User login
Update on eating disorders: Binge-eating disorder
Managing patients with binge-eating disorder (BED) often requires behavioral, medical, and psychiatric interventions.
These patients suffer from recurrent episodes of distressing, uncontrollable overeating, but they do not purge or show other compensatory weight-loss behaviors common to bulimia nervosa1 and anorexia nervosa.2-10 As a result, they are often overweight or obese and may have obesity-related illnesses, such as hypertension or type 2 diabetes. Mild to severe depression—unipolar or bipolar—is a common psychopathology.
Because no one treatment fits all patients with binge eating disorder, their management usually requires an individualized program of:
- behavioral weight control
- psychotherapy
- and sometimes medications.
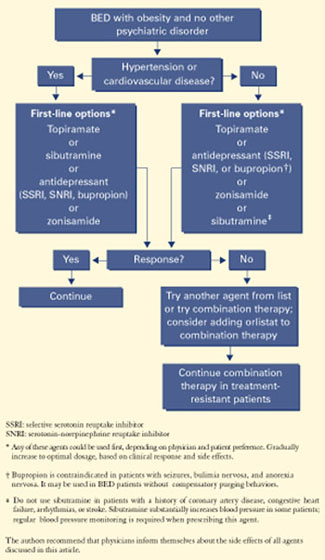
In our weight management clinic, we consider medication options based on patient preference and whether BED is uncomplicated (Figure 1) or coexists with a mood disorder (Figure 2).
This article presents the evidence on which we base our comprehensive approach. General psychiatrists with knowledge of BED can treat patients with this eating disorder, although complicated cases may require referral for specialized treatment.
Figure 1 Medication options for uncomplicated BED
Clinical characteristics
Psychiatric comorbidity. BED often occurs in patients with mood, anxiety, substance-abuse, impulsecontrol, and personality disorders.4,6,10-12 Mood disorder—particularly depression—appears to be the most common comorbidity. BED can occur with bipolar disorder12—a comorbidity that in our experience is underrecognized both clinically and in the literature.
Patients with BED and bipolar disorder show increased impulsivity and mood lability. As bipolar II disorder and other “soft-spectrum” forms are more common than bipolar I disorder, BED is also more likely to occur with hypomania than mania.
Overweight. Not surprisingly, BED is associated with overweight and obesity.5,8,9,11 Not all patients with BED are overweight or obese, but most who participate in clinical trials of BED treatments are at least overweight. BED has been reported in up to:
- 30% of participants in weight-loss programs7
- 70% of participants in groups such as Overeaters Anonymous
- 50% of patients who seek bariatric surgery.5
In our experience, patients are often more distressed by their weight than by their binge eating, depression, or anxiety. Indeed, overweight and obesity are the usual reasons patients with BED present for treatment at our center.
Diagnosis. BED’s validity as a clinical diagnosis has been controversial since the disorder was first included in DSM-IV (Table 1).3 Debate continues about some definitions in the DSM criteria, including what amount of food is “definitely larger” than most people would eat and what is “loss of control over eating.”
Nevertheless, screening for BED is relatively easy. Clinicians may use the eating disorder section of the Structured Clinical Interview for DSM-IV or the Eating Disorders Examination. Alternatively, simply ask patients if they have episodes of uncontrollable overeating, during which they eat unusually large amounts of food and their eating feels out of control.
Course. BED begins in adolescence or adulthood. Disease course is variable, with periods of remission, recurrence, and chronicity.6,7,10 Interestingly, one prospective study showed that even if the binge eating resolves, persons may still develop obesity.13
Prevalence. BED affects 1.5% to 3% of the U.S. population. It is more common in women than men, equally prevalent in whites and blacks, and more prevalent than anorexia nervosa and bulimia nervosa combined.11,14 Subthreshold BED—such as obesity with infrequent or nondistressing binge eating—appears to be much more common,10 although no data are available.
Theories of binge eating
BED’s cause is unknown, but biological, familial, and psychosocial factors have been implicated.
Biological factors. The neurotransmitters serotonin (5-HT) and dopamine—as well as various peptides—have been shown to help regulate feeding behavior.10
Table 1
Diagnostic criteria for binge-eating disorder*
|
| * Research criteria, DSM-IV-TR appendix B. |
| Source: Reprinted with permission from the Diagnostic and statistical manual of mental disorders, 4th edition, text revision. Copyright 2000. American Psychiatric Association. |
Serotonin. Reduced 5-HT transporter binding has been shown in obese women with BED.15 Their 5-HT binding improved and binge eating subsided with group psychotherapy and fluoxetine, although the women continued to gain weight.
Figure 2 Medication options for BED with obesity and a mood disorder*

Dopamine. Obese patients who compulsively overeat may have lower levels of dopamine D2 receptors than do normal-weight controls.16
Genetic factors. In severely obese patients (body mass index 44±2), those with a DSM-IV diagnosis of BED exhibited mutations of the melanocortin 4 receptor gene, which affects the anorectic properties of alpha melanocyte-stimulating hormone.17
Familial factors associated with BED include parental depression and obesity.18
Psychosocial correlates include physical and sexual abuse, bullying by peers, and discrimination because of being overweight.19
Treatment recommendations
Few systematic studies have examined BED treatment. Emerging research suggests that behavioral weight-loss treatment, specialized psychotherapies, and medications may be effective in some patients with BED.4,6,8
Behavioral weight-loss treatment’s main goal is to manage the patient’s weight with a lower-calorie, healthy diet and to increase exercise.20,21
Over the short term (<1 year), behavioral weight-loss treatment produces similar weight loss in obese patients with or without BED; long-term results in both groups, however, have not been satisfactory.20,21 No studies have examined the efficacy of specialized diets (such as low-carbohydrate regimens) in patients with BED.
Specialized psychotherapy’s goal is to modify bingeeating behavior with behavioral self-management strategies, reducing interpersonal dysfunction and stress, and/or managing affective dysregulation.
Cognitive-behavioral therapy (CBT) and interpersonal therapy (IPT) have been effective in reducing binge eating, both acutely and for up to 12 months4,20-24 but less effective in achieving and maintaining weight loss. Patients who achieve remission in binge eating after undergoing CBT or IPI often experience modest but stable weight loss.20-22 For example, in a comparison study of CBT and IPT:
- After 20 weekly sessions, patients whose binge eating was in remission lost weight (mean body mass index [BMI] −0.5 ± 1.5 kg/m2), whereas those who continued to binge gained weight (mean BMI +0.4 ±2.0 kg/m2).
- At 12 months’ follow-up, patients still in remission continued to lose weight (mean BMI −1.0 ± 3.0 kg/m2), whereas those no longer in remission gained weight (mean BMI +0.7 ±2.9 kg/m2[P = 0.01]).22
Self-help and dialectical behavioral therapy (DBT) may also help reduce binge eating in BED. As with CBT and IPT, they are less effective in weight loss. In the only controlled study of DBT,24 patients achieved an average 2.5-lb weight loss after 20 weeks of DBT, compared with an average 0.6-lb weight gain in the control group. This difference was not significant, and the report did not include data on weight loss maintenance.
In summary, CBT may be more effective than behavioral weight loss treatment for reducing binge eating, but behavioral weight loss is more effective for weight loss.
Medications for BED
Medications that have been tried for BED include antidepressants, appetite suppressants, and anticonvulsants.25,26 Antidepressants are used to treat BED because:
- BED is often associated with depressive symptoms and disorders.
- BED is related to bulimia nervosa, and placebo-controlled trials have shown that the binge eating of bulimia nervosa responds to several classes of antidepressants. The selective serotonin reuptake inhibitor (SSRI) fluoxetine is the only medication indicated for treating any eating disorder (bulimia nervosa).
- Bupropion and venlafaxine—a serotonin-norepinephrine reuptake inhibitor (SNRI)—have weight-loss properties.
SSRIs are the most extensively studied antidepressants for treating BED. SSRIs have weightloss properties, but only short term.25-26 Citalopram, fluoxetine, fluvoxamine, and sertraline have reduced binge eating and body weight more effectively than placebo during 6 to 9 weeks of treatment (Table 2).25-26 However, one controlled study23 showed that fluoxetine was not significantly more effective than placebo in reducing binge frequency or body weight after 16 weeks.
TCAs. Studies of tricyclic antidepressants (TCAs) for BED are sparse, and results have been mixed. In one trial, imipramine was similar to placebo in reducing binge frequency and body weight. In a placebo-controlled study of patients with nonpurging bulimia nervosa, desipramine reduced binge eating but had no effect on body weight.25,26
Table 2
Drug therapies shown to be effective for BED*
| Medication | Binge eating | Weight | Depression | Study size | Duration (weeks) | Dosage (mg/d) |
|---|---|---|---|---|---|---|
| Antidepressants | ||||||
| Citalopram | + | + | − | 38 | 6 | 20 to 60 |
| Fluoxetine † | + | + | + | 60 | 6 | 20 to 80 |
| Fluvoxamine | + | + | − | 85 | 9 | 50 to 300 |
| Sertraline | + | + | − | 34 | 6 | 50 to 200 |
| Appetite suppressant | ||||||
| Sibutramine | + | + | + | 60 | 12 | 15 |
| Anticonvulsant | ||||||
| Topiramate | + | + | − | 61 | 14 | 50 to 600 |
| + Improvement | ||||||
| − No improvement | ||||||
| * Randomized, controlled trials. Antidepressants were studied in patients with BED; sibutramine and topiramate were studied in patients with BED and associated obesity. | ||||||
| † One 16-week trial of fluoxetine for BED (reference 23) did not show statistically significant differences in post-treatment binge frequency or body-mass index. | ||||||
Venlafaxine. In a retrospective review of 35 consecutive obese women with BED, venlafaxine, mean 222 mg/d for 28 to 300 days (median 120 days), reduced binge eating, body weight, and depressive symptoms.27
Bupropion has been more effective than placebo for treating:
- uncomplicated obesity (short- and long-term)
- obesity associated with depressive symptoms
- bulimia nervosa (although bupropion is contraindicated in these patients because of seizure risk).26,28,29
No controlled trials have studied bupropion for BED. When using dosages effective in depressive disorders, we find bupropion helpful in reducing binge eating, body weight, and depressive symptoms in BED patients.
Appetite suppressants decrease appetite and weight, may increase satiety, and may reduce depressive symptoms.
Sibutramine—a serotonin, norepinephrine, and dopamine reuptake inhibitor indicated for managing obesity—has been reported effective in BED in a 12-week, randomized, double-blind, placebo-controlled trial. A 15-mg/d dosage reduced binge frequency, body weight, and depressive symptoms more effectively than placebo in 60 obese patients with BED.30 Most-frequent adverse effects (dry mouth and constipation) were mild and benign, and no significant complications were observed.
Sibutramine’s mechanism of action in BED is unknown. However, it suppressed food intake during binge-eating episodes in patients with BED in a randomized, controlled, cross-over laboratory study.31
Orlistat. We know of no published controlled studies of the lipase inhibitor orlistat in treating BED. In our experience, some patients do well with this agent, though we have observed infrequent purging episodes with it in patients with BED.
With orlistat, 120 mg tid, our BED patients have experienced weight loss comparable to that seen in uncomplicated obesity at similar dosages. Orlistat seems most effective for:
- patients whose binge eating is in remission
- those who responded to behavioral weightloss treatment, a psychological treatment, or another medication.
Anticonvulsants such as topiramate and zonisamide have been shown effective in treating obesity32,33 and are sometimes used to treat BED. Obese BED patients with mood disorders often do best with psychotherapy plus medication
Topiramate at dosages of 50 to 600 mg/d (median 212 mg/d) reduced binge-eating frequency, obsessive-compulsive features of binge eating, and body weight more effectively than placebo in a 14-week study of 61 obese patients with BED. These effects were maintained across 48 weeks in an open-label extension trial.34
Zonisamide, mean 513 mg/d, produced similar results during a prospective, open-label, 12-week trial in 15 patients with BED.35 A controlled trial to replicate these findings is ongoing.
BED may respond to anticonvulsant therapy for several reasons:
- Some anticonvulsants are effective in treating bipolar disorder, which may occur with BED.12
- Some anticonvulsants have shown benefit in conditions associated with pathologic impulsivity, such as substance abuse, impulse-control, and cluster B disorders.10
Growing evidence shows that bulimia nervosa and BED may be associated with pathologic impulsivity.
Combination therapies are generally more effective than monotherapies in patients with mood disorders, uncomplicated obesity, and possibly bulimia nervosa. Even so, few trials have systematically studied combination therapy in managing patients with BED.
Two studies compared psychotherapy and antidepressants alone and in combination in treating BED.21,23 Both showed that CBT alone was more effective in decreasing binge frequency than desipramine alone,21 fluoxetine alone,23 and the combination of CBT and medication. On the other hand, patients who took desipramine either alone or in combination experienced a greater degree of weight loss than those who did not take desipramine.21
In another combination therapy, exercise has been shown to be an effective adjunct to CBT in maintenance treatment of obese women with BED.36
No studies have compared behavioral weight management or a specialized psychotherapy in combination with an antiobesity drug or a weight-loss anticonvulsant in treating BED.
Treatment recommendations
In our experience, BED patients—particularly those with obesity and psychopathology—often do best with some combination of psychological treatment and medication:
- The psychological component may be behavioral weight-loss treatment, a specialized psychotherapy such as CBT or IPT, or some combination of behavioral weight-loss treatment and specialized psychotherapy.
- The medication component may consist of an antidepressant, anticonvulsant, antiobesity drug, or multiple drugs (such as an SSRI or sibutramine with topiramate for BED with major depression, or topiramate with lithium for BED with bipolar disorder).
Although combination therapies may be optimal for some patients, this approach remains unproven in controlled trials.
Patient preference. In addition to comorbidities, patient preference is an important consideration when choosing BED treatments. We determine our patients’ preferences by educating them as much as possible about their options. We explain the benefits and weaknesses of all treatments and encourage them to participate in forming their individualized treatment plans.
Patients sometimes have strong treatment preferences. Some prefer psychological treatments, whereas others prefer medications. Working with patient preferences enhances treatment adherence. For example, patients who fail a preferred treatment are often more willing to adhere to another treatment modality about which they initially were skeptical.
Related resources
- Bray GA, Bouchard C (eds). Handbook of obesity: clinical applications (2nd ed). New York, NY: Marcel Dekker, 2004.
- Cooper Z, Zairburn CG, Hawker DM. Cognitive behavioral treatment of obesity. A clinician’s guide. New York: Guilford Press, 2003.
- Carter WP, Hudson JI, Lalonde JK, et al. Pharmacologic treatment of binge eating disorder. Int J Eat Disord 2003;34(suppl):S74-88.
Drug brand names
- Bupropion • Wellbutrin
- Citalopram • Celexa
- Desipramine • Norpramin
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Imipramine • Tofranil
- Lamotrigine • Lamictal
- Lithium • Eskalith, others
- Orlistat • Xenical
- Sertraline • Zoloft
- Sibutramine • Meridia
- Topiramate • Topamax
- Venlafaxine • Effexor
- Zonisamide • Zonegran
Disclosure
Dr. Kotwal receives grant support from Elan Corporation and is a speaker for Ortho-McNeil Pharmaceutical and Pfizer Inc.
Dr. Kaneria and Ms. Guerdjikova report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. McElroy is a consultant to Abbott Laboratories, Bristol-Myers Squibb Co., Elan Corporation, GlaxoSmithKline, Janssen Pharmaceutica, Eli Lilly and Co., and Ortho-McNeil Pharmaceutical. She receives grant/research support from Elan Pharmaceuticals, Forest Pharmaceuticals, Merck & Co., Ortho-McNeil Pharmaceutical, and Sanofi-Synthelabo and is a speaker for Eli Lilly and Co. and Ortho-McNeil Pharmaceutical.
1. Pope HG, Hudson JI. Bulimia nervosa: Persistent disorders requires equally persistent treatment. Current Psychiatry 2004;3(1):13-22.
2. Halmi KA. Anorexia nervosa: Dual therapy can bring patients back from the brink. Current Psychiatry 2004;3(3):39-56.
3. American Psychiatric Association. Diagnostic and statistical manual of mental disorders (4th ed). Washington, DC: American Psychiatric Association, 1994.
4. Agras WS. Treatment of binge eating disorder. In: Gabbard GO (ed). Treatments of psychiatric disorders (3rd ed). Washington, DC: American Psychiatric Press, 2001;2209-19.
5. de Zwaan M. Binge eating disorder and obesity. Int J Obes Relat Metab Disord 2001;25(suppl 1):S51-5.
6. Dingemans AE, Bruna MJ, van Furth EF. Binge eating disorder: a review. Int J Obes Relat Metab Disord 2002;26:299-307.
7. Fairburn CG, Harrison PJ. Eating disorders. Lancet 2003;361:407-16.
8. Walsh BT (ed). The current status of binge eating disorder. Int J Eat Disord 2003;34(suppl):S1-120.
9. Devlin MJ, Goldfein JA, Dobrow I. What is this thing called BED? Current status of binge eating disorder nosology. Int J Eat Disord 2003;34(suppl):S2-18.
10. McElroy SL, Kotwal R. Binge eating. In: Hollander E, Stein D (eds). Handbook of impulse control disorders Washington, DC: American Psychiatric Press (in press).
11. Smith DE, Marcus MD, Lewis CE, et al. Prevalence of binge eating disorder, obesity, and depression in a biracial cohort of young adults. Ann Behav Med 1998;20:227-32.
12. Kruger S, Shugar G, Cooke RG. Comorbidity of binge eating disorder and the partial binge eating syndrome with bipolar disorder. Int J Eat Disord 1996;19:45-52.
13. Fairburn CG, Cooper Z, Doll H, et al. The natural course of bulimia nervosa and binge eating disorder in young women. Arch Gen Psychiatry 2000;57:659-65.
14. Striegel-Moore RH, Franko DL. Epidemiology of binge eating disorder. Int J Eat Disord 2003;34(suppl):S19-29.
15. Tammela LI, Rissanen A, Kuikka JT, et al. Treatment improves serotonin transporter binding and reduces binge eating. Psychopharmacology (Berl) 2003;170:89-93.
16. Wang GJ, Volkow ND, Logan J, et al. Brain dopamine and obesity. Lancet 2001;357:354-7.
17. Branson R, Potoczna N, Kral JG, et al. Binge eating as a major phenotype of melanocortin 4 receptor gene mutations. N Engl J Med 2003;348:1096-103.
18. Fairburn CG, Doll HA, Welch SL, et al. Risk factors for binge eating disorder: a community-based, case-control study. Arch Gen Psychiatry 1998;55:425-32.
19. Striegel-Moore RH, Dohm FA, Pike KM, et al. Abuse, bullying, and discrimination as risk factors for binge eating disorder. Am J Psychiatry 2002;159:1902-7.
20. Wonderlich SA, de Zwaan M, Mitchell JE, et al. Psychological and dietary treatments of binge eating disorder: conceptual implications. Int J Eat Disord 2003;34(suppl):S58-78.
21. Agras WS, Telch DF, Arnow B, et al. Weight loss, cognitive-behavioral, and desipramine treatments in binge eating disorder. An additive design. Behav Ther 1994;25:225-38.
22. Wilfley DE, Welch RR, Stein RI, et al. A randomized comparison of group cognitive-behavioral therapy and group interpersonal psychotherapy for the treatment of overweight individuals with binge eating disorder. Arch Gen Psychiatry 2002;59:713-21.
23. Grilo CM. A controlled study of cognitive behavioral therapy and fluoxetine for binge eating disorder (presentation) Charleston, SC: Eating Disorders Research Society annual meeting, 2002.
24. Telch CF, Agras WS, Linehan MM. Dialectical behavior therapy for binge eating disorder. J Consult Clin Psychol 2001;69:1061-5.
25. Carter WP, Hudson JI, Lalonde JK, et al. Pharmacologic treatment of binge eating disorder. Int J Eat Disord 2003;34(suppl):S74-88.
26. Appolinario JC, McElroy SL. Pharmacologic approaches in the treatment of binge eating disorder. Curr Drug Targets (in press).
27. Malhotra S, King KH, Welge JA, et al. Venlafaxine treatment of binge-eating disorder associated with obesity: a series of 35 patients. J Clin Psychiatry 2002;63:802-6.
28. Anderson JW, Greenway FL, Fujioka K, et al. Bupropion SR enhances weight loss: a 48-week double-blind, placebo-controlled trial. Obes Res 2002;10:633-41.
29. McElroy SL, Kotwal R, Malhotra S, et al. Are mood disorders and obesity related? A review for the mental health professional. J Clin Psychiatry (in press).
30. Appolinario JC, Bacaltchuk J, Sichieri R, et al. A randomized, double-blind, placebo-controlled study of sibutramine in the treatment of binge-eating disorder. Arch Gen Psychiatry 2003;60:1109-16.
31. Mitchell JE, Gosnell BA, Roerig JL, et al. Effects of sibutramine on binge eating, hunger, and fullness in a laboratory human feeding paradigm. Obes Res 2003;11:599-602.
32. Bray GA, Hollander P, Klein S, et al. A 6-month randomized, placebo-controlled, dose-ranging trial of topiramate for weight loss in obesity. Obes Res 2003;11:722-33.
33. Gadde KM, Franciscy DM, Wagner HR, 2nd, Krishnan KR. Zonisamide for weight loss in obese adults: a randomized controlled trial. JAMA 2003;289:1820-5.
34. McElroy SL, Arnold LM, Shapira NA, et al. Topiramate in the treatment of binge eating disorder associated with obesity: a randomized, placebo-controlled trial. Am J Psychiatry 2003;160:255-61.
35. McElroy SL, Kotwal R, Hudson JI, et al. Zonisamide in the treatment of binge-eating disorder: an open-label, prospective trial. J Clin Psychiatry 2004;65:50-6.
36. Pendleton VR, Goodrick GK, Poston WSC, et al. Exercise augments the effects of cognitive-behavioral therapy in the treatment of binge eating. Int J Eat Disord 2002;31(2):172-84.
Managing patients with binge-eating disorder (BED) often requires behavioral, medical, and psychiatric interventions.
These patients suffer from recurrent episodes of distressing, uncontrollable overeating, but they do not purge or show other compensatory weight-loss behaviors common to bulimia nervosa1 and anorexia nervosa.2-10 As a result, they are often overweight or obese and may have obesity-related illnesses, such as hypertension or type 2 diabetes. Mild to severe depression—unipolar or bipolar—is a common psychopathology.
Because no one treatment fits all patients with binge eating disorder, their management usually requires an individualized program of:
- behavioral weight control
- psychotherapy
- and sometimes medications.
In our weight management clinic, we consider medication options based on patient preference and whether BED is uncomplicated (Figure 1) or coexists with a mood disorder (Figure 2).
This article presents the evidence on which we base our comprehensive approach. General psychiatrists with knowledge of BED can treat patients with this eating disorder, although complicated cases may require referral for specialized treatment.
Figure 1 Medication options for uncomplicated BED
Clinical characteristics
Psychiatric comorbidity. BED often occurs in patients with mood, anxiety, substance-abuse, impulsecontrol, and personality disorders.4,6,10-12 Mood disorder—particularly depression—appears to be the most common comorbidity. BED can occur with bipolar disorder12—a comorbidity that in our experience is underrecognized both clinically and in the literature.
Patients with BED and bipolar disorder show increased impulsivity and mood lability. As bipolar II disorder and other “soft-spectrum” forms are more common than bipolar I disorder, BED is also more likely to occur with hypomania than mania.
Overweight. Not surprisingly, BED is associated with overweight and obesity.5,8,9,11 Not all patients with BED are overweight or obese, but most who participate in clinical trials of BED treatments are at least overweight. BED has been reported in up to:
- 30% of participants in weight-loss programs7
- 70% of participants in groups such as Overeaters Anonymous
- 50% of patients who seek bariatric surgery.5
In our experience, patients are often more distressed by their weight than by their binge eating, depression, or anxiety. Indeed, overweight and obesity are the usual reasons patients with BED present for treatment at our center.
Diagnosis. BED’s validity as a clinical diagnosis has been controversial since the disorder was first included in DSM-IV (Table 1).3 Debate continues about some definitions in the DSM criteria, including what amount of food is “definitely larger” than most people would eat and what is “loss of control over eating.”
Nevertheless, screening for BED is relatively easy. Clinicians may use the eating disorder section of the Structured Clinical Interview for DSM-IV or the Eating Disorders Examination. Alternatively, simply ask patients if they have episodes of uncontrollable overeating, during which they eat unusually large amounts of food and their eating feels out of control.
Course. BED begins in adolescence or adulthood. Disease course is variable, with periods of remission, recurrence, and chronicity.6,7,10 Interestingly, one prospective study showed that even if the binge eating resolves, persons may still develop obesity.13
Prevalence. BED affects 1.5% to 3% of the U.S. population. It is more common in women than men, equally prevalent in whites and blacks, and more prevalent than anorexia nervosa and bulimia nervosa combined.11,14 Subthreshold BED—such as obesity with infrequent or nondistressing binge eating—appears to be much more common,10 although no data are available.
Theories of binge eating
BED’s cause is unknown, but biological, familial, and psychosocial factors have been implicated.
Biological factors. The neurotransmitters serotonin (5-HT) and dopamine—as well as various peptides—have been shown to help regulate feeding behavior.10
Table 1
Diagnostic criteria for binge-eating disorder*
|
| * Research criteria, DSM-IV-TR appendix B. |
| Source: Reprinted with permission from the Diagnostic and statistical manual of mental disorders, 4th edition, text revision. Copyright 2000. American Psychiatric Association. |
Serotonin. Reduced 5-HT transporter binding has been shown in obese women with BED.15 Their 5-HT binding improved and binge eating subsided with group psychotherapy and fluoxetine, although the women continued to gain weight.
Figure 2 Medication options for BED with obesity and a mood disorder*
Dopamine. Obese patients who compulsively overeat may have lower levels of dopamine D2 receptors than do normal-weight controls.16
Genetic factors. In severely obese patients (body mass index 44±2), those with a DSM-IV diagnosis of BED exhibited mutations of the melanocortin 4 receptor gene, which affects the anorectic properties of alpha melanocyte-stimulating hormone.17
Familial factors associated with BED include parental depression and obesity.18
Psychosocial correlates include physical and sexual abuse, bullying by peers, and discrimination because of being overweight.19
Treatment recommendations
Few systematic studies have examined BED treatment. Emerging research suggests that behavioral weight-loss treatment, specialized psychotherapies, and medications may be effective in some patients with BED.4,6,8
Behavioral weight-loss treatment’s main goal is to manage the patient’s weight with a lower-calorie, healthy diet and to increase exercise.20,21
Over the short term (<1 year), behavioral weight-loss treatment produces similar weight loss in obese patients with or without BED; long-term results in both groups, however, have not been satisfactory.20,21 No studies have examined the efficacy of specialized diets (such as low-carbohydrate regimens) in patients with BED.
Specialized psychotherapy’s goal is to modify bingeeating behavior with behavioral self-management strategies, reducing interpersonal dysfunction and stress, and/or managing affective dysregulation.
Cognitive-behavioral therapy (CBT) and interpersonal therapy (IPT) have been effective in reducing binge eating, both acutely and for up to 12 months4,20-24 but less effective in achieving and maintaining weight loss. Patients who achieve remission in binge eating after undergoing CBT or IPI often experience modest but stable weight loss.20-22 For example, in a comparison study of CBT and IPT:
- After 20 weekly sessions, patients whose binge eating was in remission lost weight (mean body mass index [BMI] −0.5 ± 1.5 kg/m2), whereas those who continued to binge gained weight (mean BMI +0.4 ±2.0 kg/m2).
- At 12 months’ follow-up, patients still in remission continued to lose weight (mean BMI −1.0 ± 3.0 kg/m2), whereas those no longer in remission gained weight (mean BMI +0.7 ±2.9 kg/m2[P = 0.01]).22
Self-help and dialectical behavioral therapy (DBT) may also help reduce binge eating in BED. As with CBT and IPT, they are less effective in weight loss. In the only controlled study of DBT,24 patients achieved an average 2.5-lb weight loss after 20 weeks of DBT, compared with an average 0.6-lb weight gain in the control group. This difference was not significant, and the report did not include data on weight loss maintenance.
In summary, CBT may be more effective than behavioral weight loss treatment for reducing binge eating, but behavioral weight loss is more effective for weight loss.
Medications for BED
Medications that have been tried for BED include antidepressants, appetite suppressants, and anticonvulsants.25,26 Antidepressants are used to treat BED because:
- BED is often associated with depressive symptoms and disorders.
- BED is related to bulimia nervosa, and placebo-controlled trials have shown that the binge eating of bulimia nervosa responds to several classes of antidepressants. The selective serotonin reuptake inhibitor (SSRI) fluoxetine is the only medication indicated for treating any eating disorder (bulimia nervosa).
- Bupropion and venlafaxine—a serotonin-norepinephrine reuptake inhibitor (SNRI)—have weight-loss properties.
SSRIs are the most extensively studied antidepressants for treating BED. SSRIs have weightloss properties, but only short term.25-26 Citalopram, fluoxetine, fluvoxamine, and sertraline have reduced binge eating and body weight more effectively than placebo during 6 to 9 weeks of treatment (Table 2).25-26 However, one controlled study23 showed that fluoxetine was not significantly more effective than placebo in reducing binge frequency or body weight after 16 weeks.
TCAs. Studies of tricyclic antidepressants (TCAs) for BED are sparse, and results have been mixed. In one trial, imipramine was similar to placebo in reducing binge frequency and body weight. In a placebo-controlled study of patients with nonpurging bulimia nervosa, desipramine reduced binge eating but had no effect on body weight.25,26
Table 2
Drug therapies shown to be effective for BED*
| Medication | Binge eating | Weight | Depression | Study size | Duration (weeks) | Dosage (mg/d) |
|---|---|---|---|---|---|---|
| Antidepressants | ||||||
| Citalopram | + | + | − | 38 | 6 | 20 to 60 |
| Fluoxetine † | + | + | + | 60 | 6 | 20 to 80 |
| Fluvoxamine | + | + | − | 85 | 9 | 50 to 300 |
| Sertraline | + | + | − | 34 | 6 | 50 to 200 |
| Appetite suppressant | ||||||
| Sibutramine | + | + | + | 60 | 12 | 15 |
| Anticonvulsant | ||||||
| Topiramate | + | + | − | 61 | 14 | 50 to 600 |
| + Improvement | ||||||
| − No improvement | ||||||
| * Randomized, controlled trials. Antidepressants were studied in patients with BED; sibutramine and topiramate were studied in patients with BED and associated obesity. | ||||||
| † One 16-week trial of fluoxetine for BED (reference 23) did not show statistically significant differences in post-treatment binge frequency or body-mass index. | ||||||
Venlafaxine. In a retrospective review of 35 consecutive obese women with BED, venlafaxine, mean 222 mg/d for 28 to 300 days (median 120 days), reduced binge eating, body weight, and depressive symptoms.27
Bupropion has been more effective than placebo for treating:
- uncomplicated obesity (short- and long-term)
- obesity associated with depressive symptoms
- bulimia nervosa (although bupropion is contraindicated in these patients because of seizure risk).26,28,29
No controlled trials have studied bupropion for BED. When using dosages effective in depressive disorders, we find bupropion helpful in reducing binge eating, body weight, and depressive symptoms in BED patients.
Appetite suppressants decrease appetite and weight, may increase satiety, and may reduce depressive symptoms.
Sibutramine—a serotonin, norepinephrine, and dopamine reuptake inhibitor indicated for managing obesity—has been reported effective in BED in a 12-week, randomized, double-blind, placebo-controlled trial. A 15-mg/d dosage reduced binge frequency, body weight, and depressive symptoms more effectively than placebo in 60 obese patients with BED.30 Most-frequent adverse effects (dry mouth and constipation) were mild and benign, and no significant complications were observed.
Sibutramine’s mechanism of action in BED is unknown. However, it suppressed food intake during binge-eating episodes in patients with BED in a randomized, controlled, cross-over laboratory study.31
Orlistat. We know of no published controlled studies of the lipase inhibitor orlistat in treating BED. In our experience, some patients do well with this agent, though we have observed infrequent purging episodes with it in patients with BED.
With orlistat, 120 mg tid, our BED patients have experienced weight loss comparable to that seen in uncomplicated obesity at similar dosages. Orlistat seems most effective for:
- patients whose binge eating is in remission
- those who responded to behavioral weightloss treatment, a psychological treatment, or another medication.
Anticonvulsants such as topiramate and zonisamide have been shown effective in treating obesity32,33 and are sometimes used to treat BED. Obese BED patients with mood disorders often do best with psychotherapy plus medication
Topiramate at dosages of 50 to 600 mg/d (median 212 mg/d) reduced binge-eating frequency, obsessive-compulsive features of binge eating, and body weight more effectively than placebo in a 14-week study of 61 obese patients with BED. These effects were maintained across 48 weeks in an open-label extension trial.34
Zonisamide, mean 513 mg/d, produced similar results during a prospective, open-label, 12-week trial in 15 patients with BED.35 A controlled trial to replicate these findings is ongoing.
BED may respond to anticonvulsant therapy for several reasons:
- Some anticonvulsants are effective in treating bipolar disorder, which may occur with BED.12
- Some anticonvulsants have shown benefit in conditions associated with pathologic impulsivity, such as substance abuse, impulse-control, and cluster B disorders.10
Growing evidence shows that bulimia nervosa and BED may be associated with pathologic impulsivity.
Combination therapies are generally more effective than monotherapies in patients with mood disorders, uncomplicated obesity, and possibly bulimia nervosa. Even so, few trials have systematically studied combination therapy in managing patients with BED.
Two studies compared psychotherapy and antidepressants alone and in combination in treating BED.21,23 Both showed that CBT alone was more effective in decreasing binge frequency than desipramine alone,21 fluoxetine alone,23 and the combination of CBT and medication. On the other hand, patients who took desipramine either alone or in combination experienced a greater degree of weight loss than those who did not take desipramine.21
In another combination therapy, exercise has been shown to be an effective adjunct to CBT in maintenance treatment of obese women with BED.36
No studies have compared behavioral weight management or a specialized psychotherapy in combination with an antiobesity drug or a weight-loss anticonvulsant in treating BED.
Treatment recommendations
In our experience, BED patients—particularly those with obesity and psychopathology—often do best with some combination of psychological treatment and medication:
- The psychological component may be behavioral weight-loss treatment, a specialized psychotherapy such as CBT or IPT, or some combination of behavioral weight-loss treatment and specialized psychotherapy.
- The medication component may consist of an antidepressant, anticonvulsant, antiobesity drug, or multiple drugs (such as an SSRI or sibutramine with topiramate for BED with major depression, or topiramate with lithium for BED with bipolar disorder).
Although combination therapies may be optimal for some patients, this approach remains unproven in controlled trials.
Patient preference. In addition to comorbidities, patient preference is an important consideration when choosing BED treatments. We determine our patients’ preferences by educating them as much as possible about their options. We explain the benefits and weaknesses of all treatments and encourage them to participate in forming their individualized treatment plans.
Patients sometimes have strong treatment preferences. Some prefer psychological treatments, whereas others prefer medications. Working with patient preferences enhances treatment adherence. For example, patients who fail a preferred treatment are often more willing to adhere to another treatment modality about which they initially were skeptical.
Related resources
- Bray GA, Bouchard C (eds). Handbook of obesity: clinical applications (2nd ed). New York, NY: Marcel Dekker, 2004.
- Cooper Z, Zairburn CG, Hawker DM. Cognitive behavioral treatment of obesity. A clinician’s guide. New York: Guilford Press, 2003.
- Carter WP, Hudson JI, Lalonde JK, et al. Pharmacologic treatment of binge eating disorder. Int J Eat Disord 2003;34(suppl):S74-88.
Drug brand names
- Bupropion • Wellbutrin
- Citalopram • Celexa
- Desipramine • Norpramin
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Imipramine • Tofranil
- Lamotrigine • Lamictal
- Lithium • Eskalith, others
- Orlistat • Xenical
- Sertraline • Zoloft
- Sibutramine • Meridia
- Topiramate • Topamax
- Venlafaxine • Effexor
- Zonisamide • Zonegran
Disclosure
Dr. Kotwal receives grant support from Elan Corporation and is a speaker for Ortho-McNeil Pharmaceutical and Pfizer Inc.
Dr. Kaneria and Ms. Guerdjikova report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. McElroy is a consultant to Abbott Laboratories, Bristol-Myers Squibb Co., Elan Corporation, GlaxoSmithKline, Janssen Pharmaceutica, Eli Lilly and Co., and Ortho-McNeil Pharmaceutical. She receives grant/research support from Elan Pharmaceuticals, Forest Pharmaceuticals, Merck & Co., Ortho-McNeil Pharmaceutical, and Sanofi-Synthelabo and is a speaker for Eli Lilly and Co. and Ortho-McNeil Pharmaceutical.
Managing patients with binge-eating disorder (BED) often requires behavioral, medical, and psychiatric interventions.
These patients suffer from recurrent episodes of distressing, uncontrollable overeating, but they do not purge or show other compensatory weight-loss behaviors common to bulimia nervosa1 and anorexia nervosa.2-10 As a result, they are often overweight or obese and may have obesity-related illnesses, such as hypertension or type 2 diabetes. Mild to severe depression—unipolar or bipolar—is a common psychopathology.
Because no one treatment fits all patients with binge eating disorder, their management usually requires an individualized program of:
- behavioral weight control
- psychotherapy
- and sometimes medications.
In our weight management clinic, we consider medication options based on patient preference and whether BED is uncomplicated (Figure 1) or coexists with a mood disorder (Figure 2).
This article presents the evidence on which we base our comprehensive approach. General psychiatrists with knowledge of BED can treat patients with this eating disorder, although complicated cases may require referral for specialized treatment.
Figure 1 Medication options for uncomplicated BED
Clinical characteristics
Psychiatric comorbidity. BED often occurs in patients with mood, anxiety, substance-abuse, impulsecontrol, and personality disorders.4,6,10-12 Mood disorder—particularly depression—appears to be the most common comorbidity. BED can occur with bipolar disorder12—a comorbidity that in our experience is underrecognized both clinically and in the literature.
Patients with BED and bipolar disorder show increased impulsivity and mood lability. As bipolar II disorder and other “soft-spectrum” forms are more common than bipolar I disorder, BED is also more likely to occur with hypomania than mania.
Overweight. Not surprisingly, BED is associated with overweight and obesity.5,8,9,11 Not all patients with BED are overweight or obese, but most who participate in clinical trials of BED treatments are at least overweight. BED has been reported in up to:
- 30% of participants in weight-loss programs7
- 70% of participants in groups such as Overeaters Anonymous
- 50% of patients who seek bariatric surgery.5
In our experience, patients are often more distressed by their weight than by their binge eating, depression, or anxiety. Indeed, overweight and obesity are the usual reasons patients with BED present for treatment at our center.
Diagnosis. BED’s validity as a clinical diagnosis has been controversial since the disorder was first included in DSM-IV (Table 1).3 Debate continues about some definitions in the DSM criteria, including what amount of food is “definitely larger” than most people would eat and what is “loss of control over eating.”
Nevertheless, screening for BED is relatively easy. Clinicians may use the eating disorder section of the Structured Clinical Interview for DSM-IV or the Eating Disorders Examination. Alternatively, simply ask patients if they have episodes of uncontrollable overeating, during which they eat unusually large amounts of food and their eating feels out of control.
Course. BED begins in adolescence or adulthood. Disease course is variable, with periods of remission, recurrence, and chronicity.6,7,10 Interestingly, one prospective study showed that even if the binge eating resolves, persons may still develop obesity.13
Prevalence. BED affects 1.5% to 3% of the U.S. population. It is more common in women than men, equally prevalent in whites and blacks, and more prevalent than anorexia nervosa and bulimia nervosa combined.11,14 Subthreshold BED—such as obesity with infrequent or nondistressing binge eating—appears to be much more common,10 although no data are available.
Theories of binge eating
BED’s cause is unknown, but biological, familial, and psychosocial factors have been implicated.
Biological factors. The neurotransmitters serotonin (5-HT) and dopamine—as well as various peptides—have been shown to help regulate feeding behavior.10
Table 1
Diagnostic criteria for binge-eating disorder*
|
| * Research criteria, DSM-IV-TR appendix B. |
| Source: Reprinted with permission from the Diagnostic and statistical manual of mental disorders, 4th edition, text revision. Copyright 2000. American Psychiatric Association. |
Serotonin. Reduced 5-HT transporter binding has been shown in obese women with BED.15 Their 5-HT binding improved and binge eating subsided with group psychotherapy and fluoxetine, although the women continued to gain weight.
Figure 2 Medication options for BED with obesity and a mood disorder*
Dopamine. Obese patients who compulsively overeat may have lower levels of dopamine D2 receptors than do normal-weight controls.16
Genetic factors. In severely obese patients (body mass index 44±2), those with a DSM-IV diagnosis of BED exhibited mutations of the melanocortin 4 receptor gene, which affects the anorectic properties of alpha melanocyte-stimulating hormone.17
Familial factors associated with BED include parental depression and obesity.18
Psychosocial correlates include physical and sexual abuse, bullying by peers, and discrimination because of being overweight.19
Treatment recommendations
Few systematic studies have examined BED treatment. Emerging research suggests that behavioral weight-loss treatment, specialized psychotherapies, and medications may be effective in some patients with BED.4,6,8
Behavioral weight-loss treatment’s main goal is to manage the patient’s weight with a lower-calorie, healthy diet and to increase exercise.20,21
Over the short term (<1 year), behavioral weight-loss treatment produces similar weight loss in obese patients with or without BED; long-term results in both groups, however, have not been satisfactory.20,21 No studies have examined the efficacy of specialized diets (such as low-carbohydrate regimens) in patients with BED.
Specialized psychotherapy’s goal is to modify bingeeating behavior with behavioral self-management strategies, reducing interpersonal dysfunction and stress, and/or managing affective dysregulation.
Cognitive-behavioral therapy (CBT) and interpersonal therapy (IPT) have been effective in reducing binge eating, both acutely and for up to 12 months4,20-24 but less effective in achieving and maintaining weight loss. Patients who achieve remission in binge eating after undergoing CBT or IPI often experience modest but stable weight loss.20-22 For example, in a comparison study of CBT and IPT:
- After 20 weekly sessions, patients whose binge eating was in remission lost weight (mean body mass index [BMI] −0.5 ± 1.5 kg/m2), whereas those who continued to binge gained weight (mean BMI +0.4 ±2.0 kg/m2).
- At 12 months’ follow-up, patients still in remission continued to lose weight (mean BMI −1.0 ± 3.0 kg/m2), whereas those no longer in remission gained weight (mean BMI +0.7 ±2.9 kg/m2[P = 0.01]).22
Self-help and dialectical behavioral therapy (DBT) may also help reduce binge eating in BED. As with CBT and IPT, they are less effective in weight loss. In the only controlled study of DBT,24 patients achieved an average 2.5-lb weight loss after 20 weeks of DBT, compared with an average 0.6-lb weight gain in the control group. This difference was not significant, and the report did not include data on weight loss maintenance.
In summary, CBT may be more effective than behavioral weight loss treatment for reducing binge eating, but behavioral weight loss is more effective for weight loss.
Medications for BED
Medications that have been tried for BED include antidepressants, appetite suppressants, and anticonvulsants.25,26 Antidepressants are used to treat BED because:
- BED is often associated with depressive symptoms and disorders.
- BED is related to bulimia nervosa, and placebo-controlled trials have shown that the binge eating of bulimia nervosa responds to several classes of antidepressants. The selective serotonin reuptake inhibitor (SSRI) fluoxetine is the only medication indicated for treating any eating disorder (bulimia nervosa).
- Bupropion and venlafaxine—a serotonin-norepinephrine reuptake inhibitor (SNRI)—have weight-loss properties.
SSRIs are the most extensively studied antidepressants for treating BED. SSRIs have weightloss properties, but only short term.25-26 Citalopram, fluoxetine, fluvoxamine, and sertraline have reduced binge eating and body weight more effectively than placebo during 6 to 9 weeks of treatment (Table 2).25-26 However, one controlled study23 showed that fluoxetine was not significantly more effective than placebo in reducing binge frequency or body weight after 16 weeks.
TCAs. Studies of tricyclic antidepressants (TCAs) for BED are sparse, and results have been mixed. In one trial, imipramine was similar to placebo in reducing binge frequency and body weight. In a placebo-controlled study of patients with nonpurging bulimia nervosa, desipramine reduced binge eating but had no effect on body weight.25,26
Table 2
Drug therapies shown to be effective for BED*
| Medication | Binge eating | Weight | Depression | Study size | Duration (weeks) | Dosage (mg/d) |
|---|---|---|---|---|---|---|
| Antidepressants | ||||||
| Citalopram | + | + | − | 38 | 6 | 20 to 60 |
| Fluoxetine † | + | + | + | 60 | 6 | 20 to 80 |
| Fluvoxamine | + | + | − | 85 | 9 | 50 to 300 |
| Sertraline | + | + | − | 34 | 6 | 50 to 200 |
| Appetite suppressant | ||||||
| Sibutramine | + | + | + | 60 | 12 | 15 |
| Anticonvulsant | ||||||
| Topiramate | + | + | − | 61 | 14 | 50 to 600 |
| + Improvement | ||||||
| − No improvement | ||||||
| * Randomized, controlled trials. Antidepressants were studied in patients with BED; sibutramine and topiramate were studied in patients with BED and associated obesity. | ||||||
| † One 16-week trial of fluoxetine for BED (reference 23) did not show statistically significant differences in post-treatment binge frequency or body-mass index. | ||||||
Venlafaxine. In a retrospective review of 35 consecutive obese women with BED, venlafaxine, mean 222 mg/d for 28 to 300 days (median 120 days), reduced binge eating, body weight, and depressive symptoms.27
Bupropion has been more effective than placebo for treating:
- uncomplicated obesity (short- and long-term)
- obesity associated with depressive symptoms
- bulimia nervosa (although bupropion is contraindicated in these patients because of seizure risk).26,28,29
No controlled trials have studied bupropion for BED. When using dosages effective in depressive disorders, we find bupropion helpful in reducing binge eating, body weight, and depressive symptoms in BED patients.
Appetite suppressants decrease appetite and weight, may increase satiety, and may reduce depressive symptoms.
Sibutramine—a serotonin, norepinephrine, and dopamine reuptake inhibitor indicated for managing obesity—has been reported effective in BED in a 12-week, randomized, double-blind, placebo-controlled trial. A 15-mg/d dosage reduced binge frequency, body weight, and depressive symptoms more effectively than placebo in 60 obese patients with BED.30 Most-frequent adverse effects (dry mouth and constipation) were mild and benign, and no significant complications were observed.
Sibutramine’s mechanism of action in BED is unknown. However, it suppressed food intake during binge-eating episodes in patients with BED in a randomized, controlled, cross-over laboratory study.31
Orlistat. We know of no published controlled studies of the lipase inhibitor orlistat in treating BED. In our experience, some patients do well with this agent, though we have observed infrequent purging episodes with it in patients with BED.
With orlistat, 120 mg tid, our BED patients have experienced weight loss comparable to that seen in uncomplicated obesity at similar dosages. Orlistat seems most effective for:
- patients whose binge eating is in remission
- those who responded to behavioral weightloss treatment, a psychological treatment, or another medication.
Anticonvulsants such as topiramate and zonisamide have been shown effective in treating obesity32,33 and are sometimes used to treat BED. Obese BED patients with mood disorders often do best with psychotherapy plus medication
Topiramate at dosages of 50 to 600 mg/d (median 212 mg/d) reduced binge-eating frequency, obsessive-compulsive features of binge eating, and body weight more effectively than placebo in a 14-week study of 61 obese patients with BED. These effects were maintained across 48 weeks in an open-label extension trial.34
Zonisamide, mean 513 mg/d, produced similar results during a prospective, open-label, 12-week trial in 15 patients with BED.35 A controlled trial to replicate these findings is ongoing.
BED may respond to anticonvulsant therapy for several reasons:
- Some anticonvulsants are effective in treating bipolar disorder, which may occur with BED.12
- Some anticonvulsants have shown benefit in conditions associated with pathologic impulsivity, such as substance abuse, impulse-control, and cluster B disorders.10
Growing evidence shows that bulimia nervosa and BED may be associated with pathologic impulsivity.
Combination therapies are generally more effective than monotherapies in patients with mood disorders, uncomplicated obesity, and possibly bulimia nervosa. Even so, few trials have systematically studied combination therapy in managing patients with BED.
