User login
Acute aortic syndromes: Time to talk of many things
“The time has come,” the Walrus said,
“To talk of many things:
Of shoes—and ships—and sealing-wax—
Of cabbages—and kings—
And why the sea is boiling hot
And whether pigs have wings.”
—Lewis Carroll, The Walrus and the Carpenter (from Through the Looking-Glass and What Alice Found There, 1872).
Lewis Carroll's poem of 1872 is a useful starting point for identifying issues resulting from confusion over the variously described acute aortic syndromes—and, for oysters, the dangers of listening to walruses.
TALK OF MANY THINGS
In cases of aortic dissection (splitting or separation of the layers of the aortic wall), it is important to establish the type (ie, the location and extent) and class (ie, the structure) of the dissection, because these distinctions determine the treatment.1 Similarly, in cases of painful or leaking degenerative aneurysms, we need to know the location of the aneurysm and whether the presenting pain is from compression of surrounding tissue, particularly of the vertebral bodies, or from leakage.
The location and extent of an aortic dissection can be classified in three ways (see Figure 3 in Smith and Schoenhagen’s excellent review of the use of computed tomography [CT] in acute aortic syndromes in this issue of the Cleveland Clinic Journal of Medicine2):
- The DeBakey system (type I, II, or III)
- The Stanford system (type A or B)
- Distal or proximal to the left subclavian artery.
Of note, the DeBakey system does not include tears in the arch that extend distally without ascending involvement. The original Stanford system included arch tears with distal extension in type B; hence, type B excluded all patients without ascending involvement.
The importance of the extent of dissection is that most patients with Stanford type A or DeBakey type I or II dissections should undergo immediate surgery, as most of them would die without it. Surgery is also indicated for arch tears (non-DeBakey, original Stanford type B).
Because these classifications are somewhat confusing, the simplest approach is to note whether the dissection extends proximal or distal to the left subclavian artery, because proximal dissections need surgery and distal ones are first managed medically.
The classes of dissection also have bearing on treatment.1 These are:
- Class I—classic aortic dissection in the media with two lumens separated by a “flap” or septum
- Class II—intramural hematoma in the aortic wall from dissection in which the intimal tear cannot be imaged (these are nearly always found duringsurgery or autopsy)
- Class III—localized confined intimal tears without extensive undermining of the intima or flap formation. These are often seen with Marfan syndrome and can rupture or cause tamponade, as can any type of proximal dissection. The typical appearance is of a bulging bubble in the aortic wall.
- Class IV—penetrating atherosclerotic ulcers with localized dissections or wall hematomas, often with calcium at the base of a mushroom-shaped area of extraluminal contrast. Of note, the plane of dissection is often between the media and adventitia.
- Class V—iatrogenic or posttraumatic dissection.
All class I to class IV tears of the proximal aorta require surgery, whereas distal class IV and V tears may require either open or endovascular surgical intervention. Surgery is also indicated for patients with distal dissections who have severe narrowing of the true lumen, distal ischemia, uncontrolled pain, severe hypertension, or evidence of leaking, particularly with class IV tears.
In distal dissections that are subacute (2–6 week sold), the Investigation of Stent grafts in Patients With Type B Aortic Dissection (INSTEAD) trial found that inserting a stent prophylactically provided no benefit. Further-more, there is no proof that stenting is beneficial if the aortic dissection is chronic, ie, more than 6 weeks old.1,3–5
WHICH SHOE FITS?
There is no ideal procedure to detect dissection, although the trend is towards CT angiography, as Smith and Schoenhagen report.2 Although some investigators have optimistically estimated CT’s sensitivity and specificity as 100%, cardiovascular surgeons are well aware of both false-positive and false-negative CT studies. Thus, for emergency repairs of proximal dissections, transesophageal echocardiography should be done after intubation and before opening a patient’s chest if time allows. Magnetic resonance imaging, CT, and transesophageal echocardiography may all miss class III tears, but these are frequently evidenced by eccentric “bubbles”or “ballooning.”1
SHIPS
Patients with either acute aortic dissection or severe pain associated with degenerative aneurysms need to be “shipped” promptly to a tertiary medical center after diagnosis, since larger volumes of procedures appear to be associated with better outcomes.
SEALING WAX
Using current surgical methods, the aortic valve can be preserved during aortic dissection repair unless the valve is bicuspid or the patient has Marfan syndrome.1,3,4,6–8
Sealing wax in the form of biological glues, rather than for letters, is a new innovation. A caveat remains, however: we have seen patients who have required reoperation for false aneurysms or infection. Hence, glues should be used with caution.
CABBAGES
A dilemma is whether patients should undergo coronary catheterization (or CT angiography—a separate question) and subsequent coronary artery bypass grafting (CABG), if needed, at the time of aortic dissection repair. The problem is that approximately one-third of patients have coronary artery disease that may require CABG, but the delay for catheterization increases the risk of rupture or tamponade before surgery.
Indeed, 40% of patients with proximal dissections die immediately, and 1% to 3% die in the hour before surgery. The short-term (in-hospital and 30-day) mortality rates range from 3.4% (Cleveland Clinic 2006 data) to 25%, and of the survivors only about 50% area live 5 years after surgery.
Though dismal, the prognosis is improving. In 162 patients with aortic dissection and Marfan syndrome or connective tissue disorders who underwent surgery at Cleveland Clinic in the years 1978–2003, the 5-year survival rate in those with aortic dissection was 75% and the 10-year rate was 55%.7 In those without dissection, the 10-year survival rate was approximately 90% (P < .001).
KINGS
Noted personalities who have had aortic dissection include King George II of England (who died in 1760), Lucille Ball, Conway Twitty, Jan Larson, and most recently John Ritter. None of these famous people survived their aortic dissections. Indeed, dissection and diseases of the aorta or its branches cause between 43,000 and 47,000 deaths annually,9 more than from breast cancer, murders, or motor vehicle accidents. The main reason for these dismal statistics is that the disease is often misdiagnosed at the time of presentation.
BOILING SEA
Careful studies from Olmsted County, Minnesota,10 have shown a tripling of the incidence of aortic disease, particularly in women, even though the rate of deaths from coronary artery disease has been decreasing. Furthermore, Olsson et al11 report that the incidence of aortic dissection in men in Sweden increased to approximately16 per 100,000 per year from 1987 to 2002, a 52% increase. The aging of the population must play a large role, but other factors may exist that are not well understood or defined and require further research.
PIGS HAVE WINGS
Will it be possible to overcome this rising problem? The answer is a definite yes. The results of aortic surgery have never been better. Many new innovations are available, such as aortic root preservation and endovascular stenting procedures. It may be possible to slow the growth of or prevent some aneurysms and aortic dissections, particularly with beta-blockers and, potentially, with losartan (Cozaar) for Marfan syndrome patients.
One of the keys to preventing aortic catastrophes and aortic dissection is to repair aortic aneurysms. The threshold for surgery, however, depends on a surgeon’s experience and results, the underlying pathology, and the aortic size.
We observed that 12.5% of dissections in patients with bicuspid valves and 15% of those in patients with Marfan syndrome were in aortas smaller than 5.0 cm in diameter, that aortic dissection occurred at smaller diameters in shorter patients, and that the risk of dissection increased exponentially with the size of the aorta. Subsequently, we found that a better measure of risk is the maximal aortic cross-sectional area in cm2 divided by the patient’s height in meters; if this ratio exceeds 10, then surgery is recommended.12
Results of surgery are good in experienced hands. In patients who undergo surgical repair of bicuspid aortic valves with or without concurrent repair of the ascending aorta (mostly in patients with an aortic cross-section-to-height ratio > 10), the perioperative mortality rate is about 1.0% for both groups, and at 10 years about 98% of patients are free from re-operation on the aorta and more than 90% are free from re-operation on the aortic valve.8 This is important because these are typically young patients who would do better without biological replacement valves (which are not very durable) or mechanical valves (which necessitate lifelong anticoagulation). Results are also good in surgery of the aortic arch and even better in patients with tricuspid aortic valves.4,6,8
Increasingly, in patients at high risk, we are inserting thoracic, abdominal, and thoracoabdominal stent grafts, with excellent early results. An even newer innovation is to replace the aortic valve in high-risk patients via a transcatheter balloon-expandable valve stent inserted through the groin or left ventricular apex.
These treatment innovations have been big strides, but aortic disease continues to increase. Indeed, our volume of thoracic aortic surgery at Cleveland Clinic increased from 190 procedures in 1999 to 717 in 2006. Early detection—before acute emergency surgery is required, with its concomitant high risk of death—is the key to successful surgical outcome and long-term survival.
- Svensson LG, Labib SB, Eisenhauer AC, Butterly JR. Intimal tear without hematoma: an important variant of aortic dissection that can elude current imaging techniques. Circulation 1999; 99:1331–1336.
- Smith AD, Schoenhagen P. CT imaging for acute aortic syndrome. Cleve Clin J Med 2008; 75:7–24.
- Svensson LG, Nadolny EM, Kimmel WA. Multimodal protocol influence on stroke and neurocognitive deficit prevention after ascending/arch aortic operations. Ann Thorac Surg 2002; 74:2040–2046.
- Svensson LG, Kim KH, Blackstone EH, et al. Elephant trunk procedure: newer indications and uses. Ann Thorac Surg 2004; 78:109–116.
- Greenberg RK, Haddad F, Svensson L, et al. Hybrid approaches to thoracic aortic aneurysms: the role of endovascular elephant trunk completion. Circulation 2005; 112:2619–2626.
- Svensson LG. Sizing for modified David’s reimplantation procedure. Ann Thorac Surg 2003; 76:1751–1753.
- Svensson LG, Blackstone EH, Feng J, et al. Are Marfan syndrome and marfanoid patients distinguishable on long-term follow-up? Ann Thorac Surg 2007; 83:1067–1074.
- Svensson LG, Blackstone EH, Cosgrove DM 3rd. Surgical options in young adults with aortic valve disease. Curr Probl Cardiol 2003; 28:417–480.
- Svensson LG, Rodriguez ER. Aortic organ disease epidemic, and why do balloons pop? Circulation 2005; 112:1082–1084.
- Clouse WD, Hallett JW Jr, Schaff HV, Gayari MM, Ilstrup DM, Melton LJ 3rd. Improved prognosis of thoracic aortic aneurysms: a population-based study. JAMA 1998; 280:1926–1929.
- Olsson C, Thelin S, Ståhle E, Ekbom A, Granath F. Thoracic aortic aneurysm and dissection: increasing prevalence and improved outcomes reported in a nationwide population-based study of more than 14,000 cases from 1987 to 2002. Circulation 2006; 114:2611–2618.
- Svensson LG, Kim KH, Lytle BW, Cosgrove DM. Relationship of aortic cross-sectional area to height ratio and the risk of aortic dissection inpatients with bicuspid aortic valves. J Thorac Cardiovasc Surg 2003;126:892–893.
“The time has come,” the Walrus said,
“To talk of many things:
Of shoes—and ships—and sealing-wax—
Of cabbages—and kings—
And why the sea is boiling hot
And whether pigs have wings.”
—Lewis Carroll, The Walrus and the Carpenter (from Through the Looking-Glass and What Alice Found There, 1872).
Lewis Carroll's poem of 1872 is a useful starting point for identifying issues resulting from confusion over the variously described acute aortic syndromes—and, for oysters, the dangers of listening to walruses.
TALK OF MANY THINGS
In cases of aortic dissection (splitting or separation of the layers of the aortic wall), it is important to establish the type (ie, the location and extent) and class (ie, the structure) of the dissection, because these distinctions determine the treatment.1 Similarly, in cases of painful or leaking degenerative aneurysms, we need to know the location of the aneurysm and whether the presenting pain is from compression of surrounding tissue, particularly of the vertebral bodies, or from leakage.
The location and extent of an aortic dissection can be classified in three ways (see Figure 3 in Smith and Schoenhagen’s excellent review of the use of computed tomography [CT] in acute aortic syndromes in this issue of the Cleveland Clinic Journal of Medicine2):
- The DeBakey system (type I, II, or III)
- The Stanford system (type A or B)
- Distal or proximal to the left subclavian artery.
Of note, the DeBakey system does not include tears in the arch that extend distally without ascending involvement. The original Stanford system included arch tears with distal extension in type B; hence, type B excluded all patients without ascending involvement.
The importance of the extent of dissection is that most patients with Stanford type A or DeBakey type I or II dissections should undergo immediate surgery, as most of them would die without it. Surgery is also indicated for arch tears (non-DeBakey, original Stanford type B).
Because these classifications are somewhat confusing, the simplest approach is to note whether the dissection extends proximal or distal to the left subclavian artery, because proximal dissections need surgery and distal ones are first managed medically.
The classes of dissection also have bearing on treatment.1 These are:
- Class I—classic aortic dissection in the media with two lumens separated by a “flap” or septum
- Class II—intramural hematoma in the aortic wall from dissection in which the intimal tear cannot be imaged (these are nearly always found duringsurgery or autopsy)
- Class III—localized confined intimal tears without extensive undermining of the intima or flap formation. These are often seen with Marfan syndrome and can rupture or cause tamponade, as can any type of proximal dissection. The typical appearance is of a bulging bubble in the aortic wall.
- Class IV—penetrating atherosclerotic ulcers with localized dissections or wall hematomas, often with calcium at the base of a mushroom-shaped area of extraluminal contrast. Of note, the plane of dissection is often between the media and adventitia.
- Class V—iatrogenic or posttraumatic dissection.
All class I to class IV tears of the proximal aorta require surgery, whereas distal class IV and V tears may require either open or endovascular surgical intervention. Surgery is also indicated for patients with distal dissections who have severe narrowing of the true lumen, distal ischemia, uncontrolled pain, severe hypertension, or evidence of leaking, particularly with class IV tears.
In distal dissections that are subacute (2–6 week sold), the Investigation of Stent grafts in Patients With Type B Aortic Dissection (INSTEAD) trial found that inserting a stent prophylactically provided no benefit. Further-more, there is no proof that stenting is beneficial if the aortic dissection is chronic, ie, more than 6 weeks old.1,3–5
WHICH SHOE FITS?
There is no ideal procedure to detect dissection, although the trend is towards CT angiography, as Smith and Schoenhagen report.2 Although some investigators have optimistically estimated CT’s sensitivity and specificity as 100%, cardiovascular surgeons are well aware of both false-positive and false-negative CT studies. Thus, for emergency repairs of proximal dissections, transesophageal echocardiography should be done after intubation and before opening a patient’s chest if time allows. Magnetic resonance imaging, CT, and transesophageal echocardiography may all miss class III tears, but these are frequently evidenced by eccentric “bubbles”or “ballooning.”1
SHIPS
Patients with either acute aortic dissection or severe pain associated with degenerative aneurysms need to be “shipped” promptly to a tertiary medical center after diagnosis, since larger volumes of procedures appear to be associated with better outcomes.
SEALING WAX
Using current surgical methods, the aortic valve can be preserved during aortic dissection repair unless the valve is bicuspid or the patient has Marfan syndrome.1,3,4,6–8
Sealing wax in the form of biological glues, rather than for letters, is a new innovation. A caveat remains, however: we have seen patients who have required reoperation for false aneurysms or infection. Hence, glues should be used with caution.
CABBAGES
A dilemma is whether patients should undergo coronary catheterization (or CT angiography—a separate question) and subsequent coronary artery bypass grafting (CABG), if needed, at the time of aortic dissection repair. The problem is that approximately one-third of patients have coronary artery disease that may require CABG, but the delay for catheterization increases the risk of rupture or tamponade before surgery.
Indeed, 40% of patients with proximal dissections die immediately, and 1% to 3% die in the hour before surgery. The short-term (in-hospital and 30-day) mortality rates range from 3.4% (Cleveland Clinic 2006 data) to 25%, and of the survivors only about 50% area live 5 years after surgery.
Though dismal, the prognosis is improving. In 162 patients with aortic dissection and Marfan syndrome or connective tissue disorders who underwent surgery at Cleveland Clinic in the years 1978–2003, the 5-year survival rate in those with aortic dissection was 75% and the 10-year rate was 55%.7 In those without dissection, the 10-year survival rate was approximately 90% (P < .001).
KINGS
Noted personalities who have had aortic dissection include King George II of England (who died in 1760), Lucille Ball, Conway Twitty, Jan Larson, and most recently John Ritter. None of these famous people survived their aortic dissections. Indeed, dissection and diseases of the aorta or its branches cause between 43,000 and 47,000 deaths annually,9 more than from breast cancer, murders, or motor vehicle accidents. The main reason for these dismal statistics is that the disease is often misdiagnosed at the time of presentation.
BOILING SEA
Careful studies from Olmsted County, Minnesota,10 have shown a tripling of the incidence of aortic disease, particularly in women, even though the rate of deaths from coronary artery disease has been decreasing. Furthermore, Olsson et al11 report that the incidence of aortic dissection in men in Sweden increased to approximately16 per 100,000 per year from 1987 to 2002, a 52% increase. The aging of the population must play a large role, but other factors may exist that are not well understood or defined and require further research.
PIGS HAVE WINGS
Will it be possible to overcome this rising problem? The answer is a definite yes. The results of aortic surgery have never been better. Many new innovations are available, such as aortic root preservation and endovascular stenting procedures. It may be possible to slow the growth of or prevent some aneurysms and aortic dissections, particularly with beta-blockers and, potentially, with losartan (Cozaar) for Marfan syndrome patients.
One of the keys to preventing aortic catastrophes and aortic dissection is to repair aortic aneurysms. The threshold for surgery, however, depends on a surgeon’s experience and results, the underlying pathology, and the aortic size.
We observed that 12.5% of dissections in patients with bicuspid valves and 15% of those in patients with Marfan syndrome were in aortas smaller than 5.0 cm in diameter, that aortic dissection occurred at smaller diameters in shorter patients, and that the risk of dissection increased exponentially with the size of the aorta. Subsequently, we found that a better measure of risk is the maximal aortic cross-sectional area in cm2 divided by the patient’s height in meters; if this ratio exceeds 10, then surgery is recommended.12
Results of surgery are good in experienced hands. In patients who undergo surgical repair of bicuspid aortic valves with or without concurrent repair of the ascending aorta (mostly in patients with an aortic cross-section-to-height ratio > 10), the perioperative mortality rate is about 1.0% for both groups, and at 10 years about 98% of patients are free from re-operation on the aorta and more than 90% are free from re-operation on the aortic valve.8 This is important because these are typically young patients who would do better without biological replacement valves (which are not very durable) or mechanical valves (which necessitate lifelong anticoagulation). Results are also good in surgery of the aortic arch and even better in patients with tricuspid aortic valves.4,6,8
Increasingly, in patients at high risk, we are inserting thoracic, abdominal, and thoracoabdominal stent grafts, with excellent early results. An even newer innovation is to replace the aortic valve in high-risk patients via a transcatheter balloon-expandable valve stent inserted through the groin or left ventricular apex.
These treatment innovations have been big strides, but aortic disease continues to increase. Indeed, our volume of thoracic aortic surgery at Cleveland Clinic increased from 190 procedures in 1999 to 717 in 2006. Early detection—before acute emergency surgery is required, with its concomitant high risk of death—is the key to successful surgical outcome and long-term survival.
“The time has come,” the Walrus said,
“To talk of many things:
Of shoes—and ships—and sealing-wax—
Of cabbages—and kings—
And why the sea is boiling hot
And whether pigs have wings.”
—Lewis Carroll, The Walrus and the Carpenter (from Through the Looking-Glass and What Alice Found There, 1872).
Lewis Carroll's poem of 1872 is a useful starting point for identifying issues resulting from confusion over the variously described acute aortic syndromes—and, for oysters, the dangers of listening to walruses.
TALK OF MANY THINGS
In cases of aortic dissection (splitting or separation of the layers of the aortic wall), it is important to establish the type (ie, the location and extent) and class (ie, the structure) of the dissection, because these distinctions determine the treatment.1 Similarly, in cases of painful or leaking degenerative aneurysms, we need to know the location of the aneurysm and whether the presenting pain is from compression of surrounding tissue, particularly of the vertebral bodies, or from leakage.
The location and extent of an aortic dissection can be classified in three ways (see Figure 3 in Smith and Schoenhagen’s excellent review of the use of computed tomography [CT] in acute aortic syndromes in this issue of the Cleveland Clinic Journal of Medicine2):
- The DeBakey system (type I, II, or III)
- The Stanford system (type A or B)
- Distal or proximal to the left subclavian artery.
Of note, the DeBakey system does not include tears in the arch that extend distally without ascending involvement. The original Stanford system included arch tears with distal extension in type B; hence, type B excluded all patients without ascending involvement.
The importance of the extent of dissection is that most patients with Stanford type A or DeBakey type I or II dissections should undergo immediate surgery, as most of them would die without it. Surgery is also indicated for arch tears (non-DeBakey, original Stanford type B).
Because these classifications are somewhat confusing, the simplest approach is to note whether the dissection extends proximal or distal to the left subclavian artery, because proximal dissections need surgery and distal ones are first managed medically.
The classes of dissection also have bearing on treatment.1 These are:
- Class I—classic aortic dissection in the media with two lumens separated by a “flap” or septum
- Class II—intramural hematoma in the aortic wall from dissection in which the intimal tear cannot be imaged (these are nearly always found duringsurgery or autopsy)
- Class III—localized confined intimal tears without extensive undermining of the intima or flap formation. These are often seen with Marfan syndrome and can rupture or cause tamponade, as can any type of proximal dissection. The typical appearance is of a bulging bubble in the aortic wall.
- Class IV—penetrating atherosclerotic ulcers with localized dissections or wall hematomas, often with calcium at the base of a mushroom-shaped area of extraluminal contrast. Of note, the plane of dissection is often between the media and adventitia.
- Class V—iatrogenic or posttraumatic dissection.
All class I to class IV tears of the proximal aorta require surgery, whereas distal class IV and V tears may require either open or endovascular surgical intervention. Surgery is also indicated for patients with distal dissections who have severe narrowing of the true lumen, distal ischemia, uncontrolled pain, severe hypertension, or evidence of leaking, particularly with class IV tears.
In distal dissections that are subacute (2–6 week sold), the Investigation of Stent grafts in Patients With Type B Aortic Dissection (INSTEAD) trial found that inserting a stent prophylactically provided no benefit. Further-more, there is no proof that stenting is beneficial if the aortic dissection is chronic, ie, more than 6 weeks old.1,3–5
WHICH SHOE FITS?
There is no ideal procedure to detect dissection, although the trend is towards CT angiography, as Smith and Schoenhagen report.2 Although some investigators have optimistically estimated CT’s sensitivity and specificity as 100%, cardiovascular surgeons are well aware of both false-positive and false-negative CT studies. Thus, for emergency repairs of proximal dissections, transesophageal echocardiography should be done after intubation and before opening a patient’s chest if time allows. Magnetic resonance imaging, CT, and transesophageal echocardiography may all miss class III tears, but these are frequently evidenced by eccentric “bubbles”or “ballooning.”1
SHIPS
Patients with either acute aortic dissection or severe pain associated with degenerative aneurysms need to be “shipped” promptly to a tertiary medical center after diagnosis, since larger volumes of procedures appear to be associated with better outcomes.
SEALING WAX
Using current surgical methods, the aortic valve can be preserved during aortic dissection repair unless the valve is bicuspid or the patient has Marfan syndrome.1,3,4,6–8
Sealing wax in the form of biological glues, rather than for letters, is a new innovation. A caveat remains, however: we have seen patients who have required reoperation for false aneurysms or infection. Hence, glues should be used with caution.
CABBAGES
A dilemma is whether patients should undergo coronary catheterization (or CT angiography—a separate question) and subsequent coronary artery bypass grafting (CABG), if needed, at the time of aortic dissection repair. The problem is that approximately one-third of patients have coronary artery disease that may require CABG, but the delay for catheterization increases the risk of rupture or tamponade before surgery.
Indeed, 40% of patients with proximal dissections die immediately, and 1% to 3% die in the hour before surgery. The short-term (in-hospital and 30-day) mortality rates range from 3.4% (Cleveland Clinic 2006 data) to 25%, and of the survivors only about 50% area live 5 years after surgery.
Though dismal, the prognosis is improving. In 162 patients with aortic dissection and Marfan syndrome or connective tissue disorders who underwent surgery at Cleveland Clinic in the years 1978–2003, the 5-year survival rate in those with aortic dissection was 75% and the 10-year rate was 55%.7 In those without dissection, the 10-year survival rate was approximately 90% (P < .001).
KINGS
Noted personalities who have had aortic dissection include King George II of England (who died in 1760), Lucille Ball, Conway Twitty, Jan Larson, and most recently John Ritter. None of these famous people survived their aortic dissections. Indeed, dissection and diseases of the aorta or its branches cause between 43,000 and 47,000 deaths annually,9 more than from breast cancer, murders, or motor vehicle accidents. The main reason for these dismal statistics is that the disease is often misdiagnosed at the time of presentation.
BOILING SEA
Careful studies from Olmsted County, Minnesota,10 have shown a tripling of the incidence of aortic disease, particularly in women, even though the rate of deaths from coronary artery disease has been decreasing. Furthermore, Olsson et al11 report that the incidence of aortic dissection in men in Sweden increased to approximately16 per 100,000 per year from 1987 to 2002, a 52% increase. The aging of the population must play a large role, but other factors may exist that are not well understood or defined and require further research.
PIGS HAVE WINGS
Will it be possible to overcome this rising problem? The answer is a definite yes. The results of aortic surgery have never been better. Many new innovations are available, such as aortic root preservation and endovascular stenting procedures. It may be possible to slow the growth of or prevent some aneurysms and aortic dissections, particularly with beta-blockers and, potentially, with losartan (Cozaar) for Marfan syndrome patients.
One of the keys to preventing aortic catastrophes and aortic dissection is to repair aortic aneurysms. The threshold for surgery, however, depends on a surgeon’s experience and results, the underlying pathology, and the aortic size.
We observed that 12.5% of dissections in patients with bicuspid valves and 15% of those in patients with Marfan syndrome were in aortas smaller than 5.0 cm in diameter, that aortic dissection occurred at smaller diameters in shorter patients, and that the risk of dissection increased exponentially with the size of the aorta. Subsequently, we found that a better measure of risk is the maximal aortic cross-sectional area in cm2 divided by the patient’s height in meters; if this ratio exceeds 10, then surgery is recommended.12
Results of surgery are good in experienced hands. In patients who undergo surgical repair of bicuspid aortic valves with or without concurrent repair of the ascending aorta (mostly in patients with an aortic cross-section-to-height ratio > 10), the perioperative mortality rate is about 1.0% for both groups, and at 10 years about 98% of patients are free from re-operation on the aorta and more than 90% are free from re-operation on the aortic valve.8 This is important because these are typically young patients who would do better without biological replacement valves (which are not very durable) or mechanical valves (which necessitate lifelong anticoagulation). Results are also good in surgery of the aortic arch and even better in patients with tricuspid aortic valves.4,6,8
Increasingly, in patients at high risk, we are inserting thoracic, abdominal, and thoracoabdominal stent grafts, with excellent early results. An even newer innovation is to replace the aortic valve in high-risk patients via a transcatheter balloon-expandable valve stent inserted through the groin or left ventricular apex.
These treatment innovations have been big strides, but aortic disease continues to increase. Indeed, our volume of thoracic aortic surgery at Cleveland Clinic increased from 190 procedures in 1999 to 717 in 2006. Early detection—before acute emergency surgery is required, with its concomitant high risk of death—is the key to successful surgical outcome and long-term survival.
- Svensson LG, Labib SB, Eisenhauer AC, Butterly JR. Intimal tear without hematoma: an important variant of aortic dissection that can elude current imaging techniques. Circulation 1999; 99:1331–1336.
- Smith AD, Schoenhagen P. CT imaging for acute aortic syndrome. Cleve Clin J Med 2008; 75:7–24.
- Svensson LG, Nadolny EM, Kimmel WA. Multimodal protocol influence on stroke and neurocognitive deficit prevention after ascending/arch aortic operations. Ann Thorac Surg 2002; 74:2040–2046.
- Svensson LG, Kim KH, Blackstone EH, et al. Elephant trunk procedure: newer indications and uses. Ann Thorac Surg 2004; 78:109–116.
- Greenberg RK, Haddad F, Svensson L, et al. Hybrid approaches to thoracic aortic aneurysms: the role of endovascular elephant trunk completion. Circulation 2005; 112:2619–2626.
- Svensson LG. Sizing for modified David’s reimplantation procedure. Ann Thorac Surg 2003; 76:1751–1753.
- Svensson LG, Blackstone EH, Feng J, et al. Are Marfan syndrome and marfanoid patients distinguishable on long-term follow-up? Ann Thorac Surg 2007; 83:1067–1074.
- Svensson LG, Blackstone EH, Cosgrove DM 3rd. Surgical options in young adults with aortic valve disease. Curr Probl Cardiol 2003; 28:417–480.
- Svensson LG, Rodriguez ER. Aortic organ disease epidemic, and why do balloons pop? Circulation 2005; 112:1082–1084.
- Clouse WD, Hallett JW Jr, Schaff HV, Gayari MM, Ilstrup DM, Melton LJ 3rd. Improved prognosis of thoracic aortic aneurysms: a population-based study. JAMA 1998; 280:1926–1929.
- Olsson C, Thelin S, Ståhle E, Ekbom A, Granath F. Thoracic aortic aneurysm and dissection: increasing prevalence and improved outcomes reported in a nationwide population-based study of more than 14,000 cases from 1987 to 2002. Circulation 2006; 114:2611–2618.
- Svensson LG, Kim KH, Lytle BW, Cosgrove DM. Relationship of aortic cross-sectional area to height ratio and the risk of aortic dissection inpatients with bicuspid aortic valves. J Thorac Cardiovasc Surg 2003;126:892–893.
- Svensson LG, Labib SB, Eisenhauer AC, Butterly JR. Intimal tear without hematoma: an important variant of aortic dissection that can elude current imaging techniques. Circulation 1999; 99:1331–1336.
- Smith AD, Schoenhagen P. CT imaging for acute aortic syndrome. Cleve Clin J Med 2008; 75:7–24.
- Svensson LG, Nadolny EM, Kimmel WA. Multimodal protocol influence on stroke and neurocognitive deficit prevention after ascending/arch aortic operations. Ann Thorac Surg 2002; 74:2040–2046.
- Svensson LG, Kim KH, Blackstone EH, et al. Elephant trunk procedure: newer indications and uses. Ann Thorac Surg 2004; 78:109–116.
- Greenberg RK, Haddad F, Svensson L, et al. Hybrid approaches to thoracic aortic aneurysms: the role of endovascular elephant trunk completion. Circulation 2005; 112:2619–2626.
- Svensson LG. Sizing for modified David’s reimplantation procedure. Ann Thorac Surg 2003; 76:1751–1753.
- Svensson LG, Blackstone EH, Feng J, et al. Are Marfan syndrome and marfanoid patients distinguishable on long-term follow-up? Ann Thorac Surg 2007; 83:1067–1074.
- Svensson LG, Blackstone EH, Cosgrove DM 3rd. Surgical options in young adults with aortic valve disease. Curr Probl Cardiol 2003; 28:417–480.
- Svensson LG, Rodriguez ER. Aortic organ disease epidemic, and why do balloons pop? Circulation 2005; 112:1082–1084.
- Clouse WD, Hallett JW Jr, Schaff HV, Gayari MM, Ilstrup DM, Melton LJ 3rd. Improved prognosis of thoracic aortic aneurysms: a population-based study. JAMA 1998; 280:1926–1929.
- Olsson C, Thelin S, Ståhle E, Ekbom A, Granath F. Thoracic aortic aneurysm and dissection: increasing prevalence and improved outcomes reported in a nationwide population-based study of more than 14,000 cases from 1987 to 2002. Circulation 2006; 114:2611–2618.
- Svensson LG, Kim KH, Lytle BW, Cosgrove DM. Relationship of aortic cross-sectional area to height ratio and the risk of aortic dissection inpatients with bicuspid aortic valves. J Thorac Cardiovasc Surg 2003;126:892–893.
What is the most important public health problem facing the world today and how should it be addressed?
Urticarial Vasculitis in an Infant
Sigh syndrome: Is it a sign of trouble?
- Sigh syndrome is a genuine medical diagnosis with distinct criteria, conferring significant stress for those affected. Despite outward signs of an abnormal breathing pattern, this symptomatology is unrelated to any respiratory or organic pathology.
- Ancillary testing and medication seem unnecessary; supporting reassurance appears sufficient, since the syndrome has a favorable outcome.
Objective The goal of this study was to identify the characteristics and clinical course of patients presenting with considerable stress regarding irrepressible persistent sighing, and to determine whether any association exists between this syndrome and respiratory or other organic disease during the acute or follow-up period.
Study design We conducted a case series review of patients diagnosed with a defined symptom complex and gathered relevant data.
Population Forty patients who presented to 3 clinics in Israel met our 10 criteria for sigh syndrome: recurrent sighing (at least once a minute, for varying lengths of time throughout the day); otherwise shallow respiration; patient conviction that deep breaths are obstructed; intensity of episodes provokes stress leading to consultation; no obvious trigger; episodes last a few days to several weeks; no interference with speech; sighing is absent during sleep; no correlation with physical activity or rest; and self-limited.
Outcomes measured We assessed demographic and health status information, as well as recent circumstances that could have served as triggers for the symptoms. We also performed systematic diagnoses of acute and chronic organic disease.
Results Physicians diagnosed “sigh syndrome” in 40 subjects (19 men [47.5%]), mean age 31.8 years, during the 3-year study period. All patients conformed to 10 sigh syndrome criteria. In 13 patients (32.5%), a significant traumatic event preceded onset of symptoms. Ten (25%) had previous anxiety or somatoform-related disorders. For 23 patients (57.5%), the sigh syndrome episode repeated itself after an initial episode. We found no association in any of the cases with any form of organic disease. Likewise, during the follow-up period (on average, 18 months), we did not observe the development of a specific organic disorder in any case.
Conclusions The “sigh syndrome” runs a benign course; it mainly demands the support and understanding of the treating physician to allay any patient concerns.
In our clinical practices, we have repeatedly cared for patients who came into our clinics because of a worrisome irregular breathing pattern characterized by a deep inspiration, and followed by a noisy expiration. We have referred to the set of clinical signs that these patients present with as “sigh syndrome.”
We have long suspected that sigh syndrome is an underdiagnosed and self-limited condition that is often mistaken for a serious respiratory disorder. In our experience, this syndrome runs a benign course. However, we believed that this syndrome had characteristic and consistent features, and should not be considered a diagnosis of exclusion.
Thus, we undertook a study to observe a group of subjects with these features to judge whether this subjectively alarming symptom complex is in fact harmless, and whether it is appropriate to respond to it as we had, by taking a stress-alleviating approach alone.
What is sigh syndrome?
Patients with sigh syndrome exhibit a compulsion to perform single but repeated deep inspirations, accompanied by a sensation of difficulty in inhaling a sufficient quantity of air. Each inspiration is followed by a prolonged, sometimes noisy expiration—namely, a sigh. Observing such abnormal breaths and confirming that the patient feels a concomitant inability to fill his lungs to capacity is sufficient to make the diagnosis.
This breathing compulsion is irregular in nature: It may occur once a minute or several times a minute, and this breathing pattern may continue—on and off throughout the day—for a few days to several weeks. In our experience, it provokes significant anxiety in patients, prompting them to seek medical advice. It does not occur when the patient is asleep, and it is not triggered by physical activity.
Both patient and doctor may, at first, be convinced that the problem reflects a serious illness. The 10 features of sigh syndrome (TABLE 1) constitute a proposed definition. All of our study subjects exhibited these 10 features.
TABLE 1
10 features of sigh syndrome
|
Sighing as an illness marker
Sighing has been described as one member of a group of signs exhibited by depressed or anxiety-ridden patients.1 While Perin et al2 were the first to point out the importance of distinguishing between sighing and respiratory disease, sighing per se has never been identified as a discrete illness marker.
A number of psychiatric disorders are already well known to incorporate breathing and chest symptoms along with widespread somatization. These include globus hystericus, neurocirculatory asthenia, and Tietze syndrome.3-6 As such, the acute pain of precordial catch syndrome stands out as an example of a distinguishable, clear-cut clinical state devoid of any apparent organic basis.7,8
Methods
How we recruited the patients
Data was collected from 3 family practice clinics in Israel from February 2002 to February 2005. We requested that these practices contribute data of consecutive clinical cases presenting with the 10 set symptoms of sigh syndrome (TABLE 1).
Data collected included basic demographics, the circumstances of the onset of symptoms, concurrent medical conditions, and any associated symptoms. We assessed the patients’ education level by asking questions pertaining to their years of schooling and college degrees. Patients rated their own economic status as being below, average, or above-average income.
The main outcome we examined was the clinical course of the sighing episodes during the ensuing months after their visit, in order to determine whether any patients developed a form of significant organic disease or a disorder that led to hospitalization.
Results
40 cases that cut across the socioeconomic spectrum
Forty patients were recruited for this study. Nineteen (47.5%) were male; their ages ranged from 7 to 53 (mean, 31.8; standard deviation, 13.7). Two patients (5%) were Ashkenazi Jews; 34 (85%) were of North African ethnicity (Sephardic Jews); the other 4 were of varied Asian and European ethnicity. The number of patients with North African ethnicity overrepresents that of the population in their communities. Additionally, 3 members of this group were from the same family.
There was no predilection toward any specific education level or socioeconomic status. The occupations of the subjects were diverse.
Their clinical characteristics
The clinical characteristics of the 40 patients are presented in TABLE 2. The subjects’ sighing began at various times of the day, without relationship to eating or any other activity, and disappeared during sleep. All patients reported the same feeling: that of an extra effort demanded to perform full inspiration. In many cases, adult patients were certain their complaints were a sign of cardiac or respiratory disease, and they were very concerned that there was some grave, underlying disorder.
History and examination failed to reveal evidence of any somatic findings related to breathing difficulty. Breathing rate was within normal limits in all cases.
The physicians’ initial encounters with these patients led to further examination in many cases: electrocardiography, blood oxygen saturation, and complete blood counts. However, no abnormalities were found on any of these tests. Medications, if prescribed at all during these consultations, were usually given to alleviate insomnia or anxiety. Further ancillary investigations or referrals were not ordered.
The sole notable finding on physical examination was a typical murmur (which had already been diagnosed) in a young girl with a congenital atrial septal defect. This 7-year-old developed repeated episodes of sigh syndrome just before her annual visit to the pediatric cardiologist; her mother believed that the child was frightened by the thought of possible future surgery.
TABLE 2
Clinical characteristics of the 40 patients studied—One third experienced a traumatic event
| CHARACTERISTIC | YES | NO |
|---|---|---|
| Smoker | 2 (5%) | 38 (95%) |
| History of anxiety or somatoform disorder | 10 (25%) | 30 (75%) |
| Taking prescription medication at time of diagnosis | 4 (10%) | 36 (90%) |
| Recurrence of sighing episodes during follow-up period | 24 (60%) | 16 (40%) |
| Trigger event (eg, exposure to traumatic event 1 month before presentation with syndrome) | 13 (32.5%) | 27 (67.5%) |
Traumatic events, anxiety disorders suggest stress as a cause
Thirteen patient histories disclosed a definite, recent, significant traumatic event that may have triggered the onset of sigh syndrome. Examples of 2 triggering events are the terrorist murder of several members of a neighbor’s family, and a near-miss with a mortar shell. One subject—a teenager—had recently been left alone in the dark with 2 younger siblings during a power blackout; another young woman said that the sighing episodes began when she decided to get married.
Ten patients had previously diagnosed neurotic disorders, mainly generalized anxiety; these included 2 cases of somatization disorder and 1 case of posttraumatic stress disorder. This information from the patients’ histories was documented in their medical files.
Episodes appear to be self-limited
In all patients, the episodes were self-limited. During the follow-up period, lasting an average of 18 months, none of the patients showed additional medical conditions—respiratory or otherwise—that could be linked to episodes of sigh syndrome. Recurrences of sighing episodes were reported by 24 subjects (60%) after the marker episode. One patient was diagnosed with carcinoma of the pancreas 2 years into follow-up, and later died.
Discussion
A benign, transient disorder
Aside from the solitary and unrelated death noted above, examination and follow-up in all 40 cases did not lead to an alternative diagnosis. Sigh syndrome thus seems to be an entirely benign and transient condition with no sequelae aside from possible recurrences.
Although the pathophysiology is unclear, our finding that 32.5% of patients had a recent traumatic incident strongly suggests a stress-related condition. Furthermore, 25% of the patients were already known to suffer from intermittent anxiety or somatoform disorders, although none were taking medications for these conditions. This adds support to the assumption that a mind-body interaction is underpinning the disorder. Large-scale migration, recent war or terrorist acts, or natural disaster are likely to increase the chances that the average physician will see a patient with sigh syndrome.
A tendency towards North African/Sephardic ethnicity, rather than European ethnicity—in addition to the cluster of 3 cases belonging to the same family—suggests the presentation may be a subconscious cultural, learned, or adopted expression of uneasiness.
Making your evaluation: History and physical are enough
The diagnostic evaluation of sigh syndrome—consisting of careful history-taking and a thorough physical examination—should be sufficient to differentiate it from an array of organic diseases. A physical examination is imperative to exclude other causes for this breathing abnormality.
Ancillary testing is rarely, if ever, indicated. It can perhaps be justified only if the condition is accompanied by an additional (if serendipitous) finding such as the cardiac murmur in the 7-year-old girl noted earlier. Physicians sometimes perform unnecessary investigations, being reluctant to base their diagnoses solely on their clinical expertise.9 A patient may interpret this testing as uncertainty or begin to doubt the diagnosis, thus augmenting—rather than reducing—any anxiety.10 The additional burden of the costs and possible side effects compound the futility of testing indiscriminately.11
Identifying these symptoms with the name “sigh syndrome,” and basing this diagnosis on the history and physical examination, stresses certainty and familiarity with the diagnosis.9 Not only does this reassure the patient, but it eases communication between professionals and forms a basis for research.
Management: Reassure your patient
Management of sigh syndrome consists largely of providing reassurances to your patient. You should emphasize that the condition is real, albeit benign, and that you understand the concern it causes.
Further treatment is unnecessary, aside perhaps from addressing any associated anxiety. A self-limiting (if sometimes recurrent) course can be confidently predicted, and follow-up visits can safely be left to the patient’s own discretion. Since the major correlation with sigh syndrome seems to be stress and the experience of a recent traumatic event, you should always investigate these 2 possibilities when taking the history of a patient with suspected sigh syndrome.
