User login
AVAHO
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
div[contains(@class, 'main-prefix')]
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
Immunotherapy stewardship could save tens of millions a year
Implementing stewardship strategies for immune checkpoint inhibitor (ICI) therapy, including personalized weight-based dosing, dose rounding, and pharmacy-level vial sharing, could generate savings of as much as $74 million each year for the Veterans Health Administration (VHA), a new analysis suggests.
That $74 million in savings would translate to nearly 14% less spent on ICI therapy annually.
first author Alex Bryant, MD, University of Michigan, Ann Arbor, said in an interview.
The study was published in Health Affairs.
ICI therapy is used in about 40 unique cancer indications and, in 2020, accounted for more than $6 billion in Medicare Part B spending.
Two of the most prescribed ICIs – pembrolizumab and nivolumab – initially received their U.S. approval at personalized weight-based doses. But at the request of the manufacturers, the Food and Drug Administration approved “one-size-fits-all” flat doses, despite a lack of data to support this strategy compared with weight-based dosing.
With a fixed dose strategy, “patients with cancer not only tend to get too high a dose of the drug, but costs go up significantly,” Daniel Goldstein, MD, a medical oncologist at the Rabin Medical Center, Petah Tikva, Israel, told this news organization last year. “Why should we give a higher dose with the same efficacy when that dose will cost significantly more and has the potential to increase adverse events?”
To compare the cost of a weight-based vs. fixed-dose strategy, Dr. Bryant and colleagues conducted a simulation analysis under four stewardship scenarios, using data from the VHA and Medicare drug prices. Strategy one looked at weight-based dosing; strategy two combined weight-based dosing and dose rounding but not single-use vial sharing; strategy three used weight-based dosing and single-use vial sharing but not dose rounding; and strategy four, the most aggressive, combined all three.
ICIs in the VHA national formulary included pembrolizumab, nivolumab, atezolizumab, durvalumab, and cemiplimab-rwlc.
Using an algorithm to extract data, the team identified 49,851 administration events in 8,276 unique patients in 2021 – just over half were pembrolizumab, nearly 23% were nivolumab, and the remaining 26% largely included atezolizumab (12.1%) and durvalumab (11.9%).
The team found that the VHA spends roughly $537 million annually on ICIs. But implementing the stewardship measures that combined weight-based dosing, dose rounding, and vial sharing could save the VHA $74 million, or about 14%, annually on ICIs.
Most of the savings came from dosing changes to pembrolizumab and nivolumab, with greater savings achieved by combining more stewardship strategies. For instance, using strategy one (weight-based dosing alone) could lead to annual pembrolizumab savings of $14 million. Adding dose rounding (strategy two) could reduce pembrolizumab spending by $24 million. And using strategy four, with an unlimited window for vial sharing, could mean annual savings of nearly $60 million.
“Our results should prompt cost-conscious systems and payers to ask whether the amounts of drugs they’re providing to patients and how they go about making those doses are the most cost-effective approaches,” said corresponding author Garth W. Strohbehn, MD, of the University of Michigan and the VA Ann Arbor Healthcare System.
Dr. Strohbehn said the prospect of adopting these strategies hinges on several factors, with financial incentives at the prescriber and medical center level likely being the most influential.
“In fee-for-service systems, reimbursement scales with the amount of drug administered, so there can be a financial disincentive to decreasing overall drug usage,” Dr. Strohbehn explained.
“Conversely, integrated systems such as Kaiser Permanente or the VHA and large self-insured employers are incentivized to contain costs and take great care of patients, so they may be more inclined to promote these strategies,” he added.
However, Adam C. Powell, PhD, president, Payer+Provider Syndicate, who wasn’t involved in the analysis, cautioned that such a shift may come with unintended consequences.
The Infrastructure, Investment, and Jobs Act of 2021 let the Centers for Medicare and Medicaid Services seek reimbursement for discarded drugs – in effect, changing the reimbursement model for medications. That led pharmaceutical manufacturers to respond in kind by changing the dosing model, Dr. Powell said.
“Drugs that previously had personalized weight-based dosing were moved to uniform flat dosing, eliminating the potential for the manufacturer to have to issue a reimbursement if the patient’s personalized dose fell short of the amount in the single-use vial,” Dr. Powell added.
If there is a substantial migration to weight-based dosing, “it is possible that pharmaceutical manufacturers will rethink their dosing and pricing models, just as happened previously,” he cautioned.
However, these strategies could also provide relief for another escalating issue: drug shortages. Especially in the current moment, having a stewardship mindset, “might be helpful in navigating drug shortages,” Dr. Strohbehn said.
This research had no commercial funding. Dr. Bryant, Dr. Strohbehn, and Dr. Powell report no relevant financial relationships.
A version of this article appeared on Medscape.com.
Implementing stewardship strategies for immune checkpoint inhibitor (ICI) therapy, including personalized weight-based dosing, dose rounding, and pharmacy-level vial sharing, could generate savings of as much as $74 million each year for the Veterans Health Administration (VHA), a new analysis suggests.
That $74 million in savings would translate to nearly 14% less spent on ICI therapy annually.
first author Alex Bryant, MD, University of Michigan, Ann Arbor, said in an interview.
The study was published in Health Affairs.
ICI therapy is used in about 40 unique cancer indications and, in 2020, accounted for more than $6 billion in Medicare Part B spending.
Two of the most prescribed ICIs – pembrolizumab and nivolumab – initially received their U.S. approval at personalized weight-based doses. But at the request of the manufacturers, the Food and Drug Administration approved “one-size-fits-all” flat doses, despite a lack of data to support this strategy compared with weight-based dosing.
With a fixed dose strategy, “patients with cancer not only tend to get too high a dose of the drug, but costs go up significantly,” Daniel Goldstein, MD, a medical oncologist at the Rabin Medical Center, Petah Tikva, Israel, told this news organization last year. “Why should we give a higher dose with the same efficacy when that dose will cost significantly more and has the potential to increase adverse events?”
To compare the cost of a weight-based vs. fixed-dose strategy, Dr. Bryant and colleagues conducted a simulation analysis under four stewardship scenarios, using data from the VHA and Medicare drug prices. Strategy one looked at weight-based dosing; strategy two combined weight-based dosing and dose rounding but not single-use vial sharing; strategy three used weight-based dosing and single-use vial sharing but not dose rounding; and strategy four, the most aggressive, combined all three.
ICIs in the VHA national formulary included pembrolizumab, nivolumab, atezolizumab, durvalumab, and cemiplimab-rwlc.
Using an algorithm to extract data, the team identified 49,851 administration events in 8,276 unique patients in 2021 – just over half were pembrolizumab, nearly 23% were nivolumab, and the remaining 26% largely included atezolizumab (12.1%) and durvalumab (11.9%).
The team found that the VHA spends roughly $537 million annually on ICIs. But implementing the stewardship measures that combined weight-based dosing, dose rounding, and vial sharing could save the VHA $74 million, or about 14%, annually on ICIs.
Most of the savings came from dosing changes to pembrolizumab and nivolumab, with greater savings achieved by combining more stewardship strategies. For instance, using strategy one (weight-based dosing alone) could lead to annual pembrolizumab savings of $14 million. Adding dose rounding (strategy two) could reduce pembrolizumab spending by $24 million. And using strategy four, with an unlimited window for vial sharing, could mean annual savings of nearly $60 million.
“Our results should prompt cost-conscious systems and payers to ask whether the amounts of drugs they’re providing to patients and how they go about making those doses are the most cost-effective approaches,” said corresponding author Garth W. Strohbehn, MD, of the University of Michigan and the VA Ann Arbor Healthcare System.
Dr. Strohbehn said the prospect of adopting these strategies hinges on several factors, with financial incentives at the prescriber and medical center level likely being the most influential.
“In fee-for-service systems, reimbursement scales with the amount of drug administered, so there can be a financial disincentive to decreasing overall drug usage,” Dr. Strohbehn explained.
“Conversely, integrated systems such as Kaiser Permanente or the VHA and large self-insured employers are incentivized to contain costs and take great care of patients, so they may be more inclined to promote these strategies,” he added.
However, Adam C. Powell, PhD, president, Payer+Provider Syndicate, who wasn’t involved in the analysis, cautioned that such a shift may come with unintended consequences.
The Infrastructure, Investment, and Jobs Act of 2021 let the Centers for Medicare and Medicaid Services seek reimbursement for discarded drugs – in effect, changing the reimbursement model for medications. That led pharmaceutical manufacturers to respond in kind by changing the dosing model, Dr. Powell said.
“Drugs that previously had personalized weight-based dosing were moved to uniform flat dosing, eliminating the potential for the manufacturer to have to issue a reimbursement if the patient’s personalized dose fell short of the amount in the single-use vial,” Dr. Powell added.
If there is a substantial migration to weight-based dosing, “it is possible that pharmaceutical manufacturers will rethink their dosing and pricing models, just as happened previously,” he cautioned.
However, these strategies could also provide relief for another escalating issue: drug shortages. Especially in the current moment, having a stewardship mindset, “might be helpful in navigating drug shortages,” Dr. Strohbehn said.
This research had no commercial funding. Dr. Bryant, Dr. Strohbehn, and Dr. Powell report no relevant financial relationships.
A version of this article appeared on Medscape.com.
Implementing stewardship strategies for immune checkpoint inhibitor (ICI) therapy, including personalized weight-based dosing, dose rounding, and pharmacy-level vial sharing, could generate savings of as much as $74 million each year for the Veterans Health Administration (VHA), a new analysis suggests.
That $74 million in savings would translate to nearly 14% less spent on ICI therapy annually.
first author Alex Bryant, MD, University of Michigan, Ann Arbor, said in an interview.
The study was published in Health Affairs.
ICI therapy is used in about 40 unique cancer indications and, in 2020, accounted for more than $6 billion in Medicare Part B spending.
Two of the most prescribed ICIs – pembrolizumab and nivolumab – initially received their U.S. approval at personalized weight-based doses. But at the request of the manufacturers, the Food and Drug Administration approved “one-size-fits-all” flat doses, despite a lack of data to support this strategy compared with weight-based dosing.
With a fixed dose strategy, “patients with cancer not only tend to get too high a dose of the drug, but costs go up significantly,” Daniel Goldstein, MD, a medical oncologist at the Rabin Medical Center, Petah Tikva, Israel, told this news organization last year. “Why should we give a higher dose with the same efficacy when that dose will cost significantly more and has the potential to increase adverse events?”
To compare the cost of a weight-based vs. fixed-dose strategy, Dr. Bryant and colleagues conducted a simulation analysis under four stewardship scenarios, using data from the VHA and Medicare drug prices. Strategy one looked at weight-based dosing; strategy two combined weight-based dosing and dose rounding but not single-use vial sharing; strategy three used weight-based dosing and single-use vial sharing but not dose rounding; and strategy four, the most aggressive, combined all three.
ICIs in the VHA national formulary included pembrolizumab, nivolumab, atezolizumab, durvalumab, and cemiplimab-rwlc.
Using an algorithm to extract data, the team identified 49,851 administration events in 8,276 unique patients in 2021 – just over half were pembrolizumab, nearly 23% were nivolumab, and the remaining 26% largely included atezolizumab (12.1%) and durvalumab (11.9%).
The team found that the VHA spends roughly $537 million annually on ICIs. But implementing the stewardship measures that combined weight-based dosing, dose rounding, and vial sharing could save the VHA $74 million, or about 14%, annually on ICIs.
Most of the savings came from dosing changes to pembrolizumab and nivolumab, with greater savings achieved by combining more stewardship strategies. For instance, using strategy one (weight-based dosing alone) could lead to annual pembrolizumab savings of $14 million. Adding dose rounding (strategy two) could reduce pembrolizumab spending by $24 million. And using strategy four, with an unlimited window for vial sharing, could mean annual savings of nearly $60 million.