Two studies compared psychotherapy and antidepressants alone and in combination in treating BED.21,23 Both showed that CBT alone was more effective in decreasing binge frequency than desipramine alone,21 fluoxetine alone,23 and the combination of CBT and medication. On the other hand, patients who took desipramine either alone or in combination experienced a greater degree of weight loss than those who did not take desipramine.21
In another combination therapy, exercise has been shown to be an effective adjunct to CBT in maintenance treatment of obese women with BED.36
No studies have compared behavioral weight management or a specialized psychotherapy in combination with an antiobesity drug or a weight-loss anticonvulsant in treating BED.
Treatment recommendations
In our experience, BED patients—particularly those with obesity and psychopathology—often do best with some combination of psychological treatment and medication:
- The psychological component may be behavioral weight-loss treatment, a specialized psychotherapy such as CBT or IPT, or some combination of behavioral weight-loss treatment and specialized psychotherapy.
- The medication component may consist of an antidepressant, anticonvulsant, antiobesity drug, or multiple drugs (such as an SSRI or sibutramine with topiramate for BED with major depression, or topiramate with lithium for BED with bipolar disorder).
Although combination therapies may be optimal for some patients, this approach remains unproven in controlled trials.
Patient preference. In addition to comorbidities, patient preference is an important consideration when choosing BED treatments. We determine our patients’ preferences by educating them as much as possible about their options. We explain the benefits and weaknesses of all treatments and encourage them to participate in forming their individualized treatment plans.
Patients sometimes have strong treatment preferences. Some prefer psychological treatments, whereas others prefer medications. Working with patient preferences enhances treatment adherence. For example, patients who fail a preferred treatment are often more willing to adhere to another treatment modality about which they initially were skeptical.
Related resources
- Bray GA, Bouchard C (eds). Handbook of obesity: clinical applications (2nd ed). New York, NY: Marcel Dekker, 2004.
- Cooper Z, Zairburn CG, Hawker DM. Cognitive behavioral treatment of obesity. A clinician’s guide. New York: Guilford Press, 2003.
- Carter WP, Hudson JI, Lalonde JK, et al. Pharmacologic treatment of binge eating disorder. Int J Eat Disord 2003;34(suppl):S74-88.
Drug brand names
- Bupropion • Wellbutrin
- Citalopram • Celexa
- Desipramine • Norpramin
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Imipramine • Tofranil
- Lamotrigine • Lamictal
- Lithium • Eskalith, others
- Orlistat • Xenical
- Sertraline • Zoloft
- Sibutramine • Meridia
- Topiramate • Topamax
- Venlafaxine • Effexor
- Zonisamide • Zonegran
Disclosure
Dr. Kotwal receives grant support from Elan Corporation and is a speaker for Ortho-McNeil Pharmaceutical and Pfizer Inc.
Dr. Kaneria and Ms. Guerdjikova report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. McElroy is a consultant to Abbott Laboratories, Bristol-Myers Squibb Co., Elan Corporation, GlaxoSmithKline, Janssen Pharmaceutica, Eli Lilly and Co., and Ortho-McNeil Pharmaceutical. She receives grant/research support from Elan Pharmaceuticals, Forest Pharmaceuticals, Merck & Co., Ortho-McNeil Pharmaceutical, and Sanofi-Synthelabo and is a speaker for Eli Lilly and Co. and Ortho-McNeil Pharmaceutical.
1. Pope HG, Hudson JI. Bulimia nervosa: Persistent disorders requires equally persistent treatment. Current Psychiatry 2004;3(1):13-22.
2. Halmi KA. Anorexia nervosa: Dual therapy can bring patients back from the brink. Current Psychiatry 2004;3(3):39-56.
3. American Psychiatric Association. Diagnostic and statistical manual of mental disorders (4th ed). Washington, DC: American Psychiatric Association, 1994.
4. Agras WS. Treatment of binge eating disorder. In: Gabbard GO (ed). Treatments of psychiatric disorders (3rd ed). Washington, DC: American Psychiatric Press, 2001;2209-19.
5. de Zwaan M. Binge eating disorder and obesity. Int J Obes Relat Metab Disord 2001;25(suppl 1):S51-5.
6. Dingemans AE, Bruna MJ, van Furth EF. Binge eating disorder: a review. Int J Obes Relat Metab Disord 2002;26:299-307.
7. Fairburn CG, Harrison PJ. Eating disorders. Lancet 2003;361:407-16.
8. Walsh BT (ed). The current status of binge eating disorder. Int J Eat Disord 2003;34(suppl):S1-120.
9. Devlin MJ, Goldfein JA, Dobrow I. What is this thing called BED? Current status of binge eating disorder nosology. Int J Eat Disord 2003;34(suppl):S2-18.
10. McElroy SL, Kotwal R. Binge eating. In: Hollander E, Stein D (eds). Handbook of impulse control disorders Washington, DC: American Psychiatric Press (in press).
11. Smith DE, Marcus MD, Lewis CE, et al. Prevalence of binge eating disorder, obesity, and depression in a biracial cohort of young adults. Ann Behav Med 1998;20:227-32.
12. Kruger S, Shugar G, Cooke RG. Comorbidity of binge eating disorder and the partial binge eating syndrome with bipolar disorder. Int J Eat Disord 1996;19:45-52.
13. Fairburn CG, Cooper Z, Doll H, et al. The natural course of bulimia nervosa and binge eating disorder in young women. Arch Gen Psychiatry 2000;57:659-65.
14. Striegel-Moore RH, Franko DL. Epidemiology of binge eating disorder. Int J Eat Disord 2003;34(suppl):S19-29.
15. Tammela LI, Rissanen A, Kuikka JT, et al. Treatment improves serotonin transporter binding and reduces binge eating. Psychopharmacology (Berl) 2003;170:89-93.
16. Wang GJ, Volkow ND, Logan J, et al. Brain dopamine and obesity. Lancet 2001;357:354-7.
17. Branson R, Potoczna N, Kral JG, et al. Binge eating as a major phenotype of melanocortin 4 receptor gene mutations. N Engl J Med 2003;348:1096-103.
18. Fairburn CG, Doll HA, Welch SL, et al. Risk factors for binge eating disorder: a community-based, case-control study. Arch Gen Psychiatry 1998;55:425-32.
19. Striegel-Moore RH, Dohm FA, Pike KM, et al. Abuse, bullying, and discrimination as risk factors for binge eating disorder. Am J Psychiatry 2002;159:1902-7.
20. Wonderlich SA, de Zwaan M, Mitchell JE, et al. Psychological and dietary treatments of binge eating disorder: conceptual implications. Int J Eat Disord 2003;34(suppl):S58-78.
21. Agras WS, Telch DF, Arnow B, et al. Weight loss, cognitive-behavioral, and desipramine treatments in binge eating disorder. An additive design. Behav Ther 1994;25:225-38.
22. Wilfley DE, Welch RR, Stein RI, et al. A randomized comparison of group cognitive-behavioral therapy and group interpersonal psychotherapy for the treatment of overweight individuals with binge eating disorder. Arch Gen Psychiatry 2002;59:713-21.
23. Grilo CM. A controlled study of cognitive behavioral therapy and fluoxetine for binge eating disorder (presentation) Charleston, SC: Eating Disorders Research Society annual meeting, 2002.
24. Telch CF, Agras WS, Linehan MM. Dialectical behavior therapy for binge eating disorder. J Consult Clin Psychol 2001;69:1061-5.
25. Carter WP, Hudson JI, Lalonde JK, et al. Pharmacologic treatment of binge eating disorder. Int J Eat Disord 2003;34(suppl):S74-88.
26. Appolinario JC, McElroy SL. Pharmacologic approaches in the treatment of binge eating disorder. Curr Drug Targets (in press).
27. Malhotra S, King KH, Welge JA, et al. Venlafaxine treatment of binge-eating disorder associated with obesity: a series of 35 patients. J Clin Psychiatry 2002;63:802-6.
28. Anderson JW, Greenway FL, Fujioka K, et al. Bupropion SR enhances weight loss: a 48-week double-blind, placebo-controlled trial. Obes Res 2002;10:633-41.
29. McElroy SL, Kotwal R, Malhotra S, et al. Are mood disorders and obesity related? A review for the mental health professional. J Clin Psychiatry (in press).
30. Appolinario JC, Bacaltchuk J, Sichieri R, et al. A randomized, double-blind, placebo-controlled study of sibutramine in the treatment of binge-eating disorder. Arch Gen Psychiatry 2003;60:1109-16.
31. Mitchell JE, Gosnell BA, Roerig JL, et al. Effects of sibutramine on binge eating, hunger, and fullness in a laboratory human feeding paradigm. Obes Res 2003;11:599-602.
32. Bray GA, Hollander P, Klein S, et al. A 6-month randomized, placebo-controlled, dose-ranging trial of topiramate for weight loss in obesity. Obes Res 2003;11:722-33.
33. Gadde KM, Franciscy DM, Wagner HR, 2nd, Krishnan KR. Zonisamide for weight loss in obese adults: a randomized controlled trial. JAMA 2003;289:1820-5.
34. McElroy SL, Arnold LM, Shapira NA, et al. Topiramate in the treatment of binge eating disorder associated with obesity: a randomized, placebo-controlled trial. Am J Psychiatry 2003;160:255-61.
35. McElroy SL, Kotwal R, Hudson JI, et al. Zonisamide in the treatment of binge-eating disorder: an open-label, prospective trial. J Clin Psychiatry 2004;65:50-6.
36. Pendleton VR, Goodrick GK, Poston WSC, et al. Exercise augments the effects of cognitive-behavioral therapy in the treatment of binge eating. Int J Eat Disord 2002;31(2):172-84.
1. Pope HG, Hudson JI. Bulimia nervosa: Persistent disorders requires equally persistent treatment. Current Psychiatry 2004;3(1):13-22.
2. Halmi KA. Anorexia nervosa: Dual therapy can bring patients back from the brink. Current Psychiatry 2004;3(3):39-56.
3. American Psychiatric Association. Diagnostic and statistical manual of mental disorders (4th ed). Washington, DC: American Psychiatric Association, 1994.
4. Agras WS. Treatment of binge eating disorder. In: Gabbard GO (ed). Treatments of psychiatric disorders (3rd ed). Washington, DC: American Psychiatric Press, 2001;2209-19.
5. de Zwaan M. Binge eating disorder and obesity. Int J Obes Relat Metab Disord 2001;25(suppl 1):S51-5.
6. Dingemans AE, Bruna MJ, van Furth EF. Binge eating disorder: a review. Int J Obes Relat Metab Disord 2002;26:299-307.
7. Fairburn CG, Harrison PJ. Eating disorders. Lancet 2003;361:407-16.
8. Walsh BT (ed). The current status of binge eating disorder. Int J Eat Disord 2003;34(suppl):S1-120.
9. Devlin MJ, Goldfein JA, Dobrow I. What is this thing called BED? Current status of binge eating disorder nosology. Int J Eat Disord 2003;34(suppl):S2-18.
10. McElroy SL, Kotwal R. Binge eating. In: Hollander E, Stein D (eds). Handbook of impulse control disorders Washington, DC: American Psychiatric Press (in press).
11. Smith DE, Marcus MD, Lewis CE, et al. Prevalence of binge eating disorder, obesity, and depression in a biracial cohort of young adults. Ann Behav Med 1998;20:227-32.
12. Kruger S, Shugar G, Cooke RG. Comorbidity of binge eating disorder and the partial binge eating syndrome with bipolar disorder. Int J Eat Disord 1996;19:45-52.
13. Fairburn CG, Cooper Z, Doll H, et al. The natural course of bulimia nervosa and binge eating disorder in young women. Arch Gen Psychiatry 2000;57:659-65.
14. Striegel-Moore RH, Franko DL. Epidemiology of binge eating disorder. Int J Eat Disord 2003;34(suppl):S19-29.
15. Tammela LI, Rissanen A, Kuikka JT, et al. Treatment improves serotonin transporter binding and reduces binge eating. Psychopharmacology (Berl) 2003;170:89-93.
16. Wang GJ, Volkow ND, Logan J, et al. Brain dopamine and obesity. Lancet 2001;357:354-7.
17. Branson R, Potoczna N, Kral JG, et al. Binge eating as a major phenotype of melanocortin 4 receptor gene mutations. N Engl J Med 2003;348:1096-103.
18. Fairburn CG, Doll HA, Welch SL, et al. Risk factors for binge eating disorder: a community-based, case-control study. Arch Gen Psychiatry 1998;55:425-32.
19. Striegel-Moore RH, Dohm FA, Pike KM, et al. Abuse, bullying, and discrimination as risk factors for binge eating disorder. Am J Psychiatry 2002;159:1902-7.
20. Wonderlich SA, de Zwaan M, Mitchell JE, et al. Psychological and dietary treatments of binge eating disorder: conceptual implications. Int J Eat Disord 2003;34(suppl):S58-78.
21. Agras WS, Telch DF, Arnow B, et al. Weight loss, cognitive-behavioral, and desipramine treatments in binge eating disorder. An additive design. Behav Ther 1994;25:225-38.
22. Wilfley DE, Welch RR, Stein RI, et al. A randomized comparison of group cognitive-behavioral therapy and group interpersonal psychotherapy for the treatment of overweight individuals with binge eating disorder. Arch Gen Psychiatry 2002;59:713-21.
23. Grilo CM. A controlled study of cognitive behavioral therapy and fluoxetine for binge eating disorder (presentation) Charleston, SC: Eating Disorders Research Society annual meeting, 2002.
24. Telch CF, Agras WS, Linehan MM. Dialectical behavior therapy for binge eating disorder. J Consult Clin Psychol 2001;69:1061-5.
25. Carter WP, Hudson JI, Lalonde JK, et al. Pharmacologic treatment of binge eating disorder. Int J Eat Disord 2003;34(suppl):S74-88.
26. Appolinario JC, McElroy SL. Pharmacologic approaches in the treatment of binge eating disorder. Curr Drug Targets (in press).
27. Malhotra S, King KH, Welge JA, et al. Venlafaxine treatment of binge-eating disorder associated with obesity: a series of 35 patients. J Clin Psychiatry 2002;63:802-6.
28. Anderson JW, Greenway FL, Fujioka K, et al. Bupropion SR enhances weight loss: a 48-week double-blind, placebo-controlled trial. Obes Res 2002;10:633-41.
29. McElroy SL, Kotwal R, Malhotra S, et al. Are mood disorders and obesity related? A review for the mental health professional. J Clin Psychiatry (in press).
30. Appolinario JC, Bacaltchuk J, Sichieri R, et al. A randomized, double-blind, placebo-controlled study of sibutramine in the treatment of binge-eating disorder. Arch Gen Psychiatry 2003;60:1109-16.
31. Mitchell JE, Gosnell BA, Roerig JL, et al. Effects of sibutramine on binge eating, hunger, and fullness in a laboratory human feeding paradigm. Obes Res 2003;11:599-602.
32. Bray GA, Hollander P, Klein S, et al. A 6-month randomized, placebo-controlled, dose-ranging trial of topiramate for weight loss in obesity. Obes Res 2003;11:722-33.
33. Gadde KM, Franciscy DM, Wagner HR, 2nd, Krishnan KR. Zonisamide for weight loss in obese adults: a randomized controlled trial. JAMA 2003;289:1820-5.
34. McElroy SL, Arnold LM, Shapira NA, et al. Topiramate in the treatment of binge eating disorder associated with obesity: a randomized, placebo-controlled trial. Am J Psychiatry 2003;160:255-61.
35. McElroy SL, Kotwal R, Hudson JI, et al. Zonisamide in the treatment of binge-eating disorder: an open-label, prospective trial. J Clin Psychiatry 2004;65:50-6.
36. Pendleton VR, Goodrick GK, Poston WSC, et al. Exercise augments the effects of cognitive-behavioral therapy in the treatment of binge eating. Int J Eat Disord 2002;31(2):172-84.
Brain/body connection: Treating depression in patients with cardiovascular disease
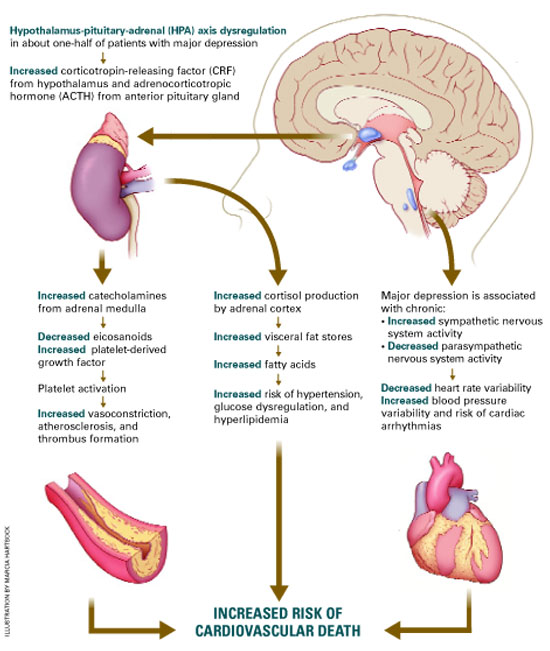
Depression can exacerbate cardiovascular disease (CVD), and CVD can exacerbate depression (Figure). Thus, effectively treating depression enhances heart disease treatment, particularly if psychiatrists and medical physicians collaborate in providing patient care.
This article describes a patient with risk factors for heart disease, illustrates the physiologic pathways that link depression and CVD, and offers clinical tips to help you improve outcomes for patients with both disorders.
Case report: Trying to ‘get going’
Mr. D, age 51, presents with vegetative symptoms and a personal and family history of CVD, depression, and substance abuse disorders. He was born in a small town in Kentucky and raised in Louisville’s poorest neighborhood. After his mother died at age 42 of “hardening of the arteries,” his father started drinking more, working less, and “never really got going again.”
Figure Neuroendocrine pathways by which depression may cause or promote CVD
Among patients with a recent myocardial infarction (MI), as many as two-thirds report depressive symptoms.1 Major depression has been reported in:
- 16% to 22% of patients hospitalized post-MI,2,3 compared with 5% in the general population and 10% in the primary care population4
- 15% of patients with unstable angina5 and 20% of patients undergoing coronary artery bypass (CABG) surgery.6
Among the annual 1.5 million Americans who have an acute MI or unstable angina, 40% develop depression immediately thereafter. These 600,000 depressed patients are three times more likely to die within 6 months, compared with post-MI patients who are not depressed.7
Mr. D worked 20 years as a construction contractor, often running several work crews at once. At age 41, he slid into a depressive episode after his second divorce. He struggled with low energy, disturbed sleep, hopelessness, and increased smoking and drinking for 1 year, but he did not seek help.
Two years later, he suffered an inferior wall transmural myocardial infarction. His CVD risk factors included family history of early heart disease, smoking for 32 years, and elevated low-density lipoprotein (LDL) cholesterol. After subsequent episodes of unstable angina, stents were placed in two coronary arteries. Though his cardiologist cleared him to return to work, he felt able to work only part-time and erratically.
During a visit to their family doctor several years later, Mr. D’s wife suggested that her husband might be depressed. Reluctantly, Mr. D consulted a psychiatrist.
The psychiatrist diagnosed major depressive disorder and prescribed sertraline, 50 mg/d. Within 2 months, Mr. D’s symptoms had dropped by 50% on a symptom severity measure. He did not refill his prescription, however, because of concerns about sexual side effects. Two months later he was hospitalized for another episode of unstable angina. His depression had returned within 1 month of stopping sertraline.
The psychiatrist switched him to citalopram, 20 mg/d, and carefully monitored depressive symptoms, side effects, and medication adherence. Aside from talking with the psychiatrist for a half-hour in his family doctor’s office every few weeks, Mr. D refused to undergo psychotherapy. He eventually achieved depression remission with a combination of citalopram, 20 mg/d, and nefazodone, 200 mg/d.
Depression-CVD connection
As in Mr. D’s case, depression and CVD commonly occur together, often with serious consequences (Box). 1-7 The association between depression and CVD is not limited to depression’s effect on existing disease, however. Depression often precedes coronary disease by about 30 years—suggesting possible cause and effect. Two systematic reviews8,9 found that depression increased CVD risk by 64%.
Seven well-controlled studies5-7,10-13 compared the relative effect of depression on the cardiovascular system with that of established CVD predictors. All seven found depression’s independent effect to be significant and comparable to or greater than that of ejection fraction, previous MI history, or number of vessels with >50% narrowing.
Comorbid depression and CVD usually persists months or years,14 and most studies indicate a dose-response relationship; the more severe the depression, the greater the risk for CVD to develop or progress.8,15
The link between depression treatment and CVD risk has not been well-studied. The only randomized, controlled trial found that cognitive therapy for depression did not significantly reduce cardiac events among patients with known CVD.16
Possible mechanisms
Depression’s effect on CVD. How does depression affect CVD development and progression? Both behavioral and biological pathways may be involved.17 The behavioral pathway proposes that depression triggers behaviors—such as smoking, overeating, and sedentary lifestyles—that increase the risk of developing or worsening CVD. The biological pathway proposes that neuroendocrine changes during depression accelerate CVD development.
About one-half of persons with major depression exhibit hypothalamic-pituitary-adrenal (HPA) axis dysregulation, with excessive secretion of corticotropin releasing factor (CRF) and chronically elevated cortisol.18 This HPA dysregulation is related to defective negative feedback at the paraventricular nucleus of the hypothalamus. Chronic HPA axis dysregulation promotes vascular inflammation, and several studies have reported C-reactive protein elevation and cytokine changes in patients with major depression.19,20
Major depression is also associated with excessive sympathetic and diminished parasym-pathetic nervous system activity, potentially contributing to hypertension, increased resting heart rate, decreased heart rate variability, and altered endothelial function.2,21,22 Each of these factors facilitates arterial plaque formation.
Depression may also exacerbate chronic anxiety and other forms of distress. The combined effects of an overtaxed central nervous system, neuroendocrine dysregulation, and unhealthy behaviors may eventually overwhelm the cardiovascular system.
CVD’s effect on depression. How does CVD contribute to depression? The vascular depression hypothesis23 proposes that diffuse heart and brain atherosclerosis restricts perfusion of limbic and cortical structures that regulate mood. A first depressive episode after acute MI or CABG probably represents exacerbation of cerebrovascular insufficiency that preceded the coronary event.
Table
Four keys to effectively treat depression in patients with heart disease
|
In practical terms, this means that pathways linking depression and heart disease include not only biological factors but also:
- psychological factors such as depression, anxiety, and chronic stress
- behavioral factors such as smoking, physical inactivity, and high-fat diet.
How to improve outcomes
Patients with CVD commonly do not receive effective depression treatment:
- Internists and family physicians give preferential attention to physical illness.
- Patients may have insufficient access to mental health specialists.
- Physicians do not adequately monitor depression treatment.
- Patients are reluctant to accept the stigma of mental illness.
By collaborating with primary care physicians, you can improve the likelihood that depression treatment will achieve remission and prevent relapse (Table).
Risk factors for CVD. Depression contributes to heart disease by exacerbating four major CVD risk factors—smoking, diabetes, obesity, and physical inactivity. By effectively treating depression, you may help patients avoid common depressive symptoms—such as overeating and sedentary behaviors—that are related to low energy or fatigue.
Educate middle-aged patients with depression about CVD’s associated risk. Prochaska’s “stages of change” (see Related resources) can help them stop smoking, lose weight, and exercise.
Access to cardiac care. Depressed patients may be less motivated than nondepressed patients to pursue cardiac care.24 Therefore, you may need to:
- encourage your patients to take advantage of indicated state-of-the-art care, including stents, bypass surgery, and medications
- understand patients’ complex cardiac regimens and help them adhere when depression interferes with their motivation.
Effective depression treatment
Patient history. For depressed patients older than 40, take a careful inventory of CVD risk factors:
- family history of heart disease before age 60 for men and age 70 for women
- personal history of smoking, blood pressure >140/90 mm Hg, LDL cholesterol >100 mg/dL, type 2 diabetes, body mass index >30, or physical inactivity (<30 minutes of walking 3 days a week).
In general, the more risk factors, the greater the risk of CVD.
Antidepressant selection. Selective serotonin reuptake inhibitors (SSRIs) are safe and effective for treating major depression in CVD and congestive heart failure.25 Venlafaxine at doses >300 mg/d may increase blood pressure, so use this drug with caution in depressed patients with hypertension.
No controlled clinical trials have gauged the safety and efficacy of bupropion or mirtazapine in patients with CVD.
Tricyclic antidepressants are contraindicated for 6 months post-MI because they may contribute to arrhythmias. Avoid using them in depressed patients with CVD or conduction defects because of their quinidine-like effects on conduction.
Cardiac medications. Contrary to folk wisdom, beta blockers do not cause depression.26 Whether or not a patient is depressed, our primary care and cardiology colleagues can use beta blockers to help regulate the peripheral autonomic nervous system, reducing high blood pressure and the risk of arrhythmias.
SSRIs may increase blood levels of beta blockers, warfarin, and other cardiac medications via cytochrome P-450 isoenzyme inhibition. Make sure warfarin levels and other cardiac drug effects are well monitored when you adjust psychotropic dosages.
Divalproex and SSRIs also may reduce platelet aggregation. Patients who are receiving concomitant aspirin or warfarin may bruise or bleed easily and require dosage reductions or medication changes.
Psychotherapy. All patients with major or minor depression and CVD are considered high-risk and are candidates for a trial of brief psychotherapy. Therapeutic goals are to achieve full remission of depressive symptoms as rapidly as possible, prevent relapse, and maximize adherence to cardiac and depression drug regimens.
Collaborate closely with the cardiologist or primary care physician during the patient’s depressive episode and occasionally during maintenance treatment. Discuss or share notes on the patient’s depressive and cardiac disorders, medication management, symptom monitoring, and behavior changes needed to reduce cardiac risk.
With your added support, patients with depression and CVD are more likely to adhere to antidepressant medications and achieve symptom remission.
- National Institute of Mental Health. Depression and heart disease. www.nimh.nih.gov/publicat/depheart.cfm.
- Dewan NA, Suresh DP, Blomkalns A. Selecting safe psychotropics for post-MI patients. Current Psychiatry. 2003;2(3):15-21.
- Prochaska JO, Norcross JC, DiClemente CC. Changing for good. New York: Avon, 1994.
Drug brand names
- Bupropion • Wellbutrin
- Citalopram • Celexa
- Escitalopram • Lexapro
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Paroxetine • Paxil
- Mirtazapine • Remeron
- Nefazodone • Serzone
- Sertraline • Zoloft
- Venlafaxine • Effexor
Disclosure
Dr. Wulsin is a consultant to Pfizer Inc. and Janssen Pharmaceutica.
Dr. Vieweg is a speaker for Janssen Pharmaceutica, Eli Lilly and Co., Pfizer Inc., Wyeth Pharmaceuticals, Forest Pharmaceuticals, and GlaxoSmithKline.
Dr. Fernandez reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Cassem N, Hackett T. Psychiatric condition in a coronary care unit. Ann Intern Med 1971;75:9-14.
2. Glassman A, Shapiro P. Depression and the course of coronary artery disease. Am J Psychiatry 1998;155:4-11.
3. Carney R, Freedland K, Sheline Y, Weiss E. Depression and coronary heart disease: a review for cardiologists. Clin Cardiol 1997;20:196-200.
4. Katon W, Schulbert H. Epidemiology of depression in primary care. Gen Hosp Psychiatry 1992;14:237-47.
5. Lesperance F, Frasure-Smith N, Theroux P. Depression and 1-year prognosis in unstable angina. Arch Intern Med 2000;160:1354-60.
6. Connerney I, Shapiro P, McLaughlin J, et al. Relation between depression after coronary artery bypass surgery and 12-month outcome: a prospective study. Lancet 2001;358:1766-71.
7. Frasure-Smith N, Lesperance F, Talajic M. Depression and 18-month prognosis after myocardial infarction. Circulation 1995;91:999-1005.
8. Rugulies R. Depression as a predictor for coronary heart disease. Am J Prev Med 2002;23:51-61.
9. Wulsin L, Singal B. Do depressive symptoms increase the risk for the onset of coronary disease? A systematic quantitative review. Psychosom Med 2003;65:201-10.
10. Carney R, Rich M, Freedland K, et al. Major depressive disorder predicts cardiac events in patients with coronary artery disease. Psychosom Med 1988;50:627-33.
11. Ladwig K, Roll G, Breithardt G, Borggrefe M. Extracardiac contributions to chest pain perception in patients 6 months after acute myocardial infarction. Am Heart J 1999;137:528-34.
12. Levine J, Covino N, Slack W, et al. Psychological predictors of subsequent medical care among patients hospitalized with cardiac disease. J Cardiopulm Rehabil 1996;16:109-16.
13. Lesperance F, Frasure-Smith N, Talajic M, Bourassa M. Five-year risk of cardiac mortality in relation to initial severity and one-year changes in depression symptoms after myocardial infarction. Circulation 2002;105:1049-53.
14. Dwight M, Stoudemire A. Effects of depressive disorders on coronary artery disease: a review. Harv Rev Psychiatry 1997;5:115-122.
15. Penninx B, Beekman A, Honig A, et al. Depression and cardiac mortality. Arch Gen Psychiatry 2001;58:221-7.
16. Writing committee of the ENRICHD investigators. Effects of treating depression and low perceived social support on clinical events after myocardial infarction. JAMA 2003;289:3106-16.
17. Carney RM, Freedland K, Miller G, Jaffe AS. Depression as a risk factor for cardiac mortality and morbidity: a review of potential mechanisms. J Psychosom Res 2002;53:897-902.
18. Musselman D, Evans D, Nemeroff C. The relationship of depression to cardiovascular disease. Arch Gen Psychiatry 1998;55:580-92.
19. Kop WJ. Chronic and acute psychological risk factors for clinical manifestations of coronary artery disease. Psychosom Med 1999;61:476-86.
20. Miller G, Cohen S, Herbert T. Pathways linking major depression and immunity in ambulatory female patients. Psychosom Med 1999;61:850-60.
21. Carney R, Freedland K, Stein P. Change in heart rate and heart rate variability during treatment for depression in patients with coronary heart disease. Psychosom Med 2000;62:639-47.
22. Carney R, Freedland K, Miller G, Jaffe A. Depression as a risk factor for cardiac mortality and morbidity: a review of potential mechanisms. J Psychosom Res 2002;53:897-902.
23. Alexopoulos G, Meyers B, Young R, et al. Vascular depression hypothesis. Psychosom Med 1997;58:113-121.
24. Ziegelstein R, Fauerbach J, Stevens S, et al. Patients with depression are less likely to follow recommendations to reduce cardiac risk during recovery from a myocardial infarction. Arch Intern Med 2000;160:1818-23.
25. Glassman AH, O’Connor C, Califf RM, et al. Sertraline treatment of major depression in patients with acute MI or unstable angina. JAMA 2002;288:701-9.
26. Ko D, Hebert P, Coffey C, et al. B-blocker therapy and symptoms of depression, fatigue, and sexual dysfunction. JAMA 2002;288:351-7.
Depression can exacerbate cardiovascular disease (CVD), and CVD can exacerbate depression (Figure). Thus, effectively treating depression enhances heart disease treatment, particularly if psychiatrists and medical physicians collaborate in providing patient care.
This article describes a patient with risk factors for heart disease, illustrates the physiologic pathways that link depression and CVD, and offers clinical tips to help you improve outcomes for patients with both disorders.
Case report: Trying to ‘get going’
Mr. D, age 51, presents with vegetative symptoms and a personal and family history of CVD, depression, and substance abuse disorders. He was born in a small town in Kentucky and raised in Louisville’s poorest neighborhood. After his mother died at age 42 of “hardening of the arteries,” his father started drinking more, working less, and “never really got going again.”
Figure Neuroendocrine pathways by which depression may cause or promote CVD
Among patients with a recent myocardial infarction (MI), as many as two-thirds report depressive symptoms.1 Major depression has been reported in:
- 16% to 22% of patients hospitalized post-MI,2,3 compared with 5% in the general population and 10% in the primary care population4
- 15% of patients with unstable angina5 and 20% of patients undergoing coronary artery bypass (CABG) surgery.6
Among the annual 1.5 million Americans who have an acute MI or unstable angina, 40% develop depression immediately thereafter. These 600,000 depressed patients are three times more likely to die within 6 months, compared with post-MI patients who are not depressed.7
Mr. D worked 20 years as a construction contractor, often running several work crews at once. At age 41, he slid into a depressive episode after his second divorce. He struggled with low energy, disturbed sleep, hopelessness, and increased smoking and drinking for 1 year, but he did not seek help.
Two years later, he suffered an inferior wall transmural myocardial infarction. His CVD risk factors included family history of early heart disease, smoking for 32 years, and elevated low-density lipoprotein (LDL) cholesterol. After subsequent episodes of unstable angina, stents were placed in two coronary arteries. Though his cardiologist cleared him to return to work, he felt able to work only part-time and erratically.
During a visit to their family doctor several years later, Mr. D’s wife suggested that her husband might be depressed. Reluctantly, Mr. D consulted a psychiatrist.
The psychiatrist diagnosed major depressive disorder and prescribed sertraline, 50 mg/d. Within 2 months, Mr. D’s symptoms had dropped by 50% on a symptom severity measure. He did not refill his prescription, however, because of concerns about sexual side effects. Two months later he was hospitalized for another episode of unstable angina. His depression had returned within 1 month of stopping sertraline.
The psychiatrist switched him to citalopram, 20 mg/d, and carefully monitored depressive symptoms, side effects, and medication adherence. Aside from talking with the psychiatrist for a half-hour in his family doctor’s office every few weeks, Mr. D refused to undergo psychotherapy. He eventually achieved depression remission with a combination of citalopram, 20 mg/d, and nefazodone, 200 mg/d.
Depression-CVD connection
As in Mr. D’s case, depression and CVD commonly occur together, often with serious consequences (Box). 1-7 The association between depression and CVD is not limited to depression’s effect on existing disease, however. Depression often precedes coronary disease by about 30 years—suggesting possible cause and effect. Two systematic reviews8,9 found that depression increased CVD risk by 64%.
Seven well-controlled studies5-7,10-13 compared the relative effect of depression on the cardiovascular system with that of established CVD predictors. All seven found depression’s independent effect to be significant and comparable to or greater than that of ejection fraction, previous MI history, or number of vessels with >50% narrowing.
Comorbid depression and CVD usually persists months or years,14 and most studies indicate a dose-response relationship; the more severe the depression, the greater the risk for CVD to develop or progress.8,15
The link between depression treatment and CVD risk has not been well-studied. The only randomized, controlled trial found that cognitive therapy for depression did not significantly reduce cardiac events among patients with known CVD.16
Possible mechanisms
Depression’s effect on CVD. How does depression affect CVD development and progression? Both behavioral and biological pathways may be involved.17 The behavioral pathway proposes that depression triggers behaviors—such as smoking, overeating, and sedentary lifestyles—that increase the risk of developing or worsening CVD. The biological pathway proposes that neuroendocrine changes during depression accelerate CVD development.
About one-half of persons with major depression exhibit hypothalamic-pituitary-adrenal (HPA) axis dysregulation, with excessive secretion of corticotropin releasing factor (CRF) and chronically elevated cortisol.18 This HPA dysregulation is related to defective negative feedback at the paraventricular nucleus of the hypothalamus. Chronic HPA axis dysregulation promotes vascular inflammation, and several studies have reported C-reactive protein elevation and cytokine changes in patients with major depression.19,20
Major depression is also associated with excessive sympathetic and diminished parasym-pathetic nervous system activity, potentially contributing to hypertension, increased resting heart rate, decreased heart rate variability, and altered endothelial function.2,21,22 Each of these factors facilitates arterial plaque formation.
Depression may also exacerbate chronic anxiety and other forms of distress. The combined effects of an overtaxed central nervous system, neuroendocrine dysregulation, and unhealthy behaviors may eventually overwhelm the cardiovascular system.
CVD’s effect on depression. How does CVD contribute to depression? The vascular depression hypothesis23 proposes that diffuse heart and brain atherosclerosis restricts perfusion of limbic and cortical structures that regulate mood. A first depressive episode after acute MI or CABG probably represents exacerbation of cerebrovascular insufficiency that preceded the coronary event.
Table
Four keys to effectively treat depression in patients with heart disease
|
In practical terms, this means that pathways linking depression and heart disease include not only biological factors but also:
- psychological factors such as depression, anxiety, and chronic stress
- behavioral factors such as smoking, physical inactivity, and high-fat diet.
How to improve outcomes
Patients with CVD commonly do not receive effective depression treatment:
- Internists and family physicians give preferential attention to physical illness.
- Patients may have insufficient access to mental health specialists.
- Physicians do not adequately monitor depression treatment.
- Patients are reluctant to accept the stigma of mental illness.
By collaborating with primary care physicians, you can improve the likelihood that depression treatment will achieve remission and prevent relapse (Table).
Risk factors for CVD. Depression contributes to heart disease by exacerbating four major CVD risk factors—smoking, diabetes, obesity, and physical inactivity. By effectively treating depression, you may help patients avoid common depressive symptoms—such as overeating and sedentary behaviors—that are related to low energy or fatigue.
Educate middle-aged patients with depression about CVD’s associated risk. Prochaska’s “stages of change” (see Related resources) can help them stop smoking, lose weight, and exercise.
Access to cardiac care. Depressed patients may be less motivated than nondepressed patients to pursue cardiac care.24 Therefore, you may need to:
- encourage your patients to take advantage of indicated state-of-the-art care, including stents, bypass surgery, and medications
- understand patients’ complex cardiac regimens and help them adhere when depression interferes with their motivation.
Effective depression treatment
Patient history. For depressed patients older than 40, take a careful inventory of CVD risk factors:
- family history of heart disease before age 60 for men and age 70 for women
- personal history of smoking, blood pressure >140/90 mm Hg, LDL cholesterol >100 mg/dL, type 2 diabetes, body mass index >30, or physical inactivity (<30 minutes of walking 3 days a week).
In general, the more risk factors, the greater the risk of CVD.
Antidepressant selection. Selective serotonin reuptake inhibitors (SSRIs) are safe and effective for treating major depression in CVD and congestive heart failure.25 Venlafaxine at doses >300 mg/d may increase blood pressure, so use this drug with caution in depressed patients with hypertension.
No controlled clinical trials have gauged the safety and efficacy of bupropion or mirtazapine in patients with CVD.
Tricyclic antidepressants are contraindicated for 6 months post-MI because they may contribute to arrhythmias. Avoid using them in depressed patients with CVD or conduction defects because of their quinidine-like effects on conduction.
Cardiac medications. Contrary to folk wisdom, beta blockers do not cause depression.26 Whether or not a patient is depressed, our primary care and cardiology colleagues can use beta blockers to help regulate the peripheral autonomic nervous system, reducing high blood pressure and the risk of arrhythmias.
SSRIs may increase blood levels of beta blockers, warfarin, and other cardiac medications via cytochrome P-450 isoenzyme inhibition. Make sure warfarin levels and other cardiac drug effects are well monitored when you adjust psychotropic dosages.
Divalproex and SSRIs also may reduce platelet aggregation. Patients who are receiving concomitant aspirin or warfarin may bruise or bleed easily and require dosage reductions or medication changes.
Psychotherapy. All patients with major or minor depression and CVD are considered high-risk and are candidates for a trial of brief psychotherapy. Therapeutic goals are to achieve full remission of depressive symptoms as rapidly as possible, prevent relapse, and maximize adherence to cardiac and depression drug regimens.
Collaborate closely with the cardiologist or primary care physician during the patient’s depressive episode and occasionally during maintenance treatment. Discuss or share notes on the patient’s depressive and cardiac disorders, medication management, symptom monitoring, and behavior changes needed to reduce cardiac risk.
With your added support, patients with depression and CVD are more likely to adhere to antidepressant medications and achieve symptom remission.
- National Institute of Mental Health. Depression and heart disease. www.nimh.nih.gov/publicat/depheart.cfm.
- Dewan NA, Suresh DP, Blomkalns A. Selecting safe psychotropics for post-MI patients. Current Psychiatry. 2003;2(3):15-21.
- Prochaska JO, Norcross JC, DiClemente CC. Changing for good. New York: Avon, 1994.
Drug brand names
- Bupropion • Wellbutrin
- Citalopram • Celexa
- Escitalopram • Lexapro
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Paroxetine • Paxil
- Mirtazapine • Remeron
- Nefazodone • Serzone
- Sertraline • Zoloft
- Venlafaxine • Effexor
Disclosure
Dr. Wulsin is a consultant to Pfizer Inc. and Janssen Pharmaceutica.
Dr. Vieweg is a speaker for Janssen Pharmaceutica, Eli Lilly and Co., Pfizer Inc., Wyeth Pharmaceuticals, Forest Pharmaceuticals, and GlaxoSmithKline.
Dr. Fernandez reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Depression can exacerbate cardiovascular disease (CVD), and CVD can exacerbate depression (Figure). Thus, effectively treating depression enhances heart disease treatment, particularly if psychiatrists and medical physicians collaborate in providing patient care.
This article describes a patient with risk factors for heart disease, illustrates the physiologic pathways that link depression and CVD, and offers clinical tips to help you improve outcomes for patients with both disorders.
Case report: Trying to ‘get going’
Mr. D, age 51, presents with vegetative symptoms and a personal and family history of CVD, depression, and substance abuse disorders. He was born in a small town in Kentucky and raised in Louisville’s poorest neighborhood. After his mother died at age 42 of “hardening of the arteries,” his father started drinking more, working less, and “never really got going again.”
Figure Neuroendocrine pathways by which depression may cause or promote CVD
Among patients with a recent myocardial infarction (MI), as many as two-thirds report depressive symptoms.1 Major depression has been reported in:
- 16% to 22% of patients hospitalized post-MI,2,3 compared with 5% in the general population and 10% in the primary care population4
- 15% of patients with unstable angina5 and 20% of patients undergoing coronary artery bypass (CABG) surgery.6
Among the annual 1.5 million Americans who have an acute MI or unstable angina, 40% develop depression immediately thereafter. These 600,000 depressed patients are three times more likely to die within 6 months, compared with post-MI patients who are not depressed.7
Mr. D worked 20 years as a construction contractor, often running several work crews at once. At age 41, he slid into a depressive episode after his second divorce. He struggled with low energy, disturbed sleep, hopelessness, and increased smoking and drinking for 1 year, but he did not seek help.
Two years later, he suffered an inferior wall transmural myocardial infarction. His CVD risk factors included family history of early heart disease, smoking for 32 years, and elevated low-density lipoprotein (LDL) cholesterol. After subsequent episodes of unstable angina, stents were placed in two coronary arteries. Though his cardiologist cleared him to return to work, he felt able to work only part-time and erratically.
During a visit to their family doctor several years later, Mr. D’s wife suggested that her husband might be depressed. Reluctantly, Mr. D consulted a psychiatrist.
The psychiatrist diagnosed major depressive disorder and prescribed sertraline, 50 mg/d. Within 2 months, Mr. D’s symptoms had dropped by 50% on a symptom severity measure. He did not refill his prescription, however, because of concerns about sexual side effects. Two months later he was hospitalized for another episode of unstable angina. His depression had returned within 1 month of stopping sertraline.
The psychiatrist switched him to citalopram, 20 mg/d, and carefully monitored depressive symptoms, side effects, and medication adherence. Aside from talking with the psychiatrist for a half-hour in his family doctor’s office every few weeks, Mr. D refused to undergo psychotherapy. He eventually achieved depression remission with a combination of citalopram, 20 mg/d, and nefazodone, 200 mg/d.
Depression-CVD connection
As in Mr. D’s case, depression and CVD commonly occur together, often with serious consequences (Box). 1-7 The association between depression and CVD is not limited to depression’s effect on existing disease, however. Depression often precedes coronary disease by about 30 years—suggesting possible cause and effect. Two systematic reviews8,9 found that depression increased CVD risk by 64%.
Seven well-controlled studies5-7,10-13 compared the relative effect of depression on the cardiovascular system with that of established CVD predictors. All seven found depression’s independent effect to be significant and comparable to or greater than that of ejection fraction, previous MI history, or number of vessels with >50% narrowing.
Comorbid depression and CVD usually persists months or years,14 and most studies indicate a dose-response relationship; the more severe the depression, the greater the risk for CVD to develop or progress.8,15
The link between depression treatment and CVD risk has not been well-studied. The only randomized, controlled trial found that cognitive therapy for depression did not significantly reduce cardiac events among patients with known CVD.16
Possible mechanisms
Depression’s effect on CVD. How does depression affect CVD development and progression? Both behavioral and biological pathways may be involved.17 The behavioral pathway proposes that depression triggers behaviors—such as smoking, overeating, and sedentary lifestyles—that increase the risk of developing or worsening CVD. The biological pathway proposes that neuroendocrine changes during depression accelerate CVD development.
About one-half of persons with major depression exhibit hypothalamic-pituitary-adrenal (HPA) axis dysregulation, with excessive secretion of corticotropin releasing factor (CRF) and chronically elevated cortisol.18 This HPA dysregulation is related to defective negative feedback at the paraventricular nucleus of the hypothalamus. Chronic HPA axis dysregulation promotes vascular inflammation, and several studies have reported C-reactive protein elevation and cytokine changes in patients with major depression.19,20
Major depression is also associated with excessive sympathetic and diminished parasym-pathetic nervous system activity, potentially contributing to hypertension, increased resting heart rate, decreased heart rate variability, and altered endothelial function.2,21,22 Each of these factors facilitates arterial plaque formation.
Depression may also exacerbate chronic anxiety and other forms of distress. The combined effects of an overtaxed central nervous system, neuroendocrine dysregulation, and unhealthy behaviors may eventually overwhelm the cardiovascular system.
CVD’s effect on depression. How does CVD contribute to depression? The vascular depression hypothesis23 proposes that diffuse heart and brain atherosclerosis restricts perfusion of limbic and cortical structures that regulate mood. A first depressive episode after acute MI or CABG probably represents exacerbation of cerebrovascular insufficiency that preceded the coronary event.
Table
Four keys to effectively treat depression in patients with heart disease
|
In practical terms, this means that pathways linking depression and heart disease include not only biological factors but also:
- psychological factors such as depression, anxiety, and chronic stress
- behavioral factors such as smoking, physical inactivity, and high-fat diet.
How to improve outcomes
Patients with CVD commonly do not receive effective depression treatment:
- Internists and family physicians give preferential attention to physical illness.
- Patients may have insufficient access to mental health specialists.
- Physicians do not adequately monitor depression treatment.
- Patients are reluctant to accept the stigma of mental illness.
By collaborating with primary care physicians, you can improve the likelihood that depression treatment will achieve remission and prevent relapse (Table).
Risk factors for CVD. Depression contributes to heart disease by exacerbating four major CVD risk factors—smoking, diabetes, obesity, and physical inactivity. By effectively treating depression, you may help patients avoid common depressive symptoms—such as overeating and sedentary behaviors—that are related to low energy or fatigue.
Educate middle-aged patients with depression about CVD’s associated risk. Prochaska’s “stages of change” (see Related resources) can help them stop smoking, lose weight, and exercise.
Access to cardiac care. Depressed patients may be less motivated than nondepressed patients to pursue cardiac care.24 Therefore, you may need to:
- encourage your patients to take advantage of indicated state-of-the-art care, including stents, bypass surgery, and medications
- understand patients’ complex cardiac regimens and help them adhere when depression interferes with their motivation.
Effective depression treatment
Patient history. For depressed patients older than 40, take a careful inventory of CVD risk factors:
- family history of heart disease before age 60 for men and age 70 for women
- personal history of smoking, blood pressure >140/90 mm Hg, LDL cholesterol >100 mg/dL, type 2 diabetes, body mass index >30, or physical inactivity (<30 minutes of walking 3 days a week).
In general, the more risk factors, the greater the risk of CVD.
Antidepressant selection. Selective serotonin reuptake inhibitors (SSRIs) are safe and effective for treating major depression in CVD and congestive heart failure.25 Venlafaxine at doses >300 mg/d may increase blood pressure, so use this drug with caution in depressed patients with hypertension.
No controlled clinical trials have gauged the safety and efficacy of bupropion or mirtazapine in patients with CVD.
Tricyclic antidepressants are contraindicated for 6 months post-MI because they may contribute to arrhythmias. Avoid using them in depressed patients with CVD or conduction defects because of their quinidine-like effects on conduction.
Cardiac medications. Contrary to folk wisdom, beta blockers do not cause depression.26 Whether or not a patient is depressed, our primary care and cardiology colleagues can use beta blockers to help regulate the peripheral autonomic nervous system, reducing high blood pressure and the risk of arrhythmias.
SSRIs may increase blood levels of beta blockers, warfarin, and other cardiac medications via cytochrome P-450 isoenzyme inhibition. Make sure warfarin levels and other cardiac drug effects are well monitored when you adjust psychotropic dosages.
