User login
Hypertension in the ED
Case Scenarios
Case 1
You had just started your shift, and your first patient presented with symptoms of headache and dizziness, and a blood pressure (BP) of 240/130 mm Hg, without any vomiting or visual symptoms. Physical examination revealed an alert, pleasant 65-year-old black man whose ocular, neurological, and cardiovascular (CV) examinations were normal. The patient reported a history of borderline hypertension, but had never taken any medications for it.
After placing some initial orders, including an electrocardiogram (ECG), basic metabolic panel (BMP), and head computed tomography (CT) scan, and ordering 10 mg intravenous (IV) prochlorperazine and 25 mg IV diphenhydramine to treat the patient’s headache, you are left asking yourself what steps you should take next.
Case 2
Your next patient was a 90-year-old white woman who had been referred to the ED by her primary care physician (PCP) for “hypertensive urgency.” She had no complaints to report. Similar to the first patient, this patient’s physical examination was also normal, with the exception of a persistently elevated BP of 220/140 mm Hg. Her history was significant for congestive heart failure (CHF), but she exhibited no current CV signs or symptoms. The patient had been taking furosemide but was not on any other antihypertensive medications.
Case 3
In the room next to your 90-year-old patient is a 32-year-old uninsured hypertensive white woman. During the history taking, the patient stated that she was trying to become pregnant and was not currently using any form of contraception. Similar to the second patient, she had no complaints to report. Regarding her reason for presentation, the patient stated that when she had her BP checked at a pharmacy earlier that day, the reading was “too high,” and the pharmacist had advised her to go to the ED. She seemed anxious but otherwise well. Her initial BP at presentation was 240/100 mm Hg, but her physical examination was otherwise normal.
Hypertensive Emergencies
As emergency physicians (EPs), we see hypertensive patients every day. According to the US Centers for Disease Control and Prevention, 33% of American adults have hypertension, which is defined by a BP of ≥140/90 mm Hg (Table 1). 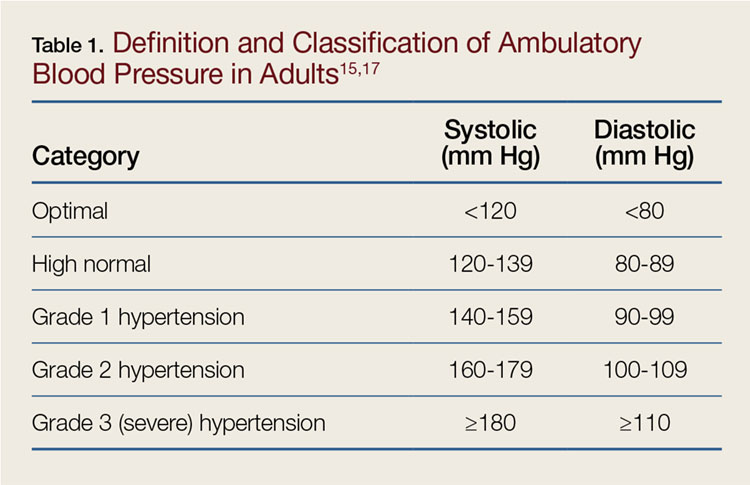
Almost 25% of total annual US adult ED visits are directly or indirectly related to hypertension, and about 1% of all ED visits are due solely to elevated BP.3 In an ambulatory care survey for 2007, moderate or severe hypertensive BP readings were found to be more common in patients presenting to the ED (43.5%) than to primary care clinics (27%).4 Patients presenting to the ED with hypertensive BP readings disproportionately represented patients who were older, male, non-Hispanic black, Medicare beneficiaries, or uninsured. Certainly, some patients presenting to the ED have hypertensive BP readings due to pain or anxiety, but multiple studies have suggested that 50% to 70% of ED patients who have hypertensive BP readings will be diagnosed with hypertension on office follow-up.5,6 While a minority of these patients present to the ED with hypertensive emergencies, the majority present either without symptoms of hypertension or with only mild headache. Given the disease burden of hypertension combined with the benefits of treatment, it is worthwhile for the practicing EP to review the most up-to-date guidelines on outpatient management of hypertension.
When a patient presents to the ED with a hypertensive BP reading, the initial priority of the EP is to exclude hypertensive emergency. Hypertensive emergencies are defined by the presence of hypertension (generally grade 3/severe hypertension with BP ≥180/110 mm Hg; see Table 1) in conjunction with evidence of target organ damage. 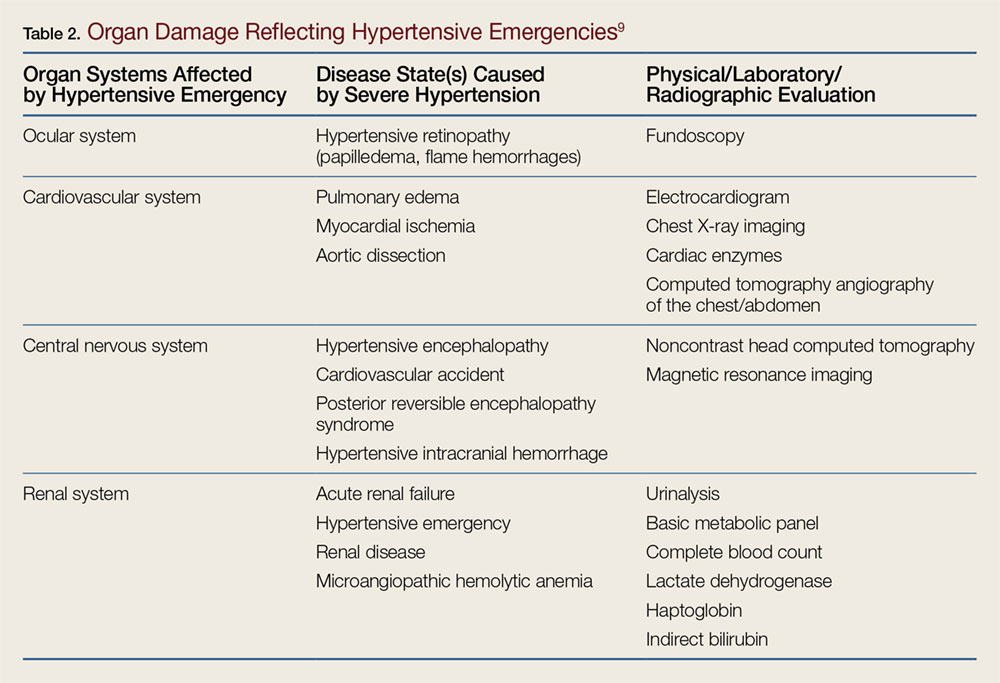
Target Organ Manifestations
The acuity and/or presence of target organ damage are not always clear on initial ED evaluation. For instance, when a patient who has no history of primary care presents to the ED with severe hypertension, laboratory evaluation may demonstrate protein and blood in his or her urine and an elevated serum creatinine level. In the absence of values from past laboratory studies, it is difficult to determine whether these test results represent normal laboratory parameters for this patient due to longstanding hypertensive kidney disease (ie, hypertensive nephrosclerosis) or if they represent a true hypertensive emergency, (ie, hypertensive emergency-related nephropathy).7 In patients with severe hypertension and possibly new acute kidney injury, it is probably safest to either assume hypertensive emergency-related nephropathy and to treat accordingly or consult with nephrology services. The picture of hypertensive emergency-related nephropathy often only becomes clear after renal biopsy results and improvement in renal parameters with BP control.
The ocular manifestations of hypertensive emergency require detailed fundoscopy, which at times can be challenging in the ED. In assessing for cardiac target organ damage, at our institution, we typically ask patients if they have experienced symptoms of dyspnea and chest pain or pressure. Generally, we also evaluate cardiac enzymes, B-type natriuretic peptide, and order ECG and chest X-ray studies when suggested by history or physical examination. Alarmingly, a study of 161 ED hypertensive (average BP of 183/109 mm Hg), asymptomatic, predominantly black patients found that 146 (90.7%) had subclinical hypertensive heart disease on point-of-care echocardiogram.8
Neurological/Hypertensive Encephalopathy
Hypertensive encephalopathy is a diagnosis of exclusion as alternate causes of confusion and headache, such as intracranial hemorrhage, are excluded and mental status improves with titrated BP control. Nonetheless, it is difficult to confidently state from the literature that patients who present with headache but have a normal mental status in the presence of severe hypertension are not on an early spectrum of hypertensive encephalopathy. Therefore, it is likely that the degree of symptoms should define whether target organ damage exists, though there is certainly a spectrum of hypertensive emergency—the strict definition of which is not always clear.
When a hypertensive emergency is diagnosed, management typically involves the use of antihypertensive IV medication in the intensive care unit. While such management is outside the scope of this paper, Adebayo and Rogers9 have published an excellent review of the care of hypertensive emergencies.
Asymptomatic Hypertension
The American College of Emergency Physicians (ACEP) has developed two clinical policies on the evaluation and management of asymptomatic hypertension in the ED. The original, published in 2006, advised that initially high BP readings of ED patients should be repeated: two separate high readings are adequate for screening, and those patients with hypertension should be referred for follow-up. Furthermore, ACEP policies note that initiating treatment in the ED is not necessary when patients are referred for follow-up. If treatment for hypertension is initiated in the ED, ACEP recommends that such management should attempt only to gradually lower BP, and not to normalize it during the initial ED visit.10
The 2013 update to ACEP’s clinical policy on managing asymptomatic hypertension expanded on the original policy. The updated policy advised against routine testing for target organ damage in patients who have asymptomatic severe hypertension. However, ACEP policy notes that evaluating serum creatinine in these patients with poor follow-up may influence patient disposition.11
The 2013 policy further stated that medical intervention is not required in ED patients who have asymptomatic severe hypertension, but may be considered in patients with poor follow-up. The policies emphasize that all asymptomatic hypertensive patients should be referred for follow-up. The literature cited for the recommendation that ED patients with asymptomatic severe hypertension do not require routine investigation stems from two observational studies. These studies found that screening asymptomatic ED patients who presented with severe hypertension revealed serum creatinine abnormalities in approximately 6%, which impacted patient disposition, though it was not clear from the study results whether admission correlated to meaningful patient outcomes.12,13
Patient Disposition
Since ACEP’s 2013 clinical policy, a study from the Cleveland Clinic has been published. This retrospective cohort study reviewed 6 years of data looking at all patients in its system with a BP of ≥180/110 mm Hg, and compared those office patients discharged to home to those referred to the ED or directly admitted to the inpatient hospital solely on the basis of severe hypertension.14 The study found that 0.5% of 387 patients referred to the ED by primary care clinics for asymptomatic severe hypertension had confirmed acute kidney injury on BMP.14 The Cleveland Clinic study also found that 2.1% of patients had evidence of target organ damage and 5.5% had any abnormal results.14 In addition, referral to the ED from the clinic for hypertension was associated with a slightly higher rate of major adverse CV events at 7 days (2 of 426 [0.5%] versus 61 of 58,109 [0.1%]; P = .02).14
The results of the Cleveland Clinic study confirm that in the absence of target organ damage, hypertension is probably best managed in the outpatient setting. The European Task Force hypertensive guidelines state “hospitalization for hypertension is regarded as inappropriate in most European countries.”15 However, from 2006 to 2012, 26% of US ED patients with primary diagnoses of hypertension were admitted to the hospital.3 In Canada’s most populous province of Ontario, from 2002 to 2011, approximately 8% of hypertensive patients were admitted.16 Part of this discrepancy may be due to the sometimes ambiguous nature of the presentation of patients with hypertension, making it unclear whether a true hypertensive emergency exists. Many patients perceive visual symptoms, headache, dizziness, and even chest pressure as the result of their elevated BP—without clear findings on fundoscopy, ECG, or cardiac marker testing. Perhaps more of these patients would be discharged if EPs felt comfortable initiating appropriate initial antihypertensive treatment.
Management
Initiating Antihypertensive Treatment
Some EPs may feel that an accurate diagnosis of hypertension requires repeat BP testing in the primary care office setting, and for this reason are reluctant to initiate antihypertensive treatment in the ED. The most recent guidelines by the Joint National Committee (JNC 8) do not address how many BP readings are necessary to diagnose hypertension, but JNC 7 suggested that diagnosis of hypertension requires two separate office visits.17 Evidence cited in ACEP’s first clinical policy states that two separate BP measurements in the ED are adequate for screening—but not necessarily for initiating treatment.10 However, European and British outpatient clinical recommendations advocate initiation of antihypertensive medication for a single visit in patients who have an elevated BP categorized as grade 3/severe hypertension (BP of ≥180/110 mm Hg).15,18 Furthermore, for patients with severe hypertension seen in the ED, as many as 97% are likely to have true hypertension at office follow-up.6 Those ED patients presenting with severe hypertension are very likely to have a true diagnosis of hypertension.
A recent retrospective analysis of a group of hypertensive ED patients by Brody et al19 found that patients prescribed BP medications by an EP were more likely to have improved BP control at follow-up 2 weeks later. In their study, the decision to prescribe antihypertensive medications were at the discretion of the EP. Seventy-six patients were given one or more prescriptions for antihypertensive therapy, compared to a control group of 141 patients who were not given a prescription. On follow-up at 2 weeks, there was an 11 mm Hg greater reduction of BP in the group who received prescriptions compared to the control group. None of the patients in either group on follow-up had experienced any new neurological deficits, ischemic events, life-threatening anaphylactic reactions, or clinically significant hypotension.
The Cleveland Clinic study14 also reported on those patents given who received new prescriptions from the ED. Similar to the study by Brody et al,19 none of the 82 patients discharged to home from the ED with a new antihypertensive prescription had any major adverse event at 30-day follow-up.14
Pharmacological Treatment Recommendations
When choosing to treat patients with new prescriptions for antihypertensives, it is important to follow the most current outpatient treatment recommendations. In 2014, JNC 8 released new guidelines for the outpatient management of adults with hypertension.20 The panel issued recommendations based on its systematic review of randomized controlled trials on antihypertensive treatments. The key recommendations are as follows:
- In patients aged 60 years or older, initiate pharmacological treatment at a BP of ≥150/90 mm Hg.
- In patients aged 18 to 59 years, initiate pharmacological treatment at a BP of ≥140/90 mm Hg.
- In the general nonblack population, initial antihypertensive treatment should include a thiazide-type diuretic, a calcium channel blocker (CCB), an angiotensin-converting enzyme inhibitor (ACE-I), or an angiotensin receptor blocker (ARB).
