User login
Cancer cell lines predict drug response, study shows

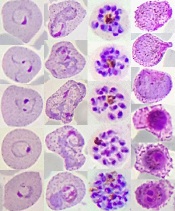
Image from PNAS
A study published in Cell has shown that patient-derived cancer cell lines harbor most of the same genetic changes found in patients’ tumors and could therefore be used to learn how cancers are likely to respond to new drugs.
Researchers believe this discovery could help advance personalized cancer medicine by leading to results that help doctors predict the best available drugs or the most suitable clinical trials for each individual patient.
“We need better ways to figure out which groups of patients are more likely to respond to a new drug before we run complex and expensive clinical trials,” said study author Ultan McDermott, MD, PhD, of the Wellcome Trust Sanger Institute in Cambridge, UK.
“Our research shows that cancer cell lines do capture the molecular alterations found in tumors and so can be predictive of how a tumor will respond to a drug. This means the cell lines could tell us much more about how a tumor is likely to respond to a new drug before we try to test it in patients. We hope this information will ultimately help in the design of clinical trials that target those patients with the greatest likelihood of benefiting from treatment.”
The researchers said this is the first systematic, large-scale study to combine molecular data from patients, cancer cell lines, and drug sensitivity.
For the study, the team looked at genetic mutations known to cause cancer in more than 11,000 patient samples of 29 different cancer types, including acute lymphoblastic leukemia, acute myeloid leukemia, chronic lymphocytic leukemia, chronic myelogenous leukemia, diffuse large B-cell lymphoma, and multiple myeloma.
The researchers built a catalogue of the genetic changes that cause cancer in patients and mapped these alterations onto 1000 cancer cell lines. Next, they tested the cell lines for sensitivity to 265 different cancer drugs to understand which of these changes affect sensitivity.
This revealed that the majority of molecular abnormalities found in patients’ cancers are also found in cancer cells in the laboratory.
The work also showed that many of the molecular abnormalities detected in the thousands of patient samples can, both individually and in combination, have a strong effect on whether a particular drug affects a cancer cell’s survival.
The results suggest cancer cell lines could be better exploited to learn which drugs offer the most effective treatment to which patients.
“If a cell line has the same genetic features as a patient’s tumor, and that cell line responded to a specific drug, we can focus new research on this finding,” said study author Francesco Iorio, PhD, of the European Bioinformatics Institute in Cambridge, UK.
“This could ultimately help assign cancer patients into more precise groups based on how likely they are to respond to therapy. This resource can really help cancer research. Most importantly, it can be used to create tools for doctors to select a clinical trial which is most promising for their cancer patient. That is still a way off, but we are heading in the right direction.” ![]()
Image from PNAS
A study published in Cell has shown that patient-derived cancer cell lines harbor most of the same genetic changes found in patients’ tumors and could therefore be used to learn how cancers are likely to respond to new drugs.
Researchers believe this discovery could help advance personalized cancer medicine by leading to results that help doctors predict the best available drugs or the most suitable clinical trials for each individual patient.
“We need better ways to figure out which groups of patients are more likely to respond to a new drug before we run complex and expensive clinical trials,” said study author Ultan McDermott, MD, PhD, of the Wellcome Trust Sanger Institute in Cambridge, UK.
“Our research shows that cancer cell lines do capture the molecular alterations found in tumors and so can be predictive of how a tumor will respond to a drug. This means the cell lines could tell us much more about how a tumor is likely to respond to a new drug before we try to test it in patients. We hope this information will ultimately help in the design of clinical trials that target those patients with the greatest likelihood of benefiting from treatment.”
The researchers said this is the first systematic, large-scale study to combine molecular data from patients, cancer cell lines, and drug sensitivity.
For the study, the team looked at genetic mutations known to cause cancer in more than 11,000 patient samples of 29 different cancer types, including acute lymphoblastic leukemia, acute myeloid leukemia, chronic lymphocytic leukemia, chronic myelogenous leukemia, diffuse large B-cell lymphoma, and multiple myeloma.
The researchers built a catalogue of the genetic changes that cause cancer in patients and mapped these alterations onto 1000 cancer cell lines. Next, they tested the cell lines for sensitivity to 265 different cancer drugs to understand which of these changes affect sensitivity.
This revealed that the majority of molecular abnormalities found in patients’ cancers are also found in cancer cells in the laboratory.
The work also showed that many of the molecular abnormalities detected in the thousands of patient samples can, both individually and in combination, have a strong effect on whether a particular drug affects a cancer cell’s survival.
The results suggest cancer cell lines could be better exploited to learn which drugs offer the most effective treatment to which patients.
“If a cell line has the same genetic features as a patient’s tumor, and that cell line responded to a specific drug, we can focus new research on this finding,” said study author Francesco Iorio, PhD, of the European Bioinformatics Institute in Cambridge, UK.
“This could ultimately help assign cancer patients into more precise groups based on how likely they are to respond to therapy. This resource can really help cancer research. Most importantly, it can be used to create tools for doctors to select a clinical trial which is most promising for their cancer patient. That is still a way off, but we are heading in the right direction.” ![]()
Image from PNAS
A study published in Cell has shown that patient-derived cancer cell lines harbor most of the same genetic changes found in patients’ tumors and could therefore be used to learn how cancers are likely to respond to new drugs.
Researchers believe this discovery could help advance personalized cancer medicine by leading to results that help doctors predict the best available drugs or the most suitable clinical trials for each individual patient.
“We need better ways to figure out which groups of patients are more likely to respond to a new drug before we run complex and expensive clinical trials,” said study author Ultan McDermott, MD, PhD, of the Wellcome Trust Sanger Institute in Cambridge, UK.
“Our research shows that cancer cell lines do capture the molecular alterations found in tumors and so can be predictive of how a tumor will respond to a drug. This means the cell lines could tell us much more about how a tumor is likely to respond to a new drug before we try to test it in patients. We hope this information will ultimately help in the design of clinical trials that target those patients with the greatest likelihood of benefiting from treatment.”
The researchers said this is the first systematic, large-scale study to combine molecular data from patients, cancer cell lines, and drug sensitivity.
For the study, the team looked at genetic mutations known to cause cancer in more than 11,000 patient samples of 29 different cancer types, including acute lymphoblastic leukemia, acute myeloid leukemia, chronic lymphocytic leukemia, chronic myelogenous leukemia, diffuse large B-cell lymphoma, and multiple myeloma.
The researchers built a catalogue of the genetic changes that cause cancer in patients and mapped these alterations onto 1000 cancer cell lines. Next, they tested the cell lines for sensitivity to 265 different cancer drugs to understand which of these changes affect sensitivity.
This revealed that the majority of molecular abnormalities found in patients’ cancers are also found in cancer cells in the laboratory.
The work also showed that many of the molecular abnormalities detected in the thousands of patient samples can, both individually and in combination, have a strong effect on whether a particular drug affects a cancer cell’s survival.
The results suggest cancer cell lines could be better exploited to learn which drugs offer the most effective treatment to which patients.
“If a cell line has the same genetic features as a patient’s tumor, and that cell line responded to a specific drug, we can focus new research on this finding,” said study author Francesco Iorio, PhD, of the European Bioinformatics Institute in Cambridge, UK.
“This could ultimately help assign cancer patients into more precise groups based on how likely they are to respond to therapy. This resource can really help cancer research. Most importantly, it can be used to create tools for doctors to select a clinical trial which is most promising for their cancer patient. That is still a way off, but we are heading in the right direction.” ![]()
Mutations may be a ‘missing link’ in AML

Research published in Nature Communications suggests that mutations in the ZBTB7A gene are associated with t(8;21)-rearranged acute myeloid leukemia (AML).
Investigators believe these mutations may be one of the “missing links” in RUNX1/RUNX1T1-driven leukemogenesis.
The team analyzed samples from 56 patients with t(8;21)-rearranged AML and identified recurring ZBTB7A mutations in 23% of those samples.
This included missense and truncating mutations that resulted in alteration or loss of the C-terminal zinc-finger domain of ZBTB7A.
