User login
Psychiatrists urged to take lead in recognizing physician burnout
NEW YORK – The proportion of physicians who commit suicide each year is greater than the proportion of Americans who die of an opioid overdose, according to a series of sobering statistics on physician burnout presented at the American Psychiatric Association annual meeting.
“There are about 400 physician suicides very year, which is proportional rate that is about twice the suicide rate in the general population,” reported Darrell G. Kirch, MD, president and chief executive officer of the Association of American Medical Colleges, Washington.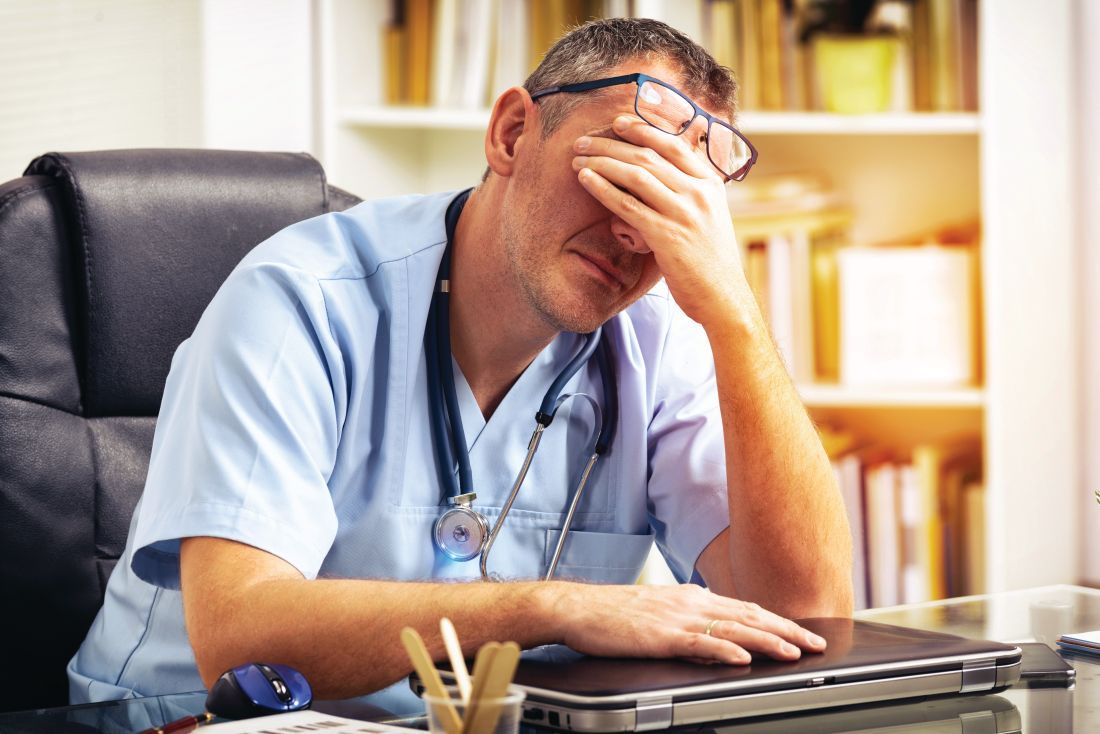
Burnout is variably defined, but characterizations typically include emotional exhaustion, a high sense of depersonalization, and a low sense of personal accomplishment. In the 2015 study, the overall rate of burnout when assessed via the Maslach Burnout Inventory was 54.4%.
At 40%, the rate of burnout found among psychiatrists is lower than the mean and places them toward the bottom of the list in the rank order among specialists. Yet, 40% is still a large proportion. Moreover, Dr. Kirch believes that psychiatrists have an important role to play in recognizing and addressing this condition in others.
“ in the organization you work in,” Dr. Kirch said. The campaign to which he referred was a call to action launched last year by the National Academy of Medicine (NAM), the Association of American Medical Colleges, and the Accreditation Council for Graduate Medical Education. Led by NAM, it is called the Action Collaborative on Clinician Well-Being and Resilience.
In the 18 months since it was launched, “more than 150 organizations, including the APA, have made commitment statements and are supporting the work of the collaborative around improving clinician well-being,” Dr. Kirch reported.
Many tools already generated by this collaboration can be found in the NAM website at nam.edu/clinicianwellbeing. This section of the website not only includes data about burnout as well as presentation slides for download on the topic, but it is expected to be “a growing repository for solutions that work,” Dr. Kirch said.
