro J, Peikes DN. Enhancing the primary care team to provide redesigned care: the roles of practice facilitators and care managers. Ann Fam Med. 2013;11(1):80-83.
8. Liddy C, Laferriere D, Baskerville B, Dahrouge S, Knox L, Hogg W. An overview of practice facilitation programs in Canada: current perspectives and future directions. Healthc Policy. 2013;8(3):58-67.
9. Birken SA, Lee SY, Weiner BJ, Chin MH, Schaefer CT. Improving the effectiveness of health care innovation implementation: middle managers as change agents. Med Care Res Rev. 2013;70(1):29-45.
10. Ahluwalia S, Offredy M. A qualitative study of the impact of the implementation of advanced access in primary healthcare on the working lives of general practice staff. BMC Fam Pract. 2005;6:39.
11. Damschroder LJ, Aron DC, Keith RE, Kirsh SR, Alexander JA, Lowery JC. Fostering implementation of health services research findings into practice: a consolidated framework for advancing implementation science. Implement Sci. 2009;4:50.
12. Elo S, Kyngäs H. The qualitative content analysis process. J Adv Nurs. 2008;62(1):107-115.
13. Stefl ME. Common competencies for all healthcare managers: the Healthcare Leadership Alliance model. J Healthc Manag. 2008;53(6):360-374.
1. US Department of Veterans Affairs. Veterans Health Administration. https://www.va.gov/health. Updated October 25, 2019. Accessed January 8, 2020.
2. Veterans Access, Choice, and Accountability Act of 2014. 38 CFR § 17.1500 (2014).
3. Fahmy N, Aprikian A, Al-Otaibi M, et al. Impact of treatment delay in patients with bladder cancer managed with partial cystectomy in Quebec: a population-based study. Can Urol Assoc J. 2009;3(2):131-135.
4. Hill CJ, Joonas K. The impact of unacceptable wait time on health care patients’ attitudes and actions. Health Mark Q. 2005;23(2):69-87.
5. Ansell D, Crispo JAG, Simard B, Bjerre LM. Interventions to reduce wait times for primary care appointments: a systematic review. BMC Health Serv Res. 2017;17(1):295.
6. Kotecha J, Han H, Green M, Russell G, Martin MI, Birtwhistle R. The role of the practice facilitators in Ontario primary healthcare quality improvement. BMC Fam Pract. 2015;16:93.
7. Taylor EF, Machta RM, Meyers DS, Genevro J, Peikes DN. Enhancing the primary care team to provide redesigned care: the roles of practice facilitators and care managers. Ann Fam Med. 2013;11(1):80-83.
8. Liddy C, Laferriere D, Baskerville B, Dahrouge S, Knox L, Hogg W. An overview of practice facilitation programs in Canada: current perspectives and future directions. Healthc Policy. 2013;8(3):58-67.
9. Birken SA, Lee SY, Weiner BJ, Chin MH, Schaefer CT. Improving the effectiveness of health care innovation implementation: middle managers as change agents. Med Care Res Rev. 2013;70(1):29-45.
10. Ahluwalia S, Offredy M. A qualitative study of the impact of the implementation of advanced access in primary healthcare on the working lives of general practice staff. BMC Fam Pract. 2005;6:39.
11. Damschroder LJ, Aron DC, Keith RE, Kirsh SR, Alexander JA, Lowery JC. Fostering implementation of health services research findings into practice: a consolidated framework for advancing implementation science. Implement Sci. 2009;4:50.
12. Elo S, Kyngäs H. The qualitative content analysis process. J Adv Nurs. 2008;62(1):107-115.
13. Stefl ME. Common competencies for all healthcare managers: the Healthcare Leadership Alliance model. J Healthc Manag. 2008;53(6):360-374.