User login
Welcome to Current Psychiatry, a leading source of information, online and in print, for practitioners of psychiatry and its related subspecialties, including addiction psychiatry, child and adolescent psychiatry, and geriatric psychiatry. This Web site contains evidence-based reviews of the prevention, diagnosis, and treatment of mental illness and psychological disorders; case reports; updates on psychopharmacology; news about the specialty of psychiatry; pearls for practice; and other topics of interest and use to this audience.
Dear Drupal User: You're seeing this because you're logged in to Drupal, and not redirected to MDedge.com/psychiatry.
Depression
adolescent depression
adolescent major depressive disorder
adolescent schizophrenia
adolescent with major depressive disorder
animals
autism
baby
brexpiprazole
child
child bipolar
child depression
child schizophrenia
children with bipolar disorder
children with depression
children with major depressive disorder
compulsive behaviors
cure
elderly bipolar
elderly depression
elderly major depressive disorder
elderly schizophrenia
elderly with dementia
first break
first episode
gambling
gaming
geriatric depression
geriatric major depressive disorder
geriatric schizophrenia
infant
kid
major depressive disorder
major depressive disorder in adolescents
major depressive disorder in children
parenting
pediatric
pediatric bipolar
pediatric depression
pediatric major depressive disorder
pediatric schizophrenia
pregnancy
pregnant
rexulti
skin care
teen
wine
section[contains(@class, 'nav-hidden')]
footer[@id='footer']
div[contains(@class, 'pane-pub-article-current-psychiatry')]
div[contains(@class, 'pane-pub-home-current-psychiatry')]
div[contains(@class, 'pane-pub-topic-current-psychiatry')]
div[contains(@class, 'panel-panel-inner')]
div[contains(@class, 'pane-node-field-article-topics')]
section[contains(@class, 'footer-nav-section-wrapper')]
Conversion disorder? One patient’s ‘moving’ story
History: 3 ‘Uncontrollable’ months
Ms. M, age 57, presents to the ER complaining of coordination problems and involuntary limb movements that have gradually worsened over 3 months.
Two months ago, Ms. M’s primary care physician and neurologist diagnosed her with conversion disorder. Brain MRI at the time showed mild chronic ischemic changes; cervical spinal cord MRI was normal. The neurologist referred Ms. M to a psychiatrist, who prescribed duloxetine, dosage unknown. She started having suicidal thoughts and trembling after starting the medication, so she stopped taking it after 1 week.
Physical exam shows upbeat nystagmus, inconsistent sensory findings, limb ataxia that is more pronounced on the right side, and uncontrollable limb movements, particularly of the right arm.
Ms. M is divorced, lives alone, and works as a medical secretary. Four months ago, she marked the fifth anniversary of her daughter’s death from a drug overdose at age 20. Her parents, whom she cared for, died within the last 3 years. Her son recently left home to attend graduate school, and she is estranged from the rest of her family. She endorses depressed mood and grief over her daughter’s death but says she has no one with whom to talk. She also feels persistent guilt, as she was out on a date when her daughter tried to call home shortly before her death.
The limb movements and lack of coordination are increasingly interfering with Ms. M’s life. She often uses her left hand to stop the right from moving and to guide it in simple tasks, such as opening doors. She can no longer hold a cup of coffee in her right hand or stand on stools at work to reach overhead shelves. At presentation, Ms. M’s imbalance and involuntary movements are so severe that she cannot walk. A coworker drove her to the ER.
poll here
The authors’ observations
A neurologist who evaluates Ms. M in the ER is concerned about her vertical nystagmus, which, unlike horizontal nystagmus, is almost always pathologic. The neurology service admits her for further evaluation.
Ms. M’s age, recent normal MRIs, physical presentation, and lack of other findings suggest a paraneoplastic syndrome. Ataxia associated with subacute cerebellar degeneration can indicate an occult malignancy and is closely linked to gynecologic and breast cancers. Cerebellar degeneration often begins with loss of coordination, can be unilateral, and can appear as intention myoclonus.1
Also considered are:
- opsoclonus-myoclonus, which presents with ataxia, myoclonus, and random chaotic eye movements. This paraneoplastic disorder is less common in adults than in children, however.1
- alien hand/limb syndrome, in which the limb unintentionally performs seemingly purposeful movements, often prompting the patient to restrain the limb with the other hand. This syndrome, however, usually localizes to a lesion in the medial frontal lobe or corpus callosum. Ms. M’s brain MRIs show no such lesion.
poll here
Treatment: Searching for answers
We order an extensive neurologic workup for Ms. M, focusing on causes of inherited and acquired ataxias. The evaluation includes:
- brain and cervical spine MRIs to check for focal cerebral and spinal lesions
- EEG to search for seizure activity and slowing characteristic of encephalopathies
- urine heavy metal testing for toxic processes
- thyroid-stimulating hormone testing for hypothyroid-associated ataxia.
Paraneoplastic workup includes chest, pelvic, and abdominal CT; a gynecologic exam; and a mammogram. All results are negative or equivocal.
We also order blood tests for paraneoplastic antibodies, evidence of opsoclonus/myoclonus, and spinocerebellar ataxia genetic testing; and a CSF check for protein 14-3-3 levels suggestive of prion disease. These tests, run at specialized laboratories, take 4 to 6 weeks.
Ms. M remains hospitalized for 7 days for evaluation. Her movement problems persist, though they often abate when she is distracted. Her upbeat nystagmus appears intermittent. Her affect is diverse, often shifting between tearfulness and inappropriate laughter.
Based on interviews with Ms. M, the C/L team sees prominent depressive symptoms including marked difficulty sleeping, appetite loss, and excessive guilt over her daughter’s death. She also seems indifferent towards her disabling motor symptoms.
The C/L team diagnoses Ms. M with chronic and acute adjustment disorder and major depressive disorder. She is initially hesitant to take another antidepressant but agrees to try mirtazapine, 15 mg nightly, to treat her depression, decreased appetite, and sleep problems. After 2 days, mirtazapine is increased to 30 mg nightly as she is tolerating it and is willing to try a higher dosage.
poll here
The authors’ observations
No neurologic or pathologic explanation is found for Ms. M’s symptoms. Imaging reveals no lesions to explain her intermittent upbeat nystagmus, which localizes to the pons and caudal medulla.2
Conversion disorder. Ms. M, however, appears to meet DSM-IV-TR criteria for conversion disorder (Box), which is thought to result from intense psychological distress in persons who can only express such emotions somatically. Her complaints had specific precursors: she was newly separated from her son and had marked the anniversary of her daughter’s death, which intensified her persistent mourning. We link both circumstances temporally to symptom onset. Also, lack of interest in her serious motor symptoms could be the “la belle indifference” typical of conversion disorder.
Ms. M, however, appears highly suggestible. Her physical symptoms improve soon after her attending psychiatrist suggests that treating her depression will decrease her movements. The neurologists also notice day-to-day fluctuations in her gait disturbance and jerking movements. Distraction techniques produce objective improvement in both symptoms.
- One or more symptoms or deficits affecting voluntary motor or sensory function that suggest a neurological or other general medical condition.
- Psychological factors are judged to be associated with the symptom or deficit because the initiation or exacerbation of the symptom or deficit is preceded by conflicts or other stressors.
- The symptoms or deficit is not intentionally produced or feigned (as in factitious disorder or malingering).
- The symptom or deficit cannot, after appropriate investigation, be fully explained by a general medical condition, or by the direct effects of a substance, or as a culturally sanctioned behavior or experience.
- The symptom or deficit causes clinically significant distress or impairment in social, occupational, or other important areas of functioning or warrants medical evaluation.
- The symptom or deficit is not limited to pain or sexual dysfunction, does not occur exclusively during the course of somatization disorder, and is not better accounted for by another mental disorder.
Specify type of symptom or deficit:
With motor symptom or deficit
With sensory symptom or deficit
With seizures or convulsions
With mixed presentation
Source: Diagnostic and statistical manual of mental disorders (4th ed-text rev). Copyright 2000.
American Psychiatric Association. Reprinted with permission.
In malingering, the patient seeks external incentives for feigned behavior. The role of secondary gain must be considered, as Ms. M’s illness has reunited her with her son, who visits her regularly at the hospital.
Ms. M’s evaluation, however, uncovers no evidence that she is intentionally producing symptoms.
Follow-up: The answer becomes clear
One month after discharge to inpatient rehabilitation, Ms. M is readmitted to the neurology unit. Her uncontrollable limb jerks and ataxia are worse, and she appears demented and near mute. At that time, we learn that the CSF sample sent during her first admission is positive for protein 14-3-3.
Ms. M is diagnosed with Creutzfeldt-Jakob disease (CJD), a spongiform encephalopathy secondary to prion disease. She dies 6 days later. Sporadic CJD is confirmed at autopsy.
The authors’ observations
The literature lists no comprehensive differential diagnosis for conversion disorder, probably because presentations are diverse and the symptoms overlap with innumerable neurologic and medical conditions. This is underscored by the broad differential diagnosis for Ms. M’s ataxia.
In a study to identify organic syndromes initially diagnosed as conversion disorder,4 10 of 85 patients (11.8%) were initially misdiagnosed and later found to have dyskinesia, amyotrophic lateral sclerosis, multiple system atrophy, extrapyramidal syndrome, multiple sclerosis, dementia, Parkinson’s disease with psychogenic aggravation, lung cancer with cerebral metastases, and radicular syndrome. CJD and conversion disorder also share many symptoms (Table).
Correct diagnosis of conversion disorder calls for ruling out neurologic and medical conditions. Ms. M’s upbeat nystagmus prompted aggressive neurologic evaluation. Although horizontal nystagmus has been reported rarely in conversion disorder,5 vertical nystagmus has not. One case report6 describes vertical nystagmus as the first clinical sign of CJD.
Leading clinical symptoms of CJD include progressive dementia, myoclonus, cerebellar ataxia, visual problems, and extrapyramidal signs.7 Ms. M’s uncontrollable movements and jerks, although not classically myoclonic, were similar to this common finding. She did not present with dementia, but her rapidly progressive end-stage mental status changes were characteristic of CJD.
Sporadic CJD accounts for 84% of transmissible spongiform encephalopathies. Genetic, iatrogenic, and variant CJD forms (linked to bovine spongiform encephalopathy, or “mad-cow disease”) account for other cases.8 Psychiatric symptoms are a more-common manifestation of variant CJD9 but have been reported in sporadic CJD.10
Eventually, Ms. M’s upbeat nystagmus, persistent abnormal movements, rapidly progressive dementia, and elevated CSF protein 14-3-3 made the CJD diagnosis. Protein 14-3-3 is 94% sensitive and 84% specific for diagnosing CJD.11 Ms. M’s EEG findings did not suggest CJD, but these findings are less sensitive and occur later than the CSF findings.11
Finally, conversion disorder is almost always acute, not slowly progressive as with Ms. M.
Table
Conversion disorder, sporadic Creutzfeldt-Jakob disease share many symptoms
| Complaint | Conversion disorder | Sporadic CJD |
|---|---|---|
| Paralysis | May not follow motor pathways | No |
| Myoclonus | Yes | Cardinal manifestation |
| Ataxia | May be bizarre in character | Present in 25% to 30% of patients, reflecting multiple disease subtypes |
| Hyperreflexia | No | Yes (40% to 80% of patients) |
| Dysphagia | Yes | No |
| Vomiting | Yes | No |
| Aphonia | Yes | No |
| Diplopia | Yes | Rare |
| Nystagmus | Rare | Yes |
| Blindness | Hysterical blindness detectable by ophthalmologic examination | Rare |
| Deafness | Yes | Rare |
| Anesthesia | Yes | No |
| Paresthesia | Yes | No |
| Depression | Yes | Yes |
| Other psychiatry diagnoses | Yes | More common in variant CJD |
| Progressive dementia | No | Cardinal manifestation |
| Temporal relationship with stress | Yes | No |
| Left-side symptoms more common | Yes | No |
Getting the diagnosis right
DSM-IV-TR criteria state that conversion disorder symptoms cannot be otherwise explained “after appropriate investigation,” but what constitutes “appropriate” is unclear. Extensive inpatient evaluation eventually produced the correct diagnosis for Ms. M, but such a detailed evaluation may be too expensive and expansive for every patient with conversion disorder symptoms.
In the conversion disorder study,4 the 10 misdiagnosed patients received one to eight supplemental diagnostic techniques before being correctly diagnosed. In five of the patients, however, the general neurologic examination was identified as the diagnostic technique responsible for final diagnosis.
These findings suggest that a neurologic examination is key to evaluating complaints that suggest conversion disorder and to identify neurologic conditions. The results can also suggest somatic disorders, as exam findings will reflect patients’ perceptions of neurologic processes. For example:
- patients with conversion motor symptoms may have tonic contractures of antagonistic muscles to “paralyze” certain joints
- those with conversion sensory symptoms rarely have sensory impairments that follow known innervation patterns.
Motor complaints, such as localized paralysis or abnormal movements, should be evaluated with a brain MRI to look for lesions along the motor or cerebellar tracts. Sensory pathways can be further investigated with brain MRI and the relevant evoked potential(s) (visual, brainstem, or somatosensory).
Order EEG for patients with convulsions, particularly prolonged EEG monitoring with a video component, and measure serum prolactin immediately after an episode. In some cases, the neurologic exam alone or in conjunction with these initial studies can make the diagnosis. If the clinical situation warrants, more-detailed evaluations may be necessary.
Related resources
- Wise MG, Rundell JR. Clinical manual of psychosomatic medicine: a guide to consultation-liaison psychiatry. Arlington, VA: American Psychiatric Publishing; 2005.
- National Institute of Neurological Disorders and Stroke. Creutzfeldt-Jakob disease fact sheet. www.ninds.nih.gov/disorders/cjd/detail_cjd.htm.
- Duloxetine • Cymbalta
- Mirtazapine • Remeron
The authors report no financial relationship with any company whose products are mentioned in this article, or with manufacturers of competing products.
1. Dropcho EJ, Dalmau J, Greenlee JE, et al. Paraneoplastic disorders: Central nervous system disorders. Continuum 1999;5:25-40.
2. Zingler VC, Strupp M, Jahn K, et al. Upbeat nystagmus as the initial clinical sign of Creutzfeldt-Jakob disease. Ann Neurol 2005;57:607-8.
3. Phillips KA (ed). Somatoform and factitious disorders. Washington, DC: American Psychiatric Publishing; 2001.
4. Moene FC, Landberg EH, Hoogduin KA, et al. Organic syndromes diagnosed as conversion disorder: identification and frequency in a study of 85 patients. J Psychosom Res 2000;49:7-12.
5. Smith CH, Beck RW, Mills RP. Functional disease in neuroophthalmology. Neurol Clin 1983;1:955-71.
6. Pierrot-Deseilligny C, Milea D. Vertical nystagmus: clinical facts and hypotheses. Brain 2005;128(Pt 6):1237-46.
7. Glatzel M, Stoeck K, Seeger H, et al. Human prion diseases: molecular and clinical aspects. Arch Neurol 2005;62:545-52.
8. Ladogana A, Puopolo M, Croes EA, et al. Mortality from Creutzfeldt-Jakob disease and related disorders in Europe, Australia, and Canada. Neurology 2005;64:1586-91.
9. Spencer MD, Knight RSG, Will RG. First hundred cases of variant Creutzfeldt-Jakob disease: retrospective case note review of early psychiatric and neurological features. BMJ 2002;324:1479-82.
10. Jiang TT, Moses H, Gordon H, Obah E. Sporadic Creuztfeldt-Jakob disease presenting as major depression. South Med J 1999;92:807-8.
11. Zerr I, Pocchiari M, Collins S, et al. Analysis of EEG and CSF 14-3-3 proteins as aids to the diagnosis of Creutzfeldt-Jakob disease. Neurology 2000;55:811-15.
History: 3 ‘Uncontrollable’ months
Ms. M, age 57, presents to the ER complaining of coordination problems and involuntary limb movements that have gradually worsened over 3 months.
Two months ago, Ms. M’s primary care physician and neurologist diagnosed her with conversion disorder. Brain MRI at the time showed mild chronic ischemic changes; cervical spinal cord MRI was normal. The neurologist referred Ms. M to a psychiatrist, who prescribed duloxetine, dosage unknown. She started having suicidal thoughts and trembling after starting the medication, so she stopped taking it after 1 week.
Physical exam shows upbeat nystagmus, inconsistent sensory findings, limb ataxia that is more pronounced on the right side, and uncontrollable limb movements, particularly of the right arm.
Ms. M is divorced, lives alone, and works as a medical secretary. Four months ago, she marked the fifth anniversary of her daughter’s death from a drug overdose at age 20. Her parents, whom she cared for, died within the last 3 years. Her son recently left home to attend graduate school, and she is estranged from the rest of her family. She endorses depressed mood and grief over her daughter’s death but says she has no one with whom to talk. She also feels persistent guilt, as she was out on a date when her daughter tried to call home shortly before her death.
The limb movements and lack of coordination are increasingly interfering with Ms. M’s life. She often uses her left hand to stop the right from moving and to guide it in simple tasks, such as opening doors. She can no longer hold a cup of coffee in her right hand or stand on stools at work to reach overhead shelves. At presentation, Ms. M’s imbalance and involuntary movements are so severe that she cannot walk. A coworker drove her to the ER.
poll here
The authors’ observations
A neurologist who evaluates Ms. M in the ER is concerned about her vertical nystagmus, which, unlike horizontal nystagmus, is almost always pathologic. The neurology service admits her for further evaluation.
Ms. M’s age, recent normal MRIs, physical presentation, and lack of other findings suggest a paraneoplastic syndrome. Ataxia associated with subacute cerebellar degeneration can indicate an occult malignancy and is closely linked to gynecologic and breast cancers. Cerebellar degeneration often begins with loss of coordination, can be unilateral, and can appear as intention myoclonus.1
Also considered are:
- opsoclonus-myoclonus, which presents with ataxia, myoclonus, and random chaotic eye movements. This paraneoplastic disorder is less common in adults than in children, however.1
- alien hand/limb syndrome, in which the limb unintentionally performs seemingly purposeful movements, often prompting the patient to restrain the limb with the other hand. This syndrome, however, usually localizes to a lesion in the medial frontal lobe or corpus callosum. Ms. M’s brain MRIs show no such lesion.
poll here
Treatment: Searching for answers
We order an extensive neurologic workup for Ms. M, focusing on causes of inherited and acquired ataxias. The evaluation includes:
- brain and cervical spine MRIs to check for focal cerebral and spinal lesions
- EEG to search for seizure activity and slowing characteristic of encephalopathies
- urine heavy metal testing for toxic processes
- thyroid-stimulating hormone testing for hypothyroid-associated ataxia.
Paraneoplastic workup includes chest, pelvic, and abdominal CT; a gynecologic exam; and a mammogram. All results are negative or equivocal.
We also order blood tests for paraneoplastic antibodies, evidence of opsoclonus/myoclonus, and spinocerebellar ataxia genetic testing; and a CSF check for protein 14-3-3 levels suggestive of prion disease. These tests, run at specialized laboratories, take 4 to 6 weeks.
Ms. M remains hospitalized for 7 days for evaluation. Her movement problems persist, though they often abate when she is distracted. Her upbeat nystagmus appears intermittent. Her affect is diverse, often shifting between tearfulness and inappropriate laughter.
Based on interviews with Ms. M, the C/L team sees prominent depressive symptoms including marked difficulty sleeping, appetite loss, and excessive guilt over her daughter’s death. She also seems indifferent towards her disabling motor symptoms.
The C/L team diagnoses Ms. M with chronic and acute adjustment disorder and major depressive disorder. She is initially hesitant to take another antidepressant but agrees to try mirtazapine, 15 mg nightly, to treat her depression, decreased appetite, and sleep problems. After 2 days, mirtazapine is increased to 30 mg nightly as she is tolerating it and is willing to try a higher dosage.
poll here
The authors’ observations
No neurologic or pathologic explanation is found for Ms. M’s symptoms. Imaging reveals no lesions to explain her intermittent upbeat nystagmus, which localizes to the pons and caudal medulla.2
Conversion disorder. Ms. M, however, appears to meet DSM-IV-TR criteria for conversion disorder (Box), which is thought to result from intense psychological distress in persons who can only express such emotions somatically. Her complaints had specific precursors: she was newly separated from her son and had marked the anniversary of her daughter’s death, which intensified her persistent mourning. We link both circumstances temporally to symptom onset. Also, lack of interest in her serious motor symptoms could be the “la belle indifference” typical of conversion disorder.
Ms. M, however, appears highly suggestible. Her physical symptoms improve soon after her attending psychiatrist suggests that treating her depression will decrease her movements. The neurologists also notice day-to-day fluctuations in her gait disturbance and jerking movements. Distraction techniques produce objective improvement in both symptoms.
- One or more symptoms or deficits affecting voluntary motor or sensory function that suggest a neurological or other general medical condition.
- Psychological factors are judged to be associated with the symptom or deficit because the initiation or exacerbation of the symptom or deficit is preceded by conflicts or other stressors.
- The symptoms or deficit is not intentionally produced or feigned (as in factitious disorder or malingering).
- The symptom or deficit cannot, after appropriate investigation, be fully explained by a general medical condition, or by the direct effects of a substance, or as a culturally sanctioned behavior or experience.
- The symptom or deficit causes clinically significant distress or impairment in social, occupational, or other important areas of functioning or warrants medical evaluation.
- The symptom or deficit is not limited to pain or sexual dysfunction, does not occur exclusively during the course of somatization disorder, and is not better accounted for by another mental disorder.
Specify type of symptom or deficit:
With motor symptom or deficit
With sensory symptom or deficit
With seizures or convulsions
With mixed presentation
Source: Diagnostic and statistical manual of mental disorders (4th ed-text rev). Copyright 2000.
American Psychiatric Association. Reprinted with permission.
In malingering, the patient seeks external incentives for feigned behavior. The role of secondary gain must be considered, as Ms. M’s illness has reunited her with her son, who visits her regularly at the hospital.
Ms. M’s evaluation, however, uncovers no evidence that she is intentionally producing symptoms.
Follow-up: The answer becomes clear
One month after discharge to inpatient rehabilitation, Ms. M is readmitted to the neurology unit. Her uncontrollable limb jerks and ataxia are worse, and she appears demented and near mute. At that time, we learn that the CSF sample sent during her first admission is positive for protein 14-3-3.
Ms. M is diagnosed with Creutzfeldt-Jakob disease (CJD), a spongiform encephalopathy secondary to prion disease. She dies 6 days later. Sporadic CJD is confirmed at autopsy.
The authors’ observations
The literature lists no comprehensive differential diagnosis for conversion disorder, probably because presentations are diverse and the symptoms overlap with innumerable neurologic and medical conditions. This is underscored by the broad differential diagnosis for Ms. M’s ataxia.
In a study to identify organic syndromes initially diagnosed as conversion disorder,4 10 of 85 patients (11.8%) were initially misdiagnosed and later found to have dyskinesia, amyotrophic lateral sclerosis, multiple system atrophy, extrapyramidal syndrome, multiple sclerosis, dementia, Parkinson’s disease with psychogenic aggravation, lung cancer with cerebral metastases, and radicular syndrome. CJD and conversion disorder also share many symptoms (Table).
Correct diagnosis of conversion disorder calls for ruling out neurologic and medical conditions. Ms. M’s upbeat nystagmus prompted aggressive neurologic evaluation. Although horizontal nystagmus has been reported rarely in conversion disorder,5 vertical nystagmus has not. One case report6 describes vertical nystagmus as the first clinical sign of CJD.
Leading clinical symptoms of CJD include progressive dementia, myoclonus, cerebellar ataxia, visual problems, and extrapyramidal signs.7 Ms. M’s uncontrollable movements and jerks, although not classically myoclonic, were similar to this common finding. She did not present with dementia, but her rapidly progressive end-stage mental status changes were characteristic of CJD.
Sporadic CJD accounts for 84% of transmissible spongiform encephalopathies. Genetic, iatrogenic, and variant CJD forms (linked to bovine spongiform encephalopathy, or “mad-cow disease”) account for other cases.8 Psychiatric symptoms are a more-common manifestation of variant CJD9 but have been reported in sporadic CJD.10
Eventually, Ms. M’s upbeat nystagmus, persistent abnormal movements, rapidly progressive dementia, and elevated CSF protein 14-3-3 made the CJD diagnosis. Protein 14-3-3 is 94% sensitive and 84% specific for diagnosing CJD.11 Ms. M’s EEG findings did not suggest CJD, but these findings are less sensitive and occur later than the CSF findings.11
Finally, conversion disorder is almost always acute, not slowly progressive as with Ms. M.
Table
Conversion disorder, sporadic Creutzfeldt-Jakob disease share many symptoms
| Complaint | Conversion disorder | Sporadic CJD |
|---|---|---|
| Paralysis | May not follow motor pathways | No |
| Myoclonus | Yes | Cardinal manifestation |
| Ataxia | May be bizarre in character | Present in 25% to 30% of patients, reflecting multiple disease subtypes |
| Hyperreflexia | No | Yes (40% to 80% of patients) |
| Dysphagia | Yes | No |
| Vomiting | Yes | No |
| Aphonia | Yes | No |
| Diplopia | Yes | Rare |
| Nystagmus | Rare | Yes |
| Blindness | Hysterical blindness detectable by ophthalmologic examination | Rare |
| Deafness | Yes | Rare |
| Anesthesia | Yes | No |
| Paresthesia | Yes | No |
| Depression | Yes | Yes |
| Other psychiatry diagnoses | Yes | More common in variant CJD |
| Progressive dementia | No | Cardinal manifestation |
| Temporal relationship with stress | Yes | No |
| Left-side symptoms more common | Yes | No |
Getting the diagnosis right
DSM-IV-TR criteria state that conversion disorder symptoms cannot be otherwise explained “after appropriate investigation,” but what constitutes “appropriate” is unclear. Extensive inpatient evaluation eventually produced the correct diagnosis for Ms. M, but such a detailed evaluation may be too expensive and expansive for every patient with conversion disorder symptoms.
In the conversion disorder study,4 the 10 misdiagnosed patients received one to eight supplemental diagnostic techniques before being correctly diagnosed. In five of the patients, however, the general neurologic examination was identified as the diagnostic technique responsible for final diagnosis.
These findings suggest that a neurologic examination is key to evaluating complaints that suggest conversion disorder and to identify neurologic conditions. The results can also suggest somatic disorders, as exam findings will reflect patients’ perceptions of neurologic processes. For example:
- patients with conversion motor symptoms may have tonic contractures of antagonistic muscles to “paralyze” certain joints
- those with conversion sensory symptoms rarely have sensory impairments that follow known innervation patterns.
Motor complaints, such as localized paralysis or abnormal movements, should be evaluated with a brain MRI to look for lesions along the motor or cerebellar tracts. Sensory pathways can be further investigated with brain MRI and the relevant evoked potential(s) (visual, brainstem, or somatosensory).
Order EEG for patients with convulsions, particularly prolonged EEG monitoring with a video component, and measure serum prolactin immediately after an episode. In some cases, the neurologic exam alone or in conjunction with these initial studies can make the diagnosis. If the clinical situation warrants, more-detailed evaluations may be necessary.
Related resources
- Wise MG, Rundell JR. Clinical manual of psychosomatic medicine: a guide to consultation-liaison psychiatry. Arlington, VA: American Psychiatric Publishing; 2005.
- National Institute of Neurological Disorders and Stroke. Creutzfeldt-Jakob disease fact sheet. www.ninds.nih.gov/disorders/cjd/detail_cjd.htm.
- Duloxetine • Cymbalta
- Mirtazapine • Remeron
The authors report no financial relationship with any company whose products are mentioned in this article, or with manufacturers of competing products.
History: 3 ‘Uncontrollable’ months
Ms. M, age 57, presents to the ER complaining of coordination problems and involuntary limb movements that have gradually worsened over 3 months.
Two months ago, Ms. M’s primary care physician and neurologist diagnosed her with conversion disorder. Brain MRI at the time showed mild chronic ischemic changes; cervical spinal cord MRI was normal. The neurologist referred Ms. M to a psychiatrist, who prescribed duloxetine, dosage unknown. She started having suicidal thoughts and trembling after starting the medication, so she stopped taking it after 1 week.
Physical exam shows upbeat nystagmus, inconsistent sensory findings, limb ataxia that is more pronounced on the right side, and uncontrollable limb movements, particularly of the right arm.
Ms. M is divorced, lives alone, and works as a medical secretary. Four months ago, she marked the fifth anniversary of her daughter’s death from a drug overdose at age 20. Her parents, whom she cared for, died within the last 3 years. Her son recently left home to attend graduate school, and she is estranged from the rest of her family. She endorses depressed mood and grief over her daughter’s death but says she has no one with whom to talk. She also feels persistent guilt, as she was out on a date when her daughter tried to call home shortly before her death.
