User login
Official news magazine of the Society of Hospital Medicine
Copyright by Society of Hospital Medicine or related companies. All rights reserved. ISSN 1553-085X
nav[contains(@class, 'nav-ce-stack nav-ce-stack__large-screen')]
header[@id='header']
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'main-prefix')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
div[contains(@class, 'view-medstat-quiz-listing-panes')]
div[contains(@class, 'pane-article-sidebar-latest-news')]
div[contains(@class, 'pane-pub-article-hospitalist')]

Utah Health Sciences Center Realizes Significant Savings from Cost-Analysis Tool
Most healthcare systems don’t know or understand their cost of care at the unit that matters, i.e., the actual cost of care for an individual patient. Knowing this, University of Utah Health Sciences Center (UHSC) sought to develop methodologies using clinical data that would enable it to determine cost of care. Ultimately, a team led by systems, data, and analytics personnel, and including hospitalists, created an analytics framework known as value driven outcomes (VDO) using an agile methodology. Evaluation consisted of measurement against project objectives, including implementation timeliness, system performance, completeness, accuracy, extensibility, adoption, satisfaction, and the ability to support value improvement.1

“The initial results of employing the cost-savings tool have been exciting. For example, a 30% reduction in the cost of an orthopedic joint replacement—an inpatient hospital procedure—was realized,” says Robert C. Pendleton, MD, chief medical quality officer and professor of medicine at the University of Utah in Salt Lake City.
In another instance, hospitalists at UHSC led an initiative to reduce the use of unnecessary laboratory tests. That resulted in $400,000 in cost savings in the first year.
Another UHSC hospitalist used data to reduce unnecessary telemetry utilization by 60% on the hospitalist service.
“The accumulative impact of these initiatives, among others, will be a savings of millions of dollars annually by making process changes,” says Dr. Pendleton, a hospitalist who served on the executive steering committee that designed the web-based tool. “Our early experience shows that there is a lot of waste in the healthcare system.”
Along with the costing tool, quality and outcome measures were integrated so that the actual value of care (best outcomes at the lowest cost) could be assessed and incrementally improved.
Widespread Use?
Dr. Pendleton believes the tool could become popular among hospitalists, explaining that the field is known as the “leading system thinkers in healthcare.”
“By their nature, if you give them meaningful data and they can compare themselves to their peers, they are highly engaged to determine where waste in their hospitals exists and to lead improvement efforts,” he says.
UHSC is currently in the process of rolling out the VDO tool systemwide to its 1,200 faculty members. The rollout will take six to 12 months. In the next year, it’s also working to define and integrate outcome measures for the top 50 medical conditions it treats, which will allow it to robustly assess the value of care delivery.
“Success will equally be to increase quality without an increase in cost,” he says.
What’s more, Dr. Pendleton says efforts are in the works to make the self-intuitive system available to institutions nationwide. For example, the center is working to address technical complexities resulting from the use of multiple electronic health record vendors.
“The goal is to make it usable in every environment so we can support other organizations in the most effective ways,” he says.
Although the tool is very easy to use, stakeholders are providing feedback that allows for continuous improvements in how data are presented.
“Anyone with basic computer skills and the ability to interpret bar charts and basic graphs can use it,” Dr. Pendleton says. The center also offers a 15-minute, confidential, training module and a one-hour, one-on-one training session with an analyst. TH
Karen Appold is a freelance author in Pennsylvania.
Reference
- Kawamoto K, Martin CJ, Williams K, et al. Value driven outcomes (VDO): a pragmatic, modular, and extensible software framework for understanding and improving health care costs and outcomes. J Am Med Inform Assoc. 2015;22(1):223-235.
Most healthcare systems don’t know or understand their cost of care at the unit that matters, i.e., the actual cost of care for an individual patient. Knowing this, University of Utah Health Sciences Center (UHSC) sought to develop methodologies using clinical data that would enable it to determine cost of care. Ultimately, a team led by systems, data, and analytics personnel, and including hospitalists, created an analytics framework known as value driven outcomes (VDO) using an agile methodology. Evaluation consisted of measurement against project objectives, including implementation timeliness, system performance, completeness, accuracy, extensibility, adoption, satisfaction, and the ability to support value improvement.1
“The initial results of employing the cost-savings tool have been exciting. For example, a 30% reduction in the cost of an orthopedic joint replacement—an inpatient hospital procedure—was realized,” says Robert C. Pendleton, MD, chief medical quality officer and professor of medicine at the University of Utah in Salt Lake City.
In another instance, hospitalists at UHSC led an initiative to reduce the use of unnecessary laboratory tests. That resulted in $400,000 in cost savings in the first year.
Another UHSC hospitalist used data to reduce unnecessary telemetry utilization by 60% on the hospitalist service.
“The accumulative impact of these initiatives, among others, will be a savings of millions of dollars annually by making process changes,” says Dr. Pendleton, a hospitalist who served on the executive steering committee that designed the web-based tool. “Our early experience shows that there is a lot of waste in the healthcare system.”
Along with the costing tool, quality and outcome measures were integrated so that the actual value of care (best outcomes at the lowest cost) could be assessed and incrementally improved.
Widespread Use?
Dr. Pendleton believes the tool could become popular among hospitalists, explaining that the field is known as the “leading system thinkers in healthcare.”
“By their nature, if you give them meaningful data and they can compare themselves to their peers, they are highly engaged to determine where waste in their hospitals exists and to lead improvement efforts,” he says.
UHSC is currently in the process of rolling out the VDO tool systemwide to its 1,200 faculty members. The rollout will take six to 12 months. In the next year, it’s also working to define and integrate outcome measures for the top 50 medical conditions it treats, which will allow it to robustly assess the value of care delivery.
“Success will equally be to increase quality without an increase in cost,” he says.
What’s more, Dr. Pendleton says efforts are in the works to make the self-intuitive system available to institutions nationwide. For example, the center is working to address technical complexities resulting from the use of multiple electronic health record vendors.
“The goal is to make it usable in every environment so we can support other organizations in the most effective ways,” he says.
Although the tool is very easy to use, stakeholders are providing feedback that allows for continuous improvements in how data are presented.
“Anyone with basic computer skills and the ability to interpret bar charts and basic graphs can use it,” Dr. Pendleton says. The center also offers a 15-minute, confidential, training module and a one-hour, one-on-one training session with an analyst. TH
Karen Appold is a freelance author in Pennsylvania.
Reference
- Kawamoto K, Martin CJ, Williams K, et al. Value driven outcomes (VDO): a pragmatic, modular, and extensible software framework for understanding and improving health care costs and outcomes. J Am Med Inform Assoc. 2015;22(1):223-235.
Most healthcare systems don’t know or understand their cost of care at the unit that matters, i.e., the actual cost of care for an individual patient. Knowing this, University of Utah Health Sciences Center (UHSC) sought to develop methodologies using clinical data that would enable it to determine cost of care. Ultimately, a team led by systems, data, and analytics personnel, and including hospitalists, created an analytics framework known as value driven outcomes (VDO) using an agile methodology. Evaluation consisted of measurement against project objectives, including implementation timeliness, system performance, completeness, accuracy, extensibility, adoption, satisfaction, and the ability to support value improvement.1
“The initial results of employing the cost-savings tool have been exciting. For example, a 30% reduction in the cost of an orthopedic joint replacement—an inpatient hospital procedure—was realized,” says Robert C. Pendleton, MD, chief medical quality officer and professor of medicine at the University of Utah in Salt Lake City.
In another instance, hospitalists at UHSC led an initiative to reduce the use of unnecessary laboratory tests. That resulted in $400,000 in cost savings in the first year.
Another UHSC hospitalist used data to reduce unnecessary telemetry utilization by 60% on the hospitalist service.
“The accumulative impact of these initiatives, among others, will be a savings of millions of dollars annually by making process changes,” says Dr. Pendleton, a hospitalist who served on the executive steering committee that designed the web-based tool. “Our early experience shows that there is a lot of waste in the healthcare system.”
Along with the costing tool, quality and outcome measures were integrated so that the actual value of care (best outcomes at the lowest cost) could be assessed and incrementally improved.
Widespread Use?
Dr. Pendleton believes the tool could become popular among hospitalists, explaining that the field is known as the “leading system thinkers in healthcare.”
“By their nature, if you give them meaningful data and they can compare themselves to their peers, they are highly engaged to determine where waste in their hospitals exists and to lead improvement efforts,” he says.
UHSC is currently in the process of rolling out the VDO tool systemwide to its 1,200 faculty members. The rollout will take six to 12 months. In the next year, it’s also working to define and integrate outcome measures for the top 50 medical conditions it treats, which will allow it to robustly assess the value of care delivery.
“Success will equally be to increase quality without an increase in cost,” he says.
What’s more, Dr. Pendleton says efforts are in the works to make the self-intuitive system available to institutions nationwide. For example, the center is working to address technical complexities resulting from the use of multiple electronic health record vendors.
“The goal is to make it usable in every environment so we can support other organizations in the most effective ways,” he says.
Although the tool is very easy to use, stakeholders are providing feedback that allows for continuous improvements in how data are presented.
“Anyone with basic computer skills and the ability to interpret bar charts and basic graphs can use it,” Dr. Pendleton says. The center also offers a 15-minute, confidential, training module and a one-hour, one-on-one training session with an analyst. TH
Karen Appold is a freelance author in Pennsylvania.
Reference
- Kawamoto K, Martin CJ, Williams K, et al. Value driven outcomes (VDO): a pragmatic, modular, and extensible software framework for understanding and improving health care costs and outcomes. J Am Med Inform Assoc. 2015;22(1):223-235.
Risk of Chronic Kidney Disease is Increased If You Have Sleep Apnea
(Reuters Health) - Having sleep apnea may increase the risk of chronic kidney disease, according to a report from Taiwan.
Researchers analyzed data from 2000 through 2010 on 8,600 adults diagnosed with sleep apnea and four times as many adults of similar age, sex and monthly income without sleep apnea, using Taiwan's National Health Insurance Research Database.
They found 157 new cases of chronic kidney disease among people with sleep apnea and 298 cases in the comparison group, according to Yung-Tai Chen of Taipei City Hospital Heping Fuyou Branch in Taiwan and coauthors.
After taking other health factors into account, sleep apnea increased the risk of kidney disease by 58%. By comparison, hypertension (a known risk factor for kidney disease) increased the risk by 17%. Diabetes was a stronger predictor than both other factors, more than doubling the risk of kidney disease, the research team reported online February 1 in Respirology.
Intermittent low oxygen levels during the night and fragmented sleep patterns may activate higher blood pressure, which would damage the kidneys and could make individuals more susceptible to chronic kidney disease, said Tetyana Kendzerska of the University of Toronto Institute for Clinical Evaluative Sciences, who was not part of the study in Taiwan.
But, "the findings from this study are limited by lack of information on sleep apnea and chronic kidney disease severity given that these conditions were defined through the health administrative data," Kendzerska said.
Factors like obesity and smoking status are also important for kidney risk but were not included in the assessment, she told Reuters Health by email.
"So, instead of concluding that sleep apnea has the same impact as high blood pressure on the kidney, I would rather conclude that this study suggests that the association between sleep apnea and chronic kidney disease may exist," and should be validated with more powerful studies, she said.
Moderate to severe obstructive sleep apnea can be treated with continuous positive airway pressure (CPAP) at night which may decrease high blood pressure and mitigate kidney risk, Kendzerska said.
"These findings raise the issue of whether the relationship between sleep apnea and chronic kidney disease is unidirectional or bidirectional," she said. "If the importance of sleep apnea and preventive effect of treatment will be confirmed in further studies, sleep apnea should be added to the list of modifiable risk factors considered in (chronic kidney disease) risk assessment."
The authors of the study did not respond to a request for comment.
(Reuters Health) - Having sleep apnea may increase the risk of chronic kidney disease, according to a report from Taiwan.
Researchers analyzed data from 2000 through 2010 on 8,600 adults diagnosed with sleep apnea and four times as many adults of similar age, sex and monthly income without sleep apnea, using Taiwan's National Health Insurance Research Database.
They found 157 new cases of chronic kidney disease among people with sleep apnea and 298 cases in the comparison group, according to Yung-Tai Chen of Taipei City Hospital Heping Fuyou Branch in Taiwan and coauthors.
After taking other health factors into account, sleep apnea increased the risk of kidney disease by 58%. By comparison, hypertension (a known risk factor for kidney disease) increased the risk by 17%. Diabetes was a stronger predictor than both other factors, more than doubling the risk of kidney disease, the research team reported online February 1 in Respirology.
