User login
Sleep and Circadian Misalignment
For hospitalists, patient care is 24 hours a day. To provide continual patient care, shift work has become a way of life for hospitalists, similar to hospital nurses, residents in training, and emergency medicine physicians. Notably, they belong to a substantial minority of the workforce as shift workers, starting after 6 PM or before 6 AM, approximately one‐fifth of the total work force in industrialized nations.1, 2 Unfortunately, shift workers suffer from misalignment of their endogenous circadian system, which regulates daily sleep and alertness patterns, and work obligations beyond daylight hours. Such a misalignment can lead to fatigue, sleep loss, and excessive sleepiness, which can adversely affect personal health and safety, as well as the quality of medical care delivered.3
The relationship between shift work, extended work hours, and medical safety is a topic currently under intense scrutiny, as reviewed in the Institute of Medicine's (IOM) controversial report on residents and sleep.4 This publication led the Accreditation Council of Graduate Medical Education (ACGME) to mandate more changes to residents' work hours,5 adding to those first implemented in 2003.6 These restrictions forbid residents from working more than 30 consecutive hours, and required at least 10 hours off between shifts and an average of 1 day off in 7. Subsequent studies suggested that the reduction in resident work hours led to greater resident well‐being, fewer attention failures. and fewer medical errors.3, 7
In 2007, amid growing public concern over sleep‐deprived residents and patient safety, Congress requested the IOM investigate additional safeguards for residents.8 In 2008, the IOM published a report calling for more protection against resident fatigue.4 They recommended integrating a protected sleep period into any 24‐hour shift. If residents cannot get protected sleep time, then the maximal shift duration should not exceed 16 hoursreduced from the previous ACGME recommendation of 30. Further provisions to allow adequate sleep include capping the number of consecutive night shifts at 4, and extending the time off after a night shift. In response, the ACGME recently updated their recommendations effective July 1, 2011,5 though not following all the IOM's recommendations (Table 1).
| 2003 ACGME Limits | 2008 IOM Recommendation | 2010 ACGME Limits | |
|---|---|---|---|
| |||
| Maximum work hours per week | 80 hr, averaged over 4 wk | No change | No change |
| Maximum shift length | 30 hr (admitting patients up to 24 hr, with 6 hr of transition activities) | 30 hr (admitting patients up to 16 hr, with 5 hr protected sleep between 10 PM to 8 AM, and remaining hours for transition activities) | PGY‐1: 16 hr; PGY‐2 and above: 28 hr (admitting patients up to 24 hr, with 4 hr of transition activities) |
| Minimum time off between shifts | 10 hr after shift | 10 hr after day shift; 12 hr after night shift; 14 hr after any extended shift of 30 hr and not return until 6 AM the next day | 10 hr after shift; 14 hr free after 24‐hr shift for intermediate level residents |
| Maximum frequency of in‐hospital night shifts | No limits | 4 night maximum, with 48 hr off after 3 or 4 consecutive shifts | 6 consecutive night maximum |
The growing nationwide emphasis on fatigue prevention within healthcare settings now clearly impacts residents and their training schedule. But why focus only on residents? Why not other physicians, such as hospitalists, who work shifts to cover 24 hours each day? Are they any less prone to making medical errors when fatigued? Given that hospitalists' represent the fastest growing specialty in the history of American medicine,9 we sought to inform decisions about their scheduling by reviewing normal regulation of sleep and wake patterns, addressing the problems associated with misalignment between sleep and work, and identifying strategies to realign circadian schedules.
NORMAL SLEEP AND CIRCADIAN RHYTHMS
An understanding of sleep physiology begins with the endogenous circadian timekeeping system. At the center of this timekeeping system is a master circadian clock, located in the suprachiasmatic nucleus (SCN) of the hypothalamus. Cells within the SCN generate a near 24‐hour rhythm, transmitted through neural connections, to rhythmically influence the entire central nervous system and other bodily systems.10
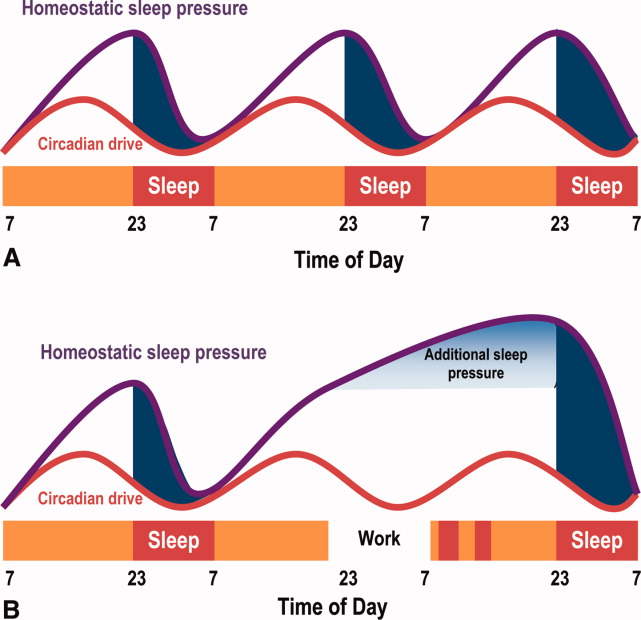
The SCN and the circadian rhythm interact with the need to sleep (sleep homeostasis) to form the 2‐process model of sleepwakefulness.11 In this model, progression of biological day (a time when wakefulness and its associated functions are promoted) coincides with a rise in homeostatic pressure to sleep (see Figure 1). Daytime alertness is maintained by increasing SCN neuronal activity to counterbalance rising sleep pressure. After peaking in the early evening, SCN activity falls to begin biological night (a time when sleep and its associated functions are promoted). To facilitate the onset of biological night, the SCN coordinates the activity of sleep‐promoting centers and the release of melatonin from the pineal gland which promotes sleep.
This endogenous circadian clock runs slightly longer than 24 hours and must be resynchronized daily to the 24‐hour day, a process known as entrainment. This occurs primarily through environmental exposure of retinalhypothalamic links to the lightdark cycle. The intensity, duration, and wave length of light all influence the circadian system,12 but perhaps most importantly is the timing. In general, light exposure in the evening will shift the circadian clock later (phase delay shift), whereas light exposure in the morning will shift the clock earlier (phase advance shift). Exogenous melatonin can also shift the circadian system. However, when endogenous levels of melatonin are high, ingested melatonin has little influence on sleep.13
Balancing sleep and wakefulness requires an interweaving of endogenous and exogenous factors. This balance is disturbed if we try to sleep or be wakeful during incorrect endogenous biological times, a process called circadian misalignment.
DELETERIOUS EFFECTS OF CIRCADIAN MISALIGNMENT
Hospitalists and other shift workers required to work during the biological night risk circadian misalignment and, consequently, poor sleep, shift work disorder, errors on the job, and possibly long‐term health consequences.
Chronic Sleep Loss
When working at night or in the early morning, nearly 75% of shift workers encounter some amount of at‐work fatigue and sleepiness.14 After the shift is over, objective assessments among rotating shift workers15, 16 and interns7 demonstrated that day sleep is 1 to 4 hours shorter than night sleep. Chronic or recurring night shifts can therefore lead to chronic sleep loss. While it seems reasonable that permanent night shift workers have greater circadian adjustment to suit their work schedule, little evidence supports this argument.17 Permanent night shift workers may sleep a little longer during the day than rotating shift workers. Yet, the sleep quality does not match night sleep, presumably from conflict between external factors, such as light and activity, and the scheduled sleep period.
Shift Work Disorder
If severe and chronic, sleepiness and impaired performance during work hours and poor sleep during the day can be enough to warrant a diagnosis of shift work disorder (SWD), one of the several circadian rhythm sleep disorders (CRSD). The prevalence of SWD among rotating and night workers is estimated to be 10%25%.18 Patients with SWD can experience similar levels of nighttime sleepiness as patients with narcolepsy and sleep apnea.19 These patients experience reduced satisfaction with the work schedule, and suffer higher rates of depression, ulcers, and sleepiness‐related accidents, compared to other shift workers.18 What distinguishes those shift workers who suffer from normal fatigue and those with SWD is not easily identified. The International Classification of Sleep Disorders‐2 (ICSD‐2) lists the diagnostic criteria for SWD20:
-
Symptoms of insomnia associated with a work schedule that overlaps the usual time for sleep.
-
Symptoms are directly associated with shift work schedule over the course of at least 1 month.
-
Sleep log monitoring for at least 7 days demonstrates circadian and sleep‐time misalignment.
-
Sleep disturbance is not better explained by another sleep disorder or by a medical, neurological, or mental disorder; medication use; or substance‐use disorder.
Symptoms must be present for at least 1 month, and comorbid mood or sleep/wake disorders (commonly found in this disorder) need to be treated. SWD is more common among night shift workers, although those workers starting shifts between 4 AM and 7 AM (early morning shift) are also subject to SWD.21 Type of work schedule, along with physical or mental disorders, domestic responsibilities, and commute times are examples of factors that may increase vulnerability for SWD.18 In addition, genetic factors may explain the considerable inter‐individual differences in susceptibility to SWD. For example, a polymorphism in the circadian gene, PER 3, present in 10%15% of the population, is believed to decrease tolerability to acute sleep loss,22 while genetic variation in the adenosine A2A receptor may be associated with resistance to the effects of sleep loss.23 If a hospitalist suspects a diagnosis SWD, they should seek evaluation by a physician specializing in sleep medicine.
Errors
Disruption of the circadian rhythm influences neurocognitive and psychomotor function, and can lead to human error. Human errors that result in serious accidents or injuries typically result from interaction of circadian rhythm misalignment with multiple other factors, including task duration and complexity, motivation and proficiency, and level of sleep deprivation.24 Though difficult to isolate from the environmental and work experience factors, consistent evidence identifies circadian misalignment as a cause of errors and serious accidents. Most evidence comes from night shift workers trying to remain awake when the circadian signal for alertness is low, or attempting sleep when the circadian alerting signal is high. Compared to day workers, night shift workers are 1.63 times more likely to suffer a fatal accident.25 A study of critical care nurses revealed a prominent circadian pattern of inadvertent sleep episodes during work with the highest peak between 2 AM and 6 AM.26 In addition, nurses working the night shift have been shown to commit more medication administration errors than day workers.27
Medical errors among resident physicians during extended shift durations is well documented.28 On the other hand, not much research has examined error rates among attending physicians. In 1 small study, attending surgeons made more cognitive errors using a simulated laparoscopic exercise as the amount of on‐call overnight sleep decreased.29 A large, single‐center review reported an increased rate of complications among post‐nighttime surgical procedures performed by attendings who slept 6 hours or less the preceding night.30 Notably, proposed legislation would require physicians who have been awake 22 of the preceding 24 hours to inform patients of the potential safety impact of their sleep deprivation prior to providing clinical care.31
Chronic Health Morbidity
Several studies reveal the effect of shift work on chronic health conditions among healthcare workers, such as obesity, cardiovascular disease, and certain cancers (eg, breast, colorectal). These results are summarized in Table 2, with the largest evaluation of healthcare shift workers coming from the Nurses' Health Study.3234
| Disease | Study Design | Population | Comparison | Health Risk | Adjusted Risk Factors |
|---|---|---|---|---|---|
| |||||
| Acute myocardial infarction | Prospective cohort32 | 79,109 US nurses | Working 3 night shifts/mo for 6 yr | RR 1.51 | CAD risk factors, aspirin use, hormone replacement therapy |
| 95% CI (1.12‐2.03) | |||||
| Obesity (BMI 30) | Cross‐sectional72 | 27,485 Swedish workers | Shift‐workers vs day workers | OR 1.41 | Age, socioeconomic status |
| 95% CI (1.25‐1.59) | |||||
| Breast cancer | Prospective cohort33 | 116,087 US nurses | Working 3 night shifts/mo for 20 yr | RR 1.79 | Breast cancer risk factors |
| 95% CI (1.06‐3.01) | |||||
| Colon cancer | Prospective cohort34 | 78,586 US nurses | Working 3 night shifts/mo for 15 yr | RR 1.35 | Family history of colon cancer, dietary intake, activity |
| 95% CI (1.03‐1.77) | |||||
Some believe that adverse health outcomes in shift workers derive from circadian stressan alteration of psychosocial and physiological homeostasis (eg, increased cortisol and catecholamine output) resulting from circadian misalignment.35 Based on data suggesting an increased risk for certain cancers among shift workers, the International Agency for Research of Cancer, a unit of the World Health Organization, announced that shift work resulting in circadian misalignment is probably carcinogenic.36 Researchers propose several biologic mechanisms to explain the increased cancer riskmost revolve around the alteration of the melatonin circadian cycle, found in night shift workers,37 and subsequent disruption of its believed cancer‐protective biologic pathways.
Overall, however, the heterogeneous nature of shift work limits conclusions regarding the long‐term health of shift workers. That is, as the shift work intensity and composition varies, and as the number and timing of these shifts change, so too can the adverse health consequences.
HOSPITALISTS AND NIGHT SHIFTS
Hospital medicine is the fastest growing specialty in the history of medicine, with an estimated 30,000 practicing hospitalists in 2010.38 Survey results from 2009 indicate that hospitalists staff 58% of hospitals; 89% of hospitals with more than 200 beds (J. Miller, Society of Hospital Medicine, personal communication). One reason for the growth in the number of hospitalists at academic medical centers has been the imposed work‐hour restrictions for residents.39
Across the county, hospitalist programs use a variety of shift work systems to ensure 24‐hour patient care. Among those programs that provide continuous on‐site coverage, many staff 3 shiftsday, late afternoon/evening (swing), and night shifts. Some permanently partition the scheduling, with dedicated night hospitalists or nocturnists.40
Hospitalists do not have mandated work‐hour restrictions and, in general, are older than resident physicians. Whether or not hospitalists who trained before the era of work‐hour regulations are better prepared for practicing in a real‐world, after‐hours scenario than hospitalists with previous work‐hour restrictions is a matter of debate. That said, hospitalists who are fatigued, just like residents, may be at increased risk for committing medical errors, particularly when the fatigue is unrecognized. Yet, limiting hospitalists' work hours would have obvious financial implications, likely similar those from resident work‐hour reductions.41 As part of the ACGME 2011 recommendations, faculty and residents now must be trained to recognize signs of fatigue and sleep deprivation, and adopt management strategies such as naps or backup call schedules. Fatigue that results in excessive sleepiness while at work may manifest as weariness, difficulty concentrating, headache, irritability or depressed mood, and feeling unrefreshed after sleeping.42
STRATEGIES TO IMPROVE CIRCADIAN ADAPTATION
Hospitalists can help limit fatigue and improve performance and safety through circadian adaptation: a multimodal approach to realign work and circadian schedules. Depending on whether the shift starts at night or in the early morning (4 AM to 7 AM), circadian adaptation aims may differ. For night shift workers, the overall aim is to delay the timing of circadian rhythms such that the highest propensity of wakefulness occurs during the night work period, while the highest propensity for sleep occurs during the day.17, 43 For early morning shift workers, circadian rhythms for wakefulness and sleep propensity should be shifted earlier. Circadian adaptation involves not only sleeping well before work, but also preventing dips in wakefulness during work. Adaptation strategies are listed in Table 3.
| Night Shift60 | Early Day Shift (Starting at 4 AM‐7 AM) | |
|---|---|---|
| Prior to shift | Avoid sleep debt | Avoid sleep debt |
| Proper sleep hygiene | Proper sleep hygiene | |
| Planned napping | Bright light exposure | |
| Caffeine use | ||
| During the shift | Bright light exposure | Caffeine use |
| Planned napping | ||
| After the shift | Avoid bright light | Avoid late evening bright light (when applicable) |
| Melatonin prior to sleep | ||
| Careful use of other hypnotics | Initiate sleep early |
Improved Sleep Before Work
As an essential first step, hospitalists must get a full night's rest before starting a night shift, as sleep debt will worsen fatigue while at work. Tips for proper sleep hygiene are listed in Table 4. Some shift workers stay up late the night before a scheduled night shift, in order to sleep during the day and awaken shortly before their scheduled night shift, to combat fatigue at work. Such an approach to shift work is typically met with 3 barriers. First, environmental factors often prevent 6 hours of uninterrupted day sleep. Second, 6 hours of continual day sleep is typically difficult because rising circadian activity often limits the sleep period to just a few hours. Third, an adequate amount of sleep prior to a night shift will itself not be enough to prevent sleepiness from occurring after midnightreducing the fall in circadian activity is also essential to maintaining alertness and performance.
| Physical | Adhere to regular wake and sleep schedule |
| activities73 | Engage in regular exercise early in the day |
| Avoid caffeine, nicotine, and alcohol use 6 hr prior to sleeping | |
| Avoid stimulating or stressful activities 30 min prior to sleeping | |
| Proper sleep | Well ventilated, temperature‐controlled bedroom |
| environment | Use heavy curtains to provide as much darkness as possible |
| Comfortable mattress and pillow | |
| Remove television and pets from the bedroom | |
| Housemates should help provide quiet sleep environment |
Napping
Napping prior to a night shift, or during the work shift, can improve alertness and performance and decrease accident rates.44, 45 During shift work, naps of 20 to 50 minutes in duration have demonstrated improvements in reaction time, and restoration of performance to that seen at the start of the shift. Napping early in the night shift can improve objective measures of alertness.44 To avoid increased drowsiness that sometimes occurs when waking from a nap, naps should not be longer than 50 minutes, and can be as short as 10 to 15 minutes.44, 46 Although effective, napping may be impractical for many workers due to time or space constraints. To facilitate brief naps, hospitalist practices should ensure they have a dark, quiet call room for use by overnight hospitalists.
Bright Light Exposure
Studies demonstrate that light exposure during the night shift improves circadian alignment, mood, and performance during the night shift.47, 48 Light exposure ranged from 6 hours to 5 light treatments of 15 minutes each, with brightness ranging from 2,500 to 10,000 lux (approximating outdoor daylight; typical office lighting provides 200‐500 lux).47, 49 Results demonstrate that bright light exposure during the night shift acutely improves alertness and performance, though not to daytime levels.50 The greatest circadian adjustments occur in groups using both bright light during the night shift and light avoidance the following morning.51 Dark sunglasses and a dark home environment can decrease bright light exposure during the day. Though little evidence exists to support widespread application of bright light devices in hospitalists' call‐rooms, a hospitalist practice should consider installing one to promote circadian adaptation if physicians working overnight have multiple consecutive shifts. Likewise, these physicians should be vigilant and wear dark sunglasses during the day after their night shifteven a few minutes of light exposure at the wrong time of the day may disrupt the intended circadian adaptation.
Wake‐Promoting Agents
Numerous studies demonstrate that 150 mg to 400 mg of caffeine (a 16 oz grande cup of coffee from Starbucks contains between 200 to 500 mg of caffeine52; a Diet Coke contains 46 mg/12 oz53) reduces sleepiness, increases alertness, and improves performance during the night shift.54, 55 Thus, judicious use of caffeine may be recommended in hospital practices during extended work hours. Other wake‐promoting agents, such as modafinil and armodafinil, are US Food and Drug Administration (FDA)‐approved in the treatment of excessive sleepiness associated with SWD. Typically taken 3060 minutes before the start of the night shift, these medications have been shown in trials, enrolling mostly permanent night shift workers, to reduce excessive nighttime sleepiness and improve performance.19, 56 Armodafinil used to treat SWD‐associated excessive sleepiness, has been safely tolerated for durations of 1 year or more.57 However, these agents are not approved for use in patients without a diagnosed sleep disorder.
Melatonin
Exogenous melatonin has been used to reset circadian rhythms in patients with CRSDs.58 Melatonin administered in the late afternoon to early evening directs the largest phase advance. In contrast, melatonin given in the morning produces the largest phase delays.59 When taken after a night shift, melatonin (at a dose 1.8 to 3.0 mg) can improve day sleep quality and duration.60 Despite this result, melatonin's effectiveness in improving circadian adaptation has been mixed.61 For example, improvements in nighttime alertness during the night shift were not seen, despite the use of melatonin to facilitate daytime sleep beforehand.62 Hospitalists may consider a trial of melatonin to improve circadian alignment and facilitate daytime sleep, but its chronic use and long‐term safety has not been adequately studied.
Hypnotics After Work
Hypnotics such as temazepam 20 mg,63 triazolam,64 and zolpidem65 taken after night shift work have been shown to improve day sleep quality under simulated conditions, but do not improve shift work performance. These medications should be reserved for judicious short‐term use in patients with insomnia associated with SWD.
NIGHT SHIFT SCHEDULING TO REDUCE CIRCADIAN MISALIGNMENT
When providing 24‐hour, on‐site medical care, questions may arise about how to incorporate circadian adaptation into the daily schedule.
How Should Shifts Be Rotated?
When scheduling shifts with different start times, evidence suggests that sleep disturbance is reduced with a clockwise progression in shifts (eg, day shift to evening shift to night shift). This reduction in sleep disturbance is thought due to increased time between shifts and the circadian timekeeping tendency to extend beyond 24 hours.66
When Should the Night Shift Start?
Those hospitalist programs using an evening swing shift from afternoon to late evening may have the option of using a 12‐hour night shift starting around 7 PM, or a shorter night shift beginning later at night. Though there are no data among hospitalists to suggest which night shift start time and duration would lead to the least amount of fatigue and errors, healthcare providers working a 12‐hour night shift may have increased morale due to fewer shifts, but may suffer a reduction in the quality of care provided compared with working an 8‐hour night shift.67 In either case, shift workers given flexibility in scheduling have been shown to have positive effects on sleep.68
Should Night Shifts Be Bunched?
The decision to bunch night shifts together depends on how many night shifts are required, and how quickly circadian adaptation can occur. Under simulated conditions, circadian adaptation can yield significant changes in sleep/wake cycles in as little as 4 days.48 In real‐world settings, more time may be required to achieve significant shifts in the circadian cycle. Therefore, hospitalists who have 7 or fewer night shifts during the academic year may want to space the shifts out to prevent sleep debt on consecutive shifts, since significant circadian adaptation would be difficult to achieve in less than a week. In this situation, after a night shift, the hospitalist should have at least one 9‐hour sleep period at night to relieve their sleep debt before staffing another night shift.69 Consecutive night shifts require at least 2 nighttime sleep periods of 9 hours to recover from sleep debt.70 The IOM recommends setting a limit of 4 consecutive night float shifts for resident physicians, however, a recent systematic review of resident night float models did not find data supporting use of a 4‐night‐maximum model.28
If more than 7 night shifts are required, then scheduling the shifts close together with use of circadian adaptation techniques may result in increased nighttime alertness, less fatigue, and fewer errors while at work than widely spacing out the shifts. For example, 1 recent study simulated 8 night shifts over a 10‐day period, and compared circadian schedules and work performance between those subjects who used circadian adaptation strategies and those that did not.71 Circadian adaptation techniques included: four 15‐minute bright light pulses during each night shift, dark sunglasses when outside, dark bedrooms and delayed sleeping until 3 AM on the nights off in between the night shift blocks. The group who shifted their circadian schedule improved night shift alertness and performance as measured by neurophysiological testing, while permitting sufficient daytime sleep after work, as well as late‐night sleep on days off. The group without circadian interventions did not shift their circadian schedule as significantly as the intervention group, and performed worse on the performance testing.
CONCLUSIONS
The nationwide use of hospitalists to provide 24‐hour patient care continues to expand, thus subjecting more hospitalists to work hours asynchronous with the lightdark cycle. Resultant circadian misalignment can result in fatigue while at work, shift work disorder, and, potentially, an increased rate of medical errors. Recognition of these dangers among resident physicians has prompted the ACGME to intensify their regulations on work hours, shift schedules, and time off between shifts. However, no such recommendations exist for hospitalists or emergency physicians and nurses.
Given the potential risk to both physicians and patients, we recommend more research examining the effects of circadian misalignment within the hospitalist community. Sample research questions are offered in Table 5. More information is urgently needed to provide evidence‐based practice guidelines to ensure the safety of this growing workforce and the patients they treat.
| Are hospitalists more immune to fatigue than resident physicians? |
| Are hospitalists better able to recognize fatigue while at work than resident physicians? |
| Does 1 shift work schedule promote better circadian alignment than other shift schedules? |
| Do consistent nighttime hours of nocturnists make them more prone to commit medical errors than hospitalists rotating their shifts? |
- .Job, family, and gender: determinants of nonstandard work schedules among employed Americans in 1991.Demography.1995;32:577–598.
- ,.Shift work among dual‐earner couples with children.Science.1983;219:876–879.
- ,,, et al.Effect of reducing interns' work hours on serious medical errors in intensive care units.N Engl J Med.2004;351:1838–1848.
- Institute of Medicine. Resident Duty Hours: Enhancing Sleep, Supervision and Safety. Released December 15,2008. Available at: http://www.iom.edu/Reports/2008/Resident‐Duty‐Hours‐Enhancing‐Sleep‐Supervision‐and‐Safety.aspx. Accessed on October 20, 2010.
- ACGME. ACGME Approved Standards. Effective July2011. Available at: http://acgme‐2010standards.org/. Accessed on January 6, 2011
- ACGME. Common Program Requirements: Resident Duty Hours in the Learning and Work Environment. Effective July 1, 2007. Available at: http://www.acgme.org/acWebsite/dutyHours/dh_ComProgrRequirmentsDutyHours0707.pdf. Accessed October 20,2010.
- ,,, et al.Effect of reducing interns' weekly work hours on sleep and attentional failures.N Engl J Med.2004;351:1829–1837.
- Letter written to William Munier, Agency for Healthcare Research and Quality.Washington, DC:US House of Representatives, Committee on Energy and Commerce, March 29,2007. Available at: http://energycommerce.house.gov/Press_110/110‐ltr.032907.HHS.Munier.pdf. Accessed on October 24, 2010.
- ,.The evolution and future of hospital medicine.Mt Sinai J Med.2008;75:418–423.
- .Brain structures and receptors involved in alertness.Sleep Med.2005;6(suppl 1):S3–S7.
- .A two process model of sleep regulation.Hum Neurobiol.1982;1:195–204.
- ,.Entrainment of the human circadian system by light.J Biol Rhythms.2005;20:326–338.
- ,.Sleep‐promoting and hypothermic effects of daytime melatonin administration in humans.Sleep.1997;20:124–131.
- .Sleepiness as a consequence of shift work.Sleep.1988;11:17–34.
- ,,,,.The sleep of long‐haul truck drivers.N Engl J Med.1997;337:755–761.
- ,,,.Sleep on the night shift: 24‐hour EEG monitoring of spontaneous sleep/wake behavior.Psychophysiology.1989;26:352–358.
- .Do permanent night workers show circadian adjustment? A review based on the endogenous melatonin rhythm.Chronobiol Int.2008;25:215–224.
- ,,,,.Shift work sleep disorder: prevalence and consequences beyond that of symptomatic day workers.Sleep.2004;27:1453–1462.
- ,,, et al.Modafinil for excessive sleepiness associated with shift‐work sleep disorder.N Engl J Med.2005;353:476–486.
- American Academy of Sleep Medicine.The International Classification of Sleep Disorders (ICSD).2nd ed.Chicago, IL:American Academy of Sleep Medicine;2005.
- ,.Circadian rhythm sleep disorders.Chest.2006;130:1915–1923.
- ,,,,,.Early morning executive functioning during sleep deprivation is compromised by a PERIOD3 polymorphism.Sleep.2008;31:1159–1167.
- ,,,,,.Genetic variation in the adenosine A2A receptor gene modulates performance on the psychomotor vigilance task.Sleep Biol Rhythms.2007;5:A47.
- ,.Circadian rhythms in cognitive performance: methodological constraints, protocols, theoretical underpinnings.Physiol Behav.2007;90:196–208.
- ,,,.A prospective study of fatal occupational accidents—relationship to sleeping difficulties and occupational factors.J Sleep Res.2002;11:69–71.
- ,,,.Effects of critical care nurses' work hours on vigilance and patients' safety.Am J Crit Care.2006;15:30–37.
- ,,,,.Daytime sleepiness, sleep habits and occupational accidents among hospital nurses.J Adv Nurs.2005;52:445–453.
- ,,.Systematic review: association of shift length, protected sleep time, and night float with patient care, residents' health, and education.Ann Intern Med.2010;153:829–842.
- ,,,,.Jack Barney Award: the effect of fatigue on cognitive and psychomotor skills of trauma residents and attending surgeons.Am J Surg.2008;196:813–819; discussion 9–20.
- ,,, et al.Risks of complications by attending physicians after performing nighttime procedures.JAMA.2009;302:1565–1572.
- ,,.Sleep deprivation, elective surgical procedures, and informed consent.N Engl J Med.2010;363:2577–2579.
- ,,,,.A prospective study of anger and coronary heart disease. The Normative Aging Study.Circulation.1996;94:2090–2095.
- ,,,.Night work and risk of breast cancer.Epidemiology.2006;17:108–111.
- ,,, et al.Night‐shift work and risk of colorectal cancer in the nurses' health study.J Natl Cancer Inst.2003;95:825–828.
- ,,.Shift work and cardiovascular disease—pathways from circadian stress to morbidity.Scand J Work Environ Health.2010;36:96–108.
- IARC. IARC monographs on the evalutaion of carcinogenic risks to humans. Vol 98. Painting, firefighting, and shiftwork. 2007. Available at: monographs.iarc.fr/ENG/Monographs/vol98/mono98.pdf. Accessed January 16,2011.
- ,,,.Influence of melatonin on invasive and metastatic properties of MCF‐7 human breast cancer cells.Cancer Res.1998;58:4383–4390.
- Society of Hospital Medicine. Society of Hospital Medicine releases results of the 2007–2008 survey on the state of the hospital medicine movement. 2008. Available at: http://www.hospitalmedicine.org/AM/Template.cfm?Section=Press_Releases3:247–255.
- ,,.Hospitalists: A Guide to Building and Sustaining a Successful Program.Chicago, IL:Health Administration Press;2008.
- ,,,,.The increased financial burden of further proposed orthopaedic resident work‐hour reductions.J Bone Joint Surg Am.2011;93:e31.
- ,,,,,.Fatigue and shift work.J Sleep Res.2006;15:1–5.
- ,,, et al.Rapid shift in peak melatonin secretion associated with improved performance in short shift work schedule.Sleep.1997;20:1145–1150.
- ,,.The impact of a nap opportunity during the night shift on the performance and alertness of 12‐h shift workers.J Sleep Res.2002;11:219–227.
- ,,, et al.Improving alertness and performance in emergency department physicians and nurses: the use of planned naps.Ann Emerg Med.2006;48:596–604, e1‐e3.
- ,,,,.Promoting alertness with a short nap during a night shift.J Sleep Res.1998;7:240–247.
- ,.Circadian adaptation to night‐shift work by judicious light and darkness exposure.J Biol Rhythms.2002;17:556–567.
- ,,,,,.Exposure to bright light and darkness to treat physiologic maladaptation to night work.N Engl J Med.1990;322:1253–1259.
- ,.Night shift performance is improved by a compromise circadian phase position: study 3. Circadian phase after 7 night shifts with an intervening weekend off.Sleep.2008;31:1639–1645.
- ,,,.Dose‐response relationship for light intensity and ocular and electroencephalographic correlates of human alertness.Behav Brain Res.2000;115:75–83.
- ,,,,.Dark goggles and bright light improve circadian rhythm adaptation to night‐shift work.Sleep.1994;17:535–543.
- ,,.Caffeine content of specialty coffees.J Anal Toxicol.2003;27:520–522.
- ,.Caffeine content of prepackaged national‐brand and private‐label carbonated beverages.J Food Sci.2007;72:C337–C342.
- ,,, et al.The effects of coffee and napping on nighttime highway driving: a randomized trial.Ann Intern Med.2006;144:785–791.
- ,,,,.Laboratory and field studies of naps and caffeine as practical countermeasures for sleep‐wake problems associated with night work.Sleep.2006;29:39–50.
