User login
Firing
Last month’s column on good hiring practices, which stressed the importance of replacing marginal employees with excellent ones, triggered an interesting round of discussion. “Isn’t it true,” asked one contributor, “that most physicians tolerate marginal employees because it’s less painful than firing them?”
Indeed it is. Firing someone is never easy, and it is particularly tough on physicians. Sometimes, however, it is unavoidable if you want to preserve the efficiency and morale of your other employees, as well as your own.
Before you do it, however, be sure that you have legitimate grounds, and assemble as much documentation as you can. Record all terminatable transgressions in the employee’s permanent record, and document all verbal and written warnings. This is essential. You must be prepared to prove that your reasons for termination were legal.
Former employees will sometimes charge that any of a number of their civil rights was violated. For example, federal law prohibits you from firing anyone because of race, gender, national origin, disability, religion, or age (if the employee is over 40). You cannot fire a woman because she is pregnant or recently gave birth. Other illegal reasons include assertion of antidiscrimination rights, refusal to take a lie detector test, and report of OSHA violations.
You also can’t terminate someone for refusing to commit an illegal act, such as filing false insurance claims, or for exercising a legal right, such as voting or participating in a political demonstration. You cannot fire an alcohol abuser unless he or she is caught drinking at work, but many forms of illegal drug use are legitimate cause for termination. Other laws may apply, depending on where you live. When in doubt, contact your state labor department or fair employment office.
If a fired employee alleges that he or she was fired for any of these illegal reasons and you do not have convincing documentation to counter the charge, you may find yourself defending your actions in court. If you anticipate such problems, you can ask the employee to sign a waver of future litigation in exchange for a concession from you – such as extra severance pay or a promise not to contest an unemployment application. Also, consider adding employment practices liability insurance (EPLI) to your umbrella policy, since lawsuits are always a possibility despite all efforts to prevent them.
Once you have all your legal ducks in a row, don’t procrastinate. Get it over with first thing on Monday morning. If you wait until Friday afternoon (as many do), you will worry about the dreaded task all week long, and the fired employee will stew about it all weekend.
Explain the performance you have expected, the steps you have taken to help correct the problems you have seen, and the fact that the problems persist. Try to limit the conversation to a minute or two, have the final paycheck ready, and make it clear that the decision has already been made, so begging and pleading will not change anything.
I’ve been asked to share exactly what I say, so, for what it’s worth: “I have called you in to discuss a difficult issue. You know that we have not been happy with your performance. We are still not happy with it, despite all the discussions we have had, and we feel that you can do better elsewhere. So, today, we will part company, and I wish you the best of luck in your future endeavors. Here is your severance check. I hope there are no hard feelings.”
There will, of course, be hard feelings, but that cannot be helped. The point is to be quick, firm, and decisive. Get it over with and allow everyone to move on.
Be sure to get all your office keys back – or change the locks if you cannot. Back up all important computer files, and change all your passwords. Most employees know more of them than you would ever suspect.
Finally, call the staff together and explain what you have done. They should hear the real story from you, not some distorted version via the rumor mill. You don’t have to explain your reasoning or divulge every detail, but do explain how the termination will affect everyone else. Responsibilities will need to be shifted until a replacement can be hired, and all employees should understand that.
If you are asked in the future to give a reference or write a letter of recommendation for the terminated employee, be sure that everything you say is truthful and well documented.

Last month’s column on good hiring practices, which stressed the importance of replacing marginal employees with excellent ones, triggered an interesting round of discussion. “Isn’t it true,” asked one contributor, “that most physicians tolerate marginal employees because it’s less painful than firing them?”
Indeed it is. Firing someone is never easy, and it is particularly tough on physicians. Sometimes, however, it is unavoidable if you want to preserve the efficiency and morale of your other employees, as well as your own.
Before you do it, however, be sure that you have legitimate grounds, and assemble as much documentation as you can. Record all terminatable transgressions in the employee’s permanent record, and document all verbal and written warnings. This is essential. You must be prepared to prove that your reasons for termination were legal.
Former employees will sometimes charge that any of a number of their civil rights was violated. For example, federal law prohibits you from firing anyone because of race, gender, national origin, disability, religion, or age (if the employee is over 40). You cannot fire a woman because she is pregnant or recently gave birth. Other illegal reasons include assertion of antidiscrimination rights, refusal to take a lie detector test, and report of OSHA violations.
You also can’t terminate someone for refusing to commit an illegal act, such as filing false insurance claims, or for exercising a legal right, such as voting or participating in a political demonstration. You cannot fire an alcohol abuser unless he or she is caught drinking at work, but many forms of illegal drug use are legitimate cause for termination. Other laws may apply, depending on where you live. When in doubt, contact your state labor department or fair employment office.
If a fired employee alleges that he or she was fired for any of these illegal reasons and you do not have convincing documentation to counter the charge, you may find yourself defending your actions in court. If you anticipate such problems, you can ask the employee to sign a waver of future litigation in exchange for a concession from you – such as extra severance pay or a promise not to contest an unemployment application. Also, consider adding employment practices liability insurance (EPLI) to your umbrella policy, since lawsuits are always a possibility despite all efforts to prevent them.
Once you have all your legal ducks in a row, don’t procrastinate. Get it over with first thing on Monday morning. If you wait until Friday afternoon (as many do), you will worry about the dreaded task all week long, and the fired employee will stew about it all weekend.
Explain the performance you have expected, the steps you have taken to help correct the problems you have seen, and the fact that the problems persist. Try to limit the conversation to a minute or two, have the final paycheck ready, and make it clear that the decision has already been made, so begging and pleading will not change anything.
I’ve been asked to share exactly what I say, so, for what it’s worth: “I have called you in to discuss a difficult issue. You know that we have not been happy with your performance. We are still not happy with it, despite all the discussions we have had, and we feel that you can do better elsewhere. So, today, we will part company, and I wish you the best of luck in your future endeavors. Here is your severance check. I hope there are no hard feelings.”
There will, of course, be hard feelings, but that cannot be helped. The point is to be quick, firm, and decisive. Get it over with and allow everyone to move on.
Be sure to get all your office keys back – or change the locks if you cannot. Back up all important computer files, and change all your passwords. Most employees know more of them than you would ever suspect.
Finally, call the staff together and explain what you have done. They should hear the real story from you, not some distorted version via the rumor mill. You don’t have to explain your reasoning or divulge every detail, but do explain how the termination will affect everyone else. Responsibilities will need to be shifted until a replacement can be hired, and all employees should understand that.
If you are asked in the future to give a reference or write a letter of recommendation for the terminated employee, be sure that everything you say is truthful and well documented.
Last month’s column on good hiring practices, which stressed the importance of replacing marginal employees with excellent ones, triggered an interesting round of discussion. “Isn’t it true,” asked one contributor, “that most physicians tolerate marginal employees because it’s less painful than firing them?”
Indeed it is. Firing someone is never easy, and it is particularly tough on physicians. Sometimes, however, it is unavoidable if you want to preserve the efficiency and morale of your other employees, as well as your own.
Before you do it, however, be sure that you have legitimate grounds, and assemble as much documentation as you can. Record all terminatable transgressions in the employee’s permanent record, and document all verbal and written warnings. This is essential. You must be prepared to prove that your reasons for termination were legal.
Former employees will sometimes charge that any of a number of their civil rights was violated. For example, federal law prohibits you from firing anyone because of race, gender, national origin, disability, religion, or age (if the employee is over 40). You cannot fire a woman because she is pregnant or recently gave birth. Other illegal reasons include assertion of antidiscrimination rights, refusal to take a lie detector test, and report of OSHA violations.
You also can’t terminate someone for refusing to commit an illegal act, such as filing false insurance claims, or for exercising a legal right, such as voting or participating in a political demonstration. You cannot fire an alcohol abuser unless he or she is caught drinking at work, but many forms of illegal drug use are legitimate cause for termination. Other laws may apply, depending on where you live. When in doubt, contact your state labor department or fair employment office.
If a fired employee alleges that he or she was fired for any of these illegal reasons and you do not have convincing documentation to counter the charge, you may find yourself defending your actions in court. If you anticipate such problems, you can ask the employee to sign a waver of future litigation in exchange for a concession from you – such as extra severance pay or a promise not to contest an unemployment application. Also, consider adding employment practices liability insurance (EPLI) to your umbrella policy, since lawsuits are always a possibility despite all efforts to prevent them.
Once you have all your legal ducks in a row, don’t procrastinate. Get it over with first thing on Monday morning. If you wait until Friday afternoon (as many do), you will worry about the dreaded task all week long, and the fired employee will stew about it all weekend.
Explain the performance you have expected, the steps you have taken to help correct the problems you have seen, and the fact that the problems persist. Try to limit the conversation to a minute or two, have the final paycheck ready, and make it clear that the decision has already been made, so begging and pleading will not change anything.
I’ve been asked to share exactly what I say, so, for what it’s worth: “I have called you in to discuss a difficult issue. You know that we have not been happy with your performance. We are still not happy with it, despite all the discussions we have had, and we feel that you can do better elsewhere. So, today, we will part company, and I wish you the best of luck in your future endeavors. Here is your severance check. I hope there are no hard feelings.”
There will, of course, be hard feelings, but that cannot be helped. The point is to be quick, firm, and decisive. Get it over with and allow everyone to move on.
Be sure to get all your office keys back – or change the locks if you cannot. Back up all important computer files, and change all your passwords. Most employees know more of them than you would ever suspect.
Finally, call the staff together and explain what you have done. They should hear the real story from you, not some distorted version via the rumor mill. You don’t have to explain your reasoning or divulge every detail, but do explain how the termination will affect everyone else. Responsibilities will need to be shifted until a replacement can be hired, and all employees should understand that.
If you are asked in the future to give a reference or write a letter of recommendation for the terminated employee, be sure that everything you say is truthful and well documented.

Hiring the right employees
Many of the personnel questions I receive concern the dreaded “marginal employee” – a person who has never done anything truly heinous to merit firing but also hasn’t done anything special to merit continued employment. I always advise getting rid of such people and then changing the hiring criteria that all too often result in poor hires.
Most bad hires come about because employers do not have a clear vision of the kind of employee they want. Many office manuals do not contain detailed job descriptions. If you don’t know exactly what you are looking for, your entire selection process will be inadequate from initial screening of applicants through assessments of their skills and personalities. Many physicians compound the problem with poor interview techniques and inadequate checking of references.
Once you have a clear job description in mind (and in print), take all the time you need to find the best possible match for it. This is not a place to cut corners. Screen your candidates carefully, and avoid lowering your expectations. This is the point at which it might be tempting to settle for a marginal candidate just to get the process over with.
It is also sometimes tempting to hire the candidate that you have the “best feeling” about, even though he or she is a poor match for the job, and then try to mold the job to that person. Every doctor knows that hunches are no substitute for hard data.
Be alert for red flags in resumes: significant time gaps between jobs, positions at companies that are no longer in business or are otherwise impossible to verify, job titles that don’t make sense given the applicant’s qualifications.
Background checks are a dicey subject, but publicly available information can be found, cheap or free, on multiple web sites created for that purpose. Be sure to tell applicants that you will be verifying facts in their resumes. It’s usually wise to get their written consent to do so.
Many employers skip the essential step of calling references, and many applicants know that. Some old bosses will be reluctant to tell you anything substantive, so I always ask, “Would you hire this person again?” You can interpret a lot from the answer – or lack of one.
Interviews often get short shrift as well. Many doctors tend to do all the talking. As I’ve observed numerous times, listening is not our strong suit, as a general rule. The purpose of an interview is to allow you to size up the prospective employee, not to deliver a lecture on the sterling attributes of your office. Important interview topics include educational background, skills, experience, and unrelated job history.
By law, you cannot ask an applicant’s age, date of birth, gender, creed, color, religion, or national origin. Other forbidden subjects include disabilities, marital status, military record, number of children (or who cares for them), addiction history, citizenship, criminal record, psychiatric history, absenteeism, or workman’s compensation.