“Our results should prompt cost-conscious systems and payers to ask whether the amounts of drugs they’re providing to patients and how they go about making those doses are the most cost-effective approaches,” said corresponding author Garth W. Strohbehn, MD, of the University of Michigan and the VA Ann Arbor Healthcare System.
Dr. Strohbehn said the prospect of adopting these strategies hinges on several factors, with financial incentives at the prescriber and medical center level likely being the most influential.
“In fee-for-service systems, reimbursement scales with the amount of drug administered, so there can be a financial disincentive to decreasing overall drug usage,” Dr. Strohbehn explained.
“Conversely, integrated systems such as Kaiser Permanente or the VHA and large self-insured employers are incentivized to contain costs and take great care of patients, so they may be more inclined to promote these strategies,” he added.
However, Adam C. Powell, PhD, president, Payer+Provider Syndicate, who wasn’t involved in the analysis, cautioned that such a shift may come with unintended consequences.
The Infrastructure, Investment, and Jobs Act of 2021 let the Centers for Medicare and Medicaid Services seek reimbursement for discarded drugs – in effect, changing the reimbursement model for medications. That led pharmaceutical manufacturers to respond in kind by changing the dosing model, Dr. Powell said.
“Drugs that previously had personalized weight-based dosing were moved to uniform flat dosing, eliminating the potential for the manufacturer to have to issue a reimbursement if the patient’s personalized dose fell short of the amount in the single-use vial,” Dr. Powell added.
If there is a substantial migration to weight-based dosing, “it is possible that pharmaceutical manufacturers will rethink their dosing and pricing models, just as happened previously,” he cautioned.
However, these strategies could also provide relief for another escalating issue: drug shortages. Especially in the current moment, having a stewardship mindset, “might be helpful in navigating drug shortages,” Dr. Strohbehn said.
This research had no commercial funding. Dr. Bryant, Dr. Strohbehn, and Dr. Powell report no relevant financial relationships.
A version of this article appeared on Medscape.com.
FROM HEALTH AFFAIRS
Metachronous CRC risk after colonoscopy for positive FIT
TOPLINE:
a study suggests.
,
METHODOLOGY:
- Investigators conducted a retrospective analysis of 253,833 colonoscopies performed after FIT-positive screens in a Dutch CRC screening program.
- A Cox regression analysis assessed the association between the findings at baseline colonoscopy and metachronous CRC risk.
- Investigators categorized patients into subgroups based on removed polyp subtypes and used groups without polyps as a reference.
- High-risk subgroups included those with high-risk serrated polyps, which were defined as a serrated polyp of at least 10 mm, sessile serrated lesions with dysplasia, or traditional serrated adenomas, as well as high-risk adenomas, which were defined as an adenoma of at least 10 mm or containing high-grade dysplasia.
TAKEAWAY:
- Over a median follow-up of 36 months, 504 metachronous CRCs were identified.
- Individuals with high-risk serrated polyps without co-occurring high-risk adenomas had an increased risk for metachronous CRC (hazard ratio, 1.70).
- The highest risk was seen in individuals with both high-risk serrated polyps and high-risk adenomas (HR, 2.0), as well as those with villous adenomas (HR, 2.07).
- Individuals with only high-risk adenomas did not show a significantly increased risk for metachronous CRC (HR, 1.22).
IN PRACTICE:
“Our results suggest that individuals with high-risk serrated polyps might comprise the higher CRC risk in the first years after colonoscopy. Results of this study could contribute to establish more restrictive polyp surveillance guidelines in a quality-assured setting,” the authors wrote.
SOURCE:
The study was led by David E. F. W. M. van Toledo, MD, department of gastroenterology and hepatology, Amsterdam University Medical Centers. It was published online July 5, 2023, in eClinicalMedicine. The study received no funding.
LIMITATIONS:
The relatively short median follow-up time of 3 years may limit the assessment of long-term metachronous CRC risk. The study population consisted of FIT-positive individuals, which may introduce selection bias. The incidence of metachronous CRC in the study was lower compared with other studies, potentially affecting the risk estimates. The limited number of cases in some subgroups may result in unreliable risk estimations.
DISCLOSURES:
Dr. van Toledo declared no relevant financial relationships.
A version of this article first appeared on Medscape.com.
TOPLINE:
a study suggests.
,
METHODOLOGY:
- Investigators conducted a retrospective analysis of 253,833 colonoscopies performed after FIT-positive screens in a Dutch CRC screening program.
- A Cox regression analysis assessed the association between the findings at baseline colonoscopy and metachronous CRC risk.
- Investigators categorized patients into subgroups based on removed polyp subtypes and used groups without polyps as a reference.
- High-risk subgroups included those with high-risk serrated polyps, which were defined as a serrated polyp of at least 10 mm, sessile serrated lesions with dysplasia, or traditional serrated adenomas, as well as high-risk adenomas, which were defined as an adenoma of at least 10 mm or containing high-grade dysplasia.
TAKEAWAY:
- Over a median follow-up of 36 months, 504 metachronous CRCs were identified.
- Individuals with high-risk serrated polyps without co-occurring high-risk adenomas had an increased risk for metachronous CRC (hazard ratio, 1.70).
- The highest risk was seen in individuals with both high-risk serrated polyps and high-risk adenomas (HR, 2.0), as well as those with villous adenomas (HR, 2.07).
- Individuals with only high-risk adenomas did not show a significantly increased risk for metachronous CRC (HR, 1.22).
IN PRACTICE:
“Our results suggest that individuals with high-risk serrated polyps might comprise the higher CRC risk in the first years after colonoscopy. Results of this study could contribute to establish more restrictive polyp surveillance guidelines in a quality-assured setting,” the authors wrote.
SOURCE:
The study was led by David E. F. W. M. van Toledo, MD, department of gastroenterology and hepatology, Amsterdam University Medical Centers. It was published online July 5, 2023, in eClinicalMedicine. The study received no funding.
LIMITATIONS:
The relatively short median follow-up time of 3 years may limit the assessment of long-term metachronous CRC risk. The study population consisted of FIT-positive individuals, which may introduce selection bias. The incidence of metachronous CRC in the study was lower compared with other studies, potentially affecting the risk estimates. The limited number of cases in some subgroups may result in unreliable risk estimations.
DISCLOSURES:
Dr. van Toledo declared no relevant financial relationships.
A version of this article first appeared on Medscape.com.
TOPLINE:
a study suggests.
,
METHODOLOGY:
- Investigators conducted a retrospective analysis of 253,833 colonoscopies performed after FIT-positive screens in a Dutch CRC screening program.
- A Cox regression analysis assessed the association between the findings at baseline colonoscopy and metachronous CRC risk.
- Investigators categorized patients into subgroups based on removed polyp subtypes and used groups without polyps as a reference.
- High-risk subgroups included those with high-risk serrated polyps, which were defined as a serrated polyp of at least 10 mm, sessile serrated lesions with dysplasia, or traditional serrated adenomas, as well as high-risk adenomas, which were defined as an adenoma of at least 10 mm or containing high-grade dysplasia.
TAKEAWAY:
- Over a median follow-up of 36 months, 504 metachronous CRCs were identified.
- Individuals with high-risk serrated polyps without co-occurring high-risk adenomas had an increased risk for metachronous CRC (hazard ratio, 1.70).
- The highest risk was seen in individuals with both high-risk serrated polyps and high-risk adenomas (HR, 2.0), as well as those with villous adenomas (HR, 2.07).
- Individuals with only high-risk adenomas did not show a significantly increased risk for metachronous CRC (HR, 1.22).
IN PRACTICE:
“Our results suggest that individuals with high-risk serrated polyps might comprise the higher CRC risk in the first years after colonoscopy. Results of this study could contribute to establish more restrictive polyp surveillance guidelines in a quality-assured setting,” the authors wrote.
SOURCE:
The study was led by David E. F. W. M. van Toledo, MD, department of gastroenterology and hepatology, Amsterdam University Medical Centers. It was published online July 5, 2023, in eClinicalMedicine. The study received no funding.
LIMITATIONS:
The relatively short median follow-up time of 3 years may limit the assessment of long-term metachronous CRC risk. The study population consisted of FIT-positive individuals, which may introduce selection bias. The incidence of metachronous CRC in the study was lower compared with other studies, potentially affecting the risk estimates. The limited number of cases in some subgroups may result in unreliable risk estimations.
DISCLOSURES:
Dr. van Toledo declared no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Liquid biopsy shows big promise in oropharyngeal cancer
In a retrospective observational cohort study, a commercially available blood test used to evaluate tumor tissue–modified viral-HPV DNA demonstrated 100% specificity for both diagnosis of oropharyngeal cancer and surveillance for recurrence. Sensitivity was 91.5% for correctly identifying patients who have the disease and 88.4% for surveillance.
“A positive result appeared to confirm the presence of disease, [but] approximately 1 in 10 negative results in patients with pathologically confirmed HPV-associated oropharyngeal squamous cell carcinoma were falsely negative,” lead investigator Rocco Ferrandino, MD, with Mount Sinai, New York, said in an interview.
“Therefore, further workup should still be pursued when clinical suspicion for HPV-associated oropharynx cancer is high,” Dr. Ferrandino said.
The study was published online, in JAMA Otolaryngology–Head and Neck Surgery, to coincide with presentation at the annual meeting of the American Head and Neck Society in Montreal.
‘Remarkable promise’
The diagnosis of HPV-associated oropharyngeal cancer currently relies on a tissue-based biopsy of the primary site or a regional lymph node; however, there has been growing interest in the potential of liquid biopsy for diagnosis and surveillance.
The commercially available assay that was evaluated in the study uses a distinct method to identify and quantify a tumor-associated or tumor-modified pattern of DNA fragments that significantly increases the specificity for identifying an HPV-associated malignant tumor. However, evaluation of the assay has been limited to small cohort studies and clinical trials.
In the current study, Dr. Ferrandino and colleagues evaluated the performance of the assay used during routine clinical practice at their high-volume institution over a period of nearly 3 years.
The study included 163 patients in the diagnostic cohort and 290 in the surveillance cohort. In the diagnostic cohort, 152 had HPV-associated oropharyngeal cancer, and 11 had HPV-negative oropharyngeal cancer. The sensitivity of the assay in pretreatment diagnosis was 91.5% (139 of 152 tests), and the specificity was 100% (11 of 11 tests).
In the surveillance cohort of 290 patients, 591 tests were evaluated. A total of 23 patients developed pathologically confirmed recurrences over a median follow-up of 40.5 months. The assay demonstrated sensitivity of 88.4% (38 of 43 tests) and specificity of 100% (548 of 548 tests) in detecting recurrences.
The median lead time from positive test to pathologic confirmation was 47 days.
“The lead time provided by positive assay results may allow a window of opportunity for salvage treatment or for the application of adjuvant systemic therapy,” Dr. Ferrandino and colleagues explain.
“While these results are exciting and may support adjunctive use of circulating tumor DNA testing for diagnosis and surveillance, we really need more prospective and multicenter studies to validate these findings,” Dr. Ferrandino said in an interview.
In an accompanying commentary, Miriam Lango, MD, department of head and neck surgery, the University of Texas MD Anderson Cancer Center, Houston, said she agrees that a prospective clinical validation study is needed.
“Nevertheless, the use of this technology shows remarkable promise to transform the ability to identify and follow patients with HPV-related disease. Testing is likely to be increasingly used in routine clinical care, as it is commercially available,” Dr. Lango writes.
Still, she noted, “It is incumbent on us to establish evidence for strong and detailed surveillance guidelines to share among the cancer community.”
