User login
Welcome to Current Psychiatry, a leading source of information, online and in print, for practitioners of psychiatry and its related subspecialties, including addiction psychiatry, child and adolescent psychiatry, and geriatric psychiatry. This Web site contains evidence-based reviews of the prevention, diagnosis, and treatment of mental illness and psychological disorders; case reports; updates on psychopharmacology; news about the specialty of psychiatry; pearls for practice; and other topics of interest and use to this audience.
Dear Drupal User: You're seeing this because you're logged in to Drupal, and not redirected to MDedge.com/psychiatry.
Depression
adolescent depression
adolescent major depressive disorder
adolescent schizophrenia
adolescent with major depressive disorder
animals
autism
baby
brexpiprazole
child
child bipolar
child depression
child schizophrenia
children with bipolar disorder
children with depression
children with major depressive disorder
compulsive behaviors
cure
elderly bipolar
elderly depression
elderly major depressive disorder
elderly schizophrenia
elderly with dementia
first break
first episode
gambling
gaming
geriatric depression
geriatric major depressive disorder
geriatric schizophrenia
infant
kid
major depressive disorder
major depressive disorder in adolescents
major depressive disorder in children
parenting
pediatric
pediatric bipolar
pediatric depression
pediatric major depressive disorder
pediatric schizophrenia
pregnancy
pregnant
rexulti
skin care
teen
wine
section[contains(@class, 'nav-hidden')]
footer[@id='footer']
div[contains(@class, 'pane-pub-article-current-psychiatry')]
div[contains(@class, 'pane-pub-home-current-psychiatry')]
div[contains(@class, 'pane-pub-topic-current-psychiatry')]
div[contains(@class, 'panel-panel-inner')]
div[contains(@class, 'pane-node-field-article-topics')]
section[contains(@class, 'footer-nav-section-wrapper')]
What to tell patients about side effects
Man taking trazodone claims he was not told about priapism risk
Unknown Massachusetts venue
A 52-year-old man saw a psychiatrist for acute anxiety, panic attacks, and difficulty sleeping. The psychiatrist prescribed the alprazolam, 0.25 mg/d, for the anxiety symptoms and one or two tablets of trazodone, 50 mg at bedtime, to aid sleep.
At follow-up 2 weeks later, the patient reported he was feeling better, and the psychiatrist increased alprazolam to 0.5 mg tid.
The next morning, the patient woke with a painless partial erection, but was unconcerned because he had experienced this in the past. The erection persisted for 2 days. On the third morning, the patient went to the emergency department because the erection had become painful.
A urologist diagnosed the patient’s condition as priapism. After less-invasive treatment measures failed, the urologist performed surgery to extract clotted blood and inserted shunts to facilitate blood flow.
The patient was transferred to another facility and prescribed pain medication and an antiandrogen hormone to diminish the erection. Within 2 weeks following surgery, a black eschar covered the entire glans penis and necrotic tissue closed the meatus. Pain, eschar formation, and necrotic tissue on the patient’s glans penis persisted as long-term complications from priapism, resulting in permanent scarring, penile disfigurement, and inability to achieve an erection or have intercourse.
The patient claimed the psychiatrist never informed him of the risk of priapism associated with trazodone and failed to recommend immediate medical attention if this condition developed.
The psychiatrist maintained that although he had no memory of informing the patient of priapism risk, it would have been his custom to do so. The psychiatrist also contended that the length of time between the patient noticing the condition and seeking medical care constituted comparative negligence by the patient.
- A $300,000 settlement was reached.
Errant lamotrigine course
caused fatal hypersensitivity, estate alleges
Fairfax Country (VA) Circuit Court
A 43-year-old woman sought treatment for emotional difficulties. The psychiatrist diagnosed her with bipolar type II disorder and prescribed lamotrigine. Within 5 weeks, the patient developed Stevens-Johnson syndrome and died from its complications.
The patient’s estate claimed
- that the psychiatrist misdiagnosed the patient, who the estate alleged had posttraumatic stress disorder (PTSD).
- that prescribing lamotrigine was inappropriate because the patient didn’t have bipolar disorder and the drug is not first-line treatment for bipolar II disorder.
- the psychiatrist failed to inform the patient that lamotrigine may cause hypersensitivity reactions and neglected to obtain informed consent to use the drug.
- The jury awarded the defendant $3 million. This was reduced to $1.65 million because of a statutory capitation.
Dr. Grant’s observations
These cases raise three potential malpractice issues:
- What happens if you misdiagnose a patient?
- Is it OK to use a treatment that is not “first-line”?
- How much do you have to tell patients about potential side effects?
A successful malpractice claim of misdiagnosis against a psychiatrist would likely be based on:
- failure to recognize the disorder
- improper treatment based on the misdiagnosis
- resultant harm caused by improper treatment.
To be valid in court, informed consent must be documented in the patient’s chart. One study of 30 psychiatrists treating patients with antipsychotics found that only 23% of their patients’ charts had documentation of informed consent.7 Without proper documentation (Table 2), negligence claims are more likely to be successful.
Informed consent is a continuous process. After each visit summarize discussions about medications you had with the patient, document his or her response to medication, and note your reasons for continuing medication.9
Informed consent does not shield a psychiatrist from liability. For example, if the patient’s condition does not justify the risks of a certain medication, negligence could be proven even though the patient consented to the treatment. Having consent, however, provides evidence that the psychiatrist advised the patient of consequences of possible side effects.
Table 2
What to include when documenting informed consent
| Diagnosis |
| Nature and purpose of the proposed treatment |
| Risks Infrequent risks that pose a significant possibility of harm Frequent risks that pose less danger |
| Reasonably expected benefits |
| Alternate treatments, their risks and benefits |
| Risks of no treatment |
| Source: Reference 8 |
1. American Psychiatric Association. Practice guidelines. Available at: http://www.psych.org/psych_pract/treatg/pg/prac_guide.cfm. Accessed Dec. 27, 2005.
2. Slovenko R. Update on legal issues associated with tardive dyskinesia. J Clin Psychiatry 2000;61(suppl 4):45-57.
3. American Psychiatric Association. Principles of informed consent in psychiatry. Available at: http://www.psych.org/edu/other_res/lib_archives/archives/199601.pdf. Accessed Dec. 27, 2005
4. Sard v Hardy, 379 A2d 1014 (1977).
5. Wilkinson v Vesey, 295 A2d 676 (1972).
6. Canterbury v Spence, 464 F2d 772,755 (DC Cir 1972).
7. Schachter D, Kleinman I. Psychiatrists’ documentation of informed consent. Can J Psychiatry 1998;43:1012-7.
8. Berner M. Informed consent. In: Lifson LE, Simon RI (eds). The mental health practitioner and the law. Cambridge, MA: Harvard University Press; 1998:23-43.
9. Hinton M. Experts urge caution in prescribing medications for off-label use. Psychiatric News Sept. 1, 2000. Available at: http://www.psych.org/pnews/00-09-01/experts.html. Accessed Dec. 27, 2005.
Cases are selected by Current Psychiatry’s editors from Medical Malpractice Verdicts, Settlements & Experts, with permission of its editor, Lewis Laska of Nashville, TN (www.verdictslaska.com). Information may be incomplete in some instances, but these cases represent clinical situations that typically result in litigation.
Man taking trazodone claims he was not told about priapism risk
Unknown Massachusetts venue
A 52-year-old man saw a psychiatrist for acute anxiety, panic attacks, and difficulty sleeping. The psychiatrist prescribed the alprazolam, 0.25 mg/d, for the anxiety symptoms and one or two tablets of trazodone, 50 mg at bedtime, to aid sleep.
At follow-up 2 weeks later, the patient reported he was feeling better, and the psychiatrist increased alprazolam to 0.5 mg tid.
The next morning, the patient woke with a painless partial erection, but was unconcerned because he had experienced this in the past. The erection persisted for 2 days. On the third morning, the patient went to the emergency department because the erection had become painful.
A urologist diagnosed the patient’s condition as priapism. After less-invasive treatment measures failed, the urologist performed surgery to extract clotted blood and inserted shunts to facilitate blood flow.
The patient was transferred to another facility and prescribed pain medication and an antiandrogen hormone to diminish the erection. Within 2 weeks following surgery, a black eschar covered the entire glans penis and necrotic tissue closed the meatus. Pain, eschar formation, and necrotic tissue on the patient’s glans penis persisted as long-term complications from priapism, resulting in permanent scarring, penile disfigurement, and inability to achieve an erection or have intercourse.
The patient claimed the psychiatrist never informed him of the risk of priapism associated with trazodone and failed to recommend immediate medical attention if this condition developed.
The psychiatrist maintained that although he had no memory of informing the patient of priapism risk, it would have been his custom to do so. The psychiatrist also contended that the length of time between the patient noticing the condition and seeking medical care constituted comparative negligence by the patient.
- A $300,000 settlement was reached.
Errant lamotrigine course
caused fatal hypersensitivity, estate alleges
Fairfax Country (VA) Circuit Court
A 43-year-old woman sought treatment for emotional difficulties. The psychiatrist diagnosed her with bipolar type II disorder and prescribed lamotrigine. Within 5 weeks, the patient developed Stevens-Johnson syndrome and died from its complications.
The patient’s estate claimed
- that the psychiatrist misdiagnosed the patient, who the estate alleged had posttraumatic stress disorder (PTSD).
- that prescribing lamotrigine was inappropriate because the patient didn’t have bipolar disorder and the drug is not first-line treatment for bipolar II disorder.
- the psychiatrist failed to inform the patient that lamotrigine may cause hypersensitivity reactions and neglected to obtain informed consent to use the drug.
- The jury awarded the defendant $3 million. This was reduced to $1.65 million because of a statutory capitation.
Dr. Grant’s observations
These cases raise three potential malpractice issues:
- What happens if you misdiagnose a patient?
- Is it OK to use a treatment that is not “first-line”?
- How much do you have to tell patients about potential side effects?
A successful malpractice claim of misdiagnosis against a psychiatrist would likely be based on:
- failure to recognize the disorder
- improper treatment based on the misdiagnosis
- resultant harm caused by improper treatment.
To be valid in court, informed consent must be documented in the patient’s chart. One study of 30 psychiatrists treating patients with antipsychotics found that only 23% of their patients’ charts had documentation of informed consent.7 Without proper documentation (Table 2), negligence claims are more likely to be successful.
Informed consent is a continuous process. After each visit summarize discussions about medications you had with the patient, document his or her response to medication, and note your reasons for continuing medication.9
Informed consent does not shield a psychiatrist from liability. For example, if the patient’s condition does not justify the risks of a certain medication, negligence could be proven even though the patient consented to the treatment. Having consent, however, provides evidence that the psychiatrist advised the patient of consequences of possible side effects.
Table 2
What to include when documenting informed consent
| Diagnosis |
| Nature and purpose of the proposed treatment |
| Risks Infrequent risks that pose a significant possibility of harm Frequent risks that pose less danger |
| Reasonably expected benefits |
| Alternate treatments, their risks and benefits |
| Risks of no treatment |
| Source: Reference 8 |
Man taking trazodone claims he was not told about priapism risk
Unknown Massachusetts venue
A 52-year-old man saw a psychiatrist for acute anxiety, panic attacks, and difficulty sleeping. The psychiatrist prescribed the alprazolam, 0.25 mg/d, for the anxiety symptoms and one or two tablets of trazodone, 50 mg at bedtime, to aid sleep.
At follow-up 2 weeks later, the patient reported he was feeling better, and the psychiatrist increased alprazolam to 0.5 mg tid.
The next morning, the patient woke with a painless partial erection, but was unconcerned because he had experienced this in the past. The erection persisted for 2 days. On the third morning, the patient went to the emergency department because the erection had become painful.
A urologist diagnosed the patient’s condition as priapism. After less-invasive treatment measures failed, the urologist performed surgery to extract clotted blood and inserted shunts to facilitate blood flow.
The patient was transferred to another facility and prescribed pain medication and an antiandrogen hormone to diminish the erection. Within 2 weeks following surgery, a black eschar covered the entire glans penis and necrotic tissue closed the meatus. Pain, eschar formation, and necrotic tissue on the patient’s glans penis persisted as long-term complications from priapism, resulting in permanent scarring, penile disfigurement, and inability to achieve an erection or have intercourse.
The patient claimed the psychiatrist never informed him of the risk of priapism associated with trazodone and failed to recommend immediate medical attention if this condition developed.
The psychiatrist maintained that although he had no memory of informing the patient of priapism risk, it would have been his custom to do so. The psychiatrist also contended that the length of time between the patient noticing the condition and seeking medical care constituted comparative negligence by the patient.
- A $300,000 settlement was reached.
Errant lamotrigine course
caused fatal hypersensitivity, estate alleges
Fairfax Country (VA) Circuit Court
A 43-year-old woman sought treatment for emotional difficulties. The psychiatrist diagnosed her with bipolar type II disorder and prescribed lamotrigine. Within 5 weeks, the patient developed Stevens-Johnson syndrome and died from its complications.
The patient’s estate claimed
- that the psychiatrist misdiagnosed the patient, who the estate alleged had posttraumatic stress disorder (PTSD).
- that prescribing lamotrigine was inappropriate because the patient didn’t have bipolar disorder and the drug is not first-line treatment for bipolar II disorder.
- the psychiatrist failed to inform the patient that lamotrigine may cause hypersensitivity reactions and neglected to obtain informed consent to use the drug.
- The jury awarded the defendant $3 million. This was reduced to $1.65 million because of a statutory capitation.
Dr. Grant’s observations
These cases raise three potential malpractice issues:
- What happens if you misdiagnose a patient?
- Is it OK to use a treatment that is not “first-line”?
- How much do you have to tell patients about potential side effects?
A successful malpractice claim of misdiagnosis against a psychiatrist would likely be based on:
- failure to recognize the disorder
- improper treatment based on the misdiagnosis
- resultant harm caused by improper treatment.
To be valid in court, informed consent must be documented in the patient’s chart. One study of 30 psychiatrists treating patients with antipsychotics found that only 23% of their patients’ charts had documentation of informed consent.7 Without proper documentation (Table 2), negligence claims are more likely to be successful.
Informed consent is a continuous process. After each visit summarize discussions about medications you had with the patient, document his or her response to medication, and note your reasons for continuing medication.9
Informed consent does not shield a psychiatrist from liability. For example, if the patient’s condition does not justify the risks of a certain medication, negligence could be proven even though the patient consented to the treatment. Having consent, however, provides evidence that the psychiatrist advised the patient of consequences of possible side effects.
Table 2
What to include when documenting informed consent
| Diagnosis |
| Nature and purpose of the proposed treatment |
| Risks Infrequent risks that pose a significant possibility of harm Frequent risks that pose less danger |
| Reasonably expected benefits |
| Alternate treatments, their risks and benefits |
| Risks of no treatment |
| Source: Reference 8 |
1. American Psychiatric Association. Practice guidelines. Available at: http://www.psych.org/psych_pract/treatg/pg/prac_guide.cfm. Accessed Dec. 27, 2005.
2. Slovenko R. Update on legal issues associated with tardive dyskinesia. J Clin Psychiatry 2000;61(suppl 4):45-57.
3. American Psychiatric Association. Principles of informed consent in psychiatry. Available at: http://www.psych.org/edu/other_res/lib_archives/archives/199601.pdf. Accessed Dec. 27, 2005
4. Sard v Hardy, 379 A2d 1014 (1977).
5. Wilkinson v Vesey, 295 A2d 676 (1972).
6. Canterbury v Spence, 464 F2d 772,755 (DC Cir 1972).
7. Schachter D, Kleinman I. Psychiatrists’ documentation of informed consent. Can J Psychiatry 1998;43:1012-7.
8. Berner M. Informed consent. In: Lifson LE, Simon RI (eds). The mental health practitioner and the law. Cambridge, MA: Harvard University Press; 1998:23-43.
9. Hinton M. Experts urge caution in prescribing medications for off-label use. Psychiatric News Sept. 1, 2000. Available at: http://www.psych.org/pnews/00-09-01/experts.html. Accessed Dec. 27, 2005.
Cases are selected by Current Psychiatry’s editors from Medical Malpractice Verdicts, Settlements & Experts, with permission of its editor, Lewis Laska of Nashville, TN (www.verdictslaska.com). Information may be incomplete in some instances, but these cases represent clinical situations that typically result in litigation.
1. American Psychiatric Association. Practice guidelines. Available at: http://www.psych.org/psych_pract/treatg/pg/prac_guide.cfm. Accessed Dec. 27, 2005.
2. Slovenko R. Update on legal issues associated with tardive dyskinesia. J Clin Psychiatry 2000;61(suppl 4):45-57.
3. American Psychiatric Association. Principles of informed consent in psychiatry. Available at: http://www.psych.org/edu/other_res/lib_archives/archives/199601.pdf. Accessed Dec. 27, 2005
4. Sard v Hardy, 379 A2d 1014 (1977).
5. Wilkinson v Vesey, 295 A2d 676 (1972).
6. Canterbury v Spence, 464 F2d 772,755 (DC Cir 1972).
7. Schachter D, Kleinman I. Psychiatrists’ documentation of informed consent. Can J Psychiatry 1998;43:1012-7.
8. Berner M. Informed consent. In: Lifson LE, Simon RI (eds). The mental health practitioner and the law. Cambridge, MA: Harvard University Press; 1998:23-43.
9. Hinton M. Experts urge caution in prescribing medications for off-label use. Psychiatric News Sept. 1, 2000. Available at: http://www.psych.org/pnews/00-09-01/experts.html. Accessed Dec. 27, 2005.
Cases are selected by Current Psychiatry’s editors from Medical Malpractice Verdicts, Settlements & Experts, with permission of its editor, Lewis Laska of Nashville, TN (www.verdictslaska.com). Information may be incomplete in some instances, but these cases represent clinical situations that typically result in litigation.
The ‘date’ that changed her life
History: From sociable to sullen
Julie, a Hispanic/Native American, was adopted by a Caucasian couple when she was 6 weeks old. Before age 12, she had no psychiatric problems and was medically healthy though slightly overweight.
At age 12, Julie started having episodes of brooding depression, verbal and physical aggression, and impulsive suicidal behavior. She also began suffering intermittent migraines and having trouble falling asleep. She insisted on sleeping with her parents or with a nightlight in her room.
Once a sociable girl who enjoyed being in the middle school chorus and band, Julie suddenly became sullen and defiant. She dropped out of afterschool activities and stopped socializing with peers except for her best friend, Sheila, age 12, and Mark, age 13, an “almost boyfriend” who lived next door.
Julie also started arguing with her mother, often yelling and screaming when approached with minor requests. Sometimes, Julie hit and pushed her. A psychiatrist diagnosed the 12-year-old with major depressive disorder and prescribed fluoxetine, dosage unknown.
Soon after Julie’s symptoms surfaced, her adoptive father, a sales representative, was laid off. He found work in another state; the family left an ethnically diverse city for a predominantly Caucasian rural area. There, Julie completed middle school and her freshman year of high school, and lost contact with Sheila and Mark.
Midway through her freshman year, Julie tried to induce vomiting after eating so that she would lose weight and “fit in better with the other girls.” She stopped this at the end of the school year.
The following fall, 5 weeks into her sophomore year, she dropped out of high school and was ultimately enrolled in home school.
Treatment: 4 hospitalizations in 3 years
Between ages 12 and 15, Julie was hospitalized four times for outbursts of violence with impulsive self-harm. She “overdosed” on eight aceta-minophen/diphenhydramine tablets on one occasion and superficially cut her forearm on another. During these episodes, she said, she heard voices telling her to harm her mother and herself.
During this period, Julie was diagnosed as having schizophrenia, major depressive disorder, attention-deficit/hyperactivity disorder (ADHD), and oppositional defiant disorder (ODD). Numerous antidepressant and mood stabilizer regimens produced no lasting improvement, though her angry and violent episodes became less frequent.
poll here
The authors’ observations
Although Julie’s psychotic symptoms might suggest an evolving disorder such as schizophrenia, no clear pattern supports this diagnosis. Also:
- Onset at age 12 is unusual. Schizophrenia typically begins in late teens to early adulthood.
- Julie showed no premorbid personality problems—found in up to one-third of patients with chronic schizophrenia—and no premorbid adjustment difficulties resulting from negative symptoms, cognitive deficits, or poor social function.1
Julie’s birth parents’ mental health history would offer crucial information, but this was not available.
Continued history: ‘I left my body’
Shortly after her 15th birthday, Julie broke down and told her parents that 3 years earlier, four boys had gang-raped her while she was “on a first date” with one of them at a school football game. She said one attacker held a knife to her throat, and they threatened to kill her friend Sheila if anyone was told. Julie said she felt so terrorized that “I left my body and watched what was happening.”
After the rape, Julie went home, showered, and went to bed. She said she felt “emotionally numb” for 2 months, during which she threw herself into schoolwork, stopped attending after-school events, and began arguing with her parents. She developed nightmares of the trauma and, eventually, auditory command hallucinations. When stressed, she has “out of body” feelings lasting several minutes.
The parents, though angry at Julie‘s attackers, did not seek legal counsel or report the rape to authorities because they felt too much time had passed. They sought support from a counselor, who referred their daughter to a male psychiatrist for medication management. Julie, now age 16, preferred to be treated by a woman, so her care was transferred to our clinic.
Based on clinical observations, Julie gets along well with her father. She complains that her mother is overprotective yet Julie cannot bear to be separated from her for even a couple hours. She resents her mother’s overinvolvement but relies on it for emotional regulation. Her mother has been treated for major depressive disorder, generalized anxiety disorder, and alcohol dependence. These were in sustained remission when Julie presented to us.
At presentation, we diagnosed Julie as having chronic posttraumatic stress disorder (PTSD), recurrent major depressive disorder, and eating disorder not otherwise specified. At 5 feet, 7 inches and 190 pounds, her body mass index is 30 kg/m2, indicating clinical obesity. She has been taking duloxetine, 60 mg/d, extended release dextroamphetamine, 20 mg/d, aripiprazole, 20 mg/d, and amitriptyline, 10 mg/d nightly. She also has been taking sumatriptan, 100 mg as needed, for migraines.
poll here
The authors’ observations
After a life-threatening sexual assault, Julie suddenly became irritable and hostile. She could not keep relationships, yet she feared being alone. She impulsively hurt herself, experienced nightmares, and systematically avoided school activities. These behaviors suggest PTSD,1 which is prevalent among sexual assault victims (Box 1). For 3 years, however, psychiatrists kept missing the diagnosis as Julie kept her shame a secret.
Julie tells us that she re-experiences trauma-related dysphoria when exposed to cues, such as the anniversary of the rape. She endorses avoidance symptoms, including feelings of estrangement from her family and friends. She shuns thoughts, feelings, places, and conversations associated with the trauma, which partly explains her refusal to stay in school. She reports arousal symptoms, including difficulty falling and staying asleep and fears of harm if left alone, even during the day. At night she has rituals for checking windows and doors to ensure they are locked.
Julie’s decision to hide her trauma was understandable given her age and developmental phase. For a teenager trying to separate from her parents and fit in at school, the humiliation was overwhelming. She lacked the cognitive tools to process and describe her experience. She was assaulted while on a date, normally a positive rite of passage. Further, as a young Hispanic/Native American, Julie feared disappointing her Caucasian parents by not fitting in at school.
When a previously well-adjusted teenager presents with sudden-onset behavioral problems, ask about past or recent trauma. Watch for contextual, developmental, and sociocultural factors that may prevent the youth from disclosing embarrassing events.
Also question the diagnosis if several adequate medication trials have failed. Check for comorbidities, lack of adherence, or other circumstances that can hamper response to treatment.
The National Comorbidity Survey estimates lifetime prevalence of PTSD at 7.8%.2 Sexual assault victims face a high risk of PTSD among persons exposed to trauma.3,4
Factors that may influence whether trauma exposure progresses to PTSD:
Natural resiliency
Genetic loading
Type of trauma
Whether the trauma is natural or man-made
Past traumas
Psychiatric comorbidities
When a patient presents immediately after a life-threatening trauma:
Ensure physical and psychological safety
Screen for prior traumas that may increase risk of developing PTSD
Refer for physical examination, particularly for victims of rape or physical violence
PTSD checklists can help confirm the diagnosis (see Related resources)
Factors that may signal ptsd
American Psychiatric Association (APA) practice guidelines for treating PTSD list several factors to consider if you suspect this diagnosis:5
Impulsive and episodic aggression can result from an anticipatory bias that increases readiness for “fight, flight, or freeze.” For Julie, this turned previously comfortable interactions into dissonance and conflict.
Self-injurious and suicidal behaviors often occur when trauma creates stigma, shame, or guilt. Julie felt these emotions while trying to establish herself in a new community and school. Her obesity and ethnic background further set her apart from peers. She also left behind friends who provided emotional support outside the home and helped her differentiate from her mother.
Trauma during early adolescence can impair age-appropriate development, making it difficult to develop a stable self-image, consolidate and integrate the personality, and form relationships. At age 16, poor self-image and maladaptive coping strategies were an enduring pattern in Julie’s life.
Psychiatric comorbidities. Many patients with PTSD develop psychiatric comorbidities that exaggerate symptoms, making the disorder more difficult to detect and treat. Julie’s depression increased her avoidance tendencies and rein-forced her isolation. Difficulty concentrating—misdiagnosed as ADHD—deterred her from engaging in school. Dissociative symptoms related to PTSD impaired her reality testing, diminishing her ability to interact with others.
Treatment: Medication change
We continued extended-release dextroamphetamine, 20 mg/d, as Julie felt the medication helped her focus on her schoolwork. We also:
- weaned her off aripiprazole, which was not helping her symptoms
- stopped amitriptyline and duloxetine because of her history of impulsive overdose and to reduce side-effect risk from polypharmacy
- titrated fluoxetine to 40 mg/d to treat her ongoing chronic depression and added trazodone, 50 mg/d as needed, to help her sleep
- stopped sumatriptan, as the headaches remitted after Julie’s eyes were tested and eyeglasses prescribed.
poll here
The authors’ observations
Medication. APA treatment guidelines support using SSRIs to treat all three PTSD symptom clusters—re-experiencing, avoidance, and hyperarousal—as well as coexisting depression. Evidence also supports use of the tricyclics amitriptyline and imipramine and some monoamine oxidase inhibitors (MAOIs).6-10 Dietary restrictions associated with MAOIs, however, can pose a problem for teenagers.
Benzodiazepines can decrease anxiety and improve sleep, but they can be addictive and their efficacy in treating PTSD has not been established. Alpha-2-adrenergic agonists such as prazosin and clonidine may decrease hyperarousal and trauma-related nightmares.11,12
Obtain informed parental consent before starting a child or adolescent on an antidepressant. These medications contain a black-box warning that the drug may increase suicide risk in youths.
Psychotherapy. Varying levels of evidence support psychotherapy models in PTSD (Box 2). Julie can benefit from psychoeducation, supportive therapy, psychodynamic psychotherapy, and cautious re-exposure to trauma where possible.
Psychoeducation provided a safe starting point for Julie’s therapy, engaged her parents and select school counselors and teachers, and helped her understand PTSD’s effects. This allowed us to teach stress reduction and coping strategies.
Supportive techniques helped Julie contain painful affects. She could then network with community resources such as AlaTeen and a peer support group via a local Native American mental health program. This approach helped us gain Julie’s trust, and we anticipate more in-depth work with time.
Trauma re-exposure helps some patients but worsens others’ symptoms. For Julie, trauma re-exposure has been minimal because of the many other issues she was facing.
Developing a trusting relationship over time is crucial to successful trauma re-exposure. Re-exposure should be gradual to keep affective arousal moderate. This will minimize dissociation and affective flooding, which can frustrate treatment.
Cognitive-behavioral therapy (CBT) might help Julie understand the automatic thoughts of failure and defeat that flood her when she is stressed. CBT could help her master her feelings and lay a foundation for improved coping.
Psychodynamic psychotherapy may be started later to help Julie verbalize feelings and modulate how she expresses affect. This model could promote her development, improve her self-image, and treat her depression.
Recommended with substantial clinical confidence (Level I)
Cognitive-behavioral therapy
Psychoeducation
Supportive techniques
Recommended with moderate clinical confidence (Level II)
Exposure techniques
Eye movement desensitization and reprocessing
Imagery rehearsal
Psychodynamic therapy
Stress inoculation
May be recommended in some cases (Level III)
Present-centered group therapy
Trauma-focused group therapy
Not recommended (no evidence)
Psychological debriefings
Single-session techniques
Source: APA practice guideline for PTSD (see Related resources)
Follow-up: Back to school
After 2 months under our care, Julie begins to show improvement. Because of her progress and the fact that her parents drive 45 minutes each way to get to our clinic, we reduce visit frequency from weekly to biweekly.
Julie now attends school 2 hours daily, is earning additional credits through home study, and plans to graduate early and attend community college. Her depression has lifted, and she continues to take fluoxetine, 40 mg/d and extended-release dextroamphetamine, 20 mg/d. She still struggles with social isolation, failure to reach age-appropriate developmental milestones, and a poor body image.
- American Psychiatric Association. Practice guideline for treating acute stress disorder and posttraumatic stress disorder. www.psych.org/psych_pract/treatg/pg/PTSD-PG-PartsA-B-C-New.pdf
- National Center for Post-Traumatic Stress Disorder. Information on obtaining Impact of Events Scale and Davidson Trauma Scale. www.ncptsd.va.gov/publications/assessment/adult_self_report.html
- Amitriptyline • Elavil
- Aripiprazole • Abilify
- Clonidine • Catapres
- Dextroamphetamine (extended-release) • Adderall XR
- Duloxetine • Cymbalta
- Fluoxetine • Prozac
- Imipramine • Tofranil
- Phenelzine • Nardil
- Prazosin • Minipress
- Sumatriptan • Imitrex
- Trazodone • Desyrel
Dr. Matthews is an American Psychiatric Association Bristol-Myers Squibb Co. fellow in public and community psychiatry.
Dr. Mossefin reports no financial relationship with any company whose products are mentioned in this article, or with manufacturers of competing products.
Acknowledgements
The authors thank Larry Schwartz, MD, for his help in preparing this article for publication.
1. Ho BC, Black DW, Andreasen NC. Schizophrenia and other psychotic disorders. In: Hales RE, Yudofsky SC (eds). Textbook of clinical psychiatry (4th ed). Washington, DC: American Psychiatric Publishing; 2003.
2. Kessler RC, Sonnega A, Bromet E, et al. Posttraumatic stress disorder in the National Comorbidity Survey. Arch Gen Psychiatry 1995;52:1048-60.
3. Breslau N, Kessler RC, Chilcoat HD, et al. Trauma and posttraumatic stress disorder in the community: the 1996 Detroit Area Survey of Trauma. Arch Gen Psychiatry 1998;55:626-32.
4. Brewin CR, Andrews B, Valentine JD. Meta-analysis of risk factors for posttraumatic stress disorder in trauma-exposed adults. J Consult Clin Psychol 2000;68:748-66.
5. Ursano RJ, Bell C, Eth S, et al. Work Group on ASD and PTSD. Steering Committee on Practice Guidelines. Practice guideline for the treatment of patients with acute stress disorder and posttraumatic stress disorder. Am J Psychiatry 2004;161(11 suppl):3-31.
6. Kosten TR, Frank JB, Dan E, et al. Pharmacotherapy for posttraumatic stress disorder using phenelzine or imipramine. J Nerv Ment Dis 1991;179:366-70.
7. Davidson J, Kudler H, Smith R, et al. Treatment of posttraumatic stress disorder with amitriptyline and placebo. Arch Gen Psychiatry 1990;47:259-66.
8. Reist C, Kauffmann CD, Haier RJ, et al. A controlled trial of desipramine in 18 men with posttraumatic stress disorder. Am J Psychiatry 1989;146:513-16.
9. Katz RJ, Lott MH, Arbus P, et al. Pharmacotherapy of post-traumatic stress disorder with a novel psychotropic. Anxiety 1994-95;1:169-74.
10. Baker DG, Diamond BI, Gillette GM, et al. A double-blind, randomized, placebo-controlled, multi-center study of brofaromine in the treatment of post-traumatic stress disorder. Psychopharmacology 1995;122:386-9.
11. Raskind MA, Peskind ER, Kanter ED, et al. Reduction of nightmares and other PTSD symptoms in combat veterans by prazosin: a placebo-controlled study. Am J Psychiatry 2003;160:371-3.
12. Kinzie JD, Leung P. Clonidine in Cambodian patients with posttraumatic stress disorder. J Nerv Ment Dis 1989;177:546-50.
History: From sociable to sullen
Julie, a Hispanic/Native American, was adopted by a Caucasian couple when she was 6 weeks old. Before age 12, she had no psychiatric problems and was medically healthy though slightly overweight.
At age 12, Julie started having episodes of brooding depression, verbal and physical aggression, and impulsive suicidal behavior. She also began suffering intermittent migraines and having trouble falling asleep. She insisted on sleeping with her parents or with a nightlight in her room.
Once a sociable girl who enjoyed being in the middle school chorus and band, Julie suddenly became sullen and defiant. She dropped out of afterschool activities and stopped socializing with peers except for her best friend, Sheila, age 12, and Mark, age 13, an “almost boyfriend” who lived next door.
Julie also started arguing with her mother, often yelling and screaming when approached with minor requests. Sometimes, Julie hit and pushed her. A psychiatrist diagnosed the 12-year-old with major depressive disorder and prescribed fluoxetine, dosage unknown.
Soon after Julie’s symptoms surfaced, her adoptive father, a sales representative, was laid off. He found work in another state; the family left an ethnically diverse city for a predominantly Caucasian rural area. There, Julie completed middle school and her freshman year of high school, and lost contact with Sheila and Mark.
Midway through her freshman year, Julie tried to induce vomiting after eating so that she would lose weight and “fit in better with the other girls.” She stopped this at the end of the school year.
The following fall, 5 weeks into her sophomore year, she dropped out of high school and was ultimately enrolled in home school.
Treatment: 4 hospitalizations in 3 years
Between ages 12 and 15, Julie was hospitalized four times for outbursts of violence with impulsive self-harm. She “overdosed” on eight aceta-minophen/diphenhydramine tablets on one occasion and superficially cut her forearm on another. During these episodes, she said, she heard voices telling her to harm her mother and herself.
During this period, Julie was diagnosed as having schizophrenia, major depressive disorder, attention-deficit/hyperactivity disorder (ADHD), and oppositional defiant disorder (ODD). Numerous antidepressant and mood stabilizer regimens produced no lasting improvement, though her angry and violent episodes became less frequent.
poll here
The authors’ observations
Although Julie’s psychotic symptoms might suggest an evolving disorder such as schizophrenia, no clear pattern supports this diagnosis. Also:
- Onset at age 12 is unusual. Schizophrenia typically begins in late teens to early adulthood.
- Julie showed no premorbid personality problems—found in up to one-third of patients with chronic schizophrenia—and no premorbid adjustment difficulties resulting from negative symptoms, cognitive deficits, or poor social function.1
Julie’s birth parents’ mental health history would offer crucial information, but this was not available.
Continued history: ‘I left my body’
Shortly after her 15th birthday, Julie broke down and told her parents that 3 years earlier, four boys had gang-raped her while she was “on a first date” with one of them at a school football game. She said one attacker held a knife to her throat, and they threatened to kill her friend Sheila if anyone was told. Julie said she felt so terrorized that “I left my body and watched what was happening.”
After the rape, Julie went home, showered, and went to bed. She said she felt “emotionally numb” for 2 months, during which she threw herself into schoolwork, stopped attending after-school events, and began arguing with her parents. She developed nightmares of the trauma and, eventually, auditory command hallucinations. When stressed, she has “out of body” feelings lasting several minutes.
The parents, though angry at Julie‘s attackers, did not seek legal counsel or report the rape to authorities because they felt too much time had passed. They sought support from a counselor, who referred their daughter to a male psychiatrist for medication management. Julie, now age 16, preferred to be treated by a woman, so her care was transferred to our clinic.
Based on clinical observations, Julie gets along well with her father. She complains that her mother is overprotective yet Julie cannot bear to be separated from her for even a couple hours. She resents her mother’s overinvolvement but relies on it for emotional regulation. Her mother has been treated for major depressive disorder, generalized anxiety disorder, and alcohol dependence. These were in sustained remission when Julie presented to us.
At presentation, we diagnosed Julie as having chronic posttraumatic stress disorder (PTSD), recurrent major depressive disorder, and eating disorder not otherwise specified. At 5 feet, 7 inches and 190 pounds, her body mass index is 30 kg/m2, indicating clinical obesity. She has been taking duloxetine, 60 mg/d, extended release dextroamphetamine, 20 mg/d, aripiprazole, 20 mg/d, and amitriptyline, 10 mg/d nightly. She also has been taking sumatriptan, 100 mg as needed, for migraines.
poll here
The authors’ observations
After a life-threatening sexual assault, Julie suddenly became irritable and hostile. She could not keep relationships, yet she feared being alone. She impulsively hurt herself, experienced nightmares, and systematically avoided school activities. These behaviors suggest PTSD,1 which is prevalent among sexual assault victims (Box 1). For 3 years, however, psychiatrists kept missing the diagnosis as Julie kept her shame a secret.
Julie tells us that she re-experiences trauma-related dysphoria when exposed to cues, such as the anniversary of the rape. She endorses avoidance symptoms, including feelings of estrangement from her family and friends. She shuns thoughts, feelings, places, and conversations associated with the trauma, which partly explains her refusal to stay in school. She reports arousal symptoms, including difficulty falling and staying asleep and fears of harm if left alone, even during the day. At night she has rituals for checking windows and doors to ensure they are locked.
Julie’s decision to hide her trauma was understandable given her age and developmental phase. For a teenager trying to separate from her parents and fit in at school, the humiliation was overwhelming. She lacked the cognitive tools to process and describe her experience. She was assaulted while on a date, normally a positive rite of passage. Further, as a young Hispanic/Native American, Julie feared disappointing her Caucasian parents by not fitting in at school.
When a previously well-adjusted teenager presents with sudden-onset behavioral problems, ask about past or recent trauma. Watch for contextual, developmental, and sociocultural factors that may prevent the youth from disclosing embarrassing events.
Also question the diagnosis if several adequate medication trials have failed. Check for comorbidities, lack of adherence, or other circumstances that can hamper response to treatment.
The National Comorbidity Survey estimates lifetime prevalence of PTSD at 7.8%.2 Sexual assault victims face a high risk of PTSD among persons exposed to trauma.3,4
Factors that may influence whether trauma exposure progresses to PTSD:
Natural resiliency
Genetic loading
Type of trauma
Whether the trauma is natural or man-made
Past traumas
Psychiatric comorbidities
When a patient presents immediately after a life-threatening trauma:
Ensure physical and psychological safety
Screen for prior traumas that may increase risk of developing PTSD
Refer for physical examination, particularly for victims of rape or physical violence
PTSD checklists can help confirm the diagnosis (see Related resources)
Factors that may signal ptsd
American Psychiatric Association (APA) practice guidelines for treating PTSD list several factors to consider if you suspect this diagnosis:5
Impulsive and episodic aggression can result from an anticipatory bias that increases readiness for “fight, flight, or freeze.” For Julie, this turned previously comfortable interactions into dissonance and conflict.
Self-injurious and suicidal behaviors often occur when trauma creates stigma, shame, or guilt. Julie felt these emotions while trying to establish herself in a new community and school. Her obesity and ethnic background further set her apart from peers. She also left behind friends who provided emotional support outside the home and helped her differentiate from her mother.
Trauma during early adolescence can impair age-appropriate development, making it difficult to develop a stable self-image, consolidate and integrate the personality, and form relationships. At age 16, poor self-image and maladaptive coping strategies were an enduring pattern in Julie’s life.
Psychiatric comorbidities. Many patients with PTSD develop psychiatric comorbidities that exaggerate symptoms, making the disorder more difficult to detect and treat. Julie’s depression increased her avoidance tendencies and rein-forced her isolation. Difficulty concentrating—misdiagnosed as ADHD—deterred her from engaging in school. Dissociative symptoms related to PTSD impaired her reality testing, diminishing her ability to interact with others.
Treatment: Medication change
We continued extended-release dextroamphetamine, 20 mg/d, as Julie felt the medication helped her focus on her schoolwork. We also:
- weaned her off aripiprazole, which was not helping her symptoms
- stopped amitriptyline and duloxetine because of her history of impulsive overdose and to reduce side-effect risk from polypharmacy
- titrated fluoxetine to 40 mg/d to treat her ongoing chronic depression and added trazodone, 50 mg/d as needed, to help her sleep
- stopped sumatriptan, as the headaches remitted after Julie’s eyes were tested and eyeglasses prescribed.
poll here
The authors’ observations
Medication. APA treatment guidelines support using SSRIs to treat all three PTSD symptom clusters—re-experiencing, avoidance, and hyperarousal—as well as coexisting depression. Evidence also supports use of the tricyclics amitriptyline and imipramine and some monoamine oxidase inhibitors (MAOIs).6-10 Dietary restrictions associated with MAOIs, however, can pose a problem for teenagers.
Benzodiazepines can decrease anxiety and improve sleep, but they can be addictive and their efficacy in treating PTSD has not been established. Alpha-2-adrenergic agonists such as prazosin and clonidine may decrease hyperarousal and trauma-related nightmares.11,12
Obtain informed parental consent before starting a child or adolescent on an antidepressant. These medications contain a black-box warning that the drug may increase suicide risk in youths.
Psychotherapy. Varying levels of evidence support psychotherapy models in PTSD (Box 2). Julie can benefit from psychoeducation, supportive therapy, psychodynamic psychotherapy, and cautious re-exposure to trauma where possible.
Psychoeducation provided a safe starting point for Julie’s therapy, engaged her parents and select school counselors and teachers, and helped her understand PTSD’s effects. This allowed us to teach stress reduction and coping strategies.
Supportive techniques helped Julie contain painful affects. She could then network with community resources such as AlaTeen and a peer support group via a local Native American mental health program. This approach helped us gain Julie’s trust, and we anticipate more in-depth work with time.
Trauma re-exposure helps some patients but worsens others’ symptoms. For Julie, trauma re-exposure has been minimal because of the many other issues she was facing.
Developing a trusting relationship over time is crucial to successful trauma re-exposure. Re-exposure should be gradual to keep affective arousal moderate. This will minimize dissociation and affective flooding, which can frustrate treatment.
Cognitive-behavioral therapy (CBT) might help Julie understand the automatic thoughts of failure and defeat that flood her when she is stressed. CBT could help her master her feelings and lay a foundation for improved coping.
Psychodynamic psychotherapy may be started later to help Julie verbalize feelings and modulate how she expresses affect. This model could promote her development, improve her self-image, and treat her depression.
Recommended with substantial clinical confidence (Level I)
Cognitive-behavioral therapy
Psychoeducation
Supportive techniques
Recommended with moderate clinical confidence (Level II)
Exposure techniques
Eye movement desensitization and reprocessing
Imagery rehearsal
Psychodynamic therapy
Stress inoculation
May be recommended in some cases (Level III)
Present-centered group therapy
Trauma-focused group therapy
Not recommended (no evidence)
Psychological debriefings
Single-session techniques
Source: APA practice guideline for PTSD (see Related resources)
Follow-up: Back to school
After 2 months under our care, Julie begins to show improvement. Because of her progress and the fact that her parents drive 45 minutes each way to get to our clinic, we reduce visit frequency from weekly to biweekly.
Julie now attends school 2 hours daily, is earning additional credits through home study, and plans to graduate early and attend community college. Her depression has lifted, and she continues to take fluoxetine, 40 mg/d and extended-release dextroamphetamine, 20 mg/d. She still struggles with social isolation, failure to reach age-appropriate developmental milestones, and a poor body image.
- American Psychiatric Association. Practice guideline for treating acute stress disorder and posttraumatic stress disorder. www.psych.org/psych_pract/treatg/pg/PTSD-PG-PartsA-B-C-New.pdf
- National Center for Post-Traumatic Stress Disorder. Information on obtaining Impact of Events Scale and Davidson Trauma Scale. www.ncptsd.va.gov/publications/assessment/adult_self_report.html
- Amitriptyline • Elavil
- Aripiprazole • Abilify
- Clonidine • Catapres
- Dextroamphetamine (extended-release) • Adderall XR
- Duloxetine • Cymbalta
- Fluoxetine • Prozac
- Imipramine • Tofranil
- Phenelzine • Nardil
- Prazosin • Minipress
- Sumatriptan • Imitrex
- Trazodone • Desyrel
Dr. Matthews is an American Psychiatric Association Bristol-Myers Squibb Co. fellow in public and community psychiatry.
