User login
Official news magazine of the Society of Hospital Medicine
Copyright by Society of Hospital Medicine or related companies. All rights reserved. ISSN 1553-085X
nav[contains(@class, 'nav-ce-stack nav-ce-stack__large-screen')]
header[@id='header']
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'main-prefix')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
div[contains(@class, 'view-medstat-quiz-listing-panes')]
div[contains(@class, 'pane-article-sidebar-latest-news')]
div[contains(@class, 'pane-pub-article-hospitalist')]

UK Report Shows Prevalence of Antibiotic Resistance in Pediatric Urinary Tract Infection
NEW YORK (Reuters Health) - The prevalence of antibiotic resistance in pediatric urinary tract infection (UTI) has reached such high levels in many countries that existing empiric therapies may no longer be effective, researchers from UK report."
Prevalence of resistance to commonly prescribed antibiotics in primary care in children with urinary tract infections caused by E. coli is high, and there was remarkable variability in E. coli resistance among countries in the study, particularly in countries outside the OECD (Organization for Economic Cooperation and Development), where one possible explanation is the availability of antibiotics over the counter," Ashley Bryce from the University of Bristol in the U.K. and Dr. Céire E. Costelloe from Imperial College London told Reuters Health in a joint email.
"This could render some antibiotics ineffective as first-line treatments for urinary tract infection," they said.
E. coli is responsible for more than 80% of all UTIs and is also the most common cause of bacteremia and foodborne infections and one cause of meningitis in neonates.
Bryce, Dr. Costelloe, and colleagues investigated the prevalence of resistance in community-acquired E. coli UTI to the most commonly prescribed antibiotics given to children in primary care in their systematic review of 58 published reports.
For all antibiotics tested, the prevalence of antibiotic resistance was higher in non-OECD countries than in OECD countries, the team reports in an article online March 15 in The BMJ.
The prevalence of resistance was highest for ampicillin, ranging from 41% in Switzerland to 100% in Ghana and Nigeria.
Resistance to co-trimoxazole and trimethoprim was 30% in OECD countries and 67% in Saudi Arabia, the only non-OECD country for which rates were available.
Pooled prevalences of resistance to ciprofloxacin and ceftazidime were around 2% in OECD countries but over 26% in non-OECD countries.
For all time periods analyzed, the odds of resistance were greater in children exposed to antibiotics than in those who were unexposed.
"The Infectious Diseases Society of America (IDSA) in collaboration with the European Society for Microbiology and Infectious Diseases (ESCMID) recommend that an antibiotic should be selected for first line empirical treatment of urinary tract infection only if the local prevalence of resistance is less than 20%," the researchers note.
"According to these guidelines, our review suggests ampicillin, co-trimoxazole, and trimethoprim are no longer suitable first line treatment options for urinary tract infection in many OECD countries and that as a result many guidelines, such as those published by the National Institute for Health and Care Excellence (NICE), might need updating," they write. "In non-OECD countries, resistance to all first line antibiotics specified for urinary tract infections was in excess of 20%, suggesting that choices of first line treatment might need to be re-evaluated in less well developed countries."
"We are not able to advise clinicians on which antibiotic is best to prescribe as this often depends on the individual case," Bryce and Dr. Costelloe said. "Clinicians should, however, adhere to local or national guidelines wherever possible, which is why it is of great importance that such guidelines are kept up to date and reflect current resistance rates."
"Clinicians may also wish to consider the antibiotic history of the child when they present to primary care with symptoms of an infection, especially in light of the suggestion of our results that previous treatment with an antibiotic is associated with resistance to that same antibiotic, and that this association may be present up to 6 months post treatment," they added.
Dr. Grant Russell from Monash University in Melbourne, Australia, wrote an editorial accompanying the report. He told Reuters Health by email, "I found the extent of the resistance (and the fact that it covered all of the regularly used empiric antibiotics) both concerning and surprising. The fact that choices are diminishing is disturbing, and the fact that the situation is dire in the developing world is deeply troubling."
"We need to do what we can do to prevent bacterial infections, and when treating them to consider that effective antibiotics are a finite resource," he said. "We all have a responsibility in attempting to conserve that resource."
"No new classes of antibiotics have been developed in the last 30 years - this and the dire situation in both the developed and the developing world suggests that the 'global problem' of antibiotic resistance is going to become more and more of an issue in years and decades to come," Dr. Russell concluded.
NEW YORK (Reuters Health) - The prevalence of antibiotic resistance in pediatric urinary tract infection (UTI) has reached such high levels in many countries that existing empiric therapies may no longer be effective, researchers from UK report."
Prevalence of resistance to commonly prescribed antibiotics in primary care in children with urinary tract infections caused by E. coli is high, and there was remarkable variability in E. coli resistance among countries in the study, particularly in countries outside the OECD (Organization for Economic Cooperation and Development), where one possible explanation is the availability of antibiotics over the counter," Ashley Bryce from the University of Bristol in the U.K. and Dr. Céire E. Costelloe from Imperial College London told Reuters Health in a joint email.
"This could render some antibiotics ineffective as first-line treatments for urinary tract infection," they said.
E. coli is responsible for more than 80% of all UTIs and is also the most common cause of bacteremia and foodborne infections and one cause of meningitis in neonates.
Bryce, Dr. Costelloe, and colleagues investigated the prevalence of resistance in community-acquired E. coli UTI to the most commonly prescribed antibiotics given to children in primary care in their systematic review of 58 published reports.
For all antibiotics tested, the prevalence of antibiotic resistance was higher in non-OECD countries than in OECD countries, the team reports in an article online March 15 in The BMJ.
The prevalence of resistance was highest for ampicillin, ranging from 41% in Switzerland to 100% in Ghana and Nigeria.
Resistance to co-trimoxazole and trimethoprim was 30% in OECD countries and 67% in Saudi Arabia, the only non-OECD country for which rates were available.
Pooled prevalences of resistance to ciprofloxacin and ceftazidime were around 2% in OECD countries but over 26% in non-OECD countries.
For all time periods analyzed, the odds of resistance were greater in children exposed to antibiotics than in those who were unexposed.
"The Infectious Diseases Society of America (IDSA) in collaboration with the European Society for Microbiology and Infectious Diseases (ESCMID) recommend that an antibiotic should be selected for first line empirical treatment of urinary tract infection only if the local prevalence of resistance is less than 20%," the researchers note.
"According to these guidelines, our review suggests ampicillin, co-trimoxazole, and trimethoprim are no longer suitable first line treatment options for urinary tract infection in many OECD countries and that as a result many guidelines, such as those published by the National Institute for Health and Care Excellence (NICE), might need updating," they write. "In non-OECD countries, resistance to all first line antibiotics specified for urinary tract infections was in excess of 20%, suggesting that choices of first line treatment might need to be re-evaluated in less well developed countries."
"We are not able to advise clinicians on which antibiotic is best to prescribe as this often depends on the individual case," Bryce and Dr. Costelloe said. "Clinicians should, however, adhere to local or national guidelines wherever possible, which is why it is of great importance that such guidelines are kept up to date and reflect current resistance rates."
"Clinicians may also wish to consider the antibiotic history of the child when they present to primary care with symptoms of an infection, especially in light of the suggestion of our results that previous treatment with an antibiotic is associated with resistance to that same antibiotic, and that this association may be present up to 6 months post treatment," they added.
Dr. Grant Russell from Monash University in Melbourne, Australia, wrote an editorial accompanying the report. He told Reuters Health by email, "I found the extent of the resistance (and the fact that it covered all of the regularly used empiric antibiotics) both concerning and surprising. The fact that choices are diminishing is disturbing, and the fact that the situation is dire in the developing world is deeply troubling."
"We need to do what we can do to prevent bacterial infections, and when treating them to consider that effective antibiotics are a finite resource," he said. "We all have a responsibility in attempting to conserve that resource."
"No new classes of antibiotics have been developed in the last 30 years - this and the dire situation in both the developed and the developing world suggests that the 'global problem' of antibiotic resistance is going to become more and more of an issue in years and decades to come," Dr. Russell concluded.
NEW YORK (Reuters Health) - The prevalence of antibiotic resistance in pediatric urinary tract infection (UTI) has reached such high levels in many countries that existing empiric therapies may no longer be effective, researchers from UK report."
Prevalence of resistance to commonly prescribed antibiotics in primary care in children with urinary tract infections caused by E. coli is high, and there was remarkable variability in E. coli resistance among countries in the study, particularly in countries outside the OECD (Organization for Economic Cooperation and Development), where one possible explanation is the availability of antibiotics over the counter," Ashley Bryce from the University of Bristol in the U.K. and Dr. Céire E. Costelloe from Imperial College London told Reuters Health in a joint email.
"This could render some antibiotics ineffective as first-line treatments for urinary tract infection," they said.
E. coli is responsible for more than 80% of all UTIs and is also the most common cause of bacteremia and foodborne infections and one cause of meningitis in neonates.
Bryce, Dr. Costelloe, and colleagues investigated the prevalence of resistance in community-acquired E. coli UTI to the most commonly prescribed antibiotics given to children in primary care in their systematic review of 58 published reports.
For all antibiotics tested, the prevalence of antibiotic resistance was higher in non-OECD countries than in OECD countries, the team reports in an article online March 15 in The BMJ.
The prevalence of resistance was highest for ampicillin, ranging from 41% in Switzerland to 100% in Ghana and Nigeria.
Resistance to co-trimoxazole and trimethoprim was 30% in OECD countries and 67% in Saudi Arabia, the only non-OECD country for which rates were available.
Pooled prevalences of resistance to ciprofloxacin and ceftazidime were around 2% in OECD countries but over 26% in non-OECD countries.
For all time periods analyzed, the odds of resistance were greater in children exposed to antibiotics than in those who were unexposed.
"The Infectious Diseases Society of America (IDSA) in collaboration with the European Society for Microbiology and Infectious Diseases (ESCMID) recommend that an antibiotic should be selected for first line empirical treatment of urinary tract infection only if the local prevalence of resistance is less than 20%," the researchers note.
"According to these guidelines, our review suggests ampicillin, co-trimoxazole, and trimethoprim are no longer suitable first line treatment options for urinary tract infection in many OECD countries and that as a result many guidelines, such as those published by the National Institute for Health and Care Excellence (NICE), might need updating," they write. "In non-OECD countries, resistance to all first line antibiotics specified for urinary tract infections was in excess of 20%, suggesting that choices of first line treatment might need to be re-evaluated in less well developed countries."
"We are not able to advise clinicians on which antibiotic is best to prescribe as this often depends on the individual case," Bryce and Dr. Costelloe said. "Clinicians should, however, adhere to local or national guidelines wherever possible, which is why it is of great importance that such guidelines are kept up to date and reflect current resistance rates."
"Clinicians may also wish to consider the antibiotic history of the child when they present to primary care with symptoms of an infection, especially in light of the suggestion of our results that previous treatment with an antibiotic is associated with resistance to that same antibiotic, and that this association may be present up to 6 months post treatment," they added.
Dr. Grant Russell from Monash University in Melbourne, Australia, wrote an editorial accompanying the report. He told Reuters Health by email, "I found the extent of the resistance (and the fact that it covered all of the regularly used empiric antibiotics) both concerning and surprising. The fact that choices are diminishing is disturbing, and the fact that the situation is dire in the developing world is deeply troubling."
