User login
Welcome to Current Psychiatry, a leading source of information, online and in print, for practitioners of psychiatry and its related subspecialties, including addiction psychiatry, child and adolescent psychiatry, and geriatric psychiatry. This Web site contains evidence-based reviews of the prevention, diagnosis, and treatment of mental illness and psychological disorders; case reports; updates on psychopharmacology; news about the specialty of psychiatry; pearls for practice; and other topics of interest and use to this audience.
Dear Drupal User: You're seeing this because you're logged in to Drupal, and not redirected to MDedge.com/psychiatry.
Depression
adolescent depression
adolescent major depressive disorder
adolescent schizophrenia
adolescent with major depressive disorder
animals
autism
baby
brexpiprazole
child
child bipolar
child depression
child schizophrenia
children with bipolar disorder
children with depression
children with major depressive disorder
compulsive behaviors
cure
elderly bipolar
elderly depression
elderly major depressive disorder
elderly schizophrenia
elderly with dementia
first break
first episode
gambling
gaming
geriatric depression
geriatric major depressive disorder
geriatric schizophrenia
infant
kid
major depressive disorder
major depressive disorder in adolescents
major depressive disorder in children
parenting
pediatric
pediatric bipolar
pediatric depression
pediatric major depressive disorder
pediatric schizophrenia
pregnancy
pregnant
rexulti
skin care
teen
wine
section[contains(@class, 'nav-hidden')]
footer[@id='footer']
div[contains(@class, 'pane-pub-article-current-psychiatry')]
div[contains(@class, 'pane-pub-home-current-psychiatry')]
div[contains(@class, 'pane-pub-topic-current-psychiatry')]
div[contains(@class, 'panel-panel-inner')]
div[contains(@class, 'pane-node-field-article-topics')]
section[contains(@class, 'footer-nav-section-wrapper')]
Our mission: ‘Operation Healing’
Three years after the U.S.-led invasion of Iraq, psychiatrists on the home front are dealing with the war’s neuropsychiatric casualties. We are seeing veterans, their families, friends, and acquaintances, whether we practice in VA medical centers, military medicine, or the community.
To help us, Drs. Timothy Lineberry, Sriram Ramaswamy, J. Michael Bostwick, and James Rundell offer tools to screen for and treat combat-related posttraumatic stress disorder, including PTSD of military sexual trauma. Dr. John Daniels tells which medications may do more harm than good for patients with traumatic brain injury.
World War II brought psychiatric disorders home, showing that not just “crazy people” develop psychiatric symptoms. A half-million U.S. troops were admitted for psychiatric care in overseas hospitals alone.1 Americans began to accept that anyone under extreme conditions could become psychiatrically ill.
Today, there are many ways to feel about our involvement in “Operation Iraqi Freedom” but only one way to feel about the dedicated men and women serving there. They deserve our respect, our love, and all our knowledge and skill to help them deal with the trauma they have endured for us all.
1. Ursano RJ, Holloway HC. Military psychiatry. In: Kaplan HI, Sadock BJ (eds). Comprehensive textbook of psychiatry, 4th ed. Baltimore: Williams and Wilkins; 1985:1904.

James Randolph Hillard, MD
James Randolph Hillard, MD
James Randolph Hillard, MD
Three years after the U.S.-led invasion of Iraq, psychiatrists on the home front are dealing with the war’s neuropsychiatric casualties. We are seeing veterans, their families, friends, and acquaintances, whether we practice in VA medical centers, military medicine, or the community.
To help us, Drs. Timothy Lineberry, Sriram Ramaswamy, J. Michael Bostwick, and James Rundell offer tools to screen for and treat combat-related posttraumatic stress disorder, including PTSD of military sexual trauma. Dr. John Daniels tells which medications may do more harm than good for patients with traumatic brain injury.
World War II brought psychiatric disorders home, showing that not just “crazy people” develop psychiatric symptoms. A half-million U.S. troops were admitted for psychiatric care in overseas hospitals alone.1 Americans began to accept that anyone under extreme conditions could become psychiatrically ill.
Today, there are many ways to feel about our involvement in “Operation Iraqi Freedom” but only one way to feel about the dedicated men and women serving there. They deserve our respect, our love, and all our knowledge and skill to help them deal with the trauma they have endured for us all.
Three years after the U.S.-led invasion of Iraq, psychiatrists on the home front are dealing with the war’s neuropsychiatric casualties. We are seeing veterans, their families, friends, and acquaintances, whether we practice in VA medical centers, military medicine, or the community.
To help us, Drs. Timothy Lineberry, Sriram Ramaswamy, J. Michael Bostwick, and James Rundell offer tools to screen for and treat combat-related posttraumatic stress disorder, including PTSD of military sexual trauma. Dr. John Daniels tells which medications may do more harm than good for patients with traumatic brain injury.
World War II brought psychiatric disorders home, showing that not just “crazy people” develop psychiatric symptoms. A half-million U.S. troops were admitted for psychiatric care in overseas hospitals alone.1 Americans began to accept that anyone under extreme conditions could become psychiatrically ill.
Today, there are many ways to feel about our involvement in “Operation Iraqi Freedom” but only one way to feel about the dedicated men and women serving there. They deserve our respect, our love, and all our knowledge and skill to help them deal with the trauma they have endured for us all.
1. Ursano RJ, Holloway HC. Military psychiatry. In: Kaplan HI, Sadock BJ (eds). Comprehensive textbook of psychiatry, 4th ed. Baltimore: Williams and Wilkins; 1985:1904.
1. Ursano RJ, Holloway HC. Military psychiatry. In: Kaplan HI, Sadock BJ (eds). Comprehensive textbook of psychiatry, 4th ed. Baltimore: Williams and Wilkins; 1985:1904.
It’s not easy being emperor
Tiberius Claudius Germanicus, age 64 and the third emperor of Rome’s Julio-Claudian dynasty, presents to you and reports, “I have severe stomach cramps. I think my wife is poisoning me, but no one believes me. I need your help.”
Retrospective diagnoses are difficult and sometimes ill-advised, but pondering the psychiatric diagnoses of historical figures can alert us to possible differential diagnoses in today’s patients. Consider this imaginary interview between Claudius and a psychiatrist, which suggests several possible diagnoses.
History: terrible royal childhood
Though born into royalty, Claudius was such a sickly infant that his family was ashamed of him and kept him out of their home. He was raised by servants. As a child, he limped and was ridiculed.
He tells you he received little formal education but had many tutors. He learned several languages and became a distinguished historian, scholar, and writer. He served in the military, both in Rome and overseas. For 13 years he has ruled the Roman Empire but fears he will soon be overthrown.
Claudius’ reign began well. He treated his freedmen advisors well, diligently attended to court proceedings, built an aqueduct, and reorganized the Roman government. Recently, however, he has ruled more eccentrically and harshly. He has ordered capricious and costly public works, such as the futile attempt to drain the 12-mile-long Fucine Lake so that the land could be farmed. He has become fond of gladiatorial games and enjoys ordering the execution of political foes. He drinks several liters of wine daily and gorges himself at imperial banquets.
This patient’s family history is complex (Box) and fraught with antisocial behavior and mental illness. Three previous marriages failed, and he describes his current wife, Agrippina, as powerful and manipulative. She has a son, Nero, from an earlier marriage. Claudius fears being poisoned by Agrippina after she instigates a relationship between Nero and Claudius’ daughter.
Claudius lived from 10 BC to 54 AD and ruled the Roman Empire from 41 AD until his death during a feast. Some historians believe that Agrippina poisoned him after her son, Nero, married Claudius’ daughter, Octavia. Because this marriage ensured Nero’s ascendancy to the throne, power-hungry Agrippina no longer needed Claudius.
Claudius was the son of Drusus Claudius Nero and Antonia (the daughter of Mark Antony). His older brother was Germanicus, father of Caligula and Agrippina. Even though Claudius succeeded Caligula as emperor, Claudius was Caligula’s uncle
Nero, in addition to being Claudius’ adopted son, was also his great nephew. When Claudius married Agrippina, he was marrying his niece.
Interview: ‘surrounded by enemies’
Claudius is uncooperative during the interview. He is irritable, tends to bark orders, smells of alcohol, stutters severely, and drools. He admits that he is depressed over myriad family problems.
He also believes that he will become a deity when he dies. He reminds you that he has the power to order executions and wonders if he should have Agrippina and her minions killed. He claims to have written 43 books and numerous historical monographs and to be the last person in the world to speak fluent Etruscan, but laments that no one appreciates his scholarly work. He says he is “surrounded by enemies” and rambles on about family intrigue, cabals, and executions.
He is oriented and shows no florid psychotic symptoms or signs of suicidality. His insight and judgment are severely impaired, and he rejects the idea that he might have a psychiatric disorder.
Claudius refuses a physical exam and abruptly terminates the interview after about 20 minutes, saying he must attend to important affairs of state.
Follow-up: claudius’ ‘last supper’
You want to get more information from family members but wonder if it is safe to do so. It becomes moot: Claudius dies one evening at dinner, days after the interview.
poll here
The authors’ observations
Lead poisoning can cause a range of medical and neuropsychological problems, including attention deficits, antisocial behavior, and irritability.1-4 Romans—particularly the upper class—were exposed to lead from numerous sources:
- Drinking water was contaminated because lead was used extensively to build ancient Rome’s water transportation systems.
- Grape juice fermented to become wine was often preserved in lead vessels, which made it sweeter. The elite drank wine more profusely than did lower-class Romans, who probably could not afford wine. Lead-sweetened grape juice was also used in delicacies eaten by the wealthy.
- The rich also favored expensive, lead-lined bronze bowls and plates, whereas commoners used cheap earthenware. Thus, ancient Rome’s ruling class was ingesting lead-contaminated drink and food.
Some scholars, noting the relative sterility of many Roman emperors, have suggested that lead poisoning, which can decrease sperm count and cause miscarriage, may have contributed to the fall of the Roman Empire.5
Jerome Nriagu, a geochemist who has studied lead’s toxic effects, attributed many of Claudius’ symptoms and negative traits to lead poisoning: “He had disturbed speech, weak limbs, an ungainly gait, tremors, fits of excessive and inappropriate laughter, and unseemly anger, and he often slobbered…his contracting of plumbism would not be surprising, since he was an intemperate glutton.”6 Nriagu also argued that the neuropsychological sequelae of lead poisoning might have clouded the judgment of many Roman emperors.6
Yet some scholars, notably Robert Graves,7,8 have argued that Claudius was highly intelligent and that his copious writing showcased his scholarly interests, hard work, and sound judgment in young adulthood. Based on Graves’ assessment, Claudius probably did not suffer severe plumbism as a child.
Birth injury or cerebral palsy might have caused Claudius’ poor gait and drooling, which were present from childhood. As his drinking and gluttony worsened later in life, alcoholism and lead poisoning could have shortened Claudius’ temper and blurred his judgment, particularly in marrying Agrippina.
Claudius’ belief that he would become a god does not strongly indicate psychosis, because his contemporaries believed that emperors could be deified after death. Opler et al,9 however, found that prenatal lead exposure, as suggested by elevated D-aminolevulinic acid, may be a risk factor for schizophrenia and other psychiatric disorders that manifest in late adolescence or adulthood.
Although we know little about Claudius’ medical problems, abdominal pain has a broad differential diagnosis. Poisoning at Agrippina’s hands or alcohol-induced gastritis, as well as lead-induced abdominal colic, could have caused his intolerable pain.
Bipolar disorder. Claudius’ unrestrained spending, irritability, impulsivity, grandiosity, and mood lability suggest bipolar disorder. Hypomania could have fueled his vast literary output, which has been lost. His belief that he would be deified could also be a manic symptom.
Hypomania was prevalent among Claudius’ family. Two close relatives—his nephew Caligula and great-nephew/adopted son Nero—had marked mood swings. These two emperors were more antisocial than Claudius and showed behavior more consistent with frank mania.
Caligula, who preceded Claudius as emperor, was well known for his excessive behaviors. He was vicious and promiscuous, having sex in public with men, wives of others, and his sisters. Most famously, he considered making his horse, Incitatus, a consul. He gave this horse a “marble stable…a house and a household of slaves and furniture.”10
Nero, who succeeded Claudius, was an alcoholic who frequently indulged his appetites. He believed he was a great singer and became infamous for playing his fiddle while Rome burned. Some of his last words are supposed to have been, “What an artist dies with me!”10
Alcoholism. Some historians have estimated that two-thirds of Roman emperors who reigned from 30 BC (Augustus) to 220 AD (Elegabalus) drank heavily.6 Claudius was reputedly a heavy drinker, and many features displayed by him and his relatives—bad temper, poor judgment, paranoia, impulsivity, violence, and sexual indiscretions—can result from alcohol abuse.
Psychosocial stressors. Claudius was raised and surrounded by malevolent people, then given almost limitless power. That mix of circumstances, plus fear fostered by persistent intrigue, may explain some of his behavior, particularly his brutality.
poll here
The authors’ observations
Had laboratories been available in ancient Rome, a blood test would have determined whether Claudius suffered lead poisoning. Diagnosing bipolar disorder and/or alcoholism is much more difficult. Differentiating these disorders from each other and from other psychiatric disorders is challenging, as no laboratory tests confirm the diagnosis. Ongoing clinical observation of the illness and response to medication are crucial.
In some cases, having the patient list his or her depressive and manic episodes on a “life chart” might clarify the diagnosis. This exercise can also help the patient recognize bipolar symptoms and accept that he or she has the illness, which is critical to ensuring treatment adherence. Also start medication at this time.
Treatment
Treat bipolar disorder and alcoholism simultaneously, as either disorder could worsen the other’s course.11,12
Lithium or valproate would be probable first-line treatments for Claudius. Discuss the medication’s risks and benefits with the patient and involved family members/caretakers. Inform them that you might have to change or add medication if the patient does not respond or experiences side effects.
Psychotherapy and/or psychoeducation are integral to treating comorbid bipolar disorder and alcoholism. Claudius also could have benefited from:
- education about healthy dieting
- counseling against high-risk behaviors associated with alcoholism, such as domestic violence and gambling
- a support group for patients with bipolar disorder or a 12-step program.
What claudius can teach us
Although Claudius’ symptoms cannot be diagnosed with certainty, the information and perspective available today offer insight into his likely psychiatric problems. His case reminds us that:
- Patients often have multiple diagnoses. Bipolar disorder is strongly associated with substance abuse disorder—particularly alcoholism.
- Lead-containing alcoholic beverages are still a public health concern. Morgan et al13 tested 115 samples of moonshine from nine southeastern, south central, and north central U.S. states. One-third of samples contained lead >300 μg/dL. The authors estimated that excessive consumption of 25% of the samples could lead to blood lead levels consistent with lead poisoning (≥25 μg/dL).
Related resources
- Schwartz BS, Stewart WF, Bolla KO, et al. Past adult lead exposure is associated with longitudinal decline in cognitive function. Neurology 2000;55:1144-50.
- Canfield RL, Henderson CR Jr, Cory-Slechta DA, et al. Intellectual impairment in children with blood lead concentrations below 10 microg per deciliter. N Engl J Med 2003;348:1517-26.
- Salloum IM, Thase ME. Impact of substance abuse on the course and treatment of bipolar disorder. Bipolar Disord 2000;2:269-80.
- Nriagu JO. Lead and lead poisoning in antiquity. New York: John Wiley and Sons; 1983.
- Lithium • Eskalith, others
- Valproate • Depakene
Dr. Frankenburg reports no financial relationship with any company whose products are mentioned in this article, or with manufacturers of competing products.
1. Needleman HL, Gunnoe C, Leviton A, et al. Deficits in psychologic and classroom performance of children with elevated dentine lead levels. N Engl J Med 1979;300:689-95.
2. Needleman HL, Gatsonis CA. Low-level lead exposure and the IQ of children. A meta-analysis of modern studies. JAMA 1990;263:673-8.
3. Bellinger DC. Lead. Pediatrics 2004;113:1016-22.
4. Lindgren KN, Ford DP, Bleecker ML. Pattern of blood lead levels over working lifetime and neuropsychological performance. Arch Environ Health 2003;58:373-9.
5. Gilfillan SC. Lead poisoning and the fall of Rome. J Occup Med 1965;7:53-60.
6. Nriagu JO. Lead and lead poisoning in antiquity. New York: John Wiley & Sons; 1983:399-415.
7. Graves R. I, Claudius. From the autobiography of Tiberius Claudius. New York: Vintage Books; 1934; 1989.
8. Graves R. Claudius the god. And his wife Messalina. New York: Vintage Books; 1935; 1989.
9. Opler MG, Brown AS, Graziano J, et al. Prenatal lead exposure, delta-aminolevulinic acid, and schizophrenia. Environ Health Perspect 2004;112:548-52.
10. Suetonius. Lives of the Caesars. Edwards C, trans-ed. New York: Oxford University Press; 2000.
11. Salloum IM, Thase ME. Impact of substance abuse on the course and treatment of bipolar disorder. Bipolar Disord 2000;2:269-80.
12. Cassidy F, Ahearn EP, Carroll BJ. Substance abuse in bipolar disorder. Bipolar Disord 2001;3:181-8.
13. Morgan BW, Parramore CS, Ethridge M. Lead contaminated moonshine: a report of Bureau of Alcohol, Tobacco and Firearms analyzed samples. Vet Hum Toxicol 2004;46:89-90.
14. De Smet PA. Herbal remedies. N Engl J Med 2002;347:2046-56.
Tiberius Claudius Germanicus, age 64 and the third emperor of Rome’s Julio-Claudian dynasty, presents to you and reports, “I have severe stomach cramps. I think my wife is poisoning me, but no one believes me. I need your help.”
Retrospective diagnoses are difficult and sometimes ill-advised, but pondering the psychiatric diagnoses of historical figures can alert us to possible differential diagnoses in today’s patients. Consider this imaginary interview between Claudius and a psychiatrist, which suggests several possible diagnoses.
History: terrible royal childhood
Though born into royalty, Claudius was such a sickly infant that his family was ashamed of him and kept him out of their home. He was raised by servants. As a child, he limped and was ridiculed.
He tells you he received little formal education but had many tutors. He learned several languages and became a distinguished historian, scholar, and writer. He served in the military, both in Rome and overseas. For 13 years he has ruled the Roman Empire but fears he will soon be overthrown.
Claudius’ reign began well. He treated his freedmen advisors well, diligently attended to court proceedings, built an aqueduct, and reorganized the Roman government. Recently, however, he has ruled more eccentrically and harshly. He has ordered capricious and costly public works, such as the futile attempt to drain the 12-mile-long Fucine Lake so that the land could be farmed. He has become fond of gladiatorial games and enjoys ordering the execution of political foes. He drinks several liters of wine daily and gorges himself at imperial banquets.
This patient’s family history is complex (Box) and fraught with antisocial behavior and mental illness. Three previous marriages failed, and he describes his current wife, Agrippina, as powerful and manipulative. She has a son, Nero, from an earlier marriage. Claudius fears being poisoned by Agrippina after she instigates a relationship between Nero and Claudius’ daughter.
Claudius lived from 10 BC to 54 AD and ruled the Roman Empire from 41 AD until his death during a feast. Some historians believe that Agrippina poisoned him after her son, Nero, married Claudius’ daughter, Octavia. Because this marriage ensured Nero’s ascendancy to the throne, power-hungry Agrippina no longer needed Claudius.
Claudius was the son of Drusus Claudius Nero and Antonia (the daughter of Mark Antony). His older brother was Germanicus, father of Caligula and Agrippina. Even though Claudius succeeded Caligula as emperor, Claudius was Caligula’s uncle
Nero, in addition to being Claudius’ adopted son, was also his great nephew. When Claudius married Agrippina, he was marrying his niece.
Interview: ‘surrounded by enemies’
Claudius is uncooperative during the interview. He is irritable, tends to bark orders, smells of alcohol, stutters severely, and drools. He admits that he is depressed over myriad family problems.
He also believes that he will become a deity when he dies. He reminds you that he has the power to order executions and wonders if he should have Agrippina and her minions killed. He claims to have written 43 books and numerous historical monographs and to be the last person in the world to speak fluent Etruscan, but laments that no one appreciates his scholarly work. He says he is “surrounded by enemies” and rambles on about family intrigue, cabals, and executions.
He is oriented and shows no florid psychotic symptoms or signs of suicidality. His insight and judgment are severely impaired, and he rejects the idea that he might have a psychiatric disorder.
Claudius refuses a physical exam and abruptly terminates the interview after about 20 minutes, saying he must attend to important affairs of state.
Follow-up: claudius’ ‘last supper’
You want to get more information from family members but wonder if it is safe to do so. It becomes moot: Claudius dies one evening at dinner, days after the interview.
poll here
The authors’ observations
Lead poisoning can cause a range of medical and neuropsychological problems, including attention deficits, antisocial behavior, and irritability.1-4 Romans—particularly the upper class—were exposed to lead from numerous sources:
- Drinking water was contaminated because lead was used extensively to build ancient Rome’s water transportation systems.
- Grape juice fermented to become wine was often preserved in lead vessels, which made it sweeter. The elite drank wine more profusely than did lower-class Romans, who probably could not afford wine. Lead-sweetened grape juice was also used in delicacies eaten by the wealthy.
- The rich also favored expensive, lead-lined bronze bowls and plates, whereas commoners used cheap earthenware. Thus, ancient Rome’s ruling class was ingesting lead-contaminated drink and food.
Some scholars, noting the relative sterility of many Roman emperors, have suggested that lead poisoning, which can decrease sperm count and cause miscarriage, may have contributed to the fall of the Roman Empire.5
Jerome Nriagu, a geochemist who has studied lead’s toxic effects, attributed many of Claudius’ symptoms and negative traits to lead poisoning: “He had disturbed speech, weak limbs, an ungainly gait, tremors, fits of excessive and inappropriate laughter, and unseemly anger, and he often slobbered…his contracting of plumbism would not be surprising, since he was an intemperate glutton.”6 Nriagu also argued that the neuropsychological sequelae of lead poisoning might have clouded the judgment of many Roman emperors.6
Yet some scholars, notably Robert Graves,7,8 have argued that Claudius was highly intelligent and that his copious writing showcased his scholarly interests, hard work, and sound judgment in young adulthood. Based on Graves’ assessment, Claudius probably did not suffer severe plumbism as a child.
Birth injury or cerebral palsy might have caused Claudius’ poor gait and drooling, which were present from childhood. As his drinking and gluttony worsened later in life, alcoholism and lead poisoning could have shortened Claudius’ temper and blurred his judgment, particularly in marrying Agrippina.
Claudius’ belief that he would become a god does not strongly indicate psychosis, because his contemporaries believed that emperors could be deified after death. Opler et al,9 however, found that prenatal lead exposure, as suggested by elevated D-aminolevulinic acid, may be a risk factor for schizophrenia and other psychiatric disorders that manifest in late adolescence or adulthood.
Although we know little about Claudius’ medical problems, abdominal pain has a broad differential diagnosis. Poisoning at Agrippina’s hands or alcohol-induced gastritis, as well as lead-induced abdominal colic, could have caused his intolerable pain.
Bipolar disorder. Claudius’ unrestrained spending, irritability, impulsivity, grandiosity, and mood lability suggest bipolar disorder. Hypomania could have fueled his vast literary output, which has been lost. His belief that he would be deified could also be a manic symptom.
Hypomania was prevalent among Claudius’ family. Two close relatives—his nephew Caligula and great-nephew/adopted son Nero—had marked mood swings. These two emperors were more antisocial than Claudius and showed behavior more consistent with frank mania.
Caligula, who preceded Claudius as emperor, was well known for his excessive behaviors. He was vicious and promiscuous, having sex in public with men, wives of others, and his sisters. Most famously, he considered making his horse, Incitatus, a consul. He gave this horse a “marble stable…a house and a household of slaves and furniture.”10
Nero, who succeeded Claudius, was an alcoholic who frequently indulged his appetites. He believed he was a great singer and became infamous for playing his fiddle while Rome burned. Some of his last words are supposed to have been, “What an artist dies with me!”10
Alcoholism. Some historians have estimated that two-thirds of Roman emperors who reigned from 30 BC (Augustus) to 220 AD (Elegabalus) drank heavily.6 Claudius was reputedly a heavy drinker, and many features displayed by him and his relatives—bad temper, poor judgment, paranoia, impulsivity, violence, and sexual indiscretions—can result from alcohol abuse.
Psychosocial stressors. Claudius was raised and surrounded by malevolent people, then given almost limitless power. That mix of circumstances, plus fear fostered by persistent intrigue, may explain some of his behavior, particularly his brutality.
poll here
The authors’ observations
Had laboratories been available in ancient Rome, a blood test would have determined whether Claudius suffered lead poisoning. Diagnosing bipolar disorder and/or alcoholism is much more difficult. Differentiating these disorders from each other and from other psychiatric disorders is challenging, as no laboratory tests confirm the diagnosis. Ongoing clinical observation of the illness and response to medication are crucial.
In some cases, having the patient list his or her depressive and manic episodes on a “life chart” might clarify the diagnosis. This exercise can also help the patient recognize bipolar symptoms and accept that he or she has the illness, which is critical to ensuring treatment adherence. Also start medication at this time.
Treatment
Treat bipolar disorder and alcoholism simultaneously, as either disorder could worsen the other’s course.11,12
Lithium or valproate would be probable first-line treatments for Claudius. Discuss the medication’s risks and benefits with the patient and involved family members/caretakers. Inform them that you might have to change or add medication if the patient does not respond or experiences side effects.
Psychotherapy and/or psychoeducation are integral to treating comorbid bipolar disorder and alcoholism. Claudius also could have benefited from:
- education about healthy dieting
- counseling against high-risk behaviors associated with alcoholism, such as domestic violence and gambling
- a support group for patients with bipolar disorder or a 12-step program.
What claudius can teach us
Although Claudius’ symptoms cannot be diagnosed with certainty, the information and perspective available today offer insight into his likely psychiatric problems. His case reminds us that:
- Patients often have multiple diagnoses. Bipolar disorder is strongly associated with substance abuse disorder—particularly alcoholism.
- Lead-containing alcoholic beverages are still a public health concern. Morgan et al13 tested 115 samples of moonshine from nine southeastern, south central, and north central U.S. states. One-third of samples contained lead >300 μg/dL. The authors estimated that excessive consumption of 25% of the samples could lead to blood lead levels consistent with lead poisoning (≥25 μg/dL).
Related resources
- Schwartz BS, Stewart WF, Bolla KO, et al. Past adult lead exposure is associated with longitudinal decline in cognitive function. Neurology 2000;55:1144-50.
- Canfield RL, Henderson CR Jr, Cory-Slechta DA, et al. Intellectual impairment in children with blood lead concentrations below 10 microg per deciliter. N Engl J Med 2003;348:1517-26.
- Salloum IM, Thase ME. Impact of substance abuse on the course and treatment of bipolar disorder. Bipolar Disord 2000;2:269-80.
- Nriagu JO. Lead and lead poisoning in antiquity. New York: John Wiley and Sons; 1983.
- Lithium • Eskalith, others
- Valproate • Depakene
Dr. Frankenburg reports no financial relationship with any company whose products are mentioned in this article, or with manufacturers of competing products.
Tiberius Claudius Germanicus, age 64 and the third emperor of Rome’s Julio-Claudian dynasty, presents to you and reports, “I have severe stomach cramps. I think my wife is poisoning me, but no one believes me. I need your help.”
Retrospective diagnoses are difficult and sometimes ill-advised, but pondering the psychiatric diagnoses of historical figures can alert us to possible differential diagnoses in today’s patients. Consider this imaginary interview between Claudius and a psychiatrist, which suggests several possible diagnoses.
History: terrible royal childhood
Though born into royalty, Claudius was such a sickly infant that his family was ashamed of him and kept him out of their home. He was raised by servants. As a child, he limped and was ridiculed.
He tells you he received little formal education but had many tutors. He learned several languages and became a distinguished historian, scholar, and writer. He served in the military, both in Rome and overseas. For 13 years he has ruled the Roman Empire but fears he will soon be overthrown.
Claudius’ reign began well. He treated his freedmen advisors well, diligently attended to court proceedings, built an aqueduct, and reorganized the Roman government. Recently, however, he has ruled more eccentrically and harshly. He has ordered capricious and costly public works, such as the futile attempt to drain the 12-mile-long Fucine Lake so that the land could be farmed. He has become fond of gladiatorial games and enjoys ordering the execution of political foes. He drinks several liters of wine daily and gorges himself at imperial banquets.
This patient’s family history is complex (Box) and fraught with antisocial behavior and mental illness. Three previous marriages failed, and he describes his current wife, Agrippina, as powerful and manipulative. She has a son, Nero, from an earlier marriage. Claudius fears being poisoned by Agrippina after she instigates a relationship between Nero and Claudius’ daughter.
Claudius lived from 10 BC to 54 AD and ruled the Roman Empire from 41 AD until his death during a feast. Some historians believe that Agrippina poisoned him after her son, Nero, married Claudius’ daughter, Octavia. Because this marriage ensured Nero’s ascendancy to the throne, power-hungry Agrippina no longer needed Claudius.
Claudius was the son of Drusus Claudius Nero and Antonia (the daughter of Mark Antony). His older brother was Germanicus, father of Caligula and Agrippina. Even though Claudius succeeded Caligula as emperor, Claudius was Caligula’s uncle
Nero, in addition to being Claudius’ adopted son, was also his great nephew. When Claudius married Agrippina, he was marrying his niece.
Interview: ‘surrounded by enemies’
Claudius is uncooperative during the interview. He is irritable, tends to bark orders, smells of alcohol, stutters severely, and drools. He admits that he is depressed over myriad family problems.
He also believes that he will become a deity when he dies. He reminds you that he has the power to order executions and wonders if he should have Agrippina and her minions killed. He claims to have written 43 books and numerous historical monographs and to be the last person in the world to speak fluent Etruscan, but laments that no one appreciates his scholarly work. He says he is “surrounded by enemies” and rambles on about family intrigue, cabals, and executions.
He is oriented and shows no florid psychotic symptoms or signs of suicidality. His insight and judgment are severely impaired, and he rejects the idea that he might have a psychiatric disorder.
Claudius refuses a physical exam and abruptly terminates the interview after about 20 minutes, saying he must attend to important affairs of state.
Follow-up: claudius’ ‘last supper’
You want to get more information from family members but wonder if it is safe to do so. It becomes moot: Claudius dies one evening at dinner, days after the interview.
poll here
The authors’ observations
Lead poisoning can cause a range of medical and neuropsychological problems, including attention deficits, antisocial behavior, and irritability.1-4 Romans—particularly the upper class—were exposed to lead from numerous sources:
- Drinking water was contaminated because lead was used extensively to build ancient Rome’s water transportation systems.
- Grape juice fermented to become wine was often preserved in lead vessels, which made it sweeter. The elite drank wine more profusely than did lower-class Romans, who probably could not afford wine. Lead-sweetened grape juice was also used in delicacies eaten by the wealthy.
- The rich also favored expensive, lead-lined bronze bowls and plates, whereas commoners used cheap earthenware. Thus, ancient Rome’s ruling class was ingesting lead-contaminated drink and food.
Some scholars, noting the relative sterility of many Roman emperors, have suggested that lead poisoning, which can decrease sperm count and cause miscarriage, may have contributed to the fall of the Roman Empire.5
Jerome Nriagu, a geochemist who has studied lead’s toxic effects, attributed many of Claudius’ symptoms and negative traits to lead poisoning: “He had disturbed speech, weak limbs, an ungainly gait, tremors, fits of excessive and inappropriate laughter, and unseemly anger, and he often slobbered…his contracting of plumbism would not be surprising, since he was an intemperate glutton.”6 Nriagu also argued that the neuropsychological sequelae of lead poisoning might have clouded the judgment of many Roman emperors.6
Yet some scholars, notably Robert Graves,7,8 have argued that Claudius was highly intelligent and that his copious writing showcased his scholarly interests, hard work, and sound judgment in young adulthood. Based on Graves’ assessment, Claudius probably did not suffer severe plumbism as a child.
Birth injury or cerebral palsy might have caused Claudius’ poor gait and drooling, which were present from childhood. As his drinking and gluttony worsened later in life, alcoholism and lead poisoning could have shortened Claudius’ temper and blurred his judgment, particularly in marrying Agrippina.
Claudius’ belief that he would become a god does not strongly indicate psychosis, because his contemporaries believed that emperors could be deified after death. Opler et al,9 however, found that prenatal lead exposure, as suggested by elevated D-aminolevulinic acid, may be a risk factor for schizophrenia and other psychiatric disorders that manifest in late adolescence or adulthood.
Although we know little about Claudius’ medical problems, abdominal pain has a broad differential diagnosis. Poisoning at Agrippina’s hands or alcohol-induced gastritis, as well as lead-induced abdominal colic, could have caused his intolerable pain.
Bipolar disorder. Claudius’ unrestrained spending, irritability, impulsivity, grandiosity, and mood lability suggest bipolar disorder. Hypomania could have fueled his vast literary output, which has been lost. His belief that he would be deified could also be a manic symptom.
Hypomania was prevalent among Claudius’ family. Two close relatives—his nephew Caligula and great-nephew/adopted son Nero—had marked mood swings. These two emperors were more antisocial than Claudius and showed behavior more consistent with frank mania.
Caligula, who preceded Claudius as emperor, was well known for his excessive behaviors. He was vicious and promiscuous, having sex in public with men, wives of others, and his sisters. Most famously, he considered making his horse, Incitatus, a consul. He gave this horse a “marble stable…a house and a household of slaves and furniture.”10
Nero, who succeeded Claudius, was an alcoholic who frequently indulged his appetites. He believed he was a great singer and became infamous for playing his fiddle while Rome burned. Some of his last words are supposed to have been, “What an artist dies with me!”10
Alcoholism. Some historians have estimated that two-thirds of Roman emperors who reigned from 30 BC (Augustus) to 220 AD (Elegabalus) drank heavily.6 Claudius was reputedly a heavy drinker, and many features displayed by him and his relatives—bad temper, poor judgment, paranoia, impulsivity, violence, and sexual indiscretions—can result from alcohol abuse.
Psychosocial stressors. Claudius was raised and surrounded by malevolent people, then given almost limitless power. That mix of circumstances, plus fear fostered by persistent intrigue, may explain some of his behavior, particularly his brutality.
poll here
The authors’ observations
Had laboratories been available in ancient Rome, a blood test would have determined whether Claudius suffered lead poisoning. Diagnosing bipolar disorder and/or alcoholism is much more difficult. Differentiating these disorders from each other and from other psychiatric disorders is challenging, as no laboratory tests confirm the diagnosis. Ongoing clinical observation of the illness and response to medication are crucial.
In some cases, having the patient list his or her depressive and manic episodes on a “life chart” might clarify the diagnosis. This exercise can also help the patient recognize bipolar symptoms and accept that he or she has the illness, which is critical to ensuring treatment adherence. Also start medication at this time.
Treatment
Treat bipolar disorder and alcoholism simultaneously, as either disorder could worsen the other’s course.11,12
Lithium or valproate would be probable first-line treatments for Claudius. Discuss the medication’s risks and benefits with the patient and involved family members/caretakers. Inform them that you might have to change or add medication if the patient does not respond or experiences side effects.
Psychotherapy and/or psychoeducation are integral to treating comorbid bipolar disorder and alcoholism. Claudius also could have benefited from:
- education about healthy dieting
- counseling against high-risk behaviors associated with alcoholism, such as domestic violence and gambling
- a support group for patients with bipolar disorder or a 12-step program.
What claudius can teach us
Although Claudius’ symptoms cannot be diagnosed with certainty, the information and perspective available today offer insight into his likely psychiatric problems. His case reminds us that:
- Patients often have multiple diagnoses. Bipolar disorder is strongly associated with substance abuse disorder—particularly alcoholism.
- Lead-containing alcoholic beverages are still a public health concern. Morgan et al13 tested 115 samples of moonshine from nine southeastern, south central, and north central U.S. states. One-third of samples contained lead >300 μg/dL. The authors estimated that excessive consumption of 25% of the samples could lead to blood lead levels consistent with lead poisoning (≥25 μg/dL).
Related resources
- Schwartz BS, Stewart WF, Bolla KO, et al. Past adult lead exposure is associated with longitudinal decline in cognitive function. Neurology 2000;55:1144-50.
- Canfield RL, Henderson CR Jr, Cory-Slechta DA, et al. Intellectual impairment in children with blood lead concentrations below 10 microg per deciliter. N Engl J Med 2003;348:1517-26.