Dr. Mossefin reports no financial relationship with any company whose products are mentioned in this article, or with manufacturers of competing products.
Acknowledgements
The authors thank Larry Schwartz, MD, for his help in preparing this article for publication.
History: From sociable to sullen
Julie, a Hispanic/Native American, was adopted by a Caucasian couple when she was 6 weeks old. Before age 12, she had no psychiatric problems and was medically healthy though slightly overweight.
At age 12, Julie started having episodes of brooding depression, verbal and physical aggression, and impulsive suicidal behavior. She also began suffering intermittent migraines and having trouble falling asleep. She insisted on sleeping with her parents or with a nightlight in her room.
Once a sociable girl who enjoyed being in the middle school chorus and band, Julie suddenly became sullen and defiant. She dropped out of afterschool activities and stopped socializing with peers except for her best friend, Sheila, age 12, and Mark, age 13, an “almost boyfriend” who lived next door.
Julie also started arguing with her mother, often yelling and screaming when approached with minor requests. Sometimes, Julie hit and pushed her. A psychiatrist diagnosed the 12-year-old with major depressive disorder and prescribed fluoxetine, dosage unknown.
Soon after Julie’s symptoms surfaced, her adoptive father, a sales representative, was laid off. He found work in another state; the family left an ethnically diverse city for a predominantly Caucasian rural area. There, Julie completed middle school and her freshman year of high school, and lost contact with Sheila and Mark.
Midway through her freshman year, Julie tried to induce vomiting after eating so that she would lose weight and “fit in better with the other girls.” She stopped this at the end of the school year.
The following fall, 5 weeks into her sophomore year, she dropped out of high school and was ultimately enrolled in home school.
Treatment: 4 hospitalizations in 3 years
Between ages 12 and 15, Julie was hospitalized four times for outbursts of violence with impulsive self-harm. She “overdosed” on eight aceta-minophen/diphenhydramine tablets on one occasion and superficially cut her forearm on another. During these episodes, she said, she heard voices telling her to harm her mother and herself.
During this period, Julie was diagnosed as having schizophrenia, major depressive disorder, attention-deficit/hyperactivity disorder (ADHD), and oppositional defiant disorder (ODD). Numerous antidepressant and mood stabilizer regimens produced no lasting improvement, though her angry and violent episodes became less frequent.
poll here
The authors’ observations
Although Julie’s psychotic symptoms might suggest an evolving disorder such as schizophrenia, no clear pattern supports this diagnosis. Also:
- Onset at age 12 is unusual. Schizophrenia typically begins in late teens to early adulthood.
- Julie showed no premorbid personality problems—found in up to one-third of patients with chronic schizophrenia—and no premorbid adjustment difficulties resulting from negative symptoms, cognitive deficits, or poor social function.1
Julie’s birth parents’ mental health history would offer crucial information, but this was not available.
Continued history: ‘I left my body’
Shortly after her 15th birthday, Julie broke down and told her parents that 3 years earlier, four boys had gang-raped her while she was “on a first date” with one of them at a school football game. She said one attacker held a knife to her throat, and they threatened to kill her friend Sheila if anyone was told. Julie said she felt so terrorized that “I left my body and watched what was happening.”
After the rape, Julie went home, showered, and went to bed. She said she felt “emotionally numb” for 2 months, during which she threw herself into schoolwork, stopped attending after-school events, and began arguing with her parents. She developed nightmares of the trauma and, eventually, auditory command hallucinations. When stressed, she has “out of body” feelings lasting several minutes.
The parents, though angry at Julie‘s attackers, did not seek legal counsel or report the rape to authorities because they felt too much time had passed. They sought support from a counselor, who referred their daughter to a male psychiatrist for medication management. Julie, now age 16, preferred to be treated by a woman, so her care was transferred to our clinic.
Based on clinical observations, Julie gets along well with her father. She complains that her mother is overprotective yet Julie cannot bear to be separated from her for even a couple hours. She resents her mother’s overinvolvement but relies on it for emotional regulation. Her mother has been treated for major depressive disorder, generalized anxiety disorder, and alcohol dependence. These were in sustained remission when Julie presented to us.
At presentation, we diagnosed Julie as having chronic posttraumatic stress disorder (PTSD), recurrent major depressive disorder, and eating disorder not otherwise specified. At 5 feet, 7 inches and 190 pounds, her body mass index is 30 kg/m2, indicating clinical obesity. She has been taking duloxetine, 60 mg/d, extended release dextroamphetamine, 20 mg/d, aripiprazole, 20 mg/d, and amitriptyline, 10 mg/d nightly. She also has been taking sumatriptan, 100 mg as needed, for migraines.
poll here
The authors’ observations
After a life-threatening sexual assault, Julie suddenly became irritable and hostile. She could not keep relationships, yet she feared being alone. She impulsively hurt herself, experienced nightmares, and systematically avoided school activities. These behaviors suggest PTSD,1 which is prevalent among sexual assault victims (Box 1). For 3 years, however, psychiatrists kept missing the diagnosis as Julie kept her shame a secret.
Julie tells us that she re-experiences trauma-related dysphoria when exposed to cues, such as the anniversary of the rape. She endorses avoidance symptoms, including feelings of estrangement from her family and friends. She shuns thoughts, feelings, places, and conversations associated with the trauma, which partly explains her refusal to stay in school. She reports arousal symptoms, including difficulty falling and staying asleep and fears of harm if left alone, even during the day. At night she has rituals for checking windows and doors to ensure they are locked.
Julie’s decision to hide her trauma was understandable given her age and developmental phase. For a teenager trying to separate from her parents and fit in at school, the humiliation was overwhelming. She lacked the cognitive tools to process and describe her experience. She was assaulted while on a date, normally a positive rite of passage. Further, as a young Hispanic/Native American, Julie feared disappointing her Caucasian parents by not fitting in at school.
When a previously well-adjusted teenager presents with sudden-onset behavioral problems, ask about past or recent trauma. Watch for contextual, developmental, and sociocultural factors that may prevent the youth from disclosing embarrassing events.
Also question the diagnosis if several adequate medication trials have failed. Check for comorbidities, lack of adherence, or other circumstances that can hamper response to treatment.
The National Comorbidity Survey estimates lifetime prevalence of PTSD at 7.8%.2 Sexual assault victims face a high risk of PTSD among persons exposed to trauma.3,4
Factors that may influence whether trauma exposure progresses to PTSD:
Natural resiliency
Genetic loading
Type of trauma
Whether the trauma is natural or man-made
Past traumas
Psychiatric comorbidities
When a patient presents immediately after a life-threatening trauma:
Ensure physical and psychological safety
Screen for prior traumas that may increase risk of developing PTSD
Refer for physical examination, particularly for victims of rape or physical violence
PTSD checklists can help confirm the diagnosis (see Related resources)
Factors that may signal ptsd
American Psychiatric Association (APA) practice guidelines for treating PTSD list several factors to consider if you suspect this diagnosis:5
Impulsive and episodic aggression can result from an anticipatory bias that increases readiness for “fight, flight, or freeze.” For Julie, this turned previously comfortable interactions into dissonance and conflict.
Self-injurious and suicidal behaviors often occur when trauma creates stigma, shame, or guilt. Julie felt these emotions while trying to establish herself in a new community and school. Her obesity and ethnic background further set her apart from peers. She also left behind friends who provided emotional support outside the home and helped her differentiate from her mother.
Trauma during early adolescence can impair age-appropriate development, making it difficult to develop a stable self-image, consolidate and integrate the personality, and form relationships. At age 16, poor self-image and maladaptive coping strategies were an enduring pattern in Julie’s life.
Psychiatric comorbidities. Many patients with PTSD develop psychiatric comorbidities that exaggerate symptoms, making the disorder more difficult to detect and treat. Julie’s depression increased her avoidance tendencies and rein-forced her isolation. Difficulty concentrating—misdiagnosed as ADHD—deterred her from engaging in school. Dissociative symptoms related to PTSD impaired her reality testing, diminishing her ability to interact with others.
Treatment: Medication change
We continued extended-release dextroamphetamine, 20 mg/d, as Julie felt the medication helped her focus on her schoolwork. We also:
- weaned her off aripiprazole, which was not helping her symptoms
- stopped amitriptyline and duloxetine because of her history of impulsive overdose and to reduce side-effect risk from polypharmacy
- titrated fluoxetine to 40 mg/d to treat her ongoing chronic depression and added trazodone, 50 mg/d as needed, to help her sleep
- stopped sumatriptan, as the headaches remitted after Julie’s eyes were tested and eyeglasses prescribed.
poll here
The authors’ observations
Medication. APA treatment guidelines support using SSRIs to treat all three PTSD symptom clusters—re-experiencing, avoidance, and hyperarousal—as well as coexisting depression. Evidence also supports use of the tricyclics amitriptyline and imipramine and some monoamine oxidase inhibitors (MAOIs).6-10 Dietary restrictions associated with MAOIs, however, can pose a problem for teenagers.
Benzodiazepines can decrease anxiety and improve sleep, but they can be addictive and their efficacy in treating PTSD has not been established. Alpha-2-adrenergic agonists such as prazosin and clonidine may decrease hyperarousal and trauma-related nightmares.11,12
Obtain informed parental consent before starting a child or adolescent on an antidepressant. These medications contain a black-box warning that the drug may increase suicide risk in youths.
Psychotherapy. Varying levels of evidence support psychotherapy models in PTSD (Box 2). Julie can benefit from psychoeducation, supportive therapy, psychodynamic psychotherapy, and cautious re-exposure to trauma where possible.
Psychoeducation provided a safe starting point for Julie’s therapy, engaged her parents and select school counselors and teachers, and helped her understand PTSD’s effects. This allowed us to teach stress reduction and coping strategies.
Supportive techniques helped Julie contain painful affects. She could then network with community resources such as AlaTeen and a peer support group via a local Native American mental health program. This approach helped us gain Julie’s trust, and we anticipate more in-depth work with time.
Trauma re-exposure helps some patients but worsens others’ symptoms. For Julie, trauma re-exposure has been minimal because of the many other issues she was facing.
Developing a trusting relationship over time is crucial to successful trauma re-exposure. Re-exposure should be gradual to keep affective arousal moderate. This will minimize dissociation and affective flooding, which can frustrate treatment.
Cognitive-behavioral therapy (CBT) might help Julie understand the automatic thoughts of failure and defeat that flood her when she is stressed. CBT could help her master her feelings and lay a foundation for improved coping.
Psychodynamic psychotherapy may be started later to help Julie verbalize feelings and modulate how she expresses affect. This model could promote her development, improve her self-image, and treat her depression.
Recommended with substantial clinical confidence (Level I)
Cognitive-behavioral therapy
Psychoeducation
Supportive techniques
Recommended with moderate clinical confidence (Level II)
Exposure techniques
Eye movement desensitization and reprocessing
Imagery rehearsal
Psychodynamic therapy
Stress inoculation
May be recommended in some cases (Level III)
Present-centered group therapy
Trauma-focused group therapy
Not recommended (no evidence)
Psychological debriefings
Single-session techniques
Source: APA practice guideline for PTSD (see Related resources)
Follow-up: Back to school
After 2 months under our care, Julie begins to show improvement. Because of her progress and the fact that her parents drive 45 minutes each way to get to our clinic, we reduce visit frequency from weekly to biweekly.
Julie now attends school 2 hours daily, is earning additional credits through home study, and plans to graduate early and attend community college. Her depression has lifted, and she continues to take fluoxetine, 40 mg/d and extended-release dextroamphetamine, 20 mg/d. She still struggles with social isolation, failure to reach age-appropriate developmental milestones, and a poor body image.
- American Psychiatric Association. Practice guideline for treating acute stress disorder and posttraumatic stress disorder. www.psych.org/psych_pract/treatg/pg/PTSD-PG-PartsA-B-C-New.pdf
- National Center for Post-Traumatic Stress Disorder. Information on obtaining Impact of Events Scale and Davidson Trauma Scale. www.ncptsd.va.gov/publications/assessment/adult_self_report.html
- Amitriptyline • Elavil
- Aripiprazole • Abilify
- Clonidine • Catapres
- Dextroamphetamine (extended-release) • Adderall XR
- Duloxetine • Cymbalta
- Fluoxetine • Prozac
- Imipramine • Tofranil
- Phenelzine • Nardil
- Prazosin • Minipress
- Sumatriptan • Imitrex
- Trazodone • Desyrel
Dr. Matthews is an American Psychiatric Association Bristol-Myers Squibb Co. fellow in public and community psychiatry.
Dr. Mossefin reports no financial relationship with any company whose products are mentioned in this article, or with manufacturers of competing products.
Acknowledgements
The authors thank Larry Schwartz, MD, for his help in preparing this article for publication.
1. Ho BC, Black DW, Andreasen NC. Schizophrenia and other psychotic disorders. In: Hales RE, Yudofsky SC (eds). Textbook of clinical psychiatry (4th ed). Washington, DC: American Psychiatric Publishing; 2003.
2. Kessler RC, Sonnega A, Bromet E, et al. Posttraumatic stress disorder in the National Comorbidity Survey. Arch Gen Psychiatry 1995;52:1048-60.
3. Breslau N, Kessler RC, Chilcoat HD, et al. Trauma and posttraumatic stress disorder in the community: the 1996 Detroit Area Survey of Trauma. Arch Gen Psychiatry 1998;55:626-32.
4. Brewin CR, Andrews B, Valentine JD. Meta-analysis of risk factors for posttraumatic stress disorder in trauma-exposed adults. J Consult Clin Psychol 2000;68:748-66.
5. Ursano RJ, Bell C, Eth S, et al. Work Group on ASD and PTSD. Steering Committee on Practice Guidelines. Practice guideline for the treatment of patients with acute stress disorder and posttraumatic stress disorder. Am J Psychiatry 2004;161(11 suppl):3-31.
6. Kosten TR, Frank JB, Dan E, et al. Pharmacotherapy for posttraumatic stress disorder using phenelzine or imipramine. J Nerv Ment Dis 1991;179:366-70.
7. Davidson J, Kudler H, Smith R, et al. Treatment of posttraumatic stress disorder with amitriptyline and placebo. Arch Gen Psychiatry 1990;47:259-66.
8. Reist C, Kauffmann CD, Haier RJ, et al. A controlled trial of desipramine in 18 men with posttraumatic stress disorder. Am J Psychiatry 1989;146:513-16.
9. Katz RJ, Lott MH, Arbus P, et al. Pharmacotherapy of post-traumatic stress disorder with a novel psychotropic. Anxiety 1994-95;1:169-74.
10. Baker DG, Diamond BI, Gillette GM, et al. A double-blind, randomized, placebo-controlled, multi-center study of brofaromine in the treatment of post-traumatic stress disorder. Psychopharmacology 1995;122:386-9.
11. Raskind MA, Peskind ER, Kanter ED, et al. Reduction of nightmares and other PTSD symptoms in combat veterans by prazosin: a placebo-controlled study. Am J Psychiatry 2003;160:371-3.
12. Kinzie JD, Leung P. Clonidine in Cambodian patients with posttraumatic stress disorder. J Nerv Ment Dis 1989;177:546-50.
1. Ho BC, Black DW, Andreasen NC. Schizophrenia and other psychotic disorders. In: Hales RE, Yudofsky SC (eds). Textbook of clinical psychiatry (4th ed). Washington, DC: American Psychiatric Publishing; 2003.
2. Kessler RC, Sonnega A, Bromet E, et al. Posttraumatic stress disorder in the National Comorbidity Survey. Arch Gen Psychiatry 1995;52:1048-60.
3. Breslau N, Kessler RC, Chilcoat HD, et al. Trauma and posttraumatic stress disorder in the community: the 1996 Detroit Area Survey of Trauma. Arch Gen Psychiatry 1998;55:626-32.
4. Brewin CR, Andrews B, Valentine JD. Meta-analysis of risk factors for posttraumatic stress disorder in trauma-exposed adults. J Consult Clin Psychol 2000;68:748-66.
5. Ursano RJ, Bell C, Eth S, et al. Work Group on ASD and PTSD. Steering Committee on Practice Guidelines. Practice guideline for the treatment of patients with acute stress disorder and posttraumatic stress disorder. Am J Psychiatry 2004;161(11 suppl):3-31.
6. Kosten TR, Frank JB, Dan E, et al. Pharmacotherapy for posttraumatic stress disorder using phenelzine or imipramine. J Nerv Ment Dis 1991;179:366-70.
7. Davidson J, Kudler H, Smith R, et al. Treatment of posttraumatic stress disorder with amitriptyline and placebo. Arch Gen Psychiatry 1990;47:259-66.
8. Reist C, Kauffmann CD, Haier RJ, et al. A controlled trial of desipramine in 18 men with posttraumatic stress disorder. Am J Psychiatry 1989;146:513-16.
9. Katz RJ, Lott MH, Arbus P, et al. Pharmacotherapy of post-traumatic stress disorder with a novel psychotropic. Anxiety 1994-95;1:169-74.
10. Baker DG, Diamond BI, Gillette GM, et al. A double-blind, randomized, placebo-controlled, multi-center study of brofaromine in the treatment of post-traumatic stress disorder. Psychopharmacology 1995;122:386-9.
11. Raskind MA, Peskind ER, Kanter ED, et al. Reduction of nightmares and other PTSD symptoms in combat veterans by prazosin: a placebo-controlled study. Am J Psychiatry 2003;160:371-3.
12. Kinzie JD, Leung P. Clonidine in Cambodian patients with posttraumatic stress disorder. J Nerv Ment Dis 1989;177:546-50.
CATIE’s surprises: In antipsychotics’ square-off, were there winners or losers?
Investigators faced a dilemma while designing the Clinical Antipsychotic Trials of Intervention Effectiveness (CATIE). More than 200 enrollees with chronic schizophrenia had pre-existing tardive dyskinesia (TD). Would it be ethical to give them the antipsychotic most likely to worsen their TD? Would exempting them from taking that drug influence the trial’s outcome?
This issue and others had to be resolved before the largest controlled study of “real world” schizophrenia could begin. Now that data are unfolding, groups with diverse agendas are debating CATIE’s methods and surprising results. This article describes how the trial’s design and findings could transform public policy and clinical practice.
poll here
Efficacy vs Effectiveness
The National Institute of Mental Health funded the prospective CATIE schizophrenia study to compare the effectiveness of atypical antipsychotics versus each other and versus a first-generation (typical) antipsychotic.
All approved atypicals have shown similar efficacy compared with placebo in short-term trials (usually 6 weeks).1 The CATIE trial’s rationale is that short-term efficacy studies required for FDA approval may not necessarily reflect the drugs’ effectiveness in long-term schizophrenia management. Effectiveness measures take into account efficacy as well as safety, tolerability, and unpredictable patient behaviors in the real world.
CATIE’s ‘Real World’ Patients
CATIE investigators enrolled a community sample of chronic schizophrenia patients similar to those many psychiatrists see. Very liberal inclusion and exclusion criteria (Table 1) allowed enrollees to have a history of substance abuse, comorbid psychiatric or medical disorders, be receiving other medications, or show evidence of TD. Their schizophrenia ranged from minimal to severe.2,3
The 1,493 patients who completed the study (Table 2) were enrolled at 57 outpatient treatment settings. One site’s 33 patients were eliminated from analysis because of doubts about the integrity of the data, leaving a total of 1,460 subjects.4
Table 1
Criteria for enrolling patients in the CATIE schizophrenia trial
| Inclusion criteria | Ages 18 to 65 yrs |
| DSM-IV diagnosis of schizophrenia | |
| Able to take oral medication | |
| Able to give informed consent | |
| Exclusion criteria | Diagnosis of schizoaffective disorder, mental retardation, or other cognitive disorders |
| History of serious adverse reactions to one of the study medications | |
| Had only one schizophrenic episode | |
| History of treatment resistance, defined as persistence of severe symptoms despite adequate trials of one of the study antipsychotics or prior treatment with clozapine | |
| Pregnant or breast feeding | |
| Serious and unstable medical conditions |
Table 2
CATIE’s 1,460 ‘real world’ schizophrenia patients at trial entry
| Mean age | 40.6±11.1 yrs |
| Mean age of first treatment | 24.0±8.9 yrs |
| Mean duration of treatment | 14.4±10.7 yrs |
| Gender | 74% male |
| Race | 60% white, 35% black, 5% other |
| Mean education | 12.1±2.3 years |
| Marital status | 59% never married |
| 29% previously married | |
| 11% married | |
| Employment status | 85% unemployed |
| Mean PANSS total score | 75.7±17.6 |
| Mean CGI | 4.0±0.9 |
| Psychiatric comorbidities | 29% drug dependence/abuse |
| 28% depression | |
| 25% alcohol dependence/abuse | |
| 14% anxiety disorder | |
| 5% obsessive-compulsive disorder | |
| Illness severity | 4% severe |
| 20% marked | |
| 47% moderate | |
| 23% mild | |
| 6% minimal | |
| PANSS: Positive and Negative Syndrome Scale | |
| CGI: Clinician-rated Clinical Global Impressions severity score | |
| Source: Reference 5. | |
Medications. Before randomization, 28% of enrollees were not receiving antipsychotics. The remainder were receiving:
- olanzapine (22%)
- risperidone (19%)
- quetiapine (7%)
- ziprasidone (0%; approved after the trial began)
- any combination of olanzapine, risperidone, and quetiapine (7%)
- typical antipsychotics (16%).
Metabolic profile. These outpatients had a high rate of metabolic disorders: 42%—twice the rate in the general population—met criteria for metabolic syndrome,5 putting them at high risk to die of cardiovascular causes within 10 years.6 They had relatively poor physical health self-ratings and increased somatic preoccupation.7 Most worrisome, many were receiving no medications for their metabolic disorders, including 45% of those with diabetes, 89% with hyperlipidemia, and 62% with hypertension.8
Substance abuse. At enrollment, 40% of patients were abstinent from substance use, 22% were using substances without abuse or dependence, and 37% had substance abuse or dependence. Compared with nonusers, substance abusers tended to be male with more childhood problems, higher positive symptoms on the Positive and Negative Syndrome Scale (PANSS), and more likely to have had a recent illness exacerbation.9
Tardive dyskinesia. The 231 subjects who met criteria for probable TD10 were older than the overall sample with more years of antipsychotic treatment, especially with conventional neuroleptics and anticholinergics. Substance abuse was associated with TD, as were severity of psychopathology, extrapyramidal symptoms (EPS), and akathisia.11
Violent behavior. A history of serious violent behavior was reported in:
- 5.4% of patients with high positive and low negative PANSS symptom scores
- 1.7% of patients with low positive and high negative PANSS symptom scores.
Consent. Patients’ capacity to give consent to participate in the study was assessed with the MacArthur Competence Assessment Tool for Clinical Research (MacCAT-CR). Psychosis severity (PANSS positive symptom scale) was not found to affect decision-making capacity, but negative symptoms and diminished working memory did.12
CATIE’s Unique Design
Defining effectiveness. CATIE was designed in three phases (Figure). Phase 1—discussed here—was a blinded, controlled comparison of four atypical antipsychotics and perphenazine. Results of phases 2 and 3 have yet to be published. The primary effectiveness endpoint, “all-cause discontinuation,” was defined as:
- lack of efficacy (patient was switched to another drug assigned at random)
- lack of tolerability (patient requested a drug change)
- safety problem (investigator initiated a switch)
- patient’s decision for any reason (often dropping out of the study).
The longer subjects stayed on the first antipsychotic they received, the more effective that drug was considered to be.
Figure CATIE schizophrenia trial design
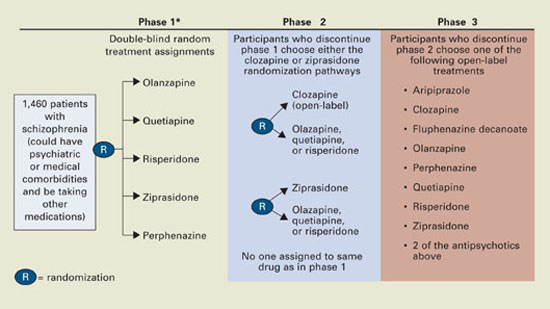
* Phase 1A: participants with tardive dyskinesia (N=231) do not get randomized to perphenazine; phase 1B: participants who fail perphenazine will be randomized to an atypical (olanzapine, quetiapine, or risperidone) before eligibility for phase 2.
Source: Reference 2.Medications. Three atypicals—risperidone, olanzapine, and quetiapine—were approved for schizophrenia when the trial began in 1999. Recruitment ended in June 2003, the last subject completed the 18-month trial in December 2004, and data analysis began in January 2005. Ziprasidone was added to phase 1 after 40% of the sample had been enrolled, and aripiprazole was included as an option in the unblinded phase 3.
Perphenazine was chosen to represent typical antipsychotics because it has medium potency and less risk of EPS than high-potency drugs such as haloperidol and is associated with less weight gain than low-potency drugs such as thioridazine.
Dosing. Pharmaceutical manufacturers donated the antipsychotics and were invited to recommend their respective drugs’ starting dosages, dose increments, and maximum dosages. Olanzapine’s maker requested a higher starting dosage (7.5 mg/d instead of 5.0 mg/d) and a maximum dosage 50% higher than the FDA-approved range (30 mg/d instead of 20 mg/d). The others recommended the FDA-approved dosage ranges or less:
- quetiapine, 200 to 800 mg/d
- risperidone, 1.5 to 6 mg/d
- ziprasidone, 40 to 160 mg/d
- perphenazine, 8 to 32 mg/d.
The study team accepted their recommendations.
The medications were packaged in identical capsules. Quetiapine and ziprasidone were given twice daily because of product labeling; risperidone, olanzapine, and perphenazine were given once daily to one-half the patients assigned to them and twice daily to the others to prevent raters from guessing which drug a patient was receiving.
Tardive dyskinesia. For ethical reasons, the 231 patients with TD at enrollment were randomly assigned in phase 1 to atypicals but not to perphenazine because of the well-established link between typical antipsychotics and TD. This exception could have contributed to the closer-than-expected differences in EPS and perhaps in efficacy, given reports that TD patients have more negative symptoms and cognitive dysfunction.13 However, a statistical analysis took that into account.
CATIE’s Key Findings
Discontinuation. A disappointingly high discontinuation rate (74% overall) within a few months was the most important finding (Table 3). A recent effectiveness study with a design similar to the CATIE trial found a similarly high rate of all-cause discontinuation (70%) in patients with first-episode psychosis.14 Thus, patient-initiated drug discontinuation appears to be a core illness behavior from schizophrenia onset to chronic illness.
The high discontinuation rate shows that we need to modify our approach to schizophrenia, emphasizing full adherence to antipsychotic therapy from the onset of the illness.
Table 3
All-cause discontinuation rates in the CATIE trial
| Antipsychotic | Percent discontinued | Duration on antipsychotic (months)* | Dosage (mg/d)* |
| Olanzapine | 64% | 9.2 | 20.1 |
| Perphenazine | 75% | 4.6 | 20.8 |
| Quetiapine | 82% | 4.8 | 543.4 |
| Risperidone | 74% | 5.6 | 3.9 |
| Ziprasidone | 79% | 3.5 | 112.8 |
| Overall | 74% | Median 6.0; mean 8.3 | |
| Notes | |||
| *Mean modal | |||
| Olanzapine’s discontinuation rate was significantly lower than those of perphenazine, quetiapine, and risperidone but not of ziprasidone. | |||
| Olanzapine’s maximum dosage was 30 mg/d (50% higher than FDA-approved 20 mg/d); other agents were dosed within approved ranges. | |||
| Patients reached maximum daily antipsychotic dosages at these rates: 40% with olanzapine, 40% with perphenazine, 44% with quetiapine, 40% with risperidone, and 48% with ziprasidone. | |||
Effectiveness—measured as all-cause discontinuation or switching—was the primary outcome of phase 1. The unexpected finding that perphenazine and the atypicals had similar effectiveness could influence clinical practice. Insurers, for example, might consider promoting cheaper typical antipsychotics for first-line use. CATIE’s cost-effectiveness arm (Rosenheck et al, submitted for publication) will provide additional data on this issue.
Before rushing to use older antipsychotics as first-line treatments for schizophrenia, however, policymakers should consider three factors in the study design that could have enhanced perphenazine’s efficacy and safety profiles.
First, perphenazine was given at lower dosages (up to 32 mg/d) than “real world” clinicians used a decade ago (up to 64 mg/d). Thus, lower rates of serious side effects, especially TD, might have occurred in the study than in past clinical practice. Since atypical antipsychotics were approved, clinicians see far fewer psychiatric patients with pill-rolling tremors, rigid posture, or a shuffling gait, compared with 10 to 15 years ago when typical antipsychotics were widely used.
Second, perphenazine was associated with the highest EPS rate (17%), though its mean modal dosage (20.8 mg/d) is considered moderate. Discontinuation because of EPS was highest with perphenazine and lowest with quetiapine.
Third, excluding enrollees with TD from perphenazine may have increased perphenazine’s effectiveness, whereas including them in the atypicals groups may have reduced the atypicals’ effectiveness. TD patients are at increased risk to develop EPS; they had more-severe illness and a higher substance abuse rate among CATIE patients.11 Even so, investigators did control for TD in the data analysis and found no significant difference between typical and atypical antipsychotics.
No ‘Winners’ or ‘Losers’
Effectiveness, tolerability, and safety findings for each antipsychotic are compared in Tables 4A and 4B. Careful review shows no clear “winners” or “losers;” each agent has weaknesses but also strengths that may benefit individual patients.
Efficacy. Olanzapine showed a relatively higher efficacy and lower discontinuation rate but also had the highest risk of adverse metabolic effects. Some have attributed its greater efficacy to its higher dosing compared with the other antipsychotics. Some also have argued that the antipsychotics that showed lower efficacy, such as quetiapine and ziprasidone, were underdosed in this chronic schizophrenia population with a mean duration of illness of 14 years. Perphenazine, too, was dosed at the lower end of its range (mean modal dose 20.8 mg/d) compared with the old community standard of 36 to 64 mg/d.
Generally, a mean modal dosage of 20.1 mg/d for olanzapine is considered equivalent to ziprasidone, 160 mg; quetiapine, 800 mg; and risperidone, 6 mg. In CATIE phase 1, mean modal dosages were:
- ziprasidone, 112.8 mg/d (30% below 160 mg)
- quetiapine, 543.4 mg/d (32% below 800)
- risperidone, 3.9 mg/d (35% below 6 mg).
Olanzapine’s starting dosage of 7.5 mg/d was relatively higher than those of the other atypicals, which may have produced more-rapid onset of efficacy.
Switching. Another potential “advantage” for olanzapine was that 22% of subjects were taking it when they enrolled. By random assignment, 23% of patients who were taking olanzapine stayed on olanzapine and did not switch. By comparison:
- No patients assigned to ziprasidone were taking it before entering the trial.
- Only 5% of those taking quetiapine stayed on that drug after randomization.
- Few were receiving perphenazine before enrollment.
Switching antipsychotics may increase side effect risk or efficacy problems. For example, a patient switched from olanzapine or quetiapine to ziprasidone or perphenazine may experience insomnia during the transition, which may lead to tolerability complaints.
Metabolic side effects seen in this trial support past observations and reports that olanzapine is associated with higher risk for weight gain, hyperglycemia, and hyperlipidemia than other antipsychotics.15 Data on metabolic changes in CATIE patients taking olanzapine are being analyzed.
Hyperprolactinemia was most common with risperidone and practically nonexistent with other antipsychotics—even perphenazine. On the other hand, risperidone had the most favorable tolerability profile. This implies that elevated prolactin does not necessarily lead to antipsychotic discontinuation because of tolerability among patients with schizophrenia.
QTC interval and cataract data were benign across all antipsychotics. These findings appear to exonerate ziprasidone and quetiapine, respectively, which have been perceived as associated with these side effects.
When data become available, the next article in this series will discuss CATIE phase 2 findings. This phase includes patients who did not improve with the phase 1 regimens because of efficacy or tolerability problems and were switched to other antipsychotic therapies.
Related resources
- Clinical Antipsychotic Trials of Intervention Effectiveness (CATIE) schizophrenia study. www.catie.unc.edu/schizophrenia
- Schizophrenia Research Forum. NARSAD, The Mental Health Research Association.www.schizophreniaforum.org
Drug brand names
- Aripiprazole • Abilify
- Olanzapine • Zyprexa
- Perphenazine • Trilafon
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Ziprasidone • Geodon
Disclosures
Dr Nasrallah receives grants/research support from AstraZeneca, Janssen Pharmaceutica, Eli Lilly & Co., and Pfizer. He is a consultant, advisory board member, and speaker for Abbott Laboratories, AstraZeneca, Janssen Pharmaceutica, Pfizer, and Shire Pharmaceuticals Group.
1. Tandon R, Jibson MD. Efficacy of newer generation antipsychotics in the treatment of schizophrenia. Psychoneuroendocrinol 2003;28(suppl 1):9-26.
2. Stroup TS, McEvoy JP, Swartz MS, et al. The National Institute of Mental Health Clinical Antipsychotic Trial of Intervention Effectiveness (CATIE). Project: schizophrenia trial design and protocol development. Schizophr Bull 2003;29:15-31.
3. Swartz MS, Perkins DO, Stroup TS, et al. Assessing clinical and functional outcomes in the Clinical Antipsychotic Trials of Intervention Effectiveness (CATIE) schizophrenia trial. Schizophr Bull 2003;29:33-43.
4. Lieberman JA, Stroup TS, McEvoy JP, et al. Effectiveness of antipsychotic drugs in patients with chronic schizophrenia. N Engl J Med 2005;353:1209-23.
5. McEvoy JP, Meyer JM, Goff DC, et al. Prevalence of the metabolic syndrome in patients with schizophrenia: baseline results from the CATIE schizophrenia trial and comparison with national estimates from NHANES III. Schizophr Res 2005;80:19-32.
6. Goff D, Sullivan LM, McEvoy JP, et al. A comparison of ten-year cardiac risk estimates in schizophrenia patients from the CATIE study and matched controls. Schizophr Res 2005;80:45-53.
7. Meyer JM, Nasrallah HA, McEvoy JP, et al. The Clinical Antipsychotic Trial of Intervention Effectiveness (CATIE) schizophrenia trial: clinical comparison of subgroups with and without the metabolic syndrome. Schizophr Res 2005;80:9-18.
8. Nasrallah HA, McEvoy JP, Meyer JM, et al. Low rates of treatment for metabolic disorders in the CATIE schizophrenia trial. Neuropsychopharmacol 2005;(suppl 1):204.-
9. Swartz MS, et al. (unpublished data).
10. Schooler NR, Kane JM. Research diagnosis for tardive dyskinesia. Arch Gen Psychiatry 1982;39:486-7.
11. Miller DD, McEvoy JP, Davis SM, et al. Clinical correlates of tardive dyskinesia in schizophrenia: baseline data from the CATIE schizophrenia trial. Schizophr Res 2005;80:33-43.
12. Stroup TS, Applebaum P, Swartz M, et al. Decision-making capacity for research participation among individuals in the CATIE schizophrenia trial. Schizophr Res 2005;80:1-8.
13. Waddington JL, Youssef HA, Dolphin C, et al. Cognitive function, negative symptoms and tardive dyskinesia in schizophrenia. Their association in relation to topography of involuntary movements and criterion of their abnormality. Arch Gen Psychiatry 1987;44:907-12.
14. Keefe R. The CAFÉ effectiveness study. Amsterdam: European College of Neuropsychopharmacology annual meeting, 2005;
15. American Diabetes Association, American Psychiatric Association, American Association of Clinical Endocrinologists, and North American Association for the Study of Obesity. Consensus development conference on antipsychotic drugs, obesity, and diabetes. Diabetes Care 2004;27:596-601.
Investigators faced a dilemma while designing the Clinical Antipsychotic Trials of Intervention Effectiveness (CATIE). More than 200 enrollees with chronic schizophrenia had pre-existing tardive dyskinesia (TD). Would it be ethical to give them the antipsychotic most likely to worsen their TD? Would exempting them from taking that drug influence the trial’s outcome?
This issue and others had to be resolved before the largest controlled study of “real world” schizophrenia could begin. Now that data are unfolding, groups with diverse agendas are debating CATIE’s methods and surprising results. This article describes how the trial’s design and findings could transform public policy and clinical practice.
poll here
Efficacy vs Effectiveness
The National Institute of Mental Health funded the prospective CATIE schizophrenia study to compare the effectiveness of atypical antipsychotics versus each other and versus a first-generation (typical) antipsychotic.
All approved atypicals have shown similar efficacy compared with placebo in short-term trials (usually 6 weeks).1 The CATIE trial’s rationale is that short-term efficacy studies required for FDA approval may not necessarily reflect the drugs’ effectiveness in long-term schizophrenia management. Effectiveness measures take into account efficacy as well as safety, tolerability, and unpredictable patient behaviors in the real world.
CATIE’s ‘Real World’ Patients
CATIE investigators enrolled a community sample of chronic schizophrenia patients similar to those many psychiatrists see. Very liberal inclusion and exclusion criteria (Table 1) allowed enrollees to have a history of substance abuse, comorbid psychiatric or medical disorders, be receiving other medications, or show evidence of TD. Their schizophrenia ranged from minimal to severe.2,3
The 1,493 patients who completed the study (Table 2) were enrolled at 57 outpatient treatment settings. One site’s 33 patients were eliminated from analysis because of doubts about the integrity of the data, leaving a total of 1,460 subjects.4
Table 1
Criteria for enrolling patients in the CATIE schizophrenia trial
| Inclusion criteria | Ages 18 to 65 yrs |
| DSM-IV diagnosis of schizophrenia | |
| Able to take oral medication | |
| Able to give informed consent | |
| Exclusion criteria | Diagnosis of schizoaffective disorder, mental retardation, or other cognitive disorders |
| History of serious adverse reactions to one of the study medications | |
| Had only one schizophrenic episode | |
| History of treatment resistance, defined as persistence of severe symptoms despite adequate trials of one of the study antipsychotics or prior treatment with clozapine | |
| Pregnant or breast feeding | |
| Serious and unstable medical conditions |
Table 2
CATIE’s 1,460 ‘real world’ schizophrenia patients at trial entry
| Mean age | 40.6±11.1 yrs |
| Mean age of first treatment | 24.0±8.9 yrs |
| Mean duration of treatment | 14.4±10.7 yrs |
| Gender | 74% male |
| Race | 60% white, 35% black, 5% other |
| Mean education | 12.1±2.3 years |
| Marital status | 59% never married |
| 29% previously married | |
| 11% married | |
| Employment status | 85% unemployed |
| Mean PANSS total score | 75.7±17.6 |
| Mean CGI | 4.0±0.9 |
| Psychiatric comorbidities | 29% drug dependence/abuse |
| 28% depression | |
| 25% alcohol dependence/abuse | |
| 14% anxiety disorder | |
| 5% obsessive-compulsive disorder | |
| Illness severity | 4% severe |
| 20% marked | |
| 47% moderate | |
| 23% mild | |
| 6% minimal | |
| PANSS: Positive and Negative Syndrome Scale | |
| CGI: Clinician-rated Clinical Global Impressions severity score | |
| Source: Reference 5. | |
Medications. Before randomization, 28% of enrollees were not receiving antipsychotics. The remainder were receiving:
- olanzapine (22%)
- risperidone (19%)
- quetiapine (7%)
- ziprasidone (0%; approved after the trial began)
- any combination of olanzapine, risperidone, and quetiapine (7%)
- typical antipsychotics (16%).
Metabolic profile. These outpatients had a high rate of metabolic disorders: 42%—twice the rate in the general population—met criteria for metabolic syndrome,5 putting them at high risk to die of cardiovascular causes within 10 years.6 They had relatively poor physical health self-ratings and increased somatic preoccupation.7 Most worrisome, many were receiving no medications for their metabolic disorders, including 45% of those with diabetes, 89% with hyperlipidemia, and 62% with hypertension.8
Substance abuse. At enrollment, 40% of patients were abstinent from substance use, 22% were using substances without abuse or dependence, and 37% had substance abuse or dependence. Compared with nonusers, substance abusers tended to be male with more childhood problems, higher positive symptoms on the Positive and Negative Syndrome Scale (PANSS), and more likely to have had a recent illness exacerbation.9
Tardive dyskinesia. The 231 subjects who met criteria for probable TD10 were older than the overall sample with more years of antipsychotic treatment, especially with conventional neuroleptics and anticholinergics. Substance abuse was associated with TD, as were severity of psychopathology, extrapyramidal symptoms (EPS), and akathisia.11
Violent behavior. A history of serious violent behavior was reported in:
- 5.4% of patients with high positive and low negative PANSS symptom scores
- 1.7% of patients with low positive and high negative PANSS symptom scores.
Consent. Patients’ capacity to give consent to participate in the study was assessed with the MacArthur Competence Assessment Tool for Clinical Research (MacCAT-CR). Psychosis severity (PANSS positive symptom scale) was not found to affect decision-making capacity, but negative symptoms and diminished working memory did.12
CATIE’s Unique Design
Defining effectiveness. CATIE was designed in three phases (Figure). Phase 1—discussed here—was a blinded, controlled comparison of four atypical antipsychotics and perphenazine. Results of phases 2 and 3 have yet to be published. The primary effectiveness endpoint, “all-cause discontinuation,” was defined as:
- lack of efficacy (patient was switched to another drug assigned at random)
- lack of tolerability (patient requested a drug change)
- safety problem (investigator initiated a switch)
- patient’s decision for any reason (often dropping out of the study).
The longer subjects stayed on the first antipsychotic they received, the more effective that drug was considered to be.
Figure CATIE schizophrenia trial design
* Phase 1A: participants with tardive dyskinesia (N=231) do not get randomized to perphenazine; phase 1B: participants who fail perphenazine will be randomized to an atypical (olanzapine, quetiapine, or risperidone) before eligibility for phase 2.
Source: Reference 2.Medications. Three atypicals—risperidone, olanzapine, and quetiapine—were approved for schizophrenia when the trial began in 1999. Recruitment ended in June 2003, the last subject completed the 18-month trial in December 2004, and data analysis began in January 2005. Ziprasidone was added to phase 1 after 40% of the sample had been enrolled, and aripiprazole was included as an option in the unblinded phase 3.
Perphenazine was chosen to represent typical antipsychotics because it has medium potency and less risk of EPS than high-potency drugs such as haloperidol and is associated with less weight gain than low-potency drugs such as thioridazine.
Dosing. Pharmaceutical manufacturers donated the antipsychotics and were invited to recommend their respective drugs’ starting dosages, dose increments, and maximum dosages. Olanzapine’s maker requested a higher starting dosage (7.5 mg/d instead of 5.0 mg/d) and a maximum dosage 50% higher than the FDA-approved range (30 mg/d instead of 20 mg/d). The others recommended the FDA-approved dosage ranges or less:
- quetiapine, 200 to 800 mg/d
- risperidone, 1.5 to 6 mg/d
- ziprasidone, 40 to 160 mg/d
- perphenazine, 8 to 32 mg/d.
The study team accepted their recommendations.
The medications were packaged in identical capsules. Quetiapine and ziprasidone were given twice daily because of product labeling; risperidone, olanzapine, and perphenazine were given once daily to one-half the patients assigned to them and twice daily to the others to prevent raters from guessing which drug a patient was receiving.
Tardive dyskinesia. For ethical reasons, the 231 patients with TD at enrollment were randomly assigned in phase 1 to atypicals but not to perphenazine because of the well-established link between typical antipsychotics and TD. This exception could have contributed to the closer-than-expected differences in EPS and perhaps in efficacy, given reports that TD patients have more negative symptoms and cognitive dysfunction.13 However, a statistical analysis took that into account.
CATIE’s Key Findings
Discontinuation. A disappointingly high discontinuation rate (74% overall) within a few months was the most important finding (Table 3). A recent effectiveness study with a design similar to the CATIE trial found a similarly high rate of all-cause discontinuation (70%) in patients with first-episode psychosis.14 Thus, patient-initiated drug discontinuation appears to be a core illness behavior from schizophrenia onset to chronic illness.
The high discontinuation rate shows that we need to modify our approach to schizophrenia, emphasizing full adherence to antipsychotic therapy from the onset of the illness.