This was not news to those who attended the APA symposium. When Dr. Kirch asked the audience who had treated a colleague for burnout, almost every hand was raised. This would not be surprising, except that the leaders in this field so far have typically not been psychiatrists, Dr. Kirch said.
For example, an increasing number of medical centers are following the lead of Stanford (Calif.) University, which appointed Tate D. Shanafelt, MD, as its first chief wellness officer. However, to the knowledge of Dr. Kirch, none of the appointments have gone to a psychiatrist.
“It strikes me that if you need a chief wellness officer who not only can understand the dynamics of burnout but can understand what a short path it is from being burned out to being depressed, suicidal, or addicted, who would be better suited than a psychiatrist? I really think that in many ways, this may be a career path for psychiatrists,” Dr. Kirch said.
Even with the appointment of chief wellness officers, the problem will not soon go away. Although Dr. Kirch believes interventions are needed from the beginning of medical training, he acknowledged that eliminating burnout “is a heavy lift, because there is no single solution.” Listing regulatory burdens, administrative burdens, lack of support staff, and a sense of isolation among documented causes of burnout, he believes identifying all of the solutions to relieve stress and improve clinical satisfaction “will be a journey.”
Dr. Kirch reported no potential conflicts of interest.
NEW YORK – The proportion of physicians who commit suicide each year is greater than the proportion of Americans who die of an opioid overdose, according to a series of sobering statistics on physician burnout presented at the American Psychiatric Association annual meeting.
“There are about 400 physician suicides very year, which is proportional rate that is about twice the suicide rate in the general population,” reported Darrell G. Kirch, MD, president and chief executive officer of the Association of American Medical Colleges, Washington.
Burnout is variably defined, but characterizations typically include emotional exhaustion, a high sense of depersonalization, and a low sense of personal accomplishment. In the 2015 study, the overall rate of burnout when assessed via the Maslach Burnout Inventory was 54.4%.
At 40%, the rate of burnout found among psychiatrists is lower than the mean and places them toward the bottom of the list in the rank order among specialists. Yet, 40% is still a large proportion. Moreover, Dr. Kirch believes that psychiatrists have an important role to play in recognizing and addressing this condition in others.
“ in the organization you work in,” Dr. Kirch said. The campaign to which he referred was a call to action launched last year by the National Academy of Medicine (NAM), the Association of American Medical Colleges, and the Accreditation Council for Graduate Medical Education. Led by NAM, it is called the Action Collaborative on Clinician Well-Being and Resilience.
In the 18 months since it was launched, “more than 150 organizations, including the APA, have made commitment statements and are supporting the work of the collaborative around improving clinician well-being,” Dr. Kirch reported.
Many tools already generated by this collaboration can be found in the NAM website at nam.edu/clinicianwellbeing. This section of the website not only includes data about burnout as well as presentation slides for download on the topic, but it is expected to be “a growing repository for solutions that work,” Dr. Kirch said.
This was not news to those who attended the APA symposium. When Dr. Kirch asked the audience who had treated a colleague for burnout, almost every hand was raised. This would not be surprising, except that the leaders in this field so far have typically not been psychiatrists, Dr. Kirch said.
For example, an increasing number of medical centers are following the lead of Stanford (Calif.) University, which appointed Tate D. Shanafelt, MD, as its first chief wellness officer. However, to the knowledge of Dr. Kirch, none of the appointments have gone to a psychiatrist.
“It strikes me that if you need a chief wellness officer who not only can understand the dynamics of burnout but can understand what a short path it is from being burned out to being depressed, suicidal, or addicted, who would be better suited than a psychiatrist? I really think that in many ways, this may be a career path for psychiatrists,” Dr. Kirch said.
Even with the appointment of chief wellness officers, the problem will not soon go away. Although Dr. Kirch believes interventions are needed from the beginning of medical training, he acknowledged that eliminating burnout “is a heavy lift, because there is no single solution.” Listing regulatory burdens, administrative burdens, lack of support staff, and a sense of isolation among documented causes of burnout, he believes identifying all of the solutions to relieve stress and improve clinical satisfaction “will be a journey.”
Dr. Kirch reported no potential conflicts of interest.
NEW YORK – The proportion of physicians who commit suicide each year is greater than the proportion of Americans who die of an opioid overdose, according to a series of sobering statistics on physician burnout presented at the American Psychiatric Association annual meeting.
“There are about 400 physician suicides very year, which is proportional rate that is about twice the suicide rate in the general population,” reported Darrell G. Kirch, MD, president and chief executive officer of the Association of American Medical Colleges, Washington.