- In the general black population, initial treatment should include a thiazide-type diuretic or a CCB.
- In patients with chronic kidney disease (CKD) (including black patients), initial (or add-on) antihypertensive treatment should include an ACE-I or ARB to improve kidney outcomes—but not both.
- If goal BP is not reached within 1 month of initial treatment, increase the dose of the initial drug or add a second agent (eg, thiazide-type diuretic, CCB, ACE-I, or ARB). If goal is not reached with two drugs, use the third drug from that list if no contraindications exist, but do not use both an ACE-I and an ARB together in the same patient.
Of note, JNC 8, in departure from JNC 7, no longer recommends beta-blockers as first-line therapy for isolated hypertension (there may be compelling alternate indications, such as atrial fibrillation or postmyocardial infarction (MI), such that a beta-blocker would still be the first medication considered). The reason for this stems from a single randomized controlled trial of 9,193 patients that found that despite equivalent BP reduction, use of a beta-blocker in comparison to an ARB resulted in a higher rate of a composite outcome of death, MI, or stroke.21 The main difference was a 25% relative risk reduction for stroke with use of an ARB (losartan) in comparison to a beta-blocker (atenolol). The most recent European guidelines still include beta-blockers among its first-line recommended BP medications, but do acknowledge that they are not as effective in reducing stroke incidence as other alternative medications.15 The European guidelines otherwise include the same list of first-line agents. The British guidelines mirror JNC 8 in terms of first-line antihypertensive medication choices.18
Since the release of JNC 8, the Systolic Blood Pressure Intervention Trial (SPRINT) has been published, and will likely impact future national recommendations on BP management. The SPRINT study was a randomized controlled trial enrolling over 9,000 hypertensive nondiabetic patients older than age 50 years that treated individuals to a standard BP goal (systolic BP of 140 mm Hg) versus an intensive BP goal (systolic BP of 120 mm Hg) over a 3.5-year period. The trial was stopped early for safety as a 25% mortality reduction was observed in the intensive treatment group (1.65 vs 2.19 deaths/y).22 This was in contrast to previous trials that had mostly failed to show this sort of benefit, though previous trials were smaller in number or included only diabetic patients.23 While it is likely that this trial may influence lowering treatment thresholds from the office, it is not likely to impact care from the ED.
The recommendations of JNC 8 do not necessarily coincide with current US EP practice. In the study by Brody et al,19 of patients provided ED antihypertensive prescriptions, 54% received thiazide-type diuretics, 26% ACE-I, 10% CCBs, and 6% beta-blockers. This is noteworthy because 96% of those in the study were black patients who would benefit most from either a thiazide or a CCB. Another recent study of ED patients showed that of patients who were both treated in the ED and discharged with antihypertensive medications, 34% received a diuretic prescription, 32% clonidine, 15% a beta-blocker, 19% an ARB or ACE-I, 12% a CCB, and 2% hydrazine.24 These results are important because according to many published guidelines, including JNC 8, clonidine is only considered one of several fourth-line options for severe resistant hypertension.15,18,20 Since clonidine use can be complicated by rebound hypertension, it is not an ideal agent to be prescribed de novo to patients in the ED. This is particularly true if these patients are not already on maximum doses of the three most recommended agents previously noted, or if there are concerns over patient compliance.
Of the drug classes recommended by JNC 8, Table 3 lists the absolute and relative contraindications. 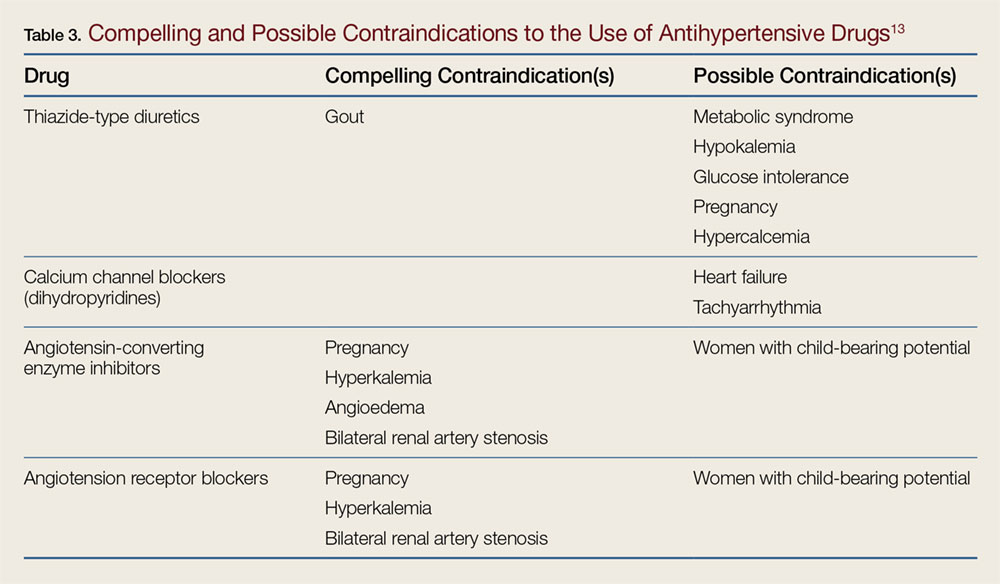
In clinical trials, amlodipine is among the most effective BP medications and is considered first-line therapy for all groups of patients with hypertension.15,18,20 A simplistic approach for most patients presenting with severe asymptomatic hypertension (BP of ≥180/110 mm Hg) not currently on treatment would be to recheck the BP and assure it remains elevated over the period of the ED visit. 
Conclusion
Hypertension is among the most common medical conditions for which emergency patients seek care. The ACEP clinical policies provide guidance on the appropriate work-up and treatment of these patients. Given the occasional lack of clarity on whether a patient’s presentation is on the spectrum of more acute/serious, EPs may feel more comfortable in discharging patients with poor follow-up if they are able to safely prescribe antihypertensive treatment. Prior to prescribing treatment, EPs should refer to the JNC 8 guidelines to appropriately start antihypertensive treatment in select patient groups in the ED. The guidelines of JNC 8 are therefore worth referring to in order to appropriately start treatment in select patient groups from the ED.
Case Scenarios Continued
Case 1
[The 65-year-old black man who presented with headache and dizziness, and had an initial BP of 240/130 mm Hg.]
After treating the patient with prochlorperazine and diphenhydramine, his headache resolved. His BP improved but remained elevated at 190/120 mm Hg. On further questioning, the patient reported a history of similar headaches and wondered whether it was related to his BP. The head CT scan was negative for any acute hemorrhage, infarct, or mass; the ECG only showed evidence of left ventricular hypertrophy; and the BMP showed normal renal function.
After a long discussion with the patient, you agreed to start him on amlodipine 5 mg/d and referred him for follow-up with a local PCP.
Case 2
[The 90-year-old white woman with a history of CHF and an initial BP of 220/140 mm Hg at presentation.]
The BMP evaluation showed a baseline creatinine level of 1.3 mg/dL. Given this patient’s history of CHF, amlodipine would not be the ideal next agent to prescribe. After discussion with her PCP, you elected to start her on losartan at 25 mg/d, and instructed her to follow-up with her PCP within 1 week.
Case 3
[The 32-year-old white woman who presented at the advice of a pharmacist and had an initial BP of 240/100 mm Hg.]While reviewing the patient’s work-up and history, you noted her plans to become pregnant, and recalled a recent review on BP management, noting the contraindications associated with ARB or ACE-I in pregnancy. Based on the patient’s uninsured status and poor follow-up, you considered prescribing amlodipine. Prior to issuing the prescription, you performed a repeat BP check and noted that the patient’s BP had decreased to 130/85 mm Hg. Given the marked improvement in the patient’s BP during her ED course, you were not convinced that she truly had hypertension.
Instead of prescribing an antihypertensive agent, which may not ultimately benefit this patient, you advised her to seek follow-up care at an outpatient clinic to have her BP rechecked. The patient agreed, and you referred her to a local free clinic.
1. Nwankwo T, Yoon SS, Burt V, Gu Q. Hypertension among adults in the United States: National Health and Nutrition Examination Survey, 2011-2012. NCHS Data Brief. 2013;(133):1-8.
2. Turnbull F; Blood Pressure Lowering Treatment Trialists’ Collaboration. Effects of different blood-pressure-lowering regimens on major cardiovascular events: results of prospectively-designed overviews of randomised trials. Lancet. 2013;362(9395):1527-1535.
3. McNaughton CD, Self WH, Zhu Y, Janke AT, Storrow AB, Levy P. Incidence of hypertension-related emergency department visits in the United States, 2006 to 2012. Am J Cardiol. 2015;116(11):1717-1723. doi: 10.1016/j.amjcard.2015.09.007.
4. Niska RW. Blood pressure measurements at emergency department visits by adults: United States, 2007-2008. NCHS Data Brief. 2011;(72):1-8.
5. Chernow SM, Iserson KV, Criss E. Use of the emergency department for hypertension screening: a prospective study. Ann Emerg Med. 1987;16(2):180-182.
6. Backer HD, Decker L, Ackerson L. Reproducibility of increased blood pressure during an emergency department or urgent care visit. Ann Emerg Med. 2003.41(4):507-512.
7. Nonaka K, Ubara Y, Sumida K, et al. Clinical and pathological evaluation of hypertensive emergency-related nephropathy. Intern Med. 2013;52(1):45-53.
8. Levy P, Ye H, Compton S, et al. Subclinical hypertensive heart disease in black patients with elevated blood pressure in an inner-city emergency department. Ann Emerg Med. 2012;60(4):467-474.e1. doi: 10.1016/j.annemergmed.2012.03.030.
9. Adebayo O, Rogers RL. Hypertensive emergencies in the emergency department. Emerg Med Clin North Am. 2015;33(3):539-551. doi: 10.1016/j.emc.2015.04.005.
10. Decker WW, Godwin SA, Hess EP, Lenamond CC, Jagoda AS; American College of Emergency Physicians Clinical Policies Subcommittee (Writing Committee) on Asymptomatic Hypertension in the ED. Clinical policy: critical issues in the evaluation and management of adult patients with asymptomatic hypertension in the emergency department. Ann Emerg Med. 2006;47(3):237-234. doi: 10.1016/j.annemergmed.2005.10.003
11. Wolf SJ, Lo B, Shih RD, Smith MD, Fesmire FM; American College of Emergency Physicians Clinical Policies Committee. Clinical policy: critical issues in the evaluation and management of adult patients in the emergency department with asymptomatic elevated blood pressure. Ann Emerg Med. 2013;62(1):59-68. doi: 10.1016/j.annemergmed.2013.05.012.
12. Karras DJ, Kruus LK, Cienki JJ, et al. Evaluation and treatment of patients with severely elevated blood pressure in academic emergency departments: a multicenter study. Ann Emerg Med. 2006;47(3):230-236.
13. Nishijima DK, Paladino L, Sinert R. Routine testing in patients with asymptomatic elevated blood pressure in the ED. Am J Emerg Med. 2010;28(2):235-242. doi: 10.1016/j.ajem.2008.11.015.
14. Patel KK, Young L, Howell EH, et al. Characteristics and outcomes of patients presenting with hypertensive urgency in the office setting. JAMA Intern Med. 2016;176(7):981-988. doi: 10.1001/jamainternmed.2016.1509.
15. Mancia G, Fagard R, Narkiewicz K, et al. 2013 ESH/ESC guidelines for the management of arterial hypertension: the Task Force for the Management of Arterial Hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). Eur Heart J. 2013;34(28):2159-2219. doi: 10.1093/eurheartj/eht151.
16. Masood S, Austin PC, Atzema CL. A population-based analysis of outcomes in patients with a primary diagnosis of hypertension in the emergency department. Ann Emerg Med. 2016;68(3):258-267.e5. doi: 10.1016/j.annemergmed.2016.04.060.
17. Chobanian AV, Bakris GL, Black HR, et al; National Heart, Lung, and Blood Institute Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure; National High Blood Pressure Education Program Coordinating Committee. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure: the JNC 7 report. JAMA. 2003;289(19):2560-2572. Erratum in: JAMA. 2003;290(2):197.
18. Krause T, Lovibond K, Caulfield M, McCormack T, Williams B; Guideline Development Group. Management of hypertension: summary of NICE guidance. BMJ. 2011;343:d4891. doi: 10.1136/bmj.d4891.
19. Brody A, Rahman T, Reed B, et al. Safety and efficacy of antihypertensive prescription at emergency department discharge. Acad Emerg Med. 2015;22(5):632-635. doi: 10.1111/acem.12660.
20. James PA, Oparil S, Carter BL, et al. 2014 evidence-based guideline for the management of high blood pressure in adults: report from the panel members appointed to the Eighth Joint National Committee (JNC 8). JAMA. 2014;311(5):507-520. doi: 10.1001/jama.2013.284427. Erratum in: JAMA. 2014;311(17):1809.
21. Dahlöf B, Devereux RB, Kjeldsen SE, et al; LIFE Study Group. Cardiovascular morbidity and mortality in the Losartan Intervention For Endpoint reduction in hypertension study (LIFE): a randomised trial against atenolol. Lancet. 2002;359(9311):995-1003.
22. PRINT Research Group, Wright JT Jr, Williamson JD, Whelton PK, et al. A randomized trial of intensive versus standard blood-pressure control. N Engl J Med. 2015;373(22):2103-2116. doi: 10.1056/NEJMoa1511939.
23. ACCORD Study Group, Cushman WC, Evans GW, Byington RP, et al. Effects of intensive blood-pressure control in type 2 diabetes mellitus. N Engl J Med. 2010;362(17):1575-1585. doi: 10.1056/NEJMoa1001286.
24. Levy PD, Mahn JJ, Miller J, et al. Blood pressure treatment and outcomes in hypertensive patients without acute target organ damage: a retrospective cohort. Am J Emerg Med. 2015;33(9):1219-1224. doi: 10.1016/j.ajem.2015.05.036.
25. Leung AA, Wright A, Pazo V, Karson A, Bates DW. Risk of thiazide-induced hyponatremia in patients with hypertension. Am J Med. 2011;124(11):1064-1072. doi: 10.1016/j.amjmed.2011.06.031.
