User login
Counseling is a must with this smoking cessation aid
Inform patients who are interested in taking varenicline (Chantix) that there is a small cardiovascular (CV) risk associated with it, as well as neuropsychiatric risks—and consider recommending that smokers with a history of cardiovascular disease (CVD) use nicotine replacement therapy (NRT) or bupropion instead.1
STRENGTH OF RECOMMENDATION
A: Based on a meta-analysis.
Singh S, Loke YK, Spangler JG, et al. Risk of serious adverse cardiovascular events associated with varenicline: a systematic review and meta-analysis. CMAJ. 2011;183:1359-1366.
ILLUSTRATIVE CASE
A 53-year-old man asks you to prescribe Chantix to help him stop smoking. He has made several attempts to quit in the past, but never managed to stop for more than 6 months— and has smoked a pack a day for 30 years. The patient does not have a history of heart disease, but he is on statin therapy for hyperlipidemia. What should you tell him about varenicline’s potential benefits and risks?
Tobacco use remains the largest preventable contributor to death and disease in the United States.2 In smokers with coronary heart disease, smoking cessation is associated with a 36% reduction in all-cause mortality (relative risk [RR], 0.64; 95% confidence interval [CI], 0.58-0.71)—a risk reduction greater than that of statins (29%), aspirin (15%), beta-blockers (23%), or ACE inhibitors (23%).3
Varenicline now has 2 black box warnings
In its 2009 update on recommendations for smoking cessation, the United States Preventive Services Task Force cited NRT and controlled-release bupropion, as well as varenicline, as effective smoking cessation aids.4 Varenicline received US Food and Drug Administration (FDA) approval in 2006. In 2009, the FDA added a black box warning based on evidence of its adverse neuropsychiatric effects, including suicidality.5
In July 2011, the FDA required another label change,6 based on a double-blind RCT published in 2010 showing that for patients with CVD, varenicline is associated with an increased risk.7 As a partial nicotine agonist, varenicline could confer some of the CV risk associated with nicotine abuse.8 The FDA has asked its manufacturer, Pfizer Inc, to conduct further studies.6 The meta-analysis reviewed below—which was not associated with Pfizer or the FDA—was published in September 2011, just a couple of months after the label change.1
STUDY SUMMARY: Risk of ischemic or arrhythmic event is small but significant
Singh et al searched for double-blind RCTs that tested varenicline against a control in tobacco users.1 All included studies had to have reported adverse CV events. The primary outcome was any ischemic or arrhythmic CV event.
The researchers found 15 such studies (n=8216), which ranged in duration from 7 to 52 weeks. Most used a placebo control, but some included bupropion or NRT. The researchers used a Peto odds ratio (OR) for the meta-analysis, useful when combining uncommon events and including studies with no events.9
Compared with placebo, varenicline significantly increased the risk of CV events (odds ratio [OR], 1.72; 95% CI, 1.09-2.71). The incidence of CV events was 1.06% (52 of 4908) among varenicline users vs 0.82% (27 of 3308) in the controls (number needed to harm [NNH]=417).
The limited number of deaths (1.4% among patients taking varenicline vs 2.1% in the placebo groups) prevented analysis of mortality risk. The study with the most statistical power, which accounted for 57% of the overall effect, was the only one that included patients with known stable CV disease. (None included patients with unstable CV disease, whose risk may be greater.) Even when this study was removed, however, the outcome (OR, 2.54; 95% CI, 1.26-5.12) was consistent with the primary result for CV events. A sensitivity analysis comparing the risk associated with varenicline with that of either NRT or bupropion yielded similar results (OR, 1.67; 95% CI, 1.07-26.2). For a higher risk population with stable CVD (5.6% annual risk at baseline), the authors estimated an overall NNH of 28 per year (95% CI, 13-213).
WHAT’S NEW: Evidence of CV risk is cause for concern
This meta-analysis provides evidence that varenicline is associated with a small but significant harmful effect on CV outcomes. The methods Singh et al used for review and article selection appear to be sound, and analysis of the included studies reveals little likelihood of publication bias.
CAVEATS: For many, benefits of quitting outweigh the risks
The absolute risk of a CV event found in this meta-analysis was small—just 0.24%. What’s more, the primary outcome was a composite of a diverse group of outcomes, some more serious than others. And, when compared with the highly positive effects of smoking cessation, the benefit-harm analysis still appears to favor varenicline for most patients. The estimated number needed to treat to get one person to stop smoking for ≥24 weeks is about 10 (95% CI, 8-13).8
CHALLENGES TO IMPLEMENTATION: Finding time to educate patients
The additional time needed to discuss the CV and neuropsychiatric risks of varenicline will be a challenge to physicians working in busy outpatient settings. Proper documentation of this discussion is prudent, however, given the increase in risk with this medication.
Acknowledgement
The Purls Surveillance System is supported in part by Grant Number UL1RR024999 from the National Center for Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center for Research Resources or the National Institutes of Health.
Click here to view PURL METHODOLOGY
1. Singh S, Loke YK, Spangler JG, et al. Risk of serious adverse cardiovascular events associated with varenicline: a systematic review and meta-analysis. CMAJ. 2011;183:1359-1366.
2. Centers for Disease Control and Prevention. Smoking-attributable mortality, years of potential life lost, and productivity Losses-United States, 2000-2004. MMWR Morbidity and Mortality Weekly Report. 2008;57:1226-1228.
3. Critchley JA, Capewell S. Mortality risk reduction associated with smoking cessation in patients with coronary heart disease. JAMA. 2003;290:86-97.
4. US Preventive Services Task Force. Counseling and interventions to prevent tobacco use and tobacco-caused disease in adults and pregnant women. Ann Intern Med. 2009;150:551-555.
5. US Food and Drug Administration. Boxed warning on serious mental health events to be required for Chantix and Zyban [press release]. July 1, 2009. Available at: http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm170100.htm#.Ttab-ZCbYtE. Accessed January 21, 2012.
6. US Food and Drug Administration. Chantix (varenicline): label change - risk of certain cardiovascular adverse events. 2011. Available at: http://www.fda.gov/Safety/MedWatch/SafetyInformation/SafetyAlertsforHumanMedicalProducts/ucm259469.htm. Accessed January 21, 2012.
7. Rigotti NA, Pipe AL, Benowitz NL, et al. Efficacy and safety of varenicline for smoking cessation in patients with cardiovascular disease: a randomized trial. Circulation. 2010;121:221-229.
8. Cahill K, Stead LF, Lancaster T. Nicotine receptor partial agonists for smoking cessation. Cochrane Database Syst Rev. 2011;(2):CD006103.
9. Singh S, Loke YK, Spangler JG, et al. Authors’ response. CMAJ. 2011;183:1405, 1407.
Inform patients who are interested in taking varenicline (Chantix) that there is a small cardiovascular (CV) risk associated with it, as well as neuropsychiatric risks—and consider recommending that smokers with a history of cardiovascular disease (CVD) use nicotine replacement therapy (NRT) or bupropion instead.1
STRENGTH OF RECOMMENDATION
A: Based on a meta-analysis.
Singh S, Loke YK, Spangler JG, et al. Risk of serious adverse cardiovascular events associated with varenicline: a systematic review and meta-analysis. CMAJ. 2011;183:1359-1366.
ILLUSTRATIVE CASE
A 53-year-old man asks you to prescribe Chantix to help him stop smoking. He has made several attempts to quit in the past, but never managed to stop for more than 6 months— and has smoked a pack a day for 30 years. The patient does not have a history of heart disease, but he is on statin therapy for hyperlipidemia. What should you tell him about varenicline’s potential benefits and risks?
Tobacco use remains the largest preventable contributor to death and disease in the United States.2 In smokers with coronary heart disease, smoking cessation is associated with a 36% reduction in all-cause mortality (relative risk [RR], 0.64; 95% confidence interval [CI], 0.58-0.71)—a risk reduction greater than that of statins (29%), aspirin (15%), beta-blockers (23%), or ACE inhibitors (23%).3
Varenicline now has 2 black box warnings
In its 2009 update on recommendations for smoking cessation, the United States Preventive Services Task Force cited NRT and controlled-release bupropion, as well as varenicline, as effective smoking cessation aids.4 Varenicline received US Food and Drug Administration (FDA) approval in 2006. In 2009, the FDA added a black box warning based on evidence of its adverse neuropsychiatric effects, including suicidality.5
In July 2011, the FDA required another label change,6 based on a double-blind RCT published in 2010 showing that for patients with CVD, varenicline is associated with an increased risk.7 As a partial nicotine agonist, varenicline could confer some of the CV risk associated with nicotine abuse.8 The FDA has asked its manufacturer, Pfizer Inc, to conduct further studies.6 The meta-analysis reviewed below—which was not associated with Pfizer or the FDA—was published in September 2011, just a couple of months after the label change.1
STUDY SUMMARY: Risk of ischemic or arrhythmic event is small but significant
Singh et al searched for double-blind RCTs that tested varenicline against a control in tobacco users.1 All included studies had to have reported adverse CV events. The primary outcome was any ischemic or arrhythmic CV event.
The researchers found 15 such studies (n=8216), which ranged in duration from 7 to 52 weeks. Most used a placebo control, but some included bupropion or NRT. The researchers used a Peto odds ratio (OR) for the meta-analysis, useful when combining uncommon events and including studies with no events.9
Compared with placebo, varenicline significantly increased the risk of CV events (odds ratio [OR], 1.72; 95% CI, 1.09-2.71). The incidence of CV events was 1.06% (52 of 4908) among varenicline users vs 0.82% (27 of 3308) in the controls (number needed to harm [NNH]=417).
The limited number of deaths (1.4% among patients taking varenicline vs 2.1% in the placebo groups) prevented analysis of mortality risk. The study with the most statistical power, which accounted for 57% of the overall effect, was the only one that included patients with known stable CV disease. (None included patients with unstable CV disease, whose risk may be greater.) Even when this study was removed, however, the outcome (OR, 2.54; 95% CI, 1.26-5.12) was consistent with the primary result for CV events. A sensitivity analysis comparing the risk associated with varenicline with that of either NRT or bupropion yielded similar results (OR, 1.67; 95% CI, 1.07-26.2). For a higher risk population with stable CVD (5.6% annual risk at baseline), the authors estimated an overall NNH of 28 per year (95% CI, 13-213).
WHAT’S NEW: Evidence of CV risk is cause for concern
This meta-analysis provides evidence that varenicline is associated with a small but significant harmful effect on CV outcomes. The methods Singh et al used for review and article selection appear to be sound, and analysis of the included studies reveals little likelihood of publication bias.
CAVEATS: For many, benefits of quitting outweigh the risks
The absolute risk of a CV event found in this meta-analysis was small—just 0.24%. What’s more, the primary outcome was a composite of a diverse group of outcomes, some more serious than others. And, when compared with the highly positive effects of smoking cessation, the benefit-harm analysis still appears to favor varenicline for most patients. The estimated number needed to treat to get one person to stop smoking for ≥24 weeks is about 10 (95% CI, 8-13).8
CHALLENGES TO IMPLEMENTATION: Finding time to educate patients
The additional time needed to discuss the CV and neuropsychiatric risks of varenicline will be a challenge to physicians working in busy outpatient settings. Proper documentation of this discussion is prudent, however, given the increase in risk with this medication.
Acknowledgement
The Purls Surveillance System is supported in part by Grant Number UL1RR024999 from the National Center for Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center for Research Resources or the National Institutes of Health.
Click here to view PURL METHODOLOGY
Inform patients who are interested in taking varenicline (Chantix) that there is a small cardiovascular (CV) risk associated with it, as well as neuropsychiatric risks—and consider recommending that smokers with a history of cardiovascular disease (CVD) use nicotine replacement therapy (NRT) or bupropion instead.1
STRENGTH OF RECOMMENDATION
A: Based on a meta-analysis.
Singh S, Loke YK, Spangler JG, et al. Risk of serious adverse cardiovascular events associated with varenicline: a systematic review and meta-analysis. CMAJ. 2011;183:1359-1366.
ILLUSTRATIVE CASE
A 53-year-old man asks you to prescribe Chantix to help him stop smoking. He has made several attempts to quit in the past, but never managed to stop for more than 6 months— and has smoked a pack a day for 30 years. The patient does not have a history of heart disease, but he is on statin therapy for hyperlipidemia. What should you tell him about varenicline’s potential benefits and risks?
Tobacco use remains the largest preventable contributor to death and disease in the United States.2 In smokers with coronary heart disease, smoking cessation is associated with a 36% reduction in all-cause mortality (relative risk [RR], 0.64; 95% confidence interval [CI], 0.58-0.71)—a risk reduction greater than that of statins (29%), aspirin (15%), beta-blockers (23%), or ACE inhibitors (23%).3
Varenicline now has 2 black box warnings
In its 2009 update on recommendations for smoking cessation, the United States Preventive Services Task Force cited NRT and controlled-release bupropion, as well as varenicline, as effective smoking cessation aids.4 Varenicline received US Food and Drug Administration (FDA) approval in 2006. In 2009, the FDA added a black box warning based on evidence of its adverse neuropsychiatric effects, including suicidality.5
In July 2011, the FDA required another label change,6 based on a double-blind RCT published in 2010 showing that for patients with CVD, varenicline is associated with an increased risk.7 As a partial nicotine agonist, varenicline could confer some of the CV risk associated with nicotine abuse.8 The FDA has asked its manufacturer, Pfizer Inc, to conduct further studies.6 The meta-analysis reviewed below—which was not associated with Pfizer or the FDA—was published in September 2011, just a couple of months after the label change.1
STUDY SUMMARY: Risk of ischemic or arrhythmic event is small but significant
Singh et al searched for double-blind RCTs that tested varenicline against a control in tobacco users.1 All included studies had to have reported adverse CV events. The primary outcome was any ischemic or arrhythmic CV event.
The researchers found 15 such studies (n=8216), which ranged in duration from 7 to 52 weeks. Most used a placebo control, but some included bupropion or NRT. The researchers used a Peto odds ratio (OR) for the meta-analysis, useful when combining uncommon events and including studies with no events.9
Compared with placebo, varenicline significantly increased the risk of CV events (odds ratio [OR], 1.72; 95% CI, 1.09-2.71). The incidence of CV events was 1.06% (52 of 4908) among varenicline users vs 0.82% (27 of 3308) in the controls (number needed to harm [NNH]=417).
The limited number of deaths (1.4% among patients taking varenicline vs 2.1% in the placebo groups) prevented analysis of mortality risk. The study with the most statistical power, which accounted for 57% of the overall effect, was the only one that included patients with known stable CV disease. (None included patients with unstable CV disease, whose risk may be greater.) Even when this study was removed, however, the outcome (OR, 2.54; 95% CI, 1.26-5.12) was consistent with the primary result for CV events. A sensitivity analysis comparing the risk associated with varenicline with that of either NRT or bupropion yielded similar results (OR, 1.67; 95% CI, 1.07-26.2). For a higher risk population with stable CVD (5.6% annual risk at baseline), the authors estimated an overall NNH of 28 per year (95% CI, 13-213).
WHAT’S NEW: Evidence of CV risk is cause for concern
This meta-analysis provides evidence that varenicline is associated with a small but significant harmful effect on CV outcomes. The methods Singh et al used for review and article selection appear to be sound, and analysis of the included studies reveals little likelihood of publication bias.
CAVEATS: For many, benefits of quitting outweigh the risks
The absolute risk of a CV event found in this meta-analysis was small—just 0.24%. What’s more, the primary outcome was a composite of a diverse group of outcomes, some more serious than others. And, when compared with the highly positive effects of smoking cessation, the benefit-harm analysis still appears to favor varenicline for most patients. The estimated number needed to treat to get one person to stop smoking for ≥24 weeks is about 10 (95% CI, 8-13).8
CHALLENGES TO IMPLEMENTATION: Finding time to educate patients
The additional time needed to discuss the CV and neuropsychiatric risks of varenicline will be a challenge to physicians working in busy outpatient settings. Proper documentation of this discussion is prudent, however, given the increase in risk with this medication.
Acknowledgement
The Purls Surveillance System is supported in part by Grant Number UL1RR024999 from the National Center for Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center for Research Resources or the National Institutes of Health.
Click here to view PURL METHODOLOGY
1. Singh S, Loke YK, Spangler JG, et al. Risk of serious adverse cardiovascular events associated with varenicline: a systematic review and meta-analysis. CMAJ. 2011;183:1359-1366.
2. Centers for Disease Control and Prevention. Smoking-attributable mortality, years of potential life lost, and productivity Losses-United States, 2000-2004. MMWR Morbidity and Mortality Weekly Report. 2008;57:1226-1228.
3. Critchley JA, Capewell S. Mortality risk reduction associated with smoking cessation in patients with coronary heart disease. JAMA. 2003;290:86-97.
4. US Preventive Services Task Force. Counseling and interventions to prevent tobacco use and tobacco-caused disease in adults and pregnant women. Ann Intern Med. 2009;150:551-555.
5. US Food and Drug Administration. Boxed warning on serious mental health events to be required for Chantix and Zyban [press release]. July 1, 2009. Available at: http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm170100.htm#.Ttab-ZCbYtE. Accessed January 21, 2012.
6. US Food and Drug Administration. Chantix (varenicline): label change - risk of certain cardiovascular adverse events. 2011. Available at: http://www.fda.gov/Safety/MedWatch/SafetyInformation/SafetyAlertsforHumanMedicalProducts/ucm259469.htm. Accessed January 21, 2012.
7. Rigotti NA, Pipe AL, Benowitz NL, et al. Efficacy and safety of varenicline for smoking cessation in patients with cardiovascular disease: a randomized trial. Circulation. 2010;121:221-229.
8. Cahill K, Stead LF, Lancaster T. Nicotine receptor partial agonists for smoking cessation. Cochrane Database Syst Rev. 2011;(2):CD006103.
9. Singh S, Loke YK, Spangler JG, et al. Authors’ response. CMAJ. 2011;183:1405, 1407.
1. Singh S, Loke YK, Spangler JG, et al. Risk of serious adverse cardiovascular events associated with varenicline: a systematic review and meta-analysis. CMAJ. 2011;183:1359-1366.
2. Centers for Disease Control and Prevention. Smoking-attributable mortality, years of potential life lost, and productivity Losses-United States, 2000-2004. MMWR Morbidity and Mortality Weekly Report. 2008;57:1226-1228.
3. Critchley JA, Capewell S. Mortality risk reduction associated with smoking cessation in patients with coronary heart disease. JAMA. 2003;290:86-97.
4. US Preventive Services Task Force. Counseling and interventions to prevent tobacco use and tobacco-caused disease in adults and pregnant women. Ann Intern Med. 2009;150:551-555.
5. US Food and Drug Administration. Boxed warning on serious mental health events to be required for Chantix and Zyban [press release]. July 1, 2009. Available at: http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm170100.htm#.Ttab-ZCbYtE. Accessed January 21, 2012.
6. US Food and Drug Administration. Chantix (varenicline): label change - risk of certain cardiovascular adverse events. 2011. Available at: http://www.fda.gov/Safety/MedWatch/SafetyInformation/SafetyAlertsforHumanMedicalProducts/ucm259469.htm. Accessed January 21, 2012.
7. Rigotti NA, Pipe AL, Benowitz NL, et al. Efficacy and safety of varenicline for smoking cessation in patients with cardiovascular disease: a randomized trial. Circulation. 2010;121:221-229.
8. Cahill K, Stead LF, Lancaster T. Nicotine receptor partial agonists for smoking cessation. Cochrane Database Syst Rev. 2011;(2):CD006103.
9. Singh S, Loke YK, Spangler JG, et al. Authors’ response. CMAJ. 2011;183:1405, 1407.
Copyright © 2012 The Family Physicians Inquiries Network.
All rights reserved.
Fatty liver disease in type 2 diabetes: Common and often unmanaged
Purpose The objective of this pilot study was to evaluate the prevalence and management of nonalcoholic fatty liver disease in a rural type 2 diabetes population.
Methods We randomly selected 100 patients with type 2 diabetes from a large rural clinic/hospital system in the upper Midwest and conducted a chart review to determine the prevalence of abnormal results of serum liver function tests and liver imaging (eg, computed tomography, ultrasound, magnetic resonance imaging). We also determined the number of patients who were given a diagnosis of fatty liver disease and who among those were subsequently managed for the condition.
Results Of the 100 subjects, 40 had abnormal serum liver function testing, and half of those individuals underwent imaging. This resulted in a diagnosis of fatty liver disease in 11 (27.5% of the 40 with abnormal liver function). Only 4 patients received specific interventions for fatty liver disease.
Conclusion In this rural population, fatty liver disease was common and untreated, suggesting a possible need for a change in screening and management protocols.
Nonalcoholic fatty liver disease (NAFLD) is the most common chronic liver disease in the United States.1 In particular, NAFLD and the related inflammatory nonalcoholic steatohepatitis (NASH) often develop in individuals who are obese or who have prediabetes or type 2 diabetes, affecting up to 75% of patients with these conditions.2
In addition to NAFLD and NASH, other liver diseases associated with type 2 diabetes include cirrhosis, hepatocellular carcinoma, liver failure, and hepatitis.1,3,4 Of patients with type 2 diabetes, more than 600,000 have cirrhosis; 4.4% of diabetes-related deaths have been attributed to cirrhosis.4,5
NAFLD and NASH share a common pathophysiology in type 2 diabetes with respect to insulin resistance, which results in hyperlipidemias that enhance fatty deposits in the liver.1,2 Hepatic fat accumulation is also associated with increasing measures of inflammation, including C-reactive protein.6
Resultant liver function test abnormalities and characteristic appearance on imaging studies (ultrasound, computed tomography [CT], or magnetic resonance imaging [MRI]) may be similar in NAFLD and NASH.1-3 Liver biopsy therefore is necessary to distinguish NAFLD from NASH, with NASH showing characteristic inflammatory and fibrotic changes.1,2 Evaluations of patients with minor liver test abnormalities reveal that up to 98% may have liver disease, most often fatty liver disease.7
Weight loss is a strategy for managing NAFLD and NASH, although large randomized controlled trials are lacking.8-10 Several agents used for diabetes and dyslipidemias, including glucagon-like peptide-1 (GLP-1) mimetics, metformin, thiazolidinediones, and statins, have been studied as possible treatments for NAFLD and NASH.8-13 Currently, these medications carry cautions or warnings about using them in patients with liver disease and are not indicated as treatments for NAFLD or NASH.
SUBJECTS AND METHODS
One hundred patients were randomly selected from a type 2 diabetes patient database at the Altru Health System (Grand Forks, ND) for cross-sectional analysis. Manual data extraction from “paper charts” was necessary in some cases, limiting the size of the study.
All subjects had a diagnosis of type 2 diabetes confirmed by American Diabetes Association criteria, were between the ages of 18 and 64 years, and had no known liver disease other than that associated with their diabetes. Other criteria included visiting a health care provider regarding diabetes management within the last year and having undergone laboratory blood testing of liver function within the last 5 years. The study population comprised an equal number of men and women.
We collected data about abnormal liver function from blood test results, including levels of aspartate transaminase (AST), alanine aminotransferase (ALT), and alkaline phosphatase (ALP); results of radiologic imaging of the liver (ultrasound, MRI, or CT) and liver biopsy; any interventions (medication changes, lifestyle management, or surgery); and referral to a specialist (gastroenterologist or surgeon).