However, there are acceptable alternatives to some of those questions. You can ask if applicants have ever gone by another name (for your background check), for example. You can ask if they are legally authorized to work in this country and whether they will be physically able to perform the duties specified in the job description. While past addictions are off limits, you do have a right to know about current addictions to illegal substances.
Once you have hired people whose skills and personalities best fit your needs, train them well. Then, give them the opportunity to succeed. “The best executive,” wrote Theodore Roosevelt, “is one who has sense enough to pick good people to do what he [or she] wants done and self-restraint enough to keep from meddling with them while they do it.” ”
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters and is a longtime monthly columnist for Dermatology News. Write to him at [email protected].
Many of the personnel questions I receive concern the dreaded “marginal employee” – a person who has never done anything truly heinous to merit firing but also hasn’t done anything special to merit continued employment. I always advise getting rid of such people and then changing the hiring criteria that all too often result in poor hires.
Most bad hires come about because employers do not have a clear vision of the kind of employee they want. Many office manuals do not contain detailed job descriptions. If you don’t know exactly what you are looking for, your entire selection process will be inadequate from initial screening of applicants through assessments of their skills and personalities. Many physicians compound the problem with poor interview techniques and inadequate checking of references.
Once you have a clear job description in mind (and in print), take all the time you need to find the best possible match for it. This is not a place to cut corners. Screen your candidates carefully, and avoid lowering your expectations. This is the point at which it might be tempting to settle for a marginal candidate just to get the process over with.
It is also sometimes tempting to hire the candidate that you have the “best feeling” about, even though he or she is a poor match for the job, and then try to mold the job to that person. Every doctor knows that hunches are no substitute for hard data.
Be alert for red flags in resumes: significant time gaps between jobs, positions at companies that are no longer in business or are otherwise impossible to verify, job titles that don’t make sense given the applicant’s qualifications.
Background checks are a dicey subject, but publicly available information can be found, cheap or free, on multiple web sites created for that purpose. Be sure to tell applicants that you will be verifying facts in their resumes. It’s usually wise to get their written consent to do so.
Many employers skip the essential step of calling references, and many applicants know that. Some old bosses will be reluctant to tell you anything substantive, so I always ask, “Would you hire this person again?” You can interpret a lot from the answer – or lack of one.
Interviews often get short shrift as well. Many doctors tend to do all the talking. As I’ve observed numerous times, listening is not our strong suit, as a general rule. The purpose of an interview is to allow you to size up the prospective employee, not to deliver a lecture on the sterling attributes of your office. Important interview topics include educational background, skills, experience, and unrelated job history.
By law, you cannot ask an applicant’s age, date of birth, gender, creed, color, religion, or national origin. Other forbidden subjects include disabilities, marital status, military record, number of children (or who cares for them), addiction history, citizenship, criminal record, psychiatric history, absenteeism, or workman’s compensation.
However, there are acceptable alternatives to some of those questions. You can ask if applicants have ever gone by another name (for your background check), for example. You can ask if they are legally authorized to work in this country and whether they will be physically able to perform the duties specified in the job description. While past addictions are off limits, you do have a right to know about current addictions to illegal substances.
Once you have hired people whose skills and personalities best fit your needs, train them well. Then, give them the opportunity to succeed. “The best executive,” wrote Theodore Roosevelt, “is one who has sense enough to pick good people to do what he [or she] wants done and self-restraint enough to keep from meddling with them while they do it.” ”
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters and is a longtime monthly columnist for Dermatology News. Write to him at [email protected].
Many of the personnel questions I receive concern the dreaded “marginal employee” – a person who has never done anything truly heinous to merit firing but also hasn’t done anything special to merit continued employment. I always advise getting rid of such people and then changing the hiring criteria that all too often result in poor hires.
Most bad hires come about because employers do not have a clear vision of the kind of employee they want. Many office manuals do not contain detailed job descriptions. If you don’t know exactly what you are looking for, your entire selection process will be inadequate from initial screening of applicants through assessments of their skills and personalities. Many physicians compound the problem with poor interview techniques and inadequate checking of references.
Once you have a clear job description in mind (and in print), take all the time you need to find the best possible match for it. This is not a place to cut corners. Screen your candidates carefully, and avoid lowering your expectations. This is the point at which it might be tempting to settle for a marginal candidate just to get the process over with.
It is also sometimes tempting to hire the candidate that you have the “best feeling” about, even though he or she is a poor match for the job, and then try to mold the job to that person. Every doctor knows that hunches are no substitute for hard data.
Be alert for red flags in resumes: significant time gaps between jobs, positions at companies that are no longer in business or are otherwise impossible to verify, job titles that don’t make sense given the applicant’s qualifications.
Background checks are a dicey subject, but publicly available information can be found, cheap or free, on multiple web sites created for that purpose. Be sure to tell applicants that you will be verifying facts in their resumes. It’s usually wise to get their written consent to do so.
Many employers skip the essential step of calling references, and many applicants know that. Some old bosses will be reluctant to tell you anything substantive, so I always ask, “Would you hire this person again?” You can interpret a lot from the answer – or lack of one.
Interviews often get short shrift as well. Many doctors tend to do all the talking. As I’ve observed numerous times, listening is not our strong suit, as a general rule. The purpose of an interview is to allow you to size up the prospective employee, not to deliver a lecture on the sterling attributes of your office. Important interview topics include educational background, skills, experience, and unrelated job history.
By law, you cannot ask an applicant’s age, date of birth, gender, creed, color, religion, or national origin. Other forbidden subjects include disabilities, marital status, military record, number of children (or who cares for them), addiction history, citizenship, criminal record, psychiatric history, absenteeism, or workman’s compensation.
However, there are acceptable alternatives to some of those questions. You can ask if applicants have ever gone by another name (for your background check), for example. You can ask if they are legally authorized to work in this country and whether they will be physically able to perform the duties specified in the job description. While past addictions are off limits, you do have a right to know about current addictions to illegal substances.
Once you have hired people whose skills and personalities best fit your needs, train them well. Then, give them the opportunity to succeed. “The best executive,” wrote Theodore Roosevelt, “is one who has sense enough to pick good people to do what he [or she] wants done and self-restraint enough to keep from meddling with them while they do it.” ”
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters and is a longtime monthly columnist for Dermatology News. Write to him at [email protected].
No-shows
Of all the headaches inherent in a private medical practice, few are more frustrating than patients who make appointments and then fail to keep them.
No-shows are a problem for all physicians but especially for dermatologists. In one study, the no-show rate in dermatology offices averaged 10% – almost double the average for medical offices as a whole.
Why the higher rate? One reason is a lag between appointment and visit. Many dermatologists are booked well in advance, so, by the time the appointment arrives, some patients’ complaints will have resolved spontaneously, while other patients will have found other offices willing to see them sooner. Another reason is lack of insurance coverage. Studies have shown that the no-show rate is highest when the patient is paying out-of-pocket for the visit.
Whatever the reasons, no-shows are an economic and medicolegal liability. It is worth the considerable effort it often takes to minimize them.
Deal with simple forgetfulness by calling your patients the day before to remind them of their appointments. Reasonably-priced phone software is available from a variety of vendors to automate this process. You could also hire a teenager to do it after school each day.
Whenever possible, use cell phone numbers for reminder calls. Patients often aren’t home during the day, and many don’t listen to their messages when they come in. Patients who have moved will often have a new home phone number, but their cell phone numbers will be the same.
Decrease the wait for new appointments. Keep some slots open each week for new patients, who will often “shop around” for a faster appointment while they’re waiting for an appointment they already have elsewhere.
If your no-shows are incorrigible, consider charging them. One increasingly popular mechanism is a fee ($20 seems to be popular) that must be paid at the time of the next appointment before being seen. Some patients will respond to that by never showing up again. Fine. You need to reserve your appointment slots for patients who plan to keep them. Those more contrite will pay and, hopefully, learn their lesson. Give your receptionists the power to override the charge since there are, obviously, legitimate reasons for missing an appointment.
One physician in my area told me he seldom actually collects the fee, which is okay with him. “After all,” he said, “the purpose is not to generate income. It’s to encourage patients to keep their appointments.”
If you go this route, be sure to post notices in your office and on your website clearly delineating your policy. Emphasize that it is not a service fee and cannot be billed to insurance. Remind patients about it during reminder calls. If you have a high no-show rate for cosmetic and other noninsurance procedures, consider collecting a nonrefundable deposit in advance.
Above all, seek to maximize the strength of your physician-patient relationships. Try not to shuttle patients between different physicians or PAs, and make it clear that you are genuinely concerned about their health. Impress upon them the crucial role they play in their own care, which includes keeping all their appointments.
In our office, significant no-shows (for example, a patient with a melanoma who misses the visit for re-excision) receive a phone call and a certified letter, and their records go into a special file for close follow-up by the nursing staff.
All missed appointments should be documented in the patient’s record – it’s important clinical and medicolegal information. A second missed appointment should prompt a written warning that measures will be taken if it happens again. Make sure to spell out what those measures are, and stick to them. Habitual no-shows should be dismissed from your practice. You cannot afford them.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters and is a longtime monthly columnist for Dermatology News. Write to him at [email protected].
Of all the headaches inherent in a private medical practice, few are more frustrating than patients who make appointments and then fail to keep them.
No-shows are a problem for all physicians but especially for dermatologists. In one study, the no-show rate in dermatology offices averaged 10% – almost double the average for medical offices as a whole.
Why the higher rate? One reason is a lag between appointment and visit. Many dermatologists are booked well in advance, so, by the time the appointment arrives, some patients’ complaints will have resolved spontaneously, while other patients will have found other offices willing to see them sooner. Another reason is lack of insurance coverage. Studies have shown that the no-show rate is highest when the patient is paying out-of-pocket for the visit.
Whatever the reasons, no-shows are an economic and medicolegal liability. It is worth the considerable effort it often takes to minimize them.
Deal with simple forgetfulness by calling your patients the day before to remind them of their appointments. Reasonably-priced phone software is available from a variety of vendors to automate this process. You could also hire a teenager to do it after school each day.
Whenever possible, use cell phone numbers for reminder calls. Patients often aren’t home during the day, and many don’t listen to their messages when they come in. Patients who have moved will often have a new home phone number, but their cell phone numbers will be the same.
Decrease the wait for new appointments. Keep some slots open each week for new patients, who will often “shop around” for a faster appointment while they’re waiting for an appointment they already have elsewhere.
If your no-shows are incorrigible, consider charging them. One increasingly popular mechanism is a fee ($20 seems to be popular) that must be paid at the time of the next appointment before being seen. Some patients will respond to that by never showing up again. Fine. You need to reserve your appointment slots for patients who plan to keep them. Those more contrite will pay and, hopefully, learn their lesson. Give your receptionists the power to override the charge since there are, obviously, legitimate reasons for missing an appointment.
One physician in my area told me he seldom actually collects the fee, which is okay with him. “After all,” he said, “the purpose is not to generate income. It’s to encourage patients to keep their appointments.”
If you go this route, be sure to post notices in your office and on your website clearly delineating your policy. Emphasize that it is not a service fee and cannot be billed to insurance. Remind patients about it during reminder calls. If you have a high no-show rate for cosmetic and other noninsurance procedures, consider collecting a nonrefundable deposit in advance.
Above all, seek to maximize the strength of your physician-patient relationships. Try not to shuttle patients between different physicians or PAs, and make it clear that you are genuinely concerned about their health. Impress upon them the crucial role they play in their own care, which includes keeping all their appointments.
In our office, significant no-shows (for example, a patient with a melanoma who misses the visit for re-excision) receive a phone call and a certified letter, and their records go into a special file for close follow-up by the nursing staff.
All missed appointments should be documented in the patient’s record – it’s important clinical and medicolegal information. A second missed appointment should prompt a written warning that measures will be taken if it happens again. Make sure to spell out what those measures are, and stick to them. Habitual no-shows should be dismissed from your practice. You cannot afford them.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters and is a longtime monthly columnist for Dermatology News. Write to him at [email protected].
Of all the headaches inherent in a private medical practice, few are more frustrating than patients who make appointments and then fail to keep them.