The limb movements and lack of coordination are increasingly interfering with Ms. M’s life. She often uses her left hand to stop the right from moving and to guide it in simple tasks, such as opening doors. She can no longer hold a cup of coffee in her right hand or stand on stools at work to reach overhead shelves. At presentation, Ms. M’s imbalance and involuntary movements are so severe that she cannot walk. A coworker drove her to the ER.
poll here
The authors’ observations
A neurologist who evaluates Ms. M in the ER is concerned about her vertical nystagmus, which, unlike horizontal nystagmus, is almost always pathologic. The neurology service admits her for further evaluation.
Ms. M’s age, recent normal MRIs, physical presentation, and lack of other findings suggest a paraneoplastic syndrome. Ataxia associated with subacute cerebellar degeneration can indicate an occult malignancy and is closely linked to gynecologic and breast cancers. Cerebellar degeneration often begins with loss of coordination, can be unilateral, and can appear as intention myoclonus.1
Also considered are:
- opsoclonus-myoclonus, which presents with ataxia, myoclonus, and random chaotic eye movements. This paraneoplastic disorder is less common in adults than in children, however.1
- alien hand/limb syndrome, in which the limb unintentionally performs seemingly purposeful movements, often prompting the patient to restrain the limb with the other hand. This syndrome, however, usually localizes to a lesion in the medial frontal lobe or corpus callosum. Ms. M’s brain MRIs show no such lesion.
poll here
Treatment: Searching for answers
We order an extensive neurologic workup for Ms. M, focusing on causes of inherited and acquired ataxias. The evaluation includes:
- brain and cervical spine MRIs to check for focal cerebral and spinal lesions
- EEG to search for seizure activity and slowing characteristic of encephalopathies
- urine heavy metal testing for toxic processes
- thyroid-stimulating hormone testing for hypothyroid-associated ataxia.
Paraneoplastic workup includes chest, pelvic, and abdominal CT; a gynecologic exam; and a mammogram. All results are negative or equivocal.
We also order blood tests for paraneoplastic antibodies, evidence of opsoclonus/myoclonus, and spinocerebellar ataxia genetic testing; and a CSF check for protein 14-3-3 levels suggestive of prion disease. These tests, run at specialized laboratories, take 4 to 6 weeks.
Ms. M remains hospitalized for 7 days for evaluation. Her movement problems persist, though they often abate when she is distracted. Her upbeat nystagmus appears intermittent. Her affect is diverse, often shifting between tearfulness and inappropriate laughter.
Based on interviews with Ms. M, the C/L team sees prominent depressive symptoms including marked difficulty sleeping, appetite loss, and excessive guilt over her daughter’s death. She also seems indifferent towards her disabling motor symptoms.
The C/L team diagnoses Ms. M with chronic and acute adjustment disorder and major depressive disorder. She is initially hesitant to take another antidepressant but agrees to try mirtazapine, 15 mg nightly, to treat her depression, decreased appetite, and sleep problems. After 2 days, mirtazapine is increased to 30 mg nightly as she is tolerating it and is willing to try a higher dosage.
poll here
The authors’ observations
No neurologic or pathologic explanation is found for Ms. M’s symptoms. Imaging reveals no lesions to explain her intermittent upbeat nystagmus, which localizes to the pons and caudal medulla.2
Conversion disorder. Ms. M, however, appears to meet DSM-IV-TR criteria for conversion disorder (Box), which is thought to result from intense psychological distress in persons who can only express such emotions somatically. Her complaints had specific precursors: she was newly separated from her son and had marked the anniversary of her daughter’s death, which intensified her persistent mourning. We link both circumstances temporally to symptom onset. Also, lack of interest in her serious motor symptoms could be the “la belle indifference” typical of conversion disorder.
Ms. M, however, appears highly suggestible. Her physical symptoms improve soon after her attending psychiatrist suggests that treating her depression will decrease her movements. The neurologists also notice day-to-day fluctuations in her gait disturbance and jerking movements. Distraction techniques produce objective improvement in both symptoms.
- One or more symptoms or deficits affecting voluntary motor or sensory function that suggest a neurological or other general medical condition.
- Psychological factors are judged to be associated with the symptom or deficit because the initiation or exacerbation of the symptom or deficit is preceded by conflicts or other stressors.
- The symptoms or deficit is not intentionally produced or feigned (as in factitious disorder or malingering).
- The symptom or deficit cannot, after appropriate investigation, be fully explained by a general medical condition, or by the direct effects of a substance, or as a culturally sanctioned behavior or experience.
- The symptom or deficit causes clinically significant distress or impairment in social, occupational, or other important areas of functioning or warrants medical evaluation.
- The symptom or deficit is not limited to pain or sexual dysfunction, does not occur exclusively during the course of somatization disorder, and is not better accounted for by another mental disorder.
Specify type of symptom or deficit:
With motor symptom or deficit
With sensory symptom or deficit
With seizures or convulsions
With mixed presentation
Source: Diagnostic and statistical manual of mental disorders (4th ed-text rev). Copyright 2000.
American Psychiatric Association. Reprinted with permission.
In malingering, the patient seeks external incentives for feigned behavior. The role of secondary gain must be considered, as Ms. M’s illness has reunited her with her son, who visits her regularly at the hospital.
Ms. M’s evaluation, however, uncovers no evidence that she is intentionally producing symptoms.
Follow-up: The answer becomes clear
One month after discharge to inpatient rehabilitation, Ms. M is readmitted to the neurology unit. Her uncontrollable limb jerks and ataxia are worse, and she appears demented and near mute. At that time, we learn that the CSF sample sent during her first admission is positive for protein 14-3-3.
Ms. M is diagnosed with Creutzfeldt-Jakob disease (CJD), a spongiform encephalopathy secondary to prion disease. She dies 6 days later. Sporadic CJD is confirmed at autopsy.
The authors’ observations
The literature lists no comprehensive differential diagnosis for conversion disorder, probably because presentations are diverse and the symptoms overlap with innumerable neurologic and medical conditions. This is underscored by the broad differential diagnosis for Ms. M’s ataxia.
In a study to identify organic syndromes initially diagnosed as conversion disorder,4 10 of 85 patients (11.8%) were initially misdiagnosed and later found to have dyskinesia, amyotrophic lateral sclerosis, multiple system atrophy, extrapyramidal syndrome, multiple sclerosis, dementia, Parkinson’s disease with psychogenic aggravation, lung cancer with cerebral metastases, and radicular syndrome. CJD and conversion disorder also share many symptoms (Table).
Correct diagnosis of conversion disorder calls for ruling out neurologic and medical conditions. Ms. M’s upbeat nystagmus prompted aggressive neurologic evaluation. Although horizontal nystagmus has been reported rarely in conversion disorder,5 vertical nystagmus has not. One case report6 describes vertical nystagmus as the first clinical sign of CJD.
Leading clinical symptoms of CJD include progressive dementia, myoclonus, cerebellar ataxia, visual problems, and extrapyramidal signs.7 Ms. M’s uncontrollable movements and jerks, although not classically myoclonic, were similar to this common finding. She did not present with dementia, but her rapidly progressive end-stage mental status changes were characteristic of CJD.
Sporadic CJD accounts for 84% of transmissible spongiform encephalopathies. Genetic, iatrogenic, and variant CJD forms (linked to bovine spongiform encephalopathy, or “mad-cow disease”) account for other cases.8 Psychiatric symptoms are a more-common manifestation of variant CJD9 but have been reported in sporadic CJD.10
Eventually, Ms. M’s upbeat nystagmus, persistent abnormal movements, rapidly progressive dementia, and elevated CSF protein 14-3-3 made the CJD diagnosis. Protein 14-3-3 is 94% sensitive and 84% specific for diagnosing CJD.11 Ms. M’s EEG findings did not suggest CJD, but these findings are less sensitive and occur later than the CSF findings.11
Finally, conversion disorder is almost always acute, not slowly progressive as with Ms. M.
Table
Conversion disorder, sporadic Creutzfeldt-Jakob disease share many symptoms
| Complaint | Conversion disorder | Sporadic CJD |
|---|---|---|
| Paralysis | May not follow motor pathways | No |
| Myoclonus | Yes | Cardinal manifestation |
| Ataxia | May be bizarre in character | Present in 25% to 30% of patients, reflecting multiple disease subtypes |
| Hyperreflexia | No | Yes (40% to 80% of patients) |
| Dysphagia | Yes | No |
| Vomiting | Yes | No |
| Aphonia | Yes | No |
| Diplopia | Yes | Rare |
| Nystagmus | Rare | Yes |
| Blindness | Hysterical blindness detectable by ophthalmologic examination | Rare |
| Deafness | Yes | Rare |
| Anesthesia | Yes | No |
| Paresthesia | Yes | No |
| Depression | Yes | Yes |
| Other psychiatry diagnoses | Yes | More common in variant CJD |
| Progressive dementia | No | Cardinal manifestation |
| Temporal relationship with stress | Yes | No |
| Left-side symptoms more common | Yes | No |
Getting the diagnosis right
DSM-IV-TR criteria state that conversion disorder symptoms cannot be otherwise explained “after appropriate investigation,” but what constitutes “appropriate” is unclear. Extensive inpatient evaluation eventually produced the correct diagnosis for Ms. M, but such a detailed evaluation may be too expensive and expansive for every patient with conversion disorder symptoms.
In the conversion disorder study,4 the 10 misdiagnosed patients received one to eight supplemental diagnostic techniques before being correctly diagnosed. In five of the patients, however, the general neurologic examination was identified as the diagnostic technique responsible for final diagnosis.
These findings suggest that a neurologic examination is key to evaluating complaints that suggest conversion disorder and to identify neurologic conditions. The results can also suggest somatic disorders, as exam findings will reflect patients’ perceptions of neurologic processes. For example:
- patients with conversion motor symptoms may have tonic contractures of antagonistic muscles to “paralyze” certain joints
- those with conversion sensory symptoms rarely have sensory impairments that follow known innervation patterns.
Motor complaints, such as localized paralysis or abnormal movements, should be evaluated with a brain MRI to look for lesions along the motor or cerebellar tracts. Sensory pathways can be further investigated with brain MRI and the relevant evoked potential(s) (visual, brainstem, or somatosensory).
Order EEG for patients with convulsions, particularly prolonged EEG monitoring with a video component, and measure serum prolactin immediately after an episode. In some cases, the neurologic exam alone or in conjunction with these initial studies can make the diagnosis. If the clinical situation warrants, more-detailed evaluations may be necessary.
Related resources
- Wise MG, Rundell JR. Clinical manual of psychosomatic medicine: a guide to consultation-liaison psychiatry. Arlington, VA: American Psychiatric Publishing; 2005.
- National Institute of Neurological Disorders and Stroke. Creutzfeldt-Jakob disease fact sheet. www.ninds.nih.gov/disorders/cjd/detail_cjd.htm.
- Duloxetine • Cymbalta
- Mirtazapine • Remeron
The authors report no financial relationship with any company whose products are mentioned in this article, or with manufacturers of competing products.
1. Dropcho EJ, Dalmau J, Greenlee JE, et al. Paraneoplastic disorders: Central nervous system disorders. Continuum 1999;5:25-40.
2. Zingler VC, Strupp M, Jahn K, et al. Upbeat nystagmus as the initial clinical sign of Creutzfeldt-Jakob disease. Ann Neurol 2005;57:607-8.
3. Phillips KA (ed). Somatoform and factitious disorders. Washington, DC: American Psychiatric Publishing; 2001.
4. Moene FC, Landberg EH, Hoogduin KA, et al. Organic syndromes diagnosed as conversion disorder: identification and frequency in a study of 85 patients. J Psychosom Res 2000;49:7-12.
5. Smith CH, Beck RW, Mills RP. Functional disease in neuroophthalmology. Neurol Clin 1983;1:955-71.
6. Pierrot-Deseilligny C, Milea D. Vertical nystagmus: clinical facts and hypotheses. Brain 2005;128(Pt 6):1237-46.
7. Glatzel M, Stoeck K, Seeger H, et al. Human prion diseases: molecular and clinical aspects. Arch Neurol 2005;62:545-52.
8. Ladogana A, Puopolo M, Croes EA, et al. Mortality from Creutzfeldt-Jakob disease and related disorders in Europe, Australia, and Canada. Neurology 2005;64:1586-91.
9. Spencer MD, Knight RSG, Will RG. First hundred cases of variant Creutzfeldt-Jakob disease: retrospective case note review of early psychiatric and neurological features. BMJ 2002;324:1479-82.
10. Jiang TT, Moses H, Gordon H, Obah E. Sporadic Creuztfeldt-Jakob disease presenting as major depression. South Med J 1999;92:807-8.
11. Zerr I, Pocchiari M, Collins S, et al. Analysis of EEG and CSF 14-3-3 proteins as aids to the diagnosis of Creutzfeldt-Jakob disease. Neurology 2000;55:811-15.
1. Dropcho EJ, Dalmau J, Greenlee JE, et al. Paraneoplastic disorders: Central nervous system disorders. Continuum 1999;5:25-40.
2. Zingler VC, Strupp M, Jahn K, et al. Upbeat nystagmus as the initial clinical sign of Creutzfeldt-Jakob disease. Ann Neurol 2005;57:607-8.
3. Phillips KA (ed). Somatoform and factitious disorders. Washington, DC: American Psychiatric Publishing; 2001.
4. Moene FC, Landberg EH, Hoogduin KA, et al. Organic syndromes diagnosed as conversion disorder: identification and frequency in a study of 85 patients. J Psychosom Res 2000;49:7-12.
5. Smith CH, Beck RW, Mills RP. Functional disease in neuroophthalmology. Neurol Clin 1983;1:955-71.
6. Pierrot-Deseilligny C, Milea D. Vertical nystagmus: clinical facts and hypotheses. Brain 2005;128(Pt 6):1237-46.
7. Glatzel M, Stoeck K, Seeger H, et al. Human prion diseases: molecular and clinical aspects. Arch Neurol 2005;62:545-52.
8. Ladogana A, Puopolo M, Croes EA, et al. Mortality from Creutzfeldt-Jakob disease and related disorders in Europe, Australia, and Canada. Neurology 2005;64:1586-91.
9. Spencer MD, Knight RSG, Will RG. First hundred cases of variant Creutzfeldt-Jakob disease: retrospective case note review of early psychiatric and neurological features. BMJ 2002;324:1479-82.
10. Jiang TT, Moses H, Gordon H, Obah E. Sporadic Creuztfeldt-Jakob disease presenting as major depression. South Med J 1999;92:807-8.
11. Zerr I, Pocchiari M, Collins S, et al. Analysis of EEG and CSF 14-3-3 proteins as aids to the diagnosis of Creutzfeldt-Jakob disease. Neurology 2000;55:811-15.
2 NAMES, 1 DISEASE: Does schizophrenia = psychotic bipolar disorder?
When a patient presents with psychotic symptoms, you might not recognize or pursue hints of bipolarity if you assume psychosis means schizophrenia. Yet psychotic bipolar disorder can explain every sign, symptom, course, and other characteristic traditionally assumed to indicate schizophrenia (Table 1). The literature, including recent genetic data,1-6 marshals a persuasive argument that patients diagnosed with schizophrenia usually suffer from a psychotic bipolar disorder.
Consider here how a cascade of changing signs and symptoms, initially unrecognized, caused five sequential re-evaluations of one psychotic patient’s primary Axis I diagnosis. His case highlights why the correct initial diagnosis of the disease causing psychosis is essential to effective treatment.4,7-9
Table 1
DSM-IV-TR criteria for schizophrenia vs. psychotic mood disorder
| Schizophrenia diagnosis6 | Seen in psychotic mood disorders |
|---|---|
| Criterion A | |
| Hallucinations and delusions | 50% to 80% explained by mood16,21 |
| Paranoia | Hides grandiosity4 |
| Catatonia | 75% explained by mood7,8 |
| Disorganized speech and behavior | All patients with moderate to severe mania1-5 |
| Negative symptoms | All patients with moderate to severe depression4 |
| Criterion B | |
| Social and job dysfunction | All patients with moderate to severe bipolar disorder5,13 |
| Criterion C | |
| Chronic continuous symptoms | Patients can have psychotic symptoms continuously for 2 years to life5,6,13 |
Case: Carved in stone
Police officers carry Mr. C, age 30, into the emergency department. He is mentally disorganized and arrives in a rigid, catatonic posture. According to a neighbor, Mr. C was kneeling motionless on his mother’s front lawn, alternating between mutism and inappropriately loud, disorganized religious preaching. When his arm is lifted, it remains as placed. He is admitted to the acute care inpatient unit.
Mr. C’s most striking symptoms are catatonia and psychosis. Postural rigidity, waxy flexibility, and automatic obedience are characteristics of catatonia.6-8 An organic cause is first considered, such as hyperthyroidism, cerebrovascular accident, cerebral neoplasm, head trauma, seizure disorder, dementia, neuroleptic malignant syndrome, pheochromocytoma, or—especially—intoxication from illegal drugs.7
While awaiting results from physical, mental status, and lab exams and imaging studies, staff assign him two admitting diagnoses: catatonic disorder due to a general medical condition and psychotic disorder not otherwise specified.6
Case: Inconclusive workup
Mr. C denies using illegal substances or alcohol, which his mother confirms. He has no history of seizures or other medical conditions. His distractibility prevents him from focusing on a formal mental status exam. Physical exam, urine drug screen, lab results, and imaging studies are unremarkable except for an admitting blood pressure of 145/95 mm Hg and pulse of 115 beats per minute. These readings normalize within 1 hour. IM haloperidol and lorazepam are given as needed for agitation, but physicians withhold scheduled medications to allow staff to observe his symptoms.
Organic causes of catatonia now seem less likely, though past use of drugs such as phencyclidine that can cause chronic psychosis cannot be ruled out. Schizophrenia is considered likely because catatonia is one of schizophrenia’s five core diagnostic symptoms.6 Catatonia can also be a symptom of bipolar disorder.6-9 Staff make a preliminary diagnosis of schizophrenia, catatonic type.
Case: ‘Hit men are after me’
Staff observe Mr. C responding to threatening auditory hallucinations. His affect is “fearful to terrified.” He says he hears the voice of God warning him of danger and continuing a running commentary on his actions. He fears for his life because “hit men have been sent to kill me” and have “infiltrated” the inpatient ward. He does not eat, saying his food is poisoned. He says these beliefs have escalated over the past year.
Mr. C’s catatonic symptoms resolve overnight, but obtaining additional history is difficult because of his paranoia. He denies any history of bizarre behavior or past contact with mental health services. He claims not to be especially religious. He is unmarried and lives with his mother, is college-educated, but has held only menial jobs.
Inpatient staff shifts its diagnostic focus to functional disorders associated with auditory hallucinations, paranoid delusions, and gross disorganization. According to Schneider and the DSM-IV-TR,6,10 hearing a voice “keeping up a running commentary on one’s behavior” is especially diagnostic of schizophrenia.
Because of the rapid resolution of his “catatonic” symptoms and prominence of paranoia, they change his diagnosis on day 2 to schizophrenia, paranoid type. Mr. C meets all diagnostic criteria for schizophrenia except one: the staff has overlooked and has not adequately excluded a psychotic mood disorder.
Case: A turn for the worse
That night, nursing staff find Mr. C naked and cowering in the fetal position in a corner of his room. He has smeared his feces on his face and in his hair and mouth. While being cleaned up, he suddenly begins quoting scripture in a loud, disorganized voice. His expressed thoughts are incomprehensible. He is given haloperidol and lorazepam immediately; oral haloperidol is continued at 10 mg bid.
Both Bleuler and Kraepelin concluded “coprophilia and coprophagia are unique to children and patients with schizophrenia.”11,12 The DSM casebook cites Kraepelin’s description of a catatonic patient who “smeared feces about” as a “classic, textbook case” of schizophrenia.11 The casebook goes on to say: “In the absence of any known general medical condition, the combination of coprophilia, disorganized speech, and catatonic behavior clearly indicates the diagnosis of schizophrenia.”
Mr. C shows each of these. Staff changes his diagnosis again—to schizophrenia, disorganized type, which carries a poor prognosis.11,12
Case: Banking and ray guns
By day 5, Mr. C’s mental status is normalizing and his psychosis improving. He volunteers for a weekly student case conference. There, he reveals additional information that staff could have discovered at admission with more-focused questions.
He reports that 2 years earlier he suffered severe suicidal depression. Six months later, during a hypomanic episode, he began “toying with the idea” that he might become part owner of his local bank. He believes “the Secret Service decided to transfer ownership to me.”
His plans upon acquiring the bank include buying three houses and six cars valued at several million dollars and running for state governor. For weeks before admission, he did not need sleep, experienced an increase in energy and activities, and his mind was racing. His job seemed so “trivial” that he quit. Immediately before his hospital admission, his delusions intensified to include an “evil conspiracy” to murder him for ownership of the bank and he feared his execution was imminent.
He explains his catatonic behavior on the lawn by his belief that “hit men” hiding across the street aimed a “motion-detecting, heat-seeking ray gun” at him so that if he had “moved an inch,” he would die. He says the “feces incident” was an effort to get himself transferred to the state hospital, where he thought he would be safer because his present caretakers were “infiltrated.” He also says his mother received electroconvulsive therapy in her 20s.
These symptoms—especially the striking grandiosity, lack of need for sleep, racing thoughts, hallucinations and delusions—define a manic episode with psychotic features. Only one manic episode as described here is diagnostic of bipolar disorder, type I.2,6,13 Staff changes his diagnosis to schizoaffective disorder, a compromise used to include patients with bipolar and psychotic (schizophrenic) features. Some authors contend schizoaffective disorder is psychotic bipolar disorder and not a separate disease.3,4,9
Case: From SSRI to lithium
After 2 weeks, Mr. C is discharged on haloperidol, 5 mg bid, but no mood stabilizer. He receives follow-up care at a community mental health center. When he develops severe depressive symptoms 6 months after discharge, the attending psychiatrist starts him on a selective serotonin reuptake inhibitor (SSRI). Within 2 weeks, Mr. C switches from depression to a mixed, dysphoric mania. After the SSRI is discontinued and lithium is added to his haloperidol, his mood gradually stabilizes to moderate depression. He develops rigidity, masked faces, and a fine tremor in his hands.
About 10% of bipolar depressed patients given an antidepressant—especially without a mood stabilizer—switch to mania, and their cycle frequency increases.2,13-15 A correct initial diagnosis and treatment with a mood stabilizer might have avoided Mr. C’s switch.
Mixed bipolar disorder with overlapping depressive and manic symptoms is often resistant to monotherapy, requiring two or more mood stabilizers such as lithium and an anticonvulsant.14 Without a mood-stabilizing combination, the mixed, rapid-cycling type of bipolar disorder is likely to progress, with more-rapid and more-severe episodes.2,13-15 Adding lamotrigine, a mood stabilizer with antidepressant effects, can help.2,14
Stopping the SSRI is correct, despite Mr. C’s severe depression, to avoid increasing the cycle frequency.13-15 Some authors recommend tapering the antipsychotic, using it only as needed for psychotic features after psychosis has resolved.14-17 Continuing antipsychotic drugs after psychosis has remitted increases rates of cycling to depression, depressive and extrapyramidal symptoms, and medication discontinuation.17 Lithium may have aggravated Mr. C’s antipsychotic-induced parkinsonism, but discontinuing haloperidol may have been the most therapeutic decision.
The community mental health staff changes his diagnosis again, this time to bipolar disorder, type I, mixed, severe with psychotic features. We concur that this is correct.
Case: A diagnostic step back
Two years later, Mr. C is working and continues to take lithium and haloperidol prescribed at the mental health center. His intermittent depressive episodes persist, but—apparently because he has not had another manic episode—the staff switches his diagnosis back to schizoaffective disorder.
We disagree with this change. A diagnosis of schizoaffective disorder precludes ideal pharmacotherapy for Mr. C’s rapid-cycling bipolar disorder and increases the risk of adverse drug effects and stigma. Persuasive evidence shows that schizoaffective disorder is psychotic bipolar disorder; there is no schizoaffective disorder (Box).3,4,16-18
Three disorders—schizophrenia, schizoaffective disorder, and psychotic bipolar disorder—have been evoked to account for the variance in severity in psychotic patients, but psychotic bipolar disorder expresses the entire spectrum. We concur with others that psychotic bipolar disorder includes patient populations typically diagnosed as having schizophrenia and schizoaffective disorder.3,4,9,16-18 In other words, there is no schizophrenia or schizoaffective disorder.4,19
Based on these data, we advocate re-evaluating all patients diagnosed with schizoaffective disorder and schizophrenia, with detailed inquiry for personal and family histories of mania or hypomania. A mood stabilizer may be warranted in some patients with psychosis but without clear manic symptoms. In such cases, we suggest using a provisional DSM-IV-TR diagnosis of psychotic disorder not otherwise specified while you seek obscure mood and/or organic causes.
Misdiagnosis of psychosis
Bipolar disorder can be missed when patients present with psychotic symptoms, but clinicians could have initially recognized Mr. C’s bipolar disorder. His diagnostic trail illustrates important points about psychotic presentations:
- Predominant psychotic symptoms can obscure mood disturbances.
- Mistakenly believing that psychosis means schizophrenia can jeopardize patient care.
- When paranoia and fear hide grandiosity, then mania—not schizophrenia—is likely.
- Psychotic mood disorders—not schizophrenia—cause functional psychosis; there is no schizophrenia (Box).
- Pursuing mood symptoms in psychotic presentations is critical in an initial diagnostic interview.
Bipolar disorder has a broad spectrum of severity and course; it frequently reaches psychotic levels that can become chronic.2,5,21 Psychotic symptoms of rigorously diagnosed bipolar patients can deteriorate until their overwhelming psychosis obscures bipolar symptoms.5,6,13,21 Like most, if not all, acutely psychotic bipolar patients, Mr. C shows all diagnostic criteria for schizophrenia.1-6,21
Patients with severe, psychotic bipolar disorder can stop responding to medication and suffer chronic deterioration without remission.5,21 They can lose their jobs, families, friends, and health until they are homeless, hungry, sick, and psychotic. A deteriorating course such as this has typically defined the schizophrenic process, but this concept has been reassessed.1-6,13,15
Most, but not all, bipolar type I patients experience psychosis. Mr. C’s bipolar symptoms were not initially obvious because of predominant psychosis and were revealed only with specific, focused questions. Without the student case conference, his diagnosis might have remained schizophrenia. His treatment would have remained substandard because of the conventional belief that schizophrenia requires lifelong antipsychotics, usually without mood stabilizers.
Our patient satisfied all DSM-IV-TR criteria for both schizophrenia and psychotic bipolar. Bleuler and Schneider would have diagnosed him as having schizophrenia because they thought all psychotic disorders were schizophrenic.10,12 They were incorrect, as psychotic symptoms are common in patients with severe bipolar disorder.1-6,13,22
Cinical implications
Our observations about this case suggest four important clinical questions:
- Do data justify diagnosing patients such as Mr. C with bipolar disorder and not schizophrenia?
- Do data substantiate either diagnosis as valid?
- Does the diagnosis matter?
- What is standard-of-care treatment for these patients?
Evidence for validity? Bipolar disorder’s two extremes in mood and behavior are so different from those in persons without bipolar disorder or with any other condition that homogeneous bipolar populations can be identified and studied with confidence.2,5,13,21 DSM-IV-TR diagnostic symptoms for bipolar disorder are unique (Table 2).
For a psychiatric disorder to be considered valid, patients must share other characteristics. Bipolar disorder has been validated as a specific disease by consistent genetic,1,13,23,24 pharmacologic,2,14,15 and epidemiologic1 data accumulated across 30 years. The concordance for bipolar disorder in monozygotic twins is approximately 75%, and susceptibility loci for bipolar disorder are established.23,24
Table 2
Characteristics indicating a mood disorder, not schizophrenia*
| History | Past diagnosis or symptoms of a mood disorder; family history of mood disorder or alcoholism |
| Past medications | Lithium, valproic acid, or other mood stabilizers |
| Periods of uncharacteristic and excessive goal-directed activities | Political, religious, legal, sexual, business, criminal, medical, physical, spending, calling, writing, preaching, cleaning, planning, exercise |
| Presence of uncharacteristic emotions or conflict | Irritability, anger, violence, conflict with law enforcement, elation, grandiosity (paranoia), sadness, hopelessness, crying, suicidal ideation |
| Periods of appropriate affect | Smiles, laughs, cries, irritable, angry |
| Mood-congruent delusions and/or hallucinations | Consider grandiosity when there is paranoia and fear |
| Episodes of relatively normal function/remission; premorbid personality positive | Friends, dating, team sports, group activities, election to an office/title, club or gang memberships |
| Current social interactions | Enjoys a friendship, active interactions with spouse and own children, regular interactions with others |
| *Absence of any or all does not rule out mood disorder. | |
Does the diagnosis matter? Failing to make an accurate initial diagnosis can worsen the course of patients who present with psychosis (Table 3):
- Bipolar illness not treated with mood stabilizers progresses, with episodes becoming more frequent and severe.2,14,15
- Antipsychotics are given longer and in higher dosages for schizophrenia than for psychotic bipolar disorder and tend to have more common, chronic, and disabling adverse effects than do antidepressants and mood stabilizers.14,16
- Mr. C was given an antidepressant without mood stabilization, which is contraindicated in bipolar I disorder (especially mixed type) because the cycling rate increases.2,14,15
Several initial signs could have raised suspicion that Mr. C had psychotic bipolar disorder (Table 4). Standard-of-care treatment in psychotic patients is predicated on early and correct diagnosis. On the basis of the evidence and our experience, we recommend that you look for bipolar symptoms when a patient:
- presents for the first time with psychosis, and you rule out an organic cause
- is readmitted for treatment of psychotic symptoms after having been diagnosed with schizophrenia.
