HM15 presenters: Joshua D. Lenchus, DO, FACP, SFHM, and Nilam Soni, MD, FHM
Summary: Drs. Lenchus and Soni focused on the forces that are driving the value and success of established procedure teams in hospital medicine groups (HMGs). These stem from a need to rapidly address the growing shortage of skilled internists who can perform diagnostic and therapeutic procedures, thus leading to a subset of hospitalists who are willing to provide these services, particularly with the assistance of bedside ultrasonography.
They stressed the importance of providing a platform that is preemptive, proprietary, and scalable. With a defined set of value-creating metrics such as faster turn-around times, a reduction in complication rates, and ultimately a reduction in cost, LOS, and utilization, data must be collected to adequately measure the impact of these services on the institution.
They also discussed the key components necessary to create a procedure service, starting with the logistics of adequate training and demonstration of competence, proper staffing, supplies and equipment, ultrasound image archiving, and the use of documentation templates. The process is followed by the development of pre-procedure and post-procedure guidelines, as well as standardized procedural techniques.
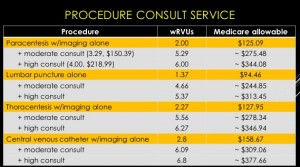
The session also reviewed billing practices and professional fees. An analysis was made comparing Medicare reimbursement and work RVUs for each procedure service with and without a full procedure consultation. A complete consultation significantly increases the allowable fee and associated wRVU. The caveat is that billing for consults is limited to services rendered for patients that are not cared for by the same hospitalist group.
Furthermore, sub-specialists historically perform these procedures. The argument can be made that hospitalists will reduce an unnecessary burden on interventional radiologists, thereby enabling them to focus on more acomplex invasive and highly technical procedures.
The key to success is the ability to find a strategic partner in the C-suite who will directly or indirectly provide the financial and political support. Other sources of funding include private foundations, medical schools, the Department of Veteran Affairs, and such patient safety organizations as AHRQ, IOM, and IHI. HMG leaders also should consider scalability across other hospitalist groups.
“If you build it, they will come."
HM takeaways
Create a business plan;
Find institutional financial and political support;
Start small and selective;
Plan for standardization and training of colleagues;
Create a credentialing/privileging process;
Bill for services and consider billing for full consults; and
HM15 presenters: Joshua D. Lenchus, DO, FACP, SFHM, and Nilam Soni, MD, FHM
Summary: Drs. Lenchus and Soni focused on the forces that are driving the value and success of established procedure teams in hospital medicine groups (HMGs). These stem from a need to rapidly address the growing shortage of skilled internists who can perform diagnostic and therapeutic procedures, thus leading to a subset of hospitalists who are willing to provide these services, particularly with the assistance of bedside ultrasonography.
They stressed the importance of providing a platform that is preemptive, proprietary, and scalable. With a defined set of value-creating metrics such as faster turn-around times, a reduction in complication rates, and ultimately a reduction in cost, LOS, and utilization, data must be collected to adequately measure the impact of these services on the institution.
They also discussed the key components necessary to create a procedure service, starting with the logistics of adequate training and demonstration of competence, proper staffing, supplies and equipment, ultrasound image archiving, and the use of documentation templates. The process is followed by the development of pre-procedure and post-procedure guidelines, as well as standardized procedural techniques.
The session also reviewed billing practices and professional fees. An analysis was made comparing Medicare reimbursement and work RVUs for each procedure service with and without a full procedure consultation. A complete consultation significantly increases the allowable fee and associated wRVU. The caveat is that billing for consults is limited to services rendered for patients that are not cared for by the same hospitalist group.
Furthermore, sub-specialists historically perform these procedures. The argument can be made that hospitalists will reduce an unnecessary burden on interventional radiologists, thereby enabling them to focus on more acomplex invasive and highly technical procedures.
The key to success is the ability to find a strategic partner in the C-suite who will directly or indirectly provide the financial and political support. Other sources of funding include private foundations, medical schools, the Department of Veteran Affairs, and such patient safety organizations as AHRQ, IOM, and IHI. HMG leaders also should consider scalability across other hospitalist groups.
“If you build it, they will come."
HM takeaways
Create a business plan;
Find institutional financial and political support;
Start small and selective;
Plan for standardization and training of colleagues;
Create a credentialing/privileging process;
Bill for services and consider billing for full consults; and
Gather baseline and follow-up data.
HM15 presenters: Joshua D. Lenchus, DO, FACP, SFHM, and Nilam Soni, MD, FHM
Summary: Drs. Lenchus and Soni focused on the forces that are driving the value and success of established procedure teams in hospital medicine groups (HMGs). These stem from a need to rapidly address the growing shortage of skilled internists who can perform diagnostic and therapeutic procedures, thus leading to a subset of hospitalists who are willing to provide these services, particularly with the assistance of bedside ultrasonography.
They stressed the importance of providing a platform that is preemptive, proprietary, and scalable. With a defined set of value-creating metrics such as faster turn-around times, a reduction in complication rates, and ultimately a reduction in cost, LOS, and utilization, data must be collected to adequately measure the impact of these services on the institution.
