User login
Genes may be targets for AML therapy

Two genes are critical to the development of acute myeloid leukemia (AML), according to research published in Cancer Cell.
Previous research suggested the genes, KDM4C and PRMT1, are key players in transcription regulation during both normal and disease development.
The new study showed that, during AML development, KDM4C and PRMT1 are recruited to enable the transformation of blood cells into cancer cells.
The genes work in tandem, and, if either is not fully active, AML does not develop.
The researchers made these discoveries by inhibiting KDM4C and PRMT1—either genetically or pharmacologically—in mice with AML.
When either gene was silenced via genetic means, the majority of the mice were still alive at the end of the researchers’ 60-day experiment. However, the majority of control mice died in less than 40 days.
The team observed similarly favorable results when they inhibited either gene with drugs—the PRMT1 inhibitor AMI-408 and the KDM4C inhibitor SD70.
The median disease latency was 48 days in mice that received AMI-408 and 36 days in control mice. The median disease latency was 62 days in mice that received SD70 and 55 days in control mice.
“The demonstration of how critical these genes are to cancer transformation and treatment could be highly significant for the design of new drugs,” said study author Eric So, PhD, of King’s College London in the UK.
“Further work is needed to develop and refine drugs to maximize their effects and so that they are suitable for patients. Clinical trials will then be needed to see how leukemia patients respond to these drugs and how use of them can be optimized.” ![]()
Two genes are critical to the development of acute myeloid leukemia (AML), according to research published in Cancer Cell.
Previous research suggested the genes, KDM4C and PRMT1, are key players in transcription regulation during both normal and disease development.
The new study showed that, during AML development, KDM4C and PRMT1 are recruited to enable the transformation of blood cells into cancer cells.
The genes work in tandem, and, if either is not fully active, AML does not develop.
The researchers made these discoveries by inhibiting KDM4C and PRMT1—either genetically or pharmacologically—in mice with AML.
When either gene was silenced via genetic means, the majority of the mice were still alive at the end of the researchers’ 60-day experiment. However, the majority of control mice died in less than 40 days.
The team observed similarly favorable results when they inhibited either gene with drugs—the PRMT1 inhibitor AMI-408 and the KDM4C inhibitor SD70.
The median disease latency was 48 days in mice that received AMI-408 and 36 days in control mice. The median disease latency was 62 days in mice that received SD70 and 55 days in control mice.
“The demonstration of how critical these genes are to cancer transformation and treatment could be highly significant for the design of new drugs,” said study author Eric So, PhD, of King’s College London in the UK.
“Further work is needed to develop and refine drugs to maximize their effects and so that they are suitable for patients. Clinical trials will then be needed to see how leukemia patients respond to these drugs and how use of them can be optimized.” ![]()
Two genes are critical to the development of acute myeloid leukemia (AML), according to research published in Cancer Cell.
Previous research suggested the genes, KDM4C and PRMT1, are key players in transcription regulation during both normal and disease development.
The new study showed that, during AML development, KDM4C and PRMT1 are recruited to enable the transformation of blood cells into cancer cells.
The genes work in tandem, and, if either is not fully active, AML does not develop.
The researchers made these discoveries by inhibiting KDM4C and PRMT1—either genetically or pharmacologically—in mice with AML.
When either gene was silenced via genetic means, the majority of the mice were still alive at the end of the researchers’ 60-day experiment. However, the majority of control mice died in less than 40 days.
The team observed similarly favorable results when they inhibited either gene with drugs—the PRMT1 inhibitor AMI-408 and the KDM4C inhibitor SD70.
The median disease latency was 48 days in mice that received AMI-408 and 36 days in control mice. The median disease latency was 62 days in mice that received SD70 and 55 days in control mice.
“The demonstration of how critical these genes are to cancer transformation and treatment could be highly significant for the design of new drugs,” said study author Eric So, PhD, of King’s College London in the UK.
“Further work is needed to develop and refine drugs to maximize their effects and so that they are suitable for patients. Clinical trials will then be needed to see how leukemia patients respond to these drugs and how use of them can be optimized.” ![]()
Forces driving leukemia differ in kids and adults

New research suggests childhood leukemias are forged by different evolutionary forces than leukemias in older adults.
Researchers used a computational model to characterize the population dynamics of hematopoietic stem cells (HSCs) that give rise to leukemias.
And they found the evolutionary force known as “drift” contributes to leukemia development in young children but not in older adults.
“Basically, leukemia risk early in life may be more dictated by chance than by the typical ‘survival of the fittest’ that characterizes leukemia formation in older adults,” explained study author James DeGregori, PhD, of the University of Colorado School of Medicine in Aurora.
He and his colleagues recounted this discovery in PNAS.
With previous work, the DeGregori lab showed that the inevitable tissue decline associated with aging benefits HSCs with mutations that allow the cells to better adapt to the new ecosystem.
In contrast, the ecosystem of young tissue favors healthy cells. Optimized by millions of years of co-evolution, most mutations make cells less fit for the ecosystem of young, healthy tissue and lead to purging of mutant cells from the tissue.
With the current study, Dr DeGregori and his colleagues made a surprising discovery. Despite the ability of young tissue to select against cells with cancer-causing mutations, the computational model showed increased proportions of specific, mutation-bearing HSCs in the first few years after birth.
And these mutated cells were not dependent on the effect of the mutation on cell fitness. In other words, the mutation-bearing cells were not more fit than cells without the mutations. Instead of the survival-of-the-fittest form of natural selection that drives the evolution of cancer in older adults, there was another force at work.
In fact, the researchers discovered 2 factors that influence the development of childhood leukemia: the small HSC pool size at birth and the high rate of cell division necessary for body growth early in life.
The high rate of cell division increases the risk of leukemia because mutations largely happen during cell divisions. More cell divisions mean more mutations, and this increases the risk that some of these mutations could contribute to leukemia development.
The small HSC pool size influences leukemia development via the evolutionary force known as drift. Drift is the role of chance—the possibility that, despite being less fit, an animal, organism, or HSC with an oncogenic mutation will survive to shift the genetic makeup of the population.
The influence of drift is greater in small populations and, in this case, small stem cell pools. In the small HSC pools of young children, drift becomes important as a lucky genotype may end up with a larger share of the total HSC pool than warranted by its fitness status.
If this lucky cell clone happens to have a mutation that can start the HSC down the path toward leukemia, this drift-driven expansion should increase the risk of leukemia by increasing the number of HSCs with this mutation.
“Thus, early somatic evolution in HSC pools is significantly impacted by drift, with selection playing a lesser role,” Dr DeGregori and his colleagues wrote.
On the other hand, the impact of drift lessens as the HSC pool grows along with an infant’s body to reach adult size. The larger HSC pool size decreases the role of drift in the success of particular cells in the tissue.
In addition, as the pool size reaches its maximum, the HSC division rate slows to a crawl (as these stem cells enter the maintenance rather than growth phase). With a landscape of healthy, youthful tissues and low rates of mutation due to low cell division rates, the odds of leukemia diminish.
“With a large population of healthy cells optimized to young, healthy tissue, the ability of mutations, including cancerous mutations, to drive uncontrolled cell proliferation is reduced,” Dr DeGregori said.
However, in old age, tissue decline promotes selection for adaptive mutations, leading to the expansion of potentially oncogenic HSC clones that will again increase the risk of leukemia.
Thus, this research shows that, in early life, leukemias are driven by mutation and drift. And in later life, leukemias are driven by mutation and selection.
“We show that leukemias of children and older adults are different diseases, forged by different evolutionary forces and propagated under different circumstances,” Dr DeGregori said.
He and his colleagues believe this understanding raises the possibility of a new approach to cancer treatment. Perhaps researchers could find a way to manipulate the parameters of cell evolution or manipulate the tissue ecosystem to decrease cancer risk. ![]()
New research suggests childhood leukemias are forged by different evolutionary forces than leukemias in older adults.
Researchers used a computational model to characterize the population dynamics of hematopoietic stem cells (HSCs) that give rise to leukemias.
And they found the evolutionary force known as “drift” contributes to leukemia development in young children but not in older adults.
“Basically, leukemia risk early in life may be more dictated by chance than by the typical ‘survival of the fittest’ that characterizes leukemia formation in older adults,” explained study author James DeGregori, PhD, of the University of Colorado School of Medicine in Aurora.
He and his colleagues recounted this discovery in PNAS.
With previous work, the DeGregori lab showed that the inevitable tissue decline associated with aging benefits HSCs with mutations that allow the cells to better adapt to the new ecosystem.
In contrast, the ecosystem of young tissue favors healthy cells. Optimized by millions of years of co-evolution, most mutations make cells less fit for the ecosystem of young, healthy tissue and lead to purging of mutant cells from the tissue.
With the current study, Dr DeGregori and his colleagues made a surprising discovery. Despite the ability of young tissue to select against cells with cancer-causing mutations, the computational model showed increased proportions of specific, mutation-bearing HSCs in the first few years after birth.
And these mutated cells were not dependent on the effect of the mutation on cell fitness. In other words, the mutation-bearing cells were not more fit than cells without the mutations. Instead of the survival-of-the-fittest form of natural selection that drives the evolution of cancer in older adults, there was another force at work.
In fact, the researchers discovered 2 factors that influence the development of childhood leukemia: the small HSC pool size at birth and the high rate of cell division necessary for body growth early in life.
The high rate of cell division increases the risk of leukemia because mutations largely happen during cell divisions. More cell divisions mean more mutations, and this increases the risk that some of these mutations could contribute to leukemia development.
The small HSC pool size influences leukemia development via the evolutionary force known as drift. Drift is the role of chance—the possibility that, despite being less fit, an animal, organism, or HSC with an oncogenic mutation will survive to shift the genetic makeup of the population.
The influence of drift is greater in small populations and, in this case, small stem cell pools. In the small HSC pools of young children, drift becomes important as a lucky genotype may end up with a larger share of the total HSC pool than warranted by its fitness status.