Burnout is variably defined, but characterizations typically include emotional exhaustion, a high sense of depersonalization, and a low sense of personal accomplishment. In the 2015 study, the overall rate of burnout when assessed via the Maslach Burnout Inventory was 54.4%.
At 40%, the rate of burnout found among psychiatrists is lower than the mean and places them toward the bottom of the list in the rank order among specialists. Yet, 40% is still a large proportion. Moreover, Dr. Kirch believes that psychiatrists have an important role to play in recognizing and addressing this condition in others.
“ in the organization you work in,” Dr. Kirch said. The campaign to which he referred was a call to action launched last year by the National Academy of Medicine (NAM), the Association of American Medical Colleges, and the Accreditation Council for Graduate Medical Education. Led by NAM, it is called the Action Collaborative on Clinician Well-Being and Resilience.
In the 18 months since it was launched, “more than 150 organizations, including the APA, have made commitment statements and are supporting the work of the collaborative around improving clinician well-being,” Dr. Kirch reported.
Many tools already generated by this collaboration can be found in the NAM website at nam.edu/clinicianwellbeing. This section of the website not only includes data about burnout as well as presentation slides for download on the topic, but it is expected to be “a growing repository for solutions that work,” Dr. Kirch said.
This was not news to those who attended the APA symposium. When Dr. Kirch asked the audience who had treated a colleague for burnout, almost every hand was raised. This would not be surprising, except that the leaders in this field so far have typically not been psychiatrists, Dr. Kirch said.
For example, an increasing number of medical centers are following the lead of Stanford (Calif.) University, which appointed Tate D. Shanafelt, MD, as its first chief wellness officer. However, to the knowledge of Dr. Kirch, none of the appointments have gone to a psychiatrist.
“It strikes me that if you need a chief wellness officer who not only can understand the dynamics of burnout but can understand what a short path it is from being burned out to being depressed, suicidal, or addicted, who would be better suited than a psychiatrist? I really think that in many ways, this may be a career path for psychiatrists,” Dr. Kirch said.
Even with the appointment of chief wellness officers, the problem will not soon go away. Although Dr. Kirch believes interventions are needed from the beginning of medical training, he acknowledged that eliminating burnout “is a heavy lift, because there is no single solution.” Listing regulatory burdens, administrative burdens, lack of support staff, and a sense of isolation among documented causes of burnout, he believes identifying all of the solutions to relieve stress and improve clinical satisfaction “will be a journey.”
Dr. Kirch reported no potential conflicts of interest.
REPORTING FROM APA

Consider heterogeneous experiences among veteran cohorts when treating PTSD
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
NEW YORK – Veterans are not a homogeneous group, and when treating them for posttraumatic stress, it helps to consider their specific cohort, according to Elspeth Cameron Ritchie, MD.
Veterans from the first Gulf War, for example, have lingering concerns regarding medical illness (Gulf War syndrome); those from Vietnam are aging and might have medical problems or find that while they did well while working, now they are experiencing PTSD symptoms for the first time; and those returning from the conflicts in Iraq and Afghanistan might have physical injuries from blasts – the “signature weapon” of those wars. Such blasts can cause amputations, genital injuries, head trauma, and PTSD, said Dr. Ritchie, of the Uniformed Services University of the Health Sciences, Bethesda, Md.
In this video interview, Dr. Ritchie discusses these and other issues related to the treatment of PTSD among veterans as presented during a workshop entitled “Psychiatry and U.S. Veterans,” which she chaired at the annual meeting of the American Psychiatric Association.
The workshop covered the spectrum of treatments that might be helpful for veterans.
“ They don’t want it to just be the doctor giving them a pill,” she said. “Veterans are resilient; they’re tough; they don’t like to be thought of as victims ... and when you’re working with them, it’s very important to link into that dynamic resilient piece and capitalize on their strengths.”
Dr. Ritchie reported having no disclosures.
SOURCE: Ritchie EC et al. APA Workshop.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
NEW YORK – Veterans are not a homogeneous group, and when treating them for posttraumatic stress, it helps to consider their specific cohort, according to Elspeth Cameron Ritchie, MD.
Veterans from the first Gulf War, for example, have lingering concerns regarding medical illness (Gulf War syndrome); those from Vietnam are aging and might have medical problems or find that while they did well while working, now they are experiencing PTSD symptoms for the first time; and those returning from the conflicts in Iraq and Afghanistan might have physical injuries from blasts – the “signature weapon” of those wars. Such blasts can cause amputations, genital injuries, head trauma, and PTSD, said Dr. Ritchie, of the Uniformed Services University of the Health Sciences, Bethesda, Md.
