User login
Painful leg mass
A 61-year-old Caucasian man sought care at our emergency department for a painful mass on his right leg that had appeared and progressively enlarged over the past 3 weeks. The patient denied trauma prior to the appearance of the mass, but did note extensive varicosities spanning from the right groin to the right foot a few weeks before the lesion appeared.
He also indicated that he’d had progressive dyspnea and intermittent chest pain for the past 4 months, a 30-lb weight loss in the past 6 months without change in appetite or diet, a depressed mood, and generalized weakness.
The patient’s past medical history was notable for hypertension and coronary artery disease. He reported a 30 pack-year smoking history, but had quit 12 years earlier. He denied alcohol use, although there was a family history of alcoholism and chronic obstructive pulmonary disease.
Physical examination revealed a frail, pale, unkempt man. His vital signs were normal except for mild tachycardia. Additional findings included:
- nonicteric, pale palpebral conjunctivae
- a 3/6 nonradiating holosystolic murmur heard along the left upper sternal border
- a large friable 3.5-cm pedunculated mass on a 2-cm stalk located on right lower leg (FIGURE 1); the lesion was moist, purple, and exophytic
- bilateral enlargement of the inguinal lymph nodes.
Lab work revealed microcytic anemia with a hemoglobin count of 5.8 g/dL and mild hyponatremia. The patient’s liver and renal function were normal. Urinalysis showed 3 red blood cells (RBCs) and a chest x-ray revealed bilateral hilar lymphadenopathy.
FIGURE 1
Exophytic mass on right lower leg
WHAT IS YOUR DIAGNOSIS?
HOW WOULD YOU TREAT THIS PATIENT?
Diagnosis: Renal cell carcinoma
The patient was admitted and stabilized with packed RBCs for symptomatic anemia. He underwent biopsy of the right leg lesion and computed tomography (CT) imaging of his chest, abdomen, and pelvis.
The biopsy report from the resected right leg mass revealed metastatic clear cell renal cell carcinoma (RCC). The CT scan showed a large exophytic mass involving the right kidney measuring 12 × 11 × 9 cm. Additionally, the scan revealed multiple noncalcified nodules of both lungs with enlarged bilateral hilar and paratracheal lymph nodes, lytic bone lesions, and multiple enhancing round lesions throughout the liver, suggesting metastatic involvement (FIGURE 2).
FIGURE 2
Abdominal CT scan reveals a 12-cm mass on right kidney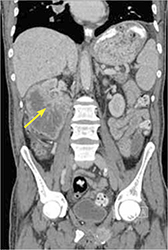
Metastases on initial presentation? It’s not uncommon
More than 64,000 new cases of renal cancer are expected to be diagnosed in 2012 and 92% of them are expected to be cases of RCC.1 Interestingly, the incidence and mortality rates of RCC have been on the rise.2 Part of this increased incidence is likely secondary to increased detection of asymptomatic renal masses noted on imaging studies done for other reasons; however, the increased overall mortality from renal cancer is not fully understood.
Renal cancer risk factors include tobacco use, obesity, renal cystic disease, and toxic occupational exposures (eg, cadmium). A genetic predisposition also appears to play a role.2 The classic presenting symptoms of renal malignancy include hematuria, a flank mass, and abdominal pain. Patients may experience a single symptom but rarely all 3, and many patients come in with nonspecific complaints of fever, sweats, weight loss, and fatigue.2
RCC also has a propensity for paraneoplastic syndromes that may present with anemia, hypercalcemia, or hepatic dysfunction.2 Unfortunately, many smaller renal lesions are asymptomatic, so as many as 55% of patients may present with metastatic disease at the time of initial presentation.3
The most common sites for renal metastatic disease are the lungs, bone, lymph nodes, brain, and contralateral kidney.2 Skin metastases, occurring in 2% to 10% of RCC cases, are less common and are often a sign of poorer prognosis.4 Men who have RCC are more likely to have skin metastases than women; the typical locations are the head, neck, and trunk.4
Is it RCC, or something else?