If this lucky cell clone happens to have a mutation that can start the HSC down the path toward leukemia, this drift-driven expansion should increase the risk of leukemia by increasing the number of HSCs with this mutation.
“Thus, early somatic evolution in HSC pools is significantly impacted by drift, with selection playing a lesser role,” Dr DeGregori and his colleagues wrote.
On the other hand, the impact of drift lessens as the HSC pool grows along with an infant’s body to reach adult size. The larger HSC pool size decreases the role of drift in the success of particular cells in the tissue.
In addition, as the pool size reaches its maximum, the HSC division rate slows to a crawl (as these stem cells enter the maintenance rather than growth phase). With a landscape of healthy, youthful tissues and low rates of mutation due to low cell division rates, the odds of leukemia diminish.
“With a large population of healthy cells optimized to young, healthy tissue, the ability of mutations, including cancerous mutations, to drive uncontrolled cell proliferation is reduced,” Dr DeGregori said.
However, in old age, tissue decline promotes selection for adaptive mutations, leading to the expansion of potentially oncogenic HSC clones that will again increase the risk of leukemia.
Thus, this research shows that, in early life, leukemias are driven by mutation and drift. And in later life, leukemias are driven by mutation and selection.
“We show that leukemias of children and older adults are different diseases, forged by different evolutionary forces and propagated under different circumstances,” Dr DeGregori said.
He and his colleagues believe this understanding raises the possibility of a new approach to cancer treatment. Perhaps researchers could find a way to manipulate the parameters of cell evolution or manipulate the tissue ecosystem to decrease cancer risk. ![]()
New research suggests childhood leukemias are forged by different evolutionary forces than leukemias in older adults.
Researchers used a computational model to characterize the population dynamics of hematopoietic stem cells (HSCs) that give rise to leukemias.
And they found the evolutionary force known as “drift” contributes to leukemia development in young children but not in older adults.
“Basically, leukemia risk early in life may be more dictated by chance than by the typical ‘survival of the fittest’ that characterizes leukemia formation in older adults,” explained study author James DeGregori, PhD, of the University of Colorado School of Medicine in Aurora.
He and his colleagues recounted this discovery in PNAS.
With previous work, the DeGregori lab showed that the inevitable tissue decline associated with aging benefits HSCs with mutations that allow the cells to better adapt to the new ecosystem.
In contrast, the ecosystem of young tissue favors healthy cells. Optimized by millions of years of co-evolution, most mutations make cells less fit for the ecosystem of young, healthy tissue and lead to purging of mutant cells from the tissue.
With the current study, Dr DeGregori and his colleagues made a surprising discovery. Despite the ability of young tissue to select against cells with cancer-causing mutations, the computational model showed increased proportions of specific, mutation-bearing HSCs in the first few years after birth.
And these mutated cells were not dependent on the effect of the mutation on cell fitness. In other words, the mutation-bearing cells were not more fit than cells without the mutations. Instead of the survival-of-the-fittest form of natural selection that drives the evolution of cancer in older adults, there was another force at work.
In fact, the researchers discovered 2 factors that influence the development of childhood leukemia: the small HSC pool size at birth and the high rate of cell division necessary for body growth early in life.
The high rate of cell division increases the risk of leukemia because mutations largely happen during cell divisions. More cell divisions mean more mutations, and this increases the risk that some of these mutations could contribute to leukemia development.
The small HSC pool size influences leukemia development via the evolutionary force known as drift. Drift is the role of chance—the possibility that, despite being less fit, an animal, organism, or HSC with an oncogenic mutation will survive to shift the genetic makeup of the population.
The influence of drift is greater in small populations and, in this case, small stem cell pools. In the small HSC pools of young children, drift becomes important as a lucky genotype may end up with a larger share of the total HSC pool than warranted by its fitness status.
If this lucky cell clone happens to have a mutation that can start the HSC down the path toward leukemia, this drift-driven expansion should increase the risk of leukemia by increasing the number of HSCs with this mutation.
“Thus, early somatic evolution in HSC pools is significantly impacted by drift, with selection playing a lesser role,” Dr DeGregori and his colleagues wrote.
On the other hand, the impact of drift lessens as the HSC pool grows along with an infant’s body to reach adult size. The larger HSC pool size decreases the role of drift in the success of particular cells in the tissue.
In addition, as the pool size reaches its maximum, the HSC division rate slows to a crawl (as these stem cells enter the maintenance rather than growth phase). With a landscape of healthy, youthful tissues and low rates of mutation due to low cell division rates, the odds of leukemia diminish.
“With a large population of healthy cells optimized to young, healthy tissue, the ability of mutations, including cancerous mutations, to drive uncontrolled cell proliferation is reduced,” Dr DeGregori said.
However, in old age, tissue decline promotes selection for adaptive mutations, leading to the expansion of potentially oncogenic HSC clones that will again increase the risk of leukemia.
Thus, this research shows that, in early life, leukemias are driven by mutation and drift. And in later life, leukemias are driven by mutation and selection.
“We show that leukemias of children and older adults are different diseases, forged by different evolutionary forces and propagated under different circumstances,” Dr DeGregori said.
He and his colleagues believe this understanding raises the possibility of a new approach to cancer treatment. Perhaps researchers could find a way to manipulate the parameters of cell evolution or manipulate the tissue ecosystem to decrease cancer risk. ![]()
Microcapsules could provide targeted drug delivery
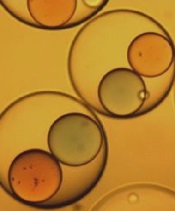
Image courtesy of Ronald Xu
& The Ohio State University
Researchers say they have developed a quick and controllable method for getting 2 or more ingredients into the same tiny drug capsule and having them mix only when triggered by a signal like vibrations or heat.
This work was inspired by the search for targeted drug delivery options to treat cancers.
The idea with this multi-ingredient capsule is that the ingredients must be mixed for the drug to work, and the mixing could be triggered in targeted areas of the body, thereby boosting drug efficiency while reducing side effects.
While the researchers found they could use their technique to create multi-ingredient microcapsules, they have not yet used it to encapsulate cancer treatments.
They described their work in Applied Physics Letters.
“One of the limitations of chemotherapy is that less than 5% of the drugs typically get to the tumor, while the rest can be absorbed by other organs,” said study author Ronald Xu, PhD, of The Ohio State University in Columbus.
He and his colleagues thought one possible way to address this problem could be to make the drugs non-toxic when injected into the body and trigger mixing that would produce a toxic product only near the tumor site.
The researchers knew that, for such drugs to work on a large scale, there must be a way to quickly, controllably, and cost-effectively produce capsules with 2 or more active ingredients. If the drugs are to be injected and spread through the body via the bloodstream, the capsules should also be small.
With that in mind, Dr Xu and his colleagues developed a device that can produce tiny capsules approximately 100 microns across with multiple inner ingredients.
The device works by funneling different ingredients through 2 inner needles. These needles run parallel to each other and are both enclosed in a larger outer needle, which contains an ingredient for making the outer shell of the capsule.
As all the ingredients exit the needles through a single nozzle, a high-speed gas forces the liquids into a narrow stream that breaks into individual droplets. An electric field stabilizes the flow so that uniform droplets are created.
Depending on the relative flow rates, each droplet may contain 2 or more smaller inner droplets made from the ingredients in the inner needles.
The researchers tested their device with colored paraffin wax—red in one needle and blue in the other. The outer shell was made from sodium alginate, a material extracted from seaweed that turned gelatinous when the droplets fell into a calcium chloride solution.
Depending on the experimental conditions, the team was able to produce between 1000 and 100,000 capsules per second, and nearly 100% of the inner liquids were incorporated into the capsules without any waste.
Once encapsulated, the 2 colors of wax did not mix because of surface tension. But the researchers found they could force the red and blue wax to merge by vibrating the capsules. The team also discovered they could release the inner droplets by dissolving the outer shell.
The key features of the new device are its high efficiency and yield, and the fact that the size of the droplets can be uniformly controlled, Dr Xu said.
He added that, by further fine-tuning the device’s operation, the team could make capsules that are 3-5 microns across, about the size of a red blood cell. The process can also be scaled up by building an array of nozzles and could be modified to encapsulate 3 or more active ingredients by adding additional inner needles.
While Dr Xu and his colleagues were motivated by drug delivery, they believe their device might also find wider use in a range of applications that require controlled reactions, such as regenerative medicine and nuclear and chemical engineering. ![]()
Image courtesy of Ronald Xu
& The Ohio State University
Researchers say they have developed a quick and controllable method for getting 2 or more ingredients into the same tiny drug capsule and having them mix only when triggered by a signal like vibrations or heat.
This work was inspired by the search for targeted drug delivery options to treat cancers.
The idea with this multi-ingredient capsule is that the ingredients must be mixed for the drug to work, and the mixing could be triggered in targeted areas of the body, thereby boosting drug efficiency while reducing side effects.
While the researchers found they could use their technique to create multi-ingredient microcapsules, they have not yet used it to encapsulate cancer treatments.
They described their work in Applied Physics Letters.
“One of the limitations of chemotherapy is that less than 5% of the drugs typically get to the tumor, while the rest can be absorbed by other organs,” said study author Ronald Xu, PhD, of The Ohio State University in Columbus.
He and his colleagues thought one possible way to address this problem could be to make the drugs non-toxic when injected into the body and trigger mixing that would produce a toxic product only near the tumor site.
The researchers knew that, for such drugs to work on a large scale, there must be a way to quickly, controllably, and cost-effectively produce capsules with 2 or more active ingredients. If the drugs are to be injected and spread through the body via the bloodstream, the capsules should also be small.
With that in mind, Dr Xu and his colleagues developed a device that can produce tiny capsules approximately 100 microns across with multiple inner ingredients.
The device works by funneling different ingredients through 2 inner needles. These needles run parallel to each other and are both enclosed in a larger outer needle, which contains an ingredient for making the outer shell of the capsule.