In this video interview, Dr. Ritchie discusses these and other issues related to the treatment of PTSD among veterans as presented during a workshop entitled “Psychiatry and U.S. Veterans,” which she chaired at the annual meeting of the American Psychiatric Association.
The workshop covered the spectrum of treatments that might be helpful for veterans.
“ They don’t want it to just be the doctor giving them a pill,” she said. “Veterans are resilient; they’re tough; they don’t like to be thought of as victims ... and when you’re working with them, it’s very important to link into that dynamic resilient piece and capitalize on their strengths.”
Dr. Ritchie reported having no disclosures.
SOURCE: Ritchie EC et al. APA Workshop.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
NEW YORK – Veterans are not a homogeneous group, and when treating them for posttraumatic stress, it helps to consider their specific cohort, according to Elspeth Cameron Ritchie, MD.
Veterans from the first Gulf War, for example, have lingering concerns regarding medical illness (Gulf War syndrome); those from Vietnam are aging and might have medical problems or find that while they did well while working, now they are experiencing PTSD symptoms for the first time; and those returning from the conflicts in Iraq and Afghanistan might have physical injuries from blasts – the “signature weapon” of those wars. Such blasts can cause amputations, genital injuries, head trauma, and PTSD, said Dr. Ritchie, of the Uniformed Services University of the Health Sciences, Bethesda, Md.
In this video interview, Dr. Ritchie discusses these and other issues related to the treatment of PTSD among veterans as presented during a workshop entitled “Psychiatry and U.S. Veterans,” which she chaired at the annual meeting of the American Psychiatric Association.
The workshop covered the spectrum of treatments that might be helpful for veterans.
“ They don’t want it to just be the doctor giving them a pill,” she said. “Veterans are resilient; they’re tough; they don’t like to be thought of as victims ... and when you’re working with them, it’s very important to link into that dynamic resilient piece and capitalize on their strengths.”
Dr. Ritchie reported having no disclosures.
SOURCE: Ritchie EC et al. APA Workshop.
REPORTING FROM APA

Climate change expected to impose major burden on mental health
NEW YORK – Of the broad range of direct and indirect threats to public health anticipated from climate change, those involving mental health will place psychiatrists on the front lines of efforts to mitigate the impact, a member of the Climate Psychiatry Alliance said at the annual meeting of the American Psychiatric Association.
“One thing climate changes mean for us in psychiatry is more work,” reported Janet L. Lewis, MD, an assistant clinical professor of psychiatry at the University of Rochester (N.Y.).
Mental health is sensitive to climate. “Psychiatric patients can be particularly vulnerable to the medical effects of climate change,” Dr. Lewis said. “People with schizophrenia exhibit impaired thermoregulatory functioning, and many of our medications can impair the body’s normal heat regulation.”
The evidence of increased death rates among schizophrenia patients during heat waves has been attributed to this phenomenon as well as to the failure of patients with mental disorders to seek or obtain relief from heat, according to Dr. Lewis, but she noted that These links are true for the individual, and they affect trends in communities.
As a cause of societal stresses, such as food and water insecurity, climate change also has the very real potential of producing traumatic disruptions commensurate with disasters such as hurricanes or earthquakes. Noting that the rate of PTSD after such natural disasters typically runs at around 30%, Dr. Lewis suggested that psychiatrists might face large challenges from major upheavals induced by climate change.
However, even in the absence of catastrophic consequences, significant psychiatric morbidity may be generated by climate change in the form of “ecoanxieties” or “solastalgia,” a term coined about 10 years ago to describe psychic anxiety induced by environmental change. While many individuals continue to function normally despite fear or anxiety about climate change, Dr. Lewis said that there are many reports in the literature now show that psychoterratic illness, another term for this phenomenon, is associated with degraded or threatened environments linked to climate change.
The Climate Psychiatry Alliance is one of several professional psychiatry groups that is engaged in evaluating how psychiatry as a profession should react to climate change. The Climate Psychiatry committee of the Group for the Advancement of Psychiatry is another. Dr. Lewis, addressing the potential criticism that climate is a political issue, said that “we bring some very particular things to this 21st-century disaster … hopefully, everything I have said about the mental effects of climate change convinces you that it is not just a political problem.”
It is, however, a problem that is complex. Differentiating complex problems from complicated problems – which can be solved eventually with sufficient information – Dr. Lewis explained that complex problems are dynamic with an interplay between components that make solutions uncertain without experimentation and continual reassessment. She believes both mitigation of the problem and adaption to the inevitability of rising temperatures will be necessary.
