User login
Anaphylactic Reaction to Bacitracin Ointment
The treatment-resistant catatonia patient
Case: Worsening psychosis
Ms. R, age 21, is admitted to our psychiatric facility while experiencing paranoid delusions and auditory hallucinations. Upon admission, she is agitated and her mood is labile.
Ms. R has 4 previous brief psychiatric admissions and was diagnosed with schizoaffective disorder, bipolar type and moderate mental retardation. Her family history is positive for psychiatric illness, as her mother was diagnosed with schizophrenia. Prior to admission, Ms. R was taking ziprasidone, 160 mg/d, and lithium, 450 mg/d, for 11 months. Both were discontinued during the first week of admission because Ms. R was not responding.
During this admission, the treating psychiatrist assesses Ms. R using the Schedules for Clinicians’ Interview in Psychiatry (SCIP), an instrument developed by the lead author (AA) for psychiatrists to use in conjunction with their routine clinical interviews in inpatient and outpatient settings (see Related Resources). The SCIP includes a 25-question screening section and a diagnostic section that consists of 7 modules that represent major psychiatric diagnoses defined by DSM and International Classification of Diseases criteria.1
During the first week of admission, we monitor Ms. R and administer haloperidol as needed, 10 mg total. Eight days after admission, she develops severe catatonia. On the catatonia scale of the SCIP, Ms. R scores the maximum on measures of immobility, catalepsy/waxy flexibility, and mutism (Table).
How would you treat Ms. R’s catatonia?
Table
Patient’s catatonia symptoms: Response to pharmacotherapy
| Lorazepam only | Lorazepam + risperidone | Risperidone oral only | Risperidone long-acting injection only | |
|---|---|---|---|---|
| Dosage(s) | 7 mg total over 7 days | Lorazepam: 4 mg/d Risperidone: 4 mg/d | 8 mg/d | 37.5 mg every 2 weeks |
| Scores on SCIP catatonia scale:* | ||||
| Immobility | 2 | 1 | 0 | 0 |
| Catalepsy/waxy flexibility† | 2 | 1 | 0 | 0 |
| Mutism | 2 | 0 | 0 | 0 |
| Total score | 6 | 2 | 0 | 0 |
| *Scale of 0 to 2, with 0=none, 1=less than half the time, and 2=more than half the time. Symptoms are evaluated over a 1-day period | ||||
| †For this category, 0=none, 1=brief (usually 1 minute | ||||
| SCIP: Schedules for Clinicians’ Interview in Psychiatry | ||||
The authors’ observations
DSM-IV-TR recognizes catatonia as a schizophrenia subtype, as a descriptor for mania and major depression, and as being caused by various medical conditions, such as neuroleptic malignant syndrome, encephalopathy, or renal failure.2 Kahlbaum initially described catatonia in 1873 as a brain disease characterized by motor abnormalities such as akinesia, rigidity, negativism, mutism, grimacing, posturing, catalepsy, waxy flexibility, and verbigerations.3 Catatonia is characterized by hypo- and hyperkinetic features. Catalepsy, stupor, rigidity, and catatonic posturing with waxy flexibility might alternate with violent catatonic excitement.4
Catatonia can be life-threatening; patients might not be able to eat or chew food, which puts them at risk for aspiration. Those with immobility might not move to urinate or defecate. During the first half of the 20th century, catatonia was documented in up to 50% of patients with schizophrenia.5 Since then, the incidence of catatonia has decreased, possibly the result of advances in psychopharmacology.6
Two days after Ms. R develops catatonia, we transfer her to a local hospital for evaluation to rule out a medical cause of her catatonic symptoms.
EVALUATION: No medical cause
At the hospital, physical examination, electroencephalography, drug screening, and liver and thyroid function tests are within normal limits, eliminating an organic cause of Ms. R’s catatonia. MRI of the head shows a 3-mm mass at the base of the infundibulum, which is unchanged from a prior MRI. Ms. R received 7 mg total of lorazepam over 4 days without relief of her catatonia. She is transferred back to our facility.
The authors’ observations
Benzodiazepines and ECT are effective treatments for catatonia.7 Benzodiazepines are considered first-line treatment because of their efficacy and favorable side-effect profile.7 Lorazepam frequently is used to treat catatonia in the short term.8 Long-term use of benzodiazepines, however, is associated with tolerance, addiction, and rebound phenomena.8,9
Patients with catatonia who do not respond to benzodiazepines may benefit from ECT.9 ECT can cause serious side effects, however, including memory impairment, confusion, delirium, and cardiac arrhythmias.10
Atypical antipsychotics may alleviate motor symptoms of catatonia by virtue of their 5-HT2A receptor antagonistic action.9 In 2 case reports, risperidone successfully treated catatonia.4,11 Kopala et al11 found risperidone, 4 mg/d, was effective in treating severe, first-episode catatonic schizophrenia in a neuroleptic-naive young man. This efficacy was sustained over a 3.5-year outpatient follow-up.
In another report, risperidone, 6 mg/d, effectively treated catatonia and prevented further episodes in a patient with schizophrenia who developed severe catatonia after receiving adequate treatment for Lyme disease with encephalitis.4 Two relapses of catatonic syndrome occurred when risperidone was reduced to 2 mg/d, and remission occurred after risperidone was increased to 6 mg/d. Risperidone’s antagonistic activity of the 5-HT2/D2 receptors may be relevant to its anticatatonic effect.12
Other atypical antipsychotics—ziprasidone and olanzapine—also have been shown to be effective in treating catatonia. Levy et al13 reported successful treatment of a catatonic state (with catalepsy, stupor, and mutism) using intramuscular ziprasidone followed by oral ziprasidone. A data analysis by Martenyi et al14 showed olanzapine to be effective in treating nonspecific signs and symptoms of catatonia, as measured by the Positive and Negative Syndrome Scale.
TREATMENT: Trying risperidone
Based on case reports showing risperidone’s efficacy for catatonia, we start Ms. R on risperidone, 4 mg/d, and lorazepam, 4 mg/d. Eight days later, her catatonic symptoms decrease substantially—she scores 2/6 on the SCIP catatonia scale (Table)—and she starts to talk with the staff.
We continue this regimen for 30 days, then discontinue lorazepam to avoid long-term side effects—such as dependence—and titrate risperidone to 8 mg/d. Ms. R continues to improve while taking risperidone only. Twenty-three days after stopping lorazepam, she is free of catatonic symptoms, scoring 0/6 on the SCIP catatonia scale.
We discharge Ms. R on risperidone. Because she has a history of medication nonadherence, we prescribe risperidone long-acting injection, 37.5 mg every 2 weeks, while continuing oral risperidone for 3 weeks after the first injection. She does well on this medication, experiencing no catatonic symptoms or adverse effects over the next 15 months as measured by the SCIP assessment.
The authors’ observations
This is the third case report in the literature to show that risperidone is effective in short- and long-term treatment of catatonia.4,11 Although Ms. R’s initial response can be attributed at least partially to lorazepam—which is known to be effective in treating catatonia—she continued to show improvement while taking risperidone only and remained free from catatonic symptoms for 15 months, until she was readmitted for reasons unrelated to catatonia.
We recommend using risperidone to treat catatonia in patients who do not respond to a benzodiazepine, especially those with other psychotic symptoms such as delusions or hallucinations. While administering risperidone, watch for long-term side effects, such as hyperlipidemia, weight gain, and diabetes. For catatonia in patients who cannot tolerate risperidone, consider olanzapine or ziprasidone.
- Schedules for Clinicians’ Interview in Psychiatry (SCIP). Available from Ahmed Aboraya, [email protected].
- Valevski A, Loebl T, Keren T, et al. Response of catatonia to risperidone: two case reports. Clin Neuropharmacol. 2001;24(4):228-231.
- Van Den Eede F, Van Hecke J, Van Dalfsen A, et al. The use of atypical antipsychotics in the treatment of catatonia. Eur Psychiatry. 2005;20(5-6):422-429.
- Haloperidol • Haldol
- Lithium • Eskalith, Lithobid
- Lorazepam • Ativan
- Olanzapine • Zyprexa
- Risperidone • Risperdal
- Risperidone long-acting injection • Risperdal Consta
- Ziprasidone • Geodon
The authors have no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Aboraya A, Tien A. Schedules for Clinicians’ Interviews in Psychiatry (SCIP): work in progress. International Journal of Mental Health and Addiction. Available at: http://www.ijma-journal.com/pdf/c01a09.pdf. Accessed February 4, 2009.
2. Diagnostic and statistical manual of disorders, 4th ed, text rev. Washington, DC: American Psychiatric Association; 2000.
3. Kahlbaum KL. In: Levi Y, Pridon T, trans. Catatonia. Baltimore, MD: Johns Hopkins University Press; 1973.
4. Hesslinger B, Walden J, Normann C. Acute and long-term treatment of catatonia with risperidone. Pharmacopsychiatry. 2001;34(1):25-26.
5. Bleuler E. Dementia praecox. New York, NY: International University Press; 1950.
6. Blumer D. Catatonia and the neuroleptics: psychobiologic significance of remote and recent findings. Compr Psychiatry. 1997;38(4):193-201.
7. Bush G, Fink M, Petrides G, et al. Catatonia. II Treatment with lorazepam and electroconvulsive therapy. Acta Psychiatr Scand. 1996;93(2):137-143.
8. Duggal HS, Gandotra G. Risperidone treatment of periodic catatonia. Can J Psychiatry. 2005;50(4):241-242.
9. Duggal HS. Risperidone treatment of febrile catatonia in first-episode psychosis. Gen Hosp Psychiatry. 2005;27(1):80-81.
10. Rudorfer M, Henry M, Sackeim H. Electroconvulsive therapy. In: Tasman A, Kay J, Lieberman JA, eds. Psychiatry: therapeutics. London, UK: John Wiley & Sons; 2003:167-203.
11. Kopala LC, Caudle C. Acute and longer-term effects of risperidone in a case of first-episode catatonic schizophrenia. J Psychopharmacol. 1998;12(3):314-317.
12. Poyurousky M, Bergman J, Weizman A. Risperidone in the treatment of catatonia in a schizophrenic patient. Isr J Psychiatry Relat Sci. 1997;34(4):323-324.
13. Levy WO, Nunez CY. Use of ziprasidone to treat bipolar-associated catatonia. Bipolar Disord. 2004;6(2):166-167.
14. Martenyi F, Metcalfe S, Schausberger B, et al. An efficacy analysis of olanzapine treatment data in schizophrenia patients with catatonic signs and symptoms. J Clin Psychiatry. 2001;62(suppl 2):225-227.
Case: Worsening psychosis
Ms. R, age 21, is admitted to our psychiatric facility while experiencing paranoid delusions and auditory hallucinations. Upon admission, she is agitated and her mood is labile.
Ms. R has 4 previous brief psychiatric admissions and was diagnosed with schizoaffective disorder, bipolar type and moderate mental retardation. Her family history is positive for psychiatric illness, as her mother was diagnosed with schizophrenia. Prior to admission, Ms. R was taking ziprasidone, 160 mg/d, and lithium, 450 mg/d, for 11 months. Both were discontinued during the first week of admission because Ms. R was not responding.
During this admission, the treating psychiatrist assesses Ms. R using the Schedules for Clinicians’ Interview in Psychiatry (SCIP), an instrument developed by the lead author (AA) for psychiatrists to use in conjunction with their routine clinical interviews in inpatient and outpatient settings (see Related Resources). The SCIP includes a 25-question screening section and a diagnostic section that consists of 7 modules that represent major psychiatric diagnoses defined by DSM and International Classification of Diseases criteria.1
During the first week of admission, we monitor Ms. R and administer haloperidol as needed, 10 mg total. Eight days after admission, she develops severe catatonia. On the catatonia scale of the SCIP, Ms. R scores the maximum on measures of immobility, catalepsy/waxy flexibility, and mutism (Table).
How would you treat Ms. R’s catatonia?
Table
Patient’s catatonia symptoms: Response to pharmacotherapy
| Lorazepam only | Lorazepam + risperidone | Risperidone oral only | Risperidone long-acting injection only | |
|---|---|---|---|---|
| Dosage(s) | 7 mg total over 7 days | Lorazepam: 4 mg/d Risperidone: 4 mg/d | 8 mg/d | 37.5 mg every 2 weeks |
| Scores on SCIP catatonia scale:* | ||||
| Immobility | 2 | 1 | 0 | 0 |
| Catalepsy/waxy flexibility† | 2 | 1 | 0 | 0 |
| Mutism | 2 | 0 | 0 | 0 |
| Total score | 6 | 2 | 0 | 0 |
| *Scale of 0 to 2, with 0=none, 1=less than half the time, and 2=more than half the time. Symptoms are evaluated over a 1-day period | ||||
| †For this category, 0=none, 1=brief (usually 1 minute | ||||
| SCIP: Schedules for Clinicians’ Interview in Psychiatry | ||||
The authors’ observations
DSM-IV-TR recognizes catatonia as a schizophrenia subtype, as a descriptor for mania and major depression, and as being caused by various medical conditions, such as neuroleptic malignant syndrome, encephalopathy, or renal failure.2 Kahlbaum initially described catatonia in 1873 as a brain disease characterized by motor abnormalities such as akinesia, rigidity, negativism, mutism, grimacing, posturing, catalepsy, waxy flexibility, and verbigerations.3 Catatonia is characterized by hypo- and hyperkinetic features. Catalepsy, stupor, rigidity, and catatonic posturing with waxy flexibility might alternate with violent catatonic excitement.4
Catatonia can be life-threatening; patients might not be able to eat or chew food, which puts them at risk for aspiration. Those with immobility might not move to urinate or defecate. During the first half of the 20th century, catatonia was documented in up to 50% of patients with schizophrenia.5 Since then, the incidence of catatonia has decreased, possibly the result of advances in psychopharmacology.6
Two days after Ms. R develops catatonia, we transfer her to a local hospital for evaluation to rule out a medical cause of her catatonic symptoms.
EVALUATION: No medical cause
At the hospital, physical examination, electroencephalography, drug screening, and liver and thyroid function tests are within normal limits, eliminating an organic cause of Ms. R’s catatonia. MRI of the head shows a 3-mm mass at the base of the infundibulum, which is unchanged from a prior MRI. Ms. R received 7 mg total of lorazepam over 4 days without relief of her catatonia. She is transferred back to our facility.
The authors’ observations
Benzodiazepines and ECT are effective treatments for catatonia.7 Benzodiazepines are considered first-line treatment because of their efficacy and favorable side-effect profile.7 Lorazepam frequently is used to treat catatonia in the short term.8 Long-term use of benzodiazepines, however, is associated with tolerance, addiction, and rebound phenomena.8,9
Patients with catatonia who do not respond to benzodiazepines may benefit from ECT.9 ECT can cause serious side effects, however, including memory impairment, confusion, delirium, and cardiac arrhythmias.10
Atypical antipsychotics may alleviate motor symptoms of catatonia by virtue of their 5-HT2A receptor antagonistic action.9 In 2 case reports, risperidone successfully treated catatonia.4,11 Kopala et al11 found risperidone, 4 mg/d, was effective in treating severe, first-episode catatonic schizophrenia in a neuroleptic-naive young man. This efficacy was sustained over a 3.5-year outpatient follow-up.
In another report, risperidone, 6 mg/d, effectively treated catatonia and prevented further episodes in a patient with schizophrenia who developed severe catatonia after receiving adequate treatment for Lyme disease with encephalitis.4 Two relapses of catatonic syndrome occurred when risperidone was reduced to 2 mg/d, and remission occurred after risperidone was increased to 6 mg/d. Risperidone’s antagonistic activity of the 5-HT2/D2 receptors may be relevant to its anticatatonic effect.12
Other atypical antipsychotics—ziprasidone and olanzapine—also have been shown to be effective in treating catatonia. Levy et al13 reported successful treatment of a catatonic state (with catalepsy, stupor, and mutism) using intramuscular ziprasidone followed by oral ziprasidone. A data analysis by Martenyi et al14 showed olanzapine to be effective in treating nonspecific signs and symptoms of catatonia, as measured by the Positive and Negative Syndrome Scale.
TREATMENT: Trying risperidone
Based on case reports showing risperidone’s efficacy for catatonia, we start Ms. R on risperidone, 4 mg/d, and lorazepam, 4 mg/d. Eight days later, her catatonic symptoms decrease substantially—she scores 2/6 on the SCIP catatonia scale (Table)—and she starts to talk with the staff.
We continue this regimen for 30 days, then discontinue lorazepam to avoid long-term side effects—such as dependence—and titrate risperidone to 8 mg/d. Ms. R continues to improve while taking risperidone only. Twenty-three days after stopping lorazepam, she is free of catatonic symptoms, scoring 0/6 on the SCIP catatonia scale.
We discharge Ms. R on risperidone. Because she has a history of medication nonadherence, we prescribe risperidone long-acting injection, 37.5 mg every 2 weeks, while continuing oral risperidone for 3 weeks after the first injection. She does well on this medication, experiencing no catatonic symptoms or adverse effects over the next 15 months as measured by the SCIP assessment.
The authors’ observations
This is the third case report in the literature to show that risperidone is effective in short- and long-term treatment of catatonia.4,11 Although Ms. R’s initial response can be attributed at least partially to lorazepam—which is known to be effective in treating catatonia—she continued to show improvement while taking risperidone only and remained free from catatonic symptoms for 15 months, until she was readmitted for reasons unrelated to catatonia.
We recommend using risperidone to treat catatonia in patients who do not respond to a benzodiazepine, especially those with other psychotic symptoms such as delusions or hallucinations. While administering risperidone, watch for long-term side effects, such as hyperlipidemia, weight gain, and diabetes. For catatonia in patients who cannot tolerate risperidone, consider olanzapine or ziprasidone.
- Schedules for Clinicians’ Interview in Psychiatry (SCIP). Available from Ahmed Aboraya, [email protected].
- Valevski A, Loebl T, Keren T, et al. Response of catatonia to risperidone: two case reports. Clin Neuropharmacol. 2001;24(4):228-231.
- Van Den Eede F, Van Hecke J, Van Dalfsen A, et al. The use of atypical antipsychotics in the treatment of catatonia. Eur Psychiatry. 2005;20(5-6):422-429.
- Haloperidol • Haldol
- Lithium • Eskalith, Lithobid
- Lorazepam • Ativan
- Olanzapine • Zyprexa
- Risperidone • Risperdal
- Risperidone long-acting injection • Risperdal Consta
- Ziprasidone • Geodon
The authors have no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Case: Worsening psychosis
Ms. R, age 21, is admitted to our psychiatric facility while experiencing paranoid delusions and auditory hallucinations. Upon admission, she is agitated and her mood is labile.
Ms. R has 4 previous brief psychiatric admissions and was diagnosed with schizoaffective disorder, bipolar type and moderate mental retardation. Her family history is positive for psychiatric illness, as her mother was diagnosed with schizophrenia. Prior to admission, Ms. R was taking ziprasidone, 160 mg/d, and lithium, 450 mg/d, for 11 months. Both were discontinued during the first week of admission because Ms. R was not responding.
During this admission, the treating psychiatrist assesses Ms. R using the Schedules for Clinicians’ Interview in Psychiatry (SCIP), an instrument developed by the lead author (AA) for psychiatrists to use in conjunction with their routine clinical interviews in inpatient and outpatient settings (see Related Resources). The SCIP includes a 25-question screening section and a diagnostic section that consists of 7 modules that represent major psychiatric diagnoses defined by DSM and International Classification of Diseases criteria.1
During the first week of admission, we monitor Ms. R and administer haloperidol as needed, 10 mg total. Eight days after admission, she develops severe catatonia. On the catatonia scale of the SCIP, Ms. R scores the maximum on measures of immobility, catalepsy/waxy flexibility, and mutism (Table).
How would you treat Ms. R’s catatonia?
Table
Patient’s catatonia symptoms: Response to pharmacotherapy
| Lorazepam only | Lorazepam + risperidone | Risperidone oral only | Risperidone long-acting injection only | |
|---|---|---|---|---|
| Dosage(s) | 7 mg total over 7 days | Lorazepam: 4 mg/d Risperidone: 4 mg/d | 8 mg/d | 37.5 mg every 2 weeks |
| Scores on SCIP catatonia scale:* | ||||
| Immobility | 2 | 1 | 0 | 0 |
| Catalepsy/waxy flexibility† | 2 | 1 | 0 | 0 |
| Mutism | 2 | 0 | 0 | 0 |
| Total score | 6 | 2 | 0 | 0 |
| *Scale of 0 to 2, with 0=none, 1=less than half the time, and 2=more than half the time. Symptoms are evaluated over a 1-day period | ||||
| †For this category, 0=none, 1=brief (usually 1 minute | ||||
| SCIP: Schedules for Clinicians’ Interview in Psychiatry | ||||
The authors’ observations
DSM-IV-TR recognizes catatonia as a schizophrenia subtype, as a descriptor for mania and major depression, and as being caused by various medical conditions, such as neuroleptic malignant syndrome, encephalopathy, or renal failure.2 Kahlbaum initially described catatonia in 1873 as a brain disease characterized by motor abnormalities such as akinesia, rigidity, negativism, mutism, grimacing, posturing, catalepsy, waxy flexibility, and verbigerations.3 Catatonia is characterized by hypo- and hyperkinetic features. Catalepsy, stupor, rigidity, and catatonic posturing with waxy flexibility might alternate with violent catatonic excitement.4
Catatonia can be life-threatening; patients might not be able to eat or chew food, which puts them at risk for aspiration. Those with immobility might not move to urinate or defecate. During the first half of the 20th century, catatonia was documented in up to 50% of patients with schizophrenia.5 Since then, the incidence of catatonia has decreased, possibly the result of advances in psychopharmacology.6
Two days after Ms. R develops catatonia, we transfer her to a local hospital for evaluation to rule out a medical cause of her catatonic symptoms.
EVALUATION: No medical cause
At the hospital, physical examination, electroencephalography, drug screening, and liver and thyroid function tests are within normal limits, eliminating an organic cause of Ms. R’s catatonia. MRI of the head shows a 3-mm mass at the base of the infundibulum, which is unchanged from a prior MRI. Ms. R received 7 mg total of lorazepam over 4 days without relief of her catatonia. She is transferred back to our facility.
The authors’ observations
Benzodiazepines and ECT are effective treatments for catatonia.7 Benzodiazepines are considered first-line treatment because of their efficacy and favorable side-effect profile.7 Lorazepam frequently is used to treat catatonia in the short term.8 Long-term use of benzodiazepines, however, is associated with tolerance, addiction, and rebound phenomena.8,9
Patients with catatonia who do not respond to benzodiazepines may benefit from ECT.9 ECT can cause serious side effects, however, including memory impairment, confusion, delirium, and cardiac arrhythmias.10
Atypical antipsychotics may alleviate motor symptoms of catatonia by virtue of their 5-HT2A receptor antagonistic action.9 In 2 case reports, risperidone successfully treated catatonia.4,11 Kopala et al11 found risperidone, 4 mg/d, was effective in treating severe, first-episode catatonic schizophrenia in a neuroleptic-naive young man. This efficacy was sustained over a 3.5-year outpatient follow-up.
In another report, risperidone, 6 mg/d, effectively treated catatonia and prevented further episodes in a patient with schizophrenia who developed severe catatonia after receiving adequate treatment for Lyme disease with encephalitis.4 Two relapses of catatonic syndrome occurred when risperidone was reduced to 2 mg/d, and remission occurred after risperidone was increased to 6 mg/d. Risperidone’s antagonistic activity of the 5-HT2/D2 receptors may be relevant to its anticatatonic effect.12
Other atypical antipsychotics—ziprasidone and olanzapine—also have been shown to be effective in treating catatonia. Levy et al13 reported successful treatment of a catatonic state (with catalepsy, stupor, and mutism) using intramuscular ziprasidone followed by oral ziprasidone. A data analysis by Martenyi et al14 showed olanzapine to be effective in treating nonspecific signs and symptoms of catatonia, as measured by the Positive and Negative Syndrome Scale.
TREATMENT: Trying risperidone
Based on case reports showing risperidone’s efficacy for catatonia, we start Ms. R on risperidone, 4 mg/d, and lorazepam, 4 mg/d. Eight days later, her catatonic symptoms decrease substantially—she scores 2/6 on the SCIP catatonia scale (Table)—and she starts to talk with the staff.
We continue this regimen for 30 days, then discontinue lorazepam to avoid long-term side effects—such as dependence—and titrate risperidone to 8 mg/d. Ms. R continues to improve while taking risperidone only. Twenty-three days after stopping lorazepam, she is free of catatonic symptoms, scoring 0/6 on the SCIP catatonia scale.
We discharge Ms. R on risperidone. Because she has a history of medication nonadherence, we prescribe risperidone long-acting injection, 37.5 mg every 2 weeks, while continuing oral risperidone for 3 weeks after the first injection. She does well on this medication, experiencing no catatonic symptoms or adverse effects over the next 15 months as measured by the SCIP assessment.
The authors’ observations
This is the third case report in the literature to show that risperidone is effective in short- and long-term treatment of catatonia.4,11 Although Ms. R’s initial response can be attributed at least partially to lorazepam—which is known to be effective in treating catatonia—she continued to show improvement while taking risperidone only and remained free from catatonic symptoms for 15 months, until she was readmitted for reasons unrelated to catatonia.
We recommend using risperidone to treat catatonia in patients who do not respond to a benzodiazepine, especially those with other psychotic symptoms such as delusions or hallucinations. While administering risperidone, watch for long-term side effects, such as hyperlipidemia, weight gain, and diabetes. For catatonia in patients who cannot tolerate risperidone, consider olanzapine or ziprasidone.
- Schedules for Clinicians’ Interview in Psychiatry (SCIP). Available from Ahmed Aboraya, [email protected].
- Valevski A, Loebl T, Keren T, et al. Response of catatonia to risperidone: two case reports. Clin Neuropharmacol. 2001;24(4):228-231.
- Van Den Eede F, Van Hecke J, Van Dalfsen A, et al. The use of atypical antipsychotics in the treatment of catatonia. Eur Psychiatry. 2005;20(5-6):422-429.
- Haloperidol • Haldol
- Lithium • Eskalith, Lithobid
- Lorazepam • Ativan
- Olanzapine • Zyprexa
- Risperidone • Risperdal
- Risperidone long-acting injection • Risperdal Consta
- Ziprasidone • Geodon
The authors have no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Aboraya A, Tien A. Schedules for Clinicians’ Interviews in Psychiatry (SCIP): work in progress. International Journal of Mental Health and Addiction. Available at: http://www.ijma-journal.com/pdf/c01a09.pdf. Accessed February 4, 2009.
2. Diagnostic and statistical manual of disorders, 4th ed, text rev. Washington, DC: American Psychiatric Association; 2000.
3. Kahlbaum KL. In: Levi Y, Pridon T, trans. Catatonia. Baltimore, MD: Johns Hopkins University Press; 1973.
4. Hesslinger B, Walden J, Normann C. Acute and long-term treatment of catatonia with risperidone. Pharmacopsychiatry. 2001;34(1):25-26.
5. Bleuler E. Dementia praecox. New York, NY: International University Press; 1950.
6. Blumer D. Catatonia and the neuroleptics: psychobiologic significance of remote and recent findings. Compr Psychiatry. 1997;38(4):193-201.
7. Bush G, Fink M, Petrides G, et al. Catatonia. II Treatment with lorazepam and electroconvulsive therapy. Acta Psychiatr Scand. 1996;93(2):137-143.
8. Duggal HS, Gandotra G. Risperidone treatment of periodic catatonia. Can J Psychiatry. 2005;50(4):241-242.
9. Duggal HS. Risperidone treatment of febrile catatonia in first-episode psychosis. Gen Hosp Psychiatry. 2005;27(1):80-81.
10. Rudorfer M, Henry M, Sackeim H. Electroconvulsive therapy. In: Tasman A, Kay J, Lieberman JA, eds. Psychiatry: therapeutics. London, UK: John Wiley & Sons; 2003:167-203.
11. Kopala LC, Caudle C. Acute and longer-term effects of risperidone in a case of first-episode catatonic schizophrenia. J Psychopharmacol. 1998;12(3):314-317.
12. Poyurousky M, Bergman J, Weizman A. Risperidone in the treatment of catatonia in a schizophrenic patient. Isr J Psychiatry Relat Sci. 1997;34(4):323-324.
13. Levy WO, Nunez CY. Use of ziprasidone to treat bipolar-associated catatonia. Bipolar Disord. 2004;6(2):166-167.
14. Martenyi F, Metcalfe S, Schausberger B, et al. An efficacy analysis of olanzapine treatment data in schizophrenia patients with catatonic signs and symptoms. J Clin Psychiatry. 2001;62(suppl 2):225-227.
1. Aboraya A, Tien A. Schedules for Clinicians’ Interviews in Psychiatry (SCIP): work in progress. International Journal of Mental Health and Addiction. Available at: http://www.ijma-journal.com/pdf/c01a09.pdf. Accessed February 4, 2009.
2. Diagnostic and statistical manual of disorders, 4th ed, text rev. Washington, DC: American Psychiatric Association; 2000.
3. Kahlbaum KL. In: Levi Y, Pridon T, trans. Catatonia. Baltimore, MD: Johns Hopkins University Press; 1973.
4. Hesslinger B, Walden J, Normann C. Acute and long-term treatment of catatonia with risperidone. Pharmacopsychiatry. 2001;34(1):25-26.
5. Bleuler E. Dementia praecox. New York, NY: International University Press; 1950.
6. Blumer D. Catatonia and the neuroleptics: psychobiologic significance of remote and recent findings. Compr Psychiatry. 1997;38(4):193-201.
7. Bush G, Fink M, Petrides G, et al. Catatonia. II Treatment with lorazepam and electroconvulsive therapy. Acta Psychiatr Scand. 1996;93(2):137-143.
8. Duggal HS, Gandotra G. Risperidone treatment of periodic catatonia. Can J Psychiatry. 2005;50(4):241-242.
9. Duggal HS. Risperidone treatment of febrile catatonia in first-episode psychosis. Gen Hosp Psychiatry. 2005;27(1):80-81.
10. Rudorfer M, Henry M, Sackeim H. Electroconvulsive therapy. In: Tasman A, Kay J, Lieberman JA, eds. Psychiatry: therapeutics. London, UK: John Wiley & Sons; 2003:167-203.
11. Kopala LC, Caudle C. Acute and longer-term effects of risperidone in a case of first-episode catatonic schizophrenia. J Psychopharmacol. 1998;12(3):314-317.
12. Poyurousky M, Bergman J, Weizman A. Risperidone in the treatment of catatonia in a schizophrenic patient. Isr J Psychiatry Relat Sci. 1997;34(4):323-324.
13. Levy WO, Nunez CY. Use of ziprasidone to treat bipolar-associated catatonia. Bipolar Disord. 2004;6(2):166-167.
14. Martenyi F, Metcalfe S, Schausberger B, et al. An efficacy analysis of olanzapine treatment data in schizophrenia patients with catatonic signs and symptoms. J Clin Psychiatry. 2001;62(suppl 2):225-227.
The angry patient with Asperger’s
CASE ‘Sad, worried, and angry’
Mr. A, age 24, is referred to our university psychiatric clinic. He reports that he’s sad, worried, angry, and wants to hurt people. He endorses having chronic depressive episodes that last >2 weeks and consist of poor sleep, low energy, anhedonia, poor concentration, and psychomotor retardation.
He is developmentally disabled and has been living in a group home for almost 1 year. In former group homes, Mr. A threatened and assaulted other patients and staff. In 1 incident Mr. A broke a patient’s nose and was incarcerated for 4 days. With the help of a job coach, Mr. A has been working in a department store for 8 months. He was fired from other jobs because he threatened co-workers.
The author’s observations
Problem behaviors in patients with pervasive developmental disorders include aggression and self-injury. These behaviors may improve with behavioral or pharmacologic interventions.1 For example, risperidone is FDA-approved to treat irritability associated with autistic disorder in children and adolescents age 5 to 16 years.2 Violence has been reported in patients with pervasive developmental disorders, and such symptoms can lead to psychiatric referral.1
HISTORY Difficult childhood
Mr. A’s medical history is unremarkable. He has no history of hypomania, mania, psychosis, substance use, tics, seizures, genetic illnesses, head trauma, or physical or sexual abuse. He has never attempted suicide nor been hospitalized for psychiatric illness.
With Mr. A’s permission, his mother is consulted. She says that as a child Mr. A would become extremely interested in various topics—including Pokémon, Magic cards, and video games—and had a strong desire to tell everyone the details of each. However, he rocked back and forth, had few friends, and would bite other children.
Mr. A has no history of language delay but received speech therapy during his childhood to help him “work on eye contact and social skills.” He is estranged from and angry with his father, who has difficulty accepting his son’s developmental disability.
At the time of referral, Mr. A is receiving paroxetine, 30 mg/d, for depression, risperidone, 1.5 mg/d, for aggression, and dextroamphetamine/amphetamine extended-release, 30 mg/d, for hyperactivity/inattention. The efficacy of these medications, which were prescribed by an outside psychiatrist, is unclear.
Table 1
Diagnostic criteria for Asperger’s disorder
A. Qualitative impairment in social interaction, as manifested by ≥2 of the following:
|
B. Restricted repetitive and stereotyped patterns of behavior, interests, and activities, as manifested by ≥1 of the following:
|
| C. The disturbance causes clinically significant impairment in social, occupational, or other important areas of functioning. |
| D. There is no clinically significant general delay in language (eg, single words used by age 2 years, communicative phrases used by age 3 years). |
| E. There is no clinically significant delay in cognitive development or in the development of age-appropriate self-help skills, adaptive behavior (other than in social interaction), and curiosity about the environment in childhood. |
| F. Criteria are not met for another specific pervasive developmental disorder or schizophrenia. |
| Source: Diagnostic and statistical manual of mental disorders, 4th ed, text rev. Washington, DC: American Psychiatric Association; 2000 |
Based on Mr. A’s impaired social interaction, repetitive interests and behaviors, and lack of language delay, Mr. A meets criteria for Asperger’s disorder (Table 1). He also meets criteria for major depressive disorder, recurrent, moderate.
The author’s observations
Psychosocial interventions for patients with an autism-spectrum disorder consist of educational, vocational, behavioral, and family interventions. Individual, group, and family psychotherapy may benefit patients with Asperger’s disorder who have comorbid depression.1
TREATMENT A rocky start
At Mr. A’s initial assessment, the clinic psychiatrist increases risperidone to 1 mg twice daily to target aggression. Even after receiving this dosage for 1 month, however, Mr. A continues to display physical aggression toward peers in the group home whenever he becomes angry.
The psychiatrist refers Mr. A to a social worker for supportive therapy to help him cope with worry and chronic sadness. The social worker uses general cognitive-behavioral strategies for anxiety and aggression for 12 sessions over 8 months until scheduling conflicts end therapy. The efficacy of this therapy is minimal; Mr. A remains depressed, anxious, and aggressive. During this time, the psychiatrist increases paroxetine to 40 mg/d, but Mr. A continues to feel depressed after 1 month. Mr. A is cross-tapered to duloxetine, but continues to feel depressed after receiving duloxetine, 60 mg/d, for 1 month.