Table 3
All-cause discontinuation rates in the CATIE trial
| Antipsychotic | Percent discontinued | Duration on antipsychotic (months)* | Dosage (mg/d)* |
| Olanzapine | 64% | 9.2 | 20.1 |
| Perphenazine | 75% | 4.6 | 20.8 |
| Quetiapine | 82% | 4.8 | 543.4 |
| Risperidone | 74% | 5.6 | 3.9 |
| Ziprasidone | 79% | 3.5 | 112.8 |
| Overall | 74% | Median 6.0; mean 8.3 | |
| Notes | |||
| *Mean modal | |||
| Olanzapine’s discontinuation rate was significantly lower than those of perphenazine, quetiapine, and risperidone but not of ziprasidone. | |||
| Olanzapine’s maximum dosage was 30 mg/d (50% higher than FDA-approved 20 mg/d); other agents were dosed within approved ranges. | |||
| Patients reached maximum daily antipsychotic dosages at these rates: 40% with olanzapine, 40% with perphenazine, 44% with quetiapine, 40% with risperidone, and 48% with ziprasidone. | |||
Effectiveness—measured as all-cause discontinuation or switching—was the primary outcome of phase 1. The unexpected finding that perphenazine and the atypicals had similar effectiveness could influence clinical practice. Insurers, for example, might consider promoting cheaper typical antipsychotics for first-line use. CATIE’s cost-effectiveness arm (Rosenheck et al, submitted for publication) will provide additional data on this issue.
Before rushing to use older antipsychotics as first-line treatments for schizophrenia, however, policymakers should consider three factors in the study design that could have enhanced perphenazine’s efficacy and safety profiles.
First, perphenazine was given at lower dosages (up to 32 mg/d) than “real world” clinicians used a decade ago (up to 64 mg/d). Thus, lower rates of serious side effects, especially TD, might have occurred in the study than in past clinical practice. Since atypical antipsychotics were approved, clinicians see far fewer psychiatric patients with pill-rolling tremors, rigid posture, or a shuffling gait, compared with 10 to 15 years ago when typical antipsychotics were widely used.
Second, perphenazine was associated with the highest EPS rate (17%), though its mean modal dosage (20.8 mg/d) is considered moderate. Discontinuation because of EPS was highest with perphenazine and lowest with quetiapine.
Third, excluding enrollees with TD from perphenazine may have increased perphenazine’s effectiveness, whereas including them in the atypicals groups may have reduced the atypicals’ effectiveness. TD patients are at increased risk to develop EPS; they had more-severe illness and a higher substance abuse rate among CATIE patients.11 Even so, investigators did control for TD in the data analysis and found no significant difference between typical and atypical antipsychotics.
No ‘Winners’ or ‘Losers’
Effectiveness, tolerability, and safety findings for each antipsychotic are compared in Tables 4A and 4B. Careful review shows no clear “winners” or “losers;” each agent has weaknesses but also strengths that may benefit individual patients.
Efficacy. Olanzapine showed a relatively higher efficacy and lower discontinuation rate but also had the highest risk of adverse metabolic effects. Some have attributed its greater efficacy to its higher dosing compared with the other antipsychotics. Some also have argued that the antipsychotics that showed lower efficacy, such as quetiapine and ziprasidone, were underdosed in this chronic schizophrenia population with a mean duration of illness of 14 years. Perphenazine, too, was dosed at the lower end of its range (mean modal dose 20.8 mg/d) compared with the old community standard of 36 to 64 mg/d.
Generally, a mean modal dosage of 20.1 mg/d for olanzapine is considered equivalent to ziprasidone, 160 mg; quetiapine, 800 mg; and risperidone, 6 mg. In CATIE phase 1, mean modal dosages were:
- ziprasidone, 112.8 mg/d (30% below 160 mg)
- quetiapine, 543.4 mg/d (32% below 800)
- risperidone, 3.9 mg/d (35% below 6 mg).
Olanzapine’s starting dosage of 7.5 mg/d was relatively higher than those of the other atypicals, which may have produced more-rapid onset of efficacy.
Switching. Another potential “advantage” for olanzapine was that 22% of subjects were taking it when they enrolled. By random assignment, 23% of patients who were taking olanzapine stayed on olanzapine and did not switch. By comparison:
- No patients assigned to ziprasidone were taking it before entering the trial.
- Only 5% of those taking quetiapine stayed on that drug after randomization.
- Few were receiving perphenazine before enrollment.
Switching antipsychotics may increase side effect risk or efficacy problems. For example, a patient switched from olanzapine or quetiapine to ziprasidone or perphenazine may experience insomnia during the transition, which may lead to tolerability complaints.
Metabolic side effects seen in this trial support past observations and reports that olanzapine is associated with higher risk for weight gain, hyperglycemia, and hyperlipidemia than other antipsychotics.15 Data on metabolic changes in CATIE patients taking olanzapine are being analyzed.
Hyperprolactinemia was most common with risperidone and practically nonexistent with other antipsychotics—even perphenazine. On the other hand, risperidone had the most favorable tolerability profile. This implies that elevated prolactin does not necessarily lead to antipsychotic discontinuation because of tolerability among patients with schizophrenia.
QTC interval and cataract data were benign across all antipsychotics. These findings appear to exonerate ziprasidone and quetiapine, respectively, which have been perceived as associated with these side effects.
When data become available, the next article in this series will discuss CATIE phase 2 findings. This phase includes patients who did not improve with the phase 1 regimens because of efficacy or tolerability problems and were switched to other antipsychotic therapies.
Related resources
- Clinical Antipsychotic Trials of Intervention Effectiveness (CATIE) schizophrenia study. www.catie.unc.edu/schizophrenia
- Schizophrenia Research Forum. NARSAD, The Mental Health Research Association.www.schizophreniaforum.org
Drug brand names
- Aripiprazole • Abilify
- Olanzapine • Zyprexa
- Perphenazine • Trilafon
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Ziprasidone • Geodon
Disclosures
Dr Nasrallah receives grants/research support from AstraZeneca, Janssen Pharmaceutica, Eli Lilly & Co., and Pfizer. He is a consultant, advisory board member, and speaker for Abbott Laboratories, AstraZeneca, Janssen Pharmaceutica, Pfizer, and Shire Pharmaceuticals Group.
Investigators faced a dilemma while designing the Clinical Antipsychotic Trials of Intervention Effectiveness (CATIE). More than 200 enrollees with chronic schizophrenia had pre-existing tardive dyskinesia (TD). Would it be ethical to give them the antipsychotic most likely to worsen their TD? Would exempting them from taking that drug influence the trial’s outcome?
This issue and others had to be resolved before the largest controlled study of “real world” schizophrenia could begin. Now that data are unfolding, groups with diverse agendas are debating CATIE’s methods and surprising results. This article describes how the trial’s design and findings could transform public policy and clinical practice.
poll here
Efficacy vs Effectiveness
The National Institute of Mental Health funded the prospective CATIE schizophrenia study to compare the effectiveness of atypical antipsychotics versus each other and versus a first-generation (typical) antipsychotic.
All approved atypicals have shown similar efficacy compared with placebo in short-term trials (usually 6 weeks).1 The CATIE trial’s rationale is that short-term efficacy studies required for FDA approval may not necessarily reflect the drugs’ effectiveness in long-term schizophrenia management. Effectiveness measures take into account efficacy as well as safety, tolerability, and unpredictable patient behaviors in the real world.
CATIE’s ‘Real World’ Patients
CATIE investigators enrolled a community sample of chronic schizophrenia patients similar to those many psychiatrists see. Very liberal inclusion and exclusion criteria (Table 1) allowed enrollees to have a history of substance abuse, comorbid psychiatric or medical disorders, be receiving other medications, or show evidence of TD. Their schizophrenia ranged from minimal to severe.2,3
The 1,493 patients who completed the study (Table 2) were enrolled at 57 outpatient treatment settings. One site’s 33 patients were eliminated from analysis because of doubts about the integrity of the data, leaving a total of 1,460 subjects.4
Table 1
Criteria for enrolling patients in the CATIE schizophrenia trial
| Inclusion criteria | Ages 18 to 65 yrs |
| DSM-IV diagnosis of schizophrenia | |
| Able to take oral medication | |
| Able to give informed consent | |
| Exclusion criteria | Diagnosis of schizoaffective disorder, mental retardation, or other cognitive disorders |
| History of serious adverse reactions to one of the study medications | |
| Had only one schizophrenic episode | |
| History of treatment resistance, defined as persistence of severe symptoms despite adequate trials of one of the study antipsychotics or prior treatment with clozapine | |
| Pregnant or breast feeding | |
| Serious and unstable medical conditions |
Table 2
CATIE’s 1,460 ‘real world’ schizophrenia patients at trial entry
| Mean age | 40.6±11.1 yrs |
| Mean age of first treatment | 24.0±8.9 yrs |
| Mean duration of treatment | 14.4±10.7 yrs |
| Gender | 74% male |
| Race | 60% white, 35% black, 5% other |
| Mean education | 12.1±2.3 years |
| Marital status | 59% never married |
| 29% previously married | |
| 11% married | |
| Employment status | 85% unemployed |
| Mean PANSS total score | 75.7±17.6 |
| Mean CGI | 4.0±0.9 |
| Psychiatric comorbidities | 29% drug dependence/abuse |
| 28% depression | |
| 25% alcohol dependence/abuse | |
| 14% anxiety disorder | |
| 5% obsessive-compulsive disorder | |
| Illness severity | 4% severe |
| 20% marked | |
| 47% moderate | |
| 23% mild | |
| 6% minimal | |
| PANSS: Positive and Negative Syndrome Scale | |
| CGI: Clinician-rated Clinical Global Impressions severity score | |
| Source: Reference 5. | |
Medications. Before randomization, 28% of enrollees were not receiving antipsychotics. The remainder were receiving:
- olanzapine (22%)
- risperidone (19%)
- quetiapine (7%)
- ziprasidone (0%; approved after the trial began)
- any combination of olanzapine, risperidone, and quetiapine (7%)
- typical antipsychotics (16%).
Metabolic profile. These outpatients had a high rate of metabolic disorders: 42%—twice the rate in the general population—met criteria for metabolic syndrome,5 putting them at high risk to die of cardiovascular causes within 10 years.6 They had relatively poor physical health self-ratings and increased somatic preoccupation.7 Most worrisome, many were receiving no medications for their metabolic disorders, including 45% of those with diabetes, 89% with hyperlipidemia, and 62% with hypertension.8
Substance abuse. At enrollment, 40% of patients were abstinent from substance use, 22% were using substances without abuse or dependence, and 37% had substance abuse or dependence. Compared with nonusers, substance abusers tended to be male with more childhood problems, higher positive symptoms on the Positive and Negative Syndrome Scale (PANSS), and more likely to have had a recent illness exacerbation.9
Tardive dyskinesia. The 231 subjects who met criteria for probable TD10 were older than the overall sample with more years of antipsychotic treatment, especially with conventional neuroleptics and anticholinergics. Substance abuse was associated with TD, as were severity of psychopathology, extrapyramidal symptoms (EPS), and akathisia.11
Violent behavior. A history of serious violent behavior was reported in:
- 5.4% of patients with high positive and low negative PANSS symptom scores
- 1.7% of patients with low positive and high negative PANSS symptom scores.
Consent. Patients’ capacity to give consent to participate in the study was assessed with the MacArthur Competence Assessment Tool for Clinical Research (MacCAT-CR). Psychosis severity (PANSS positive symptom scale) was not found to affect decision-making capacity, but negative symptoms and diminished working memory did.12
CATIE’s Unique Design
Defining effectiveness. CATIE was designed in three phases (Figure). Phase 1—discussed here—was a blinded, controlled comparison of four atypical antipsychotics and perphenazine. Results of phases 2 and 3 have yet to be published. The primary effectiveness endpoint, “all-cause discontinuation,” was defined as:
- lack of efficacy (patient was switched to another drug assigned at random)
- lack of tolerability (patient requested a drug change)
- safety problem (investigator initiated a switch)
- patient’s decision for any reason (often dropping out of the study).
The longer subjects stayed on the first antipsychotic they received, the more effective that drug was considered to be.
Figure CATIE schizophrenia trial design
* Phase 1A: participants with tardive dyskinesia (N=231) do not get randomized to perphenazine; phase 1B: participants who fail perphenazine will be randomized to an atypical (olanzapine, quetiapine, or risperidone) before eligibility for phase 2.
Source: Reference 2.Medications. Three atypicals—risperidone, olanzapine, and quetiapine—were approved for schizophrenia when the trial began in 1999. Recruitment ended in June 2003, the last subject completed the 18-month trial in December 2004, and data analysis began in January 2005. Ziprasidone was added to phase 1 after 40% of the sample had been enrolled, and aripiprazole was included as an option in the unblinded phase 3.
Perphenazine was chosen to represent typical antipsychotics because it has medium potency and less risk of EPS than high-potency drugs such as haloperidol and is associated with less weight gain than low-potency drugs such as thioridazine.
Dosing. Pharmaceutical manufacturers donated the antipsychotics and were invited to recommend their respective drugs’ starting dosages, dose increments, and maximum dosages. Olanzapine’s maker requested a higher starting dosage (7.5 mg/d instead of 5.0 mg/d) and a maximum dosage 50% higher than the FDA-approved range (30 mg/d instead of 20 mg/d). The others recommended the FDA-approved dosage ranges or less:
- quetiapine, 200 to 800 mg/d
- risperidone, 1.5 to 6 mg/d
- ziprasidone, 40 to 160 mg/d
- perphenazine, 8 to 32 mg/d.
The study team accepted their recommendations.
The medications were packaged in identical capsules. Quetiapine and ziprasidone were given twice daily because of product labeling; risperidone, olanzapine, and perphenazine were given once daily to one-half the patients assigned to them and twice daily to the others to prevent raters from guessing which drug a patient was receiving.
Tardive dyskinesia. For ethical reasons, the 231 patients with TD at enrollment were randomly assigned in phase 1 to atypicals but not to perphenazine because of the well-established link between typical antipsychotics and TD. This exception could have contributed to the closer-than-expected differences in EPS and perhaps in efficacy, given reports that TD patients have more negative symptoms and cognitive dysfunction.13 However, a statistical analysis took that into account.
CATIE’s Key Findings
Discontinuation. A disappointingly high discontinuation rate (74% overall) within a few months was the most important finding (Table 3). A recent effectiveness study with a design similar to the CATIE trial found a similarly high rate of all-cause discontinuation (70%) in patients with first-episode psychosis.14 Thus, patient-initiated drug discontinuation appears to be a core illness behavior from schizophrenia onset to chronic illness.
The high discontinuation rate shows that we need to modify our approach to schizophrenia, emphasizing full adherence to antipsychotic therapy from the onset of the illness.
Table 3
All-cause discontinuation rates in the CATIE trial
| Antipsychotic | Percent discontinued | Duration on antipsychotic (months)* | Dosage (mg/d)* |
| Olanzapine | 64% | 9.2 | 20.1 |
| Perphenazine | 75% | 4.6 | 20.8 |
| Quetiapine | 82% | 4.8 | 543.4 |
| Risperidone | 74% | 5.6 | 3.9 |
| Ziprasidone | 79% | 3.5 | 112.8 |
| Overall | 74% | Median 6.0; mean 8.3 | |
| Notes | |||
| *Mean modal | |||
| Olanzapine’s discontinuation rate was significantly lower than those of perphenazine, quetiapine, and risperidone but not of ziprasidone. | |||
| Olanzapine’s maximum dosage was 30 mg/d (50% higher than FDA-approved 20 mg/d); other agents were dosed within approved ranges. | |||
| Patients reached maximum daily antipsychotic dosages at these rates: 40% with olanzapine, 40% with perphenazine, 44% with quetiapine, 40% with risperidone, and 48% with ziprasidone. | |||
Effectiveness—measured as all-cause discontinuation or switching—was the primary outcome of phase 1. The unexpected finding that perphenazine and the atypicals had similar effectiveness could influence clinical practice. Insurers, for example, might consider promoting cheaper typical antipsychotics for first-line use. CATIE’s cost-effectiveness arm (Rosenheck et al, submitted for publication) will provide additional data on this issue.
Before rushing to use older antipsychotics as first-line treatments for schizophrenia, however, policymakers should consider three factors in the study design that could have enhanced perphenazine’s efficacy and safety profiles.
First, perphenazine was given at lower dosages (up to 32 mg/d) than “real world” clinicians used a decade ago (up to 64 mg/d). Thus, lower rates of serious side effects, especially TD, might have occurred in the study than in past clinical practice. Since atypical antipsychotics were approved, clinicians see far fewer psychiatric patients with pill-rolling tremors, rigid posture, or a shuffling gait, compared with 10 to 15 years ago when typical antipsychotics were widely used.
Second, perphenazine was associated with the highest EPS rate (17%), though its mean modal dosage (20.8 mg/d) is considered moderate. Discontinuation because of EPS was highest with perphenazine and lowest with quetiapine.
Third, excluding enrollees with TD from perphenazine may have increased perphenazine’s effectiveness, whereas including them in the atypicals groups may have reduced the atypicals’ effectiveness. TD patients are at increased risk to develop EPS; they had more-severe illness and a higher substance abuse rate among CATIE patients.11 Even so, investigators did control for TD in the data analysis and found no significant difference between typical and atypical antipsychotics.
No ‘Winners’ or ‘Losers’
Effectiveness, tolerability, and safety findings for each antipsychotic are compared in Tables 4A and 4B. Careful review shows no clear “winners” or “losers;” each agent has weaknesses but also strengths that may benefit individual patients.
Efficacy. Olanzapine showed a relatively higher efficacy and lower discontinuation rate but also had the highest risk of adverse metabolic effects. Some have attributed its greater efficacy to its higher dosing compared with the other antipsychotics. Some also have argued that the antipsychotics that showed lower efficacy, such as quetiapine and ziprasidone, were underdosed in this chronic schizophrenia population with a mean duration of illness of 14 years. Perphenazine, too, was dosed at the lower end of its range (mean modal dose 20.8 mg/d) compared with the old community standard of 36 to 64 mg/d.
Generally, a mean modal dosage of 20.1 mg/d for olanzapine is considered equivalent to ziprasidone, 160 mg; quetiapine, 800 mg; and risperidone, 6 mg. In CATIE phase 1, mean modal dosages were:
- ziprasidone, 112.8 mg/d (30% below 160 mg)
- quetiapine, 543.4 mg/d (32% below 800)
- risperidone, 3.9 mg/d (35% below 6 mg).
Olanzapine’s starting dosage of 7.5 mg/d was relatively higher than those of the other atypicals, which may have produced more-rapid onset of efficacy.
Switching. Another potential “advantage” for olanzapine was that 22% of subjects were taking it when they enrolled. By random assignment, 23% of patients who were taking olanzapine stayed on olanzapine and did not switch. By comparison:
- No patients assigned to ziprasidone were taking it before entering the trial.
- Only 5% of those taking quetiapine stayed on that drug after randomization.
- Few were receiving perphenazine before enrollment.
Switching antipsychotics may increase side effect risk or efficacy problems. For example, a patient switched from olanzapine or quetiapine to ziprasidone or perphenazine may experience insomnia during the transition, which may lead to tolerability complaints.
Metabolic side effects seen in this trial support past observations and reports that olanzapine is associated with higher risk for weight gain, hyperglycemia, and hyperlipidemia than other antipsychotics.15 Data on metabolic changes in CATIE patients taking olanzapine are being analyzed.
Hyperprolactinemia was most common with risperidone and practically nonexistent with other antipsychotics—even perphenazine. On the other hand, risperidone had the most favorable tolerability profile. This implies that elevated prolactin does not necessarily lead to antipsychotic discontinuation because of tolerability among patients with schizophrenia.
QTC interval and cataract data were benign across all antipsychotics. These findings appear to exonerate ziprasidone and quetiapine, respectively, which have been perceived as associated with these side effects.
When data become available, the next article in this series will discuss CATIE phase 2 findings. This phase includes patients who did not improve with the phase 1 regimens because of efficacy or tolerability problems and were switched to other antipsychotic therapies.
Related resources
- Clinical Antipsychotic Trials of Intervention Effectiveness (CATIE) schizophrenia study. www.catie.unc.edu/schizophrenia
- Schizophrenia Research Forum. NARSAD, The Mental Health Research Association.www.schizophreniaforum.org
Drug brand names
- Aripiprazole • Abilify
- Olanzapine • Zyprexa
- Perphenazine • Trilafon
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Ziprasidone • Geodon
Disclosures
Dr Nasrallah receives grants/research support from AstraZeneca, Janssen Pharmaceutica, Eli Lilly & Co., and Pfizer. He is a consultant, advisory board member, and speaker for Abbott Laboratories, AstraZeneca, Janssen Pharmaceutica, Pfizer, and Shire Pharmaceuticals Group.
1. Tandon R, Jibson MD. Efficacy of newer generation antipsychotics in the treatment of schizophrenia. Psychoneuroendocrinol 2003;28(suppl 1):9-26.
2. Stroup TS, McEvoy JP, Swartz MS, et al. The National Institute of Mental Health Clinical Antipsychotic Trial of Intervention Effectiveness (CATIE). Project: schizophrenia trial design and protocol development. Schizophr Bull 2003;29:15-31.
3. Swartz MS, Perkins DO, Stroup TS, et al. Assessing clinical and functional outcomes in the Clinical Antipsychotic Trials of Intervention Effectiveness (CATIE) schizophrenia trial. Schizophr Bull 2003;29:33-43.
4. Lieberman JA, Stroup TS, McEvoy JP, et al. Effectiveness of antipsychotic drugs in patients with chronic schizophrenia. N Engl J Med 2005;353:1209-23.
5. McEvoy JP, Meyer JM, Goff DC, et al. Prevalence of the metabolic syndrome in patients with schizophrenia: baseline results from the CATIE schizophrenia trial and comparison with national estimates from NHANES III. Schizophr Res 2005;80:19-32.
6. Goff D, Sullivan LM, McEvoy JP, et al. A comparison of ten-year cardiac risk estimates in schizophrenia patients from the CATIE study and matched controls. Schizophr Res 2005;80:45-53.
7. Meyer JM, Nasrallah HA, McEvoy JP, et al. The Clinical Antipsychotic Trial of Intervention Effectiveness (CATIE) schizophrenia trial: clinical comparison of subgroups with and without the metabolic syndrome. Schizophr Res 2005;80:9-18.
8. Nasrallah HA, McEvoy JP, Meyer JM, et al. Low rates of treatment for metabolic disorders in the CATIE schizophrenia trial. Neuropsychopharmacol 2005;(suppl 1):204.-
9. Swartz MS, et al. (unpublished data).
10. Schooler NR, Kane JM. Research diagnosis for tardive dyskinesia. Arch Gen Psychiatry 1982;39:486-7.
11. Miller DD, McEvoy JP, Davis SM, et al. Clinical correlates of tardive dyskinesia in schizophrenia: baseline data from the CATIE schizophrenia trial. Schizophr Res 2005;80:33-43.
12. Stroup TS, Applebaum P, Swartz M, et al. Decision-making capacity for research participation among individuals in the CATIE schizophrenia trial. Schizophr Res 2005;80:1-8.
13. Waddington JL, Youssef HA, Dolphin C, et al. Cognitive function, negative symptoms and tardive dyskinesia in schizophrenia. Their association in relation to topography of involuntary movements and criterion of their abnormality. Arch Gen Psychiatry 1987;44:907-12.
14. Keefe R. The CAFÉ effectiveness study. Amsterdam: European College of Neuropsychopharmacology annual meeting, 2005;
15. American Diabetes Association, American Psychiatric Association, American Association of Clinical Endocrinologists, and North American Association for the Study of Obesity. Consensus development conference on antipsychotic drugs, obesity, and diabetes. Diabetes Care 2004;27:596-601.
1. Tandon R, Jibson MD. Efficacy of newer generation antipsychotics in the treatment of schizophrenia. Psychoneuroendocrinol 2003;28(suppl 1):9-26.
2. Stroup TS, McEvoy JP, Swartz MS, et al. The National Institute of Mental Health Clinical Antipsychotic Trial of Intervention Effectiveness (CATIE). Project: schizophrenia trial design and protocol development. Schizophr Bull 2003;29:15-31.
3. Swartz MS, Perkins DO, Stroup TS, et al. Assessing clinical and functional outcomes in the Clinical Antipsychotic Trials of Intervention Effectiveness (CATIE) schizophrenia trial. Schizophr Bull 2003;29:33-43.
4. Lieberman JA, Stroup TS, McEvoy JP, et al. Effectiveness of antipsychotic drugs in patients with chronic schizophrenia. N Engl J Med 2005;353:1209-23.
5. McEvoy JP, Meyer JM, Goff DC, et al. Prevalence of the metabolic syndrome in patients with schizophrenia: baseline results from the CATIE schizophrenia trial and comparison with national estimates from NHANES III. Schizophr Res 2005;80:19-32.
6. Goff D, Sullivan LM, McEvoy JP, et al. A comparison of ten-year cardiac risk estimates in schizophrenia patients from the CATIE study and matched controls. Schizophr Res 2005;80:45-53.
7. Meyer JM, Nasrallah HA, McEvoy JP, et al. The Clinical Antipsychotic Trial of Intervention Effectiveness (CATIE) schizophrenia trial: clinical comparison of subgroups with and without the metabolic syndrome. Schizophr Res 2005;80:9-18.
8. Nasrallah HA, McEvoy JP, Meyer JM, et al. Low rates of treatment for metabolic disorders in the CATIE schizophrenia trial. Neuropsychopharmacol 2005;(suppl 1):204.-
9. Swartz MS, et al. (unpublished data).
10. Schooler NR, Kane JM. Research diagnosis for tardive dyskinesia. Arch Gen Psychiatry 1982;39:486-7.
11. Miller DD, McEvoy JP, Davis SM, et al. Clinical correlates of tardive dyskinesia in schizophrenia: baseline data from the CATIE schizophrenia trial. Schizophr Res 2005;80:33-43.
12. Stroup TS, Applebaum P, Swartz M, et al. Decision-making capacity for research participation among individuals in the CATIE schizophrenia trial. Schizophr Res 2005;80:1-8.
13. Waddington JL, Youssef HA, Dolphin C, et al. Cognitive function, negative symptoms and tardive dyskinesia in schizophrenia. Their association in relation to topography of involuntary movements and criterion of their abnormality. Arch Gen Psychiatry 1987;44:907-12.
14. Keefe R. The CAFÉ effectiveness study. Amsterdam: European College of Neuropsychopharmacology annual meeting, 2005;
15. American Diabetes Association, American Psychiatric Association, American Association of Clinical Endocrinologists, and North American Association for the Study of Obesity. Consensus development conference on antipsychotic drugs, obesity, and diabetes. Diabetes Care 2004;27:596-601.
Psychosis: 6 steps rule out medical causes in kids
John, age 16, is admitted to our inpatient psychiatric unit, complaining of “a 2-week constant headache” caused by “voices arguing in my head.” He has lived in Mexico with an uncle for 6 months but returned home last week for medical evaluation of his headaches.
His parents report that John developed normally until 3 years ago, when he gradually lost interest in his favorite activities and became socially withdrawn. He has not attended school in 2 years. He has no history of illicit drug use and is not taking prescription or over the-counter medications.
Complete physical examination, neurologic exam, and routine screening lab test results are normal. Thinking that a high lead content of cookware used in Mexico might be causing John’s symptoms, we order a lead level: result-0.2 mg/dL (
We diagnose schizophreniform disorder, but John’s parents refuse to accept this diagnosis. They repeatedly ask if we can do more to identify a medical cause of their son’s psychiatric symptoms.
As in John’s case, young patients or their parents may resist the diagnosis of a chronic mental illness such as schizophrenia. Understandably, they may be invested in trying to identify “medically treatable” causes. You can address their anxieties by showing them that you have systematically evaluated medical causes of psychosis.
We offer such a tool: an algorithm and tables to help you identify common and rare medical conditions that may cause or exacerbate psychotic symptoms in patients ages 3 to 18.
An evidence-based algorithm
Multiple factors—developmental, psychological, family, environmental, or medical—typically cause psychotic symptoms in a child or adolescent. Evaluating all possibilities is essential, but guidelines tend to minimize medical causes. American Academy of Child and Adolescent Psychiatry guidelines, for example, recommend that “all medical disorders (including general medical conditions and substance-induced disorders) are ruled out,”1 but they do not specify which medical conditions to consider.
To supplement existing guidelines, we searched the literature and developed an evidence-based algorithm to help you systematically consider medical causes of pediatric psychotic symptoms. We excluded children age 2
How to use it. The algorithm walks you through a medical systems review. You begin with a complete history, then address six causes of psychotic symptoms: substance abuse, medication reactions, general medical conditions, unexplained somatic symptoms (such as from toxic environmental exposures), developmental and learning disabilities, and atypical presentations.
Don’t stop if you find one possible cause of psychotic symptoms; continue to the end of the algorithm. The more factors you identify, the greater your chance of finding a treatable cause that may ameliorate your patient’s symptoms.
To make the algorithm clinically useful, we listed conditions in order of decreasing probability of causing psychotic symptoms. For example, the first cause listed is substance-induced disorders,3 which are most common among adolescent patients. We also “triaged” medical conditions from common to rare (based on estimated prevalence of association with psychotic symptoms), listing rare causes only in cases of atypical presentation or treatment resistance.
Supporting tables. The following discussion summarizes data that support the algorithm and its tables:
- medications reported to cause psychosis (Table 1)
- medical conditions most likely to cause psychosis (Table 2)
- medical conditions that rarely cause psychosis (Table 3).
Drugs that may cause psychotic symptoms
| Drug class | Psychotic symptoms | |
|---|---|---|
| Bizarre behavior/delusions | Auditory or visual hallucinations | |
| Amphetamine-like drugs | X | X |
| Anabolic steroids | X | |
| Angiotensin-converting enzyme (ACE) inhibitors | X | |
| Anticholinergics and atropine | X | X |
| Antidepressants, tricyclic | X | |
| Antiepileptics | X | |
| Barbiturates | X | X |
| Benzodiazepines | X | X |
| Beta-adrenergic blockers | X | X |
| Calcium channel blockers | X | |
| Cephalosporins | X | X |
| Corticosteroids | X | |
| Dopamine receptor agonists | X | X |
| Fluoroquinolone antibiotics | X | X |
| Histamine H1 receptor blockers | X | |
| Histamine H2 receptor blockers | X | |
| HMG-CoA reductase inhibitors | X | |
| Nonsteroidal anti-inflammatory drugs | X | |
| Opioids | X | X |
| Procaine derivatives (procainamide, procaine penicillin G) | X | X |
| Salicylates | X | X |
| Selective serotonin reuptake inhibitors | X | |
| Sulfonamides | X | |
| Source: Adapted from reference 10. | ||
Common medical conditions that may cause pediatric psychosis symptoms*
| Category | Conditions not to forget | Common symptoms/comments |
|---|---|---|
| Rheumatologic | Lupus erythematosus | Joint pain, fever, facial butterfly rash, prolonged fatigue |
| Infectious | Viral encephalitis | Fever, headache, mental status change; may occur in perinatal period |
| Neurologic | Multiple sclerosis | Varied neurologic deficits, especially ophthalmologic changes and weakness |
| Neurosyphilis | Personality change, ataxia, stroke, ophthalmic symptoms | |
| Seizure (temporal lobe epilepsy, interictal psychosis) | Paroxysmal periods of sudden change in mood, behavior, or motor activity with or without loss of consciousness | |
| Toxicologic | Carbon monoxide poisoning | Shortness of breath, mild nausea, headache, dizziness |
| * Clinically significant symptoms that meet DSM-IV-TR criteria for a primary psychiatric disorder. | ||
| Click here to view citations supporting statements in this table | ||
Medical conditions that rarely cause pediatric psychosis symptoms*
| Category/condition | Symptoms/comments |
|---|---|
| Endocrine | |
| Hyperthyroidism | Tachycardia, weight loss, excessive sweating, tiredness, inability to sleep, diarrhea, shakiness, muscle weakness |
| Thymoma/myasthenia gravis | Shortness of breath, swelling of face, muscle weakness (especially around eyes) |
| Hematologic | |
| Porphyria (acute intermittent porphyria, porphyria variegate) | Intermittent abdominal pain (severe) accompanied by dark urine |
| Genetic | |
| Fabry’s disease | Burning sensations in hands and feet that worsen with exercise and hot weather |
| Niemann-Pick disease, type C | Vertical gaze palsy, hepatosplenomegaly, jaundice, ataxia |
| Prader-Willi syndrome | Obesity, hyperphagia, mild to moderate mental retardation, hypogonadism, tantrums, obsessive-compulsive disorder |
| Infectious | |
| Epstein-Barr virus | Fever, sore throat, adenopathy, fatigue, poor concentration |
| Lyme disease | Target lesion, fever; high-risk geographic area |
| Malaria/typhoid fever | Fever, mental status change; endemic area |
| Mycoplasma pneumonia | Fever, mental status change; may occur in absence of pneumonia |
| Rabies | History of exposure |
| Metabolic | |
| Citrullinemia | Mental status change, high plasma citrulline and ammonia |
| Tay-Sachs disease | Unsteadiness of gait and progressive neurologic deterioration |
| Homocystinuria | Dislocated lenses, blood clots, tall stature, some mental retardation |
| Juvenile metachromatic leukodystrophy | Cognitive decline, ataxia, pyramidal signs, peripheral neuropathy, dystonia; 60% of cases present before age 3 |
| Neurologic | |
| Central pontine myelinolysis | Suspect in patient with pathogenic polydipsia |
| Huntington’s disease | Chorea, myoclonic seizures, poor coordination, emotional lability |
| Moyamoya disease | Paresis, syncopal episodes |
| Narcolepsy | Excessive daytime sleepiness, cataplexy |
| Subacute sclerosing panencephalitis | Visual hallucinations, loss of developmental milestones |
| Traumatic brain injury | Occurring 4 to 5 years after a loss of consciousness >30 minutes |
| Wilson’s disease | Tremors, muscle spasticity, possible liver inflammation |
| Nutritional | |
| Pellagra (vitamin B6 deficiency) | Redness, swelling of mouth and tongue, diarrhea, rash, abnormal mental functioning; seen with isoniazid treatment for tuberculosis |
| Oncologic | |
| Cancers (pancreatic, CNS papilloma, germinoma) | Postural headache, neurologic signs, increased intracranial pressure, early morning nausea, vomiting |
| Toxicologic | |
| Lead intoxication | Headache, fatigue, mental status change |
| Mercury poisoning | Abdominal pain, bleeding gums, metallic taste; history of exposure |
| * Clinically significant symptoms that meet DSM-IV-TR criteria for a primary psychiatric disorder. | |
| Click here to view citations supporting statements in this table | |
Substance abuse
Substance abuse is common among adolescents and adults with psychotic illnesses.4 Drug-induced states can cause delusions, hallucinations, paranoia, and disorganized behavior,5 which are reported most commonly during intoxication and withdrawal.6 Diagnosis is often straightforward because of the temporal association between the substance abuse and onset of psychotic symptoms.
Little evidence supports a causal relationship between drug use and the development of chronic psychotic symptoms, however. Case reports link use of 3,4-methylenedioxymethamphetamine (“Ecstasy”), lysergic acid diethylamide (LSD), and marijuana to chronic schizophrenia-like symptoms.7 The strongest evidence links long-term methamphetamine and cocaine use to chronic psychotic symptoms.8,9
Medications
Side effects of at least 25 drug classes have been reported to mimic psychosis (Table 1),10 but little is known about the incidence and prevalence of this problem. Case reports and chart reviews provide the only data that associate most medications with psychotic symptoms. These disagree on what defines a “psychotic symptom,” and most fail to rule out delirium as a possible cause.
The relationship between glucocorticosteroids and psychotic symptoms has been studied extensively. A clear link has been found between corticosteroids at dosages >40 mg/d and a markedly elevated risk for transient psychotic symptoms.11
Medical conditions
We identified 27 medical conditions that may cause or worsen clinical symptoms of psychosis (Tables 2 and 3) by searching PubMed, psychiatric journals, and neuropsychiatry and consult-liaison textbooks. We included only conditions:
- shown to cause significant morbidity in pediatric populations
- shown to have a statistically significant association with psychotic symptoms, or patients’ symptoms consistently resolved when the condition was treated.
Endocrine disorders. Behavioral disturbances (including psychosis) may be the earliest manifestation of an endocrine disorder.17 Cushing’s syndrome,18 hyperthyroidism,19 and hypothyroidism20—met our inclusion criteria.
Cushing’s syndrome—caused by long-term systemic glucocorticoids and thyroid disorders—is not uncommon in children and adolescents but rarely presents with psychotic behaviors. For each endocrine disorder we included, however, at least one case report described delayed diagnosis because of prominent psychosis. Treating the endocrinopathies resolved the psychotic symptoms.
Genetic disorders. Genetically determined neurodevelopmental disorders usually present in very young children, but some may appear later. Genetic conditions that co-occur with psychotic symptoms at rates significantly greater than the population prevalence include Prader-Willi syndrome,21 metachromatic leukodystrophy,22 Turner’s syndrome,21 velocardiofacial syndrome,23 and Wilson’s disease.15
Acute intermittent porphyria, GM2 gangliosidosis (Tay-Sachs disease), and homocystinuria are rare conditions with unknown prevalence in patients with psychotic disorders. Still, they are important to consider when evaluating youths with psychosis because case reports link their treatment with psychotic symptom resolution.24-26
Infectious disease. An infectious CNS disease does not usually present with psychotic symptoms only. When this does happen, making the correct diagnosis as soon as possible is critical because early treatment is associated with better outcomes.27 Misdiagnosis as a primary psychotic disorder may expose a patient to psychotropics that may adversely affect clinical outcome.
Viruses that affect the CNS (viral encephalopathies) are the infections most likely to cause psychotic symptoms. By decreasing frequency, they are human simian virus, HIV, influenza, measles, Epstein-Barr virus, mumps, and rabies.27,28 Bacterial infections that cause psychosis include mycoplasma pneumonia,29 syphilis,30 typhoid fever,31 and Lyme disease.32
Brain tumor. Childhood brain tumors often present with behavioral symptoms associated with headache, vomiting, visual changes, and motor and cognitive symptoms. A CNS tumor rarely presents with isolated neuropsychiatric symptoms.33 A few case reports describe intracranial tumors initially misdiagnosed as primary psychotic illness because of prominent psychotic symptoms.34,35 In each case, these symptoms resolved with tumor resection.
A temporal relationship does not necessarily equate to a “causal” relationship, however. Tatter et al36 describe a case of “reoccurrence” of manic symptoms initially thought to be caused by an arteriovenous malformation (AVM) 10 years after the AVM was successfully removed. The important point is that, although rarely, pediatric brain tumor can present with prominent psychotic symptoms.
Environmental toxin exposure may cause well-defined psychiatric syndromes,37 although frank psychosis is uncommon at presentation. Most often, environmental toxins produce an encephalopathic process of which psychosis may be one symptom. A few toxic exposures—such as lead,38 carbon monoxide,39 and elemental mercury40 —have presented with prominent psychotic symptoms without other encephalopathic symptoms.
Collagen vascular disease is associated with significantly elevated rates of psychiatric illness, especially depression, but only systemic lupus erythematosus (SLE) is known to be associated with prominent psychosis. Case series report delayed SLE diagnosis in patients with this presentation.41
High-dose pulse corticosteroids have been reported to effectively treat SLE-related psychotic symptoms,42 although high-dose corticosteroids can also cause psychotic symptoms. The timing and character of the symptoms can help you determine whether using corticosteroids is helping or making the patient worse.
Using the algorithm
John’s mother and father fear that the inpatient team’s diagnosis of a primary psychotic disorder means that a medical cause has been permanently “ruled out.” To reassure them, we use the algorithm to explain in concrete terms the thought process that led us to John’s psychiatric diagnosis. We walk them through the algorithm and its tables, explaining how we used evidence to rationally rule out all known medical causes of psychotic symptoms in pediatric patients.
John’s parents are relieved to know that the case is not closed, even though we found no medical cause for their son’s condition. If more clinical data become available, we remain open to considering the possibility that medical conditions could be causing or worsening their son’s symptoms.
Related resources
- American Academy of Child and Adolescent Psychiatry. Practice parameter for the assessment and treatment of children and adolescents with schizophrenia. J Am Acad Child Adolesc Psychiatry 2001;40(7 Suppl):4S-23S.
- Schiffer RB, Klein RF, Sider RC. The medical evaluation of psychiatric patients. New York: Plenum Medical Book Co.; 1998.
- National Organization for Rare Disorders (NORD). www.rarediseases.org.
1. American Academy of Child and Adolescent Psychiatry. Summary of the practice parameters for the assessment and treatment of children and adolescents with schizophrenia. J Am Acad Child Adolesc Psychiatry 2000;39(12):1580-92.
2. Behrman RE (ed). Nelson textbook of pediatrics (17th ed). Philadelphia: WB Saunders; 2003:397-518.
3. Dalmau A, Bergman B, Brismar B. Psychotic disorders among inpatients with abuse of cannabis, amphetamine and opiates. Do dopaminergic stimulants facilitate psychiatric illness? Eur Psychiatry 1999;14(7):366-71.
4. Breslow RE, Klinger BI, Erickson BJ. Acute intoxication and substance abuse among patients presenting to a psychiatric emergency service. Gen Hosp Psychiatry 1996;18(3):183-91.
5. Poole R, Brabbins C. Drug-induced psychosis. Br J Psychiatry 1996;168:137.-
6. DiSclafani A, 2nd, Hall RC, Gardner ER. Drug-induced psychosis: emergency diagnosis and management. Psychosomatics 1981;22(10):845-55.
7. Cohen SI. Substance-induced psychosis. Br J Psychiatry 1996;168(5):651-2.
8. Farrell M, Boys A, Bebbington P, et al. Psychosis and drug dependence: results from a national survey of prisoners. Br J Psychiatry 2002;181:393-8.
9. Ujike H, Sato M. Clinical features of sensitization to methamphetamine observed in patients with methamphetamine dependence and psychosis. Ann NY Acad Sci 2004;1025:279-87.
10. Drugs that may cause psychiatric symptoms. Med Lett Drugs Ther 2002;44:29-62.
11. Lewis DA, Smith RE. Steroid-induced psychiatric symptoms; a report of 14 cases and a review of the literature. J Affect Disord 1983;5(4):319-32.
12. Cummings JL. Organic psychosis. Psychosomatics 1988;29(1):16-26.
13. Roy AK, Rajesh SV, Iby N, et al. A study of epilepsy-related psychosis. Neurol India 2003;51(3):359-60.
14. Mendez MF. Huntington’s disease: update and review of neuropsychiatric aspects. Int J Psychiatry Med 1994;24:189-208.
15. Brewer GJ. Recognition and management of Wilson’s disease. Proc Soc Exp Biol Med 2000;223:39-46.
16. Mendhekar DN, Mehta R, Puri V. Successful steroid therapy in multiple sclerosis presented as acute psychosis. J Assoc Physicians India 2004;52:512-3.
17. Reus VI. Behavioral disturbances associated with endocrine disorders. Ann Rev Med 1986;37:205-14.
18. Hirsch D, Orr G, Kantarovich V, et al. Cushing’s syndrome presenting as a schizophrenia-like psychotic state. Isr J Psychiatry Relat Sci 2000;37(1):46-50.
19. Lu CL, Lee YC, Tsai SJ, et al. Psychiatric disturbances associated with hyperthyroidism: an analysis report of 30 cases. Zhonghua Yi Xue Za Zhi (Taipei) 1995;56(6):393-8.
20. Bhatara V, Alshari MG, Warhol P, et al. Coexistent hypothyroidism, psychosis, and severe obsessions in an adolescent: a 10-year follow-up. J Child Adolesc Psychopharmacol 2004;14(2):315-23.
21. Prior TI, Chue PS, Tibbo P. Investigation of Turner syndrome in schizophrenia. Am J Med Genet 2000;96(3):373-8.
22. Hyde TM, Ziegler JC, Weinberger DR. Psychiatric disturbances in metachromatic leukodystrophy. Insights into the neurobiology of psychosis. Arch Neurol 1992;49(4):401-6.
23. Briegel W, Cohen M. Chromosome 22q11 deletion syndrome and its relevance for child and adolescent psychiatry. An overview of etiology, physical symptoms, aspects of child development and psychiatric disorders. Z Kinder Jugendpsychiatr Psychother 2004;32(2):107-15.