As all the ingredients exit the needles through a single nozzle, a high-speed gas forces the liquids into a narrow stream that breaks into individual droplets. An electric field stabilizes the flow so that uniform droplets are created.
Depending on the relative flow rates, each droplet may contain 2 or more smaller inner droplets made from the ingredients in the inner needles.
The researchers tested their device with colored paraffin wax—red in one needle and blue in the other. The outer shell was made from sodium alginate, a material extracted from seaweed that turned gelatinous when the droplets fell into a calcium chloride solution.
Depending on the experimental conditions, the team was able to produce between 1000 and 100,000 capsules per second, and nearly 100% of the inner liquids were incorporated into the capsules without any waste.
Once encapsulated, the 2 colors of wax did not mix because of surface tension. But the researchers found they could force the red and blue wax to merge by vibrating the capsules. The team also discovered they could release the inner droplets by dissolving the outer shell.
The key features of the new device are its high efficiency and yield, and the fact that the size of the droplets can be uniformly controlled, Dr Xu said.
He added that, by further fine-tuning the device’s operation, the team could make capsules that are 3-5 microns across, about the size of a red blood cell. The process can also be scaled up by building an array of nozzles and could be modified to encapsulate 3 or more active ingredients by adding additional inner needles.
While Dr Xu and his colleagues were motivated by drug delivery, they believe their device might also find wider use in a range of applications that require controlled reactions, such as regenerative medicine and nuclear and chemical engineering. ![]()
Image courtesy of Ronald Xu
& The Ohio State University
Researchers say they have developed a quick and controllable method for getting 2 or more ingredients into the same tiny drug capsule and having them mix only when triggered by a signal like vibrations or heat.
This work was inspired by the search for targeted drug delivery options to treat cancers.
The idea with this multi-ingredient capsule is that the ingredients must be mixed for the drug to work, and the mixing could be triggered in targeted areas of the body, thereby boosting drug efficiency while reducing side effects.
While the researchers found they could use their technique to create multi-ingredient microcapsules, they have not yet used it to encapsulate cancer treatments.
They described their work in Applied Physics Letters.
“One of the limitations of chemotherapy is that less than 5% of the drugs typically get to the tumor, while the rest can be absorbed by other organs,” said study author Ronald Xu, PhD, of The Ohio State University in Columbus.
He and his colleagues thought one possible way to address this problem could be to make the drugs non-toxic when injected into the body and trigger mixing that would produce a toxic product only near the tumor site.
The researchers knew that, for such drugs to work on a large scale, there must be a way to quickly, controllably, and cost-effectively produce capsules with 2 or more active ingredients. If the drugs are to be injected and spread through the body via the bloodstream, the capsules should also be small.
With that in mind, Dr Xu and his colleagues developed a device that can produce tiny capsules approximately 100 microns across with multiple inner ingredients.
The device works by funneling different ingredients through 2 inner needles. These needles run parallel to each other and are both enclosed in a larger outer needle, which contains an ingredient for making the outer shell of the capsule.
As all the ingredients exit the needles through a single nozzle, a high-speed gas forces the liquids into a narrow stream that breaks into individual droplets. An electric field stabilizes the flow so that uniform droplets are created.
Depending on the relative flow rates, each droplet may contain 2 or more smaller inner droplets made from the ingredients in the inner needles.
The researchers tested their device with colored paraffin wax—red in one needle and blue in the other. The outer shell was made from sodium alginate, a material extracted from seaweed that turned gelatinous when the droplets fell into a calcium chloride solution.
Depending on the experimental conditions, the team was able to produce between 1000 and 100,000 capsules per second, and nearly 100% of the inner liquids were incorporated into the capsules without any waste.
Once encapsulated, the 2 colors of wax did not mix because of surface tension. But the researchers found they could force the red and blue wax to merge by vibrating the capsules. The team also discovered they could release the inner droplets by dissolving the outer shell.
The key features of the new device are its high efficiency and yield, and the fact that the size of the droplets can be uniformly controlled, Dr Xu said.
He added that, by further fine-tuning the device’s operation, the team could make capsules that are 3-5 microns across, about the size of a red blood cell. The process can also be scaled up by building an array of nozzles and could be modified to encapsulate 3 or more active ingredients by adding additional inner needles.
While Dr Xu and his colleagues were motivated by drug delivery, they believe their device might also find wider use in a range of applications that require controlled reactions, such as regenerative medicine and nuclear and chemical engineering. ![]()
ATG can reduce risk, severity of chronic GVHD

Image courtesy of PLOS ONE
Results of a phase 3 study suggest that administering antihuman T-lymphocyte immune globulin (ATG) prior to hematopoietic stem cell transplant (HSCT) can decrease the risk and severity of chronic graft-versus-host disease (GVHD).
Study investigators included ATG in the conditioning regimens of leukemia patients receiving peripheral blood stem cells from an HLA-identical sibling donor.
Two years after HSCT, these patients had less than half the rate of chronic GVHD of patients who did not receive ATG.
In addition, patients who received ATG were less likely to have severe chronic GVHD.
Nicolaus Kroger, MD, of the University Medical Center Hamburg-Eppendorf in Hamburg, Germany, and his colleagues reported these results in NEJM.
The investigators enrolled 168 patients undergoing HSCT at 27 centers. They were randomized in a 1:1 ratio to receive ATG or not.
One hundred and fifty-five patients were randomized and evaluable—83 in the ATG group and 72 in the non-ATG group.
The only significant difference in baseline characteristics was age. The median age was 39 (range, 18-64) in the ATG group and 43.5 (range, 21-61) in the non-ATG group (P=0.04).
Most patients in both groups were male (63.9% and 55.6%, respectively), and most had acute myeloid leukemia (66.3% and 76.4%, respectively) rather than acute lymphoblastic leukemia (33.8% and 23.6%, respectively).
Most patients had intermediate-risk disease (75.9% and 82.1%, respectively), and a minority had high-risk cytogenetics (37.3% and 30.6%, respectively).
The median time between diagnosis and HSCT was about 5 months in both groups. Both groups had a median of 2 courses of chemotherapy before transplant (overall range, 1-8).
Most patients in both groups received busulfan plus cyclophosphamide as conditioning—67.5% of the ATG group and 70.8% of the non-ATG group. Some received total-body irradiation plus cyclophosphamide (27.7% and 25.0%, respectively), and a few received total-body irradiation plus etoposide (4.8% and 4.2%, respectively).
Results
After a median follow-up of 24 months, the cumulative incidence of chronic GVHD was significantly lower in the ATG group than the non-ATG group—32.2% and 68.7%, respectively (P<0.001).
In addition, patients in the ATG group were significantly less likely to have severe or extensive chronic GVHD.
According to revised Seattle criteria, the rate of limited chronic GVHD was 20.5% in the ATG group and 30.6% in the non-ATG group. And the rates of extensive chronic GVHD were 6% and 33.3%, respectively (P<0.001).
According to revised NIH criteria, the rate of mild chronic GVHD was 15.7% in the ATG group and 16.7% in the non-ATG group. The rates of moderate chronic GVHD were 8.4% and 25%, respectively. And the rates of severe chronic GVHD were 2.4% and 22.2%, respectively (P<0.001).
However, all other outcomes, when assessed alone, were similar between the treatment groups.
The rate of 2-year relapse-free survival was 59.4% in the ATG group and 64.6% in the non-ATG group (P=0.21). The overall survival rates were 74.1% and 77.9%, respectively (P=0.46).
The incidence of relapse was 32.2% and 35.5%, respectively (P=0.17). Infectious complications occurred in 57.8% and 54.2%, respectively (P=0.65). And the rates of acute GVHD were 10.8% and 18.1%, respectively (P=0.13).
However, the rate of a composite endpoint of chronic GVHD-free and relapse-free survival at 2 years was significantly higher in the ATG group than the non-ATG group—36.6% and 16.8%, respectively (P=0.005). ![]()
Image courtesy of PLOS ONE
Results of a phase 3 study suggest that administering antihuman T-lymphocyte immune globulin (ATG) prior to hematopoietic stem cell transplant (HSCT) can decrease the risk and severity of chronic graft-versus-host disease (GVHD).
Study investigators included ATG in the conditioning regimens of leukemia patients receiving peripheral blood stem cells from an HLA-identical sibling donor.
Two years after HSCT, these patients had less than half the rate of chronic GVHD of patients who did not receive ATG.
In addition, patients who received ATG were less likely to have severe chronic GVHD.
Nicolaus Kroger, MD, of the University Medical Center Hamburg-Eppendorf in Hamburg, Germany, and his colleagues reported these results in NEJM.
The investigators enrolled 168 patients undergoing HSCT at 27 centers. They were randomized in a 1:1 ratio to receive ATG or not.
One hundred and fifty-five patients were randomized and evaluable—83 in the ATG group and 72 in the non-ATG group.
The only significant difference in baseline characteristics was age. The median age was 39 (range, 18-64) in the ATG group and 43.5 (range, 21-61) in the non-ATG group (P=0.04).
Most patients in both groups were male (63.9% and 55.6%, respectively), and most had acute myeloid leukemia (66.3% and 76.4%, respectively) rather than acute lymphoblastic leukemia (33.8% and 23.6%, respectively).
Most patients had intermediate-risk disease (75.9% and 82.1%, respectively), and a minority had high-risk cytogenetics (37.3% and 30.6%, respectively).
The median time between diagnosis and HSCT was about 5 months in both groups. Both groups had a median of 2 courses of chemotherapy before transplant (overall range, 1-8).
Most patients in both groups received busulfan plus cyclophosphamide as conditioning—67.5% of the ATG group and 70.8% of the non-ATG group. Some received total-body irradiation plus cyclophosphamide (27.7% and 25.0%, respectively), and a few received total-body irradiation plus etoposide (4.8% and 4.2%, respectively).
Results
After a median follow-up of 24 months, the cumulative incidence of chronic GVHD was significantly lower in the ATG group than the non-ATG group—32.2% and 68.7%, respectively (P<0.001).