Divalproex and SSRIs also may reduce platelet aggregation. Patients who are receiving concomitant aspirin or warfarin may bruise or bleed easily and require dosage reductions or medication changes.
Psychotherapy. All patients with major or minor depression and CVD are considered high-risk and are candidates for a trial of brief psychotherapy. Therapeutic goals are to achieve full remission of depressive symptoms as rapidly as possible, prevent relapse, and maximize adherence to cardiac and depression drug regimens.
Collaborate closely with the cardiologist or primary care physician during the patient’s depressive episode and occasionally during maintenance treatment. Discuss or share notes on the patient’s depressive and cardiac disorders, medication management, symptom monitoring, and behavior changes needed to reduce cardiac risk.
With your added support, patients with depression and CVD are more likely to adhere to antidepressant medications and achieve symptom remission.
- National Institute of Mental Health. Depression and heart disease. www.nimh.nih.gov/publicat/depheart.cfm.
- Dewan NA, Suresh DP, Blomkalns A. Selecting safe psychotropics for post-MI patients. Current Psychiatry. 2003;2(3):15-21.
- Prochaska JO, Norcross JC, DiClemente CC. Changing for good. New York: Avon, 1994.
Drug brand names
- Bupropion • Wellbutrin
- Citalopram • Celexa
- Escitalopram • Lexapro
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Paroxetine • Paxil
- Mirtazapine • Remeron
- Nefazodone • Serzone
- Sertraline • Zoloft
- Venlafaxine • Effexor
Disclosure
Dr. Wulsin is a consultant to Pfizer Inc. and Janssen Pharmaceutica.
Dr. Vieweg is a speaker for Janssen Pharmaceutica, Eli Lilly and Co., Pfizer Inc., Wyeth Pharmaceuticals, Forest Pharmaceuticals, and GlaxoSmithKline.
Dr. Fernandez reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Cassem N, Hackett T. Psychiatric condition in a coronary care unit. Ann Intern Med 1971;75:9-14.
2. Glassman A, Shapiro P. Depression and the course of coronary artery disease. Am J Psychiatry 1998;155:4-11.
3. Carney R, Freedland K, Sheline Y, Weiss E. Depression and coronary heart disease: a review for cardiologists. Clin Cardiol 1997;20:196-200.
4. Katon W, Schulbert H. Epidemiology of depression in primary care. Gen Hosp Psychiatry 1992;14:237-47.
5. Lesperance F, Frasure-Smith N, Theroux P. Depression and 1-year prognosis in unstable angina. Arch Intern Med 2000;160:1354-60.
6. Connerney I, Shapiro P, McLaughlin J, et al. Relation between depression after coronary artery bypass surgery and 12-month outcome: a prospective study. Lancet 2001;358:1766-71.
7. Frasure-Smith N, Lesperance F, Talajic M. Depression and 18-month prognosis after myocardial infarction. Circulation 1995;91:999-1005.
8. Rugulies R. Depression as a predictor for coronary heart disease. Am J Prev Med 2002;23:51-61.
9. Wulsin L, Singal B. Do depressive symptoms increase the risk for the onset of coronary disease? A systematic quantitative review. Psychosom Med 2003;65:201-10.
10. Carney R, Rich M, Freedland K, et al. Major depressive disorder predicts cardiac events in patients with coronary artery disease. Psychosom Med 1988;50:627-33.
11. Ladwig K, Roll G, Breithardt G, Borggrefe M. Extracardiac contributions to chest pain perception in patients 6 months after acute myocardial infarction. Am Heart J 1999;137:528-34.
12. Levine J, Covino N, Slack W, et al. Psychological predictors of subsequent medical care among patients hospitalized with cardiac disease. J Cardiopulm Rehabil 1996;16:109-16.
13. Lesperance F, Frasure-Smith N, Talajic M, Bourassa M. Five-year risk of cardiac mortality in relation to initial severity and one-year changes in depression symptoms after myocardial infarction. Circulation 2002;105:1049-53.
14. Dwight M, Stoudemire A. Effects of depressive disorders on coronary artery disease: a review. Harv Rev Psychiatry 1997;5:115-122.
15. Penninx B, Beekman A, Honig A, et al. Depression and cardiac mortality. Arch Gen Psychiatry 2001;58:221-7.
16. Writing committee of the ENRICHD investigators. Effects of treating depression and low perceived social support on clinical events after myocardial infarction. JAMA 2003;289:3106-16.
17. Carney RM, Freedland K, Miller G, Jaffe AS. Depression as a risk factor for cardiac mortality and morbidity: a review of potential mechanisms. J Psychosom Res 2002;53:897-902.
18. Musselman D, Evans D, Nemeroff C. The relationship of depression to cardiovascular disease. Arch Gen Psychiatry 1998;55:580-92.
19. Kop WJ. Chronic and acute psychological risk factors for clinical manifestations of coronary artery disease. Psychosom Med 1999;61:476-86.
20. Miller G, Cohen S, Herbert T. Pathways linking major depression and immunity in ambulatory female patients. Psychosom Med 1999;61:850-60.
21. Carney R, Freedland K, Stein P. Change in heart rate and heart rate variability during treatment for depression in patients with coronary heart disease. Psychosom Med 2000;62:639-47.
22. Carney R, Freedland K, Miller G, Jaffe A. Depression as a risk factor for cardiac mortality and morbidity: a review of potential mechanisms. J Psychosom Res 2002;53:897-902.
23. Alexopoulos G, Meyers B, Young R, et al. Vascular depression hypothesis. Psychosom Med 1997;58:113-121.
24. Ziegelstein R, Fauerbach J, Stevens S, et al. Patients with depression are less likely to follow recommendations to reduce cardiac risk during recovery from a myocardial infarction. Arch Intern Med 2000;160:1818-23.
25. Glassman AH, O’Connor C, Califf RM, et al. Sertraline treatment of major depression in patients with acute MI or unstable angina. JAMA 2002;288:701-9.
26. Ko D, Hebert P, Coffey C, et al. B-blocker therapy and symptoms of depression, fatigue, and sexual dysfunction. JAMA 2002;288:351-7.
1. Cassem N, Hackett T. Psychiatric condition in a coronary care unit. Ann Intern Med 1971;75:9-14.
2. Glassman A, Shapiro P. Depression and the course of coronary artery disease. Am J Psychiatry 1998;155:4-11.
3. Carney R, Freedland K, Sheline Y, Weiss E. Depression and coronary heart disease: a review for cardiologists. Clin Cardiol 1997;20:196-200.
4. Katon W, Schulbert H. Epidemiology of depression in primary care. Gen Hosp Psychiatry 1992;14:237-47.
5. Lesperance F, Frasure-Smith N, Theroux P. Depression and 1-year prognosis in unstable angina. Arch Intern Med 2000;160:1354-60.
6. Connerney I, Shapiro P, McLaughlin J, et al. Relation between depression after coronary artery bypass surgery and 12-month outcome: a prospective study. Lancet 2001;358:1766-71.
7. Frasure-Smith N, Lesperance F, Talajic M. Depression and 18-month prognosis after myocardial infarction. Circulation 1995;91:999-1005.
8. Rugulies R. Depression as a predictor for coronary heart disease. Am J Prev Med 2002;23:51-61.
9. Wulsin L, Singal B. Do depressive symptoms increase the risk for the onset of coronary disease? A systematic quantitative review. Psychosom Med 2003;65:201-10.
10. Carney R, Rich M, Freedland K, et al. Major depressive disorder predicts cardiac events in patients with coronary artery disease. Psychosom Med 1988;50:627-33.
11. Ladwig K, Roll G, Breithardt G, Borggrefe M. Extracardiac contributions to chest pain perception in patients 6 months after acute myocardial infarction. Am Heart J 1999;137:528-34.
12. Levine J, Covino N, Slack W, et al. Psychological predictors of subsequent medical care among patients hospitalized with cardiac disease. J Cardiopulm Rehabil 1996;16:109-16.
13. Lesperance F, Frasure-Smith N, Talajic M, Bourassa M. Five-year risk of cardiac mortality in relation to initial severity and one-year changes in depression symptoms after myocardial infarction. Circulation 2002;105:1049-53.
14. Dwight M, Stoudemire A. Effects of depressive disorders on coronary artery disease: a review. Harv Rev Psychiatry 1997;5:115-122.
15. Penninx B, Beekman A, Honig A, et al. Depression and cardiac mortality. Arch Gen Psychiatry 2001;58:221-7.
16. Writing committee of the ENRICHD investigators. Effects of treating depression and low perceived social support on clinical events after myocardial infarction. JAMA 2003;289:3106-16.
17. Carney RM, Freedland K, Miller G, Jaffe AS. Depression as a risk factor for cardiac mortality and morbidity: a review of potential mechanisms. J Psychosom Res 2002;53:897-902.
18. Musselman D, Evans D, Nemeroff C. The relationship of depression to cardiovascular disease. Arch Gen Psychiatry 1998;55:580-92.
19. Kop WJ. Chronic and acute psychological risk factors for clinical manifestations of coronary artery disease. Psychosom Med 1999;61:476-86.
20. Miller G, Cohen S, Herbert T. Pathways linking major depression and immunity in ambulatory female patients. Psychosom Med 1999;61:850-60.
21. Carney R, Freedland K, Stein P. Change in heart rate and heart rate variability during treatment for depression in patients with coronary heart disease. Psychosom Med 2000;62:639-47.
22. Carney R, Freedland K, Miller G, Jaffe A. Depression as a risk factor for cardiac mortality and morbidity: a review of potential mechanisms. J Psychosom Res 2002;53:897-902.
23. Alexopoulos G, Meyers B, Young R, et al. Vascular depression hypothesis. Psychosom Med 1997;58:113-121.
24. Ziegelstein R, Fauerbach J, Stevens S, et al. Patients with depression are less likely to follow recommendations to reduce cardiac risk during recovery from a myocardial infarction. Arch Intern Med 2000;160:1818-23.
25. Glassman AH, O’Connor C, Califf RM, et al. Sertraline treatment of major depression in patients with acute MI or unstable angina. JAMA 2002;288:701-9.
26. Ko D, Hebert P, Coffey C, et al. B-blocker therapy and symptoms of depression, fatigue, and sexual dysfunction. JAMA 2002;288:351-7.
SSRIs in children and adolescents: Where do we stand?
Caitlin McIntosh, 12, hanged herself with shoelaces weeks after starting treatment for depression with a selective serotonin reuptake inhibitor (SSRI). Matt Miller, 13, hanged himself in his bedroom closet after taking his seventh SSRI dose. Michael Shivak, 11, slashed his wrists in class—but survived—while taking an SSRI.
These adolescents’ parents testified at an FDA hearing Feb. 2 about possible increased risk of suicidality with SSRIs in depressed children and adolescents.
Other families related positive experiences. Sherri Walton said her daughter, Jordan, 14, has achieved “enormous benefit” from taking SSRIs for obsessive-compulsive disorder. Suzanne Vogel-Scibilia told the FDA panel she is convinced that her two children with psychiatric disorders lead full lives because of SSRIs.
Sensitive to the anguish of grieving families but not wanting to deprive seriously depressed children of effective treatment, the FDA is proceeding methodically with its inquiry—probably at least until summer.
In the meantime, this article offers resources to help you answer questions from parents concerned about their children starting or continuing SSRIs. We include pediatric antidepressant dosing recommendations and data on benefits and risks of SSRIs and other reuptake inhibitors in young patients.
Why the FDA inquiry?
SSRI-associated behavioral activation and suicidal ideation in children and adolescents were reported anecdotally, as case reports, in the early 1990s,1 and more recently.2 No convincing evidence has shown, however, that SSRIs increase the risk of suicide. In fact, widespread use of SSRIs has been associated with reduced suicide rates.3
In May 2003, unpublished data submitted to the FDA from placebo-controlled trials suggested an increased risk of “possibly suicide-related” events and “suicide attempts” in pediatric patients taking paroxetine for major depression. No suicides were reported.
The Medicines and Healthcare Products Regulatory Agency (MHRA)—the United Kingdom’s equivalent of the Food and Drug Administration—responded by warning British physicians against prescribing paroxetine for depressed patients younger than 18. It also ordered a labeling change for paroxetine, contraindicating its use in pediatric major depression.
The FDA advised U.S. doctors against using paroxetine for children under age 18 with major depressive disorder and began investigating data on pediatric use of antidepressants, including all approved SSRIs. Since then:
- In the United States, venlafaxine’s manufacturer changed the drug’s labeling to include increased reports of hostility and suicidality in pediatric trial data. A “Dear Health Care Professional” letter in August 2003 indicated that venlafaxine is not recommended in depressed pediatric patients.
- Britain’s MHRA added pediatric con-traindications to labeling of venlafaxine, sertraline, citalopram, and escitalopram in December 2003. The agency opined that fluoxetine is the only SSRI with a favorable risk-benefit profile for pediatric major depression.
- At press time, the FDA had not changed any SSRI labeling.
At the Feb. 2 public hearing, the FDA’s Psycho-pharmacological Drugs Advisory Committee and Pediatric Subcommittee of the Anti-Infective Drugs Advisory Committee heard public comments from patients, families, and physicians and reviewed the inquiry’s progress. To locate the Web site containing the FDA’s memorandum on this hearing, see Related resources.
For the next several months, an expert group at Columbia University is under contract with the FDA to develop a system to classify events that might represent suicidality. The group will then analyze data from 24 studies involving more than 4,000 depressed pediatric patients and nine antidepressants (paroxetine, fluoxetine, sertraline, fluvoxamine, citalopram, bupropion, venlafaxine, nefazodone, and mirtazapine).
Independent findings. In January, an American College of Neuropsychopharmacology (ACNP) report concluded that SSRIs do not increase suicidal thoughts or suicide attempts in youth (Table 1). An ACNP task force examined the use of SSRIs in more than 2,000 children and adolescents, including all published clinical trial data, unpublished data from several pharmaceutical companies, and data reported to Britain’s MHRA. An executive summary is available on the ACNP’s Web site (see Related resources).
Table 1
Suicide deaths, behavior, or ideation in clinical trials of youth with major depressive disorder
| Medication | Total youth* in trials | No. of suicide deaths | % of youth with suicidal behavior or ideation** | P value | Statistical significance | |
|---|---|---|---|---|---|---|
| Antidepressant | Placebo | |||||
| Citalopram | 418 | 0 | 8.9%(19) | 7.3% (15) | 0.5 | No |
| Fluoxetine | 458 | 0 | 3.6%(9) | 3.8% (8) | 0.9 | No |
| Paroxetine | 669 | 0 | 3.7%(14) | 2.5% (7) | 0.4 | No |
| Sertraline | 376 | 0 | 2.7%(5) | 1.1% (2) | 0.3 | No |
| Venlafaxine | 334 | 0 | 2%(NA) | 0% | 0.25 | No |
| * Total number of youth given antidepressants and placebo | ||||||
| ** Number inside parenthesis is actual number of youth | ||||||
| NA = Not available | ||||||
| Source: Data from published clinical trials, unpublished clinical trials provided by drug sponsor, and clinical data compiled by the Medicines and Healthcare Products Regulatory Agency of the United Kingdom. | ||||||
| Reprinted with permission of the American College of Neuropsychopharmacology from Preliminary report of the Task Force on SSRIs and Suicidal Behavior in Youth (executive summary), January 2004:18. | ||||||
Depression’s impact on children
The prevalence of depression in youth age 18 and younger is 8.3%,4 and the rate increases with patient age. Before puberty, common signs of depression include somatic symptoms such as abdominal pain, headaches, and irritability, whereas adolescents are more likely to express feelings of depression and exhibit suicidal behavior. Girls and boys are equally at risk for depression until puberty, when girls begin to outnumber boys and the presentation begins to resemble adult depression.
Untreated pediatric depression is associated with substantial morbidity, including reduced academic performance, substance abuse, interpersonal problems, social withdrawal, and a poor quality of life,4,5 It also increases the risk of suicide.
Early-onset depression is considered a more malignant illness than adult-onset depression because of its effect on development, potential for recurrence,6 and chronicity into adulthood.7 The quest to develop appropriate treatment for depressed children and adolescents has been spurred by:
- the substantial risks of morbidity and mortality from childhood depression
- advances in drug treatments for adult-onset depression
- recognition that early-onset depression is treatable.
Physiologically, children are not “mini-adults.” Thus, practicing evidence-based medicine requires separate empirical research for pediatric conditions.
Despite some efforts by the National Institute of Mental Health (NIMH) and the pharmaceutical industry, research in pediatric psychopharmacology and ancillary treatments lags decades behind evidence-based treatment in adults.
Table 2
Efficacy of SSRIs and other newer antidepressants in short-term, placebo-controlled pediatric studies in major depressive disorder
| Drug | Age range | Outcome* (drug vs. placebo) |
|---|---|---|
| Paroxetine | ||
| Study 1 Study 2 Study 3 | 12 to 18 13 to 18 7 to 17 | Negative† Negative Negative |
| Fluoxetine | ||
| Study 1 Study 2 | 8 to 17 8 to 17 | Positive Positive |
| Sertraline | ||
| Study 1 Study 2 | 6 to 17 6 to 17 | Trend Negative§ |
| Venlafaxine | ||
| Study 1 Study 2 | 7 to 17 7 to 17 | Negative Negative |
| Citalopram | ||
| Study 1 Study 2 | 7 to 17 13 to 18 | Positive Negative |
| Nefazodone | ||
| Study 1 Study 2 | 12 to 18 7 to 17 | Trend Negative |
| Mirtazapine | ||
| Study 1 Study 2 | 7 to 17 7 to 17 | Negative Negative |
| * Positive (P 0.05); Negative (P >0.10; Trend (0.05 | ||
| † Positive on most secondary endpoints | ||
| § Positive on pooling of 2 studies | ||
| Source: Adapted and reprinted from Laughren TP. Memorandum: Background comments for Feb. 2, 2004 meeting of Psychopharmacological Drugs Advisory Committee and Pediatric Subcommittee of the Anti-Infective Drugs Advisory Committee. Appendix I. Center for Drug Evaluation and Research. Food and Drug Administration, Public Health Service, Department of Health and Human Services. | ||
From tricyclics to SSRIS
Tricyclic antidepressants (TCAs) were the mainstay in treating childhood depression two decades ago, based on clinical and anecdotal evidence. However, double blind, placebo-controlled studies failed to show that TCAs were effective in treating depressed children and adolescents. The few controlled studies included small samples of children and adolescents, and the methodologies were often flawed.
In the late 1980s, TCA use in children dropped precipitously because of:
- episodes of sudden death in pediatric patients taking desipramine
- introduction of SSRIs as safer alternatives.
The causal link between sudden death and desipramine was tenuous; Biederman’s article comparing children exposed versus not exposed to TCAs did not demonstrate a statistically significant difference in sudden death.8 Even so, fear of cardiotoxicity in children curtailed TCAs’ use.
SSRIs are now are now usually considered firstline antidepressants for children and adolescents because they are presumed to be safer than TCAs. SSRIs are associated with minimal cardiotoxicity and anticholinergic effects, a wider margin of safety in overdose than TCAs, and demonstrated efficacy.
A 12-week, double-blind study compared paroxetine, 20 to 40 mg/d, imipramine, up to 300 mg/d, and placebo in 275 adolescents with major depression.9 Patients receiving paroxetine improved significantly more than patients receiving placebo, as measured by reductions in the Hamilton Rating Scale for Depression (HAM-D) total scores and other scales. Response to imipramine was not significantly different from placebo.
Discontinuation rates because of side effects were 9.7% for paroxetine and 31.5% (nearly one-third because of cardiovascular side effects) for imipramine. The average imipramine dosage of 200 mg/d was higher than usual, however.
Table 3
Recommended antidepressant dosages for children and adolescents
| Selective serotonin reuptake inhibitors | ||
| Drug | Dosage | Comments |
| Citalopram | Once-daily Children: 10 to 20 mg Adolescents: 10 to 40 mg | Antianxiety component Limited pediatric data Less effect on P-450 isoenzyme systems than other SSRIs, with fewer drug-drug interactions claimed |
| Escitalopram | Once-daily Children: 5 to 10 mg Adolescents: 10 mg | L-isomer of citalopram, purported to have lesser side effects than parent compound No data in children |
| Fluoxetine | Once-daily Children: 5 to 20 mg Adolescents: 10 to 60 mg | Antianxiety properties More effective than placebo in trials of adolescent depression11-12 Long half-life; watch for drug-drug interactions |
| Fluvoxamine | Divided Children: 50 to 100 mg/d Adolescents: 50 to 200 mg/d | Useful in depression with comorbid obsessive-compulsive symptoms No data for pediatric depression |
| Paroxetine | Once-daily Children: 10 to 20 mg Adolescents: 10 to 40 mg | Similar profile as fluoxetine but shorter half-life Not recommended in pediatric patients (FDA advisory) |
| Sertraline | Divided Children: 25 to100 mg/d Adolescents: 50 to 200 mg/d | Less activating and shorter half-life than fluoxetine |
| Other reuptake inhibitors | ||
| Drug | Dosage | Comment |
| Bupropion | Divided Children: 75 to 250 mg/d Adolescents: 75 to 400 mg/d | Useful in depression with comorbid attention- deficit/hyperactivity disorder No controlled data in children |
| Nefazodone | Divided Children: 100 to 300 mg/d Adolescents: 200 to 600 mg/d | 5HT2-receptor and serotonin-reuptake blocker |
| Venlafaxine | Divided or once-daily Children: 18.75 to 75 mg/d Adolescents: 37.5 to 150 mg/d | Noradrenergic and serotonergic effects Limited pediatric data; not recommended in depressed pediatric patients (manufacturer advisory) |
| Source: Adapted and reprinted with permission from Sood B, Sood R. Depression in children and adolescents. In: Levenson JL (ed). Depression: key diseases series. Philadelphia: American College of Physicians, 2000:244. | ||
Head-to-head studies of children with obsessive-compulsive disorder have shown fewer side effects with paroxetine compared with clomipramine. Paroxetine’s side effects included anxiety and headaches; clomipra-ALmine’s included headache, tremor, nausea, insomnia, dry mouth and anxiety.10
Efficacy data. Two double-blind, placebo-controlled studies have shown fluoxetine to be more effective than placebo in treating children and adolescents with depression.11-13 In general, however, not all SSRIs have shown consistent efficacy in placebo-controlled trials of pediatric major depression. Among 15 such trials submitted to the FDA, three (20%) showed positive results (Table 2). The success rate of drug therapy trials for adult major depression is about 50%.
The FDA’s Feb. 2 hearing memorandum notes several reasons why the agency does not view these findings as proof that SSRIs lack benefit for pediatric patients. For one, the FDA’s program allowing drug companies to apply for pediatric marketing exclusivity—for which the 15 studies were submitted—did not require positive efficacy results.
Clearly, more research is needed to demonstrate the benefits and risks of SSRIs in children and adolescents with major depression and other disorders.
Using SSRIs safely in youth
During its inquiry, the FDA recommended that prescribers observe standard antidepressant labeling language:
- Be cautious when using SSRIs or related antidepressants in major depressive disorder in children and adolescents.
- Supervise high-risk patients, especially during initial drug therapy.
Monitor suicidality. When treating depressed youth with SSRIs and other antidepressants, ask about suicide attempts, suicidal thinking, and plans for suicide. As part of informed consent, discuss with parents the potential for suicidal behavior in youth with untreated depression.
Discuss antidepressant side effects, which may include disinhibition and impulsivity. Individualize treatment plans; for example, aggressive and impulsive children require especially careful monitoring for risky or suicidal behavior.
Rule out bipolar depression and mixed episodes that are often characterized by marked irritability before prescribing antidepressants to depressed children and adolescents. Early-onset depression is a marker for bipolar disorder in pediatric populations, and bipolar illness may be a possible explanation for behavioral activation and dysphoria when antidepressants are prescribed.
Minimize side effects. Children can tolerate moderately high SSRI dosages but are usually started on lower dosages than are used in adolescents and adults (Table 3). SSRIs do not show a clear dose-response relationship, but their side effects are considered dose-dependent.14
Most-frequent SSRI side effects are nausea, diarrhea, decreased or increased appetite, headaches, restlessness, tremor, and insomnia or hypersomnia. Rare side effects include ecchymoses.15 Reduced growth, possibly related to growth hormone suppression, has been reported in four boys treated with SSRIs.16
Prevent drug interactions. SSRIs are rarely used as monotherapy in pediatric patients because of the high rates of comorbidity and severity of mental illness that presents in childhood. Using two or more medications is the rule, not the exception.17
SSRIs are highly protein-bound and are metabolized by the cytochrome P-450 isoenzyme system, which increases the likelihood of drug-drug interactions. Thus, be aware of the potential impact of combining SSRIs with other agents.
Some researchers suggest that paroxetine, sertraline, and citalopram’s relatively short half-lives (14 to 16 hours) in children may be a rationale for giving the medications twice daily.18
Avoid withdrawal. The withdrawal syndrome following abrupt cessation of paroxetine, venlafaxine, or fluvoxamine is well known, and its irritability and depression-like symptoms can be quite distressing for patients. Thus, make decisions thoughtfully when discontinuing SSRIs, and plan to taper for 1 to 2 weeks.
- Food and Drug Administration. Report prepared for public hearing Feb. 2, 2004. www.fda.gov/ohrms/dockets/ac/04/briefing/4006b1.htm (click on “Background Memorandum”)
- Preliminary report of the task force on SSRIs and suicidal behavior in youth, Jan. 21, 2004. American College of Neuropsychopharmacology. www.acnp.org/exec_summary.pdf
- Sood B, Sood R. Depression in children and adolescents. In: Levenson JL (ed). Depression: key diseases series. Philadelphia: American College of Physicians, 2000.
Drug brand names
- Bupropion • Wellbutrin
- Citalopram • Celexa
- Escitalopram • Lexapro
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Nefazodone • Serzone
- Paroxetine • Paxil
- Sertraline • Zoloft
- Venlafaxine • Effexor
Disclosure
Dr. Sood is a speaker for AstraZeneca, Shire Pharmaceutical Group, and Eli Lilly and Co.
Dr. Elizabeth Weller has received research/grant support from Forest Pharmaceuticals, Organon, and Wyeth Pharmaceuticals and is a consultant to Johnson & Johnson, Novartis, AstraZeneca, and Otsuka Pharmaceutical.
Dr. Ronald Weller receives research/grant support from Wyeth Pharmaceuticals, Organon, and Forest Pharmaceuticals.
1. King RA, Riddle MA, Chappell PB, et al. Emergence of self-destructive phenomena in children and adolescents during fluoxetine treatment. J Am Acad Child Adolesc Psychiatry 1991;30:179-86.
2. Vorstman J, Lahuis B, Buitelaar JK. SSRIs associated with behavioral activation and suicidal ideation. J Am Acad Child Adolesc Psychiatry 2001;40:1364-5.
3. Hall WD, Mant A, Mitchell PB, et al. Association between antidepressant prescribing and suicide in Australia, 1991-2000. BMJ 2003;326(7397):1008.-
4. Shaffer D, Fisher P, Dulcan MK, et al. The NIMH Diagnostic Interview Schedule, Version 2.3 (DISC 2.3): description, acceptability, prevalence rates and performance of the MECA Study. Methods for the Epidemiology of Child and Adolescent Mental Disorders Study. J Am Acad Child Adolesc Psychiatry 1996a;35:865-77.
5. Harrington R, Bredenkamp D, Groothues C, et al. Adult outcomes of child and adolescent depression, III: Links with suicidal behaviors. J Child Psychol Psychiatry 1994;35:1309-19.
6. Kovacs M. Presentation of course and major depressive disorder during childhood and later years of the life span. J Am Acad Child Adolesc Psychiatry 1996;35:705-15.
7. Rao U, Hammen C, Daley SE. Continuity of depression during the transition through adulthood: a five-year longitudinal study of young women. J Am Acad Child Adolesc Psychiatry 1999;38:908-15.
8. Biederman J. Sudden death in children with a tricyclic antidepressant. J Am Acad Child Adolesc Psychiatry 1991;30(3):495-8.
9. Keller MB, Ryan ND, Strober M, et al. Efficacy of paroxetine in the treatment of adolescent major depression: a randomized, controlled study. J Am Acad Child Adolesc Psychiatry 2001;40:762-72.
10. Flament M, Cohen D. Childhood obsessive compulsive disorder. In: Maj M, Sartorius N (eds). Obsessive compulsive disorder: evidence and practice New York: World Psychiatric Association 2000;147-83.
11. Simeon J, Dinicola V, Ferguson H, Copping W. Adolescent depression: a placebo-controlled fluoxetine treatment study and follow up. Prog Neuropsychopharmacol Biol Psychiatry 1990;14:791-5.
12. Emslie G, Rush AJ, Weinberg AW, et al. A double-blind, randomized, placebo-controlled trial of fluoxetine in depressed children and adolescents. Arch Gen Psychiatry 1997;54:1031-7.
13. Emslie GJ, Heiligenstein JH, Wagner KD, et al. Fluoxetine for acute treatment of depression in children and adolescents: a placebo-controlled, randomized, clinical trial. J Am Acad Child Adolesc Psychiatry 2002;41(10):1205-15.
14. Preskorn SH. Outpatient management of depression: a guide for the practitioner (2nd ed). Caddo, OK: Professional Communications, 1999.
15. Lake MB, Birmaher B, Wassick S, et al. Bleeding and selective serotonin reuptake inhibitors in childhood and adolescence. J Child Adolesc Psychopharmacol 2000;10:35-8.
16. Weintrob N, Cohen D, Klipper-Aurbach Y, et al. Decreased growth during therapy with selective serotonin reuptake inhibitors. Arch Pediatr Adolesc Med 2002;156:696-701.
17. Rushton JL, Whitmire JT. Pediatric stimulant and selective serotonin reuptake inhibitor prescription trends. Arch Pediatr Adolesc Med 2001;155:560-5.
18. Axelson D, Perel J, Rudolph G, et al. Significant differences in pharmacokinetic/dynamics of citalopram between adolescents and adults: implications for clinical dosing (abstract). San Juan, PR: American College of Neuropsychopharmacology annual meeting, 2000.
Caitlin McIntosh, 12, hanged herself with shoelaces weeks after starting treatment for depression with a selective serotonin reuptake inhibitor (SSRI). Matt Miller, 13, hanged himself in his bedroom closet after taking his seventh SSRI dose. Michael Shivak, 11, slashed his wrists in class—but survived—while taking an SSRI.
These adolescents’ parents testified at an FDA hearing Feb. 2 about possible increased risk of suicidality with SSRIs in depressed children and adolescents.
Other families related positive experiences. Sherri Walton said her daughter, Jordan, 14, has achieved “enormous benefit” from taking SSRIs for obsessive-compulsive disorder. Suzanne Vogel-Scibilia told the FDA panel she is convinced that her two children with psychiatric disorders lead full lives because of SSRIs.
Sensitive to the anguish of grieving families but not wanting to deprive seriously depressed children of effective treatment, the FDA is proceeding methodically with its inquiry—probably at least until summer.
In the meantime, this article offers resources to help you answer questions from parents concerned about their children starting or continuing SSRIs. We include pediatric antidepressant dosing recommendations and data on benefits and risks of SSRIs and other reuptake inhibitors in young patients.
Why the FDA inquiry?
SSRI-associated behavioral activation and suicidal ideation in children and adolescents were reported anecdotally, as case reports, in the early 1990s,1 and more recently.2 No convincing evidence has shown, however, that SSRIs increase the risk of suicide. In fact, widespread use of SSRIs has been associated with reduced suicide rates.3
In May 2003, unpublished data submitted to the FDA from placebo-controlled trials suggested an increased risk of “possibly suicide-related” events and “suicide attempts” in pediatric patients taking paroxetine for major depression. No suicides were reported.
The Medicines and Healthcare Products Regulatory Agency (MHRA)—the United Kingdom’s equivalent of the Food and Drug Administration—responded by warning British physicians against prescribing paroxetine for depressed patients younger than 18. It also ordered a labeling change for paroxetine, contraindicating its use in pediatric major depression.
The FDA advised U.S. doctors against using paroxetine for children under age 18 with major depressive disorder and began investigating data on pediatric use of antidepressants, including all approved SSRIs. Since then:
- In the United States, venlafaxine’s manufacturer changed the drug’s labeling to include increased reports of hostility and suicidality in pediatric trial data. A “Dear Health Care Professional” letter in August 2003 indicated that venlafaxine is not recommended in depressed pediatric patients.
- Britain’s MHRA added pediatric con-traindications to labeling of venlafaxine, sertraline, citalopram, and escitalopram in December 2003. The agency opined that fluoxetine is the only SSRI with a favorable risk-benefit profile for pediatric major depression.
- At press time, the FDA had not changed any SSRI labeling.
At the Feb. 2 public hearing, the FDA’s Psycho-pharmacological Drugs Advisory Committee and Pediatric Subcommittee of the Anti-Infective Drugs Advisory Committee heard public comments from patients, families, and physicians and reviewed the inquiry’s progress. To locate the Web site containing the FDA’s memorandum on this hearing, see Related resources.
For the next several months, an expert group at Columbia University is under contract with the FDA to develop a system to classify events that might represent suicidality. The group will then analyze data from 24 studies involving more than 4,000 depressed pediatric patients and nine antidepressants (paroxetine, fluoxetine, sertraline, fluvoxamine, citalopram, bupropion, venlafaxine, nefazodone, and mirtazapine).
Independent findings. In January, an American College of Neuropsychopharmacology (ACNP) report concluded that SSRIs do not increase suicidal thoughts or suicide attempts in youth (Table 1). An ACNP task force examined the use of SSRIs in more than 2,000 children and adolescents, including all published clinical trial data, unpublished data from several pharmaceutical companies, and data reported to Britain’s MHRA. An executive summary is available on the ACNP’s Web site (see Related resources).
Table 1
Suicide deaths, behavior, or ideation in clinical trials of youth with major depressive disorder
| Medication | Total youth* in trials | No. of suicide deaths | % of youth with suicidal behavior or ideation** | P value | Statistical significance | |
|---|---|---|---|---|---|---|
| Antidepressant | Placebo | |||||
| Citalopram | 418 | 0 | 8.9%(19) | 7.3% (15) | 0.5 | No |
| Fluoxetine | 458 | 0 | 3.6%(9) | 3.8% (8) | 0.9 | No |
| Paroxetine | 669 | 0 | 3.7%(14) | 2.5% (7) | 0.4 | No |
| Sertraline | 376 | 0 | 2.7%(5) | 1.1% (2) | 0.3 | No |
| Venlafaxine | 334 | 0 | 2%(NA) | 0% | 0.25 | No |
| * Total number of youth given antidepressants and placebo | ||||||
| ** Number inside parenthesis is actual number of youth | ||||||
| NA = Not available | ||||||
| Source: Data from published clinical trials, unpublished clinical trials provided by drug sponsor, and clinical data compiled by the Medicines and Healthcare Products Regulatory Agency of the United Kingdom. | ||||||
| Reprinted with permission of the American College of Neuropsychopharmacology from Preliminary report of the Task Force on SSRIs and Suicidal Behavior in Youth (executive summary), January 2004:18. | ||||||
Depression’s impact on children
The prevalence of depression in youth age 18 and younger is 8.3%,4 and the rate increases with patient age. Before puberty, common signs of depression include somatic symptoms such as abdominal pain, headaches, and irritability, whereas adolescents are more likely to express feelings of depression and exhibit suicidal behavior. Girls and boys are equally at risk for depression until puberty, when girls begin to outnumber boys and the presentation begins to resemble adult depression.
Untreated pediatric depression is associated with substantial morbidity, including reduced academic performance, substance abuse, interpersonal problems, social withdrawal, and a poor quality of life,4,5 It also increases the risk of suicide.
Early-onset depression is considered a more malignant illness than adult-onset depression because of its effect on development, potential for recurrence,6 and chronicity into adulthood.7 The quest to develop appropriate treatment for depressed children and adolescents has been spurred by:
- the substantial risks of morbidity and mortality from childhood depression
- advances in drug treatments for adult-onset depression
- recognition that early-onset depression is treatable.
Physiologically, children are not “mini-adults.” Thus, practicing evidence-based medicine requires separate empirical research for pediatric conditions.
Despite some efforts by the National Institute of Mental Health (NIMH) and the pharmaceutical industry, research in pediatric psychopharmacology and ancillary treatments lags decades behind evidence-based treatment in adults.
Table 2
Efficacy of SSRIs and other newer antidepressants in short-term, placebo-controlled pediatric studies in major depressive disorder
| Drug | Age range | Outcome* (drug vs. placebo) |
|---|---|---|
| Paroxetine | ||
| Study 1 Study 2 Study 3 | 12 to 18 13 to 18 7 to 17 | Negative† Negative Negative |
| Fluoxetine | ||
| Study 1 Study 2 | 8 to 17 8 to 17 | Positive Positive |
| Sertraline | ||
| Study 1 Study 2 | 6 to 17 6 to 17 | Trend Negative§ |
| Venlafaxine | ||
| Study 1 Study 2 | 7 to 17 7 to 17 | Negative Negative |
| Citalopram | ||
| Study 1 Study 2 | 7 to 17 13 to 18 | Positive Negative |
| Nefazodone | ||
| Study 1 Study 2 | 12 to 18 7 to 17 | Trend Negative |
| Mirtazapine | ||
| Study 1 Study 2 | 7 to 17 7 to 17 | Negative Negative |
| * Positive (P 0.05); Negative (P >0.10; Trend (0.05 | ||
| † Positive on most secondary endpoints | ||
| § Positive on pooling of 2 studies | ||
| Source: Adapted and reprinted from Laughren TP. Memorandum: Background comments for Feb. 2, 2004 meeting of Psychopharmacological Drugs Advisory Committee and Pediatric Subcommittee of the Anti-Infective Drugs Advisory Committee. Appendix I. Center for Drug Evaluation and Research. Food and Drug Administration, Public Health Service, Department of Health and Human Services. | ||
From tricyclics to SSRIS
Tricyclic antidepressants (TCAs) were the mainstay in treating childhood depression two decades ago, based on clinical and anecdotal evidence. However, double blind, placebo-controlled studies failed to show that TCAs were effective in treating depressed children and adolescents. The few controlled studies included small samples of children and adolescents, and the methodologies were often flawed.
In the late 1980s, TCA use in children dropped precipitously because of:
- episodes of sudden death in pediatric patients taking desipramine
- introduction of SSRIs as safer alternatives.
The causal link between sudden death and desipramine was tenuous; Biederman’s article comparing children exposed versus not exposed to TCAs did not demonstrate a statistically significant difference in sudden death.8 Even so, fear of cardiotoxicity in children curtailed TCAs’ use.
SSRIs are now are now usually considered firstline antidepressants for children and adolescents because they are presumed to be safer than TCAs. SSRIs are associated with minimal cardiotoxicity and anticholinergic effects, a wider margin of safety in overdose than TCAs, and demonstrated efficacy.
A 12-week, double-blind study compared paroxetine, 20 to 40 mg/d, imipramine, up to 300 mg/d, and placebo in 275 adolescents with major depression.9 Patients receiving paroxetine improved significantly more than patients receiving placebo, as measured by reductions in the Hamilton Rating Scale for Depression (HAM-D) total scores and other scales. Response to imipramine was not significantly different from placebo.
Discontinuation rates because of side effects were 9.7% for paroxetine and 31.5% (nearly one-third because of cardiovascular side effects) for imipramine. The average imipramine dosage of 200 mg/d was higher than usual, however.
Table 3
Recommended antidepressant dosages for children and adolescents
| Selective serotonin reuptake inhibitors | ||
| Drug | Dosage | Comments |
| Citalopram | Once-daily Children: 10 to 20 mg Adolescents: 10 to 40 mg | Antianxiety component Limited pediatric data Less effect on P-450 isoenzyme systems than other SSRIs, with fewer drug-drug interactions claimed |
| Escitalopram | Once-daily Children: 5 to 10 mg Adolescents: 10 mg | L-isomer of citalopram, purported to have lesser side effects than parent compound No data in children |
| Fluoxetine | Once-daily Children: 5 to 20 mg Adolescents: 10 to 60 mg | Antianxiety properties More effective than placebo in trials of adolescent depression11-12 Long half-life; watch for drug-drug interactions |
| Fluvoxamine | Divided Children: 50 to 100 mg/d Adolescents: 50 to 200 mg/d | Useful in depression with comorbid obsessive-compulsive symptoms No data for pediatric depression |
| Paroxetine | Once-daily Children: 10 to 20 mg Adolescents: 10 to 40 mg | Similar profile as fluoxetine but shorter half-life Not recommended in pediatric patients (FDA advisory) |
| Sertraline | Divided Children: 25 to100 mg/d Adolescents: 50 to 200 mg/d | Less activating and shorter half-life than fluoxetine |
| Other reuptake inhibitors | ||
| Drug | Dosage | Comment |
| Bupropion | Divided Children: 75 to 250 mg/d Adolescents: 75 to 400 mg/d | Useful in depression with comorbid attention- deficit/hyperactivity disorder No controlled data in children |
| Nefazodone | Divided Children: 100 to 300 mg/d Adolescents: 200 to 600 mg/d | 5HT2-receptor and serotonin-reuptake blocker |
| Venlafaxine | Divided or once-daily Children: 18.75 to 75 mg/d Adolescents: 37.5 to 150 mg/d | Noradrenergic and serotonergic effects Limited pediatric data; not recommended in depressed pediatric patients (manufacturer advisory) |
| Source: Adapted and reprinted with permission from Sood B, Sood R. Depression in children and adolescents. In: Levenson JL (ed). Depression: key diseases series. Philadelphia: American College of Physicians, 2000:244. | ||
Head-to-head studies of children with obsessive-compulsive disorder have shown fewer side effects with paroxetine compared with clomipramine. Paroxetine’s side effects included anxiety and headaches; clomipra-ALmine’s included headache, tremor, nausea, insomnia, dry mouth and anxiety.10
Efficacy data. Two double-blind, placebo-controlled studies have shown fluoxetine to be more effective than placebo in treating children and adolescents with depression.11-13 In general, however, not all SSRIs have shown consistent efficacy in placebo-controlled trials of pediatric major depression. Among 15 such trials submitted to the FDA, three (20%) showed positive results (Table 2). The success rate of drug therapy trials for adult major depression is about 50%.
The FDA’s Feb. 2 hearing memorandum notes several reasons why the agency does not view these findings as proof that SSRIs lack benefit for pediatric patients. For one, the FDA’s program allowing drug companies to apply for pediatric marketing exclusivity—for which the 15 studies were submitted—did not require positive efficacy results.
Clearly, more research is needed to demonstrate the benefits and risks of SSRIs in children and adolescents with major depression and other disorders.
Using SSRIs safely in youth
During its inquiry, the FDA recommended that prescribers observe standard antidepressant labeling language:
- Be cautious when using SSRIs or related antidepressants in major depressive disorder in children and adolescents.
- Supervise high-risk patients, especially during initial drug therapy.
Monitor suicidality. When treating depressed youth with SSRIs and other antidepressants, ask about suicide attempts, suicidal thinking, and plans for suicide. As part of informed consent, discuss with parents the potential for suicidal behavior in youth with untreated depression.
Discuss antidepressant side effects, which may include disinhibition and impulsivity. Individualize treatment plans; for example, aggressive and impulsive children require especially careful monitoring for risky or suicidal behavior.
Rule out bipolar depression and mixed episodes that are often characterized by marked irritability before prescribing antidepressants to depressed children and adolescents. Early-onset depression is a marker for bipolar disorder in pediatric populations, and bipolar illness may be a possible explanation for behavioral activation and dysphoria when antidepressants are prescribed.
Minimize side effects. Children can tolerate moderately high SSRI dosages but are usually started on lower dosages than are used in adolescents and adults (Table 3). SSRIs do not show a clear dose-response relationship, but their side effects are considered dose-dependent.14
Most-frequent SSRI side effects are nausea, diarrhea, decreased or increased appetite, headaches, restlessness, tremor, and insomnia or hypersomnia. Rare side effects include ecchymoses.15 Reduced growth, possibly related to growth hormone suppression, has been reported in four boys treated with SSRIs.16
Prevent drug interactions. SSRIs are rarely used as monotherapy in pediatric patients because of the high rates of comorbidity and severity of mental illness that presents in childhood. Using two or more medications is the rule, not the exception.17
SSRIs are highly protein-bound and are metabolized by the cytochrome P-450 isoenzyme system, which increases the likelihood of drug-drug interactions. Thus, be aware of the potential impact of combining SSRIs with other agents.
Some researchers suggest that paroxetine, sertraline, and citalopram’s relatively short half-lives (14 to 16 hours) in children may be a rationale for giving the medications twice daily.18
Avoid withdrawal. The withdrawal syndrome following abrupt cessation of paroxetine, venlafaxine, or fluvoxamine is well known, and its irritability and depression-like symptoms can be quite distressing for patients. Thus, make decisions thoughtfully when discontinuing SSRIs, and plan to taper for 1 to 2 weeks.
- Food and Drug Administration. Report prepared for public hearing Feb. 2, 2004. www.fda.gov/ohrms/dockets/ac/04/briefing/4006b1.htm (click on “Background Memorandum”)
- Preliminary report of the task force on SSRIs and suicidal behavior in youth, Jan. 21, 2004. American College of Neuropsychopharmacology. www.acnp.org/exec_summary.pdf
- Sood B, Sood R. Depression in children and adolescents. In: Levenson JL (ed). Depression: key diseases series. Philadelphia: American College of Physicians, 2000.
Drug brand names
- Bupropion • Wellbutrin
- Citalopram • Celexa
- Escitalopram • Lexapro
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Nefazodone • Serzone
- Paroxetine • Paxil
- Sertraline • Zoloft
- Venlafaxine • Effexor
Disclosure
Dr. Sood is a speaker for AstraZeneca, Shire Pharmaceutical Group, and Eli Lilly and Co.
Dr. Elizabeth Weller has received research/grant support from Forest Pharmaceuticals, Organon, and Wyeth Pharmaceuticals and is a consultant to Johnson & Johnson, Novartis, AstraZeneca, and Otsuka Pharmaceutical.
Dr. Ronald Weller receives research/grant support from Wyeth Pharmaceuticals, Organon, and Forest Pharmaceuticals.
Caitlin McIntosh, 12, hanged herself with shoelaces weeks after starting treatment for depression with a selective serotonin reuptake inhibitor (SSRI). Matt Miller, 13, hanged himself in his bedroom closet after taking his seventh SSRI dose. Michael Shivak, 11, slashed his wrists in class—but survived—while taking an SSRI.
These adolescents’ parents testified at an FDA hearing Feb. 2 about possible increased risk of suicidality with SSRIs in depressed children and adolescents.
Other families related positive experiences. Sherri Walton said her daughter, Jordan, 14, has achieved “enormous benefit” from taking SSRIs for obsessive-compulsive disorder. Suzanne Vogel-Scibilia told the FDA panel she is convinced that her two children with psychiatric disorders lead full lives because of SSRIs.
Sensitive to the anguish of grieving families but not wanting to deprive seriously depressed children of effective treatment, the FDA is proceeding methodically with its inquiry—probably at least until summer.
In the meantime, this article offers resources to help you answer questions from parents concerned about their children starting or continuing SSRIs. We include pediatric antidepressant dosing recommendations and data on benefits and risks of SSRIs and other reuptake inhibitors in young patients.
Why the FDA inquiry?
SSRI-associated behavioral activation and suicidal ideation in children and adolescents were reported anecdotally, as case reports, in the early 1990s,1 and more recently.2 No convincing evidence has shown, however, that SSRIs increase the risk of suicide. In fact, widespread use of SSRIs has been associated with reduced suicide rates.3
In May 2003, unpublished data submitted to the FDA from placebo-controlled trials suggested an increased risk of “possibly suicide-related” events and “suicide attempts” in pediatric patients taking paroxetine for major depression. No suicides were reported.
The Medicines and Healthcare Products Regulatory Agency (MHRA)—the United Kingdom’s equivalent of the Food and Drug Administration—responded by warning British physicians against prescribing paroxetine for depressed patients younger than 18. It also ordered a labeling change for paroxetine, contraindicating its use in pediatric major depression.
The FDA advised U.S. doctors against using paroxetine for children under age 18 with major depressive disorder and began investigating data on pediatric use of antidepressants, including all approved SSRIs. Since then:
- In the United States, venlafaxine’s manufacturer changed the drug’s labeling to include increased reports of hostility and suicidality in pediatric trial data. A “Dear Health Care Professional” letter in August 2003 indicated that venlafaxine is not recommended in depressed pediatric patients.
- Britain’s MHRA added pediatric con-traindications to labeling of venlafaxine, sertraline, citalopram, and escitalopram in December 2003. The agency opined that fluoxetine is the only SSRI with a favorable risk-benefit profile for pediatric major depression.
