User login
Maximum Rosuvastatin, Atorvastatin Dosages Shrink Atheroma Equally
ORLANDO – Results from a head-to-head comparison of the two top statins on the U.S. market, rosuvastatin and atorvastatin, in more than 1,000 patients with coronary disease – a study apparently designed to more definitively prove rosuvastatin’s superiority – instead showed that atorvastatin was statistically indistinguishable from its somewhat more potent rival for the study’s primary end point.
With this finding coming just 2 weeks before atorvastatin’s expected availability as a substantially cheaper generic drug, the study – funded by AstraZeneca, the company that markets rosuvastatin (Crestor) – appeared to have the ironic consequence of convincing experts, as well as likely payers and patients, that generic atorvastatin will do just fine for most clinical situations.

And by testing maximum dosages of both drugs for 2 years of therapy and showing that both were "amazingly well tolerated" by patients, in the words of the study’s leader, Dr. Stephen J. Nicholls, the trial also added to existing evidence that intensive therapy using either agent was safe and should be accepted more readily by physicians and patients.
The results "add to the body of evidence that these two statins are safe and quite effective for reducing risk," commented Dr. Daniel J. Rader, professor of medicine and director of the preventive cardiology program at the University of Pennsylvania in Philadelphia.
"These were very high doses. Physicians don’t like to prescribe the highest doses, and patients don’t like to take them, because they don’t think they’re safe and that they don’t have added benefit. [This study] was a good opportunity to show, in more than 1,000 patients, that if you treat patients for 24 months, [these drugs] are actually very well tolerated, the safety profile looks very good, [and] you can regress disease and get very good lipid changes," said Dr. Nicholls, clinical director of the Cleveland Clinic Center for Clinical Research.
Dr. Nicholls also highlighted the "unprecedented" regression of coronary atheroma (the study’s primary efficacy measure) that was achieved in most study patients after 2 years of treatment with maximum dosages of either of the two statins. "It’s quite profound, the ability of the high doses of these therapies to remove lipid and reduce inflammation," he said at the annual scientific sessions of the American Heart Association. "It’s not a clinical marker," he acknowledged, "but it’s a reasonable surrogate, in that [coronary atheroma] is the pathology that ultimately causes events."
Until now, rosuvastatin was known to hold a modest but consistent edge over atorvastatin in its ability to lower blood levels of LDL cholesterol and also to produce a higher rise in HDL cholesterol, but the clinical meaning of these differences had not been established. Dr. Nicholls and his associates ran SATURN (Study of Coronary Atheroma by Intravascular Ultrasound: Effect of Rosuvastatin vs. Atorvastatin) to "compare the effect of maximal dosages of the most efficacious statin regimens on progression of coronary atherosclerosis," a 40-mg/day dosage or rosuvastatin and an 80-mg/day dosage of atorvastatin.
Simultaneously with Dr. Nicholls’ report at the meeting, the results appeared in an article online (N. Engl. J. Med. 2011 Nov. 15 [doi:10.1056/NEJMoa1110874]).
From January 2008 through June 2009, the researchers enrolled 1,578 patients with coronary disease at 208 centers. After randomization, patients underwent a 2-week run-in phase of treatment, receiving their assigned drug at half the study dose. This phase eliminated nearly 200 patients, although Dr. Nicholls said that most did not continue because of investigators’ inability to obtain a usable, baseline intravascular ultrasound (IVUS) image of the patient’s target artery, and not because of adverse effects of treatment. The 1,385 patients who remained in the study (691 on atorvastatin and 694 on rosuvastatin) had their dosage scaled up to the full study level and then remained on treatment for 104 weeks, after which they underwent follow-up IVUS imaging of their index coronary artery. The study’s primary end point was the change in percent atheroma volume from baseline to follow-up IVUS.
The results showed that this primary end point decreased by an average of 0.99% in the atorvastatin-treated patients, and by an average of 1.22% in those on rosuvastatin. Although each group had statistically significant atheroma shrinkage, compared with baseline, the two groups did not significantly differ from each other. The percentage of patients with atheroma shrinkage was 69% in the rosuvastatin group and 63% in the atorvastatin group, a difference that neared – but did not reach – statistical significance.

After 2 years of treatment, average LDL cholesterol levels were 70.2 mg/dL on atorvastatin and 62.6 mg/dL on rosuvastatin, a statistically significant difference. By the end of the study, the mean HDL cholesterol levels in the two groups stood at 48.6 mg/dL for those on atorvastatin and 50.4 mg/dL for those on rosuvastatin. Although this difference in HDL also was statistically significant, "we were somewhat surprised [that] the difference in HDL was not quite as large as we suspected," Dr. Nicholls said. "At the highest doses, the difference in HDL effect appears to dissipate."
Based on the primary end point results, "the study provides no basis to infer differential clinical benefit between atorvastatin and rosuvastatin," commented Dr. Darwin R. Labarthe, professor of preventive medicine at Northwestern University in Chicago and the designated discussant for the report at the meeting.
The study showed "a low number of clinical and biochemical adverse events in both groups," said Dr. Nicholls. An elevated ALT level occurred in 2.0% of the atorvastatin patients and in 0.7% of the rosuvastatin patients, a statistically significant difference. Proteinuria occurred in 3.8% of the rosuvastatin patients and in 1.7% of those on atorvastatin, also a statistically significant difference. No patient had rhabdomyolysis, and the two groups did not differ significantly in their rates of major adverse cardiovascular events, which occurred in 7.1% of the atorvastatin patients and in 7.5% of those on rosuvastatin.
Although Dr. Nicholls highlighted the high level of coronary-atheroma regression seen among most patients in both study arms, some experts dismissed the immediate importance of this finding without evidence for the association of this regression with clinical end points.

"The question is whether plaque stability is any different," commented Dr. Robert H. Eckel, professor of medicine and an atherosclerosis specialist at the University of Colorado at Denver, Aurora. "It is possible that with regression the plaque is more stable, but it is a surrogate marker. We don’t know whether that will translate into a clinical benefit." The U.S. cholesterol-treatment goals set by the National Heart, Lung, and Blood Institute, which are now in late stages of revision, "are directed by evidence-based outcomes," and hence the findings from SATURN "will not influence" goal revisions, he said in an interview.
Dr. Eckel and other experts also said they believe that the results would prod insurers and patients to focus more on treatment with generic atorvastatin and less on treatment with a pricier, proprietary rosuvastatin. "Price will drive treatment decisions," Dr. Eckel said. "In many cases, third-party payers and patients won’t pay for Crestor."
The SATURN study was sponsored by AstraZeneca, which markets rosuvastatin (Crestor). Dr. Nicholls said that he has been a consultant to and has received honoraria from AstraZeneca, Eli Lilly, Anthera, Omthera, Merck, Takeda, Resverlogix, Sanofi-Aventis, CSL Behring, Esperion, and Boehringer Ingelheim. He said he has received research support from AstraZeneca, Anthera, Eli Lilly, Novartis, Resverlogix, Roche, and LipoScience. Dr. Rader has been a consultant or advisor to Genentech, Merck, and Roche, and he has spoken on behalf of and has received research grants from Merck. Dr. Labarthe, Dr. Eckel, and Dr. Lloyd-Jones said that they had no relevant disclosures.
One of the most important things we can do for patients with cardiovascular disease is to get them on an intensive dosage of a potent statin. That’s the most effective way to reduce their risk for secondary events.
We already have substantial evidence on the safety of high-dose statins, particularly atorvastatin and increasingly with rosuvastatin as well. My hope is that by piling on here with additional safety data, physicians will become increasingly comfortable with using these medications at potent doses to achieve maximal LDL cholesterol lowering and really benefit patients. In SATURN, we see that intensive dosages of very potent statins are safe and effective [for lowering LDL cholesterol]. In SATURN, we did not see incremental benefit from one of the tested statins over the other.
Having generic atorvastatin available soon will be a real game changer. If payers then include atorvastatin among their class 1 medications that we can easily prescribe to patients, we’ll be able to get more patients to lower [LDL cholesterol levels] with a safe and well-tolerated drug.
The SATURN results don’t really change anything in clinical practice. The study looked at an intermediate marker of coronary disease – plaque volume – that does not really correlate well with the risk for secondary events. I would be more interested in seeing data on changes in the quality of the coronary plaque [such as] changes in the fibrous cap and lipid core. Those measures tend to correlate with events.
Donald M. Lloyd-Jones, M.D., is a cardiologist and chairman of the department of preventive medicine at Northwestern University in Chicago. He said that he has no disclosures. He made these comments in an interview.
One of the most important things we can do for patients with cardiovascular disease is to get them on an intensive dosage of a potent statin. That’s the most effective way to reduce their risk for secondary events.
We already have substantial evidence on the safety of high-dose statins, particularly atorvastatin and increasingly with rosuvastatin as well. My hope is that by piling on here with additional safety data, physicians will become increasingly comfortable with using these medications at potent doses to achieve maximal LDL cholesterol lowering and really benefit patients. In SATURN, we see that intensive dosages of very potent statins are safe and effective [for lowering LDL cholesterol]. In SATURN, we did not see incremental benefit from one of the tested statins over the other.
Having generic atorvastatin available soon will be a real game changer. If payers then include atorvastatin among their class 1 medications that we can easily prescribe to patients, we’ll be able to get more patients to lower [LDL cholesterol levels] with a safe and well-tolerated drug.
The SATURN results don’t really change anything in clinical practice. The study looked at an intermediate marker of coronary disease – plaque volume – that does not really correlate well with the risk for secondary events. I would be more interested in seeing data on changes in the quality of the coronary plaque [such as] changes in the fibrous cap and lipid core. Those measures tend to correlate with events.
Donald M. Lloyd-Jones, M.D., is a cardiologist and chairman of the department of preventive medicine at Northwestern University in Chicago. He said that he has no disclosures. He made these comments in an interview.
One of the most important things we can do for patients with cardiovascular disease is to get them on an intensive dosage of a potent statin. That’s the most effective way to reduce their risk for secondary events.
We already have substantial evidence on the safety of high-dose statins, particularly atorvastatin and increasingly with rosuvastatin as well. My hope is that by piling on here with additional safety data, physicians will become increasingly comfortable with using these medications at potent doses to achieve maximal LDL cholesterol lowering and really benefit patients. In SATURN, we see that intensive dosages of very potent statins are safe and effective [for lowering LDL cholesterol]. In SATURN, we did not see incremental benefit from one of the tested statins over the other.
Having generic atorvastatin available soon will be a real game changer. If payers then include atorvastatin among their class 1 medications that we can easily prescribe to patients, we’ll be able to get more patients to lower [LDL cholesterol levels] with a safe and well-tolerated drug.
The SATURN results don’t really change anything in clinical practice. The study looked at an intermediate marker of coronary disease – plaque volume – that does not really correlate well with the risk for secondary events. I would be more interested in seeing data on changes in the quality of the coronary plaque [such as] changes in the fibrous cap and lipid core. Those measures tend to correlate with events.
Donald M. Lloyd-Jones, M.D., is a cardiologist and chairman of the department of preventive medicine at Northwestern University in Chicago. He said that he has no disclosures. He made these comments in an interview.
ORLANDO – Results from a head-to-head comparison of the two top statins on the U.S. market, rosuvastatin and atorvastatin, in more than 1,000 patients with coronary disease – a study apparently designed to more definitively prove rosuvastatin’s superiority – instead showed that atorvastatin was statistically indistinguishable from its somewhat more potent rival for the study’s primary end point.
With this finding coming just 2 weeks before atorvastatin’s expected availability as a substantially cheaper generic drug, the study – funded by AstraZeneca, the company that markets rosuvastatin (Crestor) – appeared to have the ironic consequence of convincing experts, as well as likely payers and patients, that generic atorvastatin will do just fine for most clinical situations.
And by testing maximum dosages of both drugs for 2 years of therapy and showing that both were "amazingly well tolerated" by patients, in the words of the study’s leader, Dr. Stephen J. Nicholls, the trial also added to existing evidence that intensive therapy using either agent was safe and should be accepted more readily by physicians and patients.
The results "add to the body of evidence that these two statins are safe and quite effective for reducing risk," commented Dr. Daniel J. Rader, professor of medicine and director of the preventive cardiology program at the University of Pennsylvania in Philadelphia.
"These were very high doses. Physicians don’t like to prescribe the highest doses, and patients don’t like to take them, because they don’t think they’re safe and that they don’t have added benefit. [This study] was a good opportunity to show, in more than 1,000 patients, that if you treat patients for 24 months, [these drugs] are actually very well tolerated, the safety profile looks very good, [and] you can regress disease and get very good lipid changes," said Dr. Nicholls, clinical director of the Cleveland Clinic Center for Clinical Research.
Dr. Nicholls also highlighted the "unprecedented" regression of coronary atheroma (the study’s primary efficacy measure) that was achieved in most study patients after 2 years of treatment with maximum dosages of either of the two statins. "It’s quite profound, the ability of the high doses of these therapies to remove lipid and reduce inflammation," he said at the annual scientific sessions of the American Heart Association. "It’s not a clinical marker," he acknowledged, "but it’s a reasonable surrogate, in that [coronary atheroma] is the pathology that ultimately causes events."
Until now, rosuvastatin was known to hold a modest but consistent edge over atorvastatin in its ability to lower blood levels of LDL cholesterol and also to produce a higher rise in HDL cholesterol, but the clinical meaning of these differences had not been established. Dr. Nicholls and his associates ran SATURN (Study of Coronary Atheroma by Intravascular Ultrasound: Effect of Rosuvastatin vs. Atorvastatin) to "compare the effect of maximal dosages of the most efficacious statin regimens on progression of coronary atherosclerosis," a 40-mg/day dosage or rosuvastatin and an 80-mg/day dosage of atorvastatin.
Simultaneously with Dr. Nicholls’ report at the meeting, the results appeared in an article online (N. Engl. J. Med. 2011 Nov. 15 [doi:10.1056/NEJMoa1110874]).
From January 2008 through June 2009, the researchers enrolled 1,578 patients with coronary disease at 208 centers. After randomization, patients underwent a 2-week run-in phase of treatment, receiving their assigned drug at half the study dose. This phase eliminated nearly 200 patients, although Dr. Nicholls said that most did not continue because of investigators’ inability to obtain a usable, baseline intravascular ultrasound (IVUS) image of the patient’s target artery, and not because of adverse effects of treatment. The 1,385 patients who remained in the study (691 on atorvastatin and 694 on rosuvastatin) had their dosage scaled up to the full study level and then remained on treatment for 104 weeks, after which they underwent follow-up IVUS imaging of their index coronary artery. The study’s primary end point was the change in percent atheroma volume from baseline to follow-up IVUS.
The results showed that this primary end point decreased by an average of 0.99% in the atorvastatin-treated patients, and by an average of 1.22% in those on rosuvastatin. Although each group had statistically significant atheroma shrinkage, compared with baseline, the two groups did not significantly differ from each other. The percentage of patients with atheroma shrinkage was 69% in the rosuvastatin group and 63% in the atorvastatin group, a difference that neared – but did not reach – statistical significance.
After 2 years of treatment, average LDL cholesterol levels were 70.2 mg/dL on atorvastatin and 62.6 mg/dL on rosuvastatin, a statistically significant difference. By the end of the study, the mean HDL cholesterol levels in the two groups stood at 48.6 mg/dL for those on atorvastatin and 50.4 mg/dL for those on rosuvastatin. Although this difference in HDL also was statistically significant, "we were somewhat surprised [that] the difference in HDL was not quite as large as we suspected," Dr. Nicholls said. "At the highest doses, the difference in HDL effect appears to dissipate."
Based on the primary end point results, "the study provides no basis to infer differential clinical benefit between atorvastatin and rosuvastatin," commented Dr. Darwin R. Labarthe, professor of preventive medicine at Northwestern University in Chicago and the designated discussant for the report at the meeting.
The study showed "a low number of clinical and biochemical adverse events in both groups," said Dr. Nicholls. An elevated ALT level occurred in 2.0% of the atorvastatin patients and in 0.7% of the rosuvastatin patients, a statistically significant difference. Proteinuria occurred in 3.8% of the rosuvastatin patients and in 1.7% of those on atorvastatin, also a statistically significant difference. No patient had rhabdomyolysis, and the two groups did not differ significantly in their rates of major adverse cardiovascular events, which occurred in 7.1% of the atorvastatin patients and in 7.5% of those on rosuvastatin.
Although Dr. Nicholls highlighted the high level of coronary-atheroma regression seen among most patients in both study arms, some experts dismissed the immediate importance of this finding without evidence for the association of this regression with clinical end points.
"The question is whether plaque stability is any different," commented Dr. Robert H. Eckel, professor of medicine and an atherosclerosis specialist at the University of Colorado at Denver, Aurora. "It is possible that with regression the plaque is more stable, but it is a surrogate marker. We don’t know whether that will translate into a clinical benefit." The U.S. cholesterol-treatment goals set by the National Heart, Lung, and Blood Institute, which are now in late stages of revision, "are directed by evidence-based outcomes," and hence the findings from SATURN "will not influence" goal revisions, he said in an interview.
Dr. Eckel and other experts also said they believe that the results would prod insurers and patients to focus more on treatment with generic atorvastatin and less on treatment with a pricier, proprietary rosuvastatin. "Price will drive treatment decisions," Dr. Eckel said. "In many cases, third-party payers and patients won’t pay for Crestor."
The SATURN study was sponsored by AstraZeneca, which markets rosuvastatin (Crestor). Dr. Nicholls said that he has been a consultant to and has received honoraria from AstraZeneca, Eli Lilly, Anthera, Omthera, Merck, Takeda, Resverlogix, Sanofi-Aventis, CSL Behring, Esperion, and Boehringer Ingelheim. He said he has received research support from AstraZeneca, Anthera, Eli Lilly, Novartis, Resverlogix, Roche, and LipoScience. Dr. Rader has been a consultant or advisor to Genentech, Merck, and Roche, and he has spoken on behalf of and has received research grants from Merck. Dr. Labarthe, Dr. Eckel, and Dr. Lloyd-Jones said that they had no relevant disclosures.
ORLANDO – Results from a head-to-head comparison of the two top statins on the U.S. market, rosuvastatin and atorvastatin, in more than 1,000 patients with coronary disease – a study apparently designed to more definitively prove rosuvastatin’s superiority – instead showed that atorvastatin was statistically indistinguishable from its somewhat more potent rival for the study’s primary end point.
With this finding coming just 2 weeks before atorvastatin’s expected availability as a substantially cheaper generic drug, the study – funded by AstraZeneca, the company that markets rosuvastatin (Crestor) – appeared to have the ironic consequence of convincing experts, as well as likely payers and patients, that generic atorvastatin will do just fine for most clinical situations.
And by testing maximum dosages of both drugs for 2 years of therapy and showing that both were "amazingly well tolerated" by patients, in the words of the study’s leader, Dr. Stephen J. Nicholls, the trial also added to existing evidence that intensive therapy using either agent was safe and should be accepted more readily by physicians and patients.
The results "add to the body of evidence that these two statins are safe and quite effective for reducing risk," commented Dr. Daniel J. Rader, professor of medicine and director of the preventive cardiology program at the University of Pennsylvania in Philadelphia.
"These were very high doses. Physicians don’t like to prescribe the highest doses, and patients don’t like to take them, because they don’t think they’re safe and that they don’t have added benefit. [This study] was a good opportunity to show, in more than 1,000 patients, that if you treat patients for 24 months, [these drugs] are actually very well tolerated, the safety profile looks very good, [and] you can regress disease and get very good lipid changes," said Dr. Nicholls, clinical director of the Cleveland Clinic Center for Clinical Research.
Dr. Nicholls also highlighted the "unprecedented" regression of coronary atheroma (the study’s primary efficacy measure) that was achieved in most study patients after 2 years of treatment with maximum dosages of either of the two statins. "It’s quite profound, the ability of the high doses of these therapies to remove lipid and reduce inflammation," he said at the annual scientific sessions of the American Heart Association. "It’s not a clinical marker," he acknowledged, "but it’s a reasonable surrogate, in that [coronary atheroma] is the pathology that ultimately causes events."