- ,,,,.Armodafinil for treatment of excessive sleepiness associated with shift work disorder: a randomized controlled study.Mayo Clin Proc.2009;84:958–972.
- ,,,,.The long‐term tolerability and efficacy of armodafinil in patients with excessive sleepiness associated with treated obstructive sleep apnea, shift work disorder, or narcolepsy: an open‐label extension study.J Clin Sleep Med.2010;6:458–466.
- ,,.Circadian rhythm sleep disorders.Med Clin North Am.2004;88:631–651, viii.
- ,,.A three pulse phase response curve to three milligrams of melatonin in humans.J Physiol.2008;586:639–647.
- ,,, et al.Practice parameters for the clinical evaluation and treatment of circadian rhythm sleep disorders. An American Academy of Sleep Medicine report.Sleep.2007;30:1445–1459.
- ,,, et al.Efficacy and safety of exogenous melatonin for secondary sleep disorders and sleep disorders accompanying sleep restriction: meta‐analysis.BMJ.2006;332:385–393.
- ,,.Effects of melatonin administration on daytime sleep after simulated night shift work.J Sleep Res.2001;10:181–192.
- ,,,.Performance, ability to stay awake, and tendency to fall asleep during the night after a diurnal sleep with temazepam or placebo.Sleep.1997;20:535–541.
- ,,,,,.Sleepiness/alertness on a simulated night shift following sleep at home with triazolam.Sleep.1991;14:140–146.
- ,,,.Zolpidem‐related effects on performance and mood during simulated night‐shift work.Exp Clin Psychopharmacol.2003;11:259–268.
- ,,,,.Intrinsic near‐24‐h pacemaker period determines limits of circadian entrainment to a weak synchronizer in humans.Proc Natl Acad Sci USA.2001;98:14027–14032.
- ,,,.Work shift duration: a review comparing eight hour and 12 hour shift systems.Occup Environ Med.1998;55:217–229.
- ,,.Influence of flexibility and variability of working hours on health and well‐being.Chronobiol Int.2006;23:1125–1137.
- ,,.Impact of night‐float rotation on sleep, mood, and alertness: the resident's perception.Chronobiol Int.2002;19:893–902.
- ,,,,,.The characteristics of recovery sleep when recovery opportunity is restricted.Sleep.2007;30:353–360.
- ,,.Practical interventions to promote circadian adaptation to permanent night shift work: study 4.J Biol Rhythms.2009;24:161–172.
- ,,.Is there an association between shift work and having a metabolic syndrome? Results from a population based study of 27,485 people.Occup Environ Med.2001;58:747–752.
- ,.Use of sleep hygiene in the treatment of insomnia.Sleep Med Rev.2003;7:215–225.
For hospitalists, patient care is 24 hours a day. To provide continual patient care, shift work has become a way of life for hospitalists, similar to hospital nurses, residents in training, and emergency medicine physicians. Notably, they belong to a substantial minority of the workforce as shift workers, starting after 6 PM or before 6 AM, approximately one‐fifth of the total work force in industrialized nations.1, 2 Unfortunately, shift workers suffer from misalignment of their endogenous circadian system, which regulates daily sleep and alertness patterns, and work obligations beyond daylight hours. Such a misalignment can lead to fatigue, sleep loss, and excessive sleepiness, which can adversely affect personal health and safety, as well as the quality of medical care delivered.3
The relationship between shift work, extended work hours, and medical safety is a topic currently under intense scrutiny, as reviewed in the Institute of Medicine's (IOM) controversial report on residents and sleep.4 This publication led the Accreditation Council of Graduate Medical Education (ACGME) to mandate more changes to residents' work hours,5 adding to those first implemented in 2003.6 These restrictions forbid residents from working more than 30 consecutive hours, and required at least 10 hours off between shifts and an average of 1 day off in 7. Subsequent studies suggested that the reduction in resident work hours led to greater resident well‐being, fewer attention failures. and fewer medical errors.3, 7
In 2007, amid growing public concern over sleep‐deprived residents and patient safety, Congress requested the IOM investigate additional safeguards for residents.8 In 2008, the IOM published a report calling for more protection against resident fatigue.4 They recommended integrating a protected sleep period into any 24‐hour shift. If residents cannot get protected sleep time, then the maximal shift duration should not exceed 16 hoursreduced from the previous ACGME recommendation of 30. Further provisions to allow adequate sleep include capping the number of consecutive night shifts at 4, and extending the time off after a night shift. In response, the ACGME recently updated their recommendations effective July 1, 2011,5 though not following all the IOM's recommendations (Table 1).
| 2003 ACGME Limits | 2008 IOM Recommendation | 2010 ACGME Limits | |
|---|---|---|---|
| |||
| Maximum work hours per week | 80 hr, averaged over 4 wk | No change | No change |
| Maximum shift length | 30 hr (admitting patients up to 24 hr, with 6 hr of transition activities) | 30 hr (admitting patients up to 16 hr, with 5 hr protected sleep between 10 PM to 8 AM, and remaining hours for transition activities) | PGY‐1: 16 hr; PGY‐2 and above: 28 hr (admitting patients up to 24 hr, with 4 hr of transition activities) |
| Minimum time off between shifts | 10 hr after shift | 10 hr after day shift; 12 hr after night shift; 14 hr after any extended shift of 30 hr and not return until 6 AM the next day | 10 hr after shift; 14 hr free after 24‐hr shift for intermediate level residents |
| Maximum frequency of in‐hospital night shifts | No limits | 4 night maximum, with 48 hr off after 3 or 4 consecutive shifts | 6 consecutive night maximum |
The growing nationwide emphasis on fatigue prevention within healthcare settings now clearly impacts residents and their training schedule. But why focus only on residents? Why not other physicians, such as hospitalists, who work shifts to cover 24 hours each day? Are they any less prone to making medical errors when fatigued? Given that hospitalists' represent the fastest growing specialty in the history of American medicine,9 we sought to inform decisions about their scheduling by reviewing normal regulation of sleep and wake patterns, addressing the problems associated with misalignment between sleep and work, and identifying strategies to realign circadian schedules.
NORMAL SLEEP AND CIRCADIAN RHYTHMS
An understanding of sleep physiology begins with the endogenous circadian timekeeping system. At the center of this timekeeping system is a master circadian clock, located in the suprachiasmatic nucleus (SCN) of the hypothalamus. Cells within the SCN generate a near 24‐hour rhythm, transmitted through neural connections, to rhythmically influence the entire central nervous system and other bodily systems.10
The SCN and the circadian rhythm interact with the need to sleep (sleep homeostasis) to form the 2‐process model of sleepwakefulness.11 In this model, progression of biological day (a time when wakefulness and its associated functions are promoted) coincides with a rise in homeostatic pressure to sleep (see Figure 1). Daytime alertness is maintained by increasing SCN neuronal activity to counterbalance rising sleep pressure. After peaking in the early evening, SCN activity falls to begin biological night (a time when sleep and its associated functions are promoted). To facilitate the onset of biological night, the SCN coordinates the activity of sleep‐promoting centers and the release of melatonin from the pineal gland which promotes sleep.
This endogenous circadian clock runs slightly longer than 24 hours and must be resynchronized daily to the 24‐hour day, a process known as entrainment. This occurs primarily through environmental exposure of retinalhypothalamic links to the lightdark cycle. The intensity, duration, and wave length of light all influence the circadian system,12 but perhaps most importantly is the timing. In general, light exposure in the evening will shift the circadian clock later (phase delay shift), whereas light exposure in the morning will shift the clock earlier (phase advance shift). Exogenous melatonin can also shift the circadian system. However, when endogenous levels of melatonin are high, ingested melatonin has little influence on sleep.13
Balancing sleep and wakefulness requires an interweaving of endogenous and exogenous factors. This balance is disturbed if we try to sleep or be wakeful during incorrect endogenous biological times, a process called circadian misalignment.
DELETERIOUS EFFECTS OF CIRCADIAN MISALIGNMENT
Hospitalists and other shift workers required to work during the biological night risk circadian misalignment and, consequently, poor sleep, shift work disorder, errors on the job, and possibly long‐term health consequences.
Chronic Sleep Loss
When working at night or in the early morning, nearly 75% of shift workers encounter some amount of at‐work fatigue and sleepiness.14 After the shift is over, objective assessments among rotating shift workers15, 16 and interns7 demonstrated that day sleep is 1 to 4 hours shorter than night sleep. Chronic or recurring night shifts can therefore lead to chronic sleep loss. While it seems reasonable that permanent night shift workers have greater circadian adjustment to suit their work schedule, little evidence supports this argument.17 Permanent night shift workers may sleep a little longer during the day than rotating shift workers. Yet, the sleep quality does not match night sleep, presumably from conflict between external factors, such as light and activity, and the scheduled sleep period.
Shift Work Disorder
If severe and chronic, sleepiness and impaired performance during work hours and poor sleep during the day can be enough to warrant a diagnosis of shift work disorder (SWD), one of the several circadian rhythm sleep disorders (CRSD). The prevalence of SWD among rotating and night workers is estimated to be 10%25%.18 Patients with SWD can experience similar levels of nighttime sleepiness as patients with narcolepsy and sleep apnea.19 These patients experience reduced satisfaction with the work schedule, and suffer higher rates of depression, ulcers, and sleepiness‐related accidents, compared to other shift workers.18 What distinguishes those shift workers who suffer from normal fatigue and those with SWD is not easily identified. The International Classification of Sleep Disorders‐2 (ICSD‐2) lists the diagnostic criteria for SWD20:
-
Symptoms of insomnia associated with a work schedule that overlaps the usual time for sleep.
-
Symptoms are directly associated with shift work schedule over the course of at least 1 month.
-
Sleep log monitoring for at least 7 days demonstrates circadian and sleep‐time misalignment.
-
Sleep disturbance is not better explained by another sleep disorder or by a medical, neurological, or mental disorder; medication use; or substance‐use disorder.
Symptoms must be present for at least 1 month, and comorbid mood or sleep/wake disorders (commonly found in this disorder) need to be treated. SWD is more common among night shift workers, although those workers starting shifts between 4 AM and 7 AM (early morning shift) are also subject to SWD.21 Type of work schedule, along with physical or mental disorders, domestic responsibilities, and commute times are examples of factors that may increase vulnerability for SWD.18 In addition, genetic factors may explain the considerable inter‐individual differences in susceptibility to SWD. For example, a polymorphism in the circadian gene, PER 3, present in 10%15% of the population, is believed to decrease tolerability to acute sleep loss,22 while genetic variation in the adenosine A2A receptor may be associated with resistance to the effects of sleep loss.23 If a hospitalist suspects a diagnosis SWD, they should seek evaluation by a physician specializing in sleep medicine.
Errors
Disruption of the circadian rhythm influences neurocognitive and psychomotor function, and can lead to human error. Human errors that result in serious accidents or injuries typically result from interaction of circadian rhythm misalignment with multiple other factors, including task duration and complexity, motivation and proficiency, and level of sleep deprivation.24 Though difficult to isolate from the environmental and work experience factors, consistent evidence identifies circadian misalignment as a cause of errors and serious accidents. Most evidence comes from night shift workers trying to remain awake when the circadian signal for alertness is low, or attempting sleep when the circadian alerting signal is high. Compared to day workers, night shift workers are 1.63 times more likely to suffer a fatal accident.25 A study of critical care nurses revealed a prominent circadian pattern of inadvertent sleep episodes during work with the highest peak between 2 AM and 6 AM.26 In addition, nurses working the night shift have been shown to commit more medication administration errors than day workers.27
Medical errors among resident physicians during extended shift durations is well documented.28 On the other hand, not much research has examined error rates among attending physicians. In 1 small study, attending surgeons made more cognitive errors using a simulated laparoscopic exercise as the amount of on‐call overnight sleep decreased.29 A large, single‐center review reported an increased rate of complications among post‐nighttime surgical procedures performed by attendings who slept 6 hours or less the preceding night.30 Notably, proposed legislation would require physicians who have been awake 22 of the preceding 24 hours to inform patients of the potential safety impact of their sleep deprivation prior to providing clinical care.31
Chronic Health Morbidity
Several studies reveal the effect of shift work on chronic health conditions among healthcare workers, such as obesity, cardiovascular disease, and certain cancers (eg, breast, colorectal). These results are summarized in Table 2, with the largest evaluation of healthcare shift workers coming from the Nurses' Health Study.3234
| Disease | Study Design | Population | Comparison | Health Risk | Adjusted Risk Factors |
|---|---|---|---|---|---|
| |||||
| Acute myocardial infarction | Prospective cohort32 | 79,109 US nurses | Working 3 night shifts/mo for 6 yr | RR 1.51 | CAD risk factors, aspirin use, hormone replacement therapy |
| 95% CI (1.12‐2.03) | |||||
| Obesity (BMI 30) | Cross‐sectional72 | 27,485 Swedish workers | Shift‐workers vs day workers | OR 1.41 | Age, socioeconomic status |
| 95% CI (1.25‐1.59) | |||||
| Breast cancer | Prospective cohort33 | 116,087 US nurses | Working 3 night shifts/mo for 20 yr | RR 1.79 | Breast cancer risk factors |
| 95% CI (1.06‐3.01) | |||||
| Colon cancer | Prospective cohort34 | 78,586 US nurses | Working 3 night shifts/mo for 15 yr | RR 1.35 | Family history of colon cancer, dietary intake, activity |
| 95% CI (1.03‐1.77) | |||||
Some believe that adverse health outcomes in shift workers derive from circadian stressan alteration of psychosocial and physiological homeostasis (eg, increased cortisol and catecholamine output) resulting from circadian misalignment.35 Based on data suggesting an increased risk for certain cancers among shift workers, the International Agency for Research of Cancer, a unit of the World Health Organization, announced that shift work resulting in circadian misalignment is probably carcinogenic.36 Researchers propose several biologic mechanisms to explain the increased cancer riskmost revolve around the alteration of the melatonin circadian cycle, found in night shift workers,37 and subsequent disruption of its believed cancer‐protective biologic pathways.
Overall, however, the heterogeneous nature of shift work limits conclusions regarding the long‐term health of shift workers. That is, as the shift work intensity and composition varies, and as the number and timing of these shifts change, so too can the adverse health consequences.
HOSPITALISTS AND NIGHT SHIFTS
Hospital medicine is the fastest growing specialty in the history of medicine, with an estimated 30,000 practicing hospitalists in 2010.38 Survey results from 2009 indicate that hospitalists staff 58% of hospitals; 89% of hospitals with more than 200 beds (J. Miller, Society of Hospital Medicine, personal communication). One reason for the growth in the number of hospitalists at academic medical centers has been the imposed work‐hour restrictions for residents.39
Across the county, hospitalist programs use a variety of shift work systems to ensure 24‐hour patient care. Among those programs that provide continuous on‐site coverage, many staff 3 shiftsday, late afternoon/evening (swing), and night shifts. Some permanently partition the scheduling, with dedicated night hospitalists or nocturnists.40
Hospitalists do not have mandated work‐hour restrictions and, in general, are older than resident physicians. Whether or not hospitalists who trained before the era of work‐hour regulations are better prepared for practicing in a real‐world, after‐hours scenario than hospitalists with previous work‐hour restrictions is a matter of debate. That said, hospitalists who are fatigued, just like residents, may be at increased risk for committing medical errors, particularly when the fatigue is unrecognized. Yet, limiting hospitalists' work hours would have obvious financial implications, likely similar those from resident work‐hour reductions.41 As part of the ACGME 2011 recommendations, faculty and residents now must be trained to recognize signs of fatigue and sleep deprivation, and adopt management strategies such as naps or backup call schedules. Fatigue that results in excessive sleepiness while at work may manifest as weariness, difficulty concentrating, headache, irritability or depressed mood, and feeling unrefreshed after sleeping.42
STRATEGIES TO IMPROVE CIRCADIAN ADAPTATION
Hospitalists can help limit fatigue and improve performance and safety through circadian adaptation: a multimodal approach to realign work and circadian schedules. Depending on whether the shift starts at night or in the early morning (4 AM to 7 AM), circadian adaptation aims may differ. For night shift workers, the overall aim is to delay the timing of circadian rhythms such that the highest propensity of wakefulness occurs during the night work period, while the highest propensity for sleep occurs during the day.17, 43 For early morning shift workers, circadian rhythms for wakefulness and sleep propensity should be shifted earlier. Circadian adaptation involves not only sleeping well before work, but also preventing dips in wakefulness during work. Adaptation strategies are listed in Table 3.
| Night Shift60 | Early Day Shift (Starting at 4 AM‐7 AM) | |
|---|---|---|
| Prior to shift | Avoid sleep debt | Avoid sleep debt |
| Proper sleep hygiene | Proper sleep hygiene | |
| Planned napping | Bright light exposure | |
| Caffeine use | ||
| During the shift | Bright light exposure | Caffeine use |
| Planned napping | ||
| After the shift | Avoid bright light | Avoid late evening bright light (when applicable) |
| Melatonin prior to sleep | ||
| Careful use of other hypnotics | Initiate sleep early |
Improved Sleep Before Work
As an essential first step, hospitalists must get a full night's rest before starting a night shift, as sleep debt will worsen fatigue while at work. Tips for proper sleep hygiene are listed in Table 4. Some shift workers stay up late the night before a scheduled night shift, in order to sleep during the day and awaken shortly before their scheduled night shift, to combat fatigue at work. Such an approach to shift work is typically met with 3 barriers. First, environmental factors often prevent 6 hours of uninterrupted day sleep. Second, 6 hours of continual day sleep is typically difficult because rising circadian activity often limits the sleep period to just a few hours. Third, an adequate amount of sleep prior to a night shift will itself not be enough to prevent sleepiness from occurring after midnightreducing the fall in circadian activity is also essential to maintaining alertness and performance.
| Physical | Adhere to regular wake and sleep schedule |
| activities73 | Engage in regular exercise early in the day |
| Avoid caffeine, nicotine, and alcohol use 6 hr prior to sleeping | |
| Avoid stimulating or stressful activities 30 min prior to sleeping | |
| Proper sleep | Well ventilated, temperature‐controlled bedroom |
| environment | Use heavy curtains to provide as much darkness as possible |
| Comfortable mattress and pillow | |
| Remove television and pets from the bedroom | |
| Housemates should help provide quiet sleep environment |
Napping
Napping prior to a night shift, or during the work shift, can improve alertness and performance and decrease accident rates.44, 45 During shift work, naps of 20 to 50 minutes in duration have demonstrated improvements in reaction time, and restoration of performance to that seen at the start of the shift. Napping early in the night shift can improve objective measures of alertness.44 To avoid increased drowsiness that sometimes occurs when waking from a nap, naps should not be longer than 50 minutes, and can be as short as 10 to 15 minutes.44, 46 Although effective, napping may be impractical for many workers due to time or space constraints. To facilitate brief naps, hospitalist practices should ensure they have a dark, quiet call room for use by overnight hospitalists.
Bright Light Exposure
Studies demonstrate that light exposure during the night shift improves circadian alignment, mood, and performance during the night shift.47, 48 Light exposure ranged from 6 hours to 5 light treatments of 15 minutes each, with brightness ranging from 2,500 to 10,000 lux (approximating outdoor daylight; typical office lighting provides 200‐500 lux).47, 49 Results demonstrate that bright light exposure during the night shift acutely improves alertness and performance, though not to daytime levels.50 The greatest circadian adjustments occur in groups using both bright light during the night shift and light avoidance the following morning.51 Dark sunglasses and a dark home environment can decrease bright light exposure during the day. Though little evidence exists to support widespread application of bright light devices in hospitalists' call‐rooms, a hospitalist practice should consider installing one to promote circadian adaptation if physicians working overnight have multiple consecutive shifts. Likewise, these physicians should be vigilant and wear dark sunglasses during the day after their night shifteven a few minutes of light exposure at the wrong time of the day may disrupt the intended circadian adaptation.
Wake‐Promoting Agents
Numerous studies demonstrate that 150 mg to 400 mg of caffeine (a 16 oz grande cup of coffee from Starbucks contains between 200 to 500 mg of caffeine52; a Diet Coke contains 46 mg/12 oz53) reduces sleepiness, increases alertness, and improves performance during the night shift.54, 55 Thus, judicious use of caffeine may be recommended in hospital practices during extended work hours. Other wake‐promoting agents, such as modafinil and armodafinil, are US Food and Drug Administration (FDA)‐approved in the treatment of excessive sleepiness associated with SWD. Typically taken 3060 minutes before the start of the night shift, these medications have been shown in trials, enrolling mostly permanent night shift workers, to reduce excessive nighttime sleepiness and improve performance.19, 56 Armodafinil used to treat SWD‐associated excessive sleepiness, has been safely tolerated for durations of 1 year or more.57 However, these agents are not approved for use in patients without a diagnosed sleep disorder.
Melatonin
Exogenous melatonin has been used to reset circadian rhythms in patients with CRSDs.58 Melatonin administered in the late afternoon to early evening directs the largest phase advance. In contrast, melatonin given in the morning produces the largest phase delays.59 When taken after a night shift, melatonin (at a dose 1.8 to 3.0 mg) can improve day sleep quality and duration.60 Despite this result, melatonin's effectiveness in improving circadian adaptation has been mixed.61 For example, improvements in nighttime alertness during the night shift were not seen, despite the use of melatonin to facilitate daytime sleep beforehand.62 Hospitalists may consider a trial of melatonin to improve circadian alignment and facilitate daytime sleep, but its chronic use and long‐term safety has not been adequately studied.
Hypnotics After Work
Hypnotics such as temazepam 20 mg,63 triazolam,64 and zolpidem65 taken after night shift work have been shown to improve day sleep quality under simulated conditions, but do not improve shift work performance. These medications should be reserved for judicious short‐term use in patients with insomnia associated with SWD.
NIGHT SHIFT SCHEDULING TO REDUCE CIRCADIAN MISALIGNMENT
When providing 24‐hour, on‐site medical care, questions may arise about how to incorporate circadian adaptation into the daily schedule.
How Should Shifts Be Rotated?
When scheduling shifts with different start times, evidence suggests that sleep disturbance is reduced with a clockwise progression in shifts (eg, day shift to evening shift to night shift). This reduction in sleep disturbance is thought due to increased time between shifts and the circadian timekeeping tendency to extend beyond 24 hours.66
When Should the Night Shift Start?
Those hospitalist programs using an evening swing shift from afternoon to late evening may have the option of using a 12‐hour night shift starting around 7 PM, or a shorter night shift beginning later at night. Though there are no data among hospitalists to suggest which night shift start time and duration would lead to the least amount of fatigue and errors, healthcare providers working a 12‐hour night shift may have increased morale due to fewer shifts, but may suffer a reduction in the quality of care provided compared with working an 8‐hour night shift.67 In either case, shift workers given flexibility in scheduling have been shown to have positive effects on sleep.68
Should Night Shifts Be Bunched?
The decision to bunch night shifts together depends on how many night shifts are required, and how quickly circadian adaptation can occur. Under simulated conditions, circadian adaptation can yield significant changes in sleep/wake cycles in as little as 4 days.48 In real‐world settings, more time may be required to achieve significant shifts in the circadian cycle. Therefore, hospitalists who have 7 or fewer night shifts during the academic year may want to space the shifts out to prevent sleep debt on consecutive shifts, since significant circadian adaptation would be difficult to achieve in less than a week. In this situation, after a night shift, the hospitalist should have at least one 9‐hour sleep period at night to relieve their sleep debt before staffing another night shift.69 Consecutive night shifts require at least 2 nighttime sleep periods of 9 hours to recover from sleep debt.70 The IOM recommends setting a limit of 4 consecutive night float shifts for resident physicians, however, a recent systematic review of resident night float models did not find data supporting use of a 4‐night‐maximum model.28
If more than 7 night shifts are required, then scheduling the shifts close together with use of circadian adaptation techniques may result in increased nighttime alertness, less fatigue, and fewer errors while at work than widely spacing out the shifts. For example, 1 recent study simulated 8 night shifts over a 10‐day period, and compared circadian schedules and work performance between those subjects who used circadian adaptation strategies and those that did not.71 Circadian adaptation techniques included: four 15‐minute bright light pulses during each night shift, dark sunglasses when outside, dark bedrooms and delayed sleeping until 3 AM on the nights off in between the night shift blocks. The group who shifted their circadian schedule improved night shift alertness and performance as measured by neurophysiological testing, while permitting sufficient daytime sleep after work, as well as late‐night sleep on days off. The group without circadian interventions did not shift their circadian schedule as significantly as the intervention group, and performed worse on the performance testing.
CONCLUSIONS
The nationwide use of hospitalists to provide 24‐hour patient care continues to expand, thus subjecting more hospitalists to work hours asynchronous with the lightdark cycle. Resultant circadian misalignment can result in fatigue while at work, shift work disorder, and, potentially, an increased rate of medical errors. Recognition of these dangers among resident physicians has prompted the ACGME to intensify their regulations on work hours, shift schedules, and time off between shifts. However, no such recommendations exist for hospitalists or emergency physicians and nurses.
Given the potential risk to both physicians and patients, we recommend more research examining the effects of circadian misalignment within the hospitalist community. Sample research questions are offered in Table 5. More information is urgently needed to provide evidence‐based practice guidelines to ensure the safety of this growing workforce and the patients they treat.
| Are hospitalists more immune to fatigue than resident physicians? |
| Are hospitalists better able to recognize fatigue while at work than resident physicians? |
| Does 1 shift work schedule promote better circadian alignment than other shift schedules? |
| Do consistent nighttime hours of nocturnists make them more prone to commit medical errors than hospitalists rotating their shifts? |
For hospitalists, patient care is 24 hours a day. To provide continual patient care, shift work has become a way of life for hospitalists, similar to hospital nurses, residents in training, and emergency medicine physicians. Notably, they belong to a substantial minority of the workforce as shift workers, starting after 6 PM or before 6 AM, approximately one‐fifth of the total work force in industrialized nations.1, 2 Unfortunately, shift workers suffer from misalignment of their endogenous circadian system, which regulates daily sleep and alertness patterns, and work obligations beyond daylight hours. Such a misalignment can lead to fatigue, sleep loss, and excessive sleepiness, which can adversely affect personal health and safety, as well as the quality of medical care delivered.3
The relationship between shift work, extended work hours, and medical safety is a topic currently under intense scrutiny, as reviewed in the Institute of Medicine's (IOM) controversial report on residents and sleep.4 This publication led the Accreditation Council of Graduate Medical Education (ACGME) to mandate more changes to residents' work hours,5 adding to those first implemented in 2003.6 These restrictions forbid residents from working more than 30 consecutive hours, and required at least 10 hours off between shifts and an average of 1 day off in 7. Subsequent studies suggested that the reduction in resident work hours led to greater resident well‐being, fewer attention failures. and fewer medical errors.3, 7
In 2007, amid growing public concern over sleep‐deprived residents and patient safety, Congress requested the IOM investigate additional safeguards for residents.8 In 2008, the IOM published a report calling for more protection against resident fatigue.4 They recommended integrating a protected sleep period into any 24‐hour shift. If residents cannot get protected sleep time, then the maximal shift duration should not exceed 16 hoursreduced from the previous ACGME recommendation of 30. Further provisions to allow adequate sleep include capping the number of consecutive night shifts at 4, and extending the time off after a night shift. In response, the ACGME recently updated their recommendations effective July 1, 2011,5 though not following all the IOM's recommendations (Table 1).
| 2003 ACGME Limits | 2008 IOM Recommendation | 2010 ACGME Limits | |
|---|---|---|---|
| |||
| Maximum work hours per week | 80 hr, averaged over 4 wk | No change | No change |
| Maximum shift length | 30 hr (admitting patients up to 24 hr, with 6 hr of transition activities) | 30 hr (admitting patients up to 16 hr, with 5 hr protected sleep between 10 PM to 8 AM, and remaining hours for transition activities) | PGY‐1: 16 hr; PGY‐2 and above: 28 hr (admitting patients up to 24 hr, with 4 hr of transition activities) |
| Minimum time off between shifts | 10 hr after shift | 10 hr after day shift; 12 hr after night shift; 14 hr after any extended shift of 30 hr and not return until 6 AM the next day | 10 hr after shift; 14 hr free after 24‐hr shift for intermediate level residents |
| Maximum frequency of in‐hospital night shifts | No limits | 4 night maximum, with 48 hr off after 3 or 4 consecutive shifts | 6 consecutive night maximum |
The growing nationwide emphasis on fatigue prevention within healthcare settings now clearly impacts residents and their training schedule. But why focus only on residents? Why not other physicians, such as hospitalists, who work shifts to cover 24 hours each day? Are they any less prone to making medical errors when fatigued? Given that hospitalists' represent the fastest growing specialty in the history of American medicine,9 we sought to inform decisions about their scheduling by reviewing normal regulation of sleep and wake patterns, addressing the problems associated with misalignment between sleep and work, and identifying strategies to realign circadian schedules.
NORMAL SLEEP AND CIRCADIAN RHYTHMS
An understanding of sleep physiology begins with the endogenous circadian timekeeping system. At the center of this timekeeping system is a master circadian clock, located in the suprachiasmatic nucleus (SCN) of the hypothalamus. Cells within the SCN generate a near 24‐hour rhythm, transmitted through neural connections, to rhythmically influence the entire central nervous system and other bodily systems.10
The SCN and the circadian rhythm interact with the need to sleep (sleep homeostasis) to form the 2‐process model of sleepwakefulness.11 In this model, progression of biological day (a time when wakefulness and its associated functions are promoted) coincides with a rise in homeostatic pressure to sleep (see Figure 1). Daytime alertness is maintained by increasing SCN neuronal activity to counterbalance rising sleep pressure. After peaking in the early evening, SCN activity falls to begin biological night (a time when sleep and its associated functions are promoted). To facilitate the onset of biological night, the SCN coordinates the activity of sleep‐promoting centers and the release of melatonin from the pineal gland which promotes sleep.
This endogenous circadian clock runs slightly longer than 24 hours and must be resynchronized daily to the 24‐hour day, a process known as entrainment. This occurs primarily through environmental exposure of retinalhypothalamic links to the lightdark cycle. The intensity, duration, and wave length of light all influence the circadian system,12 but perhaps most importantly is the timing. In general, light exposure in the evening will shift the circadian clock later (phase delay shift), whereas light exposure in the morning will shift the clock earlier (phase advance shift). Exogenous melatonin can also shift the circadian system. However, when endogenous levels of melatonin are high, ingested melatonin has little influence on sleep.13
Balancing sleep and wakefulness requires an interweaving of endogenous and exogenous factors. This balance is disturbed if we try to sleep or be wakeful during incorrect endogenous biological times, a process called circadian misalignment.
DELETERIOUS EFFECTS OF CIRCADIAN MISALIGNMENT
Hospitalists and other shift workers required to work during the biological night risk circadian misalignment and, consequently, poor sleep, shift work disorder, errors on the job, and possibly long‐term health consequences.
Chronic Sleep Loss
When working at night or in the early morning, nearly 75% of shift workers encounter some amount of at‐work fatigue and sleepiness.14 After the shift is over, objective assessments among rotating shift workers15, 16 and interns7 demonstrated that day sleep is 1 to 4 hours shorter than night sleep. Chronic or recurring night shifts can therefore lead to chronic sleep loss. While it seems reasonable that permanent night shift workers have greater circadian adjustment to suit their work schedule, little evidence supports this argument.17 Permanent night shift workers may sleep a little longer during the day than rotating shift workers. Yet, the sleep quality does not match night sleep, presumably from conflict between external factors, such as light and activity, and the scheduled sleep period.
