User login
Infants with an undescended testis should be referred between ages 6 and 15 months, since almost all who experience spontaneous descent do so by 6 months (strength of recommendation [SOR]: A, extrapolation from cohort studies).
The incidence of germ cell aplasia in undescended testes begins to rise at 15 months (SOR: C, extrapolation of observational studies); however, evidence is inconclusive that orchiopexy at this age results in higher rates of paternity success (SOR: B, retrospective cohort study).
Orchiopexy may allow earlier detection of testicular tumors (SOR: C, expert opinion), but it has not been shown to reduce the risk of testicular cancer (SOR: B, retrospective cohort study) or improve 5-year survival rates for those patients diagnosed with testicular cancer (SOR: B, retrospective cohort study).
Periodically evaluate a newborn’s scrotum for either an undescended or reascended testicle
Danny Thomason, DO
Oklahoma State University, Tulsa
This Inquiry highlights 2 important considerations regarding the child with a cryptorchid testis. First, periodically evaluate the newborn and infant patient’s scrotum for either an undescended or reascended testicle. In my practice at Oklahoma State University Family Medicine Residency, I ask residents to perform the scrotal examination at birth, at every well-child visit up to 1 year of age, and then yearly thereafter. During puberty, these exams serve as opportunities to educate patients about testicular self-examination.
Secondly, as the authors indicate, there is some disagreement in the literature as to the risk of testicular cancer following orchiopexy for cryptorchidism. However, surgical repair is likely to facilitate regular testicular self-examination, which could increase the likelihood of detection of cancer during young adulthood.
Evidence summary
Three large cohort studies determined that cryptorchidism (FIGURE) is present at birth in approximately 3% of term infants (higher in preterm infants), with spontaneous descent occurring in two thirds of cases by age 3 to 6 months. One study1 of 10,730 consecutive male term infants found cryptorchidism at birth in 2.7%, dropping to 1.22% by 6 months of age, but without further change at 1 year. A similar study2 followed 6935 infant boys, finding cryptorchidism at birth in 3.7%, which decreased to 1% at 3 months and remained unchanged at 1 year. A third study3 found cryptorchidism at birth in 90 of 6414 (2.7%) infant boys. At follow-up, 45 of 90 had testicular descent at 1 month, 60 of 90 at 3 months, 67 of 90 at 9 months and at 1 year.
The 2 main indications for orchiopexy are potential avoidance of infertility and early detection and treatment of testicular cancer. A literature review4 of fertility after orchiopexy for undescended testis found inconclusive results. While epidemiological and pathological data (testicular biopsy, hormonal analysis, and sperm counts performed after orchiopexy) predict diminished fertility potential for men with unilaterally undescended testes, studies evaluating paternity find no difference from normal men. Biopsy studies of undescended testes at the time of orchiopexy show increased incidence of germ cell aplasia with older age at surgery (0.5%, 2%, 20%, and 45% at 6, 12, 24, and 48 months, respectively).4 A retrospective cohort study5 found 87% successful paternity after orchiopexy for 24 patients with unilateral undescended testis and 33% success for 9 with bilateral undescended testes but there was no normal control group. The boys were aged 1 to 14 years (mean, 7 years) at surgery, and there was no relationship between timing of orchiopexy and paternity success.5
The benefits of orchiopexy for testicular cancer are also unclear; expert opinion suggests that orchiopexy may allow earlier detection of testicular tumors.6 A cohort study7 of boys with cryptorchidism showed an increased risk of testicular cancer (relative risk=5.2). However, risk did not decrease after orchiopexy in early childhood. A retrospective cohort study8 of 137 men with cryptorchidism who developed testicular cancer found no difference in 5-year survival between those who had orchiopexy (at ages 2 to 42) and those who had not (61% vs 63%, respectively).
FIGURE
Cryptorchidism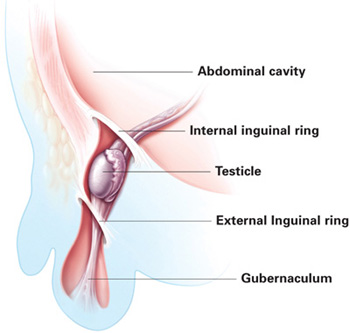
In most cases of cryptorchidism, the testis will be inguinal or prescrotal. A smaller number of cases are ectopic (have left the inguinal ring), abdominal, or absent. ILLUSTRATION BY RICH LaROCCO
Recommendations from others
The American Academy of Pediatrics policy section on urology says that spontaneous descent after 6 months is unlikely and recommends orchiopexy by 1 year of age.9
1. Ghirri P, Ciulli C, Vuerich M, et al. Incidence at birth and natural history of cryptorchidism: a study of 10,730 consecutive male infants. J Endocrinol Invest 2002;25:709-715.