Until now, rosuvastatin was known to hold a modest but consistent edge over atorvastatin in its ability to lower blood levels of LDL cholesterol and also to produce a higher rise in HDL cholesterol, but the clinical meaning of these differences had not been established. Dr. Nicholls and his associates ran SATURN (Study of Coronary Atheroma by Intravascular Ultrasound: Effect of Rosuvastatin vs. Atorvastatin) to "compare the effect of maximal dosages of the most efficacious statin regimens on progression of coronary atherosclerosis," a 40-mg/day dosage or rosuvastatin and an 80-mg/day dosage of atorvastatin.
Simultaneously with Dr. Nicholls’ report at the meeting, the results appeared in an article online (N. Engl. J. Med. 2011 Nov. 15 [doi:10.1056/NEJMoa1110874]).
From January 2008 through June 2009, the researchers enrolled 1,578 patients with coronary disease at 208 centers. After randomization, patients underwent a 2-week run-in phase of treatment, receiving their assigned drug at half the study dose. This phase eliminated nearly 200 patients, although Dr. Nicholls said that most did not continue because of investigators’ inability to obtain a usable, baseline intravascular ultrasound (IVUS) image of the patient’s target artery, and not because of adverse effects of treatment. The 1,385 patients who remained in the study (691 on atorvastatin and 694 on rosuvastatin) had their dosage scaled up to the full study level and then remained on treatment for 104 weeks, after which they underwent follow-up IVUS imaging of their index coronary artery. The study’s primary end point was the change in percent atheroma volume from baseline to follow-up IVUS.
The results showed that this primary end point decreased by an average of 0.99% in the atorvastatin-treated patients, and by an average of 1.22% in those on rosuvastatin. Although each group had statistically significant atheroma shrinkage, compared with baseline, the two groups did not significantly differ from each other. The percentage of patients with atheroma shrinkage was 69% in the rosuvastatin group and 63% in the atorvastatin group, a difference that neared – but did not reach – statistical significance.
After 2 years of treatment, average LDL cholesterol levels were 70.2 mg/dL on atorvastatin and 62.6 mg/dL on rosuvastatin, a statistically significant difference. By the end of the study, the mean HDL cholesterol levels in the two groups stood at 48.6 mg/dL for those on atorvastatin and 50.4 mg/dL for those on rosuvastatin. Although this difference in HDL also was statistically significant, "we were somewhat surprised [that] the difference in HDL was not quite as large as we suspected," Dr. Nicholls said. "At the highest doses, the difference in HDL effect appears to dissipate."
Based on the primary end point results, "the study provides no basis to infer differential clinical benefit between atorvastatin and rosuvastatin," commented Dr. Darwin R. Labarthe, professor of preventive medicine at Northwestern University in Chicago and the designated discussant for the report at the meeting.
The study showed "a low number of clinical and biochemical adverse events in both groups," said Dr. Nicholls. An elevated ALT level occurred in 2.0% of the atorvastatin patients and in 0.7% of the rosuvastatin patients, a statistically significant difference. Proteinuria occurred in 3.8% of the rosuvastatin patients and in 1.7% of those on atorvastatin, also a statistically significant difference. No patient had rhabdomyolysis, and the two groups did not differ significantly in their rates of major adverse cardiovascular events, which occurred in 7.1% of the atorvastatin patients and in 7.5% of those on rosuvastatin.
Although Dr. Nicholls highlighted the high level of coronary-atheroma regression seen among most patients in both study arms, some experts dismissed the immediate importance of this finding without evidence for the association of this regression with clinical end points.
"The question is whether plaque stability is any different," commented Dr. Robert H. Eckel, professor of medicine and an atherosclerosis specialist at the University of Colorado at Denver, Aurora. "It is possible that with regression the plaque is more stable, but it is a surrogate marker. We don’t know whether that will translate into a clinical benefit." The U.S. cholesterol-treatment goals set by the National Heart, Lung, and Blood Institute, which are now in late stages of revision, "are directed by evidence-based outcomes," and hence the findings from SATURN "will not influence" goal revisions, he said in an interview.
Dr. Eckel and other experts also said they believe that the results would prod insurers and patients to focus more on treatment with generic atorvastatin and less on treatment with a pricier, proprietary rosuvastatin. "Price will drive treatment decisions," Dr. Eckel said. "In many cases, third-party payers and patients won’t pay for Crestor."
The SATURN study was sponsored by AstraZeneca, which markets rosuvastatin (Crestor). Dr. Nicholls said that he has been a consultant to and has received honoraria from AstraZeneca, Eli Lilly, Anthera, Omthera, Merck, Takeda, Resverlogix, Sanofi-Aventis, CSL Behring, Esperion, and Boehringer Ingelheim. He said he has received research support from AstraZeneca, Anthera, Eli Lilly, Novartis, Resverlogix, Roche, and LipoScience. Dr. Rader has been a consultant or advisor to Genentech, Merck, and Roche, and he has spoken on behalf of and has received research grants from Merck. Dr. Labarthe, Dr. Eckel, and Dr. Lloyd-Jones said that they had no relevant disclosures.
FROM THE ANNUAL SCIENTIFIC SESSIONS OF THE AMERICAN HEART ASSOCIATION
Major Finding: At their maximal labeled dosages, 2 years of treatment with rosuvastatin or atorvastatin led to similar average levels of coronary atheroma volume shrinkage (1.22% and 0.99%, respectively), and were both safe and well tolerated.
Data Source: The SATURN study, which randomized 1,385 patients with coronary artery disease to 2 years of treatment with 40-mg/day rosuvastatin or 80-mg/day atorvastatin.
Disclosures: The SATURN study was sponsored by AstraZeneca, which markets rosuvastatin (Crestor). Dr. Nicholls said that he has been a consultant to and has received honoraria from AstraZeneca, Eli Lilly, Anthera, Omthera, Merck, Takeda, Resverlogix, Sanofi-Aventis, CSL Behring, Esperion, and Boehringer Ingelheim. He said he has received research support from AstraZeneca, Anthera, Eli Lilly, Novartis, Resverlogix, Roche, and LipoScience. Dr. Rader has been a consultant or advisor to Genentech, Merck, and Roche, and he has spoken on behalf of and has received research grants from Merck. Dr. Labarthe and Dr. Eckel said that they had no relevant disclosures.
Bone Marrow Cell Therapy Failed to Change Post-MI Outcomes
ORLANDO – Intracoronary delivery of bone marrow cell therapy 2 to 3 weeks after a first myocardial infarction is safe, but does not improve global or regional function at 6 months follow-up, results from a prospective, randomized controlled trial suggest.
Early trials dating back to 2006 suggested that the delivery of autologous bone marrow mononuclear cells (BMC) was feasible in clinical practice, safe, and potentially effective in increasing cardiac function. Predictors of efficacy appeared to be low ejection fraction and relatively late timing of BMC infusion at about 5 to 7 days post-myocardial infarction (MI), explained Dr. Thomas Eschenhagen, of the Hamburg (Germany) Institute of Experimental Pharmacology and Toxicology, who discussed the findings presented at the annual scientific sessions of the American Heart Association.
He suggested that possible reasons for the lack efficacy of BMC therapy in this latest trial, known as Late TIME (Use of Adult Autologous Stem Cells in Treating People 2 to 3 Weeks After Having a Heart Attack), may be the timing of the infusion more than 2 weeks after percutaneous intervention. In addition, the trial was small (87 patients), and the cells were not tested for efficiency in an animal model, although the in vitro data were convincing. But, he added, "It could as well mean that bone marrow cell therapy is inefficient."
Dr. Eschenhagen made a back-of-the-envelope calculation based on 11 BMC studies including Late TIME conducted from 2004 to 2011 that showed a mean weighted gain in left ventricle function of just 0.43%. The best results were reported early on in BOOST (BNP Therapy Observation Unit Outcomes Study), finding a 6% improvement in left ventricle ejection fraction (LVEF) between BMC and controls, while the 2011 BONAMI (BOne Marrow in Acute Myocardial Infarction) trial came in at the bottom of the list with an LVEF loss of 0.3%.
"Late TIME adds to a number of recent BMC trials with neutral outcome, arguing against the therapeutic efficacy of BMC therapy in acute or subacute MI," he concluded.

Among the 87 patients randomized in Late TIME, bone marrow aspiration and intracoronary infusion of 150 x 106 total nucleated cells was performed at a median of 17.4 days in the BMC group and 16.8 days in the placebo group following primary percutaneous intervention. It was thought that later delivery may be particularly important for patients initially too sick or who present to hospitals without the capacity to perform cell therapy, said study author, Dr. Jay Traverse, with the Minneapolis Heart Institute at Abbott Northwestern Hospital.
The high-risk cohort had predominantly large, anterior MIs and a mean LVEF of 36.4% in the 58 BMC patients and 35% in the 29 placebo patients. Their mean peak creatine kinase MB fraction was 234 and 318, respectively, two-third received a drug-eluting stent, and more than half were smokers or had hyperlipidemia.
At 6 months, there was a gain in LVEF of just 0.5% (48.7% to 49.2%) in the BMC group, compared with 3.5% (45.3% to 48.8%) in the placebo group, which was not significantly different (P value = .14), Dr. Traverse said.
The coprimary end point of change in wall motion also was similar at 6 months among the 81 evaluable patients. Wall motion in the infarct zone changed from a mean of 6.2 mm to 6.5 mm in the BMC group and from 4.9 mm to 5.9 mm in the placebo group. Wall motion in the border zone changed from a mean of 16 mm to 16.6 mm in the BMC group and from 16.1 mm to 19.3 mm in the placebo group.
Both groups experienced a similar change in infarct size and left ventricular volumes at 6 months, he said.
Only one death occurred in the placebo group and one repeat MI in the BMC group. Repeat revascularization was required in three placebo-treated patients and one patient receiving BMC therapy. Two patients in the placebo group required placement of an implantable cardioverter defibrillator and one BMC patient was hospitalized for heart failure. Total events significantly favored the BMC group at 5% vs. 17%, Dr. Traverse said.
The study was simultaneously published online (JAMA 2011 Nov. 14 [doi: doi:10.1001/jama.2011.1670]).
Late TIME was sponsored by the National Heart, Lung, and Blood Institute. Dr. Traverse reported no conflicts, and a coauthor reported serving as a consultant for Juventas Therapeutics and Aastrom Biosciences and grant funding from Athersys.
ORLANDO – Intracoronary delivery of bone marrow cell therapy 2 to 3 weeks after a first myocardial infarction is safe, but does not improve global or regional function at 6 months follow-up, results from a prospective, randomized controlled trial suggest.
Early trials dating back to 2006 suggested that the delivery of autologous bone marrow mononuclear cells (BMC) was feasible in clinical practice, safe, and potentially effective in increasing cardiac function. Predictors of efficacy appeared to be low ejection fraction and relatively late timing of BMC infusion at about 5 to 7 days post-myocardial infarction (MI), explained Dr. Thomas Eschenhagen, of the Hamburg (Germany) Institute of Experimental Pharmacology and Toxicology, who discussed the findings presented at the annual scientific sessions of the American Heart Association.
He suggested that possible reasons for the lack efficacy of BMC therapy in this latest trial, known as Late TIME (Use of Adult Autologous Stem Cells in Treating People 2 to 3 Weeks After Having a Heart Attack), may be the timing of the infusion more than 2 weeks after percutaneous intervention. In addition, the trial was small (87 patients), and the cells were not tested for efficiency in an animal model, although the in vitro data were convincing. But, he added, "It could as well mean that bone marrow cell therapy is inefficient."
Dr. Eschenhagen made a back-of-the-envelope calculation based on 11 BMC studies including Late TIME conducted from 2004 to 2011 that showed a mean weighted gain in left ventricle function of just 0.43%. The best results were reported early on in BOOST (BNP Therapy Observation Unit Outcomes Study), finding a 6% improvement in left ventricle ejection fraction (LVEF) between BMC and controls, while the 2011 BONAMI (BOne Marrow in Acute Myocardial Infarction) trial came in at the bottom of the list with an LVEF loss of 0.3%.
"Late TIME adds to a number of recent BMC trials with neutral outcome, arguing against the therapeutic efficacy of BMC therapy in acute or subacute MI," he concluded.
Among the 87 patients randomized in Late TIME, bone marrow aspiration and intracoronary infusion of 150 x 106 total nucleated cells was performed at a median of 17.4 days in the BMC group and 16.8 days in the placebo group following primary percutaneous intervention. It was thought that later delivery may be particularly important for patients initially too sick or who present to hospitals without the capacity to perform cell therapy, said study author, Dr. Jay Traverse, with the Minneapolis Heart Institute at Abbott Northwestern Hospital.
The high-risk cohort had predominantly large, anterior MIs and a mean LVEF of 36.4% in the 58 BMC patients and 35% in the 29 placebo patients. Their mean peak creatine kinase MB fraction was 234 and 318, respectively, two-third received a drug-eluting stent, and more than half were smokers or had hyperlipidemia.
At 6 months, there was a gain in LVEF of just 0.5% (48.7% to 49.2%) in the BMC group, compared with 3.5% (45.3% to 48.8%) in the placebo group, which was not significantly different (P value = .14), Dr. Traverse said.
The coprimary end point of change in wall motion also was similar at 6 months among the 81 evaluable patients. Wall motion in the infarct zone changed from a mean of 6.2 mm to 6.5 mm in the BMC group and from 4.9 mm to 5.9 mm in the placebo group. Wall motion in the border zone changed from a mean of 16 mm to 16.6 mm in the BMC group and from 16.1 mm to 19.3 mm in the placebo group.
Both groups experienced a similar change in infarct size and left ventricular volumes at 6 months, he said.
Only one death occurred in the placebo group and one repeat MI in the BMC group. Repeat revascularization was required in three placebo-treated patients and one patient receiving BMC therapy. Two patients in the placebo group required placement of an implantable cardioverter defibrillator and one BMC patient was hospitalized for heart failure. Total events significantly favored the BMC group at 5% vs. 17%, Dr. Traverse said.
The study was simultaneously published online (JAMA 2011 Nov. 14 [doi: doi:10.1001/jama.2011.1670]).
Late TIME was sponsored by the National Heart, Lung, and Blood Institute. Dr. Traverse reported no conflicts, and a coauthor reported serving as a consultant for Juventas Therapeutics and Aastrom Biosciences and grant funding from Athersys.
ORLANDO – Intracoronary delivery of bone marrow cell therapy 2 to 3 weeks after a first myocardial infarction is safe, but does not improve global or regional function at 6 months follow-up, results from a prospective, randomized controlled trial suggest.
Early trials dating back to 2006 suggested that the delivery of autologous bone marrow mononuclear cells (BMC) was feasible in clinical practice, safe, and potentially effective in increasing cardiac function. Predictors of efficacy appeared to be low ejection fraction and relatively late timing of BMC infusion at about 5 to 7 days post-myocardial infarction (MI), explained Dr. Thomas Eschenhagen, of the Hamburg (Germany) Institute of Experimental Pharmacology and Toxicology, who discussed the findings presented at the annual scientific sessions of the American Heart Association.
He suggested that possible reasons for the lack efficacy of BMC therapy in this latest trial, known as Late TIME (Use of Adult Autologous Stem Cells in Treating People 2 to 3 Weeks After Having a Heart Attack), may be the timing of the infusion more than 2 weeks after percutaneous intervention. In addition, the trial was small (87 patients), and the cells were not tested for efficiency in an animal model, although the in vitro data were convincing. But, he added, "It could as well mean that bone marrow cell therapy is inefficient."
Dr. Eschenhagen made a back-of-the-envelope calculation based on 11 BMC studies including Late TIME conducted from 2004 to 2011 that showed a mean weighted gain in left ventricle function of just 0.43%. The best results were reported early on in BOOST (BNP Therapy Observation Unit Outcomes Study), finding a 6% improvement in left ventricle ejection fraction (LVEF) between BMC and controls, while the 2011 BONAMI (BOne Marrow in Acute Myocardial Infarction) trial came in at the bottom of the list with an LVEF loss of 0.3%.
"Late TIME adds to a number of recent BMC trials with neutral outcome, arguing against the therapeutic efficacy of BMC therapy in acute or subacute MI," he concluded.
Among the 87 patients randomized in Late TIME, bone marrow aspiration and intracoronary infusion of 150 x 106 total nucleated cells was performed at a median of 17.4 days in the BMC group and 16.8 days in the placebo group following primary percutaneous intervention. It was thought that later delivery may be particularly important for patients initially too sick or who present to hospitals without the capacity to perform cell therapy, said study author, Dr. Jay Traverse, with the Minneapolis Heart Institute at Abbott Northwestern Hospital.
The high-risk cohort had predominantly large, anterior MIs and a mean LVEF of 36.4% in the 58 BMC patients and 35% in the 29 placebo patients. Their mean peak creatine kinase MB fraction was 234 and 318, respectively, two-third received a drug-eluting stent, and more than half were smokers or had hyperlipidemia.
At 6 months, there was a gain in LVEF of just 0.5% (48.7% to 49.2%) in the BMC group, compared with 3.5% (45.3% to 48.8%) in the placebo group, which was not significantly different (P value = .14), Dr. Traverse said.
The coprimary end point of change in wall motion also was similar at 6 months among the 81 evaluable patients. Wall motion in the infarct zone changed from a mean of 6.2 mm to 6.5 mm in the BMC group and from 4.9 mm to 5.9 mm in the placebo group. Wall motion in the border zone changed from a mean of 16 mm to 16.6 mm in the BMC group and from 16.1 mm to 19.3 mm in the placebo group.
Both groups experienced a similar change in infarct size and left ventricular volumes at 6 months, he said.
Only one death occurred in the placebo group and one repeat MI in the BMC group. Repeat revascularization was required in three placebo-treated patients and one patient receiving BMC therapy. Two patients in the placebo group required placement of an implantable cardioverter defibrillator and one BMC patient was hospitalized for heart failure. Total events significantly favored the BMC group at 5% vs. 17%, Dr. Traverse said.
The study was simultaneously published online (JAMA 2011 Nov. 14 [doi: doi:10.1001/jama.2011.1670]).
Late TIME was sponsored by the National Heart, Lung, and Blood Institute. Dr. Traverse reported no conflicts, and a coauthor reported serving as a consultant for Juventas Therapeutics and Aastrom Biosciences and grant funding from Athersys.
FROM THE ANNUAL SCIENTIFIC SESSIONS OF THE AMERICAN HEART ASSOCIATION
Major Finding: At 6 months, there was a gain in LVEF of just 0.5% (48.7% to 49.2%) in the BMC group, compared with 3.5% (45.3% to 48.8%) in the placebo group, which was not significantly different.
Data Source: A randomized, placebo-controlled trial involving 87 patients.
Disclosures: Late TIME was sponsored by the National Heart, Lung, and Blood Institute. Dr. Traverse reported no conflicts, and a coauthor reported serving as a consultant for Juventas Therapeutics and Aastrom Biosciences and grant funding from Athersys.
PALLAS Trial Demotes Dronedarone for Atrial Fibrillation
ORLANDO – A giant question mark now surrounds the antiarrhythmic agent dronedarone because of the drug’s surprisingly poor performance in a major randomized trial involving patients with permanent atrial fibrillation.
The hypothesis in the study known as PALLAS (Permanent Atrial fibriLLAtion Study) was that dronedarone (Multaq) would reduce major vascular events in patients with high-risk permanent atrial fibrillation (AF). Quite the opposite occurred. As a result, the international trial came to a screeching halt for safety reasons after only 30% of the planned 10,800 subjects were enrolled.
Prompting early termination of PALLAS was a disturbing 2.3-fold increase in the composite coprimary outcome consisting of stroke, MI, systemic embolism, or death from cardiovascular causes in the dronedarone group, compared with placebo-treated controls.
"It’s clear from our data that dronedarone should not be used in patients with permanent AF who have a high burden of vascular disease," Dr. Stuart J. Connolly, chair of the PALLAS steering committee, said in presenting the study results at the annual scientific sessions of the American Heart Association.