They also discussed the key components necessary to create a procedure service, starting with the logistics of adequate training and demonstration of competence, proper staffing, supplies and equipment, ultrasound image archiving, and the use of documentation templates. The process is followed by the development of pre-procedure and post-procedure guidelines, as well as standardized procedural techniques.
The session also reviewed billing practices and professional fees. An analysis was made comparing Medicare reimbursement and work RVUs for each procedure service with and without a full procedure consultation. A complete consultation significantly increases the allowable fee and associated wRVU. The caveat is that billing for consults is limited to services rendered for patients that are not cared for by the same hospitalist group.
Furthermore, sub-specialists historically perform these procedures. The argument can be made that hospitalists will reduce an unnecessary burden on interventional radiologists, thereby enabling them to focus on more acomplex invasive and highly technical procedures.
The key to success is the ability to find a strategic partner in the C-suite who will directly or indirectly provide the financial and political support. Other sources of funding include private foundations, medical schools, the Department of Veteran Affairs, and such patient safety organizations as AHRQ, IOM, and IHI. HMG leaders also should consider scalability across other hospitalist groups.
“If you build it, they will come."
HM takeaways
Create a business plan;
Find institutional financial and political support;
Start small and selective;
Plan for standardization and training of colleagues;
Create a credentialing/privileging process;
Bill for services and consider billing for full consults; and
HM15 presenters: Verity Schaye, Michael Janjigian, Frank Volpicelli, Susan Hunt.
Performing a physical exam is the standard of care for evaluating patients. It has been shown to have higher diagnostic utility than many technology based tests. The physical exam is the Gold Standard for dermatological and mental status assessment for which technological tests are not readily available. The tradition “laying on of hands” has important benefits for the physician patient relationship.
The teaching of physical exam skills is increasingly problematic. Barriers include attending time, comfort and skill level as well as challenges of patient comfort and potential isolation issues.
The Peyton Model provides a better means of teaching physical exam skills than the traditional “See one, do one, teach one” model. The Peyton Model has four steps:
Demonstration. The teacher performs the exam at normal speed without commentary.
Deconstruction. The teacher performs the exam while describing the steps.
Comprehension. The teacher performs the exam while the learner describes the steps.
Performance. The learner performs the exam while also describing the steps.
This approach can be abbreviated for more advanced learners with the middle two steps being combined to a discussion between the teacher and learner to highlight any differences or changes in technique. TH
HM15 presenters: Verity Schaye, Michael Janjigian, Frank Volpicelli, Susan Hunt.
Performing a physical exam is the standard of care for evaluating patients. It has been shown to have higher diagnostic utility than many technology based tests. The physical exam is the Gold Standard for dermatological and mental status assessment for which technological tests are not readily available. The tradition “laying on of hands” has important benefits for the physician patient relationship.
The teaching of physical exam skills is increasingly problematic. Barriers include attending time, comfort and skill level as well as challenges of patient comfort and potential isolation issues.
The Peyton Model provides a better means of teaching physical exam skills than the traditional “See one, do one, teach one” model. The Peyton Model has four steps:
Demonstration. The teacher performs the exam at normal speed without commentary.
Deconstruction. The teacher performs the exam while describing the steps.
Comprehension. The teacher performs the exam while the learner describes the steps.
Performance. The learner performs the exam while also describing the steps.
This approach can be abbreviated for more advanced learners with the middle two steps being combined to a discussion between the teacher and learner to highlight any differences or changes in technique. TH
HM15 presenters: Verity Schaye, Michael Janjigian, Frank Volpicelli, Susan Hunt.
Performing a physical exam is the standard of care for evaluating patients. It has been shown to have higher diagnostic utility than many technology based tests. The physical exam is the Gold Standard for dermatological and mental status assessment for which technological tests are not readily available. The tradition “laying on of hands” has important benefits for the physician patient relationship.
The teaching of physical exam skills is increasingly problematic. Barriers include attending time, comfort and skill level as well as challenges of patient comfort and potential isolation issues.
The Peyton Model provides a better means of teaching physical exam skills than the traditional “See one, do one, teach one” model. The Peyton Model has four steps:
Demonstration. The teacher performs the exam at normal speed without commentary.
Deconstruction. The teacher performs the exam while describing the steps.
Comprehension. The teacher performs the exam while the learner describes the steps.
Performance. The learner performs the exam while also describing the steps.
This approach can be abbreviated for more advanced learners with the middle two steps being combined to a discussion between the teacher and learner to highlight any differences or changes in technique. TH
Kathleen Finn, MD, FHM and Jeffrey Greenwald, MD, SFHM engaged the audience with their playful banter while reviewing medical literature of clinical significance for the hospitalist in Update in Hospital Medicine. The studies presented were high-quality, practical and addressed questions that arise in our day-to-day practice. A wide variety of topics were addressed and key points are summarized below.
Key takeaways
In the PARADIGM-HF study, Angiotensin Receptor Blocker (ARB) + Neprilysin Inhibitor decreased cardiovascular mortality and reduced CHF hospitalization by 20% when compared to Enalapril alone in heart failure patients. The combination drug is an alternative choice to ACE inhibitors. FDA approval is forthcoming.