26. Mann JFE, Hilgers KF. Renin-angiotensin system inhibition in the treatment of hypertension. http://www.uptodate.com/contents/renin-angiotensin-system-inhibition-in-the-treatment-of-hypertension. Accessed September 21, 2016.
Case Scenarios
Case 1
You had just started your shift, and your first patient presented with symptoms of headache and dizziness, and a blood pressure (BP) of 240/130 mm Hg, without any vomiting or visual symptoms. Physical examination revealed an alert, pleasant 65-year-old black man whose ocular, neurological, and cardiovascular (CV) examinations were normal. The patient reported a history of borderline hypertension, but had never taken any medications for it.
After placing some initial orders, including an electrocardiogram (ECG), basic metabolic panel (BMP), and head computed tomography (CT) scan, and ordering 10 mg intravenous (IV) prochlorperazine and 25 mg IV diphenhydramine to treat the patient’s headache, you are left asking yourself what steps you should take next.
Case 2
Your next patient was a 90-year-old white woman who had been referred to the ED by her primary care physician (PCP) for “hypertensive urgency.” She had no complaints to report. Similar to the first patient, this patient’s physical examination was also normal, with the exception of a persistently elevated BP of 220/140 mm Hg. Her history was significant for congestive heart failure (CHF), but she exhibited no current CV signs or symptoms. The patient had been taking furosemide but was not on any other antihypertensive medications.
Case 3
In the room next to your 90-year-old patient is a 32-year-old uninsured hypertensive white woman. During the history taking, the patient stated that she was trying to become pregnant and was not currently using any form of contraception. Similar to the second patient, she had no complaints to report. Regarding her reason for presentation, the patient stated that when she had her BP checked at a pharmacy earlier that day, the reading was “too high,” and the pharmacist had advised her to go to the ED. She seemed anxious but otherwise well. Her initial BP at presentation was 240/100 mm Hg, but her physical examination was otherwise normal.
Hypertensive Emergencies
As emergency physicians (EPs), we see hypertensive patients every day. According to the US Centers for Disease Control and Prevention, 33% of American adults have hypertension, which is defined by a BP of ≥140/90 mm Hg (Table 1).
Almost 25% of total annual US adult ED visits are directly or indirectly related to hypertension, and about 1% of all ED visits are due solely to elevated BP.3 In an ambulatory care survey for 2007, moderate or severe hypertensive BP readings were found to be more common in patients presenting to the ED (43.5%) than to primary care clinics (27%).4 Patients presenting to the ED with hypertensive BP readings disproportionately represented patients who were older, male, non-Hispanic black, Medicare beneficiaries, or uninsured. Certainly, some patients presenting to the ED have hypertensive BP readings due to pain or anxiety, but multiple studies have suggested that 50% to 70% of ED patients who have hypertensive BP readings will be diagnosed with hypertension on office follow-up.5,6 While a minority of these patients present to the ED with hypertensive emergencies, the majority present either without symptoms of hypertension or with only mild headache. Given the disease burden of hypertension combined with the benefits of treatment, it is worthwhile for the practicing EP to review the most up-to-date guidelines on outpatient management of hypertension.
When a patient presents to the ED with a hypertensive BP reading, the initial priority of the EP is to exclude hypertensive emergency. Hypertensive emergencies are defined by the presence of hypertension (generally grade 3/severe hypertension with BP ≥180/110 mm Hg; see Table 1) in conjunction with evidence of target organ damage.
Target Organ Manifestations
The acuity and/or presence of target organ damage are not always clear on initial ED evaluation. For instance, when a patient who has no history of primary care presents to the ED with severe hypertension, laboratory evaluation may demonstrate protein and blood in his or her urine and an elevated serum creatinine level. In the absence of values from past laboratory studies, it is difficult to determine whether these test results represent normal laboratory parameters for this patient due to longstanding hypertensive kidney disease (ie, hypertensive nephrosclerosis) or if they represent a true hypertensive emergency, (ie, hypertensive emergency-related nephropathy).7 In patients with severe hypertension and possibly new acute kidney injury, it is probably safest to either assume hypertensive emergency-related nephropathy and to treat accordingly or consult with nephrology services. The picture of hypertensive emergency-related nephropathy often only becomes clear after renal biopsy results and improvement in renal parameters with BP control.
The ocular manifestations of hypertensive emergency require detailed fundoscopy, which at times can be challenging in the ED. In assessing for cardiac target organ damage, at our institution, we typically ask patients if they have experienced symptoms of dyspnea and chest pain or pressure. Generally, we also evaluate cardiac enzymes, B-type natriuretic peptide, and order ECG and chest X-ray studies when suggested by history or physical examination. Alarmingly, a study of 161 ED hypertensive (average BP of 183/109 mm Hg), asymptomatic, predominantly black patients found that 146 (90.7%) had subclinical hypertensive heart disease on point-of-care echocardiogram.8
Neurological/Hypertensive Encephalopathy
Hypertensive encephalopathy is a diagnosis of exclusion as alternate causes of confusion and headache, such as intracranial hemorrhage, are excluded and mental status improves with titrated BP control. Nonetheless, it is difficult to confidently state from the literature that patients who present with headache but have a normal mental status in the presence of severe hypertension are not on an early spectrum of hypertensive encephalopathy. Therefore, it is likely that the degree of symptoms should define whether target organ damage exists, though there is certainly a spectrum of hypertensive emergency—the strict definition of which is not always clear.
When a hypertensive emergency is diagnosed, management typically involves the use of antihypertensive IV medication in the intensive care unit. While such management is outside the scope of this paper, Adebayo and Rogers9 have published an excellent review of the care of hypertensive emergencies.
Asymptomatic Hypertension
The American College of Emergency Physicians (ACEP) has developed two clinical policies on the evaluation and management of asymptomatic hypertension in the ED. The original, published in 2006, advised that initially high BP readings of ED patients should be repeated: two separate high readings are adequate for screening, and those patients with hypertension should be referred for follow-up. Furthermore, ACEP policies note that initiating treatment in the ED is not necessary when patients are referred for follow-up. If treatment for hypertension is initiated in the ED, ACEP recommends that such management should attempt only to gradually lower BP, and not to normalize it during the initial ED visit.10
The 2013 update to ACEP’s clinical policy on managing asymptomatic hypertension expanded on the original policy. The updated policy advised against routine testing for target organ damage in patients who have asymptomatic severe hypertension. However, ACEP policy notes that evaluating serum creatinine in these patients with poor follow-up may influence patient disposition.11
The 2013 policy further stated that medical intervention is not required in ED patients who have asymptomatic severe hypertension, but may be considered in patients with poor follow-up. The policies emphasize that all asymptomatic hypertensive patients should be referred for follow-up. The literature cited for the recommendation that ED patients with asymptomatic severe hypertension do not require routine investigation stems from two observational studies. These studies found that screening asymptomatic ED patients who presented with severe hypertension revealed serum creatinine abnormalities in approximately 6%, which impacted patient disposition, though it was not clear from the study results whether admission correlated to meaningful patient outcomes.12,13
Patient Disposition
Since ACEP’s 2013 clinical policy, a study from the Cleveland Clinic has been published. This retrospective cohort study reviewed 6 years of data looking at all patients in its system with a BP of ≥180/110 mm Hg, and compared those office patients discharged to home to those referred to the ED or directly admitted to the inpatient hospital solely on the basis of severe hypertension.14 The study found that 0.5% of 387 patients referred to the ED by primary care clinics for asymptomatic severe hypertension had confirmed acute kidney injury on BMP.14 The Cleveland Clinic study also found that 2.1% of patients had evidence of target organ damage and 5.5% had any abnormal results.14 In addition, referral to the ED from the clinic for hypertension was associated with a slightly higher rate of major adverse CV events at 7 days (2 of 426 [0.5%] versus 61 of 58,109 [0.1%]; P = .02).14
The results of the Cleveland Clinic study confirm that in the absence of target organ damage, hypertension is probably best managed in the outpatient setting. The European Task Force hypertensive guidelines state “hospitalization for hypertension is regarded as inappropriate in most European countries.”15 However, from 2006 to 2012, 26% of US ED patients with primary diagnoses of hypertension were admitted to the hospital.3 In Canada’s most populous province of Ontario, from 2002 to 2011, approximately 8% of hypertensive patients were admitted.16 Part of this discrepancy may be due to the sometimes ambiguous nature of the presentation of patients with hypertension, making it unclear whether a true hypertensive emergency exists. Many patients perceive visual symptoms, headache, dizziness, and even chest pressure as the result of their elevated BP—without clear findings on fundoscopy, ECG, or cardiac marker testing. Perhaps more of these patients would be discharged if EPs felt comfortable initiating appropriate initial antihypertensive treatment.
Management
Initiating Antihypertensive Treatment
Some EPs may feel that an accurate diagnosis of hypertension requires repeat BP testing in the primary care office setting, and for this reason are reluctant to initiate antihypertensive treatment in the ED. The most recent guidelines by the Joint National Committee (JNC 8) do not address how many BP readings are necessary to diagnose hypertension, but JNC 7 suggested that diagnosis of hypertension requires two separate office visits.17 Evidence cited in ACEP’s first clinical policy states that two separate BP measurements in the ED are adequate for screening—but not necessarily for initiating treatment.10 However, European and British outpatient clinical recommendations advocate initiation of antihypertensive medication for a single visit in patients who have an elevated BP categorized as grade 3/severe hypertension (BP of ≥180/110 mm Hg).15,18 Furthermore, for patients with severe hypertension seen in the ED, as many as 97% are likely to have true hypertension at office follow-up.6 Those ED patients presenting with severe hypertension are very likely to have a true diagnosis of hypertension.
A recent retrospective analysis of a group of hypertensive ED patients by Brody et al19 found that patients prescribed BP medications by an EP were more likely to have improved BP control at follow-up 2 weeks later. In their study, the decision to prescribe antihypertensive medications were at the discretion of the EP. Seventy-six patients were given one or more prescriptions for antihypertensive therapy, compared to a control group of 141 patients who were not given a prescription. On follow-up at 2 weeks, there was an 11 mm Hg greater reduction of BP in the group who received prescriptions compared to the control group. None of the patients in either group on follow-up had experienced any new neurological deficits, ischemic events, life-threatening anaphylactic reactions, or clinically significant hypotension.
The Cleveland Clinic study14 also reported on those patents given who received new prescriptions from the ED. Similar to the study by Brody et al,19 none of the 82 patients discharged to home from the ED with a new antihypertensive prescription had any major adverse event at 30-day follow-up.14
Pharmacological Treatment Recommendations
When choosing to treat patients with new prescriptions for antihypertensives, it is important to follow the most current outpatient treatment recommendations. In 2014, JNC 8 released new guidelines for the outpatient management of adults with hypertension.20 The panel issued recommendations based on its systematic review of randomized controlled trials on antihypertensive treatments. The key recommendations are as follows:
- In patients aged 60 years or older, initiate pharmacological treatment at a BP of ≥150/90 mm Hg.
- In patients aged 18 to 59 years, initiate pharmacological treatment at a BP of ≥140/90 mm Hg.
- In the general nonblack population, initial antihypertensive treatment should include a thiazide-type diuretic, a calcium channel blocker (CCB), an angiotensin-converting enzyme inhibitor (ACE-I), or an angiotensin receptor blocker (ARB).
- In the general black population, initial treatment should include a thiazide-type diuretic or a CCB.
- In patients with chronic kidney disease (CKD) (including black patients), initial (or add-on) antihypertensive treatment should include an ACE-I or ARB to improve kidney outcomes—but not both.
- If goal BP is not reached within 1 month of initial treatment, increase the dose of the initial drug or add a second agent (eg, thiazide-type diuretic, CCB, ACE-I, or ARB). If goal is not reached with two drugs, use the third drug from that list if no contraindications exist, but do not use both an ACE-I and an ARB together in the same patient.
Of note, JNC 8, in departure from JNC 7, no longer recommends beta-blockers as first-line therapy for isolated hypertension (there may be compelling alternate indications, such as atrial fibrillation or postmyocardial infarction (MI), such that a beta-blocker would still be the first medication considered). The reason for this stems from a single randomized controlled trial of 9,193 patients that found that despite equivalent BP reduction, use of a beta-blocker in comparison to an ARB resulted in a higher rate of a composite outcome of death, MI, or stroke.21 The main difference was a 25% relative risk reduction for stroke with use of an ARB (losartan) in comparison to a beta-blocker (atenolol). The most recent European guidelines still include beta-blockers among its first-line recommended BP medications, but do acknowledge that they are not as effective in reducing stroke incidence as other alternative medications.15 The European guidelines otherwise include the same list of first-line agents. The British guidelines mirror JNC 8 in terms of first-line antihypertensive medication choices.18
Since the release of JNC 8, the Systolic Blood Pressure Intervention Trial (SPRINT) has been published, and will likely impact future national recommendations on BP management. The SPRINT study was a randomized controlled trial enrolling over 9,000 hypertensive nondiabetic patients older than age 50 years that treated individuals to a standard BP goal (systolic BP of 140 mm Hg) versus an intensive BP goal (systolic BP of 120 mm Hg) over a 3.5-year period. The trial was stopped early for safety as a 25% mortality reduction was observed in the intensive treatment group (1.65 vs 2.19 deaths/y).22 This was in contrast to previous trials that had mostly failed to show this sort of benefit, though previous trials were smaller in number or included only diabetic patients.23 While it is likely that this trial may influence lowering treatment thresholds from the office, it is not likely to impact care from the ED.
The recommendations of JNC 8 do not necessarily coincide with current US EP practice. In the study by Brody et al,19 of patients provided ED antihypertensive prescriptions, 54% received thiazide-type diuretics, 26% ACE-I, 10% CCBs, and 6% beta-blockers. This is noteworthy because 96% of those in the study were black patients who would benefit most from either a thiazide or a CCB. Another recent study of ED patients showed that of patients who were both treated in the ED and discharged with antihypertensive medications, 34% received a diuretic prescription, 32% clonidine, 15% a beta-blocker, 19% an ARB or ACE-I, 12% a CCB, and 2% hydrazine.24 These results are important because according to many published guidelines, including JNC 8, clonidine is only considered one of several fourth-line options for severe resistant hypertension.15,18,20 Since clonidine use can be complicated by rebound hypertension, it is not an ideal agent to be prescribed de novo to patients in the ED. This is particularly true if these patients are not already on maximum doses of the three most recommended agents previously noted, or if there are concerns over patient compliance.