DATA ANALYSIS
Of the 100 subjects, 40 had at least one abnormal serum liver function test (AST, ALT, or ALP), although we could find no record of tests for one of the 100 subjects. Of the 40 with abnormal test results, 17 (42.5%) were women and 23 (57.5%) were men. None of these patients had highly elevated levels of AST, ALT, or ALP.
Of the 40 patients with abnormal serum liver function tests, only 10 (25%) were specifically referred for imaging studies related to a possible diagnosis of fatty liver disease. Four of these 10 patients (1 woman and 3 men) had both ultrasound and CT imaging. Another 10 subjects (25%) had incidental findings of fatty liver disease on imaging performed for another presumed diagnosis or symptom, eg, abdominal pain. Overall, 11 (6 men, 5 women) of the 40 subjects (27.5%) with at least one abnormal liver function test received a diagnosis of fatty liver disease based on imaging findings. None of the subjects had a diagnosis of cirrhosis or other end-stage liver disease.
A medical intervention was offered to 4 of the 11 patients (2 women and 2 men) who received a diagnosis of fatty liver disease. Practitioners specifically referred one woman for medical weight loss management and another for weight loss surgery. One man was advised to stop taking metformin, and another was referred to a dietician for lifestyle weight loss management. No patient was referred to a gastroenterologist or any other specialist for further evaluation or biopsy.
DISCUSSION
Although a small sample size limits the strength of this pilot study, the finding that fatty liver disease is common in patients with type 2 diabetes in a rural community hospital population supports other published data. As only half of the subjects with abnormal liver function tests had imaging studies, it’s likely that some patients in the study group who did not undergo imaging also had NAFLD, NASH, or other liver disease, but it was not diagnosed.
While no specific screening guidelines for fatty liver disease in patients with type 2 diabetes have been issued, clinical interest in this area has been growing, and this study suggests some avenues for further exploration.3 In the institution where this study was conducted, it appears that liver function tests were most likely to be performed in conjunction with routine monitoring of the use of statins, metformin, or other medications or because of a symptom such as abdominal pain. Yet given the widespread availability and relatively low cost of such tests, periodic monitoring of serum liver function in patients with type 2 diabetes may be warranted.14
Patients found to have persistent or recurrent abnormal liver function tests could then be referred for further evaluation with ultrasound, CT, or MRI.14 Ultrasound has the benefit of lower cost and avoidance of intravenous contrast, which may be important for patients with renal dysfunction.14 Based on the results of these tests, appropriate medical interventions could then follow.
·Acknowledgements·
The author thanks Bonnie Lee and Diane Vold for their assistance in the design of this study and its preparation for publication. The author also thanks William Zaks, MD, PhD, and James Brosseau, MD, MPH, for their guidance and feedback.
1. Caldwell SH, Oelsner DH, Iezzoni JC, et al. Cryptogenic cirrhosis: clinical characterization and risk factors for underlying disease. Hepatology. 1999;29:664-669.
2. Pagano G, Pacini G, Musso G, et al. Nonalcoholic steatohepatitis, insulin resistance, and metabolic syndrome: further evidence for an etiologic association. Hepatology. 2002;35:367-372.
3. Tolman KG, Fonseca V, Dalpiaz A, et al. Spectrum of liver disease in type 2 diabetes and management of patients with diabetes and liver disease. Diabetes Care. 2007;30:734-743.
4. de Marco R, Locatelli F, Zoppini G, et al. Cause-specific mortality in type 2 diabetes: the Verona Diabetes Study. Diabetes Care. 1999;22:756-761.
5. Koehler E, Watt K, Charlton M. Fatty liver and liver transplantation. Clin Liver Dis. 2009;13:621-630.
6. Saremi A, Allison M, Ditomasso D, et al. Preliminary report: hepatic fat and inflammation in type 2 diabetes mellitus. Metabolism. 2010;59:430-432.
7. Hultcrantz R, Glaumann H, Lindberg G, et al. Liver investigation in 149 asymptomatic patients with moderately elevated activities of serum aminotransferases. Scand J Gastroenterol. 1986;21:109-113.
8. Schreuder TC, Verwer BJ, van Nieuwkerk CM, et al. Nonalcoholic fatty liver disease: an overview of current insights in pathogenesis, diagnosis and treatment. World J Gastroenterol. 2008;14:2474-2486.
9. Chavez-Tapia NC, Tellez-Avila FI, Barrientos-Gutierrez T, et al. Bariatric surgery for non-alcoholic steatohepatitis in obese patients. Cochrane Database Syst Rev. 2010;(1):CD007340.-
10. Medina J, Fernández-Salazar LI, García-Buey L, et al. Approach to the pathogenesis and treatment of nonalcoholic steatohepatitis. Diabetes Care. 2004;27:2057-2066.
11. Khashab M, Chalasani N. Use of insulin sensitizers in NASH. Endocrinol Metab Clin North Am. 2007;36:1067-1087.
12. Ding X, Saxena NK, Lin S, et al. Exendin-4, a glucagon-like protein (GLP-1) receptor agonist, reverses hepatic steatosis in ob/ob mice. Hepatology. 2006;43:173-181.
13. Matafome P, Nunes E, Louro T, et al. A role for atorvastatin and insulin combination in protecting from liver injury in a model of type 2 diabetes with hyperlipidemia. Naunyn Schmiedebergs Arch Pharmacol. 2009;379:241-251.
14. Ratziu V, Bellentani S, Cortez-Pinto H, et al. A position statement on NAFLD/NASH based on the EASL 2009 special conference. J Hepatol. 2010;53:372-384.
CORRESPONDENCE Eric L. Johnson, MD, 501 N. Columbia Road, Stop 9037, Grand Forks, ND 58202; [email protected]
Purpose The objective of this pilot study was to evaluate the prevalence and management of nonalcoholic fatty liver disease in a rural type 2 diabetes population.
Methods We randomly selected 100 patients with type 2 diabetes from a large rural clinic/hospital system in the upper Midwest and conducted a chart review to determine the prevalence of abnormal results of serum liver function tests and liver imaging (eg, computed tomography, ultrasound, magnetic resonance imaging). We also determined the number of patients who were given a diagnosis of fatty liver disease and who among those were subsequently managed for the condition.
Results Of the 100 subjects, 40 had abnormal serum liver function testing, and half of those individuals underwent imaging. This resulted in a diagnosis of fatty liver disease in 11 (27.5% of the 40 with abnormal liver function). Only 4 patients received specific interventions for fatty liver disease.
Conclusion In this rural population, fatty liver disease was common and untreated, suggesting a possible need for a change in screening and management protocols.
Nonalcoholic fatty liver disease (NAFLD) is the most common chronic liver disease in the United States.1 In particular, NAFLD and the related inflammatory nonalcoholic steatohepatitis (NASH) often develop in individuals who are obese or who have prediabetes or type 2 diabetes, affecting up to 75% of patients with these conditions.2
In addition to NAFLD and NASH, other liver diseases associated with type 2 diabetes include cirrhosis, hepatocellular carcinoma, liver failure, and hepatitis.1,3,4 Of patients with type 2 diabetes, more than 600,000 have cirrhosis; 4.4% of diabetes-related deaths have been attributed to cirrhosis.4,5
NAFLD and NASH share a common pathophysiology in type 2 diabetes with respect to insulin resistance, which results in hyperlipidemias that enhance fatty deposits in the liver.1,2 Hepatic fat accumulation is also associated with increasing measures of inflammation, including C-reactive protein.6
Resultant liver function test abnormalities and characteristic appearance on imaging studies (ultrasound, computed tomography [CT], or magnetic resonance imaging [MRI]) may be similar in NAFLD and NASH.1-3 Liver biopsy therefore is necessary to distinguish NAFLD from NASH, with NASH showing characteristic inflammatory and fibrotic changes.1,2 Evaluations of patients with minor liver test abnormalities reveal that up to 98% may have liver disease, most often fatty liver disease.7
Weight loss is a strategy for managing NAFLD and NASH, although large randomized controlled trials are lacking.8-10 Several agents used for diabetes and dyslipidemias, including glucagon-like peptide-1 (GLP-1) mimetics, metformin, thiazolidinediones, and statins, have been studied as possible treatments for NAFLD and NASH.8-13 Currently, these medications carry cautions or warnings about using them in patients with liver disease and are not indicated as treatments for NAFLD or NASH.
SUBJECTS AND METHODS
One hundred patients were randomly selected from a type 2 diabetes patient database at the Altru Health System (Grand Forks, ND) for cross-sectional analysis. Manual data extraction from “paper charts” was necessary in some cases, limiting the size of the study.
All subjects had a diagnosis of type 2 diabetes confirmed by American Diabetes Association criteria, were between the ages of 18 and 64 years, and had no known liver disease other than that associated with their diabetes. Other criteria included visiting a health care provider regarding diabetes management within the last year and having undergone laboratory blood testing of liver function within the last 5 years. The study population comprised an equal number of men and women.
We collected data about abnormal liver function from blood test results, including levels of aspartate transaminase (AST), alanine aminotransferase (ALT), and alkaline phosphatase (ALP); results of radiologic imaging of the liver (ultrasound, MRI, or CT) and liver biopsy; any interventions (medication changes, lifestyle management, or surgery); and referral to a specialist (gastroenterologist or surgeon).
DATA ANALYSIS
Of the 100 subjects, 40 had at least one abnormal serum liver function test (AST, ALT, or ALP), although we could find no record of tests for one of the 100 subjects. Of the 40 with abnormal test results, 17 (42.5%) were women and 23 (57.5%) were men. None of these patients had highly elevated levels of AST, ALT, or ALP.
Of the 40 patients with abnormal serum liver function tests, only 10 (25%) were specifically referred for imaging studies related to a possible diagnosis of fatty liver disease. Four of these 10 patients (1 woman and 3 men) had both ultrasound and CT imaging. Another 10 subjects (25%) had incidental findings of fatty liver disease on imaging performed for another presumed diagnosis or symptom, eg, abdominal pain. Overall, 11 (6 men, 5 women) of the 40 subjects (27.5%) with at least one abnormal liver function test received a diagnosis of fatty liver disease based on imaging findings. None of the subjects had a diagnosis of cirrhosis or other end-stage liver disease.
A medical intervention was offered to 4 of the 11 patients (2 women and 2 men) who received a diagnosis of fatty liver disease. Practitioners specifically referred one woman for medical weight loss management and another for weight loss surgery. One man was advised to stop taking metformin, and another was referred to a dietician for lifestyle weight loss management. No patient was referred to a gastroenterologist or any other specialist for further evaluation or biopsy.
DISCUSSION
Although a small sample size limits the strength of this pilot study, the finding that fatty liver disease is common in patients with type 2 diabetes in a rural community hospital population supports other published data. As only half of the subjects with abnormal liver function tests had imaging studies, it’s likely that some patients in the study group who did not undergo imaging also had NAFLD, NASH, or other liver disease, but it was not diagnosed.
While no specific screening guidelines for fatty liver disease in patients with type 2 diabetes have been issued, clinical interest in this area has been growing, and this study suggests some avenues for further exploration.3 In the institution where this study was conducted, it appears that liver function tests were most likely to be performed in conjunction with routine monitoring of the use of statins, metformin, or other medications or because of a symptom such as abdominal pain. Yet given the widespread availability and relatively low cost of such tests, periodic monitoring of serum liver function in patients with type 2 diabetes may be warranted.14
Patients found to have persistent or recurrent abnormal liver function tests could then be referred for further evaluation with ultrasound, CT, or MRI.14 Ultrasound has the benefit of lower cost and avoidance of intravenous contrast, which may be important for patients with renal dysfunction.14 Based on the results of these tests, appropriate medical interventions could then follow.
·Acknowledgements·
The author thanks Bonnie Lee and Diane Vold for their assistance in the design of this study and its preparation for publication. The author also thanks William Zaks, MD, PhD, and James Brosseau, MD, MPH, for their guidance and feedback.
Purpose The objective of this pilot study was to evaluate the prevalence and management of nonalcoholic fatty liver disease in a rural type 2 diabetes population.
Methods We randomly selected 100 patients with type 2 diabetes from a large rural clinic/hospital system in the upper Midwest and conducted a chart review to determine the prevalence of abnormal results of serum liver function tests and liver imaging (eg, computed tomography, ultrasound, magnetic resonance imaging). We also determined the number of patients who were given a diagnosis of fatty liver disease and who among those were subsequently managed for the condition.
Results Of the 100 subjects, 40 had abnormal serum liver function testing, and half of those individuals underwent imaging. This resulted in a diagnosis of fatty liver disease in 11 (27.5% of the 40 with abnormal liver function). Only 4 patients received specific interventions for fatty liver disease.
Conclusion In this rural population, fatty liver disease was common and untreated, suggesting a possible need for a change in screening and management protocols.
Nonalcoholic fatty liver disease (NAFLD) is the most common chronic liver disease in the United States.1 In particular, NAFLD and the related inflammatory nonalcoholic steatohepatitis (NASH) often develop in individuals who are obese or who have prediabetes or type 2 diabetes, affecting up to 75% of patients with these conditions.2
In addition to NAFLD and NASH, other liver diseases associated with type 2 diabetes include cirrhosis, hepatocellular carcinoma, liver failure, and hepatitis.1,3,4 Of patients with type 2 diabetes, more than 600,000 have cirrhosis; 4.4% of diabetes-related deaths have been attributed to cirrhosis.4,5
NAFLD and NASH share a common pathophysiology in type 2 diabetes with respect to insulin resistance, which results in hyperlipidemias that enhance fatty deposits in the liver.1,2 Hepatic fat accumulation is also associated with increasing measures of inflammation, including C-reactive protein.6
Resultant liver function test abnormalities and characteristic appearance on imaging studies (ultrasound, computed tomography [CT], or magnetic resonance imaging [MRI]) may be similar in NAFLD and NASH.1-3 Liver biopsy therefore is necessary to distinguish NAFLD from NASH, with NASH showing characteristic inflammatory and fibrotic changes.1,2 Evaluations of patients with minor liver test abnormalities reveal that up to 98% may have liver disease, most often fatty liver disease.7
Weight loss is a strategy for managing NAFLD and NASH, although large randomized controlled trials are lacking.8-10 Several agents used for diabetes and dyslipidemias, including glucagon-like peptide-1 (GLP-1) mimetics, metformin, thiazolidinediones, and statins, have been studied as possible treatments for NAFLD and NASH.8-13 Currently, these medications carry cautions or warnings about using them in patients with liver disease and are not indicated as treatments for NAFLD or NASH.
SUBJECTS AND METHODS
One hundred patients were randomly selected from a type 2 diabetes patient database at the Altru Health System (Grand Forks, ND) for cross-sectional analysis. Manual data extraction from “paper charts” was necessary in some cases, limiting the size of the study.
All subjects had a diagnosis of type 2 diabetes confirmed by American Diabetes Association criteria, were between the ages of 18 and 64 years, and had no known liver disease other than that associated with their diabetes. Other criteria included visiting a health care provider regarding diabetes management within the last year and having undergone laboratory blood testing of liver function within the last 5 years. The study population comprised an equal number of men and women.
We collected data about abnormal liver function from blood test results, including levels of aspartate transaminase (AST), alanine aminotransferase (ALT), and alkaline phosphatase (ALP); results of radiologic imaging of the liver (ultrasound, MRI, or CT) and liver biopsy; any interventions (medication changes, lifestyle management, or surgery); and referral to a specialist (gastroenterologist or surgeon).
DATA ANALYSIS
Of the 100 subjects, 40 had at least one abnormal serum liver function test (AST, ALT, or ALP), although we could find no record of tests for one of the 100 subjects. Of the 40 with abnormal test results, 17 (42.5%) were women and 23 (57.5%) were men. None of these patients had highly elevated levels of AST, ALT, or ALP.
Of the 40 patients with abnormal serum liver function tests, only 10 (25%) were specifically referred for imaging studies related to a possible diagnosis of fatty liver disease. Four of these 10 patients (1 woman and 3 men) had both ultrasound and CT imaging. Another 10 subjects (25%) had incidental findings of fatty liver disease on imaging performed for another presumed diagnosis or symptom, eg, abdominal pain. Overall, 11 (6 men, 5 women) of the 40 subjects (27.5%) with at least one abnormal liver function test received a diagnosis of fatty liver disease based on imaging findings. None of the subjects had a diagnosis of cirrhosis or other end-stage liver disease.
A medical intervention was offered to 4 of the 11 patients (2 women and 2 men) who received a diagnosis of fatty liver disease. Practitioners specifically referred one woman for medical weight loss management and another for weight loss surgery. One man was advised to stop taking metformin, and another was referred to a dietician for lifestyle weight loss management. No patient was referred to a gastroenterologist or any other specialist for further evaluation or biopsy.
DISCUSSION
Although a small sample size limits the strength of this pilot study, the finding that fatty liver disease is common in patients with type 2 diabetes in a rural community hospital population supports other published data. As only half of the subjects with abnormal liver function tests had imaging studies, it’s likely that some patients in the study group who did not undergo imaging also had NAFLD, NASH, or other liver disease, but it was not diagnosed.
While no specific screening guidelines for fatty liver disease in patients with type 2 diabetes have been issued, clinical interest in this area has been growing, and this study suggests some avenues for further exploration.3 In the institution where this study was conducted, it appears that liver function tests were most likely to be performed in conjunction with routine monitoring of the use of statins, metformin, or other medications or because of a symptom such as abdominal pain. Yet given the widespread availability and relatively low cost of such tests, periodic monitoring of serum liver function in patients with type 2 diabetes may be warranted.14
Patients found to have persistent or recurrent abnormal liver function tests could then be referred for further evaluation with ultrasound, CT, or MRI.14 Ultrasound has the benefit of lower cost and avoidance of intravenous contrast, which may be important for patients with renal dysfunction.14 Based on the results of these tests, appropriate medical interventions could then follow.
·Acknowledgements·
The author thanks Bonnie Lee and Diane Vold for their assistance in the design of this study and its preparation for publication. The author also thanks William Zaks, MD, PhD, and James Brosseau, MD, MPH, for their guidance and feedback.
1. Caldwell SH, Oelsner DH, Iezzoni JC, et al. Cryptogenic cirrhosis: clinical characterization and risk factors for underlying disease. Hepatology. 1999;29:664-669.
2. Pagano G, Pacini G, Musso G, et al. Nonalcoholic steatohepatitis, insulin resistance, and metabolic syndrome: further evidence for an etiologic association. Hepatology. 2002;35:367-372.
3. Tolman KG, Fonseca V, Dalpiaz A, et al. Spectrum of liver disease in type 2 diabetes and management of patients with diabetes and liver disease. Diabetes Care. 2007;30:734-743.
4. de Marco R, Locatelli F, Zoppini G, et al. Cause-specific mortality in type 2 diabetes: the Verona Diabetes Study. Diabetes Care. 1999;22:756-761.
5. Koehler E, Watt K, Charlton M. Fatty liver and liver transplantation. Clin Liver Dis. 2009;13:621-630.
6. Saremi A, Allison M, Ditomasso D, et al. Preliminary report: hepatic fat and inflammation in type 2 diabetes mellitus. Metabolism. 2010;59:430-432.
7. Hultcrantz R, Glaumann H, Lindberg G, et al. Liver investigation in 149 asymptomatic patients with moderately elevated activities of serum aminotransferases. Scand J Gastroenterol. 1986;21:109-113.
8. Schreuder TC, Verwer BJ, van Nieuwkerk CM, et al. Nonalcoholic fatty liver disease: an overview of current insights in pathogenesis, diagnosis and treatment. World J Gastroenterol. 2008;14:2474-2486.
9. Chavez-Tapia NC, Tellez-Avila FI, Barrientos-Gutierrez T, et al. Bariatric surgery for non-alcoholic steatohepatitis in obese patients. Cochrane Database Syst Rev. 2010;(1):CD007340.-
10. Medina J, Fernández-Salazar LI, García-Buey L, et al. Approach to the pathogenesis and treatment of nonalcoholic steatohepatitis. Diabetes Care. 2004;27:2057-2066.
11. Khashab M, Chalasani N. Use of insulin sensitizers in NASH. Endocrinol Metab Clin North Am. 2007;36:1067-1087.
12. Ding X, Saxena NK, Lin S, et al. Exendin-4, a glucagon-like protein (GLP-1) receptor agonist, reverses hepatic steatosis in ob/ob mice. Hepatology. 2006;43:173-181.
13. Matafome P, Nunes E, Louro T, et al. A role for atorvastatin and insulin combination in protecting from liver injury in a model of type 2 diabetes with hyperlipidemia. Naunyn Schmiedebergs Arch Pharmacol. 2009;379:241-251.
14. Ratziu V, Bellentani S, Cortez-Pinto H, et al. A position statement on NAFLD/NASH based on the EASL 2009 special conference. J Hepatol. 2010;53:372-384.
CORRESPONDENCE Eric L. Johnson, MD, 501 N. Columbia Road, Stop 9037, Grand Forks, ND 58202; [email protected]
1. Caldwell SH, Oelsner DH, Iezzoni JC, et al. Cryptogenic cirrhosis: clinical characterization and risk factors for underlying disease. Hepatology. 1999;29:664-669.
2. Pagano G, Pacini G, Musso G, et al. Nonalcoholic steatohepatitis, insulin resistance, and metabolic syndrome: further evidence for an etiologic association. Hepatology. 2002;35:367-372.
3. Tolman KG, Fonseca V, Dalpiaz A, et al. Spectrum of liver disease in type 2 diabetes and management of patients with diabetes and liver disease. Diabetes Care. 2007;30:734-743.
4. de Marco R, Locatelli F, Zoppini G, et al. Cause-specific mortality in type 2 diabetes: the Verona Diabetes Study. Diabetes Care. 1999;22:756-761.
5. Koehler E, Watt K, Charlton M. Fatty liver and liver transplantation. Clin Liver Dis. 2009;13:621-630.
6. Saremi A, Allison M, Ditomasso D, et al. Preliminary report: hepatic fat and inflammation in type 2 diabetes mellitus. Metabolism. 2010;59:430-432.
7. Hultcrantz R, Glaumann H, Lindberg G, et al. Liver investigation in 149 asymptomatic patients with moderately elevated activities of serum aminotransferases. Scand J Gastroenterol. 1986;21:109-113.
8. Schreuder TC, Verwer BJ, van Nieuwkerk CM, et al. Nonalcoholic fatty liver disease: an overview of current insights in pathogenesis, diagnosis and treatment. World J Gastroenterol. 2008;14:2474-2486.
9. Chavez-Tapia NC, Tellez-Avila FI, Barrientos-Gutierrez T, et al. Bariatric surgery for non-alcoholic steatohepatitis in obese patients. Cochrane Database Syst Rev. 2010;(1):CD007340.-
10. Medina J, Fernández-Salazar LI, García-Buey L, et al. Approach to the pathogenesis and treatment of nonalcoholic steatohepatitis. Diabetes Care. 2004;27:2057-2066.
11. Khashab M, Chalasani N. Use of insulin sensitizers in NASH. Endocrinol Metab Clin North Am. 2007;36:1067-1087.
12. Ding X, Saxena NK, Lin S, et al. Exendin-4, a glucagon-like protein (GLP-1) receptor agonist, reverses hepatic steatosis in ob/ob mice. Hepatology. 2006;43:173-181.
