User login
Rising Migraine Prevalence Observed in Denmark
LOS ANGELES – The lifetime prevalence of self-reported migraine in the general population rose considerably in a recent 8-year period, suggested a study of roughly 37,000 middle-aged adults in Denmark.
From 1994 to 2002, the proportion reporting that they had ever had migraine rose by 32%, from a prevalence of 18.5% to 24.5% (P less than .001), Dr. Han Le of the University of Copenhagen reported at the annual meeting of the American Headache Society.

By type, there was a 68% increase in the prevalence of migraine with aura (from 5.6% to 9.4%; P less than .001) and a 16% increase in the prevalence of migraine without aura (from 13% to 15.1%; P less than .001), although the latter remained considerably more common (BMJ 2012 July 2 [doi:10.1136/bmjopen-2012-000962]).
"So are we having a micro-epidemic? ... We do believe that there is an increase, but [it] may not be as high as we are finding," Dr. Le commented, noting that that short time span over which the change took place would favor environmental explanations over genetic ones.
"Some part may be explained by more awareness or increased medical consultation. We do know for a fact that medical consultation has increased in Denmark. But there aren’t any campaigns to make people more aware of migraine," she elaborated. "A small part of the subjects participated in both surveys, so perhaps when they saw the migraine questions for the first time, they kind of thought more about it and went to a physician. That’s hard to tell."
In additional study findings, low education and high physical workload and activity increased the risk only of migraine without aura, whereas low body mass index increased the risk only of migraine with aura. Thus "different environmental factors seem to increase the development of migraine with aura and migraine without aura," she commented.
The investigators analyzed data from the Danish Twin Study, in which 20- to 41-year-olds in the general population were asked if they had ever experienced migraine and, if so, if they had had antecedent visual disturbances. Analyses were based on data from 22,053 adults in 1994 and from 14,810 adults in 2002.
Age-stratified analyses showed that most of the increase occurred among individuals aged older than 32 years. There was a significant increase among men and women individually, with the relative increase comparable for the sexes.
The investigators conducted an additional analysis of migraine risk factors among 13,498 adults aged 18-41 years who were free of migraine in 1994 and completed surveys in both study years.
Results showed that these adults were more likely to develop migraine if they had low back pain (odds ratio, 1.3), low education (OR, 1.3), hard physical workload (OR, 1.1), hard physical activity (OR, 1.2), and a body mass index of less than 18.5 kg/m2 (OR, 1.3).
In stratified analyses, only one of these factors (low back pain) was a risk factor for both types of migraine, according to Dr. Le. Low education as well as high physical workload and activity were risk factors only for migraine without aura, whereas low BMI was a risk factor only for migraine with aura.
Dr. Le disclosed no relevant conflicts of interest.
LOS ANGELES – The lifetime prevalence of self-reported migraine in the general population rose considerably in a recent 8-year period, suggested a study of roughly 37,000 middle-aged adults in Denmark.
From 1994 to 2002, the proportion reporting that they had ever had migraine rose by 32%, from a prevalence of 18.5% to 24.5% (P less than .001), Dr. Han Le of the University of Copenhagen reported at the annual meeting of the American Headache Society.
By type, there was a 68% increase in the prevalence of migraine with aura (from 5.6% to 9.4%; P less than .001) and a 16% increase in the prevalence of migraine without aura (from 13% to 15.1%; P less than .001), although the latter remained considerably more common (BMJ 2012 July 2 [doi:10.1136/bmjopen-2012-000962]).
"So are we having a micro-epidemic? ... We do believe that there is an increase, but [it] may not be as high as we are finding," Dr. Le commented, noting that that short time span over which the change took place would favor environmental explanations over genetic ones.
"Some part may be explained by more awareness or increased medical consultation. We do know for a fact that medical consultation has increased in Denmark. But there aren’t any campaigns to make people more aware of migraine," she elaborated. "A small part of the subjects participated in both surveys, so perhaps when they saw the migraine questions for the first time, they kind of thought more about it and went to a physician. That’s hard to tell."
In additional study findings, low education and high physical workload and activity increased the risk only of migraine without aura, whereas low body mass index increased the risk only of migraine with aura. Thus "different environmental factors seem to increase the development of migraine with aura and migraine without aura," she commented.
The investigators analyzed data from the Danish Twin Study, in which 20- to 41-year-olds in the general population were asked if they had ever experienced migraine and, if so, if they had had antecedent visual disturbances. Analyses were based on data from 22,053 adults in 1994 and from 14,810 adults in 2002.
Age-stratified analyses showed that most of the increase occurred among individuals aged older than 32 years. There was a significant increase among men and women individually, with the relative increase comparable for the sexes.
The investigators conducted an additional analysis of migraine risk factors among 13,498 adults aged 18-41 years who were free of migraine in 1994 and completed surveys in both study years.
Results showed that these adults were more likely to develop migraine if they had low back pain (odds ratio, 1.3), low education (OR, 1.3), hard physical workload (OR, 1.1), hard physical activity (OR, 1.2), and a body mass index of less than 18.5 kg/m2 (OR, 1.3).
In stratified analyses, only one of these factors (low back pain) was a risk factor for both types of migraine, according to Dr. Le. Low education as well as high physical workload and activity were risk factors only for migraine without aura, whereas low BMI was a risk factor only for migraine with aura.
Dr. Le disclosed no relevant conflicts of interest.
LOS ANGELES – The lifetime prevalence of self-reported migraine in the general population rose considerably in a recent 8-year period, suggested a study of roughly 37,000 middle-aged adults in Denmark.
From 1994 to 2002, the proportion reporting that they had ever had migraine rose by 32%, from a prevalence of 18.5% to 24.5% (P less than .001), Dr. Han Le of the University of Copenhagen reported at the annual meeting of the American Headache Society.
By type, there was a 68% increase in the prevalence of migraine with aura (from 5.6% to 9.4%; P less than .001) and a 16% increase in the prevalence of migraine without aura (from 13% to 15.1%; P less than .001), although the latter remained considerably more common (BMJ 2012 July 2 [doi:10.1136/bmjopen-2012-000962]).
"So are we having a micro-epidemic? ... We do believe that there is an increase, but [it] may not be as high as we are finding," Dr. Le commented, noting that that short time span over which the change took place would favor environmental explanations over genetic ones.
"Some part may be explained by more awareness or increased medical consultation. We do know for a fact that medical consultation has increased in Denmark. But there aren’t any campaigns to make people more aware of migraine," she elaborated. "A small part of the subjects participated in both surveys, so perhaps when they saw the migraine questions for the first time, they kind of thought more about it and went to a physician. That’s hard to tell."
In additional study findings, low education and high physical workload and activity increased the risk only of migraine without aura, whereas low body mass index increased the risk only of migraine with aura. Thus "different environmental factors seem to increase the development of migraine with aura and migraine without aura," she commented.
The investigators analyzed data from the Danish Twin Study, in which 20- to 41-year-olds in the general population were asked if they had ever experienced migraine and, if so, if they had had antecedent visual disturbances. Analyses were based on data from 22,053 adults in 1994 and from 14,810 adults in 2002.
Age-stratified analyses showed that most of the increase occurred among individuals aged older than 32 years. There was a significant increase among men and women individually, with the relative increase comparable for the sexes.
The investigators conducted an additional analysis of migraine risk factors among 13,498 adults aged 18-41 years who were free of migraine in 1994 and completed surveys in both study years.
Results showed that these adults were more likely to develop migraine if they had low back pain (odds ratio, 1.3), low education (OR, 1.3), hard physical workload (OR, 1.1), hard physical activity (OR, 1.2), and a body mass index of less than 18.5 kg/m2 (OR, 1.3).
In stratified analyses, only one of these factors (low back pain) was a risk factor for both types of migraine, according to Dr. Le. Low education as well as high physical workload and activity were risk factors only for migraine without aura, whereas low BMI was a risk factor only for migraine with aura.
Dr. Le disclosed no relevant conflicts of interest.
AT THE ANNUAL MEETING OF THE AMERICAN HEADACHE SOCIETY
Major Finding: From 1994 to 2002, the lifetime prevalence of self-reported migraine increased from 18.5% to 24.5% (P less than .001), with increases for both migraine with aura and migraine without aura individually.
Data Source: This was an observational study of 36,863 young and middle-aged adults from the Danish general population.
Disclosures: Dr. Le disclosed no relevant conflicts of interest.

Secondary Headaches Flag Medical Conditions in Pregnancy
LOS ANGELES – Secondary headaches in pregnant women are likely to be associated with an additional medical complaint, according to a retrospective study of patients who presented to a tertiary-care center.
A team led by Dr. Matthew S. Robbins of Montefiore Headache Center in the Bronx, N.Y., assessed characteristics of 68 consecutive women who had an inpatient neurologic consultation for acute headache in pregnancy over a 2.5-year period at Montefiore Medical Center.
Secondary headaches were diagnosed in 57% of these women. Women with secondary headaches were more likely to have hypertension and some other chief complaint along with headache. Women with primary headaches were more likely to have a history of migraine and to have photophobia, phonophobia, and lacrimation on exam.
Three cases (4%) were noteworthy in that the headache led to discovery of an unrecognized pregnancy. All of these patients had secondary headache, and life-threatening but treatable medical conditions.
"In the acute care setting, vigilance for secondary headache in the pregnant population should be heightened, particularly in those patients who may have headache in addition to other symptoms, the lack of a migraine history, and elevated blood pressure acutely," Dr. Robbins recommended. "Because of our sad corollary [of three cases], we should ... always consider a pregnancy test in all women presenting with headache during childbearing years."
He acknowledged that a study limitation was the highly selected patient population. "This is not only patients presenting to the acute care setting, but patients who are then referred by the [emergency department] doctors or obstetricians for a neurologic consultation. So we are probably not capturing the routine cases of preeclampsia that are obvious, or other diagnoses that, in our center, the obstetricians don’t feel warrant neurologic consultation," he commented at the annual meeting of the American Headache Society.
Session attendee Dr. Peter J. Goadsby of the University of California, San Francisco, noted that about a fifth of patients with primary headache were classified as having an abnormal neurologic exam. "That wouldn’t be consistent with primary headache, would it? So what’s abnormal mean?" he asked.
"Most of the abnormal exam findings in the primary headache group were sensory abnormalities," such as unilateral facial numbness, which – although documented as abnormal – might not be clinically relevant. "It was up to the discretion of the treating team whether that patient had a primary or secondary diagnosis with the exam and abnormality combined," Dr. Robbins replied.
"Clinical experience, at least ours, suggests that consultation in the acute care setting for headache in pregnant women is not such an uncommon experience," he noted, explaining the study’s rationale. However, "there are very few guidelines that address this. It is mostly review articles in the obstetrics and gynecology literature that are not really validated, and clinical series are not well reported."
On average, the 68 women the investigators studied were 29 years old, and they were predominantly Hispanic (43%) and black (41%). The mean gestational age was 28.6 weeks, with 60% of women in their third trimester.
In terms of diagnoses, made via the ICHD-II (International Classification of Headache Disorders, second edition) system, 57% of the women had secondary headache and 43% had primary headache.
Headache class was predominantly migraine (43%), preeclampsia or eclampsia (25%), intercurrent infection (7%), and pituitary adenoma/apoplexy (6%).
The patients with primary headache and the patients with secondary headache were statistically indistinguishable in terms of most demographic, pregnancy, and clinical characteristics, according to Dr. Robbins.
But patients in the secondary headache group were less likely to have a history of migraine (39% vs. 90%; P less than .0001) and, on exam, photophobia (67% vs. 93%; P = .02), phonophobia (36% vs. 79%; P = .0004), and lacrimation (0% vs. 17%; P = .01).
On the flip side, those in the secondary headache group were more likely to have headache plus some other chief complaint such as seizure, shortness of breath, or visual disturbances (54% vs. 14%; P = .0009) and hypertension (49% vs. 0%; P less than .0001).
Of the three cases in which headache led to the discovery of an unrecognized pregnancy, one had diagnoses of PRES (posterior reversible encephalopathy syndrome) and eclampsia; one had diagnoses of PRES, RCVS (reversible cerebral vasoconstriction syndrome), and eclampsia; and one had diagnoses of hyperkalemia and renal failure in systemic lupus erythematous.
Dr. Robbins disclosed no relevant conflicts of interest.
LOS ANGELES – Secondary headaches in pregnant women are likely to be associated with an additional medical complaint, according to a retrospective study of patients who presented to a tertiary-care center.
A team led by Dr. Matthew S. Robbins of Montefiore Headache Center in the Bronx, N.Y., assessed characteristics of 68 consecutive women who had an inpatient neurologic consultation for acute headache in pregnancy over a 2.5-year period at Montefiore Medical Center.
Secondary headaches were diagnosed in 57% of these women. Women with secondary headaches were more likely to have hypertension and some other chief complaint along with headache. Women with primary headaches were more likely to have a history of migraine and to have photophobia, phonophobia, and lacrimation on exam.
Three cases (4%) were noteworthy in that the headache led to discovery of an unrecognized pregnancy. All of these patients had secondary headache, and life-threatening but treatable medical conditions.
"In the acute care setting, vigilance for secondary headache in the pregnant population should be heightened, particularly in those patients who may have headache in addition to other symptoms, the lack of a migraine history, and elevated blood pressure acutely," Dr. Robbins recommended. "Because of our sad corollary [of three cases], we should ... always consider a pregnancy test in all women presenting with headache during childbearing years."
He acknowledged that a study limitation was the highly selected patient population. "This is not only patients presenting to the acute care setting, but patients who are then referred by the [emergency department] doctors or obstetricians for a neurologic consultation. So we are probably not capturing the routine cases of preeclampsia that are obvious, or other diagnoses that, in our center, the obstetricians don’t feel warrant neurologic consultation," he commented at the annual meeting of the American Headache Society.
Session attendee Dr. Peter J. Goadsby of the University of California, San Francisco, noted that about a fifth of patients with primary headache were classified as having an abnormal neurologic exam. "That wouldn’t be consistent with primary headache, would it? So what’s abnormal mean?" he asked.
"Most of the abnormal exam findings in the primary headache group were sensory abnormalities," such as unilateral facial numbness, which – although documented as abnormal – might not be clinically relevant. "It was up to the discretion of the treating team whether that patient had a primary or secondary diagnosis with the exam and abnormality combined," Dr. Robbins replied.
"Clinical experience, at least ours, suggests that consultation in the acute care setting for headache in pregnant women is not such an uncommon experience," he noted, explaining the study’s rationale. However, "there are very few guidelines that address this. It is mostly review articles in the obstetrics and gynecology literature that are not really validated, and clinical series are not well reported."
On average, the 68 women the investigators studied were 29 years old, and they were predominantly Hispanic (43%) and black (41%). The mean gestational age was 28.6 weeks, with 60% of women in their third trimester.
In terms of diagnoses, made via the ICHD-II (International Classification of Headache Disorders, second edition) system, 57% of the women had secondary headache and 43% had primary headache.
Headache class was predominantly migraine (43%), preeclampsia or eclampsia (25%), intercurrent infection (7%), and pituitary adenoma/apoplexy (6%).
The patients with primary headache and the patients with secondary headache were statistically indistinguishable in terms of most demographic, pregnancy, and clinical characteristics, according to Dr. Robbins.
But patients in the secondary headache group were less likely to have a history of migraine (39% vs. 90%; P less than .0001) and, on exam, photophobia (67% vs. 93%; P = .02), phonophobia (36% vs. 79%; P = .0004), and lacrimation (0% vs. 17%; P = .01).
On the flip side, those in the secondary headache group were more likely to have headache plus some other chief complaint such as seizure, shortness of breath, or visual disturbances (54% vs. 14%; P = .0009) and hypertension (49% vs. 0%; P less than .0001).
Of the three cases in which headache led to the discovery of an unrecognized pregnancy, one had diagnoses of PRES (posterior reversible encephalopathy syndrome) and eclampsia; one had diagnoses of PRES, RCVS (reversible cerebral vasoconstriction syndrome), and eclampsia; and one had diagnoses of hyperkalemia and renal failure in systemic lupus erythematous.
Dr. Robbins disclosed no relevant conflicts of interest.
LOS ANGELES – Secondary headaches in pregnant women are likely to be associated with an additional medical complaint, according to a retrospective study of patients who presented to a tertiary-care center.
A team led by Dr. Matthew S. Robbins of Montefiore Headache Center in the Bronx, N.Y., assessed characteristics of 68 consecutive women who had an inpatient neurologic consultation for acute headache in pregnancy over a 2.5-year period at Montefiore Medical Center.
Secondary headaches were diagnosed in 57% of these women. Women with secondary headaches were more likely to have hypertension and some other chief complaint along with headache. Women with primary headaches were more likely to have a history of migraine and to have photophobia, phonophobia, and lacrimation on exam.
Three cases (4%) were noteworthy in that the headache led to discovery of an unrecognized pregnancy. All of these patients had secondary headache, and life-threatening but treatable medical conditions.
"In the acute care setting, vigilance for secondary headache in the pregnant population should be heightened, particularly in those patients who may have headache in addition to other symptoms, the lack of a migraine history, and elevated blood pressure acutely," Dr. Robbins recommended. "Because of our sad corollary [of three cases], we should ... always consider a pregnancy test in all women presenting with headache during childbearing years."
He acknowledged that a study limitation was the highly selected patient population. "This is not only patients presenting to the acute care setting, but patients who are then referred by the [emergency department] doctors or obstetricians for a neurologic consultation. So we are probably not capturing the routine cases of preeclampsia that are obvious, or other diagnoses that, in our center, the obstetricians don’t feel warrant neurologic consultation," he commented at the annual meeting of the American Headache Society.
Session attendee Dr. Peter J. Goadsby of the University of California, San Francisco, noted that about a fifth of patients with primary headache were classified as having an abnormal neurologic exam. "That wouldn’t be consistent with primary headache, would it? So what’s abnormal mean?" he asked.
"Most of the abnormal exam findings in the primary headache group were sensory abnormalities," such as unilateral facial numbness, which – although documented as abnormal – might not be clinically relevant. "It was up to the discretion of the treating team whether that patient had a primary or secondary diagnosis with the exam and abnormality combined," Dr. Robbins replied.
"Clinical experience, at least ours, suggests that consultation in the acute care setting for headache in pregnant women is not such an uncommon experience," he noted, explaining the study’s rationale. However, "there are very few guidelines that address this. It is mostly review articles in the obstetrics and gynecology literature that are not really validated, and clinical series are not well reported."
On average, the 68 women the investigators studied were 29 years old, and they were predominantly Hispanic (43%) and black (41%). The mean gestational age was 28.6 weeks, with 60% of women in their third trimester.
In terms of diagnoses, made via the ICHD-II (International Classification of Headache Disorders, second edition) system, 57% of the women had secondary headache and 43% had primary headache.
Headache class was predominantly migraine (43%), preeclampsia or eclampsia (25%), intercurrent infection (7%), and pituitary adenoma/apoplexy (6%).
The patients with primary headache and the patients with secondary headache were statistically indistinguishable in terms of most demographic, pregnancy, and clinical characteristics, according to Dr. Robbins.
But patients in the secondary headache group were less likely to have a history of migraine (39% vs. 90%; P less than .0001) and, on exam, photophobia (67% vs. 93%; P = .02), phonophobia (36% vs. 79%; P = .0004), and lacrimation (0% vs. 17%; P = .01).
On the flip side, those in the secondary headache group were more likely to have headache plus some other chief complaint such as seizure, shortness of breath, or visual disturbances (54% vs. 14%; P = .0009) and hypertension (49% vs. 0%; P less than .0001).
Of the three cases in which headache led to the discovery of an unrecognized pregnancy, one had diagnoses of PRES (posterior reversible encephalopathy syndrome) and eclampsia; one had diagnoses of PRES, RCVS (reversible cerebral vasoconstriction syndrome), and eclampsia; and one had diagnoses of hyperkalemia and renal failure in systemic lupus erythematous.
Dr. Robbins disclosed no relevant conflicts of interest.
AT THE ANNUAL MEETING OF THE AMERICAN HEADACHE SOCIETY
Major Finding: Secondary headaches were seen in 57% of 68 consecutive women who had an inpatient neurologic consultation for acute headache in pregnancy.
Data Source: Researchers conducted a retrospective study of 68 women who were referred for inpatient neurologic consultation because of acute headache in pregnancy.
Disclosures: Dr. Robbins disclosed no relevant conflicts of interest.
Doubt Cast on Discrete-Phase Nature of Migraine With Aura
LOS ANGELES – Contrasting with current classification criteria and the usual wisdom that attacks of migraine with aura have discrete phases, new data suggest that headache is more often than not already present during the aura phase.
In a prospective, diary-based study of 201 adults experiencing 861 attacks of migraine with aura, headache was reported within 15 minutes of the onset of aura in 61% of attacks, researchers reported at the annual meeting of the American Headache Society.