Dronedarone’s approved indication, based upon the results of the earlier ATHENA (A placebo-controlled, double-blind, parallel arm Trial to assess the efficacy of dronedarone 400 mg bid for the prevention of cardiovascular Hospitalization or death from any cause in patiENts with Atrial fibrillation/atrial flutter) trial, is to restore sinus rhythm and reduce hospitalizations for cardiovascular causes in patients with paroxysmal or persistent AF (N. Engl. J. Med. 2009;360:668-78). It is not approved for permanent AF.
The critical question now is whether the adverse results seen in PALLAS in patients with permanent AF apply to patients on dronedarone for the approved indication. Further data are needed in order to answer that question, but caution is appropriate, according to discussant Dr. Mark Estes III, professor of medicine at Tufts University and director of the cardiac arrhythmia center at Tufts Medical Center, Boston.
If physicians elect to initiate therapy with dronedarone, he said, they’d better make sure that patients possess the clinical profile of ATHENA-type patients: that is, paroxysmal or persistent AF and a low burden of vascular disease.
"Currently, I think patients taking dronedarone who fit the ATHENA profile should be monitored regularly – at least every 6 months – to ensure that they remain within the approved indication and don’t progress to permanent AF or new or worsening heart failure," Dr. Estes added.

Monitoring for progression from intermittent to permanent AF can be done quite easily by ECG, noted Dr. Connolly, chair of the PALLAS steering committee and professor of cardiology at McMaster University in Hamilton, Ont.
The impetus for organizing PALLAS was the finding in ATHENA that dronedarone not only decreased cardiovascular hospitalizations, it also reduced rates of death, MI, stroke, and systemic embolism in patients with intermittent AF, including the subgroup which developed permanent AF during the course of the study. These findings, along with dronedarone’s blood pressure–lowering and adrenergic blockade effects, encouraged investigators to think that the drug might also be beneficial in patients with permanent AF, a group for which there has been no effective therapy. And so PALLAS came about.
PALLAS participants had to be at least 65 years old and have had permanent AF for at least 6 months. They also had to have coronary artery disease, symptomatic heart failure, prior stroke or transient ischemic attack, peripheral arterial disease, and/or a left ventricular ejection fraction of 40% or less. Indeed, 69% of PALLAS participants had a history of symptomatic heart failure, compared with just 20% in ATHENA.
One possible contributor to the unfavorable outcomes in PALLAS was the fact that about one-third of study participants were on digoxin. Dronedarone increases the serum digoxin level, sometimes into a potentially toxic range. That could have played a causative role in the increased cardiovascular death rate, but it does not explain the puzzling increased risks of stroke and heart failure episodes, according to Dr. Connolly.
An important lesson provided by PALLAS, the cardiologist continued, is that the patient population with permanent AF is fundamentally different from others with AF.
"As cardiologists we’ve tended to think of AF as running along a continuum from short, intermittent episodes to more persistent episodes and finally to permanent AF, with some progression of vascular disease along the way. We think of it all as one disease process. This trial really makes us see that this is not the case. Something rather unique seems to have changed between the ATHENA-type population and the PALLAS population because of their dramatically different response to the same drug," he observed.
Simultaneous with Dr. Connolly’s presentation at the AHA meeting, the PALLAS results were published (N. Engl. J. Med. 2011 Nov. 14 [doi:10.1056/NEJMoa1109867]).
"It’s clear ... that dronedarone should not be used in patients with permanent AF who have a high burden of vascular disease."
In an accompanying editorial, Dr. Stanley Nattel of the Montreal Heart Institute referred to dronedarone in AF as a "Jekyll and Hyde" drug (N. Engl. J. Med. 2011 Nov. 14 [doi:10.1056/NEJMe1111997]). He said that exactly why dronedarone was so harmful in PALLAS and yet so beneficial in ATHENA may never be known for certain. Was the key factor in PALLAS the permanent AF, the high burden of vascular disease overall, the substantial prevalence of heart failure, or something else? Regardless, the PALLAS experience warrants a revised, far more limited role for dronedarone moving forward, according to Dr. Nattel.
Not only should dronedarone absolutely be avoided in patients with permanent AF, it should also be avoided in high-risk patients with intermittent AF, particularly if they have heart failure. If dronedarone is to be prescribed in patients on digoxin, dose adjustment of the digoxin is now clearly mandatory, he continued.
And the major guidelines for management of AF need to be reexamined. Since receiving marketing approval, dronedarone has figured prominently in the treatment algorithms for patients with paroxysmal or persistent AF. Now, however, it seems appropriate to reserve the antiarrhythmic for selected low-risk patients, and perhaps only those in whom other antiarrhythmic drugs have failed, Dr. Nattel said.
Dr. Estes disagreed. The latest AHA/American College of Cardiology guidelines characterize dronedarone as a reasonable drug for maintaining sinus rhythm in patients with recurrent paroxysmal or persistent AF who have no structural heart disease, or who have hypertension without left ventricular hypertrophy, or in those with CAD without heart failure (Circulation 2011;123:104-23).
"I think that these guidelines still apply," he said.
Dr. Connolly disclosed having received research grants and honoraria from Sanofi-Aventis, which sponsored PALLAS. Dr. Estes and Dr. Nattel reported no relevant financial interests.
ORLANDO – A giant question mark now surrounds the antiarrhythmic agent dronedarone because of the drug’s surprisingly poor performance in a major randomized trial involving patients with permanent atrial fibrillation.
The hypothesis in the study known as PALLAS (Permanent Atrial fibriLLAtion Study) was that dronedarone (Multaq) would reduce major vascular events in patients with high-risk permanent atrial fibrillation (AF). Quite the opposite occurred. As a result, the international trial came to a screeching halt for safety reasons after only 30% of the planned 10,800 subjects were enrolled.
Prompting early termination of PALLAS was a disturbing 2.3-fold increase in the composite coprimary outcome consisting of stroke, MI, systemic embolism, or death from cardiovascular causes in the dronedarone group, compared with placebo-treated controls.
"It’s clear from our data that dronedarone should not be used in patients with permanent AF who have a high burden of vascular disease," Dr. Stuart J. Connolly, chair of the PALLAS steering committee, said in presenting the study results at the annual scientific sessions of the American Heart Association.
Dronedarone’s approved indication, based upon the results of the earlier ATHENA (A placebo-controlled, double-blind, parallel arm Trial to assess the efficacy of dronedarone 400 mg bid for the prevention of cardiovascular Hospitalization or death from any cause in patiENts with Atrial fibrillation/atrial flutter) trial, is to restore sinus rhythm and reduce hospitalizations for cardiovascular causes in patients with paroxysmal or persistent AF (N. Engl. J. Med. 2009;360:668-78). It is not approved for permanent AF.
The critical question now is whether the adverse results seen in PALLAS in patients with permanent AF apply to patients on dronedarone for the approved indication. Further data are needed in order to answer that question, but caution is appropriate, according to discussant Dr. Mark Estes III, professor of medicine at Tufts University and director of the cardiac arrhythmia center at Tufts Medical Center, Boston.
If physicians elect to initiate therapy with dronedarone, he said, they’d better make sure that patients possess the clinical profile of ATHENA-type patients: that is, paroxysmal or persistent AF and a low burden of vascular disease.
"Currently, I think patients taking dronedarone who fit the ATHENA profile should be monitored regularly – at least every 6 months – to ensure that they remain within the approved indication and don’t progress to permanent AF or new or worsening heart failure," Dr. Estes added.
Monitoring for progression from intermittent to permanent AF can be done quite easily by ECG, noted Dr. Connolly, chair of the PALLAS steering committee and professor of cardiology at McMaster University in Hamilton, Ont.
The impetus for organizing PALLAS was the finding in ATHENA that dronedarone not only decreased cardiovascular hospitalizations, it also reduced rates of death, MI, stroke, and systemic embolism in patients with intermittent AF, including the subgroup which developed permanent AF during the course of the study. These findings, along with dronedarone’s blood pressure–lowering and adrenergic blockade effects, encouraged investigators to think that the drug might also be beneficial in patients with permanent AF, a group for which there has been no effective therapy. And so PALLAS came about.
PALLAS participants had to be at least 65 years old and have had permanent AF for at least 6 months. They also had to have coronary artery disease, symptomatic heart failure, prior stroke or transient ischemic attack, peripheral arterial disease, and/or a left ventricular ejection fraction of 40% or less. Indeed, 69% of PALLAS participants had a history of symptomatic heart failure, compared with just 20% in ATHENA.
One possible contributor to the unfavorable outcomes in PALLAS was the fact that about one-third of study participants were on digoxin. Dronedarone increases the serum digoxin level, sometimes into a potentially toxic range. That could have played a causative role in the increased cardiovascular death rate, but it does not explain the puzzling increased risks of stroke and heart failure episodes, according to Dr. Connolly.
An important lesson provided by PALLAS, the cardiologist continued, is that the patient population with permanent AF is fundamentally different from others with AF.
"As cardiologists we’ve tended to think of AF as running along a continuum from short, intermittent episodes to more persistent episodes and finally to permanent AF, with some progression of vascular disease along the way. We think of it all as one disease process. This trial really makes us see that this is not the case. Something rather unique seems to have changed between the ATHENA-type population and the PALLAS population because of their dramatically different response to the same drug," he observed.
Simultaneous with Dr. Connolly’s presentation at the AHA meeting, the PALLAS results were published (N. Engl. J. Med. 2011 Nov. 14 [doi:10.1056/NEJMoa1109867]).
"It’s clear ... that dronedarone should not be used in patients with permanent AF who have a high burden of vascular disease."
In an accompanying editorial, Dr. Stanley Nattel of the Montreal Heart Institute referred to dronedarone in AF as a "Jekyll and Hyde" drug (N. Engl. J. Med. 2011 Nov. 14 [doi:10.1056/NEJMe1111997]). He said that exactly why dronedarone was so harmful in PALLAS and yet so beneficial in ATHENA may never be known for certain. Was the key factor in PALLAS the permanent AF, the high burden of vascular disease overall, the substantial prevalence of heart failure, or something else? Regardless, the PALLAS experience warrants a revised, far more limited role for dronedarone moving forward, according to Dr. Nattel.
Not only should dronedarone absolutely be avoided in patients with permanent AF, it should also be avoided in high-risk patients with intermittent AF, particularly if they have heart failure. If dronedarone is to be prescribed in patients on digoxin, dose adjustment of the digoxin is now clearly mandatory, he continued.
And the major guidelines for management of AF need to be reexamined. Since receiving marketing approval, dronedarone has figured prominently in the treatment algorithms for patients with paroxysmal or persistent AF. Now, however, it seems appropriate to reserve the antiarrhythmic for selected low-risk patients, and perhaps only those in whom other antiarrhythmic drugs have failed, Dr. Nattel said.
Dr. Estes disagreed. The latest AHA/American College of Cardiology guidelines characterize dronedarone as a reasonable drug for maintaining sinus rhythm in patients with recurrent paroxysmal or persistent AF who have no structural heart disease, or who have hypertension without left ventricular hypertrophy, or in those with CAD without heart failure (Circulation 2011;123:104-23).
"I think that these guidelines still apply," he said.
Dr. Connolly disclosed having received research grants and honoraria from Sanofi-Aventis, which sponsored PALLAS. Dr. Estes and Dr. Nattel reported no relevant financial interests.
ORLANDO – A giant question mark now surrounds the antiarrhythmic agent dronedarone because of the drug’s surprisingly poor performance in a major randomized trial involving patients with permanent atrial fibrillation.
The hypothesis in the study known as PALLAS (Permanent Atrial fibriLLAtion Study) was that dronedarone (Multaq) would reduce major vascular events in patients with high-risk permanent atrial fibrillation (AF). Quite the opposite occurred. As a result, the international trial came to a screeching halt for safety reasons after only 30% of the planned 10,800 subjects were enrolled.
Prompting early termination of PALLAS was a disturbing 2.3-fold increase in the composite coprimary outcome consisting of stroke, MI, systemic embolism, or death from cardiovascular causes in the dronedarone group, compared with placebo-treated controls.
"It’s clear from our data that dronedarone should not be used in patients with permanent AF who have a high burden of vascular disease," Dr. Stuart J. Connolly, chair of the PALLAS steering committee, said in presenting the study results at the annual scientific sessions of the American Heart Association.
Dronedarone’s approved indication, based upon the results of the earlier ATHENA (A placebo-controlled, double-blind, parallel arm Trial to assess the efficacy of dronedarone 400 mg bid for the prevention of cardiovascular Hospitalization or death from any cause in patiENts with Atrial fibrillation/atrial flutter) trial, is to restore sinus rhythm and reduce hospitalizations for cardiovascular causes in patients with paroxysmal or persistent AF (N. Engl. J. Med. 2009;360:668-78). It is not approved for permanent AF.
The critical question now is whether the adverse results seen in PALLAS in patients with permanent AF apply to patients on dronedarone for the approved indication. Further data are needed in order to answer that question, but caution is appropriate, according to discussant Dr. Mark Estes III, professor of medicine at Tufts University and director of the cardiac arrhythmia center at Tufts Medical Center, Boston.
If physicians elect to initiate therapy with dronedarone, he said, they’d better make sure that patients possess the clinical profile of ATHENA-type patients: that is, paroxysmal or persistent AF and a low burden of vascular disease.
"Currently, I think patients taking dronedarone who fit the ATHENA profile should be monitored regularly – at least every 6 months – to ensure that they remain within the approved indication and don’t progress to permanent AF or new or worsening heart failure," Dr. Estes added.
Monitoring for progression from intermittent to permanent AF can be done quite easily by ECG, noted Dr. Connolly, chair of the PALLAS steering committee and professor of cardiology at McMaster University in Hamilton, Ont.
The impetus for organizing PALLAS was the finding in ATHENA that dronedarone not only decreased cardiovascular hospitalizations, it also reduced rates of death, MI, stroke, and systemic embolism in patients with intermittent AF, including the subgroup which developed permanent AF during the course of the study. These findings, along with dronedarone’s blood pressure–lowering and adrenergic blockade effects, encouraged investigators to think that the drug might also be beneficial in patients with permanent AF, a group for which there has been no effective therapy. And so PALLAS came about.
PALLAS participants had to be at least 65 years old and have had permanent AF for at least 6 months. They also had to have coronary artery disease, symptomatic heart failure, prior stroke or transient ischemic attack, peripheral arterial disease, and/or a left ventricular ejection fraction of 40% or less. Indeed, 69% of PALLAS participants had a history of symptomatic heart failure, compared with just 20% in ATHENA.
One possible contributor to the unfavorable outcomes in PALLAS was the fact that about one-third of study participants were on digoxin. Dronedarone increases the serum digoxin level, sometimes into a potentially toxic range. That could have played a causative role in the increased cardiovascular death rate, but it does not explain the puzzling increased risks of stroke and heart failure episodes, according to Dr. Connolly.
An important lesson provided by PALLAS, the cardiologist continued, is that the patient population with permanent AF is fundamentally different from others with AF.
"As cardiologists we’ve tended to think of AF as running along a continuum from short, intermittent episodes to more persistent episodes and finally to permanent AF, with some progression of vascular disease along the way. We think of it all as one disease process. This trial really makes us see that this is not the case. Something rather unique seems to have changed between the ATHENA-type population and the PALLAS population because of their dramatically different response to the same drug," he observed.
Simultaneous with Dr. Connolly’s presentation at the AHA meeting, the PALLAS results were published (N. Engl. J. Med. 2011 Nov. 14 [doi:10.1056/NEJMoa1109867]).
"It’s clear ... that dronedarone should not be used in patients with permanent AF who have a high burden of vascular disease."
In an accompanying editorial, Dr. Stanley Nattel of the Montreal Heart Institute referred to dronedarone in AF as a "Jekyll and Hyde" drug (N. Engl. J. Med. 2011 Nov. 14 [doi:10.1056/NEJMe1111997]). He said that exactly why dronedarone was so harmful in PALLAS and yet so beneficial in ATHENA may never be known for certain. Was the key factor in PALLAS the permanent AF, the high burden of vascular disease overall, the substantial prevalence of heart failure, or something else? Regardless, the PALLAS experience warrants a revised, far more limited role for dronedarone moving forward, according to Dr. Nattel.
Not only should dronedarone absolutely be avoided in patients with permanent AF, it should also be avoided in high-risk patients with intermittent AF, particularly if they have heart failure. If dronedarone is to be prescribed in patients on digoxin, dose adjustment of the digoxin is now clearly mandatory, he continued.
And the major guidelines for management of AF need to be reexamined. Since receiving marketing approval, dronedarone has figured prominently in the treatment algorithms for patients with paroxysmal or persistent AF. Now, however, it seems appropriate to reserve the antiarrhythmic for selected low-risk patients, and perhaps only those in whom other antiarrhythmic drugs have failed, Dr. Nattel said.
Dr. Estes disagreed. The latest AHA/American College of Cardiology guidelines characterize dronedarone as a reasonable drug for maintaining sinus rhythm in patients with recurrent paroxysmal or persistent AF who have no structural heart disease, or who have hypertension without left ventricular hypertrophy, or in those with CAD without heart failure (Circulation 2011;123:104-23).
"I think that these guidelines still apply," he said.
Dr. Connolly disclosed having received research grants and honoraria from Sanofi-Aventis, which sponsored PALLAS. Dr. Estes and Dr. Nattel reported no relevant financial interests.
FROM THE ANNUAL SCIENTIFIC SESSIONS OF THE AMERICAN HEART ASSOCIATION
Major Finding: Treatment with the antiarrhythmic agent dronedarone in patients with permanent atrial fibrillation resulted in roughly a 2.29-fold increase in the coprimary end point of stroke, MI, embolism, or cardiovascular death events, compared to placebo, and led to a halt in a planned 10,800-patient international randomized trial.
Data Source: PALLAS (Permanent Atrial fibriLLation Study), comprising 3,236 patients with permanent AF and major cardiovascular risk factors.
Disclosures: Dr. Connolly disclosed having received research grants and honoraria from Sanofi-Aventis, which sponsored PALLAS. Dr. Estes and Dr. Nattel reported no relevant financial interests.
Vitamin C Deficiency Ups Heart Risk
ORLANDO – Low vitamin C intake may worsen heart failure and put patients at a higher risk for cardiac events, according to a study conducted in three U.S. clinics.
The findings showed that patients who had low intakes of vitamin C were 2.4 times as likely to have higher levels of high-sensitivity C-reactive protein (hsCRP) – a marker for inflammation – compared with those who had high vitamin C intake. They also had shorter intervals without cardiac events.

In other words, "adequate intake of vitamin C was associated with longer survival in patients with heart failure," said Eun Kyeung Song, Ph.D., of the University of Ulsan (South Korea), who is the lead author of the study and a registered nurse.
The study, which is the first of its kind, was "provocative," and could lead to more investigations and larger studies to verify the findings, said Dr. Roger S. Blumenthal, director of preventive cardiology at Johns Hopkins University, Baltimore. He was not involved in the study.
"We generally attribute high CRP to increased weight in the midsection," said Dr. Blumenthal. "But this study suggests that it may be dietary inadequacies that may also increase inflammation and may be even a stronger predictor than just the CRP blood test by itself."
After taking a detailed, 4-day food diary, the authors measured the serum hsCRP of 212 patients at three outpatient heart failure clinics in Kentucky, Indiana, and Georgia during a 12-month follow-up.
Of the cohort, 82 patients (39%) had low vitamin C intake, as defined by the Institute of Medicine’s guidelines. In all, 98 (46%) had hsCRP greater than 3 mg/L, which is the cut-off point for being at high risk of having cardiac events. The patients with low vitamin C were 2.4 times more likely to have a high hsCRP level.
During the follow-up, 61 patients (29%) had cardiac events. After the authors controlled for age, sex, body mass index, New York Heart Association class, ejection fraction, comorbidities, total caloric intake, and medications, the results showed that the patients with low vitamin C levels were exactly twice as likely as those with adequate levels to have shorter cumulative cardiac event–free survival. Furthermore, those with hsCRP levels of at least 3 mg/L were 1.9 times as likely to have that outcome. Both differences were significant.
"Adequate intake of vitamin C was associated with longer survival in patients with heart failure."