2. Berkowitz GS, Lapinski RH, Dolgin MD, et al. Prevalence and natural history of cryptorchidism. Pediatrics 1993;92:44-49.
3. Scorer CG. The descent of the testis. Arch Dis Childhood 1964;39:605-609.
4. Husmann DA. Cryptorchidism. In: Belman AB, King LR, Kramer SA, eds. Clinical Pediatric Urology. 4th ed. London, UK: Martin Dunitz Ltd.; 2002: 1125–1154.
5. Cendron M, Keating MA, Huff DS, Koop CE, Snyder HM, 3rd, Duckett JW. Cryptorchidism, orchiopexy and infertility: a critical long-term retrospective analysis. J Urol 1989;142(2 pt 2):559-562.
6. Docimo SG, Silver RI, Cromie W. The undescended testicle: diagnosis and management. Am Fam Physician 2000;62:2037-2048.
7. Prener A, Engholm G, Jensen OM. Genital anomalies and risk for testicular cancer in Danish men. Epidemiology 1996;7:14-19.
8. Batata MA, Chu FC, Hilaris BS, Whitmore WF, Golbey RB. Testicular cancer in cryptorchids. Cancer 1982;49:1023-1030.
9. American Academy of Pediatrics Policy Statement. Timing of elective surgery on the genitalia of male children with particular reference to the risks, benefits, and psychological effects of surgery and anesthesia. Pediatrics 1996;97:590-594.
Infants with an undescended testis should be referred between ages 6 and 15 months, since almost all who experience spontaneous descent do so by 6 months (strength of recommendation [SOR]: A, extrapolation from cohort studies).
The incidence of germ cell aplasia in undescended testes begins to rise at 15 months (SOR: C, extrapolation of observational studies); however, evidence is inconclusive that orchiopexy at this age results in higher rates of paternity success (SOR: B, retrospective cohort study).
Orchiopexy may allow earlier detection of testicular tumors (SOR: C, expert opinion), but it has not been shown to reduce the risk of testicular cancer (SOR: B, retrospective cohort study) or improve 5-year survival rates for those patients diagnosed with testicular cancer (SOR: B, retrospective cohort study).
Periodically evaluate a newborn’s scrotum for either an undescended or reascended testicle
Danny Thomason, DO
Oklahoma State University, Tulsa
This Inquiry highlights 2 important considerations regarding the child with a cryptorchid testis. First, periodically evaluate the newborn and infant patient’s scrotum for either an undescended or reascended testicle. In my practice at Oklahoma State University Family Medicine Residency, I ask residents to perform the scrotal examination at birth, at every well-child visit up to 1 year of age, and then yearly thereafter. During puberty, these exams serve as opportunities to educate patients about testicular self-examination.
Secondly, as the authors indicate, there is some disagreement in the literature as to the risk of testicular cancer following orchiopexy for cryptorchidism. However, surgical repair is likely to facilitate regular testicular self-examination, which could increase the likelihood of detection of cancer during young adulthood.
Evidence summary
Three large cohort studies determined that cryptorchidism (FIGURE) is present at birth in approximately 3% of term infants (higher in preterm infants), with spontaneous descent occurring in two thirds of cases by age 3 to 6 months. One study1 of 10,730 consecutive male term infants found cryptorchidism at birth in 2.7%, dropping to 1.22% by 6 months of age, but without further change at 1 year. A similar study2 followed 6935 infant boys, finding cryptorchidism at birth in 3.7%, which decreased to 1% at 3 months and remained unchanged at 1 year. A third study3 found cryptorchidism at birth in 90 of 6414 (2.7%) infant boys. At follow-up, 45 of 90 had testicular descent at 1 month, 60 of 90 at 3 months, 67 of 90 at 9 months and at 1 year.