Additionally, more than half of the attacks met formal diagnostic criteria for migraine or pragmatic criteria for probable migraine within this time frame.
"These results do not seem to be consistent with the current ICHD-2 [International Classification of Headache Disorders, second edition] classification that states that migraine headache usually follows the aura symptoms; that’s not the case here," commented lead researcher Dr. Jakob M. Hansen of the headache research and treatment program at the University of California, Los Angeles and the Danish Headache Center at the University of Copenhagen.
"Furthermore, we have already headache at the onset of aura, and that does seem to conflict with the idea that you have to have a [cortical] spreading depression to activate the trigeminovascular system to cause headache."
"These data suggest that the phases of migraine attack may not be as discrete as originally believed. This is food for thought," he added.
Session attendee Dr. Jes Olesen, also of the University of Copenhagen, was skeptical of the findings, however, noting that they contrast with those of large studies in which careful histories were taken. "Always when you find something that is clearly in contrast to what is sort of conventional wisdom, we have to think about possible sources of error. ... My idea is it could be because people are mixing up a little bit attacks with and without aura ... because patients tend to mix these things up if you don’t instruct them very, very carefully," he said.
"The good thing is, for [patients] to report anything during the study, they should have an aura that they were familiar with to include an attack. I think it’s highly unlikely that people were having a migraine attack without aura. They were asked in the electronic diary, ‘Do you have an aura right now?’ " Dr. Hansen explained. "Of course it’s possible that they answered, ‘Yes, I do,’ because we reminded them. But I think it’s unlikely that so many patients would respond wrongly to a very simple question like that."
Dr. Werner Becker of the University of Calgary (Alta.), who also attended the session, commented that "migraine patients who have premonitory symptoms will often report nausea or photophobia or phonophobia even during their premonitory phase, so I’m not all that surprised that maybe symptoms are occurring during the aura as well.
"Having said that, your findings of so much headache during the aura are very interesting. But I suppose your results are consistent with the idea that the hypothalamus activation is perhaps the first part of the migraine attack," he added.

Dr. Hansen and his coinvestigators studied patients who were enrolled in a randomized therapeutic trial and had migraine with aura.
In the first phase of the study (456 attacks), patients reported the time elapsed since aura onset in quarter hours, as well as pain intensity and associated symptoms. In the second phase (405 attacks), they reported baseline pain and associated symptoms within 1 hour of aura onset, immediately before treatment.
Results showed that for 61% of attacks in the study’s first phase, headache was already present at 0-15 minutes after aura onset, Dr. Hansen reported. Patients also commonly had nausea (40%), photophobia (84%), and phonophobia (67%) at this very early phase.
Additionally, a large proportion of attacks met criteria for migraine with aura within 15 minutes of the onset of aura: 22% with use of the stricter ICHD-2 criteria for migraine with aura, and 54% with use of less strict, pragmatic criteria for probable migraine with aura (defined as migraine aura plus any-intensity headache plus at least one associated symptom among nausea/vomiting, photophobia, and phonophobia).
"These results were, of course, somewhat surprising to us because of the conflict with many of the firmly held beliefs" on migraine with aura, Dr. Hansen commented. Nonetheless, "it seems that headache and migraine symptoms are present during the aura phase."
(For all attacks studied, headache occurred within an hour of aura onset in 73%; some 31% met the ICHD-2 criteria for migraine with aura, whereas 65% met the pragmatic criteria for probable migraine with aura.)
Dr. Hansen disclosed no relevant financial conflicts of interest.
LOS ANGELES – Contrasting with current classification criteria and the usual wisdom that attacks of migraine with aura have discrete phases, new data suggest that headache is more often than not already present during the aura phase.
In a prospective, diary-based study of 201 adults experiencing 861 attacks of migraine with aura, headache was reported within 15 minutes of the onset of aura in 61% of attacks, researchers reported at the annual meeting of the American Headache Society.
Additionally, more than half of the attacks met formal diagnostic criteria for migraine or pragmatic criteria for probable migraine within this time frame.
"These results do not seem to be consistent with the current ICHD-2 [International Classification of Headache Disorders, second edition] classification that states that migraine headache usually follows the aura symptoms; that’s not the case here," commented lead researcher Dr. Jakob M. Hansen of the headache research and treatment program at the University of California, Los Angeles and the Danish Headache Center at the University of Copenhagen.
"Furthermore, we have already headache at the onset of aura, and that does seem to conflict with the idea that you have to have a [cortical] spreading depression to activate the trigeminovascular system to cause headache."
"These data suggest that the phases of migraine attack may not be as discrete as originally believed. This is food for thought," he added.
Session attendee Dr. Jes Olesen, also of the University of Copenhagen, was skeptical of the findings, however, noting that they contrast with those of large studies in which careful histories were taken. "Always when you find something that is clearly in contrast to what is sort of conventional wisdom, we have to think about possible sources of error. ... My idea is it could be because people are mixing up a little bit attacks with and without aura ... because patients tend to mix these things up if you don’t instruct them very, very carefully," he said.
"The good thing is, for [patients] to report anything during the study, they should have an aura that they were familiar with to include an attack. I think it’s highly unlikely that people were having a migraine attack without aura. They were asked in the electronic diary, ‘Do you have an aura right now?’ " Dr. Hansen explained. "Of course it’s possible that they answered, ‘Yes, I do,’ because we reminded them. But I think it’s unlikely that so many patients would respond wrongly to a very simple question like that."
Dr. Werner Becker of the University of Calgary (Alta.), who also attended the session, commented that "migraine patients who have premonitory symptoms will often report nausea or photophobia or phonophobia even during their premonitory phase, so I’m not all that surprised that maybe symptoms are occurring during the aura as well.
"Having said that, your findings of so much headache during the aura are very interesting. But I suppose your results are consistent with the idea that the hypothalamus activation is perhaps the first part of the migraine attack," he added.
Dr. Hansen and his coinvestigators studied patients who were enrolled in a randomized therapeutic trial and had migraine with aura.
In the first phase of the study (456 attacks), patients reported the time elapsed since aura onset in quarter hours, as well as pain intensity and associated symptoms. In the second phase (405 attacks), they reported baseline pain and associated symptoms within 1 hour of aura onset, immediately before treatment.
Results showed that for 61% of attacks in the study’s first phase, headache was already present at 0-15 minutes after aura onset, Dr. Hansen reported. Patients also commonly had nausea (40%), photophobia (84%), and phonophobia (67%) at this very early phase.
Additionally, a large proportion of attacks met criteria for migraine with aura within 15 minutes of the onset of aura: 22% with use of the stricter ICHD-2 criteria for migraine with aura, and 54% with use of less strict, pragmatic criteria for probable migraine with aura (defined as migraine aura plus any-intensity headache plus at least one associated symptom among nausea/vomiting, photophobia, and phonophobia).
"These results were, of course, somewhat surprising to us because of the conflict with many of the firmly held beliefs" on migraine with aura, Dr. Hansen commented. Nonetheless, "it seems that headache and migraine symptoms are present during the aura phase."
(For all attacks studied, headache occurred within an hour of aura onset in 73%; some 31% met the ICHD-2 criteria for migraine with aura, whereas 65% met the pragmatic criteria for probable migraine with aura.)
Dr. Hansen disclosed no relevant financial conflicts of interest.
LOS ANGELES – Contrasting with current classification criteria and the usual wisdom that attacks of migraine with aura have discrete phases, new data suggest that headache is more often than not already present during the aura phase.
In a prospective, diary-based study of 201 adults experiencing 861 attacks of migraine with aura, headache was reported within 15 minutes of the onset of aura in 61% of attacks, researchers reported at the annual meeting of the American Headache Society.
Additionally, more than half of the attacks met formal diagnostic criteria for migraine or pragmatic criteria for probable migraine within this time frame.
"These results do not seem to be consistent with the current ICHD-2 [International Classification of Headache Disorders, second edition] classification that states that migraine headache usually follows the aura symptoms; that’s not the case here," commented lead researcher Dr. Jakob M. Hansen of the headache research and treatment program at the University of California, Los Angeles and the Danish Headache Center at the University of Copenhagen.
"Furthermore, we have already headache at the onset of aura, and that does seem to conflict with the idea that you have to have a [cortical] spreading depression to activate the trigeminovascular system to cause headache."
"These data suggest that the phases of migraine attack may not be as discrete as originally believed. This is food for thought," he added.
Session attendee Dr. Jes Olesen, also of the University of Copenhagen, was skeptical of the findings, however, noting that they contrast with those of large studies in which careful histories were taken. "Always when you find something that is clearly in contrast to what is sort of conventional wisdom, we have to think about possible sources of error. ... My idea is it could be because people are mixing up a little bit attacks with and without aura ... because patients tend to mix these things up if you don’t instruct them very, very carefully," he said.
"The good thing is, for [patients] to report anything during the study, they should have an aura that they were familiar with to include an attack. I think it’s highly unlikely that people were having a migraine attack without aura. They were asked in the electronic diary, ‘Do you have an aura right now?’ " Dr. Hansen explained. "Of course it’s possible that they answered, ‘Yes, I do,’ because we reminded them. But I think it’s unlikely that so many patients would respond wrongly to a very simple question like that."
Dr. Werner Becker of the University of Calgary (Alta.), who also attended the session, commented that "migraine patients who have premonitory symptoms will often report nausea or photophobia or phonophobia even during their premonitory phase, so I’m not all that surprised that maybe symptoms are occurring during the aura as well.
"Having said that, your findings of so much headache during the aura are very interesting. But I suppose your results are consistent with the idea that the hypothalamus activation is perhaps the first part of the migraine attack," he added.
Dr. Hansen and his coinvestigators studied patients who were enrolled in a randomized therapeutic trial and had migraine with aura.
In the first phase of the study (456 attacks), patients reported the time elapsed since aura onset in quarter hours, as well as pain intensity and associated symptoms. In the second phase (405 attacks), they reported baseline pain and associated symptoms within 1 hour of aura onset, immediately before treatment.
Results showed that for 61% of attacks in the study’s first phase, headache was already present at 0-15 minutes after aura onset, Dr. Hansen reported. Patients also commonly had nausea (40%), photophobia (84%), and phonophobia (67%) at this very early phase.
Additionally, a large proportion of attacks met criteria for migraine with aura within 15 minutes of the onset of aura: 22% with use of the stricter ICHD-2 criteria for migraine with aura, and 54% with use of less strict, pragmatic criteria for probable migraine with aura (defined as migraine aura plus any-intensity headache plus at least one associated symptom among nausea/vomiting, photophobia, and phonophobia).
"These results were, of course, somewhat surprising to us because of the conflict with many of the firmly held beliefs" on migraine with aura, Dr. Hansen commented. Nonetheless, "it seems that headache and migraine symptoms are present during the aura phase."
(For all attacks studied, headache occurred within an hour of aura onset in 73%; some 31% met the ICHD-2 criteria for migraine with aura, whereas 65% met the pragmatic criteria for probable migraine with aura.)
Dr. Hansen disclosed no relevant financial conflicts of interest.
AT THE ANNUAL MEETING OF THE AMERICAN HEADACHE SOCIETY
Major Finding: In 61% of attacks, headache was already present within 15 minutes of the onset of aura.
Data Source: This was a prospective, diary-based study of 201 adult patients experiencing 861 attacks of migraine with aura.
Disclosures: Dr. Hansen disclosed no relevant financial conflicts of interest.