The investigators noted that the transcription factor ZBTB7A is important for hematopoietic lineage fate decisions and for the regulation of glycolysis.
So the team was not surprised to find that ZBTB7A mutations boosted the energy metabolism in leukemia cells.
“In healthy cells, the active ZBTB7A gene acts like a parking brake on metabolism,” said study author Philipp Greif, MD, of Ludwig-Maximilians-Universität München in Munich, Germany.
“If the gene is defective, cancer cells get more energy to use for proliferation.”
Dr Greif and his colleagues also found they could reduce the growth rate of AML cells by increasing levels of active ZBTB7A.
And the team observed an indication of ZBTB7A’s growth-inhibiting effects in the clinic. Leukemia patients with higher levels of ZBTB7A expression had significantly better chances of survival than patients in whom the gene was hardly active or not active at all.
Now, the investigators plan to explore whether ZBTB7A expression can be used to customize therapies for individual patients. They also believe their discovery is a promising starting point for developing new approaches to treat AML.
“It might be possible to use specially modified glucose molecules to block the energy production process in AML cells,” said study author Luise Hartmann, of Ludwig-Maximilians-Universität München.
“Initial clinical trials in other cancers have already shown that these agents are well-tolerated by patients.” ![]()
Research published in Nature Communications suggests that mutations in the ZBTB7A gene are associated with t(8;21)-rearranged acute myeloid leukemia (AML).
Investigators believe these mutations may be one of the “missing links” in RUNX1/RUNX1T1-driven leukemogenesis.
The team analyzed samples from 56 patients with t(8;21)-rearranged AML and identified recurring ZBTB7A mutations in 23% of those samples.
This included missense and truncating mutations that resulted in alteration or loss of the C-terminal zinc-finger domain of ZBTB7A.
The investigators noted that the transcription factor ZBTB7A is important for hematopoietic lineage fate decisions and for the regulation of glycolysis.
So the team was not surprised to find that ZBTB7A mutations boosted the energy metabolism in leukemia cells.
“In healthy cells, the active ZBTB7A gene acts like a parking brake on metabolism,” said study author Philipp Greif, MD, of Ludwig-Maximilians-Universität München in Munich, Germany.
“If the gene is defective, cancer cells get more energy to use for proliferation.”
Dr Greif and his colleagues also found they could reduce the growth rate of AML cells by increasing levels of active ZBTB7A.
And the team observed an indication of ZBTB7A’s growth-inhibiting effects in the clinic. Leukemia patients with higher levels of ZBTB7A expression had significantly better chances of survival than patients in whom the gene was hardly active or not active at all.
Now, the investigators plan to explore whether ZBTB7A expression can be used to customize therapies for individual patients. They also believe their discovery is a promising starting point for developing new approaches to treat AML.
“It might be possible to use specially modified glucose molecules to block the energy production process in AML cells,” said study author Luise Hartmann, of Ludwig-Maximilians-Universität München.
“Initial clinical trials in other cancers have already shown that these agents are well-tolerated by patients.” ![]()
Research published in Nature Communications suggests that mutations in the ZBTB7A gene are associated with t(8;21)-rearranged acute myeloid leukemia (AML).
Investigators believe these mutations may be one of the “missing links” in RUNX1/RUNX1T1-driven leukemogenesis.
The team analyzed samples from 56 patients with t(8;21)-rearranged AML and identified recurring ZBTB7A mutations in 23% of those samples.
This included missense and truncating mutations that resulted in alteration or loss of the C-terminal zinc-finger domain of ZBTB7A.
The investigators noted that the transcription factor ZBTB7A is important for hematopoietic lineage fate decisions and for the regulation of glycolysis.
So the team was not surprised to find that ZBTB7A mutations boosted the energy metabolism in leukemia cells.
“In healthy cells, the active ZBTB7A gene acts like a parking brake on metabolism,” said study author Philipp Greif, MD, of Ludwig-Maximilians-Universität München in Munich, Germany.
“If the gene is defective, cancer cells get more energy to use for proliferation.”
Dr Greif and his colleagues also found they could reduce the growth rate of AML cells by increasing levels of active ZBTB7A.
And the team observed an indication of ZBTB7A’s growth-inhibiting effects in the clinic. Leukemia patients with higher levels of ZBTB7A expression had significantly better chances of survival than patients in whom the gene was hardly active or not active at all.
Now, the investigators plan to explore whether ZBTB7A expression can be used to customize therapies for individual patients. They also believe their discovery is a promising starting point for developing new approaches to treat AML.
“It might be possible to use specially modified glucose molecules to block the energy production process in AML cells,” said study author Luise Hartmann, of Ludwig-Maximilians-Universität München.
“Initial clinical trials in other cancers have already shown that these agents are well-tolerated by patients.” ![]()
Material can dissolve blood clots more efficiently, team says

Image by Kevin MacKenzie
Researchers say they have developed a thrombolytic material that can be condensed on a blood clot by means of a magnetic field.
Experiments suggest the material can dissolve clots up to 4000 times more efficiently than thrombolytic agents currently in use.
Vladimir Vinogradov, PhD, of ITMO University in St Petersburg, Russia, and his colleagues described the material in Scientific Reports.
“We prepared a thrombolytic colloid and tested its effects on an artificial blood clot obtained from plasma and blood of humans and thrombus extracted from patients,” Dr Vinogradov said.
“The results may soon allow us to try out the new thrombolytic system on mammals. Now, we are preparing for preclinical studies.”
Specifically, Dr Vinogradov and his colleagues produced a composite material that can deliver thrombolytic enzymes in a targeted manner. The material is composed of a porous magnetite framework and molecules of urokinase, an enzyme frequently used as a thrombolytic agent.
The composite can be used to create thrombolytic coating for artificial blood vessels and stable injectable solutions made of nanoparticles that can be localized near the clot by means of an external magnetic field.
The magnetite framework also protects enzymes from various inhibitors that are present in the blood and can deactivate thrombolytic medications.
“Usually, in order to achieve a prolonged effect for such drugs, the enzyme is placed inside a polymeric matrix,” said study author Andrey Drozdov, of ITMO University.
“The enzyme is then gradually released from the matrix and eventually loses all activity. We, on the other hand, experimentally demonstrated that enzymes protected using our approach do not lose therapeutic properties over extended periods of time and even after repeated use. The rate at which the new drug can dissolve the clot outperforms unprotected enzymes by about 4000 times.”
The researchers also believe the material is safe for humans because it is made of components that are already approved for intravenous injection. ![]()
Image by Kevin MacKenzie
Researchers say they have developed a thrombolytic material that can be condensed on a blood clot by means of a magnetic field.
Experiments suggest the material can dissolve clots up to 4000 times more efficiently than thrombolytic agents currently in use.
Vladimir Vinogradov, PhD, of ITMO University in St Petersburg, Russia, and his colleagues described the material in Scientific Reports.
“We prepared a thrombolytic colloid and tested its effects on an artificial blood clot obtained from plasma and blood of humans and thrombus extracted from patients,” Dr Vinogradov said.
“The results may soon allow us to try out the new thrombolytic system on mammals. Now, we are preparing for preclinical studies.”
Specifically, Dr Vinogradov and his colleagues produced a composite material that can deliver thrombolytic enzymes in a targeted manner. The material is composed of a porous magnetite framework and molecules of urokinase, an enzyme frequently used as a thrombolytic agent.
The composite can be used to create thrombolytic coating for artificial blood vessels and stable injectable solutions made of nanoparticles that can be localized near the clot by means of an external magnetic field.
The magnetite framework also protects enzymes from various inhibitors that are present in the blood and can deactivate thrombolytic medications.
“Usually, in order to achieve a prolonged effect for such drugs, the enzyme is placed inside a polymeric matrix,” said study author Andrey Drozdov, of ITMO University.
“The enzyme is then gradually released from the matrix and eventually loses all activity. We, on the other hand, experimentally demonstrated that enzymes protected using our approach do not lose therapeutic properties over extended periods of time and even after repeated use. The rate at which the new drug can dissolve the clot outperforms unprotected enzymes by about 4000 times.”