This is relevant for psychiatrists who also must adapt to the environmental changes and develop resilience that will help them deal objectively with the mental health consequences of climate change. She noted that environmentalists recognize two traps in approaching solutions to climate change. The first is proposing overly simplistic solutions that fail to address the profound implications of climate change. The second is being rendered inactive by the overwhelming complexity of this growing problem.
Ultimately, Dr. Lewis called for psychiatrists to be proactive in dealing the mental health consequences of climate change. She noted that the APA issued a position statement in 2017, which emphasized that individuals with mental health disorders are disproportionately affected by climate change.
“We as psychiatrists know what it is to deal with complex systems, and we understand through our own work with traumatized patients how to manage patients with trauma responses and how to get empowered and engaged in the rebuilding of realistic lives,” Dr. Lewis said. She believes those skills will be important as the impact of climate change on mental health unfolds.
NEW YORK – Of the broad range of direct and indirect threats to public health anticipated from climate change, those involving mental health will place psychiatrists on the front lines of efforts to mitigate the impact, a member of the Climate Psychiatry Alliance said at the annual meeting of the American Psychiatric Association.
“One thing climate changes mean for us in psychiatry is more work,” reported Janet L. Lewis, MD, an assistant clinical professor of psychiatry at the University of Rochester (N.Y.).
Mental health is sensitive to climate. “Psychiatric patients can be particularly vulnerable to the medical effects of climate change,” Dr. Lewis said. “People with schizophrenia exhibit impaired thermoregulatory functioning, and many of our medications can impair the body’s normal heat regulation.”
The evidence of increased death rates among schizophrenia patients during heat waves has been attributed to this phenomenon as well as to the failure of patients with mental disorders to seek or obtain relief from heat, according to Dr. Lewis, but she noted that These links are true for the individual, and they affect trends in communities.
As a cause of societal stresses, such as food and water insecurity, climate change also has the very real potential of producing traumatic disruptions commensurate with disasters such as hurricanes or earthquakes. Noting that the rate of PTSD after such natural disasters typically runs at around 30%, Dr. Lewis suggested that psychiatrists might face large challenges from major upheavals induced by climate change.
However, even in the absence of catastrophic consequences, significant psychiatric morbidity may be generated by climate change in the form of “ecoanxieties” or “solastalgia,” a term coined about 10 years ago to describe psychic anxiety induced by environmental change. While many individuals continue to function normally despite fear or anxiety about climate change, Dr. Lewis said that there are many reports in the literature now show that psychoterratic illness, another term for this phenomenon, is associated with degraded or threatened environments linked to climate change.
The Climate Psychiatry Alliance is one of several professional psychiatry groups that is engaged in evaluating how psychiatry as a profession should react to climate change. The Climate Psychiatry committee of the Group for the Advancement of Psychiatry is another. Dr. Lewis, addressing the potential criticism that climate is a political issue, said that “we bring some very particular things to this 21st-century disaster … hopefully, everything I have said about the mental effects of climate change convinces you that it is not just a political problem.”
It is, however, a problem that is complex. Differentiating complex problems from complicated problems – which can be solved eventually with sufficient information – Dr. Lewis explained that complex problems are dynamic with an interplay between components that make solutions uncertain without experimentation and continual reassessment. She believes both mitigation of the problem and adaption to the inevitability of rising temperatures will be necessary.
This is relevant for psychiatrists who also must adapt to the environmental changes and develop resilience that will help them deal objectively with the mental health consequences of climate change. She noted that environmentalists recognize two traps in approaching solutions to climate change. The first is proposing overly simplistic solutions that fail to address the profound implications of climate change. The second is being rendered inactive by the overwhelming complexity of this growing problem.
Ultimately, Dr. Lewis called for psychiatrists to be proactive in dealing the mental health consequences of climate change. She noted that the APA issued a position statement in 2017, which emphasized that individuals with mental health disorders are disproportionately affected by climate change.
“We as psychiatrists know what it is to deal with complex systems, and we understand through our own work with traumatized patients how to manage patients with trauma responses and how to get empowered and engaged in the rebuilding of realistic lives,” Dr. Lewis said. She believes those skills will be important as the impact of climate change on mental health unfolds.
NEW YORK – Of the broad range of direct and indirect threats to public health anticipated from climate change, those involving mental health will place psychiatrists on the front lines of efforts to mitigate the impact, a member of the Climate Psychiatry Alliance said at the annual meeting of the American Psychiatric Association.