Posttraumatic Headache More Common When Injury Is Mild
LOS ANGELES – The likelihood of headache after traumatic brain injury was inversely related to the severity of injury in a longitudinal study of 598 patients.
The patients with mild injury were about 70% more likely than were their counterparts with moderate or severe injury to develop new headache or have a worsening of preexisting headache over the next year, first author Dr. Sylvia Lucas reported at the annual meeting of the American Headache Society.
The majority of headaches were migraine or probable migraine according to the ICHD-2 (International Classification of Headache Disorders, second edition) system, but a large share – roughly a quarter – had features that defied classification. Patients with preexisting headache and female patients had a higher risk of posttraumatic headache.
"Using symptom-based criteria for headache after TBI [traumatic brain injury] hopefully may serve as a framework from which to provide evidence-based treatment," commented Dr. Lucas, clinical professor of neurology, rehabilitation medicine, and neurosurgery at the University of Washington in Seattle.
Session attendee Dr. Werner Becker of the University of Calgary (Alta.) asked, "Any thoughts as to why the patients with milder injuries have more headache?"
"I don’t know. It has to have something to do with the mechanics of the hit, I suspect," Dr. Lucas replied. "We’re just now trying to look at the types of injury. We’re trying to separate subarachnoid hemorrhage, depressed skull fracture, intracerebral hemorrhage, and trying to look at how they relate to the chronicity of the headache. But, as of now, I can’t answer that."
Dr. James R. Couch of the University of Oklahoma, Oklahoma City, who also attended the session, noted that he and his colleagues found a similar pattern in a previous study. "I was very gratified to see that what you are finding is the less severely injured people seem to have a greater propensity for headache," he said. "Maybe the severe brain injury takes out some kind of center that is involved in generating headache, whereas the mild head injury just irritates it."
The investigators studied a single-center cohort of 220 patients with mild TBI who were enrolled within a week of injury and a seven-center cohort of 378 patients with moderate to severe TBI who were admitted to inpatient rehabilitation facilities. All patients were evaluated with the same questionnaire, in person at baseline, and prospectively by telephone over a year, to gain a better understanding of headache incidence, characteristics, and predictors, and treatment effectiveness.
"We feel that the ICHD-2 criteria, both in the civilian and military populations, really don’t contribute to treatment planning," Dr. Lucas commented. "They also don’t account for the latency of posttraumatic headache following trauma," with experience suggesting that almost a third of headache cases do not come to clinical attention until more than 1 week after the injury, even though that is the window typically used to define posttraumatic headache.
Patients in both groups were about 43 years old, on average, and roughly three-quarters each were male and white, and had completed high school. The leading cause of injury was vehicular accident (58%) followed by falls (25%).
Study results showed that the mild TBI group and the moderate or severe TBI group had an identical prevalence of headache before injury (17%). But the former had a higher incidence of new or worsened headache at baseline (56% vs. 40%), at 3 months (63% vs. 37%), at 6 months (69% vs. 33%), and at 12 months (58% vs. 34%).
Headache was classified according to ICHD-2 criteria for primary headache, with only a single class permitted per patient, based on the predominant features, according to Dr. Lucas. "The idea behind classification of a secondary headache using primary headache criteria is really to try to find some defining features that may allow us to do what we want in the future, which is to get some evidence-based medicine treatment or management protocols," she explained.
At all time points and in both groups, the largest share of headaches (39%-67%) was of the migraine or probable migraine type. Tension headaches were the next most common type. "Surprisingly, cervicogenic was not very [common], particularly considering that many of these were motor vehicle accidents and probably involved whiplash-type injuries," she observed.
Roughly a quarter of headaches were unclassifiable. "We felt that rather than trying to use a shoehorn to fit the headache into a classification, if it didn’t fit, we just stayed with it and deemed it unclassifiable," Dr. Lucas commented.
In both the mild TBI group and the moderate to severe TBI group, the migraine and probable migraine headaches, in addition to being most common, were more likely than the other types of headache to occur daily or several times weekly.
Also, in both groups, patients who had a prior history of headache and female patients were more likely to have headache at follow-up. For example, in the mild TBI group, about 70% of patients who had preexisting headache had headache at all time points during follow-up, compared with about 50% of patients who did not have preexisting headache.
Dr. Lucas disclosed no relevant conflicts of interest.
LOS ANGELES – The likelihood of headache after traumatic brain injury was inversely related to the severity of injury in a longitudinal study of 598 patients.
The patients with mild injury were about 70% more likely than were their counterparts with moderate or severe injury to develop new headache or have a worsening of preexisting headache over the next year, first author Dr. Sylvia Lucas reported at the annual meeting of the American Headache Society.
The majority of headaches were migraine or probable migraine according to the ICHD-2 (International Classification of Headache Disorders, second edition) system, but a large share – roughly a quarter – had features that defied classification. Patients with preexisting headache and female patients had a higher risk of posttraumatic headache.
"Using symptom-based criteria for headache after TBI [traumatic brain injury] hopefully may serve as a framework from which to provide evidence-based treatment," commented Dr. Lucas, clinical professor of neurology, rehabilitation medicine, and neurosurgery at the University of Washington in Seattle.
Session attendee Dr. Werner Becker of the University of Calgary (Alta.) asked, "Any thoughts as to why the patients with milder injuries have more headache?"
"I don’t know. It has to have something to do with the mechanics of the hit, I suspect," Dr. Lucas replied. "We’re just now trying to look at the types of injury. We’re trying to separate subarachnoid hemorrhage, depressed skull fracture, intracerebral hemorrhage, and trying to look at how they relate to the chronicity of the headache. But, as of now, I can’t answer that."
Dr. James R. Couch of the University of Oklahoma, Oklahoma City, who also attended the session, noted that he and his colleagues found a similar pattern in a previous study. "I was very gratified to see that what you are finding is the less severely injured people seem to have a greater propensity for headache," he said. "Maybe the severe brain injury takes out some kind of center that is involved in generating headache, whereas the mild head injury just irritates it."
The investigators studied a single-center cohort of 220 patients with mild TBI who were enrolled within a week of injury and a seven-center cohort of 378 patients with moderate to severe TBI who were admitted to inpatient rehabilitation facilities. All patients were evaluated with the same questionnaire, in person at baseline, and prospectively by telephone over a year, to gain a better understanding of headache incidence, characteristics, and predictors, and treatment effectiveness.
"We feel that the ICHD-2 criteria, both in the civilian and military populations, really don’t contribute to treatment planning," Dr. Lucas commented. "They also don’t account for the latency of posttraumatic headache following trauma," with experience suggesting that almost a third of headache cases do not come to clinical attention until more than 1 week after the injury, even though that is the window typically used to define posttraumatic headache.
Patients in both groups were about 43 years old, on average, and roughly three-quarters each were male and white, and had completed high school. The leading cause of injury was vehicular accident (58%) followed by falls (25%).
Study results showed that the mild TBI group and the moderate or severe TBI group had an identical prevalence of headache before injury (17%). But the former had a higher incidence of new or worsened headache at baseline (56% vs. 40%), at 3 months (63% vs. 37%), at 6 months (69% vs. 33%), and at 12 months (58% vs. 34%).
Headache was classified according to ICHD-2 criteria for primary headache, with only a single class permitted per patient, based on the predominant features, according to Dr. Lucas. "The idea behind classification of a secondary headache using primary headache criteria is really to try to find some defining features that may allow us to do what we want in the future, which is to get some evidence-based medicine treatment or management protocols," she explained.
At all time points and in both groups, the largest share of headaches (39%-67%) was of the migraine or probable migraine type. Tension headaches were the next most common type. "Surprisingly, cervicogenic was not very [common], particularly considering that many of these were motor vehicle accidents and probably involved whiplash-type injuries," she observed.
Roughly a quarter of headaches were unclassifiable. "We felt that rather than trying to use a shoehorn to fit the headache into a classification, if it didn’t fit, we just stayed with it and deemed it unclassifiable," Dr. Lucas commented.
In both the mild TBI group and the moderate to severe TBI group, the migraine and probable migraine headaches, in addition to being most common, were more likely than the other types of headache to occur daily or several times weekly.
Also, in both groups, patients who had a prior history of headache and female patients were more likely to have headache at follow-up. For example, in the mild TBI group, about 70% of patients who had preexisting headache had headache at all time points during follow-up, compared with about 50% of patients who did not have preexisting headache.
Dr. Lucas disclosed no relevant conflicts of interest.
LOS ANGELES – The likelihood of headache after traumatic brain injury was inversely related to the severity of injury in a longitudinal study of 598 patients.
The patients with mild injury were about 70% more likely than were their counterparts with moderate or severe injury to develop new headache or have a worsening of preexisting headache over the next year, first author Dr. Sylvia Lucas reported at the annual meeting of the American Headache Society.
The majority of headaches were migraine or probable migraine according to the ICHD-2 (International Classification of Headache Disorders, second edition) system, but a large share – roughly a quarter – had features that defied classification. Patients with preexisting headache and female patients had a higher risk of posttraumatic headache.
"Using symptom-based criteria for headache after TBI [traumatic brain injury] hopefully may serve as a framework from which to provide evidence-based treatment," commented Dr. Lucas, clinical professor of neurology, rehabilitation medicine, and neurosurgery at the University of Washington in Seattle.
Session attendee Dr. Werner Becker of the University of Calgary (Alta.) asked, "Any thoughts as to why the patients with milder injuries have more headache?"
"I don’t know. It has to have something to do with the mechanics of the hit, I suspect," Dr. Lucas replied. "We’re just now trying to look at the types of injury. We’re trying to separate subarachnoid hemorrhage, depressed skull fracture, intracerebral hemorrhage, and trying to look at how they relate to the chronicity of the headache. But, as of now, I can’t answer that."
Dr. James R. Couch of the University of Oklahoma, Oklahoma City, who also attended the session, noted that he and his colleagues found a similar pattern in a previous study. "I was very gratified to see that what you are finding is the less severely injured people seem to have a greater propensity for headache," he said. "Maybe the severe brain injury takes out some kind of center that is involved in generating headache, whereas the mild head injury just irritates it."
The investigators studied a single-center cohort of 220 patients with mild TBI who were enrolled within a week of injury and a seven-center cohort of 378 patients with moderate to severe TBI who were admitted to inpatient rehabilitation facilities. All patients were evaluated with the same questionnaire, in person at baseline, and prospectively by telephone over a year, to gain a better understanding of headache incidence, characteristics, and predictors, and treatment effectiveness.
"We feel that the ICHD-2 criteria, both in the civilian and military populations, really don’t contribute to treatment planning," Dr. Lucas commented. "They also don’t account for the latency of posttraumatic headache following trauma," with experience suggesting that almost a third of headache cases do not come to clinical attention until more than 1 week after the injury, even though that is the window typically used to define posttraumatic headache.
Patients in both groups were about 43 years old, on average, and roughly three-quarters each were male and white, and had completed high school. The leading cause of injury was vehicular accident (58%) followed by falls (25%).
Study results showed that the mild TBI group and the moderate or severe TBI group had an identical prevalence of headache before injury (17%). But the former had a higher incidence of new or worsened headache at baseline (56% vs. 40%), at 3 months (63% vs. 37%), at 6 months (69% vs. 33%), and at 12 months (58% vs. 34%).
Headache was classified according to ICHD-2 criteria for primary headache, with only a single class permitted per patient, based on the predominant features, according to Dr. Lucas. "The idea behind classification of a secondary headache using primary headache criteria is really to try to find some defining features that may allow us to do what we want in the future, which is to get some evidence-based medicine treatment or management protocols," she explained.
At all time points and in both groups, the largest share of headaches (39%-67%) was of the migraine or probable migraine type. Tension headaches were the next most common type. "Surprisingly, cervicogenic was not very [common], particularly considering that many of these were motor vehicle accidents and probably involved whiplash-type injuries," she observed.
Roughly a quarter of headaches were unclassifiable. "We felt that rather than trying to use a shoehorn to fit the headache into a classification, if it didn’t fit, we just stayed with it and deemed it unclassifiable," Dr. Lucas commented.
In both the mild TBI group and the moderate to severe TBI group, the migraine and probable migraine headaches, in addition to being most common, were more likely than the other types of headache to occur daily or several times weekly.
Also, in both groups, patients who had a prior history of headache and female patients were more likely to have headache at follow-up. For example, in the mild TBI group, about 70% of patients who had preexisting headache had headache at all time points during follow-up, compared with about 50% of patients who did not have preexisting headache.
Dr. Lucas disclosed no relevant conflicts of interest.
AT THE ANNUAL MEETING OF THE AMERICAN HEADACHE SOCIETY
Major Finding: The prevalence of new or worsened headache at 1 year after TBI was 58% in the cohort with mild injury, compared with 34% in the cohort with moderate or severe injury.
Data Source: This was a longitudinal study of two cohorts having a total of 598 patients with TBI.
Disclosures: Dr. Lucas disclosed no relevant conflicts of interest.
Acute Use of Rizatriptan for Migraine Safe, Effective in Teens
LOS ANGELES – Rizatriptan is safe and effective when used for intermittent treatment of migraine in adolescents on a long-term basis, according to a year-long, multicenter, open-label trial presented at the annual meeting of the American Headache Society.
Less than 1% of the 606 patients studied experienced serious drug-related adverse events. And all of these events were classified as serious because they occurred after accidental use of an extra dose of rizatriptan in a 24-hour period.