24. Crimlisk HL. The great imitator-porphyria: a neuropsychiatric disorder. J Neurol Neurosurg Psychiatry 2001;62(4):319-28.
25. Ryan MM, Sidhu RK, Alexander J, Megerian JT. Homocystinuria presenting as psychosis in an adolescent. J Child Neurol 2002;17(11):859-60.
26. MacQueen GM, Rosebush PI, Mazurek MF. Neuropsychiatric aspects of the adult variant of Tay-Sachs disease. J Neuropsychiatry Clin Neurosci 1998;10(1):10-9.
27. Caroff SN, Mann SC, Gliatto MF, et al. Psychiatric manifestations of acute viral encephalitis. Psych Annals 2001;31(3):193-204.
28. Caplan R, Tanguay PE, Szekely AG. Subacute sclerosing panencephalitis presenting as childhood psychosis. J Am Acad Child Adolesc Psychiatry 1987;26(3):440-3.
29. Gillberg C. Schizophreniform psychosis in a case of mycoplasma pneumoniae encephalitis. J Autism Dev Disord 1980;10(2):153-8.
30. Gliatto MF, Caroff SN. Neurosyphilis: a history and clinical review. Psych Annals 2001;31(3):153-61.
31. Venkatesh S, Grell GA. Neuropsychiatric manifestations of typhoid fever. West Indian Med J 1989;38(3):137-41.
32. Tager FA, Fallon B. Psychiatric and cognitive features of Lyme disease. Psych Annals 2001;31(3):173-92.
33. Stein MT, Duffner PK, Wery JS, Trauner D. School refusal and emotional liability in a 6 year old boy. J Dev Behav Pediatr 2001;22(suppl):29-32.
34. Carson BS, Weingart JD, Guarnieri M, Fisher PG. Third ventricular choroid plexus papilloma with psychosis. Case report. J Neurosurg 1997;87(1):103-5.
35. Craven C. Pineal germinoma and psychosis. J Am Acad Child Adolesc Psychiatry 2001;40(1):6.-
36. Tatter SB, Ogilvy CS. Recurrent manic episode 10 years after arteriovenous malformation resection. J Clin Psychiatry 1995;56(2):83.-
37. Hartman DE. Missed diagnosis and misdiagnosis of environmental toxicants exposure: the psychiatry of toxic exposure and multiple chemical sensitivity. Psychiatr Clin North Am 1998;21(3):659-70.
38. Bahiga LM, Kotb NA, El-Dessoukey EA. Neurological syndromes produced by some toxic metals encountered industrially or environmentally. Z Ernahrungswiss 1978;17(2):84-8.
39. Olson KR. Carbon monoxide poisoning: mechanisms, presentation, and controversies in management. J Emerg Med 1984;1(3):233-43.
40. Fagala GE, Wigg CL. Psychiatric manifestations of mercury poisoning. J Am Acad Child Adolesc Psychiatry 1992;31(2):306-11.
41. Turkel SB, Miller JH, Reiff A. Case series: neuropsychiatric symptoms with pediatric systemic lupus erythematosus. J Am Acad Child Adolesc Psychiatry 2001;40(4):482-5.
42. Baca V, Lavalle C, Garcia R, et al. Favorable response to intravenous methylprednisolone and cyclophosphamide in children with severe neuropsychiatric lupus. J Rheumatol 1999;26(2):432-9.
John, age 16, is admitted to our inpatient psychiatric unit, complaining of “a 2-week constant headache” caused by “voices arguing in my head.” He has lived in Mexico with an uncle for 6 months but returned home last week for medical evaluation of his headaches.
His parents report that John developed normally until 3 years ago, when he gradually lost interest in his favorite activities and became socially withdrawn. He has not attended school in 2 years. He has no history of illicit drug use and is not taking prescription or over the-counter medications.
Complete physical examination, neurologic exam, and routine screening lab test results are normal. Thinking that a high lead content of cookware used in Mexico might be causing John’s symptoms, we order a lead level: result-0.2 mg/dL (
We diagnose schizophreniform disorder, but John’s parents refuse to accept this diagnosis. They repeatedly ask if we can do more to identify a medical cause of their son’s psychiatric symptoms.
As in John’s case, young patients or their parents may resist the diagnosis of a chronic mental illness such as schizophrenia. Understandably, they may be invested in trying to identify “medically treatable” causes. You can address their anxieties by showing them that you have systematically evaluated medical causes of psychosis.
We offer such a tool: an algorithm and tables to help you identify common and rare medical conditions that may cause or exacerbate psychotic symptoms in patients ages 3 to 18.
An evidence-based algorithm
Multiple factors—developmental, psychological, family, environmental, or medical—typically cause psychotic symptoms in a child or adolescent. Evaluating all possibilities is essential, but guidelines tend to minimize medical causes. American Academy of Child and Adolescent Psychiatry guidelines, for example, recommend that “all medical disorders (including general medical conditions and substance-induced disorders) are ruled out,”1 but they do not specify which medical conditions to consider.
To supplement existing guidelines, we searched the literature and developed an evidence-based algorithm to help you systematically consider medical causes of pediatric psychotic symptoms. We excluded children age 2
How to use it. The algorithm walks you through a medical systems review. You begin with a complete history, then address six causes of psychotic symptoms: substance abuse, medication reactions, general medical conditions, unexplained somatic symptoms (such as from toxic environmental exposures), developmental and learning disabilities, and atypical presentations.
Don’t stop if you find one possible cause of psychotic symptoms; continue to the end of the algorithm. The more factors you identify, the greater your chance of finding a treatable cause that may ameliorate your patient’s symptoms.
To make the algorithm clinically useful, we listed conditions in order of decreasing probability of causing psychotic symptoms. For example, the first cause listed is substance-induced disorders,3 which are most common among adolescent patients. We also “triaged” medical conditions from common to rare (based on estimated prevalence of association with psychotic symptoms), listing rare causes only in cases of atypical presentation or treatment resistance.
Supporting tables. The following discussion summarizes data that support the algorithm and its tables:
- medications reported to cause psychosis (Table 1)
- medical conditions most likely to cause psychosis (Table 2)
- medical conditions that rarely cause psychosis (Table 3).
Drugs that may cause psychotic symptoms
| Drug class | Psychotic symptoms | |
|---|---|---|
| Bizarre behavior/delusions | Auditory or visual hallucinations | |
| Amphetamine-like drugs | X | X |
| Anabolic steroids | X | |
| Angiotensin-converting enzyme (ACE) inhibitors | X | |
| Anticholinergics and atropine | X | X |
| Antidepressants, tricyclic | X | |
| Antiepileptics | X | |
| Barbiturates | X | X |
| Benzodiazepines | X | X |
| Beta-adrenergic blockers | X | X |
| Calcium channel blockers | X | |
| Cephalosporins | X | X |
| Corticosteroids | X | |
| Dopamine receptor agonists | X | X |
| Fluoroquinolone antibiotics | X | X |
| Histamine H1 receptor blockers | X | |
| Histamine H2 receptor blockers | X | |
| HMG-CoA reductase inhibitors | X | |
| Nonsteroidal anti-inflammatory drugs | X | |
| Opioids | X | X |
| Procaine derivatives (procainamide, procaine penicillin G) | X | X |
| Salicylates | X | X |
| Selective serotonin reuptake inhibitors | X | |
| Sulfonamides | X | |
| Source: Adapted from reference 10. | ||
Common medical conditions that may cause pediatric psychosis symptoms*
| Category | Conditions not to forget | Common symptoms/comments |
|---|---|---|
| Rheumatologic | Lupus erythematosus | Joint pain, fever, facial butterfly rash, prolonged fatigue |
| Infectious | Viral encephalitis | Fever, headache, mental status change; may occur in perinatal period |
| Neurologic | Multiple sclerosis | Varied neurologic deficits, especially ophthalmologic changes and weakness |
| Neurosyphilis | Personality change, ataxia, stroke, ophthalmic symptoms | |
| Seizure (temporal lobe epilepsy, interictal psychosis) | Paroxysmal periods of sudden change in mood, behavior, or motor activity with or without loss of consciousness | |
| Toxicologic | Carbon monoxide poisoning | Shortness of breath, mild nausea, headache, dizziness |
| * Clinically significant symptoms that meet DSM-IV-TR criteria for a primary psychiatric disorder. | ||
| Click here to view citations supporting statements in this table | ||
Medical conditions that rarely cause pediatric psychosis symptoms*
| Category/condition | Symptoms/comments |
|---|---|
| Endocrine | |
| Hyperthyroidism | Tachycardia, weight loss, excessive sweating, tiredness, inability to sleep, diarrhea, shakiness, muscle weakness |
| Thymoma/myasthenia gravis | Shortness of breath, swelling of face, muscle weakness (especially around eyes) |
| Hematologic | |
| Porphyria (acute intermittent porphyria, porphyria variegate) | Intermittent abdominal pain (severe) accompanied by dark urine |
| Genetic | |
| Fabry’s disease | Burning sensations in hands and feet that worsen with exercise and hot weather |
| Niemann-Pick disease, type C | Vertical gaze palsy, hepatosplenomegaly, jaundice, ataxia |
| Prader-Willi syndrome | Obesity, hyperphagia, mild to moderate mental retardation, hypogonadism, tantrums, obsessive-compulsive disorder |
| Infectious | |
| Epstein-Barr virus | Fever, sore throat, adenopathy, fatigue, poor concentration |
| Lyme disease | Target lesion, fever; high-risk geographic area |
| Malaria/typhoid fever | Fever, mental status change; endemic area |
| Mycoplasma pneumonia | Fever, mental status change; may occur in absence of pneumonia |
| Rabies | History of exposure |
| Metabolic | |
| Citrullinemia | Mental status change, high plasma citrulline and ammonia |
| Tay-Sachs disease | Unsteadiness of gait and progressive neurologic deterioration |
| Homocystinuria | Dislocated lenses, blood clots, tall stature, some mental retardation |
| Juvenile metachromatic leukodystrophy | Cognitive decline, ataxia, pyramidal signs, peripheral neuropathy, dystonia; 60% of cases present before age 3 |
| Neurologic | |
| Central pontine myelinolysis | Suspect in patient with pathogenic polydipsia |
| Huntington’s disease | Chorea, myoclonic seizures, poor coordination, emotional lability |
| Moyamoya disease | Paresis, syncopal episodes |
| Narcolepsy | Excessive daytime sleepiness, cataplexy |
| Subacute sclerosing panencephalitis | Visual hallucinations, loss of developmental milestones |
| Traumatic brain injury | Occurring 4 to 5 years after a loss of consciousness >30 minutes |
| Wilson’s disease | Tremors, muscle spasticity, possible liver inflammation |
| Nutritional | |
| Pellagra (vitamin B6 deficiency) | Redness, swelling of mouth and tongue, diarrhea, rash, abnormal mental functioning; seen with isoniazid treatment for tuberculosis |
| Oncologic | |
| Cancers (pancreatic, CNS papilloma, germinoma) | Postural headache, neurologic signs, increased intracranial pressure, early morning nausea, vomiting |
| Toxicologic | |
| Lead intoxication | Headache, fatigue, mental status change |
| Mercury poisoning | Abdominal pain, bleeding gums, metallic taste; history of exposure |
| * Clinically significant symptoms that meet DSM-IV-TR criteria for a primary psychiatric disorder. | |
| Click here to view citations supporting statements in this table | |
Substance abuse
Substance abuse is common among adolescents and adults with psychotic illnesses.4 Drug-induced states can cause delusions, hallucinations, paranoia, and disorganized behavior,5 which are reported most commonly during intoxication and withdrawal.6 Diagnosis is often straightforward because of the temporal association between the substance abuse and onset of psychotic symptoms.
Little evidence supports a causal relationship between drug use and the development of chronic psychotic symptoms, however. Case reports link use of 3,4-methylenedioxymethamphetamine (“Ecstasy”), lysergic acid diethylamide (LSD), and marijuana to chronic schizophrenia-like symptoms.7 The strongest evidence links long-term methamphetamine and cocaine use to chronic psychotic symptoms.8,9
Medications
Side effects of at least 25 drug classes have been reported to mimic psychosis (Table 1),10 but little is known about the incidence and prevalence of this problem. Case reports and chart reviews provide the only data that associate most medications with psychotic symptoms. These disagree on what defines a “psychotic symptom,” and most fail to rule out delirium as a possible cause.
The relationship between glucocorticosteroids and psychotic symptoms has been studied extensively. A clear link has been found between corticosteroids at dosages >40 mg/d and a markedly elevated risk for transient psychotic symptoms.11
Medical conditions
We identified 27 medical conditions that may cause or worsen clinical symptoms of psychosis (Tables 2 and 3) by searching PubMed, psychiatric journals, and neuropsychiatry and consult-liaison textbooks. We included only conditions:
- shown to cause significant morbidity in pediatric populations
- shown to have a statistically significant association with psychotic symptoms, or patients’ symptoms consistently resolved when the condition was treated.
Endocrine disorders. Behavioral disturbances (including psychosis) may be the earliest manifestation of an endocrine disorder.17 Cushing’s syndrome,18 hyperthyroidism,19 and hypothyroidism20—met our inclusion criteria.
Cushing’s syndrome—caused by long-term systemic glucocorticoids and thyroid disorders—is not uncommon in children and adolescents but rarely presents with psychotic behaviors. For each endocrine disorder we included, however, at least one case report described delayed diagnosis because of prominent psychosis. Treating the endocrinopathies resolved the psychotic symptoms.
Genetic disorders. Genetically determined neurodevelopmental disorders usually present in very young children, but some may appear later. Genetic conditions that co-occur with psychotic symptoms at rates significantly greater than the population prevalence include Prader-Willi syndrome,21 metachromatic leukodystrophy,22 Turner’s syndrome,21 velocardiofacial syndrome,23 and Wilson’s disease.15
Acute intermittent porphyria, GM2 gangliosidosis (Tay-Sachs disease), and homocystinuria are rare conditions with unknown prevalence in patients with psychotic disorders. Still, they are important to consider when evaluating youths with psychosis because case reports link their treatment with psychotic symptom resolution.24-26
Infectious disease. An infectious CNS disease does not usually present with psychotic symptoms only. When this does happen, making the correct diagnosis as soon as possible is critical because early treatment is associated with better outcomes.27 Misdiagnosis as a primary psychotic disorder may expose a patient to psychotropics that may adversely affect clinical outcome.
Viruses that affect the CNS (viral encephalopathies) are the infections most likely to cause psychotic symptoms. By decreasing frequency, they are human simian virus, HIV, influenza, measles, Epstein-Barr virus, mumps, and rabies.27,28 Bacterial infections that cause psychosis include mycoplasma pneumonia,29 syphilis,30 typhoid fever,31 and Lyme disease.32
Brain tumor. Childhood brain tumors often present with behavioral symptoms associated with headache, vomiting, visual changes, and motor and cognitive symptoms. A CNS tumor rarely presents with isolated neuropsychiatric symptoms.33 A few case reports describe intracranial tumors initially misdiagnosed as primary psychotic illness because of prominent psychotic symptoms.34,35 In each case, these symptoms resolved with tumor resection.
A temporal relationship does not necessarily equate to a “causal” relationship, however. Tatter et al36 describe a case of “reoccurrence” of manic symptoms initially thought to be caused by an arteriovenous malformation (AVM) 10 years after the AVM was successfully removed. The important point is that, although rarely, pediatric brain tumor can present with prominent psychotic symptoms.
Environmental toxin exposure may cause well-defined psychiatric syndromes,37 although frank psychosis is uncommon at presentation. Most often, environmental toxins produce an encephalopathic process of which psychosis may be one symptom. A few toxic exposures—such as lead,38 carbon monoxide,39 and elemental mercury40 —have presented with prominent psychotic symptoms without other encephalopathic symptoms.
Collagen vascular disease is associated with significantly elevated rates of psychiatric illness, especially depression, but only systemic lupus erythematosus (SLE) is known to be associated with prominent psychosis. Case series report delayed SLE diagnosis in patients with this presentation.41
High-dose pulse corticosteroids have been reported to effectively treat SLE-related psychotic symptoms,42 although high-dose corticosteroids can also cause psychotic symptoms. The timing and character of the symptoms can help you determine whether using corticosteroids is helping or making the patient worse.
Using the algorithm
John’s mother and father fear that the inpatient team’s diagnosis of a primary psychotic disorder means that a medical cause has been permanently “ruled out.” To reassure them, we use the algorithm to explain in concrete terms the thought process that led us to John’s psychiatric diagnosis. We walk them through the algorithm and its tables, explaining how we used evidence to rationally rule out all known medical causes of psychotic symptoms in pediatric patients.
John’s parents are relieved to know that the case is not closed, even though we found no medical cause for their son’s condition. If more clinical data become available, we remain open to considering the possibility that medical conditions could be causing or worsening their son’s symptoms.
Related resources
- American Academy of Child and Adolescent Psychiatry. Practice parameter for the assessment and treatment of children and adolescents with schizophrenia. J Am Acad Child Adolesc Psychiatry 2001;40(7 Suppl):4S-23S.
- Schiffer RB, Klein RF, Sider RC. The medical evaluation of psychiatric patients. New York: Plenum Medical Book Co.; 1998.
- National Organization for Rare Disorders (NORD). www.rarediseases.org.
John, age 16, is admitted to our inpatient psychiatric unit, complaining of “a 2-week constant headache” caused by “voices arguing in my head.” He has lived in Mexico with an uncle for 6 months but returned home last week for medical evaluation of his headaches.
His parents report that John developed normally until 3 years ago, when he gradually lost interest in his favorite activities and became socially withdrawn. He has not attended school in 2 years. He has no history of illicit drug use and is not taking prescription or over the-counter medications.
Complete physical examination, neurologic exam, and routine screening lab test results are normal. Thinking that a high lead content of cookware used in Mexico might be causing John’s symptoms, we order a lead level: result-0.2 mg/dL (
We diagnose schizophreniform disorder, but John’s parents refuse to accept this diagnosis. They repeatedly ask if we can do more to identify a medical cause of their son’s psychiatric symptoms.
As in John’s case, young patients or their parents may resist the diagnosis of a chronic mental illness such as schizophrenia. Understandably, they may be invested in trying to identify “medically treatable” causes. You can address their anxieties by showing them that you have systematically evaluated medical causes of psychosis.
We offer such a tool: an algorithm and tables to help you identify common and rare medical conditions that may cause or exacerbate psychotic symptoms in patients ages 3 to 18.
An evidence-based algorithm
Multiple factors—developmental, psychological, family, environmental, or medical—typically cause psychotic symptoms in a child or adolescent. Evaluating all possibilities is essential, but guidelines tend to minimize medical causes. American Academy of Child and Adolescent Psychiatry guidelines, for example, recommend that “all medical disorders (including general medical conditions and substance-induced disorders) are ruled out,”1 but they do not specify which medical conditions to consider.
To supplement existing guidelines, we searched the literature and developed an evidence-based algorithm to help you systematically consider medical causes of pediatric psychotic symptoms. We excluded children age 2
How to use it. The algorithm walks you through a medical systems review. You begin with a complete history, then address six causes of psychotic symptoms: substance abuse, medication reactions, general medical conditions, unexplained somatic symptoms (such as from toxic environmental exposures), developmental and learning disabilities, and atypical presentations.
Don’t stop if you find one possible cause of psychotic symptoms; continue to the end of the algorithm. The more factors you identify, the greater your chance of finding a treatable cause that may ameliorate your patient’s symptoms.
To make the algorithm clinically useful, we listed conditions in order of decreasing probability of causing psychotic symptoms. For example, the first cause listed is substance-induced disorders,3 which are most common among adolescent patients. We also “triaged” medical conditions from common to rare (based on estimated prevalence of association with psychotic symptoms), listing rare causes only in cases of atypical presentation or treatment resistance.
Supporting tables. The following discussion summarizes data that support the algorithm and its tables:
- medications reported to cause psychosis (Table 1)
- medical conditions most likely to cause psychosis (Table 2)
- medical conditions that rarely cause psychosis (Table 3).
Drugs that may cause psychotic symptoms
| Drug class | Psychotic symptoms | |
|---|---|---|
| Bizarre behavior/delusions | Auditory or visual hallucinations | |
| Amphetamine-like drugs | X | X |
| Anabolic steroids | X | |
| Angiotensin-converting enzyme (ACE) inhibitors | X | |
| Anticholinergics and atropine | X | X |
| Antidepressants, tricyclic | X | |
| Antiepileptics | X | |
| Barbiturates | X | X |
| Benzodiazepines | X | X |
| Beta-adrenergic blockers | X | X |
| Calcium channel blockers | X | |
| Cephalosporins | X | X |
| Corticosteroids | X | |
| Dopamine receptor agonists | X | X |
| Fluoroquinolone antibiotics | X | X |
| Histamine H1 receptor blockers | X | |
| Histamine H2 receptor blockers | X | |
| HMG-CoA reductase inhibitors | X | |
| Nonsteroidal anti-inflammatory drugs | X | |
| Opioids | X | X |
| Procaine derivatives (procainamide, procaine penicillin G) | X | X |
| Salicylates | X | X |
| Selective serotonin reuptake inhibitors | X | |
| Sulfonamides | X | |
| Source: Adapted from reference 10. | ||
Common medical conditions that may cause pediatric psychosis symptoms*
| Category | Conditions not to forget | Common symptoms/comments |
|---|---|---|
| Rheumatologic | Lupus erythematosus | Joint pain, fever, facial butterfly rash, prolonged fatigue |
| Infectious | Viral encephalitis | Fever, headache, mental status change; may occur in perinatal period |
| Neurologic | Multiple sclerosis | Varied neurologic deficits, especially ophthalmologic changes and weakness |
| Neurosyphilis | Personality change, ataxia, stroke, ophthalmic symptoms | |
| Seizure (temporal lobe epilepsy, interictal psychosis) | Paroxysmal periods of sudden change in mood, behavior, or motor activity with or without loss of consciousness | |
| Toxicologic | Carbon monoxide poisoning | Shortness of breath, mild nausea, headache, dizziness |
| * Clinically significant symptoms that meet DSM-IV-TR criteria for a primary psychiatric disorder. | ||
| Click here to view citations supporting statements in this table | ||
Medical conditions that rarely cause pediatric psychosis symptoms*
| Category/condition | Symptoms/comments |
|---|---|
| Endocrine | |
| Hyperthyroidism | Tachycardia, weight loss, excessive sweating, tiredness, inability to sleep, diarrhea, shakiness, muscle weakness |
| Thymoma/myasthenia gravis | Shortness of breath, swelling of face, muscle weakness (especially around eyes) |
| Hematologic | |
| Porphyria (acute intermittent porphyria, porphyria variegate) | Intermittent abdominal pain (severe) accompanied by dark urine |
| Genetic | |
| Fabry’s disease | Burning sensations in hands and feet that worsen with exercise and hot weather |
| Niemann-Pick disease, type C | Vertical gaze palsy, hepatosplenomegaly, jaundice, ataxia |
| Prader-Willi syndrome | Obesity, hyperphagia, mild to moderate mental retardation, hypogonadism, tantrums, obsessive-compulsive disorder |
| Infectious | |
| Epstein-Barr virus | Fever, sore throat, adenopathy, fatigue, poor concentration |
| Lyme disease | Target lesion, fever; high-risk geographic area |
| Malaria/typhoid fever | Fever, mental status change; endemic area |
| Mycoplasma pneumonia | Fever, mental status change; may occur in absence of pneumonia |
| Rabies | History of exposure |
| Metabolic | |
| Citrullinemia | Mental status change, high plasma citrulline and ammonia |
| Tay-Sachs disease | Unsteadiness of gait and progressive neurologic deterioration |
| Homocystinuria | Dislocated lenses, blood clots, tall stature, some mental retardation |
| Juvenile metachromatic leukodystrophy | Cognitive decline, ataxia, pyramidal signs, peripheral neuropathy, dystonia; 60% of cases present before age 3 |
| Neurologic | |
| Central pontine myelinolysis | Suspect in patient with pathogenic polydipsia |
| Huntington’s disease | Chorea, myoclonic seizures, poor coordination, emotional lability |
| Moyamoya disease | Paresis, syncopal episodes |
| Narcolepsy | Excessive daytime sleepiness, cataplexy |
| Subacute sclerosing panencephalitis | Visual hallucinations, loss of developmental milestones |
| Traumatic brain injury | Occurring 4 to 5 years after a loss of consciousness >30 minutes |
| Wilson’s disease | Tremors, muscle spasticity, possible liver inflammation |
| Nutritional | |
| Pellagra (vitamin B6 deficiency) | Redness, swelling of mouth and tongue, diarrhea, rash, abnormal mental functioning; seen with isoniazid treatment for tuberculosis |
| Oncologic | |
| Cancers (pancreatic, CNS papilloma, germinoma) | Postural headache, neurologic signs, increased intracranial pressure, early morning nausea, vomiting |
| Toxicologic | |
| Lead intoxication | Headache, fatigue, mental status change |
| Mercury poisoning | Abdominal pain, bleeding gums, metallic taste; history of exposure |
| * Clinically significant symptoms that meet DSM-IV-TR criteria for a primary psychiatric disorder. | |
| Click here to view citations supporting statements in this table | |
Substance abuse
Substance abuse is common among adolescents and adults with psychotic illnesses.4 Drug-induced states can cause delusions, hallucinations, paranoia, and disorganized behavior,5 which are reported most commonly during intoxication and withdrawal.6 Diagnosis is often straightforward because of the temporal association between the substance abuse and onset of psychotic symptoms.
Little evidence supports a causal relationship between drug use and the development of chronic psychotic symptoms, however. Case reports link use of 3,4-methylenedioxymethamphetamine (“Ecstasy”), lysergic acid diethylamide (LSD), and marijuana to chronic schizophrenia-like symptoms.7 The strongest evidence links long-term methamphetamine and cocaine use to chronic psychotic symptoms.8,9
Medications
Side effects of at least 25 drug classes have been reported to mimic psychosis (Table 1),10 but little is known about the incidence and prevalence of this problem. Case reports and chart reviews provide the only data that associate most medications with psychotic symptoms. These disagree on what defines a “psychotic symptom,” and most fail to rule out delirium as a possible cause.
The relationship between glucocorticosteroids and psychotic symptoms has been studied extensively. A clear link has been found between corticosteroids at dosages >40 mg/d and a markedly elevated risk for transient psychotic symptoms.11
Medical conditions
We identified 27 medical conditions that may cause or worsen clinical symptoms of psychosis (Tables 2 and 3) by searching PubMed, psychiatric journals, and neuropsychiatry and consult-liaison textbooks. We included only conditions:
- shown to cause significant morbidity in pediatric populations
- shown to have a statistically significant association with psychotic symptoms, or patients’ symptoms consistently resolved when the condition was treated.
Endocrine disorders. Behavioral disturbances (including psychosis) may be the earliest manifestation of an endocrine disorder.17 Cushing’s syndrome,18 hyperthyroidism,19 and hypothyroidism20—met our inclusion criteria.
Cushing’s syndrome—caused by long-term systemic glucocorticoids and thyroid disorders—is not uncommon in children and adolescents but rarely presents with psychotic behaviors. For each endocrine disorder we included, however, at least one case report described delayed diagnosis because of prominent psychosis. Treating the endocrinopathies resolved the psychotic symptoms.
Genetic disorders. Genetically determined neurodevelopmental disorders usually present in very young children, but some may appear later. Genetic conditions that co-occur with psychotic symptoms at rates significantly greater than the population prevalence include Prader-Willi syndrome,21 metachromatic leukodystrophy,22 Turner’s syndrome,21 velocardiofacial syndrome,23 and Wilson’s disease.15
Acute intermittent porphyria, GM2 gangliosidosis (Tay-Sachs disease), and homocystinuria are rare conditions with unknown prevalence in patients with psychotic disorders. Still, they are important to consider when evaluating youths with psychosis because case reports link their treatment with psychotic symptom resolution.24-26
Infectious disease. An infectious CNS disease does not usually present with psychotic symptoms only. When this does happen, making the correct diagnosis as soon as possible is critical because early treatment is associated with better outcomes.27 Misdiagnosis as a primary psychotic disorder may expose a patient to psychotropics that may adversely affect clinical outcome.
Viruses that affect the CNS (viral encephalopathies) are the infections most likely to cause psychotic symptoms. By decreasing frequency, they are human simian virus, HIV, influenza, measles, Epstein-Barr virus, mumps, and rabies.27,28 Bacterial infections that cause psychosis include mycoplasma pneumonia,29 syphilis,30 typhoid fever,31 and Lyme disease.32
Brain tumor. Childhood brain tumors often present with behavioral symptoms associated with headache, vomiting, visual changes, and motor and cognitive symptoms. A CNS tumor rarely presents with isolated neuropsychiatric symptoms.33 A few case reports describe intracranial tumors initially misdiagnosed as primary psychotic illness because of prominent psychotic symptoms.34,35 In each case, these symptoms resolved with tumor resection.
A temporal relationship does not necessarily equate to a “causal” relationship, however. Tatter et al36 describe a case of “reoccurrence” of manic symptoms initially thought to be caused by an arteriovenous malformation (AVM) 10 years after the AVM was successfully removed. The important point is that, although rarely, pediatric brain tumor can present with prominent psychotic symptoms.
Environmental toxin exposure may cause well-defined psychiatric syndromes,37 although frank psychosis is uncommon at presentation. Most often, environmental toxins produce an encephalopathic process of which psychosis may be one symptom. A few toxic exposures—such as lead,38 carbon monoxide,39 and elemental mercury40 —have presented with prominent psychotic symptoms without other encephalopathic symptoms.
Collagen vascular disease is associated with significantly elevated rates of psychiatric illness, especially depression, but only systemic lupus erythematosus (SLE) is known to be associated with prominent psychosis. Case series report delayed SLE diagnosis in patients with this presentation.41
High-dose pulse corticosteroids have been reported to effectively treat SLE-related psychotic symptoms,42 although high-dose corticosteroids can also cause psychotic symptoms. The timing and character of the symptoms can help you determine whether using corticosteroids is helping or making the patient worse.
Using the algorithm
John’s mother and father fear that the inpatient team’s diagnosis of a primary psychotic disorder means that a medical cause has been permanently “ruled out.” To reassure them, we use the algorithm to explain in concrete terms the thought process that led us to John’s psychiatric diagnosis. We walk them through the algorithm and its tables, explaining how we used evidence to rationally rule out all known medical causes of psychotic symptoms in pediatric patients.
John’s parents are relieved to know that the case is not closed, even though we found no medical cause for their son’s condition. If more clinical data become available, we remain open to considering the possibility that medical conditions could be causing or worsening their son’s symptoms.
Related resources
- American Academy of Child and Adolescent Psychiatry. Practice parameter for the assessment and treatment of children and adolescents with schizophrenia. J Am Acad Child Adolesc Psychiatry 2001;40(7 Suppl):4S-23S.
- Schiffer RB, Klein RF, Sider RC. The medical evaluation of psychiatric patients. New York: Plenum Medical Book Co.; 1998.
- National Organization for Rare Disorders (NORD). www.rarediseases.org.
1. American Academy of Child and Adolescent Psychiatry. Summary of the practice parameters for the assessment and treatment of children and adolescents with schizophrenia. J Am Acad Child Adolesc Psychiatry 2000;39(12):1580-92.
2. Behrman RE (ed). Nelson textbook of pediatrics (17th ed). Philadelphia: WB Saunders; 2003:397-518.
3. Dalmau A, Bergman B, Brismar B. Psychotic disorders among inpatients with abuse of cannabis, amphetamine and opiates. Do dopaminergic stimulants facilitate psychiatric illness? Eur Psychiatry 1999;14(7):366-71.
4. Breslow RE, Klinger BI, Erickson BJ. Acute intoxication and substance abuse among patients presenting to a psychiatric emergency service. Gen Hosp Psychiatry 1996;18(3):183-91.
5. Poole R, Brabbins C. Drug-induced psychosis. Br J Psychiatry 1996;168:137.-
6. DiSclafani A, 2nd, Hall RC, Gardner ER. Drug-induced psychosis: emergency diagnosis and management. Psychosomatics 1981;22(10):845-55.
7. Cohen SI. Substance-induced psychosis. Br J Psychiatry 1996;168(5):651-2.
8. Farrell M, Boys A, Bebbington P, et al. Psychosis and drug dependence: results from a national survey of prisoners. Br J Psychiatry 2002;181:393-8.
9. Ujike H, Sato M. Clinical features of sensitization to methamphetamine observed in patients with methamphetamine dependence and psychosis. Ann NY Acad Sci 2004;1025:279-87.
10. Drugs that may cause psychiatric symptoms. Med Lett Drugs Ther 2002;44:29-62.
11. Lewis DA, Smith RE. Steroid-induced psychiatric symptoms; a report of 14 cases and a review of the literature. J Affect Disord 1983;5(4):319-32.
12. Cummings JL. Organic psychosis. Psychosomatics 1988;29(1):16-26.
13. Roy AK, Rajesh SV, Iby N, et al. A study of epilepsy-related psychosis. Neurol India 2003;51(3):359-60.
14. Mendez MF. Huntington’s disease: update and review of neuropsychiatric aspects. Int J Psychiatry Med 1994;24:189-208.
15. Brewer GJ. Recognition and management of Wilson’s disease. Proc Soc Exp Biol Med 2000;223:39-46.
16. Mendhekar DN, Mehta R, Puri V. Successful steroid therapy in multiple sclerosis presented as acute psychosis. J Assoc Physicians India 2004;52:512-3.
17. Reus VI. Behavioral disturbances associated with endocrine disorders. Ann Rev Med 1986;37:205-14.
18. Hirsch D, Orr G, Kantarovich V, et al. Cushing’s syndrome presenting as a schizophrenia-like psychotic state. Isr J Psychiatry Relat Sci 2000;37(1):46-50.
19. Lu CL, Lee YC, Tsai SJ, et al. Psychiatric disturbances associated with hyperthyroidism: an analysis report of 30 cases. Zhonghua Yi Xue Za Zhi (Taipei) 1995;56(6):393-8.
20. Bhatara V, Alshari MG, Warhol P, et al. Coexistent hypothyroidism, psychosis, and severe obsessions in an adolescent: a 10-year follow-up. J Child Adolesc Psychopharmacol 2004;14(2):315-23.
21. Prior TI, Chue PS, Tibbo P. Investigation of Turner syndrome in schizophrenia. Am J Med Genet 2000;96(3):373-8.
22. Hyde TM, Ziegler JC, Weinberger DR. Psychiatric disturbances in metachromatic leukodystrophy. Insights into the neurobiology of psychosis. Arch Neurol 1992;49(4):401-6.
23. Briegel W, Cohen M. Chromosome 22q11 deletion syndrome and its relevance for child and adolescent psychiatry. An overview of etiology, physical symptoms, aspects of child development and psychiatric disorders. Z Kinder Jugendpsychiatr Psychother 2004;32(2):107-15.
24. Crimlisk HL. The great imitator-porphyria: a neuropsychiatric disorder. J Neurol Neurosurg Psychiatry 2001;62(4):319-28.
25. Ryan MM, Sidhu RK, Alexander J, Megerian JT. Homocystinuria presenting as psychosis in an adolescent. J Child Neurol 2002;17(11):859-60.
26. MacQueen GM, Rosebush PI, Mazurek MF. Neuropsychiatric aspects of the adult variant of Tay-Sachs disease. J Neuropsychiatry Clin Neurosci 1998;10(1):10-9.
27. Caroff SN, Mann SC, Gliatto MF, et al. Psychiatric manifestations of acute viral encephalitis. Psych Annals 2001;31(3):193-204.
28. Caplan R, Tanguay PE, Szekely AG. Subacute sclerosing panencephalitis presenting as childhood psychosis. J Am Acad Child Adolesc Psychiatry 1987;26(3):440-3.
29. Gillberg C. Schizophreniform psychosis in a case of mycoplasma pneumoniae encephalitis. J Autism Dev Disord 1980;10(2):153-8.
30. Gliatto MF, Caroff SN. Neurosyphilis: a history and clinical review. Psych Annals 2001;31(3):153-61.
31. Venkatesh S, Grell GA. Neuropsychiatric manifestations of typhoid fever. West Indian Med J 1989;38(3):137-41.
32. Tager FA, Fallon B. Psychiatric and cognitive features of Lyme disease. Psych Annals 2001;31(3):173-92.
33. Stein MT, Duffner PK, Wery JS, Trauner D. School refusal and emotional liability in a 6 year old boy. J Dev Behav Pediatr 2001;22(suppl):29-32.
34. Carson BS, Weingart JD, Guarnieri M, Fisher PG. Third ventricular choroid plexus papilloma with psychosis. Case report. J Neurosurg 1997;87(1):103-5.
35. Craven C. Pineal germinoma and psychosis. J Am Acad Child Adolesc Psychiatry 2001;40(1):6.-
36. Tatter SB, Ogilvy CS. Recurrent manic episode 10 years after arteriovenous malformation resection. J Clin Psychiatry 1995;56(2):83.-
37. Hartman DE. Missed diagnosis and misdiagnosis of environmental toxicants exposure: the psychiatry of toxic exposure and multiple chemical sensitivity. Psychiatr Clin North Am 1998;21(3):659-70.
38. Bahiga LM, Kotb NA, El-Dessoukey EA. Neurological syndromes produced by some toxic metals encountered industrially or environmentally. Z Ernahrungswiss 1978;17(2):84-8.
39. Olson KR. Carbon monoxide poisoning: mechanisms, presentation, and controversies in management. J Emerg Med 1984;1(3):233-43.
40. Fagala GE, Wigg CL. Psychiatric manifestations of mercury poisoning. J Am Acad Child Adolesc Psychiatry 1992;31(2):306-11.
41. Turkel SB, Miller JH, Reiff A. Case series: neuropsychiatric symptoms with pediatric systemic lupus erythematosus. J Am Acad Child Adolesc Psychiatry 2001;40(4):482-5.
42. Baca V, Lavalle C, Garcia R, et al. Favorable response to intravenous methylprednisolone and cyclophosphamide in children with severe neuropsychiatric lupus. J Rheumatol 1999;26(2):432-9.
1. American Academy of Child and Adolescent Psychiatry. Summary of the practice parameters for the assessment and treatment of children and adolescents with schizophrenia. J Am Acad Child Adolesc Psychiatry 2000;39(12):1580-92.
2. Behrman RE (ed). Nelson textbook of pediatrics (17th ed). Philadelphia: WB Saunders; 2003:397-518.
3. Dalmau A, Bergman B, Brismar B. Psychotic disorders among inpatients with abuse of cannabis, amphetamine and opiates. Do dopaminergic stimulants facilitate psychiatric illness? Eur Psychiatry 1999;14(7):366-71.
4. Breslow RE, Klinger BI, Erickson BJ. Acute intoxication and substance abuse among patients presenting to a psychiatric emergency service. Gen Hosp Psychiatry 1996;18(3):183-91.
5. Poole R, Brabbins C. Drug-induced psychosis. Br J Psychiatry 1996;168:137.-
6. DiSclafani A, 2nd, Hall RC, Gardner ER. Drug-induced psychosis: emergency diagnosis and management. Psychosomatics 1981;22(10):845-55.
7. Cohen SI. Substance-induced psychosis. Br J Psychiatry 1996;168(5):651-2.
8. Farrell M, Boys A, Bebbington P, et al. Psychosis and drug dependence: results from a national survey of prisoners. Br J Psychiatry 2002;181:393-8.
9. Ujike H, Sato M. Clinical features of sensitization to methamphetamine observed in patients with methamphetamine dependence and psychosis. Ann NY Acad Sci 2004;1025:279-87.
10. Drugs that may cause psychiatric symptoms. Med Lett Drugs Ther 2002;44:29-62.
11. Lewis DA, Smith RE. Steroid-induced psychiatric symptoms; a report of 14 cases and a review of the literature. J Affect Disord 1983;5(4):319-32.
12. Cummings JL. Organic psychosis. Psychosomatics 1988;29(1):16-26.
13. Roy AK, Rajesh SV, Iby N, et al. A study of epilepsy-related psychosis. Neurol India 2003;51(3):359-60.
14. Mendez MF. Huntington’s disease: update and review of neuropsychiatric aspects. Int J Psychiatry Med 1994;24:189-208.
15. Brewer GJ. Recognition and management of Wilson’s disease. Proc Soc Exp Biol Med 2000;223:39-46.
16. Mendhekar DN, Mehta R, Puri V. Successful steroid therapy in multiple sclerosis presented as acute psychosis. J Assoc Physicians India 2004;52:512-3.
17. Reus VI. Behavioral disturbances associated with endocrine disorders. Ann Rev Med 1986;37:205-14.
18. Hirsch D, Orr G, Kantarovich V, et al. Cushing’s syndrome presenting as a schizophrenia-like psychotic state. Isr J Psychiatry Relat Sci 2000;37(1):46-50.
19. Lu CL, Lee YC, Tsai SJ, et al. Psychiatric disturbances associated with hyperthyroidism: an analysis report of 30 cases. Zhonghua Yi Xue Za Zhi (Taipei) 1995;56(6):393-8.
20. Bhatara V, Alshari MG, Warhol P, et al. Coexistent hypothyroidism, psychosis, and severe obsessions in an adolescent: a 10-year follow-up. J Child Adolesc Psychopharmacol 2004;14(2):315-23.
21. Prior TI, Chue PS, Tibbo P. Investigation of Turner syndrome in schizophrenia. Am J Med Genet 2000;96(3):373-8.
22. Hyde TM, Ziegler JC, Weinberger DR. Psychiatric disturbances in metachromatic leukodystrophy. Insights into the neurobiology of psychosis. Arch Neurol 1992;49(4):401-6.
23. Briegel W, Cohen M. Chromosome 22q11 deletion syndrome and its relevance for child and adolescent psychiatry. An overview of etiology, physical symptoms, aspects of child development and psychiatric disorders. Z Kinder Jugendpsychiatr Psychother 2004;32(2):107-15.
24. Crimlisk HL. The great imitator-porphyria: a neuropsychiatric disorder. J Neurol Neurosurg Psychiatry 2001;62(4):319-28.
25. Ryan MM, Sidhu RK, Alexander J, Megerian JT. Homocystinuria presenting as psychosis in an adolescent. J Child Neurol 2002;17(11):859-60.
26. MacQueen GM, Rosebush PI, Mazurek MF. Neuropsychiatric aspects of the adult variant of Tay-Sachs disease. J Neuropsychiatry Clin Neurosci 1998;10(1):10-9.
27. Caroff SN, Mann SC, Gliatto MF, et al. Psychiatric manifestations of acute viral encephalitis. Psych Annals 2001;31(3):193-204.
28. Caplan R, Tanguay PE, Szekely AG. Subacute sclerosing panencephalitis presenting as childhood psychosis. J Am Acad Child Adolesc Psychiatry 1987;26(3):440-3.
29. Gillberg C. Schizophreniform psychosis in a case of mycoplasma pneumoniae encephalitis. J Autism Dev Disord 1980;10(2):153-8.
30. Gliatto MF, Caroff SN. Neurosyphilis: a history and clinical review. Psych Annals 2001;31(3):153-61.
31. Venkatesh S, Grell GA. Neuropsychiatric manifestations of typhoid fever. West Indian Med J 1989;38(3):137-41.
32. Tager FA, Fallon B. Psychiatric and cognitive features of Lyme disease. Psych Annals 2001;31(3):173-92.
33. Stein MT, Duffner PK, Wery JS, Trauner D. School refusal and emotional liability in a 6 year old boy. J Dev Behav Pediatr 2001;22(suppl):29-32.
34. Carson BS, Weingart JD, Guarnieri M, Fisher PG. Third ventricular choroid plexus papilloma with psychosis. Case report. J Neurosurg 1997;87(1):103-5.
35. Craven C. Pineal germinoma and psychosis. J Am Acad Child Adolesc Psychiatry 2001;40(1):6.-
36. Tatter SB, Ogilvy CS. Recurrent manic episode 10 years after arteriovenous malformation resection. J Clin Psychiatry 1995;56(2):83.-
37. Hartman DE. Missed diagnosis and misdiagnosis of environmental toxicants exposure: the psychiatry of toxic exposure and multiple chemical sensitivity. Psychiatr Clin North Am 1998;21(3):659-70.
38. Bahiga LM, Kotb NA, El-Dessoukey EA. Neurological syndromes produced by some toxic metals encountered industrially or environmentally. Z Ernahrungswiss 1978;17(2):84-8.