Acknowledgments
This work was inspired and developed by arthur Furst, MD, who died following the submission of this manuscript. Dr Furst was a distinguished and dedicated family physician, a thorough researcher, and a renowned tutor. We dedicate this article to the fond memory of a true leader in the field of rural medicine, and an exceptionally funny and amicable colleague.
Correspondence
Abby Naimer Sody, MD, Gush Katif Health Center, Neve Dekalim, Goosh Katif, Israel 79779; [email protected]
1. Rakel RE. Textbook of Family Practice. 6th ed. St louis, Mo: WB Saunders; 2002.
2. Perin PV, Perin RJ, Rooklin AR. When a sigh is just a sigh…and not asthma. Ann Allergy 1993;71:478-480.
3. Wilhelm FH, Gevirtz R, Roth WT. Respiratory dys-regulation in anxiety, functional cardiac, and pain disorders. Assessment, phenomenology, and treatment. Behav Modif 2001;25:513-45.
4. Malcomson KG. Globus hystericus vel pharyngis (a reconnaissance of proximal vagal modalities). J Laryngol Otol 1968;82:219-230.
5. Ravich WJ, Wilson RS, Jones B, Donner MW. Psychogenic dysphagia and globus: reevaluation of 23 patients. Dysphagia 1989;4:35-38.
6. Eifert GHB. Cardiophobia: a paradigmatic behavioural model of heart-focused anxiety and non-anginal chest pain. Behav Res Ther 1992;30:329-345.
7. Miller AJ, Texidor TA. “Precordial catch,” a syndrome of anterior chest pain. Ann Intern Med 1959;51:461-467.
8. Sparrow MJ, Bird EL. “Precordial catch”: a benign syndrome of chest pain in young persons. NZ Med J 1978;88:325-326.
9. Balint M. The Doctor, his Patient and the Illness. 2nd ed. London: Sir Isaac Pitman & Sons, 1964.
10. Salmon P. The potentially somatizing effect of clinical consultation. CNS Spectr 2006;11:190-200.
11. Hajioff D, Lowe D. The diagnostic value of barium swallow in globus syndrome. Int J Clin Pract 2004;58:86-89.
- Sigh syndrome is a genuine medical diagnosis with distinct criteria, conferring significant stress for those affected. Despite outward signs of an abnormal breathing pattern, this symptomatology is unrelated to any respiratory or organic pathology.
- Ancillary testing and medication seem unnecessary; supporting reassurance appears sufficient, since the syndrome has a favorable outcome.
Objective The goal of this study was to identify the characteristics and clinical course of patients presenting with considerable stress regarding irrepressible persistent sighing, and to determine whether any association exists between this syndrome and respiratory or other organic disease during the acute or follow-up period.
Study design We conducted a case series review of patients diagnosed with a defined symptom complex and gathered relevant data.
Population Forty patients who presented to 3 clinics in Israel met our 10 criteria for sigh syndrome: recurrent sighing (at least once a minute, for varying lengths of time throughout the day); otherwise shallow respiration; patient conviction that deep breaths are obstructed; intensity of episodes provokes stress leading to consultation; no obvious trigger; episodes last a few days to several weeks; no interference with speech; sighing is absent during sleep; no correlation with physical activity or rest; and self-limited.
Outcomes measured We assessed demographic and health status information, as well as recent circumstances that could have served as triggers for the symptoms. We also performed systematic diagnoses of acute and chronic organic disease.
Results Physicians diagnosed “sigh syndrome” in 40 subjects (19 men [47.5%]), mean age 31.8 years, during the 3-year study period. All patients conformed to 10 sigh syndrome criteria. In 13 patients (32.5%), a significant traumatic event preceded onset of symptoms. Ten (25%) had previous anxiety or somatoform-related disorders. For 23 patients (57.5%), the sigh syndrome episode repeated itself after an initial episode. We found no association in any of the cases with any form of organic disease. Likewise, during the follow-up period (on average, 18 months), we did not observe the development of a specific organic disorder in any case.
Conclusions The “sigh syndrome” runs a benign course; it mainly demands the support and understanding of the treating physician to allay any patient concerns.
In our clinical practices, we have repeatedly cared for patients who came into our clinics because of a worrisome irregular breathing pattern characterized by a deep inspiration, and followed by a noisy expiration. We have referred to the set of clinical signs that these patients present with as “sigh syndrome.”
We have long suspected that sigh syndrome is an underdiagnosed and self-limited condition that is often mistaken for a serious respiratory disorder. In our experience, this syndrome runs a benign course. However, we believed that this syndrome had characteristic and consistent features, and should not be considered a diagnosis of exclusion.
Thus, we undertook a study to observe a group of subjects with these features to judge whether this subjectively alarming symptom complex is in fact harmless, and whether it is appropriate to respond to it as we had, by taking a stress-alleviating approach alone.
What is sigh syndrome?
Patients with sigh syndrome exhibit a compulsion to perform single but repeated deep inspirations, accompanied by a sensation of difficulty in inhaling a sufficient quantity of air. Each inspiration is followed by a prolonged, sometimes noisy expiration—namely, a sigh. Observing such abnormal breaths and confirming that the patient feels a concomitant inability to fill his lungs to capacity is sufficient to make the diagnosis.
This breathing compulsion is irregular in nature: It may occur once a minute or several times a minute, and this breathing pattern may continue—on and off throughout the day—for a few days to several weeks. In our experience, it provokes significant anxiety in patients, prompting them to seek medical advice. It does not occur when the patient is asleep, and it is not triggered by physical activity.
Both patient and doctor may, at first, be convinced that the problem reflects a serious illness. The 10 features of sigh syndrome (TABLE 1) constitute a proposed definition. All of our study subjects exhibited these 10 features.
TABLE 1
10 features of sigh syndrome
|
Sighing as an illness marker
Sighing has been described as one member of a group of signs exhibited by depressed or anxiety-ridden patients.1 While Perin et al2 were the first to point out the importance of distinguishing between sighing and respiratory disease, sighing per se has never been identified as a discrete illness marker.
A number of psychiatric disorders are already well known to incorporate breathing and chest symptoms along with widespread somatization. These include globus hystericus, neurocirculatory asthenia, and Tietze syndrome.3-6 As such, the acute pain of precordial catch syndrome stands out as an example of a distinguishable, clear-cut clinical state devoid of any apparent organic basis.7,8
Methods
How we recruited the patients
Data was collected from 3 family practice clinics in Israel from February 2002 to February 2005. We requested that these practices contribute data of consecutive clinical cases presenting with the 10 set symptoms of sigh syndrome (TABLE 1).
Data collected included basic demographics, the circumstances of the onset of symptoms, concurrent medical conditions, and any associated symptoms. We assessed the patients’ education level by asking questions pertaining to their years of schooling and college degrees. Patients rated their own economic status as being below, average, or above-average income.
The main outcome we examined was the clinical course of the sighing episodes during the ensuing months after their visit, in order to determine whether any patients developed a form of significant organic disease or a disorder that led to hospitalization.
Results
40 cases that cut across the socioeconomic spectrum
Forty patients were recruited for this study. Nineteen (47.5%) were male; their ages ranged from 7 to 53 (mean, 31.8; standard deviation, 13.7). Two patients (5%) were Ashkenazi Jews; 34 (85%) were of North African ethnicity (Sephardic Jews); the other 4 were of varied Asian and European ethnicity. The number of patients with North African ethnicity overrepresents that of the population in their communities. Additionally, 3 members of this group were from the same family.
There was no predilection toward any specific education level or socioeconomic status. The occupations of the subjects were diverse.
Their clinical characteristics
The clinical characteristics of the 40 patients are presented in TABLE 2. The subjects’ sighing began at various times of the day, without relationship to eating or any other activity, and disappeared during sleep. All patients reported the same feeling: that of an extra effort demanded to perform full inspiration. In many cases, adult patients were certain their complaints were a sign of cardiac or respiratory disease, and they were very concerned that there was some grave, underlying disorder.
History and examination failed to reveal evidence of any somatic findings related to breathing difficulty. Breathing rate was within normal limits in all cases.
The physicians’ initial encounters with these patients led to further examination in many cases: electrocardiography, blood oxygen saturation, and complete blood counts. However, no abnormalities were found on any of these tests. Medications, if prescribed at all during these consultations, were usually given to alleviate insomnia or anxiety. Further ancillary investigations or referrals were not ordered.
The sole notable finding on physical examination was a typical murmur (which had already been diagnosed) in a young girl with a congenital atrial septal defect. This 7-year-old developed repeated episodes of sigh syndrome just before her annual visit to the pediatric cardiologist; her mother believed that the child was frightened by the thought of possible future surgery.
TABLE 2
Clinical characteristics of the 40 patients studied—One third experienced a traumatic event
| CHARACTERISTIC | YES | NO |
|---|---|---|
| Smoker | 2 (5%) | 38 (95%) |
| History of anxiety or somatoform disorder | 10 (25%) | 30 (75%) |
| Taking prescription medication at time of diagnosis | 4 (10%) | 36 (90%) |
| Recurrence of sighing episodes during follow-up period | 24 (60%) | 16 (40%) |
| Trigger event (eg, exposure to traumatic event 1 month before presentation with syndrome) | 13 (32.5%) | 27 (67.5%) |
Traumatic events, anxiety disorders suggest stress as a cause
Thirteen patient histories disclosed a definite, recent, significant traumatic event that may have triggered the onset of sigh syndrome. Examples of 2 triggering events are the terrorist murder of several members of a neighbor’s family, and a near-miss with a mortar shell. One subject—a teenager—had recently been left alone in the dark with 2 younger siblings during a power blackout; another young woman said that the sighing episodes began when she decided to get married.
Ten patients had previously diagnosed neurotic disorders, mainly generalized anxiety; these included 2 cases of somatization disorder and 1 case of posttraumatic stress disorder. This information from the patients’ histories was documented in their medical files.
Episodes appear to be self-limited
In all patients, the episodes were self-limited. During the follow-up period, lasting an average of 18 months, none of the patients showed additional medical conditions—respiratory or otherwise—that could be linked to episodes of sigh syndrome. Recurrences of sighing episodes were reported by 24 subjects (60%) after the marker episode. One patient was diagnosed with carcinoma of the pancreas 2 years into follow-up, and later died.
Discussion
A benign, transient disorder
Aside from the solitary and unrelated death noted above, examination and follow-up in all 40 cases did not lead to an alternative diagnosis. Sigh syndrome thus seems to be an entirely benign and transient condition with no sequelae aside from possible recurrences.
Although the pathophysiology is unclear, our finding that 32.5% of patients had a recent traumatic incident strongly suggests a stress-related condition. Furthermore, 25% of the patients were already known to suffer from intermittent anxiety or somatoform disorders, although none were taking medications for these conditions. This adds support to the assumption that a mind-body interaction is underpinning the disorder. Large-scale migration, recent war or terrorist acts, or natural disaster are likely to increase the chances that the average physician will see a patient with sigh syndrome.
A tendency towards North African/Sephardic ethnicity, rather than European ethnicity—in addition to the cluster of 3 cases belonging to the same family—suggests the presentation may be a subconscious cultural, learned, or adopted expression of uneasiness.
Making your evaluation: History and physical are enough
The diagnostic evaluation of sigh syndrome—consisting of careful history-taking and a thorough physical examination—should be sufficient to differentiate it from an array of organic diseases. A physical examination is imperative to exclude other causes for this breathing abnormality.
Ancillary testing is rarely, if ever, indicated. It can perhaps be justified only if the condition is accompanied by an additional (if serendipitous) finding such as the cardiac murmur in the 7-year-old girl noted earlier. Physicians sometimes perform unnecessary investigations, being reluctant to base their diagnoses solely on their clinical expertise.9 A patient may interpret this testing as uncertainty or begin to doubt the diagnosis, thus augmenting—rather than reducing—any anxiety.10 The additional burden of the costs and possible side effects compound the futility of testing indiscriminately.11
Identifying these symptoms with the name “sigh syndrome,” and basing this diagnosis on the history and physical examination, stresses certainty and familiarity with the diagnosis.9 Not only does this reassure the patient, but it eases communication between professionals and forms a basis for research.
Management: Reassure your patient
Management of sigh syndrome consists largely of providing reassurances to your patient. You should emphasize that the condition is real, albeit benign, and that you understand the concern it causes.
Further treatment is unnecessary, aside perhaps from addressing any associated anxiety. A self-limiting (if sometimes recurrent) course can be confidently predicted, and follow-up visits can safely be left to the patient’s own discretion. Since the major correlation with sigh syndrome seems to be stress and the experience of a recent traumatic event, you should always investigate these 2 possibilities when taking the history of a patient with suspected sigh syndrome.
Acknowledgments
This work was inspired and developed by arthur Furst, MD, who died following the submission of this manuscript. Dr Furst was a distinguished and dedicated family physician, a thorough researcher, and a renowned tutor. We dedicate this article to the fond memory of a true leader in the field of rural medicine, and an exceptionally funny and amicable colleague.
Correspondence
Abby Naimer Sody, MD, Gush Katif Health Center, Neve Dekalim, Goosh Katif, Israel 79779; [email protected]
- Sigh syndrome is a genuine medical diagnosis with distinct criteria, conferring significant stress for those affected. Despite outward signs of an abnormal breathing pattern, this symptomatology is unrelated to any respiratory or organic pathology.
- Ancillary testing and medication seem unnecessary; supporting reassurance appears sufficient, since the syndrome has a favorable outcome.
Objective The goal of this study was to identify the characteristics and clinical course of patients presenting with considerable stress regarding irrepressible persistent sighing, and to determine whether any association exists between this syndrome and respiratory or other organic disease during the acute or follow-up period.
Study design We conducted a case series review of patients diagnosed with a defined symptom complex and gathered relevant data.
Population Forty patients who presented to 3 clinics in Israel met our 10 criteria for sigh syndrome: recurrent sighing (at least once a minute, for varying lengths of time throughout the day); otherwise shallow respiration; patient conviction that deep breaths are obstructed; intensity of episodes provokes stress leading to consultation; no obvious trigger; episodes last a few days to several weeks; no interference with speech; sighing is absent during sleep; no correlation with physical activity or rest; and self-limited.
Outcomes measured We assessed demographic and health status information, as well as recent circumstances that could have served as triggers for the symptoms. We also performed systematic diagnoses of acute and chronic organic disease.
Results Physicians diagnosed “sigh syndrome” in 40 subjects (19 men [47.5%]), mean age 31.8 years, during the 3-year study period. All patients conformed to 10 sigh syndrome criteria. In 13 patients (32.5%), a significant traumatic event preceded onset of symptoms. Ten (25%) had previous anxiety or somatoform-related disorders. For 23 patients (57.5%), the sigh syndrome episode repeated itself after an initial episode. We found no association in any of the cases with any form of organic disease. Likewise, during the follow-up period (on average, 18 months), we did not observe the development of a specific organic disorder in any case.
Conclusions The “sigh syndrome” runs a benign course; it mainly demands the support and understanding of the treating physician to allay any patient concerns.
In our clinical practices, we have repeatedly cared for patients who came into our clinics because of a worrisome irregular breathing pattern characterized by a deep inspiration, and followed by a noisy expiration. We have referred to the set of clinical signs that these patients present with as “sigh syndrome.”
We have long suspected that sigh syndrome is an underdiagnosed and self-limited condition that is often mistaken for a serious respiratory disorder. In our experience, this syndrome runs a benign course. However, we believed that this syndrome had characteristic and consistent features, and should not be considered a diagnosis of exclusion.
Thus, we undertook a study to observe a group of subjects with these features to judge whether this subjectively alarming symptom complex is in fact harmless, and whether it is appropriate to respond to it as we had, by taking a stress-alleviating approach alone.
What is sigh syndrome?
Patients with sigh syndrome exhibit a compulsion to perform single but repeated deep inspirations, accompanied by a sensation of difficulty in inhaling a sufficient quantity of air. Each inspiration is followed by a prolonged, sometimes noisy expiration—namely, a sigh. Observing such abnormal breaths and confirming that the patient feels a concomitant inability to fill his lungs to capacity is sufficient to make the diagnosis.
This breathing compulsion is irregular in nature: It may occur once a minute or several times a minute, and this breathing pattern may continue—on and off throughout the day—for a few days to several weeks. In our experience, it provokes significant anxiety in patients, prompting them to seek medical advice. It does not occur when the patient is asleep, and it is not triggered by physical activity.
Both patient and doctor may, at first, be convinced that the problem reflects a serious illness. The 10 features of sigh syndrome (TABLE 1) constitute a proposed definition. All of our study subjects exhibited these 10 features.
TABLE 1
10 features of sigh syndrome
|
Sighing as an illness marker
Sighing has been described as one member of a group of signs exhibited by depressed or anxiety-ridden patients.1 While Perin et al2 were the first to point out the importance of distinguishing between sighing and respiratory disease, sighing per se has never been identified as a discrete illness marker.
A number of psychiatric disorders are already well known to incorporate breathing and chest symptoms along with widespread somatization. These include globus hystericus, neurocirculatory asthenia, and Tietze syndrome.3-6 As such, the acute pain of precordial catch syndrome stands out as an example of a distinguishable, clear-cut clinical state devoid of any apparent organic basis.7,8
Methods
How we recruited the patients
Data was collected from 3 family practice clinics in Israel from February 2002 to February 2005. We requested that these practices contribute data of consecutive clinical cases presenting with the 10 set symptoms of sigh syndrome (TABLE 1).
Data collected included basic demographics, the circumstances of the onset of symptoms, concurrent medical conditions, and any associated symptoms. We assessed the patients’ education level by asking questions pertaining to their years of schooling and college degrees. Patients rated their own economic status as being below, average, or above-average income.
The main outcome we examined was the clinical course of the sighing episodes during the ensuing months after their visit, in order to determine whether any patients developed a form of significant organic disease or a disorder that led to hospitalization.
Results
40 cases that cut across the socioeconomic spectrum
Forty patients were recruited for this study. Nineteen (47.5%) were male; their ages ranged from 7 to 53 (mean, 31.8; standard deviation, 13.7). Two patients (5%) were Ashkenazi Jews; 34 (85%) were of North African ethnicity (Sephardic Jews); the other 4 were of varied Asian and European ethnicity. The number of patients with North African ethnicity overrepresents that of the population in their communities. Additionally, 3 members of this group were from the same family.
There was no predilection toward any specific education level or socioeconomic status. The occupations of the subjects were diverse.
Their clinical characteristics
The clinical characteristics of the 40 patients are presented in TABLE 2. The subjects’ sighing began at various times of the day, without relationship to eating or any other activity, and disappeared during sleep. All patients reported the same feeling: that of an extra effort demanded to perform full inspiration. In many cases, adult patients were certain their complaints were a sign of cardiac or respiratory disease, and they were very concerned that there was some grave, underlying disorder.
History and examination failed to reveal evidence of any somatic findings related to breathing difficulty. Breathing rate was within normal limits in all cases.
The physicians’ initial encounters with these patients led to further examination in many cases: electrocardiography, blood oxygen saturation, and complete blood counts. However, no abnormalities were found on any of these tests. Medications, if prescribed at all during these consultations, were usually given to alleviate insomnia or anxiety. Further ancillary investigations or referrals were not ordered.
The sole notable finding on physical examination was a typical murmur (which had already been diagnosed) in a young girl with a congenital atrial septal defect. This 7-year-old developed repeated episodes of sigh syndrome just before her annual visit to the pediatric cardiologist; her mother believed that the child was frightened by the thought of possible future surgery.
TABLE 2
Clinical characteristics of the 40 patients studied—One third experienced a traumatic event
| CHARACTERISTIC | YES | NO |
|---|---|---|
| Smoker | 2 (5%) | 38 (95%) |
| History of anxiety or somatoform disorder | 10 (25%) | 30 (75%) |
| Taking prescription medication at time of diagnosis | 4 (10%) | 36 (90%) |
| Recurrence of sighing episodes during follow-up period | 24 (60%) | 16 (40%) |
| Trigger event (eg, exposure to traumatic event 1 month before presentation with syndrome) | 13 (32.5%) | 27 (67.5%) |
Traumatic events, anxiety disorders suggest stress as a cause
Thirteen patient histories disclosed a definite, recent, significant traumatic event that may have triggered the onset of sigh syndrome. Examples of 2 triggering events are the terrorist murder of several members of a neighbor’s family, and a near-miss with a mortar shell. One subject—a teenager—had recently been left alone in the dark with 2 younger siblings during a power blackout; another young woman said that the sighing episodes began when she decided to get married.
Ten patients had previously diagnosed neurotic disorders, mainly generalized anxiety; these included 2 cases of somatization disorder and 1 case of posttraumatic stress disorder. This information from the patients’ histories was documented in their medical files.
Episodes appear to be self-limited
In all patients, the episodes were self-limited. During the follow-up period, lasting an average of 18 months, none of the patients showed additional medical conditions—respiratory or otherwise—that could be linked to episodes of sigh syndrome. Recurrences of sighing episodes were reported by 24 subjects (60%) after the marker episode. One patient was diagnosed with carcinoma of the pancreas 2 years into follow-up, and later died.
Discussion
A benign, transient disorder
Aside from the solitary and unrelated death noted above, examination and follow-up in all 40 cases did not lead to an alternative diagnosis. Sigh syndrome thus seems to be an entirely benign and transient condition with no sequelae aside from possible recurrences.
Although the pathophysiology is unclear, our finding that 32.5% of patients had a recent traumatic incident strongly suggests a stress-related condition. Furthermore, 25% of the patients were already known to suffer from intermittent anxiety or somatoform disorders, although none were taking medications for these conditions. This adds support to the assumption that a mind-body interaction is underpinning the disorder. Large-scale migration, recent war or terrorist acts, or natural disaster are likely to increase the chances that the average physician will see a patient with sigh syndrome.
A tendency towards North African/Sephardic ethnicity, rather than European ethnicity—in addition to the cluster of 3 cases belonging to the same family—suggests the presentation may be a subconscious cultural, learned, or adopted expression of uneasiness.
Making your evaluation: History and physical are enough
The diagnostic evaluation of sigh syndrome—consisting of careful history-taking and a thorough physical examination—should be sufficient to differentiate it from an array of organic diseases. A physical examination is imperative to exclude other causes for this breathing abnormality.
Ancillary testing is rarely, if ever, indicated. It can perhaps be justified only if the condition is accompanied by an additional (if serendipitous) finding such as the cardiac murmur in the 7-year-old girl noted earlier. Physicians sometimes perform unnecessary investigations, being reluctant to base their diagnoses solely on their clinical expertise.9 A patient may interpret this testing as uncertainty or begin to doubt the diagnosis, thus augmenting—rather than reducing—any anxiety.10 The additional burden of the costs and possible side effects compound the futility of testing indiscriminately.11
Identifying these symptoms with the name “sigh syndrome,” and basing this diagnosis on the history and physical examination, stresses certainty and familiarity with the diagnosis.9 Not only does this reassure the patient, but it eases communication between professionals and forms a basis for research.
Management: Reassure your patient
Management of sigh syndrome consists largely of providing reassurances to your patient. You should emphasize that the condition is real, albeit benign, and that you understand the concern it causes.
Further treatment is unnecessary, aside perhaps from addressing any associated anxiety. A self-limiting (if sometimes recurrent) course can be confidently predicted, and follow-up visits can safely be left to the patient’s own discretion. Since the major correlation with sigh syndrome seems to be stress and the experience of a recent traumatic event, you should always investigate these 2 possibilities when taking the history of a patient with suspected sigh syndrome.
Acknowledgments
This work was inspired and developed by arthur Furst, MD, who died following the submission of this manuscript. Dr Furst was a distinguished and dedicated family physician, a thorough researcher, and a renowned tutor. We dedicate this article to the fond memory of a true leader in the field of rural medicine, and an exceptionally funny and amicable colleague.
Correspondence
Abby Naimer Sody, MD, Gush Katif Health Center, Neve Dekalim, Goosh Katif, Israel 79779; [email protected]
1. Rakel RE. Textbook of Family Practice. 6th ed. St louis, Mo: WB Saunders; 2002.
2. Perin PV, Perin RJ, Rooklin AR. When a sigh is just a sigh…and not asthma. Ann Allergy 1993;71:478-480.
3. Wilhelm FH, Gevirtz R, Roth WT. Respiratory dys-regulation in anxiety, functional cardiac, and pain disorders. Assessment, phenomenology, and treatment. Behav Modif 2001;25:513-45.
4. Malcomson KG. Globus hystericus vel pharyngis (a reconnaissance of proximal vagal modalities). J Laryngol Otol 1968;82:219-230.
5. Ravich WJ, Wilson RS, Jones B, Donner MW. Psychogenic dysphagia and globus: reevaluation of 23 patients. Dysphagia 1989;4:35-38.
6. Eifert GHB. Cardiophobia: a paradigmatic behavioural model of heart-focused anxiety and non-anginal chest pain. Behav Res Ther 1992;30:329-345.
7. Miller AJ, Texidor TA. “Precordial catch,” a syndrome of anterior chest pain. Ann Intern Med 1959;51:461-467.
8. Sparrow MJ, Bird EL. “Precordial catch”: a benign syndrome of chest pain in young persons. NZ Med J 1978;88:325-326.
9. Balint M. The Doctor, his Patient and the Illness. 2nd ed. London: Sir Isaac Pitman & Sons, 1964.
10. Salmon P. The potentially somatizing effect of clinical consultation. CNS Spectr 2006;11:190-200.
11. Hajioff D, Lowe D. The diagnostic value of barium swallow in globus syndrome. Int J Clin Pract 2004;58:86-89.
1. Rakel RE. Textbook of Family Practice. 6th ed. St louis, Mo: WB Saunders; 2002.
2. Perin PV, Perin RJ, Rooklin AR. When a sigh is just a sigh…and not asthma. Ann Allergy 1993;71:478-480.
3. Wilhelm FH, Gevirtz R, Roth WT. Respiratory dys-regulation in anxiety, functional cardiac, and pain disorders. Assessment, phenomenology, and treatment. Behav Modif 2001;25:513-45.
4. Malcomson KG. Globus hystericus vel pharyngis (a reconnaissance of proximal vagal modalities). J Laryngol Otol 1968;82:219-230.
5. Ravich WJ, Wilson RS, Jones B, Donner MW. Psychogenic dysphagia and globus: reevaluation of 23 patients. Dysphagia 1989;4:35-38.
6. Eifert GHB. Cardiophobia: a paradigmatic behavioural model of heart-focused anxiety and non-anginal chest pain. Behav Res Ther 1992;30:329-345.
7. Miller AJ, Texidor TA. “Precordial catch,” a syndrome of anterior chest pain. Ann Intern Med 1959;51:461-467.
8. Sparrow MJ, Bird EL. “Precordial catch”: a benign syndrome of chest pain in young persons. NZ Med J 1978;88:325-326.
9. Balint M. The Doctor, his Patient and the Illness. 2nd ed. London: Sir Isaac Pitman & Sons, 1964.
10. Salmon P. The potentially somatizing effect of clinical consultation. CNS Spectr 2006;11:190-200.
11. Hajioff D, Lowe D. The diagnostic value of barium swallow in globus syndrome. Int J Clin Pract 2004;58:86-89.
Codes for phone and online counseling, team meetings
Old codes 99371–99373 that were used to report a call you made to a patient, or to consult or coordinate medical management with other health-care professionals, are deleted in 2008. In their place? A series of new codes that cover not only physician–patient contact but nonphysician–patient contact on the telephone.
Additional codes have also been added for non–face-to-face physician– provider contact regarding the care of a patient. Although these new codes may not be reimbursed by many payers, they do allow you to bill the patient for such services in many instances. They’ll also help the practice better track the care given by its providers.
Patient-initiated telephone contact
99441 Telephone evaluation and management service provided by a physician to an established patient, parent, or guardian not originating from a related E/M service provided within the previous 7 days nor leading to an E/M service or procedure within the next 24 hours or soonest available appointment; 5–10 minutes of medical discussion
99442 …11–20 minutes of medical discussion
99443 …21–30 minutes of medical discussion
98966 Telephone assessment and management service provided by a qualified nonphysician health care professional to an established patient, parent, or guardian not originating from a related assessment and management service provided within the previous seven days nor leading to an assessment and management service or procedure within the next 24 hours or soonest available appointment; 5–10 minutes of medical discussion
98967 …11–20 minutes of medical discussion
98968 …21–30 minutes of medical discussion
To use these codes, keep in mind a few rules:
- Contact must be initiated by the patient or the established patient’s guardian
- Don’t report the new codes if the patient is then seen for the problem within 24 hours after the call or at the next available urgent appointment. When that happens, the call is considered part of the pre-service work and may be counted as part of the billable E/M service
- Don’t report the new codes if the call relates to an E/M service that was reported by the provider within the prior 7 days—whether the provider did or did not request that the call be made
- Don’t report the new codes for any follow-up regarding a procedure that was performed while the patient is still in the postop period.
Conferring with the medical team
99367 Medical team conference with interdisciplinary team of health care professionals, patient and/or family not present, 30 minutes or more; participation by physician
99368 …participation by nonphysician qualified health care professional
The interactions of an interdisciplinary team are more comprehensive and complex than the conversations that might take place during a regular E/M service. So, the rules for these codes are somewhat different:
- The patient must be an established patient who has a chronic health condition or multiple health conditions that require a team approach to manage
- The participants in the conference are familiar with the patient and have seen the patient within 60 days prior to the conference call
- Only one provider from the same specialty may report these codes for each conference
- The conference must be at least 30 minutes long; the clock starts at the beginning of the review of the patient’s case and ends at the conclusion of that review. Time spent writing reports on the conference can’t be counted.
Providing your services online
99444 Online evaluation and management service provided by a physician to an established patient, guardian, or health care provider not originating from a related E/M service provided within the previous 7 days, using the Internet or similar electronic communications network
98969 Online assessment and management service provided by a qualified nonphysician health care professional to an established patient, guardian, or health care provider not originating from a related assessment and management service provided within the previous 7 days, using the Internet or similar electronic communications network
Just as telephone calls are becoming a more common method of communicating with providers, online medical services are tracing a similar pattern of use. The Internet has allowed many patients to contact their physician (or nonphysician provider) directly; with assurances of privacy offered by current Internet communications systems, information can be readily shared between patient and physician.
Criteria for using these new codes are:
- The established patient or her guardian must have initiated the online evaluation request
- The provider’s response must be timely and must include permanent electronic or hard-copy documentation of the encounter
- The online service can only be reported once during a 7-day period for the same problem, but more than one provider can report his (her) separate online communication with the patient
- As with the rules for telephone contact with a patient, do not report the new codes if the provider has billed an E/M service related to the online query within the prior 7 days or within the postop period of a procedure.
Old codes 99371–99373 that were used to report a call you made to a patient, or to consult or coordinate medical management with other health-care professionals, are deleted in 2008. In their place? A series of new codes that cover not only physician–patient contact but nonphysician–patient contact on the telephone.
Additional codes have also been added for non–face-to-face physician– provider contact regarding the care of a patient. Although these new codes may not be reimbursed by many payers, they do allow you to bill the patient for such services in many instances. They’ll also help the practice better track the care given by its providers.
Patient-initiated telephone contact
99441 Telephone evaluation and management service provided by a physician to an established patient, parent, or guardian not originating from a related E/M service provided within the previous 7 days nor leading to an E/M service or procedure within the next 24 hours or soonest available appointment; 5–10 minutes of medical discussion
99442 …11–20 minutes of medical discussion
99443 …21–30 minutes of medical discussion
98966 Telephone assessment and management service provided by a qualified nonphysician health care professional to an established patient, parent, or guardian not originating from a related assessment and management service provided within the previous seven days nor leading to an assessment and management service or procedure within the next 24 hours or soonest available appointment; 5–10 minutes of medical discussion
98967 …11–20 minutes of medical discussion
98968 …21–30 minutes of medical discussion
To use these codes, keep in mind a few rules:
- Contact must be initiated by the patient or the established patient’s guardian
- Don’t report the new codes if the patient is then seen for the problem within 24 hours after the call or at the next available urgent appointment. When that happens, the call is considered part of the pre-service work and may be counted as part of the billable E/M service
- Don’t report the new codes if the call relates to an E/M service that was reported by the provider within the prior 7 days—whether the provider did or did not request that the call be made
- Don’t report the new codes for any follow-up regarding a procedure that was performed while the patient is still in the postop period.
Conferring with the medical team
99367 Medical team conference with interdisciplinary team of health care professionals, patient and/or family not present, 30 minutes or more; participation by physician
99368 …participation by nonphysician qualified health care professional
The interactions of an interdisciplinary team are more comprehensive and complex than the conversations that might take place during a regular E/M service. So, the rules for these codes are somewhat different:
- The patient must be an established patient who has a chronic health condition or multiple health conditions that require a team approach to manage
- The participants in the conference are familiar with the patient and have seen the patient within 60 days prior to the conference call
- Only one provider from the same specialty may report these codes for each conference
- The conference must be at least 30 minutes long; the clock starts at the beginning of the review of the patient’s case and ends at the conclusion of that review. Time spent writing reports on the conference can’t be counted.
Providing your services online
99444 Online evaluation and management service provided by a physician to an established patient, guardian, or health care provider not originating from a related E/M service provided within the previous 7 days, using the Internet or similar electronic communications network
98969 Online assessment and management service provided by a qualified nonphysician health care professional to an established patient, guardian, or health care provider not originating from a related assessment and management service provided within the previous 7 days, using the Internet or similar electronic communications network
Just as telephone calls are becoming a more common method of communicating with providers, online medical services are tracing a similar pattern of use. The Internet has allowed many patients to contact their physician (or nonphysician provider) directly; with assurances of privacy offered by current Internet communications systems, information can be readily shared between patient and physician.
Criteria for using these new codes are:
- The established patient or her guardian must have initiated the online evaluation request
- The provider’s response must be timely and must include permanent electronic or hard-copy documentation of the encounter
- The online service can only be reported once during a 7-day period for the same problem, but more than one provider can report his (her) separate online communication with the patient
- As with the rules for telephone contact with a patient, do not report the new codes if the provider has billed an E/M service related to the online query within the prior 7 days or within the postop period of a procedure.
Old codes 99371–99373 that were used to report a call you made to a patient, or to consult or coordinate medical management with other health-care professionals, are deleted in 2008. In their place? A series of new codes that cover not only physician–patient contact but nonphysician–patient contact on the telephone.
Additional codes have also been added for non–face-to-face physician– provider contact regarding the care of a patient. Although these new codes may not be reimbursed by many payers, they do allow you to bill the patient for such services in many instances. They’ll also help the practice better track the care given by its providers.
Patient-initiated telephone contact
99441 Telephone evaluation and management service provided by a physician to an established patient, parent, or guardian not originating from a related E/M service provided within the previous 7 days nor leading to an E/M service or procedure within the next 24 hours or soonest available appointment; 5–10 minutes of medical discussion
99442 …11–20 minutes of medical discussion
99443 …21–30 minutes of medical discussion
98966 Telephone assessment and management service provided by a qualified nonphysician health care professional to an established patient, parent, or guardian not originating from a related assessment and management service provided within the previous seven days nor leading to an assessment and management service or procedure within the next 24 hours or soonest available appointment; 5–10 minutes of medical discussion
98967 …11–20 minutes of medical discussion
98968 …21–30 minutes of medical discussion
To use these codes, keep in mind a few rules:
- Contact must be initiated by the patient or the established patient’s guardian
- Don’t report the new codes if the patient is then seen for the problem within 24 hours after the call or at the next available urgent appointment. When that happens, the call is considered part of the pre-service work and may be counted as part of the billable E/M service
- Don’t report the new codes if the call relates to an E/M service that was reported by the provider within the prior 7 days—whether the provider did or did not request that the call be made
- Don’t report the new codes for any follow-up regarding a procedure that was performed while the patient is still in the postop period.
Conferring with the medical team
99367 Medical team conference with interdisciplinary team of health care professionals, patient and/or family not present, 30 minutes or more; participation by physician
99368 …participation by nonphysician qualified health care professional
The interactions of an interdisciplinary team are more comprehensive and complex than the conversations that might take place during a regular E/M service. So, the rules for these codes are somewhat different:
- The patient must be an established patient who has a chronic health condition or multiple health conditions that require a team approach to manage
- The participants in the conference are familiar with the patient and have seen the patient within 60 days prior to the conference call
- Only one provider from the same specialty may report these codes for each conference
- The conference must be at least 30 minutes long; the clock starts at the beginning of the review of the patient’s case and ends at the conclusion of that review. Time spent writing reports on the conference can’t be counted.
Providing your services online
99444 Online evaluation and management service provided by a physician to an established patient, guardian, or health care provider not originating from a related E/M service provided within the previous 7 days, using the Internet or similar electronic communications network
98969 Online assessment and management service provided by a qualified nonphysician health care professional to an established patient, guardian, or health care provider not originating from a related assessment and management service provided within the previous 7 days, using the Internet or similar electronic communications network
Just as telephone calls are becoming a more common method of communicating with providers, online medical services are tracing a similar pattern of use. The Internet has allowed many patients to contact their physician (or nonphysician provider) directly; with assurances of privacy offered by current Internet communications systems, information can be readily shared between patient and physician.
Criteria for using these new codes are:
- The established patient or her guardian must have initiated the online evaluation request
- The provider’s response must be timely and must include permanent electronic or hard-copy documentation of the encounter
- The online service can only be reported once during a 7-day period for the same problem, but more than one provider can report his (her) separate online communication with the patient
- As with the rules for telephone contact with a patient, do not report the new codes if the provider has billed an E/M service related to the online query within the prior 7 days or within the postop period of a procedure.
When not to use beta-blockers in seniors with hypertension
Beta-blockers should not be used to treat hypertension in patients older than age 60 unless they have another compelling indication to use these agents, such as heart failure or ischemic heart disease.1,2
Strength of recommendation
A: Based on a well-done meta-analyses
Khan N, Mcalister FA. Re-examining the efficacy of beta-blockers for the treatment of hypertension: a meta-analysis. CMAJ 2006; 174:1737– 1742.1
Wiysonge CS, Bradley H, Mayosi BM, et al. Beta-blockers for hypertension. Cochrane Database Syst Rev 2007; (1):CD002003.2
Illustrative case
A 70-year-old man with newly diagnosed hypertension comes to your office. You don’t want to prescribe a diuretic due to his history of gout. He has no history of coronary artery disease or heart failure.
What is the best antihypertensive agent for him?
Background: Guidelines do not reflect new evidence
Guidelines for the use of beta-blockers in the elderly do not reflect current evidence.
JNC recommendations
The 2003 JNC 7 Report recommended the same antihypertensive medications for adults of all ages.3 (JNC 7 is the most recent report from the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure.)
JNC 7 recommends thiazide diuretics for first-line treatment of hypertension, and recommends other drugs—including beta-blockers, calcium-channel blockers, angiotensin-converting enzyme (ACE) inhibitors, and angiotensin receptor blockers (ARBs)—for first-line therapy if a thiazide is contraindicated, or in combination with thiazides for higher initial blood pressure.
Compelling indications. Beta-blockers are recommended in the JNC 7 Report as first-line therapy in patients with “compelling indications” such as ischemic heart disease and heart failure.
Clinical context: Seniors taking beta-blockers to their detriment?
Many elderly patients are on beta-blockers, perhaps to their detriment. Treatment choices for hypertension can have an enormous impact on outcomes among older patients:
Two thirds of US adults 60 years of age and older have hypertension, mostly isolated systolic hypertension.4,5
Multiple studies, including the Systolic Hypertension in the Elderly Program and the Systolic Hypertension in Europe, have shown that lowering blood pressure with pharmacologic interventions in older patients can reduce the risk of cardiovascular events and possibly dementia.6
Beta-blockers have been a mainstay of hypertension treatment for many decades and we suspect continue to be widely used as first-line therapy in patients for whom the evidence now indicates they are inferior.
Heart failure and angina are indications for beta-blockers
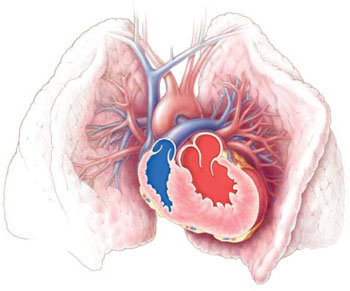
New evidence does not alter the 2003 JNC 7 recommendations to use beta-blockers as first-line therapy in patients with “compelling indications” such as ischemic heart disease and heart failure.
Study summaries
Two well-done reviews of beta-blocker trials show that they are inferior for first-line hypertension treatment in the elderly who do not have heart failure or angina.
2007 Cochrane review
The 2007 Cochrane review2 analyzed randomized trials that compared beta-blockers for hypertension in adults 18 years of age and older to each of the other major classes of antihypertensives.
Conclusion. This meta-analysis showed a “relatively weak effect of beta-blockers to reduce stroke, and the absence of effect on coronary heart disease when compared with placebo or no treatment” and a “trend toward worse outcomes in comparison with calcium channel blockers, renin-angiotensin system inhibitors, and thiazide diuretics.”
This meta-analysis included all adults and did not make any conclusions based on age.
2006 CMAJ meta-analysis
The Kahn and McAlister meta-analysis1 pooled data from 21 randomized hyper-tension trials (including 6 placebo-controlled trials) that evaluated the efficacy of beta-blockers as first-line therapy for hypertension in preventing major cardiovascular outcomes (death, nonfatal MI, or nonfatal stroke).
The results were analyzed by age group: trials enrolling patients with a mean age of 60 years or older at baseline vs trials enrolling patients with a mean age of under 60 years.
Conclusion. They concluded that in trials comparing other antihypertensive medications with beta-blockers, all agents showed similar efficacy in younger patients, while in older patients, beta-blockers were associated with a higher risk of both composite events and strokes ( TABLE ).
TABLE
Adverse outcomes more likely in seniors taking a beta-blocker vs other antihypertensives1
| ADVERSE OUTCOME | PATIENTS UNDER AGE 60 | PATIENTS AGE 60 AND OVER |
|---|---|---|
| ADVERSE OUTCOMES LESS LIKELY WITH A BETA-BLOCKER | ADVERSE OUTCOMES MORE LIKELY WITH A BETA-BLOCKER | |
| Composite outcomes (death, stroke, or MI) | RR=0.97 (95% CI, 0.88–1.07) | RR=1.06 (95% CI, 1.01–1.1) |
| Stroke | RR=0.99 (95% CI, 0.67–1.44) | RR=1.18 (95% CI, 1.07–1.3) |
| RR, relative risk of adverse outcomes, in randomized clinical trials of hypertensive patients treated with beta-blockers, compared with other antihypertensive drugs. | ||
What’s new?: The age distinction
These 2 meta-analyses1,2 help overturn a long-held belief about the value of beta-blockers for the treatment of hypertension. Beta-blockers may not be a good first-line choice for any hypertensive patient—and the evidence clearly shows they are not a good first-line choice for patients over 60 years old.