13. Matafome P, Nunes E, Louro T, et al. A role for atorvastatin and insulin combination in protecting from liver injury in a model of type 2 diabetes with hyperlipidemia. Naunyn Schmiedebergs Arch Pharmacol. 2009;379:241-251.
14. Ratziu V, Bellentani S, Cortez-Pinto H, et al. A position statement on NAFLD/NASH based on the EASL 2009 special conference. J Hepatol. 2010;53:372-384.
CORRESPONDENCE Eric L. Johnson, MD, 501 N. Columbia Road, Stop 9037, Grand Forks, ND 58202; [email protected]
ACIP immunization update
In February, the Centers for Disease Control and Prevention (CDC) published the 2012 immunization schedules for infants and children, adolescents, and adults.1,2 The schedules, which are available at http://www.cdc.gov/vaccines/recs/schedules/default.htm, are updated annually and incorporate additions and changes recommended by the Advisory Committee on Immunization Practices (ACIP) over the past year. While there were no major advances in new vaccines in 2011, there were a number of new indications for existing ones.
Human papillomavirus vaccine for males
Quadrivalent vaccine against human papillomavirus is now recommended for routine use for males ages 11 to 12 years to prevent genital warts and anal intraepithelial neoplasia.3,4 Catch-up vaccination is also recommended for males ages 13 to 21 who have not received it. In addition, routine use is recommended for males ages 22 to 26 years who have sex with men or are HIV positive or immuno-compromised.
Tetanus toxoid, reduced strength diphtheria toxoid, and acellular pertussis (Tdap)
Indications for the routine use of Tdap were expanded to include children ages 7 to 10 years, pregnant women, and adults age 65 and older who have contact with infants.5,6 Children ages 7 to 10 years who have not had the full series of DTaP should receive Td/Tdap according to the catch-up schedule,1 with one of the doses being Tdap. Adults older than 65 who have never received Tdap and who have close contact with infants should receive one dose. No minimum interval is required between receipt of the Td and Tdap vaccines. Other older adults who ask for Tdap vaccination should receive it. Use of Tdap in those ages 7 to 10 years or 65 and older is off label.5
Pregnant women who have not received Tdap should receive 1 dose after week 20 of pregnancy, although receiving it earlier is not contraindicated if tetanus toxoid is needed for tetanus prevention following a wound.6
Hepatitis B virus (HBV) vaccine
Added to the list of high-risk adults who should receive HBV vaccine routinely are those ages 19 through 59 years with diabetes.7 Vaccinate as soon as possible after the diabetes diagnosis is confirmed. The decision as to whether to vaccinate patients ≥60 years with diabetes should be based on the likelihood that they will become infected. Considerations include the risks associated with an increased need for help with blood-glucose monitoring in long-term care facilities, the likelihood that the patient will experience chronic sequelae if infected, and the likelihood that the patient will mount a proper immune response to the vaccine.7 (The more frail patients are, the less likely they are to achieve adequate immunity.7)
Meningococcal conjugate vaccine, quadrivalent (MCV4)
An MCV4 vaccine (Menactra) has now been licensed for use in children as young as 9 months.8 At this time, however, neither Menactra nor its competitor, Menveo (licensed for use in those 2 years and older), is recommended for routine administration until the age of 11 to 12 years. Infants and children ages 9 through 23 months with complement deficiencies, or who will be traveling to countries with endemic high levels of meningococcus, should be vaccinated with 2 doses of Menactra 3 months apart, and with a booster dose after 3 years if risk persists. The recommendations regarding the use of MCV4 in those ≤2 years with high-risk conditions are listed in TABLE 1.
In February 2012, the CDC announced results of the 2010 National Health Interview Survey. Increases in immunization coverage occurred only with Tdap vaccination for individuals 19 to 64 years of age (from 6.6% to 8.2%), herpes zoster vaccination among those ≥60 years (from 10% to 14.4%), and ≥1 dose of HPV vaccination for women 19 to 26 years (from 17.1% to 20.7%). Rates of immunization were unchanged for other vaccines. The CDC said a substantial improvement in coverage is needed to reduce vaccine-preventable diseases among adults.
Source: CDC. Adult vaccination coverage—United States, 2010. MMWR Morb Mortal Wkly Rep. 2012;61:66-72.
Another change regarding the use of MCV4 is a recommended booster dose for those age 16 and older who were first vaccinated at age 11 or 12 years.9 For those vaccinated at ages 13 to 15, a booster should be received at ages 16 to 18. No booster is needed if the first MCV4 dose is received at or after age 16. Recommendations for MCV4 use and booster doses for those 2 years and older are listed in TABLE 2.
TABLE 1
Recommended Menactra schedule for young children at high risk for invasive meningococcal disease8
| Risk group | Primary vaccination series | Booster dose, if child remains at increased risk |
|---|---|---|
| Children ages 9-23 months at high risk for invasive meningococcal disease,* except those with functional or anatomic asplenia | 2 doses, 3 months apart Catch-up dose at earliest opportunity if dose 2 is not given on schedule | Initial booster 3 years after completing primary series At 5-year intervals after initial booster |
| Children with functional or anatomic asplenia at high risk for invasive meningococcal disease | 2 doses, 2 months apart, starting at age 2 years and ≥4 weeks after completing the PCV13 vaccine series | |
| PCV, pneumococcal conjugate vaccine. *Children who have persistent complement component deficiencies (eg, C5–C9, properdin, factor H, or factor D); those traveling to (or residents of) countries where meningococcal disease is hyperendemic or epidemic; or those who are in a defined risk group during a community or institutional meningococcal outbreak. | ||
TABLE 2
Recommended schedule for meningococcal conjugate vaccine in those ≥2 years, according to risk9
| Risk group | Primary vaccination series | Booster dose |
|---|---|---|
| Individuals ages 11-18 years | 1 dose, preferably at 11 or 12 years | At age 16 years, if primary dose given at age 11 or 12 years Age 16-18 years, if primary dose given at age 13-15 years No booster needed if primary dose given on or after age 16 years |
| Individuals ages 11-18 years infected with HIV | 2 doses, 2 months apart | |
| Individuals ages 2-55 years with persistent complement component deficiency (eg, C5–C9, properdin, or factor D) or functional or anatomical asplenia | 2 doses, 2 months apart | Every 5 years At the earliest opportunity if only 1 primary dose; every 5 years thereafter |
| Individuals ages 2-55 years with prolonged increased risk for exposure, such as microbiologists routinely working with Neisseria meningitides, and travelers to, or residents of, countries where meningococcal disease is hyperendemic or epidemic | 1 dose | After 3 years, if primary dose given at age 2-6 years After 5 years, if primary dose given at ≥7 years and the individual remains at risk Every 5 years thereafter, as long as the risk persists |
| HIV, human immunodeficiency virus. | ||
Herpes zoster vaccine
The herpes zoster vaccine was initially licensed for those 60 years and older. Last year the FDA approved lowering the age to 50 years and older. At this time, however, the ACIP continues to recommend that the vaccine be used routinely starting at age 60 years. The age was not lowered because of a concern about vaccine supply and the uncertainty about the possible need for a booster dose if administered at age 50.10
Influenza vaccine
As described in a previous Practice Alert,11 a history of egg allergy is no longer a strict contraindication for receipt of the influenza vaccine. The other major adjustment is a simplified recommendation on how to determine the required number of doses for a child younger than 9 years. If the child received 1 or both doses of the 2010-2011 vaccine, give just a single dose of the 2011-2012 vaccine. If the history is uncertain, give 2 doses of the new vaccine at least 4 weeks apart.12
1. CDC. Recommended immunization schedules for persons aged 0 through 18 years—United States, 2012. MMWR Morb Mortal Wkly Rep. 2012;61(5):1-4.
2. CDC. Recommended adult immunization schedule—United States, 2012. MMWR Morb Mortal Wkly Rep. 2012;61(4):1-7.
3. Campos-Outcalt D. Human papilloma virus: Vaccine is now routinely indicated for males. J Fam Pract. 2012;61:38-40.
4. CDC. Recommendations on the use of quadrivalent human papillomavirus vaccine in males—Advisory Committee on Immunization Practices (ACIP), 2011. MMWR Morb Mortal Wkly Rep. 2011;60:1705-1708.
5. CDC. Updated recommendations for use of tetanus toxoid, reduced diphtheria toxoid and acellular pertussis (Tdap) vaccine from the Advisory Committee on Immunization Practices, 2010. MMWR Morb Mortal Wkly Rep. 2011;60:13-15.
6. CDC. Updated recommendations for use of tetanus toxoid, reduced diphtheria toxoid and acellular pertussis vaccine (Tdap) in pregnant women and persons who have or anticipate having close contact with an infant aged <12 months—Advisory Committee on Immunization Practices (ACIP), 2011. MMWR Morb Mortal Wkly Rep. 2011;60:1424-1426.
7. CDC. Use of hepatitis B vaccination for adults with diabetes mellitus: recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Morb Mortal Wkly Rep. 2011;60:1709-1711.
8. CDC. Recommendation of the Advisory Committee on Immunization Practices (ACIP) for use of quadrivalent meningococcal conjugate vaccine (MenACWY-D) among children aged 9 through 23 months at increased risk for invasive meningococcal disease. MMWR Morb Mortal Wkly Rep. 2011;60:1391-1392.
9. CDC. Updated recommendations for use of meningococcal conjugate vaccines—Advisory Committee on Immunization Practices (ACIP), 2010. MMWR Morb Mortal Wkly Rep. 2011;60:72-76.
10. CDC. Update on herpes zoster vaccine: licensure for persons aged 50 through 59 years. MMWR Morb Mortal Wkly Rep. 2011;60:1528-
11. Campos-Outcalt D. Ready for flu season? The 2011-2012 ACIP recommendations. J Fam Pract. 2011;60:543-544.
12. CDC. Prevention and control of influenza with vaccines: recommendations of the advisory committee on immunization practices (ACIP), 2011. MMWR Morb Mortal Wkly Rep. 2011;60:1128-1132.
| Another reason to recommend the HPV vaccine Doug Campos-Outcalt, MD, MPA |
Doug Campos-Outcalt, MD, MPA
Department of Family and Community Medicine, University of Arizona College of Medicine, Phoenix
[email protected]
| Another reason to recommend the HPV vaccine Doug Campos-Outcalt, MD, MPA |
Doug Campos-Outcalt, MD, MPA
Department of Family and Community Medicine, University of Arizona College of Medicine, Phoenix
[email protected]
| Another reason to recommend the HPV vaccine Doug Campos-Outcalt, MD, MPA |
Doug Campos-Outcalt, MD, MPA
Department of Family and Community Medicine, University of Arizona College of Medicine, Phoenix
[email protected]
In February, the Centers for Disease Control and Prevention (CDC) published the 2012 immunization schedules for infants and children, adolescents, and adults.1,2 The schedules, which are available at http://www.cdc.gov/vaccines/recs/schedules/default.htm, are updated annually and incorporate additions and changes recommended by the Advisory Committee on Immunization Practices (ACIP) over the past year. While there were no major advances in new vaccines in 2011, there were a number of new indications for existing ones.
Human papillomavirus vaccine for males
Quadrivalent vaccine against human papillomavirus is now recommended for routine use for males ages 11 to 12 years to prevent genital warts and anal intraepithelial neoplasia.3,4 Catch-up vaccination is also recommended for males ages 13 to 21 who have not received it. In addition, routine use is recommended for males ages 22 to 26 years who have sex with men or are HIV positive or immuno-compromised.
Tetanus toxoid, reduced strength diphtheria toxoid, and acellular pertussis (Tdap)
Indications for the routine use of Tdap were expanded to include children ages 7 to 10 years, pregnant women, and adults age 65 and older who have contact with infants.5,6 Children ages 7 to 10 years who have not had the full series of DTaP should receive Td/Tdap according to the catch-up schedule,1 with one of the doses being Tdap. Adults older than 65 who have never received Tdap and who have close contact with infants should receive one dose. No minimum interval is required between receipt of the Td and Tdap vaccines. Other older adults who ask for Tdap vaccination should receive it. Use of Tdap in those ages 7 to 10 years or 65 and older is off label.5
Pregnant women who have not received Tdap should receive 1 dose after week 20 of pregnancy, although receiving it earlier is not contraindicated if tetanus toxoid is needed for tetanus prevention following a wound.6
Hepatitis B virus (HBV) vaccine
Added to the list of high-risk adults who should receive HBV vaccine routinely are those ages 19 through 59 years with diabetes.7 Vaccinate as soon as possible after the diabetes diagnosis is confirmed. The decision as to whether to vaccinate patients ≥60 years with diabetes should be based on the likelihood that they will become infected. Considerations include the risks associated with an increased need for help with blood-glucose monitoring in long-term care facilities, the likelihood that the patient will experience chronic sequelae if infected, and the likelihood that the patient will mount a proper immune response to the vaccine.7 (The more frail patients are, the less likely they are to achieve adequate immunity.7)
Meningococcal conjugate vaccine, quadrivalent (MCV4)
An MCV4 vaccine (Menactra) has now been licensed for use in children as young as 9 months.8 At this time, however, neither Menactra nor its competitor, Menveo (licensed for use in those 2 years and older), is recommended for routine administration until the age of 11 to 12 years. Infants and children ages 9 through 23 months with complement deficiencies, or who will be traveling to countries with endemic high levels of meningococcus, should be vaccinated with 2 doses of Menactra 3 months apart, and with a booster dose after 3 years if risk persists. The recommendations regarding the use of MCV4 in those ≤2 years with high-risk conditions are listed in TABLE 1.
In February 2012, the CDC announced results of the 2010 National Health Interview Survey. Increases in immunization coverage occurred only with Tdap vaccination for individuals 19 to 64 years of age (from 6.6% to 8.2%), herpes zoster vaccination among those ≥60 years (from 10% to 14.4%), and ≥1 dose of HPV vaccination for women 19 to 26 years (from 17.1% to 20.7%). Rates of immunization were unchanged for other vaccines. The CDC said a substantial improvement in coverage is needed to reduce vaccine-preventable diseases among adults.
Source: CDC. Adult vaccination coverage—United States, 2010. MMWR Morb Mortal Wkly Rep. 2012;61:66-72.
Another change regarding the use of MCV4 is a recommended booster dose for those age 16 and older who were first vaccinated at age 11 or 12 years.9 For those vaccinated at ages 13 to 15, a booster should be received at ages 16 to 18. No booster is needed if the first MCV4 dose is received at or after age 16. Recommendations for MCV4 use and booster doses for those 2 years and older are listed in TABLE 2.
TABLE 1
Recommended Menactra schedule for young children at high risk for invasive meningococcal disease8
| Risk group | Primary vaccination series | Booster dose, if child remains at increased risk |
|---|---|---|
| Children ages 9-23 months at high risk for invasive meningococcal disease,* except those with functional or anatomic asplenia | 2 doses, 3 months apart Catch-up dose at earliest opportunity if dose 2 is not given on schedule | Initial booster 3 years after completing primary series At 5-year intervals after initial booster |
| Children with functional or anatomic asplenia at high risk for invasive meningococcal disease | 2 doses, 2 months apart, starting at age 2 years and ≥4 weeks after completing the PCV13 vaccine series | |
| PCV, pneumococcal conjugate vaccine. *Children who have persistent complement component deficiencies (eg, C5–C9, properdin, factor H, or factor D); those traveling to (or residents of) countries where meningococcal disease is hyperendemic or epidemic; or those who are in a defined risk group during a community or institutional meningococcal outbreak. | ||
TABLE 2
Recommended schedule for meningococcal conjugate vaccine in those ≥2 years, according to risk9
| Risk group | Primary vaccination series | Booster dose |
|---|---|---|
| Individuals ages 11-18 years | 1 dose, preferably at 11 or 12 years | At age 16 years, if primary dose given at age 11 or 12 years Age 16-18 years, if primary dose given at age 13-15 years No booster needed if primary dose given on or after age 16 years |
| Individuals ages 11-18 years infected with HIV | 2 doses, 2 months apart | |
| Individuals ages 2-55 years with persistent complement component deficiency (eg, C5–C9, properdin, or factor D) or functional or anatomical asplenia | 2 doses, 2 months apart | Every 5 years At the earliest opportunity if only 1 primary dose; every 5 years thereafter |
| Individuals ages 2-55 years with prolonged increased risk for exposure, such as microbiologists routinely working with Neisseria meningitides, and travelers to, or residents of, countries where meningococcal disease is hyperendemic or epidemic | 1 dose | After 3 years, if primary dose given at age 2-6 years After 5 years, if primary dose given at ≥7 years and the individual remains at risk Every 5 years thereafter, as long as the risk persists |
| HIV, human immunodeficiency virus. | ||
Herpes zoster vaccine
The herpes zoster vaccine was initially licensed for those 60 years and older. Last year the FDA approved lowering the age to 50 years and older. At this time, however, the ACIP continues to recommend that the vaccine be used routinely starting at age 60 years. The age was not lowered because of a concern about vaccine supply and the uncertainty about the possible need for a booster dose if administered at age 50.10
Influenza vaccine
As described in a previous Practice Alert,11 a history of egg allergy is no longer a strict contraindication for receipt of the influenza vaccine. The other major adjustment is a simplified recommendation on how to determine the required number of doses for a child younger than 9 years. If the child received 1 or both doses of the 2010-2011 vaccine, give just a single dose of the 2011-2012 vaccine. If the history is uncertain, give 2 doses of the new vaccine at least 4 weeks apart.12
In February, the Centers for Disease Control and Prevention (CDC) published the 2012 immunization schedules for infants and children, adolescents, and adults.1,2 The schedules, which are available at http://www.cdc.gov/vaccines/recs/schedules/default.htm, are updated annually and incorporate additions and changes recommended by the Advisory Committee on Immunization Practices (ACIP) over the past year. While there were no major advances in new vaccines in 2011, there were a number of new indications for existing ones.
Human papillomavirus vaccine for males
Quadrivalent vaccine against human papillomavirus is now recommended for routine use for males ages 11 to 12 years to prevent genital warts and anal intraepithelial neoplasia.3,4 Catch-up vaccination is also recommended for males ages 13 to 21 who have not received it. In addition, routine use is recommended for males ages 22 to 26 years who have sex with men or are HIV positive or immuno-compromised.
Tetanus toxoid, reduced strength diphtheria toxoid, and acellular pertussis (Tdap)
Indications for the routine use of Tdap were expanded to include children ages 7 to 10 years, pregnant women, and adults age 65 and older who have contact with infants.5,6 Children ages 7 to 10 years who have not had the full series of DTaP should receive Td/Tdap according to the catch-up schedule,1 with one of the doses being Tdap. Adults older than 65 who have never received Tdap and who have close contact with infants should receive one dose. No minimum interval is required between receipt of the Td and Tdap vaccines. Other older adults who ask for Tdap vaccination should receive it. Use of Tdap in those ages 7 to 10 years or 65 and older is off label.5
Pregnant women who have not received Tdap should receive 1 dose after week 20 of pregnancy, although receiving it earlier is not contraindicated if tetanus toxoid is needed for tetanus prevention following a wound.6
Hepatitis B virus (HBV) vaccine
Added to the list of high-risk adults who should receive HBV vaccine routinely are those ages 19 through 59 years with diabetes.7 Vaccinate as soon as possible after the diabetes diagnosis is confirmed. The decision as to whether to vaccinate patients ≥60 years with diabetes should be based on the likelihood that they will become infected. Considerations include the risks associated with an increased need for help with blood-glucose monitoring in long-term care facilities, the likelihood that the patient will experience chronic sequelae if infected, and the likelihood that the patient will mount a proper immune response to the vaccine.7 (The more frail patients are, the less likely they are to achieve adequate immunity.7)
Meningococcal conjugate vaccine, quadrivalent (MCV4)
An MCV4 vaccine (Menactra) has now been licensed for use in children as young as 9 months.8 At this time, however, neither Menactra nor its competitor, Menveo (licensed for use in those 2 years and older), is recommended for routine administration until the age of 11 to 12 years. Infants and children ages 9 through 23 months with complement deficiencies, or who will be traveling to countries with endemic high levels of meningococcus, should be vaccinated with 2 doses of Menactra 3 months apart, and with a booster dose after 3 years if risk persists. The recommendations regarding the use of MCV4 in those ≤2 years with high-risk conditions are listed in TABLE 1.
In February 2012, the CDC announced results of the 2010 National Health Interview Survey. Increases in immunization coverage occurred only with Tdap vaccination for individuals 19 to 64 years of age (from 6.6% to 8.2%), herpes zoster vaccination among those ≥60 years (from 10% to 14.4%), and ≥1 dose of HPV vaccination for women 19 to 26 years (from 17.1% to 20.7%). Rates of immunization were unchanged for other vaccines. The CDC said a substantial improvement in coverage is needed to reduce vaccine-preventable diseases among adults.
Source: CDC. Adult vaccination coverage—United States, 2010. MMWR Morb Mortal Wkly Rep. 2012;61:66-72.
Another change regarding the use of MCV4 is a recommended booster dose for those age 16 and older who were first vaccinated at age 11 or 12 years.9 For those vaccinated at ages 13 to 15, a booster should be received at ages 16 to 18. No booster is needed if the first MCV4 dose is received at or after age 16. Recommendations for MCV4 use and booster doses for those 2 years and older are listed in TABLE 2.
TABLE 1
Recommended Menactra schedule for young children at high risk for invasive meningococcal disease8
| Risk group | Primary vaccination series | Booster dose, if child remains at increased risk |
|---|---|---|
| Children ages 9-23 months at high risk for invasive meningococcal disease,* except those with functional or anatomic asplenia | 2 doses, 3 months apart Catch-up dose at earliest opportunity if dose 2 is not given on schedule | Initial booster 3 years after completing primary series At 5-year intervals after initial booster |
| Children with functional or anatomic asplenia at high risk for invasive meningococcal disease | 2 doses, 2 months apart, starting at age 2 years and ≥4 weeks after completing the PCV13 vaccine series | |
| PCV, pneumococcal conjugate vaccine. *Children who have persistent complement component deficiencies (eg, C5–C9, properdin, factor H, or factor D); those traveling to (or residents of) countries where meningococcal disease is hyperendemic or epidemic; or those who are in a defined risk group during a community or institutional meningococcal outbreak. | ||
TABLE 2
Recommended schedule for meningococcal conjugate vaccine in those ≥2 years, according to risk9
| Risk group | Primary vaccination series | Booster dose |
|---|---|---|
| Individuals ages 11-18 years | 1 dose, preferably at 11 or 12 years | At age 16 years, if primary dose given at age 11 or 12 years Age 16-18 years, if primary dose given at age 13-15 years No booster needed if primary dose given on or after age 16 years |
| Individuals ages 11-18 years infected with HIV | 2 doses, 2 months apart | |
| Individuals ages 2-55 years with persistent complement component deficiency (eg, C5–C9, properdin, or factor D) or functional or anatomical asplenia | 2 doses, 2 months apart | Every 5 years At the earliest opportunity if only 1 primary dose; every 5 years thereafter |
| Individuals ages 2-55 years with prolonged increased risk for exposure, such as microbiologists routinely working with Neisseria meningitides, and travelers to, or residents of, countries where meningococcal disease is hyperendemic or epidemic | 1 dose | After 3 years, if primary dose given at age 2-6 years After 5 years, if primary dose given at ≥7 years and the individual remains at risk Every 5 years thereafter, as long as the risk persists |
| HIV, human immunodeficiency virus. | ||
Herpes zoster vaccine
The herpes zoster vaccine was initially licensed for those 60 years and older. Last year the FDA approved lowering the age to 50 years and older. At this time, however, the ACIP continues to recommend that the vaccine be used routinely starting at age 60 years. The age was not lowered because of a concern about vaccine supply and the uncertainty about the possible need for a booster dose if administered at age 50.10
Influenza vaccine
As described in a previous Practice Alert,11 a history of egg allergy is no longer a strict contraindication for receipt of the influenza vaccine. The other major adjustment is a simplified recommendation on how to determine the required number of doses for a child younger than 9 years. If the child received 1 or both doses of the 2010-2011 vaccine, give just a single dose of the 2011-2012 vaccine. If the history is uncertain, give 2 doses of the new vaccine at least 4 weeks apart.12
1. CDC. Recommended immunization schedules for persons aged 0 through 18 years—United States, 2012. MMWR Morb Mortal Wkly Rep. 2012;61(5):1-4.