No-shows are a problem for all physicians but especially for dermatologists. In one study, the no-show rate in dermatology offices averaged 10% – almost double the average for medical offices as a whole.
Why the higher rate? One reason is a lag between appointment and visit. Many dermatologists are booked well in advance, so, by the time the appointment arrives, some patients’ complaints will have resolved spontaneously, while other patients will have found other offices willing to see them sooner. Another reason is lack of insurance coverage. Studies have shown that the no-show rate is highest when the patient is paying out-of-pocket for the visit.
Whatever the reasons, no-shows are an economic and medicolegal liability. It is worth the considerable effort it often takes to minimize them.
Deal with simple forgetfulness by calling your patients the day before to remind them of their appointments. Reasonably-priced phone software is available from a variety of vendors to automate this process. You could also hire a teenager to do it after school each day.
Whenever possible, use cell phone numbers for reminder calls. Patients often aren’t home during the day, and many don’t listen to their messages when they come in. Patients who have moved will often have a new home phone number, but their cell phone numbers will be the same.
Decrease the wait for new appointments. Keep some slots open each week for new patients, who will often “shop around” for a faster appointment while they’re waiting for an appointment they already have elsewhere.
If your no-shows are incorrigible, consider charging them. One increasingly popular mechanism is a fee ($20 seems to be popular) that must be paid at the time of the next appointment before being seen. Some patients will respond to that by never showing up again. Fine. You need to reserve your appointment slots for patients who plan to keep them. Those more contrite will pay and, hopefully, learn their lesson. Give your receptionists the power to override the charge since there are, obviously, legitimate reasons for missing an appointment.
One physician in my area told me he seldom actually collects the fee, which is okay with him. “After all,” he said, “the purpose is not to generate income. It’s to encourage patients to keep their appointments.”
If you go this route, be sure to post notices in your office and on your website clearly delineating your policy. Emphasize that it is not a service fee and cannot be billed to insurance. Remind patients about it during reminder calls. If you have a high no-show rate for cosmetic and other noninsurance procedures, consider collecting a nonrefundable deposit in advance.
Above all, seek to maximize the strength of your physician-patient relationships. Try not to shuttle patients between different physicians or PAs, and make it clear that you are genuinely concerned about their health. Impress upon them the crucial role they play in their own care, which includes keeping all their appointments.
In our office, significant no-shows (for example, a patient with a melanoma who misses the visit for re-excision) receive a phone call and a certified letter, and their records go into a special file for close follow-up by the nursing staff.
All missed appointments should be documented in the patient’s record – it’s important clinical and medicolegal information. A second missed appointment should prompt a written warning that measures will be taken if it happens again. Make sure to spell out what those measures are, and stick to them. Habitual no-shows should be dismissed from your practice. You cannot afford them.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters and is a longtime monthly columnist for Dermatology News. Write to him at [email protected].
Don’t forget HIPAA
In the struggle to understand and comply with new regulations, it’s easy to neglect older ones. Recently, I suggested reviewing your practice for potential Occupational Safety and Health Administration violations, which can be far more costly than anything MACRA has in store.
The same goes for HIPAA since HIPAA violations can be just as costly, in view of renewed governmental enforcement and some disturbing trends in completely unrelated government agencies.
Your most basic review should be a yearly examination of every part of your office where patient information is handled to identify potential violations. Examples discovered in my office included computers at our front desk whose screens were visible to patients checking in or out; laptops that were left on counters overnight; emails between staff involving patients or their care; and documents slated for shredding that remained in a “to shred” bin for days. All of these issues were easily solved at minimal cost – respectively, screen protectors, locking all laptops after hours, new email rules, and eliminating the “to shred” bin, forcing immediate shredding of all sensitive documents. Make sure you correct any problems you find before the OCR auditors come calling. You can compare your office’s compliance status against the recommendations listed on the OCR website.
Where safeguarding protected health information is concerned, you must now assume the worst-case scenario: Previously, when protected health information was compromised, you would have to notify the affected patients (and the government) only if there was a “significant risk of financial or reputational harm.” But now, any incident involving patient records is assumed to be a breach, and must be reported. Failure to do so could subject your practice to significant fines.
The biggest vulnerability in most practices is probably mobile devices carrying patient data; and that’s where the disturbing new trend comes in: Governments, both foreign and domestic, have developed an interest in the personal data on your devices. Travelers, including American citizens, now are being pressured into giving Customs and Border Protection officers access to their cellphones and laptops at airports.
As a physician, you can invoke HIPAA in such situations, since your devices likely contain patient data in some form. But rules may vary depending on where you are traveling to or from, and officials in other countries are not bound by U.S. HIPAA constraints.
So, how do you protect patients’ (and your personal) information from invasive searches? First, encrypt all of your data; encryption software is cheap, readily available, and easy to use. (I recently posted a list of inexpensive encryption applications on the website.) Desktop apps such as BitLocker or Apple’s FileVault let you encrypt your entire hard drive, requiring a password for decryption. (As always, I have no financial interest in anything I mention here.) To avoid surrendering the password, write it down and give it to a friend, then contact that person after crossing the border. It is easier to say you didn’t memorize it, as opposed to refusing to provide it – and nobody can compel you to reveal a password you don’t know.
Experts also recommend disabling the fingerprint sensor on your smartphone; customs officials have successfully used warrants to compel people to unlock their cellphones with a fingerprint. Because of your right to remain silent, it would be difficult (but not impossible) for them to force you to share your phone’s passcode.
A better alternative, in my view, is to travel with devices that have never contained any of your patient or personal data in the first place. Invest in a cheap phone and computer to use only when you are abroad; you don’t want your nice equipment lost or stolen, anyway. A budget Android phone that works with foreign SIM cards can be had for about $100; basic laptops run $500 or less.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at [email protected].
In the struggle to understand and comply with new regulations, it’s easy to neglect older ones. Recently, I suggested reviewing your practice for potential Occupational Safety and Health Administration violations, which can be far more costly than anything MACRA has in store.
The same goes for HIPAA since HIPAA violations can be just as costly, in view of renewed governmental enforcement and some disturbing trends in completely unrelated government agencies.
Your most basic review should be a yearly examination of every part of your office where patient information is handled to identify potential violations. Examples discovered in my office included computers at our front desk whose screens were visible to patients checking in or out; laptops that were left on counters overnight; emails between staff involving patients or their care; and documents slated for shredding that remained in a “to shred” bin for days. All of these issues were easily solved at minimal cost – respectively, screen protectors, locking all laptops after hours, new email rules, and eliminating the “to shred” bin, forcing immediate shredding of all sensitive documents. Make sure you correct any problems you find before the OCR auditors come calling. You can compare your office’s compliance status against the recommendations listed on the OCR website.
Where safeguarding protected health information is concerned, you must now assume the worst-case scenario: Previously, when protected health information was compromised, you would have to notify the affected patients (and the government) only if there was a “significant risk of financial or reputational harm.” But now, any incident involving patient records is assumed to be a breach, and must be reported. Failure to do so could subject your practice to significant fines.
The biggest vulnerability in most practices is probably mobile devices carrying patient data; and that’s where the disturbing new trend comes in: Governments, both foreign and domestic, have developed an interest in the personal data on your devices. Travelers, including American citizens, now are being pressured into giving Customs and Border Protection officers access to their cellphones and laptops at airports.
As a physician, you can invoke HIPAA in such situations, since your devices likely contain patient data in some form. But rules may vary depending on where you are traveling to or from, and officials in other countries are not bound by U.S. HIPAA constraints.
So, how do you protect patients’ (and your personal) information from invasive searches? First, encrypt all of your data; encryption software is cheap, readily available, and easy to use. (I recently posted a list of inexpensive encryption applications on the website.) Desktop apps such as BitLocker or Apple’s FileVault let you encrypt your entire hard drive, requiring a password for decryption. (As always, I have no financial interest in anything I mention here.) To avoid surrendering the password, write it down and give it to a friend, then contact that person after crossing the border. It is easier to say you didn’t memorize it, as opposed to refusing to provide it – and nobody can compel you to reveal a password you don’t know.
Experts also recommend disabling the fingerprint sensor on your smartphone; customs officials have successfully used warrants to compel people to unlock their cellphones with a fingerprint. Because of your right to remain silent, it would be difficult (but not impossible) for them to force you to share your phone’s passcode.
A better alternative, in my view, is to travel with devices that have never contained any of your patient or personal data in the first place. Invest in a cheap phone and computer to use only when you are abroad; you don’t want your nice equipment lost or stolen, anyway. A budget Android phone that works with foreign SIM cards can be had for about $100; basic laptops run $500 or less.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at [email protected].
In the struggle to understand and comply with new regulations, it’s easy to neglect older ones. Recently, I suggested reviewing your practice for potential Occupational Safety and Health Administration violations, which can be far more costly than anything MACRA has in store.
The same goes for HIPAA since HIPAA violations can be just as costly, in view of renewed governmental enforcement and some disturbing trends in completely unrelated government agencies.
Your most basic review should be a yearly examination of every part of your office where patient information is handled to identify potential violations. Examples discovered in my office included computers at our front desk whose screens were visible to patients checking in or out; laptops that were left on counters overnight; emails between staff involving patients or their care; and documents slated for shredding that remained in a “to shred” bin for days. All of these issues were easily solved at minimal cost – respectively, screen protectors, locking all laptops after hours, new email rules, and eliminating the “to shred” bin, forcing immediate shredding of all sensitive documents. Make sure you correct any problems you find before the OCR auditors come calling. You can compare your office’s compliance status against the recommendations listed on the OCR website.
Where safeguarding protected health information is concerned, you must now assume the worst-case scenario: Previously, when protected health information was compromised, you would have to notify the affected patients (and the government) only if there was a “significant risk of financial or reputational harm.” But now, any incident involving patient records is assumed to be a breach, and must be reported. Failure to do so could subject your practice to significant fines.
The biggest vulnerability in most practices is probably mobile devices carrying patient data; and that’s where the disturbing new trend comes in: Governments, both foreign and domestic, have developed an interest in the personal data on your devices. Travelers, including American citizens, now are being pressured into giving Customs and Border Protection officers access to their cellphones and laptops at airports.
As a physician, you can invoke HIPAA in such situations, since your devices likely contain patient data in some form. But rules may vary depending on where you are traveling to or from, and officials in other countries are not bound by U.S. HIPAA constraints.
So, how do you protect patients’ (and your personal) information from invasive searches? First, encrypt all of your data; encryption software is cheap, readily available, and easy to use. (I recently posted a list of inexpensive encryption applications on the website.) Desktop apps such as BitLocker or Apple’s FileVault let you encrypt your entire hard drive, requiring a password for decryption. (As always, I have no financial interest in anything I mention here.) To avoid surrendering the password, write it down and give it to a friend, then contact that person after crossing the border. It is easier to say you didn’t memorize it, as opposed to refusing to provide it – and nobody can compel you to reveal a password you don’t know.
Experts also recommend disabling the fingerprint sensor on your smartphone; customs officials have successfully used warrants to compel people to unlock their cellphones with a fingerprint. Because of your right to remain silent, it would be difficult (but not impossible) for them to force you to share your phone’s passcode.
A better alternative, in my view, is to travel with devices that have never contained any of your patient or personal data in the first place. Invest in a cheap phone and computer to use only when you are abroad; you don’t want your nice equipment lost or stolen, anyway. A budget Android phone that works with foreign SIM cards can be had for about $100; basic laptops run $500 or less.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at [email protected].
Contract negotiations
As more and more physicians, both young and experienced, choose to merge with larger practices or join multispecialty groups, I am getting numerous questions about the contracts they are being asked to sign. Obviously, every circumstance will be unique; but some common issues and avoidable mistakes are worth mentioning.
The most common error I see is failing to retain an attorney in a timely manner. Incredibly, many physicians try to do their own negotiating, and call a lawyer only when unpleasant discoveries are made after the contract has been signed. You will need counsel from the very beginning – and not your brother-in-law, or a family friend. Get referrals from colleagues who have gone through the process and are happy with their contracts.