Intermittent low oxygen levels during the night and fragmented sleep patterns may activate higher blood pressure, which would damage the kidneys and could make individuals more susceptible to chronic kidney disease, said Tetyana Kendzerska of the University of Toronto Institute for Clinical Evaluative Sciences, who was not part of the study in Taiwan.
But, "the findings from this study are limited by lack of information on sleep apnea and chronic kidney disease severity given that these conditions were defined through the health administrative data," Kendzerska said.
Factors like obesity and smoking status are also important for kidney risk but were not included in the assessment, she told Reuters Health by email.
"So, instead of concluding that sleep apnea has the same impact as high blood pressure on the kidney, I would rather conclude that this study suggests that the association between sleep apnea and chronic kidney disease may exist," and should be validated with more powerful studies, she said.
Moderate to severe obstructive sleep apnea can be treated with continuous positive airway pressure (CPAP) at night which may decrease high blood pressure and mitigate kidney risk, Kendzerska said.
"These findings raise the issue of whether the relationship between sleep apnea and chronic kidney disease is unidirectional or bidirectional," she said. "If the importance of sleep apnea and preventive effect of treatment will be confirmed in further studies, sleep apnea should be added to the list of modifiable risk factors considered in (chronic kidney disease) risk assessment."
The authors of the study did not respond to a request for comment.
(Reuters Health) - Having sleep apnea may increase the risk of chronic kidney disease, according to a report from Taiwan.
Researchers analyzed data from 2000 through 2010 on 8,600 adults diagnosed with sleep apnea and four times as many adults of similar age, sex and monthly income without sleep apnea, using Taiwan's National Health Insurance Research Database.
They found 157 new cases of chronic kidney disease among people with sleep apnea and 298 cases in the comparison group, according to Yung-Tai Chen of Taipei City Hospital Heping Fuyou Branch in Taiwan and coauthors.
After taking other health factors into account, sleep apnea increased the risk of kidney disease by 58%. By comparison, hypertension (a known risk factor for kidney disease) increased the risk by 17%. Diabetes was a stronger predictor than both other factors, more than doubling the risk of kidney disease, the research team reported online February 1 in Respirology.
Intermittent low oxygen levels during the night and fragmented sleep patterns may activate higher blood pressure, which would damage the kidneys and could make individuals more susceptible to chronic kidney disease, said Tetyana Kendzerska of the University of Toronto Institute for Clinical Evaluative Sciences, who was not part of the study in Taiwan.
But, "the findings from this study are limited by lack of information on sleep apnea and chronic kidney disease severity given that these conditions were defined through the health administrative data," Kendzerska said.
Factors like obesity and smoking status are also important for kidney risk but were not included in the assessment, she told Reuters Health by email.
"So, instead of concluding that sleep apnea has the same impact as high blood pressure on the kidney, I would rather conclude that this study suggests that the association between sleep apnea and chronic kidney disease may exist," and should be validated with more powerful studies, she said.
Moderate to severe obstructive sleep apnea can be treated with continuous positive airway pressure (CPAP) at night which may decrease high blood pressure and mitigate kidney risk, Kendzerska said.
"These findings raise the issue of whether the relationship between sleep apnea and chronic kidney disease is unidirectional or bidirectional," she said. "If the importance of sleep apnea and preventive effect of treatment will be confirmed in further studies, sleep apnea should be added to the list of modifiable risk factors considered in (chronic kidney disease) risk assessment."
The authors of the study did not respond to a request for comment.
A Closer Look at Characteristics of High-Performing HM Groups
Early in 2015, SHM published the updated edition of the “Key Principles and Characteristics of an Effective Hospital Medicine Group,” which is a free download via the SHM website. Every hospitalist group should use this comprehensive list of attributes as one important frame of reference to guide ongoing improvement efforts and long-range planning.
In this column and the next two, I’ll split the difference between the very brief list of top success factors for hospitalist groups I wrote about in my March 2011 column and the very comprehensive “Key Characteristics” document. I think these attributes are among the most important to support a high-performing group, yet they are sometimes overlooked or implemented poorly. They are of roughly equal importance and are listed in no particular order.
Deliberately Cultivating a Culture (or Mindset) of Practice Ownership
It’s easy for hospitalists to think of themselves as employees who just work shifts but have no need or opportunity to attend to the bigger picture of the practice or the hospital in which they operate. After all, being a good doctor for your patients is an awfully big job itself, and lots of recruitment ads tell you doctoring is all that will be expected of you. Someone else will handle everything necessary to ensure your practice is successful.
This line of thinking will limit the success of your group.
Your group will perform much better and you’re likely to find your career much more rewarding if you and your hospitalist colleagues think of yourselves as owning your practice and take an active role in managing it. You’ll still need others to manage day-to-day business affairs, but at least a portion of the hospitalists in the group should be actively involved in planning and making decisions about the group’s operations and future evolution.
I encounter hospitalist groups that have become convinced they don’t even have the opportunity to shape or influence their practice. “No one ever listens,” they say. “The hospital executives just do what they want regardless of what we say.” But in nearly every case, that is an exaggeration. Most administrative leaders desperately want hospitalist engagement and thoughtful participation in planning and decision making.
I wrote additional thoughts about the importance of a culture, or mindset, of practice ownership in August 2008. The print version of that column included a short list of questions you could ask yourself to assess whether your own group has such a culture, but it is missing from the web version and can be found at nelsonflores.com/html/quiz.html.
A Formal System of Group ‘Governance’
So many hospitalist groups rely almost entirely on consensus to make decisions. This might work well enough for a very small group (e.g., four or five doctors), but for large groups, it means just one or two dissenters can block a decision and nothing much gets done.
Disagreements about practice operations and future direction are common, so every group should commit to writing some method of how votes will be taken in the absence of consensus. For example, the group might be divided about whether to adopt unit-based assignments or change the hours of an evening (“swing”) shift, and a formal vote might be the only way to make a decision. It’s best if you have decided in advance issues such as what constitutes a quorum, who is eligible to vote, and whether the winning vote requires a simple or super-majority. And a formalized system of voting helps support a culture ownership.
I wrote about this originally in December 2007 and provided sample bylaws your group could modify as needed. Of course, you should keep in mind that if you are indeed employed by a larger entity such as a hospital or staffing company, you don’t have the ability to make all decisions by a vote of the group. Pay raises, staff additions, and similar decisions require support of the employer, and while a vote in support of them might influence what actually happens, it still requires the support of the employer. But there are lots of things, like the work schedule, system of allocating patients across providers, etc., that are usually best made by the group itself, and sometimes they might come down to a vote of the group.
Never Stop Recruiting and Ensure Hospitalists Themselves Are Actively Engaged in Recruiting
I wrote about recruiting originally in July 2008 when there was a shortage of hospitalists everywhere. Since then, the supply of doctors seeking work as a hospitalist has caught up with demand in many major metropolitan areas like Minneapolis and Washington, D.C.
But outside of large markets—that is, in most of the country—demand for hospitalists still far exceeds supply, and groups face ongoing staffing deficits that come with the need for existing doctors to work extra shifts and use locum tenens or other forms of temporary staffing. The potential excess supply of hospitalists in major markets may eventually trickle out and ease the shortages elsewhere, but that hasn’t happened in a big way yet. So for these places, it is crucial to devote a lot of energy and resources to recruiting.
A vital component of successful recruiting is participation in the effort by the hospitalists themselves. I think the best mindset for the hospitalists is to think of themselves as leading recruitment efforts assisted by recruiters rather than the other way around. For example, the lead hospitalist or some other designated doctor should try to respond by phone (if that’s impractical, then respond by email) to every reasonable inquiry from a new candidate within 24 hours and serve as the candidate’s principle point of communication throughout the recruitment process. The recruiter can handle details of things like arranging travel for an interview, but a hospitalist in the group should be the main source of information regarding things like the work schedule, patient volume, compensation, etc. And a hospitalist should serve as the main host during a candidate’s on-site interview.
More to Come …
Next month, I’ll address things like a written policy and procedure manual, clear reporting relationships for the hospitalist group, and roles for advanced practice clinicians (NPs and PAs). TH

Early in 2015, SHM published the updated edition of the “Key Principles and Characteristics of an Effective Hospital Medicine Group,” which is a free download via the SHM website. Every hospitalist group should use this comprehensive list of attributes as one important frame of reference to guide ongoing improvement efforts and long-range planning.
In this column and the next two, I’ll split the difference between the very brief list of top success factors for hospitalist groups I wrote about in my March 2011 column and the very comprehensive “Key Characteristics” document. I think these attributes are among the most important to support a high-performing group, yet they are sometimes overlooked or implemented poorly. They are of roughly equal importance and are listed in no particular order.
Deliberately Cultivating a Culture (or Mindset) of Practice Ownership
It’s easy for hospitalists to think of themselves as employees who just work shifts but have no need or opportunity to attend to the bigger picture of the practice or the hospital in which they operate. After all, being a good doctor for your patients is an awfully big job itself, and lots of recruitment ads tell you doctoring is all that will be expected of you. Someone else will handle everything necessary to ensure your practice is successful.
This line of thinking will limit the success of your group.
Your group will perform much better and you’re likely to find your career much more rewarding if you and your hospitalist colleagues think of yourselves as owning your practice and take an active role in managing it. You’ll still need others to manage day-to-day business affairs, but at least a portion of the hospitalists in the group should be actively involved in planning and making decisions about the group’s operations and future evolution.
I encounter hospitalist groups that have become convinced they don’t even have the opportunity to shape or influence their practice. “No one ever listens,” they say. “The hospital executives just do what they want regardless of what we say.” But in nearly every case, that is an exaggeration. Most administrative leaders desperately want hospitalist engagement and thoughtful participation in planning and decision making.
I wrote additional thoughts about the importance of a culture, or mindset, of practice ownership in August 2008. The print version of that column included a short list of questions you could ask yourself to assess whether your own group has such a culture, but it is missing from the web version and can be found at nelsonflores.com/html/quiz.html.
A Formal System of Group ‘Governance’
So many hospitalist groups rely almost entirely on consensus to make decisions. This might work well enough for a very small group (e.g., four or five doctors), but for large groups, it means just one or two dissenters can block a decision and nothing much gets done.
Disagreements about practice operations and future direction are common, so every group should commit to writing some method of how votes will be taken in the absence of consensus. For example, the group might be divided about whether to adopt unit-based assignments or change the hours of an evening (“swing”) shift, and a formal vote might be the only way to make a decision. It’s best if you have decided in advance issues such as what constitutes a quorum, who is eligible to vote, and whether the winning vote requires a simple or super-majority. And a formalized system of voting helps support a culture ownership.
I wrote about this originally in December 2007 and provided sample bylaws your group could modify as needed. Of course, you should keep in mind that if you are indeed employed by a larger entity such as a hospital or staffing company, you don’t have the ability to make all decisions by a vote of the group. Pay raises, staff additions, and similar decisions require support of the employer, and while a vote in support of them might influence what actually happens, it still requires the support of the employer. But there are lots of things, like the work schedule, system of allocating patients across providers, etc., that are usually best made by the group itself, and sometimes they might come down to a vote of the group.
Never Stop Recruiting and Ensure Hospitalists Themselves Are Actively Engaged in Recruiting
I wrote about recruiting originally in July 2008 when there was a shortage of hospitalists everywhere. Since then, the supply of doctors seeking work as a hospitalist has caught up with demand in many major metropolitan areas like Minneapolis and Washington, D.C.
But outside of large markets—that is, in most of the country—demand for hospitalists still far exceeds supply, and groups face ongoing staffing deficits that come with the need for existing doctors to work extra shifts and use locum tenens or other forms of temporary staffing. The potential excess supply of hospitalists in major markets may eventually trickle out and ease the shortages elsewhere, but that hasn’t happened in a big way yet. So for these places, it is crucial to devote a lot of energy and resources to recruiting.
A vital component of successful recruiting is participation in the effort by the hospitalists themselves. I think the best mindset for the hospitalists is to think of themselves as leading recruitment efforts assisted by recruiters rather than the other way around. For example, the lead hospitalist or some other designated doctor should try to respond by phone (if that’s impractical, then respond by email) to every reasonable inquiry from a new candidate within 24 hours and serve as the candidate’s principle point of communication throughout the recruitment process. The recruiter can handle details of things like arranging travel for an interview, but a hospitalist in the group should be the main source of information regarding things like the work schedule, patient volume, compensation, etc. And a hospitalist should serve as the main host during a candidate’s on-site interview.
More to Come …
Next month, I’ll address things like a written policy and procedure manual, clear reporting relationships for the hospitalist group, and roles for advanced practice clinicians (NPs and PAs). TH
Early in 2015, SHM published the updated edition of the “Key Principles and Characteristics of an Effective Hospital Medicine Group,” which is a free download via the SHM website. Every hospitalist group should use this comprehensive list of attributes as one important frame of reference to guide ongoing improvement efforts and long-range planning.