"We need to do what we can do to prevent bacterial infections, and when treating them to consider that effective antibiotics are a finite resource," he said. "We all have a responsibility in attempting to conserve that resource."
"No new classes of antibiotics have been developed in the last 30 years - this and the dire situation in both the developed and the developing world suggests that the 'global problem' of antibiotic resistance is going to become more and more of an issue in years and decades to come," Dr. Russell concluded.
New Sepsis Definition, Bedside Screening to Identify Patients at High-Mortality Risk
Clinical question: What are the best criteria to identify sepsis and septic shock?
Bottom line: An international task force of experts has updated the definitions of sepsis and septic shock and created a new bedside scoring tool to identify patients with suspected infection who may be at high risk for poor outcomes. Based on the Sequential Organ Failure Assessment (SOFA) score, the new quickSOFA states that meeting 2 of 3 clinical criteria (respiratory rate of 22 per minute or greater, systolic blood pressure of 100 mg Hg or less, and altered mental status) identifies patients at high risk of poor outcomes from sepsis. This score will need to be validated further in multiple health care settings before it can be widely accepted in clinical practice. (LOE = 5)
References: Singer M, Deutschman CS, Seymour CW, et al. The third international consensus definitions for sepsis and septic shock (Sepsis-3). JAMA 2016;315(8):801-810.
Seymour CW, Liu VX, Iwashyna TJ, et al. Assessment of clinical criteria for sepsis (Sepsis-3). JAMA 2016;315(8):762-774.
Shankar-Hari M, Phillips GS, Levy ML, et al. Developing a new definition and assessing new clinical criteria for septic shock (Sepsis-3). JAMA 2016;315(8):775-787.
Study design: Other
Funding source: Foundation
Allocation: Uncertain
Setting: Inpatient (ward only)
Synopsis: Systemic inflammatory response syndrome (SIRS) criteria are present in many hospitalized patients, even those without infections or life-threatening illnesses. The use of these criteria to identify sepsis may lead to misdiagnosis. Funded by the European Society of Intensive Care Medicine and the Society of Critical Care Medicine, an international task force consisting of 19 critical care, infectious disease, surgical, and pulmonary specialists convened to update the definitions of sepsis and septic shock and identify clinical criteria that can be used to recognize patients at high risk for mortality. Researchers conducted a systematic review and meta-analysis of observational studies followed by a Delphi consensus process to determine appropriate criteria for identifying septic shock. Furthermore, they validated and confirmed the ability of different clinical criteria, including the SIRS criteria and the SOFA score, to predict poor outcomes in patients with suspected infection.
Per the task force's recommendations, sepsis should be defined as life-threatening organ dysfunction caused by a dysregulated host response to infection. Septic shock is a subset of sepsis in which there is an increased risk of mortality due to profound circulatory and cellular metabolism abnormalities. Sepsis can be identified by an increase in the SOFA score of 2 points or more. This is associated with an in-hospital mortality exceeding 10%. Septic shock can be identified by a vasopressor requirement to maintain a mean arterial pressure of 65 mm Hg or greater and a serum lactate level greater than 18 mg/dL (> 2 mmol/L) after adequate fluid resuscitation. This combination of clinical criteria is associated with a hospital mortality rate of 40%.
Using a derivation and validation cohort of approximately 75,000 patients, the group also developed a new bedside clinical measure termed quickSOFA, or qSOFA, which consists of a respiratory rate of 22 per minute or greater, altered mental status, and systolic blood pressure of 100 mm Hg or less. Patients with suspected infection who are not in the intensive care unit and have at least 2 of these 3 criteria are at higher risk of poor outcomes from sepsis (area under receiver operating characteristics curve = 0.81).
Dr. Kulkarni is an assistant professor of hospital medicine at Northwestern University in Chicago.
Clinical question: What are the best criteria to identify sepsis and septic shock?
Bottom line: An international task force of experts has updated the definitions of sepsis and septic shock and created a new bedside scoring tool to identify patients with suspected infection who may be at high risk for poor outcomes. Based on the Sequential Organ Failure Assessment (SOFA) score, the new quickSOFA states that meeting 2 of 3 clinical criteria (respiratory rate of 22 per minute or greater, systolic blood pressure of 100 mg Hg or less, and altered mental status) identifies patients at high risk of poor outcomes from sepsis. This score will need to be validated further in multiple health care settings before it can be widely accepted in clinical practice. (LOE = 5)
References: Singer M, Deutschman CS, Seymour CW, et al. The third international consensus definitions for sepsis and septic shock (Sepsis-3). JAMA 2016;315(8):801-810.
Seymour CW, Liu VX, Iwashyna TJ, et al. Assessment of clinical criteria for sepsis (Sepsis-3). JAMA 2016;315(8):762-774.
Shankar-Hari M, Phillips GS, Levy ML, et al. Developing a new definition and assessing new clinical criteria for septic shock (Sepsis-3). JAMA 2016;315(8):775-787.
Study design: Other
Funding source: Foundation
Allocation: Uncertain
Setting: Inpatient (ward only)
Synopsis: Systemic inflammatory response syndrome (SIRS) criteria are present in many hospitalized patients, even those without infections or life-threatening illnesses. The use of these criteria to identify sepsis may lead to misdiagnosis. Funded by the European Society of Intensive Care Medicine and the Society of Critical Care Medicine, an international task force consisting of 19 critical care, infectious disease, surgical, and pulmonary specialists convened to update the definitions of sepsis and septic shock and identify clinical criteria that can be used to recognize patients at high risk for mortality. Researchers conducted a systematic review and meta-analysis of observational studies followed by a Delphi consensus process to determine appropriate criteria for identifying septic shock. Furthermore, they validated and confirmed the ability of different clinical criteria, including the SIRS criteria and the SOFA score, to predict poor outcomes in patients with suspected infection.
Per the task force's recommendations, sepsis should be defined as life-threatening organ dysfunction caused by a dysregulated host response to infection. Septic shock is a subset of sepsis in which there is an increased risk of mortality due to profound circulatory and cellular metabolism abnormalities. Sepsis can be identified by an increase in the SOFA score of 2 points or more. This is associated with an in-hospital mortality exceeding 10%. Septic shock can be identified by a vasopressor requirement to maintain a mean arterial pressure of 65 mm Hg or greater and a serum lactate level greater than 18 mg/dL (> 2 mmol/L) after adequate fluid resuscitation. This combination of clinical criteria is associated with a hospital mortality rate of 40%.
Using a derivation and validation cohort of approximately 75,000 patients, the group also developed a new bedside clinical measure termed quickSOFA, or qSOFA, which consists of a respiratory rate of 22 per minute or greater, altered mental status, and systolic blood pressure of 100 mm Hg or less. Patients with suspected infection who are not in the intensive care unit and have at least 2 of these 3 criteria are at higher risk of poor outcomes from sepsis (area under receiver operating characteristics curve = 0.81).
Dr. Kulkarni is an assistant professor of hospital medicine at Northwestern University in Chicago.
Clinical question: What are the best criteria to identify sepsis and septic shock?
Bottom line: An international task force of experts has updated the definitions of sepsis and septic shock and created a new bedside scoring tool to identify patients with suspected infection who may be at high risk for poor outcomes. Based on the Sequential Organ Failure Assessment (SOFA) score, the new quickSOFA states that meeting 2 of 3 clinical criteria (respiratory rate of 22 per minute or greater, systolic blood pressure of 100 mg Hg or less, and altered mental status) identifies patients at high risk of poor outcomes from sepsis. This score will need to be validated further in multiple health care settings before it can be widely accepted in clinical practice. (LOE = 5)
References: Singer M, Deutschman CS, Seymour CW, et al. The third international consensus definitions for sepsis and septic shock (Sepsis-3). JAMA 2016;315(8):801-810.
Seymour CW, Liu VX, Iwashyna TJ, et al. Assessment of clinical criteria for sepsis (Sepsis-3). JAMA 2016;315(8):762-774.
Shankar-Hari M, Phillips GS, Levy ML, et al. Developing a new definition and assessing new clinical criteria for septic shock (Sepsis-3). JAMA 2016;315(8):775-787.
Study design: Other
Funding source: Foundation
Allocation: Uncertain
Setting: Inpatient (ward only)
Synopsis: Systemic inflammatory response syndrome (SIRS) criteria are present in many hospitalized patients, even those without infections or life-threatening illnesses. The use of these criteria to identify sepsis may lead to misdiagnosis. Funded by the European Society of Intensive Care Medicine and the Society of Critical Care Medicine, an international task force consisting of 19 critical care, infectious disease, surgical, and pulmonary specialists convened to update the definitions of sepsis and septic shock and identify clinical criteria that can be used to recognize patients at high risk for mortality. Researchers conducted a systematic review and meta-analysis of observational studies followed by a Delphi consensus process to determine appropriate criteria for identifying septic shock. Furthermore, they validated and confirmed the ability of different clinical criteria, including the SIRS criteria and the SOFA score, to predict poor outcomes in patients with suspected infection.
Per the task force's recommendations, sepsis should be defined as life-threatening organ dysfunction caused by a dysregulated host response to infection. Septic shock is a subset of sepsis in which there is an increased risk of mortality due to profound circulatory and cellular metabolism abnormalities. Sepsis can be identified by an increase in the SOFA score of 2 points or more. This is associated with an in-hospital mortality exceeding 10%. Septic shock can be identified by a vasopressor requirement to maintain a mean arterial pressure of 65 mm Hg or greater and a serum lactate level greater than 18 mg/dL (> 2 mmol/L) after adequate fluid resuscitation. This combination of clinical criteria is associated with a hospital mortality rate of 40%.
Using a derivation and validation cohort of approximately 75,000 patients, the group also developed a new bedside clinical measure termed quickSOFA, or qSOFA, which consists of a respiratory rate of 22 per minute or greater, altered mental status, and systolic blood pressure of 100 mm Hg or less. Patients with suspected infection who are not in the intensive care unit and have at least 2 of these 3 criteria are at higher risk of poor outcomes from sepsis (area under receiver operating characteristics curve = 0.81).
Dr. Kulkarni is an assistant professor of hospital medicine at Northwestern University in Chicago.
Research Reaffirms Management of Hospitalized Patients with Community-Acquired Pneumonia
Clinical question: What is the best antibiotic strategy to improve outcomes in patients hospitalized with community-acquired pneumonia?
Bottom line: For patients hospitalized with community-acquired pneumonia (CAP), start antibiotics early, use either fluoroquinolone monotherapy or beta-lactam/macrolide combination therapy, and switch to oral antibiotics as soon as patients are hemodynamically stable and can take oral medications. Although the evidence is mostly of low quality, this review reaffirms what we already do. (LOE = 2a)
Reference: Lee JS, Giesler DL, Gellad WF, Fine MJ. Antibiotic therapy for adults hospitalized with community-acquired pneumonia. JAMA 2016;315(6):593-602.
Study design: Systematic review
Funding source: Unknown/not stated
Allocation: Uncertain
Setting: Inpatient (ward only)
Synopsis: These investigators searched MEDLINE, EMBASE, and the Cochrane databases to identify studies that evaluated outcomes for patients hospitalized with CAP with regard to optimal timing of antibiotic initiation, initial antibiotic selection, and criteria for transition from intravenous to oral antibiotic therapy. Two authors independently reviewed studies for inclusion and assessed study quality.