The study had no specific funding. Dr. Ferrandino and Dr. Lango have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
In a retrospective observational cohort study, a commercially available blood test used to evaluate tumor tissue–modified viral-HPV DNA demonstrated 100% specificity for both diagnosis of oropharyngeal cancer and surveillance for recurrence. Sensitivity was 91.5% for correctly identifying patients who have the disease and 88.4% for surveillance.
“A positive result appeared to confirm the presence of disease, [but] approximately 1 in 10 negative results in patients with pathologically confirmed HPV-associated oropharyngeal squamous cell carcinoma were falsely negative,” lead investigator Rocco Ferrandino, MD, with Mount Sinai, New York, said in an interview.
“Therefore, further workup should still be pursued when clinical suspicion for HPV-associated oropharynx cancer is high,” Dr. Ferrandino said.
The study was published online, in JAMA Otolaryngology–Head and Neck Surgery, to coincide with presentation at the annual meeting of the American Head and Neck Society in Montreal.
‘Remarkable promise’
The diagnosis of HPV-associated oropharyngeal cancer currently relies on a tissue-based biopsy of the primary site or a regional lymph node; however, there has been growing interest in the potential of liquid biopsy for diagnosis and surveillance.
The commercially available assay that was evaluated in the study uses a distinct method to identify and quantify a tumor-associated or tumor-modified pattern of DNA fragments that significantly increases the specificity for identifying an HPV-associated malignant tumor. However, evaluation of the assay has been limited to small cohort studies and clinical trials.
In the current study, Dr. Ferrandino and colleagues evaluated the performance of the assay used during routine clinical practice at their high-volume institution over a period of nearly 3 years.
The study included 163 patients in the diagnostic cohort and 290 in the surveillance cohort. In the diagnostic cohort, 152 had HPV-associated oropharyngeal cancer, and 11 had HPV-negative oropharyngeal cancer. The sensitivity of the assay in pretreatment diagnosis was 91.5% (139 of 152 tests), and the specificity was 100% (11 of 11 tests).
In the surveillance cohort of 290 patients, 591 tests were evaluated. A total of 23 patients developed pathologically confirmed recurrences over a median follow-up of 40.5 months. The assay demonstrated sensitivity of 88.4% (38 of 43 tests) and specificity of 100% (548 of 548 tests) in detecting recurrences.
The median lead time from positive test to pathologic confirmation was 47 days.
“The lead time provided by positive assay results may allow a window of opportunity for salvage treatment or for the application of adjuvant systemic therapy,” Dr. Ferrandino and colleagues explain.
“While these results are exciting and may support adjunctive use of circulating tumor DNA testing for diagnosis and surveillance, we really need more prospective and multicenter studies to validate these findings,” Dr. Ferrandino said in an interview.
In an accompanying commentary, Miriam Lango, MD, department of head and neck surgery, the University of Texas MD Anderson Cancer Center, Houston, said she agrees that a prospective clinical validation study is needed.
“Nevertheless, the use of this technology shows remarkable promise to transform the ability to identify and follow patients with HPV-related disease. Testing is likely to be increasingly used in routine clinical care, as it is commercially available,” Dr. Lango writes.
Still, she noted, “It is incumbent on us to establish evidence for strong and detailed surveillance guidelines to share among the cancer community.”
The study had no specific funding. Dr. Ferrandino and Dr. Lango have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
In a retrospective observational cohort study, a commercially available blood test used to evaluate tumor tissue–modified viral-HPV DNA demonstrated 100% specificity for both diagnosis of oropharyngeal cancer and surveillance for recurrence. Sensitivity was 91.5% for correctly identifying patients who have the disease and 88.4% for surveillance.
“A positive result appeared to confirm the presence of disease, [but] approximately 1 in 10 negative results in patients with pathologically confirmed HPV-associated oropharyngeal squamous cell carcinoma were falsely negative,” lead investigator Rocco Ferrandino, MD, with Mount Sinai, New York, said in an interview.
“Therefore, further workup should still be pursued when clinical suspicion for HPV-associated oropharynx cancer is high,” Dr. Ferrandino said.
The study was published online, in JAMA Otolaryngology–Head and Neck Surgery, to coincide with presentation at the annual meeting of the American Head and Neck Society in Montreal.
‘Remarkable promise’
The diagnosis of HPV-associated oropharyngeal cancer currently relies on a tissue-based biopsy of the primary site or a regional lymph node; however, there has been growing interest in the potential of liquid biopsy for diagnosis and surveillance.
The commercially available assay that was evaluated in the study uses a distinct method to identify and quantify a tumor-associated or tumor-modified pattern of DNA fragments that significantly increases the specificity for identifying an HPV-associated malignant tumor. However, evaluation of the assay has been limited to small cohort studies and clinical trials.
In the current study, Dr. Ferrandino and colleagues evaluated the performance of the assay used during routine clinical practice at their high-volume institution over a period of nearly 3 years.
The study included 163 patients in the diagnostic cohort and 290 in the surveillance cohort. In the diagnostic cohort, 152 had HPV-associated oropharyngeal cancer, and 11 had HPV-negative oropharyngeal cancer. The sensitivity of the assay in pretreatment diagnosis was 91.5% (139 of 152 tests), and the specificity was 100% (11 of 11 tests).
In the surveillance cohort of 290 patients, 591 tests were evaluated. A total of 23 patients developed pathologically confirmed recurrences over a median follow-up of 40.5 months. The assay demonstrated sensitivity of 88.4% (38 of 43 tests) and specificity of 100% (548 of 548 tests) in detecting recurrences.
The median lead time from positive test to pathologic confirmation was 47 days.
“The lead time provided by positive assay results may allow a window of opportunity for salvage treatment or for the application of adjuvant systemic therapy,” Dr. Ferrandino and colleagues explain.
“While these results are exciting and may support adjunctive use of circulating tumor DNA testing for diagnosis and surveillance, we really need more prospective and multicenter studies to validate these findings,” Dr. Ferrandino said in an interview.
In an accompanying commentary, Miriam Lango, MD, department of head and neck surgery, the University of Texas MD Anderson Cancer Center, Houston, said she agrees that a prospective clinical validation study is needed.
“Nevertheless, the use of this technology shows remarkable promise to transform the ability to identify and follow patients with HPV-related disease. Testing is likely to be increasingly used in routine clinical care, as it is commercially available,” Dr. Lango writes.
Still, she noted, “It is incumbent on us to establish evidence for strong and detailed surveillance guidelines to share among the cancer community.”
The study had no specific funding. Dr. Ferrandino and Dr. Lango have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM JAMA OTOLARYNGOLOGY–HEAD AND NECK SURGERY
Does timing of surgery affect rectal cancer outcomes?
TOPLINE:
METHODOLOGY:
- A total of 1,506 patients with locally advanced rectal cancer who underwent neoadjuvant therapy followed by total mesorectal excision were divided into three groups based on the time interval between therapy and surgery: short (8 weeks), intermediate (> 8 to 12 weeks), and long (> 12 weeks).
- The primary outcome was pathologic complete response, and secondary outcomes included other histopathologic results, perioperative events, and survival outcomes.
- Median follow-up was 33 months.
TAKEAWAY:
- Overall, a pathologic complete response was observed in 255 patients (17.2%).
- Compared with the intermediate interval (reference) group, investigators found no association between time interval and pathologic complete response in the short-interval (odds ratio, 0.74; 95% CI, 0.55-1.01) or long-interval groups (OR, 1.07; P = .70).
- A long interval was significantly associated with a lower risk of a bad response as measured by tumor regression grade 2-3, compared with the reference category (OR, 0.47), but a higher risk of minor postoperative complications (OR, 1.43), conversion to open surgery (OR, 3.14), and longer operative time.
- The long-interval group was associated with a significantly reduced risk of systemic recurrence, compared with the reference group (hazard ratio, 0.59; P = .04), but not improved overall survival (HR, 1.38; P = .11) or locoregional recurrence (HR, 0.53; P = .18); no significant findings occurred for the short versus intermediate group.
IN PRACTICE:
“Findings suggest that delaying surgery may improve tumor regression and decrease risk of distant metastasis but increase surgical complexity,” the authors conclude. “Nonetheless, the reported improvements in tumor regression and systemic recurrence in the long-interval group were unexpectedly not followed by improved [overall survival].”
SOURCE:
F. Borja de Lacy, MD, PhD, Hospital Clinic of Barcelona, University of Barcelona, led the study, published online in JAMA Surgery, with an accompanying editorial.
LIMITATIONS:
- The study’s main limitation was its retrospective design, which could have resulted in missing or inconsistent data, as well as the short follow-up time.
- Decisions about time interval were based more on professional preference rather than specific tumor characteristics.
DISCLOSURES:
Dr. de Lacy has reported no relevant financial relationships. No outside funding source was disclosed.
A version of this article first appeared on Medscape.com.
TOPLINE:
METHODOLOGY:
- A total of 1,506 patients with locally advanced rectal cancer who underwent neoadjuvant therapy followed by total mesorectal excision were divided into three groups based on the time interval between therapy and surgery: short (8 weeks), intermediate (> 8 to 12 weeks), and long (> 12 weeks).
- The primary outcome was pathologic complete response, and secondary outcomes included other histopathologic results, perioperative events, and survival outcomes.
- Median follow-up was 33 months.
TAKEAWAY:
- Overall, a pathologic complete response was observed in 255 patients (17.2%).
- Compared with the intermediate interval (reference) group, investigators found no association between time interval and pathologic complete response in the short-interval (odds ratio, 0.74; 95% CI, 0.55-1.01) or long-interval groups (OR, 1.07; P = .70).
- A long interval was significantly associated with a lower risk of a bad response as measured by tumor regression grade 2-3, compared with the reference category (OR, 0.47), but a higher risk of minor postoperative complications (OR, 1.43), conversion to open surgery (OR, 3.14), and longer operative time.
- The long-interval group was associated with a significantly reduced risk of systemic recurrence, compared with the reference group (hazard ratio, 0.59; P = .04), but not improved overall survival (HR, 1.38; P = .11) or locoregional recurrence (HR, 0.53; P = .18); no significant findings occurred for the short versus intermediate group.
IN PRACTICE:
“Findings suggest that delaying surgery may improve tumor regression and decrease risk of distant metastasis but increase surgical complexity,” the authors conclude. “Nonetheless, the reported improvements in tumor regression and systemic recurrence in the long-interval group were unexpectedly not followed by improved [overall survival].”
SOURCE:
F. Borja de Lacy, MD, PhD, Hospital Clinic of Barcelona, University of Barcelona, led the study, published online in JAMA Surgery, with an accompanying editorial.
LIMITATIONS:
- The study’s main limitation was its retrospective design, which could have resulted in missing or inconsistent data, as well as the short follow-up time.
- Decisions about time interval were based more on professional preference rather than specific tumor characteristics.
DISCLOSURES:
Dr. de Lacy has reported no relevant financial relationships. No outside funding source was disclosed.
A version of this article first appeared on Medscape.com.
TOPLINE:
METHODOLOGY:
- A total of 1,506 patients with locally advanced rectal cancer who underwent neoadjuvant therapy followed by total mesorectal excision were divided into three groups based on the time interval between therapy and surgery: short (8 weeks), intermediate (> 8 to 12 weeks), and long (> 12 weeks).
- The primary outcome was pathologic complete response, and secondary outcomes included other histopathologic results, perioperative events, and survival outcomes.
- Median follow-up was 33 months.
TAKEAWAY:
- Overall, a pathologic complete response was observed in 255 patients (17.2%).
- Compared with the intermediate interval (reference) group, investigators found no association between time interval and pathologic complete response in the short-interval (odds ratio, 0.74; 95% CI, 0.55-1.01) or long-interval groups (OR, 1.07; P = .70).