- Salloum IM, Thase ME. Impact of substance abuse on the course and treatment of bipolar disorder. Bipolar Disord 2000;2:269-80.
- Nriagu JO. Lead and lead poisoning in antiquity. New York: John Wiley and Sons; 1983.
- Lithium • Eskalith, others
- Valproate • Depakene
Dr. Frankenburg reports no financial relationship with any company whose products are mentioned in this article, or with manufacturers of competing products.
1. Needleman HL, Gunnoe C, Leviton A, et al. Deficits in psychologic and classroom performance of children with elevated dentine lead levels. N Engl J Med 1979;300:689-95.
2. Needleman HL, Gatsonis CA. Low-level lead exposure and the IQ of children. A meta-analysis of modern studies. JAMA 1990;263:673-8.
3. Bellinger DC. Lead. Pediatrics 2004;113:1016-22.
4. Lindgren KN, Ford DP, Bleecker ML. Pattern of blood lead levels over working lifetime and neuropsychological performance. Arch Environ Health 2003;58:373-9.
5. Gilfillan SC. Lead poisoning and the fall of Rome. J Occup Med 1965;7:53-60.
6. Nriagu JO. Lead and lead poisoning in antiquity. New York: John Wiley & Sons; 1983:399-415.
7. Graves R. I, Claudius. From the autobiography of Tiberius Claudius. New York: Vintage Books; 1934; 1989.
8. Graves R. Claudius the god. And his wife Messalina. New York: Vintage Books; 1935; 1989.
9. Opler MG, Brown AS, Graziano J, et al. Prenatal lead exposure, delta-aminolevulinic acid, and schizophrenia. Environ Health Perspect 2004;112:548-52.
10. Suetonius. Lives of the Caesars. Edwards C, trans-ed. New York: Oxford University Press; 2000.
11. Salloum IM, Thase ME. Impact of substance abuse on the course and treatment of bipolar disorder. Bipolar Disord 2000;2:269-80.
12. Cassidy F, Ahearn EP, Carroll BJ. Substance abuse in bipolar disorder. Bipolar Disord 2001;3:181-8.
13. Morgan BW, Parramore CS, Ethridge M. Lead contaminated moonshine: a report of Bureau of Alcohol, Tobacco and Firearms analyzed samples. Vet Hum Toxicol 2004;46:89-90.
14. De Smet PA. Herbal remedies. N Engl J Med 2002;347:2046-56.
1. Needleman HL, Gunnoe C, Leviton A, et al. Deficits in psychologic and classroom performance of children with elevated dentine lead levels. N Engl J Med 1979;300:689-95.
2. Needleman HL, Gatsonis CA. Low-level lead exposure and the IQ of children. A meta-analysis of modern studies. JAMA 1990;263:673-8.
3. Bellinger DC. Lead. Pediatrics 2004;113:1016-22.
4. Lindgren KN, Ford DP, Bleecker ML. Pattern of blood lead levels over working lifetime and neuropsychological performance. Arch Environ Health 2003;58:373-9.
5. Gilfillan SC. Lead poisoning and the fall of Rome. J Occup Med 1965;7:53-60.
6. Nriagu JO. Lead and lead poisoning in antiquity. New York: John Wiley & Sons; 1983:399-415.
7. Graves R. I, Claudius. From the autobiography of Tiberius Claudius. New York: Vintage Books; 1934; 1989.
8. Graves R. Claudius the god. And his wife Messalina. New York: Vintage Books; 1935; 1989.
9. Opler MG, Brown AS, Graziano J, et al. Prenatal lead exposure, delta-aminolevulinic acid, and schizophrenia. Environ Health Perspect 2004;112:548-52.
10. Suetonius. Lives of the Caesars. Edwards C, trans-ed. New York: Oxford University Press; 2000.
11. Salloum IM, Thase ME. Impact of substance abuse on the course and treatment of bipolar disorder. Bipolar Disord 2000;2:269-80.
12. Cassidy F, Ahearn EP, Carroll BJ. Substance abuse in bipolar disorder. Bipolar Disord 2001;3:181-8.
13. Morgan BW, Parramore CS, Ethridge M. Lead contaminated moonshine: a report of Bureau of Alcohol, Tobacco and Firearms analyzed samples. Vet Hum Toxicol 2004;46:89-90.
14. De Smet PA. Herbal remedies. N Engl J Med 2002;347:2046-56.
Get creative to manage dementia-related behaviors
Mrs. A, age 82, has advanced Alzheimer’s disease and has resided in a nursing home for 2 years. She does not recognize that she lives in a nursing home and waits by the door for her son to take her home. She spends her days weeping, telling visitors and staff she has been abandoned and must go home to care for her children.
Recently she has been wandering from the facility. When staff attempt to direct her away from the door, she resists, becomes physically aggressive, and hollers loudly. Her behavior bothers visitors and other patients, who frequently complain.
Her primary care physician prescribes a trial of olanzapine, 10 mg/d, but she becomes confused and suffers a fall. Staff report that Mrs. A is sleeping poorly and losing weight.
Deciding how to manage agitation, aggression, or psychotic symptoms of dementia is dicey at best. You can try an atypical antipsychotic despite the FDA’s black-box warning (Risks of using vs. not using atypical antipsychotics. Current Psychiatry 2005;4(8):14-28.
- Carbamazepine • Carbatrol
- Donepezil • Aricept
- Lorazepam • Ativan
- Memantine • Namenda
- Mirtazapine • Remeron
- Olanzapine • Zyprexa
- Oxazepam • Serax
- Trazodone • Desyrel
- Valproic acid • Depakote
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Alexopoulos GS, Jeste DV, Chung H, et al. The expert consensus guideline series: Treatment of dementia and its behavioral disturbances. Minneapolis, MN: McGraw-Hill; 2005.
2. Schneider LS, Dagerman LS, Insel P. Risk of death with atypical antipsychotic drug treatment for dementia: Meta-analysis of randomized placebo-controlled trials. JAMA 2005;294:1934-43.
3. FDA Talk Paper. FDA issues public health advisory for antipsychotic drugs used for treatment of behavioral disorders in elderly patients. U.S. Food and Drug Administration. Available at: http://www.fda.gov/bbs/topics/ANSWERS/2005/ANS01350.html. Accessed March 10, 2006.
4. Treatment of agitation in older persons with dementia. The Expert Consensus Panel for Agitation in Dementia. Postgrad Med 1998;SPEC NO:1-88.
5. Sutor B, Rummans TA, Smith GE. Assessment and management of behavioral disturbances in nursing home patients with dementia. Mayo Clin Proc 2001;76:540-50.
6. McKeith IG, Dickson DW, Lowe J, et al. Diagnosis and management of dementia in Lewy bodies: Third report of the DLB consortium. Neurology 2005;65:1863-72.
7. Feldman H, Lyketsos LD, Steinberg QM, et al. A 24-week, randomized, double-blind study of donepezil in moderate to severe Alzheimer’s disease. Arch Gen Psychiatry 2003;60:737-46.
8. Sink KM, Holden KF, Yaffe K. Pharmacologic treatment of neuropsychiatric symptoms of dementia: A review of the evidence. JAMA 2005;293:596-608.
9. Gauthier S, Wirth Y, Mobius HJ. Effects of memantine on behavioral symptoms in Alzheimer’s disease patients: An analysis of the Neuropsychiatric Inventory (NPI) data of two randomized controlled studies. Int J Geriatr Psychiatry 2005;20:259-62.
10. Porsteinsson AP, Tariot PN, Jakimovich LJ, et al. Valproate therapy for agitation in dementia: Open-label extension of a double-blind trial. Am J Geriatr Psychiatry 2003;11:434-40.
11. Tariot PN, Raman R, Jakimovich L, et al. Divalproex sodium in nursing home residents with possible or probable Alzheimer’s disease complicated by agitation: A randomized controlled trial. Am J Geriatr Psychiatry 2005;13:942-9.
Mrs. A, age 82, has advanced Alzheimer’s disease and has resided in a nursing home for 2 years. She does not recognize that she lives in a nursing home and waits by the door for her son to take her home. She spends her days weeping, telling visitors and staff she has been abandoned and must go home to care for her children.
Recently she has been wandering from the facility. When staff attempt to direct her away from the door, she resists, becomes physically aggressive, and hollers loudly. Her behavior bothers visitors and other patients, who frequently complain.
Her primary care physician prescribes a trial of olanzapine, 10 mg/d, but she becomes confused and suffers a fall. Staff report that Mrs. A is sleeping poorly and losing weight.
Deciding how to manage agitation, aggression, or psychotic symptoms of dementia is dicey at best. You can try an atypical antipsychotic despite the FDA’s black-box warning (Risks of using vs. not using atypical antipsychotics. Current Psychiatry 2005;4(8):14-28.
- Carbamazepine • Carbatrol
- Donepezil • Aricept
- Lorazepam • Ativan
- Memantine • Namenda
- Mirtazapine • Remeron
- Olanzapine • Zyprexa
- Oxazepam • Serax
- Trazodone • Desyrel
- Valproic acid • Depakote
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Mrs. A, age 82, has advanced Alzheimer’s disease and has resided in a nursing home for 2 years. She does not recognize that she lives in a nursing home and waits by the door for her son to take her home. She spends her days weeping, telling visitors and staff she has been abandoned and must go home to care for her children.
Recently she has been wandering from the facility. When staff attempt to direct her away from the door, she resists, becomes physically aggressive, and hollers loudly. Her behavior bothers visitors and other patients, who frequently complain.
Her primary care physician prescribes a trial of olanzapine, 10 mg/d, but she becomes confused and suffers a fall. Staff report that Mrs. A is sleeping poorly and losing weight.
Deciding how to manage agitation, aggression, or psychotic symptoms of dementia is dicey at best. You can try an atypical antipsychotic despite the FDA’s black-box warning (Risks of using vs. not using atypical antipsychotics. Current Psychiatry 2005;4(8):14-28.
- Carbamazepine • Carbatrol
- Donepezil • Aricept
- Lorazepam • Ativan
- Memantine • Namenda
- Mirtazapine • Remeron
- Olanzapine • Zyprexa
- Oxazepam • Serax
- Trazodone • Desyrel
- Valproic acid • Depakote
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Alexopoulos GS, Jeste DV, Chung H, et al. The expert consensus guideline series: Treatment of dementia and its behavioral disturbances. Minneapolis, MN: McGraw-Hill; 2005.
2. Schneider LS, Dagerman LS, Insel P. Risk of death with atypical antipsychotic drug treatment for dementia: Meta-analysis of randomized placebo-controlled trials. JAMA 2005;294:1934-43.
3. FDA Talk Paper. FDA issues public health advisory for antipsychotic drugs used for treatment of behavioral disorders in elderly patients. U.S. Food and Drug Administration. Available at: http://www.fda.gov/bbs/topics/ANSWERS/2005/ANS01350.html. Accessed March 10, 2006.
4. Treatment of agitation in older persons with dementia. The Expert Consensus Panel for Agitation in Dementia. Postgrad Med 1998;SPEC NO:1-88.
5. Sutor B, Rummans TA, Smith GE. Assessment and management of behavioral disturbances in nursing home patients with dementia. Mayo Clin Proc 2001;76:540-50.
6. McKeith IG, Dickson DW, Lowe J, et al. Diagnosis and management of dementia in Lewy bodies: Third report of the DLB consortium. Neurology 2005;65:1863-72.
7. Feldman H, Lyketsos LD, Steinberg QM, et al. A 24-week, randomized, double-blind study of donepezil in moderate to severe Alzheimer’s disease. Arch Gen Psychiatry 2003;60:737-46.
8. Sink KM, Holden KF, Yaffe K. Pharmacologic treatment of neuropsychiatric symptoms of dementia: A review of the evidence. JAMA 2005;293:596-608.
9. Gauthier S, Wirth Y, Mobius HJ. Effects of memantine on behavioral symptoms in Alzheimer’s disease patients: An analysis of the Neuropsychiatric Inventory (NPI) data of two randomized controlled studies. Int J Geriatr Psychiatry 2005;20:259-62.
10. Porsteinsson AP, Tariot PN, Jakimovich LJ, et al. Valproate therapy for agitation in dementia: Open-label extension of a double-blind trial. Am J Geriatr Psychiatry 2003;11:434-40.
11. Tariot PN, Raman R, Jakimovich L, et al. Divalproex sodium in nursing home residents with possible or probable Alzheimer’s disease complicated by agitation: A randomized controlled trial. Am J Geriatr Psychiatry 2005;13:942-9.
1. Alexopoulos GS, Jeste DV, Chung H, et al. The expert consensus guideline series: Treatment of dementia and its behavioral disturbances. Minneapolis, MN: McGraw-Hill; 2005.
2. Schneider LS, Dagerman LS, Insel P. Risk of death with atypical antipsychotic drug treatment for dementia: Meta-analysis of randomized placebo-controlled trials. JAMA 2005;294:1934-43.
3. FDA Talk Paper. FDA issues public health advisory for antipsychotic drugs used for treatment of behavioral disorders in elderly patients. U.S. Food and Drug Administration. Available at: http://www.fda.gov/bbs/topics/ANSWERS/2005/ANS01350.html. Accessed March 10, 2006.
4. Treatment of agitation in older persons with dementia. The Expert Consensus Panel for Agitation in Dementia. Postgrad Med 1998;SPEC NO:1-88.
5. Sutor B, Rummans TA, Smith GE. Assessment and management of behavioral disturbances in nursing home patients with dementia. Mayo Clin Proc 2001;76:540-50.
6. McKeith IG, Dickson DW, Lowe J, et al. Diagnosis and management of dementia in Lewy bodies: Third report of the DLB consortium. Neurology 2005;65:1863-72.
7. Feldman H, Lyketsos LD, Steinberg QM, et al. A 24-week, randomized, double-blind study of donepezil in moderate to severe Alzheimer’s disease. Arch Gen Psychiatry 2003;60:737-46.
8. Sink KM, Holden KF, Yaffe K. Pharmacologic treatment of neuropsychiatric symptoms of dementia: A review of the evidence. JAMA 2005;293:596-608.
9. Gauthier S, Wirth Y, Mobius HJ. Effects of memantine on behavioral symptoms in Alzheimer’s disease patients: An analysis of the Neuropsychiatric Inventory (NPI) data of two randomized controlled studies. Int J Geriatr Psychiatry 2005;20:259-62.
10. Porsteinsson AP, Tariot PN, Jakimovich LJ, et al. Valproate therapy for agitation in dementia: Open-label extension of a double-blind trial. Am J Geriatr Psychiatry 2003;11:434-40.
11. Tariot PN, Raman R, Jakimovich L, et al. Divalproex sodium in nursing home residents with possible or probable Alzheimer’s disease complicated by agitation: A randomized controlled trial. Am J Geriatr Psychiatry 2005;13:942-9.
Traumatic brain injury: Choosing drugs to assist recovery
Choosing medications for patients with traumatic brain injury (TBI) requires caution; some drugs slow their recovery, and no standard post-TBI treatment exists.
As consulting psychiatrist on a TBI rehabilitation team, I am asked to manage enduring cognitive and emotional problems—aggression, apathy, learning disabilities, dementia—in patients with moderate to severe head injuries. This article describes how we apply available evidence to treat neurobehavioral symptoms in these patients.
Case: An iraq war casualty
The physical medicine and rehabilitation service asks for help in managing agitation, anxiety, and nightmares in Mr. N, age 20, a U.S. combat soldier. While on patrol 2 months ago in Iraq, he suffered a penetrating right frontoparietal brain injury from an improvised explosive device.
Mr. N has undergone a right temporoparietal craniectomy with debridement, ventriculostomy placement, and scalp flap closure. He has had seizures and then pancreatitis—thought to be caused by divalproex prescribed to treat the seizures. Divalproex was replaced with phenytoin at our hospital, and the pancreatitis resolved.
How serious an injury?
TBI ranges from self-limited concussion to devastating, permanent CNS impairment and life-long disability. Brain injuries from sudden impact—from assaults, falls, motor vehicle accidents, combat, or sports—can cause diffuse axonal injury and confusion or unconsciousness, even without radiographic evidence of cerebral bleeding, edema, or mass effect.
No hierarchy or nomenclature is universally accepted for TBI. The term “concussion” is generally used for milder injury and TBI for more-severe injuries.
Concussion. The American Academy of Neurology defines concussion as a trauma-induced alteration in mental status that may or may not involve loss of consciousness. Confusion and amnesia—the hallmarks of concussion—may occur immediately after the head trauma or several minutes later.1 This definition recognizes three concussion grades:
- Grade 1: confusion lasts
- Grade 2: confusion persists >15 minutes but without LOC
- Grade 3: concussion with LOC. The confusional state is marked by disorientation, delayed verbal and motor responses, inattention, incoordination, emotional lability, and slurred or incoherent speech.
- Mild TBI: GCS 13 to 15, LOC 1,3
- Moderate TBI: GCS 9 to 12, LOC 30 minutes to 7 days, and PTA 24 hours to 7 days.
- Severe TBI: GCS ≤8, LOC, and PTA >7 days,4 or any focal neuroimaging abnormalities.3
Using Glasgow Coma Scale scores to evaluate brain injury severity
| Component | Response | Score |
|---|---|---|
| Best eye response | No eye opening | 1 |
| Eye opening to pain | 2 | |
| Eye opening to verbal command | 3 | |
| Eyes open spontaneously | 4 | |
| Best verbal response | No verbal response | 1 |
| Incomprehensible sounds | 2 | |
| Inappropriate words | 3 | |
| Confused | 4 | |
| Oriented | 5 | |
| Best motor response | No motor response | 1 |
| Extension to pain | 2 | |
| Flexion to pain | 3 | |
| Withdrawal from pain | 4 | |
| Localizing pain | 5 | |
| Obeys commands | 6 | |
| GCS total score ≥12 is mild injury, 9 to 11 is moderate, and ≤8 is severe (90% of patients with scores ≤8 are in a coma). Coma is defined as not opening eyes, not obeying commands, and not saying understandable words. Composite scores with eye, verbal, and motor responses (such as E3V3M5) are clinically more useful than totals. | ||
| Source: Reference 2. | ||
Case continued: ‘They’re hurting me’
Mr. N meets criteria for severe TBI. He is periodically agitated and aggressive and refuses to return to physical therapy, complaining that rehabilitation nurses are intentionally hurting him. He occasionally hits the staff and throws things. His medications include:
- phenytoin, 100 mg every 6 hours for seizure prophylaxis
- lamotrigine, 50 mg bid for seizure prophylaxis
- zolpidem, 5 mg as needed at bedtime for pain
- methadone, 10 mg/d for pain
- oxycodone, 5 mg every 4 hours as needed for breakthrough pain.
Assessing progress
For patients such as Mr. N, TBI recovery progress is measured with the Rancho Los Amigos Scale.
The original Rancho scale—developed in 1972 by staff at the Rancho Los Amigos rehabilitation hospital in Downey, CA—described eight levels of cognitive and adaptive functioning, from coma and total care through normal cognition and independence. A 1997 revised version separates the highest cognitive functioning level (VIII, purposeful, appropriate function) into three parts, expanding the scale to 10 levels (Table 2).5
Of course, not all TBI patients begin recovery at Rancho level I, and unfortunately not all achieve level X. Some experience dementia caused by head trauma, with persistent memory impairment and cognitive deficits in language, apraxia, agnosia, or executive function.6
Most patients recover as predicted by the initial injury’s severity. Others experience diffuse cerebral swelling with sudden, rapid deterioration after what appeared to be a grade 1 or grade 2 concussion. Diffuse cerebral swelling is sometimes considered a “second-impact syndrome,” but it can also occur after a single impact.7 A second TBI is not universally believed to cause the precipitous decline, but animal studies suggest an additive effect of rapid sequential TBI.8
Table 2
10-level Rancho Los Amigos Scale for assessing TBI recovery
| Level | Cognitive and adaptive function | Assistance required |
|---|---|---|
| I | No response | Total assistance |
| II | Generalized response | Total assistance |
| III | Localized response | Total assistance |
| IV | Confused/agitated | Maximal assistance |
| V | Confused, inappropriate non-agitated | Maximal assistance |
| VI | Confused, appropriate | Moderate assistance |
| VII | Automatic, appropriate | Minimal assistance |
| VIII | Purposeful, appropriate | Stand-by assistance |
| IX | Purposeful, appropriate | Stand-by assistanceon request |
| X | Purposeful, appropriate | Modified independent |
| Source: Traumatic Brain Injury Resource Guide. www.neuroskills.com. | ||
Recovery for a patient such as Mr. N with Rancho level IV to V TBI may be complicated by marked mood lability, spontaneous aggression, psychomotor agitation, extremely short attention with marked distractibility, little to no short-term memory, and noncooperation with treatment and care. Patients may also show disorders of diminished motivation, characterized by normal consciousness but decreased goal-directed behavior and affective flattening.9
Case continued: Calling in reinforcements
Besides combat nightmares, Mr. N is experiencing other signs of posttraumatic stress disorder (PTSD): intrusive memories of dead comrades, anhedonia, insomnia, irritability, and hypervigilance. We recommend a trial of citalopram, 10 mg/d, but within 1 week he becomes more irritable, agitated, and aggressive, with worsening sleep. We arrange a meeting to obtain collateral information from Mr. N’s aunt, mother, and clinical psychologist. We learn that a first-degree relative had bipolar disorder, and Mr. N lived with various relatives during childhood.
As a child, Mr. N was easily angered, hyperactive, unpredictably aggressive with peers, and impulsive. He was diagnosed with “explosive disorder” at age 8. A psychiatrist prescribed methylphenidate (which helped) and paroxetine (which worsened his behavior and aggression). Based on this history, we make a presumptive diagnosis of comorbid bipolar disorder.
Treating psychopathology
Comorbidities. Adolescents and adults with pre-existing attention-deficit/hyperactivity disorder or bipolar disorder may be predisposed to carelessness or risk taking that lead to accidents and TBI. Likewise, alcoholism and substance use disorders are risk factors for head injuries. These pre-existing conditions will complicate the post-TBI course and must be treated concurrently.
Depression and PTSD may follow a head injury and complicate recovery. In fact, post-TBI symptoms—poor sleep, poor memory and concentration, and irritability—are common to both depression and PTSD.
A team approach. Regardless of its severity or recovery stage, TBI requires multidisciplinary treatment. Physical, occupational, and speech therapies are essential initially. As recovery progresses, vocational rehabilitation may need to be added. Throughout rehabilitation, supportive individual and family therapy can help patients reintegrate into the community. Psychologists, neuropsychologists, and clinical social workers are indispensable to the treatment team.
Medication precautions
Using medications to manage post-TBI syndromes is difficult and controversial. No standard regimen exists, and few clinical trials guide treatment. Small, uncontrolled studies (human and animal) suggest commonly prescribed drugs may worsen outcomes (Table 3).10,11 For example:
- Cognitive function improved in three TBI patients after thioridazine was discontinued in two and haloperidol in one.12
- Haloperidol given to 11 patients with TBI made no difference in rehabilitation outcomes when compared with 15 patients who did not receive the antipsychotic. Those receiving haloperidol also had longer post-trauma amnesia (5 to 30 weeks), compared with the untreated group (1 to 18 weeks).13
- In animal studies of TBI, motor recovery was slowed with haloperidol but not olanzapine,14,15 and with clonidine,16 phenytoin,17 and trazodone.18 Phenobarbitol.19 and diazepam20 have been associated with delayed behavioral recovery and chronic behavior problems, respectively, in rats with TBI. How these agents might affect human patients is speculative.
Medications with potential to impede TBI recovery*
| Class | Medications |
|---|---|
| Alpha-2 agonist | Clonidine |
| Antidepressant | Trazodone |
| Antiepileptic | Phenytoin, phenobarbital |
| Benzodiazepine | Diazepam |
| Neuroleptic | Haloperidol, thioridazine |
| *Suggested by animal or clinical studies | |
| Source: References 11-20 | |
- Psychostimulants have improved recovery of motor function in animal trials if given before physical therapy.14
- Stimulants and dopaminergic agonists such as bromocriptine and amantadine might help disorders of diminished motivation.22
- Dextroamphetamine and methylphenidate have improved impulsivity, memory, and concentration in a patient with TBI.23
Table 4
Drugs considered safe and effective
for TBI neurobehavioral symptoms
| Target symptom(s) | Drug | Usual daily dosage* |
|---|---|---|
| Apathy | Amantadine | 100 to 400 mg |
| Bromocriptine | 1.25 to 100 mg | |
| Cognition | Donepezil | |
| Inattention | Dextroamphetamine | 5 to 60 mg |
| Methylphenidate | 10 to 60 mg | |
| Depression, PTSD symptoms | Fluoxetine | 20 to 80 mg |
| Agitation, mood stabilization | Anticonvulsants | |
| Lamotrigine | 25 to 200 mg | |
| Divalproex sodium | 10 to 15 mg/kg/day† | |
| Carbamazepine | 400 to 1,600 mg‡ | |
| Atypical antipsychotics | ||
| Olanzapine | 2.5 to 20 mg | |
| Quetiapine | 50 to 800 mg | |
| Risperidone | 0.5 to 6 mg | |
| Ziprasidone | 20 to 160 mg | |
| Beta blocker | ||
| Propranolol | 20 to 480 mg | |
| PTSD: posttraumatic stress disorder | ||
| * Dosage may be divided; see full prescribing information. | ||
| † Adjust dosage to achieve serum level of 50 to 100 mcg/mL. | ||
| ‡ Adjust dosage to achieve serum level of 4 to 12 mcg/mL. | ||
Small studies of anticonvulsants for post-TBI agitation report:
- valproic acid might improve behavioral control and decrease aggression, and it did not worsen performance on neuropsychological testing
- carbamazepine reduced agitation in seven TBI patients and reduced anger outbursts in 8 of 10 others
- gabapentin caused paradoxical effects in two TBI patients25
- lamotrigine improved agitation in one TBI patient.26
- propranolol, 420 to 520 mg/d
- pindolol, 60 mg/d
- metoprolol, 200 mg/d.21
Dosing atypical antipsychotics
for agitation and aggression in TBI
| Drug | Initial daily dosage* | Maximum daily dosage* |
|---|---|---|
| Aripiprazole | 2.5 to 5 mg | 30 mg |
| Olanzapine | 2.5 mg | 20 mg |
| Quetiapine | 12.5 to 50 mg | 800 mg |
| Risperidone | 0.25 mg | 8 mg |
| Ziprasidone | 20 mg | 160 mg |
| *Daily dosages may be divided | ||
Depression and PTSD in TBI patients are considered indications for selective serotonin reuptake inhibitors (SSRIs). Animal data suggest that fluoxetine is safe for patients with TBI,27 though no human data have been published.
For PTSD with bipolar depression, we usually prescribe lamotrigine or combine an atypical antipsychotic with an SSRI. Lithium would be second-line therapy. PTSD with bipolar mania is more difficult to treat because little evidence guides medication choices. As with depression and PTSD, we usually combine an atypical antipsychotic with an SSRI. We try to control manic and psychotic symptoms first, then add the SSRI for anxiety after the mood becomes more stable.
Cognitive impairment. A dozen published studies and case reports indicate that donepezil improves cognition in subacute and chronic TBI. For example:
- An open-label trial showed subjective improvement in cognitive functions in 8 of 10 patients given donepezil.28
- In a double-blind, placebo-controlled, crossover trial, short-term memory and attention improved with donepezil in 18 patients with post-acute TBI, as shown by neuropsychological test scores.29
- A retrospective case-control study showed no significant difference in cognitive outcome between controls and 18 patients prescribed donepezil but did suggest that cognition improved more rapidly when patients started donepezil earlier in recovery.30
Case continued: Back to rehab
We replace Mr. N’s phenytoin with carbamazepine, 700 mg/d (serum level about 12 mcg/mL), discontinue citalopram, and start him on quetiapine as a mood stabilizer, titrating the dosage to 600 mg/d over 3 weeks. We select quetiapine based on experience using it as a mood stabilizer and carbamazepine for additional mood stabilization and seizure prophylaxis.
We continue methadone and oxycodone at the same dosages for pain management, with good results. We eventually switch him from zolpidem to trazodone, 50 mg as needed at bedtime. We discontinue lamotrigine because he is no longer having seizures.
Mr. N tolerates quetiapine and carbamazepine well. The nursing staff reports he is much less irritable and aggressive and his sleep has improved, but he is not oversedated. He returns to and participates in physical, occupational, and speech therapies.
Tips for using medications
Many TBI patients are unusually sensitive to or intolerant of medication side effects. Because no randomized, controlled clinical trials support using any medication in these patients, be cautious. The following recommendations can help:
- Use psychotropics with a low risk of complications.
- Start with low dosages and increase gradually to assess side effects and efficacy of medication trials.
- Give full trials and adequate dosing before you decide a medication has not improved symptoms sufficiently.
- Monitor closely for side effects.
- Seek information from family members to evaluate a medication’s effectiveness, as patients’ cognitive deficits may limit their ability to reliably report symptoms.
Related resources
- Silver JM, McAllister TW, Yudofsky SC (eds). Textbook of traumatic brain injury. Arlington, VA: American Psychiatric Press, 2005.
- Traumatic Brain Injury Resource Guide. www.neuroskills.com
- Amantadine • Symmetrel
- Bromocriptine • Parlodel
- Carbamazepine • Tegretol
- Citalopram • Celexa
- Clonidine • Catapres
- Dextroamphetamine • Dexedrine
- Diazepam • Valium
- Divalproex sodium • Depakote
- Donepezil • Aricept
- Fluoxetine • Prozac
- Gabapentin • Neurontin
- Haloperidol • Haldol
- Lamotrigine • Lamictal
- Methadone • Dolophine
- Methylphenidate • Ritalin
- Metoprolol • Lopressor
- Olanzapine • Zyprexa
- Oxycodone • Oxycontin
- Paroxetine • Paxil
- Phenobarbital • Luminal
- Phenytoin • Dilantin
- Pindolol • Visken
- Propranolol • Inderal
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Thioridazine • Mellaril
- Trazodone • Desyrel
- Ziprasidone • Geodon
- Zolpidem • Ambien
The author reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. American Academy of Neurology. Practice parameter: The management of concussion in sports. Neurology 1997;48:581-5.
2. Teasdale G, Jennett B. Assessment of coma and impaired consciousness. A practical scale. Lancet 1974;2(7872):81-4.
3. Alexander MP. Mild traumatic brain injury: Pathophysiology, natural history, and clinical management. Neurology 1995;45:1253-60.
4. Arlinghaus KA, Shoaib AM, Price TRP. Neuropsychiatric assessment. In: Silver JM, McAllister TW, Yudofsky SC (eds). Textbook of traumatic brain injury. Arlington, VA: American Psychiatric Press; 2005:59-78.
5. Hagen C, Malkmus D, Durham P. Communication Disorders Service, Rancho Los Amigos Rehabilitation Hospital, Downey, CA, 1972 (rev. 1997).
6. Diagnostic and statistical manual of mental disorders (4th ed, text rev). Washington, DC: American Psychiatric Association; 2000.
7. McCrory P. Does second impact syndrome exist? Clin J Sport Med 2001;11:144-9.
8. Vagnozzi R, Signoretti S, Tavazzi B, et al. Hypothesis of the postconcussive vulnerable brain: experimental evidence of its metabolic occurrence. Neurosurgery 2005;57:164-71.
9. Marin RS, Chakravorty S. Disorders of diminished motivation. In: Silver JM, McAllister TW, Yudofsky SC (eds). Textbook of traumatic brain injury. Arlington, VA; American Psychiatric Press; 2005:337-52.
10. Goldstein LB. Prescribing of potentially harmful drugs to patients admitted to hospital after head injury. J Neurol Neurosurg Psychiatry 1995;58:753-5.
11. Phillips JP, Devier DJ, Feeney DM. Rehabilitation pharmacology bridging laboratory work to clinical application. J Head Trauma Rehabil 2003;18:342-56.
12. Stanislaw SL. Cognitive effects of antipsychotic agents in persons with traumatic brain injury. Brain Injury 1997;11:335-41.
13. Rao N, Jellinek HM, Woolston DC. Agitation in closed head injury: haloperidol effects on rehabilitation outcome. Arch Phys Med Rehabil 1985;66:30-4.
14. Feeney DM, Gonzalez A, Law WA. Amphetamine, haloperidol, and experience interact to affect rate of recovery after motor cortex injury. Science 1982;217:855-7.
15. Wilson MS, Gibson CL, Hamm RJ. Haloperidol, but not olanzapine, impairs cognitive performance after traumatic brain injury in rats. Am J Phys Med Rehabil 2003;82:871-9.
16. Goldstein LB, Davis JN. Clonidine impairs recovery of beamwalking after a sensorimotor cortex lesion in the rat. Brain Research 1990;508:305-9.
17. Brailowsky S, Knight RT, Efron R. Phenytoin increases the severity of cortical hemiplegia in rats. Brain Research 1986;376:71-7.
18. Boyeson MG, Harmon RL. Effects of trazodone and desipramine on motor recovery in brain-injured rats. Am J Phys Med Rehabil 1993;72:286-93.
19. Hernandez TD, Holling LC. Disruption of behavioral recovery by the anticonvulsant phenobarbital. Brain Research 1994;635:300-6.
20. Schallert T, Hernandez TD, Barth TM. Recovery of function after brain damage: severe and chronic disruption by diazepam. Brain Research 1986;379:104-11.
21. Deb S, Crownshaw T. The role of pharmacotherapy in the management of behavior disorders in traumatic brain injury patients. Brain Injury 2004;18:1-31.
22. Campbell JJ, Duffy JD. Treatment strategies in amotivated patients. Psychiatric Annals 1997;27(1):44-9.
23. Evans RW, Gualtieri CT, Patterson D. Treatment of chronic closed head injury with psychostimulant drugs: a controlled case study and an appropriate evaluation procedure. J Nerv Ment Dis 1987;175:106-10.
24. Elovic EP, Lansang R, Li Y, Ricker JH. The use of atypical antipsychotics in traumatic brain injury. J Head Trauma Rehabil 2003;18:177-95.
25. Lombard LA, Zafonte RD. Agitation after traumatic brain injury: considerations and treatment options. Am J Phys Med Rehabil 2005;84:797-812.
26. Pachet A, Friesen S, Winkelaar D, Gray S. Beneficial behavioural effects of lamotrigine in traumatic brain injury. Brain Injury 2003;17:715-22.
27. Boyeson MG, Harmon RL, Jones JL. Comparative effects of fluoxetine, amitriptyline, and serotonin on functional motor recovery after sensorimotor cortex injury. Am J Phys Med Rehabil 1994;73:76-83.
28. Khateb A, Ammann J, Annoni JM, Diserens K. Cognition enhancing effects of onepezil in traumatic brain injury (abstract). Eur Neurol 2005;54:39-45.
29. Zhang L, Plotkin RC, Wang G, et al. Cholinergic augmentation with donepezil enhances recovery in short-term memory and sustained attention after traumatic brain injury. Arch Phys Med Rehabil 2004;85:1005-55.
30. Walker W, Seel R, Gibellato M, et al. The effects of donepezil on traumatic brain injury acute rehabilitation outcomes. Brain Inj 2004;18:739-50.
Choosing medications for patients with traumatic brain injury (TBI) requires caution; some drugs slow their recovery, and no standard post-TBI treatment exists.
As consulting psychiatrist on a TBI rehabilitation team, I am asked to manage enduring cognitive and emotional problems—aggression, apathy, learning disabilities, dementia—in patients with moderate to severe head injuries. This article describes how we apply available evidence to treat neurobehavioral symptoms in these patients.
Case: An iraq war casualty
The physical medicine and rehabilitation service asks for help in managing agitation, anxiety, and nightmares in Mr. N, age 20, a U.S. combat soldier. While on patrol 2 months ago in Iraq, he suffered a penetrating right frontoparietal brain injury from an improvised explosive device.
Mr. N has undergone a right temporoparietal craniectomy with debridement, ventriculostomy placement, and scalp flap closure. He has had seizures and then pancreatitis—thought to be caused by divalproex prescribed to treat the seizures. Divalproex was replaced with phenytoin at our hospital, and the pancreatitis resolved.
How serious an injury?
TBI ranges from self-limited concussion to devastating, permanent CNS impairment and life-long disability. Brain injuries from sudden impact—from assaults, falls, motor vehicle accidents, combat, or sports—can cause diffuse axonal injury and confusion or unconsciousness, even without radiographic evidence of cerebral bleeding, edema, or mass effect.