Of the drug classes recommended by JNC 8, Table 3 lists the absolute and relative contraindications.
In clinical trials, amlodipine is among the most effective BP medications and is considered first-line therapy for all groups of patients with hypertension.15,18,20 A simplistic approach for most patients presenting with severe asymptomatic hypertension (BP of ≥180/110 mm Hg) not currently on treatment would be to recheck the BP and assure it remains elevated over the period of the ED visit.
Conclusion
Hypertension is among the most common medical conditions for which emergency patients seek care. The ACEP clinical policies provide guidance on the appropriate work-up and treatment of these patients. Given the occasional lack of clarity on whether a patient’s presentation is on the spectrum of more acute/serious, EPs may feel more comfortable in discharging patients with poor follow-up if they are able to safely prescribe antihypertensive treatment. Prior to prescribing treatment, EPs should refer to the JNC 8 guidelines to appropriately start antihypertensive treatment in select patient groups in the ED. The guidelines of JNC 8 are therefore worth referring to in order to appropriately start treatment in select patient groups from the ED.
Case Scenarios Continued
Case 1
[The 65-year-old black man who presented with headache and dizziness, and had an initial BP of 240/130 mm Hg.]
After treating the patient with prochlorperazine and diphenhydramine, his headache resolved. His BP improved but remained elevated at 190/120 mm Hg. On further questioning, the patient reported a history of similar headaches and wondered whether it was related to his BP. The head CT scan was negative for any acute hemorrhage, infarct, or mass; the ECG only showed evidence of left ventricular hypertrophy; and the BMP showed normal renal function.
After a long discussion with the patient, you agreed to start him on amlodipine 5 mg/d and referred him for follow-up with a local PCP.
Case 2
[The 90-year-old white woman with a history of CHF and an initial BP of 220/140 mm Hg at presentation.]
The BMP evaluation showed a baseline creatinine level of 1.3 mg/dL. Given this patient’s history of CHF, amlodipine would not be the ideal next agent to prescribe. After discussion with her PCP, you elected to start her on losartan at 25 mg/d, and instructed her to follow-up with her PCP within 1 week.
Case 3
[The 32-year-old white woman who presented at the advice of a pharmacist and had an initial BP of 240/100 mm Hg.]While reviewing the patient’s work-up and history, you noted her plans to become pregnant, and recalled a recent review on BP management, noting the contraindications associated with ARB or ACE-I in pregnancy. Based on the patient’s uninsured status and poor follow-up, you considered prescribing amlodipine. Prior to issuing the prescription, you performed a repeat BP check and noted that the patient’s BP had decreased to 130/85 mm Hg. Given the marked improvement in the patient’s BP during her ED course, you were not convinced that she truly had hypertension.
Instead of prescribing an antihypertensive agent, which may not ultimately benefit this patient, you advised her to seek follow-up care at an outpatient clinic to have her BP rechecked. The patient agreed, and you referred her to a local free clinic.
Case Scenarios
Case 1
You had just started your shift, and your first patient presented with symptoms of headache and dizziness, and a blood pressure (BP) of 240/130 mm Hg, without any vomiting or visual symptoms. Physical examination revealed an alert, pleasant 65-year-old black man whose ocular, neurological, and cardiovascular (CV) examinations were normal. The patient reported a history of borderline hypertension, but had never taken any medications for it.
After placing some initial orders, including an electrocardiogram (ECG), basic metabolic panel (BMP), and head computed tomography (CT) scan, and ordering 10 mg intravenous (IV) prochlorperazine and 25 mg IV diphenhydramine to treat the patient’s headache, you are left asking yourself what steps you should take next.
Case 2
Your next patient was a 90-year-old white woman who had been referred to the ED by her primary care physician (PCP) for “hypertensive urgency.” She had no complaints to report. Similar to the first patient, this patient’s physical examination was also normal, with the exception of a persistently elevated BP of 220/140 mm Hg. Her history was significant for congestive heart failure (CHF), but she exhibited no current CV signs or symptoms. The patient had been taking furosemide but was not on any other antihypertensive medications.
Case 3
In the room next to your 90-year-old patient is a 32-year-old uninsured hypertensive white woman. During the history taking, the patient stated that she was trying to become pregnant and was not currently using any form of contraception. Similar to the second patient, she had no complaints to report. Regarding her reason for presentation, the patient stated that when she had her BP checked at a pharmacy earlier that day, the reading was “too high,” and the pharmacist had advised her to go to the ED. She seemed anxious but otherwise well. Her initial BP at presentation was 240/100 mm Hg, but her physical examination was otherwise normal.
Hypertensive Emergencies
As emergency physicians (EPs), we see hypertensive patients every day. According to the US Centers for Disease Control and Prevention, 33% of American adults have hypertension, which is defined by a BP of ≥140/90 mm Hg (Table 1).
Almost 25% of total annual US adult ED visits are directly or indirectly related to hypertension, and about 1% of all ED visits are due solely to elevated BP.3 In an ambulatory care survey for 2007, moderate or severe hypertensive BP readings were found to be more common in patients presenting to the ED (43.5%) than to primary care clinics (27%).4 Patients presenting to the ED with hypertensive BP readings disproportionately represented patients who were older, male, non-Hispanic black, Medicare beneficiaries, or uninsured. Certainly, some patients presenting to the ED have hypertensive BP readings due to pain or anxiety, but multiple studies have suggested that 50% to 70% of ED patients who have hypertensive BP readings will be diagnosed with hypertension on office follow-up.5,6 While a minority of these patients present to the ED with hypertensive emergencies, the majority present either without symptoms of hypertension or with only mild headache. Given the disease burden of hypertension combined with the benefits of treatment, it is worthwhile for the practicing EP to review the most up-to-date guidelines on outpatient management of hypertension.
When a patient presents to the ED with a hypertensive BP reading, the initial priority of the EP is to exclude hypertensive emergency. Hypertensive emergencies are defined by the presence of hypertension (generally grade 3/severe hypertension with BP ≥180/110 mm Hg; see Table 1) in conjunction with evidence of target organ damage.
Target Organ Manifestations
The acuity and/or presence of target organ damage are not always clear on initial ED evaluation. For instance, when a patient who has no history of primary care presents to the ED with severe hypertension, laboratory evaluation may demonstrate protein and blood in his or her urine and an elevated serum creatinine level. In the absence of values from past laboratory studies, it is difficult to determine whether these test results represent normal laboratory parameters for this patient due to longstanding hypertensive kidney disease (ie, hypertensive nephrosclerosis) or if they represent a true hypertensive emergency, (ie, hypertensive emergency-related nephropathy).7 In patients with severe hypertension and possibly new acute kidney injury, it is probably safest to either assume hypertensive emergency-related nephropathy and to treat accordingly or consult with nephrology services. The picture of hypertensive emergency-related nephropathy often only becomes clear after renal biopsy results and improvement in renal parameters with BP control.
The ocular manifestations of hypertensive emergency require detailed fundoscopy, which at times can be challenging in the ED. In assessing for cardiac target organ damage, at our institution, we typically ask patients if they have experienced symptoms of dyspnea and chest pain or pressure. Generally, we also evaluate cardiac enzymes, B-type natriuretic peptide, and order ECG and chest X-ray studies when suggested by history or physical examination. Alarmingly, a study of 161 ED hypertensive (average BP of 183/109 mm Hg), asymptomatic, predominantly black patients found that 146 (90.7%) had subclinical hypertensive heart disease on point-of-care echocardiogram.8
Neurological/Hypertensive Encephalopathy
Hypertensive encephalopathy is a diagnosis of exclusion as alternate causes of confusion and headache, such as intracranial hemorrhage, are excluded and mental status improves with titrated BP control. Nonetheless, it is difficult to confidently state from the literature that patients who present with headache but have a normal mental status in the presence of severe hypertension are not on an early spectrum of hypertensive encephalopathy. Therefore, it is likely that the degree of symptoms should define whether target organ damage exists, though there is certainly a spectrum of hypertensive emergency—the strict definition of which is not always clear.
When a hypertensive emergency is diagnosed, management typically involves the use of antihypertensive IV medication in the intensive care unit. While such management is outside the scope of this paper, Adebayo and Rogers9 have published an excellent review of the care of hypertensive emergencies.
Asymptomatic Hypertension
The American College of Emergency Physicians (ACEP) has developed two clinical policies on the evaluation and management of asymptomatic hypertension in the ED. The original, published in 2006, advised that initially high BP readings of ED patients should be repeated: two separate high readings are adequate for screening, and those patients with hypertension should be referred for follow-up. Furthermore, ACEP policies note that initiating treatment in the ED is not necessary when patients are referred for follow-up. If treatment for hypertension is initiated in the ED, ACEP recommends that such management should attempt only to gradually lower BP, and not to normalize it during the initial ED visit.10
The 2013 update to ACEP’s clinical policy on managing asymptomatic hypertension expanded on the original policy. The updated policy advised against routine testing for target organ damage in patients who have asymptomatic severe hypertension. However, ACEP policy notes that evaluating serum creatinine in these patients with poor follow-up may influence patient disposition.11
The 2013 policy further stated that medical intervention is not required in ED patients who have asymptomatic severe hypertension, but may be considered in patients with poor follow-up. The policies emphasize that all asymptomatic hypertensive patients should be referred for follow-up. The literature cited for the recommendation that ED patients with asymptomatic severe hypertension do not require routine investigation stems from two observational studies. These studies found that screening asymptomatic ED patients who presented with severe hypertension revealed serum creatinine abnormalities in approximately 6%, which impacted patient disposition, though it was not clear from the study results whether admission correlated to meaningful patient outcomes.12,13
Patient Disposition
Since ACEP’s 2013 clinical policy, a study from the Cleveland Clinic has been published. This retrospective cohort study reviewed 6 years of data looking at all patients in its system with a BP of ≥180/110 mm Hg, and compared those office patients discharged to home to those referred to the ED or directly admitted to the inpatient hospital solely on the basis of severe hypertension.14 The study found that 0.5% of 387 patients referred to the ED by primary care clinics for asymptomatic severe hypertension had confirmed acute kidney injury on BMP.14 The Cleveland Clinic study also found that 2.1% of patients had evidence of target organ damage and 5.5% had any abnormal results.14 In addition, referral to the ED from the clinic for hypertension was associated with a slightly higher rate of major adverse CV events at 7 days (2 of 426 [0.5%] versus 61 of 58,109 [0.1%]; P = .02).14
The results of the Cleveland Clinic study confirm that in the absence of target organ damage, hypertension is probably best managed in the outpatient setting. The European Task Force hypertensive guidelines state “hospitalization for hypertension is regarded as inappropriate in most European countries.”15 However, from 2006 to 2012, 26% of US ED patients with primary diagnoses of hypertension were admitted to the hospital.3 In Canada’s most populous province of Ontario, from 2002 to 2011, approximately 8% of hypertensive patients were admitted.16 Part of this discrepancy may be due to the sometimes ambiguous nature of the presentation of patients with hypertension, making it unclear whether a true hypertensive emergency exists. Many patients perceive visual symptoms, headache, dizziness, and even chest pressure as the result of their elevated BP—without clear findings on fundoscopy, ECG, or cardiac marker testing. Perhaps more of these patients would be discharged if EPs felt comfortable initiating appropriate initial antihypertensive treatment.
Management
Initiating Antihypertensive Treatment
Some EPs may feel that an accurate diagnosis of hypertension requires repeat BP testing in the primary care office setting, and for this reason are reluctant to initiate antihypertensive treatment in the ED. The most recent guidelines by the Joint National Committee (JNC 8) do not address how many BP readings are necessary to diagnose hypertension, but JNC 7 suggested that diagnosis of hypertension requires two separate office visits.17 Evidence cited in ACEP’s first clinical policy states that two separate BP measurements in the ED are adequate for screening—but not necessarily for initiating treatment.10 However, European and British outpatient clinical recommendations advocate initiation of antihypertensive medication for a single visit in patients who have an elevated BP categorized as grade 3/severe hypertension (BP of ≥180/110 mm Hg).15,18 Furthermore, for patients with severe hypertension seen in the ED, as many as 97% are likely to have true hypertension at office follow-up.6 Those ED patients presenting with severe hypertension are very likely to have a true diagnosis of hypertension.
A recent retrospective analysis of a group of hypertensive ED patients by Brody et al19 found that patients prescribed BP medications by an EP were more likely to have improved BP control at follow-up 2 weeks later. In their study, the decision to prescribe antihypertensive medications were at the discretion of the EP. Seventy-six patients were given one or more prescriptions for antihypertensive therapy, compared to a control group of 141 patients who were not given a prescription. On follow-up at 2 weeks, there was an 11 mm Hg greater reduction of BP in the group who received prescriptions compared to the control group. None of the patients in either group on follow-up had experienced any new neurological deficits, ischemic events, life-threatening anaphylactic reactions, or clinically significant hypotension.
The Cleveland Clinic study14 also reported on those patents given who received new prescriptions from the ED. Similar to the study by Brody et al,19 none of the 82 patients discharged to home from the ED with a new antihypertensive prescription had any major adverse event at 30-day follow-up.14
Pharmacological Treatment Recommendations
When choosing to treat patients with new prescriptions for antihypertensives, it is important to follow the most current outpatient treatment recommendations. In 2014, JNC 8 released new guidelines for the outpatient management of adults with hypertension.20 The panel issued recommendations based on its systematic review of randomized controlled trials on antihypertensive treatments. The key recommendations are as follows:
- In patients aged 60 years or older, initiate pharmacological treatment at a BP of ≥150/90 mm Hg.
- In patients aged 18 to 59 years, initiate pharmacological treatment at a BP of ≥140/90 mm Hg.
- In the general nonblack population, initial antihypertensive treatment should include a thiazide-type diuretic, a calcium channel blocker (CCB), an angiotensin-converting enzyme inhibitor (ACE-I), or an angiotensin receptor blocker (ARB).
- In the general black population, initial treatment should include a thiazide-type diuretic or a CCB.
- In patients with chronic kidney disease (CKD) (including black patients), initial (or add-on) antihypertensive treatment should include an ACE-I or ARB to improve kidney outcomes—but not both.
- If goal BP is not reached within 1 month of initial treatment, increase the dose of the initial drug or add a second agent (eg, thiazide-type diuretic, CCB, ACE-I, or ARB). If goal is not reached with two drugs, use the third drug from that list if no contraindications exist, but do not use both an ACE-I and an ARB together in the same patient.