"The data suggest that one possible mechanism by which vitamin C deficiency contributed to poor health outcomes is through inflammatory pathways in [heart failure] patients," they concluded.
"Diet is the best source of vitamin C," said Terry Lennie, Ph.D., one of the study authors and an associate dean at the University of Kentucky in Lexington. "Eating the recommended five servings of fruits and vegetables a day provides an adequate amount."
Dr. Blumenthal added that "sometimes we just talk to our patients about avoiding fast foods, and we don’t give as much positive reinforcement for things that are good for them to eat. ... We should go back to what our mothers and grandmothers told us, and try to have a more balanced diet and have more fruits and vegetables."
Dr. Lennie has received research grant from multiple extramural funders in the research area. Dr. Song and Dr. Blumenthal had no disclosures.
ORLANDO – Low vitamin C intake may worsen heart failure and put patients at a higher risk for cardiac events, according to a study conducted in three U.S. clinics.
The findings showed that patients who had low intakes of vitamin C were 2.4 times as likely to have higher levels of high-sensitivity C-reactive protein (hsCRP) – a marker for inflammation – compared with those who had high vitamin C intake. They also had shorter intervals without cardiac events.
In other words, "adequate intake of vitamin C was associated with longer survival in patients with heart failure," said Eun Kyeung Song, Ph.D., of the University of Ulsan (South Korea), who is the lead author of the study and a registered nurse.
The study, which is the first of its kind, was "provocative," and could lead to more investigations and larger studies to verify the findings, said Dr. Roger S. Blumenthal, director of preventive cardiology at Johns Hopkins University, Baltimore. He was not involved in the study.
"We generally attribute high CRP to increased weight in the midsection," said Dr. Blumenthal. "But this study suggests that it may be dietary inadequacies that may also increase inflammation and may be even a stronger predictor than just the CRP blood test by itself."
After taking a detailed, 4-day food diary, the authors measured the serum hsCRP of 212 patients at three outpatient heart failure clinics in Kentucky, Indiana, and Georgia during a 12-month follow-up.
Of the cohort, 82 patients (39%) had low vitamin C intake, as defined by the Institute of Medicine’s guidelines. In all, 98 (46%) had hsCRP greater than 3 mg/L, which is the cut-off point for being at high risk of having cardiac events. The patients with low vitamin C were 2.4 times more likely to have a high hsCRP level.
During the follow-up, 61 patients (29%) had cardiac events. After the authors controlled for age, sex, body mass index, New York Heart Association class, ejection fraction, comorbidities, total caloric intake, and medications, the results showed that the patients with low vitamin C levels were exactly twice as likely as those with adequate levels to have shorter cumulative cardiac event–free survival. Furthermore, those with hsCRP levels of at least 3 mg/L were 1.9 times as likely to have that outcome. Both differences were significant.
"Adequate intake of vitamin C was associated with longer survival in patients with heart failure."
"The data suggest that one possible mechanism by which vitamin C deficiency contributed to poor health outcomes is through inflammatory pathways in [heart failure] patients," they concluded.
"Diet is the best source of vitamin C," said Terry Lennie, Ph.D., one of the study authors and an associate dean at the University of Kentucky in Lexington. "Eating the recommended five servings of fruits and vegetables a day provides an adequate amount."
Dr. Blumenthal added that "sometimes we just talk to our patients about avoiding fast foods, and we don’t give as much positive reinforcement for things that are good for them to eat. ... We should go back to what our mothers and grandmothers told us, and try to have a more balanced diet and have more fruits and vegetables."
Dr. Lennie has received research grant from multiple extramural funders in the research area. Dr. Song and Dr. Blumenthal had no disclosures.
ORLANDO – Low vitamin C intake may worsen heart failure and put patients at a higher risk for cardiac events, according to a study conducted in three U.S. clinics.
The findings showed that patients who had low intakes of vitamin C were 2.4 times as likely to have higher levels of high-sensitivity C-reactive protein (hsCRP) – a marker for inflammation – compared with those who had high vitamin C intake. They also had shorter intervals without cardiac events.
In other words, "adequate intake of vitamin C was associated with longer survival in patients with heart failure," said Eun Kyeung Song, Ph.D., of the University of Ulsan (South Korea), who is the lead author of the study and a registered nurse.
The study, which is the first of its kind, was "provocative," and could lead to more investigations and larger studies to verify the findings, said Dr. Roger S. Blumenthal, director of preventive cardiology at Johns Hopkins University, Baltimore. He was not involved in the study.
"We generally attribute high CRP to increased weight in the midsection," said Dr. Blumenthal. "But this study suggests that it may be dietary inadequacies that may also increase inflammation and may be even a stronger predictor than just the CRP blood test by itself."
After taking a detailed, 4-day food diary, the authors measured the serum hsCRP of 212 patients at three outpatient heart failure clinics in Kentucky, Indiana, and Georgia during a 12-month follow-up.
Of the cohort, 82 patients (39%) had low vitamin C intake, as defined by the Institute of Medicine’s guidelines. In all, 98 (46%) had hsCRP greater than 3 mg/L, which is the cut-off point for being at high risk of having cardiac events. The patients with low vitamin C were 2.4 times more likely to have a high hsCRP level.
During the follow-up, 61 patients (29%) had cardiac events. After the authors controlled for age, sex, body mass index, New York Heart Association class, ejection fraction, comorbidities, total caloric intake, and medications, the results showed that the patients with low vitamin C levels were exactly twice as likely as those with adequate levels to have shorter cumulative cardiac event–free survival. Furthermore, those with hsCRP levels of at least 3 mg/L were 1.9 times as likely to have that outcome. Both differences were significant.
"Adequate intake of vitamin C was associated with longer survival in patients with heart failure."
"The data suggest that one possible mechanism by which vitamin C deficiency contributed to poor health outcomes is through inflammatory pathways in [heart failure] patients," they concluded.
"Diet is the best source of vitamin C," said Terry Lennie, Ph.D., one of the study authors and an associate dean at the University of Kentucky in Lexington. "Eating the recommended five servings of fruits and vegetables a day provides an adequate amount."
Dr. Blumenthal added that "sometimes we just talk to our patients about avoiding fast foods, and we don’t give as much positive reinforcement for things that are good for them to eat. ... We should go back to what our mothers and grandmothers told us, and try to have a more balanced diet and have more fruits and vegetables."
Dr. Lennie has received research grant from multiple extramural funders in the research area. Dr. Song and Dr. Blumenthal had no disclosures.
FROM THE ANNUAL SCIENTIFIC SESSIONS OF THE AMERICAN HEART ASSOCIATION
Major Finding: Patients who had low intakes of vitamin C were 2.4 times as likely to have higher levels of hsCRP – a marker for inflammation – compared with those who had high vitamin C intake. They also had shorter intervals without cardiac events.
Data Source: A study based on a detailed, 4-day food diary and measurement of serum hsCRP levels in 212 patients in three outpatient heart failure clinics during a 12-month follow-up.
Disclosures: Dr. Lennie has received research grants from multiple extramural funders in the research area. Dr. Song and Dr. Blumenthal had no disclosures.
Stem Cell Treatment of MI Yields 5-Year Benefit
ORLANDO – After 5-years of follow-up, the largest randomized trial done to date of stem cells placed into patients’ hearts following an acute myocardial infarction showed stable but modest improvement in ejection fraction as well as significant improvement in a combined clinical end point, a finding made possible by the lengthy follow-up.
"The improvement in global left ventricular function was sustained over 5 years, due to profound recovery of contractile function in infracted segments 5 years after administration of bone marrow cells," Dr. David M. Leistner said at the annual scientific sessions of the American Heart Association.

He reported 5-year follow-up data on 200 of the 204 acute MI patients initially enrolled in the Remodeling in Acute Myocardial Infarction (REPAIR-AMI) study, which randomized patients 3-7 days after successful reperfusion to receive an intracoronary infusion of autologous progenitor, mononuclear bone marrow cells (BMC) infused into the patient’s infarct-related artery, or a placebo infusion.
After 5 years, 16 BMC recipients who underwent measurement of their left ventricular ejection fraction had an average 5.9% improvement, compared with their baseline levels. In contrast, the 10 placebo patients who underwent ejection-fraction measurement at the 5-year follow-up had an average 3.3% decline in ejection fraction, compared with their baseline level, a statistically significant difference compared with the BMC-treated patients. These ejection fraction changes relative to baseline closely matched the 4-month follow-up findings, the primary end point from REPAIR-AMI, that the researchers previously reported (N. Engl. J. Med. 2006;355:1210-21).
Dr. Leistner and his associates had 5-year follow-up data for the clinical outcomes of 100 of the 101 patients originally randomized to BMC treatment and for 100 of the 103 patients originally in the placebo control group. After 5 years, the combined rate of death, MI, or need for revascularization was 64% in the placebo patients and 42% in the BMC patients, a statistically significant difference in a prespecified end point.
In a multivariate analysis, the patient’s change in left ventricular ejection infraction at 4 months after treatment was the only measured variable to significantly link with this combined clinical outcome. Patients with significant ejection fraction improvement after 4 months had a 19% reduced rate of the combined clinical end point event at 5 years, said Dr. Leistner, a cardiologist at Goethe University in Frankfurt am Main, Germany.
The 5-year clinical follow-up also showed suggestive trends of reduced rates of death from congestive heart failure and reduced heart failure hospitalization among the BMC patients. Three of the control patients and none of the BMC patients died from heart failure, and nine control patients and five BMC patients required hospitalization for heart failure during the follow-up period, he said.
The prolonged follow-up also showed no signs of increased rates of cancer, cardiac arrhythmia, syncope, or need for a pacemaker or implantable cardioverter defibrillator. "Initially, we were apprehensive about these potential adverse events," Dr. Leistner said.
A MRI assessment done in a subgroup of 16 BMC and 10 control patients also showed significantly more systolic wall thickening in the BMC-treated patients compared with the controls, extending an observation first made at the 4-month follow-up.
Based on these promising outcomes, the Frankfurt group will launch in January a new study of the same treatment protocol that plans to randomize about 3,000 patients and will have clinical outcomes after 2-3 years as the study’s primary end point. It will also include a MRI substudy that may be large enough to address how the BMC infusion acts, Dr. Leistner said.
The Bone Marrow Cells in Acute Myocardial Infarction (BAMI) study will be run at several centers throughout Europe, with funding coming from the European Union, said the lead investigator for this program, Dr. Andreas M. Zeiher, professor and chairman of the department of medicine at Goethe University.
Dr. Zeiher noted that several research groups have reported results from about 20 studies of stem cell therapy delivered into the myocardium of acute MI patients in an effort to improve ejection fraction and prevent heart failure development. Not only is the REPAIR-AMI study the largest of these and the one with the longest reported follow-up, but it is one of only four studies to report treatment efficacy.
A key problem with many of the failed studies was their use of heparin during delivery of the cells into the coronary circulation, Dr. Zeiher said in an interview.
Heparin treatment completely blocks the ability of cells to respond to cytokines and to enter the myocardium from coronary blood. Heparin-treated cells pass through the heart without adhering. The Frankfurt protocol uses heparin when withdrawing bone marrow cells, but after the researchers separate out the mononuclear cells they use serum to neutralize the heparin. When the cells are infused into the coronary circulation no heparin is used in the cell mixture nor is heparin administered to the patient. To prevent clotting during the treatment catheterization, the Frankfurt group administers bivalirudin, he explained.
Dr. Leistner said that he had no disclosures. Dr. Zeiher said he is a cofounder of and scientific advisor to t2cure, a company set up to run the BAMI trial, sponsored by the European Union.
The Frankfurt group’s report that the early, 4-month improvement in left ventricular ejection fraction that they reported several years ago was associated with better clinical outcomes after 5 years is an important finding. It’s notable that they found this association even though the improvement at 4 months was modest. In addition, this study remains the largest study of bone-marrow cell treatment of acute MI patients and now is also the study with the longest reported follow-up.
Investigators have reported mixed results over the past 10 years from several pilot studies that assessed stem cell treatment of myocardium following an acute MI. As recently as last week, at Transcatheter Cardiovascular Therapeutics 2011 in San Francisco, Wöhrle and his associates reported results from a study very similar to the design of the REPAIR-AMI study but without similar evidence of efficacy. The only apparent difference in the two protocols was that the Wöhrle study infused heparin-treated bone marrow–derived cells, while the Frankfurt group specifically avoided exposing these cells to heparin. Heparin treatment also may have played a role in other negative studies. Heparin changes cell surface receptors, perhaps preventing them from localizing in the myocardium.

|
|
Another recent report found positive short-term, 4-month results in a study that randomized 23 patients to an intracoronary infusion of cardiac stem cells (Lancet 2011; doi:10.1016/S0140-6736(11)61590-0).
A key issue currently unresolved is the mechanism by which the infused bone-marrow monocytes produce a beneficial effect. We know these cells do not differentiate into myocytes, nor do they trigger cardiomyogenesis. The cells may augment natural healing or activate endogenous repair, activate resident cardiac stem cells, stimulate angiogenesis, or mediate repair by a paracrine mechanism.
Stem cell treatment of the myocardium following an acute MI is a potentially exciting intervention. I encourage the Frankfurt researchers to pursue this potential in the expanded BAMI trial they have planned. But in addition to this attempt to obtain additional evidence for a clinical benefit from bone marrow cell treatment, further research is also needed to better define the mechanism by which this treatment leads to benefit.
Robert O. Bonow, M.D., is professor of cardiology at Northwestern University in Chicago. He said that he had no disclosures. He made these comments as the invited discussant for the report by Dr. Leistner and in an interview.
The Frankfurt group’s report that the early, 4-month improvement in left ventricular ejection fraction that they reported several years ago was associated with better clinical outcomes after 5 years is an important finding. It’s notable that they found this association even though the improvement at 4 months was modest. In addition, this study remains the largest study of bone-marrow cell treatment of acute MI patients and now is also the study with the longest reported follow-up.
Investigators have reported mixed results over the past 10 years from several pilot studies that assessed stem cell treatment of myocardium following an acute MI. As recently as last week, at Transcatheter Cardiovascular Therapeutics 2011 in San Francisco, Wöhrle and his associates reported results from a study very similar to the design of the REPAIR-AMI study but without similar evidence of efficacy. The only apparent difference in the two protocols was that the Wöhrle study infused heparin-treated bone marrow–derived cells, while the Frankfurt group specifically avoided exposing these cells to heparin. Heparin treatment also may have played a role in other negative studies. Heparin changes cell surface receptors, perhaps preventing them from localizing in the myocardium.
|
|
|
Another recent report found positive short-term, 4-month results in a study that randomized 23 patients to an intracoronary infusion of cardiac stem cells (Lancet 2011; doi:10.1016/S0140-6736(11)61590-0).
A key issue currently unresolved is the mechanism by which the infused bone-marrow monocytes produce a beneficial effect. We know these cells do not differentiate into myocytes, nor do they trigger cardiomyogenesis. The cells may augment natural healing or activate endogenous repair, activate resident cardiac stem cells, stimulate angiogenesis, or mediate repair by a paracrine mechanism.
Stem cell treatment of the myocardium following an acute MI is a potentially exciting intervention. I encourage the Frankfurt researchers to pursue this potential in the expanded BAMI trial they have planned. But in addition to this attempt to obtain additional evidence for a clinical benefit from bone marrow cell treatment, further research is also needed to better define the mechanism by which this treatment leads to benefit.
Robert O. Bonow, M.D., is professor of cardiology at Northwestern University in Chicago. He said that he had no disclosures. He made these comments as the invited discussant for the report by Dr. Leistner and in an interview.
The Frankfurt group’s report that the early, 4-month improvement in left ventricular ejection fraction that they reported several years ago was associated with better clinical outcomes after 5 years is an important finding. It’s notable that they found this association even though the improvement at 4 months was modest. In addition, this study remains the largest study of bone-marrow cell treatment of acute MI patients and now is also the study with the longest reported follow-up.
Investigators have reported mixed results over the past 10 years from several pilot studies that assessed stem cell treatment of myocardium following an acute MI. As recently as last week, at Transcatheter Cardiovascular Therapeutics 2011 in San Francisco, Wöhrle and his associates reported results from a study very similar to the design of the REPAIR-AMI study but without similar evidence of efficacy. The only apparent difference in the two protocols was that the Wöhrle study infused heparin-treated bone marrow–derived cells, while the Frankfurt group specifically avoided exposing these cells to heparin. Heparin treatment also may have played a role in other negative studies. Heparin changes cell surface receptors, perhaps preventing them from localizing in the myocardium.
|
|
|
Another recent report found positive short-term, 4-month results in a study that randomized 23 patients to an intracoronary infusion of cardiac stem cells (Lancet 2011; doi:10.1016/S0140-6736(11)61590-0).
A key issue currently unresolved is the mechanism by which the infused bone-marrow monocytes produce a beneficial effect. We know these cells do not differentiate into myocytes, nor do they trigger cardiomyogenesis. The cells may augment natural healing or activate endogenous repair, activate resident cardiac stem cells, stimulate angiogenesis, or mediate repair by a paracrine mechanism.
Stem cell treatment of the myocardium following an acute MI is a potentially exciting intervention. I encourage the Frankfurt researchers to pursue this potential in the expanded BAMI trial they have planned. But in addition to this attempt to obtain additional evidence for a clinical benefit from bone marrow cell treatment, further research is also needed to better define the mechanism by which this treatment leads to benefit.
Robert O. Bonow, M.D., is professor of cardiology at Northwestern University in Chicago. He said that he had no disclosures. He made these comments as the invited discussant for the report by Dr. Leistner and in an interview.
ORLANDO – After 5-years of follow-up, the largest randomized trial done to date of stem cells placed into patients’ hearts following an acute myocardial infarction showed stable but modest improvement in ejection fraction as well as significant improvement in a combined clinical end point, a finding made possible by the lengthy follow-up.
"The improvement in global left ventricular function was sustained over 5 years, due to profound recovery of contractile function in infracted segments 5 years after administration of bone marrow cells," Dr. David M. Leistner said at the annual scientific sessions of the American Heart Association.
He reported 5-year follow-up data on 200 of the 204 acute MI patients initially enrolled in the Remodeling in Acute Myocardial Infarction (REPAIR-AMI) study, which randomized patients 3-7 days after successful reperfusion to receive an intracoronary infusion of autologous progenitor, mononuclear bone marrow cells (BMC) infused into the patient’s infarct-related artery, or a placebo infusion.
After 5 years, 16 BMC recipients who underwent measurement of their left ventricular ejection fraction had an average 5.9% improvement, compared with their baseline levels. In contrast, the 10 placebo patients who underwent ejection-fraction measurement at the 5-year follow-up had an average 3.3% decline in ejection fraction, compared with their baseline level, a statistically significant difference compared with the BMC-treated patients. These ejection fraction changes relative to baseline closely matched the 4-month follow-up findings, the primary end point from REPAIR-AMI, that the researchers previously reported (N. Engl. J. Med. 2006;355:1210-21).
Dr. Leistner and his associates had 5-year follow-up data for the clinical outcomes of 100 of the 101 patients originally randomized to BMC treatment and for 100 of the 103 patients originally in the placebo control group. After 5 years, the combined rate of death, MI, or need for revascularization was 64% in the placebo patients and 42% in the BMC patients, a statistically significant difference in a prespecified end point.
In a multivariate analysis, the patient’s change in left ventricular ejection infraction at 4 months after treatment was the only measured variable to significantly link with this combined clinical outcome. Patients with significant ejection fraction improvement after 4 months had a 19% reduced rate of the combined clinical end point event at 5 years, said Dr. Leistner, a cardiologist at Goethe University in Frankfurt am Main, Germany.
The 5-year clinical follow-up also showed suggestive trends of reduced rates of death from congestive heart failure and reduced heart failure hospitalization among the BMC patients. Three of the control patients and none of the BMC patients died from heart failure, and nine control patients and five BMC patients required hospitalization for heart failure during the follow-up period, he said.
The prolonged follow-up also showed no signs of increased rates of cancer, cardiac arrhythmia, syncope, or need for a pacemaker or implantable cardioverter defibrillator. "Initially, we were apprehensive about these potential adverse events," Dr. Leistner said.