The researchers also believe the material is safe for humans because it is made of components that are already approved for intravenous injection. ![]()
Image by Kevin MacKenzie
Researchers say they have developed a thrombolytic material that can be condensed on a blood clot by means of a magnetic field.
Experiments suggest the material can dissolve clots up to 4000 times more efficiently than thrombolytic agents currently in use.
Vladimir Vinogradov, PhD, of ITMO University in St Petersburg, Russia, and his colleagues described the material in Scientific Reports.
“We prepared a thrombolytic colloid and tested its effects on an artificial blood clot obtained from plasma and blood of humans and thrombus extracted from patients,” Dr Vinogradov said.
“The results may soon allow us to try out the new thrombolytic system on mammals. Now, we are preparing for preclinical studies.”
Specifically, Dr Vinogradov and his colleagues produced a composite material that can deliver thrombolytic enzymes in a targeted manner. The material is composed of a porous magnetite framework and molecules of urokinase, an enzyme frequently used as a thrombolytic agent.
The composite can be used to create thrombolytic coating for artificial blood vessels and stable injectable solutions made of nanoparticles that can be localized near the clot by means of an external magnetic field.
The magnetite framework also protects enzymes from various inhibitors that are present in the blood and can deactivate thrombolytic medications.
“Usually, in order to achieve a prolonged effect for such drugs, the enzyme is placed inside a polymeric matrix,” said study author Andrey Drozdov, of ITMO University.
“The enzyme is then gradually released from the matrix and eventually loses all activity. We, on the other hand, experimentally demonstrated that enzymes protected using our approach do not lose therapeutic properties over extended periods of time and even after repeated use. The rate at which the new drug can dissolve the clot outperforms unprotected enzymes by about 4000 times.”
The researchers also believe the material is safe for humans because it is made of components that are already approved for intravenous injection. ![]()
NICE recommends approval for bosutinib

Photo courtesy of CDC
The National Institute for Health and Care Excellence (NICE) has issued a final draft guidance recommending approval for bosutinib (Bosulif), a tyrosine kinase inhibitor used to treat certain patients with chronic myeloid leukemia (CML).
NICE is recommending that bosutinib be made available through normal National Health Service (NHS) funding channels so patients don’t have to apply to the Cancer Drugs Fund (CDF) to obtain it.
The CDF is money the government sets aside to pay for cancer drugs that haven’t been approved by NICE and aren’t available within the NHS in England.
Following the decision to reform the CDF earlier this year, NICE began to reappraise all drugs currently in the CDF in April. Bosutinib is the first drug to be looked at through this reconsideration process.
Bosutinib has conditional approval from the European Commission to treat adults with Philadelphia-chromosome-positive CML in chronic phase, accelerated phase, or blast phase, but only if those patients have previously received one or more tyrosine kinase inhibitors and are not considered eligible for treatment with imatinib, nilotinib, or dasatinib.
“People with this type of chronic myeloid leukemia, who haven’t responded to first- and second-line treatment or who experience severe side effects, have few or no treatment options left,” said Carole Longson, director of the Centre for Health Technology Evaluation at NICE.
“New patients who need this drug can be reassured that bosutinib should be made available for routine use within the NHS.”
The current list price of bosutinib is £45,000 per patient per year. However, the NHS has been offered a discount by Pfizer, the drug’s manufacturer.
NICE previously looked at bosutinib in 2013 but did not recommend the drug for use on the NHS at that time, saying the drug was not cost-effective. Bosutinib was then made available to patients via the CDF.
As part of the reappraisal process, Pfizer offered a discount for bosutinib. Taking this discount into consideration, as well as the limited treatment options for CML patients, NICE decided bosutinib is cost-effective.
“The company positively engaged with our CDF reconsideration process and demonstrated that their drug can be cost-effective, which resulted in a positive recommendation,” Longson said. “This decision, when implemented, frees up funding in the CDF, which can be spent on other new and innovative cancer treatments.”
NICE’s final draft guidance is now with consultees who have the opportunity to appeal against the decision or notify NICE of any factual errors. The appeal period will close at 5 pm on July 21, 2016.
Until the final decision is published, bosutinib will still be available to new and existing patients through the old CDF. ![]()
Photo courtesy of CDC
The National Institute for Health and Care Excellence (NICE) has issued a final draft guidance recommending approval for bosutinib (Bosulif), a tyrosine kinase inhibitor used to treat certain patients with chronic myeloid leukemia (CML).
NICE is recommending that bosutinib be made available through normal National Health Service (NHS) funding channels so patients don’t have to apply to the Cancer Drugs Fund (CDF) to obtain it.
The CDF is money the government sets aside to pay for cancer drugs that haven’t been approved by NICE and aren’t available within the NHS in England.
Following the decision to reform the CDF earlier this year, NICE began to reappraise all drugs currently in the CDF in April. Bosutinib is the first drug to be looked at through this reconsideration process.
Bosutinib has conditional approval from the European Commission to treat adults with Philadelphia-chromosome-positive CML in chronic phase, accelerated phase, or blast phase, but only if those patients have previously received one or more tyrosine kinase inhibitors and are not considered eligible for treatment with imatinib, nilotinib, or dasatinib.
“People with this type of chronic myeloid leukemia, who haven’t responded to first- and second-line treatment or who experience severe side effects, have few or no treatment options left,” said Carole Longson, director of the Centre for Health Technology Evaluation at NICE.
“New patients who need this drug can be reassured that bosutinib should be made available for routine use within the NHS.”
The current list price of bosutinib is £45,000 per patient per year. However, the NHS has been offered a discount by Pfizer, the drug’s manufacturer.
NICE previously looked at bosutinib in 2013 but did not recommend the drug for use on the NHS at that time, saying the drug was not cost-effective. Bosutinib was then made available to patients via the CDF.
As part of the reappraisal process, Pfizer offered a discount for bosutinib. Taking this discount into consideration, as well as the limited treatment options for CML patients, NICE decided bosutinib is cost-effective.
“The company positively engaged with our CDF reconsideration process and demonstrated that their drug can be cost-effective, which resulted in a positive recommendation,” Longson said. “This decision, when implemented, frees up funding in the CDF, which can be spent on other new and innovative cancer treatments.”
NICE’s final draft guidance is now with consultees who have the opportunity to appeal against the decision or notify NICE of any factual errors. The appeal period will close at 5 pm on July 21, 2016.
Until the final decision is published, bosutinib will still be available to new and existing patients through the old CDF. ![]()
Photo courtesy of CDC
The National Institute for Health and Care Excellence (NICE) has issued a final draft guidance recommending approval for bosutinib (Bosulif), a tyrosine kinase inhibitor used to treat certain patients with chronic myeloid leukemia (CML).
NICE is recommending that bosutinib be made available through normal National Health Service (NHS) funding channels so patients don’t have to apply to the Cancer Drugs Fund (CDF) to obtain it.
The CDF is money the government sets aside to pay for cancer drugs that haven’t been approved by NICE and aren’t available within the NHS in England.
Following the decision to reform the CDF earlier this year, NICE began to reappraise all drugs currently in the CDF in April. Bosutinib is the first drug to be looked at through this reconsideration process.
Bosutinib has conditional approval from the European Commission to treat adults with Philadelphia-chromosome-positive CML in chronic phase, accelerated phase, or blast phase, but only if those patients have previously received one or more tyrosine kinase inhibitors and are not considered eligible for treatment with imatinib, nilotinib, or dasatinib.
“People with this type of chronic myeloid leukemia, who haven’t responded to first- and second-line treatment or who experience severe side effects, have few or no treatment options left,” said Carole Longson, director of the Centre for Health Technology Evaluation at NICE.
“New patients who need this drug can be reassured that bosutinib should be made available for routine use within the NHS.”
The current list price of bosutinib is £45,000 per patient per year. However, the NHS has been offered a discount by Pfizer, the drug’s manufacturer.