Of note, JNC 8, in departure from JNC 7, no longer recommends beta-blockers as first-line therapy for isolated hypertension (there may be compelling alternate indications, such as atrial fibrillation or postmyocardial infarction (MI), such that a beta-blocker would still be the first medication considered). The reason for this stems from a single randomized controlled trial of 9,193 patients that found that despite equivalent BP reduction, use of a beta-blocker in comparison to an ARB resulted in a higher rate of a composite outcome of death, MI, or stroke.21 The main difference was a 25% relative risk reduction for stroke with use of an ARB (losartan) in comparison to a beta-blocker (atenolol). The most recent European guidelines still include beta-blockers among its first-line recommended BP medications, but do acknowledge that they are not as effective in reducing stroke incidence as other alternative medications.15 The European guidelines otherwise include the same list of first-line agents. The British guidelines mirror JNC 8 in terms of first-line antihypertensive medication choices.18
Since the release of JNC 8, the Systolic Blood Pressure Intervention Trial (SPRINT) has been published, and will likely impact future national recommendations on BP management. The SPRINT study was a randomized controlled trial enrolling over 9,000 hypertensive nondiabetic patients older than age 50 years that treated individuals to a standard BP goal (systolic BP of 140 mm Hg) versus an intensive BP goal (systolic BP of 120 mm Hg) over a 3.5-year period. The trial was stopped early for safety as a 25% mortality reduction was observed in the intensive treatment group (1.65 vs 2.19 deaths/y).22 This was in contrast to previous trials that had mostly failed to show this sort of benefit, though previous trials were smaller in number or included only diabetic patients.23 While it is likely that this trial may influence lowering treatment thresholds from the office, it is not likely to impact care from the ED.
The recommendations of JNC 8 do not necessarily coincide with current US EP practice. In the study by Brody et al,19 of patients provided ED antihypertensive prescriptions, 54% received thiazide-type diuretics, 26% ACE-I, 10% CCBs, and 6% beta-blockers. This is noteworthy because 96% of those in the study were black patients who would benefit most from either a thiazide or a CCB. Another recent study of ED patients showed that of patients who were both treated in the ED and discharged with antihypertensive medications, 34% received a diuretic prescription, 32% clonidine, 15% a beta-blocker, 19% an ARB or ACE-I, 12% a CCB, and 2% hydrazine.24 These results are important because according to many published guidelines, including JNC 8, clonidine is only considered one of several fourth-line options for severe resistant hypertension.15,18,20 Since clonidine use can be complicated by rebound hypertension, it is not an ideal agent to be prescribed de novo to patients in the ED. This is particularly true if these patients are not already on maximum doses of the three most recommended agents previously noted, or if there are concerns over patient compliance.
Of the drug classes recommended by JNC 8, Table 3 lists the absolute and relative contraindications.
In clinical trials, amlodipine is among the most effective BP medications and is considered first-line therapy for all groups of patients with hypertension.15,18,20 A simplistic approach for most patients presenting with severe asymptomatic hypertension (BP of ≥180/110 mm Hg) not currently on treatment would be to recheck the BP and assure it remains elevated over the period of the ED visit.
Conclusion
Hypertension is among the most common medical conditions for which emergency patients seek care. The ACEP clinical policies provide guidance on the appropriate work-up and treatment of these patients. Given the occasional lack of clarity on whether a patient’s presentation is on the spectrum of more acute/serious, EPs may feel more comfortable in discharging patients with poor follow-up if they are able to safely prescribe antihypertensive treatment. Prior to prescribing treatment, EPs should refer to the JNC 8 guidelines to appropriately start antihypertensive treatment in select patient groups in the ED. The guidelines of JNC 8 are therefore worth referring to in order to appropriately start treatment in select patient groups from the ED.
Case Scenarios Continued
Case 1
[The 65-year-old black man who presented with headache and dizziness, and had an initial BP of 240/130 mm Hg.]
After treating the patient with prochlorperazine and diphenhydramine, his headache resolved. His BP improved but remained elevated at 190/120 mm Hg. On further questioning, the patient reported a history of similar headaches and wondered whether it was related to his BP. The head CT scan was negative for any acute hemorrhage, infarct, or mass; the ECG only showed evidence of left ventricular hypertrophy; and the BMP showed normal renal function.
After a long discussion with the patient, you agreed to start him on amlodipine 5 mg/d and referred him for follow-up with a local PCP.
Case 2
[The 90-year-old white woman with a history of CHF and an initial BP of 220/140 mm Hg at presentation.]
The BMP evaluation showed a baseline creatinine level of 1.3 mg/dL. Given this patient’s history of CHF, amlodipine would not be the ideal next agent to prescribe. After discussion with her PCP, you elected to start her on losartan at 25 mg/d, and instructed her to follow-up with her PCP within 1 week.
Case 3
[The 32-year-old white woman who presented at the advice of a pharmacist and had an initial BP of 240/100 mm Hg.]While reviewing the patient’s work-up and history, you noted her plans to become pregnant, and recalled a recent review on BP management, noting the contraindications associated with ARB or ACE-I in pregnancy. Based on the patient’s uninsured status and poor follow-up, you considered prescribing amlodipine. Prior to issuing the prescription, you performed a repeat BP check and noted that the patient’s BP had decreased to 130/85 mm Hg. Given the marked improvement in the patient’s BP during her ED course, you were not convinced that she truly had hypertension.
Instead of prescribing an antihypertensive agent, which may not ultimately benefit this patient, you advised her to seek follow-up care at an outpatient clinic to have her BP rechecked. The patient agreed, and you referred her to a local free clinic.
1. Nwankwo T, Yoon SS, Burt V, Gu Q. Hypertension among adults in the United States: National Health and Nutrition Examination Survey, 2011-2012. NCHS Data Brief. 2013;(133):1-8.
2. Turnbull F; Blood Pressure Lowering Treatment Trialists’ Collaboration. Effects of different blood-pressure-lowering regimens on major cardiovascular events: results of prospectively-designed overviews of randomised trials. Lancet. 2013;362(9395):1527-1535.
3. McNaughton CD, Self WH, Zhu Y, Janke AT, Storrow AB, Levy P. Incidence of hypertension-related emergency department visits in the United States, 2006 to 2012. Am J Cardiol. 2015;116(11):1717-1723. doi: 10.1016/j.amjcard.2015.09.007.
4. Niska RW. Blood pressure measurements at emergency department visits by adults: United States, 2007-2008. NCHS Data Brief. 2011;(72):1-8.
5. Chernow SM, Iserson KV, Criss E. Use of the emergency department for hypertension screening: a prospective study. Ann Emerg Med. 1987;16(2):180-182.
6. Backer HD, Decker L, Ackerson L. Reproducibility of increased blood pressure during an emergency department or urgent care visit. Ann Emerg Med. 2003.41(4):507-512.
7. Nonaka K, Ubara Y, Sumida K, et al. Clinical and pathological evaluation of hypertensive emergency-related nephropathy. Intern Med. 2013;52(1):45-53.
8. Levy P, Ye H, Compton S, et al. Subclinical hypertensive heart disease in black patients with elevated blood pressure in an inner-city emergency department. Ann Emerg Med. 2012;60(4):467-474.e1. doi: 10.1016/j.annemergmed.2012.03.030.
9. Adebayo O, Rogers RL. Hypertensive emergencies in the emergency department. Emerg Med Clin North Am. 2015;33(3):539-551. doi: 10.1016/j.emc.2015.04.005.
10. Decker WW, Godwin SA, Hess EP, Lenamond CC, Jagoda AS; American College of Emergency Physicians Clinical Policies Subcommittee (Writing Committee) on Asymptomatic Hypertension in the ED. Clinical policy: critical issues in the evaluation and management of adult patients with asymptomatic hypertension in the emergency department. Ann Emerg Med. 2006;47(3):237-234. doi: 10.1016/j.annemergmed.2005.10.003
11. Wolf SJ, Lo B, Shih RD, Smith MD, Fesmire FM; American College of Emergency Physicians Clinical Policies Committee. Clinical policy: critical issues in the evaluation and management of adult patients in the emergency department with asymptomatic elevated blood pressure. Ann Emerg Med. 2013;62(1):59-68. doi: 10.1016/j.annemergmed.2013.05.012.
12. Karras DJ, Kruus LK, Cienki JJ, et al. Evaluation and treatment of patients with severely elevated blood pressure in academic emergency departments: a multicenter study. Ann Emerg Med. 2006;47(3):230-236.
13. Nishijima DK, Paladino L, Sinert R. Routine testing in patients with asymptomatic elevated blood pressure in the ED. Am J Emerg Med. 2010;28(2):235-242. doi: 10.1016/j.ajem.2008.11.015.
14. Patel KK, Young L, Howell EH, et al. Characteristics and outcomes of patients presenting with hypertensive urgency in the office setting. JAMA Intern Med. 2016;176(7):981-988. doi: 10.1001/jamainternmed.2016.1509.
15. Mancia G, Fagard R, Narkiewicz K, et al. 2013 ESH/ESC guidelines for the management of arterial hypertension: the Task Force for the Management of Arterial Hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). Eur Heart J. 2013;34(28):2159-2219. doi: 10.1093/eurheartj/eht151.
16. Masood S, Austin PC, Atzema CL. A population-based analysis of outcomes in patients with a primary diagnosis of hypertension in the emergency department. Ann Emerg Med. 2016;68(3):258-267.e5. doi: 10.1016/j.annemergmed.2016.04.060.
17. Chobanian AV, Bakris GL, Black HR, et al; National Heart, Lung, and Blood Institute Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure; National High Blood Pressure Education Program Coordinating Committee. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure: the JNC 7 report. JAMA. 2003;289(19):2560-2572. Erratum in: JAMA. 2003;290(2):197.
18. Krause T, Lovibond K, Caulfield M, McCormack T, Williams B; Guideline Development Group. Management of hypertension: summary of NICE guidance. BMJ. 2011;343:d4891. doi: 10.1136/bmj.d4891.
19. Brody A, Rahman T, Reed B, et al. Safety and efficacy of antihypertensive prescription at emergency department discharge. Acad Emerg Med. 2015;22(5):632-635. doi: 10.1111/acem.12660.
20. James PA, Oparil S, Carter BL, et al. 2014 evidence-based guideline for the management of high blood pressure in adults: report from the panel members appointed to the Eighth Joint National Committee (JNC 8). JAMA. 2014;311(5):507-520. doi: 10.1001/jama.2013.284427. Erratum in: JAMA. 2014;311(17):1809.
21. Dahlöf B, Devereux RB, Kjeldsen SE, et al; LIFE Study Group. Cardiovascular morbidity and mortality in the Losartan Intervention For Endpoint reduction in hypertension study (LIFE): a randomised trial against atenolol. Lancet. 2002;359(9311):995-1003.
22. PRINT Research Group, Wright JT Jr, Williamson JD, Whelton PK, et al. A randomized trial of intensive versus standard blood-pressure control. N Engl J Med. 2015;373(22):2103-2116. doi: 10.1056/NEJMoa1511939.
23. ACCORD Study Group, Cushman WC, Evans GW, Byington RP, et al. Effects of intensive blood-pressure control in type 2 diabetes mellitus. N Engl J Med. 2010;362(17):1575-1585. doi: 10.1056/NEJMoa1001286.
24. Levy PD, Mahn JJ, Miller J, et al. Blood pressure treatment and outcomes in hypertensive patients without acute target organ damage: a retrospective cohort. Am J Emerg Med. 2015;33(9):1219-1224. doi: 10.1016/j.ajem.2015.05.036.
25. Leung AA, Wright A, Pazo V, Karson A, Bates DW. Risk of thiazide-induced hyponatremia in patients with hypertension. Am J Med. 2011;124(11):1064-1072. doi: 10.1016/j.amjmed.2011.06.031.
26. Mann JFE, Hilgers KF. Renin-angiotensin system inhibition in the treatment of hypertension. http://www.uptodate.com/contents/renin-angiotensin-system-inhibition-in-the-treatment-of-hypertension. Accessed September 21, 2016.
1. Nwankwo T, Yoon SS, Burt V, Gu Q. Hypertension among adults in the United States: National Health and Nutrition Examination Survey, 2011-2012. NCHS Data Brief. 2013;(133):1-8.
2. Turnbull F; Blood Pressure Lowering Treatment Trialists’ Collaboration. Effects of different blood-pressure-lowering regimens on major cardiovascular events: results of prospectively-designed overviews of randomised trials. Lancet. 2013;362(9395):1527-1535.
3. McNaughton CD, Self WH, Zhu Y, Janke AT, Storrow AB, Levy P. Incidence of hypertension-related emergency department visits in the United States, 2006 to 2012. Am J Cardiol. 2015;116(11):1717-1723. doi: 10.1016/j.amjcard.2015.09.007.
4. Niska RW. Blood pressure measurements at emergency department visits by adults: United States, 2007-2008. NCHS Data Brief. 2011;(72):1-8.
5. Chernow SM, Iserson KV, Criss E. Use of the emergency department for hypertension screening: a prospective study. Ann Emerg Med. 1987;16(2):180-182.
6. Backer HD, Decker L, Ackerson L. Reproducibility of increased blood pressure during an emergency department or urgent care visit. Ann Emerg Med. 2003.41(4):507-512.
7. Nonaka K, Ubara Y, Sumida K, et al. Clinical and pathological evaluation of hypertensive emergency-related nephropathy. Intern Med. 2013;52(1):45-53.
8. Levy P, Ye H, Compton S, et al. Subclinical hypertensive heart disease in black patients with elevated blood pressure in an inner-city emergency department. Ann Emerg Med. 2012;60(4):467-474.e1. doi: 10.1016/j.annemergmed.2012.03.030.
9. Adebayo O, Rogers RL. Hypertensive emergencies in the emergency department. Emerg Med Clin North Am. 2015;33(3):539-551. doi: 10.1016/j.emc.2015.04.005.
10. Decker WW, Godwin SA, Hess EP, Lenamond CC, Jagoda AS; American College of Emergency Physicians Clinical Policies Subcommittee (Writing Committee) on Asymptomatic Hypertension in the ED. Clinical policy: critical issues in the evaluation and management of adult patients with asymptomatic hypertension in the emergency department. Ann Emerg Med. 2006;47(3):237-234. doi: 10.1016/j.annemergmed.2005.10.003
11. Wolf SJ, Lo B, Shih RD, Smith MD, Fesmire FM; American College of Emergency Physicians Clinical Policies Committee. Clinical policy: critical issues in the evaluation and management of adult patients in the emergency department with asymptomatic elevated blood pressure. Ann Emerg Med. 2013;62(1):59-68. doi: 10.1016/j.annemergmed.2013.05.012.