My first visit with Mr. A occurs 3 months after his last visit with the social worker. He states he does not remember anything from those sessions. Mr. A’s goals for therapy are to reduce anxiety, manage anger, and improve relationship skills.
I begin the first 4 months of Mr. A’s therapy with cognitive-behavioral interventions based on the Treatment of Adolescents Depression Study (TADS) manual.3 Although Mr. A is an adult, I choose a manual that targets adolescents because my clinical impression is that his cognitive developmental level is more like an adolescent’s than an adult’s.
I assign homework such as mood monitoring. I ask him to use a form from the TADS manual to rate his mood on a scale of 0 to 10 every morning, afternoon, and evening, and write down what he is doing that makes him feel that way at the time he rates his mood. Mr. A never completes any homework; during each session he states he “just forgot to do it.”
I discuss concepts such as goal setting, for a novel Mr. A says he wants to write, and relaxation strategies to address anger; in session, I work with him on filling out the “What Helps Me to Relax?” form from the TADS manual. Mr. A lists “play games,” “write my book,” “listen to music,” “go outside,” and “exercise” as strategies to help him relax. We also work on visual handouts—such as “Safety Plan” and “What Can I Do to Relax”—to post in his room.
Mr. A does not show up for 3 sessions. When I call the group home, a staff member tells me they were busy with other patients and forgot about Mr. A. I decide to call the group home the day before each appointment as a reminder. This increases Mr. A’s attendance rate.
During each session, Mr. A complains about the quality of the group home, the staff, and other patients. To get my own perspective of Mr. A’s living environment, I consider visiting his group home, similar to how a geriatric psychiatrist sees patients in a nursing home or an assertive community treatment team psychiatrist sees patients in their home environments. Because I am concerned about boundary crossings/violations, I first discuss this action with 2 psychotherapists not involved in Mr. A’s treatment. They recommend that I limit this action to a one-time visit.
I visit Mr. A’s group home 2 months after my first session with him. Located in front of a dairy farm in a rural part of the state about 1 hour from our clinic, the isolated facility has a secured keypad entry. When I meet Mr. A there, he says he feels as if he is in jail. I meet the staff and find them willing to help with various aspects of Mr. A’s treatment, such as discussing events, reporting behaviors, and helping carry out interventions.
For example, I ask staff to remind Mr. A of his relaxation strategies when he becomes angry. On the “Safety Plan” handout, I had Mr. A identify 5 people he could talk to when he becomes angry; I ask staff to remind him of those people when Mr. A becomes angry. I also ask staff to ask Mr. A every day if he is writing the novel he wants to complete. After my visit, Mr. A starts putting more effort into therapy. When I set a daily goal of working on his novel for 15 minutes, he starts bringing pages of his writings to sessions.
Table 2
Social skills training for patients with Asperger’s disorde
| Starting a conversation: “Hi, how was your day?” |
| Staying on topic: “Oh, that sounds interesting. Tell me more about…” |
| Making eye contact: Look at people’s eyes when talking to them |
| Greetings: “Hi, how are you?” |
| Ending a conversation: “Well, I have to go now. I’ll see you later!” |
| Shifting topics: “Speaking of…, did you hear about…?” |
| Source:Reference 7 |
The author’s observations
In a study in rural Appalachia, telephone reminders increased attendance at psychiatric intake appointments.4 Calling the group home before each of Mr. A’s appointments took extra time out of my schedule but improved Mr. A’s attendance rate.
In residential treatment of children, Monahan notes that childcare workers could contribute useful observations and benefit from the therapist’s advice.5 Establishing rapport with the staff at Mr. A’s group home helped me proceed with therapy.
TREATMENT Social skills training
In the second 4 months of therapy, Mr. A changes jobs to become a greeter in a local video game store. He is happy, and group home staff members are pleased they no longer spend 2 hours each day transporting him to his previous job.
Soon after, during a reminder phone call, a staff member tells me that Mr. A’s brother and father were murdered the prior week. Three staff members attend Mr. A’s brother’s funeral, which he appreciates. Mr. A refuses to attend his father’s funeral because of continued anger toward him.
When I ask Mr. A if he wants to talk about the deaths, he declines. I subsequently spend half a session discussing strategies to address grief,6 such as imagining a conversation with his deceased brother.
I decide to review Mr. A’s therapy goals because he still has a lot of anger toward his recently deceased father. I am concerned he might discharge this anger onto a staff member, coworker, or fellow patient. Mr. A states he wants to focus on relationships, especially his anxiety around women. He discusses his anxiety with starting and maintaining conversations with women.
I begin role-playing in sessions by pretending to be a woman for Mr. A to speak with, but he feels this is silly. I teach him exercises from a social skills training workbook developed for patients with Asperger’s, such as “Starting a conversation,” “Staying on topic,” and “Making eye contact” (Table 2).7 Mr. A says group home staff members occasionally take him out to a nearby nightclub and encourage him to talk to women.
To see how Mr. A behaves in public, during our sessions I take him to different parts of the hospital, such as the gift shop, library, and deli. I instruct him to ask various women non-threatening questions, such as how much a certain entrée costs. I note his body language, such as tilting his head down and fidgeting during conversations. I provide him with immediate feedback, which slowly increases his awareness of these behaviors.
With Mr. A’s permission, I educate the group home staff about how to point out these behaviors when Mr. A is in public. I ask them to focus on body language and emphasize that Mr. A needs to apply what I teach him to other settings.
The author’s observations
Patients with Asperger’s disorder need specific training to build a repertoire of social skills.7 Teaching in real-life settings helps patients generalize these skills.1
Zimmerman8 discusses how caregivers might have an unrealistic, “magical” view of psychotherapy and feel suspicious of the process. With Mr. A’s permission, I ask group home staff members to meet with me for 10 minutes at the end of each of Mr. A’s sessions to make them aware of what is happening with his therapy. I want them to feel that they are an important part of Mr. A’s therapy. These meetings may have alleviated staff members’ fears about my time with him. Even though Mr. A granted me permission to disclose all details of our sessions with the staff, I was careful to not disclose sensitive issues, such as the patient’s dreams and fantasies.
TREATMENT ‘Fear’
Mr. A rates his anxiety as a 4/10 whenever he speaks with women. To more specifically understand his underlying cognitions, I use Kendall’s FEAR plan (Table 3).9
I ask him to divide his automatic “E” thoughts into “she” and “I” thoughts. Examples of automatic “she” thoughts include “She probably won’t like me” and “She thinks I’m not cute.” Examples of automatic “I” thoughts include “I’m probably not smart enough for her” and “I think we won’t have anything in common.”
Table 3
The FEAR plan*
| F=feeling anxious | |
| E=expecting bad things to happen | |
| A=attitudes and actions that can help | |
| R=results and rewards | |
| Developed to help anxious children and adolescents recognize signs of anxiety, relax, and modify anxious self-talk and thinking. | |
| Source:Reference 9 | |
The author’s observations
Schwartz10 discusses countertransference challenges in nursing home patients, where therapists identify with patients’ hopelessness. Schwartz recommends addressing these challenges by thinking of realistic expectations. Even though a facility might be far from perfect, it may be “good enough.”
Mr. A’s group home was far from perfect and located in an isolated setting. Even so, I was able to help him complete psychotherapy at our clinic by adapting my practice to his needs, including:
- making reminder phone calls for appointments
- visiting the group home
- enlisting the help of caregivers with therapeutic techniques.
OUTCOME Improving
In the final 4 months of therapy, we continue to work on social skills lessons, practice exercises in the hospital, and the FEAR acronym. I continue to include caregivers in these efforts.
During 1 session, I tell Mr. A I will be leaving at the end of my fellowship. In the final month, I gradually transition him to a new therapist. I decided to transition him to a male therapist so Mr. A will continue to feel comfortable sharing his feelings, rather than shutting down from anxiety with a female therapist. As I end therapy, Mr. A is promoted to a cashier at the video game store and enrolls in classes to study for a General Education Development (GED) certificate.
Related resource
- National Institute of Mental Health. Autism spectrum disorders. www.nimh.nih.gov/health/publications/autism/complete-publication.shtml.
- Bupropion extended-release • Wellbutrin XL
- Dextroamphetamine/amphetamine extended-release • Adderall XR
- Duloxetine • Cymbalta
- Paroxetine • Paxil
- Risperidone • Risperdal
- Ziprasidone • Geodon
The author reports no financial relationships with any company whose products are mentioned in this article or with manufacturers of competing products.
Acknowledgment
The author thanks Dr. Ann Lagges, PhD, for her assistance with this patient’s treatment.
1. American Association of Child and Adolescent Psychiatry. Practice parameters for autism in children, adolescents, and adults. Available at: http://www.aacap.org/galleries/PracticeParameters/Autism.pdf. Accessed December 25, 2008.
2. Risperdal [package insert]. Titusville, NJ: Janssen Pharmaceuticals, Inc; 2008. Available at: http://www.risperdal.com/risperdal/shared/pi/risperdal.pdf. Accessed December 25, 2008.
3. Curry JF, Wells KC, Brent DA, et al. Treatment for adolescents with depression study (TADS): cognitive behavior therapy manual. Available at: https://trialweb.dcri.duke.edu/tads/tad/manuals/TADS_CBT.pdf. Accessed August 2, 2007.
4. Shoffner J, Staudt M, Marcus S, et al. Using telephone reminders to increase attendance at psychiatric appointments: findings of a pilot study in rural Appalachia. Psychiatr Serv. 2007;58(6):872-875.
5. Monahan RT. Individual and group psychotherapy. In: Lyman RD, Prentice-Dunn S, Gabel S, eds. Residential and inpatient treatment of children and adolescents. New York, NY: Plenum Publishing; 1989:192.
6. Shear K, Frank E, Houck PR, et al. Treatment of complicated grief: a randomized controlled trial. JAMA. 2005;293(1):2601-2608.
7. Baker JE. Social skills training for children and adolescents with Asperger syndrome and social-communication problems. Shawnee Mission, KS: Autism Asperger Publishing Company; 2003.
8. Zimmerman DP. Psychotherapy in residential treatment: historical development and critical issues. Child Adolesc Psychiatr Clin N Am. 2004;13(2):347-361.
9. Kendall PC, Hedtke A. Coping cat workbook. 2nd ed. Ardmore, PA: Workbook Publishing; 2006.
10. Schwartz K. Remembering the forgotten: psychotherapy groups for the nursing home resident. Int J Group Psychother. 2007;57(4):497-514.
CASE ‘Sad, worried, and angry’
Mr. A, age 24, is referred to our university psychiatric clinic. He reports that he’s sad, worried, angry, and wants to hurt people. He endorses having chronic depressive episodes that last >2 weeks and consist of poor sleep, low energy, anhedonia, poor concentration, and psychomotor retardation.
He is developmentally disabled and has been living in a group home for almost 1 year. In former group homes, Mr. A threatened and assaulted other patients and staff. In 1 incident Mr. A broke a patient’s nose and was incarcerated for 4 days. With the help of a job coach, Mr. A has been working in a department store for 8 months. He was fired from other jobs because he threatened co-workers.
The author’s observations
Problem behaviors in patients with pervasive developmental disorders include aggression and self-injury. These behaviors may improve with behavioral or pharmacologic interventions.1 For example, risperidone is FDA-approved to treat irritability associated with autistic disorder in children and adolescents age 5 to 16 years.2 Violence has been reported in patients with pervasive developmental disorders, and such symptoms can lead to psychiatric referral.1
HISTORY Difficult childhood
Mr. A’s medical history is unremarkable. He has no history of hypomania, mania, psychosis, substance use, tics, seizures, genetic illnesses, head trauma, or physical or sexual abuse. He has never attempted suicide nor been hospitalized for psychiatric illness.
With Mr. A’s permission, his mother is consulted. She says that as a child Mr. A would become extremely interested in various topics—including Pokémon, Magic cards, and video games—and had a strong desire to tell everyone the details of each. However, he rocked back and forth, had few friends, and would bite other children.
Mr. A has no history of language delay but received speech therapy during his childhood to help him “work on eye contact and social skills.” He is estranged from and angry with his father, who has difficulty accepting his son’s developmental disability.
At the time of referral, Mr. A is receiving paroxetine, 30 mg/d, for depression, risperidone, 1.5 mg/d, for aggression, and dextroamphetamine/amphetamine extended-release, 30 mg/d, for hyperactivity/inattention. The efficacy of these medications, which were prescribed by an outside psychiatrist, is unclear.
Table 1
Diagnostic criteria for Asperger’s disorder
A. Qualitative impairment in social interaction, as manifested by ≥2 of the following:
|
B. Restricted repetitive and stereotyped patterns of behavior, interests, and activities, as manifested by ≥1 of the following:
|
| C. The disturbance causes clinically significant impairment in social, occupational, or other important areas of functioning. |
| D. There is no clinically significant general delay in language (eg, single words used by age 2 years, communicative phrases used by age 3 years). |
| E. There is no clinically significant delay in cognitive development or in the development of age-appropriate self-help skills, adaptive behavior (other than in social interaction), and curiosity about the environment in childhood. |
| F. Criteria are not met for another specific pervasive developmental disorder or schizophrenia. |
| Source: Diagnostic and statistical manual of mental disorders, 4th ed, text rev. Washington, DC: American Psychiatric Association; 2000 |
Based on Mr. A’s impaired social interaction, repetitive interests and behaviors, and lack of language delay, Mr. A meets criteria for Asperger’s disorder (Table 1). He also meets criteria for major depressive disorder, recurrent, moderate.
The author’s observations
Psychosocial interventions for patients with an autism-spectrum disorder consist of educational, vocational, behavioral, and family interventions. Individual, group, and family psychotherapy may benefit patients with Asperger’s disorder who have comorbid depression.1
TREATMENT A rocky start
At Mr. A’s initial assessment, the clinic psychiatrist increases risperidone to 1 mg twice daily to target aggression. Even after receiving this dosage for 1 month, however, Mr. A continues to display physical aggression toward peers in the group home whenever he becomes angry.
The psychiatrist refers Mr. A to a social worker for supportive therapy to help him cope with worry and chronic sadness. The social worker uses general cognitive-behavioral strategies for anxiety and aggression for 12 sessions over 8 months until scheduling conflicts end therapy. The efficacy of this therapy is minimal; Mr. A remains depressed, anxious, and aggressive. During this time, the psychiatrist increases paroxetine to 40 mg/d, but Mr. A continues to feel depressed after 1 month. Mr. A is cross-tapered to duloxetine, but continues to feel depressed after receiving duloxetine, 60 mg/d, for 1 month.
My first visit with Mr. A occurs 3 months after his last visit with the social worker. He states he does not remember anything from those sessions. Mr. A’s goals for therapy are to reduce anxiety, manage anger, and improve relationship skills.
I begin the first 4 months of Mr. A’s therapy with cognitive-behavioral interventions based on the Treatment of Adolescents Depression Study (TADS) manual.3 Although Mr. A is an adult, I choose a manual that targets adolescents because my clinical impression is that his cognitive developmental level is more like an adolescent’s than an adult’s.
I assign homework such as mood monitoring. I ask him to use a form from the TADS manual to rate his mood on a scale of 0 to 10 every morning, afternoon, and evening, and write down what he is doing that makes him feel that way at the time he rates his mood. Mr. A never completes any homework; during each session he states he “just forgot to do it.”
I discuss concepts such as goal setting, for a novel Mr. A says he wants to write, and relaxation strategies to address anger; in session, I work with him on filling out the “What Helps Me to Relax?” form from the TADS manual. Mr. A lists “play games,” “write my book,” “listen to music,” “go outside,” and “exercise” as strategies to help him relax. We also work on visual handouts—such as “Safety Plan” and “What Can I Do to Relax”—to post in his room.
Mr. A does not show up for 3 sessions. When I call the group home, a staff member tells me they were busy with other patients and forgot about Mr. A. I decide to call the group home the day before each appointment as a reminder. This increases Mr. A’s attendance rate.
During each session, Mr. A complains about the quality of the group home, the staff, and other patients. To get my own perspective of Mr. A’s living environment, I consider visiting his group home, similar to how a geriatric psychiatrist sees patients in a nursing home or an assertive community treatment team psychiatrist sees patients in their home environments. Because I am concerned about boundary crossings/violations, I first discuss this action with 2 psychotherapists not involved in Mr. A’s treatment. They recommend that I limit this action to a one-time visit.
I visit Mr. A’s group home 2 months after my first session with him. Located in front of a dairy farm in a rural part of the state about 1 hour from our clinic, the isolated facility has a secured keypad entry. When I meet Mr. A there, he says he feels as if he is in jail. I meet the staff and find them willing to help with various aspects of Mr. A’s treatment, such as discussing events, reporting behaviors, and helping carry out interventions.
For example, I ask staff to remind Mr. A of his relaxation strategies when he becomes angry. On the “Safety Plan” handout, I had Mr. A identify 5 people he could talk to when he becomes angry; I ask staff to remind him of those people when Mr. A becomes angry. I also ask staff to ask Mr. A every day if he is writing the novel he wants to complete. After my visit, Mr. A starts putting more effort into therapy. When I set a daily goal of working on his novel for 15 minutes, he starts bringing pages of his writings to sessions.
Table 2
Social skills training for patients with Asperger’s disorde
| Starting a conversation: “Hi, how was your day?” |
| Staying on topic: “Oh, that sounds interesting. Tell me more about…” |
| Making eye contact: Look at people’s eyes when talking to them |
| Greetings: “Hi, how are you?” |
| Ending a conversation: “Well, I have to go now. I’ll see you later!” |
| Shifting topics: “Speaking of…, did you hear about…?” |
| Source:Reference 7 |
The author’s observations
In a study in rural Appalachia, telephone reminders increased attendance at psychiatric intake appointments.4 Calling the group home before each of Mr. A’s appointments took extra time out of my schedule but improved Mr. A’s attendance rate.
In residential treatment of children, Monahan notes that childcare workers could contribute useful observations and benefit from the therapist’s advice.5 Establishing rapport with the staff at Mr. A’s group home helped me proceed with therapy.
TREATMENT Social skills training
In the second 4 months of therapy, Mr. A changes jobs to become a greeter in a local video game store. He is happy, and group home staff members are pleased they no longer spend 2 hours each day transporting him to his previous job.
Soon after, during a reminder phone call, a staff member tells me that Mr. A’s brother and father were murdered the prior week. Three staff members attend Mr. A’s brother’s funeral, which he appreciates. Mr. A refuses to attend his father’s funeral because of continued anger toward him.
When I ask Mr. A if he wants to talk about the deaths, he declines. I subsequently spend half a session discussing strategies to address grief,6 such as imagining a conversation with his deceased brother.
I decide to review Mr. A’s therapy goals because he still has a lot of anger toward his recently deceased father. I am concerned he might discharge this anger onto a staff member, coworker, or fellow patient. Mr. A states he wants to focus on relationships, especially his anxiety around women. He discusses his anxiety with starting and maintaining conversations with women.
I begin role-playing in sessions by pretending to be a woman for Mr. A to speak with, but he feels this is silly. I teach him exercises from a social skills training workbook developed for patients with Asperger’s, such as “Starting a conversation,” “Staying on topic,” and “Making eye contact” (Table 2).7 Mr. A says group home staff members occasionally take him out to a nearby nightclub and encourage him to talk to women.
To see how Mr. A behaves in public, during our sessions I take him to different parts of the hospital, such as the gift shop, library, and deli. I instruct him to ask various women non-threatening questions, such as how much a certain entrée costs. I note his body language, such as tilting his head down and fidgeting during conversations. I provide him with immediate feedback, which slowly increases his awareness of these behaviors.
With Mr. A’s permission, I educate the group home staff about how to point out these behaviors when Mr. A is in public. I ask them to focus on body language and emphasize that Mr. A needs to apply what I teach him to other settings.
The author’s observations
Patients with Asperger’s disorder need specific training to build a repertoire of social skills.7 Teaching in real-life settings helps patients generalize these skills.1
Zimmerman8 discusses how caregivers might have an unrealistic, “magical” view of psychotherapy and feel suspicious of the process. With Mr. A’s permission, I ask group home staff members to meet with me for 10 minutes at the end of each of Mr. A’s sessions to make them aware of what is happening with his therapy. I want them to feel that they are an important part of Mr. A’s therapy. These meetings may have alleviated staff members’ fears about my time with him. Even though Mr. A granted me permission to disclose all details of our sessions with the staff, I was careful to not disclose sensitive issues, such as the patient’s dreams and fantasies.
TREATMENT ‘Fear’
Mr. A rates his anxiety as a 4/10 whenever he speaks with women. To more specifically understand his underlying cognitions, I use Kendall’s FEAR plan (Table 3).9
I ask him to divide his automatic “E” thoughts into “she” and “I” thoughts. Examples of automatic “she” thoughts include “She probably won’t like me” and “She thinks I’m not cute.” Examples of automatic “I” thoughts include “I’m probably not smart enough for her” and “I think we won’t have anything in common.”
Table 3
The FEAR plan*
| F=feeling anxious | |
| E=expecting bad things to happen | |
| A=attitudes and actions that can help | |
| R=results and rewards | |
| Developed to help anxious children and adolescents recognize signs of anxiety, relax, and modify anxious self-talk and thinking. | |
| Source:Reference 9 | |
The author’s observations
Schwartz10 discusses countertransference challenges in nursing home patients, where therapists identify with patients’ hopelessness. Schwartz recommends addressing these challenges by thinking of realistic expectations. Even though a facility might be far from perfect, it may be “good enough.”
Mr. A’s group home was far from perfect and located in an isolated setting. Even so, I was able to help him complete psychotherapy at our clinic by adapting my practice to his needs, including:
- making reminder phone calls for appointments
- visiting the group home
- enlisting the help of caregivers with therapeutic techniques.
OUTCOME Improving
In the final 4 months of therapy, we continue to work on social skills lessons, practice exercises in the hospital, and the FEAR acronym. I continue to include caregivers in these efforts.
During 1 session, I tell Mr. A I will be leaving at the end of my fellowship. In the final month, I gradually transition him to a new therapist. I decided to transition him to a male therapist so Mr. A will continue to feel comfortable sharing his feelings, rather than shutting down from anxiety with a female therapist. As I end therapy, Mr. A is promoted to a cashier at the video game store and enrolls in classes to study for a General Education Development (GED) certificate.
Related resource
- National Institute of Mental Health. Autism spectrum disorders. www.nimh.nih.gov/health/publications/autism/complete-publication.shtml.
- Bupropion extended-release • Wellbutrin XL
- Dextroamphetamine/amphetamine extended-release • Adderall XR
- Duloxetine • Cymbalta
- Paroxetine • Paxil
- Risperidone • Risperdal
- Ziprasidone • Geodon
The author reports no financial relationships with any company whose products are mentioned in this article or with manufacturers of competing products.
Acknowledgment
The author thanks Dr. Ann Lagges, PhD, for her assistance with this patient’s treatment.
CASE ‘Sad, worried, and angry’
Mr. A, age 24, is referred to our university psychiatric clinic. He reports that he’s sad, worried, angry, and wants to hurt people. He endorses having chronic depressive episodes that last >2 weeks and consist of poor sleep, low energy, anhedonia, poor concentration, and psychomotor retardation.
He is developmentally disabled and has been living in a group home for almost 1 year. In former group homes, Mr. A threatened and assaulted other patients and staff. In 1 incident Mr. A broke a patient’s nose and was incarcerated for 4 days. With the help of a job coach, Mr. A has been working in a department store for 8 months. He was fired from other jobs because he threatened co-workers.
The author’s observations
Problem behaviors in patients with pervasive developmental disorders include aggression and self-injury. These behaviors may improve with behavioral or pharmacologic interventions.1 For example, risperidone is FDA-approved to treat irritability associated with autistic disorder in children and adolescents age 5 to 16 years.2 Violence has been reported in patients with pervasive developmental disorders, and such symptoms can lead to psychiatric referral.1
HISTORY Difficult childhood
Mr. A’s medical history is unremarkable. He has no history of hypomania, mania, psychosis, substance use, tics, seizures, genetic illnesses, head trauma, or physical or sexual abuse. He has never attempted suicide nor been hospitalized for psychiatric illness.
With Mr. A’s permission, his mother is consulted. She says that as a child Mr. A would become extremely interested in various topics—including Pokémon, Magic cards, and video games—and had a strong desire to tell everyone the details of each. However, he rocked back and forth, had few friends, and would bite other children.
Mr. A has no history of language delay but received speech therapy during his childhood to help him “work on eye contact and social skills.” He is estranged from and angry with his father, who has difficulty accepting his son’s developmental disability.
At the time of referral, Mr. A is receiving paroxetine, 30 mg/d, for depression, risperidone, 1.5 mg/d, for aggression, and dextroamphetamine/amphetamine extended-release, 30 mg/d, for hyperactivity/inattention. The efficacy of these medications, which were prescribed by an outside psychiatrist, is unclear.
Table 1
Diagnostic criteria for Asperger’s disorder
A. Qualitative impairment in social interaction, as manifested by ≥2 of the following:
|
B. Restricted repetitive and stereotyped patterns of behavior, interests, and activities, as manifested by ≥1 of the following:
|
| C. The disturbance causes clinically significant impairment in social, occupational, or other important areas of functioning. |
| D. There is no clinically significant general delay in language (eg, single words used by age 2 years, communicative phrases used by age 3 years). |
| E. There is no clinically significant delay in cognitive development or in the development of age-appropriate self-help skills, adaptive behavior (other than in social interaction), and curiosity about the environment in childhood. |
| F. Criteria are not met for another specific pervasive developmental disorder or schizophrenia. |
| Source: Diagnostic and statistical manual of mental disorders, 4th ed, text rev. Washington, DC: American Psychiatric Association; 2000 |
Based on Mr. A’s impaired social interaction, repetitive interests and behaviors, and lack of language delay, Mr. A meets criteria for Asperger’s disorder (Table 1). He also meets criteria for major depressive disorder, recurrent, moderate.
The author’s observations
Psychosocial interventions for patients with an autism-spectrum disorder consist of educational, vocational, behavioral, and family interventions. Individual, group, and family psychotherapy may benefit patients with Asperger’s disorder who have comorbid depression.1
TREATMENT A rocky start
At Mr. A’s initial assessment, the clinic psychiatrist increases risperidone to 1 mg twice daily to target aggression. Even after receiving this dosage for 1 month, however, Mr. A continues to display physical aggression toward peers in the group home whenever he becomes angry.
The psychiatrist refers Mr. A to a social worker for supportive therapy to help him cope with worry and chronic sadness. The social worker uses general cognitive-behavioral strategies for anxiety and aggression for 12 sessions over 8 months until scheduling conflicts end therapy. The efficacy of this therapy is minimal; Mr. A remains depressed, anxious, and aggressive. During this time, the psychiatrist increases paroxetine to 40 mg/d, but Mr. A continues to feel depressed after 1 month. Mr. A is cross-tapered to duloxetine, but continues to feel depressed after receiving duloxetine, 60 mg/d, for 1 month.
My first visit with Mr. A occurs 3 months after his last visit with the social worker. He states he does not remember anything from those sessions. Mr. A’s goals for therapy are to reduce anxiety, manage anger, and improve relationship skills.
I begin the first 4 months of Mr. A’s therapy with cognitive-behavioral interventions based on the Treatment of Adolescents Depression Study (TADS) manual.3 Although Mr. A is an adult, I choose a manual that targets adolescents because my clinical impression is that his cognitive developmental level is more like an adolescent’s than an adult’s.
I assign homework such as mood monitoring. I ask him to use a form from the TADS manual to rate his mood on a scale of 0 to 10 every morning, afternoon, and evening, and write down what he is doing that makes him feel that way at the time he rates his mood. Mr. A never completes any homework; during each session he states he “just forgot to do it.”
I discuss concepts such as goal setting, for a novel Mr. A says he wants to write, and relaxation strategies to address anger; in session, I work with him on filling out the “What Helps Me to Relax?” form from the TADS manual. Mr. A lists “play games,” “write my book,” “listen to music,” “go outside,” and “exercise” as strategies to help him relax. We also work on visual handouts—such as “Safety Plan” and “What Can I Do to Relax”—to post in his room.
Mr. A does not show up for 3 sessions. When I call the group home, a staff member tells me they were busy with other patients and forgot about Mr. A. I decide to call the group home the day before each appointment as a reminder. This increases Mr. A’s attendance rate.
During each session, Mr. A complains about the quality of the group home, the staff, and other patients. To get my own perspective of Mr. A’s living environment, I consider visiting his group home, similar to how a geriatric psychiatrist sees patients in a nursing home or an assertive community treatment team psychiatrist sees patients in their home environments. Because I am concerned about boundary crossings/violations, I first discuss this action with 2 psychotherapists not involved in Mr. A’s treatment. They recommend that I limit this action to a one-time visit.
I visit Mr. A’s group home 2 months after my first session with him. Located in front of a dairy farm in a rural part of the state about 1 hour from our clinic, the isolated facility has a secured keypad entry. When I meet Mr. A there, he says he feels as if he is in jail. I meet the staff and find them willing to help with various aspects of Mr. A’s treatment, such as discussing events, reporting behaviors, and helping carry out interventions.
For example, I ask staff to remind Mr. A of his relaxation strategies when he becomes angry. On the “Safety Plan” handout, I had Mr. A identify 5 people he could talk to when he becomes angry; I ask staff to remind him of those people when Mr. A becomes angry. I also ask staff to ask Mr. A every day if he is writing the novel he wants to complete. After my visit, Mr. A starts putting more effort into therapy. When I set a daily goal of working on his novel for 15 minutes, he starts bringing pages of his writings to sessions.
Table 2
Social skills training for patients with Asperger’s disorde
| Starting a conversation: “Hi, how was your day?” |
| Staying on topic: “Oh, that sounds interesting. Tell me more about…” |
| Making eye contact: Look at people’s eyes when talking to them |
| Greetings: “Hi, how are you?” |
| Ending a conversation: “Well, I have to go now. I’ll see you later!” |
| Shifting topics: “Speaking of…, did you hear about…?” |
| Source:Reference 7 |
The author’s observations
In a study in rural Appalachia, telephone reminders increased attendance at psychiatric intake appointments.4 Calling the group home before each of Mr. A’s appointments took extra time out of my schedule but improved Mr. A’s attendance rate.
In residential treatment of children, Monahan notes that childcare workers could contribute useful observations and benefit from the therapist’s advice.5 Establishing rapport with the staff at Mr. A’s group home helped me proceed with therapy.
TREATMENT Social skills training
In the second 4 months of therapy, Mr. A changes jobs to become a greeter in a local video game store. He is happy, and group home staff members are pleased they no longer spend 2 hours each day transporting him to his previous job.
Soon after, during a reminder phone call, a staff member tells me that Mr. A’s brother and father were murdered the prior week. Three staff members attend Mr. A’s brother’s funeral, which he appreciates. Mr. A refuses to attend his father’s funeral because of continued anger toward him.
When I ask Mr. A if he wants to talk about the deaths, he declines. I subsequently spend half a session discussing strategies to address grief,6 such as imagining a conversation with his deceased brother.
I decide to review Mr. A’s therapy goals because he still has a lot of anger toward his recently deceased father. I am concerned he might discharge this anger onto a staff member, coworker, or fellow patient. Mr. A states he wants to focus on relationships, especially his anxiety around women. He discusses his anxiety with starting and maintaining conversations with women.
I begin role-playing in sessions by pretending to be a woman for Mr. A to speak with, but he feels this is silly. I teach him exercises from a social skills training workbook developed for patients with Asperger’s, such as “Starting a conversation,” “Staying on topic,” and “Making eye contact” (Table 2).7 Mr. A says group home staff members occasionally take him out to a nearby nightclub and encourage him to talk to women.
To see how Mr. A behaves in public, during our sessions I take him to different parts of the hospital, such as the gift shop, library, and deli. I instruct him to ask various women non-threatening questions, such as how much a certain entrée costs. I note his body language, such as tilting his head down and fidgeting during conversations. I provide him with immediate feedback, which slowly increases his awareness of these behaviors.
With Mr. A’s permission, I educate the group home staff about how to point out these behaviors when Mr. A is in public. I ask them to focus on body language and emphasize that Mr. A needs to apply what I teach him to other settings.
The author’s observations
Patients with Asperger’s disorder need specific training to build a repertoire of social skills.7 Teaching in real-life settings helps patients generalize these skills.1
Zimmerman8 discusses how caregivers might have an unrealistic, “magical” view of psychotherapy and feel suspicious of the process. With Mr. A’s permission, I ask group home staff members to meet with me for 10 minutes at the end of each of Mr. A’s sessions to make them aware of what is happening with his therapy. I want them to feel that they are an important part of Mr. A’s therapy. These meetings may have alleviated staff members’ fears about my time with him. Even though Mr. A granted me permission to disclose all details of our sessions with the staff, I was careful to not disclose sensitive issues, such as the patient’s dreams and fantasies.
TREATMENT ‘Fear’
Mr. A rates his anxiety as a 4/10 whenever he speaks with women. To more specifically understand his underlying cognitions, I use Kendall’s FEAR plan (Table 3).9
I ask him to divide his automatic “E” thoughts into “she” and “I” thoughts. Examples of automatic “she” thoughts include “She probably won’t like me” and “She thinks I’m not cute.” Examples of automatic “I” thoughts include “I’m probably not smart enough for her” and “I think we won’t have anything in common.”
Table 3
The FEAR plan*
| F=feeling anxious | |
| E=expecting bad things to happen | |
| A=attitudes and actions that can help | |
| R=results and rewards | |
| Developed to help anxious children and adolescents recognize signs of anxiety, relax, and modify anxious self-talk and thinking. | |
| Source:Reference 9 | |
The author’s observations
Schwartz10 discusses countertransference challenges in nursing home patients, where therapists identify with patients’ hopelessness. Schwartz recommends addressing these challenges by thinking of realistic expectations. Even though a facility might be far from perfect, it may be “good enough.”
Mr. A’s group home was far from perfect and located in an isolated setting. Even so, I was able to help him complete psychotherapy at our clinic by adapting my practice to his needs, including:
- making reminder phone calls for appointments
- visiting the group home
- enlisting the help of caregivers with therapeutic techniques.
OUTCOME Improving
In the final 4 months of therapy, we continue to work on social skills lessons, practice exercises in the hospital, and the FEAR acronym. I continue to include caregivers in these efforts.
During 1 session, I tell Mr. A I will be leaving at the end of my fellowship. In the final month, I gradually transition him to a new therapist. I decided to transition him to a male therapist so Mr. A will continue to feel comfortable sharing his feelings, rather than shutting down from anxiety with a female therapist. As I end therapy, Mr. A is promoted to a cashier at the video game store and enrolls in classes to study for a General Education Development (GED) certificate.
Related resource
- National Institute of Mental Health. Autism spectrum disorders. www.nimh.nih.gov/health/publications/autism/complete-publication.shtml.
- Bupropion extended-release • Wellbutrin XL
- Dextroamphetamine/amphetamine extended-release • Adderall XR
- Duloxetine • Cymbalta
- Paroxetine • Paxil
- Risperidone • Risperdal
- Ziprasidone • Geodon
The author reports no financial relationships with any company whose products are mentioned in this article or with manufacturers of competing products.
Acknowledgment
The author thanks Dr. Ann Lagges, PhD, for her assistance with this patient’s treatment.