In addition, patients in the ATG group were significantly less likely to have severe or extensive chronic GVHD.
According to revised Seattle criteria, the rate of limited chronic GVHD was 20.5% in the ATG group and 30.6% in the non-ATG group. And the rates of extensive chronic GVHD were 6% and 33.3%, respectively (P<0.001).
According to revised NIH criteria, the rate of mild chronic GVHD was 15.7% in the ATG group and 16.7% in the non-ATG group. The rates of moderate chronic GVHD were 8.4% and 25%, respectively. And the rates of severe chronic GVHD were 2.4% and 22.2%, respectively (P<0.001).
However, all other outcomes, when assessed alone, were similar between the treatment groups.
The rate of 2-year relapse-free survival was 59.4% in the ATG group and 64.6% in the non-ATG group (P=0.21). The overall survival rates were 74.1% and 77.9%, respectively (P=0.46).
The incidence of relapse was 32.2% and 35.5%, respectively (P=0.17). Infectious complications occurred in 57.8% and 54.2%, respectively (P=0.65). And the rates of acute GVHD were 10.8% and 18.1%, respectively (P=0.13).
However, the rate of a composite endpoint of chronic GVHD-free and relapse-free survival at 2 years was significantly higher in the ATG group than the non-ATG group—36.6% and 16.8%, respectively (P=0.005). ![]()
Image courtesy of PLOS ONE
Results of a phase 3 study suggest that administering antihuman T-lymphocyte immune globulin (ATG) prior to hematopoietic stem cell transplant (HSCT) can decrease the risk and severity of chronic graft-versus-host disease (GVHD).
Study investigators included ATG in the conditioning regimens of leukemia patients receiving peripheral blood stem cells from an HLA-identical sibling donor.
Two years after HSCT, these patients had less than half the rate of chronic GVHD of patients who did not receive ATG.
In addition, patients who received ATG were less likely to have severe chronic GVHD.
Nicolaus Kroger, MD, of the University Medical Center Hamburg-Eppendorf in Hamburg, Germany, and his colleagues reported these results in NEJM.
The investigators enrolled 168 patients undergoing HSCT at 27 centers. They were randomized in a 1:1 ratio to receive ATG or not.
One hundred and fifty-five patients were randomized and evaluable—83 in the ATG group and 72 in the non-ATG group.
The only significant difference in baseline characteristics was age. The median age was 39 (range, 18-64) in the ATG group and 43.5 (range, 21-61) in the non-ATG group (P=0.04).
Most patients in both groups were male (63.9% and 55.6%, respectively), and most had acute myeloid leukemia (66.3% and 76.4%, respectively) rather than acute lymphoblastic leukemia (33.8% and 23.6%, respectively).
Most patients had intermediate-risk disease (75.9% and 82.1%, respectively), and a minority had high-risk cytogenetics (37.3% and 30.6%, respectively).
The median time between diagnosis and HSCT was about 5 months in both groups. Both groups had a median of 2 courses of chemotherapy before transplant (overall range, 1-8).
Most patients in both groups received busulfan plus cyclophosphamide as conditioning—67.5% of the ATG group and 70.8% of the non-ATG group. Some received total-body irradiation plus cyclophosphamide (27.7% and 25.0%, respectively), and a few received total-body irradiation plus etoposide (4.8% and 4.2%, respectively).
Results
After a median follow-up of 24 months, the cumulative incidence of chronic GVHD was significantly lower in the ATG group than the non-ATG group—32.2% and 68.7%, respectively (P<0.001).
In addition, patients in the ATG group were significantly less likely to have severe or extensive chronic GVHD.
According to revised Seattle criteria, the rate of limited chronic GVHD was 20.5% in the ATG group and 30.6% in the non-ATG group. And the rates of extensive chronic GVHD were 6% and 33.3%, respectively (P<0.001).
According to revised NIH criteria, the rate of mild chronic GVHD was 15.7% in the ATG group and 16.7% in the non-ATG group. The rates of moderate chronic GVHD were 8.4% and 25%, respectively. And the rates of severe chronic GVHD were 2.4% and 22.2%, respectively (P<0.001).
However, all other outcomes, when assessed alone, were similar between the treatment groups.
The rate of 2-year relapse-free survival was 59.4% in the ATG group and 64.6% in the non-ATG group (P=0.21). The overall survival rates were 74.1% and 77.9%, respectively (P=0.46).
The incidence of relapse was 32.2% and 35.5%, respectively (P=0.17). Infectious complications occurred in 57.8% and 54.2%, respectively (P=0.65). And the rates of acute GVHD were 10.8% and 18.1%, respectively (P=0.13).
However, the rate of a composite endpoint of chronic GVHD-free and relapse-free survival at 2 years was significantly higher in the ATG group than the non-ATG group—36.6% and 16.8%, respectively (P=0.005). ![]()
Hodgkin lymphoma going untreated in patients with HIV
cultured lymphocyte
Image courtesy of the CDC
Patients with HIV-associated Hodgkin lymphoma may not be getting potentially curative treatment, according to a study published in the journal AIDS.
The study showed that 16% of HIV-positive patients did not receive treatment for their lymphoma, compared to 9% of Hodgkin lymphoma patients who were HIV-negative.
“Hodgkin lymphoma is generally believed to be highly curable,” said study author Adam Olszewski, MD, of Brown University in Providence, Rhode Island.
“We have an expectation to cure over 90% of early stage patients and even 70% to 80% of quite advanced cases.”
It hasn’t been clear whether HIV-positive patients with Hodgkin lymphoma survive the cancer as well as people who are HIV-negative. While some small studies, particularly in Europe, have shown that HIV status makes no difference to survival, observations in the US population suggest that being HIV-positive makes survival less likely.
The new study, which is the largest of its kind to date, may reconcile that conflict. It suggests that, in the US, the reason people with HIV seem to fare worse with the cancer is because they are less likely to be treated for it.
The study included 2090 cases of HIV-associated Hodgkin lymphoma recorded in the National Cancer Data Base between 2004 and 2012, as well as 41,846 cases of Hodgkin lymphoma in patients who were HIV-negative.
The unadjusted 5-year overall survival was 66% for HIV-positive patients and 80% for the HIV-negative population.
Among the HIV-positive patients, 81% received chemotherapy (12% in combination with radiation), 13% received any radiation therapy, and 16% received no treatment for their lymphoma. The corresponding numbers for HIV-negative patients were 87%, 31%, and 9%, respectively (P<0.00001 for all comparisons).
The researchers assessed patient- and disease-related factors associated with the risk of not receiving chemotherapy in the HIV-positive population.
And they found the risk was significantly higher for patients who were older than 40, male, “nonwhite” (black, Hispanic, or Asian/”other”), did not have health insurance, lived in areas with the lowest median income, and had early stage Hodgkin lymphoma or an undetermined histology.
Dr Olszewski said the lack of treatment among HIV-positive patients could be due to a lingering assumption that they won’t tolerate the treatment well. Or some patients may be declining treatment, either for HIV (thereby making them seem more vulnerable) or for the lymphoma itself.
He noted, however, that lymphoma treatment can be effective for and tolerated by HIV-positive patients, especially when the lymphoma subtype is known.
Among the patients who received chemotherapy in this study, there was no significant difference in the hazard of death between HIV-positive and HIV-negative patients who had one of the defined classical histologic subtypes: nodular sclerosis, mixed cellularity, lymphocyte-rich, or lymphocyte-depleted Hodgkin lymphoma. However, mortality was significantly higher for HIV-positive patients with an undetermined histologic subtype. ![]()
cultured lymphocyte
Image courtesy of the CDC
Patients with HIV-associated Hodgkin lymphoma may not be getting potentially curative treatment, according to a study published in the journal AIDS.
The study showed that 16% of HIV-positive patients did not receive treatment for their lymphoma, compared to 9% of Hodgkin lymphoma patients who were HIV-negative.
“Hodgkin lymphoma is generally believed to be highly curable,” said study author Adam Olszewski, MD, of Brown University in Providence, Rhode Island.
“We have an expectation to cure over 90% of early stage patients and even 70% to 80% of quite advanced cases.”
It hasn’t been clear whether HIV-positive patients with Hodgkin lymphoma survive the cancer as well as people who are HIV-negative. While some small studies, particularly in Europe, have shown that HIV status makes no difference to survival, observations in the US population suggest that being HIV-positive makes survival less likely.
The new study, which is the largest of its kind to date, may reconcile that conflict. It suggests that, in the US, the reason people with HIV seem to fare worse with the cancer is because they are less likely to be treated for it.
The study included 2090 cases of HIV-associated Hodgkin lymphoma recorded in the National Cancer Data Base between 2004 and 2012, as well as 41,846 cases of Hodgkin lymphoma in patients who were HIV-negative.
The unadjusted 5-year overall survival was 66% for HIV-positive patients and 80% for the HIV-negative population.
Among the HIV-positive patients, 81% received chemotherapy (12% in combination with radiation), 13% received any radiation therapy, and 16% received no treatment for their lymphoma. The corresponding numbers for HIV-negative patients were 87%, 31%, and 9%, respectively (P<0.00001 for all comparisons).
The researchers assessed patient- and disease-related factors associated with the risk of not receiving chemotherapy in the HIV-positive population.
And they found the risk was significantly higher for patients who were older than 40, male, “nonwhite” (black, Hispanic, or Asian/”other”), did not have health insurance, lived in areas with the lowest median income, and had early stage Hodgkin lymphoma or an undetermined histology.
Dr Olszewski said the lack of treatment among HIV-positive patients could be due to a lingering assumption that they won’t tolerate the treatment well. Or some patients may be declining treatment, either for HIV (thereby making them seem more vulnerable) or for the lymphoma itself.
He noted, however, that lymphoma treatment can be effective for and tolerated by HIV-positive patients, especially when the lymphoma subtype is known.