The 2 main indications for orchiopexy are potential avoidance of infertility and early detection and treatment of testicular cancer. A literature review4 of fertility after orchiopexy for undescended testis found inconclusive results. While epidemiological and pathological data (testicular biopsy, hormonal analysis, and sperm counts performed after orchiopexy) predict diminished fertility potential for men with unilaterally undescended testes, studies evaluating paternity find no difference from normal men. Biopsy studies of undescended testes at the time of orchiopexy show increased incidence of germ cell aplasia with older age at surgery (0.5%, 2%, 20%, and 45% at 6, 12, 24, and 48 months, respectively).4 A retrospective cohort study5 found 87% successful paternity after orchiopexy for 24 patients with unilateral undescended testis and 33% success for 9 with bilateral undescended testes but there was no normal control group. The boys were aged 1 to 14 years (mean, 7 years) at surgery, and there was no relationship between timing of orchiopexy and paternity success.5
The benefits of orchiopexy for testicular cancer are also unclear; expert opinion suggests that orchiopexy may allow earlier detection of testicular tumors.6 A cohort study7 of boys with cryptorchidism showed an increased risk of testicular cancer (relative risk=5.2). However, risk did not decrease after orchiopexy in early childhood. A retrospective cohort study8 of 137 men with cryptorchidism who developed testicular cancer found no difference in 5-year survival between those who had orchiopexy (at ages 2 to 42) and those who had not (61% vs 63%, respectively).
FIGURE
Cryptorchidism
In most cases of cryptorchidism, the testis will be inguinal or prescrotal. A smaller number of cases are ectopic (have left the inguinal ring), abdominal, or absent. ILLUSTRATION BY RICH LaROCCO
Recommendations from others
The American Academy of Pediatrics policy section on urology says that spontaneous descent after 6 months is unlikely and recommends orchiopexy by 1 year of age.9
Infants with an undescended testis should be referred between ages 6 and 15 months, since almost all who experience spontaneous descent do so by 6 months (strength of recommendation [SOR]: A, extrapolation from cohort studies).
The incidence of germ cell aplasia in undescended testes begins to rise at 15 months (SOR: C, extrapolation of observational studies); however, evidence is inconclusive that orchiopexy at this age results in higher rates of paternity success (SOR: B, retrospective cohort study).
Orchiopexy may allow earlier detection of testicular tumors (SOR: C, expert opinion), but it has not been shown to reduce the risk of testicular cancer (SOR: B, retrospective cohort study) or improve 5-year survival rates for those patients diagnosed with testicular cancer (SOR: B, retrospective cohort study).
Periodically evaluate a newborn’s scrotum for either an undescended or reascended testicle
Danny Thomason, DO
Oklahoma State University, Tulsa
This Inquiry highlights 2 important considerations regarding the child with a cryptorchid testis. First, periodically evaluate the newborn and infant patient’s scrotum for either an undescended or reascended testicle. In my practice at Oklahoma State University Family Medicine Residency, I ask residents to perform the scrotal examination at birth, at every well-child visit up to 1 year of age, and then yearly thereafter. During puberty, these exams serve as opportunities to educate patients about testicular self-examination.
Secondly, as the authors indicate, there is some disagreement in the literature as to the risk of testicular cancer following orchiopexy for cryptorchidism. However, surgical repair is likely to facilitate regular testicular self-examination, which could increase the likelihood of detection of cancer during young adulthood.
Evidence summary
Three large cohort studies determined that cryptorchidism (FIGURE) is present at birth in approximately 3% of term infants (higher in preterm infants), with spontaneous descent occurring in two thirds of cases by age 3 to 6 months. One study1 of 10,730 consecutive male term infants found cryptorchidism at birth in 2.7%, dropping to 1.22% by 6 months of age, but without further change at 1 year. A similar study2 followed 6935 infant boys, finding cryptorchidism at birth in 3.7%, which decreased to 1% at 3 months and remained unchanged at 1 year. A third study3 found cryptorchidism at birth in 90 of 6414 (2.7%) infant boys. At follow-up, 45 of 90 had testicular descent at 1 month, 60 of 90 at 3 months, 67 of 90 at 9 months and at 1 year.