12. Karras DJ, Kruus LK, Cienki JJ, et al. Evaluation and treatment of patients with severely elevated blood pressure in academic emergency departments: a multicenter study. Ann Emerg Med. 2006;47(3):230-236.
13. Nishijima DK, Paladino L, Sinert R. Routine testing in patients with asymptomatic elevated blood pressure in the ED. Am J Emerg Med. 2010;28(2):235-242. doi: 10.1016/j.ajem.2008.11.015.
14. Patel KK, Young L, Howell EH, et al. Characteristics and outcomes of patients presenting with hypertensive urgency in the office setting. JAMA Intern Med. 2016;176(7):981-988. doi: 10.1001/jamainternmed.2016.1509.
15. Mancia G, Fagard R, Narkiewicz K, et al. 2013 ESH/ESC guidelines for the management of arterial hypertension: the Task Force for the Management of Arterial Hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). Eur Heart J. 2013;34(28):2159-2219. doi: 10.1093/eurheartj/eht151.
16. Masood S, Austin PC, Atzema CL. A population-based analysis of outcomes in patients with a primary diagnosis of hypertension in the emergency department. Ann Emerg Med. 2016;68(3):258-267.e5. doi: 10.1016/j.annemergmed.2016.04.060.
17. Chobanian AV, Bakris GL, Black HR, et al; National Heart, Lung, and Blood Institute Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure; National High Blood Pressure Education Program Coordinating Committee. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure: the JNC 7 report. JAMA. 2003;289(19):2560-2572. Erratum in: JAMA. 2003;290(2):197.
18. Krause T, Lovibond K, Caulfield M, McCormack T, Williams B; Guideline Development Group. Management of hypertension: summary of NICE guidance. BMJ. 2011;343:d4891. doi: 10.1136/bmj.d4891.
19. Brody A, Rahman T, Reed B, et al. Safety and efficacy of antihypertensive prescription at emergency department discharge. Acad Emerg Med. 2015;22(5):632-635. doi: 10.1111/acem.12660.
20. James PA, Oparil S, Carter BL, et al. 2014 evidence-based guideline for the management of high blood pressure in adults: report from the panel members appointed to the Eighth Joint National Committee (JNC 8). JAMA. 2014;311(5):507-520. doi: 10.1001/jama.2013.284427. Erratum in: JAMA. 2014;311(17):1809.
21. Dahlöf B, Devereux RB, Kjeldsen SE, et al; LIFE Study Group. Cardiovascular morbidity and mortality in the Losartan Intervention For Endpoint reduction in hypertension study (LIFE): a randomised trial against atenolol. Lancet. 2002;359(9311):995-1003.
22. PRINT Research Group, Wright JT Jr, Williamson JD, Whelton PK, et al. A randomized trial of intensive versus standard blood-pressure control. N Engl J Med. 2015;373(22):2103-2116. doi: 10.1056/NEJMoa1511939.
23. ACCORD Study Group, Cushman WC, Evans GW, Byington RP, et al. Effects of intensive blood-pressure control in type 2 diabetes mellitus. N Engl J Med. 2010;362(17):1575-1585. doi: 10.1056/NEJMoa1001286.
24. Levy PD, Mahn JJ, Miller J, et al. Blood pressure treatment and outcomes in hypertensive patients without acute target organ damage: a retrospective cohort. Am J Emerg Med. 2015;33(9):1219-1224. doi: 10.1016/j.ajem.2015.05.036.
25. Leung AA, Wright A, Pazo V, Karson A, Bates DW. Risk of thiazide-induced hyponatremia in patients with hypertension. Am J Med. 2011;124(11):1064-1072. doi: 10.1016/j.amjmed.2011.06.031.
26. Mann JFE, Hilgers KF. Renin-angiotensin system inhibition in the treatment of hypertension. http://www.uptodate.com/contents/renin-angiotensin-system-inhibition-in-the-treatment-of-hypertension. Accessed September 21, 2016.

Diabetes Mellitus: Diagnosis and Management in the Emergency Department
According to the US Centers for Disease Control and Prevention (CDC), in 2011 there were 25.8 million people in the United States living with diabetes mellitus (DM), 90% to 95% of whom had type 2 DM.1 Seven million of those with DM are undiagnosed. In addition, an estimated 79 million adults in the United States have prediabetes, a condition in which glycated hemoglobin (HbA1c) levels are above normal but do not yet meet the diagnostic threshold for DM (≥6.5%).1 This large population with prediabetes, defined by HbA1c levels of 5.7% to 6.4%, has a 5-year risk of progression to diabetes ranging from 9% to 50%; the higher risk is associated with higher HbA1c levels as the disease represents a continuum.2
The benefits of diagnosis and treatment of diabetes—preventing the progression of microvascular complications—are well established. Through medication, exercise, and dietary interventions, the progression of both prediabetes and diabetes can be halted and in many cases reversed.
Given the prevalence of DM in the United States and the clear benefits of treatment, the ability to diagnose DM is important for any physician who may encounter patients with undiagnosed diabetes or prediabetes. This article reviews the management of hyperglycemia relevant to the emergency physician (EP) and discusses the criteria used in diagnosing DM.
The American College of Emergency Physicians (ACEP) currently does not have a clinical policy for the initial treatment of patients with DM that is newly diagnosed in the ED. A 2007 survey of 152 EPs in the United States found that 52% would leave initiation of outpatient treatment of diabetes to a patient’s primary care physician (PCP), regardless of the degree of hyperglycemia noted in the ED.3 Almost paradoxically, among these same EPs, the most common reason for not screening for diabetes (cited by 69%) was the inability to secure follow-up for newly diagnosed patients. Given the fragmentary care many emergency patients receive and the difficulty in assuring close ED follow-up, reviewing the American Diabetes Association (ADA) recommendations for initiation of diabetes management is worthwhile.
ADA Treatment Guidelines
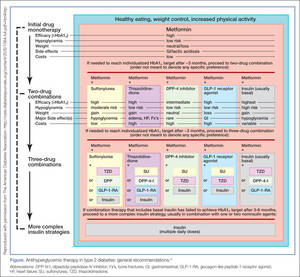
Metformin
Metformin, if tolerated and without contraindications, is the preferred initial pharmacologic agent for all patients with newly diagnosed DM. This drug typically lowers HbA1c by 1.5%, and does not cause weight gain or hypoglycemia associated with some other oral agents (eg, sulfonylureas). Metformin therapy, however, is contraindicated in patients with chronic kidney disease (CKD) (Cr >1.5 in males and >1.4 in females), liver disease, a history of lactic acidosis, and a low-perfusion state. Metformin also should not be used for 48 hours following an intravenous (IV) contrast-enhanced study.
When starting metformin or increasing the dose, patients frequently experience abdominal symptoms, including cramping, nausea, vomiting, and diarrhea. These side effects are usually mild and self-limiting, and they usually resolve within a week. However, patients should be warned of these complications and advised to take metformin with meals to limit side effects. They also should be encouraged to continue the medication through the initial symptoms, if possible.
For a patient with newly diagnosed type 2 DM, a reasonable ED discharge plan is to start metformin at 500 mg daily, taken with a meal. If the patient develops abdominal symptoms, the dose can be reduced to 250 mg daily. Patients should additionally be advised to follow up with their PCP as soon as feasible. Patients can be instructed to increase the dose of metformin on their own. Because the development of gastrointestinal symptoms is the main dose-limiting effect of metformin therapy, it is generally safe to give patients instructions on weekly dose escalation by 500 mg/day to the optimal dose of 1,000 mg twice daily. Although metformin therapy is associated with rare cases of lactic acidosis in patients with CKD, it does not, on its own, cause acute kidney injury; therefore, intense monitoring is not required while doses are increased. Metformin therapy can decrease vitamin B12 absorption, though it rarely results in megaloblastic anemia, and it takes 5 to 10 years for neurological symptoms to manifest.5
Other Treatment Options
The Figure highlights the ADA guidelines on additional pharmacologic agents beyond metformin. When these additional agents are used, the patient should follow-up with a PCP every 3 months to determine how far HbA1c has been lowered. For most patients with DM, the goal for HbA1c is less than 7%. This goal may be raised for elderly patients and those with a history of cardiovascular disease, as these patients are at higher risk for cardiovascular mortality from an episode of hypoglycemia.
The secondary medication options include sulfonylureas, thiazolidinediones, dipeptidyl peptidase-IV inhibitors, glucagon-like peptide-1 (GLP-1) agonists, sodium-glucose cotransporter-2 inhibitors, and insulin. Insulin therapy is the final medication step for all patients with DM who are willing and able to comply with daily injections and who have failed to meet goals through alternative agents.
Before using additional agents beyond metformin, the PCP or endocrinologist should discuss in detail factors such as side effects (ie, weight gain, risk of hypoglycemia), medication delivery (GLP-1 agonists and insulin require injections), and cost with the patient. It is generally advisable not to try to accomplish this medication adjustment in the ED without consultation with a PCP or endocrinologist.
Diagnosis
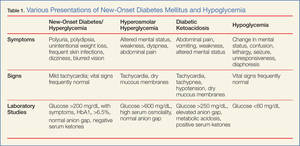
The clinical presentation of new-onset DM can range from the relatively benign (eg, polyuria, polydipsia, frequent skin infections) to the life-threatening (eg, diabetic ketoacidosis) (Table 1). The classic symptoms of hyperglycemia include polyuria, polydipsia, unexplained weight loss, easy fatigability, dizziness, and blurred vision. Any one of these symptoms should prompt consideration of DM in the differential diagnosis.
Four abnormal laboratory results comprise the ADA’s diagnostic criteria for DM6:
- HbA1c ≥6.5%;
- 8-hour fasting plasma glucose ≥126 mg/dL;
- 2-hour oral glucose tolerance test (OGTT) ≥200 mg/dL (Patient is given 75 g sugar orally; then plasma glucose is drawn 2 hours later); and
- A random plasma glucose of ≥200 mg/dL in association with “classic symptoms” of DM, defined as polyuria, polydipsia, and unexplained weight loss.
In the absence of an unequivocal indicator, such as the patient presenting in diabetic ketoacidosis, the formal diagnosis of DM should not be made unless at least 2 abnormal test results are obtained simultaneously (from a 2-hour OGTT test and an HbA1c panel, for example, or when the same test is repeated one month later and both test results indicate DM).
Limitations of Glucometers
When interpreting test results, keep in mind that the US Food and Drug Administration allows point-of-care (POC) glucometers to have an accuracy of +/- 20%. The POC glucometers measure whole-blood glucose rather than plasma glucose; generally the amount of glucose in plasma is about 10% to 15% higher than the amount in whole blood.7 Therefore, the formal diagnosis of DM relies on laboratory plasma glucose results; POC glucometer results may guide the EP in initiating a workup for DM but should not be among the diagnostic criteria.
HbA1c Testing
The HbA1c percentage represents the preceding 3-month average plasma glucose level. This is due to nonenzymatic glycosylation of Hb, a reaction driven by higher concentrations of circulating plasma glucose. The HbA1c can be falsely low in states of high red blood cell (RBC) turnover, such as ongoing blood loss or the RBC fragility seen in hemoglobinopathies. Patients who have had RBC transfusions in the preceding months will have inaccurate HbA1c test results as well.
Keeping these test characteristics in mind, the HbA1c test may be more useful than glucose-based testing strategies in diagnosing diabetes in the ED. Hyperglycemia can be observed in nondiabetic emergency patients undergoing a stress response, since gluconeogenesis and glycogenolysis are normal hepatic stress responses to circulating epinephrine and cortisol. Unless a patient is on chronic steroids, the HbA1c is not similarly affected.
A recent study of ED patients using HbA1c as the sole screening modality found that test characteristics for ED patients were similar to those for patients in typical outpatient settings. HbA1c of 6.5 or greater yielded a sensitivity of 54% and a specificity of 96% in diagnosing diabetes.8 The availability of test results at the time of the emergency visit depends upon the individual hospital laboratory, but most labs run the test itself in less than an hour. Emergency physicians working in hospitals that perform the test will often have the test results prior to patient discharge.
Inpatient Management
Managing a patient with newly diagnosed DM that requires admission to the hospital is different from managing a patient who can be treated as an outpatient. The ADA-recommended treatment regimen for DM in the inpatient setting focuses on the use of insulin. While type 1 DM, by definition, requires insulin treatment, many patients with type 2 DM are treated with oral agents only as outpatients. However, because of complications associated with the use of oral agents in low renal perfusion states (such as during surgery, during IV contrast-enhanced studies, or when the admitting condition causes shock), the ADA generally does not prefer oral agents for inpatient glycemic control. Metformin particularly should not be used in the inpatient setting, due to increased risk of lactic acidosis.
The preferred insulin regimen for noncritically ill diabetic inpatients consists of scheduled subcutaneous therapy with basal, nutritional, and correctional components.9 Because absorption from subcutaneous tissue varies among critically ill patients, the ADA recommends an IV insulin therapy protocol for ICU patients with diabetes. The NICE SUGAR trial found that the overall risk of death was 2.6% higher among patients treated with an intensive insulin therapy regimen (finger stick blood glucose goal 80-108 mg/dL) than it was among patients treated using standard therapy with a goal of less than 180 mg/dL, a statistically significant difference.10 These results form the basis for the ADA-recommended inpatient glycemic target of 140 to 180 mg/dL among critically ill patients.11 While no definitive evidence exists to guide glycemic control among noncritically ill inpatients, the strategy applied to critically ill patients can be extrapolated to other hospitalized patients because the ADA recommends treatment to keep finger stick blood glucose values below 180 mg/dL.
Hypoglycemia
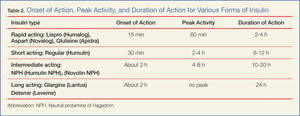
Often a hypoglycemic event can clearly be correlated to a missed meal. This may only require re-education of the patient about the need to be consistent in the timing of his or her dietary regimen. However, often a hypoglycemic event is not clearly related to a missed meal. When a patient has recently taken a long-acting insulin or sulfonylurea or has new renal failure, prolonged observation or admission may be required. In most other cases of medication-induced hypoglycemia, the patients are expediently sent home. As many such patient encounters occur in the early morning hours, EPs need to know how to manage insulin regimens if these patients are to be safely discharged home. Additionally, worsening renal function is a common cause of potentiation of both oral agents and insulin; it is generally worthwhile to check renal function on patients presenting with significant hypoglycemia.