1. American Association of Child and Adolescent Psychiatry. Practice parameters for autism in children, adolescents, and adults. Available at: http://www.aacap.org/galleries/PracticeParameters/Autism.pdf. Accessed December 25, 2008.
2. Risperdal [package insert]. Titusville, NJ: Janssen Pharmaceuticals, Inc; 2008. Available at: http://www.risperdal.com/risperdal/shared/pi/risperdal.pdf. Accessed December 25, 2008.
3. Curry JF, Wells KC, Brent DA, et al. Treatment for adolescents with depression study (TADS): cognitive behavior therapy manual. Available at: https://trialweb.dcri.duke.edu/tads/tad/manuals/TADS_CBT.pdf. Accessed August 2, 2007.
4. Shoffner J, Staudt M, Marcus S, et al. Using telephone reminders to increase attendance at psychiatric appointments: findings of a pilot study in rural Appalachia. Psychiatr Serv. 2007;58(6):872-875.
5. Monahan RT. Individual and group psychotherapy. In: Lyman RD, Prentice-Dunn S, Gabel S, eds. Residential and inpatient treatment of children and adolescents. New York, NY: Plenum Publishing; 1989:192.
6. Shear K, Frank E, Houck PR, et al. Treatment of complicated grief: a randomized controlled trial. JAMA. 2005;293(1):2601-2608.
7. Baker JE. Social skills training for children and adolescents with Asperger syndrome and social-communication problems. Shawnee Mission, KS: Autism Asperger Publishing Company; 2003.
8. Zimmerman DP. Psychotherapy in residential treatment: historical development and critical issues. Child Adolesc Psychiatr Clin N Am. 2004;13(2):347-361.
9. Kendall PC, Hedtke A. Coping cat workbook. 2nd ed. Ardmore, PA: Workbook Publishing; 2006.
10. Schwartz K. Remembering the forgotten: psychotherapy groups for the nursing home resident. Int J Group Psychother. 2007;57(4):497-514.
1. American Association of Child and Adolescent Psychiatry. Practice parameters for autism in children, adolescents, and adults. Available at: http://www.aacap.org/galleries/PracticeParameters/Autism.pdf. Accessed December 25, 2008.
2. Risperdal [package insert]. Titusville, NJ: Janssen Pharmaceuticals, Inc; 2008. Available at: http://www.risperdal.com/risperdal/shared/pi/risperdal.pdf. Accessed December 25, 2008.
3. Curry JF, Wells KC, Brent DA, et al. Treatment for adolescents with depression study (TADS): cognitive behavior therapy manual. Available at: https://trialweb.dcri.duke.edu/tads/tad/manuals/TADS_CBT.pdf. Accessed August 2, 2007.
4. Shoffner J, Staudt M, Marcus S, et al. Using telephone reminders to increase attendance at psychiatric appointments: findings of a pilot study in rural Appalachia. Psychiatr Serv. 2007;58(6):872-875.
5. Monahan RT. Individual and group psychotherapy. In: Lyman RD, Prentice-Dunn S, Gabel S, eds. Residential and inpatient treatment of children and adolescents. New York, NY: Plenum Publishing; 1989:192.
6. Shear K, Frank E, Houck PR, et al. Treatment of complicated grief: a randomized controlled trial. JAMA. 2005;293(1):2601-2608.
7. Baker JE. Social skills training for children and adolescents with Asperger syndrome and social-communication problems. Shawnee Mission, KS: Autism Asperger Publishing Company; 2003.
8. Zimmerman DP. Psychotherapy in residential treatment: historical development and critical issues. Child Adolesc Psychiatr Clin N Am. 2004;13(2):347-361.
9. Kendall PC, Hedtke A. Coping cat workbook. 2nd ed. Ardmore, PA: Workbook Publishing; 2006.
10. Schwartz K. Remembering the forgotten: psychotherapy groups for the nursing home resident. Int J Group Psychother. 2007;57(4):497-514.
A pacemaker patient’s electrical dilemma
CASE: Relapsing depression
Mrs. A, age 41, presents with worsening depression and suicidal ideation with a plan to take an overdose of her medications. She describes herself as “tense, anxious, and worrying all the time.” She reports worsening mood, loss of interest in previously pleasurable activities, lack of energy and drive, and difficulties performing routine household tasks. She also endorses a combination of initial and middle insomnia. According to her husband, the patient has been slow in movement and speech and has not been taking adequate care of herself.
Mrs. A denies auditory or visual hallucinations, thought insertion, thought withdrawal, thought broadcast, ideas of reference, or paranoid ideation. She also denies recent or past symptoms of mania or hypomania.
Mrs. A has a history of alcohol abuse and major depressive disorder. For her first depressive episode 5 years ago, she was treated with paroxetine, 20 to 80 mg/d, with good results. Following a depressive relapse, she was switched to fluoxetine, 80 mg/d, which improved her depressive symptoms. Approximately 2 years later, she experienced another depressive relapse that resulted in hospitalization. During hospitalization and subsequent outpatient visits, she was treated with citalopram, 20 mg/d, ziprasidone, 80 mg bid, and lorazepam, 1 mg tid. Her depressive symptoms were in partial remission for 2 years until her current relapse.
Her medical history includes syncope of unexplained origin, for which she received an implanted cardiac pacemaker 3 years ago. She takes sertraline, 150 mg/d, methylphenidate, 15 mg/d, and trazodone, 200 mg at night. Laboratory testing is unremarkable.
On mental status examination, Mrs. A’s mood is sad and her affect constricted. Her speech is fluent but slow, and she speaks only when spoken to. We note that Mrs. A has thought blocking but no hallucinations or delusions. She is alert and oriented, but her attention and concentration are impaired. Her insight is fair, and judgment is poor.
The authors’ observations
Somatic therapy for severe major depressive disorders has been limited principally to pharmacotherapy. Despite the availability of effective antidepressants and aggressive treatment, for many patients—such as Mrs. A—the course of depression is characterized by relapse, recurrence, and chronicity.1,2
Because Mrs. A has treatment-refractory depression, we decide to treat her with ECT. ECT has few contraindications and typically is well tolerated. It commonly is used to treat depression in patients with cardiac conditions and generally is quite safe in this population.3,4
ECT in patients with cardiac pacemakers in situ theoretically presents an increased risk of complications, however.5 Specific concerns of administering ECT to pacemaker patients include electrical interference from ECT stimulus and pacemaker sensing of:
- myopotentials that originate from succinylcholine-induced fasciculation (muscular twitching of contiguous groups of muscle fibers)
- muscle contractions that result in incomplete muscle paralysis
- dysrhythmias during the seizure.
Skeletal muscle can generate significant electrical potentials that are well within the sensing capabilities of most newer pulse generators. This happens most frequently in some dual-chamber pacemakers that can automatically perform mode switching or adapt their sensing and pacing thresholds to new situations, which might make them more sensitive to interference by ECT.
Similar concerns apply to administering ECT to patients receiving vagus nerve stimulation (VNS) therapy, as both VNS pulse generators and cardiac pacemakers are battery-powered, electrical signal-producing mechanisms housed in a metal case. The safety of concurrent ECT and VNS therapy is unknown (Box).6,7
Although vagus nerve stimulation (VNS) and electroconvulsive therapy (ECT) are not mutually exclusive, the safety of concurrent use of these 2 therapies is uncertain.6 The manufacturer of the VNS device recommends turning off the VNS pulse generator before administering ECT. In at least 1 case report, however, ECT was administered safely without the VNS pulse generator turned off.7
No case reports describe the safety of VNS in patients with an implanted device such as a pacemaker or automatic cardioverter defibrillator. According to the manufacturer, the VNS system may affect the operation of other devices. For VNS patients who require an implantable pacemaker, defibrillator therapy, or other types of stimulators, the VNS manufacturer advises careful programming of each system and implanting the 2 stimulators at least 10 centimeters (4 inches) apart to avoid communication interference.
What the evidence says
In evidence-based medicine, we tend to say: “In God we trust; all the others have to bring their data.” Unfortunately, it is difficult to conduct a trial of patients with multiple medical issues. Based on anecdotal reports, it appears that ECT use in patients with an implanted cardiac device such as a pacemaker or automatic internal cardioverter-defibrillator (AICD) generally is safe.8-12
One case report describes successful administration of ECT in a treatment-refractory depressed patient with an AICD. The AICD was deactivated during ECT and re-activated immediately upon completion of each treatment. The case report’s authors concluded that the presence of an AICD should not be a contraindication to ECT.13
A chart review of 3 patients with ICDs who received concurrent ECT found treatment was generally uneventful.12 One patient developed tachycardia with a rate-dependent left bundle branch block and hypotension in the recovery room, which responded promptly to esmolol. She did not experience similar events after subsequent ECT treatments.
Minimizing risk
In the absence of controlled data about the use of ECT in patients with implanted cardiac devices, crucial therapeutic decisions depend on the physician’s skill and judgment. Risk strategies can minimize complications (Algorithm).12 An internist or cardiologist experienced in pacemaker management should conduct a device interrogation—evaluating thresholds, lead impedance, and battery voltage and reviewing histograms, mode switch episodes, and stored electrograms—before the first ECT session and after the final one.
Most modern implantable pacemakers work in the synchronous (demand), rate-adaptive mode. In a patient in whom non-cardiac electrical signals cause bradycardia or asystole during ECT, the pacemaker can be reprogrammed to be less sensitive by placing a magnet over the pulse generator, which converts the pacemaker to an asynchronous (fixed), non-sensing mode. It is important to keep in mind that magnet application will not “turn off” a pacemaker; although each pacemaker is programmed to respond to a magnet in a specific fashion, the main response is asynchronous pacing.
Careful cardiac monitoring during ECT is essential (Table). The cardiologist or internist should be available during the first few ECT sessions to monitor for potential pacemaker interference or malfunction. This physician should be familiar with the pacemaker model and type of lead system so he or she can deactivate, reactivate, or reprogram the device.
Algorithm
Reducing risk when administering ECT to cardiac pacemaker patients
| Step 1 | |
| Evaluate the patient to ensure medical suitability for ECT and associated anesthesia | |
| Step 2 | ↓ |
| Conduct pacemaker interrogation (evaluating thresholds, lead impedance, and battery voltage and reviewing histograms, mode switch episodes, and stored electrograms) prior to first ECT treatment and after completion of full ECT course | |
| Step 3 | ↓ |
| Perform cardiac monitoring during and immediately after administering ECT | |
| Step 4 | ↓ |
| Have a magnet available to reprogram the pacemaker in the event of pacemaker inhibition or symptomatic bradycardia during ECT | |
| Step 5 | ↓ |
| Check that all monitoring devices are properly grounded, insulate the patient’s stretcher, and ensure that the patient does not touch anyone who is in contact with the ground during presentation of the ECT electrical stimulus | |
| ECT: electroconvulsive therapy | |
| Source: Reference 12 | |
Guidelines for monitoring cardiac pacemaker patients during ECT
| Use multilead ECG monitoring |
| Have equipment available to rapidly obtain central access (if vasoactive medications or transvenous pacing is needed) |
| Assess the plethysmography tracing of the pulse oximeter (a useful surrogate if the patient experiences dysrhythmias) |
| Have ready an external defibrillator |
TREATMENT: Successful ECT
We seek a medical consultation before initiating ECT. An internist performs device interrogation before the first ECT treatment and is present in the ECT treatment suite to ensure proper pacemaker conversion and to monitor for cardiac complications. The internist conducts another device interrogation after the acute series of ECT treatments.
Mrs. A tolerates the ECT sessions without cardiac complications. Her depressive symptoms respond well to 12 ECT sessions. She is more interactive and reports better attention and concentration. Although Mrs. A still has middle and initial insomnia, she denies thoughts of harming herself or anyone else.
Related resources
- Yarlagadda C. Pacemaker failure. www.emedicine.com/med/TOPIC1704.HTM.
- Atracurium • Tracrium
- Citalopram • Celexa
- Esmolol • Brevibloc
- Fluoxetine • Prozac
- Lorazepam • Ativan
- Methylphenidate • Ritalin, Concerta, others
- Nortriptyline • Aventyl, Pamelor, others
- Paroxetine • Paxil
- Sertraline • Zoloft
- Succinylcholine • Anectine
- Trazodone • Desyrel
- Venlafaxine • Effexor
- Ziprasidone • Geodon
Dr. Romanowicz reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Ramaswamy receives research support from Bristol-Myers Squibb, Shire, and Forest Pharmaceuticals and is a consultant to Dainippon Sumitomo Pharma.
1. American Psychiatric Association Committee on ECT. The practice of electroconvulsive therapy: recommendations for treatment, training, and privileging. 2nd ed. Washington, D.C: American Psychiatric Association; 2001.
2. Russell JC, Rasmussen KG, O’Connor MK, et al. Long-term maintenance ECT: a retrospective review of efficacy and cognitive outcome. J ECT. 2003;19(1):4-9.
3. Alexopoulos GS, Shamoian CJ, Lucas J, et al. Medical problems of geriatric psychiatric patients and younger controls during electroconvulsive therapy. J Am Geriatr Soc. 1984;32(9):651-654.
4. Rasmussen KG, Rummans TA, Richardson JR. Electroconvulsive therapy in the medically ill. Psychiatric Clin North Am. 2002;25:177-193.
5. MacPherson RD, Loo CK, Barrett N. Electroconvulsive therapy in patients with cardiac pacemakers. Anaesth Intensive Care. 2006;34(4):470-474.
6. Burke MJ, Husain MM. Concomitant use of vagus nerve stimulation and electroconvulsive therapy for treatment-resistant depression. J ECT. 2006;22(3):218-222.
7. Husain MM, Montgomery JH, Fernandes P, et al. Safety of vagus nerve stimulation with ECT. Am J Psychiatry. 2002;159:1243.-
8. Alexopoulos GS, Frances RJ. ECT and cardiac patients with pacemakers. Am J Psychiatry. 1980;137(9):1111-1112.
9. Stone KR, McPherson CA. Assessment and management of patients with pacemakers and implantable cardioverter defibrillators. Crit Care Med. 2004;32(4 suppl):S155-S165.
10. Maisel WH, Sweeney MO, Stevenson WG, et al. Recalls and safety alerts involving pacemakers and implantable cardioverter-defibrillator generators. JAMA. 2001;286(7):793-799.
11. Gibson TC, Leaman DM, Devors J, et al. Pacemaker function in relation to electroconvulsive therapy. Chest. 1973;63(6):1025-1027.
12. Dolenc TJ, Barnes RD, Hayes DL, et al. Electroconvulsive therapy in patients with cardiac pacemakers and implantable cardioverter defibrillators. Pacing Clin Electrophysiol. 2004;27(9):1257-1263.
13. Lapid MI, Rummans TA, Hofmann VE, et al. ECT and automatic internal cardioverter-defibrillator. J ECT. 2001;17(2):146-148.
CASE: Relapsing depression
Mrs. A, age 41, presents with worsening depression and suicidal ideation with a plan to take an overdose of her medications. She describes herself as “tense, anxious, and worrying all the time.” She reports worsening mood, loss of interest in previously pleasurable activities, lack of energy and drive, and difficulties performing routine household tasks. She also endorses a combination of initial and middle insomnia. According to her husband, the patient has been slow in movement and speech and has not been taking adequate care of herself.
Mrs. A denies auditory or visual hallucinations, thought insertion, thought withdrawal, thought broadcast, ideas of reference, or paranoid ideation. She also denies recent or past symptoms of mania or hypomania.
Mrs. A has a history of alcohol abuse and major depressive disorder. For her first depressive episode 5 years ago, she was treated with paroxetine, 20 to 80 mg/d, with good results. Following a depressive relapse, she was switched to fluoxetine, 80 mg/d, which improved her depressive symptoms. Approximately 2 years later, she experienced another depressive relapse that resulted in hospitalization. During hospitalization and subsequent outpatient visits, she was treated with citalopram, 20 mg/d, ziprasidone, 80 mg bid, and lorazepam, 1 mg tid. Her depressive symptoms were in partial remission for 2 years until her current relapse.
Her medical history includes syncope of unexplained origin, for which she received an implanted cardiac pacemaker 3 years ago. She takes sertraline, 150 mg/d, methylphenidate, 15 mg/d, and trazodone, 200 mg at night. Laboratory testing is unremarkable.
On mental status examination, Mrs. A’s mood is sad and her affect constricted. Her speech is fluent but slow, and she speaks only when spoken to. We note that Mrs. A has thought blocking but no hallucinations or delusions. She is alert and oriented, but her attention and concentration are impaired. Her insight is fair, and judgment is poor.
The authors’ observations
Somatic therapy for severe major depressive disorders has been limited principally to pharmacotherapy. Despite the availability of effective antidepressants and aggressive treatment, for many patients—such as Mrs. A—the course of depression is characterized by relapse, recurrence, and chronicity.1,2
Because Mrs. A has treatment-refractory depression, we decide to treat her with ECT. ECT has few contraindications and typically is well tolerated. It commonly is used to treat depression in patients with cardiac conditions and generally is quite safe in this population.3,4
ECT in patients with cardiac pacemakers in situ theoretically presents an increased risk of complications, however.5 Specific concerns of administering ECT to pacemaker patients include electrical interference from ECT stimulus and pacemaker sensing of:
- myopotentials that originate from succinylcholine-induced fasciculation (muscular twitching of contiguous groups of muscle fibers)
- muscle contractions that result in incomplete muscle paralysis
- dysrhythmias during the seizure.
Skeletal muscle can generate significant electrical potentials that are well within the sensing capabilities of most newer pulse generators. This happens most frequently in some dual-chamber pacemakers that can automatically perform mode switching or adapt their sensing and pacing thresholds to new situations, which might make them more sensitive to interference by ECT.
Similar concerns apply to administering ECT to patients receiving vagus nerve stimulation (VNS) therapy, as both VNS pulse generators and cardiac pacemakers are battery-powered, electrical signal-producing mechanisms housed in a metal case. The safety of concurrent ECT and VNS therapy is unknown (Box).6,7
Although vagus nerve stimulation (VNS) and electroconvulsive therapy (ECT) are not mutually exclusive, the safety of concurrent use of these 2 therapies is uncertain.6 The manufacturer of the VNS device recommends turning off the VNS pulse generator before administering ECT. In at least 1 case report, however, ECT was administered safely without the VNS pulse generator turned off.7
No case reports describe the safety of VNS in patients with an implanted device such as a pacemaker or automatic cardioverter defibrillator. According to the manufacturer, the VNS system may affect the operation of other devices. For VNS patients who require an implantable pacemaker, defibrillator therapy, or other types of stimulators, the VNS manufacturer advises careful programming of each system and implanting the 2 stimulators at least 10 centimeters (4 inches) apart to avoid communication interference.
What the evidence says
In evidence-based medicine, we tend to say: “In God we trust; all the others have to bring their data.” Unfortunately, it is difficult to conduct a trial of patients with multiple medical issues. Based on anecdotal reports, it appears that ECT use in patients with an implanted cardiac device such as a pacemaker or automatic internal cardioverter-defibrillator (AICD) generally is safe.8-12
One case report describes successful administration of ECT in a treatment-refractory depressed patient with an AICD. The AICD was deactivated during ECT and re-activated immediately upon completion of each treatment. The case report’s authors concluded that the presence of an AICD should not be a contraindication to ECT.13
A chart review of 3 patients with ICDs who received concurrent ECT found treatment was generally uneventful.12 One patient developed tachycardia with a rate-dependent left bundle branch block and hypotension in the recovery room, which responded promptly to esmolol. She did not experience similar events after subsequent ECT treatments.
Minimizing risk
In the absence of controlled data about the use of ECT in patients with implanted cardiac devices, crucial therapeutic decisions depend on the physician’s skill and judgment. Risk strategies can minimize complications (Algorithm).12 An internist or cardiologist experienced in pacemaker management should conduct a device interrogation—evaluating thresholds, lead impedance, and battery voltage and reviewing histograms, mode switch episodes, and stored electrograms—before the first ECT session and after the final one.
Most modern implantable pacemakers work in the synchronous (demand), rate-adaptive mode. In a patient in whom non-cardiac electrical signals cause bradycardia or asystole during ECT, the pacemaker can be reprogrammed to be less sensitive by placing a magnet over the pulse generator, which converts the pacemaker to an asynchronous (fixed), non-sensing mode. It is important to keep in mind that magnet application will not “turn off” a pacemaker; although each pacemaker is programmed to respond to a magnet in a specific fashion, the main response is asynchronous pacing.
Careful cardiac monitoring during ECT is essential (Table). The cardiologist or internist should be available during the first few ECT sessions to monitor for potential pacemaker interference or malfunction. This physician should be familiar with the pacemaker model and type of lead system so he or she can deactivate, reactivate, or reprogram the device.
Algorithm
Reducing risk when administering ECT to cardiac pacemaker patients
| Step 1 | |
| Evaluate the patient to ensure medical suitability for ECT and associated anesthesia | |
| Step 2 | ↓ |
| Conduct pacemaker interrogation (evaluating thresholds, lead impedance, and battery voltage and reviewing histograms, mode switch episodes, and stored electrograms) prior to first ECT treatment and after completion of full ECT course | |
| Step 3 | ↓ |
| Perform cardiac monitoring during and immediately after administering ECT | |
| Step 4 | ↓ |
| Have a magnet available to reprogram the pacemaker in the event of pacemaker inhibition or symptomatic bradycardia during ECT | |
| Step 5 | ↓ |
| Check that all monitoring devices are properly grounded, insulate the patient’s stretcher, and ensure that the patient does not touch anyone who is in contact with the ground during presentation of the ECT electrical stimulus | |
| ECT: electroconvulsive therapy | |
| Source: Reference 12 | |
Guidelines for monitoring cardiac pacemaker patients during ECT
| Use multilead ECG monitoring |
| Have equipment available to rapidly obtain central access (if vasoactive medications or transvenous pacing is needed) |
| Assess the plethysmography tracing of the pulse oximeter (a useful surrogate if the patient experiences dysrhythmias) |
| Have ready an external defibrillator |
TREATMENT: Successful ECT
We seek a medical consultation before initiating ECT. An internist performs device interrogation before the first ECT treatment and is present in the ECT treatment suite to ensure proper pacemaker conversion and to monitor for cardiac complications. The internist conducts another device interrogation after the acute series of ECT treatments.
Mrs. A tolerates the ECT sessions without cardiac complications. Her depressive symptoms respond well to 12 ECT sessions. She is more interactive and reports better attention and concentration. Although Mrs. A still has middle and initial insomnia, she denies thoughts of harming herself or anyone else.
Related resources
- Yarlagadda C. Pacemaker failure. www.emedicine.com/med/TOPIC1704.HTM.
- Atracurium • Tracrium
- Citalopram • Celexa
- Esmolol • Brevibloc
- Fluoxetine • Prozac
- Lorazepam • Ativan
- Methylphenidate • Ritalin, Concerta, others
- Nortriptyline • Aventyl, Pamelor, others
- Paroxetine • Paxil
- Sertraline • Zoloft
- Succinylcholine • Anectine
- Trazodone • Desyrel
- Venlafaxine • Effexor
- Ziprasidone • Geodon
Dr. Romanowicz reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Ramaswamy receives research support from Bristol-Myers Squibb, Shire, and Forest Pharmaceuticals and is a consultant to Dainippon Sumitomo Pharma.
CASE: Relapsing depression
Mrs. A, age 41, presents with worsening depression and suicidal ideation with a plan to take an overdose of her medications. She describes herself as “tense, anxious, and worrying all the time.” She reports worsening mood, loss of interest in previously pleasurable activities, lack of energy and drive, and difficulties performing routine household tasks. She also endorses a combination of initial and middle insomnia. According to her husband, the patient has been slow in movement and speech and has not been taking adequate care of herself.
Mrs. A denies auditory or visual hallucinations, thought insertion, thought withdrawal, thought broadcast, ideas of reference, or paranoid ideation. She also denies recent or past symptoms of mania or hypomania.
Mrs. A has a history of alcohol abuse and major depressive disorder. For her first depressive episode 5 years ago, she was treated with paroxetine, 20 to 80 mg/d, with good results. Following a depressive relapse, she was switched to fluoxetine, 80 mg/d, which improved her depressive symptoms. Approximately 2 years later, she experienced another depressive relapse that resulted in hospitalization. During hospitalization and subsequent outpatient visits, she was treated with citalopram, 20 mg/d, ziprasidone, 80 mg bid, and lorazepam, 1 mg tid. Her depressive symptoms were in partial remission for 2 years until her current relapse.
Her medical history includes syncope of unexplained origin, for which she received an implanted cardiac pacemaker 3 years ago. She takes sertraline, 150 mg/d, methylphenidate, 15 mg/d, and trazodone, 200 mg at night. Laboratory testing is unremarkable.
On mental status examination, Mrs. A’s mood is sad and her affect constricted. Her speech is fluent but slow, and she speaks only when spoken to. We note that Mrs. A has thought blocking but no hallucinations or delusions. She is alert and oriented, but her attention and concentration are impaired. Her insight is fair, and judgment is poor.
The authors’ observations
Somatic therapy for severe major depressive disorders has been limited principally to pharmacotherapy. Despite the availability of effective antidepressants and aggressive treatment, for many patients—such as Mrs. A—the course of depression is characterized by relapse, recurrence, and chronicity.1,2
Because Mrs. A has treatment-refractory depression, we decide to treat her with ECT. ECT has few contraindications and typically is well tolerated. It commonly is used to treat depression in patients with cardiac conditions and generally is quite safe in this population.3,4
ECT in patients with cardiac pacemakers in situ theoretically presents an increased risk of complications, however.5 Specific concerns of administering ECT to pacemaker patients include electrical interference from ECT stimulus and pacemaker sensing of:
- myopotentials that originate from succinylcholine-induced fasciculation (muscular twitching of contiguous groups of muscle fibers)
- muscle contractions that result in incomplete muscle paralysis
- dysrhythmias during the seizure.
Skeletal muscle can generate significant electrical potentials that are well within the sensing capabilities of most newer pulse generators. This happens most frequently in some dual-chamber pacemakers that can automatically perform mode switching or adapt their sensing and pacing thresholds to new situations, which might make them more sensitive to interference by ECT.
Similar concerns apply to administering ECT to patients receiving vagus nerve stimulation (VNS) therapy, as both VNS pulse generators and cardiac pacemakers are battery-powered, electrical signal-producing mechanisms housed in a metal case. The safety of concurrent ECT and VNS therapy is unknown (Box).6,7
Although vagus nerve stimulation (VNS) and electroconvulsive therapy (ECT) are not mutually exclusive, the safety of concurrent use of these 2 therapies is uncertain.6 The manufacturer of the VNS device recommends turning off the VNS pulse generator before administering ECT. In at least 1 case report, however, ECT was administered safely without the VNS pulse generator turned off.7
No case reports describe the safety of VNS in patients with an implanted device such as a pacemaker or automatic cardioverter defibrillator. According to the manufacturer, the VNS system may affect the operation of other devices. For VNS patients who require an implantable pacemaker, defibrillator therapy, or other types of stimulators, the VNS manufacturer advises careful programming of each system and implanting the 2 stimulators at least 10 centimeters (4 inches) apart to avoid communication interference.
What the evidence says
In evidence-based medicine, we tend to say: “In God we trust; all the others have to bring their data.” Unfortunately, it is difficult to conduct a trial of patients with multiple medical issues. Based on anecdotal reports, it appears that ECT use in patients with an implanted cardiac device such as a pacemaker or automatic internal cardioverter-defibrillator (AICD) generally is safe.8-12
One case report describes successful administration of ECT in a treatment-refractory depressed patient with an AICD. The AICD was deactivated during ECT and re-activated immediately upon completion of each treatment. The case report’s authors concluded that the presence of an AICD should not be a contraindication to ECT.13
A chart review of 3 patients with ICDs who received concurrent ECT found treatment was generally uneventful.12 One patient developed tachycardia with a rate-dependent left bundle branch block and hypotension in the recovery room, which responded promptly to esmolol. She did not experience similar events after subsequent ECT treatments.
Minimizing risk
In the absence of controlled data about the use of ECT in patients with implanted cardiac devices, crucial therapeutic decisions depend on the physician’s skill and judgment. Risk strategies can minimize complications (Algorithm).12 An internist or cardiologist experienced in pacemaker management should conduct a device interrogation—evaluating thresholds, lead impedance, and battery voltage and reviewing histograms, mode switch episodes, and stored electrograms—before the first ECT session and after the final one.
Most modern implantable pacemakers work in the synchronous (demand), rate-adaptive mode. In a patient in whom non-cardiac electrical signals cause bradycardia or asystole during ECT, the pacemaker can be reprogrammed to be less sensitive by placing a magnet over the pulse generator, which converts the pacemaker to an asynchronous (fixed), non-sensing mode. It is important to keep in mind that magnet application will not “turn off” a pacemaker; although each pacemaker is programmed to respond to a magnet in a specific fashion, the main response is asynchronous pacing.
Careful cardiac monitoring during ECT is essential (Table). The cardiologist or internist should be available during the first few ECT sessions to monitor for potential pacemaker interference or malfunction. This physician should be familiar with the pacemaker model and type of lead system so he or she can deactivate, reactivate, or reprogram the device.
Algorithm
Reducing risk when administering ECT to cardiac pacemaker patients
| Step 1 | |
| Evaluate the patient to ensure medical suitability for ECT and associated anesthesia | |
| Step 2 | ↓ |
| Conduct pacemaker interrogation (evaluating thresholds, lead impedance, and battery voltage and reviewing histograms, mode switch episodes, and stored electrograms) prior to first ECT treatment and after completion of full ECT course | |
| Step 3 | ↓ |
| Perform cardiac monitoring during and immediately after administering ECT | |
| Step 4 | ↓ |
| Have a magnet available to reprogram the pacemaker in the event of pacemaker inhibition or symptomatic bradycardia during ECT | |
| Step 5 | ↓ |
| Check that all monitoring devices are properly grounded, insulate the patient’s stretcher, and ensure that the patient does not touch anyone who is in contact with the ground during presentation of the ECT electrical stimulus | |
| ECT: electroconvulsive therapy | |
| Source: Reference 12 | |
Guidelines for monitoring cardiac pacemaker patients during ECT
| Use multilead ECG monitoring |
| Have equipment available to rapidly obtain central access (if vasoactive medications or transvenous pacing is needed) |
| Assess the plethysmography tracing of the pulse oximeter (a useful surrogate if the patient experiences dysrhythmias) |
| Have ready an external defibrillator |
TREATMENT: Successful ECT
We seek a medical consultation before initiating ECT. An internist performs device interrogation before the first ECT treatment and is present in the ECT treatment suite to ensure proper pacemaker conversion and to monitor for cardiac complications. The internist conducts another device interrogation after the acute series of ECT treatments.
Mrs. A tolerates the ECT sessions without cardiac complications. Her depressive symptoms respond well to 12 ECT sessions. She is more interactive and reports better attention and concentration. Although Mrs. A still has middle and initial insomnia, she denies thoughts of harming herself or anyone else.
Related resources
- Yarlagadda C. Pacemaker failure. www.emedicine.com/med/TOPIC1704.HTM.
- Atracurium • Tracrium
- Citalopram • Celexa
- Esmolol • Brevibloc
- Fluoxetine • Prozac
- Lorazepam • Ativan
- Methylphenidate • Ritalin, Concerta, others
- Nortriptyline • Aventyl, Pamelor, others
- Paroxetine • Paxil
- Sertraline • Zoloft
- Succinylcholine • Anectine
- Trazodone • Desyrel
- Venlafaxine • Effexor
- Ziprasidone • Geodon
Dr. Romanowicz reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Ramaswamy receives research support from Bristol-Myers Squibb, Shire, and Forest Pharmaceuticals and is a consultant to Dainippon Sumitomo Pharma.
1. American Psychiatric Association Committee on ECT. The practice of electroconvulsive therapy: recommendations for treatment, training, and privileging. 2nd ed. Washington, D.C: American Psychiatric Association; 2001.
2. Russell JC, Rasmussen KG, O’Connor MK, et al. Long-term maintenance ECT: a retrospective review of efficacy and cognitive outcome. J ECT. 2003;19(1):4-9.
3. Alexopoulos GS, Shamoian CJ, Lucas J, et al. Medical problems of geriatric psychiatric patients and younger controls during electroconvulsive therapy. J Am Geriatr Soc. 1984;32(9):651-654.
4. Rasmussen KG, Rummans TA, Richardson JR. Electroconvulsive therapy in the medically ill. Psychiatric Clin North Am. 2002;25:177-193.
5. MacPherson RD, Loo CK, Barrett N. Electroconvulsive therapy in patients with cardiac pacemakers. Anaesth Intensive Care. 2006;34(4):470-474.
6. Burke MJ, Husain MM. Concomitant use of vagus nerve stimulation and electroconvulsive therapy for treatment-resistant depression. J ECT. 2006;22(3):218-222.
7. Husain MM, Montgomery JH, Fernandes P, et al. Safety of vagus nerve stimulation with ECT. Am J Psychiatry. 2002;159:1243.-
8. Alexopoulos GS, Frances RJ. ECT and cardiac patients with pacemakers. Am J Psychiatry. 1980;137(9):1111-1112.
9. Stone KR, McPherson CA. Assessment and management of patients with pacemakers and implantable cardioverter defibrillators. Crit Care Med. 2004;32(4 suppl):S155-S165.
10. Maisel WH, Sweeney MO, Stevenson WG, et al. Recalls and safety alerts involving pacemakers and implantable cardioverter-defibrillator generators. JAMA. 2001;286(7):793-799.
11. Gibson TC, Leaman DM, Devors J, et al. Pacemaker function in relation to electroconvulsive therapy. Chest. 1973;63(6):1025-1027.
12. Dolenc TJ, Barnes RD, Hayes DL, et al. Electroconvulsive therapy in patients with cardiac pacemakers and implantable cardioverter defibrillators. Pacing Clin Electrophysiol. 2004;27(9):1257-1263.
13. Lapid MI, Rummans TA, Hofmann VE, et al. ECT and automatic internal cardioverter-defibrillator. J ECT. 2001;17(2):146-148.
1. American Psychiatric Association Committee on ECT. The practice of electroconvulsive therapy: recommendations for treatment, training, and privileging. 2nd ed. Washington, D.C: American Psychiatric Association; 2001.
2. Russell JC, Rasmussen KG, O’Connor MK, et al. Long-term maintenance ECT: a retrospective review of efficacy and cognitive outcome. J ECT. 2003;19(1):4-9.
3. Alexopoulos GS, Shamoian CJ, Lucas J, et al. Medical problems of geriatric psychiatric patients and younger controls during electroconvulsive therapy. J Am Geriatr Soc. 1984;32(9):651-654.
4. Rasmussen KG, Rummans TA, Richardson JR. Electroconvulsive therapy in the medically ill. Psychiatric Clin North Am. 2002;25:177-193.
5. MacPherson RD, Loo CK, Barrett N. Electroconvulsive therapy in patients with cardiac pacemakers. Anaesth Intensive Care. 2006;34(4):470-474.
6. Burke MJ, Husain MM. Concomitant use of vagus nerve stimulation and electroconvulsive therapy for treatment-resistant depression. J ECT. 2006;22(3):218-222.