Two earlier systematic reviews did raise the concern about using beta-blockers as first-line treatment for hypertension (even when thiazides are not contraindicated).
The first systematic review to raise this concern was a 1998 study of 10 hypertension trials in more than 16,000 patients, ages 60 and older. This review showed that diuretics were superior to beta-blockers in reducing cardiovascular and all-cause mortality—which supports the JNC 7 recommendation to choose a thiazide diuretic as the first-line drug of choice.7
The second study, a meta-analysis published in 2005, also concluded that beta-blockers should no longer be considered first-line therapy for hypertension, due to a 16% increase in the relative risk of stroke compared with other agents. This meta-analysis, however, did not report outcomes by patient age.8
Beta-blockers are not 1st-line, even if thiazides are contraindicated
What is new about the Kahn and McAlister evidence is that beta-blockers should not be the first-line drug of choice even when thiazide diuretics are contraindicated. Their study included a larger number of trials (21 trials vs 13 in the 2005 meta-analysis), which allowed the investigators to examine outcomes in patients younger than 60 and in those 60 years and older.
Caveats: Continue beta-blockers for the right reasons
Patients over 60 with ischemic heart disease or heart failure should still be prescribed beta-blockers for heart failure and angina. Also, in older patients with hypertension who need multiple agents to control their blood pressure, a beta-blocker could be added as a third or fourth agent in addition to a diuretic, ACE inhibitor, ARB, or calcium-channel blocker. Metoprolol is a good choice, as it is inexpensive and proven to reduce mortality in patients with a history of MI or heart failure.
Atenolol may underperform
In a meta-analysis of 31 trials, Freemantle9 found that after MI, acebutolol, metoprolol, propranolol, and timolol significantly reduced mortality, while there was no mortality reduction with atenolol. Similarly, in heart failure, only bisoprolol, metoprolol, and carvedilol have evidence to support a reduction in mortality.10
Although atenolol is one of the most commonly prescribed beta-blockers due to its low cost and once-daily dosing, it may be the least effective. In a systematic review of 9 hypertension studies, Carlberg11 showed that atenolol was no more effective than placebo at reducing MI, cardiovascular mortality, or all-cause mortality, and that patients on atenolol had significantly higher mortality than those taking other antihypertensives. Khan and McAlister do not differentiate between atenolol and other beta-blockers in their meta-analysis.1
Challenges to implementation: Letting go
The evidence supporting this change in practice has been accumulating over time. The change itself represents a significant reversal of long-standing belief in the value of beta-blockers as an antihypertensive agent. For each individual patient, the risk is not dramatic even though the cumulative “harm” from using a beta-blocker compared to other options is potentially staggering because so many people over 60 have hypertension.
We suspect that the main challenge will be changing the beliefs of both physicians and patients. Once doctors are convinced that beta-blockers are not indicated for uncomplicated hypertension in patients over 60, changing medications in the millions of older patients who have been taking a beta-blocker for some time and have become comfortable with it will take tact and excellent communication skills.
Providing patient information may help. Sources for patients are available free or at low cost at www.nhlbi.nih.gov/health/public/heart/index.htm#hbp. These materials explain that diuretics are inexpensive and are the preferred drugs for initial treatment of hypertension.
In patients over 60 who can’t tolerate a thiazide, the least expensive option is an ACE inhibitor. For example, in the Target and Walmart discount generic programs, benazepril, captopril, enalapril, and lisinopril are all available for $4 per month.
PURLs methodology
This study was selected and evaluated using FPIN’s Priority Updates from the Research Literature (PURL) Surveillance System methodology. The criteria and findings leading to the selection of this study as a PURL can be accessed at www.jfponline.com/purls.
1. Khan N, McAlister FA. Re-examining the efficacy of beta-blockers for the treatment of hypertension: a meta-analysis. CMAJ 2006;174:1737-1742.
2. Wiysonge CS, Bradley H, Mayosi BM, et al. Beta-blockers for hypertension. Cochrane Database Syst Rev 2007;(1):CD002003.-
3. The Seventh report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. US Department of Health and Human Services/National Heart, Lung and Blood Institute; 2003. Available at: www.nhlbi.nih.gov/guidelines/hypertension. Accessed on Dec 11, 2007.
4. Ostchega Y, Dillon CF, Hughes JP, Carroll M, Yoon S. Trends in hypertension prevalence, awareness, treatment, and control in older US adults: data from the National Health and Nutrition Examination Survey 1988 to 2004. J Am Geriatr Soc 2007;55:1056-1065.
5. Chobanian A. Isolated systolic hypertension in the elderly. N Engl J Med 2007;357:789-796.
6. Waeber B. Trials in isolated systolic hypertension: an update. Curr Hypertens Rep 2003;5:329-336.
7. Messerli FH, Grossman E, Goldbourt U. Are beta-blockers efficacious as first-line therapy for hypertension in the elderly? a systematic review. JAMA 1998;279:1903-1907.
8. Lindholm LH, Carlberg B, Samuelsson O. Should beta blockers remain first choice in the treatment of primary hypertension? A meta-analysis. Lancet 2005;366:1545-1553.
9. Freemantle N, Cleland J, Young P, Mason J, Harrison J. Beta blockade after myocardial infarction: systematic review and meta regression analysis. BMJ 1999;318:1730-1737.
10. Ong HT. Beta blockers in hypertension and cardiovascular disease. BMJ 2007;334:946-949.
11. Carlberg B, Samuelsson O, Lindholm LH. Atenolol in hypertension: is it a wise choice? Lancet 2004;364:1684-1689.
Beta-blockers should not be used to treat hypertension in patients older than age 60 unless they have another compelling indication to use these agents, such as heart failure or ischemic heart disease.1,2
Strength of recommendation
A: Based on a well-done meta-analyses
Khan N, Mcalister FA. Re-examining the efficacy of beta-blockers for the treatment of hypertension: a meta-analysis. CMAJ 2006; 174:1737– 1742.1
Wiysonge CS, Bradley H, Mayosi BM, et al. Beta-blockers for hypertension. Cochrane Database Syst Rev 2007; (1):CD002003.2
Illustrative case
A 70-year-old man with newly diagnosed hypertension comes to your office. You don’t want to prescribe a diuretic due to his history of gout. He has no history of coronary artery disease or heart failure.
What is the best antihypertensive agent for him?
Background: Guidelines do not reflect new evidence
Guidelines for the use of beta-blockers in the elderly do not reflect current evidence.
JNC recommendations
The 2003 JNC 7 Report recommended the same antihypertensive medications for adults of all ages.3 (JNC 7 is the most recent report from the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure.)
JNC 7 recommends thiazide diuretics for first-line treatment of hypertension, and recommends other drugs—including beta-blockers, calcium-channel blockers, angiotensin-converting enzyme (ACE) inhibitors, and angiotensin receptor blockers (ARBs)—for first-line therapy if a thiazide is contraindicated, or in combination with thiazides for higher initial blood pressure.
Compelling indications. Beta-blockers are recommended in the JNC 7 Report as first-line therapy in patients with “compelling indications” such as ischemic heart disease and heart failure.
Clinical context: Seniors taking beta-blockers to their detriment?
Many elderly patients are on beta-blockers, perhaps to their detriment. Treatment choices for hypertension can have an enormous impact on outcomes among older patients:
Two thirds of US adults 60 years of age and older have hypertension, mostly isolated systolic hypertension.4,5
Multiple studies, including the Systolic Hypertension in the Elderly Program and the Systolic Hypertension in Europe, have shown that lowering blood pressure with pharmacologic interventions in older patients can reduce the risk of cardiovascular events and possibly dementia.6
Beta-blockers have been a mainstay of hypertension treatment for many decades and we suspect continue to be widely used as first-line therapy in patients for whom the evidence now indicates they are inferior.
Heart failure and angina are indications for beta-blockers
New evidence does not alter the 2003 JNC 7 recommendations to use beta-blockers as first-line therapy in patients with “compelling indications” such as ischemic heart disease and heart failure.
Study summaries
Two well-done reviews of beta-blocker trials show that they are inferior for first-line hypertension treatment in the elderly who do not have heart failure or angina.
2007 Cochrane review
The 2007 Cochrane review2 analyzed randomized trials that compared beta-blockers for hypertension in adults 18 years of age and older to each of the other major classes of antihypertensives.
Conclusion. This meta-analysis showed a “relatively weak effect of beta-blockers to reduce stroke, and the absence of effect on coronary heart disease when compared with placebo or no treatment” and a “trend toward worse outcomes in comparison with calcium channel blockers, renin-angiotensin system inhibitors, and thiazide diuretics.”
This meta-analysis included all adults and did not make any conclusions based on age.
2006 CMAJ meta-analysis
The Kahn and McAlister meta-analysis1 pooled data from 21 randomized hyper-tension trials (including 6 placebo-controlled trials) that evaluated the efficacy of beta-blockers as first-line therapy for hypertension in preventing major cardiovascular outcomes (death, nonfatal MI, or nonfatal stroke).
The results were analyzed by age group: trials enrolling patients with a mean age of 60 years or older at baseline vs trials enrolling patients with a mean age of under 60 years.
Conclusion. They concluded that in trials comparing other antihypertensive medications with beta-blockers, all agents showed similar efficacy in younger patients, while in older patients, beta-blockers were associated with a higher risk of both composite events and strokes ( TABLE ).
TABLE
Adverse outcomes more likely in seniors taking a beta-blocker vs other antihypertensives1
| ADVERSE OUTCOME | PATIENTS UNDER AGE 60 | PATIENTS AGE 60 AND OVER |
|---|---|---|
| ADVERSE OUTCOMES LESS LIKELY WITH A BETA-BLOCKER | ADVERSE OUTCOMES MORE LIKELY WITH A BETA-BLOCKER | |
| Composite outcomes (death, stroke, or MI) | RR=0.97 (95% CI, 0.88–1.07) | RR=1.06 (95% CI, 1.01–1.1) |
| Stroke | RR=0.99 (95% CI, 0.67–1.44) | RR=1.18 (95% CI, 1.07–1.3) |
| RR, relative risk of adverse outcomes, in randomized clinical trials of hypertensive patients treated with beta-blockers, compared with other antihypertensive drugs. | ||
What’s new?: The age distinction
These 2 meta-analyses1,2 help overturn a long-held belief about the value of beta-blockers for the treatment of hypertension. Beta-blockers may not be a good first-line choice for any hypertensive patient—and the evidence clearly shows they are not a good first-line choice for patients over 60 years old.
Two earlier systematic reviews did raise the concern about using beta-blockers as first-line treatment for hypertension (even when thiazides are not contraindicated).
The first systematic review to raise this concern was a 1998 study of 10 hypertension trials in more than 16,000 patients, ages 60 and older. This review showed that diuretics were superior to beta-blockers in reducing cardiovascular and all-cause mortality—which supports the JNC 7 recommendation to choose a thiazide diuretic as the first-line drug of choice.7
The second study, a meta-analysis published in 2005, also concluded that beta-blockers should no longer be considered first-line therapy for hypertension, due to a 16% increase in the relative risk of stroke compared with other agents. This meta-analysis, however, did not report outcomes by patient age.8
Beta-blockers are not 1st-line, even if thiazides are contraindicated
What is new about the Kahn and McAlister evidence is that beta-blockers should not be the first-line drug of choice even when thiazide diuretics are contraindicated. Their study included a larger number of trials (21 trials vs 13 in the 2005 meta-analysis), which allowed the investigators to examine outcomes in patients younger than 60 and in those 60 years and older.
Caveats: Continue beta-blockers for the right reasons
Patients over 60 with ischemic heart disease or heart failure should still be prescribed beta-blockers for heart failure and angina. Also, in older patients with hypertension who need multiple agents to control their blood pressure, a beta-blocker could be added as a third or fourth agent in addition to a diuretic, ACE inhibitor, ARB, or calcium-channel blocker. Metoprolol is a good choice, as it is inexpensive and proven to reduce mortality in patients with a history of MI or heart failure.
Atenolol may underperform
In a meta-analysis of 31 trials, Freemantle9 found that after MI, acebutolol, metoprolol, propranolol, and timolol significantly reduced mortality, while there was no mortality reduction with atenolol. Similarly, in heart failure, only bisoprolol, metoprolol, and carvedilol have evidence to support a reduction in mortality.10
Although atenolol is one of the most commonly prescribed beta-blockers due to its low cost and once-daily dosing, it may be the least effective. In a systematic review of 9 hypertension studies, Carlberg11 showed that atenolol was no more effective than placebo at reducing MI, cardiovascular mortality, or all-cause mortality, and that patients on atenolol had significantly higher mortality than those taking other antihypertensives. Khan and McAlister do not differentiate between atenolol and other beta-blockers in their meta-analysis.1
Challenges to implementation: Letting go
The evidence supporting this change in practice has been accumulating over time. The change itself represents a significant reversal of long-standing belief in the value of beta-blockers as an antihypertensive agent. For each individual patient, the risk is not dramatic even though the cumulative “harm” from using a beta-blocker compared to other options is potentially staggering because so many people over 60 have hypertension.
We suspect that the main challenge will be changing the beliefs of both physicians and patients. Once doctors are convinced that beta-blockers are not indicated for uncomplicated hypertension in patients over 60, changing medications in the millions of older patients who have been taking a beta-blocker for some time and have become comfortable with it will take tact and excellent communication skills.
Providing patient information may help. Sources for patients are available free or at low cost at www.nhlbi.nih.gov/health/public/heart/index.htm#hbp. These materials explain that diuretics are inexpensive and are the preferred drugs for initial treatment of hypertension.
In patients over 60 who can’t tolerate a thiazide, the least expensive option is an ACE inhibitor. For example, in the Target and Walmart discount generic programs, benazepril, captopril, enalapril, and lisinopril are all available for $4 per month.
PURLs methodology
This study was selected and evaluated using FPIN’s Priority Updates from the Research Literature (PURL) Surveillance System methodology. The criteria and findings leading to the selection of this study as a PURL can be accessed at www.jfponline.com/purls.
Beta-blockers should not be used to treat hypertension in patients older than age 60 unless they have another compelling indication to use these agents, such as heart failure or ischemic heart disease.1,2
Strength of recommendation
A: Based on a well-done meta-analyses
Khan N, Mcalister FA. Re-examining the efficacy of beta-blockers for the treatment of hypertension: a meta-analysis. CMAJ 2006; 174:1737– 1742.1
Wiysonge CS, Bradley H, Mayosi BM, et al. Beta-blockers for hypertension. Cochrane Database Syst Rev 2007; (1):CD002003.2
Illustrative case
A 70-year-old man with newly diagnosed hypertension comes to your office. You don’t want to prescribe a diuretic due to his history of gout. He has no history of coronary artery disease or heart failure.
What is the best antihypertensive agent for him?
Background: Guidelines do not reflect new evidence
Guidelines for the use of beta-blockers in the elderly do not reflect current evidence.
JNC recommendations
The 2003 JNC 7 Report recommended the same antihypertensive medications for adults of all ages.3 (JNC 7 is the most recent report from the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure.)
JNC 7 recommends thiazide diuretics for first-line treatment of hypertension, and recommends other drugs—including beta-blockers, calcium-channel blockers, angiotensin-converting enzyme (ACE) inhibitors, and angiotensin receptor blockers (ARBs)—for first-line therapy if a thiazide is contraindicated, or in combination with thiazides for higher initial blood pressure.
Compelling indications. Beta-blockers are recommended in the JNC 7 Report as first-line therapy in patients with “compelling indications” such as ischemic heart disease and heart failure.
Clinical context: Seniors taking beta-blockers to their detriment?
Many elderly patients are on beta-blockers, perhaps to their detriment. Treatment choices for hypertension can have an enormous impact on outcomes among older patients:
Two thirds of US adults 60 years of age and older have hypertension, mostly isolated systolic hypertension.4,5
Multiple studies, including the Systolic Hypertension in the Elderly Program and the Systolic Hypertension in Europe, have shown that lowering blood pressure with pharmacologic interventions in older patients can reduce the risk of cardiovascular events and possibly dementia.6
Beta-blockers have been a mainstay of hypertension treatment for many decades and we suspect continue to be widely used as first-line therapy in patients for whom the evidence now indicates they are inferior.
Heart failure and angina are indications for beta-blockers
New evidence does not alter the 2003 JNC 7 recommendations to use beta-blockers as first-line therapy in patients with “compelling indications” such as ischemic heart disease and heart failure.
Study summaries
Two well-done reviews of beta-blocker trials show that they are inferior for first-line hypertension treatment in the elderly who do not have heart failure or angina.
2007 Cochrane review
The 2007 Cochrane review2 analyzed randomized trials that compared beta-blockers for hypertension in adults 18 years of age and older to each of the other major classes of antihypertensives.
Conclusion. This meta-analysis showed a “relatively weak effect of beta-blockers to reduce stroke, and the absence of effect on coronary heart disease when compared with placebo or no treatment” and a “trend toward worse outcomes in comparison with calcium channel blockers, renin-angiotensin system inhibitors, and thiazide diuretics.”
This meta-analysis included all adults and did not make any conclusions based on age.
2006 CMAJ meta-analysis
The Kahn and McAlister meta-analysis1 pooled data from 21 randomized hyper-tension trials (including 6 placebo-controlled trials) that evaluated the efficacy of beta-blockers as first-line therapy for hypertension in preventing major cardiovascular outcomes (death, nonfatal MI, or nonfatal stroke).
The results were analyzed by age group: trials enrolling patients with a mean age of 60 years or older at baseline vs trials enrolling patients with a mean age of under 60 years.
Conclusion. They concluded that in trials comparing other antihypertensive medications with beta-blockers, all agents showed similar efficacy in younger patients, while in older patients, beta-blockers were associated with a higher risk of both composite events and strokes ( TABLE ).
TABLE
Adverse outcomes more likely in seniors taking a beta-blocker vs other antihypertensives1
| ADVERSE OUTCOME | PATIENTS UNDER AGE 60 | PATIENTS AGE 60 AND OVER |
|---|---|---|
| ADVERSE OUTCOMES LESS LIKELY WITH A BETA-BLOCKER | ADVERSE OUTCOMES MORE LIKELY WITH A BETA-BLOCKER | |
| Composite outcomes (death, stroke, or MI) | RR=0.97 (95% CI, 0.88–1.07) | RR=1.06 (95% CI, 1.01–1.1) |
| Stroke | RR=0.99 (95% CI, 0.67–1.44) | RR=1.18 (95% CI, 1.07–1.3) |
| RR, relative risk of adverse outcomes, in randomized clinical trials of hypertensive patients treated with beta-blockers, compared with other antihypertensive drugs. | ||
What’s new?: The age distinction
These 2 meta-analyses1,2 help overturn a long-held belief about the value of beta-blockers for the treatment of hypertension. Beta-blockers may not be a good first-line choice for any hypertensive patient—and the evidence clearly shows they are not a good first-line choice for patients over 60 years old.
Two earlier systematic reviews did raise the concern about using beta-blockers as first-line treatment for hypertension (even when thiazides are not contraindicated).
The first systematic review to raise this concern was a 1998 study of 10 hypertension trials in more than 16,000 patients, ages 60 and older. This review showed that diuretics were superior to beta-blockers in reducing cardiovascular and all-cause mortality—which supports the JNC 7 recommendation to choose a thiazide diuretic as the first-line drug of choice.7
The second study, a meta-analysis published in 2005, also concluded that beta-blockers should no longer be considered first-line therapy for hypertension, due to a 16% increase in the relative risk of stroke compared with other agents. This meta-analysis, however, did not report outcomes by patient age.8
Beta-blockers are not 1st-line, even if thiazides are contraindicated
What is new about the Kahn and McAlister evidence is that beta-blockers should not be the first-line drug of choice even when thiazide diuretics are contraindicated. Their study included a larger number of trials (21 trials vs 13 in the 2005 meta-analysis), which allowed the investigators to examine outcomes in patients younger than 60 and in those 60 years and older.
Caveats: Continue beta-blockers for the right reasons
Patients over 60 with ischemic heart disease or heart failure should still be prescribed beta-blockers for heart failure and angina. Also, in older patients with hypertension who need multiple agents to control their blood pressure, a beta-blocker could be added as a third or fourth agent in addition to a diuretic, ACE inhibitor, ARB, or calcium-channel blocker. Metoprolol is a good choice, as it is inexpensive and proven to reduce mortality in patients with a history of MI or heart failure.
Atenolol may underperform
In a meta-analysis of 31 trials, Freemantle9 found that after MI, acebutolol, metoprolol, propranolol, and timolol significantly reduced mortality, while there was no mortality reduction with atenolol. Similarly, in heart failure, only bisoprolol, metoprolol, and carvedilol have evidence to support a reduction in mortality.10
Although atenolol is one of the most commonly prescribed beta-blockers due to its low cost and once-daily dosing, it may be the least effective. In a systematic review of 9 hypertension studies, Carlberg11 showed that atenolol was no more effective than placebo at reducing MI, cardiovascular mortality, or all-cause mortality, and that patients on atenolol had significantly higher mortality than those taking other antihypertensives. Khan and McAlister do not differentiate between atenolol and other beta-blockers in their meta-analysis.1
Challenges to implementation: Letting go
The evidence supporting this change in practice has been accumulating over time. The change itself represents a significant reversal of long-standing belief in the value of beta-blockers as an antihypertensive agent. For each individual patient, the risk is not dramatic even though the cumulative “harm” from using a beta-blocker compared to other options is potentially staggering because so many people over 60 have hypertension.
We suspect that the main challenge will be changing the beliefs of both physicians and patients. Once doctors are convinced that beta-blockers are not indicated for uncomplicated hypertension in patients over 60, changing medications in the millions of older patients who have been taking a beta-blocker for some time and have become comfortable with it will take tact and excellent communication skills.
Providing patient information may help. Sources for patients are available free or at low cost at www.nhlbi.nih.gov/health/public/heart/index.htm#hbp. These materials explain that diuretics are inexpensive and are the preferred drugs for initial treatment of hypertension.
In patients over 60 who can’t tolerate a thiazide, the least expensive option is an ACE inhibitor. For example, in the Target and Walmart discount generic programs, benazepril, captopril, enalapril, and lisinopril are all available for $4 per month.
PURLs methodology
This study was selected and evaluated using FPIN’s Priority Updates from the Research Literature (PURL) Surveillance System methodology. The criteria and findings leading to the selection of this study as a PURL can be accessed at www.jfponline.com/purls.
1. Khan N, McAlister FA. Re-examining the efficacy of beta-blockers for the treatment of hypertension: a meta-analysis. CMAJ 2006;174:1737-1742.
2. Wiysonge CS, Bradley H, Mayosi BM, et al. Beta-blockers for hypertension. Cochrane Database Syst Rev 2007;(1):CD002003.-
3. The Seventh report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. US Department of Health and Human Services/National Heart, Lung and Blood Institute; 2003. Available at: www.nhlbi.nih.gov/guidelines/hypertension. Accessed on Dec 11, 2007.
4. Ostchega Y, Dillon CF, Hughes JP, Carroll M, Yoon S. Trends in hypertension prevalence, awareness, treatment, and control in older US adults: data from the National Health and Nutrition Examination Survey 1988 to 2004. J Am Geriatr Soc 2007;55:1056-1065.
5. Chobanian A. Isolated systolic hypertension in the elderly. N Engl J Med 2007;357:789-796.
6. Waeber B. Trials in isolated systolic hypertension: an update. Curr Hypertens Rep 2003;5:329-336.
7. Messerli FH, Grossman E, Goldbourt U. Are beta-blockers efficacious as first-line therapy for hypertension in the elderly? a systematic review. JAMA 1998;279:1903-1907.
8. Lindholm LH, Carlberg B, Samuelsson O. Should beta blockers remain first choice in the treatment of primary hypertension? A meta-analysis. Lancet 2005;366:1545-1553.
9. Freemantle N, Cleland J, Young P, Mason J, Harrison J. Beta blockade after myocardial infarction: systematic review and meta regression analysis. BMJ 1999;318:1730-1737.
10. Ong HT. Beta blockers in hypertension and cardiovascular disease. BMJ 2007;334:946-949.
11. Carlberg B, Samuelsson O, Lindholm LH. Atenolol in hypertension: is it a wise choice? Lancet 2004;364:1684-1689.
1. Khan N, McAlister FA. Re-examining the efficacy of beta-blockers for the treatment of hypertension: a meta-analysis. CMAJ 2006;174:1737-1742.
2. Wiysonge CS, Bradley H, Mayosi BM, et al. Beta-blockers for hypertension. Cochrane Database Syst Rev 2007;(1):CD002003.-
3. The Seventh report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. US Department of Health and Human Services/National Heart, Lung and Blood Institute; 2003. Available at: www.nhlbi.nih.gov/guidelines/hypertension. Accessed on Dec 11, 2007.
4. Ostchega Y, Dillon CF, Hughes JP, Carroll M, Yoon S. Trends in hypertension prevalence, awareness, treatment, and control in older US adults: data from the National Health and Nutrition Examination Survey 1988 to 2004. J Am Geriatr Soc 2007;55:1056-1065.
5. Chobanian A. Isolated systolic hypertension in the elderly. N Engl J Med 2007;357:789-796.
6. Waeber B. Trials in isolated systolic hypertension: an update. Curr Hypertens Rep 2003;5:329-336.
7. Messerli FH, Grossman E, Goldbourt U. Are beta-blockers efficacious as first-line therapy for hypertension in the elderly? a systematic review. JAMA 1998;279:1903-1907.
8. Lindholm LH, Carlberg B, Samuelsson O. Should beta blockers remain first choice in the treatment of primary hypertension? A meta-analysis. Lancet 2005;366:1545-1553.
9. Freemantle N, Cleland J, Young P, Mason J, Harrison J. Beta blockade after myocardial infarction: systematic review and meta regression analysis. BMJ 1999;318:1730-1737.
10. Ong HT. Beta blockers in hypertension and cardiovascular disease. BMJ 2007;334:946-949.
11. Carlberg B, Samuelsson O, Lindholm LH. Atenolol in hypertension: is it a wise choice? Lancet 2004;364:1684-1689.
Copyright © 2008 The Family Physicians Inquiries Network.
All rights reserved.
If you don’t ask (about memory), they probably won’t tell
- Ask elderly patients whether they’re having any memory problems, since they are unlikely to volunteer this information on their own. Doing so may help to identify potentially frail patients (C).
Strength of recommendation (SOR)
- Good-quality patient-oriented evidence
- Inconsistent or limited-quality patient-oriented evidence
- Consensus, usual practice, opinion, disease-oriented evidence, case series
Objectives To investigate the prevalence and potential clinical implications of self-reported memory impairment among elderly patients in general practice.
Methods This was a cross-sectional study in 17 general practices serving 40,865 patients, of whom 2934 were 65 years of age or older. Outcome measures were self-reported memory impairment, health-related quality of life, and cognition.
Results In total, 177 (23.4%) out of 758 elderly patients consulting their physician reported impaired memory. Only 33 (18.6%) had consulted their physician for memory problems. The only independent predictor for impaired memory was a lower quality-of-life score: scores on the EuroQol-5D-VAS of 0 to 49 and 50–74 points both correlated with memory complaints (odds ratios=4.8 and 4.1, respectively).
Conclusions Memory impairment is a common complaint among elderly patients in general practice, but many patients will not present with these symptoms. It may be useful for general practitioners (GPs) to ask about memory problems in order to identify potentially frail patients. Prospective trials are warranted.
In studies of older patients, the prevalence of subjective memory complaints in community-based populations varies from 11% to 56%,1,2 depending on sample selection and on how the complaints are assessed.1 Subjective memory complaints may be associated with psychiatric symptoms—in particular, depression3,4 and anxiety—as well as older age, lower education, and female gender.1 In these studies, some association has been found between memory complaints and cognitive impairment on testing, even after adjustment for depressive symptoms.4,5
Researchers have suggested that subjective memory complaints may be an early indicator for dementia,1 and could therefore be considered as a marker for identification of dementia in general practice. However, these complaints may be the result of a wide range of conditions; longitudinal studies assessing the value of memory complaints in predicting dementia or cognitive decline have shown varying results.6-8
The prevalence of subjective memory complaints among elderly patients consulting their GP is not known, and the clinical implication of these complaints is not well established. We conducted this study in order to investigate the prevalence and potential clinical implications of subjective memory complaints among elderly patients in general practice.
Methods
Recruiting the subjects
Seventeen general medical practices with 24 GPs located in the central district of Copenhagen, Denmark, participated in this study. These practices served a total of 40,865 patients, 2934 of whom were 65 years of age or older.
We asked all patients 65 years of age or older who consulted their GP in October and November 2002 to participate in the study, regardless of the reason for the encounter. We excluded patients who were not able to read Danish or not able to sign an informed consent form. We also excluded those with severe acute or terminal illness or a diagnosis of dementia.
Assessment of the patients
Participant questionnaire. Before the visit with their GP, we asked all qualifying patients to complete a questionnaire with items about self-reported health and memory status, as well as demographic questions. The item regarding memory status was phrased: “How would you evaluate your memory?” The categories were “excellent,” “good,” “less good,” “poor,” and “miserable.” Patients rating their memory as “less good,” “poor,” or “miserable” were classified as patients with subjective memory complaints, whereas patients rating their memory as “excellent” or “good” were defined as patients without subjective memory complaints.
Quality-of-life assessment. During their visit, the patients also completed the Danish Validated Version of EuroQoL-5D, which includes a visual analogue scale (VAS). EuroQoL-5D is a standardized instrument for use as a measure of health outcomes.9 Patients are asked to assess their health—in regards to mobility, self-care, everyday activities, pain, and anxiety—by checking 1 of 3 boxes. They are then asked to assess their general state of health on a VAS ranging from 0 to 100.
GP questionnaire. A questionnaire dealing with the GP’s clinical impression of dementia was developed together with 2 of the GPs and tested in a pilot survey. This questionnaire was completed by the GP for each patient before they administered the Mini Mental State Examination (MMSE), with no information from the completed participant questionnaire. The GPs could complete the questionnaire before or during the office visit.
MMSE. The MMSE, recommended in GP guidelines as a cognitive screening test, was given to the patients after the GPs completed their own questionnaires.10 The test is a 30-point questionnaire that assesses cognition; it includes simple questions and problems in a number of areas: time and place of the test, repeating lists of words, math problems, language use and comprehension, and copying a drawing. An MMSE score <24 has been widely used as an indication of the presence of cognitive impairment in population-based studies.
Registry data and ethics
The Danish National Health Register provided the information regarding the physicians and their practices.11 The municipality of Copenhagen provided information regarding the nursing home status of patients.
The Scientific Ethical Committee for Copenhagen and Frederiksberg Municipalities evaluated the project. The Danish Data Protection Agency and the Danish College of General Practitioners Study Committee approved the project.
How we analyzed the data
All statistical analyses were performed using SAS, version 9.1 (SAS Institute Inc, Cary, NC). To avoid a possible cluster effect between the 17 practices, probabilities and corresponding 95% confidence intervals were estimated using a Generalized Estimating Equation (GEE) regression model. We used this method so that we could compare participants to nonparticipants, as well as to patients with subjective memory complaints and those without them. A backward elimination and a significance level of 5% to stay in model were used. Pearson’s chi-square was used to evaluate Goodness of Fit for the reduced model.
In the hypothesis-generating analysis, the following variables were included: age, gender, living with partner, receiving home care, school education, MMSE score, and EuroQoL-5D-VAS score. The EuroQoL-5D results were categorized into 3 groups: severe impairment (0 to 49 points), mild to moderate impairment (50 to 74), and normal (75 to 100). The MMSE was adjusted for age and education.
Results
Only quality-of-life scores predicted memory complaints
A total of 1180 patients 65 years of age and older consulted their GPs in the study period. From this group, we excluded 133 patients. Of the eligible 1047 patients, 775 (74.0%) patients agreed to participate in the study. These patents had a mean age of 74.8 years (standard deviation [SD], 7.1), and an average relationship with their GP of 11 years. Those who refused to participate in the study were more likely to be female and were less likely to complain about memory problems, according to the GP surveys.
The average MMSE score for these 775 patients was 28.2 (SD, 2.0), and the average EuroQoL-5D-VAS score was 70.9 (SD, 18.9). A total of 758 patients responded to the patient questionnaire regarding memory. Of these 758 patients, 177 (23.4%) reported memory complaints (that is, indicated their memory was “less good,” “poor,” or “miserable”). Only 33 (18.6%) of these 177 patients had previously consulted their GP regarding memory problems. The TABLE shows the characteristics of participants based on self-reported memory complaints.
In a hypothesis-generating analysis, we found that the only predictor for subjective memory complaints, as compared with those patients with good memory (stated as “excellent” or “good”), was an impairment of EuroQoL-5D-VAS: for a score of 0–49 points, the odds ratio (OR) for subjective memory complaints was 4.8; for a score of 50–74 points, the OR was 4.1. The patients’ gender, education, MMSE score, whether they lived alone or with a partner, and whether they were receiving home care did not seem to be independent predictors.
TABLE
Quality-of-life score was the only predictor of self-reported memory problems
| SELF-RATED MEMORY (n=758)* | ||
|---|---|---|
| EXCELLENT OR GOOD (N=581) | LESS GOOD, POOR, OR MISERABLE (N=177) | |
| Age, years (95% CI) | 74.5 (73.9–75.1) | 75.7 (74.6–76.8) |
| Female, n (%) | 348/581 (59.9%) | 116/177 (65.5%) |
| 8 years or less schooling, n (%) | 203/558 (36.4%) | 60/168 (35.7%) |
| Living without partner, n (%) | 340/580 (58.6%) | 115/175 (65.7%) |
| Receiving home care, n (%) | 106/579 (18.3%) | 49/175 (28.0%) |
| Cognition | ||
| Participant had previously complained about memory (per GP survey), n (%) | 16/567 (2.8%) | 33/175 (18.9%) |
| MMSE score (95% CI) | 28.3 (28.2–28.5) | 27.8 (27.3–28.0) |
| Quality of life: EuroQol-5D-VAS score (95% CI) | 73.8 (72.3–75.4) | 61.4 (58.5–64.2) |
| *We did not obtain self-rated memory status from 17 participants. Of the 758 subjects who took the survey, not everyone answered every question. | ||
Discussion
Other predictors of memory problems remain to be discovered
Depression,12 other psychiatric conditions,3,4 as well as certain medications may be associated with self-reported memory problems in elderly patients. These associations may explain why we found a correlation between reports of a lower quality of life and subjective memory complaints. Advanced age, female gender, and a low level of education have also been associated with a higher prevalence of memory complaints in other studies, but our study did not confirm any of these findings.
Limitations of this study
This study had several limitations. It had some selection bias, which may decrease its generalizability. In addition, this study was not designed to clarify whether memory complaints could be an early indicator for onset of dementia, or whether these complaints are associated with mild cognitive impairment or existing dementia.
The collection of data was monitored on a weekly basis by site visits from a study nurse. However, we did not monitor the actual exams.
An MMSE score of <24 has been widely used as an indication of the presence of cognitive impairment in population-based studies.12 However, research has shown that MMSE scores are affected by age, education, and cultural background; this may explain why the MMSE by itself is not sufficient to diagnose dementia.12
Future studies should focus on clinically relevant outcomes
Further prospective studies in GP settings are needed to examine the potential implications of subjective memory complaints. We suggest that in future studies, clinically relevant outcomes—such as death, nursing home placement, medication usage, or health care usage—be used as possible correlating factors.
Correspondence
Frans Boch Waldorff, MD, PhD, Research Unit of General Practice, Kommunehospitalet, Øster Farimagsgade 5, DK-1014 Copenhagen, Denmark; [email protected]
1. Jonker C, Geerlings MI, Schmand B. Are memory complaints predictive for dementia? A review of clinical and population-based studies. Int J Geriatr Psychiatry 2000;15:983-991.
2. Jungwirth S, Fischer P, Weissgram S, Kirchmeyr W, Bauer P, Tragl KH. Subjective memory complaints and objective memory impairment in the Vienna-Transdanube aging community. J Am Geriatr Soc 2004;52:263-268.
3. Zandi T. Relationship between subjective memory complaints, objective memory performance, and depression among older adults. Am J Alzheimers Dis Other Demen 2004;19:353-360.
4. Gagnon M, Dartigues JF, Mazaux JM, et al. Self-reported memory complaints and memory performance in elderly French community residents: results of the PAQUID Research Program. Neuroepidemiology 1994;13:145-154.
5. O’Connor DW, Pollitt PA, Roth M, Brook PB, Reiss BB. Memory complaints and impairment in normal, depressed, and demented elderly persons identified in a community survey. Arch Gen Psychiatry 1990;47:224-227.
6. Mol ME, van Boxtel MP, Willems D, Jolles J. Do subjective memory complaints predict cognitive dysfunction over time? A six-year follow-up of the Maastricht aging Study. Int J Geriatr Psychiatry 2006;21:432-441.
7. Geerlings MI, Jonker C, Bouter lM, Ader HJ, Schmand B. Association between memory complaints and incident alzheimer’s disease in elderly people with normal baseline cognition. Am J Psychiatry 1999;156:531-537.
8. Schmand B, Jonker C, Hooijer C, lindeboom J. Subjective memory complaints may announce dementia. Neurology 1996;46:121-125.
9. Rabin R, De Charro F. EQ-5D: a measure of health status from the EuroQol Group. Ann Med 2001;33:337-343.
10. Folstein MF, Folstein SE, McHugh PR. “Mini-mental state.” A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res 1975;12:189-198.
11. Olivarius NF, Hollnagel H, Krasnik A, Pedersen PA, Thorsen H. The Danish National Health Service Register. A tool for primary health care research. Dan Med Bull 1997;44:449-453.
12. Tombaugh TN, McIntyre NJ. The mini-mental state examination: a comprehensive review. J Am Geriatr Soc 1992;40:922-935.
- Ask elderly patients whether they’re having any memory problems, since they are unlikely to volunteer this information on their own. Doing so may help to identify potentially frail patients (C).
Strength of recommendation (SOR)
- Good-quality patient-oriented evidence
- Inconsistent or limited-quality patient-oriented evidence
- Consensus, usual practice, opinion, disease-oriented evidence, case series
Objectives To investigate the prevalence and potential clinical implications of self-reported memory impairment among elderly patients in general practice.
Methods This was a cross-sectional study in 17 general practices serving 40,865 patients, of whom 2934 were 65 years of age or older. Outcome measures were self-reported memory impairment, health-related quality of life, and cognition.
Results In total, 177 (23.4%) out of 758 elderly patients consulting their physician reported impaired memory. Only 33 (18.6%) had consulted their physician for memory problems. The only independent predictor for impaired memory was a lower quality-of-life score: scores on the EuroQol-5D-VAS of 0 to 49 and 50–74 points both correlated with memory complaints (odds ratios=4.8 and 4.1, respectively).
Conclusions Memory impairment is a common complaint among elderly patients in general practice, but many patients will not present with these symptoms. It may be useful for general practitioners (GPs) to ask about memory problems in order to identify potentially frail patients. Prospective trials are warranted.
In studies of older patients, the prevalence of subjective memory complaints in community-based populations varies from 11% to 56%,1,2 depending on sample selection and on how the complaints are assessed.1 Subjective memory complaints may be associated with psychiatric symptoms—in particular, depression3,4 and anxiety—as well as older age, lower education, and female gender.1 In these studies, some association has been found between memory complaints and cognitive impairment on testing, even after adjustment for depressive symptoms.4,5
Researchers have suggested that subjective memory complaints may be an early indicator for dementia,1 and could therefore be considered as a marker for identification of dementia in general practice. However, these complaints may be the result of a wide range of conditions; longitudinal studies assessing the value of memory complaints in predicting dementia or cognitive decline have shown varying results.6-8
The prevalence of subjective memory complaints among elderly patients consulting their GP is not known, and the clinical implication of these complaints is not well established. We conducted this study in order to investigate the prevalence and potential clinical implications of subjective memory complaints among elderly patients in general practice.
Methods
Recruiting the subjects
Seventeen general medical practices with 24 GPs located in the central district of Copenhagen, Denmark, participated in this study. These practices served a total of 40,865 patients, 2934 of whom were 65 years of age or older.
We asked all patients 65 years of age or older who consulted their GP in October and November 2002 to participate in the study, regardless of the reason for the encounter. We excluded patients who were not able to read Danish or not able to sign an informed consent form. We also excluded those with severe acute or terminal illness or a diagnosis of dementia.
Assessment of the patients
Participant questionnaire. Before the visit with their GP, we asked all qualifying patients to complete a questionnaire with items about self-reported health and memory status, as well as demographic questions. The item regarding memory status was phrased: “How would you evaluate your memory?” The categories were “excellent,” “good,” “less good,” “poor,” and “miserable.” Patients rating their memory as “less good,” “poor,” or “miserable” were classified as patients with subjective memory complaints, whereas patients rating their memory as “excellent” or “good” were defined as patients without subjective memory complaints.
Quality-of-life assessment. During their visit, the patients also completed the Danish Validated Version of EuroQoL-5D, which includes a visual analogue scale (VAS). EuroQoL-5D is a standardized instrument for use as a measure of health outcomes.9 Patients are asked to assess their health—in regards to mobility, self-care, everyday activities, pain, and anxiety—by checking 1 of 3 boxes. They are then asked to assess their general state of health on a VAS ranging from 0 to 100.
GP questionnaire. A questionnaire dealing with the GP’s clinical impression of dementia was developed together with 2 of the GPs and tested in a pilot survey. This questionnaire was completed by the GP for each patient before they administered the Mini Mental State Examination (MMSE), with no information from the completed participant questionnaire. The GPs could complete the questionnaire before or during the office visit.
MMSE. The MMSE, recommended in GP guidelines as a cognitive screening test, was given to the patients after the GPs completed their own questionnaires.10 The test is a 30-point questionnaire that assesses cognition; it includes simple questions and problems in a number of areas: time and place of the test, repeating lists of words, math problems, language use and comprehension, and copying a drawing. An MMSE score <24 has been widely used as an indication of the presence of cognitive impairment in population-based studies.