Shift Work Disorder
If severe and chronic, sleepiness and impaired performance during work hours and poor sleep during the day can be enough to warrant a diagnosis of shift work disorder (SWD), one of the several circadian rhythm sleep disorders (CRSD). The prevalence of SWD among rotating and night workers is estimated to be 10%25%.18 Patients with SWD can experience similar levels of nighttime sleepiness as patients with narcolepsy and sleep apnea.19 These patients experience reduced satisfaction with the work schedule, and suffer higher rates of depression, ulcers, and sleepiness‐related accidents, compared to other shift workers.18 What distinguishes those shift workers who suffer from normal fatigue and those with SWD is not easily identified. The International Classification of Sleep Disorders‐2 (ICSD‐2) lists the diagnostic criteria for SWD20:
-
Symptoms of insomnia associated with a work schedule that overlaps the usual time for sleep.
-
Symptoms are directly associated with shift work schedule over the course of at least 1 month.
-
Sleep log monitoring for at least 7 days demonstrates circadian and sleep‐time misalignment.
-
Sleep disturbance is not better explained by another sleep disorder or by a medical, neurological, or mental disorder; medication use; or substance‐use disorder.
Symptoms must be present for at least 1 month, and comorbid mood or sleep/wake disorders (commonly found in this disorder) need to be treated. SWD is more common among night shift workers, although those workers starting shifts between 4 AM and 7 AM (early morning shift) are also subject to SWD.21 Type of work schedule, along with physical or mental disorders, domestic responsibilities, and commute times are examples of factors that may increase vulnerability for SWD.18 In addition, genetic factors may explain the considerable inter‐individual differences in susceptibility to SWD. For example, a polymorphism in the circadian gene, PER 3, present in 10%15% of the population, is believed to decrease tolerability to acute sleep loss,22 while genetic variation in the adenosine A2A receptor may be associated with resistance to the effects of sleep loss.23 If a hospitalist suspects a diagnosis SWD, they should seek evaluation by a physician specializing in sleep medicine.
Errors
Disruption of the circadian rhythm influences neurocognitive and psychomotor function, and can lead to human error. Human errors that result in serious accidents or injuries typically result from interaction of circadian rhythm misalignment with multiple other factors, including task duration and complexity, motivation and proficiency, and level of sleep deprivation.24 Though difficult to isolate from the environmental and work experience factors, consistent evidence identifies circadian misalignment as a cause of errors and serious accidents. Most evidence comes from night shift workers trying to remain awake when the circadian signal for alertness is low, or attempting sleep when the circadian alerting signal is high. Compared to day workers, night shift workers are 1.63 times more likely to suffer a fatal accident.25 A study of critical care nurses revealed a prominent circadian pattern of inadvertent sleep episodes during work with the highest peak between 2 AM and 6 AM.26 In addition, nurses working the night shift have been shown to commit more medication administration errors than day workers.27
Medical errors among resident physicians during extended shift durations is well documented.28 On the other hand, not much research has examined error rates among attending physicians. In 1 small study, attending surgeons made more cognitive errors using a simulated laparoscopic exercise as the amount of on‐call overnight sleep decreased.29 A large, single‐center review reported an increased rate of complications among post‐nighttime surgical procedures performed by attendings who slept 6 hours or less the preceding night.30 Notably, proposed legislation would require physicians who have been awake 22 of the preceding 24 hours to inform patients of the potential safety impact of their sleep deprivation prior to providing clinical care.31
Chronic Health Morbidity
Several studies reveal the effect of shift work on chronic health conditions among healthcare workers, such as obesity, cardiovascular disease, and certain cancers (eg, breast, colorectal). These results are summarized in Table 2, with the largest evaluation of healthcare shift workers coming from the Nurses' Health Study.3234
| Disease | Study Design | Population | Comparison | Health Risk | Adjusted Risk Factors |
|---|---|---|---|---|---|
| |||||
| Acute myocardial infarction | Prospective cohort32 | 79,109 US nurses | Working 3 night shifts/mo for 6 yr | RR 1.51 | CAD risk factors, aspirin use, hormone replacement therapy |
| 95% CI (1.12‐2.03) | |||||
| Obesity (BMI 30) | Cross‐sectional72 | 27,485 Swedish workers | Shift‐workers vs day workers | OR 1.41 | Age, socioeconomic status |
| 95% CI (1.25‐1.59) | |||||
| Breast cancer | Prospective cohort33 | 116,087 US nurses | Working 3 night shifts/mo for 20 yr | RR 1.79 | Breast cancer risk factors |
| 95% CI (1.06‐3.01) | |||||
| Colon cancer | Prospective cohort34 | 78,586 US nurses | Working 3 night shifts/mo for 15 yr | RR 1.35 | Family history of colon cancer, dietary intake, activity |
| 95% CI (1.03‐1.77) | |||||
Some believe that adverse health outcomes in shift workers derive from circadian stressan alteration of psychosocial and physiological homeostasis (eg, increased cortisol and catecholamine output) resulting from circadian misalignment.35 Based on data suggesting an increased risk for certain cancers among shift workers, the International Agency for Research of Cancer, a unit of the World Health Organization, announced that shift work resulting in circadian misalignment is probably carcinogenic.36 Researchers propose several biologic mechanisms to explain the increased cancer riskmost revolve around the alteration of the melatonin circadian cycle, found in night shift workers,37 and subsequent disruption of its believed cancer‐protective biologic pathways.
Overall, however, the heterogeneous nature of shift work limits conclusions regarding the long‐term health of shift workers. That is, as the shift work intensity and composition varies, and as the number and timing of these shifts change, so too can the adverse health consequences.
HOSPITALISTS AND NIGHT SHIFTS
Hospital medicine is the fastest growing specialty in the history of medicine, with an estimated 30,000 practicing hospitalists in 2010.38 Survey results from 2009 indicate that hospitalists staff 58% of hospitals; 89% of hospitals with more than 200 beds (J. Miller, Society of Hospital Medicine, personal communication). One reason for the growth in the number of hospitalists at academic medical centers has been the imposed work‐hour restrictions for residents.39
Across the county, hospitalist programs use a variety of shift work systems to ensure 24‐hour patient care. Among those programs that provide continuous on‐site coverage, many staff 3 shiftsday, late afternoon/evening (swing), and night shifts. Some permanently partition the scheduling, with dedicated night hospitalists or nocturnists.40
Hospitalists do not have mandated work‐hour restrictions and, in general, are older than resident physicians. Whether or not hospitalists who trained before the era of work‐hour regulations are better prepared for practicing in a real‐world, after‐hours scenario than hospitalists with previous work‐hour restrictions is a matter of debate. That said, hospitalists who are fatigued, just like residents, may be at increased risk for committing medical errors, particularly when the fatigue is unrecognized. Yet, limiting hospitalists' work hours would have obvious financial implications, likely similar those from resident work‐hour reductions.41 As part of the ACGME 2011 recommendations, faculty and residents now must be trained to recognize signs of fatigue and sleep deprivation, and adopt management strategies such as naps or backup call schedules. Fatigue that results in excessive sleepiness while at work may manifest as weariness, difficulty concentrating, headache, irritability or depressed mood, and feeling unrefreshed after sleeping.42
STRATEGIES TO IMPROVE CIRCADIAN ADAPTATION
Hospitalists can help limit fatigue and improve performance and safety through circadian adaptation: a multimodal approach to realign work and circadian schedules. Depending on whether the shift starts at night or in the early morning (4 AM to 7 AM), circadian adaptation aims may differ. For night shift workers, the overall aim is to delay the timing of circadian rhythms such that the highest propensity of wakefulness occurs during the night work period, while the highest propensity for sleep occurs during the day.17, 43 For early morning shift workers, circadian rhythms for wakefulness and sleep propensity should be shifted earlier. Circadian adaptation involves not only sleeping well before work, but also preventing dips in wakefulness during work. Adaptation strategies are listed in Table 3.
| Night Shift60 | Early Day Shift (Starting at 4 AM‐7 AM) | |
|---|---|---|
| Prior to shift | Avoid sleep debt | Avoid sleep debt |
| Proper sleep hygiene | Proper sleep hygiene | |
| Planned napping | Bright light exposure | |
| Caffeine use | ||
| During the shift | Bright light exposure | Caffeine use |
| Planned napping | ||
| After the shift | Avoid bright light | Avoid late evening bright light (when applicable) |
| Melatonin prior to sleep | ||
| Careful use of other hypnotics | Initiate sleep early |
Improved Sleep Before Work
As an essential first step, hospitalists must get a full night's rest before starting a night shift, as sleep debt will worsen fatigue while at work. Tips for proper sleep hygiene are listed in Table 4. Some shift workers stay up late the night before a scheduled night shift, in order to sleep during the day and awaken shortly before their scheduled night shift, to combat fatigue at work. Such an approach to shift work is typically met with 3 barriers. First, environmental factors often prevent 6 hours of uninterrupted day sleep. Second, 6 hours of continual day sleep is typically difficult because rising circadian activity often limits the sleep period to just a few hours. Third, an adequate amount of sleep prior to a night shift will itself not be enough to prevent sleepiness from occurring after midnightreducing the fall in circadian activity is also essential to maintaining alertness and performance.
| Physical | Adhere to regular wake and sleep schedule |
| activities73 | Engage in regular exercise early in the day |
| Avoid caffeine, nicotine, and alcohol use 6 hr prior to sleeping | |
| Avoid stimulating or stressful activities 30 min prior to sleeping | |
| Proper sleep | Well ventilated, temperature‐controlled bedroom |
| environment | Use heavy curtains to provide as much darkness as possible |
| Comfortable mattress and pillow | |
| Remove television and pets from the bedroom | |
| Housemates should help provide quiet sleep environment |
Napping
Napping prior to a night shift, or during the work shift, can improve alertness and performance and decrease accident rates.44, 45 During shift work, naps of 20 to 50 minutes in duration have demonstrated improvements in reaction time, and restoration of performance to that seen at the start of the shift. Napping early in the night shift can improve objective measures of alertness.44 To avoid increased drowsiness that sometimes occurs when waking from a nap, naps should not be longer than 50 minutes, and can be as short as 10 to 15 minutes.44, 46 Although effective, napping may be impractical for many workers due to time or space constraints. To facilitate brief naps, hospitalist practices should ensure they have a dark, quiet call room for use by overnight hospitalists.
Bright Light Exposure
Studies demonstrate that light exposure during the night shift improves circadian alignment, mood, and performance during the night shift.47, 48 Light exposure ranged from 6 hours to 5 light treatments of 15 minutes each, with brightness ranging from 2,500 to 10,000 lux (approximating outdoor daylight; typical office lighting provides 200‐500 lux).47, 49 Results demonstrate that bright light exposure during the night shift acutely improves alertness and performance, though not to daytime levels.50 The greatest circadian adjustments occur in groups using both bright light during the night shift and light avoidance the following morning.51 Dark sunglasses and a dark home environment can decrease bright light exposure during the day. Though little evidence exists to support widespread application of bright light devices in hospitalists' call‐rooms, a hospitalist practice should consider installing one to promote circadian adaptation if physicians working overnight have multiple consecutive shifts. Likewise, these physicians should be vigilant and wear dark sunglasses during the day after their night shifteven a few minutes of light exposure at the wrong time of the day may disrupt the intended circadian adaptation.
Wake‐Promoting Agents
Numerous studies demonstrate that 150 mg to 400 mg of caffeine (a 16 oz grande cup of coffee from Starbucks contains between 200 to 500 mg of caffeine52; a Diet Coke contains 46 mg/12 oz53) reduces sleepiness, increases alertness, and improves performance during the night shift.54, 55 Thus, judicious use of caffeine may be recommended in hospital practices during extended work hours. Other wake‐promoting agents, such as modafinil and armodafinil, are US Food and Drug Administration (FDA)‐approved in the treatment of excessive sleepiness associated with SWD. Typically taken 3060 minutes before the start of the night shift, these medications have been shown in trials, enrolling mostly permanent night shift workers, to reduce excessive nighttime sleepiness and improve performance.19, 56 Armodafinil used to treat SWD‐associated excessive sleepiness, has been safely tolerated for durations of 1 year or more.57 However, these agents are not approved for use in patients without a diagnosed sleep disorder.
Melatonin
Exogenous melatonin has been used to reset circadian rhythms in patients with CRSDs.58 Melatonin administered in the late afternoon to early evening directs the largest phase advance. In contrast, melatonin given in the morning produces the largest phase delays.59 When taken after a night shift, melatonin (at a dose 1.8 to 3.0 mg) can improve day sleep quality and duration.60 Despite this result, melatonin's effectiveness in improving circadian adaptation has been mixed.61 For example, improvements in nighttime alertness during the night shift were not seen, despite the use of melatonin to facilitate daytime sleep beforehand.62 Hospitalists may consider a trial of melatonin to improve circadian alignment and facilitate daytime sleep, but its chronic use and long‐term safety has not been adequately studied.
Hypnotics After Work
Hypnotics such as temazepam 20 mg,63 triazolam,64 and zolpidem65 taken after night shift work have been shown to improve day sleep quality under simulated conditions, but do not improve shift work performance. These medications should be reserved for judicious short‐term use in patients with insomnia associated with SWD.
NIGHT SHIFT SCHEDULING TO REDUCE CIRCADIAN MISALIGNMENT
When providing 24‐hour, on‐site medical care, questions may arise about how to incorporate circadian adaptation into the daily schedule.
How Should Shifts Be Rotated?
When scheduling shifts with different start times, evidence suggests that sleep disturbance is reduced with a clockwise progression in shifts (eg, day shift to evening shift to night shift). This reduction in sleep disturbance is thought due to increased time between shifts and the circadian timekeeping tendency to extend beyond 24 hours.66
When Should the Night Shift Start?
Those hospitalist programs using an evening swing shift from afternoon to late evening may have the option of using a 12‐hour night shift starting around 7 PM, or a shorter night shift beginning later at night. Though there are no data among hospitalists to suggest which night shift start time and duration would lead to the least amount of fatigue and errors, healthcare providers working a 12‐hour night shift may have increased morale due to fewer shifts, but may suffer a reduction in the quality of care provided compared with working an 8‐hour night shift.67 In either case, shift workers given flexibility in scheduling have been shown to have positive effects on sleep.68
Should Night Shifts Be Bunched?
The decision to bunch night shifts together depends on how many night shifts are required, and how quickly circadian adaptation can occur. Under simulated conditions, circadian adaptation can yield significant changes in sleep/wake cycles in as little as 4 days.48 In real‐world settings, more time may be required to achieve significant shifts in the circadian cycle. Therefore, hospitalists who have 7 or fewer night shifts during the academic year may want to space the shifts out to prevent sleep debt on consecutive shifts, since significant circadian adaptation would be difficult to achieve in less than a week. In this situation, after a night shift, the hospitalist should have at least one 9‐hour sleep period at night to relieve their sleep debt before staffing another night shift.69 Consecutive night shifts require at least 2 nighttime sleep periods of 9 hours to recover from sleep debt.70 The IOM recommends setting a limit of 4 consecutive night float shifts for resident physicians, however, a recent systematic review of resident night float models did not find data supporting use of a 4‐night‐maximum model.28
If more than 7 night shifts are required, then scheduling the shifts close together with use of circadian adaptation techniques may result in increased nighttime alertness, less fatigue, and fewer errors while at work than widely spacing out the shifts. For example, 1 recent study simulated 8 night shifts over a 10‐day period, and compared circadian schedules and work performance between those subjects who used circadian adaptation strategies and those that did not.71 Circadian adaptation techniques included: four 15‐minute bright light pulses during each night shift, dark sunglasses when outside, dark bedrooms and delayed sleeping until 3 AM on the nights off in between the night shift blocks. The group who shifted their circadian schedule improved night shift alertness and performance as measured by neurophysiological testing, while permitting sufficient daytime sleep after work, as well as late‐night sleep on days off. The group without circadian interventions did not shift their circadian schedule as significantly as the intervention group, and performed worse on the performance testing.
CONCLUSIONS
The nationwide use of hospitalists to provide 24‐hour patient care continues to expand, thus subjecting more hospitalists to work hours asynchronous with the lightdark cycle. Resultant circadian misalignment can result in fatigue while at work, shift work disorder, and, potentially, an increased rate of medical errors. Recognition of these dangers among resident physicians has prompted the ACGME to intensify their regulations on work hours, shift schedules, and time off between shifts. However, no such recommendations exist for hospitalists or emergency physicians and nurses.
Given the potential risk to both physicians and patients, we recommend more research examining the effects of circadian misalignment within the hospitalist community. Sample research questions are offered in Table 5. More information is urgently needed to provide evidence‐based practice guidelines to ensure the safety of this growing workforce and the patients they treat.
| Are hospitalists more immune to fatigue than resident physicians? |
| Are hospitalists better able to recognize fatigue while at work than resident physicians? |
| Does 1 shift work schedule promote better circadian alignment than other shift schedules? |
| Do consistent nighttime hours of nocturnists make them more prone to commit medical errors than hospitalists rotating their shifts? |
- .Job, family, and gender: determinants of nonstandard work schedules among employed Americans in 1991.Demography.1995;32:577–598.
- ,.Shift work among dual‐earner couples with children.Science.1983;219:876–879.
- ,,, et al.Effect of reducing interns' work hours on serious medical errors in intensive care units.N Engl J Med.2004;351:1838–1848.
- Institute of Medicine. Resident Duty Hours: Enhancing Sleep, Supervision and Safety. Released December 15,2008. Available at: http://www.iom.edu/Reports/2008/Resident‐Duty‐Hours‐Enhancing‐Sleep‐Supervision‐and‐Safety.aspx. Accessed on October 20, 2010.
- ACGME. ACGME Approved Standards. Effective July2011. Available at: http://acgme‐2010standards.org/. Accessed on January 6, 2011
- ACGME. Common Program Requirements: Resident Duty Hours in the Learning and Work Environment. Effective July 1, 2007. Available at: http://www.acgme.org/acWebsite/dutyHours/dh_ComProgrRequirmentsDutyHours0707.pdf. Accessed October 20,2010.
- ,,, et al.Effect of reducing interns' weekly work hours on sleep and attentional failures.N Engl J Med.2004;351:1829–1837.
- Letter written to William Munier, Agency for Healthcare Research and Quality.Washington, DC:US House of Representatives, Committee on Energy and Commerce, March 29,2007. Available at: http://energycommerce.house.gov/Press_110/110‐ltr.032907.HHS.Munier.pdf. Accessed on October 24, 2010.
- ,.The evolution and future of hospital medicine.Mt Sinai J Med.2008;75:418–423.
- .Brain structures and receptors involved in alertness.Sleep Med.2005;6(suppl 1):S3–S7.
- .A two process model of sleep regulation.Hum Neurobiol.1982;1:195–204.
- ,.Entrainment of the human circadian system by light.J Biol Rhythms.2005;20:326–338.
- ,.Sleep‐promoting and hypothermic effects of daytime melatonin administration in humans.Sleep.1997;20:124–131.
- .Sleepiness as a consequence of shift work.Sleep.1988;11:17–34.
- ,,,,.The sleep of long‐haul truck drivers.N Engl J Med.1997;337:755–761.
- ,,,.Sleep on the night shift: 24‐hour EEG monitoring of spontaneous sleep/wake behavior.Psychophysiology.1989;26:352–358.
- .Do permanent night workers show circadian adjustment? A review based on the endogenous melatonin rhythm.Chronobiol Int.2008;25:215–224.
- ,,,,.Shift work sleep disorder: prevalence and consequences beyond that of symptomatic day workers.Sleep.2004;27:1453–1462.
- ,,, et al.Modafinil for excessive sleepiness associated with shift‐work sleep disorder.N Engl J Med.2005;353:476–486.
- American Academy of Sleep Medicine.The International Classification of Sleep Disorders (ICSD).2nd ed.Chicago, IL:American Academy of Sleep Medicine;2005.
- ,.Circadian rhythm sleep disorders.Chest.2006;130:1915–1923.
- ,,,,,.Early morning executive functioning during sleep deprivation is compromised by a PERIOD3 polymorphism.Sleep.2008;31:1159–1167.
- ,,,,,.Genetic variation in the adenosine A2A receptor gene modulates performance on the psychomotor vigilance task.Sleep Biol Rhythms.2007;5:A47.
- ,.Circadian rhythms in cognitive performance: methodological constraints, protocols, theoretical underpinnings.Physiol Behav.2007;90:196–208.
- ,,,.A prospective study of fatal occupational accidents—relationship to sleeping difficulties and occupational factors.J Sleep Res.2002;11:69–71.
- ,,,.Effects of critical care nurses' work hours on vigilance and patients' safety.Am J Crit Care.2006;15:30–37.
- ,,,,.Daytime sleepiness, sleep habits and occupational accidents among hospital nurses.J Adv Nurs.2005;52:445–453.
- ,,.Systematic review: association of shift length, protected sleep time, and night float with patient care, residents' health, and education.Ann Intern Med.2010;153:829–842.
- ,,,,.Jack Barney Award: the effect of fatigue on cognitive and psychomotor skills of trauma residents and attending surgeons.Am J Surg.2008;196:813–819; discussion 9–20.
- ,,, et al.Risks of complications by attending physicians after performing nighttime procedures.JAMA.2009;302:1565–1572.
- ,,.Sleep deprivation, elective surgical procedures, and informed consent.N Engl J Med.2010;363:2577–2579.
- ,,,,.A prospective study of anger and coronary heart disease. The Normative Aging Study.Circulation.1996;94:2090–2095.
- ,,,.Night work and risk of breast cancer.Epidemiology.2006;17:108–111.
- ,,, et al.Night‐shift work and risk of colorectal cancer in the nurses' health study.J Natl Cancer Inst.2003;95:825–828.
- ,,.Shift work and cardiovascular disease—pathways from circadian stress to morbidity.Scand J Work Environ Health.2010;36:96–108.
- IARC. IARC monographs on the evalutaion of carcinogenic risks to humans. Vol 98. Painting, firefighting, and shiftwork. 2007. Available at: monographs.iarc.fr/ENG/Monographs/vol98/mono98.pdf. Accessed January 16,2011.
- ,,,.Influence of melatonin on invasive and metastatic properties of MCF‐7 human breast cancer cells.Cancer Res.1998;58:4383–4390.
- Society of Hospital Medicine. Society of Hospital Medicine releases results of the 2007–2008 survey on the state of the hospital medicine movement. 2008. Available at: http://www.hospitalmedicine.org/AM/Template.cfm?Section=Press_Releases3:247–255.
- ,,.Hospitalists: A Guide to Building and Sustaining a Successful Program.Chicago, IL:Health Administration Press;2008.
- ,,,,.The increased financial burden of further proposed orthopaedic resident work‐hour reductions.J Bone Joint Surg Am.2011;93:e31.
- ,,,,,.Fatigue and shift work.J Sleep Res.2006;15:1–5.
- ,,, et al.Rapid shift in peak melatonin secretion associated with improved performance in short shift work schedule.Sleep.1997;20:1145–1150.
- ,,.The impact of a nap opportunity during the night shift on the performance and alertness of 12‐h shift workers.J Sleep Res.2002;11:219–227.
- ,,, et al.Improving alertness and performance in emergency department physicians and nurses: the use of planned naps.Ann Emerg Med.2006;48:596–604, e1‐e3.
- ,,,,.Promoting alertness with a short nap during a night shift.J Sleep Res.1998;7:240–247.
- ,.Circadian adaptation to night‐shift work by judicious light and darkness exposure.J Biol Rhythms.2002;17:556–567.
- ,,,,,.Exposure to bright light and darkness to treat physiologic maladaptation to night work.N Engl J Med.1990;322:1253–1259.
- ,.Night shift performance is improved by a compromise circadian phase position: study 3. Circadian phase after 7 night shifts with an intervening weekend off.Sleep.2008;31:1639–1645.
- ,,,.Dose‐response relationship for light intensity and ocular and electroencephalographic correlates of human alertness.Behav Brain Res.2000;115:75–83.
- ,,,,.Dark goggles and bright light improve circadian rhythm adaptation to night‐shift work.Sleep.1994;17:535–543.
- ,,.Caffeine content of specialty coffees.J Anal Toxicol.2003;27:520–522.
- ,.Caffeine content of prepackaged national‐brand and private‐label carbonated beverages.J Food Sci.2007;72:C337–C342.
- ,,, et al.The effects of coffee and napping on nighttime highway driving: a randomized trial.Ann Intern Med.2006;144:785–791.
- ,,,,.Laboratory and field studies of naps and caffeine as practical countermeasures for sleep‐wake problems associated with night work.Sleep.2006;29:39–50.
- ,,,,.Armodafinil for treatment of excessive sleepiness associated with shift work disorder: a randomized controlled study.Mayo Clin Proc.2009;84:958–972.
- ,,,,.The long‐term tolerability and efficacy of armodafinil in patients with excessive sleepiness associated with treated obstructive sleep apnea, shift work disorder, or narcolepsy: an open‐label extension study.J Clin Sleep Med.2010;6:458–466.
- ,,.Circadian rhythm sleep disorders.Med Clin North Am.2004;88:631–651, viii.
- ,,.A three pulse phase response curve to three milligrams of melatonin in humans.J Physiol.2008;586:639–647.
- ,,, et al.Practice parameters for the clinical evaluation and treatment of circadian rhythm sleep disorders. An American Academy of Sleep Medicine report.Sleep.2007;30:1445–1459.
- ,,, et al.Efficacy and safety of exogenous melatonin for secondary sleep disorders and sleep disorders accompanying sleep restriction: meta‐analysis.BMJ.2006;332:385–393.
- ,,.Effects of melatonin administration on daytime sleep after simulated night shift work.J Sleep Res.2001;10:181–192.
- ,,,.Performance, ability to stay awake, and tendency to fall asleep during the night after a diurnal sleep with temazepam or placebo.Sleep.1997;20:535–541.
- ,,,,,.Sleepiness/alertness on a simulated night shift following sleep at home with triazolam.Sleep.1991;14:140–146.
- ,,,.Zolpidem‐related effects on performance and mood during simulated night‐shift work.Exp Clin Psychopharmacol.2003;11:259–268.
- ,,,,.Intrinsic near‐24‐h pacemaker period determines limits of circadian entrainment to a weak synchronizer in humans.Proc Natl Acad Sci USA.2001;98:14027–14032.
- ,,,.Work shift duration: a review comparing eight hour and 12 hour shift systems.Occup Environ Med.1998;55:217–229.
- ,,.Influence of flexibility and variability of working hours on health and well‐being.Chronobiol Int.2006;23:1125–1137.
- ,,.Impact of night‐float rotation on sleep, mood, and alertness: the resident's perception.Chronobiol Int.2002;19:893–902.
- ,,,,,.The characteristics of recovery sleep when recovery opportunity is restricted.Sleep.2007;30:353–360.
- ,,.Practical interventions to promote circadian adaptation to permanent night shift work: study 4.J Biol Rhythms.2009;24:161–172.
- ,,.Is there an association between shift work and having a metabolic syndrome? Results from a population based study of 27,485 people.Occup Environ Med.2001;58:747–752.
- ,.Use of sleep hygiene in the treatment of insomnia.Sleep Med Rev.2003;7:215–225.
- .Job, family, and gender: determinants of nonstandard work schedules among employed Americans in 1991.Demography.1995;32:577–598.
- ,.Shift work among dual‐earner couples with children.Science.1983;219:876–879.
- ,,, et al.Effect of reducing interns' work hours on serious medical errors in intensive care units.N Engl J Med.2004;351:1838–1848.
- Institute of Medicine. Resident Duty Hours: Enhancing Sleep, Supervision and Safety. Released December 15,2008. Available at: http://www.iom.edu/Reports/2008/Resident‐Duty‐Hours‐Enhancing‐Sleep‐Supervision‐and‐Safety.aspx. Accessed on October 20, 2010.
- ACGME. ACGME Approved Standards. Effective July2011. Available at: http://acgme‐2010standards.org/. Accessed on January 6, 2011
- ACGME. Common Program Requirements: Resident Duty Hours in the Learning and Work Environment. Effective July 1, 2007. Available at: http://www.acgme.org/acWebsite/dutyHours/dh_ComProgrRequirmentsDutyHours0707.pdf. Accessed October 20,2010.
- ,,, et al.Effect of reducing interns' weekly work hours on sleep and attentional failures.N Engl J Med.2004;351:1829–1837.
- Letter written to William Munier, Agency for Healthcare Research and Quality.Washington, DC:US House of Representatives, Committee on Energy and Commerce, March 29,2007. Available at: http://energycommerce.house.gov/Press_110/110‐ltr.032907.HHS.Munier.pdf. Accessed on October 24, 2010.
- ,.The evolution and future of hospital medicine.Mt Sinai J Med.2008;75:418–423.
- .Brain structures and receptors involved in alertness.Sleep Med.2005;6(suppl 1):S3–S7.
- .A two process model of sleep regulation.Hum Neurobiol.1982;1:195–204.
- ,.Entrainment of the human circadian system by light.J Biol Rhythms.2005;20:326–338.
- ,.Sleep‐promoting and hypothermic effects of daytime melatonin administration in humans.Sleep.1997;20:124–131.
- .Sleepiness as a consequence of shift work.Sleep.1988;11:17–34.
- ,,,,.The sleep of long‐haul truck drivers.N Engl J Med.1997;337:755–761.
- ,,,.Sleep on the night shift: 24‐hour EEG monitoring of spontaneous sleep/wake behavior.Psychophysiology.1989;26:352–358.
- .Do permanent night workers show circadian adjustment? A review based on the endogenous melatonin rhythm.Chronobiol Int.2008;25:215–224.
- ,,,,.Shift work sleep disorder: prevalence and consequences beyond that of symptomatic day workers.Sleep.2004;27:1453–1462.
- ,,, et al.Modafinil for excessive sleepiness associated with shift‐work sleep disorder.N Engl J Med.2005;353:476–486.
- American Academy of Sleep Medicine.The International Classification of Sleep Disorders (ICSD).2nd ed.Chicago, IL:American Academy of Sleep Medicine;2005.
- ,.Circadian rhythm sleep disorders.Chest.2006;130:1915–1923.
- ,,,,,.Early morning executive functioning during sleep deprivation is compromised by a PERIOD3 polymorphism.Sleep.2008;31:1159–1167.
- ,,,,,.Genetic variation in the adenosine A2A receptor gene modulates performance on the psychomotor vigilance task.Sleep Biol Rhythms.2007;5:A47.
- ,.Circadian rhythms in cognitive performance: methodological constraints, protocols, theoretical underpinnings.Physiol Behav.2007;90:196–208.
- ,,,.A prospective study of fatal occupational accidents—relationship to sleeping difficulties and occupational factors.J Sleep Res.2002;11:69–71.
- ,,,.Effects of critical care nurses' work hours on vigilance and patients' safety.Am J Crit Care.2006;15:30–37.
- ,,,,.Daytime sleepiness, sleep habits and occupational accidents among hospital nurses.J Adv Nurs.2005;52:445–453.
- ,,.Systematic review: association of shift length, protected sleep time, and night float with patient care, residents' health, and education.Ann Intern Med.2010;153:829–842.
- ,,,,.Jack Barney Award: the effect of fatigue on cognitive and psychomotor skills of trauma residents and attending surgeons.Am J Surg.2008;196:813–819; discussion 9–20.
- ,,, et al.Risks of complications by attending physicians after performing nighttime procedures.JAMA.2009;302:1565–1572.
- ,,.Sleep deprivation, elective surgical procedures, and informed consent.N Engl J Med.2010;363:2577–2579.
- ,,,,.A prospective study of anger and coronary heart disease. The Normative Aging Study.Circulation.1996;94:2090–2095.
- ,,,.Night work and risk of breast cancer.Epidemiology.2006;17:108–111.
- ,,, et al.Night‐shift work and risk of colorectal cancer in the nurses' health study.J Natl Cancer Inst.2003;95:825–828.
- ,,.Shift work and cardiovascular disease—pathways from circadian stress to morbidity.Scand J Work Environ Health.2010;36:96–108.
- IARC. IARC monographs on the evalutaion of carcinogenic risks to humans. Vol 98. Painting, firefighting, and shiftwork. 2007. Available at: monographs.iarc.fr/ENG/Monographs/vol98/mono98.pdf. Accessed January 16,2011.