Signs and symptoms suggestive of possible renal malignancy (eg, hematuria, flank pain, weight loss, flank mass on exam) should prompt a work-up that includes abdominal imaging. The preferred imaging modality is a CT scan. Final tissue diagnosis is made on review of biopsy specimens obtained from the renal mass.
Skin metastases in RCC may be mistaken for other skin lesions, such as pyogenic granulomas, melanomas, or dermatofibromas.5 Histopathological analysis (and sometimes even special immunohistochemical staining and cytogenic analysis) can be used to make a definitive diagnosis.
Management options include radical nephrectomy
Treatment options and the prognosis for RCC are dependent on the extent of disease involvement at diagnosis. Radical nephrectomy is the gold standard therapy for patients with local, locally advanced, and even minimally metastatic disease.6
Other therapies include immunotherapy, interferons, interleukins, and gene therapy.6 Chemotherapy and radiation therapy have a limited role, as RCC is generally resistant to them. However, with more advanced metastatic disease, most treatment is palliative. The median survival time after diagnosis of metastatic RCC is about 20 months.6
Patient opts for treatment, then discontinues it
My patient was transferred to a local hospital with oncology support for further evaluation and management. He was ultimately diagnosed with metastatic renal carcinoma with bony, cutaneous, liver, and lung metastases. His hospital course was complicated by the development of hematuria and anemia, which required additional blood transfusions.
The patient was initially started on immunotherapy with sorafenib but upon acceptance of his metastatic disease and poor prognosis, he opted to discontinue therapy and enter an inpatient hospice facility.
CORRESPONDENCE Lesli M. Lucas, MD, Naval Branch Health Clinic Dahlgren, 17457 Caffee Road, Dahlgren, VA 22448; [email protected]
1. American Cancer Society. Cancer facts and figures 2012. Available at: http://www.cancer.org/acs/groups/content/@epidemiologysurveilance/documents/document/acspc-031941.pdf. Accessed April 6, 2012.
2. Gillenwater JY. Renal tumors. In: Gillenwater JY, Grayhack JT, Howards SS, Mitchell ME, eds. Adult and Pediatric Urology. 4th ed. Philadelphia, Pa: Lippincott Williams & Wilkins; 2002: 612-641.
3. Cuckow P, Doyle P. Renal cell carcinoma presenting in the skin. J R Soc Med. 1991;84:497-498.
4. Preetha R. Cutaneous metastasis from silent renal cell carcinoma. J Postgrad Med. 2004;50:287-288.
5. Garcia TM. Skin metastases from a renal cell carcinoma [in Spanish]. Actas Urol Esp. 2007;31:556-558.
6. Vogelzang NJ, Stadler WM. Kidney cancer. Lancet. 1998;352:1691-1696.
A 61-year-old Caucasian man sought care at our emergency department for a painful mass on his right leg that had appeared and progressively enlarged over the past 3 weeks. The patient denied trauma prior to the appearance of the mass, but did note extensive varicosities spanning from the right groin to the right foot a few weeks before the lesion appeared.
He also indicated that he’d had progressive dyspnea and intermittent chest pain for the past 4 months, a 30-lb weight loss in the past 6 months without change in appetite or diet, a depressed mood, and generalized weakness.
The patient’s past medical history was notable for hypertension and coronary artery disease. He reported a 30 pack-year smoking history, but had quit 12 years earlier. He denied alcohol use, although there was a family history of alcoholism and chronic obstructive pulmonary disease.
Physical examination revealed a frail, pale, unkempt man. His vital signs were normal except for mild tachycardia. Additional findings included:
- nonicteric, pale palpebral conjunctivae
- a 3/6 nonradiating holosystolic murmur heard along the left upper sternal border
- a large friable 3.5-cm pedunculated mass on a 2-cm stalk located on right lower leg (FIGURE 1); the lesion was moist, purple, and exophytic
- bilateral enlargement of the inguinal lymph nodes.