Among the patients who received chemotherapy in this study, there was no significant difference in the hazard of death between HIV-positive and HIV-negative patients who had one of the defined classical histologic subtypes: nodular sclerosis, mixed cellularity, lymphocyte-rich, or lymphocyte-depleted Hodgkin lymphoma. However, mortality was significantly higher for HIV-positive patients with an undetermined histologic subtype. ![]()
cultured lymphocyte
Image courtesy of the CDC
Patients with HIV-associated Hodgkin lymphoma may not be getting potentially curative treatment, according to a study published in the journal AIDS.
The study showed that 16% of HIV-positive patients did not receive treatment for their lymphoma, compared to 9% of Hodgkin lymphoma patients who were HIV-negative.
“Hodgkin lymphoma is generally believed to be highly curable,” said study author Adam Olszewski, MD, of Brown University in Providence, Rhode Island.
“We have an expectation to cure over 90% of early stage patients and even 70% to 80% of quite advanced cases.”
It hasn’t been clear whether HIV-positive patients with Hodgkin lymphoma survive the cancer as well as people who are HIV-negative. While some small studies, particularly in Europe, have shown that HIV status makes no difference to survival, observations in the US population suggest that being HIV-positive makes survival less likely.
The new study, which is the largest of its kind to date, may reconcile that conflict. It suggests that, in the US, the reason people with HIV seem to fare worse with the cancer is because they are less likely to be treated for it.
The study included 2090 cases of HIV-associated Hodgkin lymphoma recorded in the National Cancer Data Base between 2004 and 2012, as well as 41,846 cases of Hodgkin lymphoma in patients who were HIV-negative.
The unadjusted 5-year overall survival was 66% for HIV-positive patients and 80% for the HIV-negative population.
Among the HIV-positive patients, 81% received chemotherapy (12% in combination with radiation), 13% received any radiation therapy, and 16% received no treatment for their lymphoma. The corresponding numbers for HIV-negative patients were 87%, 31%, and 9%, respectively (P<0.00001 for all comparisons).
The researchers assessed patient- and disease-related factors associated with the risk of not receiving chemotherapy in the HIV-positive population.
And they found the risk was significantly higher for patients who were older than 40, male, “nonwhite” (black, Hispanic, or Asian/”other”), did not have health insurance, lived in areas with the lowest median income, and had early stage Hodgkin lymphoma or an undetermined histology.
Dr Olszewski said the lack of treatment among HIV-positive patients could be due to a lingering assumption that they won’t tolerate the treatment well. Or some patients may be declining treatment, either for HIV (thereby making them seem more vulnerable) or for the lymphoma itself.
He noted, however, that lymphoma treatment can be effective for and tolerated by HIV-positive patients, especially when the lymphoma subtype is known.
Among the patients who received chemotherapy in this study, there was no significant difference in the hazard of death between HIV-positive and HIV-negative patients who had one of the defined classical histologic subtypes: nodular sclerosis, mixed cellularity, lymphocyte-rich, or lymphocyte-depleted Hodgkin lymphoma. However, mortality was significantly higher for HIV-positive patients with an undetermined histologic subtype. ![]()
Watchdog says trial was unethical

Photo courtesy of
The Medicines Company
The watchdog group Public Citizen is alleging that ethics violations were made during the CHAMPION PHOENIX trial, in which researchers compared cangrelor and clopidogrel as thromboprophylaxis for patients undergoing coronary stent procedures.
Public Citizen said the trial “needlessly threatened” the lives of subjects assigned to the control group, and trial participants may not have been informed about the potential risks of enrollment.
Public Citizen sent a letter to the Office of Research Oversight (ORO) at the US Department of Veterans Affairs (VA) asserting that the CHAMPION PHOENIX trial unnecessarily increased the risk of death, heart attack, and other adverse cardiac events for subjects placed in the control group.
The trial was conducted at 153 institutions around the world, including 3 VA facilities: the Dallas VA Medical Center, the Jesse Brown VA Medical Center in Chicago, and the VA Boston Healthcare System. The study involved more than 11,000 subjects, 84 of whom were patients at the 3 VA medical centers.
The primary goal of the trial was to determine whether cangrelor is more effective than clopidogrel at preventing death, heart attacks, and other serious cardiac complications in patients undergoing coronary artery stent procedures.
Public Citizen said the increased risk to subjects in the control group resulted from failure to ensure they were treated with clopidogrel prior to their coronary stent procedures.
An analysis by a senior medical reviewer at the US Food and Drug Administration revealed that failure to administer the necessary antiplatelet treatment occurred in 89% of subjects enrolled at the 3 VA facilities, compared with 30% of subjects enrolled at non-VA facilities.
“The seriously flawed trial protocol paved the way for inappropriate and shocking delays in antiplatelet therapy for subjects enrolled in the control group at all trial institutions,” said Michael Carome, MD, director of Public Citizen’s Health Research Group.
“Inexplicably, the rate of such delays was extraordinarily high at the VA trial sites, making participation in the trial even more hazardous for subjects randomized to the control group at those sites compared with other sites.”
Public Citizen’s complaint contends that the trial’s research protocol was unethical because it failed to require that control group subjects receive lifesaving antiplatelet medications as soon as possible prior to undergoing coronary artery stent procedures.
Prior research conducted by the same research team, expert clinical practice guidelines, and other data available to the researchers established that withholding clopidogrel until after the coronary stent procedures constitutes substandard care.
Indeed, one of the two lead researchers for the trial stated publicly before the trial’s initiation, “If you ask the experts, they will all tell you to give antiplatelet therapy upfront before the PCI [coronary stent] procedure.”
Public Citizen is calling on the ORO to investigate why the institutional review boards responsible for reviewing human research at the 3 VA medical facilities approved the trial given a design that was unethical and failed to minimize the risks to the control group subjects.
The complaint also urges the ORO to investigate whether proper consent of the subjects was obtained in light of the risks, as required by the VA’s human subjects protection rules.
Public Citizen said another issue that requires further inquiry—but falls outside the scope of the ORO’s jurisdiction—is whether inappropriate delays in antiplatelet therapy were more widespread at VA healthcare facilities for patients who did not participate in the trial.
In a separate letter, Public Citizen urged the VA’s Office of Inspector General to launch an investigation to find out. ![]()
Photo courtesy of
The Medicines Company
The watchdog group Public Citizen is alleging that ethics violations were made during the CHAMPION PHOENIX trial, in which researchers compared cangrelor and clopidogrel as thromboprophylaxis for patients undergoing coronary stent procedures.
Public Citizen said the trial “needlessly threatened” the lives of subjects assigned to the control group, and trial participants may not have been informed about the potential risks of enrollment.
Public Citizen sent a letter to the Office of Research Oversight (ORO) at the US Department of Veterans Affairs (VA) asserting that the CHAMPION PHOENIX trial unnecessarily increased the risk of death, heart attack, and other adverse cardiac events for subjects placed in the control group.
The trial was conducted at 153 institutions around the world, including 3 VA facilities: the Dallas VA Medical Center, the Jesse Brown VA Medical Center in Chicago, and the VA Boston Healthcare System. The study involved more than 11,000 subjects, 84 of whom were patients at the 3 VA medical centers.
The primary goal of the trial was to determine whether cangrelor is more effective than clopidogrel at preventing death, heart attacks, and other serious cardiac complications in patients undergoing coronary artery stent procedures.
Public Citizen said the increased risk to subjects in the control group resulted from failure to ensure they were treated with clopidogrel prior to their coronary stent procedures.
An analysis by a senior medical reviewer at the US Food and Drug Administration revealed that failure to administer the necessary antiplatelet treatment occurred in 89% of subjects enrolled at the 3 VA facilities, compared with 30% of subjects enrolled at non-VA facilities.
“The seriously flawed trial protocol paved the way for inappropriate and shocking delays in antiplatelet therapy for subjects enrolled in the control group at all trial institutions,” said Michael Carome, MD, director of Public Citizen’s Health Research Group.
“Inexplicably, the rate of such delays was extraordinarily high at the VA trial sites, making participation in the trial even more hazardous for subjects randomized to the control group at those sites compared with other sites.”
Public Citizen’s complaint contends that the trial’s research protocol was unethical because it failed to require that control group subjects receive lifesaving antiplatelet medications as soon as possible prior to undergoing coronary artery stent procedures.
Prior research conducted by the same research team, expert clinical practice guidelines, and other data available to the researchers established that withholding clopidogrel until after the coronary stent procedures constitutes substandard care.
Indeed, one of the two lead researchers for the trial stated publicly before the trial’s initiation, “If you ask the experts, they will all tell you to give antiplatelet therapy upfront before the PCI [coronary stent] procedure.”
Public Citizen is calling on the ORO to investigate why the institutional review boards responsible for reviewing human research at the 3 VA medical facilities approved the trial given a design that was unethical and failed to minimize the risks to the control group subjects.
The complaint also urges the ORO to investigate whether proper consent of the subjects was obtained in light of the risks, as required by the VA’s human subjects protection rules.
Public Citizen said another issue that requires further inquiry—but falls outside the scope of the ORO’s jurisdiction—is whether inappropriate delays in antiplatelet therapy were more widespread at VA healthcare facilities for patients who did not participate in the trial.
In a separate letter, Public Citizen urged the VA’s Office of Inspector General to launch an investigation to find out. ![]()
Photo courtesy of
The Medicines Company
The watchdog group Public Citizen is alleging that ethics violations were made during the CHAMPION PHOENIX trial, in which researchers compared cangrelor and clopidogrel as thromboprophylaxis for patients undergoing coronary stent procedures.
Public Citizen said the trial “needlessly threatened” the lives of subjects assigned to the control group, and trial participants may not have been informed about the potential risks of enrollment.
Public Citizen sent a letter to the Office of Research Oversight (ORO) at the US Department of Veterans Affairs (VA) asserting that the CHAMPION PHOENIX trial unnecessarily increased the risk of death, heart attack, and other adverse cardiac events for subjects placed in the control group.