Registry data and ethics
The Danish National Health Register provided the information regarding the physicians and their practices.11 The municipality of Copenhagen provided information regarding the nursing home status of patients.
The Scientific Ethical Committee for Copenhagen and Frederiksberg Municipalities evaluated the project. The Danish Data Protection Agency and the Danish College of General Practitioners Study Committee approved the project.
How we analyzed the data
All statistical analyses were performed using SAS, version 9.1 (SAS Institute Inc, Cary, NC). To avoid a possible cluster effect between the 17 practices, probabilities and corresponding 95% confidence intervals were estimated using a Generalized Estimating Equation (GEE) regression model. We used this method so that we could compare participants to nonparticipants, as well as to patients with subjective memory complaints and those without them. A backward elimination and a significance level of 5% to stay in model were used. Pearson’s chi-square was used to evaluate Goodness of Fit for the reduced model.
In the hypothesis-generating analysis, the following variables were included: age, gender, living with partner, receiving home care, school education, MMSE score, and EuroQoL-5D-VAS score. The EuroQoL-5D results were categorized into 3 groups: severe impairment (0 to 49 points), mild to moderate impairment (50 to 74), and normal (75 to 100). The MMSE was adjusted for age and education.
Results
Only quality-of-life scores predicted memory complaints
A total of 1180 patients 65 years of age and older consulted their GPs in the study period. From this group, we excluded 133 patients. Of the eligible 1047 patients, 775 (74.0%) patients agreed to participate in the study. These patents had a mean age of 74.8 years (standard deviation [SD], 7.1), and an average relationship with their GP of 11 years. Those who refused to participate in the study were more likely to be female and were less likely to complain about memory problems, according to the GP surveys.
The average MMSE score for these 775 patients was 28.2 (SD, 2.0), and the average EuroQoL-5D-VAS score was 70.9 (SD, 18.9). A total of 758 patients responded to the patient questionnaire regarding memory. Of these 758 patients, 177 (23.4%) reported memory complaints (that is, indicated their memory was “less good,” “poor,” or “miserable”). Only 33 (18.6%) of these 177 patients had previously consulted their GP regarding memory problems. The TABLE shows the characteristics of participants based on self-reported memory complaints.
In a hypothesis-generating analysis, we found that the only predictor for subjective memory complaints, as compared with those patients with good memory (stated as “excellent” or “good”), was an impairment of EuroQoL-5D-VAS: for a score of 0–49 points, the odds ratio (OR) for subjective memory complaints was 4.8; for a score of 50–74 points, the OR was 4.1. The patients’ gender, education, MMSE score, whether they lived alone or with a partner, and whether they were receiving home care did not seem to be independent predictors.
TABLE
Quality-of-life score was the only predictor of self-reported memory problems
| SELF-RATED MEMORY (n=758)* | ||
|---|---|---|
| EXCELLENT OR GOOD (N=581) | LESS GOOD, POOR, OR MISERABLE (N=177) | |
| Age, years (95% CI) | 74.5 (73.9–75.1) | 75.7 (74.6–76.8) |
| Female, n (%) | 348/581 (59.9%) | 116/177 (65.5%) |
| 8 years or less schooling, n (%) | 203/558 (36.4%) | 60/168 (35.7%) |
| Living without partner, n (%) | 340/580 (58.6%) | 115/175 (65.7%) |
| Receiving home care, n (%) | 106/579 (18.3%) | 49/175 (28.0%) |
| Cognition | ||
| Participant had previously complained about memory (per GP survey), n (%) | 16/567 (2.8%) | 33/175 (18.9%) |
| MMSE score (95% CI) | 28.3 (28.2–28.5) | 27.8 (27.3–28.0) |
| Quality of life: EuroQol-5D-VAS score (95% CI) | 73.8 (72.3–75.4) | 61.4 (58.5–64.2) |
| *We did not obtain self-rated memory status from 17 participants. Of the 758 subjects who took the survey, not everyone answered every question. | ||
Discussion
Other predictors of memory problems remain to be discovered
Depression,12 other psychiatric conditions,3,4 as well as certain medications may be associated with self-reported memory problems in elderly patients. These associations may explain why we found a correlation between reports of a lower quality of life and subjective memory complaints. Advanced age, female gender, and a low level of education have also been associated with a higher prevalence of memory complaints in other studies, but our study did not confirm any of these findings.
Limitations of this study
This study had several limitations. It had some selection bias, which may decrease its generalizability. In addition, this study was not designed to clarify whether memory complaints could be an early indicator for onset of dementia, or whether these complaints are associated with mild cognitive impairment or existing dementia.
The collection of data was monitored on a weekly basis by site visits from a study nurse. However, we did not monitor the actual exams.
An MMSE score of <24 has been widely used as an indication of the presence of cognitive impairment in population-based studies.12 However, research has shown that MMSE scores are affected by age, education, and cultural background; this may explain why the MMSE by itself is not sufficient to diagnose dementia.12
Future studies should focus on clinically relevant outcomes
Further prospective studies in GP settings are needed to examine the potential implications of subjective memory complaints. We suggest that in future studies, clinically relevant outcomes—such as death, nursing home placement, medication usage, or health care usage—be used as possible correlating factors.
Correspondence
Frans Boch Waldorff, MD, PhD, Research Unit of General Practice, Kommunehospitalet, Øster Farimagsgade 5, DK-1014 Copenhagen, Denmark; [email protected]
- Ask elderly patients whether they’re having any memory problems, since they are unlikely to volunteer this information on their own. Doing so may help to identify potentially frail patients (C).
Strength of recommendation (SOR)
- Good-quality patient-oriented evidence
- Inconsistent or limited-quality patient-oriented evidence
- Consensus, usual practice, opinion, disease-oriented evidence, case series
Objectives To investigate the prevalence and potential clinical implications of self-reported memory impairment among elderly patients in general practice.
Methods This was a cross-sectional study in 17 general practices serving 40,865 patients, of whom 2934 were 65 years of age or older. Outcome measures were self-reported memory impairment, health-related quality of life, and cognition.
Results In total, 177 (23.4%) out of 758 elderly patients consulting their physician reported impaired memory. Only 33 (18.6%) had consulted their physician for memory problems. The only independent predictor for impaired memory was a lower quality-of-life score: scores on the EuroQol-5D-VAS of 0 to 49 and 50–74 points both correlated with memory complaints (odds ratios=4.8 and 4.1, respectively).
Conclusions Memory impairment is a common complaint among elderly patients in general practice, but many patients will not present with these symptoms. It may be useful for general practitioners (GPs) to ask about memory problems in order to identify potentially frail patients. Prospective trials are warranted.
In studies of older patients, the prevalence of subjective memory complaints in community-based populations varies from 11% to 56%,1,2 depending on sample selection and on how the complaints are assessed.1 Subjective memory complaints may be associated with psychiatric symptoms—in particular, depression3,4 and anxiety—as well as older age, lower education, and female gender.1 In these studies, some association has been found between memory complaints and cognitive impairment on testing, even after adjustment for depressive symptoms.4,5
Researchers have suggested that subjective memory complaints may be an early indicator for dementia,1 and could therefore be considered as a marker for identification of dementia in general practice. However, these complaints may be the result of a wide range of conditions; longitudinal studies assessing the value of memory complaints in predicting dementia or cognitive decline have shown varying results.6-8
The prevalence of subjective memory complaints among elderly patients consulting their GP is not known, and the clinical implication of these complaints is not well established. We conducted this study in order to investigate the prevalence and potential clinical implications of subjective memory complaints among elderly patients in general practice.
Methods
Recruiting the subjects
Seventeen general medical practices with 24 GPs located in the central district of Copenhagen, Denmark, participated in this study. These practices served a total of 40,865 patients, 2934 of whom were 65 years of age or older.
We asked all patients 65 years of age or older who consulted their GP in October and November 2002 to participate in the study, regardless of the reason for the encounter. We excluded patients who were not able to read Danish or not able to sign an informed consent form. We also excluded those with severe acute or terminal illness or a diagnosis of dementia.
Assessment of the patients
Participant questionnaire. Before the visit with their GP, we asked all qualifying patients to complete a questionnaire with items about self-reported health and memory status, as well as demographic questions. The item regarding memory status was phrased: “How would you evaluate your memory?” The categories were “excellent,” “good,” “less good,” “poor,” and “miserable.” Patients rating their memory as “less good,” “poor,” or “miserable” were classified as patients with subjective memory complaints, whereas patients rating their memory as “excellent” or “good” were defined as patients without subjective memory complaints.
Quality-of-life assessment. During their visit, the patients also completed the Danish Validated Version of EuroQoL-5D, which includes a visual analogue scale (VAS). EuroQoL-5D is a standardized instrument for use as a measure of health outcomes.9 Patients are asked to assess their health—in regards to mobility, self-care, everyday activities, pain, and anxiety—by checking 1 of 3 boxes. They are then asked to assess their general state of health on a VAS ranging from 0 to 100.
GP questionnaire. A questionnaire dealing with the GP’s clinical impression of dementia was developed together with 2 of the GPs and tested in a pilot survey. This questionnaire was completed by the GP for each patient before they administered the Mini Mental State Examination (MMSE), with no information from the completed participant questionnaire. The GPs could complete the questionnaire before or during the office visit.
MMSE. The MMSE, recommended in GP guidelines as a cognitive screening test, was given to the patients after the GPs completed their own questionnaires.10 The test is a 30-point questionnaire that assesses cognition; it includes simple questions and problems in a number of areas: time and place of the test, repeating lists of words, math problems, language use and comprehension, and copying a drawing. An MMSE score <24 has been widely used as an indication of the presence of cognitive impairment in population-based studies.
Registry data and ethics
The Danish National Health Register provided the information regarding the physicians and their practices.11 The municipality of Copenhagen provided information regarding the nursing home status of patients.
The Scientific Ethical Committee for Copenhagen and Frederiksberg Municipalities evaluated the project. The Danish Data Protection Agency and the Danish College of General Practitioners Study Committee approved the project.
How we analyzed the data
All statistical analyses were performed using SAS, version 9.1 (SAS Institute Inc, Cary, NC). To avoid a possible cluster effect between the 17 practices, probabilities and corresponding 95% confidence intervals were estimated using a Generalized Estimating Equation (GEE) regression model. We used this method so that we could compare participants to nonparticipants, as well as to patients with subjective memory complaints and those without them. A backward elimination and a significance level of 5% to stay in model were used. Pearson’s chi-square was used to evaluate Goodness of Fit for the reduced model.
In the hypothesis-generating analysis, the following variables were included: age, gender, living with partner, receiving home care, school education, MMSE score, and EuroQoL-5D-VAS score. The EuroQoL-5D results were categorized into 3 groups: severe impairment (0 to 49 points), mild to moderate impairment (50 to 74), and normal (75 to 100). The MMSE was adjusted for age and education.
Results
Only quality-of-life scores predicted memory complaints
A total of 1180 patients 65 years of age and older consulted their GPs in the study period. From this group, we excluded 133 patients. Of the eligible 1047 patients, 775 (74.0%) patients agreed to participate in the study. These patents had a mean age of 74.8 years (standard deviation [SD], 7.1), and an average relationship with their GP of 11 years. Those who refused to participate in the study were more likely to be female and were less likely to complain about memory problems, according to the GP surveys.
The average MMSE score for these 775 patients was 28.2 (SD, 2.0), and the average EuroQoL-5D-VAS score was 70.9 (SD, 18.9). A total of 758 patients responded to the patient questionnaire regarding memory. Of these 758 patients, 177 (23.4%) reported memory complaints (that is, indicated their memory was “less good,” “poor,” or “miserable”). Only 33 (18.6%) of these 177 patients had previously consulted their GP regarding memory problems. The TABLE shows the characteristics of participants based on self-reported memory complaints.
In a hypothesis-generating analysis, we found that the only predictor for subjective memory complaints, as compared with those patients with good memory (stated as “excellent” or “good”), was an impairment of EuroQoL-5D-VAS: for a score of 0–49 points, the odds ratio (OR) for subjective memory complaints was 4.8; for a score of 50–74 points, the OR was 4.1. The patients’ gender, education, MMSE score, whether they lived alone or with a partner, and whether they were receiving home care did not seem to be independent predictors.
TABLE
Quality-of-life score was the only predictor of self-reported memory problems
| SELF-RATED MEMORY (n=758)* | ||
|---|---|---|
| EXCELLENT OR GOOD (N=581) | LESS GOOD, POOR, OR MISERABLE (N=177) | |
| Age, years (95% CI) | 74.5 (73.9–75.1) | 75.7 (74.6–76.8) |
| Female, n (%) | 348/581 (59.9%) | 116/177 (65.5%) |
| 8 years or less schooling, n (%) | 203/558 (36.4%) | 60/168 (35.7%) |
| Living without partner, n (%) | 340/580 (58.6%) | 115/175 (65.7%) |
| Receiving home care, n (%) | 106/579 (18.3%) | 49/175 (28.0%) |
| Cognition | ||
| Participant had previously complained about memory (per GP survey), n (%) | 16/567 (2.8%) | 33/175 (18.9%) |
| MMSE score (95% CI) | 28.3 (28.2–28.5) | 27.8 (27.3–28.0) |
| Quality of life: EuroQol-5D-VAS score (95% CI) | 73.8 (72.3–75.4) | 61.4 (58.5–64.2) |
| *We did not obtain self-rated memory status from 17 participants. Of the 758 subjects who took the survey, not everyone answered every question. | ||
Discussion
Other predictors of memory problems remain to be discovered
Depression,12 other psychiatric conditions,3,4 as well as certain medications may be associated with self-reported memory problems in elderly patients. These associations may explain why we found a correlation between reports of a lower quality of life and subjective memory complaints. Advanced age, female gender, and a low level of education have also been associated with a higher prevalence of memory complaints in other studies, but our study did not confirm any of these findings.
Limitations of this study
This study had several limitations. It had some selection bias, which may decrease its generalizability. In addition, this study was not designed to clarify whether memory complaints could be an early indicator for onset of dementia, or whether these complaints are associated with mild cognitive impairment or existing dementia.
The collection of data was monitored on a weekly basis by site visits from a study nurse. However, we did not monitor the actual exams.
An MMSE score of <24 has been widely used as an indication of the presence of cognitive impairment in population-based studies.12 However, research has shown that MMSE scores are affected by age, education, and cultural background; this may explain why the MMSE by itself is not sufficient to diagnose dementia.12
Future studies should focus on clinically relevant outcomes
Further prospective studies in GP settings are needed to examine the potential implications of subjective memory complaints. We suggest that in future studies, clinically relevant outcomes—such as death, nursing home placement, medication usage, or health care usage—be used as possible correlating factors.
Correspondence
Frans Boch Waldorff, MD, PhD, Research Unit of General Practice, Kommunehospitalet, Øster Farimagsgade 5, DK-1014 Copenhagen, Denmark; [email protected]
1. Jonker C, Geerlings MI, Schmand B. Are memory complaints predictive for dementia? A review of clinical and population-based studies. Int J Geriatr Psychiatry 2000;15:983-991.
2. Jungwirth S, Fischer P, Weissgram S, Kirchmeyr W, Bauer P, Tragl KH. Subjective memory complaints and objective memory impairment in the Vienna-Transdanube aging community. J Am Geriatr Soc 2004;52:263-268.
3. Zandi T. Relationship between subjective memory complaints, objective memory performance, and depression among older adults. Am J Alzheimers Dis Other Demen 2004;19:353-360.
4. Gagnon M, Dartigues JF, Mazaux JM, et al. Self-reported memory complaints and memory performance in elderly French community residents: results of the PAQUID Research Program. Neuroepidemiology 1994;13:145-154.
5. O’Connor DW, Pollitt PA, Roth M, Brook PB, Reiss BB. Memory complaints and impairment in normal, depressed, and demented elderly persons identified in a community survey. Arch Gen Psychiatry 1990;47:224-227.
6. Mol ME, van Boxtel MP, Willems D, Jolles J. Do subjective memory complaints predict cognitive dysfunction over time? A six-year follow-up of the Maastricht aging Study. Int J Geriatr Psychiatry 2006;21:432-441.
7. Geerlings MI, Jonker C, Bouter lM, Ader HJ, Schmand B. Association between memory complaints and incident alzheimer’s disease in elderly people with normal baseline cognition. Am J Psychiatry 1999;156:531-537.
8. Schmand B, Jonker C, Hooijer C, lindeboom J. Subjective memory complaints may announce dementia. Neurology 1996;46:121-125.
9. Rabin R, De Charro F. EQ-5D: a measure of health status from the EuroQol Group. Ann Med 2001;33:337-343.
10. Folstein MF, Folstein SE, McHugh PR. “Mini-mental state.” A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res 1975;12:189-198.
11. Olivarius NF, Hollnagel H, Krasnik A, Pedersen PA, Thorsen H. The Danish National Health Service Register. A tool for primary health care research. Dan Med Bull 1997;44:449-453.
12. Tombaugh TN, McIntyre NJ. The mini-mental state examination: a comprehensive review. J Am Geriatr Soc 1992;40:922-935.
1. Jonker C, Geerlings MI, Schmand B. Are memory complaints predictive for dementia? A review of clinical and population-based studies. Int J Geriatr Psychiatry 2000;15:983-991.
2. Jungwirth S, Fischer P, Weissgram S, Kirchmeyr W, Bauer P, Tragl KH. Subjective memory complaints and objective memory impairment in the Vienna-Transdanube aging community. J Am Geriatr Soc 2004;52:263-268.
3. Zandi T. Relationship between subjective memory complaints, objective memory performance, and depression among older adults. Am J Alzheimers Dis Other Demen 2004;19:353-360.
4. Gagnon M, Dartigues JF, Mazaux JM, et al. Self-reported memory complaints and memory performance in elderly French community residents: results of the PAQUID Research Program. Neuroepidemiology 1994;13:145-154.
5. O’Connor DW, Pollitt PA, Roth M, Brook PB, Reiss BB. Memory complaints and impairment in normal, depressed, and demented elderly persons identified in a community survey. Arch Gen Psychiatry 1990;47:224-227.
6. Mol ME, van Boxtel MP, Willems D, Jolles J. Do subjective memory complaints predict cognitive dysfunction over time? A six-year follow-up of the Maastricht aging Study. Int J Geriatr Psychiatry 2006;21:432-441.
7. Geerlings MI, Jonker C, Bouter lM, Ader HJ, Schmand B. Association between memory complaints and incident alzheimer’s disease in elderly people with normal baseline cognition. Am J Psychiatry 1999;156:531-537.
8. Schmand B, Jonker C, Hooijer C, lindeboom J. Subjective memory complaints may announce dementia. Neurology 1996;46:121-125.
9. Rabin R, De Charro F. EQ-5D: a measure of health status from the EuroQol Group. Ann Med 2001;33:337-343.
10. Folstein MF, Folstein SE, McHugh PR. “Mini-mental state.” A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res 1975;12:189-198.
11. Olivarius NF, Hollnagel H, Krasnik A, Pedersen PA, Thorsen H. The Danish National Health Service Register. A tool for primary health care research. Dan Med Bull 1997;44:449-453.
12. Tombaugh TN, McIntyre NJ. The mini-mental state examination: a comprehensive review. J Am Geriatr Soc 1992;40:922-935.
Varicella vaccination: 2 doses now the standard
The varicella vaccine has had tremendous success over the last few years, but its success has stalled.
The widespread use of the varicella vaccine has led to a coverage rate of 88%, and the vaccine has proven to be 85% effective. As a result, between 1995 and 2001 there was an 87% decline in hospitalizations, 66% decline in deaths, and an 87% decline in costs attributed to varicella.
However, the number of varicella cases has remained at a constant level over the past few years and sporadic outbreaks continue to occur in schools—even where high rates of immunization are achieved.1,2
Varicella outbreaks involve both infections in unvaccinated children and “breakthrough disease” in those who have been vaccinated. If a vaccinated person is exposed to varicella, the risk of suffering a breakthrough infection is about 15%.2 A 2-dose series of varicella vaccine reduces the risk by about 75%1 (Figure).
Breakthrough disease is usually milder than infection in the unvaccinated, with fewer skin lesions, milder symptoms, and fewer complications. Those affected, though, are still infectious to others.
It was this ongoing risk of varicella that prompted the Advisory Committee on Immunization Practices (ACIP) to recommend new control measures, reported on in 2007.1
- All children should now receive 2 doses of varicella vaccine. The timing of the first and second dose should correspond with the administration of the MMR vaccine.
- Children older than 6 years of age and adults who previously received only 1 dose of vaccine should receive 1 more dose.
- Health care workers should ensure that they are immune to varicella by blood titers or receiving 2 doses of the vaccine.
- Pregnant women should be screened for immunity to varicella. They should be vaccinated postpartum if they are not immune.
FIGURE
2 doses of varicella vaccine reduce risk of breakthrough infection by about 75%1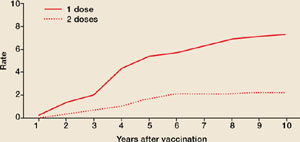
Cumulative breakthrough rates for 1 and 2 doses of single-antigen varicella vaccine among children (ages 12 months to 12 years) by number of years after vaccination. Breakthrough rates are per 100 person-years at risk.
ACIP now recommends 2 doses of the vaccine
ACIP recommends the following:
- Universal administration of 2 doses of varicella vaccine; the first at ages 12 to 15 months and the second at age 4 to 6 years. (This is the same schedule as immunization against mumps, measles, and rubella.)
- Two doses of varicella vaccine, 4 to 8 weeks apart, for all adolescents and adults without evidence of immunity. (See “New criteria to prove immunity” at right.)
- A catch-up second dose for everyone who received one dose previously.
- Screening for varicella immunity in pregnant women and postpartum vaccination for those who are not immune, with 2 doses 4 to 8 weeks apart. The first dose should be administered before discharge.
Which HIV patients can get the vaccine?
ACIP has also clarified when HIV patients can be vaccinated, noting that single antigen varicella vaccine can be administered to HIV positive children if their CD4+ Tlymphocyte % is ≥15%. HIV positive adolescents and adults can be vaccinated if their CD4+ T-lymphocyte count ≥200/μL and, if 2 doses are indicated, they should be separated by at least 3 months.
ACIP has approved new criteria for establishing proof of immunity to varicella. ACIP now includes laboratory confirmation of disease or birth in the US prior to 1980 as evidence of immunity. Another change to ACIP’s criteria: A reported varicella history alone does not suffice; it needs to be verified by a provider.
ACIP’s new criteria include:
- Documentation of age appropriate vaccination (1 dose for preschool children ≥12 months of age, and 2 doses, 1 month apart, for school-age children, adolescents, and adults)
- Laboratory evidence of immunity or laboratory confirmation of disease
- A history of varicella disease or varicella zoster verified by a health care provider
- 4. Birth in the US prior to 1980. This criterion does not apply to health care providers, pregnant women, or the immune-suppressed.
2 options: Varivax and ProQuad
Two varicella vaccines contain modified live varicella virus antigen. Varivax, a single antigen vaccine, is approved for use in adults, adolescents, and children ≥12 months of age. The second vaccine, ProQuad, is approved for use in patients who are between 12 months and 12 years of age, and contains 4 viral antigens: mumps, measles, rubella, and varicella.
The quadrivalent MMRV vaccine is currently unavailable, however, and isn’t expected to be available until early 2009.3 Once the supply is stabilized, though, it will facilitate vaccination of children by decreasing the number of injections needed to achieve full immunization status.

29-year-old patient with varicellaThese 2 varicella vaccines should not be confused with the varicella zoster vaccine, Zostavax, which is approved for use in adults who are 60 years of age and older for the prevention of shingles and postherpetic neuralgia.4
- Can the varicella vaccine be co-administered with other childhood vaccines?
Yes. - What if a nonimmune pregnant women is exposed to chicken-pox?
You’ll need to consult your local health department about the possibility of administering varicella immune globulin. - Can the vaccine be administered to mothers who are breastfeeding their babies?
yes. - Can the vaccine be administered to those who live in a household with an immune-suppressed person?
yes, the risk of transmission of vaccine virus is very low. - What if a woman is inadvertently vaccinated while pregnant?
The risk during pregnancy is theoretical and to date, no cases of congenital varicella have resulted from inadvertent vaccination during pregnancy. - Will the vaccine prevent shingles later in life?
No one knows for sure. Surveillance is currently in progress, but long-term results are not available.
Pregnancy precludes vaccination
Varicella vaccine is contraindicated during pregnancy and in those who have had a severe allergic reaction to any vaccine component, including gelatin; have a malignancy of the blood, bone marrow, or lymphatic system; have a congenital or hereditary immunodeficiency; or are receiving systemic immunosuppressive therapy including those on the equivalent of 2 mg/kg, or >20 mg/day, of prednisone.
You should delay giving the vaccine to patients with an acute, severe illness. There is a potential for immune globulin containing products to interfere with the effectiveness of live virus vaccines. As a result, if a patient has received blood, plasma, or immune globulin, you should wait 3 to 11 months before giving the varicella vaccine. These products should also be avoided, if possible, for 2 weeks after the vaccine has been administered.
Avoid using quadrivalent MMRV in patients with HIV infection because it contains a higher quantity of varicella antigen than the single antigen product.
One final precaution: Patients should avoid taking salicylates for 6 weeks following vaccination because of the theoretical risk of Reye’s syndrome.
1. CDC. Prevention of varicella: Recommendations of the Advisory Committee on Immunization Practices. MMWR Recomm Rep 2007; 56(rr-4):1–40. Available at: www.cdc.gov/mmwr/PDF/rr/rr5604.pdf. Accessed on November 27, 2007.
2. CDC. Varicella disease. Available at: www.cdc.gov/vaccines/vpd-vac/varicella/dis-faqs-clinic.htm. Accessed on November 27, 2007.
3. Public Affairs Department, Merck & Co, Inc. Personal communication; December 4, 2007.
4. Zostavax [package insert]. Whitehouse Sation, NJ: Merck & Co, Inc; 2006. Available at: www.fda.gov/cber/label/zostavaxlB.pdf. Accessed on November 27, 2007.
The varicella vaccine has had tremendous success over the last few years, but its success has stalled.
The widespread use of the varicella vaccine has led to a coverage rate of 88%, and the vaccine has proven to be 85% effective. As a result, between 1995 and 2001 there was an 87% decline in hospitalizations, 66% decline in deaths, and an 87% decline in costs attributed to varicella.
However, the number of varicella cases has remained at a constant level over the past few years and sporadic outbreaks continue to occur in schools—even where high rates of immunization are achieved.1,2
Varicella outbreaks involve both infections in unvaccinated children and “breakthrough disease” in those who have been vaccinated. If a vaccinated person is exposed to varicella, the risk of suffering a breakthrough infection is about 15%.2 A 2-dose series of varicella vaccine reduces the risk by about 75%1 (Figure).
Breakthrough disease is usually milder than infection in the unvaccinated, with fewer skin lesions, milder symptoms, and fewer complications. Those affected, though, are still infectious to others.
It was this ongoing risk of varicella that prompted the Advisory Committee on Immunization Practices (ACIP) to recommend new control measures, reported on in 2007.1
- All children should now receive 2 doses of varicella vaccine. The timing of the first and second dose should correspond with the administration of the MMR vaccine.
- Children older than 6 years of age and adults who previously received only 1 dose of vaccine should receive 1 more dose.
- Health care workers should ensure that they are immune to varicella by blood titers or receiving 2 doses of the vaccine.
- Pregnant women should be screened for immunity to varicella. They should be vaccinated postpartum if they are not immune.
FIGURE
2 doses of varicella vaccine reduce risk of breakthrough infection by about 75%1
Cumulative breakthrough rates for 1 and 2 doses of single-antigen varicella vaccine among children (ages 12 months to 12 years) by number of years after vaccination. Breakthrough rates are per 100 person-years at risk.
ACIP now recommends 2 doses of the vaccine
ACIP recommends the following:
- Universal administration of 2 doses of varicella vaccine; the first at ages 12 to 15 months and the second at age 4 to 6 years. (This is the same schedule as immunization against mumps, measles, and rubella.)
- Two doses of varicella vaccine, 4 to 8 weeks apart, for all adolescents and adults without evidence of immunity. (See “New criteria to prove immunity” at right.)
- A catch-up second dose for everyone who received one dose previously.
- Screening for varicella immunity in pregnant women and postpartum vaccination for those who are not immune, with 2 doses 4 to 8 weeks apart. The first dose should be administered before discharge.
Which HIV patients can get the vaccine?
ACIP has also clarified when HIV patients can be vaccinated, noting that single antigen varicella vaccine can be administered to HIV positive children if their CD4+ Tlymphocyte % is ≥15%. HIV positive adolescents and adults can be vaccinated if their CD4+ T-lymphocyte count ≥200/μL and, if 2 doses are indicated, they should be separated by at least 3 months.
ACIP has approved new criteria for establishing proof of immunity to varicella. ACIP now includes laboratory confirmation of disease or birth in the US prior to 1980 as evidence of immunity. Another change to ACIP’s criteria: A reported varicella history alone does not suffice; it needs to be verified by a provider.
ACIP’s new criteria include:
- Documentation of age appropriate vaccination (1 dose for preschool children ≥12 months of age, and 2 doses, 1 month apart, for school-age children, adolescents, and adults)
- Laboratory evidence of immunity or laboratory confirmation of disease
- A history of varicella disease or varicella zoster verified by a health care provider
- 4. Birth in the US prior to 1980. This criterion does not apply to health care providers, pregnant women, or the immune-suppressed.
2 options: Varivax and ProQuad
Two varicella vaccines contain modified live varicella virus antigen. Varivax, a single antigen vaccine, is approved for use in adults, adolescents, and children ≥12 months of age. The second vaccine, ProQuad, is approved for use in patients who are between 12 months and 12 years of age, and contains 4 viral antigens: mumps, measles, rubella, and varicella.
The quadrivalent MMRV vaccine is currently unavailable, however, and isn’t expected to be available until early 2009.3 Once the supply is stabilized, though, it will facilitate vaccination of children by decreasing the number of injections needed to achieve full immunization status.
29-year-old patient with varicellaThese 2 varicella vaccines should not be confused with the varicella zoster vaccine, Zostavax, which is approved for use in adults who are 60 years of age and older for the prevention of shingles and postherpetic neuralgia.4
- Can the varicella vaccine be co-administered with other childhood vaccines?
Yes. - What if a nonimmune pregnant women is exposed to chicken-pox?
You’ll need to consult your local health department about the possibility of administering varicella immune globulin. - Can the vaccine be administered to mothers who are breastfeeding their babies?
yes. - Can the vaccine be administered to those who live in a household with an immune-suppressed person?
yes, the risk of transmission of vaccine virus is very low. - What if a woman is inadvertently vaccinated while pregnant?
The risk during pregnancy is theoretical and to date, no cases of congenital varicella have resulted from inadvertent vaccination during pregnancy. - Will the vaccine prevent shingles later in life?
No one knows for sure. Surveillance is currently in progress, but long-term results are not available.
Pregnancy precludes vaccination
Varicella vaccine is contraindicated during pregnancy and in those who have had a severe allergic reaction to any vaccine component, including gelatin; have a malignancy of the blood, bone marrow, or lymphatic system; have a congenital or hereditary immunodeficiency; or are receiving systemic immunosuppressive therapy including those on the equivalent of 2 mg/kg, or >20 mg/day, of prednisone.
You should delay giving the vaccine to patients with an acute, severe illness. There is a potential for immune globulin containing products to interfere with the effectiveness of live virus vaccines. As a result, if a patient has received blood, plasma, or immune globulin, you should wait 3 to 11 months before giving the varicella vaccine. These products should also be avoided, if possible, for 2 weeks after the vaccine has been administered.
Avoid using quadrivalent MMRV in patients with HIV infection because it contains a higher quantity of varicella antigen than the single antigen product.
One final precaution: Patients should avoid taking salicylates for 6 weeks following vaccination because of the theoretical risk of Reye’s syndrome.
The varicella vaccine has had tremendous success over the last few years, but its success has stalled.
The widespread use of the varicella vaccine has led to a coverage rate of 88%, and the vaccine has proven to be 85% effective. As a result, between 1995 and 2001 there was an 87% decline in hospitalizations, 66% decline in deaths, and an 87% decline in costs attributed to varicella.
However, the number of varicella cases has remained at a constant level over the past few years and sporadic outbreaks continue to occur in schools—even where high rates of immunization are achieved.1,2
Varicella outbreaks involve both infections in unvaccinated children and “breakthrough disease” in those who have been vaccinated. If a vaccinated person is exposed to varicella, the risk of suffering a breakthrough infection is about 15%.2 A 2-dose series of varicella vaccine reduces the risk by about 75%1 (Figure).
Breakthrough disease is usually milder than infection in the unvaccinated, with fewer skin lesions, milder symptoms, and fewer complications. Those affected, though, are still infectious to others.
It was this ongoing risk of varicella that prompted the Advisory Committee on Immunization Practices (ACIP) to recommend new control measures, reported on in 2007.1
- All children should now receive 2 doses of varicella vaccine. The timing of the first and second dose should correspond with the administration of the MMR vaccine.
- Children older than 6 years of age and adults who previously received only 1 dose of vaccine should receive 1 more dose.
- Health care workers should ensure that they are immune to varicella by blood titers or receiving 2 doses of the vaccine.
- Pregnant women should be screened for immunity to varicella. They should be vaccinated postpartum if they are not immune.
FIGURE
2 doses of varicella vaccine reduce risk of breakthrough infection by about 75%1
Cumulative breakthrough rates for 1 and 2 doses of single-antigen varicella vaccine among children (ages 12 months to 12 years) by number of years after vaccination. Breakthrough rates are per 100 person-years at risk.
ACIP now recommends 2 doses of the vaccine
ACIP recommends the following:
- Universal administration of 2 doses of varicella vaccine; the first at ages 12 to 15 months and the second at age 4 to 6 years. (This is the same schedule as immunization against mumps, measles, and rubella.)
- Two doses of varicella vaccine, 4 to 8 weeks apart, for all adolescents and adults without evidence of immunity. (See “New criteria to prove immunity” at right.)
- A catch-up second dose for everyone who received one dose previously.
- Screening for varicella immunity in pregnant women and postpartum vaccination for those who are not immune, with 2 doses 4 to 8 weeks apart. The first dose should be administered before discharge.
Which HIV patients can get the vaccine?
ACIP has also clarified when HIV patients can be vaccinated, noting that single antigen varicella vaccine can be administered to HIV positive children if their CD4+ Tlymphocyte % is ≥15%. HIV positive adolescents and adults can be vaccinated if their CD4+ T-lymphocyte count ≥200/μL and, if 2 doses are indicated, they should be separated by at least 3 months.
ACIP has approved new criteria for establishing proof of immunity to varicella. ACIP now includes laboratory confirmation of disease or birth in the US prior to 1980 as evidence of immunity. Another change to ACIP’s criteria: A reported varicella history alone does not suffice; it needs to be verified by a provider.
ACIP’s new criteria include:
- Documentation of age appropriate vaccination (1 dose for preschool children ≥12 months of age, and 2 doses, 1 month apart, for school-age children, adolescents, and adults)
- Laboratory evidence of immunity or laboratory confirmation of disease
- A history of varicella disease or varicella zoster verified by a health care provider
- 4. Birth in the US prior to 1980. This criterion does not apply to health care providers, pregnant women, or the immune-suppressed.
2 options: Varivax and ProQuad
Two varicella vaccines contain modified live varicella virus antigen. Varivax, a single antigen vaccine, is approved for use in adults, adolescents, and children ≥12 months of age. The second vaccine, ProQuad, is approved for use in patients who are between 12 months and 12 years of age, and contains 4 viral antigens: mumps, measles, rubella, and varicella.
The quadrivalent MMRV vaccine is currently unavailable, however, and isn’t expected to be available until early 2009.3 Once the supply is stabilized, though, it will facilitate vaccination of children by decreasing the number of injections needed to achieve full immunization status.
29-year-old patient with varicellaThese 2 varicella vaccines should not be confused with the varicella zoster vaccine, Zostavax, which is approved for use in adults who are 60 years of age and older for the prevention of shingles and postherpetic neuralgia.4
- Can the varicella vaccine be co-administered with other childhood vaccines?
Yes. - What if a nonimmune pregnant women is exposed to chicken-pox?
You’ll need to consult your local health department about the possibility of administering varicella immune globulin. - Can the vaccine be administered to mothers who are breastfeeding their babies?
yes. - Can the vaccine be administered to those who live in a household with an immune-suppressed person?
yes, the risk of transmission of vaccine virus is very low. - What if a woman is inadvertently vaccinated while pregnant?
The risk during pregnancy is theoretical and to date, no cases of congenital varicella have resulted from inadvertent vaccination during pregnancy. - Will the vaccine prevent shingles later in life?
No one knows for sure. Surveillance is currently in progress, but long-term results are not available.
Pregnancy precludes vaccination
Varicella vaccine is contraindicated during pregnancy and in those who have had a severe allergic reaction to any vaccine component, including gelatin; have a malignancy of the blood, bone marrow, or lymphatic system; have a congenital or hereditary immunodeficiency; or are receiving systemic immunosuppressive therapy including those on the equivalent of 2 mg/kg, or >20 mg/day, of prednisone.
You should delay giving the vaccine to patients with an acute, severe illness. There is a potential for immune globulin containing products to interfere with the effectiveness of live virus vaccines. As a result, if a patient has received blood, plasma, or immune globulin, you should wait 3 to 11 months before giving the varicella vaccine. These products should also be avoided, if possible, for 2 weeks after the vaccine has been administered.
Avoid using quadrivalent MMRV in patients with HIV infection because it contains a higher quantity of varicella antigen than the single antigen product.
One final precaution: Patients should avoid taking salicylates for 6 weeks following vaccination because of the theoretical risk of Reye’s syndrome.
1. CDC. Prevention of varicella: Recommendations of the Advisory Committee on Immunization Practices. MMWR Recomm Rep 2007; 56(rr-4):1–40. Available at: www.cdc.gov/mmwr/PDF/rr/rr5604.pdf. Accessed on November 27, 2007.
2. CDC. Varicella disease. Available at: www.cdc.gov/vaccines/vpd-vac/varicella/dis-faqs-clinic.htm. Accessed on November 27, 2007.
3. Public Affairs Department, Merck & Co, Inc. Personal communication; December 4, 2007.
4. Zostavax [package insert]. Whitehouse Sation, NJ: Merck & Co, Inc; 2006. Available at: www.fda.gov/cber/label/zostavaxlB.pdf. Accessed on November 27, 2007.
1. CDC. Prevention of varicella: Recommendations of the Advisory Committee on Immunization Practices. MMWR Recomm Rep 2007; 56(rr-4):1–40. Available at: www.cdc.gov/mmwr/PDF/rr/rr5604.pdf. Accessed on November 27, 2007.
2. CDC. Varicella disease. Available at: www.cdc.gov/vaccines/vpd-vac/varicella/dis-faqs-clinic.htm. Accessed on November 27, 2007.
3. Public Affairs Department, Merck & Co, Inc. Personal communication; December 4, 2007.
4. Zostavax [package insert]. Whitehouse Sation, NJ: Merck & Co, Inc; 2006. Available at: www.fda.gov/cber/label/zostavaxlB.pdf. Accessed on November 27, 2007.
Geriatric Syndromes in Older Cardiology Patients
Utilizing hospitalist physicians as the primary providers of inpatient care is a rapidly growing trend. In the United States the number of hospitalists now approaches 12,000 and may reach 30,000 by 2010.1 Simultaneously, by 2030 the proportion of adults aged 65 and older will have more than doubled to make up 20% of the U.S. population. Currently, patients aged 65 and older account for approximately 49% of hospital days.2 Congestive heart failure is the most common discharge diagnosis and cardiovascular disease is the leading cause of death of these older adults.3 Given current trends in aging demographics, hospitalists can expect an increasing proportion of their practices to consist of frail older adults with cardiovascular disease.
Hospitalization for any acute illness predisposes elderly patients to increased disability.4 Studies have demonstrated that underrecognition of geriatric syndromes is common and contributes to hospitalized older adults having poor outcomes.5, 6, 7 Between 35% and 50% of elderly patients will experience functional decline while hospitalized,4, 8 and up to 50% will develop hospital‐acquired delirium.6 The risk of experiencing an iatrogenic event while hospitalized is 2‐fold higher for older adults than for those younger than age 65.7, 9 These adverse outcomes lead to longer length of stay (LOS), higher hospital costs, and, for patients able to live at home prior to admission, increased risk of temporary or permanent institutionalization.10, 11
The objective of this study was to characterize a population of acutely ill older adults with known cardiovascular disease admitted to a specialty cardiac ward, to determine the prevalence of geriatric syndromes (ie, functional impairment, cognitive impairment, depression, polypharmacy), and to record the incidence of hospital‐acquired adverse events (urinary tract infection, falls, use of restraints). We hypothesized that these syndromes would be prevalent and underrecognized by the patients' physicians.
METHODS
At Barnes‐Jewish Hospital, an academic medical center in St. Louis, Missouri, patients hospitalized for an acute cardiovascular disorder are preferentially admitted to a cardiac ward with a cardiologist as the attending physician. We conducted a prospective cohort study of 100 patients aged 70 and older admitted to the cardiac ward between January and December of 2003. Participation in the study was not offered to patients who were nonverbal, non‐English‐speaking, or unavailable for screening because of being hospitalized on weekends, holidays, or other days when the research nurse was not available. Participants provided written informed consent. If a patient did not demonstrate an understanding of his or her role in the study, a surrogate decision maker was identified who provided consent in addition to the patient's assent. If a surrogate decision maker was not present, the patient was not enrolled in the study. In addition, patients could decline to continue participating in the study at any time. The institutional review board of the Human Studies Committee at Washington University School of Medicine approved this study.