Consequences of misdiagnosing psychotic mood disorder as schizophrenia
For patient
|
For clinician
|
Mr. C’s symptoms that indicated bipolar disorder
| Religiosity | Loud preaching and no past special interest in religion |
| Catatonia | Most frequently associated with bipolar disorder |
| Paranoia; fear | Usually hides grandiosity, which is diagnostic of mania |
| Distractibility | Could not stay focused in the diagnostic interview; showed ‘flight of ideas’ |
| Pressured speech | Rapid, disorganized thoughts |
| Disorganization | Hallmark of mania; present in all patients with severe mania |
| Functional psychosis | If an organic cause is ruled out, a psychotic mood disorder is the most likely diagnosis |
| Trouble with the law | Police found patient disturbing neighborhood and escorted him to hospital |
| Patient history | Severe depression |
| Family history | Mother was treated for depression with ECT |
| ECT: electroconvulsive therapy | |
- an antipsychotic, with or without a benzodiazepine for sedation, to enhance ward safety and treat acute psychotic symptoms
- and a first-line mood stabilizer such as valproate, carbamazepine, lithium, or lamotrigine, followed by atypical antipsychotics.
The idea that “symptoms should be treated, not the diagnosis” is inaccurate and provides substandard care. When psychotic symptoms overwhelm and obscure bipolar symptoms, giving only antipsychotics is beyond standard of care.
Related resources
- Berrettini WH. Molecular linkage studies of bipolar disorders. Bipolar Disord 2001;3:276-83.
- Lake CR, Hurwitz N. Schizoaffective disorders are psychotic mood disorders; there are no schizoaffective disorders. Psychiatry Res 2006 (in press).
- Pope HG, Lipinski JF. Diagnosis in schizophrenia and manic-depressive illness, a reassessment of the specificity of “schizophrenic” symptoms in the light of current research. Arch Gen Psychiatry 1978;35:811-28.
- Post RM. Transduction of psychosocial stress into the neurobiology of recurrent affective disorder. Am J Psychiatry 1992;149:999-1010.
- Haloperidol • Haldol
- Lamotrigine • Lamictal
- Lithium • Lithobid
- Lorazepam • Ativan
- Carbamazepine • Tegretol
- Valproate • Depakote
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Acknowledgements
The patient described in this case report gave informed, written consent to interviews and to the anonymous publication of his treatment.
The authors thank Anita Swisher for technical assistance.
1. Berrettini WH. Molecular linkage studies of bipolar disorders. Bipolar Disord 2001;3:276-83.
2. Belmaker RH. Bipolar disorder. N Engl J Med 2004;351:476-86.
3. Pope HG, Lipinski JF. Diagnosis in schizophrenia and manic-depressive illness, a reassessment of the specificity of “schizophrenic” symptoms in the light of current research. Arch Gen Psychiatry 1978;35:811-28.
4. Lake CR, Hurwitz N. Schizoaffective disorders are psychotic mood disorders; there are no schizoaffective disorders. Psychiatry Res 2006 (in press).
5. Post RM. Transduction of psychosocial stress into the neurobiology of recurrent affective disorder. Am J Psychiatry 1992;149:999-1010.
6. Diagnostic and statistical manual of mental disorders 4th ed text rev. Washington, DC: American Psychiatric Association; 2000.
7. Carroll BT, Thomas C, Jayanti K, et al. Treating persistent catatonia when benzodiazepines fail. Current Psychiatry 2005;4:56-64.
8. Abrams R, Taylor MA. Catatonia, a prospective clinical study. Arch Gen Psychiatry 1976;33:579-81.
9. Pope HG. Distinguishing bipolar disorder from schizophrenia in clinical practice: Guidelines and case reports. Hosp Com Psychiatry 1983;34:322-8.
10. Schneider K. Clinical psychopathology. New York: Grune & Stratton; 1959.
11. Kraepelin E. Clinical psychiatry. New York: William Wood Co; 1913.
12. Bleuler E. Dementia praecox or the group of schizophrenias. New York: International Universities Press; 1911/1950.
13. Goodwin FK, Jamison KR. Manic-depressive illness. New York: Oxford University Press; 1990.
14. Calabrese JR, Shelton MD, Bowden CL, et al. Bipolar rapid cycling: Focus on depression as its hallmark. J Clin Psychiatry 2001;62:34-41.
15. Goodwin FK. The biology of recurrence: new directions for the pharmacologic bridge. J Clin Psychiatry 1989;50:40-4.
16. Dieperink ME, Sands JR. Bipolar mania with psychotic features: diagnosis and treatment. Psychiatr Ann 1996;26:633-7.
17. Zarate CA, Tohen M. Double-blind comparison of the continued use of antipsychotic treatment versus its discontinuation in remitted manic patients. Am J Psychiatry 2004;161:169-71.
18. Fowler RC, McCabe MS, Cadoret RJ, Winokur G. The validity of good prognosis schizophrenia. Arch Gen Psychiatry 1972;26:182-5.
19. Harrow M, Grossman LS, Silverstein ML, Meltzer HY. Thought pathology in manic and schizophrenic patients. Its occurrence at hospital admission and 7 weeks later. Arch Gen Psychiatry 1982;39:665-71.
20. Szasz TS. Schizophrenia: the sacred symbol of psychiatry. Br J Psychiatry 1976;129:308-16.
21. Carlson GA, Goodwin FK. The stages of mania. Arch Gen Psychiatry 1973;28:221-8.
22. Pini S, Cassano GB, Dell’Osso L, Amador XF. Insight into illness in schizophrenia, schizoaffective disorder, and mood disorders with psychotic features. Am J Psychiatry 2001;158:122-5.
23. Bertelsen A, Harvald B, Hauge M. A Danish twin study of manic-depressive illness. Br J Psychiatry 1977;130:330-51.
24. Green E, Elvidge G, Jacobson N, et al. Localization of bipolar susceptibility locus by molecular genetic analysis of the chromosome 12q23-q24 region in two pedigrees with bipolar disorder and Darier’s disease. Am J Psychiatry 2005;162:35-42.
When a patient presents with psychotic symptoms, you might not recognize or pursue hints of bipolarity if you assume psychosis means schizophrenia. Yet psychotic bipolar disorder can explain every sign, symptom, course, and other characteristic traditionally assumed to indicate schizophrenia (Table 1). The literature, including recent genetic data,1-6 marshals a persuasive argument that patients diagnosed with schizophrenia usually suffer from a psychotic bipolar disorder.
Consider here how a cascade of changing signs and symptoms, initially unrecognized, caused five sequential re-evaluations of one psychotic patient’s primary Axis I diagnosis. His case highlights why the correct initial diagnosis of the disease causing psychosis is essential to effective treatment.4,7-9
Table 1
DSM-IV-TR criteria for schizophrenia vs. psychotic mood disorder
| Schizophrenia diagnosis6 | Seen in psychotic mood disorders |
|---|---|
| Criterion A | |
| Hallucinations and delusions | 50% to 80% explained by mood16,21 |
| Paranoia | Hides grandiosity4 |
| Catatonia | 75% explained by mood7,8 |
| Disorganized speech and behavior | All patients with moderate to severe mania1-5 |
| Negative symptoms | All patients with moderate to severe depression4 |
| Criterion B | |
| Social and job dysfunction | All patients with moderate to severe bipolar disorder5,13 |
| Criterion C | |
| Chronic continuous symptoms | Patients can have psychotic symptoms continuously for 2 years to life5,6,13 |
Case: Carved in stone
Police officers carry Mr. C, age 30, into the emergency department. He is mentally disorganized and arrives in a rigid, catatonic posture. According to a neighbor, Mr. C was kneeling motionless on his mother’s front lawn, alternating between mutism and inappropriately loud, disorganized religious preaching. When his arm is lifted, it remains as placed. He is admitted to the acute care inpatient unit.
Mr. C’s most striking symptoms are catatonia and psychosis. Postural rigidity, waxy flexibility, and automatic obedience are characteristics of catatonia.6-8 An organic cause is first considered, such as hyperthyroidism, cerebrovascular accident, cerebral neoplasm, head trauma, seizure disorder, dementia, neuroleptic malignant syndrome, pheochromocytoma, or—especially—intoxication from illegal drugs.7
While awaiting results from physical, mental status, and lab exams and imaging studies, staff assign him two admitting diagnoses: catatonic disorder due to a general medical condition and psychotic disorder not otherwise specified.6
Case: Inconclusive workup
Mr. C denies using illegal substances or alcohol, which his mother confirms. He has no history of seizures or other medical conditions. His distractibility prevents him from focusing on a formal mental status exam. Physical exam, urine drug screen, lab results, and imaging studies are unremarkable except for an admitting blood pressure of 145/95 mm Hg and pulse of 115 beats per minute. These readings normalize within 1 hour. IM haloperidol and lorazepam are given as needed for agitation, but physicians withhold scheduled medications to allow staff to observe his symptoms.
Organic causes of catatonia now seem less likely, though past use of drugs such as phencyclidine that can cause chronic psychosis cannot be ruled out. Schizophrenia is considered likely because catatonia is one of schizophrenia’s five core diagnostic symptoms.6 Catatonia can also be a symptom of bipolar disorder.6-9 Staff make a preliminary diagnosis of schizophrenia, catatonic type.
Case: ‘Hit men are after me’
Staff observe Mr. C responding to threatening auditory hallucinations. His affect is “fearful to terrified.” He says he hears the voice of God warning him of danger and continuing a running commentary on his actions. He fears for his life because “hit men have been sent to kill me” and have “infiltrated” the inpatient ward. He does not eat, saying his food is poisoned. He says these beliefs have escalated over the past year.
Mr. C’s catatonic symptoms resolve overnight, but obtaining additional history is difficult because of his paranoia. He denies any history of bizarre behavior or past contact with mental health services. He claims not to be especially religious. He is unmarried and lives with his mother, is college-educated, but has held only menial jobs.
Inpatient staff shifts its diagnostic focus to functional disorders associated with auditory hallucinations, paranoid delusions, and gross disorganization. According to Schneider and the DSM-IV-TR,6,10 hearing a voice “keeping up a running commentary on one’s behavior” is especially diagnostic of schizophrenia.
Because of the rapid resolution of his “catatonic” symptoms and prominence of paranoia, they change his diagnosis on day 2 to schizophrenia, paranoid type. Mr. C meets all diagnostic criteria for schizophrenia except one: the staff has overlooked and has not adequately excluded a psychotic mood disorder.
Case: A turn for the worse
That night, nursing staff find Mr. C naked and cowering in the fetal position in a corner of his room. He has smeared his feces on his face and in his hair and mouth. While being cleaned up, he suddenly begins quoting scripture in a loud, disorganized voice. His expressed thoughts are incomprehensible. He is given haloperidol and lorazepam immediately; oral haloperidol is continued at 10 mg bid.
Both Bleuler and Kraepelin concluded “coprophilia and coprophagia are unique to children and patients with schizophrenia.”11,12 The DSM casebook cites Kraepelin’s description of a catatonic patient who “smeared feces about” as a “classic, textbook case” of schizophrenia.11 The casebook goes on to say: “In the absence of any known general medical condition, the combination of coprophilia, disorganized speech, and catatonic behavior clearly indicates the diagnosis of schizophrenia.”
Mr. C shows each of these. Staff changes his diagnosis again—to schizophrenia, disorganized type, which carries a poor prognosis.11,12
Case: Banking and ray guns
By day 5, Mr. C’s mental status is normalizing and his psychosis improving. He volunteers for a weekly student case conference. There, he reveals additional information that staff could have discovered at admission with more-focused questions.
He reports that 2 years earlier he suffered severe suicidal depression. Six months later, during a hypomanic episode, he began “toying with the idea” that he might become part owner of his local bank. He believes “the Secret Service decided to transfer ownership to me.”
His plans upon acquiring the bank include buying three houses and six cars valued at several million dollars and running for state governor. For weeks before admission, he did not need sleep, experienced an increase in energy and activities, and his mind was racing. His job seemed so “trivial” that he quit. Immediately before his hospital admission, his delusions intensified to include an “evil conspiracy” to murder him for ownership of the bank and he feared his execution was imminent.
He explains his catatonic behavior on the lawn by his belief that “hit men” hiding across the street aimed a “motion-detecting, heat-seeking ray gun” at him so that if he had “moved an inch,” he would die. He says the “feces incident” was an effort to get himself transferred to the state hospital, where he thought he would be safer because his present caretakers were “infiltrated.” He also says his mother received electroconvulsive therapy in her 20s.
These symptoms—especially the striking grandiosity, lack of need for sleep, racing thoughts, hallucinations and delusions—define a manic episode with psychotic features. Only one manic episode as described here is diagnostic of bipolar disorder, type I.2,6,13 Staff changes his diagnosis to schizoaffective disorder, a compromise used to include patients with bipolar and psychotic (schizophrenic) features. Some authors contend schizoaffective disorder is psychotic bipolar disorder and not a separate disease.3,4,9
Case: From SSRI to lithium
After 2 weeks, Mr. C is discharged on haloperidol, 5 mg bid, but no mood stabilizer. He receives follow-up care at a community mental health center. When he develops severe depressive symptoms 6 months after discharge, the attending psychiatrist starts him on a selective serotonin reuptake inhibitor (SSRI). Within 2 weeks, Mr. C switches from depression to a mixed, dysphoric mania. After the SSRI is discontinued and lithium is added to his haloperidol, his mood gradually stabilizes to moderate depression. He develops rigidity, masked faces, and a fine tremor in his hands.
About 10% of bipolar depressed patients given an antidepressant—especially without a mood stabilizer—switch to mania, and their cycle frequency increases.2,13-15 A correct initial diagnosis and treatment with a mood stabilizer might have avoided Mr. C’s switch.
Mixed bipolar disorder with overlapping depressive and manic symptoms is often resistant to monotherapy, requiring two or more mood stabilizers such as lithium and an anticonvulsant.14 Without a mood-stabilizing combination, the mixed, rapid-cycling type of bipolar disorder is likely to progress, with more-rapid and more-severe episodes.2,13-15 Adding lamotrigine, a mood stabilizer with antidepressant effects, can help.2,14
Stopping the SSRI is correct, despite Mr. C’s severe depression, to avoid increasing the cycle frequency.13-15 Some authors recommend tapering the antipsychotic, using it only as needed for psychotic features after psychosis has resolved.14-17 Continuing antipsychotic drugs after psychosis has remitted increases rates of cycling to depression, depressive and extrapyramidal symptoms, and medication discontinuation.17 Lithium may have aggravated Mr. C’s antipsychotic-induced parkinsonism, but discontinuing haloperidol may have been the most therapeutic decision.
The community mental health staff changes his diagnosis again, this time to bipolar disorder, type I, mixed, severe with psychotic features. We concur that this is correct.
Case: A diagnostic step back
Two years later, Mr. C is working and continues to take lithium and haloperidol prescribed at the mental health center. His intermittent depressive episodes persist, but—apparently because he has not had another manic episode—the staff switches his diagnosis back to schizoaffective disorder.
We disagree with this change. A diagnosis of schizoaffective disorder precludes ideal pharmacotherapy for Mr. C’s rapid-cycling bipolar disorder and increases the risk of adverse drug effects and stigma. Persuasive evidence shows that schizoaffective disorder is psychotic bipolar disorder; there is no schizoaffective disorder (Box).3,4,16-18
Three disorders—schizophrenia, schizoaffective disorder, and psychotic bipolar disorder—have been evoked to account for the variance in severity in psychotic patients, but psychotic bipolar disorder expresses the entire spectrum. We concur with others that psychotic bipolar disorder includes patient populations typically diagnosed as having schizophrenia and schizoaffective disorder.3,4,9,16-18 In other words, there is no schizophrenia or schizoaffective disorder.4,19
Based on these data, we advocate re-evaluating all patients diagnosed with schizoaffective disorder and schizophrenia, with detailed inquiry for personal and family histories of mania or hypomania. A mood stabilizer may be warranted in some patients with psychosis but without clear manic symptoms. In such cases, we suggest using a provisional DSM-IV-TR diagnosis of psychotic disorder not otherwise specified while you seek obscure mood and/or organic causes.
Misdiagnosis of psychosis
Bipolar disorder can be missed when patients present with psychotic symptoms, but clinicians could have initially recognized Mr. C’s bipolar disorder. His diagnostic trail illustrates important points about psychotic presentations:
- Predominant psychotic symptoms can obscure mood disturbances.
- Mistakenly believing that psychosis means schizophrenia can jeopardize patient care.
- When paranoia and fear hide grandiosity, then mania—not schizophrenia—is likely.
- Psychotic mood disorders—not schizophrenia—cause functional psychosis; there is no schizophrenia (Box).
- Pursuing mood symptoms in psychotic presentations is critical in an initial diagnostic interview.
Bipolar disorder has a broad spectrum of severity and course; it frequently reaches psychotic levels that can become chronic.2,5,21 Psychotic symptoms of rigorously diagnosed bipolar patients can deteriorate until their overwhelming psychosis obscures bipolar symptoms.5,6,13,21 Like most, if not all, acutely psychotic bipolar patients, Mr. C shows all diagnostic criteria for schizophrenia.1-6,21
Patients with severe, psychotic bipolar disorder can stop responding to medication and suffer chronic deterioration without remission.5,21 They can lose their jobs, families, friends, and health until they are homeless, hungry, sick, and psychotic. A deteriorating course such as this has typically defined the schizophrenic process, but this concept has been reassessed.1-6,13,15
Most, but not all, bipolar type I patients experience psychosis. Mr. C’s bipolar symptoms were not initially obvious because of predominant psychosis and were revealed only with specific, focused questions. Without the student case conference, his diagnosis might have remained schizophrenia. His treatment would have remained substandard because of the conventional belief that schizophrenia requires lifelong antipsychotics, usually without mood stabilizers.
Our patient satisfied all DSM-IV-TR criteria for both schizophrenia and psychotic bipolar. Bleuler and Schneider would have diagnosed him as having schizophrenia because they thought all psychotic disorders were schizophrenic.10,12 They were incorrect, as psychotic symptoms are common in patients with severe bipolar disorder.1-6,13,22
Cinical implications
Our observations about this case suggest four important clinical questions:
- Do data justify diagnosing patients such as Mr. C with bipolar disorder and not schizophrenia?
- Do data substantiate either diagnosis as valid?
- Does the diagnosis matter?
- What is standard-of-care treatment for these patients?
Evidence for validity? Bipolar disorder’s two extremes in mood and behavior are so different from those in persons without bipolar disorder or with any other condition that homogeneous bipolar populations can be identified and studied with confidence.2,5,13,21 DSM-IV-TR diagnostic symptoms for bipolar disorder are unique (Table 2).
For a psychiatric disorder to be considered valid, patients must share other characteristics. Bipolar disorder has been validated as a specific disease by consistent genetic,1,13,23,24 pharmacologic,2,14,15 and epidemiologic1 data accumulated across 30 years. The concordance for bipolar disorder in monozygotic twins is approximately 75%, and susceptibility loci for bipolar disorder are established.23,24
Table 2
Characteristics indicating a mood disorder, not schizophrenia*
| History | Past diagnosis or symptoms of a mood disorder; family history of mood disorder or alcoholism |
| Past medications | Lithium, valproic acid, or other mood stabilizers |
| Periods of uncharacteristic and excessive goal-directed activities | Political, religious, legal, sexual, business, criminal, medical, physical, spending, calling, writing, preaching, cleaning, planning, exercise |
| Presence of uncharacteristic emotions or conflict | Irritability, anger, violence, conflict with law enforcement, elation, grandiosity (paranoia), sadness, hopelessness, crying, suicidal ideation |
| Periods of appropriate affect | Smiles, laughs, cries, irritable, angry |
| Mood-congruent delusions and/or hallucinations | Consider grandiosity when there is paranoia and fear |
| Episodes of relatively normal function/remission; premorbid personality positive | Friends, dating, team sports, group activities, election to an office/title, club or gang memberships |
| Current social interactions | Enjoys a friendship, active interactions with spouse and own children, regular interactions with others |
| *Absence of any or all does not rule out mood disorder. | |
Does the diagnosis matter? Failing to make an accurate initial diagnosis can worsen the course of patients who present with psychosis (Table 3):
- Bipolar illness not treated with mood stabilizers progresses, with episodes becoming more frequent and severe.2,14,15
- Antipsychotics are given longer and in higher dosages for schizophrenia than for psychotic bipolar disorder and tend to have more common, chronic, and disabling adverse effects than do antidepressants and mood stabilizers.14,16
- Mr. C was given an antidepressant without mood stabilization, which is contraindicated in bipolar I disorder (especially mixed type) because the cycling rate increases.2,14,15
Several initial signs could have raised suspicion that Mr. C had psychotic bipolar disorder (Table 4). Standard-of-care treatment in psychotic patients is predicated on early and correct diagnosis. On the basis of the evidence and our experience, we recommend that you look for bipolar symptoms when a patient:
- presents for the first time with psychosis, and you rule out an organic cause
- is readmitted for treatment of psychotic symptoms after having been diagnosed with schizophrenia.
Consequences of misdiagnosing psychotic mood disorder as schizophrenia
For patient
|
For clinician
|
Mr. C’s symptoms that indicated bipolar disorder
| Religiosity | Loud preaching and no past special interest in religion |
| Catatonia | Most frequently associated with bipolar disorder |
| Paranoia; fear | Usually hides grandiosity, which is diagnostic of mania |
| Distractibility | Could not stay focused in the diagnostic interview; showed ‘flight of ideas’ |
| Pressured speech | Rapid, disorganized thoughts |
| Disorganization | Hallmark of mania; present in all patients with severe mania |
| Functional psychosis | If an organic cause is ruled out, a psychotic mood disorder is the most likely diagnosis |
| Trouble with the law | Police found patient disturbing neighborhood and escorted him to hospital |
| Patient history | Severe depression |
| Family history | Mother was treated for depression with ECT |
| ECT: electroconvulsive therapy | |
- an antipsychotic, with or without a benzodiazepine for sedation, to enhance ward safety and treat acute psychotic symptoms
- and a first-line mood stabilizer such as valproate, carbamazepine, lithium, or lamotrigine, followed by atypical antipsychotics.
The idea that “symptoms should be treated, not the diagnosis” is inaccurate and provides substandard care. When psychotic symptoms overwhelm and obscure bipolar symptoms, giving only antipsychotics is beyond standard of care.
Related resources
- Berrettini WH. Molecular linkage studies of bipolar disorders. Bipolar Disord 2001;3:276-83.
- Lake CR, Hurwitz N. Schizoaffective disorders are psychotic mood disorders; there are no schizoaffective disorders. Psychiatry Res 2006 (in press).
- Pope HG, Lipinski JF. Diagnosis in schizophrenia and manic-depressive illness, a reassessment of the specificity of “schizophrenic” symptoms in the light of current research. Arch Gen Psychiatry 1978;35:811-28.
- Post RM. Transduction of psychosocial stress into the neurobiology of recurrent affective disorder. Am J Psychiatry 1992;149:999-1010.
- Haloperidol • Haldol
- Lamotrigine • Lamictal
- Lithium • Lithobid
- Lorazepam • Ativan
- Carbamazepine • Tegretol
- Valproate • Depakote
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Acknowledgements
The patient described in this case report gave informed, written consent to interviews and to the anonymous publication of his treatment.
The authors thank Anita Swisher for technical assistance.
When a patient presents with psychotic symptoms, you might not recognize or pursue hints of bipolarity if you assume psychosis means schizophrenia. Yet psychotic bipolar disorder can explain every sign, symptom, course, and other characteristic traditionally assumed to indicate schizophrenia (Table 1). The literature, including recent genetic data,1-6 marshals a persuasive argument that patients diagnosed with schizophrenia usually suffer from a psychotic bipolar disorder.
Consider here how a cascade of changing signs and symptoms, initially unrecognized, caused five sequential re-evaluations of one psychotic patient’s primary Axis I diagnosis. His case highlights why the correct initial diagnosis of the disease causing psychosis is essential to effective treatment.4,7-9
Table 1
DSM-IV-TR criteria for schizophrenia vs. psychotic mood disorder
| Schizophrenia diagnosis6 | Seen in psychotic mood disorders |
|---|---|
| Criterion A | |
| Hallucinations and delusions | 50% to 80% explained by mood16,21 |
| Paranoia | Hides grandiosity4 |
| Catatonia | 75% explained by mood7,8 |
| Disorganized speech and behavior | All patients with moderate to severe mania1-5 |
| Negative symptoms | All patients with moderate to severe depression4 |
| Criterion B | |
| Social and job dysfunction | All patients with moderate to severe bipolar disorder5,13 |
| Criterion C | |
| Chronic continuous symptoms | Patients can have psychotic symptoms continuously for 2 years to life5,6,13 |
Case: Carved in stone
Police officers carry Mr. C, age 30, into the emergency department. He is mentally disorganized and arrives in a rigid, catatonic posture. According to a neighbor, Mr. C was kneeling motionless on his mother’s front lawn, alternating between mutism and inappropriately loud, disorganized religious preaching. When his arm is lifted, it remains as placed. He is admitted to the acute care inpatient unit.
Mr. C’s most striking symptoms are catatonia and psychosis. Postural rigidity, waxy flexibility, and automatic obedience are characteristics of catatonia.6-8 An organic cause is first considered, such as hyperthyroidism, cerebrovascular accident, cerebral neoplasm, head trauma, seizure disorder, dementia, neuroleptic malignant syndrome, pheochromocytoma, or—especially—intoxication from illegal drugs.7
While awaiting results from physical, mental status, and lab exams and imaging studies, staff assign him two admitting diagnoses: catatonic disorder due to a general medical condition and psychotic disorder not otherwise specified.6
Case: Inconclusive workup
Mr. C denies using illegal substances or alcohol, which his mother confirms. He has no history of seizures or other medical conditions. His distractibility prevents him from focusing on a formal mental status exam. Physical exam, urine drug screen, lab results, and imaging studies are unremarkable except for an admitting blood pressure of 145/95 mm Hg and pulse of 115 beats per minute. These readings normalize within 1 hour. IM haloperidol and lorazepam are given as needed for agitation, but physicians withhold scheduled medications to allow staff to observe his symptoms.
Organic causes of catatonia now seem less likely, though past use of drugs such as phencyclidine that can cause chronic psychosis cannot be ruled out. Schizophrenia is considered likely because catatonia is one of schizophrenia’s five core diagnostic symptoms.6 Catatonia can also be a symptom of bipolar disorder.6-9 Staff make a preliminary diagnosis of schizophrenia, catatonic type.
Case: ‘Hit men are after me’
Staff observe Mr. C responding to threatening auditory hallucinations. His affect is “fearful to terrified.” He says he hears the voice of God warning him of danger and continuing a running commentary on his actions. He fears for his life because “hit men have been sent to kill me” and have “infiltrated” the inpatient ward. He does not eat, saying his food is poisoned. He says these beliefs have escalated over the past year.
Mr. C’s catatonic symptoms resolve overnight, but obtaining additional history is difficult because of his paranoia. He denies any history of bizarre behavior or past contact with mental health services. He claims not to be especially religious. He is unmarried and lives with his mother, is college-educated, but has held only menial jobs.
Inpatient staff shifts its diagnostic focus to functional disorders associated with auditory hallucinations, paranoid delusions, and gross disorganization. According to Schneider and the DSM-IV-TR,6,10 hearing a voice “keeping up a running commentary on one’s behavior” is especially diagnostic of schizophrenia.
Because of the rapid resolution of his “catatonic” symptoms and prominence of paranoia, they change his diagnosis on day 2 to schizophrenia, paranoid type. Mr. C meets all diagnostic criteria for schizophrenia except one: the staff has overlooked and has not adequately excluded a psychotic mood disorder.
Case: A turn for the worse
That night, nursing staff find Mr. C naked and cowering in the fetal position in a corner of his room. He has smeared his feces on his face and in his hair and mouth. While being cleaned up, he suddenly begins quoting scripture in a loud, disorganized voice. His expressed thoughts are incomprehensible. He is given haloperidol and lorazepam immediately; oral haloperidol is continued at 10 mg bid.
Both Bleuler and Kraepelin concluded “coprophilia and coprophagia are unique to children and patients with schizophrenia.”11,12 The DSM casebook cites Kraepelin’s description of a catatonic patient who “smeared feces about” as a “classic, textbook case” of schizophrenia.11 The casebook goes on to say: “In the absence of any known general medical condition, the combination of coprophilia, disorganized speech, and catatonic behavior clearly indicates the diagnosis of schizophrenia.”
Mr. C shows each of these. Staff changes his diagnosis again—to schizophrenia, disorganized type, which carries a poor prognosis.11,12
Case: Banking and ray guns
By day 5, Mr. C’s mental status is normalizing and his psychosis improving. He volunteers for a weekly student case conference. There, he reveals additional information that staff could have discovered at admission with more-focused questions.