In this column and the next two, I’ll split the difference between the very brief list of top success factors for hospitalist groups I wrote about in my March 2011 column and the very comprehensive “Key Characteristics” document. I think these attributes are among the most important to support a high-performing group, yet they are sometimes overlooked or implemented poorly. They are of roughly equal importance and are listed in no particular order.
Deliberately Cultivating a Culture (or Mindset) of Practice Ownership
It’s easy for hospitalists to think of themselves as employees who just work shifts but have no need or opportunity to attend to the bigger picture of the practice or the hospital in which they operate. After all, being a good doctor for your patients is an awfully big job itself, and lots of recruitment ads tell you doctoring is all that will be expected of you. Someone else will handle everything necessary to ensure your practice is successful.
This line of thinking will limit the success of your group.
Your group will perform much better and you’re likely to find your career much more rewarding if you and your hospitalist colleagues think of yourselves as owning your practice and take an active role in managing it. You’ll still need others to manage day-to-day business affairs, but at least a portion of the hospitalists in the group should be actively involved in planning and making decisions about the group’s operations and future evolution.
I encounter hospitalist groups that have become convinced they don’t even have the opportunity to shape or influence their practice. “No one ever listens,” they say. “The hospital executives just do what they want regardless of what we say.” But in nearly every case, that is an exaggeration. Most administrative leaders desperately want hospitalist engagement and thoughtful participation in planning and decision making.
I wrote additional thoughts about the importance of a culture, or mindset, of practice ownership in August 2008. The print version of that column included a short list of questions you could ask yourself to assess whether your own group has such a culture, but it is missing from the web version and can be found at nelsonflores.com/html/quiz.html.
A Formal System of Group ‘Governance’
So many hospitalist groups rely almost entirely on consensus to make decisions. This might work well enough for a very small group (e.g., four or five doctors), but for large groups, it means just one or two dissenters can block a decision and nothing much gets done.
Disagreements about practice operations and future direction are common, so every group should commit to writing some method of how votes will be taken in the absence of consensus. For example, the group might be divided about whether to adopt unit-based assignments or change the hours of an evening (“swing”) shift, and a formal vote might be the only way to make a decision. It’s best if you have decided in advance issues such as what constitutes a quorum, who is eligible to vote, and whether the winning vote requires a simple or super-majority. And a formalized system of voting helps support a culture ownership.
I wrote about this originally in December 2007 and provided sample bylaws your group could modify as needed. Of course, you should keep in mind that if you are indeed employed by a larger entity such as a hospital or staffing company, you don’t have the ability to make all decisions by a vote of the group. Pay raises, staff additions, and similar decisions require support of the employer, and while a vote in support of them might influence what actually happens, it still requires the support of the employer. But there are lots of things, like the work schedule, system of allocating patients across providers, etc., that are usually best made by the group itself, and sometimes they might come down to a vote of the group.
Never Stop Recruiting and Ensure Hospitalists Themselves Are Actively Engaged in Recruiting
I wrote about recruiting originally in July 2008 when there was a shortage of hospitalists everywhere. Since then, the supply of doctors seeking work as a hospitalist has caught up with demand in many major metropolitan areas like Minneapolis and Washington, D.C.
But outside of large markets—that is, in most of the country—demand for hospitalists still far exceeds supply, and groups face ongoing staffing deficits that come with the need for existing doctors to work extra shifts and use locum tenens or other forms of temporary staffing. The potential excess supply of hospitalists in major markets may eventually trickle out and ease the shortages elsewhere, but that hasn’t happened in a big way yet. So for these places, it is crucial to devote a lot of energy and resources to recruiting.
A vital component of successful recruiting is participation in the effort by the hospitalists themselves. I think the best mindset for the hospitalists is to think of themselves as leading recruitment efforts assisted by recruiters rather than the other way around. For example, the lead hospitalist or some other designated doctor should try to respond by phone (if that’s impractical, then respond by email) to every reasonable inquiry from a new candidate within 24 hours and serve as the candidate’s principle point of communication throughout the recruitment process. The recruiter can handle details of things like arranging travel for an interview, but a hospitalist in the group should be the main source of information regarding things like the work schedule, patient volume, compensation, etc. And a hospitalist should serve as the main host during a candidate’s on-site interview.
More to Come …
Next month, I’ll address things like a written policy and procedure manual, clear reporting relationships for the hospitalist group, and roles for advanced practice clinicians (NPs and PAs). TH
Researchers Report Opioid Modulation with the Combination of Buprenorphine and Samidorphan Improves Symptoms in Patients with Depression
NEW YORK (Reuters Health) - Opioid modulation with the combination of buprenorphine and samidorphan (ALKS 5461) improves symptoms in patients whose depression has not responded adequately to antidepressant treatment, researchers report.
"If the findings are confirmed in phase 3 studies, ALKS 5461 could be used as an augmenting agent in patients not responding to standard antidepressant therapies as an alternative to the atypical antipsychotic agents currently approved for the treatment of this population," Dr. Maurizio Fava, from Massachusetts General Hospital and Harvard Medical School, Boston, told Reuters Health by email.
Buprenorphine is a mu- and kappa-opioid partial agonist, and samidorphan blocks the mu agonist effects of buprenorphine associated with its abuse and addictive potential. A growing body of evidence implicates dysregulation of the endogenous mu- and kappa-opioid system in mood disorders.
Dr. Fava and colleagues at 31 sites in the U.S. used a sequential parallel comparison design to investigate the efficacy of buprenorphine/samidorphan (2 mg/2 mg or 8 mg/8 mg) in 142 patients with major depression inadequately responsive to antidepressant therapy.
At the end of four weeks of treatment, patients in the ALKS 5461 2 mg/2 mg group showed significantly greater improvements in Hamilton Depression Rating Scale (HAM-D), Montgomery-Asberg Depression Rating Scale (MADRS), and Clinical Global Impression severity scores, compared with patients in the placebo group. The ALKS 5461 8 mg/8 mg group showed smaller, nonsignificant improvements.
"The overall effect sizes for the 2/2 dosage were 0.50 for HAM-D and 0.54 for MADRS," the researchers noted. "The result compares favorably with results from a meta-analysis of 14 studies with atypical antipsychotics as adjunctive therapy for major depression, with reported effect sizes of 0.35 to 0.48 for individual drugs."
Treatment response rates according to HAM-D and MADRS (at least 50% reduction in scores) were highest with ALKS 5461 2 mg/2 mg treatment group, according to the February 12 onlinereport in the American Journal of Psychiatry.
Two patients (1.6%) in the placebo group and 17 patients (19.3%) in the ALKS 5461 groups discontinued because of treatment-emergent adverse events, but there was no evidence of opioid withdrawal in any patient.
"When depressed patients do not respond to standard monoamine-based therapies for depression, consider the use of an augmenting agent that modulates other systems, such as the opioid one," Dr. Fava concluded.
Dr. Jeffrey F. Scherrer, from Saint Louis University School of Medicine, St. Louis, Missouri, recently examined the association between opioid use and increased depression rates. He told Reuters Health by email, "Our analysis of opioid use and depression did not include buprenorphine among the opioid exposure variable. Therefore, it is difficult to extrapolate our results to a trial of buprenorphine/samidorphan and major depression."
"As the authors noted, the clinical trial was of short duration and the risks of depression that we have observed appears to be greatest among those patients remaining on opioids for more than 90 days," he explained. "Additional work is currently being done to determine if some opioid medications have a greater depressogenic effect than others, which further limits direct comparison of our findings to the current study."
"I will say that it is unlikely for oxycodone, codeine, and hydrocodone (which together account for more than 90% of prescribed opioids) would help depressed patients and be more likely to worsen their depression with chronic treatment," Dr. Scherrer concluded.
Alkermes sponsored the trial, employed seven coauthors, and had various relationships with the other four coauthors.
NEW YORK (Reuters Health) - Opioid modulation with the combination of buprenorphine and samidorphan (ALKS 5461) improves symptoms in patients whose depression has not responded adequately to antidepressant treatment, researchers report.
"If the findings are confirmed in phase 3 studies, ALKS 5461 could be used as an augmenting agent in patients not responding to standard antidepressant therapies as an alternative to the atypical antipsychotic agents currently approved for the treatment of this population," Dr. Maurizio Fava, from Massachusetts General Hospital and Harvard Medical School, Boston, told Reuters Health by email.
Buprenorphine is a mu- and kappa-opioid partial agonist, and samidorphan blocks the mu agonist effects of buprenorphine associated with its abuse and addictive potential. A growing body of evidence implicates dysregulation of the endogenous mu- and kappa-opioid system in mood disorders.
Dr. Fava and colleagues at 31 sites in the U.S. used a sequential parallel comparison design to investigate the efficacy of buprenorphine/samidorphan (2 mg/2 mg or 8 mg/8 mg) in 142 patients with major depression inadequately responsive to antidepressant therapy.
At the end of four weeks of treatment, patients in the ALKS 5461 2 mg/2 mg group showed significantly greater improvements in Hamilton Depression Rating Scale (HAM-D), Montgomery-Asberg Depression Rating Scale (MADRS), and Clinical Global Impression severity scores, compared with patients in the placebo group. The ALKS 5461 8 mg/8 mg group showed smaller, nonsignificant improvements.
"The overall effect sizes for the 2/2 dosage were 0.50 for HAM-D and 0.54 for MADRS," the researchers noted. "The result compares favorably with results from a meta-analysis of 14 studies with atypical antipsychotics as adjunctive therapy for major depression, with reported effect sizes of 0.35 to 0.48 for individual drugs."
Treatment response rates according to HAM-D and MADRS (at least 50% reduction in scores) were highest with ALKS 5461 2 mg/2 mg treatment group, according to the February 12 onlinereport in the American Journal of Psychiatry.
Two patients (1.6%) in the placebo group and 17 patients (19.3%) in the ALKS 5461 groups discontinued because of treatment-emergent adverse events, but there was no evidence of opioid withdrawal in any patient.
"When depressed patients do not respond to standard monoamine-based therapies for depression, consider the use of an augmenting agent that modulates other systems, such as the opioid one," Dr. Fava concluded.
Dr. Jeffrey F. Scherrer, from Saint Louis University School of Medicine, St. Louis, Missouri, recently examined the association between opioid use and increased depression rates. He told Reuters Health by email, "Our analysis of opioid use and depression did not include buprenorphine among the opioid exposure variable. Therefore, it is difficult to extrapolate our results to a trial of buprenorphine/samidorphan and major depression."
"As the authors noted, the clinical trial was of short duration and the risks of depression that we have observed appears to be greatest among those patients remaining on opioids for more than 90 days," he explained. "Additional work is currently being done to determine if some opioid medications have a greater depressogenic effect than others, which further limits direct comparison of our findings to the current study."
"I will say that it is unlikely for oxycodone, codeine, and hydrocodone (which together account for more than 90% of prescribed opioids) would help depressed patients and be more likely to worsen their depression with chronic treatment," Dr. Scherrer concluded.
Alkermes sponsored the trial, employed seven coauthors, and had various relationships with the other four coauthors.
NEW YORK (Reuters Health) - Opioid modulation with the combination of buprenorphine and samidorphan (ALKS 5461) improves symptoms in patients whose depression has not responded adequately to antidepressant treatment, researchers report.
"If the findings are confirmed in phase 3 studies, ALKS 5461 could be used as an augmenting agent in patients not responding to standard antidepressant therapies as an alternative to the atypical antipsychotic agents currently approved for the treatment of this population," Dr. Maurizio Fava, from Massachusetts General Hospital and Harvard Medical School, Boston, told Reuters Health by email.
Buprenorphine is a mu- and kappa-opioid partial agonist, and samidorphan blocks the mu agonist effects of buprenorphine associated with its abuse and addictive potential. A growing body of evidence implicates dysregulation of the endogenous mu- and kappa-opioid system in mood disorders.
Dr. Fava and colleagues at 31 sites in the U.S. used a sequential parallel comparison design to investigate the efficacy of buprenorphine/samidorphan (2 mg/2 mg or 8 mg/8 mg) in 142 patients with major depression inadequately responsive to antidepressant therapy.
At the end of four weeks of treatment, patients in the ALKS 5461 2 mg/2 mg group showed significantly greater improvements in Hamilton Depression Rating Scale (HAM-D), Montgomery-Asberg Depression Rating Scale (MADRS), and Clinical Global Impression severity scores, compared with patients in the placebo group. The ALKS 5461 8 mg/8 mg group showed smaller, nonsignificant improvements.