Data Collection
A trained research nurse administered the following geriatric screening questionnaires: (1) the Katz Index of basic activities of daily living (ADLs)12; (2) the Vulnerable Elders Survey (VES)13; (3) the Short Blessed Test of Orientation, Memory, and Concentration (SBT)14; (4) the Clock Completion Test (CCT)15; and (5) the 15‐item Yesavage Geriatric Depression Scale (GDS).16 The Katz Index (score range 6‐18) assesses the performance of 6 basic ADLs (bathing, continence, dressing, feeding, toileting, and transferring) based on a report by the patient or a collateral source about the patient's level of dependence. Performance of each activity is rated on a scale from 1 (completely dependent) to 3 (completely independent). For this study, patients were considered dependent in any activity if the performance score was less than 3. The Vulnerable Elders Survey (score range 0‐10) utilizes patient age and self‐reported health and functional status to identify frail older adults. A VES score of 3 or greater correlates with a 4‐fold increased risk of death or functional decline over a 2‐year period. Cognition was assessed with the Short Blessed Test of Orientation, Memory, and Concentration and the Clock Completion Test. The Short Blessed Test score ranges from 0 to 28, with a score of 9 or greater indicating increasing severity of cognitive impairment. The Clock Completion Test is scored by evaluating whether the digits in the 4 quadrants of a predrawn circle are accurately placed. The CCT score can range from 0 to 7, with a score of 4 or more indicating cognitive impairment. The 15‐item Geriatric Depression Scale was administered to screen for depressive symptoms. The GDS score can range from 0 to 15, with a score of 6 or more indicating increasing severity of depressive symptoms.
Demographic, psychosocial, and medical data were abstracted by review of patients' hospital records (A.R., C.L.). Medical data obtained from the medical charts included medical diagnoses, number and classes of medications prescribed, and physician documentation of prior or newly diagnosed geriatric syndromes. These geriatric syndromes included dementia, delirium, depression, falls, malnutrition/weight loss, pressure sores, osteoporosis and/or hip fracture, urinary incontinence, and polypharmacy (4 routine medications). A patient was recorded as having documented dementia and/or delirium if the terms dementia, memory loss, cognitive impairment, delirium/delirious, confusion, mental status change, or similar were recorded in physician notes. Admission and discharge orders were reviewed for classes of medications cited in Beers criteria as potentially inappropriate medications for older adults.17 For this study, these high‐risk medications included benzodiazepines, diphenhydramine, propoxyphene, hypnotics, anticholingeric/antidopaminergic medications, and tricyclic antidepressants. Patients' medical charts were reviewed for adverse events such as falls and development of pressure sores or use of restraints. A patient was recorded as having a urinary tract infection (UTI) if a physician documented a UTI in the medical record at any time during hospitalization.
Statistical Analysis
Descriptive statistics were generated using SPSS version 12.0. For continuous measures, values were dichotomized for analytic purposes using standard cutoff scores. Fisher's exact test was used to compare the UTI rate of patients who received a Foley catheter with that of those who did not.
A P value < .05 was considered statistically significant.
RESULTS
Sample Characteristics
Descriptive characteristics for the population are summarized in Table 1. The mean age of the patients was 79.2 5.5 years. The sample was predominantly female and white and had an average stay of 7 days on the cardiac ward. Most patients were admitted for management of heart failure, an arrhythmia, acute myocardial infarction, or angina. Twelve patients had a history of cardiovascular disease (CVD) but were admitted for a noncardiovascular complaint. Only 4 patients did not have a history of CVD.
| Patient characteristic | |
|---|---|
| |
| Age, years (mean SD) | 79.2 5.5 |
| Sex (% female) | 61% |
| Race (% white) | 68% |
| Percent admitted to cardiac ward from: | |
| Home | 69% |
| Outside hospital | 21% |
| Nursing home/skilled nursing facility | 8% |
| ICU | 2% |
| Discharged home from cardiac ward (%) | 84% |
| Length of hospital stay (days), mean SD | 7.4 5.9 |
| Length of cardiac ward stay (days), mean SD | 7.0 5.5 |
| Died during hospitalization (%) | 3% |
| Admitting diagnoses as determined by ICD9 codes (%) | |
| Heart failure | 23% |
| Arrhythmia | 19% |
| Acute myocardial infarction | 10% |
| Chest pain/stable or unstable angina | 10% |
| Coronary artery disease | 9% |
| Syncope | 6% |
| Other cardiovascular diagnoses* | 7% |
| Noncardiovascular diagnoses in patients with history of CVD | 12% |
| Noncardiovascular diagnoses in patients without history of CVD | 4% |
| Comorbidities (%) | |
| Hypertension | 83% |
| Coronary artery disease | 67% |
| History of CABG and/or percutaneous intervention | 54% |
| Hyperlipidemia | 53% |
| Atrial fibrillation | 50% |
| Heart failure | 46% |
| Myocardial infarction | 38% |
| Diabetes mellitus | 37% |
| Chronic renal insufficiency | 29% |
| Stroke or transient ischemic attack | 25% |
| Chronic obstructive pulmonary disease | 23% |
Functional Status and Geriatric Syndromes
Forty‐one percent of patients had a history of 2 or more geriatric syndromes, as documented in their medical record (Table 2). Thirty‐five percent of patients were dependent in at least 1 basic ADL, and 85% had a VES score that indicated an increased risk of functional decline and mortality over the next 2 years. Only 6% of all patients had dementia and only 9% had delirium documented by their physicians in the medical record. Abnormal cognition as detected by screening tests was prevalent. Screening showed that 19% of the patients who completed the SBT and 59% of those who completed the CCT had cognitive impairment. Only 14% of patients with an abnormal CCT and 42% with an abnormal SBT had dementia and/or delirium documented in their hospital chart.
| |
| Katz Index of Basic Activities of Daily Living* (n = 100) | |
| Mean score SD (range 0‐18) | 17.0 1.9 |
| Dependent in 1 ADL (%) | 35% |
| Dependent in 2 ADLs (%) | 20% |
| Vulnerable Elders Survey (n = 100) | |
| Mean score SD (range 0‐10) | 4.6 3.0 |
| Patients with score 3 (%) | 85% |
| Abnormal geriatric screens (%) | |
| Short Blessed Test score 9 (n = 98) | 19% |
| Clock Construction Test score 4 (n = 95) | 59% |
| Geriatric Depression Scale score‖ 6 (n = 99) | 7% |
| Geriatric syndromes documented in cardiology physician notes (%) | |
| Polypharmacy | 95% |
| Depression | 18% |
| History of a prior fall | 17% |
| Delirium | 9% |
| Dementia | 6% |
| Other | 21% |
| Patients with 2 geriatric syndromes | 41% |
| Polypharmacy | |
| Routine medications (range 0‐17) on admission, (n = 100), mean SD | 8.2 3.2 |
| Routine medications (range 3‐17) at discharge, (n = 97), mean SD | 9.0 3.0 |
| Patients taking 12 routine medications on admission (%) | 15% |
| Patients taking 12 routine medications at discharge (%) | 19% |
| Patients with 1 potentially inappropriate medication# ordered on admission or discharge, routine or PRN (%) | 37% |
Polypharmacy was also prevalent. Patients had an average of 9 routine discharge medications, with 19% of patients prescribed at least 12 routine medications at discharge. Thirty‐seven percent of patients were prescribed at least 1 high‐risk medication. Of the 6 patients prescribed a tricyclic antidepressant, 3 had a history of atrial fibrillation/flutter, and 4 had a history of coronary artery disease.
Adverse Events
Thirty‐eight of the 100 patients in the study received a Foley catheter during hospitalization (Table 3). These patients were significantly more likely to have a UTI during their hospitalization than those who did not have a catheter placed (risk ratio 6.0, 95% CI 1.8‐20, P = .002). Other adverse events were rare. Three patients experienced a fall while hospitalized, and 1 patient was restrained (soft limb restraint applied to left upper extremity).
| Developed a UTI (n) | Did not develop a UTI (n) | Risk ratio* (95% confidence interval) | |
|---|---|---|---|
| |||
| Received a Foley | |||
| Yes | 11 | 27 | 6.0 (1.8‐20) |
| No | 3 | 59 | P = .002 (Fisher's exact test) |
DISCUSSION
The goal of this pilot study was to determine the prevalence of geriatric syndromes and the incidence of selected adverse events in hospitalized older patients with cardiovascular disease. We are unaware of another study documenting these syndromes specifically in hospitalized elderly patients with cardiovascular disease. We found that geriatric syndromes were prevalent in this patient population and often unrecognized by physicians. In 1 study of hospitalized frail elderly cardiovascular patients with long hospital stays, physician failure to recognize poor functional status on admission was an independent predictor of patients experiencing a preventable iatrogenic event.7 Brown et al. documented the prevalence and impact of poor mobility in hospitalized adults aged 70 and older. In this study, low mobility was associated with increased risk of further decline in ADL performance, institutionalization, and death; however, it was common for these patients to have bed rest orders (33%), usually without medical indication (60%), indicating underrecognition of functional impairment by attending physicians.18 The proportion of our patients with dependence in at least 1 ADL (35%) and/or at increased risk of functional decline and death based on VES scores (85%) indicates that our patients were already experiencing significant disability at the time of admission, yet these disabilities were rarely documented in the medical record.
In addition to physical frailty, elderly patients with cardiovascular disease may be at increased risk of cognitive impairment. The ongoing Cognitive and Emotional Health Project survey of 36 large cohort studies noted shared risk factors for cardiovascular disease and cognitive impairment in older adults.19 In our study abnormal scores were found for 19% and 59% of the patients who completed the SBT and the CCT, respectively. Several factors may explain the difference in the proportion of patients scoring abnormally on these 2 cognitive screens. We did not measure the visual acuity of our participants, so the number of patients with an abnormal CCT (which relies more on visual cues than the SBT does) may overrepresent the true prevalence of cognitive impairment in our sample. Also, the CCT is a more sensitive indicator of impairments in the visuospatial and executive function domains of cognition than is the SBT and is more likely to be abnormal in vascular dementia.20 Thus, differences in the SBT and CCT scores in our sample may also reflect a higher proportion of patients with a vascular component to their dementia. However, even the number of patients with an abnormal SBT score likely underrepresents the prevalence of underlying cognitive impairment in this sample because of selection bias introduced in obtaining informed consent (ie, the most cognitively impaired patients and/or those deemed to not have decision‐making capacity were excluded or were more likely to decline participation in this study). Consistent with the results of studies of other inpatient populations, cognitive impairment (dementia and/or delirium) was documented in our patients' medical charts far less frequently than detected by either cognitive screen.5, 21 Patients with unrecognized dementia are at increased risk for incident delirium during hospitalization.6
Another common geriatric syndrome in patients with cardiovascular disease is polypharmacy. According to current guidelines, heart failure and coronary artery disease each require multiple medications for optimal therapy. Our patient population were prescribed an average of 9 routine medications at discharge, with nearly 20% prescribed 12 or more routine medications (in addition to as‐needed medications). In comparison, a cohort of hospitalized elderly oncology patients were prescribed an average of 6 routine medications at discharge.22 Thirty‐seven percent of the patients in our study had at least 1 potentially inappropriate medication ordered on admission or at discharge. Although this study was not able to monitor prospectively for adverse drug events, the potential for harm from drug prescribing is substantial in this sample of frail older adult patients. This remains a fruitful area for research.
Thirty‐eight percent of patients in our study received a Foley catheter and were therefore at increased risk of developing a UTI. We did not document the indications for catheterization in this patient population. Studies indicate that up to 20% of urinary catheters are placed without a specific medical indication23 and that hospitalized older adults receiving unwarranted urinary catheterization are at increased risk of prolonged length of stay and death.24
Interventions that increase recognition of geriatric syndromes have been shown to improve the outcomes of hospitalized older adults. The Hospital Elder Life Program demonstrated a 40% reduction in hospital‐acquired delirium in patients aged 70 and older by enhancing recognition and management of geriatric syndromes such as cognitive impairment, immobility, visual/hearing impairment, and polypharmacy.6, 8 Other studies have demonstrated that use of inappropriate medications in hospitalized older adults can be reduced with nonpharmacologic and physician‐education interventions.25, 26 In a broader effort to address multiple geriatric syndromes simultaneously, Acute Care for Elders (ACE) Units have been developed in medical centers worldwide. The ACE Unit model of care emphasizes patient‐centered care, nurse‐driven prevention protocols, frequent interdisciplinary team rounds addressing geriatric syndromes, and discharge planning beginning the day of admission. Studies evaluating outcomes in patients admitted to an ACE Unit have found preservation of physical functioning and independence in ADLs,27, 28 reduced LOS,21 improved patient and provider satisfaction,29 and reduced rates of restraint use,29, 30 institutionalization,27, 29 and mortality.31 This model should be considered for older adults admitted to a cardiac ward. However, other care models could include utilization of inpatient geriatric consultation, hiring a gerontological nurse specialist, or educational programs focused on recognizing and managing geriatric syndromes and designed for the physicians and nurses who care for these patients.
Our study had several limitations. The sample size and number of serious adverse outcomes were small. We did not have adequate power to detect clinically significant differences in length of stay between patients with and without selected geriatric syndromes (0.5 days). The process of informed consent likely selected for a greater number of cognitively intact and fewer depressed patients. The results of the ADL screens may be limited because they were mostly based on patient self‐report of functional status without informant corroboration. Specifically, self‐report may overestimate functional status.
Despite these limitations, we found that functional dependence and geriatric syndromes were prevalent in older cardiovascular patients and that these conditions were rarely documented by the attending physicians or house staff. Over the next decades, an increasing proportion of older adults will be admitted and cared for by hospitalist physicians. Interventions utilizing comprehensive geriatric assessments and interdisciplinary models of care could assist hospitalists in recognizing and managing geriatric syndromes in their frail elderly patients. Future studies are needed to confirm the prevalence of geriatric syndromes and to evaluate the impact of an interdisciplinary model of care on clinical outcomes in hospitalized elderly cardiovascular patients.
Acknowledgements
The authors thank Valerie Emory for her invaluable assistance in collecting data for this study.
- ,.The expanding role of hospitalists in the United States.Swiss Med Wkly.2006;136:591–596.
- American Association of Retired Persons and the Administration on Aging.A Profile of Older Americans: 1999.Washington, DC:American Association of Retired Persons;1999.
- Federal Interagency Forum on Aging Related Statistics. Older Americans 2004: key indicators of well‐being. Available at: http://www.agingstats.gov
- ,,,.Hospitalization, restricted activity, and the development of disability among older persons.JAMA.2004;292:2115–2124.
- ,,,.Cognitively impaired older adults: From hospital to home.Am J Nurs.2005;105:52–61.
- .Prevention of delirium in hospitalized older patients: risk factors and targeted intervention strategies.Ann Med.2000;32:257–263.
- ,,, et al.Iatrogenic complications in high‐risk, elderly patients.Arch Intern Med.1992;152:2074–2080.
- ,,,,.The hospital elder life program: A model of care to prevent cognitive and functional decline in older hospitalized patients.J Am Geriatr Soc.2000;48:1697–1706.
- ,.Incidence and types of preventable adverse events in elderly patients: population based review of medical records.BMJ.2000;320:741–744.
- ,Landefeld S: Improving care for hospitalized elders.Ann Long Term Care: Clin Care Aging.2001;9:35–40.
- :Acute hospital care of the elderly: minimizing the risk of functional decline.Cleve Clin J Med.1995;62:117–128.
- ,,,,.Studies of illness in the aged: the index of ADL: a standardized measure of biological and psychosocial function.JAMA.1963;185:914–919.
- ,,, et al.The Vulnerable Elders Survey: a tool for identifying vulnerable older people in the community.J Am Geriatr Soc.2001;49:1691–1699.
- ,,,,,.Validation of a short orientation memory‐concentration test of cognitive impairment.Am J Psychiatry.1983;140:734–739.
- ,,.Clock completion: an objective screening test for dementia.J Am Geriatr Soc.1993;41:1235–1240.
- .Geriatric depression scale.Psychopharmacol Bull.1988;24:709–711.
- ,,,,,.Updating the Beers Criteria for potentially inappropriate medication use in older adults.Arch Intern Med.2003;163:2716–2724.
- ,,.Prevalence and outcomes of low mobility in hospitalized older patients.J Am Geriatr Soc.2004;52:1263–1270.
- ,,, et al.The NIH cognitive and emotional health project: Report of the critical evaluation study committee.Alzheimers Dement.2006;2:12–32.
- ,,,.Can clock drawing test help to differentiate between dementia of the Alzheimer's type and vascular dementia? A preliminary study.Int J Geriatr Psychiatry.2002;17:699–703.
- ,,, et al.Geriatric‐based versus general wards for older acute medical patients: a randomized comparison of outcomes and use of resources.J Am Geriatr Soc.2000;48:1381–1388.
- ,,,,,.Geriatric syndromes in elderly patients admitted to an oncology‐acute care for elders unit.J Clin Oncol.2006;24:2298–2303.
- ,,,.Overuse of the indwelling urinary tract catheter in hospitalized medical patients.Arch Intern Med.1995;155:1425–1429.
- ,,, et al.The relationship of indwelling urinary catheters to death, length of hospital stay, functional decline, and nursing home admission in hospitalized older medical patients.J Am Geriatr Soc.2007;55:227–233.
- ,,,.A strategy to decrease the use of risky drugs in the elderly.Cleve Clin J Med.2004;71:561–568.
- ,,,,,.A multifactorial intervention to reduce prevalence of delirium and shorten hospital length of stay.J Am Geriatr Soc.2005;53:18–23.
- ,,,,.A randomized trial of care in a hospital medical unit especially designed to improve the functional outcomes of acutely ill older patients.N Engl J Med.1995;332:1338–1344.
- ,,, et al.A controlled trial of inpatient and outpatient geriatric evaluation and management.N Engl J Med.2002;346:905–912.
- ,,, et al.Effects of a multicomponent intervention on functional outcomes and process of care in hospitalized older patients: A randomized controlled trial of Acute Care for Elders (ACE) in a community hospital.J Am Geriatr Soc.2000;48:1572–1581.
- ,,,,,.A model for managing delirious older inpatients.J Am Geriatr Soc.2003;51:1031–1035.
- ,,,,.Reduced mortality in treating acutely sick, frail older patients in a geriatric evaluation and management unit. A prospective randomized trial.J Am Geriatr Soc.2002;50:792–798.
Utilizing hospitalist physicians as the primary providers of inpatient care is a rapidly growing trend. In the United States the number of hospitalists now approaches 12,000 and may reach 30,000 by 2010.1 Simultaneously, by 2030 the proportion of adults aged 65 and older will have more than doubled to make up 20% of the U.S. population. Currently, patients aged 65 and older account for approximately 49% of hospital days.2 Congestive heart failure is the most common discharge diagnosis and cardiovascular disease is the leading cause of death of these older adults.3 Given current trends in aging demographics, hospitalists can expect an increasing proportion of their practices to consist of frail older adults with cardiovascular disease.
Hospitalization for any acute illness predisposes elderly patients to increased disability.4 Studies have demonstrated that underrecognition of geriatric syndromes is common and contributes to hospitalized older adults having poor outcomes.5, 6, 7 Between 35% and 50% of elderly patients will experience functional decline while hospitalized,4, 8 and up to 50% will develop hospital‐acquired delirium.6 The risk of experiencing an iatrogenic event while hospitalized is 2‐fold higher for older adults than for those younger than age 65.7, 9 These adverse outcomes lead to longer length of stay (LOS), higher hospital costs, and, for patients able to live at home prior to admission, increased risk of temporary or permanent institutionalization.10, 11
The objective of this study was to characterize a population of acutely ill older adults with known cardiovascular disease admitted to a specialty cardiac ward, to determine the prevalence of geriatric syndromes (ie, functional impairment, cognitive impairment, depression, polypharmacy), and to record the incidence of hospital‐acquired adverse events (urinary tract infection, falls, use of restraints). We hypothesized that these syndromes would be prevalent and underrecognized by the patients' physicians.
METHODS
At Barnes‐Jewish Hospital, an academic medical center in St. Louis, Missouri, patients hospitalized for an acute cardiovascular disorder are preferentially admitted to a cardiac ward with a cardiologist as the attending physician. We conducted a prospective cohort study of 100 patients aged 70 and older admitted to the cardiac ward between January and December of 2003. Participation in the study was not offered to patients who were nonverbal, non‐English‐speaking, or unavailable for screening because of being hospitalized on weekends, holidays, or other days when the research nurse was not available. Participants provided written informed consent. If a patient did not demonstrate an understanding of his or her role in the study, a surrogate decision maker was identified who provided consent in addition to the patient's assent. If a surrogate decision maker was not present, the patient was not enrolled in the study. In addition, patients could decline to continue participating in the study at any time. The institutional review board of the Human Studies Committee at Washington University School of Medicine approved this study.
Data Collection
A trained research nurse administered the following geriatric screening questionnaires: (1) the Katz Index of basic activities of daily living (ADLs)12; (2) the Vulnerable Elders Survey (VES)13; (3) the Short Blessed Test of Orientation, Memory, and Concentration (SBT)14; (4) the Clock Completion Test (CCT)15; and (5) the 15‐item Yesavage Geriatric Depression Scale (GDS).16 The Katz Index (score range 6‐18) assesses the performance of 6 basic ADLs (bathing, continence, dressing, feeding, toileting, and transferring) based on a report by the patient or a collateral source about the patient's level of dependence. Performance of each activity is rated on a scale from 1 (completely dependent) to 3 (completely independent). For this study, patients were considered dependent in any activity if the performance score was less than 3. The Vulnerable Elders Survey (score range 0‐10) utilizes patient age and self‐reported health and functional status to identify frail older adults. A VES score of 3 or greater correlates with a 4‐fold increased risk of death or functional decline over a 2‐year period. Cognition was assessed with the Short Blessed Test of Orientation, Memory, and Concentration and the Clock Completion Test. The Short Blessed Test score ranges from 0 to 28, with a score of 9 or greater indicating increasing severity of cognitive impairment. The Clock Completion Test is scored by evaluating whether the digits in the 4 quadrants of a predrawn circle are accurately placed. The CCT score can range from 0 to 7, with a score of 4 or more indicating cognitive impairment. The 15‐item Geriatric Depression Scale was administered to screen for depressive symptoms. The GDS score can range from 0 to 15, with a score of 6 or more indicating increasing severity of depressive symptoms.
Demographic, psychosocial, and medical data were abstracted by review of patients' hospital records (A.R., C.L.). Medical data obtained from the medical charts included medical diagnoses, number and classes of medications prescribed, and physician documentation of prior or newly diagnosed geriatric syndromes. These geriatric syndromes included dementia, delirium, depression, falls, malnutrition/weight loss, pressure sores, osteoporosis and/or hip fracture, urinary incontinence, and polypharmacy (4 routine medications). A patient was recorded as having documented dementia and/or delirium if the terms dementia, memory loss, cognitive impairment, delirium/delirious, confusion, mental status change, or similar were recorded in physician notes. Admission and discharge orders were reviewed for classes of medications cited in Beers criteria as potentially inappropriate medications for older adults.17 For this study, these high‐risk medications included benzodiazepines, diphenhydramine, propoxyphene, hypnotics, anticholingeric/antidopaminergic medications, and tricyclic antidepressants. Patients' medical charts were reviewed for adverse events such as falls and development of pressure sores or use of restraints. A patient was recorded as having a urinary tract infection (UTI) if a physician documented a UTI in the medical record at any time during hospitalization.
Statistical Analysis
Descriptive statistics were generated using SPSS version 12.0. For continuous measures, values were dichotomized for analytic purposes using standard cutoff scores. Fisher's exact test was used to compare the UTI rate of patients who received a Foley catheter with that of those who did not.
A P value < .05 was considered statistically significant.
RESULTS
Sample Characteristics
Descriptive characteristics for the population are summarized in Table 1. The mean age of the patients was 79.2 5.5 years. The sample was predominantly female and white and had an average stay of 7 days on the cardiac ward. Most patients were admitted for management of heart failure, an arrhythmia, acute myocardial infarction, or angina. Twelve patients had a history of cardiovascular disease (CVD) but were admitted for a noncardiovascular complaint. Only 4 patients did not have a history of CVD.
| Patient characteristic | |
|---|---|
| |
| Age, years (mean SD) | 79.2 5.5 |
| Sex (% female) | 61% |
| Race (% white) | 68% |
| Percent admitted to cardiac ward from: | |
| Home | 69% |
| Outside hospital | 21% |
| Nursing home/skilled nursing facility | 8% |
| ICU | 2% |
| Discharged home from cardiac ward (%) | 84% |
| Length of hospital stay (days), mean SD | 7.4 5.9 |
| Length of cardiac ward stay (days), mean SD | 7.0 5.5 |
| Died during hospitalization (%) | 3% |
| Admitting diagnoses as determined by ICD9 codes (%) | |
| Heart failure | 23% |
| Arrhythmia | 19% |
| Acute myocardial infarction | 10% |
| Chest pain/stable or unstable angina | 10% |
| Coronary artery disease | 9% |
| Syncope | 6% |
| Other cardiovascular diagnoses* | 7% |
| Noncardiovascular diagnoses in patients with history of CVD | 12% |
| Noncardiovascular diagnoses in patients without history of CVD | 4% |
| Comorbidities (%) | |
| Hypertension | 83% |
| Coronary artery disease | 67% |
| History of CABG and/or percutaneous intervention | 54% |
| Hyperlipidemia | 53% |
| Atrial fibrillation | 50% |
| Heart failure | 46% |
| Myocardial infarction | 38% |
| Diabetes mellitus | 37% |
| Chronic renal insufficiency | 29% |
| Stroke or transient ischemic attack | 25% |
| Chronic obstructive pulmonary disease | 23% |
Functional Status and Geriatric Syndromes
Forty‐one percent of patients had a history of 2 or more geriatric syndromes, as documented in their medical record (Table 2). Thirty‐five percent of patients were dependent in at least 1 basic ADL, and 85% had a VES score that indicated an increased risk of functional decline and mortality over the next 2 years. Only 6% of all patients had dementia and only 9% had delirium documented by their physicians in the medical record. Abnormal cognition as detected by screening tests was prevalent. Screening showed that 19% of the patients who completed the SBT and 59% of those who completed the CCT had cognitive impairment. Only 14% of patients with an abnormal CCT and 42% with an abnormal SBT had dementia and/or delirium documented in their hospital chart.
| |
| Katz Index of Basic Activities of Daily Living* (n = 100) | |
| Mean score SD (range 0‐18) | 17.0 1.9 |
| Dependent in 1 ADL (%) | 35% |
| Dependent in 2 ADLs (%) | 20% |
| Vulnerable Elders Survey (n = 100) | |
| Mean score SD (range 0‐10) | 4.6 3.0 |
| Patients with score 3 (%) | 85% |
| Abnormal geriatric screens (%) | |
| Short Blessed Test score 9 (n = 98) | 19% |
| Clock Construction Test score 4 (n = 95) | 59% |
| Geriatric Depression Scale score‖ 6 (n = 99) | 7% |
| Geriatric syndromes documented in cardiology physician notes (%) | |
| Polypharmacy | 95% |
| Depression | 18% |
| History of a prior fall | 17% |
| Delirium | 9% |
| Dementia | 6% |
| Other | 21% |
| Patients with 2 geriatric syndromes | 41% |
| Polypharmacy | |
| Routine medications (range 0‐17) on admission, (n = 100), mean SD | 8.2 3.2 |
| Routine medications (range 3‐17) at discharge, (n = 97), mean SD | 9.0 3.0 |
| Patients taking 12 routine medications on admission (%) | 15% |
| Patients taking 12 routine medications at discharge (%) | 19% |
| Patients with 1 potentially inappropriate medication# ordered on admission or discharge, routine or PRN (%) | 37% |
Polypharmacy was also prevalent. Patients had an average of 9 routine discharge medications, with 19% of patients prescribed at least 12 routine medications at discharge. Thirty‐seven percent of patients were prescribed at least 1 high‐risk medication. Of the 6 patients prescribed a tricyclic antidepressant, 3 had a history of atrial fibrillation/flutter, and 4 had a history of coronary artery disease.
Adverse Events
Thirty‐eight of the 100 patients in the study received a Foley catheter during hospitalization (Table 3). These patients were significantly more likely to have a UTI during their hospitalization than those who did not have a catheter placed (risk ratio 6.0, 95% CI 1.8‐20, P = .002). Other adverse events were rare. Three patients experienced a fall while hospitalized, and 1 patient was restrained (soft limb restraint applied to left upper extremity).
| Developed a UTI (n) | Did not develop a UTI (n) | Risk ratio* (95% confidence interval) | |
|---|---|---|---|
| |||
| Received a Foley | |||
| Yes | 11 | 27 | 6.0 (1.8‐20) |
| No | 3 | 59 | P = .002 (Fisher's exact test) |
DISCUSSION
The goal of this pilot study was to determine the prevalence of geriatric syndromes and the incidence of selected adverse events in hospitalized older patients with cardiovascular disease. We are unaware of another study documenting these syndromes specifically in hospitalized elderly patients with cardiovascular disease. We found that geriatric syndromes were prevalent in this patient population and often unrecognized by physicians. In 1 study of hospitalized frail elderly cardiovascular patients with long hospital stays, physician failure to recognize poor functional status on admission was an independent predictor of patients experiencing a preventable iatrogenic event.7 Brown et al. documented the prevalence and impact of poor mobility in hospitalized adults aged 70 and older. In this study, low mobility was associated with increased risk of further decline in ADL performance, institutionalization, and death; however, it was common for these patients to have bed rest orders (33%), usually without medical indication (60%), indicating underrecognition of functional impairment by attending physicians.18 The proportion of our patients with dependence in at least 1 ADL (35%) and/or at increased risk of functional decline and death based on VES scores (85%) indicates that our patients were already experiencing significant disability at the time of admission, yet these disabilities were rarely documented in the medical record.
In addition to physical frailty, elderly patients with cardiovascular disease may be at increased risk of cognitive impairment. The ongoing Cognitive and Emotional Health Project survey of 36 large cohort studies noted shared risk factors for cardiovascular disease and cognitive impairment in older adults.19 In our study abnormal scores were found for 19% and 59% of the patients who completed the SBT and the CCT, respectively. Several factors may explain the difference in the proportion of patients scoring abnormally on these 2 cognitive screens. We did not measure the visual acuity of our participants, so the number of patients with an abnormal CCT (which relies more on visual cues than the SBT does) may overrepresent the true prevalence of cognitive impairment in our sample. Also, the CCT is a more sensitive indicator of impairments in the visuospatial and executive function domains of cognition than is the SBT and is more likely to be abnormal in vascular dementia.20 Thus, differences in the SBT and CCT scores in our sample may also reflect a higher proportion of patients with a vascular component to their dementia. However, even the number of patients with an abnormal SBT score likely underrepresents the prevalence of underlying cognitive impairment in this sample because of selection bias introduced in obtaining informed consent (ie, the most cognitively impaired patients and/or those deemed to not have decision‐making capacity were excluded or were more likely to decline participation in this study). Consistent with the results of studies of other inpatient populations, cognitive impairment (dementia and/or delirium) was documented in our patients' medical charts far less frequently than detected by either cognitive screen.5, 21 Patients with unrecognized dementia are at increased risk for incident delirium during hospitalization.6
Another common geriatric syndrome in patients with cardiovascular disease is polypharmacy. According to current guidelines, heart failure and coronary artery disease each require multiple medications for optimal therapy. Our patient population were prescribed an average of 9 routine medications at discharge, with nearly 20% prescribed 12 or more routine medications (in addition to as‐needed medications). In comparison, a cohort of hospitalized elderly oncology patients were prescribed an average of 6 routine medications at discharge.22 Thirty‐seven percent of the patients in our study had at least 1 potentially inappropriate medication ordered on admission or at discharge. Although this study was not able to monitor prospectively for adverse drug events, the potential for harm from drug prescribing is substantial in this sample of frail older adult patients. This remains a fruitful area for research.
Thirty‐eight percent of patients in our study received a Foley catheter and were therefore at increased risk of developing a UTI. We did not document the indications for catheterization in this patient population. Studies indicate that up to 20% of urinary catheters are placed without a specific medical indication23 and that hospitalized older adults receiving unwarranted urinary catheterization are at increased risk of prolonged length of stay and death.24
Interventions that increase recognition of geriatric syndromes have been shown to improve the outcomes of hospitalized older adults. The Hospital Elder Life Program demonstrated a 40% reduction in hospital‐acquired delirium in patients aged 70 and older by enhancing recognition and management of geriatric syndromes such as cognitive impairment, immobility, visual/hearing impairment, and polypharmacy.6, 8 Other studies have demonstrated that use of inappropriate medications in hospitalized older adults can be reduced with nonpharmacologic and physician‐education interventions.25, 26 In a broader effort to address multiple geriatric syndromes simultaneously, Acute Care for Elders (ACE) Units have been developed in medical centers worldwide. The ACE Unit model of care emphasizes patient‐centered care, nurse‐driven prevention protocols, frequent interdisciplinary team rounds addressing geriatric syndromes, and discharge planning beginning the day of admission. Studies evaluating outcomes in patients admitted to an ACE Unit have found preservation of physical functioning and independence in ADLs,27, 28 reduced LOS,21 improved patient and provider satisfaction,29 and reduced rates of restraint use,29, 30 institutionalization,27, 29 and mortality.31 This model should be considered for older adults admitted to a cardiac ward. However, other care models could include utilization of inpatient geriatric consultation, hiring a gerontological nurse specialist, or educational programs focused on recognizing and managing geriatric syndromes and designed for the physicians and nurses who care for these patients.
Our study had several limitations. The sample size and number of serious adverse outcomes were small. We did not have adequate power to detect clinically significant differences in length of stay between patients with and without selected geriatric syndromes (0.5 days). The process of informed consent likely selected for a greater number of cognitively intact and fewer depressed patients. The results of the ADL screens may be limited because they were mostly based on patient self‐report of functional status without informant corroboration. Specifically, self‐report may overestimate functional status.
Despite these limitations, we found that functional dependence and geriatric syndromes were prevalent in older cardiovascular patients and that these conditions were rarely documented by the attending physicians or house staff. Over the next decades, an increasing proportion of older adults will be admitted and cared for by hospitalist physicians. Interventions utilizing comprehensive geriatric assessments and interdisciplinary models of care could assist hospitalists in recognizing and managing geriatric syndromes in their frail elderly patients. Future studies are needed to confirm the prevalence of geriatric syndromes and to evaluate the impact of an interdisciplinary model of care on clinical outcomes in hospitalized elderly cardiovascular patients.
Acknowledgements
The authors thank Valerie Emory for her invaluable assistance in collecting data for this study.
Utilizing hospitalist physicians as the primary providers of inpatient care is a rapidly growing trend. In the United States the number of hospitalists now approaches 12,000 and may reach 30,000 by 2010.1 Simultaneously, by 2030 the proportion of adults aged 65 and older will have more than doubled to make up 20% of the U.S. population. Currently, patients aged 65 and older account for approximately 49% of hospital days.2 Congestive heart failure is the most common discharge diagnosis and cardiovascular disease is the leading cause of death of these older adults.3 Given current trends in aging demographics, hospitalists can expect an increasing proportion of their practices to consist of frail older adults with cardiovascular disease.
Hospitalization for any acute illness predisposes elderly patients to increased disability.4 Studies have demonstrated that underrecognition of geriatric syndromes is common and contributes to hospitalized older adults having poor outcomes.5, 6, 7 Between 35% and 50% of elderly patients will experience functional decline while hospitalized,4, 8 and up to 50% will develop hospital‐acquired delirium.6 The risk of experiencing an iatrogenic event while hospitalized is 2‐fold higher for older adults than for those younger than age 65.7, 9 These adverse outcomes lead to longer length of stay (LOS), higher hospital costs, and, for patients able to live at home prior to admission, increased risk of temporary or permanent institutionalization.10, 11
The objective of this study was to characterize a population of acutely ill older adults with known cardiovascular disease admitted to a specialty cardiac ward, to determine the prevalence of geriatric syndromes (ie, functional impairment, cognitive impairment, depression, polypharmacy), and to record the incidence of hospital‐acquired adverse events (urinary tract infection, falls, use of restraints). We hypothesized that these syndromes would be prevalent and underrecognized by the patients' physicians.
METHODS
At Barnes‐Jewish Hospital, an academic medical center in St. Louis, Missouri, patients hospitalized for an acute cardiovascular disorder are preferentially admitted to a cardiac ward with a cardiologist as the attending physician. We conducted a prospective cohort study of 100 patients aged 70 and older admitted to the cardiac ward between January and December of 2003. Participation in the study was not offered to patients who were nonverbal, non‐English‐speaking, or unavailable for screening because of being hospitalized on weekends, holidays, or other days when the research nurse was not available. Participants provided written informed consent. If a patient did not demonstrate an understanding of his or her role in the study, a surrogate decision maker was identified who provided consent in addition to the patient's assent. If a surrogate decision maker was not present, the patient was not enrolled in the study. In addition, patients could decline to continue participating in the study at any time. The institutional review board of the Human Studies Committee at Washington University School of Medicine approved this study.
Data Collection
A trained research nurse administered the following geriatric screening questionnaires: (1) the Katz Index of basic activities of daily living (ADLs)12; (2) the Vulnerable Elders Survey (VES)13; (3) the Short Blessed Test of Orientation, Memory, and Concentration (SBT)14; (4) the Clock Completion Test (CCT)15; and (5) the 15‐item Yesavage Geriatric Depression Scale (GDS).16 The Katz Index (score range 6‐18) assesses the performance of 6 basic ADLs (bathing, continence, dressing, feeding, toileting, and transferring) based on a report by the patient or a collateral source about the patient's level of dependence. Performance of each activity is rated on a scale from 1 (completely dependent) to 3 (completely independent). For this study, patients were considered dependent in any activity if the performance score was less than 3. The Vulnerable Elders Survey (score range 0‐10) utilizes patient age and self‐reported health and functional status to identify frail older adults. A VES score of 3 or greater correlates with a 4‐fold increased risk of death or functional decline over a 2‐year period. Cognition was assessed with the Short Blessed Test of Orientation, Memory, and Concentration and the Clock Completion Test. The Short Blessed Test score ranges from 0 to 28, with a score of 9 or greater indicating increasing severity of cognitive impairment. The Clock Completion Test is scored by evaluating whether the digits in the 4 quadrants of a predrawn circle are accurately placed. The CCT score can range from 0 to 7, with a score of 4 or more indicating cognitive impairment. The 15‐item Geriatric Depression Scale was administered to screen for depressive symptoms. The GDS score can range from 0 to 15, with a score of 6 or more indicating increasing severity of depressive symptoms.
Demographic, psychosocial, and medical data were abstracted by review of patients' hospital records (A.R., C.L.). Medical data obtained from the medical charts included medical diagnoses, number and classes of medications prescribed, and physician documentation of prior or newly diagnosed geriatric syndromes. These geriatric syndromes included dementia, delirium, depression, falls, malnutrition/weight loss, pressure sores, osteoporosis and/or hip fracture, urinary incontinence, and polypharmacy (4 routine medications). A patient was recorded as having documented dementia and/or delirium if the terms dementia, memory loss, cognitive impairment, delirium/delirious, confusion, mental status change, or similar were recorded in physician notes. Admission and discharge orders were reviewed for classes of medications cited in Beers criteria as potentially inappropriate medications for older adults.17 For this study, these high‐risk medications included benzodiazepines, diphenhydramine, propoxyphene, hypnotics, anticholingeric/antidopaminergic medications, and tricyclic antidepressants. Patients' medical charts were reviewed for adverse events such as falls and development of pressure sores or use of restraints. A patient was recorded as having a urinary tract infection (UTI) if a physician documented a UTI in the medical record at any time during hospitalization.
Statistical Analysis
Descriptive statistics were generated using SPSS version 12.0. For continuous measures, values were dichotomized for analytic purposes using standard cutoff scores. Fisher's exact test was used to compare the UTI rate of patients who received a Foley catheter with that of those who did not.
A P value < .05 was considered statistically significant.
RESULTS
Sample Characteristics
Descriptive characteristics for the population are summarized in Table 1. The mean age of the patients was 79.2 5.5 years. The sample was predominantly female and white and had an average stay of 7 days on the cardiac ward. Most patients were admitted for management of heart failure, an arrhythmia, acute myocardial infarction, or angina. Twelve patients had a history of cardiovascular disease (CVD) but were admitted for a noncardiovascular complaint. Only 4 patients did not have a history of CVD.
| Patient characteristic | |
|---|---|
| |
| Age, years (mean SD) | 79.2 5.5 |
| Sex (% female) | 61% |
| Race (% white) | 68% |
| Percent admitted to cardiac ward from: | |
| Home | 69% |
| Outside hospital | 21% |
| Nursing home/skilled nursing facility | 8% |
| ICU | 2% |
| Discharged home from cardiac ward (%) | 84% |
| Length of hospital stay (days), mean SD | 7.4 5.9 |
| Length of cardiac ward stay (days), mean SD | 7.0 5.5 |
| Died during hospitalization (%) | 3% |
| Admitting diagnoses as determined by ICD9 codes (%) | |
| Heart failure | 23% |
| Arrhythmia | 19% |
| Acute myocardial infarction | 10% |
| Chest pain/stable or unstable angina | 10% |
| Coronary artery disease | 9% |
| Syncope | 6% |
| Other cardiovascular diagnoses* | 7% |
| Noncardiovascular diagnoses in patients with history of CVD | 12% |
| Noncardiovascular diagnoses in patients without history of CVD | 4% |
| Comorbidities (%) | |
| Hypertension | 83% |
| Coronary artery disease | 67% |
| History of CABG and/or percutaneous intervention | 54% |
| Hyperlipidemia | 53% |
| Atrial fibrillation | 50% |
| Heart failure | 46% |
| Myocardial infarction | 38% |
| Diabetes mellitus | 37% |
| Chronic renal insufficiency | 29% |
| Stroke or transient ischemic attack | 25% |
| Chronic obstructive pulmonary disease | 23% |
Functional Status and Geriatric Syndromes
Forty‐one percent of patients had a history of 2 or more geriatric syndromes, as documented in their medical record (Table 2). Thirty‐five percent of patients were dependent in at least 1 basic ADL, and 85% had a VES score that indicated an increased risk of functional decline and mortality over the next 2 years. Only 6% of all patients had dementia and only 9% had delirium documented by their physicians in the medical record. Abnormal cognition as detected by screening tests was prevalent. Screening showed that 19% of the patients who completed the SBT and 59% of those who completed the CCT had cognitive impairment. Only 14% of patients with an abnormal CCT and 42% with an abnormal SBT had dementia and/or delirium documented in their hospital chart.
| |
| Katz Index of Basic Activities of Daily Living* (n = 100) | |
| Mean score SD (range 0‐18) | 17.0 1.9 |
| Dependent in 1 ADL (%) | 35% |
| Dependent in 2 ADLs (%) | 20% |
| Vulnerable Elders Survey (n = 100) | |
| Mean score SD (range 0‐10) | 4.6 3.0 |
| Patients with score 3 (%) | 85% |
| Abnormal geriatric screens (%) | |
| Short Blessed Test score 9 (n = 98) | 19% |
| Clock Construction Test score 4 (n = 95) | 59% |
| Geriatric Depression Scale score‖ 6 (n = 99) | 7% |
| Geriatric syndromes documented in cardiology physician notes (%) | |
| Polypharmacy | 95% |
| Depression | 18% |
| History of a prior fall | 17% |
| Delirium | 9% |
| Dementia | 6% |
| Other | 21% |
| Patients with 2 geriatric syndromes | 41% |
| Polypharmacy | |
| Routine medications (range 0‐17) on admission, (n = 100), mean SD | 8.2 3.2 |
| Routine medications (range 3‐17) at discharge, (n = 97), mean SD | 9.0 3.0 |
| Patients taking 12 routine medications on admission (%) | 15% |
| Patients taking 12 routine medications at discharge (%) | 19% |
| Patients with 1 potentially inappropriate medication# ordered on admission or discharge, routine or PRN (%) | 37% |
Polypharmacy was also prevalent. Patients had an average of 9 routine discharge medications, with 19% of patients prescribed at least 12 routine medications at discharge. Thirty‐seven percent of patients were prescribed at least 1 high‐risk medication. Of the 6 patients prescribed a tricyclic antidepressant, 3 had a history of atrial fibrillation/flutter, and 4 had a history of coronary artery disease.