A MRI assessment done in a subgroup of 16 BMC and 10 control patients also showed significantly more systolic wall thickening in the BMC-treated patients compared with the controls, extending an observation first made at the 4-month follow-up.
Based on these promising outcomes, the Frankfurt group will launch in January a new study of the same treatment protocol that plans to randomize about 3,000 patients and will have clinical outcomes after 2-3 years as the study’s primary end point. It will also include a MRI substudy that may be large enough to address how the BMC infusion acts, Dr. Leistner said.
The Bone Marrow Cells in Acute Myocardial Infarction (BAMI) study will be run at several centers throughout Europe, with funding coming from the European Union, said the lead investigator for this program, Dr. Andreas M. Zeiher, professor and chairman of the department of medicine at Goethe University.
Dr. Zeiher noted that several research groups have reported results from about 20 studies of stem cell therapy delivered into the myocardium of acute MI patients in an effort to improve ejection fraction and prevent heart failure development. Not only is the REPAIR-AMI study the largest of these and the one with the longest reported follow-up, but it is one of only four studies to report treatment efficacy.
A key problem with many of the failed studies was their use of heparin during delivery of the cells into the coronary circulation, Dr. Zeiher said in an interview.
Heparin treatment completely blocks the ability of cells to respond to cytokines and to enter the myocardium from coronary blood. Heparin-treated cells pass through the heart without adhering. The Frankfurt protocol uses heparin when withdrawing bone marrow cells, but after the researchers separate out the mononuclear cells they use serum to neutralize the heparin. When the cells are infused into the coronary circulation no heparin is used in the cell mixture nor is heparin administered to the patient. To prevent clotting during the treatment catheterization, the Frankfurt group administers bivalirudin, he explained.
Dr. Leistner said that he had no disclosures. Dr. Zeiher said he is a cofounder of and scientific advisor to t2cure, a company set up to run the BAMI trial, sponsored by the European Union.
ORLANDO – After 5-years of follow-up, the largest randomized trial done to date of stem cells placed into patients’ hearts following an acute myocardial infarction showed stable but modest improvement in ejection fraction as well as significant improvement in a combined clinical end point, a finding made possible by the lengthy follow-up.
"The improvement in global left ventricular function was sustained over 5 years, due to profound recovery of contractile function in infracted segments 5 years after administration of bone marrow cells," Dr. David M. Leistner said at the annual scientific sessions of the American Heart Association.
He reported 5-year follow-up data on 200 of the 204 acute MI patients initially enrolled in the Remodeling in Acute Myocardial Infarction (REPAIR-AMI) study, which randomized patients 3-7 days after successful reperfusion to receive an intracoronary infusion of autologous progenitor, mononuclear bone marrow cells (BMC) infused into the patient’s infarct-related artery, or a placebo infusion.
After 5 years, 16 BMC recipients who underwent measurement of their left ventricular ejection fraction had an average 5.9% improvement, compared with their baseline levels. In contrast, the 10 placebo patients who underwent ejection-fraction measurement at the 5-year follow-up had an average 3.3% decline in ejection fraction, compared with their baseline level, a statistically significant difference compared with the BMC-treated patients. These ejection fraction changes relative to baseline closely matched the 4-month follow-up findings, the primary end point from REPAIR-AMI, that the researchers previously reported (N. Engl. J. Med. 2006;355:1210-21).
Dr. Leistner and his associates had 5-year follow-up data for the clinical outcomes of 100 of the 101 patients originally randomized to BMC treatment and for 100 of the 103 patients originally in the placebo control group. After 5 years, the combined rate of death, MI, or need for revascularization was 64% in the placebo patients and 42% in the BMC patients, a statistically significant difference in a prespecified end point.
In a multivariate analysis, the patient’s change in left ventricular ejection infraction at 4 months after treatment was the only measured variable to significantly link with this combined clinical outcome. Patients with significant ejection fraction improvement after 4 months had a 19% reduced rate of the combined clinical end point event at 5 years, said Dr. Leistner, a cardiologist at Goethe University in Frankfurt am Main, Germany.
The 5-year clinical follow-up also showed suggestive trends of reduced rates of death from congestive heart failure and reduced heart failure hospitalization among the BMC patients. Three of the control patients and none of the BMC patients died from heart failure, and nine control patients and five BMC patients required hospitalization for heart failure during the follow-up period, he said.
The prolonged follow-up also showed no signs of increased rates of cancer, cardiac arrhythmia, syncope, or need for a pacemaker or implantable cardioverter defibrillator. "Initially, we were apprehensive about these potential adverse events," Dr. Leistner said.
A MRI assessment done in a subgroup of 16 BMC and 10 control patients also showed significantly more systolic wall thickening in the BMC-treated patients compared with the controls, extending an observation first made at the 4-month follow-up.
Based on these promising outcomes, the Frankfurt group will launch in January a new study of the same treatment protocol that plans to randomize about 3,000 patients and will have clinical outcomes after 2-3 years as the study’s primary end point. It will also include a MRI substudy that may be large enough to address how the BMC infusion acts, Dr. Leistner said.
The Bone Marrow Cells in Acute Myocardial Infarction (BAMI) study will be run at several centers throughout Europe, with funding coming from the European Union, said the lead investigator for this program, Dr. Andreas M. Zeiher, professor and chairman of the department of medicine at Goethe University.
Dr. Zeiher noted that several research groups have reported results from about 20 studies of stem cell therapy delivered into the myocardium of acute MI patients in an effort to improve ejection fraction and prevent heart failure development. Not only is the REPAIR-AMI study the largest of these and the one with the longest reported follow-up, but it is one of only four studies to report treatment efficacy.
A key problem with many of the failed studies was their use of heparin during delivery of the cells into the coronary circulation, Dr. Zeiher said in an interview.
Heparin treatment completely blocks the ability of cells to respond to cytokines and to enter the myocardium from coronary blood. Heparin-treated cells pass through the heart without adhering. The Frankfurt protocol uses heparin when withdrawing bone marrow cells, but after the researchers separate out the mononuclear cells they use serum to neutralize the heparin. When the cells are infused into the coronary circulation no heparin is used in the cell mixture nor is heparin administered to the patient. To prevent clotting during the treatment catheterization, the Frankfurt group administers bivalirudin, he explained.
Dr. Leistner said that he had no disclosures. Dr. Zeiher said he is a cofounder of and scientific advisor to t2cure, a company set up to run the BAMI trial, sponsored by the European Union.
FROM THE ANNUAL SCIENTIFIC SESSIONS OF THE AMERICAN HEART ASSOCIATION
Major Finding: At 5-year follow-up, 100 acute MI patients treated with an intracoronary infusion of autologous bone-marrow derived mononuclear cells had a statistically significant one-third relative reduction in the incidence of death, incident MI, or need for revascularization compared with 100 patients who had received a placebo infusion.
Data Source: Five-year follow-up of the REPAIR-AMI study, which had clinical follow-up for 200 of the 204 acute MI patients randomized to treatment with an intracoronary infusion of autologous bone marrow-derived mononuclear cells or placebo.
Disclosures: Dr. Leistner said that he had no disclosures. Dr. Zeiher said he is a cofounder of and scientific advisor to t2cure, a company set up to run the BAMI trial, sponsored by the European Union.
Free Meds Boost Post-MI Outcomes, Rx Adherence
ORLANDO – Eliminating drug copayments for patients following a myocardial infarction reduced vascular events without increasing overall costs for insurers in the prospective randomized MI FREEE trial.
Although the Post-Myocardial Infarction Free Rx Event and Economic Evaluation trial had only a "modest" impact on medication adherence and missed its primary end point, the findings were dramatic enough that study sponsor Aetna has announced it will waive copayments for its post-MI patients beginning January 2013, lead author Dr. Niteesh Choudhry said at the annual scientific sessions of the American Heart Association.

"As the very first step in the idea of translation into practice, it’s not a flippant comment to say this could be translated tomorrow," he said. "The mechanisms we used are widely generalizable."
The trial randomly assigned 5,855 post-MI patients covered by Aetna to usual prescription coverage or full coverage so patients faced no copays for all brand and generic statins, beta-blockers, ACE inhibitors, or angiotensin-receptor blockers. Randomization occurred at about 49 days post discharge.
The trial’s primary composite end point of rate of major vascular event or revascularization was similar at 17.6 per 100 person-years for patients in the full coverage group vs. 18.8 per 100 person-years in the usual care group.
When evaluated separately, however, patients given free drugs had a statistically significant 14% decrease in major vascular events, defined as fatal or nonfatal MI, unstable angina, congestive heart failure or stroke, said Dr. Choudhry, an internist and researcher at Harvard Medical School in Boston.
The rate of stroke was also significantly reduced (HR 0.69).
In the full-coverage group, rates of medication adherence, defined as the number of days covered, increased 4.4% for beta-blockers, 6.2% for statins, 5.6% for ACE/ARBs, and by 5.4% to 43.9% for all three classes. Rates for full adherence, defined as the number of patients taking 80% of their medications, increased significantly, by 32%, 37%, 31% and 41%, respectively.
The low baseline adherence and small improvement in adherence in what should have been a highly motivated group of patients after MI was described as perhaps "the most sobering findings" of the trial in an editorial (N. Engl. J. Med. 2011 [doi:10.1056/NEJMe1111558]) that accompanied the simultaneous publication of the study (N. Engl. J. Med. 2011 [doi:10.1056/NEJMsa1107913]).
Invited discussant Dr. Eric Peterson, professor of medicine in cardiology and associate director of the Duke Clinical Research Institute in Durham, N.C., said MI FREEE highlights the huge challenge for post-MI secondary prevention, even when medications are given gratis.
"Adherence rates for any one of these medicines that can alter the course of disease with myocardial infarction was under 50%, and [when] combined, only one in 10 patients consistently took all three of these medicines," he said. "Thus, as Dr. Chaudhry noted, we need to get much better and have novel interventions to improve adherence long term."
Dr. Choudhry said the next step in their research is to provide financial incentives to patients to remain medication adherent.
"There are some concerns about paying patients, but providing positive financial incentives is the next step in the game," he said. "If you call this value-based insurance, we call that VBI 2.0. It’s the next innovation.
"From an economic perspective, you could come up with the amount of money that you’ve saved in copays and instead give that as a positive incentive."
Dr. Mariell Jessup, medical director of the Penn Heart and Vascular Center in Philadelphia, suggested that the trial may have had a better outcome if patients were notified the day they left the hospital that they were getting free drugs.
"I think that resets something," she said in an interview. "People are overwhelmed if they have a whole lot of pills to take and then they go to the drug store for the first time and get the bill, and we lose them."
One of the gaps in the study, however, is the failure to include clopidogrel (Plavix) and atorvastatin (Lipitor) in the equation, Dr. Jessup noted.
During a panel discussion of the study, AHA immediate past president Dr. Clyde Yancy, chief of cardiology at Northwestern University in Chicago, said clinicians and patients don’t always value the same clinical trial end points and that patients would likely view an intervention that is safe, effective, and saves them money as more than just a "modest" improvement.
"There are some concerns about paying patients, but providing positive financial incentives is the next step in the game."
As expected, rates of patient out-of-pocket spending in the full-coverage group dropped by 30% for drugs, but were also significantly cut for medical services by 18% and for total overall spending by 26%. This translated into a savings of $526 per patient over the trial, Dr. Chaudhry said.
Not surprisingly, pharmacy costs went up significantly for insurers in the full-coverage group by 8%, but there was also a nonsignificant decrease of 14% in spending for medical services and an 11% decrease in total spending. This translated into a savings of $18,254 for insurers.
While Aetna may have been impressed by MI FREEE, Dr. Yancy asked whether the researchers have taken the value-based insurance strategy to the Centers for Medicaid and Medicare Services.
Dr. Chaudhry responded that the CMS is the "big bear in the room," but suggested they see this as a "winning strategy" because they are on the hook for the same drugs, despite spending slightly less than private insurers on medical services.
Aetna and the Commonwealth Fund to Brigham and Women’s Hospital funded the trial. Dr. Choudhry reported receiving consulting fees from Mercer Health and Benefits and grants from CVS Caremark. Some of his coauthors are employees of, and have an equity interest in, Aetna.
ORLANDO – Eliminating drug copayments for patients following a myocardial infarction reduced vascular events without increasing overall costs for insurers in the prospective randomized MI FREEE trial.
Although the Post-Myocardial Infarction Free Rx Event and Economic Evaluation trial had only a "modest" impact on medication adherence and missed its primary end point, the findings were dramatic enough that study sponsor Aetna has announced it will waive copayments for its post-MI patients beginning January 2013, lead author Dr. Niteesh Choudhry said at the annual scientific sessions of the American Heart Association.
"As the very first step in the idea of translation into practice, it’s not a flippant comment to say this could be translated tomorrow," he said. "The mechanisms we used are widely generalizable."
The trial randomly assigned 5,855 post-MI patients covered by Aetna to usual prescription coverage or full coverage so patients faced no copays for all brand and generic statins, beta-blockers, ACE inhibitors, or angiotensin-receptor blockers. Randomization occurred at about 49 days post discharge.
The trial’s primary composite end point of rate of major vascular event or revascularization was similar at 17.6 per 100 person-years for patients in the full coverage group vs. 18.8 per 100 person-years in the usual care group.
When evaluated separately, however, patients given free drugs had a statistically significant 14% decrease in major vascular events, defined as fatal or nonfatal MI, unstable angina, congestive heart failure or stroke, said Dr. Choudhry, an internist and researcher at Harvard Medical School in Boston.
The rate of stroke was also significantly reduced (HR 0.69).
In the full-coverage group, rates of medication adherence, defined as the number of days covered, increased 4.4% for beta-blockers, 6.2% for statins, 5.6% for ACE/ARBs, and by 5.4% to 43.9% for all three classes. Rates for full adherence, defined as the number of patients taking 80% of their medications, increased significantly, by 32%, 37%, 31% and 41%, respectively.
The low baseline adherence and small improvement in adherence in what should have been a highly motivated group of patients after MI was described as perhaps "the most sobering findings" of the trial in an editorial (N. Engl. J. Med. 2011 [doi:10.1056/NEJMe1111558]) that accompanied the simultaneous publication of the study (N. Engl. J. Med. 2011 [doi:10.1056/NEJMsa1107913]).
Invited discussant Dr. Eric Peterson, professor of medicine in cardiology and associate director of the Duke Clinical Research Institute in Durham, N.C., said MI FREEE highlights the huge challenge for post-MI secondary prevention, even when medications are given gratis.
"Adherence rates for any one of these medicines that can alter the course of disease with myocardial infarction was under 50%, and [when] combined, only one in 10 patients consistently took all three of these medicines," he said. "Thus, as Dr. Chaudhry noted, we need to get much better and have novel interventions to improve adherence long term."
Dr. Choudhry said the next step in their research is to provide financial incentives to patients to remain medication adherent.
"There are some concerns about paying patients, but providing positive financial incentives is the next step in the game," he said. "If you call this value-based insurance, we call that VBI 2.0. It’s the next innovation.
"From an economic perspective, you could come up with the amount of money that you’ve saved in copays and instead give that as a positive incentive."
Dr. Mariell Jessup, medical director of the Penn Heart and Vascular Center in Philadelphia, suggested that the trial may have had a better outcome if patients were notified the day they left the hospital that they were getting free drugs.
"I think that resets something," she said in an interview. "People are overwhelmed if they have a whole lot of pills to take and then they go to the drug store for the first time and get the bill, and we lose them."
One of the gaps in the study, however, is the failure to include clopidogrel (Plavix) and atorvastatin (Lipitor) in the equation, Dr. Jessup noted.
During a panel discussion of the study, AHA immediate past president Dr. Clyde Yancy, chief of cardiology at Northwestern University in Chicago, said clinicians and patients don’t always value the same clinical trial end points and that patients would likely view an intervention that is safe, effective, and saves them money as more than just a "modest" improvement.
"There are some concerns about paying patients, but providing positive financial incentives is the next step in the game."
As expected, rates of patient out-of-pocket spending in the full-coverage group dropped by 30% for drugs, but were also significantly cut for medical services by 18% and for total overall spending by 26%. This translated into a savings of $526 per patient over the trial, Dr. Chaudhry said.
Not surprisingly, pharmacy costs went up significantly for insurers in the full-coverage group by 8%, but there was also a nonsignificant decrease of 14% in spending for medical services and an 11% decrease in total spending. This translated into a savings of $18,254 for insurers.
While Aetna may have been impressed by MI FREEE, Dr. Yancy asked whether the researchers have taken the value-based insurance strategy to the Centers for Medicaid and Medicare Services.
Dr. Chaudhry responded that the CMS is the "big bear in the room," but suggested they see this as a "winning strategy" because they are on the hook for the same drugs, despite spending slightly less than private insurers on medical services.
Aetna and the Commonwealth Fund to Brigham and Women’s Hospital funded the trial. Dr. Choudhry reported receiving consulting fees from Mercer Health and Benefits and grants from CVS Caremark. Some of his coauthors are employees of, and have an equity interest in, Aetna.
ORLANDO – Eliminating drug copayments for patients following a myocardial infarction reduced vascular events without increasing overall costs for insurers in the prospective randomized MI FREEE trial.
Although the Post-Myocardial Infarction Free Rx Event and Economic Evaluation trial had only a "modest" impact on medication adherence and missed its primary end point, the findings were dramatic enough that study sponsor Aetna has announced it will waive copayments for its post-MI patients beginning January 2013, lead author Dr. Niteesh Choudhry said at the annual scientific sessions of the American Heart Association.
"As the very first step in the idea of translation into practice, it’s not a flippant comment to say this could be translated tomorrow," he said. "The mechanisms we used are widely generalizable."
The trial randomly assigned 5,855 post-MI patients covered by Aetna to usual prescription coverage or full coverage so patients faced no copays for all brand and generic statins, beta-blockers, ACE inhibitors, or angiotensin-receptor blockers. Randomization occurred at about 49 days post discharge.
The trial’s primary composite end point of rate of major vascular event or revascularization was similar at 17.6 per 100 person-years for patients in the full coverage group vs. 18.8 per 100 person-years in the usual care group.
When evaluated separately, however, patients given free drugs had a statistically significant 14% decrease in major vascular events, defined as fatal or nonfatal MI, unstable angina, congestive heart failure or stroke, said Dr. Choudhry, an internist and researcher at Harvard Medical School in Boston.
The rate of stroke was also significantly reduced (HR 0.69).
In the full-coverage group, rates of medication adherence, defined as the number of days covered, increased 4.4% for beta-blockers, 6.2% for statins, 5.6% for ACE/ARBs, and by 5.4% to 43.9% for all three classes. Rates for full adherence, defined as the number of patients taking 80% of their medications, increased significantly, by 32%, 37%, 31% and 41%, respectively.
The low baseline adherence and small improvement in adherence in what should have been a highly motivated group of patients after MI was described as perhaps "the most sobering findings" of the trial in an editorial (N. Engl. J. Med. 2011 [doi:10.1056/NEJMe1111558]) that accompanied the simultaneous publication of the study (N. Engl. J. Med. 2011 [doi:10.1056/NEJMsa1107913]).
Invited discussant Dr. Eric Peterson, professor of medicine in cardiology and associate director of the Duke Clinical Research Institute in Durham, N.C., said MI FREEE highlights the huge challenge for post-MI secondary prevention, even when medications are given gratis.
"Adherence rates for any one of these medicines that can alter the course of disease with myocardial infarction was under 50%, and [when] combined, only one in 10 patients consistently took all three of these medicines," he said. "Thus, as Dr. Chaudhry noted, we need to get much better and have novel interventions to improve adherence long term."
Dr. Choudhry said the next step in their research is to provide financial incentives to patients to remain medication adherent.
"There are some concerns about paying patients, but providing positive financial incentives is the next step in the game," he said. "If you call this value-based insurance, we call that VBI 2.0. It’s the next innovation.
"From an economic perspective, you could come up with the amount of money that you’ve saved in copays and instead give that as a positive incentive."