- ,,,.Influence of melatonin on invasive and metastatic properties of MCF‐7 human breast cancer cells.Cancer Res.1998;58:4383–4390.
- Society of Hospital Medicine. Society of Hospital Medicine releases results of the 2007–2008 survey on the state of the hospital medicine movement. 2008. Available at: http://www.hospitalmedicine.org/AM/Template.cfm?Section=Press_Releases3:247–255.
- ,,.Hospitalists: A Guide to Building and Sustaining a Successful Program.Chicago, IL:Health Administration Press;2008.
- ,,,,.The increased financial burden of further proposed orthopaedic resident work‐hour reductions.J Bone Joint Surg Am.2011;93:e31.
- ,,,,,.Fatigue and shift work.J Sleep Res.2006;15:1–5.
- ,,, et al.Rapid shift in peak melatonin secretion associated with improved performance in short shift work schedule.Sleep.1997;20:1145–1150.
- ,,.The impact of a nap opportunity during the night shift on the performance and alertness of 12‐h shift workers.J Sleep Res.2002;11:219–227.
- ,,, et al.Improving alertness and performance in emergency department physicians and nurses: the use of planned naps.Ann Emerg Med.2006;48:596–604, e1‐e3.
- ,,,,.Promoting alertness with a short nap during a night shift.J Sleep Res.1998;7:240–247.
- ,.Circadian adaptation to night‐shift work by judicious light and darkness exposure.J Biol Rhythms.2002;17:556–567.
- ,,,,,.Exposure to bright light and darkness to treat physiologic maladaptation to night work.N Engl J Med.1990;322:1253–1259.
- ,.Night shift performance is improved by a compromise circadian phase position: study 3. Circadian phase after 7 night shifts with an intervening weekend off.Sleep.2008;31:1639–1645.
- ,,,.Dose‐response relationship for light intensity and ocular and electroencephalographic correlates of human alertness.Behav Brain Res.2000;115:75–83.
- ,,,,.Dark goggles and bright light improve circadian rhythm adaptation to night‐shift work.Sleep.1994;17:535–543.
- ,,.Caffeine content of specialty coffees.J Anal Toxicol.2003;27:520–522.
- ,.Caffeine content of prepackaged national‐brand and private‐label carbonated beverages.J Food Sci.2007;72:C337–C342.
- ,,, et al.The effects of coffee and napping on nighttime highway driving: a randomized trial.Ann Intern Med.2006;144:785–791.
- ,,,,.Laboratory and field studies of naps and caffeine as practical countermeasures for sleep‐wake problems associated with night work.Sleep.2006;29:39–50.
- ,,,,.Armodafinil for treatment of excessive sleepiness associated with shift work disorder: a randomized controlled study.Mayo Clin Proc.2009;84:958–972.
- ,,,,.The long‐term tolerability and efficacy of armodafinil in patients with excessive sleepiness associated with treated obstructive sleep apnea, shift work disorder, or narcolepsy: an open‐label extension study.J Clin Sleep Med.2010;6:458–466.
- ,,.Circadian rhythm sleep disorders.Med Clin North Am.2004;88:631–651, viii.
- ,,.A three pulse phase response curve to three milligrams of melatonin in humans.J Physiol.2008;586:639–647.
- ,,, et al.Practice parameters for the clinical evaluation and treatment of circadian rhythm sleep disorders. An American Academy of Sleep Medicine report.Sleep.2007;30:1445–1459.
- ,,, et al.Efficacy and safety of exogenous melatonin for secondary sleep disorders and sleep disorders accompanying sleep restriction: meta‐analysis.BMJ.2006;332:385–393.
- ,,.Effects of melatonin administration on daytime sleep after simulated night shift work.J Sleep Res.2001;10:181–192.
- ,,,.Performance, ability to stay awake, and tendency to fall asleep during the night after a diurnal sleep with temazepam or placebo.Sleep.1997;20:535–541.
- ,,,,,.Sleepiness/alertness on a simulated night shift following sleep at home with triazolam.Sleep.1991;14:140–146.
- ,,,.Zolpidem‐related effects on performance and mood during simulated night‐shift work.Exp Clin Psychopharmacol.2003;11:259–268.
- ,,,,.Intrinsic near‐24‐h pacemaker period determines limits of circadian entrainment to a weak synchronizer in humans.Proc Natl Acad Sci USA.2001;98:14027–14032.
- ,,,.Work shift duration: a review comparing eight hour and 12 hour shift systems.Occup Environ Med.1998;55:217–229.
- ,,.Influence of flexibility and variability of working hours on health and well‐being.Chronobiol Int.2006;23:1125–1137.
- ,,.Impact of night‐float rotation on sleep, mood, and alertness: the resident's perception.Chronobiol Int.2002;19:893–902.
- ,,,,,.The characteristics of recovery sleep when recovery opportunity is restricted.Sleep.2007;30:353–360.
- ,,.Practical interventions to promote circadian adaptation to permanent night shift work: study 4.J Biol Rhythms.2009;24:161–172.
- ,,.Is there an association between shift work and having a metabolic syndrome? Results from a population based study of 27,485 people.Occup Environ Med.2001;58:747–752.
- ,.Use of sleep hygiene in the treatment of insomnia.Sleep Med Rev.2003;7:215–225.
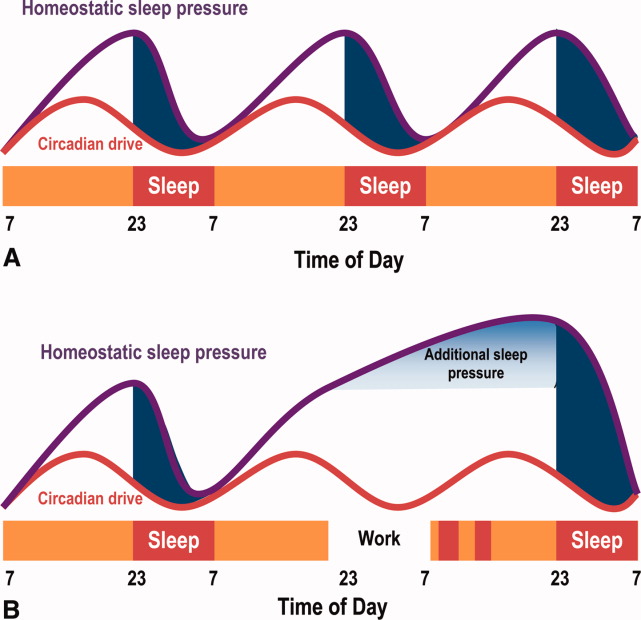
FDA Approves Long-Acting Form of Diabetes Drug Exenatide
The first once weekly diabetes drug has been approved by the Food and Drug Administration. An extended-release formulation of the type 2 diabetes medication exenatide, a glucagon-like peptide-1 (GLP-1) receptor, was approved on Jan. 27, the manufacturer announced.
The formulation, called Bydureon, is administered once a week in a subcutaneous injection, and is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes. The regular formulation of exenatide (Byetta), approved in 2005, is administered twice a day.
Approval was based on the results of the DURATION-5 study, which compared treatment with the two formulations in 252 patients with type 2 diabetes and inadequate glycemic control (mean baseline hemoglobin A1c was 8.4%) with diet and exercise alone or with oral therapy, including metformin, a sulfonylurea, a thiazolidinedione, or a combination of two of these treatments.
The mean reduction in HbA1c was 1.6 percentage points among those treated with 2 mg of extended-release exenatide once weekly, compared with a mean reduction of 0.9 percentage points among those treated with the regular form of exenatide (starting at 5 mcg twice daily increasing to 10 mcg twice daily after 4 weeks), a statistically significant difference, according to the prescribing information and the press release.
Extended-release exenatide has been approved with a Risk Evaluation and Mitigation Strategy (REMS), to ensure that the benefits of the drug outweigh the risks of acute pancreatitis and the "potential" risk of medullary thyroid cancer with treatment. There have been postmarketing reports of pancreatitis associated with exenatide, including nonfatal hemorrhagic or necrotizing pancreatitis.
In rats, extended-release exenatide causes thyroid C-cell tumors at clinically relevant exposures, but at this point, the relevance to humans is not known, according to a boxed warning in the prescribing information. It is contraindicated in people with a personal or family history of medullary thyroid cancer or those with Multiple Endocrine Neoplasia syndrome type 2 (MEN2).
The first once weekly diabetes drug has been approved by the Food and Drug Administration. An extended-release formulation of the type 2 diabetes medication exenatide, a glucagon-like peptide-1 (GLP-1) receptor, was approved on Jan. 27, the manufacturer announced.
The formulation, called Bydureon, is administered once a week in a subcutaneous injection, and is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes. The regular formulation of exenatide (Byetta), approved in 2005, is administered twice a day.
Approval was based on the results of the DURATION-5 study, which compared treatment with the two formulations in 252 patients with type 2 diabetes and inadequate glycemic control (mean baseline hemoglobin A1c was 8.4%) with diet and exercise alone or with oral therapy, including metformin, a sulfonylurea, a thiazolidinedione, or a combination of two of these treatments.
The mean reduction in HbA1c was 1.6 percentage points among those treated with 2 mg of extended-release exenatide once weekly, compared with a mean reduction of 0.9 percentage points among those treated with the regular form of exenatide (starting at 5 mcg twice daily increasing to 10 mcg twice daily after 4 weeks), a statistically significant difference, according to the prescribing information and the press release.
Extended-release exenatide has been approved with a Risk Evaluation and Mitigation Strategy (REMS), to ensure that the benefits of the drug outweigh the risks of acute pancreatitis and the "potential" risk of medullary thyroid cancer with treatment. There have been postmarketing reports of pancreatitis associated with exenatide, including nonfatal hemorrhagic or necrotizing pancreatitis.
In rats, extended-release exenatide causes thyroid C-cell tumors at clinically relevant exposures, but at this point, the relevance to humans is not known, according to a boxed warning in the prescribing information. It is contraindicated in people with a personal or family history of medullary thyroid cancer or those with Multiple Endocrine Neoplasia syndrome type 2 (MEN2).
The first once weekly diabetes drug has been approved by the Food and Drug Administration. An extended-release formulation of the type 2 diabetes medication exenatide, a glucagon-like peptide-1 (GLP-1) receptor, was approved on Jan. 27, the manufacturer announced.
The formulation, called Bydureon, is administered once a week in a subcutaneous injection, and is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes. The regular formulation of exenatide (Byetta), approved in 2005, is administered twice a day.
Approval was based on the results of the DURATION-5 study, which compared treatment with the two formulations in 252 patients with type 2 diabetes and inadequate glycemic control (mean baseline hemoglobin A1c was 8.4%) with diet and exercise alone or with oral therapy, including metformin, a sulfonylurea, a thiazolidinedione, or a combination of two of these treatments.
The mean reduction in HbA1c was 1.6 percentage points among those treated with 2 mg of extended-release exenatide once weekly, compared with a mean reduction of 0.9 percentage points among those treated with the regular form of exenatide (starting at 5 mcg twice daily increasing to 10 mcg twice daily after 4 weeks), a statistically significant difference, according to the prescribing information and the press release.
Extended-release exenatide has been approved with a Risk Evaluation and Mitigation Strategy (REMS), to ensure that the benefits of the drug outweigh the risks of acute pancreatitis and the "potential" risk of medullary thyroid cancer with treatment. There have been postmarketing reports of pancreatitis associated with exenatide, including nonfatal hemorrhagic or necrotizing pancreatitis.
In rats, extended-release exenatide causes thyroid C-cell tumors at clinically relevant exposures, but at this point, the relevance to humans is not known, according to a boxed warning in the prescribing information. It is contraindicated in people with a personal or family history of medullary thyroid cancer or those with Multiple Endocrine Neoplasia syndrome type 2 (MEN2).
Study: Booster Seat Use During Carpooling Inconsistent
Only 55% of parents with children aged 4-8 years always have their child use a car booster seat when driving with other children in the car, according to a study published Jan. 30 in Pediatrics.
The researchers surveyed 681 parents with 4- to 8-year-old children to ask about their safety seat practices, especially when carpooling. They found that most parents – 76% – reported using a booster seat when riding in the family car.
However, among the 64% of parents who carpool, 45% said they do not always have their child use their booster seat when driving with friends who don’t have boosters. "These findings suggest that social norms and self-efficacy for booster seat use may be influential in carpooling situations," wrote Dr. Michelle L. Macy of the University of Michigan, Ann Arbor, and her associates (Pediatrics 2012;129:290-98).
Still, 54% of parents who frequently carpool said they would always ask another driver to use a booster seat for their child; that percentage rose to 64% in parents who occasionally carpool. In addition, parents who occasionally carpool were significantly more likely than were parents who carpool frequently to report their child always uses a booster seat, they found.
Physician should ask not just about use of size-appropriate child safety seats during office visits, but also whether parents consistently use them for their children and if there are any barriers to their use, such as perceived difficulty making arrangements to have booster seats available for other people’s children or problems transferring child safety seats between vehicles, Dr. Macy and her colleagues said.
Dr. Macy and her associates said they had no relevant financial disclosures. This research was conducted as part of the C.S. Mott Children’s Hospital National Poll on Children’s Health, sponsored by the department of pediatrics and communicable diseases at the University of Michigan and the University of Michigan Health System. The study was funded by a grant from the Michigan Center for Advancing Safe Transportation Throughout the Lifespan.
Only 55% of parents with children aged 4-8 years always have their child use a car booster seat when driving with other children in the car, according to a study published Jan. 30 in Pediatrics.
The researchers surveyed 681 parents with 4- to 8-year-old children to ask about their safety seat practices, especially when carpooling. They found that most parents – 76% – reported using a booster seat when riding in the family car.
However, among the 64% of parents who carpool, 45% said they do not always have their child use their booster seat when driving with friends who don’t have boosters. "These findings suggest that social norms and self-efficacy for booster seat use may be influential in carpooling situations," wrote Dr. Michelle L. Macy of the University of Michigan, Ann Arbor, and her associates (Pediatrics 2012;129:290-98).
Still, 54% of parents who frequently carpool said they would always ask another driver to use a booster seat for their child; that percentage rose to 64% in parents who occasionally carpool. In addition, parents who occasionally carpool were significantly more likely than were parents who carpool frequently to report their child always uses a booster seat, they found.
Physician should ask not just about use of size-appropriate child safety seats during office visits, but also whether parents consistently use them for their children and if there are any barriers to their use, such as perceived difficulty making arrangements to have booster seats available for other people’s children or problems transferring child safety seats between vehicles, Dr. Macy and her colleagues said.
Dr. Macy and her associates said they had no relevant financial disclosures. This research was conducted as part of the C.S. Mott Children’s Hospital National Poll on Children’s Health, sponsored by the department of pediatrics and communicable diseases at the University of Michigan and the University of Michigan Health System. The study was funded by a grant from the Michigan Center for Advancing Safe Transportation Throughout the Lifespan.
Only 55% of parents with children aged 4-8 years always have their child use a car booster seat when driving with other children in the car, according to a study published Jan. 30 in Pediatrics.
The researchers surveyed 681 parents with 4- to 8-year-old children to ask about their safety seat practices, especially when carpooling. They found that most parents – 76% – reported using a booster seat when riding in the family car.
However, among the 64% of parents who carpool, 45% said they do not always have their child use their booster seat when driving with friends who don’t have boosters. "These findings suggest that social norms and self-efficacy for booster seat use may be influential in carpooling situations," wrote Dr. Michelle L. Macy of the University of Michigan, Ann Arbor, and her associates (Pediatrics 2012;129:290-98).
Still, 54% of parents who frequently carpool said they would always ask another driver to use a booster seat for their child; that percentage rose to 64% in parents who occasionally carpool. In addition, parents who occasionally carpool were significantly more likely than were parents who carpool frequently to report their child always uses a booster seat, they found.
Physician should ask not just about use of size-appropriate child safety seats during office visits, but also whether parents consistently use them for their children and if there are any barriers to their use, such as perceived difficulty making arrangements to have booster seats available for other people’s children or problems transferring child safety seats between vehicles, Dr. Macy and her colleagues said.
Dr. Macy and her associates said they had no relevant financial disclosures. This research was conducted as part of the C.S. Mott Children’s Hospital National Poll on Children’s Health, sponsored by the department of pediatrics and communicable diseases at the University of Michigan and the University of Michigan Health System. The study was funded by a grant from the Michigan Center for Advancing Safe Transportation Throughout the Lifespan.
FROM PEDIATRICS
Major Finding: Only 55% of parents with children aged 4-8 years always have their child use a booster seat when carpooling.
Data Source: Cross-sectional Web-based survey of 681 U.S. parents.
Disclosures: Dr. Macy and her associates said they had no relevant financial disclosures. This research was conducted as part of the C.S. Mott Children’s Hospital National Poll on Children Health, sponsored by the department of pediatrics and communicable diseases at the University of Michigan and the University of Michigan Health System. The study was funded by a grant from the Michigan Center for Advancing Safe Transportation Throughout the Lifespan.
Vytorin Falls Short of New Indication for CKD Patients
The Food and Drug Administration approved a revised label for Vytorin that now includes data from a study showing a benefit of treatment in patients with moderate to severe kidney disease, but the agency did not approve a new indication that reflects these findings for Vytorin or for ezetemibe, one of the components of the combination product, according to Merck.
In a Jan. 25 press release, Merck, the manufacturer of ezetimibe (Zetia) and Vytorin – a combination of ezetimibe and simvastatin – said that the FDA had approved the new labeling that now includes data from the Study of Heart and Renal Protection (SHARP). Themultinational, randomized, double-blind placebo controlled study of almost 9,500 patients with moderate to severe chronic kidney disease who did not have a history of myocardial infarction or coronary revascularization found that the lipid-lowering treatment reduced the risk of major vascular events, compared with placebo.
However, the FDA did not approve a new indication to reflect these results, because SHARP compared the combination of the two drugs with placebo and "was not designed to assess the independent contributions of each drug to the observed effect," the Merck release said, adding: "For this reason, the FDA did not approve a new indication for Vytorin or for Zetia," and the SHARP results have not been added to the ezetimibe label.
This was despite the unanimous recommendation of the FDA’s Endocrinologic and Metabolic Drugs Advisory Committee in November to approve Vytorin for reducing major cardiovascular events in patients with CKD who are not on dialysis. The panel also voted 10-6 that the data did not support approval of the combination for the same indication in patients with end-stage renal disease who are on dialysis.
Merck had filed for approval of the claim that 10 mg of ezetimibe plus 20 mg of simvastatin (in the fixed-dose combination pill or taken separately) reduces the risk of major cardiovascular events in patients with chronic kidney disease on the basis of the SHARP results.
About two-thirds of the patients enrolled in SHARP were not on dialysis at baseline, and in these patients, there was a 23% reduction in the primary end point – the risk of a major vascular event (nonfatal MI or cardiac death, stroke, or a revascularization procedure that excluded dialysis access–related procedures) – compared with those on placebo over a mean of 5 years (Lancet 2011;377:2181-92).
Among the patients who were on dialysis at baseline, the risk reduction was less (about 6% over placebo).
The two drugs remain approved for lipid-lowering indications only: Ezetimibe, a selective inhibitor of the absorption of intestinal cholesterol and related phytosterol, was approved in 2002; Vytorin, a combination of ezetimibe and the HMG-CoA reductase inhibitor simvastatin was approved in 2004; simvastatin was approved in 1991.
In an interview, Dr. William Hiatt, one of the members of the FDA panel that reviewed the SHARP data, said that "by allowing Merck to add the information from the SHARP trial to the product label, physicians will be able to use that information to help guide their decisions to use this medication for their CKD patients." Dr. Hiatt is professor of medicine, division of cardiology, University of Colorado, Denver. Members of FDA advisory panels are cleared of potential conflicts related to the topic of the meeting.
The agency usually follows FDA panel recommendations, which are not binding. At press time, no statement was available from the FDA to explain the decision.
SHARP was funded by Merck and Schering-Plough, but was independently conducted by the Oxford (England) University Clinical Trials Service Unit.
The Food and Drug Administration approved a revised label for Vytorin that now includes data from a study showing a benefit of treatment in patients with moderate to severe kidney disease, but the agency did not approve a new indication that reflects these findings for Vytorin or for ezetemibe, one of the components of the combination product, according to Merck.
In a Jan. 25 press release, Merck, the manufacturer of ezetimibe (Zetia) and Vytorin – a combination of ezetimibe and simvastatin – said that the FDA had approved the new labeling that now includes data from the Study of Heart and Renal Protection (SHARP). Themultinational, randomized, double-blind placebo controlled study of almost 9,500 patients with moderate to severe chronic kidney disease who did not have a history of myocardial infarction or coronary revascularization found that the lipid-lowering treatment reduced the risk of major vascular events, compared with placebo.
However, the FDA did not approve a new indication to reflect these results, because SHARP compared the combination of the two drugs with placebo and "was not designed to assess the independent contributions of each drug to the observed effect," the Merck release said, adding: "For this reason, the FDA did not approve a new indication for Vytorin or for Zetia," and the SHARP results have not been added to the ezetimibe label.
This was despite the unanimous recommendation of the FDA’s Endocrinologic and Metabolic Drugs Advisory Committee in November to approve Vytorin for reducing major cardiovascular events in patients with CKD who are not on dialysis. The panel also voted 10-6 that the data did not support approval of the combination for the same indication in patients with end-stage renal disease who are on dialysis.
Merck had filed for approval of the claim that 10 mg of ezetimibe plus 20 mg of simvastatin (in the fixed-dose combination pill or taken separately) reduces the risk of major cardiovascular events in patients with chronic kidney disease on the basis of the SHARP results.
About two-thirds of the patients enrolled in SHARP were not on dialysis at baseline, and in these patients, there was a 23% reduction in the primary end point – the risk of a major vascular event (nonfatal MI or cardiac death, stroke, or a revascularization procedure that excluded dialysis access–related procedures) – compared with those on placebo over a mean of 5 years (Lancet 2011;377:2181-92).
Among the patients who were on dialysis at baseline, the risk reduction was less (about 6% over placebo).
The two drugs remain approved for lipid-lowering indications only: Ezetimibe, a selective inhibitor of the absorption of intestinal cholesterol and related phytosterol, was approved in 2002; Vytorin, a combination of ezetimibe and the HMG-CoA reductase inhibitor simvastatin was approved in 2004; simvastatin was approved in 1991.
In an interview, Dr. William Hiatt, one of the members of the FDA panel that reviewed the SHARP data, said that "by allowing Merck to add the information from the SHARP trial to the product label, physicians will be able to use that information to help guide their decisions to use this medication for their CKD patients." Dr. Hiatt is professor of medicine, division of cardiology, University of Colorado, Denver. Members of FDA advisory panels are cleared of potential conflicts related to the topic of the meeting.
The agency usually follows FDA panel recommendations, which are not binding. At press time, no statement was available from the FDA to explain the decision.
SHARP was funded by Merck and Schering-Plough, but was independently conducted by the Oxford (England) University Clinical Trials Service Unit.
The Food and Drug Administration approved a revised label for Vytorin that now includes data from a study showing a benefit of treatment in patients with moderate to severe kidney disease, but the agency did not approve a new indication that reflects these findings for Vytorin or for ezetemibe, one of the components of the combination product, according to Merck.
In a Jan. 25 press release, Merck, the manufacturer of ezetimibe (Zetia) and Vytorin – a combination of ezetimibe and simvastatin – said that the FDA had approved the new labeling that now includes data from the Study of Heart and Renal Protection (SHARP). Themultinational, randomized, double-blind placebo controlled study of almost 9,500 patients with moderate to severe chronic kidney disease who did not have a history of myocardial infarction or coronary revascularization found that the lipid-lowering treatment reduced the risk of major vascular events, compared with placebo.
However, the FDA did not approve a new indication to reflect these results, because SHARP compared the combination of the two drugs with placebo and "was not designed to assess the independent contributions of each drug to the observed effect," the Merck release said, adding: "For this reason, the FDA did not approve a new indication for Vytorin or for Zetia," and the SHARP results have not been added to the ezetimibe label.
This was despite the unanimous recommendation of the FDA’s Endocrinologic and Metabolic Drugs Advisory Committee in November to approve Vytorin for reducing major cardiovascular events in patients with CKD who are not on dialysis. The panel also voted 10-6 that the data did not support approval of the combination for the same indication in patients with end-stage renal disease who are on dialysis.
Merck had filed for approval of the claim that 10 mg of ezetimibe plus 20 mg of simvastatin (in the fixed-dose combination pill or taken separately) reduces the risk of major cardiovascular events in patients with chronic kidney disease on the basis of the SHARP results.
About two-thirds of the patients enrolled in SHARP were not on dialysis at baseline, and in these patients, there was a 23% reduction in the primary end point – the risk of a major vascular event (nonfatal MI or cardiac death, stroke, or a revascularization procedure that excluded dialysis access–related procedures) – compared with those on placebo over a mean of 5 years (Lancet 2011;377:2181-92).
Among the patients who were on dialysis at baseline, the risk reduction was less (about 6% over placebo).
The two drugs remain approved for lipid-lowering indications only: Ezetimibe, a selective inhibitor of the absorption of intestinal cholesterol and related phytosterol, was approved in 2002; Vytorin, a combination of ezetimibe and the HMG-CoA reductase inhibitor simvastatin was approved in 2004; simvastatin was approved in 1991.
In an interview, Dr. William Hiatt, one of the members of the FDA panel that reviewed the SHARP data, said that "by allowing Merck to add the information from the SHARP trial to the product label, physicians will be able to use that information to help guide their decisions to use this medication for their CKD patients." Dr. Hiatt is professor of medicine, division of cardiology, University of Colorado, Denver. Members of FDA advisory panels are cleared of potential conflicts related to the topic of the meeting.
The agency usually follows FDA panel recommendations, which are not binding. At press time, no statement was available from the FDA to explain the decision.
SHARP was funded by Merck and Schering-Plough, but was independently conducted by the Oxford (England) University Clinical Trials Service Unit.
Physician Involvement in Hospital Quality and Safety Programs

Should or must? That was the sticking point. After months of hard work, it had come down to this.
In a sense, these words are synonyms. In reality, they are words, and they are worlds apart.
This discourse occurred within a task force I am working with to clinically transform our medical center—that is, making an institutional commitment to quality improvement (QI), patient safety, and clinical efficiency. The effort, in part, is driven by value-based purchasing, public reporting, payment reform, and the like. But mostly it’s being driven by the fundamental premise of doing right by our patients.
We all agreed that we have to change, that it will be hard and even what types of change are needed. The struggle came down to “should” or “must.”
I’ve used several columns imploring hospitalists to lead the quality evolution. I’ve spent less time explaining how to do this. It’s one thing to say, “Hospitalists are perfectly positioned to fundamentally change the quality, safety, and efficiency of hospital care.” It’s another to fundamentally change the quality, safety, and efficiency of hospital care. So, with the disclaimer that my HM group’s efforts to improve quality have only begun to scratch the surface of success, here are some of the lessons I’ve learned.
Start Urgently
Change is very hard for hominids. We favor the devil we know. Therefore, change requires establishing a sense of urgency for the change. Conceptually, QI is enticing—until it gets hard. Then the inevitable changes in workflow start to feel like a lot of work, often without obvious or immediate benefit.
As such, people have to believe there is a problem before they can muster the energy it takes to change. I’d submit to you that the problem with patient safety and quality in healthcare is that most of us don’t think there is a problem.
It takes someone to show us there is a problem before we can change. If you cannot create this sense of urgency for change, you should stop. Don’t continue to try to lead change. You will fail. Guaranteed.
Thus, the most important step in transformation toward quality is convincing people of the need to change. This is hard to do and requires our second step.
Leading The Ship
Leadership. By which I’m not talking about the person in charge, the autocrat, the boss. Leadership is getting people to go somewhere they otherwise wouldn’t have gone. A boss can do this, but most often this is done by the people in the trenches, by front-line people who see a problem and aspire for change, by people like you.
Quality needs leadership; we are its leaders.
20/20 Vision
A vision is the end game; it’s the finish line, that thing we are all striving for. It’s a big, inspirational, audacious goal that we can all rally behind. It’s things like “zero harm” or “no avoidable errors.”
The vision should not be confused with the plan. Plans are great. But plans that don’t tie back to a vision are destined to fail. Why? Because change is hard, and as soon as a plan (e.g. call PCPs on each discharge, reconcile 24 medications in a demented patient) gets hard, people stop doing it.
Show them, however, how the plan (often something they don’t want to do) ties back to the vision (something they want to do), and people are more likely to follow. I’ll put in the extra effort for medication reconciliation (plan) if I believe there is a problem (sense of urgency) and that this plan helps achieve the vision (no avoidable errors).
Have Patience
Administrators rightly want solutions yesterday. But clinical transformation of this type takes time. We will not unfurl the “Mission Accomplished” banner in three months. This will take years, probably a decade. For two reasons:
- This requires culture change, which takes time.
- We need bench strength.
A focus on quality cannot be accomplished with five or even 50 people working on this. Rather, it requires 500 to 5,000 people—indeed, the entire organization. It takes time to change the culture, engage the people, and make the mistakes that success requires.
Make It Easier To Do The Right Thing
We have to remove the barriers that limit success. This means not asking high-paid physicians to do chart abstraction, analyze data, and coordinate meetings—support staff should perform these tasks.
We also need institution- and provider-level data. Without valid and timely provider-level data, it is exceptionally difficult to create the needed sense of urgency for change. Show me I’m not meeting my expectations, and I’ll do what it takes to change. Leave me to believe that I’m the best doctor in the world—as we all are, of course—and I have no impetus to improve.
Success requires the infrastructure that makes it harder to do the wrong thing and easier to do the right thing.
Show Me The Money
Quality cannot be an unfunded mandate. Infrastructure needs to be built, support staff hired, and physician time protected to devote to this work.
That being said, I’d submit that if after five years an institution doesn’t see a return on investment (in cost avoidance and increased revenue) of at least 5:1 for every dollar spent, then either you’ve built it wrong or we are all misreading the tea leaves in terms of value-based purchasing. I wouldn’t bet on the latter.
Partner With Your Partners
Medicine is a team sport. True success hinges on a multiprofessional approach. Our success will be directly proportional to the degree to which we engage our clinical-care partners.
This is a less autonomous way of thinking than most of us were taught. We studied alone, took tests alone, saw patients alone. To engage nurses, therapists, pharmacists, and hospital administrators in a dynamic team is outside most of our comfort zones.
Culturing Change
We cannot mend our broken system until we begin to do things differently. Success demands that we work in teams, partner with our hospital administrators, and agree to be measured. We must better communicate with other providers, reduce variability, forgo some autonomy, and shift from physician- to patient-centric care models. This will be hard. This will be uncomfortable. This will require tough decisions.
Failure or Success
Which brings me back to our task force’s definitional divide. The issue was how strongly we push physician involvement in our quality and safety program. Do we encourage all doctors to participate (doctors “should”), or do we require all doctors to participate (doctors “must”)? The task force was divided.
On the one hand, it’s hard to mandate involvement. This would be a huge physician commitment. It would take a lot of training, time, effort, and money. There would be innumerable challenges, perhaps physician turnover.
Was this a battle worth fighting? The difference between “should” and “must” is quite small. They say nearly the same thing. Except they don’t. “Should” says it’s optional; “must” is a mandate. “Should” says it’d be nice if you’d do this; “must” states it’s an institutional priority.
This distinction is not small. It is the difference between indifference and commitment, between our present and our future, between failure and success.
Dr. Glasheen is physician editor of The Hospitalist.
For more tips on getting quality programs started at your hospital, visit www.hospitalmedicine.org/thecenter.
Should or must? That was the sticking point. After months of hard work, it had come down to this.
In a sense, these words are synonyms. In reality, they are words, and they are worlds apart.