NICE previously looked at bosutinib in 2013 but did not recommend the drug for use on the NHS at that time, saying the drug was not cost-effective. Bosutinib was then made available to patients via the CDF.
As part of the reappraisal process, Pfizer offered a discount for bosutinib. Taking this discount into consideration, as well as the limited treatment options for CML patients, NICE decided bosutinib is cost-effective.
“The company positively engaged with our CDF reconsideration process and demonstrated that their drug can be cost-effective, which resulted in a positive recommendation,” Longson said. “This decision, when implemented, frees up funding in the CDF, which can be spent on other new and innovative cancer treatments.”
NICE’s final draft guidance is now with consultees who have the opportunity to appeal against the decision or notify NICE of any factual errors. The appeal period will close at 5 pm on July 21, 2016.
Until the final decision is published, bosutinib will still be available to new and existing patients through the old CDF. ![]()
EC extends marketing authorization for brentuximab vedotin

Photo from Business Wire
The European Commission (EC) has extended the current conditional marketing authorization of brentuximab vedotin (Adcetris) to include the treatment of adults with CD30+ Hodgkin lymphoma (HL) who are at an increased risk of relapse or progression following autologous stem cell transplant (ASCT).
Conditional marketing authorizations are valid for 1 year and are reviewed annually.
The company developing the drug is required to provide comprehensive data confirming the drug’s benefit-risk balance is positive. Once these data are available, the marketing authorization may be converted into a standard marketing authorization.
Drugs are eligible for conditional marketing authorization if they are designated as orphan medicines, intended for use in emergency situations, or designed to treat, prevent, or diagnose seriously debilitating or life-threatening diseases.
The EC previously granted brentuximab vedotin conditional marketing authorization for 2 indications:
- To treat adults with relapsed or refractory CD30+ HL after ASCT or following at least 2 prior therapies when ASCT or multi-agent chemotherapy is not a treatment option
- To treat adults with relapsed or refractory systemic anaplastic large-cell lymphoma (sALCL).
In January 2016, the EC approved a Type II variation to include data on the retreatment of adult patients with HL or sALCL who previously responded to brentuximab vedotin and later relapsed.
Brentuximab vedotin is under joint development by Seattle Genetics and Takeda Pharmaceutical Company Limited.
AETHERA trial
The EC’s decision to extend the conditional marketing authorization of brentuximab vedotin is based on results from the phase 3 AETHERA trial.
The trial was designed to compare brentuximab vedotin to placebo, both administered for up to 16 cycles (approximately 1 year) every 3 weeks following ASCT. Results from the trial were published in The Lancet in March 2015 and presented at the 2014 ASH Annual Meeting.
The study enrolled 329 HL patients at risk of relapse or progression, including 165 on the brentuximab vedotin arm and 164 on the placebo arm.
Patients were eligible for enrollment if they had a history of primary refractory HL, relapsed within a year of receiving frontline chemotherapy, and/or had disease outside of the lymph nodes at the time of pre-ASCT relapse.
Brentuximab vedotin conferred a significant increase in progression-free survival over placebo, with a hazard ratio of 0.57 (P=0.001). The median progression-free survival was 43 months for patients who received brentuximab vedotin and 24 months for those who received placebo.
The most common adverse events (≥20%), of any grade and regardless of causality, in the brentuximab vedotin arm were neutropenia (78%), peripheral sensory neuropathy (56%), thrombocytopenia (41%), anemia (27%), upper respiratory tract infection (26%), fatigue (24%), peripheral motor neuropathy (23%), nausea (22%), cough (21%), and diarrhea (20%).
The most common adverse events (≥20%), of any grade and regardless of causality, in the placebo arm were neutropenia (34%), upper respiratory tract infection (23%), and thrombocytopenia (20%).
In all, 67% of patients on the brentuximab vedotin arm experienced peripheral neuropathy. Of those patients, 85% had resolution (59%) or partial improvement (26%) in symptoms at the time of their last evaluation, with a median time to improvement of 23 weeks (range, 0.1-138). ![]()
Photo from Business Wire
The European Commission (EC) has extended the current conditional marketing authorization of brentuximab vedotin (Adcetris) to include the treatment of adults with CD30+ Hodgkin lymphoma (HL) who are at an increased risk of relapse or progression following autologous stem cell transplant (ASCT).
Conditional marketing authorizations are valid for 1 year and are reviewed annually.
The company developing the drug is required to provide comprehensive data confirming the drug’s benefit-risk balance is positive. Once these data are available, the marketing authorization may be converted into a standard marketing authorization.
Drugs are eligible for conditional marketing authorization if they are designated as orphan medicines, intended for use in emergency situations, or designed to treat, prevent, or diagnose seriously debilitating or life-threatening diseases.
The EC previously granted brentuximab vedotin conditional marketing authorization for 2 indications:
- To treat adults with relapsed or refractory CD30+ HL after ASCT or following at least 2 prior therapies when ASCT or multi-agent chemotherapy is not a treatment option
- To treat adults with relapsed or refractory systemic anaplastic large-cell lymphoma (sALCL).
In January 2016, the EC approved a Type II variation to include data on the retreatment of adult patients with HL or sALCL who previously responded to brentuximab vedotin and later relapsed.
Brentuximab vedotin is under joint development by Seattle Genetics and Takeda Pharmaceutical Company Limited.
AETHERA trial
The EC’s decision to extend the conditional marketing authorization of brentuximab vedotin is based on results from the phase 3 AETHERA trial.
The trial was designed to compare brentuximab vedotin to placebo, both administered for up to 16 cycles (approximately 1 year) every 3 weeks following ASCT. Results from the trial were published in The Lancet in March 2015 and presented at the 2014 ASH Annual Meeting.
The study enrolled 329 HL patients at risk of relapse or progression, including 165 on the brentuximab vedotin arm and 164 on the placebo arm.
Patients were eligible for enrollment if they had a history of primary refractory HL, relapsed within a year of receiving frontline chemotherapy, and/or had disease outside of the lymph nodes at the time of pre-ASCT relapse.
Brentuximab vedotin conferred a significant increase in progression-free survival over placebo, with a hazard ratio of 0.57 (P=0.001). The median progression-free survival was 43 months for patients who received brentuximab vedotin and 24 months for those who received placebo.
The most common adverse events (≥20%), of any grade and regardless of causality, in the brentuximab vedotin arm were neutropenia (78%), peripheral sensory neuropathy (56%), thrombocytopenia (41%), anemia (27%), upper respiratory tract infection (26%), fatigue (24%), peripheral motor neuropathy (23%), nausea (22%), cough (21%), and diarrhea (20%).
The most common adverse events (≥20%), of any grade and regardless of causality, in the placebo arm were neutropenia (34%), upper respiratory tract infection (23%), and thrombocytopenia (20%).
In all, 67% of patients on the brentuximab vedotin arm experienced peripheral neuropathy. Of those patients, 85% had resolution (59%) or partial improvement (26%) in symptoms at the time of their last evaluation, with a median time to improvement of 23 weeks (range, 0.1-138). ![]()
Photo from Business Wire
The European Commission (EC) has extended the current conditional marketing authorization of brentuximab vedotin (Adcetris) to include the treatment of adults with CD30+ Hodgkin lymphoma (HL) who are at an increased risk of relapse or progression following autologous stem cell transplant (ASCT).
Conditional marketing authorizations are valid for 1 year and are reviewed annually.
The company developing the drug is required to provide comprehensive data confirming the drug’s benefit-risk balance is positive. Once these data are available, the marketing authorization may be converted into a standard marketing authorization.
Drugs are eligible for conditional marketing authorization if they are designated as orphan medicines, intended for use in emergency situations, or designed to treat, prevent, or diagnose seriously debilitating or life-threatening diseases.
The EC previously granted brentuximab vedotin conditional marketing authorization for 2 indications:
- To treat adults with relapsed or refractory CD30+ HL after ASCT or following at least 2 prior therapies when ASCT or multi-agent chemotherapy is not a treatment option
- To treat adults with relapsed or refractory systemic anaplastic large-cell lymphoma (sALCL).