He reports that 2 years earlier he suffered severe suicidal depression. Six months later, during a hypomanic episode, he began “toying with the idea” that he might become part owner of his local bank. He believes “the Secret Service decided to transfer ownership to me.”
His plans upon acquiring the bank include buying three houses and six cars valued at several million dollars and running for state governor. For weeks before admission, he did not need sleep, experienced an increase in energy and activities, and his mind was racing. His job seemed so “trivial” that he quit. Immediately before his hospital admission, his delusions intensified to include an “evil conspiracy” to murder him for ownership of the bank and he feared his execution was imminent.
He explains his catatonic behavior on the lawn by his belief that “hit men” hiding across the street aimed a “motion-detecting, heat-seeking ray gun” at him so that if he had “moved an inch,” he would die. He says the “feces incident” was an effort to get himself transferred to the state hospital, where he thought he would be safer because his present caretakers were “infiltrated.” He also says his mother received electroconvulsive therapy in her 20s.
These symptoms—especially the striking grandiosity, lack of need for sleep, racing thoughts, hallucinations and delusions—define a manic episode with psychotic features. Only one manic episode as described here is diagnostic of bipolar disorder, type I.2,6,13 Staff changes his diagnosis to schizoaffective disorder, a compromise used to include patients with bipolar and psychotic (schizophrenic) features. Some authors contend schizoaffective disorder is psychotic bipolar disorder and not a separate disease.3,4,9
Case: From SSRI to lithium
After 2 weeks, Mr. C is discharged on haloperidol, 5 mg bid, but no mood stabilizer. He receives follow-up care at a community mental health center. When he develops severe depressive symptoms 6 months after discharge, the attending psychiatrist starts him on a selective serotonin reuptake inhibitor (SSRI). Within 2 weeks, Mr. C switches from depression to a mixed, dysphoric mania. After the SSRI is discontinued and lithium is added to his haloperidol, his mood gradually stabilizes to moderate depression. He develops rigidity, masked faces, and a fine tremor in his hands.
About 10% of bipolar depressed patients given an antidepressant—especially without a mood stabilizer—switch to mania, and their cycle frequency increases.2,13-15 A correct initial diagnosis and treatment with a mood stabilizer might have avoided Mr. C’s switch.
Mixed bipolar disorder with overlapping depressive and manic symptoms is often resistant to monotherapy, requiring two or more mood stabilizers such as lithium and an anticonvulsant.14 Without a mood-stabilizing combination, the mixed, rapid-cycling type of bipolar disorder is likely to progress, with more-rapid and more-severe episodes.2,13-15 Adding lamotrigine, a mood stabilizer with antidepressant effects, can help.2,14
Stopping the SSRI is correct, despite Mr. C’s severe depression, to avoid increasing the cycle frequency.13-15 Some authors recommend tapering the antipsychotic, using it only as needed for psychotic features after psychosis has resolved.14-17 Continuing antipsychotic drugs after psychosis has remitted increases rates of cycling to depression, depressive and extrapyramidal symptoms, and medication discontinuation.17 Lithium may have aggravated Mr. C’s antipsychotic-induced parkinsonism, but discontinuing haloperidol may have been the most therapeutic decision.
The community mental health staff changes his diagnosis again, this time to bipolar disorder, type I, mixed, severe with psychotic features. We concur that this is correct.
Case: A diagnostic step back
Two years later, Mr. C is working and continues to take lithium and haloperidol prescribed at the mental health center. His intermittent depressive episodes persist, but—apparently because he has not had another manic episode—the staff switches his diagnosis back to schizoaffective disorder.
We disagree with this change. A diagnosis of schizoaffective disorder precludes ideal pharmacotherapy for Mr. C’s rapid-cycling bipolar disorder and increases the risk of adverse drug effects and stigma. Persuasive evidence shows that schizoaffective disorder is psychotic bipolar disorder; there is no schizoaffective disorder (Box).3,4,16-18
Three disorders—schizophrenia, schizoaffective disorder, and psychotic bipolar disorder—have been evoked to account for the variance in severity in psychotic patients, but psychotic bipolar disorder expresses the entire spectrum. We concur with others that psychotic bipolar disorder includes patient populations typically diagnosed as having schizophrenia and schizoaffective disorder.3,4,9,16-18 In other words, there is no schizophrenia or schizoaffective disorder.4,19
Based on these data, we advocate re-evaluating all patients diagnosed with schizoaffective disorder and schizophrenia, with detailed inquiry for personal and family histories of mania or hypomania. A mood stabilizer may be warranted in some patients with psychosis but without clear manic symptoms. In such cases, we suggest using a provisional DSM-IV-TR diagnosis of psychotic disorder not otherwise specified while you seek obscure mood and/or organic causes.
Misdiagnosis of psychosis
Bipolar disorder can be missed when patients present with psychotic symptoms, but clinicians could have initially recognized Mr. C’s bipolar disorder. His diagnostic trail illustrates important points about psychotic presentations:
- Predominant psychotic symptoms can obscure mood disturbances.
- Mistakenly believing that psychosis means schizophrenia can jeopardize patient care.
- When paranoia and fear hide grandiosity, then mania—not schizophrenia—is likely.
- Psychotic mood disorders—not schizophrenia—cause functional psychosis; there is no schizophrenia (Box).
- Pursuing mood symptoms in psychotic presentations is critical in an initial diagnostic interview.
Bipolar disorder has a broad spectrum of severity and course; it frequently reaches psychotic levels that can become chronic.2,5,21 Psychotic symptoms of rigorously diagnosed bipolar patients can deteriorate until their overwhelming psychosis obscures bipolar symptoms.5,6,13,21 Like most, if not all, acutely psychotic bipolar patients, Mr. C shows all diagnostic criteria for schizophrenia.1-6,21
Patients with severe, psychotic bipolar disorder can stop responding to medication and suffer chronic deterioration without remission.5,21 They can lose their jobs, families, friends, and health until they are homeless, hungry, sick, and psychotic. A deteriorating course such as this has typically defined the schizophrenic process, but this concept has been reassessed.1-6,13,15
Most, but not all, bipolar type I patients experience psychosis. Mr. C’s bipolar symptoms were not initially obvious because of predominant psychosis and were revealed only with specific, focused questions. Without the student case conference, his diagnosis might have remained schizophrenia. His treatment would have remained substandard because of the conventional belief that schizophrenia requires lifelong antipsychotics, usually without mood stabilizers.
Our patient satisfied all DSM-IV-TR criteria for both schizophrenia and psychotic bipolar. Bleuler and Schneider would have diagnosed him as having schizophrenia because they thought all psychotic disorders were schizophrenic.10,12 They were incorrect, as psychotic symptoms are common in patients with severe bipolar disorder.1-6,13,22
Cinical implications
Our observations about this case suggest four important clinical questions:
- Do data justify diagnosing patients such as Mr. C with bipolar disorder and not schizophrenia?
- Do data substantiate either diagnosis as valid?
- Does the diagnosis matter?
- What is standard-of-care treatment for these patients?
Evidence for validity? Bipolar disorder’s two extremes in mood and behavior are so different from those in persons without bipolar disorder or with any other condition that homogeneous bipolar populations can be identified and studied with confidence.2,5,13,21 DSM-IV-TR diagnostic symptoms for bipolar disorder are unique (Table 2).
For a psychiatric disorder to be considered valid, patients must share other characteristics. Bipolar disorder has been validated as a specific disease by consistent genetic,1,13,23,24 pharmacologic,2,14,15 and epidemiologic1 data accumulated across 30 years. The concordance for bipolar disorder in monozygotic twins is approximately 75%, and susceptibility loci for bipolar disorder are established.23,24
Table 2
Characteristics indicating a mood disorder, not schizophrenia*
| History | Past diagnosis or symptoms of a mood disorder; family history of mood disorder or alcoholism |
| Past medications | Lithium, valproic acid, or other mood stabilizers |
| Periods of uncharacteristic and excessive goal-directed activities | Political, religious, legal, sexual, business, criminal, medical, physical, spending, calling, writing, preaching, cleaning, planning, exercise |
| Presence of uncharacteristic emotions or conflict | Irritability, anger, violence, conflict with law enforcement, elation, grandiosity (paranoia), sadness, hopelessness, crying, suicidal ideation |
| Periods of appropriate affect | Smiles, laughs, cries, irritable, angry |
| Mood-congruent delusions and/or hallucinations | Consider grandiosity when there is paranoia and fear |
| Episodes of relatively normal function/remission; premorbid personality positive | Friends, dating, team sports, group activities, election to an office/title, club or gang memberships |
| Current social interactions | Enjoys a friendship, active interactions with spouse and own children, regular interactions with others |
| *Absence of any or all does not rule out mood disorder. | |
Does the diagnosis matter? Failing to make an accurate initial diagnosis can worsen the course of patients who present with psychosis (Table 3):
- Bipolar illness not treated with mood stabilizers progresses, with episodes becoming more frequent and severe.2,14,15
- Antipsychotics are given longer and in higher dosages for schizophrenia than for psychotic bipolar disorder and tend to have more common, chronic, and disabling adverse effects than do antidepressants and mood stabilizers.14,16
- Mr. C was given an antidepressant without mood stabilization, which is contraindicated in bipolar I disorder (especially mixed type) because the cycling rate increases.2,14,15
Several initial signs could have raised suspicion that Mr. C had psychotic bipolar disorder (Table 4). Standard-of-care treatment in psychotic patients is predicated on early and correct diagnosis. On the basis of the evidence and our experience, we recommend that you look for bipolar symptoms when a patient:
- presents for the first time with psychosis, and you rule out an organic cause
- is readmitted for treatment of psychotic symptoms after having been diagnosed with schizophrenia.
Consequences of misdiagnosing psychotic mood disorder as schizophrenia
For patient
|
For clinician
|
Mr. C’s symptoms that indicated bipolar disorder
| Religiosity | Loud preaching and no past special interest in religion |
| Catatonia | Most frequently associated with bipolar disorder |
| Paranoia; fear | Usually hides grandiosity, which is diagnostic of mania |
| Distractibility | Could not stay focused in the diagnostic interview; showed ‘flight of ideas’ |
| Pressured speech | Rapid, disorganized thoughts |
| Disorganization | Hallmark of mania; present in all patients with severe mania |
| Functional psychosis | If an organic cause is ruled out, a psychotic mood disorder is the most likely diagnosis |
| Trouble with the law | Police found patient disturbing neighborhood and escorted him to hospital |
| Patient history | Severe depression |
| Family history | Mother was treated for depression with ECT |
| ECT: electroconvulsive therapy | |
- an antipsychotic, with or without a benzodiazepine for sedation, to enhance ward safety and treat acute psychotic symptoms
- and a first-line mood stabilizer such as valproate, carbamazepine, lithium, or lamotrigine, followed by atypical antipsychotics.
The idea that “symptoms should be treated, not the diagnosis” is inaccurate and provides substandard care. When psychotic symptoms overwhelm and obscure bipolar symptoms, giving only antipsychotics is beyond standard of care.
Related resources
- Berrettini WH. Molecular linkage studies of bipolar disorders. Bipolar Disord 2001;3:276-83.
- Lake CR, Hurwitz N. Schizoaffective disorders are psychotic mood disorders; there are no schizoaffective disorders. Psychiatry Res 2006 (in press).
- Pope HG, Lipinski JF. Diagnosis in schizophrenia and manic-depressive illness, a reassessment of the specificity of “schizophrenic” symptoms in the light of current research. Arch Gen Psychiatry 1978;35:811-28.
- Post RM. Transduction of psychosocial stress into the neurobiology of recurrent affective disorder. Am J Psychiatry 1992;149:999-1010.
- Haloperidol • Haldol
- Lamotrigine • Lamictal
- Lithium • Lithobid
- Lorazepam • Ativan
- Carbamazepine • Tegretol
- Valproate • Depakote
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Acknowledgements
The patient described in this case report gave informed, written consent to interviews and to the anonymous publication of his treatment.
The authors thank Anita Swisher for technical assistance.
1. Berrettini WH. Molecular linkage studies of bipolar disorders. Bipolar Disord 2001;3:276-83.
2. Belmaker RH. Bipolar disorder. N Engl J Med 2004;351:476-86.
3. Pope HG, Lipinski JF. Diagnosis in schizophrenia and manic-depressive illness, a reassessment of the specificity of “schizophrenic” symptoms in the light of current research. Arch Gen Psychiatry 1978;35:811-28.
4. Lake CR, Hurwitz N. Schizoaffective disorders are psychotic mood disorders; there are no schizoaffective disorders. Psychiatry Res 2006 (in press).
5. Post RM. Transduction of psychosocial stress into the neurobiology of recurrent affective disorder. Am J Psychiatry 1992;149:999-1010.
6. Diagnostic and statistical manual of mental disorders 4th ed text rev. Washington, DC: American Psychiatric Association; 2000.
7. Carroll BT, Thomas C, Jayanti K, et al. Treating persistent catatonia when benzodiazepines fail. Current Psychiatry 2005;4:56-64.
8. Abrams R, Taylor MA. Catatonia, a prospective clinical study. Arch Gen Psychiatry 1976;33:579-81.
9. Pope HG. Distinguishing bipolar disorder from schizophrenia in clinical practice: Guidelines and case reports. Hosp Com Psychiatry 1983;34:322-8.
10. Schneider K. Clinical psychopathology. New York: Grune & Stratton; 1959.
11. Kraepelin E. Clinical psychiatry. New York: William Wood Co; 1913.
12. Bleuler E. Dementia praecox or the group of schizophrenias. New York: International Universities Press; 1911/1950.
13. Goodwin FK, Jamison KR. Manic-depressive illness. New York: Oxford University Press; 1990.
14. Calabrese JR, Shelton MD, Bowden CL, et al. Bipolar rapid cycling: Focus on depression as its hallmark. J Clin Psychiatry 2001;62:34-41.
15. Goodwin FK. The biology of recurrence: new directions for the pharmacologic bridge. J Clin Psychiatry 1989;50:40-4.
16. Dieperink ME, Sands JR. Bipolar mania with psychotic features: diagnosis and treatment. Psychiatr Ann 1996;26:633-7.
17. Zarate CA, Tohen M. Double-blind comparison of the continued use of antipsychotic treatment versus its discontinuation in remitted manic patients. Am J Psychiatry 2004;161:169-71.
18. Fowler RC, McCabe MS, Cadoret RJ, Winokur G. The validity of good prognosis schizophrenia. Arch Gen Psychiatry 1972;26:182-5.
19. Harrow M, Grossman LS, Silverstein ML, Meltzer HY. Thought pathology in manic and schizophrenic patients. Its occurrence at hospital admission and 7 weeks later. Arch Gen Psychiatry 1982;39:665-71.
20. Szasz TS. Schizophrenia: the sacred symbol of psychiatry. Br J Psychiatry 1976;129:308-16.
21. Carlson GA, Goodwin FK. The stages of mania. Arch Gen Psychiatry 1973;28:221-8.
22. Pini S, Cassano GB, Dell’Osso L, Amador XF. Insight into illness in schizophrenia, schizoaffective disorder, and mood disorders with psychotic features. Am J Psychiatry 2001;158:122-5.
23. Bertelsen A, Harvald B, Hauge M. A Danish twin study of manic-depressive illness. Br J Psychiatry 1977;130:330-51.
24. Green E, Elvidge G, Jacobson N, et al. Localization of bipolar susceptibility locus by molecular genetic analysis of the chromosome 12q23-q24 region in two pedigrees with bipolar disorder and Darier’s disease. Am J Psychiatry 2005;162:35-42.
1. Berrettini WH. Molecular linkage studies of bipolar disorders. Bipolar Disord 2001;3:276-83.
2. Belmaker RH. Bipolar disorder. N Engl J Med 2004;351:476-86.
3. Pope HG, Lipinski JF. Diagnosis in schizophrenia and manic-depressive illness, a reassessment of the specificity of “schizophrenic” symptoms in the light of current research. Arch Gen Psychiatry 1978;35:811-28.
4. Lake CR, Hurwitz N. Schizoaffective disorders are psychotic mood disorders; there are no schizoaffective disorders. Psychiatry Res 2006 (in press).
5. Post RM. Transduction of psychosocial stress into the neurobiology of recurrent affective disorder. Am J Psychiatry 1992;149:999-1010.
6. Diagnostic and statistical manual of mental disorders 4th ed text rev. Washington, DC: American Psychiatric Association; 2000.
7. Carroll BT, Thomas C, Jayanti K, et al. Treating persistent catatonia when benzodiazepines fail. Current Psychiatry 2005;4:56-64.
8. Abrams R, Taylor MA. Catatonia, a prospective clinical study. Arch Gen Psychiatry 1976;33:579-81.
9. Pope HG. Distinguishing bipolar disorder from schizophrenia in clinical practice: Guidelines and case reports. Hosp Com Psychiatry 1983;34:322-8.
10. Schneider K. Clinical psychopathology. New York: Grune & Stratton; 1959.
11. Kraepelin E. Clinical psychiatry. New York: William Wood Co; 1913.
12. Bleuler E. Dementia praecox or the group of schizophrenias. New York: International Universities Press; 1911/1950.
13. Goodwin FK, Jamison KR. Manic-depressive illness. New York: Oxford University Press; 1990.
14. Calabrese JR, Shelton MD, Bowden CL, et al. Bipolar rapid cycling: Focus on depression as its hallmark. J Clin Psychiatry 2001;62:34-41.
15. Goodwin FK. The biology of recurrence: new directions for the pharmacologic bridge. J Clin Psychiatry 1989;50:40-4.
16. Dieperink ME, Sands JR. Bipolar mania with psychotic features: diagnosis and treatment. Psychiatr Ann 1996;26:633-7.
17. Zarate CA, Tohen M. Double-blind comparison of the continued use of antipsychotic treatment versus its discontinuation in remitted manic patients. Am J Psychiatry 2004;161:169-71.
18. Fowler RC, McCabe MS, Cadoret RJ, Winokur G. The validity of good prognosis schizophrenia. Arch Gen Psychiatry 1972;26:182-5.
19. Harrow M, Grossman LS, Silverstein ML, Meltzer HY. Thought pathology in manic and schizophrenic patients. Its occurrence at hospital admission and 7 weeks later. Arch Gen Psychiatry 1982;39:665-71.
20. Szasz TS. Schizophrenia: the sacred symbol of psychiatry. Br J Psychiatry 1976;129:308-16.
21. Carlson GA, Goodwin FK. The stages of mania. Arch Gen Psychiatry 1973;28:221-8.
22. Pini S, Cassano GB, Dell’Osso L, Amador XF. Insight into illness in schizophrenia, schizoaffective disorder, and mood disorders with psychotic features. Am J Psychiatry 2001;158:122-5.
23. Bertelsen A, Harvald B, Hauge M. A Danish twin study of manic-depressive illness. Br J Psychiatry 1977;130:330-51.
24. Green E, Elvidge G, Jacobson N, et al. Localization of bipolar susceptibility locus by molecular genetic analysis of the chromosome 12q23-q24 region in two pedigrees with bipolar disorder and Darier’s disease. Am J Psychiatry 2005;162:35-42.
When a child can’t sleep, start by treating the parents
Sleep problems are very common in children but more complicated to manage than in adults. That’s because you usually must consider the parents’ opinions in making the child’s diagnosis and change the parents’ behavior for the treatment to succeed.
This article describes sleep disorders of children and adolescents, the most effective behavioral therapies, and the limited situations when hypnotic therapy may be appropriate.
A Symptom, Not a Diagnosis
Pediatric insomnia is significant difficulty in initiating and/or maintaining sleep that impairs a child’s or caregiver’s daytime function (Table 1).1-4 Childhood sleep disorders may manifest primarily as daytime sleepiness and neurobehavioral symptoms or occur with comorbid psychiatric diagnoses such as depression, anxiety, or attention-deficit/hyperactivity disorder (ADHD).
It is important to view insomnia as a symptom—not a diagnosis. Causes of insomnia in children may be medical (drug-related, pain-induced, or obstructive sleep apnea syndrome), behavioral (poor sleep hygiene or negative sleep-onset associations), or multiple factors (Table 2).
Sleep hygiene. Before starting therapy, educate parents and children about normal sleep development and sleep hygiene, which includes:
- environmental factors (temperature, noise, ambient light)
- scheduling (regular sleep-wake schedule)
- sleep practice (bedtime routine)
- physiologic factors (exercise, timing of meals, caffeine intake).
- insufficient sleep for individual physiologic needs (“lifestyle” sleep restriction, delayed sleep onset related to behavioral insomnia)
- adequate sleep but fragmented or disrupted by conditions such as obstructive sleep apnea or periodic limb movement disorder that cause frequent or prolonged arousals
- primary disorders of excessive daytime sleepiness such as narcolepsy (less common than in adults but under-recognized in children and adolescents)
- circadian rhythm disorders in which sleep is usually normal in structure and duration but occurs at an undesired time (delayed sleep phase syndrome).
Table 1
Insomnia’s negative effects on children and adolescents
| Problem | Manifestations |
|---|---|
| Daytime sleepiness | Yawning, rubbing eyes, resting head on desk |
| Neurocognitive dysfunction | Decreased cognitive flexibility and verbal creativity |
| Poor abstract reasoning | |
| Impaired motor skills | |
| Decreased attention and vigilance | |
| Memory impairment | |
| Externalizing behaviors | Increased impulsivity, hyperactivity, and aggressiveness |
| Mood dysregulation | Increased irritability |
| Decreased positive mood | |
| Poor affect modulation | |
| Source: References 1-4 | |
Diagnostic types of pediatric insomnia
| Diagnosis | Characteristics |
|---|---|
| Behavioral insomnia of childhood | Learned behaviors that interfere with sleep onset or maintenance |
| Sleep-onset association | Prolonged nighttime arousals because child can fall asleep only with certain sleep associations, such as being soothed by parent |
| Limit-setting subtype | Active resistance, verbal protests, and repeated demands by child at bedtime |
| Psychophysiologic insomnia | Conditioned anxiety about sleep difficulty heightens physiologic and emotional arousal, further compromising ability to sleep |
| Delayed sleep phase disorder | Common in adolescents; persistent phase shift in sleep-wake schedule (later bedtime and wake time) that conflicts with school and lifestyle demands |
| Secondary insomnia | Not primary; related to other diagnoses or factors |
| Psychiatric disorders | Depression, anxiety, posttraumatic stress disorder, attention-deficit/hyperactivity disorder |
| Medical disorders | Obstructive sleep apnea syndrome, pain |
| Medication | Psychostimulants used to treat ADHD and antidepressants used for major depression may cause sleep-onset delay |
With Psychiatric Disorders
Sleep disturbances can profoundly affect the clinical presentation, severity, and management of psychiatric disorders in children and adolescents.5-7 Up to 75% of children with a major depressive disorder have insomnia (severe in 30%), and one-third of depressed adolescents have delayed sleep-onset. Sleep complaints—especially bedtime resistance, refusal to sleep alone, increased nighttime fears, and nightmares—are also common in anxious children and those who have experienced severe trauma (including physical and sexual abuse).
Growing evidence suggests that pediatric “primary” insomnia with no concurrent psychiatric disorder is a risk factor for developing psychiatric conditions later in life—particularly depressive and anxiety disorders. Psychotropics such as psychostimulants and antidepressants also may interfere with sleep.
ADHD. Parents often report that children with ADHD have sleep disturbances, especially difficulty initiating sleep, poor sleep quality, restless sleep, frequent nighttime arousals, and shortened sleep duration.8 Parental observations notwithstanding, most objective methods of examining sleep and sleep architecture (polysomnography, actigraphy) have shown few or inconsistent differences between children with ADHD and controls.
Sleep problems in children with ADHD are often multifactorial. Potential causes include:
- psychostimulant-mediated sleep-onset delay
- bedtime resistance related to comorbid anxiety, oppositional defiant disorder, or circadian phase delay
- settling difficulties related to deficits in sensory integration associated with ADHD.
When managing a child with ADHD, evaluate comorbid sleep problems and provide diagnostically driven behavioral and/or drug therapy.
Behavioral Insomnia of Childhood
Behavioral insomnia of childhood may manifest as sleep-onset association and limit-setting types.9 The two often coexist, and many children present with both bedtime delays and nighttime arousals.
Sleep-onset association type. The presenting problem is usually prolonged nighttime arousals resulting in insufficient sleep. The child has learned to fall asleep only with sleep associations, such as being soothed by a parent, that usually are available at bedtime.
During the night, when the child experiences the type of brief arousal that normally occurs at the end of each sleep cycle (every 60 to 90 minutes) or awakens for other reasons, he is unable to get back to sleep (“self-soothe”) unless those same conditions are available to him. The child then “signals” the caregiver by crying (or coming into the parents’ bedroom) until the necessary associations are provided.
Limit-setting type is characterized by active resistance, verbal protests, and repeated demands at bedtime (“curtain calls”) rather than nighttime arousals. If sufficiently prolonged, the sleep-onset delay may result in inadequate sleep duration.
Sometimes bedtime resistance is related to:
- an underlying problem (a medical condition such as asthma or medication use, a sleep disorder such as restless legs, or anxiety)
- a mismatch between the child’s intrinsic circadian preferences (“night owl”) and parental expectations.
Behavioral therapy can alleviate bedtime resistance and nighttime arousals in young children.10 Controlled group studies strongly support three techniques: unmodified extinction, graduated extinction, and preventive parental education (Table 3).
To use graduated extinction, tell parents to ignore bedtime crying and tantrums for specified periods before checking. Tailor the duration or interval between check-ins to the child’s age and temperament; the limiting factor is how much crying the parents can tolerate, as checking is often more to reassure them than the child.
For younger children, parents might check every 2 minutes initially, then gradually lengthen to 5-, 10-, and 15-minute intervals. A common scenario is to double the time between each successive check-in (2 minutes, 4 minutes, 8 minutes, etc.). For older children, checking could start at 5- or 10-minute intervals.
During check-ins, the parents briefly comfort the child (usually 15 seconds to 1 minute). Advise parents to minimize interactions that may reinforce the child’s attention-seeking behavior.
To treat limit-setting sleep problems, recommend a combination of:
- decreased parental attention to bedtime-delaying behavior
- establishing a consistent bedtime routine that does not include stimulating activities such as television viewing
- bedtime “fading” (temporarily setting bedtime to the current sleep-onset time and then gradually advancing bedtime)
- positive reinforcement (sticker charts) for appropriate behavior at bedtime.
Behavioral treatment strategies require parental consistency to avoid inadvertently reinforcing nighttime arousals. Warn parents that children’s protests frequently escalate temporarily as treatment begins (“postextinction burst”).
How parents define a sleep “problem” and how well they accept your treatment recommendations can depend on their cultural values and beliefs about sleep’s meaning, importance, and role in daily life. Family attitudes vary about solitary sleep versus co-sleeping and about offering children transitional objects such as a blanket or toy to help them sleep.
Parents who repeatedly fail to start or enforce behavioral management may have other issues to address, such as depression or marital conflict.
Table 3
3 treatments for behavioral insomnia of childhood
| Treatment | Definition/examples |
|---|---|
| Extinction | Withdrawing parental assistance at sleep onset and during the night (‘systematic ignoring’) |
| Graduated extinction | Gradual rather than abrupt extinction treatment |
| For toddlers, parents check child briefly at successively longer intervals during wake-sleep transition | |
| For older children, parents introduce transitional sleep association objects (a blanket or toy) and use positive reinforcement (stickers for remaining in bed) | |
| Preventive parental education | Parents must consistently use behavioral treatment strategies to avoid reinforcing the child’s nighttime arousals |
Psychophysiologic Insomnia
Psychophysiologic insomnia (sleep onset and/or maintenance) occurs primarily in older children and adolescents and results from:
- predisposing factors (genetic vulnerability, underlying medical or psychiatric conditions)
- precipitating factors (acute stress)
- perpetuating factors (poor sleep habits, caffeine use, maladaptive thoughts about sleep).
- using the bed only for sleep
- getting out of bed if unable to fall asleep (stimulus control)
- restricting time in bed to actual time asleep (sleep restriction)
- learning relaxation techniques to reduce anxiety.
12 The problem is the timing rather than quality of sleep.
Sleep quantity may be compromised if the individual must arise before obtaining adequate sleep. Sleep-onset delays resolve, however, when the patient is allowed to follow his or her preferred later bedtime and wake time.
The typical DSPS sleep-wake pattern is a consistently preferred bedtime/sleep-onset time after midnight and wake time after 10 AM on weekdays and weekends. Adolescents with DSPS often complain of sleep-onset insomnia, extreme difficulty waking in the morning, and profound daytime sleepiness.
A 1- to 2-hour phase shift to a later bedtime and wake time is part of normal pubertal development and has been cited as a rationale for delaying high school start times. The phase shift in DSPS is typically much more dramatic and intractable than the norm.