"The overall effect sizes for the 2/2 dosage were 0.50 for HAM-D and 0.54 for MADRS," the researchers noted. "The result compares favorably with results from a meta-analysis of 14 studies with atypical antipsychotics as adjunctive therapy for major depression, with reported effect sizes of 0.35 to 0.48 for individual drugs."
Treatment response rates according to HAM-D and MADRS (at least 50% reduction in scores) were highest with ALKS 5461 2 mg/2 mg treatment group, according to the February 12 onlinereport in the American Journal of Psychiatry.
Two patients (1.6%) in the placebo group and 17 patients (19.3%) in the ALKS 5461 groups discontinued because of treatment-emergent adverse events, but there was no evidence of opioid withdrawal in any patient.
"When depressed patients do not respond to standard monoamine-based therapies for depression, consider the use of an augmenting agent that modulates other systems, such as the opioid one," Dr. Fava concluded.
Dr. Jeffrey F. Scherrer, from Saint Louis University School of Medicine, St. Louis, Missouri, recently examined the association between opioid use and increased depression rates. He told Reuters Health by email, "Our analysis of opioid use and depression did not include buprenorphine among the opioid exposure variable. Therefore, it is difficult to extrapolate our results to a trial of buprenorphine/samidorphan and major depression."
"As the authors noted, the clinical trial was of short duration and the risks of depression that we have observed appears to be greatest among those patients remaining on opioids for more than 90 days," he explained. "Additional work is currently being done to determine if some opioid medications have a greater depressogenic effect than others, which further limits direct comparison of our findings to the current study."
"I will say that it is unlikely for oxycodone, codeine, and hydrocodone (which together account for more than 90% of prescribed opioids) would help depressed patients and be more likely to worsen their depression with chronic treatment," Dr. Scherrer concluded.
Alkermes sponsored the trial, employed seven coauthors, and had various relationships with the other four coauthors.
No Change in Duration of Mechanical Ventilation with Acetazolamide for COPD Patients with Metabolic Alkalosis
Clinical question: Does acetazolamide decrease the duration of mechanical ventilation for patients with chronic obstructive pulmonary disease and metabolic alkalosis?
Bottom line: Although acetazolamide effectively decreased the levels of serum bicarbonate and the number of days with metabolic alkalosis in critically ill patients with chronic obstructive pulmonary disease (COPD) on mechanical ventilation, it did not produce a statistically significant difference in the duration of mechanical ventilation. However, this lack of statistical significance may have been due to an underpowered study. (LOE = 1b-)
Reference: Faisy C, Meziani F, Planquette B, et al, for the DIABOLO Investigators. Effect of acetazolamide vs placebo on duration of invasive mechanical ventilation among patients with chronic obstructive pulmonary disease. JAMA 2016;315(5):480-488.
Study design: Randomized controlled trial (double-blinded)
Funding source: Industry + govt
Allocation: Concealed
Setting: Inpatient (ICU only)
Synopsis:
Acetazolamide is used as a respiratory stimulant for patients with COPD and metabolic alkalosis because of its ability to reduce serum bicarbonate, which may lead to a rise in minute ventilation. However, its clinical benefit has not been demonstrated previously in controlled trials.
Using concealed allocation, these investigators randomized patients with COPD who required invasive mechanical ventilation to receive either acetazolamide 500 mg intravenously twice daily (1000 mg if loop diuretics were also prescribed) or matching placebo up to 28 days. Only those patients found to have pure or mixed metabolic alkalosis received the treatment. The intention-to-treat population consisted of 380 patients and baseline characteristics were similar in both groups. The use of acetazolamide led to decreased levels of serum bicarbonate and fewer days with metabolic alkalosis but did not improve respiratory parameters such as respiratory rate, tidal volume, or minute ventilation.
For the primary outcome of duration of mechanical ventilation, the magnitude of the difference between the 2 groups was large, suggesting a clinically important effect, but the difference did not reach statistical significance (between-group difference -16 hours with acetazolamide; 95% CI -36.5 to 4.0 hours). The lack of statistical significance may be due to an underpowered study because of fewer-than-expected patients who received the treatment (more than 20% of patients in each group did not receive the assigned treatment because of lack of metabolic alkalosis or temporary contraindications) and a shorter-than-anticipated duration of mechanical ventilation in the placebo group.
Dr. Kulkarni is an assistant professor of hospital medicine at Northwestern University in Chicago.
Clinical question: Does acetazolamide decrease the duration of mechanical ventilation for patients with chronic obstructive pulmonary disease and metabolic alkalosis?
Bottom line: Although acetazolamide effectively decreased the levels of serum bicarbonate and the number of days with metabolic alkalosis in critically ill patients with chronic obstructive pulmonary disease (COPD) on mechanical ventilation, it did not produce a statistically significant difference in the duration of mechanical ventilation. However, this lack of statistical significance may have been due to an underpowered study. (LOE = 1b-)
Reference: Faisy C, Meziani F, Planquette B, et al, for the DIABOLO Investigators. Effect of acetazolamide vs placebo on duration of invasive mechanical ventilation among patients with chronic obstructive pulmonary disease. JAMA 2016;315(5):480-488.
Study design: Randomized controlled trial (double-blinded)
Funding source: Industry + govt
Allocation: Concealed
Setting: Inpatient (ICU only)
Synopsis:
Acetazolamide is used as a respiratory stimulant for patients with COPD and metabolic alkalosis because of its ability to reduce serum bicarbonate, which may lead to a rise in minute ventilation. However, its clinical benefit has not been demonstrated previously in controlled trials.
Using concealed allocation, these investigators randomized patients with COPD who required invasive mechanical ventilation to receive either acetazolamide 500 mg intravenously twice daily (1000 mg if loop diuretics were also prescribed) or matching placebo up to 28 days. Only those patients found to have pure or mixed metabolic alkalosis received the treatment. The intention-to-treat population consisted of 380 patients and baseline characteristics were similar in both groups. The use of acetazolamide led to decreased levels of serum bicarbonate and fewer days with metabolic alkalosis but did not improve respiratory parameters such as respiratory rate, tidal volume, or minute ventilation.
For the primary outcome of duration of mechanical ventilation, the magnitude of the difference between the 2 groups was large, suggesting a clinically important effect, but the difference did not reach statistical significance (between-group difference -16 hours with acetazolamide; 95% CI -36.5 to 4.0 hours). The lack of statistical significance may be due to an underpowered study because of fewer-than-expected patients who received the treatment (more than 20% of patients in each group did not receive the assigned treatment because of lack of metabolic alkalosis or temporary contraindications) and a shorter-than-anticipated duration of mechanical ventilation in the placebo group.
Dr. Kulkarni is an assistant professor of hospital medicine at Northwestern University in Chicago.
Clinical question: Does acetazolamide decrease the duration of mechanical ventilation for patients with chronic obstructive pulmonary disease and metabolic alkalosis?
Bottom line: Although acetazolamide effectively decreased the levels of serum bicarbonate and the number of days with metabolic alkalosis in critically ill patients with chronic obstructive pulmonary disease (COPD) on mechanical ventilation, it did not produce a statistically significant difference in the duration of mechanical ventilation. However, this lack of statistical significance may have been due to an underpowered study. (LOE = 1b-)
Reference: Faisy C, Meziani F, Planquette B, et al, for the DIABOLO Investigators. Effect of acetazolamide vs placebo on duration of invasive mechanical ventilation among patients with chronic obstructive pulmonary disease. JAMA 2016;315(5):480-488.
Study design: Randomized controlled trial (double-blinded)
Funding source: Industry + govt
Allocation: Concealed
Setting: Inpatient (ICU only)
Synopsis:
Acetazolamide is used as a respiratory stimulant for patients with COPD and metabolic alkalosis because of its ability to reduce serum bicarbonate, which may lead to a rise in minute ventilation. However, its clinical benefit has not been demonstrated previously in controlled trials.
Using concealed allocation, these investigators randomized patients with COPD who required invasive mechanical ventilation to receive either acetazolamide 500 mg intravenously twice daily (1000 mg if loop diuretics were also prescribed) or matching placebo up to 28 days. Only those patients found to have pure or mixed metabolic alkalosis received the treatment. The intention-to-treat population consisted of 380 patients and baseline characteristics were similar in both groups. The use of acetazolamide led to decreased levels of serum bicarbonate and fewer days with metabolic alkalosis but did not improve respiratory parameters such as respiratory rate, tidal volume, or minute ventilation.
For the primary outcome of duration of mechanical ventilation, the magnitude of the difference between the 2 groups was large, suggesting a clinically important effect, but the difference did not reach statistical significance (between-group difference -16 hours with acetazolamide; 95% CI -36.5 to 4.0 hours). The lack of statistical significance may be due to an underpowered study because of fewer-than-expected patients who received the treatment (more than 20% of patients in each group did not receive the assigned treatment because of lack of metabolic alkalosis or temporary contraindications) and a shorter-than-anticipated duration of mechanical ventilation in the placebo group.
Dr. Kulkarni is an assistant professor of hospital medicine at Northwestern University in Chicago.
Tamsulosin Effective as Expulsion Therapy for Distal Ureteric Stones
Clinical question: Is tamsulosin effective in the management of distal ureteric stones?
Bottom line: Tamsulosin promotes stone passage of ureteric stones that are 5 mm to 10 mm. You would need to treat 5 patients with tamsulosin to cause the expulsion of one such stone. Stones smaller than 5 mm have a high rate of spontaneous passage without any intervention. (LOE = 1b-)
Reference: Furyk JS, Chu K, Banks C et al. Distal ureteric stones and tamsulosin: a double-blind, placebo-controlled, randomized, multicenter trial. Ann Emerg Med 2016;67(1):86-95.
Study design: Randomized controlled trial (double-blinded)
Funding source: Foundation
Allocation: Concealed
Setting: Outpatient (primary care)
Synopsis: These authors recruited adult patients who presented to the emergency department with symptoms and imaging consistent with distal ureteric stones. Patients with fever, hypotension, stones larger than 10 mm, or kidney disease were excluded. Using concealed allocation, the investigators randomized the patients to receive either tamsulosin 0.4 mg daily or matching placebo for 28 days or until stone passage. The 2 groups had similar baseline characteristics and analysis was by intention to treat.
The primary outcome was stone expulsion as confirmed by computed tomography (CT) and time to stone expulsion was defined by self-reported passage of stone or 48-hour pain-free period. Compliance to the study medications was poor in both groups, and almost one-fifth of the patients did not have follow-up imaging. Of the approximately 80% of patients in each group who underwent follow-up CT, there was no difference in the percentage of patients with passed stones (87% in the tamsulosin group vs 82% in the placebo group; P = .22). In the subset of patients with larger stones (5 mm -10 mm), the tamsulosin group had a significantly higher rate of stone passage than the placebo group (83% vs 61%; P = .03). There were no significant differences detected in time to stone passage, pain, analgesia requirements, need for urological intervention, or adverse events.
Dr. Kulkarni is an assistant professor of hospital medicine at Northwestern University in Chicago.
Clinical question: Is tamsulosin effective in the management of distal ureteric stones?
Bottom line: Tamsulosin promotes stone passage of ureteric stones that are 5 mm to 10 mm. You would need to treat 5 patients with tamsulosin to cause the expulsion of one such stone. Stones smaller than 5 mm have a high rate of spontaneous passage without any intervention. (LOE = 1b-)
Reference: Furyk JS, Chu K, Banks C et al. Distal ureteric stones and tamsulosin: a double-blind, placebo-controlled, randomized, multicenter trial. Ann Emerg Med 2016;67(1):86-95.
Study design: Randomized controlled trial (double-blinded)
Funding source: Foundation
Allocation: Concealed
Setting: Outpatient (primary care)
Synopsis: These authors recruited adult patients who presented to the emergency department with symptoms and imaging consistent with distal ureteric stones. Patients with fever, hypotension, stones larger than 10 mm, or kidney disease were excluded. Using concealed allocation, the investigators randomized the patients to receive either tamsulosin 0.4 mg daily or matching placebo for 28 days or until stone passage. The 2 groups had similar baseline characteristics and analysis was by intention to treat.
The primary outcome was stone expulsion as confirmed by computed tomography (CT) and time to stone expulsion was defined by self-reported passage of stone or 48-hour pain-free period. Compliance to the study medications was poor in both groups, and almost one-fifth of the patients did not have follow-up imaging. Of the approximately 80% of patients in each group who underwent follow-up CT, there was no difference in the percentage of patients with passed stones (87% in the tamsulosin group vs 82% in the placebo group; P = .22). In the subset of patients with larger stones (5 mm -10 mm), the tamsulosin group had a significantly higher rate of stone passage than the placebo group (83% vs 61%; P = .03). There were no significant differences detected in time to stone passage, pain, analgesia requirements, need for urological intervention, or adverse events.