Of 8 low-quality observational studies, 4 showed a significant association between initiating antibiotic therapy within 4 hours to 8 hours of hospital arrival and reduced mortality. When comparing 2 different antibiotic strategies, 6 of 8 observational studies showed mortality benefit with the use of beta-lactams plus macrolides as compared with beta-lactam monotherapy, though the 2 recent high-quality randomized trials had conflicting results. All three observational studies that compared fluoroquinolones with beta-lactam monotherapy for the treatment of CAP showed an association with fluoroquinolone use and decreased mortality.
Finally, one high-quality trial showed that transitioning patients to oral antibiotics once they meet clinical criteria for stability (stable vital signs, lack of confusion, ability to tolerate oral medications) leads to a shorter length of stay.
Dr. Kulkarni is an assistant professor of hospital medicine at Northwestern University in Chicago.
Clinical question: What is the best antibiotic strategy to improve outcomes in patients hospitalized with community-acquired pneumonia?
Bottom line: For patients hospitalized with community-acquired pneumonia (CAP), start antibiotics early, use either fluoroquinolone monotherapy or beta-lactam/macrolide combination therapy, and switch to oral antibiotics as soon as patients are hemodynamically stable and can take oral medications. Although the evidence is mostly of low quality, this review reaffirms what we already do. (LOE = 2a)
Reference: Lee JS, Giesler DL, Gellad WF, Fine MJ. Antibiotic therapy for adults hospitalized with community-acquired pneumonia. JAMA 2016;315(6):593-602.
Study design: Systematic review
Funding source: Unknown/not stated
Allocation: Uncertain
Setting: Inpatient (ward only)
Synopsis: These investigators searched MEDLINE, EMBASE, and the Cochrane databases to identify studies that evaluated outcomes for patients hospitalized with CAP with regard to optimal timing of antibiotic initiation, initial antibiotic selection, and criteria for transition from intravenous to oral antibiotic therapy. Two authors independently reviewed studies for inclusion and assessed study quality.
Of 8 low-quality observational studies, 4 showed a significant association between initiating antibiotic therapy within 4 hours to 8 hours of hospital arrival and reduced mortality. When comparing 2 different antibiotic strategies, 6 of 8 observational studies showed mortality benefit with the use of beta-lactams plus macrolides as compared with beta-lactam monotherapy, though the 2 recent high-quality randomized trials had conflicting results. All three observational studies that compared fluoroquinolones with beta-lactam monotherapy for the treatment of CAP showed an association with fluoroquinolone use and decreased mortality.
Finally, one high-quality trial showed that transitioning patients to oral antibiotics once they meet clinical criteria for stability (stable vital signs, lack of confusion, ability to tolerate oral medications) leads to a shorter length of stay.
Dr. Kulkarni is an assistant professor of hospital medicine at Northwestern University in Chicago.
Clinical question: What is the best antibiotic strategy to improve outcomes in patients hospitalized with community-acquired pneumonia?
Bottom line: For patients hospitalized with community-acquired pneumonia (CAP), start antibiotics early, use either fluoroquinolone monotherapy or beta-lactam/macrolide combination therapy, and switch to oral antibiotics as soon as patients are hemodynamically stable and can take oral medications. Although the evidence is mostly of low quality, this review reaffirms what we already do. (LOE = 2a)
Reference: Lee JS, Giesler DL, Gellad WF, Fine MJ. Antibiotic therapy for adults hospitalized with community-acquired pneumonia. JAMA 2016;315(6):593-602.
Study design: Systematic review
Funding source: Unknown/not stated
Allocation: Uncertain
Setting: Inpatient (ward only)
Synopsis: These investigators searched MEDLINE, EMBASE, and the Cochrane databases to identify studies that evaluated outcomes for patients hospitalized with CAP with regard to optimal timing of antibiotic initiation, initial antibiotic selection, and criteria for transition from intravenous to oral antibiotic therapy. Two authors independently reviewed studies for inclusion and assessed study quality.
Of 8 low-quality observational studies, 4 showed a significant association between initiating antibiotic therapy within 4 hours to 8 hours of hospital arrival and reduced mortality. When comparing 2 different antibiotic strategies, 6 of 8 observational studies showed mortality benefit with the use of beta-lactams plus macrolides as compared with beta-lactam monotherapy, though the 2 recent high-quality randomized trials had conflicting results. All three observational studies that compared fluoroquinolones with beta-lactam monotherapy for the treatment of CAP showed an association with fluoroquinolone use and decreased mortality.
Finally, one high-quality trial showed that transitioning patients to oral antibiotics once they meet clinical criteria for stability (stable vital signs, lack of confusion, ability to tolerate oral medications) leads to a shorter length of stay.
Dr. Kulkarni is an assistant professor of hospital medicine at Northwestern University in Chicago.
When Should Harm-Reduction Strategies Be Used for Inpatients with Opioid Misuse?
Case
A 33-year-old male with a history of opioid overdose and opioid use disorder is admitted with IV heroin use complicated by injection site cellulitis. He is started on antibiotics with improvement in his cellulitis; however, his hospitalization is complicated by acute opioid withdrawal. Despite his history of opioid overdose and opioid use disorder, he has never seen a substance use disorder specialist nor received any education or treatment for his addiction. He reports that he will stop using illicit drugs but declines any further addiction treatment.
What strategies can be employed to reduce his risk of future harm from opioid misuse?
Background
Over the past decade, the U.S. has experienced a rapid increase in the rates of opioid prescriptions and opioid misuse.1 Consequently, the number of ED visits and hospitalizations for opioid-related complications has also increased.2 Many complications result from the practice of injection drug use (IDU), which predisposes individuals to serious blood-borne viral infections such as human immunodeficiency virus (HIV) and hepatitis C virus (HCV) as well as bacterial infections such as infective endocarditis. In addition, individuals who misuse opioids are at risk of death related to opioid overdose. In 2013, there were more than 24,000 deaths in the U.S. due to opioid overdose (see Figure 1).3
In response to the opioid epidemic, there have been a number of local, state, and federal public health initiatives to monitor and secure the opioid drug supply, improve treatment resources, and promulgate harm-reduction interventions. At a more individual level, hospitalists have an important role to play in combating the opioid epidemic. As frontline providers, hospitalists have access to hospitalized individuals with opioid misuse who may not otherwise be exposed to the healthcare system. Therefore, inpatient hospitalizations serve as a unique and important opportunity to engage individuals in the management of their addiction.
There are a number of interventions that hospitalists and substance use disorder specialists can pursue. Psychiatric evaluation and initiation of medication-assisted treatment often aim to aid patients in abstaining from further opioid misuse. However, many individuals with opioid use disorder are not ready for treatment or experience relapses of opioid misuse despite treatment. Given this, a secondary goal is to reduce any harm that may result from opioid misuse. This is done through the implementation of harm-reduction strategies. These strategies include teaching safe injection practices, facilitating the use of syringe exchange programs, and providing opioid overdose education and naloxone distribution.
Overview of Data
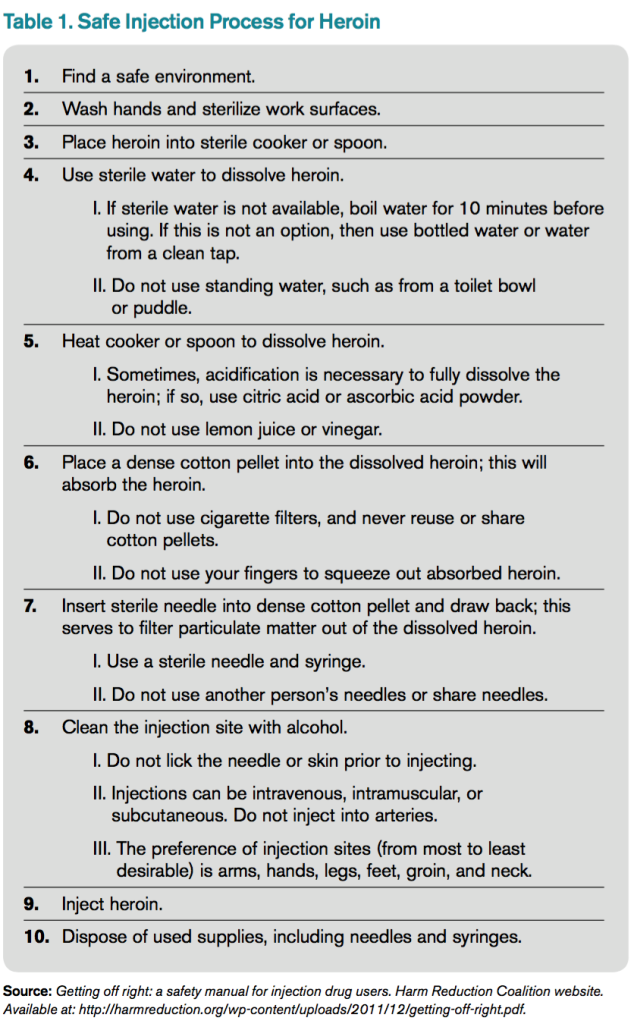
Safe Injection Education. People who inject drugs are at risk for viral, bacterial, and fungal infections. These infections are often the result of nonsterile injection and may be minimized by the utilization of safe injection practices. In order to educate people who inject drugs on safe injection practices, the hospitalist must first understand the process involved in injecting drugs. In Table 1, the process of injecting heroin is outlined (of note, other illicit drugs can be injected, and processes may vary).4

As evidenced by Table 1, the process of sterile injection can be complicated, especially for an individual who may be withdrawing from opioids. Table 1 is also optimistic in that it recommends new and sterile products be used with every injection. If new and sterile equipment is not available, another option is to clean the equipment after every use, which can be done by using bleach and water. This may mitigate the risk of viral, bacterial, and fungal infections. However, the risk is still present, so users should not share or use another individual’s equipment even if it has been cleaned. Due to the risk of viral, bacterial, and fungal infections, all hospitalized individuals who inject drugs should receive education on safe injection practices.
Syringe Exchange Programs. IDU accounts for up to 15% of all new HIV infections and is the primary risk factor for the transmission of HCV.5 These infections occur when people inject using equipment contaminated with blood that contains HIV and/or HCV. Given this, if people who inject drugs could access and consistently use sterile syringes and other injection paraphernalia, the risk of transmitting blood-borne infections would be dramatically reduced. This is the concept behind syringe exchange programs (also known as needle exchange programs), which serve to increase access to sterile syringes while removing contaminated or used syringes from the community.
There is compelling evidence that syringe exchange programs decrease the rate of HIV transmission and likely reduce the rate of HCV transmission as well.6 In addition, syringe exchange programs often provide other beneficial services, such as counseling, testing, and prevention efforts for HIV, HCV, and sexually transmitted infections; distribution of condoms; and referrals to treatment services for substance use disorder.5
Unfortunately, in the U.S., restrictive state laws and lack of funding limit the number of established syringe exchange programs. According to the North American Syringe Exchange Network, there are only 226 programs in 33 states and the District of Columbia. Hospitalists and social workers should be aware of available local resources, including syringe exchange programs, and distribute this information to hospitalized individuals who inject drugs.