Dr. Mariell Jessup, medical director of the Penn Heart and Vascular Center in Philadelphia, suggested that the trial may have had a better outcome if patients were notified the day they left the hospital that they were getting free drugs.
"I think that resets something," she said in an interview. "People are overwhelmed if they have a whole lot of pills to take and then they go to the drug store for the first time and get the bill, and we lose them."
One of the gaps in the study, however, is the failure to include clopidogrel (Plavix) and atorvastatin (Lipitor) in the equation, Dr. Jessup noted.
During a panel discussion of the study, AHA immediate past president Dr. Clyde Yancy, chief of cardiology at Northwestern University in Chicago, said clinicians and patients don’t always value the same clinical trial end points and that patients would likely view an intervention that is safe, effective, and saves them money as more than just a "modest" improvement.
"There are some concerns about paying patients, but providing positive financial incentives is the next step in the game."
As expected, rates of patient out-of-pocket spending in the full-coverage group dropped by 30% for drugs, but were also significantly cut for medical services by 18% and for total overall spending by 26%. This translated into a savings of $526 per patient over the trial, Dr. Chaudhry said.
Not surprisingly, pharmacy costs went up significantly for insurers in the full-coverage group by 8%, but there was also a nonsignificant decrease of 14% in spending for medical services and an 11% decrease in total spending. This translated into a savings of $18,254 for insurers.
While Aetna may have been impressed by MI FREEE, Dr. Yancy asked whether the researchers have taken the value-based insurance strategy to the Centers for Medicaid and Medicare Services.
Dr. Chaudhry responded that the CMS is the "big bear in the room," but suggested they see this as a "winning strategy" because they are on the hook for the same drugs, despite spending slightly less than private insurers on medical services.
Aetna and the Commonwealth Fund to Brigham and Women’s Hospital funded the trial. Dr. Choudhry reported receiving consulting fees from Mercer Health and Benefits and grants from CVS Caremark. Some of his coauthors are employees of, and have an equity interest in, Aetna.
FROM THE ANNUAL SCIENTIFIC SESSIONS OF THE AMERICAN HEART ASSOCIATION
Major Finding: Post-MI patients given free drugs had a statistically significant 14% decrease in major vascular events, defined as fatal or nonfatal MI, unstable angina, congestive heart failure, or stroke.
Data Source: Randomized trial involving 5,855 patients covered by Aetna recently hospitalized with a myocardial infarction.
Disclosures: Aetna and the Commonwealth Fund to Brigham and Women’s Hospital funded the trial. Dr. Choudhry reported receiving consulting fees from Mercer Health and Benefits and grants from CVS Caremark. Some of his coauthors are employees of, and have an equity interest in, Aetna.
Weight Loss Modest With Primary Care Program
Enhanced brief lifestyle counseling by a primary care team helped about one-third of obese patients lose and keep off 5% or more of their baseline weight after 2 years, according to a study published online Nov. 14 in the New England Journal of Medicine and simultaneously presented at the annual meeting of the American Heart Association.
However, many of the patients during the study’s second year regained at least some of the lost weight, confirming "the problem of weight regain despite ongoing counseling for weight-loss maintenance," the study’s authors noted.
The intervention involved quarterly visits with a primary care physician, brief lifestyle coaching delivered monthly by a medical assistant, and the use of meal replacements or weight-loss medication.
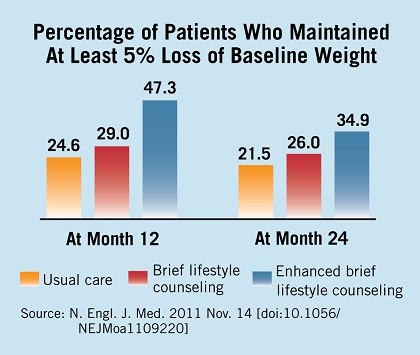
The average weight loss of 4.7%, most of which was maintained for 2 years and was accompanied by improvements in some cardiovascular risk factors, was greater than that observed in other primary care trials, said Thomas A. Wadden, Ph.D., of the department of psychiatry at the University of Pennsylvania, Philadelphia, and his associates (N. Engl. J. Med. 2011 Nov. 14 [doi:10.1056/NEJMoa1109220]).
The results of the 2-year study of 390 obese patients demonstrate that "primary care physicians could help a considerable minority of obese persons achieve clinically meaningful weight loss, which they may not achieve if they were simply told to reduce their weight on their own," the investigators noted.
Dr. Wadden and his colleagues conducted the POWER-UP (Practice-based Opportunities for Weight Reduction trial at the University of Pennsylvania) study at three primary care practices in urban settings and three in suburban settings. A total of 30 primary care physicians took part.
The study enrolled 311 women and 79 men, with a mean age of 52 years, a mean body weight of 108 kg, and a mean body mass index of 39 kg/m2 at baseline. By patient self-report, approximately 59% were white, 38.5% were black, and 4.6% were Hispanic.
The study participants all had the same dietary and activity goals but were given different levels of support to achieve them.
All were instructed to gradually increase their physical activity to 180 min/wk. Those who weighed less than 113 kg were prescribed a diet of 1,200-1,500 kcal/day, while those who were heavier were prescribed 1,500-1,800 kcal/day.
A total of 130 patients were randomly assigned to receive usual care, which consisted of quarterly visits in which their primary care physician spent 5-7 minutes discussing the weight-loss information and reviewing any weight change.
Another 131 were randomly assigned to that same care plus brief lifestyle counseling, in which they spent 10-15 min/mo with a medical assistant, called a "lifestyle coach," who conducted a weigh-in, reviewed a diary of food intake, reviewed a physical activity diary, and delivered abbreviated lessons from the Diabetes Prevention Program.
Another 129 patients were randomly assigned to receive enhanced lifestyle counseling, which included that same intervention plus their choice of taking sibutramine, orlistat, or meal replacements under the guidance of the primary care physician. Sibutramine was withdrawn from the market during the trial, and patients in that group were switched to orlistat or meal replacements.
Patients taking meal replacements were instructed to substitute two meals and one snack every day with Slim-Fast shakes or meal bars for the first 4 months, and to replace one meal and one snack each day for the remainder of the study.
The primary outcome was weight loss at 2 years. Enhanced lifestyle counseling produced significantly greater weight loss (mean, 4.6 kg) than either lifestyle counseling (2.9 kg) or usual care (1.7 kg). Within the group receiving enhanced lifestyle counseling, there were no significant differences in weight loss among those taking meal replacements (67 patients), sibutramine (38 patients), or orlistat (24 patients).
The differences among the groups were first evident at 6 months, and maximal weight loss was achieved at 12 months. Between year 1 and year 2, however, most patients regained at least some of the weight they had lost.
Secondary outcomes also were significantly better in the group that received enhanced lifestyle counseling than in the usual-care group, including the percentage of patients whose weight was at or below their baseline weight at 1 year (72.1% vs. 59.2%) and 2 years (67.4% vs. 53.1%); the percentages who lost 5% or more of their baseline weight at 1 year (47.3% vs. 24.6%) and 2 years (34.9% vs. 21.5%); and the percentages who lost 10% or more of their baseline weight at 1 year (25.6% vs. 3.9%) and 2 years (17.8% vs. 6.2%).
Patients who received enhanced lifestyle counseling showed significantly greater improvements in waist circumference, HDL cholesterol levels, and triglyceride levels, but not in LDL cholesterol levels or blood pressure.
There were 73 hospitalizations for severe adverse events, with no significant differences among the three study groups. Only three such events were deemed to be possibly related to the intervention: two cholecystectomies, and one case of syncope. In addition, sibutramine was discontinued in seven patients because of blood pressure elevation, tachycardia, or anxiety; and orlistat was discontinued in five patients because of gastrointestinal symptoms.
"Although our study has shown that primary care personnel can provide effective weight-management support, it has not addressed the more challenging question of who will pay for these or related weight-loss interventions," the researchers noted.
The National Heart, Lung, and Blood Institute funded the study. Dr. Wadden reported ties to Novo Nordisk, Orexigen, Vivus, Nutrisystem, Guilford Press, and the Cardiometabolic Support Network. His associates reported ties to numerous industry sources. Orlistat and Slim-Fast products were provided free of charge by the manufacturers, GlaxoSmithKline and Unilever.
Enhanced brief lifestyle counseling by a primary care team helped about one-third of obese patients lose and keep off 5% or more of their baseline weight after 2 years, according to a study published online Nov. 14 in the New England Journal of Medicine and simultaneously presented at the annual meeting of the American Heart Association.
However, many of the patients during the study’s second year regained at least some of the lost weight, confirming "the problem of weight regain despite ongoing counseling for weight-loss maintenance," the study’s authors noted.
The intervention involved quarterly visits with a primary care physician, brief lifestyle coaching delivered monthly by a medical assistant, and the use of meal replacements or weight-loss medication.
The average weight loss of 4.7%, most of which was maintained for 2 years and was accompanied by improvements in some cardiovascular risk factors, was greater than that observed in other primary care trials, said Thomas A. Wadden, Ph.D., of the department of psychiatry at the University of Pennsylvania, Philadelphia, and his associates (N. Engl. J. Med. 2011 Nov. 14 [doi:10.1056/NEJMoa1109220]).
The results of the 2-year study of 390 obese patients demonstrate that "primary care physicians could help a considerable minority of obese persons achieve clinically meaningful weight loss, which they may not achieve if they were simply told to reduce their weight on their own," the investigators noted.
Dr. Wadden and his colleagues conducted the POWER-UP (Practice-based Opportunities for Weight Reduction trial at the University of Pennsylvania) study at three primary care practices in urban settings and three in suburban settings. A total of 30 primary care physicians took part.
The study enrolled 311 women and 79 men, with a mean age of 52 years, a mean body weight of 108 kg, and a mean body mass index of 39 kg/m2 at baseline. By patient self-report, approximately 59% were white, 38.5% were black, and 4.6% were Hispanic.
The study participants all had the same dietary and activity goals but were given different levels of support to achieve them.
All were instructed to gradually increase their physical activity to 180 min/wk. Those who weighed less than 113 kg were prescribed a diet of 1,200-1,500 kcal/day, while those who were heavier were prescribed 1,500-1,800 kcal/day.
A total of 130 patients were randomly assigned to receive usual care, which consisted of quarterly visits in which their primary care physician spent 5-7 minutes discussing the weight-loss information and reviewing any weight change.
Another 131 were randomly assigned to that same care plus brief lifestyle counseling, in which they spent 10-15 min/mo with a medical assistant, called a "lifestyle coach," who conducted a weigh-in, reviewed a diary of food intake, reviewed a physical activity diary, and delivered abbreviated lessons from the Diabetes Prevention Program.
Another 129 patients were randomly assigned to receive enhanced lifestyle counseling, which included that same intervention plus their choice of taking sibutramine, orlistat, or meal replacements under the guidance of the primary care physician. Sibutramine was withdrawn from the market during the trial, and patients in that group were switched to orlistat or meal replacements.
Patients taking meal replacements were instructed to substitute two meals and one snack every day with Slim-Fast shakes or meal bars for the first 4 months, and to replace one meal and one snack each day for the remainder of the study.
The primary outcome was weight loss at 2 years. Enhanced lifestyle counseling produced significantly greater weight loss (mean, 4.6 kg) than either lifestyle counseling (2.9 kg) or usual care (1.7 kg). Within the group receiving enhanced lifestyle counseling, there were no significant differences in weight loss among those taking meal replacements (67 patients), sibutramine (38 patients), or orlistat (24 patients).
The differences among the groups were first evident at 6 months, and maximal weight loss was achieved at 12 months. Between year 1 and year 2, however, most patients regained at least some of the weight they had lost.
Secondary outcomes also were significantly better in the group that received enhanced lifestyle counseling than in the usual-care group, including the percentage of patients whose weight was at or below their baseline weight at 1 year (72.1% vs. 59.2%) and 2 years (67.4% vs. 53.1%); the percentages who lost 5% or more of their baseline weight at 1 year (47.3% vs. 24.6%) and 2 years (34.9% vs. 21.5%); and the percentages who lost 10% or more of their baseline weight at 1 year (25.6% vs. 3.9%) and 2 years (17.8% vs. 6.2%).
Patients who received enhanced lifestyle counseling showed significantly greater improvements in waist circumference, HDL cholesterol levels, and triglyceride levels, but not in LDL cholesterol levels or blood pressure.
There were 73 hospitalizations for severe adverse events, with no significant differences among the three study groups. Only three such events were deemed to be possibly related to the intervention: two cholecystectomies, and one case of syncope. In addition, sibutramine was discontinued in seven patients because of blood pressure elevation, tachycardia, or anxiety; and orlistat was discontinued in five patients because of gastrointestinal symptoms.
"Although our study has shown that primary care personnel can provide effective weight-management support, it has not addressed the more challenging question of who will pay for these or related weight-loss interventions," the researchers noted.
The National Heart, Lung, and Blood Institute funded the study. Dr. Wadden reported ties to Novo Nordisk, Orexigen, Vivus, Nutrisystem, Guilford Press, and the Cardiometabolic Support Network. His associates reported ties to numerous industry sources. Orlistat and Slim-Fast products were provided free of charge by the manufacturers, GlaxoSmithKline and Unilever.
Enhanced brief lifestyle counseling by a primary care team helped about one-third of obese patients lose and keep off 5% or more of their baseline weight after 2 years, according to a study published online Nov. 14 in the New England Journal of Medicine and simultaneously presented at the annual meeting of the American Heart Association.
However, many of the patients during the study’s second year regained at least some of the lost weight, confirming "the problem of weight regain despite ongoing counseling for weight-loss maintenance," the study’s authors noted.
The intervention involved quarterly visits with a primary care physician, brief lifestyle coaching delivered monthly by a medical assistant, and the use of meal replacements or weight-loss medication.
The average weight loss of 4.7%, most of which was maintained for 2 years and was accompanied by improvements in some cardiovascular risk factors, was greater than that observed in other primary care trials, said Thomas A. Wadden, Ph.D., of the department of psychiatry at the University of Pennsylvania, Philadelphia, and his associates (N. Engl. J. Med. 2011 Nov. 14 [doi:10.1056/NEJMoa1109220]).
The results of the 2-year study of 390 obese patients demonstrate that "primary care physicians could help a considerable minority of obese persons achieve clinically meaningful weight loss, which they may not achieve if they were simply told to reduce their weight on their own," the investigators noted.
Dr. Wadden and his colleagues conducted the POWER-UP (Practice-based Opportunities for Weight Reduction trial at the University of Pennsylvania) study at three primary care practices in urban settings and three in suburban settings. A total of 30 primary care physicians took part.
The study enrolled 311 women and 79 men, with a mean age of 52 years, a mean body weight of 108 kg, and a mean body mass index of 39 kg/m2 at baseline. By patient self-report, approximately 59% were white, 38.5% were black, and 4.6% were Hispanic.
The study participants all had the same dietary and activity goals but were given different levels of support to achieve them.
All were instructed to gradually increase their physical activity to 180 min/wk. Those who weighed less than 113 kg were prescribed a diet of 1,200-1,500 kcal/day, while those who were heavier were prescribed 1,500-1,800 kcal/day.
A total of 130 patients were randomly assigned to receive usual care, which consisted of quarterly visits in which their primary care physician spent 5-7 minutes discussing the weight-loss information and reviewing any weight change.
Another 131 were randomly assigned to that same care plus brief lifestyle counseling, in which they spent 10-15 min/mo with a medical assistant, called a "lifestyle coach," who conducted a weigh-in, reviewed a diary of food intake, reviewed a physical activity diary, and delivered abbreviated lessons from the Diabetes Prevention Program.
Another 129 patients were randomly assigned to receive enhanced lifestyle counseling, which included that same intervention plus their choice of taking sibutramine, orlistat, or meal replacements under the guidance of the primary care physician. Sibutramine was withdrawn from the market during the trial, and patients in that group were switched to orlistat or meal replacements.
Patients taking meal replacements were instructed to substitute two meals and one snack every day with Slim-Fast shakes or meal bars for the first 4 months, and to replace one meal and one snack each day for the remainder of the study.
The primary outcome was weight loss at 2 years. Enhanced lifestyle counseling produced significantly greater weight loss (mean, 4.6 kg) than either lifestyle counseling (2.9 kg) or usual care (1.7 kg). Within the group receiving enhanced lifestyle counseling, there were no significant differences in weight loss among those taking meal replacements (67 patients), sibutramine (38 patients), or orlistat (24 patients).
The differences among the groups were first evident at 6 months, and maximal weight loss was achieved at 12 months. Between year 1 and year 2, however, most patients regained at least some of the weight they had lost.
Secondary outcomes also were significantly better in the group that received enhanced lifestyle counseling than in the usual-care group, including the percentage of patients whose weight was at or below their baseline weight at 1 year (72.1% vs. 59.2%) and 2 years (67.4% vs. 53.1%); the percentages who lost 5% or more of their baseline weight at 1 year (47.3% vs. 24.6%) and 2 years (34.9% vs. 21.5%); and the percentages who lost 10% or more of their baseline weight at 1 year (25.6% vs. 3.9%) and 2 years (17.8% vs. 6.2%).
Patients who received enhanced lifestyle counseling showed significantly greater improvements in waist circumference, HDL cholesterol levels, and triglyceride levels, but not in LDL cholesterol levels or blood pressure.
There were 73 hospitalizations for severe adverse events, with no significant differences among the three study groups. Only three such events were deemed to be possibly related to the intervention: two cholecystectomies, and one case of syncope. In addition, sibutramine was discontinued in seven patients because of blood pressure elevation, tachycardia, or anxiety; and orlistat was discontinued in five patients because of gastrointestinal symptoms.
"Although our study has shown that primary care personnel can provide effective weight-management support, it has not addressed the more challenging question of who will pay for these or related weight-loss interventions," the researchers noted.
The National Heart, Lung, and Blood Institute funded the study. Dr. Wadden reported ties to Novo Nordisk, Orexigen, Vivus, Nutrisystem, Guilford Press, and the Cardiometabolic Support Network. His associates reported ties to numerous industry sources. Orlistat and Slim-Fast products were provided free of charge by the manufacturers, GlaxoSmithKline and Unilever.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Major Finding: Enhanced lifestyle counseling produced significantly greater weight loss (mean, 4.6 kg) than did either brief lifestyle counseling (2.9 kg) or usual care (1.7 kg).
Data Source: A randomized clinical trial comparing weight loss in 390 obese patients after 2 years of usual care, brief lifestyle counseling, and enhanced lifestyle counseling delivered by a primary care physician and staff medical assistants.
Disclosures: The study was supported by the National Heart, Lung, and Blood Institute. Dr. Wadden reported ties to Novo Nordisk, Orexigen, Vivus, Nutrisystem, Guilford Press, and the Cardiometabolic Support Network. His associates reported ties to numerous industry sources. Orlistat and Slim-Fast products were provided free of charge by the manufacturers, GlaxoSmithKline and Unilever.
Triple Therapy With Vorapaxar Fails in ACS
ORLANDO – Adding the investigational agent vorapaxar to dual-antiplatelet therapy did not impact the primary end point and significantly increased bleeding among high-risk patients with non–ST elevation acute coronary syndrome in the prospective phase III TRACER trial.
Use of the oral protease-activated receptor-1 (PAR-1) antagonist was associated with a significant, 35% increased risk of moderate to severe bleeding based on GUSTO (Global Use of Strategies to Open Occluded Coronary Arteries) criteria, compared with placebo (7.2% vs. 5.2%; hazard ratio, 1.35), as well as a 43% increase in the risk of clinically significant TIMI (Thrombolysis in Myocardial Infarction) bleeding (20.2% vs. 14.6%; HR, 1.43), also a significant difference.

Fatal bleeding was not significantly increased, but intracranial hemorrhage was 3.4-fold higher with vorapaxar, senior author Dr. Kenneth Mahaffey said at the annual scientific sessions of the American Heart Association.
Excess moderate and severe bleeding based on GUSTO criteria and intracranial hemorrhage with vorapaxar occurred early and continued to accrue over time in the phase III TRACER (Thrombin Receptor Antagonist for Clinical Event Reduction in Acute Coronary Syndrome) trial.