- At press time, the FDA had not changed any SSRI labeling.
At the Feb. 2 public hearing, the FDA’s Psycho-pharmacological Drugs Advisory Committee and Pediatric Subcommittee of the Anti-Infective Drugs Advisory Committee heard public comments from patients, families, and physicians and reviewed the inquiry’s progress. To locate the Web site containing the FDA’s memorandum on this hearing, see Related resources.
For the next several months, an expert group at Columbia University is under contract with the FDA to develop a system to classify events that might represent suicidality. The group will then analyze data from 24 studies involving more than 4,000 depressed pediatric patients and nine antidepressants (paroxetine, fluoxetine, sertraline, fluvoxamine, citalopram, bupropion, venlafaxine, nefazodone, and mirtazapine).
Independent findings. In January, an American College of Neuropsychopharmacology (ACNP) report concluded that SSRIs do not increase suicidal thoughts or suicide attempts in youth (Table 1). An ACNP task force examined the use of SSRIs in more than 2,000 children and adolescents, including all published clinical trial data, unpublished data from several pharmaceutical companies, and data reported to Britain’s MHRA. An executive summary is available on the ACNP’s Web site (see Related resources).
Table 1
Suicide deaths, behavior, or ideation in clinical trials of youth with major depressive disorder
| Medication | Total youth* in trials | No. of suicide deaths | % of youth with suicidal behavior or ideation** | P value | Statistical significance | |
|---|---|---|---|---|---|---|
| Antidepressant | Placebo | |||||
| Citalopram | 418 | 0 | 8.9%(19) | 7.3% (15) | 0.5 | No |
| Fluoxetine | 458 | 0 | 3.6%(9) | 3.8% (8) | 0.9 | No |
| Paroxetine | 669 | 0 | 3.7%(14) | 2.5% (7) | 0.4 | No |
| Sertraline | 376 | 0 | 2.7%(5) | 1.1% (2) | 0.3 | No |
| Venlafaxine | 334 | 0 | 2%(NA) | 0% | 0.25 | No |
| * Total number of youth given antidepressants and placebo | ||||||
| ** Number inside parenthesis is actual number of youth | ||||||
| NA = Not available | ||||||
| Source: Data from published clinical trials, unpublished clinical trials provided by drug sponsor, and clinical data compiled by the Medicines and Healthcare Products Regulatory Agency of the United Kingdom. | ||||||
| Reprinted with permission of the American College of Neuropsychopharmacology from Preliminary report of the Task Force on SSRIs and Suicidal Behavior in Youth (executive summary), January 2004:18. | ||||||
Depression’s impact on children
The prevalence of depression in youth age 18 and younger is 8.3%,4 and the rate increases with patient age. Before puberty, common signs of depression include somatic symptoms such as abdominal pain, headaches, and irritability, whereas adolescents are more likely to express feelings of depression and exhibit suicidal behavior. Girls and boys are equally at risk for depression until puberty, when girls begin to outnumber boys and the presentation begins to resemble adult depression.
Untreated pediatric depression is associated with substantial morbidity, including reduced academic performance, substance abuse, interpersonal problems, social withdrawal, and a poor quality of life,4,5 It also increases the risk of suicide.
Early-onset depression is considered a more malignant illness than adult-onset depression because of its effect on development, potential for recurrence,6 and chronicity into adulthood.7 The quest to develop appropriate treatment for depressed children and adolescents has been spurred by:
- the substantial risks of morbidity and mortality from childhood depression
- advances in drug treatments for adult-onset depression
- recognition that early-onset depression is treatable.
Physiologically, children are not “mini-adults.” Thus, practicing evidence-based medicine requires separate empirical research for pediatric conditions.
Despite some efforts by the National Institute of Mental Health (NIMH) and the pharmaceutical industry, research in pediatric psychopharmacology and ancillary treatments lags decades behind evidence-based treatment in adults.
Table 2
Efficacy of SSRIs and other newer antidepressants in short-term, placebo-controlled pediatric studies in major depressive disorder
| Drug | Age range | Outcome* (drug vs. placebo) |
|---|---|---|
| Paroxetine | ||
| Study 1 Study 2 Study 3 | 12 to 18 13 to 18 7 to 17 | Negative† Negative Negative |
| Fluoxetine | ||
| Study 1 Study 2 | 8 to 17 8 to 17 | Positive Positive |
| Sertraline | ||
| Study 1 Study 2 | 6 to 17 6 to 17 | Trend Negative§ |
| Venlafaxine | ||
| Study 1 Study 2 | 7 to 17 7 to 17 | Negative Negative |
| Citalopram | ||
| Study 1 Study 2 | 7 to 17 13 to 18 | Positive Negative |
| Nefazodone | ||
| Study 1 Study 2 | 12 to 18 7 to 17 | Trend Negative |
| Mirtazapine | ||
| Study 1 Study 2 | 7 to 17 7 to 17 | Negative Negative |
| * Positive (P 0.05); Negative (P >0.10; Trend (0.05 | ||
| † Positive on most secondary endpoints | ||
| § Positive on pooling of 2 studies | ||
| Source: Adapted and reprinted from Laughren TP. Memorandum: Background comments for Feb. 2, 2004 meeting of Psychopharmacological Drugs Advisory Committee and Pediatric Subcommittee of the Anti-Infective Drugs Advisory Committee. Appendix I. Center for Drug Evaluation and Research. Food and Drug Administration, Public Health Service, Department of Health and Human Services. | ||
From tricyclics to SSRIS
Tricyclic antidepressants (TCAs) were the mainstay in treating childhood depression two decades ago, based on clinical and anecdotal evidence. However, double blind, placebo-controlled studies failed to show that TCAs were effective in treating depressed children and adolescents. The few controlled studies included small samples of children and adolescents, and the methodologies were often flawed.
In the late 1980s, TCA use in children dropped precipitously because of:
- episodes of sudden death in pediatric patients taking desipramine
- introduction of SSRIs as safer alternatives.
The causal link between sudden death and desipramine was tenuous; Biederman’s article comparing children exposed versus not exposed to TCAs did not demonstrate a statistically significant difference in sudden death.8 Even so, fear of cardiotoxicity in children curtailed TCAs’ use.
SSRIs are now are now usually considered firstline antidepressants for children and adolescents because they are presumed to be safer than TCAs. SSRIs are associated with minimal cardiotoxicity and anticholinergic effects, a wider margin of safety in overdose than TCAs, and demonstrated efficacy.
A 12-week, double-blind study compared paroxetine, 20 to 40 mg/d, imipramine, up to 300 mg/d, and placebo in 275 adolescents with major depression.9 Patients receiving paroxetine improved significantly more than patients receiving placebo, as measured by reductions in the Hamilton Rating Scale for Depression (HAM-D) total scores and other scales. Response to imipramine was not significantly different from placebo.
Discontinuation rates because of side effects were 9.7% for paroxetine and 31.5% (nearly one-third because of cardiovascular side effects) for imipramine. The average imipramine dosage of 200 mg/d was higher than usual, however.
Table 3
Recommended antidepressant dosages for children and adolescents
| Selective serotonin reuptake inhibitors | ||
| Drug | Dosage | Comments |
| Citalopram | Once-daily Children: 10 to 20 mg Adolescents: 10 to 40 mg | Antianxiety component Limited pediatric data Less effect on P-450 isoenzyme systems than other SSRIs, with fewer drug-drug interactions claimed |
| Escitalopram | Once-daily Children: 5 to 10 mg Adolescents: 10 mg | L-isomer of citalopram, purported to have lesser side effects than parent compound No data in children |
| Fluoxetine | Once-daily Children: 5 to 20 mg Adolescents: 10 to 60 mg | Antianxiety properties More effective than placebo in trials of adolescent depression11-12 Long half-life; watch for drug-drug interactions |
| Fluvoxamine | Divided Children: 50 to 100 mg/d Adolescents: 50 to 200 mg/d | Useful in depression with comorbid obsessive-compulsive symptoms No data for pediatric depression |
| Paroxetine | Once-daily Children: 10 to 20 mg Adolescents: 10 to 40 mg | Similar profile as fluoxetine but shorter half-life Not recommended in pediatric patients (FDA advisory) |
| Sertraline | Divided Children: 25 to100 mg/d Adolescents: 50 to 200 mg/d | Less activating and shorter half-life than fluoxetine |
| Other reuptake inhibitors | ||
| Drug | Dosage | Comment |
| Bupropion | Divided Children: 75 to 250 mg/d Adolescents: 75 to 400 mg/d | Useful in depression with comorbid attention- deficit/hyperactivity disorder No controlled data in children |
| Nefazodone | Divided Children: 100 to 300 mg/d Adolescents: 200 to 600 mg/d | 5HT2-receptor and serotonin-reuptake blocker |
| Venlafaxine | Divided or once-daily Children: 18.75 to 75 mg/d Adolescents: 37.5 to 150 mg/d | Noradrenergic and serotonergic effects Limited pediatric data; not recommended in depressed pediatric patients (manufacturer advisory) |
| Source: Adapted and reprinted with permission from Sood B, Sood R. Depression in children and adolescents. In: Levenson JL (ed). Depression: key diseases series. Philadelphia: American College of Physicians, 2000:244. | ||
Head-to-head studies of children with obsessive-compulsive disorder have shown fewer side effects with paroxetine compared with clomipramine. Paroxetine’s side effects included anxiety and headaches; clomipra-ALmine’s included headache, tremor, nausea, insomnia, dry mouth and anxiety.10
Efficacy data. Two double-blind, placebo-controlled studies have shown fluoxetine to be more effective than placebo in treating children and adolescents with depression.11-13 In general, however, not all SSRIs have shown consistent efficacy in placebo-controlled trials of pediatric major depression. Among 15 such trials submitted to the FDA, three (20%) showed positive results (Table 2). The success rate of drug therapy trials for adult major depression is about 50%.
The FDA’s Feb. 2 hearing memorandum notes several reasons why the agency does not view these findings as proof that SSRIs lack benefit for pediatric patients. For one, the FDA’s program allowing drug companies to apply for pediatric marketing exclusivity—for which the 15 studies were submitted—did not require positive efficacy results.
Clearly, more research is needed to demonstrate the benefits and risks of SSRIs in children and adolescents with major depression and other disorders.
Using SSRIs safely in youth
During its inquiry, the FDA recommended that prescribers observe standard antidepressant labeling language:
- Be cautious when using SSRIs or related antidepressants in major depressive disorder in children and adolescents.
- Supervise high-risk patients, especially during initial drug therapy.
Monitor suicidality. When treating depressed youth with SSRIs and other antidepressants, ask about suicide attempts, suicidal thinking, and plans for suicide. As part of informed consent, discuss with parents the potential for suicidal behavior in youth with untreated depression.
Discuss antidepressant side effects, which may include disinhibition and impulsivity. Individualize treatment plans; for example, aggressive and impulsive children require especially careful monitoring for risky or suicidal behavior.
Rule out bipolar depression and mixed episodes that are often characterized by marked irritability before prescribing antidepressants to depressed children and adolescents. Early-onset depression is a marker for bipolar disorder in pediatric populations, and bipolar illness may be a possible explanation for behavioral activation and dysphoria when antidepressants are prescribed.
Minimize side effects. Children can tolerate moderately high SSRI dosages but are usually started on lower dosages than are used in adolescents and adults (Table 3). SSRIs do not show a clear dose-response relationship, but their side effects are considered dose-dependent.14
Most-frequent SSRI side effects are nausea, diarrhea, decreased or increased appetite, headaches, restlessness, tremor, and insomnia or hypersomnia. Rare side effects include ecchymoses.15 Reduced growth, possibly related to growth hormone suppression, has been reported in four boys treated with SSRIs.16
Prevent drug interactions. SSRIs are rarely used as monotherapy in pediatric patients because of the high rates of comorbidity and severity of mental illness that presents in childhood. Using two or more medications is the rule, not the exception.17
SSRIs are highly protein-bound and are metabolized by the cytochrome P-450 isoenzyme system, which increases the likelihood of drug-drug interactions. Thus, be aware of the potential impact of combining SSRIs with other agents.
Some researchers suggest that paroxetine, sertraline, and citalopram’s relatively short half-lives (14 to 16 hours) in children may be a rationale for giving the medications twice daily.18
Avoid withdrawal. The withdrawal syndrome following abrupt cessation of paroxetine, venlafaxine, or fluvoxamine is well known, and its irritability and depression-like symptoms can be quite distressing for patients. Thus, make decisions thoughtfully when discontinuing SSRIs, and plan to taper for 1 to 2 weeks.
- Food and Drug Administration. Report prepared for public hearing Feb. 2, 2004. www.fda.gov/ohrms/dockets/ac/04/briefing/4006b1.htm (click on “Background Memorandum”)
- Preliminary report of the task force on SSRIs and suicidal behavior in youth, Jan. 21, 2004. American College of Neuropsychopharmacology. www.acnp.org/exec_summary.pdf
- Sood B, Sood R. Depression in children and adolescents. In: Levenson JL (ed). Depression: key diseases series. Philadelphia: American College of Physicians, 2000.
Drug brand names
- Bupropion • Wellbutrin
- Citalopram • Celexa
- Escitalopram • Lexapro
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Nefazodone • Serzone
- Paroxetine • Paxil
- Sertraline • Zoloft
- Venlafaxine • Effexor
Disclosure
Dr. Sood is a speaker for AstraZeneca, Shire Pharmaceutical Group, and Eli Lilly and Co.
Dr. Elizabeth Weller has received research/grant support from Forest Pharmaceuticals, Organon, and Wyeth Pharmaceuticals and is a consultant to Johnson & Johnson, Novartis, AstraZeneca, and Otsuka Pharmaceutical.
Dr. Ronald Weller receives research/grant support from Wyeth Pharmaceuticals, Organon, and Forest Pharmaceuticals.
1. King RA, Riddle MA, Chappell PB, et al. Emergence of self-destructive phenomena in children and adolescents during fluoxetine treatment. J Am Acad Child Adolesc Psychiatry 1991;30:179-86.
2. Vorstman J, Lahuis B, Buitelaar JK. SSRIs associated with behavioral activation and suicidal ideation. J Am Acad Child Adolesc Psychiatry 2001;40:1364-5.
3. Hall WD, Mant A, Mitchell PB, et al. Association between antidepressant prescribing and suicide in Australia, 1991-2000. BMJ 2003;326(7397):1008.-
4. Shaffer D, Fisher P, Dulcan MK, et al. The NIMH Diagnostic Interview Schedule, Version 2.3 (DISC 2.3): description, acceptability, prevalence rates and performance of the MECA Study. Methods for the Epidemiology of Child and Adolescent Mental Disorders Study. J Am Acad Child Adolesc Psychiatry 1996a;35:865-77.
5. Harrington R, Bredenkamp D, Groothues C, et al. Adult outcomes of child and adolescent depression, III: Links with suicidal behaviors. J Child Psychol Psychiatry 1994;35:1309-19.
6. Kovacs M. Presentation of course and major depressive disorder during childhood and later years of the life span. J Am Acad Child Adolesc Psychiatry 1996;35:705-15.
7. Rao U, Hammen C, Daley SE. Continuity of depression during the transition through adulthood: a five-year longitudinal study of young women. J Am Acad Child Adolesc Psychiatry 1999;38:908-15.
8. Biederman J. Sudden death in children with a tricyclic antidepressant. J Am Acad Child Adolesc Psychiatry 1991;30(3):495-8.
9. Keller MB, Ryan ND, Strober M, et al. Efficacy of paroxetine in the treatment of adolescent major depression: a randomized, controlled study. J Am Acad Child Adolesc Psychiatry 2001;40:762-72.
10. Flament M, Cohen D. Childhood obsessive compulsive disorder. In: Maj M, Sartorius N (eds). Obsessive compulsive disorder: evidence and practice New York: World Psychiatric Association 2000;147-83.
11. Simeon J, Dinicola V, Ferguson H, Copping W. Adolescent depression: a placebo-controlled fluoxetine treatment study and follow up. Prog Neuropsychopharmacol Biol Psychiatry 1990;14:791-5.
12. Emslie G, Rush AJ, Weinberg AW, et al. A double-blind, randomized, placebo-controlled trial of fluoxetine in depressed children and adolescents. Arch Gen Psychiatry 1997;54:1031-7.
13. Emslie GJ, Heiligenstein JH, Wagner KD, et al. Fluoxetine for acute treatment of depression in children and adolescents: a placebo-controlled, randomized, clinical trial. J Am Acad Child Adolesc Psychiatry 2002;41(10):1205-15.
14. Preskorn SH. Outpatient management of depression: a guide for the practitioner (2nd ed). Caddo, OK: Professional Communications, 1999.
15. Lake MB, Birmaher B, Wassick S, et al. Bleeding and selective serotonin reuptake inhibitors in childhood and adolescence. J Child Adolesc Psychopharmacol 2000;10:35-8.
16. Weintrob N, Cohen D, Klipper-Aurbach Y, et al. Decreased growth during therapy with selective serotonin reuptake inhibitors. Arch Pediatr Adolesc Med 2002;156:696-701.
17. Rushton JL, Whitmire JT. Pediatric stimulant and selective serotonin reuptake inhibitor prescription trends. Arch Pediatr Adolesc Med 2001;155:560-5.
18. Axelson D, Perel J, Rudolph G, et al. Significant differences in pharmacokinetic/dynamics of citalopram between adolescents and adults: implications for clinical dosing (abstract). San Juan, PR: American College of Neuropsychopharmacology annual meeting, 2000.
1. King RA, Riddle MA, Chappell PB, et al. Emergence of self-destructive phenomena in children and adolescents during fluoxetine treatment. J Am Acad Child Adolesc Psychiatry 1991;30:179-86.
2. Vorstman J, Lahuis B, Buitelaar JK. SSRIs associated with behavioral activation and suicidal ideation. J Am Acad Child Adolesc Psychiatry 2001;40:1364-5.
3. Hall WD, Mant A, Mitchell PB, et al. Association between antidepressant prescribing and suicide in Australia, 1991-2000. BMJ 2003;326(7397):1008.-
4. Shaffer D, Fisher P, Dulcan MK, et al. The NIMH Diagnostic Interview Schedule, Version 2.3 (DISC 2.3): description, acceptability, prevalence rates and performance of the MECA Study. Methods for the Epidemiology of Child and Adolescent Mental Disorders Study. J Am Acad Child Adolesc Psychiatry 1996a;35:865-77.
5. Harrington R, Bredenkamp D, Groothues C, et al. Adult outcomes of child and adolescent depression, III: Links with suicidal behaviors. J Child Psychol Psychiatry 1994;35:1309-19.
6. Kovacs M. Presentation of course and major depressive disorder during childhood and later years of the life span. J Am Acad Child Adolesc Psychiatry 1996;35:705-15.
7. Rao U, Hammen C, Daley SE. Continuity of depression during the transition through adulthood: a five-year longitudinal study of young women. J Am Acad Child Adolesc Psychiatry 1999;38:908-15.
8. Biederman J. Sudden death in children with a tricyclic antidepressant. J Am Acad Child Adolesc Psychiatry 1991;30(3):495-8.
9. Keller MB, Ryan ND, Strober M, et al. Efficacy of paroxetine in the treatment of adolescent major depression: a randomized, controlled study. J Am Acad Child Adolesc Psychiatry 2001;40:762-72.
10. Flament M, Cohen D. Childhood obsessive compulsive disorder. In: Maj M, Sartorius N (eds). Obsessive compulsive disorder: evidence and practice New York: World Psychiatric Association 2000;147-83.
11. Simeon J, Dinicola V, Ferguson H, Copping W. Adolescent depression: a placebo-controlled fluoxetine treatment study and follow up. Prog Neuropsychopharmacol Biol Psychiatry 1990;14:791-5.
12. Emslie G, Rush AJ, Weinberg AW, et al. A double-blind, randomized, placebo-controlled trial of fluoxetine in depressed children and adolescents. Arch Gen Psychiatry 1997;54:1031-7.
13. Emslie GJ, Heiligenstein JH, Wagner KD, et al. Fluoxetine for acute treatment of depression in children and adolescents: a placebo-controlled, randomized, clinical trial. J Am Acad Child Adolesc Psychiatry 2002;41(10):1205-15.
14. Preskorn SH. Outpatient management of depression: a guide for the practitioner (2nd ed). Caddo, OK: Professional Communications, 1999.
15. Lake MB, Birmaher B, Wassick S, et al. Bleeding and selective serotonin reuptake inhibitors in childhood and adolescence. J Child Adolesc Psychopharmacol 2000;10:35-8.
16. Weintrob N, Cohen D, Klipper-Aurbach Y, et al. Decreased growth during therapy with selective serotonin reuptake inhibitors. Arch Pediatr Adolesc Med 2002;156:696-701.
17. Rushton JL, Whitmire JT. Pediatric stimulant and selective serotonin reuptake inhibitor prescription trends. Arch Pediatr Adolesc Med 2001;155:560-5.
18. Axelson D, Perel J, Rudolph G, et al. Significant differences in pharmacokinetic/dynamics of citalopram between adolescents and adults: implications for clinical dosing (abstract). San Juan, PR: American College of Neuropsychopharmacology annual meeting, 2000.
Treatment-resistant depression: Switch or augment? Choices that improve response rates
When depression fails to respond to initial therapy—as it commonly does—we have many options but little evidence to guide our choices. We often wonder:
- Is this patient’s depression treatment-resistant?
- Would switching medications or augmenting the initial drug be more likely to achieve an adequate response?
- How effective is psychotherapy compared with medication for treatment-resistant depression?
This article offers insights into each question, based on available trial data, algorithmic approaches to major depressive disorder, and clinical experience. Included is a preview of an ongoing multicenter, treatment-resistant depression study that mimics clinical practice and a look at vagus nerve stimulation (VNS)—a novel somatic therapy being considered by the FDA.
Measuring treatment response
Sustained symptom remission—with normalization of function—is the aim of treating major depressive disorder. Outcomes are categorized as:
- remission (virtual absence of depressive symptoms)
- response with residual symptoms (>50% reduction in baseline symptom severity that does not qualify for remission)
- partial response (>25% but <50% decrease in baseline symptom severity)
- nonresponse (<25% reduction in baseline symptoms).
Major depressive disorder (MDD) is typically recurrent or chronic and characterized by marked disability and a life expectancy shortened by suicide and increased mortality from associated medical conditions. Lifetime prevalence is 16.2%.6
MDD is twice as likely to affect women as men and is common among adolescents, young adults, and persons with concurrent medical conditions.
Major depression’s course is characterized by:
- recurrent episodes (approximately every 5 years)
- or a persistent level of waxing and waning depressive symptoms (in 20% to 35% of cases).
Dysthymic disorder often heralds major depression. Within 1 year, 5% to 20% of persons with dysthymic disorder develop major depression.7
Disability associated with major depression
often exceeds that of other general medical conditions. Depression is the fourth most disabling condition worldwide and is projected to rank number two by 2020 because of its chronic and recurrent nature, high prevalence, and life-shortening effects.8
Consequences of unremitting depression include:
- poor day-to-day function (work, family)
- increased likelihood of recurrence
- psychiatric or medical complications, including substance abuse
- high use of mental health and general medical resources
- worsened prognosis of medical conditions
- high family burden.
In 8-week acute-phase trials, 7% to 15% of patients do not tolerate the initial medication, 25% show no response, 15% show partial response, 10% to 20% exhibit response with residual symptoms, and 30% to 40% achieve remission. Complicated depressions that may not respond as well include those concurrent with Axis I conditions—such as panic disorder or substance abuse—or Axis II or III conditions.1
Time-limited psychotherapies targeted at depressive symptoms (such as cognitive, interpersonal, and behavioral therapies) also typically achieve a 50% response rate in uncomplicated depression that is not treatment-resistant.
Recommendation. When treating depression, assess response at least every 4 weeks (preferably at each visit), using a self-report or clinician rating such as:
- Quick Inventory of Depressive Symptomatology2 (see Related resources)
- Beck Depression Inventory3,4
- Patient Health Questionnaire.5
Defining treatment resistance
A patient may not achieve remission for a variety of reasons, including poor adherence, inadequate medication trial or dosing, occult substance abuse, undiagnosed medical conditions (Box),6-8 concurrent Axis I or II disorders, or treatment resistance.
The general consensus is to consider depression “treatment-resistant” when at least two adequately delivered treatments do not achieve at least a response. A stricter definition—failure to achieve sustained remission with two or more treatments—has also been suggested.
Several schemes have proposed treatment resistance levels, such as the five stages identified in the Table. Recent studies9,10 suggest that increasing treatment resistance is associated with decreasing response or remission rates.
Therefore, when a patient’s treatment resistance is high, two appropriate strategies are to:
- persist with and use maximally tolerated dosages of the treatment you select
- aim for response because high resistance lowers the likelihood of remission.
Predicting response. A major clinical issue is determining whether remission will occur during an acute treatment trial. It is important to not declare treatment resistance unless there has been:
- adequate exposure (dosing and duration) to the treatment
- and adequate adherence.
Patients often have apparent but not actual resistance, meaning that the agent was not used long enough (at least 6 weeks) or at high enough doses. Remission typically follows response by several weeks or even 1 to 2 months for more-chronic depressions.11 Thus, treatment trials should continue at least 12 weeks to determine whether remission will occur.
On the other hand, not obtaining at least a signal of minimal benefit (at least a 20% reduction in baseline symptom severity) in 4 to 6 weeks often portends a low likelihood of response in the long run.12,13 Thus, continue a treatment at least 6 weeks before you decide that it will not achieve a response.
Recommendation. Measure symptoms at key decision points. If modest improvement (such as 20% reduction in baseline symptoms) is found at 4 to 6 weeks, continue treating another 4 to 6 weeks, increasing the dosage as tolerated.
Table
Simple system for staging antidepressant resistance
| Stage | Definition |
|---|---|
| I | Failure of at least one adequate trial of one major antidepressant class |
| II | Stage I resistance plus failure of an adequate trial of an antidepressant in a distinctly different class from that used in Stage I |
| III | Stage II resistance plus failure of an adequate trial of a tricyclic antidepressant |
| IV | Stage III resistance plus failure of an adequate trial of a monoamine oxidase inhibitor |
| V | Stage IV resistance plus failure of a course of bilateral electroconvulsive therapy |
| Source: Reprinted with permission from Thase ME, Rush AJ. When at first you don’t succeed: sequential strategies for antidepressant nonresponders. J Clin Psychiatry 1997;58(suppl 13):24. | |
Treatment options
When initial antidepressant treatment fails to achieve an adequate response—as it does in more than onehalf of major depression cases—the next step is to add a second agent or switch to another agent.
Available evidence14 relies almost exclusively on open, uncontrolled trials, which do not provide definitive answers. Even so, these trials indicate that nonresponse (or nonremission) with one agent does not predict nonresponse/nonremission with another.
Switching strategies. When a selective serotonin reuptake inhibitor (SSRI) is the first treatment, several open trials reveal an approximately 50% response rate to a second SSRI. However, opentrial evidence and retrospective chart review reports also indicate that switching out of class (such as from an SSRI to bupropion) is also approximately 50% effective.15
Some post hoc analyses of acute 8-week trials indicate that the dual-action agent venlafaxine at higher dosages (up to 225 mg/d of venlafaxine XR) is associated with higher remission rates than the more-selective SSRIs.16,17 On the other hand, unpublished data indicate that escitalopram, 10 mg/d, and venlafaxine XR, up to 150 mg/d, did not differ in efficacy among outpatients treated by primary care physicians.18
On the other hand, sertraline and imipramine (a dual-action agent) were equally effective in a 12-week acute-phase trial.19 Furthermore, response and remission rates were similar when nonresponders in each group switched to the other antidepressant.20 This suggests that the dual-action agent (imipramine) was not more effective than the more selective agent (sertraline) in this population.
Well-controlled trials show that monoamine oxidase inhibitors (MAOIs) can be effective when tricyclic antidepressants (TCAs) are not. Switches among the TCAs are associated with a 30% response rate, whereas switching from a TCA to an MAOI typically results in a 50% response rate.21
Controlled prospective comparisons of two or more alternate switch or augment treatments are needed to establish comparative efficacy and tolerability.
Augmentation strategies may include lithium, buspirone, thyroid hormone (T3), stimulants, or atypical antipsychotics. Although head-to-head comparisons are rare, a randomized, controlled trial found that combining olanzapine (mean 50 mg/d), with fluoxetine (mean 15 mg/d) was more effective than each agent used alone.22
Risperidone augmentation is supported by open trials, as is the use of modafinil, other stimulants, and bupropion. An important unanswered question with most augmentation strategies is how long to continue them if they are successful.
Psychotherapy may also play a key role in augmenting medication’s effects. Keller et al23 found in chronically depressed outpatients that 12 weeks of nefazodone, up to 600 mg/d, plus cognitive behavioral analytic system psychotherapy (CBASP) produced higher response and remission rates compared with either treatment alone. A subsequent report24 found that 50% of nefa-zodone and CBASP monotherapy nonresponders did respond when switched to the alternate treatment.
Thus, CBASP may be useful at least in chronic depression to augment medication or as a “switch” to monotherapy if medication alone fails. Interestingly, Nemeroff et al25 found CBASP more effective than nefazodone for patients with chronic major depression who had a childhood history of parental loss or physical, sexual, or emotional abuse.
Antidepressant tachyphylaxis—commonly referred to as “poop-out”—is reported with all antidepressants. That is, even while apparently taking their medications for 6 to 18 months, some patients lose the antidepressant effect, such that some symptoms return or a full relapse/recurrence ensues. Mechanisms of this phenomenon are unknown.
Clinically, some believe that “poop out” is more common with SSRIs than with other antidepressant classes, but no long-term comparative data support or challenge this view. Treatment options include a dosage increase, dosage reduction (especially for long half-life SSRIs such as fluoxetine), or augmentation with the options noted above (such as bupropion, buspirone, etc.).
Benefit of using algorithms
Algorithms (such as the Texas Medication Algorithm Project26 ) have suggested multiple treatment steps for major depression after initial treatment fails, with several options available at each step. Using medication algorithms has been found more effective than treatment-as-usual in outpatients with major depressive disorder.27 No studies have compared different algorithms.
STAR*D trial. The ongoing National Institute of Mental Health (NIMH) Sequenced Treatment Alternatives to Relieve Depression (STAR*D) trial may offer a new algorithmic approach to treating major depression.14,28 NIMH launched STAR*D in 1999, enrollment began in 2001, and results are expecte by May 2005 (see Related resources).
STAR*D—of which I am the study director—is a randomized, controlled, raterblinded, multisite trial of outpatients ages 18 to 75 with nonpsychotic major depression (17-item Hamilton Rating Scale for Depression score 14). The trial design includes four treatment levels and numerous antidepressant options (Figure).
The study’s aim is to enroll 4,000 patients into level 1, with 1,500 entering level 2. Patients who achieve an adequate response based on clinician judgment may continue the effective treatment for 12 months, during which their symptoms and other relevant information are monitored monthly by telephone. Patients who do not achieve an acceptable response in level 1 (or in subsequent levels) may proceed to the next level, which involves a randomized assignment.
STAR*D has an innovative design that mimics clinical practice and ensures high levels of patient participation. When patients agree to randomization, they may elect to exclude groups of treatments but may not pick a particular treatment (they must accept randomization to stay in the study).
Figure STAR*D treatment levels for major depressive disorder
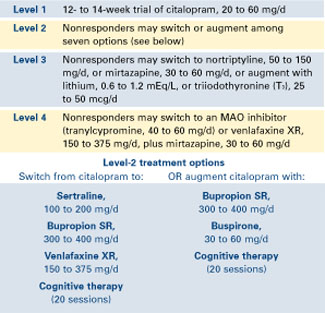
For example, patient A entering level 2 may exclude switch treatments and elect to accept randomization to citalopram plus bupropion SR, citalopram plus buspirone, or citalopram and cognitive therapy. Conversely, patient B may exclude all augment options at level 2, and accept randomization to the four switch options.
Patients may exclude cognitive psychotherapy as an augment and/or switch option as long as they accept randomization to all available medication switches, or augments, or both. They may also choose cognitive therapy and exclude all medication switch and augment options. These patients must accept randomization to either cognitive therapy switch or cognitive therapy augmentation.
This so-called equipoise stratified randomized design29 allows us to compare all participants randomized to the treatments being compared. To date, only 1% of subjects have accepted randomization to all seven level-2 treatments. About one-half elect only the switch options, and about one-half elect only the augment options.
STAR*D’s goal is to determine whether there is a preferred next step for varying types and degrees of treatment-resistant repression.
Vagus nerve stimulation
Somatic therapies being investigated to expand our therapeutic options for major depressive disorder include magnetic seizure therapy, repetitive transcranial magnetic stimulation, and vagus nerve stimulation (VNS).
VNS—now indicated for treatment-resistant epilepsy—is being investigated as a potential augmentation for treatment-resistant depression. An application for this supplemental indication was submitted to the FDA in October 2003.
With VNS, a device implanted in the patient’s chest provides intermittent stimulation to the left vagus nerve (typically 30 seconds on and 5 minutes off, 24 hours a day). In an open trial10 and follow-up report,30 VNS was associated with a 30% to 45% response rate in 59 depressed patients with high levels of treatment resistance (inadequate response to an average of 16 treatment trials).
VNS is well tolerated, though it has not been prospectively studied in patients with diagnosed cardiovascular disease. Side effects that may occur when the stimulation is “on” include:
- voice alteration in about 60% of patients (the voice becomes more hoarse when the left recurrent laryngeal nerve is activated)
- paresthesias in the neck
- shortness of breath on heavy exertion.
These effects are usually absent in the 5-minute “off” phase.
- National Institute of Mental Health. Sequenced Treatment Alternatives to Relieve Depression (STAR*D) trial. Includes the Quick Inventory of Depressive Symptomatology. www.star-d.org
- HealthyPlace.Com Depression Community. Vagus nerve stimulation for treating depression. www.healthyplace.com/communities/depression/treatment/vns
Drug brand names
- Bupropion • Wellbutrin, Wellbutrin SR
- Buspirone • BuSpar
- Citalopram • Celexa
- Fluoxetine • Prozac
- Imipramine • Tofranil
- Mirtazapine • Remeron
- Modafinil • Provigil
- Nefazodone • Serzone
- Nortriptyline • Pamelor, Aventyl
- Olanzapine • Zyprexa
- Risperidone • Risperdal
- Sertraline • Zoloft
- Tranylcypromine • Parnate
- Venlafaxine • Effexor, Effexor XR
Disclosure
Dr. Rush receives grant/research support from the Robert Wood Johnson Foundation, National Institute of Mental Health, and The Stanley Foundation. He is a consultant to Bristol-Myers Squibb Co., Cyberonics, Eli Lilly & Co., Forest Laboratories, and GlaxoSmithKline, and a speaker for Bristol-Myers Squibb Co., Cyberonics, Eli Lilly & Co., Forest Laboratories, GlaxoSmithKline, and Wyeth Pharmaceuticals.
1. Depression Guideline Panel. Clinical practice guideline, number 5: depression in primary care: vol. 2. Treatment of major depression Rockville, MD: U.S. Department of Health and Human Services, Public Health Service, Agency for Health Care Policy and Research. AHCPR publication no. 93-0551, 1993.
2. Rush AJ, Trivedi MH, Ibrahim HM, et al. The 16-Item Quick Inventory of Depressive Symptomatology (QIDS), clinician rating (QIDS-C), and self-report (QIDS-SR): a psychometric evaluation in patients with chronic major depression. Biol Psychiatry 2003;54:573-83.
3. Beck AT, Steer RA, Brown GK. Beck Depression Inventory (2nd ed. manual). San Antonio, TX: The Psychological Corporation, 1996.
4. Beck AT, Ward CH, Mendelson M, et al. An inventory for measuring depression. Arch Gen Psychiatry 1961;4:561-71.
5. Kroenke K, Spitzer RL, Williams JBW. The PHQ-9. Validity of a brief depression severity measure. J Gen Intern Med 2001;16:606-13.
6. Kessler RC, Berglund P, Demler O, et al. The epidemiology of major depressive disorder: results from the National Comorbidity Survey Replication (NCS-R). JAMA 2003;289(23):3095-105.
7. Depression Guideline Panel. Clinical practice guideline, number 5: Depression in primary care, vol. 1: detection and diagnosis Rockville, MD: U.S. Department of Health and Human Services, Public Health Service, Agency for Health Care Policy and Research. AHCPR publication no. 93-0550, 1993.
8. Murray CJ, Lopez AD. (eds) The global burden of disease Boston: Harvard School of Public Health, 1996.
9. Barbee JG, Jamhour NJ. Lamotrigine as an augmentation agent in treatment-resistant depression. J Clin Psychiatry 2002;63(8):737-41.
10. Sackeim HA, Rush AJ, George MS, et al. Vagus nerve stimulation (VNS) for treatment-resistant depression: efficacy, side effects, and predictors of outcome. Neuropsychopharmacology 2001;25(5):713-28.
11. Koran LM, Gelenberg AJ, Kornstein SG, et al. Sertraline versus imipramine to prevent relapse in chronic depression. J Affect Disord 2001;65(1):27-36.
12. Nierenberg AA, Feighner JP, Rudolph R, et al. Venlafaxine for treatment-resistant unipolar depression. J Clin Psychopharmacol 1994;14(6):419-23.
13. Quitkin FM, Petkova E, McGrath PJ, et al. When should a trial of fluoxetine for major depression be declared failed? Am J Psychiatry 2003;160(4):734-40.
14. Fava M, Rush AJ, Trivedi MH, et al. Background and rationale for the sequenced treatment alternatives to relieve depression (STAR*D) study. Psychiatr Clin North Am 2003;26(2):457-94.
15. Fava M, Papakostas GI, Petersen T, et al. Switching to bupropion in fluoxetine-resistant major depressive disorder. Ann Clin Psychiatry 2003;15:17-22.
16. Entsuah AR, Huang H, Thase ME. Response and remission rates in different subpopulations with major depressive disorder administered venlafaxine, selective serotonin reuptake inhibitors, or placebo. J Clin Psychiatry 2001;62:869-77.
17. Thase ME, Entsuah AR, Rudolph RL. Remission rates during treatment with venlafaxine or selective serotonin reuptake inhibitors. Br J Psychiatry 2001;178:234-41.
18. Montgomery SA, Huusom A, Bothmer J. Flexible dose comparison of s-citalopram and venlafaxine XR. J Eur Neuropsychopharmacol 2002;12(suppl 3):S-254.
19. Keller MB, Gelenberg AJ, Hirschfeld RM, et al. The treatment of chronic depression, part 2: a double-blind, randomized trial of sertraline and imipramine. J Clin Psychiatry 1998;59(11):598-607.
20. Thase ME, Rush AJ, Howland RH, et al. Double-blind switch study of imipramine or sertraline treatment of antidepressant-resistant chronic depression. Arch Gen Psychiatry 2002;59(3):233-9.
21. Thase ME, Rush AJ. Treatment resistant depression. In: Bloom FE, Kupfer DJ (eds). Psychopharmacology: the fourth generation of progress New York: Raven Press, 1995;1081-97.
22. Shelton RC, Tollefson GD, Tohen M, et al. A novel augmentation strategy for treating resistant major depression. Am J Psychiatry 2001;158:131-4.
23. Keller MB, McCullough JP, Klein DN, et al. A comparison of nefazodone, the cognitive behavioral-analysis system of psychotherapy, and their combination for the treatment of chronic depression. N Engl J Med 2000;342:1462-70.
24. Schatzberg AF, Rush AJ, Arnow BA, et al. Medication or psychotherapy is effective when the other is not in chronic depression: empirical support. Arch Gen Psychiatry (submitted).
25. Nemeroff CB, Heim CM, Thase ME, et al. Differential responses to psychotherapy versus pharmacotherapy in patients with chronic forms of major depression and childhood trauma. Proc Natl Acad Sci USA 2003;100(24):14293-6.
26. Crismon ML, Trivedi M, Pigott TA, et al. The Texas Medication Algorithm Project: report of the Texas Consensus Conference Panel on Medication Treatment of Major Depressive Disorder. J Clin Psychiatry 1999;60(3):142-56.
27. Trivedi MH, Rush AJ, Crismon ML, et al. The Texas Medication Algorithm Project (TMAP): clinical results for patients with major depressive disorder. Arch Gen Psychiatry (in press).
28. Rush AJ, Fava M, Wisniewski SR, et al. for the STAR*D Investigators Group. Sequenced Treatment Alternatives to Relieve Depression (STAR*D): rationale and design. Control Clin Trials 2004;25(1):118-41.
29. Lavori PW, Rush AJ, Wisniewski SR, et al. Strengthening clinical effectiveness trials: equipoise-stratified randomization. Biol Psychiatry 2001;50:792-801.
30. Marangell LB, Rush AJ, George MS, et al. Vagus nerve stimulation (VNS) for major depressive episodes: one-year outcomes. Biol Psychiatry 2002;51(4):280-7.
When depression fails to respond to initial therapy—as it commonly does—we have many options but little evidence to guide our choices. We often wonder:
- Is this patient’s depression treatment-resistant?
- Would switching medications or augmenting the initial drug be more likely to achieve an adequate response?
- How effective is psychotherapy compared with medication for treatment-resistant depression?
This article offers insights into each question, based on available trial data, algorithmic approaches to major depressive disorder, and clinical experience. Included is a preview of an ongoing multicenter, treatment-resistant depression study that mimics clinical practice and a look at vagus nerve stimulation (VNS)—a novel somatic therapy being considered by the FDA.
Measuring treatment response
Sustained symptom remission—with normalization of function—is the aim of treating major depressive disorder. Outcomes are categorized as:
- remission (virtual absence of depressive symptoms)
- response with residual symptoms (>50% reduction in baseline symptom severity that does not qualify for remission)
- partial response (>25% but <50% decrease in baseline symptom severity)
- nonresponse (<25% reduction in baseline symptoms).
Major depressive disorder (MDD) is typically recurrent or chronic and characterized by marked disability and a life expectancy shortened by suicide and increased mortality from associated medical conditions. Lifetime prevalence is 16.2%.6
MDD is twice as likely to affect women as men and is common among adolescents, young adults, and persons with concurrent medical conditions.
Major depression’s course is characterized by:
- recurrent episodes (approximately every 5 years)
- or a persistent level of waxing and waning depressive symptoms (in 20% to 35% of cases).
Dysthymic disorder often heralds major depression. Within 1 year, 5% to 20% of persons with dysthymic disorder develop major depression.7
Disability associated with major depression
often exceeds that of other general medical conditions. Depression is the fourth most disabling condition worldwide and is projected to rank number two by 2020 because of its chronic and recurrent nature, high prevalence, and life-shortening effects.8
Consequences of unremitting depression include:
- poor day-to-day function (work, family)
- increased likelihood of recurrence
- psychiatric or medical complications, including substance abuse
- high use of mental health and general medical resources
- worsened prognosis of medical conditions
- high family burden.
In 8-week acute-phase trials, 7% to 15% of patients do not tolerate the initial medication, 25% show no response, 15% show partial response, 10% to 20% exhibit response with residual symptoms, and 30% to 40% achieve remission. Complicated depressions that may not respond as well include those concurrent with Axis I conditions—such as panic disorder or substance abuse—or Axis II or III conditions.1
Time-limited psychotherapies targeted at depressive symptoms (such as cognitive, interpersonal, and behavioral therapies) also typically achieve a 50% response rate in uncomplicated depression that is not treatment-resistant.
Recommendation. When treating depression, assess response at least every 4 weeks (preferably at each visit), using a self-report or clinician rating such as:
- Quick Inventory of Depressive Symptomatology2 (see Related resources)
- Beck Depression Inventory3,4
- Patient Health Questionnaire.5
Defining treatment resistance
A patient may not achieve remission for a variety of reasons, including poor adherence, inadequate medication trial or dosing, occult substance abuse, undiagnosed medical conditions (Box),6-8 concurrent Axis I or II disorders, or treatment resistance.
The general consensus is to consider depression “treatment-resistant” when at least two adequately delivered treatments do not achieve at least a response. A stricter definition—failure to achieve sustained remission with two or more treatments—has also been suggested.
Several schemes have proposed treatment resistance levels, such as the five stages identified in the Table. Recent studies9,10 suggest that increasing treatment resistance is associated with decreasing response or remission rates.
Therefore, when a patient’s treatment resistance is high, two appropriate strategies are to:
- persist with and use maximally tolerated dosages of the treatment you select
- aim for response because high resistance lowers the likelihood of remission.
Predicting response. A major clinical issue is determining whether remission will occur during an acute treatment trial. It is important to not declare treatment resistance unless there has been:
- adequate exposure (dosing and duration) to the treatment
- and adequate adherence.
Patients often have apparent but not actual resistance, meaning that the agent was not used long enough (at least 6 weeks) or at high enough doses. Remission typically follows response by several weeks or even 1 to 2 months for more-chronic depressions.11 Thus, treatment trials should continue at least 12 weeks to determine whether remission will occur.
On the other hand, not obtaining at least a signal of minimal benefit (at least a 20% reduction in baseline symptom severity) in 4 to 6 weeks often portends a low likelihood of response in the long run.12,13 Thus, continue a treatment at least 6 weeks before you decide that it will not achieve a response.
Recommendation. Measure symptoms at key decision points. If modest improvement (such as 20% reduction in baseline symptoms) is found at 4 to 6 weeks, continue treating another 4 to 6 weeks, increasing the dosage as tolerated.
Table
Simple system for staging antidepressant resistance
| Stage | Definition |
|---|---|
| I | Failure of at least one adequate trial of one major antidepressant class |
| II | Stage I resistance plus failure of an adequate trial of an antidepressant in a distinctly different class from that used in Stage I |
| III | Stage II resistance plus failure of an adequate trial of a tricyclic antidepressant |
| IV | Stage III resistance plus failure of an adequate trial of a monoamine oxidase inhibitor |
| V | Stage IV resistance plus failure of a course of bilateral electroconvulsive therapy |
| Source: Reprinted with permission from Thase ME, Rush AJ. When at first you don’t succeed: sequential strategies for antidepressant nonresponders. J Clin Psychiatry 1997;58(suppl 13):24. | |
Treatment options
When initial antidepressant treatment fails to achieve an adequate response—as it does in more than onehalf of major depression cases—the next step is to add a second agent or switch to another agent.
Available evidence14 relies almost exclusively on open, uncontrolled trials, which do not provide definitive answers. Even so, these trials indicate that nonresponse (or nonremission) with one agent does not predict nonresponse/nonremission with another.
Switching strategies. When a selective serotonin reuptake inhibitor (SSRI) is the first treatment, several open trials reveal an approximately 50% response rate to a second SSRI. However, opentrial evidence and retrospective chart review reports also indicate that switching out of class (such as from an SSRI to bupropion) is also approximately 50% effective.15
Some post hoc analyses of acute 8-week trials indicate that the dual-action agent venlafaxine at higher dosages (up to 225 mg/d of venlafaxine XR) is associated with higher remission rates than the more-selective SSRIs.16,17 On the other hand, unpublished data indicate that escitalopram, 10 mg/d, and venlafaxine XR, up to 150 mg/d, did not differ in efficacy among outpatients treated by primary care physicians.18
On the other hand, sertraline and imipramine (a dual-action agent) were equally effective in a 12-week acute-phase trial.19 Furthermore, response and remission rates were similar when nonresponders in each group switched to the other antidepressant.20 This suggests that the dual-action agent (imipramine) was not more effective than the more selective agent (sertraline) in this population.
Well-controlled trials show that monoamine oxidase inhibitors (MAOIs) can be effective when tricyclic antidepressants (TCAs) are not. Switches among the TCAs are associated with a 30% response rate, whereas switching from a TCA to an MAOI typically results in a 50% response rate.21
Controlled prospective comparisons of two or more alternate switch or augment treatments are needed to establish comparative efficacy and tolerability.
Augmentation strategies may include lithium, buspirone, thyroid hormone (T3), stimulants, or atypical antipsychotics. Although head-to-head comparisons are rare, a randomized, controlled trial found that combining olanzapine (mean 50 mg/d), with fluoxetine (mean 15 mg/d) was more effective than each agent used alone.22
Risperidone augmentation is supported by open trials, as is the use of modafinil, other stimulants, and bupropion. An important unanswered question with most augmentation strategies is how long to continue them if they are successful.
Psychotherapy may also play a key role in augmenting medication’s effects. Keller et al23 found in chronically depressed outpatients that 12 weeks of nefazodone, up to 600 mg/d, plus cognitive behavioral analytic system psychotherapy (CBASP) produced higher response and remission rates compared with either treatment alone. A subsequent report24 found that 50% of nefa-zodone and CBASP monotherapy nonresponders did respond when switched to the alternate treatment.