No hierarchy or nomenclature is universally accepted for TBI. The term “concussion” is generally used for milder injury and TBI for more-severe injuries.
Concussion. The American Academy of Neurology defines concussion as a trauma-induced alteration in mental status that may or may not involve loss of consciousness. Confusion and amnesia—the hallmarks of concussion—may occur immediately after the head trauma or several minutes later.1 This definition recognizes three concussion grades:
- Grade 1: confusion lasts
- Grade 2: confusion persists >15 minutes but without LOC
- Grade 3: concussion with LOC. The confusional state is marked by disorientation, delayed verbal and motor responses, inattention, incoordination, emotional lability, and slurred or incoherent speech.
- Mild TBI: GCS 13 to 15, LOC 1,3
- Moderate TBI: GCS 9 to 12, LOC 30 minutes to 7 days, and PTA 24 hours to 7 days.
- Severe TBI: GCS ≤8, LOC, and PTA >7 days,4 or any focal neuroimaging abnormalities.3
Using Glasgow Coma Scale scores to evaluate brain injury severity
| Component | Response | Score |
|---|---|---|
| Best eye response | No eye opening | 1 |
| Eye opening to pain | 2 | |
| Eye opening to verbal command | 3 | |
| Eyes open spontaneously | 4 | |
| Best verbal response | No verbal response | 1 |
| Incomprehensible sounds | 2 | |
| Inappropriate words | 3 | |
| Confused | 4 | |
| Oriented | 5 | |
| Best motor response | No motor response | 1 |
| Extension to pain | 2 | |
| Flexion to pain | 3 | |
| Withdrawal from pain | 4 | |
| Localizing pain | 5 | |
| Obeys commands | 6 | |
| GCS total score ≥12 is mild injury, 9 to 11 is moderate, and ≤8 is severe (90% of patients with scores ≤8 are in a coma). Coma is defined as not opening eyes, not obeying commands, and not saying understandable words. Composite scores with eye, verbal, and motor responses (such as E3V3M5) are clinically more useful than totals. | ||
| Source: Reference 2. | ||
Case continued: ‘They’re hurting me’
Mr. N meets criteria for severe TBI. He is periodically agitated and aggressive and refuses to return to physical therapy, complaining that rehabilitation nurses are intentionally hurting him. He occasionally hits the staff and throws things. His medications include:
- phenytoin, 100 mg every 6 hours for seizure prophylaxis
- lamotrigine, 50 mg bid for seizure prophylaxis
- zolpidem, 5 mg as needed at bedtime for pain
- methadone, 10 mg/d for pain
- oxycodone, 5 mg every 4 hours as needed for breakthrough pain.
Assessing progress
For patients such as Mr. N, TBI recovery progress is measured with the Rancho Los Amigos Scale.
The original Rancho scale—developed in 1972 by staff at the Rancho Los Amigos rehabilitation hospital in Downey, CA—described eight levels of cognitive and adaptive functioning, from coma and total care through normal cognition and independence. A 1997 revised version separates the highest cognitive functioning level (VIII, purposeful, appropriate function) into three parts, expanding the scale to 10 levels (Table 2).5
Of course, not all TBI patients begin recovery at Rancho level I, and unfortunately not all achieve level X. Some experience dementia caused by head trauma, with persistent memory impairment and cognitive deficits in language, apraxia, agnosia, or executive function.6
Most patients recover as predicted by the initial injury’s severity. Others experience diffuse cerebral swelling with sudden, rapid deterioration after what appeared to be a grade 1 or grade 2 concussion. Diffuse cerebral swelling is sometimes considered a “second-impact syndrome,” but it can also occur after a single impact.7 A second TBI is not universally believed to cause the precipitous decline, but animal studies suggest an additive effect of rapid sequential TBI.8
Table 2
10-level Rancho Los Amigos Scale for assessing TBI recovery
| Level | Cognitive and adaptive function | Assistance required |
|---|---|---|
| I | No response | Total assistance |
| II | Generalized response | Total assistance |
| III | Localized response | Total assistance |
| IV | Confused/agitated | Maximal assistance |
| V | Confused, inappropriate non-agitated | Maximal assistance |
| VI | Confused, appropriate | Moderate assistance |
| VII | Automatic, appropriate | Minimal assistance |
| VIII | Purposeful, appropriate | Stand-by assistance |
| IX | Purposeful, appropriate | Stand-by assistanceon request |
| X | Purposeful, appropriate | Modified independent |
| Source: Traumatic Brain Injury Resource Guide. www.neuroskills.com. | ||
Recovery for a patient such as Mr. N with Rancho level IV to V TBI may be complicated by marked mood lability, spontaneous aggression, psychomotor agitation, extremely short attention with marked distractibility, little to no short-term memory, and noncooperation with treatment and care. Patients may also show disorders of diminished motivation, characterized by normal consciousness but decreased goal-directed behavior and affective flattening.9
Case continued: Calling in reinforcements
Besides combat nightmares, Mr. N is experiencing other signs of posttraumatic stress disorder (PTSD): intrusive memories of dead comrades, anhedonia, insomnia, irritability, and hypervigilance. We recommend a trial of citalopram, 10 mg/d, but within 1 week he becomes more irritable, agitated, and aggressive, with worsening sleep. We arrange a meeting to obtain collateral information from Mr. N’s aunt, mother, and clinical psychologist. We learn that a first-degree relative had bipolar disorder, and Mr. N lived with various relatives during childhood.
As a child, Mr. N was easily angered, hyperactive, unpredictably aggressive with peers, and impulsive. He was diagnosed with “explosive disorder” at age 8. A psychiatrist prescribed methylphenidate (which helped) and paroxetine (which worsened his behavior and aggression). Based on this history, we make a presumptive diagnosis of comorbid bipolar disorder.
Treating psychopathology
Comorbidities. Adolescents and adults with pre-existing attention-deficit/hyperactivity disorder or bipolar disorder may be predisposed to carelessness or risk taking that lead to accidents and TBI. Likewise, alcoholism and substance use disorders are risk factors for head injuries. These pre-existing conditions will complicate the post-TBI course and must be treated concurrently.
Depression and PTSD may follow a head injury and complicate recovery. In fact, post-TBI symptoms—poor sleep, poor memory and concentration, and irritability—are common to both depression and PTSD.
A team approach. Regardless of its severity or recovery stage, TBI requires multidisciplinary treatment. Physical, occupational, and speech therapies are essential initially. As recovery progresses, vocational rehabilitation may need to be added. Throughout rehabilitation, supportive individual and family therapy can help patients reintegrate into the community. Psychologists, neuropsychologists, and clinical social workers are indispensable to the treatment team.
Medication precautions
Using medications to manage post-TBI syndromes is difficult and controversial. No standard regimen exists, and few clinical trials guide treatment. Small, uncontrolled studies (human and animal) suggest commonly prescribed drugs may worsen outcomes (Table 3).10,11 For example:
- Cognitive function improved in three TBI patients after thioridazine was discontinued in two and haloperidol in one.12
- Haloperidol given to 11 patients with TBI made no difference in rehabilitation outcomes when compared with 15 patients who did not receive the antipsychotic. Those receiving haloperidol also had longer post-trauma amnesia (5 to 30 weeks), compared with the untreated group (1 to 18 weeks).13
- In animal studies of TBI, motor recovery was slowed with haloperidol but not olanzapine,14,15 and with clonidine,16 phenytoin,17 and trazodone.18 Phenobarbitol.19 and diazepam20 have been associated with delayed behavioral recovery and chronic behavior problems, respectively, in rats with TBI. How these agents might affect human patients is speculative.
Medications with potential to impede TBI recovery*
| Class | Medications |
|---|---|
| Alpha-2 agonist | Clonidine |
| Antidepressant | Trazodone |
| Antiepileptic | Phenytoin, phenobarbital |
| Benzodiazepine | Diazepam |
| Neuroleptic | Haloperidol, thioridazine |
| *Suggested by animal or clinical studies | |
| Source: References 11-20 | |
- Psychostimulants have improved recovery of motor function in animal trials if given before physical therapy.14
- Stimulants and dopaminergic agonists such as bromocriptine and amantadine might help disorders of diminished motivation.22
- Dextroamphetamine and methylphenidate have improved impulsivity, memory, and concentration in a patient with TBI.23
Table 4
Drugs considered safe and effective
for TBI neurobehavioral symptoms
| Target symptom(s) | Drug | Usual daily dosage* |
|---|---|---|
| Apathy | Amantadine | 100 to 400 mg |
| Bromocriptine | 1.25 to 100 mg | |
| Cognition | Donepezil | |
| Inattention | Dextroamphetamine | 5 to 60 mg |
| Methylphenidate | 10 to 60 mg | |
| Depression, PTSD symptoms | Fluoxetine | 20 to 80 mg |
| Agitation, mood stabilization | Anticonvulsants | |
| Lamotrigine | 25 to 200 mg | |
| Divalproex sodium | 10 to 15 mg/kg/day† | |
| Carbamazepine | 400 to 1,600 mg‡ | |
| Atypical antipsychotics | ||
| Olanzapine | 2.5 to 20 mg | |
| Quetiapine | 50 to 800 mg | |
| Risperidone | 0.5 to 6 mg | |
| Ziprasidone | 20 to 160 mg | |
| Beta blocker | ||
| Propranolol | 20 to 480 mg | |
| PTSD: posttraumatic stress disorder | ||
| * Dosage may be divided; see full prescribing information. | ||
| † Adjust dosage to achieve serum level of 50 to 100 mcg/mL. | ||
| ‡ Adjust dosage to achieve serum level of 4 to 12 mcg/mL. | ||
Small studies of anticonvulsants for post-TBI agitation report:
- valproic acid might improve behavioral control and decrease aggression, and it did not worsen performance on neuropsychological testing
- carbamazepine reduced agitation in seven TBI patients and reduced anger outbursts in 8 of 10 others
- gabapentin caused paradoxical effects in two TBI patients25
- lamotrigine improved agitation in one TBI patient.26
- propranolol, 420 to 520 mg/d
- pindolol, 60 mg/d
- metoprolol, 200 mg/d.21
Dosing atypical antipsychotics
for agitation and aggression in TBI
| Drug | Initial daily dosage* | Maximum daily dosage* |
|---|---|---|
| Aripiprazole | 2.5 to 5 mg | 30 mg |
| Olanzapine | 2.5 mg | 20 mg |
| Quetiapine | 12.5 to 50 mg | 800 mg |
| Risperidone | 0.25 mg | 8 mg |
| Ziprasidone | 20 mg | 160 mg |
| *Daily dosages may be divided | ||
Depression and PTSD in TBI patients are considered indications for selective serotonin reuptake inhibitors (SSRIs). Animal data suggest that fluoxetine is safe for patients with TBI,27 though no human data have been published.
For PTSD with bipolar depression, we usually prescribe lamotrigine or combine an atypical antipsychotic with an SSRI. Lithium would be second-line therapy. PTSD with bipolar mania is more difficult to treat because little evidence guides medication choices. As with depression and PTSD, we usually combine an atypical antipsychotic with an SSRI. We try to control manic and psychotic symptoms first, then add the SSRI for anxiety after the mood becomes more stable.
Cognitive impairment. A dozen published studies and case reports indicate that donepezil improves cognition in subacute and chronic TBI. For example:
- An open-label trial showed subjective improvement in cognitive functions in 8 of 10 patients given donepezil.28
- In a double-blind, placebo-controlled, crossover trial, short-term memory and attention improved with donepezil in 18 patients with post-acute TBI, as shown by neuropsychological test scores.29
- A retrospective case-control study showed no significant difference in cognitive outcome between controls and 18 patients prescribed donepezil but did suggest that cognition improved more rapidly when patients started donepezil earlier in recovery.30
Case continued: Back to rehab
We replace Mr. N’s phenytoin with carbamazepine, 700 mg/d (serum level about 12 mcg/mL), discontinue citalopram, and start him on quetiapine as a mood stabilizer, titrating the dosage to 600 mg/d over 3 weeks. We select quetiapine based on experience using it as a mood stabilizer and carbamazepine for additional mood stabilization and seizure prophylaxis.
We continue methadone and oxycodone at the same dosages for pain management, with good results. We eventually switch him from zolpidem to trazodone, 50 mg as needed at bedtime. We discontinue lamotrigine because he is no longer having seizures.
Mr. N tolerates quetiapine and carbamazepine well. The nursing staff reports he is much less irritable and aggressive and his sleep has improved, but he is not oversedated. He returns to and participates in physical, occupational, and speech therapies.
Tips for using medications
Many TBI patients are unusually sensitive to or intolerant of medication side effects. Because no randomized, controlled clinical trials support using any medication in these patients, be cautious. The following recommendations can help:
- Use psychotropics with a low risk of complications.
- Start with low dosages and increase gradually to assess side effects and efficacy of medication trials.
- Give full trials and adequate dosing before you decide a medication has not improved symptoms sufficiently.
- Monitor closely for side effects.
- Seek information from family members to evaluate a medication’s effectiveness, as patients’ cognitive deficits may limit their ability to reliably report symptoms.
Related resources
- Silver JM, McAllister TW, Yudofsky SC (eds). Textbook of traumatic brain injury. Arlington, VA: American Psychiatric Press, 2005.
- Traumatic Brain Injury Resource Guide. www.neuroskills.com
- Amantadine • Symmetrel
- Bromocriptine • Parlodel
- Carbamazepine • Tegretol
- Citalopram • Celexa
- Clonidine • Catapres
- Dextroamphetamine • Dexedrine
- Diazepam • Valium
- Divalproex sodium • Depakote
- Donepezil • Aricept
- Fluoxetine • Prozac
- Gabapentin • Neurontin
- Haloperidol • Haldol
- Lamotrigine • Lamictal
- Methadone • Dolophine
- Methylphenidate • Ritalin
- Metoprolol • Lopressor
- Olanzapine • Zyprexa
- Oxycodone • Oxycontin
- Paroxetine • Paxil
- Phenobarbital • Luminal
- Phenytoin • Dilantin
- Pindolol • Visken
- Propranolol • Inderal
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Thioridazine • Mellaril
- Trazodone • Desyrel
- Ziprasidone • Geodon
- Zolpidem • Ambien
The author reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Choosing medications for patients with traumatic brain injury (TBI) requires caution; some drugs slow their recovery, and no standard post-TBI treatment exists.
As consulting psychiatrist on a TBI rehabilitation team, I am asked to manage enduring cognitive and emotional problems—aggression, apathy, learning disabilities, dementia—in patients with moderate to severe head injuries. This article describes how we apply available evidence to treat neurobehavioral symptoms in these patients.
Case: An iraq war casualty
The physical medicine and rehabilitation service asks for help in managing agitation, anxiety, and nightmares in Mr. N, age 20, a U.S. combat soldier. While on patrol 2 months ago in Iraq, he suffered a penetrating right frontoparietal brain injury from an improvised explosive device.
Mr. N has undergone a right temporoparietal craniectomy with debridement, ventriculostomy placement, and scalp flap closure. He has had seizures and then pancreatitis—thought to be caused by divalproex prescribed to treat the seizures. Divalproex was replaced with phenytoin at our hospital, and the pancreatitis resolved.
How serious an injury?
TBI ranges from self-limited concussion to devastating, permanent CNS impairment and life-long disability. Brain injuries from sudden impact—from assaults, falls, motor vehicle accidents, combat, or sports—can cause diffuse axonal injury and confusion or unconsciousness, even without radiographic evidence of cerebral bleeding, edema, or mass effect.
No hierarchy or nomenclature is universally accepted for TBI. The term “concussion” is generally used for milder injury and TBI for more-severe injuries.
Concussion. The American Academy of Neurology defines concussion as a trauma-induced alteration in mental status that may or may not involve loss of consciousness. Confusion and amnesia—the hallmarks of concussion—may occur immediately after the head trauma or several minutes later.1 This definition recognizes three concussion grades:
- Grade 1: confusion lasts
- Grade 2: confusion persists >15 minutes but without LOC
- Grade 3: concussion with LOC. The confusional state is marked by disorientation, delayed verbal and motor responses, inattention, incoordination, emotional lability, and slurred or incoherent speech.
- Mild TBI: GCS 13 to 15, LOC 1,3
- Moderate TBI: GCS 9 to 12, LOC 30 minutes to 7 days, and PTA 24 hours to 7 days.
- Severe TBI: GCS ≤8, LOC, and PTA >7 days,4 or any focal neuroimaging abnormalities.3
Using Glasgow Coma Scale scores to evaluate brain injury severity
| Component | Response | Score |
|---|---|---|
| Best eye response | No eye opening | 1 |
| Eye opening to pain | 2 | |
| Eye opening to verbal command | 3 | |
| Eyes open spontaneously | 4 | |
| Best verbal response | No verbal response | 1 |
| Incomprehensible sounds | 2 | |
| Inappropriate words | 3 | |
| Confused | 4 | |
| Oriented | 5 | |
| Best motor response | No motor response | 1 |
| Extension to pain | 2 | |
| Flexion to pain | 3 | |
| Withdrawal from pain | 4 | |
| Localizing pain | 5 | |
| Obeys commands | 6 | |
| GCS total score ≥12 is mild injury, 9 to 11 is moderate, and ≤8 is severe (90% of patients with scores ≤8 are in a coma). Coma is defined as not opening eyes, not obeying commands, and not saying understandable words. Composite scores with eye, verbal, and motor responses (such as E3V3M5) are clinically more useful than totals. | ||
| Source: Reference 2. | ||
Case continued: ‘They’re hurting me’
Mr. N meets criteria for severe TBI. He is periodically agitated and aggressive and refuses to return to physical therapy, complaining that rehabilitation nurses are intentionally hurting him. He occasionally hits the staff and throws things. His medications include:
- phenytoin, 100 mg every 6 hours for seizure prophylaxis
- lamotrigine, 50 mg bid for seizure prophylaxis
- zolpidem, 5 mg as needed at bedtime for pain
- methadone, 10 mg/d for pain
- oxycodone, 5 mg every 4 hours as needed for breakthrough pain.
Assessing progress
For patients such as Mr. N, TBI recovery progress is measured with the Rancho Los Amigos Scale.
The original Rancho scale—developed in 1972 by staff at the Rancho Los Amigos rehabilitation hospital in Downey, CA—described eight levels of cognitive and adaptive functioning, from coma and total care through normal cognition and independence. A 1997 revised version separates the highest cognitive functioning level (VIII, purposeful, appropriate function) into three parts, expanding the scale to 10 levels (Table 2).5
Of course, not all TBI patients begin recovery at Rancho level I, and unfortunately not all achieve level X. Some experience dementia caused by head trauma, with persistent memory impairment and cognitive deficits in language, apraxia, agnosia, or executive function.6
Most patients recover as predicted by the initial injury’s severity. Others experience diffuse cerebral swelling with sudden, rapid deterioration after what appeared to be a grade 1 or grade 2 concussion. Diffuse cerebral swelling is sometimes considered a “second-impact syndrome,” but it can also occur after a single impact.7 A second TBI is not universally believed to cause the precipitous decline, but animal studies suggest an additive effect of rapid sequential TBI.8
Table 2
10-level Rancho Los Amigos Scale for assessing TBI recovery
| Level | Cognitive and adaptive function | Assistance required |
|---|---|---|
| I | No response | Total assistance |
| II | Generalized response | Total assistance |
| III | Localized response | Total assistance |
| IV | Confused/agitated | Maximal assistance |
| V | Confused, inappropriate non-agitated | Maximal assistance |
| VI | Confused, appropriate | Moderate assistance |
| VII | Automatic, appropriate | Minimal assistance |
| VIII | Purposeful, appropriate | Stand-by assistance |
| IX | Purposeful, appropriate | Stand-by assistanceon request |
| X | Purposeful, appropriate | Modified independent |
| Source: Traumatic Brain Injury Resource Guide. www.neuroskills.com. | ||
Recovery for a patient such as Mr. N with Rancho level IV to V TBI may be complicated by marked mood lability, spontaneous aggression, psychomotor agitation, extremely short attention with marked distractibility, little to no short-term memory, and noncooperation with treatment and care. Patients may also show disorders of diminished motivation, characterized by normal consciousness but decreased goal-directed behavior and affective flattening.9
Case continued: Calling in reinforcements
Besides combat nightmares, Mr. N is experiencing other signs of posttraumatic stress disorder (PTSD): intrusive memories of dead comrades, anhedonia, insomnia, irritability, and hypervigilance. We recommend a trial of citalopram, 10 mg/d, but within 1 week he becomes more irritable, agitated, and aggressive, with worsening sleep. We arrange a meeting to obtain collateral information from Mr. N’s aunt, mother, and clinical psychologist. We learn that a first-degree relative had bipolar disorder, and Mr. N lived with various relatives during childhood.
As a child, Mr. N was easily angered, hyperactive, unpredictably aggressive with peers, and impulsive. He was diagnosed with “explosive disorder” at age 8. A psychiatrist prescribed methylphenidate (which helped) and paroxetine (which worsened his behavior and aggression). Based on this history, we make a presumptive diagnosis of comorbid bipolar disorder.
Treating psychopathology
Comorbidities. Adolescents and adults with pre-existing attention-deficit/hyperactivity disorder or bipolar disorder may be predisposed to carelessness or risk taking that lead to accidents and TBI. Likewise, alcoholism and substance use disorders are risk factors for head injuries. These pre-existing conditions will complicate the post-TBI course and must be treated concurrently.
Depression and PTSD may follow a head injury and complicate recovery. In fact, post-TBI symptoms—poor sleep, poor memory and concentration, and irritability—are common to both depression and PTSD.
A team approach. Regardless of its severity or recovery stage, TBI requires multidisciplinary treatment. Physical, occupational, and speech therapies are essential initially. As recovery progresses, vocational rehabilitation may need to be added. Throughout rehabilitation, supportive individual and family therapy can help patients reintegrate into the community. Psychologists, neuropsychologists, and clinical social workers are indispensable to the treatment team.
Medication precautions
Using medications to manage post-TBI syndromes is difficult and controversial. No standard regimen exists, and few clinical trials guide treatment. Small, uncontrolled studies (human and animal) suggest commonly prescribed drugs may worsen outcomes (Table 3).10,11 For example:
- Cognitive function improved in three TBI patients after thioridazine was discontinued in two and haloperidol in one.12
- Haloperidol given to 11 patients with TBI made no difference in rehabilitation outcomes when compared with 15 patients who did not receive the antipsychotic. Those receiving haloperidol also had longer post-trauma amnesia (5 to 30 weeks), compared with the untreated group (1 to 18 weeks).13
- In animal studies of TBI, motor recovery was slowed with haloperidol but not olanzapine,14,15 and with clonidine,16 phenytoin,17 and trazodone.18 Phenobarbitol.19 and diazepam20 have been associated with delayed behavioral recovery and chronic behavior problems, respectively, in rats with TBI. How these agents might affect human patients is speculative.
Medications with potential to impede TBI recovery*
| Class | Medications |
|---|---|
| Alpha-2 agonist | Clonidine |
| Antidepressant | Trazodone |
| Antiepileptic | Phenytoin, phenobarbital |
| Benzodiazepine | Diazepam |
| Neuroleptic | Haloperidol, thioridazine |
| *Suggested by animal or clinical studies | |
| Source: References 11-20 | |
- Psychostimulants have improved recovery of motor function in animal trials if given before physical therapy.14
- Stimulants and dopaminergic agonists such as bromocriptine and amantadine might help disorders of diminished motivation.22
- Dextroamphetamine and methylphenidate have improved impulsivity, memory, and concentration in a patient with TBI.23
Table 4
Drugs considered safe and effective
for TBI neurobehavioral symptoms
| Target symptom(s) | Drug | Usual daily dosage* |
|---|---|---|
| Apathy | Amantadine | 100 to 400 mg |
| Bromocriptine | 1.25 to 100 mg | |
| Cognition | Donepezil | |
| Inattention | Dextroamphetamine | 5 to 60 mg |
| Methylphenidate | 10 to 60 mg | |
| Depression, PTSD symptoms | Fluoxetine | 20 to 80 mg |
| Agitation, mood stabilization | Anticonvulsants | |
| Lamotrigine | 25 to 200 mg | |
| Divalproex sodium | 10 to 15 mg/kg/day† | |
| Carbamazepine | 400 to 1,600 mg‡ | |
| Atypical antipsychotics | ||
| Olanzapine | 2.5 to 20 mg | |
| Quetiapine | 50 to 800 mg | |
| Risperidone | 0.5 to 6 mg | |
| Ziprasidone | 20 to 160 mg | |
| Beta blocker | ||
| Propranolol | 20 to 480 mg | |
| PTSD: posttraumatic stress disorder | ||
| * Dosage may be divided; see full prescribing information. | ||
| † Adjust dosage to achieve serum level of 50 to 100 mcg/mL. | ||
| ‡ Adjust dosage to achieve serum level of 4 to 12 mcg/mL. | ||
Small studies of anticonvulsants for post-TBI agitation report:
- valproic acid might improve behavioral control and decrease aggression, and it did not worsen performance on neuropsychological testing
- carbamazepine reduced agitation in seven TBI patients and reduced anger outbursts in 8 of 10 others
- gabapentin caused paradoxical effects in two TBI patients25
- lamotrigine improved agitation in one TBI patient.26
- propranolol, 420 to 520 mg/d
- pindolol, 60 mg/d
- metoprolol, 200 mg/d.21
Dosing atypical antipsychotics
for agitation and aggression in TBI
| Drug | Initial daily dosage* | Maximum daily dosage* |
|---|---|---|
| Aripiprazole | 2.5 to 5 mg | 30 mg |
| Olanzapine | 2.5 mg | 20 mg |
| Quetiapine | 12.5 to 50 mg | 800 mg |
| Risperidone | 0.25 mg | 8 mg |
| Ziprasidone | 20 mg | 160 mg |
| *Daily dosages may be divided | ||
Depression and PTSD in TBI patients are considered indications for selective serotonin reuptake inhibitors (SSRIs). Animal data suggest that fluoxetine is safe for patients with TBI,27 though no human data have been published.
For PTSD with bipolar depression, we usually prescribe lamotrigine or combine an atypical antipsychotic with an SSRI. Lithium would be second-line therapy. PTSD with bipolar mania is more difficult to treat because little evidence guides medication choices. As with depression and PTSD, we usually combine an atypical antipsychotic with an SSRI. We try to control manic and psychotic symptoms first, then add the SSRI for anxiety after the mood becomes more stable.
Cognitive impairment. A dozen published studies and case reports indicate that donepezil improves cognition in subacute and chronic TBI. For example:
- An open-label trial showed subjective improvement in cognitive functions in 8 of 10 patients given donepezil.28
- In a double-blind, placebo-controlled, crossover trial, short-term memory and attention improved with donepezil in 18 patients with post-acute TBI, as shown by neuropsychological test scores.29
- A retrospective case-control study showed no significant difference in cognitive outcome between controls and 18 patients prescribed donepezil but did suggest that cognition improved more rapidly when patients started donepezil earlier in recovery.30
Case continued: Back to rehab
We replace Mr. N’s phenytoin with carbamazepine, 700 mg/d (serum level about 12 mcg/mL), discontinue citalopram, and start him on quetiapine as a mood stabilizer, titrating the dosage to 600 mg/d over 3 weeks. We select quetiapine based on experience using it as a mood stabilizer and carbamazepine for additional mood stabilization and seizure prophylaxis.
We continue methadone and oxycodone at the same dosages for pain management, with good results. We eventually switch him from zolpidem to trazodone, 50 mg as needed at bedtime. We discontinue lamotrigine because he is no longer having seizures.
Mr. N tolerates quetiapine and carbamazepine well. The nursing staff reports he is much less irritable and aggressive and his sleep has improved, but he is not oversedated. He returns to and participates in physical, occupational, and speech therapies.
Tips for using medications
Many TBI patients are unusually sensitive to or intolerant of medication side effects. Because no randomized, controlled clinical trials support using any medication in these patients, be cautious. The following recommendations can help:
- Use psychotropics with a low risk of complications.
- Start with low dosages and increase gradually to assess side effects and efficacy of medication trials.
- Give full trials and adequate dosing before you decide a medication has not improved symptoms sufficiently.
- Monitor closely for side effects.
- Seek information from family members to evaluate a medication’s effectiveness, as patients’ cognitive deficits may limit their ability to reliably report symptoms.
Related resources
- Silver JM, McAllister TW, Yudofsky SC (eds). Textbook of traumatic brain injury. Arlington, VA: American Psychiatric Press, 2005.
- Traumatic Brain Injury Resource Guide. www.neuroskills.com
- Amantadine • Symmetrel
- Bromocriptine • Parlodel
- Carbamazepine • Tegretol
- Citalopram • Celexa
- Clonidine • Catapres
- Dextroamphetamine • Dexedrine
- Diazepam • Valium
- Divalproex sodium • Depakote
- Donepezil • Aricept
- Fluoxetine • Prozac
- Gabapentin • Neurontin
- Haloperidol • Haldol
- Lamotrigine • Lamictal
- Methadone • Dolophine
- Methylphenidate • Ritalin
- Metoprolol • Lopressor
- Olanzapine • Zyprexa
- Oxycodone • Oxycontin
- Paroxetine • Paxil
- Phenobarbital • Luminal
- Phenytoin • Dilantin
- Pindolol • Visken
- Propranolol • Inderal
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Thioridazine • Mellaril
- Trazodone • Desyrel
- Ziprasidone • Geodon
- Zolpidem • Ambien
The author reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. American Academy of Neurology. Practice parameter: The management of concussion in sports. Neurology 1997;48:581-5.
2. Teasdale G, Jennett B. Assessment of coma and impaired consciousness. A practical scale. Lancet 1974;2(7872):81-4.
3. Alexander MP. Mild traumatic brain injury: Pathophysiology, natural history, and clinical management. Neurology 1995;45:1253-60.
4. Arlinghaus KA, Shoaib AM, Price TRP. Neuropsychiatric assessment. In: Silver JM, McAllister TW, Yudofsky SC (eds). Textbook of traumatic brain injury. Arlington, VA: American Psychiatric Press; 2005:59-78.
5. Hagen C, Malkmus D, Durham P. Communication Disorders Service, Rancho Los Amigos Rehabilitation Hospital, Downey, CA, 1972 (rev. 1997).
6. Diagnostic and statistical manual of mental disorders (4th ed, text rev). Washington, DC: American Psychiatric Association; 2000.
7. McCrory P. Does second impact syndrome exist? Clin J Sport Med 2001;11:144-9.
8. Vagnozzi R, Signoretti S, Tavazzi B, et al. Hypothesis of the postconcussive vulnerable brain: experimental evidence of its metabolic occurrence. Neurosurgery 2005;57:164-71.
9. Marin RS, Chakravorty S. Disorders of diminished motivation. In: Silver JM, McAllister TW, Yudofsky SC (eds). Textbook of traumatic brain injury. Arlington, VA; American Psychiatric Press; 2005:337-52.
10. Goldstein LB. Prescribing of potentially harmful drugs to patients admitted to hospital after head injury. J Neurol Neurosurg Psychiatry 1995;58:753-5.
11. Phillips JP, Devier DJ, Feeney DM. Rehabilitation pharmacology bridging laboratory work to clinical application. J Head Trauma Rehabil 2003;18:342-56.
12. Stanislaw SL. Cognitive effects of antipsychotic agents in persons with traumatic brain injury. Brain Injury 1997;11:335-41.
13. Rao N, Jellinek HM, Woolston DC. Agitation in closed head injury: haloperidol effects on rehabilitation outcome. Arch Phys Med Rehabil 1985;66:30-4.
14. Feeney DM, Gonzalez A, Law WA. Amphetamine, haloperidol, and experience interact to affect rate of recovery after motor cortex injury. Science 1982;217:855-7.
15. Wilson MS, Gibson CL, Hamm RJ. Haloperidol, but not olanzapine, impairs cognitive performance after traumatic brain injury in rats. Am J Phys Med Rehabil 2003;82:871-9.
16. Goldstein LB, Davis JN. Clonidine impairs recovery of beamwalking after a sensorimotor cortex lesion in the rat. Brain Research 1990;508:305-9.
17. Brailowsky S, Knight RT, Efron R. Phenytoin increases the severity of cortical hemiplegia in rats. Brain Research 1986;376:71-7.
18. Boyeson MG, Harmon RL. Effects of trazodone and desipramine on motor recovery in brain-injured rats. Am J Phys Med Rehabil 1993;72:286-93.
19. Hernandez TD, Holling LC. Disruption of behavioral recovery by the anticonvulsant phenobarbital. Brain Research 1994;635:300-6.
20. Schallert T, Hernandez TD, Barth TM. Recovery of function after brain damage: severe and chronic disruption by diazepam. Brain Research 1986;379:104-11.
21. Deb S, Crownshaw T. The role of pharmacotherapy in the management of behavior disorders in traumatic brain injury patients. Brain Injury 2004;18:1-31.
22. Campbell JJ, Duffy JD. Treatment strategies in amotivated patients. Psychiatric Annals 1997;27(1):44-9.
23. Evans RW, Gualtieri CT, Patterson D. Treatment of chronic closed head injury with psychostimulant drugs: a controlled case study and an appropriate evaluation procedure. J Nerv Ment Dis 1987;175:106-10.
24. Elovic EP, Lansang R, Li Y, Ricker JH. The use of atypical antipsychotics in traumatic brain injury. J Head Trauma Rehabil 2003;18:177-95.
25. Lombard LA, Zafonte RD. Agitation after traumatic brain injury: considerations and treatment options. Am J Phys Med Rehabil 2005;84:797-812.
26. Pachet A, Friesen S, Winkelaar D, Gray S. Beneficial behavioural effects of lamotrigine in traumatic brain injury. Brain Injury 2003;17:715-22.
27. Boyeson MG, Harmon RL, Jones JL. Comparative effects of fluoxetine, amitriptyline, and serotonin on functional motor recovery after sensorimotor cortex injury. Am J Phys Med Rehabil 1994;73:76-83.
28. Khateb A, Ammann J, Annoni JM, Diserens K. Cognition enhancing effects of onepezil in traumatic brain injury (abstract). Eur Neurol 2005;54:39-45.
29. Zhang L, Plotkin RC, Wang G, et al. Cholinergic augmentation with donepezil enhances recovery in short-term memory and sustained attention after traumatic brain injury. Arch Phys Med Rehabil 2004;85:1005-55.
30. Walker W, Seel R, Gibellato M, et al. The effects of donepezil on traumatic brain injury acute rehabilitation outcomes. Brain Inj 2004;18:739-50.
1. American Academy of Neurology. Practice parameter: The management of concussion in sports. Neurology 1997;48:581-5.
2. Teasdale G, Jennett B. Assessment of coma and impaired consciousness. A practical scale. Lancet 1974;2(7872):81-4.
3. Alexander MP. Mild traumatic brain injury: Pathophysiology, natural history, and clinical management. Neurology 1995;45:1253-60.
4. Arlinghaus KA, Shoaib AM, Price TRP. Neuropsychiatric assessment. In: Silver JM, McAllister TW, Yudofsky SC (eds). Textbook of traumatic brain injury. Arlington, VA: American Psychiatric Press; 2005:59-78.
5. Hagen C, Malkmus D, Durham P. Communication Disorders Service, Rancho Los Amigos Rehabilitation Hospital, Downey, CA, 1972 (rev. 1997).
6. Diagnostic and statistical manual of mental disorders (4th ed, text rev). Washington, DC: American Psychiatric Association; 2000.
7. McCrory P. Does second impact syndrome exist? Clin J Sport Med 2001;11:144-9.
8. Vagnozzi R, Signoretti S, Tavazzi B, et al. Hypothesis of the postconcussive vulnerable brain: experimental evidence of its metabolic occurrence. Neurosurgery 2005;57:164-71.
9. Marin RS, Chakravorty S. Disorders of diminished motivation. In: Silver JM, McAllister TW, Yudofsky SC (eds). Textbook of traumatic brain injury. Arlington, VA; American Psychiatric Press; 2005:337-52.
10. Goldstein LB. Prescribing of potentially harmful drugs to patients admitted to hospital after head injury. J Neurol Neurosurg Psychiatry 1995;58:753-5.
11. Phillips JP, Devier DJ, Feeney DM. Rehabilitation pharmacology bridging laboratory work to clinical application. J Head Trauma Rehabil 2003;18:342-56.