- A long interval was significantly associated with a lower risk of a bad response as measured by tumor regression grade 2-3, compared with the reference category (OR, 0.47), but a higher risk of minor postoperative complications (OR, 1.43), conversion to open surgery (OR, 3.14), and longer operative time.
- The long-interval group was associated with a significantly reduced risk of systemic recurrence, compared with the reference group (hazard ratio, 0.59; P = .04), but not improved overall survival (HR, 1.38; P = .11) or locoregional recurrence (HR, 0.53; P = .18); no significant findings occurred for the short versus intermediate group.
IN PRACTICE:
“Findings suggest that delaying surgery may improve tumor regression and decrease risk of distant metastasis but increase surgical complexity,” the authors conclude. “Nonetheless, the reported improvements in tumor regression and systemic recurrence in the long-interval group were unexpectedly not followed by improved [overall survival].”
SOURCE:
F. Borja de Lacy, MD, PhD, Hospital Clinic of Barcelona, University of Barcelona, led the study, published online in JAMA Surgery, with an accompanying editorial.
LIMITATIONS:
- The study’s main limitation was its retrospective design, which could have resulted in missing or inconsistent data, as well as the short follow-up time.
- Decisions about time interval were based more on professional preference rather than specific tumor characteristics.
DISCLOSURES:
Dr. de Lacy has reported no relevant financial relationships. No outside funding source was disclosed.
A version of this article first appeared on Medscape.com.
Brisk walking: No-cost option for patients to improve cancer outcomes
This transcript has been edited for clarity.
I’m Maurie Markman, MD, from Cancer Treatment Centers of America in Philadelphia. I wanted to discuss a highly provocative paper that I think deserves attention. It was published in the Journal of Clinical Oncology, titled Physical Activity in Stage III Colon Cancer: CALGB/SWOG 80702 (Alliance).
This is an incredibly important paper that highlights something that has not been emphasized enough in oncology practice. What are the things that we can recommend to our patients that are not expensive, but which they can do for themselves to impact a potential for adding to a positive outcome? In this case, we’re talking about physical activity.
This was an extremely well-conducted study. It was a prospective cohort study that was built into an ongoing phase 3 randomized, multicenter study looking at adjuvant therapy of stage III colon cancer. The median follow-up in this population was almost 6 years. We’re talking about 1,696 patients.
The investigators did a survey, asking patients when they started treatment and then a short time after that, and measured the level of recreational physical activity. They didn’t do a design. They asked the individuals how much activity they had.
There were a number of analyses done in terms of looking at this that were reported in the paper. I want to highlight one because it’s so simple. The investigators looked at brisk walking. For brisk walking, the 3-year disease-free survival was 81.7% for individuals who had less than 1 hour per week of brisk walking versus 88.4% for individuals who walked briskly more than 3 hours per week.
There is no additional expense. It’s walking. There were other activities that were looked at here, including aerobic activities.
The bottom line is that physical activity is positive, is not expensive, and focuses on what the individual patient can do for themselves. It’s something I believe that, in the oncology community, we need to emphasize more.
I encourage you to review this paper and use your own opinion as to what you want to do with this information, but I strongly urge you to look at this – and other types of activities – that we can recommend that individuals do themselves to impact their outcomes related to cancer.
Dr. Markman is a clinical professor of medicine at Drexel University, Philadelphia. He reported conflicts of interest with Genentech, AstraZeneca, Celgene, Clovis, and Amgen.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
I’m Maurie Markman, MD, from Cancer Treatment Centers of America in Philadelphia. I wanted to discuss a highly provocative paper that I think deserves attention. It was published in the Journal of Clinical Oncology, titled Physical Activity in Stage III Colon Cancer: CALGB/SWOG 80702 (Alliance).
This is an incredibly important paper that highlights something that has not been emphasized enough in oncology practice. What are the things that we can recommend to our patients that are not expensive, but which they can do for themselves to impact a potential for adding to a positive outcome? In this case, we’re talking about physical activity.
This was an extremely well-conducted study. It was a prospective cohort study that was built into an ongoing phase 3 randomized, multicenter study looking at adjuvant therapy of stage III colon cancer. The median follow-up in this population was almost 6 years. We’re talking about 1,696 patients.
The investigators did a survey, asking patients when they started treatment and then a short time after that, and measured the level of recreational physical activity. They didn’t do a design. They asked the individuals how much activity they had.
There were a number of analyses done in terms of looking at this that were reported in the paper. I want to highlight one because it’s so simple. The investigators looked at brisk walking. For brisk walking, the 3-year disease-free survival was 81.7% for individuals who had less than 1 hour per week of brisk walking versus 88.4% for individuals who walked briskly more than 3 hours per week.
There is no additional expense. It’s walking. There were other activities that were looked at here, including aerobic activities.
The bottom line is that physical activity is positive, is not expensive, and focuses on what the individual patient can do for themselves. It’s something I believe that, in the oncology community, we need to emphasize more.
I encourage you to review this paper and use your own opinion as to what you want to do with this information, but I strongly urge you to look at this – and other types of activities – that we can recommend that individuals do themselves to impact their outcomes related to cancer.
Dr. Markman is a clinical professor of medicine at Drexel University, Philadelphia. He reported conflicts of interest with Genentech, AstraZeneca, Celgene, Clovis, and Amgen.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
I’m Maurie Markman, MD, from Cancer Treatment Centers of America in Philadelphia. I wanted to discuss a highly provocative paper that I think deserves attention. It was published in the Journal of Clinical Oncology, titled Physical Activity in Stage III Colon Cancer: CALGB/SWOG 80702 (Alliance).
This is an incredibly important paper that highlights something that has not been emphasized enough in oncology practice. What are the things that we can recommend to our patients that are not expensive, but which they can do for themselves to impact a potential for adding to a positive outcome? In this case, we’re talking about physical activity.
This was an extremely well-conducted study. It was a prospective cohort study that was built into an ongoing phase 3 randomized, multicenter study looking at adjuvant therapy of stage III colon cancer. The median follow-up in this population was almost 6 years. We’re talking about 1,696 patients.
The investigators did a survey, asking patients when they started treatment and then a short time after that, and measured the level of recreational physical activity. They didn’t do a design. They asked the individuals how much activity they had.
There were a number of analyses done in terms of looking at this that were reported in the paper. I want to highlight one because it’s so simple. The investigators looked at brisk walking. For brisk walking, the 3-year disease-free survival was 81.7% for individuals who had less than 1 hour per week of brisk walking versus 88.4% for individuals who walked briskly more than 3 hours per week.
There is no additional expense. It’s walking. There were other activities that were looked at here, including aerobic activities.
The bottom line is that physical activity is positive, is not expensive, and focuses on what the individual patient can do for themselves. It’s something I believe that, in the oncology community, we need to emphasize more.
I encourage you to review this paper and use your own opinion as to what you want to do with this information, but I strongly urge you to look at this – and other types of activities – that we can recommend that individuals do themselves to impact their outcomes related to cancer.
Dr. Markman is a clinical professor of medicine at Drexel University, Philadelphia. He reported conflicts of interest with Genentech, AstraZeneca, Celgene, Clovis, and Amgen.
A version of this article first appeared on Medscape.com.
Lower-dose FOLFIRINOX effective, safer for pancreatic cancer
TOPLINE:
Although practice patterns vary widely, and it is less likely to cause febrile neutropenia.
METHODOLOGY:
- No randomized controlled trials have directly compared modified FOLFIRINOX to standard FOLFIRINOX; this meta-analysis aims to fill the evidence gap.
- The investigators winnowed hundreds of first-line FOLFIRINOX studies down to 37 – 11 prospective and 26 retrospective analyses – to assess practice patterns and clinical outcomes.
- Dose information was grouped into four categories: planned dose in the standard FOLFIRINOX group; actual administered dose in the standard group; planned dose in the modified group; actual administered dose in the modified group.
TAKEAWAY:
- There were 12 types of “planned” dose reductions in FOLFIRINOX: 75%-100% oxaliplatin, 75%-100% irinotecan, 0%-100% 5-fluorouracil (5-FU) bolus, and 75%-133% 5-FU continuous injection.
- Doses actually delivered fell further to 54%-96% for oxaliplatin, 61%-88% for irinotecan, 0%-92% for 5-FU bolus, and 63%-98% 5-FU continuous injection.
- Despite the variations in dosing, reduced doses of FOLFIRINOX were associated with a slightly but not significantly higher objective response rate: 33.8% versus 28.2% for standard dosing (P = .1).
- The incidence of febrile neutropenia was significantly lower in the reduced-dose groups: 5.5% with modified FOLFIRINOX versus 11.6% with standard (P = .03).
IN PRACTICE:
Although the study supports reduced-dose regimens, it also shows that there is “still no consensus” on appropriate dose modification, the authors said. “The best dose modification protocol” remains to be determined and standardized for metastatic pancreatic cancer.
SOURCE:
The study was led by Kwangrok Jung at Seoul (South Korea) National University, and was published June 29 in Therapeutic Advances in Medical Oncology.
LIMITATIONS:
- Only 11 of the 37 studies were prospective.
- The studies often lacked key information, including the reason for dose reductions or detailed dose reduction protocols.
- Studies were also inconsistent in how they reported FOLFIRINOX dose modifications.
DISCLOSURES:
There was no funding for the study, and the investigators had no disclosures.
A version of this article first appeared on Medscape.com.
TOPLINE:
Although practice patterns vary widely, and it is less likely to cause febrile neutropenia.
METHODOLOGY:
- No randomized controlled trials have directly compared modified FOLFIRINOX to standard FOLFIRINOX; this meta-analysis aims to fill the evidence gap.
- The investigators winnowed hundreds of first-line FOLFIRINOX studies down to 37 – 11 prospective and 26 retrospective analyses – to assess practice patterns and clinical outcomes.
- Dose information was grouped into four categories: planned dose in the standard FOLFIRINOX group; actual administered dose in the standard group; planned dose in the modified group; actual administered dose in the modified group.
TAKEAWAY:
- There were 12 types of “planned” dose reductions in FOLFIRINOX: 75%-100% oxaliplatin, 75%-100% irinotecan, 0%-100% 5-fluorouracil (5-FU) bolus, and 75%-133% 5-FU continuous injection.
- Doses actually delivered fell further to 54%-96% for oxaliplatin, 61%-88% for irinotecan, 0%-92% for 5-FU bolus, and 63%-98% 5-FU continuous injection.
- Despite the variations in dosing, reduced doses of FOLFIRINOX were associated with a slightly but not significantly higher objective response rate: 33.8% versus 28.2% for standard dosing (P = .1).
- The incidence of febrile neutropenia was significantly lower in the reduced-dose groups: 5.5% with modified FOLFIRINOX versus 11.6% with standard (P = .03).
IN PRACTICE:
Although the study supports reduced-dose regimens, it also shows that there is “still no consensus” on appropriate dose modification, the authors said. “The best dose modification protocol” remains to be determined and standardized for metastatic pancreatic cancer.
SOURCE:
The study was led by Kwangrok Jung at Seoul (South Korea) National University, and was published June 29 in Therapeutic Advances in Medical Oncology.
LIMITATIONS:
- Only 11 of the 37 studies were prospective.
- The studies often lacked key information, including the reason for dose reductions or detailed dose reduction protocols.
- Studies were also inconsistent in how they reported FOLFIRINOX dose modifications.
DISCLOSURES:
There was no funding for the study, and the investigators had no disclosures.
A version of this article first appeared on Medscape.com.
TOPLINE:
Although practice patterns vary widely, and it is less likely to cause febrile neutropenia.