Additionally, in 46% of treated attacks, the patients were pain free at 2 hours after taking the medication, reported lead investigator Dr. Eric M. Pearlman of Children’s Hospital at Memorial University Medical Center, Savannah, Ga.
"Rizatriptan was generally safe and well tolerated in the long-term acute treatment of migraine in this adolescent population," he maintained. And "at least in an open-label fashion, it was effective."
Session attendee Dr. James R. Couch of the University of Oklahoma, Oklahoma City, commented, "That’s a very impressive pain-free number. ... The usual triptan gives us between 25% and 30% pain freedom. Do you have any comments on why children seem to respond much better?"
"I think it was because it was open label," Dr. Pearlman replied. "But this was done in conjunction with a single-attack, double-blind, placebo-controlled trial," he added. That trial, which led to regulatory approval of the drug for adolescents, had a run-in phase aimed at identifying and excluding placebo responders; the rate of pain freedom at 2 hours was 31% with rizatriptan.
Dr. Pearlman and his colleagues studied 12- to 17-years-olds in the United States and Europe who met diagnostic criteria for migraine and had not achieved a satisfactory response to treatment with nonsteroidal anti-inflammatory drugs or acetaminophen.
They were assigned to the orally disintegrating tablet formulation of rizatriptan (Maxalt-MLT) based on weight: 5 mg if they weighed less than 40 kg, and 10 mg if they weighed 40 kg or more.
Patients were instructed to use the medication to treat up to eight migraines of any severity per month. But they also were told to use only a single dose of the medication in a 24-hour period (additional nontriptan rescue medication was permitted if necessary).
Overall, 23 patients were treated with the 5-mg dose, and 583 were treated with the 10-mg dose. The average age was about 13 years in the former group and 15 years in the latter group.
As far as migraine history, in the 3 months before the study, the patients had experienced on average four attacks monthly. The majority had migraines lasting more than 6 hours. Twelve percent were on preventive therapies. "For an adolescent trial, these are fairly disabling characteristics," Dr. Pearlman noted.
A total of 12,284 attacks (most either moderate or severe) were treated during the study. The mean number of doses of study medication taken by treated patients was 20.
The leading adverse event by far was accidental overdose (seen in 24% of patients overall), defined as taking more than one dose of rizatriptan in 24 hours. Possible reasons for these overdoses may have been previous experience with triptans for which two doses are allowed in this time period, and confusing a 24-hour day with a calendar day, Dr. Pearlman speculated. The next most common adverse events were dizziness (8%), somnolence (7%), and nausea (6%).
The rate of serious drug-related adverse events was 0% in the 5-mg group and 0.5% in the 10-mg group. "All three adverse events that were classified as serious occurred in the setting of an accidental overdose, and any adverse event that occurred in conjunction with an overdose per protocol was defined as serious," he explained.
In terms of efficacy, the rate of freedom from pain at 2 hours was 46% for all treated attacks, and it appeared to be consistent over time. In a post hoc analysis, the rate of pain relief at 2 hours was 65% for treated attacks. Rescue medications were used in only 6% of treated attacks.
Dr. Pearlman disclosed that he has received consulting fees from Merck, maker of Maxalt. The study was funded by Merck.
LOS ANGELES – Rizatriptan is safe and effective when used for intermittent treatment of migraine in adolescents on a long-term basis, according to a year-long, multicenter, open-label trial presented at the annual meeting of the American Headache Society.
Less than 1% of the 606 patients studied experienced serious drug-related adverse events. And all of these events were classified as serious because they occurred after accidental use of an extra dose of rizatriptan in a 24-hour period.
Additionally, in 46% of treated attacks, the patients were pain free at 2 hours after taking the medication, reported lead investigator Dr. Eric M. Pearlman of Children’s Hospital at Memorial University Medical Center, Savannah, Ga.
"Rizatriptan was generally safe and well tolerated in the long-term acute treatment of migraine in this adolescent population," he maintained. And "at least in an open-label fashion, it was effective."
Session attendee Dr. James R. Couch of the University of Oklahoma, Oklahoma City, commented, "That’s a very impressive pain-free number. ... The usual triptan gives us between 25% and 30% pain freedom. Do you have any comments on why children seem to respond much better?"
"I think it was because it was open label," Dr. Pearlman replied. "But this was done in conjunction with a single-attack, double-blind, placebo-controlled trial," he added. That trial, which led to regulatory approval of the drug for adolescents, had a run-in phase aimed at identifying and excluding placebo responders; the rate of pain freedom at 2 hours was 31% with rizatriptan.
Dr. Pearlman and his colleagues studied 12- to 17-years-olds in the United States and Europe who met diagnostic criteria for migraine and had not achieved a satisfactory response to treatment with nonsteroidal anti-inflammatory drugs or acetaminophen.
They were assigned to the orally disintegrating tablet formulation of rizatriptan (Maxalt-MLT) based on weight: 5 mg if they weighed less than 40 kg, and 10 mg if they weighed 40 kg or more.
Patients were instructed to use the medication to treat up to eight migraines of any severity per month. But they also were told to use only a single dose of the medication in a 24-hour period (additional nontriptan rescue medication was permitted if necessary).
Overall, 23 patients were treated with the 5-mg dose, and 583 were treated with the 10-mg dose. The average age was about 13 years in the former group and 15 years in the latter group.
As far as migraine history, in the 3 months before the study, the patients had experienced on average four attacks monthly. The majority had migraines lasting more than 6 hours. Twelve percent were on preventive therapies. "For an adolescent trial, these are fairly disabling characteristics," Dr. Pearlman noted.
A total of 12,284 attacks (most either moderate or severe) were treated during the study. The mean number of doses of study medication taken by treated patients was 20.
The leading adverse event by far was accidental overdose (seen in 24% of patients overall), defined as taking more than one dose of rizatriptan in 24 hours. Possible reasons for these overdoses may have been previous experience with triptans for which two doses are allowed in this time period, and confusing a 24-hour day with a calendar day, Dr. Pearlman speculated. The next most common adverse events were dizziness (8%), somnolence (7%), and nausea (6%).
The rate of serious drug-related adverse events was 0% in the 5-mg group and 0.5% in the 10-mg group. "All three adverse events that were classified as serious occurred in the setting of an accidental overdose, and any adverse event that occurred in conjunction with an overdose per protocol was defined as serious," he explained.
In terms of efficacy, the rate of freedom from pain at 2 hours was 46% for all treated attacks, and it appeared to be consistent over time. In a post hoc analysis, the rate of pain relief at 2 hours was 65% for treated attacks. Rescue medications were used in only 6% of treated attacks.
Dr. Pearlman disclosed that he has received consulting fees from Merck, maker of Maxalt. The study was funded by Merck.
LOS ANGELES – Rizatriptan is safe and effective when used for intermittent treatment of migraine in adolescents on a long-term basis, according to a year-long, multicenter, open-label trial presented at the annual meeting of the American Headache Society.
Less than 1% of the 606 patients studied experienced serious drug-related adverse events. And all of these events were classified as serious because they occurred after accidental use of an extra dose of rizatriptan in a 24-hour period.
Additionally, in 46% of treated attacks, the patients were pain free at 2 hours after taking the medication, reported lead investigator Dr. Eric M. Pearlman of Children’s Hospital at Memorial University Medical Center, Savannah, Ga.
"Rizatriptan was generally safe and well tolerated in the long-term acute treatment of migraine in this adolescent population," he maintained. And "at least in an open-label fashion, it was effective."
Session attendee Dr. James R. Couch of the University of Oklahoma, Oklahoma City, commented, "That’s a very impressive pain-free number. ... The usual triptan gives us between 25% and 30% pain freedom. Do you have any comments on why children seem to respond much better?"
"I think it was because it was open label," Dr. Pearlman replied. "But this was done in conjunction with a single-attack, double-blind, placebo-controlled trial," he added. That trial, which led to regulatory approval of the drug for adolescents, had a run-in phase aimed at identifying and excluding placebo responders; the rate of pain freedom at 2 hours was 31% with rizatriptan.
Dr. Pearlman and his colleagues studied 12- to 17-years-olds in the United States and Europe who met diagnostic criteria for migraine and had not achieved a satisfactory response to treatment with nonsteroidal anti-inflammatory drugs or acetaminophen.
They were assigned to the orally disintegrating tablet formulation of rizatriptan (Maxalt-MLT) based on weight: 5 mg if they weighed less than 40 kg, and 10 mg if they weighed 40 kg or more.
Patients were instructed to use the medication to treat up to eight migraines of any severity per month. But they also were told to use only a single dose of the medication in a 24-hour period (additional nontriptan rescue medication was permitted if necessary).
Overall, 23 patients were treated with the 5-mg dose, and 583 were treated with the 10-mg dose. The average age was about 13 years in the former group and 15 years in the latter group.
As far as migraine history, in the 3 months before the study, the patients had experienced on average four attacks monthly. The majority had migraines lasting more than 6 hours. Twelve percent were on preventive therapies. "For an adolescent trial, these are fairly disabling characteristics," Dr. Pearlman noted.
A total of 12,284 attacks (most either moderate or severe) were treated during the study. The mean number of doses of study medication taken by treated patients was 20.
The leading adverse event by far was accidental overdose (seen in 24% of patients overall), defined as taking more than one dose of rizatriptan in 24 hours. Possible reasons for these overdoses may have been previous experience with triptans for which two doses are allowed in this time period, and confusing a 24-hour day with a calendar day, Dr. Pearlman speculated. The next most common adverse events were dizziness (8%), somnolence (7%), and nausea (6%).
The rate of serious drug-related adverse events was 0% in the 5-mg group and 0.5% in the 10-mg group. "All three adverse events that were classified as serious occurred in the setting of an accidental overdose, and any adverse event that occurred in conjunction with an overdose per protocol was defined as serious," he explained.
In terms of efficacy, the rate of freedom from pain at 2 hours was 46% for all treated attacks, and it appeared to be consistent over time. In a post hoc analysis, the rate of pain relief at 2 hours was 65% for treated attacks. Rescue medications were used in only 6% of treated attacks.
Dr. Pearlman disclosed that he has received consulting fees from Merck, maker of Maxalt. The study was funded by Merck.
AT THE ANNUAL MEETING OF THE AMERICAN HEADACHE SOCIETY
'Visual Snow' May Be a Distinct Clinical Entity
LOS ANGELES – So-called visual snow, characterized by myriad persistent tiny dots throughout the visual field, commonly occurs in patients with migraine, but it is usually accompanied by other visual symptoms and appears to be a distinct entity, according to combined data from two cross-sectional studies.
In a two-part study among 240 patients with visual snow, nearly all had other visual symptoms such as after-images or poor night vision, reported lead investigator Christoph Schankin, Ph.D., a postdoctoral clinical research fellow at the University of California at San Francisco Headache Center. Slightly more than half also had migraine, but the visual snow did not have any of the features of typical aura. Also, only a small minority of affected patients had used illicit drugs.

"Visual snow is almost always associated with additional visual symptoms. It therefore represents a unique clinical syndrome – the visual snow syndrome," he said at the annual meeting of the American Headache Society. "It is distinct from visual aura in migraine; migraine with and without aura are common comorbidities, but we don’t actually know at the moment what is the pathological link between those two conditions. And the intake of illicit drugs is not relevant."
Dr. Schankin went one step further, proposing new diagnostic criteria for the visual snow syndrome: visual snow plus at least three additional visual symptoms out of nine identified in the study, in the context where these symptoms are not consistent with typical migraine aura and cannot be attributed to some other disorder.
A session attendee congratulated the investigators on the research, noting, "These patients, for those who haven’t seen them, are devastated and lonely. Some can’t drive, some can’t work, some can’t read books, some can’t use computers. They are a wreck ... and there is nobody out there who is owning this condition – I don’t know if it falls in the realm of neuro-ophthalmology or neurology or headache, and what to do with these poor folks. ...They have been banished to the realms of psychiatry and have been told they have functional disorders and other things, when it is very clearly a widespread neurological perceptual disturbance."
He said his own experience with affected patients affirms the existence of the visual snow syndrome. "The more you talk to them, the more you appreciate that they really do have these features in common ... So I just want to thank you for bringing attention to this sort of orphan disorder, and hope it raises awareness, and that some people will take interest in it and studying the biophysiology and treatment options."
Session chair Dr. R. Allan Purdy, a neurologist at Dalhousie University in Halifax, N.S., asked the neuro-ophthalmologists present to weigh in with their thoughts on the possible pathophysiology of visual snow.
"I think this is a somewhat migrainous phenomenon in people with very sensitive brains," one replied. "We have done EEGs on these people and they are normal, at least in adults that we have seen with this. It is definitely real – these people are not making this up. And we have seen quite a few of these cases in neuro-ophthalmology."
Another concurred, saying "I think it’s real." Moreover, in her opinion, the presence of visual snow alone would be sufficient for diagnosis. "I suspect it’s migrainous because most of these people have migraines. But it’s not aura. I don’t know really what it is. It’s incredibly frustrating because nothing works. You can try every antiepileptic known to mankind, and nothing works. So I agree that this is something we need to pay attention to and help these people."
Dr. Schankin noted that research on visual snow is scarce, and affected individuals suffer in part because of a lack of knowledge about the condition in the medical community. "Patients are commonly given the diagnosis of persistent migraine aura or a posthallucinogen perceptual disorder, especially after LSD intake," he noted.
He and his coinvestigators studied members of an online support group for visual snow (Eye on Vision). In the first part of the study, they analyzed data from an Internet survey among 120 patients that asked about visual symptoms. They were 26 years old on average and about two-thirds were men.
Results showed that in addition to visual snow, nearly all patients reported other visual symptoms, such floaters (73%); persistent visual images (63%); difficulty seeing at night (58%); tiny objects moving on the blue sky (57%); sensitivity to light (54%); trails behind moving objects (48%); bright flashes (44%); and colored swirls, clouds, or waves when their eyes were closed (41%).
Dr. Schankin noted that some of these symptoms map onto the well defined clinical phenomena of palinopsia (trailing and prolonged after-images), photophobia, and impaired night vision.
And others fall into a category of entoptic phenomena, or visual symptoms originating in the eyes themselves, namely, floaters (likely protein aggregations in the vitreous fluid that cast a shadow on photoreceptors); photopsia (bright flashes typically elicited by mechanical stimulation of the eyes); Scheerer’s phenomenon (small moving objects against the sky thought to be due to blood cells moving in the retinal vessels that cast a shadow on the photoreceptors); and self-light of the eye (the colored swirls, clouds, and waves), whose etiology is unknown.
In the second part of the study, the investigators conducted telephone interviews with another 120 patients with visual snow to further explore the nature of symptoms and antecedent events. These patients were 31 years old on average and nearly evenly split between men and women.
Results showed that the textural patterns described for the snow varied considerably. The most common pattern reported was dots alternating from black (on light backgrounds) to white (on dark backgrounds) (48%), while some patients reported flashing dots, transparent dots, or other patterns. "We don’t know what that means – whether that has some pathophysiologic relevance," Dr. Schankin commented.
Analyses restricted to the subset reporting black and white dots showed that 98% had at least one additional visual symptom, and 93% had three or more. In this part of the study, another symptom identified was halos or starbursts, seen in 65% of cases.
Of the 40 patients with onset of visual snow later in life, 54% had a history of migraine. However, when asked about events in the week before the onset of visual snow, only 33% reported headache, and just 10% reported aura symptoms. But none had classic features of visual aura, such as unilaterality, zig-zag lines, or scotoma, during visual snow. Additionally, only 8% had used illicit drugs, mainly marijuana, in the week leading up to the start of visual snow, and none had significant ophthalmologic findings.
Dr. Schankin disclosed no relevant conflicts of interest.
LOS ANGELES – So-called visual snow, characterized by myriad persistent tiny dots throughout the visual field, commonly occurs in patients with migraine, but it is usually accompanied by other visual symptoms and appears to be a distinct entity, according to combined data from two cross-sectional studies.
In a two-part study among 240 patients with visual snow, nearly all had other visual symptoms such as after-images or poor night vision, reported lead investigator Christoph Schankin, Ph.D., a postdoctoral clinical research fellow at the University of California at San Francisco Headache Center. Slightly more than half also had migraine, but the visual snow did not have any of the features of typical aura. Also, only a small minority of affected patients had used illicit drugs.
"Visual snow is almost always associated with additional visual symptoms. It therefore represents a unique clinical syndrome – the visual snow syndrome," he said at the annual meeting of the American Headache Society. "It is distinct from visual aura in migraine; migraine with and without aura are common comorbidities, but we don’t actually know at the moment what is the pathological link between those two conditions. And the intake of illicit drugs is not relevant."
Dr. Schankin went one step further, proposing new diagnostic criteria for the visual snow syndrome: visual snow plus at least three additional visual symptoms out of nine identified in the study, in the context where these symptoms are not consistent with typical migraine aura and cannot be attributed to some other disorder.
A session attendee congratulated the investigators on the research, noting, "These patients, for those who haven’t seen them, are devastated and lonely. Some can’t drive, some can’t work, some can’t read books, some can’t use computers. They are a wreck ... and there is nobody out there who is owning this condition – I don’t know if it falls in the realm of neuro-ophthalmology or neurology or headache, and what to do with these poor folks. ...They have been banished to the realms of psychiatry and have been told they have functional disorders and other things, when it is very clearly a widespread neurological perceptual disturbance."
He said his own experience with affected patients affirms the existence of the visual snow syndrome. "The more you talk to them, the more you appreciate that they really do have these features in common ... So I just want to thank you for bringing attention to this sort of orphan disorder, and hope it raises awareness, and that some people will take interest in it and studying the biophysiology and treatment options."
Session chair Dr. R. Allan Purdy, a neurologist at Dalhousie University in Halifax, N.S., asked the neuro-ophthalmologists present to weigh in with their thoughts on the possible pathophysiology of visual snow.
"I think this is a somewhat migrainous phenomenon in people with very sensitive brains," one replied. "We have done EEGs on these people and they are normal, at least in adults that we have seen with this. It is definitely real – these people are not making this up. And we have seen quite a few of these cases in neuro-ophthalmology."
Another concurred, saying "I think it’s real." Moreover, in her opinion, the presence of visual snow alone would be sufficient for diagnosis. "I suspect it’s migrainous because most of these people have migraines. But it’s not aura. I don’t know really what it is. It’s incredibly frustrating because nothing works. You can try every antiepileptic known to mankind, and nothing works. So I agree that this is something we need to pay attention to and help these people."
Dr. Schankin noted that research on visual snow is scarce, and affected individuals suffer in part because of a lack of knowledge about the condition in the medical community. "Patients are commonly given the diagnosis of persistent migraine aura or a posthallucinogen perceptual disorder, especially after LSD intake," he noted.
He and his coinvestigators studied members of an online support group for visual snow (Eye on Vision). In the first part of the study, they analyzed data from an Internet survey among 120 patients that asked about visual symptoms. They were 26 years old on average and about two-thirds were men.
Results showed that in addition to visual snow, nearly all patients reported other visual symptoms, such floaters (73%); persistent visual images (63%); difficulty seeing at night (58%); tiny objects moving on the blue sky (57%); sensitivity to light (54%); trails behind moving objects (48%); bright flashes (44%); and colored swirls, clouds, or waves when their eyes were closed (41%).
Dr. Schankin noted that some of these symptoms map onto the well defined clinical phenomena of palinopsia (trailing and prolonged after-images), photophobia, and impaired night vision.
And others fall into a category of entoptic phenomena, or visual symptoms originating in the eyes themselves, namely, floaters (likely protein aggregations in the vitreous fluid that cast a shadow on photoreceptors); photopsia (bright flashes typically elicited by mechanical stimulation of the eyes); Scheerer’s phenomenon (small moving objects against the sky thought to be due to blood cells moving in the retinal vessels that cast a shadow on the photoreceptors); and self-light of the eye (the colored swirls, clouds, and waves), whose etiology is unknown.
In the second part of the study, the investigators conducted telephone interviews with another 120 patients with visual snow to further explore the nature of symptoms and antecedent events. These patients were 31 years old on average and nearly evenly split between men and women.
Results showed that the textural patterns described for the snow varied considerably. The most common pattern reported was dots alternating from black (on light backgrounds) to white (on dark backgrounds) (48%), while some patients reported flashing dots, transparent dots, or other patterns. "We don’t know what that means – whether that has some pathophysiologic relevance," Dr. Schankin commented.
Analyses restricted to the subset reporting black and white dots showed that 98% had at least one additional visual symptom, and 93% had three or more. In this part of the study, another symptom identified was halos or starbursts, seen in 65% of cases.
Of the 40 patients with onset of visual snow later in life, 54% had a history of migraine. However, when asked about events in the week before the onset of visual snow, only 33% reported headache, and just 10% reported aura symptoms. But none had classic features of visual aura, such as unilaterality, zig-zag lines, or scotoma, during visual snow. Additionally, only 8% had used illicit drugs, mainly marijuana, in the week leading up to the start of visual snow, and none had significant ophthalmologic findings.
Dr. Schankin disclosed no relevant conflicts of interest.
LOS ANGELES – So-called visual snow, characterized by myriad persistent tiny dots throughout the visual field, commonly occurs in patients with migraine, but it is usually accompanied by other visual symptoms and appears to be a distinct entity, according to combined data from two cross-sectional studies.
In a two-part study among 240 patients with visual snow, nearly all had other visual symptoms such as after-images or poor night vision, reported lead investigator Christoph Schankin, Ph.D., a postdoctoral clinical research fellow at the University of California at San Francisco Headache Center. Slightly more than half also had migraine, but the visual snow did not have any of the features of typical aura. Also, only a small minority of affected patients had used illicit drugs.
"Visual snow is almost always associated with additional visual symptoms. It therefore represents a unique clinical syndrome – the visual snow syndrome," he said at the annual meeting of the American Headache Society. "It is distinct from visual aura in migraine; migraine with and without aura are common comorbidities, but we don’t actually know at the moment what is the pathological link between those two conditions. And the intake of illicit drugs is not relevant."
Dr. Schankin went one step further, proposing new diagnostic criteria for the visual snow syndrome: visual snow plus at least three additional visual symptoms out of nine identified in the study, in the context where these symptoms are not consistent with typical migraine aura and cannot be attributed to some other disorder.
A session attendee congratulated the investigators on the research, noting, "These patients, for those who haven’t seen them, are devastated and lonely. Some can’t drive, some can’t work, some can’t read books, some can’t use computers. They are a wreck ... and there is nobody out there who is owning this condition – I don’t know if it falls in the realm of neuro-ophthalmology or neurology or headache, and what to do with these poor folks. ...They have been banished to the realms of psychiatry and have been told they have functional disorders and other things, when it is very clearly a widespread neurological perceptual disturbance."
He said his own experience with affected patients affirms the existence of the visual snow syndrome. "The more you talk to them, the more you appreciate that they really do have these features in common ... So I just want to thank you for bringing attention to this sort of orphan disorder, and hope it raises awareness, and that some people will take interest in it and studying the biophysiology and treatment options."
Session chair Dr. R. Allan Purdy, a neurologist at Dalhousie University in Halifax, N.S., asked the neuro-ophthalmologists present to weigh in with their thoughts on the possible pathophysiology of visual snow.
"I think this is a somewhat migrainous phenomenon in people with very sensitive brains," one replied. "We have done EEGs on these people and they are normal, at least in adults that we have seen with this. It is definitely real – these people are not making this up. And we have seen quite a few of these cases in neuro-ophthalmology."
Another concurred, saying "I think it’s real." Moreover, in her opinion, the presence of visual snow alone would be sufficient for diagnosis. "I suspect it’s migrainous because most of these people have migraines. But it’s not aura. I don’t know really what it is. It’s incredibly frustrating because nothing works. You can try every antiepileptic known to mankind, and nothing works. So I agree that this is something we need to pay attention to and help these people."
Dr. Schankin noted that research on visual snow is scarce, and affected individuals suffer in part because of a lack of knowledge about the condition in the medical community. "Patients are commonly given the diagnosis of persistent migraine aura or a posthallucinogen perceptual disorder, especially after LSD intake," he noted.
He and his coinvestigators studied members of an online support group for visual snow (Eye on Vision). In the first part of the study, they analyzed data from an Internet survey among 120 patients that asked about visual symptoms. They were 26 years old on average and about two-thirds were men.
Results showed that in addition to visual snow, nearly all patients reported other visual symptoms, such floaters (73%); persistent visual images (63%); difficulty seeing at night (58%); tiny objects moving on the blue sky (57%); sensitivity to light (54%); trails behind moving objects (48%); bright flashes (44%); and colored swirls, clouds, or waves when their eyes were closed (41%).
Dr. Schankin noted that some of these symptoms map onto the well defined clinical phenomena of palinopsia (trailing and prolonged after-images), photophobia, and impaired night vision.
And others fall into a category of entoptic phenomena, or visual symptoms originating in the eyes themselves, namely, floaters (likely protein aggregations in the vitreous fluid that cast a shadow on photoreceptors); photopsia (bright flashes typically elicited by mechanical stimulation of the eyes); Scheerer’s phenomenon (small moving objects against the sky thought to be due to blood cells moving in the retinal vessels that cast a shadow on the photoreceptors); and self-light of the eye (the colored swirls, clouds, and waves), whose etiology is unknown.
In the second part of the study, the investigators conducted telephone interviews with another 120 patients with visual snow to further explore the nature of symptoms and antecedent events. These patients were 31 years old on average and nearly evenly split between men and women.
Results showed that the textural patterns described for the snow varied considerably. The most common pattern reported was dots alternating from black (on light backgrounds) to white (on dark backgrounds) (48%), while some patients reported flashing dots, transparent dots, or other patterns. "We don’t know what that means – whether that has some pathophysiologic relevance," Dr. Schankin commented.
Analyses restricted to the subset reporting black and white dots showed that 98% had at least one additional visual symptom, and 93% had three or more. In this part of the study, another symptom identified was halos or starbursts, seen in 65% of cases.
Of the 40 patients with onset of visual snow later in life, 54% had a history of migraine. However, when asked about events in the week before the onset of visual snow, only 33% reported headache, and just 10% reported aura symptoms. But none had classic features of visual aura, such as unilaterality, zig-zag lines, or scotoma, during visual snow. Additionally, only 8% had used illicit drugs, mainly marijuana, in the week leading up to the start of visual snow, and none had significant ophthalmologic findings.
Dr. Schankin disclosed no relevant conflicts of interest.
AT THE ANNUAL MEETING OF THE AMERICAN HEADACHE SOCIETY
Major Finding: Slightly more than half of patients with ‘visual snow’ have migraine, and the patients nearly always have other visual symptoms, such as floaters (73%); persistent visual images (63%); difficulty seeing at night (58%); tiny objects moving on the blue sky (57%); sensitivity to light (54%); trails behind moving objects (48%); bright flashes (44%); and colored swirls, clouds, or waves when their eyes were closed (41%).
Data Source: A pair of cross-sectional studies among 240 patients with visual snow.
Disclosures: Dr. Schankin disclosed no relevant conflicts of interest.