12. Stanislaw SL. Cognitive effects of antipsychotic agents in persons with traumatic brain injury. Brain Injury 1997;11:335-41.
13. Rao N, Jellinek HM, Woolston DC. Agitation in closed head injury: haloperidol effects on rehabilitation outcome. Arch Phys Med Rehabil 1985;66:30-4.
14. Feeney DM, Gonzalez A, Law WA. Amphetamine, haloperidol, and experience interact to affect rate of recovery after motor cortex injury. Science 1982;217:855-7.
15. Wilson MS, Gibson CL, Hamm RJ. Haloperidol, but not olanzapine, impairs cognitive performance after traumatic brain injury in rats. Am J Phys Med Rehabil 2003;82:871-9.
16. Goldstein LB, Davis JN. Clonidine impairs recovery of beamwalking after a sensorimotor cortex lesion in the rat. Brain Research 1990;508:305-9.
17. Brailowsky S, Knight RT, Efron R. Phenytoin increases the severity of cortical hemiplegia in rats. Brain Research 1986;376:71-7.
18. Boyeson MG, Harmon RL. Effects of trazodone and desipramine on motor recovery in brain-injured rats. Am J Phys Med Rehabil 1993;72:286-93.
19. Hernandez TD, Holling LC. Disruption of behavioral recovery by the anticonvulsant phenobarbital. Brain Research 1994;635:300-6.
20. Schallert T, Hernandez TD, Barth TM. Recovery of function after brain damage: severe and chronic disruption by diazepam. Brain Research 1986;379:104-11.
21. Deb S, Crownshaw T. The role of pharmacotherapy in the management of behavior disorders in traumatic brain injury patients. Brain Injury 2004;18:1-31.
22. Campbell JJ, Duffy JD. Treatment strategies in amotivated patients. Psychiatric Annals 1997;27(1):44-9.
23. Evans RW, Gualtieri CT, Patterson D. Treatment of chronic closed head injury with psychostimulant drugs: a controlled case study and an appropriate evaluation procedure. J Nerv Ment Dis 1987;175:106-10.
24. Elovic EP, Lansang R, Li Y, Ricker JH. The use of atypical antipsychotics in traumatic brain injury. J Head Trauma Rehabil 2003;18:177-95.
25. Lombard LA, Zafonte RD. Agitation after traumatic brain injury: considerations and treatment options. Am J Phys Med Rehabil 2005;84:797-812.
26. Pachet A, Friesen S, Winkelaar D, Gray S. Beneficial behavioural effects of lamotrigine in traumatic brain injury. Brain Injury 2003;17:715-22.
27. Boyeson MG, Harmon RL, Jones JL. Comparative effects of fluoxetine, amitriptyline, and serotonin on functional motor recovery after sensorimotor cortex injury. Am J Phys Med Rehabil 1994;73:76-83.
28. Khateb A, Ammann J, Annoni JM, Diserens K. Cognition enhancing effects of onepezil in traumatic brain injury (abstract). Eur Neurol 2005;54:39-45.
29. Zhang L, Plotkin RC, Wang G, et al. Cholinergic augmentation with donepezil enhances recovery in short-term memory and sustained attention after traumatic brain injury. Arch Phys Med Rehabil 2004;85:1005-55.
30. Walker W, Seel R, Gibellato M, et al. The effects of donepezil on traumatic brain injury acute rehabilitation outcomes. Brain Inj 2004;18:739-50.
Protect against drug-drug interactions with anxiolytics
Patients with anxiety disorders are at risk for drug-drug interactions (DDIs) with anxiolytics because they often take medications for comorbid medical or psychiatric illnesses.1-3 Prescribing anxiolytics for them without contemplating both physiology and chemistry leads to what Osler called “popgun pharmacy, hitting now the malady and again the patient,” while “not knowing which.”4
To help you “hit” the anxiety instead of the patient,1 we explain the pharmacokinetics and pharmacodynamics of benzodiazepines, buspirone, and propranolol. Practical tables provide information at a glance about which combinations to avoid and which have potential clinical effects (Box 1) you could use to your patients’ advantage.
Clinical effect=Affinity for site of action (pharmacodynamics)×Concentration at site of action (pharmacokinetics)×Patient’s biology (genetics, age, disease, internal environment)
Pharmacodynamics
What a drug does to the body (actions that mediate its efficacy and adverse effects)
Pharmacokinetics
What the body does to a drug (absorption, distribution, metabolism, elimination) that determines its concentration at the site of action
Patient’s biology
Why patients respond differently to the same dose of the same medication (internal environment includes what patients consume, such as foods and co-prescribed drugs)
Benzodiazepines
Benzodiazepines provide an anxiolytic effect by increasing the relative efficiency of the gamma-aminobutyric acid (GABA) receptor when it is stimulated by GABA.5 As a class, benzodiazepines are efficacious for treating panic disorder, social anxiety disorder, generalized anxiety disorder, alcohol withdrawal, and situational anxiety.
Oxidative metabolism. Some benzodiazepines require bio-transformation in the liver by oxidative metabolism; others—such as lorazepam, oxazepam, and emazepam—undergo only glucuronidation reactions and do not have active metabolites (Table 1).6-8
Table 1
Benzodiazepines: How metabolized and half-lives
| Benzodiazepine | Metabolism | Half-life (includes metabolites) |
|---|---|---|
| Alprazolam | Oxidation 3A3/4 | 8 to 12 hrs |
| Chlordiazepoxide | Oxidation 3A3/4 | 10 to 20 hrs |
| Clonazepam | Oxidation 3A3/4 | 18 to 50 hrs |
| Clorazepate | Oxidation 3A3/4 | 40 to 100 hrs |
| Diazepam | Oxidation 1A2, 2C8/9, 2C19, 3A3/4 | 20 to 70 hrs |
| Lorazepam | Conjugation | 10 to 20 hrs |
| Oxazepam | Conjugation | 5 to 15 hrs |
| Source: References 5-7. | ||
Benzodiazepines that undergo oxidative metabolism are more likely than those that do not to be influenced by old age, liver disease, or co-administration of other drugs that increase or decrease hepatic CYP enzyme function. Some (midazolam and triazolam) have high first-pass metabolism before reaching systemic circulation.
Pharmacodynamic DDIs. Giving benzodiazepines with other CNS depressants—such as barbiturates, tricyclics and tetracyclics, dopamine receptor antagonists, opioids, or antihistamines, or alcohol—can cause potentially serious oversedation and respiratory depression (Table 2).
Table 2
Clinical effects of drug-drug interactions with benzodiazepines
| Pharmacodynamic |
| Respiratory depression with alcohol, barbiturates, tricyclic and tetracyclic drugs, dopamine receptor antagonists, opioids, antihistamines |
| With mirtazapine ↑ sedation |
| With lithium, antipsychotics, and clonazepam → ataxia and dysarthria |
| With clozapine → delirium |
| Pharmacokinetic |
| Cimetidine, disulfiram, isoniazid, estrogen, oral contraceptives ↑ diazepam, chlordiazepoxide plasma concentrations |
| Nefazodone and fluvoxamine ↑ plasma concentration of triazolam, alprazolam |
| Carbamazepine ↓ alprazolam plasma concentration |
| Food, antacids ↓ benzodiazepine plasma concentrations |
| Cigarette smoking ↑ benzodiazepine metabolism |
| Benzodiazepines ↑ plasma concentrations of digoxin, phenytoin |
Using benzodiazepines with lithium or antipsychotics may cause ataxia and dysarthria, and benzodiazepines with clozapine can cause delirium.
At-risk patients. Benzodiazepine use is a significant predictor of falling, especially in elderly persons taking more than one sedative. In a controlled study of hospitalized older patients, 84 (46%) of 181 who fell were taking one or more benzodiazepine, compared with 48 (27%) of 181 age-matched controls who did not fall.10 The message: seek an alternative to benzodiazepines to sedate older patients, especially those taking another CNS depressant.
Alprazolam and DDIs. Alprazolam is commonly prescribed, despite its high potential for abuse and association with dangerous DDIs:
- A study of 172 deaths involving oxycodone showed that 117 patients died from combined drug toxicity. Benzodiazepines (detected in 96 cases) were the most common co-intoxicants and were led by alprazolam.11
- Benzodiazepine abuse is common among clients at methadone maintenance clinics and was reported in 3 fatal drug overdoses caused by co-ingestion of methadone and alprazolam.12
- Cocaine and methadone were the most common co-intoxicants with alprazolam in a study of 87 deaths attributed to combined drug toxicity.13
- In a study of patients who overdosed with benzodiazepines, 22% of those who took alprazolam required ICU admission. This was twice the rate of ICU admission after overdose with other benzodiazepines.14
These studies indicate that alprazolam may be more toxic than other benzodiazepines in overdose and when used with other drugs. We recommend that you exercise great care when prescribing alprazolam, particularly for patients who may be at risk of deliberate self-poisoning and lethal DDIs.
Pharmacokinetic DDIs. Diazepam and chlordiazepoxide plasma concentrations increase in combination with drugs that inhibit CYP enzymes, including cimetidine, disulfiram, isoniazid, estrogen, and oral contraceptives.15
Nefazodone—a CYP 3A3/4 inhibitor—can increase plasma concentrations of triazolam and alprazolam to potentially toxic levels. Nefazodone’s manufacturer recommends lowering triazolam dosages by 75% and alprazolam dosages by 50% when used with nefazodone.3
Carbamazepine—a CYP 3A3/4 inducer—induces both its own and other drugs’ metabolism. It can lower plasma concentrations of alprazolam, clonazepam, midazolam, and triazolam, which are metabolized by 3A3/4. Smoking, food, and antacids also may decrease benzodiazepine plasma concentrations.
As perpetuator drugs, benzodiazepines might increase digoxin plasma concentration, probably because of reduced digoxin renal clearance.16 Diazepam may inhibit CYP 2C9 and/or 2C19 by being an alternate substrate for enzymebinding sites,15,17 increasing the concentration of other drugs such as phenytoin.
Buspirone: Complicated pharmacology
One of buspirone’s major clinical advantages is that it does not pharmacodynamically or pharmacokinetically affect benzodiazepines. Buspirone, the only azaspirodecanedione marketed in the United States, has complex central 5-HT effects.18,19 Because it is a partial 5-HT1A agonist, buspirone’s net effect depends on 5-HT concentration at the receptor:
- If 5-HT concentration is low, buspirone will act as an agonist.
- If 5-HT concentration is high, buspirone—being a partial agonist—will antagonize the effect of excessive 5-HT.
Buspirone’s pharmacology is further complicated by its conversion via oxidative metabolism into an active metabolite—1-pheyl-piperazine (1-PP). Buspirone is a CYP 3A3/4 enzyme substrate, so it is extensively metabolized as it crosses the duodenum and passes through the liver. As a result, the parent drug has low bioavailability and is principally converted into 1-PP before entering systemic circulation.6
1-PP works differently than the parent drug. As an alpha-2-adrenergic antagonist, 1-PP increases the firing rate of adrenergic neurons in the locus ceruleus by blocking a receptor in presynaptic feedback system.
Which traits of buspirone and its active metabolite produce the drug’s anxiolytic effect? It might be one of these, all of them, or some other unknown trait.
Pharmacodynamic DDIs. Presumably because of its effects on serotonin release at 5-HT1A receptors, buspirone may cause hypertensive episodes when used with monoamine oxidase inhibitors (MAOIs) (Table 3). This is why a 2-week washout is recommended between discontinuing an MAOIs and starting buspirone.21
Table 3
Clinical effects of drug-drug interactions with buspirone
| Pharmacodynamic |
| DO NOT use buspirone with monoamine oxidase inhibitors (MAOIs); allow 2-week washout after stopping an MAOI before starting buspirone |
| Pharmacokinetic |
| Food ↑ buspirone Cmax and AUC 2-fold |
| Renal impairment ↑ buspirone plasma concentration 2-fold |
| Hepatic impairment ↑ buspirone Cmax and AUC 15-fold and ↑ half-life 2-fold |
| Verapamil, diltiazem, erythromycin, itraconazole ↑ buspirone plasma concentration |
| Rifampicin ↓ buspirone plasma concentration 10-fold |
| Buspirone ↑ haloperidol plasma concentration |
| Erythromycin, itraconazole, nefazodone, grapefruit juice ↑ buspirone plasma concentration |
| Cmax: maximum drug concentration |
| AUC: area under the curve (mathematical calculation of the body’s total exposure to a drug over time) |
- buspirone affects 5-HT mechanisms
- drugs that affect serotonin reuptake inhibition, 5HT1A receptors, and 5HT2 receptors may have synergy.20
Some SSRIs—such as high-dose fluoxetine and usual doses of fluvoxamine—may increase buspirone serum concentration by inhibiting CYP 3A4.6 Consider this clinical effect before you combine an SSRI with buspirone. Using buspirone with fluoxetine, paroxetine, or bupropion also increases serum 1-PP. This increase, which occurs when CYP 2D6 slows 1-PP clearance, could cause euphoria, mania, or seizures.20
Coadministering rifampin can lower buspirone plasma concentrations almost 10-fold because rifampin induces CYP 3A3/4.22
As a perpetuator, buspirone can increase haloperidol plasma concentrations, but probably not to a clinically important extent. In an open trial, Goff23 added buspirone, mean dosage 23.8 mg/d, to a stable regimen of haloperidol in 7 patients with schizophrenia. Although haloperidol’s mean plasma concentration increased by 26% after 6 weeks, this modest change would be difficult to detect in clinical practice.
Huang et al24 found no clinically significant pharmacokinetic interaction between buspirone, 10 mg tid, and haloperidol, 10 to 40 mg/d, during 6 weeks of coadministration in 27 patients with schizophrenia.
Propranolol: Beta-blocking anxiolytic
Propranolol is prescribed off-label for anxiety disorders more often than other beta blockers. It may help patients with situational or performance anxiety.
Beta-adrenergic blockers competitively antagonize norepinephrine and epinephrine at the beta-adrenergic receptor. These cardiovascular agents can reduce many of anxiety’s peripheral manifestations, such as tachycardia, diaphoresis, trembling, and blushing. All beta blockers share this pharmacologic effect, but their pharmacokinetics differ greatly. Some depend on a single CYP enzyme for clearance (metoprolol, by CYP 2D6), whereas others, such as propranolol, are metabolized by multiple CYP enzymes.
Pharmacodynamic DDIs. Drugs that block alpha-1 adrenergic receptors potentiate beta blockers’ blood pressure-lowering effects and increase the risk of orthostatic hypotension. This is probably why haloperidol can potentiate propranolol’s hypotensive effects.6 Other alpha-1 adrenergic antagonists—though not normally classified as such—include some tertiary amine tricyclic antidepressants (amitriptyline and imipramine) and some antipsychotics (quetiapine).
Reports have associated hypertensive crises and bradycardia with coadministration of beta blockers and MAOIs.21 Depressed myocardial contractility and A-V nodal conduction may occur when beta blockers are combined with calcium channel inhibitors.21 Beta blockers also can decrease IV anesthetic dose requirements because they decrease cardiac output.25
In patients using insulin for diabetes mellitus, propranolol inhibits recovery from insulin-induced hypoglycemia and may cause hypertension and bradycardia. Beta blockers also can mask the tachycardia that usually accompanies insulin-induced hypoglycemia.
Pharmacokinetic DDIs. Propranolol has an extensive first-pass effect, being etabolized in the liver to active and inactive compounds that interact with CYP enzymes 1A2, 2C18, 2C19 and 2D6.6
Coadministering strong CYP 2D6 inhibitors such as bupropion, fluoxetine, or paroxetine can reduce propanolol clearance, increasing its effect and risking cardiac toxicity6 (Table 4). CYP 1A2 inhibitors such as amiodarone and fluoroquinolones or CYP 2C19 inhibitors such as fluvoxamine also increase serum concentrations of propranolol.
Table 4
How to avoid drug interactions with three common anxiolytics*
| When prescribing benzodiazepines… | |
| DO | DO NOT |
| Advise patients not to combine benzodiazepines with alcohol | Use with other CNS depressants or nefazodone |
| Talk to patients about potential for abuse/dependency, and monitor benzodiazepine use | Use in elderly patients or in patients with high potential for substance abuse |
| When prescribing buspirone… | |
| DO | DO NOT |
| Allow a 2-week washout between discontinuing an MAOI and starting buspirone | Use with MAOIs, verapamil, diltiazem, erythromycin, or itraconazole |
| Consider adding buspirone when SSRI monotherapy has not adequately helped patients with anxiety | Co-administer with rifampin |
| Combine with benzodiazepines, if needed | |
| When prescribing propranolol… | |
| DO | DO NOT |
| Educate patients using insulin for diabetes mellitus that propranolol may inhibit recovery from insulin-induced hypoglycemia, cause bradycardia, or mask tachycardia | Combine with medications with strong hypotensive effects |
| Coadminister with strong CYP 2D6 or 1A2 inhibitors | |
| Recheck anticonvulsant plasma concentrations after starting propranolol | Add to calcium inhibitors for patients with ↓ myocardial contractility and A-V nodal conduction |
| * Before prescribing any anxiolytic, review all co-prescribed medications for potential DDIs | |
| DDI: drug-drug interaction | |
| MAOI: monoamine oxidase inhibitor | |
| SSRI: selective serotonin reuptake inhibitor | |
As a perpetuator, propranolol produces small increases in diazepam concentration, suggesting that the beta-blocker inhibits diazepam metabolism. This interaction can impair kinetic visual acuity, which is correlated with the ability to discriminate moving objects in space.26
Propranolol increases plasma concentrations of antipsychotics, anticonvulsants, theophylline, and levothyroxine (Table 5)—possibly because of the beta blocker’s negative inotropic effects (decreased cardiac output reduces hepatic and renal blood flow).
Table 5
Clinical effects of drug-drug interactions with propranolol
| Pharmacodynamic |
| With MAO inhibitors → hypertensive crisis and bradycardia |
| With calcium channel inhibitors → ↓ myocardial contractility and A-V nodal conduction |
| ↓ intravenous anesthetic dose requirements |
| ↓ diazepam metabolism |
| ↓ median effective dosage of valproate and diazepam; might improve antiepileptic potential of valproate |
| Pharmacokinetic |
| ↑ plasma concentration of antipsychotics, anticonvulsants, theophylline, levothyroxine |
| Barbiturates, phenytoin, and cigarette smoking ↑ propranolol elimination |
- Cytochrome P450 interactions. www.drug-interaction.com.
- FDA. Food and drug interactions. http://vm.cfsan.fda.gov/~lrd/fdinter.html.
- Psychiatric drug interactions. www.preskorn.com.
- Alprazolam • Xanax
- Bupropion • Wellbutrin
- Buspirone • BuSpar
- Carbamazepine • Carbatrol, others
- Chlordiazepoxide • Librium
- Cimetidine • Tagamet
- Clonazepam • Klonopin
- Clorazepate • Tranxene
- Clozapine • Clozaril
- Diazepam • Valium
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Haloperidol • Haldol
- Itraconazole • Sporanox
- Lorazepam • Ativan
- Midazolam • Versed
- Mirtazapine • Remeron
- Oxazepam • Serax
- Paroxetine • Paxil
- Phenytoin • Dilantin
- Propranolol • Inderal
- Quetiapine • Seroquel
- Rifampin • Rifadin, Rimactane
- Triazolam • Halcion
- Valproate • various
- Verapamil • Calan, Isoptin
Drs. Ramadan and Werder report no financial relationships with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Preskorn has received grants or has been a consultant or speaker for Abbott Laboratories, AstraZeneca Pharmaceuticals, Boehringer-Ingelheim, Bristol-Myers Squibb Co., Merck & Co., Eisai, Eli Lilly and Co., GlaxoSmithKline, Janssen Pharmaceutica, Johnson & Johnson, Novartis Pharmaceuticals Corp., Organon, Otsuka America Pharmaceutical, Pfizer, Solvay Pharmaceuticals, Sanofi-Aventis, and Wyeth.
1. Preskorn S, Flockhart D. Psychiatric drug interactions guide. New York: MBL Communications.; 2004.
2. Bruce SE, Yonkers KA, Otto MW, et al. Influence of psychiatric comorbidity on recovery and recurrence in generalized anxiety disorder, social phobia, and panic disorder 12-year prospective study. Am J Psychiatry 2005;162:1179-87.
3. Nemeroff CB. Use of atypical antipsychotics in refractory depression and anxiety. J Clin Psychiatry 2005;66(Suppl 8):13-21.
4. Bean RB, Bean WB. Sir William Osler: Aphorisms from his bedside teaching and writing. Springfield, IL: Charles C. Thomas; 1961:53.
5. Tasman A, Kay J, Lieberman JA. Psychiatry Therapeutics. 2nd ed. West Sussex, UK: John Wiley & Sons; 2003:347.
6. Fuller M, Sajatovic M. Drug information for mental health. 3rd ed. Hudson, OH: Lexi-Comp; 2001.
7. Stahl SM. Essential psychopharmacology: Neuroscientific basis and practical applications. 2nd ed. New York: Cambridge University Press; 2000.
8. Janicak PG, Davis JM, Preskorn SH, Ayad FJ. Principles and practice of psychopharmacology. 3rd ed. Philadelphia, PA: Lippincott Williams and Wilkins; 2001.
9. Tanaka E. Toxicological interactions involving psychiatric drugs and alcohol: an update. J Clin Pharm Ther 2003;28(2):81-95.
10. Frels C, Williams P, Narayanan S, Gariballa SE. Iatrogenic causes of falls in hospitalised elderly patients: a case-control study. Postgrad Med 2002;78(922):487-9.
11. Wolf BC, Lavezzi WA, Sullivan LM, Flannagan LM. One hundred seventy two deaths involving the use of oxycodone in Palm Beach County. J Forensic Sci 2005;50(1):192-5.
12. Rogers WO, Hall MA, Brissie RM, Robinson CA. Detection of alprazolam in three cases of methadone/benzodiazepine overdose. J Forensic Sci 1997;42(1):155-6.
13. Wolf BC, Lavezzi WA, Sullivan LM, et al. Alprazolam-related deaths in Palm Beach County. Am J Forensic Med Pathol 2005;26(1):24-7.
14. Isbister GK, O’Regan L, Sibbritt D, et al. Alprazolam is relatively more toxic than other benzodiazepines in overdose. Br J Clin Pharmacol 2004;58(1):88-95.
15. Sadock BJ, Sadock VA. Kaplan and Sadock’s pocket handbook of psychiatric drug treatment. 3rd ed. Philadelphia: Lippincott Williams & Wilkins; 2001.
16. Tollefson G, Lesar T, Grothe D, et al. Alprazolam-related digoxin toxicity. Am J Psychiatry 1984;141(12):1612-3.
17. Murphy A, Wilbur K. Phenytoin-diazepam interaction. Ann Pharmacother 2003;37(5):659-3.
18. Sharp T, McQuade R, Bramwell S, et al. Effect of acute and repeated administration of 5-HT1A receptor agonists on 5-HT release in rat brain in vivo. Naunhyn Schmiedebergs Arch Pharmacol 1993;348(4):339-46.
19. Van den Hooff P, Galvan M. Actions of 5-hydroxytryptamine and 5-HT1A receptor ligands on rat dorso-lateral septal neurons in vitro. Br J Pharmacol 1992;106(4):893-9.
20. Preskorn SH Do you believe in magic? Journal of Practical Psychiatry and Behavioral Health March 1997;99-103
21. Physicians’ Desk Reference. 59th ed. Montvale, NJ: Thomson PDR; 2005.
22. Mahmood I, Sahajwalla C. Clinical pharmacokinetics and pharmacodynamics of buspirone, an anxiolytic drug. Clin Pharmacokinet 1999;36(4):277-87.
23. Goff DC, Midha KK, Brotman AW, et al. An open trial of buspirone added to neuroleptics in schizophrenic patients. J Clin Psychopharmacol 1991;11(3):193-7.
24. Huang HF, Jann MW, Wei FC, et al. Lack of pharmacokinetic interaction between buspirone and haloperidol in patients with schizophrenia. J Clin Pharmacol 1996;36(10):963-9.
25. Avram MJ, Krejcie TC, Henthorn TK, et al. Beta-adrenergic blockade affects initial drug distribution due to decreased cardiac output and altered blood flow distribution. J Pharmacol Exp Ther 2004;311(2):617-24.
26. Hawksworth G, Betts T, Crowe A, et al. Diazepam/beta-adrenoceptor antagonist interactions. Br J Clin Pharmacol 1984;17(Suppl 1):69S-76S.
27. Hallengren B, Nilsson OR, Karlberg BE, et al. Influence of hyperthyroidism on the kinetics of methimazole, propranolol, metoprolol and atenolol. Eur J Clin Pharmacol 1982;21(5):379-84.
Patients with anxiety disorders are at risk for drug-drug interactions (DDIs) with anxiolytics because they often take medications for comorbid medical or psychiatric illnesses.1-3 Prescribing anxiolytics for them without contemplating both physiology and chemistry leads to what Osler called “popgun pharmacy, hitting now the malady and again the patient,” while “not knowing which.”4
To help you “hit” the anxiety instead of the patient,1 we explain the pharmacokinetics and pharmacodynamics of benzodiazepines, buspirone, and propranolol. Practical tables provide information at a glance about which combinations to avoid and which have potential clinical effects (Box 1) you could use to your patients’ advantage.
Clinical effect=Affinity for site of action (pharmacodynamics)×Concentration at site of action (pharmacokinetics)×Patient’s biology (genetics, age, disease, internal environment)
Pharmacodynamics
What a drug does to the body (actions that mediate its efficacy and adverse effects)
Pharmacokinetics
What the body does to a drug (absorption, distribution, metabolism, elimination) that determines its concentration at the site of action
Patient’s biology
Why patients respond differently to the same dose of the same medication (internal environment includes what patients consume, such as foods and co-prescribed drugs)
Benzodiazepines
Benzodiazepines provide an anxiolytic effect by increasing the relative efficiency of the gamma-aminobutyric acid (GABA) receptor when it is stimulated by GABA.5 As a class, benzodiazepines are efficacious for treating panic disorder, social anxiety disorder, generalized anxiety disorder, alcohol withdrawal, and situational anxiety.
Oxidative metabolism. Some benzodiazepines require bio-transformation in the liver by oxidative metabolism; others—such as lorazepam, oxazepam, and emazepam—undergo only glucuronidation reactions and do not have active metabolites (Table 1).6-8
Table 1
Benzodiazepines: How metabolized and half-lives
| Benzodiazepine | Metabolism | Half-life (includes metabolites) |
|---|---|---|
| Alprazolam | Oxidation 3A3/4 | 8 to 12 hrs |
| Chlordiazepoxide | Oxidation 3A3/4 | 10 to 20 hrs |
| Clonazepam | Oxidation 3A3/4 | 18 to 50 hrs |
| Clorazepate | Oxidation 3A3/4 | 40 to 100 hrs |
| Diazepam | Oxidation 1A2, 2C8/9, 2C19, 3A3/4 | 20 to 70 hrs |
| Lorazepam | Conjugation | 10 to 20 hrs |
| Oxazepam | Conjugation | 5 to 15 hrs |
| Source: References 5-7. | ||
Benzodiazepines that undergo oxidative metabolism are more likely than those that do not to be influenced by old age, liver disease, or co-administration of other drugs that increase or decrease hepatic CYP enzyme function. Some (midazolam and triazolam) have high first-pass metabolism before reaching systemic circulation.
Pharmacodynamic DDIs. Giving benzodiazepines with other CNS depressants—such as barbiturates, tricyclics and tetracyclics, dopamine receptor antagonists, opioids, or antihistamines, or alcohol—can cause potentially serious oversedation and respiratory depression (Table 2).
Table 2
Clinical effects of drug-drug interactions with benzodiazepines
| Pharmacodynamic |
| Respiratory depression with alcohol, barbiturates, tricyclic and tetracyclic drugs, dopamine receptor antagonists, opioids, antihistamines |
| With mirtazapine ↑ sedation |
| With lithium, antipsychotics, and clonazepam → ataxia and dysarthria |
| With clozapine → delirium |
| Pharmacokinetic |
| Cimetidine, disulfiram, isoniazid, estrogen, oral contraceptives ↑ diazepam, chlordiazepoxide plasma concentrations |
| Nefazodone and fluvoxamine ↑ plasma concentration of triazolam, alprazolam |
| Carbamazepine ↓ alprazolam plasma concentration |
| Food, antacids ↓ benzodiazepine plasma concentrations |
| Cigarette smoking ↑ benzodiazepine metabolism |
| Benzodiazepines ↑ plasma concentrations of digoxin, phenytoin |
Using benzodiazepines with lithium or antipsychotics may cause ataxia and dysarthria, and benzodiazepines with clozapine can cause delirium.
At-risk patients. Benzodiazepine use is a significant predictor of falling, especially in elderly persons taking more than one sedative. In a controlled study of hospitalized older patients, 84 (46%) of 181 who fell were taking one or more benzodiazepine, compared with 48 (27%) of 181 age-matched controls who did not fall.10 The message: seek an alternative to benzodiazepines to sedate older patients, especially those taking another CNS depressant.
Alprazolam and DDIs. Alprazolam is commonly prescribed, despite its high potential for abuse and association with dangerous DDIs:
- A study of 172 deaths involving oxycodone showed that 117 patients died from combined drug toxicity. Benzodiazepines (detected in 96 cases) were the most common co-intoxicants and were led by alprazolam.11
- Benzodiazepine abuse is common among clients at methadone maintenance clinics and was reported in 3 fatal drug overdoses caused by co-ingestion of methadone and alprazolam.12
- Cocaine and methadone were the most common co-intoxicants with alprazolam in a study of 87 deaths attributed to combined drug toxicity.13
- In a study of patients who overdosed with benzodiazepines, 22% of those who took alprazolam required ICU admission. This was twice the rate of ICU admission after overdose with other benzodiazepines.14
These studies indicate that alprazolam may be more toxic than other benzodiazepines in overdose and when used with other drugs. We recommend that you exercise great care when prescribing alprazolam, particularly for patients who may be at risk of deliberate self-poisoning and lethal DDIs.
Pharmacokinetic DDIs. Diazepam and chlordiazepoxide plasma concentrations increase in combination with drugs that inhibit CYP enzymes, including cimetidine, disulfiram, isoniazid, estrogen, and oral contraceptives.15
Nefazodone—a CYP 3A3/4 inhibitor—can increase plasma concentrations of triazolam and alprazolam to potentially toxic levels. Nefazodone’s manufacturer recommends lowering triazolam dosages by 75% and alprazolam dosages by 50% when used with nefazodone.3
Carbamazepine—a CYP 3A3/4 inducer—induces both its own and other drugs’ metabolism. It can lower plasma concentrations of alprazolam, clonazepam, midazolam, and triazolam, which are metabolized by 3A3/4. Smoking, food, and antacids also may decrease benzodiazepine plasma concentrations.
As perpetuator drugs, benzodiazepines might increase digoxin plasma concentration, probably because of reduced digoxin renal clearance.16 Diazepam may inhibit CYP 2C9 and/or 2C19 by being an alternate substrate for enzymebinding sites,15,17 increasing the concentration of other drugs such as phenytoin.
Buspirone: Complicated pharmacology
One of buspirone’s major clinical advantages is that it does not pharmacodynamically or pharmacokinetically affect benzodiazepines. Buspirone, the only azaspirodecanedione marketed in the United States, has complex central 5-HT effects.18,19 Because it is a partial 5-HT1A agonist, buspirone’s net effect depends on 5-HT concentration at the receptor:
- If 5-HT concentration is low, buspirone will act as an agonist.
- If 5-HT concentration is high, buspirone—being a partial agonist—will antagonize the effect of excessive 5-HT.
Buspirone’s pharmacology is further complicated by its conversion via oxidative metabolism into an active metabolite—1-pheyl-piperazine (1-PP). Buspirone is a CYP 3A3/4 enzyme substrate, so it is extensively metabolized as it crosses the duodenum and passes through the liver. As a result, the parent drug has low bioavailability and is principally converted into 1-PP before entering systemic circulation.6
1-PP works differently than the parent drug. As an alpha-2-adrenergic antagonist, 1-PP increases the firing rate of adrenergic neurons in the locus ceruleus by blocking a receptor in presynaptic feedback system.
Which traits of buspirone and its active metabolite produce the drug’s anxiolytic effect? It might be one of these, all of them, or some other unknown trait.
Pharmacodynamic DDIs. Presumably because of its effects on serotonin release at 5-HT1A receptors, buspirone may cause hypertensive episodes when used with monoamine oxidase inhibitors (MAOIs) (Table 3). This is why a 2-week washout is recommended between discontinuing an MAOIs and starting buspirone.21
Table 3
Clinical effects of drug-drug interactions with buspirone
| Pharmacodynamic |
| DO NOT use buspirone with monoamine oxidase inhibitors (MAOIs); allow 2-week washout after stopping an MAOI before starting buspirone |
| Pharmacokinetic |
| Food ↑ buspirone Cmax and AUC 2-fold |
| Renal impairment ↑ buspirone plasma concentration 2-fold |
| Hepatic impairment ↑ buspirone Cmax and AUC 15-fold and ↑ half-life 2-fold |
| Verapamil, diltiazem, erythromycin, itraconazole ↑ buspirone plasma concentration |
| Rifampicin ↓ buspirone plasma concentration 10-fold |
| Buspirone ↑ haloperidol plasma concentration |
| Erythromycin, itraconazole, nefazodone, grapefruit juice ↑ buspirone plasma concentration |
| Cmax: maximum drug concentration |
| AUC: area under the curve (mathematical calculation of the body’s total exposure to a drug over time) |
- buspirone affects 5-HT mechanisms
- drugs that affect serotonin reuptake inhibition, 5HT1A receptors, and 5HT2 receptors may have synergy.20
Some SSRIs—such as high-dose fluoxetine and usual doses of fluvoxamine—may increase buspirone serum concentration by inhibiting CYP 3A4.6 Consider this clinical effect before you combine an SSRI with buspirone. Using buspirone with fluoxetine, paroxetine, or bupropion also increases serum 1-PP. This increase, which occurs when CYP 2D6 slows 1-PP clearance, could cause euphoria, mania, or seizures.20
Coadministering rifampin can lower buspirone plasma concentrations almost 10-fold because rifampin induces CYP 3A3/4.22
As a perpetuator, buspirone can increase haloperidol plasma concentrations, but probably not to a clinically important extent. In an open trial, Goff23 added buspirone, mean dosage 23.8 mg/d, to a stable regimen of haloperidol in 7 patients with schizophrenia. Although haloperidol’s mean plasma concentration increased by 26% after 6 weeks, this modest change would be difficult to detect in clinical practice.
Huang et al24 found no clinically significant pharmacokinetic interaction between buspirone, 10 mg tid, and haloperidol, 10 to 40 mg/d, during 6 weeks of coadministration in 27 patients with schizophrenia.
Propranolol: Beta-blocking anxiolytic
Propranolol is prescribed off-label for anxiety disorders more often than other beta blockers. It may help patients with situational or performance anxiety.
Beta-adrenergic blockers competitively antagonize norepinephrine and epinephrine at the beta-adrenergic receptor. These cardiovascular agents can reduce many of anxiety’s peripheral manifestations, such as tachycardia, diaphoresis, trembling, and blushing. All beta blockers share this pharmacologic effect, but their pharmacokinetics differ greatly. Some depend on a single CYP enzyme for clearance (metoprolol, by CYP 2D6), whereas others, such as propranolol, are metabolized by multiple CYP enzymes.
Pharmacodynamic DDIs. Drugs that block alpha-1 adrenergic receptors potentiate beta blockers’ blood pressure-lowering effects and increase the risk of orthostatic hypotension. This is probably why haloperidol can potentiate propranolol’s hypotensive effects.6 Other alpha-1 adrenergic antagonists—though not normally classified as such—include some tertiary amine tricyclic antidepressants (amitriptyline and imipramine) and some antipsychotics (quetiapine).
Reports have associated hypertensive crises and bradycardia with coadministration of beta blockers and MAOIs.21 Depressed myocardial contractility and A-V nodal conduction may occur when beta blockers are combined with calcium channel inhibitors.21 Beta blockers also can decrease IV anesthetic dose requirements because they decrease cardiac output.25
In patients using insulin for diabetes mellitus, propranolol inhibits recovery from insulin-induced hypoglycemia and may cause hypertension and bradycardia. Beta blockers also can mask the tachycardia that usually accompanies insulin-induced hypoglycemia.