The trial was conducted at 153 institutions around the world, including 3 VA facilities: the Dallas VA Medical Center, the Jesse Brown VA Medical Center in Chicago, and the VA Boston Healthcare System. The study involved more than 11,000 subjects, 84 of whom were patients at the 3 VA medical centers.
The primary goal of the trial was to determine whether cangrelor is more effective than clopidogrel at preventing death, heart attacks, and other serious cardiac complications in patients undergoing coronary artery stent procedures.
Public Citizen said the increased risk to subjects in the control group resulted from failure to ensure they were treated with clopidogrel prior to their coronary stent procedures.
An analysis by a senior medical reviewer at the US Food and Drug Administration revealed that failure to administer the necessary antiplatelet treatment occurred in 89% of subjects enrolled at the 3 VA facilities, compared with 30% of subjects enrolled at non-VA facilities.
“The seriously flawed trial protocol paved the way for inappropriate and shocking delays in antiplatelet therapy for subjects enrolled in the control group at all trial institutions,” said Michael Carome, MD, director of Public Citizen’s Health Research Group.
“Inexplicably, the rate of such delays was extraordinarily high at the VA trial sites, making participation in the trial even more hazardous for subjects randomized to the control group at those sites compared with other sites.”
Public Citizen’s complaint contends that the trial’s research protocol was unethical because it failed to require that control group subjects receive lifesaving antiplatelet medications as soon as possible prior to undergoing coronary artery stent procedures.
Prior research conducted by the same research team, expert clinical practice guidelines, and other data available to the researchers established that withholding clopidogrel until after the coronary stent procedures constitutes substandard care.
Indeed, one of the two lead researchers for the trial stated publicly before the trial’s initiation, “If you ask the experts, they will all tell you to give antiplatelet therapy upfront before the PCI [coronary stent] procedure.”
Public Citizen is calling on the ORO to investigate why the institutional review boards responsible for reviewing human research at the 3 VA medical facilities approved the trial given a design that was unethical and failed to minimize the risks to the control group subjects.
The complaint also urges the ORO to investigate whether proper consent of the subjects was obtained in light of the risks, as required by the VA’s human subjects protection rules.
Public Citizen said another issue that requires further inquiry—but falls outside the scope of the ORO’s jurisdiction—is whether inappropriate delays in antiplatelet therapy were more widespread at VA healthcare facilities for patients who did not participate in the trial.
In a separate letter, Public Citizen urged the VA’s Office of Inspector General to launch an investigation to find out. ![]()
Study confirms resistant malaria in Cambodia
Image by Ute Frevert
and Margaret Shear
Results of a new study confirm that dihydroartemisinin-piperaquine, the first-line treatment for Plasmodium falciparum malaria infection in Cambodia, has failed in certain provinces due to parasite resistance to both artemisinin and piperaquine.
Dihydroartemisinin-piperaquine is an artemisinin combination therapy (ACT) that combines fast-acting artemisinin with a long-acting partner drug, piperaquine.
Resistance to artemisinin in parts of Southeast Asia is well-documented, but, until now, only a few studies have presented clear evidence of piperaquine resistance.
Additional results from this study suggest that artesunate, a form of artemisinin, plus mefloquine, a different long-acting partner drug, should be the first-line ACT in areas where dihydroartemisinin-piperaquine treatment has failed.
Chanaki Amaratunga, PhD, of the National Institute of Allergy and Infectious Diseases in Rockville, Maryland, and colleagues reported these results in The Lancet Infectious Diseases.
The researchers assessed the efficacy of dihydroartemisinin-piperaquine treatment in 241 malaria-afflicted participants ages 2 to 65. The subjects lived in 3 different Cambodian provinces with varying levels of artemisinin resistance.
After monitoring parasite levels in the blood for 63 days, the researchers found that parasites had reemerged despite initial clearance in 45.7% of participants in Pursat, 15.9% of participants in Preah Vihear, and 1.67% of participants in Ratanakiri.
The results indicate the ACT is failing in Pursat and Preah Vihear, where artemisinin resistance is common, but remains highly efficacious in Ratanakiri, where resistance is uncommon.
Laboratory tests showed the parasites from dihydroartemisinin-piperaquine failures contained a genetic marker of artemisinin resistance and had a decreased susceptibility to piperaquine, demonstrating that both artemisinin and piperaquine resistance contributed to treatment failures.
However, the parasites also showed an increased susceptibility to mefloquine and completely lacked the molecular marker for mefloquine resistance.
These findings informed new World Health Organization guidelines reinstating artesunate plus mefloquine as the first-line ACT in Cambodia where dihydroartemisinin-piperaquine treatment has failed.
The researchers said the findings also provide evidence to initiate surveillance programs to track the spread of piperaquine resistance and clinical trials to test alternative combination therapies. ![]()
Image by Ute Frevert
and Margaret Shear
Results of a new study confirm that dihydroartemisinin-piperaquine, the first-line treatment for Plasmodium falciparum malaria infection in Cambodia, has failed in certain provinces due to parasite resistance to both artemisinin and piperaquine.
Dihydroartemisinin-piperaquine is an artemisinin combination therapy (ACT) that combines fast-acting artemisinin with a long-acting partner drug, piperaquine.
Resistance to artemisinin in parts of Southeast Asia is well-documented, but, until now, only a few studies have presented clear evidence of piperaquine resistance.
Additional results from this study suggest that artesunate, a form of artemisinin, plus mefloquine, a different long-acting partner drug, should be the first-line ACT in areas where dihydroartemisinin-piperaquine treatment has failed.
Chanaki Amaratunga, PhD, of the National Institute of Allergy and Infectious Diseases in Rockville, Maryland, and colleagues reported these results in The Lancet Infectious Diseases.
The researchers assessed the efficacy of dihydroartemisinin-piperaquine treatment in 241 malaria-afflicted participants ages 2 to 65. The subjects lived in 3 different Cambodian provinces with varying levels of artemisinin resistance.
After monitoring parasite levels in the blood for 63 days, the researchers found that parasites had reemerged despite initial clearance in 45.7% of participants in Pursat, 15.9% of participants in Preah Vihear, and 1.67% of participants in Ratanakiri.
The results indicate the ACT is failing in Pursat and Preah Vihear, where artemisinin resistance is common, but remains highly efficacious in Ratanakiri, where resistance is uncommon.
Laboratory tests showed the parasites from dihydroartemisinin-piperaquine failures contained a genetic marker of artemisinin resistance and had a decreased susceptibility to piperaquine, demonstrating that both artemisinin and piperaquine resistance contributed to treatment failures.
However, the parasites also showed an increased susceptibility to mefloquine and completely lacked the molecular marker for mefloquine resistance.
These findings informed new World Health Organization guidelines reinstating artesunate plus mefloquine as the first-line ACT in Cambodia where dihydroartemisinin-piperaquine treatment has failed.
The researchers said the findings also provide evidence to initiate surveillance programs to track the spread of piperaquine resistance and clinical trials to test alternative combination therapies. ![]()
Image by Ute Frevert
and Margaret Shear
Results of a new study confirm that dihydroartemisinin-piperaquine, the first-line treatment for Plasmodium falciparum malaria infection in Cambodia, has failed in certain provinces due to parasite resistance to both artemisinin and piperaquine.
Dihydroartemisinin-piperaquine is an artemisinin combination therapy (ACT) that combines fast-acting artemisinin with a long-acting partner drug, piperaquine.
Resistance to artemisinin in parts of Southeast Asia is well-documented, but, until now, only a few studies have presented clear evidence of piperaquine resistance.
Additional results from this study suggest that artesunate, a form of artemisinin, plus mefloquine, a different long-acting partner drug, should be the first-line ACT in areas where dihydroartemisinin-piperaquine treatment has failed.
Chanaki Amaratunga, PhD, of the National Institute of Allergy and Infectious Diseases in Rockville, Maryland, and colleagues reported these results in The Lancet Infectious Diseases.
The researchers assessed the efficacy of dihydroartemisinin-piperaquine treatment in 241 malaria-afflicted participants ages 2 to 65. The subjects lived in 3 different Cambodian provinces with varying levels of artemisinin resistance.
After monitoring parasite levels in the blood for 63 days, the researchers found that parasites had reemerged despite initial clearance in 45.7% of participants in Pursat, 15.9% of participants in Preah Vihear, and 1.67% of participants in Ratanakiri.
The results indicate the ACT is failing in Pursat and Preah Vihear, where artemisinin resistance is common, but remains highly efficacious in Ratanakiri, where resistance is uncommon.
Laboratory tests showed the parasites from dihydroartemisinin-piperaquine failures contained a genetic marker of artemisinin resistance and had a decreased susceptibility to piperaquine, demonstrating that both artemisinin and piperaquine resistance contributed to treatment failures.
However, the parasites also showed an increased susceptibility to mefloquine and completely lacked the molecular marker for mefloquine resistance.
These findings informed new World Health Organization guidelines reinstating artesunate plus mefloquine as the first-line ACT in Cambodia where dihydroartemisinin-piperaquine treatment has failed.
The researchers said the findings also provide evidence to initiate surveillance programs to track the spread of piperaquine resistance and clinical trials to test alternative combination therapies.
HSPCs shape their own environment, team says

in the bone marrow
New research has revealed a mechanism through which hematopoietic stem and progenitor cells (HSPCs) control both their own proliferation and the characteristics of the niche that houses them.
Researchers detected high expression of the protein E-selectin ligand-1 (ESL-1) in HSPCs and also found that ESL-1 controls HSPCs’ production of the cytokine TGF-β.
The team said this is important because TGF-β has antiproliferative properties and is essential for impeding the loss of HSPCs in some diseases, such as some types of anemia.
The researchers also showed that HSPCs lacking ESL-1 are resistant to chemotherapeutic and cytotoxic agents.
These results suggest ESL-1 is a potential target for therapies aimed at improving bone marrow regeneration after chemotherapy or for expanding the HSPC population in preparation for donation.