Thus, CBASP may be useful at least in chronic depression to augment medication or as a “switch” to monotherapy if medication alone fails. Interestingly, Nemeroff et al25 found CBASP more effective than nefazodone for patients with chronic major depression who had a childhood history of parental loss or physical, sexual, or emotional abuse.
Antidepressant tachyphylaxis—commonly referred to as “poop-out”—is reported with all antidepressants. That is, even while apparently taking their medications for 6 to 18 months, some patients lose the antidepressant effect, such that some symptoms return or a full relapse/recurrence ensues. Mechanisms of this phenomenon are unknown.
Clinically, some believe that “poop out” is more common with SSRIs than with other antidepressant classes, but no long-term comparative data support or challenge this view. Treatment options include a dosage increase, dosage reduction (especially for long half-life SSRIs such as fluoxetine), or augmentation with the options noted above (such as bupropion, buspirone, etc.).
Benefit of using algorithms
Algorithms (such as the Texas Medication Algorithm Project26 ) have suggested multiple treatment steps for major depression after initial treatment fails, with several options available at each step. Using medication algorithms has been found more effective than treatment-as-usual in outpatients with major depressive disorder.27 No studies have compared different algorithms.
STAR*D trial. The ongoing National Institute of Mental Health (NIMH) Sequenced Treatment Alternatives to Relieve Depression (STAR*D) trial may offer a new algorithmic approach to treating major depression.14,28 NIMH launched STAR*D in 1999, enrollment began in 2001, and results are expecte by May 2005 (see Related resources).
STAR*D—of which I am the study director—is a randomized, controlled, raterblinded, multisite trial of outpatients ages 18 to 75 with nonpsychotic major depression (17-item Hamilton Rating Scale for Depression score 14). The trial design includes four treatment levels and numerous antidepressant options (Figure).
The study’s aim is to enroll 4,000 patients into level 1, with 1,500 entering level 2. Patients who achieve an adequate response based on clinician judgment may continue the effective treatment for 12 months, during which their symptoms and other relevant information are monitored monthly by telephone. Patients who do not achieve an acceptable response in level 1 (or in subsequent levels) may proceed to the next level, which involves a randomized assignment.
STAR*D has an innovative design that mimics clinical practice and ensures high levels of patient participation. When patients agree to randomization, they may elect to exclude groups of treatments but may not pick a particular treatment (they must accept randomization to stay in the study).
Figure STAR*D treatment levels for major depressive disorder
For example, patient A entering level 2 may exclude switch treatments and elect to accept randomization to citalopram plus bupropion SR, citalopram plus buspirone, or citalopram and cognitive therapy. Conversely, patient B may exclude all augment options at level 2, and accept randomization to the four switch options.
Patients may exclude cognitive psychotherapy as an augment and/or switch option as long as they accept randomization to all available medication switches, or augments, or both. They may also choose cognitive therapy and exclude all medication switch and augment options. These patients must accept randomization to either cognitive therapy switch or cognitive therapy augmentation.
This so-called equipoise stratified randomized design29 allows us to compare all participants randomized to the treatments being compared. To date, only 1% of subjects have accepted randomization to all seven level-2 treatments. About one-half elect only the switch options, and about one-half elect only the augment options.
STAR*D’s goal is to determine whether there is a preferred next step for varying types and degrees of treatment-resistant repression.
Vagus nerve stimulation
Somatic therapies being investigated to expand our therapeutic options for major depressive disorder include magnetic seizure therapy, repetitive transcranial magnetic stimulation, and vagus nerve stimulation (VNS).
VNS—now indicated for treatment-resistant epilepsy—is being investigated as a potential augmentation for treatment-resistant depression. An application for this supplemental indication was submitted to the FDA in October 2003.
With VNS, a device implanted in the patient’s chest provides intermittent stimulation to the left vagus nerve (typically 30 seconds on and 5 minutes off, 24 hours a day). In an open trial10 and follow-up report,30 VNS was associated with a 30% to 45% response rate in 59 depressed patients with high levels of treatment resistance (inadequate response to an average of 16 treatment trials).
VNS is well tolerated, though it has not been prospectively studied in patients with diagnosed cardiovascular disease. Side effects that may occur when the stimulation is “on” include:
- voice alteration in about 60% of patients (the voice becomes more hoarse when the left recurrent laryngeal nerve is activated)
- paresthesias in the neck
- shortness of breath on heavy exertion.
These effects are usually absent in the 5-minute “off” phase.
- National Institute of Mental Health. Sequenced Treatment Alternatives to Relieve Depression (STAR*D) trial. Includes the Quick Inventory of Depressive Symptomatology. www.star-d.org
- HealthyPlace.Com Depression Community. Vagus nerve stimulation for treating depression. www.healthyplace.com/communities/depression/treatment/vns
Drug brand names
- Bupropion • Wellbutrin, Wellbutrin SR
- Buspirone • BuSpar
- Citalopram • Celexa
- Fluoxetine • Prozac
- Imipramine • Tofranil
- Mirtazapine • Remeron
- Modafinil • Provigil
- Nefazodone • Serzone
- Nortriptyline • Pamelor, Aventyl
- Olanzapine • Zyprexa
- Risperidone • Risperdal
- Sertraline • Zoloft
- Tranylcypromine • Parnate
- Venlafaxine • Effexor, Effexor XR
Disclosure
Dr. Rush receives grant/research support from the Robert Wood Johnson Foundation, National Institute of Mental Health, and The Stanley Foundation. He is a consultant to Bristol-Myers Squibb Co., Cyberonics, Eli Lilly & Co., Forest Laboratories, and GlaxoSmithKline, and a speaker for Bristol-Myers Squibb Co., Cyberonics, Eli Lilly & Co., Forest Laboratories, GlaxoSmithKline, and Wyeth Pharmaceuticals.
When depression fails to respond to initial therapy—as it commonly does—we have many options but little evidence to guide our choices. We often wonder:
- Is this patient’s depression treatment-resistant?
- Would switching medications or augmenting the initial drug be more likely to achieve an adequate response?
- How effective is psychotherapy compared with medication for treatment-resistant depression?
This article offers insights into each question, based on available trial data, algorithmic approaches to major depressive disorder, and clinical experience. Included is a preview of an ongoing multicenter, treatment-resistant depression study that mimics clinical practice and a look at vagus nerve stimulation (VNS)—a novel somatic therapy being considered by the FDA.
Measuring treatment response
Sustained symptom remission—with normalization of function—is the aim of treating major depressive disorder. Outcomes are categorized as:
- remission (virtual absence of depressive symptoms)
- response with residual symptoms (>50% reduction in baseline symptom severity that does not qualify for remission)
- partial response (>25% but <50% decrease in baseline symptom severity)
- nonresponse (<25% reduction in baseline symptoms).
Major depressive disorder (MDD) is typically recurrent or chronic and characterized by marked disability and a life expectancy shortened by suicide and increased mortality from associated medical conditions. Lifetime prevalence is 16.2%.6
MDD is twice as likely to affect women as men and is common among adolescents, young adults, and persons with concurrent medical conditions.
Major depression’s course is characterized by:
- recurrent episodes (approximately every 5 years)
- or a persistent level of waxing and waning depressive symptoms (in 20% to 35% of cases).
Dysthymic disorder often heralds major depression. Within 1 year, 5% to 20% of persons with dysthymic disorder develop major depression.7
Disability associated with major depression
often exceeds that of other general medical conditions. Depression is the fourth most disabling condition worldwide and is projected to rank number two by 2020 because of its chronic and recurrent nature, high prevalence, and life-shortening effects.8
Consequences of unremitting depression include:
- poor day-to-day function (work, family)
- increased likelihood of recurrence
- psychiatric or medical complications, including substance abuse
- high use of mental health and general medical resources
- worsened prognosis of medical conditions
- high family burden.
In 8-week acute-phase trials, 7% to 15% of patients do not tolerate the initial medication, 25% show no response, 15% show partial response, 10% to 20% exhibit response with residual symptoms, and 30% to 40% achieve remission. Complicated depressions that may not respond as well include those concurrent with Axis I conditions—such as panic disorder or substance abuse—or Axis II or III conditions.1
Time-limited psychotherapies targeted at depressive symptoms (such as cognitive, interpersonal, and behavioral therapies) also typically achieve a 50% response rate in uncomplicated depression that is not treatment-resistant.
Recommendation. When treating depression, assess response at least every 4 weeks (preferably at each visit), using a self-report or clinician rating such as:
- Quick Inventory of Depressive Symptomatology2 (see Related resources)
- Beck Depression Inventory3,4
- Patient Health Questionnaire.5
Defining treatment resistance
A patient may not achieve remission for a variety of reasons, including poor adherence, inadequate medication trial or dosing, occult substance abuse, undiagnosed medical conditions (Box),6-8 concurrent Axis I or II disorders, or treatment resistance.
The general consensus is to consider depression “treatment-resistant” when at least two adequately delivered treatments do not achieve at least a response. A stricter definition—failure to achieve sustained remission with two or more treatments—has also been suggested.
Several schemes have proposed treatment resistance levels, such as the five stages identified in the Table. Recent studies9,10 suggest that increasing treatment resistance is associated with decreasing response or remission rates.
Therefore, when a patient’s treatment resistance is high, two appropriate strategies are to:
- persist with and use maximally tolerated dosages of the treatment you select
- aim for response because high resistance lowers the likelihood of remission.
Predicting response. A major clinical issue is determining whether remission will occur during an acute treatment trial. It is important to not declare treatment resistance unless there has been:
- adequate exposure (dosing and duration) to the treatment
- and adequate adherence.
Patients often have apparent but not actual resistance, meaning that the agent was not used long enough (at least 6 weeks) or at high enough doses. Remission typically follows response by several weeks or even 1 to 2 months for more-chronic depressions.11 Thus, treatment trials should continue at least 12 weeks to determine whether remission will occur.
On the other hand, not obtaining at least a signal of minimal benefit (at least a 20% reduction in baseline symptom severity) in 4 to 6 weeks often portends a low likelihood of response in the long run.12,13 Thus, continue a treatment at least 6 weeks before you decide that it will not achieve a response.
Recommendation. Measure symptoms at key decision points. If modest improvement (such as 20% reduction in baseline symptoms) is found at 4 to 6 weeks, continue treating another 4 to 6 weeks, increasing the dosage as tolerated.
Table
Simple system for staging antidepressant resistance
| Stage | Definition |
|---|---|
| I | Failure of at least one adequate trial of one major antidepressant class |
| II | Stage I resistance plus failure of an adequate trial of an antidepressant in a distinctly different class from that used in Stage I |
| III | Stage II resistance plus failure of an adequate trial of a tricyclic antidepressant |
| IV | Stage III resistance plus failure of an adequate trial of a monoamine oxidase inhibitor |
| V | Stage IV resistance plus failure of a course of bilateral electroconvulsive therapy |
| Source: Reprinted with permission from Thase ME, Rush AJ. When at first you don’t succeed: sequential strategies for antidepressant nonresponders. J Clin Psychiatry 1997;58(suppl 13):24. | |
Treatment options
When initial antidepressant treatment fails to achieve an adequate response—as it does in more than onehalf of major depression cases—the next step is to add a second agent or switch to another agent.
Available evidence14 relies almost exclusively on open, uncontrolled trials, which do not provide definitive answers. Even so, these trials indicate that nonresponse (or nonremission) with one agent does not predict nonresponse/nonremission with another.
Switching strategies. When a selective serotonin reuptake inhibitor (SSRI) is the first treatment, several open trials reveal an approximately 50% response rate to a second SSRI. However, opentrial evidence and retrospective chart review reports also indicate that switching out of class (such as from an SSRI to bupropion) is also approximately 50% effective.15
Some post hoc analyses of acute 8-week trials indicate that the dual-action agent venlafaxine at higher dosages (up to 225 mg/d of venlafaxine XR) is associated with higher remission rates than the more-selective SSRIs.16,17 On the other hand, unpublished data indicate that escitalopram, 10 mg/d, and venlafaxine XR, up to 150 mg/d, did not differ in efficacy among outpatients treated by primary care physicians.18
On the other hand, sertraline and imipramine (a dual-action agent) were equally effective in a 12-week acute-phase trial.19 Furthermore, response and remission rates were similar when nonresponders in each group switched to the other antidepressant.20 This suggests that the dual-action agent (imipramine) was not more effective than the more selective agent (sertraline) in this population.
Well-controlled trials show that monoamine oxidase inhibitors (MAOIs) can be effective when tricyclic antidepressants (TCAs) are not. Switches among the TCAs are associated with a 30% response rate, whereas switching from a TCA to an MAOI typically results in a 50% response rate.21
Controlled prospective comparisons of two or more alternate switch or augment treatments are needed to establish comparative efficacy and tolerability.
Augmentation strategies may include lithium, buspirone, thyroid hormone (T3), stimulants, or atypical antipsychotics. Although head-to-head comparisons are rare, a randomized, controlled trial found that combining olanzapine (mean 50 mg/d), with fluoxetine (mean 15 mg/d) was more effective than each agent used alone.22
Risperidone augmentation is supported by open trials, as is the use of modafinil, other stimulants, and bupropion. An important unanswered question with most augmentation strategies is how long to continue them if they are successful.
Psychotherapy may also play a key role in augmenting medication’s effects. Keller et al23 found in chronically depressed outpatients that 12 weeks of nefazodone, up to 600 mg/d, plus cognitive behavioral analytic system psychotherapy (CBASP) produced higher response and remission rates compared with either treatment alone. A subsequent report24 found that 50% of nefa-zodone and CBASP monotherapy nonresponders did respond when switched to the alternate treatment.
Thus, CBASP may be useful at least in chronic depression to augment medication or as a “switch” to monotherapy if medication alone fails. Interestingly, Nemeroff et al25 found CBASP more effective than nefazodone for patients with chronic major depression who had a childhood history of parental loss or physical, sexual, or emotional abuse.
Antidepressant tachyphylaxis—commonly referred to as “poop-out”—is reported with all antidepressants. That is, even while apparently taking their medications for 6 to 18 months, some patients lose the antidepressant effect, such that some symptoms return or a full relapse/recurrence ensues. Mechanisms of this phenomenon are unknown.
Clinically, some believe that “poop out” is more common with SSRIs than with other antidepressant classes, but no long-term comparative data support or challenge this view. Treatment options include a dosage increase, dosage reduction (especially for long half-life SSRIs such as fluoxetine), or augmentation with the options noted above (such as bupropion, buspirone, etc.).
Benefit of using algorithms
Algorithms (such as the Texas Medication Algorithm Project26 ) have suggested multiple treatment steps for major depression after initial treatment fails, with several options available at each step. Using medication algorithms has been found more effective than treatment-as-usual in outpatients with major depressive disorder.27 No studies have compared different algorithms.
STAR*D trial. The ongoing National Institute of Mental Health (NIMH) Sequenced Treatment Alternatives to Relieve Depression (STAR*D) trial may offer a new algorithmic approach to treating major depression.14,28 NIMH launched STAR*D in 1999, enrollment began in 2001, and results are expecte by May 2005 (see Related resources).
STAR*D—of which I am the study director—is a randomized, controlled, raterblinded, multisite trial of outpatients ages 18 to 75 with nonpsychotic major depression (17-item Hamilton Rating Scale for Depression score 14). The trial design includes four treatment levels and numerous antidepressant options (Figure).
The study’s aim is to enroll 4,000 patients into level 1, with 1,500 entering level 2. Patients who achieve an adequate response based on clinician judgment may continue the effective treatment for 12 months, during which their symptoms and other relevant information are monitored monthly by telephone. Patients who do not achieve an acceptable response in level 1 (or in subsequent levels) may proceed to the next level, which involves a randomized assignment.
STAR*D has an innovative design that mimics clinical practice and ensures high levels of patient participation. When patients agree to randomization, they may elect to exclude groups of treatments but may not pick a particular treatment (they must accept randomization to stay in the study).
Figure STAR*D treatment levels for major depressive disorder
For example, patient A entering level 2 may exclude switch treatments and elect to accept randomization to citalopram plus bupropion SR, citalopram plus buspirone, or citalopram and cognitive therapy. Conversely, patient B may exclude all augment options at level 2, and accept randomization to the four switch options.
Patients may exclude cognitive psychotherapy as an augment and/or switch option as long as they accept randomization to all available medication switches, or augments, or both. They may also choose cognitive therapy and exclude all medication switch and augment options. These patients must accept randomization to either cognitive therapy switch or cognitive therapy augmentation.
This so-called equipoise stratified randomized design29 allows us to compare all participants randomized to the treatments being compared. To date, only 1% of subjects have accepted randomization to all seven level-2 treatments. About one-half elect only the switch options, and about one-half elect only the augment options.
STAR*D’s goal is to determine whether there is a preferred next step for varying types and degrees of treatment-resistant repression.
Vagus nerve stimulation
Somatic therapies being investigated to expand our therapeutic options for major depressive disorder include magnetic seizure therapy, repetitive transcranial magnetic stimulation, and vagus nerve stimulation (VNS).
VNS—now indicated for treatment-resistant epilepsy—is being investigated as a potential augmentation for treatment-resistant depression. An application for this supplemental indication was submitted to the FDA in October 2003.
With VNS, a device implanted in the patient’s chest provides intermittent stimulation to the left vagus nerve (typically 30 seconds on and 5 minutes off, 24 hours a day). In an open trial10 and follow-up report,30 VNS was associated with a 30% to 45% response rate in 59 depressed patients with high levels of treatment resistance (inadequate response to an average of 16 treatment trials).
VNS is well tolerated, though it has not been prospectively studied in patients with diagnosed cardiovascular disease. Side effects that may occur when the stimulation is “on” include:
- voice alteration in about 60% of patients (the voice becomes more hoarse when the left recurrent laryngeal nerve is activated)
- paresthesias in the neck
- shortness of breath on heavy exertion.
These effects are usually absent in the 5-minute “off” phase.
- National Institute of Mental Health. Sequenced Treatment Alternatives to Relieve Depression (STAR*D) trial. Includes the Quick Inventory of Depressive Symptomatology. www.star-d.org
- HealthyPlace.Com Depression Community. Vagus nerve stimulation for treating depression. www.healthyplace.com/communities/depression/treatment/vns
Drug brand names
- Bupropion • Wellbutrin, Wellbutrin SR
- Buspirone • BuSpar
- Citalopram • Celexa
- Fluoxetine • Prozac
- Imipramine • Tofranil
- Mirtazapine • Remeron
- Modafinil • Provigil
- Nefazodone • Serzone
- Nortriptyline • Pamelor, Aventyl
- Olanzapine • Zyprexa
- Risperidone • Risperdal
- Sertraline • Zoloft
- Tranylcypromine • Parnate
- Venlafaxine • Effexor, Effexor XR
Disclosure
Dr. Rush receives grant/research support from the Robert Wood Johnson Foundation, National Institute of Mental Health, and The Stanley Foundation. He is a consultant to Bristol-Myers Squibb Co., Cyberonics, Eli Lilly & Co., Forest Laboratories, and GlaxoSmithKline, and a speaker for Bristol-Myers Squibb Co., Cyberonics, Eli Lilly & Co., Forest Laboratories, GlaxoSmithKline, and Wyeth Pharmaceuticals.
1. Depression Guideline Panel. Clinical practice guideline, number 5: depression in primary care: vol. 2. Treatment of major depression Rockville, MD: U.S. Department of Health and Human Services, Public Health Service, Agency for Health Care Policy and Research. AHCPR publication no. 93-0551, 1993.
2. Rush AJ, Trivedi MH, Ibrahim HM, et al. The 16-Item Quick Inventory of Depressive Symptomatology (QIDS), clinician rating (QIDS-C), and self-report (QIDS-SR): a psychometric evaluation in patients with chronic major depression. Biol Psychiatry 2003;54:573-83.
3. Beck AT, Steer RA, Brown GK. Beck Depression Inventory (2nd ed. manual). San Antonio, TX: The Psychological Corporation, 1996.
4. Beck AT, Ward CH, Mendelson M, et al. An inventory for measuring depression. Arch Gen Psychiatry 1961;4:561-71.
5. Kroenke K, Spitzer RL, Williams JBW. The PHQ-9. Validity of a brief depression severity measure. J Gen Intern Med 2001;16:606-13.
6. Kessler RC, Berglund P, Demler O, et al. The epidemiology of major depressive disorder: results from the National Comorbidity Survey Replication (NCS-R). JAMA 2003;289(23):3095-105.
7. Depression Guideline Panel. Clinical practice guideline, number 5: Depression in primary care, vol. 1: detection and diagnosis Rockville, MD: U.S. Department of Health and Human Services, Public Health Service, Agency for Health Care Policy and Research. AHCPR publication no. 93-0550, 1993.
8. Murray CJ, Lopez AD. (eds) The global burden of disease Boston: Harvard School of Public Health, 1996.
9. Barbee JG, Jamhour NJ. Lamotrigine as an augmentation agent in treatment-resistant depression. J Clin Psychiatry 2002;63(8):737-41.
10. Sackeim HA, Rush AJ, George MS, et al. Vagus nerve stimulation (VNS) for treatment-resistant depression: efficacy, side effects, and predictors of outcome. Neuropsychopharmacology 2001;25(5):713-28.
11. Koran LM, Gelenberg AJ, Kornstein SG, et al. Sertraline versus imipramine to prevent relapse in chronic depression. J Affect Disord 2001;65(1):27-36.
12. Nierenberg AA, Feighner JP, Rudolph R, et al. Venlafaxine for treatment-resistant unipolar depression. J Clin Psychopharmacol 1994;14(6):419-23.
13. Quitkin FM, Petkova E, McGrath PJ, et al. When should a trial of fluoxetine for major depression be declared failed? Am J Psychiatry 2003;160(4):734-40.
14. Fava M, Rush AJ, Trivedi MH, et al. Background and rationale for the sequenced treatment alternatives to relieve depression (STAR*D) study. Psychiatr Clin North Am 2003;26(2):457-94.
15. Fava M, Papakostas GI, Petersen T, et al. Switching to bupropion in fluoxetine-resistant major depressive disorder. Ann Clin Psychiatry 2003;15:17-22.
16. Entsuah AR, Huang H, Thase ME. Response and remission rates in different subpopulations with major depressive disorder administered venlafaxine, selective serotonin reuptake inhibitors, or placebo. J Clin Psychiatry 2001;62:869-77.
17. Thase ME, Entsuah AR, Rudolph RL. Remission rates during treatment with venlafaxine or selective serotonin reuptake inhibitors. Br J Psychiatry 2001;178:234-41.
18. Montgomery SA, Huusom A, Bothmer J. Flexible dose comparison of s-citalopram and venlafaxine XR. J Eur Neuropsychopharmacol 2002;12(suppl 3):S-254.
19. Keller MB, Gelenberg AJ, Hirschfeld RM, et al. The treatment of chronic depression, part 2: a double-blind, randomized trial of sertraline and imipramine. J Clin Psychiatry 1998;59(11):598-607.
20. Thase ME, Rush AJ, Howland RH, et al. Double-blind switch study of imipramine or sertraline treatment of antidepressant-resistant chronic depression. Arch Gen Psychiatry 2002;59(3):233-9.
21. Thase ME, Rush AJ. Treatment resistant depression. In: Bloom FE, Kupfer DJ (eds). Psychopharmacology: the fourth generation of progress New York: Raven Press, 1995;1081-97.
22. Shelton RC, Tollefson GD, Tohen M, et al. A novel augmentation strategy for treating resistant major depression. Am J Psychiatry 2001;158:131-4.
23. Keller MB, McCullough JP, Klein DN, et al. A comparison of nefazodone, the cognitive behavioral-analysis system of psychotherapy, and their combination for the treatment of chronic depression. N Engl J Med 2000;342:1462-70.
24. Schatzberg AF, Rush AJ, Arnow BA, et al. Medication or psychotherapy is effective when the other is not in chronic depression: empirical support. Arch Gen Psychiatry (submitted).
25. Nemeroff CB, Heim CM, Thase ME, et al. Differential responses to psychotherapy versus pharmacotherapy in patients with chronic forms of major depression and childhood trauma. Proc Natl Acad Sci USA 2003;100(24):14293-6.
26. Crismon ML, Trivedi M, Pigott TA, et al. The Texas Medication Algorithm Project: report of the Texas Consensus Conference Panel on Medication Treatment of Major Depressive Disorder. J Clin Psychiatry 1999;60(3):142-56.
27. Trivedi MH, Rush AJ, Crismon ML, et al. The Texas Medication Algorithm Project (TMAP): clinical results for patients with major depressive disorder. Arch Gen Psychiatry (in press).
28. Rush AJ, Fava M, Wisniewski SR, et al. for the STAR*D Investigators Group. Sequenced Treatment Alternatives to Relieve Depression (STAR*D): rationale and design. Control Clin Trials 2004;25(1):118-41.
29. Lavori PW, Rush AJ, Wisniewski SR, et al. Strengthening clinical effectiveness trials: equipoise-stratified randomization. Biol Psychiatry 2001;50:792-801.
30. Marangell LB, Rush AJ, George MS, et al. Vagus nerve stimulation (VNS) for major depressive episodes: one-year outcomes. Biol Psychiatry 2002;51(4):280-7.
1. Depression Guideline Panel. Clinical practice guideline, number 5: depression in primary care: vol. 2. Treatment of major depression Rockville, MD: U.S. Department of Health and Human Services, Public Health Service, Agency for Health Care Policy and Research. AHCPR publication no. 93-0551, 1993.
2. Rush AJ, Trivedi MH, Ibrahim HM, et al. The 16-Item Quick Inventory of Depressive Symptomatology (QIDS), clinician rating (QIDS-C), and self-report (QIDS-SR): a psychometric evaluation in patients with chronic major depression. Biol Psychiatry 2003;54:573-83.
3. Beck AT, Steer RA, Brown GK. Beck Depression Inventory (2nd ed. manual). San Antonio, TX: The Psychological Corporation, 1996.
4. Beck AT, Ward CH, Mendelson M, et al. An inventory for measuring depression. Arch Gen Psychiatry 1961;4:561-71.
5. Kroenke K, Spitzer RL, Williams JBW. The PHQ-9. Validity of a brief depression severity measure. J Gen Intern Med 2001;16:606-13.
6. Kessler RC, Berglund P, Demler O, et al. The epidemiology of major depressive disorder: results from the National Comorbidity Survey Replication (NCS-R). JAMA 2003;289(23):3095-105.
7. Depression Guideline Panel. Clinical practice guideline, number 5: Depression in primary care, vol. 1: detection and diagnosis Rockville, MD: U.S. Department of Health and Human Services, Public Health Service, Agency for Health Care Policy and Research. AHCPR publication no. 93-0550, 1993.
8. Murray CJ, Lopez AD. (eds) The global burden of disease Boston: Harvard School of Public Health, 1996.
9. Barbee JG, Jamhour NJ. Lamotrigine as an augmentation agent in treatment-resistant depression. J Clin Psychiatry 2002;63(8):737-41.
10. Sackeim HA, Rush AJ, George MS, et al. Vagus nerve stimulation (VNS) for treatment-resistant depression: efficacy, side effects, and predictors of outcome. Neuropsychopharmacology 2001;25(5):713-28.
11. Koran LM, Gelenberg AJ, Kornstein SG, et al. Sertraline versus imipramine to prevent relapse in chronic depression. J Affect Disord 2001;65(1):27-36.
12. Nierenberg AA, Feighner JP, Rudolph R, et al. Venlafaxine for treatment-resistant unipolar depression. J Clin Psychopharmacol 1994;14(6):419-23.
13. Quitkin FM, Petkova E, McGrath PJ, et al. When should a trial of fluoxetine for major depression be declared failed? Am J Psychiatry 2003;160(4):734-40.
14. Fava M, Rush AJ, Trivedi MH, et al. Background and rationale for the sequenced treatment alternatives to relieve depression (STAR*D) study. Psychiatr Clin North Am 2003;26(2):457-94.
15. Fava M, Papakostas GI, Petersen T, et al. Switching to bupropion in fluoxetine-resistant major depressive disorder. Ann Clin Psychiatry 2003;15:17-22.
16. Entsuah AR, Huang H, Thase ME. Response and remission rates in different subpopulations with major depressive disorder administered venlafaxine, selective serotonin reuptake inhibitors, or placebo. J Clin Psychiatry 2001;62:869-77.
17. Thase ME, Entsuah AR, Rudolph RL. Remission rates during treatment with venlafaxine or selective serotonin reuptake inhibitors. Br J Psychiatry 2001;178:234-41.
18. Montgomery SA, Huusom A, Bothmer J. Flexible dose comparison of s-citalopram and venlafaxine XR. J Eur Neuropsychopharmacol 2002;12(suppl 3):S-254.
19. Keller MB, Gelenberg AJ, Hirschfeld RM, et al. The treatment of chronic depression, part 2: a double-blind, randomized trial of sertraline and imipramine. J Clin Psychiatry 1998;59(11):598-607.
20. Thase ME, Rush AJ, Howland RH, et al. Double-blind switch study of imipramine or sertraline treatment of antidepressant-resistant chronic depression. Arch Gen Psychiatry 2002;59(3):233-9.
21. Thase ME, Rush AJ. Treatment resistant depression. In: Bloom FE, Kupfer DJ (eds). Psychopharmacology: the fourth generation of progress New York: Raven Press, 1995;1081-97.
22. Shelton RC, Tollefson GD, Tohen M, et al. A novel augmentation strategy for treating resistant major depression. Am J Psychiatry 2001;158:131-4.
23. Keller MB, McCullough JP, Klein DN, et al. A comparison of nefazodone, the cognitive behavioral-analysis system of psychotherapy, and their combination for the treatment of chronic depression. N Engl J Med 2000;342:1462-70.
24. Schatzberg AF, Rush AJ, Arnow BA, et al. Medication or psychotherapy is effective when the other is not in chronic depression: empirical support. Arch Gen Psychiatry (submitted).
25. Nemeroff CB, Heim CM, Thase ME, et al. Differential responses to psychotherapy versus pharmacotherapy in patients with chronic forms of major depression and childhood trauma. Proc Natl Acad Sci USA 2003;100(24):14293-6.
26. Crismon ML, Trivedi M, Pigott TA, et al. The Texas Medication Algorithm Project: report of the Texas Consensus Conference Panel on Medication Treatment of Major Depressive Disorder. J Clin Psychiatry 1999;60(3):142-56.
27. Trivedi MH, Rush AJ, Crismon ML, et al. The Texas Medication Algorithm Project (TMAP): clinical results for patients with major depressive disorder. Arch Gen Psychiatry (in press).
28. Rush AJ, Fava M, Wisniewski SR, et al. for the STAR*D Investigators Group. Sequenced Treatment Alternatives to Relieve Depression (STAR*D): rationale and design. Control Clin Trials 2004;25(1):118-41.
29. Lavori PW, Rush AJ, Wisniewski SR, et al. Strengthening clinical effectiveness trials: equipoise-stratified randomization. Biol Psychiatry 2001;50:792-801.
30. Marangell LB, Rush AJ, George MS, et al. Vagus nerve stimulation (VNS) for major depressive episodes: one-year outcomes. Biol Psychiatry 2002;51(4):280-7.
Prescribing to preserve or restore sexual function
Many psychotropics can cause erectile dysfunction (ED) and other sexual problems (Tables 1 and 2). This side effect can discourage treatment compliance and jeopardize outcomes.
This article offers evidence-based strategies for preventing and treating psychotropic-induced ED. We also review information psychiatrists need to share with primary care physicians when treating a patient with ED.
Case report: A good relationship
Mr. A, age 52, has experienced diminishing erectile function for 6 months and now cannot achieve an erection. His relationship with his wife is good; he attributes loss of libido to his erection problem.
A pack-a-day smoker since age 18, Mr. A has type 2 diabetes and has been taking metformin, 850 mg bid, for 2 years. For about 2 months he has been taking sertraline, 50 mg, for depression and reports significantly improved mood, sleep, concentration, and appetite. He also has been taking lisinopril, 20 mg/d, for hypertension, and simvastatin, 40 mg nightly, for hyperlipidemia.
Table 1
Antidepressants associated with sexual dysfunction
| Drug class/agent | Proposed mechanism | Dysfunction |
|---|---|---|
| Monoamine oxidase inhibitors | Unknown | ED (rare), retarded ejaculation(rare) |
| Selective serotonin reuptake inhibitors | Increased serum prolactin (possible) Increased relative dopamine-to-serotonin reuptake inhibition Increased central serotonin | Decreased libido ED Anorgasmia Delayed/retarded ejaculation |
| Tricyclic antidepressants | CNS depression Anticholinergic activity | Decreased libido ED |
| Venlafaxine | Increased relative dopamine-to-serotonin reuptake inhibition Increased central serotonin | ED Anorgasmia Delayed/retarded ejaculation |
| ED: Erectile dysfunction | ||
Mr. A’s hemoglobin A1C is 9.8%, indicating poor diabetes control. His blood pressure is 168/94 mm Hg, well above his goal of <135/80. He has no chest pain or history of myocardial infarction; a recent exercise stress test indicated no coronary disease.
Discussion. Several medical causes—diabetes, hypertension, hyperlipidemia, and 34 years of heavy smoking—could explain Mr. A’s ED. Vascular disease is suspected, although the stress test was negative.
Identifying a specific cause is crucial to treating ED but may be difficult. Up to 80% of cases can be traced to one or more organic causes.1 Mr. A’s depression could be a factor, although psychogenic ED is not common. Adding the selective serotonin reuptake inhibitor (SSRI) sertraline may also have worsened his ED.
Other possible causes of ED include:
- nonpsychotropic drugs (to view a list of agents, see this article at currentpsychiatry.com)
- decreased libido, delayed orgasm, and anorgasmia. Decreased libido and anorgasmia are often misdiagnosed as primary ED because the presenting symptoms are similar.
ED treatment begins with managing underlying medical problems, although optimal control alone may not alleviate ED. Encourage the patient to stop smoking and offer smoking cessation strategies.
Alert the primary care physician and patient when prescribing a psychotropic associated with sexual side effects, and explain the drug’s potential benefits. Assess baseline sexual function before starting the psychotropic so that changes in sexual function can be detected. Report your findings to the referring physician after each visit.
If ED is believed to be psychotropic-induced:
- maintain the psychotropic regimen for 6 to 8 weeksto see if the patient builds a tolerance to its sexual side effects.
- lower the psychotropic dosage. In one study,2 nearly 75% of patients whose SSRI dosages were reduced by one-half reported improved sexual function with sustained antidepressant effectiveness. This SSRIeffect has been replicated and has also been demonstrated with imipramine.3-5
- schedule 1- to 2-day drug “holidays” (on weekends, for example) for medications with a short halflife (such as sertraline or paroxetine) if the underlying condition permits.7
Table 2
Other psychotropics associated with sexual dysfunction
| Drug class/agent | Proposed mechanism | Dysfunction |
|---|---|---|
| Amphetamines | Increased relative sympathetic nervous syndrome/parasympathetic nervous system activity | ED |
| Anticholinergics | Anticholinergic activity | ED |
| Antipsychotics (typical and atypical) | CNS depression, increased serum prolactin Anticholinergic activity Alpha1-receptor blockade Decreased internal urethral sphincter closure | Decreased libido ED Retarded ejaculation Retrograde ejaculation |
| Barbiturates, benzodiazepines, CNS depressants | CNS depression | Decreased libido |
| Carbamazepine, gabapentin | Decreased androgenic activity | Decreased libido, ED, retarded ejaculation |
| Disulfiram | Unknown | ED |
| Dopamine-receptor agonists | Unknown | ED |
| Dopamine-receptor antagonists | Increased serum prolactin | Decreased libido |
| ED: Erectile dysfunction | ||
If these measures do not work, individualized treatment of the sexual dysfunction becomes necessary. For some patients, switching psychotropics may be necessary to ensure compliance and preserve response. In cases such as Mr. A’s, however, the physician and patient may not want to stop a psychotropic that is working. For these patients, consider adding a drug to restore sexual function.
If ED persists after treatment, the primary care physician may refer the patient to a urologist.
Case report:Continued
Mr. A was advised to quit smoking and control his blood pressure and diabetes. His primary care doctor restarted lisinopril, 20 mg/d, increased his metformin to 1,000 mg bid, and added sildenafil, 50 mg before anticipated sexual activity. Mr. A says sildenafil has worked well.
Psychotropics and sexual dysfunction
Several physiologic processes contribute to psychotropics’ sexual side effects.
Libido is primarily a function of hormonal and CNS control. By contrast, erectile functions are mediated through local parasympathetic stimulation and ejaculation, which are controlled by norepinephrine. Orgasm is a cerebral cortical event distinct from ejaculation; either process can be disturbed independently. Elevated central serotonin levels inhibit orgasm and, to a lesser extent, ejaculation. Dopamine elevation over time leads to hyperprolactinemia and resultant hypotestosteronemia, decreasing libido.
SSRIs have been associated with ED and ejaculatory disturbances. A high serotonin-to-dopamine reuptake inhibition ratio associated with these agents may contribute to ED. Paroxetine has a higher serotonin-to-dopamine reuptake inhibition ratio—and is associated with a higher incidence of sexual dysfunction—than other SSRIs.7
Elevated central serotonin concentrations associated with SSRIs may also inhibit orgasm. SSRIs have been used to prolong orgasm in patients experiencing premature ejaculation.8
Venlafaxine, a serotonin/norepinephrine reuptake inhibitor, exhibits similar effects on sexual function as SSRIs, probably via the same serotonin/dopamine reuptake mechanisms. The lowest effective dosage can still cause sexual dysfunction but may reduce the likelihood.
TCAs. Tricyclic antidepressants may have fewer effects on sexual function than SSRIs. The mechanisms by which TCAs decrease libido and cause ED seem to be mediated through their CNS sedative and local anticholinergic effects.
MAOIs. Monoamine oxidase inhibitors have fewer effects on sexual function than SSRIs or TCAs, but these agents are rarely used to treat depression because of their adverse effects and drug-drug interactions.
Other antidepressants. Trazodone and nefazodone exhibit similar mechanisms of antidepressant action as SSRIs, but neither agent causes significant ED or ejaculatory disturbances. Priapism has been described with use of these agents, however.
Avoid using nefazodone in patients with hepatic dysfunction and in those who have taken an MAOI within 14 days.
Mirtazapine, a novel antidepressant with antiserotonergic actions, and bupropion, a dopamine and norepinephrine reuptake inhibitor, are not associated with significant sexual dysfunction compared with placebo. These agents are good alternatives to SSRIs9-11 and may alleviate sexual dysfunction when used to augment SSRIs.12,13
Lithium has been shown to decrease libido and cause ED. Lithium-mediated CNS sedation contributes to decreased libido; other mechanisms of lithium’s sexual side effects are not known. It is unclear whether lower dosages reduce the likelihood of sexual dysfunction.
Anticonvulsants. In two small studies, phenytoin increased sex hormone-binding globulin, resulting in lower free testosterone levels, which may lead to sexual dysfunction.18,19 Barbiturates have been shown to decrease libido, probably because of CNS sedation. Carbamazepine and gabapentin exhibit antiandrogenic effects, leading to various types of sexual dysfunction. These effects have not been observed with oxcarbazepine, however.
Lamotrigine may be an effective alternative in patients exhibiting sexual dysfunction with gabapentin.20
Typical antipsychotics can impair all aspects of sexual function:14
- CNS sedation and hyperprolactinemia account for decreased libido.
- Local anticholinergic effects may cause ED. Thus, the greater the anticholinergic effects, the presumably higher the incidence of ED.
- Alpha-receptor blockade and inhibition of inner urethral sphincter closure may cause retarded and retrograde ejaculation, respectively.
Of the conventional antipsychotics, thioridazine is associated with the highest incidence of sexual dysfunction.15
Table 3
Side effects, drug interactions associated with PDE-5 inhibitors
| Drug | Adverse effects | Drug interactions |
|---|---|---|
| Sildenafil | Dyspepsia, flushing, headache, hypotension, myocardial infarction (rare), nasal congestion, rash, visual disturbances | CYP-2C9 inducers and inhibitors (minor alterations in sildenafil plasma concentration) CYP-3A4 inducers and inhibitors (major alterations in sildenafil plasma concentration) Dihydrocodeine (rare priapism) Nitrates (severe hypotension) |
| Tadalafil* | Headache, dyspepsia, back pain, myalgia, nasal congestion, flushing, pain in limb, visual disturbances | CYP-3A4 inhibitors (increase tadalafil exposure) Alpha blockers other than tamsulosin (hypotension) Nitrates (severe hypotension) |
| Vardenafil* | Dizziness, dyspepsia, headache, hypotension | CYP-3A4 inducers and inhibitors (altered vardenafil plasma concentration) Nitrates (severe hypotension) |
| * Tadalafil and vardenafil are still undergoing post-marketing surveillance. This explains in part why fewer adverse effects and drug-drug interactions have been reported with these agents than with sildenafil. | ||
Atypical antipsychotics exhibit fewer adverse effects on sexual function than their typical counterparts, but the mechanisms that mediate these effects are the same.
Of these agents, risperidone causes the greatest prolactin elevation.16 Aripiprazole may also be associated with minimal sexual dysfunction.17 Other atypicals decrease prolactin levels or raise them transiently,16,17 so consider switching to one of these agents if a patient experiences ED.
Anxiolytics. Benzodiazepines, with their CNS sedative effects, are associated with decreased libido. Their potential for abuse may augment this effect. Buspirone, a novel anxiolytic that exhibits serotonergic and dopaminergic effects, is not associated with significant sexual dysfunction and may be a viable alternative.
Others. Amphetamines can increase the local sympathetic-to-parasympathetic activity ratio, resulting in ED. This effect is more pronounced with long-term use, though it is also seen with short-term use.
ED also has been reported in patients taking disulfiram, though it is unclear whether the drug or long-term alcohol use caused the dysfunction.
Drug treatment of ED
Because primary ED is a quality-of-life issue and not a health risk, few comparative trials have tested medications that improve erectile function. Thus, ED drug treatment may require trials of two or more agents.
Adverse effects and drug-drug interactions of selected agents used for ED treatment are listed in Tables 3 and 4.
Phosphodiesterase (PDE-5) inhibitors have become widely used as first-line oral medications for ED secondary to numerous causes. Sildenafil has demonstrated effectiveness in treating SSRI-induced ED compared with placebo. Tadalafil and vardenafil have not been studied in patients taking SSRIs.
Table 4
Side effects, drug interactions associated with other ED agents
| Drug | Adverse effects | Drug interactions |
|---|---|---|
| Amantadine | Aggression, altered mentation, anxiety, heart failure (rare), insomnia, leukopenia (rare), nausea Livedo reticularis (with extended use), neuroleptic malignant syndrome (upon discontinuation), orthostatic hypotension, psychoses | Bupropion (increased adverse events) Triamterene (may increase amantadine plasma concentration) |
| Bethanechol | Cholinergic effects (increased GI motility, lacrimation, miosis, urinary frequency) Diaphoresis, flushing, headache, hypotension, tachycardia | Anticholinergics (decreased effects of both agents) Cholinesterase inhibitors (increased cholinergic effects), Ganglionic blockers (severe hypotension) |
| Bupropion | Agitation, amblyopia, arrhythmias (rare), constipation, diaphoresis, dizziness, extrapyramidal symptoms (rare), headache, hypertension Hypoprolactinemia, insomnia, leukopenia (minor), nausea/vomiting Alcohol psychoses (rare), seizures, serum sickness (rare), taste perversion, tinnitus, tremor, urinary frequency Urticaria, weight gain (rare), weight loss, xerostomia | CYP-2D6 inducers and inhibitors (altered bupropion plasma concentration) Dopamine-receptor agonists (increased adverse effects) MAOIs (increased seizures and psychoses) QT-prolonging agents (increased QT-prolongation) Alcohol, systemic steroids, theophylline (increased seizures) |
| Mirtazapine | Somnolence, constipation, xerostomia, increased appetite, weight gain, dizziness, abnormal dreams, confusion Hyperlipidemia, flu-like symptoms, back pain | MAO inhibitors, linezolid, CNS depressants (increased sedative effects) Alcohol (may increase CNS depression) St John’s wort (may decrease mirtazapine levels) |
| Ropinirole | Abdominal pain, anxiety, arthralgias, confusion, constipation, diaphoresis, dyskinesias, dyspepsia, headache Hallucinations, insomnia, nausea/vomiting, orthostatic hypotension, peripheral edema Somnolence, tremor, upper respiratory infection, urinary tract infection, visual disturbances, xerostomia | CYP-1A2 inducers and inhibitors (altered ropinirole plasma concentration) Dopamine-receptor antagonists (decreased efficacy of both agents) |
In one 6-week study,21 54.4% of patients taking both an SSRI and sildenafil, up to 100 mg, showed significantly improved erectile function, arousal, ejaculation, orgasm, and overall satisfaction. In another study,22 SSRI-treated patients receiving sildenafil, 5 to 200 mg before sexual activity, reported noticeably improved ability to achieve and maintain erection, ejaculate, and achieve orgasm.
Sildenafil should not be taken concomitantly with agents or products containing nitrates. Use sildenafil with caution in patients with a blood pressure >170/110 mm Hg or <90/50 mm Hg, unstable angina, or retinitis pigmentosa. Also use sildenafil cautiously in patients who have suffered myocardial infarction, stroke, or life-threatening arrhythmia within the last 6 months.
Bupropion. In double-blind trials,11,12 the agent’s sustained-release form has shown effectiveness as an alternative or adjunct to SSRIs in treating SSRI-induced ED. Prescribe at 150 mg nightly when used as an adjunct.
Bupropion is contraindicated in patients with bulimia, anorexia nervosa, and seizure disorders, and in patients taking MAOIs. Use bupropion cautiously in patients with cranial trauma, renal or hepatic insufficiency, uncontrolled hypertension, myocardial infarction, unstable cardiovascular disease, psychosis, and bipolar disorder, and in patients abusing alcohol or taking warfarin.
Amantadine, an oral dopamine-receptor agonist with innate cholinergic effects, has shown effectiveness against SSRI-induced ED when given at 200 mg bid in a small trial.23
Avoid using amantadine in patients with closed-angle glaucoma, and use with caution in patients with heart failure and in persons age 65 and older.
Mirtazapine, 15 mg/d, has shown effectiveness as an SSRI alternative and as SSRI augmentation therapy to alleviate sexual dysfunction.12,13
Mirtazapine is contraindicated in patients with hypersensitivity or in patients who have used an MAOI within 14 days. Be careful when combining mirtazapine with an SSRI as the combination may increase the risk of serotonin syndrome.
Ropinirole, an oral dopamine 2-receptor agonist used to treat Parkinson’s disease, has shown effectiveness against antidepressant-induced ED when given at 0.25 mg/d and titrated across 4 weeks to 2 to 4 mg/d.24 Use ropinirole carefully in patients with bradycardia, dyskinesias, hallucinations, renal or hepatic insufficiency, and hypotension.
Bethanechol, an oral cholinergic agent used to treat urinary retention, has been described in case reports to alleviate TCA-induced ED when given at 20 mg 1 to 2 hours before sexual activity.25,26 Bethanechol is contraindicated in patients with hyperthyroidism, peptic ulcer disease, asthma, bradycardia, hypotension, coronary artery disease, epilepsy, Parkinson’s disease, urinary bladder neck obstruction, spastic GI disturbances, acute inflammatory GI lesions, peritonitis, and vagotonia.
Related resources
- Miller TA. Diagnostic evaluation of erectile dysfunction. Am Fam Physician 2000;61:95-110.
- Viera AJ, Clenney TL, Shenenberger DW, Green GF. Newer pharmacologic alternatives for erectile dysfunction. Am Fam Physician 1999;60:1159-72.
- British Medical Journal Web site search: erectile dysfunction. http://bmj.bmjjournals.com/cgi/collection/erectile_dysfunction
Drug brand names
- Amantadine • Symmetrel
- Aripiprazole • Abilify
- Bethanechol • Urecholine
- Bupropion • Wellbutrin
- Buspirone • BuSpar
- Carbamazepine • Tegretol
- Dihydrocodeine • Synalgos
- Disulfiram • Antabuse
- Gabapentin • Neurontin
- Lamotrigine • Lamictal
- Linezolid • Zyvox
- Lisinopril • Prinivil, others
- Lithium • Eskalith, others
- Metformin • Glucophage
- Mirtazapine • Remeron
- Nefazodone • Serzone
- Oxcarbazepine • Trileptal
- Paroxetine • Paxil
- Phenytoin • Dilantin
- Risperidone • Risperdal
- Ropinirole • Requip
- Sertraline • Zoloft
- Sildenafil • Viagra
- Simvastatin • Zocor
- Tadalafil • Cialis
- Triamterene • Dyazide, others
- Trazodone • Desyrel, others
- Vardenafil • Levitra
- Warfarin • Coumadin
Disclosure
Dr. Viera and Mr. Conrad report no financial relationship with any company whose products are mentioned in this article, or with manufacturers of competing products.