Dr. Kulkarni is an assistant professor of hospital medicine at Northwestern University in Chicago.
Clinical question: Is tamsulosin effective in the management of distal ureteric stones?
Bottom line: Tamsulosin promotes stone passage of ureteric stones that are 5 mm to 10 mm. You would need to treat 5 patients with tamsulosin to cause the expulsion of one such stone. Stones smaller than 5 mm have a high rate of spontaneous passage without any intervention. (LOE = 1b-)
Reference: Furyk JS, Chu K, Banks C et al. Distal ureteric stones and tamsulosin: a double-blind, placebo-controlled, randomized, multicenter trial. Ann Emerg Med 2016;67(1):86-95.
Study design: Randomized controlled trial (double-blinded)
Funding source: Foundation
Allocation: Concealed
Setting: Outpatient (primary care)
Synopsis: These authors recruited adult patients who presented to the emergency department with symptoms and imaging consistent with distal ureteric stones. Patients with fever, hypotension, stones larger than 10 mm, or kidney disease were excluded. Using concealed allocation, the investigators randomized the patients to receive either tamsulosin 0.4 mg daily or matching placebo for 28 days or until stone passage. The 2 groups had similar baseline characteristics and analysis was by intention to treat.
The primary outcome was stone expulsion as confirmed by computed tomography (CT) and time to stone expulsion was defined by self-reported passage of stone or 48-hour pain-free period. Compliance to the study medications was poor in both groups, and almost one-fifth of the patients did not have follow-up imaging. Of the approximately 80% of patients in each group who underwent follow-up CT, there was no difference in the percentage of patients with passed stones (87% in the tamsulosin group vs 82% in the placebo group; P = .22). In the subset of patients with larger stones (5 mm -10 mm), the tamsulosin group had a significantly higher rate of stone passage than the placebo group (83% vs 61%; P = .03). There were no significant differences detected in time to stone passage, pain, analgesia requirements, need for urological intervention, or adverse events.
Dr. Kulkarni is an assistant professor of hospital medicine at Northwestern University in Chicago.
SHM Offering Webinars on Reducing Readmissions, Optimizing Glycemic Control
This April, the Society of Hospital Medicine (SHM) will offer two free live webinars on how two of its signature mentored implementation programs are changing the way hospitals manage two key issues: readmissions and glycemic control.
Project BOOST is an evidence-based approach to reduce preventable admissions, decrease average length of stay, and improve patient satisfaction. It includes one year of individualized mentoring from a physician leader with expertise in clinical quality, on-site mentoring and training from leaders in the field, access to an online tool kit with clinical resources, and more. Find out how to get involved with Project BOOST and take the first steps toward reducing readmissions with our complimentary webinar in April.
Learn more at www.hospitalmedicine.org/BOOST.
Another signature program, SHM’s Glycemic Control Mentored Implementation Program, has supported the development and implementation of glycemic control in more than 100 hospitals nationwide. Added benefits include data collection and analysis tools, monthly coaching calls with mentors, SHM-facilitated calls and live webinars, and access to an online web-based glycemic control collaborative to share best practices.
Join more than 100 hospitals working with SHM to improve glycemic control at an upcoming free live webinar. More information is available at www.hospitalmedicine.org/gc.
A comprehensive suite of mentored implementation programs offered through SHM’s Center for Hospital Innovation and Improvement is designed to provide institutions with coaching by national physician experts to map current processes, identify root causes of deficiencies, and tailor interventions to the unique needs of the institution for sustainable results.
For more information, visit www.hospitalmedicine.org and click on Quality & Innovation.
This April, the Society of Hospital Medicine (SHM) will offer two free live webinars on how two of its signature mentored implementation programs are changing the way hospitals manage two key issues: readmissions and glycemic control.
Project BOOST is an evidence-based approach to reduce preventable admissions, decrease average length of stay, and improve patient satisfaction. It includes one year of individualized mentoring from a physician leader with expertise in clinical quality, on-site mentoring and training from leaders in the field, access to an online tool kit with clinical resources, and more. Find out how to get involved with Project BOOST and take the first steps toward reducing readmissions with our complimentary webinar in April.
Learn more at www.hospitalmedicine.org/BOOST.
Another signature program, SHM’s Glycemic Control Mentored Implementation Program, has supported the development and implementation of glycemic control in more than 100 hospitals nationwide. Added benefits include data collection and analysis tools, monthly coaching calls with mentors, SHM-facilitated calls and live webinars, and access to an online web-based glycemic control collaborative to share best practices.
Join more than 100 hospitals working with SHM to improve glycemic control at an upcoming free live webinar. More information is available at www.hospitalmedicine.org/gc.
A comprehensive suite of mentored implementation programs offered through SHM’s Center for Hospital Innovation and Improvement is designed to provide institutions with coaching by national physician experts to map current processes, identify root causes of deficiencies, and tailor interventions to the unique needs of the institution for sustainable results.
For more information, visit www.hospitalmedicine.org and click on Quality & Innovation.
This April, the Society of Hospital Medicine (SHM) will offer two free live webinars on how two of its signature mentored implementation programs are changing the way hospitals manage two key issues: readmissions and glycemic control.
Project BOOST is an evidence-based approach to reduce preventable admissions, decrease average length of stay, and improve patient satisfaction. It includes one year of individualized mentoring from a physician leader with expertise in clinical quality, on-site mentoring and training from leaders in the field, access to an online tool kit with clinical resources, and more. Find out how to get involved with Project BOOST and take the first steps toward reducing readmissions with our complimentary webinar in April.
Learn more at www.hospitalmedicine.org/BOOST.
Another signature program, SHM’s Glycemic Control Mentored Implementation Program, has supported the development and implementation of glycemic control in more than 100 hospitals nationwide. Added benefits include data collection and analysis tools, monthly coaching calls with mentors, SHM-facilitated calls and live webinars, and access to an online web-based glycemic control collaborative to share best practices.
Join more than 100 hospitals working with SHM to improve glycemic control at an upcoming free live webinar. More information is available at www.hospitalmedicine.org/gc.
A comprehensive suite of mentored implementation programs offered through SHM’s Center for Hospital Innovation and Improvement is designed to provide institutions with coaching by national physician experts to map current processes, identify root causes of deficiencies, and tailor interventions to the unique needs of the institution for sustainable results.
For more information, visit www.hospitalmedicine.org and click on Quality & Innovation.
Study Shows Non-diabetics can Benefit from Taking the Diabetes Drug Pioglitaztione
NEW YORK (Reuters Health) - The diabetes drug pioglitazone, given to non-diabetics with a recent history of stroke or transient ischemic attack (TIA), prevented subsequent strokes and reduced their odds of developing type 2 diabetes, a long-term multicenter study has concluded.
But the drug also increased the risk of fracture, weight gain, and edema.
After nearly five years of follow-up, the rate of stroke or heart attack was 11.8% with placebo and 9.0% with the drug (p=0.007). The target dose was 45 mg daily.
"That 25% relative reduction is a huge effect for a stroke trial," coauthor Dr. Wayne Clark, director of the Oregon Stroke Center at Oregon Health and Science University, told Reuters Health by phone. "That's on the same realm as aspirin and a big effect for stroke.
"We're always expecting negative results these days," because so many stroke drugs have failed in previous tests, he said. "This was a positive surprise."
Dr. Clark said he was particularly taken aback by the rate that diabetes developed in pioglitazone recipients. It manifested in 3.8% of drug recipients versus 7.7% of placebo
recipients (p<0.001).
"I didn't expect that at all," he said. "That has much wider implications and might take confirmatory studies."
The 3,876 volunteers studied at 179 sites worldwide were not diabetic but they had developed insulin resistance at the time of enrollment.
Drug therapy did not reduce mortality.The results of the study, known as IRIS, were presented February 17 at the American Heart Association and the American
Stroke Association's International Stroke Conference in Los Angeles, and online in the New England Journal of Medicine.
"The findings suggest that the administration of pioglitazone in 100 patients similar to those in our trial for about five years could prevent three patients from having a
stroke or myocardial infarction," the researchers wrote in the Journal. "However, during the same period, the treatment would be expected to result in bone fractures requiring surgery or hospitalization in two patients.
"It seems reasonable to consider individual treatment preference and risk of drug-related adverse events in addition to potential benefits when making patient-specific decisions regarding therapy," they concluded.
Serious fractures occurred in 5.1% of drug recipients versus 3.2% among placebo patients (p=0.003). A weight gain of more than 4.5 kg was seen in 52.2% of pioglitazone recipientscompared with 33.7% for placebo, and rates of edema were 35.6% with the drug versus 24.9% with placebo (both p<0.001).
The drug has been plagued by suspicions that it might increase the risk of heart failure and bladder cancer. In this study, 74 pioglitazone recipients developed heart failure versus 71 in the placebo group (p=0.80). A dozen drug recipients were diagnosed with bladder cancer compared with eight cases in the placebo group (p=0.37).
Dr. Clark said, "All of the stuff we're doing for risk-factor reduction -- blood pressure reduction, stop smoking and giving aspirin -- they're all on the same level of relative improvement, and all of those are widely used. Aspirin has a list of side effects that will fill up three pages."
At the start of the study, all of the volunteers were insulin resistant, at least 40 years old, and had experienced an ischemic stroke or TIA in the previous six months. Diabetics were excluded as were patients with heart failure, active liver disease, and an increased risk of bladder cancer.
By the end of the study, 60% of the pioglitazone patients were still taking their medicine compared with 67% of placebo recipients. The most common reason for discontinuing was edema or weight gain.
The National Institute of Neurological Disorders and Stroke funded this study. Eleven coauthors reported disclosures.
NEW YORK (Reuters Health) - The diabetes drug pioglitazone, given to non-diabetics with a recent history of stroke or transient ischemic attack (TIA), prevented subsequent strokes and reduced their odds of developing type 2 diabetes, a long-term multicenter study has concluded.
But the drug also increased the risk of fracture, weight gain, and edema.
After nearly five years of follow-up, the rate of stroke or heart attack was 11.8% with placebo and 9.0% with the drug (p=0.007). The target dose was 45 mg daily.
"That 25% relative reduction is a huge effect for a stroke trial," coauthor Dr. Wayne Clark, director of the Oregon Stroke Center at Oregon Health and Science University, told Reuters Health by phone. "That's on the same realm as aspirin and a big effect for stroke.
"We're always expecting negative results these days," because so many stroke drugs have failed in previous tests, he said. "This was a positive surprise."
Dr. Clark said he was particularly taken aback by the rate that diabetes developed in pioglitazone recipients. It manifested in 3.8% of drug recipients versus 7.7% of placebo
recipients (p<0.001).
"I didn't expect that at all," he said. "That has much wider implications and might take confirmatory studies."
The 3,876 volunteers studied at 179 sites worldwide were not diabetic but they had developed insulin resistance at the time of enrollment.
Drug therapy did not reduce mortality.The results of the study, known as IRIS, were presented February 17 at the American Heart Association and the American
Stroke Association's International Stroke Conference in Los Angeles, and online in the New England Journal of Medicine.
"The findings suggest that the administration of pioglitazone in 100 patients similar to those in our trial for about five years could prevent three patients from having a
stroke or myocardial infarction," the researchers wrote in the Journal. "However, during the same period, the treatment would be expected to result in bone fractures requiring surgery or hospitalization in two patients.
"It seems reasonable to consider individual treatment preference and risk of drug-related adverse events in addition to potential benefits when making patient-specific decisions regarding therapy," they concluded.
Serious fractures occurred in 5.1% of drug recipients versus 3.2% among placebo patients (p=0.003). A weight gain of more than 4.5 kg was seen in 52.2% of pioglitazone recipientscompared with 33.7% for placebo, and rates of edema were 35.6% with the drug versus 24.9% with placebo (both p<0.001).
The drug has been plagued by suspicions that it might increase the risk of heart failure and bladder cancer. In this study, 74 pioglitazone recipients developed heart failure versus 71 in the placebo group (p=0.80). A dozen drug recipients were diagnosed with bladder cancer compared with eight cases in the placebo group (p=0.37).
Dr. Clark said, "All of the stuff we're doing for risk-factor reduction -- blood pressure reduction, stop smoking and giving aspirin -- they're all on the same level of relative improvement, and all of those are widely used. Aspirin has a list of side effects that will fill up three pages."
At the start of the study, all of the volunteers were insulin resistant, at least 40 years old, and had experienced an ischemic stroke or TIA in the previous six months. Diabetics were excluded as were patients with heart failure, active liver disease, and an increased risk of bladder cancer.
By the end of the study, 60% of the pioglitazone patients were still taking their medicine compared with 67% of placebo recipients. The most common reason for discontinuing was edema or weight gain.