39. Olson KR. Carbon monoxide poisoning: mechanisms, presentation, and controversies in management. J Emerg Med 1984;1(3):233-43.
40. Fagala GE, Wigg CL. Psychiatric manifestations of mercury poisoning. J Am Acad Child Adolesc Psychiatry 1992;31(2):306-11.
41. Turkel SB, Miller JH, Reiff A. Case series: neuropsychiatric symptoms with pediatric systemic lupus erythematosus. J Am Acad Child Adolesc Psychiatry 2001;40(4):482-5.
42. Baca V, Lavalle C, Garcia R, et al. Favorable response to intravenous methylprednisolone and cyclophosphamide in children with severe neuropsychiatric lupus. J Rheumatol 1999;26(2):432-9.
Adult with ADHD? Try medication + psychotherapy
Mr. B, age 50, dreams of becoming a computer programmer but fears he will embarrass himself—as he has in many classrooms before. He is seeking evaluation because his teenage son was recently diagnosed with attention-deficit/hyperactivity disorder (ADHD), and he recognizes similar symptoms in himself.
Mr. B received a college degree with great difficulty, putting off assignments until the last minute and “squeaking by.” For years he has changed occupations often, never progressing beyond entry level, and now works as a personal care provider and limousine driver. He reports problems keeping up with work and managing time.
His history includes early childhood hyperactivity, difficulty sitting through classes, sloppy handwriting, disorganization, short attention span, and distractibility. He is restless, fidgety, and has trouble staying on topic. His disorganization has caused marital difficulties, for which he has sought counseling.
After careful evaluation, you determine that Mr. B meets criteria for ADHD, combined type, and for anxiety disorder not otherwise specified. His treatment goals are to increase his ability to focus; procrastinate less; improve his planning, prioritizing, and self-esteem; and to become less sensitive to criticism and less anxious about handling work demands.
Like Mr. B, adults with ADHD need treatment for the disorder’s core symptoms as well as its psychiatric comorbidities and psychosocial consequences. Comprehensive treatment with medications, cognitive-behavioral therapy (CBT), and environmental adaptations is usually recommended.
Comorbidity rules
Core symptoms. ADHD is a lifespan disorder with multiple behavioral, cognitive, and emotional manifestations that impair relationships and academic and vocational functioning. ADHD-like symptoms are seen in other conditions such as mood disorders or substance abuse, but complaints of inattention, distractibility, procrastination, restlessness, and impulsivity—particularly when pervasive and chronic—are highly indicative of ADHD.
In treating adults with ADHD, we have noticed common behavioral patterns that contribute to their psychosocial problems (Table 1). Dysfunctional coping behaviors have short-term advantages, but patients readily admit they would rather accomplish tasks through greater thought and planning.
Chronic frustrations—often associated with deep shame—are typical of adult ADHD. Many patients have maladaptive core beliefs of failure, self-mistrust, and inadequacy (Table 2).
Table 1
Common dysfunctional behavioral patterns in adults with ADHD
| Behavior | Description | Short-term gain/long-term loss |
|---|---|---|
| Anticipatory avoidance | Magnifying the difficulty of a pending task and doubts about being able to complete it; results in rationalizations to justify procrastination | Defers short-term stress, but often creates a self-fulfilling prophecy because the task looms and may seem overwhelming when facing a deadline |
| Brinksmanship | Waiting until the last moment (eg, the night before) to complete a task, often when facing an impending deadline | Deadline-associated stress can be focusing, but this tactic leaves little room for error and may yield a substandard result |
| Pseudoefficiency | Completing several low-priority, manageable tasks (eg, checking e-mail) but avoiding high-priority tasks (eg, a project for work) | Creates sense of productivity by reducing items on to-do list but defers a more difficult project |
| Juggling | Taking on new, exciting projects and feeling ‘busy’ without completing projects already started | It is easier to become motivated to start a novel project than to complete an ongoing one; pattern usually results in several incomplete projects |
Table 2
5 common maladaptive core beliefs of adults with ADHD
| Self-mistrust | ‘I cannot rely on myself to do what I need to do. I let myself down’ |
| Failure | ‘I always have failed and always will fail at what I set out to do.’ |
| Inadequacy | ‘I am basically a bad and defective person.’ |
| Incompetence | ‘I am too inept to handle life’s basic demands.’ |
| Instability | ‘My life will always be chaotic and in turmoil.’ |
Psychiatric comorbidity is the rule in adults with ADHD (Table 3). For example, among 43 patients who received combined medication and CBT at the University of Pennsylvania Adult ADHD Treatment and Research Program, 75% reported at least one comorbid condition, including:
- 27 (63%) with mood disorder
- 23 (54%) with anxiety disorder
- 5 (12%) with substance abuse.1
Other treatment studies have reported similar comorbidity rates in adults with ADHD.2-4
Table 3
Psychiatric comorbidity in adult ADHD
| Disorder | Prevalence |
|---|---|
| Mood disorders | 50% to 65% |
| Recurrent depression | |
| Bipolar disorder | |
| Cyclothymia | |
| Dysthymia | |
| Depressive disorder NOS | |
| Anxiety disorders | 40% to 55% |
| Generalized anxiety disorder | |
| Anxiety disorder NOS | |
| Others | Various |
| Substance use disorder | |
| Learning disabilities | |
| Intermittent explosive disorder | |
| Tourette syndrome | |
| Antisocial personality | |
| Borderline personality disorder | |
| Dependent personality | |
| NOS: Not otherwise specified | |
Making the diagnosis
Diagnosis of adult ADHD is based on a comprehensive assessment, including:
- careful history of presenting complaints
- thorough review of educational, occupational, and family history
- standardized rating scales (such as the Barkley ADHD Behavior Checklists, the Conners’ Adult ADHD Rating Scale, or the Brown Attention Deficit Disorder Scales)
- collateral information
- assessment of mood, anxiety, substance use, and learning/organizational skills. For details, consult references on adult ADHD.5-8
Case continued: Self-fulfilling prophesies
On standardized rating scales, Mr. B meets criteria for combined ADHD for childhood and current symptoms. Information from his wife and brother also confirms the ADHD diagnosis.
He is motivated, resilient, optimistic, and has a good support system. However, his negative automatic thoughts about his ability to succeed in school and to handle increasing time demands suggest deeper beliefs of inadequacy and failure.
Mr. B struggled academically. Without guidance about how to change his approach to difficult situations, he has repeated old thinking and behavior patterns. Believing he will embarrass himself and fail to learn required material, Mr. B procrastinates and avoids doing assignments. In class, his feelings of inadequacy make him self-conscious, which causes him to lose focus and have trouble concentrating.
See the world through the patient’s eyes
Understanding your patient. Before you start treatment, we recommend that you conceptualize how ADHD has influenced your patient’s life, including:
- developmental experiences
- family-of-origin issues, such as conflicts with parents stemming from ADHD symptoms or reciprocal interactions with an ADHD parent
- world view (“schemata”)
- patterns of coping with (or avoiding) stress
- attitudes toward self and important others
- readiness to change.
Developing a working case conceptualization is a dynamic, collaborative process. You talk with patients, and encourage them to reflect on how ADHD affects their view of themselves and their important relationships. The conceptualization takes shape as you:
- observe patients’ behaviors
- elicit how they think and feel
- assess with them the relevance and accuracies of their belief systems and response patterns.
Seeing the world “through their eyes” prepares you to help them accept the diagnosis and learn to manage ADHD symptoms. Then, by providing a blueprint to manage what patients may see as uncontrollable responses, you can help them take charge of their automatic reactions.
Psychoeducation. To set the stage for treatment, encourage patients to learn about ADHD by reading articles and books and consulting Web sites for adults with ADHD (see Related resources). Psychoeducation helps patients:
- review possible treatment approaches, including organizational (environmental) management, medication, and psychotherapy (individual or group)
- become informed participants in setting treatment goals.
Explain the relative contribution of each treatment component. For example, medications can reduce distractibility and improve attention, organizational strategies can reduce disorganization and improve time management, and structured psychotherapy can help the patient develop more effective coping skills.
Case continued: Planning combined treatment
You discuss diagnosis and treatment options with Mr. B, and he agrees to start the methylphenidate compound Concerta, initially at 18 mg/d, and weekly CBT sessions. You recommended a stimulant based on efficacy studies and your clinical experience in treating adults with ADHD. Mr. B wants a medication that will help him focus while working or studying, and he says Concerta has improved his son’s ADHD symptoms.
You instruct Mr. B to increase the dosage by 18 mg each week until he reaches 72 mg/d. You also tell him to keep a medication response log and to note any positive changes and side effects.
If an adult with ADHD expresses preference for a particular medication, we usually prescribe that one first. Most patients to whom we offer both medication and psychotherapy agree to this “top-down” and “bottom-up” approach. “Top down” means giving patients new ways of thinking to help them understand and modify their responses. “Bottom up” refers to the medication reducing their impulsivity, distractibility, and inattentiveness.
CBT for adult ADHD
Medications can ameliorate key symptoms of adult ADHD, but adjunctive interventions are needed to improve functioning and quality of life. Evidence supporting psychosocial treatment for adults with ADHD is limited, but CBT has been studied the most.1,9-13 Safren et al13 found a four-fold greater therapeutic response when patients received adjunctive CBT for residual ADHD symptoms, compared with patients who received medication alone.
We usually provide CBT weekly for 12 weeks and then taper to 8 additional sessions over 3 months (total 20 sessions). We may extend CBT with additional sessions to address complicated issues. CBT helps adults with ADHD to:
- identify dysfunctional thinking, feeling, and behaving patterns
- recognize contexts in which patterns arise
- systematically change these patterns.
CBT can reduce ADHD-associated anxiety and depression and improve coping skills and sense of well-being.1,9,11 Its flexibility allows you to address family issues with patients’ partners, children and other relatives to improve communication, reduce conflict, and develop healthier interactions.
We focus CBT sessions on finding alternate coping strategies. We might try role playing, rehearsing, creating “thought experiments,” and anticipating and preparing to modify typical patterns of avoidance. These approaches have been described elsewhere.10,11,14
We adopt an active stance during therapy to keep ADHD patients’ distractibility from disrupting our conversation. For example, we set the therapeutic agenda, provide feedback about patients’ behaviors, and encourage them to clarify rewards and consequences of using (or avoiding) problem-solving strategies.
Although we typically assign between-session homework, we expect patients to have difficulty completing it. We remain nonjudgmental and collaborative, viewing incomplete assignments as opportunities to learn about patients’ unproductive problem solving and to help them develop more-effective patterns.
Challenging maladaptive beliefs. A strong therapeutic relationship allows adults with ADHD to discuss their chronic frustrations, which often are associated with deep shame. We then shift CBT’s focus to deeper ADHD-related schemata that perpetuate dysfunctional patterns.
We work with patients to elucidate and challenge their maladaptive core beliefs and encourage new ways to view themselves and others. Allowing patients to grieve about the limitations ADHD imposes on their lives also helps to reduce chronic negative self-esteem.
Case continued: ‘less frenetic’
Mr. B achieves good results within 3 weeks of an increasing titration of stimulant medication, reporting significantly less restlessness and greater concentration without significant side effects. His wife confirms that he is less frenetic, can converse without interruptions, and is better at managing his complicated work schedule.
Which medications?
Drug therapy for adult ADHD is not as well-studied as in children and adolescents, but American Academy of Child and Adolescent Psychiatry guidelines and others15-18 recommend stimulant and nonstimulant medications. Your choice depends on the patient’s clinical profile (including risk factors and comorbid conditions), past medication use, treatment goals, preferred medication effects and dosing patterns (once-daily versus multiple times), and potential side effects. Stimulants or atomoxetine are first-line choices for adult ADHD without psychiatric comorbidity.
Stimulants work quickly and are cleared relatively rapidly from the brain without causing euphoria or dependency. They are effective (80% to 90% response rate) and well-tolerated, though long-term effects have not been studied in adults (Table 4).
Stimulants’ effect size of 0.9 is considered substantial. Effect size—a statistical method of reporting an intervention’s effect across different studies—is typically rated as:
- <0.32 very small
- 0.33 to 0.54, moderate
- >0.55, significant or very strong.
When choosing a medication, we usually try methylphenidate and amphetamine first, one after the other. We explain to the patient how stimulants work in the brain and the need for a comparative trial to determine which might work best for him or her. If the patient has tried a stimulant and found it helpful, we start with that class. Similarly, if he/she has not had good results with one type, we start with the other. Approximately one-third of our patients respond equally well to methylphenidate or amphetamine, one-third respond better to methylphenidate, and one-third respond better to amphetamine.
To determine the optimal dosage, we usually titrate up from 10 to 30 mg per dose of an immediate-release preparation. We begin with this form to help patients notice the medication’s onset and duration of action. After we find the optimal dosage, we switch to a longer-acting preparation.
Insomnia, mood instability, and euphoria are unacceptable stimulant side effects, although many patients welcome others such as appetite suppression and weight loss. Closely monitor cardiovascular effects, and review potential interactions with other medications, such as antihypertensives or bronchodilators. Because sudden death has been reported with stimulants in persons with structural cardiac lesions,19 obtain a cardiology consultation for patients with a history of heart disease.
We encourage patients to keep daily medication logs (Box), which we review at each visit and use to make dosing or medication changes. Dosing guidelines resemble those used for children and adolescents, although adults usually tolerate higher maximum dosages (such as methylphenidate, 80 to 100 mg/d).
Because of stimulants’ potential for recreational misuse and abuse, remain wary about choosing stimulants for patients with whom you lack a solid doctor-patient relationship.
Table 4
Stimulant dosages used in treating adult ADHD
| Class (brand name) | Daily dosing | Typical dosing schedule |
|---|---|---|
| Methylphenidate | ||
| Short-acting (Metadate, Ritadex, Ritalin) | Two to four times | 10 to 40 mg bid to qid |
| Intermediate-acting (Metadate SR, Ritalin SR) | Once or twice | 20 to 60 mg qd to bid |
| Extended-release (Concerta, Metadate CD, Ritalin LA) | Once or twice | 18 to 108 mg qd (Concerta) 20 to 40 mg bid (Ritalin LA, Metadate CD) |
| Dextromethylphenidate | ||
| Short-acting (Focalin) | Two to four times | 5 to 20 mg bid to qid |
| Long-acting (Focalin XR) | Once or twice | 10 to 20 mg qd or bid |
| Dextroamphetamine | ||
| Short-acting (Dexedrine) | Twice or three times | 10 to 30 mg bid or tid |
| Intermediate-acting (Dexedrine spansules) | Once or twice | 10 to 30 mg bid |
| Mixed amphetamine salts | ||
| Intermediate-acting (Adderall) | Once or twice | 10 to 30 mg bid or tid |
| Extended-release (Adderall XR) | Once or twice | 10 to 40 mg qd or bid |
Atomoxetine, a nonstimulant, norepinephrine re-uptake inhibitor, is approved for ADHD in adults.20-22 In two double-blind, controlled, randomized trials totalling 536 adults, Michaelson et al20 found significantly reduced ADHD symptoms after 10 weeks of atomoxetine treatment. Effect sizes of 0.35 and 0.40 were reported, with 10% of patients discontinuing because of side effects.
Atomoxetine has a long duration of action (>12 hours) but a more gradual onset (4 to 6 weeks) than that of stimulants. Approximately 60% of patients respond to atomoxetine, though effect sizes are less than those of stimulants. We have found atomoxetine works well for patients who:
- do not tolerate or are uncomfortable with taking stimulants
- are highly anxious
- report emotional dysregulation as a major target symptom.
To reduce risk of common side effects (nausea, GI upset, headache, sedation, reduced sex drive), we start with low dosages (such as 25 mg bid) and increase weekly by 25 mg to a target of 80 to 100 mg/d.
Treating complicated ADHD
Bupropion or tricyclic antidepressants are reasonable options for ADHD with depression. Atomoxetine, a tricyclic, or a stimulant plus a selective serotonin reuptake inhibitor (SSRI) can provide good symptom relief for adults with ADHD and comorbid anxiety and/or depression.
Bupropion. Approximately 50% of adults with ADHD respond to bupropion,23,24 with a treatment effect size of 0.6. Bupropion’s efficacy in smoking cessation adds value for those trying to quit.
We usually start extended-release bupropion at 150 mg/d and increase after 2 weeks to 300 mg/d if response is suboptimal. Headache, dry mouth, insomnia, and nausea are the most common adverse effects. Agitation or irritability is sometimes serious enough to warrant stopping bupropion.
Combining medications. Using SSRIs with stimulants can help adults with ADHD and comorbid anxiety or depression. Any SSRI can be safely combined with stimulants, though we tend to pick:
- more-sedating agents such as paroxetine or sertraline when patients report difficulty with insomnia or overactivation
- less-sedating compounds such as fluoxetine or citalopram when patients complain of being too tired or underactive.
When patients taking SSRIs seek help for ADHD, adding a stimulant usually reduces inattention, distractibility, impulsivity, and/or subjective feelings of restlessness. We prescribe usual dosages because stimulants and SSRIs do not interact. We have not seen serious side effects, but some patients report feeling oversedated.
Tricyclics. We use tricyclics when a stimulant/SSRI combination does not relieve symptoms satisfactorily or a patient complains of side effects. We usually have good results with desipramine or imipramine, 150 to 300 mg/d, or nortriptyline, 50 to 150 mg/d. Spencer et al have reported a response rate of 68% with nortriptyline or desipramine in a retrospective chart review25 and a prospective placebo-controlled trial26 of adults with ADHD.
Case continued: Closer to dream job
After 6 months of combined treatment, Mr. B reports much-improved ADHD symptoms, with minimal stimulant-related side effects. He has made some realistic plans for computer programming school and is taking preliminary courses. Keeping a schedule book has reduced his tardiness and tendency to procrastinate.
He is more comfortable in the classroom and better able to challenge self-critical thinking. When routine difficulties arise, he is using more-adaptive coping strategies. To maintain gains achieved in therapy, he chooses to continue periodic CBT booster sessions.
Long-term treatment
Even with medication and CBT, patients may require referral for organizational coaching, academic counseling, school or workplace accommodations, vocational counseling, cognitive remediation, group therapy, or social skills classes. You can help them obtain quality adjunctive care by collaborating with professionals who offer these services.
No studies have examined long-term care of adults with ADHD. In our experience, ongoing medication and intermittent therapy can sustain symptom control and coping skills for years. Most patients are initially skeptical about staying on medication, but after they experience the benefits most seem willing to continue as long as the medication helps.
Most of our patients sustain changes in thinking, feeling, and behaving that they learn through BT. They may seek additional sessions to meet a challenge, such as a new job or starting a family.
Books
- Kolberg J, Nadeau K. ADD-friendly ways to organize your life. New York: Brunner-Routledge; 2002.
- Hallowell EM, Ratey JJ. Driven to distraction. New York: Touchstone; 1994.
- Hallowell E, Ratey J. Delivered from distraction. New York: Ballantine Books; 2005.
Organizations
- Children and Adults with Attention-Deficit/Hyperactivity Disorder (CHADD). National Resource Center on AD/HD. www.chadd.org.
- Attention Deficit Disorder Association (ADDA). Resources and membership organization for adults with ADHD. www.add.org.
Drug brand names
- Amphetamine • Adderall, Dexedrine
- Atomoxetine • Strattera
- Bupropion • Wellbutrin
- Desipramine • Norpramin
- Imipramine • Tofranil
- Methylphenidate • Concerta, Focalin, Metadate, Ritalin
- Nortriptyline • Aventyl, Pamelor
Disclosures
Dr. Rostain is a consultant to Shire Pharamaceuticals Group and a speaker for Eli Lilly & Co. and Ortho-McNeil Pharmaceutical
Dr. Ramsay reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Rostain AL, Ramsay JR. A combined treatment approach for adults with attention-deficit/hyperactivity disorder. Results of an open study of 43 patients J Attention Disorders. In press.
2. Shekim WO, Asarnow RF, Hess E, et al. A clinical and demographic profile of a sample of adults with attention deficit hyperactivity disorder, residual state. Comp Psychiatry 1990;31:416-25.
3. Biederman J, Faraone SV, Spencer T, et al. Patterns of psychiatric comorbidity, cognition and psychosocial functioning in adults with attention deficit hyperactivity disorder. Am J Psychiatry 1993;150:1792-8.
4. Wilens TE, Biederman J, Spencer T. Attention-deficit/hyperactivity disorder across the lifespan. Ann Rev Medicine 2002;53:113-31.
5. Barkley RA. Attention deficit hyperactivity disorder: a handbook for diagnosis and treatment. New York: Guilford Press; 1998.
6. Wender PH. ADHD: Attention-deficit hyperactivity disorder in children and adults. New York: Oxford University Press; 2000.
7. Goldstein S, Ellison AT. Clinician’s guide to adult ADHD. San Diego: Academic Press; 2000.
8. Brown TE. Attention-deficit disorder: the unfocused mind in children and adults. New Haven, CT: Yale University Press; 2005.
9. Wilens TE, McDermott SP, Biederman J, et al. Cognitive therapy in the treatment of adults with ADHD: a systematic chart review of 26 cases. J Cogn Ther 1999;13:215-26.
10. Ramsay JR, Rostain AL. A cognitive therapy approach for adult attention-deficit/hyperactivity disorder. J Cogn Psychother 2003;17:319-34.
11. Safren SA, Sprich S, Chulvick S, Otto MW. Psychosocial treatments for adults with attention-deficit/hyperactivity disorder. Psychiatr Clin North Am 2004;27:349-60.
12. Ramsay JR, Rostain AL. Adapting psychotherapy to meet the needs of adults with attention-deficit/hyperactivity disorder. Psychotherapy: Theory, Research, Practice, Training 2005;42:72-84.
13. Safren SA, Otto MW, Sprich S, et al. Cognitive-behavior therapy for ADHD in medication-treated adults with continued symptoms. Behav Res Ther 2005;43:831-42.
14. Ramsay JR, Rostain AL. Girl, repeatedly interrupted: The case of a young adult woman with ADHD. Clinical Case Studies 2005;4:329-46.
15. American Academy of Child and Adolescent Psychiatry. Practice parameters for the use of stimulant medications in the treatment of children, adolescents, and adults. J Am Acad Child Adolesc Psychiatry 2002;42(suppl 2):26S-49S.
16. Weiss M, Murray C, Weiss G. Adults with attention-deficit/hyperactivity disorder: Current concepts. J Psychiatr Pract 2002;8:99-111.
17. Wilens TE. Drug therapy for adults with attention-deficit hyperactivity disorder. Drugs 2003;63:2395-411.
18. Dodson WW. Pharmacotherapy of adult ADHD. J Clin Psychol 2005;61:589-606.
19. Francis PD. Effects of psychotropic medications on the pediatric electrocardiogram and recommendations for monitoring. Curr Opin Pediatr 2002;14(2):224-30
20. Michaelson D, Adler L, Spencer T. Atomoxetine in adults: Two randomized, placebo-controlled studies. Biol Psychiatry 2003;53:112-20.
21. Simpson D, Plosker GL. Atomoxetine: a review of its use in adults with attention deficit hyperactivity disorder. Drugs 2004;64:205-22.
22. Reimherr FW, Marchant BK, Strong RE, et al. Emotional dysregulation in adult ADHD and response to atomoxetine. Biol Psychiatry 2005;58:125-31.
23. Wilens TE, Spencer T, Biederman J. A controlled clinical trial of bupropion for attention-deficit/hyperactivity disorder in adults. Am J Psychiatry 2001;158:282-8.
24. Wilens TE, Haight BR, Horrigan JP, et al. Bupropion XL in adults with attention-deficit/hyperactivity disorder: a randomized, placebo-controlled study. Biol Psychiatry 2005;57:793-801.
25. Wilens TE, Biederman JB, Mick E, Spencer TJ. A systematic assessment of tricyclic antidepressants in the treatment of adult attention deficit/hyperactivity disorder. J Nerv Ment Dis 1995;183:48-50.
26. Wilens TE, Biederman JB, Prince J, et al. Six-week, double-blind, placebo-controlled study of desipramine for adult attention deficit hyperactivity disorder. Am J Psychiatry 1996;153:1147-53.
Mr. B, age 50, dreams of becoming a computer programmer but fears he will embarrass himself—as he has in many classrooms before. He is seeking evaluation because his teenage son was recently diagnosed with attention-deficit/hyperactivity disorder (ADHD), and he recognizes similar symptoms in himself.
Mr. B received a college degree with great difficulty, putting off assignments until the last minute and “squeaking by.” For years he has changed occupations often, never progressing beyond entry level, and now works as a personal care provider and limousine driver. He reports problems keeping up with work and managing time.
His history includes early childhood hyperactivity, difficulty sitting through classes, sloppy handwriting, disorganization, short attention span, and distractibility. He is restless, fidgety, and has trouble staying on topic. His disorganization has caused marital difficulties, for which he has sought counseling.
After careful evaluation, you determine that Mr. B meets criteria for ADHD, combined type, and for anxiety disorder not otherwise specified. His treatment goals are to increase his ability to focus; procrastinate less; improve his planning, prioritizing, and self-esteem; and to become less sensitive to criticism and less anxious about handling work demands.
Like Mr. B, adults with ADHD need treatment for the disorder’s core symptoms as well as its psychiatric comorbidities and psychosocial consequences. Comprehensive treatment with medications, cognitive-behavioral therapy (CBT), and environmental adaptations is usually recommended.
Comorbidity rules
Core symptoms. ADHD is a lifespan disorder with multiple behavioral, cognitive, and emotional manifestations that impair relationships and academic and vocational functioning. ADHD-like symptoms are seen in other conditions such as mood disorders or substance abuse, but complaints of inattention, distractibility, procrastination, restlessness, and impulsivity—particularly when pervasive and chronic—are highly indicative of ADHD.
In treating adults with ADHD, we have noticed common behavioral patterns that contribute to their psychosocial problems (Table 1). Dysfunctional coping behaviors have short-term advantages, but patients readily admit they would rather accomplish tasks through greater thought and planning.
Chronic frustrations—often associated with deep shame—are typical of adult ADHD. Many patients have maladaptive core beliefs of failure, self-mistrust, and inadequacy (Table 2).
Table 1
Common dysfunctional behavioral patterns in adults with ADHD
| Behavior | Description | Short-term gain/long-term loss |
|---|---|---|
| Anticipatory avoidance | Magnifying the difficulty of a pending task and doubts about being able to complete it; results in rationalizations to justify procrastination | Defers short-term stress, but often creates a self-fulfilling prophecy because the task looms and may seem overwhelming when facing a deadline |
| Brinksmanship | Waiting until the last moment (eg, the night before) to complete a task, often when facing an impending deadline | Deadline-associated stress can be focusing, but this tactic leaves little room for error and may yield a substandard result |
| Pseudoefficiency | Completing several low-priority, manageable tasks (eg, checking e-mail) but avoiding high-priority tasks (eg, a project for work) | Creates sense of productivity by reducing items on to-do list but defers a more difficult project |
| Juggling | Taking on new, exciting projects and feeling ‘busy’ without completing projects already started | It is easier to become motivated to start a novel project than to complete an ongoing one; pattern usually results in several incomplete projects |
Table 2
5 common maladaptive core beliefs of adults with ADHD
| Self-mistrust | ‘I cannot rely on myself to do what I need to do. I let myself down’ |
| Failure | ‘I always have failed and always will fail at what I set out to do.’ |
| Inadequacy | ‘I am basically a bad and defective person.’ |
| Incompetence | ‘I am too inept to handle life’s basic demands.’ |
| Instability | ‘My life will always be chaotic and in turmoil.’ |
Psychiatric comorbidity is the rule in adults with ADHD (Table 3). For example, among 43 patients who received combined medication and CBT at the University of Pennsylvania Adult ADHD Treatment and Research Program, 75% reported at least one comorbid condition, including:
- 27 (63%) with mood disorder
- 23 (54%) with anxiety disorder
- 5 (12%) with substance abuse.1
Other treatment studies have reported similar comorbidity rates in adults with ADHD.2-4
Table 3
Psychiatric comorbidity in adult ADHD
| Disorder | Prevalence |
|---|---|
| Mood disorders | 50% to 65% |
| Recurrent depression | |
| Bipolar disorder | |
| Cyclothymia | |
| Dysthymia | |
| Depressive disorder NOS | |
| Anxiety disorders | 40% to 55% |
| Generalized anxiety disorder | |
| Anxiety disorder NOS | |
| Others | Various |
| Substance use disorder | |
| Learning disabilities | |
| Intermittent explosive disorder | |
| Tourette syndrome | |
| Antisocial personality | |
| Borderline personality disorder | |
| Dependent personality | |
| NOS: Not otherwise specified | |
Making the diagnosis
Diagnosis of adult ADHD is based on a comprehensive assessment, including:
- careful history of presenting complaints
- thorough review of educational, occupational, and family history
- standardized rating scales (such as the Barkley ADHD Behavior Checklists, the Conners’ Adult ADHD Rating Scale, or the Brown Attention Deficit Disorder Scales)
- collateral information
- assessment of mood, anxiety, substance use, and learning/organizational skills. For details, consult references on adult ADHD.5-8
Case continued: Self-fulfilling prophesies
On standardized rating scales, Mr. B meets criteria for combined ADHD for childhood and current symptoms. Information from his wife and brother also confirms the ADHD diagnosis.
He is motivated, resilient, optimistic, and has a good support system. However, his negative automatic thoughts about his ability to succeed in school and to handle increasing time demands suggest deeper beliefs of inadequacy and failure.
Mr. B struggled academically. Without guidance about how to change his approach to difficult situations, he has repeated old thinking and behavior patterns. Believing he will embarrass himself and fail to learn required material, Mr. B procrastinates and avoids doing assignments. In class, his feelings of inadequacy make him self-conscious, which causes him to lose focus and have trouble concentrating.
See the world through the patient’s eyes
Understanding your patient. Before you start treatment, we recommend that you conceptualize how ADHD has influenced your patient’s life, including:
- developmental experiences
- family-of-origin issues, such as conflicts with parents stemming from ADHD symptoms or reciprocal interactions with an ADHD parent
- world view (“schemata”)
- patterns of coping with (or avoiding) stress
- attitudes toward self and important others
- readiness to change.
Developing a working case conceptualization is a dynamic, collaborative process. You talk with patients, and encourage them to reflect on how ADHD affects their view of themselves and their important relationships. The conceptualization takes shape as you:
- observe patients’ behaviors
- elicit how they think and feel
- assess with them the relevance and accuracies of their belief systems and response patterns.
Seeing the world “through their eyes” prepares you to help them accept the diagnosis and learn to manage ADHD symptoms. Then, by providing a blueprint to manage what patients may see as uncontrollable responses, you can help them take charge of their automatic reactions.
Psychoeducation. To set the stage for treatment, encourage patients to learn about ADHD by reading articles and books and consulting Web sites for adults with ADHD (see Related resources). Psychoeducation helps patients:
- review possible treatment approaches, including organizational (environmental) management, medication, and psychotherapy (individual or group)
- become informed participants in setting treatment goals.
Explain the relative contribution of each treatment component. For example, medications can reduce distractibility and improve attention, organizational strategies can reduce disorganization and improve time management, and structured psychotherapy can help the patient develop more effective coping skills.
Case continued: Planning combined treatment
You discuss diagnosis and treatment options with Mr. B, and he agrees to start the methylphenidate compound Concerta, initially at 18 mg/d, and weekly CBT sessions. You recommended a stimulant based on efficacy studies and your clinical experience in treating adults with ADHD. Mr. B wants a medication that will help him focus while working or studying, and he says Concerta has improved his son’s ADHD symptoms.
You instruct Mr. B to increase the dosage by 18 mg each week until he reaches 72 mg/d. You also tell him to keep a medication response log and to note any positive changes and side effects.
If an adult with ADHD expresses preference for a particular medication, we usually prescribe that one first. Most patients to whom we offer both medication and psychotherapy agree to this “top-down” and “bottom-up” approach. “Top down” means giving patients new ways of thinking to help them understand and modify their responses. “Bottom up” refers to the medication reducing their impulsivity, distractibility, and inattentiveness.
CBT for adult ADHD
Medications can ameliorate key symptoms of adult ADHD, but adjunctive interventions are needed to improve functioning and quality of life. Evidence supporting psychosocial treatment for adults with ADHD is limited, but CBT has been studied the most.1,9-13 Safren et al13 found a four-fold greater therapeutic response when patients received adjunctive CBT for residual ADHD symptoms, compared with patients who received medication alone.
We usually provide CBT weekly for 12 weeks and then taper to 8 additional sessions over 3 months (total 20 sessions). We may extend CBT with additional sessions to address complicated issues. CBT helps adults with ADHD to:
- identify dysfunctional thinking, feeling, and behaving patterns
- recognize contexts in which patterns arise
- systematically change these patterns.
CBT can reduce ADHD-associated anxiety and depression and improve coping skills and sense of well-being.1,9,11 Its flexibility allows you to address family issues with patients’ partners, children and other relatives to improve communication, reduce conflict, and develop healthier interactions.
We focus CBT sessions on finding alternate coping strategies. We might try role playing, rehearsing, creating “thought experiments,” and anticipating and preparing to modify typical patterns of avoidance. These approaches have been described elsewhere.10,11,14
We adopt an active stance during therapy to keep ADHD patients’ distractibility from disrupting our conversation. For example, we set the therapeutic agenda, provide feedback about patients’ behaviors, and encourage them to clarify rewards and consequences of using (or avoiding) problem-solving strategies.
Although we typically assign between-session homework, we expect patients to have difficulty completing it. We remain nonjudgmental and collaborative, viewing incomplete assignments as opportunities to learn about patients’ unproductive problem solving and to help them develop more-effective patterns.
Challenging maladaptive beliefs. A strong therapeutic relationship allows adults with ADHD to discuss their chronic frustrations, which often are associated with deep shame. We then shift CBT’s focus to deeper ADHD-related schemata that perpetuate dysfunctional patterns.
We work with patients to elucidate and challenge their maladaptive core beliefs and encourage new ways to view themselves and others. Allowing patients to grieve about the limitations ADHD imposes on their lives also helps to reduce chronic negative self-esteem.
Case continued: ‘less frenetic’
Mr. B achieves good results within 3 weeks of an increasing titration of stimulant medication, reporting significantly less restlessness and greater concentration without significant side effects. His wife confirms that he is less frenetic, can converse without interruptions, and is better at managing his complicated work schedule.
Which medications?
Drug therapy for adult ADHD is not as well-studied as in children and adolescents, but American Academy of Child and Adolescent Psychiatry guidelines and others15-18 recommend stimulant and nonstimulant medications. Your choice depends on the patient’s clinical profile (including risk factors and comorbid conditions), past medication use, treatment goals, preferred medication effects and dosing patterns (once-daily versus multiple times), and potential side effects. Stimulants or atomoxetine are first-line choices for adult ADHD without psychiatric comorbidity.
Stimulants work quickly and are cleared relatively rapidly from the brain without causing euphoria or dependency. They are effective (80% to 90% response rate) and well-tolerated, though long-term effects have not been studied in adults (Table 4).
Stimulants’ effect size of 0.9 is considered substantial. Effect size—a statistical method of reporting an intervention’s effect across different studies—is typically rated as:
- <0.32 very small
- 0.33 to 0.54, moderate
- >0.55, significant or very strong.
When choosing a medication, we usually try methylphenidate and amphetamine first, one after the other. We explain to the patient how stimulants work in the brain and the need for a comparative trial to determine which might work best for him or her. If the patient has tried a stimulant and found it helpful, we start with that class. Similarly, if he/she has not had good results with one type, we start with the other. Approximately one-third of our patients respond equally well to methylphenidate or amphetamine, one-third respond better to methylphenidate, and one-third respond better to amphetamine.
To determine the optimal dosage, we usually titrate up from 10 to 30 mg per dose of an immediate-release preparation. We begin with this form to help patients notice the medication’s onset and duration of action. After we find the optimal dosage, we switch to a longer-acting preparation.
Insomnia, mood instability, and euphoria are unacceptable stimulant side effects, although many patients welcome others such as appetite suppression and weight loss. Closely monitor cardiovascular effects, and review potential interactions with other medications, such as antihypertensives or bronchodilators. Because sudden death has been reported with stimulants in persons with structural cardiac lesions,19 obtain a cardiology consultation for patients with a history of heart disease.
We encourage patients to keep daily medication logs (Box), which we review at each visit and use to make dosing or medication changes. Dosing guidelines resemble those used for children and adolescents, although adults usually tolerate higher maximum dosages (such as methylphenidate, 80 to 100 mg/d).
Because of stimulants’ potential for recreational misuse and abuse, remain wary about choosing stimulants for patients with whom you lack a solid doctor-patient relationship.
Table 4
Stimulant dosages used in treating adult ADHD
| Class (brand name) | Daily dosing | Typical dosing schedule |
|---|---|---|
| Methylphenidate | ||
| Short-acting (Metadate, Ritadex, Ritalin) | Two to four times | 10 to 40 mg bid to qid |
| Intermediate-acting (Metadate SR, Ritalin SR) | Once or twice | 20 to 60 mg qd to bid |
| Extended-release (Concerta, Metadate CD, Ritalin LA) | Once or twice | 18 to 108 mg qd (Concerta) 20 to 40 mg bid (Ritalin LA, Metadate CD) |
| Dextromethylphenidate | ||
| Short-acting (Focalin) | Two to four times | 5 to 20 mg bid to qid |
| Long-acting (Focalin XR) | Once or twice | 10 to 20 mg qd or bid |
| Dextroamphetamine | ||
| Short-acting (Dexedrine) | Twice or three times | 10 to 30 mg bid or tid |
| Intermediate-acting (Dexedrine spansules) | Once or twice | 10 to 30 mg bid |
| Mixed amphetamine salts | ||
| Intermediate-acting (Adderall) | Once or twice | 10 to 30 mg bid or tid |
| Extended-release (Adderall XR) | Once or twice | 10 to 40 mg qd or bid |
Atomoxetine, a nonstimulant, norepinephrine re-uptake inhibitor, is approved for ADHD in adults.20-22 In two double-blind, controlled, randomized trials totalling 536 adults, Michaelson et al20 found significantly reduced ADHD symptoms after 10 weeks of atomoxetine treatment. Effect sizes of 0.35 and 0.40 were reported, with 10% of patients discontinuing because of side effects.
Atomoxetine has a long duration of action (>12 hours) but a more gradual onset (4 to 6 weeks) than that of stimulants. Approximately 60% of patients respond to atomoxetine, though effect sizes are less than those of stimulants. We have found atomoxetine works well for patients who:
- do not tolerate or are uncomfortable with taking stimulants
- are highly anxious
- report emotional dysregulation as a major target symptom.
To reduce risk of common side effects (nausea, GI upset, headache, sedation, reduced sex drive), we start with low dosages (such as 25 mg bid) and increase weekly by 25 mg to a target of 80 to 100 mg/d.
Treating complicated ADHD
Bupropion or tricyclic antidepressants are reasonable options for ADHD with depression. Atomoxetine, a tricyclic, or a stimulant plus a selective serotonin reuptake inhibitor (SSRI) can provide good symptom relief for adults with ADHD and comorbid anxiety and/or depression.
Bupropion. Approximately 50% of adults with ADHD respond to bupropion,23,24 with a treatment effect size of 0.6. Bupropion’s efficacy in smoking cessation adds value for those trying to quit.
We usually start extended-release bupropion at 150 mg/d and increase after 2 weeks to 300 mg/d if response is suboptimal. Headache, dry mouth, insomnia, and nausea are the most common adverse effects. Agitation or irritability is sometimes serious enough to warrant stopping bupropion.
Combining medications. Using SSRIs with stimulants can help adults with ADHD and comorbid anxiety or depression. Any SSRI can be safely combined with stimulants, though we tend to pick:
- more-sedating agents such as paroxetine or sertraline when patients report difficulty with insomnia or overactivation
- less-sedating compounds such as fluoxetine or citalopram when patients complain of being too tired or underactive.
When patients taking SSRIs seek help for ADHD, adding a stimulant usually reduces inattention, distractibility, impulsivity, and/or subjective feelings of restlessness. We prescribe usual dosages because stimulants and SSRIs do not interact. We have not seen serious side effects, but some patients report feeling oversedated.
Tricyclics. We use tricyclics when a stimulant/SSRI combination does not relieve symptoms satisfactorily or a patient complains of side effects. We usually have good results with desipramine or imipramine, 150 to 300 mg/d, or nortriptyline, 50 to 150 mg/d. Spencer et al have reported a response rate of 68% with nortriptyline or desipramine in a retrospective chart review25 and a prospective placebo-controlled trial26 of adults with ADHD.
Case continued: Closer to dream job
After 6 months of combined treatment, Mr. B reports much-improved ADHD symptoms, with minimal stimulant-related side effects. He has made some realistic plans for computer programming school and is taking preliminary courses. Keeping a schedule book has reduced his tardiness and tendency to procrastinate.
He is more comfortable in the classroom and better able to challenge self-critical thinking. When routine difficulties arise, he is using more-adaptive coping strategies. To maintain gains achieved in therapy, he chooses to continue periodic CBT booster sessions.
Long-term treatment
Even with medication and CBT, patients may require referral for organizational coaching, academic counseling, school or workplace accommodations, vocational counseling, cognitive remediation, group therapy, or social skills classes. You can help them obtain quality adjunctive care by collaborating with professionals who offer these services.
No studies have examined long-term care of adults with ADHD. In our experience, ongoing medication and intermittent therapy can sustain symptom control and coping skills for years. Most patients are initially skeptical about staying on medication, but after they experience the benefits most seem willing to continue as long as the medication helps.
Most of our patients sustain changes in thinking, feeling, and behaving that they learn through BT. They may seek additional sessions to meet a challenge, such as a new job or starting a family.
Books
- Kolberg J, Nadeau K. ADD-friendly ways to organize your life. New York: Brunner-Routledge; 2002.
- Hallowell EM, Ratey JJ. Driven to distraction. New York: Touchstone; 1994.
- Hallowell E, Ratey J. Delivered from distraction. New York: Ballantine Books; 2005.
Organizations
- Children and Adults with Attention-Deficit/Hyperactivity Disorder (CHADD). National Resource Center on AD/HD. www.chadd.org.
- Attention Deficit Disorder Association (ADDA). Resources and membership organization for adults with ADHD. www.add.org.
Drug brand names
- Amphetamine • Adderall, Dexedrine
- Atomoxetine • Strattera
- Bupropion • Wellbutrin
- Desipramine • Norpramin
- Imipramine • Tofranil
- Methylphenidate • Concerta, Focalin, Metadate, Ritalin
- Nortriptyline • Aventyl, Pamelor
Disclosures
Dr. Rostain is a consultant to Shire Pharamaceuticals Group and a speaker for Eli Lilly & Co. and Ortho-McNeil Pharmaceutical
Dr. Ramsay reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Mr. B, age 50, dreams of becoming a computer programmer but fears he will embarrass himself—as he has in many classrooms before. He is seeking evaluation because his teenage son was recently diagnosed with attention-deficit/hyperactivity disorder (ADHD), and he recognizes similar symptoms in himself.
Mr. B received a college degree with great difficulty, putting off assignments until the last minute and “squeaking by.” For years he has changed occupations often, never progressing beyond entry level, and now works as a personal care provider and limousine driver. He reports problems keeping up with work and managing time.
His history includes early childhood hyperactivity, difficulty sitting through classes, sloppy handwriting, disorganization, short attention span, and distractibility. He is restless, fidgety, and has trouble staying on topic. His disorganization has caused marital difficulties, for which he has sought counseling.
After careful evaluation, you determine that Mr. B meets criteria for ADHD, combined type, and for anxiety disorder not otherwise specified. His treatment goals are to increase his ability to focus; procrastinate less; improve his planning, prioritizing, and self-esteem; and to become less sensitive to criticism and less anxious about handling work demands.
Like Mr. B, adults with ADHD need treatment for the disorder’s core symptoms as well as its psychiatric comorbidities and psychosocial consequences. Comprehensive treatment with medications, cognitive-behavioral therapy (CBT), and environmental adaptations is usually recommended.
Comorbidity rules
Core symptoms. ADHD is a lifespan disorder with multiple behavioral, cognitive, and emotional manifestations that impair relationships and academic and vocational functioning. ADHD-like symptoms are seen in other conditions such as mood disorders or substance abuse, but complaints of inattention, distractibility, procrastination, restlessness, and impulsivity—particularly when pervasive and chronic—are highly indicative of ADHD.