Opioid Overdose Education and Naloxone Distribution. Syringe exchange programs and safe injection education aim to reduce harm by decreasing the transmission of infections; however, they do not address the problem of deaths related to opioid overdose. The primary harm-reduction strategy used to address deaths related to opioid overdose in the U.S is opioid overdose education and naloxone distribution (OEND). Naloxone is an opioid antagonist that reverses the respiratory depression and decreased consciousness caused by opioids. The OEND strategy involves educating first responders— including individuals and friends and family of individuals who use opioids—to recognize the signs of an opioid overdose, seek help, provide rescue breathing, administer naloxone, and stay with the individual until emergency medical services arrive.7 This strategy has been observed to decrease rates of death related to opioid overdose.7
Given the evolving opioid epidemic and effectiveness of the OEND strategy, it is not surprising that the number of local opioid overdose prevention programs adopting OEND has risen dramatically. As of 2014, there were 140 organizations, with 644 local sites providing naloxone in 29 states and the District of Columbia. These organizations have distributed 152,000 naloxone kits and have reported more than 26,000 reversals.8 Certainly, OEND has prevented morbidity and mortality in some of these patients.
The adoption of OEND can be performed by individual prescribers as well. Naloxone is U.S. FDA-approved for the treatment of opioid overdose, and thus the liability to prescribers is similar to that of other FDA-approved drugs. However, the distribution of naloxone to third parties, such as friends and family of individuals with opioid misuse, is more complex and regulated by state laws. Many states have created liability protection for naloxone prescription to third parties. Individual state laws and additional information can be found at prescribetoprevent.org.
Hospitalists should provide opioid overdose education to all individuals with opioid misuse and friends and family of individuals with opioid misuse. In addition, hospitalists should prescribe naloxone to individuals with opioid misuse and, in states where the law allows, distribute naloxone to friends and family of individuals with opioid misuse as well.
Controversies. In general, opioid use disorder treatment providers; public health officials; and local, state, and federal government agencies have increasingly embraced harm-reduction strategies. However, some feel that harm-reduction strategies are misguided or even detrimental due to concern that they implicitly condone or enable the use of illicit substances. There have been a number of studies to evaluate the potential unintended consequences of harm-reduction strategies, and overwhelmingly, these have been either neutral or have shown the benefit of harm-reduction interventions. At this point, there is no good evidence to prevent the widespread adoption of harm-reduction strategies for hospitalists.
Back to the Case
The case involves an individual who has already had at least two complications of his IV heroin use, including cellulitis and opioid overdose. Ideally, this individual would be willing to see an addiction specialist and start medication-assisted treatment. Unfortunately, he is unwilling to be further evaluated by a specialist at this time. Regardless, he remains at risk of future complications, and it is the hospitalist’s responsibility to intervene with a goal of reducing future harm that may result from his IV heroin use.
The hospitalist in this case advises the patient to abstain from heroin and IDU, encourages him to seek treatment for his opioid use disorder, and gives him resources for linkage to care if he becomes interested. In addition, the hospitalist educates the patient on safe injection practices and provides a list of local syringe exchange programs to decrease future risk of viral, bacterial, and fungal infections. Furthermore, the hospitalist provides opioid overdose education and distributes naloxone to the patient, along with friends and family of the patient, to reduce the risk of death related to opioid overdose.
Bottom Line
Hospitalists should utilize harm-reduction interventions in individuals hospitalized with opioid misuse. TH
Dr. Theisen-Toupal is a hospitalist at the Veterans Affairs Medical Center and assistant professor of medicine at the George Washington University School of Medicine & Health Sciences, both in Washington, D.C.
References
- Vital signs: overdoses of prescription opioid pain relievers—United States, 1999–2008. Morbidity and Mortality Weekly Report. Centers for Disease Control and Prevention website. Available at: http://www.cdc.gov/mmwr/preview/mmwrhtml/mm6043a4.htm. Published November 4, 2011.
- Drug abuse warning network, 2011: national estimates of drug-related emergency department visits. Substance Abuse and Mental Health Services Administration website. Available at: http://www.samhsa.gov/data/2k13/DAWN2k11ED/DAWN2k11ED.htm#5. Accessed July 29, 2015.
- Hedergaard H, Chen LH, Warner M. Drug-poisoning deaths involving heroin: United States, 2000–2013. National Center for Health Statistics Data Brief. Centers for Disease Control and Prevention website. Available at: http://www.cdc.gov/nchs/data/databriefs/db190.htm. Published March 2015.
- Getting off right: a safety manual for injection drug users. Harm Reduction Coalition website. Available at: http://harmreduction.org/wp-content/uploads/2011/12/getting-off-right.pdf.
- Syringe exchange programs—United States, 2008. Morbidity and Mortality Weekly Report. Centers for Disease Control and Prevention website. Available at: http://www.cdc.gov/mmwr/preview/mmwrhtml/mm5945a4.htm/Syringe-Exchange-Programs-United-States-2008. Published November 19, 2010.
- Wodak A, Conney A. Effectiveness of sterile needle and syringe programming in reducing HIV/AIDS among injecting drug users. World Health Organization website. Available at: http://apps.who.int/iris/bitstream/10665/43107/1/9241591641.pdf. Published 2004.
- Walley AY, Xuan Z, Hackman HH, et al. Opioid overdose rates and implementation of overdose education and nasal naloxone distribution in Massachusetts: interrupted time series analysis. BMJ. 2013;346:f174.
- Wheeler E, Jones TS, Gilbert MK, Davidson PJ. Opioid overdose prevention programs providing naloxone to laypersons—United States, 2014. Morbidity and Mortality Weekly Report. Centers for Disease Control and Prevention website. Available at: http://www.cdc.gov/mmwr/preview/mmwrhtml/mm6423a2.htm. Published June 19, 2015.
Case
A 33-year-old male with a history of opioid overdose and opioid use disorder is admitted with IV heroin use complicated by injection site cellulitis. He is started on antibiotics with improvement in his cellulitis; however, his hospitalization is complicated by acute opioid withdrawal. Despite his history of opioid overdose and opioid use disorder, he has never seen a substance use disorder specialist nor received any education or treatment for his addiction. He reports that he will stop using illicit drugs but declines any further addiction treatment.
What strategies can be employed to reduce his risk of future harm from opioid misuse?
Background
Over the past decade, the U.S. has experienced a rapid increase in the rates of opioid prescriptions and opioid misuse.1 Consequently, the number of ED visits and hospitalizations for opioid-related complications has also increased.2 Many complications result from the practice of injection drug use (IDU), which predisposes individuals to serious blood-borne viral infections such as human immunodeficiency virus (HIV) and hepatitis C virus (HCV) as well as bacterial infections such as infective endocarditis. In addition, individuals who misuse opioids are at risk of death related to opioid overdose. In 2013, there were more than 24,000 deaths in the U.S. due to opioid overdose (see Figure 1).3
In response to the opioid epidemic, there have been a number of local, state, and federal public health initiatives to monitor and secure the opioid drug supply, improve treatment resources, and promulgate harm-reduction interventions. At a more individual level, hospitalists have an important role to play in combating the opioid epidemic. As frontline providers, hospitalists have access to hospitalized individuals with opioid misuse who may not otherwise be exposed to the healthcare system. Therefore, inpatient hospitalizations serve as a unique and important opportunity to engage individuals in the management of their addiction.
There are a number of interventions that hospitalists and substance use disorder specialists can pursue. Psychiatric evaluation and initiation of medication-assisted treatment often aim to aid patients in abstaining from further opioid misuse. However, many individuals with opioid use disorder are not ready for treatment or experience relapses of opioid misuse despite treatment. Given this, a secondary goal is to reduce any harm that may result from opioid misuse. This is done through the implementation of harm-reduction strategies. These strategies include teaching safe injection practices, facilitating the use of syringe exchange programs, and providing opioid overdose education and naloxone distribution.
Overview of Data
Safe Injection Education. People who inject drugs are at risk for viral, bacterial, and fungal infections. These infections are often the result of nonsterile injection and may be minimized by the utilization of safe injection practices. In order to educate people who inject drugs on safe injection practices, the hospitalist must first understand the process involved in injecting drugs. In Table 1, the process of injecting heroin is outlined (of note, other illicit drugs can be injected, and processes may vary).4
As evidenced by Table 1, the process of sterile injection can be complicated, especially for an individual who may be withdrawing from opioids. Table 1 is also optimistic in that it recommends new and sterile products be used with every injection. If new and sterile equipment is not available, another option is to clean the equipment after every use, which can be done by using bleach and water. This may mitigate the risk of viral, bacterial, and fungal infections. However, the risk is still present, so users should not share or use another individual’s equipment even if it has been cleaned. Due to the risk of viral, bacterial, and fungal infections, all hospitalized individuals who inject drugs should receive education on safe injection practices.
Syringe Exchange Programs. IDU accounts for up to 15% of all new HIV infections and is the primary risk factor for the transmission of HCV.5 These infections occur when people inject using equipment contaminated with blood that contains HIV and/or HCV. Given this, if people who inject drugs could access and consistently use sterile syringes and other injection paraphernalia, the risk of transmitting blood-borne infections would be dramatically reduced. This is the concept behind syringe exchange programs (also known as needle exchange programs), which serve to increase access to sterile syringes while removing contaminated or used syringes from the community.
There is compelling evidence that syringe exchange programs decrease the rate of HIV transmission and likely reduce the rate of HCV transmission as well.6 In addition, syringe exchange programs often provide other beneficial services, such as counseling, testing, and prevention efforts for HIV, HCV, and sexually transmitted infections; distribution of condoms; and referrals to treatment services for substance use disorder.5
Unfortunately, in the U.S., restrictive state laws and lack of funding limit the number of established syringe exchange programs. According to the North American Syringe Exchange Network, there are only 226 programs in 33 states and the District of Columbia. Hospitalists and social workers should be aware of available local resources, including syringe exchange programs, and distribute this information to hospitalized individuals who inject drugs.
Opioid Overdose Education and Naloxone Distribution. Syringe exchange programs and safe injection education aim to reduce harm by decreasing the transmission of infections; however, they do not address the problem of deaths related to opioid overdose. The primary harm-reduction strategy used to address deaths related to opioid overdose in the U.S is opioid overdose education and naloxone distribution (OEND). Naloxone is an opioid antagonist that reverses the respiratory depression and decreased consciousness caused by opioids. The OEND strategy involves educating first responders— including individuals and friends and family of individuals who use opioids—to recognize the signs of an opioid overdose, seek help, provide rescue breathing, administer naloxone, and stay with the individual until emergency medical services arrive.7 This strategy has been observed to decrease rates of death related to opioid overdose.7
Given the evolving opioid epidemic and effectiveness of the OEND strategy, it is not surprising that the number of local opioid overdose prevention programs adopting OEND has risen dramatically. As of 2014, there were 140 organizations, with 644 local sites providing naloxone in 29 states and the District of Columbia. These organizations have distributed 152,000 naloxone kits and have reported more than 26,000 reversals.8 Certainly, OEND has prevented morbidity and mortality in some of these patients.
The adoption of OEND can be performed by individual prescribers as well. Naloxone is U.S. FDA-approved for the treatment of opioid overdose, and thus the liability to prescribers is similar to that of other FDA-approved drugs. However, the distribution of naloxone to third parties, such as friends and family of individuals with opioid misuse, is more complex and regulated by state laws. Many states have created liability protection for naloxone prescription to third parties. Individual state laws and additional information can be found at prescribetoprevent.org.