Lab work revealed microcytic anemia with a hemoglobin count of 5.8 g/dL and mild hyponatremia. The patient’s liver and renal function were normal. Urinalysis showed 3 red blood cells (RBCs) and a chest x-ray revealed bilateral hilar lymphadenopathy.
FIGURE 1
Exophytic mass on right lower leg
WHAT IS YOUR DIAGNOSIS?
HOW WOULD YOU TREAT THIS PATIENT?
Diagnosis: Renal cell carcinoma
The patient was admitted and stabilized with packed RBCs for symptomatic anemia. He underwent biopsy of the right leg lesion and computed tomography (CT) imaging of his chest, abdomen, and pelvis.
The biopsy report from the resected right leg mass revealed metastatic clear cell renal cell carcinoma (RCC). The CT scan showed a large exophytic mass involving the right kidney measuring 12 × 11 × 9 cm. Additionally, the scan revealed multiple noncalcified nodules of both lungs with enlarged bilateral hilar and paratracheal lymph nodes, lytic bone lesions, and multiple enhancing round lesions throughout the liver, suggesting metastatic involvement (FIGURE 2).
FIGURE 2
Abdominal CT scan reveals a 12-cm mass on right kidney
Metastases on initial presentation? It’s not uncommon
More than 64,000 new cases of renal cancer are expected to be diagnosed in 2012 and 92% of them are expected to be cases of RCC.1 Interestingly, the incidence and mortality rates of RCC have been on the rise.2 Part of this increased incidence is likely secondary to increased detection of asymptomatic renal masses noted on imaging studies done for other reasons; however, the increased overall mortality from renal cancer is not fully understood.
Renal cancer risk factors include tobacco use, obesity, renal cystic disease, and toxic occupational exposures (eg, cadmium). A genetic predisposition also appears to play a role.2 The classic presenting symptoms of renal malignancy include hematuria, a flank mass, and abdominal pain. Patients may experience a single symptom but rarely all 3, and many patients come in with nonspecific complaints of fever, sweats, weight loss, and fatigue.2
RCC also has a propensity for paraneoplastic syndromes that may present with anemia, hypercalcemia, or hepatic dysfunction.2 Unfortunately, many smaller renal lesions are asymptomatic, so as many as 55% of patients may present with metastatic disease at the time of initial presentation.3
The most common sites for renal metastatic disease are the lungs, bone, lymph nodes, brain, and contralateral kidney.2 Skin metastases, occurring in 2% to 10% of RCC cases, are less common and are often a sign of poorer prognosis.4 Men who have RCC are more likely to have skin metastases than women; the typical locations are the head, neck, and trunk.4
Is it RCC, or something else?
Signs and symptoms suggestive of possible renal malignancy (eg, hematuria, flank pain, weight loss, flank mass on exam) should prompt a work-up that includes abdominal imaging. The preferred imaging modality is a CT scan. Final tissue diagnosis is made on review of biopsy specimens obtained from the renal mass.
Skin metastases in RCC may be mistaken for other skin lesions, such as pyogenic granulomas, melanomas, or dermatofibromas.5 Histopathological analysis (and sometimes even special immunohistochemical staining and cytogenic analysis) can be used to make a definitive diagnosis.
Management options include radical nephrectomy
Treatment options and the prognosis for RCC are dependent on the extent of disease involvement at diagnosis. Radical nephrectomy is the gold standard therapy for patients with local, locally advanced, and even minimally metastatic disease.6
Other therapies include immunotherapy, interferons, interleukins, and gene therapy.6 Chemotherapy and radiation therapy have a limited role, as RCC is generally resistant to them. However, with more advanced metastatic disease, most treatment is palliative. The median survival time after diagnosis of metastatic RCC is about 20 months.6
Patient opts for treatment, then discontinues it
My patient was transferred to a local hospital with oncology support for further evaluation and management. He was ultimately diagnosed with metastatic renal carcinoma with bony, cutaneous, liver, and lung metastases. His hospital course was complicated by the development of hematuria and anemia, which required additional blood transfusions.