METHODOLOGY:
- No randomized controlled trials have directly compared modified FOLFIRINOX to standard FOLFIRINOX; this meta-analysis aims to fill the evidence gap.
- The investigators winnowed hundreds of first-line FOLFIRINOX studies down to 37 – 11 prospective and 26 retrospective analyses – to assess practice patterns and clinical outcomes.
- Dose information was grouped into four categories: planned dose in the standard FOLFIRINOX group; actual administered dose in the standard group; planned dose in the modified group; actual administered dose in the modified group.
TAKEAWAY:
- There were 12 types of “planned” dose reductions in FOLFIRINOX: 75%-100% oxaliplatin, 75%-100% irinotecan, 0%-100% 5-fluorouracil (5-FU) bolus, and 75%-133% 5-FU continuous injection.
- Doses actually delivered fell further to 54%-96% for oxaliplatin, 61%-88% for irinotecan, 0%-92% for 5-FU bolus, and 63%-98% 5-FU continuous injection.
- Despite the variations in dosing, reduced doses of FOLFIRINOX were associated with a slightly but not significantly higher objective response rate: 33.8% versus 28.2% for standard dosing (P = .1).
- The incidence of febrile neutropenia was significantly lower in the reduced-dose groups: 5.5% with modified FOLFIRINOX versus 11.6% with standard (P = .03).
IN PRACTICE:
Although the study supports reduced-dose regimens, it also shows that there is “still no consensus” on appropriate dose modification, the authors said. “The best dose modification protocol” remains to be determined and standardized for metastatic pancreatic cancer.
SOURCE:
The study was led by Kwangrok Jung at Seoul (South Korea) National University, and was published June 29 in Therapeutic Advances in Medical Oncology.
LIMITATIONS:
- Only 11 of the 37 studies were prospective.
- The studies often lacked key information, including the reason for dose reductions or detailed dose reduction protocols.
- Studies were also inconsistent in how they reported FOLFIRINOX dose modifications.
DISCLOSURES:
There was no funding for the study, and the investigators had no disclosures.
A version of this article first appeared on Medscape.com.
No benefit to adding limited radiation in advanced cancer
TOPLINE:
METHODOLOGY:
- In the phase 2 CHEERS trial, 52 patients with advanced solid tumors were randomized to anti-PD-1/PD-L1 monotherapy and 47 patients to the same treatment plus stereotactic body radiotherapy (3 x 8 Gy) to a maximum of three lesions before the second or third cycle of an immune checkpoint inhibitor.
- Patients had locally advanced or metastatic melanoma, renal cell carcinoma, urothelial carcinoma, non-small cell lung carcinoma, or head and neck squamous cell carcinoma and were treated at five Belgian hospitals.
- Most patients had more than three lesions.
- Seven patients in the experimental group did not complete radiotherapy because of early progression or intercurrent illness.
TAKEAWAY:
- Over a median follow-up of 12.5 months, median progression-free survival was 4.4 months in the radiotherapy group versus 2.8 months in the control group (hazard ratio, 0.95; P = .82).
- Median overall survival was not significantly better with radiotherapy, compared with the control group (14.3 vs. 11 months; HR, 0.82; P = .47), nor was the objective response rate (27% vs. 22%; P = .56).
- However, a post hoc analysis demonstrated a significant association between the number of irradiated lesions and overall survival among patients receiving radiotherapy (HR, 0.31; P = .002).
- The incidence of grade 3 or worse treatment-related adverse events was 18% in both groups.
IN PRACTICE:
Although the study was negative overall, the post hoc analysis coupled with “recent evidence suggests that treating all active disease sites with higher radiation doses ... may be a more promising strategy to optimize systemic disease control,” the authors concluded.
SOURCE:
The study was led by Mathieu Spaas, MD, department of radiation oncology, Ghent (Bellgium) University, and published online in JAMA Oncology.
LIMITATIONS:
- There was insufficient power to detect if certain cancers benefited more from add-on radiation because of the small sample size.
- More than half of patients in the control group had already received some form of radiotherapy before study inclusion, which may mean the study underestimated the benefit of radiotherapy.
DISCLOSURES:
The work was funded by Kom Op Tegen Kanker and Varian Medical Systems.
Investigators disclosed numerous industry ties, including Merck, Novartis, and Bristol Myers Squibb.
A version of this article first appeared on Medscape.com.
TOPLINE:
METHODOLOGY:
- In the phase 2 CHEERS trial, 52 patients with advanced solid tumors were randomized to anti-PD-1/PD-L1 monotherapy and 47 patients to the same treatment plus stereotactic body radiotherapy (3 x 8 Gy) to a maximum of three lesions before the second or third cycle of an immune checkpoint inhibitor.
- Patients had locally advanced or metastatic melanoma, renal cell carcinoma, urothelial carcinoma, non-small cell lung carcinoma, or head and neck squamous cell carcinoma and were treated at five Belgian hospitals.
- Most patients had more than three lesions.
- Seven patients in the experimental group did not complete radiotherapy because of early progression or intercurrent illness.
TAKEAWAY:
- Over a median follow-up of 12.5 months, median progression-free survival was 4.4 months in the radiotherapy group versus 2.8 months in the control group (hazard ratio, 0.95; P = .82).
- Median overall survival was not significantly better with radiotherapy, compared with the control group (14.3 vs. 11 months; HR, 0.82; P = .47), nor was the objective response rate (27% vs. 22%; P = .56).
- However, a post hoc analysis demonstrated a significant association between the number of irradiated lesions and overall survival among patients receiving radiotherapy (HR, 0.31; P = .002).
- The incidence of grade 3 or worse treatment-related adverse events was 18% in both groups.
IN PRACTICE:
Although the study was negative overall, the post hoc analysis coupled with “recent evidence suggests that treating all active disease sites with higher radiation doses ... may be a more promising strategy to optimize systemic disease control,” the authors concluded.
SOURCE:
The study was led by Mathieu Spaas, MD, department of radiation oncology, Ghent (Bellgium) University, and published online in JAMA Oncology.
LIMITATIONS:
- There was insufficient power to detect if certain cancers benefited more from add-on radiation because of the small sample size.
- More than half of patients in the control group had already received some form of radiotherapy before study inclusion, which may mean the study underestimated the benefit of radiotherapy.
DISCLOSURES:
The work was funded by Kom Op Tegen Kanker and Varian Medical Systems.
Investigators disclosed numerous industry ties, including Merck, Novartis, and Bristol Myers Squibb.
A version of this article first appeared on Medscape.com.
TOPLINE:
METHODOLOGY:
- In the phase 2 CHEERS trial, 52 patients with advanced solid tumors were randomized to anti-PD-1/PD-L1 monotherapy and 47 patients to the same treatment plus stereotactic body radiotherapy (3 x 8 Gy) to a maximum of three lesions before the second or third cycle of an immune checkpoint inhibitor.
- Patients had locally advanced or metastatic melanoma, renal cell carcinoma, urothelial carcinoma, non-small cell lung carcinoma, or head and neck squamous cell carcinoma and were treated at five Belgian hospitals.
- Most patients had more than three lesions.
- Seven patients in the experimental group did not complete radiotherapy because of early progression or intercurrent illness.
TAKEAWAY:
- Over a median follow-up of 12.5 months, median progression-free survival was 4.4 months in the radiotherapy group versus 2.8 months in the control group (hazard ratio, 0.95; P = .82).
- Median overall survival was not significantly better with radiotherapy, compared with the control group (14.3 vs. 11 months; HR, 0.82; P = .47), nor was the objective response rate (27% vs. 22%; P = .56).
- However, a post hoc analysis demonstrated a significant association between the number of irradiated lesions and overall survival among patients receiving radiotherapy (HR, 0.31; P = .002).
- The incidence of grade 3 or worse treatment-related adverse events was 18% in both groups.
IN PRACTICE:
Although the study was negative overall, the post hoc analysis coupled with “recent evidence suggests that treating all active disease sites with higher radiation doses ... may be a more promising strategy to optimize systemic disease control,” the authors concluded.
SOURCE:
The study was led by Mathieu Spaas, MD, department of radiation oncology, Ghent (Bellgium) University, and published online in JAMA Oncology.
LIMITATIONS:
- There was insufficient power to detect if certain cancers benefited more from add-on radiation because of the small sample size.
- More than half of patients in the control group had already received some form of radiotherapy before study inclusion, which may mean the study underestimated the benefit of radiotherapy.
DISCLOSURES:
The work was funded by Kom Op Tegen Kanker and Varian Medical Systems.
Investigators disclosed numerous industry ties, including Merck, Novartis, and Bristol Myers Squibb.
A version of this article first appeared on Medscape.com.
A teenage girl refuses more cancer treatment; her father disagrees
This transcript has been edited for clarity.
Hi. I’m Art Caplan, PhD. I’m director of the division of medical ethics at the New York University Grossman School of Medicine.
Every once in a while at my school, I get referrals about interesting or difficult clinical cases where doctors would like some input or advice that they can consider in managing a patient. Sometimes those requests come from other hospitals to me. I’ve been doing that kind of ethics consulting, both as a member of various ethics committees and sometimes individually, when, for various reasons, doctors don’t want to go to the Ethics Committee as a first stop.
There was a very interesting case recently involving a young woman I’m going to call Tinslee. She was 17 years old and she suffered, sadly, from recurrent metastatic osteogenic sarcoma. She had bone cancer. It had first been diagnosed at the age of 9. She had received chemotherapy and been under that treatment for a while.
If osteosarcoma is treated before it spreads outside the area where it began, the 5-year survival rate for people like her is about 75%. If the cancer spreads outside of the bones and gets into surrounding tissues, organs, or – worse – into the lymph nodes and starts traveling around, the 5-year survival rate drops to about 60%. The two approaches are chemotherapy and amputation. That’s what we have to offer patients like Tinslee.
Initially, her chemotherapy worked. She went to school and enjoyed sports. She was a real fan of softball and tried to manage the team and be involved. At the time I learned about her, she was planning to go to college. Her love of softball remained, but given the recurrence of the cancer, she had no chance to pursue her athletic interests, not only as a player, but also as a manager or even as a coach for younger players. That was all off the table.
She’d been very compliant up until this time with her chemotherapy. When the recommendation came in that she undergo nonstandard chemotherapy because of the reoccurrence, with experimental drugs using an experimental protocol, she said to her family and the doctors that she didn’t want to do it. She would rather die. She couldn’t take any more chemotherapy and she certainly didn’t want to do it if it was experimental, with the outcomes of this intervention being uncertain.
Her mother said, “Her input matters. I want to listen to her.” Her mom wasn’t as adamant about doing it or not, but she really felt that Tinslee should be heard loudly because she felt she was mature enough or old enough, even though a minor, to really have a position about what it is to undergo chemotherapy.
Time matters in trying to control the spread, and the doctors were pushing for experimental intervention. I should add, by the way, that although it didn’t really drive the decision about whether to do it or not do it, experimental care like this is not covered by most insurance, and it wasn’t covered by their insurance, so they were facing a big bill if the experimental intervention was administered.
There was some money in a grant to cover some of it, but they were going to face some big financial costs. It never came up in my discussions with the doctors about what to do. I’m not sure whether it ever came up with the family’s discussion with the doctors about what to do, or even whether Tinslee was worrying and didn’t want her family to face a financial burden.
I suggested that we bring the family in. We did some counseling. We had a social worker and we brought in a pastor because these people were fairly religious. We talked about all scenarios, including accepting death, knowing that this disease was not likely to go into remission with the experimental effort; maybe it would, but the doctors were not optimistic.
We tried to talk about how much we should listen to what this young woman wanted. We knew there was the possibility of going to court and having a judge decide this, but in my experience, I do not like going to judges and courts because I know what they’re going to say. They almost always say “administer the intervention.” They don’t want to be in a position of saying don’t do something. They’re a little less willing to do that if something is experimental, but generally speaking, if you’re headed to court, it’s because you’ve decided that you want this to happen.