Hospitalists should provide opioid overdose education to all individuals with opioid misuse and friends and family of individuals with opioid misuse. In addition, hospitalists should prescribe naloxone to individuals with opioid misuse and, in states where the law allows, distribute naloxone to friends and family of individuals with opioid misuse as well.
Controversies. In general, opioid use disorder treatment providers; public health officials; and local, state, and federal government agencies have increasingly embraced harm-reduction strategies. However, some feel that harm-reduction strategies are misguided or even detrimental due to concern that they implicitly condone or enable the use of illicit substances. There have been a number of studies to evaluate the potential unintended consequences of harm-reduction strategies, and overwhelmingly, these have been either neutral or have shown the benefit of harm-reduction interventions. At this point, there is no good evidence to prevent the widespread adoption of harm-reduction strategies for hospitalists.
Back to the Case
The case involves an individual who has already had at least two complications of his IV heroin use, including cellulitis and opioid overdose. Ideally, this individual would be willing to see an addiction specialist and start medication-assisted treatment. Unfortunately, he is unwilling to be further evaluated by a specialist at this time. Regardless, he remains at risk of future complications, and it is the hospitalist’s responsibility to intervene with a goal of reducing future harm that may result from his IV heroin use.
The hospitalist in this case advises the patient to abstain from heroin and IDU, encourages him to seek treatment for his opioid use disorder, and gives him resources for linkage to care if he becomes interested. In addition, the hospitalist educates the patient on safe injection practices and provides a list of local syringe exchange programs to decrease future risk of viral, bacterial, and fungal infections. Furthermore, the hospitalist provides opioid overdose education and distributes naloxone to the patient, along with friends and family of the patient, to reduce the risk of death related to opioid overdose.
Bottom Line
Hospitalists should utilize harm-reduction interventions in individuals hospitalized with opioid misuse. TH
Dr. Theisen-Toupal is a hospitalist at the Veterans Affairs Medical Center and assistant professor of medicine at the George Washington University School of Medicine & Health Sciences, both in Washington, D.C.
References
- Vital signs: overdoses of prescription opioid pain relievers—United States, 1999–2008. Morbidity and Mortality Weekly Report. Centers for Disease Control and Prevention website. Available at: http://www.cdc.gov/mmwr/preview/mmwrhtml/mm6043a4.htm. Published November 4, 2011.
- Drug abuse warning network, 2011: national estimates of drug-related emergency department visits. Substance Abuse and Mental Health Services Administration website. Available at: http://www.samhsa.gov/data/2k13/DAWN2k11ED/DAWN2k11ED.htm#5. Accessed July 29, 2015.
- Hedergaard H, Chen LH, Warner M. Drug-poisoning deaths involving heroin: United States, 2000–2013. National Center for Health Statistics Data Brief. Centers for Disease Control and Prevention website. Available at: http://www.cdc.gov/nchs/data/databriefs/db190.htm. Published March 2015.
- Getting off right: a safety manual for injection drug users. Harm Reduction Coalition website. Available at: http://harmreduction.org/wp-content/uploads/2011/12/getting-off-right.pdf.
- Syringe exchange programs—United States, 2008. Morbidity and Mortality Weekly Report. Centers for Disease Control and Prevention website. Available at: http://www.cdc.gov/mmwr/preview/mmwrhtml/mm5945a4.htm/Syringe-Exchange-Programs-United-States-2008. Published November 19, 2010.
- Wodak A, Conney A. Effectiveness of sterile needle and syringe programming in reducing HIV/AIDS among injecting drug users. World Health Organization website. Available at: http://apps.who.int/iris/bitstream/10665/43107/1/9241591641.pdf. Published 2004.
- Walley AY, Xuan Z, Hackman HH, et al. Opioid overdose rates and implementation of overdose education and nasal naloxone distribution in Massachusetts: interrupted time series analysis. BMJ. 2013;346:f174.
- Wheeler E, Jones TS, Gilbert MK, Davidson PJ. Opioid overdose prevention programs providing naloxone to laypersons—United States, 2014. Morbidity and Mortality Weekly Report. Centers for Disease Control and Prevention website. Available at: http://www.cdc.gov/mmwr/preview/mmwrhtml/mm6423a2.htm. Published June 19, 2015.
Case
A 33-year-old male with a history of opioid overdose and opioid use disorder is admitted with IV heroin use complicated by injection site cellulitis. He is started on antibiotics with improvement in his cellulitis; however, his hospitalization is complicated by acute opioid withdrawal. Despite his history of opioid overdose and opioid use disorder, he has never seen a substance use disorder specialist nor received any education or treatment for his addiction. He reports that he will stop using illicit drugs but declines any further addiction treatment.
What strategies can be employed to reduce his risk of future harm from opioid misuse?
Background
Over the past decade, the U.S. has experienced a rapid increase in the rates of opioid prescriptions and opioid misuse.1 Consequently, the number of ED visits and hospitalizations for opioid-related complications has also increased.2 Many complications result from the practice of injection drug use (IDU), which predisposes individuals to serious blood-borne viral infections such as human immunodeficiency virus (HIV) and hepatitis C virus (HCV) as well as bacterial infections such as infective endocarditis. In addition, individuals who misuse opioids are at risk of death related to opioid overdose. In 2013, there were more than 24,000 deaths in the U.S. due to opioid overdose (see Figure 1).3
In response to the opioid epidemic, there have been a number of local, state, and federal public health initiatives to monitor and secure the opioid drug supply, improve treatment resources, and promulgate harm-reduction interventions. At a more individual level, hospitalists have an important role to play in combating the opioid epidemic. As frontline providers, hospitalists have access to hospitalized individuals with opioid misuse who may not otherwise be exposed to the healthcare system. Therefore, inpatient hospitalizations serve as a unique and important opportunity to engage individuals in the management of their addiction.
There are a number of interventions that hospitalists and substance use disorder specialists can pursue. Psychiatric evaluation and initiation of medication-assisted treatment often aim to aid patients in abstaining from further opioid misuse. However, many individuals with opioid use disorder are not ready for treatment or experience relapses of opioid misuse despite treatment. Given this, a secondary goal is to reduce any harm that may result from opioid misuse. This is done through the implementation of harm-reduction strategies. These strategies include teaching safe injection practices, facilitating the use of syringe exchange programs, and providing opioid overdose education and naloxone distribution.
Overview of Data
Safe Injection Education. People who inject drugs are at risk for viral, bacterial, and fungal infections. These infections are often the result of nonsterile injection and may be minimized by the utilization of safe injection practices. In order to educate people who inject drugs on safe injection practices, the hospitalist must first understand the process involved in injecting drugs. In Table 1, the process of injecting heroin is outlined (of note, other illicit drugs can be injected, and processes may vary).4
As evidenced by Table 1, the process of sterile injection can be complicated, especially for an individual who may be withdrawing from opioids. Table 1 is also optimistic in that it recommends new and sterile products be used with every injection. If new and sterile equipment is not available, another option is to clean the equipment after every use, which can be done by using bleach and water. This may mitigate the risk of viral, bacterial, and fungal infections. However, the risk is still present, so users should not share or use another individual’s equipment even if it has been cleaned. Due to the risk of viral, bacterial, and fungal infections, all hospitalized individuals who inject drugs should receive education on safe injection practices.
Syringe Exchange Programs. IDU accounts for up to 15% of all new HIV infections and is the primary risk factor for the transmission of HCV.5 These infections occur when people inject using equipment contaminated with blood that contains HIV and/or HCV. Given this, if people who inject drugs could access and consistently use sterile syringes and other injection paraphernalia, the risk of transmitting blood-borne infections would be dramatically reduced. This is the concept behind syringe exchange programs (also known as needle exchange programs), which serve to increase access to sterile syringes while removing contaminated or used syringes from the community.
There is compelling evidence that syringe exchange programs decrease the rate of HIV transmission and likely reduce the rate of HCV transmission as well.6 In addition, syringe exchange programs often provide other beneficial services, such as counseling, testing, and prevention efforts for HIV, HCV, and sexually transmitted infections; distribution of condoms; and referrals to treatment services for substance use disorder.5
Unfortunately, in the U.S., restrictive state laws and lack of funding limit the number of established syringe exchange programs. According to the North American Syringe Exchange Network, there are only 226 programs in 33 states and the District of Columbia. Hospitalists and social workers should be aware of available local resources, including syringe exchange programs, and distribute this information to hospitalized individuals who inject drugs.
Opioid Overdose Education and Naloxone Distribution. Syringe exchange programs and safe injection education aim to reduce harm by decreasing the transmission of infections; however, they do not address the problem of deaths related to opioid overdose. The primary harm-reduction strategy used to address deaths related to opioid overdose in the U.S is opioid overdose education and naloxone distribution (OEND). Naloxone is an opioid antagonist that reverses the respiratory depression and decreased consciousness caused by opioids. The OEND strategy involves educating first responders— including individuals and friends and family of individuals who use opioids—to recognize the signs of an opioid overdose, seek help, provide rescue breathing, administer naloxone, and stay with the individual until emergency medical services arrive.7 This strategy has been observed to decrease rates of death related to opioid overdose.7
Given the evolving opioid epidemic and effectiveness of the OEND strategy, it is not surprising that the number of local opioid overdose prevention programs adopting OEND has risen dramatically. As of 2014, there were 140 organizations, with 644 local sites providing naloxone in 29 states and the District of Columbia. These organizations have distributed 152,000 naloxone kits and have reported more than 26,000 reversals.8 Certainly, OEND has prevented morbidity and mortality in some of these patients.
The adoption of OEND can be performed by individual prescribers as well. Naloxone is U.S. FDA-approved for the treatment of opioid overdose, and thus the liability to prescribers is similar to that of other FDA-approved drugs. However, the distribution of naloxone to third parties, such as friends and family of individuals with opioid misuse, is more complex and regulated by state laws. Many states have created liability protection for naloxone prescription to third parties. Individual state laws and additional information can be found at prescribetoprevent.org.
Hospitalists should provide opioid overdose education to all individuals with opioid misuse and friends and family of individuals with opioid misuse. In addition, hospitalists should prescribe naloxone to individuals with opioid misuse and, in states where the law allows, distribute naloxone to friends and family of individuals with opioid misuse as well.
Controversies. In general, opioid use disorder treatment providers; public health officials; and local, state, and federal government agencies have increasingly embraced harm-reduction strategies. However, some feel that harm-reduction strategies are misguided or even detrimental due to concern that they implicitly condone or enable the use of illicit substances. There have been a number of studies to evaluate the potential unintended consequences of harm-reduction strategies, and overwhelmingly, these have been either neutral or have shown the benefit of harm-reduction interventions. At this point, there is no good evidence to prevent the widespread adoption of harm-reduction strategies for hospitalists.
Back to the Case
The case involves an individual who has already had at least two complications of his IV heroin use, including cellulitis and opioid overdose. Ideally, this individual would be willing to see an addiction specialist and start medication-assisted treatment. Unfortunately, he is unwilling to be further evaluated by a specialist at this time. Regardless, he remains at risk of future complications, and it is the hospitalist’s responsibility to intervene with a goal of reducing future harm that may result from his IV heroin use.