Adverse Events
Thirty‐eight of the 100 patients in the study received a Foley catheter during hospitalization (Table 3). These patients were significantly more likely to have a UTI during their hospitalization than those who did not have a catheter placed (risk ratio 6.0, 95% CI 1.8‐20, P = .002). Other adverse events were rare. Three patients experienced a fall while hospitalized, and 1 patient was restrained (soft limb restraint applied to left upper extremity).
| Developed a UTI (n) | Did not develop a UTI (n) | Risk ratio* (95% confidence interval) | |
|---|---|---|---|
| |||
| Received a Foley | |||
| Yes | 11 | 27 | 6.0 (1.8‐20) |
| No | 3 | 59 | P = .002 (Fisher's exact test) |
DISCUSSION
The goal of this pilot study was to determine the prevalence of geriatric syndromes and the incidence of selected adverse events in hospitalized older patients with cardiovascular disease. We are unaware of another study documenting these syndromes specifically in hospitalized elderly patients with cardiovascular disease. We found that geriatric syndromes were prevalent in this patient population and often unrecognized by physicians. In 1 study of hospitalized frail elderly cardiovascular patients with long hospital stays, physician failure to recognize poor functional status on admission was an independent predictor of patients experiencing a preventable iatrogenic event.7 Brown et al. documented the prevalence and impact of poor mobility in hospitalized adults aged 70 and older. In this study, low mobility was associated with increased risk of further decline in ADL performance, institutionalization, and death; however, it was common for these patients to have bed rest orders (33%), usually without medical indication (60%), indicating underrecognition of functional impairment by attending physicians.18 The proportion of our patients with dependence in at least 1 ADL (35%) and/or at increased risk of functional decline and death based on VES scores (85%) indicates that our patients were already experiencing significant disability at the time of admission, yet these disabilities were rarely documented in the medical record.
In addition to physical frailty, elderly patients with cardiovascular disease may be at increased risk of cognitive impairment. The ongoing Cognitive and Emotional Health Project survey of 36 large cohort studies noted shared risk factors for cardiovascular disease and cognitive impairment in older adults.19 In our study abnormal scores were found for 19% and 59% of the patients who completed the SBT and the CCT, respectively. Several factors may explain the difference in the proportion of patients scoring abnormally on these 2 cognitive screens. We did not measure the visual acuity of our participants, so the number of patients with an abnormal CCT (which relies more on visual cues than the SBT does) may overrepresent the true prevalence of cognitive impairment in our sample. Also, the CCT is a more sensitive indicator of impairments in the visuospatial and executive function domains of cognition than is the SBT and is more likely to be abnormal in vascular dementia.20 Thus, differences in the SBT and CCT scores in our sample may also reflect a higher proportion of patients with a vascular component to their dementia. However, even the number of patients with an abnormal SBT score likely underrepresents the prevalence of underlying cognitive impairment in this sample because of selection bias introduced in obtaining informed consent (ie, the most cognitively impaired patients and/or those deemed to not have decision‐making capacity were excluded or were more likely to decline participation in this study). Consistent with the results of studies of other inpatient populations, cognitive impairment (dementia and/or delirium) was documented in our patients' medical charts far less frequently than detected by either cognitive screen.5, 21 Patients with unrecognized dementia are at increased risk for incident delirium during hospitalization.6
Another common geriatric syndrome in patients with cardiovascular disease is polypharmacy. According to current guidelines, heart failure and coronary artery disease each require multiple medications for optimal therapy. Our patient population were prescribed an average of 9 routine medications at discharge, with nearly 20% prescribed 12 or more routine medications (in addition to as‐needed medications). In comparison, a cohort of hospitalized elderly oncology patients were prescribed an average of 6 routine medications at discharge.22 Thirty‐seven percent of the patients in our study had at least 1 potentially inappropriate medication ordered on admission or at discharge. Although this study was not able to monitor prospectively for adverse drug events, the potential for harm from drug prescribing is substantial in this sample of frail older adult patients. This remains a fruitful area for research.
Thirty‐eight percent of patients in our study received a Foley catheter and were therefore at increased risk of developing a UTI. We did not document the indications for catheterization in this patient population. Studies indicate that up to 20% of urinary catheters are placed without a specific medical indication23 and that hospitalized older adults receiving unwarranted urinary catheterization are at increased risk of prolonged length of stay and death.24
Interventions that increase recognition of geriatric syndromes have been shown to improve the outcomes of hospitalized older adults. The Hospital Elder Life Program demonstrated a 40% reduction in hospital‐acquired delirium in patients aged 70 and older by enhancing recognition and management of geriatric syndromes such as cognitive impairment, immobility, visual/hearing impairment, and polypharmacy.6, 8 Other studies have demonstrated that use of inappropriate medications in hospitalized older adults can be reduced with nonpharmacologic and physician‐education interventions.25, 26 In a broader effort to address multiple geriatric syndromes simultaneously, Acute Care for Elders (ACE) Units have been developed in medical centers worldwide. The ACE Unit model of care emphasizes patient‐centered care, nurse‐driven prevention protocols, frequent interdisciplinary team rounds addressing geriatric syndromes, and discharge planning beginning the day of admission. Studies evaluating outcomes in patients admitted to an ACE Unit have found preservation of physical functioning and independence in ADLs,27, 28 reduced LOS,21 improved patient and provider satisfaction,29 and reduced rates of restraint use,29, 30 institutionalization,27, 29 and mortality.31 This model should be considered for older adults admitted to a cardiac ward. However, other care models could include utilization of inpatient geriatric consultation, hiring a gerontological nurse specialist, or educational programs focused on recognizing and managing geriatric syndromes and designed for the physicians and nurses who care for these patients.
Our study had several limitations. The sample size and number of serious adverse outcomes were small. We did not have adequate power to detect clinically significant differences in length of stay between patients with and without selected geriatric syndromes (0.5 days). The process of informed consent likely selected for a greater number of cognitively intact and fewer depressed patients. The results of the ADL screens may be limited because they were mostly based on patient self‐report of functional status without informant corroboration. Specifically, self‐report may overestimate functional status.
Despite these limitations, we found that functional dependence and geriatric syndromes were prevalent in older cardiovascular patients and that these conditions were rarely documented by the attending physicians or house staff. Over the next decades, an increasing proportion of older adults will be admitted and cared for by hospitalist physicians. Interventions utilizing comprehensive geriatric assessments and interdisciplinary models of care could assist hospitalists in recognizing and managing geriatric syndromes in their frail elderly patients. Future studies are needed to confirm the prevalence of geriatric syndromes and to evaluate the impact of an interdisciplinary model of care on clinical outcomes in hospitalized elderly cardiovascular patients.
Acknowledgements
The authors thank Valerie Emory for her invaluable assistance in collecting data for this study.
- ,.The expanding role of hospitalists in the United States.Swiss Med Wkly.2006;136:591–596.
- American Association of Retired Persons and the Administration on Aging.A Profile of Older Americans: 1999.Washington, DC:American Association of Retired Persons;1999.
- Federal Interagency Forum on Aging Related Statistics. Older Americans 2004: key indicators of well‐being. Available at: http://www.agingstats.gov
- ,,,.Hospitalization, restricted activity, and the development of disability among older persons.JAMA.2004;292:2115–2124.
- ,,,.Cognitively impaired older adults: From hospital to home.Am J Nurs.2005;105:52–61.
- .Prevention of delirium in hospitalized older patients: risk factors and targeted intervention strategies.Ann Med.2000;32:257–263.
- ,,, et al.Iatrogenic complications in high‐risk, elderly patients.Arch Intern Med.1992;152:2074–2080.
- ,,,,.The hospital elder life program: A model of care to prevent cognitive and functional decline in older hospitalized patients.J Am Geriatr Soc.2000;48:1697–1706.
- ,.Incidence and types of preventable adverse events in elderly patients: population based review of medical records.BMJ.2000;320:741–744.
- ,Landefeld S: Improving care for hospitalized elders.Ann Long Term Care: Clin Care Aging.2001;9:35–40.
- :Acute hospital care of the elderly: minimizing the risk of functional decline.Cleve Clin J Med.1995;62:117–128.
- ,,,,.Studies of illness in the aged: the index of ADL: a standardized measure of biological and psychosocial function.JAMA.1963;185:914–919.
- ,,, et al.The Vulnerable Elders Survey: a tool for identifying vulnerable older people in the community.J Am Geriatr Soc.2001;49:1691–1699.
- ,,,,,.Validation of a short orientation memory‐concentration test of cognitive impairment.Am J Psychiatry.1983;140:734–739.
- ,,.Clock completion: an objective screening test for dementia.J Am Geriatr Soc.1993;41:1235–1240.
- .Geriatric depression scale.Psychopharmacol Bull.1988;24:709–711.
- ,,,,,.Updating the Beers Criteria for potentially inappropriate medication use in older adults.Arch Intern Med.2003;163:2716–2724.
- ,,.Prevalence and outcomes of low mobility in hospitalized older patients.J Am Geriatr Soc.2004;52:1263–1270.
- ,,, et al.The NIH cognitive and emotional health project: Report of the critical evaluation study committee.Alzheimers Dement.2006;2:12–32.
- ,,,.Can clock drawing test help to differentiate between dementia of the Alzheimer's type and vascular dementia? A preliminary study.Int J Geriatr Psychiatry.2002;17:699–703.
- ,,, et al.Geriatric‐based versus general wards for older acute medical patients: a randomized comparison of outcomes and use of resources.J Am Geriatr Soc.2000;48:1381–1388.
- ,,,,,.Geriatric syndromes in elderly patients admitted to an oncology‐acute care for elders unit.J Clin Oncol.2006;24:2298–2303.
- ,,,.Overuse of the indwelling urinary tract catheter in hospitalized medical patients.Arch Intern Med.1995;155:1425–1429.
- ,,, et al.The relationship of indwelling urinary catheters to death, length of hospital stay, functional decline, and nursing home admission in hospitalized older medical patients.J Am Geriatr Soc.2007;55:227–233.
- ,,,.A strategy to decrease the use of risky drugs in the elderly.Cleve Clin J Med.2004;71:561–568.
- ,,,,,.A multifactorial intervention to reduce prevalence of delirium and shorten hospital length of stay.J Am Geriatr Soc.2005;53:18–23.
- ,,,,.A randomized trial of care in a hospital medical unit especially designed to improve the functional outcomes of acutely ill older patients.N Engl J Med.1995;332:1338–1344.
- ,,, et al.A controlled trial of inpatient and outpatient geriatric evaluation and management.N Engl J Med.2002;346:905–912.
- ,,, et al.Effects of a multicomponent intervention on functional outcomes and process of care in hospitalized older patients: A randomized controlled trial of Acute Care for Elders (ACE) in a community hospital.J Am Geriatr Soc.2000;48:1572–1581.
- ,,,,,.A model for managing delirious older inpatients.J Am Geriatr Soc.2003;51:1031–1035.
- ,,,,.Reduced mortality in treating acutely sick, frail older patients in a geriatric evaluation and management unit. A prospective randomized trial.J Am Geriatr Soc.2002;50:792–798.
- ,.The expanding role of hospitalists in the United States.Swiss Med Wkly.2006;136:591–596.
- American Association of Retired Persons and the Administration on Aging.A Profile of Older Americans: 1999.Washington, DC:American Association of Retired Persons;1999.
- Federal Interagency Forum on Aging Related Statistics. Older Americans 2004: key indicators of well‐being. Available at: http://www.agingstats.gov
- ,,,.Hospitalization, restricted activity, and the development of disability among older persons.JAMA.2004;292:2115–2124.
- ,,,.Cognitively impaired older adults: From hospital to home.Am J Nurs.2005;105:52–61.
- .Prevention of delirium in hospitalized older patients: risk factors and targeted intervention strategies.Ann Med.2000;32:257–263.
- ,,, et al.Iatrogenic complications in high‐risk, elderly patients.Arch Intern Med.1992;152:2074–2080.
- ,,,,.The hospital elder life program: A model of care to prevent cognitive and functional decline in older hospitalized patients.J Am Geriatr Soc.2000;48:1697–1706.
- ,.Incidence and types of preventable adverse events in elderly patients: population based review of medical records.BMJ.2000;320:741–744.
- ,Landefeld S: Improving care for hospitalized elders.Ann Long Term Care: Clin Care Aging.2001;9:35–40.
- :Acute hospital care of the elderly: minimizing the risk of functional decline.Cleve Clin J Med.1995;62:117–128.
- ,,,,.Studies of illness in the aged: the index of ADL: a standardized measure of biological and psychosocial function.JAMA.1963;185:914–919.
- ,,, et al.The Vulnerable Elders Survey: a tool for identifying vulnerable older people in the community.J Am Geriatr Soc.2001;49:1691–1699.
- ,,,,,.Validation of a short orientation memory‐concentration test of cognitive impairment.Am J Psychiatry.1983;140:734–739.
- ,,.Clock completion: an objective screening test for dementia.J Am Geriatr Soc.1993;41:1235–1240.
- .Geriatric depression scale.Psychopharmacol Bull.1988;24:709–711.
- ,,,,,.Updating the Beers Criteria for potentially inappropriate medication use in older adults.Arch Intern Med.2003;163:2716–2724.
- ,,.Prevalence and outcomes of low mobility in hospitalized older patients.J Am Geriatr Soc.2004;52:1263–1270.
- ,,, et al.The NIH cognitive and emotional health project: Report of the critical evaluation study committee.Alzheimers Dement.2006;2:12–32.
- ,,,.Can clock drawing test help to differentiate between dementia of the Alzheimer's type and vascular dementia? A preliminary study.Int J Geriatr Psychiatry.2002;17:699–703.
- ,,, et al.Geriatric‐based versus general wards for older acute medical patients: a randomized comparison of outcomes and use of resources.J Am Geriatr Soc.2000;48:1381–1388.
- ,,,,,.Geriatric syndromes in elderly patients admitted to an oncology‐acute care for elders unit.J Clin Oncol.2006;24:2298–2303.
- ,,,.Overuse of the indwelling urinary tract catheter in hospitalized medical patients.Arch Intern Med.1995;155:1425–1429.
- ,,, et al.The relationship of indwelling urinary catheters to death, length of hospital stay, functional decline, and nursing home admission in hospitalized older medical patients.J Am Geriatr Soc.2007;55:227–233.
- ,,,.A strategy to decrease the use of risky drugs in the elderly.Cleve Clin J Med.2004;71:561–568.
- ,,,,,.A multifactorial intervention to reduce prevalence of delirium and shorten hospital length of stay.J Am Geriatr Soc.2005;53:18–23.
- ,,,,.A randomized trial of care in a hospital medical unit especially designed to improve the functional outcomes of acutely ill older patients.N Engl J Med.1995;332:1338–1344.
- ,,, et al.A controlled trial of inpatient and outpatient geriatric evaluation and management.N Engl J Med.2002;346:905–912.
- ,,, et al.Effects of a multicomponent intervention on functional outcomes and process of care in hospitalized older patients: A randomized controlled trial of Acute Care for Elders (ACE) in a community hospital.J Am Geriatr Soc.2000;48:1572–1581.
- ,,,,,.A model for managing delirious older inpatients.J Am Geriatr Soc.2003;51:1031–1035.
- ,,,,.Reduced mortality in treating acutely sick, frail older patients in a geriatric evaluation and management unit. A prospective randomized trial.J Am Geriatr Soc.2002;50:792–798.
Copyright © 2007 Society of Hospital Medicine
Systematic Review of Rapid Response Systems
A medical emergency team1 is a group of clinicians trained to quickly assess and treat hospitalized patients showing acute signs of clinical deterioration. Equivalent terms used are rapid response team,2 critical care outreach team,3 and patient‐at‐risk team.4 A consensus panel5 recently endorsed use of the term rapid response system (RRS) to denote any system that uses a standard set of clinical criteria to summon caregivers to the bedside of a patient who is deemed unstable but not in cardiopulmonary arrest (in which case a standard resuscitation team would be summoned). Such teams primarily evaluate patients on general hospital wards.
RRSs have been developed in response to data indicating that patients frequently demonstrate premonitory signs or receive inadequate care prior to unanticipated intensive care unit (ICU) admission, cardiopulmonary arrest, or death outside the ICU.614 Earlier identification and treatment of such patients could prevent adverse clinical outcomes. The structure of RRSs varies but generally includes a physician and nurse and may also include other staff such as respiratory therapists.5 Teams are summoned by hospital staff to assess patients meeting specific clinical criteria (see box) about whom the bedside staff has significant concern.150
| Any staff member may call the team if 1 of the following criteria is met: |
| Heart rate > 140/min or 40/min |
| Respiratory rate > 28/min or 8/min |
| Systolic blood pressure > 180 mmHg or 90 mm Hg |
| Oxygen saturation 90% despite supplementation |
| Acute change in mental status |
| Urine output 50 cc over 4 hours |
| Staff member has significant concern about patient's condition |
| Additional criteria used at some institutions: |
| Chest pain unrelieved by nitroglycerin |
| Threatened airway |
| Seizure |
| Uncontrolled pain |
Initial studies of RRSs, performed primarily in Australia and the United Kingdom, showed promising reductions in unanticipated ICU admissions, cardiac arrests, and even overall inpatient mortality.1, 16, 17 The considerable enthusiasm generated by these studies18, 19 resulted in the Institute for Healthcare Improvement (IHI) incorporating RRSs into its 100,000 Lives campaign,2 and RRSs are now being implemented in the more than 3000 U.S. hospitals that joined the campaign. However, a recent commentary on rapid response teams20 and a systematic review of critical care outreach teams21 have raised concerns that this widespread implementation may not be justified by the available evidence. We performed a systematic review of studies of all variations of RRSs in order to determine their effect on patient outcomes and to characterize variations in their organization and implementation.
METHODS
Literature Search and Inclusion and Exclusion Criteria
We systematically searched MEDLINE, CINAHL, and BIOSIS through August 2006 for relevant studies using the various terms for RRSs (eg, medical emergency team, rapid response team, critical care outreach) and medical subject headings relevant to inpatient care and critical illness (eg, patient care team and resuscitation; the full search strategy is given in the Appendix). We also reviewed the abstract lists from the 2004 and 2005 American Thoracic Society and Society of Critical Care Medicine annual meetings and scanned reference lists from key articles.
We screened the abstracts of the articles identified by the search, and 2 independent reviewers abstracted potentially relevant articles using a standardized data abstraction form. Disagreements between the reviewers were resolved by consensus and, if necessary, discussion with a third reviewer. We included randomized controlled trials (RCTs), controlled before‐after studies, and interrupted time series, including simple before‐after studies with no contemporaneous control group, though we planned to separately analyze data from controlled studies if possible. We included only English‐language articles.
On the basis of RRS features in widely cited articles2224 and the recommendations of a recent consensus statement,5 we defined an RRS as having the following characteristics: (1) its primary responsibility is to intervene whenever hospitalized patients become unstable before cardiopulmonary arrest occurs; (2) it must primarily provide care outside the ICU and emergency department; (3) specific clinical criteria must be in place that define instability and trigger a call to the team; and (4) it must be expected to respond within a specified time. We defined these criteria in order to distinguish studies of RRSs from studies of cardiac arrest (code blue) teams or traditional consulting services.
To be included in the analysis, articles had to report the effects of a rapid response system on at least 1 of these outcomes: inpatient mortality, inpatient cardiac arrest, or unscheduled ICU transfer. We used the definitions of cardiac arrest and unscheduled ICU transfer given in the primary studies. In addition to these outcomes, we abstracted information on the number of admissions and the number of RRS calls during the study period. To maximize the comparability of study outcomes, we calculated the rates of mortality, cardiac arrest, unscheduled ICU transfer, and RRS calls per 1000 admissions for studies that did not supply data in this fashion.
Assessment of Study Quality
Quality scoring instruments for studies included in systematic reviews generally focus on randomized controlled trials, which we anticipated would account for a minority of included studies. On the basis of recommendations for the assessment of methodology for nonrandomized study designs,25, 26 we identified and abstracted 4 important determinants of internal validity (Table 1). The consensus statement5 recommends monitoring the effectiveness of RRSs by measuring the rate of unscheduled ICU admissions (defined as an unplanned admission to the ICU from a general ward27) and cardiac arrests of patients who were not listed as do not resuscitate (DNR). As the definition of unscheduled ICU admission allows room for subjectivity, we considered the blinding of assessment of this outcome to study group assignment to be important, especially for retrospective studies. Measurement of cardiac arrests should be less susceptible to blinding issues, but one of the functions of an RRS can be to initiate discussions that result in changes in the goals of care and code status.22 Thus, excluding patients made DNR by the team from cardiac arrest calculations could falsely lower the cardiac arrest rate.
| Quality measures |
|---|
|
| A. Internal validity |
| 1. Did the study have a contemporaneous control group? |
| 2. If there was no contemporaneous control group, did the study report data for more than 1 time point before and after the intervention? |
| 3. Were nonobjective primary outcomes (eg, unplanned ICU transfer) measured in a blinded fashion? |
| 4. Were patients made DNR by the RRS included in calculations of the cardiac arrest and mortality rates? |
| B. Generalizability |
| 5. Was the intervention performed independent of other quality improvement interventions targeting the care of critically ill patients? |
| 6. Did the study report the number of admissions and RRS calls during the study period? |
| 7. Did the study report the availability of intensivists before and after the intervention? |
We also abstracted 3 separate elements of study quality pertaining to the external validity or generalizability of included studies (Table 1). These elements were defined a priori by consensus reached by discussion among the reviewers. These elements were intended to provide a framework for interpreting the included studies and to guide subgroup analyses. They were not used to form a composite quality score.
Statistical Analysis
We performed a random‐effects meta‐analysis to calculate summary risk ratios with 95% confidence intervals for the effects of RRSs on inpatient mortality, cardiopulmonary arrest, and unscheduled ICU admission. Included in the meta‐analysis were the studies that reported total number of admissions and incidence of each outcome before and after institution of the RRS. For randomized trials that reported pre‐ and postintervention data, we treated the intervention and control groups as separate trials in order to be able to compare their effects with the before‐after trials. For studies that reported results adjusted for clustering (ie, by hospital), we back‐calculated the unadjusted results by multiplying the standard error by the square of the design factor coefficient.28, 29 We calculated the I2 statistic to assess heterogeneity.30 All analyses were performed using Stata version 8.2 (Stata Corporation, College Station, TX).
RESULTS
The database searches identified 861 citations, and 1 additional prepublication study was supplied by the study's first author31; 89 articles underwent full‐text review (Fig. 1). Most studies excluded during the full‐text review did not meet our criteria for a study of an RRS or were observational studies or review articles. For instance, Sebat et al.32 published a study of a shock team at a community hospital that intervened when any patient suffered nontraumatic shock; the study did not meet our inclusion criteria as all patients were admitted to the ICU, most directly from the emergency department. Another frequently cited study, by Bristow et al.,16 was excluded as it was a case‐control study. Thirteen studies,3, 2224, 31, 334011 full‐length studies and 2 abstractsmet all criteria for inclusion.
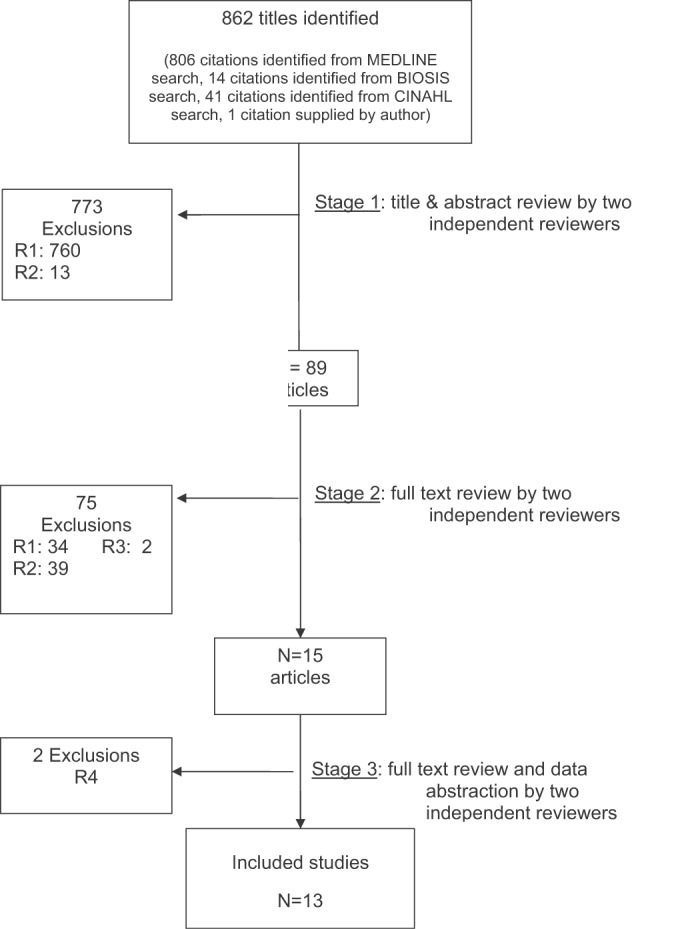
Characteristics of Included Trials
The characteristics of included studies are outlined in Table 2. Five studies were performed in Australia, 4 in the United States, and 4 in the United Kingdom. All were conducted in academic teaching hospitals. Two studies37, 38 focused on pediatric inpatients, and the remainder involved hospitalized adults. The RRS intervened for all hospitalized patients in all but 2 studies (1 of which focused on surgical inpatients33 and the other in which the RRS evaluated only patients discharged from the ICU3). In 2 studies,31, 39 the RRS was available to evaluate outpatients, such as hospital visitors, in addition to inpatients.0
| Study | Location | Hospital type | Patient population | RRS composition | Measured outcomes | Definition of unscheduled ICU admission | Definition of cardiac arrest |
|---|---|---|---|---|---|---|---|
| |||||||
| Buist et al., 200220 | Australia | Tertiary‐care academic hospital | Adult inpatients | ICU registrar | DNR status | Not supplied | Any code blue team activation |
| Medical registrar | Cardiac arrest | ||||||
| ICU nurse | Unscheduled ICU admission | ||||||
| Mortality | |||||||
| Bellomo et al., 200321 | Australia | Tertiary‐care academic hospital | Adult inpatients | ICU nurse and ICU fellow attended all calls; ICU attending (8 AM‐8 PM) and medical registrar attended if requested | Mortality | NA | Unresponsive, with no pulse or blood pressure, and basic life support initiated |
| Cardiac arrest | |||||||
| DNR status | |||||||
| Pittard et al., 200322 | United Kingdom | Tertiary‐care academic hospital | Adult inpatients on surgical wards | Senior critical care nurses and medical staff | Unscheduled ICU admission | Any patient not admitted directly from operating theater after elective surgery | NA |
| Bellomo et al., 200431 | Australia | Tertiary‐care academic hospital | Adult postoperative patients | ICU attending | Mortality Unscheduled ICU admission ICU length of stay DNR status | Postoperative admission to ICU because of a clinical complication | NA |
| ICU fellow | Unscheduled ICU admission | ||||||
| ICU registered nurse | ICU length of stay | ||||||
| Medical fellow | DNR status | ||||||
| DeVita et al., 200432 | United States | Tertiary‐care academic hospital | Adult inpatients | ICU physician | Cardiac arrest | NA | Any code blue team activation |
| Anesthesiologist | |||||||
| 2 other physicians | |||||||
| 2 ICU nurses | |||||||
| Floor nurse | |||||||
| Respiratory therapist | |||||||
| Garcea et al., 20043 | United Kingdom | Teaching hospital | Adult patients discharged from ICU | 2 ICU nurses | Mortality | Emergency readmissions to ICU | NA |
| 1 ICU nurse specialist | Unscheduled ICU admission | ||||||
| ICU consultant physician (if needed) | |||||||
| Kenward et al., 200438 | United Kingdom | Teaching hospital | Adult inpatients | Not stated | Mortality | NA | Loss of spontaneous circulation |
| Cardiac arrest | |||||||
| Priestley et al., 200433 | United Kingdom | Teaching hospital | Adult inpatients | ICU nurse consultant | Mortality | NA | NA |
| ICU physician available if needed | Overall length of stay | ||||||
| Hillman et al., 200534 | Australia | 23 hospitals (17 academic, 6 nonacademic) | Adult inpatients | Varied between study hospitals; required to have at least 1 MD and 1 RN from ED or ICU | Mortality | Any unscheduled admission to ICU from general ward | No palpable pulse |
| Cardiac arrest | |||||||
| Unscheduled ICU admission | |||||||
| DNR status | |||||||
| Hunt et al., 2005 (abstract)36 | United States | Pediatric tertiary‐care academic hospital | Pediatric inpatients | Not provided | Cardiac arrest | NA | Not provided |
| Meredith et al., 2005 (abstract)37 | United States | Tertiary‐care academic hospital | Adult inpatients, outpatients, and visitors | ICU registered nurse | Mortality | NA | Not provided |
| Respiratory therapist | |||||||
| Tibballs et al., 200535 | Australia | Pediatric tertiary‐care academic hospital | Pediatric inpatients | ICU physician | Cardiac arrest | Not supplied | Not provided |
| Medical registrar | Unscheduled ICU admission | ||||||
| ED physician | |||||||
| ICU nurse | |||||||
| King et al., 200629 | United States | Tertiary‐care academic hospital | Adult inpatients, outpatients, and visitors | Hospitalist | Cardiac arrest | NA | Not provided |
| Internal medicine resident | |||||||
| ICU nurse | |||||||
| Ward nurse | |||||||
| Pharmacist | |||||||
RRS Structure, Calling Criteria, and Responsibilities
Seven studies22, 23, 31, 33, 34, 36, 37 that described the team composition used variants of the medical emergency team model, a physician‐led team (Table 2). In 6 of these 7 studies, the team included a critical care physician (attending or fellow) and an ICU nurse; in the sole RCT (the MERIT study36), the team structure varied between hospitals, consisting of a nurse and physician from either the emergency department or ICU. Hospitalists, who are involved in RRS responses at many U.S. hospitals, were primary team leaders of the RRS in only 1 study.31 In 2 studies34, 37 the RRS also responded to code blue calls, and in 4 studies23, 31, 33, 39 the RRS and the code blue team had separate personnel; the remaining studies did not define the distinction between RRS and code blue team.
| Study | Contemporaneous control group | Data reported at more than 1 time before/after intervention | RRS calling rate reported | Outcomes analysis included patients made DNR by team | Blind measurement of nonobjective outcomes | Intensivist always available | Other QI efforts during study |
|---|---|---|---|---|---|---|---|
| |||||||
| Buist et al., 200220 | No | No | Yes | No (mortality) | No | NR | NR |
| Bellomo et al., 200321 | No | No | Yes | Yes (mortality) | NA | Yes (ICU fellow) | No |
| Pittard et al., 200322 | No | No | Yes | NA | No | NR | NR |
| Bellomo et al., 200431 | No | No | Yes | Yes (mortality) | No | Yes (ICU fellow) | No |
| DeVita et al., 200432 | No | Yes | Yes | NA | No | Yes (critical care attending physician) | NR |
| Garcea et al., 200433 | No | No | No | Unclear | No | NR | NR |
| Kenward et al., 200438 | No | No | Yes | Unclear | No | NR | NR |
| Priestley et al., 200433 | No (interrupted time series) | Yes | No | NA | No | NR | NR |
| Hillman et al., 200534 | Yes | No | Yes | Unclear | Yes | NR | No |
| Hunt et al., 2005 (abstract)36 | No | No | Yes | NA | NR | NR | NR |
| Meredith et al., 2005 (abstract)37 | No | No | Yes | No | NA | No | No |
| Tibballs et al., 200535 | No | No | Yes | Unclear | No | NR | Yes (educational workshops/more training in APLS) |
| King et al., 200629 | No | Yes | Yes | NA | No | Yes | No |
In 4 studies the RRSs were led by nurses. One study published in abstract form39 used the rapid response team model, consisting of a critical care nurse and a respiratory therapist, with assistance as needed from the primary medical staff and a critical care physician. Three studies3, 24, 35 from UK hospitals used the critical care outreach (CCO) model, in which ICU‐trained nurses respond initially with assistance from intensivists. The CCO model also involves follow‐up on patients discharged from the ICU and proactive rounding on unstable ward patients.
The hospitals used broadly similar approaches to determining when to summon the RRS, relying on combinations of objective clinical criteria (eg, vital sign abnormalities) and subjective criteria (eg, acute mental status change, staff member concerned about patient's condition). Three studies3, 24, 35 used a formal clinical score (the Patient‐At‐Risk score or the Modified Early Warning score) to trigger calls to the RRS. Three studies, 2 of them from the same institution,23, 33 reported the frequency of specific triggers for RRS activation. Concern by bedside staff and respiratory distress were the most frequent activators of the RRS.
Study Internal Validity and Generalizability
One study,36 the MERIT trial, conducted in Australia, was a cluster‐randomized RCT (randomized by hospital) that adhered to recommended elements of design and reporting for studies of this type.41 In this study, hospitals in the control group received an educational intervention on caring for deteriorating patients only; hospitals in the intervention group received the educational module and started an RRS. An additional study35 identified itself as a randomized trial, but randomization occurred at the hospital ward level, with introduction of the intervention (critical care outreach) staggered so that at different points an individual ward could have been in either the control or intervention group; therefore, this study was considered an interrupted time series. All other trials included were before‐after studies with no contemporaneous control group
Most studies did not meet criteria for internal validity or generalizability (Table 2). Two studies3, 35 did not report the number of RRS calls during the study period. One study22 omitted patients whose resuscitation status was changed after RRS evaluation from the calculation of inpatient mortality; thus, the patients who had been made do not resuscitate by the RRS did not contribute to the calculated mortality rate. The disposition of these patients was unclear in another study.36 All studies measured clinical outcomes retrospectively, and no studies reported blinding of outcomes assessors for nonobjective outcomes (eg, unplanned ICU admission). Studies generally did not report on the availability of intensivists or if other quality improvement interventions targeting critically ill patients were implemented along with the RRS.
RRS Usage and Effects on Patient Outcomes
Seven studies2224, 34, 3638 reported enough information to calculate the RRS calling rate (4 studies24, 31, 39, 40 reported the total number of calls but not the number of admissions, and 2 studies3, 35 did not report either). In these 7 studies, the calling rate varied from 4.5 to 25.8 calls per 1000 admissions. Three studies documented the calling rate before and after the intervention: a study at a hospital with a preexisting RRS34 reported that the calling rate increased from 13.7 to 25.8 calls per 1000 admissions after an intensive education and publicity program; in a pediatric trial,38 the overall emergency calling rate (for cardiac arrests and medical emergencies) was reported to increase from 6.6 to 10.4 per 1000 admissions; and in the MERIT trial,36 calls increased from 3.1 to 8.7 per 1000 admissions.
Effects of RRS on Clinical Outcomes
Nine studies3, 22, 23, 33, 3537, 39, 40 reported the effect of an RRS on inpatient mortality, 9 studies22, 23, 31, 33, 34, 3638, 40 reported its effect on cardiopulmonary arrests, and 6 studies3, 22, 24, 33, 36, 37 reported its effect on unscheduled ICU admissions. Of these, 7 trials that reported mortality and cardiopulmonary arrests and 6 studies that reported unscheduled ICU admissions supplied sufficient data for meta‐analysis.
Observational studies demonstrated improvement in inpatient mortality, with a summary risk ratio of 0.82 (95% CI: 0.74‐0.91, heterogeneity I2 62.1%; Fig. 2). However, the magnitude of these improvements was very similar to that seen in the control group of the MERIT trial (RR 0.73, 95% CI: 0.53‐1.02). The intervention group of the MERIT trial also demonstrated a reduction in mortality that was not significantly different from that of the control group (RR 0.65, 95% CI: 0.48‐0.87). We found a similar pattern in studies reporting RRS effects on cardiopulmonary arrests (Fig. 3). The observational studies did not show any effect on the risk of unscheduled ICU admissions (summary RR 1.08, 95% CI: 0.96‐1.22, heterogeneity I2 79.1%) nor did the MERIT trial (Fig. 4).
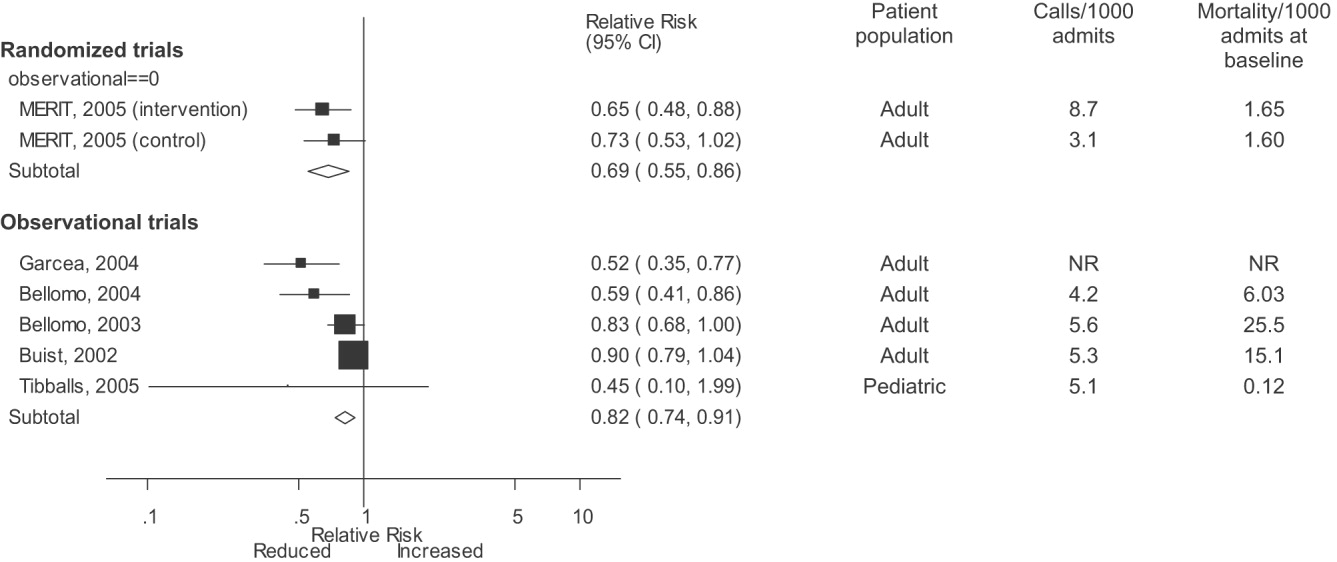
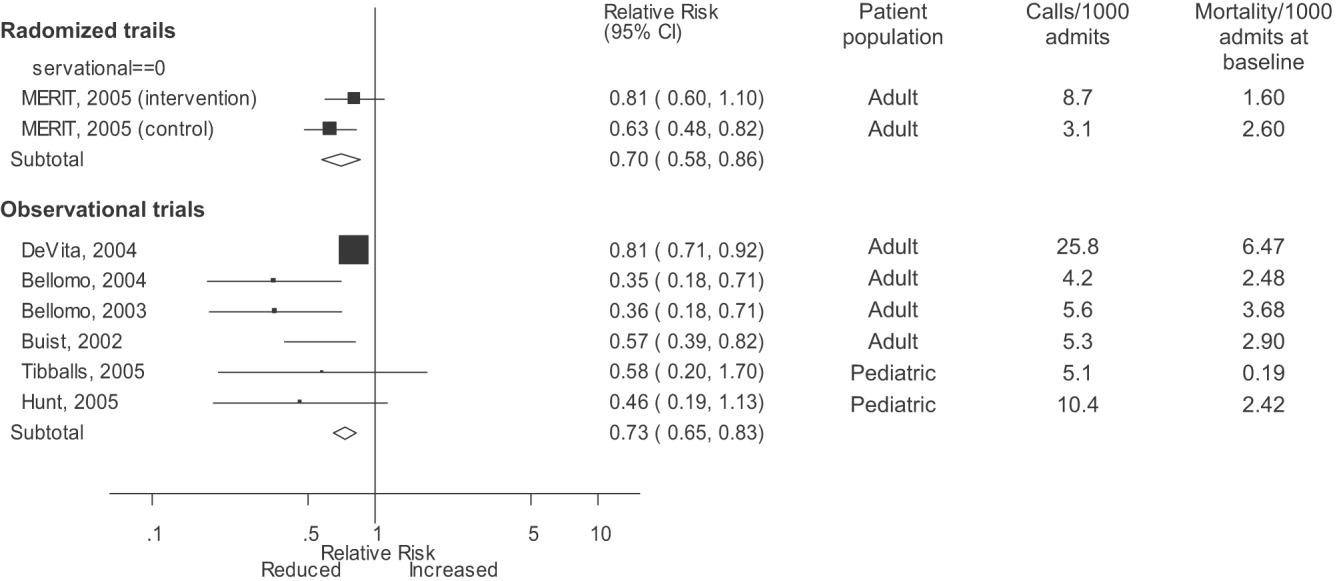
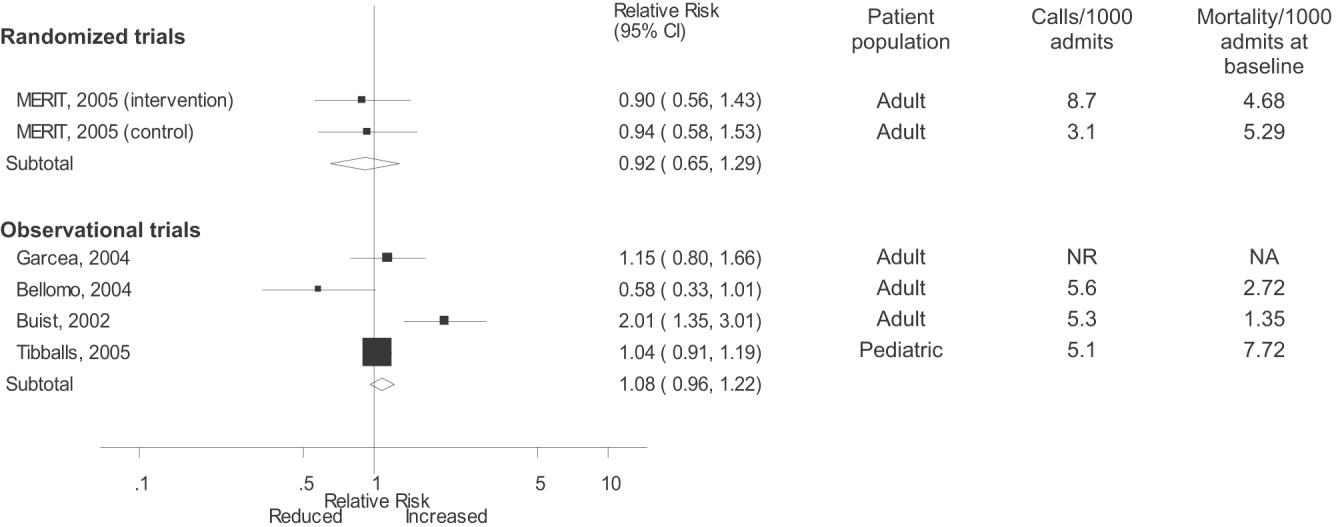
DISCUSSION
Despite the strong face validity of the RRS concept, the current literature on medical emergency teams, rapid response teams, and critical care outreach suffers from substantial flaws that make it difficult to determine the effect of an RRS on patient outcomes. These flaws include the use of suboptimal study designs, failure to report important cointerventions, the methods in which outcomes were defined, and lack of verification of the validity of the outcomes measured. As a result, very little empiric data are available to define the effectiveness of RRSs or to provide guidance for hospitals planning to implement an RRS.