After a significant hypoglycemic event, many guidelines recommend decreasing the daily insulin dose by 10% to 20%. However, with a careful medication history and knowledge of each insulin dose’s activity profile, a physician can often discern which individual insulin dose is responsible for a given hypoglycemic event. That individual daily dose can then be decreased by 20% to better target the cause of the hypoglycemic event.
Conclusion
Diabetes mellitus is one of the most common chronic medical conditions in the United States, and more than 7 million Americans may be living with undiagnosed DM. In the ED setting, physicians regularly encounter patients with undiagnosed type 2 DM. Since treatment is known to prevent the microvascular complications associated with DM, EPs should know the diagnostic criteria and understand the ADA’s inpatient and outpatient treatment recommendations.
- Centers for Disease Control and Prevention. National Diabetes Fact Sheet: National Estimates and General Information on Diabetes and Prediabetes in the United States, 2011. Atlanta, GA: Centers for Disease Control and Prevention, US Department of Health and Human Services; 2011.
- Zhang X, Gregg EW, Williamson DF, et al. A1C level and future risk of diabetes: a systematic review. Diabetes Care. 2010;33(7):1665-1673.
- Ginde AA, Delaney KE, Pallin DJ, Camargo CA Jr. Multicenter survey of emergency physician management and referral for hyperglycemia. J Emerg Med. 2010;38(2):264-270.
- Inzucchi SE, Bergenstal RM, Buse JB, et al; American Diabetes Association (ADA); EuropeanAssociation for the Study of Diabetes (EASD).Management of hyperglycemia in type 2 diabetes:a patient-centered approach. Position statementf the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care. 2012;35(6):1364-1379.
- Mazokopakis EE, Starakis IK. Recommendations for diagnosis and management of metformin-induced vitamin B12 (Cbl) deficiency. Diabetes Res Clin Pract. 2012;97(3):359-367.
- American Diabetes Association. Diagnosis and classification of diabetes mellitus. Diabetes Care. 2014;37(Suppl 1):S81-S90.
- Kotwal N, Pandit A. Variability of capillary blood glucose monitoring measured on home glucose monitoring devices. Indian J Endocrinol Metab. 2012;16(Suppl 2):S248-S251.
- Silverman RA, Thakker U, Ellman T, et al. Hemoglobin A1c as a screen for previously undiagnosed prediabetes and diabetes in an acute-care setting. Diabetes Care. 2011;34(9):1908-1912.
- American Diabetes Association Executive Summary: Standards of medical care in diabetes—2014. Diabetes Care. 2014;37(Supp 1):S5-S13.
- Finfer S, Chittock DR, Su SY, et al; NICE-SUGAR Study Investigators. Intensive versus conventional glucose control in critically ill patients. N Engl J Med. 2009;360(13):1283-1297.
- American Diabetes Association. Standards of medical care in diabetes—2014. Diabetes Care. 2014;37(Suppl 1):S14-S80.
According to the US Centers for Disease Control and Prevention (CDC), in 2011 there were 25.8 million people in the United States living with diabetes mellitus (DM), 90% to 95% of whom had type 2 DM.1 Seven million of those with DM are undiagnosed. In addition, an estimated 79 million adults in the United States have prediabetes, a condition in which glycated hemoglobin (HbA1c) levels are above normal but do not yet meet the diagnostic threshold for DM (≥6.5%).1 This large population with prediabetes, defined by HbA1c levels of 5.7% to 6.4%, has a 5-year risk of progression to diabetes ranging from 9% to 50%; the higher risk is associated with higher HbA1c levels as the disease represents a continuum.2
The benefits of diagnosis and treatment of diabetes—preventing the progression of microvascular complications—are well established. Through medication, exercise, and dietary interventions, the progression of both prediabetes and diabetes can be halted and in many cases reversed.
Given the prevalence of DM in the United States and the clear benefits of treatment, the ability to diagnose DM is important for any physician who may encounter patients with undiagnosed diabetes or prediabetes. This article reviews the management of hyperglycemia relevant to the emergency physician (EP) and discusses the criteria used in diagnosing DM.
The American College of Emergency Physicians (ACEP) currently does not have a clinical policy for the initial treatment of patients with DM that is newly diagnosed in the ED. A 2007 survey of 152 EPs in the United States found that 52% would leave initiation of outpatient treatment of diabetes to a patient’s primary care physician (PCP), regardless of the degree of hyperglycemia noted in the ED.3 Almost paradoxically, among these same EPs, the most common reason for not screening for diabetes (cited by 69%) was the inability to secure follow-up for newly diagnosed patients. Given the fragmentary care many emergency patients receive and the difficulty in assuring close ED follow-up, reviewing the American Diabetes Association (ADA) recommendations for initiation of diabetes management is worthwhile.
ADA Treatment Guidelines
Metformin
Metformin, if tolerated and without contraindications, is the preferred initial pharmacologic agent for all patients with newly diagnosed DM. This drug typically lowers HbA1c by 1.5%, and does not cause weight gain or hypoglycemia associated with some other oral agents (eg, sulfonylureas). Metformin therapy, however, is contraindicated in patients with chronic kidney disease (CKD) (Cr >1.5 in males and >1.4 in females), liver disease, a history of lactic acidosis, and a low-perfusion state. Metformin also should not be used for 48 hours following an intravenous (IV) contrast-enhanced study.
When starting metformin or increasing the dose, patients frequently experience abdominal symptoms, including cramping, nausea, vomiting, and diarrhea. These side effects are usually mild and self-limiting, and they usually resolve within a week. However, patients should be warned of these complications and advised to take metformin with meals to limit side effects. They also should be encouraged to continue the medication through the initial symptoms, if possible.
For a patient with newly diagnosed type 2 DM, a reasonable ED discharge plan is to start metformin at 500 mg daily, taken with a meal. If the patient develops abdominal symptoms, the dose can be reduced to 250 mg daily. Patients should additionally be advised to follow up with their PCP as soon as feasible. Patients can be instructed to increase the dose of metformin on their own. Because the development of gastrointestinal symptoms is the main dose-limiting effect of metformin therapy, it is generally safe to give patients instructions on weekly dose escalation by 500 mg/day to the optimal dose of 1,000 mg twice daily. Although metformin therapy is associated with rare cases of lactic acidosis in patients with CKD, it does not, on its own, cause acute kidney injury; therefore, intense monitoring is not required while doses are increased. Metformin therapy can decrease vitamin B12 absorption, though it rarely results in megaloblastic anemia, and it takes 5 to 10 years for neurological symptoms to manifest.5
Other Treatment Options
The Figure highlights the ADA guidelines on additional pharmacologic agents beyond metformin. When these additional agents are used, the patient should follow-up with a PCP every 3 months to determine how far HbA1c has been lowered. For most patients with DM, the goal for HbA1c is less than 7%. This goal may be raised for elderly patients and those with a history of cardiovascular disease, as these patients are at higher risk for cardiovascular mortality from an episode of hypoglycemia.
The secondary medication options include sulfonylureas, thiazolidinediones, dipeptidyl peptidase-IV inhibitors, glucagon-like peptide-1 (GLP-1) agonists, sodium-glucose cotransporter-2 inhibitors, and insulin. Insulin therapy is the final medication step for all patients with DM who are willing and able to comply with daily injections and who have failed to meet goals through alternative agents.
Before using additional agents beyond metformin, the PCP or endocrinologist should discuss in detail factors such as side effects (ie, weight gain, risk of hypoglycemia), medication delivery (GLP-1 agonists and insulin require injections), and cost with the patient. It is generally advisable not to try to accomplish this medication adjustment in the ED without consultation with a PCP or endocrinologist.
Diagnosis
The clinical presentation of new-onset DM can range from the relatively benign (eg, polyuria, polydipsia, frequent skin infections) to the life-threatening (eg, diabetic ketoacidosis) (Table 1). The classic symptoms of hyperglycemia include polyuria, polydipsia, unexplained weight loss, easy fatigability, dizziness, and blurred vision. Any one of these symptoms should prompt consideration of DM in the differential diagnosis.
Four abnormal laboratory results comprise the ADA’s diagnostic criteria for DM6:
- HbA1c ≥6.5%;
- 8-hour fasting plasma glucose ≥126 mg/dL;
- 2-hour oral glucose tolerance test (OGTT) ≥200 mg/dL (Patient is given 75 g sugar orally; then plasma glucose is drawn 2 hours later); and
- A random plasma glucose of ≥200 mg/dL in association with “classic symptoms” of DM, defined as polyuria, polydipsia, and unexplained weight loss.
In the absence of an unequivocal indicator, such as the patient presenting in diabetic ketoacidosis, the formal diagnosis of DM should not be made unless at least 2 abnormal test results are obtained simultaneously (from a 2-hour OGTT test and an HbA1c panel, for example, or when the same test is repeated one month later and both test results indicate DM).
Limitations of Glucometers
When interpreting test results, keep in mind that the US Food and Drug Administration allows point-of-care (POC) glucometers to have an accuracy of +/- 20%. The POC glucometers measure whole-blood glucose rather than plasma glucose; generally the amount of glucose in plasma is about 10% to 15% higher than the amount in whole blood.7 Therefore, the formal diagnosis of DM relies on laboratory plasma glucose results; POC glucometer results may guide the EP in initiating a workup for DM but should not be among the diagnostic criteria.
HbA1c Testing
The HbA1c percentage represents the preceding 3-month average plasma glucose level. This is due to nonenzymatic glycosylation of Hb, a reaction driven by higher concentrations of circulating plasma glucose. The HbA1c can be falsely low in states of high red blood cell (RBC) turnover, such as ongoing blood loss or the RBC fragility seen in hemoglobinopathies. Patients who have had RBC transfusions in the preceding months will have inaccurate HbA1c test results as well.
Keeping these test characteristics in mind, the HbA1c test may be more useful than glucose-based testing strategies in diagnosing diabetes in the ED. Hyperglycemia can be observed in nondiabetic emergency patients undergoing a stress response, since gluconeogenesis and glycogenolysis are normal hepatic stress responses to circulating epinephrine and cortisol. Unless a patient is on chronic steroids, the HbA1c is not similarly affected.
A recent study of ED patients using HbA1c as the sole screening modality found that test characteristics for ED patients were similar to those for patients in typical outpatient settings. HbA1c of 6.5 or greater yielded a sensitivity of 54% and a specificity of 96% in diagnosing diabetes.8 The availability of test results at the time of the emergency visit depends upon the individual hospital laboratory, but most labs run the test itself in less than an hour. Emergency physicians working in hospitals that perform the test will often have the test results prior to patient discharge.
Inpatient Management
Managing a patient with newly diagnosed DM that requires admission to the hospital is different from managing a patient who can be treated as an outpatient. The ADA-recommended treatment regimen for DM in the inpatient setting focuses on the use of insulin. While type 1 DM, by definition, requires insulin treatment, many patients with type 2 DM are treated with oral agents only as outpatients. However, because of complications associated with the use of oral agents in low renal perfusion states (such as during surgery, during IV contrast-enhanced studies, or when the admitting condition causes shock), the ADA generally does not prefer oral agents for inpatient glycemic control. Metformin particularly should not be used in the inpatient setting, due to increased risk of lactic acidosis.
The preferred insulin regimen for noncritically ill diabetic inpatients consists of scheduled subcutaneous therapy with basal, nutritional, and correctional components.9 Because absorption from subcutaneous tissue varies among critically ill patients, the ADA recommends an IV insulin therapy protocol for ICU patients with diabetes. The NICE SUGAR trial found that the overall risk of death was 2.6% higher among patients treated with an intensive insulin therapy regimen (finger stick blood glucose goal 80-108 mg/dL) than it was among patients treated using standard therapy with a goal of less than 180 mg/dL, a statistically significant difference.10 These results form the basis for the ADA-recommended inpatient glycemic target of 140 to 180 mg/dL among critically ill patients.11 While no definitive evidence exists to guide glycemic control among noncritically ill inpatients, the strategy applied to critically ill patients can be extrapolated to other hospitalized patients because the ADA recommends treatment to keep finger stick blood glucose values below 180 mg/dL.
Hypoglycemia
Often a hypoglycemic event can clearly be correlated to a missed meal. This may only require re-education of the patient about the need to be consistent in the timing of his or her dietary regimen. However, often a hypoglycemic event is not clearly related to a missed meal. When a patient has recently taken a long-acting insulin or sulfonylurea or has new renal failure, prolonged observation or admission may be required. In most other cases of medication-induced hypoglycemia, the patients are expediently sent home. As many such patient encounters occur in the early morning hours, EPs need to know how to manage insulin regimens if these patients are to be safely discharged home. Additionally, worsening renal function is a common cause of potentiation of both oral agents and insulin; it is generally worthwhile to check renal function on patients presenting with significant hypoglycemia.
After a significant hypoglycemic event, many guidelines recommend decreasing the daily insulin dose by 10% to 20%. However, with a careful medication history and knowledge of each insulin dose’s activity profile, a physician can often discern which individual insulin dose is responsible for a given hypoglycemic event. That individual daily dose can then be decreased by 20% to better target the cause of the hypoglycemic event.
Conclusion
Diabetes mellitus is one of the most common chronic medical conditions in the United States, and more than 7 million Americans may be living with undiagnosed DM. In the ED setting, physicians regularly encounter patients with undiagnosed type 2 DM. Since treatment is known to prevent the microvascular complications associated with DM, EPs should know the diagnostic criteria and understand the ADA’s inpatient and outpatient treatment recommendations.
According to the US Centers for Disease Control and Prevention (CDC), in 2011 there were 25.8 million people in the United States living with diabetes mellitus (DM), 90% to 95% of whom had type 2 DM.1 Seven million of those with DM are undiagnosed. In addition, an estimated 79 million adults in the United States have prediabetes, a condition in which glycated hemoglobin (HbA1c) levels are above normal but do not yet meet the diagnostic threshold for DM (≥6.5%).1 This large population with prediabetes, defined by HbA1c levels of 5.7% to 6.4%, has a 5-year risk of progression to diabetes ranging from 9% to 50%; the higher risk is associated with higher HbA1c levels as the disease represents a continuum.2
The benefits of diagnosis and treatment of diabetes—preventing the progression of microvascular complications—are well established. Through medication, exercise, and dietary interventions, the progression of both prediabetes and diabetes can be halted and in many cases reversed.