Is the risk of contrast-induced nephrotoxicity really as great as we have come to believe? Review of propensity matched studies suggests that AKI, 30 day need for emergent hemodi
alysis and death are unrelated to contrast. If CT with contrast makes a difference to the patient, consider using it if GFR>30 ml/min.
SAGES trial and Project Recovery developed a delirium screening method in hospitalized patients. The CAM (Confusion Assessment Method) scoring system assesses delirium severity in elderly patients (70+). Hospital and post-hospital outcomes in delirious vs. non-delirious patients showed that the more severe the delirium, the longer the patient stayed in the hospital. Further, the rate of new SNF placement and 90 day mortality was higher in the delirious group. The CAM score correlates with prognosis in medical patients. Addressing long-term goals of care in this patient population may be warranted.
A randomized placebo-controlled trail looked at the preventive effects of Ramelteon (melatonin receptor agonist) on delirium. Ramelteon 8mg was given to patients at 9pm for 7 days (or d/c). Although this was a small and short study, Ramelteon appears to reduce incident delirium in medical and non-intubated ICU patients.
The HELP randomized clinical trial compared Lactulose vs. Polyethylene Glycol (PEG) electrolyte solution for treatment of overt hepatic encephalopathy. Patients received either PEG (4L in 4 hours) or Lactulose (20-30g 3+doses/24hrs). Primary outcome was an improvement in HESA (Hepatic Encephalopathy Scoring Algorithm ) score by 1 at 24 hours. HESA score improved and patients had a shorter length of stay in the PEG group. In addition, patients requested PEG at discharge because it tasted better.
A retrospective study looked at Nonselective beta blockers (NSBB) in patients with Spontaneous Bacterial Peritonitis (SBP). It suggests that the use of NSBB after SBP onset increases the risk of AKI, Hepatorenal Syndrome and mortality by 58%. NSBB appear beneficial before SBP onset suggesting that as cirrhosis becomes more severe, NSBB may not be effective.
A retrospective cohort trial (Michigan Hospital Medicine Safety Consortium) assessed hospital performance of VTE prophylaxis. The rate of clinically evident, confirmed VTE was measured. There was no difference in VTE occurrence during hospitalization, 90 day VTE rates and PE vs. DVT rates. No clear benefit was evident from VTE prophylaxis for medical patients. This could indicate the need to risk stratify patients’ VTE risk.
Direct oral anticoagulants (DOACs) were compared with Vitamin K antagonists (VKA) for treatment of acute VTE in a meta-analysis reviewed by the speakers. Death, safety and bleeding were assessed. DOACs seem to work as well as VKAs for VTE. They also had a better safety profile. In cancer patients, DOACs vs. LMWH study is still needed. In patients with atrial fibrillation (AF), DOACs prevent AF-associated strokes better than VKAs. They also reduce hemorrhagic stroke and intracranial hemorrhage.
In the elderly (75 or older) patient, DOACs are as safe as VKAs and LMWH for AF and VTE treatment.
Randomized control trails compared once weekly Dalbavancin or single-dose Oritavancin vs. daily conventional therapy for acute bacterial skin infections (cellulitis, major abscess, wound infection, 75cm² erythema). Outcomes measured were cessation of spread of erythema and no fever X3 readings in 48-72 hours. Dalbavancin once weekly was non-inferior to Vancomycin in safety profile and outcome measures. Direct cost of Dalbavancin was higher although patients on this drug had shorter length of stays which is cost effective. FDA approved for skin infections.
The presence of family during CPR decreased PTSD, anxiety and depression symptoms in family members. Outcomes were similar when participants were assesses at 90 days and 1 year. While this study was conducted in an out of hospital setting, it may be worthwhile to assess if it is applicable to patients who code in the hospital.
Kathleen Finn, MD, FHM and Jeffrey Greenwald, MD, SFHM engaged the audience with their playful banter while reviewing medical literature of clinical significance for the hospitalist in Update in Hospital Medicine. The studies presented were high-quality, practical and addressed questions that arise in our day-to-day practice. A wide variety of topics were addressed and key points are summarized below.
Key takeaways
In the PARADIGM-HF study, Angiotensin Receptor Blocker (ARB) + Neprilysin Inhibitor decreased cardiovascular mortality and reduced CHF hospitalization by 20% when compared to Enalapril alone in heart failure patients. The combination drug is an alternative choice to ACE inhibitors. FDA approval is forthcoming.
Is the risk of contrast-induced nephrotoxicity really as great as we have come to believe? Review of propensity matched studies suggests that AKI, 30 day need for emergent hemodi
alysis and death are unrelated to contrast. If CT with contrast makes a difference to the patient, consider using it if GFR>30 ml/min.
SAGES trial and Project Recovery developed a delirium screening method in hospitalized patients. The CAM (Confusion Assessment Method) scoring system assesses delirium severity in elderly patients (70+). Hospital and post-hospital outcomes in delirious vs. non-delirious patients showed that the more severe the delirium, the longer the patient stayed in the hospital. Further, the rate of new SNF placement and 90 day mortality was higher in the delirious group. The CAM score correlates with prognosis in medical patients. Addressing long-term goals of care in this patient population may be warranted.