2. CDC. Recommended adult immunization schedule—United States, 2012. MMWR Morb Mortal Wkly Rep. 2012;61(4):1-7.
3. Campos-Outcalt D. Human papilloma virus: Vaccine is now routinely indicated for males. J Fam Pract. 2012;61:38-40.
4. CDC. Recommendations on the use of quadrivalent human papillomavirus vaccine in males—Advisory Committee on Immunization Practices (ACIP), 2011. MMWR Morb Mortal Wkly Rep. 2011;60:1705-1708.
5. CDC. Updated recommendations for use of tetanus toxoid, reduced diphtheria toxoid and acellular pertussis (Tdap) vaccine from the Advisory Committee on Immunization Practices, 2010. MMWR Morb Mortal Wkly Rep. 2011;60:13-15.
6. CDC. Updated recommendations for use of tetanus toxoid, reduced diphtheria toxoid and acellular pertussis vaccine (Tdap) in pregnant women and persons who have or anticipate having close contact with an infant aged <12 months—Advisory Committee on Immunization Practices (ACIP), 2011. MMWR Morb Mortal Wkly Rep. 2011;60:1424-1426.
7. CDC. Use of hepatitis B vaccination for adults with diabetes mellitus: recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Morb Mortal Wkly Rep. 2011;60:1709-1711.
8. CDC. Recommendation of the Advisory Committee on Immunization Practices (ACIP) for use of quadrivalent meningococcal conjugate vaccine (MenACWY-D) among children aged 9 through 23 months at increased risk for invasive meningococcal disease. MMWR Morb Mortal Wkly Rep. 2011;60:1391-1392.
9. CDC. Updated recommendations for use of meningococcal conjugate vaccines—Advisory Committee on Immunization Practices (ACIP), 2010. MMWR Morb Mortal Wkly Rep. 2011;60:72-76.
10. CDC. Update on herpes zoster vaccine: licensure for persons aged 50 through 59 years. MMWR Morb Mortal Wkly Rep. 2011;60:1528-
11. Campos-Outcalt D. Ready for flu season? The 2011-2012 ACIP recommendations. J Fam Pract. 2011;60:543-544.
12. CDC. Prevention and control of influenza with vaccines: recommendations of the advisory committee on immunization practices (ACIP), 2011. MMWR Morb Mortal Wkly Rep. 2011;60:1128-1132.
1. CDC. Recommended immunization schedules for persons aged 0 through 18 years—United States, 2012. MMWR Morb Mortal Wkly Rep. 2012;61(5):1-4.
2. CDC. Recommended adult immunization schedule—United States, 2012. MMWR Morb Mortal Wkly Rep. 2012;61(4):1-7.
3. Campos-Outcalt D. Human papilloma virus: Vaccine is now routinely indicated for males. J Fam Pract. 2012;61:38-40.
4. CDC. Recommendations on the use of quadrivalent human papillomavirus vaccine in males—Advisory Committee on Immunization Practices (ACIP), 2011. MMWR Morb Mortal Wkly Rep. 2011;60:1705-1708.
5. CDC. Updated recommendations for use of tetanus toxoid, reduced diphtheria toxoid and acellular pertussis (Tdap) vaccine from the Advisory Committee on Immunization Practices, 2010. MMWR Morb Mortal Wkly Rep. 2011;60:13-15.
6. CDC. Updated recommendations for use of tetanus toxoid, reduced diphtheria toxoid and acellular pertussis vaccine (Tdap) in pregnant women and persons who have or anticipate having close contact with an infant aged <12 months—Advisory Committee on Immunization Practices (ACIP), 2011. MMWR Morb Mortal Wkly Rep. 2011;60:1424-1426.
7. CDC. Use of hepatitis B vaccination for adults with diabetes mellitus: recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Morb Mortal Wkly Rep. 2011;60:1709-1711.
8. CDC. Recommendation of the Advisory Committee on Immunization Practices (ACIP) for use of quadrivalent meningococcal conjugate vaccine (MenACWY-D) among children aged 9 through 23 months at increased risk for invasive meningococcal disease. MMWR Morb Mortal Wkly Rep. 2011;60:1391-1392.
9. CDC. Updated recommendations for use of meningococcal conjugate vaccines—Advisory Committee on Immunization Practices (ACIP), 2010. MMWR Morb Mortal Wkly Rep. 2011;60:72-76.
10. CDC. Update on herpes zoster vaccine: licensure for persons aged 50 through 59 years. MMWR Morb Mortal Wkly Rep. 2011;60:1528-
11. Campos-Outcalt D. Ready for flu season? The 2011-2012 ACIP recommendations. J Fam Pract. 2011;60:543-544.
12. CDC. Prevention and control of influenza with vaccines: recommendations of the advisory committee on immunization practices (ACIP), 2011. MMWR Morb Mortal Wkly Rep. 2011;60:1128-1132.
Facebook: Social networking meets professional duty
Discuss this article at www.facebook.com/CurrentPsychiatry
Dear Dr. Mossman:
A patient has invited me to “friend” her on Facebook. I’m uncomfortable with this request, but I don’t want her to feel rejected. How should I respond?—Submitted by “Dr. V”
Among the many cultural developments that characterize the Internet era, few have had the impact of the social networking Web site Facebook. Because of Facebook, “friend” has become a transitive verb, and “like,” “wall,” “poke,” and “post” have acquired meanings that reflect new modes of communication and interpersonal connection. As of early 2012, Facebook had >800 million users.1 If you’re like most medical students, residents, and junior faculty members,2 you have a Facebook page.
The ubiquity of Facebook has added new dimensions to defining, teaching, and modeling professionalism in medicine.3,4 Facebook can be used to rapidly disseminate medical information through status updates and medical support groups.5 Professionals can create profiles, post their curricula vitae, and “like” professional journals—including Current Psychiatry.
But social media such as Facebook also present clinicians with new ethical and professional challenges.6 If you use Facebook personally or professionally, you need to decide how you will separate your personal and professional identities in a forum that rapidly distributes information across the Web for all to see. Sound, responsible decisions about your online profile can let you and your employing institutions prosper from the many benefits that accrue to savvy Facebook users—while avoiding potential embarrassments and liability.
Before you create a profile or “post” your next “status update” on your “wall,” you should:
- understand potential boundary violations
- know how to activate your security and privacy settings
- remember that you represent not only yourself but your profession.
Boundary crossings, violations
Feelings of online closeness and informality make receiving “friend” requests from patients far from uncommon.7 The Internet lets individuals quickly check out people and learn personal information (eg, where they live and what their homes cost) that was hard to discover 15 years ago. But the information on a person’s Facebook page usually is much more personal than what Internet searches reveal—and often much less dignified.
A quick Internet search of the phrase “professional boundaries” will show that concern about maintaining proper relationships between professionals and service recipients is not restricted to psychiatry. Yet the special, intensely personal nature of mental health care—especially psychotherapy—traditionally has made psychiatrists place special constraints on their relationships with patients.
Because psychiatrists recognize that even brief comments about ourselves can affect how patients feel, we refrain from forms of self-disclosure that non-psychiatric colleagues view as innocent.8 Psychiatrists also do not freely socialize with patients or provide care to persons we know well. We avoid blurring therapeutic and other types of relationships because such “boundary crossings” can cause problems and because “crossings” can be precursors to serious “boundary violations”—eg, sexual contact with patients.
Most doctors decline “friend” requests from patients because friending them could adversely affect the treatment relationship and could lead to new relationships that might interfere with patient care.9 The American Medical Association’s social media guidelines do not forbid friending patients, but physicians are advised to “consider separating personal and professional content online” and “maintain appropriate boundaries” with patients.10 The British Medical Association simply tells physicians to “politely refuse” patients’ friend requests.11
Privacy problems
Psychiatrists who friend patients need to be aware of potential privacy breeches among Facebook users. Individuals whose presence among a psychiatrist’s friends becomes known (eg, via a wall post) are revealing their connection to the psychiatrist, and other friends may surmise that an individual is a patient.
Also, Facebook’s “find friends” feature ostensibly lets Facebook locate individuals who are common to pairs of people and who can then be suggested as potential friends to others, but “find friends” imports members’ entire e-mail address books. If doctors who are on Facebook have patients in their webmail address books and have allowed “find friends,” then Facebook will import e-mail addresses, potentially disclosing associations between patients and their doctors.12
Facebook has tools that let users block their profiles from public view, but these privacy settings can be difficult to access and understand. Although social networking among medical trainees and new graduates is common in the culture of emerging professionals, most Facebook users allow anyone to view their profile—the default privacy setting.2,13 Even if you don’t friend patients, failing to privatize your account leaves your Facebook information readily available to the public, including your patients.
Professionalism in cyberspace
Under some circumstances, medical advice given in casual, outside-the-office contexts can establish a doctor-patient relationship, with all its accompanying obligations and liability risks. This is true of Facebook communications. If you communicate medical information or advice to someone in a form specific enough to be relied upon, you may be establishing a doctor-patient relationship. If harm comes to a person who relied upon your information, a negligence lawsuit could result—even though you never saw or spoke to the “patient.”14
Medical training programs have found that medical students and residents have posted work-related comments on Facebook that directly referenced specific patient situations or other patient care matters. Such actions can breach the Health Insurance Portability and Accountability Act of 1996 and can jeopardize careers.15 Medical professionals also have posted uncouth, inappropriate, and embarrassing content—profanity, frankly discriminatory language, tales of intoxication, and sexually explicit information. In a recent survey of 78 medical schools, 60% responded that their students had posted unprofessional online content.16 In 45 cases, schools reported such incidents and responded to follow-up questions about disciplinary actions; 30 schools gave informal warnings, and 2 schools reported student dismissals.
Using Facebook
Should psychiatrists stay off Facebook? Of course not. Many prominent American psychiatrists are on Facebook because, like everyone else, they enjoy keeping in contact with friends and family.17 Thousands of professional groups (eg, the American Psychiatric Association) and physician practices have Facebook pages. Institutions, schools, and agencies use social media to promote their curricula, notify students and staff of course changes, or organize meetings. Professionals join groups or “like” groups associated with their specialty to affiliate with each other, and they use Facebook to promote their practices, disseminate information, and network with colleagues.
Psychiatrists need not shy away from establishing an account on Facebook,18 but they should do so with greater circumspection than most persons, including physicians in other specialties. Table 1 lists several examples of Facebook behavior that all physicians should avoid.2,13,16,19,20
What about using Facebook to learn about your patients? Medical reports about checking Facebook to resolve emergencies have appeared,20 and forensic psychiatrists can use Facebook and other Internet resources to learn about evaluees.21 But if doctors search for information about a patient’s out-of-office behavior or statements, it may be like “driving down a patient’s street to see what he or she is up to,” which, although legal, seems inappropriate in a professional relationship.22
Recent experience suggests that medical schools and residencies should include “e-professionalism” in their curricula, emphasizing instruction and guidance on where personal and professional identities may intersect and where they should be kept separate. Table 2 lists several responses to the new challenges to medical professionalism posed by Facebook and other social media.5,6
Table 1
Facebook errors: What to avoid
| Category | Pitfalls |
|---|---|
| Information | Relationships, religious views, home address, and telephone number all may be readily viewable to the general public and patients if privacy settings are not properly configured |
| Photos | Intoxication, sexually explicit material, risk-taking behavior |
| “Wall posts” | Blatant comments about patients, disgruntlement with institution or supervisors |
| Security settings | Lack of privacy restrictions |
| “Friends” | Friending patients and supervisors |
| “Like” | “Liking” groups that contain pornographic material or other controversial topics |
| Source: References 2,13,16,19,20 | |
Table 2
Promoting e-professionalism
| Understand and activate all relevant privacy and security settings on social networking sites |
| Recognize the need to teach e-professionalism in the curricula of medical schools and residency training programs |
| Combine instruction on professional use of Facebook with teaching about relevant legal regulations in medicine (eg, HIPAA) |
| Guidance in online professionalism should come from faculty supervisors or program directors |
| Faculty should model appropriate Facebook behaviors for employees, medical students, and residents |
| Users of social media are well-advised to conduct Web searches on themselves and modify their pages to conform with professional standards |
| Politely decline patients’ “friend” requests |
| Discussions of medical professionalism, involving students, faculty, and employers, can help identify issues and define responses |
| Institutions should establish and enforce guidelines for Facebook professionalism |
| HIPAA: Health Insurance Portability and Accountability Act of 1996 Source: References 5,6 |
Responding to Dr. V
Psychiatrists should not “friend” patients. If you receive a “friend” request, you should proceed in 1 of the following ways:17
- Simply ignore the request. If your patient asks why you didn’t respond, explain that you use Facebook only for personal matters
- Ignore the request, and at the patient’s next appointment, mention the request and politely explain that you do not “friend” patients
- Ignore the request, but ask the patient about it at your next meeting. This is especially important for a patient whose treatment examines the doctor-patient relationship (eg, psychodynamic therapy), but may be valuable even in medication-focused care.
- Facebook. www.facebook.com.
- Foreman J. Think before you click. Boston Globe. April 12, 2010.
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Facebook. Statistics. http://www.facebook.com/press/info.php?statistics. Accessed January 30, 2012.
2. MacDonald J, Sohn S, Ellis P. Privacy professionalism and Facebook: a dilemma for young doctors. Med Educ. 2010;44(8):805-813.
3. Gorrindo T, Gorrindo PC, Groves JE. Intersection of online social networking with medical professionalism: can medicine police the Facebook boom? J Gen Intern Med. 2008;23(12):2155.-
4. Baer W, Schwartz AC. Teaching professionalism in the digital age on the psychiatric consultation-liaison service. Psychosomatics. 2011;52(4):303-309.
5. Landman MP, Shelton J, Kauffmann RM, et al. Guidelines for maintaining a professional compass in the era of social networking. J Surg Educ. 2010;67(6):381-386.
6. Guseh JS 2nd, Brendel RW, Brendel DH. Medical professionalism in the age of online social networking. J Med Ethics. 2009;35(9):584-586.
7. Devi S. Facebook friend request from a patient? Lancet. 2011;377(9772):1141-1142.
8. Gruenberg PB. Boundary violations. In: Wahl DS Polster DS, eds. Ethics primer. Arlington, VA: American Psychiatric Association; 2001. http://www.psych.org/Departments/EDU/residentmit/dl01.aspx. Accessed January 4, 2012.
9. Moubarak G, Guiot A, Benhamou Y, et al. Facebook activity of residents and fellows and its impact on the doctor-patient relationship. J Med Ethics. 2011;37(2):101-104.
10. American Medical Association. AMA policy: professionalism in the use of social media. http://www.ama-assn.org/ama/pub/meeting/professionalism-social-media.shtml. Accessed January 4 2012.
11. British Medical Association. Using social media: practical and ethical guidance for doctors and medical students. http://www.bma.org.uk/press_centre/video_social_media/socialmediaguidance2011.jsp. Accessed January 4 2012.
12. Wilson S. A bigger threat to patient privacy when doctors use Facebook. J Med Ethics. http://jme.bmj.com/content/37/2/101.abstract/reply#medethics_el_3625. Published December 20 2010. Accessed January 4, 2012.
13. Thompson LA, Dawson K, Ferdig R, et al. The intersection of online social networking with medical professionalism. J Gen Intern Med. 2008;23(7):954-957.
14. Reisman N. Avoid being too social when using social media. Plastic Surgery News. September 13 2011. http://www.psnextra.org/Columns/OLG-September-11.html. Accessed January 4, 2012.
15. Greysen SR, Kind T, Chretien KC. Online professionalism and the mirror of social media. J Gen Intern Med. 2010;25(11):1227-1229.
16. Chretien KC, Greysen SR, Chretien JP, et al. Online posting of unprofessional content by medical students. JAMA. 2009;302(12):1309-1315.
17. Arehart-Treichel J. Facebook can be useful–if you use common sense. Psychiatric News. 2011;46(22):5A.-
18. O’Hanlon S, Shannon B. Comments further to: privacy professionalism and Facebook: a dilemma for young doctors. Med Educ. 2011;45(2):209.-
19. Metzger AH, Finley KN, Ulbrich TR, et al. Pharmacy faculty members’ perspectives on the student/faculty relationship in online social networks. Am J Pharm Educ. 2010;74(10):188.-
20. Ben-Yakov M, Snider C. How Facebook saved our day! Acad Emerg Med. 2011;18(11):1217-1219.
21. Metzner JL, Ash P. Commentary: the mental status examination in the age of the internet—challenges and opportunities. J Am Acad Psychiatry Law. 2010;38(1):27-31.
22. Bosslet GT. Commentary: the good the bad, and the ugly of social media. Acad Emerg Med. 2011;18(11):1221-1222.

Douglas Mossman, MD
Dr. Mossman is administrative director, Glenn M. Weaver Institute of Law and Psychiatry, University of Cincinnati College of Law, and Adjunct Professor of Clinical Psychiatry and Training Director for the University of Cincinnati Forensic Psychiatry Fellowship, Cincinnati, OH
Helen M. Farrell, MD
Dr. Farrell is an instructor at Harvard Medical School and a staff psychiatrist at Beth Israel Deaconess Medical Center, Boston, MA
Douglas Mossman, MD
Dr. Mossman is administrative director, Glenn M. Weaver Institute of Law and Psychiatry, University of Cincinnati College of Law, and Adjunct Professor of Clinical Psychiatry and Training Director for the University of Cincinnati Forensic Psychiatry Fellowship, Cincinnati, OH
Helen M. Farrell, MD
Dr. Farrell is an instructor at Harvard Medical School and a staff psychiatrist at Beth Israel Deaconess Medical Center, Boston, MA
Douglas Mossman, MD
Dr. Mossman is administrative director, Glenn M. Weaver Institute of Law and Psychiatry, University of Cincinnati College of Law, and Adjunct Professor of Clinical Psychiatry and Training Director for the University of Cincinnati Forensic Psychiatry Fellowship, Cincinnati, OH
Helen M. Farrell, MD
Dr. Farrell is an instructor at Harvard Medical School and a staff psychiatrist at Beth Israel Deaconess Medical Center, Boston, MA
Discuss this article at www.facebook.com/CurrentPsychiatry
Dear Dr. Mossman:
A patient has invited me to “friend” her on Facebook. I’m uncomfortable with this request, but I don’t want her to feel rejected. How should I respond?—Submitted by “Dr. V”
Among the many cultural developments that characterize the Internet era, few have had the impact of the social networking Web site Facebook. Because of Facebook, “friend” has become a transitive verb, and “like,” “wall,” “poke,” and “post” have acquired meanings that reflect new modes of communication and interpersonal connection. As of early 2012, Facebook had >800 million users.1 If you’re like most medical students, residents, and junior faculty members,2 you have a Facebook page.
The ubiquity of Facebook has added new dimensions to defining, teaching, and modeling professionalism in medicine.3,4 Facebook can be used to rapidly disseminate medical information through status updates and medical support groups.5 Professionals can create profiles, post their curricula vitae, and “like” professional journals—including Current Psychiatry.
But social media such as Facebook also present clinicians with new ethical and professional challenges.6 If you use Facebook personally or professionally, you need to decide how you will separate your personal and professional identities in a forum that rapidly distributes information across the Web for all to see. Sound, responsible decisions about your online profile can let you and your employing institutions prosper from the many benefits that accrue to savvy Facebook users—while avoiding potential embarrassments and liability.
Before you create a profile or “post” your next “status update” on your “wall,” you should:
- understand potential boundary violations
- know how to activate your security and privacy settings
- remember that you represent not only yourself but your profession.
Boundary crossings, violations
Feelings of online closeness and informality make receiving “friend” requests from patients far from uncommon.7 The Internet lets individuals quickly check out people and learn personal information (eg, where they live and what their homes cost) that was hard to discover 15 years ago. But the information on a person’s Facebook page usually is much more personal than what Internet searches reveal—and often much less dignified.
A quick Internet search of the phrase “professional boundaries” will show that concern about maintaining proper relationships between professionals and service recipients is not restricted to psychiatry. Yet the special, intensely personal nature of mental health care—especially psychotherapy—traditionally has made psychiatrists place special constraints on their relationships with patients.
Because psychiatrists recognize that even brief comments about ourselves can affect how patients feel, we refrain from forms of self-disclosure that non-psychiatric colleagues view as innocent.8 Psychiatrists also do not freely socialize with patients or provide care to persons we know well. We avoid blurring therapeutic and other types of relationships because such “boundary crossings” can cause problems and because “crossings” can be precursors to serious “boundary violations”—eg, sexual contact with patients.
Most doctors decline “friend” requests from patients because friending them could adversely affect the treatment relationship and could lead to new relationships that might interfere with patient care.9 The American Medical Association’s social media guidelines do not forbid friending patients, but physicians are advised to “consider separating personal and professional content online” and “maintain appropriate boundaries” with patients.10 The British Medical Association simply tells physicians to “politely refuse” patients’ friend requests.11
Privacy problems
Psychiatrists who friend patients need to be aware of potential privacy breeches among Facebook users. Individuals whose presence among a psychiatrist’s friends becomes known (eg, via a wall post) are revealing their connection to the psychiatrist, and other friends may surmise that an individual is a patient.
Also, Facebook’s “find friends” feature ostensibly lets Facebook locate individuals who are common to pairs of people and who can then be suggested as potential friends to others, but “find friends” imports members’ entire e-mail address books. If doctors who are on Facebook have patients in their webmail address books and have allowed “find friends,” then Facebook will import e-mail addresses, potentially disclosing associations between patients and their doctors.12
Facebook has tools that let users block their profiles from public view, but these privacy settings can be difficult to access and understand. Although social networking among medical trainees and new graduates is common in the culture of emerging professionals, most Facebook users allow anyone to view their profile—the default privacy setting.2,13 Even if you don’t friend patients, failing to privatize your account leaves your Facebook information readily available to the public, including your patients.
Professionalism in cyberspace
Under some circumstances, medical advice given in casual, outside-the-office contexts can establish a doctor-patient relationship, with all its accompanying obligations and liability risks. This is true of Facebook communications. If you communicate medical information or advice to someone in a form specific enough to be relied upon, you may be establishing a doctor-patient relationship. If harm comes to a person who relied upon your information, a negligence lawsuit could result—even though you never saw or spoke to the “patient.”14
Medical training programs have found that medical students and residents have posted work-related comments on Facebook that directly referenced specific patient situations or other patient care matters. Such actions can breach the Health Insurance Portability and Accountability Act of 1996 and can jeopardize careers.15 Medical professionals also have posted uncouth, inappropriate, and embarrassing content—profanity, frankly discriminatory language, tales of intoxication, and sexually explicit information. In a recent survey of 78 medical schools, 60% responded that their students had posted unprofessional online content.16 In 45 cases, schools reported such incidents and responded to follow-up questions about disciplinary actions; 30 schools gave informal warnings, and 2 schools reported student dismissals.