Treatment options for DSPS include:
- strict sleep-wake schedule (such as 9:30 or 10 PM to 6:30 AM on school nights, with no more than a 1-hour discrepancy on non-school nights)
- melatonin, 3 to 5 mg, given 3 to 4 hours before the desired bedtime, if sleep schedule strategies are unsuccessful
- bright-light therapy in the morning to suppress melatonin secretion and “reset” the body clock, especially if morning waking is particularly difficult.13
If the adolescent also has school avoidance or a mood disorder—which is often the case—noncompliance with treatment is common. More-intensive behavioral and medication approaches may be needed.
Use Hypnotics?
Most insomnia in children and adolescents can be managed from infancy on with behavior therapy alone. If not, combined behavioral and drug interventions may be appropriate, such as when:
- the family is overwhelmed by the sleep problem and cannot execute behavioral strategies
- the child’s safety is at risk (engaging in dangerous activities during night awakenings, for example)
- treating specific populations (such as children with ADHD or autistic disorders).
- antihistamines such as diphenhydramine
- tricyclic antidepressants (amitriptyline, trazodone, and others)
- benzodiazepines (clonazepam)
- nonbenzodiazepine hypnotics (zolpidem, zaleplon)
- alpha-agonists (clonidine).14,15
Use these medications with caution in children, as safety and tolerability are unknown. Prescribe the lowest dosage for the briefest time possible, and use in combination with behavioral management strategies. Choose the shortest-acting agents to avoid morning grogginess. Chloral hydrate and barbiturates are rarely indicated in children because of side effects.
Over-the-counter products. Parents often use nonprescription products such as diphenhydramine, melatonin, and herbal preparations to treat children’s sleep problems, with or without a clinician’s recommendation. Most herbal preparations are generally safe but remain untested in pediatric patients.
Antihistamines such as diphenhydramine are generally well-tolerated, but they may have a paradoxical agitating effect. Tolerance also tends to develop, leading to increasing doses. Parents may inadvertently overdose a child by giving multiple nonprescription products with diphenhydramine as the active ingredient (such as combining Benadryl with Tylenol PM).
Related resources
- National Sleep Foundation. Information for patients and clinicians. www.sleepfoundation.org.
- American Academy of Sleep Medicine. Professional and patient resources and links. www.aasmnet.org.
- Mindell J, Owens J. A clinical guide to pediatric sleep: diagnosis and management of sleep problems in children and adolescents. Philadelphia: Lippincott Williams and Wilkins; 2003.
- Owens J, Mindell J. Take charge of your child’s sleep: the all-in-one resource for solving sleep problems in kids and teens. New York: Marlowe & Co.; 2005.
- Amitriptyline • Elavil
- Clonazepam • Klonopin
- Clonidine • Catapres
- Diphenhydramine • Benadryl and others (nonprescription)
- Divalproex sodium • Depakote
- Mirtazapine • Remeron
- Risperidone • Risperdal
- Trazodone • Desyrel
- Zaleplon • Sonata
- Zolpidem • Ambien
Dr. Owens receives research support from Sepracor, Eli Lilly & Co., and Cephalon; is a consultant to Eli Lilly & Co., Cephalon, and Shire; and is a speaker for Eli Lilly & Co., Cephalon, and Johnson & Johnson.
1. Fallone G, Owens J, Deane J. Sleepiness in children and adolescents: clinical implications. Sleep Med Rev 2002;6(2):287-306.
2. Smedje H, Broman JE, Hetta J. Associations between disturbed sleep and behavioural difficulties in 635 children aged 6-8 years: a study based on parents’ perceptions. Eur Child Adolesc Psychiatry 2001;10(1):1-9.
3. Dahl RE. The regulation of sleep and arousal: development and psychopathology. Dev Psychopathol 1996;8:3-27.
4. Randazzo AC, Muehlbach MJ, Schweitzer PK, Walsh JK. Cognitive function following acute sleep restriction in children ages 10-14. Sleep 1998;21:861-8.
5. Sadeh A, McGuire JP, Sachs H. Sleep and psychological characteristics of children on a psychiatric inpatient unit. J Am Acad Child Adolesc Psychiatry 1995;33:1303-46.
6. Sachs H, McGuire J, Sadeh A, et al. Cognitive and behavioural correlates of mother-reported sleep problems in psychiatrically hospitalized children. Sleep Res 1994;23:207-13.
7. Dahl RE, Ryan ND, Matty MK, et al. Sleep onset abnormalities in depressed adolescents. Biol Psychiatry 1996;39:400-10.
8. Owens J. The ADHD and sleep conundrum: A review. J Develop Behav Pediatr 2005;26(4):312-22.
9. The International Classification of Sleep Disorders. Diagnosis and Coding Manual (ICSD-2) (2nd ed). Westchester, IL: American Academy of Sleep Medicine; 2005.
10. Mindell J, Kuhn B, Lewin D, et al. Behavioral treatment of bedtime problems and night wakings in infants and young children. An American Academy of Sleep Medicine Review. Sleep. In press.
11. Hohagen F. Nonpharmacologic treatment of insomnia. Sleep 1996;19(8):S50-51.
12. Garcia J, Rosen G, Mahowald M. Circadian rhythms and circadian rhythm disturbances in children and adolescents. Semin Pediatr Neurol 2001;8:229-40.
13. Sack RL, Lewy AJ, Hughes RJ. Use of melatonin for sleep and circadian rhythm disorders. Ann Med 1998;30:115-21.
14. Owens J, Rosen C, Mindell J. Medication use in the treatment of pediatric insomnia: results of a survey of community-based pediatricians. Pediatrics 2003;111(5):e628-35.
15. Owens J, Babcock D, Blumer J, et al. The use of pharmacotherapy in the treatment of pediatric insomnia in primary care: rational approaches. A consensus meeting summary. J Clin Sleep Med 2005;1(1):49-59.
Sleep problems are very common in children but more complicated to manage than in adults. That’s because you usually must consider the parents’ opinions in making the child’s diagnosis and change the parents’ behavior for the treatment to succeed.
This article describes sleep disorders of children and adolescents, the most effective behavioral therapies, and the limited situations when hypnotic therapy may be appropriate.
A Symptom, Not a Diagnosis
Pediatric insomnia is significant difficulty in initiating and/or maintaining sleep that impairs a child’s or caregiver’s daytime function (Table 1).1-4 Childhood sleep disorders may manifest primarily as daytime sleepiness and neurobehavioral symptoms or occur with comorbid psychiatric diagnoses such as depression, anxiety, or attention-deficit/hyperactivity disorder (ADHD).
It is important to view insomnia as a symptom—not a diagnosis. Causes of insomnia in children may be medical (drug-related, pain-induced, or obstructive sleep apnea syndrome), behavioral (poor sleep hygiene or negative sleep-onset associations), or multiple factors (Table 2).
Sleep hygiene. Before starting therapy, educate parents and children about normal sleep development and sleep hygiene, which includes:
- environmental factors (temperature, noise, ambient light)
- scheduling (regular sleep-wake schedule)
- sleep practice (bedtime routine)
- physiologic factors (exercise, timing of meals, caffeine intake).
- insufficient sleep for individual physiologic needs (“lifestyle” sleep restriction, delayed sleep onset related to behavioral insomnia)
- adequate sleep but fragmented or disrupted by conditions such as obstructive sleep apnea or periodic limb movement disorder that cause frequent or prolonged arousals
- primary disorders of excessive daytime sleepiness such as narcolepsy (less common than in adults but under-recognized in children and adolescents)
- circadian rhythm disorders in which sleep is usually normal in structure and duration but occurs at an undesired time (delayed sleep phase syndrome).
Table 1
Insomnia’s negative effects on children and adolescents
| Problem | Manifestations |
|---|---|
| Daytime sleepiness | Yawning, rubbing eyes, resting head on desk |
| Neurocognitive dysfunction | Decreased cognitive flexibility and verbal creativity |
| Poor abstract reasoning | |
| Impaired motor skills | |
| Decreased attention and vigilance | |
| Memory impairment | |
| Externalizing behaviors | Increased impulsivity, hyperactivity, and aggressiveness |
| Mood dysregulation | Increased irritability |
| Decreased positive mood | |
| Poor affect modulation | |
| Source: References 1-4 | |
Diagnostic types of pediatric insomnia
| Diagnosis | Characteristics |
|---|---|
| Behavioral insomnia of childhood | Learned behaviors that interfere with sleep onset or maintenance |
| Sleep-onset association | Prolonged nighttime arousals because child can fall asleep only with certain sleep associations, such as being soothed by parent |
| Limit-setting subtype | Active resistance, verbal protests, and repeated demands by child at bedtime |
| Psychophysiologic insomnia | Conditioned anxiety about sleep difficulty heightens physiologic and emotional arousal, further compromising ability to sleep |
| Delayed sleep phase disorder | Common in adolescents; persistent phase shift in sleep-wake schedule (later bedtime and wake time) that conflicts with school and lifestyle demands |
| Secondary insomnia | Not primary; related to other diagnoses or factors |
| Psychiatric disorders | Depression, anxiety, posttraumatic stress disorder, attention-deficit/hyperactivity disorder |
| Medical disorders | Obstructive sleep apnea syndrome, pain |
| Medication | Psychostimulants used to treat ADHD and antidepressants used for major depression may cause sleep-onset delay |
With Psychiatric Disorders
Sleep disturbances can profoundly affect the clinical presentation, severity, and management of psychiatric disorders in children and adolescents.5-7 Up to 75% of children with a major depressive disorder have insomnia (severe in 30%), and one-third of depressed adolescents have delayed sleep-onset. Sleep complaints—especially bedtime resistance, refusal to sleep alone, increased nighttime fears, and nightmares—are also common in anxious children and those who have experienced severe trauma (including physical and sexual abuse).
Growing evidence suggests that pediatric “primary” insomnia with no concurrent psychiatric disorder is a risk factor for developing psychiatric conditions later in life—particularly depressive and anxiety disorders. Psychotropics such as psychostimulants and antidepressants also may interfere with sleep.
ADHD. Parents often report that children with ADHD have sleep disturbances, especially difficulty initiating sleep, poor sleep quality, restless sleep, frequent nighttime arousals, and shortened sleep duration.8 Parental observations notwithstanding, most objective methods of examining sleep and sleep architecture (polysomnography, actigraphy) have shown few or inconsistent differences between children with ADHD and controls.
Sleep problems in children with ADHD are often multifactorial. Potential causes include:
- psychostimulant-mediated sleep-onset delay
- bedtime resistance related to comorbid anxiety, oppositional defiant disorder, or circadian phase delay
- settling difficulties related to deficits in sensory integration associated with ADHD.
When managing a child with ADHD, evaluate comorbid sleep problems and provide diagnostically driven behavioral and/or drug therapy.
Behavioral Insomnia of Childhood
Behavioral insomnia of childhood may manifest as sleep-onset association and limit-setting types.9 The two often coexist, and many children present with both bedtime delays and nighttime arousals.
Sleep-onset association type. The presenting problem is usually prolonged nighttime arousals resulting in insufficient sleep. The child has learned to fall asleep only with sleep associations, such as being soothed by a parent, that usually are available at bedtime.
During the night, when the child experiences the type of brief arousal that normally occurs at the end of each sleep cycle (every 60 to 90 minutes) or awakens for other reasons, he is unable to get back to sleep (“self-soothe”) unless those same conditions are available to him. The child then “signals” the caregiver by crying (or coming into the parents’ bedroom) until the necessary associations are provided.
Limit-setting type is characterized by active resistance, verbal protests, and repeated demands at bedtime (“curtain calls”) rather than nighttime arousals. If sufficiently prolonged, the sleep-onset delay may result in inadequate sleep duration.
Sometimes bedtime resistance is related to:
- an underlying problem (a medical condition such as asthma or medication use, a sleep disorder such as restless legs, or anxiety)
- a mismatch between the child’s intrinsic circadian preferences (“night owl”) and parental expectations.
Behavioral therapy can alleviate bedtime resistance and nighttime arousals in young children.10 Controlled group studies strongly support three techniques: unmodified extinction, graduated extinction, and preventive parental education (Table 3).
To use graduated extinction, tell parents to ignore bedtime crying and tantrums for specified periods before checking. Tailor the duration or interval between check-ins to the child’s age and temperament; the limiting factor is how much crying the parents can tolerate, as checking is often more to reassure them than the child.
For younger children, parents might check every 2 minutes initially, then gradually lengthen to 5-, 10-, and 15-minute intervals. A common scenario is to double the time between each successive check-in (2 minutes, 4 minutes, 8 minutes, etc.). For older children, checking could start at 5- or 10-minute intervals.
During check-ins, the parents briefly comfort the child (usually 15 seconds to 1 minute). Advise parents to minimize interactions that may reinforce the child’s attention-seeking behavior.
To treat limit-setting sleep problems, recommend a combination of:
- decreased parental attention to bedtime-delaying behavior
- establishing a consistent bedtime routine that does not include stimulating activities such as television viewing
- bedtime “fading” (temporarily setting bedtime to the current sleep-onset time and then gradually advancing bedtime)
- positive reinforcement (sticker charts) for appropriate behavior at bedtime.
Behavioral treatment strategies require parental consistency to avoid inadvertently reinforcing nighttime arousals. Warn parents that children’s protests frequently escalate temporarily as treatment begins (“postextinction burst”).
How parents define a sleep “problem” and how well they accept your treatment recommendations can depend on their cultural values and beliefs about sleep’s meaning, importance, and role in daily life. Family attitudes vary about solitary sleep versus co-sleeping and about offering children transitional objects such as a blanket or toy to help them sleep.
Parents who repeatedly fail to start or enforce behavioral management may have other issues to address, such as depression or marital conflict.
Table 3
3 treatments for behavioral insomnia of childhood
| Treatment | Definition/examples |
|---|---|
| Extinction | Withdrawing parental assistance at sleep onset and during the night (‘systematic ignoring’) |
| Graduated extinction | Gradual rather than abrupt extinction treatment |
| For toddlers, parents check child briefly at successively longer intervals during wake-sleep transition | |
| For older children, parents introduce transitional sleep association objects (a blanket or toy) and use positive reinforcement (stickers for remaining in bed) | |
| Preventive parental education | Parents must consistently use behavioral treatment strategies to avoid reinforcing the child’s nighttime arousals |
Psychophysiologic Insomnia
Psychophysiologic insomnia (sleep onset and/or maintenance) occurs primarily in older children and adolescents and results from:
- predisposing factors (genetic vulnerability, underlying medical or psychiatric conditions)
- precipitating factors (acute stress)
- perpetuating factors (poor sleep habits, caffeine use, maladaptive thoughts about sleep).
- using the bed only for sleep
- getting out of bed if unable to fall asleep (stimulus control)
- restricting time in bed to actual time asleep (sleep restriction)
- learning relaxation techniques to reduce anxiety.
12 The problem is the timing rather than quality of sleep.
Sleep quantity may be compromised if the individual must arise before obtaining adequate sleep. Sleep-onset delays resolve, however, when the patient is allowed to follow his or her preferred later bedtime and wake time.
The typical DSPS sleep-wake pattern is a consistently preferred bedtime/sleep-onset time after midnight and wake time after 10 AM on weekdays and weekends. Adolescents with DSPS often complain of sleep-onset insomnia, extreme difficulty waking in the morning, and profound daytime sleepiness.
A 1- to 2-hour phase shift to a later bedtime and wake time is part of normal pubertal development and has been cited as a rationale for delaying high school start times. The phase shift in DSPS is typically much more dramatic and intractable than the norm.
Treatment options for DSPS include:
- strict sleep-wake schedule (such as 9:30 or 10 PM to 6:30 AM on school nights, with no more than a 1-hour discrepancy on non-school nights)
- melatonin, 3 to 5 mg, given 3 to 4 hours before the desired bedtime, if sleep schedule strategies are unsuccessful
- bright-light therapy in the morning to suppress melatonin secretion and “reset” the body clock, especially if morning waking is particularly difficult.13
If the adolescent also has school avoidance or a mood disorder—which is often the case—noncompliance with treatment is common. More-intensive behavioral and medication approaches may be needed.
Use Hypnotics?
Most insomnia in children and adolescents can be managed from infancy on with behavior therapy alone. If not, combined behavioral and drug interventions may be appropriate, such as when:
- the family is overwhelmed by the sleep problem and cannot execute behavioral strategies
- the child’s safety is at risk (engaging in dangerous activities during night awakenings, for example)
- treating specific populations (such as children with ADHD or autistic disorders).
- antihistamines such as diphenhydramine
- tricyclic antidepressants (amitriptyline, trazodone, and others)
- benzodiazepines (clonazepam)
- nonbenzodiazepine hypnotics (zolpidem, zaleplon)
- alpha-agonists (clonidine).14,15
Use these medications with caution in children, as safety and tolerability are unknown. Prescribe the lowest dosage for the briefest time possible, and use in combination with behavioral management strategies. Choose the shortest-acting agents to avoid morning grogginess. Chloral hydrate and barbiturates are rarely indicated in children because of side effects.
Over-the-counter products. Parents often use nonprescription products such as diphenhydramine, melatonin, and herbal preparations to treat children’s sleep problems, with or without a clinician’s recommendation. Most herbal preparations are generally safe but remain untested in pediatric patients.
Antihistamines such as diphenhydramine are generally well-tolerated, but they may have a paradoxical agitating effect. Tolerance also tends to develop, leading to increasing doses. Parents may inadvertently overdose a child by giving multiple nonprescription products with diphenhydramine as the active ingredient (such as combining Benadryl with Tylenol PM).
Related resources
- National Sleep Foundation. Information for patients and clinicians. www.sleepfoundation.org.
- American Academy of Sleep Medicine. Professional and patient resources and links. www.aasmnet.org.
- Mindell J, Owens J. A clinical guide to pediatric sleep: diagnosis and management of sleep problems in children and adolescents. Philadelphia: Lippincott Williams and Wilkins; 2003.
- Owens J, Mindell J. Take charge of your child’s sleep: the all-in-one resource for solving sleep problems in kids and teens. New York: Marlowe & Co.; 2005.
- Amitriptyline • Elavil
- Clonazepam • Klonopin
- Clonidine • Catapres
- Diphenhydramine • Benadryl and others (nonprescription)
- Divalproex sodium • Depakote
- Mirtazapine • Remeron
- Risperidone • Risperdal
- Trazodone • Desyrel
- Zaleplon • Sonata
- Zolpidem • Ambien
Dr. Owens receives research support from Sepracor, Eli Lilly & Co., and Cephalon; is a consultant to Eli Lilly & Co., Cephalon, and Shire; and is a speaker for Eli Lilly & Co., Cephalon, and Johnson & Johnson.
Sleep problems are very common in children but more complicated to manage than in adults. That’s because you usually must consider the parents’ opinions in making the child’s diagnosis and change the parents’ behavior for the treatment to succeed.
This article describes sleep disorders of children and adolescents, the most effective behavioral therapies, and the limited situations when hypnotic therapy may be appropriate.
A Symptom, Not a Diagnosis
Pediatric insomnia is significant difficulty in initiating and/or maintaining sleep that impairs a child’s or caregiver’s daytime function (Table 1).1-4 Childhood sleep disorders may manifest primarily as daytime sleepiness and neurobehavioral symptoms or occur with comorbid psychiatric diagnoses such as depression, anxiety, or attention-deficit/hyperactivity disorder (ADHD).
It is important to view insomnia as a symptom—not a diagnosis. Causes of insomnia in children may be medical (drug-related, pain-induced, or obstructive sleep apnea syndrome), behavioral (poor sleep hygiene or negative sleep-onset associations), or multiple factors (Table 2).
Sleep hygiene. Before starting therapy, educate parents and children about normal sleep development and sleep hygiene, which includes:
- environmental factors (temperature, noise, ambient light)
- scheduling (regular sleep-wake schedule)
- sleep practice (bedtime routine)
- physiologic factors (exercise, timing of meals, caffeine intake).
- insufficient sleep for individual physiologic needs (“lifestyle” sleep restriction, delayed sleep onset related to behavioral insomnia)
- adequate sleep but fragmented or disrupted by conditions such as obstructive sleep apnea or periodic limb movement disorder that cause frequent or prolonged arousals
- primary disorders of excessive daytime sleepiness such as narcolepsy (less common than in adults but under-recognized in children and adolescents)
- circadian rhythm disorders in which sleep is usually normal in structure and duration but occurs at an undesired time (delayed sleep phase syndrome).
Table 1
Insomnia’s negative effects on children and adolescents
| Problem | Manifestations |
|---|---|
| Daytime sleepiness | Yawning, rubbing eyes, resting head on desk |
| Neurocognitive dysfunction | Decreased cognitive flexibility and verbal creativity |
| Poor abstract reasoning | |
| Impaired motor skills | |
| Decreased attention and vigilance | |
| Memory impairment | |
| Externalizing behaviors | Increased impulsivity, hyperactivity, and aggressiveness |
| Mood dysregulation | Increased irritability |
| Decreased positive mood | |
| Poor affect modulation | |
| Source: References 1-4 | |
Diagnostic types of pediatric insomnia
| Diagnosis | Characteristics |
|---|---|
| Behavioral insomnia of childhood | Learned behaviors that interfere with sleep onset or maintenance |
| Sleep-onset association | Prolonged nighttime arousals because child can fall asleep only with certain sleep associations, such as being soothed by parent |
| Limit-setting subtype | Active resistance, verbal protests, and repeated demands by child at bedtime |
| Psychophysiologic insomnia | Conditioned anxiety about sleep difficulty heightens physiologic and emotional arousal, further compromising ability to sleep |
| Delayed sleep phase disorder | Common in adolescents; persistent phase shift in sleep-wake schedule (later bedtime and wake time) that conflicts with school and lifestyle demands |
| Secondary insomnia | Not primary; related to other diagnoses or factors |
| Psychiatric disorders | Depression, anxiety, posttraumatic stress disorder, attention-deficit/hyperactivity disorder |
| Medical disorders | Obstructive sleep apnea syndrome, pain |
| Medication | Psychostimulants used to treat ADHD and antidepressants used for major depression may cause sleep-onset delay |
With Psychiatric Disorders
Sleep disturbances can profoundly affect the clinical presentation, severity, and management of psychiatric disorders in children and adolescents.5-7 Up to 75% of children with a major depressive disorder have insomnia (severe in 30%), and one-third of depressed adolescents have delayed sleep-onset. Sleep complaints—especially bedtime resistance, refusal to sleep alone, increased nighttime fears, and nightmares—are also common in anxious children and those who have experienced severe trauma (including physical and sexual abuse).
Growing evidence suggests that pediatric “primary” insomnia with no concurrent psychiatric disorder is a risk factor for developing psychiatric conditions later in life—particularly depressive and anxiety disorders. Psychotropics such as psychostimulants and antidepressants also may interfere with sleep.
ADHD. Parents often report that children with ADHD have sleep disturbances, especially difficulty initiating sleep, poor sleep quality, restless sleep, frequent nighttime arousals, and shortened sleep duration.8 Parental observations notwithstanding, most objective methods of examining sleep and sleep architecture (polysomnography, actigraphy) have shown few or inconsistent differences between children with ADHD and controls.
Sleep problems in children with ADHD are often multifactorial. Potential causes include:
- psychostimulant-mediated sleep-onset delay
- bedtime resistance related to comorbid anxiety, oppositional defiant disorder, or circadian phase delay
- settling difficulties related to deficits in sensory integration associated with ADHD.
When managing a child with ADHD, evaluate comorbid sleep problems and provide diagnostically driven behavioral and/or drug therapy.
Behavioral Insomnia of Childhood
Behavioral insomnia of childhood may manifest as sleep-onset association and limit-setting types.9 The two often coexist, and many children present with both bedtime delays and nighttime arousals.
Sleep-onset association type. The presenting problem is usually prolonged nighttime arousals resulting in insufficient sleep. The child has learned to fall asleep only with sleep associations, such as being soothed by a parent, that usually are available at bedtime.
During the night, when the child experiences the type of brief arousal that normally occurs at the end of each sleep cycle (every 60 to 90 minutes) or awakens for other reasons, he is unable to get back to sleep (“self-soothe”) unless those same conditions are available to him. The child then “signals” the caregiver by crying (or coming into the parents’ bedroom) until the necessary associations are provided.
Limit-setting type is characterized by active resistance, verbal protests, and repeated demands at bedtime (“curtain calls”) rather than nighttime arousals. If sufficiently prolonged, the sleep-onset delay may result in inadequate sleep duration.
Sometimes bedtime resistance is related to:
- an underlying problem (a medical condition such as asthma or medication use, a sleep disorder such as restless legs, or anxiety)
- a mismatch between the child’s intrinsic circadian preferences (“night owl”) and parental expectations.
Behavioral therapy can alleviate bedtime resistance and nighttime arousals in young children.10 Controlled group studies strongly support three techniques: unmodified extinction, graduated extinction, and preventive parental education (Table 3).
To use graduated extinction, tell parents to ignore bedtime crying and tantrums for specified periods before checking. Tailor the duration or interval between check-ins to the child’s age and temperament; the limiting factor is how much crying the parents can tolerate, as checking is often more to reassure them than the child.
For younger children, parents might check every 2 minutes initially, then gradually lengthen to 5-, 10-, and 15-minute intervals. A common scenario is to double the time between each successive check-in (2 minutes, 4 minutes, 8 minutes, etc.). For older children, checking could start at 5- or 10-minute intervals.
During check-ins, the parents briefly comfort the child (usually 15 seconds to 1 minute). Advise parents to minimize interactions that may reinforce the child’s attention-seeking behavior.
To treat limit-setting sleep problems, recommend a combination of:
- decreased parental attention to bedtime-delaying behavior
- establishing a consistent bedtime routine that does not include stimulating activities such as television viewing
- bedtime “fading” (temporarily setting bedtime to the current sleep-onset time and then gradually advancing bedtime)
- positive reinforcement (sticker charts) for appropriate behavior at bedtime.
Behavioral treatment strategies require parental consistency to avoid inadvertently reinforcing nighttime arousals. Warn parents that children’s protests frequently escalate temporarily as treatment begins (“postextinction burst”).
How parents define a sleep “problem” and how well they accept your treatment recommendations can depend on their cultural values and beliefs about sleep’s meaning, importance, and role in daily life. Family attitudes vary about solitary sleep versus co-sleeping and about offering children transitional objects such as a blanket or toy to help them sleep.
Parents who repeatedly fail to start or enforce behavioral management may have other issues to address, such as depression or marital conflict.
Table 3
3 treatments for behavioral insomnia of childhood
| Treatment | Definition/examples |
|---|---|
| Extinction | Withdrawing parental assistance at sleep onset and during the night (‘systematic ignoring’) |
| Graduated extinction | Gradual rather than abrupt extinction treatment |
| For toddlers, parents check child briefly at successively longer intervals during wake-sleep transition | |
| For older children, parents introduce transitional sleep association objects (a blanket or toy) and use positive reinforcement (stickers for remaining in bed) | |
| Preventive parental education | Parents must consistently use behavioral treatment strategies to avoid reinforcing the child’s nighttime arousals |
Psychophysiologic Insomnia
Psychophysiologic insomnia (sleep onset and/or maintenance) occurs primarily in older children and adolescents and results from:
- predisposing factors (genetic vulnerability, underlying medical or psychiatric conditions)
- precipitating factors (acute stress)
- perpetuating factors (poor sleep habits, caffeine use, maladaptive thoughts about sleep).
- using the bed only for sleep
- getting out of bed if unable to fall asleep (stimulus control)
- restricting time in bed to actual time asleep (sleep restriction)
- learning relaxation techniques to reduce anxiety.
12 The problem is the timing rather than quality of sleep.
Sleep quantity may be compromised if the individual must arise before obtaining adequate sleep. Sleep-onset delays resolve, however, when the patient is allowed to follow his or her preferred later bedtime and wake time.
The typical DSPS sleep-wake pattern is a consistently preferred bedtime/sleep-onset time after midnight and wake time after 10 AM on weekdays and weekends. Adolescents with DSPS often complain of sleep-onset insomnia, extreme difficulty waking in the morning, and profound daytime sleepiness.
A 1- to 2-hour phase shift to a later bedtime and wake time is part of normal pubertal development and has been cited as a rationale for delaying high school start times. The phase shift in DSPS is typically much more dramatic and intractable than the norm.
Treatment options for DSPS include:
- strict sleep-wake schedule (such as 9:30 or 10 PM to 6:30 AM on school nights, with no more than a 1-hour discrepancy on non-school nights)
- melatonin, 3 to 5 mg, given 3 to 4 hours before the desired bedtime, if sleep schedule strategies are unsuccessful
- bright-light therapy in the morning to suppress melatonin secretion and “reset” the body clock, especially if morning waking is particularly difficult.13
If the adolescent also has school avoidance or a mood disorder—which is often the case—noncompliance with treatment is common. More-intensive behavioral and medication approaches may be needed.
Use Hypnotics?
Most insomnia in children and adolescents can be managed from infancy on with behavior therapy alone. If not, combined behavioral and drug interventions may be appropriate, such as when:
- the family is overwhelmed by the sleep problem and cannot execute behavioral strategies
- the child’s safety is at risk (engaging in dangerous activities during night awakenings, for example)
- treating specific populations (such as children with ADHD or autistic disorders).