The National Institute of Neurological Disorders and Stroke funded this study. Eleven coauthors reported disclosures.
NEW YORK (Reuters Health) - The diabetes drug pioglitazone, given to non-diabetics with a recent history of stroke or transient ischemic attack (TIA), prevented subsequent strokes and reduced their odds of developing type 2 diabetes, a long-term multicenter study has concluded.
But the drug also increased the risk of fracture, weight gain, and edema.
After nearly five years of follow-up, the rate of stroke or heart attack was 11.8% with placebo and 9.0% with the drug (p=0.007). The target dose was 45 mg daily.
"That 25% relative reduction is a huge effect for a stroke trial," coauthor Dr. Wayne Clark, director of the Oregon Stroke Center at Oregon Health and Science University, told Reuters Health by phone. "That's on the same realm as aspirin and a big effect for stroke.
"We're always expecting negative results these days," because so many stroke drugs have failed in previous tests, he said. "This was a positive surprise."
Dr. Clark said he was particularly taken aback by the rate that diabetes developed in pioglitazone recipients. It manifested in 3.8% of drug recipients versus 7.7% of placebo
recipients (p<0.001).
"I didn't expect that at all," he said. "That has much wider implications and might take confirmatory studies."
The 3,876 volunteers studied at 179 sites worldwide were not diabetic but they had developed insulin resistance at the time of enrollment.
Drug therapy did not reduce mortality.The results of the study, known as IRIS, were presented February 17 at the American Heart Association and the American
Stroke Association's International Stroke Conference in Los Angeles, and online in the New England Journal of Medicine.
"The findings suggest that the administration of pioglitazone in 100 patients similar to those in our trial for about five years could prevent three patients from having a
stroke or myocardial infarction," the researchers wrote in the Journal. "However, during the same period, the treatment would be expected to result in bone fractures requiring surgery or hospitalization in two patients.
"It seems reasonable to consider individual treatment preference and risk of drug-related adverse events in addition to potential benefits when making patient-specific decisions regarding therapy," they concluded.
Serious fractures occurred in 5.1% of drug recipients versus 3.2% among placebo patients (p=0.003). A weight gain of more than 4.5 kg was seen in 52.2% of pioglitazone recipientscompared with 33.7% for placebo, and rates of edema were 35.6% with the drug versus 24.9% with placebo (both p<0.001).
The drug has been plagued by suspicions that it might increase the risk of heart failure and bladder cancer. In this study, 74 pioglitazone recipients developed heart failure versus 71 in the placebo group (p=0.80). A dozen drug recipients were diagnosed with bladder cancer compared with eight cases in the placebo group (p=0.37).
Dr. Clark said, "All of the stuff we're doing for risk-factor reduction -- blood pressure reduction, stop smoking and giving aspirin -- they're all on the same level of relative improvement, and all of those are widely used. Aspirin has a list of side effects that will fill up three pages."
At the start of the study, all of the volunteers were insulin resistant, at least 40 years old, and had experienced an ischemic stroke or TIA in the previous six months. Diabetics were excluded as were patients with heart failure, active liver disease, and an increased risk of bladder cancer.
By the end of the study, 60% of the pioglitazone patients were still taking their medicine compared with 67% of placebo recipients. The most common reason for discontinuing was edema or weight gain.
The National Institute of Neurological Disorders and Stroke funded this study. Eleven coauthors reported disclosures.
Key Elements of Critical Care
Code 99291 is used for critical care, evaluation, and management of the critically ill or critically injured patient, first 30–74 minutes.1 It is to be reported only once per day per physician or group member of the same specialty.

Code 99292 is for critical care, evaluation, and management of the critically ill or critically injured patient, each additional 30 minutes. It is to be listed separately in addition to the code for primary service.1 Code 99292 is categorized as an add-on code. It must be reported on the same invoice as its primary code, 99291. Multiple units of code 99292 can be reported per day per physician/group.
Despite the increased resources and references for critical care billing, critical care reporting issues persist. Medicare data analysis continues to identify 99291 as high risk for claim payment errors, perpetuating prepayment claim edits for outlier utilization and location discrepancies (i.e., settings other than inpatient hospital, outpatient hospital, or the emergency department). 2,3,4
Bolster your documentation with these three key elements.
Critical Illness, Injury Management
Current Procedural Terminology (CPT) and the Centers for Medicare & Medicaid Services (CMS) define “critical illness or injury” as a condition that acutely impairs one or more vital organ systems such that there is a high probability of imminent or life-threatening deterioration in the patient’s condition (e.g., central nervous system failure; circulatory failure; shock; renal, hepatic, metabolic, and/or respiratory failure).5
Hospitalists providing care to the critically ill patient must perform highly complex decision making and interventions of high intensity that are required to prevent the patient’s inevitable decline. CMS further elaborates that “the patient shall be critically ill or injured at the time of the physician’s visit.”6 This is to ensure that hospitalists and other specialists support the medical necessity of the service and do not continue to report critical care codes on days after the patient has become stable and improved.
Consider the following scenarios:
CMS examples of patients whose medical condition may warrant critical care services (99291, 99292):6
- An 81-year-old male patient is admitted to the ICU following abdominal aortic aneurysm resection. Two days after surgery, he requires fluids and pressors to maintain adequate perfusion and arterial pressures. He remains ventilator dependent.
- A 67-year-old female patient is three days post mitral valve repair. She develops petechiae, hypotension, and hypoxia requiring respiratory and circulatory support.
- A 70-year-old admitted for right lower lobe pneumococcal pneumonia with a history of COPD becomes hypoxic and hypotensive two days after admission.
- A 68-year-old admitted for an acute anterior wall myocardial infarction continues to have symptomatic ventricular tachycardia that is marginally responsive to antiarrhythmic therapy.
CMS examples of patients who may not satisfy Medicare medical necessity criteria, or do not meet critical care criteria, or who do not have a critical care illness or injury and, therefore, are not eligible for critical care payment but may be reported using another appropriate hospital care code, such as subsequent hospital care codes (99231–99233), initial hospital care codes (99221–99223), or hospital consultation codes (99251–99255) when applicable:1,6
- Patients admitted to a critical care unit because no other hospital beds were available;
- Patients admitted to a critical care unit for close nursing observation and/or frequent monitoring of vital signs (e.g., drug toxicity or overdose);
- Patients admitted to a critical care unit because hospital rules require certain treatments (e.g., insulin infusions) to be administered in the critical care unit; and
- Patients receiving only care of a chronic illness in absence of care for a critical illness (e.g., daily management of a chronic ventilator patient, management of or care related to dialysis for end-stage renal disease). Services considered palliative in nature as this type of care do not meet the definition of critical care services.7
Concurrent Care
Critically ill patients often require the care of hospitalists and other specialists throughout the course of treatment. Payors are sensitive to the multiple hours billed by multiple providers for a single patient on a given day. Claim logic provides an automated response to only allow reimbursement for 99291 once per day when reported by physicians of the same group and specialty.8 Physicians of different specialties can separately report critical care hours as long as they are caring for a condition that meets the definition of critical care.
The CMS example of this: A dermatologist evaluates and treats a rash on an ICU patient who is maintained on a ventilator and nitroglycerine infusion that are being managed by an intensivist. The dermatologist should not report a service for critical care.6
Similarly for hospitalists, if an intensivist is taking care of the critical condition and there is nothing more for the hospitalist to add to the plan of care for the critical condition, critical care services may not be justified.
When different specialists are reporting critical care on the same day, it is imperative for the documentation to demonstrate that care is not duplicative of any other provider’s care (i.e., identify management of different conditions or revising elements of the plan). The care cannot overlap the same time period of any other physician reporting critical care services.
Calculating Time
Critical care time constitutes bedside time and time spent on the patient’s unit/floor where the physician is immediately available to the patient (see Table 1). Certain labs, diagnostic studies, and procedures are considered inherent to critical care services and are not reported separately on the claim form: cardiac output measurements (93561, 93562); chest X-rays (71010, 71015, 71020); pulse oximetry (94760, 94761, 94762); blood gases and interpretation of data stored in computers, such as ECGs, blood pressures, and hematologic data (99090); gastric intubation (43752, 43753); temporary transcutaneous pacing (92953); ventilation management (94002–94004, 94660, 94662); and vascular access procedures (36000, 36410, 36415, 36591, 36600).1

Instead, physician time associated with the performance and/or interpretation of these services is toward the cumulative critical care time of the day. Services or procedures that are considered separately billable (e.g., central line placement, intubation, CPR) cannot contribute to critical care time.
When separately billable procedures are performed by the same provider/specialty group on the same day as critical care, physicians should make a notation in the medical record indicating the non-overlapping service times (e.g., “central line insertion is not included as critical care time”). This may assist with securing reimbursement when the payor requests the documentation for each reported claim item.
Activities on the floor/unit that do not directly contribute to patient care or management (e.g., review of literature, teaching rounds) cannot be counted toward critical care time. Do not count time associated with indirect care provided outside of the patient’s unit/floor (e.g., reviewing data or calling the family from the office) toward critical care time.
Family discussions can be counted toward critical care time but must take place at bedside or on the patient’s unit/floor. The patient must participate in the discussion unless medically unable or clinically incompetent to participate. If unable to participate, a notation in the chart must delineate the patient’s inability to participate and the reason.
Credited time can only involve obtaining a medical history and/or discussing treatment options or limitation(s) of treatment. The conversation must bear directly on patient management.1,7 Do not count time associated with providing periodic condition updates to the family, answering questions about the patient’s condition that are unrelated to decision making, or counseling the family during their grief process. If the conversation must take place via phone, it may be counted toward critical care time if the physician is calling from the patient’s unit/floor and the conversation involves the same criterion identified for face-to-face family meetings.10
Physicians should keep track of their critical care time throughout the day. Since critical care time is a cumulative service, each entry should include the total time that critical care services were provided (e.g., 45 minutes).10 Some payors may still impose the notation of “start-and-stop time” per encounter (e.g., 2–2:50 a.m.).
Same-specialty physicians (i.e., two hospitalists from the same group practice) may require separate claims. The initial critical care hour (99291) must be met by a single physician. Medically necessary critical care time beyond the first hour (99292) may be met individually by the same physician or collectively with another physician from the same group. The physician performing the additional time, beyond the first hour, reports the appropriate units of 99292 (see Table 1) under the corresponding NPI.11
CMS has issued instructions for contractors to recognize this atypical reporting method. However, non-Medicare payors may not recognize this newer reporting method and maintain that the cumulative service (by the same-specialty physician in the same provider group) should be reported under one physician name. Be sure to query the payors for appropriate reporting methods. TH
References
- Abraham M, Ahlman J, Boudreau A, Connelly J, Crosslin, R. Current Procedural Terminology 2015 Professional Edition. Chicago: American Medical Association Press; 2014. 23-25.
- Widespread prepayment targeted review notification—CPT 99291. Cahaba website. Available at: www.cahabagba.com/news/widespread-prepayment-targeted-review-notification-part-b/. Accessed December 17, 2015.
- Critical care CPT 99291 widespread prepayment targeted review results. Cahaba website. Available at: https://www.cahabagba.com/news/critical-care-cpt-99291-widespread-prepayment-targeted-review-results-2/. Accessed December 17, 2015.
- Prepayment edit of evaluation and management (E/M) code 99291. First Coast Service Options, Inc. website. Available at: medicare.fcso.com/Publications_B/2013/251608.pdf. Accessed December 17, 2015.
- Medicare claims processing manual: chapter 12, section 30.6.12A. Centers for Medicare & Medicaid Services website. Available at: www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/downloads/clm104c12.pdf. Accessed December 17, 2015.
- Medicare claims processing manual: chapter 12, section 30.6.12B. Centers for Medicare & Medicaid Services website. Available at: www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/downloads/clm104c12.pdf. Accessed December 17, 2015.
- Critical care fact sheet. CGS Administrators, LLC website. Available at: www.cgsmedicare.com/partb/mr/pdf/critical_care_fact_sheet.pdf. Accessed December 17, 2015.
- Same day same service policy. United Healthcare website. Available at: www.unitedhealthcareonline.com/ccmcontent/ProviderII/UHC/en-US/Main%20Menu/Tools%20&%20Resources/Policies%20and%20Protocols/Medicare%20Advantage%20Reimbursement%20Policies/S/SameDaySameService.pdf. Accessed December 17, 2015.
- Medicare claims processing manual: chapter 12, section 30.6.12G. Centers for Medicare & Medicaid Services website. Available at: www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/downloads/clm104c12.pdf. Accessed December 17, 2015.