Notably, patients were on vorapaxar for much longer than in previous dual-antiplatelet trials, at a median of 379 days, he said.
Invited discussant Dr. Keith A. Fox, professor of cardiology at the University of Edinburgh, said there is an absolute excess at 2 years of about two moderate or severe bleeds, almost five clinically significant TIMI bleeds, and almost one additional intracranial hemorrhage per 100 patients treated, without an impact on the primary end point.
"The potential I think still remains to reduce thrombotic events after [acute coronary syndrome], but I would argue that TRACER has missed the ‘sweet spot’ between efficacy and safety," he said.
TRACER was halted early this year after meeting the prerequisite number of events. It enrolled 12,944 patients with non–ST elevation ACS within 24 hours of presentation who had elevated troponin levels, elevated creatine kinase MB levels, or new ST-segment changes, and at least one other high-risk feature such as diabetes, previous MI, or coronary artery bypass graft surgery.
Patients were randomized to placebo or vorapaxar at a loading dose of 40 mg and maintained at 2.5 mg daily.
Clopidogrel was given to 92% of patients during the index hospitalization; 88% of patients underwent cardiac stenting, and 10% underwent coronary artery bypass grafting. About 87% of patients in each arm were on a thienopyridine, and 40% were taking at least 100 mg/day of aspirin.
At 2 years, the composite primary end point of cardiovascular death, MI, stroke, hospitalization for recurrent ischemia, or urgent revascularization was reported in 18.5% of patients on vorapaxar and 19.9% on placebo, a nonsignificant difference (P = .072; hazard ratio, 0.92), said Dr. Mahaffey, codirector of cardiovascular research at Duke Clinical Research Institute in Durham, N.C.
There was a nominal yet significant relative risk reduction of 11% in the secondary end point of reduced cardiovascular death, MI, or stroke with vorapaxar at 14.7%, compared with 16.4% with placebo, that was primarily driven by a decrease in spontaneous MI.
Interestingly, the subgroup of patients not on a thienopyridine at baseline had a trend toward improved efficacy with vorapaxar and less risk of GUSTO moderate to severe bleeding than those receiving a thienopyridine, he noted.
Session comoderator Dr. Jeffrey Weitz, holder of the Canada Research Chair in Thrombosis and professor of medicine at McMaster University in Hamilton, Ont., said the subgroup analysis suggests that clinicians are "reaching a ceiling" in terms of what they can do with triple therapy and should instead be looking at this class of drugs to substitute one antiplatelet or anticoagulant therapy for another.
Dr. Mahaffey responded that "we are on the precipice of a paradigm shift in how we think about antiplatelets and antithrombins" and that the challenge is to find "what drug, what dosages, and now for how long."
Additional insights are expected to come from ongoing analyses and from the companion phase III TRA-2P TIMI-50 (Thrombin-Receptor Antagonist in Secondary Prevention of Atherothrombotic Ischemic Events) trial, Dr. Mahaffey said. TRA-2P TIMI-50 is evaluating vorapaxar in addition to standard of care as chronic therapy in patients with a history of coronary artery disease and peripheral artery disease, with results expected in 2012.
The full results of TRACER were simultaneously published in the New England Journal of Medicine (2011 Nov. 13 [doi:10.1056/NEJMoa1109719}).
Merck funded the trial. Dr. Mahaffey is a consultant to and has received grants from Merck and numerous other drug companies. At press time, disclosures were not available for Dr. Cox and Dr. Weitz.
ORLANDO – Adding the investigational agent vorapaxar to dual-antiplatelet therapy did not impact the primary end point and significantly increased bleeding among high-risk patients with non–ST elevation acute coronary syndrome in the prospective phase III TRACER trial.
Use of the oral protease-activated receptor-1 (PAR-1) antagonist was associated with a significant, 35% increased risk of moderate to severe bleeding based on GUSTO (Global Use of Strategies to Open Occluded Coronary Arteries) criteria, compared with placebo (7.2% vs. 5.2%; hazard ratio, 1.35), as well as a 43% increase in the risk of clinically significant TIMI (Thrombolysis in Myocardial Infarction) bleeding (20.2% vs. 14.6%; HR, 1.43), also a significant difference.
Fatal bleeding was not significantly increased, but intracranial hemorrhage was 3.4-fold higher with vorapaxar, senior author Dr. Kenneth Mahaffey said at the annual scientific sessions of the American Heart Association.
Excess moderate and severe bleeding based on GUSTO criteria and intracranial hemorrhage with vorapaxar occurred early and continued to accrue over time in the phase III TRACER (Thrombin Receptor Antagonist for Clinical Event Reduction in Acute Coronary Syndrome) trial.
Notably, patients were on vorapaxar for much longer than in previous dual-antiplatelet trials, at a median of 379 days, he said.
Invited discussant Dr. Keith A. Fox, professor of cardiology at the University of Edinburgh, said there is an absolute excess at 2 years of about two moderate or severe bleeds, almost five clinically significant TIMI bleeds, and almost one additional intracranial hemorrhage per 100 patients treated, without an impact on the primary end point.
"The potential I think still remains to reduce thrombotic events after [acute coronary syndrome], but I would argue that TRACER has missed the ‘sweet spot’ between efficacy and safety," he said.
TRACER was halted early this year after meeting the prerequisite number of events. It enrolled 12,944 patients with non–ST elevation ACS within 24 hours of presentation who had elevated troponin levels, elevated creatine kinase MB levels, or new ST-segment changes, and at least one other high-risk feature such as diabetes, previous MI, or coronary artery bypass graft surgery.
Patients were randomized to placebo or vorapaxar at a loading dose of 40 mg and maintained at 2.5 mg daily.
Clopidogrel was given to 92% of patients during the index hospitalization; 88% of patients underwent cardiac stenting, and 10% underwent coronary artery bypass grafting. About 87% of patients in each arm were on a thienopyridine, and 40% were taking at least 100 mg/day of aspirin.
At 2 years, the composite primary end point of cardiovascular death, MI, stroke, hospitalization for recurrent ischemia, or urgent revascularization was reported in 18.5% of patients on vorapaxar and 19.9% on placebo, a nonsignificant difference (P = .072; hazard ratio, 0.92), said Dr. Mahaffey, codirector of cardiovascular research at Duke Clinical Research Institute in Durham, N.C.
There was a nominal yet significant relative risk reduction of 11% in the secondary end point of reduced cardiovascular death, MI, or stroke with vorapaxar at 14.7%, compared with 16.4% with placebo, that was primarily driven by a decrease in spontaneous MI.
Interestingly, the subgroup of patients not on a thienopyridine at baseline had a trend toward improved efficacy with vorapaxar and less risk of GUSTO moderate to severe bleeding than those receiving a thienopyridine, he noted.
Session comoderator Dr. Jeffrey Weitz, holder of the Canada Research Chair in Thrombosis and professor of medicine at McMaster University in Hamilton, Ont., said the subgroup analysis suggests that clinicians are "reaching a ceiling" in terms of what they can do with triple therapy and should instead be looking at this class of drugs to substitute one antiplatelet or anticoagulant therapy for another.
Dr. Mahaffey responded that "we are on the precipice of a paradigm shift in how we think about antiplatelets and antithrombins" and that the challenge is to find "what drug, what dosages, and now for how long."
Additional insights are expected to come from ongoing analyses and from the companion phase III TRA-2P TIMI-50 (Thrombin-Receptor Antagonist in Secondary Prevention of Atherothrombotic Ischemic Events) trial, Dr. Mahaffey said. TRA-2P TIMI-50 is evaluating vorapaxar in addition to standard of care as chronic therapy in patients with a history of coronary artery disease and peripheral artery disease, with results expected in 2012.
The full results of TRACER were simultaneously published in the New England Journal of Medicine (2011 Nov. 13 [doi:10.1056/NEJMoa1109719}).
Merck funded the trial. Dr. Mahaffey is a consultant to and has received grants from Merck and numerous other drug companies. At press time, disclosures were not available for Dr. Cox and Dr. Weitz.
ORLANDO – Adding the investigational agent vorapaxar to dual-antiplatelet therapy did not impact the primary end point and significantly increased bleeding among high-risk patients with non–ST elevation acute coronary syndrome in the prospective phase III TRACER trial.
Use of the oral protease-activated receptor-1 (PAR-1) antagonist was associated with a significant, 35% increased risk of moderate to severe bleeding based on GUSTO (Global Use of Strategies to Open Occluded Coronary Arteries) criteria, compared with placebo (7.2% vs. 5.2%; hazard ratio, 1.35), as well as a 43% increase in the risk of clinically significant TIMI (Thrombolysis in Myocardial Infarction) bleeding (20.2% vs. 14.6%; HR, 1.43), also a significant difference.
Fatal bleeding was not significantly increased, but intracranial hemorrhage was 3.4-fold higher with vorapaxar, senior author Dr. Kenneth Mahaffey said at the annual scientific sessions of the American Heart Association.
Excess moderate and severe bleeding based on GUSTO criteria and intracranial hemorrhage with vorapaxar occurred early and continued to accrue over time in the phase III TRACER (Thrombin Receptor Antagonist for Clinical Event Reduction in Acute Coronary Syndrome) trial.
Notably, patients were on vorapaxar for much longer than in previous dual-antiplatelet trials, at a median of 379 days, he said.
Invited discussant Dr. Keith A. Fox, professor of cardiology at the University of Edinburgh, said there is an absolute excess at 2 years of about two moderate or severe bleeds, almost five clinically significant TIMI bleeds, and almost one additional intracranial hemorrhage per 100 patients treated, without an impact on the primary end point.
"The potential I think still remains to reduce thrombotic events after [acute coronary syndrome], but I would argue that TRACER has missed the ‘sweet spot’ between efficacy and safety," he said.
TRACER was halted early this year after meeting the prerequisite number of events. It enrolled 12,944 patients with non–ST elevation ACS within 24 hours of presentation who had elevated troponin levels, elevated creatine kinase MB levels, or new ST-segment changes, and at least one other high-risk feature such as diabetes, previous MI, or coronary artery bypass graft surgery.
Patients were randomized to placebo or vorapaxar at a loading dose of 40 mg and maintained at 2.5 mg daily.
Clopidogrel was given to 92% of patients during the index hospitalization; 88% of patients underwent cardiac stenting, and 10% underwent coronary artery bypass grafting. About 87% of patients in each arm were on a thienopyridine, and 40% were taking at least 100 mg/day of aspirin.
At 2 years, the composite primary end point of cardiovascular death, MI, stroke, hospitalization for recurrent ischemia, or urgent revascularization was reported in 18.5% of patients on vorapaxar and 19.9% on placebo, a nonsignificant difference (P = .072; hazard ratio, 0.92), said Dr. Mahaffey, codirector of cardiovascular research at Duke Clinical Research Institute in Durham, N.C.
There was a nominal yet significant relative risk reduction of 11% in the secondary end point of reduced cardiovascular death, MI, or stroke with vorapaxar at 14.7%, compared with 16.4% with placebo, that was primarily driven by a decrease in spontaneous MI.
Interestingly, the subgroup of patients not on a thienopyridine at baseline had a trend toward improved efficacy with vorapaxar and less risk of GUSTO moderate to severe bleeding than those receiving a thienopyridine, he noted.
Session comoderator Dr. Jeffrey Weitz, holder of the Canada Research Chair in Thrombosis and professor of medicine at McMaster University in Hamilton, Ont., said the subgroup analysis suggests that clinicians are "reaching a ceiling" in terms of what they can do with triple therapy and should instead be looking at this class of drugs to substitute one antiplatelet or anticoagulant therapy for another.
Dr. Mahaffey responded that "we are on the precipice of a paradigm shift in how we think about antiplatelets and antithrombins" and that the challenge is to find "what drug, what dosages, and now for how long."
Additional insights are expected to come from ongoing analyses and from the companion phase III TRA-2P TIMI-50 (Thrombin-Receptor Antagonist in Secondary Prevention of Atherothrombotic Ischemic Events) trial, Dr. Mahaffey said. TRA-2P TIMI-50 is evaluating vorapaxar in addition to standard of care as chronic therapy in patients with a history of coronary artery disease and peripheral artery disease, with results expected in 2012.
The full results of TRACER were simultaneously published in the New England Journal of Medicine (2011 Nov. 13 [doi:10.1056/NEJMoa1109719}).
Merck funded the trial. Dr. Mahaffey is a consultant to and has received grants from Merck and numerous other drug companies. At press time, disclosures were not available for Dr. Cox and Dr. Weitz.
FROM THE ANNUAL SCIENTIFIC SESSIONS OF THE AMERICAN HEART ASSOCIATION
Major Finding: The primary end point occurred in 18.5% of patients treated with vorapaxar and 19.9% with placebo (P = .072; hazard ratio, 0.92).
Data Source: TRACER, a prospective double-blind randomized trial in 6,473 patients with acute coronary syndromes.
Disclosures: Merck funded the trial. At press time, disclosures were not available for Dr. Cox and Dr. Weitz.
SCD Screenings in Young Athletes Often Miss the Mark
ORLANDO – Although guidelines for assessing the risk of sudden cardiac death in high school athletes were first issued 15 years ago, less than 6% of physicians fully follow those guidelines, according to a survey conducted in Washington State.
Preparticipation physical evaluation is the main mechanism of screening for sudden cardiac death (SCD) in the United States, and is recognized by all national medical organizations, according to Dr. Nicolas Madsen, the survey’s lead author and a pediatric cardiology fellow at Seattle Children’s Hospital and the University of Washington School of Medicine.
The American Heart Association’s (AHA’s) guidelines, issued in 1996 and reaffirmed in 2007, recommend 12 elements for SCD screening of competitive athletes (Circulation 2007;115:1643-55). There are also websites such as ppesportsevaluation.org that provide screening forms for free.
Yet, according to the survey, 47% of physicians and only 6% of high school athletic directors were aware of the guidelines. And although 60% used a screening form, they incorporated only 8 of the 12 recommended elements. Not a single school surveyed was in complete compliance with the AHA guidelines, Dr. Madsen reported at the annual scientific sessions of the American Heart Association.
Lack of compliance with the guidelines was driven mainly by lack of knowledge, and not by location, experience, or physician specialty, said Dr. Madsen.
"New directions for provider education and policy requirements are needed to improve this implementation gap," he and his coauthors wrote.
Dr. Madsen had no disclosures. Dr. G. Paul Matherne (featured in video above) also had no disclosures.
ORLANDO – Although guidelines for assessing the risk of sudden cardiac death in high school athletes were first issued 15 years ago, less than 6% of physicians fully follow those guidelines, according to a survey conducted in Washington State.
Preparticipation physical evaluation is the main mechanism of screening for sudden cardiac death (SCD) in the United States, and is recognized by all national medical organizations, according to Dr. Nicolas Madsen, the survey’s lead author and a pediatric cardiology fellow at Seattle Children’s Hospital and the University of Washington School of Medicine.
The American Heart Association’s (AHA’s) guidelines, issued in 1996 and reaffirmed in 2007, recommend 12 elements for SCD screening of competitive athletes (Circulation 2007;115:1643-55). There are also websites such as ppesportsevaluation.org that provide screening forms for free.
Yet, according to the survey, 47% of physicians and only 6% of high school athletic directors were aware of the guidelines. And although 60% used a screening form, they incorporated only 8 of the 12 recommended elements. Not a single school surveyed was in complete compliance with the AHA guidelines, Dr. Madsen reported at the annual scientific sessions of the American Heart Association.
Lack of compliance with the guidelines was driven mainly by lack of knowledge, and not by location, experience, or physician specialty, said Dr. Madsen.
"New directions for provider education and policy requirements are needed to improve this implementation gap," he and his coauthors wrote.
Dr. Madsen had no disclosures. Dr. G. Paul Matherne (featured in video above) also had no disclosures.
ORLANDO – Although guidelines for assessing the risk of sudden cardiac death in high school athletes were first issued 15 years ago, less than 6% of physicians fully follow those guidelines, according to a survey conducted in Washington State.
Preparticipation physical evaluation is the main mechanism of screening for sudden cardiac death (SCD) in the United States, and is recognized by all national medical organizations, according to Dr. Nicolas Madsen, the survey’s lead author and a pediatric cardiology fellow at Seattle Children’s Hospital and the University of Washington School of Medicine.
The American Heart Association’s (AHA’s) guidelines, issued in 1996 and reaffirmed in 2007, recommend 12 elements for SCD screening of competitive athletes (Circulation 2007;115:1643-55). There are also websites such as ppesportsevaluation.org that provide screening forms for free.
Yet, according to the survey, 47% of physicians and only 6% of high school athletic directors were aware of the guidelines. And although 60% used a screening form, they incorporated only 8 of the 12 recommended elements. Not a single school surveyed was in complete compliance with the AHA guidelines, Dr. Madsen reported at the annual scientific sessions of the American Heart Association.
Lack of compliance with the guidelines was driven mainly by lack of knowledge, and not by location, experience, or physician specialty, said Dr. Madsen.
"New directions for provider education and policy requirements are needed to improve this implementation gap," he and his coauthors wrote.
Dr. Madsen had no disclosures. Dr. G. Paul Matherne (featured in video above) also had no disclosures.
FROM THE ANNUAL SCIENTIFIC SESSIONS OF THE AMERICAN HEART ASSOCIATION
Rivaroxaban Shows Net Benefit for Acute Coronary Syndrome
ORLANDO – A new era in the management of patients with a recent episode of acute coronary syndrome arrived with the report that adding a low dose of the oral anticoagulant drug rivaroxaban to standard medical therapy with aspirin and clopidogrel produced a striking mortality-rate improvement over as much as 2 years of follow-up at a price of only a modest increase in major bleeds.
"Very low-dose anticoagulation with rivaroxaban, 2.5 mg b.i.d., in addition to antiplatelet therapies, represents an effective strategy to reduce cardiovascular events in patients with a recent ACS" [acute coronary syndrome] event, Dr. C. Michael Gibson said at the meeting. "Rivaroxaban reduced the risk of cardiovascular death, myocardial infarction, or stroke in patients across the spectrum of ACS, ST-elevation myocardial infarction, non-ST-elevation myocardial infarction, or unstable angina."

Rates of major bleeding and intracranial hemorrhage were higher with rivaroxaban; however, there was no excess of fatal intracranial hemorrhage or fatal bleeding with rivaroxaban compared with placebo, particularly the twice-daily 2.5 mg dosage.
"There was increased major bleeding and intracranial hemorrhage, but this kind of mortality benefit bleeding seems to trump the nonfatal bleeds," he said. In addition, among patients who developed intracranial hemorrhages or ischemic strokes, "Rankin scores after strokes were significantly better in the rivaroxaban-treated patients. They had better functional status," compared with placebo-treated patients who had a stroke, said Dr. Gibson, chief of clinical research in the division of cardiology at Beth Israel Deaconess Medical Center in Boston.
The efficacy result showed that among the 93% of patients enrolled in the trial who were maintained on concurrent treatment with aspirin plus clopidogrel, the lower rivaroxaban dosage resulted in the prevention of one death for every 56 patients treated for 2 years.
Concurrent with Dr. Gibson’s report at the meeting the results from the Anti-Xa Therapy to Lower Cardiovascular Events in Addition to Standard Therapy in Subjects with Acute Coronary Syndrome-Thrombolysis in Myocardial Infarction 51 trial (ATLAS ACS-2 TIMI 51) appeared online (N. Engl. J. Med. 2011;365:doi:10.1056.NEJMoa1112277).
Although rivaroxaban received Food and Drug Administration approval earlier this year for the indications of preventing stroke in patients with atrial fibrillation, and for preventing venous thromboembolism in patients following hip or knee replacement surgery, a 10-mg pill is the smallest formulation now sold in the United States, which would make it difficult for physicians to prescribe a 2.5-mg twice-daily dosage until the ACS indication goes through FDA review, Dr. Gibson cautioned.