I felt, in all honesty, that this young woman should have some real respect of her position because the treatment was experimental. She is approaching the age of competency and consent, and she’s been through many interventions. She knows what’s involved. I think you really have to listen hard to what she’s saying.
By the way, after this case, I looked and there have been some surveys of residents in pediatrics. A large number of them said that they hadn’t received any training about what to do when mature minors refuse experimental treatments. The study I saw said that 30% had not undergone any training about this, so we certainly want to introduce that into the appropriate areas of medicine and talk about this with residents and fellows.
Long story short, we had the family meeting, we had another meeting with dad and mom and Tinslee, and the dad began to come around and he began to listen hard. Tinslee said what she wanted was to go to her prom. She wanted to get to her sister’s junior high school softball championship game. If you will, setting some smaller goals that seemed to make her very, very happy began to satisfy mom and dad and they could accept her refusal.
Ultimately, an agreement was reached that she would not undergo the experimental intervention. We agreed on a course of palliative care, recommended that as what the doctors follow, and they decided to do so. Sadly, Tinslee died. She died at home. She did make it to her prom.
I think the outcome, while difficult, sad, tragic, and a close call, was correct. Mature minors who have been through a rough life of interventions and know the price to pay – and for those who have recurrent disease and now face only experimental options – if they say no, that’s something we really have to listen to very hard.
Dr. Kaplan is director, division of medical ethics, New York University Langone Medical Center, New York. He reported a conflict of interest with Johnson & Johnson’s Panel for Compassionate Drug Use.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
Hi. I’m Art Caplan, PhD. I’m director of the division of medical ethics at the New York University Grossman School of Medicine.
Every once in a while at my school, I get referrals about interesting or difficult clinical cases where doctors would like some input or advice that they can consider in managing a patient. Sometimes those requests come from other hospitals to me. I’ve been doing that kind of ethics consulting, both as a member of various ethics committees and sometimes individually, when, for various reasons, doctors don’t want to go to the Ethics Committee as a first stop.
There was a very interesting case recently involving a young woman I’m going to call Tinslee. She was 17 years old and she suffered, sadly, from recurrent metastatic osteogenic sarcoma. She had bone cancer. It had first been diagnosed at the age of 9. She had received chemotherapy and been under that treatment for a while.
If osteosarcoma is treated before it spreads outside the area where it began, the 5-year survival rate for people like her is about 75%. If the cancer spreads outside of the bones and gets into surrounding tissues, organs, or – worse – into the lymph nodes and starts traveling around, the 5-year survival rate drops to about 60%. The two approaches are chemotherapy and amputation. That’s what we have to offer patients like Tinslee.
Initially, her chemotherapy worked. She went to school and enjoyed sports. She was a real fan of softball and tried to manage the team and be involved. At the time I learned about her, she was planning to go to college. Her love of softball remained, but given the recurrence of the cancer, she had no chance to pursue her athletic interests, not only as a player, but also as a manager or even as a coach for younger players. That was all off the table.
She’d been very compliant up until this time with her chemotherapy. When the recommendation came in that she undergo nonstandard chemotherapy because of the reoccurrence, with experimental drugs using an experimental protocol, she said to her family and the doctors that she didn’t want to do it. She would rather die. She couldn’t take any more chemotherapy and she certainly didn’t want to do it if it was experimental, with the outcomes of this intervention being uncertain.
Her mother said, “Her input matters. I want to listen to her.” Her mom wasn’t as adamant about doing it or not, but she really felt that Tinslee should be heard loudly because she felt she was mature enough or old enough, even though a minor, to really have a position about what it is to undergo chemotherapy.
Time matters in trying to control the spread, and the doctors were pushing for experimental intervention. I should add, by the way, that although it didn’t really drive the decision about whether to do it or not do it, experimental care like this is not covered by most insurance, and it wasn’t covered by their insurance, so they were facing a big bill if the experimental intervention was administered.
There was some money in a grant to cover some of it, but they were going to face some big financial costs. It never came up in my discussions with the doctors about what to do. I’m not sure whether it ever came up with the family’s discussion with the doctors about what to do, or even whether Tinslee was worrying and didn’t want her family to face a financial burden.
I suggested that we bring the family in. We did some counseling. We had a social worker and we brought in a pastor because these people were fairly religious. We talked about all scenarios, including accepting death, knowing that this disease was not likely to go into remission with the experimental effort; maybe it would, but the doctors were not optimistic.
We tried to talk about how much we should listen to what this young woman wanted. We knew there was the possibility of going to court and having a judge decide this, but in my experience, I do not like going to judges and courts because I know what they’re going to say. They almost always say “administer the intervention.” They don’t want to be in a position of saying don’t do something. They’re a little less willing to do that if something is experimental, but generally speaking, if you’re headed to court, it’s because you’ve decided that you want this to happen.
I felt, in all honesty, that this young woman should have some real respect of her position because the treatment was experimental. She is approaching the age of competency and consent, and she’s been through many interventions. She knows what’s involved. I think you really have to listen hard to what she’s saying.
By the way, after this case, I looked and there have been some surveys of residents in pediatrics. A large number of them said that they hadn’t received any training about what to do when mature minors refuse experimental treatments. The study I saw said that 30% had not undergone any training about this, so we certainly want to introduce that into the appropriate areas of medicine and talk about this with residents and fellows.
Long story short, we had the family meeting, we had another meeting with dad and mom and Tinslee, and the dad began to come around and he began to listen hard. Tinslee said what she wanted was to go to her prom. She wanted to get to her sister’s junior high school softball championship game. If you will, setting some smaller goals that seemed to make her very, very happy began to satisfy mom and dad and they could accept her refusal.
Ultimately, an agreement was reached that she would not undergo the experimental intervention. We agreed on a course of palliative care, recommended that as what the doctors follow, and they decided to do so. Sadly, Tinslee died. She died at home. She did make it to her prom.
I think the outcome, while difficult, sad, tragic, and a close call, was correct. Mature minors who have been through a rough life of interventions and know the price to pay – and for those who have recurrent disease and now face only experimental options – if they say no, that’s something we really have to listen to very hard.
Dr. Kaplan is director, division of medical ethics, New York University Langone Medical Center, New York. He reported a conflict of interest with Johnson & Johnson’s Panel for Compassionate Drug Use.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
Hi. I’m Art Caplan, PhD. I’m director of the division of medical ethics at the New York University Grossman School of Medicine.
Every once in a while at my school, I get referrals about interesting or difficult clinical cases where doctors would like some input or advice that they can consider in managing a patient. Sometimes those requests come from other hospitals to me. I’ve been doing that kind of ethics consulting, both as a member of various ethics committees and sometimes individually, when, for various reasons, doctors don’t want to go to the Ethics Committee as a first stop.
There was a very interesting case recently involving a young woman I’m going to call Tinslee. She was 17 years old and she suffered, sadly, from recurrent metastatic osteogenic sarcoma. She had bone cancer. It had first been diagnosed at the age of 9. She had received chemotherapy and been under that treatment for a while.
If osteosarcoma is treated before it spreads outside the area where it began, the 5-year survival rate for people like her is about 75%. If the cancer spreads outside of the bones and gets into surrounding tissues, organs, or – worse – into the lymph nodes and starts traveling around, the 5-year survival rate drops to about 60%. The two approaches are chemotherapy and amputation. That’s what we have to offer patients like Tinslee.
Initially, her chemotherapy worked. She went to school and enjoyed sports. She was a real fan of softball and tried to manage the team and be involved. At the time I learned about her, she was planning to go to college. Her love of softball remained, but given the recurrence of the cancer, she had no chance to pursue her athletic interests, not only as a player, but also as a manager or even as a coach for younger players. That was all off the table.
She’d been very compliant up until this time with her chemotherapy. When the recommendation came in that she undergo nonstandard chemotherapy because of the reoccurrence, with experimental drugs using an experimental protocol, she said to her family and the doctors that she didn’t want to do it. She would rather die. She couldn’t take any more chemotherapy and she certainly didn’t want to do it if it was experimental, with the outcomes of this intervention being uncertain.
Her mother said, “Her input matters. I want to listen to her.” Her mom wasn’t as adamant about doing it or not, but she really felt that Tinslee should be heard loudly because she felt she was mature enough or old enough, even though a minor, to really have a position about what it is to undergo chemotherapy.
Time matters in trying to control the spread, and the doctors were pushing for experimental intervention. I should add, by the way, that although it didn’t really drive the decision about whether to do it or not do it, experimental care like this is not covered by most insurance, and it wasn’t covered by their insurance, so they were facing a big bill if the experimental intervention was administered.
There was some money in a grant to cover some of it, but they were going to face some big financial costs. It never came up in my discussions with the doctors about what to do. I’m not sure whether it ever came up with the family’s discussion with the doctors about what to do, or even whether Tinslee was worrying and didn’t want her family to face a financial burden.
I suggested that we bring the family in. We did some counseling. We had a social worker and we brought in a pastor because these people were fairly religious. We talked about all scenarios, including accepting death, knowing that this disease was not likely to go into remission with the experimental effort; maybe it would, but the doctors were not optimistic.
We tried to talk about how much we should listen to what this young woman wanted. We knew there was the possibility of going to court and having a judge decide this, but in my experience, I do not like going to judges and courts because I know what they’re going to say. They almost always say “administer the intervention.” They don’t want to be in a position of saying don’t do something. They’re a little less willing to do that if something is experimental, but generally speaking, if you’re headed to court, it’s because you’ve decided that you want this to happen.
I felt, in all honesty, that this young woman should have some real respect of her position because the treatment was experimental. She is approaching the age of competency and consent, and she’s been through many interventions. She knows what’s involved. I think you really have to listen hard to what she’s saying.
By the way, after this case, I looked and there have been some surveys of residents in pediatrics. A large number of them said that they hadn’t received any training about what to do when mature minors refuse experimental treatments. The study I saw said that 30% had not undergone any training about this, so we certainly want to introduce that into the appropriate areas of medicine and talk about this with residents and fellows.
Long story short, we had the family meeting, we had another meeting with dad and mom and Tinslee, and the dad began to come around and he began to listen hard. Tinslee said what she wanted was to go to her prom. She wanted to get to her sister’s junior high school softball championship game. If you will, setting some smaller goals that seemed to make her very, very happy began to satisfy mom and dad and they could accept her refusal.
Ultimately, an agreement was reached that she would not undergo the experimental intervention. We agreed on a course of palliative care, recommended that as what the doctors follow, and they decided to do so. Sadly, Tinslee died. She died at home. She did make it to her prom.
I think the outcome, while difficult, sad, tragic, and a close call, was correct. Mature minors who have been through a rough life of interventions and know the price to pay – and for those who have recurrent disease and now face only experimental options – if they say no, that’s something we really have to listen to very hard.
Dr. Kaplan is director, division of medical ethics, New York University Langone Medical Center, New York. He reported a conflict of interest with Johnson & Johnson’s Panel for Compassionate Drug Use.
A version of this article first appeared on Medscape.com.
Can a biodegradable brain implant deliver lifesaving cancer meds?
It’s the latest advance in a rapidly growing field using ultrasound – high-frequency sound waves undetectable to humans – to fight cancer and other diseases.
The problem addressed by the researchers is the blood-brain barrier, a nearly impenetrable blood vessel lining that keeps harmful molecules from passing into the brain from the blood. But this lining can also block chemo drugs from reaching cancer cells.
So the scientists implanted 1-cm2 devices into the skulls of mice, directly behind the tumor site. The implants generate ultrasound waves, loosening the barrier and allowing the drugs to reach the tumor. The sound waves leave healthy tissue undamaged.