The patient was initially started on immunotherapy with sorafenib but upon acceptance of his metastatic disease and poor prognosis, he opted to discontinue therapy and enter an inpatient hospice facility.
CORRESPONDENCE Lesli M. Lucas, MD, Naval Branch Health Clinic Dahlgren, 17457 Caffee Road, Dahlgren, VA 22448; [email protected]
A 61-year-old Caucasian man sought care at our emergency department for a painful mass on his right leg that had appeared and progressively enlarged over the past 3 weeks. The patient denied trauma prior to the appearance of the mass, but did note extensive varicosities spanning from the right groin to the right foot a few weeks before the lesion appeared.
He also indicated that he’d had progressive dyspnea and intermittent chest pain for the past 4 months, a 30-lb weight loss in the past 6 months without change in appetite or diet, a depressed mood, and generalized weakness.
The patient’s past medical history was notable for hypertension and coronary artery disease. He reported a 30 pack-year smoking history, but had quit 12 years earlier. He denied alcohol use, although there was a family history of alcoholism and chronic obstructive pulmonary disease.
Physical examination revealed a frail, pale, unkempt man. His vital signs were normal except for mild tachycardia. Additional findings included:
- nonicteric, pale palpebral conjunctivae
- a 3/6 nonradiating holosystolic murmur heard along the left upper sternal border
- a large friable 3.5-cm pedunculated mass on a 2-cm stalk located on right lower leg (FIGURE 1); the lesion was moist, purple, and exophytic
- bilateral enlargement of the inguinal lymph nodes.
Lab work revealed microcytic anemia with a hemoglobin count of 5.8 g/dL and mild hyponatremia. The patient’s liver and renal function were normal. Urinalysis showed 3 red blood cells (RBCs) and a chest x-ray revealed bilateral hilar lymphadenopathy.
FIGURE 1
Exophytic mass on right lower leg
WHAT IS YOUR DIAGNOSIS?
HOW WOULD YOU TREAT THIS PATIENT?
Diagnosis: Renal cell carcinoma
The patient was admitted and stabilized with packed RBCs for symptomatic anemia. He underwent biopsy of the right leg lesion and computed tomography (CT) imaging of his chest, abdomen, and pelvis.
The biopsy report from the resected right leg mass revealed metastatic clear cell renal cell carcinoma (RCC). The CT scan showed a large exophytic mass involving the right kidney measuring 12 × 11 × 9 cm. Additionally, the scan revealed multiple noncalcified nodules of both lungs with enlarged bilateral hilar and paratracheal lymph nodes, lytic bone lesions, and multiple enhancing round lesions throughout the liver, suggesting metastatic involvement (FIGURE 2).
FIGURE 2
Abdominal CT scan reveals a 12-cm mass on right kidney
Metastases on initial presentation? It’s not uncommon
More than 64,000 new cases of renal cancer are expected to be diagnosed in 2012 and 92% of them are expected to be cases of RCC.1 Interestingly, the incidence and mortality rates of RCC have been on the rise.2 Part of this increased incidence is likely secondary to increased detection of asymptomatic renal masses noted on imaging studies done for other reasons; however, the increased overall mortality from renal cancer is not fully understood.
Renal cancer risk factors include tobacco use, obesity, renal cystic disease, and toxic occupational exposures (eg, cadmium). A genetic predisposition also appears to play a role.2 The classic presenting symptoms of renal malignancy include hematuria, a flank mass, and abdominal pain. Patients may experience a single symptom but rarely all 3, and many patients come in with nonspecific complaints of fever, sweats, weight loss, and fatigue.2
RCC also has a propensity for paraneoplastic syndromes that may present with anemia, hypercalcemia, or hepatic dysfunction.2 Unfortunately, many smaller renal lesions are asymptomatic, so as many as 55% of patients may present with metastatic disease at the time of initial presentation.3
The most common sites for renal metastatic disease are the lungs, bone, lymph nodes, brain, and contralateral kidney.2 Skin metastases, occurring in 2% to 10% of RCC cases, are less common and are often a sign of poorer prognosis.4 Men who have RCC are more likely to have skin metastases than women; the typical locations are the head, neck, and trunk.4
Is it RCC, or something else?