This discourse occurred within a task force I am working with to clinically transform our medical center—that is, making an institutional commitment to quality improvement (QI), patient safety, and clinical efficiency. The effort, in part, is driven by value-based purchasing, public reporting, payment reform, and the like. But mostly it’s being driven by the fundamental premise of doing right by our patients.
We all agreed that we have to change, that it will be hard and even what types of change are needed. The struggle came down to “should” or “must.”
I’ve used several columns imploring hospitalists to lead the quality evolution. I’ve spent less time explaining how to do this. It’s one thing to say, “Hospitalists are perfectly positioned to fundamentally change the quality, safety, and efficiency of hospital care.” It’s another to fundamentally change the quality, safety, and efficiency of hospital care. So, with the disclaimer that my HM group’s efforts to improve quality have only begun to scratch the surface of success, here are some of the lessons I’ve learned.
Start Urgently
Change is very hard for hominids. We favor the devil we know. Therefore, change requires establishing a sense of urgency for the change. Conceptually, QI is enticing—until it gets hard. Then the inevitable changes in workflow start to feel like a lot of work, often without obvious or immediate benefit.
As such, people have to believe there is a problem before they can muster the energy it takes to change. I’d submit to you that the problem with patient safety and quality in healthcare is that most of us don’t think there is a problem.
It takes someone to show us there is a problem before we can change. If you cannot create this sense of urgency for change, you should stop. Don’t continue to try to lead change. You will fail. Guaranteed.
Thus, the most important step in transformation toward quality is convincing people of the need to change. This is hard to do and requires our second step.
Leading The Ship
Leadership. By which I’m not talking about the person in charge, the autocrat, the boss. Leadership is getting people to go somewhere they otherwise wouldn’t have gone. A boss can do this, but most often this is done by the people in the trenches, by front-line people who see a problem and aspire for change, by people like you.
Quality needs leadership; we are its leaders.
20/20 Vision
A vision is the end game; it’s the finish line, that thing we are all striving for. It’s a big, inspirational, audacious goal that we can all rally behind. It’s things like “zero harm” or “no avoidable errors.”
The vision should not be confused with the plan. Plans are great. But plans that don’t tie back to a vision are destined to fail. Why? Because change is hard, and as soon as a plan (e.g. call PCPs on each discharge, reconcile 24 medications in a demented patient) gets hard, people stop doing it.
Show them, however, how the plan (often something they don’t want to do) ties back to the vision (something they want to do), and people are more likely to follow. I’ll put in the extra effort for medication reconciliation (plan) if I believe there is a problem (sense of urgency) and that this plan helps achieve the vision (no avoidable errors).
Have Patience
Administrators rightly want solutions yesterday. But clinical transformation of this type takes time. We will not unfurl the “Mission Accomplished” banner in three months. This will take years, probably a decade. For two reasons:
- This requires culture change, which takes time.
- We need bench strength.
A focus on quality cannot be accomplished with five or even 50 people working on this. Rather, it requires 500 to 5,000 people—indeed, the entire organization. It takes time to change the culture, engage the people, and make the mistakes that success requires.
Make It Easier To Do The Right Thing
We have to remove the barriers that limit success. This means not asking high-paid physicians to do chart abstraction, analyze data, and coordinate meetings—support staff should perform these tasks.
We also need institution- and provider-level data. Without valid and timely provider-level data, it is exceptionally difficult to create the needed sense of urgency for change. Show me I’m not meeting my expectations, and I’ll do what it takes to change. Leave me to believe that I’m the best doctor in the world—as we all are, of course—and I have no impetus to improve.
Success requires the infrastructure that makes it harder to do the wrong thing and easier to do the right thing.
Show Me The Money
Quality cannot be an unfunded mandate. Infrastructure needs to be built, support staff hired, and physician time protected to devote to this work.
That being said, I’d submit that if after five years an institution doesn’t see a return on investment (in cost avoidance and increased revenue) of at least 5:1 for every dollar spent, then either you’ve built it wrong or we are all misreading the tea leaves in terms of value-based purchasing. I wouldn’t bet on the latter.
Partner With Your Partners
Medicine is a team sport. True success hinges on a multiprofessional approach. Our success will be directly proportional to the degree to which we engage our clinical-care partners.
This is a less autonomous way of thinking than most of us were taught. We studied alone, took tests alone, saw patients alone. To engage nurses, therapists, pharmacists, and hospital administrators in a dynamic team is outside most of our comfort zones.
Culturing Change
We cannot mend our broken system until we begin to do things differently. Success demands that we work in teams, partner with our hospital administrators, and agree to be measured. We must better communicate with other providers, reduce variability, forgo some autonomy, and shift from physician- to patient-centric care models. This will be hard. This will be uncomfortable. This will require tough decisions.
Failure or Success
Which brings me back to our task force’s definitional divide. The issue was how strongly we push physician involvement in our quality and safety program. Do we encourage all doctors to participate (doctors “should”), or do we require all doctors to participate (doctors “must”)? The task force was divided.
On the one hand, it’s hard to mandate involvement. This would be a huge physician commitment. It would take a lot of training, time, effort, and money. There would be innumerable challenges, perhaps physician turnover.
Was this a battle worth fighting? The difference between “should” and “must” is quite small. They say nearly the same thing. Except they don’t. “Should” says it’s optional; “must” is a mandate. “Should” says it’d be nice if you’d do this; “must” states it’s an institutional priority.
This distinction is not small. It is the difference between indifference and commitment, between our present and our future, between failure and success.
Dr. Glasheen is physician editor of The Hospitalist.
For more tips on getting quality programs started at your hospital, visit www.hospitalmedicine.org/thecenter.
Should or must? That was the sticking point. After months of hard work, it had come down to this.
In a sense, these words are synonyms. In reality, they are words, and they are worlds apart.
This discourse occurred within a task force I am working with to clinically transform our medical center—that is, making an institutional commitment to quality improvement (QI), patient safety, and clinical efficiency. The effort, in part, is driven by value-based purchasing, public reporting, payment reform, and the like. But mostly it’s being driven by the fundamental premise of doing right by our patients.
We all agreed that we have to change, that it will be hard and even what types of change are needed. The struggle came down to “should” or “must.”
I’ve used several columns imploring hospitalists to lead the quality evolution. I’ve spent less time explaining how to do this. It’s one thing to say, “Hospitalists are perfectly positioned to fundamentally change the quality, safety, and efficiency of hospital care.” It’s another to fundamentally change the quality, safety, and efficiency of hospital care. So, with the disclaimer that my HM group’s efforts to improve quality have only begun to scratch the surface of success, here are some of the lessons I’ve learned.
Start Urgently
Change is very hard for hominids. We favor the devil we know. Therefore, change requires establishing a sense of urgency for the change. Conceptually, QI is enticing—until it gets hard. Then the inevitable changes in workflow start to feel like a lot of work, often without obvious or immediate benefit.
As such, people have to believe there is a problem before they can muster the energy it takes to change. I’d submit to you that the problem with patient safety and quality in healthcare is that most of us don’t think there is a problem.
It takes someone to show us there is a problem before we can change. If you cannot create this sense of urgency for change, you should stop. Don’t continue to try to lead change. You will fail. Guaranteed.
Thus, the most important step in transformation toward quality is convincing people of the need to change. This is hard to do and requires our second step.
Leading The Ship
Leadership. By which I’m not talking about the person in charge, the autocrat, the boss. Leadership is getting people to go somewhere they otherwise wouldn’t have gone. A boss can do this, but most often this is done by the people in the trenches, by front-line people who see a problem and aspire for change, by people like you.
Quality needs leadership; we are its leaders.
20/20 Vision
A vision is the end game; it’s the finish line, that thing we are all striving for. It’s a big, inspirational, audacious goal that we can all rally behind. It’s things like “zero harm” or “no avoidable errors.”
The vision should not be confused with the plan. Plans are great. But plans that don’t tie back to a vision are destined to fail. Why? Because change is hard, and as soon as a plan (e.g. call PCPs on each discharge, reconcile 24 medications in a demented patient) gets hard, people stop doing it.
Show them, however, how the plan (often something they don’t want to do) ties back to the vision (something they want to do), and people are more likely to follow. I’ll put in the extra effort for medication reconciliation (plan) if I believe there is a problem (sense of urgency) and that this plan helps achieve the vision (no avoidable errors).
Have Patience
Administrators rightly want solutions yesterday. But clinical transformation of this type takes time. We will not unfurl the “Mission Accomplished” banner in three months. This will take years, probably a decade. For two reasons:
- This requires culture change, which takes time.
- We need bench strength.
A focus on quality cannot be accomplished with five or even 50 people working on this. Rather, it requires 500 to 5,000 people—indeed, the entire organization. It takes time to change the culture, engage the people, and make the mistakes that success requires.
Make It Easier To Do The Right Thing
We have to remove the barriers that limit success. This means not asking high-paid physicians to do chart abstraction, analyze data, and coordinate meetings—support staff should perform these tasks.
We also need institution- and provider-level data. Without valid and timely provider-level data, it is exceptionally difficult to create the needed sense of urgency for change. Show me I’m not meeting my expectations, and I’ll do what it takes to change. Leave me to believe that I’m the best doctor in the world—as we all are, of course—and I have no impetus to improve.
Success requires the infrastructure that makes it harder to do the wrong thing and easier to do the right thing.
Show Me The Money
Quality cannot be an unfunded mandate. Infrastructure needs to be built, support staff hired, and physician time protected to devote to this work.
That being said, I’d submit that if after five years an institution doesn’t see a return on investment (in cost avoidance and increased revenue) of at least 5:1 for every dollar spent, then either you’ve built it wrong or we are all misreading the tea leaves in terms of value-based purchasing. I wouldn’t bet on the latter.
Partner With Your Partners
Medicine is a team sport. True success hinges on a multiprofessional approach. Our success will be directly proportional to the degree to which we engage our clinical-care partners.
This is a less autonomous way of thinking than most of us were taught. We studied alone, took tests alone, saw patients alone. To engage nurses, therapists, pharmacists, and hospital administrators in a dynamic team is outside most of our comfort zones.
Culturing Change
We cannot mend our broken system until we begin to do things differently. Success demands that we work in teams, partner with our hospital administrators, and agree to be measured. We must better communicate with other providers, reduce variability, forgo some autonomy, and shift from physician- to patient-centric care models. This will be hard. This will be uncomfortable. This will require tough decisions.
Failure or Success
Which brings me back to our task force’s definitional divide. The issue was how strongly we push physician involvement in our quality and safety program. Do we encourage all doctors to participate (doctors “should”), or do we require all doctors to participate (doctors “must”)? The task force was divided.
On the one hand, it’s hard to mandate involvement. This would be a huge physician commitment. It would take a lot of training, time, effort, and money. There would be innumerable challenges, perhaps physician turnover.
Was this a battle worth fighting? The difference between “should” and “must” is quite small. They say nearly the same thing. Except they don’t. “Should” says it’s optional; “must” is a mandate. “Should” says it’d be nice if you’d do this; “must” states it’s an institutional priority.
This distinction is not small. It is the difference between indifference and commitment, between our present and our future, between failure and success.
Dr. Glasheen is physician editor of The Hospitalist.
For more tips on getting quality programs started at your hospital, visit www.hospitalmedicine.org/thecenter.
Appropriate Patient Census: Hospital Medicine's Holy Grail
Ellis Knight, MD, MBA, FHM, senior vice president for physician and clinical integration at Palmetto Health in Columbia, S.C., recalls conducting root cause analyses after every serious adverse event when he was vice president for medical affairs at a large teaching hospital. “For every one of them—it was just like a broken record—every one of them, the nursing staff or the physicians involved would start the recount by saying, ‘It was a very, very busy day; we had a very high census,’” Dr. Knight says. “When that happens, when you get those, what I call tsunami waves of patients coming into a unit or being admitted at one time, it can really wreak havoc and it can make even the best clinicians get rushed, take shortcuts, and make mistakes.”
Researchers have long studied the consequences of temporary and longer-term workload imbalances for other healthcare providers; a recent in-depth study of one hospital found that the risk of inpatient patient mortality increased during shifts with below-target nurse staffing or higher patient turnover.1
Few studies, however, have specifically examined the repercussions of a patient census that is either too high or too low for a hospitalist service. At many facilities, that census can be influenced by an increasing threshold for hospitalization, meaning that the average inpatient is becoming sicker and more complicated, requiring more time during a hospitalist’s daily rounds. HM providers might report having better or worse electronic health records, support staff, and other ancillary services; different schedules; and mixes of clinical, administrative, and teaching responsibilities.

Even then, David M. Mitchell, MD, PhD, a hospitalist at Sibley Memorial Hospital in Washington, D.C., and a member of the SHM Performance Standards Committee, cautions that the ability of a doctor to churn through a higher patient count in no way ensures quality. “You don’t want to confuse efficiency with sloppiness,” he says.
In the absence of clear precedents and solid guidelines, hospitalist groups are struggling to come up with their own formulas for ensuring that workloads balance high productivity with sustainable quality—no easy feat. Nonetheless, first-hand accounts and survey data suggest that more providers are identifying common warning signs and devising tailored solutions to help the rapidly maturing field stay on track.
Henry Michtalik, MD, MPH, assistant professor of medicine at Johns Hopkins University School of Medicine, led one of the only surveys that has directly asked hospitalists how they perceive their own workloads. The survey, conducted through an online community of hospitalists and first presented at HM11, revealed several intriguing findings.2
On average, hospitalists reported seeing about 15 patients per shift or day, not including nights, weekends, or holidays. Apart from a few outliers, the range extended from the low teens to the mid-20s, Dr. Michtalik says. According to the survey, 40% of physicians said that more than once a month, their typical inpatient census exceeded the level that they deemed safe and appropriate for specific work settings; 36.1% of physicians reported that was true more than once per week.
Providers often reported that their average workload contributed to incomplete discussions with patients and families, the ordering of unnecessary tests or procedures, a delay in admissions or discharges, worsened patient satisfaction, poorer handoffs, and other problems. “We might be in a situation where we’re focusing on increasing the number of patients being seen or having high census numbers, which could be, paradoxically, actually increasing the costs of healthcare,” Dr. Michtalik says.
For a recent survey posted on the-hospitalist.org, 51% of respondents picked 11 to 15 as the most appropriate patient census for a full-time hospitalist, while another 35% selected 16 to 20. Far fewer deemed it appropriate to see either more than 20 patients a day or 10 or less, suggesting that hospitalists recognize the need for equilibrium.
A “Resounding” Success Story
David Yu, MD, MBA, SFHM, FACP, medical director of the adult inpatient medicine service at Presbyterian Medical Group in Albuquerque, N.M., says there’s no “magic number” for an ideal daily patient census, and cautions against fixating on national averages and metrics.
“For example, seeing 15 patients in an inner-city hospital—like we are, where the patients are ill and they have really incredibly high levels of social and medical issues like placement—versus seeing 15 patients in an affluent suburban hospital, it’s comparing apples and oranges,” he says.
When Dr. Yu became medical director in January 2010, he says, “we were in crisis,” with the rounding team’s average patient census ranging from 18 to 20 per day. Some hospitalists weren’t seeing their last patients until 4 or 5 p.m., losing the opportunity for timely discussions with specialists to help reduce their patients’ length of stay. By neglecting to send patients home when appropriate, Dr. Yu says, the hospital was losing thousands of dollars in revenue through the failure to open up beds for new admissions. “That’s the classic example of dropping a dollar to pick up a quarter,” he says.
Dr. Yu and his team launched a comprehensive quality-improvement (QI) project that incorporated unit-based rounding centered on the hospital’s geography, and hired more full-time equivalents. As a result, the service now employs 46 FTEs, making it one of the largest nonacademic HM programs in the country. Meanwhile, the average daily census has dropped to a more manageable 11 to 13 patients, plus a few admissions.

—Ruth M. Kleinpell, PhD, RN, FAAN, FCCM, professor of nursing, Rush University Medical Center, nurse practitioner, Mercy Hospital and Medical Center, Chicago
Most significantly, average length of stay has decreased from 4.9 to 4.6 days with increased patient satisfaction and no significant change in the readmission rate, even as the hospital has added $2.5 million to the contribution margin (the revenue minus the variable costs). “So we took the focus on productivity and just elevated it higher to overall organizational finance,” Dr. Yu says. “We answered the age-old question: Is it better and financially more productive for the organization to lower the average starting census and to pay for the extra physician? And the answer is a resounding yes for us.”
The Flip Side
Adam Singer, MD, CEO of North Hollywood, Calif.-based IPC: The Hospitalist Company, points out that an overly low census can prove just as problematic, contributing to revenue and efficiency concerns. A hospitalist’s core ability to drive a delivery system, he says, requires sufficient exposure to a facility’s range of patients and contact with enough other staff members to propel a process of positive change.
“If you only have a few patients and your rounds are done in an hour, how engaged are you?” he asks.
Dr. Singer says his company’s more than 2,000 HM providers see roughly 15 to 18 patients on any given day. Even so, he says, the appropriate census for each practice can vary widely based on its structure, patient population, and the quality and experience of individual providers.
To ensure the numbers remain in the right range, Dr. Singer says, the company provides “complete transparency across the medical group, so that every doctor in the group sees exactly how many people everybody else is seeing.” If one doctor is seeing six patients and another is seeing 20, the group can self-regulate its census.
IPC also closely monitors a core series of clinical measures to ensure quality, ranging from ACE inhibitor use to length of stay and readmission rates. If one of the clinical measures starts to degrade, Dr. Singer says, the company can spot the problem and provide counseling or staffing assistance to right the ship. Hiring more doctors might be the most effective solution, but if a facility cannot afford more FTEs and quality is diminishing, he suggests collaborating with local primary-care physicians or even a less-busy hospitalist group to help share the load.
Safe Patients, Satisfied Providers
Ruth M. Kleinpell, PhD, RN, FAAN, FCCM, professor of nursing at Rush University Medical Center in Chicago and a nurse practitioner at Mercy Hospital and Medical Center, says each institution needs to do a self-assessment based on clinician feedback. Is the workload manageable? Can the providers take breaks? What do their satisfaction surveys suggest? What are the turnover and burnout rates?
“We have clinicians who report that they don’t even get a lunch break,” Kleinpell says. “That’s not safe, and that’s not lending itself to a work environment that’s satisfying for the practitioners.”

—David Yu, MD, MBA, SFHM, FACP, medical director, adult inpatient medicine service, Presbyterian Medical Group, Albuquerque, N.M.
Dr. Mitchell has seen overwhelmed hospitalists defer the care of patients they could normally handle to specialists, which leads to higher costs. Ultimately, Dr. Mitchell says, group leaders, administrators, and staff can all help set the right tone. “In the group I’m with now, there’s positive peer pressure to do the right thing, to be efficient, to communicate,” he says, “and if someone doesn’t do it, then it kind of stands out.”
Truly overwhelmed hospitalists can’t continue working well at an unsustainable pace. “It’s an extremely tricky situation, and I think for me it comes down to working with doctors that I trust and working with an administration that trusts us to say, ‘This is what’s best for patient care,’” Dr. Mitchell says. “And you need to prove that by getting the patient feedback and staff feedback that says, ‘Hey these guys are doing a good job.’”
Dr. Yu says many medical directors see the administration’s chief financial officer as an adversary when they should be working together. That kind of collaboration means coming up with strategies, metrics, and models that a financial department can relate to.
“You can’t just complain,” he says. “If your hospital is losing money, your program is going to shut down. But if you provide bad care, the hospital is going to do badly. Both sides have very legitimate points, and one of the jobs of a good medical director is to bridge those two worlds.”
Once the administration is on board, though, each facility must devise the right remedy for a chronically frenetic workload. John Nelson, MD, MHM, FACP, medical director of the hospitalist practice at Overlake Hospital Medical Center in Bellevue, Wash., says facilities can relieve overworked doctors by relieving them of tasks that other staff members could easily do.
“There are places I go where the hospitalists are doing things like arranging follow-up appointments themselves. That’s just nuts,” says Dr. Nelson, a co-founder and past president of SHM, practice management consultant, and columnist for The Hospitalist. “Or the hospitalists themselves are tasked with printing out a copy of their discharge summary and faxing it themselves.”
Other solutions depend on the makeup of clinical teams. “Do you have the ability to integrate nurse practitioners or physician assistants into the team?” Kleinpell asks. “Because certainly they can help maximize the hospitalist’s efficiency by seeing patients who maybe are less severely ill, or new admissions.”
Calling upon other providers to do patient histories, physical exams, or discharges, she says, also removes some of the burden.
Geographical rounding at one facility where he still occasionally practices, Dr. Knight says, “has made all the difference in the world” in improved efficiency. Responsibilities can be subdivided based on more than geography, too. At Palmetto, a team of nurse practitioners does all of the day-to-day management of stroke patients, helping to provide more standardized, reliable care.
A more evolved strategy, Dr. Singer says, is to develop hospitalist-only floors, which allow providers to see a higher volume of patients very effectively. Yet another technique is to assign a case manager to a specific provider instead of by disease or floor. That way, Dr. Singer says, a hospitalist facing a high patient census can round with the same case manager and much more effectively direct management resources.
Like other hospitalists, Dr. Nelson says hard caps should be considered “only in the most dire circumstances or only when all other options have been exhausted.” Sending patients away during peak times, he says, does nothing to address unusually slow days. Apart from the economic consequences, instituting a cap also can fuel the perception that an HM group isn’t pulling its own weight and raises questions about who else will have to take the group’s patients.
There may not be any one-size-fits-all solution, but observers say they are seeing a growing maturity and sophistication in how hospitals are dealing with patient censuses. At first, facilities may view volume and production as the most important considerations.
“Over time, they realize that’s a self-defeating way to operate because it does lead to more errors, it leads to more complications, it leads to longer length of stay,” says Dr. Knight. Eventually, he adds, most organizations come around to the realization that a more modest number of patients, perhaps 15 to 20 per day, may be more realistic for achieving quality and efficiency.
“Common sense tells you that if you’re running around trying to see 40 patients a day, you can’t just pay attention to the things you need to provide high-quality and efficient care,” Dr. Knight says. “You’re just running around and putting out fires.”
Bryn Nelson is a freelance medical writer in Seattle.
for additional resources visit the free SHM Practice Management Online Resource at www.hospitalmedicine.org/pmi
References
- Needleman J, Buerhaus P, Pankratz S, Leibson CL, Stevens SR, Harris M. Nurse staffing and inpatient hospital mortality. N Engl J Med. 2011;364(11): 037-1045.
- Michtalik H, Pronovost P, Driscoll B, Paskavitz M, Brotman D. Impact of workload on patient safety and quality of care: a survey of an online community of hospitalists. J Hosp Med. 2011;6(4):S50.
Ellis Knight, MD, MBA, FHM, senior vice president for physician and clinical integration at Palmetto Health in Columbia, S.C., recalls conducting root cause analyses after every serious adverse event when he was vice president for medical affairs at a large teaching hospital. “For every one of them—it was just like a broken record—every one of them, the nursing staff or the physicians involved would start the recount by saying, ‘It was a very, very busy day; we had a very high census,’” Dr. Knight says. “When that happens, when you get those, what I call tsunami waves of patients coming into a unit or being admitted at one time, it can really wreak havoc and it can make even the best clinicians get rushed, take shortcuts, and make mistakes.”
Researchers have long studied the consequences of temporary and longer-term workload imbalances for other healthcare providers; a recent in-depth study of one hospital found that the risk of inpatient patient mortality increased during shifts with below-target nurse staffing or higher patient turnover.1
Few studies, however, have specifically examined the repercussions of a patient census that is either too high or too low for a hospitalist service. At many facilities, that census can be influenced by an increasing threshold for hospitalization, meaning that the average inpatient is becoming sicker and more complicated, requiring more time during a hospitalist’s daily rounds. HM providers might report having better or worse electronic health records, support staff, and other ancillary services; different schedules; and mixes of clinical, administrative, and teaching responsibilities.
Even then, David M. Mitchell, MD, PhD, a hospitalist at Sibley Memorial Hospital in Washington, D.C., and a member of the SHM Performance Standards Committee, cautions that the ability of a doctor to churn through a higher patient count in no way ensures quality. “You don’t want to confuse efficiency with sloppiness,” he says.
In the absence of clear precedents and solid guidelines, hospitalist groups are struggling to come up with their own formulas for ensuring that workloads balance high productivity with sustainable quality—no easy feat. Nonetheless, first-hand accounts and survey data suggest that more providers are identifying common warning signs and devising tailored solutions to help the rapidly maturing field stay on track.
Henry Michtalik, MD, MPH, assistant professor of medicine at Johns Hopkins University School of Medicine, led one of the only surveys that has directly asked hospitalists how they perceive their own workloads. The survey, conducted through an online community of hospitalists and first presented at HM11, revealed several intriguing findings.2
On average, hospitalists reported seeing about 15 patients per shift or day, not including nights, weekends, or holidays. Apart from a few outliers, the range extended from the low teens to the mid-20s, Dr. Michtalik says. According to the survey, 40% of physicians said that more than once a month, their typical inpatient census exceeded the level that they deemed safe and appropriate for specific work settings; 36.1% of physicians reported that was true more than once per week.
Providers often reported that their average workload contributed to incomplete discussions with patients and families, the ordering of unnecessary tests or procedures, a delay in admissions or discharges, worsened patient satisfaction, poorer handoffs, and other problems. “We might be in a situation where we’re focusing on increasing the number of patients being seen or having high census numbers, which could be, paradoxically, actually increasing the costs of healthcare,” Dr. Michtalik says.
For a recent survey posted on the-hospitalist.org, 51% of respondents picked 11 to 15 as the most appropriate patient census for a full-time hospitalist, while another 35% selected 16 to 20. Far fewer deemed it appropriate to see either more than 20 patients a day or 10 or less, suggesting that hospitalists recognize the need for equilibrium.
A “Resounding” Success Story
David Yu, MD, MBA, SFHM, FACP, medical director of the adult inpatient medicine service at Presbyterian Medical Group in Albuquerque, N.M., says there’s no “magic number” for an ideal daily patient census, and cautions against fixating on national averages and metrics.
“For example, seeing 15 patients in an inner-city hospital—like we are, where the patients are ill and they have really incredibly high levels of social and medical issues like placement—versus seeing 15 patients in an affluent suburban hospital, it’s comparing apples and oranges,” he says.
When Dr. Yu became medical director in January 2010, he says, “we were in crisis,” with the rounding team’s average patient census ranging from 18 to 20 per day. Some hospitalists weren’t seeing their last patients until 4 or 5 p.m., losing the opportunity for timely discussions with specialists to help reduce their patients’ length of stay. By neglecting to send patients home when appropriate, Dr. Yu says, the hospital was losing thousands of dollars in revenue through the failure to open up beds for new admissions. “That’s the classic example of dropping a dollar to pick up a quarter,” he says.
Dr. Yu and his team launched a comprehensive quality-improvement (QI) project that incorporated unit-based rounding centered on the hospital’s geography, and hired more full-time equivalents. As a result, the service now employs 46 FTEs, making it one of the largest nonacademic HM programs in the country. Meanwhile, the average daily census has dropped to a more manageable 11 to 13 patients, plus a few admissions.
—Ruth M. Kleinpell, PhD, RN, FAAN, FCCM, professor of nursing, Rush University Medical Center, nurse practitioner, Mercy Hospital and Medical Center, Chicago
Most significantly, average length of stay has decreased from 4.9 to 4.6 days with increased patient satisfaction and no significant change in the readmission rate, even as the hospital has added $2.5 million to the contribution margin (the revenue minus the variable costs). “So we took the focus on productivity and just elevated it higher to overall organizational finance,” Dr. Yu says. “We answered the age-old question: Is it better and financially more productive for the organization to lower the average starting census and to pay for the extra physician? And the answer is a resounding yes for us.”
The Flip Side
Adam Singer, MD, CEO of North Hollywood, Calif.-based IPC: The Hospitalist Company, points out that an overly low census can prove just as problematic, contributing to revenue and efficiency concerns. A hospitalist’s core ability to drive a delivery system, he says, requires sufficient exposure to a facility’s range of patients and contact with enough other staff members to propel a process of positive change.
“If you only have a few patients and your rounds are done in an hour, how engaged are you?” he asks.
Dr. Singer says his company’s more than 2,000 HM providers see roughly 15 to 18 patients on any given day. Even so, he says, the appropriate census for each practice can vary widely based on its structure, patient population, and the quality and experience of individual providers.
To ensure the numbers remain in the right range, Dr. Singer says, the company provides “complete transparency across the medical group, so that every doctor in the group sees exactly how many people everybody else is seeing.” If one doctor is seeing six patients and another is seeing 20, the group can self-regulate its census.
IPC also closely monitors a core series of clinical measures to ensure quality, ranging from ACE inhibitor use to length of stay and readmission rates. If one of the clinical measures starts to degrade, Dr. Singer says, the company can spot the problem and provide counseling or staffing assistance to right the ship. Hiring more doctors might be the most effective solution, but if a facility cannot afford more FTEs and quality is diminishing, he suggests collaborating with local primary-care physicians or even a less-busy hospitalist group to help share the load.
Safe Patients, Satisfied Providers
Ruth M. Kleinpell, PhD, RN, FAAN, FCCM, professor of nursing at Rush University Medical Center in Chicago and a nurse practitioner at Mercy Hospital and Medical Center, says each institution needs to do a self-assessment based on clinician feedback. Is the workload manageable? Can the providers take breaks? What do their satisfaction surveys suggest? What are the turnover and burnout rates?
“We have clinicians who report that they don’t even get a lunch break,” Kleinpell says. “That’s not safe, and that’s not lending itself to a work environment that’s satisfying for the practitioners.”
—David Yu, MD, MBA, SFHM, FACP, medical director, adult inpatient medicine service, Presbyterian Medical Group, Albuquerque, N.M.
Dr. Mitchell has seen overwhelmed hospitalists defer the care of patients they could normally handle to specialists, which leads to higher costs. Ultimately, Dr. Mitchell says, group leaders, administrators, and staff can all help set the right tone. “In the group I’m with now, there’s positive peer pressure to do the right thing, to be efficient, to communicate,” he says, “and if someone doesn’t do it, then it kind of stands out.”
Truly overwhelmed hospitalists can’t continue working well at an unsustainable pace. “It’s an extremely tricky situation, and I think for me it comes down to working with doctors that I trust and working with an administration that trusts us to say, ‘This is what’s best for patient care,’” Dr. Mitchell says. “And you need to prove that by getting the patient feedback and staff feedback that says, ‘Hey these guys are doing a good job.’”
Dr. Yu says many medical directors see the administration’s chief financial officer as an adversary when they should be working together. That kind of collaboration means coming up with strategies, metrics, and models that a financial department can relate to.
“You can’t just complain,” he says. “If your hospital is losing money, your program is going to shut down. But if you provide bad care, the hospital is going to do badly. Both sides have very legitimate points, and one of the jobs of a good medical director is to bridge those two worlds.”
Once the administration is on board, though, each facility must devise the right remedy for a chronically frenetic workload. John Nelson, MD, MHM, FACP, medical director of the hospitalist practice at Overlake Hospital Medical Center in Bellevue, Wash., says facilities can relieve overworked doctors by relieving them of tasks that other staff members could easily do.
“There are places I go where the hospitalists are doing things like arranging follow-up appointments themselves. That’s just nuts,” says Dr. Nelson, a co-founder and past president of SHM, practice management consultant, and columnist for The Hospitalist. “Or the hospitalists themselves are tasked with printing out a copy of their discharge summary and faxing it themselves.”
Other solutions depend on the makeup of clinical teams. “Do you have the ability to integrate nurse practitioners or physician assistants into the team?” Kleinpell asks. “Because certainly they can help maximize the hospitalist’s efficiency by seeing patients who maybe are less severely ill, or new admissions.”
Calling upon other providers to do patient histories, physical exams, or discharges, she says, also removes some of the burden.