In treating adults with ADHD, we have noticed common behavioral patterns that contribute to their psychosocial problems (Table 1). Dysfunctional coping behaviors have short-term advantages, but patients readily admit they would rather accomplish tasks through greater thought and planning.
Chronic frustrations—often associated with deep shame—are typical of adult ADHD. Many patients have maladaptive core beliefs of failure, self-mistrust, and inadequacy (Table 2).
Table 1
Common dysfunctional behavioral patterns in adults with ADHD
| Behavior | Description | Short-term gain/long-term loss |
|---|---|---|
| Anticipatory avoidance | Magnifying the difficulty of a pending task and doubts about being able to complete it; results in rationalizations to justify procrastination | Defers short-term stress, but often creates a self-fulfilling prophecy because the task looms and may seem overwhelming when facing a deadline |
| Brinksmanship | Waiting until the last moment (eg, the night before) to complete a task, often when facing an impending deadline | Deadline-associated stress can be focusing, but this tactic leaves little room for error and may yield a substandard result |
| Pseudoefficiency | Completing several low-priority, manageable tasks (eg, checking e-mail) but avoiding high-priority tasks (eg, a project for work) | Creates sense of productivity by reducing items on to-do list but defers a more difficult project |
| Juggling | Taking on new, exciting projects and feeling ‘busy’ without completing projects already started | It is easier to become motivated to start a novel project than to complete an ongoing one; pattern usually results in several incomplete projects |
Table 2
5 common maladaptive core beliefs of adults with ADHD
| Self-mistrust | ‘I cannot rely on myself to do what I need to do. I let myself down’ |
| Failure | ‘I always have failed and always will fail at what I set out to do.’ |
| Inadequacy | ‘I am basically a bad and defective person.’ |
| Incompetence | ‘I am too inept to handle life’s basic demands.’ |
| Instability | ‘My life will always be chaotic and in turmoil.’ |
Psychiatric comorbidity is the rule in adults with ADHD (Table 3). For example, among 43 patients who received combined medication and CBT at the University of Pennsylvania Adult ADHD Treatment and Research Program, 75% reported at least one comorbid condition, including:
- 27 (63%) with mood disorder
- 23 (54%) with anxiety disorder
- 5 (12%) with substance abuse.1
Other treatment studies have reported similar comorbidity rates in adults with ADHD.2-4
Table 3
Psychiatric comorbidity in adult ADHD
| Disorder | Prevalence |
|---|---|
| Mood disorders | 50% to 65% |
| Recurrent depression | |
| Bipolar disorder | |
| Cyclothymia | |
| Dysthymia | |
| Depressive disorder NOS | |
| Anxiety disorders | 40% to 55% |
| Generalized anxiety disorder | |
| Anxiety disorder NOS | |
| Others | Various |
| Substance use disorder | |
| Learning disabilities | |
| Intermittent explosive disorder | |
| Tourette syndrome | |
| Antisocial personality | |
| Borderline personality disorder | |
| Dependent personality | |
| NOS: Not otherwise specified | |
Making the diagnosis
Diagnosis of adult ADHD is based on a comprehensive assessment, including:
- careful history of presenting complaints
- thorough review of educational, occupational, and family history
- standardized rating scales (such as the Barkley ADHD Behavior Checklists, the Conners’ Adult ADHD Rating Scale, or the Brown Attention Deficit Disorder Scales)
- collateral information
- assessment of mood, anxiety, substance use, and learning/organizational skills. For details, consult references on adult ADHD.5-8
Case continued: Self-fulfilling prophesies
On standardized rating scales, Mr. B meets criteria for combined ADHD for childhood and current symptoms. Information from his wife and brother also confirms the ADHD diagnosis.
He is motivated, resilient, optimistic, and has a good support system. However, his negative automatic thoughts about his ability to succeed in school and to handle increasing time demands suggest deeper beliefs of inadequacy and failure.
Mr. B struggled academically. Without guidance about how to change his approach to difficult situations, he has repeated old thinking and behavior patterns. Believing he will embarrass himself and fail to learn required material, Mr. B procrastinates and avoids doing assignments. In class, his feelings of inadequacy make him self-conscious, which causes him to lose focus and have trouble concentrating.
See the world through the patient’s eyes
Understanding your patient. Before you start treatment, we recommend that you conceptualize how ADHD has influenced your patient’s life, including:
- developmental experiences
- family-of-origin issues, such as conflicts with parents stemming from ADHD symptoms or reciprocal interactions with an ADHD parent
- world view (“schemata”)
- patterns of coping with (or avoiding) stress
- attitudes toward self and important others
- readiness to change.
Developing a working case conceptualization is a dynamic, collaborative process. You talk with patients, and encourage them to reflect on how ADHD affects their view of themselves and their important relationships. The conceptualization takes shape as you:
- observe patients’ behaviors
- elicit how they think and feel
- assess with them the relevance and accuracies of their belief systems and response patterns.
Seeing the world “through their eyes” prepares you to help them accept the diagnosis and learn to manage ADHD symptoms. Then, by providing a blueprint to manage what patients may see as uncontrollable responses, you can help them take charge of their automatic reactions.
Psychoeducation. To set the stage for treatment, encourage patients to learn about ADHD by reading articles and books and consulting Web sites for adults with ADHD (see Related resources). Psychoeducation helps patients:
- review possible treatment approaches, including organizational (environmental) management, medication, and psychotherapy (individual or group)
- become informed participants in setting treatment goals.
Explain the relative contribution of each treatment component. For example, medications can reduce distractibility and improve attention, organizational strategies can reduce disorganization and improve time management, and structured psychotherapy can help the patient develop more effective coping skills.
Case continued: Planning combined treatment
You discuss diagnosis and treatment options with Mr. B, and he agrees to start the methylphenidate compound Concerta, initially at 18 mg/d, and weekly CBT sessions. You recommended a stimulant based on efficacy studies and your clinical experience in treating adults with ADHD. Mr. B wants a medication that will help him focus while working or studying, and he says Concerta has improved his son’s ADHD symptoms.
You instruct Mr. B to increase the dosage by 18 mg each week until he reaches 72 mg/d. You also tell him to keep a medication response log and to note any positive changes and side effects.
If an adult with ADHD expresses preference for a particular medication, we usually prescribe that one first. Most patients to whom we offer both medication and psychotherapy agree to this “top-down” and “bottom-up” approach. “Top down” means giving patients new ways of thinking to help them understand and modify their responses. “Bottom up” refers to the medication reducing their impulsivity, distractibility, and inattentiveness.
CBT for adult ADHD
Medications can ameliorate key symptoms of adult ADHD, but adjunctive interventions are needed to improve functioning and quality of life. Evidence supporting psychosocial treatment for adults with ADHD is limited, but CBT has been studied the most.1,9-13 Safren et al13 found a four-fold greater therapeutic response when patients received adjunctive CBT for residual ADHD symptoms, compared with patients who received medication alone.
We usually provide CBT weekly for 12 weeks and then taper to 8 additional sessions over 3 months (total 20 sessions). We may extend CBT with additional sessions to address complicated issues. CBT helps adults with ADHD to:
- identify dysfunctional thinking, feeling, and behaving patterns
- recognize contexts in which patterns arise
- systematically change these patterns.
CBT can reduce ADHD-associated anxiety and depression and improve coping skills and sense of well-being.1,9,11 Its flexibility allows you to address family issues with patients’ partners, children and other relatives to improve communication, reduce conflict, and develop healthier interactions.
We focus CBT sessions on finding alternate coping strategies. We might try role playing, rehearsing, creating “thought experiments,” and anticipating and preparing to modify typical patterns of avoidance. These approaches have been described elsewhere.10,11,14
We adopt an active stance during therapy to keep ADHD patients’ distractibility from disrupting our conversation. For example, we set the therapeutic agenda, provide feedback about patients’ behaviors, and encourage them to clarify rewards and consequences of using (or avoiding) problem-solving strategies.
Although we typically assign between-session homework, we expect patients to have difficulty completing it. We remain nonjudgmental and collaborative, viewing incomplete assignments as opportunities to learn about patients’ unproductive problem solving and to help them develop more-effective patterns.
Challenging maladaptive beliefs. A strong therapeutic relationship allows adults with ADHD to discuss their chronic frustrations, which often are associated with deep shame. We then shift CBT’s focus to deeper ADHD-related schemata that perpetuate dysfunctional patterns.
We work with patients to elucidate and challenge their maladaptive core beliefs and encourage new ways to view themselves and others. Allowing patients to grieve about the limitations ADHD imposes on their lives also helps to reduce chronic negative self-esteem.
Case continued: ‘less frenetic’
Mr. B achieves good results within 3 weeks of an increasing titration of stimulant medication, reporting significantly less restlessness and greater concentration without significant side effects. His wife confirms that he is less frenetic, can converse without interruptions, and is better at managing his complicated work schedule.
Which medications?
Drug therapy for adult ADHD is not as well-studied as in children and adolescents, but American Academy of Child and Adolescent Psychiatry guidelines and others15-18 recommend stimulant and nonstimulant medications. Your choice depends on the patient’s clinical profile (including risk factors and comorbid conditions), past medication use, treatment goals, preferred medication effects and dosing patterns (once-daily versus multiple times), and potential side effects. Stimulants or atomoxetine are first-line choices for adult ADHD without psychiatric comorbidity.
Stimulants work quickly and are cleared relatively rapidly from the brain without causing euphoria or dependency. They are effective (80% to 90% response rate) and well-tolerated, though long-term effects have not been studied in adults (Table 4).
Stimulants’ effect size of 0.9 is considered substantial. Effect size—a statistical method of reporting an intervention’s effect across different studies—is typically rated as:
- <0.32 very small
- 0.33 to 0.54, moderate
- >0.55, significant or very strong.
When choosing a medication, we usually try methylphenidate and amphetamine first, one after the other. We explain to the patient how stimulants work in the brain and the need for a comparative trial to determine which might work best for him or her. If the patient has tried a stimulant and found it helpful, we start with that class. Similarly, if he/she has not had good results with one type, we start with the other. Approximately one-third of our patients respond equally well to methylphenidate or amphetamine, one-third respond better to methylphenidate, and one-third respond better to amphetamine.
To determine the optimal dosage, we usually titrate up from 10 to 30 mg per dose of an immediate-release preparation. We begin with this form to help patients notice the medication’s onset and duration of action. After we find the optimal dosage, we switch to a longer-acting preparation.
Insomnia, mood instability, and euphoria are unacceptable stimulant side effects, although many patients welcome others such as appetite suppression and weight loss. Closely monitor cardiovascular effects, and review potential interactions with other medications, such as antihypertensives or bronchodilators. Because sudden death has been reported with stimulants in persons with structural cardiac lesions,19 obtain a cardiology consultation for patients with a history of heart disease.
We encourage patients to keep daily medication logs (Box), which we review at each visit and use to make dosing or medication changes. Dosing guidelines resemble those used for children and adolescents, although adults usually tolerate higher maximum dosages (such as methylphenidate, 80 to 100 mg/d).
Because of stimulants’ potential for recreational misuse and abuse, remain wary about choosing stimulants for patients with whom you lack a solid doctor-patient relationship.
Table 4
Stimulant dosages used in treating adult ADHD
| Class (brand name) | Daily dosing | Typical dosing schedule |
|---|---|---|
| Methylphenidate | ||
| Short-acting (Metadate, Ritadex, Ritalin) | Two to four times | 10 to 40 mg bid to qid |
| Intermediate-acting (Metadate SR, Ritalin SR) | Once or twice | 20 to 60 mg qd to bid |
| Extended-release (Concerta, Metadate CD, Ritalin LA) | Once or twice | 18 to 108 mg qd (Concerta) 20 to 40 mg bid (Ritalin LA, Metadate CD) |
| Dextromethylphenidate | ||
| Short-acting (Focalin) | Two to four times | 5 to 20 mg bid to qid |
| Long-acting (Focalin XR) | Once or twice | 10 to 20 mg qd or bid |
| Dextroamphetamine | ||
| Short-acting (Dexedrine) | Twice or three times | 10 to 30 mg bid or tid |
| Intermediate-acting (Dexedrine spansules) | Once or twice | 10 to 30 mg bid |
| Mixed amphetamine salts | ||
| Intermediate-acting (Adderall) | Once or twice | 10 to 30 mg bid or tid |
| Extended-release (Adderall XR) | Once or twice | 10 to 40 mg qd or bid |
Atomoxetine, a nonstimulant, norepinephrine re-uptake inhibitor, is approved for ADHD in adults.20-22 In two double-blind, controlled, randomized trials totalling 536 adults, Michaelson et al20 found significantly reduced ADHD symptoms after 10 weeks of atomoxetine treatment. Effect sizes of 0.35 and 0.40 were reported, with 10% of patients discontinuing because of side effects.
Atomoxetine has a long duration of action (>12 hours) but a more gradual onset (4 to 6 weeks) than that of stimulants. Approximately 60% of patients respond to atomoxetine, though effect sizes are less than those of stimulants. We have found atomoxetine works well for patients who:
- do not tolerate or are uncomfortable with taking stimulants
- are highly anxious
- report emotional dysregulation as a major target symptom.
To reduce risk of common side effects (nausea, GI upset, headache, sedation, reduced sex drive), we start with low dosages (such as 25 mg bid) and increase weekly by 25 mg to a target of 80 to 100 mg/d.
Treating complicated ADHD
Bupropion or tricyclic antidepressants are reasonable options for ADHD with depression. Atomoxetine, a tricyclic, or a stimulant plus a selective serotonin reuptake inhibitor (SSRI) can provide good symptom relief for adults with ADHD and comorbid anxiety and/or depression.
Bupropion. Approximately 50% of adults with ADHD respond to bupropion,23,24 with a treatment effect size of 0.6. Bupropion’s efficacy in smoking cessation adds value for those trying to quit.
We usually start extended-release bupropion at 150 mg/d and increase after 2 weeks to 300 mg/d if response is suboptimal. Headache, dry mouth, insomnia, and nausea are the most common adverse effects. Agitation or irritability is sometimes serious enough to warrant stopping bupropion.
Combining medications. Using SSRIs with stimulants can help adults with ADHD and comorbid anxiety or depression. Any SSRI can be safely combined with stimulants, though we tend to pick:
- more-sedating agents such as paroxetine or sertraline when patients report difficulty with insomnia or overactivation
- less-sedating compounds such as fluoxetine or citalopram when patients complain of being too tired or underactive.
When patients taking SSRIs seek help for ADHD, adding a stimulant usually reduces inattention, distractibility, impulsivity, and/or subjective feelings of restlessness. We prescribe usual dosages because stimulants and SSRIs do not interact. We have not seen serious side effects, but some patients report feeling oversedated.
Tricyclics. We use tricyclics when a stimulant/SSRI combination does not relieve symptoms satisfactorily or a patient complains of side effects. We usually have good results with desipramine or imipramine, 150 to 300 mg/d, or nortriptyline, 50 to 150 mg/d. Spencer et al have reported a response rate of 68% with nortriptyline or desipramine in a retrospective chart review25 and a prospective placebo-controlled trial26 of adults with ADHD.
Case continued: Closer to dream job
After 6 months of combined treatment, Mr. B reports much-improved ADHD symptoms, with minimal stimulant-related side effects. He has made some realistic plans for computer programming school and is taking preliminary courses. Keeping a schedule book has reduced his tardiness and tendency to procrastinate.
He is more comfortable in the classroom and better able to challenge self-critical thinking. When routine difficulties arise, he is using more-adaptive coping strategies. To maintain gains achieved in therapy, he chooses to continue periodic CBT booster sessions.
Long-term treatment
Even with medication and CBT, patients may require referral for organizational coaching, academic counseling, school or workplace accommodations, vocational counseling, cognitive remediation, group therapy, or social skills classes. You can help them obtain quality adjunctive care by collaborating with professionals who offer these services.
No studies have examined long-term care of adults with ADHD. In our experience, ongoing medication and intermittent therapy can sustain symptom control and coping skills for years. Most patients are initially skeptical about staying on medication, but after they experience the benefits most seem willing to continue as long as the medication helps.
Most of our patients sustain changes in thinking, feeling, and behaving that they learn through BT. They may seek additional sessions to meet a challenge, such as a new job or starting a family.
Books
- Kolberg J, Nadeau K. ADD-friendly ways to organize your life. New York: Brunner-Routledge; 2002.
- Hallowell EM, Ratey JJ. Driven to distraction. New York: Touchstone; 1994.
- Hallowell E, Ratey J. Delivered from distraction. New York: Ballantine Books; 2005.
Organizations
- Children and Adults with Attention-Deficit/Hyperactivity Disorder (CHADD). National Resource Center on AD/HD. www.chadd.org.
- Attention Deficit Disorder Association (ADDA). Resources and membership organization for adults with ADHD. www.add.org.
Drug brand names
- Amphetamine • Adderall, Dexedrine
- Atomoxetine • Strattera
- Bupropion • Wellbutrin
- Desipramine • Norpramin
- Imipramine • Tofranil
- Methylphenidate • Concerta, Focalin, Metadate, Ritalin
- Nortriptyline • Aventyl, Pamelor
Disclosures
Dr. Rostain is a consultant to Shire Pharamaceuticals Group and a speaker for Eli Lilly & Co. and Ortho-McNeil Pharmaceutical
Dr. Ramsay reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Rostain AL, Ramsay JR. A combined treatment approach for adults with attention-deficit/hyperactivity disorder. Results of an open study of 43 patients J Attention Disorders. In press.
2. Shekim WO, Asarnow RF, Hess E, et al. A clinical and demographic profile of a sample of adults with attention deficit hyperactivity disorder, residual state. Comp Psychiatry 1990;31:416-25.
3. Biederman J, Faraone SV, Spencer T, et al. Patterns of psychiatric comorbidity, cognition and psychosocial functioning in adults with attention deficit hyperactivity disorder. Am J Psychiatry 1993;150:1792-8.
4. Wilens TE, Biederman J, Spencer T. Attention-deficit/hyperactivity disorder across the lifespan. Ann Rev Medicine 2002;53:113-31.
5. Barkley RA. Attention deficit hyperactivity disorder: a handbook for diagnosis and treatment. New York: Guilford Press; 1998.
6. Wender PH. ADHD: Attention-deficit hyperactivity disorder in children and adults. New York: Oxford University Press; 2000.
7. Goldstein S, Ellison AT. Clinician’s guide to adult ADHD. San Diego: Academic Press; 2000.
8. Brown TE. Attention-deficit disorder: the unfocused mind in children and adults. New Haven, CT: Yale University Press; 2005.
9. Wilens TE, McDermott SP, Biederman J, et al. Cognitive therapy in the treatment of adults with ADHD: a systematic chart review of 26 cases. J Cogn Ther 1999;13:215-26.
10. Ramsay JR, Rostain AL. A cognitive therapy approach for adult attention-deficit/hyperactivity disorder. J Cogn Psychother 2003;17:319-34.
11. Safren SA, Sprich S, Chulvick S, Otto MW. Psychosocial treatments for adults with attention-deficit/hyperactivity disorder. Psychiatr Clin North Am 2004;27:349-60.
12. Ramsay JR, Rostain AL. Adapting psychotherapy to meet the needs of adults with attention-deficit/hyperactivity disorder. Psychotherapy: Theory, Research, Practice, Training 2005;42:72-84.
13. Safren SA, Otto MW, Sprich S, et al. Cognitive-behavior therapy for ADHD in medication-treated adults with continued symptoms. Behav Res Ther 2005;43:831-42.
14. Ramsay JR, Rostain AL. Girl, repeatedly interrupted: The case of a young adult woman with ADHD. Clinical Case Studies 2005;4:329-46.
15. American Academy of Child and Adolescent Psychiatry. Practice parameters for the use of stimulant medications in the treatment of children, adolescents, and adults. J Am Acad Child Adolesc Psychiatry 2002;42(suppl 2):26S-49S.
16. Weiss M, Murray C, Weiss G. Adults with attention-deficit/hyperactivity disorder: Current concepts. J Psychiatr Pract 2002;8:99-111.
17. Wilens TE. Drug therapy for adults with attention-deficit hyperactivity disorder. Drugs 2003;63:2395-411.
18. Dodson WW. Pharmacotherapy of adult ADHD. J Clin Psychol 2005;61:589-606.
19. Francis PD. Effects of psychotropic medications on the pediatric electrocardiogram and recommendations for monitoring. Curr Opin Pediatr 2002;14(2):224-30
20. Michaelson D, Adler L, Spencer T. Atomoxetine in adults: Two randomized, placebo-controlled studies. Biol Psychiatry 2003;53:112-20.
21. Simpson D, Plosker GL. Atomoxetine: a review of its use in adults with attention deficit hyperactivity disorder. Drugs 2004;64:205-22.
22. Reimherr FW, Marchant BK, Strong RE, et al. Emotional dysregulation in adult ADHD and response to atomoxetine. Biol Psychiatry 2005;58:125-31.
23. Wilens TE, Spencer T, Biederman J. A controlled clinical trial of bupropion for attention-deficit/hyperactivity disorder in adults. Am J Psychiatry 2001;158:282-8.
24. Wilens TE, Haight BR, Horrigan JP, et al. Bupropion XL in adults with attention-deficit/hyperactivity disorder: a randomized, placebo-controlled study. Biol Psychiatry 2005;57:793-801.
25. Wilens TE, Biederman JB, Mick E, Spencer TJ. A systematic assessment of tricyclic antidepressants in the treatment of adult attention deficit/hyperactivity disorder. J Nerv Ment Dis 1995;183:48-50.
26. Wilens TE, Biederman JB, Prince J, et al. Six-week, double-blind, placebo-controlled study of desipramine for adult attention deficit hyperactivity disorder. Am J Psychiatry 1996;153:1147-53.
1. Rostain AL, Ramsay JR. A combined treatment approach for adults with attention-deficit/hyperactivity disorder. Results of an open study of 43 patients J Attention Disorders. In press.
2. Shekim WO, Asarnow RF, Hess E, et al. A clinical and demographic profile of a sample of adults with attention deficit hyperactivity disorder, residual state. Comp Psychiatry 1990;31:416-25.
3. Biederman J, Faraone SV, Spencer T, et al. Patterns of psychiatric comorbidity, cognition and psychosocial functioning in adults with attention deficit hyperactivity disorder. Am J Psychiatry 1993;150:1792-8.
4. Wilens TE, Biederman J, Spencer T. Attention-deficit/hyperactivity disorder across the lifespan. Ann Rev Medicine 2002;53:113-31.
5. Barkley RA. Attention deficit hyperactivity disorder: a handbook for diagnosis and treatment. New York: Guilford Press; 1998.
6. Wender PH. ADHD: Attention-deficit hyperactivity disorder in children and adults. New York: Oxford University Press; 2000.
7. Goldstein S, Ellison AT. Clinician’s guide to adult ADHD. San Diego: Academic Press; 2000.
8. Brown TE. Attention-deficit disorder: the unfocused mind in children and adults. New Haven, CT: Yale University Press; 2005.
9. Wilens TE, McDermott SP, Biederman J, et al. Cognitive therapy in the treatment of adults with ADHD: a systematic chart review of 26 cases. J Cogn Ther 1999;13:215-26.
10. Ramsay JR, Rostain AL. A cognitive therapy approach for adult attention-deficit/hyperactivity disorder. J Cogn Psychother 2003;17:319-34.
11. Safren SA, Sprich S, Chulvick S, Otto MW. Psychosocial treatments for adults with attention-deficit/hyperactivity disorder. Psychiatr Clin North Am 2004;27:349-60.
12. Ramsay JR, Rostain AL. Adapting psychotherapy to meet the needs of adults with attention-deficit/hyperactivity disorder. Psychotherapy: Theory, Research, Practice, Training 2005;42:72-84.
13. Safren SA, Otto MW, Sprich S, et al. Cognitive-behavior therapy for ADHD in medication-treated adults with continued symptoms. Behav Res Ther 2005;43:831-42.
14. Ramsay JR, Rostain AL. Girl, repeatedly interrupted: The case of a young adult woman with ADHD. Clinical Case Studies 2005;4:329-46.
15. American Academy of Child and Adolescent Psychiatry. Practice parameters for the use of stimulant medications in the treatment of children, adolescents, and adults. J Am Acad Child Adolesc Psychiatry 2002;42(suppl 2):26S-49S.
16. Weiss M, Murray C, Weiss G. Adults with attention-deficit/hyperactivity disorder: Current concepts. J Psychiatr Pract 2002;8:99-111.
17. Wilens TE. Drug therapy for adults with attention-deficit hyperactivity disorder. Drugs 2003;63:2395-411.
18. Dodson WW. Pharmacotherapy of adult ADHD. J Clin Psychol 2005;61:589-606.
19. Francis PD. Effects of psychotropic medications on the pediatric electrocardiogram and recommendations for monitoring. Curr Opin Pediatr 2002;14(2):224-30
20. Michaelson D, Adler L, Spencer T. Atomoxetine in adults: Two randomized, placebo-controlled studies. Biol Psychiatry 2003;53:112-20.
21. Simpson D, Plosker GL. Atomoxetine: a review of its use in adults with attention deficit hyperactivity disorder. Drugs 2004;64:205-22.
22. Reimherr FW, Marchant BK, Strong RE, et al. Emotional dysregulation in adult ADHD and response to atomoxetine. Biol Psychiatry 2005;58:125-31.
23. Wilens TE, Spencer T, Biederman J. A controlled clinical trial of bupropion for attention-deficit/hyperactivity disorder in adults. Am J Psychiatry 2001;158:282-8.
24. Wilens TE, Haight BR, Horrigan JP, et al. Bupropion XL in adults with attention-deficit/hyperactivity disorder: a randomized, placebo-controlled study. Biol Psychiatry 2005;57:793-801.
25. Wilens TE, Biederman JB, Mick E, Spencer TJ. A systematic assessment of tricyclic antidepressants in the treatment of adult attention deficit/hyperactivity disorder. J Nerv Ment Dis 1995;183:48-50.
26. Wilens TE, Biederman JB, Prince J, et al. Six-week, double-blind, placebo-controlled study of desipramine for adult attention deficit hyperactivity disorder. Am J Psychiatry 1996;153:1147-53.
New Year’s resolutions: Hazardous to your health?
Do you make New Year’s resolutions? At least 60% of Americans do, according to a Kaiser Permanente “New Year’s and Health Issues Survey” of 1,000 U.S. adults. Rather depressingly, the survey also found that for every 10 respondents who kept their resolutions all year, 99 did not.
Going online to learn more, my Google search for “new year resolutions” yielded 1,360,000 results (by comparison, a search for “alien abduction” found 711,000). The U.S. government Web portal FirstGov.gov lists as the “most popular” resolutions: drink less alcohol, eat right, get a better education, get a better job, get fit, lose weight, quit smoking, reduce stress, save money, take a trip, and volunteer to help others.
Is it mentally healthy to make New Year’s resolutions? I suppose so, if they motivate you to make positive changes. For example, in this issue, Drs. Phil Bohnert and Anne O’Connell describe how to make changes in your life to prevent or recover from burnout. But the 10% New Year’s resolution “compliance rate” in the Kaiser Permanente survey suggests that fundamental lifestyle changes are uncommon, despite our good intentions.
If we make resolutions but don’t keep them, how could that be good? Maybe taking on health and moral issues once a year is countertherapeutic. Making resolutions, not keeping them, and then feeling guilty probably does more harm than good.
My resolution for 2005 was not to let anything drive me crazy during the year. That clearly proved overly ambitious. For 2006, I have resolved to try to watch more TV and to gain a few pounds. At least these resolutions should not leave me feeling guilty.
Best wishes for a healthy and happy new year from me and the Current Psychiatry family!
Do you make New Year’s resolutions? At least 60% of Americans do, according to a Kaiser Permanente “New Year’s and Health Issues Survey” of 1,000 U.S. adults. Rather depressingly, the survey also found that for every 10 respondents who kept their resolutions all year, 99 did not.
Going online to learn more, my Google search for “new year resolutions” yielded 1,360,000 results (by comparison, a search for “alien abduction” found 711,000). The U.S. government Web portal FirstGov.gov lists as the “most popular” resolutions: drink less alcohol, eat right, get a better education, get a better job, get fit, lose weight, quit smoking, reduce stress, save money, take a trip, and volunteer to help others.
Is it mentally healthy to make New Year’s resolutions? I suppose so, if they motivate you to make positive changes. For example, in this issue, Drs. Phil Bohnert and Anne O’Connell describe how to make changes in your life to prevent or recover from burnout. But the 10% New Year’s resolution “compliance rate” in the Kaiser Permanente survey suggests that fundamental lifestyle changes are uncommon, despite our good intentions.
If we make resolutions but don’t keep them, how could that be good? Maybe taking on health and moral issues once a year is countertherapeutic. Making resolutions, not keeping them, and then feeling guilty probably does more harm than good.
My resolution for 2005 was not to let anything drive me crazy during the year. That clearly proved overly ambitious. For 2006, I have resolved to try to watch more TV and to gain a few pounds. At least these resolutions should not leave me feeling guilty.
Best wishes for a healthy and happy new year from me and the Current Psychiatry family!
Do you make New Year’s resolutions? At least 60% of Americans do, according to a Kaiser Permanente “New Year’s and Health Issues Survey” of 1,000 U.S. adults. Rather depressingly, the survey also found that for every 10 respondents who kept their resolutions all year, 99 did not.
Going online to learn more, my Google search for “new year resolutions” yielded 1,360,000 results (by comparison, a search for “alien abduction” found 711,000). The U.S. government Web portal FirstGov.gov lists as the “most popular” resolutions: drink less alcohol, eat right, get a better education, get a better job, get fit, lose weight, quit smoking, reduce stress, save money, take a trip, and volunteer to help others.
Is it mentally healthy to make New Year’s resolutions? I suppose so, if they motivate you to make positive changes. For example, in this issue, Drs. Phil Bohnert and Anne O’Connell describe how to make changes in your life to prevent or recover from burnout. But the 10% New Year’s resolution “compliance rate” in the Kaiser Permanente survey suggests that fundamental lifestyle changes are uncommon, despite our good intentions.
If we make resolutions but don’t keep them, how could that be good? Maybe taking on health and moral issues once a year is countertherapeutic. Making resolutions, not keeping them, and then feeling guilty probably does more harm than good.
My resolution for 2005 was not to let anything drive me crazy during the year. That clearly proved overly ambitious. For 2006, I have resolved to try to watch more TV and to gain a few pounds. At least these resolutions should not leave me feeling guilty.
Best wishes for a healthy and happy new year from me and the Current Psychiatry family!
Medical problem or psychosis?
Distinguishing the cause of a patient’s psychotic symptoms can be clinically challenging in a primary care practice. This case was submitted by Matthew Rosenberg, MD, who practices family medicine at Sacramento (CA) County Primary Care Clinic. This month’s consultant is Bezalel Dantz, MD.
How would you have advised Dr. Rosenberg?
Case: ‘you’re just gonna die’
I was seeing Mr. J, age 31, weekly to monitor abdominal complaints. For 3 weeks he experienced increasing epigastric pain, and he had been evaluated twice in the emergency room for this complaint. Plain films, ultrasound, CT, and an elevated lipase reading suggested an inconclusive diagnosis of pancreatitis.
During his second office visit, Mr. J also complained of “hearing voices.” Further questioning revealed that he had been hearing voices—often male—making degrading comments for several years. The voices have increased in frequency during his illness, and their negative comments include, “What do you have to live for?” and “You’re just gonna die.”
Mr. J blames the voices on distant drug use, claiming his parents “forced” him as a young teen to take hallucinogens. He often thinks he is being followed and does not trust others. He said both parents had mental illnesses but does not know the diagnoses or seriousness of their disorders.
His thoughts are well-organized with clear content. He shows no signs of depression or mania. He plays guitar in a band and appears to be a thoughtful and high-functioning individual.
I need help with the differential diagnosis and suggestions of possible treatment options.
Dr. Dantz’s consultation
The first step in evaluating psychosis is to determine whether it indicates a medical disorder, substanceinduced disorder, or primary psychiatric illness. The chronicity and nature of Mr. J’s psychotic symptoms (auditory hallucinations and paranoid delusions), his age, and a family history of psychiatric illness suggest a primary psychiatric disorder. The elevated lipase might explain his abdominal pain but is likely independent of his psychosis.
Medical workup. Conduct a comprehensive physical exam and medical and psychiatric history. Obtain collateral information from the family about the patient’s psychiatric symptoms, family history, recreational drug use, and stressors. Acute onset, age >40, comorbid medical conditions, lack of acute psychosocial stressors, and a negative personal or family psychiatric history suggest a medical cause (The skinny on one patient’s psychosis,” November 2005.) Also assess for use of alcohol, marijuana, hallucinogens, narcotics, stimulants, and inhalants. Until any drug has been stopped for at least 1 week, its contribution to psychosis may be unclear.
Table 1
Medical conditions that may present as psychosis
| Type of condition | Examples |
|---|---|
| CNS infection | HIV, neurosyphilis, cycticercosis, encephalitis, prion disease |
| Neoplasm | Primary or metastatic, paraneoplastic syndromes |
| Endocrinopathies | Thyroid, parathyroid, adrenal |
| Degenerative diseases | Alzheimer’s disease, frontotemporal dementia, Huntington’s disease, Parkinson’s disease, Wilson’s disease, Lewy body dementia |
| Demyelinating disorders | Multiple sclerosis, adrenal leukodystrophy |
| Metabolic disorders | Cirrhosis, vitamin deficiency, uremia, porphyria, heavy metal poisoning |
| Vasculitis | Systemic lupus erythematosus |
| Others | Seizures, migraine aura, hypnagogic and hypnopompic hallucinations, neurosarcoidosis |
Lab testing. When signs or symptoms do not suggest an organic disease, laboratory tests have a low yield and are of questionable value.2 In primary care practice, however, many psychotic patients complain of somatic symptoms. Given the devastating impact of psychotic illness, one can argue that even a yield <5% justifies a workup.
A urine toxicology screen is by far the most important lab test. CBC, comprehensive metabolic panel, thyroid function tests, erythrocyte sedimentation rate, and calcium level may reveal a medical cause. Consider HIV antibody and syphilis tests in at-risk individuals.
Findings on physical exam or abnormal lab results would guide further testing. Because of Mr. J’s GI and neurologic symptoms, a 24-hour urine test may be reasonable, particularly if he has had episodes of acute intermittent porphyria.
Neuroimaging. Consider a scan when psychosis is comorbid with:
- age >40
- neurologic complaints (such as headache, numbness, vertigo, seizures)
- focal neurologic findings (such as weakness, gait abnormality, clonus, or spasticity)
- confusion, cognitive deficit, history of malignancy
- head trauma
- immunocompromised state
- atypical psychotic symptoms (such as visual or olfactory hallucinations).
Psychiatric workup. If the history and physical exam reveal no organic basis, the next step is to determine the nature of this patient’s psychosis. The two most common psychiatric conditions associated with psychosis are:
- schizophrenic spectrum disorders (such as schizophreniform, schizophrenia and schizoaffective disorder)
- affective disorders (such as psychotic depression and bipolar disorder).
Distinguishing among these conditions can be challenging (Table 2) because patients rarely present with typical syndromes.
For example, a bipolar patient may present in a mixed state with both depressive and manic features. Psychosis in schizophrenia may be brief (<6 months in schizophreniform disorder) and may be characterized by manic-like grandiose delusions or negative symptoms (flat affect, poverty of speech) that mimic affective symptoms. Finally, some patients have both an affective disorder and schizophrenia, as in schizoaffective disorder.
For Mr. J, years of uninterrupted hallucinations, longstanding paranoid delusions, and absence of prominent affective symptoms suggest schizophrenia. His hallucinations are typical of those reported in schizophrenia. Voices giving a running commentary on a person’s thoughts and actions and derogatory comments are two of the most common auditory hallucinations.
Somatic concerns are also prominent in schizophrenia. Patients may describe symptoms in bizarre terms, such as “electric shocks in my head” or “there’s a fire in my spleen.”
Supporting evidence for a schizophrenia diagnosis would include a history of social isolation, lack of interest in work, and poor social interaction. Mr. J has a supportive partner, and we are told he appears to be high-functioning and active as a guitarist in a band. These factors might support an alternate diagnosis of affective psychosis. Finally, his past drug use and somatic symptoms raise the possibility of active substance abuse.
Table 2
Differential diagnosis of primary psychosis: Typical features
| Affective disorder | Schizophrenic spectrum disorder | |
|---|---|---|
| Symptom onset | Acute or subacute | Prolonged period (months to years) of self-neglect, social isolation, odd beliefs, eccentric behaviors |
| Course | Episodic, with periods of normal social and occupational functioning between episodes | Chronic, with exacerbations superimposed on gradually deteriorating social and occupational functioning |
| Associated symptoms | Mania (irritability, insomnia, rapid speech, labile mood, psychomotor agitation, racing thoughts) | Flat or inappropriate affect, thought blocking, apathy |
| Depression (anhedonia, psychomotor retardation, sleep problems, poor appetite) |
Suicide risk. Ask psychotic patients if they think about harming themselves. Lifetime risk of suicide in schizophrenia is 10% to 15%, and rates in bipolar disorder are higher. If patients deny suicidality, ask them why. Reassuring responses include religious prohibition, hopefulness about the future, concern about suicide’s effect on a loved one, fear of dying, or lack of means.
Candidates for emergent psychiatric consultation or hospitalization include patients with violent or homicidal thoughts and any patient who has attempted suicide, has a family history of suicide, has access to means, and lacks compelling reasons against suicide. Consider immediate psychiatric evaluation and admission of patients whose delusions or behaviors put them at risk for harm.
Abdominal pain workup. Although Mr. J’s abdominal pain may be functional, also seek an organic cause. His first-time disclosure of psychotic symptoms suggests that a serious medical stressor may be exacerbating a chronic psychiatric illness. Because the elevated lipase may indicate pancreatitis, consider an endoscopic or MRI examination of the pancreas and bile ducts. In consultation with a gastroenterologist, evaluate other causes such as peptic ulcer disease, ischemic bowel (perhaps as a result of cocaine use), inflammatory bowel disease, vasculitis, porphyria, and abdominal migraine.
Managing psychosis
Psychiatric consultation is strongly recommended for patients beginning therapy for psychotic disorders who have shown a particularly high risk for suicide. Uncontrolled symptoms, unanticipated psychiatric side effects, and the humiliation that results from the insight gained through treatment may contribute to this risk.
Assuming that Mr. J does not meet criteria for acute psychiatric hospitalization, the primary care clinician can stabilize the psychotic symptoms while awaiting psychiatric referral. Any atypical antipsychotic would be appropriate (Table 3).
Table 3
Starting an atypical antipsychotic* for primary psychosis
| Drug | Starting and maintenance dosages1 | Most-common adverse effects |
|---|---|---|
| Aripiprazole | 7.5 to 15 mg daily; 15 to 30 mg daily | EPS (+), agitation (++) |
| Olanzapine | 5 to 15 mg nightly; 10 to 20 mg nightly | Sedation (+++), weight gain (++++) hyperglycemia (++++), anticholinergic |
| Quetiapine | 50 to 100 mg bid; 600 to 800 mg nightly | Sedation (++++), weight gain (+++), hyperglycemia (++) |
| Risperidone | 0.5 to 2 mg bid; 2 to 4 mg bid | EPS (++), sedation (++), weight gain (++), hyperglycemia (++), elevated prolactin |
| Ziprasidone | 20 to 40 mg bid; 60 to 80 mg bid | EPS (+), agitation (++), sedation (+), QTc prolongation2 |
| EPS: Extrapyramidal symptoms | ||
| + small risk ++ moderate risk +++ high risk ++++ most risk | ||
| * All atypical antipsychotics have been associated with rare cases of neuroleptic malignant syndrome. Tardive dyskinesia is estimated to occur in 0.5% of adults and 2.5% of geriatric patients for each year on therapy. FDA requires a warning on increased risks of hyperlipidemia, hyperglycemia, and diabetes mellitus on the labels of all atypical antipsychotics. Monitoring weight, glucose, and lipids is recommended. | ||
| 1 In clinical practice, dosages may be increased beyond maximum dosages listed. Doses may be given solely at night or bid, depending on sedation and agitation. Low dosages are recommended in geriatric patients or those with renal or hepatic disease. Review potential drug-drug interactions before dosing. | ||
| 2 Despite earlier concerns, no cases of torsade de pointes or sudden death have been reported with ziprasidone. Not recommended for patients with cardiac risk. | ||
| Source: Adapted from reference 4. | ||
Patients who refuse treatment pose a quandary. If the patient is not acutely ill, try to establish an alliance over several visits rather than endangering the therapeutic relationship through confrontation or overzealous persuasion (Table 4).
Table 4
Strategies to build a therapeutic alliance with psychotic patients
| Enlist support of the patient’s family or loved ones |
| Do not argue with the patient’s delusions |
| Focus on what is bothering the patient most, and treat identified symptoms |
| Refer to the “stress” the patient suffers because of the unusual experiences he is describing |
| Commiserate with the anxiety he feels when others (such as his family) ridicule or reject his beliefs |
| Describe the medication as a “tranquilizer” rather than an antipsychotic. Use terms such as “nerves,” “stress,” “depression,” “anxiety,” or “insomnia,” which are often preferred by psychotic patients |
| Normalize treatment by suggesting “many of my patients with fatigue or lack of sleep find this medication very helpful” |
| Use medical terms to destigmatize the illness. Suggest that the patient suffers from a chemical disturbance that can be treated, similar to patients with diabetes who require insulin |
Monitoring. The primary care physician’s role after the patient begins antipsychotic therapy is to:
- assess his or her symptoms (particularly suicidality) and adherence to psychiatric visits and treatment
- monitor for adverse effects from medications.
Atypical antipsychotics have been associated with weight gain, hyperglycemia, and hyperlipidemia. Check fasting glucose and lipids quarterly for the first year of antipsychotic therapy and annually thereafter.5 Watch for drug-drug interactions whenever a new medication is added. Monitor for abnormal movements, even though the risk of extrapyramidal symptoms and tardive dyskinesia is lower with atypical antipsychotics than with traditional agents.
For Mr. J’s psychiatric symptoms, I would:
- assess his willingness to start medication to reduce or eliminate the voices
- suggest he accept psychiatric referral
- assure him that I will remain involved in his care and continue to evaluate his abdominal symptoms.
I would also request permission to discuss his case with his partner and a family member to gather pertinent history and enlist their support for treatment. I would then start Mr. J on any drug listed in Table 3.
1. The Medical Letter. Drugs that may cause psychiatric symptoms. July 8, 2002;1134:59-62.
2. Anfinson TJ, Kathol RG. Screening laboratory evaluation in psychiatric patients: a review. Gen Hosp Psychiatry 1992;14(4):248-57.
3. Mann JJ. A current perspective of suicide and attempted suicide. Ann Intern Med 2002;136(4):302-11.
4. McIntyre RS, Konarski JZ. Tolerability profiles of atypical antipsychotics in the treatment of bipolar disorder. J Clin Psychiatry 2005;66(suppl 3):28-36.
5. Kane JM, Leucht S, Carpenter D, Docherty JP. Expert consensus guideline series. Optimizing pharmacologic treatment of psychotic disorders. Introduction: methods, commentary, and summary. J Clin Psychiatry 2003;64(suppl 12):5-19.
Dr. Dantz is a board-certified internist and psychiatrist who is assistant professor of internal medicine and psychiatry, Rush University, Chicago. He specializes in treating psychiatric disorders in the medical setting.
Distinguishing the cause of a patient’s psychotic symptoms can be clinically challenging in a primary care practice. This case was submitted by Matthew Rosenberg, MD, who practices family medicine at Sacramento (CA) County Primary Care Clinic. This month’s consultant is Bezalel Dantz, MD.
How would you have advised Dr. Rosenberg?
Case: ‘you’re just gonna die’
I was seeing Mr. J, age 31, weekly to monitor abdominal complaints. For 3 weeks he experienced increasing epigastric pain, and he had been evaluated twice in the emergency room for this complaint. Plain films, ultrasound, CT, and an elevated lipase reading suggested an inconclusive diagnosis of pancreatitis.
During his second office visit, Mr. J also complained of “hearing voices.” Further questioning revealed that he had been hearing voices—often male—making degrading comments for several years. The voices have increased in frequency during his illness, and their negative comments include, “What do you have to live for?” and “You’re just gonna die.”