A randomized placebo-controlled trail looked at the preventive effects of Ramelteon (melatonin receptor agonist) on delirium. Ramelteon 8mg was given to patients at 9pm for 7 days (or d/c). Although this was a small and short study, Ramelteon appears to reduce incident delirium in medical and non-intubated ICU patients.
The HELP randomized clinical trial compared Lactulose vs. Polyethylene Glycol (PEG) electrolyte solution for treatment of overt hepatic encephalopathy. Patients received either PEG (4L in 4 hours) or Lactulose (20-30g 3+doses/24hrs). Primary outcome was an improvement in HESA (Hepatic Encephalopathy Scoring Algorithm ) score by 1 at 24 hours. HESA score improved and patients had a shorter length of stay in the PEG group. In addition, patients requested PEG at discharge because it tasted better.
A retrospective study looked at Nonselective beta blockers (NSBB) in patients with Spontaneous Bacterial Peritonitis (SBP). It suggests that the use of NSBB after SBP onset increases the risk of AKI, Hepatorenal Syndrome and mortality by 58%. NSBB appear beneficial before SBP onset suggesting that as cirrhosis becomes more severe, NSBB may not be effective.
A retrospective cohort trial (Michigan Hospital Medicine Safety Consortium) assessed hospital performance of VTE prophylaxis. The rate of clinically evident, confirmed VTE was measured. There was no difference in VTE occurrence during hospitalization, 90 day VTE rates and PE vs. DVT rates. No clear benefit was evident from VTE prophylaxis for medical patients. This could indicate the need to risk stratify patients’ VTE risk.
Direct oral anticoagulants (DOACs) were compared with Vitamin K antagonists (VKA) for treatment of acute VTE in a meta-analysis reviewed by the speakers. Death, safety and bleeding were assessed. DOACs seem to work as well as VKAs for VTE. They also had a better safety profile. In cancer patients, DOACs vs. LMWH study is still needed. In patients with atrial fibrillation (AF), DOACs prevent AF-associated strokes better than VKAs. They also reduce hemorrhagic stroke and intracranial hemorrhage.
In the elderly (75 or older) patient, DOACs are as safe as VKAs and LMWH for AF and VTE treatment.
Randomized control trails compared once weekly Dalbavancin or single-dose Oritavancin vs. daily conventional therapy for acute bacterial skin infections (cellulitis, major abscess, wound infection, 75cm² erythema). Outcomes measured were cessation of spread of erythema and no fever X3 readings in 48-72 hours. Dalbavancin once weekly was non-inferior to Vancomycin in safety profile and outcome measures. Direct cost of Dalbavancin was higher although patients on this drug had shorter length of stays which is cost effective. FDA approved for skin infections.
The presence of family during CPR decreased PTSD, anxiety and depression symptoms in family members. Outcomes were similar when participants were assesses at 90 days and 1 year. While this study was conducted in an out of hospital setting, it may be worthwhile to assess if it is applicable to patients who code in the hospital.
Kathleen Finn, MD, FHM and Jeffrey Greenwald, MD, SFHM engaged the audience with their playful banter while reviewing medical literature of clinical significance for the hospitalist in Update in Hospital Medicine. The studies presented were high-quality, practical and addressed questions that arise in our day-to-day practice. A wide variety of topics were addressed and key points are summarized below.
Key takeaways
In the PARADIGM-HF study, Angiotensin Receptor Blocker (ARB) + Neprilysin Inhibitor decreased cardiovascular mortality and reduced CHF hospitalization by 20% when compared to Enalapril alone in heart failure patients. The combination drug is an alternative choice to ACE inhibitors. FDA approval is forthcoming.
Is the risk of contrast-induced nephrotoxicity really as great as we have come to believe? Review of propensity matched studies suggests that AKI, 30 day need for emergent hemodi
alysis and death are unrelated to contrast. If CT with contrast makes a difference to the patient, consider using it if GFR>30 ml/min.
SAGES trial and Project Recovery developed a delirium screening method in hospitalized patients. The CAM (Confusion Assessment Method) scoring system assesses delirium severity in elderly patients (70+). Hospital and post-hospital outcomes in delirious vs. non-delirious patients showed that the more severe the delirium, the longer the patient stayed in the hospital. Further, the rate of new SNF placement and 90 day mortality was higher in the delirious group. The CAM score correlates with prognosis in medical patients. Addressing long-term goals of care in this patient population may be warranted.
A randomized placebo-controlled trail looked at the preventive effects of Ramelteon (melatonin receptor agonist) on delirium. Ramelteon 8mg was given to patients at 9pm for 7 days (or d/c). Although this was a small and short study, Ramelteon appears to reduce incident delirium in medical and non-intubated ICU patients.
The HELP randomized clinical trial compared Lactulose vs. Polyethylene Glycol (PEG) electrolyte solution for treatment of overt hepatic encephalopathy. Patients received either PEG (4L in 4 hours) or Lactulose (20-30g 3+doses/24hrs). Primary outcome was an improvement in HESA (Hepatic Encephalopathy Scoring Algorithm ) score by 1 at 24 hours. HESA score improved and patients had a shorter length of stay in the PEG group. In addition, patients requested PEG at discharge because it tasted better.