- antihistamines such as diphenhydramine
- tricyclic antidepressants (amitriptyline, trazodone, and others)
- benzodiazepines (clonazepam)
- nonbenzodiazepine hypnotics (zolpidem, zaleplon)
- alpha-agonists (clonidine).14,15
Use these medications with caution in children, as safety and tolerability are unknown. Prescribe the lowest dosage for the briefest time possible, and use in combination with behavioral management strategies. Choose the shortest-acting agents to avoid morning grogginess. Chloral hydrate and barbiturates are rarely indicated in children because of side effects.
Over-the-counter products. Parents often use nonprescription products such as diphenhydramine, melatonin, and herbal preparations to treat children’s sleep problems, with or without a clinician’s recommendation. Most herbal preparations are generally safe but remain untested in pediatric patients.
Antihistamines such as diphenhydramine are generally well-tolerated, but they may have a paradoxical agitating effect. Tolerance also tends to develop, leading to increasing doses. Parents may inadvertently overdose a child by giving multiple nonprescription products with diphenhydramine as the active ingredient (such as combining Benadryl with Tylenol PM).
Related resources
- National Sleep Foundation. Information for patients and clinicians. www.sleepfoundation.org.
- American Academy of Sleep Medicine. Professional and patient resources and links. www.aasmnet.org.
- Mindell J, Owens J. A clinical guide to pediatric sleep: diagnosis and management of sleep problems in children and adolescents. Philadelphia: Lippincott Williams and Wilkins; 2003.
- Owens J, Mindell J. Take charge of your child’s sleep: the all-in-one resource for solving sleep problems in kids and teens. New York: Marlowe & Co.; 2005.
- Amitriptyline • Elavil
- Clonazepam • Klonopin
- Clonidine • Catapres
- Diphenhydramine • Benadryl and others (nonprescription)
- Divalproex sodium • Depakote
- Mirtazapine • Remeron
- Risperidone • Risperdal
- Trazodone • Desyrel
- Zaleplon • Sonata
- Zolpidem • Ambien
Dr. Owens receives research support from Sepracor, Eli Lilly & Co., and Cephalon; is a consultant to Eli Lilly & Co., Cephalon, and Shire; and is a speaker for Eli Lilly & Co., Cephalon, and Johnson & Johnson.
1. Fallone G, Owens J, Deane J. Sleepiness in children and adolescents: clinical implications. Sleep Med Rev 2002;6(2):287-306.
2. Smedje H, Broman JE, Hetta J. Associations between disturbed sleep and behavioural difficulties in 635 children aged 6-8 years: a study based on parents’ perceptions. Eur Child Adolesc Psychiatry 2001;10(1):1-9.
3. Dahl RE. The regulation of sleep and arousal: development and psychopathology. Dev Psychopathol 1996;8:3-27.
4. Randazzo AC, Muehlbach MJ, Schweitzer PK, Walsh JK. Cognitive function following acute sleep restriction in children ages 10-14. Sleep 1998;21:861-8.
5. Sadeh A, McGuire JP, Sachs H. Sleep and psychological characteristics of children on a psychiatric inpatient unit. J Am Acad Child Adolesc Psychiatry 1995;33:1303-46.
6. Sachs H, McGuire J, Sadeh A, et al. Cognitive and behavioural correlates of mother-reported sleep problems in psychiatrically hospitalized children. Sleep Res 1994;23:207-13.
7. Dahl RE, Ryan ND, Matty MK, et al. Sleep onset abnormalities in depressed adolescents. Biol Psychiatry 1996;39:400-10.
8. Owens J. The ADHD and sleep conundrum: A review. J Develop Behav Pediatr 2005;26(4):312-22.
9. The International Classification of Sleep Disorders. Diagnosis and Coding Manual (ICSD-2) (2nd ed). Westchester, IL: American Academy of Sleep Medicine; 2005.
10. Mindell J, Kuhn B, Lewin D, et al. Behavioral treatment of bedtime problems and night wakings in infants and young children. An American Academy of Sleep Medicine Review. Sleep. In press.
11. Hohagen F. Nonpharmacologic treatment of insomnia. Sleep 1996;19(8):S50-51.
12. Garcia J, Rosen G, Mahowald M. Circadian rhythms and circadian rhythm disturbances in children and adolescents. Semin Pediatr Neurol 2001;8:229-40.
13. Sack RL, Lewy AJ, Hughes RJ. Use of melatonin for sleep and circadian rhythm disorders. Ann Med 1998;30:115-21.
14. Owens J, Rosen C, Mindell J. Medication use in the treatment of pediatric insomnia: results of a survey of community-based pediatricians. Pediatrics 2003;111(5):e628-35.
15. Owens J, Babcock D, Blumer J, et al. The use of pharmacotherapy in the treatment of pediatric insomnia in primary care: rational approaches. A consensus meeting summary. J Clin Sleep Med 2005;1(1):49-59.
1. Fallone G, Owens J, Deane J. Sleepiness in children and adolescents: clinical implications. Sleep Med Rev 2002;6(2):287-306.
2. Smedje H, Broman JE, Hetta J. Associations between disturbed sleep and behavioural difficulties in 635 children aged 6-8 years: a study based on parents’ perceptions. Eur Child Adolesc Psychiatry 2001;10(1):1-9.
3. Dahl RE. The regulation of sleep and arousal: development and psychopathology. Dev Psychopathol 1996;8:3-27.
4. Randazzo AC, Muehlbach MJ, Schweitzer PK, Walsh JK. Cognitive function following acute sleep restriction in children ages 10-14. Sleep 1998;21:861-8.
5. Sadeh A, McGuire JP, Sachs H. Sleep and psychological characteristics of children on a psychiatric inpatient unit. J Am Acad Child Adolesc Psychiatry 1995;33:1303-46.
6. Sachs H, McGuire J, Sadeh A, et al. Cognitive and behavioural correlates of mother-reported sleep problems in psychiatrically hospitalized children. Sleep Res 1994;23:207-13.
7. Dahl RE, Ryan ND, Matty MK, et al. Sleep onset abnormalities in depressed adolescents. Biol Psychiatry 1996;39:400-10.
8. Owens J. The ADHD and sleep conundrum: A review. J Develop Behav Pediatr 2005;26(4):312-22.
9. The International Classification of Sleep Disorders. Diagnosis and Coding Manual (ICSD-2) (2nd ed). Westchester, IL: American Academy of Sleep Medicine; 2005.
10. Mindell J, Kuhn B, Lewin D, et al. Behavioral treatment of bedtime problems and night wakings in infants and young children. An American Academy of Sleep Medicine Review. Sleep. In press.
11. Hohagen F. Nonpharmacologic treatment of insomnia. Sleep 1996;19(8):S50-51.
12. Garcia J, Rosen G, Mahowald M. Circadian rhythms and circadian rhythm disturbances in children and adolescents. Semin Pediatr Neurol 2001;8:229-40.
13. Sack RL, Lewy AJ, Hughes RJ. Use of melatonin for sleep and circadian rhythm disorders. Ann Med 1998;30:115-21.
14. Owens J, Rosen C, Mindell J. Medication use in the treatment of pediatric insomnia: results of a survey of community-based pediatricians. Pediatrics 2003;111(5):e628-35.
15. Owens J, Babcock D, Blumer J, et al. The use of pharmacotherapy in the treatment of pediatric insomnia in primary care: rational approaches. A consensus meeting summary. J Clin Sleep Med 2005;1(1):49-59.
Is your patient making the ‘wrong’ treatment choice?
Consultation/liaison (C/L) psychiatrists assess capacity in 1 of 6 consults,1 and these evaluations must be quick but systematic. Hospital time is precious, and asking for a psychiatry consult inevitably slows down the medical team’s efforts to care for sick or injured patients.
We suggest an approach our C/L service developed to rapidly weigh capacity’s three dimensions—risks, benefits, and patient decisions—to formulate appropriate opinions for the medical team.
A standard for capacity
In most cases, capacity must be assessed and considered adequate before a patient can provide informed consent for a medical intervention. Because a patient might be capable of making some decisions but not others, the standard for determining capacity is not black and white but a sliding scale that depends on the magnitude of the decision being made.
As physicians, psychiatrists understand doctors’ frustrations when they believe a patient is making the wrong treatment choice. When the primary team turns to us, they want us to help determine the most appropriate course of action.
Capacity is determined by weighing whether the patient is competent to exercise his or her autonomy in making a decision about medical treatment. We do not assess global capacity; the goal is to provide an unbiased opinion about specific capacity for a given situation–“Does Mr. X have the ability to accept/refuse this treatment option presented to him?”
Capacity’s three dimensions. The means to achieve this goal are often complex. Roth et al2 proposed that capacity could be measured on a sliding scale. Wise and Rundell3 agreed and developed a two-dimension table to show that capacity can be evaluated at different thresholds, depending on the patient’s clinical situation. We expanded this model (Figure) to include three dimensions to consider when you evaluate capacity:
- risk of the proposed treatment (high vs. low)
- benefit of the treatment (high vs. low)
- the patient’s decision about the treatment (accept vs. refuse).
If a treatment’s benefits far outweigh the risks and the patient accepts that treatment, he is probably capable of making that decision and a lenient (low) threshold to establish capacity applies. If the same patient refuses the high-benefit, low-risk treatment, then he might be incapable of making that decision and a stringent (high) threshold to establish capacity comes into play. Our C/L service often uses this model when discussing capacity evaluations with the primary team. It explains why some capacity evaluations—when a patient agrees to a low-risk, high-benefit procedure—might take minutes, whereas others—those that fall into the medium threshold for capacity—take hours. Consider the following cases.
Figure 3-dimension model for evaluating capacity
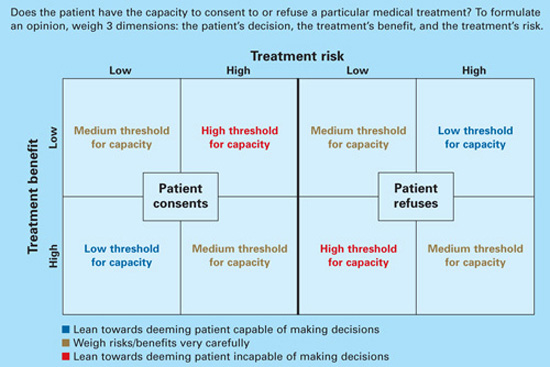
Three cases: Is capacity evaluation needed?
Mr. X, age 25, was in a motor vehicle accident that caused trauma to his esophagus. He requires a feeding tube because he will be unable to eat for several weeks. The risk of the procedure (feeding tube placement) is low, and the benefit (getting possibly life-saving nutrition) is high.
If Mr. X refuses the feeding tube, he may be incapable of making this decision and would require a rigorous capacity evaluation (high-threshold capacity). If he consents, he is making a choice with which most reasonable people would agree, and establishing capacity would be less important (low-threshold capacity).
Mr. J, age 95, has congestive heart failure, diabetes, and liver disease. If he consents to a liver transplant—a treatment likely to be low-benefit and high-risk—he would require a rigorous capacity evaluation. If he refuses this surgical intervention, then more-lenient capacity criteria would apply.
Mrs. F, age 59, has breast cancer with metastases. Her oncologist is recommending bilateral mastectomy, radiation, chemotherapy, and an experimental treatment that has shown favorable results. The risk of treatment is high, and the benefit is unknown but most likely high. Since this is a high-risk, high-benefit intervention, the capacity threshold is medium. Whether she consents to or refuses treatment, you must weigh risks and benefits very carefully with her.
The primary team’s role
A common myth holds that only psychiatrists can determine capacity, but any physician can.4 The primary team may feel comfortable deciding a patient’s capacity without seeking consultation after asking the screening questions in Table 1.5,6 A patient who gives consistent and appropriate answers to these screening questions usually also can answer the more detailed questions psychiatrists would ask and thus has sufficient capacity.
When uncertainties remain after screening, we recommend that the primary team ask psychiatry for an opinion. Knowing what the primary team is thinking about a difficult case often helps the psychiatric consultant. So when consulting with psychiatry, we suggest that the primary team:
- clarify the question (such as, “Does Mrs. Z have the capacity to refuse dialysis?”)
- give an opinion about whether the patient does or does not have capacity and why.
When sharing of opinions was studied at institutions trying this idea, C/L teams agreed with the primary teams’ initial impression of patients’ capacity 80% of the time.4 Most consults occurred because the patient was refusing an intervention the primary team felt was “essential,” or the patient and primary team disagreed on code status. At our institution, anecdotal evidence shows that if the primary team spends a few minutes asking screening questions, the C/L service and primary team agree on the patient’s capacity >90% of the time.
Table 1
Primary team capacity evaluation: 5 W’s
Explain to the patient the treatment you recommend. Review risks and benefits of accepting and of refusing the treatment. Describe alternatives. Then ask these screening questions to assess capacity:
|
| Source: References 5,6 |
Tips for the psychiatrist
C/L psychiatrists are usually asked to evaluate capacity in complicated cases, such as when the:
- family disagrees with the patient’s decision
- patient changes his mind several times
- patient has a formidable psychiatric history.
Determining capacity requires that you assess the patient’s ability to communicate choices, understand and retain information about his condition and proposed treatment, appreciate likely consequences, and rationally manipulate information (Table 2).7
You can often gauge a patient’s attitude the moment you walk into his or her room. Those who feel insulted or defensive about being evaluated by a psychiatrist say things like:
- “I’m not crazy; I don’t need to talk to you.”
- “I think you need to evaluate my doctors, not me.”
- “Why is it so hard to believe that I’m ready to die? You can’t change my mind. Get out!”
To put the patient at ease, consider an inoffensive introduction such as: “My name is Dr. Y and I’m one of the psychiatrists who work here. I’m often called by the primary team to help explain the pros and cons of the various treatments we can provide to you. I’m not here to change your mind; I just want to make sure you are aware of all your options.”
Table 2
Psychiatry C/L service capacity evaluation
Ability to communicate choices
|
Ability to understand information about a treatment
|
Appreciation of likely consequences
|
Rational manipulation of information
|
| Source: References 5,6 |
Is it ever ok not to assess capacity?
In rare situations, informed consent does not need to be pursued and neither does capacity. Informed consent occurs when a capable patient receives adequate information to make a decision and voluntarily consents to the proposed intervention.8 Informed consent is not required in emergency, patient waiver, or therapeutic privilege situations.8,9
Emergency exception is permitted if the patient lacks the capacity to consent and the harm of postponing therapy is imminent and outweighs the proposed intervention’s risks. These cases are usually life-threatening situations in the emergency department, such as when a patient suffers severe physical trauma in a motor vehicle accident and is unable to communicate. Although capacity cannot be established, patients are taken immediately to the operating room.
If a patient with capacity refuses emergent treatment, however, the treating physician cannot override the patient’s wishes simply because it is an emergency. For example:
Mrs. L, age 32, lost several liters of blood during a complicated vaginal delivery. Her obstetrician felt she needed an emergent blood transfusion to avoid further medical complications. Mrs. L—a Jehovah’s Witness—refused the transfusion because of her religious beliefs. She was deemed capable of making this decision, and the transfusion was deferred.8-10
Patient waiver applies when a patient does not want to know all the relevant information about a procedure; he or she may wish for the physician (or another person) to make decisions.
Therapeutic privilege, a controversial idea, allows the physician to make decisions for the patient without informed consent when the physician believes the risk of giving pertinent information poses a serious detriment to the patient. In the rare cases when this is invoked, obtain family input if possible. For example:
Mrs. J, age 70, has severe health anxiety. When the primary care physician she has seen for 30 years tries to discuss treatments with her, Mrs. J fixates on potential harms and refuses treatments with even minimal risk. Her doctor tells her that it may be in her best interest to not hear the risks of treatment. Mrs. J agrees and gives her doctor permission to discusses treatment risks and benefits with her daughter, who is intricately involved in her mother’s health care.
Related resources
- Harvard Medical School department of psychiatry. Web site on forensic psychiatry and medicine. www.forensic-psych.com.
- Stern TA, Fricchione GL, Cassem, NH, et al (eds). Massachusetts General Hospital handbook of general hospital psychiatry (5th ed). Philadelphia: CV Mosby; 2004:355-9.
1. Viswanathan R, Schindler B, Brendel RW, et al. Should APM develop practice guidelines for decisional capacity assessments in the medical setting? Presented at: Annual Meeting of the Academy of Psychosomatic Medicine; November 16-20, 2005; Santa Ana Pueblo, NM.
2. Roth LH, Meisel A, Lidz CW. Tests of competency to consent to treatment. Am J Psychiatry 1977;124:279-84.
3. Wise MG, Rundell JR. Medicolegal issues in consultation. In: Clinical manual of psychosomatic medicine: a guide to consultation-liaison psychiatry. Arlington, VA: American Psychiatric Publishing; 2005:254-67.
4. Muskin PR, Kornfeld DS, Aladjem A, Tahil F. Determining capacity: Is it just capacity? Plenary workshop at: Annual Meeting of the Academy of Psychosomatic Medicine; November 16-20, 2005; Santa Ana Pueblo, NM.
5. Malin PJ. Creighton University. Educational handout (adapted with permission).
6. Poole K, Singh M, Murphy J. Law and medicine: the dilemmas of capacity, consultation/liaison psychiatry. Presented at: The Mayo Clinic; February 15, 2001; Rochester, MN.
7. Grisso T, Appelbaum PS. Assessing competence to consent to treatment: A guide for physicians and other health professionals. New York: Oxford University Press; 1998.
8. Nora LM, Benvenuti RJ. Iatrogenic disorders: medicolegal aspects of informed consent. Neurol Clin 1998;16:207-16.
9. Coulson KM, Glasser BL, Liang BA. Informed consent: issues for providers. Hematol Oncol Clin North Am 2002;16:1365-80.
10. Magid M, Reichenberg JS, Philbrick KL. To cut or not to cut: that was the question. Poster presented at: Meeting of the American Academy of Psychiatry and the Law; October 2005; Montreal, Canada.
Consultation/liaison (C/L) psychiatrists assess capacity in 1 of 6 consults,1 and these evaluations must be quick but systematic. Hospital time is precious, and asking for a psychiatry consult inevitably slows down the medical team’s efforts to care for sick or injured patients.
We suggest an approach our C/L service developed to rapidly weigh capacity’s three dimensions—risks, benefits, and patient decisions—to formulate appropriate opinions for the medical team.
A standard for capacity
In most cases, capacity must be assessed and considered adequate before a patient can provide informed consent for a medical intervention. Because a patient might be capable of making some decisions but not others, the standard for determining capacity is not black and white but a sliding scale that depends on the magnitude of the decision being made.
As physicians, psychiatrists understand doctors’ frustrations when they believe a patient is making the wrong treatment choice. When the primary team turns to us, they want us to help determine the most appropriate course of action.
Capacity is determined by weighing whether the patient is competent to exercise his or her autonomy in making a decision about medical treatment. We do not assess global capacity; the goal is to provide an unbiased opinion about specific capacity for a given situation–“Does Mr. X have the ability to accept/refuse this treatment option presented to him?”
Capacity’s three dimensions. The means to achieve this goal are often complex. Roth et al2 proposed that capacity could be measured on a sliding scale. Wise and Rundell3 agreed and developed a two-dimension table to show that capacity can be evaluated at different thresholds, depending on the patient’s clinical situation. We expanded this model (Figure) to include three dimensions to consider when you evaluate capacity:
- risk of the proposed treatment (high vs. low)
- benefit of the treatment (high vs. low)
- the patient’s decision about the treatment (accept vs. refuse).
If a treatment’s benefits far outweigh the risks and the patient accepts that treatment, he is probably capable of making that decision and a lenient (low) threshold to establish capacity applies. If the same patient refuses the high-benefit, low-risk treatment, then he might be incapable of making that decision and a stringent (high) threshold to establish capacity comes into play. Our C/L service often uses this model when discussing capacity evaluations with the primary team. It explains why some capacity evaluations—when a patient agrees to a low-risk, high-benefit procedure—might take minutes, whereas others—those that fall into the medium threshold for capacity—take hours. Consider the following cases.
Figure 3-dimension model for evaluating capacity
Three cases: Is capacity evaluation needed?
Mr. X, age 25, was in a motor vehicle accident that caused trauma to his esophagus. He requires a feeding tube because he will be unable to eat for several weeks. The risk of the procedure (feeding tube placement) is low, and the benefit (getting possibly life-saving nutrition) is high.
If Mr. X refuses the feeding tube, he may be incapable of making this decision and would require a rigorous capacity evaluation (high-threshold capacity). If he consents, he is making a choice with which most reasonable people would agree, and establishing capacity would be less important (low-threshold capacity).
Mr. J, age 95, has congestive heart failure, diabetes, and liver disease. If he consents to a liver transplant—a treatment likely to be low-benefit and high-risk—he would require a rigorous capacity evaluation. If he refuses this surgical intervention, then more-lenient capacity criteria would apply.
Mrs. F, age 59, has breast cancer with metastases. Her oncologist is recommending bilateral mastectomy, radiation, chemotherapy, and an experimental treatment that has shown favorable results. The risk of treatment is high, and the benefit is unknown but most likely high. Since this is a high-risk, high-benefit intervention, the capacity threshold is medium. Whether she consents to or refuses treatment, you must weigh risks and benefits very carefully with her.
The primary team’s role
A common myth holds that only psychiatrists can determine capacity, but any physician can.4 The primary team may feel comfortable deciding a patient’s capacity without seeking consultation after asking the screening questions in Table 1.5,6 A patient who gives consistent and appropriate answers to these screening questions usually also can answer the more detailed questions psychiatrists would ask and thus has sufficient capacity.
When uncertainties remain after screening, we recommend that the primary team ask psychiatry for an opinion. Knowing what the primary team is thinking about a difficult case often helps the psychiatric consultant. So when consulting with psychiatry, we suggest that the primary team:
- clarify the question (such as, “Does Mrs. Z have the capacity to refuse dialysis?”)
- give an opinion about whether the patient does or does not have capacity and why.
When sharing of opinions was studied at institutions trying this idea, C/L teams agreed with the primary teams’ initial impression of patients’ capacity 80% of the time.4 Most consults occurred because the patient was refusing an intervention the primary team felt was “essential,” or the patient and primary team disagreed on code status. At our institution, anecdotal evidence shows that if the primary team spends a few minutes asking screening questions, the C/L service and primary team agree on the patient’s capacity >90% of the time.
Table 1
Primary team capacity evaluation: 5 W’s
Explain to the patient the treatment you recommend. Review risks and benefits of accepting and of refusing the treatment. Describe alternatives. Then ask these screening questions to assess capacity:
|
| Source: References 5,6 |
Tips for the psychiatrist
C/L psychiatrists are usually asked to evaluate capacity in complicated cases, such as when the:
- family disagrees with the patient’s decision
- patient changes his mind several times
- patient has a formidable psychiatric history.
Determining capacity requires that you assess the patient’s ability to communicate choices, understand and retain information about his condition and proposed treatment, appreciate likely consequences, and rationally manipulate information (Table 2).7
You can often gauge a patient’s attitude the moment you walk into his or her room. Those who feel insulted or defensive about being evaluated by a psychiatrist say things like:
- “I’m not crazy; I don’t need to talk to you.”
- “I think you need to evaluate my doctors, not me.”
- “Why is it so hard to believe that I’m ready to die? You can’t change my mind. Get out!”
To put the patient at ease, consider an inoffensive introduction such as: “My name is Dr. Y and I’m one of the psychiatrists who work here. I’m often called by the primary team to help explain the pros and cons of the various treatments we can provide to you. I’m not here to change your mind; I just want to make sure you are aware of all your options.”
Table 2
Psychiatry C/L service capacity evaluation
Ability to communicate choices
|
Ability to understand information about a treatment
|
Appreciation of likely consequences
|
Rational manipulation of information
|
| Source: References 5,6 |
Is it ever ok not to assess capacity?
In rare situations, informed consent does not need to be pursued and neither does capacity. Informed consent occurs when a capable patient receives adequate information to make a decision and voluntarily consents to the proposed intervention.8 Informed consent is not required in emergency, patient waiver, or therapeutic privilege situations.8,9
Emergency exception is permitted if the patient lacks the capacity to consent and the harm of postponing therapy is imminent and outweighs the proposed intervention’s risks. These cases are usually life-threatening situations in the emergency department, such as when a patient suffers severe physical trauma in a motor vehicle accident and is unable to communicate. Although capacity cannot be established, patients are taken immediately to the operating room.
If a patient with capacity refuses emergent treatment, however, the treating physician cannot override the patient’s wishes simply because it is an emergency. For example:
Mrs. L, age 32, lost several liters of blood during a complicated vaginal delivery. Her obstetrician felt she needed an emergent blood transfusion to avoid further medical complications. Mrs. L—a Jehovah’s Witness—refused the transfusion because of her religious beliefs. She was deemed capable of making this decision, and the transfusion was deferred.8-10
Patient waiver applies when a patient does not want to know all the relevant information about a procedure; he or she may wish for the physician (or another person) to make decisions.
Therapeutic privilege, a controversial idea, allows the physician to make decisions for the patient without informed consent when the physician believes the risk of giving pertinent information poses a serious detriment to the patient. In the rare cases when this is invoked, obtain family input if possible. For example:
Mrs. J, age 70, has severe health anxiety. When the primary care physician she has seen for 30 years tries to discuss treatments with her, Mrs. J fixates on potential harms and refuses treatments with even minimal risk. Her doctor tells her that it may be in her best interest to not hear the risks of treatment. Mrs. J agrees and gives her doctor permission to discusses treatment risks and benefits with her daughter, who is intricately involved in her mother’s health care.
Related resources
- Harvard Medical School department of psychiatry. Web site on forensic psychiatry and medicine. www.forensic-psych.com.
- Stern TA, Fricchione GL, Cassem, NH, et al (eds). Massachusetts General Hospital handbook of general hospital psychiatry (5th ed). Philadelphia: CV Mosby; 2004:355-9.
Consultation/liaison (C/L) psychiatrists assess capacity in 1 of 6 consults,1 and these evaluations must be quick but systematic. Hospital time is precious, and asking for a psychiatry consult inevitably slows down the medical team’s efforts to care for sick or injured patients.
We suggest an approach our C/L service developed to rapidly weigh capacity’s three dimensions—risks, benefits, and patient decisions—to formulate appropriate opinions for the medical team.
A standard for capacity
In most cases, capacity must be assessed and considered adequate before a patient can provide informed consent for a medical intervention. Because a patient might be capable of making some decisions but not others, the standard for determining capacity is not black and white but a sliding scale that depends on the magnitude of the decision being made.
As physicians, psychiatrists understand doctors’ frustrations when they believe a patient is making the wrong treatment choice. When the primary team turns to us, they want us to help determine the most appropriate course of action.
Capacity is determined by weighing whether the patient is competent to exercise his or her autonomy in making a decision about medical treatment. We do not assess global capacity; the goal is to provide an unbiased opinion about specific capacity for a given situation–“Does Mr. X have the ability to accept/refuse this treatment option presented to him?”
Capacity’s three dimensions. The means to achieve this goal are often complex. Roth et al2 proposed that capacity could be measured on a sliding scale. Wise and Rundell3 agreed and developed a two-dimension table to show that capacity can be evaluated at different thresholds, depending on the patient’s clinical situation. We expanded this model (Figure) to include three dimensions to consider when you evaluate capacity:
- risk of the proposed treatment (high vs. low)
- benefit of the treatment (high vs. low)
- the patient’s decision about the treatment (accept vs. refuse).
If a treatment’s benefits far outweigh the risks and the patient accepts that treatment, he is probably capable of making that decision and a lenient (low) threshold to establish capacity applies. If the same patient refuses the high-benefit, low-risk treatment, then he might be incapable of making that decision and a stringent (high) threshold to establish capacity comes into play. Our C/L service often uses this model when discussing capacity evaluations with the primary team. It explains why some capacity evaluations—when a patient agrees to a low-risk, high-benefit procedure—might take minutes, whereas others—those that fall into the medium threshold for capacity—take hours. Consider the following cases.
Figure 3-dimension model for evaluating capacity
Three cases: Is capacity evaluation needed?
Mr. X, age 25, was in a motor vehicle accident that caused trauma to his esophagus. He requires a feeding tube because he will be unable to eat for several weeks. The risk of the procedure (feeding tube placement) is low, and the benefit (getting possibly life-saving nutrition) is high.
If Mr. X refuses the feeding tube, he may be incapable of making this decision and would require a rigorous capacity evaluation (high-threshold capacity). If he consents, he is making a choice with which most reasonable people would agree, and establishing capacity would be less important (low-threshold capacity).
Mr. J, age 95, has congestive heart failure, diabetes, and liver disease. If he consents to a liver transplant—a treatment likely to be low-benefit and high-risk—he would require a rigorous capacity evaluation. If he refuses this surgical intervention, then more-lenient capacity criteria would apply.
Mrs. F, age 59, has breast cancer with metastases. Her oncologist is recommending bilateral mastectomy, radiation, chemotherapy, and an experimental treatment that has shown favorable results. The risk of treatment is high, and the benefit is unknown but most likely high. Since this is a high-risk, high-benefit intervention, the capacity threshold is medium. Whether she consents to or refuses treatment, you must weigh risks and benefits very carefully with her.