Though early studies reported that RRSs appeared to reduce mortality and cardiac arrest rates, the sole randomized trial of an RRS (the MERIT trial36) showed no differences between intervention and control hospitals for any clinical outcome. Both inpatient mortality and cardiac arrest rates declined in the intervention and control groups of the MERIT trial, and the reductions in these outcomes in observational trials were similar to those seen in the MERIT control group. This strongly implies that other factors besides the RRS were responsible for the results of previous before‐after studies. These studies, which have been widely cited by proponents of the RRS, suffer from methodological limitations intrinsic to the study design and issues with outcome measurement that may have introduced systematic bias; these factors likely explain the contrast between the generally positive results of the before‐after studies and the negative results of the MERIT trial.
Most early RRS trials used an uncontrolled before‐after study design, as is common in quality improvement studies.42 This study design cannot account for secular trends or other factors, including other QI interventions, that could influence the effect of an intervention.26 The statistically significant reduction in impatient mortality in the control arm of the MERIT trial is an instructive example; this decline could have been a result of the educational intervention on caring for deteriorating patients, other ongoing QI projects at the individual hospitals, or simply random variation during the relatively short (6‐month) follow‐up period. Such factors could also entirely account for the impressive results seen in the initial uncontrolled RRS studies. Nearly all the studies we reviewed also did not discuss any aspects of the hospital context that could influence outcomes for critically ill patients, such as the nurse‐staffing ratio,43 ICU bed availability,4446 overall hospital census,47 or availability of intensivists48 or hospitalists.49 Failure to control foror at least report important aspects ofthe environment in which the intervention was performed is akin to failing to report baseline patient comorbidities or concurrent therapies in a study of a drug's effectiveness.
Our review also suggests how bias in the measurement of clinical outcomes may have contributed to the apparent effect of RRSs. In 1 before‐after study, patients for whom RRS activation resulted in a change code status to do not resuscitate (DNR) were excluded from calculations of mortality,22, 50 resulting in underreporting of mortality after RRS implementation. Disposition of such patients was unclear in 3 other studies.3, 36, 40 Some studies22, 34 defined cardiopulmonary arrest as any activation of the code blue team, regardless of whether the patient was actually in cardiac arrest. This almost inevitably would result in fewer arrests after implementation of the RRS, as the indications for calling the code blue team would be narrower. Finally, nearly all studies used trends in nonobjective primary outcomes (eg, unplanned ICU transfer) to support RRS effects but did not validate any of these outcomes (eg, how often did reviewers agree an ICU transfer was preventable), and none of the assessors of these outcomes were blinded.
Some have attributed the MERIT trial not finding the RRS beneficial to inadequate implementation, as the RRS calling rate of 8.7 calls per 1000 admissions was less than the 15 calls per 1000 admissions cited as optimal in a mature RRS.51 However, published studies generally reported a calling rate of 4‐5 calls per 1000 admissions,22, 23, 37 with only 1 trial reporting a higher calling rate.34
A recent commentary20 and a systematic review of critical care outreach teams21 both addressed the effectiveness of RRSs. We sought to examine the effects of all RRS subtypes and using quantitative analysis and analysis of methodological quality, to determine the overall effect of RRSs. The results of our analysis (which included data from several newer studies31, 38, 39) support and extend the conclusion of prior reviews that RRSs, although a potentially promising intervention, do not unequivocally benefit patients and are not worthy of more widespread use until more evidence becomes available. Our analysis also demonstrates that many studies widely cited as supporting wide implementation of RRSs are flawed and probably not generalizable.
Despite these caveats, RRSs remain an intuitively attractive concept and may be of benefit at some hospitals. Further studies in this area should focus on identifying which patient populations are at high risk for clinical decompensation, identifying the role of clinical structures of care (eg, nurse‐staffing ratio, presence of hospitalists) in preventing adverse outcomes and determining which specific RRS model is most effective. As well, more information is needed about educating bedside staff and RRS team members, as this is likely critical to success of the team. Unfortunately, only the article by King et al.31 provided sufficient detail about the implementation process to assist hospitals in planning an RRS. The remaining articles had only scant details about the intervention and its implementation, a common problem noted in the quality improvement literature.42, 52, 53
Our analysis had several limitations. We attempted to identify as many RRS trials as possible by searching multiple databases and reviewing abstract proceedings, but as the RRS literature is in its infancy, we may not have located other unpublished studies or gray literature. There is no validated system for evaluating the methodological strength of nonrandomized studies; therefore, we assessed study quality on the basis of prespecified criteria for internal and external validity. Finally, we found significant statistical heterogeneity in our quantitative analyses, indicating that the variability between individual studies in treatment effects was greater than that expected by chance. As the primary reasons we conducted a meta‐analysis was to compare the results of before‐after trials with those of the randomized MERIT trial, we did not further explore the reasons for this heterogeneity, although variation in patient populations and RRS structure likely accounts for a significant proportion of the heterogeneity.
Although there is a theoretical basis for implementing a rapid response system, the published literature shows inconsistent benefits to patients and suffers from serious methodological flaws. Future studies of RRSs should attempt to define which patient populations are at risk, the essential characteristics of RRSs, effective implementation strategies, andmost importantwhether any RRS improves clinical outcomes. Until such evidence is available, hospitals should not be mandated to establish an RRS and should consider prioritizing quality improvement resources for interventions with a stronger evidence base.
Acknowledgements
The authors thank Emmanuel King, MD, for graciously providing a copy of his manuscript prior to publication and Alexis Meredith, MD, for providing additional information regarding his study. Dr. Shojania holds a Government of Canada Research Chair in Patient Safety and Quality Improvement.
APPENDIX
| Search terms | Citations | |
|---|---|---|
| 1 | {(rapid [ti] AND (response [ti] OR resuscitation [ti]) OR (patient at risk [ti])} AND (program [ti] OR team* [ti] OR service* [ti]) | 23 |
| 2 | medical emergency team* [ti] OR medical crisis team* [ti] OR {(critical [ti] OR intensive [ti]) AND care [ti] AND outreach [ti]} | 87 |
| 3 | hospital [ti] AND resuscitation [ti] AND team* [ti] | 11 |
| 4 | medical emergency team* [ab] OR rapid response team [ab] OR medical crisis team* [ab] | 89 |
| 5 | #1 OR #2 OR #3 OR #4 | 158 |
| 6 | Resuscitation [mh] OR heart arrest [mh] OR hospital mortality [mh] | 72,488 |
| 7 | (patient care team [mh] OR critical care [mh] OR intensive care units [mh]) AND (patient readmission [mh] OR organization and administration [mh]) | 20,321 |
| 8 | #6 AND #7 | 1,419 |
| 9 | {(randomised[ti] OR randomized[ti] OR controlled[ti] OR intervention[ti] OR evaluation[ti] OR comparative[ti] OR effectiveness[ti] OR evaluation[ti] OR feasibility[ti]) AND (trial[ti] OR studies[ti] OR study[ti] OR program[ti] OR design[ti])} OR clinical trial[pt] OR randomized controlled trial[pt] OR epidemiologic studies[mh] OR evaluation studies[mh] OR comparative study[mh] OR feasibility studies[mh] OR intervention studies[mh] OR program evaluation[mh] OR epidemiologic research design[mh] OR systematic5 | 2,688,847 |
| 10 | #8 AND #9 | 748 |
| 11 | #5 OR #10 | 806 |
- ,,,.The medical emergency team.Anaesth Intensive Care.1995;23(2):183–186.
- ,,,.The 100 000 Lives Campaign: setting a goal and a deadline for improving health care quality.JAMA.2006;295(3):324–7.
- ,,,,.Impact of a critical care outreach team on critical care readmissions and mortality.Acta Anaesthesiol Scand2004;48:1096–1100.
- ,.The patient‐at‐risk team.Anaesthesia.2000;55(2):198.
- ,,, et al.Findings of the First Consensus Conference on Medical Emergency Teams.Crit Care Med.2006;34:2463–2478.
- .Recognition of patients who require emergency assistance: a descriptive study.Heart Lung.2000;29(4):262–268.
- ,,, et al.Antecedents to hospital deaths.Intern Med J.2001;31:343–348.
- ,,, et al.Duration of life‐threatening antecedents prior to intensive care admission.Intensive Care Med.2002;28:1629–1634.
- ,,,,.The identification of risk factors for cardiac arrest and formulation of activation criteria to alert a medical emergency team.Resuscitation.2002;54:125–131.
- ,,,,,.A comparison of antecedents to cardiac arrests, deaths and emergency intensive care admissions in Australia and New Zealand, and the United Kingdom—the ACADEMIA study.Resuscitation.2004;62:275–282.
- ,,,.Validation of a modified Early Warning Score in medical admissions.QJM.2001;94:521–526.
- ,,,,.Inpatient transfers to the intensive care unit: delays are associated with increased mortality and morbidity.J Gen Intern Med.2003;18(2):77–83.
- ,,,,.Clinical antecedents to in‐hospital cardiopulmonary arrest.Chest.1990;98:1388–1392.
- ,.Developing strategies to prevent inhospital cardiac arrest: analyzing responses of physicians and nurses in the hours before the event.Crit Care Med.1994;22(2):244–247.
- ,,.Introduction to the rapid response systems series.Jt Comm J Qual Patient Saf.2006;32:359–360.
- ,,, et al.Rates of in‐hospital arrests, deaths and intensive care admissions: the effect of a medical emergency team.Med J Aust.2000;173:236–240.
- ,,,,.The patient‐at‐risk team: identifying and managing seriously ill ward patients.Anaesthesia.1999;54:853–860.
- .The medical emergency team: no evidence to justify not implementing change.Med J Aust.2000;173:228–229.
- ,.The medical emergency team, evidence‐based medicine and ethics.Med J Aust.2003;179:313–315.
- ,,.Rapid response teams—walk, don't run.JAMA.2006;296:1645–1647.
- ,,, et al.Investigating the effectiveness of critical care outreach services: a systematic review.Intensive Care Med.2006;32:1713–1721.
- ,,,,,.Effects of a medical emergency team on reduction of incidence of and mortality from unexpected cardiac arrests in hospital: preliminary study.BMJ.2002;324:387–390.
- ,,, et al.A prospective before‐and‐after trial of a medical emergency team.Med J Aust.2003;179:283–287.
- .Out of our reach? Assessing the impact of introducing a critical care outreach service.Anaesthesia.2003;58:882–885.
- Cochrane Collaboration Effective Practice and Organisation of Care group. Available at: http://www.epoc.uottawa.ca/inttime.pdf.Accessed August 4,2006.
- ,,.Experimental and Quasi‐Experimental Designs for Generalized Causal Inference.Boston, MA:Houghton Mifflin;2002.
- ,,, et al.Guidelines for the uniform reporting of data for Medical Emergency Teams.Resuscitation.2006;68(1):11–25.
- ,.The intracluster correlation coefficient in cluster randomisation.BMJ.1998;316:1455.
- ,.Issues in the meta‐analysis of cluster randomized trials.Stat Med.2002;21:2971–2980.
- ,,,.Measuring inconsistency in meta‐analyses.BMJ.2003;327:557–560.
- ,,.Establishing a rapid response team (RRT) in an academic hospital: one year's experience.J Hosp Med.2006;1:296–305.
- ,,, et al.A multidisciplinary community hospital program for early and rapid resuscitation of shock in nontrauma patients.Chest.2005;127:1729–1743.
- ,,, et al.Prospective controlled trial of effect of medical emergency team on postoperative morbidity and mortality rates.Crit Care Med.2004;32:916–921.
- ,,,,,.Use of medical emergency team responses to reduce hospital cardiopulmonary arrests.Qual Saf Health Care.2004;13:251–254.
- ,,, et al.Introducing critical care outreach: a ward‐randomised trial of phased introduction in a general hospital.Intensive Care Med.2004;30:1398–1404.
- ,,, et al.Introduction of the medical emergency team (MET) system: a cluster‐randomised controlled trial.Lancet.2005;365:2091–2097.
- ,,,,.Reduction of paediatric in‐patient cardiac arrest and death with a medical emergency team: preliminary results.Arch Dis Child.2005;90:1148–1152.
- ,,, et al.The effect of transition from a traditional code team to a rapid response team in a children's center: a before and after intervention trial [abstract].Crit Care Med.2005;33(12 suppl):A17.
- ,,,,.Improved hospital mortality by institution of a rapid response team in a university hospital.Chest.2005;128(suppl S):182S.
- ,,,.Evaluation of a medical emergency team one year after implementation.Resuscitation.2004;61(3):257–263.
- ,,.CONSORT statement: extension to cluster randomised trials.BMJ.2004;328:702–708.
- ,.Evidence‐Based Quality Improvement: The State Of The Science.Health Aff.2005;24(1):138–150.
- ,,,,.Hospital nurse staffing and patient mortality, nurse burnout, and job dissatisfaction.JAMA.2002;288:1987–1993.
- ,,, et al.Evaluation of triage decisions for intensive care admission.Crit Care Med.1999;27:1073–1079.
- ,,,,.Rationing of intensive care unit services. An everyday occurrence.JAMA.1986;255:1143–1146.
- ,,,.How do physicians adapt when the coronary care unit is full? A prospective multicenter study.JAMA.1987;257:1181–1185.
- ,,,,.The association between hospital overcrowding and mortality among patients admitted via Western Australian emergency departments.Med J Aust.2006;184:208–212.
- ,,,,,.Physician staffing patterns and clinical outcomes in critically ill patients: a systematic review.JAMA.2002;288:2151–2'62.
- ,,,,,.Implementation of a voluntary hospitalist service at a community teaching hospital: improved clinical efficiency and patient outcomes.Ann Intern Med.2002;137:859–865.
- .Critical care outreach team's effect on patient outcome: other conclusions are possible.BMJ.2004;328:347; author reply
- The “MERIT” Trial of medical emergency teams in Australia: an analysis of findings and implications for the 100,000 Lives Campaign. Institute for Healthcare Improvement,2006. Available at: http://www.ihi.org/NR/rdonlyres/F3401FEF‐2179‐4403‐8F67–B9255C57E207/0/LancetAnalysis81505.pdf. Accessed August 17, 2006.
- ,,, et al.Toward evidence‐based quality improvement. evidence (and its limitations) of the effectiveness of guideline dissemination and implementation strategies 1966‐1998.J Gen Intern Med.2006;21(suppl 2):S14–S20.
- ,,, et al.lessons learned about implementing research evidence into clinical practice. Experiences from VA QUERI.J Gen Intern Med.2006;21(suppl 2):S21–S24.
- ,,,,,.Improving the quality of reports of meta‐analyses of randomised controlled trials: the QUOROM statement. Quality of reporting of meta‐analyses.Lancet.1999;354:1896–1900.
- ,,,,,.Improving the utilization of medical crisis teams (Condition C) at an urban tertiary care hospital.J Crit Care.2003;18(2):87–94.
- ,,, et al.Long term effect of a medical emergency team on cardiac arrests in a teaching hospital.Crit Care.2005;9:R808–R815.
A medical emergency team1 is a group of clinicians trained to quickly assess and treat hospitalized patients showing acute signs of clinical deterioration. Equivalent terms used are rapid response team,2 critical care outreach team,3 and patient‐at‐risk team.4 A consensus panel5 recently endorsed use of the term rapid response system (RRS) to denote any system that uses a standard set of clinical criteria to summon caregivers to the bedside of a patient who is deemed unstable but not in cardiopulmonary arrest (in which case a standard resuscitation team would be summoned). Such teams primarily evaluate patients on general hospital wards.
RRSs have been developed in response to data indicating that patients frequently demonstrate premonitory signs or receive inadequate care prior to unanticipated intensive care unit (ICU) admission, cardiopulmonary arrest, or death outside the ICU.614 Earlier identification and treatment of such patients could prevent adverse clinical outcomes. The structure of RRSs varies but generally includes a physician and nurse and may also include other staff such as respiratory therapists.5 Teams are summoned by hospital staff to assess patients meeting specific clinical criteria (see box) about whom the bedside staff has significant concern.150
| Any staff member may call the team if 1 of the following criteria is met: |
| Heart rate > 140/min or 40/min |
| Respiratory rate > 28/min or 8/min |
| Systolic blood pressure > 180 mmHg or 90 mm Hg |
| Oxygen saturation 90% despite supplementation |
| Acute change in mental status |
| Urine output 50 cc over 4 hours |
| Staff member has significant concern about patient's condition |
| Additional criteria used at some institutions: |
| Chest pain unrelieved by nitroglycerin |
| Threatened airway |
| Seizure |
| Uncontrolled pain |
Initial studies of RRSs, performed primarily in Australia and the United Kingdom, showed promising reductions in unanticipated ICU admissions, cardiac arrests, and even overall inpatient mortality.1, 16, 17 The considerable enthusiasm generated by these studies18, 19 resulted in the Institute for Healthcare Improvement (IHI) incorporating RRSs into its 100,000 Lives campaign,2 and RRSs are now being implemented in the more than 3000 U.S. hospitals that joined the campaign. However, a recent commentary on rapid response teams20 and a systematic review of critical care outreach teams21 have raised concerns that this widespread implementation may not be justified by the available evidence. We performed a systematic review of studies of all variations of RRSs in order to determine their effect on patient outcomes and to characterize variations in their organization and implementation.
METHODS
Literature Search and Inclusion and Exclusion Criteria
We systematically searched MEDLINE, CINAHL, and BIOSIS through August 2006 for relevant studies using the various terms for RRSs (eg, medical emergency team, rapid response team, critical care outreach) and medical subject headings relevant to inpatient care and critical illness (eg, patient care team and resuscitation; the full search strategy is given in the Appendix). We also reviewed the abstract lists from the 2004 and 2005 American Thoracic Society and Society of Critical Care Medicine annual meetings and scanned reference lists from key articles.
We screened the abstracts of the articles identified by the search, and 2 independent reviewers abstracted potentially relevant articles using a standardized data abstraction form. Disagreements between the reviewers were resolved by consensus and, if necessary, discussion with a third reviewer. We included randomized controlled trials (RCTs), controlled before‐after studies, and interrupted time series, including simple before‐after studies with no contemporaneous control group, though we planned to separately analyze data from controlled studies if possible. We included only English‐language articles.
On the basis of RRS features in widely cited articles2224 and the recommendations of a recent consensus statement,5 we defined an RRS as having the following characteristics: (1) its primary responsibility is to intervene whenever hospitalized patients become unstable before cardiopulmonary arrest occurs; (2) it must primarily provide care outside the ICU and emergency department; (3) specific clinical criteria must be in place that define instability and trigger a call to the team; and (4) it must be expected to respond within a specified time. We defined these criteria in order to distinguish studies of RRSs from studies of cardiac arrest (code blue) teams or traditional consulting services.
To be included in the analysis, articles had to report the effects of a rapid response system on at least 1 of these outcomes: inpatient mortality, inpatient cardiac arrest, or unscheduled ICU transfer. We used the definitions of cardiac arrest and unscheduled ICU transfer given in the primary studies. In addition to these outcomes, we abstracted information on the number of admissions and the number of RRS calls during the study period. To maximize the comparability of study outcomes, we calculated the rates of mortality, cardiac arrest, unscheduled ICU transfer, and RRS calls per 1000 admissions for studies that did not supply data in this fashion.
Assessment of Study Quality
Quality scoring instruments for studies included in systematic reviews generally focus on randomized controlled trials, which we anticipated would account for a minority of included studies. On the basis of recommendations for the assessment of methodology for nonrandomized study designs,25, 26 we identified and abstracted 4 important determinants of internal validity (Table 1). The consensus statement5 recommends monitoring the effectiveness of RRSs by measuring the rate of unscheduled ICU admissions (defined as an unplanned admission to the ICU from a general ward27) and cardiac arrests of patients who were not listed as do not resuscitate (DNR). As the definition of unscheduled ICU admission allows room for subjectivity, we considered the blinding of assessment of this outcome to study group assignment to be important, especially for retrospective studies. Measurement of cardiac arrests should be less susceptible to blinding issues, but one of the functions of an RRS can be to initiate discussions that result in changes in the goals of care and code status.22 Thus, excluding patients made DNR by the team from cardiac arrest calculations could falsely lower the cardiac arrest rate.
| Quality measures |
|---|
|
| A. Internal validity |
| 1. Did the study have a contemporaneous control group? |
| 2. If there was no contemporaneous control group, did the study report data for more than 1 time point before and after the intervention? |
| 3. Were nonobjective primary outcomes (eg, unplanned ICU transfer) measured in a blinded fashion? |
| 4. Were patients made DNR by the RRS included in calculations of the cardiac arrest and mortality rates? |
| B. Generalizability |
| 5. Was the intervention performed independent of other quality improvement interventions targeting the care of critically ill patients? |
| 6. Did the study report the number of admissions and RRS calls during the study period? |
| 7. Did the study report the availability of intensivists before and after the intervention? |
We also abstracted 3 separate elements of study quality pertaining to the external validity or generalizability of included studies (Table 1). These elements were defined a priori by consensus reached by discussion among the reviewers. These elements were intended to provide a framework for interpreting the included studies and to guide subgroup analyses. They were not used to form a composite quality score.
Statistical Analysis
We performed a random‐effects meta‐analysis to calculate summary risk ratios with 95% confidence intervals for the effects of RRSs on inpatient mortality, cardiopulmonary arrest, and unscheduled ICU admission. Included in the meta‐analysis were the studies that reported total number of admissions and incidence of each outcome before and after institution of the RRS. For randomized trials that reported pre‐ and postintervention data, we treated the intervention and control groups as separate trials in order to be able to compare their effects with the before‐after trials. For studies that reported results adjusted for clustering (ie, by hospital), we back‐calculated the unadjusted results by multiplying the standard error by the square of the design factor coefficient.28, 29 We calculated the I2 statistic to assess heterogeneity.30 All analyses were performed using Stata version 8.2 (Stata Corporation, College Station, TX).
RESULTS
The database searches identified 861 citations, and 1 additional prepublication study was supplied by the study's first author31; 89 articles underwent full‐text review (Fig. 1). Most studies excluded during the full‐text review did not meet our criteria for a study of an RRS or were observational studies or review articles. For instance, Sebat et al.32 published a study of a shock team at a community hospital that intervened when any patient suffered nontraumatic shock; the study did not meet our inclusion criteria as all patients were admitted to the ICU, most directly from the emergency department. Another frequently cited study, by Bristow et al.,16 was excluded as it was a case‐control study. Thirteen studies,3, 2224, 31, 334011 full‐length studies and 2 abstractsmet all criteria for inclusion.
Characteristics of Included Trials
The characteristics of included studies are outlined in Table 2. Five studies were performed in Australia, 4 in the United States, and 4 in the United Kingdom. All were conducted in academic teaching hospitals. Two studies37, 38 focused on pediatric inpatients, and the remainder involved hospitalized adults. The RRS intervened for all hospitalized patients in all but 2 studies (1 of which focused on surgical inpatients33 and the other in which the RRS evaluated only patients discharged from the ICU3). In 2 studies,31, 39 the RRS was available to evaluate outpatients, such as hospital visitors, in addition to inpatients.0
| Study | Location | Hospital type | Patient population | RRS composition | Measured outcomes | Definition of unscheduled ICU admission | Definition of cardiac arrest |
|---|---|---|---|---|---|---|---|
| |||||||
| Buist et al., 200220 | Australia | Tertiary‐care academic hospital | Adult inpatients | ICU registrar | DNR status | Not supplied | Any code blue team activation |
| Medical registrar | Cardiac arrest | ||||||
| ICU nurse | Unscheduled ICU admission | ||||||
| Mortality | |||||||
| Bellomo et al., 200321 | Australia | Tertiary‐care academic hospital | Adult inpatients | ICU nurse and ICU fellow attended all calls; ICU attending (8 AM‐8 PM) and medical registrar attended if requested | Mortality | NA | Unresponsive, with no pulse or blood pressure, and basic life support initiated |
| Cardiac arrest | |||||||
| DNR status | |||||||
| Pittard et al., 200322 | United Kingdom | Tertiary‐care academic hospital | Adult inpatients on surgical wards | Senior critical care nurses and medical staff | Unscheduled ICU admission | Any patient not admitted directly from operating theater after elective surgery | NA |
| Bellomo et al., 200431 | Australia | Tertiary‐care academic hospital | Adult postoperative patients | ICU attending | Mortality Unscheduled ICU admission ICU length of stay DNR status | Postoperative admission to ICU because of a clinical complication | NA |
| ICU fellow | Unscheduled ICU admission | ||||||
| ICU registered nurse | ICU length of stay | ||||||
| Medical fellow | DNR status | ||||||
| DeVita et al., 200432 | United States | Tertiary‐care academic hospital | Adult inpatients | ICU physician | Cardiac arrest | NA | Any code blue team activation |
| Anesthesiologist | |||||||
| 2 other physicians | |||||||
| 2 ICU nurses | |||||||
| Floor nurse | |||||||
| Respiratory therapist | |||||||
| Garcea et al., 20043 | United Kingdom | Teaching hospital | Adult patients discharged from ICU | 2 ICU nurses | Mortality | Emergency readmissions to ICU | NA |
| 1 ICU nurse specialist | Unscheduled ICU admission | ||||||
| ICU consultant physician (if needed) | |||||||
| Kenward et al., 200438 | United Kingdom | Teaching hospital | Adult inpatients | Not stated | Mortality | NA | Loss of spontaneous circulation |
| Cardiac arrest | |||||||
| Priestley et al., 200433 | United Kingdom | Teaching hospital | Adult inpatients | ICU nurse consultant | Mortality | NA | NA |
| ICU physician available if needed | Overall length of stay | ||||||
| Hillman et al., 200534 | Australia | 23 hospitals (17 academic, 6 nonacademic) | Adult inpatients | Varied between study hospitals; required to have at least 1 MD and 1 RN from ED or ICU | Mortality | Any unscheduled admission to ICU from general ward | No palpable pulse |
| Cardiac arrest | |||||||
| Unscheduled ICU admission | |||||||
| DNR status | |||||||
| Hunt et al., 2005 (abstract)36 | United States | Pediatric tertiary‐care academic hospital | Pediatric inpatients | Not provided | Cardiac arrest | NA | Not provided |
| Meredith et al., 2005 (abstract)37 | United States | Tertiary‐care academic hospital | Adult inpatients, outpatients, and visitors | ICU registered nurse | Mortality | NA | Not provided |
| Respiratory therapist | |||||||
| Tibballs et al., 200535 | Australia | Pediatric tertiary‐care academic hospital | Pediatric inpatients | ICU physician | Cardiac arrest | Not supplied | Not provided |
| Medical registrar | Unscheduled ICU admission | ||||||
| ED physician | |||||||
| ICU nurse | |||||||
| King et al., 200629 | United States | Tertiary‐care academic hospital | Adult inpatients, outpatients, and visitors | Hospitalist | Cardiac arrest | NA | Not provided |
| Internal medicine resident | |||||||
| ICU nurse | |||||||
| Ward nurse | |||||||
| Pharmacist | |||||||
RRS Structure, Calling Criteria, and Responsibilities
Seven studies22, 23, 31, 33, 34, 36, 37 that described the team composition used variants of the medical emergency team model, a physician‐led team (Table 2). In 6 of these 7 studies, the team included a critical care physician (attending or fellow) and an ICU nurse; in the sole RCT (the MERIT study36), the team structure varied between hospitals, consisting of a nurse and physician from either the emergency department or ICU. Hospitalists, who are involved in RRS responses at many U.S. hospitals, were primary team leaders of the RRS in only 1 study.31 In 2 studies34, 37 the RRS also responded to code blue calls, and in 4 studies23, 31, 33, 39 the RRS and the code blue team had separate personnel; the remaining studies did not define the distinction between RRS and code blue team.
| Study | Contemporaneous control group | Data reported at more than 1 time before/after intervention | RRS calling rate reported | Outcomes analysis included patients made DNR by team | Blind measurement of nonobjective outcomes | Intensivist always available | Other QI efforts during study |
|---|---|---|---|---|---|---|---|
| |||||||
| Buist et al., 200220 | No | No | Yes | No (mortality) | No | NR | NR |
| Bellomo et al., 200321 | No | No | Yes | Yes (mortality) | NA | Yes (ICU fellow) | No |
| Pittard et al., 200322 | No | No | Yes | NA | No | NR | NR |
| Bellomo et al., 200431 | No | No | Yes | Yes (mortality) | No | Yes (ICU fellow) | No |
| DeVita et al., 200432 | No | Yes | Yes | NA | No | Yes (critical care attending physician) | NR |
| Garcea et al., 200433 | No | No | No | Unclear | No | NR | NR |
| Kenward et al., 200438 | No | No | Yes | Unclear | No | NR | NR |
| Priestley et al., 200433 | No (interrupted time series) | Yes | No | NA | No | NR | NR |
| Hillman et al., 200534 | Yes | No | Yes | Unclear | Yes | NR | No |
| Hunt et al., 2005 (abstract)36 | No | No | Yes | NA | NR | NR | NR |
| Meredith et al., 2005 (abstract)37 | No | No | Yes | No | NA | No | No |
| Tibballs et al., 200535 | No | No | Yes | Unclear | No | NR | Yes (educational workshops/more training in APLS) |
| King et al., 200629 | No | Yes | Yes | NA | No | Yes | No |
In 4 studies the RRSs were led by nurses. One study published in abstract form39 used the rapid response team model, consisting of a critical care nurse and a respiratory therapist, with assistance as needed from the primary medical staff and a critical care physician. Three studies3, 24, 35 from UK hospitals used the critical care outreach (CCO) model, in which ICU‐trained nurses respond initially with assistance from intensivists. The CCO model also involves follow‐up on patients discharged from the ICU and proactive rounding on unstable ward patients.
The hospitals used broadly similar approaches to determining when to summon the RRS, relying on combinations of objective clinical criteria (eg, vital sign abnormalities) and subjective criteria (eg, acute mental status change, staff member concerned about patient's condition). Three studies3, 24, 35 used a formal clinical score (the Patient‐At‐Risk score or the Modified Early Warning score) to trigger calls to the RRS. Three studies, 2 of them from the same institution,23, 33 reported the frequency of specific triggers for RRS activation. Concern by bedside staff and respiratory distress were the most frequent activators of the RRS.
Study Internal Validity and Generalizability
One study,36 the MERIT trial, conducted in Australia, was a cluster‐randomized RCT (randomized by hospital) that adhered to recommended elements of design and reporting for studies of this type.41 In this study, hospitals in the control group received an educational intervention on caring for deteriorating patients only; hospitals in the intervention group received the educational module and started an RRS. An additional study35 identified itself as a randomized trial, but randomization occurred at the hospital ward level, with introduction of the intervention (critical care outreach) staggered so that at different points an individual ward could have been in either the control or intervention group; therefore, this study was considered an interrupted time series. All other trials included were before‐after studies with no contemporaneous control group
Most studies did not meet criteria for internal validity or generalizability (Table 2). Two studies3, 35 did not report the number of RRS calls during the study period. One study22 omitted patients whose resuscitation status was changed after RRS evaluation from the calculation of inpatient mortality; thus, the patients who had been made do not resuscitate by the RRS did not contribute to the calculated mortality rate. The disposition of these patients was unclear in another study.36 All studies measured clinical outcomes retrospectively, and no studies reported blinding of outcomes assessors for nonobjective outcomes (eg, unplanned ICU admission). Studies generally did not report on the availability of intensivists or if other quality improvement interventions targeting critically ill patients were implemented along with the RRS.
RRS Usage and Effects on Patient Outcomes
Seven studies2224, 34, 3638 reported enough information to calculate the RRS calling rate (4 studies24, 31, 39, 40 reported the total number of calls but not the number of admissions, and 2 studies3, 35 did not report either). In these 7 studies, the calling rate varied from 4.5 to 25.8 calls per 1000 admissions. Three studies documented the calling rate before and after the intervention: a study at a hospital with a preexisting RRS34 reported that the calling rate increased from 13.7 to 25.8 calls per 1000 admissions after an intensive education and publicity program; in a pediatric trial,38 the overall emergency calling rate (for cardiac arrests and medical emergencies) was reported to increase from 6.6 to 10.4 per 1000 admissions; and in the MERIT trial,36 calls increased from 3.1 to 8.7 per 1000 admissions.
Effects of RRS on Clinical Outcomes
Nine studies3, 22, 23, 33, 3537, 39, 40 reported the effect of an RRS on inpatient mortality, 9 studies22, 23, 31, 33, 34, 3638, 40 reported its effect on cardiopulmonary arrests, and 6 studies3, 22, 24, 33, 36, 37 reported its effect on unscheduled ICU admissions. Of these, 7 trials that reported mortality and cardiopulmonary arrests and 6 studies that reported unscheduled ICU admissions supplied sufficient data for meta‐analysis.
Observational studies demonstrated improvement in inpatient mortality, with a summary risk ratio of 0.82 (95% CI: 0.74‐0.91, heterogeneity I2 62.1%; Fig. 2). However, the magnitude of these improvements was very similar to that seen in the control group of the MERIT trial (RR 0.73, 95% CI: 0.53‐1.02). The intervention group of the MERIT trial also demonstrated a reduction in mortality that was not significantly different from that of the control group (RR 0.65, 95% CI: 0.48‐0.87). We found a similar pattern in studies reporting RRS effects on cardiopulmonary arrests (Fig. 3). The observational studies did not show any effect on the risk of unscheduled ICU admissions (summary RR 1.08, 95% CI: 0.96‐1.22, heterogeneity I2 79.1%) nor did the MERIT trial (Fig. 4).
DISCUSSION
Despite the strong face validity of the RRS concept, the current literature on medical emergency teams, rapid response teams, and critical care outreach suffers from substantial flaws that make it difficult to determine the effect of an RRS on patient outcomes. These flaws include the use of suboptimal study designs, failure to report important cointerventions, the methods in which outcomes were defined, and lack of verification of the validity of the outcomes measured. As a result, very little empiric data are available to define the effectiveness of RRSs or to provide guidance for hospitals planning to implement an RRS.
Though early studies reported that RRSs appeared to reduce mortality and cardiac arrest rates, the sole randomized trial of an RRS (the MERIT trial36) showed no differences between intervention and control hospitals for any clinical outcome. Both inpatient mortality and cardiac arrest rates declined in the intervention and control groups of the MERIT trial, and the reductions in these outcomes in observational trials were similar to those seen in the MERIT control group. This strongly implies that other factors besides the RRS were responsible for the results of previous before‐after studies. These studies, which have been widely cited by proponents of the RRS, suffer from methodological limitations intrinsic to the study design and issues with outcome measurement that may have introduced systematic bias; these factors likely explain the contrast between the generally positive results of the before‐after studies and the negative results of the MERIT trial.
Most early RRS trials used an uncontrolled before‐after study design, as is common in quality improvement studies.42 This study design cannot account for secular trends or other factors, including other QI interventions, that could influence the effect of an intervention.26 The statistically significant reduction in impatient mortality in the control arm of the MERIT trial is an instructive example; this decline could have been a result of the educational intervention on caring for deteriorating patients, other ongoing QI projects at the individual hospitals, or simply random variation during the relatively short (6‐month) follow‐up period. Such factors could also entirely account for the impressive results seen in the initial uncontrolled RRS studies. Nearly all the studies we reviewed also did not discuss any aspects of the hospital context that could influence outcomes for critically ill patients, such as the nurse‐staffing ratio,43 ICU bed availability,4446 overall hospital census,47 or availability of intensivists48 or hospitalists.49 Failure to control foror at least report important aspects ofthe environment in which the intervention was performed is akin to failing to report baseline patient comorbidities or concurrent therapies in a study of a drug's effectiveness.
Our review also suggests how bias in the measurement of clinical outcomes may have contributed to the apparent effect of RRSs. In 1 before‐after study, patients for whom RRS activation resulted in a change code status to do not resuscitate (DNR) were excluded from calculations of mortality,22, 50 resulting in underreporting of mortality after RRS implementation. Disposition of such patients was unclear in 3 other studies.3, 36, 40 Some studies22, 34 defined cardiopulmonary arrest as any activation of the code blue team, regardless of whether the patient was actually in cardiac arrest. This almost inevitably would result in fewer arrests after implementation of the RRS, as the indications for calling the code blue team would be narrower. Finally, nearly all studies used trends in nonobjective primary outcomes (eg, unplanned ICU transfer) to support RRS effects but did not validate any of these outcomes (eg, how often did reviewers agree an ICU transfer was preventable), and none of the assessors of these outcomes were blinded.
Some have attributed the MERIT trial not finding the RRS beneficial to inadequate implementation, as the RRS calling rate of 8.7 calls per 1000 admissions was less than the 15 calls per 1000 admissions cited as optimal in a mature RRS.51 However, published studies generally reported a calling rate of 4‐5 calls per 1000 admissions,22, 23, 37 with only 1 trial reporting a higher calling rate.34
A recent commentary20 and a systematic review of critical care outreach teams21 both addressed the effectiveness of RRSs. We sought to examine the effects of all RRS subtypes and using quantitative analysis and analysis of methodological quality, to determine the overall effect of RRSs. The results of our analysis (which included data from several newer studies31, 38, 39) support and extend the conclusion of prior reviews that RRSs, although a potentially promising intervention, do not unequivocally benefit patients and are not worthy of more widespread use until more evidence becomes available. Our analysis also demonstrates that many studies widely cited as supporting wide implementation of RRSs are flawed and probably not generalizable.
Despite these caveats, RRSs remain an intuitively attractive concept and may be of benefit at some hospitals. Further studies in this area should focus on identifying which patient populations are at high risk for clinical decompensation, identifying the role of clinical structures of care (eg, nurse‐staffing ratio, presence of hospitalists) in preventing adverse outcomes and determining which specific RRS model is most effective. As well, more information is needed about educating bedside staff and RRS team members, as this is likely critical to success of the team. Unfortunately, only the article by King et al.31 provided sufficient detail about the implementation process to assist hospitals in planning an RRS. The remaining articles had only scant details about the intervention and its implementation, a common problem noted in the quality improvement literature.42, 52, 53
Our analysis had several limitations. We attempted to identify as many RRS trials as possible by searching multiple databases and reviewing abstract proceedings, but as the RRS literature is in its infancy, we may not have located other unpublished studies or gray literature. There is no validated system for evaluating the methodological strength of nonrandomized studies; therefore, we assessed study quality on the basis of prespecified criteria for internal and external validity. Finally, we found significant statistical heterogeneity in our quantitative analyses, indicating that the variability between individual studies in treatment effects was greater than that expected by chance. As the primary reasons we conducted a meta‐analysis was to compare the results of before‐after trials with those of the randomized MERIT trial, we did not further explore the reasons for this heterogeneity, although variation in patient populations and RRS structure likely accounts for a significant proportion of the heterogeneity.
Although there is a theoretical basis for implementing a rapid response system, the published literature shows inconsistent benefits to patients and suffers from serious methodological flaws. Future studies of RRSs should attempt to define which patient populations are at risk, the essential characteristics of RRSs, effective implementation strategies, andmost importantwhether any RRS improves clinical outcomes. Until such evidence is available, hospitals should not be mandated to establish an RRS and should consider prioritizing quality improvement resources for interventions with a stronger evidence base.
Acknowledgements
The authors thank Emmanuel King, MD, for graciously providing a copy of his manuscript prior to publication and Alexis Meredith, MD, for providing additional information regarding his study. Dr. Shojania holds a Government of Canada Research Chair in Patient Safety and Quality Improvement.