In January 2016, the EC approved a Type II variation to include data on the retreatment of adult patients with HL or sALCL who previously responded to brentuximab vedotin and later relapsed.
Brentuximab vedotin is under joint development by Seattle Genetics and Takeda Pharmaceutical Company Limited.
AETHERA trial
The EC’s decision to extend the conditional marketing authorization of brentuximab vedotin is based on results from the phase 3 AETHERA trial.
The trial was designed to compare brentuximab vedotin to placebo, both administered for up to 16 cycles (approximately 1 year) every 3 weeks following ASCT. Results from the trial were published in The Lancet in March 2015 and presented at the 2014 ASH Annual Meeting.
The study enrolled 329 HL patients at risk of relapse or progression, including 165 on the brentuximab vedotin arm and 164 on the placebo arm.
Patients were eligible for enrollment if they had a history of primary refractory HL, relapsed within a year of receiving frontline chemotherapy, and/or had disease outside of the lymph nodes at the time of pre-ASCT relapse.
Brentuximab vedotin conferred a significant increase in progression-free survival over placebo, with a hazard ratio of 0.57 (P=0.001). The median progression-free survival was 43 months for patients who received brentuximab vedotin and 24 months for those who received placebo.
The most common adverse events (≥20%), of any grade and regardless of causality, in the brentuximab vedotin arm were neutropenia (78%), peripheral sensory neuropathy (56%), thrombocytopenia (41%), anemia (27%), upper respiratory tract infection (26%), fatigue (24%), peripheral motor neuropathy (23%), nausea (22%), cough (21%), and diarrhea (20%).
The most common adverse events (≥20%), of any grade and regardless of causality, in the placebo arm were neutropenia (34%), upper respiratory tract infection (23%), and thrombocytopenia (20%).
In all, 67% of patients on the brentuximab vedotin arm experienced peripheral neuropathy. Of those patients, 85% had resolution (59%) or partial improvement (26%) in symptoms at the time of their last evaluation, with a median time to improvement of 23 weeks (range, 0.1-138). ![]()
NHL patients may have higher risk of second cancer

Photo courtesy of NIH
Compared to patients with other common cancers, patients with non-Hodgkin lymphoma (NHL) have a higher risk of developing a second, unrelated malignancy, according to a new study.
Researchers looked at data on more than 2.1 million patients with 10 of the most common cancers and found that patients with NHL or bladder cancer had the highest risk of developing a second malignancy.
The researchers reported these findings in Cancer.
For this study, Karim Chamie, MD, of the University of California, Los Angeles, and his colleagues looked at data from Surveillance, Epidemiology, and End Results database.
The team identified patients age 18 and older who were diagnosed with one of the 10 most common cancers—NHL, melanoma, and prostate, breast, lung, colon, rectal, bladder, uterine, and kidney cancers—between 1992 and 2008.
Of the 2,116,163 patients identified, 170,865 (8.1%) developed a second primary malignancy.
In multivariable analysis, patients with NHL or bladder cancer had the highest risk of developing a second malignancy.
The hazard ratios for patients with NHL were 2.70 for men and 2.88 for women. The hazard ratios for bladder cancer were 1.88 for men and 1.66 for women.
Lung cancer was a common second malignancy for both NHL and bladder cancer patients. NHL patients also tended to develop prostate and breast cancer.
Among patients with 2 incident cancers, 13% died of their initial cancer, and 55% died of their second primary malignancy. Lung cancer was the cause of death in 12% of the patients.
“As clinicians, we can become so focused on surveilling our patients to see if a primary cancer recurs that we sometimes may not be aware that patients can be at risk of developing a second, unrelated cancer,” Dr Chamie said.
He and his colleagues believe this study makes a case for monitoring cancer patients for second malignancies. ![]()
Photo courtesy of NIH
Compared to patients with other common cancers, patients with non-Hodgkin lymphoma (NHL) have a higher risk of developing a second, unrelated malignancy, according to a new study.
Researchers looked at data on more than 2.1 million patients with 10 of the most common cancers and found that patients with NHL or bladder cancer had the highest risk of developing a second malignancy.
The researchers reported these findings in Cancer.
For this study, Karim Chamie, MD, of the University of California, Los Angeles, and his colleagues looked at data from Surveillance, Epidemiology, and End Results database.
The team identified patients age 18 and older who were diagnosed with one of the 10 most common cancers—NHL, melanoma, and prostate, breast, lung, colon, rectal, bladder, uterine, and kidney cancers—between 1992 and 2008.
Of the 2,116,163 patients identified, 170,865 (8.1%) developed a second primary malignancy.
In multivariable analysis, patients with NHL or bladder cancer had the highest risk of developing a second malignancy.
The hazard ratios for patients with NHL were 2.70 for men and 2.88 for women. The hazard ratios for bladder cancer were 1.88 for men and 1.66 for women.
Lung cancer was a common second malignancy for both NHL and bladder cancer patients. NHL patients also tended to develop prostate and breast cancer.
Among patients with 2 incident cancers, 13% died of their initial cancer, and 55% died of their second primary malignancy. Lung cancer was the cause of death in 12% of the patients.
“As clinicians, we can become so focused on surveilling our patients to see if a primary cancer recurs that we sometimes may not be aware that patients can be at risk of developing a second, unrelated cancer,” Dr Chamie said.
He and his colleagues believe this study makes a case for monitoring cancer patients for second malignancies. ![]()
Photo courtesy of NIH
Compared to patients with other common cancers, patients with non-Hodgkin lymphoma (NHL) have a higher risk of developing a second, unrelated malignancy, according to a new study.
Researchers looked at data on more than 2.1 million patients with 10 of the most common cancers and found that patients with NHL or bladder cancer had the highest risk of developing a second malignancy.
The researchers reported these findings in Cancer.
For this study, Karim Chamie, MD, of the University of California, Los Angeles, and his colleagues looked at data from Surveillance, Epidemiology, and End Results database.
The team identified patients age 18 and older who were diagnosed with one of the 10 most common cancers—NHL, melanoma, and prostate, breast, lung, colon, rectal, bladder, uterine, and kidney cancers—between 1992 and 2008.
Of the 2,116,163 patients identified, 170,865 (8.1%) developed a second primary malignancy.
In multivariable analysis, patients with NHL or bladder cancer had the highest risk of developing a second malignancy.
The hazard ratios for patients with NHL were 2.70 for men and 2.88 for women. The hazard ratios for bladder cancer were 1.88 for men and 1.66 for women.
Lung cancer was a common second malignancy for both NHL and bladder cancer patients. NHL patients also tended to develop prostate and breast cancer.
Among patients with 2 incident cancers, 13% died of their initial cancer, and 55% died of their second primary malignancy. Lung cancer was the cause of death in 12% of the patients.
“As clinicians, we can become so focused on surveilling our patients to see if a primary cancer recurs that we sometimes may not be aware that patients can be at risk of developing a second, unrelated cancer,” Dr Chamie said.
He and his colleagues believe this study makes a case for monitoring cancer patients for second malignancies. ![]()
Study reveals global variations of P vivax
from patients in Thailand
Image by Wanlapa Roobsoong
Researchers say they have uncovered the global, evolving, and historic make-up of the malaria parasite Plasmodium vivax.
The group’s study revealed 4 genetically distinct populations of P vivax that provide insight into the movement of the parasite over time and
show how it is still adapting to regional variations in the mosquitoes that transmit P vivax, the humans infected with the parasite, and the drugs used to fight it.
“Our findings show it is evolving in response to antimalarial drugs and adapting to regional differences, indicating a wide range of approaches will likely be necessary to eliminate it globally,” said Jane Carlton, PhD, of New York University in New York, New York.
Dr Carlton and her colleagues reported these findings in Nature Genetics.
The researchers sequenced 182 DNA samples of P vivax collected from patients in 11 countries. The team said this provided new insights into the nature of P vivax as it exists today and also served as a “genetic history book” of the studied regions.