The 2 main indications for orchiopexy are potential avoidance of infertility and early detection and treatment of testicular cancer. A literature review4 of fertility after orchiopexy for undescended testis found inconclusive results. While epidemiological and pathological data (testicular biopsy, hormonal analysis, and sperm counts performed after orchiopexy) predict diminished fertility potential for men with unilaterally undescended testes, studies evaluating paternity find no difference from normal men. Biopsy studies of undescended testes at the time of orchiopexy show increased incidence of germ cell aplasia with older age at surgery (0.5%, 2%, 20%, and 45% at 6, 12, 24, and 48 months, respectively).4 A retrospective cohort study5 found 87% successful paternity after orchiopexy for 24 patients with unilateral undescended testis and 33% success for 9 with bilateral undescended testes but there was no normal control group. The boys were aged 1 to 14 years (mean, 7 years) at surgery, and there was no relationship between timing of orchiopexy and paternity success.5
The benefits of orchiopexy for testicular cancer are also unclear; expert opinion suggests that orchiopexy may allow earlier detection of testicular tumors.6 A cohort study7 of boys with cryptorchidism showed an increased risk of testicular cancer (relative risk=5.2). However, risk did not decrease after orchiopexy in early childhood. A retrospective cohort study8 of 137 men with cryptorchidism who developed testicular cancer found no difference in 5-year survival between those who had orchiopexy (at ages 2 to 42) and those who had not (61% vs 63%, respectively).
FIGURE
Cryptorchidism
In most cases of cryptorchidism, the testis will be inguinal or prescrotal. A smaller number of cases are ectopic (have left the inguinal ring), abdominal, or absent. ILLUSTRATION BY RICH LaROCCO
Recommendations from others
The American Academy of Pediatrics policy section on urology says that spontaneous descent after 6 months is unlikely and recommends orchiopexy by 1 year of age.9
1. Ghirri P, Ciulli C, Vuerich M, et al. Incidence at birth and natural history of cryptorchidism: a study of 10,730 consecutive male infants. J Endocrinol Invest 2002;25:709-715.
2. Berkowitz GS, Lapinski RH, Dolgin MD, et al. Prevalence and natural history of cryptorchidism. Pediatrics 1993;92:44-49.
3. Scorer CG. The descent of the testis. Arch Dis Childhood 1964;39:605-609.
4. Husmann DA. Cryptorchidism. In: Belman AB, King LR, Kramer SA, eds. Clinical Pediatric Urology. 4th ed. London, UK: Martin Dunitz Ltd.; 2002: 1125–1154.
5. Cendron M, Keating MA, Huff DS, Koop CE, Snyder HM, 3rd, Duckett JW. Cryptorchidism, orchiopexy and infertility: a critical long-term retrospective analysis. J Urol 1989;142(2 pt 2):559-562.
6. Docimo SG, Silver RI, Cromie W. The undescended testicle: diagnosis and management. Am Fam Physician 2000;62:2037-2048.
7. Prener A, Engholm G, Jensen OM. Genital anomalies and risk for testicular cancer in Danish men. Epidemiology 1996;7:14-19.
8. Batata MA, Chu FC, Hilaris BS, Whitmore WF, Golbey RB. Testicular cancer in cryptorchids. Cancer 1982;49:1023-1030.
9. American Academy of Pediatrics Policy Statement. Timing of elective surgery on the genitalia of male children with particular reference to the risks, benefits, and psychological effects of surgery and anesthesia. Pediatrics 1996;97:590-594.
1. Ghirri P, Ciulli C, Vuerich M, et al. Incidence at birth and natural history of cryptorchidism: a study of 10,730 consecutive male infants. J Endocrinol Invest 2002;25:709-715.
2. Berkowitz GS, Lapinski RH, Dolgin MD, et al. Prevalence and natural history of cryptorchidism. Pediatrics 1993;92:44-49.
3. Scorer CG. The descent of the testis. Arch Dis Childhood 1964;39:605-609.
4. Husmann DA. Cryptorchidism. In: Belman AB, King LR, Kramer SA, eds. Clinical Pediatric Urology. 4th ed. London, UK: Martin Dunitz Ltd.; 2002: 1125–1154.
5. Cendron M, Keating MA, Huff DS, Koop CE, Snyder HM, 3rd, Duckett JW. Cryptorchidism, orchiopexy and infertility: a critical long-term retrospective analysis. J Urol 1989;142(2 pt 2):559-562.
6. Docimo SG, Silver RI, Cromie W. The undescended testicle: diagnosis and management. Am Fam Physician 2000;62:2037-2048.
7. Prener A, Engholm G, Jensen OM. Genital anomalies and risk for testicular cancer in Danish men. Epidemiology 1996;7:14-19.
8. Batata MA, Chu FC, Hilaris BS, Whitmore WF, Golbey RB. Testicular cancer in cryptorchids. Cancer 1982;49:1023-1030.
9. American Academy of Pediatrics Policy Statement. Timing of elective surgery on the genitalia of male children with particular reference to the risks, benefits, and psychological effects of surgery and anesthesia. Pediatrics 1996;97:590-594.
Evidence-based answers from the Family Physicians Inquiries Network