Geographical rounding at one facility where he still occasionally practices, Dr. Knight says, “has made all the difference in the world” in improved efficiency. Responsibilities can be subdivided based on more than geography, too. At Palmetto, a team of nurse practitioners does all of the day-to-day management of stroke patients, helping to provide more standardized, reliable care.
A more evolved strategy, Dr. Singer says, is to develop hospitalist-only floors, which allow providers to see a higher volume of patients very effectively. Yet another technique is to assign a case manager to a specific provider instead of by disease or floor. That way, Dr. Singer says, a hospitalist facing a high patient census can round with the same case manager and much more effectively direct management resources.
Like other hospitalists, Dr. Nelson says hard caps should be considered “only in the most dire circumstances or only when all other options have been exhausted.” Sending patients away during peak times, he says, does nothing to address unusually slow days. Apart from the economic consequences, instituting a cap also can fuel the perception that an HM group isn’t pulling its own weight and raises questions about who else will have to take the group’s patients.
There may not be any one-size-fits-all solution, but observers say they are seeing a growing maturity and sophistication in how hospitals are dealing with patient censuses. At first, facilities may view volume and production as the most important considerations.
“Over time, they realize that’s a self-defeating way to operate because it does lead to more errors, it leads to more complications, it leads to longer length of stay,” says Dr. Knight. Eventually, he adds, most organizations come around to the realization that a more modest number of patients, perhaps 15 to 20 per day, may be more realistic for achieving quality and efficiency.
“Common sense tells you that if you’re running around trying to see 40 patients a day, you can’t just pay attention to the things you need to provide high-quality and efficient care,” Dr. Knight says. “You’re just running around and putting out fires.”
Bryn Nelson is a freelance medical writer in Seattle.
for additional resources visit the free SHM Practice Management Online Resource at www.hospitalmedicine.org/pmi
References
- Needleman J, Buerhaus P, Pankratz S, Leibson CL, Stevens SR, Harris M. Nurse staffing and inpatient hospital mortality. N Engl J Med. 2011;364(11): 037-1045.
- Michtalik H, Pronovost P, Driscoll B, Paskavitz M, Brotman D. Impact of workload on patient safety and quality of care: a survey of an online community of hospitalists. J Hosp Med. 2011;6(4):S50.
Ellis Knight, MD, MBA, FHM, senior vice president for physician and clinical integration at Palmetto Health in Columbia, S.C., recalls conducting root cause analyses after every serious adverse event when he was vice president for medical affairs at a large teaching hospital. “For every one of them—it was just like a broken record—every one of them, the nursing staff or the physicians involved would start the recount by saying, ‘It was a very, very busy day; we had a very high census,’” Dr. Knight says. “When that happens, when you get those, what I call tsunami waves of patients coming into a unit or being admitted at one time, it can really wreak havoc and it can make even the best clinicians get rushed, take shortcuts, and make mistakes.”
Researchers have long studied the consequences of temporary and longer-term workload imbalances for other healthcare providers; a recent in-depth study of one hospital found that the risk of inpatient patient mortality increased during shifts with below-target nurse staffing or higher patient turnover.1
Few studies, however, have specifically examined the repercussions of a patient census that is either too high or too low for a hospitalist service. At many facilities, that census can be influenced by an increasing threshold for hospitalization, meaning that the average inpatient is becoming sicker and more complicated, requiring more time during a hospitalist’s daily rounds. HM providers might report having better or worse electronic health records, support staff, and other ancillary services; different schedules; and mixes of clinical, administrative, and teaching responsibilities.
Even then, David M. Mitchell, MD, PhD, a hospitalist at Sibley Memorial Hospital in Washington, D.C., and a member of the SHM Performance Standards Committee, cautions that the ability of a doctor to churn through a higher patient count in no way ensures quality. “You don’t want to confuse efficiency with sloppiness,” he says.
In the absence of clear precedents and solid guidelines, hospitalist groups are struggling to come up with their own formulas for ensuring that workloads balance high productivity with sustainable quality—no easy feat. Nonetheless, first-hand accounts and survey data suggest that more providers are identifying common warning signs and devising tailored solutions to help the rapidly maturing field stay on track.
Henry Michtalik, MD, MPH, assistant professor of medicine at Johns Hopkins University School of Medicine, led one of the only surveys that has directly asked hospitalists how they perceive their own workloads. The survey, conducted through an online community of hospitalists and first presented at HM11, revealed several intriguing findings.2
On average, hospitalists reported seeing about 15 patients per shift or day, not including nights, weekends, or holidays. Apart from a few outliers, the range extended from the low teens to the mid-20s, Dr. Michtalik says. According to the survey, 40% of physicians said that more than once a month, their typical inpatient census exceeded the level that they deemed safe and appropriate for specific work settings; 36.1% of physicians reported that was true more than once per week.
Providers often reported that their average workload contributed to incomplete discussions with patients and families, the ordering of unnecessary tests or procedures, a delay in admissions or discharges, worsened patient satisfaction, poorer handoffs, and other problems. “We might be in a situation where we’re focusing on increasing the number of patients being seen or having high census numbers, which could be, paradoxically, actually increasing the costs of healthcare,” Dr. Michtalik says.
For a recent survey posted on the-hospitalist.org, 51% of respondents picked 11 to 15 as the most appropriate patient census for a full-time hospitalist, while another 35% selected 16 to 20. Far fewer deemed it appropriate to see either more than 20 patients a day or 10 or less, suggesting that hospitalists recognize the need for equilibrium.
A “Resounding” Success Story
David Yu, MD, MBA, SFHM, FACP, medical director of the adult inpatient medicine service at Presbyterian Medical Group in Albuquerque, N.M., says there’s no “magic number” for an ideal daily patient census, and cautions against fixating on national averages and metrics.
“For example, seeing 15 patients in an inner-city hospital—like we are, where the patients are ill and they have really incredibly high levels of social and medical issues like placement—versus seeing 15 patients in an affluent suburban hospital, it’s comparing apples and oranges,” he says.
When Dr. Yu became medical director in January 2010, he says, “we were in crisis,” with the rounding team’s average patient census ranging from 18 to 20 per day. Some hospitalists weren’t seeing their last patients until 4 or 5 p.m., losing the opportunity for timely discussions with specialists to help reduce their patients’ length of stay. By neglecting to send patients home when appropriate, Dr. Yu says, the hospital was losing thousands of dollars in revenue through the failure to open up beds for new admissions. “That’s the classic example of dropping a dollar to pick up a quarter,” he says.
Dr. Yu and his team launched a comprehensive quality-improvement (QI) project that incorporated unit-based rounding centered on the hospital’s geography, and hired more full-time equivalents. As a result, the service now employs 46 FTEs, making it one of the largest nonacademic HM programs in the country. Meanwhile, the average daily census has dropped to a more manageable 11 to 13 patients, plus a few admissions.
—Ruth M. Kleinpell, PhD, RN, FAAN, FCCM, professor of nursing, Rush University Medical Center, nurse practitioner, Mercy Hospital and Medical Center, Chicago
Most significantly, average length of stay has decreased from 4.9 to 4.6 days with increased patient satisfaction and no significant change in the readmission rate, even as the hospital has added $2.5 million to the contribution margin (the revenue minus the variable costs). “So we took the focus on productivity and just elevated it higher to overall organizational finance,” Dr. Yu says. “We answered the age-old question: Is it better and financially more productive for the organization to lower the average starting census and to pay for the extra physician? And the answer is a resounding yes for us.”
The Flip Side
Adam Singer, MD, CEO of North Hollywood, Calif.-based IPC: The Hospitalist Company, points out that an overly low census can prove just as problematic, contributing to revenue and efficiency concerns. A hospitalist’s core ability to drive a delivery system, he says, requires sufficient exposure to a facility’s range of patients and contact with enough other staff members to propel a process of positive change.
“If you only have a few patients and your rounds are done in an hour, how engaged are you?” he asks.
Dr. Singer says his company’s more than 2,000 HM providers see roughly 15 to 18 patients on any given day. Even so, he says, the appropriate census for each practice can vary widely based on its structure, patient population, and the quality and experience of individual providers.
To ensure the numbers remain in the right range, Dr. Singer says, the company provides “complete transparency across the medical group, so that every doctor in the group sees exactly how many people everybody else is seeing.” If one doctor is seeing six patients and another is seeing 20, the group can self-regulate its census.
IPC also closely monitors a core series of clinical measures to ensure quality, ranging from ACE inhibitor use to length of stay and readmission rates. If one of the clinical measures starts to degrade, Dr. Singer says, the company can spot the problem and provide counseling or staffing assistance to right the ship. Hiring more doctors might be the most effective solution, but if a facility cannot afford more FTEs and quality is diminishing, he suggests collaborating with local primary-care physicians or even a less-busy hospitalist group to help share the load.
Safe Patients, Satisfied Providers
Ruth M. Kleinpell, PhD, RN, FAAN, FCCM, professor of nursing at Rush University Medical Center in Chicago and a nurse practitioner at Mercy Hospital and Medical Center, says each institution needs to do a self-assessment based on clinician feedback. Is the workload manageable? Can the providers take breaks? What do their satisfaction surveys suggest? What are the turnover and burnout rates?
“We have clinicians who report that they don’t even get a lunch break,” Kleinpell says. “That’s not safe, and that’s not lending itself to a work environment that’s satisfying for the practitioners.”
—David Yu, MD, MBA, SFHM, FACP, medical director, adult inpatient medicine service, Presbyterian Medical Group, Albuquerque, N.M.
Dr. Mitchell has seen overwhelmed hospitalists defer the care of patients they could normally handle to specialists, which leads to higher costs. Ultimately, Dr. Mitchell says, group leaders, administrators, and staff can all help set the right tone. “In the group I’m with now, there’s positive peer pressure to do the right thing, to be efficient, to communicate,” he says, “and if someone doesn’t do it, then it kind of stands out.”
Truly overwhelmed hospitalists can’t continue working well at an unsustainable pace. “It’s an extremely tricky situation, and I think for me it comes down to working with doctors that I trust and working with an administration that trusts us to say, ‘This is what’s best for patient care,’” Dr. Mitchell says. “And you need to prove that by getting the patient feedback and staff feedback that says, ‘Hey these guys are doing a good job.’”
Dr. Yu says many medical directors see the administration’s chief financial officer as an adversary when they should be working together. That kind of collaboration means coming up with strategies, metrics, and models that a financial department can relate to.
“You can’t just complain,” he says. “If your hospital is losing money, your program is going to shut down. But if you provide bad care, the hospital is going to do badly. Both sides have very legitimate points, and one of the jobs of a good medical director is to bridge those two worlds.”
Once the administration is on board, though, each facility must devise the right remedy for a chronically frenetic workload. John Nelson, MD, MHM, FACP, medical director of the hospitalist practice at Overlake Hospital Medical Center in Bellevue, Wash., says facilities can relieve overworked doctors by relieving them of tasks that other staff members could easily do.
“There are places I go where the hospitalists are doing things like arranging follow-up appointments themselves. That’s just nuts,” says Dr. Nelson, a co-founder and past president of SHM, practice management consultant, and columnist for The Hospitalist. “Or the hospitalists themselves are tasked with printing out a copy of their discharge summary and faxing it themselves.”
Other solutions depend on the makeup of clinical teams. “Do you have the ability to integrate nurse practitioners or physician assistants into the team?” Kleinpell asks. “Because certainly they can help maximize the hospitalist’s efficiency by seeing patients who maybe are less severely ill, or new admissions.”
Calling upon other providers to do patient histories, physical exams, or discharges, she says, also removes some of the burden.
Geographical rounding at one facility where he still occasionally practices, Dr. Knight says, “has made all the difference in the world” in improved efficiency. Responsibilities can be subdivided based on more than geography, too. At Palmetto, a team of nurse practitioners does all of the day-to-day management of stroke patients, helping to provide more standardized, reliable care.
A more evolved strategy, Dr. Singer says, is to develop hospitalist-only floors, which allow providers to see a higher volume of patients very effectively. Yet another technique is to assign a case manager to a specific provider instead of by disease or floor. That way, Dr. Singer says, a hospitalist facing a high patient census can round with the same case manager and much more effectively direct management resources.
Like other hospitalists, Dr. Nelson says hard caps should be considered “only in the most dire circumstances or only when all other options have been exhausted.” Sending patients away during peak times, he says, does nothing to address unusually slow days. Apart from the economic consequences, instituting a cap also can fuel the perception that an HM group isn’t pulling its own weight and raises questions about who else will have to take the group’s patients.
There may not be any one-size-fits-all solution, but observers say they are seeing a growing maturity and sophistication in how hospitals are dealing with patient censuses. At first, facilities may view volume and production as the most important considerations.
“Over time, they realize that’s a self-defeating way to operate because it does lead to more errors, it leads to more complications, it leads to longer length of stay,” says Dr. Knight. Eventually, he adds, most organizations come around to the realization that a more modest number of patients, perhaps 15 to 20 per day, may be more realistic for achieving quality and efficiency.
“Common sense tells you that if you’re running around trying to see 40 patients a day, you can’t just pay attention to the things you need to provide high-quality and efficient care,” Dr. Knight says. “You’re just running around and putting out fires.”
Bryn Nelson is a freelance medical writer in Seattle.
for additional resources visit the free SHM Practice Management Online Resource at www.hospitalmedicine.org/pmi
References
- Needleman J, Buerhaus P, Pankratz S, Leibson CL, Stevens SR, Harris M. Nurse staffing and inpatient hospital mortality. N Engl J Med. 2011;364(11): 037-1045.
- Michtalik H, Pronovost P, Driscoll B, Paskavitz M, Brotman D. Impact of workload on patient safety and quality of care: a survey of an online community of hospitalists. J Hosp Med. 2011;6(4):S50.
In the Literature: Physician Reviews of HM-Related Research
In This Edition
Literature At A Glance
A guide to this month’s studies
- Hospitalist views on readmission prevention
- Characteristics of hospital ICU readmission
- Effect of clopidogrel on bleeding outcomes in vascular surgery
- Time-versus tissue-based diagnosis of TIA
- ETT versus ETT with imaging for the diagnosis of CAD in women
- Effect of high urine output with adequate hydration on contrast-induced nephropathy
- Stroke rate in CABG patients with severe carotid artery stenosis
- Effect of cardiac arrest on long-term cognition
Hospitalists View Readmissions as Potentially Preventable by Team-Based Care
Clinical question: How do front-line hospitalists perceive the preventability of early hospital readmissions?
Background: Hospital readmission has received national attention as an indicator of poor healthcare quality and unnecessary costs. While some studies suggest that some readmissions are preventable, the exact number is unknown. Understanding preventability and the views of front-line clinicians might help hospitalists balance multifactorial compromise between throughput and length of stay.
Study design: Retrospective cohort study.
Setting: Two community tertiary-care hospitals and two suburban hospitals staffed by a single hospitalist group in Portland, Ore.
Synopsis: A group of 17 hospitalists analyzed the inpatient and outpatient charts of 300 consecutive patients readmitted within 21 days of discharge using a structured data collection tool to record patient characteristics, process measures, and perceived preventability of the readmission. Patients were either discharged by internal-medicine hospitalists or had an internal-medicine consultation during their initial stay.
Characteristics of readmitted patients and initial hospital stays were similar to those previously reported in other studies. More than 60% of readmissions were deemed preventable (15%) or possibly preventable (46%). As prevention strategies for these readmissions, hospitalists most frequently suggested interventions under their control, such as longer initial hospital stay (23%). Other potential interventions focused on system approaches, including outpatient appointments, case management, palliative care, and home health.
In most cases (96%), the reviewer was not the discharging hospitalist. Only six hospitalists performed 83% of the reviews, and inter-reviewer reliability was not assessed. Other limitations included confounding biases, such as timing of review, source hospital reviewed, reviewer optimism, and previous primary-care experience of reviewer.
Bottom line: Prevention of hospital readmissions will require a balance between increased length of stay and system-based team approaches beyond the direct control of hospitalists.
Citation: Koekkoek D, Bayley KB, Brown A, Rustvold DL. Hospitalists assess the causes of early hospital readmissions. J Hosp Med. 2011;6:383-388.
Patients with Complex, Severe Illnesses and Persistent Physiologic Abnormalities Have Higher Risk of Intensive-Care-Unit Readmission
Clinical question: Which patient characteristics increase the risk for intensive-care-unit (ICU) readmission?
Background: Patients are often discharged from the ICU based on subjective criteria, workload, and bed demand, making ICU readmission a tempting quality indicator. Studies have examined institutional characteristics leading to ICU readmission, but few have shown how patient case mix affects longer lengths of ICU and hospital stays and higher in-hospital mortality.
Study design: Retrospective observational cohort study using a large, multi-institutional U.S. database.
Setting: Computerized data collection and analysis system from 97 intensive- and cardiac-care units at 35 hospitals in the United States.
Synopsis: Patient-level characteristics and outcomes of 229,375 initial ICU admissions from 2001 to 2009 were compared for patients with and without ICU readmission using the Acute Physiology and Chronic Health Evaluation (APACHE) IV database (Cerner Corporation, Kansas City, Mo.). Multivariable logistic regression analysis identified potential characteristics increasing the risk for ICU readmission. Case-mix adjusted outcomes for mortality and length of stay were calculated.
A total of 13,980 (6.1%) patients were readmitted to the ICUs. Characteristics associated with ICU readmission were similar to those previously reported. In addition to illness severity at initial admission, readmission was associated with complications, poor response to therapy, or persistent physiologic abnormalities at ICU discharge. Patients who were readmitted to the ICU had a risk-adjusted, fourfold greater probability of in-hospital mortality and a 2.5-fold increase in length of hospital stay.
Data were obtained solely from hospitals with an APACHE system, and included only one hospital from the Northeast. Not all ICUs from a single-study hospital were included. DNR orders were not available in the database for analysis.
Bottom line: Persistent physiologic derangements at ICU discharge are as influential on ICU readmission and poor outcomes as other known risk factors, potentially warranting slightly longer ICU stays for these specific patients.
Citation: Kramer AA, Higgins TL, Zimmerman JE. Intensive care unit readmissions in U.S. hospitals: patient characteristics, risk factors, and outcomes. Crit Care Med. 2012;40:3-10.
Clopidogrel Might Not Worsen Bleeding Complications During Surgery
Clinical question: Does clopidogrel cause bleeding complications during vascular surgery?
Background: There is no consensus and few large trials to decide if preoperative clopidogrel use causes bleeding complications in vascular surgeries.
Study design: Prospective.
Setting: New England academic and community centers.
Synopsis: The authors enrolled 10,406 patients from 15 academic and community centers in New England. These patients underwent carotid endarterectomy, lower-extremity bypass, and abdominal aortic aneurysm repair. Ruptured aortic aneurysms were excluded. The use of aspirin, clopidogrel, both, or no anti-platelet therapy within 48 hours before surgery was recorded. The outcomes measured were postoperative bleeding requiring reoperation and the need for packed red blood cell transfusions.
Clopidogrel therapy (n=229) compared with no anti-platelet therapy (n=2,010) did well when measured by reoperation (clopidogrel 0.9%, none 1.5%, P=0.74), incidence of transfusion (clopidogrel 0%, none 18%, P=0.1), and volume of transfusion (clopidogrel 0 units, none 0.7 units, P=0.1). However, the significance, especially for reoperation, is not impressive.
The power of the study could be improved with more clopidogrel users. Another limitation is that the aspirin and clopidogrel platelet effect lasts longer than the 48-hour cutoff. As there were more bleeding complications in the no-anti-platelet group, there is a concern for bias in how the patients were selected and treated.
Bottom line: Clopidogrel might be safe to continue in vascular surgeries, but larger and more valid studies are needed.
Citation: Stone DH, Goodney PP, Schanzer A, et al. Clopidogrel is not associated with major bleeding complications during peripheral arterial surgery. J Vasc Surg. 2011;54:779-784.
Tissue-Defined TIAs Have Better Prognostic Benefits Than Time-Defined TIAs
Citation: Is risk stratification for recurrent stroke better when brain imaging is performed after a transient ischemic attack (TIA)?
Background: The presence of a TIA is a known risk factor for recurrent stroke. There is debate in changing the definition of TIA from time-based to tissue-based. However, it is not known if this will improve management.
Study design: Multicenter observation cohort.
Setting: Twelve independent international research centers.
Synopsis: The current definition of a TIA is a neurological deficit that resolves within 24 hours. To determine the urgency of an admission and work-up, the ABCD2 score (age, blood pressure, clinical symptoms, duration, and diabetes) is often used as a prognostic tool for recurrent stroke. The authors enrolled 4,574 patients with the traditional diagnosis of TIA. In addition to calculating their ABCD2 score, they were then classified as tissue-positive (infarction) or tissue-negative per MRI or CT. At both seven and 90 days after TIA, both imaging modalities when combined with ABCD2 were able to identify risk for recurrent stroke better than if they were used alone.
Limitations included the images being interpreted by their individual healthcare centers and that the stroke centers had lower recurrent rates of stroke compared with community centers. If only a CT can be used, it should be noted that the sensitivity is lower when compared with an MRI in this study.
Bottom line: This categorization of tissue- or non-tissue-positive TIAs improved the prognostic information provided by the ABCD2 score and might improve management decisions.
Citation: Giles MF, Albers GW, Amarenco P, et al. Early stroke risk and ABCD2 score performance in tissue- vs time-defined TIA: a multicenter study. Neurology. 2011;77:1222-1228.
ETT Comparable to MPI as Initial Diagnostic Test for Women Suspected of CAD
Clinical question: Is the exercise treadmill test (ETT) equivalent to myocardial perfusion imaging (MPI) as an initial diagnostic test for low-risk women capable of exercising with suspected coronary artery disease (CAD)?
Background: To date, the evidence base for diagnostic testing in women with suspected CAD has been limited, with no randomized trials to guide appropriate clinical decision-making in the choice of noninvasive testing strategies. The aim of this trial was to provide comparative-effectiveness data for women capable of performing exercise testing with regard to whether the addition of imaging to standard ETT provided incremental clinical benefit over index ETT alone.
Study design: Prospective randomized.
Settings: Forty-three cardiology practices across the U.S.
Synopsis: A total of 824 women 40 years of age or older with intermediate pretest CAD likelihood were randomized to ETT or MPI. All the women included in the study were symptomatic with suspected CAD, had an interpretable ECG, and were >5 on DASI (Duke Activity Status Index). A total of 17 primary end points were confirmed, including three nonfatal myocardial infarctions, one heart failure hospitalization, 12 acute coronary syndrome hospitalizations, and only one sudden cardiac death reported in 772 women.
At two years, major adverse cardiovascular events (MACE)-free survival was identical (98%) for women randomized to the ETT or exercise MPI arm (P=0.59). The observed two-year MACE rate was 1.7% for ETT and 2.3% for exercise MPI. For secondary end points, the overall rate of hospitalization for chest pain was 3%. By randomization, the two-year rate of hospitalization for chest pain symptoms was 3% for women in the ETT arm and 4% for those in the exercise MPI arm (P=0.39). An additional six women died from non-cardiac causes (ETT arm, 0.5%; exercise MPI arm, 1%; P=0.39).
Bottom line: ETT is of comparable diagnostic efficacy to MPI as an initial diagnostic test for women suspected of CAD, capable of exercising, based on two-year outcome of cardiac death, nonfatal myocardial infarction, or hospital admission for acute coronary syndrome or heart failure.
Citation: Shaw LJ, Mieres JH, Hendel RH, et al. Comparative effectiveness of exercise electrocardiography with or without myocardial perfusion single photon emission computed tomography in women with suspected coronary artery disease: results from the What Is the Optimal Method for Ischemia Evaluation in Women (WOMEN) trial. Circulation. 2011;124:1239-1249.
Controlled Forced Diuresis Is More Effective in High-Risk Patients for CI-AKI Prevention
Clinical question: Is a system of hydration that creates high urine output while maintaining fluid balance better than routine hydration in high-risk patients for preventing contrast-induced acute kidney injury (CI-AKI)?
Background: Hydration with sodium bicarbonate solution and administration of N-acetylcysteine (NAC) help prevent CI-AKI in low- to medium-risk patients. A recent study (PRINCE) suggests that increasing the urine flow rate (≥150 mL/hr) reduces the toxic effect of contrast, but this regimen requires forced diuresis with high doses of furosemide that may result in further renal damage due to negative fluid balance. The RenalGuard system (PLC Medical Systems Inc., Franklin, Mass.) can simultaneously achieve high urine output and maintain fluid balance.
Study design: Randomized, investigator-driven, open-label study comparing two different hydration strategies.
Setting: Multicenter trial in Italy involving patients with chronic kidney disease scheduled for angiography who met the inclusion and exclusion criteria for high risk of developing CI-AKI.
Synopsis: The study included 292 patients randomized to receive sodium bicarbonate solution (control group) versus hydration with saline controlled by the RenalGuard system with furosemide. Both groups received NAC, though at different doses and routes of administration. CI-AKI occurred in 20.5% (30 of 146) in the control group versus 11% (16 of 146) in the RenalGuard group.
Bottom line: Controlled forced diuresis to achieve high urine flow rate is more effective than conventional hydration with sodium bicarbonate solution in high-risk patients for preventing CI-AKI. Larger studies are needed to confirm and define the role of the RenalGuard system.
Citation: Briguori C, Visconti G, Focaccio A, et al. Renal insufficiency after contrast media administration trial II (REMEDIAL II). Circulation. 2011;124:1260-1269.
Severe Asymptomatic Carotid Artery Stenosis Does Not Increase Stroke or Mortality Risks after CAB Surgery
Clinical question: What is the risk for stroke in patients with asymptomatic carotid artery stenosis (CAS) who are undergoing coronary artery bypass grafting (CABG)?
Background: Stroke occurs as a complication of CABG in approximately 2% of patients. The vast majority occur within the first 24 hours of surgery and are associated with a high mortality rate.
Study design: Retrospective cohort.
Setting: A single institution in Washington, D.C.
Synopsis: Data were collected on 878 consecutive patients who had undergone carotid ultrasound before CABG over a six-year period. Patients with severe CAS of >75% (n=117) were compared with those with <75% stenosis (n=761) to assess the rates of in-hospital stroke and mortality.
Patients with severe CAS had similar rates of stroke compared with those without severe CAS (3.4% vs. 3.6%). Additionally, there was no difference in the incidence of in-hospital complications or mortality between the two groups.
Bottom line: The cause of stroke after CABG is complex and multifactorial, but severe CAS alone appears to not be the biggest risk factor for stroke in patients undergoing CABG.
Citation: Mahmoudi M, Hill PC, Xue Z, et al. Patients with severe asymptomatic carotid artery stenosis do not have a higher risk of stroke and mortality after coronary artery bypass surgery. Stroke. 2011;42:2801-2805.
Cardiac Arrest Survivors Have Long-Term Memory Deficits
Clinical question: Are there any lasting cognitive deficits in patients surviving out-of-hospital cardiac arrest (OHCA) from ventricular fibrillation (VF)?
Background: Although advances have been made in the rapid intervention of OHCAs, there are no population-based, age-adjusted studies of the cognitive and neurologic outcomes of long-term survivors when the “chain of survival” is used (rapid emergency services, bystander CPR, early defibrillation, and advanced care).
Study design: Prospective population-based, age-adjusted study.
Setting: Single hospital in Olmsted County, Minn.
Synopsis: Of 332 OHCA patients, 47 survivors were enrolled for neurologic and neuropsychological testing at least six months after a near-death experience (median time since arrest, 7.8 years). Neurologic examination did not reveal any focal deficits related to the event, but long-term survivors had lower scores on measures of long-term memory and learning efficiency (P=0.001). Nearly all survivors were functionally independent at the time of testing. Interestingly, there was no correlation between prolonged call-to-shock time and cognitive ability, suggesting that there is a possibility of positive neurologic outcomes with a call-to-shock time as late as 10 minutes in OHCA. Older age was also not identified as a negative prognostic factor.
A limitation of the study was the small sample size, though larger populations of survivors are difficult to find. The precise meaning of “cognitive impairment” was also controversial and should be better defined for any future studies.
Bottom line: Long-term survivors of OHCA from VF have long-term memory impairment compared with the normal population at the same age and education level.
Citation: Mateen FJ, Josephs KA, Trenerry MR, et al. Long-term cognitive outcomes following out-of-hospital cardiac arrest. Neurology. 2011;77:1438-1445.
In This Edition
Literature At A Glance
A guide to this month’s studies
- Hospitalist views on readmission prevention
- Characteristics of hospital ICU readmission
- Effect of clopidogrel on bleeding outcomes in vascular surgery
- Time-versus tissue-based diagnosis of TIA
- ETT versus ETT with imaging for the diagnosis of CAD in women
- Effect of high urine output with adequate hydration on contrast-induced nephropathy
- Stroke rate in CABG patients with severe carotid artery stenosis
- Effect of cardiac arrest on long-term cognition
Hospitalists View Readmissions as Potentially Preventable by Team-Based Care
Clinical question: How do front-line hospitalists perceive the preventability of early hospital readmissions?
Background: Hospital readmission has received national attention as an indicator of poor healthcare quality and unnecessary costs. While some studies suggest that some readmissions are preventable, the exact number is unknown. Understanding preventability and the views of front-line clinicians might help hospitalists balance multifactorial compromise between throughput and length of stay.
Study design: Retrospective cohort study.
Setting: Two community tertiary-care hospitals and two suburban hospitals staffed by a single hospitalist group in Portland, Ore.
Synopsis: A group of 17 hospitalists analyzed the inpatient and outpatient charts of 300 consecutive patients readmitted within 21 days of discharge using a structured data collection tool to record patient characteristics, process measures, and perceived preventability of the readmission. Patients were either discharged by internal-medicine hospitalists or had an internal-medicine consultation during their initial stay.
Characteristics of readmitted patients and initial hospital stays were similar to those previously reported in other studies. More than 60% of readmissions were deemed preventable (15%) or possibly preventable (46%). As prevention strategies for these readmissions, hospitalists most frequently suggested interventions under their control, such as longer initial hospital stay (23%). Other potential interventions focused on system approaches, including outpatient appointments, case management, palliative care, and home health.
In most cases (96%), the reviewer was not the discharging hospitalist. Only six hospitalists performed 83% of the reviews, and inter-reviewer reliability was not assessed. Other limitations included confounding biases, such as timing of review, source hospital reviewed, reviewer optimism, and previous primary-care experience of reviewer.
Bottom line: Prevention of hospital readmissions will require a balance between increased length of stay and system-based team approaches beyond the direct control of hospitalists.
Citation: Koekkoek D, Bayley KB, Brown A, Rustvold DL. Hospitalists assess the causes of early hospital readmissions. J Hosp Med. 2011;6:383-388.
Patients with Complex, Severe Illnesses and Persistent Physiologic Abnormalities Have Higher Risk of Intensive-Care-Unit Readmission
Clinical question: Which patient characteristics increase the risk for intensive-care-unit (ICU) readmission?
Background: Patients are often discharged from the ICU based on subjective criteria, workload, and bed demand, making ICU readmission a tempting quality indicator. Studies have examined institutional characteristics leading to ICU readmission, but few have shown how patient case mix affects longer lengths of ICU and hospital stays and higher in-hospital mortality.
Study design: Retrospective observational cohort study using a large, multi-institutional U.S. database.
Setting: Computerized data collection and analysis system from 97 intensive- and cardiac-care units at 35 hospitals in the United States.
Synopsis: Patient-level characteristics and outcomes of 229,375 initial ICU admissions from 2001 to 2009 were compared for patients with and without ICU readmission using the Acute Physiology and Chronic Health Evaluation (APACHE) IV database (Cerner Corporation, Kansas City, Mo.). Multivariable logistic regression analysis identified potential characteristics increasing the risk for ICU readmission. Case-mix adjusted outcomes for mortality and length of stay were calculated.