Signs and symptoms suggestive of possible renal malignancy (eg, hematuria, flank pain, weight loss, flank mass on exam) should prompt a work-up that includes abdominal imaging. The preferred imaging modality is a CT scan. Final tissue diagnosis is made on review of biopsy specimens obtained from the renal mass.
Skin metastases in RCC may be mistaken for other skin lesions, such as pyogenic granulomas, melanomas, or dermatofibromas.5 Histopathological analysis (and sometimes even special immunohistochemical staining and cytogenic analysis) can be used to make a definitive diagnosis.
Management options include radical nephrectomy
Treatment options and the prognosis for RCC are dependent on the extent of disease involvement at diagnosis. Radical nephrectomy is the gold standard therapy for patients with local, locally advanced, and even minimally metastatic disease.6
Other therapies include immunotherapy, interferons, interleukins, and gene therapy.6 Chemotherapy and radiation therapy have a limited role, as RCC is generally resistant to them. However, with more advanced metastatic disease, most treatment is palliative. The median survival time after diagnosis of metastatic RCC is about 20 months.6
Patient opts for treatment, then discontinues it
My patient was transferred to a local hospital with oncology support for further evaluation and management. He was ultimately diagnosed with metastatic renal carcinoma with bony, cutaneous, liver, and lung metastases. His hospital course was complicated by the development of hematuria and anemia, which required additional blood transfusions.
The patient was initially started on immunotherapy with sorafenib but upon acceptance of his metastatic disease and poor prognosis, he opted to discontinue therapy and enter an inpatient hospice facility.
CORRESPONDENCE Lesli M. Lucas, MD, Naval Branch Health Clinic Dahlgren, 17457 Caffee Road, Dahlgren, VA 22448; [email protected]
1. American Cancer Society. Cancer facts and figures 2012. Available at: http://www.cancer.org/acs/groups/content/@epidemiologysurveilance/documents/document/acspc-031941.pdf. Accessed April 6, 2012.
2. Gillenwater JY. Renal tumors. In: Gillenwater JY, Grayhack JT, Howards SS, Mitchell ME, eds. Adult and Pediatric Urology. 4th ed. Philadelphia, Pa: Lippincott Williams & Wilkins; 2002: 612-641.
3. Cuckow P, Doyle P. Renal cell carcinoma presenting in the skin. J R Soc Med. 1991;84:497-498.
4. Preetha R. Cutaneous metastasis from silent renal cell carcinoma. J Postgrad Med. 2004;50:287-288.
5. Garcia TM. Skin metastases from a renal cell carcinoma [in Spanish]. Actas Urol Esp. 2007;31:556-558.
6. Vogelzang NJ, Stadler WM. Kidney cancer. Lancet. 1998;352:1691-1696.
1. American Cancer Society. Cancer facts and figures 2012. Available at: http://www.cancer.org/acs/groups/content/@epidemiologysurveilance/documents/document/acspc-031941.pdf. Accessed April 6, 2012.
2. Gillenwater JY. Renal tumors. In: Gillenwater JY, Grayhack JT, Howards SS, Mitchell ME, eds. Adult and Pediatric Urology. 4th ed. Philadelphia, Pa: Lippincott Williams & Wilkins; 2002: 612-641.
3. Cuckow P, Doyle P. Renal cell carcinoma presenting in the skin. J R Soc Med. 1991;84:497-498.
4. Preetha R. Cutaneous metastasis from silent renal cell carcinoma. J Postgrad Med. 2004;50:287-288.
5. Garcia TM. Skin metastases from a renal cell carcinoma [in Spanish]. Actas Urol Esp. 2007;31:556-558.
6. Vogelzang NJ, Stadler WM. Kidney cancer. Lancet. 1998;352:1691-1696.