Dr. Choksi is a regional scientific manager for cardiovascular medicine with Novartis Pharmaceuticals Corp. When he co-wrote this article he was clinical coordinator, pharmacy department, Naval Hospital, Jacksonville, FL.
1. National Institutes of Health consensus conference on impotence. JAMA 1993;270:83-90.
2. Montejo-Gonzalez AL, Llorca G, Izquierdo JA, et al. SSRI-induced sexual dysfunction: fluoxetine, paroxetine, sertraline, and fluvoxamine in a prospective, multicenter, and descriptive clinical study of 344 patients. J Sex Marital Ther 1997;23:176-94.
3. Harrison WM, Rabkin JG, Ehrhardt AA, et al. Effects of antidepressant medication on sexual function: a controlled study. J Clin Psychopharmacol 1986;6:144-9.
4. Benazzi F, Mazzoli M. Fluoxetine-induced sexual dysfunction: a dose-dependent effect? Pharmacopsychiatry 1994;27:246.-
5. Clinical management of depression: bupropion—an update. Monograph series, vol.1, no. 1. Proceedings of a closed symposium: Antidepressant drug therapy: bupropion—an update meeting, Boca Raton, FL, October 30-31, 1992.
6. Rothschild AJ. Selective serotonin reuptake inhibitor-induced sexual dysfunction: efficacy of a drug holiday. Am J Psychiatry 1995;152:1514-16.
7. Rosen RC, Lane RM, Menza M. Effects of SSRIs on sexual function: a critical review. J Clin Psychopharmacol 1999;19:67-85.
8. Waldinger MD, Hengeveld MW, Zwinderman AH, Olivier B. Effect of SSRI antidepressants on ejaculation: a double-blind, randomized, placebo-controlled study with fluoxetine, fluvoxamine, paroxetine, and sertraline. J Clin Psychopharmacol 1998;18:274-81.
9. Koutouvidis N, Pratikakis M, Fotiadou A. The use of mirtazapine in a group of 11 patients following poor compliance to selective serotonin reuptake inhibitor treatment due to sexual dysfunction. Int Clin Psychopharmacol 1999;14:253-5.
10. Gelenberg AJ, McGahuey C, Laukes C, et al. Mirtazapine substitution in SSRI-induced sexual dysfunction. J Clin Psychiatry 2000;61:356-60.
11. Segraves RT, Kavoussi R, Hughes AR, et al. Evaluation of sexual functioning in depressed outpatients: a double-blind comparison of sustained-release bupropion and sertraline treatment. J Clin Psychopharmacol 2000;20:122-8.
12. Masand PS, Ashton AK, Gupta S, Frank B. Sustained-release bupropion for selective serotonin reuptake inhibitor-induced sexual dysfunction: a randomized, double-blind, placebo-controlled, parallel-group study. Am J Psychiatry 2001;158:805-7.
13. Farah A. Relief of SSRI-induced sexual dysfunction with mirtazapine treatment. J Clin Psychiatry 1999;60:260-1.
14. Smith SM, O’Keane V, Murray R. Sexual dysfunction in patients taking conventional antipsychotic medication. Br J Psychiatry 2002;181:49-55.
15. Kotin J, Wilbert DE, Verburg D, Soldinger SM. Thioridazine and sexual dysfunction. Am J Psychiatry 1976;133:82-5.
16. Guthrie SK. Clinical issues associated with maintenance treatment of patients with schizophrenia. Am J Health-Syst Pharm 2002;59(suppl 5):519-24.
17. Goodnick PJ, Rodriguez L, Santana O. Antipsychotics: impact on prolactin levels. Expert Opin Pharmacother 2002;3:1381-91.
18. Brunet M, Rodamilans M, Martinez-Osaba MJ, et al. Effects of long-term antiepileptic therapy on the catabolism of testosterone. Pharmacol Toxicol 1995;76:371-5.
19. Heroz AG, Levesque LA, Drislane FW, et al. Phenytoin-induced elevation of serum estradiol and reproductive dysfunction in men with epilepsy. Epilepsia 1991;32:550-3.
20. Husain AM, Carwile ST, Miller PP, Radtke RA. Improved sexual function in three men taking lamotrigine for epilepsy. South Med J 2000;93:335-6.
21. Nurnberg HG, Hensley PL, Gelenberg AJ, et al. Treatment of antidepressant-associated sexual dysfunction with sildenafil. A randomized controlled trial. JAMA 2003;289:56-64.
22. Nurnberg HG, Gelenberg A, Hargreave TB, et al. Efficacy of sildenafil citrate for the treatment of erectile dysfunction in men taking serotonin reuptake inhibitors. Am J Psychiatry 2001;158:1926-8.
23. Shrivastava RK, Shrivastava S, Overweg N, Schmitt M. Amantadine in the treatment of sexual dysfunction associated with selective serotonin reuptake inhibitors. J Clin Psychopharmacol 1995;15:83-4.
24. Worthington JJ, 3rd, Simon NM, Korbly NB, et al. Ropinirole for antidepressant-induced sexual dysfunction. Int Clin Psychopharmacol 2002;17:307-10.
25. Gross MD. Reversal by bethanechol of sexual dysfunction caused by anticholinergic antidepressants. Am J Psychiatry 1982;139:1193-4.
26. Yager J. Bethanechol chloride can reverse erectile and ejaculatory dysfunction induced by tricyclic antidepressants and mazindol: case report. J Clin Psychiatry 1986;47:210-11.
Many psychotropics can cause erectile dysfunction (ED) and other sexual problems (Tables 1 and 2). This side effect can discourage treatment compliance and jeopardize outcomes.
This article offers evidence-based strategies for preventing and treating psychotropic-induced ED. We also review information psychiatrists need to share with primary care physicians when treating a patient with ED.
Case report: A good relationship
Mr. A, age 52, has experienced diminishing erectile function for 6 months and now cannot achieve an erection. His relationship with his wife is good; he attributes loss of libido to his erection problem.
A pack-a-day smoker since age 18, Mr. A has type 2 diabetes and has been taking metformin, 850 mg bid, for 2 years. For about 2 months he has been taking sertraline, 50 mg, for depression and reports significantly improved mood, sleep, concentration, and appetite. He also has been taking lisinopril, 20 mg/d, for hypertension, and simvastatin, 40 mg nightly, for hyperlipidemia.
Table 1
Antidepressants associated with sexual dysfunction
| Drug class/agent | Proposed mechanism | Dysfunction |
|---|---|---|
| Monoamine oxidase inhibitors | Unknown | ED (rare), retarded ejaculation(rare) |
| Selective serotonin reuptake inhibitors | Increased serum prolactin (possible) Increased relative dopamine-to-serotonin reuptake inhibition Increased central serotonin | Decreased libido ED Anorgasmia Delayed/retarded ejaculation |
| Tricyclic antidepressants | CNS depression Anticholinergic activity | Decreased libido ED |
| Venlafaxine | Increased relative dopamine-to-serotonin reuptake inhibition Increased central serotonin | ED Anorgasmia Delayed/retarded ejaculation |
| ED: Erectile dysfunction | ||
Mr. A’s hemoglobin A1C is 9.8%, indicating poor diabetes control. His blood pressure is 168/94 mm Hg, well above his goal of <135/80. He has no chest pain or history of myocardial infarction; a recent exercise stress test indicated no coronary disease.
Discussion. Several medical causes—diabetes, hypertension, hyperlipidemia, and 34 years of heavy smoking—could explain Mr. A’s ED. Vascular disease is suspected, although the stress test was negative.
Identifying a specific cause is crucial to treating ED but may be difficult. Up to 80% of cases can be traced to one or more organic causes.1 Mr. A’s depression could be a factor, although psychogenic ED is not common. Adding the selective serotonin reuptake inhibitor (SSRI) sertraline may also have worsened his ED.
Other possible causes of ED include:
- nonpsychotropic drugs (to view a list of agents, see this article at currentpsychiatry.com)
- decreased libido, delayed orgasm, and anorgasmia. Decreased libido and anorgasmia are often misdiagnosed as primary ED because the presenting symptoms are similar.
ED treatment begins with managing underlying medical problems, although optimal control alone may not alleviate ED. Encourage the patient to stop smoking and offer smoking cessation strategies.
Alert the primary care physician and patient when prescribing a psychotropic associated with sexual side effects, and explain the drug’s potential benefits. Assess baseline sexual function before starting the psychotropic so that changes in sexual function can be detected. Report your findings to the referring physician after each visit.
If ED is believed to be psychotropic-induced:
- maintain the psychotropic regimen for 6 to 8 weeksto see if the patient builds a tolerance to its sexual side effects.
- lower the psychotropic dosage. In one study,2 nearly 75% of patients whose SSRI dosages were reduced by one-half reported improved sexual function with sustained antidepressant effectiveness. This SSRIeffect has been replicated and has also been demonstrated with imipramine.3-5
- schedule 1- to 2-day drug “holidays” (on weekends, for example) for medications with a short halflife (such as sertraline or paroxetine) if the underlying condition permits.7
Table 2
Other psychotropics associated with sexual dysfunction
| Drug class/agent | Proposed mechanism | Dysfunction |
|---|---|---|
| Amphetamines | Increased relative sympathetic nervous syndrome/parasympathetic nervous system activity | ED |
| Anticholinergics | Anticholinergic activity | ED |
| Antipsychotics (typical and atypical) | CNS depression, increased serum prolactin Anticholinergic activity Alpha1-receptor blockade Decreased internal urethral sphincter closure | Decreased libido ED Retarded ejaculation Retrograde ejaculation |
| Barbiturates, benzodiazepines, CNS depressants | CNS depression | Decreased libido |
| Carbamazepine, gabapentin | Decreased androgenic activity | Decreased libido, ED, retarded ejaculation |
| Disulfiram | Unknown | ED |
| Dopamine-receptor agonists | Unknown | ED |
| Dopamine-receptor antagonists | Increased serum prolactin | Decreased libido |
| ED: Erectile dysfunction | ||
If these measures do not work, individualized treatment of the sexual dysfunction becomes necessary. For some patients, switching psychotropics may be necessary to ensure compliance and preserve response. In cases such as Mr. A’s, however, the physician and patient may not want to stop a psychotropic that is working. For these patients, consider adding a drug to restore sexual function.
If ED persists after treatment, the primary care physician may refer the patient to a urologist.
Case report:Continued
Mr. A was advised to quit smoking and control his blood pressure and diabetes. His primary care doctor restarted lisinopril, 20 mg/d, increased his metformin to 1,000 mg bid, and added sildenafil, 50 mg before anticipated sexual activity. Mr. A says sildenafil has worked well.
Psychotropics and sexual dysfunction
Several physiologic processes contribute to psychotropics’ sexual side effects.
Libido is primarily a function of hormonal and CNS control. By contrast, erectile functions are mediated through local parasympathetic stimulation and ejaculation, which are controlled by norepinephrine. Orgasm is a cerebral cortical event distinct from ejaculation; either process can be disturbed independently. Elevated central serotonin levels inhibit orgasm and, to a lesser extent, ejaculation. Dopamine elevation over time leads to hyperprolactinemia and resultant hypotestosteronemia, decreasing libido.
SSRIs have been associated with ED and ejaculatory disturbances. A high serotonin-to-dopamine reuptake inhibition ratio associated with these agents may contribute to ED. Paroxetine has a higher serotonin-to-dopamine reuptake inhibition ratio—and is associated with a higher incidence of sexual dysfunction—than other SSRIs.7
Elevated central serotonin concentrations associated with SSRIs may also inhibit orgasm. SSRIs have been used to prolong orgasm in patients experiencing premature ejaculation.8
Venlafaxine, a serotonin/norepinephrine reuptake inhibitor, exhibits similar effects on sexual function as SSRIs, probably via the same serotonin/dopamine reuptake mechanisms. The lowest effective dosage can still cause sexual dysfunction but may reduce the likelihood.
TCAs. Tricyclic antidepressants may have fewer effects on sexual function than SSRIs. The mechanisms by which TCAs decrease libido and cause ED seem to be mediated through their CNS sedative and local anticholinergic effects.
MAOIs. Monoamine oxidase inhibitors have fewer effects on sexual function than SSRIs or TCAs, but these agents are rarely used to treat depression because of their adverse effects and drug-drug interactions.
Other antidepressants. Trazodone and nefazodone exhibit similar mechanisms of antidepressant action as SSRIs, but neither agent causes significant ED or ejaculatory disturbances. Priapism has been described with use of these agents, however.
Avoid using nefazodone in patients with hepatic dysfunction and in those who have taken an MAOI within 14 days.
Mirtazapine, a novel antidepressant with antiserotonergic actions, and bupropion, a dopamine and norepinephrine reuptake inhibitor, are not associated with significant sexual dysfunction compared with placebo. These agents are good alternatives to SSRIs9-11 and may alleviate sexual dysfunction when used to augment SSRIs.12,13
Lithium has been shown to decrease libido and cause ED. Lithium-mediated CNS sedation contributes to decreased libido; other mechanisms of lithium’s sexual side effects are not known. It is unclear whether lower dosages reduce the likelihood of sexual dysfunction.
Anticonvulsants. In two small studies, phenytoin increased sex hormone-binding globulin, resulting in lower free testosterone levels, which may lead to sexual dysfunction.18,19 Barbiturates have been shown to decrease libido, probably because of CNS sedation. Carbamazepine and gabapentin exhibit antiandrogenic effects, leading to various types of sexual dysfunction. These effects have not been observed with oxcarbazepine, however.
Lamotrigine may be an effective alternative in patients exhibiting sexual dysfunction with gabapentin.20
Typical antipsychotics can impair all aspects of sexual function:14
- CNS sedation and hyperprolactinemia account for decreased libido.
- Local anticholinergic effects may cause ED. Thus, the greater the anticholinergic effects, the presumably higher the incidence of ED.
- Alpha-receptor blockade and inhibition of inner urethral sphincter closure may cause retarded and retrograde ejaculation, respectively.
Of the conventional antipsychotics, thioridazine is associated with the highest incidence of sexual dysfunction.15
Table 3
Side effects, drug interactions associated with PDE-5 inhibitors
| Drug | Adverse effects | Drug interactions |
|---|---|---|
| Sildenafil | Dyspepsia, flushing, headache, hypotension, myocardial infarction (rare), nasal congestion, rash, visual disturbances | CYP-2C9 inducers and inhibitors (minor alterations in sildenafil plasma concentration) CYP-3A4 inducers and inhibitors (major alterations in sildenafil plasma concentration) Dihydrocodeine (rare priapism) Nitrates (severe hypotension) |
| Tadalafil* | Headache, dyspepsia, back pain, myalgia, nasal congestion, flushing, pain in limb, visual disturbances | CYP-3A4 inhibitors (increase tadalafil exposure) Alpha blockers other than tamsulosin (hypotension) Nitrates (severe hypotension) |
| Vardenafil* | Dizziness, dyspepsia, headache, hypotension | CYP-3A4 inducers and inhibitors (altered vardenafil plasma concentration) Nitrates (severe hypotension) |
| * Tadalafil and vardenafil are still undergoing post-marketing surveillance. This explains in part why fewer adverse effects and drug-drug interactions have been reported with these agents than with sildenafil. | ||
Atypical antipsychotics exhibit fewer adverse effects on sexual function than their typical counterparts, but the mechanisms that mediate these effects are the same.
Of these agents, risperidone causes the greatest prolactin elevation.16 Aripiprazole may also be associated with minimal sexual dysfunction.17 Other atypicals decrease prolactin levels or raise them transiently,16,17 so consider switching to one of these agents if a patient experiences ED.
Anxiolytics. Benzodiazepines, with their CNS sedative effects, are associated with decreased libido. Their potential for abuse may augment this effect. Buspirone, a novel anxiolytic that exhibits serotonergic and dopaminergic effects, is not associated with significant sexual dysfunction and may be a viable alternative.
Others. Amphetamines can increase the local sympathetic-to-parasympathetic activity ratio, resulting in ED. This effect is more pronounced with long-term use, though it is also seen with short-term use.
ED also has been reported in patients taking disulfiram, though it is unclear whether the drug or long-term alcohol use caused the dysfunction.
Drug treatment of ED
Because primary ED is a quality-of-life issue and not a health risk, few comparative trials have tested medications that improve erectile function. Thus, ED drug treatment may require trials of two or more agents.
Adverse effects and drug-drug interactions of selected agents used for ED treatment are listed in Tables 3 and 4.
Phosphodiesterase (PDE-5) inhibitors have become widely used as first-line oral medications for ED secondary to numerous causes. Sildenafil has demonstrated effectiveness in treating SSRI-induced ED compared with placebo. Tadalafil and vardenafil have not been studied in patients taking SSRIs.
Table 4
Side effects, drug interactions associated with other ED agents
| Drug | Adverse effects | Drug interactions |
|---|---|---|
| Amantadine | Aggression, altered mentation, anxiety, heart failure (rare), insomnia, leukopenia (rare), nausea Livedo reticularis (with extended use), neuroleptic malignant syndrome (upon discontinuation), orthostatic hypotension, psychoses | Bupropion (increased adverse events) Triamterene (may increase amantadine plasma concentration) |
| Bethanechol | Cholinergic effects (increased GI motility, lacrimation, miosis, urinary frequency) Diaphoresis, flushing, headache, hypotension, tachycardia | Anticholinergics (decreased effects of both agents) Cholinesterase inhibitors (increased cholinergic effects), Ganglionic blockers (severe hypotension) |
| Bupropion | Agitation, amblyopia, arrhythmias (rare), constipation, diaphoresis, dizziness, extrapyramidal symptoms (rare), headache, hypertension Hypoprolactinemia, insomnia, leukopenia (minor), nausea/vomiting Alcohol psychoses (rare), seizures, serum sickness (rare), taste perversion, tinnitus, tremor, urinary frequency Urticaria, weight gain (rare), weight loss, xerostomia | CYP-2D6 inducers and inhibitors (altered bupropion plasma concentration) Dopamine-receptor agonists (increased adverse effects) MAOIs (increased seizures and psychoses) QT-prolonging agents (increased QT-prolongation) Alcohol, systemic steroids, theophylline (increased seizures) |
| Mirtazapine | Somnolence, constipation, xerostomia, increased appetite, weight gain, dizziness, abnormal dreams, confusion Hyperlipidemia, flu-like symptoms, back pain | MAO inhibitors, linezolid, CNS depressants (increased sedative effects) Alcohol (may increase CNS depression) St John’s wort (may decrease mirtazapine levels) |
| Ropinirole | Abdominal pain, anxiety, arthralgias, confusion, constipation, diaphoresis, dyskinesias, dyspepsia, headache Hallucinations, insomnia, nausea/vomiting, orthostatic hypotension, peripheral edema Somnolence, tremor, upper respiratory infection, urinary tract infection, visual disturbances, xerostomia | CYP-1A2 inducers and inhibitors (altered ropinirole plasma concentration) Dopamine-receptor antagonists (decreased efficacy of both agents) |
In one 6-week study,21 54.4% of patients taking both an SSRI and sildenafil, up to 100 mg, showed significantly improved erectile function, arousal, ejaculation, orgasm, and overall satisfaction. In another study,22 SSRI-treated patients receiving sildenafil, 5 to 200 mg before sexual activity, reported noticeably improved ability to achieve and maintain erection, ejaculate, and achieve orgasm.
Sildenafil should not be taken concomitantly with agents or products containing nitrates. Use sildenafil with caution in patients with a blood pressure >170/110 mm Hg or <90/50 mm Hg, unstable angina, or retinitis pigmentosa. Also use sildenafil cautiously in patients who have suffered myocardial infarction, stroke, or life-threatening arrhythmia within the last 6 months.
Bupropion. In double-blind trials,11,12 the agent’s sustained-release form has shown effectiveness as an alternative or adjunct to SSRIs in treating SSRI-induced ED. Prescribe at 150 mg nightly when used as an adjunct.
Bupropion is contraindicated in patients with bulimia, anorexia nervosa, and seizure disorders, and in patients taking MAOIs. Use bupropion cautiously in patients with cranial trauma, renal or hepatic insufficiency, uncontrolled hypertension, myocardial infarction, unstable cardiovascular disease, psychosis, and bipolar disorder, and in patients abusing alcohol or taking warfarin.
Amantadine, an oral dopamine-receptor agonist with innate cholinergic effects, has shown effectiveness against SSRI-induced ED when given at 200 mg bid in a small trial.23
Avoid using amantadine in patients with closed-angle glaucoma, and use with caution in patients with heart failure and in persons age 65 and older.
Mirtazapine, 15 mg/d, has shown effectiveness as an SSRI alternative and as SSRI augmentation therapy to alleviate sexual dysfunction.12,13
Mirtazapine is contraindicated in patients with hypersensitivity or in patients who have used an MAOI within 14 days. Be careful when combining mirtazapine with an SSRI as the combination may increase the risk of serotonin syndrome.
Ropinirole, an oral dopamine 2-receptor agonist used to treat Parkinson’s disease, has shown effectiveness against antidepressant-induced ED when given at 0.25 mg/d and titrated across 4 weeks to 2 to 4 mg/d.24 Use ropinirole carefully in patients with bradycardia, dyskinesias, hallucinations, renal or hepatic insufficiency, and hypotension.
Bethanechol, an oral cholinergic agent used to treat urinary retention, has been described in case reports to alleviate TCA-induced ED when given at 20 mg 1 to 2 hours before sexual activity.25,26 Bethanechol is contraindicated in patients with hyperthyroidism, peptic ulcer disease, asthma, bradycardia, hypotension, coronary artery disease, epilepsy, Parkinson’s disease, urinary bladder neck obstruction, spastic GI disturbances, acute inflammatory GI lesions, peritonitis, and vagotonia.
Related resources
- Miller TA. Diagnostic evaluation of erectile dysfunction. Am Fam Physician 2000;61:95-110.
- Viera AJ, Clenney TL, Shenenberger DW, Green GF. Newer pharmacologic alternatives for erectile dysfunction. Am Fam Physician 1999;60:1159-72.
- British Medical Journal Web site search: erectile dysfunction. http://bmj.bmjjournals.com/cgi/collection/erectile_dysfunction
Drug brand names
- Amantadine • Symmetrel
- Aripiprazole • Abilify
- Bethanechol • Urecholine
- Bupropion • Wellbutrin
- Buspirone • BuSpar
- Carbamazepine • Tegretol
- Dihydrocodeine • Synalgos
- Disulfiram • Antabuse
- Gabapentin • Neurontin
- Lamotrigine • Lamictal
- Linezolid • Zyvox
- Lisinopril • Prinivil, others
- Lithium • Eskalith, others
- Metformin • Glucophage
- Mirtazapine • Remeron
- Nefazodone • Serzone
- Oxcarbazepine • Trileptal
- Paroxetine • Paxil
- Phenytoin • Dilantin
- Risperidone • Risperdal
- Ropinirole • Requip
- Sertraline • Zoloft
- Sildenafil • Viagra
- Simvastatin • Zocor
- Tadalafil • Cialis
- Triamterene • Dyazide, others
- Trazodone • Desyrel, others
- Vardenafil • Levitra
- Warfarin • Coumadin
Disclosure
Dr. Viera and Mr. Conrad report no financial relationship with any company whose products are mentioned in this article, or with manufacturers of competing products.
Dr. Choksi is a regional scientific manager for cardiovascular medicine with Novartis Pharmaceuticals Corp. When he co-wrote this article he was clinical coordinator, pharmacy department, Naval Hospital, Jacksonville, FL.
Many psychotropics can cause erectile dysfunction (ED) and other sexual problems (Tables 1 and 2). This side effect can discourage treatment compliance and jeopardize outcomes.
This article offers evidence-based strategies for preventing and treating psychotropic-induced ED. We also review information psychiatrists need to share with primary care physicians when treating a patient with ED.
Case report: A good relationship
Mr. A, age 52, has experienced diminishing erectile function for 6 months and now cannot achieve an erection. His relationship with his wife is good; he attributes loss of libido to his erection problem.
A pack-a-day smoker since age 18, Mr. A has type 2 diabetes and has been taking metformin, 850 mg bid, for 2 years. For about 2 months he has been taking sertraline, 50 mg, for depression and reports significantly improved mood, sleep, concentration, and appetite. He also has been taking lisinopril, 20 mg/d, for hypertension, and simvastatin, 40 mg nightly, for hyperlipidemia.
Table 1
Antidepressants associated with sexual dysfunction
| Drug class/agent | Proposed mechanism | Dysfunction |
|---|---|---|
| Monoamine oxidase inhibitors | Unknown | ED (rare), retarded ejaculation(rare) |
| Selective serotonin reuptake inhibitors | Increased serum prolactin (possible) Increased relative dopamine-to-serotonin reuptake inhibition Increased central serotonin | Decreased libido ED Anorgasmia Delayed/retarded ejaculation |
| Tricyclic antidepressants | CNS depression Anticholinergic activity | Decreased libido ED |
| Venlafaxine | Increased relative dopamine-to-serotonin reuptake inhibition Increased central serotonin | ED Anorgasmia Delayed/retarded ejaculation |
| ED: Erectile dysfunction | ||
Mr. A’s hemoglobin A1C is 9.8%, indicating poor diabetes control. His blood pressure is 168/94 mm Hg, well above his goal of <135/80. He has no chest pain or history of myocardial infarction; a recent exercise stress test indicated no coronary disease.
Discussion. Several medical causes—diabetes, hypertension, hyperlipidemia, and 34 years of heavy smoking—could explain Mr. A’s ED. Vascular disease is suspected, although the stress test was negative.
Identifying a specific cause is crucial to treating ED but may be difficult. Up to 80% of cases can be traced to one or more organic causes.1 Mr. A’s depression could be a factor, although psychogenic ED is not common. Adding the selective serotonin reuptake inhibitor (SSRI) sertraline may also have worsened his ED.
Other possible causes of ED include:
- nonpsychotropic drugs (to view a list of agents, see this article at currentpsychiatry.com)
- decreased libido, delayed orgasm, and anorgasmia. Decreased libido and anorgasmia are often misdiagnosed as primary ED because the presenting symptoms are similar.
ED treatment begins with managing underlying medical problems, although optimal control alone may not alleviate ED. Encourage the patient to stop smoking and offer smoking cessation strategies.
Alert the primary care physician and patient when prescribing a psychotropic associated with sexual side effects, and explain the drug’s potential benefits. Assess baseline sexual function before starting the psychotropic so that changes in sexual function can be detected. Report your findings to the referring physician after each visit.
If ED is believed to be psychotropic-induced:
- maintain the psychotropic regimen for 6 to 8 weeksto see if the patient builds a tolerance to its sexual side effects.
- lower the psychotropic dosage. In one study,2 nearly 75% of patients whose SSRI dosages were reduced by one-half reported improved sexual function with sustained antidepressant effectiveness. This SSRIeffect has been replicated and has also been demonstrated with imipramine.3-5
- schedule 1- to 2-day drug “holidays” (on weekends, for example) for medications with a short halflife (such as sertraline or paroxetine) if the underlying condition permits.7
Table 2
Other psychotropics associated with sexual dysfunction
| Drug class/agent | Proposed mechanism | Dysfunction |
|---|---|---|
| Amphetamines | Increased relative sympathetic nervous syndrome/parasympathetic nervous system activity | ED |
| Anticholinergics | Anticholinergic activity | ED |
| Antipsychotics (typical and atypical) | CNS depression, increased serum prolactin Anticholinergic activity Alpha1-receptor blockade Decreased internal urethral sphincter closure | Decreased libido ED Retarded ejaculation Retrograde ejaculation |
| Barbiturates, benzodiazepines, CNS depressants | CNS depression | Decreased libido |
| Carbamazepine, gabapentin | Decreased androgenic activity | Decreased libido, ED, retarded ejaculation |
| Disulfiram | Unknown | ED |
| Dopamine-receptor agonists | Unknown | ED |
| Dopamine-receptor antagonists | Increased serum prolactin | Decreased libido |
| ED: Erectile dysfunction | ||
If these measures do not work, individualized treatment of the sexual dysfunction becomes necessary. For some patients, switching psychotropics may be necessary to ensure compliance and preserve response. In cases such as Mr. A’s, however, the physician and patient may not want to stop a psychotropic that is working. For these patients, consider adding a drug to restore sexual function.
If ED persists after treatment, the primary care physician may refer the patient to a urologist.
Case report:Continued
Mr. A was advised to quit smoking and control his blood pressure and diabetes. His primary care doctor restarted lisinopril, 20 mg/d, increased his metformin to 1,000 mg bid, and added sildenafil, 50 mg before anticipated sexual activity. Mr. A says sildenafil has worked well.
Psychotropics and sexual dysfunction
Several physiologic processes contribute to psychotropics’ sexual side effects.
Libido is primarily a function of hormonal and CNS control. By contrast, erectile functions are mediated through local parasympathetic stimulation and ejaculation, which are controlled by norepinephrine. Orgasm is a cerebral cortical event distinct from ejaculation; either process can be disturbed independently. Elevated central serotonin levels inhibit orgasm and, to a lesser extent, ejaculation. Dopamine elevation over time leads to hyperprolactinemia and resultant hypotestosteronemia, decreasing libido.
SSRIs have been associated with ED and ejaculatory disturbances. A high serotonin-to-dopamine reuptake inhibition ratio associated with these agents may contribute to ED. Paroxetine has a higher serotonin-to-dopamine reuptake inhibition ratio—and is associated with a higher incidence of sexual dysfunction—than other SSRIs.7
Elevated central serotonin concentrations associated with SSRIs may also inhibit orgasm. SSRIs have been used to prolong orgasm in patients experiencing premature ejaculation.8
Venlafaxine, a serotonin/norepinephrine reuptake inhibitor, exhibits similar effects on sexual function as SSRIs, probably via the same serotonin/dopamine reuptake mechanisms. The lowest effective dosage can still cause sexual dysfunction but may reduce the likelihood.
TCAs. Tricyclic antidepressants may have fewer effects on sexual function than SSRIs. The mechanisms by which TCAs decrease libido and cause ED seem to be mediated through their CNS sedative and local anticholinergic effects.
MAOIs. Monoamine oxidase inhibitors have fewer effects on sexual function than SSRIs or TCAs, but these agents are rarely used to treat depression because of their adverse effects and drug-drug interactions.
Other antidepressants. Trazodone and nefazodone exhibit similar mechanisms of antidepressant action as SSRIs, but neither agent causes significant ED or ejaculatory disturbances. Priapism has been described with use of these agents, however.
Avoid using nefazodone in patients with hepatic dysfunction and in those who have taken an MAOI within 14 days.
Mirtazapine, a novel antidepressant with antiserotonergic actions, and bupropion, a dopamine and norepinephrine reuptake inhibitor, are not associated with significant sexual dysfunction compared with placebo. These agents are good alternatives to SSRIs9-11 and may alleviate sexual dysfunction when used to augment SSRIs.12,13
Lithium has been shown to decrease libido and cause ED. Lithium-mediated CNS sedation contributes to decreased libido; other mechanisms of lithium’s sexual side effects are not known. It is unclear whether lower dosages reduce the likelihood of sexual dysfunction.
Anticonvulsants. In two small studies, phenytoin increased sex hormone-binding globulin, resulting in lower free testosterone levels, which may lead to sexual dysfunction.18,19 Barbiturates have been shown to decrease libido, probably because of CNS sedation. Carbamazepine and gabapentin exhibit antiandrogenic effects, leading to various types of sexual dysfunction. These effects have not been observed with oxcarbazepine, however.
Lamotrigine may be an effective alternative in patients exhibiting sexual dysfunction with gabapentin.20
Typical antipsychotics can impair all aspects of sexual function:14
- CNS sedation and hyperprolactinemia account for decreased libido.
- Local anticholinergic effects may cause ED. Thus, the greater the anticholinergic effects, the presumably higher the incidence of ED.
- Alpha-receptor blockade and inhibition of inner urethral sphincter closure may cause retarded and retrograde ejaculation, respectively.
Of the conventional antipsychotics, thioridazine is associated with the highest incidence of sexual dysfunction.15
Table 3
Side effects, drug interactions associated with PDE-5 inhibitors
| Drug | Adverse effects | Drug interactions |
|---|---|---|
| Sildenafil | Dyspepsia, flushing, headache, hypotension, myocardial infarction (rare), nasal congestion, rash, visual disturbances | CYP-2C9 inducers and inhibitors (minor alterations in sildenafil plasma concentration) CYP-3A4 inducers and inhibitors (major alterations in sildenafil plasma concentration) Dihydrocodeine (rare priapism) Nitrates (severe hypotension) |
| Tadalafil* | Headache, dyspepsia, back pain, myalgia, nasal congestion, flushing, pain in limb, visual disturbances | CYP-3A4 inhibitors (increase tadalafil exposure) Alpha blockers other than tamsulosin (hypotension) Nitrates (severe hypotension) |
| Vardenafil* | Dizziness, dyspepsia, headache, hypotension | CYP-3A4 inducers and inhibitors (altered vardenafil plasma concentration) Nitrates (severe hypotension) |
| * Tadalafil and vardenafil are still undergoing post-marketing surveillance. This explains in part why fewer adverse effects and drug-drug interactions have been reported with these agents than with sildenafil. | ||
Atypical antipsychotics exhibit fewer adverse effects on sexual function than their typical counterparts, but the mechanisms that mediate these effects are the same.
Of these agents, risperidone causes the greatest prolactin elevation.16 Aripiprazole may also be associated with minimal sexual dysfunction.17 Other atypicals decrease prolactin levels or raise them transiently,16,17 so consider switching to one of these agents if a patient experiences ED.
Anxiolytics. Benzodiazepines, with their CNS sedative effects, are associated with decreased libido. Their potential for abuse may augment this effect. Buspirone, a novel anxiolytic that exhibits serotonergic and dopaminergic effects, is not associated with significant sexual dysfunction and may be a viable alternative.
Others. Amphetamines can increase the local sympathetic-to-parasympathetic activity ratio, resulting in ED. This effect is more pronounced with long-term use, though it is also seen with short-term use.
ED also has been reported in patients taking disulfiram, though it is unclear whether the drug or long-term alcohol use caused the dysfunction.
Drug treatment of ED
Because primary ED is a quality-of-life issue and not a health risk, few comparative trials have tested medications that improve erectile function. Thus, ED drug treatment may require trials of two or more agents.
Adverse effects and drug-drug interactions of selected agents used for ED treatment are listed in Tables 3 and 4.
Phosphodiesterase (PDE-5) inhibitors have become widely used as first-line oral medications for ED secondary to numerous causes. Sildenafil has demonstrated effectiveness in treating SSRI-induced ED compared with placebo. Tadalafil and vardenafil have not been studied in patients taking SSRIs.
Table 4
Side effects, drug interactions associated with other ED agents
| Drug | Adverse effects | Drug interactions |
|---|---|---|
| Amantadine | Aggression, altered mentation, anxiety, heart failure (rare), insomnia, leukopenia (rare), nausea Livedo reticularis (with extended use), neuroleptic malignant syndrome (upon discontinuation), orthostatic hypotension, psychoses | Bupropion (increased adverse events) Triamterene (may increase amantadine plasma concentration) |
| Bethanechol | Cholinergic effects (increased GI motility, lacrimation, miosis, urinary frequency) Diaphoresis, flushing, headache, hypotension, tachycardia | Anticholinergics (decreased effects of both agents) Cholinesterase inhibitors (increased cholinergic effects), Ganglionic blockers (severe hypotension) |
| Bupropion | Agitation, amblyopia, arrhythmias (rare), constipation, diaphoresis, dizziness, extrapyramidal symptoms (rare), headache, hypertension Hypoprolactinemia, insomnia, leukopenia (minor), nausea/vomiting Alcohol psychoses (rare), seizures, serum sickness (rare), taste perversion, tinnitus, tremor, urinary frequency Urticaria, weight gain (rare), weight loss, xerostomia | CYP-2D6 inducers and inhibitors (altered bupropion plasma concentration) Dopamine-receptor agonists (increased adverse effects) MAOIs (increased seizures and psychoses) QT-prolonging agents (increased QT-prolongation) Alcohol, systemic steroids, theophylline (increased seizures) |
| Mirtazapine | Somnolence, constipation, xerostomia, increased appetite, weight gain, dizziness, abnormal dreams, confusion Hyperlipidemia, flu-like symptoms, back pain | MAO inhibitors, linezolid, CNS depressants (increased sedative effects) Alcohol (may increase CNS depression) St John’s wort (may decrease mirtazapine levels) |
| Ropinirole | Abdominal pain, anxiety, arthralgias, confusion, constipation, diaphoresis, dyskinesias, dyspepsia, headache Hallucinations, insomnia, nausea/vomiting, orthostatic hypotension, peripheral edema Somnolence, tremor, upper respiratory infection, urinary tract infection, visual disturbances, xerostomia | CYP-1A2 inducers and inhibitors (altered ropinirole plasma concentration) Dopamine-receptor antagonists (decreased efficacy of both agents) |
In one 6-week study,21 54.4% of patients taking both an SSRI and sildenafil, up to 100 mg, showed significantly improved erectile function, arousal, ejaculation, orgasm, and overall satisfaction. In another study,22 SSRI-treated patients receiving sildenafil, 5 to 200 mg before sexual activity, reported noticeably improved ability to achieve and maintain erection, ejaculate, and achieve orgasm.
Sildenafil should not be taken concomitantly with agents or products containing nitrates. Use sildenafil with caution in patients with a blood pressure >170/110 mm Hg or <90/50 mm Hg, unstable angina, or retinitis pigmentosa. Also use sildenafil cautiously in patients who have suffered myocardial infarction, stroke, or life-threatening arrhythmia within the last 6 months.
Bupropion. In double-blind trials,11,12 the agent’s sustained-release form has shown effectiveness as an alternative or adjunct to SSRIs in treating SSRI-induced ED. Prescribe at 150 mg nightly when used as an adjunct.
Bupropion is contraindicated in patients with bulimia, anorexia nervosa, and seizure disorders, and in patients taking MAOIs. Use bupropion cautiously in patients with cranial trauma, renal or hepatic insufficiency, uncontrolled hypertension, myocardial infarction, unstable cardiovascular disease, psychosis, and bipolar disorder, and in patients abusing alcohol or taking warfarin.
Amantadine, an oral dopamine-receptor agonist with innate cholinergic effects, has shown effectiveness against SSRI-induced ED when given at 200 mg bid in a small trial.23
Avoid using amantadine in patients with closed-angle glaucoma, and use with caution in patients with heart failure and in persons age 65 and older.
Mirtazapine, 15 mg/d, has shown effectiveness as an SSRI alternative and as SSRI augmentation therapy to alleviate sexual dysfunction.12,13
Mirtazapine is contraindicated in patients with hypersensitivity or in patients who have used an MAOI within 14 days. Be careful when combining mirtazapine with an SSRI as the combination may increase the risk of serotonin syndrome.
Ropinirole, an oral dopamine 2-receptor agonist used to treat Parkinson’s disease, has shown effectiveness against antidepressant-induced ED when given at 0.25 mg/d and titrated across 4 weeks to 2 to 4 mg/d.24 Use ropinirole carefully in patients with bradycardia, dyskinesias, hallucinations, renal or hepatic insufficiency, and hypotension.
Bethanechol, an oral cholinergic agent used to treat urinary retention, has been described in case reports to alleviate TCA-induced ED when given at 20 mg 1 to 2 hours before sexual activity.25,26 Bethanechol is contraindicated in patients with hyperthyroidism, peptic ulcer disease, asthma, bradycardia, hypotension, coronary artery disease, epilepsy, Parkinson’s disease, urinary bladder neck obstruction, spastic GI disturbances, acute inflammatory GI lesions, peritonitis, and vagotonia.
Related resources
- Miller TA. Diagnostic evaluation of erectile dysfunction. Am Fam Physician 2000;61:95-110.
- Viera AJ, Clenney TL, Shenenberger DW, Green GF. Newer pharmacologic alternatives for erectile dysfunction. Am Fam Physician 1999;60:1159-72.
- British Medical Journal Web site search: erectile dysfunction. http://bmj.bmjjournals.com/cgi/collection/erectile_dysfunction
Drug brand names
- Amantadine • Symmetrel
- Aripiprazole • Abilify
- Bethanechol • Urecholine
- Bupropion • Wellbutrin
- Buspirone • BuSpar
- Carbamazepine • Tegretol
- Dihydrocodeine • Synalgos
- Disulfiram • Antabuse
- Gabapentin • Neurontin
- Lamotrigine • Lamictal
- Linezolid • Zyvox
- Lisinopril • Prinivil, others
- Lithium • Eskalith, others
- Metformin • Glucophage
- Mirtazapine • Remeron
- Nefazodone • Serzone
- Oxcarbazepine • Trileptal
- Paroxetine • Paxil
- Phenytoin • Dilantin
- Risperidone • Risperdal
- Ropinirole • Requip
- Sertraline • Zoloft
- Sildenafil • Viagra
- Simvastatin • Zocor
- Tadalafil • Cialis
- Triamterene • Dyazide, others
- Trazodone • Desyrel, others
- Vardenafil • Levitra
- Warfarin • Coumadin
Disclosure
Dr. Viera and Mr. Conrad report no financial relationship with any company whose products are mentioned in this article, or with manufacturers of competing products.
Dr. Choksi is a regional scientific manager for cardiovascular medicine with Novartis Pharmaceuticals Corp. When he co-wrote this article he was clinical coordinator, pharmacy department, Naval Hospital, Jacksonville, FL.
1. National Institutes of Health consensus conference on impotence. JAMA 1993;270:83-90.
2. Montejo-Gonzalez AL, Llorca G, Izquierdo JA, et al. SSRI-induced sexual dysfunction: fluoxetine, paroxetine, sertraline, and fluvoxamine in a prospective, multicenter, and descriptive clinical study of 344 patients. J Sex Marital Ther 1997;23:176-94.
3. Harrison WM, Rabkin JG, Ehrhardt AA, et al. Effects of antidepressant medication on sexual function: a controlled study. J Clin Psychopharmacol 1986;6:144-9.
4. Benazzi F, Mazzoli M. Fluoxetine-induced sexual dysfunction: a dose-dependent effect? Pharmacopsychiatry 1994;27:246.-
5. Clinical management of depression: bupropion—an update. Monograph series, vol.1, no. 1. Proceedings of a closed symposium: Antidepressant drug therapy: bupropion—an update meeting, Boca Raton, FL, October 30-31, 1992.
6. Rothschild AJ. Selective serotonin reuptake inhibitor-induced sexual dysfunction: efficacy of a drug holiday. Am J Psychiatry 1995;152:1514-16.
7. Rosen RC, Lane RM, Menza M. Effects of SSRIs on sexual function: a critical review. J Clin Psychopharmacol 1999;19:67-85.
8. Waldinger MD, Hengeveld MW, Zwinderman AH, Olivier B. Effect of SSRI antidepressants on ejaculation: a double-blind, randomized, placebo-controlled study with fluoxetine, fluvoxamine, paroxetine, and sertraline. J Clin Psychopharmacol 1998;18:274-81.
9. Koutouvidis N, Pratikakis M, Fotiadou A. The use of mirtazapine in a group of 11 patients following poor compliance to selective serotonin reuptake inhibitor treatment due to sexual dysfunction. Int Clin Psychopharmacol 1999;14:253-5.
10. Gelenberg AJ, McGahuey C, Laukes C, et al. Mirtazapine substitution in SSRI-induced sexual dysfunction. J Clin Psychiatry 2000;61:356-60.
11. Segraves RT, Kavoussi R, Hughes AR, et al. Evaluation of sexual functioning in depressed outpatients: a double-blind comparison of sustained-release bupropion and sertraline treatment. J Clin Psychopharmacol 2000;20:122-8.
12. Masand PS, Ashton AK, Gupta S, Frank B. Sustained-release bupropion for selective serotonin reuptake inhibitor-induced sexual dysfunction: a randomized, double-blind, placebo-controlled, parallel-group study. Am J Psychiatry 2001;158:805-7.
13. Farah A. Relief of SSRI-induced sexual dysfunction with mirtazapine treatment. J Clin Psychiatry 1999;60:260-1.
14. Smith SM, O’Keane V, Murray R. Sexual dysfunction in patients taking conventional antipsychotic medication. Br J Psychiatry 2002;181:49-55.
15. Kotin J, Wilbert DE, Verburg D, Soldinger SM. Thioridazine and sexual dysfunction. Am J Psychiatry 1976;133:82-5.
16. Guthrie SK. Clinical issues associated with maintenance treatment of patients with schizophrenia. Am J Health-Syst Pharm 2002;59(suppl 5):519-24.
17. Goodnick PJ, Rodriguez L, Santana O. Antipsychotics: impact on prolactin levels. Expert Opin Pharmacother 2002;3:1381-91.
18. Brunet M, Rodamilans M, Martinez-Osaba MJ, et al. Effects of long-term antiepileptic therapy on the catabolism of testosterone. Pharmacol Toxicol 1995;76:371-5.
19. Heroz AG, Levesque LA, Drislane FW, et al. Phenytoin-induced elevation of serum estradiol and reproductive dysfunction in men with epilepsy. Epilepsia 1991;32:550-3.
20. Husain AM, Carwile ST, Miller PP, Radtke RA. Improved sexual function in three men taking lamotrigine for epilepsy. South Med J 2000;93:335-6.
21. Nurnberg HG, Hensley PL, Gelenberg AJ, et al. Treatment of antidepressant-associated sexual dysfunction with sildenafil. A randomized controlled trial. JAMA 2003;289:56-64.
22. Nurnberg HG, Gelenberg A, Hargreave TB, et al. Efficacy of sildenafil citrate for the treatment of erectile dysfunction in men taking serotonin reuptake inhibitors. Am J Psychiatry 2001;158:1926-8.
23. Shrivastava RK, Shrivastava S, Overweg N, Schmitt M. Amantadine in the treatment of sexual dysfunction associated with selective serotonin reuptake inhibitors. J Clin Psychopharmacol 1995;15:83-4.
24. Worthington JJ, 3rd, Simon NM, Korbly NB, et al. Ropinirole for antidepressant-induced sexual dysfunction. Int Clin Psychopharmacol 2002;17:307-10.
25. Gross MD. Reversal by bethanechol of sexual dysfunction caused by anticholinergic antidepressants. Am J Psychiatry 1982;139:1193-4.
26. Yager J. Bethanechol chloride can reverse erectile and ejaculatory dysfunction induced by tricyclic antidepressants and mazindol: case report. J Clin Psychiatry 1986;47:210-11.
1. National Institutes of Health consensus conference on impotence. JAMA 1993;270:83-90.
2. Montejo-Gonzalez AL, Llorca G, Izquierdo JA, et al. SSRI-induced sexual dysfunction: fluoxetine, paroxetine, sertraline, and fluvoxamine in a prospective, multicenter, and descriptive clinical study of 344 patients. J Sex Marital Ther 1997;23:176-94.
3. Harrison WM, Rabkin JG, Ehrhardt AA, et al. Effects of antidepressant medication on sexual function: a controlled study. J Clin Psychopharmacol 1986;6:144-9.
4. Benazzi F, Mazzoli M. Fluoxetine-induced sexual dysfunction: a dose-dependent effect? Pharmacopsychiatry 1994;27:246.-
5. Clinical management of depression: bupropion—an update. Monograph series, vol.1, no. 1. Proceedings of a closed symposium: Antidepressant drug therapy: bupropion—an update meeting, Boca Raton, FL, October 30-31, 1992.
6. Rothschild AJ. Selective serotonin reuptake inhibitor-induced sexual dysfunction: efficacy of a drug holiday. Am J Psychiatry 1995;152:1514-16.
7. Rosen RC, Lane RM, Menza M. Effects of SSRIs on sexual function: a critical review. J Clin Psychopharmacol 1999;19:67-85.
8. Waldinger MD, Hengeveld MW, Zwinderman AH, Olivier B. Effect of SSRI antidepressants on ejaculation: a double-blind, randomized, placebo-controlled study with fluoxetine, fluvoxamine, paroxetine, and sertraline. J Clin Psychopharmacol 1998;18:274-81.
9. Koutouvidis N, Pratikakis M, Fotiadou A. The use of mirtazapine in a group of 11 patients following poor compliance to selective serotonin reuptake inhibitor treatment due to sexual dysfunction. Int Clin Psychopharmacol 1999;14:253-5.
10. Gelenberg AJ, McGahuey C, Laukes C, et al. Mirtazapine substitution in SSRI-induced sexual dysfunction. J Clin Psychiatry 2000;61:356-60.