A total of 13,980 (6.1%) patients were readmitted to the ICUs. Characteristics associated with ICU readmission were similar to those previously reported. In addition to illness severity at initial admission, readmission was associated with complications, poor response to therapy, or persistent physiologic abnormalities at ICU discharge. Patients who were readmitted to the ICU had a risk-adjusted, fourfold greater probability of in-hospital mortality and a 2.5-fold increase in length of hospital stay.
Data were obtained solely from hospitals with an APACHE system, and included only one hospital from the Northeast. Not all ICUs from a single-study hospital were included. DNR orders were not available in the database for analysis.
Bottom line: Persistent physiologic derangements at ICU discharge are as influential on ICU readmission and poor outcomes as other known risk factors, potentially warranting slightly longer ICU stays for these specific patients.
Citation: Kramer AA, Higgins TL, Zimmerman JE. Intensive care unit readmissions in U.S. hospitals: patient characteristics, risk factors, and outcomes. Crit Care Med. 2012;40:3-10.
Clopidogrel Might Not Worsen Bleeding Complications During Surgery
Clinical question: Does clopidogrel cause bleeding complications during vascular surgery?
Background: There is no consensus and few large trials to decide if preoperative clopidogrel use causes bleeding complications in vascular surgeries.
Study design: Prospective.
Setting: New England academic and community centers.
Synopsis: The authors enrolled 10,406 patients from 15 academic and community centers in New England. These patients underwent carotid endarterectomy, lower-extremity bypass, and abdominal aortic aneurysm repair. Ruptured aortic aneurysms were excluded. The use of aspirin, clopidogrel, both, or no anti-platelet therapy within 48 hours before surgery was recorded. The outcomes measured were postoperative bleeding requiring reoperation and the need for packed red blood cell transfusions.
Clopidogrel therapy (n=229) compared with no anti-platelet therapy (n=2,010) did well when measured by reoperation (clopidogrel 0.9%, none 1.5%, P=0.74), incidence of transfusion (clopidogrel 0%, none 18%, P=0.1), and volume of transfusion (clopidogrel 0 units, none 0.7 units, P=0.1). However, the significance, especially for reoperation, is not impressive.
The power of the study could be improved with more clopidogrel users. Another limitation is that the aspirin and clopidogrel platelet effect lasts longer than the 48-hour cutoff. As there were more bleeding complications in the no-anti-platelet group, there is a concern for bias in how the patients were selected and treated.
Bottom line: Clopidogrel might be safe to continue in vascular surgeries, but larger and more valid studies are needed.
Citation: Stone DH, Goodney PP, Schanzer A, et al. Clopidogrel is not associated with major bleeding complications during peripheral arterial surgery. J Vasc Surg. 2011;54:779-784.
Tissue-Defined TIAs Have Better Prognostic Benefits Than Time-Defined TIAs
Citation: Is risk stratification for recurrent stroke better when brain imaging is performed after a transient ischemic attack (TIA)?
Background: The presence of a TIA is a known risk factor for recurrent stroke. There is debate in changing the definition of TIA from time-based to tissue-based. However, it is not known if this will improve management.
Study design: Multicenter observation cohort.
Setting: Twelve independent international research centers.
Synopsis: The current definition of a TIA is a neurological deficit that resolves within 24 hours. To determine the urgency of an admission and work-up, the ABCD2 score (age, blood pressure, clinical symptoms, duration, and diabetes) is often used as a prognostic tool for recurrent stroke. The authors enrolled 4,574 patients with the traditional diagnosis of TIA. In addition to calculating their ABCD2 score, they were then classified as tissue-positive (infarction) or tissue-negative per MRI or CT. At both seven and 90 days after TIA, both imaging modalities when combined with ABCD2 were able to identify risk for recurrent stroke better than if they were used alone.
Limitations included the images being interpreted by their individual healthcare centers and that the stroke centers had lower recurrent rates of stroke compared with community centers. If only a CT can be used, it should be noted that the sensitivity is lower when compared with an MRI in this study.
Bottom line: This categorization of tissue- or non-tissue-positive TIAs improved the prognostic information provided by the ABCD2 score and might improve management decisions.
Citation: Giles MF, Albers GW, Amarenco P, et al. Early stroke risk and ABCD2 score performance in tissue- vs time-defined TIA: a multicenter study. Neurology. 2011;77:1222-1228.
ETT Comparable to MPI as Initial Diagnostic Test for Women Suspected of CAD
Clinical question: Is the exercise treadmill test (ETT) equivalent to myocardial perfusion imaging (MPI) as an initial diagnostic test for low-risk women capable of exercising with suspected coronary artery disease (CAD)?
Background: To date, the evidence base for diagnostic testing in women with suspected CAD has been limited, with no randomized trials to guide appropriate clinical decision-making in the choice of noninvasive testing strategies. The aim of this trial was to provide comparative-effectiveness data for women capable of performing exercise testing with regard to whether the addition of imaging to standard ETT provided incremental clinical benefit over index ETT alone.
Study design: Prospective randomized.
Settings: Forty-three cardiology practices across the U.S.
Synopsis: A total of 824 women 40 years of age or older with intermediate pretest CAD likelihood were randomized to ETT or MPI. All the women included in the study were symptomatic with suspected CAD, had an interpretable ECG, and were >5 on DASI (Duke Activity Status Index). A total of 17 primary end points were confirmed, including three nonfatal myocardial infarctions, one heart failure hospitalization, 12 acute coronary syndrome hospitalizations, and only one sudden cardiac death reported in 772 women.
At two years, major adverse cardiovascular events (MACE)-free survival was identical (98%) for women randomized to the ETT or exercise MPI arm (P=0.59). The observed two-year MACE rate was 1.7% for ETT and 2.3% for exercise MPI. For secondary end points, the overall rate of hospitalization for chest pain was 3%. By randomization, the two-year rate of hospitalization for chest pain symptoms was 3% for women in the ETT arm and 4% for those in the exercise MPI arm (P=0.39). An additional six women died from non-cardiac causes (ETT arm, 0.5%; exercise MPI arm, 1%; P=0.39).
Bottom line: ETT is of comparable diagnostic efficacy to MPI as an initial diagnostic test for women suspected of CAD, capable of exercising, based on two-year outcome of cardiac death, nonfatal myocardial infarction, or hospital admission for acute coronary syndrome or heart failure.
Citation: Shaw LJ, Mieres JH, Hendel RH, et al. Comparative effectiveness of exercise electrocardiography with or without myocardial perfusion single photon emission computed tomography in women with suspected coronary artery disease: results from the What Is the Optimal Method for Ischemia Evaluation in Women (WOMEN) trial. Circulation. 2011;124:1239-1249.
Controlled Forced Diuresis Is More Effective in High-Risk Patients for CI-AKI Prevention
Clinical question: Is a system of hydration that creates high urine output while maintaining fluid balance better than routine hydration in high-risk patients for preventing contrast-induced acute kidney injury (CI-AKI)?
Background: Hydration with sodium bicarbonate solution and administration of N-acetylcysteine (NAC) help prevent CI-AKI in low- to medium-risk patients. A recent study (PRINCE) suggests that increasing the urine flow rate (≥150 mL/hr) reduces the toxic effect of contrast, but this regimen requires forced diuresis with high doses of furosemide that may result in further renal damage due to negative fluid balance. The RenalGuard system (PLC Medical Systems Inc., Franklin, Mass.) can simultaneously achieve high urine output and maintain fluid balance.
Study design: Randomized, investigator-driven, open-label study comparing two different hydration strategies.
Setting: Multicenter trial in Italy involving patients with chronic kidney disease scheduled for angiography who met the inclusion and exclusion criteria for high risk of developing CI-AKI.
Synopsis: The study included 292 patients randomized to receive sodium bicarbonate solution (control group) versus hydration with saline controlled by the RenalGuard system with furosemide. Both groups received NAC, though at different doses and routes of administration. CI-AKI occurred in 20.5% (30 of 146) in the control group versus 11% (16 of 146) in the RenalGuard group.
Bottom line: Controlled forced diuresis to achieve high urine flow rate is more effective than conventional hydration with sodium bicarbonate solution in high-risk patients for preventing CI-AKI. Larger studies are needed to confirm and define the role of the RenalGuard system.
Citation: Briguori C, Visconti G, Focaccio A, et al. Renal insufficiency after contrast media administration trial II (REMEDIAL II). Circulation. 2011;124:1260-1269.
Severe Asymptomatic Carotid Artery Stenosis Does Not Increase Stroke or Mortality Risks after CAB Surgery
Clinical question: What is the risk for stroke in patients with asymptomatic carotid artery stenosis (CAS) who are undergoing coronary artery bypass grafting (CABG)?
Background: Stroke occurs as a complication of CABG in approximately 2% of patients. The vast majority occur within the first 24 hours of surgery and are associated with a high mortality rate.
Study design: Retrospective cohort.
Setting: A single institution in Washington, D.C.
Synopsis: Data were collected on 878 consecutive patients who had undergone carotid ultrasound before CABG over a six-year period. Patients with severe CAS of >75% (n=117) were compared with those with <75% stenosis (n=761) to assess the rates of in-hospital stroke and mortality.
Patients with severe CAS had similar rates of stroke compared with those without severe CAS (3.4% vs. 3.6%). Additionally, there was no difference in the incidence of in-hospital complications or mortality between the two groups.
Bottom line: The cause of stroke after CABG is complex and multifactorial, but severe CAS alone appears to not be the biggest risk factor for stroke in patients undergoing CABG.
Citation: Mahmoudi M, Hill PC, Xue Z, et al. Patients with severe asymptomatic carotid artery stenosis do not have a higher risk of stroke and mortality after coronary artery bypass surgery. Stroke. 2011;42:2801-2805.
Cardiac Arrest Survivors Have Long-Term Memory Deficits
Clinical question: Are there any lasting cognitive deficits in patients surviving out-of-hospital cardiac arrest (OHCA) from ventricular fibrillation (VF)?
Background: Although advances have been made in the rapid intervention of OHCAs, there are no population-based, age-adjusted studies of the cognitive and neurologic outcomes of long-term survivors when the “chain of survival” is used (rapid emergency services, bystander CPR, early defibrillation, and advanced care).
Study design: Prospective population-based, age-adjusted study.
Setting: Single hospital in Olmsted County, Minn.
Synopsis: Of 332 OHCA patients, 47 survivors were enrolled for neurologic and neuropsychological testing at least six months after a near-death experience (median time since arrest, 7.8 years). Neurologic examination did not reveal any focal deficits related to the event, but long-term survivors had lower scores on measures of long-term memory and learning efficiency (P=0.001). Nearly all survivors were functionally independent at the time of testing. Interestingly, there was no correlation between prolonged call-to-shock time and cognitive ability, suggesting that there is a possibility of positive neurologic outcomes with a call-to-shock time as late as 10 minutes in OHCA. Older age was also not identified as a negative prognostic factor.
A limitation of the study was the small sample size, though larger populations of survivors are difficult to find. The precise meaning of “cognitive impairment” was also controversial and should be better defined for any future studies.
Bottom line: Long-term survivors of OHCA from VF have long-term memory impairment compared with the normal population at the same age and education level.
Citation: Mateen FJ, Josephs KA, Trenerry MR, et al. Long-term cognitive outcomes following out-of-hospital cardiac arrest. Neurology. 2011;77:1438-1445.
In This Edition
Literature At A Glance
A guide to this month’s studies
- Hospitalist views on readmission prevention
- Characteristics of hospital ICU readmission
- Effect of clopidogrel on bleeding outcomes in vascular surgery
- Time-versus tissue-based diagnosis of TIA
- ETT versus ETT with imaging for the diagnosis of CAD in women
- Effect of high urine output with adequate hydration on contrast-induced nephropathy
- Stroke rate in CABG patients with severe carotid artery stenosis
- Effect of cardiac arrest on long-term cognition
Hospitalists View Readmissions as Potentially Preventable by Team-Based Care
Clinical question: How do front-line hospitalists perceive the preventability of early hospital readmissions?
Background: Hospital readmission has received national attention as an indicator of poor healthcare quality and unnecessary costs. While some studies suggest that some readmissions are preventable, the exact number is unknown. Understanding preventability and the views of front-line clinicians might help hospitalists balance multifactorial compromise between throughput and length of stay.
Study design: Retrospective cohort study.
Setting: Two community tertiary-care hospitals and two suburban hospitals staffed by a single hospitalist group in Portland, Ore.
Synopsis: A group of 17 hospitalists analyzed the inpatient and outpatient charts of 300 consecutive patients readmitted within 21 days of discharge using a structured data collection tool to record patient characteristics, process measures, and perceived preventability of the readmission. Patients were either discharged by internal-medicine hospitalists or had an internal-medicine consultation during their initial stay.
Characteristics of readmitted patients and initial hospital stays were similar to those previously reported in other studies. More than 60% of readmissions were deemed preventable (15%) or possibly preventable (46%). As prevention strategies for these readmissions, hospitalists most frequently suggested interventions under their control, such as longer initial hospital stay (23%). Other potential interventions focused on system approaches, including outpatient appointments, case management, palliative care, and home health.
In most cases (96%), the reviewer was not the discharging hospitalist. Only six hospitalists performed 83% of the reviews, and inter-reviewer reliability was not assessed. Other limitations included confounding biases, such as timing of review, source hospital reviewed, reviewer optimism, and previous primary-care experience of reviewer.
Bottom line: Prevention of hospital readmissions will require a balance between increased length of stay and system-based team approaches beyond the direct control of hospitalists.
Citation: Koekkoek D, Bayley KB, Brown A, Rustvold DL. Hospitalists assess the causes of early hospital readmissions. J Hosp Med. 2011;6:383-388.
Patients with Complex, Severe Illnesses and Persistent Physiologic Abnormalities Have Higher Risk of Intensive-Care-Unit Readmission
Clinical question: Which patient characteristics increase the risk for intensive-care-unit (ICU) readmission?
Background: Patients are often discharged from the ICU based on subjective criteria, workload, and bed demand, making ICU readmission a tempting quality indicator. Studies have examined institutional characteristics leading to ICU readmission, but few have shown how patient case mix affects longer lengths of ICU and hospital stays and higher in-hospital mortality.
Study design: Retrospective observational cohort study using a large, multi-institutional U.S. database.
Setting: Computerized data collection and analysis system from 97 intensive- and cardiac-care units at 35 hospitals in the United States.
Synopsis: Patient-level characteristics and outcomes of 229,375 initial ICU admissions from 2001 to 2009 were compared for patients with and without ICU readmission using the Acute Physiology and Chronic Health Evaluation (APACHE) IV database (Cerner Corporation, Kansas City, Mo.). Multivariable logistic regression analysis identified potential characteristics increasing the risk for ICU readmission. Case-mix adjusted outcomes for mortality and length of stay were calculated.
A total of 13,980 (6.1%) patients were readmitted to the ICUs. Characteristics associated with ICU readmission were similar to those previously reported. In addition to illness severity at initial admission, readmission was associated with complications, poor response to therapy, or persistent physiologic abnormalities at ICU discharge. Patients who were readmitted to the ICU had a risk-adjusted, fourfold greater probability of in-hospital mortality and a 2.5-fold increase in length of hospital stay.
Data were obtained solely from hospitals with an APACHE system, and included only one hospital from the Northeast. Not all ICUs from a single-study hospital were included. DNR orders were not available in the database for analysis.
Bottom line: Persistent physiologic derangements at ICU discharge are as influential on ICU readmission and poor outcomes as other known risk factors, potentially warranting slightly longer ICU stays for these specific patients.
Citation: Kramer AA, Higgins TL, Zimmerman JE. Intensive care unit readmissions in U.S. hospitals: patient characteristics, risk factors, and outcomes. Crit Care Med. 2012;40:3-10.
Clopidogrel Might Not Worsen Bleeding Complications During Surgery
Clinical question: Does clopidogrel cause bleeding complications during vascular surgery?
Background: There is no consensus and few large trials to decide if preoperative clopidogrel use causes bleeding complications in vascular surgeries.
Study design: Prospective.
Setting: New England academic and community centers.
Synopsis: The authors enrolled 10,406 patients from 15 academic and community centers in New England. These patients underwent carotid endarterectomy, lower-extremity bypass, and abdominal aortic aneurysm repair. Ruptured aortic aneurysms were excluded. The use of aspirin, clopidogrel, both, or no anti-platelet therapy within 48 hours before surgery was recorded. The outcomes measured were postoperative bleeding requiring reoperation and the need for packed red blood cell transfusions.
Clopidogrel therapy (n=229) compared with no anti-platelet therapy (n=2,010) did well when measured by reoperation (clopidogrel 0.9%, none 1.5%, P=0.74), incidence of transfusion (clopidogrel 0%, none 18%, P=0.1), and volume of transfusion (clopidogrel 0 units, none 0.7 units, P=0.1). However, the significance, especially for reoperation, is not impressive.
The power of the study could be improved with more clopidogrel users. Another limitation is that the aspirin and clopidogrel platelet effect lasts longer than the 48-hour cutoff. As there were more bleeding complications in the no-anti-platelet group, there is a concern for bias in how the patients were selected and treated.
Bottom line: Clopidogrel might be safe to continue in vascular surgeries, but larger and more valid studies are needed.
Citation: Stone DH, Goodney PP, Schanzer A, et al. Clopidogrel is not associated with major bleeding complications during peripheral arterial surgery. J Vasc Surg. 2011;54:779-784.
Tissue-Defined TIAs Have Better Prognostic Benefits Than Time-Defined TIAs
Citation: Is risk stratification for recurrent stroke better when brain imaging is performed after a transient ischemic attack (TIA)?
Background: The presence of a TIA is a known risk factor for recurrent stroke. There is debate in changing the definition of TIA from time-based to tissue-based. However, it is not known if this will improve management.
Study design: Multicenter observation cohort.
Setting: Twelve independent international research centers.
Synopsis: The current definition of a TIA is a neurological deficit that resolves within 24 hours. To determine the urgency of an admission and work-up, the ABCD2 score (age, blood pressure, clinical symptoms, duration, and diabetes) is often used as a prognostic tool for recurrent stroke. The authors enrolled 4,574 patients with the traditional diagnosis of TIA. In addition to calculating their ABCD2 score, they were then classified as tissue-positive (infarction) or tissue-negative per MRI or CT. At both seven and 90 days after TIA, both imaging modalities when combined with ABCD2 were able to identify risk for recurrent stroke better than if they were used alone.
Limitations included the images being interpreted by their individual healthcare centers and that the stroke centers had lower recurrent rates of stroke compared with community centers. If only a CT can be used, it should be noted that the sensitivity is lower when compared with an MRI in this study.
Bottom line: This categorization of tissue- or non-tissue-positive TIAs improved the prognostic information provided by the ABCD2 score and might improve management decisions.
Citation: Giles MF, Albers GW, Amarenco P, et al. Early stroke risk and ABCD2 score performance in tissue- vs time-defined TIA: a multicenter study. Neurology. 2011;77:1222-1228.
ETT Comparable to MPI as Initial Diagnostic Test for Women Suspected of CAD
Clinical question: Is the exercise treadmill test (ETT) equivalent to myocardial perfusion imaging (MPI) as an initial diagnostic test for low-risk women capable of exercising with suspected coronary artery disease (CAD)?
Background: To date, the evidence base for diagnostic testing in women with suspected CAD has been limited, with no randomized trials to guide appropriate clinical decision-making in the choice of noninvasive testing strategies. The aim of this trial was to provide comparative-effectiveness data for women capable of performing exercise testing with regard to whether the addition of imaging to standard ETT provided incremental clinical benefit over index ETT alone.
Study design: Prospective randomized.
Settings: Forty-three cardiology practices across the U.S.
Synopsis: A total of 824 women 40 years of age or older with intermediate pretest CAD likelihood were randomized to ETT or MPI. All the women included in the study were symptomatic with suspected CAD, had an interpretable ECG, and were >5 on DASI (Duke Activity Status Index). A total of 17 primary end points were confirmed, including three nonfatal myocardial infarctions, one heart failure hospitalization, 12 acute coronary syndrome hospitalizations, and only one sudden cardiac death reported in 772 women.
At two years, major adverse cardiovascular events (MACE)-free survival was identical (98%) for women randomized to the ETT or exercise MPI arm (P=0.59). The observed two-year MACE rate was 1.7% for ETT and 2.3% for exercise MPI. For secondary end points, the overall rate of hospitalization for chest pain was 3%. By randomization, the two-year rate of hospitalization for chest pain symptoms was 3% for women in the ETT arm and 4% for those in the exercise MPI arm (P=0.39). An additional six women died from non-cardiac causes (ETT arm, 0.5%; exercise MPI arm, 1%; P=0.39).
Bottom line: ETT is of comparable diagnostic efficacy to MPI as an initial diagnostic test for women suspected of CAD, capable of exercising, based on two-year outcome of cardiac death, nonfatal myocardial infarction, or hospital admission for acute coronary syndrome or heart failure.
Citation: Shaw LJ, Mieres JH, Hendel RH, et al. Comparative effectiveness of exercise electrocardiography with or without myocardial perfusion single photon emission computed tomography in women with suspected coronary artery disease: results from the What Is the Optimal Method for Ischemia Evaluation in Women (WOMEN) trial. Circulation. 2011;124:1239-1249.
Controlled Forced Diuresis Is More Effective in High-Risk Patients for CI-AKI Prevention
Clinical question: Is a system of hydration that creates high urine output while maintaining fluid balance better than routine hydration in high-risk patients for preventing contrast-induced acute kidney injury (CI-AKI)?
Background: Hydration with sodium bicarbonate solution and administration of N-acetylcysteine (NAC) help prevent CI-AKI in low- to medium-risk patients. A recent study (PRINCE) suggests that increasing the urine flow rate (≥150 mL/hr) reduces the toxic effect of contrast, but this regimen requires forced diuresis with high doses of furosemide that may result in further renal damage due to negative fluid balance. The RenalGuard system (PLC Medical Systems Inc., Franklin, Mass.) can simultaneously achieve high urine output and maintain fluid balance.
Study design: Randomized, investigator-driven, open-label study comparing two different hydration strategies.
Setting: Multicenter trial in Italy involving patients with chronic kidney disease scheduled for angiography who met the inclusion and exclusion criteria for high risk of developing CI-AKI.
Synopsis: The study included 292 patients randomized to receive sodium bicarbonate solution (control group) versus hydration with saline controlled by the RenalGuard system with furosemide. Both groups received NAC, though at different doses and routes of administration. CI-AKI occurred in 20.5% (30 of 146) in the control group versus 11% (16 of 146) in the RenalGuard group.
Bottom line: Controlled forced diuresis to achieve high urine flow rate is more effective than conventional hydration with sodium bicarbonate solution in high-risk patients for preventing CI-AKI. Larger studies are needed to confirm and define the role of the RenalGuard system.
Citation: Briguori C, Visconti G, Focaccio A, et al. Renal insufficiency after contrast media administration trial II (REMEDIAL II). Circulation. 2011;124:1260-1269.
Severe Asymptomatic Carotid Artery Stenosis Does Not Increase Stroke or Mortality Risks after CAB Surgery
Clinical question: What is the risk for stroke in patients with asymptomatic carotid artery stenosis (CAS) who are undergoing coronary artery bypass grafting (CABG)?
Background: Stroke occurs as a complication of CABG in approximately 2% of patients. The vast majority occur within the first 24 hours of surgery and are associated with a high mortality rate.
Study design: Retrospective cohort.
Setting: A single institution in Washington, D.C.
Synopsis: Data were collected on 878 consecutive patients who had undergone carotid ultrasound before CABG over a six-year period. Patients with severe CAS of >75% (n=117) were compared with those with <75% stenosis (n=761) to assess the rates of in-hospital stroke and mortality.
Patients with severe CAS had similar rates of stroke compared with those without severe CAS (3.4% vs. 3.6%). Additionally, there was no difference in the incidence of in-hospital complications or mortality between the two groups.
Bottom line: The cause of stroke after CABG is complex and multifactorial, but severe CAS alone appears to not be the biggest risk factor for stroke in patients undergoing CABG.
Citation: Mahmoudi M, Hill PC, Xue Z, et al. Patients with severe asymptomatic carotid artery stenosis do not have a higher risk of stroke and mortality after coronary artery bypass surgery. Stroke. 2011;42:2801-2805.
Cardiac Arrest Survivors Have Long-Term Memory Deficits
Clinical question: Are there any lasting cognitive deficits in patients surviving out-of-hospital cardiac arrest (OHCA) from ventricular fibrillation (VF)?
Background: Although advances have been made in the rapid intervention of OHCAs, there are no population-based, age-adjusted studies of the cognitive and neurologic outcomes of long-term survivors when the “chain of survival” is used (rapid emergency services, bystander CPR, early defibrillation, and advanced care).
Study design: Prospective population-based, age-adjusted study.
Setting: Single hospital in Olmsted County, Minn.
Synopsis: Of 332 OHCA patients, 47 survivors were enrolled for neurologic and neuropsychological testing at least six months after a near-death experience (median time since arrest, 7.8 years). Neurologic examination did not reveal any focal deficits related to the event, but long-term survivors had lower scores on measures of long-term memory and learning efficiency (P=0.001). Nearly all survivors were functionally independent at the time of testing. Interestingly, there was no correlation between prolonged call-to-shock time and cognitive ability, suggesting that there is a possibility of positive neurologic outcomes with a call-to-shock time as late as 10 minutes in OHCA. Older age was also not identified as a negative prognostic factor.
A limitation of the study was the small sample size, though larger populations of survivors are difficult to find. The precise meaning of “cognitive impairment” was also controversial and should be better defined for any future studies.
Bottom line: Long-term survivors of OHCA from VF have long-term memory impairment compared with the normal population at the same age and education level.
Citation: Mateen FJ, Josephs KA, Trenerry MR, et al. Long-term cognitive outcomes following out-of-hospital cardiac arrest. Neurology. 2011;77:1438-1445.
Transitioning Pediatric Patients with Chronic Conditions
Last September, Seattle Children’s Hospital hosted a “graduation day” party for one of its longtime patients, Robyn Nichols.
Robyn first entered the hospital as a 21-month-old after a major car accident that left her a quadriplegic and ventilator-dependent. She was in a coma for nine weeks and spent many days and nights in the children’s hospital. Now 20 years old, she’s ready to be cared for in an adult hospital when the need arises.
Her mother, Amy Thompson, wrote a letter thanking the staff for their dedication. And while she’s sad to say goodbye, she’s grateful for their efforts in overseeing the shift in Robyn’s care to adult specialists.
“If I were to let a doctor know one thing about transitioning a pediatric [patient] to adult care, [it] is for them to recognize how scary it is for the patient as well as the family,” Thompson says. “After being in the adult world with a special-needs adult daughter for a couple of months, I want to go back [to the children’s hospital]. The unknown, when you are talking life and death, can be terrorizing.”
As pediatric patients with chronic medical conditions enter adolescence and the young adult years, proper transitions can make a significant difference in their inpatient and outpatient care. And with thoughtful collaboration, hospitalists can deliver solutions that lead to good outcomes.
“A safe transition provides a great deal of relief and comfort to the families of these patients,” says Moises Auron, MD, FAAP, FACP, assistant professor of medicine and pediatrics at The Cleveland Clinic.
Delayed Dangers
Anticipating a maturing adolescent’s care needs is paramount. Chronic diseases diagnosed in childhood often lead to complications in the teen years and early adulthood. Over time, more complex treatments might be necessary. For instance, Dr. Auron says, a patient living with diabetes since age 5 could require a kidney transplant at age 25.
Childhood cancer survivors also tend to encounter major health challenges as adults, according to an Oct. 13, 2011, report in the New England Journal of Medicine. Acute lymphoblastic leukemia (ALL) is the most common pediatric cancer, with a cure rate surpassing 70%. However, adult survivors of childhood leukemia have heightened risks of secondary cancers, cardiovascular disease, and other chronic illnesses.1
Assembling transitions-of-care teams is one way that hospitals can help coordinate services for such patients. As these patients mature and “quit seeing their pediatrician, they don’t usually see anybody,” says W. Benjamin Rothwell, MD, associate director of the “med-peds” residency at Tulane University School of Medicine in New Orleans. “At that point, they kind of fall off the map, so to speak, until they present to the hospital acutely ill.”

New Orleans has a large population of pediatric patients with sickle-cell anemia, a genetic disease that is more prevalent in blacks. Dr. Rothwell says he and his colleagues strive to transition these patients between the ages of 16 and 26. “The goal,” he says, “is to try to catch people in that 10-year span.”
Other conditions that add to the complexity of care for hospitalists include cerebral palsy, chromosomal abnormalities, congenital heart disease, and pregnancy in teenagers with chronic illnesses. Adult hospitalists might not be fully prepared to deal with developmentally disabled patients.
In such cases, “the family member or caregiver is a trusted ally in knowing what’s going on,” says Susan Hunt, MD, a hospitalist at Seattle Children’s Hospital and University of Washington Medical Center. “It may not be typical for adult providers to expect that kind of communication.” When put into this situation, hospitalists can enlist the caregiver’s input—for instance, asking, “How does your child show pain?”
When patients rely on medical devices, such as a gastric feeding tube, tracheotomy, or wheelchair, it helps to know where the family or previous facility obtained the specific equipment in case a replacement becomes necessary. Staying on top of the patient’s insurance coverage also is vital in a transition, Dr. Hunt says.
Communication should flow easily between providers in inpatient and outpatient settings, as adolescents with chronic conditions are “aging out of the pediatric system,” says Allen Friedland, MD, program director of the combined med-peds residency at Christiana Care Health System in Newark, Del.
Soon they are “thrust into the adult world, which has an entirely different paradigm,” Dr. Friedland says. Among the challenges is linking a hospital’s electronic health records to interface with the information given to the outpatient physicians overseeing a patient’s care.
Christiana Care Health System has collaborated with Nemours/Alfred I. duPont Hospital for Children in nearby Wilmington, Del., to transition patients with complex medical conditions into adult care. Nemours is providing comprehensive summaries, which indicate the types of subspecialty care that a patient could require in the future. “We sort of take some of the mystery out,” Dr. Friedland says. “We really anticipate the issues.”

—Emily Chapman, MD, pediatric hospitalist, Children’s Hospitals & Clinics of Minnesota, Minneapolis
Meanwhile, Christiana Care started an outpatient primary-care practice staffed by two physicians, a social worker, and a psychologist liaison. They coordinate with a physician and social worker at Nemours. Secure email also helps facilitate discussions about transitions of care between the pediatric and adult settings.
The teams have access to the transition-care practice providers for round-the-clock consultations, and Dr. Friedland assists in admitting patients to the most appropriate level of hospitalized care. “When a person goes to the ED,” he explains, “there’s already a set of expectations and orders.”
The Choice Is Yours
When staying in the hospital, some patients feel more comfortable on a pediatric floor, others in an adult environment. That’s why Keely Dwyer-Matzky, MD, and Amy Blatt, MD, both Med-Peds hospitalists, created an educational video for adolescent patients at the University of Rochester Medical Center in New York.
“There’s a lot of fear about transitioning, not knowing what it’s going to be like, what the expectations are, or the feeling of the floor itself,” Dr. Dwyer-Matzky says. The video informs viewers about the importance of keeping medical summaries of their problems and speaking up for themselves at visits to their doctors’ offices. It also mentions that the Rochester facility gives adolescents the option to tour an adult floor.

“There are a lot of variables,” says Shelley W. Collins, MD, chief of the pediatric hospitalist division at the University of Florida at Gainesville. “If their cognitive level allows them to be participants in their own care, then I think we have obligation to ask them what their preference is.”
The state law that governs where an HM group practices also factors into the equation. In an emergency, a court order could be obtained if a procedure is deemed necessary and a legal guardian has not been established or the patient will not consent, Dr. Collins says of Florida law. “But we prefer to have a patient agree to it. In fact, we like and require the assent of a teenage patient, who can give it in addition to the consent of the parents.”