“The DNA data show that P vivax has clearly had a different history of association with global human populations than other malaria parasites, indicating that unique aspects of its biology may have influenced the ways in which it spread around the world,” said Daniel Neafsey, PhD, of the Broad Institute in Cambridge, Massachusetts.
Specifically, the researchers found that Central and South American P vivax populations are genetically diverse and distinct from all other contemporary P vivax populations. The team said this suggests that New World parasites may have been introduced by colonial seafarers and represent a now-eliminated European parasite population.
The researchers also found that contemporary African and South Asian P vivax populations are genetically similar. They said this suggests that South Asian P vivax populations may have genetically mingled with European lineages during the colonial era, or it may reflect ancient connections between human populations in the Eastern Mediterranean, Middle East, and Indian subcontinent.
Another finding was the relatively homogeneous genetic makeup of P vivax in Mexico, which reflects a steady decline of the disease in this country over the last decade.
By contrast, the Papua New Guinea population of P vivax was shown to be very diverse relative to other P vivax populations.
A similar study, which also illustrated the global variations of P vivax, was recently published in Nature Genetics in as well. ![]()
from patients in Thailand
Image by Wanlapa Roobsoong
Researchers say they have uncovered the global, evolving, and historic make-up of the malaria parasite Plasmodium vivax.
The group’s study revealed 4 genetically distinct populations of P vivax that provide insight into the movement of the parasite over time and
show how it is still adapting to regional variations in the mosquitoes that transmit P vivax, the humans infected with the parasite, and the drugs used to fight it.
“Our findings show it is evolving in response to antimalarial drugs and adapting to regional differences, indicating a wide range of approaches will likely be necessary to eliminate it globally,” said Jane Carlton, PhD, of New York University in New York, New York.
Dr Carlton and her colleagues reported these findings in Nature Genetics.
The researchers sequenced 182 DNA samples of P vivax collected from patients in 11 countries. The team said this provided new insights into the nature of P vivax as it exists today and also served as a “genetic history book” of the studied regions.
“The DNA data show that P vivax has clearly had a different history of association with global human populations than other malaria parasites, indicating that unique aspects of its biology may have influenced the ways in which it spread around the world,” said Daniel Neafsey, PhD, of the Broad Institute in Cambridge, Massachusetts.
Specifically, the researchers found that Central and South American P vivax populations are genetically diverse and distinct from all other contemporary P vivax populations. The team said this suggests that New World parasites may have been introduced by colonial seafarers and represent a now-eliminated European parasite population.
The researchers also found that contemporary African and South Asian P vivax populations are genetically similar. They said this suggests that South Asian P vivax populations may have genetically mingled with European lineages during the colonial era, or it may reflect ancient connections between human populations in the Eastern Mediterranean, Middle East, and Indian subcontinent.
Another finding was the relatively homogeneous genetic makeup of P vivax in Mexico, which reflects a steady decline of the disease in this country over the last decade.
By contrast, the Papua New Guinea population of P vivax was shown to be very diverse relative to other P vivax populations.
A similar study, which also illustrated the global variations of P vivax, was recently published in Nature Genetics in as well. ![]()
from patients in Thailand
Image by Wanlapa Roobsoong
Researchers say they have uncovered the global, evolving, and historic make-up of the malaria parasite Plasmodium vivax.
The group’s study revealed 4 genetically distinct populations of P vivax that provide insight into the movement of the parasite over time and
show how it is still adapting to regional variations in the mosquitoes that transmit P vivax, the humans infected with the parasite, and the drugs used to fight it.
“Our findings show it is evolving in response to antimalarial drugs and adapting to regional differences, indicating a wide range of approaches will likely be necessary to eliminate it globally,” said Jane Carlton, PhD, of New York University in New York, New York.
Dr Carlton and her colleagues reported these findings in Nature Genetics.
The researchers sequenced 182 DNA samples of P vivax collected from patients in 11 countries. The team said this provided new insights into the nature of P vivax as it exists today and also served as a “genetic history book” of the studied regions.
“The DNA data show that P vivax has clearly had a different history of association with global human populations than other malaria parasites, indicating that unique aspects of its biology may have influenced the ways in which it spread around the world,” said Daniel Neafsey, PhD, of the Broad Institute in Cambridge, Massachusetts.
Specifically, the researchers found that Central and South American P vivax populations are genetically diverse and distinct from all other contemporary P vivax populations. The team said this suggests that New World parasites may have been introduced by colonial seafarers and represent a now-eliminated European parasite population.
The researchers also found that contemporary African and South Asian P vivax populations are genetically similar. They said this suggests that South Asian P vivax populations may have genetically mingled with European lineages during the colonial era, or it may reflect ancient connections between human populations in the Eastern Mediterranean, Middle East, and Indian subcontinent.
Another finding was the relatively homogeneous genetic makeup of P vivax in Mexico, which reflects a steady decline of the disease in this country over the last decade.
By contrast, the Papua New Guinea population of P vivax was shown to be very diverse relative to other P vivax populations.
A similar study, which also illustrated the global variations of P vivax, was recently published in Nature Genetics in as well.
Results support INR self-monitoring/management

Results of a systematic review support self-monitoring and self-management for patients on long-term oral anticoagulation therapy.
Researchers found that both self-monitoring and self-management were associated with a reduction in thromboembolic events when compared to standard monitoring.
Self-management, but not self-monitoring, was associated with a reduction in all-cause mortality.
And neither practice appeared to have an effect on major bleeding.
These results were published in the Cochrane Database of Systematic Reviews.
Point-of-care testing has made it possible for patients on long-term oral anticoagulation therapy to monitor their own international normalized ratio (INR).
Patients can either adjust their own medication according to a pre-determined dose-INR schedule, which is known as self-management, or they can call into a clinic to be told the appropriate dose adjustment, which is known as self-monitoring.
For the current review, Carl Heneghan, BM BCh, DPhil, of the University of Oxford in the UK, and his colleagues evaluated data from 28 randomized trials including 8950 patients. The trials compared self-monitoring and self-management with standard monitoring.
The researchers said pooled estimates showed a reduction in thromboembolic events with both self-management and self-monitoring, compared to standard monitoring.
Eleven studies including 3497 patients showed the relative risk (RR) of thromboembolic events was 0.47 (95% CI 0.31 to 0.70) for self-management compared to standard monitoring.
Seven studies including 4097 patients showed the RR of thromboembolic events was 0.69 (95% CI 0.49 to 0.97) for self-monitoring compared to standard monitoring.
Eight studies including 3058 patients suggested that self-management caused a reduction in all-cause mortality (RR=0.55, 95% CI 0.36 to 0.84) when compared to standard monitoring.
But 3 studies of 3300 patients indicated that self-monitoring did not reduce all-cause mortality (RR=0.94, 95% CI 0.78 to 1.15).
In 20 trials of 8018 patients, neither self-monitoring nor self-management reduced major hemorrhage (RR=0.95, 95% CI, 0.80 to 1.12) when compared to standard monitoring.
For all of these analyses, the quality of evidence was moderate.
“Our review of the latest research finds that self-monitoring alone does indeed result in a statistically significant reduction in thromboembolic events, whereas our previous review did not find this effect,” Dr Heneghan said.
“Suitable patients still need to be identified and educated for self-monitoring as it is not feasible for everyone, but the evidence clearly demonstrates that self-monitoring can improve the quality of oral anticoagulation therapy and adds weight to the argument that more patients should be given the opportunity to benefit from this treatment approach.”
The current review is an update on a previous review carried out by the same researchers in 2010. It includes 10 new studies of 4227 participants.
Results of a systematic review support self-monitoring and self-management for patients on long-term oral anticoagulation therapy.
Researchers found that both self-monitoring and self-management were associated with a reduction in thromboembolic events when compared to standard monitoring.
Self-management, but not self-monitoring, was associated with a reduction in all-cause mortality.
And neither practice appeared to have an effect on major bleeding.
These results were published in the Cochrane Database of Systematic Reviews.
Point-of-care testing has made it possible for patients on long-term oral anticoagulation therapy to monitor their own international normalized ratio (INR).