Given the prevalence of DM in the United States and the clear benefits of treatment, the ability to diagnose DM is important for any physician who may encounter patients with undiagnosed diabetes or prediabetes. This article reviews the management of hyperglycemia relevant to the emergency physician (EP) and discusses the criteria used in diagnosing DM.
The American College of Emergency Physicians (ACEP) currently does not have a clinical policy for the initial treatment of patients with DM that is newly diagnosed in the ED. A 2007 survey of 152 EPs in the United States found that 52% would leave initiation of outpatient treatment of diabetes to a patient’s primary care physician (PCP), regardless of the degree of hyperglycemia noted in the ED.3 Almost paradoxically, among these same EPs, the most common reason for not screening for diabetes (cited by 69%) was the inability to secure follow-up for newly diagnosed patients. Given the fragmentary care many emergency patients receive and the difficulty in assuring close ED follow-up, reviewing the American Diabetes Association (ADA) recommendations for initiation of diabetes management is worthwhile.
ADA Treatment Guidelines
Metformin
Metformin, if tolerated and without contraindications, is the preferred initial pharmacologic agent for all patients with newly diagnosed DM. This drug typically lowers HbA1c by 1.5%, and does not cause weight gain or hypoglycemia associated with some other oral agents (eg, sulfonylureas). Metformin therapy, however, is contraindicated in patients with chronic kidney disease (CKD) (Cr >1.5 in males and >1.4 in females), liver disease, a history of lactic acidosis, and a low-perfusion state. Metformin also should not be used for 48 hours following an intravenous (IV) contrast-enhanced study.
When starting metformin or increasing the dose, patients frequently experience abdominal symptoms, including cramping, nausea, vomiting, and diarrhea. These side effects are usually mild and self-limiting, and they usually resolve within a week. However, patients should be warned of these complications and advised to take metformin with meals to limit side effects. They also should be encouraged to continue the medication through the initial symptoms, if possible.
For a patient with newly diagnosed type 2 DM, a reasonable ED discharge plan is to start metformin at 500 mg daily, taken with a meal. If the patient develops abdominal symptoms, the dose can be reduced to 250 mg daily. Patients should additionally be advised to follow up with their PCP as soon as feasible. Patients can be instructed to increase the dose of metformin on their own. Because the development of gastrointestinal symptoms is the main dose-limiting effect of metformin therapy, it is generally safe to give patients instructions on weekly dose escalation by 500 mg/day to the optimal dose of 1,000 mg twice daily. Although metformin therapy is associated with rare cases of lactic acidosis in patients with CKD, it does not, on its own, cause acute kidney injury; therefore, intense monitoring is not required while doses are increased. Metformin therapy can decrease vitamin B12 absorption, though it rarely results in megaloblastic anemia, and it takes 5 to 10 years for neurological symptoms to manifest.5
Other Treatment Options
The Figure highlights the ADA guidelines on additional pharmacologic agents beyond metformin. When these additional agents are used, the patient should follow-up with a PCP every 3 months to determine how far HbA1c has been lowered. For most patients with DM, the goal for HbA1c is less than 7%. This goal may be raised for elderly patients and those with a history of cardiovascular disease, as these patients are at higher risk for cardiovascular mortality from an episode of hypoglycemia.
The secondary medication options include sulfonylureas, thiazolidinediones, dipeptidyl peptidase-IV inhibitors, glucagon-like peptide-1 (GLP-1) agonists, sodium-glucose cotransporter-2 inhibitors, and insulin. Insulin therapy is the final medication step for all patients with DM who are willing and able to comply with daily injections and who have failed to meet goals through alternative agents.
Before using additional agents beyond metformin, the PCP or endocrinologist should discuss in detail factors such as side effects (ie, weight gain, risk of hypoglycemia), medication delivery (GLP-1 agonists and insulin require injections), and cost with the patient. It is generally advisable not to try to accomplish this medication adjustment in the ED without consultation with a PCP or endocrinologist.
Diagnosis
The clinical presentation of new-onset DM can range from the relatively benign (eg, polyuria, polydipsia, frequent skin infections) to the life-threatening (eg, diabetic ketoacidosis) (Table 1). The classic symptoms of hyperglycemia include polyuria, polydipsia, unexplained weight loss, easy fatigability, dizziness, and blurred vision. Any one of these symptoms should prompt consideration of DM in the differential diagnosis.
Four abnormal laboratory results comprise the ADA’s diagnostic criteria for DM6:
- HbA1c ≥6.5%;
- 8-hour fasting plasma glucose ≥126 mg/dL;
- 2-hour oral glucose tolerance test (OGTT) ≥200 mg/dL (Patient is given 75 g sugar orally; then plasma glucose is drawn 2 hours later); and
- A random plasma glucose of ≥200 mg/dL in association with “classic symptoms” of DM, defined as polyuria, polydipsia, and unexplained weight loss.
In the absence of an unequivocal indicator, such as the patient presenting in diabetic ketoacidosis, the formal diagnosis of DM should not be made unless at least 2 abnormal test results are obtained simultaneously (from a 2-hour OGTT test and an HbA1c panel, for example, or when the same test is repeated one month later and both test results indicate DM).
Limitations of Glucometers
When interpreting test results, keep in mind that the US Food and Drug Administration allows point-of-care (POC) glucometers to have an accuracy of +/- 20%. The POC glucometers measure whole-blood glucose rather than plasma glucose; generally the amount of glucose in plasma is about 10% to 15% higher than the amount in whole blood.7 Therefore, the formal diagnosis of DM relies on laboratory plasma glucose results; POC glucometer results may guide the EP in initiating a workup for DM but should not be among the diagnostic criteria.
HbA1c Testing
The HbA1c percentage represents the preceding 3-month average plasma glucose level. This is due to nonenzymatic glycosylation of Hb, a reaction driven by higher concentrations of circulating plasma glucose. The HbA1c can be falsely low in states of high red blood cell (RBC) turnover, such as ongoing blood loss or the RBC fragility seen in hemoglobinopathies. Patients who have had RBC transfusions in the preceding months will have inaccurate HbA1c test results as well.
Keeping these test characteristics in mind, the HbA1c test may be more useful than glucose-based testing strategies in diagnosing diabetes in the ED. Hyperglycemia can be observed in nondiabetic emergency patients undergoing a stress response, since gluconeogenesis and glycogenolysis are normal hepatic stress responses to circulating epinephrine and cortisol. Unless a patient is on chronic steroids, the HbA1c is not similarly affected.
A recent study of ED patients using HbA1c as the sole screening modality found that test characteristics for ED patients were similar to those for patients in typical outpatient settings. HbA1c of 6.5 or greater yielded a sensitivity of 54% and a specificity of 96% in diagnosing diabetes.8 The availability of test results at the time of the emergency visit depends upon the individual hospital laboratory, but most labs run the test itself in less than an hour. Emergency physicians working in hospitals that perform the test will often have the test results prior to patient discharge.
Inpatient Management
Managing a patient with newly diagnosed DM that requires admission to the hospital is different from managing a patient who can be treated as an outpatient. The ADA-recommended treatment regimen for DM in the inpatient setting focuses on the use of insulin. While type 1 DM, by definition, requires insulin treatment, many patients with type 2 DM are treated with oral agents only as outpatients. However, because of complications associated with the use of oral agents in low renal perfusion states (such as during surgery, during IV contrast-enhanced studies, or when the admitting condition causes shock), the ADA generally does not prefer oral agents for inpatient glycemic control. Metformin particularly should not be used in the inpatient setting, due to increased risk of lactic acidosis.
The preferred insulin regimen for noncritically ill diabetic inpatients consists of scheduled subcutaneous therapy with basal, nutritional, and correctional components.9 Because absorption from subcutaneous tissue varies among critically ill patients, the ADA recommends an IV insulin therapy protocol for ICU patients with diabetes. The NICE SUGAR trial found that the overall risk of death was 2.6% higher among patients treated with an intensive insulin therapy regimen (finger stick blood glucose goal 80-108 mg/dL) than it was among patients treated using standard therapy with a goal of less than 180 mg/dL, a statistically significant difference.10 These results form the basis for the ADA-recommended inpatient glycemic target of 140 to 180 mg/dL among critically ill patients.11 While no definitive evidence exists to guide glycemic control among noncritically ill inpatients, the strategy applied to critically ill patients can be extrapolated to other hospitalized patients because the ADA recommends treatment to keep finger stick blood glucose values below 180 mg/dL.
Hypoglycemia
Often a hypoglycemic event can clearly be correlated to a missed meal. This may only require re-education of the patient about the need to be consistent in the timing of his or her dietary regimen. However, often a hypoglycemic event is not clearly related to a missed meal. When a patient has recently taken a long-acting insulin or sulfonylurea or has new renal failure, prolonged observation or admission may be required. In most other cases of medication-induced hypoglycemia, the patients are expediently sent home. As many such patient encounters occur in the early morning hours, EPs need to know how to manage insulin regimens if these patients are to be safely discharged home. Additionally, worsening renal function is a common cause of potentiation of both oral agents and insulin; it is generally worthwhile to check renal function on patients presenting with significant hypoglycemia.
After a significant hypoglycemic event, many guidelines recommend decreasing the daily insulin dose by 10% to 20%. However, with a careful medication history and knowledge of each insulin dose’s activity profile, a physician can often discern which individual insulin dose is responsible for a given hypoglycemic event. That individual daily dose can then be decreased by 20% to better target the cause of the hypoglycemic event.
Conclusion
Diabetes mellitus is one of the most common chronic medical conditions in the United States, and more than 7 million Americans may be living with undiagnosed DM. In the ED setting, physicians regularly encounter patients with undiagnosed type 2 DM. Since treatment is known to prevent the microvascular complications associated with DM, EPs should know the diagnostic criteria and understand the ADA’s inpatient and outpatient treatment recommendations.
- Centers for Disease Control and Prevention. National Diabetes Fact Sheet: National Estimates and General Information on Diabetes and Prediabetes in the United States, 2011. Atlanta, GA: Centers for Disease Control and Prevention, US Department of Health and Human Services; 2011.
- Zhang X, Gregg EW, Williamson DF, et al. A1C level and future risk of diabetes: a systematic review. Diabetes Care. 2010;33(7):1665-1673.
- Ginde AA, Delaney KE, Pallin DJ, Camargo CA Jr. Multicenter survey of emergency physician management and referral for hyperglycemia. J Emerg Med. 2010;38(2):264-270.
- Inzucchi SE, Bergenstal RM, Buse JB, et al; American Diabetes Association (ADA); EuropeanAssociation for the Study of Diabetes (EASD).Management of hyperglycemia in type 2 diabetes:a patient-centered approach. Position statementf the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care. 2012;35(6):1364-1379.
- Mazokopakis EE, Starakis IK. Recommendations for diagnosis and management of metformin-induced vitamin B12 (Cbl) deficiency. Diabetes Res Clin Pract. 2012;97(3):359-367.
- American Diabetes Association. Diagnosis and classification of diabetes mellitus. Diabetes Care. 2014;37(Suppl 1):S81-S90.
- Kotwal N, Pandit A. Variability of capillary blood glucose monitoring measured on home glucose monitoring devices. Indian J Endocrinol Metab. 2012;16(Suppl 2):S248-S251.
- Silverman RA, Thakker U, Ellman T, et al. Hemoglobin A1c as a screen for previously undiagnosed prediabetes and diabetes in an acute-care setting. Diabetes Care. 2011;34(9):1908-1912.
- American Diabetes Association Executive Summary: Standards of medical care in diabetes—2014. Diabetes Care. 2014;37(Supp 1):S5-S13.
- Finfer S, Chittock DR, Su SY, et al; NICE-SUGAR Study Investigators. Intensive versus conventional glucose control in critically ill patients. N Engl J Med. 2009;360(13):1283-1297.
- American Diabetes Association. Standards of medical care in diabetes—2014. Diabetes Care. 2014;37(Suppl 1):S14-S80.
- Centers for Disease Control and Prevention. National Diabetes Fact Sheet: National Estimates and General Information on Diabetes and Prediabetes in the United States, 2011. Atlanta, GA: Centers for Disease Control and Prevention, US Department of Health and Human Services; 2011.
- Zhang X, Gregg EW, Williamson DF, et al. A1C level and future risk of diabetes: a systematic review. Diabetes Care. 2010;33(7):1665-1673.
- Ginde AA, Delaney KE, Pallin DJ, Camargo CA Jr. Multicenter survey of emergency physician management and referral for hyperglycemia. J Emerg Med. 2010;38(2):264-270.
- Inzucchi SE, Bergenstal RM, Buse JB, et al; American Diabetes Association (ADA); EuropeanAssociation for the Study of Diabetes (EASD).Management of hyperglycemia in type 2 diabetes:a patient-centered approach. Position statementf the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care. 2012;35(6):1364-1379.
- Mazokopakis EE, Starakis IK. Recommendations for diagnosis and management of metformin-induced vitamin B12 (Cbl) deficiency. Diabetes Res Clin Pract. 2012;97(3):359-367.
- American Diabetes Association. Diagnosis and classification of diabetes mellitus. Diabetes Care. 2014;37(Suppl 1):S81-S90.
- Kotwal N, Pandit A. Variability of capillary blood glucose monitoring measured on home glucose monitoring devices. Indian J Endocrinol Metab. 2012;16(Suppl 2):S248-S251.
- Silverman RA, Thakker U, Ellman T, et al. Hemoglobin A1c as a screen for previously undiagnosed prediabetes and diabetes in an acute-care setting. Diabetes Care. 2011;34(9):1908-1912.
- American Diabetes Association Executive Summary: Standards of medical care in diabetes—2014. Diabetes Care. 2014;37(Supp 1):S5-S13.
- Finfer S, Chittock DR, Su SY, et al; NICE-SUGAR Study Investigators. Intensive versus conventional glucose control in critically ill patients. N Engl J Med. 2009;360(13):1283-1297.
- American Diabetes Association. Standards of medical care in diabetes—2014. Diabetes Care. 2014;37(Suppl 1):S14-S80.