Pharmacokinetic DDIs. Propranolol has an extensive first-pass effect, being etabolized in the liver to active and inactive compounds that interact with CYP enzymes 1A2, 2C18, 2C19 and 2D6.6
Coadministering strong CYP 2D6 inhibitors such as bupropion, fluoxetine, or paroxetine can reduce propanolol clearance, increasing its effect and risking cardiac toxicity6 (Table 4). CYP 1A2 inhibitors such as amiodarone and fluoroquinolones or CYP 2C19 inhibitors such as fluvoxamine also increase serum concentrations of propranolol.
Table 4
How to avoid drug interactions with three common anxiolytics*
| When prescribing benzodiazepines… | |
| DO | DO NOT |
| Advise patients not to combine benzodiazepines with alcohol | Use with other CNS depressants or nefazodone |
| Talk to patients about potential for abuse/dependency, and monitor benzodiazepine use | Use in elderly patients or in patients with high potential for substance abuse |
| When prescribing buspirone… | |
| DO | DO NOT |
| Allow a 2-week washout between discontinuing an MAOI and starting buspirone | Use with MAOIs, verapamil, diltiazem, erythromycin, or itraconazole |
| Consider adding buspirone when SSRI monotherapy has not adequately helped patients with anxiety | Co-administer with rifampin |
| Combine with benzodiazepines, if needed | |
| When prescribing propranolol… | |
| DO | DO NOT |
| Educate patients using insulin for diabetes mellitus that propranolol may inhibit recovery from insulin-induced hypoglycemia, cause bradycardia, or mask tachycardia | Combine with medications with strong hypotensive effects |
| Coadminister with strong CYP 2D6 or 1A2 inhibitors | |
| Recheck anticonvulsant plasma concentrations after starting propranolol | Add to calcium inhibitors for patients with ↓ myocardial contractility and A-V nodal conduction |
| * Before prescribing any anxiolytic, review all co-prescribed medications for potential DDIs | |
| DDI: drug-drug interaction | |
| MAOI: monoamine oxidase inhibitor | |
| SSRI: selective serotonin reuptake inhibitor | |
As a perpetuator, propranolol produces small increases in diazepam concentration, suggesting that the beta-blocker inhibits diazepam metabolism. This interaction can impair kinetic visual acuity, which is correlated with the ability to discriminate moving objects in space.26
Propranolol increases plasma concentrations of antipsychotics, anticonvulsants, theophylline, and levothyroxine (Table 5)—possibly because of the beta blocker’s negative inotropic effects (decreased cardiac output reduces hepatic and renal blood flow).
Table 5
Clinical effects of drug-drug interactions with propranolol
| Pharmacodynamic |
| With MAO inhibitors → hypertensive crisis and bradycardia |
| With calcium channel inhibitors → ↓ myocardial contractility and A-V nodal conduction |
| ↓ intravenous anesthetic dose requirements |
| ↓ diazepam metabolism |
| ↓ median effective dosage of valproate and diazepam; might improve antiepileptic potential of valproate |
| Pharmacokinetic |
| ↑ plasma concentration of antipsychotics, anticonvulsants, theophylline, levothyroxine |
| Barbiturates, phenytoin, and cigarette smoking ↑ propranolol elimination |
- Cytochrome P450 interactions. www.drug-interaction.com.
- FDA. Food and drug interactions. http://vm.cfsan.fda.gov/~lrd/fdinter.html.
- Psychiatric drug interactions. www.preskorn.com.
- Alprazolam • Xanax
- Bupropion • Wellbutrin
- Buspirone • BuSpar
- Carbamazepine • Carbatrol, others
- Chlordiazepoxide • Librium
- Cimetidine • Tagamet
- Clonazepam • Klonopin
- Clorazepate • Tranxene
- Clozapine • Clozaril
- Diazepam • Valium
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Haloperidol • Haldol
- Itraconazole • Sporanox
- Lorazepam • Ativan
- Midazolam • Versed
- Mirtazapine • Remeron
- Oxazepam • Serax
- Paroxetine • Paxil
- Phenytoin • Dilantin
- Propranolol • Inderal
- Quetiapine • Seroquel
- Rifampin • Rifadin, Rimactane
- Triazolam • Halcion
- Valproate • various
- Verapamil • Calan, Isoptin
Drs. Ramadan and Werder report no financial relationships with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Preskorn has received grants or has been a consultant or speaker for Abbott Laboratories, AstraZeneca Pharmaceuticals, Boehringer-Ingelheim, Bristol-Myers Squibb Co., Merck & Co., Eisai, Eli Lilly and Co., GlaxoSmithKline, Janssen Pharmaceutica, Johnson & Johnson, Novartis Pharmaceuticals Corp., Organon, Otsuka America Pharmaceutical, Pfizer, Solvay Pharmaceuticals, Sanofi-Aventis, and Wyeth.
Patients with anxiety disorders are at risk for drug-drug interactions (DDIs) with anxiolytics because they often take medications for comorbid medical or psychiatric illnesses.1-3 Prescribing anxiolytics for them without contemplating both physiology and chemistry leads to what Osler called “popgun pharmacy, hitting now the malady and again the patient,” while “not knowing which.”4
To help you “hit” the anxiety instead of the patient,1 we explain the pharmacokinetics and pharmacodynamics of benzodiazepines, buspirone, and propranolol. Practical tables provide information at a glance about which combinations to avoid and which have potential clinical effects (Box 1) you could use to your patients’ advantage.
Clinical effect=Affinity for site of action (pharmacodynamics)×Concentration at site of action (pharmacokinetics)×Patient’s biology (genetics, age, disease, internal environment)
Pharmacodynamics
What a drug does to the body (actions that mediate its efficacy and adverse effects)
Pharmacokinetics
What the body does to a drug (absorption, distribution, metabolism, elimination) that determines its concentration at the site of action
Patient’s biology
Why patients respond differently to the same dose of the same medication (internal environment includes what patients consume, such as foods and co-prescribed drugs)
Benzodiazepines
Benzodiazepines provide an anxiolytic effect by increasing the relative efficiency of the gamma-aminobutyric acid (GABA) receptor when it is stimulated by GABA.5 As a class, benzodiazepines are efficacious for treating panic disorder, social anxiety disorder, generalized anxiety disorder, alcohol withdrawal, and situational anxiety.
Oxidative metabolism. Some benzodiazepines require bio-transformation in the liver by oxidative metabolism; others—such as lorazepam, oxazepam, and emazepam—undergo only glucuronidation reactions and do not have active metabolites (Table 1).6-8
Table 1
Benzodiazepines: How metabolized and half-lives
| Benzodiazepine | Metabolism | Half-life (includes metabolites) |
|---|---|---|
| Alprazolam | Oxidation 3A3/4 | 8 to 12 hrs |
| Chlordiazepoxide | Oxidation 3A3/4 | 10 to 20 hrs |
| Clonazepam | Oxidation 3A3/4 | 18 to 50 hrs |
| Clorazepate | Oxidation 3A3/4 | 40 to 100 hrs |
| Diazepam | Oxidation 1A2, 2C8/9, 2C19, 3A3/4 | 20 to 70 hrs |
| Lorazepam | Conjugation | 10 to 20 hrs |
| Oxazepam | Conjugation | 5 to 15 hrs |
| Source: References 5-7. | ||
Benzodiazepines that undergo oxidative metabolism are more likely than those that do not to be influenced by old age, liver disease, or co-administration of other drugs that increase or decrease hepatic CYP enzyme function. Some (midazolam and triazolam) have high first-pass metabolism before reaching systemic circulation.
Pharmacodynamic DDIs. Giving benzodiazepines with other CNS depressants—such as barbiturates, tricyclics and tetracyclics, dopamine receptor antagonists, opioids, or antihistamines, or alcohol—can cause potentially serious oversedation and respiratory depression (Table 2).
Table 2
Clinical effects of drug-drug interactions with benzodiazepines
| Pharmacodynamic |
| Respiratory depression with alcohol, barbiturates, tricyclic and tetracyclic drugs, dopamine receptor antagonists, opioids, antihistamines |
| With mirtazapine ↑ sedation |
| With lithium, antipsychotics, and clonazepam → ataxia and dysarthria |
| With clozapine → delirium |
| Pharmacokinetic |
| Cimetidine, disulfiram, isoniazid, estrogen, oral contraceptives ↑ diazepam, chlordiazepoxide plasma concentrations |
| Nefazodone and fluvoxamine ↑ plasma concentration of triazolam, alprazolam |
| Carbamazepine ↓ alprazolam plasma concentration |
| Food, antacids ↓ benzodiazepine plasma concentrations |
| Cigarette smoking ↑ benzodiazepine metabolism |
| Benzodiazepines ↑ plasma concentrations of digoxin, phenytoin |
Using benzodiazepines with lithium or antipsychotics may cause ataxia and dysarthria, and benzodiazepines with clozapine can cause delirium.
At-risk patients. Benzodiazepine use is a significant predictor of falling, especially in elderly persons taking more than one sedative. In a controlled study of hospitalized older patients, 84 (46%) of 181 who fell were taking one or more benzodiazepine, compared with 48 (27%) of 181 age-matched controls who did not fall.10 The message: seek an alternative to benzodiazepines to sedate older patients, especially those taking another CNS depressant.
Alprazolam and DDIs. Alprazolam is commonly prescribed, despite its high potential for abuse and association with dangerous DDIs:
- A study of 172 deaths involving oxycodone showed that 117 patients died from combined drug toxicity. Benzodiazepines (detected in 96 cases) were the most common co-intoxicants and were led by alprazolam.11
- Benzodiazepine abuse is common among clients at methadone maintenance clinics and was reported in 3 fatal drug overdoses caused by co-ingestion of methadone and alprazolam.12
- Cocaine and methadone were the most common co-intoxicants with alprazolam in a study of 87 deaths attributed to combined drug toxicity.13
- In a study of patients who overdosed with benzodiazepines, 22% of those who took alprazolam required ICU admission. This was twice the rate of ICU admission after overdose with other benzodiazepines.14
These studies indicate that alprazolam may be more toxic than other benzodiazepines in overdose and when used with other drugs. We recommend that you exercise great care when prescribing alprazolam, particularly for patients who may be at risk of deliberate self-poisoning and lethal DDIs.
Pharmacokinetic DDIs. Diazepam and chlordiazepoxide plasma concentrations increase in combination with drugs that inhibit CYP enzymes, including cimetidine, disulfiram, isoniazid, estrogen, and oral contraceptives.15
Nefazodone—a CYP 3A3/4 inhibitor—can increase plasma concentrations of triazolam and alprazolam to potentially toxic levels. Nefazodone’s manufacturer recommends lowering triazolam dosages by 75% and alprazolam dosages by 50% when used with nefazodone.3
Carbamazepine—a CYP 3A3/4 inducer—induces both its own and other drugs’ metabolism. It can lower plasma concentrations of alprazolam, clonazepam, midazolam, and triazolam, which are metabolized by 3A3/4. Smoking, food, and antacids also may decrease benzodiazepine plasma concentrations.
As perpetuator drugs, benzodiazepines might increase digoxin plasma concentration, probably because of reduced digoxin renal clearance.16 Diazepam may inhibit CYP 2C9 and/or 2C19 by being an alternate substrate for enzymebinding sites,15,17 increasing the concentration of other drugs such as phenytoin.
Buspirone: Complicated pharmacology
One of buspirone’s major clinical advantages is that it does not pharmacodynamically or pharmacokinetically affect benzodiazepines. Buspirone, the only azaspirodecanedione marketed in the United States, has complex central 5-HT effects.18,19 Because it is a partial 5-HT1A agonist, buspirone’s net effect depends on 5-HT concentration at the receptor:
- If 5-HT concentration is low, buspirone will act as an agonist.
- If 5-HT concentration is high, buspirone—being a partial agonist—will antagonize the effect of excessive 5-HT.
Buspirone’s pharmacology is further complicated by its conversion via oxidative metabolism into an active metabolite—1-pheyl-piperazine (1-PP). Buspirone is a CYP 3A3/4 enzyme substrate, so it is extensively metabolized as it crosses the duodenum and passes through the liver. As a result, the parent drug has low bioavailability and is principally converted into 1-PP before entering systemic circulation.6
1-PP works differently than the parent drug. As an alpha-2-adrenergic antagonist, 1-PP increases the firing rate of adrenergic neurons in the locus ceruleus by blocking a receptor in presynaptic feedback system.
Which traits of buspirone and its active metabolite produce the drug’s anxiolytic effect? It might be one of these, all of them, or some other unknown trait.
Pharmacodynamic DDIs. Presumably because of its effects on serotonin release at 5-HT1A receptors, buspirone may cause hypertensive episodes when used with monoamine oxidase inhibitors (MAOIs) (Table 3). This is why a 2-week washout is recommended between discontinuing an MAOIs and starting buspirone.21
Table 3
Clinical effects of drug-drug interactions with buspirone
| Pharmacodynamic |
| DO NOT use buspirone with monoamine oxidase inhibitors (MAOIs); allow 2-week washout after stopping an MAOI before starting buspirone |
| Pharmacokinetic |
| Food ↑ buspirone Cmax and AUC 2-fold |
| Renal impairment ↑ buspirone plasma concentration 2-fold |
| Hepatic impairment ↑ buspirone Cmax and AUC 15-fold and ↑ half-life 2-fold |
| Verapamil, diltiazem, erythromycin, itraconazole ↑ buspirone plasma concentration |
| Rifampicin ↓ buspirone plasma concentration 10-fold |
| Buspirone ↑ haloperidol plasma concentration |
| Erythromycin, itraconazole, nefazodone, grapefruit juice ↑ buspirone plasma concentration |
| Cmax: maximum drug concentration |
| AUC: area under the curve (mathematical calculation of the body’s total exposure to a drug over time) |
- buspirone affects 5-HT mechanisms
- drugs that affect serotonin reuptake inhibition, 5HT1A receptors, and 5HT2 receptors may have synergy.20
Some SSRIs—such as high-dose fluoxetine and usual doses of fluvoxamine—may increase buspirone serum concentration by inhibiting CYP 3A4.6 Consider this clinical effect before you combine an SSRI with buspirone. Using buspirone with fluoxetine, paroxetine, or bupropion also increases serum 1-PP. This increase, which occurs when CYP 2D6 slows 1-PP clearance, could cause euphoria, mania, or seizures.20
Coadministering rifampin can lower buspirone plasma concentrations almost 10-fold because rifampin induces CYP 3A3/4.22
As a perpetuator, buspirone can increase haloperidol plasma concentrations, but probably not to a clinically important extent. In an open trial, Goff23 added buspirone, mean dosage 23.8 mg/d, to a stable regimen of haloperidol in 7 patients with schizophrenia. Although haloperidol’s mean plasma concentration increased by 26% after 6 weeks, this modest change would be difficult to detect in clinical practice.
Huang et al24 found no clinically significant pharmacokinetic interaction between buspirone, 10 mg tid, and haloperidol, 10 to 40 mg/d, during 6 weeks of coadministration in 27 patients with schizophrenia.
Propranolol: Beta-blocking anxiolytic
Propranolol is prescribed off-label for anxiety disorders more often than other beta blockers. It may help patients with situational or performance anxiety.
Beta-adrenergic blockers competitively antagonize norepinephrine and epinephrine at the beta-adrenergic receptor. These cardiovascular agents can reduce many of anxiety’s peripheral manifestations, such as tachycardia, diaphoresis, trembling, and blushing. All beta blockers share this pharmacologic effect, but their pharmacokinetics differ greatly. Some depend on a single CYP enzyme for clearance (metoprolol, by CYP 2D6), whereas others, such as propranolol, are metabolized by multiple CYP enzymes.
Pharmacodynamic DDIs. Drugs that block alpha-1 adrenergic receptors potentiate beta blockers’ blood pressure-lowering effects and increase the risk of orthostatic hypotension. This is probably why haloperidol can potentiate propranolol’s hypotensive effects.6 Other alpha-1 adrenergic antagonists—though not normally classified as such—include some tertiary amine tricyclic antidepressants (amitriptyline and imipramine) and some antipsychotics (quetiapine).
Reports have associated hypertensive crises and bradycardia with coadministration of beta blockers and MAOIs.21 Depressed myocardial contractility and A-V nodal conduction may occur when beta blockers are combined with calcium channel inhibitors.21 Beta blockers also can decrease IV anesthetic dose requirements because they decrease cardiac output.25
In patients using insulin for diabetes mellitus, propranolol inhibits recovery from insulin-induced hypoglycemia and may cause hypertension and bradycardia. Beta blockers also can mask the tachycardia that usually accompanies insulin-induced hypoglycemia.
Pharmacokinetic DDIs. Propranolol has an extensive first-pass effect, being etabolized in the liver to active and inactive compounds that interact with CYP enzymes 1A2, 2C18, 2C19 and 2D6.6
Coadministering strong CYP 2D6 inhibitors such as bupropion, fluoxetine, or paroxetine can reduce propanolol clearance, increasing its effect and risking cardiac toxicity6 (Table 4). CYP 1A2 inhibitors such as amiodarone and fluoroquinolones or CYP 2C19 inhibitors such as fluvoxamine also increase serum concentrations of propranolol.
Table 4
How to avoid drug interactions with three common anxiolytics*
| When prescribing benzodiazepines… | |
| DO | DO NOT |
| Advise patients not to combine benzodiazepines with alcohol | Use with other CNS depressants or nefazodone |
| Talk to patients about potential for abuse/dependency, and monitor benzodiazepine use | Use in elderly patients or in patients with high potential for substance abuse |
| When prescribing buspirone… | |
| DO | DO NOT |
| Allow a 2-week washout between discontinuing an MAOI and starting buspirone | Use with MAOIs, verapamil, diltiazem, erythromycin, or itraconazole |
| Consider adding buspirone when SSRI monotherapy has not adequately helped patients with anxiety | Co-administer with rifampin |
| Combine with benzodiazepines, if needed | |
| When prescribing propranolol… | |
| DO | DO NOT |
| Educate patients using insulin for diabetes mellitus that propranolol may inhibit recovery from insulin-induced hypoglycemia, cause bradycardia, or mask tachycardia | Combine with medications with strong hypotensive effects |
| Coadminister with strong CYP 2D6 or 1A2 inhibitors | |
| Recheck anticonvulsant plasma concentrations after starting propranolol | Add to calcium inhibitors for patients with ↓ myocardial contractility and A-V nodal conduction |
| * Before prescribing any anxiolytic, review all co-prescribed medications for potential DDIs | |
| DDI: drug-drug interaction | |
| MAOI: monoamine oxidase inhibitor | |
| SSRI: selective serotonin reuptake inhibitor | |
As a perpetuator, propranolol produces small increases in diazepam concentration, suggesting that the beta-blocker inhibits diazepam metabolism. This interaction can impair kinetic visual acuity, which is correlated with the ability to discriminate moving objects in space.26
Propranolol increases plasma concentrations of antipsychotics, anticonvulsants, theophylline, and levothyroxine (Table 5)—possibly because of the beta blocker’s negative inotropic effects (decreased cardiac output reduces hepatic and renal blood flow).
Table 5
Clinical effects of drug-drug interactions with propranolol
| Pharmacodynamic |
| With MAO inhibitors → hypertensive crisis and bradycardia |
| With calcium channel inhibitors → ↓ myocardial contractility and A-V nodal conduction |
| ↓ intravenous anesthetic dose requirements |
| ↓ diazepam metabolism |
| ↓ median effective dosage of valproate and diazepam; might improve antiepileptic potential of valproate |
| Pharmacokinetic |
| ↑ plasma concentration of antipsychotics, anticonvulsants, theophylline, levothyroxine |
| Barbiturates, phenytoin, and cigarette smoking ↑ propranolol elimination |
- Cytochrome P450 interactions. www.drug-interaction.com.
- FDA. Food and drug interactions. http://vm.cfsan.fda.gov/~lrd/fdinter.html.
- Psychiatric drug interactions. www.preskorn.com.
- Alprazolam • Xanax
- Bupropion • Wellbutrin
- Buspirone • BuSpar
- Carbamazepine • Carbatrol, others
- Chlordiazepoxide • Librium
- Cimetidine • Tagamet
- Clonazepam • Klonopin
- Clorazepate • Tranxene
- Clozapine • Clozaril
- Diazepam • Valium
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Haloperidol • Haldol
- Itraconazole • Sporanox
- Lorazepam • Ativan
- Midazolam • Versed
- Mirtazapine • Remeron
- Oxazepam • Serax
- Paroxetine • Paxil
- Phenytoin • Dilantin
- Propranolol • Inderal
- Quetiapine • Seroquel
- Rifampin • Rifadin, Rimactane
- Triazolam • Halcion
- Valproate • various
- Verapamil • Calan, Isoptin
Drs. Ramadan and Werder report no financial relationships with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Preskorn has received grants or has been a consultant or speaker for Abbott Laboratories, AstraZeneca Pharmaceuticals, Boehringer-Ingelheim, Bristol-Myers Squibb Co., Merck & Co., Eisai, Eli Lilly and Co., GlaxoSmithKline, Janssen Pharmaceutica, Johnson & Johnson, Novartis Pharmaceuticals Corp., Organon, Otsuka America Pharmaceutical, Pfizer, Solvay Pharmaceuticals, Sanofi-Aventis, and Wyeth.
1. Preskorn S, Flockhart D. Psychiatric drug interactions guide. New York: MBL Communications.; 2004.
2. Bruce SE, Yonkers KA, Otto MW, et al. Influence of psychiatric comorbidity on recovery and recurrence in generalized anxiety disorder, social phobia, and panic disorder 12-year prospective study. Am J Psychiatry 2005;162:1179-87.
3. Nemeroff CB. Use of atypical antipsychotics in refractory depression and anxiety. J Clin Psychiatry 2005;66(Suppl 8):13-21.
4. Bean RB, Bean WB. Sir William Osler: Aphorisms from his bedside teaching and writing. Springfield, IL: Charles C. Thomas; 1961:53.
5. Tasman A, Kay J, Lieberman JA. Psychiatry Therapeutics. 2nd ed. West Sussex, UK: John Wiley & Sons; 2003:347.
6. Fuller M, Sajatovic M. Drug information for mental health. 3rd ed. Hudson, OH: Lexi-Comp; 2001.
7. Stahl SM. Essential psychopharmacology: Neuroscientific basis and practical applications. 2nd ed. New York: Cambridge University Press; 2000.
8. Janicak PG, Davis JM, Preskorn SH, Ayad FJ. Principles and practice of psychopharmacology. 3rd ed. Philadelphia, PA: Lippincott Williams and Wilkins; 2001.
9. Tanaka E. Toxicological interactions involving psychiatric drugs and alcohol: an update. J Clin Pharm Ther 2003;28(2):81-95.
10. Frels C, Williams P, Narayanan S, Gariballa SE. Iatrogenic causes of falls in hospitalised elderly patients: a case-control study. Postgrad Med 2002;78(922):487-9.
11. Wolf BC, Lavezzi WA, Sullivan LM, Flannagan LM. One hundred seventy two deaths involving the use of oxycodone in Palm Beach County. J Forensic Sci 2005;50(1):192-5.
12. Rogers WO, Hall MA, Brissie RM, Robinson CA. Detection of alprazolam in three cases of methadone/benzodiazepine overdose. J Forensic Sci 1997;42(1):155-6.
13. Wolf BC, Lavezzi WA, Sullivan LM, et al. Alprazolam-related deaths in Palm Beach County. Am J Forensic Med Pathol 2005;26(1):24-7.
14. Isbister GK, O’Regan L, Sibbritt D, et al. Alprazolam is relatively more toxic than other benzodiazepines in overdose. Br J Clin Pharmacol 2004;58(1):88-95.
15. Sadock BJ, Sadock VA. Kaplan and Sadock’s pocket handbook of psychiatric drug treatment. 3rd ed. Philadelphia: Lippincott Williams & Wilkins; 2001.
16. Tollefson G, Lesar T, Grothe D, et al. Alprazolam-related digoxin toxicity. Am J Psychiatry 1984;141(12):1612-3.
17. Murphy A, Wilbur K. Phenytoin-diazepam interaction. Ann Pharmacother 2003;37(5):659-3.
18. Sharp T, McQuade R, Bramwell S, et al. Effect of acute and repeated administration of 5-HT1A receptor agonists on 5-HT release in rat brain in vivo. Naunhyn Schmiedebergs Arch Pharmacol 1993;348(4):339-46.
19. Van den Hooff P, Galvan M. Actions of 5-hydroxytryptamine and 5-HT1A receptor ligands on rat dorso-lateral septal neurons in vitro. Br J Pharmacol 1992;106(4):893-9.
20. Preskorn SH Do you believe in magic? Journal of Practical Psychiatry and Behavioral Health March 1997;99-103
21. Physicians’ Desk Reference. 59th ed. Montvale, NJ: Thomson PDR; 2005.
22. Mahmood I, Sahajwalla C. Clinical pharmacokinetics and pharmacodynamics of buspirone, an anxiolytic drug. Clin Pharmacokinet 1999;36(4):277-87.
23. Goff DC, Midha KK, Brotman AW, et al. An open trial of buspirone added to neuroleptics in schizophrenic patients. J Clin Psychopharmacol 1991;11(3):193-7.
24. Huang HF, Jann MW, Wei FC, et al. Lack of pharmacokinetic interaction between buspirone and haloperidol in patients with schizophrenia. J Clin Pharmacol 1996;36(10):963-9.
25. Avram MJ, Krejcie TC, Henthorn TK, et al. Beta-adrenergic blockade affects initial drug distribution due to decreased cardiac output and altered blood flow distribution. J Pharmacol Exp Ther 2004;311(2):617-24.
26. Hawksworth G, Betts T, Crowe A, et al. Diazepam/beta-adrenoceptor antagonist interactions. Br J Clin Pharmacol 1984;17(Suppl 1):69S-76S.
27. Hallengren B, Nilsson OR, Karlberg BE, et al. Influence of hyperthyroidism on the kinetics of methimazole, propranolol, metoprolol and atenolol. Eur J Clin Pharmacol 1982;21(5):379-84.
1. Preskorn S, Flockhart D. Psychiatric drug interactions guide. New York: MBL Communications.; 2004.
2. Bruce SE, Yonkers KA, Otto MW, et al. Influence of psychiatric comorbidity on recovery and recurrence in generalized anxiety disorder, social phobia, and panic disorder 12-year prospective study. Am J Psychiatry 2005;162:1179-87.
3. Nemeroff CB. Use of atypical antipsychotics in refractory depression and anxiety. J Clin Psychiatry 2005;66(Suppl 8):13-21.
4. Bean RB, Bean WB. Sir William Osler: Aphorisms from his bedside teaching and writing. Springfield, IL: Charles C. Thomas; 1961:53.
5. Tasman A, Kay J, Lieberman JA. Psychiatry Therapeutics. 2nd ed. West Sussex, UK: John Wiley & Sons; 2003:347.
6. Fuller M, Sajatovic M. Drug information for mental health. 3rd ed. Hudson, OH: Lexi-Comp; 2001.
7. Stahl SM. Essential psychopharmacology: Neuroscientific basis and practical applications. 2nd ed. New York: Cambridge University Press; 2000.
8. Janicak PG, Davis JM, Preskorn SH, Ayad FJ. Principles and practice of psychopharmacology. 3rd ed. Philadelphia, PA: Lippincott Williams and Wilkins; 2001.
9. Tanaka E. Toxicological interactions involving psychiatric drugs and alcohol: an update. J Clin Pharm Ther 2003;28(2):81-95.
10. Frels C, Williams P, Narayanan S, Gariballa SE. Iatrogenic causes of falls in hospitalised elderly patients: a case-control study. Postgrad Med 2002;78(922):487-9.
11. Wolf BC, Lavezzi WA, Sullivan LM, Flannagan LM. One hundred seventy two deaths involving the use of oxycodone in Palm Beach County. J Forensic Sci 2005;50(1):192-5.
12. Rogers WO, Hall MA, Brissie RM, Robinson CA. Detection of alprazolam in three cases of methadone/benzodiazepine overdose. J Forensic Sci 1997;42(1):155-6.
13. Wolf BC, Lavezzi WA, Sullivan LM, et al. Alprazolam-related deaths in Palm Beach County. Am J Forensic Med Pathol 2005;26(1):24-7.
14. Isbister GK, O’Regan L, Sibbritt D, et al. Alprazolam is relatively more toxic than other benzodiazepines in overdose. Br J Clin Pharmacol 2004;58(1):88-95.
15. Sadock BJ, Sadock VA. Kaplan and Sadock’s pocket handbook of psychiatric drug treatment. 3rd ed. Philadelphia: Lippincott Williams & Wilkins; 2001.
16. Tollefson G, Lesar T, Grothe D, et al. Alprazolam-related digoxin toxicity. Am J Psychiatry 1984;141(12):1612-3.
17. Murphy A, Wilbur K. Phenytoin-diazepam interaction. Ann Pharmacother 2003;37(5):659-3.
18. Sharp T, McQuade R, Bramwell S, et al. Effect of acute and repeated administration of 5-HT1A receptor agonists on 5-HT release in rat brain in vivo. Naunhyn Schmiedebergs Arch Pharmacol 1993;348(4):339-46.
19. Van den Hooff P, Galvan M. Actions of 5-hydroxytryptamine and 5-HT1A receptor ligands on rat dorso-lateral septal neurons in vitro. Br J Pharmacol 1992;106(4):893-9.
20. Preskorn SH Do you believe in magic? Journal of Practical Psychiatry and Behavioral Health March 1997;99-103
21. Physicians’ Desk Reference. 59th ed. Montvale, NJ: Thomson PDR; 2005.
22. Mahmood I, Sahajwalla C. Clinical pharmacokinetics and pharmacodynamics of buspirone, an anxiolytic drug. Clin Pharmacokinet 1999;36(4):277-87.
23. Goff DC, Midha KK, Brotman AW, et al. An open trial of buspirone added to neuroleptics in schizophrenic patients. J Clin Psychopharmacol 1991;11(3):193-7.
24. Huang HF, Jann MW, Wei FC, et al. Lack of pharmacokinetic interaction between buspirone and haloperidol in patients with schizophrenia. J Clin Pharmacol 1996;36(10):963-9.
25. Avram MJ, Krejcie TC, Henthorn TK, et al. Beta-adrenergic blockade affects initial drug distribution due to decreased cardiac output and altered blood flow distribution. J Pharmacol Exp Ther 2004;311(2):617-24.
26. Hawksworth G, Betts T, Crowe A, et al. Diazepam/beta-adrenoceptor antagonist interactions. Br J Clin Pharmacol 1984;17(Suppl 1):69S-76S.
27. Hallengren B, Nilsson OR, Karlberg BE, et al. Influence of hyperthyroidism on the kinetics of methimazole, propranolol, metoprolol and atenolol. Eur J Clin Pharmacol 1982;21(5):379-84.
Military sexual trauma: How to identify and treat a unique form of PTSD
Sexual trauma may cause or exacerbate posttraumatic stress disorder (PTSD).See "Traumatized Troops: How to treat combat-related PTSD"). Two recommended questions (Box) for men and women can help you start discussing MST.
Use compassion and sensitivity, recognizing the stigma of sexual assault while fastidiously preserving confidentiality. Establish a comfortable environment for disclosure, be nonjudgmental, and maintain good eye contact as you gradually introduce the questions.
The National Center for Posttraumatic Stress Disorder (Related resources) suggests two screening questions for MST:
- While you were in the military, did you experience any unwanted sexual attention, such as verbal remarks, touching, or pressure for sexual favors?
- Did anyone ever use force or threat of force to have sex with you against your will?
Recommended treatment
Comprehensive MST management includes assessing for PTSD, major depression, and substance abuse. When a veteran screens positive for MST, validation and empathy are first-line treatment. Provide MST education, assess health status, and ask them about their support systems.
Sexual trauma survivors often suffer low selfesteem, self-blame, anger, difficulties with interpersonal relationships, and sexual dysfunction. “PTSD flare-ups” can occur during medical encounters and clinical procedures. Evaluate MST survivors regularly for re-victimization, as they may be at risk to be sexually abused again outside the military.5
Referral. Consider referring veterans to a local VA facility, which all have a “military sexual trauma coordinator” to help veterans obtain treatment. Other VA resources include referrals to the women veterans program manager or mental health clinic.
Veterans living in the community can be referred to readjustment counseling service offices, which have sexual trauma counselors on staff. This may be an option for the veteran who does not want to obtain mental health services from the VA.
- Street A, Stafford J. Military sexual trauma: Issues in caring for veterans. National Center for Posttraumatic Stress Disorder. http://www.ncptsd.org//war/military_sexual_trauma.html.
1. Kang H, Dalager N, Mahan C, et al. The role of sexual assault on the risk of PTSD among Gulf War veterans. Ann Epidemiol 2005;15(3):191-5.
2. Bastian L, Lancaster A, Reyst H. Department of Defense 1995 Sexual Harassment Survey (Report No. 96-014). Arlington, VA: Defense Manpower Data Center; 1996.
3. Department of Veterans Affairs. Report to Congress on the Study of Sexual Trauma among Reservists on Active Duty for Training. According to documents provided March 30, 2006 by the Subcommittee on Health, Committee of Veterans’ Affairs, U.S. House of Representatives.
4. Street A, Stafford J. Military sexual trauma: Issues in caring for veterans. National Center for Posttraumatic Stress Disorder. Available at: http://www.ncptsd.org//war/military_sexual_trauma.html. Accessed March 13, 2006.
5. Carole T, Susane F (eds). Military sexual trauma: Veterans Health Initiative, Department of Veterans Affairs. 2004;77-83.Available at: https://www.ees-learning.net/librix/loginhtml.asp?v=librix. Accessed March 28, 2006.
Sexual trauma may cause or exacerbate posttraumatic stress disorder (PTSD).See "Traumatized Troops: How to treat combat-related PTSD"). Two recommended questions (Box) for men and women can help you start discussing MST.
Use compassion and sensitivity, recognizing the stigma of sexual assault while fastidiously preserving confidentiality. Establish a comfortable environment for disclosure, be nonjudgmental, and maintain good eye contact as you gradually introduce the questions.
The National Center for Posttraumatic Stress Disorder (Related resources) suggests two screening questions for MST:
- While you were in the military, did you experience any unwanted sexual attention, such as verbal remarks, touching, or pressure for sexual favors?
- Did anyone ever use force or threat of force to have sex with you against your will?
Recommended treatment
Comprehensive MST management includes assessing for PTSD, major depression, and substance abuse. When a veteran screens positive for MST, validation and empathy are first-line treatment. Provide MST education, assess health status, and ask them about their support systems.
Sexual trauma survivors often suffer low selfesteem, self-blame, anger, difficulties with interpersonal relationships, and sexual dysfunction. “PTSD flare-ups” can occur during medical encounters and clinical procedures. Evaluate MST survivors regularly for re-victimization, as they may be at risk to be sexually abused again outside the military.5
Referral. Consider referring veterans to a local VA facility, which all have a “military sexual trauma coordinator” to help veterans obtain treatment. Other VA resources include referrals to the women veterans program manager or mental health clinic.
Veterans living in the community can be referred to readjustment counseling service offices, which have sexual trauma counselors on staff. This may be an option for the veteran who does not want to obtain mental health services from the VA.
- Street A, Stafford J. Military sexual trauma: Issues in caring for veterans. National Center for Posttraumatic Stress Disorder. http://www.ncptsd.org//war/military_sexual_trauma.html.
Sexual trauma may cause or exacerbate posttraumatic stress disorder (PTSD).See "Traumatized Troops: How to treat combat-related PTSD"). Two recommended questions (Box) for men and women can help you start discussing MST.
Use compassion and sensitivity, recognizing the stigma of sexual assault while fastidiously preserving confidentiality. Establish a comfortable environment for disclosure, be nonjudgmental, and maintain good eye contact as you gradually introduce the questions.
The National Center for Posttraumatic Stress Disorder (Related resources) suggests two screening questions for MST:
- While you were in the military, did you experience any unwanted sexual attention, such as verbal remarks, touching, or pressure for sexual favors?
- Did anyone ever use force or threat of force to have sex with you against your will?
Recommended treatment
Comprehensive MST management includes assessing for PTSD, major depression, and substance abuse. When a veteran screens positive for MST, validation and empathy are first-line treatment. Provide MST education, assess health status, and ask them about their support systems.