The primary team’s role
A common myth holds that only psychiatrists can determine capacity, but any physician can.4 The primary team may feel comfortable deciding a patient’s capacity without seeking consultation after asking the screening questions in Table 1.5,6 A patient who gives consistent and appropriate answers to these screening questions usually also can answer the more detailed questions psychiatrists would ask and thus has sufficient capacity.
When uncertainties remain after screening, we recommend that the primary team ask psychiatry for an opinion. Knowing what the primary team is thinking about a difficult case often helps the psychiatric consultant. So when consulting with psychiatry, we suggest that the primary team:
- clarify the question (such as, “Does Mrs. Z have the capacity to refuse dialysis?”)
- give an opinion about whether the patient does or does not have capacity and why.
When sharing of opinions was studied at institutions trying this idea, C/L teams agreed with the primary teams’ initial impression of patients’ capacity 80% of the time.4 Most consults occurred because the patient was refusing an intervention the primary team felt was “essential,” or the patient and primary team disagreed on code status. At our institution, anecdotal evidence shows that if the primary team spends a few minutes asking screening questions, the C/L service and primary team agree on the patient’s capacity >90% of the time.
Table 1
Primary team capacity evaluation: 5 W’s
Explain to the patient the treatment you recommend. Review risks and benefits of accepting and of refusing the treatment. Describe alternatives. Then ask these screening questions to assess capacity:
|
| Source: References 5,6 |
Tips for the psychiatrist
C/L psychiatrists are usually asked to evaluate capacity in complicated cases, such as when the:
- family disagrees with the patient’s decision
- patient changes his mind several times
- patient has a formidable psychiatric history.
Determining capacity requires that you assess the patient’s ability to communicate choices, understand and retain information about his condition and proposed treatment, appreciate likely consequences, and rationally manipulate information (Table 2).7
You can often gauge a patient’s attitude the moment you walk into his or her room. Those who feel insulted or defensive about being evaluated by a psychiatrist say things like:
- “I’m not crazy; I don’t need to talk to you.”
- “I think you need to evaluate my doctors, not me.”
- “Why is it so hard to believe that I’m ready to die? You can’t change my mind. Get out!”
To put the patient at ease, consider an inoffensive introduction such as: “My name is Dr. Y and I’m one of the psychiatrists who work here. I’m often called by the primary team to help explain the pros and cons of the various treatments we can provide to you. I’m not here to change your mind; I just want to make sure you are aware of all your options.”
Table 2
Psychiatry C/L service capacity evaluation
Ability to communicate choices
|
Ability to understand information about a treatment
|
Appreciation of likely consequences
|
Rational manipulation of information
|
| Source: References 5,6 |
Is it ever ok not to assess capacity?
In rare situations, informed consent does not need to be pursued and neither does capacity. Informed consent occurs when a capable patient receives adequate information to make a decision and voluntarily consents to the proposed intervention.8 Informed consent is not required in emergency, patient waiver, or therapeutic privilege situations.8,9
Emergency exception is permitted if the patient lacks the capacity to consent and the harm of postponing therapy is imminent and outweighs the proposed intervention’s risks. These cases are usually life-threatening situations in the emergency department, such as when a patient suffers severe physical trauma in a motor vehicle accident and is unable to communicate. Although capacity cannot be established, patients are taken immediately to the operating room.
If a patient with capacity refuses emergent treatment, however, the treating physician cannot override the patient’s wishes simply because it is an emergency. For example:
Mrs. L, age 32, lost several liters of blood during a complicated vaginal delivery. Her obstetrician felt she needed an emergent blood transfusion to avoid further medical complications. Mrs. L—a Jehovah’s Witness—refused the transfusion because of her religious beliefs. She was deemed capable of making this decision, and the transfusion was deferred.8-10
Patient waiver applies when a patient does not want to know all the relevant information about a procedure; he or she may wish for the physician (or another person) to make decisions.
Therapeutic privilege, a controversial idea, allows the physician to make decisions for the patient without informed consent when the physician believes the risk of giving pertinent information poses a serious detriment to the patient. In the rare cases when this is invoked, obtain family input if possible. For example:
Mrs. J, age 70, has severe health anxiety. When the primary care physician she has seen for 30 years tries to discuss treatments with her, Mrs. J fixates on potential harms and refuses treatments with even minimal risk. Her doctor tells her that it may be in her best interest to not hear the risks of treatment. Mrs. J agrees and gives her doctor permission to discusses treatment risks and benefits with her daughter, who is intricately involved in her mother’s health care.
Related resources
- Harvard Medical School department of psychiatry. Web site on forensic psychiatry and medicine. www.forensic-psych.com.
- Stern TA, Fricchione GL, Cassem, NH, et al (eds). Massachusetts General Hospital handbook of general hospital psychiatry (5th ed). Philadelphia: CV Mosby; 2004:355-9.
1. Viswanathan R, Schindler B, Brendel RW, et al. Should APM develop practice guidelines for decisional capacity assessments in the medical setting? Presented at: Annual Meeting of the Academy of Psychosomatic Medicine; November 16-20, 2005; Santa Ana Pueblo, NM.
2. Roth LH, Meisel A, Lidz CW. Tests of competency to consent to treatment. Am J Psychiatry 1977;124:279-84.
3. Wise MG, Rundell JR. Medicolegal issues in consultation. In: Clinical manual of psychosomatic medicine: a guide to consultation-liaison psychiatry. Arlington, VA: American Psychiatric Publishing; 2005:254-67.
4. Muskin PR, Kornfeld DS, Aladjem A, Tahil F. Determining capacity: Is it just capacity? Plenary workshop at: Annual Meeting of the Academy of Psychosomatic Medicine; November 16-20, 2005; Santa Ana Pueblo, NM.
5. Malin PJ. Creighton University. Educational handout (adapted with permission).
6. Poole K, Singh M, Murphy J. Law and medicine: the dilemmas of capacity, consultation/liaison psychiatry. Presented at: The Mayo Clinic; February 15, 2001; Rochester, MN.
7. Grisso T, Appelbaum PS. Assessing competence to consent to treatment: A guide for physicians and other health professionals. New York: Oxford University Press; 1998.
8. Nora LM, Benvenuti RJ. Iatrogenic disorders: medicolegal aspects of informed consent. Neurol Clin 1998;16:207-16.
9. Coulson KM, Glasser BL, Liang BA. Informed consent: issues for providers. Hematol Oncol Clin North Am 2002;16:1365-80.
10. Magid M, Reichenberg JS, Philbrick KL. To cut or not to cut: that was the question. Poster presented at: Meeting of the American Academy of Psychiatry and the Law; October 2005; Montreal, Canada.
1. Viswanathan R, Schindler B, Brendel RW, et al. Should APM develop practice guidelines for decisional capacity assessments in the medical setting? Presented at: Annual Meeting of the Academy of Psychosomatic Medicine; November 16-20, 2005; Santa Ana Pueblo, NM.
2. Roth LH, Meisel A, Lidz CW. Tests of competency to consent to treatment. Am J Psychiatry 1977;124:279-84.
3. Wise MG, Rundell JR. Medicolegal issues in consultation. In: Clinical manual of psychosomatic medicine: a guide to consultation-liaison psychiatry. Arlington, VA: American Psychiatric Publishing; 2005:254-67.
4. Muskin PR, Kornfeld DS, Aladjem A, Tahil F. Determining capacity: Is it just capacity? Plenary workshop at: Annual Meeting of the Academy of Psychosomatic Medicine; November 16-20, 2005; Santa Ana Pueblo, NM.
5. Malin PJ. Creighton University. Educational handout (adapted with permission).
6. Poole K, Singh M, Murphy J. Law and medicine: the dilemmas of capacity, consultation/liaison psychiatry. Presented at: The Mayo Clinic; February 15, 2001; Rochester, MN.
7. Grisso T, Appelbaum PS. Assessing competence to consent to treatment: A guide for physicians and other health professionals. New York: Oxford University Press; 1998.
8. Nora LM, Benvenuti RJ. Iatrogenic disorders: medicolegal aspects of informed consent. Neurol Clin 1998;16:207-16.
9. Coulson KM, Glasser BL, Liang BA. Informed consent: issues for providers. Hematol Oncol Clin North Am 2002;16:1365-80.
10. Magid M, Reichenberg JS, Philbrick KL. To cut or not to cut: that was the question. Poster presented at: Meeting of the American Academy of Psychiatry and the Law; October 2005; Montreal, Canada.
Algorithms and guidelines: Superhighway road maps for treatment
Online algorithms and guidelines offer fast access to evidence-based, clinically applicable information on treating a range of psychiatric disorders (Current Psychiatry 2004;3(2):22-40.
Disclosure
Drs. Kung and Lapid report no financial relationship with any company whose products are mentioned in this article, or with manufacturers of competing products.
To comment on this article or share an algorithm that works in your practice, click here.
Online algorithms and guidelines offer fast access to evidence-based, clinically applicable information on treating a range of psychiatric disorders (Current Psychiatry 2004;3(2):22-40.
Disclosure
Drs. Kung and Lapid report no financial relationship with any company whose products are mentioned in this article, or with manufacturers of competing products.
To comment on this article or share an algorithm that works in your practice, click here.
Online algorithms and guidelines offer fast access to evidence-based, clinically applicable information on treating a range of psychiatric disorders (Current Psychiatry 2004;3(2):22-40.
Disclosure
Drs. Kung and Lapid report no financial relationship with any company whose products are mentioned in this article, or with manufacturers of competing products.
To comment on this article or share an algorithm that works in your practice, click here.
Psychologists: Trained to recognize medical problems
In her letter “ Why MDs — not psychologists — prescribe ” ( Current Psychiatry , January 2006), Dr. Susan Redge provides a brief case report to illustrate why she feels psychologists are not qualified to prescribe psychotropics.
I appreciate Dr. Redge ’ s attempt to facilitate discussion of an issue that affects both psychology and psychiatry, but I ’ m not sure that her case is a valid and representative example.
First, clinical psychologists receive on average 7 years of graduate-level training in assessing and correcting psychological and psychiatric disorders. Thus, the clinical psychologist is more than qualified to recognize the incongruence between the sample patient ’ s clinical presentation and history.
Second, the patient “ spontaneously ” disclosed that he has type I diabetes mellitus. This was not discovered through an in-depth clinical interview or laboratory analysis, so I cannot see how having a degree in medicine versus psychology applies in this example.
Finally, upon realizing that the patient ’ s blood glucose was abnormally low, Dr. Redge referred the patient to a higher level of care. Any competent clinical psychologist would do the same.
I encourage Dr. Redge to consider the extensive training clinical psychologists receive in diagnostics, assessment, and intervention. I also suggest that she review programs that provide psychopharmacology training for psychologists. She — and other psychiatrists — may be surprised.
Bret Moore, PsyD
Houston, TX
Dr. Redge responds
I did not intend to suggest that psychologists are not well-trained or extensively educated. And I did not know, as Dr. Moore suggests, that their training is equivalent to medical school.
I tried to make my letter brief and to the point, which is probably why Dr. Moore assumed that my patient “ spontaneously ” disclosed that he had type I diabetes. I asked the patient numerous questions, some of them admittedly leading. Still, eliciting the information was not easy. I did have a high index of suspicion, however, which was why I ordered a blood glucose check. I analyzed the results and identified hypoglycemia, which was why I ordered the nurse to give him some orange juice and get him to the ER.
I doubt that an “ in depth ” clinical interview would have comforted the patient ’ s family if he had slipped into a coma and died. Time can be critical.
To me, this patient dramatically showed how an organic illness may present as psychosis. It was a defining moment in my life; I felt gratified that my years of education and training allowed me to help someone, and that I had to be a physician first.
Insurance companies, and even some other physicians, do not fully appreciate the psychiatrist ’ s role in medical care. Consequently, some insurers try to save money by letting nonclinicians offer psychiatric care. They must remember that psychiatry is a medical specialty and all psychiatric illness is medical illness.
Susan Redge, MD
Rochester Hills, MI
Related resources
- American Society for the Advancement of Pharmacotherapy. Links to training programs for clinical psychologists. www.division55.org/Pages/PostdoctoralEducation.htm
- American Psychological Association. Prescriptive authority. www.apa.org/monitor/may04/prescriptive.html
In her letter “ Why MDs — not psychologists — prescribe ” ( Current Psychiatry , January 2006), Dr. Susan Redge provides a brief case report to illustrate why she feels psychologists are not qualified to prescribe psychotropics.
I appreciate Dr. Redge ’ s attempt to facilitate discussion of an issue that affects both psychology and psychiatry, but I ’ m not sure that her case is a valid and representative example.
First, clinical psychologists receive on average 7 years of graduate-level training in assessing and correcting psychological and psychiatric disorders. Thus, the clinical psychologist is more than qualified to recognize the incongruence between the sample patient ’ s clinical presentation and history.
Second, the patient “ spontaneously ” disclosed that he has type I diabetes mellitus. This was not discovered through an in-depth clinical interview or laboratory analysis, so I cannot see how having a degree in medicine versus psychology applies in this example.
Finally, upon realizing that the patient ’ s blood glucose was abnormally low, Dr. Redge referred the patient to a higher level of care. Any competent clinical psychologist would do the same.
I encourage Dr. Redge to consider the extensive training clinical psychologists receive in diagnostics, assessment, and intervention. I also suggest that she review programs that provide psychopharmacology training for psychologists. She — and other psychiatrists — may be surprised.
Bret Moore, PsyD
Houston, TX
Dr. Redge responds
I did not intend to suggest that psychologists are not well-trained or extensively educated. And I did not know, as Dr. Moore suggests, that their training is equivalent to medical school.
I tried to make my letter brief and to the point, which is probably why Dr. Moore assumed that my patient “ spontaneously ” disclosed that he had type I diabetes. I asked the patient numerous questions, some of them admittedly leading. Still, eliciting the information was not easy. I did have a high index of suspicion, however, which was why I ordered a blood glucose check. I analyzed the results and identified hypoglycemia, which was why I ordered the nurse to give him some orange juice and get him to the ER.
I doubt that an “ in depth ” clinical interview would have comforted the patient ’ s family if he had slipped into a coma and died. Time can be critical.
To me, this patient dramatically showed how an organic illness may present as psychosis. It was a defining moment in my life; I felt gratified that my years of education and training allowed me to help someone, and that I had to be a physician first.
Insurance companies, and even some other physicians, do not fully appreciate the psychiatrist ’ s role in medical care. Consequently, some insurers try to save money by letting nonclinicians offer psychiatric care. They must remember that psychiatry is a medical specialty and all psychiatric illness is medical illness.
Susan Redge, MD
Rochester Hills, MI
Related resources
- American Society for the Advancement of Pharmacotherapy. Links to training programs for clinical psychologists. www.division55.org/Pages/PostdoctoralEducation.htm
- American Psychological Association. Prescriptive authority. www.apa.org/monitor/may04/prescriptive.html
In her letter “ Why MDs — not psychologists — prescribe ” ( Current Psychiatry , January 2006), Dr. Susan Redge provides a brief case report to illustrate why she feels psychologists are not qualified to prescribe psychotropics.
I appreciate Dr. Redge ’ s attempt to facilitate discussion of an issue that affects both psychology and psychiatry, but I ’ m not sure that her case is a valid and representative example.
First, clinical psychologists receive on average 7 years of graduate-level training in assessing and correcting psychological and psychiatric disorders. Thus, the clinical psychologist is more than qualified to recognize the incongruence between the sample patient ’ s clinical presentation and history.
Second, the patient “ spontaneously ” disclosed that he has type I diabetes mellitus. This was not discovered through an in-depth clinical interview or laboratory analysis, so I cannot see how having a degree in medicine versus psychology applies in this example.
Finally, upon realizing that the patient ’ s blood glucose was abnormally low, Dr. Redge referred the patient to a higher level of care. Any competent clinical psychologist would do the same.
I encourage Dr. Redge to consider the extensive training clinical psychologists receive in diagnostics, assessment, and intervention. I also suggest that she review programs that provide psychopharmacology training for psychologists. She — and other psychiatrists — may be surprised.
Bret Moore, PsyD
Houston, TX
Dr. Redge responds
I did not intend to suggest that psychologists are not well-trained or extensively educated. And I did not know, as Dr. Moore suggests, that their training is equivalent to medical school.
I tried to make my letter brief and to the point, which is probably why Dr. Moore assumed that my patient “ spontaneously ” disclosed that he had type I diabetes. I asked the patient numerous questions, some of them admittedly leading. Still, eliciting the information was not easy. I did have a high index of suspicion, however, which was why I ordered a blood glucose check. I analyzed the results and identified hypoglycemia, which was why I ordered the nurse to give him some orange juice and get him to the ER.
I doubt that an “ in depth ” clinical interview would have comforted the patient ’ s family if he had slipped into a coma and died. Time can be critical.
To me, this patient dramatically showed how an organic illness may present as psychosis. It was a defining moment in my life; I felt gratified that my years of education and training allowed me to help someone, and that I had to be a physician first.
Insurance companies, and even some other physicians, do not fully appreciate the psychiatrist ’ s role in medical care. Consequently, some insurers try to save money by letting nonclinicians offer psychiatric care. They must remember that psychiatry is a medical specialty and all psychiatric illness is medical illness.
Susan Redge, MD
Rochester Hills, MI
Related resources
- American Society for the Advancement of Pharmacotherapy. Links to training programs for clinical psychologists. www.division55.org/Pages/PostdoctoralEducation.htm
- American Psychological Association. Prescriptive authority. www.apa.org/monitor/may04/prescriptive.html
What shall we do about CATIE?
Six years in the making, phase 1 results of the Clinical Antipsychotic Trials of Intervention Effectiveness (CATIE) in schizophrenia have confirmed my clinical observations:
- One was the 74% discontinuation rate (though I admit I take some comfort in knowing I am not the only one who has trouble keeping patients with schizophrenia in treatment).
- Another was that 42% of the patients had metabolic syndrome, and most were not being treated for diabetes, hyperlipidemia, and hypertension. I believe individuals with schizophrenia deserve better than that.
The first reported CATIE finding was that four tested atypical antipsychotics were similar in effectiveness to perphenazine, as measured by the discontinuation rate. How can this be? My experience—and probably yours, too—is that atypical antipsychotics are more effective and better tolerated than the older ones. Dr. Henry Nasrallah, a CATIE investigator, offers some explanations.
The CATIE study is sponsored by the National Institute of Mental Health. As Dr. Nasrallah describes, CATIE differs from FDA-required efficacy trials in its longer duration (18 months), larger size (nearly 1,500 patients), and less-stringent inclusion/exclusion criteria. Just about anyone with a diagnosis of schizophrenia, regardless of comorbidities, was eligible so that CATIE would reflect "real world" schizophrenia. And in that regard it succeeded; the study’s patients are much like those you and I treat.
I’m worried that this mega-study showed no agent to be clearly superior, but payers can clearly demonstrate higher costs for the newer agents. A study as huge and expensive as CATIE probably will never be repeated, so we may never have a comparable study to challenge its results.
Will our patients be deprived of treatments that our clinical experience shows are best for them? Not if we can help it; there is a lot to be learned from CATIE, and we need to be informed about its results.

James Randolph Hillard, MD
James Randolph Hillard, MD
James Randolph Hillard, MD
Six years in the making, phase 1 results of the Clinical Antipsychotic Trials of Intervention Effectiveness (CATIE) in schizophrenia have confirmed my clinical observations:
- One was the 74% discontinuation rate (though I admit I take some comfort in knowing I am not the only one who has trouble keeping patients with schizophrenia in treatment).
- Another was that 42% of the patients had metabolic syndrome, and most were not being treated for diabetes, hyperlipidemia, and hypertension. I believe individuals with schizophrenia deserve better than that.
The first reported CATIE finding was that four tested atypical antipsychotics were similar in effectiveness to perphenazine, as measured by the discontinuation rate. How can this be? My experience—and probably yours, too—is that atypical antipsychotics are more effective and better tolerated than the older ones. Dr. Henry Nasrallah, a CATIE investigator, offers some explanations.
The CATIE study is sponsored by the National Institute of Mental Health. As Dr. Nasrallah describes, CATIE differs from FDA-required efficacy trials in its longer duration (18 months), larger size (nearly 1,500 patients), and less-stringent inclusion/exclusion criteria. Just about anyone with a diagnosis of schizophrenia, regardless of comorbidities, was eligible so that CATIE would reflect "real world" schizophrenia. And in that regard it succeeded; the study’s patients are much like those you and I treat.
I’m worried that this mega-study showed no agent to be clearly superior, but payers can clearly demonstrate higher costs for the newer agents. A study as huge and expensive as CATIE probably will never be repeated, so we may never have a comparable study to challenge its results.
Will our patients be deprived of treatments that our clinical experience shows are best for them? Not if we can help it; there is a lot to be learned from CATIE, and we need to be informed about its results.
Six years in the making, phase 1 results of the Clinical Antipsychotic Trials of Intervention Effectiveness (CATIE) in schizophrenia have confirmed my clinical observations:
- One was the 74% discontinuation rate (though I admit I take some comfort in knowing I am not the only one who has trouble keeping patients with schizophrenia in treatment).
- Another was that 42% of the patients had metabolic syndrome, and most were not being treated for diabetes, hyperlipidemia, and hypertension. I believe individuals with schizophrenia deserve better than that.
The first reported CATIE finding was that four tested atypical antipsychotics were similar in effectiveness to perphenazine, as measured by the discontinuation rate. How can this be? My experience—and probably yours, too—is that atypical antipsychotics are more effective and better tolerated than the older ones. Dr. Henry Nasrallah, a CATIE investigator, offers some explanations.
The CATIE study is sponsored by the National Institute of Mental Health. As Dr. Nasrallah describes, CATIE differs from FDA-required efficacy trials in its longer duration (18 months), larger size (nearly 1,500 patients), and less-stringent inclusion/exclusion criteria. Just about anyone with a diagnosis of schizophrenia, regardless of comorbidities, was eligible so that CATIE would reflect "real world" schizophrenia. And in that regard it succeeded; the study’s patients are much like those you and I treat.
I’m worried that this mega-study showed no agent to be clearly superior, but payers can clearly demonstrate higher costs for the newer agents. A study as huge and expensive as CATIE probably will never be repeated, so we may never have a comparable study to challenge its results.
Will our patients be deprived of treatments that our clinical experience shows are best for them? Not if we can help it; there is a lot to be learned from CATIE, and we need to be informed about its results.
Get serotonin syndrome down cold with SHIVERS
Critical initial treatment of serotonin syndrome (SS) depends on its swift and accurate identification. But the diagnosis can be complicated by nonspecific laboratory markers and physical symptoms similar to other hyperthermic disorders, such as neuroleptic malignant syndrome and anticholinergic toxicity.
You can recall SS’s hallmark physical symptoms with the acronym SHIVERS (Box).
Differentiating SS from other hyperthermic states requires a thorough review of the patient’s medical and drug history, clinical findings, and laboratory results. If diagnosed shortly after symptom onset and before muscular hypertonicity and hyperthermia develop, most uncomplicated SS cases resolve uneventfully over 24 hours. The key is to discontinue the causative agents, monitor vital signs, and administer IV fluids.1
Cyproheptadine, 4 mg every 4 hours as needed, is the recommended therapy, but further investigation is needed to confirm its effectiveness in alleviating SS or preventing a more-severe, potentially fatal course.2 Try benzodiazepines such as lorazepam (1 to 2 mg slow IV push) to moderate temperature, control agitation, and blunt the syndrome’s hyperadrenergic component. Intensive care is warranted in severe cases involving hypertonicity, rhabdomyolosis, and hyperthermia (temperature >41°C).
S hivering, one of the neuromuscular symptoms unique to SS, helps distinguish it from other hyperthermic syndromes
H yperreflexia and myoclonus are frequently seen in mild to moderate cases and are especially notable in the lower extremities; muscular rigidity occurs only in more severe cases
I ncreased temperature, although variable in SS and usually observed in severe cases, is likely caused by muscular hypertonicity
V ital sign instability can present as tachycardia, tachypnea, and/or labile blood pressure
E ncephalopathy—characterized by mental status changes such as agitation, delirium, confusion, and to a lesser extent obtundation—can develop from hyperthermia
R estlessness and incoordination are common because of excess serotonin activity
S weating (diaphoresis) is an autonomic response to excessive serotonin stimulation; by comparison, anticholinergic toxicity usually manifests with hot, dry skin
1. Boyer EW, Shannon M. The serotonin syndrome. N Engl J Med 2005;353(11):1112-20.
2. Sternbach H. Serotonin syndrome: How to avoid, identify and treat dangerous drug interactions. Current Psychiatry 2003;2(5):15-24.
Dr. Christensen is associate professor of psychiatry, University of Florida College of Medicine, Jacksonville, and director of the university’s community psychiatry program.
Critical initial treatment of serotonin syndrome (SS) depends on its swift and accurate identification. But the diagnosis can be complicated by nonspecific laboratory markers and physical symptoms similar to other hyperthermic disorders, such as neuroleptic malignant syndrome and anticholinergic toxicity.
You can recall SS’s hallmark physical symptoms with the acronym SHIVERS (Box).
Differentiating SS from other hyperthermic states requires a thorough review of the patient’s medical and drug history, clinical findings, and laboratory results. If diagnosed shortly after symptom onset and before muscular hypertonicity and hyperthermia develop, most uncomplicated SS cases resolve uneventfully over 24 hours. The key is to discontinue the causative agents, monitor vital signs, and administer IV fluids.1
Cyproheptadine, 4 mg every 4 hours as needed, is the recommended therapy, but further investigation is needed to confirm its effectiveness in alleviating SS or preventing a more-severe, potentially fatal course.2 Try benzodiazepines such as lorazepam (1 to 2 mg slow IV push) to moderate temperature, control agitation, and blunt the syndrome’s hyperadrenergic component. Intensive care is warranted in severe cases involving hypertonicity, rhabdomyolosis, and hyperthermia (temperature >41°C).
S hivering, one of the neuromuscular symptoms unique to SS, helps distinguish it from other hyperthermic syndromes
H yperreflexia and myoclonus are frequently seen in mild to moderate cases and are especially notable in the lower extremities; muscular rigidity occurs only in more severe cases
I ncreased temperature, although variable in SS and usually observed in severe cases, is likely caused by muscular hypertonicity
V ital sign instability can present as tachycardia, tachypnea, and/or labile blood pressure
E ncephalopathy—characterized by mental status changes such as agitation, delirium, confusion, and to a lesser extent obtundation—can develop from hyperthermia
R estlessness and incoordination are common because of excess serotonin activity
S weating (diaphoresis) is an autonomic response to excessive serotonin stimulation; by comparison, anticholinergic toxicity usually manifests with hot, dry skin
Critical initial treatment of serotonin syndrome (SS) depends on its swift and accurate identification. But the diagnosis can be complicated by nonspecific laboratory markers and physical symptoms similar to other hyperthermic disorders, such as neuroleptic malignant syndrome and anticholinergic toxicity.
You can recall SS’s hallmark physical symptoms with the acronym SHIVERS (Box).
Differentiating SS from other hyperthermic states requires a thorough review of the patient’s medical and drug history, clinical findings, and laboratory results. If diagnosed shortly after symptom onset and before muscular hypertonicity and hyperthermia develop, most uncomplicated SS cases resolve uneventfully over 24 hours. The key is to discontinue the causative agents, monitor vital signs, and administer IV fluids.1
Cyproheptadine, 4 mg every 4 hours as needed, is the recommended therapy, but further investigation is needed to confirm its effectiveness in alleviating SS or preventing a more-severe, potentially fatal course.2 Try benzodiazepines such as lorazepam (1 to 2 mg slow IV push) to moderate temperature, control agitation, and blunt the syndrome’s hyperadrenergic component. Intensive care is warranted in severe cases involving hypertonicity, rhabdomyolosis, and hyperthermia (temperature >41°C).
S hivering, one of the neuromuscular symptoms unique to SS, helps distinguish it from other hyperthermic syndromes
H yperreflexia and myoclonus are frequently seen in mild to moderate cases and are especially notable in the lower extremities; muscular rigidity occurs only in more severe cases
I ncreased temperature, although variable in SS and usually observed in severe cases, is likely caused by muscular hypertonicity
V ital sign instability can present as tachycardia, tachypnea, and/or labile blood pressure
E ncephalopathy—characterized by mental status changes such as agitation, delirium, confusion, and to a lesser extent obtundation—can develop from hyperthermia
R estlessness and incoordination are common because of excess serotonin activity
S weating (diaphoresis) is an autonomic response to excessive serotonin stimulation; by comparison, anticholinergic toxicity usually manifests with hot, dry skin
1. Boyer EW, Shannon M. The serotonin syndrome. N Engl J Med 2005;353(11):1112-20.
2. Sternbach H. Serotonin syndrome: How to avoid, identify and treat dangerous drug interactions. Current Psychiatry 2003;2(5):15-24.
Dr. Christensen is associate professor of psychiatry, University of Florida College of Medicine, Jacksonville, and director of the university’s community psychiatry program.