Cardiologists who heard these findings hailed the 2.5-mg twice daily dosage of rivaroxaban as an important addition to standard management of most patients with a recent ACS if they could also be put on the aspirin and clopidogrel background used in the study. They also highlighted the importance of the phase III study’s design, which showed that a 5-mg twice daily dosage did not produce as clear a benefit and also led to substantially more major bleeds, intracranial hemorrhages, and fatal bleeds.

The lower tested dose of rivaroxaban "is a new standard of antithrombotic drug in ACS," commented Dr. Paul W. Armstrong, professor of medicine at the University of Alberta in Edmonton, Canada.
"The 2.5 mg b.i.d. dosage looked spectacular. A trial showing a reduction of all-cause mortality is pretty incredible," said Dr. Deepak L. Bhatt, chief of cardiology at the VA Boston Healthcare System and a co-investigator on the study.
Moreover, the results showed that "adding a little sprinkle of an anticoagulant reduced mortality, while adding more drug, 5 mg b.i.d., still reduced ischemic events but increased bleeds." In contrast, results in the recently completed APPRAISE-2 study, which used a similar design to test another oral anticoagulant, apixaban in ACS patients, administered a more potent, 5 mg b.i.d. dosage of apixaban and failed to show benefit and generated an even higher rate of bleeds (N. Engl. J. Med. 2011;365:699-708). If ATLAS "had just tested the 5 mg b.i.d. dosage, we would have been left with the issue of whether a lower dose would have worked," he said in an interview.
Continued separation of the combined-event and mortality curves between the 2.5 mg b.i.d. rivaroxaban patients and the placebo controls over time throughout the 2 years of follow-up provided another major observation that guide therapy. This finding "is a sign to continue treatment indefinitely," Dr. Bhatt said. "The platelet activation during an ACS event decreases substantially after 30 days, and after 6 months, but thrombin seems to linger, so there may be a role for prolonged anticoagulant treatment that surpasses the role for prolonged antiplatelet treatment."
ATLAS ACS-2 TIMI 51 was sponsored by Johnson & Johnson and Bayer. Dr. Gibson said that he has been a consultant to those companies and to numerous other pharmaceutical companies; has served on the speakers bureaus for Daiichi Sankyo, Eli Lilly, and The Medicines Company; and has received fees for educational presentations on behalf of Daiichi Sankyo and Eli Lilly. He has received research grants from Johnson & Johnson and Bayer. Dr. Armstrong has been a consultant to Eli Lilly, Sanofi-Aventis, Bristol-Myers Squibb, Merck, Regado, Hoffmann-LaRoche, GlaxoSmithKline, Pfizer, and Takeda, and he has received grant support from Boehringer Ingelheim, Hoffman LaRoche, Sanofi-Aventis, Schering Plough, and Merck. Dr. Bhatt said that he has received grant support from AstraZeneca, Regado, Portola, and GlaxoSmithKline.
The ATLAS results were very dramatic. The 2.5 mg b.i.d. dose, on top of standard acute coronary syndrome therapy with aspirin and clopidogrel, not only reduced the primary end point, but also significantly reduced cardiovascular mortality and total mortality. That is an effect that we really look for but rarely see in phase III trials. It’s an important finding that will catch the attention of many clinicians. This is the first trial to show a benefit of adding oral anticoagulation, at a very low dose, on top of the background regimen we give today.
The dose that appeared optimal was 2.5 mg b.i.d., which produced the efficacy benefit with a modest increase in major bleeds and no significant increase in fatal bleeding events. The results showed an overall number needed to treat to prevent one all-cause death was 63, which is pretty good, with a substantially lower number needed to harm. The balance definitely favored a net benefit from adding rivaroxaban. The researchers found rivaroxaban’s "sweet spot" for this indication at the lower dosage.
These results are relevant to the vast majority of ACS patients, who still receive aspirin and clopidogrel for antiplatelet therapy. But physicians should not extrapolate these findings to the growing number of ACS patients treated with the alternative, more powerful antiplatelet drugs prasugrel and ticagrelor. The risk for bleeding might be much greater if treatment combined rivaroxaban with one of these drugs. The safety and efficacy of rivaroxaban when added to treatment with prasugrel or ticagrelor will need testing in future studies.
Elliott M. Antman, M.D., is professor of medicine at Harvard University in Boston. He is a senior investigator for the TIMI study group, which ran the ATLAS trial, but he did not directly participate in running the trial. He also served as principal investigator for the pivotal trial of prasugrel. He said that he had no other relevant disclosures. Dr. Antman made these comments in an interview.
The ATLAS results were very dramatic. The 2.5 mg b.i.d. dose, on top of standard acute coronary syndrome therapy with aspirin and clopidogrel, not only reduced the primary end point, but also significantly reduced cardiovascular mortality and total mortality. That is an effect that we really look for but rarely see in phase III trials. It’s an important finding that will catch the attention of many clinicians. This is the first trial to show a benefit of adding oral anticoagulation, at a very low dose, on top of the background regimen we give today.
The dose that appeared optimal was 2.5 mg b.i.d., which produced the efficacy benefit with a modest increase in major bleeds and no significant increase in fatal bleeding events. The results showed an overall number needed to treat to prevent one all-cause death was 63, which is pretty good, with a substantially lower number needed to harm. The balance definitely favored a net benefit from adding rivaroxaban. The researchers found rivaroxaban’s "sweet spot" for this indication at the lower dosage.
These results are relevant to the vast majority of ACS patients, who still receive aspirin and clopidogrel for antiplatelet therapy. But physicians should not extrapolate these findings to the growing number of ACS patients treated with the alternative, more powerful antiplatelet drugs prasugrel and ticagrelor. The risk for bleeding might be much greater if treatment combined rivaroxaban with one of these drugs. The safety and efficacy of rivaroxaban when added to treatment with prasugrel or ticagrelor will need testing in future studies.
Elliott M. Antman, M.D., is professor of medicine at Harvard University in Boston. He is a senior investigator for the TIMI study group, which ran the ATLAS trial, but he did not directly participate in running the trial. He also served as principal investigator for the pivotal trial of prasugrel. He said that he had no other relevant disclosures. Dr. Antman made these comments in an interview.
The ATLAS results were very dramatic. The 2.5 mg b.i.d. dose, on top of standard acute coronary syndrome therapy with aspirin and clopidogrel, not only reduced the primary end point, but also significantly reduced cardiovascular mortality and total mortality. That is an effect that we really look for but rarely see in phase III trials. It’s an important finding that will catch the attention of many clinicians. This is the first trial to show a benefit of adding oral anticoagulation, at a very low dose, on top of the background regimen we give today.
The dose that appeared optimal was 2.5 mg b.i.d., which produced the efficacy benefit with a modest increase in major bleeds and no significant increase in fatal bleeding events. The results showed an overall number needed to treat to prevent one all-cause death was 63, which is pretty good, with a substantially lower number needed to harm. The balance definitely favored a net benefit from adding rivaroxaban. The researchers found rivaroxaban’s "sweet spot" for this indication at the lower dosage.
These results are relevant to the vast majority of ACS patients, who still receive aspirin and clopidogrel for antiplatelet therapy. But physicians should not extrapolate these findings to the growing number of ACS patients treated with the alternative, more powerful antiplatelet drugs prasugrel and ticagrelor. The risk for bleeding might be much greater if treatment combined rivaroxaban with one of these drugs. The safety and efficacy of rivaroxaban when added to treatment with prasugrel or ticagrelor will need testing in future studies.
Elliott M. Antman, M.D., is professor of medicine at Harvard University in Boston. He is a senior investigator for the TIMI study group, which ran the ATLAS trial, but he did not directly participate in running the trial. He also served as principal investigator for the pivotal trial of prasugrel. He said that he had no other relevant disclosures. Dr. Antman made these comments in an interview.
ORLANDO – A new era in the management of patients with a recent episode of acute coronary syndrome arrived with the report that adding a low dose of the oral anticoagulant drug rivaroxaban to standard medical therapy with aspirin and clopidogrel produced a striking mortality-rate improvement over as much as 2 years of follow-up at a price of only a modest increase in major bleeds.
"Very low-dose anticoagulation with rivaroxaban, 2.5 mg b.i.d., in addition to antiplatelet therapies, represents an effective strategy to reduce cardiovascular events in patients with a recent ACS" [acute coronary syndrome] event, Dr. C. Michael Gibson said at the meeting. "Rivaroxaban reduced the risk of cardiovascular death, myocardial infarction, or stroke in patients across the spectrum of ACS, ST-elevation myocardial infarction, non-ST-elevation myocardial infarction, or unstable angina."
Rates of major bleeding and intracranial hemorrhage were higher with rivaroxaban; however, there was no excess of fatal intracranial hemorrhage or fatal bleeding with rivaroxaban compared with placebo, particularly the twice-daily 2.5 mg dosage.
"There was increased major bleeding and intracranial hemorrhage, but this kind of mortality benefit bleeding seems to trump the nonfatal bleeds," he said. In addition, among patients who developed intracranial hemorrhages or ischemic strokes, "Rankin scores after strokes were significantly better in the rivaroxaban-treated patients. They had better functional status," compared with placebo-treated patients who had a stroke, said Dr. Gibson, chief of clinical research in the division of cardiology at Beth Israel Deaconess Medical Center in Boston.
The efficacy result showed that among the 93% of patients enrolled in the trial who were maintained on concurrent treatment with aspirin plus clopidogrel, the lower rivaroxaban dosage resulted in the prevention of one death for every 56 patients treated for 2 years.
Concurrent with Dr. Gibson’s report at the meeting the results from the Anti-Xa Therapy to Lower Cardiovascular Events in Addition to Standard Therapy in Subjects with Acute Coronary Syndrome-Thrombolysis in Myocardial Infarction 51 trial (ATLAS ACS-2 TIMI 51) appeared online (N. Engl. J. Med. 2011;365:doi:10.1056.NEJMoa1112277).
Although rivaroxaban received Food and Drug Administration approval earlier this year for the indications of preventing stroke in patients with atrial fibrillation, and for preventing venous thromboembolism in patients following hip or knee replacement surgery, a 10-mg pill is the smallest formulation now sold in the United States, which would make it difficult for physicians to prescribe a 2.5-mg twice-daily dosage until the ACS indication goes through FDA review, Dr. Gibson cautioned.
Cardiologists who heard these findings hailed the 2.5-mg twice daily dosage of rivaroxaban as an important addition to standard management of most patients with a recent ACS if they could also be put on the aspirin and clopidogrel background used in the study. They also highlighted the importance of the phase III study’s design, which showed that a 5-mg twice daily dosage did not produce as clear a benefit and also led to substantially more major bleeds, intracranial hemorrhages, and fatal bleeds.
The lower tested dose of rivaroxaban "is a new standard of antithrombotic drug in ACS," commented Dr. Paul W. Armstrong, professor of medicine at the University of Alberta in Edmonton, Canada.
"The 2.5 mg b.i.d. dosage looked spectacular. A trial showing a reduction of all-cause mortality is pretty incredible," said Dr. Deepak L. Bhatt, chief of cardiology at the VA Boston Healthcare System and a co-investigator on the study.
Moreover, the results showed that "adding a little sprinkle of an anticoagulant reduced mortality, while adding more drug, 5 mg b.i.d., still reduced ischemic events but increased bleeds." In contrast, results in the recently completed APPRAISE-2 study, which used a similar design to test another oral anticoagulant, apixaban in ACS patients, administered a more potent, 5 mg b.i.d. dosage of apixaban and failed to show benefit and generated an even higher rate of bleeds (N. Engl. J. Med. 2011;365:699-708). If ATLAS "had just tested the 5 mg b.i.d. dosage, we would have been left with the issue of whether a lower dose would have worked," he said in an interview.
Continued separation of the combined-event and mortality curves between the 2.5 mg b.i.d. rivaroxaban patients and the placebo controls over time throughout the 2 years of follow-up provided another major observation that guide therapy. This finding "is a sign to continue treatment indefinitely," Dr. Bhatt said. "The platelet activation during an ACS event decreases substantially after 30 days, and after 6 months, but thrombin seems to linger, so there may be a role for prolonged anticoagulant treatment that surpasses the role for prolonged antiplatelet treatment."
ATLAS ACS-2 TIMI 51 was sponsored by Johnson & Johnson and Bayer. Dr. Gibson said that he has been a consultant to those companies and to numerous other pharmaceutical companies; has served on the speakers bureaus for Daiichi Sankyo, Eli Lilly, and The Medicines Company; and has received fees for educational presentations on behalf of Daiichi Sankyo and Eli Lilly. He has received research grants from Johnson & Johnson and Bayer. Dr. Armstrong has been a consultant to Eli Lilly, Sanofi-Aventis, Bristol-Myers Squibb, Merck, Regado, Hoffmann-LaRoche, GlaxoSmithKline, Pfizer, and Takeda, and he has received grant support from Boehringer Ingelheim, Hoffman LaRoche, Sanofi-Aventis, Schering Plough, and Merck. Dr. Bhatt said that he has received grant support from AstraZeneca, Regado, Portola, and GlaxoSmithKline.
ORLANDO – A new era in the management of patients with a recent episode of acute coronary syndrome arrived with the report that adding a low dose of the oral anticoagulant drug rivaroxaban to standard medical therapy with aspirin and clopidogrel produced a striking mortality-rate improvement over as much as 2 years of follow-up at a price of only a modest increase in major bleeds.
"Very low-dose anticoagulation with rivaroxaban, 2.5 mg b.i.d., in addition to antiplatelet therapies, represents an effective strategy to reduce cardiovascular events in patients with a recent ACS" [acute coronary syndrome] event, Dr. C. Michael Gibson said at the meeting. "Rivaroxaban reduced the risk of cardiovascular death, myocardial infarction, or stroke in patients across the spectrum of ACS, ST-elevation myocardial infarction, non-ST-elevation myocardial infarction, or unstable angina."
Rates of major bleeding and intracranial hemorrhage were higher with rivaroxaban; however, there was no excess of fatal intracranial hemorrhage or fatal bleeding with rivaroxaban compared with placebo, particularly the twice-daily 2.5 mg dosage.
"There was increased major bleeding and intracranial hemorrhage, but this kind of mortality benefit bleeding seems to trump the nonfatal bleeds," he said. In addition, among patients who developed intracranial hemorrhages or ischemic strokes, "Rankin scores after strokes were significantly better in the rivaroxaban-treated patients. They had better functional status," compared with placebo-treated patients who had a stroke, said Dr. Gibson, chief of clinical research in the division of cardiology at Beth Israel Deaconess Medical Center in Boston.
The efficacy result showed that among the 93% of patients enrolled in the trial who were maintained on concurrent treatment with aspirin plus clopidogrel, the lower rivaroxaban dosage resulted in the prevention of one death for every 56 patients treated for 2 years.
Concurrent with Dr. Gibson’s report at the meeting the results from the Anti-Xa Therapy to Lower Cardiovascular Events in Addition to Standard Therapy in Subjects with Acute Coronary Syndrome-Thrombolysis in Myocardial Infarction 51 trial (ATLAS ACS-2 TIMI 51) appeared online (N. Engl. J. Med. 2011;365:doi:10.1056.NEJMoa1112277).
Although rivaroxaban received Food and Drug Administration approval earlier this year for the indications of preventing stroke in patients with atrial fibrillation, and for preventing venous thromboembolism in patients following hip or knee replacement surgery, a 10-mg pill is the smallest formulation now sold in the United States, which would make it difficult for physicians to prescribe a 2.5-mg twice-daily dosage until the ACS indication goes through FDA review, Dr. Gibson cautioned.
Cardiologists who heard these findings hailed the 2.5-mg twice daily dosage of rivaroxaban as an important addition to standard management of most patients with a recent ACS if they could also be put on the aspirin and clopidogrel background used in the study. They also highlighted the importance of the phase III study’s design, which showed that a 5-mg twice daily dosage did not produce as clear a benefit and also led to substantially more major bleeds, intracranial hemorrhages, and fatal bleeds.
The lower tested dose of rivaroxaban "is a new standard of antithrombotic drug in ACS," commented Dr. Paul W. Armstrong, professor of medicine at the University of Alberta in Edmonton, Canada.
"The 2.5 mg b.i.d. dosage looked spectacular. A trial showing a reduction of all-cause mortality is pretty incredible," said Dr. Deepak L. Bhatt, chief of cardiology at the VA Boston Healthcare System and a co-investigator on the study.
Moreover, the results showed that "adding a little sprinkle of an anticoagulant reduced mortality, while adding more drug, 5 mg b.i.d., still reduced ischemic events but increased bleeds." In contrast, results in the recently completed APPRAISE-2 study, which used a similar design to test another oral anticoagulant, apixaban in ACS patients, administered a more potent, 5 mg b.i.d. dosage of apixaban and failed to show benefit and generated an even higher rate of bleeds (N. Engl. J. Med. 2011;365:699-708). If ATLAS "had just tested the 5 mg b.i.d. dosage, we would have been left with the issue of whether a lower dose would have worked," he said in an interview.
Continued separation of the combined-event and mortality curves between the 2.5 mg b.i.d. rivaroxaban patients and the placebo controls over time throughout the 2 years of follow-up provided another major observation that guide therapy. This finding "is a sign to continue treatment indefinitely," Dr. Bhatt said. "The platelet activation during an ACS event decreases substantially after 30 days, and after 6 months, but thrombin seems to linger, so there may be a role for prolonged anticoagulant treatment that surpasses the role for prolonged antiplatelet treatment."
ATLAS ACS-2 TIMI 51 was sponsored by Johnson & Johnson and Bayer. Dr. Gibson said that he has been a consultant to those companies and to numerous other pharmaceutical companies; has served on the speakers bureaus for Daiichi Sankyo, Eli Lilly, and The Medicines Company; and has received fees for educational presentations on behalf of Daiichi Sankyo and Eli Lilly. He has received research grants from Johnson & Johnson and Bayer. Dr. Armstrong has been a consultant to Eli Lilly, Sanofi-Aventis, Bristol-Myers Squibb, Merck, Regado, Hoffmann-LaRoche, GlaxoSmithKline, Pfizer, and Takeda, and he has received grant support from Boehringer Ingelheim, Hoffman LaRoche, Sanofi-Aventis, Schering Plough, and Merck. Dr. Bhatt said that he has received grant support from AstraZeneca, Regado, Portola, and GlaxoSmithKline.
FROM THE ANNUAL SCIENTIFIC SESSIONS OF THE AMERICAN HEART ASSOCIATION
Major Finding: Adding the oral anticoagulant rivaroxaban at 2.5 mg b.i.d to standard aspirin and clopidogrel treatment of patients with a recent acute coronary syndrome event cut all-cause death by 1.6 percentage points, and the primary end point of cardiovascular death, myocardial infarction, and stroke by 1.6 percentage points, while also increasing major bleeds by 1.2 percentage points.
Data Source: The ATLAS ACS-2 TIMI 51 study, which randomized 15,526 patients a median of 4.7 days after their index event to daily treatment with 2.5 mg rivaroxaban b.i.d., 5 mg b.i.d., or placebo for a median duration of 13 months.
Disclosures: ATLAS ACS-2 TIMI 51 was sponsored by Johnson & Johnson and Bayer. Dr. Gibson said that he has been a consultant to Portola, Sanofi-Aventius, The Medicines Company, Daiichi Sankyo, Eli Lilly, Biogen Idec, Bristol-Myers Squibb, Ischemix, Johnson & Johnson, Bayer, Merck, Schering Plough, Ortho-McNeil, Medicure, Archemix, Genentech, and Boehringer Ingelheim. He has served on the speaker’s bureau for Daiichi Sankyo, Eli Lilly, and The Medicines Company, and he has received fees for educational presentations on behalf of Daiichi Sankyo and Eli Lilly. He has received research grants from Johnson & Johnson and Bayer. Dr. Armstrong has been a consultant to Eli Lilly, Sanofi-Aventis, Bristol-Myers Squibb, Merck, Regado, Hoffmann-LaRoche, GlaxoSmithKline, Pfizer, and Takeda, and he has received grant support from Boehringer Ingelheim, Hoffmann-LaRoche, Sanofi-Aventis, Schering Plough, and Merck. Dr. Bhatt said that he has received grant support from Astra Zeneca, Regado, Portola, and GlaxoSmithKline.