- Medicare claims processing manual: chapter 12, section 30.6.12E. Centers for Medicare & Medicaid Services website. Available at: www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/downloads/clm104c12.pdf. Accessed December 17, 2015.
- Medicare claims processing manual: chapter 12, section 30.6.12I. Centers for Medicare & Medicaid Services website. Available at: www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/downloads/clm104c12.pdf. Accessed December 17, 2015.
Code 99291 is used for critical care, evaluation, and management of the critically ill or critically injured patient, first 30–74 minutes.1 It is to be reported only once per day per physician or group member of the same specialty.
Code 99292 is for critical care, evaluation, and management of the critically ill or critically injured patient, each additional 30 minutes. It is to be listed separately in addition to the code for primary service.1 Code 99292 is categorized as an add-on code. It must be reported on the same invoice as its primary code, 99291. Multiple units of code 99292 can be reported per day per physician/group.
Despite the increased resources and references for critical care billing, critical care reporting issues persist. Medicare data analysis continues to identify 99291 as high risk for claim payment errors, perpetuating prepayment claim edits for outlier utilization and location discrepancies (i.e., settings other than inpatient hospital, outpatient hospital, or the emergency department). 2,3,4
Bolster your documentation with these three key elements.
Critical Illness, Injury Management
Current Procedural Terminology (CPT) and the Centers for Medicare & Medicaid Services (CMS) define “critical illness or injury” as a condition that acutely impairs one or more vital organ systems such that there is a high probability of imminent or life-threatening deterioration in the patient’s condition (e.g., central nervous system failure; circulatory failure; shock; renal, hepatic, metabolic, and/or respiratory failure).5
Hospitalists providing care to the critically ill patient must perform highly complex decision making and interventions of high intensity that are required to prevent the patient’s inevitable decline. CMS further elaborates that “the patient shall be critically ill or injured at the time of the physician’s visit.”6 This is to ensure that hospitalists and other specialists support the medical necessity of the service and do not continue to report critical care codes on days after the patient has become stable and improved.
Consider the following scenarios:
CMS examples of patients whose medical condition may warrant critical care services (99291, 99292):6
- An 81-year-old male patient is admitted to the ICU following abdominal aortic aneurysm resection. Two days after surgery, he requires fluids and pressors to maintain adequate perfusion and arterial pressures. He remains ventilator dependent.
- A 67-year-old female patient is three days post mitral valve repair. She develops petechiae, hypotension, and hypoxia requiring respiratory and circulatory support.
- A 70-year-old admitted for right lower lobe pneumococcal pneumonia with a history of COPD becomes hypoxic and hypotensive two days after admission.
- A 68-year-old admitted for an acute anterior wall myocardial infarction continues to have symptomatic ventricular tachycardia that is marginally responsive to antiarrhythmic therapy.
CMS examples of patients who may not satisfy Medicare medical necessity criteria, or do not meet critical care criteria, or who do not have a critical care illness or injury and, therefore, are not eligible for critical care payment but may be reported using another appropriate hospital care code, such as subsequent hospital care codes (99231–99233), initial hospital care codes (99221–99223), or hospital consultation codes (99251–99255) when applicable:1,6
- Patients admitted to a critical care unit because no other hospital beds were available;
- Patients admitted to a critical care unit for close nursing observation and/or frequent monitoring of vital signs (e.g., drug toxicity or overdose);
- Patients admitted to a critical care unit because hospital rules require certain treatments (e.g., insulin infusions) to be administered in the critical care unit; and
- Patients receiving only care of a chronic illness in absence of care for a critical illness (e.g., daily management of a chronic ventilator patient, management of or care related to dialysis for end-stage renal disease). Services considered palliative in nature as this type of care do not meet the definition of critical care services.7
Concurrent Care
Critically ill patients often require the care of hospitalists and other specialists throughout the course of treatment. Payors are sensitive to the multiple hours billed by multiple providers for a single patient on a given day. Claim logic provides an automated response to only allow reimbursement for 99291 once per day when reported by physicians of the same group and specialty.8 Physicians of different specialties can separately report critical care hours as long as they are caring for a condition that meets the definition of critical care.
The CMS example of this: A dermatologist evaluates and treats a rash on an ICU patient who is maintained on a ventilator and nitroglycerine infusion that are being managed by an intensivist. The dermatologist should not report a service for critical care.6
Similarly for hospitalists, if an intensivist is taking care of the critical condition and there is nothing more for the hospitalist to add to the plan of care for the critical condition, critical care services may not be justified.
When different specialists are reporting critical care on the same day, it is imperative for the documentation to demonstrate that care is not duplicative of any other provider’s care (i.e., identify management of different conditions or revising elements of the plan). The care cannot overlap the same time period of any other physician reporting critical care services.
Calculating Time
Critical care time constitutes bedside time and time spent on the patient’s unit/floor where the physician is immediately available to the patient (see Table 1). Certain labs, diagnostic studies, and procedures are considered inherent to critical care services and are not reported separately on the claim form: cardiac output measurements (93561, 93562); chest X-rays (71010, 71015, 71020); pulse oximetry (94760, 94761, 94762); blood gases and interpretation of data stored in computers, such as ECGs, blood pressures, and hematologic data (99090); gastric intubation (43752, 43753); temporary transcutaneous pacing (92953); ventilation management (94002–94004, 94660, 94662); and vascular access procedures (36000, 36410, 36415, 36591, 36600).1
Instead, physician time associated with the performance and/or interpretation of these services is toward the cumulative critical care time of the day. Services or procedures that are considered separately billable (e.g., central line placement, intubation, CPR) cannot contribute to critical care time.
When separately billable procedures are performed by the same provider/specialty group on the same day as critical care, physicians should make a notation in the medical record indicating the non-overlapping service times (e.g., “central line insertion is not included as critical care time”). This may assist with securing reimbursement when the payor requests the documentation for each reported claim item.
Activities on the floor/unit that do not directly contribute to patient care or management (e.g., review of literature, teaching rounds) cannot be counted toward critical care time. Do not count time associated with indirect care provided outside of the patient’s unit/floor (e.g., reviewing data or calling the family from the office) toward critical care time.
Family discussions can be counted toward critical care time but must take place at bedside or on the patient’s unit/floor. The patient must participate in the discussion unless medically unable or clinically incompetent to participate. If unable to participate, a notation in the chart must delineate the patient’s inability to participate and the reason.
Credited time can only involve obtaining a medical history and/or discussing treatment options or limitation(s) of treatment. The conversation must bear directly on patient management.1,7 Do not count time associated with providing periodic condition updates to the family, answering questions about the patient’s condition that are unrelated to decision making, or counseling the family during their grief process. If the conversation must take place via phone, it may be counted toward critical care time if the physician is calling from the patient’s unit/floor and the conversation involves the same criterion identified for face-to-face family meetings.10
Physicians should keep track of their critical care time throughout the day. Since critical care time is a cumulative service, each entry should include the total time that critical care services were provided (e.g., 45 minutes).10 Some payors may still impose the notation of “start-and-stop time” per encounter (e.g., 2–2:50 a.m.).
Same-specialty physicians (i.e., two hospitalists from the same group practice) may require separate claims. The initial critical care hour (99291) must be met by a single physician. Medically necessary critical care time beyond the first hour (99292) may be met individually by the same physician or collectively with another physician from the same group. The physician performing the additional time, beyond the first hour, reports the appropriate units of 99292 (see Table 1) under the corresponding NPI.11
CMS has issued instructions for contractors to recognize this atypical reporting method. However, non-Medicare payors may not recognize this newer reporting method and maintain that the cumulative service (by the same-specialty physician in the same provider group) should be reported under one physician name. Be sure to query the payors for appropriate reporting methods. TH
References
- Abraham M, Ahlman J, Boudreau A, Connelly J, Crosslin, R. Current Procedural Terminology 2015 Professional Edition. Chicago: American Medical Association Press; 2014. 23-25.
- Widespread prepayment targeted review notification—CPT 99291. Cahaba website. Available at: www.cahabagba.com/news/widespread-prepayment-targeted-review-notification-part-b/. Accessed December 17, 2015.
- Critical care CPT 99291 widespread prepayment targeted review results. Cahaba website. Available at: https://www.cahabagba.com/news/critical-care-cpt-99291-widespread-prepayment-targeted-review-results-2/. Accessed December 17, 2015.
- Prepayment edit of evaluation and management (E/M) code 99291. First Coast Service Options, Inc. website. Available at: medicare.fcso.com/Publications_B/2013/251608.pdf. Accessed December 17, 2015.
- Medicare claims processing manual: chapter 12, section 30.6.12A. Centers for Medicare & Medicaid Services website. Available at: www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/downloads/clm104c12.pdf. Accessed December 17, 2015.
- Medicare claims processing manual: chapter 12, section 30.6.12B. Centers for Medicare & Medicaid Services website. Available at: www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/downloads/clm104c12.pdf. Accessed December 17, 2015.
- Critical care fact sheet. CGS Administrators, LLC website. Available at: www.cgsmedicare.com/partb/mr/pdf/critical_care_fact_sheet.pdf. Accessed December 17, 2015.
- Same day same service policy. United Healthcare website. Available at: www.unitedhealthcareonline.com/ccmcontent/ProviderII/UHC/en-US/Main%20Menu/Tools%20&%20Resources/Policies%20and%20Protocols/Medicare%20Advantage%20Reimbursement%20Policies/S/SameDaySameService.pdf. Accessed December 17, 2015.
- Medicare claims processing manual: chapter 12, section 30.6.12G. Centers for Medicare & Medicaid Services website. Available at: www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/downloads/clm104c12.pdf. Accessed December 17, 2015.
- Medicare claims processing manual: chapter 12, section 30.6.12E. Centers for Medicare & Medicaid Services website. Available at: www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/downloads/clm104c12.pdf. Accessed December 17, 2015.
- Medicare claims processing manual: chapter 12, section 30.6.12I. Centers for Medicare & Medicaid Services website. Available at: www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/downloads/clm104c12.pdf. Accessed December 17, 2015.
Code 99291 is used for critical care, evaluation, and management of the critically ill or critically injured patient, first 30–74 minutes.1 It is to be reported only once per day per physician or group member of the same specialty.
Code 99292 is for critical care, evaluation, and management of the critically ill or critically injured patient, each additional 30 minutes. It is to be listed separately in addition to the code for primary service.1 Code 99292 is categorized as an add-on code. It must be reported on the same invoice as its primary code, 99291. Multiple units of code 99292 can be reported per day per physician/group.
Despite the increased resources and references for critical care billing, critical care reporting issues persist. Medicare data analysis continues to identify 99291 as high risk for claim payment errors, perpetuating prepayment claim edits for outlier utilization and location discrepancies (i.e., settings other than inpatient hospital, outpatient hospital, or the emergency department). 2,3,4
Bolster your documentation with these three key elements.
Critical Illness, Injury Management
Current Procedural Terminology (CPT) and the Centers for Medicare & Medicaid Services (CMS) define “critical illness or injury” as a condition that acutely impairs one or more vital organ systems such that there is a high probability of imminent or life-threatening deterioration in the patient’s condition (e.g., central nervous system failure; circulatory failure; shock; renal, hepatic, metabolic, and/or respiratory failure).5
Hospitalists providing care to the critically ill patient must perform highly complex decision making and interventions of high intensity that are required to prevent the patient’s inevitable decline. CMS further elaborates that “the patient shall be critically ill or injured at the time of the physician’s visit.”6 This is to ensure that hospitalists and other specialists support the medical necessity of the service and do not continue to report critical care codes on days after the patient has become stable and improved.
Consider the following scenarios:
CMS examples of patients whose medical condition may warrant critical care services (99291, 99292):6
- An 81-year-old male patient is admitted to the ICU following abdominal aortic aneurysm resection. Two days after surgery, he requires fluids and pressors to maintain adequate perfusion and arterial pressures. He remains ventilator dependent.
- A 67-year-old female patient is three days post mitral valve repair. She develops petechiae, hypotension, and hypoxia requiring respiratory and circulatory support.
- A 70-year-old admitted for right lower lobe pneumococcal pneumonia with a history of COPD becomes hypoxic and hypotensive two days after admission.
- A 68-year-old admitted for an acute anterior wall myocardial infarction continues to have symptomatic ventricular tachycardia that is marginally responsive to antiarrhythmic therapy.