7. Husain MM, Montgomery JH, Fernandes P, et al. Safety of vagus nerve stimulation with ECT. Am J Psychiatry. 2002;159:1243.-
8. Alexopoulos GS, Frances RJ. ECT and cardiac patients with pacemakers. Am J Psychiatry. 1980;137(9):1111-1112.
9. Stone KR, McPherson CA. Assessment and management of patients with pacemakers and implantable cardioverter defibrillators. Crit Care Med. 2004;32(4 suppl):S155-S165.
10. Maisel WH, Sweeney MO, Stevenson WG, et al. Recalls and safety alerts involving pacemakers and implantable cardioverter-defibrillator generators. JAMA. 2001;286(7):793-799.
11. Gibson TC, Leaman DM, Devors J, et al. Pacemaker function in relation to electroconvulsive therapy. Chest. 1973;63(6):1025-1027.
12. Dolenc TJ, Barnes RD, Hayes DL, et al. Electroconvulsive therapy in patients with cardiac pacemakers and implantable cardioverter defibrillators. Pacing Clin Electrophysiol. 2004;27(9):1257-1263.
13. Lapid MI, Rummans TA, Hofmann VE, et al. ECT and automatic internal cardioverter-defibrillator. J ECT. 2001;17(2):146-148.
A mysterious physical and mental decline
HISTORY: ‘Not himself’
Mr. C, age 69, presents to the emergency department complaining of intermittent fever of about 100°F, hematuria, headache, weakness, fatigue, and decreased appetite over 2 months. Testing shows acute renal failure, elevated C-reactive protein, and increased sedimentation rate. The attending internist admits Mr. C with a working diagnosis of temporal arteritis and acute renal failure, administers corticosteroids for headache, and orders a right temporal artery biopsy, which shows no signs of vasculitis.
Family members report that Mr. C has not been himself—he has become increasingly withdrawn and “emotionless.” Mr. C’s wife says her husband has needed help with dressing and eating because of short-term memory loss over 9 months. She says he has lost 20 to 30 lb.
The patient’s cognitive function appears to have worsened since he developed these physical symptoms. Mrs. C also reports that he has had weakness and fatigue for 8 months.
One month earlier, the patient was admitted to a different hospital and treated for 2 weeks with IV antibiotics for fever of unknown origin. Results of lumbar puncture and extensive rheumatologic, infectious disease, urologic, and gastroenterologic evaluations were normal.
The internal medicine physician requests a psychiatric consultation. During our interview, Mr. C is cooperative, shows no signs of acute distress, is well groomed and dressed appropriately, and maintains eye contact. Speech rate and volume are low, with normal articulation and coherence, diminished spontaneity, and paucity of language. Mrs. C tells us her husband was lively and talkative before his recent illness. His mood is euthymic, and he is pleasant and cheerful during the evaluation.
The authors’ observations
Initially, we suspect an underlying medical condition is causing Mr. C’s psychiatric symptoms.
Mr. C’s wife reports that her husband stopped drinking 2 years ago after his family expressed concern about his health. Mr. C’s past alcohol use could not be quantified. He has not abused illicit drugs and has no personal or family history of dementia, trauma, or psychiatric or neurologic disorders.
EVALUATION: Impaired memory
Mr. C is afebrile during the initial physical examination, but fever returns within several days. Neurologic examination is normal, and negative rapid plasma reagin rules out syphilis. Vitamin B12 and folate levels are normal, as is thyroid function. Other laboratory findings are outside normal limits (Table).
Urine is cloudy with 2+ protein, 3+ blood, and trace leukocyte esterase. The presence of protein and blood suggests a glomerular disease such as a glomerulonephritis.
A positive leukocyte esterase test results from the presence of white blood cells, either as whole cells or as lysed cells. An abnormal number of leukocytes may appear with upper or lower urinary tract infection or in acute glomerulonephritis.
Chest radiography shows increased bilateral pulmonary vasculature, which can indicate pulmonary hypertension.
Mr. C has fair attention and concentration but impaired recent memory. He cannot recall yesterday’s events without help.
Mr. C’s Mini-Mental State Examination score of 21/30 suggests markedly impaired executive functioning and cognitive deficits. The attending psychiatrist recommends brain MRI.
Table
Mr. C’s laboratory findings
| Value | Normal range | |
|---|---|---|
| WBC | 15.1 | 4.8 to 10.8 cells/μL |
| Hb | 9 | 13.8 to 17.5 g/dL |
| Hct | 25.9% | 40% to 54% |
| MCV | 89.7 | 80 to 94 fL |
| BUN | 119 | 7 to 18 mg/dL |
| Cr | 12.1 | 0.7 to 1.3 mg/dL |
| Na | 125 | 136 to 145 mmol/L |
| K | 6.5 | 3.5 to 5 mEq/dL |
| HCO3 | 13.5 | 22 to 29 mmol/L |
| ECR | 125 | 30 mm/hr |
| WBC: white blood cell; Hb: hemoglobin; Hct: hematocrit; MCV: mean corpuscular volume; BUN: blood urea nitrogen; Cr: creatinine; Na: sodium; K: potassium; HCO3: bicarbonate; ESR: erythrocyte sedimentation rate | ||
The authors’ observations
Mr. C shows markedly impaired cognitive function without significant impairment of attention and concentration despite his progressive deterioration and increasing disability. Urine toxicology shows no illicit substances. Given his lack of a previous mood disorder and his family’s description of him as formerly vibrant and cheerful, he likely does not have a mood disorder.
Based on the history of events, including the symptom pattern, we rule out delirium. We suspect that Mr. C has dementia secondary to a general medical condition. His symptoms seem to be directly related to his medical complaints and do not have a waxing and waning course. The internal medicine physician orders additional laboratory tests.
TESTING: Kidney, lung damage
Over 5 days, Mr. C’s intermittent low-grade fevers continue. Laboratory tests are negative for HIV antibody, hepatitis panel, and antinuclear antibodies (ANA). C-reactive protein is elevated at 27.8 mg/dL (normal range,
Renal ultrasound is normal, but preliminary renal biopsy shows rapidly progressive glomerulonephritis. The internist immediately starts dialysis, cyclophosphamide at 1.5 mg/kg, and prednisone, 1 mg/kg. The pathology report on the renal biopsy describes extensive crescentic glomerular destruction, with inflammatory cells present.
Ten days after admission, Mr. C develops hemoptysis, and chest radiography shows increasing alveolar infiltrates. The attending internist consults pulmonary and critical care services.
The consultant suspects a pulmonary-renal syndrome because of bilateral alveolar infiltrates (diffuse alveolar hemorrhage). The internal medicine team continues high-dose corticosteroids, followed by plasmapheresis.
Brain MRI shows subacute to chronic infarcts involving the right basal ganglia and corona radiate and mild to moderate small vessel ischemic changes. Old areas of hemorrhage are noted within both cerebellar lobes, left temporal lobe, right basal ganglia, right parietal lobe, and right frontal lobe.
During follow-up interviews, Mr. C often cannot recall recent dialysis or plasmapheresis and reports no physical symptoms. His short-term memory continues to deteriorate; he would forget to eat if not cued by family or nursing staff. He shows global cognitive deficits and is increasingly withdrawn and flat.
The authors’ observations
Although few case reports have associated Goodpasture’s syndrome with neurobehavioral changes, the apparent relationship of Mr. C’s medical symptoms with the worsening of his cognitive impairment suggests a link.
Mr. C’s MRI findings also might suggest CNS vasculitis, which affects small arteries of the cerebral and spinal cord leptomeninges and parenchyma, leading to CNS dys-function.6-8 CNS vasculitis can result from primary nervous system involvement or from a secondary systemic process such as Goodpasture’s syndrome.9
We rule out lupus because Mr. C is ANA-negative; this test has 99% sensitivity for lupus.10
Goodpasture’s syndrome, which afflicts 1 Patients typically present with alveolar bleeding, rapidly progressive acute renal failure with proteinuria,1 and pulmonary symptoms such as dyspnea and hemoptysis.2
Possible triggers include:
- viral upper respiratory tract infection (20% to 60% of patients)3
- exposure to hydrocarbon solvents (3,4
Mr. C was exposed to solvents during the 15 years he worked in a factory. Some researchers believe a noxious event among genetically susceptible persons damages basement membrane and exposes an antigen that triggers IgG auto-antibody production.3,4
Malaise, weight loss, and fever are atypical in Goodpasture’s syndrome but could suggest concomitant vasculitis.5
OUTCOME: Ongoing disability
Mr. C is hospitalized for 6 weeks. He receives cyclophosphamide, prednisone, and 10 sessions of plasmapheresis. We prescribe mirtazapine, 15 mg at bedtime, to treat mood symptoms. We chose mirtazapine because of the drug’s sleep-restoring and appetite-stimulating properties.
Mr. C’s fever resolves and pulmonary function soon improves, but his cognitive impairment persists. He has difficulties preparing meals, taking medications, and managing his money.
Mr. C is discharged with a referral to a psychiatrist. He continues taking mirtazapine and a lower dose of prednisone. He requires ongoing hemodialysis and assistance with activities of daily living.
The authors’ observations
Prompt multidisciplinary intervention is critical when patients present with concurrent cognitive and medical symptoms. A thorough psychiatric evaluation can help piece together the illness’ course. The psychiatrist’s role in a multidisciplinary assessment is to:
- document neurocognitive changes
- verify them through collateral information
- correlate these changes with the timing of medical symptoms.
An underlying psychiatric condition can complicate the diagnosis. In these cases, careful interviewing and collateral information can help you discern the chronology of events.
1. Bolton WK. Goodpasture’s syndrome. Kidney Int 1996;50(5):1753-66.
2. Pusey CD. Anti-glomerular basement membrane disease. Kidney Int 2003;64(4):1535-50.
3. Humes HD, DuPont HL. eds. Kelley’s textbook of internal medicine. 4th ed. New York, NY: Lippincott Williams & Wilkins; 2000.
4. Stevenson A, Yaqoob M, Mason H, et al. Biochemical markers of basement membrane disturbances and occupational exposure to hydrocarbons and mixed solvents. QJM 1995;88(1):23-8.
5. Kluth DC, Rees AJ. Anti-glomerular basement membrane disease. J Am Soc Nephrol. 1999;10(11):2446-53.
6. Rydel JJ, Rodby RA. An 18-year-old man with Goodpasture’s syndrome and ANCA-negative central nervous system vasculitis. Am J Kidney Dis 1998;31(2):345-9.
7. Gittins N, Basu A, Eyre J, et al. Cerebral vasculitis in a teenager with Goodpasture’s syndrome. Nephrol Dial Transplant 2004;19(12):3168-71.
8. Garnier P, Deprele C. Cerebral angiitis and Goodpasture’s syndrome. Rev Neurol 2003;159(1):68-70.
9. Calabrese LH, Duna GF, Lie JT. Vasculitis in the central nervous system. Arthritis Rhem 1997;40(7):1189-201.
10. Edworthy SM, Zatarain E, McShane DJ, Bloch DA. Analysis of the 1982 ARA lupus criteria data set by recursive partitioning methodology: new insights into the relative merit of individual criteria. J Rheumatol 1988;15(10):1493-8.
HISTORY: ‘Not himself’
Mr. C, age 69, presents to the emergency department complaining of intermittent fever of about 100°F, hematuria, headache, weakness, fatigue, and decreased appetite over 2 months. Testing shows acute renal failure, elevated C-reactive protein, and increased sedimentation rate. The attending internist admits Mr. C with a working diagnosis of temporal arteritis and acute renal failure, administers corticosteroids for headache, and orders a right temporal artery biopsy, which shows no signs of vasculitis.
Family members report that Mr. C has not been himself—he has become increasingly withdrawn and “emotionless.” Mr. C’s wife says her husband has needed help with dressing and eating because of short-term memory loss over 9 months. She says he has lost 20 to 30 lb.
The patient’s cognitive function appears to have worsened since he developed these physical symptoms. Mrs. C also reports that he has had weakness and fatigue for 8 months.
One month earlier, the patient was admitted to a different hospital and treated for 2 weeks with IV antibiotics for fever of unknown origin. Results of lumbar puncture and extensive rheumatologic, infectious disease, urologic, and gastroenterologic evaluations were normal.
The internal medicine physician requests a psychiatric consultation. During our interview, Mr. C is cooperative, shows no signs of acute distress, is well groomed and dressed appropriately, and maintains eye contact. Speech rate and volume are low, with normal articulation and coherence, diminished spontaneity, and paucity of language. Mrs. C tells us her husband was lively and talkative before his recent illness. His mood is euthymic, and he is pleasant and cheerful during the evaluation.
The authors’ observations
Initially, we suspect an underlying medical condition is causing Mr. C’s psychiatric symptoms.
Mr. C’s wife reports that her husband stopped drinking 2 years ago after his family expressed concern about his health. Mr. C’s past alcohol use could not be quantified. He has not abused illicit drugs and has no personal or family history of dementia, trauma, or psychiatric or neurologic disorders.
EVALUATION: Impaired memory
Mr. C is afebrile during the initial physical examination, but fever returns within several days. Neurologic examination is normal, and negative rapid plasma reagin rules out syphilis. Vitamin B12 and folate levels are normal, as is thyroid function. Other laboratory findings are outside normal limits (Table).
Urine is cloudy with 2+ protein, 3+ blood, and trace leukocyte esterase. The presence of protein and blood suggests a glomerular disease such as a glomerulonephritis.
A positive leukocyte esterase test results from the presence of white blood cells, either as whole cells or as lysed cells. An abnormal number of leukocytes may appear with upper or lower urinary tract infection or in acute glomerulonephritis.
Chest radiography shows increased bilateral pulmonary vasculature, which can indicate pulmonary hypertension.
Mr. C has fair attention and concentration but impaired recent memory. He cannot recall yesterday’s events without help.
Mr. C’s Mini-Mental State Examination score of 21/30 suggests markedly impaired executive functioning and cognitive deficits. The attending psychiatrist recommends brain MRI.
Table
Mr. C’s laboratory findings
| Value | Normal range | |
|---|---|---|
| WBC | 15.1 | 4.8 to 10.8 cells/μL |
| Hb | 9 | 13.8 to 17.5 g/dL |
| Hct | 25.9% | 40% to 54% |
| MCV | 89.7 | 80 to 94 fL |
| BUN | 119 | 7 to 18 mg/dL |
| Cr | 12.1 | 0.7 to 1.3 mg/dL |
| Na | 125 | 136 to 145 mmol/L |
| K | 6.5 | 3.5 to 5 mEq/dL |
| HCO3 | 13.5 | 22 to 29 mmol/L |
| ECR | 125 | 30 mm/hr |
| WBC: white blood cell; Hb: hemoglobin; Hct: hematocrit; MCV: mean corpuscular volume; BUN: blood urea nitrogen; Cr: creatinine; Na: sodium; K: potassium; HCO3: bicarbonate; ESR: erythrocyte sedimentation rate | ||
The authors’ observations
Mr. C shows markedly impaired cognitive function without significant impairment of attention and concentration despite his progressive deterioration and increasing disability. Urine toxicology shows no illicit substances. Given his lack of a previous mood disorder and his family’s description of him as formerly vibrant and cheerful, he likely does not have a mood disorder.
Based on the history of events, including the symptom pattern, we rule out delirium. We suspect that Mr. C has dementia secondary to a general medical condition. His symptoms seem to be directly related to his medical complaints and do not have a waxing and waning course. The internal medicine physician orders additional laboratory tests.
TESTING: Kidney, lung damage
Over 5 days, Mr. C’s intermittent low-grade fevers continue. Laboratory tests are negative for HIV antibody, hepatitis panel, and antinuclear antibodies (ANA). C-reactive protein is elevated at 27.8 mg/dL (normal range,
Renal ultrasound is normal, but preliminary renal biopsy shows rapidly progressive glomerulonephritis. The internist immediately starts dialysis, cyclophosphamide at 1.5 mg/kg, and prednisone, 1 mg/kg. The pathology report on the renal biopsy describes extensive crescentic glomerular destruction, with inflammatory cells present.
Ten days after admission, Mr. C develops hemoptysis, and chest radiography shows increasing alveolar infiltrates. The attending internist consults pulmonary and critical care services.
The consultant suspects a pulmonary-renal syndrome because of bilateral alveolar infiltrates (diffuse alveolar hemorrhage). The internal medicine team continues high-dose corticosteroids, followed by plasmapheresis.
Brain MRI shows subacute to chronic infarcts involving the right basal ganglia and corona radiate and mild to moderate small vessel ischemic changes. Old areas of hemorrhage are noted within both cerebellar lobes, left temporal lobe, right basal ganglia, right parietal lobe, and right frontal lobe.
During follow-up interviews, Mr. C often cannot recall recent dialysis or plasmapheresis and reports no physical symptoms. His short-term memory continues to deteriorate; he would forget to eat if not cued by family or nursing staff. He shows global cognitive deficits and is increasingly withdrawn and flat.
The authors’ observations
Although few case reports have associated Goodpasture’s syndrome with neurobehavioral changes, the apparent relationship of Mr. C’s medical symptoms with the worsening of his cognitive impairment suggests a link.
Mr. C’s MRI findings also might suggest CNS vasculitis, which affects small arteries of the cerebral and spinal cord leptomeninges and parenchyma, leading to CNS dys-function.6-8 CNS vasculitis can result from primary nervous system involvement or from a secondary systemic process such as Goodpasture’s syndrome.9
We rule out lupus because Mr. C is ANA-negative; this test has 99% sensitivity for lupus.10
Goodpasture’s syndrome, which afflicts 1 Patients typically present with alveolar bleeding, rapidly progressive acute renal failure with proteinuria,1 and pulmonary symptoms such as dyspnea and hemoptysis.2
Possible triggers include:
- viral upper respiratory tract infection (20% to 60% of patients)3
- exposure to hydrocarbon solvents (3,4
Mr. C was exposed to solvents during the 15 years he worked in a factory. Some researchers believe a noxious event among genetically susceptible persons damages basement membrane and exposes an antigen that triggers IgG auto-antibody production.3,4
Malaise, weight loss, and fever are atypical in Goodpasture’s syndrome but could suggest concomitant vasculitis.5
OUTCOME: Ongoing disability
Mr. C is hospitalized for 6 weeks. He receives cyclophosphamide, prednisone, and 10 sessions of plasmapheresis. We prescribe mirtazapine, 15 mg at bedtime, to treat mood symptoms. We chose mirtazapine because of the drug’s sleep-restoring and appetite-stimulating properties.
Mr. C’s fever resolves and pulmonary function soon improves, but his cognitive impairment persists. He has difficulties preparing meals, taking medications, and managing his money.
Mr. C is discharged with a referral to a psychiatrist. He continues taking mirtazapine and a lower dose of prednisone. He requires ongoing hemodialysis and assistance with activities of daily living.
The authors’ observations
Prompt multidisciplinary intervention is critical when patients present with concurrent cognitive and medical symptoms. A thorough psychiatric evaluation can help piece together the illness’ course. The psychiatrist’s role in a multidisciplinary assessment is to:
- document neurocognitive changes
- verify them through collateral information
- correlate these changes with the timing of medical symptoms.
An underlying psychiatric condition can complicate the diagnosis. In these cases, careful interviewing and collateral information can help you discern the chronology of events.
HISTORY: ‘Not himself’
Mr. C, age 69, presents to the emergency department complaining of intermittent fever of about 100°F, hematuria, headache, weakness, fatigue, and decreased appetite over 2 months. Testing shows acute renal failure, elevated C-reactive protein, and increased sedimentation rate. The attending internist admits Mr. C with a working diagnosis of temporal arteritis and acute renal failure, administers corticosteroids for headache, and orders a right temporal artery biopsy, which shows no signs of vasculitis.
Family members report that Mr. C has not been himself—he has become increasingly withdrawn and “emotionless.” Mr. C’s wife says her husband has needed help with dressing and eating because of short-term memory loss over 9 months. She says he has lost 20 to 30 lb.
The patient’s cognitive function appears to have worsened since he developed these physical symptoms. Mrs. C also reports that he has had weakness and fatigue for 8 months.
One month earlier, the patient was admitted to a different hospital and treated for 2 weeks with IV antibiotics for fever of unknown origin. Results of lumbar puncture and extensive rheumatologic, infectious disease, urologic, and gastroenterologic evaluations were normal.
The internal medicine physician requests a psychiatric consultation. During our interview, Mr. C is cooperative, shows no signs of acute distress, is well groomed and dressed appropriately, and maintains eye contact. Speech rate and volume are low, with normal articulation and coherence, diminished spontaneity, and paucity of language. Mrs. C tells us her husband was lively and talkative before his recent illness. His mood is euthymic, and he is pleasant and cheerful during the evaluation.
The authors’ observations
Initially, we suspect an underlying medical condition is causing Mr. C’s psychiatric symptoms.
Mr. C’s wife reports that her husband stopped drinking 2 years ago after his family expressed concern about his health. Mr. C’s past alcohol use could not be quantified. He has not abused illicit drugs and has no personal or family history of dementia, trauma, or psychiatric or neurologic disorders.
EVALUATION: Impaired memory
Mr. C is afebrile during the initial physical examination, but fever returns within several days. Neurologic examination is normal, and negative rapid plasma reagin rules out syphilis. Vitamin B12 and folate levels are normal, as is thyroid function. Other laboratory findings are outside normal limits (Table).
Urine is cloudy with 2+ protein, 3+ blood, and trace leukocyte esterase. The presence of protein and blood suggests a glomerular disease such as a glomerulonephritis.
A positive leukocyte esterase test results from the presence of white blood cells, either as whole cells or as lysed cells. An abnormal number of leukocytes may appear with upper or lower urinary tract infection or in acute glomerulonephritis.
Chest radiography shows increased bilateral pulmonary vasculature, which can indicate pulmonary hypertension.
Mr. C has fair attention and concentration but impaired recent memory. He cannot recall yesterday’s events without help.
Mr. C’s Mini-Mental State Examination score of 21/30 suggests markedly impaired executive functioning and cognitive deficits. The attending psychiatrist recommends brain MRI.
Table
Mr. C’s laboratory findings
| Value | Normal range | |
|---|---|---|
| WBC | 15.1 | 4.8 to 10.8 cells/μL |
| Hb | 9 | 13.8 to 17.5 g/dL |
| Hct | 25.9% | 40% to 54% |
| MCV | 89.7 | 80 to 94 fL |
| BUN | 119 | 7 to 18 mg/dL |
| Cr | 12.1 | 0.7 to 1.3 mg/dL |
| Na | 125 | 136 to 145 mmol/L |
| K | 6.5 | 3.5 to 5 mEq/dL |
| HCO3 | 13.5 | 22 to 29 mmol/L |
| ECR | 125 | 30 mm/hr |
| WBC: white blood cell; Hb: hemoglobin; Hct: hematocrit; MCV: mean corpuscular volume; BUN: blood urea nitrogen; Cr: creatinine; Na: sodium; K: potassium; HCO3: bicarbonate; ESR: erythrocyte sedimentation rate | ||
The authors’ observations
Mr. C shows markedly impaired cognitive function without significant impairment of attention and concentration despite his progressive deterioration and increasing disability. Urine toxicology shows no illicit substances. Given his lack of a previous mood disorder and his family’s description of him as formerly vibrant and cheerful, he likely does not have a mood disorder.
Based on the history of events, including the symptom pattern, we rule out delirium. We suspect that Mr. C has dementia secondary to a general medical condition. His symptoms seem to be directly related to his medical complaints and do not have a waxing and waning course. The internal medicine physician orders additional laboratory tests.
TESTING: Kidney, lung damage
Over 5 days, Mr. C’s intermittent low-grade fevers continue. Laboratory tests are negative for HIV antibody, hepatitis panel, and antinuclear antibodies (ANA). C-reactive protein is elevated at 27.8 mg/dL (normal range,
Renal ultrasound is normal, but preliminary renal biopsy shows rapidly progressive glomerulonephritis. The internist immediately starts dialysis, cyclophosphamide at 1.5 mg/kg, and prednisone, 1 mg/kg. The pathology report on the renal biopsy describes extensive crescentic glomerular destruction, with inflammatory cells present.
Ten days after admission, Mr. C develops hemoptysis, and chest radiography shows increasing alveolar infiltrates. The attending internist consults pulmonary and critical care services.
The consultant suspects a pulmonary-renal syndrome because of bilateral alveolar infiltrates (diffuse alveolar hemorrhage). The internal medicine team continues high-dose corticosteroids, followed by plasmapheresis.
Brain MRI shows subacute to chronic infarcts involving the right basal ganglia and corona radiate and mild to moderate small vessel ischemic changes. Old areas of hemorrhage are noted within both cerebellar lobes, left temporal lobe, right basal ganglia, right parietal lobe, and right frontal lobe.
During follow-up interviews, Mr. C often cannot recall recent dialysis or plasmapheresis and reports no physical symptoms. His short-term memory continues to deteriorate; he would forget to eat if not cued by family or nursing staff. He shows global cognitive deficits and is increasingly withdrawn and flat.
The authors’ observations
Although few case reports have associated Goodpasture’s syndrome with neurobehavioral changes, the apparent relationship of Mr. C’s medical symptoms with the worsening of his cognitive impairment suggests a link.
Mr. C’s MRI findings also might suggest CNS vasculitis, which affects small arteries of the cerebral and spinal cord leptomeninges and parenchyma, leading to CNS dys-function.6-8 CNS vasculitis can result from primary nervous system involvement or from a secondary systemic process such as Goodpasture’s syndrome.9
We rule out lupus because Mr. C is ANA-negative; this test has 99% sensitivity for lupus.10
Goodpasture’s syndrome, which afflicts 1 Patients typically present with alveolar bleeding, rapidly progressive acute renal failure with proteinuria,1 and pulmonary symptoms such as dyspnea and hemoptysis.2
Possible triggers include:
- viral upper respiratory tract infection (20% to 60% of patients)3
- exposure to hydrocarbon solvents (3,4
Mr. C was exposed to solvents during the 15 years he worked in a factory. Some researchers believe a noxious event among genetically susceptible persons damages basement membrane and exposes an antigen that triggers IgG auto-antibody production.3,4
Malaise, weight loss, and fever are atypical in Goodpasture’s syndrome but could suggest concomitant vasculitis.5
OUTCOME: Ongoing disability
Mr. C is hospitalized for 6 weeks. He receives cyclophosphamide, prednisone, and 10 sessions of plasmapheresis. We prescribe mirtazapine, 15 mg at bedtime, to treat mood symptoms. We chose mirtazapine because of the drug’s sleep-restoring and appetite-stimulating properties.
Mr. C’s fever resolves and pulmonary function soon improves, but his cognitive impairment persists. He has difficulties preparing meals, taking medications, and managing his money.
Mr. C is discharged with a referral to a psychiatrist. He continues taking mirtazapine and a lower dose of prednisone. He requires ongoing hemodialysis and assistance with activities of daily living.
The authors’ observations
Prompt multidisciplinary intervention is critical when patients present with concurrent cognitive and medical symptoms. A thorough psychiatric evaluation can help piece together the illness’ course. The psychiatrist’s role in a multidisciplinary assessment is to:
- document neurocognitive changes
- verify them through collateral information
- correlate these changes with the timing of medical symptoms.
An underlying psychiatric condition can complicate the diagnosis. In these cases, careful interviewing and collateral information can help you discern the chronology of events.
1. Bolton WK. Goodpasture’s syndrome. Kidney Int 1996;50(5):1753-66.
2. Pusey CD. Anti-glomerular basement membrane disease. Kidney Int 2003;64(4):1535-50.
3. Humes HD, DuPont HL. eds. Kelley’s textbook of internal medicine. 4th ed. New York, NY: Lippincott Williams & Wilkins; 2000.
4. Stevenson A, Yaqoob M, Mason H, et al. Biochemical markers of basement membrane disturbances and occupational exposure to hydrocarbons and mixed solvents. QJM 1995;88(1):23-8.
5. Kluth DC, Rees AJ. Anti-glomerular basement membrane disease. J Am Soc Nephrol. 1999;10(11):2446-53.
6. Rydel JJ, Rodby RA. An 18-year-old man with Goodpasture’s syndrome and ANCA-negative central nervous system vasculitis. Am J Kidney Dis 1998;31(2):345-9.
7. Gittins N, Basu A, Eyre J, et al. Cerebral vasculitis in a teenager with Goodpasture’s syndrome. Nephrol Dial Transplant 2004;19(12):3168-71.
8. Garnier P, Deprele C. Cerebral angiitis and Goodpasture’s syndrome. Rev Neurol 2003;159(1):68-70.
9. Calabrese LH, Duna GF, Lie JT. Vasculitis in the central nervous system. Arthritis Rhem 1997;40(7):1189-201.
10. Edworthy SM, Zatarain E, McShane DJ, Bloch DA. Analysis of the 1982 ARA lupus criteria data set by recursive partitioning methodology: new insights into the relative merit of individual criteria. J Rheumatol 1988;15(10):1493-8.
1. Bolton WK. Goodpasture’s syndrome. Kidney Int 1996;50(5):1753-66.
2. Pusey CD. Anti-glomerular basement membrane disease. Kidney Int 2003;64(4):1535-50.
3. Humes HD, DuPont HL. eds. Kelley’s textbook of internal medicine. 4th ed. New York, NY: Lippincott Williams & Wilkins; 2000.
4. Stevenson A, Yaqoob M, Mason H, et al. Biochemical markers of basement membrane disturbances and occupational exposure to hydrocarbons and mixed solvents. QJM 1995;88(1):23-8.
5. Kluth DC, Rees AJ. Anti-glomerular basement membrane disease. J Am Soc Nephrol. 1999;10(11):2446-53.
6. Rydel JJ, Rodby RA. An 18-year-old man with Goodpasture’s syndrome and ANCA-negative central nervous system vasculitis. Am J Kidney Dis 1998;31(2):345-9.
7. Gittins N, Basu A, Eyre J, et al. Cerebral vasculitis in a teenager with Goodpasture’s syndrome. Nephrol Dial Transplant 2004;19(12):3168-71.
8. Garnier P, Deprele C. Cerebral angiitis and Goodpasture’s syndrome. Rev Neurol 2003;159(1):68-70.
9. Calabrese LH, Duna GF, Lie JT. Vasculitis in the central nervous system. Arthritis Rhem 1997;40(7):1189-201.
10. Edworthy SM, Zatarain E, McShane DJ, Bloch DA. Analysis of the 1982 ARA lupus criteria data set by recursive partitioning methodology: new insights into the relative merit of individual criteria. J Rheumatol 1988;15(10):1493-8.
A Diagnostic Pearl in Allergic Contact Dermatitis to Fragrances: The Atomizer Sign (See Erratum. 2009;83:49)
The inexplicably suicidal patient
CASE: Confused and suicidal
Mr. A, age 39, becomes disoriented while walking and approaches a suspension bridge. He borrows a passerby’s cell phone and calls his sister. His sister later states that he was confused and expressed his final goodbyes, saying, “I will see Mom in heaven.” He gives back the phone and leaps of the bridge. A nearby boat rescues him almost immediately.
Mr. A is brought to the trauma unit, where he is treated for a lacerated liver. After he is stabilized, Mr. A is awake and answering questions appropriately. He is placed on suicide precautions and direct 24-hour, one-to-one supervision. Our psychiatric team evaluates him.
Mr. A reports no history of diabetes, hypertension, cardiac disorders, or neurologic disorders, but does have a history of cognitive developmental delay. He has no history of psychiatric illness, suicide attempts, or self-injurious behavior. He denies a psychiatric family history or using alcohol, tobacco, or illicit drugs; drug screen is negative. He is unemployed, collects disability, and lives with his sister.
The authors’ observations
In our initial evaluation, we find no obvious reason for Mr. A’s confusion or suicide attempt. We decide to closely review Mr. A’s history in the days leading up to his jumping off the bridge.
HISTORY: Otitis media treatment
Mr. A has a history of chronic otitis media and sought treatment for ear pain at a local emergency room (ER) 10 days before his suicide attempt. He was prescribed amoxicillin, 500 mg tid for 10 days, and meclizine, 25 mg every 8 hours as needed for dizziness.
Immediately after his first dose of both drugs, the patient told his family he was feeling “weird,” but denied being dizzy. Thinking the unusual feeling was from meclizine, Mr. A stopped taking it but continued amoxicillin. On the second day of amoxicillin, he noticed bouts of confusion. He could perform his daily activities, but with difficulty. Mr. A’s niece said he had to ask for help with minor tasks, such as opening a can of soup.
On day 3, Mr. A developed prominent auditory hallucinations. He described hearing unrecognizable male and female voices chattering and mumbling throughout the day. The voices and confusion progressively worsened, but Mr. A continued taking the antibiotic and did not mention the voices to his family.
Mr. A’s sister reports that in a phone conversation with her brother on day 7, “he wasn’t himself…he was talking about my sister and mother but what he said didn’t make sense.” She asked a neighbor to check on Mr. A; he reported that Mr. A was “OK.” On the final day of amoxicillin—day 10—Mr. A became increasingly agitated. He says us that shortly before wandering onto the bridge and jumping, he was having a difficult time dealing with the voices and confusion.
We suspect amoxicillin might have been responsible for Mr. A’s psychotic symptoms.
The authors’ observations
Treatment modalities and pharmaceutical approaches used to treat infectious diseases carry many potential adverse effects. When a patient presents with new-onset psychiatric symptoms, explore whether they are related to an underlying mood disorder or medication side effects. Three important considerations are to:
- determine whether the condition is reversible by discontinuing a drug
- identify and characterize previously unrecognized adverse drug effects
- avoid inaccurate diagnosis that leads to nonindicated psychiatric treatment.1
Antibiotic side effects vary, depending on the particular drug and its target bacteria. The most common are gastrointestinal, such as upset stomach and diarrhea. Antibiotics also can induce an anaphylactic reaction ranging from mild (pruritic rash or slight wheezing) to life-threatening (swelling of the throat, difficulty breathing, and hypotension).
Several classes of antibiotics have psychiatric side effects that range from minor confusion and irritability to severe encephalopathy and suicide (Table 1).2 Case reports have described psychotic symptoms associated with cotrimoxazole,3 trimethoprim/sulfamethoxazole,4 and ciprofloxacin.5 An older review found that amoxicillin is among the top 10 most commonly prescribed medications associated with psychiatric side effects.1
Table 1
Potential psychiatric effects of antibiotics
| Medication | Side effects |
|---|---|
| Antibacterials | |
| Penicillins | Encephalopathy, irritability, sedation, anxiety, hallucinations |
| Cephalosporins | Sleep disturbances, hallucinations |
| Cycloserine | Dose-dependent side effects, depression, irritability, psychosis |
| Quinolones | Sleep and mood disorders, psychosis |
| Nitrofurans | Euphoria, psychosis, sleep disturbances |
| Tetracyclines | Decreased concentration, mood and sleep disorders |
| Chloramphenicol | Depression |
| Trimethoprim, sulfonamides | Depression, psychosis |
| Antimycobacterials | |
| Isoniazid | Cognitive impairment, mood disorder, psychosis |
| Clofazimine | Major depression, suicide |
| Rifampin | Sedation |
| Ethionamide | Sedation, irritability, agitation, depression, psychosis |
| Ganciclovir | Sleep disturbances, anxiety, mood disorders, psychosis |
| Antifungals | |
| Amphotericin B | Delirium |
| Ketoconazole | Decreased libido, mood disorders, psychosis |
| Flucytosine | Sedation, hallucinations |
| Griseofulvin | Depression, psychosis, sleep disturbances |
| Source: Turjanski N, Lloyd GG. Psychiatric side effects of medications: recent developments. Advances in Psychiatric Treatment 2005;11:58-70. Reprinted with permission | |
Amoxicillin is a penicillin-based, broad-spectrum antibiotic (Box).1,6 Its potential psychiatric side effects include encephalopathy, irritability, sedation, anxiety, and hallucinations.2 These symptoms usually are managed by reducing the dosage or discontinuing the medication. In some cases, antipsychotics may be used to control the symptoms.