11. Segraves RT, Kavoussi R, Hughes AR, et al. Evaluation of sexual functioning in depressed outpatients: a double-blind comparison of sustained-release bupropion and sertraline treatment. J Clin Psychopharmacol 2000;20:122-8.
12. Masand PS, Ashton AK, Gupta S, Frank B. Sustained-release bupropion for selective serotonin reuptake inhibitor-induced sexual dysfunction: a randomized, double-blind, placebo-controlled, parallel-group study. Am J Psychiatry 2001;158:805-7.
13. Farah A. Relief of SSRI-induced sexual dysfunction with mirtazapine treatment. J Clin Psychiatry 1999;60:260-1.
14. Smith SM, O’Keane V, Murray R. Sexual dysfunction in patients taking conventional antipsychotic medication. Br J Psychiatry 2002;181:49-55.
15. Kotin J, Wilbert DE, Verburg D, Soldinger SM. Thioridazine and sexual dysfunction. Am J Psychiatry 1976;133:82-5.
16. Guthrie SK. Clinical issues associated with maintenance treatment of patients with schizophrenia. Am J Health-Syst Pharm 2002;59(suppl 5):519-24.
17. Goodnick PJ, Rodriguez L, Santana O. Antipsychotics: impact on prolactin levels. Expert Opin Pharmacother 2002;3:1381-91.
18. Brunet M, Rodamilans M, Martinez-Osaba MJ, et al. Effects of long-term antiepileptic therapy on the catabolism of testosterone. Pharmacol Toxicol 1995;76:371-5.
19. Heroz AG, Levesque LA, Drislane FW, et al. Phenytoin-induced elevation of serum estradiol and reproductive dysfunction in men with epilepsy. Epilepsia 1991;32:550-3.
20. Husain AM, Carwile ST, Miller PP, Radtke RA. Improved sexual function in three men taking lamotrigine for epilepsy. South Med J 2000;93:335-6.
21. Nurnberg HG, Hensley PL, Gelenberg AJ, et al. Treatment of antidepressant-associated sexual dysfunction with sildenafil. A randomized controlled trial. JAMA 2003;289:56-64.
22. Nurnberg HG, Gelenberg A, Hargreave TB, et al. Efficacy of sildenafil citrate for the treatment of erectile dysfunction in men taking serotonin reuptake inhibitors. Am J Psychiatry 2001;158:1926-8.
23. Shrivastava RK, Shrivastava S, Overweg N, Schmitt M. Amantadine in the treatment of sexual dysfunction associated with selective serotonin reuptake inhibitors. J Clin Psychopharmacol 1995;15:83-4.
24. Worthington JJ, 3rd, Simon NM, Korbly NB, et al. Ropinirole for antidepressant-induced sexual dysfunction. Int Clin Psychopharmacol 2002;17:307-10.
25. Gross MD. Reversal by bethanechol of sexual dysfunction caused by anticholinergic antidepressants. Am J Psychiatry 1982;139:1193-4.
26. Yager J. Bethanechol chloride can reverse erectile and ejaculatory dysfunction induced by tricyclic antidepressants and mazindol: case report. J Clin Psychiatry 1986;47:210-11.
Update on eating disorders Anorexia nervosa: Dual therapy can bring patients back from the brink
Ms. J started losing weight deliberately at age 14 while attending boarding school. She lost 25 lbs by jogging 6 miles per day, exercising another 2 hours, avoiding meat, abusing laxatives, and drinking large quantities of coffee.
She was referred to a school counselor because of her weight loss and returned home. She was happier at a local high school and recovered to normal weight. In college, however, she reverted to compulsive exercising and preoccupation with her weight after the break-up of her first intimate relationship.
Now at age 22, Ms. J has persistently failed to gain weight during outpatient therapy for anorexia nervosa. At 5′7″ she weighs 98 lbs. On the day she was to be hospitalized involuntarily, she took 25 diphenhydramine tablets, which her psychiatrist viewed as a suicide threat. The overdose was treated in the emergency room with ipecac syrup, and she was admitted for inpatient eating disorder treatment.
Like Ms. J, patients with anorexia nervosa resist treatment and deny having most diagnostic signs and symptoms. Based on the evidence and my 30 years of treating anorectic patients,1 this article offers suggestions to help you:
- gather accurate histories from patients and their families
- identify common psychiatric comorbidities
- gain the patient’s trust during treatment
- provide effective dual therapy, with cognitive-behavioral and pharmacologic components.
Table 1
Diagnostic criteria for anorexia nervosa
| Underweight (<85% of normal for age and height) |
| Fear of gaining weight or becoming fat, even though underweight |
| Disturbed conceptualization of body shape and weight, denial of seriousness of low body weight, or overemphasis on body shape and weight in self-evaluation |
Amenorrhea. Subtypes:
|
| Source: Adapted with permission from Diagnostic and statistical manual of mental disorders (4th ed. text revision). |
| Copyright 2000 American Psychiatric Association. |
Making the diagnosis
Anorexia nervosa is characterized by underweight, fear of gaining weight, disturbed body concept, and amenorrhea (Table 1). Its core psychological symptoms have been described as:
- relentless pursuit of thinness
- denial of cachexia
- and feelings of general ineffectiveness.2
The patient may say she feels fat even though emaciated or that parts of her body are too large. This disturbed experience of body weight or shape may represent sublimation and displacement for feelings of inadequacy. Because anorectic patients stay thin so effectively, they may feel a sense of accomplishment by evaluating themselves in terms of their thinness. Cognitive therapy focuses on correcting patients’ pervasive sense of inadequacy, as manifest in maturity fears and lack of confidence in coping with life’s problems.3
Subtypes. Anorexia nervosa has two subtypes—restricting and binge eating/purging—that differ in behavioral and medical symptoms.4 Patients with binge eating/purging show:
- higher rates of impulsivity (suicide attempts, self-mutilation, stealing, and alcohol and other substance abuse)
- more-prevalent impulsive personality disorders (borderline personality disorder, hysterical personality disorder)
- medical problems caused by purging.
Restricting-type patients are often dependent and submissive, with difficulty separating from parents. These patients may be preoccupied with orderliness, perfectionism, and control.
Recommendation. A structured interview to diagnose anorexia nervosa is summarized in Table 2. Because the patient will likely deny her symptoms, it is usually necessary to also interview family members or close friends.
Psychiatric comorbidity
Case report continued: A ‘perfectionist.’
School for Ms. J required great effort, and she spent many hours studying. Her upper-middle-class parents described her as “a perfectionist.” The family placed considerable emphasis on doing the “correct” thing.
During adolescence, Ms. J developed a major depressive episode that lasted 4 months. She also developed obsessions and compulsions unrelated to her eating disorder. She obsessively ruminated about the correct things to say in social circumstances and devoted 4 hours per day to cleaning and checking compulsions. She felt she had to wash her car every time before going out; if she could not, she would cancel her social plans.
Table 2
Diagnosis of anorexia nervosa: Questions to ask*
| Weight history | -What was her highest weight and lowest weight (after weight loss) -At what ages did these weights occur? -Ask about her present weight before you weigh her |
| Eating behavior | -What does she eat and when from morning awakening to bedtime? -Does she eat with the family less often than in the past? -Is she binging? |
| Purging behavior | -Is she inducing vomiting? -Is she using laxatives, diuretics, ipecac, or enemas? |
| Preoccupations and rituals concerning food and weight | -Does she constantly count calories and express concern about fat content in foods? -Does she often gaze in the mirror and comment about being fat? -How often does she weigh herself? -Does she express fear of being unable to stop eating? |
| Activity | -Is she jogging, bike riding, or doing aerobics? -How often, and for how long? -Is she overactive at home, such as pacing? |
| Menstrual history | -At what age did menses begin? -What was the date of her last period? -How regular is her cycle? |
| Psychiatric comorbidity | -Does she have symptoms of depression? -Impulsive behavior (suicide attempts or self-mutilation)? -Drug or alcohol abuse? -Anxiety (obsessive-compulsive behaviors, social phobia, generalized anxiety, fearfulness)? -Personality disorders? |
| * Because patients with anorexia nervosa often deny their symptoms and conceal their food intake, it is usually necessary to interview family members or close friends as well as the patient. | |
In college, she began abusing alcohol and was arrested once for driving while intoxicated.
Depression is the most common comorbidity in anorexia nervosa. Two-thirds of anorectic patients in a 10-year follow-up study reported a history of major depressive disorder.5 Suicide, starvation, and electrolyte imbalance are the three major causes of death. Among severely ill patients who require hospitalization, 10% to 20% die, though the suicide rate is undocumented.
Compulsions. Anorectics’ preoccupations about food and eating rituals have been compared with compulsions, though less than 20% of patients meet diagnostic criteria for obsessive-compulsive disorder.6
Substance abuse. Bulimic anorectics report more alcohol and substance use and abuse than restricting anorectics.7 The most common substances of abuse are cannabis, cocaine, stimulants, and over-the-counter pills such as diet aids.
Personality disorders. Up to 50% of patients with anorexia nervosa—particularly the binge/purge subtype—have personality disorders. Borderline personality disorder is especially common among binge/purge types,8 and avoidant personality disorder is more common among restricting types.
Table 3
Diagnostic signs of emaciation and purging in patients with anorexia nervosa
Emaciation
|
Purging
|
Personality disorders usually reflect instability in interpersonal relationships, poor self-image, or fluctuating affect. Patients may show a pattern of social inhibition, feelings of inadequacy, and hypersensitivity to negative evaluation.
Sexuality. Psychosocial and sexual development is often delayed in adolescent anorectics. In adults, interest in sex often plummets with anorexia onset, although binge/purge-type patients occasionally become promiscuous.
Medical signs
Case report continued: Abnormal ECG.
Ms. J was hospitalized after her weight dropped below 75% of normal for her age, height, and body build. She showed signs of electrolyte disturbance, including severe bradycardia (pulse rate 40) and ST-segment abnormalities on ECG.
Clinical signs of emaciation and purging can assist with diagnosis and in making decisions about medical treatment, including hospitalization (Table 3). Patients who purge are often weak and have puffy cheeks or parotid gland enlargement. They may have fainting spells and scars on their hands from stimulating vomiting. Laxative abuse may decrease colon motility and worsen constipation.
Neuroendocrine changes secondary to dieting and weight loss include:
- increased corticotropin-releasing hormone secretion
- blunted diurnal cortisol fluctuation
- decreased follicle-stimulating hormone (FSH) secretion
- impaired growth hormone regulation
- decreased luteinizing hormone (LH) secretion
- mildly decreased triiodothyronine
- erratic vasopressin secretion.
Measuring these changes is unnecessary, as general nutritional rehabilitation with weight gain will correct them.
Neurotransmitter function. Emaciated anorectics have a blunted response to pharmacologic probes for dopamine, reduced CSF norepinephrine turnover, and decreased CSF serotonin. Neuroimaging studies suggest that serotonin dysfunction may persist after weight is restored, although these findings require replication.
Treatment priorities
Effective therapies. Open studies indicate that multidimensional treatment—medical management, psychoeducation, and individual cognitive-behavioral therapy (CBT)—is most effective for anorexia nervosa. The fewer than 10 controlled trials that address anorexia nervosa treatment show:
- the more severe the illness, the more intense the treatment required
- outpatient therapy is most successful in patients who have had the illness <6 months, are not binging and vomiting, and have parents who participate in family therapy.
Hospitalization. An emaciated patient who is irritable, depressed, preoccupied with food, and sleep-deprived is unlikely to make progress toward behavioral change. The first goal, therefore, is to restore her nutritional state to normal.
Severely ill anorectic patients require hospitalization for daily monitoring of weight, calorie intake, urine output, and serum electrolytes and amylase (to assess purging behavior). Hospitalization is indicated for:
- loss of >20% of normal weight for age, height, and bone structure
- >6 months of repeated hospitalizations and underweight
- psychotic depression or serious suicide attempt
- incapacitating obsessions and compulsions, related or not to the eating disorder
- serious comorbid medical conditions, such as edema, hypoproteinemia, severe anemia, cardiac arrhythmia, or hypokalemic alkalosis (serum K+ < 2.5 mEq/L).
Keeping a patient in the hospital long enough to provide effective medical and psychological therapy has become difficult, however, because of medical insurance restrictions (Box). The result: poorer outcomes and increased relapse rates compared with 10 years ago.9-12
Hospital treatment of eating disorders has shifted from long-term care of a chronic disorder to stabilization of acute episodes. For some patients, this change has been deleterious and not cost-effective.
A decade ago, eating disorder hospitalizations were covered primarily by private insurance. Today, health maintenance organizations, managed care oversight of private insurance, and public funding are the primary sources of payment. These insurers often limit payment for eating disorder hospitalization, the most costly aspect of psychiatric care.
Poor outcomes and a high relapse rate have been documented in anorexia nervosa patients who left the hospital while underweight.9-11 From 1984 to 1998:
- average hospital stays for anorexia nervosa decreased from 150 days to 23.7 days
- readmissions increased from 0% to 27% of total admissions
- anorectic patients’ average body mass index at discharge dropped from 19.3 to 17.7, a statistically significant difference.12
For psychiatrists, this trend means many outpatients with anorexia nervosa will require repeated hospitalizations that will not substantially improve their anorectic behaviors.
Nutritional rehabilitation and behavior changes can often correct the medical complications of emaciation and purging. Lost bone density is seldom restored, but nutritional rehabilitation can prevent further bone loss.13 Women who remain amenorrheic for several years after weight restoration tend to be more psychologically disturbed than those who resume menses rapidly.14
Cognitive-behavioral therapy
Other authors have discussed CBT for anorexia nervosa.3,15 In general, the key tasks—operationalizing beliefs, evaluating autonomic thoughts, testing prospective hypotheses, and examining underlying assumptions—are accomplished by assessing anorexia’s distorted cognitions. No satisfactory controlled studies have examined any other type of individual psychotherapy for treating anorexia nervosa.
Alliance building. Patients with anorexia find it difficult to participate in therapeutic relationships. They are terrified of gaining weight and readily drop out of treatment. To build a therapeutic alliance:
- begin by helping the patient develop a history of her significant life events
- proceed slowly, praising her for every small attempt at changing her behavior
- set realistic therapy goals, considering her degree of resistance.
Monitoring. Behavior therapy consists primarily of positive reinforcements for weight gain. For this, we weigh outpatients weekly and inpatients daily. Outpatients are taught to keep diaries of daily food intake, stressful events, and emotional responses to them. The therapist begins each session by examining the patient’s diary with her and discussing how life events affect her eating behavior.
Cognitive restructuring helps patients identify their disturbed cognitions and challenge core beliefs about self-image. In this process, they become aware of their negative thoughts and develop arguments and evidence to support and refute the thoughts’ validity. They then form a reasoned conclusion based on the evidence.
Even if patients do not accept this logical conclusion, we encourage them to behave as if they believe it to be true. By doing this repeatedly, they eventually obtain some symptom relief.
Response-prevention techniques can help stop binging and purging. For example, we may require inpatients to sit together for 1 hour after eating. Because most patients will not vomit in front of each other, they learn how to resist vomiting and eventually experience reduced anxiety without vomiting after a meal.
Problem solving helps patients to reason through difficult food-related or interpersonal situations. The patient states the problem, then generates as many solutions as possible with the therapist’s assistance. She chooses one solution and puts it into effect, usually for 1 week. She then discusses the results with her therapist and decides whether to try another solution.
Family therapy. A family analysis—including a brief psychiatric history and evaluation of interactions—is recommended for all patients who live at home. This analysis can help you decide what type of family therapy or counseling to recommend.
Some families respond well with the parents and patient together in therapy sessions, whereas others are more comfortable with separate counseling. In a recent controlled study, anorectic patients younger than age 18 did equally well whether they were counseled with the family or separately.16
Brief therapy sessions are sometimes the most effective method to address family issues. When this is not possible, you and the patient can discuss family relationships in individual therapy.
Medications
Many medications have been used to treat anorexia nervosa, though few randomized, placebo-controlled studies exist. Because evidence does not support using psychotropics as monotherapy for anorexia nervosa, medication is considered adjunctive to CBT.
Chlorpromazine can help the hospitalized, severely ill patient who is overwhelmed with uncontrollable behavioral rituals and thoughts of losing weight. This antipsychotic helps reduce anorectic preoccupations and anxiety and helps make patients more amenable to therapy.
Start chlorpromazine at 10 mg tid and increase gradually until the patient can eat without extreme anxiety. Usual maximum dosage is 50 mg tid. Monitor blood pressure, tardive dyskinesia, and decreased white blood cell count.
Olanzapine may help induce weight gain and reduce anxiety in anorectic patients.17 Controlled and open-label studies are under way.
We start olanzapine at 2.5 mg/d and increase gradually to 10 or 15 mg/d. At this dosage, patients’ anxiety about eating is usually substantially reduced. Sedation is the most common side effect.
Anorexia patients often refuse to take olanzapine for fear of weight gain. If a patient’s emaciation is life-threatening, we may seek court permission to medicate her involuntarily. We reassure her that we will discontinue olanzapine when she reaches her target weight.
Serotonin in anorexia. Central serotonin pathways modulate feeding behavior. Serotonin antagonists—such as cyproheptadine—increase food intake and weight gain, whereas serotonin agonists—such as selective serotonin reuptake inhibitors (SSRIs)—decrease food intake.
Serotonin pathways also may modulate obsessive-compulsive and impulsive behaviors. Both serotonin agonists and antagonists can be useful adjuncts in treating anorexia nervosa.
In a double-blind, placebo-controlled trial, cyproheptadine, 4 to 8 mg tid, was associated with weight gain and reduced depressive symptoms in anorexia nervosa patients.18 Unlike tricyclic antidepressants, cyproheptadine does not reduce blood pressure or increase heart rate, which makes it attractive for emaciated anorectic patients. Dosages up to 28 mg/d can be used safely.
The SSRI fluoxetine may help prevent weight loss relapse in anorexia nervosa and reduce obsessive-compulsive behaviors.19 In open studies of low-weight anorectics, however, fluoxetine had little impact on weight or other clinically meaningful variables.20 Thus, this agent is recommended for preventing weight-loss relapse only in patients who are within 10% to 15% of ideal body weight.
Outpatient care
Case report continued: Ongoing therapy
During hospitalization, Ms. J participated in all therapeutic modalities but had difficulty eating enough to gain weight. She reached her target weight of 127 lbs in about 7 weeks but gained no sense of purpose in life.
She is starting an intensive outpatient program using CBT to maintain her weight and further address the core psychopathology of her illness. Her maintenance therapy includes attending Alcoholics Anonymous meetings, ongoing fluoxetine (20 mg/d) to prevent weight-loss relapse, and CBT for obsessions and compulsions not related to her eating disorder.
Related resources
- Halmi KA. Eating disorders: Anorexia, bulimia nervosa and obesity. In: Hales RE, Yudofsky SC (eds). Textbook of clinical psychiatry, 4th ed. Washington, DC: American Psychiatric Publishing, 2003:1001-21.
- Academy of Eating Disorders. www.aedweb.org
- Anorexia Nervosa & Associated Disorders (ANAD). www.anad.org
Drug brand names
- Chlorpromazine • Thorazine
- Cyproheptadine • Periactin
- Fluoxetine • Prozac
- Olanzapine • Zyprexa
Disclosure
The author reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Halmi KA. Anorexia nervosa: demographic and clinical features in 94 cases. Psychosom Med 1974;36:18-24.
2. Bruch AH. Eating disorders: obesity, anorexia nervosa, and the person within. New York, Basic books, 1973.
3. Kleifield E, Wagner S, Halmi KA. Cognitive behavioral treatment of anorexia nervosa. Psychiatr Clin North Am 1996;19:715-34.
4. Halmi KA. Eating disorders. In: Martin A, Scahill L, Charney DS Leckman JF (eds). Pediatric pharmacology. New York: Oxford University Press, 2002;592-602.
5. Halmi KA, Eckert E, Marci P, Cohen J. Comorbidity of psychiatric diagnoses in anorexia nervosa. Arch Gen Psychiatry 1991;48:712-18.
6. Braun DL, Sunday SR, Halmi KA. Psychiatric comorbidity in patients with eating disorders. Psychol Med 1994;24:859-67.
7. Holderness CC, Brooks-Gunn J, Warren MP. Comorbidity of eating disorders and substance abuse review of the literature. Int J Eat Disord 1994;16:1-34.
8. Herzog DB, Keller M, Lavori P. The prevalence of personality disorders in 210 women with eating disorders. J Clin Psychiatry 1992;53:147-52.
9. Baran S, Weltzin T, Kaye W. Low discharge weight and outcome in anorexia nervosa. Am J Psychiatry 1995;150:1070-2.
10. Commerford MC, Licinio J, Halmi KA. Guidelines for discharging eating disorder patients. Eat Disord 1997;5:69-74.
11. Howard W, Evans K, Quinter-Howard C, et al. Predictors of success or failure of transition to day hospital treatment for inpatients with anorexia nervosa. Am J Psychiatry 1999;156:1697-1702.
12. Wiseman C, Sunday SR, Klapper F, et al. Changing patterns of hospitalization in eating disorder patients. Int J Eat Disord 2001;30:69-74.
13. Newman M, Halmi KA. The relationship of bone density to estradiol and cortisol in anorexia nervosa and bulimia nervosa. Psychiatr Res 1989;29:105-12.
14. Falk JR, Halmi KA. Amenorrhea in anorexia nervosa: examination of the critical body hypothesis. Biol Psychiatr 1982;17:799-806.
15. Garner DM, Bemis KM. A cognitive-behavioral approach to anorexia nervosa. Cognit Ther Res 1982;6:1223-50.
16. Dare C. Eisler. Family therapy and eating disorders. In: Fairburn CR, Brownell KD (eds). Eating disorders and obesity. New York: Guilford Press, 2002;314-19.
17. Powers P, Santana CA, Bannon YS. Olanzapine in the treatment of anorexia nervosa: an open label trial. Int J Eat Disord 2002;32:146-54.
18. Halmi KA, Eckert ED, Ladu T, Cohen J. Anorexia nervosa: treatment efficacy of cyproheptadine and amitriptyline. Arch Gen Psychiatry 1986;43:177-81.
19. Kaye W. The use of fluoxetine to prevent relapse in anorexia nervosa (presentation). Pittsburgh, PA: Eating Disorder Research Society annual meeting, 1996.
20. Ferguson C, Lavia M, Crossan P. Are serotonin selective reuptake inhibitors effective in underweight anorexia nervosa? Int J Eat Disord 1999;25:11-17.
Ms. J started losing weight deliberately at age 14 while attending boarding school. She lost 25 lbs by jogging 6 miles per day, exercising another 2 hours, avoiding meat, abusing laxatives, and drinking large quantities of coffee.
She was referred to a school counselor because of her weight loss and returned home. She was happier at a local high school and recovered to normal weight. In college, however, she reverted to compulsive exercising and preoccupation with her weight after the break-up of her first intimate relationship.
Now at age 22, Ms. J has persistently failed to gain weight during outpatient therapy for anorexia nervosa. At 5′7″ she weighs 98 lbs. On the day she was to be hospitalized involuntarily, she took 25 diphenhydramine tablets, which her psychiatrist viewed as a suicide threat. The overdose was treated in the emergency room with ipecac syrup, and she was admitted for inpatient eating disorder treatment.
Like Ms. J, patients with anorexia nervosa resist treatment and deny having most diagnostic signs and symptoms. Based on the evidence and my 30 years of treating anorectic patients,1 this article offers suggestions to help you:
- gather accurate histories from patients and their families
- identify common psychiatric comorbidities
- gain the patient’s trust during treatment
- provide effective dual therapy, with cognitive-behavioral and pharmacologic components.
Table 1
Diagnostic criteria for anorexia nervosa
| Underweight (<85% of normal for age and height) |
| Fear of gaining weight or becoming fat, even though underweight |
| Disturbed conceptualization of body shape and weight, denial of seriousness of low body weight, or overemphasis on body shape and weight in self-evaluation |
Amenorrhea. Subtypes:
|
| Source: Adapted with permission from Diagnostic and statistical manual of mental disorders (4th ed. text revision). |
| Copyright 2000 American Psychiatric Association. |
Making the diagnosis
Anorexia nervosa is characterized by underweight, fear of gaining weight, disturbed body concept, and amenorrhea (Table 1). Its core psychological symptoms have been described as:
- relentless pursuit of thinness
- denial of cachexia
- and feelings of general ineffectiveness.2
The patient may say she feels fat even though emaciated or that parts of her body are too large. This disturbed experience of body weight or shape may represent sublimation and displacement for feelings of inadequacy. Because anorectic patients stay thin so effectively, they may feel a sense of accomplishment by evaluating themselves in terms of their thinness. Cognitive therapy focuses on correcting patients’ pervasive sense of inadequacy, as manifest in maturity fears and lack of confidence in coping with life’s problems.3
Subtypes. Anorexia nervosa has two subtypes—restricting and binge eating/purging—that differ in behavioral and medical symptoms.4 Patients with binge eating/purging show:
- higher rates of impulsivity (suicide attempts, self-mutilation, stealing, and alcohol and other substance abuse)
- more-prevalent impulsive personality disorders (borderline personality disorder, hysterical personality disorder)
- medical problems caused by purging.
Restricting-type patients are often dependent and submissive, with difficulty separating from parents. These patients may be preoccupied with orderliness, perfectionism, and control.
Recommendation. A structured interview to diagnose anorexia nervosa is summarized in Table 2. Because the patient will likely deny her symptoms, it is usually necessary to also interview family members or close friends.
Psychiatric comorbidity
Case report continued: A ‘perfectionist.’
School for Ms. J required great effort, and she spent many hours studying. Her upper-middle-class parents described her as “a perfectionist.” The family placed considerable emphasis on doing the “correct” thing.
During adolescence, Ms. J developed a major depressive episode that lasted 4 months. She also developed obsessions and compulsions unrelated to her eating disorder. She obsessively ruminated about the correct things to say in social circumstances and devoted 4 hours per day to cleaning and checking compulsions. She felt she had to wash her car every time before going out; if she could not, she would cancel her social plans.
Table 2
Diagnosis of anorexia nervosa: Questions to ask*
| Weight history | -What was her highest weight and lowest weight (after weight loss) -At what ages did these weights occur? -Ask about her present weight before you weigh her |
| Eating behavior | -What does she eat and when from morning awakening to bedtime? -Does she eat with the family less often than in the past? -Is she binging? |
| Purging behavior | -Is she inducing vomiting? -Is she using laxatives, diuretics, ipecac, or enemas? |
| Preoccupations and rituals concerning food and weight | -Does she constantly count calories and express concern about fat content in foods? -Does she often gaze in the mirror and comment about being fat? -How often does she weigh herself? -Does she express fear of being unable to stop eating? |
| Activity | -Is she jogging, bike riding, or doing aerobics? -How often, and for how long? -Is she overactive at home, such as pacing? |
| Menstrual history | -At what age did menses begin? -What was the date of her last period? -How regular is her cycle? |
| Psychiatric comorbidity | -Does she have symptoms of depression? -Impulsive behavior (suicide attempts or self-mutilation)? -Drug or alcohol abuse? -Anxiety (obsessive-compulsive behaviors, social phobia, generalized anxiety, fearfulness)? -Personality disorders? |
| * Because patients with anorexia nervosa often deny their symptoms and conceal their food intake, it is usually necessary to interview family members or close friends as well as the patient. | |
In college, she began abusing alcohol and was arrested once for driving while intoxicated.
Depression is the most common comorbidity in anorexia nervosa. Two-thirds of anorectic patients in a 10-year follow-up study reported a history of major depressive disorder.5 Suicide, starvation, and electrolyte imbalance are the three major causes of death. Among severely ill patients who require hospitalization, 10% to 20% die, though the suicide rate is undocumented.
Compulsions. Anorectics’ preoccupations about food and eating rituals have been compared with compulsions, though less than 20% of patients meet diagnostic criteria for obsessive-compulsive disorder.6
Substance abuse. Bulimic anorectics report more alcohol and substance use and abuse than restricting anorectics.7 The most common substances of abuse are cannabis, cocaine, stimulants, and over-the-counter pills such as diet aids.
Personality disorders. Up to 50% of patients with anorexia nervosa—particularly the binge/purge subtype—have personality disorders. Borderline personality disorder is especially common among binge/purge types,8 and avoidant personality disorder is more common among restricting types.
Table 3
Diagnostic signs of emaciation and purging in patients with anorexia nervosa
Emaciation
|
Purging
|
Personality disorders usually reflect instability in interpersonal relationships, poor self-image, or fluctuating affect. Patients may show a pattern of social inhibition, feelings of inadequacy, and hypersensitivity to negative evaluation.
Sexuality. Psychosocial and sexual development is often delayed in adolescent anorectics. In adults, interest in sex often plummets with anorexia onset, although binge/purge-type patients occasionally become promiscuous.
Medical signs
Case report continued: Abnormal ECG.
Ms. J was hospitalized after her weight dropped below 75% of normal for her age, height, and body build. She showed signs of electrolyte disturbance, including severe bradycardia (pulse rate 40) and ST-segment abnormalities on ECG.
Clinical signs of emaciation and purging can assist with diagnosis and in making decisions about medical treatment, including hospitalization (Table 3). Patients who purge are often weak and have puffy cheeks or parotid gland enlargement. They may have fainting spells and scars on their hands from stimulating vomiting. Laxative abuse may decrease colon motility and worsen constipation.
Neuroendocrine changes secondary to dieting and weight loss include:
- increased corticotropin-releasing hormone secretion
- blunted diurnal cortisol fluctuation
- decreased follicle-stimulating hormone (FSH) secretion
- impaired growth hormone regulation
- decreased luteinizing hormone (LH) secretion
- mildly decreased triiodothyronine
- erratic vasopressin secretion.
Measuring these changes is unnecessary, as general nutritional rehabilitation with weight gain will correct them.
Neurotransmitter function. Emaciated anorectics have a blunted response to pharmacologic probes for dopamine, reduced CSF norepinephrine turnover, and decreased CSF serotonin. Neuroimaging studies suggest that serotonin dysfunction may persist after weight is restored, although these findings require replication.
Treatment priorities
Effective therapies. Open studies indicate that multidimensional treatment—medical management, psychoeducation, and individual cognitive-behavioral therapy (CBT)—is most effective for anorexia nervosa. The fewer than 10 controlled trials that address anorexia nervosa treatment show:
- the more severe the illness, the more intense the treatment required
- outpatient therapy is most successful in patients who have had the illness <6 months, are not binging and vomiting, and have parents who participate in family therapy.
Hospitalization. An emaciated patient who is irritable, depressed, preoccupied with food, and sleep-deprived is unlikely to make progress toward behavioral change. The first goal, therefore, is to restore her nutritional state to normal.
Severely ill anorectic patients require hospitalization for daily monitoring of weight, calorie intake, urine output, and serum electrolytes and amylase (to assess purging behavior). Hospitalization is indicated for:
- loss of >20% of normal weight for age, height, and bone structure
- >6 months of repeated hospitalizations and underweight
- psychotic depression or serious suicide attempt
- incapacitating obsessions and compulsions, related or not to the eating disorder
- serious comorbid medical conditions, such as edema, hypoproteinemia, severe anemia, cardiac arrhythmia, or hypokalemic alkalosis (serum K+ < 2.5 mEq/L).
Keeping a patient in the hospital long enough to provide effective medical and psychological therapy has become difficult, however, because of medical insurance restrictions (Box). The result: poorer outcomes and increased relapse rates compared with 10 years ago.9-12
Hospital treatment of eating disorders has shifted from long-term care of a chronic disorder to stabilization of acute episodes. For some patients, this change has been deleterious and not cost-effective.
A decade ago, eating disorder hospitalizations were covered primarily by private insurance. Today, health maintenance organizations, managed care oversight of private insurance, and public funding are the primary sources of payment. These insurers often limit payment for eating disorder hospitalization, the most costly aspect of psychiatric care.
Poor outcomes and a high relapse rate have been documented in anorexia nervosa patients who left the hospital while underweight.9-11 From 1984 to 1998:
- average hospital stays for anorexia nervosa decreased from 150 days to 23.7 days
- readmissions increased from 0% to 27% of total admissions
- anorectic patients’ average body mass index at discharge dropped from 19.3 to 17.7, a statistically significant difference.12
For psychiatrists, this trend means many outpatients with anorexia nervosa will require repeated hospitalizations that will not substantially improve their anorectic behaviors.
Nutritional rehabilitation and behavior changes can often correct the medical complications of emaciation and purging. Lost bone density is seldom restored, but nutritional rehabilitation can prevent further bone loss.13 Women who remain amenorrheic for several years after weight restoration tend to be more psychologically disturbed than those who resume menses rapidly.14
Cognitive-behavioral therapy
Other authors have discussed CBT for anorexia nervosa.3,15 In general, the key tasks—operationalizing beliefs, evaluating autonomic thoughts, testing prospective hypotheses, and examining underlying assumptions—are accomplished by assessing anorexia’s distorted cognitions. No satisfactory controlled studies have examined any other type of individual psychotherapy for treating anorexia nervosa.
Alliance building. Patients with anorexia find it difficult to participate in therapeutic relationships. They are terrified of gaining weight and readily drop out of treatment. To build a therapeutic alliance:
- begin by helping the patient develop a history of her significant life events
- proceed slowly, praising her for every small attempt at changing her behavior
- set realistic therapy goals, considering her degree of resistance.
Monitoring. Behavior therapy consists primarily of positive reinforcements for weight gain. For this, we weigh outpatients weekly and inpatients daily. Outpatients are taught to keep diaries of daily food intake, stressful events, and emotional responses to them. The therapist begins each session by examining the patient’s diary with her and discussing how life events affect her eating behavior.
Cognitive restructuring helps patients identify their disturbed cognitions and challenge core beliefs about self-image. In this process, they become aware of their negative thoughts and develop arguments and evidence to support and refute the thoughts’ validity. They then form a reasoned conclusion based on the evidence.
Even if patients do not accept this logical conclusion, we encourage them to behave as if they believe it to be true. By doing this repeatedly, they eventually obtain some symptom relief.
Response-prevention techniques can help stop binging and purging. For example, we may require inpatients to sit together for 1 hour after eating. Because most patients will not vomit in front of each other, they learn how to resist vomiting and eventually experience reduced anxiety without vomiting after a meal.
Problem solving helps patients to reason through difficult food-related or interpersonal situations. The patient states the problem, then generates as many solutions as possible with the therapist’s assistance. She chooses one solution and puts it into effect, usually for 1 week. She then discusses the results with her therapist and decides whether to try another solution.
Family therapy. A family analysis—including a brief psychiatric history and evaluation of interactions—is recommended for all patients who live at home. This analysis can help you decide what type of family therapy or counseling to recommend.
Some families respond well with the parents and patient together in therapy sessions, whereas others are more comfortable with separate counseling. In a recent controlled study, anorectic patients younger than age 18 did equally well whether they were counseled with the family or separately.16
Brief therapy sessions are sometimes the most effective method to address family issues. When this is not possible, you and the patient can discuss family relationships in individual therapy.
Medications
Many medications have been used to treat anorexia nervosa, though few randomized, placebo-controlled studies exist. Because evidence does not support using psychotropics as monotherapy for anorexia nervosa, medication is considered adjunctive to CBT.
Chlorpromazine can help the hospitalized, severely ill patient who is overwhelmed with uncontrollable behavioral rituals and thoughts of losing weight. This antipsychotic helps reduce anorectic preoccupations and anxiety and helps make patients more amenable to therapy.
Start chlorpromazine at 10 mg tid and increase gradually until the patient can eat without extreme anxiety. Usual maximum dosage is 50 mg tid. Monitor blood pressure, tardive dyskinesia, and decreased white blood cell count.
Olanzapine may help induce weight gain and reduce anxiety in anorectic patients.17 Controlled and open-label studies are under way.
We start olanzapine at 2.5 mg/d and increase gradually to 10 or 15 mg/d. At this dosage, patients’ anxiety about eating is usually substantially reduced. Sedation is the most common side effect.
Anorexia patients often refuse to take olanzapine for fear of weight gain. If a patient’s emaciation is life-threatening, we may seek court permission to medicate her involuntarily. We reassure her that we will discontinue olanzapine when she reaches her target weight.
Serotonin in anorexia. Central serotonin pathways modulate feeding behavior. Serotonin antagonists—such as cyproheptadine—increase food intake and weight gain, whereas serotonin agonists—such as selective serotonin reuptake inhibitors (SSRIs)—decrease food intake.
Serotonin pathways also may modulate obsessive-compulsive and impulsive behaviors. Both serotonin agonists and antagonists can be useful adjuncts in treating anorexia nervosa.
In a double-blind, placebo-controlled trial, cyproheptadine, 4 to 8 mg tid, was associated with weight gain and reduced depressive symptoms in anorexia nervosa patients.18 Unlike tricyclic antidepressants, cyproheptadine does not reduce blood pressure or increase heart rate, which makes it attractive for emaciated anorectic patients. Dosages up to 28 mg/d can be used safely.
The SSRI fluoxetine may help prevent weight loss relapse in anorexia nervosa and reduce obsessive-compulsive behaviors.19 In open studies of low-weight anorectics, however, fluoxetine had little impact on weight or other clinically meaningful variables.20 Thus, this agent is recommended for preventing weight-loss relapse only in patients who are within 10% to 15% of ideal body weight.
Outpatient care
Case report continued: Ongoing therapy
During hospitalization, Ms. J participated in all therapeutic modalities but had difficulty eating enough to gain weight. She reached her target weight of 127 lbs in about 7 weeks but gained no sense of purpose in life.
She is starting an intensive outpatient program using CBT to maintain her weight and further address the core psychopathology of her illness. Her maintenance therapy includes attending Alcoholics Anonymous meetings, ongoing fluoxetine (20 mg/d) to prevent weight-loss relapse, and CBT for obsessions and compulsions not related to her eating disorder.
Related resources
- Halmi KA. Eating disorders: Anorexia, bulimia nervosa and obesity. In: Hales RE, Yudofsky SC (eds). Textbook of clinical psychiatry, 4th ed. Washington, DC: American Psychiatric Publishing, 2003:1001-21.
- Academy of Eating Disorders. www.aedweb.org
- Anorexia Nervosa & Associated Disorders (ANAD). www.anad.org
Drug brand names
- Chlorpromazine • Thorazine
- Cyproheptadine • Periactin
- Fluoxetine • Prozac
- Olanzapine • Zyprexa
Disclosure
The author reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Ms. J started losing weight deliberately at age 14 while attending boarding school. She lost 25 lbs by jogging 6 miles per day, exercising another 2 hours, avoiding meat, abusing laxatives, and drinking large quantities of coffee.
She was referred to a school counselor because of her weight loss and returned home. She was happier at a local high school and recovered to normal weight. In college, however, she reverted to compulsive exercising and preoccupation with her weight after the break-up of her first intimate relationship.
Now at age 22, Ms. J has persistently failed to gain weight during outpatient therapy for anorexia nervosa. At 5′7″ she weighs 98 lbs. On the day she was to be hospitalized involuntarily, she took 25 diphenhydramine tablets, which her psychiatrist viewed as a suicide threat. The overdose was treated in the emergency room with ipecac syrup, and she was admitted for inpatient eating disorder treatment.
Like Ms. J, patients with anorexia nervosa resist treatment and deny having most diagnostic signs and symptoms. Based on the evidence and my 30 years of treating anorectic patients,1 this article offers suggestions to help you:
- gather accurate histories from patients and their families
- identify common psychiatric comorbidities
- gain the patient’s trust during treatment
- provide effective dual therapy, with cognitive-behavioral and pharmacologic components.
Table 1
Diagnostic criteria for anorexia nervosa
| Underweight (<85% of normal for age and height) |
| Fear of gaining weight or becoming fat, even though underweight |
| Disturbed conceptualization of body shape and weight, denial of seriousness of low body weight, or overemphasis on body shape and weight in self-evaluation |
Amenorrhea. Subtypes:
|
| Source: Adapted with permission from Diagnostic and statistical manual of mental disorders (4th ed. text revision). |
| Copyright 2000 American Psychiatric Association. |
Making the diagnosis
Anorexia nervosa is characterized by underweight, fear of gaining weight, disturbed body concept, and amenorrhea (Table 1). Its core psychological symptoms have been described as:
- relentless pursuit of thinness
- denial of cachexia
- and feelings of general ineffectiveness.2
The patient may say she feels fat even though emaciated or that parts of her body are too large. This disturbed experience of body weight or shape may represent sublimation and displacement for feelings of inadequacy. Because anorectic patients stay thin so effectively, they may feel a sense of accomplishment by evaluating themselves in terms of their thinness. Cognitive therapy focuses on correcting patients’ pervasive sense of inadequacy, as manifest in maturity fears and lack of confidence in coping with life’s problems.3
Subtypes. Anorexia nervosa has two subtypes—restricting and binge eating/purging—that differ in behavioral and medical symptoms.4 Patients with binge eating/purging show:
- higher rates of impulsivity (suicide attempts, self-mutilation, stealing, and alcohol and other substance abuse)
- more-prevalent impulsive personality disorders (borderline personality disorder, hysterical personality disorder)
- medical problems caused by purging.
Restricting-type patients are often dependent and submissive, with difficulty separating from parents. These patients may be preoccupied with orderliness, perfectionism, and control.
Recommendation. A structured interview to diagnose anorexia nervosa is summarized in Table 2. Because the patient will likely deny her symptoms, it is usually necessary to also interview family members or close friends.
Psychiatric comorbidity
Case report continued: A ‘perfectionist.’
School for Ms. J required great effort, and she spent many hours studying. Her upper-middle-class parents described her as “a perfectionist.” The family placed considerable emphasis on doing the “correct” thing.
During adolescence, Ms. J developed a major depressive episode that lasted 4 months. She also developed obsessions and compulsions unrelated to her eating disorder. She obsessively ruminated about the correct things to say in social circumstances and devoted 4 hours per day to cleaning and checking compulsions. She felt she had to wash her car every time before going out; if she could not, she would cancel her social plans.
Table 2
Diagnosis of anorexia nervosa: Questions to ask*
| Weight history | -What was her highest weight and lowest weight (after weight loss) -At what ages did these weights occur? -Ask about her present weight before you weigh her |
| Eating behavior | -What does she eat and when from morning awakening to bedtime? -Does she eat with the family less often than in the past? -Is she binging? |
| Purging behavior | -Is she inducing vomiting? -Is she using laxatives, diuretics, ipecac, or enemas? |
| Preoccupations and rituals concerning food and weight | -Does she constantly count calories and express concern about fat content in foods? -Does she often gaze in the mirror and comment about being fat? -How often does she weigh herself? -Does she express fear of being unable to stop eating? |
| Activity | -Is she jogging, bike riding, or doing aerobics? -How often, and for how long? -Is she overactive at home, such as pacing? |
| Menstrual history | -At what age did menses begin? -What was the date of her last period? -How regular is her cycle? |
| Psychiatric comorbidity | -Does she have symptoms of depression? -Impulsive behavior (suicide attempts or self-mutilation)? -Drug or alcohol abuse? -Anxiety (obsessive-compulsive behaviors, social phobia, generalized anxiety, fearfulness)? -Personality disorders? |
| * Because patients with anorexia nervosa often deny their symptoms and conceal their food intake, it is usually necessary to interview family members or close friends as well as the patient. | |
In college, she began abusing alcohol and was arrested once for driving while intoxicated.
Depression is the most common comorbidity in anorexia nervosa. Two-thirds of anorectic patients in a 10-year follow-up study reported a history of major depressive disorder.5 Suicide, starvation, and electrolyte imbalance are the three major causes of death. Among severely ill patients who require hospitalization, 10% to 20% die, though the suicide rate is undocumented.
Compulsions. Anorectics’ preoccupations about food and eating rituals have been compared with compulsions, though less than 20% of patients meet diagnostic criteria for obsessive-compulsive disorder.6
Substance abuse. Bulimic anorectics report more alcohol and substance use and abuse than restricting anorectics.7 The most common substances of abuse are cannabis, cocaine, stimulants, and over-the-counter pills such as diet aids.
Personality disorders. Up to 50% of patients with anorexia nervosa—particularly the binge/purge subtype—have personality disorders. Borderline personality disorder is especially common among binge/purge types,8 and avoidant personality disorder is more common among restricting types.
Table 3
Diagnostic signs of emaciation and purging in patients with anorexia nervosa
Emaciation
|
Purging
|
Personality disorders usually reflect instability in interpersonal relationships, poor self-image, or fluctuating affect. Patients may show a pattern of social inhibition, feelings of inadequacy, and hypersensitivity to negative evaluation.
Sexuality. Psychosocial and sexual development is often delayed in adolescent anorectics. In adults, interest in sex often plummets with anorexia onset, although binge/purge-type patients occasionally become promiscuous.
Medical signs
Case report continued: Abnormal ECG.
Ms. J was hospitalized after her weight dropped below 75% of normal for her age, height, and body build. She showed signs of electrolyte disturbance, including severe bradycardia (pulse rate 40) and ST-segment abnormalities on ECG.
Clinical signs of emaciation and purging can assist with diagnosis and in making decisions about medical treatment, including hospitalization (Table 3). Patients who purge are often weak and have puffy cheeks or parotid gland enlargement. They may have fainting spells and scars on their hands from stimulating vomiting. Laxative abuse may decrease colon motility and worsen constipation.
Neuroendocrine changes secondary to dieting and weight loss include:
- increased corticotropin-releasing hormone secretion
- blunted diurnal cortisol fluctuation
- decreased follicle-stimulating hormone (FSH) secretion
- impaired growth hormone regulation
- decreased luteinizing hormone (LH) secretion
- mildly decreased triiodothyronine
- erratic vasopressin secretion.
Measuring these changes is unnecessary, as general nutritional rehabilitation with weight gain will correct them.
Neurotransmitter function. Emaciated anorectics have a blunted response to pharmacologic probes for dopamine, reduced CSF norepinephrine turnover, and decreased CSF serotonin. Neuroimaging studies suggest that serotonin dysfunction may persist after weight is restored, although these findings require replication.
Treatment priorities
Effective therapies. Open studies indicate that multidimensional treatment—medical management, psychoeducation, and individual cognitive-behavioral therapy (CBT)—is most effective for anorexia nervosa. The fewer than 10 controlled trials that address anorexia nervosa treatment show:
- the more severe the illness, the more intense the treatment required
- outpatient therapy is most successful in patients who have had the illness <6 months, are not binging and vomiting, and have parents who participate in family therapy.
Hospitalization. An emaciated patient who is irritable, depressed, preoccupied with food, and sleep-deprived is unlikely to make progress toward behavioral change. The first goal, therefore, is to restore her nutritional state to normal.
Severely ill anorectic patients require hospitalization for daily monitoring of weight, calorie intake, urine output, and serum electrolytes and amylase (to assess purging behavior). Hospitalization is indicated for:
- loss of >20% of normal weight for age, height, and bone structure
- >6 months of repeated hospitalizations and underweight
- psychotic depression or serious suicide attempt
- incapacitating obsessions and compulsions, related or not to the eating disorder
- serious comorbid medical conditions, such as edema, hypoproteinemia, severe anemia, cardiac arrhythmia, or hypokalemic alkalosis (serum K+ < 2.5 mEq/L).
Keeping a patient in the hospital long enough to provide effective medical and psychological therapy has become difficult, however, because of medical insurance restrictions (Box). The result: poorer outcomes and increased relapse rates compared with 10 years ago.9-12
Hospital treatment of eating disorders has shifted from long-term care of a chronic disorder to stabilization of acute episodes. For some patients, this change has been deleterious and not cost-effective.
A decade ago, eating disorder hospitalizations were covered primarily by private insurance. Today, health maintenance organizations, managed care oversight of private insurance, and public funding are the primary sources of payment. These insurers often limit payment for eating disorder hospitalization, the most costly aspect of psychiatric care.
Poor outcomes and a high relapse rate have been documented in anorexia nervosa patients who left the hospital while underweight.9-11 From 1984 to 1998:
- average hospital stays for anorexia nervosa decreased from 150 days to 23.7 days
- readmissions increased from 0% to 27% of total admissions
- anorectic patients’ average body mass index at discharge dropped from 19.3 to 17.7, a statistically significant difference.12
For psychiatrists, this trend means many outpatients with anorexia nervosa will require repeated hospitalizations that will not substantially improve their anorectic behaviors.
Nutritional rehabilitation and behavior changes can often correct the medical complications of emaciation and purging. Lost bone density is seldom restored, but nutritional rehabilitation can prevent further bone loss.13 Women who remain amenorrheic for several years after weight restoration tend to be more psychologically disturbed than those who resume menses rapidly.14
Cognitive-behavioral therapy
Other authors have discussed CBT for anorexia nervosa.3,15 In general, the key tasks—operationalizing beliefs, evaluating autonomic thoughts, testing prospective hypotheses, and examining underlying assumptions—are accomplished by assessing anorexia’s distorted cognitions. No satisfactory controlled studies have examined any other type of individual psychotherapy for treating anorexia nervosa.