Using Facebook
Should psychiatrists stay off Facebook? Of course not. Many prominent American psychiatrists are on Facebook because, like everyone else, they enjoy keeping in contact with friends and family.17 Thousands of professional groups (eg, the American Psychiatric Association) and physician practices have Facebook pages. Institutions, schools, and agencies use social media to promote their curricula, notify students and staff of course changes, or organize meetings. Professionals join groups or “like” groups associated with their specialty to affiliate with each other, and they use Facebook to promote their practices, disseminate information, and network with colleagues.
Psychiatrists need not shy away from establishing an account on Facebook,18 but they should do so with greater circumspection than most persons, including physicians in other specialties. Table 1 lists several examples of Facebook behavior that all physicians should avoid.2,13,16,19,20
What about using Facebook to learn about your patients? Medical reports about checking Facebook to resolve emergencies have appeared,20 and forensic psychiatrists can use Facebook and other Internet resources to learn about evaluees.21 But if doctors search for information about a patient’s out-of-office behavior or statements, it may be like “driving down a patient’s street to see what he or she is up to,” which, although legal, seems inappropriate in a professional relationship.22
Recent experience suggests that medical schools and residencies should include “e-professionalism” in their curricula, emphasizing instruction and guidance on where personal and professional identities may intersect and where they should be kept separate. Table 2 lists several responses to the new challenges to medical professionalism posed by Facebook and other social media.5,6
Table 1
Facebook errors: What to avoid
| Category | Pitfalls |
|---|---|
| Information | Relationships, religious views, home address, and telephone number all may be readily viewable to the general public and patients if privacy settings are not properly configured |
| Photos | Intoxication, sexually explicit material, risk-taking behavior |
| “Wall posts” | Blatant comments about patients, disgruntlement with institution or supervisors |
| Security settings | Lack of privacy restrictions |
| “Friends” | Friending patients and supervisors |
| “Like” | “Liking” groups that contain pornographic material or other controversial topics |
| Source: References 2,13,16,19,20 | |
Table 2
Promoting e-professionalism
| Understand and activate all relevant privacy and security settings on social networking sites |
| Recognize the need to teach e-professionalism in the curricula of medical schools and residency training programs |
| Combine instruction on professional use of Facebook with teaching about relevant legal regulations in medicine (eg, HIPAA) |
| Guidance in online professionalism should come from faculty supervisors or program directors |
| Faculty should model appropriate Facebook behaviors for employees, medical students, and residents |
| Users of social media are well-advised to conduct Web searches on themselves and modify their pages to conform with professional standards |
| Politely decline patients’ “friend” requests |
| Discussions of medical professionalism, involving students, faculty, and employers, can help identify issues and define responses |
| Institutions should establish and enforce guidelines for Facebook professionalism |
| HIPAA: Health Insurance Portability and Accountability Act of 1996 Source: References 5,6 |
Responding to Dr. V
Psychiatrists should not “friend” patients. If you receive a “friend” request, you should proceed in 1 of the following ways:17
- Simply ignore the request. If your patient asks why you didn’t respond, explain that you use Facebook only for personal matters
- Ignore the request, and at the patient’s next appointment, mention the request and politely explain that you do not “friend” patients
- Ignore the request, but ask the patient about it at your next meeting. This is especially important for a patient whose treatment examines the doctor-patient relationship (eg, psychodynamic therapy), but may be valuable even in medication-focused care.
- Facebook. www.facebook.com.
- Foreman J. Think before you click. Boston Globe. April 12, 2010.
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Discuss this article at www.facebook.com/CurrentPsychiatry
Dear Dr. Mossman:
A patient has invited me to “friend” her on Facebook. I’m uncomfortable with this request, but I don’t want her to feel rejected. How should I respond?—Submitted by “Dr. V”
Among the many cultural developments that characterize the Internet era, few have had the impact of the social networking Web site Facebook. Because of Facebook, “friend” has become a transitive verb, and “like,” “wall,” “poke,” and “post” have acquired meanings that reflect new modes of communication and interpersonal connection. As of early 2012, Facebook had >800 million users.1 If you’re like most medical students, residents, and junior faculty members,2 you have a Facebook page.
The ubiquity of Facebook has added new dimensions to defining, teaching, and modeling professionalism in medicine.3,4 Facebook can be used to rapidly disseminate medical information through status updates and medical support groups.5 Professionals can create profiles, post their curricula vitae, and “like” professional journals—including Current Psychiatry.
But social media such as Facebook also present clinicians with new ethical and professional challenges.6 If you use Facebook personally or professionally, you need to decide how you will separate your personal and professional identities in a forum that rapidly distributes information across the Web for all to see. Sound, responsible decisions about your online profile can let you and your employing institutions prosper from the many benefits that accrue to savvy Facebook users—while avoiding potential embarrassments and liability.
Before you create a profile or “post” your next “status update” on your “wall,” you should:
- understand potential boundary violations
- know how to activate your security and privacy settings
- remember that you represent not only yourself but your profession.
Boundary crossings, violations
Feelings of online closeness and informality make receiving “friend” requests from patients far from uncommon.7 The Internet lets individuals quickly check out people and learn personal information (eg, where they live and what their homes cost) that was hard to discover 15 years ago. But the information on a person’s Facebook page usually is much more personal than what Internet searches reveal—and often much less dignified.
A quick Internet search of the phrase “professional boundaries” will show that concern about maintaining proper relationships between professionals and service recipients is not restricted to psychiatry. Yet the special, intensely personal nature of mental health care—especially psychotherapy—traditionally has made psychiatrists place special constraints on their relationships with patients.
Because psychiatrists recognize that even brief comments about ourselves can affect how patients feel, we refrain from forms of self-disclosure that non-psychiatric colleagues view as innocent.8 Psychiatrists also do not freely socialize with patients or provide care to persons we know well. We avoid blurring therapeutic and other types of relationships because such “boundary crossings” can cause problems and because “crossings” can be precursors to serious “boundary violations”—eg, sexual contact with patients.
Most doctors decline “friend” requests from patients because friending them could adversely affect the treatment relationship and could lead to new relationships that might interfere with patient care.9 The American Medical Association’s social media guidelines do not forbid friending patients, but physicians are advised to “consider separating personal and professional content online” and “maintain appropriate boundaries” with patients.10 The British Medical Association simply tells physicians to “politely refuse” patients’ friend requests.11
Privacy problems
Psychiatrists who friend patients need to be aware of potential privacy breeches among Facebook users. Individuals whose presence among a psychiatrist’s friends becomes known (eg, via a wall post) are revealing their connection to the psychiatrist, and other friends may surmise that an individual is a patient.
Also, Facebook’s “find friends” feature ostensibly lets Facebook locate individuals who are common to pairs of people and who can then be suggested as potential friends to others, but “find friends” imports members’ entire e-mail address books. If doctors who are on Facebook have patients in their webmail address books and have allowed “find friends,” then Facebook will import e-mail addresses, potentially disclosing associations between patients and their doctors.12
Facebook has tools that let users block their profiles from public view, but these privacy settings can be difficult to access and understand. Although social networking among medical trainees and new graduates is common in the culture of emerging professionals, most Facebook users allow anyone to view their profile—the default privacy setting.2,13 Even if you don’t friend patients, failing to privatize your account leaves your Facebook information readily available to the public, including your patients.
Professionalism in cyberspace
Under some circumstances, medical advice given in casual, outside-the-office contexts can establish a doctor-patient relationship, with all its accompanying obligations and liability risks. This is true of Facebook communications. If you communicate medical information or advice to someone in a form specific enough to be relied upon, you may be establishing a doctor-patient relationship. If harm comes to a person who relied upon your information, a negligence lawsuit could result—even though you never saw or spoke to the “patient.”14
Medical training programs have found that medical students and residents have posted work-related comments on Facebook that directly referenced specific patient situations or other patient care matters. Such actions can breach the Health Insurance Portability and Accountability Act of 1996 and can jeopardize careers.15 Medical professionals also have posted uncouth, inappropriate, and embarrassing content—profanity, frankly discriminatory language, tales of intoxication, and sexually explicit information. In a recent survey of 78 medical schools, 60% responded that their students had posted unprofessional online content.16 In 45 cases, schools reported such incidents and responded to follow-up questions about disciplinary actions; 30 schools gave informal warnings, and 2 schools reported student dismissals.
Using Facebook
Should psychiatrists stay off Facebook? Of course not. Many prominent American psychiatrists are on Facebook because, like everyone else, they enjoy keeping in contact with friends and family.17 Thousands of professional groups (eg, the American Psychiatric Association) and physician practices have Facebook pages. Institutions, schools, and agencies use social media to promote their curricula, notify students and staff of course changes, or organize meetings. Professionals join groups or “like” groups associated with their specialty to affiliate with each other, and they use Facebook to promote their practices, disseminate information, and network with colleagues.
Psychiatrists need not shy away from establishing an account on Facebook,18 but they should do so with greater circumspection than most persons, including physicians in other specialties. Table 1 lists several examples of Facebook behavior that all physicians should avoid.2,13,16,19,20
What about using Facebook to learn about your patients? Medical reports about checking Facebook to resolve emergencies have appeared,20 and forensic psychiatrists can use Facebook and other Internet resources to learn about evaluees.21 But if doctors search for information about a patient’s out-of-office behavior or statements, it may be like “driving down a patient’s street to see what he or she is up to,” which, although legal, seems inappropriate in a professional relationship.22
Recent experience suggests that medical schools and residencies should include “e-professionalism” in their curricula, emphasizing instruction and guidance on where personal and professional identities may intersect and where they should be kept separate. Table 2 lists several responses to the new challenges to medical professionalism posed by Facebook and other social media.5,6
Table 1
Facebook errors: What to avoid
| Category | Pitfalls |
|---|---|
| Information | Relationships, religious views, home address, and telephone number all may be readily viewable to the general public and patients if privacy settings are not properly configured |
| Photos | Intoxication, sexually explicit material, risk-taking behavior |
| “Wall posts” | Blatant comments about patients, disgruntlement with institution or supervisors |
| Security settings | Lack of privacy restrictions |
| “Friends” | Friending patients and supervisors |
| “Like” | “Liking” groups that contain pornographic material or other controversial topics |
| Source: References 2,13,16,19,20 | |
Table 2
Promoting e-professionalism
| Understand and activate all relevant privacy and security settings on social networking sites |
| Recognize the need to teach e-professionalism in the curricula of medical schools and residency training programs |
| Combine instruction on professional use of Facebook with teaching about relevant legal regulations in medicine (eg, HIPAA) |
| Guidance in online professionalism should come from faculty supervisors or program directors |
| Faculty should model appropriate Facebook behaviors for employees, medical students, and residents |
| Users of social media are well-advised to conduct Web searches on themselves and modify their pages to conform with professional standards |
| Politely decline patients’ “friend” requests |
| Discussions of medical professionalism, involving students, faculty, and employers, can help identify issues and define responses |
| Institutions should establish and enforce guidelines for Facebook professionalism |
| HIPAA: Health Insurance Portability and Accountability Act of 1996 Source: References 5,6 |
Responding to Dr. V
Psychiatrists should not “friend” patients. If you receive a “friend” request, you should proceed in 1 of the following ways:17
- Simply ignore the request. If your patient asks why you didn’t respond, explain that you use Facebook only for personal matters
- Ignore the request, and at the patient’s next appointment, mention the request and politely explain that you do not “friend” patients
- Ignore the request, but ask the patient about it at your next meeting. This is especially important for a patient whose treatment examines the doctor-patient relationship (eg, psychodynamic therapy), but may be valuable even in medication-focused care.
- Facebook. www.facebook.com.
- Foreman J. Think before you click. Boston Globe. April 12, 2010.
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Facebook. Statistics. http://www.facebook.com/press/info.php?statistics. Accessed January 30, 2012.
2. MacDonald J, Sohn S, Ellis P. Privacy professionalism and Facebook: a dilemma for young doctors. Med Educ. 2010;44(8):805-813.
3. Gorrindo T, Gorrindo PC, Groves JE. Intersection of online social networking with medical professionalism: can medicine police the Facebook boom? J Gen Intern Med. 2008;23(12):2155.-
4. Baer W, Schwartz AC. Teaching professionalism in the digital age on the psychiatric consultation-liaison service. Psychosomatics. 2011;52(4):303-309.
5. Landman MP, Shelton J, Kauffmann RM, et al. Guidelines for maintaining a professional compass in the era of social networking. J Surg Educ. 2010;67(6):381-386.
6. Guseh JS 2nd, Brendel RW, Brendel DH. Medical professionalism in the age of online social networking. J Med Ethics. 2009;35(9):584-586.
7. Devi S. Facebook friend request from a patient? Lancet. 2011;377(9772):1141-1142.
8. Gruenberg PB. Boundary violations. In: Wahl DS Polster DS, eds. Ethics primer. Arlington, VA: American Psychiatric Association; 2001. http://www.psych.org/Departments/EDU/residentmit/dl01.aspx. Accessed January 4, 2012.
9. Moubarak G, Guiot A, Benhamou Y, et al. Facebook activity of residents and fellows and its impact on the doctor-patient relationship. J Med Ethics. 2011;37(2):101-104.
10. American Medical Association. AMA policy: professionalism in the use of social media. http://www.ama-assn.org/ama/pub/meeting/professionalism-social-media.shtml. Accessed January 4 2012.
11. British Medical Association. Using social media: practical and ethical guidance for doctors and medical students. http://www.bma.org.uk/press_centre/video_social_media/socialmediaguidance2011.jsp. Accessed January 4 2012.
12. Wilson S. A bigger threat to patient privacy when doctors use Facebook. J Med Ethics. http://jme.bmj.com/content/37/2/101.abstract/reply#medethics_el_3625. Published December 20 2010. Accessed January 4, 2012.
13. Thompson LA, Dawson K, Ferdig R, et al. The intersection of online social networking with medical professionalism. J Gen Intern Med. 2008;23(7):954-957.
14. Reisman N. Avoid being too social when using social media. Plastic Surgery News. September 13 2011. http://www.psnextra.org/Columns/OLG-September-11.html. Accessed January 4, 2012.
15. Greysen SR, Kind T, Chretien KC. Online professionalism and the mirror of social media. J Gen Intern Med. 2010;25(11):1227-1229.
16. Chretien KC, Greysen SR, Chretien JP, et al. Online posting of unprofessional content by medical students. JAMA. 2009;302(12):1309-1315.
17. Arehart-Treichel J. Facebook can be useful–if you use common sense. Psychiatric News. 2011;46(22):5A.-
18. O’Hanlon S, Shannon B. Comments further to: privacy professionalism and Facebook: a dilemma for young doctors. Med Educ. 2011;45(2):209.-
19. Metzger AH, Finley KN, Ulbrich TR, et al. Pharmacy faculty members’ perspectives on the student/faculty relationship in online social networks. Am J Pharm Educ. 2010;74(10):188.-
20. Ben-Yakov M, Snider C. How Facebook saved our day! Acad Emerg Med. 2011;18(11):1217-1219.
21. Metzner JL, Ash P. Commentary: the mental status examination in the age of the internet—challenges and opportunities. J Am Acad Psychiatry Law. 2010;38(1):27-31.
22. Bosslet GT. Commentary: the good the bad, and the ugly of social media. Acad Emerg Med. 2011;18(11):1221-1222.
1. Facebook. Statistics. http://www.facebook.com/press/info.php?statistics. Accessed January 30, 2012.
2. MacDonald J, Sohn S, Ellis P. Privacy professionalism and Facebook: a dilemma for young doctors. Med Educ. 2010;44(8):805-813.
3. Gorrindo T, Gorrindo PC, Groves JE. Intersection of online social networking with medical professionalism: can medicine police the Facebook boom? J Gen Intern Med. 2008;23(12):2155.-
4. Baer W, Schwartz AC. Teaching professionalism in the digital age on the psychiatric consultation-liaison service. Psychosomatics. 2011;52(4):303-309.
5. Landman MP, Shelton J, Kauffmann RM, et al. Guidelines for maintaining a professional compass in the era of social networking. J Surg Educ. 2010;67(6):381-386.
6. Guseh JS 2nd, Brendel RW, Brendel DH. Medical professionalism in the age of online social networking. J Med Ethics. 2009;35(9):584-586.
7. Devi S. Facebook friend request from a patient? Lancet. 2011;377(9772):1141-1142.
8. Gruenberg PB. Boundary violations. In: Wahl DS Polster DS, eds. Ethics primer. Arlington, VA: American Psychiatric Association; 2001. http://www.psych.org/Departments/EDU/residentmit/dl01.aspx. Accessed January 4, 2012.
9. Moubarak G, Guiot A, Benhamou Y, et al. Facebook activity of residents and fellows and its impact on the doctor-patient relationship. J Med Ethics. 2011;37(2):101-104.
10. American Medical Association. AMA policy: professionalism in the use of social media. http://www.ama-assn.org/ama/pub/meeting/professionalism-social-media.shtml. Accessed January 4 2012.
11. British Medical Association. Using social media: practical and ethical guidance for doctors and medical students. http://www.bma.org.uk/press_centre/video_social_media/socialmediaguidance2011.jsp. Accessed January 4 2012.
12. Wilson S. A bigger threat to patient privacy when doctors use Facebook. J Med Ethics. http://jme.bmj.com/content/37/2/101.abstract/reply#medethics_el_3625. Published December 20 2010. Accessed January 4, 2012.
13. Thompson LA, Dawson K, Ferdig R, et al. The intersection of online social networking with medical professionalism. J Gen Intern Med. 2008;23(7):954-957.
14. Reisman N. Avoid being too social when using social media. Plastic Surgery News. September 13 2011. http://www.psnextra.org/Columns/OLG-September-11.html. Accessed January 4, 2012.
15. Greysen SR, Kind T, Chretien KC. Online professionalism and the mirror of social media. J Gen Intern Med. 2010;25(11):1227-1229.
16. Chretien KC, Greysen SR, Chretien JP, et al. Online posting of unprofessional content by medical students. JAMA. 2009;302(12):1309-1315.
17. Arehart-Treichel J. Facebook can be useful–if you use common sense. Psychiatric News. 2011;46(22):5A.-
18. O’Hanlon S, Shannon B. Comments further to: privacy professionalism and Facebook: a dilemma for young doctors. Med Educ. 2011;45(2):209.-
19. Metzger AH, Finley KN, Ulbrich TR, et al. Pharmacy faculty members’ perspectives on the student/faculty relationship in online social networks. Am J Pharm Educ. 2010;74(10):188.-
20. Ben-Yakov M, Snider C. How Facebook saved our day! Acad Emerg Med. 2011;18(11):1217-1219.
21. Metzner JL, Ash P. Commentary: the mental status examination in the age of the internet—challenges and opportunities. J Am Acad Psychiatry Law. 2010;38(1):27-31.
22. Bosslet GT. Commentary: the good the bad, and the ugly of social media. Acad Emerg Med. 2011;18(11):1221-1222.
New Alzheimer’s disease guidelines: Implications for clinicians
Discuss this article at www.facebook.com/CurrentPsychiatry
In 2011, a workgroup of experts from the Alzheimer’s Association and the National Institute on Aging published new criteria and guidelines for diagnosing Alzheimer’s disease (AD), the first new AD guidelines since 1984.1-4 These criteria reflect data that suggest AD is not synonymous with dementia of the Alzheimer’s type (DAT) but is a disease that slowly develops over many years as a result of accumulated neuropathologic changes, with dementia representing only the final phase of the disease (Figure).1-4
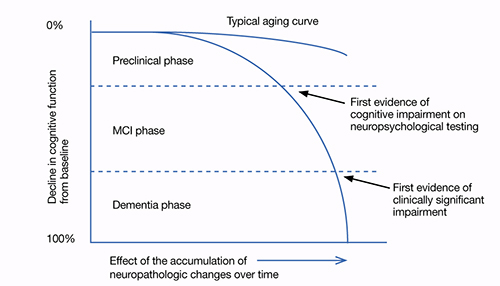
Figure: Cognitive decline in AD over time
AD: Alzheimer’s disease; MCI: mild cognitive impairment
Source: Adapted from reference 2
This article highlights the similarities and differences of the 1984 and 2011 AD diagnosis guidelines. We also discuss the new guidelines’ limitations and clinical implications.
The 1984 AD criteria
Both the 1984 AD criteria5 and DSM-IV-TR criteria6 rely on the concept that AD is a clinical diagnosis made after a patient develops dementia. That is, diagnosis rests on the physician’s clinical judgment about the etiology of the patient’s symptoms, taking into account reports from the patient, family, and friends, as well as results of neurocognitive testing and mental status evaluation. The 1984 criteria were developed with the expectation that if a patient who met clinical criteria for AD were to undergo an autopsy, he or she likely would have evidence of AD pathology as the underlying etiology. These criteria were developed before researchers discovered that in AD, pathologic changes occur over many years and clinical dementia is the end product of accumulated pathology. The 1984 criteria did not address important phases that precede clinical dementia—such as mild cognitive impairment (MCI). See the Table for a summary of the 1984 AD criteria.
Table
The 1984 NINCDS-ADRDA criteria for clinical diagnosis of AD
|
| AD: Alzheimer’s disease; NINCDS-ADRDA: National Institute of Neurological and Communicative Diseases and Stroke/Alzheimer’s Disease and Related Disorders Association Source: McKhann G, Drachman D, Folstein M, et al. Clinical diagnosis of Alzheimer’s disease: report of the NINCDS-ADRDA Work Group under the auspices of Department of Health and Human Services Task Force on Alzheimer’s Disease. Neurology. 1984;34(7):939-944 |
The 2011 AD criteria
The new AD criteria differ from the 1984 criteria in 2 major ways:
- expansion of AD into 3 phases, only 1 of which is characterized by dementia
- incorporation of biomarkers to provide information regarding pathophysiologic changes underlying the disease state (Table 1).1-5
The 3 phases. The 2011 criteria expand the definition of AD to include an asymptomatic, preclinical phase; a symptomatic, pre-dementia phase; and a dementia phase. In the initial phase, neuronal toxins such as beta-amyloid (Aβ) plaques and elevated tau first become detectable. Patients in this phase are asymptomatic or have subtle symptoms. This phase should be viewed as part of a continuum and includes patients who may, for instance, develop Aβ plaques but do not progress to further neurodegeneration.2 The diagnostic criteria of this phase are intended for research purposes only.1,2
Patients in the symptomatic, pre-dementia phase—also known as the MCI phase—exhibit mild decline in memory, attention, and thinking. Although this decline is more than what is expected for the patient’s age and education, it does not compromise everyday activity and functioning.
A patient who develops cognitive or behavioral problems that interfere with his or her ability to function at work or in everyday activities has entered the dementia phase. Similar to the 1984 guidelines, the 2011 criteria classify patients into probable and possible AD dementia. All patients who would have satisfied criteria for probable AD under the 1984 guidelines will satisfy criteria for probable AD dementia under the 2011 criteria.4 The same is not true for possible AD dementia. The 2011 criteria include 2 other major categories for patients with AD dementia: probable and possible AD dementia with evidence of the AD pathophysiological process. These categories are intended for research purposes only, whereas the criteria for the MCI and dementia phases are intended to guide diagnosis in the clinical setting.