Dr. Collins and her colleague Arwa Saidi, MD, a pediatric cardiologist, propose “a transition checklist” for hospitalists to review and update every time a pediatric or adolescent patient with a chronic condition arrives at the hospital. This aggregate of information becomes part of the medical record for hospitalists to consult in the future.
Adolescents can present with adult-related problems such as heart disease or stroke. These are the sorts of issues that pediatric hospitalist may not be as comfortable handling. Meanwhile, adult hospitalists encounter child-related issues that don’t normally enter their territory.
For instance, with a patient admitted to the hospital for an asthma flare or diabetic ketoacidosis, adult hospitalists might be unaware of school rules pertaining to inhalers and insulin injections, says Weijen Chang, MD, FAAP, FACP, a hospitalist experienced in treating both adult and pediatric patients at the University of California at San Diego (UCSD).
“They’re not used to interacting with school systems in regards to someone’s health care,” says Dr. Chang, a Team Hospitalist member. “The best solution, as always, is education.”
—Amy Thompson, parent
In April, hospitalists trained in both internal medicine and pediatrics will convene at SHM’s annual meeting in San Diego to educate their peers in managing difficult and unfamiliar situations. (The April 4 workshop, “Demystifying Medical Care of Adults with Chronic Diseases of Childhood: What the Hospitalist Should Know,” has limited seating; visit www.hospitalmedicine2012.org to register.)
At UCSD-affiliated Rady Children’s Hospital, hospitalists encountered a patient who was very agitated and combative toward staff. That wasn’t so unusual, except that the patient was quite large in size. “They were uncomfortable with the physical nature of the interaction,” Dr. Chang says.
The physicians and nurses on a pediatric floor also might not be comfortable with obstetrics, and they might lack the equipment for monitoring fetal heart tones and other vitals. In this case, a pregnant teen would be best served in an adult hospital. On the flip side, an adult hospital might not have a blood pressure cuff small enough for some adolescent patients, says Heather Toth, MD, program director of the med-peds residency at the Medical College of Wisconsin in Milwaukee. Collaboration between adult and pediatric providers is essential in ironing out these types of kinks.
Ironing out these types of kinks is crucial. “The worst mistake you can make is to put off planning for the transition,” says Emily Chapman, MD, a pediatric hospitalist at Children’s Hospitals & Clinics of Minnesota in Minneapolis. “When families are in crisis, they return to what they know, so they are likely to show up in your pediatric emergency room even though their child is now 19 or 20 years old.”
That’s why Dr. Chapman recommends introducing the family to a new health provider for a “get-acquainted visit,” she says. “The medical history can be reviewed, and the patient and doctor can begin to build a relationship.” Once that initial rapport has been established, in crisis, “they’re much more likely to seek out the new provider rather than fall back on their old support system.”
Dr. Chapman was part of a team that assisted with the move to adult care for a Down syndrome patient whom she had known since the patient was about 7 years old. “As he approached about the age of 16, we worked on transitioning his care over a few years period of time,” she explains, “to involve him with adult specialists and adult primary care that could manage him as he got older.”
However, Dr. Chapman cautions against switching the patient’s providers all at once. Instead, she says, “You would change an element of the team, have some period of overlap with the old players and new players, before transitioning the rest of the team.”
Susan Kreimer is a freelance medical writer based in New York.
Reference
- Diller L. Adult primary care after childhood acute lymphoblastic leukemia. N Engl J Med. 2011;365:1417-1424.
Last September, Seattle Children’s Hospital hosted a “graduation day” party for one of its longtime patients, Robyn Nichols.
Robyn first entered the hospital as a 21-month-old after a major car accident that left her a quadriplegic and ventilator-dependent. She was in a coma for nine weeks and spent many days and nights in the children’s hospital. Now 20 years old, she’s ready to be cared for in an adult hospital when the need arises.
Her mother, Amy Thompson, wrote a letter thanking the staff for their dedication. And while she’s sad to say goodbye, she’s grateful for their efforts in overseeing the shift in Robyn’s care to adult specialists.
“If I were to let a doctor know one thing about transitioning a pediatric [patient] to adult care, [it] is for them to recognize how scary it is for the patient as well as the family,” Thompson says. “After being in the adult world with a special-needs adult daughter for a couple of months, I want to go back [to the children’s hospital]. The unknown, when you are talking life and death, can be terrorizing.”
As pediatric patients with chronic medical conditions enter adolescence and the young adult years, proper transitions can make a significant difference in their inpatient and outpatient care. And with thoughtful collaboration, hospitalists can deliver solutions that lead to good outcomes.
“A safe transition provides a great deal of relief and comfort to the families of these patients,” says Moises Auron, MD, FAAP, FACP, assistant professor of medicine and pediatrics at The Cleveland Clinic.
Delayed Dangers
Anticipating a maturing adolescent’s care needs is paramount. Chronic diseases diagnosed in childhood often lead to complications in the teen years and early adulthood. Over time, more complex treatments might be necessary. For instance, Dr. Auron says, a patient living with diabetes since age 5 could require a kidney transplant at age 25.
Childhood cancer survivors also tend to encounter major health challenges as adults, according to an Oct. 13, 2011, report in the New England Journal of Medicine. Acute lymphoblastic leukemia (ALL) is the most common pediatric cancer, with a cure rate surpassing 70%. However, adult survivors of childhood leukemia have heightened risks of secondary cancers, cardiovascular disease, and other chronic illnesses.1
Assembling transitions-of-care teams is one way that hospitals can help coordinate services for such patients. As these patients mature and “quit seeing their pediatrician, they don’t usually see anybody,” says W. Benjamin Rothwell, MD, associate director of the “med-peds” residency at Tulane University School of Medicine in New Orleans. “At that point, they kind of fall off the map, so to speak, until they present to the hospital acutely ill.”
New Orleans has a large population of pediatric patients with sickle-cell anemia, a genetic disease that is more prevalent in blacks. Dr. Rothwell says he and his colleagues strive to transition these patients between the ages of 16 and 26. “The goal,” he says, “is to try to catch people in that 10-year span.”
Other conditions that add to the complexity of care for hospitalists include cerebral palsy, chromosomal abnormalities, congenital heart disease, and pregnancy in teenagers with chronic illnesses. Adult hospitalists might not be fully prepared to deal with developmentally disabled patients.
In such cases, “the family member or caregiver is a trusted ally in knowing what’s going on,” says Susan Hunt, MD, a hospitalist at Seattle Children’s Hospital and University of Washington Medical Center. “It may not be typical for adult providers to expect that kind of communication.” When put into this situation, hospitalists can enlist the caregiver’s input—for instance, asking, “How does your child show pain?”
When patients rely on medical devices, such as a gastric feeding tube, tracheotomy, or wheelchair, it helps to know where the family or previous facility obtained the specific equipment in case a replacement becomes necessary. Staying on top of the patient’s insurance coverage also is vital in a transition, Dr. Hunt says.
Communication should flow easily between providers in inpatient and outpatient settings, as adolescents with chronic conditions are “aging out of the pediatric system,” says Allen Friedland, MD, program director of the combined med-peds residency at Christiana Care Health System in Newark, Del.
Soon they are “thrust into the adult world, which has an entirely different paradigm,” Dr. Friedland says. Among the challenges is linking a hospital’s electronic health records to interface with the information given to the outpatient physicians overseeing a patient’s care.
Christiana Care Health System has collaborated with Nemours/Alfred I. duPont Hospital for Children in nearby Wilmington, Del., to transition patients with complex medical conditions into adult care. Nemours is providing comprehensive summaries, which indicate the types of subspecialty care that a patient could require in the future. “We sort of take some of the mystery out,” Dr. Friedland says. “We really anticipate the issues.”
—Emily Chapman, MD, pediatric hospitalist, Children’s Hospitals & Clinics of Minnesota, Minneapolis
Meanwhile, Christiana Care started an outpatient primary-care practice staffed by two physicians, a social worker, and a psychologist liaison. They coordinate with a physician and social worker at Nemours. Secure email also helps facilitate discussions about transitions of care between the pediatric and adult settings.
The teams have access to the transition-care practice providers for round-the-clock consultations, and Dr. Friedland assists in admitting patients to the most appropriate level of hospitalized care. “When a person goes to the ED,” he explains, “there’s already a set of expectations and orders.”
The Choice Is Yours
When staying in the hospital, some patients feel more comfortable on a pediatric floor, others in an adult environment. That’s why Keely Dwyer-Matzky, MD, and Amy Blatt, MD, both Med-Peds hospitalists, created an educational video for adolescent patients at the University of Rochester Medical Center in New York.
“There’s a lot of fear about transitioning, not knowing what it’s going to be like, what the expectations are, or the feeling of the floor itself,” Dr. Dwyer-Matzky says. The video informs viewers about the importance of keeping medical summaries of their problems and speaking up for themselves at visits to their doctors’ offices. It also mentions that the Rochester facility gives adolescents the option to tour an adult floor.
“There are a lot of variables,” says Shelley W. Collins, MD, chief of the pediatric hospitalist division at the University of Florida at Gainesville. “If their cognitive level allows them to be participants in their own care, then I think we have obligation to ask them what their preference is.”
The state law that governs where an HM group practices also factors into the equation. In an emergency, a court order could be obtained if a procedure is deemed necessary and a legal guardian has not been established or the patient will not consent, Dr. Collins says of Florida law. “But we prefer to have a patient agree to it. In fact, we like and require the assent of a teenage patient, who can give it in addition to the consent of the parents.”
Dr. Collins and her colleague Arwa Saidi, MD, a pediatric cardiologist, propose “a transition checklist” for hospitalists to review and update every time a pediatric or adolescent patient with a chronic condition arrives at the hospital. This aggregate of information becomes part of the medical record for hospitalists to consult in the future.
Adolescents can present with adult-related problems such as heart disease or stroke. These are the sorts of issues that pediatric hospitalist may not be as comfortable handling. Meanwhile, adult hospitalists encounter child-related issues that don’t normally enter their territory.
For instance, with a patient admitted to the hospital for an asthma flare or diabetic ketoacidosis, adult hospitalists might be unaware of school rules pertaining to inhalers and insulin injections, says Weijen Chang, MD, FAAP, FACP, a hospitalist experienced in treating both adult and pediatric patients at the University of California at San Diego (UCSD).
“They’re not used to interacting with school systems in regards to someone’s health care,” says Dr. Chang, a Team Hospitalist member. “The best solution, as always, is education.”
—Amy Thompson, parent
In April, hospitalists trained in both internal medicine and pediatrics will convene at SHM’s annual meeting in San Diego to educate their peers in managing difficult and unfamiliar situations. (The April 4 workshop, “Demystifying Medical Care of Adults with Chronic Diseases of Childhood: What the Hospitalist Should Know,” has limited seating; visit www.hospitalmedicine2012.org to register.)
At UCSD-affiliated Rady Children’s Hospital, hospitalists encountered a patient who was very agitated and combative toward staff. That wasn’t so unusual, except that the patient was quite large in size. “They were uncomfortable with the physical nature of the interaction,” Dr. Chang says.
The physicians and nurses on a pediatric floor also might not be comfortable with obstetrics, and they might lack the equipment for monitoring fetal heart tones and other vitals. In this case, a pregnant teen would be best served in an adult hospital. On the flip side, an adult hospital might not have a blood pressure cuff small enough for some adolescent patients, says Heather Toth, MD, program director of the med-peds residency at the Medical College of Wisconsin in Milwaukee. Collaboration between adult and pediatric providers is essential in ironing out these types of kinks.
Ironing out these types of kinks is crucial. “The worst mistake you can make is to put off planning for the transition,” says Emily Chapman, MD, a pediatric hospitalist at Children’s Hospitals & Clinics of Minnesota in Minneapolis. “When families are in crisis, they return to what they know, so they are likely to show up in your pediatric emergency room even though their child is now 19 or 20 years old.”
That’s why Dr. Chapman recommends introducing the family to a new health provider for a “get-acquainted visit,” she says. “The medical history can be reviewed, and the patient and doctor can begin to build a relationship.” Once that initial rapport has been established, in crisis, “they’re much more likely to seek out the new provider rather than fall back on their old support system.”
Dr. Chapman was part of a team that assisted with the move to adult care for a Down syndrome patient whom she had known since the patient was about 7 years old. “As he approached about the age of 16, we worked on transitioning his care over a few years period of time,” she explains, “to involve him with adult specialists and adult primary care that could manage him as he got older.”
However, Dr. Chapman cautions against switching the patient’s providers all at once. Instead, she says, “You would change an element of the team, have some period of overlap with the old players and new players, before transitioning the rest of the team.”
Susan Kreimer is a freelance medical writer based in New York.
Reference
- Diller L. Adult primary care after childhood acute lymphoblastic leukemia. N Engl J Med. 2011;365:1417-1424.
Last September, Seattle Children’s Hospital hosted a “graduation day” party for one of its longtime patients, Robyn Nichols.
Robyn first entered the hospital as a 21-month-old after a major car accident that left her a quadriplegic and ventilator-dependent. She was in a coma for nine weeks and spent many days and nights in the children’s hospital. Now 20 years old, she’s ready to be cared for in an adult hospital when the need arises.
Her mother, Amy Thompson, wrote a letter thanking the staff for their dedication. And while she’s sad to say goodbye, she’s grateful for their efforts in overseeing the shift in Robyn’s care to adult specialists.
“If I were to let a doctor know one thing about transitioning a pediatric [patient] to adult care, [it] is for them to recognize how scary it is for the patient as well as the family,” Thompson says. “After being in the adult world with a special-needs adult daughter for a couple of months, I want to go back [to the children’s hospital]. The unknown, when you are talking life and death, can be terrorizing.”
As pediatric patients with chronic medical conditions enter adolescence and the young adult years, proper transitions can make a significant difference in their inpatient and outpatient care. And with thoughtful collaboration, hospitalists can deliver solutions that lead to good outcomes.
“A safe transition provides a great deal of relief and comfort to the families of these patients,” says Moises Auron, MD, FAAP, FACP, assistant professor of medicine and pediatrics at The Cleveland Clinic.
Delayed Dangers
Anticipating a maturing adolescent’s care needs is paramount. Chronic diseases diagnosed in childhood often lead to complications in the teen years and early adulthood. Over time, more complex treatments might be necessary. For instance, Dr. Auron says, a patient living with diabetes since age 5 could require a kidney transplant at age 25.
Childhood cancer survivors also tend to encounter major health challenges as adults, according to an Oct. 13, 2011, report in the New England Journal of Medicine. Acute lymphoblastic leukemia (ALL) is the most common pediatric cancer, with a cure rate surpassing 70%. However, adult survivors of childhood leukemia have heightened risks of secondary cancers, cardiovascular disease, and other chronic illnesses.1
Assembling transitions-of-care teams is one way that hospitals can help coordinate services for such patients. As these patients mature and “quit seeing their pediatrician, they don’t usually see anybody,” says W. Benjamin Rothwell, MD, associate director of the “med-peds” residency at Tulane University School of Medicine in New Orleans. “At that point, they kind of fall off the map, so to speak, until they present to the hospital acutely ill.”
New Orleans has a large population of pediatric patients with sickle-cell anemia, a genetic disease that is more prevalent in blacks. Dr. Rothwell says he and his colleagues strive to transition these patients between the ages of 16 and 26. “The goal,” he says, “is to try to catch people in that 10-year span.”
Other conditions that add to the complexity of care for hospitalists include cerebral palsy, chromosomal abnormalities, congenital heart disease, and pregnancy in teenagers with chronic illnesses. Adult hospitalists might not be fully prepared to deal with developmentally disabled patients.
In such cases, “the family member or caregiver is a trusted ally in knowing what’s going on,” says Susan Hunt, MD, a hospitalist at Seattle Children’s Hospital and University of Washington Medical Center. “It may not be typical for adult providers to expect that kind of communication.” When put into this situation, hospitalists can enlist the caregiver’s input—for instance, asking, “How does your child show pain?”
When patients rely on medical devices, such as a gastric feeding tube, tracheotomy, or wheelchair, it helps to know where the family or previous facility obtained the specific equipment in case a replacement becomes necessary. Staying on top of the patient’s insurance coverage also is vital in a transition, Dr. Hunt says.
Communication should flow easily between providers in inpatient and outpatient settings, as adolescents with chronic conditions are “aging out of the pediatric system,” says Allen Friedland, MD, program director of the combined med-peds residency at Christiana Care Health System in Newark, Del.
Soon they are “thrust into the adult world, which has an entirely different paradigm,” Dr. Friedland says. Among the challenges is linking a hospital’s electronic health records to interface with the information given to the outpatient physicians overseeing a patient’s care.
Christiana Care Health System has collaborated with Nemours/Alfred I. duPont Hospital for Children in nearby Wilmington, Del., to transition patients with complex medical conditions into adult care. Nemours is providing comprehensive summaries, which indicate the types of subspecialty care that a patient could require in the future. “We sort of take some of the mystery out,” Dr. Friedland says. “We really anticipate the issues.”
—Emily Chapman, MD, pediatric hospitalist, Children’s Hospitals & Clinics of Minnesota, Minneapolis
Meanwhile, Christiana Care started an outpatient primary-care practice staffed by two physicians, a social worker, and a psychologist liaison. They coordinate with a physician and social worker at Nemours. Secure email also helps facilitate discussions about transitions of care between the pediatric and adult settings.
The teams have access to the transition-care practice providers for round-the-clock consultations, and Dr. Friedland assists in admitting patients to the most appropriate level of hospitalized care. “When a person goes to the ED,” he explains, “there’s already a set of expectations and orders.”
The Choice Is Yours
When staying in the hospital, some patients feel more comfortable on a pediatric floor, others in an adult environment. That’s why Keely Dwyer-Matzky, MD, and Amy Blatt, MD, both Med-Peds hospitalists, created an educational video for adolescent patients at the University of Rochester Medical Center in New York.
“There’s a lot of fear about transitioning, not knowing what it’s going to be like, what the expectations are, or the feeling of the floor itself,” Dr. Dwyer-Matzky says. The video informs viewers about the importance of keeping medical summaries of their problems and speaking up for themselves at visits to their doctors’ offices. It also mentions that the Rochester facility gives adolescents the option to tour an adult floor.
“There are a lot of variables,” says Shelley W. Collins, MD, chief of the pediatric hospitalist division at the University of Florida at Gainesville. “If their cognitive level allows them to be participants in their own care, then I think we have obligation to ask them what their preference is.”
The state law that governs where an HM group practices also factors into the equation. In an emergency, a court order could be obtained if a procedure is deemed necessary and a legal guardian has not been established or the patient will not consent, Dr. Collins says of Florida law. “But we prefer to have a patient agree to it. In fact, we like and require the assent of a teenage patient, who can give it in addition to the consent of the parents.”
Dr. Collins and her colleague Arwa Saidi, MD, a pediatric cardiologist, propose “a transition checklist” for hospitalists to review and update every time a pediatric or adolescent patient with a chronic condition arrives at the hospital. This aggregate of information becomes part of the medical record for hospitalists to consult in the future.
Adolescents can present with adult-related problems such as heart disease or stroke. These are the sorts of issues that pediatric hospitalist may not be as comfortable handling. Meanwhile, adult hospitalists encounter child-related issues that don’t normally enter their territory.
For instance, with a patient admitted to the hospital for an asthma flare or diabetic ketoacidosis, adult hospitalists might be unaware of school rules pertaining to inhalers and insulin injections, says Weijen Chang, MD, FAAP, FACP, a hospitalist experienced in treating both adult and pediatric patients at the University of California at San Diego (UCSD).
“They’re not used to interacting with school systems in regards to someone’s health care,” says Dr. Chang, a Team Hospitalist member. “The best solution, as always, is education.”
—Amy Thompson, parent
In April, hospitalists trained in both internal medicine and pediatrics will convene at SHM’s annual meeting in San Diego to educate their peers in managing difficult and unfamiliar situations. (The April 4 workshop, “Demystifying Medical Care of Adults with Chronic Diseases of Childhood: What the Hospitalist Should Know,” has limited seating; visit www.hospitalmedicine2012.org to register.)
At UCSD-affiliated Rady Children’s Hospital, hospitalists encountered a patient who was very agitated and combative toward staff. That wasn’t so unusual, except that the patient was quite large in size. “They were uncomfortable with the physical nature of the interaction,” Dr. Chang says.
The physicians and nurses on a pediatric floor also might not be comfortable with obstetrics, and they might lack the equipment for monitoring fetal heart tones and other vitals. In this case, a pregnant teen would be best served in an adult hospital. On the flip side, an adult hospital might not have a blood pressure cuff small enough for some adolescent patients, says Heather Toth, MD, program director of the med-peds residency at the Medical College of Wisconsin in Milwaukee. Collaboration between adult and pediatric providers is essential in ironing out these types of kinks.
Ironing out these types of kinks is crucial. “The worst mistake you can make is to put off planning for the transition,” says Emily Chapman, MD, a pediatric hospitalist at Children’s Hospitals & Clinics of Minnesota in Minneapolis. “When families are in crisis, they return to what they know, so they are likely to show up in your pediatric emergency room even though their child is now 19 or 20 years old.”
That’s why Dr. Chapman recommends introducing the family to a new health provider for a “get-acquainted visit,” she says. “The medical history can be reviewed, and the patient and doctor can begin to build a relationship.” Once that initial rapport has been established, in crisis, “they’re much more likely to seek out the new provider rather than fall back on their old support system.”
Dr. Chapman was part of a team that assisted with the move to adult care for a Down syndrome patient whom she had known since the patient was about 7 years old. “As he approached about the age of 16, we worked on transitioning his care over a few years period of time,” she explains, “to involve him with adult specialists and adult primary care that could manage him as he got older.”
However, Dr. Chapman cautions against switching the patient’s providers all at once. Instead, she says, “You would change an element of the team, have some period of overlap with the old players and new players, before transitioning the rest of the team.”
Susan Kreimer is a freelance medical writer based in New York.
Reference
- Diller L. Adult primary care after childhood acute lymphoblastic leukemia. N Engl J Med. 2011;365:1417-1424.
Wachter, Washington Insiders Ready for HM12 Keynote Addresses




SHM’s annual meeting will bring some of the top thinkers in healthcare and HM to San Diego in April to present the ideas hospitalists will be talking about for the next year. In fact, with their experience in healthcare policy, this year’s presenters will frame the conversations that hospitalists will have at HM13, outside of Washington, D.C.
HM12’s featured speakers include:
Patrick H. Conway, MD, MSc, FAAP, SFHM, chief medical officer and director of the Office of Clinical Standards and Quality for the Centers for Medicare & Medicaid Services (CMS);
Norman J. Ornstein, PhD, MA, resident scholar, American Enterprise Institute for Public Policy Research; and
Robert M. Wachter, MD, MHM, professor and associate chairman of medicine, University of California at San Francisco.
“The featured speakers at HM12 in San Diego are guaranteed to provoke conversation among hospitalists, other caregivers, and policymakers throughout the year and beyond,” says HM12 course director Jeff Glasheen, MD, SFHM. “This year’s lineup brings some of the best hospitalists, nonhospitalists, and perennial favorites to the podium. The breadth of their experience and their insight into providing the best care possible in the hospital will resonate with all of the hospitalists who come to the meeting—and will give them fresh new ideas to take back to their hospitals.”
Dr. Conway and Dr. Ornstein will present starting at 8:15 a.m. Monday, April 2 (visit www.hospitalmedicine2012.org for a complete schedule). Dr. Conway will address the implementation of the Affordable Care Act and how hospitalists can help lead the transformation of the healthcare system. Dr. Ornstein will immediately follow Dr. Conway with his featured address, “Making Health Policy in an Age of Dysfunctional Politics.”
As in years past, Dr. Wachter’s featured presentation will be one of HM12’s final events. His presentation, “The Great Physician, c. 2012: How Hospitalists Must Lead Efforts to Identify and Become This New Breed,” is set for noon Wednesday, April 4.
“If hospitalists really want to be part of the transformation of healthcare and lead their hospitals forward, the featured presentations at HM12 should be required courses,” Dr. Glasheen says.
SHM’s annual meeting will bring some of the top thinkers in healthcare and HM to San Diego in April to present the ideas hospitalists will be talking about for the next year. In fact, with their experience in healthcare policy, this year’s presenters will frame the conversations that hospitalists will have at HM13, outside of Washington, D.C.
HM12’s featured speakers include:
Patrick H. Conway, MD, MSc, FAAP, SFHM, chief medical officer and director of the Office of Clinical Standards and Quality for the Centers for Medicare & Medicaid Services (CMS);
Norman J. Ornstein, PhD, MA, resident scholar, American Enterprise Institute for Public Policy Research; and
Robert M. Wachter, MD, MHM, professor and associate chairman of medicine, University of California at San Francisco.
“The featured speakers at HM12 in San Diego are guaranteed to provoke conversation among hospitalists, other caregivers, and policymakers throughout the year and beyond,” says HM12 course director Jeff Glasheen, MD, SFHM. “This year’s lineup brings some of the best hospitalists, nonhospitalists, and perennial favorites to the podium. The breadth of their experience and their insight into providing the best care possible in the hospital will resonate with all of the hospitalists who come to the meeting—and will give them fresh new ideas to take back to their hospitals.”
Dr. Conway and Dr. Ornstein will present starting at 8:15 a.m. Monday, April 2 (visit www.hospitalmedicine2012.org for a complete schedule). Dr. Conway will address the implementation of the Affordable Care Act and how hospitalists can help lead the transformation of the healthcare system. Dr. Ornstein will immediately follow Dr. Conway with his featured address, “Making Health Policy in an Age of Dysfunctional Politics.”
As in years past, Dr. Wachter’s featured presentation will be one of HM12’s final events. His presentation, “The Great Physician, c. 2012: How Hospitalists Must Lead Efforts to Identify and Become This New Breed,” is set for noon Wednesday, April 4.
“If hospitalists really want to be part of the transformation of healthcare and lead their hospitals forward, the featured presentations at HM12 should be required courses,” Dr. Glasheen says.
SHM’s annual meeting will bring some of the top thinkers in healthcare and HM to San Diego in April to present the ideas hospitalists will be talking about for the next year. In fact, with their experience in healthcare policy, this year’s presenters will frame the conversations that hospitalists will have at HM13, outside of Washington, D.C.
HM12’s featured speakers include:
Patrick H. Conway, MD, MSc, FAAP, SFHM, chief medical officer and director of the Office of Clinical Standards and Quality for the Centers for Medicare & Medicaid Services (CMS);
Norman J. Ornstein, PhD, MA, resident scholar, American Enterprise Institute for Public Policy Research; and
Robert M. Wachter, MD, MHM, professor and associate chairman of medicine, University of California at San Francisco.
“The featured speakers at HM12 in San Diego are guaranteed to provoke conversation among hospitalists, other caregivers, and policymakers throughout the year and beyond,” says HM12 course director Jeff Glasheen, MD, SFHM. “This year’s lineup brings some of the best hospitalists, nonhospitalists, and perennial favorites to the podium. The breadth of their experience and their insight into providing the best care possible in the hospital will resonate with all of the hospitalists who come to the meeting—and will give them fresh new ideas to take back to their hospitals.”
Dr. Conway and Dr. Ornstein will present starting at 8:15 a.m. Monday, April 2 (visit www.hospitalmedicine2012.org for a complete schedule). Dr. Conway will address the implementation of the Affordable Care Act and how hospitalists can help lead the transformation of the healthcare system. Dr. Ornstein will immediately follow Dr. Conway with his featured address, “Making Health Policy in an Age of Dysfunctional Politics.”
As in years past, Dr. Wachter’s featured presentation will be one of HM12’s final events. His presentation, “The Great Physician, c. 2012: How Hospitalists Must Lead Efforts to Identify and Become This New Breed,” is set for noon Wednesday, April 4.
“If hospitalists really want to be part of the transformation of healthcare and lead their hospitals forward, the featured presentations at HM12 should be required courses,” Dr. Glasheen says.
Participate in the 2012 State of Hospital Medicine Questionnaire
Every year, hospitalist group leaders across the country look forward to SHM’s annual State of Hospital Medicine report. The report provides thousands of data points that enable hospitalists to compare their own group’s productivity and compensation against national and regional averages.
And now, hospitalists can receive the 2012 report for free when they participate in the survey.
“This is the definitive tool for hospitalists to measure their compensation, practice models, and productivity against the most up-to-date information from hundreds of similar operations,” says Leslie Flores, SHM senior advisor of practice management.
The report will be somewhat different from the last two years; so, too, will submitting information for the survey. This year, SHM and MGMA will be conducting two separate but parallel surveys (MGMA will license the data from its survey to SHM), which will then be compiled into the State of Hospital Medicine report.
“The means for this year’s report will be different, but the end product—and its utility for hospitalist programs—will not differ greatly,” Flores says.
The report is a valuable tool for hospitalist group leaders because it contains national and regional data on:
- Hospitalist demographics;
- Practice and compensation models, including academic hospital medicine practices;
- Types of hospitals and patients served;
- Coverage models, including use of nonphysician practitioners (NPPs);
- Models of practice funding; and
- Comparisons of work RVUs by practice model.
Now is the time to start the survey, Flores says. In order to provide a data-rich report, the questionnaire requires more than just a few minutes to complete. The survey closes on March 9.
To begin, visit www.hospitalmedicine.org/survey
Every year, hospitalist group leaders across the country look forward to SHM’s annual State of Hospital Medicine report. The report provides thousands of data points that enable hospitalists to compare their own group’s productivity and compensation against national and regional averages.
And now, hospitalists can receive the 2012 report for free when they participate in the survey.
“This is the definitive tool for hospitalists to measure their compensation, practice models, and productivity against the most up-to-date information from hundreds of similar operations,” says Leslie Flores, SHM senior advisor of practice management.
The report will be somewhat different from the last two years; so, too, will submitting information for the survey. This year, SHM and MGMA will be conducting two separate but parallel surveys (MGMA will license the data from its survey to SHM), which will then be compiled into the State of Hospital Medicine report.
“The means for this year’s report will be different, but the end product—and its utility for hospitalist programs—will not differ greatly,” Flores says.
The report is a valuable tool for hospitalist group leaders because it contains national and regional data on:
- Hospitalist demographics;
- Practice and compensation models, including academic hospital medicine practices;
- Types of hospitals and patients served;
- Coverage models, including use of nonphysician practitioners (NPPs);
- Models of practice funding; and
- Comparisons of work RVUs by practice model.
Now is the time to start the survey, Flores says. In order to provide a data-rich report, the questionnaire requires more than just a few minutes to complete. The survey closes on March 9.
To begin, visit www.hospitalmedicine.org/survey
Every year, hospitalist group leaders across the country look forward to SHM’s annual State of Hospital Medicine report. The report provides thousands of data points that enable hospitalists to compare their own group’s productivity and compensation against national and regional averages.
And now, hospitalists can receive the 2012 report for free when they participate in the survey.
“This is the definitive tool for hospitalists to measure their compensation, practice models, and productivity against the most up-to-date information from hundreds of similar operations,” says Leslie Flores, SHM senior advisor of practice management.
The report will be somewhat different from the last two years; so, too, will submitting information for the survey. This year, SHM and MGMA will be conducting two separate but parallel surveys (MGMA will license the data from its survey to SHM), which will then be compiled into the State of Hospital Medicine report.
“The means for this year’s report will be different, but the end product—and its utility for hospitalist programs—will not differ greatly,” Flores says.
The report is a valuable tool for hospitalist group leaders because it contains national and regional data on:
- Hospitalist demographics;
- Practice and compensation models, including academic hospital medicine practices;
- Types of hospitals and patients served;
- Coverage models, including use of nonphysician practitioners (NPPs);
- Models of practice funding; and
- Comparisons of work RVUs by practice model.
Now is the time to start the survey, Flores says. In order to provide a data-rich report, the questionnaire requires more than just a few minutes to complete. The survey closes on March 9.
To begin, visit www.hospitalmedicine.org/survey