Cortical Thickening Observed in Patients With Frequent Migraines
LOS ANGELES – The thickness and functional activation of primary somatosensory cortex mapping to the face differed according to the frequency of migraine in a small study presented at the annual meeting of the American Headache Society.
In the cross-sectional study of 20 patients, investigators conducted anatomic and functional magnetic resonance imaging in 10 patients with a low frequency of migraine attacks (mean age 40 years) and 10 with a high frequency of attacks (mean age 44 years).

Results showed that the area of the postcentral gyrus cortex representing the face was about a quarter thicker in the high-frequency group, compared with the low-frequency group. And activation of this area in response to a painful stimulus was also greater in the former.
"We think that this change that we see in high-frequency migraineurs is probably an adaptive response of the brain in order to accommodate this increased input of painful attacks, to be able to process it more and be able to handle it," commented lead investigator Nasim Maleki, Ph.D., of the Center for Pain and the Brain at Children’s Hospital Boston. Thus, the cortical thickening and increased activation might be a marker of chronification or transformation of migraine due to greater frequency of pain, triptan use, or both, she proposed.
A longitudinal study would be needed to definitively sort out cause versus effect, Dr. Maleki acknowledged. "But it could be a good hypothesis at least if somebody could do a longitudinal study, for example, looking at patients who regress from chronic to episodic migraine and then seeing if that area undergoes changes, both morphometric and functional changes."
Dr. Peter Goadsby of the University of California, San Francisco, asked, "Did you say that the BOLD [blood oxygen level–dependent] effect was being elicited from the dorsum of the hand, and the flow changes were in the face area [of the cortex]?"
"I was surprised by the same thing, too," Dr. Maleki replied. She noted that in results not shown, there was also activation of cortical areas corresponding to the hand. "But I think that maybe because that [face] area is already sensitized and responds to pain in general, the fact that we were seeing it even when we were stimulating the hand ... that’s relevant."
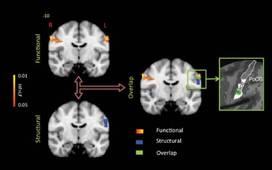
Session attendee Dr. Ronald Andiman of Cedars-Sinai Medical Center in Los Angeles asked, "What is the substance of the increased thickness of the cortex when you see it? Is it cellular? Is it neural fibers?"
It was not possible to tell given that the study used only MRI, Dr. Maleki said. "But ... we are thinking of doing the same thing in rats and seeing if there is the same pattern, and then we will be able to determine if it is density, or if it is just the number of neurons, or what exactly is going on," she said.
In a discussion of research highlights from the meeting and elsewhere, Dr. Stephen D. Silberstein of the Jefferson Headache Center in Philadelphia noted that a previous study of new London cab drivers found that their cortical thickness increased when they learned to navigate the city.
In the migraine study, "the question is, is this [thickening] cause or result?" he said. "I suspect this is like the cab drivers: If you have a lot of headaches, you learn what they are, and it affects your cortex. And I agree that this is probably a marker for migraine, not a cause of it."
Dr. Maleki and her colleagues recruited patients who had had episodic migraine for at least 3 years. On the basis of age, sex, and other migraine characteristics, they matched patients with low-frequency attacks (1-2 per month) to patients with high-frequency attacks (8-12 per month). However, she acknowledged, use of analgesic medications was unavoidably greater in the high-frequency group. The investigators also included a group of age- and sex-matched healthy individuals as controls.
Results from anatomical MRI showed that the thickness of the area of the postcentral gyrus representing the face averaged approximately 2.25 mm in patients with high-frequency migraines, compared with 1.75 mm in patients with low-frequency migraines (P less than .05) and 2.0 mm in the control participants (P less than .05).
During functional MRI performed while a noxious heat stimulus was applied to the dorsum of the hand on the migraine-dominant side, there were greater increases in BOLD signals bilaterally in the same area in the high- versus low-frequency group. "Comparing what we saw in the morphometric differences between groups and these functional contrasting results, we saw an overlap between the area that shows this structural thickening and the area that shows this functional difference," Dr. Maleki noted.
Additional functional MRI comparing somatosensory cortex connectivity between migraine groups showed that certain other areas of the brain were also more active in the high-frequency group.
"Interestingly, all of these areas ... are known areas involved in pain processing," she noted. "So again, this confirms that this thicker cortical area in high-frequency migraineurs also has stronger communication with these other areas of the brain that are also involved in pain processing."
Dr. Maleki disclosed no relevant conflicts of interest. Data analysis was supported in part by a grant from Merck.
LOS ANGELES – The thickness and functional activation of primary somatosensory cortex mapping to the face differed according to the frequency of migraine in a small study presented at the annual meeting of the American Headache Society.
In the cross-sectional study of 20 patients, investigators conducted anatomic and functional magnetic resonance imaging in 10 patients with a low frequency of migraine attacks (mean age 40 years) and 10 with a high frequency of attacks (mean age 44 years).
Results showed that the area of the postcentral gyrus cortex representing the face was about a quarter thicker in the high-frequency group, compared with the low-frequency group. And activation of this area in response to a painful stimulus was also greater in the former.
"We think that this change that we see in high-frequency migraineurs is probably an adaptive response of the brain in order to accommodate this increased input of painful attacks, to be able to process it more and be able to handle it," commented lead investigator Nasim Maleki, Ph.D., of the Center for Pain and the Brain at Children’s Hospital Boston. Thus, the cortical thickening and increased activation might be a marker of chronification or transformation of migraine due to greater frequency of pain, triptan use, or both, she proposed.
A longitudinal study would be needed to definitively sort out cause versus effect, Dr. Maleki acknowledged. "But it could be a good hypothesis at least if somebody could do a longitudinal study, for example, looking at patients who regress from chronic to episodic migraine and then seeing if that area undergoes changes, both morphometric and functional changes."
Dr. Peter Goadsby of the University of California, San Francisco, asked, "Did you say that the BOLD [blood oxygen level–dependent] effect was being elicited from the dorsum of the hand, and the flow changes were in the face area [of the cortex]?"
"I was surprised by the same thing, too," Dr. Maleki replied. She noted that in results not shown, there was also activation of cortical areas corresponding to the hand. "But I think that maybe because that [face] area is already sensitized and responds to pain in general, the fact that we were seeing it even when we were stimulating the hand ... that’s relevant."
Session attendee Dr. Ronald Andiman of Cedars-Sinai Medical Center in Los Angeles asked, "What is the substance of the increased thickness of the cortex when you see it? Is it cellular? Is it neural fibers?"
It was not possible to tell given that the study used only MRI, Dr. Maleki said. "But ... we are thinking of doing the same thing in rats and seeing if there is the same pattern, and then we will be able to determine if it is density, or if it is just the number of neurons, or what exactly is going on," she said.
In a discussion of research highlights from the meeting and elsewhere, Dr. Stephen D. Silberstein of the Jefferson Headache Center in Philadelphia noted that a previous study of new London cab drivers found that their cortical thickness increased when they learned to navigate the city.
In the migraine study, "the question is, is this [thickening] cause or result?" he said. "I suspect this is like the cab drivers: If you have a lot of headaches, you learn what they are, and it affects your cortex. And I agree that this is probably a marker for migraine, not a cause of it."
Dr. Maleki and her colleagues recruited patients who had had episodic migraine for at least 3 years. On the basis of age, sex, and other migraine characteristics, they matched patients with low-frequency attacks (1-2 per month) to patients with high-frequency attacks (8-12 per month). However, she acknowledged, use of analgesic medications was unavoidably greater in the high-frequency group. The investigators also included a group of age- and sex-matched healthy individuals as controls.
Results from anatomical MRI showed that the thickness of the area of the postcentral gyrus representing the face averaged approximately 2.25 mm in patients with high-frequency migraines, compared with 1.75 mm in patients with low-frequency migraines (P less than .05) and 2.0 mm in the control participants (P less than .05).
During functional MRI performed while a noxious heat stimulus was applied to the dorsum of the hand on the migraine-dominant side, there were greater increases in BOLD signals bilaterally in the same area in the high- versus low-frequency group. "Comparing what we saw in the morphometric differences between groups and these functional contrasting results, we saw an overlap between the area that shows this structural thickening and the area that shows this functional difference," Dr. Maleki noted.
Additional functional MRI comparing somatosensory cortex connectivity between migraine groups showed that certain other areas of the brain were also more active in the high-frequency group.
"Interestingly, all of these areas ... are known areas involved in pain processing," she noted. "So again, this confirms that this thicker cortical area in high-frequency migraineurs also has stronger communication with these other areas of the brain that are also involved in pain processing."
Dr. Maleki disclosed no relevant conflicts of interest. Data analysis was supported in part by a grant from Merck.
LOS ANGELES – The thickness and functional activation of primary somatosensory cortex mapping to the face differed according to the frequency of migraine in a small study presented at the annual meeting of the American Headache Society.
In the cross-sectional study of 20 patients, investigators conducted anatomic and functional magnetic resonance imaging in 10 patients with a low frequency of migraine attacks (mean age 40 years) and 10 with a high frequency of attacks (mean age 44 years).
Results showed that the area of the postcentral gyrus cortex representing the face was about a quarter thicker in the high-frequency group, compared with the low-frequency group. And activation of this area in response to a painful stimulus was also greater in the former.
"We think that this change that we see in high-frequency migraineurs is probably an adaptive response of the brain in order to accommodate this increased input of painful attacks, to be able to process it more and be able to handle it," commented lead investigator Nasim Maleki, Ph.D., of the Center for Pain and the Brain at Children’s Hospital Boston. Thus, the cortical thickening and increased activation might be a marker of chronification or transformation of migraine due to greater frequency of pain, triptan use, or both, she proposed.
A longitudinal study would be needed to definitively sort out cause versus effect, Dr. Maleki acknowledged. "But it could be a good hypothesis at least if somebody could do a longitudinal study, for example, looking at patients who regress from chronic to episodic migraine and then seeing if that area undergoes changes, both morphometric and functional changes."
Dr. Peter Goadsby of the University of California, San Francisco, asked, "Did you say that the BOLD [blood oxygen level–dependent] effect was being elicited from the dorsum of the hand, and the flow changes were in the face area [of the cortex]?"
"I was surprised by the same thing, too," Dr. Maleki replied. She noted that in results not shown, there was also activation of cortical areas corresponding to the hand. "But I think that maybe because that [face] area is already sensitized and responds to pain in general, the fact that we were seeing it even when we were stimulating the hand ... that’s relevant."
Session attendee Dr. Ronald Andiman of Cedars-Sinai Medical Center in Los Angeles asked, "What is the substance of the increased thickness of the cortex when you see it? Is it cellular? Is it neural fibers?"
It was not possible to tell given that the study used only MRI, Dr. Maleki said. "But ... we are thinking of doing the same thing in rats and seeing if there is the same pattern, and then we will be able to determine if it is density, or if it is just the number of neurons, or what exactly is going on," she said.
In a discussion of research highlights from the meeting and elsewhere, Dr. Stephen D. Silberstein of the Jefferson Headache Center in Philadelphia noted that a previous study of new London cab drivers found that their cortical thickness increased when they learned to navigate the city.
In the migraine study, "the question is, is this [thickening] cause or result?" he said. "I suspect this is like the cab drivers: If you have a lot of headaches, you learn what they are, and it affects your cortex. And I agree that this is probably a marker for migraine, not a cause of it."
Dr. Maleki and her colleagues recruited patients who had had episodic migraine for at least 3 years. On the basis of age, sex, and other migraine characteristics, they matched patients with low-frequency attacks (1-2 per month) to patients with high-frequency attacks (8-12 per month). However, she acknowledged, use of analgesic medications was unavoidably greater in the high-frequency group. The investigators also included a group of age- and sex-matched healthy individuals as controls.
Results from anatomical MRI showed that the thickness of the area of the postcentral gyrus representing the face averaged approximately 2.25 mm in patients with high-frequency migraines, compared with 1.75 mm in patients with low-frequency migraines (P less than .05) and 2.0 mm in the control participants (P less than .05).
During functional MRI performed while a noxious heat stimulus was applied to the dorsum of the hand on the migraine-dominant side, there were greater increases in BOLD signals bilaterally in the same area in the high- versus low-frequency group. "Comparing what we saw in the morphometric differences between groups and these functional contrasting results, we saw an overlap between the area that shows this structural thickening and the area that shows this functional difference," Dr. Maleki noted.
Additional functional MRI comparing somatosensory cortex connectivity between migraine groups showed that certain other areas of the brain were also more active in the high-frequency group.
"Interestingly, all of these areas ... are known areas involved in pain processing," she noted. "So again, this confirms that this thicker cortical area in high-frequency migraineurs also has stronger communication with these other areas of the brain that are also involved in pain processing."
Dr. Maleki disclosed no relevant conflicts of interest. Data analysis was supported in part by a grant from Merck.
AT THE ANNUAL MEETING OF THE AMERICAN HEADACHE SOCIETY
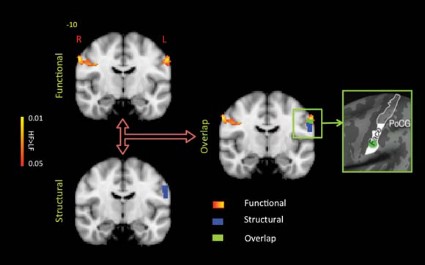
Chronic Migraine Linked to More Stressful Life Events
LOS ANGELES – Chronic migraineurs reported a greater number of stressful major life events than did those with episodic migraines in a large, cross-sectional analysis of the American Migraine Prevalence and Prevention Study.
In the study, 551 chronic migraineurs were 25% more likely report to a higher number of stressful major life events in the past year than were 7,644 episodic migraineurs, after other factors were taken into account.
"We don’t know whether the events occurred before the onset of chronic migraine or because a person was a chronic migraineur," acknowledged Aubrey N. Manack, Ph.D., an epidemiologist with Allergan Inc.