“One thing climate changes mean for us in psychiatry is more work,” reported Janet L. Lewis, MD, an assistant clinical professor of psychiatry at the University of Rochester (N.Y.).
Mental health is sensitive to climate. “Psychiatric patients can be particularly vulnerable to the medical effects of climate change,” Dr. Lewis said. “People with schizophrenia exhibit impaired thermoregulatory functioning, and many of our medications can impair the body’s normal heat regulation.”
The evidence of increased death rates among schizophrenia patients during heat waves has been attributed to this phenomenon as well as to the failure of patients with mental disorders to seek or obtain relief from heat, according to Dr. Lewis, but she noted that These links are true for the individual, and they affect trends in communities.
As a cause of societal stresses, such as food and water insecurity, climate change also has the very real potential of producing traumatic disruptions commensurate with disasters such as hurricanes or earthquakes. Noting that the rate of PTSD after such natural disasters typically runs at around 30%, Dr. Lewis suggested that psychiatrists might face large challenges from major upheavals induced by climate change.
However, even in the absence of catastrophic consequences, significant psychiatric morbidity may be generated by climate change in the form of “ecoanxieties” or “solastalgia,” a term coined about 10 years ago to describe psychic anxiety induced by environmental change. While many individuals continue to function normally despite fear or anxiety about climate change, Dr. Lewis said that there are many reports in the literature now show that psychoterratic illness, another term for this phenomenon, is associated with degraded or threatened environments linked to climate change.
The Climate Psychiatry Alliance is one of several professional psychiatry groups that is engaged in evaluating how psychiatry as a profession should react to climate change. The Climate Psychiatry committee of the Group for the Advancement of Psychiatry is another. Dr. Lewis, addressing the potential criticism that climate is a political issue, said that “we bring some very particular things to this 21st-century disaster … hopefully, everything I have said about the mental effects of climate change convinces you that it is not just a political problem.”
It is, however, a problem that is complex. Differentiating complex problems from complicated problems – which can be solved eventually with sufficient information – Dr. Lewis explained that complex problems are dynamic with an interplay between components that make solutions uncertain without experimentation and continual reassessment. She believes both mitigation of the problem and adaption to the inevitability of rising temperatures will be necessary.
This is relevant for psychiatrists who also must adapt to the environmental changes and develop resilience that will help them deal objectively with the mental health consequences of climate change. She noted that environmentalists recognize two traps in approaching solutions to climate change. The first is proposing overly simplistic solutions that fail to address the profound implications of climate change. The second is being rendered inactive by the overwhelming complexity of this growing problem.
Ultimately, Dr. Lewis called for psychiatrists to be proactive in dealing the mental health consequences of climate change. She noted that the APA issued a position statement in 2017, which emphasized that individuals with mental health disorders are disproportionately affected by climate change.
“We as psychiatrists know what it is to deal with complex systems, and we understand through our own work with traumatized patients how to manage patients with trauma responses and how to get empowered and engaged in the rebuilding of realistic lives,” Dr. Lewis said. She believes those skills will be important as the impact of climate change on mental health unfolds.
VIDEO: Consider unique stressors when treating members of peacekeeping operations
NEW YORK – Sustained peacekeeping operations are associated with unique psychological stressors, and understanding of these stressors on the part of both community and military psychiatrists can help make a difference at each stage of a deployment cycle, according to Elspeth Cameron Ritchie, MD.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
During a workshop at the annual meeting of the American Psychiatric Association entitled “War and Peace: Understanding the Psychological Stressors Associated with Sustained Peacekeeping Operations (PKOs),” chaired by Dr. Ritchie of the Uniformed Services University of the Health Sciences, Bethesda, Md., various dimensions of salient psychological stress were discussed, as were approaches for minimizing any resultant impact on the psychological health of peacekeepers.
In this video interview, Dr. Ritchie discussed the differences and similarities between peacekeeping operations and military operations with respect to stressors and their effects, and the risk of posttraumatic stress disorder among peacekeepers.
Although treatment for PTSD is “pretty much the same,” it is important to “tailor the treatment for the situation,” she said.
“Lay out the different options, explain them to the patient, and partner with the patient in terms of what is the best option for them,” she said.
Dr. Ritchie reported having no relevant disclosures.