Sexual trauma survivors often suffer low selfesteem, self-blame, anger, difficulties with interpersonal relationships, and sexual dysfunction. “PTSD flare-ups” can occur during medical encounters and clinical procedures. Evaluate MST survivors regularly for re-victimization, as they may be at risk to be sexually abused again outside the military.5
Referral. Consider referring veterans to a local VA facility, which all have a “military sexual trauma coordinator” to help veterans obtain treatment. Other VA resources include referrals to the women veterans program manager or mental health clinic.
Veterans living in the community can be referred to readjustment counseling service offices, which have sexual trauma counselors on staff. This may be an option for the veteran who does not want to obtain mental health services from the VA.
- Street A, Stafford J. Military sexual trauma: Issues in caring for veterans. National Center for Posttraumatic Stress Disorder. http://www.ncptsd.org//war/military_sexual_trauma.html.
1. Kang H, Dalager N, Mahan C, et al. The role of sexual assault on the risk of PTSD among Gulf War veterans. Ann Epidemiol 2005;15(3):191-5.
2. Bastian L, Lancaster A, Reyst H. Department of Defense 1995 Sexual Harassment Survey (Report No. 96-014). Arlington, VA: Defense Manpower Data Center; 1996.
3. Department of Veterans Affairs. Report to Congress on the Study of Sexual Trauma among Reservists on Active Duty for Training. According to documents provided March 30, 2006 by the Subcommittee on Health, Committee of Veterans’ Affairs, U.S. House of Representatives.
4. Street A, Stafford J. Military sexual trauma: Issues in caring for veterans. National Center for Posttraumatic Stress Disorder. Available at: http://www.ncptsd.org//war/military_sexual_trauma.html. Accessed March 13, 2006.
5. Carole T, Susane F (eds). Military sexual trauma: Veterans Health Initiative, Department of Veterans Affairs. 2004;77-83.Available at: https://www.ees-learning.net/librix/loginhtml.asp?v=librix. Accessed March 28, 2006.
1. Kang H, Dalager N, Mahan C, et al. The role of sexual assault on the risk of PTSD among Gulf War veterans. Ann Epidemiol 2005;15(3):191-5.
2. Bastian L, Lancaster A, Reyst H. Department of Defense 1995 Sexual Harassment Survey (Report No. 96-014). Arlington, VA: Defense Manpower Data Center; 1996.
3. Department of Veterans Affairs. Report to Congress on the Study of Sexual Trauma among Reservists on Active Duty for Training. According to documents provided March 30, 2006 by the Subcommittee on Health, Committee of Veterans’ Affairs, U.S. House of Representatives.
4. Street A, Stafford J. Military sexual trauma: Issues in caring for veterans. National Center for Posttraumatic Stress Disorder. Available at: http://www.ncptsd.org//war/military_sexual_trauma.html. Accessed March 13, 2006.
5. Carole T, Susane F (eds). Military sexual trauma: Veterans Health Initiative, Department of Veterans Affairs. 2004;77-83.Available at: https://www.ees-learning.net/librix/loginhtml.asp?v=librix. Accessed March 28, 2006.
TRAUMATIZED TROOPS How to treat combat-related PTSD
Thousands of U.S. troops are seeking mental health care after being deployed in Iraq. Among 222,000 Army and Marine Iraq veterans, 35% sought treatment in the year after returning home—many for posttraumatic stress disorder (PTSD).In a related article, we discuss the diagnosis and treatment of military sexual trauma, a form of PTSD.
Persistent pathology
The greater the intensity of an Iraq/Afghanistan veteran’s combat experiences (“firefights”), the more likely the soldier is to develop PTSD.Traumatic brain injury: Choosing medications for neurobehavioral symptoms”). Sexual trauma also may cause or exacerbate PTSD.Military sexual trauma: How to identify and treat a unique form of PTSD”).
Table 1
3 domains of posttraumatic stress disorder symptoms
| Domain | Symptoms |
|---|---|
| Re-experiencing |
|
| Avoidance and numbing |
|
| Increased arousal |
|
| Source: DSM-IV-TR | |
FigurePTSD screen for war veterans
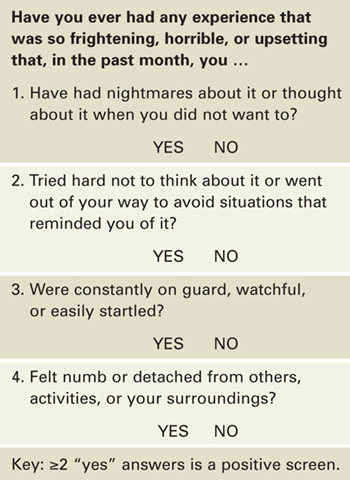
Source: U.S. Department of Veterans Affairs. Afghan & Iraq Post-Deployment Screen, Attachment B. Screening for risk factors associated with development of post-traumatic stress disorder (PTSD)
Cognitive therapy
Psychotherapy is the cornerstone of PTSD treatment; skilled therapists may achieve greater efficacy and more-durable results than medications do. Evidence strongly supports cognitive behavioral therapy—including exposure therapy, anxiety management, and cognitive therapy.U.S. troops returning home: Are you prepared? Current Psychiatry 2006;5(1):12-22.
- U.S. Department of Veterans Affairs. Seamless Transition Home. http://www.seamlesstransition.va.gov. Accessed March 13, 2006.
- American Psychiatric Association. Practice guideline for the treatment of acute stress disorder and posttraumatic stress disorder. http://www.psych.org/psych_pract/treatg/pg/PTSD-PG-PartsA-B-C-New.pdf.
Drug brand names
- Carbamazepine • Carbatrol
- Fluoxetine • Prozac
- Lamotrigine • Lamictal
- Lithium • Lithobid, others
- Mirtazapine • Remeron
- Paroxetine • Paxil
- Prazosin • Minipress
- Sertraline • Zoloft
- Trazodone • Desyrel
- Temazepam • Restoril
- Valproic acid • Divalproex, others
- Venlafaxine • Effexor
- Zolpidem • Ambien
Disclosures
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products. Drs. Lineberry, Bostwick, and Rundell served on active duty in the U.S. Air Force. Dr. Ramaswamy is staff psychiatrist, Omaha Veterans Administration. and Director of Psychopharmacology Research, Creighton University, Omaha, NE.
1. Hoge CW, Auchterlonie JL, Milliken CS. Mental health problems, use of mental health services, and attrition from military service after returning from deployment to Iraq or Afghanistan. JAMA 2006;295(9):1023-32.
2. Hoge CW, Castro CA, Messer SC, et al. Combat duty in Iraq and Afghanistan, mental health problems, and barriers to care. N Engl J Med 2004;351:13-22.
3. Schlenger WE, Kulka RA, Fairbank JA, et al. The prevalence of post-traumatic stress disorder in the Vietnam generation: a multimethod, multisource assessment of psychiatric disorder. J Trauma Stress 1992;5:333-63.
4. Prigerson HG, Maciejewski PK, Rosenheck RA. Combat trauma: trauma with highest risk of delayed onset and unresolved posttraumatic stress disorder symptoms, unemployment, and abuse among men. J Nerv Ment Dis 2001;189:99-108.
5. Prigerson HG, Maciejewski PK, Rosenheck RA. Population attributable fractions of psychiatric disorders and behavioral outcomes associated with combat exposures among U.S. men. Am J Public Health 2002;92(1):59-63.
6. Diagnostic and statistical manual of mental disorders (4th ed, text rev). Washington, DC: American Psychiatric Association; 2000.
7. Xydakis MS, Fravell MD, Nasser KE, Casler JD. Analysis of battlefield head and neck injuries in Iraq and Afghanistan. Otolaryngol Head Neck Surg 2005;133:497-504.
8. Okie S. Traumatic brain injury in the war zone. N Engl J Med 2005;352(20):2043-7.
9. Kang H, Dalager N, Mahan C, et al. The role of sexual assault on the risk of PTSD among Gulf War veterans. Ann Epidemiol 2005;15(3):191-5.
10. Bradley R, Greene J, Russ E, et al. A multidimensional metaanalysis of psychotherapy for posttraumatic stress disorder. Am J Psychiatry 2005;162:214-27.
11. Foa EB, Hembree EA, Cahill SP, et al. Randomized trial of prolonged exposure for posttraumatic stress disorder with and without cognitive restructuring: outcome at academic and community clinics. J Consult Clin Psychol 2005;73:953-64.
12. Schnurr PP, Lunney CA, Sengupta A. Risk factors for the development versus maintenance of post-traumatic stress disorder. J Trauma Stress 2004;17:85-95.
13. Friedman MJ, Donnelly CL, Mellman TA. Pharmacotherapy for PTSD. Psychiatric Annals 2003;33(8):57-62.
14. Asnis GM, Kohn SR, Henderson M, Brown NL. SSRIs versus non- SSRIs in posttraumatic stress disorder: an update with recommendations. Drugs 2004;6:383-404.
15. Simon GE, Savarino J, Operskalski B, et al. Suicide risk during antidepressant treatment. Am J Psychiatry 2006;163(1):41-7.
16. Oquendo M, Brent DA, Birmaher B, et al. Posttraumatic stress disorder comorbid with major depression: factors mediating the association with suicidal behavior. Am J Psychiatry 2005;162(3):560-6.
17. Schoenfeld FB, Marmar CR, Neylan TC. Current concepts in pharmacotherapy for posttraumatic stress disorder. Psychiatr Serv 2004;55:519-31.
18. Martenyi F, Brown EB, Zhang H, et al. Fluoxetine versus placebo in posttraumatic stress disorder. J Clin Psychiatry 2002;63:199-206.
19. Brady KT, Sonne SC, Roberts JM. Sertraline treatment of comorbid posttraumatic stress disorder and alcohol dependence J Clin Psychiatry 1995;56(11):502-5.
20. Davidson JR, Rothbaum BO, van der Kolk BA, et al. Multicenter, double-blind comparison of sertraline and placebo in the treatment of posttraumatic stress disorder. Arch Gen Psychiatry 2001;58(5):485-92.
21. Zohar J, Amital D, Miodownik C, et al. Double-blind placebocontrolled pilot study of sertraline in military veterans with posttraumatic stress disorder J Clin Psychopharmacol 2002;22(2):190-5.
22. Marshall RD, Beebe KL, Oldham M, et al. Efficacy and safety of paroxetine treatment for chronic PTSD: a fixed-dose, placebocontrolled study. Am J Psychiatr 2001;158(12):1982-8.
23. Tucker P, Zaninelli R, Yehuda R, et al. Paroxetine in the treatment of chronic posttraumatic stress disorder: results of a placebocontrolled, flexible-dosage trial. J Clin Psychiatry 2001;62(11):860-8.
24. Raskind MA, Peskind ER, Kanter ED, et al. Reduction of nightmares and other PTSD symptoms in combat veterans by prazosin: a placebo-controlled study. Am J Psychiatry 2003;160(2):371-3.
25. Hamner MB, Deitsch SE, Brodrick PS, et al. Quetiapine treatment in patients with posttraumatic stress disorder: an open trial of adjunctive therapy. J Clin Psychopharmacol 2003;23(1):15-20.
26. Villarreal G, Calais L, Pickard J, et al. Open-label aripiprazole monotherapy in the treatment of posttraumatic stress disorder. Poster presented at: annual meeting of the NIMH New Clinical Drug Evaluation Unit; June 6-9, 2005; Boca Raton FL.
27. Vieweg WVR, Julius DA, Fernandez A, et al. Posttraumatic stress disorder in male military veterans with comorbid overweight and obesity: Psychotropic, antihypertensive, and metabolic medications. Prim Care Companion J Clin Psychiatry 2006;8(1):
28. Stein MB, Kline NA, Matloff JL. Adjunctive olanzapine for SSRI-resistant combat-related PTSD: a double-blind, placebo-controlled study. Am J Psychiatry 2002;159(10):1777-9.
29. Kozaric-Kovacic D, Pivac N, Muck-Seler D, et al. Risperidone in psychotic combat-related posttraumatic stress disorder: an open trial. J Clin Psychiatry 2005;66(7):922-7.
30. Ahearn EP, Mussey M, Johnson C, et al. Quetiapine as an adjunctive treatment for post-traumatic stress disorder: an 8-week open-label study. Int Clin Psychopharmacol 2006;21(1):29-33.
31. Lambert MT. Aripiprazole in the management of post-traumatic stress disorder symptoms in returning Global War on Terrorism veterans. Int Clin Psychopharmacol 2006;21(3):185-7.
32. Warner MD, Dorn MR, Peabody CA. Survey on the usefulness of trazodone in patients with PTSD with insomnia or nightmares. Pharmacopsychiatry 2001;34(4):128-31.
33. Ocasio-Tascon ME, Alicea-Colon E, et al., Torres-Palacios A, et al. The veteran population: one at high risk for sleep-disordered breathing. Sleep Breath 2006 Feb 22;[Epub ahead of print].
34. Krakow B, Lowry C, Germain A, et al. A retrospective study on improvements in nightmares and post-traumatic stress disorder following treatment for co-morbid sleep-disordered breathing. J Psychosom Res 2000;49(5):291-8.
35. Forbes D, Creamer M, Hawthorne G, et al. Co-morbidity as a predictor of symptom changes after treatment in combat-related posttraumatic stress disorder. J Nerv Ment Dis 2003;191:93-9.
Thousands of U.S. troops are seeking mental health care after being deployed in Iraq. Among 222,000 Army and Marine Iraq veterans, 35% sought treatment in the year after returning home—many for posttraumatic stress disorder (PTSD).In a related article, we discuss the diagnosis and treatment of military sexual trauma, a form of PTSD.
Persistent pathology
The greater the intensity of an Iraq/Afghanistan veteran’s combat experiences (“firefights”), the more likely the soldier is to develop PTSD.Traumatic brain injury: Choosing medications for neurobehavioral symptoms”). Sexual trauma also may cause or exacerbate PTSD.Military sexual trauma: How to identify and treat a unique form of PTSD”).
Table 1
3 domains of posttraumatic stress disorder symptoms
| Domain | Symptoms |
|---|---|
| Re-experiencing |
|
| Avoidance and numbing |
|
| Increased arousal |
|
| Source: DSM-IV-TR | |
FigurePTSD screen for war veterans
Source: U.S. Department of Veterans Affairs. Afghan & Iraq Post-Deployment Screen, Attachment B. Screening for risk factors associated with development of post-traumatic stress disorder (PTSD)
Cognitive therapy
Psychotherapy is the cornerstone of PTSD treatment; skilled therapists may achieve greater efficacy and more-durable results than medications do. Evidence strongly supports cognitive behavioral therapy—including exposure therapy, anxiety management, and cognitive therapy.U.S. troops returning home: Are you prepared? Current Psychiatry 2006;5(1):12-22.
- U.S. Department of Veterans Affairs. Seamless Transition Home. http://www.seamlesstransition.va.gov. Accessed March 13, 2006.
- American Psychiatric Association. Practice guideline for the treatment of acute stress disorder and posttraumatic stress disorder. http://www.psych.org/psych_pract/treatg/pg/PTSD-PG-PartsA-B-C-New.pdf.
Drug brand names
- Carbamazepine • Carbatrol
- Fluoxetine • Prozac
- Lamotrigine • Lamictal
- Lithium • Lithobid, others
- Mirtazapine • Remeron
- Paroxetine • Paxil
- Prazosin • Minipress
- Sertraline • Zoloft
- Trazodone • Desyrel
- Temazepam • Restoril
- Valproic acid • Divalproex, others
- Venlafaxine • Effexor
- Zolpidem • Ambien
Disclosures
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products. Drs. Lineberry, Bostwick, and Rundell served on active duty in the U.S. Air Force. Dr. Ramaswamy is staff psychiatrist, Omaha Veterans Administration. and Director of Psychopharmacology Research, Creighton University, Omaha, NE.
Thousands of U.S. troops are seeking mental health care after being deployed in Iraq. Among 222,000 Army and Marine Iraq veterans, 35% sought treatment in the year after returning home—many for posttraumatic stress disorder (PTSD).In a related article, we discuss the diagnosis and treatment of military sexual trauma, a form of PTSD.
Persistent pathology
The greater the intensity of an Iraq/Afghanistan veteran’s combat experiences (“firefights”), the more likely the soldier is to develop PTSD.Traumatic brain injury: Choosing medications for neurobehavioral symptoms”). Sexual trauma also may cause or exacerbate PTSD.Military sexual trauma: How to identify and treat a unique form of PTSD”).
Table 1
3 domains of posttraumatic stress disorder symptoms
| Domain | Symptoms |
|---|---|
| Re-experiencing |
|
| Avoidance and numbing |
|
| Increased arousal |
|
| Source: DSM-IV-TR | |
FigurePTSD screen for war veterans
Source: U.S. Department of Veterans Affairs. Afghan & Iraq Post-Deployment Screen, Attachment B. Screening for risk factors associated with development of post-traumatic stress disorder (PTSD)
Cognitive therapy
Psychotherapy is the cornerstone of PTSD treatment; skilled therapists may achieve greater efficacy and more-durable results than medications do. Evidence strongly supports cognitive behavioral therapy—including exposure therapy, anxiety management, and cognitive therapy.U.S. troops returning home: Are you prepared? Current Psychiatry 2006;5(1):12-22.
- U.S. Department of Veterans Affairs. Seamless Transition Home. http://www.seamlesstransition.va.gov. Accessed March 13, 2006.
- American Psychiatric Association. Practice guideline for the treatment of acute stress disorder and posttraumatic stress disorder. http://www.psych.org/psych_pract/treatg/pg/PTSD-PG-PartsA-B-C-New.pdf.
Drug brand names
- Carbamazepine • Carbatrol
- Fluoxetine • Prozac
- Lamotrigine • Lamictal
- Lithium • Lithobid, others
- Mirtazapine • Remeron
- Paroxetine • Paxil
- Prazosin • Minipress
- Sertraline • Zoloft
- Trazodone • Desyrel
- Temazepam • Restoril
- Valproic acid • Divalproex, others
- Venlafaxine • Effexor
- Zolpidem • Ambien
Disclosures
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products. Drs. Lineberry, Bostwick, and Rundell served on active duty in the U.S. Air Force. Dr. Ramaswamy is staff psychiatrist, Omaha Veterans Administration. and Director of Psychopharmacology Research, Creighton University, Omaha, NE.
1. Hoge CW, Auchterlonie JL, Milliken CS. Mental health problems, use of mental health services, and attrition from military service after returning from deployment to Iraq or Afghanistan. JAMA 2006;295(9):1023-32.
2. Hoge CW, Castro CA, Messer SC, et al. Combat duty in Iraq and Afghanistan, mental health problems, and barriers to care. N Engl J Med 2004;351:13-22.
3. Schlenger WE, Kulka RA, Fairbank JA, et al. The prevalence of post-traumatic stress disorder in the Vietnam generation: a multimethod, multisource assessment of psychiatric disorder. J Trauma Stress 1992;5:333-63.
4. Prigerson HG, Maciejewski PK, Rosenheck RA. Combat trauma: trauma with highest risk of delayed onset and unresolved posttraumatic stress disorder symptoms, unemployment, and abuse among men. J Nerv Ment Dis 2001;189:99-108.
5. Prigerson HG, Maciejewski PK, Rosenheck RA. Population attributable fractions of psychiatric disorders and behavioral outcomes associated with combat exposures among U.S. men. Am J Public Health 2002;92(1):59-63.
6. Diagnostic and statistical manual of mental disorders (4th ed, text rev). Washington, DC: American Psychiatric Association; 2000.
7. Xydakis MS, Fravell MD, Nasser KE, Casler JD. Analysis of battlefield head and neck injuries in Iraq and Afghanistan. Otolaryngol Head Neck Surg 2005;133:497-504.
8. Okie S. Traumatic brain injury in the war zone. N Engl J Med 2005;352(20):2043-7.
9. Kang H, Dalager N, Mahan C, et al. The role of sexual assault on the risk of PTSD among Gulf War veterans. Ann Epidemiol 2005;15(3):191-5.
10. Bradley R, Greene J, Russ E, et al. A multidimensional metaanalysis of psychotherapy for posttraumatic stress disorder. Am J Psychiatry 2005;162:214-27.
11. Foa EB, Hembree EA, Cahill SP, et al. Randomized trial of prolonged exposure for posttraumatic stress disorder with and without cognitive restructuring: outcome at academic and community clinics. J Consult Clin Psychol 2005;73:953-64.
12. Schnurr PP, Lunney CA, Sengupta A. Risk factors for the development versus maintenance of post-traumatic stress disorder. J Trauma Stress 2004;17:85-95.
13. Friedman MJ, Donnelly CL, Mellman TA. Pharmacotherapy for PTSD. Psychiatric Annals 2003;33(8):57-62.
14. Asnis GM, Kohn SR, Henderson M, Brown NL. SSRIs versus non- SSRIs in posttraumatic stress disorder: an update with recommendations. Drugs 2004;6:383-404.
15. Simon GE, Savarino J, Operskalski B, et al. Suicide risk during antidepressant treatment. Am J Psychiatry 2006;163(1):41-7.
16. Oquendo M, Brent DA, Birmaher B, et al. Posttraumatic stress disorder comorbid with major depression: factors mediating the association with suicidal behavior. Am J Psychiatry 2005;162(3):560-6.
17. Schoenfeld FB, Marmar CR, Neylan TC. Current concepts in pharmacotherapy for posttraumatic stress disorder. Psychiatr Serv 2004;55:519-31.
18. Martenyi F, Brown EB, Zhang H, et al. Fluoxetine versus placebo in posttraumatic stress disorder. J Clin Psychiatry 2002;63:199-206.
19. Brady KT, Sonne SC, Roberts JM. Sertraline treatment of comorbid posttraumatic stress disorder and alcohol dependence J Clin Psychiatry 1995;56(11):502-5.
20. Davidson JR, Rothbaum BO, van der Kolk BA, et al. Multicenter, double-blind comparison of sertraline and placebo in the treatment of posttraumatic stress disorder. Arch Gen Psychiatry 2001;58(5):485-92.
21. Zohar J, Amital D, Miodownik C, et al. Double-blind placebocontrolled pilot study of sertraline in military veterans with posttraumatic stress disorder J Clin Psychopharmacol 2002;22(2):190-5.
22. Marshall RD, Beebe KL, Oldham M, et al. Efficacy and safety of paroxetine treatment for chronic PTSD: a fixed-dose, placebocontrolled study. Am J Psychiatr 2001;158(12):1982-8.
23. Tucker P, Zaninelli R, Yehuda R, et al. Paroxetine in the treatment of chronic posttraumatic stress disorder: results of a placebocontrolled, flexible-dosage trial. J Clin Psychiatry 2001;62(11):860-8.
24. Raskind MA, Peskind ER, Kanter ED, et al. Reduction of nightmares and other PTSD symptoms in combat veterans by prazosin: a placebo-controlled study. Am J Psychiatry 2003;160(2):371-3.
25. Hamner MB, Deitsch SE, Brodrick PS, et al. Quetiapine treatment in patients with posttraumatic stress disorder: an open trial of adjunctive therapy. J Clin Psychopharmacol 2003;23(1):15-20.
26. Villarreal G, Calais L, Pickard J, et al. Open-label aripiprazole monotherapy in the treatment of posttraumatic stress disorder. Poster presented at: annual meeting of the NIMH New Clinical Drug Evaluation Unit; June 6-9, 2005; Boca Raton FL.
27. Vieweg WVR, Julius DA, Fernandez A, et al. Posttraumatic stress disorder in male military veterans with comorbid overweight and obesity: Psychotropic, antihypertensive, and metabolic medications. Prim Care Companion J Clin Psychiatry 2006;8(1):
28. Stein MB, Kline NA, Matloff JL. Adjunctive olanzapine for SSRI-resistant combat-related PTSD: a double-blind, placebo-controlled study. Am J Psychiatry 2002;159(10):1777-9.
29. Kozaric-Kovacic D, Pivac N, Muck-Seler D, et al. Risperidone in psychotic combat-related posttraumatic stress disorder: an open trial. J Clin Psychiatry 2005;66(7):922-7.
30. Ahearn EP, Mussey M, Johnson C, et al. Quetiapine as an adjunctive treatment for post-traumatic stress disorder: an 8-week open-label study. Int Clin Psychopharmacol 2006;21(1):29-33.
31. Lambert MT. Aripiprazole in the management of post-traumatic stress disorder symptoms in returning Global War on Terrorism veterans. Int Clin Psychopharmacol 2006;21(3):185-7.
32. Warner MD, Dorn MR, Peabody CA. Survey on the usefulness of trazodone in patients with PTSD with insomnia or nightmares. Pharmacopsychiatry 2001;34(4):128-31.
33. Ocasio-Tascon ME, Alicea-Colon E, et al., Torres-Palacios A, et al. The veteran population: one at high risk for sleep-disordered breathing. Sleep Breath 2006 Feb 22;[Epub ahead of print].
34. Krakow B, Lowry C, Germain A, et al. A retrospective study on improvements in nightmares and post-traumatic stress disorder following treatment for co-morbid sleep-disordered breathing. J Psychosom Res 2000;49(5):291-8.
35. Forbes D, Creamer M, Hawthorne G, et al. Co-morbidity as a predictor of symptom changes after treatment in combat-related posttraumatic stress disorder. J Nerv Ment Dis 2003;191:93-9.
1. Hoge CW, Auchterlonie JL, Milliken CS. Mental health problems, use of mental health services, and attrition from military service after returning from deployment to Iraq or Afghanistan. JAMA 2006;295(9):1023-32.
2. Hoge CW, Castro CA, Messer SC, et al. Combat duty in Iraq and Afghanistan, mental health problems, and barriers to care. N Engl J Med 2004;351:13-22.
3. Schlenger WE, Kulka RA, Fairbank JA, et al. The prevalence of post-traumatic stress disorder in the Vietnam generation: a multimethod, multisource assessment of psychiatric disorder. J Trauma Stress 1992;5:333-63.
4. Prigerson HG, Maciejewski PK, Rosenheck RA. Combat trauma: trauma with highest risk of delayed onset and unresolved posttraumatic stress disorder symptoms, unemployment, and abuse among men. J Nerv Ment Dis 2001;189:99-108.
5. Prigerson HG, Maciejewski PK, Rosenheck RA. Population attributable fractions of psychiatric disorders and behavioral outcomes associated with combat exposures among U.S. men. Am J Public Health 2002;92(1):59-63.
6. Diagnostic and statistical manual of mental disorders (4th ed, text rev). Washington, DC: American Psychiatric Association; 2000.
7. Xydakis MS, Fravell MD, Nasser KE, Casler JD. Analysis of battlefield head and neck injuries in Iraq and Afghanistan. Otolaryngol Head Neck Surg 2005;133:497-504.
8. Okie S. Traumatic brain injury in the war zone. N Engl J Med 2005;352(20):2043-7.
9. Kang H, Dalager N, Mahan C, et al. The role of sexual assault on the risk of PTSD among Gulf War veterans. Ann Epidemiol 2005;15(3):191-5.
10. Bradley R, Greene J, Russ E, et al. A multidimensional metaanalysis of psychotherapy for posttraumatic stress disorder. Am J Psychiatry 2005;162:214-27.
11. Foa EB, Hembree EA, Cahill SP, et al. Randomized trial of prolonged exposure for posttraumatic stress disorder with and without cognitive restructuring: outcome at academic and community clinics. J Consult Clin Psychol 2005;73:953-64.
12. Schnurr PP, Lunney CA, Sengupta A. Risk factors for the development versus maintenance of post-traumatic stress disorder. J Trauma Stress 2004;17:85-95.
13. Friedman MJ, Donnelly CL, Mellman TA. Pharmacotherapy for PTSD. Psychiatric Annals 2003;33(8):57-62.
14. Asnis GM, Kohn SR, Henderson M, Brown NL. SSRIs versus non- SSRIs in posttraumatic stress disorder: an update with recommendations. Drugs 2004;6:383-404.
15. Simon GE, Savarino J, Operskalski B, et al. Suicide risk during antidepressant treatment. Am J Psychiatry 2006;163(1):41-7.
16. Oquendo M, Brent DA, Birmaher B, et al. Posttraumatic stress disorder comorbid with major depression: factors mediating the association with suicidal behavior. Am J Psychiatry 2005;162(3):560-6.
17. Schoenfeld FB, Marmar CR, Neylan TC. Current concepts in pharmacotherapy for posttraumatic stress disorder. Psychiatr Serv 2004;55:519-31.
18. Martenyi F, Brown EB, Zhang H, et al. Fluoxetine versus placebo in posttraumatic stress disorder. J Clin Psychiatry 2002;63:199-206.
19. Brady KT, Sonne SC, Roberts JM. Sertraline treatment of comorbid posttraumatic stress disorder and alcohol dependence J Clin Psychiatry 1995;56(11):502-5.
20. Davidson JR, Rothbaum BO, van der Kolk BA, et al. Multicenter, double-blind comparison of sertraline and placebo in the treatment of posttraumatic stress disorder. Arch Gen Psychiatry 2001;58(5):485-92.
21. Zohar J, Amital D, Miodownik C, et al. Double-blind placebocontrolled pilot study of sertraline in military veterans with posttraumatic stress disorder J Clin Psychopharmacol 2002;22(2):190-5.
22. Marshall RD, Beebe KL, Oldham M, et al. Efficacy and safety of paroxetine treatment for chronic PTSD: a fixed-dose, placebocontrolled study. Am J Psychiatr 2001;158(12):1982-8.
23. Tucker P, Zaninelli R, Yehuda R, et al. Paroxetine in the treatment of chronic posttraumatic stress disorder: results of a placebocontrolled, flexible-dosage trial. J Clin Psychiatry 2001;62(11):860-8.
24. Raskind MA, Peskind ER, Kanter ED, et al. Reduction of nightmares and other PTSD symptoms in combat veterans by prazosin: a placebo-controlled study. Am J Psychiatry 2003;160(2):371-3.
25. Hamner MB, Deitsch SE, Brodrick PS, et al. Quetiapine treatment in patients with posttraumatic stress disorder: an open trial of adjunctive therapy. J Clin Psychopharmacol 2003;23(1):15-20.
26. Villarreal G, Calais L, Pickard J, et al. Open-label aripiprazole monotherapy in the treatment of posttraumatic stress disorder. Poster presented at: annual meeting of the NIMH New Clinical Drug Evaluation Unit; June 6-9, 2005; Boca Raton FL.
27. Vieweg WVR, Julius DA, Fernandez A, et al. Posttraumatic stress disorder in male military veterans with comorbid overweight and obesity: Psychotropic, antihypertensive, and metabolic medications. Prim Care Companion J Clin Psychiatry 2006;8(1):
28. Stein MB, Kline NA, Matloff JL. Adjunctive olanzapine for SSRI-resistant combat-related PTSD: a double-blind, placebo-controlled study. Am J Psychiatry 2002;159(10):1777-9.
29. Kozaric-Kovacic D, Pivac N, Muck-Seler D, et al. Risperidone in psychotic combat-related posttraumatic stress disorder: an open trial. J Clin Psychiatry 2005;66(7):922-7.
30. Ahearn EP, Mussey M, Johnson C, et al. Quetiapine as an adjunctive treatment for post-traumatic stress disorder: an 8-week open-label study. Int Clin Psychopharmacol 2006;21(1):29-33.
31. Lambert MT. Aripiprazole in the management of post-traumatic stress disorder symptoms in returning Global War on Terrorism veterans. Int Clin Psychopharmacol 2006;21(3):185-7.
32. Warner MD, Dorn MR, Peabody CA. Survey on the usefulness of trazodone in patients with PTSD with insomnia or nightmares. Pharmacopsychiatry 2001;34(4):128-31.
33. Ocasio-Tascon ME, Alicea-Colon E, et al., Torres-Palacios A, et al. The veteran population: one at high risk for sleep-disordered breathing. Sleep Breath 2006 Feb 22;[Epub ahead of print].
34. Krakow B, Lowry C, Germain A, et al. A retrospective study on improvements in nightmares and post-traumatic stress disorder following treatment for co-morbid sleep-disordered breathing. J Psychosom Res 2000;49(5):291-8.
35. Forbes D, Creamer M, Hawthorne G, et al. Co-morbidity as a predictor of symptom changes after treatment in combat-related posttraumatic stress disorder. J Nerv Ment Dis 2003;191:93-9.
A prescription to improve drug regimens?
Technology companies are offering two new computerized tools to reduce the “trial and error” of prescribing. Thanks to quantitative EEG (QEEG) testing and pharmacogenetic testing, you may one day be able to consistently choose medications that offer optimal benefit and minimal adverse events—without subjecting patients to unsuccessful trials.
How quantitative eeg works
QEEG adds modern computer and statistical analyses to traditional EEG recordings. The computer creates a graphic display on a schematic map of the head. The procedure is often called brain electrical activity mapping (BEAM) or simply “mapping.”1
QEEG is nearly identical to EEG, but approximately 50% more electrodes are applied to the scalp. The additional electrodes provide better definition and about twice the data compared with traditional EEG.
The UCLA Quantitative EEG Laboratory developed cordance,2 a QEEG measure, to study regional brain activity. Cordance is calculated with reference to absolute and relative power measures from the various electrodes on the brain. It is more closely correlated than traditional EEG with regional cerebral perfusion, which may offer clues to brain activity under different conditions such as depression and medication treatment.
What the data show
Several studies suggest that QEEG can trace response to medication.
Cook et al3 used QEEG in a double-blind study comparing response to fluoxetine, 20 mg/d, and placebo across 8 weeks in 24 adults with unipolar major depression. Subjects were classified as concordant or discordant depending on how many electrodes showed discordance.
Concordant patients showed a more-robust response to fluoxetine than did the discordant group, as evidenced by lower Beck Depression Inventory and Hamilton Rating Scale for Depression (HRSD) scores. The findings suggest that cordance may identify patients who will or will not respond to an antidepressant.
Cook et al4 also used cordance to measure response to fluoxetine, 20 mg/d, venlafaxine, 150 mg/d, or placebo in 51 adults with unipolar depression. Responders to antidepressants (defined as HRSD score ≤10) showed decreased prefrontal cordance after 48 hours and 1 week, suggesting that the prefrontal region may mediate antidepressant response.
A recent study in Korea5 investigated the effects of methylphenidate, 0.7 mg/kg/d (range 15 to 35 mg/d) on QEEG patterns in 20 boys ages 6 to 12 while at work or rest. Numerous changes in band waves were seen during continuous performance tests, but none were reported while the subjects were at rest. This suggests that methylphenidate exerts greater electrophysiologic influence during attention-related tasks.
Clinical applicability
QEEG has just begun to enter mainstream practice, with vendors offering analysis services. As patients increasingly demand improved diagnostic reliability and medication effectiveness, QEEG use could become a standard of practice within 5 years.
Lexicor offers a QEEG analysis to diagnose attention-deficit/hyperactivity disorder based on theta/beta band wave ratio. Lexicor says its analysis offers 86% to 90% sensitivity and 94% to 98% specificity, both far greater than traditional methods such as the Child Behavior Checklist, Behavior Assessment System for Children, and Devereaux Scales of Mental Disorder.
Major health plans offer limited coverage of quantitative EEG testing, however, so many patients would pay $200 or more for tests out of pocket. Also, the American Academy of Neurology and American Clinical Neurophysiology Society endorse QEEG for use in screening for and assessing epilepsy, but not in mental disorders,6 making insurers less likely to cover these tests for psychiatric purposes.
Pharmacogenetic testing
With the sequencing of the human genome and improved speed of genetic analysis, pharmacogenetic testing could supplement quantitative EEG in identifying an appropriate medication.
Companies such as Genelex (www.healthanddna.com/professional/pharmacogenetics.html) and Signature Genetics (www.signaturegenetics.com) have begun offering tests to detect variants of the cytochrome-P(CYP) 2C9, 2C19, 2D6, and 1A2 genes. The findings indicate if the patient will metabolize a medication too slowly or rapidly through these pathways. Psychiatrists can then adjust the dosage accordingly or try another medication. Physicians can order any combination of gene tests, which cost about $150 to $200 each, or all available tests for a discounted price of approximately $600.
Genelex and Signature Genetics can create individualized CYP-450 function reports to facilitate prescribing and customized reports that take into account the patient’s medication and diet regimen. Genelex also offers an Internet-based software tool, GeneMedRx, which allows doctors to customize medication regimens based on potential drug-drug interactions and genomic information.