A retrospective study looked at Nonselective beta blockers (NSBB) in patients with Spontaneous Bacterial Peritonitis (SBP). It suggests that the use of NSBB after SBP onset increases the risk of AKI, Hepatorenal Syndrome and mortality by 58%. NSBB appear beneficial before SBP onset suggesting that as cirrhosis becomes more severe, NSBB may not be effective.
A retrospective cohort trial (Michigan Hospital Medicine Safety Consortium) assessed hospital performance of VTE prophylaxis. The rate of clinically evident, confirmed VTE was measured. There was no difference in VTE occurrence during hospitalization, 90 day VTE rates and PE vs. DVT rates. No clear benefit was evident from VTE prophylaxis for medical patients. This could indicate the need to risk stratify patients’ VTE risk.
Direct oral anticoagulants (DOACs) were compared with Vitamin K antagonists (VKA) for treatment of acute VTE in a meta-analysis reviewed by the speakers. Death, safety and bleeding were assessed. DOACs seem to work as well as VKAs for VTE. They also had a better safety profile. In cancer patients, DOACs vs. LMWH study is still needed. In patients with atrial fibrillation (AF), DOACs prevent AF-associated strokes better than VKAs. They also reduce hemorrhagic stroke and intracranial hemorrhage.
In the elderly (75 or older) patient, DOACs are as safe as VKAs and LMWH for AF and VTE treatment.
Randomized control trails compared once weekly Dalbavancin or single-dose Oritavancin vs. daily conventional therapy for acute bacterial skin infections (cellulitis, major abscess, wound infection, 75cm² erythema). Outcomes measured were cessation of spread of erythema and no fever X3 readings in 48-72 hours. Dalbavancin once weekly was non-inferior to Vancomycin in safety profile and outcome measures. Direct cost of Dalbavancin was higher although patients on this drug had shorter length of stays which is cost effective. FDA approved for skin infections.
The presence of family during CPR decreased PTSD, anxiety and depression symptoms in family members. Outcomes were similar when participants were assesses at 90 days and 1 year. While this study was conducted in an out of hospital setting, it may be worthwhile to assess if it is applicable to patients who code in the hospital.
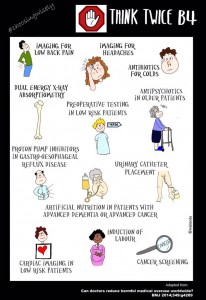
John Bulger, DO, MBA reviewed the components of the Choosing Wisely campaign and SHM’s recommendations in an era where providing high value cost-conscious care is key to optimizing the health of our patients. Choosing Wisely is an initiative of the ABIM foundation to foster communication between physicians and patients about common tests and procedures that may fail to provide value or enhance patient outcomes. It’s a partnership with 70-plus medical societies including an innovative partnership with Consumer Reports. SHM’s evidence-based recommendations are:
Don’t leave urinary catheters in place for convenience or monitoring of output for non-critically ill patients.
Don’t prescribe stress ulcer prophylaxis to hospitalized patients unless they are at high risk for GI complications.
Avoid transfusion of PRBC for arbitrary hemoglobin in the absence of CAD, CHF or CVA.
Don’t order continuous telemetry monitoring outside of the ICU without a protocol.
Don’t perform repetitive CBC and chemistry testing in a clinically stable patient.
Dr. Bulger highlighted that the Choosing Wisely campaign is designed to encourage conversations to
improve patient care. While cost-conscious care is a natural by-product of this effort, the primary focus when these guidelines were developed was to provide better healthcare for our patients. This year, SHM’s Choosing Wisely Case Competition has triggered the application of the above recommendations in institutions across the country. A summary of these efforts will be published in the near future to assist fellow hospitalists with their efforts to minimize waste and improve care in their own institutions. Look for the Hospitalist Guide to Choosing Wisely which is expected to be published in spring 2015. Choosing Wisely has now become a world-wide effort with Canada, Europe and Brazil implementing similar recommendations to improve healthcare.
Dr.Bulger concluded that while tradition is hard to change, it is of paramount importance to think differently to find innovative solutions to common problems in healthcare. Join the conversation using #ChoosingWisely or #LessIsMore on twitter.
Key Takeaways
Choosing Wisely is an ABIM campaign developed to address and promote conversations about common tests and procedures that are of low-value.
SHM’s recommendations were implemented in institutions with positive results as evidenced by the Choosing Wisely case competition at #HospMed15.
Look for a summary of these efforts to be published in the spring of 2015.
Use these guidelines to educate, provoke dialogue and achieve optimal patient outcomes in your institution.
John Bulger, DO, MBA reviewed the components of the Choosing Wisely campaign and SHM’s recommendations in an era where providing high value cost-conscious care is key to optimizing the health of our patients. Choosing Wisely is an initiative of the ABIM foundation to foster communication between physicians and patients about common tests and procedures that may fail to provide value or enhance patient outcomes. It’s a partnership with 70-plus medical societies including an innovative partnership with Consumer Reports. SHM’s evidence-based recommendations are:
Don’t leave urinary catheters in place for convenience or monitoring of output for non-critically ill patients.