Ambiguous provisions that could later become the subjects of dispute should be kept to a minimum. One example I have seen more than once is, “physician shall share call duties.” Don’t rely on the employer to be fair and reasonable with the call schedule. Get specific language that does not hinge on factors outside your control, such as the health or diligence of other physicians in the practice.
The conditions of your employment may also be inadequately defined. Office hours, administrative duties, medical record responsibilities, and access to specialized equipment and support staff are all negotiable, and should be clearly delineated, preferably prior to any discussion of compensation.
Other provisions may be defined, but not the way you might define them. When a contract puts a specific definition on a specific term, it will highlight the term in italics or boldface, then define it in the “Definitions” section. Read that section carefully! In court, the term will mean what the contract says it means, not what you may think it means. For example, if you can be terminated for “professional misconduct,” make sure you know how the agreement defines that transgression. Look carefully at any other termination provisions as well; make sure they are fair, reasonable, and well defined. Vague conditions such as “conduct detrimental to the practice” should be clarified.
When you discuss compensation, pay close attention to fringe benefits, such as vacation and sick leave, dues, allowances, profit sharing and retirement plans, and various insurances. Most are open to negotiation, even if the employers do not volunteer that they are. An experienced contract lawyer may also propose additional benefits that aren’t listed, and that you may not have thought of.
Incentive provisions require particularly close scrutiny. Beware of bonus triggers that an unscrupulous employer could manipulate against your interests. I’ve seen contracts that award a percentage of net income as a bonus; net income is subjective, and easy to manipulate. Owners can pay themselves a higher salary and drive down the practice’s net income. Such bonuses should be based on gross income numbers, which are more objective and easier to pin down. Incentive plans should protect you as well as your employer.
Be sure to include specific language protecting your rights to outside or additional income, such as lecture honoraria, writing royalties, expert witness testimony, and patent royalties. And carefully consider all of the implications of signing a noncompetition clause. Negotiate the clause cautiously; you won’t want to spend time and money litigating this issue if you leave.
Finally, don’t neglect researching your prospective employer, and colleagues already employed there. A friend of 30 years recently told me that merging his practice with a large conglomerate was “the worst mistake I’ve ever made,” largely because of important promises that were not kept. Due diligence, he now admits, would have revealed that the organization has a long history of promising the world, but failing to deliver. He also discovered – too late – a series of pending government sanctions, malpractice claims, and other litigation that diminish his own previously impeccable reputation, and may well affect his compensation and profit sharing for years.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at [email protected].
As more and more physicians, both young and experienced, choose to merge with larger practices or join multispecialty groups, I am getting numerous questions about the contracts they are being asked to sign. Obviously, every circumstance will be unique; but some common issues and avoidable mistakes are worth mentioning.
The most common error I see is failing to retain an attorney in a timely manner. Incredibly, many physicians try to do their own negotiating, and call a lawyer only when unpleasant discoveries are made after the contract has been signed. You will need counsel from the very beginning – and not your brother-in-law, or a family friend. Get referrals from colleagues who have gone through the process and are happy with their contracts.
Ambiguous provisions that could later become the subjects of dispute should be kept to a minimum. One example I have seen more than once is, “physician shall share call duties.” Don’t rely on the employer to be fair and reasonable with the call schedule. Get specific language that does not hinge on factors outside your control, such as the health or diligence of other physicians in the practice.
The conditions of your employment may also be inadequately defined. Office hours, administrative duties, medical record responsibilities, and access to specialized equipment and support staff are all negotiable, and should be clearly delineated, preferably prior to any discussion of compensation.
Other provisions may be defined, but not the way you might define them. When a contract puts a specific definition on a specific term, it will highlight the term in italics or boldface, then define it in the “Definitions” section. Read that section carefully! In court, the term will mean what the contract says it means, not what you may think it means. For example, if you can be terminated for “professional misconduct,” make sure you know how the agreement defines that transgression. Look carefully at any other termination provisions as well; make sure they are fair, reasonable, and well defined. Vague conditions such as “conduct detrimental to the practice” should be clarified.
When you discuss compensation, pay close attention to fringe benefits, such as vacation and sick leave, dues, allowances, profit sharing and retirement plans, and various insurances. Most are open to negotiation, even if the employers do not volunteer that they are. An experienced contract lawyer may also propose additional benefits that aren’t listed, and that you may not have thought of.
Incentive provisions require particularly close scrutiny. Beware of bonus triggers that an unscrupulous employer could manipulate against your interests. I’ve seen contracts that award a percentage of net income as a bonus; net income is subjective, and easy to manipulate. Owners can pay themselves a higher salary and drive down the practice’s net income. Such bonuses should be based on gross income numbers, which are more objective and easier to pin down. Incentive plans should protect you as well as your employer.
Be sure to include specific language protecting your rights to outside or additional income, such as lecture honoraria, writing royalties, expert witness testimony, and patent royalties. And carefully consider all of the implications of signing a noncompetition clause. Negotiate the clause cautiously; you won’t want to spend time and money litigating this issue if you leave.
Finally, don’t neglect researching your prospective employer, and colleagues already employed there. A friend of 30 years recently told me that merging his practice with a large conglomerate was “the worst mistake I’ve ever made,” largely because of important promises that were not kept. Due diligence, he now admits, would have revealed that the organization has a long history of promising the world, but failing to deliver. He also discovered – too late – a series of pending government sanctions, malpractice claims, and other litigation that diminish his own previously impeccable reputation, and may well affect his compensation and profit sharing for years.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at [email protected].
As more and more physicians, both young and experienced, choose to merge with larger practices or join multispecialty groups, I am getting numerous questions about the contracts they are being asked to sign. Obviously, every circumstance will be unique; but some common issues and avoidable mistakes are worth mentioning.
The most common error I see is failing to retain an attorney in a timely manner. Incredibly, many physicians try to do their own negotiating, and call a lawyer only when unpleasant discoveries are made after the contract has been signed. You will need counsel from the very beginning – and not your brother-in-law, or a family friend. Get referrals from colleagues who have gone through the process and are happy with their contracts.
Ambiguous provisions that could later become the subjects of dispute should be kept to a minimum. One example I have seen more than once is, “physician shall share call duties.” Don’t rely on the employer to be fair and reasonable with the call schedule. Get specific language that does not hinge on factors outside your control, such as the health or diligence of other physicians in the practice.
The conditions of your employment may also be inadequately defined. Office hours, administrative duties, medical record responsibilities, and access to specialized equipment and support staff are all negotiable, and should be clearly delineated, preferably prior to any discussion of compensation.
Other provisions may be defined, but not the way you might define them. When a contract puts a specific definition on a specific term, it will highlight the term in italics or boldface, then define it in the “Definitions” section. Read that section carefully! In court, the term will mean what the contract says it means, not what you may think it means. For example, if you can be terminated for “professional misconduct,” make sure you know how the agreement defines that transgression. Look carefully at any other termination provisions as well; make sure they are fair, reasonable, and well defined. Vague conditions such as “conduct detrimental to the practice” should be clarified.
When you discuss compensation, pay close attention to fringe benefits, such as vacation and sick leave, dues, allowances, profit sharing and retirement plans, and various insurances. Most are open to negotiation, even if the employers do not volunteer that they are. An experienced contract lawyer may also propose additional benefits that aren’t listed, and that you may not have thought of.
Incentive provisions require particularly close scrutiny. Beware of bonus triggers that an unscrupulous employer could manipulate against your interests. I’ve seen contracts that award a percentage of net income as a bonus; net income is subjective, and easy to manipulate. Owners can pay themselves a higher salary and drive down the practice’s net income. Such bonuses should be based on gross income numbers, which are more objective and easier to pin down. Incentive plans should protect you as well as your employer.
Be sure to include specific language protecting your rights to outside or additional income, such as lecture honoraria, writing royalties, expert witness testimony, and patent royalties. And carefully consider all of the implications of signing a noncompetition clause. Negotiate the clause cautiously; you won’t want to spend time and money litigating this issue if you leave.
Finally, don’t neglect researching your prospective employer, and colleagues already employed there. A friend of 30 years recently told me that merging his practice with a large conglomerate was “the worst mistake I’ve ever made,” largely because of important promises that were not kept. Due diligence, he now admits, would have revealed that the organization has a long history of promising the world, but failing to deliver. He also discovered – too late – a series of pending government sanctions, malpractice claims, and other litigation that diminish his own previously impeccable reputation, and may well affect his compensation and profit sharing for years.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at [email protected].
Estate planning
The latest anniversary of my birth recently passed; I am now a provider and a beneficiary in the Medicare system. Fortunately, I have learned to celebrate these annual events, and the changes they bring, rather than dread them. I now appreciate that life gets better as we get older, on all levels – except, perhaps, the physical.
But I have also learned that birthdays are a good time to pause and consider the various financial arrangements that I’ve set up over the years, and to determine whether any of them need updating.
Estate plans, in particular, need regular review and revision. Nothing important has changed in your life since you drafted your will, you say? Well, chances are the laws have changed, or other factors may have rendered your plan obsolete without your even realizing it.
I am assuming, of course, that you have in fact drafted a will. If not – regardless of your age – do it as soon as possible. Stuff happens; if you die without a will (“intestate,” in lawyer lingo), your heirs will be at the mercy of attorneys, bureaucrats, state and federal laws, and greed. Quarrels will ensue; decisions will be made that are almost certainly at variance with what you would have wanted; and a substantial chunk of your estate that could have gone to loved ones, or to charity, will be lost to taxes and legal fees.
In other words, if you don’t write a will, others will write one for you – one your heirs probably won’t like. Don’t let that happen. That said, let’s consider some variables that mandate your constant vigilance:
Laws change. Trust laws, in particular, have changed a great deal in recent years, and trust strategies have changed with them. New instruments such as perpetual trusts, trust protectors, directed trusts, and total return trusts may or may not work to your advantage, but you won’t know without asking. State laws change too.
Once a year, my wife and I meet with our estate lawyer to learn about any new legislation that may have affected our plan. A few years ago, for example, I learned that my irrevocable trust was no longer irrevocable; new laws now permit certain provisions to be modified.
Laws that don’t directly regulate wills and trusts can impact your plan as well. For instance, the ever-popular Health Insurance Portability and Accountability Act (HIPAA) applies to your estate as well as your practice; under its provisions, your family cannot access your medical information or make treatment and life-support decisions without your specific permission. So if a Health Care Power of Attorney is not already part of your will, add it. And remember to modify it if your medical status, or your philosophy of life, changes.
Financial markets change. It’s not exactly a secret that asset values and interest rates are considerably different than they were even a few years ago. Real estate or securities bequests could now be significantly larger or smaller. Your accountant and estate lawyer should take a look at your assets periodically, and their apportionment in your will, to be sure all arrangements remain as you intend. And be sure to notify them whenever the composition of your assets changes, even if their value doesn’t. Say, for example, you sell a business or property, and reinvest the proceeds in something completely different; a different set of tax laws will apply, and your will must reflect that.
Fiduciaries change. Keep track of the executor of your estate and the trustee(s) of your trust(s), and be prepared to make changes if needed. If your brother-in-law is your executor, and your sister divorces him, you may want to name a new executor. A once-vigorous trustee who is now old or sick should be replaced. Trustees are often financial institutions; if a corporate trustee goes belly up, or the employee you were working with leaves or retires, you’ll need a replacement.
Personal circumstances change. Some changes – marriage, divorce, the death of an heir, or the birth of a new one – obviously require modifications to wills and trusts. But any significant alteration of your personal or financial circumstances probably merits a phone call to your financial planners. The need for changes, and your options, are not always obvious.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at [email protected].
The latest anniversary of my birth recently passed; I am now a provider and a beneficiary in the Medicare system. Fortunately, I have learned to celebrate these annual events, and the changes they bring, rather than dread them. I now appreciate that life gets better as we get older, on all levels – except, perhaps, the physical.
But I have also learned that birthdays are a good time to pause and consider the various financial arrangements that I’ve set up over the years, and to determine whether any of them need updating.