Magdalena Leiva, PhD, of Centro Nacional de Investigaciones Cardiovasculares in Madrid, Spain, and her colleagues reported these findings in Nature Communications.
The researchers first found that ESL-1 deficiency causes HSPC quiescence and expansion, and elevated TGF-β causes quiescence in the absence of ESL-1. In addition, ESL-1 controls HSPC proliferation independently of E-selectin, and HSPCs are a relevant source of TGF-β.
The team also discovered that ESL-1 exerts local effects on distinct cell populations in the stromal niche. They found that hematopoietic-borne ESL-1 can control HSPC proliferation directly through cytokine secretion, and/or indirectly through repressive effects on supportive niche cells.
According to Dr Leiva, this finding opens the path to new therapies “that use genetically modified stem cells to treat hematological diseases, such as certain types of leukemia, in which the hematopoietic niche and HSPCs are very affected.”
The researchers made these discoveries by analyzing the bone marrow of mice deficient in ESL-1. In the absence of ESL-1, HSPCs proliferated less and were therefore of superior quality and more suitable for potential therapeutic applications, the team found.
“We see that these cells are resistant to processes associated with bone marrow damage, such as cell death triggered by cytotoxic agents,” Dr Leiva said.
She and her colleagues found that stem cells lacking ESL-1 were resistant to the deleterious effects of 5-fluorouracil and hydroxyurea. They said this suggests ESL-1 is a possible therapeutic target for improved regeneration of the bone marrow during chemotherapy.
in the bone marrow
New research has revealed a mechanism through which hematopoietic stem and progenitor cells (HSPCs) control both their own proliferation and the characteristics of the niche that houses them.
Researchers detected high expression of the protein E-selectin ligand-1 (ESL-1) in HSPCs and also found that ESL-1 controls HSPCs’ production of the cytokine TGF-β.
The team said this is important because TGF-β has antiproliferative properties and is essential for impeding the loss of HSPCs in some diseases, such as some types of anemia.
The researchers also showed that HSPCs lacking ESL-1 are resistant to chemotherapeutic and cytotoxic agents.
These results suggest ESL-1 is a potential target for therapies aimed at improving bone marrow regeneration after chemotherapy or for expanding the HSPC population in preparation for donation.
Magdalena Leiva, PhD, of Centro Nacional de Investigaciones Cardiovasculares in Madrid, Spain, and her colleagues reported these findings in Nature Communications.
The researchers first found that ESL-1 deficiency causes HSPC quiescence and expansion, and elevated TGF-β causes quiescence in the absence of ESL-1. In addition, ESL-1 controls HSPC proliferation independently of E-selectin, and HSPCs are a relevant source of TGF-β.
The team also discovered that ESL-1 exerts local effects on distinct cell populations in the stromal niche. They found that hematopoietic-borne ESL-1 can control HSPC proliferation directly through cytokine secretion, and/or indirectly through repressive effects on supportive niche cells.
According to Dr Leiva, this finding opens the path to new therapies “that use genetically modified stem cells to treat hematological diseases, such as certain types of leukemia, in which the hematopoietic niche and HSPCs are very affected.”
The researchers made these discoveries by analyzing the bone marrow of mice deficient in ESL-1. In the absence of ESL-1, HSPCs proliferated less and were therefore of superior quality and more suitable for potential therapeutic applications, the team found.
“We see that these cells are resistant to processes associated with bone marrow damage, such as cell death triggered by cytotoxic agents,” Dr Leiva said.
She and her colleagues found that stem cells lacking ESL-1 were resistant to the deleterious effects of 5-fluorouracil and hydroxyurea. They said this suggests ESL-1 is a possible therapeutic target for improved regeneration of the bone marrow during chemotherapy.
in the bone marrow
New research has revealed a mechanism through which hematopoietic stem and progenitor cells (HSPCs) control both their own proliferation and the characteristics of the niche that houses them.
Researchers detected high expression of the protein E-selectin ligand-1 (ESL-1) in HSPCs and also found that ESL-1 controls HSPCs’ production of the cytokine TGF-β.
The team said this is important because TGF-β has antiproliferative properties and is essential for impeding the loss of HSPCs in some diseases, such as some types of anemia.
The researchers also showed that HSPCs lacking ESL-1 are resistant to chemotherapeutic and cytotoxic agents.
These results suggest ESL-1 is a potential target for therapies aimed at improving bone marrow regeneration after chemotherapy or for expanding the HSPC population in preparation for donation.
Magdalena Leiva, PhD, of Centro Nacional de Investigaciones Cardiovasculares in Madrid, Spain, and her colleagues reported these findings in Nature Communications.
The researchers first found that ESL-1 deficiency causes HSPC quiescence and expansion, and elevated TGF-β causes quiescence in the absence of ESL-1. In addition, ESL-1 controls HSPC proliferation independently of E-selectin, and HSPCs are a relevant source of TGF-β.
The team also discovered that ESL-1 exerts local effects on distinct cell populations in the stromal niche. They found that hematopoietic-borne ESL-1 can control HSPC proliferation directly through cytokine secretion, and/or indirectly through repressive effects on supportive niche cells.
According to Dr Leiva, this finding opens the path to new therapies “that use genetically modified stem cells to treat hematological diseases, such as certain types of leukemia, in which the hematopoietic niche and HSPCs are very affected.”
The researchers made these discoveries by analyzing the bone marrow of mice deficient in ESL-1. In the absence of ESL-1, HSPCs proliferated less and were therefore of superior quality and more suitable for potential therapeutic applications, the team found.
“We see that these cells are resistant to processes associated with bone marrow damage, such as cell death triggered by cytotoxic agents,” Dr Leiva said.
She and her colleagues found that stem cells lacking ESL-1 were resistant to the deleterious effects of 5-fluorouracil and hydroxyurea. They said this suggests ESL-1 is a possible therapeutic target for improved regeneration of the bone marrow during chemotherapy.
Increasing eligibility for engineered T-cell therapy

Image courtesy of NIAID
A new study suggests that having a certain type of cancer or receiving certain chemotherapeutic agents
can affect T-cell function and make patients ineligible for engineered T-cell therapy.
However, researchers found that proper timing of T-cell collection can increase the number of patients eiligible for the therapy.
And the team developed a culture technique that can boost T cells’ fitness for expansion, which can increase eligibility as well.
Nathan Singh, MD, of the University of Pennsylvania in Philadelphia, and his colleagues described this work in Science Translational Medicine.
The researchers set out to determine why some patients’ T cells fail to multiply in culture. The team studied T cells from children with acute lymphoblastic leukemia (ALL) or non-Hodgkin lymphoma (NHL) who were undergoing chemotherapy. (NHL subtypes included Burkitt lymphoma, diffuse large B-cell lymphoma, primary mediastinal large B-cell lymphoma, primary lymphoma of bone, and follicular lymphoma.)
The researchers found that T cells from patients with ALL expanded better in culture than those from patients with NHL.
The team said a threshold of greater than 5-fold expansion during test expansion was associated with a high likelihood of successful clinical expansion.
Nearly 80% of patients with ALL met this threshold at diagnosis, but the rate declined over the course of therapy, falling to about 40% during maintenance therapy.
About 25% of NHL patients met the threshold at diagnosis, but few samples demonstrated any expansion after therapy began (12.5% of samples at all remaining time points tested).
The researchers said the difference in the proportion of ALL and NHL samples that met the expansion threshold was significant at all time points tested.
Analysis revealed that ALL patients had higher numbers of naïve T cells and stem central memory T cells, T cell subtypes known to be highly potent and proliferative with an enhanced capacity for self-renewal.
The researchers also found that certain chemotherapy drugs—namely, cyclophosphamide and cytarabine—selectively depleted early lineage T cells.
Fortunately, the team discovered that poor expansion can be rescued by exposing T cells to signaling molecules that stimulate T-cell activity. Culture with IL-7 and IL-15 boosted the expansion capacity of T cells from patients with NHL and those with ALL.
The researchers therefore concluded that using this culture technique or collecting T cells prior to chemotherapy can increase the number of patients eligible for engineered T-cell therapy.
Image courtesy of NIAID
A new study suggests that having a certain type of cancer or receiving certain chemotherapeutic agents
can affect T-cell function and make patients ineligible for engineered T-cell therapy.
However, researchers found that proper timing of T-cell collection can increase the number of patients eiligible for the therapy.
And the team developed a culture technique that can boost T cells’ fitness for expansion, which can increase eligibility as well.
Nathan Singh, MD, of the University of Pennsylvania in Philadelphia, and his colleagues described this work in Science Translational Medicine.
The researchers set out to determine why some patients’ T cells fail to multiply in culture. The team studied T cells from children with acute lymphoblastic leukemia (ALL) or non-Hodgkin lymphoma (NHL) who were undergoing chemotherapy. (NHL subtypes included Burkitt lymphoma, diffuse large B-cell lymphoma, primary mediastinal large B-cell lymphoma, primary lymphoma of bone, and follicular lymphoma.)
The researchers found that T cells from patients with ALL expanded better in culture than those from patients with NHL.
The team said a threshold of greater than 5-fold expansion during test expansion was associated with a high likelihood of successful clinical expansion.
Nearly 80% of patients with ALL met this threshold at diagnosis, but the rate declined over the course of therapy, falling to about 40% during maintenance therapy.
About 25% of NHL patients met the threshold at diagnosis, but few samples demonstrated any expansion after therapy began (12.5% of samples at all remaining time points tested).
The researchers said the difference in the proportion of ALL and NHL samples that met the expansion threshold was significant at all time points tested.
Analysis revealed that ALL patients had higher numbers of naïve T cells and stem central memory T cells, T cell subtypes known to be highly potent and proliferative with an enhanced capacity for self-renewal.
The researchers also found that certain chemotherapy drugs—namely, cyclophosphamide and cytarabine—selectively depleted early lineage T cells.