The hospitalist in this case advises the patient to abstain from heroin and IDU, encourages him to seek treatment for his opioid use disorder, and gives him resources for linkage to care if he becomes interested. In addition, the hospitalist educates the patient on safe injection practices and provides a list of local syringe exchange programs to decrease future risk of viral, bacterial, and fungal infections. Furthermore, the hospitalist provides opioid overdose education and distributes naloxone to the patient, along with friends and family of the patient, to reduce the risk of death related to opioid overdose.
Bottom Line
Hospitalists should utilize harm-reduction interventions in individuals hospitalized with opioid misuse. TH
Dr. Theisen-Toupal is a hospitalist at the Veterans Affairs Medical Center and assistant professor of medicine at the George Washington University School of Medicine & Health Sciences, both in Washington, D.C.
References
- Vital signs: overdoses of prescription opioid pain relievers—United States, 1999–2008. Morbidity and Mortality Weekly Report. Centers for Disease Control and Prevention website. Available at: http://www.cdc.gov/mmwr/preview/mmwrhtml/mm6043a4.htm. Published November 4, 2011.
- Drug abuse warning network, 2011: national estimates of drug-related emergency department visits. Substance Abuse and Mental Health Services Administration website. Available at: http://www.samhsa.gov/data/2k13/DAWN2k11ED/DAWN2k11ED.htm#5. Accessed July 29, 2015.
- Hedergaard H, Chen LH, Warner M. Drug-poisoning deaths involving heroin: United States, 2000–2013. National Center for Health Statistics Data Brief. Centers for Disease Control and Prevention website. Available at: http://www.cdc.gov/nchs/data/databriefs/db190.htm. Published March 2015.
- Getting off right: a safety manual for injection drug users. Harm Reduction Coalition website. Available at: http://harmreduction.org/wp-content/uploads/2011/12/getting-off-right.pdf.
- Syringe exchange programs—United States, 2008. Morbidity and Mortality Weekly Report. Centers for Disease Control and Prevention website. Available at: http://www.cdc.gov/mmwr/preview/mmwrhtml/mm5945a4.htm/Syringe-Exchange-Programs-United-States-2008. Published November 19, 2010.
- Wodak A, Conney A. Effectiveness of sterile needle and syringe programming in reducing HIV/AIDS among injecting drug users. World Health Organization website. Available at: http://apps.who.int/iris/bitstream/10665/43107/1/9241591641.pdf. Published 2004.
- Walley AY, Xuan Z, Hackman HH, et al. Opioid overdose rates and implementation of overdose education and nasal naloxone distribution in Massachusetts: interrupted time series analysis. BMJ. 2013;346:f174.
- Wheeler E, Jones TS, Gilbert MK, Davidson PJ. Opioid overdose prevention programs providing naloxone to laypersons—United States, 2014. Morbidity and Mortality Weekly Report. Centers for Disease Control and Prevention website. Available at: http://www.cdc.gov/mmwr/preview/mmwrhtml/mm6423a2.htm. Published June 19, 2015.
HM16 Q&A: What Problem Do You Hope Health IT Solves?
With the rolling out of the Health IT track on the second full day of HM16, The Hospitalist asked: What problem do you hope health IT solves or helps you solve over the next five years?

Farhanaz Chowdhury, MD, hospitalist, HSHS St. Elizabeth’s Hospital, Belleville, Ill.
“I think that hospital health systems are very primitive. When they make that software, physicians should be more involved so that in everyday life, what we see when we are facing all those problems, you have an algorithm if you want to do something. It should pop up so that you don’t have to write it down and scroll all over.”
Michael Lintner, MD, hospitalist, Aspen Valley Hospital, Colo.

“I think probably the main thing would be work flow, facilitating work flow. I think today hospitalists are just getting more and more and more work. Patient loads are getting increasingly bigger. I think with IT, [we need] systems that facilitate and help with the work flow and help the hospitalist’s day go smoother because there are so many things that we do.”
Miguel Lizardo, MD, hospitalist, University of Massachusetts Memorial Medical Center, Worcester
“It takes a lot of time to interact with the EMRs and all the technology that we have to use. If they can find a way that we can use it in a more user-friendly [way] so that it takes not a long time, that would be great. At least the EMRs that I’ve been in contact with are too cumbersome, too many clicks to get where you want, a bunch of steps to document what you need to. You really are away from the patient and spending a lot of time trying to document.”
Sandeep Palikhel, PA-C, Baylor University Medical Center, Waco, Tex.
“Definitely accuracy. In Texas, where I practice, we get a lot of transfers from rural areas because we are a Level 1 trauma hospital. We get these discharge summaries or progress notes from other hospitals that are handwritten. A lot of information gets missed whenever we’re reading it because it’s not legible, first thing, and it’s not as detail-oriented as the EHRs would be. So that definitely helps. Even going through a medication list, it helps so much to go through an EHR versus going through a handwritten medication list. That’s what I mean by accuracy.”
With the rolling out of the Health IT track on the second full day of HM16, The Hospitalist asked: What problem do you hope health IT solves or helps you solve over the next five years?
Farhanaz Chowdhury, MD, hospitalist, HSHS St. Elizabeth’s Hospital, Belleville, Ill.
“I think that hospital health systems are very primitive. When they make that software, physicians should be more involved so that in everyday life, what we see when we are facing all those problems, you have an algorithm if you want to do something. It should pop up so that you don’t have to write it down and scroll all over.”
Michael Lintner, MD, hospitalist, Aspen Valley Hospital, Colo.
“I think probably the main thing would be work flow, facilitating work flow. I think today hospitalists are just getting more and more and more work. Patient loads are getting increasingly bigger. I think with IT, [we need] systems that facilitate and help with the work flow and help the hospitalist’s day go smoother because there are so many things that we do.”
Miguel Lizardo, MD, hospitalist, University of Massachusetts Memorial Medical Center, Worcester
“It takes a lot of time to interact with the EMRs and all the technology that we have to use. If they can find a way that we can use it in a more user-friendly [way] so that it takes not a long time, that would be great. At least the EMRs that I’ve been in contact with are too cumbersome, too many clicks to get where you want, a bunch of steps to document what you need to. You really are away from the patient and spending a lot of time trying to document.”
Sandeep Palikhel, PA-C, Baylor University Medical Center, Waco, Tex.
“Definitely accuracy. In Texas, where I practice, we get a lot of transfers from rural areas because we are a Level 1 trauma hospital. We get these discharge summaries or progress notes from other hospitals that are handwritten. A lot of information gets missed whenever we’re reading it because it’s not legible, first thing, and it’s not as detail-oriented as the EHRs would be. So that definitely helps. Even going through a medication list, it helps so much to go through an EHR versus going through a handwritten medication list. That’s what I mean by accuracy.”
With the rolling out of the Health IT track on the second full day of HM16, The Hospitalist asked: What problem do you hope health IT solves or helps you solve over the next five years?
Farhanaz Chowdhury, MD, hospitalist, HSHS St. Elizabeth’s Hospital, Belleville, Ill.
“I think that hospital health systems are very primitive. When they make that software, physicians should be more involved so that in everyday life, what we see when we are facing all those problems, you have an algorithm if you want to do something. It should pop up so that you don’t have to write it down and scroll all over.”
Michael Lintner, MD, hospitalist, Aspen Valley Hospital, Colo.
“I think probably the main thing would be work flow, facilitating work flow. I think today hospitalists are just getting more and more and more work. Patient loads are getting increasingly bigger. I think with IT, [we need] systems that facilitate and help with the work flow and help the hospitalist’s day go smoother because there are so many things that we do.”
Miguel Lizardo, MD, hospitalist, University of Massachusetts Memorial Medical Center, Worcester
“It takes a lot of time to interact with the EMRs and all the technology that we have to use. If they can find a way that we can use it in a more user-friendly [way] so that it takes not a long time, that would be great. At least the EMRs that I’ve been in contact with are too cumbersome, too many clicks to get where you want, a bunch of steps to document what you need to. You really are away from the patient and spending a lot of time trying to document.”
Sandeep Palikhel, PA-C, Baylor University Medical Center, Waco, Tex.
“Definitely accuracy. In Texas, where I practice, we get a lot of transfers from rural areas because we are a Level 1 trauma hospital. We get these discharge summaries or progress notes from other hospitals that are handwritten. A lot of information gets missed whenever we’re reading it because it’s not legible, first thing, and it’s not as detail-oriented as the EHRs would be. So that definitely helps. Even going through a medication list, it helps so much to go through an EHR versus going through a handwritten medication list. That’s what I mean by accuracy.”
New Findings Show: Factors Contributing to the Prevalence in readmission for Bariatric Surgery Patients
NEW YORK (Reuters Health) - About one in 20 bariatric surgery patients are readmitted to the hospital within 30 days of having the procedure, according to new findings.
Readmissions are increasingly being used as a quality metric for surgical procedures, Dr. John Morton of Stanford University in California and colleagues note in their report, published online March 19 in the American Journal of Surgery.
"While (the Centers for Medicare and Medicaid Services) has not addressed bariatric surgery readmissions to date, other payors have made readmissions a priority," they add. "Data regarding bariatric surgery readmissions are critical to help better understand and drive quality improvement in this area.
"To investigate the prevalence, causes and risk factors for readmission following bariatric surgery, the researchers looked at data from the 2012 American College of Surgeons National Surgical Quality Improvement Program Public Use File dataset on nearly 18,300 bariatric patients, of whom 55% had laparoscopic Roux-en-Y gastric bypass (LRYGB), 10% had laparoscopic adjustable gastric banding (LAGB), and 35% had laparoscopic sleeve gastrectomy (LSG).
There were 955 readmissions (5.22%), most commonly for gastrointestinal causes (45%), dietary reasons (34%) and bleeding (7%). Readmission rates were nearly 7% for LRYGB; just under 2% for LAGB; and 4% for LSG.
The patients who were readmitted had a significantly longer average operating time (132 vs. 115 minutes) and length of stay (2.76 days vs. 2.23). Forty percent had a complication, versus 4% of patients who were not readmitted. Patients who were readmitted were also more likely to have a body mass index above 50, preoperative diabetes, chronic obstructive pulmonary disease, and hypertension.
Factors independently associated with readmission included African-American race (odds ratio, 1.53), complication (OR, 11.3) and resident involvement (OR, 0.53).
"Other studies have also demonstrated similar predictors of readmission and have also demonstrated that length of stay may also play a role in readmission rates," Dr. Morton and his team state. "This study helps demonstrate that bariatric surgery readmissions are prevalent and potentially preventable."
NEW YORK (Reuters Health) - About one in 20 bariatric surgery patients are readmitted to the hospital within 30 days of having the procedure, according to new findings.
Readmissions are increasingly being used as a quality metric for surgical procedures, Dr. John Morton of Stanford University in California and colleagues note in their report, published online March 19 in the American Journal of Surgery.
"While (the Centers for Medicare and Medicaid Services) has not addressed bariatric surgery readmissions to date, other payors have made readmissions a priority," they add. "Data regarding bariatric surgery readmissions are critical to help better understand and drive quality improvement in this area.