Estate plans, in particular, need regular review and revision. Nothing important has changed in your life since you drafted your will, you say? Well, chances are the laws have changed, or other factors may have rendered your plan obsolete without your even realizing it.
I am assuming, of course, that you have in fact drafted a will. If not – regardless of your age – do it as soon as possible. Stuff happens; if you die without a will (“intestate,” in lawyer lingo), your heirs will be at the mercy of attorneys, bureaucrats, state and federal laws, and greed. Quarrels will ensue; decisions will be made that are almost certainly at variance with what you would have wanted; and a substantial chunk of your estate that could have gone to loved ones, or to charity, will be lost to taxes and legal fees.
In other words, if you don’t write a will, others will write one for you – one your heirs probably won’t like. Don’t let that happen. That said, let’s consider some variables that mandate your constant vigilance:
Laws change. Trust laws, in particular, have changed a great deal in recent years, and trust strategies have changed with them. New instruments such as perpetual trusts, trust protectors, directed trusts, and total return trusts may or may not work to your advantage, but you won’t know without asking. State laws change too.
Once a year, my wife and I meet with our estate lawyer to learn about any new legislation that may have affected our plan. A few years ago, for example, I learned that my irrevocable trust was no longer irrevocable; new laws now permit certain provisions to be modified.
Laws that don’t directly regulate wills and trusts can impact your plan as well. For instance, the ever-popular Health Insurance Portability and Accountability Act (HIPAA) applies to your estate as well as your practice; under its provisions, your family cannot access your medical information or make treatment and life-support decisions without your specific permission. So if a Health Care Power of Attorney is not already part of your will, add it. And remember to modify it if your medical status, or your philosophy of life, changes.
Financial markets change. It’s not exactly a secret that asset values and interest rates are considerably different than they were even a few years ago. Real estate or securities bequests could now be significantly larger or smaller. Your accountant and estate lawyer should take a look at your assets periodically, and their apportionment in your will, to be sure all arrangements remain as you intend. And be sure to notify them whenever the composition of your assets changes, even if their value doesn’t. Say, for example, you sell a business or property, and reinvest the proceeds in something completely different; a different set of tax laws will apply, and your will must reflect that.
Fiduciaries change. Keep track of the executor of your estate and the trustee(s) of your trust(s), and be prepared to make changes if needed. If your brother-in-law is your executor, and your sister divorces him, you may want to name a new executor. A once-vigorous trustee who is now old or sick should be replaced. Trustees are often financial institutions; if a corporate trustee goes belly up, or the employee you were working with leaves or retires, you’ll need a replacement.
Personal circumstances change. Some changes – marriage, divorce, the death of an heir, or the birth of a new one – obviously require modifications to wills and trusts. But any significant alteration of your personal or financial circumstances probably merits a phone call to your financial planners. The need for changes, and your options, are not always obvious.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at [email protected].
The latest anniversary of my birth recently passed; I am now a provider and a beneficiary in the Medicare system. Fortunately, I have learned to celebrate these annual events, and the changes they bring, rather than dread them. I now appreciate that life gets better as we get older, on all levels – except, perhaps, the physical.
But I have also learned that birthdays are a good time to pause and consider the various financial arrangements that I’ve set up over the years, and to determine whether any of them need updating.
Estate plans, in particular, need regular review and revision. Nothing important has changed in your life since you drafted your will, you say? Well, chances are the laws have changed, or other factors may have rendered your plan obsolete without your even realizing it.
I am assuming, of course, that you have in fact drafted a will. If not – regardless of your age – do it as soon as possible. Stuff happens; if you die without a will (“intestate,” in lawyer lingo), your heirs will be at the mercy of attorneys, bureaucrats, state and federal laws, and greed. Quarrels will ensue; decisions will be made that are almost certainly at variance with what you would have wanted; and a substantial chunk of your estate that could have gone to loved ones, or to charity, will be lost to taxes and legal fees.
In other words, if you don’t write a will, others will write one for you – one your heirs probably won’t like. Don’t let that happen. That said, let’s consider some variables that mandate your constant vigilance:
Laws change. Trust laws, in particular, have changed a great deal in recent years, and trust strategies have changed with them. New instruments such as perpetual trusts, trust protectors, directed trusts, and total return trusts may or may not work to your advantage, but you won’t know without asking. State laws change too.
Once a year, my wife and I meet with our estate lawyer to learn about any new legislation that may have affected our plan. A few years ago, for example, I learned that my irrevocable trust was no longer irrevocable; new laws now permit certain provisions to be modified.
Laws that don’t directly regulate wills and trusts can impact your plan as well. For instance, the ever-popular Health Insurance Portability and Accountability Act (HIPAA) applies to your estate as well as your practice; under its provisions, your family cannot access your medical information or make treatment and life-support decisions without your specific permission. So if a Health Care Power of Attorney is not already part of your will, add it. And remember to modify it if your medical status, or your philosophy of life, changes.
Financial markets change. It’s not exactly a secret that asset values and interest rates are considerably different than they were even a few years ago. Real estate or securities bequests could now be significantly larger or smaller. Your accountant and estate lawyer should take a look at your assets periodically, and their apportionment in your will, to be sure all arrangements remain as you intend. And be sure to notify them whenever the composition of your assets changes, even if their value doesn’t. Say, for example, you sell a business or property, and reinvest the proceeds in something completely different; a different set of tax laws will apply, and your will must reflect that.
Fiduciaries change. Keep track of the executor of your estate and the trustee(s) of your trust(s), and be prepared to make changes if needed. If your brother-in-law is your executor, and your sister divorces him, you may want to name a new executor. A once-vigorous trustee who is now old or sick should be replaced. Trustees are often financial institutions; if a corporate trustee goes belly up, or the employee you were working with leaves or retires, you’ll need a replacement.
Personal circumstances change. Some changes – marriage, divorce, the death of an heir, or the birth of a new one – obviously require modifications to wills and trusts. But any significant alteration of your personal or financial circumstances probably merits a phone call to your financial planners. The need for changes, and your options, are not always obvious.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at [email protected].
Appealing rejected claims
As third-party payers become stingier and stingier with their payments, it becomes more and more important to hold them accountable for decisions that impact patient care – and your revenue. Physicians have the right to a full and fair appeal review of all rejected and underpaid claims; yet surprisingly, less than 5% of denied dermatology claims are appealed, according to one study.
Many practitioners seem to feel that appeals are simply not worth the time and effort, particularly in a high-volume field such as dermatology; but since the chance that appealing will increase your reimbursement is more than 50%, it is usually well worth the effort – particularly in the current climate of steadily decreasing reimbursements. Furthermore, once insurers become aware that you are scrutinizing your payment statements and challenging all unwarranted rejections, they will be less cavalier in denying legitimate claims.
The first thing your office manager should do is determine the reason the claim was rejected. In some cases, the benefits verification computer has ruled the patient ineligible, or decided that the provided service is not covered by the patient’s policy. If that is false, the appeal letter will be relatively simple; you can design a boilerplate form to cover those instances. If it is true, your pretreatment evaluation process needs to be examined; you should not be treating ineligible patients or performing ineligible treatments in the first place, unless such patients are made aware that their care will not be covered and that they will have to pay for it themselves. In some cases, the amount in dispute really is so small that the appeal process may indeed not be worth the bother; but such cases, in my experience, are quite rare.
Once you determine that it is worth the effort to go through the appeals process, you will need to familiarize yourself with the appeal procedure – which varies from payer to payer – and then incorporate all of the elements that comprise a successful appeal.
The basis of every appeal, obviously, is an argument against the reason given for rejecting the claim. Unfortunately, payers do not always spell out their reasoning clearly. Rejected claims often include only a cryptic statement on why the claim was denied, without explaining the motivation behind the actual denial. Explanations are often in the form of an important-sounding “code,” such as a “claim adjustment reason code” or “remittance advice remark code,” referencing a generalized, nonspecific rejection excuse. (This is a purposeful attempt, of course, to discourage you from fighting the denial.) Your manager may have to place a call to the payer, demanding more specific information.
If a valid reason is not forthcoming, the appeal process once again becomes simple. You should have another boilerplate for such circumstances; just fill in the blanks. If a specific reason behind the rejection can be identified, that will determine the basis of your appeal: coding, medical necessity, or administrative.
Coding appeals usually involve either miscoding by the practitioner, or misinterpretation of the correct code by the payer. If the fault is yours, admit it, and supply the correct code – with documentation, when necessary. If the payer has erred, clearly explain the error – again with documentation when needed – and spell out the reasons that payment is warranted (and expected) immediately.
Medical necessity appeals require you to go into detail about the patient’s medical history, condition, symptoms, and treatment. If treatment with an expensive medication has been rejected, explain the advantages of that medication over cheaper alternatives. A reference to accepted standards of care is often persuasive.
An administrative appeal may be necessary if you have a weak clinical argument. You’ll need to argue that the services you provided were consistent with how the payer defines appropriate treatment. If Medicare is the primary payer, a reference to appropriate passages in the Medicare Benefit Policy Manual is usually helpful.
If you get nowhere with written appeals, a peer-to-peer call to the payer’s medical director may solve the problem, since you can explain the patient’s specific situation in more detail, and appeal to your colleague’s empathy – and common sense.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at [email protected].
As third-party payers become stingier and stingier with their payments, it becomes more and more important to hold them accountable for decisions that impact patient care – and your revenue. Physicians have the right to a full and fair appeal review of all rejected and underpaid claims; yet surprisingly, less than 5% of denied dermatology claims are appealed, according to one study.
Many practitioners seem to feel that appeals are simply not worth the time and effort, particularly in a high-volume field such as dermatology; but since the chance that appealing will increase your reimbursement is more than 50%, it is usually well worth the effort – particularly in the current climate of steadily decreasing reimbursements. Furthermore, once insurers become aware that you are scrutinizing your payment statements and challenging all unwarranted rejections, they will be less cavalier in denying legitimate claims.
The first thing your office manager should do is determine the reason the claim was rejected. In some cases, the benefits verification computer has ruled the patient ineligible, or decided that the provided service is not covered by the patient’s policy. If that is false, the appeal letter will be relatively simple; you can design a boilerplate form to cover those instances. If it is true, your pretreatment evaluation process needs to be examined; you should not be treating ineligible patients or performing ineligible treatments in the first place, unless such patients are made aware that their care will not be covered and that they will have to pay for it themselves. In some cases, the amount in dispute really is so small that the appeal process may indeed not be worth the bother; but such cases, in my experience, are quite rare.
Once you determine that it is worth the effort to go through the appeals process, you will need to familiarize yourself with the appeal procedure – which varies from payer to payer – and then incorporate all of the elements that comprise a successful appeal.
The basis of every appeal, obviously, is an argument against the reason given for rejecting the claim. Unfortunately, payers do not always spell out their reasoning clearly. Rejected claims often include only a cryptic statement on why the claim was denied, without explaining the motivation behind the actual denial. Explanations are often in the form of an important-sounding “code,” such as a “claim adjustment reason code” or “remittance advice remark code,” referencing a generalized, nonspecific rejection excuse. (This is a purposeful attempt, of course, to discourage you from fighting the denial.) Your manager may have to place a call to the payer, demanding more specific information.
If a valid reason is not forthcoming, the appeal process once again becomes simple. You should have another boilerplate for such circumstances; just fill in the blanks. If a specific reason behind the rejection can be identified, that will determine the basis of your appeal: coding, medical necessity, or administrative.
Coding appeals usually involve either miscoding by the practitioner, or misinterpretation of the correct code by the payer. If the fault is yours, admit it, and supply the correct code – with documentation, when necessary. If the payer has erred, clearly explain the error – again with documentation when needed – and spell out the reasons that payment is warranted (and expected) immediately.
Medical necessity appeals require you to go into detail about the patient’s medical history, condition, symptoms, and treatment. If treatment with an expensive medication has been rejected, explain the advantages of that medication over cheaper alternatives. A reference to accepted standards of care is often persuasive.