"What I think is most relevant for clinical practice is that events are perceived as stressful based on an individual’s appraisal," she continued; "so cognitive behavioral interventions may be beneficial in helping individuals reframe their perception of events and in teaching more coping skills."
She recommended future study to assess whether this association is influenced by cultural factors, as well as longitudinal research to determine if stressful life events are a risk factor for or a consequence of chronic migraine.
Session attendee Dr. Gretchen Tietjen of the University of Toledo (Ohio) Medical Center noted that she and her colleagues have analyzed data from the AMPPS as well, and found that early stressful life events – in this case, childhood maltreatment – predicted more frequent headache-days. "So I think an interesting thing would be, besides controlling for all of the things you have controlled for, to look at that, since we already have the data, just to see how many of those chronic migraineurs who had perceived stressful life events had very stressful early life events," she said at the annual meeting of the American Headache Society.
Dr. Manack agreed. And Dawn Buse, Ph.D., a psychologist at the Albert Einstein College of Medicine, New York, and a coinvestigator on both studies, noted that "early stressful life events and traumatic events such as abuse and maltreatment actually in kind of an epigenetic sort of way change our responses forever – immune system responses, coping stress mechanisms. It’s very likely that individuals who had early trauma perceive an event as stressful or overwhelming compared to an individual who had a healthier childhood and who may be more hearty."

"And what’s so interesting to remember is that an event in itself inherently is not stressful," rather it is how a person perceives the event, Dr. Buse added. Therefore, "we need to help our patients perceive life events as manageable and enhance coping skills."
In the longitudinal, population-based AMPPS, questionnaires were mailed to 24,000 individuals reporting severe headache who were first identified in 2004 and then followed up annually between 2005 and 2009.
Dr. Manack’s team studied participants in 2007 who met the diagnostic criteria for migraine, and split them into an episodic migraine group (defined as having fewer than 15 headache-days monthly) and a chronic migraine group (15 or more headache-days monthly).
The participants were surveyed about major life events in the past year, including moves; changes in the status of significant relationships; work and school stressors; events related to children; deaths; and other extremely stressful situations. Those who reported experiencing at least one such event were asked to rate its stressfulness on a 1-5 scale, and events were classified as stressful if they were rated as at least 4.
Overall, 82% of patients with chronic migraine and 79% of patients with episodic migraine reported experiencing at least one major life event in the previous year.
"The difference doesn’t seem that significant, but when you look at ... the number of events that happened, you start to see greater separation," Dr. Manack noted.
Relative to their counterparts with episodic migraine, patients with chronic migraine had higher odds of reporting a greater number of major life events in unadjusted analysis (odds ratio, 1.19; P = .03) and even more so after adjustment for age, sex, race, and body mass index (OR, 1.22; P = .01).

Overall, 77% of patients with chronic migraine and 71% of patients with episodic migraine reported experiencing at least one stressful major life event in the previous year. Again, differences between groups appeared somewhat greater at higher numbers of events.
Relative to their counterparts with episodic migraine, patients with chronic migraine had higher odds of reporting a greater number of stressful major life events in both unadjusted analysis (OR, 1.25; P = .02) and adjusted analysis (OR, 1.26; P = .01).
Dr. Manack disclosed that she is a full-time employee of Allergan Inc. The AMPPS is funded through a research grant to the National Headache Foundation from Ortho-McNeil Neurologics Inc.; additional analyses and manuscript preparation were supported through a grant from Allergan Inc. to the National Headache Foundation.
LOS ANGELES – Chronic migraineurs reported a greater number of stressful major life events than did those with episodic migraines in a large, cross-sectional analysis of the American Migraine Prevalence and Prevention Study.
In the study, 551 chronic migraineurs were 25% more likely report to a higher number of stressful major life events in the past year than were 7,644 episodic migraineurs, after other factors were taken into account.
"We don’t know whether the events occurred before the onset of chronic migraine or because a person was a chronic migraineur," acknowledged Aubrey N. Manack, Ph.D., an epidemiologist with Allergan Inc.
"What I think is most relevant for clinical practice is that events are perceived as stressful based on an individual’s appraisal," she continued; "so cognitive behavioral interventions may be beneficial in helping individuals reframe their perception of events and in teaching more coping skills."
She recommended future study to assess whether this association is influenced by cultural factors, as well as longitudinal research to determine if stressful life events are a risk factor for or a consequence of chronic migraine.
Session attendee Dr. Gretchen Tietjen of the University of Toledo (Ohio) Medical Center noted that she and her colleagues have analyzed data from the AMPPS as well, and found that early stressful life events – in this case, childhood maltreatment – predicted more frequent headache-days. "So I think an interesting thing would be, besides controlling for all of the things you have controlled for, to look at that, since we already have the data, just to see how many of those chronic migraineurs who had perceived stressful life events had very stressful early life events," she said at the annual meeting of the American Headache Society.
Dr. Manack agreed. And Dawn Buse, Ph.D., a psychologist at the Albert Einstein College of Medicine, New York, and a coinvestigator on both studies, noted that "early stressful life events and traumatic events such as abuse and maltreatment actually in kind of an epigenetic sort of way change our responses forever – immune system responses, coping stress mechanisms. It’s very likely that individuals who had early trauma perceive an event as stressful or overwhelming compared to an individual who had a healthier childhood and who may be more hearty."
"And what’s so interesting to remember is that an event in itself inherently is not stressful," rather it is how a person perceives the event, Dr. Buse added. Therefore, "we need to help our patients perceive life events as manageable and enhance coping skills."
In the longitudinal, population-based AMPPS, questionnaires were mailed to 24,000 individuals reporting severe headache who were first identified in 2004 and then followed up annually between 2005 and 2009.
Dr. Manack’s team studied participants in 2007 who met the diagnostic criteria for migraine, and split them into an episodic migraine group (defined as having fewer than 15 headache-days monthly) and a chronic migraine group (15 or more headache-days monthly).
The participants were surveyed about major life events in the past year, including moves; changes in the status of significant relationships; work and school stressors; events related to children; deaths; and other extremely stressful situations. Those who reported experiencing at least one such event were asked to rate its stressfulness on a 1-5 scale, and events were classified as stressful if they were rated as at least 4.
Overall, 82% of patients with chronic migraine and 79% of patients with episodic migraine reported experiencing at least one major life event in the previous year.
"The difference doesn’t seem that significant, but when you look at ... the number of events that happened, you start to see greater separation," Dr. Manack noted.
Relative to their counterparts with episodic migraine, patients with chronic migraine had higher odds of reporting a greater number of major life events in unadjusted analysis (odds ratio, 1.19; P = .03) and even more so after adjustment for age, sex, race, and body mass index (OR, 1.22; P = .01).
Overall, 77% of patients with chronic migraine and 71% of patients with episodic migraine reported experiencing at least one stressful major life event in the previous year. Again, differences between groups appeared somewhat greater at higher numbers of events.
Relative to their counterparts with episodic migraine, patients with chronic migraine had higher odds of reporting a greater number of stressful major life events in both unadjusted analysis (OR, 1.25; P = .02) and adjusted analysis (OR, 1.26; P = .01).
Dr. Manack disclosed that she is a full-time employee of Allergan Inc. The AMPPS is funded through a research grant to the National Headache Foundation from Ortho-McNeil Neurologics Inc.; additional analyses and manuscript preparation were supported through a grant from Allergan Inc. to the National Headache Foundation.
LOS ANGELES – Chronic migraineurs reported a greater number of stressful major life events than did those with episodic migraines in a large, cross-sectional analysis of the American Migraine Prevalence and Prevention Study.
In the study, 551 chronic migraineurs were 25% more likely report to a higher number of stressful major life events in the past year than were 7,644 episodic migraineurs, after other factors were taken into account.
"We don’t know whether the events occurred before the onset of chronic migraine or because a person was a chronic migraineur," acknowledged Aubrey N. Manack, Ph.D., an epidemiologist with Allergan Inc.
"What I think is most relevant for clinical practice is that events are perceived as stressful based on an individual’s appraisal," she continued; "so cognitive behavioral interventions may be beneficial in helping individuals reframe their perception of events and in teaching more coping skills."
She recommended future study to assess whether this association is influenced by cultural factors, as well as longitudinal research to determine if stressful life events are a risk factor for or a consequence of chronic migraine.
Session attendee Dr. Gretchen Tietjen of the University of Toledo (Ohio) Medical Center noted that she and her colleagues have analyzed data from the AMPPS as well, and found that early stressful life events – in this case, childhood maltreatment – predicted more frequent headache-days. "So I think an interesting thing would be, besides controlling for all of the things you have controlled for, to look at that, since we already have the data, just to see how many of those chronic migraineurs who had perceived stressful life events had very stressful early life events," she said at the annual meeting of the American Headache Society.
Dr. Manack agreed. And Dawn Buse, Ph.D., a psychologist at the Albert Einstein College of Medicine, New York, and a coinvestigator on both studies, noted that "early stressful life events and traumatic events such as abuse and maltreatment actually in kind of an epigenetic sort of way change our responses forever – immune system responses, coping stress mechanisms. It’s very likely that individuals who had early trauma perceive an event as stressful or overwhelming compared to an individual who had a healthier childhood and who may be more hearty."
"And what’s so interesting to remember is that an event in itself inherently is not stressful," rather it is how a person perceives the event, Dr. Buse added. Therefore, "we need to help our patients perceive life events as manageable and enhance coping skills."
In the longitudinal, population-based AMPPS, questionnaires were mailed to 24,000 individuals reporting severe headache who were first identified in 2004 and then followed up annually between 2005 and 2009.
Dr. Manack’s team studied participants in 2007 who met the diagnostic criteria for migraine, and split them into an episodic migraine group (defined as having fewer than 15 headache-days monthly) and a chronic migraine group (15 or more headache-days monthly).
The participants were surveyed about major life events in the past year, including moves; changes in the status of significant relationships; work and school stressors; events related to children; deaths; and other extremely stressful situations. Those who reported experiencing at least one such event were asked to rate its stressfulness on a 1-5 scale, and events were classified as stressful if they were rated as at least 4.
Overall, 82% of patients with chronic migraine and 79% of patients with episodic migraine reported experiencing at least one major life event in the previous year.
"The difference doesn’t seem that significant, but when you look at ... the number of events that happened, you start to see greater separation," Dr. Manack noted.
Relative to their counterparts with episodic migraine, patients with chronic migraine had higher odds of reporting a greater number of major life events in unadjusted analysis (odds ratio, 1.19; P = .03) and even more so after adjustment for age, sex, race, and body mass index (OR, 1.22; P = .01).
Overall, 77% of patients with chronic migraine and 71% of patients with episodic migraine reported experiencing at least one stressful major life event in the previous year. Again, differences between groups appeared somewhat greater at higher numbers of events.
Relative to their counterparts with episodic migraine, patients with chronic migraine had higher odds of reporting a greater number of stressful major life events in both unadjusted analysis (OR, 1.25; P = .02) and adjusted analysis (OR, 1.26; P = .01).
Dr. Manack disclosed that she is a full-time employee of Allergan Inc. The AMPPS is funded through a research grant to the National Headache Foundation from Ortho-McNeil Neurologics Inc.; additional analyses and manuscript preparation were supported through a grant from Allergan Inc. to the National Headache Foundation.
AT THE ANNUAL MEETING OF THE AMERICAN HEADACHE SOCIETY
Major Finding: Relative to their counterparts with episodic migraine, patients with chronic migraine were more likely to report a greater number of stressful major life events in the past year (OR, 1.26).
Data Source: This was a cross-sectional study of 551 individuals with chronic migraine and 7,644 individuals with episodic migraine from the AMPPS.
Disclosures: Dr. Manack disclosed that she is a full-time employee of Allergan. The AMPP study is funded through a research grant to the National Headache Foundation from Ortho-McNeil Neurologics; additional analyses and manuscript preparation were supported through a grant from Allergan to the National Headache Foundation.
Neurostimulation May Work When Migraine Drugs Fail
LOS ANGELES – Occipital nerve stimulation provided relief from chronic migraine in a randomized, double-blind trial of patients who had not responded to currently available pharmacologic therapies.
The 12-week trial of 125 patients found that patients who received active neurostimulation were about four times more likely to rate their pain relief as excellent or fair than were those who received sham neurostimulation. The actively-stimulated patients also had more than double the reduction in number of days with headache each month.