"To investigate the prevalence, causes and risk factors for readmission following bariatric surgery, the researchers looked at data from the 2012 American College of Surgeons National Surgical Quality Improvement Program Public Use File dataset on nearly 18,300 bariatric patients, of whom 55% had laparoscopic Roux-en-Y gastric bypass (LRYGB), 10% had laparoscopic adjustable gastric banding (LAGB), and 35% had laparoscopic sleeve gastrectomy (LSG).
There were 955 readmissions (5.22%), most commonly for gastrointestinal causes (45%), dietary reasons (34%) and bleeding (7%). Readmission rates were nearly 7% for LRYGB; just under 2% for LAGB; and 4% for LSG.
The patients who were readmitted had a significantly longer average operating time (132 vs. 115 minutes) and length of stay (2.76 days vs. 2.23). Forty percent had a complication, versus 4% of patients who were not readmitted. Patients who were readmitted were also more likely to have a body mass index above 50, preoperative diabetes, chronic obstructive pulmonary disease, and hypertension.
Factors independently associated with readmission included African-American race (odds ratio, 1.53), complication (OR, 11.3) and resident involvement (OR, 0.53).
"Other studies have also demonstrated similar predictors of readmission and have also demonstrated that length of stay may also play a role in readmission rates," Dr. Morton and his team state. "This study helps demonstrate that bariatric surgery readmissions are prevalent and potentially preventable."
NEW YORK (Reuters Health) - About one in 20 bariatric surgery patients are readmitted to the hospital within 30 days of having the procedure, according to new findings.
Readmissions are increasingly being used as a quality metric for surgical procedures, Dr. John Morton of Stanford University in California and colleagues note in their report, published online March 19 in the American Journal of Surgery.
"While (the Centers for Medicare and Medicaid Services) has not addressed bariatric surgery readmissions to date, other payors have made readmissions a priority," they add. "Data regarding bariatric surgery readmissions are critical to help better understand and drive quality improvement in this area.
"To investigate the prevalence, causes and risk factors for readmission following bariatric surgery, the researchers looked at data from the 2012 American College of Surgeons National Surgical Quality Improvement Program Public Use File dataset on nearly 18,300 bariatric patients, of whom 55% had laparoscopic Roux-en-Y gastric bypass (LRYGB), 10% had laparoscopic adjustable gastric banding (LAGB), and 35% had laparoscopic sleeve gastrectomy (LSG).
There were 955 readmissions (5.22%), most commonly for gastrointestinal causes (45%), dietary reasons (34%) and bleeding (7%). Readmission rates were nearly 7% for LRYGB; just under 2% for LAGB; and 4% for LSG.
The patients who were readmitted had a significantly longer average operating time (132 vs. 115 minutes) and length of stay (2.76 days vs. 2.23). Forty percent had a complication, versus 4% of patients who were not readmitted. Patients who were readmitted were also more likely to have a body mass index above 50, preoperative diabetes, chronic obstructive pulmonary disease, and hypertension.
Factors independently associated with readmission included African-American race (odds ratio, 1.53), complication (OR, 11.3) and resident involvement (OR, 0.53).
"Other studies have also demonstrated similar predictors of readmission and have also demonstrated that length of stay may also play a role in readmission rates," Dr. Morton and his team state. "This study helps demonstrate that bariatric surgery readmissions are prevalent and potentially preventable."
New Analysis shows that Women who Develop Diabetes while Pregnant are Likely to Develop Fatty Liver Disease
(Reuters Health) - Women who develop diabetes while pregnant may be at elevated risk of also developing a dangerous build up of fat in their livers when they reach middle age, according to a new analysis.
The common risk factor for both gestational diabetes and non-alcoholic fatty liver disease, researchers say, is trouble making or using the hormone insulin to manage blood sugar, known as insulin resistance.
"We hope that early identification can promote healthy lifestyle changes that prevent or slow disease progression," said lead author Dr. Veeral Ajmera of the University of California, San Francisco.
"Pregnancy stresses the body in many ways, one of which is the ability to manage blood sugar," Ajmera said by email. "During pregnancy a woman's body becomes more resistant to insulin, which is the hormone required to decrease the blood sugar."
Insulin resistance is also "central to development of non-alcoholic fatty liver disease," which affects 20 percent to 30 percent of adults in the western world, the study team writes in The American Journal of Gastroenterology. Non-alcoholic fatty liver disease is the most common chronic liver disease in the United States.
Fatty liver disease is often diagnosed later in life, Ajmera told Reuters Health. So the researchers used long-term data to see if diabetes during pregnancy made a woman more likely to develop fatty liver disease 25 years later.
The researchers analyzed information about 1,115 black and white women recruited between 1985-1986 in four cities across the United States who gave birth to at least one child.
The participants did not have diabetes before becoming pregnant and the study excluded people who had liver issues related to alcohol, HIV, hepatitis or medications.
At the start of the study, women reported on whether they first experienced diabetes during pregnancy, and researchers confirmed the diagnosis with blood test results. Twenty-five years later, the women received more blood tests as well as CT scans of their livers to check if they had fatty liver disease.
At the beginning of the study, 124 women reported that they developed diabetes while they were pregnant. These women were more likely than those who did not experience gestational diabetes to be overweight. They also had higher degrees of insulin resistance when they were younger as well as at the 25-year follow up.
The women who experienced diabetes during pregnancy were also more likely to have developed diabetes again at some point in the following 25 years.
Overall, 75 women were diagnosed with non-alcoholic fatty liver disease when they were middle aged. Women who had diabetes during pregnancy were more than twice as likely as those who didn't to later develop fatty liver disease.
After researchers adjusted for diabetes that some women experienced outside of pregnancy, the risk of non-alcoholic fatty liver disease was still 50 percent higher for women who had gestational diabetes compared to those who didn't.
Fatty liver disease can have grave health effects and can even lead to cirrhosis, a condition that causes liver damage and possible failure, said Simon Taylor-Robinson, a professor of medicine at Imperial College London in the U.K. who wasn't involved in the study.
He advocates changes in diet to avoid the insulin resistance that leads to diabetes and fatty liver disease. "Many women are obese - so it is a matter of reducing weight and eating sensibly," he said.
Taylor-Robinson recommends eating fewer carbohydrates, more proteins and vegetables, and in particular, avoiding large amounts of fruit juice, which can contain a lot of sugar.
Ajmera also advised lifestyle changes, especially adding exercise. "We recommend either aerobic or resistance training for 30 minutes five times per week," he said.
"There are consequences to obesity and this includes cirrhosis, liver cancer and heart disease," Taylor-Robinson said. "Those people who become diabetic during pregnancy have strong risks of developing these complications later in life if attention isn't given to weight, diet and exercise."
(Reuters Health) - Women who develop diabetes while pregnant may be at elevated risk of also developing a dangerous build up of fat in their livers when they reach middle age, according to a new analysis.
The common risk factor for both gestational diabetes and non-alcoholic fatty liver disease, researchers say, is trouble making or using the hormone insulin to manage blood sugar, known as insulin resistance.
"We hope that early identification can promote healthy lifestyle changes that prevent or slow disease progression," said lead author Dr. Veeral Ajmera of the University of California, San Francisco.
"Pregnancy stresses the body in many ways, one of which is the ability to manage blood sugar," Ajmera said by email. "During pregnancy a woman's body becomes more resistant to insulin, which is the hormone required to decrease the blood sugar."
Insulin resistance is also "central to development of non-alcoholic fatty liver disease," which affects 20 percent to 30 percent of adults in the western world, the study team writes in The American Journal of Gastroenterology. Non-alcoholic fatty liver disease is the most common chronic liver disease in the United States.
Fatty liver disease is often diagnosed later in life, Ajmera told Reuters Health. So the researchers used long-term data to see if diabetes during pregnancy made a woman more likely to develop fatty liver disease 25 years later.
The researchers analyzed information about 1,115 black and white women recruited between 1985-1986 in four cities across the United States who gave birth to at least one child.
The participants did not have diabetes before becoming pregnant and the study excluded people who had liver issues related to alcohol, HIV, hepatitis or medications.
At the start of the study, women reported on whether they first experienced diabetes during pregnancy, and researchers confirmed the diagnosis with blood test results. Twenty-five years later, the women received more blood tests as well as CT scans of their livers to check if they had fatty liver disease.
At the beginning of the study, 124 women reported that they developed diabetes while they were pregnant. These women were more likely than those who did not experience gestational diabetes to be overweight. They also had higher degrees of insulin resistance when they were younger as well as at the 25-year follow up.
The women who experienced diabetes during pregnancy were also more likely to have developed diabetes again at some point in the following 25 years.
Overall, 75 women were diagnosed with non-alcoholic fatty liver disease when they were middle aged. Women who had diabetes during pregnancy were more than twice as likely as those who didn't to later develop fatty liver disease.
After researchers adjusted for diabetes that some women experienced outside of pregnancy, the risk of non-alcoholic fatty liver disease was still 50 percent higher for women who had gestational diabetes compared to those who didn't.
Fatty liver disease can have grave health effects and can even lead to cirrhosis, a condition that causes liver damage and possible failure, said Simon Taylor-Robinson, a professor of medicine at Imperial College London in the U.K. who wasn't involved in the study.
He advocates changes in diet to avoid the insulin resistance that leads to diabetes and fatty liver disease. "Many women are obese - so it is a matter of reducing weight and eating sensibly," he said.
Taylor-Robinson recommends eating fewer carbohydrates, more proteins and vegetables, and in particular, avoiding large amounts of fruit juice, which can contain a lot of sugar.
Ajmera also advised lifestyle changes, especially adding exercise. "We recommend either aerobic or resistance training for 30 minutes five times per week," he said.
"There are consequences to obesity and this includes cirrhosis, liver cancer and heart disease," Taylor-Robinson said. "Those people who become diabetic during pregnancy have strong risks of developing these complications later in life if attention isn't given to weight, diet and exercise."
(Reuters Health) - Women who develop diabetes while pregnant may be at elevated risk of also developing a dangerous build up of fat in their livers when they reach middle age, according to a new analysis.
The common risk factor for both gestational diabetes and non-alcoholic fatty liver disease, researchers say, is trouble making or using the hormone insulin to manage blood sugar, known as insulin resistance.
"We hope that early identification can promote healthy lifestyle changes that prevent or slow disease progression," said lead author Dr. Veeral Ajmera of the University of California, San Francisco.
"Pregnancy stresses the body in many ways, one of which is the ability to manage blood sugar," Ajmera said by email. "During pregnancy a woman's body becomes more resistant to insulin, which is the hormone required to decrease the blood sugar."
Insulin resistance is also "central to development of non-alcoholic fatty liver disease," which affects 20 percent to 30 percent of adults in the western world, the study team writes in The American Journal of Gastroenterology. Non-alcoholic fatty liver disease is the most common chronic liver disease in the United States.
Fatty liver disease is often diagnosed later in life, Ajmera told Reuters Health. So the researchers used long-term data to see if diabetes during pregnancy made a woman more likely to develop fatty liver disease 25 years later.
The researchers analyzed information about 1,115 black and white women recruited between 1985-1986 in four cities across the United States who gave birth to at least one child.
The participants did not have diabetes before becoming pregnant and the study excluded people who had liver issues related to alcohol, HIV, hepatitis or medications.
At the start of the study, women reported on whether they first experienced diabetes during pregnancy, and researchers confirmed the diagnosis with blood test results. Twenty-five years later, the women received more blood tests as well as CT scans of their livers to check if they had fatty liver disease.