By incorporating phases of AD that precede dementia into the disease spectrum, the new guidelines are designed to move clinicians toward earlier diagnosis and treatment.1-3 Similar to how early, pre-symptomatic detection and treatment of conditions such as diabetes and cancer can reduce mortality, improving diagnosis of AD in its early phases may allow clinicians to better test potential therapies and eventually use them to treat at-risk individuals.2,3 Most pharmacotherapies for AD are FDA-approved only for patients diagnosed with clinical dementia. Furthermore, current pharmacotherapies do not alter the course of AD; they have a modest effect in slowing cognitive and functional decline.7,8 If patients in the earlier phases of AD could be recruited for research studies, we may be able to develop new treatments to stop or reverse AD pathology and its clinical manifestations.
Biomarkers. The new criteria incorporate biomarkers to provide information about pathophysiologic changes underlying the disease process. These criteria define biomarkers as physiologic, biochemical, or anatomic parameters that can be measured in vivo and reflect specific features of disease-related pathophysiologic processes.1 Presently, there are no cutoff values to demarcate “normal” levels from “abnormal,” and biomarkers are proposed primarily as research tools because they have not been studied adequately in community settings and laboratory techniques to measure biomarkers have not been standardized.1-4,9
The 5 biomarkers incorporated into the new criteria are divided into 2 categories: biomarkers of Aβ accumulation and those of neuronal degeneration or injury (Table 2).1-4 In the initial, preclinical phase, biomarkers are used to detect changes in the brain—such as amyloid accumulation and nerve cell degeneration—that may already be in process in an individual whose clinical symptoms are subtle or not yet evident.1,2 In this phase, progressive evidence of biomarkers, such as both Aβ accumulation and neuronal injury rather than Aβ accumulation alone, may increase the probability that a patient will decline quickly into the MCI phase.2 Biomarkers of neuronal degeneration or injury especially correlate with the likelihood that the disease will progress to clinical dementia.1 Subtle cognitive symptoms in the preclinical phase also might predict rapid decline into MCI.2
In the MCI and dementia phases, biomarkers are used to determine the level of certainty that AD is responsible for the patient’s symptoms.1,3,4 For example, a patient could meet criteria for a non-AD dementia such as dementia with Lewy bodies, but also meet pathologic criteria for AD on autopsy.3 The diagnostic category of possible AD dementia with evidence of the AD pathophysiologic process is intended for this type of scenario.4 For the MCI phase, the criteria propose levels of certainty that a patient’s MCI syndrome is caused by AD, ranging from MCI due to AD-high likelihood to MCI-unlikely due to AD.3
Research has demonstrated that a patient’s clinical picture doesn’t necessarily reflect the extent of the underlying pathology. For example, a patient could have extensive AD pathology, such as diffuse amyloid plaques, without any obvious clinical symptoms.3 Conversely, although both Aβ deposition and elevated tau are hallmarks of AD, variations in these proteins can be seen in neuropsychiatric disorders other than AD.10 That said, it appears that worsening of clinical symptoms often parallels worsening of neurodegenerative biomarkers.1
Under the 2011 guidelines, biomarkers would not be used to diagnose or exclude AD or MCI, but instead would help improve diagnostic accuracy in individuals with cognitive decline.1,3,4 In other words, AD remains a clinical diagnosis, but these biomarkers could raise or lower the positive predictive value of a clinician’s judgment about the etiology of a patient’s symptoms.
See the Box for a description of the potential risks and benefits of using the new diagnostic criteria.
Table 1
Comparing the 1984 and 2011 AD criteria
| 1984 criteria | 2011 criteria |
|---|---|
| AD is a clinical diagnosis | AD remains a clinical diagnosis but biomarkers serve to improve the accuracy of diagnosis of the disease |
| There is only 1 phase of AD—dementia. | AD is expanded into 3 phases: an asymptomatic, preclinical phase; a symptomatic, pre-dementia phase; and a dementia phase |
| A patient who meets the clinical criteria for AD would be expected to have AD pathology as the underlying etiology were he/she to undergo a brain autopsy | Presently, biomarkers are proposed as research tools only and are not intended to be applied in the clinical setting. However, eventually clinicians will be able to diagnose AD in all 3 phases, as biomarker testing becomes standardized and reliable enough to be accurately applied in clinical settings |
| Little consideration is given to specific neuropathologic changes underlying the disease process | Biomarkers provide information regarding the pathophysiologic changes underlying the disease state |
| Little consideration is given to the idea that pathologic changes occur over many years | Inherent in dividing AD into 3 phases is the concept that AD develops slowly over many years and has a long prodromal phase that is clinically silent |
| AD: Alzheimer’s disease Source: References 1-5 | |
Table 2
5 biomarkers incorporated into the 2011 AD criteria
| Category | Biomarkers |
|---|---|
| Biomarkers of Aβ accumulation | Abnormal tracer retention on amyloid PET imaging |
| Low CSF Aβ42 | |
| Biomarkers of neuronal degeneration or injury | Elevated CSF tau (total and phosphorylated tau) |
| Decreased fluorodeoxyglucose uptake on PET | |
| Atrophy on structural magnetic resonance imaging | |
| Aβ: beta-amyloid; AD: Alzheimer’s disease; CSF: cerebrospinal fluid; PET: positron emission tomography Source: References 1-4 | |
The earlier an Alzheimer’s disease (AD) diagnosis is made, the less certain it is AD.a Biomarkers typically found in individuals with AD also can be found in patients with dementia not caused by AD, such as vascular dementia, as well as in individuals who may never develop dementia.b Additionally, there is no certainty that a patient in an early phase of AD will develop clinical dementia. Falsely diagnosing a patient with AD may lead the individual and their family to feel helpless, hopeless, depressed, anxious, or ashamed and to spend money and other resources preparing for a prognosis that may never come to fruition. Clinicians may feel compelled to assess for biomarkers using expensive, invasive tests that are not yet standardized in an attempt to support the AD diagnosis.
Early diagnosis of AD has many benefits that should not be overlooked, however. It provides patients and their families an opportunity to become familiar with the disease course, which may help some patients cope with the diagnosis. Patients diagnosed in the early stages would be able to make important decisions regarding health care, social, and financial planning before they develop pathology that limits their executive planning abilities or become functionally impaired.
Diagnosing an illness when there are no disease-modifying therapies available is not futile. Some patients with newly diagnosed AD in the pre-dementia phases may want to participate in clinical research trials to help develop therapies for AD. Some data suggest that AD treatment appears to provide the greatest benefit when initiated early in the disease course and maintained over a long duration.c Eventually, we may be able to tailor specific AD treatments in different phases of the disease. For instance, we may discover treatments for patients who show evidence of beta-amyloid plaques but not neuronal injury, or vice versa. Patients also may benefit from education on nonpharmacologic treatments, including reducing vascular risk factors to help improve brain aging,d reducing stress, and learning cognitive strategies such as using mnemonics to aid memory.
In many clinical settings, patients are being clinically diagnosed with mild cognitive impairment (MCI). Research indicates that patients with MCI are at near-term risk of developing dementia, particularly dementia of the Alzheimer’s type.d,e Presently, no definite transition points demarcate MCI from dementia; this progression is based upon clinical judgment.
In the last decade, researchers have begun to describe a syndrome of subjective cognitive impairment (SCI), which may be a phase that precedes the MCI phase of AD.f Patients with SCI report cognitive deficits (eg, forgetfulness and word-finding difficulties) but have no objective evidence of cognitive impairment on neuropsychological tests. Cognitive problems associated with SCI do not cause functional decline.g SCI may reflect the minimal cognitive complaints mentioned in the research criteria for the preclinical phase of AD. Eventually, biomarkers may be able to help clinicians more accurately predict which patients with SCI are most likely to progress to the MCI or dementia phase of AD.
References
- Albert MS, DeKosky ST, Dickson D, et al. The diagnosis of mild cognitive impairment due to Alzheimer’s disease: recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement. 2011;7(3):270-279.
- Galasko D. Biomarkers in non-Alzheimer dementias. Clinical Neuroscience Research. 2004;3(6):375-381.
- Geldmacher DS. Treatment guidelines for Alzheimer’s disease: redefining perceptions in primary care. Prim Care Companion J Clin Psychiatry. 2007;9(2):113-121.
- Chertkow H, Massoud F, Nasreddine Z, et al. Diagnosis and treatment of dementia: 3. Mild cognitive impairment and cognitive impairment without dementia. CMAJ. 2008;178(10):1273-1285.
- Rosenberg PB, Lyketsos C. Mild cognitive impairment: searching for the prodrome of Alzheimer’s disease. World Psychiatry. 2008;7(2):72-78.
- Reisberg B, Shulman MB, Torossian C, et al. Outcome over seven years of healthy adults with and without subjective cognitive impairment. Alzheimers Dement. 2010;6(1):11-24.
- Desai AK, Schwarz L. Subjective cognitive impairment: when to be concerned about ‘senior moments.’ Current Psychiatry. 2011;10(4):31-44.
Clinical applications
Although pharmacologic therapies for the early phases of AD are not yet available, research supports implementing nonpharmacologic modalities in older adults with MCI as well as those without any cognitive impairment (Table 3).8,11 Growing evidence suggests physicians should encourage patients to lead an active and socially integrated lifestyle that includes leisure activities, cognitive stimulation, meditation, a balanced diet, and daily exercise.8 Practitioners should treat vascular risk factors in geriatric patients with and without cognitive impairment to optimize healthy brain aging and reduce the risk of cardiovascular disease and stroke.11 By raising awareness of available treatments for early phases of AD, we may be able to reduce the anxiety and sense of helplessness or hopelessness that may accompany an AD diagnosis.
Depression and AD. Having depression nearly doubles one’s risk of developing AD later in life, and depression may exacerbate AD.12 Although the precise mechanism linking depression to AD is unclear, depression seems to exert a toxic effect on the hippocampus.13 Treating depression may prevent or mitigate the rate of memory impairment and overall AD severity and improve a patient’s quality of life, overall health, and ability to function.
Almost one-third of family caregivers become depressed while helping a family member with DAT.14 Directing caregivers to peer support groups and providing them with tips on how to take care of themselves physically, emotionally, and psychologically can be extremely beneficial. Data suggest that improving the psychological and emotional well-being of caretakers may delay nursing home placement of patients with DAT.15 Delaying nursing home placement can substantially improve quality of life and reduce the financial strain on patients and caregivers.
Patients and families often turn to clinicians for advice on what problems they or their loved ones may encounter if they suffer from cognitive impairment. One benefit of the new guidelines is that they can help us become educated about the early phases of AD as well as the long and often difficult course of the disease. In turn, we can better educate our patients and their families about the disease.
As early screening of AD improves, patients in the early phases will have an opportunity to take part in clinical trials for potential pharmacologic treatments of the disease. Our role as clinicians will be to guide patients and their families to such trials and give them the opportunity to help change our understanding of and approach to treating AD. It is important to keep in mind that the new guidelines should not be considered final, but rather as a work in progress that periodically will be revised as AD research progresses.3
Table 3
Promoting healthy brain aging
| Healthy diet (eg, Mediterranean diet) |
| Adequate sleep |
| Daily exercise |
| Smoking cessation |
| Active, socially integrated lifestyle |
| Leisure activities |
| Cognitive stimulation |
| Optimize treatment of depression and other mental illnesses |
| Meditation and other mindfulness strategies (eg, yoga) |
| Spiritual activities |
| Controlling vascular risk factors (hypertension, diabetes, dyslipidemia, and obesity) |
| Source: References 8,11 |
Related Resources
- Alzheimer’s Association. www.alz.org.
- National Institute on Aging. Alzheimer’s disease education and referral center. www.nia.nih.gov/alzheimers.
Disclosures
Drs. Kimchi and Desai report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Grossberg is a consultant to Baxter, Forest Laboratories, Merck, Otsuka, and Novartis.
1. Jack CR Jr, Albert MS, Knopman DS, et al. Introduction to the recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement. 2011;7(3):257-262.
2. Sperling RA, Aisen PS, Beckett LA, et al. Toward defining the preclinical stages of Alzheimer’s disease: recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement. 2011;7(3):280-292.
3. Albert MS, DeKosky ST, Dickson D, et al. The diagnosis of mild cognitive impairment due to Alzheimer’s disease: recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement. 2011;7(3):270-279.
4. McKhann GM, Knopman DS, Chertkow H, et al. The diagnosis of dementia due to Alzheimer’s disease: recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement. 2011;7(3):263-269.
5. McKhann G, Drachman D, Folstein M, et al. Clinical diagnosis of Alzheimer’s disease: report of the NINCDS-ADRDA Work Group under the auspices of Department of Health and Human Services Task Force on Alzheimer’s Disease. Neurology. 1984;34(7):939-944.
6. Diagnostic and statistical manual of mental disorders, 4th ed, text rev. Washington DC: American Psychiatric Association; 2000.
7. Ihl R, Frölich L, Winblad B, et al. World Federation of Societies of Biological Psychiatry (WFSBP) guidelines for the biological treatment of Alzheimer’s disease and other dementias. World J Biol Psychiatry. 2011;12(1):2-32.
8. Chertkow H, Massoud F, Nasreddine Z, et al. Diagnosis and treatment of dementia: 3. Mild cognitive impairment and cognitive impairment without dementia. CMAJ. 2008;178(10):1273-1285.
9. McKhann GM. Changing concepts of Alzheimer disease. JAMA. 2011;305(23):2458-2459.
10. Galasko D. Biomarkers in non-Alzheimer’s dementias. Clinical Neuroscience Research. 2004;3(6):375-381.
11. Desai AK, Grossberg GT, Chibnall JT. Healthy brain aging: a road map. Clin Geriatr Med. 2010;26(1):1-16.
12. Wilson RS, Hoganson GM, Rajan KB, et al. Temporal course of depressive symptoms during the development of Alzheimer disease. Neurology. 2010;75(1):21-26.
13. Bremner JD, Narayan M, Anderson ER, et al. Hippocampal volume reduction in major depression. Am J Psychiatry. 2000;157(1):115-118.
14. Yaffe K, Fox P, Newcomer R, et al. Patient and caregiver characteristics and nursing home placement in patients with dementia. JAMA. 2002;287(16):2090-2097.
15. Mittelman MS, Haley WE, Clay OJ, et al. Improving caregiver well-being delays nursing home placement of patients with Alzheimer disease. Neurology. 2006;67(9):1592-1599.
Discuss this article at www.facebook.com/CurrentPsychiatry
In 2011, a workgroup of experts from the Alzheimer’s Association and the National Institute on Aging published new criteria and guidelines for diagnosing Alzheimer’s disease (AD), the first new AD guidelines since 1984.1-4 These criteria reflect data that suggest AD is not synonymous with dementia of the Alzheimer’s type (DAT) but is a disease that slowly develops over many years as a result of accumulated neuropathologic changes, with dementia representing only the final phase of the disease (Figure).1-4
Figure: Cognitive decline in AD over time
AD: Alzheimer’s disease; MCI: mild cognitive impairment
Source: Adapted from reference 2
This article highlights the similarities and differences of the 1984 and 2011 AD diagnosis guidelines. We also discuss the new guidelines’ limitations and clinical implications.
The 1984 AD criteria
Both the 1984 AD criteria5 and DSM-IV-TR criteria6 rely on the concept that AD is a clinical diagnosis made after a patient develops dementia. That is, diagnosis rests on the physician’s clinical judgment about the etiology of the patient’s symptoms, taking into account reports from the patient, family, and friends, as well as results of neurocognitive testing and mental status evaluation. The 1984 criteria were developed with the expectation that if a patient who met clinical criteria for AD were to undergo an autopsy, he or she likely would have evidence of AD pathology as the underlying etiology. These criteria were developed before researchers discovered that in AD, pathologic changes occur over many years and clinical dementia is the end product of accumulated pathology. The 1984 criteria did not address important phases that precede clinical dementia—such as mild cognitive impairment (MCI). See the Table for a summary of the 1984 AD criteria.
Table
The 1984 NINCDS-ADRDA criteria for clinical diagnosis of AD
|
| AD: Alzheimer’s disease; NINCDS-ADRDA: National Institute of Neurological and Communicative Diseases and Stroke/Alzheimer’s Disease and Related Disorders Association Source: McKhann G, Drachman D, Folstein M, et al. Clinical diagnosis of Alzheimer’s disease: report of the NINCDS-ADRDA Work Group under the auspices of Department of Health and Human Services Task Force on Alzheimer’s Disease. Neurology. 1984;34(7):939-944 |
The 2011 AD criteria
The new AD criteria differ from the 1984 criteria in 2 major ways:
- expansion of AD into 3 phases, only 1 of which is characterized by dementia
- incorporation of biomarkers to provide information regarding pathophysiologic changes underlying the disease state (Table 1).1-5
The 3 phases. The 2011 criteria expand the definition of AD to include an asymptomatic, preclinical phase; a symptomatic, pre-dementia phase; and a dementia phase. In the initial phase, neuronal toxins such as beta-amyloid (Aβ) plaques and elevated tau first become detectable. Patients in this phase are asymptomatic or have subtle symptoms. This phase should be viewed as part of a continuum and includes patients who may, for instance, develop Aβ plaques but do not progress to further neurodegeneration.2 The diagnostic criteria of this phase are intended for research purposes only.1,2
Patients in the symptomatic, pre-dementia phase—also known as the MCI phase—exhibit mild decline in memory, attention, and thinking. Although this decline is more than what is expected for the patient’s age and education, it does not compromise everyday activity and functioning.
A patient who develops cognitive or behavioral problems that interfere with his or her ability to function at work or in everyday activities has entered the dementia phase. Similar to the 1984 guidelines, the 2011 criteria classify patients into probable and possible AD dementia. All patients who would have satisfied criteria for probable AD under the 1984 guidelines will satisfy criteria for probable AD dementia under the 2011 criteria.4 The same is not true for possible AD dementia. The 2011 criteria include 2 other major categories for patients with AD dementia: probable and possible AD dementia with evidence of the AD pathophysiological process. These categories are intended for research purposes only, whereas the criteria for the MCI and dementia phases are intended to guide diagnosis in the clinical setting.
By incorporating phases of AD that precede dementia into the disease spectrum, the new guidelines are designed to move clinicians toward earlier diagnosis and treatment.1-3 Similar to how early, pre-symptomatic detection and treatment of conditions such as diabetes and cancer can reduce mortality, improving diagnosis of AD in its early phases may allow clinicians to better test potential therapies and eventually use them to treat at-risk individuals.2,3 Most pharmacotherapies for AD are FDA-approved only for patients diagnosed with clinical dementia. Furthermore, current pharmacotherapies do not alter the course of AD; they have a modest effect in slowing cognitive and functional decline.7,8 If patients in the earlier phases of AD could be recruited for research studies, we may be able to develop new treatments to stop or reverse AD pathology and its clinical manifestations.
Biomarkers. The new criteria incorporate biomarkers to provide information about pathophysiologic changes underlying the disease process. These criteria define biomarkers as physiologic, biochemical, or anatomic parameters that can be measured in vivo and reflect specific features of disease-related pathophysiologic processes.1 Presently, there are no cutoff values to demarcate “normal” levels from “abnormal,” and biomarkers are proposed primarily as research tools because they have not been studied adequately in community settings and laboratory techniques to measure biomarkers have not been standardized.1-4,9
The 5 biomarkers incorporated into the new criteria are divided into 2 categories: biomarkers of Aβ accumulation and those of neuronal degeneration or injury (Table 2).1-4 In the initial, preclinical phase, biomarkers are used to detect changes in the brain—such as amyloid accumulation and nerve cell degeneration—that may already be in process in an individual whose clinical symptoms are subtle or not yet evident.1,2 In this phase, progressive evidence of biomarkers, such as both Aβ accumulation and neuronal injury rather than Aβ accumulation alone, may increase the probability that a patient will decline quickly into the MCI phase.2 Biomarkers of neuronal degeneration or injury especially correlate with the likelihood that the disease will progress to clinical dementia.1 Subtle cognitive symptoms in the preclinical phase also might predict rapid decline into MCI.2
In the MCI and dementia phases, biomarkers are used to determine the level of certainty that AD is responsible for the patient’s symptoms.1,3,4 For example, a patient could meet criteria for a non-AD dementia such as dementia with Lewy bodies, but also meet pathologic criteria for AD on autopsy.3 The diagnostic category of possible AD dementia with evidence of the AD pathophysiologic process is intended for this type of scenario.4 For the MCI phase, the criteria propose levels of certainty that a patient’s MCI syndrome is caused by AD, ranging from MCI due to AD-high likelihood to MCI-unlikely due to AD.3
Research has demonstrated that a patient’s clinical picture doesn’t necessarily reflect the extent of the underlying pathology. For example, a patient could have extensive AD pathology, such as diffuse amyloid plaques, without any obvious clinical symptoms.3 Conversely, although both Aβ deposition and elevated tau are hallmarks of AD, variations in these proteins can be seen in neuropsychiatric disorders other than AD.10 That said, it appears that worsening of clinical symptoms often parallels worsening of neurodegenerative biomarkers.1
Under the 2011 guidelines, biomarkers would not be used to diagnose or exclude AD or MCI, but instead would help improve diagnostic accuracy in individuals with cognitive decline.1,3,4 In other words, AD remains a clinical diagnosis, but these biomarkers could raise or lower the positive predictive value of a clinician’s judgment about the etiology of a patient’s symptoms.
See the Box for a description of the potential risks and benefits of using the new diagnostic criteria.
Table 1
Comparing the 1984 and 2011 AD criteria
| 1984 criteria | 2011 criteria |
|---|---|
| AD is a clinical diagnosis | AD remains a clinical diagnosis but biomarkers serve to improve the accuracy of diagnosis of the disease |
| There is only 1 phase of AD—dementia. | AD is expanded into 3 phases: an asymptomatic, preclinical phase; a symptomatic, pre-dementia phase; and a dementia phase |
| A patient who meets the clinical criteria for AD would be expected to have AD pathology as the underlying etiology were he/she to undergo a brain autopsy | Presently, biomarkers are proposed as research tools only and are not intended to be applied in the clinical setting. However, eventually clinicians will be able to diagnose AD in all 3 phases, as biomarker testing becomes standardized and reliable enough to be accurately applied in clinical settings |
| Little consideration is given to specific neuropathologic changes underlying the disease process | Biomarkers provide information regarding the pathophysiologic changes underlying the disease state |
| Little consideration is given to the idea that pathologic changes occur over many years | Inherent in dividing AD into 3 phases is the concept that AD develops slowly over many years and has a long prodromal phase that is clinically silent |
| AD: Alzheimer’s disease Source: References 1-5 | |
Table 2
5 biomarkers incorporated into the 2011 AD criteria
| Category | Biomarkers |
|---|---|
| Biomarkers of Aβ accumulation | Abnormal tracer retention on amyloid PET imaging |
| Low CSF Aβ42 | |
| Biomarkers of neuronal degeneration or injury | Elevated CSF tau (total and phosphorylated tau) |
| Decreased fluorodeoxyglucose uptake on PET | |
| Atrophy on structural magnetic resonance imaging | |
| Aβ: beta-amyloid; AD: Alzheimer’s disease; CSF: cerebrospinal fluid; PET: positron emission tomography Source: References 1-4 | |
The earlier an Alzheimer’s disease (AD) diagnosis is made, the less certain it is AD.a Biomarkers typically found in individuals with AD also can be found in patients with dementia not caused by AD, such as vascular dementia, as well as in individuals who may never develop dementia.b Additionally, there is no certainty that a patient in an early phase of AD will develop clinical dementia. Falsely diagnosing a patient with AD may lead the individual and their family to feel helpless, hopeless, depressed, anxious, or ashamed and to spend money and other resources preparing for a prognosis that may never come to fruition. Clinicians may feel compelled to assess for biomarkers using expensive, invasive tests that are not yet standardized in an attempt to support the AD diagnosis.