Beta-lactam compounds inhibit bacterial growth by interfering with cell wall synthesis. As a beta-lactam antibiotic, amoxicillin’s chemistry, mechanism of action, pharmacologic and clinical effects, and immunologic characteristics are similar to those of cephalosporins, monobactams, carbapenems, and beta-lactamase inhibitors.6
Amoxicillin is an aminopenicillin. These antibiotics retain the antibacterial spectrum of penicillin but have a broader spectrum against gram-negative organisms because of their enhanced ability to penetrate the gram-negative outer membrane. Amoxicillin causes less gastrointestinal (GI) irritation than penicillin and is stable in an acidic environment.
Amoxicillin is administered 250 to 500 mg every 8 hours for adults and 20 to 40 mg/kg of body weight every 24 hours for pediatric patients.1 Amoxicillin is more stable and better absorbed in the GI tract than most penicillins, so amoxicillin 3 times a day is as effective as 4 daily doses of other penicillins.
A literature search reveals 3 cases of amoxicillin-related psychosis (Table 2).7-9 A 30-year-old woman with a urinary tract infection (UTI) developed “confusional manic symptoms” after 10 days of amoxicillin.7 The patient’s family reported she’d had a similar reaction 14 years earlier following 9 days of ampicillin for a perforated appendix; since then she had received non-aminopenicillins without incident. In both incidents, her psychotic symptoms resolved.
A 55-year-old man developed auditory, visual, and tactile hallucinations within hours of his first dose of amoxicillin for presumed pneumonia. The patient “was able to describe what he had experienced clearly with evidence of subjective terror.”8
Most recently, a 63-year-old woman taking amoxicillin, 250 mg tid, for a UTI developed sleep disturbance after 1 day and auditory and visual hallucinations after 4 days. She had a similar episode that required hospitalization 5 years earlier. In both episodes, psychotic symptoms resolved within 3 days of antibiotic discontinuation, with no psychotropic drug treatment.9
Table 2
Amoxicillin-triggered psychosis: 3 case reports
| Study | Patient | Description |
|---|---|---|
| Beal et al7 | Woman, age 30 | Confusional manic symptoms after 10 days of treatment; symptoms resolved within 12 days of admission; patient had a similar reaction to ampicillin 14 years earlier |
| Stell et al8 | Man, age 55 | Auditory, visual, and tactile hallucinations within hours of first dose |
| Rao9 | Woman, age 63 | Auditory and visual hallucinations 1 week after taking 250 mg tid; patient had a similar reaction to amoxicillin 5 years earlier; in both cases symptoms resolved within 3 days of discontinuing amoxicillin |
Mechanism of psychiatric effects
The mechanisms of antibiotic-related neuropsychiatric sequelae are uncertain and vary with drug class and patient factors.
Hoigné’s syndrome—an acute psychotic reaction to intramuscular procaine penicillin first reported around 1950—is characterized by psychiatric symptoms, predominantly anxiety and hallucinations, almost immediately following injection. Anxiety is marked by a fear of imminent death as well as autonomic hyperactivity. This “pseudoanaphylactic reaction” persists for 5 to 30 minutes and has been noted for its resemblance to temporal lobe and limbic seizures (perceptual disturbance, sympathetic hyperactivity, and “doom anxiety”).
The underlying pathophysiology remains unclear; the reaction was originally attributed to microembolization of procaine crystals to the lungs and brain, later to direct procaine neurotoxicity, and most recently to temporolimbic kindling—the appearance of physiologic and behavioral responses to repetition of a stimulus (procaine) that initially is without effect.10
A potential mechanism for amoxicillin’s neuropsychiatric effects is less clear. Because amoxicillin is an oral medication, hypotheses regarding Hoigné’s syndrome seem inapplicable. In addition, amoxicillin is largely excreted unchanged by the kidneys; the lack of significant P450 metabolism argues against mechanisms mediated by polypharmacy or altered metabolite levels. Furthermore, penicillins are polar molecules with poor CNS penetration.6 Penicillins demonstrate known neurotoxicity, however, most often causing convulsions or myelopathy. Identified risk factors for penicillin neurotoxicity include:
- intravenous/thecal administration
- high doses
- CNS disease
- renal insufficiency
- advanced age
- use of drugs that block antibiotic export from the CNS
- conditions that increase blood-brain barrier permeability.
One hypothesis focuses on penicillins’ inhibition of both the GABAA receptor-chloride ionophore complex and the benzodiazepine receptor, yielding CNS disinhibition and decreasing the seizure threshold. Notably, GABA antagonism is considered a primary facilitator of CNS kindling. Penicillin also has been reported to cause delirium related to allergy-mediated cerebral edema.11 Beal et al7 argue for an immune-mediated cerebritis.
Psychiatric symptoms secondary to antibiotics—particularly penicillins—are likely multifactorial, suggesting certain individuals may be predisposed to “Hoigné’s syndrome” from amoxicillin. In the 3 case reports of amoxicillin-related psychosis, there is variation in duration of exposure until symptom onset, medical indication for the antibiotic, and patient age and gender. Any or all of these factors may be clinically significant. None of these patients, however, had a psychiatric history.
It is not clear whether a single 25-mg dose of meclizine—an H1-receptor antagonist—played a role in Mr. A’s psychotic symptoms. Meclizine overdose can cause extreme drowsiness, seizures, hallucinations, and decreased breathing. This anticholinergic has a half-life of only 6 hours and a duration of action of up to 24 hours, although anticholinergic toxicity from overdose can last for days.10 Mr. A ingested a single 25-mg dose of meclizine, however, and his auditory hallucinations persisted for 9 days. Furthermore, Mr. A’s previous well-tolerated meclizine use and lack of other signs and symptoms of anticholinergic toxicity do not support a substantial role for meclizine in his psychotic symptoms.
OUTCOME: Symptoms resolve
Mr. A’s confusion and auditory hallucinations resolve approximately 36 hours after he completed amoxicillin treatment. When transferred to the psychiatric unit, he denies auditory hallucinations or suicidal ideation. He also denies ear pain, tinnitus, vertigo, or ear tenderness; physical examination of the ear is unremarkable. Throughout the hospital admission, Mr. A experiences no confusion or changes in mental status and he continues to adamantly deny suicidal ideation.
He does not require treatment with anti-psychotics or other psychotropic medications and is discharged in stable condition.
Related resources
- Levenson JL, Schneider RK. Infectious diseases. In: Levenson JL, ed. The American Psychiatric Publishing textbook of psychosomatic medicine. Washington, DC: American Psychiatric Publishing; 2005:577-98.
Drug brand names
- Amoxicillin • Amoxil, Trimox, others
- Amphotericin B • Amphocin, Abelcet
- Ampicillin • Principen
- Chloramphenicol • Chloromycetin
- Ciprofloxacin • Cipro
- Clofazimine • Lamprene
- Cycloserine • Seromycin
- Ethionamide • Trecator
- Flucytosine • Ancobon
- Ganciclovir • Cytovene
- Griseofulvin • Fulvicin U/F, Grifulvin V
- Isoniazid • Nydrazid
- Ketoconazole • Nizoral
- Meclizine • Antivert, Bonine, others
- Rifampin • Rifadin, Rimactane
- Trimethoprim/sulfamethoxazole • Bactrim, Septra
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Hubbard JR, Levenson JL, Patrick GA. Psychiatric side effects associated with the ten most commonly dispensed prescription drugs: a review. J Fam Pract 1991;33(2):177-86.
2. Turjanski N, Lloyd GG. Psychiatric side effects of medications: recent developments. Advances in Psychiatric Treatment 2005;11:58-70.
3. Weis S, Karagülle D, Kornhuber J, Bayerlein K. Cotrimoxazole-induced psychosis: a case report and review of literature. Pharmacopsychiatry 2006;39:236-7.
4. Saidinejad M, Ewald MB, Shannon MW. Transient psychosis in an immune-competent patient after oral trimethoprimsulfamethoxazole administration. Pediatrics 2005;115(6):e739-41.
5. Grimm O, Alm B, Für Seelische Z. A case of ciprofloxacin-induced acute polymorphic psychosis with a distinct deficit in executive functions. Psychosomatics 2007;48(3):269.-
6. Katzung BG. Basic and clinical pharmacology. 7th ed. Stamford, CT: Appleton & Lange; 1998;726-32.
7. Beal DM, Hudson B, Zaiac M. Amoxacillin-induced psychosis? Am J Psychiatry 1986;143(2):255-6.
8. Stell IM, Ojo OA. Amoxycillin-induced hallucinations—a variant of Hoigne’s syndrome? Br J Clin Pract 1996;50(5):279.-
9. Rao R. Penicillin psychosis in later life: Hoigne’s syndrome revisited. J Neuropsychiatry Clin Neurosci 1999;11(4):517-8.
10. Araszkiewicz A, Rybakowski JK. Hoigne’s syndrome, kindling, and panic disorder. Depress Anxiety 1996-1997;4(3):139-43.
11. Sternbach H, State R. Antibiotics: neuropsychiatric effects and psychotropic interactions. Harv Rev Psychiatry 1997;5(4):214-26.
CASE: Confused and suicidal
Mr. A, age 39, becomes disoriented while walking and approaches a suspension bridge. He borrows a passerby’s cell phone and calls his sister. His sister later states that he was confused and expressed his final goodbyes, saying, “I will see Mom in heaven.” He gives back the phone and leaps of the bridge. A nearby boat rescues him almost immediately.
Mr. A is brought to the trauma unit, where he is treated for a lacerated liver. After he is stabilized, Mr. A is awake and answering questions appropriately. He is placed on suicide precautions and direct 24-hour, one-to-one supervision. Our psychiatric team evaluates him.
Mr. A reports no history of diabetes, hypertension, cardiac disorders, or neurologic disorders, but does have a history of cognitive developmental delay. He has no history of psychiatric illness, suicide attempts, or self-injurious behavior. He denies a psychiatric family history or using alcohol, tobacco, or illicit drugs; drug screen is negative. He is unemployed, collects disability, and lives with his sister.
The authors’ observations
In our initial evaluation, we find no obvious reason for Mr. A’s confusion or suicide attempt. We decide to closely review Mr. A’s history in the days leading up to his jumping off the bridge.
HISTORY: Otitis media treatment
Mr. A has a history of chronic otitis media and sought treatment for ear pain at a local emergency room (ER) 10 days before his suicide attempt. He was prescribed amoxicillin, 500 mg tid for 10 days, and meclizine, 25 mg every 8 hours as needed for dizziness.
Immediately after his first dose of both drugs, the patient told his family he was feeling “weird,” but denied being dizzy. Thinking the unusual feeling was from meclizine, Mr. A stopped taking it but continued amoxicillin. On the second day of amoxicillin, he noticed bouts of confusion. He could perform his daily activities, but with difficulty. Mr. A’s niece said he had to ask for help with minor tasks, such as opening a can of soup.
On day 3, Mr. A developed prominent auditory hallucinations. He described hearing unrecognizable male and female voices chattering and mumbling throughout the day. The voices and confusion progressively worsened, but Mr. A continued taking the antibiotic and did not mention the voices to his family.
Mr. A’s sister reports that in a phone conversation with her brother on day 7, “he wasn’t himself…he was talking about my sister and mother but what he said didn’t make sense.” She asked a neighbor to check on Mr. A; he reported that Mr. A was “OK.” On the final day of amoxicillin—day 10—Mr. A became increasingly agitated. He says us that shortly before wandering onto the bridge and jumping, he was having a difficult time dealing with the voices and confusion.
We suspect amoxicillin might have been responsible for Mr. A’s psychotic symptoms.
The authors’ observations
Treatment modalities and pharmaceutical approaches used to treat infectious diseases carry many potential adverse effects. When a patient presents with new-onset psychiatric symptoms, explore whether they are related to an underlying mood disorder or medication side effects. Three important considerations are to:
- determine whether the condition is reversible by discontinuing a drug
- identify and characterize previously unrecognized adverse drug effects
- avoid inaccurate diagnosis that leads to nonindicated psychiatric treatment.1
Antibiotic side effects vary, depending on the particular drug and its target bacteria. The most common are gastrointestinal, such as upset stomach and diarrhea. Antibiotics also can induce an anaphylactic reaction ranging from mild (pruritic rash or slight wheezing) to life-threatening (swelling of the throat, difficulty breathing, and hypotension).
Several classes of antibiotics have psychiatric side effects that range from minor confusion and irritability to severe encephalopathy and suicide (Table 1).2 Case reports have described psychotic symptoms associated with cotrimoxazole,3 trimethoprim/sulfamethoxazole,4 and ciprofloxacin.5 An older review found that amoxicillin is among the top 10 most commonly prescribed medications associated with psychiatric side effects.1
Table 1
Potential psychiatric effects of antibiotics
| Medication | Side effects |
|---|---|
| Antibacterials | |
| Penicillins | Encephalopathy, irritability, sedation, anxiety, hallucinations |
| Cephalosporins | Sleep disturbances, hallucinations |
| Cycloserine | Dose-dependent side effects, depression, irritability, psychosis |
| Quinolones | Sleep and mood disorders, psychosis |
| Nitrofurans | Euphoria, psychosis, sleep disturbances |
| Tetracyclines | Decreased concentration, mood and sleep disorders |
| Chloramphenicol | Depression |
| Trimethoprim, sulfonamides | Depression, psychosis |
| Antimycobacterials | |
| Isoniazid | Cognitive impairment, mood disorder, psychosis |
| Clofazimine | Major depression, suicide |
| Rifampin | Sedation |
| Ethionamide | Sedation, irritability, agitation, depression, psychosis |
| Ganciclovir | Sleep disturbances, anxiety, mood disorders, psychosis |
| Antifungals | |
| Amphotericin B | Delirium |
| Ketoconazole | Decreased libido, mood disorders, psychosis |
| Flucytosine | Sedation, hallucinations |
| Griseofulvin | Depression, psychosis, sleep disturbances |
| Source: Turjanski N, Lloyd GG. Psychiatric side effects of medications: recent developments. Advances in Psychiatric Treatment 2005;11:58-70. Reprinted with permission | |
Amoxicillin is a penicillin-based, broad-spectrum antibiotic (Box).1,6 Its potential psychiatric side effects include encephalopathy, irritability, sedation, anxiety, and hallucinations.2 These symptoms usually are managed by reducing the dosage or discontinuing the medication. In some cases, antipsychotics may be used to control the symptoms.
Beta-lactam compounds inhibit bacterial growth by interfering with cell wall synthesis. As a beta-lactam antibiotic, amoxicillin’s chemistry, mechanism of action, pharmacologic and clinical effects, and immunologic characteristics are similar to those of cephalosporins, monobactams, carbapenems, and beta-lactamase inhibitors.6
Amoxicillin is an aminopenicillin. These antibiotics retain the antibacterial spectrum of penicillin but have a broader spectrum against gram-negative organisms because of their enhanced ability to penetrate the gram-negative outer membrane. Amoxicillin causes less gastrointestinal (GI) irritation than penicillin and is stable in an acidic environment.
Amoxicillin is administered 250 to 500 mg every 8 hours for adults and 20 to 40 mg/kg of body weight every 24 hours for pediatric patients.1 Amoxicillin is more stable and better absorbed in the GI tract than most penicillins, so amoxicillin 3 times a day is as effective as 4 daily doses of other penicillins.
A literature search reveals 3 cases of amoxicillin-related psychosis (Table 2).7-9 A 30-year-old woman with a urinary tract infection (UTI) developed “confusional manic symptoms” after 10 days of amoxicillin.7 The patient’s family reported she’d had a similar reaction 14 years earlier following 9 days of ampicillin for a perforated appendix; since then she had received non-aminopenicillins without incident. In both incidents, her psychotic symptoms resolved.
A 55-year-old man developed auditory, visual, and tactile hallucinations within hours of his first dose of amoxicillin for presumed pneumonia. The patient “was able to describe what he had experienced clearly with evidence of subjective terror.”8
Most recently, a 63-year-old woman taking amoxicillin, 250 mg tid, for a UTI developed sleep disturbance after 1 day and auditory and visual hallucinations after 4 days. She had a similar episode that required hospitalization 5 years earlier. In both episodes, psychotic symptoms resolved within 3 days of antibiotic discontinuation, with no psychotropic drug treatment.9
Table 2
Amoxicillin-triggered psychosis: 3 case reports
| Study | Patient | Description |
|---|---|---|
| Beal et al7 | Woman, age 30 | Confusional manic symptoms after 10 days of treatment; symptoms resolved within 12 days of admission; patient had a similar reaction to ampicillin 14 years earlier |
| Stell et al8 | Man, age 55 | Auditory, visual, and tactile hallucinations within hours of first dose |
| Rao9 | Woman, age 63 | Auditory and visual hallucinations 1 week after taking 250 mg tid; patient had a similar reaction to amoxicillin 5 years earlier; in both cases symptoms resolved within 3 days of discontinuing amoxicillin |
Mechanism of psychiatric effects
The mechanisms of antibiotic-related neuropsychiatric sequelae are uncertain and vary with drug class and patient factors.
Hoigné’s syndrome—an acute psychotic reaction to intramuscular procaine penicillin first reported around 1950—is characterized by psychiatric symptoms, predominantly anxiety and hallucinations, almost immediately following injection. Anxiety is marked by a fear of imminent death as well as autonomic hyperactivity. This “pseudoanaphylactic reaction” persists for 5 to 30 minutes and has been noted for its resemblance to temporal lobe and limbic seizures (perceptual disturbance, sympathetic hyperactivity, and “doom anxiety”).
The underlying pathophysiology remains unclear; the reaction was originally attributed to microembolization of procaine crystals to the lungs and brain, later to direct procaine neurotoxicity, and most recently to temporolimbic kindling—the appearance of physiologic and behavioral responses to repetition of a stimulus (procaine) that initially is without effect.10
A potential mechanism for amoxicillin’s neuropsychiatric effects is less clear. Because amoxicillin is an oral medication, hypotheses regarding Hoigné’s syndrome seem inapplicable. In addition, amoxicillin is largely excreted unchanged by the kidneys; the lack of significant P450 metabolism argues against mechanisms mediated by polypharmacy or altered metabolite levels. Furthermore, penicillins are polar molecules with poor CNS penetration.6 Penicillins demonstrate known neurotoxicity, however, most often causing convulsions or myelopathy. Identified risk factors for penicillin neurotoxicity include:
- intravenous/thecal administration
- high doses
- CNS disease
- renal insufficiency
- advanced age
- use of drugs that block antibiotic export from the CNS
- conditions that increase blood-brain barrier permeability.
One hypothesis focuses on penicillins’ inhibition of both the GABAA receptor-chloride ionophore complex and the benzodiazepine receptor, yielding CNS disinhibition and decreasing the seizure threshold. Notably, GABA antagonism is considered a primary facilitator of CNS kindling. Penicillin also has been reported to cause delirium related to allergy-mediated cerebral edema.11 Beal et al7 argue for an immune-mediated cerebritis.
Psychiatric symptoms secondary to antibiotics—particularly penicillins—are likely multifactorial, suggesting certain individuals may be predisposed to “Hoigné’s syndrome” from amoxicillin. In the 3 case reports of amoxicillin-related psychosis, there is variation in duration of exposure until symptom onset, medical indication for the antibiotic, and patient age and gender. Any or all of these factors may be clinically significant. None of these patients, however, had a psychiatric history.
It is not clear whether a single 25-mg dose of meclizine—an H1-receptor antagonist—played a role in Mr. A’s psychotic symptoms. Meclizine overdose can cause extreme drowsiness, seizures, hallucinations, and decreased breathing. This anticholinergic has a half-life of only 6 hours and a duration of action of up to 24 hours, although anticholinergic toxicity from overdose can last for days.10 Mr. A ingested a single 25-mg dose of meclizine, however, and his auditory hallucinations persisted for 9 days. Furthermore, Mr. A’s previous well-tolerated meclizine use and lack of other signs and symptoms of anticholinergic toxicity do not support a substantial role for meclizine in his psychotic symptoms.
OUTCOME: Symptoms resolve
Mr. A’s confusion and auditory hallucinations resolve approximately 36 hours after he completed amoxicillin treatment. When transferred to the psychiatric unit, he denies auditory hallucinations or suicidal ideation. He also denies ear pain, tinnitus, vertigo, or ear tenderness; physical examination of the ear is unremarkable. Throughout the hospital admission, Mr. A experiences no confusion or changes in mental status and he continues to adamantly deny suicidal ideation.
He does not require treatment with anti-psychotics or other psychotropic medications and is discharged in stable condition.
Related resources
- Levenson JL, Schneider RK. Infectious diseases. In: Levenson JL, ed. The American Psychiatric Publishing textbook of psychosomatic medicine. Washington, DC: American Psychiatric Publishing; 2005:577-98.
Drug brand names
- Amoxicillin • Amoxil, Trimox, others
- Amphotericin B • Amphocin, Abelcet
- Ampicillin • Principen
- Chloramphenicol • Chloromycetin
- Ciprofloxacin • Cipro
- Clofazimine • Lamprene
- Cycloserine • Seromycin
- Ethionamide • Trecator
- Flucytosine • Ancobon
- Ganciclovir • Cytovene
- Griseofulvin • Fulvicin U/F, Grifulvin V
- Isoniazid • Nydrazid
- Ketoconazole • Nizoral
- Meclizine • Antivert, Bonine, others
- Rifampin • Rifadin, Rimactane
- Trimethoprim/sulfamethoxazole • Bactrim, Septra
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
CASE: Confused and suicidal
Mr. A, age 39, becomes disoriented while walking and approaches a suspension bridge. He borrows a passerby’s cell phone and calls his sister. His sister later states that he was confused and expressed his final goodbyes, saying, “I will see Mom in heaven.” He gives back the phone and leaps of the bridge. A nearby boat rescues him almost immediately.
Mr. A is brought to the trauma unit, where he is treated for a lacerated liver. After he is stabilized, Mr. A is awake and answering questions appropriately. He is placed on suicide precautions and direct 24-hour, one-to-one supervision. Our psychiatric team evaluates him.
Mr. A reports no history of diabetes, hypertension, cardiac disorders, or neurologic disorders, but does have a history of cognitive developmental delay. He has no history of psychiatric illness, suicide attempts, or self-injurious behavior. He denies a psychiatric family history or using alcohol, tobacco, or illicit drugs; drug screen is negative. He is unemployed, collects disability, and lives with his sister.
The authors’ observations
In our initial evaluation, we find no obvious reason for Mr. A’s confusion or suicide attempt. We decide to closely review Mr. A’s history in the days leading up to his jumping off the bridge.
HISTORY: Otitis media treatment
Mr. A has a history of chronic otitis media and sought treatment for ear pain at a local emergency room (ER) 10 days before his suicide attempt. He was prescribed amoxicillin, 500 mg tid for 10 days, and meclizine, 25 mg every 8 hours as needed for dizziness.
Immediately after his first dose of both drugs, the patient told his family he was feeling “weird,” but denied being dizzy. Thinking the unusual feeling was from meclizine, Mr. A stopped taking it but continued amoxicillin. On the second day of amoxicillin, he noticed bouts of confusion. He could perform his daily activities, but with difficulty. Mr. A’s niece said he had to ask for help with minor tasks, such as opening a can of soup.
On day 3, Mr. A developed prominent auditory hallucinations. He described hearing unrecognizable male and female voices chattering and mumbling throughout the day. The voices and confusion progressively worsened, but Mr. A continued taking the antibiotic and did not mention the voices to his family.
Mr. A’s sister reports that in a phone conversation with her brother on day 7, “he wasn’t himself…he was talking about my sister and mother but what he said didn’t make sense.” She asked a neighbor to check on Mr. A; he reported that Mr. A was “OK.” On the final day of amoxicillin—day 10—Mr. A became increasingly agitated. He says us that shortly before wandering onto the bridge and jumping, he was having a difficult time dealing with the voices and confusion.
We suspect amoxicillin might have been responsible for Mr. A’s psychotic symptoms.
The authors’ observations
Treatment modalities and pharmaceutical approaches used to treat infectious diseases carry many potential adverse effects. When a patient presents with new-onset psychiatric symptoms, explore whether they are related to an underlying mood disorder or medication side effects. Three important considerations are to:
- determine whether the condition is reversible by discontinuing a drug
- identify and characterize previously unrecognized adverse drug effects
- avoid inaccurate diagnosis that leads to nonindicated psychiatric treatment.1
Antibiotic side effects vary, depending on the particular drug and its target bacteria. The most common are gastrointestinal, such as upset stomach and diarrhea. Antibiotics also can induce an anaphylactic reaction ranging from mild (pruritic rash or slight wheezing) to life-threatening (swelling of the throat, difficulty breathing, and hypotension).
Several classes of antibiotics have psychiatric side effects that range from minor confusion and irritability to severe encephalopathy and suicide (Table 1).2 Case reports have described psychotic symptoms associated with cotrimoxazole,3 trimethoprim/sulfamethoxazole,4 and ciprofloxacin.5 An older review found that amoxicillin is among the top 10 most commonly prescribed medications associated with psychiatric side effects.1
Table 1
Potential psychiatric effects of antibiotics
| Medication | Side effects |
|---|---|
| Antibacterials | |
| Penicillins | Encephalopathy, irritability, sedation, anxiety, hallucinations |
| Cephalosporins | Sleep disturbances, hallucinations |
| Cycloserine | Dose-dependent side effects, depression, irritability, psychosis |
| Quinolones | Sleep and mood disorders, psychosis |
| Nitrofurans | Euphoria, psychosis, sleep disturbances |
| Tetracyclines | Decreased concentration, mood and sleep disorders |
| Chloramphenicol | Depression |
| Trimethoprim, sulfonamides | Depression, psychosis |
| Antimycobacterials | |
| Isoniazid | Cognitive impairment, mood disorder, psychosis |
| Clofazimine | Major depression, suicide |
| Rifampin | Sedation |
| Ethionamide | Sedation, irritability, agitation, depression, psychosis |
| Ganciclovir | Sleep disturbances, anxiety, mood disorders, psychosis |
| Antifungals | |
| Amphotericin B | Delirium |
| Ketoconazole | Decreased libido, mood disorders, psychosis |
| Flucytosine | Sedation, hallucinations |
| Griseofulvin | Depression, psychosis, sleep disturbances |
| Source: Turjanski N, Lloyd GG. Psychiatric side effects of medications: recent developments. Advances in Psychiatric Treatment 2005;11:58-70. Reprinted with permission | |
Amoxicillin is a penicillin-based, broad-spectrum antibiotic (Box).1,6 Its potential psychiatric side effects include encephalopathy, irritability, sedation, anxiety, and hallucinations.2 These symptoms usually are managed by reducing the dosage or discontinuing the medication. In some cases, antipsychotics may be used to control the symptoms.
Beta-lactam compounds inhibit bacterial growth by interfering with cell wall synthesis. As a beta-lactam antibiotic, amoxicillin’s chemistry, mechanism of action, pharmacologic and clinical effects, and immunologic characteristics are similar to those of cephalosporins, monobactams, carbapenems, and beta-lactamase inhibitors.6
Amoxicillin is an aminopenicillin. These antibiotics retain the antibacterial spectrum of penicillin but have a broader spectrum against gram-negative organisms because of their enhanced ability to penetrate the gram-negative outer membrane. Amoxicillin causes less gastrointestinal (GI) irritation than penicillin and is stable in an acidic environment.
Amoxicillin is administered 250 to 500 mg every 8 hours for adults and 20 to 40 mg/kg of body weight every 24 hours for pediatric patients.1 Amoxicillin is more stable and better absorbed in the GI tract than most penicillins, so amoxicillin 3 times a day is as effective as 4 daily doses of other penicillins.
A literature search reveals 3 cases of amoxicillin-related psychosis (Table 2).7-9 A 30-year-old woman with a urinary tract infection (UTI) developed “confusional manic symptoms” after 10 days of amoxicillin.7 The patient’s family reported she’d had a similar reaction 14 years earlier following 9 days of ampicillin for a perforated appendix; since then she had received non-aminopenicillins without incident. In both incidents, her psychotic symptoms resolved.
A 55-year-old man developed auditory, visual, and tactile hallucinations within hours of his first dose of amoxicillin for presumed pneumonia. The patient “was able to describe what he had experienced clearly with evidence of subjective terror.”8
Most recently, a 63-year-old woman taking amoxicillin, 250 mg tid, for a UTI developed sleep disturbance after 1 day and auditory and visual hallucinations after 4 days. She had a similar episode that required hospitalization 5 years earlier. In both episodes, psychotic symptoms resolved within 3 days of antibiotic discontinuation, with no psychotropic drug treatment.9
Table 2
Amoxicillin-triggered psychosis: 3 case reports
| Study | Patient | Description |
|---|---|---|
| Beal et al7 | Woman, age 30 | Confusional manic symptoms after 10 days of treatment; symptoms resolved within 12 days of admission; patient had a similar reaction to ampicillin 14 years earlier |
| Stell et al8 | Man, age 55 | Auditory, visual, and tactile hallucinations within hours of first dose |
| Rao9 | Woman, age 63 | Auditory and visual hallucinations 1 week after taking 250 mg tid; patient had a similar reaction to amoxicillin 5 years earlier; in both cases symptoms resolved within 3 days of discontinuing amoxicillin |
Mechanism of psychiatric effects
The mechanisms of antibiotic-related neuropsychiatric sequelae are uncertain and vary with drug class and patient factors.
Hoigné’s syndrome—an acute psychotic reaction to intramuscular procaine penicillin first reported around 1950—is characterized by psychiatric symptoms, predominantly anxiety and hallucinations, almost immediately following injection. Anxiety is marked by a fear of imminent death as well as autonomic hyperactivity. This “pseudoanaphylactic reaction” persists for 5 to 30 minutes and has been noted for its resemblance to temporal lobe and limbic seizures (perceptual disturbance, sympathetic hyperactivity, and “doom anxiety”).
The underlying pathophysiology remains unclear; the reaction was originally attributed to microembolization of procaine crystals to the lungs and brain, later to direct procaine neurotoxicity, and most recently to temporolimbic kindling—the appearance of physiologic and behavioral responses to repetition of a stimulus (procaine) that initially is without effect.10
A potential mechanism for amoxicillin’s neuropsychiatric effects is less clear. Because amoxicillin is an oral medication, hypotheses regarding Hoigné’s syndrome seem inapplicable. In addition, amoxicillin is largely excreted unchanged by the kidneys; the lack of significant P450 metabolism argues against mechanisms mediated by polypharmacy or altered metabolite levels. Furthermore, penicillins are polar molecules with poor CNS penetration.6 Penicillins demonstrate known neurotoxicity, however, most often causing convulsions or myelopathy. Identified risk factors for penicillin neurotoxicity include:
- intravenous/thecal administration
- high doses
- CNS disease
- renal insufficiency
- advanced age
- use of drugs that block antibiotic export from the CNS
- conditions that increase blood-brain barrier permeability.
One hypothesis focuses on penicillins’ inhibition of both the GABAA receptor-chloride ionophore complex and the benzodiazepine receptor, yielding CNS disinhibition and decreasing the seizure threshold. Notably, GABA antagonism is considered a primary facilitator of CNS kindling. Penicillin also has been reported to cause delirium related to allergy-mediated cerebral edema.11 Beal et al7 argue for an immune-mediated cerebritis.
Psychiatric symptoms secondary to antibiotics—particularly penicillins—are likely multifactorial, suggesting certain individuals may be predisposed to “Hoigné’s syndrome” from amoxicillin. In the 3 case reports of amoxicillin-related psychosis, there is variation in duration of exposure until symptom onset, medical indication for the antibiotic, and patient age and gender. Any or all of these factors may be clinically significant. None of these patients, however, had a psychiatric history.
It is not clear whether a single 25-mg dose of meclizine—an H1-receptor antagonist—played a role in Mr. A’s psychotic symptoms. Meclizine overdose can cause extreme drowsiness, seizures, hallucinations, and decreased breathing. This anticholinergic has a half-life of only 6 hours and a duration of action of up to 24 hours, although anticholinergic toxicity from overdose can last for days.10 Mr. A ingested a single 25-mg dose of meclizine, however, and his auditory hallucinations persisted for 9 days. Furthermore, Mr. A’s previous well-tolerated meclizine use and lack of other signs and symptoms of anticholinergic toxicity do not support a substantial role for meclizine in his psychotic symptoms.
OUTCOME: Symptoms resolve
Mr. A’s confusion and auditory hallucinations resolve approximately 36 hours after he completed amoxicillin treatment. When transferred to the psychiatric unit, he denies auditory hallucinations or suicidal ideation. He also denies ear pain, tinnitus, vertigo, or ear tenderness; physical examination of the ear is unremarkable. Throughout the hospital admission, Mr. A experiences no confusion or changes in mental status and he continues to adamantly deny suicidal ideation.
He does not require treatment with anti-psychotics or other psychotropic medications and is discharged in stable condition.
Related resources
- Levenson JL, Schneider RK. Infectious diseases. In: Levenson JL, ed. The American Psychiatric Publishing textbook of psychosomatic medicine. Washington, DC: American Psychiatric Publishing; 2005:577-98.
Drug brand names
- Amoxicillin • Amoxil, Trimox, others
- Amphotericin B • Amphocin, Abelcet
- Ampicillin • Principen
- Chloramphenicol • Chloromycetin
- Ciprofloxacin • Cipro
- Clofazimine • Lamprene
- Cycloserine • Seromycin
- Ethionamide • Trecator
- Flucytosine • Ancobon
- Ganciclovir • Cytovene
- Griseofulvin • Fulvicin U/F, Grifulvin V
- Isoniazid • Nydrazid
- Ketoconazole • Nizoral
- Meclizine • Antivert, Bonine, others
- Rifampin • Rifadin, Rimactane
- Trimethoprim/sulfamethoxazole • Bactrim, Septra
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Hubbard JR, Levenson JL, Patrick GA. Psychiatric side effects associated with the ten most commonly dispensed prescription drugs: a review. J Fam Pract 1991;33(2):177-86.
2. Turjanski N, Lloyd GG. Psychiatric side effects of medications: recent developments. Advances in Psychiatric Treatment 2005;11:58-70.
3. Weis S, Karagülle D, Kornhuber J, Bayerlein K. Cotrimoxazole-induced psychosis: a case report and review of literature. Pharmacopsychiatry 2006;39:236-7.
4. Saidinejad M, Ewald MB, Shannon MW. Transient psychosis in an immune-competent patient after oral trimethoprimsulfamethoxazole administration. Pediatrics 2005;115(6):e739-41.