At the beginning of the study, 124 women reported that they developed diabetes while they were pregnant. These women were more likely than those who did not experience gestational diabetes to be overweight. They also had higher degrees of insulin resistance when they were younger as well as at the 25-year follow up.
The women who experienced diabetes during pregnancy were also more likely to have developed diabetes again at some point in the following 25 years.
Overall, 75 women were diagnosed with non-alcoholic fatty liver disease when they were middle aged. Women who had diabetes during pregnancy were more than twice as likely as those who didn't to later develop fatty liver disease.
After researchers adjusted for diabetes that some women experienced outside of pregnancy, the risk of non-alcoholic fatty liver disease was still 50 percent higher for women who had gestational diabetes compared to those who didn't.
Fatty liver disease can have grave health effects and can even lead to cirrhosis, a condition that causes liver damage and possible failure, said Simon Taylor-Robinson, a professor of medicine at Imperial College London in the U.K. who wasn't involved in the study.
He advocates changes in diet to avoid the insulin resistance that leads to diabetes and fatty liver disease. "Many women are obese - so it is a matter of reducing weight and eating sensibly," he said.
Taylor-Robinson recommends eating fewer carbohydrates, more proteins and vegetables, and in particular, avoiding large amounts of fruit juice, which can contain a lot of sugar.
Ajmera also advised lifestyle changes, especially adding exercise. "We recommend either aerobic or resistance training for 30 minutes five times per week," he said.
"There are consequences to obesity and this includes cirrhosis, liver cancer and heart disease," Taylor-Robinson said. "Those people who become diabetic during pregnancy have strong risks of developing these complications later in life if attention isn't given to weight, diet and exercise."
The Society of Hospital Medicine is partnering with 18 U.S. Hospitals to Improve Patient Outcomes through Medication Reconciliation
The Society of Hospital Medicine Center for Hospital Innovation is supporting the implementation of a second iteration of the Multi-Center Medication Reconciliation Quality Improvement Study, or MARQUIS2. This is a mentored implementation program developed to assist hospitals and hospital clinicians with developing better ways for medications to be prescribed, recorded and reconciled accurately and safely at times of care transitions, e.g., when patients enter and leave the hospital. The ultimate goal of the study is reduce medication errors, adverse drug events and patient harm during transitions of care. The program is funded through a grant provided by the Agency for Healthcare Research and Quality (AHRQ).
Unintentional medication discrepancies during transitions in care represent a major threat to patient safety. Medication reconciliation enables healthcare providers – and hospitalists in particular – to avoid medication errors such as omissions, duplications, dosing errors and adverse drug interactions and should be completed at every transition of care, including hospital admission and discharge. Beginning in April 2016, SHM will begin working with 18 selected hospital sites to identify, implement and sustain medication reconciliation interventions with guidance from expert physician mentors. Key examples of intervention components include educating providers on how to take a best possible medication history, improving access to preadmission medication sources, encouraging patient ownership of medication lists and identifying patients at higher risk for adverse drug events in need of more intensive efforts.
The Society of Hospital Medicine Center for Hospital Innovation is supporting the implementation of a second iteration of the Multi-Center Medication Reconciliation Quality Improvement Study, or MARQUIS2. This is a mentored implementation program developed to assist hospitals and hospital clinicians with developing better ways for medications to be prescribed, recorded and reconciled accurately and safely at times of care transitions, e.g., when patients enter and leave the hospital. The ultimate goal of the study is reduce medication errors, adverse drug events and patient harm during transitions of care. The program is funded through a grant provided by the Agency for Healthcare Research and Quality (AHRQ).
Unintentional medication discrepancies during transitions in care represent a major threat to patient safety. Medication reconciliation enables healthcare providers – and hospitalists in particular – to avoid medication errors such as omissions, duplications, dosing errors and adverse drug interactions and should be completed at every transition of care, including hospital admission and discharge. Beginning in April 2016, SHM will begin working with 18 selected hospital sites to identify, implement and sustain medication reconciliation interventions with guidance from expert physician mentors. Key examples of intervention components include educating providers on how to take a best possible medication history, improving access to preadmission medication sources, encouraging patient ownership of medication lists and identifying patients at higher risk for adverse drug events in need of more intensive efforts.
The Society of Hospital Medicine Center for Hospital Innovation is supporting the implementation of a second iteration of the Multi-Center Medication Reconciliation Quality Improvement Study, or MARQUIS2. This is a mentored implementation program developed to assist hospitals and hospital clinicians with developing better ways for medications to be prescribed, recorded and reconciled accurately and safely at times of care transitions, e.g., when patients enter and leave the hospital. The ultimate goal of the study is reduce medication errors, adverse drug events and patient harm during transitions of care. The program is funded through a grant provided by the Agency for Healthcare Research and Quality (AHRQ).
Unintentional medication discrepancies during transitions in care represent a major threat to patient safety. Medication reconciliation enables healthcare providers – and hospitalists in particular – to avoid medication errors such as omissions, duplications, dosing errors and adverse drug interactions and should be completed at every transition of care, including hospital admission and discharge. Beginning in April 2016, SHM will begin working with 18 selected hospital sites to identify, implement and sustain medication reconciliation interventions with guidance from expert physician mentors. Key examples of intervention components include educating providers on how to take a best possible medication history, improving access to preadmission medication sources, encouraging patient ownership of medication lists and identifying patients at higher risk for adverse drug events in need of more intensive efforts.
Sign Up to Receive State of Hospital Medicine Report

Having credible information about how HM groups are structured and operate will benefit the entire healthcare industry and those involved in public policy and research. The survey results will be used by a wide variety of individuals and organizations to make important decisions about practice design and resource allocation.
Visit www.hospitalmedicine.org/survey and complete the notification form to be the first to know when the SOHM report becomes available this fall.
Brett Radler is SHM’s communications coordinator.
Having credible information about how HM groups are structured and operate will benefit the entire healthcare industry and those involved in public policy and research. The survey results will be used by a wide variety of individuals and organizations to make important decisions about practice design and resource allocation.
Visit www.hospitalmedicine.org/survey and complete the notification form to be the first to know when the SOHM report becomes available this fall.
Brett Radler is SHM’s communications coordinator.
Having credible information about how HM groups are structured and operate will benefit the entire healthcare industry and those involved in public policy and research. The survey results will be used by a wide variety of individuals and organizations to make important decisions about practice design and resource allocation.
Visit www.hospitalmedicine.org/survey and complete the notification form to be the first to know when the SOHM report becomes available this fall.
Brett Radler is SHM’s communications coordinator.
HM16 Q&A: How Can Hospitalists Avoid Burnout?
Robert Wachter, MD, MHM, chief of the Division of Hospital Medicine at the University of California San Francisco, in his annual address touched on some of the challenges for hospital medicine at the 20-year mark. The Hospitalist asked attendees: How can hospitalists continue to be change leaders and project leaders while also avoiding burnout?

Tamika Smith, MD, hospitalist, Alta Bates Summit Medical Center, Berkeley, Calif.
“I actually consider myself the poster child for work-life balance. I’m a nocturnist. Honestly, I think the secret is to work less. I work 12 to 14 shifts a month; that is how I make it sustainable. … I know that’s my magic number.”

Nisheeth Rai, DO, Aspirus Wausau Hospital, Wausau, Wis.
“I think you have to find a fair balance between your clinical duties. How do you balance the clinical aspect of things? How do you get into more of the management and more projects within the hospital system? We don’t know quite yet, but I think it’s an evolving thing where we’ll just see how the field evolves in the next couple years.”
Nathan Houchens, MD, hospitalist, VA Ann Arbor Healthcare System, Mich.
“It helps to know some of the fundamentals around change behavior. I think it’s also fundamental to recognize that it’s a relationship-based field and that without investment and capital in people it’s very difficult to make change sustainable.”
Janie Mathis, DO, cardiovascular hospitalist, Intermountain Medical Center, Salt Lake City
“I guess have some nonclinical time on the schedule. Schedule off from the nights and swing [shifts], and maybe have that as part of their contract and part of their job description. Have it as part of maybe your bonus, add that into your compensation, so you’re motivated to do it since you’re not going to get time off.”
Robert Wachter, MD, MHM, chief of the Division of Hospital Medicine at the University of California San Francisco, in his annual address touched on some of the challenges for hospital medicine at the 20-year mark. The Hospitalist asked attendees: How can hospitalists continue to be change leaders and project leaders while also avoiding burnout?
Tamika Smith, MD, hospitalist, Alta Bates Summit Medical Center, Berkeley, Calif.
“I actually consider myself the poster child for work-life balance. I’m a nocturnist. Honestly, I think the secret is to work less. I work 12 to 14 shifts a month; that is how I make it sustainable. … I know that’s my magic number.”
Nisheeth Rai, DO, Aspirus Wausau Hospital, Wausau, Wis.
“I think you have to find a fair balance between your clinical duties. How do you balance the clinical aspect of things? How do you get into more of the management and more projects within the hospital system? We don’t know quite yet, but I think it’s an evolving thing where we’ll just see how the field evolves in the next couple years.”
Nathan Houchens, MD, hospitalist, VA Ann Arbor Healthcare System, Mich.
“It helps to know some of the fundamentals around change behavior. I think it’s also fundamental to recognize that it’s a relationship-based field and that without investment and capital in people it’s very difficult to make change sustainable.”
Janie Mathis, DO, cardiovascular hospitalist, Intermountain Medical Center, Salt Lake City
“I guess have some nonclinical time on the schedule. Schedule off from the nights and swing [shifts], and maybe have that as part of their contract and part of their job description. Have it as part of maybe your bonus, add that into your compensation, so you’re motivated to do it since you’re not going to get time off.”
Robert Wachter, MD, MHM, chief of the Division of Hospital Medicine at the University of California San Francisco, in his annual address touched on some of the challenges for hospital medicine at the 20-year mark. The Hospitalist asked attendees: How can hospitalists continue to be change leaders and project leaders while also avoiding burnout?
Tamika Smith, MD, hospitalist, Alta Bates Summit Medical Center, Berkeley, Calif.
“I actually consider myself the poster child for work-life balance. I’m a nocturnist. Honestly, I think the secret is to work less. I work 12 to 14 shifts a month; that is how I make it sustainable. … I know that’s my magic number.”
Nisheeth Rai, DO, Aspirus Wausau Hospital, Wausau, Wis.
“I think you have to find a fair balance between your clinical duties. How do you balance the clinical aspect of things? How do you get into more of the management and more projects within the hospital system? We don’t know quite yet, but I think it’s an evolving thing where we’ll just see how the field evolves in the next couple years.”
Nathan Houchens, MD, hospitalist, VA Ann Arbor Healthcare System, Mich.
“It helps to know some of the fundamentals around change behavior. I think it’s also fundamental to recognize that it’s a relationship-based field and that without investment and capital in people it’s very difficult to make change sustainable.”
Janie Mathis, DO, cardiovascular hospitalist, Intermountain Medical Center, Salt Lake City
“I guess have some nonclinical time on the schedule. Schedule off from the nights and swing [shifts], and maybe have that as part of their contract and part of their job description. Have it as part of maybe your bonus, add that into your compensation, so you’re motivated to do it since you’re not going to get time off.”