An administrative appeal may be necessary if you have a weak clinical argument. You’ll need to argue that the services you provided were consistent with how the payer defines appropriate treatment. If Medicare is the primary payer, a reference to appropriate passages in the Medicare Benefit Policy Manual is usually helpful.
If you get nowhere with written appeals, a peer-to-peer call to the payer’s medical director may solve the problem, since you can explain the patient’s specific situation in more detail, and appeal to your colleague’s empathy – and common sense.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at [email protected].
As third-party payers become stingier and stingier with their payments, it becomes more and more important to hold them accountable for decisions that impact patient care – and your revenue. Physicians have the right to a full and fair appeal review of all rejected and underpaid claims; yet surprisingly, less than 5% of denied dermatology claims are appealed, according to one study.
Many practitioners seem to feel that appeals are simply not worth the time and effort, particularly in a high-volume field such as dermatology; but since the chance that appealing will increase your reimbursement is more than 50%, it is usually well worth the effort – particularly in the current climate of steadily decreasing reimbursements. Furthermore, once insurers become aware that you are scrutinizing your payment statements and challenging all unwarranted rejections, they will be less cavalier in denying legitimate claims.
The first thing your office manager should do is determine the reason the claim was rejected. In some cases, the benefits verification computer has ruled the patient ineligible, or decided that the provided service is not covered by the patient’s policy. If that is false, the appeal letter will be relatively simple; you can design a boilerplate form to cover those instances. If it is true, your pretreatment evaluation process needs to be examined; you should not be treating ineligible patients or performing ineligible treatments in the first place, unless such patients are made aware that their care will not be covered and that they will have to pay for it themselves. In some cases, the amount in dispute really is so small that the appeal process may indeed not be worth the bother; but such cases, in my experience, are quite rare.
Once you determine that it is worth the effort to go through the appeals process, you will need to familiarize yourself with the appeal procedure – which varies from payer to payer – and then incorporate all of the elements that comprise a successful appeal.
The basis of every appeal, obviously, is an argument against the reason given for rejecting the claim. Unfortunately, payers do not always spell out their reasoning clearly. Rejected claims often include only a cryptic statement on why the claim was denied, without explaining the motivation behind the actual denial. Explanations are often in the form of an important-sounding “code,” such as a “claim adjustment reason code” or “remittance advice remark code,” referencing a generalized, nonspecific rejection excuse. (This is a purposeful attempt, of course, to discourage you from fighting the denial.) Your manager may have to place a call to the payer, demanding more specific information.
If a valid reason is not forthcoming, the appeal process once again becomes simple. You should have another boilerplate for such circumstances; just fill in the blanks. If a specific reason behind the rejection can be identified, that will determine the basis of your appeal: coding, medical necessity, or administrative.
Coding appeals usually involve either miscoding by the practitioner, or misinterpretation of the correct code by the payer. If the fault is yours, admit it, and supply the correct code – with documentation, when necessary. If the payer has erred, clearly explain the error – again with documentation when needed – and spell out the reasons that payment is warranted (and expected) immediately.
Medical necessity appeals require you to go into detail about the patient’s medical history, condition, symptoms, and treatment. If treatment with an expensive medication has been rejected, explain the advantages of that medication over cheaper alternatives. A reference to accepted standards of care is often persuasive.
An administrative appeal may be necessary if you have a weak clinical argument. You’ll need to argue that the services you provided were consistent with how the payer defines appropriate treatment. If Medicare is the primary payer, a reference to appropriate passages in the Medicare Benefit Policy Manual is usually helpful.
If you get nowhere with written appeals, a peer-to-peer call to the payer’s medical director may solve the problem, since you can explain the patient’s specific situation in more detail, and appeal to your colleague’s empathy – and common sense.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at [email protected].
Should you continue to participate in Medicare?
Since writing about the new MACRA bureaucracy, and the Morton’s Choice facing private practitioners between Scylla (the Merit-based Incentive Payment System) and Charybdis (the still largely undefined Alternate Payment Models), a question I’ve been hearing with increasing frequency is whether it wouldn’t be better to simply opt out of Medicare participation entirely.
It is easy to see why more and more physicians are asking that question. Although the incoming administration has promised significant (but largely unspecified) changes to the health care system – as I wrote last month – reimbursements continue to decrease, onerous regulations continue to increase, and there is no evidence to suggest that either of those trends will change anytime soon. That leaves many physicians wondering whether their continued participation with Medicare (and Medicaid, for those who accept it) is ultimately worth it.
It is difficult to assign a firm answer to the basic question of whether or not opting out is a good idea. As usual, it will depend upon your unique circumstances, as well as the size and composition of your practice. This is not a decision to make lightly, or hastily – particularly if a significant percentage of your patients have federal or state health care coverage.
You will need to carefully consider the pros and cons involved, beginning with the fact that once you pull the trigger, there’s no going back for at least 2 years. (If you are opting out for the very first time, you do have 90 days to change your mind and opt back in.) And you must create a physician-patient agreement covering your treatment and billing guidelines, and make sure all of your Medicare/Medicaid patients sign it.
The obvious benefit of opting out is the freedom to do and bill what and how you wish. Once liberated from CMS compliance restrictions, you can spend your time treating patients, rather than catering to and being controlled by the government. The physician-patient relationship regains its proper priority; you can work directly with your patients in structuring their care plans and pursuing the best treatment options. Physicians with small, relatively young patient populations often find the prospect of charting their own course particularly attractive.
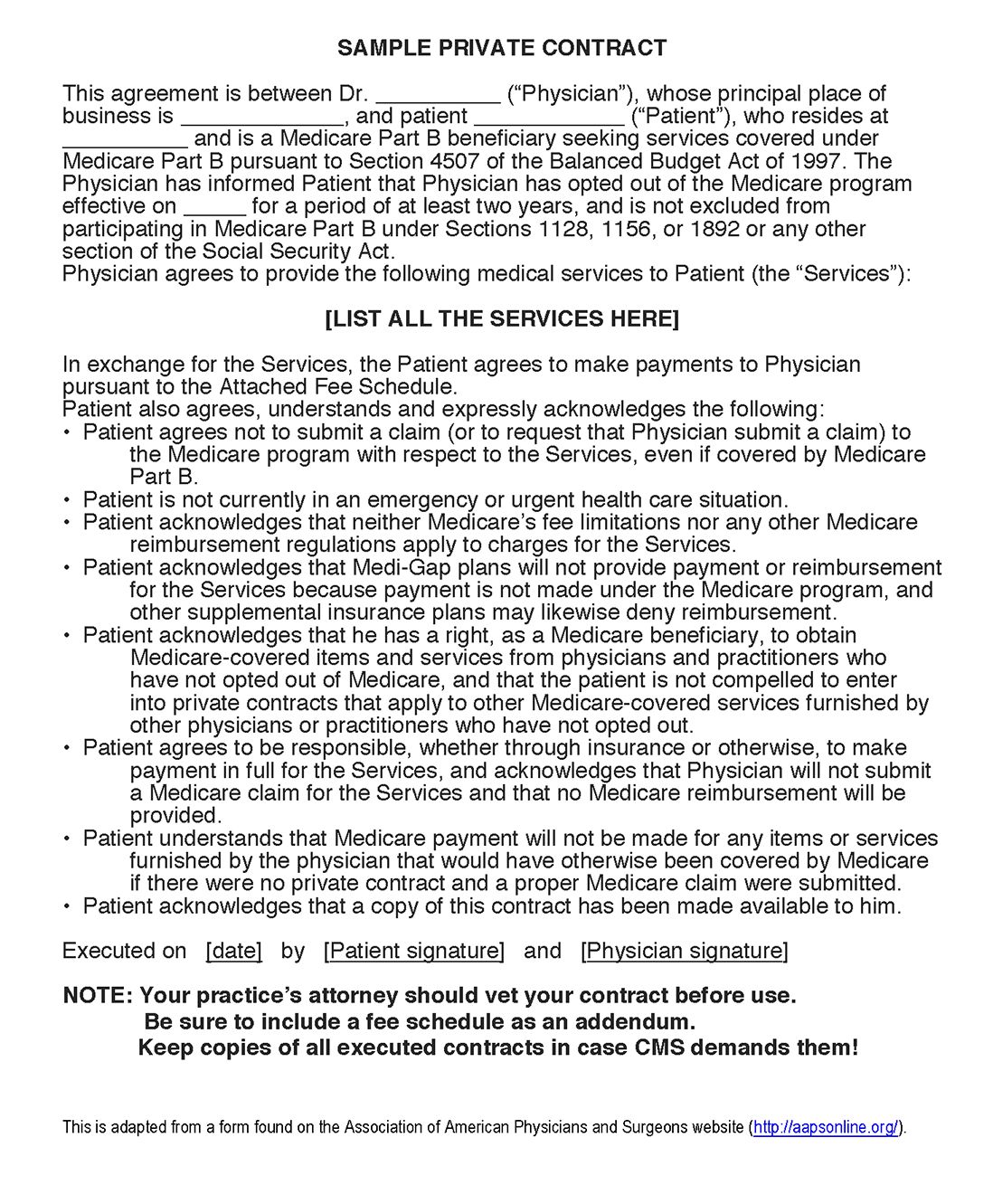
Not only that, but some commercial carriers require Medicare participation in order to maintain credentialing with them. So if you opt out of federal and state participation, you will also need to opt out of commercial plans with that requirement. Hospital admitting privileges may also be contingent on Medicare participation; be sure to check your hospitals’ bylaws.
Another challenge is pushback from patients. While few patients like dealing with insurance claims, fewer still are willing to pay for their care themselves. When drafting a physician-patient agreement, it must be made very clear that you are not going to bill Medicare or Medicaid for services rendered, and that patients cannot do so either. Inevitably, a substantial percentage of your Medicare/Medicaid-covered patients will choose to switch to a participating physician.
If you do decide to opt out, here is how you do it:
1. Notify your patients that you will be opting out by a specific date, which should be the first day of a calendar quarter.
2. File an affidavit (available at CMS.gov) with your local Medicare carrier at least 30 days before your opt-out date.
3. Draft and post a fee schedule.
4. Draft a private contract to be signed by all Medicare beneficiaries, covering all services that would normally be covered by Medicare. Be sure to run it past your attorney.
5. Install procedures to ensure that your office never files a Medicare claim, and never provides information to enable a patient to file a Medicare claim. The two exceptions – for emergency care, and for covered services that Medicare would deem unnecessary – should be used sparingly, and with caution.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at [email protected].
Since writing about the new MACRA bureaucracy, and the Morton’s Choice facing private practitioners between Scylla (the Merit-based Incentive Payment System) and Charybdis (the still largely undefined Alternate Payment Models), a question I’ve been hearing with increasing frequency is whether it wouldn’t be better to simply opt out of Medicare participation entirely.
It is easy to see why more and more physicians are asking that question. Although the incoming administration has promised significant (but largely unspecified) changes to the health care system – as I wrote last month – reimbursements continue to decrease, onerous regulations continue to increase, and there is no evidence to suggest that either of those trends will change anytime soon. That leaves many physicians wondering whether their continued participation with Medicare (and Medicaid, for those who accept it) is ultimately worth it.
It is difficult to assign a firm answer to the basic question of whether or not opting out is a good idea. As usual, it will depend upon your unique circumstances, as well as the size and composition of your practice. This is not a decision to make lightly, or hastily – particularly if a significant percentage of your patients have federal or state health care coverage.
You will need to carefully consider the pros and cons involved, beginning with the fact that once you pull the trigger, there’s no going back for at least 2 years. (If you are opting out for the very first time, you do have 90 days to change your mind and opt back in.) And you must create a physician-patient agreement covering your treatment and billing guidelines, and make sure all of your Medicare/Medicaid patients sign it.
The obvious benefit of opting out is the freedom to do and bill what and how you wish. Once liberated from CMS compliance restrictions, you can spend your time treating patients, rather than catering to and being controlled by the government. The physician-patient relationship regains its proper priority; you can work directly with your patients in structuring their care plans and pursuing the best treatment options. Physicians with small, relatively young patient populations often find the prospect of charting their own course particularly attractive.