APPENDIX
| Search terms | Citations | |
|---|---|---|
| 1 | {(rapid [ti] AND (response [ti] OR resuscitation [ti]) OR (patient at risk [ti])} AND (program [ti] OR team* [ti] OR service* [ti]) | 23 |
| 2 | medical emergency team* [ti] OR medical crisis team* [ti] OR {(critical [ti] OR intensive [ti]) AND care [ti] AND outreach [ti]} | 87 |
| 3 | hospital [ti] AND resuscitation [ti] AND team* [ti] | 11 |
| 4 | medical emergency team* [ab] OR rapid response team [ab] OR medical crisis team* [ab] | 89 |
| 5 | #1 OR #2 OR #3 OR #4 | 158 |
| 6 | Resuscitation [mh] OR heart arrest [mh] OR hospital mortality [mh] | 72,488 |
| 7 | (patient care team [mh] OR critical care [mh] OR intensive care units [mh]) AND (patient readmission [mh] OR organization and administration [mh]) | 20,321 |
| 8 | #6 AND #7 | 1,419 |
| 9 | {(randomised[ti] OR randomized[ti] OR controlled[ti] OR intervention[ti] OR evaluation[ti] OR comparative[ti] OR effectiveness[ti] OR evaluation[ti] OR feasibility[ti]) AND (trial[ti] OR studies[ti] OR study[ti] OR program[ti] OR design[ti])} OR clinical trial[pt] OR randomized controlled trial[pt] OR epidemiologic studies[mh] OR evaluation studies[mh] OR comparative study[mh] OR feasibility studies[mh] OR intervention studies[mh] OR program evaluation[mh] OR epidemiologic research design[mh] OR systematic5 | 2,688,847 |
| 10 | #8 AND #9 | 748 |
| 11 | #5 OR #10 | 806 |
A medical emergency team1 is a group of clinicians trained to quickly assess and treat hospitalized patients showing acute signs of clinical deterioration. Equivalent terms used are rapid response team,2 critical care outreach team,3 and patient‐at‐risk team.4 A consensus panel5 recently endorsed use of the term rapid response system (RRS) to denote any system that uses a standard set of clinical criteria to summon caregivers to the bedside of a patient who is deemed unstable but not in cardiopulmonary arrest (in which case a standard resuscitation team would be summoned). Such teams primarily evaluate patients on general hospital wards.
RRSs have been developed in response to data indicating that patients frequently demonstrate premonitory signs or receive inadequate care prior to unanticipated intensive care unit (ICU) admission, cardiopulmonary arrest, or death outside the ICU.614 Earlier identification and treatment of such patients could prevent adverse clinical outcomes. The structure of RRSs varies but generally includes a physician and nurse and may also include other staff such as respiratory therapists.5 Teams are summoned by hospital staff to assess patients meeting specific clinical criteria (see box) about whom the bedside staff has significant concern.150
| Any staff member may call the team if 1 of the following criteria is met: |
| Heart rate > 140/min or 40/min |
| Respiratory rate > 28/min or 8/min |
| Systolic blood pressure > 180 mmHg or 90 mm Hg |
| Oxygen saturation 90% despite supplementation |
| Acute change in mental status |
| Urine output 50 cc over 4 hours |
| Staff member has significant concern about patient's condition |
| Additional criteria used at some institutions: |
| Chest pain unrelieved by nitroglycerin |
| Threatened airway |
| Seizure |
| Uncontrolled pain |
Initial studies of RRSs, performed primarily in Australia and the United Kingdom, showed promising reductions in unanticipated ICU admissions, cardiac arrests, and even overall inpatient mortality.1, 16, 17 The considerable enthusiasm generated by these studies18, 19 resulted in the Institute for Healthcare Improvement (IHI) incorporating RRSs into its 100,000 Lives campaign,2 and RRSs are now being implemented in the more than 3000 U.S. hospitals that joined the campaign. However, a recent commentary on rapid response teams20 and a systematic review of critical care outreach teams21 have raised concerns that this widespread implementation may not be justified by the available evidence. We performed a systematic review of studies of all variations of RRSs in order to determine their effect on patient outcomes and to characterize variations in their organization and implementation.
METHODS
Literature Search and Inclusion and Exclusion Criteria
We systematically searched MEDLINE, CINAHL, and BIOSIS through August 2006 for relevant studies using the various terms for RRSs (eg, medical emergency team, rapid response team, critical care outreach) and medical subject headings relevant to inpatient care and critical illness (eg, patient care team and resuscitation; the full search strategy is given in the Appendix). We also reviewed the abstract lists from the 2004 and 2005 American Thoracic Society and Society of Critical Care Medicine annual meetings and scanned reference lists from key articles.
We screened the abstracts of the articles identified by the search, and 2 independent reviewers abstracted potentially relevant articles using a standardized data abstraction form. Disagreements between the reviewers were resolved by consensus and, if necessary, discussion with a third reviewer. We included randomized controlled trials (RCTs), controlled before‐after studies, and interrupted time series, including simple before‐after studies with no contemporaneous control group, though we planned to separately analyze data from controlled studies if possible. We included only English‐language articles.
On the basis of RRS features in widely cited articles2224 and the recommendations of a recent consensus statement,5 we defined an RRS as having the following characteristics: (1) its primary responsibility is to intervene whenever hospitalized patients become unstable before cardiopulmonary arrest occurs; (2) it must primarily provide care outside the ICU and emergency department; (3) specific clinical criteria must be in place that define instability and trigger a call to the team; and (4) it must be expected to respond within a specified time. We defined these criteria in order to distinguish studies of RRSs from studies of cardiac arrest (code blue) teams or traditional consulting services.
To be included in the analysis, articles had to report the effects of a rapid response system on at least 1 of these outcomes: inpatient mortality, inpatient cardiac arrest, or unscheduled ICU transfer. We used the definitions of cardiac arrest and unscheduled ICU transfer given in the primary studies. In addition to these outcomes, we abstracted information on the number of admissions and the number of RRS calls during the study period. To maximize the comparability of study outcomes, we calculated the rates of mortality, cardiac arrest, unscheduled ICU transfer, and RRS calls per 1000 admissions for studies that did not supply data in this fashion.
Assessment of Study Quality
Quality scoring instruments for studies included in systematic reviews generally focus on randomized controlled trials, which we anticipated would account for a minority of included studies. On the basis of recommendations for the assessment of methodology for nonrandomized study designs,25, 26 we identified and abstracted 4 important determinants of internal validity (Table 1). The consensus statement5 recommends monitoring the effectiveness of RRSs by measuring the rate of unscheduled ICU admissions (defined as an unplanned admission to the ICU from a general ward27) and cardiac arrests of patients who were not listed as do not resuscitate (DNR). As the definition of unscheduled ICU admission allows room for subjectivity, we considered the blinding of assessment of this outcome to study group assignment to be important, especially for retrospective studies. Measurement of cardiac arrests should be less susceptible to blinding issues, but one of the functions of an RRS can be to initiate discussions that result in changes in the goals of care and code status.22 Thus, excluding patients made DNR by the team from cardiac arrest calculations could falsely lower the cardiac arrest rate.
| Quality measures |
|---|
|
| A. Internal validity |
| 1. Did the study have a contemporaneous control group? |
| 2. If there was no contemporaneous control group, did the study report data for more than 1 time point before and after the intervention? |
| 3. Were nonobjective primary outcomes (eg, unplanned ICU transfer) measured in a blinded fashion? |
| 4. Were patients made DNR by the RRS included in calculations of the cardiac arrest and mortality rates? |
| B. Generalizability |
| 5. Was the intervention performed independent of other quality improvement interventions targeting the care of critically ill patients? |
| 6. Did the study report the number of admissions and RRS calls during the study period? |
| 7. Did the study report the availability of intensivists before and after the intervention? |
We also abstracted 3 separate elements of study quality pertaining to the external validity or generalizability of included studies (Table 1). These elements were defined a priori by consensus reached by discussion among the reviewers. These elements were intended to provide a framework for interpreting the included studies and to guide subgroup analyses. They were not used to form a composite quality score.
Statistical Analysis
We performed a random‐effects meta‐analysis to calculate summary risk ratios with 95% confidence intervals for the effects of RRSs on inpatient mortality, cardiopulmonary arrest, and unscheduled ICU admission. Included in the meta‐analysis were the studies that reported total number of admissions and incidence of each outcome before and after institution of the RRS. For randomized trials that reported pre‐ and postintervention data, we treated the intervention and control groups as separate trials in order to be able to compare their effects with the before‐after trials. For studies that reported results adjusted for clustering (ie, by hospital), we back‐calculated the unadjusted results by multiplying the standard error by the square of the design factor coefficient.28, 29 We calculated the I2 statistic to assess heterogeneity.30 All analyses were performed using Stata version 8.2 (Stata Corporation, College Station, TX).
RESULTS
The database searches identified 861 citations, and 1 additional prepublication study was supplied by the study's first author31; 89 articles underwent full‐text review (Fig. 1). Most studies excluded during the full‐text review did not meet our criteria for a study of an RRS or were observational studies or review articles. For instance, Sebat et al.32 published a study of a shock team at a community hospital that intervened when any patient suffered nontraumatic shock; the study did not meet our inclusion criteria as all patients were admitted to the ICU, most directly from the emergency department. Another frequently cited study, by Bristow et al.,16 was excluded as it was a case‐control study. Thirteen studies,3, 2224, 31, 334011 full‐length studies and 2 abstractsmet all criteria for inclusion.
Characteristics of Included Trials
The characteristics of included studies are outlined in Table 2. Five studies were performed in Australia, 4 in the United States, and 4 in the United Kingdom. All were conducted in academic teaching hospitals. Two studies37, 38 focused on pediatric inpatients, and the remainder involved hospitalized adults. The RRS intervened for all hospitalized patients in all but 2 studies (1 of which focused on surgical inpatients33 and the other in which the RRS evaluated only patients discharged from the ICU3). In 2 studies,31, 39 the RRS was available to evaluate outpatients, such as hospital visitors, in addition to inpatients.0
| Study | Location | Hospital type | Patient population | RRS composition | Measured outcomes | Definition of unscheduled ICU admission | Definition of cardiac arrest |
|---|---|---|---|---|---|---|---|
| |||||||
| Buist et al., 200220 | Australia | Tertiary‐care academic hospital | Adult inpatients | ICU registrar | DNR status | Not supplied | Any code blue team activation |
| Medical registrar | Cardiac arrest | ||||||
| ICU nurse | Unscheduled ICU admission | ||||||
| Mortality | |||||||
| Bellomo et al., 200321 | Australia | Tertiary‐care academic hospital | Adult inpatients | ICU nurse and ICU fellow attended all calls; ICU attending (8 AM‐8 PM) and medical registrar attended if requested | Mortality | NA | Unresponsive, with no pulse or blood pressure, and basic life support initiated |
| Cardiac arrest | |||||||
| DNR status | |||||||
| Pittard et al., 200322 | United Kingdom | Tertiary‐care academic hospital | Adult inpatients on surgical wards | Senior critical care nurses and medical staff | Unscheduled ICU admission | Any patient not admitted directly from operating theater after elective surgery | NA |
| Bellomo et al., 200431 | Australia | Tertiary‐care academic hospital | Adult postoperative patients | ICU attending | Mortality Unscheduled ICU admission ICU length of stay DNR status | Postoperative admission to ICU because of a clinical complication | NA |
| ICU fellow | Unscheduled ICU admission | ||||||
| ICU registered nurse | ICU length of stay | ||||||
| Medical fellow | DNR status | ||||||
| DeVita et al., 200432 | United States | Tertiary‐care academic hospital | Adult inpatients | ICU physician | Cardiac arrest | NA | Any code blue team activation |
| Anesthesiologist | |||||||
| 2 other physicians | |||||||
| 2 ICU nurses | |||||||
| Floor nurse | |||||||
| Respiratory therapist | |||||||
| Garcea et al., 20043 | United Kingdom | Teaching hospital | Adult patients discharged from ICU | 2 ICU nurses | Mortality | Emergency readmissions to ICU | NA |
| 1 ICU nurse specialist | Unscheduled ICU admission | ||||||
| ICU consultant physician (if needed) | |||||||
| Kenward et al., 200438 | United Kingdom | Teaching hospital | Adult inpatients | Not stated | Mortality | NA | Loss of spontaneous circulation |
| Cardiac arrest | |||||||
| Priestley et al., 200433 | United Kingdom | Teaching hospital | Adult inpatients | ICU nurse consultant | Mortality | NA | NA |
| ICU physician available if needed | Overall length of stay | ||||||
| Hillman et al., 200534 | Australia | 23 hospitals (17 academic, 6 nonacademic) | Adult inpatients | Varied between study hospitals; required to have at least 1 MD and 1 RN from ED or ICU | Mortality | Any unscheduled admission to ICU from general ward | No palpable pulse |
| Cardiac arrest | |||||||
| Unscheduled ICU admission | |||||||
| DNR status | |||||||
| Hunt et al., 2005 (abstract)36 | United States | Pediatric tertiary‐care academic hospital | Pediatric inpatients | Not provided | Cardiac arrest | NA | Not provided |
| Meredith et al., 2005 (abstract)37 | United States | Tertiary‐care academic hospital | Adult inpatients, outpatients, and visitors | ICU registered nurse | Mortality | NA | Not provided |
| Respiratory therapist | |||||||
| Tibballs et al., 200535 | Australia | Pediatric tertiary‐care academic hospital | Pediatric inpatients | ICU physician | Cardiac arrest | Not supplied | Not provided |
| Medical registrar | Unscheduled ICU admission | ||||||
| ED physician | |||||||
| ICU nurse | |||||||
| King et al., 200629 | United States | Tertiary‐care academic hospital | Adult inpatients, outpatients, and visitors | Hospitalist | Cardiac arrest | NA | Not provided |
| Internal medicine resident | |||||||
| ICU nurse | |||||||
| Ward nurse | |||||||
| Pharmacist | |||||||
RRS Structure, Calling Criteria, and Responsibilities
Seven studies22, 23, 31, 33, 34, 36, 37 that described the team composition used variants of the medical emergency team model, a physician‐led team (Table 2). In 6 of these 7 studies, the team included a critical care physician (attending or fellow) and an ICU nurse; in the sole RCT (the MERIT study36), the team structure varied between hospitals, consisting of a nurse and physician from either the emergency department or ICU. Hospitalists, who are involved in RRS responses at many U.S. hospitals, were primary team leaders of the RRS in only 1 study.31 In 2 studies34, 37 the RRS also responded to code blue calls, and in 4 studies23, 31, 33, 39 the RRS and the code blue team had separate personnel; the remaining studies did not define the distinction between RRS and code blue team.
| Study | Contemporaneous control group | Data reported at more than 1 time before/after intervention | RRS calling rate reported | Outcomes analysis included patients made DNR by team | Blind measurement of nonobjective outcomes | Intensivist always available | Other QI efforts during study |
|---|---|---|---|---|---|---|---|
| |||||||
| Buist et al., 200220 | No | No | Yes | No (mortality) | No | NR | NR |
| Bellomo et al., 200321 | No | No | Yes | Yes (mortality) | NA | Yes (ICU fellow) | No |
| Pittard et al., 200322 | No | No | Yes | NA | No | NR | NR |
| Bellomo et al., 200431 | No | No | Yes | Yes (mortality) | No | Yes (ICU fellow) | No |
| DeVita et al., 200432 | No | Yes | Yes | NA | No | Yes (critical care attending physician) | NR |
| Garcea et al., 200433 | No | No | No | Unclear | No | NR | NR |
| Kenward et al., 200438 | No | No | Yes | Unclear | No | NR | NR |
| Priestley et al., 200433 | No (interrupted time series) | Yes | No | NA | No | NR | NR |
| Hillman et al., 200534 | Yes | No | Yes | Unclear | Yes | NR | No |
| Hunt et al., 2005 (abstract)36 | No | No | Yes | NA | NR | NR | NR |
| Meredith et al., 2005 (abstract)37 | No | No | Yes | No | NA | No | No |
| Tibballs et al., 200535 | No | No | Yes | Unclear | No | NR | Yes (educational workshops/more training in APLS) |
| King et al., 200629 | No | Yes | Yes | NA | No | Yes | No |
In 4 studies the RRSs were led by nurses. One study published in abstract form39 used the rapid response team model, consisting of a critical care nurse and a respiratory therapist, with assistance as needed from the primary medical staff and a critical care physician. Three studies3, 24, 35 from UK hospitals used the critical care outreach (CCO) model, in which ICU‐trained nurses respond initially with assistance from intensivists. The CCO model also involves follow‐up on patients discharged from the ICU and proactive rounding on unstable ward patients.
The hospitals used broadly similar approaches to determining when to summon the RRS, relying on combinations of objective clinical criteria (eg, vital sign abnormalities) and subjective criteria (eg, acute mental status change, staff member concerned about patient's condition). Three studies3, 24, 35 used a formal clinical score (the Patient‐At‐Risk score or the Modified Early Warning score) to trigger calls to the RRS. Three studies, 2 of them from the same institution,23, 33 reported the frequency of specific triggers for RRS activation. Concern by bedside staff and respiratory distress were the most frequent activators of the RRS.
Study Internal Validity and Generalizability
One study,36 the MERIT trial, conducted in Australia, was a cluster‐randomized RCT (randomized by hospital) that adhered to recommended elements of design and reporting for studies of this type.41 In this study, hospitals in the control group received an educational intervention on caring for deteriorating patients only; hospitals in the intervention group received the educational module and started an RRS. An additional study35 identified itself as a randomized trial, but randomization occurred at the hospital ward level, with introduction of the intervention (critical care outreach) staggered so that at different points an individual ward could have been in either the control or intervention group; therefore, this study was considered an interrupted time series. All other trials included were before‐after studies with no contemporaneous control group
Most studies did not meet criteria for internal validity or generalizability (Table 2). Two studies3, 35 did not report the number of RRS calls during the study period. One study22 omitted patients whose resuscitation status was changed after RRS evaluation from the calculation of inpatient mortality; thus, the patients who had been made do not resuscitate by the RRS did not contribute to the calculated mortality rate. The disposition of these patients was unclear in another study.36 All studies measured clinical outcomes retrospectively, and no studies reported blinding of outcomes assessors for nonobjective outcomes (eg, unplanned ICU admission). Studies generally did not report on the availability of intensivists or if other quality improvement interventions targeting critically ill patients were implemented along with the RRS.
RRS Usage and Effects on Patient Outcomes
Seven studies2224, 34, 3638 reported enough information to calculate the RRS calling rate (4 studies24, 31, 39, 40 reported the total number of calls but not the number of admissions, and 2 studies3, 35 did not report either). In these 7 studies, the calling rate varied from 4.5 to 25.8 calls per 1000 admissions. Three studies documented the calling rate before and after the intervention: a study at a hospital with a preexisting RRS34 reported that the calling rate increased from 13.7 to 25.8 calls per 1000 admissions after an intensive education and publicity program; in a pediatric trial,38 the overall emergency calling rate (for cardiac arrests and medical emergencies) was reported to increase from 6.6 to 10.4 per 1000 admissions; and in the MERIT trial,36 calls increased from 3.1 to 8.7 per 1000 admissions.
Effects of RRS on Clinical Outcomes
Nine studies3, 22, 23, 33, 3537, 39, 40 reported the effect of an RRS on inpatient mortality, 9 studies22, 23, 31, 33, 34, 3638, 40 reported its effect on cardiopulmonary arrests, and 6 studies3, 22, 24, 33, 36, 37 reported its effect on unscheduled ICU admissions. Of these, 7 trials that reported mortality and cardiopulmonary arrests and 6 studies that reported unscheduled ICU admissions supplied sufficient data for meta‐analysis.
Observational studies demonstrated improvement in inpatient mortality, with a summary risk ratio of 0.82 (95% CI: 0.74‐0.91, heterogeneity I2 62.1%; Fig. 2). However, the magnitude of these improvements was very similar to that seen in the control group of the MERIT trial (RR 0.73, 95% CI: 0.53‐1.02). The intervention group of the MERIT trial also demonstrated a reduction in mortality that was not significantly different from that of the control group (RR 0.65, 95% CI: 0.48‐0.87). We found a similar pattern in studies reporting RRS effects on cardiopulmonary arrests (Fig. 3). The observational studies did not show any effect on the risk of unscheduled ICU admissions (summary RR 1.08, 95% CI: 0.96‐1.22, heterogeneity I2 79.1%) nor did the MERIT trial (Fig. 4).
DISCUSSION
Despite the strong face validity of the RRS concept, the current literature on medical emergency teams, rapid response teams, and critical care outreach suffers from substantial flaws that make it difficult to determine the effect of an RRS on patient outcomes. These flaws include the use of suboptimal study designs, failure to report important cointerventions, the methods in which outcomes were defined, and lack of verification of the validity of the outcomes measured. As a result, very little empiric data are available to define the effectiveness of RRSs or to provide guidance for hospitals planning to implement an RRS.
Though early studies reported that RRSs appeared to reduce mortality and cardiac arrest rates, the sole randomized trial of an RRS (the MERIT trial36) showed no differences between intervention and control hospitals for any clinical outcome. Both inpatient mortality and cardiac arrest rates declined in the intervention and control groups of the MERIT trial, and the reductions in these outcomes in observational trials were similar to those seen in the MERIT control group. This strongly implies that other factors besides the RRS were responsible for the results of previous before‐after studies. These studies, which have been widely cited by proponents of the RRS, suffer from methodological limitations intrinsic to the study design and issues with outcome measurement that may have introduced systematic bias; these factors likely explain the contrast between the generally positive results of the before‐after studies and the negative results of the MERIT trial.
Most early RRS trials used an uncontrolled before‐after study design, as is common in quality improvement studies.42 This study design cannot account for secular trends or other factors, including other QI interventions, that could influence the effect of an intervention.26 The statistically significant reduction in impatient mortality in the control arm of the MERIT trial is an instructive example; this decline could have been a result of the educational intervention on caring for deteriorating patients, other ongoing QI projects at the individual hospitals, or simply random variation during the relatively short (6‐month) follow‐up period. Such factors could also entirely account for the impressive results seen in the initial uncontrolled RRS studies. Nearly all the studies we reviewed also did not discuss any aspects of the hospital context that could influence outcomes for critically ill patients, such as the nurse‐staffing ratio,43 ICU bed availability,4446 overall hospital census,47 or availability of intensivists48 or hospitalists.49 Failure to control foror at least report important aspects ofthe environment in which the intervention was performed is akin to failing to report baseline patient comorbidities or concurrent therapies in a study of a drug's effectiveness.
Our review also suggests how bias in the measurement of clinical outcomes may have contributed to the apparent effect of RRSs. In 1 before‐after study, patients for whom RRS activation resulted in a change code status to do not resuscitate (DNR) were excluded from calculations of mortality,22, 50 resulting in underreporting of mortality after RRS implementation. Disposition of such patients was unclear in 3 other studies.3, 36, 40 Some studies22, 34 defined cardiopulmonary arrest as any activation of the code blue team, regardless of whether the patient was actually in cardiac arrest. This almost inevitably would result in fewer arrests after implementation of the RRS, as the indications for calling the code blue team would be narrower. Finally, nearly all studies used trends in nonobjective primary outcomes (eg, unplanned ICU transfer) to support RRS effects but did not validate any of these outcomes (eg, how often did reviewers agree an ICU transfer was preventable), and none of the assessors of these outcomes were blinded.
Some have attributed the MERIT trial not finding the RRS beneficial to inadequate implementation, as the RRS calling rate of 8.7 calls per 1000 admissions was less than the 15 calls per 1000 admissions cited as optimal in a mature RRS.51 However, published studies generally reported a calling rate of 4‐5 calls per 1000 admissions,22, 23, 37 with only 1 trial reporting a higher calling rate.34
A recent commentary20 and a systematic review of critical care outreach teams21 both addressed the effectiveness of RRSs. We sought to examine the effects of all RRS subtypes and using quantitative analysis and analysis of methodological quality, to determine the overall effect of RRSs. The results of our analysis (which included data from several newer studies31, 38, 39) support and extend the conclusion of prior reviews that RRSs, although a potentially promising intervention, do not unequivocally benefit patients and are not worthy of more widespread use until more evidence becomes available. Our analysis also demonstrates that many studies widely cited as supporting wide implementation of RRSs are flawed and probably not generalizable.
Despite these caveats, RRSs remain an intuitively attractive concept and may be of benefit at some hospitals. Further studies in this area should focus on identifying which patient populations are at high risk for clinical decompensation, identifying the role of clinical structures of care (eg, nurse‐staffing ratio, presence of hospitalists) in preventing adverse outcomes and determining which specific RRS model is most effective. As well, more information is needed about educating bedside staff and RRS team members, as this is likely critical to success of the team. Unfortunately, only the article by King et al.31 provided sufficient detail about the implementation process to assist hospitals in planning an RRS. The remaining articles had only scant details about the intervention and its implementation, a common problem noted in the quality improvement literature.42, 52, 53
Our analysis had several limitations. We attempted to identify as many RRS trials as possible by searching multiple databases and reviewing abstract proceedings, but as the RRS literature is in its infancy, we may not have located other unpublished studies or gray literature. There is no validated system for evaluating the methodological strength of nonrandomized studies; therefore, we assessed study quality on the basis of prespecified criteria for internal and external validity. Finally, we found significant statistical heterogeneity in our quantitative analyses, indicating that the variability between individual studies in treatment effects was greater than that expected by chance. As the primary reasons we conducted a meta‐analysis was to compare the results of before‐after trials with those of the randomized MERIT trial, we did not further explore the reasons for this heterogeneity, although variation in patient populations and RRS structure likely accounts for a significant proportion of the heterogeneity.
Although there is a theoretical basis for implementing a rapid response system, the published literature shows inconsistent benefits to patients and suffers from serious methodological flaws. Future studies of RRSs should attempt to define which patient populations are at risk, the essential characteristics of RRSs, effective implementation strategies, andmost importantwhether any RRS improves clinical outcomes. Until such evidence is available, hospitals should not be mandated to establish an RRS and should consider prioritizing quality improvement resources for interventions with a stronger evidence base.
Acknowledgements
The authors thank Emmanuel King, MD, for graciously providing a copy of his manuscript prior to publication and Alexis Meredith, MD, for providing additional information regarding his study. Dr. Shojania holds a Government of Canada Research Chair in Patient Safety and Quality Improvement.
APPENDIX
| Search terms | Citations | |
|---|---|---|
| 1 | {(rapid [ti] AND (response [ti] OR resuscitation [ti]) OR (patient at risk [ti])} AND (program [ti] OR team* [ti] OR service* [ti]) | 23 |
| 2 | medical emergency team* [ti] OR medical crisis team* [ti] OR {(critical [ti] OR intensive [ti]) AND care [ti] AND outreach [ti]} | 87 |
| 3 | hospital [ti] AND resuscitation [ti] AND team* [ti] | 11 |
| 4 | medical emergency team* [ab] OR rapid response team [ab] OR medical crisis team* [ab] | 89 |
| 5 | #1 OR #2 OR #3 OR #4 | 158 |
| 6 | Resuscitation [mh] OR heart arrest [mh] OR hospital mortality [mh] | 72,488 |
| 7 | (patient care team [mh] OR critical care [mh] OR intensive care units [mh]) AND (patient readmission [mh] OR organization and administration [mh]) | 20,321 |
| 8 | #6 AND #7 | 1,419 |
| 9 | {(randomised[ti] OR randomized[ti] OR controlled[ti] OR intervention[ti] OR evaluation[ti] OR comparative[ti] OR effectiveness[ti] OR evaluation[ti] OR feasibility[ti]) AND (trial[ti] OR studies[ti] OR study[ti] OR program[ti] OR design[ti])} OR clinical trial[pt] OR randomized controlled trial[pt] OR epidemiologic studies[mh] OR evaluation studies[mh] OR comparative study[mh] OR feasibility studies[mh] OR intervention studies[mh] OR program evaluation[mh] OR epidemiologic research design[mh] OR systematic5 | 2,688,847 |
| 10 | #8 AND #9 | 748 |
| 11 | #5 OR #10 | 806 |
- ,,,.The medical emergency team.Anaesth Intensive Care.1995;23(2):183–186.
- ,,,.The 100 000 Lives Campaign: setting a goal and a deadline for improving health care quality.JAMA.2006;295(3):324–7.
- ,,,,.Impact of a critical care outreach team on critical care readmissions and mortality.Acta Anaesthesiol Scand2004;48:1096–1100.
- ,.The patient‐at‐risk team.Anaesthesia.2000;55(2):198.
- ,,, et al.Findings of the First Consensus Conference on Medical Emergency Teams.Crit Care Med.2006;34:2463–2478.
- .Recognition of patients who require emergency assistance: a descriptive study.Heart Lung.2000;29(4):262–268.
- ,,, et al.Antecedents to hospital deaths.Intern Med J.2001;31:343–348.
- ,,, et al.Duration of life‐threatening antecedents prior to intensive care admission.Intensive Care Med.2002;28:1629–1634.
- ,,,,.The identification of risk factors for cardiac arrest and formulation of activation criteria to alert a medical emergency team.Resuscitation.2002;54:125–131.
- ,,,,,.A comparison of antecedents to cardiac arrests, deaths and emergency intensive care admissions in Australia and New Zealand, and the United Kingdom—the ACADEMIA study.Resuscitation.2004;62:275–282.
- ,,,.Validation of a modified Early Warning Score in medical admissions.QJM.2001;94:521–526.
- ,,,,.Inpatient transfers to the intensive care unit: delays are associated with increased mortality and morbidity.J Gen Intern Med.2003;18(2):77–83.
- ,,,,.Clinical antecedents to in‐hospital cardiopulmonary arrest.Chest.1990;98:1388–1392.
- ,.Developing strategies to prevent inhospital cardiac arrest: analyzing responses of physicians and nurses in the hours before the event.Crit Care Med.1994;22(2):244–247.
- ,,.Introduction to the rapid response systems series.Jt Comm J Qual Patient Saf.2006;32:359–360.
- ,,, et al.Rates of in‐hospital arrests, deaths and intensive care admissions: the effect of a medical emergency team.Med J Aust.2000;173:236–240.
- ,,,,.The patient‐at‐risk team: identifying and managing seriously ill ward patients.Anaesthesia.1999;54:853–860.
- .The medical emergency team: no evidence to justify not implementing change.Med J Aust.2000;173:228–229.
- ,.The medical emergency team, evidence‐based medicine and ethics.Med J Aust.2003;179:313–315.
- ,,.Rapid response teams—walk, don't run.JAMA.2006;296:1645–1647.
- ,,, et al.Investigating the effectiveness of critical care outreach services: a systematic review.Intensive Care Med.2006;32:1713–1721.
- ,,,,,.Effects of a medical emergency team on reduction of incidence of and mortality from unexpected cardiac arrests in hospital: preliminary study.BMJ.2002;324:387–390.
- ,,, et al.A prospective before‐and‐after trial of a medical emergency team.Med J Aust.2003;179:283–287.
- .Out of our reach? Assessing the impact of introducing a critical care outreach service.Anaesthesia.2003;58:882–885.
- Cochrane Collaboration Effective Practice and Organisation of Care group. Available at: http://www.epoc.uottawa.ca/inttime.pdf.Accessed August 4,2006.
- ,,.Experimental and Quasi‐Experimental Designs for Generalized Causal Inference.Boston, MA:Houghton Mifflin;2002.
- ,,, et al.Guidelines for the uniform reporting of data for Medical Emergency Teams.Resuscitation.2006;68(1):11–25.
- ,.The intracluster correlation coefficient in cluster randomisation.BMJ.1998;316:1455.
- ,.Issues in the meta‐analysis of cluster randomized trials.Stat Med.2002;21:2971–2980.
- ,,,.Measuring inconsistency in meta‐analyses.BMJ.2003;327:557–560.
- ,,.Establishing a rapid response team (RRT) in an academic hospital: one year's experience.J Hosp Med.2006;1:296–305.
- ,,, et al.A multidisciplinary community hospital program for early and rapid resuscitation of shock in nontrauma patients.Chest.2005;127:1729–1743.
- ,,, et al.Prospective controlled trial of effect of medical emergency team on postoperative morbidity and mortality rates.Crit Care Med.2004;32:916–921.
- ,,,,,.Use of medical emergency team responses to reduce hospital cardiopulmonary arrests.Qual Saf Health Care.2004;13:251–254.
- ,,, et al.Introducing critical care outreach: a ward‐randomised trial of phased introduction in a general hospital.Intensive Care Med.2004;30:1398–1404.
- ,,, et al.Introduction of the medical emergency team (MET) system: a cluster‐randomised controlled trial.Lancet.2005;365:2091–2097.
- ,,,,.Reduction of paediatric in‐patient cardiac arrest and death with a medical emergency team: preliminary results.Arch Dis Child.2005;90:1148–1152.
- ,,, et al.The effect of transition from a traditional code team to a rapid response team in a children's center: a before and after intervention trial [abstract].Crit Care Med.2005;33(12 suppl):A17.
- ,,,,.Improved hospital mortality by institution of a rapid response team in a university hospital.Chest.2005;128(suppl S):182S.
- ,,,.Evaluation of a medical emergency team one year after implementation.Resuscitation.2004;61(3):257–263.
- ,,.CONSORT statement: extension to cluster randomised trials.BMJ.2004;328:702–708.
- ,.Evidence‐Based Quality Improvement: The State Of The Science.Health Aff.2005;24(1):138–150.
- ,,,,.Hospital nurse staffing and patient mortality, nurse burnout, and job dissatisfaction.JAMA.2002;288:1987–1993.
- ,,, et al.Evaluation of triage decisions for intensive care admission.Crit Care Med.1999;27:1073–1079.
- ,,,,.Rationing of intensive care unit services. An everyday occurrence.JAMA.1986;255:1143–1146.
- ,,,.How do physicians adapt when the coronary care unit is full? A prospective multicenter study.JAMA.1987;257:1181–1185.
- ,,,,.The association between hospital overcrowding and mortality among patients admitted via Western Australian emergency departments.Med J Aust.2006;184:208–212.
- ,,,,,.Physician staffing patterns and clinical outcomes in critically ill patients: a systematic review.JAMA.2002;288:2151–2'62.
- ,,,,,.Implementation of a voluntary hospitalist service at a community teaching hospital: improved clinical efficiency and patient outcomes.Ann Intern Med.2002;137:859–865.
- .Critical care outreach team's effect on patient outcome: other conclusions are possible.BMJ.2004;328:347; author reply
- The “MERIT” Trial of medical emergency teams in Australia: an analysis of findings and implications for the 100,000 Lives Campaign. Institute for Healthcare Improvement,2006. Available at: http://www.ihi.org/NR/rdonlyres/F3401FEF‐2179‐4403‐8F67–B9255C57E207/0/LancetAnalysis81505.pdf. Accessed August 17, 2006.
- ,,, et al.Toward evidence‐based quality improvement. evidence (and its limitations) of the effectiveness of guideline dissemination and implementation strategies 1966‐1998.J Gen Intern Med.2006;21(suppl 2):S14–S20.
- ,,, et al.lessons learned about implementing research evidence into clinical practice. Experiences from VA QUERI.J Gen Intern Med.2006;21(suppl 2):S21–S24.
- ,,,,,.Improving the quality of reports of meta‐analyses of randomised controlled trials: the QUOROM statement. Quality of reporting of meta‐analyses.Lancet.1999;354:1896–1900.
- ,,,,,.Improving the utilization of medical crisis teams (Condition C) at an urban tertiary care hospital.J Crit Care.2003;18(2):87–94.
- ,,, et al.Long term effect of a medical emergency team on cardiac arrests in a teaching hospital.Crit Care.2005;9:R808–R815.
- ,,,.The medical emergency team.Anaesth Intensive Care.1995;23(2):183–186.
- ,,,.The 100 000 Lives Campaign: setting a goal and a deadline for improving health care quality.JAMA.2006;295(3):324–7.
- ,,,,.Impact of a critical care outreach team on critical care readmissions and mortality.Acta Anaesthesiol Scand2004;48:1096–1100.
- ,.The patient‐at‐risk team.Anaesthesia.2000;55(2):198.
- ,,, et al.Findings of the First Consensus Conference on Medical Emergency Teams.Crit Care Med.2006;34:2463–2478.
- .Recognition of patients who require emergency assistance: a descriptive study.Heart Lung.2000;29(4):262–268.
- ,,, et al.Antecedents to hospital deaths.Intern Med J.2001;31:343–348.
- ,,, et al.Duration of life‐threatening antecedents prior to intensive care admission.Intensive Care Med.2002;28:1629–1634.
- ,,,,.The identification of risk factors for cardiac arrest and formulation of activation criteria to alert a medical emergency team.Resuscitation.2002;54:125–131.
- ,,,,,.A comparison of antecedents to cardiac arrests, deaths and emergency intensive care admissions in Australia and New Zealand, and the United Kingdom—the ACADEMIA study.Resuscitation.2004;62:275–282.
- ,,,.Validation of a modified Early Warning Score in medical admissions.QJM.2001;94:521–526.
- ,,,,.Inpatient transfers to the intensive care unit: delays are associated with increased mortality and morbidity.J Gen Intern Med.2003;18(2):77–83.
- ,,,,.Clinical antecedents to in‐hospital cardiopulmonary arrest.Chest.1990;98:1388–1392.
- ,.Developing strategies to prevent inhospital cardiac arrest: analyzing responses of physicians and nurses in the hours before the event.Crit Care Med.1994;22(2):244–247.
- ,,.Introduction to the rapid response systems series.Jt Comm J Qual Patient Saf.2006;32:359–360.
- ,,, et al.Rates of in‐hospital arrests, deaths and intensive care admissions: the effect of a medical emergency team.Med J Aust.2000;173:236–240.
- ,,,,.The patient‐at‐risk team: identifying and managing seriously ill ward patients.Anaesthesia.1999;54:853–860.
- .The medical emergency team: no evidence to justify not implementing change.Med J Aust.2000;173:228–229.
- ,.The medical emergency team, evidence‐based medicine and ethics.Med J Aust.2003;179:313–315.
- ,,.Rapid response teams—walk, don't run.JAMA.2006;296:1645–1647.
- ,,, et al.Investigating the effectiveness of critical care outreach services: a systematic review.Intensive Care Med.2006;32:1713–1721.
- ,,,,,.Effects of a medical emergency team on reduction of incidence of and mortality from unexpected cardiac arrests in hospital: preliminary study.BMJ.2002;324:387–390.
- ,,, et al.A prospective before‐and‐after trial of a medical emergency team.Med J Aust.2003;179:283–287.
- .Out of our reach? Assessing the impact of introducing a critical care outreach service.Anaesthesia.2003;58:882–885.
- Cochrane Collaboration Effective Practice and Organisation of Care group. Available at: http://www.epoc.uottawa.ca/inttime.pdf.Accessed August 4,2006.
- ,,.Experimental and Quasi‐Experimental Designs for Generalized Causal Inference.Boston, MA:Houghton Mifflin;2002.
- ,,, et al.Guidelines for the uniform reporting of data for Medical Emergency Teams.Resuscitation.2006;68(1):11–25.
- ,.The intracluster correlation coefficient in cluster randomisation.BMJ.1998;316:1455.
- ,.Issues in the meta‐analysis of cluster randomized trials.Stat Med.2002;21:2971–2980.
- ,,,.Measuring inconsistency in meta‐analyses.BMJ.2003;327:557–560.
- ,,.Establishing a rapid response team (RRT) in an academic hospital: one year's experience.J Hosp Med.2006;1:296–305.
- ,,, et al.A multidisciplinary community hospital program for early and rapid resuscitation of shock in nontrauma patients.Chest.2005;127:1729–1743.
- ,,, et al.Prospective controlled trial of effect of medical emergency team on postoperative morbidity and mortality rates.Crit Care Med.2004;32:916–921.
- ,,,,,.Use of medical emergency team responses to reduce hospital cardiopulmonary arrests.Qual Saf Health Care.2004;13:251–254.
- ,,, et al.Introducing critical care outreach: a ward‐randomised trial of phased introduction in a general hospital.Intensive Care Med.2004;30:1398–1404.
- ,,, et al.Introduction of the medical emergency team (MET) system: a cluster‐randomised controlled trial.Lancet.2005;365:2091–2097.
- ,,,,.Reduction of paediatric in‐patient cardiac arrest and death with a medical emergency team: preliminary results.Arch Dis Child.2005;90:1148–1152.
- ,,, et al.The effect of transition from a traditional code team to a rapid response team in a children's center: a before and after intervention trial [abstract].Crit Care Med.2005;33(12 suppl):A17.
- ,,,,.Improved hospital mortality by institution of a rapid response team in a university hospital.Chest.2005;128(suppl S):182S.
- ,,,.Evaluation of a medical emergency team one year after implementation.Resuscitation.2004;61(3):257–263.
- ,,.CONSORT statement: extension to cluster randomised trials.BMJ.2004;328:702–708.
- ,.Evidence‐Based Quality Improvement: The State Of The Science.Health Aff.2005;24(1):138–150.
- ,,,,.Hospital nurse staffing and patient mortality, nurse burnout, and job dissatisfaction.JAMA.2002;288:1987–1993.
- ,,, et al.Evaluation of triage decisions for intensive care admission.Crit Care Med.1999;27:1073–1079.
- ,,,,.Rationing of intensive care unit services. An everyday occurrence.JAMA.1986;255:1143–1146.
- ,,,.How do physicians adapt when the coronary care unit is full? A prospective multicenter study.JAMA.1987;257:1181–1185.
- ,,,,.The association between hospital overcrowding and mortality among patients admitted via Western Australian emergency departments.Med J Aust.2006;184:208–212.
- ,,,,,.Physician staffing patterns and clinical outcomes in critically ill patients: a systematic review.JAMA.2002;288:2151–2'62.
- ,,,,,.Implementation of a voluntary hospitalist service at a community teaching hospital: improved clinical efficiency and patient outcomes.Ann Intern Med.2002;137:859–865.
- .Critical care outreach team's effect on patient outcome: other conclusions are possible.BMJ.2004;328:347; author reply
- The “MERIT” Trial of medical emergency teams in Australia: an analysis of findings and implications for the 100,000 Lives Campaign. Institute for Healthcare Improvement,2006. Available at: http://www.ihi.org/NR/rdonlyres/F3401FEF‐2179‐4403‐8F67–B9255C57E207/0/LancetAnalysis81505.pdf. Accessed August 17, 2006.
- ,,, et al.Toward evidence‐based quality improvement. evidence (and its limitations) of the effectiveness of guideline dissemination and implementation strategies 1966‐1998.J Gen Intern Med.2006;21(suppl 2):S14–S20.
- ,,, et al.lessons learned about implementing research evidence into clinical practice. Experiences from VA QUERI.J Gen Intern Med.2006;21(suppl 2):S21–S24.
- ,,,,,.Improving the quality of reports of meta‐analyses of randomised controlled trials: the QUOROM statement. Quality of reporting of meta‐analyses.Lancet.1999;354:1896–1900.
- ,,,,,.Improving the utilization of medical crisis teams (Condition C) at an urban tertiary care hospital.J Crit Care.2003;18(2):87–94.
- ,,, et al.Long term effect of a medical emergency team on cardiac arrests in a teaching hospital.Crit Care.2005;9:R808–R815.