Don’t prescribe stress ulcer prophylaxis to hospitalized patients unless they are at high risk for GI complications.
Avoid transfusion of PRBC for arbitrary hemoglobin in the absence of CAD, CHF or CVA.
Don’t order continuous telemetry monitoring outside of the ICU without a protocol.
Don’t perform repetitive CBC and chemistry testing in a clinically stable patient.
Dr. Bulger highlighted that the Choosing Wisely campaign is designed to encourage conversations to
improve patient care. While cost-conscious care is a natural by-product of this effort, the primary focus when these guidelines were developed was to provide better healthcare for our patients. This year, SHM’s Choosing Wisely Case Competition has triggered the application of the above recommendations in institutions across the country. A summary of these efforts will be published in the near future to assist fellow hospitalists with their efforts to minimize waste and improve care in their own institutions. Look for the Hospitalist Guide to Choosing Wisely which is expected to be published in spring 2015. Choosing Wisely has now become a world-wide effort with Canada, Europe and Brazil implementing similar recommendations to improve healthcare.
Dr.Bulger concluded that while tradition is hard to change, it is of paramount importance to think differently to find innovative solutions to common problems in healthcare. Join the conversation using #ChoosingWisely or #LessIsMore on twitter.
Key Takeaways
Choosing Wisely is an ABIM campaign developed to address and promote conversations about common tests and procedures that are of low-value.
SHM’s recommendations were implemented in institutions with positive results as evidenced by the Choosing Wisely case competition at #HospMed15.
Look for a summary of these efforts to be published in the spring of 2015.
Use these guidelines to educate, provoke dialogue and achieve optimal patient outcomes in your institution.
John Bulger, DO, MBA reviewed the components of the Choosing Wisely campaign and SHM’s recommendations in an era where providing high value cost-conscious care is key to optimizing the health of our patients. Choosing Wisely is an initiative of the ABIM foundation to foster communication between physicians and patients about common tests and procedures that may fail to provide value or enhance patient outcomes. It’s a partnership with 70-plus medical societies including an innovative partnership with Consumer Reports. SHM’s evidence-based recommendations are:
Don’t leave urinary catheters in place for convenience or monitoring of output for non-critically ill patients.
Don’t prescribe stress ulcer prophylaxis to hospitalized patients unless they are at high risk for GI complications.
Avoid transfusion of PRBC for arbitrary hemoglobin in the absence of CAD, CHF or CVA.
Don’t order continuous telemetry monitoring outside of the ICU without a protocol.
Don’t perform repetitive CBC and chemistry testing in a clinically stable patient.
Dr. Bulger highlighted that the Choosing Wisely campaign is designed to encourage conversations to
improve patient care. While cost-conscious care is a natural by-product of this effort, the primary focus when these guidelines were developed was to provide better healthcare for our patients. This year, SHM’s Choosing Wisely Case Competition has triggered the application of the above recommendations in institutions across the country. A summary of these efforts will be published in the near future to assist fellow hospitalists with their efforts to minimize waste and improve care in their own institutions. Look for the Hospitalist Guide to Choosing Wisely which is expected to be published in spring 2015. Choosing Wisely has now become a world-wide effort with Canada, Europe and Brazil implementing similar recommendations to improve healthcare.
Dr.Bulger concluded that while tradition is hard to change, it is of paramount importance to think differently to find innovative solutions to common problems in healthcare. Join the conversation using #ChoosingWisely or #LessIsMore on twitter.
Key Takeaways
Choosing Wisely is an ABIM campaign developed to address and promote conversations about common tests and procedures that are of low-value.
SHM’s recommendations were implemented in institutions with positive results as evidenced by the Choosing Wisely case competition at #HospMed15.
Look for a summary of these efforts to be published in the spring of 2015.
Use these guidelines to educate, provoke dialogue and achieve optimal patient outcomes in your institution.
In this session, Drs. Michelle Mourad and Christopher Moriates took a systematic approach to answer quality questions that we commonly encounter in our hospitalist practice. They reviewed current evidence including meta-analyses and systematic reviews to arrive at an answer for various quality-related questions. These are summarized below:
What are the common features of interventions that have successfully reduced re-admissions? Effective interventions that enhance patient capacity to reliably access and engage in post-discharge care has been associated with success in decreasing re-admissions.
Does patient engagement correlate with decreased resource use or readmissions? Patient activation is defined as knowledge, skills, confidence and inclination to assume responsibility for managing one’s own health. A higher patient activation score reduced the risk of 30-day hospital re-utilization.
Does patients’ report of their healthcare experience reflect quality of care? Patient satisfaction scores may be a reflection of their desires (for example, to get pain medications) regardless of clinical benefit. In these situations, quality should be based on achieving a mutual understanding of patient situation and treatment plan between the provider and patient.
Is there any relationship between quality of care and health outcomes? Positive associations were found between patient experience and safety/effectiveness. Including patient experience in quality improvement, therefore, may lead to improvements in safety and effectiveness. Reducing the trauma of hospitalization could improve patient satisfaction and outcomes. Efforts such as personalization, providing rest and nourishment, reducing stress disruption and surprises as well as providing a post discharge safety net are strategies to reduce the trauma of hospitalization, improve satisfaction and patient outcomes.