SOURCE: Ritchie EC et al. APA Workshop
NEW YORK – Sustained peacekeeping operations are associated with unique psychological stressors, and understanding of these stressors on the part of both community and military psychiatrists can help make a difference at each stage of a deployment cycle, according to Elspeth Cameron Ritchie, MD.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
During a workshop at the annual meeting of the American Psychiatric Association entitled “War and Peace: Understanding the Psychological Stressors Associated with Sustained Peacekeeping Operations (PKOs),” chaired by Dr. Ritchie of the Uniformed Services University of the Health Sciences, Bethesda, Md., various dimensions of salient psychological stress were discussed, as were approaches for minimizing any resultant impact on the psychological health of peacekeepers.
In this video interview, Dr. Ritchie discussed the differences and similarities between peacekeeping operations and military operations with respect to stressors and their effects, and the risk of posttraumatic stress disorder among peacekeepers.
Although treatment for PTSD is “pretty much the same,” it is important to “tailor the treatment for the situation,” she said.
“Lay out the different options, explain them to the patient, and partner with the patient in terms of what is the best option for them,” she said.
Dr. Ritchie reported having no relevant disclosures.
SOURCE: Ritchie EC et al. APA Workshop
NEW YORK – Sustained peacekeeping operations are associated with unique psychological stressors, and understanding of these stressors on the part of both community and military psychiatrists can help make a difference at each stage of a deployment cycle, according to Elspeth Cameron Ritchie, MD.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
During a workshop at the annual meeting of the American Psychiatric Association entitled “War and Peace: Understanding the Psychological Stressors Associated with Sustained Peacekeeping Operations (PKOs),” chaired by Dr. Ritchie of the Uniformed Services University of the Health Sciences, Bethesda, Md., various dimensions of salient psychological stress were discussed, as were approaches for minimizing any resultant impact on the psychological health of peacekeepers.
In this video interview, Dr. Ritchie discussed the differences and similarities between peacekeeping operations and military operations with respect to stressors and their effects, and the risk of posttraumatic stress disorder among peacekeepers.
Although treatment for PTSD is “pretty much the same,” it is important to “tailor the treatment for the situation,” she said.
“Lay out the different options, explain them to the patient, and partner with the patient in terms of what is the best option for them,” she said.
Dr. Ritchie reported having no relevant disclosures.
SOURCE: Ritchie EC et al. APA Workshop

VIDEO: Research underscores murky relationship between mental illness, gun violence
NEW YORK – Legislation enacted in some states in the wake of mass shootings seeks to limit access to firearms for people with mental illness, but research presented at the annual meeting of the American Psychiatric Association raises questions about the value of that approach.
During a workshop entitled “The ‘Crazed Gunman’ Myth: Examining Mental Illness and Firearm Violence,” researchers from the Yale University in New Haven, Conn., presented new findings that support existing data calling into question whether laws considered to be “common-sense approaches” to stopping gun violence really can reduce the likelihood of mass shootings.
It appears, based on the frequency and context of firearm use in more than 400 crimes that resulted in an insanity acquittal in Connecticut, for example, that individuals with mental illness are less likely than others to misuse firearms.
In this video, workshop chair Reena Kapoor, MD, also of Yale University, discusses the findings and notes that she and her colleagues seek to move past politics and ideology to focus on science that can guide policy and legislative efforts in a potentially more effective direction.
“We’ve also found that in spite of the media narrative, there has also been a slight decrease in how often [mentally ill offenders] use guns, over the years in the study,” she said. “Although the data are preliminary, it doesn’t support this idea that mentally ill people are more dangerous than ever, that they’re using guns more often in their violence; it actually says quite the opposite.”
Dr. Kapoor reported having no disclosures.
SOURCE: Kapoor R et al. APA 2018 Workshop.
NEW YORK – Legislation enacted in some states in the wake of mass shootings seeks to limit access to firearms for people with mental illness, but research presented at the annual meeting of the American Psychiatric Association raises questions about the value of that approach.
During a workshop entitled “The ‘Crazed Gunman’ Myth: Examining Mental Illness and Firearm Violence,” researchers from the Yale University in New Haven, Conn., presented new findings that support existing data calling into question whether laws considered to be “common-sense approaches” to stopping gun violence really can reduce the likelihood of mass shootings.
It appears, based on the frequency and context of firearm use in more than 400 crimes that resulted in an insanity acquittal in Connecticut, for example, that individuals with mental illness are less likely than others to misuse firearms.
In this video, workshop chair Reena Kapoor, MD, also of Yale University, discusses the findings and notes that she and her colleagues seek to move past politics and ideology to focus on science that can guide policy and legislative efforts in a potentially more effective direction.