“You inject the drug into the body and turn on the ultrasound at the same time. You’re going to hit precisely at the tumor area every single time you use it,” said lead study author Thanh Nguyen, PhD, an associate professor of mechanical engineering at the University of Connecticut, Storrs.
The drug used in the study was paclitaxel, which normally struggles to get through the blood-brain barrier. The tumors shrank, and the mice doubled their lifetime, compared with untreated mice. The mice showed no bad health effects 6 months later.
Breaking through the blood-brain barrier
The biodegradable implant is made of glycine, an amino acid that’s also strongly piezoelectric, meaning it vibrates when subjected to an electrical current. To make it, researchers cultivated glycine crystals, shattered them into pieces, and finally used a process called electrospinning, which applies a high electrical voltage to the nanocrystals.
Voltage flows to the implant via an external device. The resulting ultrasound causes the tightly adhered cells of the blood-brain barrier to vibrate, stretching them out and creating space for pores to form.
“That allows in very tiny particles, including chemo drugs,” said Dr. Nguyen.
His earlier biodegradable implant broke apart from the force, but the new glycine implant is more flexible, stable, and highly piezoelectric. It could be implanted after a patient has surgery to remove a brain tumor, to continue treating residual cancer cells. The implant dissolves harmlessly in the body over time, and doctors can control its lifespan.
A new wave of uses for ultrasound
Dr. Nguyen’s study builds on similar efforts, including a recent clinical trial of a nonbiodegradable implant for treating brain tumors. Ultrasound can focus energy on precise targets in the body.
It’s like “using a magnifying glass to focus multiple beams of light on a point and burn a hole in a leaf,” said Neal Kassell, MD, founder and chairman of the Focused Ultrasound Foundation. This approach spares adjacent normal tissue.
Doctors now understand more than 30 ways that ultrasound interacts with tissue – from destroying abnormal tissue to delivering drugs more effectively to stimulating an immune response. A decade ago, only five such interactions were known.
This opens the door for treating “a wide spectrum of medical disorders,” from neurodegenerative diseases like Alzheimer’s and Parkinson’s to difficult-to-treat cancers of the prostate and pancreas, and even addiction, said Dr. Kassell.
Dr. Kassell envisions using focused ultrasound to treat brain tumors as an alternative (or complement) to surgery, chemotherapy, immunotherapy, or radiation therapy. In the meantime, implants have helped show “the effectiveness of opening the blood-brain barrier.”
Dr. Nguyen’s team plans on testing the safety and efficacy of their implant in pigs next. Eventually, Dr. Nguyen hopes to develop a patch with an array of implants to target different areas of the brain.
One study coauthor is cofounder of PiezoBioMembrane and SingleTimeMicroneedles. The other study authors reported no conflicts of interest.
A version of this article originally appeared on WebMD.com.
It’s the latest advance in a rapidly growing field using ultrasound – high-frequency sound waves undetectable to humans – to fight cancer and other diseases.
The problem addressed by the researchers is the blood-brain barrier, a nearly impenetrable blood vessel lining that keeps harmful molecules from passing into the brain from the blood. But this lining can also block chemo drugs from reaching cancer cells.
So the scientists implanted 1-cm2 devices into the skulls of mice, directly behind the tumor site. The implants generate ultrasound waves, loosening the barrier and allowing the drugs to reach the tumor. The sound waves leave healthy tissue undamaged.
“You inject the drug into the body and turn on the ultrasound at the same time. You’re going to hit precisely at the tumor area every single time you use it,” said lead study author Thanh Nguyen, PhD, an associate professor of mechanical engineering at the University of Connecticut, Storrs.
The drug used in the study was paclitaxel, which normally struggles to get through the blood-brain barrier. The tumors shrank, and the mice doubled their lifetime, compared with untreated mice. The mice showed no bad health effects 6 months later.
Breaking through the blood-brain barrier
The biodegradable implant is made of glycine, an amino acid that’s also strongly piezoelectric, meaning it vibrates when subjected to an electrical current. To make it, researchers cultivated glycine crystals, shattered them into pieces, and finally used a process called electrospinning, which applies a high electrical voltage to the nanocrystals.
Voltage flows to the implant via an external device. The resulting ultrasound causes the tightly adhered cells of the blood-brain barrier to vibrate, stretching them out and creating space for pores to form.
“That allows in very tiny particles, including chemo drugs,” said Dr. Nguyen.
His earlier biodegradable implant broke apart from the force, but the new glycine implant is more flexible, stable, and highly piezoelectric. It could be implanted after a patient has surgery to remove a brain tumor, to continue treating residual cancer cells. The implant dissolves harmlessly in the body over time, and doctors can control its lifespan.
A new wave of uses for ultrasound
Dr. Nguyen’s study builds on similar efforts, including a recent clinical trial of a nonbiodegradable implant for treating brain tumors. Ultrasound can focus energy on precise targets in the body.
It’s like “using a magnifying glass to focus multiple beams of light on a point and burn a hole in a leaf,” said Neal Kassell, MD, founder and chairman of the Focused Ultrasound Foundation. This approach spares adjacent normal tissue.
Doctors now understand more than 30 ways that ultrasound interacts with tissue – from destroying abnormal tissue to delivering drugs more effectively to stimulating an immune response. A decade ago, only five such interactions were known.
This opens the door for treating “a wide spectrum of medical disorders,” from neurodegenerative diseases like Alzheimer’s and Parkinson’s to difficult-to-treat cancers of the prostate and pancreas, and even addiction, said Dr. Kassell.
Dr. Kassell envisions using focused ultrasound to treat brain tumors as an alternative (or complement) to surgery, chemotherapy, immunotherapy, or radiation therapy. In the meantime, implants have helped show “the effectiveness of opening the blood-brain barrier.”
Dr. Nguyen’s team plans on testing the safety and efficacy of their implant in pigs next. Eventually, Dr. Nguyen hopes to develop a patch with an array of implants to target different areas of the brain.
One study coauthor is cofounder of PiezoBioMembrane and SingleTimeMicroneedles. The other study authors reported no conflicts of interest.
A version of this article originally appeared on WebMD.com.
It’s the latest advance in a rapidly growing field using ultrasound – high-frequency sound waves undetectable to humans – to fight cancer and other diseases.
The problem addressed by the researchers is the blood-brain barrier, a nearly impenetrable blood vessel lining that keeps harmful molecules from passing into the brain from the blood. But this lining can also block chemo drugs from reaching cancer cells.
So the scientists implanted 1-cm2 devices into the skulls of mice, directly behind the tumor site. The implants generate ultrasound waves, loosening the barrier and allowing the drugs to reach the tumor. The sound waves leave healthy tissue undamaged.
“You inject the drug into the body and turn on the ultrasound at the same time. You’re going to hit precisely at the tumor area every single time you use it,” said lead study author Thanh Nguyen, PhD, an associate professor of mechanical engineering at the University of Connecticut, Storrs.
The drug used in the study was paclitaxel, which normally struggles to get through the blood-brain barrier. The tumors shrank, and the mice doubled their lifetime, compared with untreated mice. The mice showed no bad health effects 6 months later.
Breaking through the blood-brain barrier
The biodegradable implant is made of glycine, an amino acid that’s also strongly piezoelectric, meaning it vibrates when subjected to an electrical current. To make it, researchers cultivated glycine crystals, shattered them into pieces, and finally used a process called electrospinning, which applies a high electrical voltage to the nanocrystals.
Voltage flows to the implant via an external device. The resulting ultrasound causes the tightly adhered cells of the blood-brain barrier to vibrate, stretching them out and creating space for pores to form.
“That allows in very tiny particles, including chemo drugs,” said Dr. Nguyen.
His earlier biodegradable implant broke apart from the force, but the new glycine implant is more flexible, stable, and highly piezoelectric. It could be implanted after a patient has surgery to remove a brain tumor, to continue treating residual cancer cells. The implant dissolves harmlessly in the body over time, and doctors can control its lifespan.
A new wave of uses for ultrasound
Dr. Nguyen’s study builds on similar efforts, including a recent clinical trial of a nonbiodegradable implant for treating brain tumors. Ultrasound can focus energy on precise targets in the body.
It’s like “using a magnifying glass to focus multiple beams of light on a point and burn a hole in a leaf,” said Neal Kassell, MD, founder and chairman of the Focused Ultrasound Foundation. This approach spares adjacent normal tissue.
Doctors now understand more than 30 ways that ultrasound interacts with tissue – from destroying abnormal tissue to delivering drugs more effectively to stimulating an immune response. A decade ago, only five such interactions were known.
This opens the door for treating “a wide spectrum of medical disorders,” from neurodegenerative diseases like Alzheimer’s and Parkinson’s to difficult-to-treat cancers of the prostate and pancreas, and even addiction, said Dr. Kassell.
Dr. Kassell envisions using focused ultrasound to treat brain tumors as an alternative (or complement) to surgery, chemotherapy, immunotherapy, or radiation therapy. In the meantime, implants have helped show “the effectiveness of opening the blood-brain barrier.”
Dr. Nguyen’s team plans on testing the safety and efficacy of their implant in pigs next. Eventually, Dr. Nguyen hopes to develop a patch with an array of implants to target different areas of the brain.
One study coauthor is cofounder of PiezoBioMembrane and SingleTimeMicroneedles. The other study authors reported no conflicts of interest.
A version of this article originally appeared on WebMD.com.
FROM SCIENCE ADVANCES
The surprising occupations with higher-than-expected ovarian cancer rates
This transcript has been edited for clarity.
Welcome to Impact Factor, your weekly dose of commentary on a new medical study.
Basically, all cancers are caused by a mix of genetic and environmental factors, with some cancers driven more strongly by one or the other. When it comes to ovarian cancer, which kills more than 13,000 women per year in the United States, genetic factors like the BRCA gene mutations are well described.
Other risk factors, like early menarche and nulliparity, are difficult to modify. The only slam-dunk environmental toxin to be linked to ovarian cancer is asbestos. Still, the vast majority of women who develop ovarian cancer do not have a known high-risk gene or asbestos exposure, so other triggers may be out there. How do we find them? The answer may just be good old-fashioned epidemiology.
That’s just what researchers, led by Anita Koushik at the University of Montreal, did in a new study appearing in the journal Occupational and Environmental Medicine.
They identified 497 women in Montreal who had recently been diagnosed with ovarian cancer. They then matched those women to 897 women without ovarian cancer, based on age and address. (This approach would not work well in the United States, as diagnosis of ovarian cancer might depend on access to medical care, which is not universal here. In Canada, however, it’s safer to assume that anyone who could have gotten ovarian cancer in Montreal would have been detected.)
Cases and controls identified, the researchers took a detailed occupational history for each participant: every job they ever worked, and when, and for how long. Each occupation was mapped to a standardized set of industries and, interestingly, to a set of environmental exposures ranging from cosmetic talc to cooking fumes to cotton dust, in what is known as a job-exposure matrix. Of course, they also collected data on other ovarian cancer risk factors.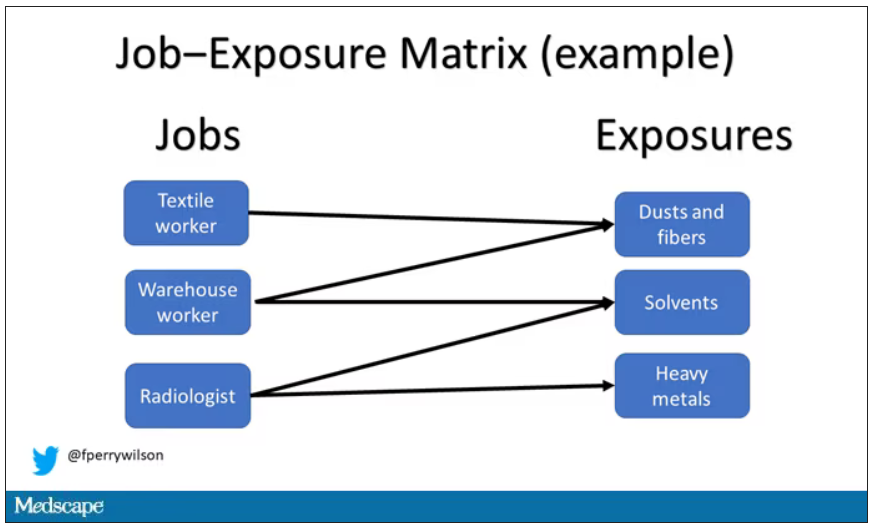
After that, it’s a simple matter of looking at the rate of ovarian cancer by occupation and occupation-associated exposures, accounting for differences in things like pregnancy rates.