Is there anything we can do to make hand-offs safer? The I-PASS hand-off bundle for a systematic hand-off process was reviewed (Illness severity, Patient summary, Action list, Situation awareness, Synthesis by receiver) as a means of reducing medical errors. When used in conjunction with training, faculty development and a culture-change campaign, this was associated with improving patient safety without negatively affecting workflow.
How can hospitalists deflate medical bills? Patient expectations of the benefits and harms of clinical interventions influences physician decision making and contributes to overuse and increased healthcare costs. Harm of excessive testing was underestimated in such situations. Conversations with patients, colleagues and the public are crucial to decreasing low value care. Physicians should discuss potential benefits and risks to address patient expectations. In addition, they should seek opportunities to better understand healthcare costs.
How big of a problem is antibiotic overuse in hospitals and can we do better? In a national database review, more than half of all patients (55.7%) discharged from a hospital received antibiotics during their stay. There is a wide variation in antibiotic use across hospital wards. Reducing this exposure to broad spectrum antibiotics would lead to a 26% reduction in C. diff infections and reduce antibiotic resistance. To improve this over-utilization, stewardship programs should actively engage and educate clinicians, encourage clear antibiotic documentation in daily progress notes and use 72-hour antibiotic time-out during multidisciplinary rounds. TH
In this session, Drs. Michelle Mourad and Christopher Moriates took a systematic approach to answer quality questions that we commonly encounter in our hospitalist practice. They reviewed current evidence including meta-analyses and systematic reviews to arrive at an answer for various quality-related questions. These are summarized below:
What are the common features of interventions that have successfully reduced re-admissions? Effective interventions that enhance patient capacity to reliably access and engage in post-discharge care has been associated with success in decreasing re-admissions.
Does patient engagement correlate with decreased resource use or readmissions? Patient activation is defined as knowledge, skills, confidence and inclination to assume responsibility for managing one’s own health. A higher patient activation score reduced the risk of 30-day hospital re-utilization.
Does patients’ report of their healthcare experience reflect quality of care? Patient satisfaction scores may be a reflection of their desires (for example, to get pain medications) regardless of clinical benefit. In these situations, quality should be based on achieving a mutual understanding of patient situation and treatment plan between the provider and patient.
Is there any relationship between quality of care and health outcomes? Positive associations were found between patient experience and safety/effectiveness. Including patient experience in quality improvement, therefore, may lead to improvements in safety and effectiveness. Reducing the trauma of hospitalization could improve patient satisfaction and outcomes. Efforts such as personalization, providing rest and nourishment, reducing stress disruption and surprises as well as providing a post discharge safety net are strategies to reduce the trauma of hospitalization, improve satisfaction and patient outcomes.
Is there anything we can do to make hand-offs safer? The I-PASS hand-off bundle for a systematic hand-off process was reviewed (Illness severity, Patient summary, Action list, Situation awareness, Synthesis by receiver) as a means of reducing medical errors. When used in conjunction with training, faculty development and a culture-change campaign, this was associated with improving patient safety without negatively affecting workflow.
How can hospitalists deflate medical bills? Patient expectations of the benefits and harms of clinical interventions influences physician decision making and contributes to overuse and increased healthcare costs. Harm of excessive testing was underestimated in such situations. Conversations with patients, colleagues and the public are crucial to decreasing low value care. Physicians should discuss potential benefits and risks to address patient expectations. In addition, they should seek opportunities to better understand healthcare costs.
How big of a problem is antibiotic overuse in hospitals and can we do better? In a national database review, more than half of all patients (55.7%) discharged from a hospital received antibiotics during their stay. There is a wide variation in antibiotic use across hospital wards. Reducing this exposure to broad spectrum antibiotics would lead to a 26% reduction in C. diff infections and reduce antibiotic resistance. To improve this over-utilization, stewardship programs should actively engage and educate clinicians, encourage clear antibiotic documentation in daily progress notes and use 72-hour antibiotic time-out during multidisciplinary rounds. TH
In this session, Drs. Michelle Mourad and Christopher Moriates took a systematic approach to answer quality questions that we commonly encounter in our hospitalist practice. They reviewed current evidence including meta-analyses and systematic reviews to arrive at an answer for various quality-related questions. These are summarized below:
What are the common features of interventions that have successfully reduced re-admissions? Effective interventions that enhance patient capacity to reliably access and engage in post-discharge care has been associated with success in decreasing re-admissions.
Does patient engagement correlate with decreased resource use or readmissions? Patient activation is defined as knowledge, skills, confidence and inclination to assume responsibility for managing one’s own health. A higher patient activation score reduced the risk of 30-day hospital re-utilization.
Does patients’ report of their healthcare experience reflect quality of care? Patient satisfaction scores may be a reflection of their desires (for example, to get pain medications) regardless of clinical benefit. In these situations, quality should be based on achieving a mutual understanding of patient situation and treatment plan between the provider and patient.