Signature Genetics offers a prospective assessment of drugs based on genetic test results. This assessment provides a comprehensive report of which medications are affected by the test results.
Genetic profiling can help psychiatrists improve the likelihood of treatment success and minimize potential drug-drug interactions and adverse reactions. Patients will be more satisfied, knowing that their medications fit their individual needs. Also, as more is learned about genetic analysis, genetic testing could one day reveal susceptibility to Alzheimer’s disease, heart attack risk, or other medical problems.
As with QEEG, however, few insurance companies cover genetic testing. Also, insurance companies might charge higher premiums to patients found to have a higher likelihood of developing certain diseases.
Related resources
- Indiana University School of Medicine. Drug interactions table. http://medicine.iupui.edu/flockhart/clinlist.htm.
Disclosure
Dr. Luo reports no financial relationship with any company whose products are mentioned in this article. The opinions expressed by Dr. Luo in this column are his own and do not necessarily reflect those of Current Psychiatry.
1. Children’s Hospital Boston. Child Health A to Z. What is qEEG? Available at: http://www.childrenshospital.org/az/Site1509/printerfriendlypageS1509P0.html. Accessed March 16, 2006.
2. UCLA Quantitative EEG Laboratory. QEEG Cordance. Available at: http://www.qeeg.npi.ucla.edu/cordance. Accessed March 16, 2006.
3. Cook IA, Leuchter AF, Witte E, et al. Neurophysiologic predictors of treatment response to fluoxetine in major depression. Psychiatry Res 1999;85:263-73.
4. Cook IA, Leuchter AF, Morgan M, et al. Early changes in prefrontal activity characterize clinical responders to antidepressants. Neuropsychopharmacology 2002;27:120-31.
5. Song DH, Shin DW, Jon DI, Ha EH. Effects of methylphenidate on quantitative EEG of boys with attention-deficit hyperactivity disorder in continuous performance test. Yonsei Med J 2005;46:34-41.
6. Nuwer M. Assessment of digital EEG, quantitative EEG, and EEG brain mapping: report of the American Academy of Neurology and the American Clinical Neurophysiology Society. Neurology 1997;49:277-92.
Technology companies are offering two new computerized tools to reduce the “trial and error” of prescribing. Thanks to quantitative EEG (QEEG) testing and pharmacogenetic testing, you may one day be able to consistently choose medications that offer optimal benefit and minimal adverse events—without subjecting patients to unsuccessful trials.
How quantitative eeg works
QEEG adds modern computer and statistical analyses to traditional EEG recordings. The computer creates a graphic display on a schematic map of the head. The procedure is often called brain electrical activity mapping (BEAM) or simply “mapping.”1
QEEG is nearly identical to EEG, but approximately 50% more electrodes are applied to the scalp. The additional electrodes provide better definition and about twice the data compared with traditional EEG.
The UCLA Quantitative EEG Laboratory developed cordance,2 a QEEG measure, to study regional brain activity. Cordance is calculated with reference to absolute and relative power measures from the various electrodes on the brain. It is more closely correlated than traditional EEG with regional cerebral perfusion, which may offer clues to brain activity under different conditions such as depression and medication treatment.
What the data show
Several studies suggest that QEEG can trace response to medication.
Cook et al3 used QEEG in a double-blind study comparing response to fluoxetine, 20 mg/d, and placebo across 8 weeks in 24 adults with unipolar major depression. Subjects were classified as concordant or discordant depending on how many electrodes showed discordance.
Concordant patients showed a more-robust response to fluoxetine than did the discordant group, as evidenced by lower Beck Depression Inventory and Hamilton Rating Scale for Depression (HRSD) scores. The findings suggest that cordance may identify patients who will or will not respond to an antidepressant.
Cook et al4 also used cordance to measure response to fluoxetine, 20 mg/d, venlafaxine, 150 mg/d, or placebo in 51 adults with unipolar depression. Responders to antidepressants (defined as HRSD score ≤10) showed decreased prefrontal cordance after 48 hours and 1 week, suggesting that the prefrontal region may mediate antidepressant response.
A recent study in Korea5 investigated the effects of methylphenidate, 0.7 mg/kg/d (range 15 to 35 mg/d) on QEEG patterns in 20 boys ages 6 to 12 while at work or rest. Numerous changes in band waves were seen during continuous performance tests, but none were reported while the subjects were at rest. This suggests that methylphenidate exerts greater electrophysiologic influence during attention-related tasks.
Clinical applicability
QEEG has just begun to enter mainstream practice, with vendors offering analysis services. As patients increasingly demand improved diagnostic reliability and medication effectiveness, QEEG use could become a standard of practice within 5 years.
Lexicor offers a QEEG analysis to diagnose attention-deficit/hyperactivity disorder based on theta/beta band wave ratio. Lexicor says its analysis offers 86% to 90% sensitivity and 94% to 98% specificity, both far greater than traditional methods such as the Child Behavior Checklist, Behavior Assessment System for Children, and Devereaux Scales of Mental Disorder.
Major health plans offer limited coverage of quantitative EEG testing, however, so many patients would pay $200 or more for tests out of pocket. Also, the American Academy of Neurology and American Clinical Neurophysiology Society endorse QEEG for use in screening for and assessing epilepsy, but not in mental disorders,6 making insurers less likely to cover these tests for psychiatric purposes.
Pharmacogenetic testing
With the sequencing of the human genome and improved speed of genetic analysis, pharmacogenetic testing could supplement quantitative EEG in identifying an appropriate medication.
Companies such as Genelex (www.healthanddna.com/professional/pharmacogenetics.html) and Signature Genetics (www.signaturegenetics.com) have begun offering tests to detect variants of the cytochrome-P(CYP) 2C9, 2C19, 2D6, and 1A2 genes. The findings indicate if the patient will metabolize a medication too slowly or rapidly through these pathways. Psychiatrists can then adjust the dosage accordingly or try another medication. Physicians can order any combination of gene tests, which cost about $150 to $200 each, or all available tests for a discounted price of approximately $600.
Genelex and Signature Genetics can create individualized CYP-450 function reports to facilitate prescribing and customized reports that take into account the patient’s medication and diet regimen. Genelex also offers an Internet-based software tool, GeneMedRx, which allows doctors to customize medication regimens based on potential drug-drug interactions and genomic information.
Signature Genetics offers a prospective assessment of drugs based on genetic test results. This assessment provides a comprehensive report of which medications are affected by the test results.
Genetic profiling can help psychiatrists improve the likelihood of treatment success and minimize potential drug-drug interactions and adverse reactions. Patients will be more satisfied, knowing that their medications fit their individual needs. Also, as more is learned about genetic analysis, genetic testing could one day reveal susceptibility to Alzheimer’s disease, heart attack risk, or other medical problems.
As with QEEG, however, few insurance companies cover genetic testing. Also, insurance companies might charge higher premiums to patients found to have a higher likelihood of developing certain diseases.
Related resources
- Indiana University School of Medicine. Drug interactions table. http://medicine.iupui.edu/flockhart/clinlist.htm.
Disclosure
Dr. Luo reports no financial relationship with any company whose products are mentioned in this article. The opinions expressed by Dr. Luo in this column are his own and do not necessarily reflect those of Current Psychiatry.
Technology companies are offering two new computerized tools to reduce the “trial and error” of prescribing. Thanks to quantitative EEG (QEEG) testing and pharmacogenetic testing, you may one day be able to consistently choose medications that offer optimal benefit and minimal adverse events—without subjecting patients to unsuccessful trials.
How quantitative eeg works
QEEG adds modern computer and statistical analyses to traditional EEG recordings. The computer creates a graphic display on a schematic map of the head. The procedure is often called brain electrical activity mapping (BEAM) or simply “mapping.”1
QEEG is nearly identical to EEG, but approximately 50% more electrodes are applied to the scalp. The additional electrodes provide better definition and about twice the data compared with traditional EEG.
The UCLA Quantitative EEG Laboratory developed cordance,2 a QEEG measure, to study regional brain activity. Cordance is calculated with reference to absolute and relative power measures from the various electrodes on the brain. It is more closely correlated than traditional EEG with regional cerebral perfusion, which may offer clues to brain activity under different conditions such as depression and medication treatment.
What the data show
Several studies suggest that QEEG can trace response to medication.
Cook et al3 used QEEG in a double-blind study comparing response to fluoxetine, 20 mg/d, and placebo across 8 weeks in 24 adults with unipolar major depression. Subjects were classified as concordant or discordant depending on how many electrodes showed discordance.
Concordant patients showed a more-robust response to fluoxetine than did the discordant group, as evidenced by lower Beck Depression Inventory and Hamilton Rating Scale for Depression (HRSD) scores. The findings suggest that cordance may identify patients who will or will not respond to an antidepressant.
Cook et al4 also used cordance to measure response to fluoxetine, 20 mg/d, venlafaxine, 150 mg/d, or placebo in 51 adults with unipolar depression. Responders to antidepressants (defined as HRSD score ≤10) showed decreased prefrontal cordance after 48 hours and 1 week, suggesting that the prefrontal region may mediate antidepressant response.
A recent study in Korea5 investigated the effects of methylphenidate, 0.7 mg/kg/d (range 15 to 35 mg/d) on QEEG patterns in 20 boys ages 6 to 12 while at work or rest. Numerous changes in band waves were seen during continuous performance tests, but none were reported while the subjects were at rest. This suggests that methylphenidate exerts greater electrophysiologic influence during attention-related tasks.
Clinical applicability
QEEG has just begun to enter mainstream practice, with vendors offering analysis services. As patients increasingly demand improved diagnostic reliability and medication effectiveness, QEEG use could become a standard of practice within 5 years.
Lexicor offers a QEEG analysis to diagnose attention-deficit/hyperactivity disorder based on theta/beta band wave ratio. Lexicor says its analysis offers 86% to 90% sensitivity and 94% to 98% specificity, both far greater than traditional methods such as the Child Behavior Checklist, Behavior Assessment System for Children, and Devereaux Scales of Mental Disorder.
Major health plans offer limited coverage of quantitative EEG testing, however, so many patients would pay $200 or more for tests out of pocket. Also, the American Academy of Neurology and American Clinical Neurophysiology Society endorse QEEG for use in screening for and assessing epilepsy, but not in mental disorders,6 making insurers less likely to cover these tests for psychiatric purposes.
Pharmacogenetic testing
With the sequencing of the human genome and improved speed of genetic analysis, pharmacogenetic testing could supplement quantitative EEG in identifying an appropriate medication.
Companies such as Genelex (www.healthanddna.com/professional/pharmacogenetics.html) and Signature Genetics (www.signaturegenetics.com) have begun offering tests to detect variants of the cytochrome-P(CYP) 2C9, 2C19, 2D6, and 1A2 genes. The findings indicate if the patient will metabolize a medication too slowly or rapidly through these pathways. Psychiatrists can then adjust the dosage accordingly or try another medication. Physicians can order any combination of gene tests, which cost about $150 to $200 each, or all available tests for a discounted price of approximately $600.
Genelex and Signature Genetics can create individualized CYP-450 function reports to facilitate prescribing and customized reports that take into account the patient’s medication and diet regimen. Genelex also offers an Internet-based software tool, GeneMedRx, which allows doctors to customize medication regimens based on potential drug-drug interactions and genomic information.
Signature Genetics offers a prospective assessment of drugs based on genetic test results. This assessment provides a comprehensive report of which medications are affected by the test results.
Genetic profiling can help psychiatrists improve the likelihood of treatment success and minimize potential drug-drug interactions and adverse reactions. Patients will be more satisfied, knowing that their medications fit their individual needs. Also, as more is learned about genetic analysis, genetic testing could one day reveal susceptibility to Alzheimer’s disease, heart attack risk, or other medical problems.
As with QEEG, however, few insurance companies cover genetic testing. Also, insurance companies might charge higher premiums to patients found to have a higher likelihood of developing certain diseases.
Related resources
- Indiana University School of Medicine. Drug interactions table. http://medicine.iupui.edu/flockhart/clinlist.htm.
Disclosure
Dr. Luo reports no financial relationship with any company whose products are mentioned in this article. The opinions expressed by Dr. Luo in this column are his own and do not necessarily reflect those of Current Psychiatry.
1. Children’s Hospital Boston. Child Health A to Z. What is qEEG? Available at: http://www.childrenshospital.org/az/Site1509/printerfriendlypageS1509P0.html. Accessed March 16, 2006.
2. UCLA Quantitative EEG Laboratory. QEEG Cordance. Available at: http://www.qeeg.npi.ucla.edu/cordance. Accessed March 16, 2006.
3. Cook IA, Leuchter AF, Witte E, et al. Neurophysiologic predictors of treatment response to fluoxetine in major depression. Psychiatry Res 1999;85:263-73.
4. Cook IA, Leuchter AF, Morgan M, et al. Early changes in prefrontal activity characterize clinical responders to antidepressants. Neuropsychopharmacology 2002;27:120-31.
5. Song DH, Shin DW, Jon DI, Ha EH. Effects of methylphenidate on quantitative EEG of boys with attention-deficit hyperactivity disorder in continuous performance test. Yonsei Med J 2005;46:34-41.
6. Nuwer M. Assessment of digital EEG, quantitative EEG, and EEG brain mapping: report of the American Academy of Neurology and the American Clinical Neurophysiology Society. Neurology 1997;49:277-92.
1. Children’s Hospital Boston. Child Health A to Z. What is qEEG? Available at: http://www.childrenshospital.org/az/Site1509/printerfriendlypageS1509P0.html. Accessed March 16, 2006.
2. UCLA Quantitative EEG Laboratory. QEEG Cordance. Available at: http://www.qeeg.npi.ucla.edu/cordance. Accessed March 16, 2006.
3. Cook IA, Leuchter AF, Witte E, et al. Neurophysiologic predictors of treatment response to fluoxetine in major depression. Psychiatry Res 1999;85:263-73.
4. Cook IA, Leuchter AF, Morgan M, et al. Early changes in prefrontal activity characterize clinical responders to antidepressants. Neuropsychopharmacology 2002;27:120-31.
5. Song DH, Shin DW, Jon DI, Ha EH. Effects of methylphenidate on quantitative EEG of boys with attention-deficit hyperactivity disorder in continuous performance test. Yonsei Med J 2005;46:34-41.
6. Nuwer M. Assessment of digital EEG, quantitative EEG, and EEG brain mapping: report of the American Academy of Neurology and the American Clinical Neurophysiology Society. Neurology 1997;49:277-92.
Smartphones: Ask 4 questions before you buy
‘Smartphones,’ hybrid cell phones and personal digital assistants (PDAs), are increasingly helping psychiatrists stay in touch on the road or manage multi-site practices.
This article reviews the capabilities of most smartphone models (Table) and offers practical advice to help you choose the right device for your practice.
What you can do with a smartphone
Make phone calls. Most smartphones integrate high-end wireless phone features such as selective call screening, Bluetooth wireless device compatibility, moderate-resolution cameras, and voice recognition for hands-free dialing. Call quality varies by device but is generally above average as cell phones go.
Smartphones cost between $100 and $500 depending on model (the more cutting-edge the smartphone, the higher the price) and whether a service activation discount is offered. A service provider’s area and coverage uniformity usually affects call quality.
Some service plans include data service (ie, e-mail) with phone service, whereas others charge an extra monthly fee depending on volume of data to be transmitted.
Send and receive e-mail. Smartphones include fully featured e-mail clients. While away from the office, you can save immeasurable time communicating with staff and colleagues via text instead of paging and waiting for callbacks.
“Pop-ups” let you quickly view and respond to e-mails without disrupting workflow. You can automatically send messages such as “will call you after this meeting” and “please call my receptionist for a meeting time” without having to type them.
Smartphones can be set to check e-mail at intervals. Many wireless service providers offer “push e-mail,” which is broadcast to your device as soon as the e-mail server receives it, but you don’t need this service if you are satisfied with receiving e-mail every 15 minutes or longer.
Search the Web. Smartphones are equipped with browsers, so you can enter key words and quickly retrieve online abstracts while away from the office. For psychiatrists practicing at multiple sites or without immediate Internet access, this point-of-care search capability can be priceless.
Organize your schedule. Datebook/calendar, address book, memo, and task list functions are cross-linked with telephony. You can make a phone call directly from an address book listing, dial by tapping on a number included in an e-mail message, and automatically add a contact to your address book after a call. You can insert contact numbers and tasks into the calendar and set reminder alarms and alerts as needed.
Task lists consolidate daily to-do lists, and reminders keep missed tasks top of mind the next day. On more-advanced models, appointment calendars can be updated wirelessly several times daily, so you can add appointments or meetings while away from the office without having to call in for a scheduling update.
Create/edit multimedia files. Recording, editing, and playing back videos, photos, audio recordings (dictation and MP3s), and even feature-length movies are becoming common handheld features.
More-advanced smartphones that are compatible with Palm OS and Pocket PC let you open and edit Microsoft Office documents, edit and play back PowerPoint presentations through a monitor or LCD projector, or create or modify Microsoft Word or Excel documents on a mobile platform. This mobile software is included with some phones and can be purchased with others.
Beat ‘belt clutter.’ Some smartphones consolidate cell phone, pager, PDA, dictation recorder, appointment book, and wristwatch functions. By taking the place of these devices, a smartphone can reduce pocket and belt clutter, a common problem among doctors.
Drawbacks
Screen size. The smartphone’s screen size and slow downloading impede its use as a stand-alone Internet browser. Smartphone screens can be similar in size to a PDA screen (4 inches diagonally) or relatively small (2 inches-by-2 inches), although resolution is usually high. Viewing full-size Web pages can be challenging, though most phones offer an option to adapt them for small-screen viewing.
Internet surfing. Broadband data transfer rates are only now appearing with service providers in different areas. Broadband will make smartphone Web surfing and data transfers much faster. By and large, however, Internet surfing is limited to analog modem speeds, so you’ll be waiting a while for Web pages to appear on your screen.
Security. Most smartphones use Bluetooth short-range radio to connect with headsets and computers. Hackers have exploited this technology in public places, so phones left open to Bluetooth ‘discovery’ by other phones can be breached.
This can spell trouble if you store medical records on your smartphone. If an unauthorized person accesses these records, you would be violating HIPAA privacy regulations because you are responsible for protecting patient information.
You can activate a password protection system using various encryption algorithms on your smartphone to guard against theft. You can also selectively encrypt some files, though having to repeatedly enter passwords to access the secure files slows daily use.
Choosing a smartphone
Your new smartphone will be your practice “companion,” so you want to get this choice right. As you shop for a smartphone, ask yourself:
- Which medical reference software do I plan to use? As with PDAs, smartphones work on the Palm OS/Windows Mobile/Pocket PC operating systems. Although most major medical reference titles—such as Lexi-Comp and Epocrates—come in Palm OS and Windows Mobile/Pocket PC versions, others are compatible with only one operating system.
- Can I read the screen display? Although text usually can be enlarged or shrunk, screen size determines how much you can see at a glance. Make sure you’re comfortable with the display before you purchase.
- Can I work the keyboard? Most smartphones integrate a small QWERTY keyboard for sending e-mail. Each smartphone keyboard has a different feel; make sure you can type comfortably and accurately.
- Which form feels most comfortable? Smartphones range from candy-bar shaped and flip phones, to slider and clamshell models.
In the end, the answers to these questions—plus a hefty dose of visceral appeal—should influence your choice. Smartphones are constantly evolving, so you’re better off taking the plunge rather than waiting for the ultimate smartphone.
Table
Smartphone models: Sample listing
| Model | Key features/cost |
|---|---|

| - Microsoft Windows Mobile 5.0 |
| - Slim form factor | |
| - Cutting-edge design | |
| - Price unknown | |
| - Available this Spring | |

| - Palm OS (650) |
| - Ergonomic design | |
| - Largest library of medical reference software available | |
| - Touch screen 320×320 pixels | |
| - $219-$548 | |

| - Windows Mobile 5.0 |
| - Ergonomic design | |
| - Touch screen 240×240 pixels | |
| - $399-$499 | |

| - Microsoft Windows Mobile for Pocket PC Phone Edition 2003 SE |
| - Runs full Microsoft Office Mobile suite | |
| - Slide-out keyboard and touch screen input | |
| - $429-$499 | |

| - RIM Blackberry OS |
| - EDGE enabled for fast Web browsing | |
| - Push e-mail (no latency) | |
| - $0-$299 | |

| - Microsoft Windows Mobile 5.0 Pocket PC Phone Edition |
| - Integrated GPS receiver with navigation software | |
| - Runs full Microsoft Office Mobile suite | |
| - Wi-Fi- and EDGE-enabled for fast Web browsing | |
| - Push e-mail | |
| - Pricing unknown | |
| - Available late spring | |
| Source: www.cnet.com | |
Related resources
Brighthand Consulting. Reviews and other information on smartphones, other handhelds. www.brighthand.com.
Cnet.com. Listing of 90 smartphone models by manufacturer, carrier, other criteria. http://reviews.cnet.com/4566-6452_7-0.html?tag=coco.
Engadget. Reviews of smartphone models. http://www.engadget.com/search/?q=smartphones.
Disclosure
Dr. Montgomery reports no financial relationship with any manufacturer whose products are mentioned in this article or with manufacturers of competing products.
‘Smartphones,’ hybrid cell phones and personal digital assistants (PDAs), are increasingly helping psychiatrists stay in touch on the road or manage multi-site practices.
This article reviews the capabilities of most smartphone models (Table) and offers practical advice to help you choose the right device for your practice.
What you can do with a smartphone
Make phone calls. Most smartphones integrate high-end wireless phone features such as selective call screening, Bluetooth wireless device compatibility, moderate-resolution cameras, and voice recognition for hands-free dialing. Call quality varies by device but is generally above average as cell phones go.
Smartphones cost between $100 and $500 depending on model (the more cutting-edge the smartphone, the higher the price) and whether a service activation discount is offered. A service provider’s area and coverage uniformity usually affects call quality.
Some service plans include data service (ie, e-mail) with phone service, whereas others charge an extra monthly fee depending on volume of data to be transmitted.
Send and receive e-mail. Smartphones include fully featured e-mail clients. While away from the office, you can save immeasurable time communicating with staff and colleagues via text instead of paging and waiting for callbacks.
“Pop-ups” let you quickly view and respond to e-mails without disrupting workflow. You can automatically send messages such as “will call you after this meeting” and “please call my receptionist for a meeting time” without having to type them.
Smartphones can be set to check e-mail at intervals. Many wireless service providers offer “push e-mail,” which is broadcast to your device as soon as the e-mail server receives it, but you don’t need this service if you are satisfied with receiving e-mail every 15 minutes or longer.
Search the Web. Smartphones are equipped with browsers, so you can enter key words and quickly retrieve online abstracts while away from the office. For psychiatrists practicing at multiple sites or without immediate Internet access, this point-of-care search capability can be priceless.
Organize your schedule. Datebook/calendar, address book, memo, and task list functions are cross-linked with telephony. You can make a phone call directly from an address book listing, dial by tapping on a number included in an e-mail message, and automatically add a contact to your address book after a call. You can insert contact numbers and tasks into the calendar and set reminder alarms and alerts as needed.
Task lists consolidate daily to-do lists, and reminders keep missed tasks top of mind the next day. On more-advanced models, appointment calendars can be updated wirelessly several times daily, so you can add appointments or meetings while away from the office without having to call in for a scheduling update.
Create/edit multimedia files. Recording, editing, and playing back videos, photos, audio recordings (dictation and MP3s), and even feature-length movies are becoming common handheld features.
More-advanced smartphones that are compatible with Palm OS and Pocket PC let you open and edit Microsoft Office documents, edit and play back PowerPoint presentations through a monitor or LCD projector, or create or modify Microsoft Word or Excel documents on a mobile platform. This mobile software is included with some phones and can be purchased with others.
Beat ‘belt clutter.’ Some smartphones consolidate cell phone, pager, PDA, dictation recorder, appointment book, and wristwatch functions. By taking the place of these devices, a smartphone can reduce pocket and belt clutter, a common problem among doctors.
Drawbacks
Screen size. The smartphone’s screen size and slow downloading impede its use as a stand-alone Internet browser. Smartphone screens can be similar in size to a PDA screen (4 inches diagonally) or relatively small (2 inches-by-2 inches), although resolution is usually high. Viewing full-size Web pages can be challenging, though most phones offer an option to adapt them for small-screen viewing.
Internet surfing. Broadband data transfer rates are only now appearing with service providers in different areas. Broadband will make smartphone Web surfing and data transfers much faster. By and large, however, Internet surfing is limited to analog modem speeds, so you’ll be waiting a while for Web pages to appear on your screen.
Security. Most smartphones use Bluetooth short-range radio to connect with headsets and computers. Hackers have exploited this technology in public places, so phones left open to Bluetooth ‘discovery’ by other phones can be breached.
This can spell trouble if you store medical records on your smartphone. If an unauthorized person accesses these records, you would be violating HIPAA privacy regulations because you are responsible for protecting patient information.
You can activate a password protection system using various encryption algorithms on your smartphone to guard against theft. You can also selectively encrypt some files, though having to repeatedly enter passwords to access the secure files slows daily use.
Choosing a smartphone
Your new smartphone will be your practice “companion,” so you want to get this choice right. As you shop for a smartphone, ask yourself:
- Which medical reference software do I plan to use? As with PDAs, smartphones work on the Palm OS/Windows Mobile/Pocket PC operating systems. Although most major medical reference titles—such as Lexi-Comp and Epocrates—come in Palm OS and Windows Mobile/Pocket PC versions, others are compatible with only one operating system.
- Can I read the screen display? Although text usually can be enlarged or shrunk, screen size determines how much you can see at a glance. Make sure you’re comfortable with the display before you purchase.
- Can I work the keyboard? Most smartphones integrate a small QWERTY keyboard for sending e-mail. Each smartphone keyboard has a different feel; make sure you can type comfortably and accurately.
- Which form feels most comfortable? Smartphones range from candy-bar shaped and flip phones, to slider and clamshell models.
In the end, the answers to these questions—plus a hefty dose of visceral appeal—should influence your choice. Smartphones are constantly evolving, so you’re better off taking the plunge rather than waiting for the ultimate smartphone.
Table
Smartphone models: Sample listing
| Model | Key features/cost |
|---|---|
|
| - Microsoft Windows Mobile 5.0 |
| - Slim form factor | |
| - Cutting-edge design | |
| - Price unknown | |
| - Available this Spring | |
|
| - Palm OS (650) |
| - Ergonomic design | |
| - Largest library of medical reference software available | |
| - Touch screen 320×320 pixels | |
| - $219-$548 | |
|
| - Windows Mobile 5.0 |
| - Ergonomic design | |
| - Touch screen 240×240 pixels | |
| - $399-$499 | |
|
| - Microsoft Windows Mobile for Pocket PC Phone Edition 2003 SE |
| - Runs full Microsoft Office Mobile suite | |
| - Slide-out keyboard and touch screen input | |
| - $429-$499 | |
|
| - RIM Blackberry OS |
| - EDGE enabled for fast Web browsing | |
| - Push e-mail (no latency) | |
| - $0-$299 | |
|
| - Microsoft Windows Mobile 5.0 Pocket PC Phone Edition |
| - Integrated GPS receiver with navigation software | |
| - Runs full Microsoft Office Mobile suite | |
| - Wi-Fi- and EDGE-enabled for fast Web browsing | |
| - Push e-mail | |
| - Pricing unknown | |
| - Available late spring | |
| Source: www.cnet.com | |
Related resources
Brighthand Consulting. Reviews and other information on smartphones, other handhelds. www.brighthand.com.
Cnet.com. Listing of 90 smartphone models by manufacturer, carrier, other criteria. http://reviews.cnet.com/4566-6452_7-0.html?tag=coco.
Engadget. Reviews of smartphone models. http://www.engadget.com/search/?q=smartphones.
Disclosure
Dr. Montgomery reports no financial relationship with any manufacturer whose products are mentioned in this article or with manufacturers of competing products.
‘Smartphones,’ hybrid cell phones and personal digital assistants (PDAs), are increasingly helping psychiatrists stay in touch on the road or manage multi-site practices.
This article reviews the capabilities of most smartphone models (Table) and offers practical advice to help you choose the right device for your practice.
What you can do with a smartphone
Make phone calls. Most smartphones integrate high-end wireless phone features such as selective call screening, Bluetooth wireless device compatibility, moderate-resolution cameras, and voice recognition for hands-free dialing. Call quality varies by device but is generally above average as cell phones go.
Smartphones cost between $100 and $500 depending on model (the more cutting-edge the smartphone, the higher the price) and whether a service activation discount is offered. A service provider’s area and coverage uniformity usually affects call quality.
Some service plans include data service (ie, e-mail) with phone service, whereas others charge an extra monthly fee depending on volume of data to be transmitted.
Send and receive e-mail. Smartphones include fully featured e-mail clients. While away from the office, you can save immeasurable time communicating with staff and colleagues via text instead of paging and waiting for callbacks.
“Pop-ups” let you quickly view and respond to e-mails without disrupting workflow. You can automatically send messages such as “will call you after this meeting” and “please call my receptionist for a meeting time” without having to type them.
Smartphones can be set to check e-mail at intervals. Many wireless service providers offer “push e-mail,” which is broadcast to your device as soon as the e-mail server receives it, but you don’t need this service if you are satisfied with receiving e-mail every 15 minutes or longer.
Search the Web. Smartphones are equipped with browsers, so you can enter key words and quickly retrieve online abstracts while away from the office. For psychiatrists practicing at multiple sites or without immediate Internet access, this point-of-care search capability can be priceless.
Organize your schedule. Datebook/calendar, address book, memo, and task list functions are cross-linked with telephony. You can make a phone call directly from an address book listing, dial by tapping on a number included in an e-mail message, and automatically add a contact to your address book after a call. You can insert contact numbers and tasks into the calendar and set reminder alarms and alerts as needed.
Task lists consolidate daily to-do lists, and reminders keep missed tasks top of mind the next day. On more-advanced models, appointment calendars can be updated wirelessly several times daily, so you can add appointments or meetings while away from the office without having to call in for a scheduling update.
Create/edit multimedia files. Recording, editing, and playing back videos, photos, audio recordings (dictation and MP3s), and even feature-length movies are becoming common handheld features.
More-advanced smartphones that are compatible with Palm OS and Pocket PC let you open and edit Microsoft Office documents, edit and play back PowerPoint presentations through a monitor or LCD projector, or create or modify Microsoft Word or Excel documents on a mobile platform. This mobile software is included with some phones and can be purchased with others.
Beat ‘belt clutter.’ Some smartphones consolidate cell phone, pager, PDA, dictation recorder, appointment book, and wristwatch functions. By taking the place of these devices, a smartphone can reduce pocket and belt clutter, a common problem among doctors.
Drawbacks
Screen size. The smartphone’s screen size and slow downloading impede its use as a stand-alone Internet browser. Smartphone screens can be similar in size to a PDA screen (4 inches diagonally) or relatively small (2 inches-by-2 inches), although resolution is usually high. Viewing full-size Web pages can be challenging, though most phones offer an option to adapt them for small-screen viewing.
Internet surfing. Broadband data transfer rates are only now appearing with service providers in different areas. Broadband will make smartphone Web surfing and data transfers much faster. By and large, however, Internet surfing is limited to analog modem speeds, so you’ll be waiting a while for Web pages to appear on your screen.
Security. Most smartphones use Bluetooth short-range radio to connect with headsets and computers. Hackers have exploited this technology in public places, so phones left open to Bluetooth ‘discovery’ by other phones can be breached.
This can spell trouble if you store medical records on your smartphone. If an unauthorized person accesses these records, you would be violating HIPAA privacy regulations because you are responsible for protecting patient information.
You can activate a password protection system using various encryption algorithms on your smartphone to guard against theft. You can also selectively encrypt some files, though having to repeatedly enter passwords to access the secure files slows daily use.
Choosing a smartphone
Your new smartphone will be your practice “companion,” so you want to get this choice right. As you shop for a smartphone, ask yourself:
- Which medical reference software do I plan to use? As with PDAs, smartphones work on the Palm OS/Windows Mobile/Pocket PC operating systems. Although most major medical reference titles—such as Lexi-Comp and Epocrates—come in Palm OS and Windows Mobile/Pocket PC versions, others are compatible with only one operating system.
- Can I read the screen display? Although text usually can be enlarged or shrunk, screen size determines how much you can see at a glance. Make sure you’re comfortable with the display before you purchase.
- Can I work the keyboard? Most smartphones integrate a small QWERTY keyboard for sending e-mail. Each smartphone keyboard has a different feel; make sure you can type comfortably and accurately.
- Which form feels most comfortable? Smartphones range from candy-bar shaped and flip phones, to slider and clamshell models.
In the end, the answers to these questions—plus a hefty dose of visceral appeal—should influence your choice. Smartphones are constantly evolving, so you’re better off taking the plunge rather than waiting for the ultimate smartphone.
Table
Smartphone models: Sample listing
| Model | Key features/cost |
|---|---|
|
| - Microsoft Windows Mobile 5.0 |
| - Slim form factor | |
| - Cutting-edge design | |
| - Price unknown | |
| - Available this Spring | |
|
| - Palm OS (650) |
| - Ergonomic design | |
| - Largest library of medical reference software available | |
| - Touch screen 320×320 pixels | |
| - $219-$548 | |
|
| - Windows Mobile 5.0 |
| - Ergonomic design | |
| - Touch screen 240×240 pixels | |
| - $399-$499 | |
|
| - Microsoft Windows Mobile for Pocket PC Phone Edition 2003 SE |
| - Runs full Microsoft Office Mobile suite | |
| - Slide-out keyboard and touch screen input | |
| - $429-$499 | |
|
| - RIM Blackberry OS |
| - EDGE enabled for fast Web browsing | |
| - Push e-mail (no latency) | |
| - $0-$299 | |
|
| - Microsoft Windows Mobile 5.0 Pocket PC Phone Edition |
| - Integrated GPS receiver with navigation software | |
| - Runs full Microsoft Office Mobile suite | |
| - Wi-Fi- and EDGE-enabled for fast Web browsing | |
| - Push e-mail | |
| - Pricing unknown | |
| - Available late spring | |
| Source: www.cnet.com | |
Related resources
Brighthand Consulting. Reviews and other information on smartphones, other handhelds. www.brighthand.com.
Cnet.com. Listing of 90 smartphone models by manufacturer, carrier, other criteria. http://reviews.cnet.com/4566-6452_7-0.html?tag=coco.
Engadget. Reviews of smartphone models. http://www.engadget.com/search/?q=smartphones.
Disclosure
Dr. Montgomery reports no financial relationship with any manufacturer whose products are mentioned in this article or with manufacturers of competing products.
Transdermal selegiline
Many psychiatrists do not prescribe monoamine oxidase inhibitors (MAOIs) for fear of causing a potentially fatal hypertensive reaction, even though restricting foods high in the amino acid tyramine usually prevents this effect.1 Consequently, most depressed patients who might respond well to MAOIs do not receive them.2,3
Transdermal selegiline, FDA-approved for treating major depressive disorder (MDD) (Table 1), offers the clinical efficacy of an MAOI but without adverse interactions with food at the 6-mg strength. Transdermal selegiline may inhibit too much gastrointestinal MAO-A at 9 mg/d and 12 mg/d to clear tyramine from foods, so tyramine-rich foods must be restricted at these dosages (Table 2).