Patients can either adjust their own medication according to a pre-determined dose-INR schedule, which is known as self-management, or they can call into a clinic to be told the appropriate dose adjustment, which is known as self-monitoring.
For the current review, Carl Heneghan, BM BCh, DPhil, of the University of Oxford in the UK, and his colleagues evaluated data from 28 randomized trials including 8950 patients. The trials compared self-monitoring and self-management with standard monitoring.
The researchers said pooled estimates showed a reduction in thromboembolic events with both self-management and self-monitoring, compared to standard monitoring.
Eleven studies including 3497 patients showed the relative risk (RR) of thromboembolic events was 0.47 (95% CI 0.31 to 0.70) for self-management compared to standard monitoring.
Seven studies including 4097 patients showed the RR of thromboembolic events was 0.69 (95% CI 0.49 to 0.97) for self-monitoring compared to standard monitoring.
Eight studies including 3058 patients suggested that self-management caused a reduction in all-cause mortality (RR=0.55, 95% CI 0.36 to 0.84) when compared to standard monitoring.
But 3 studies of 3300 patients indicated that self-monitoring did not reduce all-cause mortality (RR=0.94, 95% CI 0.78 to 1.15).
In 20 trials of 8018 patients, neither self-monitoring nor self-management reduced major hemorrhage (RR=0.95, 95% CI, 0.80 to 1.12) when compared to standard monitoring.
For all of these analyses, the quality of evidence was moderate.
“Our review of the latest research finds that self-monitoring alone does indeed result in a statistically significant reduction in thromboembolic events, whereas our previous review did not find this effect,” Dr Heneghan said.
“Suitable patients still need to be identified and educated for self-monitoring as it is not feasible for everyone, but the evidence clearly demonstrates that self-monitoring can improve the quality of oral anticoagulation therapy and adds weight to the argument that more patients should be given the opportunity to benefit from this treatment approach.”
The current review is an update on a previous review carried out by the same researchers in 2010. It includes 10 new studies of 4227 participants.
Results of a systematic review support self-monitoring and self-management for patients on long-term oral anticoagulation therapy.
Researchers found that both self-monitoring and self-management were associated with a reduction in thromboembolic events when compared to standard monitoring.
Self-management, but not self-monitoring, was associated with a reduction in all-cause mortality.
And neither practice appeared to have an effect on major bleeding.
These results were published in the Cochrane Database of Systematic Reviews.
Point-of-care testing has made it possible for patients on long-term oral anticoagulation therapy to monitor their own international normalized ratio (INR).
Patients can either adjust their own medication according to a pre-determined dose-INR schedule, which is known as self-management, or they can call into a clinic to be told the appropriate dose adjustment, which is known as self-monitoring.
For the current review, Carl Heneghan, BM BCh, DPhil, of the University of Oxford in the UK, and his colleagues evaluated data from 28 randomized trials including 8950 patients. The trials compared self-monitoring and self-management with standard monitoring.
The researchers said pooled estimates showed a reduction in thromboembolic events with both self-management and self-monitoring, compared to standard monitoring.
Eleven studies including 3497 patients showed the relative risk (RR) of thromboembolic events was 0.47 (95% CI 0.31 to 0.70) for self-management compared to standard monitoring.
Seven studies including 4097 patients showed the RR of thromboembolic events was 0.69 (95% CI 0.49 to 0.97) for self-monitoring compared to standard monitoring.
Eight studies including 3058 patients suggested that self-management caused a reduction in all-cause mortality (RR=0.55, 95% CI 0.36 to 0.84) when compared to standard monitoring.
But 3 studies of 3300 patients indicated that self-monitoring did not reduce all-cause mortality (RR=0.94, 95% CI 0.78 to 1.15).
In 20 trials of 8018 patients, neither self-monitoring nor self-management reduced major hemorrhage (RR=0.95, 95% CI, 0.80 to 1.12) when compared to standard monitoring.
For all of these analyses, the quality of evidence was moderate.
“Our review of the latest research finds that self-monitoring alone does indeed result in a statistically significant reduction in thromboembolic events, whereas our previous review did not find this effect,” Dr Heneghan said.
“Suitable patients still need to be identified and educated for self-monitoring as it is not feasible for everyone, but the evidence clearly demonstrates that self-monitoring can improve the quality of oral anticoagulation therapy and adds weight to the argument that more patients should be given the opportunity to benefit from this treatment approach.”
The current review is an update on a previous review carried out by the same researchers in 2010. It includes 10 new studies of 4227 participants.
Drugs produce comparable results in CP-CML
Long-term results from the DASISION trial suggest that dasatinib and imatinib produce similar outcomes in patients with newly diagnosed chronic phase chronic myeloid leukemia (CP-CML).
Although patients who received dasatinib experienced faster and deeper molecular responses than patients who received imatinib, the overall survival and progression-free survival rates were similar between the treatment arms.
Overall, adverse events (AEs) were similar between the arms as well.
Researchers said these results suggest that dasatinib should continue to be considered an option for patients with newly diagnosed CP-CML.
The team reported the results of this study in the Journal of Clinical Oncology. The research was sponsored by Bristol-Myers Squibb.
The trial enrolled 519 patients with newly diagnosed CP-CML. They were randomized to receive dasatinib at 100 mg once daily (n=259) or imatinib at 400 mg once daily (n=260). Baseline characteristics were well-balanced between the arms.
At 5 years of follow-up, 61% of patients in the dasatinib arm and 63% of patients in the imatinib arm remained on treatment.
Response and survival
The cumulative 5-year rate of major molecular response was 76% in the dasatinib arm and 64% in the imatinib arm (P=0.0022). The rates of MR4.5 were 42% and 33%, respectively (P=0.0251).
The estimated 5-year overall survival was 91% in the dasatinib arm and 90% in the imatinib arm (hazard ratio=1.01; 95% CI, 0.58 to 1.73).
The estimated 5-year progression-free survival was 85% and 86%, respectively (hazard ratio=1.06; 95% CI, 0.68 to 1.66).
Safety
In both treatment arms, most AEs were grade 1 or 2. Grade 3/4 AEs occurred in 15% of patients in the dasatinib arm and 11% of patients in the imatinib arm.
Rates of grade 3/4 hematologic AEs tended to be higher in the dasatinib arm than the imatinib arm.
But the rates of most drug-related, nonhematologic AEs were lower in the dasatinib arm than the imatinib arm or were comparable between the arms.
The exception was drug-related pleural effusion, which was more common with dasatinib (28%) than with imatinib (0.8%).
Drug-related AEs were largely manageable, although they led to treatment discontinuation in 16% of dasatinib-treated patients and 7% of imatinib-treated patients.
By 5 years, 26 patients (10%) in each treatment arm had died. Nine patients in the dasatinib arm died of disease progression, as did 17 patients in the imatinib arm.
Long-term results from the DASISION trial suggest that dasatinib and imatinib produce similar outcomes in patients with newly diagnosed chronic phase chronic myeloid leukemia (CP-CML).
Although patients who received dasatinib experienced faster and deeper molecular responses than patients who received imatinib, the overall survival and progression-free survival rates were similar between the treatment arms.
Overall, adverse events (AEs) were similar between the arms as well.
Researchers said these results suggest that dasatinib should continue to be considered an option for patients with newly diagnosed CP-CML.
The team reported the results of this study in the Journal of Clinical Oncology. The research was sponsored by Bristol-Myers Squibb.
The trial enrolled 519 patients with newly diagnosed CP-CML. They were randomized to receive dasatinib at 100 mg once daily (n=259) or imatinib at 400 mg once daily (n=260). Baseline characteristics were well-balanced between the arms.
At 5 years of follow-up, 61% of patients in the dasatinib arm and 63% of patients in the imatinib arm remained on treatment.
Response and survival
The cumulative 5-year rate of major molecular response was 76% in the dasatinib arm and 64% in the imatinib arm (P=0.0022). The rates of MR4.5 were 42% and 33%, respectively (P=0.0251).
The estimated 5-year overall survival was 91% in the dasatinib arm and 90% in the imatinib arm (hazard ratio=1.01; 95% CI, 0.58 to 1.73).