Is there any relationship between quality of care and health outcomes? Positive associations were found between patient experience and safety/effectiveness. Including patient experience in quality improvement, therefore, may lead to improvements in safety and effectiveness. Reducing the trauma of hospitalization could improve patient satisfaction and outcomes. Efforts such as personalization, providing rest and nourishment, reducing stress disruption and surprises as well as providing a post discharge safety net are strategies to reduce the trauma of hospitalization, improve satisfaction and patient outcomes.
Is there anything we can do to make hand-offs safer? The I-PASS hand-off bundle for a systematic hand-off process was reviewed (Illness severity, Patient summary, Action list, Situation awareness, Synthesis by receiver) as a means of reducing medical errors. When used in conjunction with training, faculty development and a culture-change campaign, this was associated with improving patient safety without negatively affecting workflow.
How can hospitalists deflate medical bills? Patient expectations of the benefits and harms of clinical interventions influences physician decision making and contributes to overuse and increased healthcare costs. Harm of excessive testing was underestimated in such situations. Conversations with patients, colleagues and the public are crucial to decreasing low value care. Physicians should discuss potential benefits and risks to address patient expectations. In addition, they should seek opportunities to better understand healthcare costs.
How big of a problem is antibiotic overuse in hospitals and can we do better? In a national database review, more than half of all patients (55.7%) discharged from a hospital received antibiotics during their stay. There is a wide variation in antibiotic use across hospital wards. Reducing this exposure to broad spectrum antibiotics would lead to a 26% reduction in C. diff infections and reduce antibiotic resistance. To improve this over-utilization, stewardship programs should actively engage and educate clinicians, encourage clear antibiotic documentation in daily progress notes and use 72-hour antibiotic time-out during multidisciplinary rounds. TH
Authors used two methods to measure continuity: the Number of Physicians Index (NPI) represented the total number of unique hospitalists caring for a patient, while the Usual Provider of Care (UPC) Index was the proportion of encounters with the most frequently encountered hospitalist.
Researchers reported that, in unadjusted models, each one-unit increase in the NPI—meaning less continuity—was significantly associated with the incidence of one or more AEs (odds ratio, 1.75; P<0.001). In addition, UPC was not associated with incidence of AEs. Across all adjusted models, neither index was "significantly associated" with the incidence of AEs.
Lead author Kevin O'Leary, MD, MS, SFHM, of Northwestern University's Feinberg School of Medicine in Chicago, says that the data could be used to help determine how best to structure handoffs.
"Where I think this has a major impact is that a whole lot of groups [are] trying to figure out how long should our rotation length be," Dr. O'Leary says. "All of those programs that are really trying to maximize continuity because they think it's the safest thing and best thing for patient outcomes, they can probably relax a little bit and swing the pendulum a little bit further toward what they think is the right model for the work-life balance of their hospitalist. [They can] worry a little bit less about the impact on the patients because there doesn't seem to be much." TH
Authors used two methods to measure continuity: the Number of Physicians Index (NPI) represented the total number of unique hospitalists caring for a patient, while the Usual Provider of Care (UPC) Index was the proportion of encounters with the most frequently encountered hospitalist.
Researchers reported that, in unadjusted models, each one-unit increase in the NPI—meaning less continuity—was significantly associated with the incidence of one or more AEs (odds ratio, 1.75; P<0.001). In addition, UPC was not associated with incidence of AEs. Across all adjusted models, neither index was "significantly associated" with the incidence of AEs.
Lead author Kevin O'Leary, MD, MS, SFHM, of Northwestern University's Feinberg School of Medicine in Chicago, says that the data could be used to help determine how best to structure handoffs.
"Where I think this has a major impact is that a whole lot of groups [are] trying to figure out how long should our rotation length be," Dr. O'Leary says. "All of those programs that are really trying to maximize continuity because they think it's the safest thing and best thing for patient outcomes, they can probably relax a little bit and swing the pendulum a little bit further toward what they think is the right model for the work-life balance of their hospitalist. [They can] worry a little bit less about the impact on the patients because there doesn't seem to be much." TH
Authors used two methods to measure continuity: the Number of Physicians Index (NPI) represented the total number of unique hospitalists caring for a patient, while the Usual Provider of Care (UPC) Index was the proportion of encounters with the most frequently encountered hospitalist.
Researchers reported that, in unadjusted models, each one-unit increase in the NPI—meaning less continuity—was significantly associated with the incidence of one or more AEs (odds ratio, 1.75; P<0.001). In addition, UPC was not associated with incidence of AEs. Across all adjusted models, neither index was "significantly associated" with the incidence of AEs.
Lead author Kevin O'Leary, MD, MS, SFHM, of Northwestern University's Feinberg School of Medicine in Chicago, says that the data could be used to help determine how best to structure handoffs.
"Where I think this has a major impact is that a whole lot of groups [are] trying to figure out how long should our rotation length be," Dr. O'Leary says. "All of those programs that are really trying to maximize continuity because they think it's the safest thing and best thing for patient outcomes, they can probably relax a little bit and swing the pendulum a little bit further toward what they think is the right model for the work-life balance of their hospitalist. [They can] worry a little bit less about the impact on the patients because there doesn't seem to be much." TH