Not only that, but some commercial carriers require Medicare participation in order to maintain credentialing with them. So if you opt out of federal and state participation, you will also need to opt out of commercial plans with that requirement. Hospital admitting privileges may also be contingent on Medicare participation; be sure to check your hospitals’ bylaws.
Another challenge is pushback from patients. While few patients like dealing with insurance claims, fewer still are willing to pay for their care themselves. When drafting a physician-patient agreement, it must be made very clear that you are not going to bill Medicare or Medicaid for services rendered, and that patients cannot do so either. Inevitably, a substantial percentage of your Medicare/Medicaid-covered patients will choose to switch to a participating physician.
If you do decide to opt out, here is how you do it:
1. Notify your patients that you will be opting out by a specific date, which should be the first day of a calendar quarter.
2. File an affidavit (available at CMS.gov) with your local Medicare carrier at least 30 days before your opt-out date.
3. Draft and post a fee schedule.
4. Draft a private contract to be signed by all Medicare beneficiaries, covering all services that would normally be covered by Medicare. Be sure to run it past your attorney.
5. Install procedures to ensure that your office never files a Medicare claim, and never provides information to enable a patient to file a Medicare claim. The two exceptions – for emergency care, and for covered services that Medicare would deem unnecessary – should be used sparingly, and with caution.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at [email protected].
Since writing about the new MACRA bureaucracy, and the Morton’s Choice facing private practitioners between Scylla (the Merit-based Incentive Payment System) and Charybdis (the still largely undefined Alternate Payment Models), a question I’ve been hearing with increasing frequency is whether it wouldn’t be better to simply opt out of Medicare participation entirely.
It is easy to see why more and more physicians are asking that question. Although the incoming administration has promised significant (but largely unspecified) changes to the health care system – as I wrote last month – reimbursements continue to decrease, onerous regulations continue to increase, and there is no evidence to suggest that either of those trends will change anytime soon. That leaves many physicians wondering whether their continued participation with Medicare (and Medicaid, for those who accept it) is ultimately worth it.
It is difficult to assign a firm answer to the basic question of whether or not opting out is a good idea. As usual, it will depend upon your unique circumstances, as well as the size and composition of your practice. This is not a decision to make lightly, or hastily – particularly if a significant percentage of your patients have federal or state health care coverage.
You will need to carefully consider the pros and cons involved, beginning with the fact that once you pull the trigger, there’s no going back for at least 2 years. (If you are opting out for the very first time, you do have 90 days to change your mind and opt back in.) And you must create a physician-patient agreement covering your treatment and billing guidelines, and make sure all of your Medicare/Medicaid patients sign it.
The obvious benefit of opting out is the freedom to do and bill what and how you wish. Once liberated from CMS compliance restrictions, you can spend your time treating patients, rather than catering to and being controlled by the government. The physician-patient relationship regains its proper priority; you can work directly with your patients in structuring their care plans and pursuing the best treatment options. Physicians with small, relatively young patient populations often find the prospect of charting their own course particularly attractive.
Not only that, but some commercial carriers require Medicare participation in order to maintain credentialing with them. So if you opt out of federal and state participation, you will also need to opt out of commercial plans with that requirement. Hospital admitting privileges may also be contingent on Medicare participation; be sure to check your hospitals’ bylaws.
Another challenge is pushback from patients. While few patients like dealing with insurance claims, fewer still are willing to pay for their care themselves. When drafting a physician-patient agreement, it must be made very clear that you are not going to bill Medicare or Medicaid for services rendered, and that patients cannot do so either. Inevitably, a substantial percentage of your Medicare/Medicaid-covered patients will choose to switch to a participating physician.
If you do decide to opt out, here is how you do it:
1. Notify your patients that you will be opting out by a specific date, which should be the first day of a calendar quarter.
2. File an affidavit (available at CMS.gov) with your local Medicare carrier at least 30 days before your opt-out date.
3. Draft and post a fee schedule.
4. Draft a private contract to be signed by all Medicare beneficiaries, covering all services that would normally be covered by Medicare. Be sure to run it past your attorney.
5. Install procedures to ensure that your office never files a Medicare claim, and never provides information to enable a patient to file a Medicare claim. The two exceptions – for emergency care, and for covered services that Medicare would deem unnecessary – should be used sparingly, and with caution.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at [email protected].
How will Donald Trump change health care?
Much speculation has already been written on what a Trump administration may look like, but comparatively little has been said about the potential impact of that administration on physicians, hospitals, and patients. While details will obviously not be available for some time, some early generalizations are possible, based on the position paper President-elect Donald Trump issued in March and the statements he has made since then.
One of Mr. Trump’s earliest and most repeated pledges was the one to repeal the Affordable Care Act and replace it with “something fantastic.” A repeal would be welcome news to many physicians, even without any idea of what its “fantastic” replacement might be; but Trump has hedged already. In mid-November, he told the Wall Street Journal that Obamacare would be “amended, or repealed and replaced,” which introduces considerable wiggle room.
In an interview with CNN, Mr. Trump indicated he would keep the individual mandate; but the next day, he tweeted – and then reiterated in his position paper – that he would remove the mandate and install a “backstop for preexisting conditions.” In the 1990s, when a few states tried to prohibit discrimination based on preexisting conditions without a corresponding mandate, premiums increased precipitously, driving away healthy customers, forcing insurers to stop selling policies in those states, and demonstrating that one cannot work without the other. Perhaps a more-informed Mr. Trump will come to see this.
Other proposals have been more enlightened. Mr. Trump has said that he favors portability of health insurance from state to state. In theory, this will introduce more competition into the system and drive premiums down. He has also proposed making health insurance premiums fully tax deductible for individuals, as they are now for businesses, further lowering premium costs.
He has proposed expanding the health savings account program, making contributions tax free, cumulative, and part of a patient’s estate. I have been a fan of HSAs since their inception because they eliminate the insurance “middleman,” which is good for physicians as well as for patients, who are more aware of what services they are receiving and what they are paying for them. Along the same lines, he has called for price transparency, so that patients can shop for the best prices for procedures and examinations, which now vary widely from one hospital or clinic to another.
Another good idea, in my opinion, is the removal of barriers to the sale of cheaper foreign-manufactured drugs in this country. Such barriers have kept drug prices higher here than anywhere else; consumers should be able to import their medications, from Canada, India, and elsewhere, as long as they are similarly safe and effective. Mr. Trump has also said that Medicare should be able to negotiate drug prices, which should have been true from the outset. The savings, particularly where biologics and other expensive new drugs are concerned, could be significant, since Medicare frequently sets the standard for prices in the industry. He also would raise the Medicare eligibility age, which I believe is a good idea as well.
Less inspired is his proposal to turn over administration of Medicaid to the states, supported by federal block grants. This plan does not take into account that Medicaid, an expensive and inefficient program with a narrow network of doctors, desperately needs an overhaul. Simply expanding it, and handing over full responsibility to the states, is not a viable solution, in my opinion.
Mr. Trump’s position paper also contains the dubious assumption that enforcing immigration laws will significantly decrease health care costs. Sealing the Southern border, he reasons, will help hospitals overburdened by the costs of services they provide to illegal immigrants who can’t pay for them and curtail the burgeoning heroin trade and its associated medical costs. There is little evidence to support either assumption – or even that the border can be effectively sealed in the first place.
So Mr. Trump has a health care plan, of sorts. How it will look by Inauguration Day, and what portion will be implemented, remains to be seen.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at [email protected].
Much speculation has already been written on what a Trump administration may look like, but comparatively little has been said about the potential impact of that administration on physicians, hospitals, and patients. While details will obviously not be available for some time, some early generalizations are possible, based on the position paper President-elect Donald Trump issued in March and the statements he has made since then.
One of Mr. Trump’s earliest and most repeated pledges was the one to repeal the Affordable Care Act and replace it with “something fantastic.” A repeal would be welcome news to many physicians, even without any idea of what its “fantastic” replacement might be; but Trump has hedged already. In mid-November, he told the Wall Street Journal that Obamacare would be “amended, or repealed and replaced,” which introduces considerable wiggle room.
In an interview with CNN, Mr. Trump indicated he would keep the individual mandate; but the next day, he tweeted – and then reiterated in his position paper – that he would remove the mandate and install a “backstop for preexisting conditions.” In the 1990s, when a few states tried to prohibit discrimination based on preexisting conditions without a corresponding mandate, premiums increased precipitously, driving away healthy customers, forcing insurers to stop selling policies in those states, and demonstrating that one cannot work without the other. Perhaps a more-informed Mr. Trump will come to see this.
Other proposals have been more enlightened. Mr. Trump has said that he favors portability of health insurance from state to state. In theory, this will introduce more competition into the system and drive premiums down. He has also proposed making health insurance premiums fully tax deductible for individuals, as they are now for businesses, further lowering premium costs.
He has proposed expanding the health savings account program, making contributions tax free, cumulative, and part of a patient’s estate. I have been a fan of HSAs since their inception because they eliminate the insurance “middleman,” which is good for physicians as well as for patients, who are more aware of what services they are receiving and what they are paying for them. Along the same lines, he has called for price transparency, so that patients can shop for the best prices for procedures and examinations, which now vary widely from one hospital or clinic to another.
Another good idea, in my opinion, is the removal of barriers to the sale of cheaper foreign-manufactured drugs in this country. Such barriers have kept drug prices higher here than anywhere else; consumers should be able to import their medications, from Canada, India, and elsewhere, as long as they are similarly safe and effective. Mr. Trump has also said that Medicare should be able to negotiate drug prices, which should have been true from the outset. The savings, particularly where biologics and other expensive new drugs are concerned, could be significant, since Medicare frequently sets the standard for prices in the industry. He also would raise the Medicare eligibility age, which I believe is a good idea as well.
Less inspired is his proposal to turn over administration of Medicaid to the states, supported by federal block grants. This plan does not take into account that Medicaid, an expensive and inefficient program with a narrow network of doctors, desperately needs an overhaul. Simply expanding it, and handing over full responsibility to the states, is not a viable solution, in my opinion.
Mr. Trump’s position paper also contains the dubious assumption that enforcing immigration laws will significantly decrease health care costs. Sealing the Southern border, he reasons, will help hospitals overburdened by the costs of services they provide to illegal immigrants who can’t pay for them and curtail the burgeoning heroin trade and its associated medical costs. There is little evidence to support either assumption – or even that the border can be effectively sealed in the first place.
So Mr. Trump has a health care plan, of sorts. How it will look by Inauguration Day, and what portion will be implemented, remains to be seen.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at [email protected].
Much speculation has already been written on what a Trump administration may look like, but comparatively little has been said about the potential impact of that administration on physicians, hospitals, and patients. While details will obviously not be available for some time, some early generalizations are possible, based on the position paper President-elect Donald Trump issued in March and the statements he has made since then.
One of Mr. Trump’s earliest and most repeated pledges was the one to repeal the Affordable Care Act and replace it with “something fantastic.” A repeal would be welcome news to many physicians, even without any idea of what its “fantastic” replacement might be; but Trump has hedged already. In mid-November, he told the Wall Street Journal that Obamacare would be “amended, or repealed and replaced,” which introduces considerable wiggle room.
In an interview with CNN, Mr. Trump indicated he would keep the individual mandate; but the next day, he tweeted – and then reiterated in his position paper – that he would remove the mandate and install a “backstop for preexisting conditions.” In the 1990s, when a few states tried to prohibit discrimination based on preexisting conditions without a corresponding mandate, premiums increased precipitously, driving away healthy customers, forcing insurers to stop selling policies in those states, and demonstrating that one cannot work without the other. Perhaps a more-informed Mr. Trump will come to see this.
Other proposals have been more enlightened. Mr. Trump has said that he favors portability of health insurance from state to state. In theory, this will introduce more competition into the system and drive premiums down. He has also proposed making health insurance premiums fully tax deductible for individuals, as they are now for businesses, further lowering premium costs.