The estimated 5-year progression-free survival was 85% and 86%, respectively (hazard ratio=1.06; 95% CI, 0.68 to 1.66).
Safety
In both treatment arms, most AEs were grade 1 or 2. Grade 3/4 AEs occurred in 15% of patients in the dasatinib arm and 11% of patients in the imatinib arm.
Rates of grade 3/4 hematologic AEs tended to be higher in the dasatinib arm than the imatinib arm.
But the rates of most drug-related, nonhematologic AEs were lower in the dasatinib arm than the imatinib arm or were comparable between the arms.
The exception was drug-related pleural effusion, which was more common with dasatinib (28%) than with imatinib (0.8%).
Drug-related AEs were largely manageable, although they led to treatment discontinuation in 16% of dasatinib-treated patients and 7% of imatinib-treated patients.
By 5 years, 26 patients (10%) in each treatment arm had died. Nine patients in the dasatinib arm died of disease progression, as did 17 patients in the imatinib arm.
Long-term results from the DASISION trial suggest that dasatinib and imatinib produce similar outcomes in patients with newly diagnosed chronic phase chronic myeloid leukemia (CP-CML).
Although patients who received dasatinib experienced faster and deeper molecular responses than patients who received imatinib, the overall survival and progression-free survival rates were similar between the treatment arms.
Overall, adverse events (AEs) were similar between the arms as well.
Researchers said these results suggest that dasatinib should continue to be considered an option for patients with newly diagnosed CP-CML.
The team reported the results of this study in the Journal of Clinical Oncology. The research was sponsored by Bristol-Myers Squibb.
The trial enrolled 519 patients with newly diagnosed CP-CML. They were randomized to receive dasatinib at 100 mg once daily (n=259) or imatinib at 400 mg once daily (n=260). Baseline characteristics were well-balanced between the arms.
At 5 years of follow-up, 61% of patients in the dasatinib arm and 63% of patients in the imatinib arm remained on treatment.
Response and survival
The cumulative 5-year rate of major molecular response was 76% in the dasatinib arm and 64% in the imatinib arm (P=0.0022). The rates of MR4.5 were 42% and 33%, respectively (P=0.0251).
The estimated 5-year overall survival was 91% in the dasatinib arm and 90% in the imatinib arm (hazard ratio=1.01; 95% CI, 0.58 to 1.73).
The estimated 5-year progression-free survival was 85% and 86%, respectively (hazard ratio=1.06; 95% CI, 0.68 to 1.66).
Safety
In both treatment arms, most AEs were grade 1 or 2. Grade 3/4 AEs occurred in 15% of patients in the dasatinib arm and 11% of patients in the imatinib arm.
Rates of grade 3/4 hematologic AEs tended to be higher in the dasatinib arm than the imatinib arm.
But the rates of most drug-related, nonhematologic AEs were lower in the dasatinib arm than the imatinib arm or were comparable between the arms.
The exception was drug-related pleural effusion, which was more common with dasatinib (28%) than with imatinib (0.8%).
Drug-related AEs were largely manageable, although they led to treatment discontinuation in 16% of dasatinib-treated patients and 7% of imatinib-treated patients.
By 5 years, 26 patients (10%) in each treatment arm had died. Nine patients in the dasatinib arm died of disease progression, as did 17 patients in the imatinib arm.
EC expands approved use of carfilzomib

Photo from Amgen
The European Commission (EC) has expanded the approved use of the proteasome inhibitor carfilzomib (Kyprolis).
The drug is now approved for use in combination with dexamethasone to treat adults with multiple myeloma (MM) who have received at least 1 prior therapy.
Carfilzomib was previously approved by the EC for use in combination with lenalidomide and dexamethasone to treat adult MM patients who have received at least 1 prior therapy.
The EC approved the extended indication for carfilzomib based on data from the phase 3 ENDEAVOR trial.
The trial included 929 MM patients whose disease had relapsed after 1 to 3 prior therapeutic regimens.
The patients received either carfilzomib plus dexamethasone (n=464) or bortezomib plus dexamethasone (n=465) until disease progression.
The primary endpoint was progression-free survival. The median progression-free survival was 18.7 months in the carfilzomib arm and 9.4 months in the bortezomib arm. The hazard ratio was 0.53 (P<0.0001).
Overall survival data were not yet mature at last follow-up.
Treatment discontinuation due to adverse events and on-study deaths were comparable between the 2 treatment arms.
However, a number of known adverse events were reported at a higher rate in the carfilzomib arm than the bortezomib arm, including dyspnea (28% vs 13%), hypertension (25% vs 3%), pyrexia (27% vs 14%), cough (25% vs 15%), cardiac failure (8% vs 3%), and acute renal failure (8% vs 5%).
Carfilzomib is marketed as Kyprolis by Onyx Pharmaceuticals, Inc., a subsidiary of Amgen that holds development and commercialization rights to the drug globally, with the exception of Japan.
Photo from Amgen
The European Commission (EC) has expanded the approved use of the proteasome inhibitor carfilzomib (Kyprolis).
The drug is now approved for use in combination with dexamethasone to treat adults with multiple myeloma (MM) who have received at least 1 prior therapy.
Carfilzomib was previously approved by the EC for use in combination with lenalidomide and dexamethasone to treat adult MM patients who have received at least 1 prior therapy.
The EC approved the extended indication for carfilzomib based on data from the phase 3 ENDEAVOR trial.
The trial included 929 MM patients whose disease had relapsed after 1 to 3 prior therapeutic regimens.
The patients received either carfilzomib plus dexamethasone (n=464) or bortezomib plus dexamethasone (n=465) until disease progression.
The primary endpoint was progression-free survival. The median progression-free survival was 18.7 months in the carfilzomib arm and 9.4 months in the bortezomib arm. The hazard ratio was 0.53 (P<0.0001).
Overall survival data were not yet mature at last follow-up.
Treatment discontinuation due to adverse events and on-study deaths were comparable between the 2 treatment arms.
However, a number of known adverse events were reported at a higher rate in the carfilzomib arm than the bortezomib arm, including dyspnea (28% vs 13%), hypertension (25% vs 3%), pyrexia (27% vs 14%), cough (25% vs 15%), cardiac failure (8% vs 3%), and acute renal failure (8% vs 5%).
Carfilzomib is marketed as Kyprolis by Onyx Pharmaceuticals, Inc., a subsidiary of Amgen that holds development and commercialization rights to the drug globally, with the exception of Japan.
Photo from Amgen
The European Commission (EC) has expanded the approved use of the proteasome inhibitor carfilzomib (Kyprolis).
The drug is now approved for use in combination with dexamethasone to treat adults with multiple myeloma (MM) who have received at least 1 prior therapy.
Carfilzomib was previously approved by the EC for use in combination with lenalidomide and dexamethasone to treat adult MM patients who have received at least 1 prior therapy.
The EC approved the extended indication for carfilzomib based on data from the phase 3 ENDEAVOR trial.
The trial included 929 MM patients whose disease had relapsed after 1 to 3 prior therapeutic regimens.
The patients received either carfilzomib plus dexamethasone (n=464) or bortezomib plus dexamethasone (n=465) until disease progression.
The primary endpoint was progression-free survival. The median progression-free survival was 18.7 months in the carfilzomib arm and 9.4 months in the bortezomib arm. The hazard ratio was 0.53 (P<0.0001).
Overall survival data were not yet mature at last follow-up.
Treatment discontinuation due to adverse events and on-study deaths were comparable between the 2 treatment arms.
However, a number of known adverse events were reported at a higher rate in the carfilzomib arm than the bortezomib arm, including dyspnea (28% vs 13%), hypertension (25% vs 3%), pyrexia (27% vs 14%), cough (25% vs 15%), cardiac failure (8% vs 3%), and acute renal failure (8% vs 5%).
Carfilzomib is marketed as Kyprolis by Onyx Pharmaceuticals, Inc., a subsidiary of Amgen that holds development and commercialization rights to the drug globally, with the exception of Japan.