Fortunately, the team discovered that poor expansion can be rescued by exposing T cells to signaling molecules that stimulate T-cell activity. Culture with IL-7 and IL-15 boosted the expansion capacity of T cells from patients with NHL and those with ALL.
The researchers therefore concluded that using this culture technique or collecting T cells prior to chemotherapy can increase the number of patients eligible for engineered T-cell therapy.
Image courtesy of NIAID
A new study suggests that having a certain type of cancer or receiving certain chemotherapeutic agents
can affect T-cell function and make patients ineligible for engineered T-cell therapy.
However, researchers found that proper timing of T-cell collection can increase the number of patients eiligible for the therapy.
And the team developed a culture technique that can boost T cells’ fitness for expansion, which can increase eligibility as well.
Nathan Singh, MD, of the University of Pennsylvania in Philadelphia, and his colleagues described this work in Science Translational Medicine.
The researchers set out to determine why some patients’ T cells fail to multiply in culture. The team studied T cells from children with acute lymphoblastic leukemia (ALL) or non-Hodgkin lymphoma (NHL) who were undergoing chemotherapy. (NHL subtypes included Burkitt lymphoma, diffuse large B-cell lymphoma, primary mediastinal large B-cell lymphoma, primary lymphoma of bone, and follicular lymphoma.)
The researchers found that T cells from patients with ALL expanded better in culture than those from patients with NHL.
The team said a threshold of greater than 5-fold expansion during test expansion was associated with a high likelihood of successful clinical expansion.
Nearly 80% of patients with ALL met this threshold at diagnosis, but the rate declined over the course of therapy, falling to about 40% during maintenance therapy.
About 25% of NHL patients met the threshold at diagnosis, but few samples demonstrated any expansion after therapy began (12.5% of samples at all remaining time points tested).
The researchers said the difference in the proportion of ALL and NHL samples that met the expansion threshold was significant at all time points tested.
Analysis revealed that ALL patients had higher numbers of naïve T cells and stem central memory T cells, T cell subtypes known to be highly potent and proliferative with an enhanced capacity for self-renewal.
The researchers also found that certain chemotherapy drugs—namely, cyclophosphamide and cytarabine—selectively depleted early lineage T cells.
Fortunately, the team discovered that poor expansion can be rescued by exposing T cells to signaling molecules that stimulate T-cell activity. Culture with IL-7 and IL-15 boosted the expansion capacity of T cells from patients with NHL and those with ALL.
The researchers therefore concluded that using this culture technique or collecting T cells prior to chemotherapy can increase the number of patients eligible for engineered T-cell therapy.
Team creates ‘more reliable’ coagulation assay

Photo courtesy of the Wyss
Institute at Harvard University
Scientists have developed a blood coagulation assay that, they say, is more reliable than existing assays and could one day be used to diagnose rare bleeding disorders and prevent toxic effects of anticoagulant and antiplatelet drugs.
The team created a microfluidic device with hollow channels through which blood is flowed and devised an algorithm for analyzing patient-specific data to predict when blood clots will form.
Together, these components make up the assay, which can monitor blood coagulation and platelet function.
Donald Ingber, MD, PhD, of the Wyss Institute for Biologically Inspired Engineering at Harvard University in Boston, Massachusetts, and his colleagues described the assay in Nature Communications.
The team developed a microfluidic device in which blood flows through a life-like network of small “vessels.” The blood is subjected to true-to-life shear stresses and force gradients of the human vascular network.
The device contains hollow channels that mimic the pathology of the narrowing of small blood vessels, which can often cause a shift in the fluid mechanics of blood flow that can lead to life-threatening blood clots or internal bleeds.
The device mimics rapid changes in blood flow dynamics associated with stenosis or narrowing of small blood vessels by pumping pressurized blood flow through the device’s microfluidic channels.
Using automated pressure sensors and a proprietary algorithm, data acquired from the device is analyzed in real-time, thereby predicting the time at which a certain blood sample will obstruct the blood vessel network.
“By combining our fabricated microfluidic device that mimics blood flow dynamics of small arterioles with our novel data analysis software, we can rapidly quantitate hemostasis in real-time and predict if blood clots will develop in an individual or blood sample,” Dr Ingber explained.
He and his colleagues found they could accurately monitor the effects of anticoagulant and antiplatelet drugs in blood samples from human subjects.
The team was able to monitor platelet function as well. In particular, they found they could detect abnormal platelet function in samples from patients with Hermansky–Pudlak syndrome, a rare bleeding disorder characterized by a deficiency of platelet-dense granules that cannot be easily identified using conventional assays.
The novel assay also proved successful in large animal experiments. The scientists integrated their device directly into a vascular access line that was inserted into the femoral vein of a living pig to measure clinical clotting parameters over time. They recorded precise predictions for clotting times that were more accurate and faster than currently used clinical assays.
The team noted that their device uses inexpensive in-line pressure sensors to measure clot formation. As a result, it does not require additional instrumentation, and it can be integrated directly into the blood lines of extracorporeal devices.
The scientists said the device’s ability to be configured for lab use or real-time patient monitoring opens the door for countless potential uses that could improve patient care.
Photo courtesy of the Wyss
Institute at Harvard University
Scientists have developed a blood coagulation assay that, they say, is more reliable than existing assays and could one day be used to diagnose rare bleeding disorders and prevent toxic effects of anticoagulant and antiplatelet drugs.
The team created a microfluidic device with hollow channels through which blood is flowed and devised an algorithm for analyzing patient-specific data to predict when blood clots will form.
Together, these components make up the assay, which can monitor blood coagulation and platelet function.
Donald Ingber, MD, PhD, of the Wyss Institute for Biologically Inspired Engineering at Harvard University in Boston, Massachusetts, and his colleagues described the assay in Nature Communications.
The team developed a microfluidic device in which blood flows through a life-like network of small “vessels.” The blood is subjected to true-to-life shear stresses and force gradients of the human vascular network.
The device contains hollow channels that mimic the pathology of the narrowing of small blood vessels, which can often cause a shift in the fluid mechanics of blood flow that can lead to life-threatening blood clots or internal bleeds.
The device mimics rapid changes in blood flow dynamics associated with stenosis or narrowing of small blood vessels by pumping pressurized blood flow through the device’s microfluidic channels.
Using automated pressure sensors and a proprietary algorithm, data acquired from the device is analyzed in real-time, thereby predicting the time at which a certain blood sample will obstruct the blood vessel network.
“By combining our fabricated microfluidic device that mimics blood flow dynamics of small arterioles with our novel data analysis software, we can rapidly quantitate hemostasis in real-time and predict if blood clots will develop in an individual or blood sample,” Dr Ingber explained.
He and his colleagues found they could accurately monitor the effects of anticoagulant and antiplatelet drugs in blood samples from human subjects.
The team was able to monitor platelet function as well. In particular, they found they could detect abnormal platelet function in samples from patients with Hermansky–Pudlak syndrome, a rare bleeding disorder characterized by a deficiency of platelet-dense granules that cannot be easily identified using conventional assays.
The novel assay also proved successful in large animal experiments. The scientists integrated their device directly into a vascular access line that was inserted into the femoral vein of a living pig to measure clinical clotting parameters over time. They recorded precise predictions for clotting times that were more accurate and faster than currently used clinical assays.
The team noted that their device uses inexpensive in-line pressure sensors to measure clot formation. As a result, it does not require additional instrumentation, and it can be integrated directly into the blood lines of extracorporeal devices.
The scientists said the device’s ability to be configured for lab use or real-time patient monitoring opens the door for countless potential uses that could improve patient care.
Photo courtesy of the Wyss
Institute at Harvard University
Scientists have developed a blood coagulation assay that, they say, is more reliable than existing assays and could one day be used to diagnose rare bleeding disorders and prevent toxic effects of anticoagulant and antiplatelet drugs.
The team created a microfluidic device with hollow channels through which blood is flowed and devised an algorithm for analyzing patient-specific data to predict when blood clots will form.
Together, these components make up the assay, which can monitor blood coagulation and platelet function.
Donald Ingber, MD, PhD, of the Wyss Institute for Biologically Inspired Engineering at Harvard University in Boston, Massachusetts, and his colleagues described the assay in Nature Communications.
The team developed a microfluidic device in which blood flows through a life-like network of small “vessels.” The blood is subjected to true-to-life shear stresses and force gradients of the human vascular network.
The device contains hollow channels that mimic the pathology of the narrowing of small blood vessels, which can often cause a shift in the fluid mechanics of blood flow that can lead to life-threatening blood clots or internal bleeds.
The device mimics rapid changes in blood flow dynamics associated with stenosis or narrowing of small blood vessels by pumping pressurized blood flow through the device’s microfluidic channels.
Using automated pressure sensors and a proprietary algorithm, data acquired from the device is analyzed in real-time, thereby predicting the time at which a certain blood sample will obstruct the blood vessel network.
“By combining our fabricated microfluidic device that mimics blood flow dynamics of small arterioles with our novel data analysis software, we can rapidly quantitate hemostasis in real-time and predict if blood clots will develop in an individual or blood sample,” Dr Ingber explained.
He and his colleagues found they could accurately monitor the effects of anticoagulant and antiplatelet drugs in blood samples from human subjects.
The team was able to monitor platelet function as well. In particular, they found they could detect abnormal platelet function in samples from patients with Hermansky–Pudlak syndrome, a rare bleeding disorder characterized by a deficiency of platelet-dense granules that cannot be easily identified using conventional assays.
The novel assay also proved successful in large animal experiments. The scientists integrated their device directly into a vascular access line that was inserted into the femoral vein of a living pig to measure clinical clotting parameters over time. They recorded precise predictions for clotting times that were more accurate and faster than currently used clinical assays.
The team noted that their device uses inexpensive in-line pressure sensors to measure clot formation. As a result, it does not require additional instrumentation, and it can be integrated directly into the blood lines of extracorporeal devices.
The scientists said the device’s ability to be configured for lab use or real-time patient monitoring opens the door for countless potential uses that could improve patient care.