Mr. J blames the voices on distant drug use, claiming his parents “forced” him as a young teen to take hallucinogens. He often thinks he is being followed and does not trust others. He said both parents had mental illnesses but does not know the diagnoses or seriousness of their disorders.
His thoughts are well-organized with clear content. He shows no signs of depression or mania. He plays guitar in a band and appears to be a thoughtful and high-functioning individual.
I need help with the differential diagnosis and suggestions of possible treatment options.
Dr. Dantz’s consultation
The first step in evaluating psychosis is to determine whether it indicates a medical disorder, substanceinduced disorder, or primary psychiatric illness. The chronicity and nature of Mr. J’s psychotic symptoms (auditory hallucinations and paranoid delusions), his age, and a family history of psychiatric illness suggest a primary psychiatric disorder. The elevated lipase might explain his abdominal pain but is likely independent of his psychosis.
Medical workup. Conduct a comprehensive physical exam and medical and psychiatric history. Obtain collateral information from the family about the patient’s psychiatric symptoms, family history, recreational drug use, and stressors. Acute onset, age >40, comorbid medical conditions, lack of acute psychosocial stressors, and a negative personal or family psychiatric history suggest a medical cause (The skinny on one patient’s psychosis,” November 2005.) Also assess for use of alcohol, marijuana, hallucinogens, narcotics, stimulants, and inhalants. Until any drug has been stopped for at least 1 week, its contribution to psychosis may be unclear.
Table 1
Medical conditions that may present as psychosis
| Type of condition | Examples |
|---|---|
| CNS infection | HIV, neurosyphilis, cycticercosis, encephalitis, prion disease |
| Neoplasm | Primary or metastatic, paraneoplastic syndromes |
| Endocrinopathies | Thyroid, parathyroid, adrenal |
| Degenerative diseases | Alzheimer’s disease, frontotemporal dementia, Huntington’s disease, Parkinson’s disease, Wilson’s disease, Lewy body dementia |
| Demyelinating disorders | Multiple sclerosis, adrenal leukodystrophy |
| Metabolic disorders | Cirrhosis, vitamin deficiency, uremia, porphyria, heavy metal poisoning |
| Vasculitis | Systemic lupus erythematosus |
| Others | Seizures, migraine aura, hypnagogic and hypnopompic hallucinations, neurosarcoidosis |
Lab testing. When signs or symptoms do not suggest an organic disease, laboratory tests have a low yield and are of questionable value.2 In primary care practice, however, many psychotic patients complain of somatic symptoms. Given the devastating impact of psychotic illness, one can argue that even a yield <5% justifies a workup.
A urine toxicology screen is by far the most important lab test. CBC, comprehensive metabolic panel, thyroid function tests, erythrocyte sedimentation rate, and calcium level may reveal a medical cause. Consider HIV antibody and syphilis tests in at-risk individuals.
Findings on physical exam or abnormal lab results would guide further testing. Because of Mr. J’s GI and neurologic symptoms, a 24-hour urine test may be reasonable, particularly if he has had episodes of acute intermittent porphyria.
Neuroimaging. Consider a scan when psychosis is comorbid with:
- age >40
- neurologic complaints (such as headache, numbness, vertigo, seizures)
- focal neurologic findings (such as weakness, gait abnormality, clonus, or spasticity)
- confusion, cognitive deficit, history of malignancy
- head trauma
- immunocompromised state
- atypical psychotic symptoms (such as visual or olfactory hallucinations).
Psychiatric workup. If the history and physical exam reveal no organic basis, the next step is to determine the nature of this patient’s psychosis. The two most common psychiatric conditions associated with psychosis are:
- schizophrenic spectrum disorders (such as schizophreniform, schizophrenia and schizoaffective disorder)
- affective disorders (such as psychotic depression and bipolar disorder).
Distinguishing among these conditions can be challenging (Table 2) because patients rarely present with typical syndromes.
For example, a bipolar patient may present in a mixed state with both depressive and manic features. Psychosis in schizophrenia may be brief (<6 months in schizophreniform disorder) and may be characterized by manic-like grandiose delusions or negative symptoms (flat affect, poverty of speech) that mimic affective symptoms. Finally, some patients have both an affective disorder and schizophrenia, as in schizoaffective disorder.
For Mr. J, years of uninterrupted hallucinations, longstanding paranoid delusions, and absence of prominent affective symptoms suggest schizophrenia. His hallucinations are typical of those reported in schizophrenia. Voices giving a running commentary on a person’s thoughts and actions and derogatory comments are two of the most common auditory hallucinations.
Somatic concerns are also prominent in schizophrenia. Patients may describe symptoms in bizarre terms, such as “electric shocks in my head” or “there’s a fire in my spleen.”
Supporting evidence for a schizophrenia diagnosis would include a history of social isolation, lack of interest in work, and poor social interaction. Mr. J has a supportive partner, and we are told he appears to be high-functioning and active as a guitarist in a band. These factors might support an alternate diagnosis of affective psychosis. Finally, his past drug use and somatic symptoms raise the possibility of active substance abuse.
Table 2
Differential diagnosis of primary psychosis: Typical features
| Affective disorder | Schizophrenic spectrum disorder | |
|---|---|---|
| Symptom onset | Acute or subacute | Prolonged period (months to years) of self-neglect, social isolation, odd beliefs, eccentric behaviors |
| Course | Episodic, with periods of normal social and occupational functioning between episodes | Chronic, with exacerbations superimposed on gradually deteriorating social and occupational functioning |
| Associated symptoms | Mania (irritability, insomnia, rapid speech, labile mood, psychomotor agitation, racing thoughts) | Flat or inappropriate affect, thought blocking, apathy |
| Depression (anhedonia, psychomotor retardation, sleep problems, poor appetite) |
Suicide risk. Ask psychotic patients if they think about harming themselves. Lifetime risk of suicide in schizophrenia is 10% to 15%, and rates in bipolar disorder are higher. If patients deny suicidality, ask them why. Reassuring responses include religious prohibition, hopefulness about the future, concern about suicide’s effect on a loved one, fear of dying, or lack of means.
Candidates for emergent psychiatric consultation or hospitalization include patients with violent or homicidal thoughts and any patient who has attempted suicide, has a family history of suicide, has access to means, and lacks compelling reasons against suicide. Consider immediate psychiatric evaluation and admission of patients whose delusions or behaviors put them at risk for harm.
Abdominal pain workup. Although Mr. J’s abdominal pain may be functional, also seek an organic cause. His first-time disclosure of psychotic symptoms suggests that a serious medical stressor may be exacerbating a chronic psychiatric illness. Because the elevated lipase may indicate pancreatitis, consider an endoscopic or MRI examination of the pancreas and bile ducts. In consultation with a gastroenterologist, evaluate other causes such as peptic ulcer disease, ischemic bowel (perhaps as a result of cocaine use), inflammatory bowel disease, vasculitis, porphyria, and abdominal migraine.
Managing psychosis
Psychiatric consultation is strongly recommended for patients beginning therapy for psychotic disorders who have shown a particularly high risk for suicide. Uncontrolled symptoms, unanticipated psychiatric side effects, and the humiliation that results from the insight gained through treatment may contribute to this risk.
Assuming that Mr. J does not meet criteria for acute psychiatric hospitalization, the primary care clinician can stabilize the psychotic symptoms while awaiting psychiatric referral. Any atypical antipsychotic would be appropriate (Table 3).
Table 3
Starting an atypical antipsychotic* for primary psychosis
| Drug | Starting and maintenance dosages1 | Most-common adverse effects |
|---|---|---|
| Aripiprazole | 7.5 to 15 mg daily; 15 to 30 mg daily | EPS (+), agitation (++) |
| Olanzapine | 5 to 15 mg nightly; 10 to 20 mg nightly | Sedation (+++), weight gain (++++) hyperglycemia (++++), anticholinergic |
| Quetiapine | 50 to 100 mg bid; 600 to 800 mg nightly | Sedation (++++), weight gain (+++), hyperglycemia (++) |
| Risperidone | 0.5 to 2 mg bid; 2 to 4 mg bid | EPS (++), sedation (++), weight gain (++), hyperglycemia (++), elevated prolactin |
| Ziprasidone | 20 to 40 mg bid; 60 to 80 mg bid | EPS (+), agitation (++), sedation (+), QTc prolongation2 |
| EPS: Extrapyramidal symptoms | ||
| + small risk ++ moderate risk +++ high risk ++++ most risk | ||
| * All atypical antipsychotics have been associated with rare cases of neuroleptic malignant syndrome. Tardive dyskinesia is estimated to occur in 0.5% of adults and 2.5% of geriatric patients for each year on therapy. FDA requires a warning on increased risks of hyperlipidemia, hyperglycemia, and diabetes mellitus on the labels of all atypical antipsychotics. Monitoring weight, glucose, and lipids is recommended. | ||
| 1 In clinical practice, dosages may be increased beyond maximum dosages listed. Doses may be given solely at night or bid, depending on sedation and agitation. Low dosages are recommended in geriatric patients or those with renal or hepatic disease. Review potential drug-drug interactions before dosing. | ||
| 2 Despite earlier concerns, no cases of torsade de pointes or sudden death have been reported with ziprasidone. Not recommended for patients with cardiac risk. | ||
| Source: Adapted from reference 4. | ||
Patients who refuse treatment pose a quandary. If the patient is not acutely ill, try to establish an alliance over several visits rather than endangering the therapeutic relationship through confrontation or overzealous persuasion (Table 4).
Table 4
Strategies to build a therapeutic alliance with psychotic patients
| Enlist support of the patient’s family or loved ones |
| Do not argue with the patient’s delusions |
| Focus on what is bothering the patient most, and treat identified symptoms |
| Refer to the “stress” the patient suffers because of the unusual experiences he is describing |
| Commiserate with the anxiety he feels when others (such as his family) ridicule or reject his beliefs |
| Describe the medication as a “tranquilizer” rather than an antipsychotic. Use terms such as “nerves,” “stress,” “depression,” “anxiety,” or “insomnia,” which are often preferred by psychotic patients |
| Normalize treatment by suggesting “many of my patients with fatigue or lack of sleep find this medication very helpful” |
| Use medical terms to destigmatize the illness. Suggest that the patient suffers from a chemical disturbance that can be treated, similar to patients with diabetes who require insulin |
Monitoring. The primary care physician’s role after the patient begins antipsychotic therapy is to:
- assess his or her symptoms (particularly suicidality) and adherence to psychiatric visits and treatment
- monitor for adverse effects from medications.
Atypical antipsychotics have been associated with weight gain, hyperglycemia, and hyperlipidemia. Check fasting glucose and lipids quarterly for the first year of antipsychotic therapy and annually thereafter.5 Watch for drug-drug interactions whenever a new medication is added. Monitor for abnormal movements, even though the risk of extrapyramidal symptoms and tardive dyskinesia is lower with atypical antipsychotics than with traditional agents.
For Mr. J’s psychiatric symptoms, I would:
- assess his willingness to start medication to reduce or eliminate the voices
- suggest he accept psychiatric referral
- assure him that I will remain involved in his care and continue to evaluate his abdominal symptoms.
I would also request permission to discuss his case with his partner and a family member to gather pertinent history and enlist their support for treatment. I would then start Mr. J on any drug listed in Table 3.
Distinguishing the cause of a patient’s psychotic symptoms can be clinically challenging in a primary care practice. This case was submitted by Matthew Rosenberg, MD, who practices family medicine at Sacramento (CA) County Primary Care Clinic. This month’s consultant is Bezalel Dantz, MD.
How would you have advised Dr. Rosenberg?
Case: ‘you’re just gonna die’
I was seeing Mr. J, age 31, weekly to monitor abdominal complaints. For 3 weeks he experienced increasing epigastric pain, and he had been evaluated twice in the emergency room for this complaint. Plain films, ultrasound, CT, and an elevated lipase reading suggested an inconclusive diagnosis of pancreatitis.
During his second office visit, Mr. J also complained of “hearing voices.” Further questioning revealed that he had been hearing voices—often male—making degrading comments for several years. The voices have increased in frequency during his illness, and their negative comments include, “What do you have to live for?” and “You’re just gonna die.”
Mr. J blames the voices on distant drug use, claiming his parents “forced” him as a young teen to take hallucinogens. He often thinks he is being followed and does not trust others. He said both parents had mental illnesses but does not know the diagnoses or seriousness of their disorders.
His thoughts are well-organized with clear content. He shows no signs of depression or mania. He plays guitar in a band and appears to be a thoughtful and high-functioning individual.
I need help with the differential diagnosis and suggestions of possible treatment options.
Dr. Dantz’s consultation
The first step in evaluating psychosis is to determine whether it indicates a medical disorder, substanceinduced disorder, or primary psychiatric illness. The chronicity and nature of Mr. J’s psychotic symptoms (auditory hallucinations and paranoid delusions), his age, and a family history of psychiatric illness suggest a primary psychiatric disorder. The elevated lipase might explain his abdominal pain but is likely independent of his psychosis.
Medical workup. Conduct a comprehensive physical exam and medical and psychiatric history. Obtain collateral information from the family about the patient’s psychiatric symptoms, family history, recreational drug use, and stressors. Acute onset, age >40, comorbid medical conditions, lack of acute psychosocial stressors, and a negative personal or family psychiatric history suggest a medical cause (The skinny on one patient’s psychosis,” November 2005.) Also assess for use of alcohol, marijuana, hallucinogens, narcotics, stimulants, and inhalants. Until any drug has been stopped for at least 1 week, its contribution to psychosis may be unclear.
Table 1
Medical conditions that may present as psychosis
| Type of condition | Examples |
|---|---|
| CNS infection | HIV, neurosyphilis, cycticercosis, encephalitis, prion disease |
| Neoplasm | Primary or metastatic, paraneoplastic syndromes |
| Endocrinopathies | Thyroid, parathyroid, adrenal |
| Degenerative diseases | Alzheimer’s disease, frontotemporal dementia, Huntington’s disease, Parkinson’s disease, Wilson’s disease, Lewy body dementia |
| Demyelinating disorders | Multiple sclerosis, adrenal leukodystrophy |
| Metabolic disorders | Cirrhosis, vitamin deficiency, uremia, porphyria, heavy metal poisoning |
| Vasculitis | Systemic lupus erythematosus |
| Others | Seizures, migraine aura, hypnagogic and hypnopompic hallucinations, neurosarcoidosis |
Lab testing. When signs or symptoms do not suggest an organic disease, laboratory tests have a low yield and are of questionable value.2 In primary care practice, however, many psychotic patients complain of somatic symptoms. Given the devastating impact of psychotic illness, one can argue that even a yield <5% justifies a workup.
A urine toxicology screen is by far the most important lab test. CBC, comprehensive metabolic panel, thyroid function tests, erythrocyte sedimentation rate, and calcium level may reveal a medical cause. Consider HIV antibody and syphilis tests in at-risk individuals.
Findings on physical exam or abnormal lab results would guide further testing. Because of Mr. J’s GI and neurologic symptoms, a 24-hour urine test may be reasonable, particularly if he has had episodes of acute intermittent porphyria.
Neuroimaging. Consider a scan when psychosis is comorbid with:
- age >40
- neurologic complaints (such as headache, numbness, vertigo, seizures)
- focal neurologic findings (such as weakness, gait abnormality, clonus, or spasticity)
- confusion, cognitive deficit, history of malignancy
- head trauma
- immunocompromised state
- atypical psychotic symptoms (such as visual or olfactory hallucinations).
Psychiatric workup. If the history and physical exam reveal no organic basis, the next step is to determine the nature of this patient’s psychosis. The two most common psychiatric conditions associated with psychosis are:
- schizophrenic spectrum disorders (such as schizophreniform, schizophrenia and schizoaffective disorder)
- affective disorders (such as psychotic depression and bipolar disorder).
Distinguishing among these conditions can be challenging (Table 2) because patients rarely present with typical syndromes.
For example, a bipolar patient may present in a mixed state with both depressive and manic features. Psychosis in schizophrenia may be brief (<6 months in schizophreniform disorder) and may be characterized by manic-like grandiose delusions or negative symptoms (flat affect, poverty of speech) that mimic affective symptoms. Finally, some patients have both an affective disorder and schizophrenia, as in schizoaffective disorder.
For Mr. J, years of uninterrupted hallucinations, longstanding paranoid delusions, and absence of prominent affective symptoms suggest schizophrenia. His hallucinations are typical of those reported in schizophrenia. Voices giving a running commentary on a person’s thoughts and actions and derogatory comments are two of the most common auditory hallucinations.
Somatic concerns are also prominent in schizophrenia. Patients may describe symptoms in bizarre terms, such as “electric shocks in my head” or “there’s a fire in my spleen.”
Supporting evidence for a schizophrenia diagnosis would include a history of social isolation, lack of interest in work, and poor social interaction. Mr. J has a supportive partner, and we are told he appears to be high-functioning and active as a guitarist in a band. These factors might support an alternate diagnosis of affective psychosis. Finally, his past drug use and somatic symptoms raise the possibility of active substance abuse.
Table 2
Differential diagnosis of primary psychosis: Typical features
| Affective disorder | Schizophrenic spectrum disorder | |
|---|---|---|
| Symptom onset | Acute or subacute | Prolonged period (months to years) of self-neglect, social isolation, odd beliefs, eccentric behaviors |
| Course | Episodic, with periods of normal social and occupational functioning between episodes | Chronic, with exacerbations superimposed on gradually deteriorating social and occupational functioning |
| Associated symptoms | Mania (irritability, insomnia, rapid speech, labile mood, psychomotor agitation, racing thoughts) | Flat or inappropriate affect, thought blocking, apathy |
| Depression (anhedonia, psychomotor retardation, sleep problems, poor appetite) |
Suicide risk. Ask psychotic patients if they think about harming themselves. Lifetime risk of suicide in schizophrenia is 10% to 15%, and rates in bipolar disorder are higher. If patients deny suicidality, ask them why. Reassuring responses include religious prohibition, hopefulness about the future, concern about suicide’s effect on a loved one, fear of dying, or lack of means.
Candidates for emergent psychiatric consultation or hospitalization include patients with violent or homicidal thoughts and any patient who has attempted suicide, has a family history of suicide, has access to means, and lacks compelling reasons against suicide. Consider immediate psychiatric evaluation and admission of patients whose delusions or behaviors put them at risk for harm.
Abdominal pain workup. Although Mr. J’s abdominal pain may be functional, also seek an organic cause. His first-time disclosure of psychotic symptoms suggests that a serious medical stressor may be exacerbating a chronic psychiatric illness. Because the elevated lipase may indicate pancreatitis, consider an endoscopic or MRI examination of the pancreas and bile ducts. In consultation with a gastroenterologist, evaluate other causes such as peptic ulcer disease, ischemic bowel (perhaps as a result of cocaine use), inflammatory bowel disease, vasculitis, porphyria, and abdominal migraine.
Managing psychosis
Psychiatric consultation is strongly recommended for patients beginning therapy for psychotic disorders who have shown a particularly high risk for suicide. Uncontrolled symptoms, unanticipated psychiatric side effects, and the humiliation that results from the insight gained through treatment may contribute to this risk.
Assuming that Mr. J does not meet criteria for acute psychiatric hospitalization, the primary care clinician can stabilize the psychotic symptoms while awaiting psychiatric referral. Any atypical antipsychotic would be appropriate (Table 3).
Table 3
Starting an atypical antipsychotic* for primary psychosis
| Drug | Starting and maintenance dosages1 | Most-common adverse effects |
|---|---|---|
| Aripiprazole | 7.5 to 15 mg daily; 15 to 30 mg daily | EPS (+), agitation (++) |
| Olanzapine | 5 to 15 mg nightly; 10 to 20 mg nightly | Sedation (+++), weight gain (++++) hyperglycemia (++++), anticholinergic |
| Quetiapine | 50 to 100 mg bid; 600 to 800 mg nightly | Sedation (++++), weight gain (+++), hyperglycemia (++) |
| Risperidone | 0.5 to 2 mg bid; 2 to 4 mg bid | EPS (++), sedation (++), weight gain (++), hyperglycemia (++), elevated prolactin |
| Ziprasidone | 20 to 40 mg bid; 60 to 80 mg bid | EPS (+), agitation (++), sedation (+), QTc prolongation2 |
| EPS: Extrapyramidal symptoms | ||
| + small risk ++ moderate risk +++ high risk ++++ most risk | ||
| * All atypical antipsychotics have been associated with rare cases of neuroleptic malignant syndrome. Tardive dyskinesia is estimated to occur in 0.5% of adults and 2.5% of geriatric patients for each year on therapy. FDA requires a warning on increased risks of hyperlipidemia, hyperglycemia, and diabetes mellitus on the labels of all atypical antipsychotics. Monitoring weight, glucose, and lipids is recommended. | ||
| 1 In clinical practice, dosages may be increased beyond maximum dosages listed. Doses may be given solely at night or bid, depending on sedation and agitation. Low dosages are recommended in geriatric patients or those with renal or hepatic disease. Review potential drug-drug interactions before dosing. | ||
| 2 Despite earlier concerns, no cases of torsade de pointes or sudden death have been reported with ziprasidone. Not recommended for patients with cardiac risk. | ||
| Source: Adapted from reference 4. | ||
Patients who refuse treatment pose a quandary. If the patient is not acutely ill, try to establish an alliance over several visits rather than endangering the therapeutic relationship through confrontation or overzealous persuasion (Table 4).
Table 4
Strategies to build a therapeutic alliance with psychotic patients
| Enlist support of the patient’s family or loved ones |
| Do not argue with the patient’s delusions |
| Focus on what is bothering the patient most, and treat identified symptoms |
| Refer to the “stress” the patient suffers because of the unusual experiences he is describing |
| Commiserate with the anxiety he feels when others (such as his family) ridicule or reject his beliefs |
| Describe the medication as a “tranquilizer” rather than an antipsychotic. Use terms such as “nerves,” “stress,” “depression,” “anxiety,” or “insomnia,” which are often preferred by psychotic patients |
| Normalize treatment by suggesting “many of my patients with fatigue or lack of sleep find this medication very helpful” |
| Use medical terms to destigmatize the illness. Suggest that the patient suffers from a chemical disturbance that can be treated, similar to patients with diabetes who require insulin |
Monitoring. The primary care physician’s role after the patient begins antipsychotic therapy is to:
- assess his or her symptoms (particularly suicidality) and adherence to psychiatric visits and treatment
- monitor for adverse effects from medications.
Atypical antipsychotics have been associated with weight gain, hyperglycemia, and hyperlipidemia. Check fasting glucose and lipids quarterly for the first year of antipsychotic therapy and annually thereafter.5 Watch for drug-drug interactions whenever a new medication is added. Monitor for abnormal movements, even though the risk of extrapyramidal symptoms and tardive dyskinesia is lower with atypical antipsychotics than with traditional agents.
For Mr. J’s psychiatric symptoms, I would:
- assess his willingness to start medication to reduce or eliminate the voices
- suggest he accept psychiatric referral
- assure him that I will remain involved in his care and continue to evaluate his abdominal symptoms.
I would also request permission to discuss his case with his partner and a family member to gather pertinent history and enlist their support for treatment. I would then start Mr. J on any drug listed in Table 3.
1. The Medical Letter. Drugs that may cause psychiatric symptoms. July 8, 2002;1134:59-62.
2. Anfinson TJ, Kathol RG. Screening laboratory evaluation in psychiatric patients: a review. Gen Hosp Psychiatry 1992;14(4):248-57.
3. Mann JJ. A current perspective of suicide and attempted suicide. Ann Intern Med 2002;136(4):302-11.
4. McIntyre RS, Konarski JZ. Tolerability profiles of atypical antipsychotics in the treatment of bipolar disorder. J Clin Psychiatry 2005;66(suppl 3):28-36.
5. Kane JM, Leucht S, Carpenter D, Docherty JP. Expert consensus guideline series. Optimizing pharmacologic treatment of psychotic disorders. Introduction: methods, commentary, and summary. J Clin Psychiatry 2003;64(suppl 12):5-19.
Dr. Dantz is a board-certified internist and psychiatrist who is assistant professor of internal medicine and psychiatry, Rush University, Chicago. He specializes in treating psychiatric disorders in the medical setting.
1. The Medical Letter. Drugs that may cause psychiatric symptoms. July 8, 2002;1134:59-62.
2. Anfinson TJ, Kathol RG. Screening laboratory evaluation in psychiatric patients: a review. Gen Hosp Psychiatry 1992;14(4):248-57.
3. Mann JJ. A current perspective of suicide and attempted suicide. Ann Intern Med 2002;136(4):302-11.
4. McIntyre RS, Konarski JZ. Tolerability profiles of atypical antipsychotics in the treatment of bipolar disorder. J Clin Psychiatry 2005;66(suppl 3):28-36.
5. Kane JM, Leucht S, Carpenter D, Docherty JP. Expert consensus guideline series. Optimizing pharmacologic treatment of psychotic disorders. Introduction: methods, commentary, and summary. J Clin Psychiatry 2003;64(suppl 12):5-19.
Dr. Dantz is a board-certified internist and psychiatrist who is assistant professor of internal medicine and psychiatry, Rush University, Chicago. He specializes in treating psychiatric disorders in the medical setting.
How to adjust drug dosing after bariatric surgery
Bariatric surgery has increased 10-fold in the United States over the past decade.1 Because one-third of bariatric candidates take psychiatric medications, psychiatric input on postoperative management is in demand.2
Despite this surgery’s rising popularity, no data exist to guide psychotropic dosing in patients with altered GI environments and who experience massive postoperative weight loss. Evidence and clinical experience support these recommendations:
Managing changes in psychotropic absorption. The most common procedure, the Roux-en-Y gastric bypass (RYGB), bypasses the duodenum, proximal jejunum, and all of the stomach except the cardia (Figure). Because ingested food is normally absorbed in the duodenum and jejunum, a bypass results in relative malabsorption of food. Orally ingested food and medications pass into the cardia, where they are not exposed to acid.
One novel in vitro study2 examined the dissolution of 22 psychotropics in a simulated GI environment of control and post-RYGB states. Twelve medications dissolved differently in a postoperative environment than in the control state; 10 dissolved much less than expected.
The effect of bariatric surgery on in vivo absorption of commonly used psychotropics has not been studied. For safe yet effective dosing immediately after surgery, try:
- Using immediate-release psychotropics.3 Time-released medications are designed to dissolve gradually within the full intestinal tract. Extended-release formulations will probably have markedly different pharmacokinetics after RYGB. Coated pills require stomach acid to release active ingredients, so crush oral medications in the immediate postoperative period.
- Monitoring serum drug levels of medications with a narrow therapeutic index. Also measure preoperative blood levels while the patient feels well. This baseline will provide a target to aim for if the patient has a postoperative relapse.
Figure Roux-en-Y gastric bypass
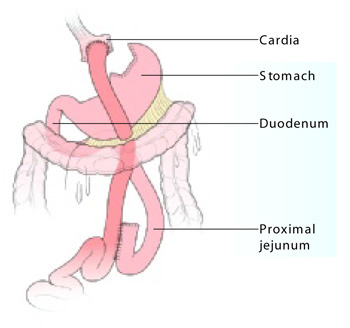
Vertical stapling of the upper stomach creates a small pouch, and a Y-shaped section of small intestine attached to the pouch allows food to bypass the duodenum and part of the jejunum.
Illustration: Jennifer Fairman
Postoperative weight loss. Many physiologic factors influence drug absorption, such as gastric emptying time and the integrity and surface area of the epithelium. The gut has an impressive capacity to compensate for loss of function, so absorption after surgery may eventually normalize. By that time, however, marked weight loss can complicate the clinical picture.
Compared with nonobese persons, obese persons have an increased proportion of adipose tissue, as well as increased total body water, lean body mass, visceral organ mass, and higher glomerular filtration rate.
Postoperative bariatric patients often lose more than 100 pounds of adipose tissue. This type of weight loss mostly affects lipid-soluble drugs with a large volume of distribution (Vd) that readily cross cell membranes, such as fluoxetine. Drugs with a large Vd, such as fluoxetine (Table), reach all major compartments of distribution, which in a normal weight individual include: plasma (5%), interstitial fluid (16%), intracellular fluid (35%), transcellular fluid (2%), and fat (20%). Because the amount of fat in an overweight patient is initially very high but rapidly decreases after bariatric surgery, drugs with a large Vd can shift into other compartments.
For drugs with a small Vd, such as lithium, a lower maintenance dosage may be required because of decreased glomerular filtration following marked weight loss.4
Table
Common drugs’ volume of distribution (Vd)
| Drug | Extent of distribution | Volume of distribution |
|---|---|---|
| Fluoxetine | Large | 10 to 103 L/kg |
| Citalopram | Moderate | 14 to 17 L/kg |
| Venlafaxine | Moderate | 6 to 7 L/kg |
| Oxcarbazepine | Small | 0.7 L/kg |
| Lithium | Small | 0.4 to 0.6 L/kg |
| Valproic acid | Small | 0.1 to 0.4 L/kg |
1. Tsao A. Weighing bariatric surgery’s risks. BusinessWeek Online. Available at: http://www.businessweek.com/bwdaily/dnflash/oct2004/nf20041028_0264_db092.htm. Accessed Nov. 28, 2005.
2. Seaman JS, Bowers SP, Dixon P, Schindler L. Dissolution of common psychiatric medications in a Roux-en-Y gastric bypass model. Psychosomatics 2005;46(3):250-3.
3. Malone M. Altered drug disposition in obesity and after bariatric surgery. Nutr Clin Pract 2003;18(2):131-5.
4. Sproule BA, Hardy BG, Shulman KI. Differential pharmacokinetics of lithium in elderly patients. Drugs Aging 2000;16(3):165-77.
Dr. McAlpine is assistant professor of psychiatry and director of eating disorders services, Mayo Clinic, Rochester, MN.
Bariatric surgery has increased 10-fold in the United States over the past decade.1 Because one-third of bariatric candidates take psychiatric medications, psychiatric input on postoperative management is in demand.2
Despite this surgery’s rising popularity, no data exist to guide psychotropic dosing in patients with altered GI environments and who experience massive postoperative weight loss. Evidence and clinical experience support these recommendations:
Managing changes in psychotropic absorption. The most common procedure, the Roux-en-Y gastric bypass (RYGB), bypasses the duodenum, proximal jejunum, and all of the stomach except the cardia (Figure). Because ingested food is normally absorbed in the duodenum and jejunum, a bypass results in relative malabsorption of food. Orally ingested food and medications pass into the cardia, where they are not exposed to acid.
One novel in vitro study2 examined the dissolution of 22 psychotropics in a simulated GI environment of control and post-RYGB states. Twelve medications dissolved differently in a postoperative environment than in the control state; 10 dissolved much less than expected.
The effect of bariatric surgery on in vivo absorption of commonly used psychotropics has not been studied. For safe yet effective dosing immediately after surgery, try:
- Using immediate-release psychotropics.3 Time-released medications are designed to dissolve gradually within the full intestinal tract. Extended-release formulations will probably have markedly different pharmacokinetics after RYGB. Coated pills require stomach acid to release active ingredients, so crush oral medications in the immediate postoperative period.
- Monitoring serum drug levels of medications with a narrow therapeutic index. Also measure preoperative blood levels while the patient feels well. This baseline will provide a target to aim for if the patient has a postoperative relapse.
Figure Roux-en-Y gastric bypass
Vertical stapling of the upper stomach creates a small pouch, and a Y-shaped section of small intestine attached to the pouch allows food to bypass the duodenum and part of the jejunum.
Illustration: Jennifer Fairman
Postoperative weight loss. Many physiologic factors influence drug absorption, such as gastric emptying time and the integrity and surface area of the epithelium. The gut has an impressive capacity to compensate for loss of function, so absorption after surgery may eventually normalize. By that time, however, marked weight loss can complicate the clinical picture.
Compared with nonobese persons, obese persons have an increased proportion of adipose tissue, as well as increased total body water, lean body mass, visceral organ mass, and higher glomerular filtration rate.
Postoperative bariatric patients often lose more than 100 pounds of adipose tissue. This type of weight loss mostly affects lipid-soluble drugs with a large volume of distribution (Vd) that readily cross cell membranes, such as fluoxetine. Drugs with a large Vd, such as fluoxetine (Table), reach all major compartments of distribution, which in a normal weight individual include: plasma (5%), interstitial fluid (16%), intracellular fluid (35%), transcellular fluid (2%), and fat (20%). Because the amount of fat in an overweight patient is initially very high but rapidly decreases after bariatric surgery, drugs with a large Vd can shift into other compartments.
For drugs with a small Vd, such as lithium, a lower maintenance dosage may be required because of decreased glomerular filtration following marked weight loss.4
Table
Common drugs’ volume of distribution (Vd)
| Drug | Extent of distribution | Volume of distribution |
|---|---|---|
| Fluoxetine | Large | 10 to 103 L/kg |
| Citalopram | Moderate | 14 to 17 L/kg |
| Venlafaxine | Moderate | 6 to 7 L/kg |
| Oxcarbazepine | Small | 0.7 L/kg |
| Lithium | Small | 0.4 to 0.6 L/kg |
| Valproic acid | Small | 0.1 to 0.4 L/kg |
Bariatric surgery has increased 10-fold in the United States over the past decade.1 Because one-third of bariatric candidates take psychiatric medications, psychiatric input on postoperative management is in demand.2
Despite this surgery’s rising popularity, no data exist to guide psychotropic dosing in patients with altered GI environments and who experience massive postoperative weight loss. Evidence and clinical experience support these recommendations:
Managing changes in psychotropic absorption. The most common procedure, the Roux-en-Y gastric bypass (RYGB), bypasses the duodenum, proximal jejunum, and all of the stomach except the cardia (Figure). Because ingested food is normally absorbed in the duodenum and jejunum, a bypass results in relative malabsorption of food. Orally ingested food and medications pass into the cardia, where they are not exposed to acid.
One novel in vitro study2 examined the dissolution of 22 psychotropics in a simulated GI environment of control and post-RYGB states. Twelve medications dissolved differently in a postoperative environment than in the control state; 10 dissolved much less than expected.
The effect of bariatric surgery on in vivo absorption of commonly used psychotropics has not been studied. For safe yet effective dosing immediately after surgery, try:
- Using immediate-release psychotropics.3 Time-released medications are designed to dissolve gradually within the full intestinal tract. Extended-release formulations will probably have markedly different pharmacokinetics after RYGB. Coated pills require stomach acid to release active ingredients, so crush oral medications in the immediate postoperative period.
- Monitoring serum drug levels of medications with a narrow therapeutic index. Also measure preoperative blood levels while the patient feels well. This baseline will provide a target to aim for if the patient has a postoperative relapse.
Figure Roux-en-Y gastric bypass
Vertical stapling of the upper stomach creates a small pouch, and a Y-shaped section of small intestine attached to the pouch allows food to bypass the duodenum and part of the jejunum.
Illustration: Jennifer Fairman
Postoperative weight loss. Many physiologic factors influence drug absorption, such as gastric emptying time and the integrity and surface area of the epithelium. The gut has an impressive capacity to compensate for loss of function, so absorption after surgery may eventually normalize. By that time, however, marked weight loss can complicate the clinical picture.
Compared with nonobese persons, obese persons have an increased proportion of adipose tissue, as well as increased total body water, lean body mass, visceral organ mass, and higher glomerular filtration rate.
Postoperative bariatric patients often lose more than 100 pounds of adipose tissue. This type of weight loss mostly affects lipid-soluble drugs with a large volume of distribution (Vd) that readily cross cell membranes, such as fluoxetine. Drugs with a large Vd, such as fluoxetine (Table), reach all major compartments of distribution, which in a normal weight individual include: plasma (5%), interstitial fluid (16%), intracellular fluid (35%), transcellular fluid (2%), and fat (20%). Because the amount of fat in an overweight patient is initially very high but rapidly decreases after bariatric surgery, drugs with a large Vd can shift into other compartments.
For drugs with a small Vd, such as lithium, a lower maintenance dosage may be required because of decreased glomerular filtration following marked weight loss.4
Table
Common drugs’ volume of distribution (Vd)
| Drug | Extent of distribution | Volume of distribution |
|---|---|---|
| Fluoxetine | Large | 10 to 103 L/kg |
| Citalopram | Moderate | 14 to 17 L/kg |
| Venlafaxine | Moderate | 6 to 7 L/kg |
| Oxcarbazepine | Small | 0.7 L/kg |
| Lithium | Small | 0.4 to 0.6 L/kg |
| Valproic acid | Small | 0.1 to 0.4 L/kg |
1. Tsao A. Weighing bariatric surgery’s risks. BusinessWeek Online. Available at: http://www.businessweek.com/bwdaily/dnflash/oct2004/nf20041028_0264_db092.htm. Accessed Nov. 28, 2005.
2. Seaman JS, Bowers SP, Dixon P, Schindler L. Dissolution of common psychiatric medications in a Roux-en-Y gastric bypass model. Psychosomatics 2005;46(3):250-3.
3. Malone M. Altered drug disposition in obesity and after bariatric surgery. Nutr Clin Pract 2003;18(2):131-5.
4. Sproule BA, Hardy BG, Shulman KI. Differential pharmacokinetics of lithium in elderly patients. Drugs Aging 2000;16(3):165-77.
Dr. McAlpine is assistant professor of psychiatry and director of eating disorders services, Mayo Clinic, Rochester, MN.
1. Tsao A. Weighing bariatric surgery’s risks. BusinessWeek Online. Available at: http://www.businessweek.com/bwdaily/dnflash/oct2004/nf20041028_0264_db092.htm. Accessed Nov. 28, 2005.
2. Seaman JS, Bowers SP, Dixon P, Schindler L. Dissolution of common psychiatric medications in a Roux-en-Y gastric bypass model. Psychosomatics 2005;46(3):250-3.
3. Malone M. Altered drug disposition in obesity and after bariatric surgery. Nutr Clin Pract 2003;18(2):131-5.
4. Sproule BA, Hardy BG, Shulman KI. Differential pharmacokinetics of lithium in elderly patients. Drugs Aging 2000;16(3):165-77.
Dr. McAlpine is assistant professor of psychiatry and director of eating disorders services, Mayo Clinic, Rochester, MN.
Think PLANT to recall vegetative symptoms
Obvious positive symptoms of schizophrenia—such as hallucinations and delusions—typically prompt treatment, but positive symptoms may be absent or clouded by the rationalizations and minimization often seen in paranoia. Negative symptoms can also escape detection because of their subtlety.
Andreasen and Olson’s criteria for negative symptoms1 provide the basis for the Schedule for the Assessment of Negative Symptoms (SANS) that includes the five As: avolition/apathy, alogia, affective flattening, anhedonia/asociality, and attentional impairment.
Many remember Bleuler’s four As of schizophrenia—autism, loosening of associations, affective disturbances, and ambivalence—but may have a harder time remembering the SANS’ five As. I find the pseudo-acronym PLANT (for the vegetative changes manifested with negative symptoms) helpful for recalling all five As (Table).
Table
Use PLANT pseudo-acronym to recall vegetative symptoms
| Symptom | Meaning | Examples |
|---|---|---|
| aPathy/avolition | Lack of drive | Poor grooming |
| Anergia | ||
| Impersistence | ||
| aLogia | Marked impairment in thought processing and/or content | Poverty of speech |
| Poverty of content | ||
| Thought blocking | ||
| Latency of response | ||
| Poor abstracting | ||
| Affective disturbances | Altered expressiveness | Poor eye contact |
| Aprosodic speech | ||
| Lack of expression | ||
| Poverty of gestures | ||
| aNhedonia/ asociality | Loss of interests and pleasures | Little interest in sex |
| Lack of closeness | ||
| Few friends | ||
| Poor capacity for rapport | ||
| aTtentional impairment | Inattentiveness | Poor concentration |
| Stereotyped thought |
1. Andreasen N, Olson SC. Negative versus positive schizophrenia: definition and validation. Arch Gen Psych 1982;39:789-94.
Dr. Wagner is assistant clinical professor, Indiana University School of Medicine, and staff psychiatrist, Richard L Roudebush VA Medical Center, Indianapolis.
Obvious positive symptoms of schizophrenia—such as hallucinations and delusions—typically prompt treatment, but positive symptoms may be absent or clouded by the rationalizations and minimization often seen in paranoia. Negative symptoms can also escape detection because of their subtlety.
Andreasen and Olson’s criteria for negative symptoms1 provide the basis for the Schedule for the Assessment of Negative Symptoms (SANS) that includes the five As: avolition/apathy, alogia, affective flattening, anhedonia/asociality, and attentional impairment.
Many remember Bleuler’s four As of schizophrenia—autism, loosening of associations, affective disturbances, and ambivalence—but may have a harder time remembering the SANS’ five As. I find the pseudo-acronym PLANT (for the vegetative changes manifested with negative symptoms) helpful for recalling all five As (Table).
Table
Use PLANT pseudo-acronym to recall vegetative symptoms
| Symptom | Meaning | Examples |
|---|---|---|
| aPathy/avolition | Lack of drive | Poor grooming |
| Anergia | ||
| Impersistence | ||
| aLogia | Marked impairment in thought processing and/or content | Poverty of speech |
| Poverty of content | ||
| Thought blocking | ||
| Latency of response | ||
| Poor abstracting | ||
| Affective disturbances | Altered expressiveness | Poor eye contact |
| Aprosodic speech | ||
| Lack of expression | ||
| Poverty of gestures | ||
| aNhedonia/ asociality | Loss of interests and pleasures | Little interest in sex |
| Lack of closeness | ||
| Few friends | ||
| Poor capacity for rapport | ||
| aTtentional impairment | Inattentiveness | Poor concentration |
| Stereotyped thought |
Obvious positive symptoms of schizophrenia—such as hallucinations and delusions—typically prompt treatment, but positive symptoms may be absent or clouded by the rationalizations and minimization often seen in paranoia. Negative symptoms can also escape detection because of their subtlety.
Andreasen and Olson’s criteria for negative symptoms1 provide the basis for the Schedule for the Assessment of Negative Symptoms (SANS) that includes the five As: avolition/apathy, alogia, affective flattening, anhedonia/asociality, and attentional impairment.
Many remember Bleuler’s four As of schizophrenia—autism, loosening of associations, affective disturbances, and ambivalence—but may have a harder time remembering the SANS’ five As. I find the pseudo-acronym PLANT (for the vegetative changes manifested with negative symptoms) helpful for recalling all five As (Table).
Table
Use PLANT pseudo-acronym to recall vegetative symptoms
| Symptom | Meaning | Examples |
|---|---|---|
| aPathy/avolition | Lack of drive | Poor grooming |
| Anergia | ||
| Impersistence | ||
| aLogia | Marked impairment in thought processing and/or content | Poverty of speech |
| Poverty of content | ||
| Thought blocking | ||
| Latency of response | ||
| Poor abstracting | ||
| Affective disturbances | Altered expressiveness | Poor eye contact |
| Aprosodic speech | ||
| Lack of expression | ||
| Poverty of gestures | ||
| aNhedonia/ asociality | Loss of interests and pleasures | Little interest in sex |
| Lack of closeness | ||
| Few friends | ||
| Poor capacity for rapport | ||
| aTtentional impairment | Inattentiveness | Poor concentration |
| Stereotyped thought |
1. Andreasen N, Olson SC. Negative versus positive schizophrenia: definition and validation. Arch Gen Psych 1982;39:789-94.
Dr. Wagner is assistant clinical professor, Indiana University School of Medicine, and staff psychiatrist, Richard L Roudebush VA Medical Center, Indianapolis.
1. Andreasen N, Olson SC. Negative versus positive schizophrenia: definition and validation. Arch Gen Psych 1982;39:789-94.
Dr. Wagner is assistant clinical professor, Indiana University School of Medicine, and staff psychiatrist, Richard L Roudebush VA Medical Center, Indianapolis.
Keeping patients physically well: A psychiatrist’s ‘CIVIC’ duty
Many patients with a severe mental disorder go years without preventive medical treatment, leaving them medically ill or at high risk for a medical illness.(See"Acute MI Risk Protecting you patients heart health" September 2005.)
Blood pressure. Check at each visit for patients with a history of hypertension and every 3 to 4 months for nonhypertensive patients. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 7)(See"Metabolic syndrome: 5 risk factors guide therapy" April 2005.)