Table 1
Transdermal selegiline: Fast facts
| Brand name: EMSAM |
| Class: Monoamine oxidase inhibitor |
| FDA-approved indication: Major depressive disorder |
| Manufacturer: Somerset Pharmaceuticals (marketed by Bristol-Myers Squibb Co.) |
| Dosing forms: 6-, 9-, and 12-mg patches |
| Recommended dosage: One 6-mg patch every 24 hours, worn on the chest, back, or stomach. Increase dosage after 2 to 3 months if clinical response is inadequate |
Table 2
Restrict these foods when prescribing transdermal selegiline at 9 or 12 mg/d
| Food/beverage class | Foods to avoid |
|---|---|
| Beverages | Tap beer |
| Beer that has not been pasteurized* | |
| Red wines | |
| Dairy | Aged cheeses |
| Meat, poultry, fish | Air-dried, aged, and fermented meats, sausages, and salamis (including cacciatore and mortadella) |
| Pickled herring | |
| Spoiled or improperly stored fish, meat, poultry, or animal livers (check for mold, discoloration, or odor) | |
| Vegetables | Broad bean pods (fava beans) |
| Miscellaneous | Concentrated yeast extract (such as Marmite) |
| Fermented soybean products (including soy sauce) | |
| Over-the-counter supplements containing tyramine | |
| Sauerkraut | |
| *Bottled and canned beer and white wine contain little or no tyramine, but more than moderate alcohol use while taking selegiline is not recommended. | |
| Source: Shulman KI, Walker SE. A reevaluation of dietary restrictions for irreversible monoamine oxidase inhibitors. Psychiatr Ann 2001;31:378-84. | |
How it works
MAO enzyme subtypes A and B metabolize CNS monoamines, but primarily MAO-A metabolizes tyramine in the gut before the amino acid enters systemic circulation. At low concentrations, selegiline selectively inhibits MAO-B.4
Oral selegiline, approved as a adjunct to levodopa/carbidopa for patients with Parkinson’s disease,5 has been shown to be effective for treating depression at ≥30 mg/d.6 Because the drug does not selectively inhibit MAOB at ≥20 mg/d, dietary tyramine must be restricted when oral selegiline is used off-label at therapeutic dosages for depression. Otherwise, selegiline has been well-tolerated up to 60 mg/d.7
The 6-mg “patch” delivers more selegiline to the bloodstream than does low-dose oral selegiline but without inhibiting gut MAO-A. This provides the brain MAO-A and MAO-B inhibition necessary for an antidepressant effect while eliminating the need for dietary restrictions at this lowest dosage.
Clinical implications
Transdermal selegiline offers an MAOI antidepressant option that might help:
- patients whose depression has not responded satisfactorily to selective serotonin reuptake inhibitors (SSRIs) or serotonin and norepinephrine reuptake inhibitors (SNRIs)
- adults and children with chronic depression marked by atypical features, including reactive mood, rejection sensitivity, anergia, and reversed vegetative symptoms—such as oversleeping, overeating, and psychomotor retardation. Although transdermal selegiline’s efficacy against these features has not been studied, patients with this depressive subtype tend to respond preferentially to MAOIs.
Pharmacokinetics
Transdermal selegiline achieves therapeutic blood levels and reaches sustained concentration within 4 to 8 hours of administration. Compared with oral selegiline, transdermal delivery results in higher plasma selegiline concentrations (1,500 pg/mL with the 6-mg patch) with much lower exposure to metabolites.8 The concentration is maintained with successive doses.
Transdermal selegiline clears rapidly upon discontinuation but MAO inhibition persists for 2 weeks, so wait 2 weeks after the last dose before starting a new antidepressant or stopping food restrictions with the 9-mg and 12-mg patches.
Efficacy
In two randomized, double-blind clinical trials,9,10 a total of 466 adults ages 18 to 65 who met DSM-IV-TR criteria for MDD received transdermal selegiline, 6 mg/d, or placebo for 6 to 8 weeks. Participants had 17-item Hamilton Rating Scale for Depression (HAM-D-17) scores ≥20 at baseline.
In the 6-week study,9 transdermal selegiline produced a 46% greater reduction in HAM-D-17 scores, a 52% greater decrease in HAM-D-28 scores, and a 79% greater drop in Montgomery-Asburg Depression Rating Scale (MADRS) scores compared with placebo. In the 8-week trial,10 HAM-D-28 and MADRS scores among the treatment group were significantly improved at endpoint compared with placebo, but HAM-D-17 scores were not.
In a 1-year, double-blind study,11 322 subjects with MDD—who had been rated as responders in a 10-week, open-label transdermal selegiline trial—received the 6-mg patch or placebo. At 6 months and 1 year, relapse was much less frequent among the treatment group compared with placebo. Relapse was defined as:
- HAM-D-17 ≥14
- Clinical Global Impressions of Severity score ≥3 with a ≥2-point increase from baseline
- and meeting DSM-IV criteria for MDD on two consecutive visits ≥11 days apart.
Side effects
Transdermal selegiline, 6 mg/d, has been well-tolerated in clinical trials. Inflammation at the application site was the most commonly reported side effect, occurring in 32% to 36% of treatment group subjects compared with 15% to 17% of the placebo groups.9,10,12 Inflammation was usually mild, but approximately 3% of patients dropped out of one study,12 citing this effect as the reason. Fair-skinned women are at highest risk for this reaction.
In the 1-year relapse prevention study,11 12% of treatment group patients reported insomnia compared with 7% of the placebo group. Insomnia incidence was the same in the selegiline and placebo groups during the 6- to 8-week clinical trials.9,10
Unlike conventional oral MAOIs,13 the 6-mg selegiline patch has not been found to impair sexual function, alter appetite, or change body weight or blood pressure compared with placebo.10-12 The toxicity of the 9- and 12-mg patches has not been studied in humans, but 8 mg/d and 12 mg/d of transdermal selegiline across 3 months were shown not to cause drug toxicity in dogs.14
Pediatric use
Although transdermal selegiline has not been studied in children and adolescents, the 6-mg patch could benefit some youths with depression. Before starting the drug, discuss with the child’s parents/guardians the FDA’s black box warning describing a possible association between selegiline and increased suicidal behavior in youths. This applies to all antidepressants.
Geriatric use
The patch might also help some older patients with depression. In a double-blind trial of high-dose oral selegiline (60 mg/d) involving 16 older patients (mean age 65.6), both the treatment and placebo groups remained almost free of side effects across 3 weeks.7 Although the sample was small, the findings suggest that older patients can tolerate selegiline at high dosages. Side effects also were minimal among treatment-group patients age ≥65 in the yearlong relapse prevention study.11
Treatment adherence rates with transdermal selegiline have been high in published studies, suggesting that the patch’s visibility might reduce the risk of forgetting to take the medication. Observing whether the patch has been changed might help older patients and family members/caregivers keep track of dosing.
Contraindications
As with the oral form, do not prescribe transdermal selegiline to patients taking SSRIs, SNRIs, tricyclic antidepressants, mirtazapine, or bupropion.
When switching antidepressants, allow enough time for the previous agent to “wash out” before starting transdermal selegiline. How much time to allow for wash-out depends on the previous agent’s half-life.
The patch is also contraindicated for patients taking:
- carbamazepine or oxcarbazepine
- meperidine
- analgesics such as tramadol, methadone, and propoxyphene
- St. John’s wort
- cough syrups containing dextromethorphan
- amphetamines, such as mixed amphetamine salts
- cyclobenzaprine
- or cold remedies or weight-loss products that contain vasoconstrictors, such as pseudoephedrine, phenylephrine, phenylpropanolamine, or ephedrine.
Do not give transdermal selegiline during pregnancy, as its effect on fetal development has not been studied.
Dosing
Start transdermal selegiline at 6 mg/d. Instruct the patient to wear the patch on the upper torso, where vascularity is richer compared with the buttocks and legs. Tell the patient to change the patch daily and to apply it to a different spot each day to prevent inflammation. Consider increasing the dosage after 2 or 3 months if response is unsatisfactory.
For treating first, second, and some third depressive episodes, continue transdermal selegiline for 6 months to 1 year of sustained recovery; consider longer-term maintenance treatment for highly recurrent depression. Transdermal selegiline has not been tapered in clinical trials, and subjects have not reported withdrawal symptoms after 1 year of continuous treatment.
Related resources
- Deniker P. The search for new antidepressants and related drugs. In: Tipton KF, Doster P, Benedetti M (eds). Monoamine oxidase and disease. London: Academic Press; 1984:2-8.
Drug brand names
- Amphetamine salts, mixed • Adderall
- Bupropion • Wellbutrin
- Carbamazepine • Tegretol, Equetro, others
- Cyclobenzaprine • Flexeril
- Meperidine • Demerol
- Mirtazapine • Remeron
- Oxcarbazepine • Trileptal
- Propoxyphene hydrochloride • Darvon
- Propoxyphene napsylate • Darvocet
- Selegiline (oral) • Eldepryl
- Selegiline (transdermal) • EMSAM
- Tramadol • Ultracet
Disclosure
Dr. Bodkin receives grant support from the National Institute of Mental Health, Eli Lilly & Co, Jazz Pharmaceuticals, Merck & Co., Organon, Sanofi-Aventis, and Somerset Pharmaceuticals; is a consultant to Bristol-Myers Squibb Co. and Somerset Pharmaceuticals; and is a speaker for Bristol-Myers Squibb Co. He has been principal investigator in several multicenter clinical trials of selegiline.
1. Blackwell B, Mabbitt LA. Tyramine in cheese related to hypertensive crises after monoamine-oxidase inhibition. Lancet 1965;62:938-40.
2. American Psychiatric Association. Practice guideline for the treatment of patients with major depressive disorder (2nd ed). Available at: http://www.psych.org/psych_pract/treatg/pg/Practice%20Guidelines8904/MajorDepressiveDisorder_2e.pdf. Accessed March 15, 2006.
3. IMS Health National Prescription Audit; 12/04-11/05. Available at: http://www.imshealth.com. Accessed March 15, 2006.
4. Johnston JP. Some observations on a new form of MAO in brain tissue. Biochem Pharmacol 1968;17:1285-97.
5. Youdim MB. Monoamine oxidase inhibitors as antidepressant drugs and as adjunct to L-dopa therapy of Parkinson’s disease. J Neural Transm Suppl 1980;(16):157-61.
6. Bodkin JA, Kwon AE. Selegiline and other atypical MAO inhibitors in depression. Ann Psychiatry 2001;31:385-91.
7. Sunderland T, Cohen RM, Molchan S, et al. High-dose selegiline in treatment-resistant older depressive patients. Arch Gen Psychiatry 1994;51:607-15.
8. Ziemniak JA, Kemper EM, Goodhear M, Azzaro AJ. Pharmacokinetics of selegiline administered via the patch, single oral dose, or intravenous infusion. Poster presented at: Annual Meeting, National Institute of Mental Health, New Clinical Drug Evaluation Unit, May 29, 2001, Phoenix, AZ.
9. Bodkin JA, Amsterdam JD. Transdermal selegiline in major depression: a double-blind, placebo-controlled, parallel-group study in outpatients. Am J Psychiatry 2002;159:1869-75.
10. Amsterdam JD. A double-blind, placebo-controlled trial of the safety and efficacy of selegiline transdermal system without dietary restrictions in patients with major depressive disorder. J Clin Psychiatry 2003;64:208-14.
11. Robinson DS, Moonsammy G, Azzaro AJ. Relapse prevention study shows the long-term safety and efficacy of transdermal selegiline, a new generation MAOI. Poster presented at: Annual Meeting, American College of Neuropsychopharmacology, Dec 11, 2002; San Juan, PR.
12. Robinson DS, Amsterdam JD. Safety and tolerability of selegiline transdermal system 20 mg for treatment of major depression. Poster presented at: Annual Meeting, American College of Neuropsychopharmacology, Dec. 13, 2005, Waikalo, HI.
13. Cole JO, Bodkin JA. Antidepressant drug side effects. J Clin Psychiatry 1990;51(Suppl):21-6.
14. Barrett JS, DiSanto AR, Thomford PJ, et al. Toxicokinetic evaluation of a selegiline transdermal system in the dog. Biopharm Drug Dispos 1997;18:165-84.
Many psychiatrists do not prescribe monoamine oxidase inhibitors (MAOIs) for fear of causing a potentially fatal hypertensive reaction, even though restricting foods high in the amino acid tyramine usually prevents this effect.1 Consequently, most depressed patients who might respond well to MAOIs do not receive them.2,3
Transdermal selegiline, FDA-approved for treating major depressive disorder (MDD) (Table 1), offers the clinical efficacy of an MAOI but without adverse interactions with food at the 6-mg strength. Transdermal selegiline may inhibit too much gastrointestinal MAO-A at 9 mg/d and 12 mg/d to clear tyramine from foods, so tyramine-rich foods must be restricted at these dosages (Table 2).
Table 1
Transdermal selegiline: Fast facts
| Brand name: EMSAM |
| Class: Monoamine oxidase inhibitor |
| FDA-approved indication: Major depressive disorder |
| Manufacturer: Somerset Pharmaceuticals (marketed by Bristol-Myers Squibb Co.) |
| Dosing forms: 6-, 9-, and 12-mg patches |
| Recommended dosage: One 6-mg patch every 24 hours, worn on the chest, back, or stomach. Increase dosage after 2 to 3 months if clinical response is inadequate |
Table 2
Restrict these foods when prescribing transdermal selegiline at 9 or 12 mg/d
| Food/beverage class | Foods to avoid |
|---|---|
| Beverages | Tap beer |
| Beer that has not been pasteurized* | |
| Red wines | |
| Dairy | Aged cheeses |
| Meat, poultry, fish | Air-dried, aged, and fermented meats, sausages, and salamis (including cacciatore and mortadella) |
| Pickled herring | |
| Spoiled or improperly stored fish, meat, poultry, or animal livers (check for mold, discoloration, or odor) | |
| Vegetables | Broad bean pods (fava beans) |
| Miscellaneous | Concentrated yeast extract (such as Marmite) |
| Fermented soybean products (including soy sauce) | |
| Over-the-counter supplements containing tyramine | |
| Sauerkraut | |
| *Bottled and canned beer and white wine contain little or no tyramine, but more than moderate alcohol use while taking selegiline is not recommended. | |
| Source: Shulman KI, Walker SE. A reevaluation of dietary restrictions for irreversible monoamine oxidase inhibitors. Psychiatr Ann 2001;31:378-84. | |
How it works
MAO enzyme subtypes A and B metabolize CNS monoamines, but primarily MAO-A metabolizes tyramine in the gut before the amino acid enters systemic circulation. At low concentrations, selegiline selectively inhibits MAO-B.4
Oral selegiline, approved as a adjunct to levodopa/carbidopa for patients with Parkinson’s disease,5 has been shown to be effective for treating depression at ≥30 mg/d.6 Because the drug does not selectively inhibit MAOB at ≥20 mg/d, dietary tyramine must be restricted when oral selegiline is used off-label at therapeutic dosages for depression. Otherwise, selegiline has been well-tolerated up to 60 mg/d.7
The 6-mg “patch” delivers more selegiline to the bloodstream than does low-dose oral selegiline but without inhibiting gut MAO-A. This provides the brain MAO-A and MAO-B inhibition necessary for an antidepressant effect while eliminating the need for dietary restrictions at this lowest dosage.
Clinical implications
Transdermal selegiline offers an MAOI antidepressant option that might help:
- patients whose depression has not responded satisfactorily to selective serotonin reuptake inhibitors (SSRIs) or serotonin and norepinephrine reuptake inhibitors (SNRIs)
- adults and children with chronic depression marked by atypical features, including reactive mood, rejection sensitivity, anergia, and reversed vegetative symptoms—such as oversleeping, overeating, and psychomotor retardation. Although transdermal selegiline’s efficacy against these features has not been studied, patients with this depressive subtype tend to respond preferentially to MAOIs.
Pharmacokinetics
Transdermal selegiline achieves therapeutic blood levels and reaches sustained concentration within 4 to 8 hours of administration. Compared with oral selegiline, transdermal delivery results in higher plasma selegiline concentrations (1,500 pg/mL with the 6-mg patch) with much lower exposure to metabolites.8 The concentration is maintained with successive doses.
Transdermal selegiline clears rapidly upon discontinuation but MAO inhibition persists for 2 weeks, so wait 2 weeks after the last dose before starting a new antidepressant or stopping food restrictions with the 9-mg and 12-mg patches.
Efficacy
In two randomized, double-blind clinical trials,9,10 a total of 466 adults ages 18 to 65 who met DSM-IV-TR criteria for MDD received transdermal selegiline, 6 mg/d, or placebo for 6 to 8 weeks. Participants had 17-item Hamilton Rating Scale for Depression (HAM-D-17) scores ≥20 at baseline.
In the 6-week study,9 transdermal selegiline produced a 46% greater reduction in HAM-D-17 scores, a 52% greater decrease in HAM-D-28 scores, and a 79% greater drop in Montgomery-Asburg Depression Rating Scale (MADRS) scores compared with placebo. In the 8-week trial,10 HAM-D-28 and MADRS scores among the treatment group were significantly improved at endpoint compared with placebo, but HAM-D-17 scores were not.
In a 1-year, double-blind study,11 322 subjects with MDD—who had been rated as responders in a 10-week, open-label transdermal selegiline trial—received the 6-mg patch or placebo. At 6 months and 1 year, relapse was much less frequent among the treatment group compared with placebo. Relapse was defined as:
- HAM-D-17 ≥14
- Clinical Global Impressions of Severity score ≥3 with a ≥2-point increase from baseline
- and meeting DSM-IV criteria for MDD on two consecutive visits ≥11 days apart.
Side effects
Transdermal selegiline, 6 mg/d, has been well-tolerated in clinical trials. Inflammation at the application site was the most commonly reported side effect, occurring in 32% to 36% of treatment group subjects compared with 15% to 17% of the placebo groups.9,10,12 Inflammation was usually mild, but approximately 3% of patients dropped out of one study,12 citing this effect as the reason. Fair-skinned women are at highest risk for this reaction.
In the 1-year relapse prevention study,11 12% of treatment group patients reported insomnia compared with 7% of the placebo group. Insomnia incidence was the same in the selegiline and placebo groups during the 6- to 8-week clinical trials.9,10
Unlike conventional oral MAOIs,13 the 6-mg selegiline patch has not been found to impair sexual function, alter appetite, or change body weight or blood pressure compared with placebo.10-12 The toxicity of the 9- and 12-mg patches has not been studied in humans, but 8 mg/d and 12 mg/d of transdermal selegiline across 3 months were shown not to cause drug toxicity in dogs.14
Pediatric use
Although transdermal selegiline has not been studied in children and adolescents, the 6-mg patch could benefit some youths with depression. Before starting the drug, discuss with the child’s parents/guardians the FDA’s black box warning describing a possible association between selegiline and increased suicidal behavior in youths. This applies to all antidepressants.
Geriatric use
The patch might also help some older patients with depression. In a double-blind trial of high-dose oral selegiline (60 mg/d) involving 16 older patients (mean age 65.6), both the treatment and placebo groups remained almost free of side effects across 3 weeks.7 Although the sample was small, the findings suggest that older patients can tolerate selegiline at high dosages. Side effects also were minimal among treatment-group patients age ≥65 in the yearlong relapse prevention study.11
Treatment adherence rates with transdermal selegiline have been high in published studies, suggesting that the patch’s visibility might reduce the risk of forgetting to take the medication. Observing whether the patch has been changed might help older patients and family members/caregivers keep track of dosing.
Contraindications
As with the oral form, do not prescribe transdermal selegiline to patients taking SSRIs, SNRIs, tricyclic antidepressants, mirtazapine, or bupropion.
When switching antidepressants, allow enough time for the previous agent to “wash out” before starting transdermal selegiline. How much time to allow for wash-out depends on the previous agent’s half-life.
The patch is also contraindicated for patients taking:
- carbamazepine or oxcarbazepine
- meperidine
- analgesics such as tramadol, methadone, and propoxyphene
- St. John’s wort
- cough syrups containing dextromethorphan
- amphetamines, such as mixed amphetamine salts
- cyclobenzaprine
- or cold remedies or weight-loss products that contain vasoconstrictors, such as pseudoephedrine, phenylephrine, phenylpropanolamine, or ephedrine.
Do not give transdermal selegiline during pregnancy, as its effect on fetal development has not been studied.
Dosing
Start transdermal selegiline at 6 mg/d. Instruct the patient to wear the patch on the upper torso, where vascularity is richer compared with the buttocks and legs. Tell the patient to change the patch daily and to apply it to a different spot each day to prevent inflammation. Consider increasing the dosage after 2 or 3 months if response is unsatisfactory.
For treating first, second, and some third depressive episodes, continue transdermal selegiline for 6 months to 1 year of sustained recovery; consider longer-term maintenance treatment for highly recurrent depression. Transdermal selegiline has not been tapered in clinical trials, and subjects have not reported withdrawal symptoms after 1 year of continuous treatment.
Related resources
- Deniker P. The search for new antidepressants and related drugs. In: Tipton KF, Doster P, Benedetti M (eds). Monoamine oxidase and disease. London: Academic Press; 1984:2-8.
Drug brand names
- Amphetamine salts, mixed • Adderall
- Bupropion • Wellbutrin
- Carbamazepine • Tegretol, Equetro, others
- Cyclobenzaprine • Flexeril
- Meperidine • Demerol
- Mirtazapine • Remeron
- Oxcarbazepine • Trileptal
- Propoxyphene hydrochloride • Darvon
- Propoxyphene napsylate • Darvocet
- Selegiline (oral) • Eldepryl
- Selegiline (transdermal) • EMSAM
- Tramadol • Ultracet
Disclosure
Dr. Bodkin receives grant support from the National Institute of Mental Health, Eli Lilly & Co, Jazz Pharmaceuticals, Merck & Co., Organon, Sanofi-Aventis, and Somerset Pharmaceuticals; is a consultant to Bristol-Myers Squibb Co. and Somerset Pharmaceuticals; and is a speaker for Bristol-Myers Squibb Co. He has been principal investigator in several multicenter clinical trials of selegiline.
Many psychiatrists do not prescribe monoamine oxidase inhibitors (MAOIs) for fear of causing a potentially fatal hypertensive reaction, even though restricting foods high in the amino acid tyramine usually prevents this effect.1 Consequently, most depressed patients who might respond well to MAOIs do not receive them.2,3
Transdermal selegiline, FDA-approved for treating major depressive disorder (MDD) (Table 1), offers the clinical efficacy of an MAOI but without adverse interactions with food at the 6-mg strength. Transdermal selegiline may inhibit too much gastrointestinal MAO-A at 9 mg/d and 12 mg/d to clear tyramine from foods, so tyramine-rich foods must be restricted at these dosages (Table 2).
Table 1
Transdermal selegiline: Fast facts
| Brand name: EMSAM |
| Class: Monoamine oxidase inhibitor |
| FDA-approved indication: Major depressive disorder |
| Manufacturer: Somerset Pharmaceuticals (marketed by Bristol-Myers Squibb Co.) |
| Dosing forms: 6-, 9-, and 12-mg patches |
| Recommended dosage: One 6-mg patch every 24 hours, worn on the chest, back, or stomach. Increase dosage after 2 to 3 months if clinical response is inadequate |
Table 2
Restrict these foods when prescribing transdermal selegiline at 9 or 12 mg/d
| Food/beverage class | Foods to avoid |
|---|---|
| Beverages | Tap beer |
| Beer that has not been pasteurized* | |
| Red wines | |
| Dairy | Aged cheeses |
| Meat, poultry, fish | Air-dried, aged, and fermented meats, sausages, and salamis (including cacciatore and mortadella) |
| Pickled herring | |
| Spoiled or improperly stored fish, meat, poultry, or animal livers (check for mold, discoloration, or odor) | |
| Vegetables | Broad bean pods (fava beans) |
| Miscellaneous | Concentrated yeast extract (such as Marmite) |
| Fermented soybean products (including soy sauce) | |
| Over-the-counter supplements containing tyramine | |
| Sauerkraut | |
| *Bottled and canned beer and white wine contain little or no tyramine, but more than moderate alcohol use while taking selegiline is not recommended. | |
| Source: Shulman KI, Walker SE. A reevaluation of dietary restrictions for irreversible monoamine oxidase inhibitors. Psychiatr Ann 2001;31:378-84. | |
How it works
MAO enzyme subtypes A and B metabolize CNS monoamines, but primarily MAO-A metabolizes tyramine in the gut before the amino acid enters systemic circulation. At low concentrations, selegiline selectively inhibits MAO-B.4
Oral selegiline, approved as a adjunct to levodopa/carbidopa for patients with Parkinson’s disease,5 has been shown to be effective for treating depression at ≥30 mg/d.6 Because the drug does not selectively inhibit MAOB at ≥20 mg/d, dietary tyramine must be restricted when oral selegiline is used off-label at therapeutic dosages for depression. Otherwise, selegiline has been well-tolerated up to 60 mg/d.7
The 6-mg “patch” delivers more selegiline to the bloodstream than does low-dose oral selegiline but without inhibiting gut MAO-A. This provides the brain MAO-A and MAO-B inhibition necessary for an antidepressant effect while eliminating the need for dietary restrictions at this lowest dosage.
Clinical implications
Transdermal selegiline offers an MAOI antidepressant option that might help:
- patients whose depression has not responded satisfactorily to selective serotonin reuptake inhibitors (SSRIs) or serotonin and norepinephrine reuptake inhibitors (SNRIs)
- adults and children with chronic depression marked by atypical features, including reactive mood, rejection sensitivity, anergia, and reversed vegetative symptoms—such as oversleeping, overeating, and psychomotor retardation. Although transdermal selegiline’s efficacy against these features has not been studied, patients with this depressive subtype tend to respond preferentially to MAOIs.
Pharmacokinetics
Transdermal selegiline achieves therapeutic blood levels and reaches sustained concentration within 4 to 8 hours of administration. Compared with oral selegiline, transdermal delivery results in higher plasma selegiline concentrations (1,500 pg/mL with the 6-mg patch) with much lower exposure to metabolites.8 The concentration is maintained with successive doses.
Transdermal selegiline clears rapidly upon discontinuation but MAO inhibition persists for 2 weeks, so wait 2 weeks after the last dose before starting a new antidepressant or stopping food restrictions with the 9-mg and 12-mg patches.
Efficacy
In two randomized, double-blind clinical trials,9,10 a total of 466 adults ages 18 to 65 who met DSM-IV-TR criteria for MDD received transdermal selegiline, 6 mg/d, or placebo for 6 to 8 weeks. Participants had 17-item Hamilton Rating Scale for Depression (HAM-D-17) scores ≥20 at baseline.
In the 6-week study,9 transdermal selegiline produced a 46% greater reduction in HAM-D-17 scores, a 52% greater decrease in HAM-D-28 scores, and a 79% greater drop in Montgomery-Asburg Depression Rating Scale (MADRS) scores compared with placebo. In the 8-week trial,10 HAM-D-28 and MADRS scores among the treatment group were significantly improved at endpoint compared with placebo, but HAM-D-17 scores were not.
In a 1-year, double-blind study,11 322 subjects with MDD—who had been rated as responders in a 10-week, open-label transdermal selegiline trial—received the 6-mg patch or placebo. At 6 months and 1 year, relapse was much less frequent among the treatment group compared with placebo. Relapse was defined as:
- HAM-D-17 ≥14
- Clinical Global Impressions of Severity score ≥3 with a ≥2-point increase from baseline
- and meeting DSM-IV criteria for MDD on two consecutive visits ≥11 days apart.
Side effects
Transdermal selegiline, 6 mg/d, has been well-tolerated in clinical trials. Inflammation at the application site was the most commonly reported side effect, occurring in 32% to 36% of treatment group subjects compared with 15% to 17% of the placebo groups.9,10,12 Inflammation was usually mild, but approximately 3% of patients dropped out of one study,12 citing this effect as the reason. Fair-skinned women are at highest risk for this reaction.
In the 1-year relapse prevention study,11 12% of treatment group patients reported insomnia compared with 7% of the placebo group. Insomnia incidence was the same in the selegiline and placebo groups during the 6- to 8-week clinical trials.9,10
Unlike conventional oral MAOIs,13 the 6-mg selegiline patch has not been found to impair sexual function, alter appetite, or change body weight or blood pressure compared with placebo.10-12 The toxicity of the 9- and 12-mg patches has not been studied in humans, but 8 mg/d and 12 mg/d of transdermal selegiline across 3 months were shown not to cause drug toxicity in dogs.14
Pediatric use
Although transdermal selegiline has not been studied in children and adolescents, the 6-mg patch could benefit some youths with depression. Before starting the drug, discuss with the child’s parents/guardians the FDA’s black box warning describing a possible association between selegiline and increased suicidal behavior in youths. This applies to all antidepressants.
Geriatric use
The patch might also help some older patients with depression. In a double-blind trial of high-dose oral selegiline (60 mg/d) involving 16 older patients (mean age 65.6), both the treatment and placebo groups remained almost free of side effects across 3 weeks.7 Although the sample was small, the findings suggest that older patients can tolerate selegiline at high dosages. Side effects also were minimal among treatment-group patients age ≥65 in the yearlong relapse prevention study.11
Treatment adherence rates with transdermal selegiline have been high in published studies, suggesting that the patch’s visibility might reduce the risk of forgetting to take the medication. Observing whether the patch has been changed might help older patients and family members/caregivers keep track of dosing.
Contraindications
As with the oral form, do not prescribe transdermal selegiline to patients taking SSRIs, SNRIs, tricyclic antidepressants, mirtazapine, or bupropion.
When switching antidepressants, allow enough time for the previous agent to “wash out” before starting transdermal selegiline. How much time to allow for wash-out depends on the previous agent’s half-life.
The patch is also contraindicated for patients taking:
- carbamazepine or oxcarbazepine
- meperidine
- analgesics such as tramadol, methadone, and propoxyphene
- St. John’s wort
- cough syrups containing dextromethorphan
- amphetamines, such as mixed amphetamine salts
- cyclobenzaprine
- or cold remedies or weight-loss products that contain vasoconstrictors, such as pseudoephedrine, phenylephrine, phenylpropanolamine, or ephedrine.
Do not give transdermal selegiline during pregnancy, as its effect on fetal development has not been studied.
Dosing
Start transdermal selegiline at 6 mg/d. Instruct the patient to wear the patch on the upper torso, where vascularity is richer compared with the buttocks and legs. Tell the patient to change the patch daily and to apply it to a different spot each day to prevent inflammation. Consider increasing the dosage after 2 or 3 months if response is unsatisfactory.
For treating first, second, and some third depressive episodes, continue transdermal selegiline for 6 months to 1 year of sustained recovery; consider longer-term maintenance treatment for highly recurrent depression. Transdermal selegiline has not been tapered in clinical trials, and subjects have not reported withdrawal symptoms after 1 year of continuous treatment.
Related resources
- Deniker P. The search for new antidepressants and related drugs. In: Tipton KF, Doster P, Benedetti M (eds). Monoamine oxidase and disease. London: Academic Press; 1984:2-8.
Drug brand names
- Amphetamine salts, mixed • Adderall
- Bupropion • Wellbutrin
- Carbamazepine • Tegretol, Equetro, others
- Cyclobenzaprine • Flexeril
- Meperidine • Demerol
- Mirtazapine • Remeron
- Oxcarbazepine • Trileptal
- Propoxyphene hydrochloride • Darvon
- Propoxyphene napsylate • Darvocet
- Selegiline (oral) • Eldepryl
- Selegiline (transdermal) • EMSAM
- Tramadol • Ultracet
Disclosure
Dr. Bodkin receives grant support from the National Institute of Mental Health, Eli Lilly & Co, Jazz Pharmaceuticals, Merck & Co., Organon, Sanofi-Aventis, and Somerset Pharmaceuticals; is a consultant to Bristol-Myers Squibb Co. and Somerset Pharmaceuticals; and is a speaker for Bristol-Myers Squibb Co. He has been principal investigator in several multicenter clinical trials of selegiline.
1. Blackwell B, Mabbitt LA. Tyramine in cheese related to hypertensive crises after monoamine-oxidase inhibition. Lancet 1965;62:938-40.
2. American Psychiatric Association. Practice guideline for the treatment of patients with major depressive disorder (2nd ed). Available at: http://www.psych.org/psych_pract/treatg/pg/Practice%20Guidelines8904/MajorDepressiveDisorder_2e.pdf. Accessed March 15, 2006.
3. IMS Health National Prescription Audit; 12/04-11/05. Available at: http://www.imshealth.com. Accessed March 15, 2006.
4. Johnston JP. Some observations on a new form of MAO in brain tissue. Biochem Pharmacol 1968;17:1285-97.
5. Youdim MB. Monoamine oxidase inhibitors as antidepressant drugs and as adjunct to L-dopa therapy of Parkinson’s disease. J Neural Transm Suppl 1980;(16):157-61.
6. Bodkin JA, Kwon AE. Selegiline and other atypical MAO inhibitors in depression. Ann Psychiatry 2001;31:385-91.
7. Sunderland T, Cohen RM, Molchan S, et al. High-dose selegiline in treatment-resistant older depressive patients. Arch Gen Psychiatry 1994;51:607-15.
8. Ziemniak JA, Kemper EM, Goodhear M, Azzaro AJ. Pharmacokinetics of selegiline administered via the patch, single oral dose, or intravenous infusion. Poster presented at: Annual Meeting, National Institute of Mental Health, New Clinical Drug Evaluation Unit, May 29, 2001, Phoenix, AZ.
9. Bodkin JA, Amsterdam JD. Transdermal selegiline in major depression: a double-blind, placebo-controlled, parallel-group study in outpatients. Am J Psychiatry 2002;159:1869-75.
10. Amsterdam JD. A double-blind, placebo-controlled trial of the safety and efficacy of selegiline transdermal system without dietary restrictions in patients with major depressive disorder. J Clin Psychiatry 2003;64:208-14.
11. Robinson DS, Moonsammy G, Azzaro AJ. Relapse prevention study shows the long-term safety and efficacy of transdermal selegiline, a new generation MAOI. Poster presented at: Annual Meeting, American College of Neuropsychopharmacology, Dec 11, 2002; San Juan, PR.
12. Robinson DS, Amsterdam JD. Safety and tolerability of selegiline transdermal system 20 mg for treatment of major depression. Poster presented at: Annual Meeting, American College of Neuropsychopharmacology, Dec. 13, 2005, Waikalo, HI.
13. Cole JO, Bodkin JA. Antidepressant drug side effects. J Clin Psychiatry 1990;51(Suppl):21-6.
14. Barrett JS, DiSanto AR, Thomford PJ, et al. Toxicokinetic evaluation of a selegiline transdermal system in the dog. Biopharm Drug Dispos 1997;18:165-84.
1. Blackwell B, Mabbitt LA. Tyramine in cheese related to hypertensive crises after monoamine-oxidase inhibition. Lancet 1965;62:938-40.
2. American Psychiatric Association. Practice guideline for the treatment of patients with major depressive disorder (2nd ed). Available at: http://www.psych.org/psych_pract/treatg/pg/Practice%20Guidelines8904/MajorDepressiveDisorder_2e.pdf. Accessed March 15, 2006.
3. IMS Health National Prescription Audit; 12/04-11/05. Available at: http://www.imshealth.com. Accessed March 15, 2006.
4. Johnston JP. Some observations on a new form of MAO in brain tissue. Biochem Pharmacol 1968;17:1285-97.
5. Youdim MB. Monoamine oxidase inhibitors as antidepressant drugs and as adjunct to L-dopa therapy of Parkinson’s disease. J Neural Transm Suppl 1980;(16):157-61.
6. Bodkin JA, Kwon AE. Selegiline and other atypical MAO inhibitors in depression. Ann Psychiatry 2001;31:385-91.
7. Sunderland T, Cohen RM, Molchan S, et al. High-dose selegiline in treatment-resistant older depressive patients. Arch Gen Psychiatry 1994;51:607-15.
8. Ziemniak JA, Kemper EM, Goodhear M, Azzaro AJ. Pharmacokinetics of selegiline administered via the patch, single oral dose, or intravenous infusion. Poster presented at: Annual Meeting, National Institute of Mental Health, New Clinical Drug Evaluation Unit, May 29, 2001, Phoenix, AZ.
9. Bodkin JA, Amsterdam JD. Transdermal selegiline in major depression: a double-blind, placebo-controlled, parallel-group study in outpatients. Am J Psychiatry 2002;159:1869-75.
10. Amsterdam JD. A double-blind, placebo-controlled trial of the safety and efficacy of selegiline transdermal system without dietary restrictions in patients with major depressive disorder. J Clin Psychiatry 2003;64:208-14.
11. Robinson DS, Moonsammy G, Azzaro AJ. Relapse prevention study shows the long-term safety and efficacy of transdermal selegiline, a new generation MAOI. Poster presented at: Annual Meeting, American College of Neuropsychopharmacology, Dec 11, 2002; San Juan, PR.
12. Robinson DS, Amsterdam JD. Safety and tolerability of selegiline transdermal system 20 mg for treatment of major depression. Poster presented at: Annual Meeting, American College of Neuropsychopharmacology, Dec. 13, 2005, Waikalo, HI.
13. Cole JO, Bodkin JA. Antidepressant drug side effects. J Clin Psychiatry 1990;51(Suppl):21-6.
14. Barrett JS, DiSanto AR, Thomford PJ, et al. Toxicokinetic evaluation of a selegiline transdermal system in the dog. Biopharm Drug Dispos 1997;18:165-84.