He has proposed expanding the health savings account program, making contributions tax free, cumulative, and part of a patient’s estate. I have been a fan of HSAs since their inception because they eliminate the insurance “middleman,” which is good for physicians as well as for patients, who are more aware of what services they are receiving and what they are paying for them. Along the same lines, he has called for price transparency, so that patients can shop for the best prices for procedures and examinations, which now vary widely from one hospital or clinic to another.
Another good idea, in my opinion, is the removal of barriers to the sale of cheaper foreign-manufactured drugs in this country. Such barriers have kept drug prices higher here than anywhere else; consumers should be able to import their medications, from Canada, India, and elsewhere, as long as they are similarly safe and effective. Mr. Trump has also said that Medicare should be able to negotiate drug prices, which should have been true from the outset. The savings, particularly where biologics and other expensive new drugs are concerned, could be significant, since Medicare frequently sets the standard for prices in the industry. He also would raise the Medicare eligibility age, which I believe is a good idea as well.
Less inspired is his proposal to turn over administration of Medicaid to the states, supported by federal block grants. This plan does not take into account that Medicaid, an expensive and inefficient program with a narrow network of doctors, desperately needs an overhaul. Simply expanding it, and handing over full responsibility to the states, is not a viable solution, in my opinion.
Mr. Trump’s position paper also contains the dubious assumption that enforcing immigration laws will significantly decrease health care costs. Sealing the Southern border, he reasons, will help hospitals overburdened by the costs of services they provide to illegal immigrants who can’t pay for them and curtail the burgeoning heroin trade and its associated medical costs. There is little evidence to support either assumption – or even that the border can be effectively sealed in the first place.
So Mr. Trump has a health care plan, of sorts. How it will look by Inauguration Day, and what portion will be implemented, remains to be seen.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at [email protected].
MACRA
Given the copious amount of printed and blog space that has been devoted in recent months to MACRA – the Medicare Access and CHIP Reauthorization Act of 2015 – I felt no particular obligation to add to the din. Then I was startled to read a recent poll from Deloitte that found that half of all private-practice physicians had never heard of MACRA. Furthermore, only 21% of solo or small-group physicians, and 9% of those employed by hospitals or larger groups, were even somewhat familiar with its financial implications.
Since yet another significant percentage of your Medicare reimbursements will be at risk under this new bureaucracy, an introduction is in order.
When the new system is implemented in 2019, physicians must choose between two payment tracks: the Merit-Based Incentive System (MIPS) or one of the so-called Alternate Payment Models (APM).
The MIPS track will use the four reporting programs just mentioned to compile a composite score between 0 and 100 each year for every practitioner, based on four performance metrics: quality measures listed in Qualified Clinical Data Registries, such as Approved Quality Improvement; total resources used by each practitioner, as measured by VBM; “improvement activities” (MOC); and MU, in some new, as-yet-undefined form. You can earn a bonus of 4% of reimbursement in 2019, rising to 5% in 2020, 7% in 2021, and 9% in 2022 – or you can be penalized those amounts (“negative adjustments”) if your performance doesn’t measure up.
The Centers for Medicare & Medicaid Services initially estimated that most physicians in groups of 24 or fewer on the MIPS track would incur a penalty in 2019; but the final MACRA regulations, issued in mid-October, allow a more gradual implementation that should decrease the penalty burden for small practices, at least initially. For example, you can avoid a penalty – but not qualify for a bonus – in 2019 by reporting your performance in only one quality-of-care or practice-improvement category, or by reporting for only a portion of the year. A decrease in penalties, however, means a smaller pot for bonuses – and reprieves will be temporary.
The alternative, APM, is difficult to discuss at present as very few models have been presented, or even defined, to date. Only Accountable Care Organizations (ACOs) have been introduced in any quantity, and most have failed miserably in real-world settings. The Episode of Care model, which pays providers a fixed amount for all services rendered in a bundle (“episode”) of care, has been discussed at some length, but remains untested, and in the end, may turn out to be just another variant of capitation.
So, which to choose? Long term, I strongly suggest that everyone prepare for the APM track as soon as better, more efficient APMs become available, as it appears that there will be more financial security, with less risk of penalties; but you will probably need to start in the MIPS program, as most projections indicate that the great majority of practitioners, particularly those in smaller operations, will do.
While some may be prompted to join a larger organization or network to decrease their risk of MIPS penalties and gain quicker access to the APM track – which may well be one of CMS’ surreptitious goals in introducing MACRA in the first place – there are steps that those individuals and small groups who choose to remain independent can take now to maximize their chances of landing on the bonus side of the MIPS ledger.
First, make sure your practice data is accurate on the Medicare Provider Enrollment, Chain, and Ownership System (PECOS) – where CMS will gather data for the VBM and Physician Feedback Reports. Study the quality benchmarks, and review your Quality Resource and Use Report (QRUR), which gathers information about each practice’s quality and performance rates for the VBM. (Both PECOS and QRUR can be downloaded at CMS.gov.) And, of course, report successfully for PQRS, which will avoid an automatic penalty of 4% 2 years hence.
If the alphabet soup above has your head swimming, join the club – you’re far from alone; but don’t be discouraged. CMS has already indicated its willingness to make changes aimed at decreasing the administrative burden and, in its words, “making the transition to MACRA as simple and as flexible as possible.”
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at [email protected] .
Given the copious amount of printed and blog space that has been devoted in recent months to MACRA – the Medicare Access and CHIP Reauthorization Act of 2015 – I felt no particular obligation to add to the din. Then I was startled to read a recent poll from Deloitte that found that half of all private-practice physicians had never heard of MACRA. Furthermore, only 21% of solo or small-group physicians, and 9% of those employed by hospitals or larger groups, were even somewhat familiar with its financial implications.
Since yet another significant percentage of your Medicare reimbursements will be at risk under this new bureaucracy, an introduction is in order.
When the new system is implemented in 2019, physicians must choose between two payment tracks: the Merit-Based Incentive System (MIPS) or one of the so-called Alternate Payment Models (APM).
The MIPS track will use the four reporting programs just mentioned to compile a composite score between 0 and 100 each year for every practitioner, based on four performance metrics: quality measures listed in Qualified Clinical Data Registries, such as Approved Quality Improvement; total resources used by each practitioner, as measured by VBM; “improvement activities” (MOC); and MU, in some new, as-yet-undefined form. You can earn a bonus of 4% of reimbursement in 2019, rising to 5% in 2020, 7% in 2021, and 9% in 2022 – or you can be penalized those amounts (“negative adjustments”) if your performance doesn’t measure up.
The Centers for Medicare & Medicaid Services initially estimated that most physicians in groups of 24 or fewer on the MIPS track would incur a penalty in 2019; but the final MACRA regulations, issued in mid-October, allow a more gradual implementation that should decrease the penalty burden for small practices, at least initially. For example, you can avoid a penalty – but not qualify for a bonus – in 2019 by reporting your performance in only one quality-of-care or practice-improvement category, or by reporting for only a portion of the year. A decrease in penalties, however, means a smaller pot for bonuses – and reprieves will be temporary.
The alternative, APM, is difficult to discuss at present as very few models have been presented, or even defined, to date. Only Accountable Care Organizations (ACOs) have been introduced in any quantity, and most have failed miserably in real-world settings. The Episode of Care model, which pays providers a fixed amount for all services rendered in a bundle (“episode”) of care, has been discussed at some length, but remains untested, and in the end, may turn out to be just another variant of capitation.
So, which to choose? Long term, I strongly suggest that everyone prepare for the APM track as soon as better, more efficient APMs become available, as it appears that there will be more financial security, with less risk of penalties; but you will probably need to start in the MIPS program, as most projections indicate that the great majority of practitioners, particularly those in smaller operations, will do.
While some may be prompted to join a larger organization or network to decrease their risk of MIPS penalties and gain quicker access to the APM track – which may well be one of CMS’ surreptitious goals in introducing MACRA in the first place – there are steps that those individuals and small groups who choose to remain independent can take now to maximize their chances of landing on the bonus side of the MIPS ledger.
First, make sure your practice data is accurate on the Medicare Provider Enrollment, Chain, and Ownership System (PECOS) – where CMS will gather data for the VBM and Physician Feedback Reports. Study the quality benchmarks, and review your Quality Resource and Use Report (QRUR), which gathers information about each practice’s quality and performance rates for the VBM. (Both PECOS and QRUR can be downloaded at CMS.gov.) And, of course, report successfully for PQRS, which will avoid an automatic penalty of 4% 2 years hence.
If the alphabet soup above has your head swimming, join the club – you’re far from alone; but don’t be discouraged. CMS has already indicated its willingness to make changes aimed at decreasing the administrative burden and, in its words, “making the transition to MACRA as simple and as flexible as possible.”
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at [email protected] .
Given the copious amount of printed and blog space that has been devoted in recent months to MACRA – the Medicare Access and CHIP Reauthorization Act of 2015 – I felt no particular obligation to add to the din. Then I was startled to read a recent poll from Deloitte that found that half of all private-practice physicians had never heard of MACRA. Furthermore, only 21% of solo or small-group physicians, and 9% of those employed by hospitals or larger groups, were even somewhat familiar with its financial implications.
Since yet another significant percentage of your Medicare reimbursements will be at risk under this new bureaucracy, an introduction is in order.
When the new system is implemented in 2019, physicians must choose between two payment tracks: the Merit-Based Incentive System (MIPS) or one of the so-called Alternate Payment Models (APM).
The MIPS track will use the four reporting programs just mentioned to compile a composite score between 0 and 100 each year for every practitioner, based on four performance metrics: quality measures listed in Qualified Clinical Data Registries, such as Approved Quality Improvement; total resources used by each practitioner, as measured by VBM; “improvement activities” (MOC); and MU, in some new, as-yet-undefined form. You can earn a bonus of 4% of reimbursement in 2019, rising to 5% in 2020, 7% in 2021, and 9% in 2022 – or you can be penalized those amounts (“negative adjustments”) if your performance doesn’t measure up.
The Centers for Medicare & Medicaid Services initially estimated that most physicians in groups of 24 or fewer on the MIPS track would incur a penalty in 2019; but the final MACRA regulations, issued in mid-October, allow a more gradual implementation that should decrease the penalty burden for small practices, at least initially. For example, you can avoid a penalty – but not qualify for a bonus – in 2019 by reporting your performance in only one quality-of-care or practice-improvement category, or by reporting for only a portion of the year. A decrease in penalties, however, means a smaller pot for bonuses – and reprieves will be temporary.
The alternative, APM, is difficult to discuss at present as very few models have been presented, or even defined, to date. Only Accountable Care Organizations (ACOs) have been introduced in any quantity, and most have failed miserably in real-world settings. The Episode of Care model, which pays providers a fixed amount for all services rendered in a bundle (“episode”) of care, has been discussed at some length, but remains untested, and in the end, may turn out to be just another variant of capitation.
So, which to choose? Long term, I strongly suggest that everyone prepare for the APM track as soon as better, more efficient APMs become available, as it appears that there will be more financial security, with less risk of penalties; but you will probably need to start in the MIPS program, as most projections indicate that the great majority of practitioners, particularly those in smaller operations, will do.
While some may be prompted to join a larger organization or network to decrease their risk of MIPS penalties and gain quicker access to the APM track – which may well be one of CMS’ surreptitious goals in introducing MACRA in the first place – there are steps that those individuals and small groups who choose to remain independent can take now to maximize their chances of landing on the bonus side of the MIPS ledger.
First, make sure your practice data is accurate on the Medicare Provider Enrollment, Chain, and Ownership System (PECOS) – where CMS will gather data for the VBM and Physician Feedback Reports. Study the quality benchmarks, and review your Quality Resource and Use Report (QRUR), which gathers information about each practice’s quality and performance rates for the VBM. (Both PECOS and QRUR can be downloaded at CMS.gov.) And, of course, report successfully for PQRS, which will avoid an automatic penalty of 4% 2 years hence.
If the alphabet soup above has your head swimming, join the club – you’re far from alone; but don’t be discouraged. CMS has already indicated its willingness to make changes aimed at decreasing the administrative burden and, in its words, “making the transition to MACRA as simple and as flexible as possible.”
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at [email protected] .