“We’ve also found that in spite of the media narrative, there has also been a slight decrease in how often [mentally ill offenders] use guns, over the years in the study,” she said. “Although the data are preliminary, it doesn’t support this idea that mentally ill people are more dangerous than ever, that they’re using guns more often in their violence; it actually says quite the opposite.”
Dr. Kapoor reported having no disclosures.
SOURCE: Kapoor R et al. APA 2018 Workshop.
NEW YORK – Legislation enacted in some states in the wake of mass shootings seeks to limit access to firearms for people with mental illness, but research presented at the annual meeting of the American Psychiatric Association raises questions about the value of that approach.
During a workshop entitled “The ‘Crazed Gunman’ Myth: Examining Mental Illness and Firearm Violence,” researchers from the Yale University in New Haven, Conn., presented new findings that support existing data calling into question whether laws considered to be “common-sense approaches” to stopping gun violence really can reduce the likelihood of mass shootings.
It appears, based on the frequency and context of firearm use in more than 400 crimes that resulted in an insanity acquittal in Connecticut, for example, that individuals with mental illness are less likely than others to misuse firearms.
In this video, workshop chair Reena Kapoor, MD, also of Yale University, discusses the findings and notes that she and her colleagues seek to move past politics and ideology to focus on science that can guide policy and legislative efforts in a potentially more effective direction.
“We’ve also found that in spite of the media narrative, there has also been a slight decrease in how often [mentally ill offenders] use guns, over the years in the study,” she said. “Although the data are preliminary, it doesn’t support this idea that mentally ill people are more dangerous than ever, that they’re using guns more often in their violence; it actually says quite the opposite.”
Dr. Kapoor reported having no disclosures.
SOURCE: Kapoor R et al. APA 2018 Workshop.
REPORTING FROM APA

Meta-analyses clarify roles for gabapentin, naltrexone, and psychotherapy in alcohol use disorder
NEW YORK – A meta-analysis of 10 studies provides at least preliminary support for the use of gabapentin for the treatment of alcohol cravings and withdrawal.
In this video interview, Ali Mahmood Khan, MD, of Kings County Hospital, New York, discusses the findings – presented in a poster at the annual meeting of the American Psychiatric Association – which show that patients treated with gabapentin have significantly reduced alcohol craving and withdrawal. While the findings require further study, he said.
Gapapentin also can be used in combination with naltrexone, which was shown in a separate poster presented by Dr. Khan and his colleagues to be useful for treating alcohol use disorders – but mainly through reducing consumption rather than cravings.
In that meta-analysis of 30 studies, no significant added benefit was seen when psychotherapy was combined with naltrexone, he said, noting, however, that additional study is warranted given that various psychotherapies were used across the studies.
Dr. Khan reported having no disclosures.
NEW YORK – A meta-analysis of 10 studies provides at least preliminary support for the use of gabapentin for the treatment of alcohol cravings and withdrawal.
In this video interview, Ali Mahmood Khan, MD, of Kings County Hospital, New York, discusses the findings – presented in a poster at the annual meeting of the American Psychiatric Association – which show that patients treated with gabapentin have significantly reduced alcohol craving and withdrawal. While the findings require further study, he said.
Gapapentin also can be used in combination with naltrexone, which was shown in a separate poster presented by Dr. Khan and his colleagues to be useful for treating alcohol use disorders – but mainly through reducing consumption rather than cravings.
In that meta-analysis of 30 studies, no significant added benefit was seen when psychotherapy was combined with naltrexone, he said, noting, however, that additional study is warranted given that various psychotherapies were used across the studies.
Dr. Khan reported having no disclosures.
NEW YORK – A meta-analysis of 10 studies provides at least preliminary support for the use of gabapentin for the treatment of alcohol cravings and withdrawal.
In this video interview, Ali Mahmood Khan, MD, of Kings County Hospital, New York, discusses the findings – presented in a poster at the annual meeting of the American Psychiatric Association – which show that patients treated with gabapentin have significantly reduced alcohol craving and withdrawal. While the findings require further study, he said.
Gapapentin also can be used in combination with naltrexone, which was shown in a separate poster presented by Dr. Khan and his colleagues to be useful for treating alcohol use disorders – but mainly through reducing consumption rather than cravings.
In that meta-analysis of 30 studies, no significant added benefit was seen when psychotherapy was combined with naltrexone, he said, noting, however, that additional study is warranted given that various psychotherapies were used across the studies.
Dr. Khan reported having no disclosures.
REPORTING FROM APA