5. Grimm O, Alm B, Für Seelische Z. A case of ciprofloxacin-induced acute polymorphic psychosis with a distinct deficit in executive functions. Psychosomatics 2007;48(3):269.-
6. Katzung BG. Basic and clinical pharmacology. 7th ed. Stamford, CT: Appleton & Lange; 1998;726-32.
7. Beal DM, Hudson B, Zaiac M. Amoxacillin-induced psychosis? Am J Psychiatry 1986;143(2):255-6.
8. Stell IM, Ojo OA. Amoxycillin-induced hallucinations—a variant of Hoigne’s syndrome? Br J Clin Pract 1996;50(5):279.-
9. Rao R. Penicillin psychosis in later life: Hoigne’s syndrome revisited. J Neuropsychiatry Clin Neurosci 1999;11(4):517-8.
10. Araszkiewicz A, Rybakowski JK. Hoigne’s syndrome, kindling, and panic disorder. Depress Anxiety 1996-1997;4(3):139-43.
11. Sternbach H, State R. Antibiotics: neuropsychiatric effects and psychotropic interactions. Harv Rev Psychiatry 1997;5(4):214-26.
1. Hubbard JR, Levenson JL, Patrick GA. Psychiatric side effects associated with the ten most commonly dispensed prescription drugs: a review. J Fam Pract 1991;33(2):177-86.
2. Turjanski N, Lloyd GG. Psychiatric side effects of medications: recent developments. Advances in Psychiatric Treatment 2005;11:58-70.
3. Weis S, Karagülle D, Kornhuber J, Bayerlein K. Cotrimoxazole-induced psychosis: a case report and review of literature. Pharmacopsychiatry 2006;39:236-7.
4. Saidinejad M, Ewald MB, Shannon MW. Transient psychosis in an immune-competent patient after oral trimethoprimsulfamethoxazole administration. Pediatrics 2005;115(6):e739-41.
5. Grimm O, Alm B, Für Seelische Z. A case of ciprofloxacin-induced acute polymorphic psychosis with a distinct deficit in executive functions. Psychosomatics 2007;48(3):269.-
6. Katzung BG. Basic and clinical pharmacology. 7th ed. Stamford, CT: Appleton & Lange; 1998;726-32.
7. Beal DM, Hudson B, Zaiac M. Amoxacillin-induced psychosis? Am J Psychiatry 1986;143(2):255-6.
8. Stell IM, Ojo OA. Amoxycillin-induced hallucinations—a variant of Hoigne’s syndrome? Br J Clin Pract 1996;50(5):279.-
9. Rao R. Penicillin psychosis in later life: Hoigne’s syndrome revisited. J Neuropsychiatry Clin Neurosci 1999;11(4):517-8.
10. Araszkiewicz A, Rybakowski JK. Hoigne’s syndrome, kindling, and panic disorder. Depress Anxiety 1996-1997;4(3):139-43.
11. Sternbach H, State R. Antibiotics: neuropsychiatric effects and psychotropic interactions. Harv Rev Psychiatry 1997;5(4):214-26.
The sailor who won’t follow orders
CASE: An unlikable patient
Mr. L, age 56, is admitted to the psychiatric unit at our Veterans Affairs Medical Center for active suicidal ideation; he has a history of self-injurious behaviors that include mutilation and overdose. He also has a history of alcohol dependence and multiple inpatient psychiatric admissions. He has never married and conflicts with his siblings—in whose home he has been staying—have led to frequent homelessness.
His affect is silly and shallow. He also shows signs of haughtiness, disinhibition, grandiosity, and confabulation. For example, he says that while in the Navy he had 82 sexual exploits and developed a drug that cured herpes.
We start Mr. L on divalproex, 1,500 mg/d, and quetiapine, titrated to 200 mg/d. After 3 days he is discharged, but this begins a cycle of repeated suicide gestures and readmissions—9 within the next 3 months. Each time he is discharged, Mr. L fails to follow through on treatment recommendations and is indifferent to our staff’s annoyed reactions.
The author’s observations
Some of our staff members regard Mr. L’s suicidal gestures as manipulative and feel angry and demoralized by his poor adherence to outpatient treatment plans. Their negative countertransference might have impacted how they evaluated Mr. L through repeated admissions and discharges. During Mr. L’s ninth admission, we decide to reevaluate his longitudinal history for clues to his noncompliant behavior.
History: Undocumented injury
Mr. L says he began drinking alcohol at age 16. He reports that he has grown marijuana but has not smoked it since 1991. He denies using heroin or other drugs.
Mr. L states that he suffered a head injury in 1975 after falling off a ladder on a Navy ship. He describes losing consciousness for a brief but uncertain duration. He reports that he has developed a seizure disorder since this fall and a history of amnesia secondary to past seizures. His medical records contain no witnessed seizures. Mr. L also says he was hospitalized a few years ago and placed on a ventilator for 7 days for an undetermined reason.
The authors’ observations
Based on Mr. L’s report of a possible traumatic brain injury (TBI), we order a neurologic evaluation. A year earlier, MRI of the brain without contrast demonstrated minimal, nonspecific periventricular and subcortical, punctuate hyperintensities on flair and T2 weighted sequences that are nonspecific. Overall, the impression was “diffuse involutional changes and mild nonspecific periventricular and subcortical white matter hyperintensities,” which might reflect covert vascular brain injury.
Our frustration over Mr. L’s repeated readmissions for suicidal gestures led us to seek outside evaluation and consultation from a senior psychiatrist for assistance with discharge and treatment planning. Unlike our staff, the consulting psychiatrist did not harbor strong negative feelings toward the patient.
Mr. L’s history of deterioration in psychosocial functioning prompted this psychiatrist to perform a thorough mental status examination that focused on cognitive elements and request formal neuropsychological testing.
Evalutation: Cognitive Deficits
During mental status examination, Mr. L has difficulty recalling 3 items and uses a memory strategy to assist himself. He fails to recollect in reverse order the last 5 U.S. presidents. He spells “world” backward, but has difficulty repeating 6 digits forward and 4 backward. He is unable to do serial 7 subtractions from 93 to 65 correctly. He adequately copies interlocking pentagons and draws a clock with the correct time. He achieves a score of 28/30 on the Folstein Mini Mental State Exam, missing the date by 4 days and recalling 2 of 3 words.
These results suggest Mr. L has difficulty with attention and working memory, short-term memory, fund of general information and long-term memory, and ability to perform simple calculations. Most important, they indicate the need for further study, especially a neuropsychological test battery.
Mr. L’s abnormal neuropsychological test results are summarized in the Table. He manifests concretization of thought. His loss of conceptual fluidity is documented formally by measures of perseverative errors and categories completed on the Wisconsin Card Sorting Test (WCST). These findings support a diagnosis of acquired dementia.
Table
Abnormal findings on Mr. L’s neuropsychological testing
| Cognitive domain | Test | Score | Interpretation |
|---|---|---|---|
| Mental status and effort | |||
| Mental status | MMSE total score | 28/30 | 2 of 3 items recalled after delay |
| Orientation | MMSE orientation questions | 9/10 | Date off by 4 days |
| Premorbid IQ estimate | WRAT-4 Reading Standard | 66th percentile | Within normal limits. Inconsistent with educational attainment, but could be impacted by temporal lobe findings |
| Verbal memory | |||
| Immediate memory | RBANS Immediate Memory Index (List and Story Learning) | 1st percentile | Severe impairment |
| Delayed memory | RBANS Delayed Memory Index | 1st percentile | Severe impairment |
| Recognition memory | List Learning | Severe impairment | |
| Visuospatial memory | |||
| Delayed memory | RBANS Figure Recall | 3rd percentile | Severe impairment |
| Executive functioning | |||
| Cognitive flexibility | Trails B | 10th percentile | Severe impairment based on educational attainment |
| WCST | Low scores: Nonperseverative errors, perseverative errors, and categories completed | ||
| * Tests of mental status effort, visuomotor processing speed, confrontation naming, visuospatial function, attention, and executive functioning fluency/initiation were within normal limits | |||
| MMSE: Mini Mental State Exam; WRAT: Wide Range Achievement Test; RBANS: Repeatable Battery for the Assessment of Neuropsychological Status; WCST: Wisconsin Card Sorting Test | |||
The authors’ observations
Mr. L’s history, cognitive testing, head imaging, and behavioral observations suggest that several pathogenic factors contribute to his impaired functioning. First, he describes a TBI of unknown severity occurring in 1975. Although brain scans did not show evidence of midline shift or encephalomalacia, a direct blow to the head after falling from a height combined with possible post-injury seizures suggests a TBI of at least moderate severity.
Second, Mr. L describes an incident in which he required inpatient respiratory assistance. Although the precipitating medical event was unclear, anoxia or hypoxia is likely. A recent CT revealed low attenuation in the left temporal region that could represent an infarct.
Mr. L’s severe memory impairment and moderate to severe impairment in cognitive flexibility are commonly reported after a TBI of moderate severity. If an ischemic incident were the primary contributor, a lateralized pattern of cognitive dysfunction—which Mr. L does not exhibit—would be expected.
Although Mr. L likely has vascular dementia, his MRI findings do not indicate sufficient disease to account for his memory scores. Vascular dementia is associated with slow, stepwise cognitive deterioration, which is not consistent with severely impaired memory in a 56-year-old patient.
Finally, alcoholism is associated with cognitive difficulty in memory, visuospatial functioning, and abstract reasoning. Mr. L demonstrated significant difficulty in memory and abstract reasoning, but his visuospatial functioning was largely intact. In the absence of Wernicke’s encephalopathy, chronic alcoholics generally do not show memory decrements in line with Mr. L’s. His MRI results indicated only minimal ventricular and sulcal enlargement. Because atrophy is present in approximately 60% of chronic alcoholics, this finding provides evidence of a contribution, but the other contributory factors are associated with more definitive medical outcomes. Thus, alcoholism must be viewed as a secondary contributor to Mr. L’s impaired functioning.
Taking into account all known contributors, TBI emerges as the primary diagnosis.
Consider neurologic injury
Recognizing and characterizing personality changes related to neurologic injury and disease is often problematic and unreliable, even when psychometrically validated instruments and structured diagnostic interviews are used (Box 1).1-5 Mr. L’s presentation differed from the more commonly reported “impulsive aggression” associated with closed head injury. Sequelae from TBI were contributing to his clinical presentation but was obscured by his shallow and silly affect, inability to accurately assess social cues, and lack of empathy.
Mr. L reported suffering a head injury from falling off a ladder. Personality changes that result from traumatic brain injury (TBI) of the sudden deceleration type—even when mild—are frequently referable to the frontal lobe, especially focal orbital and/or ventromedial damage of the prefrontal cortex.1-5 This is because of the physical proximity of the sphenoid wing to the orbitofrontal region and effects of shearing.
As a result of this damage, patients lack insight into their accompanying cognitive and behavioral abnormalities, such as the egocentricity and impaired empathy shown by Mr. L. These changes might not be detected in clinical interviews and over brief periods.2 Appreciating an acquired personality disturbance may require evaluating the patient’s behavior over months or years.2
In retrospect, Mr. L’s seeking repeated inpatient psychiatric hospitalizations is consistent with poor planning and problem-solving skills. He has a limited repertoire of adaptive behaviors and has learned that suicidal gestures lead to admission and caretaking. These are important to him because he is frequently homeless. His lack of insight is seen in his unrealistic plans for employment in jobs requiring specialized technical skills.
Mr. L’s case emphasizes the importance of considering brain injury as an etiologic factor in personality changes. It also highlights the complex—and seemingly nonoverlapping—functions and dysfunctions of the frontal lobe, including:
- source memory
- working memory
- sustained attention
- conceptual fluidity
- imaginative thinking
- impulse regulation
- planning and problem-solving skills.
Documenting Mr. L’s cognitive deficits and acquired dementia diagnosis changed our staff’s perception of his behavior, enabling us to overcome negative countertransference (Box 2). We no longer regarded him as deliberately manipulative and refer him for appropriate treatment.
Countertransference can interfere with optimal workup and treatment of patients with character changes related to traumatic brain injury and neurodegenerative processes. When we interpreted Mr. L’s suicidal gestures and hospitalizations as manipulative and deliberate, we failed to appreciate the limited number of things he could do to obtain a safe and protective environment. We also failed to recognize that his poor planning and problem-solving skills—as well as lack of insight into his illness—prevented him from adhering to outpatient treatment.
Originally, we attributed Mr. L’s egocentricity, lack of empathy, and lack of adherence to axis II pathology.
Our staff’s hostile feelings toward Mr. L led us to insufficiently consider his history—which is consistent with cognitive decline—during biopsychosocial evaluation and treatment planning. Mr. L’s status as a frequently homeless, unemployed person reflects a sharp decline for a highly educated person who served as a Navy officer and performed radiation inspections on nuclear-powered vessels.
Outome: Residential placement
We realize Mr. L needs cognitive rehabilitation—including assistance with planning and problem solving—and arrange for his placement in a residential facility for this specialized rehabilitation. Mr. L receives supportive psychotherapy and cognitive remediation from a psychologist. He also is involved in incentive work therapy with a vocational rehabilitation specialist.
Related resource
- Silver, JM, McAllister TW, Yudofsky SC, eds. Textbook of traumatic brain injury. Washington, DC: American Psychiatric Publishing; 2005.
- Divalproex • Depakote
- Quetiapine • Seroquel
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Tranel D. Functional neuroanatomy: neuropsychological correlates of cortical and subcortical damage. In: Yudofsky SC, Hales RE, eds. The American Psychiatric Publishing textbook of neuropsychiatry and clinical neurosciences. 4th ed. Washington, DC: American Psychiatric Publishing; 2002:71-113.
2. Barrash J, Tranel D, Anderson SW. Acquired personality disturbances associated with bilateral damage to the ventromedial prefrontal region. Dev Neuropsychol 2000;18(3):355-81.
3. Silver JM, Hales RE, Yudofsky SC. Neuropsychiatric aspects of traumatic brain injury. In: Yudofsky SC, Hales RE, eds. The American Psychiatric Publishing textbook of neuropsychiatry and clinical neurosciences. 4th ed. Washington, DC: American Psychiatric Publishing; 2002:625-72.
4. Damasio AR, Tranel D, Damasio HC. Somatic markers and the guidance of behavior: theory and preliminary testing. In: Levin HS, Eisenberg HM, Benton AL, eds. Frontal lobe function and dysfunction. Oxford, UK: Oxford University Press; 1991:217-29.
5. Prigatano GP. The relationship of frontal lobe damage to diminished awareness: studies in rehabilitation. In: Levin HS, Eisenberg HM, Benton AL, eds. Frontal lobe function and dysfunction. Oxford, UK: Oxford University Press; 1991:381-97.
CASE: An unlikable patient
Mr. L, age 56, is admitted to the psychiatric unit at our Veterans Affairs Medical Center for active suicidal ideation; he has a history of self-injurious behaviors that include mutilation and overdose. He also has a history of alcohol dependence and multiple inpatient psychiatric admissions. He has never married and conflicts with his siblings—in whose home he has been staying—have led to frequent homelessness.
His affect is silly and shallow. He also shows signs of haughtiness, disinhibition, grandiosity, and confabulation. For example, he says that while in the Navy he had 82 sexual exploits and developed a drug that cured herpes.
We start Mr. L on divalproex, 1,500 mg/d, and quetiapine, titrated to 200 mg/d. After 3 days he is discharged, but this begins a cycle of repeated suicide gestures and readmissions—9 within the next 3 months. Each time he is discharged, Mr. L fails to follow through on treatment recommendations and is indifferent to our staff’s annoyed reactions.
The author’s observations
Some of our staff members regard Mr. L’s suicidal gestures as manipulative and feel angry and demoralized by his poor adherence to outpatient treatment plans. Their negative countertransference might have impacted how they evaluated Mr. L through repeated admissions and discharges. During Mr. L’s ninth admission, we decide to reevaluate his longitudinal history for clues to his noncompliant behavior.
History: Undocumented injury
Mr. L says he began drinking alcohol at age 16. He reports that he has grown marijuana but has not smoked it since 1991. He denies using heroin or other drugs.
Mr. L states that he suffered a head injury in 1975 after falling off a ladder on a Navy ship. He describes losing consciousness for a brief but uncertain duration. He reports that he has developed a seizure disorder since this fall and a history of amnesia secondary to past seizures. His medical records contain no witnessed seizures. Mr. L also says he was hospitalized a few years ago and placed on a ventilator for 7 days for an undetermined reason.
The authors’ observations
Based on Mr. L’s report of a possible traumatic brain injury (TBI), we order a neurologic evaluation. A year earlier, MRI of the brain without contrast demonstrated minimal, nonspecific periventricular and subcortical, punctuate hyperintensities on flair and T2 weighted sequences that are nonspecific. Overall, the impression was “diffuse involutional changes and mild nonspecific periventricular and subcortical white matter hyperintensities,” which might reflect covert vascular brain injury.
Our frustration over Mr. L’s repeated readmissions for suicidal gestures led us to seek outside evaluation and consultation from a senior psychiatrist for assistance with discharge and treatment planning. Unlike our staff, the consulting psychiatrist did not harbor strong negative feelings toward the patient.
Mr. L’s history of deterioration in psychosocial functioning prompted this psychiatrist to perform a thorough mental status examination that focused on cognitive elements and request formal neuropsychological testing.
Evalutation: Cognitive Deficits
During mental status examination, Mr. L has difficulty recalling 3 items and uses a memory strategy to assist himself. He fails to recollect in reverse order the last 5 U.S. presidents. He spells “world” backward, but has difficulty repeating 6 digits forward and 4 backward. He is unable to do serial 7 subtractions from 93 to 65 correctly. He adequately copies interlocking pentagons and draws a clock with the correct time. He achieves a score of 28/30 on the Folstein Mini Mental State Exam, missing the date by 4 days and recalling 2 of 3 words.
These results suggest Mr. L has difficulty with attention and working memory, short-term memory, fund of general information and long-term memory, and ability to perform simple calculations. Most important, they indicate the need for further study, especially a neuropsychological test battery.
Mr. L’s abnormal neuropsychological test results are summarized in the Table. He manifests concretization of thought. His loss of conceptual fluidity is documented formally by measures of perseverative errors and categories completed on the Wisconsin Card Sorting Test (WCST). These findings support a diagnosis of acquired dementia.
Table
Abnormal findings on Mr. L’s neuropsychological testing
| Cognitive domain | Test | Score | Interpretation |
|---|---|---|---|
| Mental status and effort | |||
| Mental status | MMSE total score | 28/30 | 2 of 3 items recalled after delay |
| Orientation | MMSE orientation questions | 9/10 | Date off by 4 days |
| Premorbid IQ estimate | WRAT-4 Reading Standard | 66th percentile | Within normal limits. Inconsistent with educational attainment, but could be impacted by temporal lobe findings |
| Verbal memory | |||
| Immediate memory | RBANS Immediate Memory Index (List and Story Learning) | 1st percentile | Severe impairment |
| Delayed memory | RBANS Delayed Memory Index | 1st percentile | Severe impairment |
| Recognition memory | List Learning | Severe impairment | |
| Visuospatial memory | |||
| Delayed memory | RBANS Figure Recall | 3rd percentile | Severe impairment |
| Executive functioning | |||
| Cognitive flexibility | Trails B | 10th percentile | Severe impairment based on educational attainment |
| WCST | Low scores: Nonperseverative errors, perseverative errors, and categories completed | ||
| * Tests of mental status effort, visuomotor processing speed, confrontation naming, visuospatial function, attention, and executive functioning fluency/initiation were within normal limits | |||
| MMSE: Mini Mental State Exam; WRAT: Wide Range Achievement Test; RBANS: Repeatable Battery for the Assessment of Neuropsychological Status; WCST: Wisconsin Card Sorting Test | |||
The authors’ observations
Mr. L’s history, cognitive testing, head imaging, and behavioral observations suggest that several pathogenic factors contribute to his impaired functioning. First, he describes a TBI of unknown severity occurring in 1975. Although brain scans did not show evidence of midline shift or encephalomalacia, a direct blow to the head after falling from a height combined with possible post-injury seizures suggests a TBI of at least moderate severity.
Second, Mr. L describes an incident in which he required inpatient respiratory assistance. Although the precipitating medical event was unclear, anoxia or hypoxia is likely. A recent CT revealed low attenuation in the left temporal region that could represent an infarct.
Mr. L’s severe memory impairment and moderate to severe impairment in cognitive flexibility are commonly reported after a TBI of moderate severity. If an ischemic incident were the primary contributor, a lateralized pattern of cognitive dysfunction—which Mr. L does not exhibit—would be expected.
Although Mr. L likely has vascular dementia, his MRI findings do not indicate sufficient disease to account for his memory scores. Vascular dementia is associated with slow, stepwise cognitive deterioration, which is not consistent with severely impaired memory in a 56-year-old patient.
Finally, alcoholism is associated with cognitive difficulty in memory, visuospatial functioning, and abstract reasoning. Mr. L demonstrated significant difficulty in memory and abstract reasoning, but his visuospatial functioning was largely intact. In the absence of Wernicke’s encephalopathy, chronic alcoholics generally do not show memory decrements in line with Mr. L’s. His MRI results indicated only minimal ventricular and sulcal enlargement. Because atrophy is present in approximately 60% of chronic alcoholics, this finding provides evidence of a contribution, but the other contributory factors are associated with more definitive medical outcomes. Thus, alcoholism must be viewed as a secondary contributor to Mr. L’s impaired functioning.
Taking into account all known contributors, TBI emerges as the primary diagnosis.
Consider neurologic injury
Recognizing and characterizing personality changes related to neurologic injury and disease is often problematic and unreliable, even when psychometrically validated instruments and structured diagnostic interviews are used (Box 1).1-5 Mr. L’s presentation differed from the more commonly reported “impulsive aggression” associated with closed head injury. Sequelae from TBI were contributing to his clinical presentation but was obscured by his shallow and silly affect, inability to accurately assess social cues, and lack of empathy.
Mr. L reported suffering a head injury from falling off a ladder. Personality changes that result from traumatic brain injury (TBI) of the sudden deceleration type—even when mild—are frequently referable to the frontal lobe, especially focal orbital and/or ventromedial damage of the prefrontal cortex.1-5 This is because of the physical proximity of the sphenoid wing to the orbitofrontal region and effects of shearing.
As a result of this damage, patients lack insight into their accompanying cognitive and behavioral abnormalities, such as the egocentricity and impaired empathy shown by Mr. L. These changes might not be detected in clinical interviews and over brief periods.2 Appreciating an acquired personality disturbance may require evaluating the patient’s behavior over months or years.2
In retrospect, Mr. L’s seeking repeated inpatient psychiatric hospitalizations is consistent with poor planning and problem-solving skills. He has a limited repertoire of adaptive behaviors and has learned that suicidal gestures lead to admission and caretaking. These are important to him because he is frequently homeless. His lack of insight is seen in his unrealistic plans for employment in jobs requiring specialized technical skills.
Mr. L’s case emphasizes the importance of considering brain injury as an etiologic factor in personality changes. It also highlights the complex—and seemingly nonoverlapping—functions and dysfunctions of the frontal lobe, including:
- source memory
- working memory
- sustained attention
- conceptual fluidity
- imaginative thinking
- impulse regulation
- planning and problem-solving skills.
Documenting Mr. L’s cognitive deficits and acquired dementia diagnosis changed our staff’s perception of his behavior, enabling us to overcome negative countertransference (Box 2). We no longer regarded him as deliberately manipulative and refer him for appropriate treatment.
Countertransference can interfere with optimal workup and treatment of patients with character changes related to traumatic brain injury and neurodegenerative processes. When we interpreted Mr. L’s suicidal gestures and hospitalizations as manipulative and deliberate, we failed to appreciate the limited number of things he could do to obtain a safe and protective environment. We also failed to recognize that his poor planning and problem-solving skills—as well as lack of insight into his illness—prevented him from adhering to outpatient treatment.
Originally, we attributed Mr. L’s egocentricity, lack of empathy, and lack of adherence to axis II pathology.
Our staff’s hostile feelings toward Mr. L led us to insufficiently consider his history—which is consistent with cognitive decline—during biopsychosocial evaluation and treatment planning. Mr. L’s status as a frequently homeless, unemployed person reflects a sharp decline for a highly educated person who served as a Navy officer and performed radiation inspections on nuclear-powered vessels.
Outome: Residential placement
We realize Mr. L needs cognitive rehabilitation—including assistance with planning and problem solving—and arrange for his placement in a residential facility for this specialized rehabilitation. Mr. L receives supportive psychotherapy and cognitive remediation from a psychologist. He also is involved in incentive work therapy with a vocational rehabilitation specialist.
Related resource
- Silver, JM, McAllister TW, Yudofsky SC, eds. Textbook of traumatic brain injury. Washington, DC: American Psychiatric Publishing; 2005.
- Divalproex • Depakote
- Quetiapine • Seroquel
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
CASE: An unlikable patient
Mr. L, age 56, is admitted to the psychiatric unit at our Veterans Affairs Medical Center for active suicidal ideation; he has a history of self-injurious behaviors that include mutilation and overdose. He also has a history of alcohol dependence and multiple inpatient psychiatric admissions. He has never married and conflicts with his siblings—in whose home he has been staying—have led to frequent homelessness.
His affect is silly and shallow. He also shows signs of haughtiness, disinhibition, grandiosity, and confabulation. For example, he says that while in the Navy he had 82 sexual exploits and developed a drug that cured herpes.
We start Mr. L on divalproex, 1,500 mg/d, and quetiapine, titrated to 200 mg/d. After 3 days he is discharged, but this begins a cycle of repeated suicide gestures and readmissions—9 within the next 3 months. Each time he is discharged, Mr. L fails to follow through on treatment recommendations and is indifferent to our staff’s annoyed reactions.
The author’s observations
Some of our staff members regard Mr. L’s suicidal gestures as manipulative and feel angry and demoralized by his poor adherence to outpatient treatment plans. Their negative countertransference might have impacted how they evaluated Mr. L through repeated admissions and discharges. During Mr. L’s ninth admission, we decide to reevaluate his longitudinal history for clues to his noncompliant behavior.
History: Undocumented injury
Mr. L says he began drinking alcohol at age 16. He reports that he has grown marijuana but has not smoked it since 1991. He denies using heroin or other drugs.
Mr. L states that he suffered a head injury in 1975 after falling off a ladder on a Navy ship. He describes losing consciousness for a brief but uncertain duration. He reports that he has developed a seizure disorder since this fall and a history of amnesia secondary to past seizures. His medical records contain no witnessed seizures. Mr. L also says he was hospitalized a few years ago and placed on a ventilator for 7 days for an undetermined reason.
The authors’ observations
Based on Mr. L’s report of a possible traumatic brain injury (TBI), we order a neurologic evaluation. A year earlier, MRI of the brain without contrast demonstrated minimal, nonspecific periventricular and subcortical, punctuate hyperintensities on flair and T2 weighted sequences that are nonspecific. Overall, the impression was “diffuse involutional changes and mild nonspecific periventricular and subcortical white matter hyperintensities,” which might reflect covert vascular brain injury.
Our frustration over Mr. L’s repeated readmissions for suicidal gestures led us to seek outside evaluation and consultation from a senior psychiatrist for assistance with discharge and treatment planning. Unlike our staff, the consulting psychiatrist did not harbor strong negative feelings toward the patient.
Mr. L’s history of deterioration in psychosocial functioning prompted this psychiatrist to perform a thorough mental status examination that focused on cognitive elements and request formal neuropsychological testing.
Evalutation: Cognitive Deficits
During mental status examination, Mr. L has difficulty recalling 3 items and uses a memory strategy to assist himself. He fails to recollect in reverse order the last 5 U.S. presidents. He spells “world” backward, but has difficulty repeating 6 digits forward and 4 backward. He is unable to do serial 7 subtractions from 93 to 65 correctly. He adequately copies interlocking pentagons and draws a clock with the correct time. He achieves a score of 28/30 on the Folstein Mini Mental State Exam, missing the date by 4 days and recalling 2 of 3 words.
These results suggest Mr. L has difficulty with attention and working memory, short-term memory, fund of general information and long-term memory, and ability to perform simple calculations. Most important, they indicate the need for further study, especially a neuropsychological test battery.
Mr. L’s abnormal neuropsychological test results are summarized in the Table. He manifests concretization of thought. His loss of conceptual fluidity is documented formally by measures of perseverative errors and categories completed on the Wisconsin Card Sorting Test (WCST). These findings support a diagnosis of acquired dementia.
Table
Abnormal findings on Mr. L’s neuropsychological testing
| Cognitive domain | Test | Score | Interpretation |
|---|---|---|---|
| Mental status and effort | |||
| Mental status | MMSE total score | 28/30 | 2 of 3 items recalled after delay |
| Orientation | MMSE orientation questions | 9/10 | Date off by 4 days |
| Premorbid IQ estimate | WRAT-4 Reading Standard | 66th percentile | Within normal limits. Inconsistent with educational attainment, but could be impacted by temporal lobe findings |
| Verbal memory | |||
| Immediate memory | RBANS Immediate Memory Index (List and Story Learning) | 1st percentile | Severe impairment |
| Delayed memory | RBANS Delayed Memory Index | 1st percentile | Severe impairment |
| Recognition memory | List Learning | Severe impairment | |
| Visuospatial memory | |||
| Delayed memory | RBANS Figure Recall | 3rd percentile | Severe impairment |
| Executive functioning | |||
| Cognitive flexibility | Trails B | 10th percentile | Severe impairment based on educational attainment |
| WCST | Low scores: Nonperseverative errors, perseverative errors, and categories completed | ||
| * Tests of mental status effort, visuomotor processing speed, confrontation naming, visuospatial function, attention, and executive functioning fluency/initiation were within normal limits | |||
| MMSE: Mini Mental State Exam; WRAT: Wide Range Achievement Test; RBANS: Repeatable Battery for the Assessment of Neuropsychological Status; WCST: Wisconsin Card Sorting Test | |||
The authors’ observations
Mr. L’s history, cognitive testing, head imaging, and behavioral observations suggest that several pathogenic factors contribute to his impaired functioning. First, he describes a TBI of unknown severity occurring in 1975. Although brain scans did not show evidence of midline shift or encephalomalacia, a direct blow to the head after falling from a height combined with possible post-injury seizures suggests a TBI of at least moderate severity.
Second, Mr. L describes an incident in which he required inpatient respiratory assistance. Although the precipitating medical event was unclear, anoxia or hypoxia is likely. A recent CT revealed low attenuation in the left temporal region that could represent an infarct.
Mr. L’s severe memory impairment and moderate to severe impairment in cognitive flexibility are commonly reported after a TBI of moderate severity. If an ischemic incident were the primary contributor, a lateralized pattern of cognitive dysfunction—which Mr. L does not exhibit—would be expected.
Although Mr. L likely has vascular dementia, his MRI findings do not indicate sufficient disease to account for his memory scores. Vascular dementia is associated with slow, stepwise cognitive deterioration, which is not consistent with severely impaired memory in a 56-year-old patient.
Finally, alcoholism is associated with cognitive difficulty in memory, visuospatial functioning, and abstract reasoning. Mr. L demonstrated significant difficulty in memory and abstract reasoning, but his visuospatial functioning was largely intact. In the absence of Wernicke’s encephalopathy, chronic alcoholics generally do not show memory decrements in line with Mr. L’s. His MRI results indicated only minimal ventricular and sulcal enlargement. Because atrophy is present in approximately 60% of chronic alcoholics, this finding provides evidence of a contribution, but the other contributory factors are associated with more definitive medical outcomes. Thus, alcoholism must be viewed as a secondary contributor to Mr. L’s impaired functioning.
Taking into account all known contributors, TBI emerges as the primary diagnosis.
Consider neurologic injury
Recognizing and characterizing personality changes related to neurologic injury and disease is often problematic and unreliable, even when psychometrically validated instruments and structured diagnostic interviews are used (Box 1).1-5 Mr. L’s presentation differed from the more commonly reported “impulsive aggression” associated with closed head injury. Sequelae from TBI were contributing to his clinical presentation but was obscured by his shallow and silly affect, inability to accurately assess social cues, and lack of empathy.
Mr. L reported suffering a head injury from falling off a ladder. Personality changes that result from traumatic brain injury (TBI) of the sudden deceleration type—even when mild—are frequently referable to the frontal lobe, especially focal orbital and/or ventromedial damage of the prefrontal cortex.1-5 This is because of the physical proximity of the sphenoid wing to the orbitofrontal region and effects of shearing.
As a result of this damage, patients lack insight into their accompanying cognitive and behavioral abnormalities, such as the egocentricity and impaired empathy shown by Mr. L. These changes might not be detected in clinical interviews and over brief periods.2 Appreciating an acquired personality disturbance may require evaluating the patient’s behavior over months or years.2
In retrospect, Mr. L’s seeking repeated inpatient psychiatric hospitalizations is consistent with poor planning and problem-solving skills. He has a limited repertoire of adaptive behaviors and has learned that suicidal gestures lead to admission and caretaking. These are important to him because he is frequently homeless. His lack of insight is seen in his unrealistic plans for employment in jobs requiring specialized technical skills.
Mr. L’s case emphasizes the importance of considering brain injury as an etiologic factor in personality changes. It also highlights the complex—and seemingly nonoverlapping—functions and dysfunctions of the frontal lobe, including:
- source memory
- working memory
- sustained attention
- conceptual fluidity
- imaginative thinking
- impulse regulation
- planning and problem-solving skills.
Documenting Mr. L’s cognitive deficits and acquired dementia diagnosis changed our staff’s perception of his behavior, enabling us to overcome negative countertransference (Box 2). We no longer regarded him as deliberately manipulative and refer him for appropriate treatment.
Countertransference can interfere with optimal workup and treatment of patients with character changes related to traumatic brain injury and neurodegenerative processes. When we interpreted Mr. L’s suicidal gestures and hospitalizations as manipulative and deliberate, we failed to appreciate the limited number of things he could do to obtain a safe and protective environment. We also failed to recognize that his poor planning and problem-solving skills—as well as lack of insight into his illness—prevented him from adhering to outpatient treatment.
Originally, we attributed Mr. L’s egocentricity, lack of empathy, and lack of adherence to axis II pathology.
Our staff’s hostile feelings toward Mr. L led us to insufficiently consider his history—which is consistent with cognitive decline—during biopsychosocial evaluation and treatment planning. Mr. L’s status as a frequently homeless, unemployed person reflects a sharp decline for a highly educated person who served as a Navy officer and performed radiation inspections on nuclear-powered vessels.
Outome: Residential placement
We realize Mr. L needs cognitive rehabilitation—including assistance with planning and problem solving—and arrange for his placement in a residential facility for this specialized rehabilitation. Mr. L receives supportive psychotherapy and cognitive remediation from a psychologist. He also is involved in incentive work therapy with a vocational rehabilitation specialist.
Related resource
- Silver, JM, McAllister TW, Yudofsky SC, eds. Textbook of traumatic brain injury. Washington, DC: American Psychiatric Publishing; 2005.
- Divalproex • Depakote
- Quetiapine • Seroquel
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Tranel D. Functional neuroanatomy: neuropsychological correlates of cortical and subcortical damage. In: Yudofsky SC, Hales RE, eds. The American Psychiatric Publishing textbook of neuropsychiatry and clinical neurosciences. 4th ed. Washington, DC: American Psychiatric Publishing; 2002:71-113.
2. Barrash J, Tranel D, Anderson SW. Acquired personality disturbances associated with bilateral damage to the ventromedial prefrontal region. Dev Neuropsychol 2000;18(3):355-81.