Early diagnosis of AD has many benefits that should not be overlooked, however. It provides patients and their families an opportunity to become familiar with the disease course, which may help some patients cope with the diagnosis. Patients diagnosed in the early stages would be able to make important decisions regarding health care, social, and financial planning before they develop pathology that limits their executive planning abilities or become functionally impaired.
Diagnosing an illness when there are no disease-modifying therapies available is not futile. Some patients with newly diagnosed AD in the pre-dementia phases may want to participate in clinical research trials to help develop therapies for AD. Some data suggest that AD treatment appears to provide the greatest benefit when initiated early in the disease course and maintained over a long duration.c Eventually, we may be able to tailor specific AD treatments in different phases of the disease. For instance, we may discover treatments for patients who show evidence of beta-amyloid plaques but not neuronal injury, or vice versa. Patients also may benefit from education on nonpharmacologic treatments, including reducing vascular risk factors to help improve brain aging,d reducing stress, and learning cognitive strategies such as using mnemonics to aid memory.
In many clinical settings, patients are being clinically diagnosed with mild cognitive impairment (MCI). Research indicates that patients with MCI are at near-term risk of developing dementia, particularly dementia of the Alzheimer’s type.d,e Presently, no definite transition points demarcate MCI from dementia; this progression is based upon clinical judgment.
In the last decade, researchers have begun to describe a syndrome of subjective cognitive impairment (SCI), which may be a phase that precedes the MCI phase of AD.f Patients with SCI report cognitive deficits (eg, forgetfulness and word-finding difficulties) but have no objective evidence of cognitive impairment on neuropsychological tests. Cognitive problems associated with SCI do not cause functional decline.g SCI may reflect the minimal cognitive complaints mentioned in the research criteria for the preclinical phase of AD. Eventually, biomarkers may be able to help clinicians more accurately predict which patients with SCI are most likely to progress to the MCI or dementia phase of AD.
References
- Albert MS, DeKosky ST, Dickson D, et al. The diagnosis of mild cognitive impairment due to Alzheimer’s disease: recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement. 2011;7(3):270-279.
- Galasko D. Biomarkers in non-Alzheimer dementias. Clinical Neuroscience Research. 2004;3(6):375-381.
- Geldmacher DS. Treatment guidelines for Alzheimer’s disease: redefining perceptions in primary care. Prim Care Companion J Clin Psychiatry. 2007;9(2):113-121.
- Chertkow H, Massoud F, Nasreddine Z, et al. Diagnosis and treatment of dementia: 3. Mild cognitive impairment and cognitive impairment without dementia. CMAJ. 2008;178(10):1273-1285.
- Rosenberg PB, Lyketsos C. Mild cognitive impairment: searching for the prodrome of Alzheimer’s disease. World Psychiatry. 2008;7(2):72-78.
- Reisberg B, Shulman MB, Torossian C, et al. Outcome over seven years of healthy adults with and without subjective cognitive impairment. Alzheimers Dement. 2010;6(1):11-24.
- Desai AK, Schwarz L. Subjective cognitive impairment: when to be concerned about ‘senior moments.’ Current Psychiatry. 2011;10(4):31-44.
Clinical applications
Although pharmacologic therapies for the early phases of AD are not yet available, research supports implementing nonpharmacologic modalities in older adults with MCI as well as those without any cognitive impairment (Table 3).8,11 Growing evidence suggests physicians should encourage patients to lead an active and socially integrated lifestyle that includes leisure activities, cognitive stimulation, meditation, a balanced diet, and daily exercise.8 Practitioners should treat vascular risk factors in geriatric patients with and without cognitive impairment to optimize healthy brain aging and reduce the risk of cardiovascular disease and stroke.11 By raising awareness of available treatments for early phases of AD, we may be able to reduce the anxiety and sense of helplessness or hopelessness that may accompany an AD diagnosis.
Depression and AD. Having depression nearly doubles one’s risk of developing AD later in life, and depression may exacerbate AD.12 Although the precise mechanism linking depression to AD is unclear, depression seems to exert a toxic effect on the hippocampus.13 Treating depression may prevent or mitigate the rate of memory impairment and overall AD severity and improve a patient’s quality of life, overall health, and ability to function.
Almost one-third of family caregivers become depressed while helping a family member with DAT.14 Directing caregivers to peer support groups and providing them with tips on how to take care of themselves physically, emotionally, and psychologically can be extremely beneficial. Data suggest that improving the psychological and emotional well-being of caretakers may delay nursing home placement of patients with DAT.15 Delaying nursing home placement can substantially improve quality of life and reduce the financial strain on patients and caregivers.
Patients and families often turn to clinicians for advice on what problems they or their loved ones may encounter if they suffer from cognitive impairment. One benefit of the new guidelines is that they can help us become educated about the early phases of AD as well as the long and often difficult course of the disease. In turn, we can better educate our patients and their families about the disease.
As early screening of AD improves, patients in the early phases will have an opportunity to take part in clinical trials for potential pharmacologic treatments of the disease. Our role as clinicians will be to guide patients and their families to such trials and give them the opportunity to help change our understanding of and approach to treating AD. It is important to keep in mind that the new guidelines should not be considered final, but rather as a work in progress that periodically will be revised as AD research progresses.3
Table 3
Promoting healthy brain aging
| Healthy diet (eg, Mediterranean diet) |
| Adequate sleep |
| Daily exercise |
| Smoking cessation |
| Active, socially integrated lifestyle |
| Leisure activities |
| Cognitive stimulation |
| Optimize treatment of depression and other mental illnesses |
| Meditation and other mindfulness strategies (eg, yoga) |
| Spiritual activities |
| Controlling vascular risk factors (hypertension, diabetes, dyslipidemia, and obesity) |
| Source: References 8,11 |
Related Resources
- Alzheimer’s Association. www.alz.org.
- National Institute on Aging. Alzheimer’s disease education and referral center. www.nia.nih.gov/alzheimers.
Disclosures
Drs. Kimchi and Desai report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Grossberg is a consultant to Baxter, Forest Laboratories, Merck, Otsuka, and Novartis.
Discuss this article at www.facebook.com/CurrentPsychiatry
In 2011, a workgroup of experts from the Alzheimer’s Association and the National Institute on Aging published new criteria and guidelines for diagnosing Alzheimer’s disease (AD), the first new AD guidelines since 1984.1-4 These criteria reflect data that suggest AD is not synonymous with dementia of the Alzheimer’s type (DAT) but is a disease that slowly develops over many years as a result of accumulated neuropathologic changes, with dementia representing only the final phase of the disease (Figure).1-4
Figure: Cognitive decline in AD over time
AD: Alzheimer’s disease; MCI: mild cognitive impairment
Source: Adapted from reference 2
This article highlights the similarities and differences of the 1984 and 2011 AD diagnosis guidelines. We also discuss the new guidelines’ limitations and clinical implications.
The 1984 AD criteria
Both the 1984 AD criteria5 and DSM-IV-TR criteria6 rely on the concept that AD is a clinical diagnosis made after a patient develops dementia. That is, diagnosis rests on the physician’s clinical judgment about the etiology of the patient’s symptoms, taking into account reports from the patient, family, and friends, as well as results of neurocognitive testing and mental status evaluation. The 1984 criteria were developed with the expectation that if a patient who met clinical criteria for AD were to undergo an autopsy, he or she likely would have evidence of AD pathology as the underlying etiology. These criteria were developed before researchers discovered that in AD, pathologic changes occur over many years and clinical dementia is the end product of accumulated pathology. The 1984 criteria did not address important phases that precede clinical dementia—such as mild cognitive impairment (MCI). See the Table for a summary of the 1984 AD criteria.
Table
The 1984 NINCDS-ADRDA criteria for clinical diagnosis of AD
|
| AD: Alzheimer’s disease; NINCDS-ADRDA: National Institute of Neurological and Communicative Diseases and Stroke/Alzheimer’s Disease and Related Disorders Association Source: McKhann G, Drachman D, Folstein M, et al. Clinical diagnosis of Alzheimer’s disease: report of the NINCDS-ADRDA Work Group under the auspices of Department of Health and Human Services Task Force on Alzheimer’s Disease. Neurology. 1984;34(7):939-944 |
The 2011 AD criteria
The new AD criteria differ from the 1984 criteria in 2 major ways:
- expansion of AD into 3 phases, only 1 of which is characterized by dementia
- incorporation of biomarkers to provide information regarding pathophysiologic changes underlying the disease state (Table 1).1-5
The 3 phases. The 2011 criteria expand the definition of AD to include an asymptomatic, preclinical phase; a symptomatic, pre-dementia phase; and a dementia phase. In the initial phase, neuronal toxins such as beta-amyloid (Aβ) plaques and elevated tau first become detectable. Patients in this phase are asymptomatic or have subtle symptoms. This phase should be viewed as part of a continuum and includes patients who may, for instance, develop Aβ plaques but do not progress to further neurodegeneration.2 The diagnostic criteria of this phase are intended for research purposes only.1,2
Patients in the symptomatic, pre-dementia phase—also known as the MCI phase—exhibit mild decline in memory, attention, and thinking. Although this decline is more than what is expected for the patient’s age and education, it does not compromise everyday activity and functioning.
A patient who develops cognitive or behavioral problems that interfere with his or her ability to function at work or in everyday activities has entered the dementia phase. Similar to the 1984 guidelines, the 2011 criteria classify patients into probable and possible AD dementia. All patients who would have satisfied criteria for probable AD under the 1984 guidelines will satisfy criteria for probable AD dementia under the 2011 criteria.4 The same is not true for possible AD dementia. The 2011 criteria include 2 other major categories for patients with AD dementia: probable and possible AD dementia with evidence of the AD pathophysiological process. These categories are intended for research purposes only, whereas the criteria for the MCI and dementia phases are intended to guide diagnosis in the clinical setting.
By incorporating phases of AD that precede dementia into the disease spectrum, the new guidelines are designed to move clinicians toward earlier diagnosis and treatment.1-3 Similar to how early, pre-symptomatic detection and treatment of conditions such as diabetes and cancer can reduce mortality, improving diagnosis of AD in its early phases may allow clinicians to better test potential therapies and eventually use them to treat at-risk individuals.2,3 Most pharmacotherapies for AD are FDA-approved only for patients diagnosed with clinical dementia. Furthermore, current pharmacotherapies do not alter the course of AD; they have a modest effect in slowing cognitive and functional decline.7,8 If patients in the earlier phases of AD could be recruited for research studies, we may be able to develop new treatments to stop or reverse AD pathology and its clinical manifestations.
Biomarkers. The new criteria incorporate biomarkers to provide information about pathophysiologic changes underlying the disease process. These criteria define biomarkers as physiologic, biochemical, or anatomic parameters that can be measured in vivo and reflect specific features of disease-related pathophysiologic processes.1 Presently, there are no cutoff values to demarcate “normal” levels from “abnormal,” and biomarkers are proposed primarily as research tools because they have not been studied adequately in community settings and laboratory techniques to measure biomarkers have not been standardized.1-4,9
The 5 biomarkers incorporated into the new criteria are divided into 2 categories: biomarkers of Aβ accumulation and those of neuronal degeneration or injury (Table 2).1-4 In the initial, preclinical phase, biomarkers are used to detect changes in the brain—such as amyloid accumulation and nerve cell degeneration—that may already be in process in an individual whose clinical symptoms are subtle or not yet evident.1,2 In this phase, progressive evidence of biomarkers, such as both Aβ accumulation and neuronal injury rather than Aβ accumulation alone, may increase the probability that a patient will decline quickly into the MCI phase.2 Biomarkers of neuronal degeneration or injury especially correlate with the likelihood that the disease will progress to clinical dementia.1 Subtle cognitive symptoms in the preclinical phase also might predict rapid decline into MCI.2
In the MCI and dementia phases, biomarkers are used to determine the level of certainty that AD is responsible for the patient’s symptoms.1,3,4 For example, a patient could meet criteria for a non-AD dementia such as dementia with Lewy bodies, but also meet pathologic criteria for AD on autopsy.3 The diagnostic category of possible AD dementia with evidence of the AD pathophysiologic process is intended for this type of scenario.4 For the MCI phase, the criteria propose levels of certainty that a patient’s MCI syndrome is caused by AD, ranging from MCI due to AD-high likelihood to MCI-unlikely due to AD.3
Research has demonstrated that a patient’s clinical picture doesn’t necessarily reflect the extent of the underlying pathology. For example, a patient could have extensive AD pathology, such as diffuse amyloid plaques, without any obvious clinical symptoms.3 Conversely, although both Aβ deposition and elevated tau are hallmarks of AD, variations in these proteins can be seen in neuropsychiatric disorders other than AD.10 That said, it appears that worsening of clinical symptoms often parallels worsening of neurodegenerative biomarkers.1
Under the 2011 guidelines, biomarkers would not be used to diagnose or exclude AD or MCI, but instead would help improve diagnostic accuracy in individuals with cognitive decline.1,3,4 In other words, AD remains a clinical diagnosis, but these biomarkers could raise or lower the positive predictive value of a clinician’s judgment about the etiology of a patient’s symptoms.
See the Box for a description of the potential risks and benefits of using the new diagnostic criteria.
Table 1
Comparing the 1984 and 2011 AD criteria
| 1984 criteria | 2011 criteria |
|---|---|
| AD is a clinical diagnosis | AD remains a clinical diagnosis but biomarkers serve to improve the accuracy of diagnosis of the disease |
| There is only 1 phase of AD—dementia. | AD is expanded into 3 phases: an asymptomatic, preclinical phase; a symptomatic, pre-dementia phase; and a dementia phase |
| A patient who meets the clinical criteria for AD would be expected to have AD pathology as the underlying etiology were he/she to undergo a brain autopsy | Presently, biomarkers are proposed as research tools only and are not intended to be applied in the clinical setting. However, eventually clinicians will be able to diagnose AD in all 3 phases, as biomarker testing becomes standardized and reliable enough to be accurately applied in clinical settings |
| Little consideration is given to specific neuropathologic changes underlying the disease process | Biomarkers provide information regarding the pathophysiologic changes underlying the disease state |
| Little consideration is given to the idea that pathologic changes occur over many years | Inherent in dividing AD into 3 phases is the concept that AD develops slowly over many years and has a long prodromal phase that is clinically silent |
| AD: Alzheimer’s disease Source: References 1-5 | |
Table 2
5 biomarkers incorporated into the 2011 AD criteria
| Category | Biomarkers |
|---|---|
| Biomarkers of Aβ accumulation | Abnormal tracer retention on amyloid PET imaging |
| Low CSF Aβ42 | |
| Biomarkers of neuronal degeneration or injury | Elevated CSF tau (total and phosphorylated tau) |
| Decreased fluorodeoxyglucose uptake on PET | |
| Atrophy on structural magnetic resonance imaging | |
| Aβ: beta-amyloid; AD: Alzheimer’s disease; CSF: cerebrospinal fluid; PET: positron emission tomography Source: References 1-4 | |
The earlier an Alzheimer’s disease (AD) diagnosis is made, the less certain it is AD.a Biomarkers typically found in individuals with AD also can be found in patients with dementia not caused by AD, such as vascular dementia, as well as in individuals who may never develop dementia.b Additionally, there is no certainty that a patient in an early phase of AD will develop clinical dementia. Falsely diagnosing a patient with AD may lead the individual and their family to feel helpless, hopeless, depressed, anxious, or ashamed and to spend money and other resources preparing for a prognosis that may never come to fruition. Clinicians may feel compelled to assess for biomarkers using expensive, invasive tests that are not yet standardized in an attempt to support the AD diagnosis.
Early diagnosis of AD has many benefits that should not be overlooked, however. It provides patients and their families an opportunity to become familiar with the disease course, which may help some patients cope with the diagnosis. Patients diagnosed in the early stages would be able to make important decisions regarding health care, social, and financial planning before they develop pathology that limits their executive planning abilities or become functionally impaired.
Diagnosing an illness when there are no disease-modifying therapies available is not futile. Some patients with newly diagnosed AD in the pre-dementia phases may want to participate in clinical research trials to help develop therapies for AD. Some data suggest that AD treatment appears to provide the greatest benefit when initiated early in the disease course and maintained over a long duration.c Eventually, we may be able to tailor specific AD treatments in different phases of the disease. For instance, we may discover treatments for patients who show evidence of beta-amyloid plaques but not neuronal injury, or vice versa. Patients also may benefit from education on nonpharmacologic treatments, including reducing vascular risk factors to help improve brain aging,d reducing stress, and learning cognitive strategies such as using mnemonics to aid memory.
In many clinical settings, patients are being clinically diagnosed with mild cognitive impairment (MCI). Research indicates that patients with MCI are at near-term risk of developing dementia, particularly dementia of the Alzheimer’s type.d,e Presently, no definite transition points demarcate MCI from dementia; this progression is based upon clinical judgment.
In the last decade, researchers have begun to describe a syndrome of subjective cognitive impairment (SCI), which may be a phase that precedes the MCI phase of AD.f Patients with SCI report cognitive deficits (eg, forgetfulness and word-finding difficulties) but have no objective evidence of cognitive impairment on neuropsychological tests. Cognitive problems associated with SCI do not cause functional decline.g SCI may reflect the minimal cognitive complaints mentioned in the research criteria for the preclinical phase of AD. Eventually, biomarkers may be able to help clinicians more accurately predict which patients with SCI are most likely to progress to the MCI or dementia phase of AD.
References
- Albert MS, DeKosky ST, Dickson D, et al. The diagnosis of mild cognitive impairment due to Alzheimer’s disease: recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement. 2011;7(3):270-279.
- Galasko D. Biomarkers in non-Alzheimer dementias. Clinical Neuroscience Research. 2004;3(6):375-381.
- Geldmacher DS. Treatment guidelines for Alzheimer’s disease: redefining perceptions in primary care. Prim Care Companion J Clin Psychiatry. 2007;9(2):113-121.
- Chertkow H, Massoud F, Nasreddine Z, et al. Diagnosis and treatment of dementia: 3. Mild cognitive impairment and cognitive impairment without dementia. CMAJ. 2008;178(10):1273-1285.
- Rosenberg PB, Lyketsos C. Mild cognitive impairment: searching for the prodrome of Alzheimer’s disease. World Psychiatry. 2008;7(2):72-78.
- Reisberg B, Shulman MB, Torossian C, et al. Outcome over seven years of healthy adults with and without subjective cognitive impairment. Alzheimers Dement. 2010;6(1):11-24.
- Desai AK, Schwarz L. Subjective cognitive impairment: when to be concerned about ‘senior moments.’ Current Psychiatry. 2011;10(4):31-44.
Clinical applications
Although pharmacologic therapies for the early phases of AD are not yet available, research supports implementing nonpharmacologic modalities in older adults with MCI as well as those without any cognitive impairment (Table 3).8,11 Growing evidence suggests physicians should encourage patients to lead an active and socially integrated lifestyle that includes leisure activities, cognitive stimulation, meditation, a balanced diet, and daily exercise.8 Practitioners should treat vascular risk factors in geriatric patients with and without cognitive impairment to optimize healthy brain aging and reduce the risk of cardiovascular disease and stroke.11 By raising awareness of available treatments for early phases of AD, we may be able to reduce the anxiety and sense of helplessness or hopelessness that may accompany an AD diagnosis.
Depression and AD. Having depression nearly doubles one’s risk of developing AD later in life, and depression may exacerbate AD.12 Although the precise mechanism linking depression to AD is unclear, depression seems to exert a toxic effect on the hippocampus.13 Treating depression may prevent or mitigate the rate of memory impairment and overall AD severity and improve a patient’s quality of life, overall health, and ability to function.
Almost one-third of family caregivers become depressed while helping a family member with DAT.14 Directing caregivers to peer support groups and providing them with tips on how to take care of themselves physically, emotionally, and psychologically can be extremely beneficial. Data suggest that improving the psychological and emotional well-being of caretakers may delay nursing home placement of patients with DAT.15 Delaying nursing home placement can substantially improve quality of life and reduce the financial strain on patients and caregivers.
Patients and families often turn to clinicians for advice on what problems they or their loved ones may encounter if they suffer from cognitive impairment. One benefit of the new guidelines is that they can help us become educated about the early phases of AD as well as the long and often difficult course of the disease. In turn, we can better educate our patients and their families about the disease.
As early screening of AD improves, patients in the early phases will have an opportunity to take part in clinical trials for potential pharmacologic treatments of the disease. Our role as clinicians will be to guide patients and their families to such trials and give them the opportunity to help change our understanding of and approach to treating AD. It is important to keep in mind that the new guidelines should not be considered final, but rather as a work in progress that periodically will be revised as AD research progresses.3
Table 3
Promoting healthy brain aging
| Healthy diet (eg, Mediterranean diet) |
| Adequate sleep |
| Daily exercise |
| Smoking cessation |
| Active, socially integrated lifestyle |
| Leisure activities |
| Cognitive stimulation |
| Optimize treatment of depression and other mental illnesses |
| Meditation and other mindfulness strategies (eg, yoga) |
| Spiritual activities |
| Controlling vascular risk factors (hypertension, diabetes, dyslipidemia, and obesity) |
| Source: References 8,11 |
Related Resources
- Alzheimer’s Association. www.alz.org.
- National Institute on Aging. Alzheimer’s disease education and referral center. www.nia.nih.gov/alzheimers.
Disclosures
Drs. Kimchi and Desai report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Grossberg is a consultant to Baxter, Forest Laboratories, Merck, Otsuka, and Novartis.
1. Jack CR Jr, Albert MS, Knopman DS, et al. Introduction to the recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement. 2011;7(3):257-262.
2. Sperling RA, Aisen PS, Beckett LA, et al. Toward defining the preclinical stages of Alzheimer’s disease: recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement. 2011;7(3):280-292.
3. Albert MS, DeKosky ST, Dickson D, et al. The diagnosis of mild cognitive impairment due to Alzheimer’s disease: recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement. 2011;7(3):270-279.
4. McKhann GM, Knopman DS, Chertkow H, et al. The diagnosis of dementia due to Alzheimer’s disease: recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement. 2011;7(3):263-269.
5. McKhann G, Drachman D, Folstein M, et al. Clinical diagnosis of Alzheimer’s disease: report of the NINCDS-ADRDA Work Group under the auspices of Department of Health and Human Services Task Force on Alzheimer’s Disease. Neurology. 1984;34(7):939-944.
6. Diagnostic and statistical manual of mental disorders, 4th ed, text rev. Washington DC: American Psychiatric Association; 2000.
7. Ihl R, Frölich L, Winblad B, et al. World Federation of Societies of Biological Psychiatry (WFSBP) guidelines for the biological treatment of Alzheimer’s disease and other dementias. World J Biol Psychiatry. 2011;12(1):2-32.