1. Boyer EW, Shannon M. The serotonin syndrome. N Engl J Med 2005;353(11):1112-20.
2. Sternbach H. Serotonin syndrome: How to avoid, identify and treat dangerous drug interactions. Current Psychiatry 2003;2(5):15-24.
Dr. Christensen is associate professor of psychiatry, University of Florida College of Medicine, Jacksonville, and director of the university’s community psychiatry program.
Make tardive dyskinesia passé with PASST principle
Often disfiguring and irreversible, tardive dyskinesia (TD) remains a problem for patients on maintenance antipsychotics. Central dopamine blockade is believed to contribute to TD’s pathology, but the exact cause remains unknown and treatment results are variable.1,2
To optimally manage TD, remember the PASST principle—an acronym that includes strategies to prevent, assess, switch, suppress, and treat TD. This principle—based on clinical practice, colleague experiences, and literature reviews—has been helpful for training residents how best to manage this difficult condition.
Prevent. To lower your patient’s risk of developing TD:
- reconsider whether an antipsychotic is needed, especially in high-risk patients who are older, have negative symptoms of schizophrenia, experience acute extrapyramidal symptoms, or have affective disorders3
- prescribe atypical antipsychotics, which are less likely than the typical agents to produce TD
- use the minimum effective dosage and duration.
Assess. Screen for dyskinetic movements before you start an antipsychotic and approximately every 6 months, using the Abnormal Involuntary Movement Scale (AIMS). The AIMS is easy to administer and score and can detect subtle dyskinesias at an early stage.
Switch. If you identify TD, stop the offending antipsychotic. Switch to a different drug class if psychotic relapse is not an issue (for example, in a patient taking an antipsychotic for treatment-resistant depression).
For patients who require maintenance treatment with antipsychotics, switch from a first-generation antipsychotic to an atypical. Second-generation agents such as olanzapine carry less TD risk than conventionals such as perphenazine. There may be differential risk among atypicals as well (for example, quetiapine is probably less likely to cause TD than risperidone).1 Also, TD triggered by one atypical may respond to another.4
Suppress. It may take time for a medication switch to decrease TD symptoms, if it happens at all. If a patient experiences dangerous or bothersome symptoms such as difficulty breathing or eating, increasing the antipsychotic dosage for a few weeks often provides short-term relief; reserve this approach for urgent clinical situations where switching antipsychotics would take too long or would otherwise be impractical.
Treat. Clozapine is first-line treatment for TD.5 A variety of non-antipsychotic medications have been used to reduce TD symptoms with inconsistent results (Table). Most carry mild side-effect risks and could be considered for patients who wish to try something to help alleviate symptoms.
Informed consent and collaborative decision-making are essential to managing TD. Inform patients of TD risk before starting an antipsychotic. If TD occurs, include them in decisions by explaining the risks, benefits, and reasons for switches and treatments. Some patients choose to tolerate mild TD so they can keep taking a medication that helps them stay well. Extensively document these discussions—along with your thought processes—in the medical record.
Table
Non-antipsychotic treatments that may reduce TD symptoms
| Class | Agent | Comments |
|---|---|---|
| Antioxidants | Vitamin E | >1,200 IU/d may be best to prevent deterioration, but cardiac risks increase at dosages >400 IU/d |
| GABA agonists | Benzodiazepines | Helps some patients, but may have nonspecific sedative effect; abuse potential |
| Gabapentin | >1,200 mg/d may help TD and/or blepharospasm | |
| 5HT agonists | Buspirone | >120 mg/d |
| Calcium channel blockers | Verapamil | 160 mg/d |
| Anticholinergics | Benztropine | Worsens TD initially, may help later; recommended for tardive dystonia |
| Others | Chelated manganese | 50 mg/d, especially when combined with vitamin E |
| Vitamin B6 | 300 mg/d | |
| Melatonin | 10 mg/d | |
| Branched chain amino acid mix (Tarvil) | 222 mg/kg tid superior to placebo in one study6 |
1. Simpson GM. The treatment of tardive dyskinesia and tardive dystonia. J Clin Psychiatry 2000;61(Suppl 4):39-44.
2. Kulkarni SK, Naidu PS. Pathophysiology and drug therapy of tardive dyskinesia: Current concepts and future perspectives. Drugs Today 2003;39:19-49.
3. Gardos G. Tardive dyskinesia: How to prevent and treat a lingering nemesis. Current Psychiatry 2003;2(10):59-66.
4. Suzuki E, Obata M, Yoshida Y, Miyaoka H. Tardive dyskinesia with risperidone and anticholinergics. Am J Psychiatry 2002;159(11):1948.-
5. Louzã MR, Bassitt DP. Maintenance treatment of severe tardive dyskinesia with clozapine: 5 years’ follow-up. J Clin Psychopharmacol 2005;25(2):180-2.
6. Richardson MA, Bevans ML, Read LL, et al. Efficacy of the branched-chain amino acids in the treatment of tardive dyskinesia in men. Am J Psychiatry 2003;160:1117-24.
Dr. Rosenstock is director of medical student education, Western Psychiatric Institute and Clinic, University of Pittsburgh School of Medicine, Pennsylvania.
Often disfiguring and irreversible, tardive dyskinesia (TD) remains a problem for patients on maintenance antipsychotics. Central dopamine blockade is believed to contribute to TD’s pathology, but the exact cause remains unknown and treatment results are variable.1,2
To optimally manage TD, remember the PASST principle—an acronym that includes strategies to prevent, assess, switch, suppress, and treat TD. This principle—based on clinical practice, colleague experiences, and literature reviews—has been helpful for training residents how best to manage this difficult condition.
Prevent. To lower your patient’s risk of developing TD:
- reconsider whether an antipsychotic is needed, especially in high-risk patients who are older, have negative symptoms of schizophrenia, experience acute extrapyramidal symptoms, or have affective disorders3
- prescribe atypical antipsychotics, which are less likely than the typical agents to produce TD
- use the minimum effective dosage and duration.
Assess. Screen for dyskinetic movements before you start an antipsychotic and approximately every 6 months, using the Abnormal Involuntary Movement Scale (AIMS). The AIMS is easy to administer and score and can detect subtle dyskinesias at an early stage.
Switch. If you identify TD, stop the offending antipsychotic. Switch to a different drug class if psychotic relapse is not an issue (for example, in a patient taking an antipsychotic for treatment-resistant depression).
For patients who require maintenance treatment with antipsychotics, switch from a first-generation antipsychotic to an atypical. Second-generation agents such as olanzapine carry less TD risk than conventionals such as perphenazine. There may be differential risk among atypicals as well (for example, quetiapine is probably less likely to cause TD than risperidone).1 Also, TD triggered by one atypical may respond to another.4
Suppress. It may take time for a medication switch to decrease TD symptoms, if it happens at all. If a patient experiences dangerous or bothersome symptoms such as difficulty breathing or eating, increasing the antipsychotic dosage for a few weeks often provides short-term relief; reserve this approach for urgent clinical situations where switching antipsychotics would take too long or would otherwise be impractical.
Treat. Clozapine is first-line treatment for TD.5 A variety of non-antipsychotic medications have been used to reduce TD symptoms with inconsistent results (Table). Most carry mild side-effect risks and could be considered for patients who wish to try something to help alleviate symptoms.
Informed consent and collaborative decision-making are essential to managing TD. Inform patients of TD risk before starting an antipsychotic. If TD occurs, include them in decisions by explaining the risks, benefits, and reasons for switches and treatments. Some patients choose to tolerate mild TD so they can keep taking a medication that helps them stay well. Extensively document these discussions—along with your thought processes—in the medical record.
Table
Non-antipsychotic treatments that may reduce TD symptoms
| Class | Agent | Comments |
|---|---|---|
| Antioxidants | Vitamin E | >1,200 IU/d may be best to prevent deterioration, but cardiac risks increase at dosages >400 IU/d |
| GABA agonists | Benzodiazepines | Helps some patients, but may have nonspecific sedative effect; abuse potential |
| Gabapentin | >1,200 mg/d may help TD and/or blepharospasm | |
| 5HT agonists | Buspirone | >120 mg/d |
| Calcium channel blockers | Verapamil | 160 mg/d |
| Anticholinergics | Benztropine | Worsens TD initially, may help later; recommended for tardive dystonia |
| Others | Chelated manganese | 50 mg/d, especially when combined with vitamin E |
| Vitamin B6 | 300 mg/d | |
| Melatonin | 10 mg/d | |
| Branched chain amino acid mix (Tarvil) | 222 mg/kg tid superior to placebo in one study6 |
Often disfiguring and irreversible, tardive dyskinesia (TD) remains a problem for patients on maintenance antipsychotics. Central dopamine blockade is believed to contribute to TD’s pathology, but the exact cause remains unknown and treatment results are variable.1,2
To optimally manage TD, remember the PASST principle—an acronym that includes strategies to prevent, assess, switch, suppress, and treat TD. This principle—based on clinical practice, colleague experiences, and literature reviews—has been helpful for training residents how best to manage this difficult condition.
Prevent. To lower your patient’s risk of developing TD:
- reconsider whether an antipsychotic is needed, especially in high-risk patients who are older, have negative symptoms of schizophrenia, experience acute extrapyramidal symptoms, or have affective disorders3
- prescribe atypical antipsychotics, which are less likely than the typical agents to produce TD
- use the minimum effective dosage and duration.
Assess. Screen for dyskinetic movements before you start an antipsychotic and approximately every 6 months, using the Abnormal Involuntary Movement Scale (AIMS). The AIMS is easy to administer and score and can detect subtle dyskinesias at an early stage.
Switch. If you identify TD, stop the offending antipsychotic. Switch to a different drug class if psychotic relapse is not an issue (for example, in a patient taking an antipsychotic for treatment-resistant depression).
For patients who require maintenance treatment with antipsychotics, switch from a first-generation antipsychotic to an atypical. Second-generation agents such as olanzapine carry less TD risk than conventionals such as perphenazine. There may be differential risk among atypicals as well (for example, quetiapine is probably less likely to cause TD than risperidone).1 Also, TD triggered by one atypical may respond to another.4
Suppress. It may take time for a medication switch to decrease TD symptoms, if it happens at all. If a patient experiences dangerous or bothersome symptoms such as difficulty breathing or eating, increasing the antipsychotic dosage for a few weeks often provides short-term relief; reserve this approach for urgent clinical situations where switching antipsychotics would take too long or would otherwise be impractical.
Treat. Clozapine is first-line treatment for TD.5 A variety of non-antipsychotic medications have been used to reduce TD symptoms with inconsistent results (Table). Most carry mild side-effect risks and could be considered for patients who wish to try something to help alleviate symptoms.
Informed consent and collaborative decision-making are essential to managing TD. Inform patients of TD risk before starting an antipsychotic. If TD occurs, include them in decisions by explaining the risks, benefits, and reasons for switches and treatments. Some patients choose to tolerate mild TD so they can keep taking a medication that helps them stay well. Extensively document these discussions—along with your thought processes—in the medical record.
Table
Non-antipsychotic treatments that may reduce TD symptoms
| Class | Agent | Comments |
|---|---|---|
| Antioxidants | Vitamin E | >1,200 IU/d may be best to prevent deterioration, but cardiac risks increase at dosages >400 IU/d |
| GABA agonists | Benzodiazepines | Helps some patients, but may have nonspecific sedative effect; abuse potential |
| Gabapentin | >1,200 mg/d may help TD and/or blepharospasm | |
| 5HT agonists | Buspirone | >120 mg/d |
| Calcium channel blockers | Verapamil | 160 mg/d |
| Anticholinergics | Benztropine | Worsens TD initially, may help later; recommended for tardive dystonia |
| Others | Chelated manganese | 50 mg/d, especially when combined with vitamin E |
| Vitamin B6 | 300 mg/d | |
| Melatonin | 10 mg/d | |
| Branched chain amino acid mix (Tarvil) | 222 mg/kg tid superior to placebo in one study6 |
1. Simpson GM. The treatment of tardive dyskinesia and tardive dystonia. J Clin Psychiatry 2000;61(Suppl 4):39-44.
2. Kulkarni SK, Naidu PS. Pathophysiology and drug therapy of tardive dyskinesia: Current concepts and future perspectives. Drugs Today 2003;39:19-49.
3. Gardos G. Tardive dyskinesia: How to prevent and treat a lingering nemesis. Current Psychiatry 2003;2(10):59-66.
4. Suzuki E, Obata M, Yoshida Y, Miyaoka H. Tardive dyskinesia with risperidone and anticholinergics. Am J Psychiatry 2002;159(11):1948.-
5. Louzã MR, Bassitt DP. Maintenance treatment of severe tardive dyskinesia with clozapine: 5 years’ follow-up. J Clin Psychopharmacol 2005;25(2):180-2.
6. Richardson MA, Bevans ML, Read LL, et al. Efficacy of the branched-chain amino acids in the treatment of tardive dyskinesia in men. Am J Psychiatry 2003;160:1117-24.
Dr. Rosenstock is director of medical student education, Western Psychiatric Institute and Clinic, University of Pittsburgh School of Medicine, Pennsylvania.
1. Simpson GM. The treatment of tardive dyskinesia and tardive dystonia. J Clin Psychiatry 2000;61(Suppl 4):39-44.
2. Kulkarni SK, Naidu PS. Pathophysiology and drug therapy of tardive dyskinesia: Current concepts and future perspectives. Drugs Today 2003;39:19-49.
3. Gardos G. Tardive dyskinesia: How to prevent and treat a lingering nemesis. Current Psychiatry 2003;2(10):59-66.
4. Suzuki E, Obata M, Yoshida Y, Miyaoka H. Tardive dyskinesia with risperidone and anticholinergics. Am J Psychiatry 2002;159(11):1948.-
5. Louzã MR, Bassitt DP. Maintenance treatment of severe tardive dyskinesia with clozapine: 5 years’ follow-up. J Clin Psychopharmacol 2005;25(2):180-2.
6. Richardson MA, Bevans ML, Read LL, et al. Efficacy of the branched-chain amino acids in the treatment of tardive dyskinesia in men. Am J Psychiatry 2003;160:1117-24.
Dr. Rosenstock is director of medical student education, Western Psychiatric Institute and Clinic, University of Pittsburgh School of Medicine, Pennsylvania.
Can a vaccine prevent Alzheimer’s disease?
Deposition of amyloid-β peptide (Aβ) is believed to contribute to Alzheimer’s disease (AD) pathogenesis. Derived from a larger precursor protein, Aβ aggregates into plaques, and may promote neuronal death and, ultimately, dementia.
Current treatments alleviate symptoms without slowing underlying neurodegeneration. The prospect of harnessing the immune system to target the Aβ peptide offers an intriguing option for preventing this devastating, increasingly common disease.
Anti-a BETA antibodies
Transgenic mice bred to overexpress AD genes have responded remarkably in studies using the immune system to target the amyloid-β peptide.3 Several mouse groups have shown plaque reduction (Figure 1) and improved cognitive performance. These findings substantiate the amyloid hypothesis in AD pathogenesis.
A host could acquire anti-Aβ antibodies though two basic approaches (Figure 2):2
Figure 1 Differences in amyloid deposition between control and immunized mice
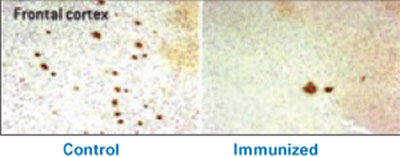
Frontal cortex of an unvaccinated mouse (left) shows more amyloid deposits (dark spots) than that of a mouse producing antibodies against the amyloid-β peptide (right).
Source: Image by Cynthia A. Lemere, PhD. Used with permission.Active immunization exposes the subject to the antigen (in this case the Aβ peptide) and allows T cells and B cells to produce anti-Aβ antibodies. This approach has been studied in humans, but adverse effects have stymied its development.
Passive immunization, which involves developing anti-Aβ antibodies in a separate source, aims to clear Aβ peptide without requiring an immunologic response from the host. Large doses of antibodies administered weekly or monthly would be needed to build adequate plasma levels in the CNS, and large quantities of circulating antibodies could cause hemorrhagic stroke.
A troublesome trial
After successful preclinical and phase 1 testing of a vaccine against the Aβ peptide (called AN-1792), a phase 2a placebo-controlled trial in 2001 followed patients with mild to moderate AD. Drug administration was halted after 18 patients (6%) developed meningoencephalitis after several months.4 However, 300 patients with AD and 72 control patients had received at least one injection, and double-blind assessments were maintained for 12 months.
Figure 2 Methods for immunizing against Aβ peptide
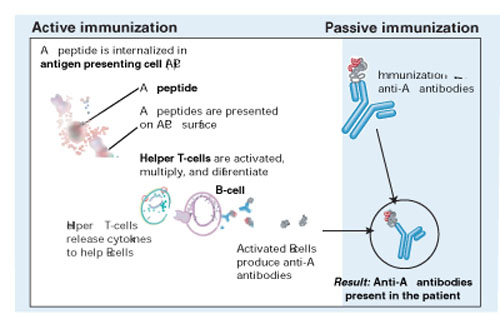
Active immunization produces anti-Aβ antibodies via immunologic response to vaccination. With passive immunization, anti-Aβ antibodies are administered directly.
Illustration by Rich LaRocco.All patients with meningoencephalitis had received the vaccine but not all developed an immune response, suggesting that something other than the antibodies—such as T cells—caused the encephalitis. Twelve patients recovered, but six had persistent cognitive and neurologic deficits.
More-optimistic news
Of the 300 patients who received an active vaccine, 20% developed an adequate antibody response.5
The responders showed no significant difference from the placebo group in most outcome measures but showed less worsening in the nine-component Neuropsychological Test Battery (NTB) (P=0.02). Of particular interest, antibody responders showed significant improvement in the NTB—s memory domain (P=0.03). Further, subjects with higher IgG antibody titers showed greater improvement than did other responders.
More work ahead
Although the outcome of this initial AN-1792 trial is disappointing because of its discontinuation and mixed results, T cell infiltration and amyloid depletion were found during postmortem examinations of two vaccine recipients.6
Pharmaceutical companies are testing two compounds for AD immunotherapy:7
- AAB-001, a human monoclonal antibody, targets all 42 Aβ amino acids via passive immunization and has entered phase 2 trials.
- ACC-001, an Aβ immuno-conjugate designed to elicit an active antibody response, began phase 1 testing last fall.
These efforts suggest that an “Alzheimer’s vaccine” could be produced, provided it could attack the Aβ peptide without inducing a significant cellular reaction.
1. Neugroschl JA, Kolevzor A, Samuels SC, Marir DB. Dementia. In: Sadock BJ, Sadock VA (eds). Kaplan & Sadock’s comprehensive text-book of psychiatry (8th ed). Philadelphia: Lippincott Williams & Wilkins; 2005:1068-93.
2. Schenk D. Amyloid-beta immunotherapy for Alzheimer’s disease: the end of the beginning. Nat Rev Neurosci 2002;3:824-8.
3. Schenk D, Hagen M, Seubert P. Current progress in beta-amyloid immunotherapy. Current Opin Immunol 2004;16:599-606.
4. Orgogozo JM, Gilman S, Dartigues JF, et al. Subacute meningoen-cephalitis in a subset of patients with AD after Abeta42 immunization. Neurology 2003;61:46-54.
5. Gilman S, Koller M, Black RS, et al. Clinical effects of Abeta immunization (AN1792) in patients with AD in an interrupted trial. Neurology 2005;64:1553-62.
6. Ferrer I, Boada Rovira M, Sanchez Guerra ML, et al. Neuropathology and pathogenesis of encephalitis following amyloid-beta immunization in Alzheimer’s disease. Brain Pathology 2004;14(1):11-20.
7. Sullivan MG. Immunotherapy studies for AD back on track. Psychiatry News 2005;33(11):69.-
Deposition of amyloid-β peptide (Aβ) is believed to contribute to Alzheimer’s disease (AD) pathogenesis. Derived from a larger precursor protein, Aβ aggregates into plaques, and may promote neuronal death and, ultimately, dementia.
Current treatments alleviate symptoms without slowing underlying neurodegeneration. The prospect of harnessing the immune system to target the Aβ peptide offers an intriguing option for preventing this devastating, increasingly common disease.
Anti-a BETA antibodies
Transgenic mice bred to overexpress AD genes have responded remarkably in studies using the immune system to target the amyloid-β peptide.3 Several mouse groups have shown plaque reduction (Figure 1) and improved cognitive performance. These findings substantiate the amyloid hypothesis in AD pathogenesis.
A host could acquire anti-Aβ antibodies though two basic approaches (Figure 2):2
Figure 1 Differences in amyloid deposition between control and immunized mice
Frontal cortex of an unvaccinated mouse (left) shows more amyloid deposits (dark spots) than that of a mouse producing antibodies against the amyloid-β peptide (right).
Source: Image by Cynthia A. Lemere, PhD. Used with permission.Active immunization exposes the subject to the antigen (in this case the Aβ peptide) and allows T cells and B cells to produce anti-Aβ antibodies. This approach has been studied in humans, but adverse effects have stymied its development.
Passive immunization, which involves developing anti-Aβ antibodies in a separate source, aims to clear Aβ peptide without requiring an immunologic response from the host. Large doses of antibodies administered weekly or monthly would be needed to build adequate plasma levels in the CNS, and large quantities of circulating antibodies could cause hemorrhagic stroke.
A troublesome trial
After successful preclinical and phase 1 testing of a vaccine against the Aβ peptide (called AN-1792), a phase 2a placebo-controlled trial in 2001 followed patients with mild to moderate AD. Drug administration was halted after 18 patients (6%) developed meningoencephalitis after several months.4 However, 300 patients with AD and 72 control patients had received at least one injection, and double-blind assessments were maintained for 12 months.
Figure 2 Methods for immunizing against Aβ peptide
Active immunization produces anti-Aβ antibodies via immunologic response to vaccination. With passive immunization, anti-Aβ antibodies are administered directly.
Illustration by Rich LaRocco.All patients with meningoencephalitis had received the vaccine but not all developed an immune response, suggesting that something other than the antibodies—such as T cells—caused the encephalitis. Twelve patients recovered, but six had persistent cognitive and neurologic deficits.
More-optimistic news
Of the 300 patients who received an active vaccine, 20% developed an adequate antibody response.5
The responders showed no significant difference from the placebo group in most outcome measures but showed less worsening in the nine-component Neuropsychological Test Battery (NTB) (P=0.02). Of particular interest, antibody responders showed significant improvement in the NTB—s memory domain (P=0.03). Further, subjects with higher IgG antibody titers showed greater improvement than did other responders.
More work ahead
Although the outcome of this initial AN-1792 trial is disappointing because of its discontinuation and mixed results, T cell infiltration and amyloid depletion were found during postmortem examinations of two vaccine recipients.6
Pharmaceutical companies are testing two compounds for AD immunotherapy:7
- AAB-001, a human monoclonal antibody, targets all 42 Aβ amino acids via passive immunization and has entered phase 2 trials.
- ACC-001, an Aβ immuno-conjugate designed to elicit an active antibody response, began phase 1 testing last fall.
These efforts suggest that an “Alzheimer’s vaccine” could be produced, provided it could attack the Aβ peptide without inducing a significant cellular reaction.
Deposition of amyloid-β peptide (Aβ) is believed to contribute to Alzheimer’s disease (AD) pathogenesis. Derived from a larger precursor protein, Aβ aggregates into plaques, and may promote neuronal death and, ultimately, dementia.
Current treatments alleviate symptoms without slowing underlying neurodegeneration. The prospect of harnessing the immune system to target the Aβ peptide offers an intriguing option for preventing this devastating, increasingly common disease.
Anti-a BETA antibodies
Transgenic mice bred to overexpress AD genes have responded remarkably in studies using the immune system to target the amyloid-β peptide.3 Several mouse groups have shown plaque reduction (Figure 1) and improved cognitive performance. These findings substantiate the amyloid hypothesis in AD pathogenesis.
A host could acquire anti-Aβ antibodies though two basic approaches (Figure 2):2
Figure 1 Differences in amyloid deposition between control and immunized mice
Frontal cortex of an unvaccinated mouse (left) shows more amyloid deposits (dark spots) than that of a mouse producing antibodies against the amyloid-β peptide (right).
Source: Image by Cynthia A. Lemere, PhD. Used with permission.Active immunization exposes the subject to the antigen (in this case the Aβ peptide) and allows T cells and B cells to produce anti-Aβ antibodies. This approach has been studied in humans, but adverse effects have stymied its development.
Passive immunization, which involves developing anti-Aβ antibodies in a separate source, aims to clear Aβ peptide without requiring an immunologic response from the host. Large doses of antibodies administered weekly or monthly would be needed to build adequate plasma levels in the CNS, and large quantities of circulating antibodies could cause hemorrhagic stroke.
A troublesome trial
After successful preclinical and phase 1 testing of a vaccine against the Aβ peptide (called AN-1792), a phase 2a placebo-controlled trial in 2001 followed patients with mild to moderate AD. Drug administration was halted after 18 patients (6%) developed meningoencephalitis after several months.4 However, 300 patients with AD and 72 control patients had received at least one injection, and double-blind assessments were maintained for 12 months.
Figure 2 Methods for immunizing against Aβ peptide
Active immunization produces anti-Aβ antibodies via immunologic response to vaccination. With passive immunization, anti-Aβ antibodies are administered directly.
Illustration by Rich LaRocco.All patients with meningoencephalitis had received the vaccine but not all developed an immune response, suggesting that something other than the antibodies—such as T cells—caused the encephalitis. Twelve patients recovered, but six had persistent cognitive and neurologic deficits.
More-optimistic news
Of the 300 patients who received an active vaccine, 20% developed an adequate antibody response.5
The responders showed no significant difference from the placebo group in most outcome measures but showed less worsening in the nine-component Neuropsychological Test Battery (NTB) (P=0.02). Of particular interest, antibody responders showed significant improvement in the NTB—s memory domain (P=0.03). Further, subjects with higher IgG antibody titers showed greater improvement than did other responders.
More work ahead
Although the outcome of this initial AN-1792 trial is disappointing because of its discontinuation and mixed results, T cell infiltration and amyloid depletion were found during postmortem examinations of two vaccine recipients.6
Pharmaceutical companies are testing two compounds for AD immunotherapy:7
- AAB-001, a human monoclonal antibody, targets all 42 Aβ amino acids via passive immunization and has entered phase 2 trials.
- ACC-001, an Aβ immuno-conjugate designed to elicit an active antibody response, began phase 1 testing last fall.
These efforts suggest that an “Alzheimer’s vaccine” could be produced, provided it could attack the Aβ peptide without inducing a significant cellular reaction.
1. Neugroschl JA, Kolevzor A, Samuels SC, Marir DB. Dementia. In: Sadock BJ, Sadock VA (eds). Kaplan & Sadock’s comprehensive text-book of psychiatry (8th ed). Philadelphia: Lippincott Williams & Wilkins; 2005:1068-93.
2. Schenk D. Amyloid-beta immunotherapy for Alzheimer’s disease: the end of the beginning. Nat Rev Neurosci 2002;3:824-8.
3. Schenk D, Hagen M, Seubert P. Current progress in beta-amyloid immunotherapy. Current Opin Immunol 2004;16:599-606.
4. Orgogozo JM, Gilman S, Dartigues JF, et al. Subacute meningoen-cephalitis in a subset of patients with AD after Abeta42 immunization. Neurology 2003;61:46-54.
5. Gilman S, Koller M, Black RS, et al. Clinical effects of Abeta immunization (AN1792) in patients with AD in an interrupted trial. Neurology 2005;64:1553-62.
6. Ferrer I, Boada Rovira M, Sanchez Guerra ML, et al. Neuropathology and pathogenesis of encephalitis following amyloid-beta immunization in Alzheimer’s disease. Brain Pathology 2004;14(1):11-20.
7. Sullivan MG. Immunotherapy studies for AD back on track. Psychiatry News 2005;33(11):69.-
1. Neugroschl JA, Kolevzor A, Samuels SC, Marir DB. Dementia. In: Sadock BJ, Sadock VA (eds). Kaplan & Sadock’s comprehensive text-book of psychiatry (8th ed). Philadelphia: Lippincott Williams & Wilkins; 2005:1068-93.
2. Schenk D. Amyloid-beta immunotherapy for Alzheimer’s disease: the end of the beginning. Nat Rev Neurosci 2002;3:824-8.
3. Schenk D, Hagen M, Seubert P. Current progress in beta-amyloid immunotherapy. Current Opin Immunol 2004;16:599-606.
4. Orgogozo JM, Gilman S, Dartigues JF, et al. Subacute meningoen-cephalitis in a subset of patients with AD after Abeta42 immunization. Neurology 2003;61:46-54.
5. Gilman S, Koller M, Black RS, et al. Clinical effects of Abeta immunization (AN1792) in patients with AD in an interrupted trial. Neurology 2005;64:1553-62.
6. Ferrer I, Boada Rovira M, Sanchez Guerra ML, et al. Neuropathology and pathogenesis of encephalitis following amyloid-beta immunization in Alzheimer’s disease. Brain Pathology 2004;14(1):11-20.
7. Sullivan MG. Immunotherapy studies for AD back on track. Psychiatry News 2005;33(11):69.-