3. Silver JM, Hales RE, Yudofsky SC. Neuropsychiatric aspects of traumatic brain injury. In: Yudofsky SC, Hales RE, eds. The American Psychiatric Publishing textbook of neuropsychiatry and clinical neurosciences. 4th ed. Washington, DC: American Psychiatric Publishing; 2002:625-72.
4. Damasio AR, Tranel D, Damasio HC. Somatic markers and the guidance of behavior: theory and preliminary testing. In: Levin HS, Eisenberg HM, Benton AL, eds. Frontal lobe function and dysfunction. Oxford, UK: Oxford University Press; 1991:217-29.
5. Prigatano GP. The relationship of frontal lobe damage to diminished awareness: studies in rehabilitation. In: Levin HS, Eisenberg HM, Benton AL, eds. Frontal lobe function and dysfunction. Oxford, UK: Oxford University Press; 1991:381-97.
1. Tranel D. Functional neuroanatomy: neuropsychological correlates of cortical and subcortical damage. In: Yudofsky SC, Hales RE, eds. The American Psychiatric Publishing textbook of neuropsychiatry and clinical neurosciences. 4th ed. Washington, DC: American Psychiatric Publishing; 2002:71-113.
2. Barrash J, Tranel D, Anderson SW. Acquired personality disturbances associated with bilateral damage to the ventromedial prefrontal region. Dev Neuropsychol 2000;18(3):355-81.
3. Silver JM, Hales RE, Yudofsky SC. Neuropsychiatric aspects of traumatic brain injury. In: Yudofsky SC, Hales RE, eds. The American Psychiatric Publishing textbook of neuropsychiatry and clinical neurosciences. 4th ed. Washington, DC: American Psychiatric Publishing; 2002:625-72.
4. Damasio AR, Tranel D, Damasio HC. Somatic markers and the guidance of behavior: theory and preliminary testing. In: Levin HS, Eisenberg HM, Benton AL, eds. Frontal lobe function and dysfunction. Oxford, UK: Oxford University Press; 1991:217-29.
5. Prigatano GP. The relationship of frontal lobe damage to diminished awareness: studies in rehabilitation. In: Levin HS, Eisenberg HM, Benton AL, eds. Frontal lobe function and dysfunction. Oxford, UK: Oxford University Press; 1991:381-97.
The puzzling self-poisoner
CASE: Unusual suicide attempt
After a friend calls 911, Ms. M, age 20, is brought to an emergency room (ER) complaining of severe leg and abdominal pain. The ER physician finds she is bleeding from her vagina and nose and has severe ecchymosis anemia. After Ms. M is admitted, clinicians discover these conditions are secondary to a suicide attempt—she ingested 15 to 16 pellets of rat poison daily for approximately 2 months.
While hospitalized, Ms. M is treated with several transfusions of fresh frozen plasma, packed red blood cells, and phytonadione (vitamin K). A consultation-liaison psychiatrist diagnoses bipolar disorder and starts Ms. M on lamotrigine, 25 mg once daily. (The justification for this diagnosis was not documented.) After physicians judge her to be medically stable, Ms. M is involuntarily committed to a short-term psychiatric care facility. Her vital signs and coagulation values are stable.
At the psychiatric facility, our team determines that her symptoms and history are consistent with major depressive disorder, recurrent. For 5 months, Ms. M had depressed mood for most of the day, diminished interest in activities, and feelings of worthlessness. She also experienced weight loss—10 lbs in 2 months—with decreased appetite and low energy for most of the day. She denies past symptoms of mania or psychosis. She says she does not know why she was diagnosed with bipolar disorder. She admits to multiple previous suicide attempts via hanging and ingesting cleaning fluid or rat poison.
We place Ms. M on suicide precautions and prescribe escitalopram, 10 mg/d, in addition to lamotrigine, 50 mg once daily. We continue lamotrigine despite a lack of documentation for Ms. M’s bipolar diagnosis because evidence suggests the drug may be an effective augmentation to antidepressants in patients with treatment-resistant depression.1
The author’s observations
Any patient transferred from a medical floor to a psychiatric inpatient unit should have documentation that clarifies any need for further medical treatment. Ms. M’s physicians told us that she was medically stable and should require little if any further treatment for her ingestion of rat poison.
TREATMENT: Coagulation concerns
We request a medical consult to monitor possible complications from the rat poison. The physician advises that rat poison essentially is the same as the anticoagulant warfarin and its effects should steadily decrease over time because its half-life is 20 to 60 hours. However, for safety reasons, we closely follow Ms. M’s coagulation values and order daily vitamin K injections, 5 mg SC.
Further medical investigation shows no evidence of complications, but Ms. M continues to request medication for pain in her left leg. The physician prescribes acetaminophen, 650 mg every 6 hours as needed for pain, which the patient takes at almost every opportunity, often 4 times a day. The physician does not choose a nonsteroidal anti-inflammatory drug (NSAID) for pain to avoid the possibility of gastrointestinal (GI) irritation that could lead to bleeding.
In the psychiatric facility, the patient’s international normalized ratio (INR) is found to be rising, indicating a lack of clotting and a risk of uncontrolled bleeding. The physician states that given the half-life of warfarin, Ms. M’s INR should be decreasing. Liver function testing does not show that liver dysfunction is contributing to the increasing INR.
Because we assume the vitamin K the patient received has been absorbed, we hypothesize that Ms. M has continued to surreptitiously ingest rat poison or another anticoagulant, which she denies. We search Ms. M and her room. She is placed on 1-to-1 observation 24 hours a day. Ms. M’s visitors also are searched, and visits are observed. We find no evidence of an anticoagulant agent.
Ms. M’s INR continues to rise. We search the facility to rule out the possibility that the patient had hidden a supply of anticoagulant outside her room. The search finds nothing. At this point we consider performing an abdominal x-ray to rule out the possibility that Ms. M may have a supply of medication hidden in her gastrointestinal tract.
The author’s observations
Patients hiding and using contraband is a common problem in involuntary inpatient units. It seemed that Ms. M was secretly ingesting rat poison. Her history showed she was determined to end her life, and she ingested rat poison daily for months. However, because an exhaustive search for contraband and 1-to-1 observation yielded no positive results, the evidence did not support this theory. Some team members thought we were not searching hard enough. I decided we needed to pursue other theories.
I was skeptical that escitalopram could be contributing to Ms. M’s rising anticoagulation values. Selective serotonin reuptake inhibitors have antiplatelet effects, but platelet function does not affect INR to the degree we were observing.
‘Superwarfarins’
Physicians had advised us that Ms. M’s INR should decrease under the assumption that rat poison is for all practical purposes the same as warfarin, but we had not investigated distinctions between the 2 compounds. A literature search revealed that several rat poisons are not simply warfarin repackaged as a pesticide. Most are “superwarfarins”—chemicals similar to warfarin but more potent and with a much longer half-life.2 Case report data suggest the plasma half-life of these chemicals is 20 to 62 days.3
Most commercial rat poisons are made of brodifacoum, which has a chemical structure similar to warfarin but with an additional long polycyclic hydrocarbon side chain (Figure 1). The potency of brodifacoum compared with warfarin is approximately 100 to 1.4-6 The chemical is highly lipophilic and can stay in the body for an extended period.4-6 Lab tests can measure serum brodifacoum levels.3
After Ms. M identifies the brand name of the rat poison she ingested, we contact the American Association of Poison Control Centers and verify the agent she used was brodifacoum. This explains why her INR was not decreasing—but does not explain the increase.
A drug interaction? Because Ms. M’s liver function is within normal limits, the next theory to investigate is if brodifacoum is interacting with any medications she is taking. I could not find any medical journal articles, programs, or Web sites describing brodifacoum’s interactions with medications. After all, brodifacoum is a pesticide, not a medication.
I considered that because brodifacoum and warfarin have a similar structure and function, they may interact with medications in a similar manner. After another literature search, only acetaminophen had evidence of interaction with warfarin that could explain her rising INR.
Documentation of interactions between warfarin and acetaminophen are sparse. In one case, a 74-year-old man receiving warfarin for atrial fibrillation experienced an abrupt increase in INR after taking acetaminophen.7 In a double-blind, placebo controlled, randomized trial of patients taking warfarin, INR rose rapidly after the start of acetaminophen and was significantly increased within 1 week compared with patients receiving placebo.8
Figure 1 Chemical structures of warfarin and rat poison
Most commercial rat poisons are made of brodifacoum, which is chemically similar to warfarin but has an additional long polycyclic hydrocarbon side chain.
FOLLOW-UP: Analgesic substitution
We suggest to the physician that Ms. M’s INR may be increasing because of an interaction between brodifacoum and acetaminophen, which she took several times a day. On day 8 of Ms. M’s hospitalization, the physician discontinues acetaminophen and prescribes ibuprofen, 400 mg tid as needed for pain, and pantoprazole, 40 mg/d, to prevent GI bleeding from possible irritation caused by ibuprofen. The team continues to monitor Ms. M’s coagulation values.
Within a day of discontinuing acetaminophen, Ms. M’s INR decreased as expected (Figure 2). The rest of her medication regimen is continued, and her INR levels continued to decrease.
One-to-one observation is discontinued. However, because of the patient’s continued determination to end her life and no significant improvement in her depression, Ms. M is considered a danger to herself and involuntary inpatient hospitalization is continued.
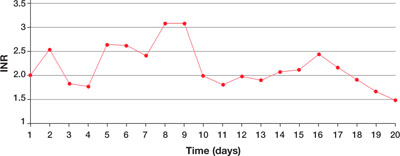
Figure 2 Ms. M’s INR values during hospitalization
The patient’s INR values began to rise mysteriously after she was transferred to the inpatient psychiatric unit. Acetaminophen was discontinued on day 8, and within a day her INR values began to drop.
INR: International normalized ratio
The author’s observations
Poisoning is a common method of attempting suicide, patients may use substances that clinicians rarely encounter. For most toxic, nonmedication substances, data on interactions with medications are sparse. if you suspect your patient has ingested a toxic substance with which the treatment team has little experience, contact the American Association of Poison Control Centers at 800-222-1222.
Suspect superwarfarin poisoning in suicidal patients with coagulopathy, prolonged prothrombin time, and elevated INR that does not respond to large amounts of vitamin K.9,10 These patients are at high risk of successfully completing suicide because of superwarfarins’ long half-life and daily maintenance required to keep coagulation levels within a safe range for at least several weeks.
The most serious complication these patients face is intracranial hemorrhage, which occurs in 2% of patients with excessive warfarin-based coagulation and is associated with a 77% mortality rate.11 GI bleeding occurs in 67% of these patients.2
Also take into account medical conditions—such as hypertension or hepatic disease—and medication side effects that can increase bleeding risk. When treating pain in these patients, consider avoiding acetaminophen but be aware of the risks of NSAIDs, such as gastritis or GI bleeding.
Related resource
- The American Association of Poison Control Centers. 800-222-1222; www.aapcc.org.
Drug brand names
- Escitalopram • Lexapro
- Lamotrigine • Lamictal
- Pantoprazole • Protonix
- Warfarin • Coumadin
Disclosure
The author reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Sharma V, Khan M, Corpse C. Role of lamotrigine in the management of treatment-resistant bipolar II depression: a chart review. J Affect Disord Epub 2008 Mar 1.
2. Su M, Hoffman R. Anticoagulants. In: Flomenbaum NE, Goldfrank LR, Hoffman RS, et al, eds. Goldfrank’s toxicologic emergencies. 8th ed. New York, NY: McGraw-Hill Medical Publishing; 2006:891-4.
3. Chua JD, Friedenberg WR. Superwarfarin poisoning. Anaesth Intensive Care 1997;25:707-9.
4. Leck JB, Park BK. A comparative study of the effect of warfarin and brodifacoum on the relationship between vitamin K1 metabolism and clotting factor activity in warfarin susceptible and warfarin resistant rats. Biochem Pharmacol 1981;30:123-9.
5. Lund M. Comparative effect of the three rodenticides warfarin, difenacoum and brodifacoum on eight rodent species in short feeding periods. J Hyg 1981;87:101-7.
6. Park BK, Scott AK, Wilson AC, et al. Plasma disposition of vitamin K antagonism by warfarin, difenacoum and brodifacoum in the rabbit. Biochem Pharmacol 1982;31:3535-639.
7. Gebauer MG, Nyfort-Hansen K, Henschke PJ, Gallus AS. Warfarin and acetaminophen interaction. Pharmacotherapy 2003;23(1):109-12.
8. Mahe I, Bertrand N, Drouet L, et al. Interaction between paracetamol and warfarin in patients: a double-blind, placebo-controlled, randomized study. Haematologica 2006;91(12):1621-7.
9. Sharma P, Bentley P. Of rats and men: superwarfarin toxicity. Lancet 2005;365:552-3.
10. Scully M. Warfarin therapy: rat poison and the prevention of thrombosis. Biochemist 2002;24:15-7.
11. Mathiesen T, Benediktsdottir K, Johnsson H, Lindqvist M. Intracranial traumatic and nontraumatic haemorrhagic complications of warfarin treatment. Acta Neurol Scan 1995;91:208-14.
CASE: Unusual suicide attempt
After a friend calls 911, Ms. M, age 20, is brought to an emergency room (ER) complaining of severe leg and abdominal pain. The ER physician finds she is bleeding from her vagina and nose and has severe ecchymosis anemia. After Ms. M is admitted, clinicians discover these conditions are secondary to a suicide attempt—she ingested 15 to 16 pellets of rat poison daily for approximately 2 months.
While hospitalized, Ms. M is treated with several transfusions of fresh frozen plasma, packed red blood cells, and phytonadione (vitamin K). A consultation-liaison psychiatrist diagnoses bipolar disorder and starts Ms. M on lamotrigine, 25 mg once daily. (The justification for this diagnosis was not documented.) After physicians judge her to be medically stable, Ms. M is involuntarily committed to a short-term psychiatric care facility. Her vital signs and coagulation values are stable.
At the psychiatric facility, our team determines that her symptoms and history are consistent with major depressive disorder, recurrent. For 5 months, Ms. M had depressed mood for most of the day, diminished interest in activities, and feelings of worthlessness. She also experienced weight loss—10 lbs in 2 months—with decreased appetite and low energy for most of the day. She denies past symptoms of mania or psychosis. She says she does not know why she was diagnosed with bipolar disorder. She admits to multiple previous suicide attempts via hanging and ingesting cleaning fluid or rat poison.
We place Ms. M on suicide precautions and prescribe escitalopram, 10 mg/d, in addition to lamotrigine, 50 mg once daily. We continue lamotrigine despite a lack of documentation for Ms. M’s bipolar diagnosis because evidence suggests the drug may be an effective augmentation to antidepressants in patients with treatment-resistant depression.1
The author’s observations
Any patient transferred from a medical floor to a psychiatric inpatient unit should have documentation that clarifies any need for further medical treatment. Ms. M’s physicians told us that she was medically stable and should require little if any further treatment for her ingestion of rat poison.
TREATMENT: Coagulation concerns
We request a medical consult to monitor possible complications from the rat poison. The physician advises that rat poison essentially is the same as the anticoagulant warfarin and its effects should steadily decrease over time because its half-life is 20 to 60 hours. However, for safety reasons, we closely follow Ms. M’s coagulation values and order daily vitamin K injections, 5 mg SC.
Further medical investigation shows no evidence of complications, but Ms. M continues to request medication for pain in her left leg. The physician prescribes acetaminophen, 650 mg every 6 hours as needed for pain, which the patient takes at almost every opportunity, often 4 times a day. The physician does not choose a nonsteroidal anti-inflammatory drug (NSAID) for pain to avoid the possibility of gastrointestinal (GI) irritation that could lead to bleeding.
In the psychiatric facility, the patient’s international normalized ratio (INR) is found to be rising, indicating a lack of clotting and a risk of uncontrolled bleeding. The physician states that given the half-life of warfarin, Ms. M’s INR should be decreasing. Liver function testing does not show that liver dysfunction is contributing to the increasing INR.
Because we assume the vitamin K the patient received has been absorbed, we hypothesize that Ms. M has continued to surreptitiously ingest rat poison or another anticoagulant, which she denies. We search Ms. M and her room. She is placed on 1-to-1 observation 24 hours a day. Ms. M’s visitors also are searched, and visits are observed. We find no evidence of an anticoagulant agent.
Ms. M’s INR continues to rise. We search the facility to rule out the possibility that the patient had hidden a supply of anticoagulant outside her room. The search finds nothing. At this point we consider performing an abdominal x-ray to rule out the possibility that Ms. M may have a supply of medication hidden in her gastrointestinal tract.
The author’s observations
Patients hiding and using contraband is a common problem in involuntary inpatient units. It seemed that Ms. M was secretly ingesting rat poison. Her history showed she was determined to end her life, and she ingested rat poison daily for months. However, because an exhaustive search for contraband and 1-to-1 observation yielded no positive results, the evidence did not support this theory. Some team members thought we were not searching hard enough. I decided we needed to pursue other theories.
I was skeptical that escitalopram could be contributing to Ms. M’s rising anticoagulation values. Selective serotonin reuptake inhibitors have antiplatelet effects, but platelet function does not affect INR to the degree we were observing.
‘Superwarfarins’
Physicians had advised us that Ms. M’s INR should decrease under the assumption that rat poison is for all practical purposes the same as warfarin, but we had not investigated distinctions between the 2 compounds. A literature search revealed that several rat poisons are not simply warfarin repackaged as a pesticide. Most are “superwarfarins”—chemicals similar to warfarin but more potent and with a much longer half-life.2 Case report data suggest the plasma half-life of these chemicals is 20 to 62 days.3
Most commercial rat poisons are made of brodifacoum, which has a chemical structure similar to warfarin but with an additional long polycyclic hydrocarbon side chain (Figure 1). The potency of brodifacoum compared with warfarin is approximately 100 to 1.4-6 The chemical is highly lipophilic and can stay in the body for an extended period.4-6 Lab tests can measure serum brodifacoum levels.3
After Ms. M identifies the brand name of the rat poison she ingested, we contact the American Association of Poison Control Centers and verify the agent she used was brodifacoum. This explains why her INR was not decreasing—but does not explain the increase.
A drug interaction? Because Ms. M’s liver function is within normal limits, the next theory to investigate is if brodifacoum is interacting with any medications she is taking. I could not find any medical journal articles, programs, or Web sites describing brodifacoum’s interactions with medications. After all, brodifacoum is a pesticide, not a medication.
I considered that because brodifacoum and warfarin have a similar structure and function, they may interact with medications in a similar manner. After another literature search, only acetaminophen had evidence of interaction with warfarin that could explain her rising INR.
Documentation of interactions between warfarin and acetaminophen are sparse. In one case, a 74-year-old man receiving warfarin for atrial fibrillation experienced an abrupt increase in INR after taking acetaminophen.7 In a double-blind, placebo controlled, randomized trial of patients taking warfarin, INR rose rapidly after the start of acetaminophen and was significantly increased within 1 week compared with patients receiving placebo.8
Figure 1 Chemical structures of warfarin and rat poison
Most commercial rat poisons are made of brodifacoum, which is chemically similar to warfarin but has an additional long polycyclic hydrocarbon side chain.
FOLLOW-UP: Analgesic substitution
We suggest to the physician that Ms. M’s INR may be increasing because of an interaction between brodifacoum and acetaminophen, which she took several times a day. On day 8 of Ms. M’s hospitalization, the physician discontinues acetaminophen and prescribes ibuprofen, 400 mg tid as needed for pain, and pantoprazole, 40 mg/d, to prevent GI bleeding from possible irritation caused by ibuprofen. The team continues to monitor Ms. M’s coagulation values.
Within a day of discontinuing acetaminophen, Ms. M’s INR decreased as expected (Figure 2). The rest of her medication regimen is continued, and her INR levels continued to decrease.
One-to-one observation is discontinued. However, because of the patient’s continued determination to end her life and no significant improvement in her depression, Ms. M is considered a danger to herself and involuntary inpatient hospitalization is continued.
Figure 2 Ms. M’s INR values during hospitalization
The patient’s INR values began to rise mysteriously after she was transferred to the inpatient psychiatric unit. Acetaminophen was discontinued on day 8, and within a day her INR values began to drop.
INR: International normalized ratio
The author’s observations
Poisoning is a common method of attempting suicide, patients may use substances that clinicians rarely encounter. For most toxic, nonmedication substances, data on interactions with medications are sparse. if you suspect your patient has ingested a toxic substance with which the treatment team has little experience, contact the American Association of Poison Control Centers at 800-222-1222.
Suspect superwarfarin poisoning in suicidal patients with coagulopathy, prolonged prothrombin time, and elevated INR that does not respond to large amounts of vitamin K.9,10 These patients are at high risk of successfully completing suicide because of superwarfarins’ long half-life and daily maintenance required to keep coagulation levels within a safe range for at least several weeks.
The most serious complication these patients face is intracranial hemorrhage, which occurs in 2% of patients with excessive warfarin-based coagulation and is associated with a 77% mortality rate.11 GI bleeding occurs in 67% of these patients.2
Also take into account medical conditions—such as hypertension or hepatic disease—and medication side effects that can increase bleeding risk. When treating pain in these patients, consider avoiding acetaminophen but be aware of the risks of NSAIDs, such as gastritis or GI bleeding.
Related resource
- The American Association of Poison Control Centers. 800-222-1222; www.aapcc.org.
Drug brand names
- Escitalopram • Lexapro
- Lamotrigine • Lamictal
- Pantoprazole • Protonix
- Warfarin • Coumadin
Disclosure
The author reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
CASE: Unusual suicide attempt
After a friend calls 911, Ms. M, age 20, is brought to an emergency room (ER) complaining of severe leg and abdominal pain. The ER physician finds she is bleeding from her vagina and nose and has severe ecchymosis anemia. After Ms. M is admitted, clinicians discover these conditions are secondary to a suicide attempt—she ingested 15 to 16 pellets of rat poison daily for approximately 2 months.
While hospitalized, Ms. M is treated with several transfusions of fresh frozen plasma, packed red blood cells, and phytonadione (vitamin K). A consultation-liaison psychiatrist diagnoses bipolar disorder and starts Ms. M on lamotrigine, 25 mg once daily. (The justification for this diagnosis was not documented.) After physicians judge her to be medically stable, Ms. M is involuntarily committed to a short-term psychiatric care facility. Her vital signs and coagulation values are stable.
At the psychiatric facility, our team determines that her symptoms and history are consistent with major depressive disorder, recurrent. For 5 months, Ms. M had depressed mood for most of the day, diminished interest in activities, and feelings of worthlessness. She also experienced weight loss—10 lbs in 2 months—with decreased appetite and low energy for most of the day. She denies past symptoms of mania or psychosis. She says she does not know why she was diagnosed with bipolar disorder. She admits to multiple previous suicide attempts via hanging and ingesting cleaning fluid or rat poison.
We place Ms. M on suicide precautions and prescribe escitalopram, 10 mg/d, in addition to lamotrigine, 50 mg once daily. We continue lamotrigine despite a lack of documentation for Ms. M’s bipolar diagnosis because evidence suggests the drug may be an effective augmentation to antidepressants in patients with treatment-resistant depression.1
The author’s observations
Any patient transferred from a medical floor to a psychiatric inpatient unit should have documentation that clarifies any need for further medical treatment. Ms. M’s physicians told us that she was medically stable and should require little if any further treatment for her ingestion of rat poison.
TREATMENT: Coagulation concerns
We request a medical consult to monitor possible complications from the rat poison. The physician advises that rat poison essentially is the same as the anticoagulant warfarin and its effects should steadily decrease over time because its half-life is 20 to 60 hours. However, for safety reasons, we closely follow Ms. M’s coagulation values and order daily vitamin K injections, 5 mg SC.
Further medical investigation shows no evidence of complications, but Ms. M continues to request medication for pain in her left leg. The physician prescribes acetaminophen, 650 mg every 6 hours as needed for pain, which the patient takes at almost every opportunity, often 4 times a day. The physician does not choose a nonsteroidal anti-inflammatory drug (NSAID) for pain to avoid the possibility of gastrointestinal (GI) irritation that could lead to bleeding.
In the psychiatric facility, the patient’s international normalized ratio (INR) is found to be rising, indicating a lack of clotting and a risk of uncontrolled bleeding. The physician states that given the half-life of warfarin, Ms. M’s INR should be decreasing. Liver function testing does not show that liver dysfunction is contributing to the increasing INR.
Because we assume the vitamin K the patient received has been absorbed, we hypothesize that Ms. M has continued to surreptitiously ingest rat poison or another anticoagulant, which she denies. We search Ms. M and her room. She is placed on 1-to-1 observation 24 hours a day. Ms. M’s visitors also are searched, and visits are observed. We find no evidence of an anticoagulant agent.
Ms. M’s INR continues to rise. We search the facility to rule out the possibility that the patient had hidden a supply of anticoagulant outside her room. The search finds nothing. At this point we consider performing an abdominal x-ray to rule out the possibility that Ms. M may have a supply of medication hidden in her gastrointestinal tract.
The author’s observations
Patients hiding and using contraband is a common problem in involuntary inpatient units. It seemed that Ms. M was secretly ingesting rat poison. Her history showed she was determined to end her life, and she ingested rat poison daily for months. However, because an exhaustive search for contraband and 1-to-1 observation yielded no positive results, the evidence did not support this theory. Some team members thought we were not searching hard enough. I decided we needed to pursue other theories.
I was skeptical that escitalopram could be contributing to Ms. M’s rising anticoagulation values. Selective serotonin reuptake inhibitors have antiplatelet effects, but platelet function does not affect INR to the degree we were observing.
‘Superwarfarins’
Physicians had advised us that Ms. M’s INR should decrease under the assumption that rat poison is for all practical purposes the same as warfarin, but we had not investigated distinctions between the 2 compounds. A literature search revealed that several rat poisons are not simply warfarin repackaged as a pesticide. Most are “superwarfarins”—chemicals similar to warfarin but more potent and with a much longer half-life.2 Case report data suggest the plasma half-life of these chemicals is 20 to 62 days.3
Most commercial rat poisons are made of brodifacoum, which has a chemical structure similar to warfarin but with an additional long polycyclic hydrocarbon side chain (Figure 1). The potency of brodifacoum compared with warfarin is approximately 100 to 1.4-6 The chemical is highly lipophilic and can stay in the body for an extended period.4-6 Lab tests can measure serum brodifacoum levels.3
After Ms. M identifies the brand name of the rat poison she ingested, we contact the American Association of Poison Control Centers and verify the agent she used was brodifacoum. This explains why her INR was not decreasing—but does not explain the increase.
A drug interaction? Because Ms. M’s liver function is within normal limits, the next theory to investigate is if brodifacoum is interacting with any medications she is taking. I could not find any medical journal articles, programs, or Web sites describing brodifacoum’s interactions with medications. After all, brodifacoum is a pesticide, not a medication.
I considered that because brodifacoum and warfarin have a similar structure and function, they may interact with medications in a similar manner. After another literature search, only acetaminophen had evidence of interaction with warfarin that could explain her rising INR.
Documentation of interactions between warfarin and acetaminophen are sparse. In one case, a 74-year-old man receiving warfarin for atrial fibrillation experienced an abrupt increase in INR after taking acetaminophen.7 In a double-blind, placebo controlled, randomized trial of patients taking warfarin, INR rose rapidly after the start of acetaminophen and was significantly increased within 1 week compared with patients receiving placebo.8
Figure 1 Chemical structures of warfarin and rat poison
Most commercial rat poisons are made of brodifacoum, which is chemically similar to warfarin but has an additional long polycyclic hydrocarbon side chain.
FOLLOW-UP: Analgesic substitution
We suggest to the physician that Ms. M’s INR may be increasing because of an interaction between brodifacoum and acetaminophen, which she took several times a day. On day 8 of Ms. M’s hospitalization, the physician discontinues acetaminophen and prescribes ibuprofen, 400 mg tid as needed for pain, and pantoprazole, 40 mg/d, to prevent GI bleeding from possible irritation caused by ibuprofen. The team continues to monitor Ms. M’s coagulation values.
Within a day of discontinuing acetaminophen, Ms. M’s INR decreased as expected (Figure 2). The rest of her medication regimen is continued, and her INR levels continued to decrease.
One-to-one observation is discontinued. However, because of the patient’s continued determination to end her life and no significant improvement in her depression, Ms. M is considered a danger to herself and involuntary inpatient hospitalization is continued.
Figure 2 Ms. M’s INR values during hospitalization
The patient’s INR values began to rise mysteriously after she was transferred to the inpatient psychiatric unit. Acetaminophen was discontinued on day 8, and within a day her INR values began to drop.
INR: International normalized ratio
The author’s observations
Poisoning is a common method of attempting suicide, patients may use substances that clinicians rarely encounter. For most toxic, nonmedication substances, data on interactions with medications are sparse. if you suspect your patient has ingested a toxic substance with which the treatment team has little experience, contact the American Association of Poison Control Centers at 800-222-1222.
Suspect superwarfarin poisoning in suicidal patients with coagulopathy, prolonged prothrombin time, and elevated INR that does not respond to large amounts of vitamin K.9,10 These patients are at high risk of successfully completing suicide because of superwarfarins’ long half-life and daily maintenance required to keep coagulation levels within a safe range for at least several weeks.
The most serious complication these patients face is intracranial hemorrhage, which occurs in 2% of patients with excessive warfarin-based coagulation and is associated with a 77% mortality rate.11 GI bleeding occurs in 67% of these patients.2
Also take into account medical conditions—such as hypertension or hepatic disease—and medication side effects that can increase bleeding risk. When treating pain in these patients, consider avoiding acetaminophen but be aware of the risks of NSAIDs, such as gastritis or GI bleeding.
Related resource
- The American Association of Poison Control Centers. 800-222-1222; www.aapcc.org.
Drug brand names
- Escitalopram • Lexapro
- Lamotrigine • Lamictal
- Pantoprazole • Protonix
- Warfarin • Coumadin
Disclosure
The author reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Sharma V, Khan M, Corpse C. Role of lamotrigine in the management of treatment-resistant bipolar II depression: a chart review. J Affect Disord Epub 2008 Mar 1.
2. Su M, Hoffman R. Anticoagulants. In: Flomenbaum NE, Goldfrank LR, Hoffman RS, et al, eds. Goldfrank’s toxicologic emergencies. 8th ed. New York, NY: McGraw-Hill Medical Publishing; 2006:891-4.
3. Chua JD, Friedenberg WR. Superwarfarin poisoning. Anaesth Intensive Care 1997;25:707-9.
4. Leck JB, Park BK. A comparative study of the effect of warfarin and brodifacoum on the relationship between vitamin K1 metabolism and clotting factor activity in warfarin susceptible and warfarin resistant rats. Biochem Pharmacol 1981;30:123-9.
5. Lund M. Comparative effect of the three rodenticides warfarin, difenacoum and brodifacoum on eight rodent species in short feeding periods. J Hyg 1981;87:101-7.
6. Park BK, Scott AK, Wilson AC, et al. Plasma disposition of vitamin K antagonism by warfarin, difenacoum and brodifacoum in the rabbit. Biochem Pharmacol 1982;31:3535-639.
7. Gebauer MG, Nyfort-Hansen K, Henschke PJ, Gallus AS. Warfarin and acetaminophen interaction. Pharmacotherapy 2003;23(1):109-12.
8. Mahe I, Bertrand N, Drouet L, et al. Interaction between paracetamol and warfarin in patients: a double-blind, placebo-controlled, randomized study. Haematologica 2006;91(12):1621-7.
9. Sharma P, Bentley P. Of rats and men: superwarfarin toxicity. Lancet 2005;365:552-3.
10. Scully M. Warfarin therapy: rat poison and the prevention of thrombosis. Biochemist 2002;24:15-7.
11. Mathiesen T, Benediktsdottir K, Johnsson H, Lindqvist M. Intracranial traumatic and nontraumatic haemorrhagic complications of warfarin treatment. Acta Neurol Scan 1995;91:208-14.
1. Sharma V, Khan M, Corpse C. Role of lamotrigine in the management of treatment-resistant bipolar II depression: a chart review. J Affect Disord Epub 2008 Mar 1.
2. Su M, Hoffman R. Anticoagulants. In: Flomenbaum NE, Goldfrank LR, Hoffman RS, et al, eds. Goldfrank’s toxicologic emergencies. 8th ed. New York, NY: McGraw-Hill Medical Publishing; 2006:891-4.
3. Chua JD, Friedenberg WR. Superwarfarin poisoning. Anaesth Intensive Care 1997;25:707-9.
4. Leck JB, Park BK. A comparative study of the effect of warfarin and brodifacoum on the relationship between vitamin K1 metabolism and clotting factor activity in warfarin susceptible and warfarin resistant rats. Biochem Pharmacol 1981;30:123-9.
5. Lund M. Comparative effect of the three rodenticides warfarin, difenacoum and brodifacoum on eight rodent species in short feeding periods. J Hyg 1981;87:101-7.
6. Park BK, Scott AK, Wilson AC, et al. Plasma disposition of vitamin K antagonism by warfarin, difenacoum and brodifacoum in the rabbit. Biochem Pharmacol 1982;31:3535-639.
7. Gebauer MG, Nyfort-Hansen K, Henschke PJ, Gallus AS. Warfarin and acetaminophen interaction. Pharmacotherapy 2003;23(1):109-12.
8. Mahe I, Bertrand N, Drouet L, et al. Interaction between paracetamol and warfarin in patients: a double-blind, placebo-controlled, randomized study. Haematologica 2006;91(12):1621-7.
9. Sharma P, Bentley P. Of rats and men: superwarfarin toxicity. Lancet 2005;365:552-3.
10. Scully M. Warfarin therapy: rat poison and the prevention of thrombosis. Biochemist 2002;24:15-7.
11. Mathiesen T, Benediktsdottir K, Johnsson H, Lindqvist M. Intracranial traumatic and nontraumatic haemorrhagic complications of warfarin treatment. Acta Neurol Scan 1995;91:208-14.
The wilting widow’s masquerading illness
CASE: Unexplained unresponsiveness
One month after being hospitalized with E coli sepsis—and just after completing a course of ciprofloxacin—Mrs. D, a 79-year-old widow, becomes withdrawn and has several days of worsening fatigue, weakness, and somnolence. Within 2 hours of being admitted to the hospital, she becomes flaccid and unresponsive, although she seems to be awake. She has decreased respirations and is intubated.
The neurology team finds her unresponsive to verbal and noxious stimuli, with some resistance to eye opening. Neurologic exam is nonfocal. Cranial nerve testing is intact, muscle strength and reflexes are normal and symmetrical, and sensory function is intact to light touch. MRI, ECG, chest radiography, and laboratory tests—including metabolic and infectious screenings—do not reveal acute pathology. Within hours, Mrs. D becomes much more responsive and is successfully extubated. Her rapid improvement rules out locked-in syndrome.
The next day, Mrs. D has another episode of reduced responsiveness that lasts several minutes and resolves quickly. The neurologist observes this episode—which occurred when Mrs. D’s daughter entered the room—and recommends a psychiatric consultation.
For the past 3 weeks Mrs. D has experienced depressed mood, low energy, poor sleep, memory complaints, and feeling as if her mind was “scattered.” She has stopped attending church, is isolating to her home, and has been hiding valuables because of an irrational fear that she would lose possessions from her estate. Her primary care physician noted markedly reduced speech during recent office visits and agrees with the family that Mrs. D seems depressed.