"This is the first large-scale study of peripheral nerve stimulation for intractable chronic migraine that showed a significant reduction in pain, number of headache-days, and migraine-related disability," said lead investigator Dr. Stephen D. Silberstein of the Jefferson Headache Center in Philadelphia.
"These results suggest that patients who have exhausted all treatment options may benefit from peripheral nerve stimulation of the occipital nerves," he added. "These results provide the strongest evidence to date to support the safety and efficacy of peripheral nerve stimulation for intractable chronic migraine."
Session attendee Dr. Peter Goadsby of the University of California, San Francisco, questioned whether the trial was truly blinded, given the challenge of concealing group assignment when using neurostimulation. "It is very difficult. ... Much of the blinding in these studies is compromised," he said at the annual meeting of the American Headache Society. "I think it’s not fair to say this is the strongest evidence for peripheral nerve, occipital nerve stimulation. I think it’s another piece of evidence, but I don’t think that we have hit a home run here. ... I don’t think this is prime time yet."
"I’m not disagreeing with you," Dr. Silberstein replied. "I am saying of all the trials, in the subset of patients we defined as intractable chronic migraine, this is the best evidence so far. ... How do you blind brain stimulation trials? That’s a fundamental problem," he acknowledged, noting that patients in the trial were told that they were receiving neurostimulation with different parameters. "It’s very difficult and very complicated to control with any active stimulation device. We tried the best we could."
In the trial, the investigators enrolled patients with chronic, intractable migraines who had headache at least 15 days a month, had experienced a failure of at least three preventive medications, and had moderate headache-related disability. Their pain had to be at least 6 cm out of 10 cm on a visual analog scale and localized to the posterior head or originating from the cervical region.
Patients were not required to have responded previously to an occipital nerve block, Dr. Silberstein noted, explaining that "there is no evidence at all that occipital nerve block is predictive of the response to stimulation." Patients who overused medication were included, but those taking opioids were not.
All patients underwent implantation of St. Jude Medical’s neurostimulation system and were randomized to the neurostimulation group (n = 88) or the control group (n = 37).
Results showed that about 70% of patients in the neurostimulation group reported excellent or fair pain relief at 12 weeks, compared with only 20% of their counterparts in the control group (P = .001).
Patients who received active neurostimulation were also more likely to achieve a reduction in mean daily pain intensity on the visual analogue scale of 10%, 20%, or 30% (P less than .05 for each). "Looking at 40%, 50%, and 60% differences in this particular trial, they were not statistically significant differences, but again, remember, this was a disabling migraine population that had failed three therapies," Dr. Silberstein commented.
The neurostimulation group also had a greater mean reduction in monthly number of headache-days (7.0 vs. 2.7 days; P = .03) and were more likely to have a 10%, 20%, 30%, and 40% reduction in the number (P less than .05 for each).
In terms of headache-related disability, patients in the neurostimulation group also had a greater reduction in MIDAS (Migraine Disability Assessment) scores (a drop of 73 points vs. a drop of 27 points; P = .001) and in Zung Pain and Distress Scale scores (by 15 vs. 6 points, P = .001).
The overall rate of adverse events was about 61% in the neurostimulation group and 49% in the control group.
The leading hardware-related adverse event was lead migration, accounting for 15% of all events, with a higher rate in the neurostimulation group. "If you have a device in and it’s actively stimulating and you are getting pain relief, and then the pain relief ceases, it’s easier to identify the fact that you have had lead migration," Dr. Silberstein explained, adding that lead migration has become much less problematic as surgical techniques have improved.
The leading biological adverse event was persistent pain and/or numbness at the implantable pulse generator or lead site, which accounted for 22% of all events.
Dr. Silberstein disclosed that he receives consulting fees/honoraria and research support from St. Jude Medical Neuromodulation Division, which funded the trial.
neurostimulation, pain relief, chronic migraine, Dr. Stephen D. Silberstein, Jefferson Headache Center in Philadelphia,
LOS ANGELES – Occipital nerve stimulation provided relief from chronic migraine in a randomized, double-blind trial of patients who had not responded to currently available pharmacologic therapies.
The 12-week trial of 125 patients found that patients who received active neurostimulation were about four times more likely to rate their pain relief as excellent or fair than were those who received sham neurostimulation. The actively-stimulated patients also had more than double the reduction in number of days with headache each month.
"This is the first large-scale study of peripheral nerve stimulation for intractable chronic migraine that showed a significant reduction in pain, number of headache-days, and migraine-related disability," said lead investigator Dr. Stephen D. Silberstein of the Jefferson Headache Center in Philadelphia.
"These results suggest that patients who have exhausted all treatment options may benefit from peripheral nerve stimulation of the occipital nerves," he added. "These results provide the strongest evidence to date to support the safety and efficacy of peripheral nerve stimulation for intractable chronic migraine."
Session attendee Dr. Peter Goadsby of the University of California, San Francisco, questioned whether the trial was truly blinded, given the challenge of concealing group assignment when using neurostimulation. "It is very difficult. ... Much of the blinding in these studies is compromised," he said at the annual meeting of the American Headache Society. "I think it’s not fair to say this is the strongest evidence for peripheral nerve, occipital nerve stimulation. I think it’s another piece of evidence, but I don’t think that we have hit a home run here. ... I don’t think this is prime time yet."
"I’m not disagreeing with you," Dr. Silberstein replied. "I am saying of all the trials, in the subset of patients we defined as intractable chronic migraine, this is the best evidence so far. ... How do you blind brain stimulation trials? That’s a fundamental problem," he acknowledged, noting that patients in the trial were told that they were receiving neurostimulation with different parameters. "It’s very difficult and very complicated to control with any active stimulation device. We tried the best we could."
In the trial, the investigators enrolled patients with chronic, intractable migraines who had headache at least 15 days a month, had experienced a failure of at least three preventive medications, and had moderate headache-related disability. Their pain had to be at least 6 cm out of 10 cm on a visual analog scale and localized to the posterior head or originating from the cervical region.
Patients were not required to have responded previously to an occipital nerve block, Dr. Silberstein noted, explaining that "there is no evidence at all that occipital nerve block is predictive of the response to stimulation." Patients who overused medication were included, but those taking opioids were not.
All patients underwent implantation of St. Jude Medical’s neurostimulation system and were randomized to the neurostimulation group (n = 88) or the control group (n = 37).
Results showed that about 70% of patients in the neurostimulation group reported excellent or fair pain relief at 12 weeks, compared with only 20% of their counterparts in the control group (P = .001).
Patients who received active neurostimulation were also more likely to achieve a reduction in mean daily pain intensity on the visual analogue scale of 10%, 20%, or 30% (P less than .05 for each). "Looking at 40%, 50%, and 60% differences in this particular trial, they were not statistically significant differences, but again, remember, this was a disabling migraine population that had failed three therapies," Dr. Silberstein commented.
The neurostimulation group also had a greater mean reduction in monthly number of headache-days (7.0 vs. 2.7 days; P = .03) and were more likely to have a 10%, 20%, 30%, and 40% reduction in the number (P less than .05 for each).
In terms of headache-related disability, patients in the neurostimulation group also had a greater reduction in MIDAS (Migraine Disability Assessment) scores (a drop of 73 points vs. a drop of 27 points; P = .001) and in Zung Pain and Distress Scale scores (by 15 vs. 6 points, P = .001).
The overall rate of adverse events was about 61% in the neurostimulation group and 49% in the control group.
The leading hardware-related adverse event was lead migration, accounting for 15% of all events, with a higher rate in the neurostimulation group. "If you have a device in and it’s actively stimulating and you are getting pain relief, and then the pain relief ceases, it’s easier to identify the fact that you have had lead migration," Dr. Silberstein explained, adding that lead migration has become much less problematic as surgical techniques have improved.
The leading biological adverse event was persistent pain and/or numbness at the implantable pulse generator or lead site, which accounted for 22% of all events.
Dr. Silberstein disclosed that he receives consulting fees/honoraria and research support from St. Jude Medical Neuromodulation Division, which funded the trial.
LOS ANGELES – Occipital nerve stimulation provided relief from chronic migraine in a randomized, double-blind trial of patients who had not responded to currently available pharmacologic therapies.
The 12-week trial of 125 patients found that patients who received active neurostimulation were about four times more likely to rate their pain relief as excellent or fair than were those who received sham neurostimulation. The actively-stimulated patients also had more than double the reduction in number of days with headache each month.
"This is the first large-scale study of peripheral nerve stimulation for intractable chronic migraine that showed a significant reduction in pain, number of headache-days, and migraine-related disability," said lead investigator Dr. Stephen D. Silberstein of the Jefferson Headache Center in Philadelphia.
"These results suggest that patients who have exhausted all treatment options may benefit from peripheral nerve stimulation of the occipital nerves," he added. "These results provide the strongest evidence to date to support the safety and efficacy of peripheral nerve stimulation for intractable chronic migraine."
Session attendee Dr. Peter Goadsby of the University of California, San Francisco, questioned whether the trial was truly blinded, given the challenge of concealing group assignment when using neurostimulation. "It is very difficult. ... Much of the blinding in these studies is compromised," he said at the annual meeting of the American Headache Society. "I think it’s not fair to say this is the strongest evidence for peripheral nerve, occipital nerve stimulation. I think it’s another piece of evidence, but I don’t think that we have hit a home run here. ... I don’t think this is prime time yet."
"I’m not disagreeing with you," Dr. Silberstein replied. "I am saying of all the trials, in the subset of patients we defined as intractable chronic migraine, this is the best evidence so far. ... How do you blind brain stimulation trials? That’s a fundamental problem," he acknowledged, noting that patients in the trial were told that they were receiving neurostimulation with different parameters. "It’s very difficult and very complicated to control with any active stimulation device. We tried the best we could."
In the trial, the investigators enrolled patients with chronic, intractable migraines who had headache at least 15 days a month, had experienced a failure of at least three preventive medications, and had moderate headache-related disability. Their pain had to be at least 6 cm out of 10 cm on a visual analog scale and localized to the posterior head or originating from the cervical region.
Patients were not required to have responded previously to an occipital nerve block, Dr. Silberstein noted, explaining that "there is no evidence at all that occipital nerve block is predictive of the response to stimulation." Patients who overused medication were included, but those taking opioids were not.
All patients underwent implantation of St. Jude Medical’s neurostimulation system and were randomized to the neurostimulation group (n = 88) or the control group (n = 37).
Results showed that about 70% of patients in the neurostimulation group reported excellent or fair pain relief at 12 weeks, compared with only 20% of their counterparts in the control group (P = .001).
Patients who received active neurostimulation were also more likely to achieve a reduction in mean daily pain intensity on the visual analogue scale of 10%, 20%, or 30% (P less than .05 for each). "Looking at 40%, 50%, and 60% differences in this particular trial, they were not statistically significant differences, but again, remember, this was a disabling migraine population that had failed three therapies," Dr. Silberstein commented.
The neurostimulation group also had a greater mean reduction in monthly number of headache-days (7.0 vs. 2.7 days; P = .03) and were more likely to have a 10%, 20%, 30%, and 40% reduction in the number (P less than .05 for each).
In terms of headache-related disability, patients in the neurostimulation group also had a greater reduction in MIDAS (Migraine Disability Assessment) scores (a drop of 73 points vs. a drop of 27 points; P = .001) and in Zung Pain and Distress Scale scores (by 15 vs. 6 points, P = .001).
The overall rate of adverse events was about 61% in the neurostimulation group and 49% in the control group.
The leading hardware-related adverse event was lead migration, accounting for 15% of all events, with a higher rate in the neurostimulation group. "If you have a device in and it’s actively stimulating and you are getting pain relief, and then the pain relief ceases, it’s easier to identify the fact that you have had lead migration," Dr. Silberstein explained, adding that lead migration has become much less problematic as surgical techniques have improved.
The leading biological adverse event was persistent pain and/or numbness at the implantable pulse generator or lead site, which accounted for 22% of all events.
Dr. Silberstein disclosed that he receives consulting fees/honoraria and research support from St. Jude Medical Neuromodulation Division, which funded the trial.
neurostimulation, pain relief, chronic migraine, Dr. Stephen D. Silberstein, Jefferson Headache Center in Philadelphia,
neurostimulation, pain relief, chronic migraine, Dr. Stephen D. Silberstein, Jefferson Headache Center in Philadelphia,
AT THE ANNUAL MEETING OF THE AMERICAN HEADACHE SOCIETY
Major Finding: About 70% of patients in the neurostimulation group reported excellent or fair pain relief at 12 weeks, compared with only 20% of their counterparts in the control group (P = .001).
Data Source: This was a multicenter, randomized, double-blind trial of 125 patients with intractable chronic migraine.
Disclosures: Dr. Silberstein disclosed that he receives consulting fees/honoraria and research support from St. Jude Medical Neuromodulation Division, which funded the trial.
Studies Examine Scenarios of Changing Triptan Regimens
LOS ANGELES – In patients using triptans for the acute treatment of migraine, the impact on headache-related disability of switching or adding medications depends on the frequency of attacks and the type of medication, new data show.
Dr. Richard B. Lipton and Dawn C. Buse, Ph.D., both of the Albert Einstein College of Medicine in New York, and their colleagues assessed associations between treatment changes and disability among more than 1,500 triptan users from the longitudinal, population-based AMPP (American Migraine Prevalence and Prevention) study, reporting their findings at the annual meeting of the American Headache Society.

In one analysis, patients switching to NSAIDs or to combination analgesics containing an opioid or a barbiturate had respective 31% and 48% worsening in scores for headache-related disability, compared with nonswitchers, but patients staying on the triptan or switching to another one did not have any significant change in score. In stratified analyses, switching to an NSAID was associated with a worsening among the subset of patients having the most frequent attacks.
The second study found that adding an NSAID to the triptan improved scores for patients with medium-frequency episodic migraines, while adding an NSAID or another triptan worsened scores for those with high-frequency episodic migraines or chronic migraines. Patients with low-frequency episodic migraines did not have any change regardless of the medication added.
"On average, the changes clinicians make in prescription drug therapy in the real world, switching from one triptan to another or adding a second triptan, are not helpful," Dr. Lipton commented. "That is not to say that when we switch individual patients, there isn’t a benefit to that or that optimized algorithms for choosing treatments have no effect on patient care. But it is to say that maybe when we think about what to do with patients who don’t respond to medications, it’s worth considering that switching triptans on average doesn’t have the benefits for disability that I certainly previously thought."
The studies may have had the bias of confounding by indication, whereby the reasons for medication changes (which were unknown) influenced outcomes, he acknowledged. "But they do have the strength of generalizability and reflecting what actually goes on in the real world."
Session attendee Dr. James Couch of the University of Oklahoma, Oklahoma City, expressed concern about the possible confounding.
"Most of us have found that all the triptans are not equal, and if you go through the whole list of seven, it’s not unlikely that you will find one that works better than others and so on," he elaborated. Thus, some patients on one triptan "may have gotten a moderate effect, and they were still looking for a triptan that was going to have that whiz-bang effect." Also, insurance company requirements may dictate medication switches in some cases.
Dr. Peter Goadsby of the University of California, San Francisco, asked whether analyses were masking the heterogeneity of response in the study sample. "It strikes me that in practice, it’s quite heterogeneous: You make a change in some patients, they do spectacularly well, or maybe it’s just luck, and other patients don’t," he commented. "So is there more than one population, and are you losing some granularity in what we do by having them all lumped together?"
"Our reason for stratifying by attack frequency was to try to reduce that heterogeneity," Dr. Lipton replied. "And when we stratify by attack frequency, we see some pretty robust effects."
Finally, session co-moderator Dr. Andrew Hershey of the Cincinnati Children’s Hospital wondered if the directionality of association was perhaps reversed, and headache-related disability had instead prompted the medication changes.
Dr. Lipton noted that the investigators assessed changes in score from before to after a medication switch, in addition to using stratification. "So that’s our attempt to take baseline differences into account, though it’s certainly imperfect," he acknowledged.
Switching Medications
Dr. Buse and her colleagues studied the impact of medication switches from one year to the next in 799 patients with migraine taking triptans for acute treatment.