A brief aside here. I was at dinner with my wife the other night and telling her about this study, and I asked, “What do you think the occupation with the highest rate of ovarian cancer is?” And without missing a beat, she said: “Hairdressers.” Which blew my mind because of how random that was, but she was also – as usual – 100% correct.
Hairdressers, at least those who had been in the industry for more than 10 years, had a threefold higher risk for ovarian cancer than matched controls who had never been hairdressers.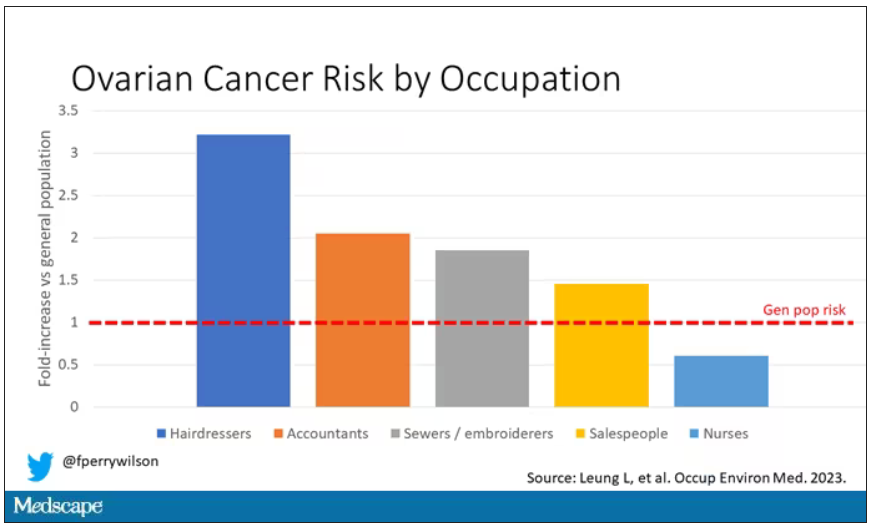
Of course, my wife is a cancer surgeon, so she has a bit of a leg up on me here. Many of you may also know that there is actually a decent body of literature showing higher rates of various cancers among hairdressers, presumably due to the variety of chemicals they are exposed to on a continuous basis.
The No. 2 highest-risk profession on the list? Accountants, with about a twofold higher risk. That one is more of a puzzler. It could be a false positive; after all, there were multiple occupations checked and random error might give a few hits that are meaningless. But there are certainly some occupational factors unique to accountants that might bear further investigation – maybe exposure to volatile organic compounds from office printers, or just a particularly sedentary office environment.
In terms of specific exposures, there were high risks seen with mononuclear aromatic hydrocarbons, bleaches, ethanol, and fluorocarbons, among others, but we have to be a bit more careful here. These exposures were not directly measured. Rather, based on the job category a woman described, the exposures were imputed based on the job-exposure matrix. As such, the correlations between the job and the particular exposure are really quite high, making it essentially impossible to tease out whether it is, for example, being a hairdresser, or being exposed to fluorocarbons as a hairdresser, or being exposed to something else as a hairdresser, that is the problem.
This is how these types of studies work; they tend to raise more questions than they answer. But in a world where a cancer diagnosis can seem to come completely out of the blue, they provide the starting point that someday may lead to a more definitive culprit agent or group of agents. Until then, it might be wise for hairdressers to make sure their workplace is well ventilated.
F. Perry Wilson, MD, MSCE, is an associate professor of medicine and director of Yale University’s Clinical and Translational Research Accelerator in New Haven, Conn. He reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
Welcome to Impact Factor, your weekly dose of commentary on a new medical study.
Basically, all cancers are caused by a mix of genetic and environmental factors, with some cancers driven more strongly by one or the other. When it comes to ovarian cancer, which kills more than 13,000 women per year in the United States, genetic factors like the BRCA gene mutations are well described.
Other risk factors, like early menarche and nulliparity, are difficult to modify. The only slam-dunk environmental toxin to be linked to ovarian cancer is asbestos. Still, the vast majority of women who develop ovarian cancer do not have a known high-risk gene or asbestos exposure, so other triggers may be out there. How do we find them? The answer may just be good old-fashioned epidemiology.
That’s just what researchers, led by Anita Koushik at the University of Montreal, did in a new study appearing in the journal Occupational and Environmental Medicine.
They identified 497 women in Montreal who had recently been diagnosed with ovarian cancer. They then matched those women to 897 women without ovarian cancer, based on age and address. (This approach would not work well in the United States, as diagnosis of ovarian cancer might depend on access to medical care, which is not universal here. In Canada, however, it’s safer to assume that anyone who could have gotten ovarian cancer in Montreal would have been detected.)
Cases and controls identified, the researchers took a detailed occupational history for each participant: every job they ever worked, and when, and for how long. Each occupation was mapped to a standardized set of industries and, interestingly, to a set of environmental exposures ranging from cosmetic talc to cooking fumes to cotton dust, in what is known as a job-exposure matrix. Of course, they also collected data on other ovarian cancer risk factors.
After that, it’s a simple matter of looking at the rate of ovarian cancer by occupation and occupation-associated exposures, accounting for differences in things like pregnancy rates.
A brief aside here. I was at dinner with my wife the other night and telling her about this study, and I asked, “What do you think the occupation with the highest rate of ovarian cancer is?” And without missing a beat, she said: “Hairdressers.” Which blew my mind because of how random that was, but she was also – as usual – 100% correct.
Hairdressers, at least those who had been in the industry for more than 10 years, had a threefold higher risk for ovarian cancer than matched controls who had never been hairdressers.
Of course, my wife is a cancer surgeon, so she has a bit of a leg up on me here. Many of you may also know that there is actually a decent body of literature showing higher rates of various cancers among hairdressers, presumably due to the variety of chemicals they are exposed to on a continuous basis.
The No. 2 highest-risk profession on the list? Accountants, with about a twofold higher risk. That one is more of a puzzler. It could be a false positive; after all, there were multiple occupations checked and random error might give a few hits that are meaningless. But there are certainly some occupational factors unique to accountants that might bear further investigation – maybe exposure to volatile organic compounds from office printers, or just a particularly sedentary office environment.
In terms of specific exposures, there were high risks seen with mononuclear aromatic hydrocarbons, bleaches, ethanol, and fluorocarbons, among others, but we have to be a bit more careful here. These exposures were not directly measured. Rather, based on the job category a woman described, the exposures were imputed based on the job-exposure matrix. As such, the correlations between the job and the particular exposure are really quite high, making it essentially impossible to tease out whether it is, for example, being a hairdresser, or being exposed to fluorocarbons as a hairdresser, or being exposed to something else as a hairdresser, that is the problem.
This is how these types of studies work; they tend to raise more questions than they answer. But in a world where a cancer diagnosis can seem to come completely out of the blue, they provide the starting point that someday may lead to a more definitive culprit agent or group of agents. Until then, it might be wise for hairdressers to make sure their workplace is well ventilated.
F. Perry Wilson, MD, MSCE, is an associate professor of medicine and director of Yale University’s Clinical and Translational Research Accelerator in New Haven, Conn. He reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
Welcome to Impact Factor, your weekly dose of commentary on a new medical study.
Basically, all cancers are caused by a mix of genetic and environmental factors, with some cancers driven more strongly by one or the other. When it comes to ovarian cancer, which kills more than 13,000 women per year in the United States, genetic factors like the BRCA gene mutations are well described.
Other risk factors, like early menarche and nulliparity, are difficult to modify. The only slam-dunk environmental toxin to be linked to ovarian cancer is asbestos. Still, the vast majority of women who develop ovarian cancer do not have a known high-risk gene or asbestos exposure, so other triggers may be out there. How do we find them? The answer may just be good old-fashioned epidemiology.
That’s just what researchers, led by Anita Koushik at the University of Montreal, did in a new study appearing in the journal Occupational and Environmental Medicine.
They identified 497 women in Montreal who had recently been diagnosed with ovarian cancer. They then matched those women to 897 women without ovarian cancer, based on age and address. (This approach would not work well in the United States, as diagnosis of ovarian cancer might depend on access to medical care, which is not universal here. In Canada, however, it’s safer to assume that anyone who could have gotten ovarian cancer in Montreal would have been detected.)
Cases and controls identified, the researchers took a detailed occupational history for each participant: every job they ever worked, and when, and for how long. Each occupation was mapped to a standardized set of industries and, interestingly, to a set of environmental exposures ranging from cosmetic talc to cooking fumes to cotton dust, in what is known as a job-exposure matrix. Of course, they also collected data on other ovarian cancer risk factors.
After that, it’s a simple matter of looking at the rate of ovarian cancer by occupation and occupation-associated exposures, accounting for differences in things like pregnancy rates.
A brief aside here. I was at dinner with my wife the other night and telling her about this study, and I asked, “What do you think the occupation with the highest rate of ovarian cancer is?” And without missing a beat, she said: “Hairdressers.” Which blew my mind because of how random that was, but she was also – as usual – 100% correct.
Hairdressers, at least those who had been in the industry for more than 10 years, had a threefold higher risk for ovarian cancer than matched controls who had never been hairdressers.
Of course, my wife is a cancer surgeon, so she has a bit of a leg up on me here. Many of you may also know that there is actually a decent body of literature showing higher rates of various cancers among hairdressers, presumably due to the variety of chemicals they are exposed to on a continuous basis.
The No. 2 highest-risk profession on the list? Accountants, with about a twofold higher risk. That one is more of a puzzler. It could be a false positive; after all, there were multiple occupations checked and random error might give a few hits that are meaningless. But there are certainly some occupational factors unique to accountants that might bear further investigation – maybe exposure to volatile organic compounds from office printers, or just a particularly sedentary office environment.
In terms of specific exposures, there were high risks seen with mononuclear aromatic hydrocarbons, bleaches, ethanol, and fluorocarbons, among others, but we have to be a bit more careful here. These exposures were not directly measured. Rather, based on the job category a woman described, the exposures were imputed based on the job-exposure matrix. As such, the correlations between the job and the particular exposure are really quite high, making it essentially impossible to tease out whether it is, for example, being a hairdresser, or being exposed to fluorocarbons as a hairdresser, or being exposed to something else as a hairdresser, that is the problem.
This is how these types of studies work; they tend to raise more questions than they answer. But in a world where a cancer diagnosis can seem to come completely out of the blue, they provide the starting point that someday may lead to a more definitive culprit agent or group of agents. Until then, it might be wise for hairdressers to make sure their workplace is well ventilated.
F. Perry Wilson, MD, MSCE, is an associate professor of medicine and director of Yale University’s Clinical and Translational Research Accelerator in New Haven, Conn. He reported no conflicts of interest.
A version of this article first appeared on Medscape.com.