Refer patients with suspected metabolic syndrome to a primary care physician or endocrinologist for management. Refer patients taking anticonvulsants if readings or symptoms suggest hepatitis or dyscrasia. Significant abnormalites include leukocites 9, platelets 14
Table 2
At what point do lipid levels indicate cardiovascular risk?
| Safe | Borderline* | Needs treatment† | Treatment options | |
|---|---|---|---|---|
| Total cholesterol | 200-239 | >240 | See LDL cholesteroltreatment options | |
| LDL cholesterol | 130-159 | >160 | Lifestyle changes | |
| Statins | ||||
| Bile sequestrants | ||||
| Nicotinic acid | ||||
| Fibrate | ||||
| HDL cholesterol | >60¶ | 59-39 | Lifestyle changes | |
| Treat triglycerides | ||||
| Add nicotinic acid or fibrate | ||||
| Triglycerides | 150-199 | >200 | Lifestyle changes | |
| Statins | ||||
| Consider nicotinic acid or fibrate | ||||
| *Treat according to risk factors. See Adult Treatment Panel III guidelines for specific regimens and cautions. | ||||
| †Three- to 6-month trial of lifestyle changes may be warranted in most cases. Urge patients to reduce saturated fat and cholesterol, eat more soluble fiber, and exercise more. | ||||
| ¶Removes one risk factor | ||||
| Source: Adapted from the Third Report of the Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) (www.nhlbi.nih.gov/guidelines/cholesterol) | ||||
VACCINATION HISTORY/INFECTION RISK
Vaccinations. Many psychiatric patients are not up to date with vaccinations against hepatitis, influenza, or pneumonia. Ask the patient to recall his or her vaccination history as accurately as possible. If he or she cannot, contact the primary care physician the patient visited most recently.
If you cannot obtain the history, refer the patient to the municipal health department for influenza vaccine and a blood test to verify hepatitis B immunization. Educate patients on the benefits of vaccination, and coordinate with a primary care doctor or case manager to ensure the patient’s immunization.
Table 3
Who needs which vaccines—and how often
| Vaccine | Targeted group/frequency |
|---|---|
| Tetanus | Two-vaccine series for intravenous drug abusers; vaccine series for adults who did not receive primary series; boosters if ≥10 years since vaccination |
| Hepatitis A | Intravenous drug users, institutionalized persons, homosexual men, and those living or working where hepatitis A is endemic |
| Hepatitis B | Three-vaccine series for health care workers, sexually active heterosexual men and women, homosexual/bisexual men, hemodialysis patients, intravenous drug abusers, institutionalized persons |
| Influenza | Annual vaccination for persons age ≥50; patients with CVD, diabetes, HIV, renal disease, or pulmonary disease; and others who are immunosuppressed, pregnant, or in a nursing home. Check updates from CDC throughout flu season |
| Pneumococcal | Persons age ≥65; institutionalized patients age ≥50; those with alcohol dependence, asplenia, HIV, chronic CVD, chronic lung disease, diabetes, chronic liver disease, renal insufficiency, or who live in settings where pneumococcal disease can spread. Repeat dose on or about 65th birthday if immunized ≥5 years earlier |
| COPD: Chronic obstructive pulmonary disease | |
| STD: Sexually transmitted disease | |
| Source: U.S. Centers for Disease Control and Prevention. Recommended adult immunization schedule, by vaccine and age group (www.cdc.gov/nip/recs/adult-schedule.pdf) | |
Sexually transmitted disease. Neglected general health or malnourishment can weaken the immune system and increase susceptibility to infections. Patients who live in urban areas or public housing—where infections tend to spread—are especially vulnerable.
In addition, mentally ill persons are more likely than the general population to have a sexually transmitted disease (STD)17,18 because:
- mental illness can cloud judgment; for example, patients with bipolar mania are at risk for impulsive, hypersexual behavior
- some mentally ill patients support themselves with prostitution.
Refer sexually active patients to a hospital or private laboratory for an HIV test and an RPR to test for syphilis. Refer sexually active women age ≤25 for DNA cervical probes for gonorrhea and chlamydia. Evidence is equivocal for screening anymptomatic women age >25 for chlamydia or gonorrhea infection. Sexually inactive women or those in monogamous relationships may not need routine screening. For sexually active men, urine testing to screen for chlamydia or gonorrhea is available.19
Consult a local health clinic or gynecologist for the DNA probe, although some clinical laboratories can check urine for signs of cervical problems. Ask sexually active patients if/when they were immunized against hepatitis B. If needed, refer for vaccination.
MANAGING DIETARY INTAKE
Obesity—defined by the National Institutes of Health as BMI ≥30 kg/m2—often precedes preventable chronic diseases and cancer. Persons with chronic severe mental illness tend to be more sedentary than nonmentally ill persons,20 and research suggests that obesity is more common among patients with severe mental illness than among the general population.21 Also, poorer patients have trouble maintaining a balanced diet.
Calculate BMI using the National Heart, Lung and Blood Institute BMI calculator (http://www.nhlbisupport.com/bmi/bmicalc.htm). Encourage patients with BMI >25 kg/m2 to eat more fruits and vegetables, eliminate empty calories (alcohol, soda pop, juices, candy), and decrease fat consumption (especially fast food). Suggest to patients age ≥50 that they incorporate calcium, 1,200 mg/d, and vitamin D, 400 to 800 IU/d, in their diet to prevent osteoporosis.22
Also encourage patients to exercise moderately for a half-hour daily, 5 days a week, to burn calories. Supplement nutritional counseling with behavioral therapy, focusing on changing eating patterns.23
CANCER PREVENTION
Many patients with chronic mental illness are not regularly screened for colon, cervical, breast, or other common early-stage cancers. In addition, their cancer rates are significantly higher than those of the general population.24
Ask men at the initial visit when they were last screened for colon or prostate cancer. Ask women when they were last screened for colon, cervical or breast cancer (Table 4). Ask again once yearly.
Colon cancer. Colonoscopy, done by a gastroenterologist, is indicated for patients age >50 every 5 to 10 years, depending on endoscopic findings. In-office fecal occult blood tests (FOBT), performed annually between colonoscopies, can identify patients who may need closer follow-up. You can do in-office FOBT or refer to a primary care physician.25
Cervical cancer is thought to be caused by human papilloma virus (HPV). Refer women with an intact cervix annually to a gynecologist or hospital clinic for a Pap smear, which usually includes testing for high-risk HPV if atypical cells are discovered. Some guidelines suggest decreasing screening frequency after several negative Pap smears for women in a monogamous sexual relationship.
Breast cancer affects 1 in 8 women, and having a first-degree relative with breast cancer increases the risk. Women should receive annual mammograms starting at age 40. The USPSTF notes that mammography’s benefits improve with increasing age between ages 40 and 70.26
Many hospital radiology departments or community health centers provide mammograms on a rotating schedule. Refer patients with abnormal findings to a general surgeon or breast center.
Table 4
Recommended intervals for cancer screening
| Type of cancer | Recommended test frequency |
|---|---|
| Colon | Asymptomatic persons age >50 should receive colonoscopy every 5 to 10 years, as directed by the gastroenterologist, and annual fecal occult blood tests |
| Cervical | Annual Pap smears for women who have ever been sexually active and still have a cervix |
| Breast | Mammography every 1 to 2 years after age 40 |
| Lung | Evidence does not support routine chest x-rays or sputum cytology in asymptomatic patients |
| Prostate | Refer men age >50 to primary care physician or hospital laboratory for PSA test; counsel patients about the results and treatment |
CASE CONTINUED: TESTING BEGINS
We schedule a battery of laboratory tests for Mrs. J at the local hospital, including a fasting plasma glucose test and lipid profile to gauge her cardiovascular risk and potential effects from olanzapine, and CBC and LFTs to check for adverse effects from oxcarbazepine.
We ask Mrs. J whether she engages in high-risk sexual activity, which she denies. She cannot recall her vaccination history, so we contact the primary care physician she had seen 5 years ago. Depending on her other comorbidities, housing situation, an early pneumococcal vaccine may be indicated.
We also suggest that Mrs. J quit smoking, but she appears to be at a pre-contemplative stage. We hope to promote a change in her attitude by discussing smoking cessation at each visit
To address Mrs. J’s obesity, we briefly review a dietary plan augmented with increased physical activity. She will bring a 3-day food diary to her next visit and promises to walk 30 minutes four to five times weekly. She says she enjoys mall walking with her children.
We strongly urge Mrs. J to schedule a mammogram, as she is past age 50 and says she has never received one. We try to refer her to a primary care physician to arrange a Pap smear and colonoscopy, but she resists, fearing the results. With continued education, exploration, and encouragement, we will briefly follow up with Mrs. J at each visit to ensure that she gets these needed tests (Box 2).
Check with patients at each visit to ensure they are following through on their test referrals. If they are not, find out why.
If the patient is procrastinating, try to uncover an underlying cause. If the patient says he or she is pressed for time, ask: “Are you going through stressful life events? Are you afraid the test will hurt or will reveal a serious disease? Did you have this test before? If so, did it make you uncomfortable?
Tell the patent, “I understand your concerns, but this test is important. You need to make it a higher priority.” To work through the patient’s resistance, start by educating him or her about preventable chronic diseases and screening or treatment resources. Then try problem-solving techniques, motivational interviewing, or dissecting cognitive distortions.
Collaboration with a case manager is key when managing an indigent mentally ill patient. Open communication, setting well-defined goals, and a clear understanding of each other’s treatment roles is crucial. Inform the case manager which target tasks, tests, or appointments the patient has agreed to. The case manager can use this information to help the patient navigate the health care system and encourage full participation in care
Finally, build a referral base for indigent and uninsured patients. Look for a nearby internist, gastroenterologist, and OB/GYN who accept uninsured patients.
- U.S. Preventative Services Task Force. Continually updated, evidence-based screening recommendations for a range of medical problems. www.ahrq.gov/clinic/uspstfix.htm.
- U.S. Public Health Service. Clinical practice guideline: treating tobacco use and dependence. www.surgeongeneral.gov/tobacco/treating_tobacco_use.pdf.
- Olanzapine • Zyprexa
- Oxcarbazepine • Trileptal
Dr. Moss recevies research/grant support from the National Institutes of Health and is a speaker for Janssen Pharmaceutica and Pfizer.
Mr. Brammer and Dr. White report no financial relationship with any company whose products are mentioned in this article, or with manufacturers of competing products.
1. Carney CP, Allen J, Doebbeling BN. Receipt of clinical preventive medical services among psychiatric patients. Psychiatr Serv 2002;53:1028-30.
2. Joukamaa M, Heliovaara M, Knekt P, et al. Mental disorders and cause-specific mortality. Br J Psychiatry 2001;179:498-502.
3. McCreadie RG. Scottish Schizophrenia Lifestyle Group. Diet, smoking and cardiovascular risk in people with schizophrenia: descriptive study. Br J Psychiatry 2003;183:534-9.
4. Cohn T, Prud’homme D, Streiner D, et al. Characterizing coronary heart disease risk in chronic schizophrenia: high prevalence of the metabolic syndrome. Can J Psychiatry 2004;49:753-60.
5. Hanson D, Gottesman I. Theories of schizophrenia: a geneticinflammatory-vascular synthesis. BMC Med Genet 2005;6:7.-
6. Chobanian AV, Bakris GL, Black HR, et al. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure: the JNC 7 report. JAMA 2003;289(19):2560-72.
7. Berg AO, Atkins D. U.S. Preventive Services Task Force: screening for lipid disorders in adults: recommendations and rationale. Am J Nurs 2002;102(6):p. 91-5.
8. Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) final report. Circulation 2002;106:3143-421.
9. Standards of medical care in diabetes. Diabetes Care 2005;28:S4-S36.
10. Clinical practice recommendations 2005. Diabetes Care 2005;28(Suppl 1):S1-S79.
11. Lasser K, Boyd JW, Woolhandler S, et al. Smoking and mental illness: a population-based prevalence study. JAMA 2000;284(20):2606-10.
12. Ockene IS, Miller NH. Cigarette smoking, cardiovascular disease, and stroke: a statement for healthcare professionals from the American Heart Association. American Heart Association Task Force on Risk Reduction. Circulation 1997;96:3243-7.
13. Fiore MC. U.S. Public Health Service clinical practice guideline: treating tobacco use and dependence. Respir Care 2000;45:1200-62.
14. Pellock JM, Willmore LJ. A rational guide to routine blood monitoring in patients receiving antiepileptic drugs. Neurology 1991;41:961-4.
15. Goodwin FK, Goldstein MA. Optimizing lithium treatment in bipolar disorder: a review of the literature and clinical recommendations. J Psychiatr Pract 2003;9:333-43.
16. Consensus development conference on antipsychotic drugs and obesity and diabetes. Diabetes Care 2004;27:596-601.
17. Erbelding EJ, Hutton HE, Zenilman JM, et al. The prevalence of psychiatric disorders in sexually transmitted disease clinic patients and their association with sexually transmitted risk. Sex Transm Dis 2004;31:8-12.
18. Rein DB, Anderson LA, Irwin KL. Mental health disorders and sexually transmitted diseases in a privately insured population. Am J Manag Care 2004;10:917-24.
19. Screening for sexually transmitted diseases. U.S.Preventive Services Task Force, Washington, DC. Am Fam Physician 1990;42:691-702.
20. Daumit GL, Goldberg RW, Anthony C, et al. Physical activity patterns in adults with severe mental illness. J Nerv Ment Dis 2005;193:641-6.
21. Daumit GL, Clark JM, Steinwachs DM, et al. Prevalence and correlates of obesity in a community sample of individuals with severe and persistent mental illness. J Nerv Ment Dis 2003;191:799-805.
22. Hodgson SF, Watts NB, Bilezikian JP, et al. American Association of Clinical Endocrinologists medical guidelines for clinical practice for the prevention and treatment of postmenopausal osteoporosis: 2001 edition, with selected updates for 2003. Endocr Pract 2003;9:544-64.
23. Jakicic JM, Clark K, Coleman E, et al. American College of Sports Medicine. American College of Sports Medicine position stand. Appropriate intervention strategies for weight loss and prevention of weight regain for adults. Med Sci Sports Exerc 2001;33:2145-56.
24. Lichtermann D, Ekelund J, Pukkala E, et al. Incidence of cancer among persons with schizophrenia and their relatives. Arch Gen Psychiatry 2001;58:573-8.
25. Colon cancer screening (USPSTF recommendation). U.S. Preventive Services Task Force. J Am Geriatr Soc 2000M;48:333-5.
26. Humphrey LL, Helfand M, Chan BK, Woolf SH. Breast cancer screening: a summary of the evidence for the U.S. Preventive Services Task Force. Ann Intern Med 2002;137(5 Part 1):347-60.
Many patients with a severe mental disorder go years without preventive medical treatment, leaving them medically ill or at high risk for a medical illness.(See"Acute MI Risk Protecting you patients heart health" September 2005.)
Blood pressure. Check at each visit for patients with a history of hypertension and every 3 to 4 months for nonhypertensive patients. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 7)(See"Metabolic syndrome: 5 risk factors guide therapy" April 2005.)
Refer patients with suspected metabolic syndrome to a primary care physician or endocrinologist for management. Refer patients taking anticonvulsants if readings or symptoms suggest hepatitis or dyscrasia. Significant abnormalites include leukocites 9, platelets 14
Table 2
At what point do lipid levels indicate cardiovascular risk?
| Safe | Borderline* | Needs treatment† | Treatment options | |
|---|---|---|---|---|
| Total cholesterol | 200-239 | >240 | See LDL cholesteroltreatment options | |
| LDL cholesterol | 130-159 | >160 | Lifestyle changes | |
| Statins | ||||
| Bile sequestrants | ||||
| Nicotinic acid | ||||
| Fibrate | ||||
| HDL cholesterol | >60¶ | 59-39 | Lifestyle changes | |
| Treat triglycerides | ||||
| Add nicotinic acid or fibrate | ||||
| Triglycerides | 150-199 | >200 | Lifestyle changes | |
| Statins | ||||
| Consider nicotinic acid or fibrate | ||||
| *Treat according to risk factors. See Adult Treatment Panel III guidelines for specific regimens and cautions. | ||||
| †Three- to 6-month trial of lifestyle changes may be warranted in most cases. Urge patients to reduce saturated fat and cholesterol, eat more soluble fiber, and exercise more. | ||||
| ¶Removes one risk factor | ||||
| Source: Adapted from the Third Report of the Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) (www.nhlbi.nih.gov/guidelines/cholesterol) | ||||
VACCINATION HISTORY/INFECTION RISK
Vaccinations. Many psychiatric patients are not up to date with vaccinations against hepatitis, influenza, or pneumonia. Ask the patient to recall his or her vaccination history as accurately as possible. If he or she cannot, contact the primary care physician the patient visited most recently.
If you cannot obtain the history, refer the patient to the municipal health department for influenza vaccine and a blood test to verify hepatitis B immunization. Educate patients on the benefits of vaccination, and coordinate with a primary care doctor or case manager to ensure the patient’s immunization.
Table 3
Who needs which vaccines—and how often
| Vaccine | Targeted group/frequency |
|---|---|
| Tetanus | Two-vaccine series for intravenous drug abusers; vaccine series for adults who did not receive primary series; boosters if ≥10 years since vaccination |
| Hepatitis A | Intravenous drug users, institutionalized persons, homosexual men, and those living or working where hepatitis A is endemic |
| Hepatitis B | Three-vaccine series for health care workers, sexually active heterosexual men and women, homosexual/bisexual men, hemodialysis patients, intravenous drug abusers, institutionalized persons |
| Influenza | Annual vaccination for persons age ≥50; patients with CVD, diabetes, HIV, renal disease, or pulmonary disease; and others who are immunosuppressed, pregnant, or in a nursing home. Check updates from CDC throughout flu season |
| Pneumococcal | Persons age ≥65; institutionalized patients age ≥50; those with alcohol dependence, asplenia, HIV, chronic CVD, chronic lung disease, diabetes, chronic liver disease, renal insufficiency, or who live in settings where pneumococcal disease can spread. Repeat dose on or about 65th birthday if immunized ≥5 years earlier |
| COPD: Chronic obstructive pulmonary disease | |
| STD: Sexually transmitted disease | |
| Source: U.S. Centers for Disease Control and Prevention. Recommended adult immunization schedule, by vaccine and age group (www.cdc.gov/nip/recs/adult-schedule.pdf) | |
Sexually transmitted disease. Neglected general health or malnourishment can weaken the immune system and increase susceptibility to infections. Patients who live in urban areas or public housing—where infections tend to spread—are especially vulnerable.
In addition, mentally ill persons are more likely than the general population to have a sexually transmitted disease (STD)17,18 because:
- mental illness can cloud judgment; for example, patients with bipolar mania are at risk for impulsive, hypersexual behavior
- some mentally ill patients support themselves with prostitution.
Refer sexually active patients to a hospital or private laboratory for an HIV test and an RPR to test for syphilis. Refer sexually active women age ≤25 for DNA cervical probes for gonorrhea and chlamydia. Evidence is equivocal for screening anymptomatic women age >25 for chlamydia or gonorrhea infection. Sexually inactive women or those in monogamous relationships may not need routine screening. For sexually active men, urine testing to screen for chlamydia or gonorrhea is available.19
Consult a local health clinic or gynecologist for the DNA probe, although some clinical laboratories can check urine for signs of cervical problems. Ask sexually active patients if/when they were immunized against hepatitis B. If needed, refer for vaccination.
MANAGING DIETARY INTAKE
Obesity—defined by the National Institutes of Health as BMI ≥30 kg/m2—often precedes preventable chronic diseases and cancer. Persons with chronic severe mental illness tend to be more sedentary than nonmentally ill persons,20 and research suggests that obesity is more common among patients with severe mental illness than among the general population.21 Also, poorer patients have trouble maintaining a balanced diet.
Calculate BMI using the National Heart, Lung and Blood Institute BMI calculator (http://www.nhlbisupport.com/bmi/bmicalc.htm). Encourage patients with BMI >25 kg/m2 to eat more fruits and vegetables, eliminate empty calories (alcohol, soda pop, juices, candy), and decrease fat consumption (especially fast food). Suggest to patients age ≥50 that they incorporate calcium, 1,200 mg/d, and vitamin D, 400 to 800 IU/d, in their diet to prevent osteoporosis.22
Also encourage patients to exercise moderately for a half-hour daily, 5 days a week, to burn calories. Supplement nutritional counseling with behavioral therapy, focusing on changing eating patterns.23
CANCER PREVENTION
Many patients with chronic mental illness are not regularly screened for colon, cervical, breast, or other common early-stage cancers. In addition, their cancer rates are significantly higher than those of the general population.24
Ask men at the initial visit when they were last screened for colon or prostate cancer. Ask women when they were last screened for colon, cervical or breast cancer (Table 4). Ask again once yearly.
Colon cancer. Colonoscopy, done by a gastroenterologist, is indicated for patients age >50 every 5 to 10 years, depending on endoscopic findings. In-office fecal occult blood tests (FOBT), performed annually between colonoscopies, can identify patients who may need closer follow-up. You can do in-office FOBT or refer to a primary care physician.25
Cervical cancer is thought to be caused by human papilloma virus (HPV). Refer women with an intact cervix annually to a gynecologist or hospital clinic for a Pap smear, which usually includes testing for high-risk HPV if atypical cells are discovered. Some guidelines suggest decreasing screening frequency after several negative Pap smears for women in a monogamous sexual relationship.
Breast cancer affects 1 in 8 women, and having a first-degree relative with breast cancer increases the risk. Women should receive annual mammograms starting at age 40. The USPSTF notes that mammography’s benefits improve with increasing age between ages 40 and 70.26
Many hospital radiology departments or community health centers provide mammograms on a rotating schedule. Refer patients with abnormal findings to a general surgeon or breast center.
Table 4
Recommended intervals for cancer screening
| Type of cancer | Recommended test frequency |
|---|---|
| Colon | Asymptomatic persons age >50 should receive colonoscopy every 5 to 10 years, as directed by the gastroenterologist, and annual fecal occult blood tests |
| Cervical | Annual Pap smears for women who have ever been sexually active and still have a cervix |
| Breast | Mammography every 1 to 2 years after age 40 |
| Lung | Evidence does not support routine chest x-rays or sputum cytology in asymptomatic patients |
| Prostate | Refer men age >50 to primary care physician or hospital laboratory for PSA test; counsel patients about the results and treatment |
CASE CONTINUED: TESTING BEGINS
We schedule a battery of laboratory tests for Mrs. J at the local hospital, including a fasting plasma glucose test and lipid profile to gauge her cardiovascular risk and potential effects from olanzapine, and CBC and LFTs to check for adverse effects from oxcarbazepine.
We ask Mrs. J whether she engages in high-risk sexual activity, which she denies. She cannot recall her vaccination history, so we contact the primary care physician she had seen 5 years ago. Depending on her other comorbidities, housing situation, an early pneumococcal vaccine may be indicated.
We also suggest that Mrs. J quit smoking, but she appears to be at a pre-contemplative stage. We hope to promote a change in her attitude by discussing smoking cessation at each visit
To address Mrs. J’s obesity, we briefly review a dietary plan augmented with increased physical activity. She will bring a 3-day food diary to her next visit and promises to walk 30 minutes four to five times weekly. She says she enjoys mall walking with her children.
We strongly urge Mrs. J to schedule a mammogram, as she is past age 50 and says she has never received one. We try to refer her to a primary care physician to arrange a Pap smear and colonoscopy, but she resists, fearing the results. With continued education, exploration, and encouragement, we will briefly follow up with Mrs. J at each visit to ensure that she gets these needed tests (Box 2).
Check with patients at each visit to ensure they are following through on their test referrals. If they are not, find out why.
If the patient is procrastinating, try to uncover an underlying cause. If the patient says he or she is pressed for time, ask: “Are you going through stressful life events? Are you afraid the test will hurt or will reveal a serious disease? Did you have this test before? If so, did it make you uncomfortable?
Tell the patent, “I understand your concerns, but this test is important. You need to make it a higher priority.” To work through the patient’s resistance, start by educating him or her about preventable chronic diseases and screening or treatment resources. Then try problem-solving techniques, motivational interviewing, or dissecting cognitive distortions.
Collaboration with a case manager is key when managing an indigent mentally ill patient. Open communication, setting well-defined goals, and a clear understanding of each other’s treatment roles is crucial. Inform the case manager which target tasks, tests, or appointments the patient has agreed to. The case manager can use this information to help the patient navigate the health care system and encourage full participation in care
Finally, build a referral base for indigent and uninsured patients. Look for a nearby internist, gastroenterologist, and OB/GYN who accept uninsured patients.
- U.S. Preventative Services Task Force. Continually updated, evidence-based screening recommendations for a range of medical problems. www.ahrq.gov/clinic/uspstfix.htm.
- U.S. Public Health Service. Clinical practice guideline: treating tobacco use and dependence. www.surgeongeneral.gov/tobacco/treating_tobacco_use.pdf.
- Olanzapine • Zyprexa
- Oxcarbazepine • Trileptal
Dr. Moss recevies research/grant support from the National Institutes of Health and is a speaker for Janssen Pharmaceutica and Pfizer.
Mr. Brammer and Dr. White report no financial relationship with any company whose products are mentioned in this article, or with manufacturers of competing products.
Many patients with a severe mental disorder go years without preventive medical treatment, leaving them medically ill or at high risk for a medical illness.(See"Acute MI Risk Protecting you patients heart health" September 2005.)
Blood pressure. Check at each visit for patients with a history of hypertension and every 3 to 4 months for nonhypertensive patients. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 7)(See"Metabolic syndrome: 5 risk factors guide therapy" April 2005.)
Refer patients with suspected metabolic syndrome to a primary care physician or endocrinologist for management. Refer patients taking anticonvulsants if readings or symptoms suggest hepatitis or dyscrasia. Significant abnormalites include leukocites 9, platelets 14
Table 2
At what point do lipid levels indicate cardiovascular risk?
| Safe | Borderline* | Needs treatment† | Treatment options | |
|---|---|---|---|---|
| Total cholesterol | 200-239 | >240 | See LDL cholesteroltreatment options | |
| LDL cholesterol | 130-159 | >160 | Lifestyle changes | |
| Statins | ||||
| Bile sequestrants | ||||
| Nicotinic acid | ||||
| Fibrate | ||||
| HDL cholesterol | >60¶ | 59-39 | Lifestyle changes | |
| Treat triglycerides | ||||
| Add nicotinic acid or fibrate | ||||
| Triglycerides | 150-199 | >200 | Lifestyle changes | |
| Statins | ||||
| Consider nicotinic acid or fibrate | ||||
| *Treat according to risk factors. See Adult Treatment Panel III guidelines for specific regimens and cautions. | ||||
| †Three- to 6-month trial of lifestyle changes may be warranted in most cases. Urge patients to reduce saturated fat and cholesterol, eat more soluble fiber, and exercise more. | ||||
| ¶Removes one risk factor | ||||
| Source: Adapted from the Third Report of the Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) (www.nhlbi.nih.gov/guidelines/cholesterol) | ||||
VACCINATION HISTORY/INFECTION RISK
Vaccinations. Many psychiatric patients are not up to date with vaccinations against hepatitis, influenza, or pneumonia. Ask the patient to recall his or her vaccination history as accurately as possible. If he or she cannot, contact the primary care physician the patient visited most recently.
If you cannot obtain the history, refer the patient to the municipal health department for influenza vaccine and a blood test to verify hepatitis B immunization. Educate patients on the benefits of vaccination, and coordinate with a primary care doctor or case manager to ensure the patient’s immunization.
Table 3
Who needs which vaccines—and how often
| Vaccine | Targeted group/frequency |
|---|---|
| Tetanus | Two-vaccine series for intravenous drug abusers; vaccine series for adults who did not receive primary series; boosters if ≥10 years since vaccination |
| Hepatitis A | Intravenous drug users, institutionalized persons, homosexual men, and those living or working where hepatitis A is endemic |
| Hepatitis B | Three-vaccine series for health care workers, sexually active heterosexual men and women, homosexual/bisexual men, hemodialysis patients, intravenous drug abusers, institutionalized persons |
| Influenza | Annual vaccination for persons age ≥50; patients with CVD, diabetes, HIV, renal disease, or pulmonary disease; and others who are immunosuppressed, pregnant, or in a nursing home. Check updates from CDC throughout flu season |
| Pneumococcal | Persons age ≥65; institutionalized patients age ≥50; those with alcohol dependence, asplenia, HIV, chronic CVD, chronic lung disease, diabetes, chronic liver disease, renal insufficiency, or who live in settings where pneumococcal disease can spread. Repeat dose on or about 65th birthday if immunized ≥5 years earlier |
| COPD: Chronic obstructive pulmonary disease | |
| STD: Sexually transmitted disease | |
| Source: U.S. Centers for Disease Control and Prevention. Recommended adult immunization schedule, by vaccine and age group (www.cdc.gov/nip/recs/adult-schedule.pdf) | |
Sexually transmitted disease. Neglected general health or malnourishment can weaken the immune system and increase susceptibility to infections. Patients who live in urban areas or public housing—where infections tend to spread—are especially vulnerable.
In addition, mentally ill persons are more likely than the general population to have a sexually transmitted disease (STD)17,18 because:
- mental illness can cloud judgment; for example, patients with bipolar mania are at risk for impulsive, hypersexual behavior
- some mentally ill patients support themselves with prostitution.
Refer sexually active patients to a hospital or private laboratory for an HIV test and an RPR to test for syphilis. Refer sexually active women age ≤25 for DNA cervical probes for gonorrhea and chlamydia. Evidence is equivocal for screening anymptomatic women age >25 for chlamydia or gonorrhea infection. Sexually inactive women or those in monogamous relationships may not need routine screening. For sexually active men, urine testing to screen for chlamydia or gonorrhea is available.19
Consult a local health clinic or gynecologist for the DNA probe, although some clinical laboratories can check urine for signs of cervical problems. Ask sexually active patients if/when they were immunized against hepatitis B. If needed, refer for vaccination.
MANAGING DIETARY INTAKE
Obesity—defined by the National Institutes of Health as BMI ≥30 kg/m2—often precedes preventable chronic diseases and cancer. Persons with chronic severe mental illness tend to be more sedentary than nonmentally ill persons,20 and research suggests that obesity is more common among patients with severe mental illness than among the general population.21 Also, poorer patients have trouble maintaining a balanced diet.
Calculate BMI using the National Heart, Lung and Blood Institute BMI calculator (http://www.nhlbisupport.com/bmi/bmicalc.htm). Encourage patients with BMI >25 kg/m2 to eat more fruits and vegetables, eliminate empty calories (alcohol, soda pop, juices, candy), and decrease fat consumption (especially fast food). Suggest to patients age ≥50 that they incorporate calcium, 1,200 mg/d, and vitamin D, 400 to 800 IU/d, in their diet to prevent osteoporosis.22
Also encourage patients to exercise moderately for a half-hour daily, 5 days a week, to burn calories. Supplement nutritional counseling with behavioral therapy, focusing on changing eating patterns.23
CANCER PREVENTION
Many patients with chronic mental illness are not regularly screened for colon, cervical, breast, or other common early-stage cancers. In addition, their cancer rates are significantly higher than those of the general population.24
Ask men at the initial visit when they were last screened for colon or prostate cancer. Ask women when they were last screened for colon, cervical or breast cancer (Table 4). Ask again once yearly.
Colon cancer. Colonoscopy, done by a gastroenterologist, is indicated for patients age >50 every 5 to 10 years, depending on endoscopic findings. In-office fecal occult blood tests (FOBT), performed annually between colonoscopies, can identify patients who may need closer follow-up. You can do in-office FOBT or refer to a primary care physician.25
Cervical cancer is thought to be caused by human papilloma virus (HPV). Refer women with an intact cervix annually to a gynecologist or hospital clinic for a Pap smear, which usually includes testing for high-risk HPV if atypical cells are discovered. Some guidelines suggest decreasing screening frequency after several negative Pap smears for women in a monogamous sexual relationship.
Breast cancer affects 1 in 8 women, and having a first-degree relative with breast cancer increases the risk. Women should receive annual mammograms starting at age 40. The USPSTF notes that mammography’s benefits improve with increasing age between ages 40 and 70.26
Many hospital radiology departments or community health centers provide mammograms on a rotating schedule. Refer patients with abnormal findings to a general surgeon or breast center.
Table 4
Recommended intervals for cancer screening
| Type of cancer | Recommended test frequency |
|---|---|
| Colon | Asymptomatic persons age >50 should receive colonoscopy every 5 to 10 years, as directed by the gastroenterologist, and annual fecal occult blood tests |
| Cervical | Annual Pap smears for women who have ever been sexually active and still have a cervix |
| Breast | Mammography every 1 to 2 years after age 40 |
| Lung | Evidence does not support routine chest x-rays or sputum cytology in asymptomatic patients |
| Prostate | Refer men age >50 to primary care physician or hospital laboratory for PSA test; counsel patients about the results and treatment |
CASE CONTINUED: TESTING BEGINS
We schedule a battery of laboratory tests for Mrs. J at the local hospital, including a fasting plasma glucose test and lipid profile to gauge her cardiovascular risk and potential effects from olanzapine, and CBC and LFTs to check for adverse effects from oxcarbazepine.
We ask Mrs. J whether she engages in high-risk sexual activity, which she denies. She cannot recall her vaccination history, so we contact the primary care physician she had seen 5 years ago. Depending on her other comorbidities, housing situation, an early pneumococcal vaccine may be indicated.
We also suggest that Mrs. J quit smoking, but she appears to be at a pre-contemplative stage. We hope to promote a change in her attitude by discussing smoking cessation at each visit
To address Mrs. J’s obesity, we briefly review a dietary plan augmented with increased physical activity. She will bring a 3-day food diary to her next visit and promises to walk 30 minutes four to five times weekly. She says she enjoys mall walking with her children.
We strongly urge Mrs. J to schedule a mammogram, as she is past age 50 and says she has never received one. We try to refer her to a primary care physician to arrange a Pap smear and colonoscopy, but she resists, fearing the results. With continued education, exploration, and encouragement, we will briefly follow up with Mrs. J at each visit to ensure that she gets these needed tests (Box 2).
Check with patients at each visit to ensure they are following through on their test referrals. If they are not, find out why.
If the patient is procrastinating, try to uncover an underlying cause. If the patient says he or she is pressed for time, ask: “Are you going through stressful life events? Are you afraid the test will hurt or will reveal a serious disease? Did you have this test before? If so, did it make you uncomfortable?
Tell the patent, “I understand your concerns, but this test is important. You need to make it a higher priority.” To work through the patient’s resistance, start by educating him or her about preventable chronic diseases and screening or treatment resources. Then try problem-solving techniques, motivational interviewing, or dissecting cognitive distortions.
Collaboration with a case manager is key when managing an indigent mentally ill patient. Open communication, setting well-defined goals, and a clear understanding of each other’s treatment roles is crucial. Inform the case manager which target tasks, tests, or appointments the patient has agreed to. The case manager can use this information to help the patient navigate the health care system and encourage full participation in care
Finally, build a referral base for indigent and uninsured patients. Look for a nearby internist, gastroenterologist, and OB/GYN who accept uninsured patients.
- U.S. Preventative Services Task Force. Continually updated, evidence-based screening recommendations for a range of medical problems. www.ahrq.gov/clinic/uspstfix.htm.
- U.S. Public Health Service. Clinical practice guideline: treating tobacco use and dependence. www.surgeongeneral.gov/tobacco/treating_tobacco_use.pdf.
- Olanzapine • Zyprexa
- Oxcarbazepine • Trileptal
Dr. Moss recevies research/grant support from the National Institutes of Health and is a speaker for Janssen Pharmaceutica and Pfizer.
Mr. Brammer and Dr. White report no financial relationship with any company whose products are mentioned in this article, or with manufacturers of competing products.
1. Carney CP, Allen J, Doebbeling BN. Receipt of clinical preventive medical services among psychiatric patients. Psychiatr Serv 2002;53:1028-30.
2. Joukamaa M, Heliovaara M, Knekt P, et al. Mental disorders and cause-specific mortality. Br J Psychiatry 2001;179:498-502.
3. McCreadie RG. Scottish Schizophrenia Lifestyle Group. Diet, smoking and cardiovascular risk in people with schizophrenia: descriptive study. Br J Psychiatry 2003;183:534-9.
4. Cohn T, Prud’homme D, Streiner D, et al. Characterizing coronary heart disease risk in chronic schizophrenia: high prevalence of the metabolic syndrome. Can J Psychiatry 2004;49:753-60.
5. Hanson D, Gottesman I. Theories of schizophrenia: a geneticinflammatory-vascular synthesis. BMC Med Genet 2005;6:7.-
6. Chobanian AV, Bakris GL, Black HR, et al. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure: the JNC 7 report. JAMA 2003;289(19):2560-72.
7. Berg AO, Atkins D. U.S. Preventive Services Task Force: screening for lipid disorders in adults: recommendations and rationale. Am J Nurs 2002;102(6):p. 91-5.
8. Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) final report. Circulation 2002;106:3143-421.
9. Standards of medical care in diabetes. Diabetes Care 2005;28:S4-S36.
10. Clinical practice recommendations 2005. Diabetes Care 2005;28(Suppl 1):S1-S79.
11. Lasser K, Boyd JW, Woolhandler S, et al. Smoking and mental illness: a population-based prevalence study. JAMA 2000;284(20):2606-10.
12. Ockene IS, Miller NH. Cigarette smoking, cardiovascular disease, and stroke: a statement for healthcare professionals from the American Heart Association. American Heart Association Task Force on Risk Reduction. Circulation 1997;96:3243-7.
13. Fiore MC. U.S. Public Health Service clinical practice guideline: treating tobacco use and dependence. Respir Care 2000;45:1200-62.
14. Pellock JM, Willmore LJ. A rational guide to routine blood monitoring in patients receiving antiepileptic drugs. Neurology 1991;41:961-4.
15. Goodwin FK, Goldstein MA. Optimizing lithium treatment in bipolar disorder: a review of the literature and clinical recommendations. J Psychiatr Pract 2003;9:333-43.
16. Consensus development conference on antipsychotic drugs and obesity and diabetes. Diabetes Care 2004;27:596-601.
17. Erbelding EJ, Hutton HE, Zenilman JM, et al. The prevalence of psychiatric disorders in sexually transmitted disease clinic patients and their association with sexually transmitted risk. Sex Transm Dis 2004;31:8-12.
18. Rein DB, Anderson LA, Irwin KL. Mental health disorders and sexually transmitted diseases in a privately insured population. Am J Manag Care 2004;10:917-24.
19. Screening for sexually transmitted diseases. U.S.Preventive Services Task Force, Washington, DC. Am Fam Physician 1990;42:691-702.
20. Daumit GL, Goldberg RW, Anthony C, et al. Physical activity patterns in adults with severe mental illness. J Nerv Ment Dis 2005;193:641-6.
21. Daumit GL, Clark JM, Steinwachs DM, et al. Prevalence and correlates of obesity in a community sample of individuals with severe and persistent mental illness. J Nerv Ment Dis 2003;191:799-805.
22. Hodgson SF, Watts NB, Bilezikian JP, et al. American Association of Clinical Endocrinologists medical guidelines for clinical practice for the prevention and treatment of postmenopausal osteoporosis: 2001 edition, with selected updates for 2003. Endocr Pract 2003;9:544-64.
23. Jakicic JM, Clark K, Coleman E, et al. American College of Sports Medicine. American College of Sports Medicine position stand. Appropriate intervention strategies for weight loss and prevention of weight regain for adults. Med Sci Sports Exerc 2001;33:2145-56.
24. Lichtermann D, Ekelund J, Pukkala E, et al. Incidence of cancer among persons with schizophrenia and their relatives. Arch Gen Psychiatry 2001;58:573-8.
25. Colon cancer screening (USPSTF recommendation). U.S. Preventive Services Task Force. J Am Geriatr Soc 2000M;48:333-5.
26. Humphrey LL, Helfand M, Chan BK, Woolf SH. Breast cancer screening: a summary of the evidence for the U.S. Preventive Services Task Force. Ann Intern Med 2002;137(5 Part 1):347-60.
1. Carney CP, Allen J, Doebbeling BN. Receipt of clinical preventive medical services among psychiatric patients. Psychiatr Serv 2002;53:1028-30.
2. Joukamaa M, Heliovaara M, Knekt P, et al. Mental disorders and cause-specific mortality. Br J Psychiatry 2001;179:498-502.
3. McCreadie RG. Scottish Schizophrenia Lifestyle Group. Diet, smoking and cardiovascular risk in people with schizophrenia: descriptive study. Br J Psychiatry 2003;183:534-9.
4. Cohn T, Prud’homme D, Streiner D, et al. Characterizing coronary heart disease risk in chronic schizophrenia: high prevalence of the metabolic syndrome. Can J Psychiatry 2004;49:753-60.
5. Hanson D, Gottesman I. Theories of schizophrenia: a geneticinflammatory-vascular synthesis. BMC Med Genet 2005;6:7.-
6. Chobanian AV, Bakris GL, Black HR, et al. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure: the JNC 7 report. JAMA 2003;289(19):2560-72.
7. Berg AO, Atkins D. U.S. Preventive Services Task Force: screening for lipid disorders in adults: recommendations and rationale. Am J Nurs 2002;102(6):p. 91-5.
8. Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) final report. Circulation 2002;106:3143-421.
9. Standards of medical care in diabetes. Diabetes Care 2005;28:S4-S36.
10. Clinical practice recommendations 2005. Diabetes Care 2005;28(Suppl 1):S1-S79.
11. Lasser K, Boyd JW, Woolhandler S, et al. Smoking and mental illness: a population-based prevalence study. JAMA 2000;284(20):2606-10.
12. Ockene IS, Miller NH. Cigarette smoking, cardiovascular disease, and stroke: a statement for healthcare professionals from the American Heart Association. American Heart Association Task Force on Risk Reduction. Circulation 1997;96:3243-7.
13. Fiore MC. U.S. Public Health Service clinical practice guideline: treating tobacco use and dependence. Respir Care 2000;45:1200-62.
14. Pellock JM, Willmore LJ. A rational guide to routine blood monitoring in patients receiving antiepileptic drugs. Neurology 1991;41:961-4.
15. Goodwin FK, Goldstein MA. Optimizing lithium treatment in bipolar disorder: a review of the literature and clinical recommendations. J Psychiatr Pract 2003;9:333-43.
16. Consensus development conference on antipsychotic drugs and obesity and diabetes. Diabetes Care 2004;27:596-601.
17. Erbelding EJ, Hutton HE, Zenilman JM, et al. The prevalence of psychiatric disorders in sexually transmitted disease clinic patients and their association with sexually transmitted risk. Sex Transm Dis 2004;31:8-12.
18. Rein DB, Anderson LA, Irwin KL. Mental health disorders and sexually transmitted diseases in a privately insured population. Am J Manag Care 2004;10:917-24.
19. Screening for sexually transmitted diseases. U.S.Preventive Services Task Force, Washington, DC. Am Fam Physician 1990;42:691-702.
20. Daumit GL, Goldberg RW, Anthony C, et al. Physical activity patterns in adults with severe mental illness. J Nerv Ment Dis 2005;193:641-6.
21. Daumit GL, Clark JM, Steinwachs DM, et al. Prevalence and correlates of obesity in a community sample of individuals with severe and persistent mental illness. J Nerv Ment Dis 2003;191:799-805.
22. Hodgson SF, Watts NB, Bilezikian JP, et al. American Association of Clinical Endocrinologists medical guidelines for clinical practice for the prevention and treatment of postmenopausal osteoporosis: 2001 edition, with selected updates for 2003. Endocr Pract 2003;9:544-64.
23. Jakicic JM, Clark K, Coleman E, et al. American College of Sports Medicine. American College of Sports Medicine position stand. Appropriate intervention strategies for weight loss and prevention of weight regain for adults. Med Sci Sports Exerc 2001;33:2145-56.
24. Lichtermann D, Ekelund J, Pukkala E, et al. Incidence of cancer among persons with schizophrenia and their relatives. Arch Gen Psychiatry 2001;58:573-8.
25. Colon cancer screening (USPSTF recommendation). U.S. Preventive Services Task Force. J Am Geriatr Soc 2000M;48:333-5.
26. Humphrey LL, Helfand M, Chan BK, Woolf SH. Breast cancer screening: a summary of the evidence for the U.S. Preventive Services Task Force. Ann Intern Med 2002;137(5 Part 1):347-60.