8. Chertkow H, Massoud F, Nasreddine Z, et al. Diagnosis and treatment of dementia: 3. Mild cognitive impairment and cognitive impairment without dementia. CMAJ. 2008;178(10):1273-1285.
9. McKhann GM. Changing concepts of Alzheimer disease. JAMA. 2011;305(23):2458-2459.
10. Galasko D. Biomarkers in non-Alzheimer’s dementias. Clinical Neuroscience Research. 2004;3(6):375-381.
11. Desai AK, Grossberg GT, Chibnall JT. Healthy brain aging: a road map. Clin Geriatr Med. 2010;26(1):1-16.
12. Wilson RS, Hoganson GM, Rajan KB, et al. Temporal course of depressive symptoms during the development of Alzheimer disease. Neurology. 2010;75(1):21-26.
13. Bremner JD, Narayan M, Anderson ER, et al. Hippocampal volume reduction in major depression. Am J Psychiatry. 2000;157(1):115-118.
14. Yaffe K, Fox P, Newcomer R, et al. Patient and caregiver characteristics and nursing home placement in patients with dementia. JAMA. 2002;287(16):2090-2097.
15. Mittelman MS, Haley WE, Clay OJ, et al. Improving caregiver well-being delays nursing home placement of patients with Alzheimer disease. Neurology. 2006;67(9):1592-1599.
1. Jack CR Jr, Albert MS, Knopman DS, et al. Introduction to the recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement. 2011;7(3):257-262.
2. Sperling RA, Aisen PS, Beckett LA, et al. Toward defining the preclinical stages of Alzheimer’s disease: recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement. 2011;7(3):280-292.
3. Albert MS, DeKosky ST, Dickson D, et al. The diagnosis of mild cognitive impairment due to Alzheimer’s disease: recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement. 2011;7(3):270-279.
4. McKhann GM, Knopman DS, Chertkow H, et al. The diagnosis of dementia due to Alzheimer’s disease: recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement. 2011;7(3):263-269.
5. McKhann G, Drachman D, Folstein M, et al. Clinical diagnosis of Alzheimer’s disease: report of the NINCDS-ADRDA Work Group under the auspices of Department of Health and Human Services Task Force on Alzheimer’s Disease. Neurology. 1984;34(7):939-944.
6. Diagnostic and statistical manual of mental disorders, 4th ed, text rev. Washington DC: American Psychiatric Association; 2000.
7. Ihl R, Frölich L, Winblad B, et al. World Federation of Societies of Biological Psychiatry (WFSBP) guidelines for the biological treatment of Alzheimer’s disease and other dementias. World J Biol Psychiatry. 2011;12(1):2-32.
8. Chertkow H, Massoud F, Nasreddine Z, et al. Diagnosis and treatment of dementia: 3. Mild cognitive impairment and cognitive impairment without dementia. CMAJ. 2008;178(10):1273-1285.
9. McKhann GM. Changing concepts of Alzheimer disease. JAMA. 2011;305(23):2458-2459.
10. Galasko D. Biomarkers in non-Alzheimer’s dementias. Clinical Neuroscience Research. 2004;3(6):375-381.
11. Desai AK, Grossberg GT, Chibnall JT. Healthy brain aging: a road map. Clin Geriatr Med. 2010;26(1):1-16.
12. Wilson RS, Hoganson GM, Rajan KB, et al. Temporal course of depressive symptoms during the development of Alzheimer disease. Neurology. 2010;75(1):21-26.
13. Bremner JD, Narayan M, Anderson ER, et al. Hippocampal volume reduction in major depression. Am J Psychiatry. 2000;157(1):115-118.
14. Yaffe K, Fox P, Newcomer R, et al. Patient and caregiver characteristics and nursing home placement in patients with dementia. JAMA. 2002;287(16):2090-2097.
15. Mittelman MS, Haley WE, Clay OJ, et al. Improving caregiver well-being delays nursing home placement of patients with Alzheimer disease. Neurology. 2006;67(9):1592-1599.
Screening for lung cancer
In one of our previous articles, we discussed a study of screening for prostate cancer.1 Now we’re going to move up a bit, at least anatomically, and discuss a study of screening for lung cancer.2 We have previously defined ourselves as curmudgeons and skeptics; to those self-descriptions we now add a new term, “chutzpahniks.” For those of you who may be unfamiliar with that Yiddish term, it means people who have chutzpah, which was defined by Leo Rosten3 as: “that quality enshrined in a man who, having killed his mother and father, throws himself on the mercy of the court because he is an orphan.” Our chutzpah stems from the fact that we are criticizing the results of a study that was published in the New England Journal of Medicine and highly praised in an editorial in that journal.4 If we had less chutzpah, we wouldn’t contemplate such a critique, but then again, if we had less chutzpah, we—a clinical psychologist and a nuclear physicist—wouldn’t be writing articles in a cancer journal. So, on to the study...
To read the full article, click on the PDF icon above.
In one of our previous articles, we discussed a study of screening for prostate cancer.1 Now we’re going to move up a bit, at least anatomically, and discuss a study of screening for lung cancer.2 We have previously defined ourselves as curmudgeons and skeptics; to those self-descriptions we now add a new term, “chutzpahniks.” For those of you who may be unfamiliar with that Yiddish term, it means people who have chutzpah, which was defined by Leo Rosten3 as: “that quality enshrined in a man who, having killed his mother and father, throws himself on the mercy of the court because he is an orphan.” Our chutzpah stems from the fact that we are criticizing the results of a study that was published in the New England Journal of Medicine and highly praised in an editorial in that journal.4 If we had less chutzpah, we wouldn’t contemplate such a critique, but then again, if we had less chutzpah, we—a clinical psychologist and a nuclear physicist—wouldn’t be writing articles in a cancer journal. So, on to the study...
To read the full article, click on the PDF icon above.
In one of our previous articles, we discussed a study of screening for prostate cancer.1 Now we’re going to move up a bit, at least anatomically, and discuss a study of screening for lung cancer.2 We have previously defined ourselves as curmudgeons and skeptics; to those self-descriptions we now add a new term, “chutzpahniks.” For those of you who may be unfamiliar with that Yiddish term, it means people who have chutzpah, which was defined by Leo Rosten3 as: “that quality enshrined in a man who, having killed his mother and father, throws himself on the mercy of the court because he is an orphan.” Our chutzpah stems from the fact that we are criticizing the results of a study that was published in the New England Journal of Medicine and highly praised in an editorial in that journal.4 If we had less chutzpah, we wouldn’t contemplate such a critique, but then again, if we had less chutzpah, we—a clinical psychologist and a nuclear physicist—wouldn’t be writing articles in a cancer journal. So, on to the study...
To read the full article, click on the PDF icon above.
Bench-to-Bedside Translation of Targeted Therapies in Multiple Myeloma
Multiple myeloma (MM) is characterized by excess monoclonal plasma cells in the bone marrow (BM), in most cases associated with monoclonal protein in blood or urine. Nearly 50 years ago, the use of combined melphalan and prednisone was shown to extend median survival of patients with MM to 2-3 years. In an approach pioneered by Prof. Tim McElwain in the 1970s, high-dose melphalan followed by BM transplantation in the 1980s and peripheral blood stem cell rescue in the 1990s further increased median survival to 3-4 years. Since 1998, MM has represented a new paradigm in drug development due to the remarkable therapeutic efficacy of targeting tumor cells in their microenvironment1,2—an approach perhaps best exemplified by the use of the proteasome inhibitor bortezomib and immunomodulatory drugs (IMiDs) thalidomide and lenalidomide to target the MM cell in the BM microenvironment. This approach has rapidly translated from bench to bedside, producing six new Food and Drug Administration (FDA)-approved treatments in the past 7 years and a doubling of patient survival from 3-4 to 7-8 years as a direct result.3 My colleagues and I have made contributions in the areas of identifying novel targets in the tumor and microenvironment, confirming the activity of inhibitors directed at these targets, and then leading clinical trials assessing the efficacy and safety of these agents...
*For a PDF of the full article, click on the link to the left of this introduction.
Multiple myeloma (MM) is characterized by excess monoclonal plasma cells in the bone marrow (BM), in most cases associated with monoclonal protein in blood or urine. Nearly 50 years ago, the use of combined melphalan and prednisone was shown to extend median survival of patients with MM to 2-3 years. In an approach pioneered by Prof. Tim McElwain in the 1970s, high-dose melphalan followed by BM transplantation in the 1980s and peripheral blood stem cell rescue in the 1990s further increased median survival to 3-4 years. Since 1998, MM has represented a new paradigm in drug development due to the remarkable therapeutic efficacy of targeting tumor cells in their microenvironment1,2—an approach perhaps best exemplified by the use of the proteasome inhibitor bortezomib and immunomodulatory drugs (IMiDs) thalidomide and lenalidomide to target the MM cell in the BM microenvironment. This approach has rapidly translated from bench to bedside, producing six new Food and Drug Administration (FDA)-approved treatments in the past 7 years and a doubling of patient survival from 3-4 to 7-8 years as a direct result.3 My colleagues and I have made contributions in the areas of identifying novel targets in the tumor and microenvironment, confirming the activity of inhibitors directed at these targets, and then leading clinical trials assessing the efficacy and safety of these agents...
*For a PDF of the full article, click on the link to the left of this introduction.
Multiple myeloma (MM) is characterized by excess monoclonal plasma cells in the bone marrow (BM), in most cases associated with monoclonal protein in blood or urine. Nearly 50 years ago, the use of combined melphalan and prednisone was shown to extend median survival of patients with MM to 2-3 years. In an approach pioneered by Prof. Tim McElwain in the 1970s, high-dose melphalan followed by BM transplantation in the 1980s and peripheral blood stem cell rescue in the 1990s further increased median survival to 3-4 years. Since 1998, MM has represented a new paradigm in drug development due to the remarkable therapeutic efficacy of targeting tumor cells in their microenvironment1,2—an approach perhaps best exemplified by the use of the proteasome inhibitor bortezomib and immunomodulatory drugs (IMiDs) thalidomide and lenalidomide to target the MM cell in the BM microenvironment. This approach has rapidly translated from bench to bedside, producing six new Food and Drug Administration (FDA)-approved treatments in the past 7 years and a doubling of patient survival from 3-4 to 7-8 years as a direct result.3 My colleagues and I have made contributions in the areas of identifying novel targets in the tumor and microenvironment, confirming the activity of inhibitors directed at these targets, and then leading clinical trials assessing the efficacy and safety of these agents...
*For a PDF of the full article, click on the link to the left of this introduction.
Therapeutic optimization of aromatase inhibitor–associated arthralgia: etiology, onset, resolution, and symptom management in early breast cancer
Third-generation aromatase inhibitors (AIs) used in the treatment of hormone-responsive breast cancer are associated with arthralgia, which is the most common reason for treatment discontinuation. This review characterizes the observed arthralgia and describes its variable definitions in key clinical trials; its typical onset and duration; symptom management strategies; and symptom resolution. The symptomatic manifestations of AI-associated arthralgia are highly variable, with typical onset occurring 2-6 months after treatment initiation. Aromatase inhibitor-associated arthralgia is most often bilateral and symmetrical, involving hands and wrists. Other common locations include knees, hips, lower back, shoulders, and feet. To improve standardization of care as well as patient quality of life, we propose a diagnostic algorithm for the management of patients who receive AIs and who develop arthralgia or worsening symptoms from preexisting joint pain. We conclude that although arthralgia is often associated with AI therapy, prompt diagnosis and management of musculoskeletal symptoms may ensure continued AI treatment and improve quality of life...
*For a PDF of the full article, click on the link to the left of this introduction.
Third-generation aromatase inhibitors (AIs) used in the treatment of hormone-responsive breast cancer are associated with arthralgia, which is the most common reason for treatment discontinuation. This review characterizes the observed arthralgia and describes its variable definitions in key clinical trials; its typical onset and duration; symptom management strategies; and symptom resolution. The symptomatic manifestations of AI-associated arthralgia are highly variable, with typical onset occurring 2-6 months after treatment initiation. Aromatase inhibitor-associated arthralgia is most often bilateral and symmetrical, involving hands and wrists. Other common locations include knees, hips, lower back, shoulders, and feet. To improve standardization of care as well as patient quality of life, we propose a diagnostic algorithm for the management of patients who receive AIs and who develop arthralgia or worsening symptoms from preexisting joint pain. We conclude that although arthralgia is often associated with AI therapy, prompt diagnosis and management of musculoskeletal symptoms may ensure continued AI treatment and improve quality of life...
*For a PDF of the full article, click on the link to the left of this introduction.
Third-generation aromatase inhibitors (AIs) used in the treatment of hormone-responsive breast cancer are associated with arthralgia, which is the most common reason for treatment discontinuation. This review characterizes the observed arthralgia and describes its variable definitions in key clinical trials; its typical onset and duration; symptom management strategies; and symptom resolution. The symptomatic manifestations of AI-associated arthralgia are highly variable, with typical onset occurring 2-6 months after treatment initiation. Aromatase inhibitor-associated arthralgia is most often bilateral and symmetrical, involving hands and wrists. Other common locations include knees, hips, lower back, shoulders, and feet. To improve standardization of care as well as patient quality of life, we propose a diagnostic algorithm for the management of patients who receive AIs and who develop arthralgia or worsening symptoms from preexisting joint pain. We conclude that although arthralgia is often associated with AI therapy, prompt diagnosis and management of musculoskeletal symptoms may ensure continued AI treatment and improve quality of life...
*For a PDF of the full article, click on the link to the left of this introduction.
Racial, Cultural Diversity Still Lacking among Hospital Executives
Less than 15% of healthcare professionals believe hospitals have closed the cultural and racial diversity gap in their leadership positions over the past five years, according to the results of a new survey (PDF).
Hospitalist leaders need to recognize the value of "cultural competence," particularly in an age when patients often tie their satisfaction to such questions as, "Does my doctor look like me?" and "Can I relate to my doctor?" according to James Gauss, senior vice president at executive search firm Witt/Kieffer, which penned the report.
Racial and ethnic disparity also will be important to address under provisions in the Affordable Care Act, which tie an economic impact to an organization's ability to deal with diverse populations of patients, says Gauss.
"We are now finally getting to a point where people might get paid correctly for dealing with these diversity issues because quality outcomes are going to be rewarded," he says.
Gauss says techniques that can help hospitals better balance the ethnic and racial makeup of their leadership include:
• implementing formal mentoring programs;
• understanding the patient and physician diversity of the geographic areas they serve; and
• establishing diversity recruiting goals.
For some groups, those goals might be as simple as recognizing that an organization is not doing enough. For others, the goals can be formal quotas.
"Some organizations set targets and they're very adamant about it," Gauss says. "But for some places, that may be two or three years down the road. … It depends on your starting point."
Less than 15% of healthcare professionals believe hospitals have closed the cultural and racial diversity gap in their leadership positions over the past five years, according to the results of a new survey (PDF).
Hospitalist leaders need to recognize the value of "cultural competence," particularly in an age when patients often tie their satisfaction to such questions as, "Does my doctor look like me?" and "Can I relate to my doctor?" according to James Gauss, senior vice president at executive search firm Witt/Kieffer, which penned the report.
Racial and ethnic disparity also will be important to address under provisions in the Affordable Care Act, which tie an economic impact to an organization's ability to deal with diverse populations of patients, says Gauss.
"We are now finally getting to a point where people might get paid correctly for dealing with these diversity issues because quality outcomes are going to be rewarded," he says.
Gauss says techniques that can help hospitals better balance the ethnic and racial makeup of their leadership include:
• implementing formal mentoring programs;
• understanding the patient and physician diversity of the geographic areas they serve; and
• establishing diversity recruiting goals.
For some groups, those goals might be as simple as recognizing that an organization is not doing enough. For others, the goals can be formal quotas.
"Some organizations set targets and they're very adamant about it," Gauss says. "But for some places, that may be two or three years down the road. … It depends on your starting point."
Less than 15% of healthcare professionals believe hospitals have closed the cultural and racial diversity gap in their leadership positions over the past five years, according to the results of a new survey (PDF).
Hospitalist leaders need to recognize the value of "cultural competence," particularly in an age when patients often tie their satisfaction to such questions as, "Does my doctor look like me?" and "Can I relate to my doctor?" according to James Gauss, senior vice president at executive search firm Witt/Kieffer, which penned the report.
Racial and ethnic disparity also will be important to address under provisions in the Affordable Care Act, which tie an economic impact to an organization's ability to deal with diverse populations of patients, says Gauss.
"We are now finally getting to a point where people might get paid correctly for dealing with these diversity issues because quality outcomes are going to be rewarded," he says.
Gauss says techniques that can help hospitals better balance the ethnic and racial makeup of their leadership include:
• implementing formal mentoring programs;
• understanding the patient and physician diversity of the geographic areas they serve; and
• establishing diversity recruiting goals.
For some groups, those goals might be as simple as recognizing that an organization is not doing enough. For others, the goals can be formal quotas.
"Some organizations set targets and they're very adamant about it," Gauss says. "But for some places, that may be two or three years down the road. … It depends on your starting point."
In the Literature: Research You Need to Know
Clinical question: How does a brief period of CPR with early analysis of rhythm compare with the strategy of a longer period of CPR with delayed analysis of rhythm in patients with out-of-hospital cardiac arrest?
Background: Based on current guidelines, emergency medical service (EMS) personnel could provide two minutes of CPR before the first analysis of cardiac rhythm. However, there is a paucity of data on the outcomes of this strategy versus the short CPR and early rhythm analysis.
Study design: The EMS groups participating in the study were cluster-randomized to one strategy or the other.
Settings: The Resuscitation Outcome Consortium (ROC) is a clinical trial consortium comprising 10 U.S. and Canadian universities and their regional EMS systems. The trial was conducted at 150 of the 260 EMS agencies participating in the ROC.
Synopsis: This is a cluster-randomized trial involving adults with out-of-hospital cardiac arrest. Patients in the early-analysis group were assigned to receive 30 to 60 seconds of EMS-administered CPR, and those in the later-analysis group were assigned to receive 180 seconds of CPR, before the initial electrocardiographic analysis. The primary outcome was survival to hospital discharge with satisfactory functional status (a modified Rankin scale score of =3, on a scale of 0 to 6, with higher scores indicating greater disability).
The study included 9,933 patients, of whom 5,290 were assigned to early analysis of cardiac rhythm and 4,643 to later analysis. A total of 273 patients (5.9%) in the later-analysis group and 310 patients (5.9%) in the early-analysis group met the criteria for the primary outcome, with a cluster-adjusted difference of -0.2 percentage points (95% confidence interval, -1.1 to 0.7; P=0.59).
Analyses of the data with adjustment for confounding factors, as well as subgroup analyses, showed no survival benefit for either study group.
Bottom line: Among patients who had an out-of-hospital cardiac arrest, there is no difference in the outcomes with a brief period, as compared with a longer period, of EMS-administered CPR before the first analysis of cardiac rhythm.
Citation: Stiell IG, Nichol G, Leroux BG, et al. Early versus later rhythm analysis in patients with out-of-hospital cardiac arrest. N Engl J Med. 2011;365;787-797.
Check out more physician reviews of HM-relevant literature on our website.
Clinical question: How does a brief period of CPR with early analysis of rhythm compare with the strategy of a longer period of CPR with delayed analysis of rhythm in patients with out-of-hospital cardiac arrest?
Background: Based on current guidelines, emergency medical service (EMS) personnel could provide two minutes of CPR before the first analysis of cardiac rhythm. However, there is a paucity of data on the outcomes of this strategy versus the short CPR and early rhythm analysis.
Study design: The EMS groups participating in the study were cluster-randomized to one strategy or the other.
Settings: The Resuscitation Outcome Consortium (ROC) is a clinical trial consortium comprising 10 U.S. and Canadian universities and their regional EMS systems. The trial was conducted at 150 of the 260 EMS agencies participating in the ROC.
Synopsis: This is a cluster-randomized trial involving adults with out-of-hospital cardiac arrest. Patients in the early-analysis group were assigned to receive 30 to 60 seconds of EMS-administered CPR, and those in the later-analysis group were assigned to receive 180 seconds of CPR, before the initial electrocardiographic analysis. The primary outcome was survival to hospital discharge with satisfactory functional status (a modified Rankin scale score of =3, on a scale of 0 to 6, with higher scores indicating greater disability).
The study included 9,933 patients, of whom 5,290 were assigned to early analysis of cardiac rhythm and 4,643 to later analysis. A total of 273 patients (5.9%) in the later-analysis group and 310 patients (5.9%) in the early-analysis group met the criteria for the primary outcome, with a cluster-adjusted difference of -0.2 percentage points (95% confidence interval, -1.1 to 0.7; P=0.59).
Analyses of the data with adjustment for confounding factors, as well as subgroup analyses, showed no survival benefit for either study group.
Bottom line: Among patients who had an out-of-hospital cardiac arrest, there is no difference in the outcomes with a brief period, as compared with a longer period, of EMS-administered CPR before the first analysis of cardiac rhythm.
Citation: Stiell IG, Nichol G, Leroux BG, et al. Early versus later rhythm analysis in patients with out-of-hospital cardiac arrest. N Engl J Med. 2011;365;787-797.
Check out more physician reviews of HM-relevant literature on our website.
Clinical question: How does a brief period of CPR with early analysis of rhythm compare with the strategy of a longer period of CPR with delayed analysis of rhythm in patients with out-of-hospital cardiac arrest?
Background: Based on current guidelines, emergency medical service (EMS) personnel could provide two minutes of CPR before the first analysis of cardiac rhythm. However, there is a paucity of data on the outcomes of this strategy versus the short CPR and early rhythm analysis.
Study design: The EMS groups participating in the study were cluster-randomized to one strategy or the other.
Settings: The Resuscitation Outcome Consortium (ROC) is a clinical trial consortium comprising 10 U.S. and Canadian universities and their regional EMS systems. The trial was conducted at 150 of the 260 EMS agencies participating in the ROC.
Synopsis: This is a cluster-randomized trial involving adults with out-of-hospital cardiac arrest. Patients in the early-analysis group were assigned to receive 30 to 60 seconds of EMS-administered CPR, and those in the later-analysis group were assigned to receive 180 seconds of CPR, before the initial electrocardiographic analysis. The primary outcome was survival to hospital discharge with satisfactory functional status (a modified Rankin scale score of =3, on a scale of 0 to 6, with higher scores indicating greater disability).
The study included 9,933 patients, of whom 5,290 were assigned to early analysis of cardiac rhythm and 4,643 to later analysis. A total of 273 patients (5.9%) in the later-analysis group and 310 patients (5.9%) in the early-analysis group met the criteria for the primary outcome, with a cluster-adjusted difference of -0.2 percentage points (95% confidence interval, -1.1 to 0.7; P=0.59).
Analyses of the data with adjustment for confounding factors, as well as subgroup analyses, showed no survival benefit for either study group.
Bottom line: Among patients who had an out-of-hospital cardiac arrest, there is no difference in the outcomes with a brief period, as compared with a longer period, of EMS-administered CPR before the first analysis of cardiac rhythm.
Citation: Stiell IG, Nichol G, Leroux BG, et al. Early versus later rhythm analysis in patients with out-of-hospital cardiac arrest. N Engl J Med. 2011;365;787-797.
Check out more physician reviews of HM-relevant literature on our website.