"Providers commonly switch patients in their acute pharmacologic regimens, we know that. We switch medications for a variety of reasons: patient preference, nonresponse, what is allowed by third-party payers," she commented. However, most studies of switching medications have looked at short-term outcomes, and few have looked at switches to or from triptans.
Fully 83% of the patients studied continued on the same triptan, 10% switched to another triptan, 4% switched to a combination analgesic containing an opioid or barbiturate, and 3% switched to an NSAID.
Results showed that headache-related disability, assessed from Migraine Disability Assessment (MIDAS) scores, was essentially unchanged from one year to the next in patients who stayed on the same triptan (14.5 vs. 14.1) or who switched from one triptan to another (16.6 vs. 16.6). In contrast, scores increased (worsened) in patients who switched to NSAIDs (16.0 vs. 20.9) and who switched to combination therapy containing opioids or barbiturates (11.9 vs. 17.6).
Additional analyses showed that the impact of switching to NSAIDs varied according to migraine frequency. Specifically, patients with high-frequency episodic migraines (10-14 headache-days monthly) or chronic migraines (15 or more headache-days monthly) had a significant increase in MIDAS scores when switching to NSAIDs relative to their counterparts with low-frequency episodic migraines (0-4 headache-days monthly) or moderate-frequency episodic migraines (5-9 headache-days monthly).
"Not only did the treatment matter, but the average number of days of headache at baseline matters quite importantly here," Dr. Buse commented.
"In this observational study, switching triptan regimens or switching from a triptan to an alternative pharmacologic therapy for acute migraine does not appear to be associated with improvements in headache-related disability and, in some cases, is associated with increased headache-related disability over the course of 1 year to the second year," she concluded.
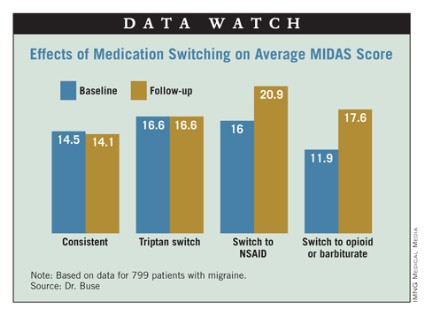
Adding medications
Dr. Lipton’s team studied the impact of medication additions from one year to the next in 960 patients with migraine taking triptans for acute treatment.
"Most people with migraine in the population use more than one acute treatment, and triptan users often use more than one triptan or use a triptan in combination with other medications, or even use combination products, such as Treximet [sumatriptan and naproxen], which contains a triptan and a nonsteroidal [anti-inflammatory drug]," he noted.
"By and large, we have not done much in terms of studying combination acute treatment in migraine, and certainly combining triptans has not been studied very often," he noted.
Most patients, 68%, did not change their acute treatment, while 13% added a combination analgesic containing opioids or barbiturates, 12% added another triptan, and 7% added an NSAID.
Results showed that among patients having low-frequency episodic migraines, adding another medication to their triptan did not significantly affect MIDAS score from one year to the next, regardless of the type of medication added.
Among patients with medium-frequency episodic migraines, adding an NSAID was associated with a significant decrease in MIDAS scores, whereas adding other medications did not affect scores.
But among patients with high-frequency episodic migraines or chronic migraines, MIDAS scores actually increased significantly with addition of an NSAID or another triptan. They were unaffected by addition of a combination analgesic containing opioids or barbiturates.
Further analyses confirmed that the impact of adding NSAIDs varied according to migraine frequency: Patients with high-frequency episodic migraines or chronic migraines had a significant increase in MIDAS scores when switching to NSAIDs relative to their counterparts with low-frequency episodic migraines.
"This is analogous to the finding in the Bigal paper [Headache 2008;48:1157-68] showing that NSAIDs are associated with an increased risk of transition to chronic migraine in people who have high-frequency episodic migraine," Dr. Lipton commented.
Dr. Lipton disclosed that he receives research grant support from the National Institutes of Health, the National Headache Foundation, and the Migraine Research Fund, and serves as a consultant or advisor to or has received honoraria from the American Headache Society and various pharmaceutical companies manufacturing drugs for migraine. Dr. Buse disclosed that she has received grant support and honoraria from Endo Pharmaceuticals and other pharmaceutical companies manufacturing drugs for migraine. The AMPP study is funded through a research grant to the National Headache Foundation from Ortho-McNeil Neurologics; additional analyses and manuscript preparation were supported through a grant from MAP Pharmaceuticals and Allergan to the National Headache Foundation.
LOS ANGELES – In patients using triptans for the acute treatment of migraine, the impact on headache-related disability of switching or adding medications depends on the frequency of attacks and the type of medication, new data show.
Dr. Richard B. Lipton and Dawn C. Buse, Ph.D., both of the Albert Einstein College of Medicine in New York, and their colleagues assessed associations between treatment changes and disability among more than 1,500 triptan users from the longitudinal, population-based AMPP (American Migraine Prevalence and Prevention) study, reporting their findings at the annual meeting of the American Headache Society.
In one analysis, patients switching to NSAIDs or to combination analgesics containing an opioid or a barbiturate had respective 31% and 48% worsening in scores for headache-related disability, compared with nonswitchers, but patients staying on the triptan or switching to another one did not have any significant change in score. In stratified analyses, switching to an NSAID was associated with a worsening among the subset of patients having the most frequent attacks.
The second study found that adding an NSAID to the triptan improved scores for patients with medium-frequency episodic migraines, while adding an NSAID or another triptan worsened scores for those with high-frequency episodic migraines or chronic migraines. Patients with low-frequency episodic migraines did not have any change regardless of the medication added.
"On average, the changes clinicians make in prescription drug therapy in the real world, switching from one triptan to another or adding a second triptan, are not helpful," Dr. Lipton commented. "That is not to say that when we switch individual patients, there isn’t a benefit to that or that optimized algorithms for choosing treatments have no effect on patient care. But it is to say that maybe when we think about what to do with patients who don’t respond to medications, it’s worth considering that switching triptans on average doesn’t have the benefits for disability that I certainly previously thought."
The studies may have had the bias of confounding by indication, whereby the reasons for medication changes (which were unknown) influenced outcomes, he acknowledged. "But they do have the strength of generalizability and reflecting what actually goes on in the real world."
Session attendee Dr. James Couch of the University of Oklahoma, Oklahoma City, expressed concern about the possible confounding.
"Most of us have found that all the triptans are not equal, and if you go through the whole list of seven, it’s not unlikely that you will find one that works better than others and so on," he elaborated. Thus, some patients on one triptan "may have gotten a moderate effect, and they were still looking for a triptan that was going to have that whiz-bang effect." Also, insurance company requirements may dictate medication switches in some cases.
Dr. Peter Goadsby of the University of California, San Francisco, asked whether analyses were masking the heterogeneity of response in the study sample. "It strikes me that in practice, it’s quite heterogeneous: You make a change in some patients, they do spectacularly well, or maybe it’s just luck, and other patients don’t," he commented. "So is there more than one population, and are you losing some granularity in what we do by having them all lumped together?"
"Our reason for stratifying by attack frequency was to try to reduce that heterogeneity," Dr. Lipton replied. "And when we stratify by attack frequency, we see some pretty robust effects."
Finally, session co-moderator Dr. Andrew Hershey of the Cincinnati Children’s Hospital wondered if the directionality of association was perhaps reversed, and headache-related disability had instead prompted the medication changes.
Dr. Lipton noted that the investigators assessed changes in score from before to after a medication switch, in addition to using stratification. "So that’s our attempt to take baseline differences into account, though it’s certainly imperfect," he acknowledged.
Switching Medications
Dr. Buse and her colleagues studied the impact of medication switches from one year to the next in 799 patients with migraine taking triptans for acute treatment.
"Providers commonly switch patients in their acute pharmacologic regimens, we know that. We switch medications for a variety of reasons: patient preference, nonresponse, what is allowed by third-party payers," she commented. However, most studies of switching medications have looked at short-term outcomes, and few have looked at switches to or from triptans.
Fully 83% of the patients studied continued on the same triptan, 10% switched to another triptan, 4% switched to a combination analgesic containing an opioid or barbiturate, and 3% switched to an NSAID.
Results showed that headache-related disability, assessed from Migraine Disability Assessment (MIDAS) scores, was essentially unchanged from one year to the next in patients who stayed on the same triptan (14.5 vs. 14.1) or who switched from one triptan to another (16.6 vs. 16.6). In contrast, scores increased (worsened) in patients who switched to NSAIDs (16.0 vs. 20.9) and who switched to combination therapy containing opioids or barbiturates (11.9 vs. 17.6).
Additional analyses showed that the impact of switching to NSAIDs varied according to migraine frequency. Specifically, patients with high-frequency episodic migraines (10-14 headache-days monthly) or chronic migraines (15 or more headache-days monthly) had a significant increase in MIDAS scores when switching to NSAIDs relative to their counterparts with low-frequency episodic migraines (0-4 headache-days monthly) or moderate-frequency episodic migraines (5-9 headache-days monthly).
"Not only did the treatment matter, but the average number of days of headache at baseline matters quite importantly here," Dr. Buse commented.
"In this observational study, switching triptan regimens or switching from a triptan to an alternative pharmacologic therapy for acute migraine does not appear to be associated with improvements in headache-related disability and, in some cases, is associated with increased headache-related disability over the course of 1 year to the second year," she concluded.
Adding medications
Dr. Lipton’s team studied the impact of medication additions from one year to the next in 960 patients with migraine taking triptans for acute treatment.
"Most people with migraine in the population use more than one acute treatment, and triptan users often use more than one triptan or use a triptan in combination with other medications, or even use combination products, such as Treximet [sumatriptan and naproxen], which contains a triptan and a nonsteroidal [anti-inflammatory drug]," he noted.
"By and large, we have not done much in terms of studying combination acute treatment in migraine, and certainly combining triptans has not been studied very often," he noted.
Most patients, 68%, did not change their acute treatment, while 13% added a combination analgesic containing opioids or barbiturates, 12% added another triptan, and 7% added an NSAID.
Results showed that among patients having low-frequency episodic migraines, adding another medication to their triptan did not significantly affect MIDAS score from one year to the next, regardless of the type of medication added.
Among patients with medium-frequency episodic migraines, adding an NSAID was associated with a significant decrease in MIDAS scores, whereas adding other medications did not affect scores.
But among patients with high-frequency episodic migraines or chronic migraines, MIDAS scores actually increased significantly with addition of an NSAID or another triptan. They were unaffected by addition of a combination analgesic containing opioids or barbiturates.
Further analyses confirmed that the impact of adding NSAIDs varied according to migraine frequency: Patients with high-frequency episodic migraines or chronic migraines had a significant increase in MIDAS scores when switching to NSAIDs relative to their counterparts with low-frequency episodic migraines.
"This is analogous to the finding in the Bigal paper [Headache 2008;48:1157-68] showing that NSAIDs are associated with an increased risk of transition to chronic migraine in people who have high-frequency episodic migraine," Dr. Lipton commented.
Dr. Lipton disclosed that he receives research grant support from the National Institutes of Health, the National Headache Foundation, and the Migraine Research Fund, and serves as a consultant or advisor to or has received honoraria from the American Headache Society and various pharmaceutical companies manufacturing drugs for migraine. Dr. Buse disclosed that she has received grant support and honoraria from Endo Pharmaceuticals and other pharmaceutical companies manufacturing drugs for migraine. The AMPP study is funded through a research grant to the National Headache Foundation from Ortho-McNeil Neurologics; additional analyses and manuscript preparation were supported through a grant from MAP Pharmaceuticals and Allergan to the National Headache Foundation.
LOS ANGELES – In patients using triptans for the acute treatment of migraine, the impact on headache-related disability of switching or adding medications depends on the frequency of attacks and the type of medication, new data show.
Dr. Richard B. Lipton and Dawn C. Buse, Ph.D., both of the Albert Einstein College of Medicine in New York, and their colleagues assessed associations between treatment changes and disability among more than 1,500 triptan users from the longitudinal, population-based AMPP (American Migraine Prevalence and Prevention) study, reporting their findings at the annual meeting of the American Headache Society.
In one analysis, patients switching to NSAIDs or to combination analgesics containing an opioid or a barbiturate had respective 31% and 48% worsening in scores for headache-related disability, compared with nonswitchers, but patients staying on the triptan or switching to another one did not have any significant change in score. In stratified analyses, switching to an NSAID was associated with a worsening among the subset of patients having the most frequent attacks.
The second study found that adding an NSAID to the triptan improved scores for patients with medium-frequency episodic migraines, while adding an NSAID or another triptan worsened scores for those with high-frequency episodic migraines or chronic migraines. Patients with low-frequency episodic migraines did not have any change regardless of the medication added.
"On average, the changes clinicians make in prescription drug therapy in the real world, switching from one triptan to another or adding a second triptan, are not helpful," Dr. Lipton commented. "That is not to say that when we switch individual patients, there isn’t a benefit to that or that optimized algorithms for choosing treatments have no effect on patient care. But it is to say that maybe when we think about what to do with patients who don’t respond to medications, it’s worth considering that switching triptans on average doesn’t have the benefits for disability that I certainly previously thought."
The studies may have had the bias of confounding by indication, whereby the reasons for medication changes (which were unknown) influenced outcomes, he acknowledged. "But they do have the strength of generalizability and reflecting what actually goes on in the real world."
Session attendee Dr. James Couch of the University of Oklahoma, Oklahoma City, expressed concern about the possible confounding.
"Most of us have found that all the triptans are not equal, and if you go through the whole list of seven, it’s not unlikely that you will find one that works better than others and so on," he elaborated. Thus, some patients on one triptan "may have gotten a moderate effect, and they were still looking for a triptan that was going to have that whiz-bang effect." Also, insurance company requirements may dictate medication switches in some cases.
Dr. Peter Goadsby of the University of California, San Francisco, asked whether analyses were masking the heterogeneity of response in the study sample. "It strikes me that in practice, it’s quite heterogeneous: You make a change in some patients, they do spectacularly well, or maybe it’s just luck, and other patients don’t," he commented. "So is there more than one population, and are you losing some granularity in what we do by having them all lumped together?"
"Our reason for stratifying by attack frequency was to try to reduce that heterogeneity," Dr. Lipton replied. "And when we stratify by attack frequency, we see some pretty robust effects."
Finally, session co-moderator Dr. Andrew Hershey of the Cincinnati Children’s Hospital wondered if the directionality of association was perhaps reversed, and headache-related disability had instead prompted the medication changes.
Dr. Lipton noted that the investigators assessed changes in score from before to after a medication switch, in addition to using stratification. "So that’s our attempt to take baseline differences into account, though it’s certainly imperfect," he acknowledged.
Switching Medications
Dr. Buse and her colleagues studied the impact of medication switches from one year to the next in 799 patients with migraine taking triptans for acute treatment.
"Providers commonly switch patients in their acute pharmacologic regimens, we know that. We switch medications for a variety of reasons: patient preference, nonresponse, what is allowed by third-party payers," she commented. However, most studies of switching medications have looked at short-term outcomes, and few have looked at switches to or from triptans.
Fully 83% of the patients studied continued on the same triptan, 10% switched to another triptan, 4% switched to a combination analgesic containing an opioid or barbiturate, and 3% switched to an NSAID.
Results showed that headache-related disability, assessed from Migraine Disability Assessment (MIDAS) scores, was essentially unchanged from one year to the next in patients who stayed on the same triptan (14.5 vs. 14.1) or who switched from one triptan to another (16.6 vs. 16.6). In contrast, scores increased (worsened) in patients who switched to NSAIDs (16.0 vs. 20.9) and who switched to combination therapy containing opioids or barbiturates (11.9 vs. 17.6).
Additional analyses showed that the impact of switching to NSAIDs varied according to migraine frequency. Specifically, patients with high-frequency episodic migraines (10-14 headache-days monthly) or chronic migraines (15 or more headache-days monthly) had a significant increase in MIDAS scores when switching to NSAIDs relative to their counterparts with low-frequency episodic migraines (0-4 headache-days monthly) or moderate-frequency episodic migraines (5-9 headache-days monthly).
"Not only did the treatment matter, but the average number of days of headache at baseline matters quite importantly here," Dr. Buse commented.
"In this observational study, switching triptan regimens or switching from a triptan to an alternative pharmacologic therapy for acute migraine does not appear to be associated with improvements in headache-related disability and, in some cases, is associated with increased headache-related disability over the course of 1 year to the second year," she concluded.
Adding medications
Dr. Lipton’s team studied the impact of medication additions from one year to the next in 960 patients with migraine taking triptans for acute treatment.
"Most people with migraine in the population use more than one acute treatment, and triptan users often use more than one triptan or use a triptan in combination with other medications, or even use combination products, such as Treximet [sumatriptan and naproxen], which contains a triptan and a nonsteroidal [anti-inflammatory drug]," he noted.
"By and large, we have not done much in terms of studying combination acute treatment in migraine, and certainly combining triptans has not been studied very often," he noted.
Most patients, 68%, did not change their acute treatment, while 13% added a combination analgesic containing opioids or barbiturates, 12% added another triptan, and 7% added an NSAID.
Results showed that among patients having low-frequency episodic migraines, adding another medication to their triptan did not significantly affect MIDAS score from one year to the next, regardless of the type of medication added.
Among patients with medium-frequency episodic migraines, adding an NSAID was associated with a significant decrease in MIDAS scores, whereas adding other medications did not affect scores.
But among patients with high-frequency episodic migraines or chronic migraines, MIDAS scores actually increased significantly with addition of an NSAID or another triptan. They were unaffected by addition of a combination analgesic containing opioids or barbiturates.
Further analyses confirmed that the impact of adding NSAIDs varied according to migraine frequency: Patients with high-frequency episodic migraines or chronic migraines had a significant increase in MIDAS scores when switching to NSAIDs relative to their counterparts with low-frequency episodic migraines.
"This is analogous to the finding in the Bigal paper [Headache 2008;48:1157-68] showing that NSAIDs are associated with an increased risk of transition to chronic migraine in people who have high-frequency episodic migraine," Dr. Lipton commented.
Dr. Lipton disclosed that he receives research grant support from the National Institutes of Health, the National Headache Foundation, and the Migraine Research Fund, and serves as a consultant or advisor to or has received honoraria from the American Headache Society and various pharmaceutical companies manufacturing drugs for migraine. Dr. Buse disclosed that she has received grant support and honoraria from Endo Pharmaceuticals and other pharmaceutical companies manufacturing drugs for migraine. The AMPP study is funded through a research grant to the National Headache Foundation from Ortho-McNeil Neurologics; additional analyses and manuscript preparation were supported through a grant from MAP Pharmaceuticals and Allergan to the National Headache Foundation.
AT THE ANNUAL MEETING OF THE AMERICAN HEADACHE SOCIETY
Major Finding: Headache-related disability among patients taking a triptan worsened by 31% in patients who switched to an NSAID and was worst among those with high-frequency episodic migraines or chronic migraines. Adding an NSAID benefited only medium-frequency patients and worsened high-frequency patients.
Data Source: A pair of studies in 799 and 960 triptan users with migraine from the longitudinal, population-based American Migraine Prevalence and Prevention (AMPP) study
Disclosures: Dr. Lipton disclosed that he receives research grant support from the National Institutes of Health, the National Headache Foundation, and the Migraine Research Fund, and serves as a consultant or advisor to or has received honoraria from the American Headache Society and various pharmaceutical companies manufacturing drugs for migraine. Dr. Buse disclosed that she has received grant support and honoraria from Endo Pharmaceuticals and other pharmaceutical companies manufacturing drugs for migraine. The AMPP study is funded through a research grant to the National Headache Foundation from Ortho-McNeil Neurologics; additional analyses and manuscript preparation were supported through a grant from MAP Pharmaceuticals and Allergan to the National Headache Foundation.