CMS examples of patients who may not satisfy Medicare medical necessity criteria, or do not meet critical care criteria, or who do not have a critical care illness or injury and, therefore, are not eligible for critical care payment but may be reported using another appropriate hospital care code, such as subsequent hospital care codes (99231–99233), initial hospital care codes (99221–99223), or hospital consultation codes (99251–99255) when applicable:1,6
- Patients admitted to a critical care unit because no other hospital beds were available;
- Patients admitted to a critical care unit for close nursing observation and/or frequent monitoring of vital signs (e.g., drug toxicity or overdose);
- Patients admitted to a critical care unit because hospital rules require certain treatments (e.g., insulin infusions) to be administered in the critical care unit; and
- Patients receiving only care of a chronic illness in absence of care for a critical illness (e.g., daily management of a chronic ventilator patient, management of or care related to dialysis for end-stage renal disease). Services considered palliative in nature as this type of care do not meet the definition of critical care services.7
Concurrent Care
Critically ill patients often require the care of hospitalists and other specialists throughout the course of treatment. Payors are sensitive to the multiple hours billed by multiple providers for a single patient on a given day. Claim logic provides an automated response to only allow reimbursement for 99291 once per day when reported by physicians of the same group and specialty.8 Physicians of different specialties can separately report critical care hours as long as they are caring for a condition that meets the definition of critical care.
The CMS example of this: A dermatologist evaluates and treats a rash on an ICU patient who is maintained on a ventilator and nitroglycerine infusion that are being managed by an intensivist. The dermatologist should not report a service for critical care.6
Similarly for hospitalists, if an intensivist is taking care of the critical condition and there is nothing more for the hospitalist to add to the plan of care for the critical condition, critical care services may not be justified.
When different specialists are reporting critical care on the same day, it is imperative for the documentation to demonstrate that care is not duplicative of any other provider’s care (i.e., identify management of different conditions or revising elements of the plan). The care cannot overlap the same time period of any other physician reporting critical care services.
Calculating Time
Critical care time constitutes bedside time and time spent on the patient’s unit/floor where the physician is immediately available to the patient (see Table 1). Certain labs, diagnostic studies, and procedures are considered inherent to critical care services and are not reported separately on the claim form: cardiac output measurements (93561, 93562); chest X-rays (71010, 71015, 71020); pulse oximetry (94760, 94761, 94762); blood gases and interpretation of data stored in computers, such as ECGs, blood pressures, and hematologic data (99090); gastric intubation (43752, 43753); temporary transcutaneous pacing (92953); ventilation management (94002–94004, 94660, 94662); and vascular access procedures (36000, 36410, 36415, 36591, 36600).1
Instead, physician time associated with the performance and/or interpretation of these services is toward the cumulative critical care time of the day. Services or procedures that are considered separately billable (e.g., central line placement, intubation, CPR) cannot contribute to critical care time.
When separately billable procedures are performed by the same provider/specialty group on the same day as critical care, physicians should make a notation in the medical record indicating the non-overlapping service times (e.g., “central line insertion is not included as critical care time”). This may assist with securing reimbursement when the payor requests the documentation for each reported claim item.
Activities on the floor/unit that do not directly contribute to patient care or management (e.g., review of literature, teaching rounds) cannot be counted toward critical care time. Do not count time associated with indirect care provided outside of the patient’s unit/floor (e.g., reviewing data or calling the family from the office) toward critical care time.
Family discussions can be counted toward critical care time but must take place at bedside or on the patient’s unit/floor. The patient must participate in the discussion unless medically unable or clinically incompetent to participate. If unable to participate, a notation in the chart must delineate the patient’s inability to participate and the reason.
Credited time can only involve obtaining a medical history and/or discussing treatment options or limitation(s) of treatment. The conversation must bear directly on patient management.1,7 Do not count time associated with providing periodic condition updates to the family, answering questions about the patient’s condition that are unrelated to decision making, or counseling the family during their grief process. If the conversation must take place via phone, it may be counted toward critical care time if the physician is calling from the patient’s unit/floor and the conversation involves the same criterion identified for face-to-face family meetings.10
Physicians should keep track of their critical care time throughout the day. Since critical care time is a cumulative service, each entry should include the total time that critical care services were provided (e.g., 45 minutes).10 Some payors may still impose the notation of “start-and-stop time” per encounter (e.g., 2–2:50 a.m.).
Same-specialty physicians (i.e., two hospitalists from the same group practice) may require separate claims. The initial critical care hour (99291) must be met by a single physician. Medically necessary critical care time beyond the first hour (99292) may be met individually by the same physician or collectively with another physician from the same group. The physician performing the additional time, beyond the first hour, reports the appropriate units of 99292 (see Table 1) under the corresponding NPI.11
CMS has issued instructions for contractors to recognize this atypical reporting method. However, non-Medicare payors may not recognize this newer reporting method and maintain that the cumulative service (by the same-specialty physician in the same provider group) should be reported under one physician name. Be sure to query the payors for appropriate reporting methods. TH
References
- Abraham M, Ahlman J, Boudreau A, Connelly J, Crosslin, R. Current Procedural Terminology 2015 Professional Edition. Chicago: American Medical Association Press; 2014. 23-25.
- Widespread prepayment targeted review notification—CPT 99291. Cahaba website. Available at: www.cahabagba.com/news/widespread-prepayment-targeted-review-notification-part-b/. Accessed December 17, 2015.
- Critical care CPT 99291 widespread prepayment targeted review results. Cahaba website. Available at: https://www.cahabagba.com/news/critical-care-cpt-99291-widespread-prepayment-targeted-review-results-2/. Accessed December 17, 2015.
- Prepayment edit of evaluation and management (E/M) code 99291. First Coast Service Options, Inc. website. Available at: medicare.fcso.com/Publications_B/2013/251608.pdf. Accessed December 17, 2015.
- Medicare claims processing manual: chapter 12, section 30.6.12A. Centers for Medicare & Medicaid Services website. Available at: www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/downloads/clm104c12.pdf. Accessed December 17, 2015.
- Medicare claims processing manual: chapter 12, section 30.6.12B. Centers for Medicare & Medicaid Services website. Available at: www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/downloads/clm104c12.pdf. Accessed December 17, 2015.
- Critical care fact sheet. CGS Administrators, LLC website. Available at: www.cgsmedicare.com/partb/mr/pdf/critical_care_fact_sheet.pdf. Accessed December 17, 2015.
- Same day same service policy. United Healthcare website. Available at: www.unitedhealthcareonline.com/ccmcontent/ProviderII/UHC/en-US/Main%20Menu/Tools%20&%20Resources/Policies%20and%20Protocols/Medicare%20Advantage%20Reimbursement%20Policies/S/SameDaySameService.pdf. Accessed December 17, 2015.
- Medicare claims processing manual: chapter 12, section 30.6.12G. Centers for Medicare & Medicaid Services website. Available at: www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/downloads/clm104c12.pdf. Accessed December 17, 2015.
- Medicare claims processing manual: chapter 12, section 30.6.12E. Centers for Medicare & Medicaid Services website. Available at: www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/downloads/clm104c12.pdf. Accessed December 17, 2015.
- Medicare claims processing manual: chapter 12, section 30.6.12I. Centers for Medicare & Medicaid Services website. Available at: www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/downloads/clm104c12.pdf. Accessed December 17, 2015.
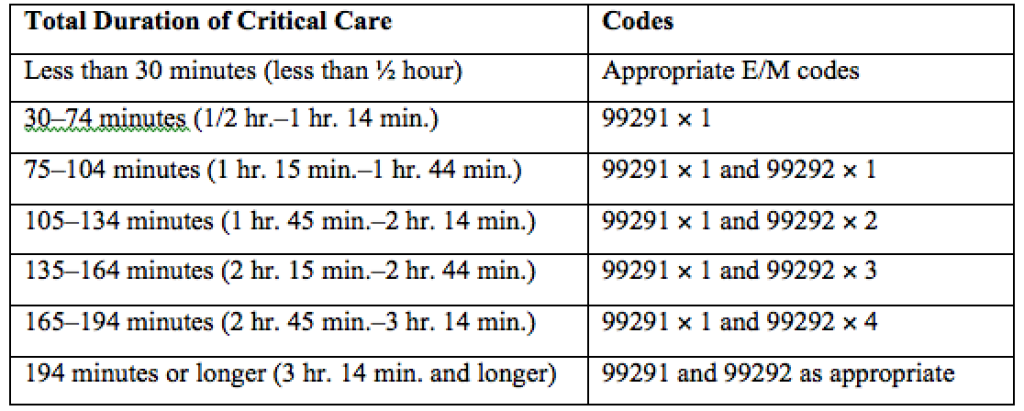
QI and Patient Safety: No Longer Just an Elective for Trainees
The demand for training in healthcare quality and patient safety, for both medical students and residents, has never been higher. The Quality and Safety Educators Academy (QSEA, sites.hospitalmedicine.org/qsea) responds to that demand by providing medical educators with the knowledge and tools to integrate quality improvement and safety concepts into their curricula.
Sponsored by the Society of Hospital Medicine (SHM) and the Alliance for Academic Internal Medicine (AAIM), QSEA 2016 is a two-and-a-half-day course designed as a faculty development program. This year, QSEA will be held at Tempe Mission Palms Hotel and Conference Center in Tempe, Ariz., from May 23 to 25.
Attendees will enjoy a hands-on, interactive learning environment with a 10-to-1 student-to-faculty ratio. Participants will develop a professional network and leave with a tool kit of educational resources and curricular tools for quality and safety education.
Think QSEA is for you? Make plans to attend now if you are:
- A program director or assistant program director interested in acquiring new curricular ideas to help meet the ACGME requirements, which require residency programs to integrate quality and safety in their curriculum
- A medical school leader or clerkship director developing quality and safety curricula for students
- A faculty member beginning a new role or expanding an existing role in quality and safety education
- A quality and safety leader who wishes to extend influence and effectiveness by learning strategies to teach and engage trainees
QSEA has sold out each of the past four years, so don’t delay. Register online at sites.hospitalmedicine.org/qsea/register.html or via phone at 800-843-3360. Questions? Email [email protected]. TH
Brett Radler is SHM’s communications coordinator.
The demand for training in healthcare quality and patient safety, for both medical students and residents, has never been higher. The Quality and Safety Educators Academy (QSEA, sites.hospitalmedicine.org/qsea) responds to that demand by providing medical educators with the knowledge and tools to integrate quality improvement and safety concepts into their curricula.
Sponsored by the Society of Hospital Medicine (SHM) and the Alliance for Academic Internal Medicine (AAIM), QSEA 2016 is a two-and-a-half-day course designed as a faculty development program. This year, QSEA will be held at Tempe Mission Palms Hotel and Conference Center in Tempe, Ariz., from May 23 to 25.
Attendees will enjoy a hands-on, interactive learning environment with a 10-to-1 student-to-faculty ratio. Participants will develop a professional network and leave with a tool kit of educational resources and curricular tools for quality and safety education.
Think QSEA is for you? Make plans to attend now if you are:
- A program director or assistant program director interested in acquiring new curricular ideas to help meet the ACGME requirements, which require residency programs to integrate quality and safety in their curriculum
- A medical school leader or clerkship director developing quality and safety curricula for students
- A faculty member beginning a new role or expanding an existing role in quality and safety education
- A quality and safety leader who wishes to extend influence and effectiveness by learning strategies to teach and engage trainees
QSEA has sold out each of the past four years, so don’t delay. Register online at sites.hospitalmedicine.org/qsea/register.html or via phone at 800-843-3360. Questions? Email [email protected]. TH
Brett Radler is SHM’s communications coordinator.
The demand for training in healthcare quality and patient safety, for both medical students and residents, has never been higher. The Quality and Safety Educators Academy (QSEA, sites.hospitalmedicine.org/qsea) responds to that demand by providing medical educators with the knowledge and tools to integrate quality improvement and safety concepts into their curricula.
Sponsored by the Society of Hospital Medicine (SHM) and the Alliance for Academic Internal Medicine (AAIM), QSEA 2016 is a two-and-a-half-day course designed as a faculty development program. This year, QSEA will be held at Tempe Mission Palms Hotel and Conference Center in Tempe, Ariz., from May 23 to 25.
Attendees will enjoy a hands-on, interactive learning environment with a 10-to-1 student-to-faculty ratio. Participants will develop a professional network and leave with a tool kit of educational resources and curricular tools for quality and safety education.
Think QSEA is for you? Make plans to attend now if you are:
- A program director or assistant program director interested in acquiring new curricular ideas to help meet the ACGME requirements, which require residency programs to integrate quality and safety in their curriculum
- A medical school leader or clerkship director developing quality and safety curricula for students
- A faculty member beginning a new role or expanding an existing role in quality and safety education
- A quality and safety leader who wishes to extend influence and effectiveness by learning strategies to teach and engage trainees
QSEA has sold out each of the past four years, so don’t delay. Register online at sites.hospitalmedicine.org/qsea/register.html or via phone at 800-843-3360. Questions? Email [email protected]. TH
Brett Radler is SHM’s communications coordinator.