On psychiatric exam, Mrs. D’s speech is quiet and slow but coherent. Her mood is depressed with a flat affect. Her thought process is goal-directed, and her Mini-Mental State Examination (MMSE) score is 27/30, indicating her cognition is grossly intact.
Mrs. D develops a low-grade fever. Although the physician does not suspect an infection, he prescribes a prophylactic course of levofloxacin, 500 mg/d. After 2 days of monitoring and assessments, the psychiatrist attributes Mrs. D’s presentation to depression, prescribes bupropion, 100 mg/d, and zolpidem, 5 mg at bedtime, and refers her for psychiatric follow-up.
Six days after discharge, Mrs. D’s family brings her to the psychiatric emergency room. They report that since discharge she has remained fatigued and seems confused intermittently. Her depressive symptoms—decreased appetite, anhedonia, poor sleep, and agitation—persist, and her personal care has deteriorated.
The authors’ observations
The psychiatrist attributes Mrs. D’s declining functioning to a worsening mood disorder. Major depression with psychotic features can include:
- fearfulness
- suspiciousness
- delusions of poverty.
Mrs. D’s cognitive and behavioral status fluctuated during her initial medical hospitalization, and on 1 occasion she required intubation. Her confusion worsened after discharge. These aspects of her history, along with worsening psychosis, can indicate seizures.
Psychiatric manifestations of seizures have been recognized for centuries. Partial complex seizures—one of the most common seizure types—have been called “psychosensory” or “psychomotor” seizures because they often include psychiatric symptoms.1
Psychiatric symptoms most often occur with seizures involving the temporal lobe, and limbic system activation adds an affective dimension to perceptual data processed by the temporal neocortex.2 Frontal and parietal lobe seizure foci also are associated with behavior change.
Psychiatric manifestations of seizures can include:
- cognitive problems
- anxiety
- mood/affect, psychotic, and dissociative symptoms
- personality changes (Table 1).2-6
As many as 30% of patients with seizures experience prominent psychiatric symptoms.7 Approximately one-half have comorbid psychiatric syndromes.8
Table 1
Seizure-related psychiatric symptoms: What to look for
| Symptom type | Characteristic features with seizures |
|---|---|
| Cognitive: intellectual function, memory, orientation | Episodic, fluctuating course of changes Amnesia occurs with complex—but not simple—seizures |
| Anxiety | Occurs most often with temporal lobe seizures May appear as full-blown panic attack Agoraphobia is rare Associated seizure features may include disturbed consciousness, automatisms, and hallucinations |
| Mood and affect | Change in affect is often episodic and profound, without many other symptoms associated with major depression or mania |
| Psychotic | Usually manifests as a single symptom, often described as incongruous, fragmentary, or out of context2 Occurs most often with temporal lobe seizures3 Delusions (paranoid, grandiose), forced thinking Hallucinations: auditory, visual, olfactory, tactile, gustatory Negative symptoms (emotional withdrawal, blunted affect) may be more common in frontal lobe seizures4 |
| Dissociative: depersonalization, déjà vu, jamais vu | Symptoms tend to be less extreme than in patients with dissociative identity disorder or PTSD May occur more often in context of panic symptoms with temporal lobe seizures5 |
| Personality changes (in epilepsy) | May be due to underlying frontal or temporal lobe damage Includes anancastic personality, emotionally unstable personality, and Geschwind syndrome (hypergraphia, hyperreligiosity, hyposexuality, and viscous personality style—perseverative and difficult to disengage from conversation)6 |
| PTSD: posttraumatic stress disorder | |
EVALUATION: Continuing decline
The emergency room staff learns Mrs. D has a history of vague auditory hallucinations and has developed more overt paranoia, including thoughts that police may be out to harm her. She has difficulty responding to questions and can not offer details of her history; her speech is soft and her thought process appears slowed.
Mrs. D is admitted to the inpatient psychiatry service. Her family reports that she has episodes of disorientation, poor memory, staring, and paranoia about the police that last minutes to 1 hour.
On a subsequent examination 1 hour later, her speech difficulties are variable. She cannot speak fluently, has limited ability to repeat phrases, and cannot follow simple verbal commands. These symptoms persist only minutes. Mrs. D slowly becomes more conversant but appears tired. During the next few hours she is disoriented and tries to walk into the nursing station. Other repetitive activity includes putting on/taking offmultiple layers of clothing.
The authors’ observations
- A normal EEG does not guarantee the absence of recent seizures; a standard scalp EEG can miss epileptiform changes that may occur earlier in the ictal phase.9
- EEG abnormalities may occur in normal subjects.
- visual, olfactory, or tactile hallucinations
- mutism
- catatonia
- poor memory not due to inattention
- episodic aphasia, apraxia, or agnosia.
Mrs. D’s confusion level and speech abnormalities varied over time. Her speech arrest early in the admission appeared to be a Broca’s or expressive aphasia because she comprehended commands but was unable to speak. Later, her speech exhibited a mixed transcortical aphasia pattern—she was unable to speak or comprehend, but retained some ability to repeat. The changing aphasia patterns and the often abrupt starting and stopping of these symptoms were the clues that an active process was occurring, suggesting that seizures should be considered.
DIAGNOSIS: Irrefutable EEG evidence
Mrs. D receives another neurology consult. An EEG shows spike and wave discharges in both frontal lobes consistent with nonconvulsive status epilepticus (NCSE). During these bursts, the neurologist notes speech arrest and altered alertness. Phenytoin loading is administered as a single 800-mg oral dose followed by 100 mg twice daily, and Mrs. D is transferred to the neurology unit for further stabilization.
The authors’ observations
When evaluating whether a psychiatric presentation reflects an underlying general medical or neurologic disorder—including seizures—consider the clinical features outlined in Table 2.12
In Mrs. D’s case, several factors supported the diagnosis of depression. She had numerous depressive symptoms, including depressed mood, social withdrawal, low energy, poor sleep, and “scattered mind,” which the psychiatrist interpreted as poor concentration. Interestingly, she attributed her dramatic episode of mutism and unresponsiveness in the hospital to being depressed. Mrs. D also had a personal and family history of depression; she had experienced a possible major depressive episode in her late 20s but was never treated, and her brother had depression.
Several features of her presentation were atypical, however, and suggested a medical etiology. Her family described the onset of her symptoms as abrupt, and she declined rapidly. Mrs. D’s concern about her estate had no connection with reality, and she became more psychotic. The dramatic episode of decreased responsiveness that led to her intubation was both peculiar and brief.
Mrs. D’s symptoms had an episodic quality with sudden onset, were repeatedly associated with aphasia, and included some automatic behavior (including dressing and undressing) suggestive of seizures. Symptoms of depression should not be surprising in this context because depression may be the most common comorbid psychiatric condition in elderly persons with epilepsy.13 Indeed, Mrs. D’s ultimate diagnosis—NCSE—is characterized by great variability in presentation, ranging from mildly impaired attention and orientation to mood disturbance, speech disturbance, and psychosis. All of these symptoms are seen with seizures.
Further, NCSE can have gradual or sudden onset, varying intensity and duration of symptoms, and fluctuating responsiveness.14 At least 10% of patients presenting with NCSE have no history of seizures.15 Precipitating factors include infection and drug toxicity.14
OUTCOME: Dual treatment
During a one-week neurology hospitalization, Mrs. D continues to receive phenytoin. Long-term EEG monitoring reveals she is no longer in status epilepticus. The patient is prescribed citalopram, 10 mg/d, and olanzapine, 2.5 mg at bedtime, to resolve mild depressive symptoms and hallucinosis. Mrs. D is referred for both neurology and psychiatry outpatient follow-up.
Table 2
Is the patient’s disorder psychiatric or medical/neurologic?
| Are the symptoms typical of a psychiatric disorder, including the severity? |
| Are the onset and course of symptoms usual? |
| Does the patient have risk factors for psychiatric illness, such as a personal or family history of psychiatric illness? |
| Are psychiatric symptoms responding poorly to treatment? |
| Does the patient have a general medical or neurologic condition commonly associated with psychiatric symptoms? |
| Does the patient exhibit abnormal cognitive functioning, including memory impairment or altered level of consciousness? |
| Did the psychiatric symptoms emerge after an abrupt change in personality? |
| Source: Reference 12 |
- Ettinger AB, Kanner AM, eds. Psychiatric issues in epilepsy: a practical guide to diagnosis and treatment. 2nd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2006.
- Bupropion • Wellbutrin
- Ciprofloxacin • Cipro
- Citalopram • Celexa
- Levofloxacin • Levaquin
- Olanzapine • Zyprexa
- Phenytoin • Dilantin
- Zolpidem • Ambien
Dr. Saragoza reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Maixner receives research/grant support from Neuronetics Inc., and is a speaker for Pfizer Inc., Bristol-Meyers Squibb, Janssen LP, and AstraZeneca.
1. Taylor M. The fundamentals of clinical neuropsychiatry. New York, NY: Oxford University Press; 1999:298-324.
2. Gloor P. The role of the limbic system in experiential phenomena of temporal lobe epilepsy. Ann Neurol 1982;12(2):129-44.
3. Scheepers M. Epilepsy and behaviour. Curr Opin Neurol 2003;16:183-7.
4. Adachi N. Inter-ictal and post-ictal psychoses in frontal lobe epilepsy: a retrospective comparison with psychoses in temporal lobe epilepsy. Seizure 2000;9:328-35.
5. Toni C. Psychosensorial and related phenomena in panic disorder and in temporal lobe epilepsy. Compr Psychiatry 1996;37(2):125-33.
6. Tucker G. Seizure disorders presenting with psychiatric symptomatology. Psychiatr Clin North Am 1998;21(3):626-35.
7. Onuma T. Classification of psychiatric symptoms in patients with epilepsy. Epilepsia 2000;41(suppl 9):43-8.
8. Marsh L, Rao V. Psychiatric complications in patients with epilepsy: a review. Epilepsy Res 2002;49(1):11-33.
9. Stern T. ed. Massachusetts General Hospital handbook of general hospital psychiatry. 5th ed. St. Louis, MO: Mosby; 2004;457-62.
10. O’Sullivan S. The role of the standard EEG in clinical psychiatry. Human Psychopharmacol Clin Exp 2006;21:265-71.
11. Gelb D. Introduction to clinical neurology. 2nd ed. London, UK: Butterworth Heinemann; 2000;133-4.
12. Marsh CM. Psychiatric presentations of medical illness. Psychiatr Clin North Am 1997;20(1):181-2.
13. Cloyd J, Hauser W, Towne A, et al. Epidemiological and medical aspects of epilepsy in the elderly. Epilepsy Res 2006;68(suppl 1):S39-48.
14. Riggio S. Nonconvulsive status epilepticus: clinical features and diagnostic challenges. Psychiatr Clin North Am 2005;28:653-64.
15. Mehlhorn AJ, Brown DA. Safety concerns with fluoroquinolones. Ann Pharmacother 2007;41:1859-66.
CASE: Unexplained unresponsiveness
One month after being hospitalized with E coli sepsis—and just after completing a course of ciprofloxacin—Mrs. D, a 79-year-old widow, becomes withdrawn and has several days of worsening fatigue, weakness, and somnolence. Within 2 hours of being admitted to the hospital, she becomes flaccid and unresponsive, although she seems to be awake. She has decreased respirations and is intubated.
The neurology team finds her unresponsive to verbal and noxious stimuli, with some resistance to eye opening. Neurologic exam is nonfocal. Cranial nerve testing is intact, muscle strength and reflexes are normal and symmetrical, and sensory function is intact to light touch. MRI, ECG, chest radiography, and laboratory tests—including metabolic and infectious screenings—do not reveal acute pathology. Within hours, Mrs. D becomes much more responsive and is successfully extubated. Her rapid improvement rules out locked-in syndrome.
The next day, Mrs. D has another episode of reduced responsiveness that lasts several minutes and resolves quickly. The neurologist observes this episode—which occurred when Mrs. D’s daughter entered the room—and recommends a psychiatric consultation.
For the past 3 weeks Mrs. D has experienced depressed mood, low energy, poor sleep, memory complaints, and feeling as if her mind was “scattered.” She has stopped attending church, is isolating to her home, and has been hiding valuables because of an irrational fear that she would lose possessions from her estate. Her primary care physician noted markedly reduced speech during recent office visits and agrees with the family that Mrs. D seems depressed.
On psychiatric exam, Mrs. D’s speech is quiet and slow but coherent. Her mood is depressed with a flat affect. Her thought process is goal-directed, and her Mini-Mental State Examination (MMSE) score is 27/30, indicating her cognition is grossly intact.
Mrs. D develops a low-grade fever. Although the physician does not suspect an infection, he prescribes a prophylactic course of levofloxacin, 500 mg/d. After 2 days of monitoring and assessments, the psychiatrist attributes Mrs. D’s presentation to depression, prescribes bupropion, 100 mg/d, and zolpidem, 5 mg at bedtime, and refers her for psychiatric follow-up.
Six days after discharge, Mrs. D’s family brings her to the psychiatric emergency room. They report that since discharge she has remained fatigued and seems confused intermittently. Her depressive symptoms—decreased appetite, anhedonia, poor sleep, and agitation—persist, and her personal care has deteriorated.
The authors’ observations
The psychiatrist attributes Mrs. D’s declining functioning to a worsening mood disorder. Major depression with psychotic features can include:
- fearfulness
- suspiciousness
- delusions of poverty.
Mrs. D’s cognitive and behavioral status fluctuated during her initial medical hospitalization, and on 1 occasion she required intubation. Her confusion worsened after discharge. These aspects of her history, along with worsening psychosis, can indicate seizures.
Psychiatric manifestations of seizures have been recognized for centuries. Partial complex seizures—one of the most common seizure types—have been called “psychosensory” or “psychomotor” seizures because they often include psychiatric symptoms.1
Psychiatric symptoms most often occur with seizures involving the temporal lobe, and limbic system activation adds an affective dimension to perceptual data processed by the temporal neocortex.2 Frontal and parietal lobe seizure foci also are associated with behavior change.
Psychiatric manifestations of seizures can include:
- cognitive problems
- anxiety
- mood/affect, psychotic, and dissociative symptoms
- personality changes (Table 1).2-6
As many as 30% of patients with seizures experience prominent psychiatric symptoms.7 Approximately one-half have comorbid psychiatric syndromes.8
Table 1
Seizure-related psychiatric symptoms: What to look for
| Symptom type | Characteristic features with seizures |
|---|---|
| Cognitive: intellectual function, memory, orientation | Episodic, fluctuating course of changes Amnesia occurs with complex—but not simple—seizures |
| Anxiety | Occurs most often with temporal lobe seizures May appear as full-blown panic attack Agoraphobia is rare Associated seizure features may include disturbed consciousness, automatisms, and hallucinations |
| Mood and affect | Change in affect is often episodic and profound, without many other symptoms associated with major depression or mania |
| Psychotic | Usually manifests as a single symptom, often described as incongruous, fragmentary, or out of context2 Occurs most often with temporal lobe seizures3 Delusions (paranoid, grandiose), forced thinking Hallucinations: auditory, visual, olfactory, tactile, gustatory Negative symptoms (emotional withdrawal, blunted affect) may be more common in frontal lobe seizures4 |
| Dissociative: depersonalization, déjà vu, jamais vu | Symptoms tend to be less extreme than in patients with dissociative identity disorder or PTSD May occur more often in context of panic symptoms with temporal lobe seizures5 |
| Personality changes (in epilepsy) | May be due to underlying frontal or temporal lobe damage Includes anancastic personality, emotionally unstable personality, and Geschwind syndrome (hypergraphia, hyperreligiosity, hyposexuality, and viscous personality style—perseverative and difficult to disengage from conversation)6 |
| PTSD: posttraumatic stress disorder | |
EVALUATION: Continuing decline
The emergency room staff learns Mrs. D has a history of vague auditory hallucinations and has developed more overt paranoia, including thoughts that police may be out to harm her. She has difficulty responding to questions and can not offer details of her history; her speech is soft and her thought process appears slowed.
Mrs. D is admitted to the inpatient psychiatry service. Her family reports that she has episodes of disorientation, poor memory, staring, and paranoia about the police that last minutes to 1 hour.
On a subsequent examination 1 hour later, her speech difficulties are variable. She cannot speak fluently, has limited ability to repeat phrases, and cannot follow simple verbal commands. These symptoms persist only minutes. Mrs. D slowly becomes more conversant but appears tired. During the next few hours she is disoriented and tries to walk into the nursing station. Other repetitive activity includes putting on/taking offmultiple layers of clothing.
The authors’ observations
- A normal EEG does not guarantee the absence of recent seizures; a standard scalp EEG can miss epileptiform changes that may occur earlier in the ictal phase.9
- EEG abnormalities may occur in normal subjects.
- visual, olfactory, or tactile hallucinations
- mutism
- catatonia
- poor memory not due to inattention
- episodic aphasia, apraxia, or agnosia.
Mrs. D’s confusion level and speech abnormalities varied over time. Her speech arrest early in the admission appeared to be a Broca’s or expressive aphasia because she comprehended commands but was unable to speak. Later, her speech exhibited a mixed transcortical aphasia pattern—she was unable to speak or comprehend, but retained some ability to repeat. The changing aphasia patterns and the often abrupt starting and stopping of these symptoms were the clues that an active process was occurring, suggesting that seizures should be considered.
DIAGNOSIS: Irrefutable EEG evidence
Mrs. D receives another neurology consult. An EEG shows spike and wave discharges in both frontal lobes consistent with nonconvulsive status epilepticus (NCSE). During these bursts, the neurologist notes speech arrest and altered alertness. Phenytoin loading is administered as a single 800-mg oral dose followed by 100 mg twice daily, and Mrs. D is transferred to the neurology unit for further stabilization.
The authors’ observations
When evaluating whether a psychiatric presentation reflects an underlying general medical or neurologic disorder—including seizures—consider the clinical features outlined in Table 2.12
In Mrs. D’s case, several factors supported the diagnosis of depression. She had numerous depressive symptoms, including depressed mood, social withdrawal, low energy, poor sleep, and “scattered mind,” which the psychiatrist interpreted as poor concentration. Interestingly, she attributed her dramatic episode of mutism and unresponsiveness in the hospital to being depressed. Mrs. D also had a personal and family history of depression; she had experienced a possible major depressive episode in her late 20s but was never treated, and her brother had depression.
Several features of her presentation were atypical, however, and suggested a medical etiology. Her family described the onset of her symptoms as abrupt, and she declined rapidly. Mrs. D’s concern about her estate had no connection with reality, and she became more psychotic. The dramatic episode of decreased responsiveness that led to her intubation was both peculiar and brief.
Mrs. D’s symptoms had an episodic quality with sudden onset, were repeatedly associated with aphasia, and included some automatic behavior (including dressing and undressing) suggestive of seizures. Symptoms of depression should not be surprising in this context because depression may be the most common comorbid psychiatric condition in elderly persons with epilepsy.13 Indeed, Mrs. D’s ultimate diagnosis—NCSE—is characterized by great variability in presentation, ranging from mildly impaired attention and orientation to mood disturbance, speech disturbance, and psychosis. All of these symptoms are seen with seizures.
Further, NCSE can have gradual or sudden onset, varying intensity and duration of symptoms, and fluctuating responsiveness.14 At least 10% of patients presenting with NCSE have no history of seizures.15 Precipitating factors include infection and drug toxicity.14
OUTCOME: Dual treatment
During a one-week neurology hospitalization, Mrs. D continues to receive phenytoin. Long-term EEG monitoring reveals she is no longer in status epilepticus. The patient is prescribed citalopram, 10 mg/d, and olanzapine, 2.5 mg at bedtime, to resolve mild depressive symptoms and hallucinosis. Mrs. D is referred for both neurology and psychiatry outpatient follow-up.
Table 2
Is the patient’s disorder psychiatric or medical/neurologic?
| Are the symptoms typical of a psychiatric disorder, including the severity? |
| Are the onset and course of symptoms usual? |
| Does the patient have risk factors for psychiatric illness, such as a personal or family history of psychiatric illness? |
| Are psychiatric symptoms responding poorly to treatment? |
| Does the patient have a general medical or neurologic condition commonly associated with psychiatric symptoms? |
| Does the patient exhibit abnormal cognitive functioning, including memory impairment or altered level of consciousness? |
| Did the psychiatric symptoms emerge after an abrupt change in personality? |
| Source: Reference 12 |
- Ettinger AB, Kanner AM, eds. Psychiatric issues in epilepsy: a practical guide to diagnosis and treatment. 2nd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2006.
- Bupropion • Wellbutrin
- Ciprofloxacin • Cipro
- Citalopram • Celexa
- Levofloxacin • Levaquin
- Olanzapine • Zyprexa
- Phenytoin • Dilantin
- Zolpidem • Ambien
Dr. Saragoza reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Maixner receives research/grant support from Neuronetics Inc., and is a speaker for Pfizer Inc., Bristol-Meyers Squibb, Janssen LP, and AstraZeneca.
CASE: Unexplained unresponsiveness
One month after being hospitalized with E coli sepsis—and just after completing a course of ciprofloxacin—Mrs. D, a 79-year-old widow, becomes withdrawn and has several days of worsening fatigue, weakness, and somnolence. Within 2 hours of being admitted to the hospital, she becomes flaccid and unresponsive, although she seems to be awake. She has decreased respirations and is intubated.
The neurology team finds her unresponsive to verbal and noxious stimuli, with some resistance to eye opening. Neurologic exam is nonfocal. Cranial nerve testing is intact, muscle strength and reflexes are normal and symmetrical, and sensory function is intact to light touch. MRI, ECG, chest radiography, and laboratory tests—including metabolic and infectious screenings—do not reveal acute pathology. Within hours, Mrs. D becomes much more responsive and is successfully extubated. Her rapid improvement rules out locked-in syndrome.
The next day, Mrs. D has another episode of reduced responsiveness that lasts several minutes and resolves quickly. The neurologist observes this episode—which occurred when Mrs. D’s daughter entered the room—and recommends a psychiatric consultation.
For the past 3 weeks Mrs. D has experienced depressed mood, low energy, poor sleep, memory complaints, and feeling as if her mind was “scattered.” She has stopped attending church, is isolating to her home, and has been hiding valuables because of an irrational fear that she would lose possessions from her estate. Her primary care physician noted markedly reduced speech during recent office visits and agrees with the family that Mrs. D seems depressed.
On psychiatric exam, Mrs. D’s speech is quiet and slow but coherent. Her mood is depressed with a flat affect. Her thought process is goal-directed, and her Mini-Mental State Examination (MMSE) score is 27/30, indicating her cognition is grossly intact.
Mrs. D develops a low-grade fever. Although the physician does not suspect an infection, he prescribes a prophylactic course of levofloxacin, 500 mg/d. After 2 days of monitoring and assessments, the psychiatrist attributes Mrs. D’s presentation to depression, prescribes bupropion, 100 mg/d, and zolpidem, 5 mg at bedtime, and refers her for psychiatric follow-up.
Six days after discharge, Mrs. D’s family brings her to the psychiatric emergency room. They report that since discharge she has remained fatigued and seems confused intermittently. Her depressive symptoms—decreased appetite, anhedonia, poor sleep, and agitation—persist, and her personal care has deteriorated.
The authors’ observations
The psychiatrist attributes Mrs. D’s declining functioning to a worsening mood disorder. Major depression with psychotic features can include:
- fearfulness
- suspiciousness
- delusions of poverty.
Mrs. D’s cognitive and behavioral status fluctuated during her initial medical hospitalization, and on 1 occasion she required intubation. Her confusion worsened after discharge. These aspects of her history, along with worsening psychosis, can indicate seizures.
Psychiatric manifestations of seizures have been recognized for centuries. Partial complex seizures—one of the most common seizure types—have been called “psychosensory” or “psychomotor” seizures because they often include psychiatric symptoms.1
Psychiatric symptoms most often occur with seizures involving the temporal lobe, and limbic system activation adds an affective dimension to perceptual data processed by the temporal neocortex.2 Frontal and parietal lobe seizure foci also are associated with behavior change.
Psychiatric manifestations of seizures can include:
- cognitive problems
- anxiety
- mood/affect, psychotic, and dissociative symptoms
- personality changes (Table 1).2-6
As many as 30% of patients with seizures experience prominent psychiatric symptoms.7 Approximately one-half have comorbid psychiatric syndromes.8
Table 1
Seizure-related psychiatric symptoms: What to look for
| Symptom type | Characteristic features with seizures |
|---|---|
| Cognitive: intellectual function, memory, orientation | Episodic, fluctuating course of changes Amnesia occurs with complex—but not simple—seizures |
| Anxiety | Occurs most often with temporal lobe seizures May appear as full-blown panic attack Agoraphobia is rare Associated seizure features may include disturbed consciousness, automatisms, and hallucinations |
| Mood and affect | Change in affect is often episodic and profound, without many other symptoms associated with major depression or mania |
| Psychotic | Usually manifests as a single symptom, often described as incongruous, fragmentary, or out of context2 Occurs most often with temporal lobe seizures3 Delusions (paranoid, grandiose), forced thinking Hallucinations: auditory, visual, olfactory, tactile, gustatory Negative symptoms (emotional withdrawal, blunted affect) may be more common in frontal lobe seizures4 |
| Dissociative: depersonalization, déjà vu, jamais vu | Symptoms tend to be less extreme than in patients with dissociative identity disorder or PTSD May occur more often in context of panic symptoms with temporal lobe seizures5 |
| Personality changes (in epilepsy) | May be due to underlying frontal or temporal lobe damage Includes anancastic personality, emotionally unstable personality, and Geschwind syndrome (hypergraphia, hyperreligiosity, hyposexuality, and viscous personality style—perseverative and difficult to disengage from conversation)6 |
| PTSD: posttraumatic stress disorder | |
EVALUATION: Continuing decline
The emergency room staff learns Mrs. D has a history of vague auditory hallucinations and has developed more overt paranoia, including thoughts that police may be out to harm her. She has difficulty responding to questions and can not offer details of her history; her speech is soft and her thought process appears slowed.
Mrs. D is admitted to the inpatient psychiatry service. Her family reports that she has episodes of disorientation, poor memory, staring, and paranoia about the police that last minutes to 1 hour.
On a subsequent examination 1 hour later, her speech difficulties are variable. She cannot speak fluently, has limited ability to repeat phrases, and cannot follow simple verbal commands. These symptoms persist only minutes. Mrs. D slowly becomes more conversant but appears tired. During the next few hours she is disoriented and tries to walk into the nursing station. Other repetitive activity includes putting on/taking offmultiple layers of clothing.
The authors’ observations
- A normal EEG does not guarantee the absence of recent seizures; a standard scalp EEG can miss epileptiform changes that may occur earlier in the ictal phase.9
- EEG abnormalities may occur in normal subjects.
- visual, olfactory, or tactile hallucinations
- mutism
- catatonia
- poor memory not due to inattention
- episodic aphasia, apraxia, or agnosia.
Mrs. D’s confusion level and speech abnormalities varied over time. Her speech arrest early in the admission appeared to be a Broca’s or expressive aphasia because she comprehended commands but was unable to speak. Later, her speech exhibited a mixed transcortical aphasia pattern—she was unable to speak or comprehend, but retained some ability to repeat. The changing aphasia patterns and the often abrupt starting and stopping of these symptoms were the clues that an active process was occurring, suggesting that seizures should be considered.
DIAGNOSIS: Irrefutable EEG evidence
Mrs. D receives another neurology consult. An EEG shows spike and wave discharges in both frontal lobes consistent with nonconvulsive status epilepticus (NCSE). During these bursts, the neurologist notes speech arrest and altered alertness. Phenytoin loading is administered as a single 800-mg oral dose followed by 100 mg twice daily, and Mrs. D is transferred to the neurology unit for further stabilization.
The authors’ observations
When evaluating whether a psychiatric presentation reflects an underlying general medical or neurologic disorder—including seizures—consider the clinical features outlined in Table 2.12
In Mrs. D’s case, several factors supported the diagnosis of depression. She had numerous depressive symptoms, including depressed mood, social withdrawal, low energy, poor sleep, and “scattered mind,” which the psychiatrist interpreted as poor concentration. Interestingly, she attributed her dramatic episode of mutism and unresponsiveness in the hospital to being depressed. Mrs. D also had a personal and family history of depression; she had experienced a possible major depressive episode in her late 20s but was never treated, and her brother had depression.
Several features of her presentation were atypical, however, and suggested a medical etiology. Her family described the onset of her symptoms as abrupt, and she declined rapidly. Mrs. D’s concern about her estate had no connection with reality, and she became more psychotic. The dramatic episode of decreased responsiveness that led to her intubation was both peculiar and brief.
Mrs. D’s symptoms had an episodic quality with sudden onset, were repeatedly associated with aphasia, and included some automatic behavior (including dressing and undressing) suggestive of seizures. Symptoms of depression should not be surprising in this context because depression may be the most common comorbid psychiatric condition in elderly persons with epilepsy.13 Indeed, Mrs. D’s ultimate diagnosis—NCSE—is characterized by great variability in presentation, ranging from mildly impaired attention and orientation to mood disturbance, speech disturbance, and psychosis. All of these symptoms are seen with seizures.
Further, NCSE can have gradual or sudden onset, varying intensity and duration of symptoms, and fluctuating responsiveness.14 At least 10% of patients presenting with NCSE have no history of seizures.15 Precipitating factors include infection and drug toxicity.14
OUTCOME: Dual treatment
During a one-week neurology hospitalization, Mrs. D continues to receive phenytoin. Long-term EEG monitoring reveals she is no longer in status epilepticus. The patient is prescribed citalopram, 10 mg/d, and olanzapine, 2.5 mg at bedtime, to resolve mild depressive symptoms and hallucinosis. Mrs. D is referred for both neurology and psychiatry outpatient follow-up.
Table 2
Is the patient’s disorder psychiatric or medical/neurologic?
| Are the symptoms typical of a psychiatric disorder, including the severity? |
| Are the onset and course of symptoms usual? |
| Does the patient have risk factors for psychiatric illness, such as a personal or family history of psychiatric illness? |
| Are psychiatric symptoms responding poorly to treatment? |
| Does the patient have a general medical or neurologic condition commonly associated with psychiatric symptoms? |
| Does the patient exhibit abnormal cognitive functioning, including memory impairment or altered level of consciousness? |
| Did the psychiatric symptoms emerge after an abrupt change in personality? |
| Source: Reference 12 |
- Ettinger AB, Kanner AM, eds. Psychiatric issues in epilepsy: a practical guide to diagnosis and treatment. 2nd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2006.
- Bupropion • Wellbutrin
- Ciprofloxacin • Cipro
- Citalopram • Celexa
- Levofloxacin • Levaquin
- Olanzapine • Zyprexa
- Phenytoin • Dilantin
- Zolpidem • Ambien
Dr. Saragoza reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Maixner receives research/grant support from Neuronetics Inc., and is a speaker for Pfizer Inc., Bristol-Meyers Squibb, Janssen LP, and AstraZeneca.
1. Taylor M. The fundamentals of clinical neuropsychiatry. New York, NY: Oxford University Press; 1999:298-324.
2. Gloor P. The role of the limbic system in experiential phenomena of temporal lobe epilepsy. Ann Neurol 1982;12(2):129-44.
3. Scheepers M. Epilepsy and behaviour. Curr Opin Neurol 2003;16:183-7.
4. Adachi N. Inter-ictal and post-ictal psychoses in frontal lobe epilepsy: a retrospective comparison with psychoses in temporal lobe epilepsy. Seizure 2000;9:328-35.
5. Toni C. Psychosensorial and related phenomena in panic disorder and in temporal lobe epilepsy. Compr Psychiatry 1996;37(2):125-33.
6. Tucker G. Seizure disorders presenting with psychiatric symptomatology. Psychiatr Clin North Am 1998;21(3):626-35.
7. Onuma T. Classification of psychiatric symptoms in patients with epilepsy. Epilepsia 2000;41(suppl 9):43-8.
8. Marsh L, Rao V. Psychiatric complications in patients with epilepsy: a review. Epilepsy Res 2002;49(1):11-33.
9. Stern T. ed. Massachusetts General Hospital handbook of general hospital psychiatry. 5th ed. St. Louis, MO: Mosby; 2004;457-62.
10. O’Sullivan S. The role of the standard EEG in clinical psychiatry. Human Psychopharmacol Clin Exp 2006;21:265-71.
11. Gelb D. Introduction to clinical neurology. 2nd ed. London, UK: Butterworth Heinemann; 2000;133-4.
12. Marsh CM. Psychiatric presentations of medical illness. Psychiatr Clin North Am 1997;20(1):181-2.
13. Cloyd J, Hauser W, Towne A, et al. Epidemiological and medical aspects of epilepsy in the elderly. Epilepsy Res 2006;68(suppl 1):S39-48.
14. Riggio S. Nonconvulsive status epilepticus: clinical features and diagnostic challenges. Psychiatr Clin North Am 2005;28:653-64.
15. Mehlhorn AJ, Brown DA. Safety concerns with fluoroquinolones. Ann Pharmacother 2007;41:1859-66.
1. Taylor M. The fundamentals of clinical neuropsychiatry. New York, NY: Oxford University Press; 1999:298-324.
2. Gloor P. The role of the limbic system in experiential phenomena of temporal lobe epilepsy. Ann Neurol 1982;12(2):129-44.
3. Scheepers M. Epilepsy and behaviour. Curr Opin Neurol 2003;16:183-7.
4. Adachi N. Inter-ictal and post-ictal psychoses in frontal lobe epilepsy: a retrospective comparison with psychoses in temporal lobe epilepsy. Seizure 2000;9:328-35.
5. Toni C. Psychosensorial and related phenomena in panic disorder and in temporal lobe epilepsy. Compr Psychiatry 1996;37(2):125-33.
6. Tucker G. Seizure disorders presenting with psychiatric symptomatology. Psychiatr Clin North Am 1998;21(3):626-35.
7. Onuma T. Classification of psychiatric symptoms in patients with epilepsy. Epilepsia 2000;41(suppl 9):43-8.
8. Marsh L, Rao V. Psychiatric complications in patients with epilepsy: a review. Epilepsy Res 2002;49(1):11-33.
9. Stern T. ed. Massachusetts General Hospital handbook of general hospital psychiatry. 5th ed. St. Louis, MO: Mosby; 2004;457-62.
10. O’Sullivan S. The role of the standard EEG in clinical psychiatry. Human Psychopharmacol Clin Exp 2006;21:265-71.
11. Gelb D. Introduction to clinical neurology. 2nd ed. London, UK: Butterworth Heinemann; 2000;133-4.
12. Marsh CM. Psychiatric presentations of medical illness. Psychiatr Clin North Am 1997;20(1):181-2.
13. Cloyd J, Hauser W, Towne A, et al. Epidemiological and medical aspects of epilepsy in the elderly. Epilepsy Res 2006;68(suppl 1):S39-48.
14. Riggio S. Nonconvulsive status epilepticus: clinical features and diagnostic challenges. Psychiatr Clin North Am 2005;28:653-64.
15. Mehlhorn AJ, Brown DA. Safety concerns with fluoroquinolones. Ann Pharmacother 2007;41:1859-66.