Alliance building. Patients with anorexia find it difficult to participate in therapeutic relationships. They are terrified of gaining weight and readily drop out of treatment. To build a therapeutic alliance:
- begin by helping the patient develop a history of her significant life events
- proceed slowly, praising her for every small attempt at changing her behavior
- set realistic therapy goals, considering her degree of resistance.
Monitoring. Behavior therapy consists primarily of positive reinforcements for weight gain. For this, we weigh outpatients weekly and inpatients daily. Outpatients are taught to keep diaries of daily food intake, stressful events, and emotional responses to them. The therapist begins each session by examining the patient’s diary with her and discussing how life events affect her eating behavior.
Cognitive restructuring helps patients identify their disturbed cognitions and challenge core beliefs about self-image. In this process, they become aware of their negative thoughts and develop arguments and evidence to support and refute the thoughts’ validity. They then form a reasoned conclusion based on the evidence.
Even if patients do not accept this logical conclusion, we encourage them to behave as if they believe it to be true. By doing this repeatedly, they eventually obtain some symptom relief.
Response-prevention techniques can help stop binging and purging. For example, we may require inpatients to sit together for 1 hour after eating. Because most patients will not vomit in front of each other, they learn how to resist vomiting and eventually experience reduced anxiety without vomiting after a meal.
Problem solving helps patients to reason through difficult food-related or interpersonal situations. The patient states the problem, then generates as many solutions as possible with the therapist’s assistance. She chooses one solution and puts it into effect, usually for 1 week. She then discusses the results with her therapist and decides whether to try another solution.
Family therapy. A family analysis—including a brief psychiatric history and evaluation of interactions—is recommended for all patients who live at home. This analysis can help you decide what type of family therapy or counseling to recommend.
Some families respond well with the parents and patient together in therapy sessions, whereas others are more comfortable with separate counseling. In a recent controlled study, anorectic patients younger than age 18 did equally well whether they were counseled with the family or separately.16
Brief therapy sessions are sometimes the most effective method to address family issues. When this is not possible, you and the patient can discuss family relationships in individual therapy.
Medications
Many medications have been used to treat anorexia nervosa, though few randomized, placebo-controlled studies exist. Because evidence does not support using psychotropics as monotherapy for anorexia nervosa, medication is considered adjunctive to CBT.
Chlorpromazine can help the hospitalized, severely ill patient who is overwhelmed with uncontrollable behavioral rituals and thoughts of losing weight. This antipsychotic helps reduce anorectic preoccupations and anxiety and helps make patients more amenable to therapy.
Start chlorpromazine at 10 mg tid and increase gradually until the patient can eat without extreme anxiety. Usual maximum dosage is 50 mg tid. Monitor blood pressure, tardive dyskinesia, and decreased white blood cell count.
Olanzapine may help induce weight gain and reduce anxiety in anorectic patients.17 Controlled and open-label studies are under way.
We start olanzapine at 2.5 mg/d and increase gradually to 10 or 15 mg/d. At this dosage, patients’ anxiety about eating is usually substantially reduced. Sedation is the most common side effect.
Anorexia patients often refuse to take olanzapine for fear of weight gain. If a patient’s emaciation is life-threatening, we may seek court permission to medicate her involuntarily. We reassure her that we will discontinue olanzapine when she reaches her target weight.
Serotonin in anorexia. Central serotonin pathways modulate feeding behavior. Serotonin antagonists—such as cyproheptadine—increase food intake and weight gain, whereas serotonin agonists—such as selective serotonin reuptake inhibitors (SSRIs)—decrease food intake.
Serotonin pathways also may modulate obsessive-compulsive and impulsive behaviors. Both serotonin agonists and antagonists can be useful adjuncts in treating anorexia nervosa.
In a double-blind, placebo-controlled trial, cyproheptadine, 4 to 8 mg tid, was associated with weight gain and reduced depressive symptoms in anorexia nervosa patients.18 Unlike tricyclic antidepressants, cyproheptadine does not reduce blood pressure or increase heart rate, which makes it attractive for emaciated anorectic patients. Dosages up to 28 mg/d can be used safely.
The SSRI fluoxetine may help prevent weight loss relapse in anorexia nervosa and reduce obsessive-compulsive behaviors.19 In open studies of low-weight anorectics, however, fluoxetine had little impact on weight or other clinically meaningful variables.20 Thus, this agent is recommended for preventing weight-loss relapse only in patients who are within 10% to 15% of ideal body weight.
Outpatient care
Case report continued: Ongoing therapy
During hospitalization, Ms. J participated in all therapeutic modalities but had difficulty eating enough to gain weight. She reached her target weight of 127 lbs in about 7 weeks but gained no sense of purpose in life.
She is starting an intensive outpatient program using CBT to maintain her weight and further address the core psychopathology of her illness. Her maintenance therapy includes attending Alcoholics Anonymous meetings, ongoing fluoxetine (20 mg/d) to prevent weight-loss relapse, and CBT for obsessions and compulsions not related to her eating disorder.
Related resources
- Halmi KA. Eating disorders: Anorexia, bulimia nervosa and obesity. In: Hales RE, Yudofsky SC (eds). Textbook of clinical psychiatry, 4th ed. Washington, DC: American Psychiatric Publishing, 2003:1001-21.
- Academy of Eating Disorders. www.aedweb.org
- Anorexia Nervosa & Associated Disorders (ANAD). www.anad.org
Drug brand names
- Chlorpromazine • Thorazine
- Cyproheptadine • Periactin
- Fluoxetine • Prozac
- Olanzapine • Zyprexa
Disclosure
The author reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Halmi KA. Anorexia nervosa: demographic and clinical features in 94 cases. Psychosom Med 1974;36:18-24.
2. Bruch AH. Eating disorders: obesity, anorexia nervosa, and the person within. New York, Basic books, 1973.
3. Kleifield E, Wagner S, Halmi KA. Cognitive behavioral treatment of anorexia nervosa. Psychiatr Clin North Am 1996;19:715-34.
4. Halmi KA. Eating disorders. In: Martin A, Scahill L, Charney DS Leckman JF (eds). Pediatric pharmacology. New York: Oxford University Press, 2002;592-602.
5. Halmi KA, Eckert E, Marci P, Cohen J. Comorbidity of psychiatric diagnoses in anorexia nervosa. Arch Gen Psychiatry 1991;48:712-18.
6. Braun DL, Sunday SR, Halmi KA. Psychiatric comorbidity in patients with eating disorders. Psychol Med 1994;24:859-67.
7. Holderness CC, Brooks-Gunn J, Warren MP. Comorbidity of eating disorders and substance abuse review of the literature. Int J Eat Disord 1994;16:1-34.
8. Herzog DB, Keller M, Lavori P. The prevalence of personality disorders in 210 women with eating disorders. J Clin Psychiatry 1992;53:147-52.
9. Baran S, Weltzin T, Kaye W. Low discharge weight and outcome in anorexia nervosa. Am J Psychiatry 1995;150:1070-2.
10. Commerford MC, Licinio J, Halmi KA. Guidelines for discharging eating disorder patients. Eat Disord 1997;5:69-74.
11. Howard W, Evans K, Quinter-Howard C, et al. Predictors of success or failure of transition to day hospital treatment for inpatients with anorexia nervosa. Am J Psychiatry 1999;156:1697-1702.
12. Wiseman C, Sunday SR, Klapper F, et al. Changing patterns of hospitalization in eating disorder patients. Int J Eat Disord 2001;30:69-74.
13. Newman M, Halmi KA. The relationship of bone density to estradiol and cortisol in anorexia nervosa and bulimia nervosa. Psychiatr Res 1989;29:105-12.
14. Falk JR, Halmi KA. Amenorrhea in anorexia nervosa: examination of the critical body hypothesis. Biol Psychiatr 1982;17:799-806.
15. Garner DM, Bemis KM. A cognitive-behavioral approach to anorexia nervosa. Cognit Ther Res 1982;6:1223-50.
16. Dare C. Eisler. Family therapy and eating disorders. In: Fairburn CR, Brownell KD (eds). Eating disorders and obesity. New York: Guilford Press, 2002;314-19.
17. Powers P, Santana CA, Bannon YS. Olanzapine in the treatment of anorexia nervosa: an open label trial. Int J Eat Disord 2002;32:146-54.
18. Halmi KA, Eckert ED, Ladu T, Cohen J. Anorexia nervosa: treatment efficacy of cyproheptadine and amitriptyline. Arch Gen Psychiatry 1986;43:177-81.
19. Kaye W. The use of fluoxetine to prevent relapse in anorexia nervosa (presentation). Pittsburgh, PA: Eating Disorder Research Society annual meeting, 1996.
20. Ferguson C, Lavia M, Crossan P. Are serotonin selective reuptake inhibitors effective in underweight anorexia nervosa? Int J Eat Disord 1999;25:11-17.
1. Halmi KA. Anorexia nervosa: demographic and clinical features in 94 cases. Psychosom Med 1974;36:18-24.
2. Bruch AH. Eating disorders: obesity, anorexia nervosa, and the person within. New York, Basic books, 1973.
3. Kleifield E, Wagner S, Halmi KA. Cognitive behavioral treatment of anorexia nervosa. Psychiatr Clin North Am 1996;19:715-34.
4. Halmi KA. Eating disorders. In: Martin A, Scahill L, Charney DS Leckman JF (eds). Pediatric pharmacology. New York: Oxford University Press, 2002;592-602.
5. Halmi KA, Eckert E, Marci P, Cohen J. Comorbidity of psychiatric diagnoses in anorexia nervosa. Arch Gen Psychiatry 1991;48:712-18.
6. Braun DL, Sunday SR, Halmi KA. Psychiatric comorbidity in patients with eating disorders. Psychol Med 1994;24:859-67.
7. Holderness CC, Brooks-Gunn J, Warren MP. Comorbidity of eating disorders and substance abuse review of the literature. Int J Eat Disord 1994;16:1-34.
8. Herzog DB, Keller M, Lavori P. The prevalence of personality disorders in 210 women with eating disorders. J Clin Psychiatry 1992;53:147-52.
9. Baran S, Weltzin T, Kaye W. Low discharge weight and outcome in anorexia nervosa. Am J Psychiatry 1995;150:1070-2.
10. Commerford MC, Licinio J, Halmi KA. Guidelines for discharging eating disorder patients. Eat Disord 1997;5:69-74.
11. Howard W, Evans K, Quinter-Howard C, et al. Predictors of success or failure of transition to day hospital treatment for inpatients with anorexia nervosa. Am J Psychiatry 1999;156:1697-1702.
12. Wiseman C, Sunday SR, Klapper F, et al. Changing patterns of hospitalization in eating disorder patients. Int J Eat Disord 2001;30:69-74.
13. Newman M, Halmi KA. The relationship of bone density to estradiol and cortisol in anorexia nervosa and bulimia nervosa. Psychiatr Res 1989;29:105-12.
14. Falk JR, Halmi KA. Amenorrhea in anorexia nervosa: examination of the critical body hypothesis. Biol Psychiatr 1982;17:799-806.
15. Garner DM, Bemis KM. A cognitive-behavioral approach to anorexia nervosa. Cognit Ther Res 1982;6:1223-50.
16. Dare C. Eisler. Family therapy and eating disorders. In: Fairburn CR, Brownell KD (eds). Eating disorders and obesity. New York: Guilford Press, 2002;314-19.
17. Powers P, Santana CA, Bannon YS. Olanzapine in the treatment of anorexia nervosa: an open label trial. Int J Eat Disord 2002;32:146-54.
18. Halmi KA, Eckert ED, Ladu T, Cohen J. Anorexia nervosa: treatment efficacy of cyproheptadine and amitriptyline. Arch Gen Psychiatry 1986;43:177-81.
19. Kaye W. The use of fluoxetine to prevent relapse in anorexia nervosa (presentation). Pittsburgh, PA: Eating Disorder Research Society annual meeting, 1996.
20. Ferguson C, Lavia M, Crossan P. Are serotonin selective reuptake inhibitors effective in underweight anorexia nervosa? Int J Eat Disord 1999;25:11-17.
Bipolar treatment update: Evidence is driving change in mania, depression algorithms
Many well-controlled trials in the past 4 years have evaluated new medications for treating bipolar disorder. It’s time to build a consensus on how this data may apply to clinical practice.
This year, our group will re-examine the Texas Medication Algorithm Project (TMAP) treatment algorithms for bipolar I disorder.
What makes TMAP unique? It is the first project to evaluate treatment algorithm use in community mental health settings for patients with a history of mania (see Box).1-5 Severely, persistently ill outpatients such as these are seldom included in research but are frequently seen in clinical practice.
To preview for psychiatrists the changes expected in 2004, this article describes the goals of TMAP and the controlled study on which the medication algorithms are based. We review the medication algorithms of 2000 as a starting point and present the evidence that is changing clinical practice.
Guiding principles of TMAP
A treatment algorithm is no substitute for clinical judgment; rather, medication guidelines and algorithms are guideposts to help the clinician and patient collaboratively develop the most effective medication strategy with the fewest side effects.
The Texas Medication Algorithm Project (TMAP)1-3 is a public and academic collaboration started in 1996 to develop evidence- and consensus-based medication treatment algorithms for schizophrenia, major depressive disorder, and bipolar disorder.
TMAP’s goal is to establish “best practices” to encourage uniformity of care, achieve the best possible patient outcomes, and use mental health care dollars most efficiently. The project includes four phases, in which the treatment algorithms were developed, compared with treatment-as-usual, put into practice, and will undergo periodic updates.4 The next update begins this year.
The comparison of algorithms for treating bipolar mania/hypomania and depression included 409 patients (mean age 38 to 40) with bipolar I disorder or schizoaffective disorder, bipolar type. These patients were severely and persistently mentally ill, from a diverse ethnic population, and significantly impaired in functioning.
During 12 months of treatment, psychiatric symptoms diminished more rapidly in patients in the algorithm group—as measured by the Brief Psychiatric Rating Scale (BPRS-24)—compared with those receiving usual treatment. After the first 3 months, the usual-treatment patients also showed diminished symptoms. At study’s end, symptom severity between the groups was not significantly different; both groups showed improvement.
Manic and psychotic symptoms—measured by Clinician-Administered Rating Scale subscales (CARS-M)5—improved significantly more in the algorithm group in the first 3 months, and this gap between the two groups was sustained for 12 months. Depressive symptoms declined, but no overall differences were noted between the two groups. Side effect rates and functioning were also similar.
TMAP’s treatment manual (see Related resources) describes clinicians’ preferred tactics and decision points, which we summarize here. The guidelines are an ongoing effort to apply evidence-based medicine to everyday practice and are meant to be adapted to patient needs.
Treatment goals that guided TMAP algorithm development are:
- symptomatic remission
- full return of psychosocial functioning
- prevention of relapse and recurrence.
Suggestions came from controlled clinical trials, open trials, retrospective data analyses, expert clinical consensus, and input from consumers.
Treatment selection. Initial algorithm stages recommend simple treatments (in terms of safety, tolerability, and side effects), whereas later stages recommend more-complicated regimens. A patient’s symptoms, comorbid conditions, and treatment history guide treatment selection. Patients may enter an algorithm at any stage, depending on their clinical presentation and medication history.
The clinician may consider patient preference when deciding among equivalent medications. The algorithm strongly encourages patients and families to participate, such as by keeping daily mood charts and completing symptom and side-effect checklists. When clinicians face a choice among medication brands, generics, or forms (such as immediate- versus slow-release), agents with greater tolerability are preferred.
Patient management. When patients enter the algorithm, clinic visits are frequent (such as every 2 weeks). Follow-up appointments address medication adherence, dosage adjustments, and side effects or adverse reactions.
If a patient’s symptoms show no change after two treatment stages, re-evaluate the diagnosis and consider mitigating factors such as substance abuse. Patients who complete acute treatment should receive continuation treatment.
Documentation. Clinicians are advised to document decision points and the rationale for treatment choices made outside the algorithm package.
Treating mania or hypomania
After clinical evaluation confirms the diagnosis of bipolar illness,4 the TMAP mania/hypomania algorithm (Algorithm 1) splits into three treatment pathways:
- euphoric mania/hypomania
- mixed or dysphoric mania/hypomania
- psychotic mania.
These pathways recognize the need for differing approaches to initial monotherapy and later two-drug combinations. If a patient develops persistent or severe depressive symptoms, the bipolar algorithm for a major depressive episode (Algorithm 2) is used during depressive periods with the primary mania algorithm.
Treatment recommendations. The key to using mood stabilizers is to achieve the optimum response—assuming good tolerability—before switching to another agent. Adjust medication dosages one at a time to allow adequate response and assessment.
When switching medications, use an overlap-and-taper strategy, assuming there is no medical necessity to stop a drug abruptly. Add the new medication, then gradually taper the one that is being discontinued. Monitor serum levels.
Discontinue antidepressants when appropriate in patients with hypomania/mania or rapid cycling, and continually evaluate suicide and homicide potential of patients in mixed or depressive states.
Stage 1: Monotherapy. First medication choices are lithium, divalproex, or olanzapine. For mixed or dysphoric mania, the algorithm recommends divalproex (preferred over valproic acid because of tolerability and side effects) or olanzapine.6 Data suggest dysphoric manic patients are less likely to respond to lithium.7 A Consensus Panel minority expressed concern about using olanzapine as first-line monotherapy for acute mania because of limited data on the drug’s long-term safety. Patients with partial response or residual symptoms may move to stage 2 or switch to other medication options within stage 1.
Patients with psychotic mania move directly to stage 4 for a broader range of combination therapy.
Stage 2: Combination therapy. Combination therapy has become the standard of care in treating most patients with bipolar disorder. The algorithm recommends using two agents:
- lithium or an anticonvulsant plus another anticonvulsant ([Li or AC]+AC)
- or lithium or an anticonvulsant plus an atypical antipsychotic ([Li or AC]+AAP).8
Recommended agents include lithium, divalproex, oxcarbazepine, olanzapine, or risperidone. The experts recommended oxcarbazepine as first choice because it is better tolerated and interacts with fewer drugs than carbamazepine and does not require serum level monitoring.9
A Consensus Panel minority expressed concern that few studies had examined using oxcarbazepine in bipolar disorder. Carbamazepine was also considered an option.
Stages 3 and 4: Other two-drug combinations. Other two-drug combinations are tried at these stages, drawing from the same pool of medication classes described in stage 2.
Stage 4 broadens the choice of atypical antipsychotic by adding quetiapine10 and ziprasidone11 to the recommended stage-2 agents olanzapine and risperidone. When the 2000 algorithm was developed, limited data were available on using some newer atypicals in patients with bipolar mania. Based on recent, high-quality studies of mono- and combination therapy—including quetiapine,10 ziprasidone,11 risperidone,12,13 and aripiprazole14 —the 2004 algorithm update panel will likely recommend using atypicals earlier, including at stage 1.
Algorithm 1 Treating mania/hypomania in patients with bipolar I disorder
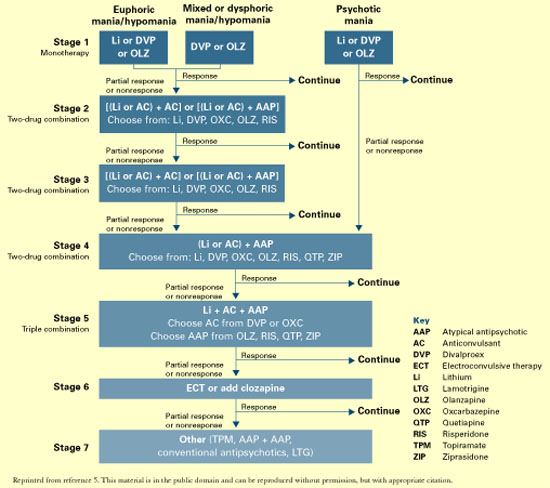
Stage 5: Triple-drug combination. Lithium, an anticonvulsant (divalproex or oxcarbazepine), and an atypical antipsychotic (olanzapine, risperidone, quetiapine, or ziprasidone) is a recommended triple-drug combination. In the 2004 update, the choices will likely expand to include all the newer atypicals and will list carbamazepine as an option.
Stage 6: ECT or clozapine. For patients with inadequate response to triple-drug combinations, the algorithm recommends adding electroconvulsive therapy (ECT) or clozapine.
ECT15 is recommended three times a week until the patient achieves remission of manic symptoms or fails to achieve a sustained response over three to six treatment cycles. Treatment resistance is declared if no response is seen after 6 to 10 treatment cycles.
Clozapine’s16 recommendation at this stage is consistent with its use in patients who fail to respond to other atypical antipsychotics. Blood monitoring for agranulocytosis is required; other adverse effects include an increased risk of seizures, myocarditis, and orthostatic hypotension.
Stage 7: Other. Treatment options such as topiramate17,18 and lamotrigine19 are recommended at this stage. These recommendations also will be reviewed and likely revised.
Treating bipolar depression
The TMAP algorithm for treating depression in bipolar disorder (Algorithm 2) assumes that anti-depressants will be used only with optimum mood-stabilizer levels because of the risk of inducing manic symptoms. The bipolar depression algorithm is always used with the primary algorithm for mania/hypomania.
The patient’s clinical presentation guides medication selection. For the “pure” bipolar I patient with a major depressive episode but little mood lability or hypomania, starting an antide-pressant is a clear decision. On the other hand, patients with predominant depressive symptoms plus dysphoric hypomania, mood lability, and irritability need a balance of mood-stabilizing drugs and antidepressants.
Stage 1: Mood stabilizer. Initiate a mood stabilizer and optimize the dosage. Choices are the same mood stabilizers listed in the hypomania/mania treatment algorithm.
Stage 2: Antidepressant. Adding an antidepressant implies that depressive symptoms are severe enough to change treatment. Antidepressant options include a selective serotonin reuptake inhibitor (SSRI), sustained-release bupropion, or lamotrigine.20
Using SSRIs is supported by widespread clinical experience and offers the convenience of once-daily dosing. Recommended SSRIs include fluoxetine, paroxetine, fluvoxamine, sertraline, and citalopram. The SSRI escitalopram was introduced after the 2000 algorithms were published; evidence for using it and other newer medications will be reviewed for the 2004 update.
The recommendation for sustained-release bupropion is consistent with the algorithm principle to use medications in the most well-tolerated form when accessible and available.
With lamotrigine, review with patients the risk of serious rash. To minimize rash risk, start lamotrigine slowly and follow the recommended titration schedule.
Stage 3: Multiple choices. At this stage, no definitive studies, safety data, or tolerability issues are available to rank the medication choices. The algorithm suggests:
- adding lithium21 or a second antidepressant
- or switching to an alternate antidepressant such as venlafaxine or nefazodone.
If a patient moves to stage 3 because of side effects with one antidepressant class, a different class—preferably with a contrasting side-effect profile—is recommended.
Algorithm 2 Treating depression in bipolar I disorder*
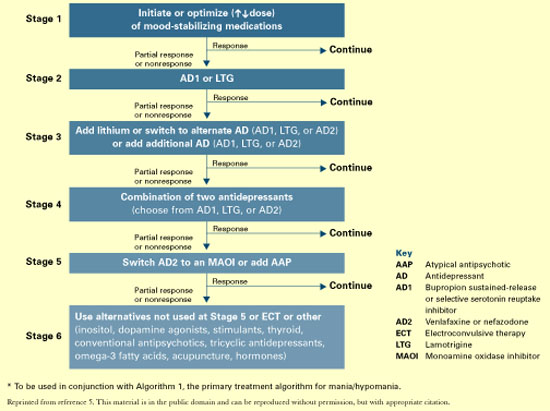
Stage 4: Two antidepressants. To enhance clinical response, the algorithm recommends combining two antidepressants, preferably from different classes. Monitor patients closely for side effects.
Stage 5. Antipsychotic or MAOI. At this stage, the algorithm recommends adding an atypical antipsychotic22 or switching to a monoamine oxidase inhibitor (MAOI).
Early evidence supported the efficacy of MAOIs in bipolar depression. However, the panel ranked MAOIs lower in the algorithm because they are associated with more bothersome side effects than SSRIs and other antidepressants. When using MAOIs, provide patients with dietary restriction guidelines.
Stage 6. Other therapies. Therapies such as ECT or “other” interventions are recommended at this stage. ECT has proven efficacy in bipolar depression and is appropriate for patients with limited medication response. The panel gave ECT a low ranking because of limited availability, lack of patient acceptance, and newer options.
Medication options include experimental treatments with limited evidence, such as inositol, dopamine agonists, stimulants, thyroid supplementation, conventional antipsychotics, and tri-cyclic antidepressants.
Acute to maintenance treatment
Adjunctive treatments for agitation, insomnia, GI upset, sedation, headache, and tremor are recommended in the physician manual supporting the TMAP guidelines (see Related resources). The manual also suggests ways to manage medication side effects and modify the algorithms for inpatients.
Patient and family psychoeducation plays an important role in helping the patient:
- identify prodromal bipolar symptoms
- understand the need to take medications as prescribed.
Continuation treatment. After mania or hypomania remits, continue medication(s) at the effective acute-phase dosages for at least 3 months. Use follow-up visits to enhance patient adherence, detect early symptoms of relapse, and monitor for side effects.
During the late continuation phase, after a period of sustained stability, clinicians can try to simplify the medications. When discontinuing a medication, taper the dosage by no more than 25% per week. If symptoms recur, promptly return to acute-phase treatment. Consider restarting medications and titrating up to the dosage(s) that resulted in remission.
In a depressive episode, continue the antidepressant(s) for 1 to 3 months at the effective acutephase dosage(s). Follow up frequently, and educate patients to watch for symptom recurrence and to communicate with you to assess when medication changes are needed.
Maintenance treatment. Relatively few well-controlled studies on long-term management of bipolar patients were available for the 2000 algorithm update.23 In general, all patients need mood stabilizer(s) to prevent relapse, using the lowest dosage that maintains therapeutic efficacy. Based on new evidence for lamotrigine and atypical antipsychotics—including FDAapproval of olanzapine for bipolar maintenace therapy—we anticipate recommendations will be expanded and more delineated in the 2004 update.
Discontinuing antidepressants after 3 to 6 months of initial treatment is now recommended. However, a recent retrospective case series suggests that continuing antidepressants at least 1 year after initial successful therapy may protect against depressive relapse. During this study, continuing antidepressants more than 3 to 6 months did not appear to increase the risk of switching to mania.24
Should antidepressants be continued or discontinued after successful acute treatment of a bipolar I depressive episode? This is an active area of research and debate as to the most appropriate strategy. The 2004 algorithm update panel will consider recent evidence that supports continuing antidepressants after symptom remission.24
- Texas Medication Algorithm Project algorithms and physician manual. Texas Department of Mental Health and Mental Retardation. http://www.mhmr.state.tx.us/centraloffice/medicaldirector/TIMA.html
- American Psychiatric Association. Practice guidelines for the treatment of patients with bipolar disorder. Am J Psychiatry 2002; 159(4):suppl 2.
- Depression and Bipolar Support Alliance. www.dbsalliance.org
Drug brand names
- Bupropion • Wellbutrin SR
- Carbamazepine • Tegretol
- Citalopram • Celexa
- Clozapine • Clozaril
- Divalproex sodium • Depakote
- Escitalopram • Lexapro
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Inositol • Various
- Lamotrigine • Lamictal
- Nefazodone • Serzone
- Olanzapine • Zyprexa
- Oxcarbazepine • Trileptal
- Paroxetine • Paxil
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Sertraline • Zoloft
- Topiramate • Topamax
- Tranylcypromine • Parnate
- Valproic acid • Depakene
- Venlafaxine • Effexor
- Ziprasidone • Geodon
Disclosure
Dr. Shivakumar reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Suppes receives research support from or is a consultant to Abbott Laboratories, AstraZeneca Pharmaceuticals, Bristol-Myers Squibb, Eli Lilly and Co., GlaxoSmithKline, Janssen Pharmaceutica, Johnson & Johnson, National Institutes of Mental Health, Novartis Pharmaceuticals Corp., Pfizer Inc., Pharmaceutical Research Institute, Ortho-McNeil Pharmaceutical, Robert Wood Johnson Pharmaceutical Research Institute, The Stanley Medical Research Institute, and UCB Pharma.
1. Gilbert DA, Altshuler KZ, Rago WV, et al. Texas Medication Algorithm Project: definitions, rationale, and methods to develop medication algorithms. J Clin Psychiatry 1998;59:345-51.
2. Altshuler KZ, Rush AJ. Computerized Texas Medication Algorithm Project undergoes testing. Outcomes Accountability Alert 1999;4(1):10-11.
3. Rush AJ, Crismon ML, Kashner TM, et al. Texas Medication Algorithm Project, Phase 3 (TMAP-3): rationale and study design. J Clin Psychiatry 2003;64(4):357-69.
4. Altman E, Hedeker D, Janicak P, et al. The Clinician-Administered Rating Scale For Mania (CARS-M): development, reliability, and validity. Biol Psychiatry 1994;36:124-34.
5. Suppes T, Dennehy EB, Swann AC, et al. Report of the Texas consensus conference panel on medication treatment of bipolar disorder 2000. J Clin Psychiatry 2002;63:288-99.
6. Dennehy EB, Doyle K, Suppes T. The efficacy of olanzapine monotherapy for acute hypomania or mania in an outpatient setting. Int Clin Psychopharmacol 2003;18(3):143-5.
7. Dilsaver SC, Swann AC, Shoaib AM, et al. The manic syndrome: factors which may predict a patient’s response to lithium, carbamazepine and valproate. J Psych Neurosci 1993;18:61-6.
8. Tohen M, Chengappa KNR, Suppes T, et al. Efficacy of olanzapine in combination with valproate or lithium in the treatment of mania in patients partially nonresponsive to valproate or lithium monotherapy. Arch Gen Psychiatry 2002;59(1):62-9.
9. Emrich HM. Studies with oxcarbazepine (Trileptal) in acute mania. Int Clin Psychopharmacol 1990;190(5,suppl):83-8.
10. Vieta E, Parramon G, Padrell E, et al. Quetiapine in the treatment of rapid cycling bipolar disorder. Bipolar Disord 2002;4(5):335-40.
11. Keck PE, Versiani M, Potkin S, et al. Ziprasidone in the treatment of acute bipolar mania: a three week placebo-controlled, double-blinded randomized trial. Am J Psychiatry 2003;160(4):741-8.
12. Yatham LN, Grossman F, Augustyns I, et al. Mood stabilisers plus risperidone or placebo in the treatment of acute mania. International, double-blinded, randomised controlled trial. Br J Psychiatry 2003;182:141-7.
13. Sachs GS, Grossman F, Ghaemi SN, et al. Combination of a mood stabilizer with risperidone or haloperidol for treatment of acute mania: a double-blind, placebo-controlled comparison of efficacy and safety. Am J Psychiatry 2002;159(7):1146-54.
14. Keck PE, Jr, Marcus R, Tourkodimitris S, et al. Aripiprazole study group. A placebo-controlled, double-blind study of the efficacy and safety of aripiprazole in patients with acute bipolar mania. Am J Psychiatry 2003;160(9):1651-8.
15. Mukherjee S, Sackeim HA, Schnur DB. Electroconvulsive therapy of acute manic episode: a review of 50 years’ experience. Am J Psychiatry 1988;45:727-32.
16. Suppes T, Webb A, Paul B, et al. Clinical outcome in a randomized 1-year trail of clozapine versus treatment as usual for patients with treatment-resistant illness and a history of mania. Am J Psychiatry 1999;156(8):1164-9.
17. Guille C, Sachs G. Clinical outcome of adjunctive topiramate treatment in a sample of refractory bipolar patients with comorbid conditions. Prog Neuropsychopharmacol Biol Psychiatry 2002;26(6):1035-9.
18. Vieta E, Torrent C, Garcia-Ribas G, et al. Use of topiramate in treatment-resistant bipolar spectrum disorders. J Clin Psychopharmacol 2002;22(4):431-5.
19. Calabrese JR, Suppes T, Bowden CL, et al. A double blinded, placebo-controlled, prophylaxis study of lamotrigine in rapid-cycling bipolar disorder. J Clin Psychiatry 2000;61:841-50.
20. Calabrese JR, Bowden CL, Sachs GS, et al. A placebo-controlled 18-month trial of lamotrigine and lithium maintenance treatment in recently depressed patients with bipolar I disorder. J Clin Psychiatry 2003;64(9):1013-24.
21. Bauer M, Dopfmer S. Lithium augmentation in treatment-resistant depression: meta-analysis of placebo-controlled studies. J Clin Psychopharmacology 1999;19:427-34.
22. Shelton RC, Tollefson GD, Tohen M, et al. A novel augmentation strategy for treating resistant major depression. Am J Psychiatry 2001;158:131-4.
23. Baldessarini RJ, Tohen M, Tondo L. Maintenance treatment in bipolar disorder (comment). Arch Gen Psychiatry 2000;57:490-2.
24. Altshuler L, Suppes T, Black D, et al. Impact of antidepressant discontinuation after acute bipolar depression remission on rates of depressive relapse at 1-year follow-up. Am J Psychiatry 2003;160:1252-62.
Many well-controlled trials in the past 4 years have evaluated new medications for treating bipolar disorder. It’s time to build a consensus on how this data may apply to clinical practice.
This year, our group will re-examine the Texas Medication Algorithm Project (TMAP) treatment algorithms for bipolar I disorder.
What makes TMAP unique? It is the first project to evaluate treatment algorithm use in community mental health settings for patients with a history of mania (see Box).1-5 Severely, persistently ill outpatients such as these are seldom included in research but are frequently seen in clinical practice.
To preview for psychiatrists the changes expected in 2004, this article describes the goals of TMAP and the controlled study on which the medication algorithms are based. We review the medication algorithms of 2000 as a starting point and present the evidence that is changing clinical practice.
Guiding principles of TMAP
A treatment algorithm is no substitute for clinical judgment; rather, medication guidelines and algorithms are guideposts to help the clinician and patient collaboratively develop the most effective medication strategy with the fewest side effects.
The Texas Medication Algorithm Project (TMAP)1-3 is a public and academic collaboration started in 1996 to develop evidence- and consensus-based medication treatment algorithms for schizophrenia, major depressive disorder, and bipolar disorder.
TMAP’s goal is to establish “best practices” to encourage uniformity of care, achieve the best possible patient outcomes, and use mental health care dollars most efficiently. The project includes four phases, in which the treatment algorithms were developed, compared with treatment-as-usual, put into practice, and will undergo periodic updates.4 The next update begins this year.
The comparison of algorithms for treating bipolar mania/hypomania and depression included 409 patients (mean age 38 to 40) with bipolar I disorder or schizoaffective disorder, bipolar type. These patients were severely and persistently mentally ill, from a diverse ethnic population, and significantly impaired in functioning.
During 12 months of treatment, psychiatric symptoms diminished more rapidly in patients in the algorithm group—as measured by the Brief Psychiatric Rating Scale (BPRS-24)—compared with those receiving usual treatment. After the first 3 months, the usual-treatment patients also showed diminished symptoms. At study’s end, symptom severity between the groups was not significantly different; both groups showed improvement.
Manic and psychotic symptoms—measured by Clinician-Administered Rating Scale subscales (CARS-M)5—improved significantly more in the algorithm group in the first 3 months, and this gap between the two groups was sustained for 12 months. Depressive symptoms declined, but no overall differences were noted between the two groups. Side effect rates and functioning were also similar.
TMAP’s treatment manual (see Related resources) describes clinicians’ preferred tactics and decision points, which we summarize here. The guidelines are an ongoing effort to apply evidence-based medicine to everyday practice and are meant to be adapted to patient needs.
Treatment goals that guided TMAP algorithm development are:
- symptomatic remission
- full return of psychosocial functioning
- prevention of relapse and recurrence.
Suggestions came from controlled clinical trials, open trials, retrospective data analyses, expert clinical consensus, and input from consumers.
Treatment selection. Initial algorithm stages recommend simple treatments (in terms of safety, tolerability, and side effects), whereas later stages recommend more-complicated regimens. A patient’s symptoms, comorbid conditions, and treatment history guide treatment selection. Patients may enter an algorithm at any stage, depending on their clinical presentation and medication history.
The clinician may consider patient preference when deciding among equivalent medications. The algorithm strongly encourages patients and families to participate, such as by keeping daily mood charts and completing symptom and side-effect checklists. When clinicians face a choice among medication brands, generics, or forms (such as immediate- versus slow-release), agents with greater tolerability are preferred.
Patient management. When patients enter the algorithm, clinic visits are frequent (such as every 2 weeks). Follow-up appointments address medication adherence, dosage adjustments, and side effects or adverse reactions.
If a patient’s symptoms show no change after two treatment stages, re-evaluate the diagnosis and consider mitigating factors such as substance abuse. Patients who complete acute treatment should receive continuation treatment.
Documentation. Clinicians are advised to document decision points and the rationale for treatment choices made outside the algorithm package.
Treating mania or hypomania
After clinical evaluation confirms the diagnosis of bipolar illness,4 the TMAP mania/hypomania algorithm (Algorithm 1) splits into three treatment pathways:
- euphoric mania/hypomania
- mixed or dysphoric mania/hypomania
- psychotic mania.
These pathways recognize the need for differing approaches to initial monotherapy and later two-drug combinations. If a patient develops persistent or severe depressive symptoms, the bipolar algorithm for a major depressive episode (Algorithm 2) is used during depressive periods with the primary mania algorithm.
Treatment recommendations. The key to using mood stabilizers is to achieve the optimum response—assuming good tolerability—before switching to another agent. Adjust medication dosages one at a time to allow adequate response and assessment.
When switching medications, use an overlap-and-taper strategy, assuming there is no medical necessity to stop a drug abruptly. Add the new medication, then gradually taper the one that is being discontinued. Monitor serum levels.
Discontinue antidepressants when appropriate in patients with hypomania/mania or rapid cycling, and continually evaluate suicide and homicide potential of patients in mixed or depressive states.
Stage 1: Monotherapy. First medication choices are lithium, divalproex, or olanzapine. For mixed or dysphoric mania, the algorithm recommends divalproex (preferred over valproic acid because of tolerability and side effects) or olanzapine.6 Data suggest dysphoric manic patients are less likely to respond to lithium.7 A Consensus Panel minority expressed concern about using olanzapine as first-line monotherapy for acute mania because of limited data on the drug’s long-term safety. Patients with partial response or residual symptoms may move to stage 2 or switch to other medication options within stage 1.
Patients with psychotic mania move directly to stage 4 for a broader range of combination therapy.
Stage 2: Combination therapy. Combination therapy has become the standard of care in treating most patients with bipolar disorder. The algorithm recommends using two agents:
- lithium or an anticonvulsant plus another anticonvulsant ([Li or AC]+AC)
- or lithium or an anticonvulsant plus an atypical antipsychotic ([Li or AC]+AAP).8
Recommended agents include lithium, divalproex, oxcarbazepine, olanzapine, or risperidone. The experts recommended oxcarbazepine as first choice because it is better tolerated and interacts with fewer drugs than carbamazepine and does not require serum level monitoring.9
A Consensus Panel minority expressed concern that few studies had examined using oxcarbazepine in bipolar disorder. Carbamazepine was also considered an option.
Stages 3 and 4: Other two-drug combinations. Other two-drug combinations are tried at these stages, drawing from the same pool of medication classes described in stage 2.
Stage 4 broadens the choice of atypical antipsychotic by adding quetiapine10 and ziprasidone11 to the recommended stage-2 agents olanzapine and risperidone. When the 2000 algorithm was developed, limited data were available on using some newer atypicals in patients with bipolar mania. Based on recent, high-quality studies of mono- and combination therapy—including quetiapine,10 ziprasidone,11 risperidone,12,13 and aripiprazole14 —the 2004 algorithm update panel will likely recommend using atypicals earlier, including at stage 1.
Algorithm 1 Treating mania/hypomania in patients with bipolar I disorder
Stage 5: Triple-drug combination. Lithium, an anticonvulsant (divalproex or oxcarbazepine), and an atypical antipsychotic (olanzapine, risperidone, quetiapine, or ziprasidone) is a recommended triple-drug combination. In the 2004 update, the choices will likely expand to include all the newer atypicals and will list carbamazepine as an option.
Stage 6: ECT or clozapine. For patients with inadequate response to triple-drug combinations, the algorithm recommends adding electroconvulsive therapy (ECT) or clozapine.
ECT15 is recommended three times a week until the patient achieves remission of manic symptoms or fails to achieve a sustained response over three to six treatment cycles. Treatment resistance is declared if no response is seen after 6 to 10 treatment cycles.
Clozapine’s16 recommendation at this stage is consistent with its use in patients who fail to respond to other atypical antipsychotics. Blood monitoring for agranulocytosis is required; other adverse effects include an increased risk of seizures, myocarditis, and orthostatic hypotension.
Stage 7: Other. Treatment options such as topiramate17,18 and lamotrigine19 are recommended at this stage. These recommendations also will be reviewed and likely revised.
Treating bipolar depression
The TMAP algorithm for treating depression in bipolar disorder (Algorithm 2) assumes that anti-depressants will be used only with optimum mood-stabilizer levels because of the risk of inducing manic symptoms. The bipolar depression algorithm is always used with the primary algorithm for mania/hypomania.
The patient’s clinical presentation guides medication selection. For the “pure” bipolar I patient with a major depressive episode but little mood lability or hypomania, starting an antide-pressant is a clear decision. On the other hand, patients with predominant depressive symptoms plus dysphoric hypomania, mood lability, and irritability need a balance of mood-stabilizing drugs and antidepressants.
Stage 1: Mood stabilizer. Initiate a mood stabilizer and optimize the dosage. Choices are the same mood stabilizers listed in the hypomania/mania treatment algorithm.
Stage 2: Antidepressant. Adding an antidepressant implies that depressive symptoms are severe enough to change treatment. Antidepressant options include a selective serotonin reuptake inhibitor (SSRI), sustained-release bupropion, or lamotrigine.20
Using SSRIs is supported by widespread clinical experience and offers the convenience of once-daily dosing. Recommended SSRIs include fluoxetine, paroxetine, fluvoxamine, sertraline, and citalopram. The SSRI escitalopram was introduced after the 2000 algorithms were published; evidence for using it and other newer medications will be reviewed for the 2004 update.
The recommendation for sustained-release bupropion is consistent with the algorithm principle to use medications in the most well-tolerated form when accessible and available.
With lamotrigine, review with patients the risk of serious rash. To minimize rash risk, start lamotrigine slowly and follow the recommended titration schedule.
Stage 3: Multiple choices. At this stage, no definitive studies, safety data, or tolerability issues are available to rank the medication choices. The algorithm suggests:
- adding lithium21 or a second antidepressant
- or switching to an alternate antidepressant such as venlafaxine or nefazodone.
If a patient moves to stage 3 because of side effects with one antidepressant class, a different class—preferably with a contrasting side-effect profile—is recommended.
Algorithm 2 Treating depression in bipolar I disorder*
Stage 4: Two antidepressants. To enhance clinical response, the algorithm recommends combining two antidepressants, preferably from different classes. Monitor patients closely for side effects.
Stage 5. Antipsychotic or MAOI. At this stage, the algorithm recommends adding an atypical antipsychotic22 or switching to a monoamine oxidase inhibitor (MAOI).
Early evidence supported the efficacy of MAOIs in bipolar depression. However, the panel ranked MAOIs lower in the algorithm because they are associated with more bothersome side effects than SSRIs and other antidepressants. When using MAOIs, provide patients with dietary restriction guidelines.
Stage 6. Other therapies. Therapies such as ECT or “other” interventions are recommended at this stage. ECT has proven efficacy in bipolar depression and is appropriate for patients with limited medication response. The panel gave ECT a low ranking because of limited availability, lack of patient acceptance, and newer options.
Medication options include experimental treatments with limited evidence, such as inositol, dopamine agonists, stimulants, thyroid supplementation, conventional antipsychotics, and tri-cyclic antidepressants.
Acute to maintenance treatment
Adjunctive treatments for agitation, insomnia, GI upset, sedation, headache, and tremor are recommended in the physician manual supporting the TMAP guidelines (see Related resources). The manual also suggests ways to manage medication side effects and modify the algorithms for inpatients.
Patient and family psychoeducation plays an important role in helping the patient:
- identify prodromal bipolar symptoms
- understand the need to take medications as prescribed.
Continuation treatment. After mania or hypomania remits, continue medication(s) at the effective acute-phase dosages for at least 3 months. Use follow-up visits to enhance patient adherence, detect early symptoms of relapse, and monitor for side effects.
During the late continuation phase, after a period of sustained stability, clinicians can try to simplify the medications. When discontinuing a medication, taper the dosage by no more than 25% per week. If symptoms recur, promptly return to acute-phase treatment. Consider restarting medications and titrating up to the dosage(s) that resulted in remission.
In a depressive episode, continue the antidepressant(s) for 1 to 3 months at the effective acutephase dosage(s). Follow up frequently, and educate patients to watch for symptom recurrence and to communicate with you to assess when medication changes are needed.
Maintenance treatment. Relatively few well-controlled studies on long-term management of bipolar patients were available for the 2000 algorithm update.23 In general, all patients need mood stabilizer(s) to prevent relapse, using the lowest dosage that maintains therapeutic efficacy. Based on new evidence for lamotrigine and atypical antipsychotics—including FDAapproval of olanzapine for bipolar maintenace therapy—we anticipate recommendations will be expanded and more delineated in the 2004 update.
Discontinuing antidepressants after 3 to 6 months of initial treatment is now recommended. However, a recent retrospective case series suggests that continuing antidepressants at least 1 year after initial successful therapy may protect against depressive relapse. During this study, continuing antidepressants more than 3 to 6 months did not appear to increase the risk of switching to mania.24
Should antidepressants be continued or discontinued after successful acute treatment of a bipolar I depressive episode? This is an active area of research and debate as to the most appropriate strategy. The 2004 algorithm update panel will consider recent evidence that supports continuing antidepressants after symptom remission.24
- Texas Medication Algorithm Project algorithms and physician manual. Texas Department of Mental Health and Mental Retardation. http://www.mhmr.state.tx.us/centraloffice/medicaldirector/TIMA.html
- American Psychiatric Association. Practice guidelines for the treatment of patients with bipolar disorder. Am J Psychiatry 2002; 159(4):suppl 2.
- Depression and Bipolar Support Alliance. www.dbsalliance.org
Drug brand names
- Bupropion • Wellbutrin SR
- Carbamazepine • Tegretol
- Citalopram • Celexa
- Clozapine • Clozaril
- Divalproex sodium • Depakote
- Escitalopram • Lexapro
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Inositol • Various
- Lamotrigine • Lamictal
- Nefazodone • Serzone
- Olanzapine • Zyprexa
- Oxcarbazepine • Trileptal
- Paroxetine • Paxil
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Sertraline • Zoloft
- Topiramate • Topamax
- Tranylcypromine • Parnate
- Valproic acid • Depakene
- Venlafaxine • Effexor
- Ziprasidone • Geodon
Disclosure
Dr. Shivakumar reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Suppes receives research support from or is a consultant to Abbott Laboratories, AstraZeneca Pharmaceuticals, Bristol-Myers Squibb, Eli Lilly and Co., GlaxoSmithKline, Janssen Pharmaceutica, Johnson & Johnson, National Institutes of Mental Health, Novartis Pharmaceuticals Corp., Pfizer Inc., Pharmaceutical Research Institute, Ortho-McNeil Pharmaceutical, Robert Wood Johnson Pharmaceutical Research Institute, The Stanley Medical Research Institute, and UCB Pharma.
Many well-controlled trials in the past 4 years have evaluated new medications for treating bipolar disorder. It’s time to build a consensus on how this data may apply to clinical practice.
This year, our group will re-examine the Texas Medication Algorithm Project (TMAP) treatment algorithms for bipolar I disorder.
What makes TMAP unique? It is the first project to evaluate treatment algorithm use in community mental health settings for patients with a history of mania (see Box).1-5 Severely, persistently ill outpatients such as these are seldom included in research but are frequently seen in clinical practice.
To preview for psychiatrists the changes expected in 2004, this article describes the goals of TMAP and the controlled study on which the medication algorithms are based. We review the medication algorithms of 2000 as a starting point and present the evidence that is changing clinical practice.
Guiding principles of TMAP
A treatment algorithm is no substitute for clinical judgment; rather, medication guidelines and algorithms are guideposts to help the clinician and patient collaboratively develop the most effective medication strategy with the fewest side effects.
The Texas Medication Algorithm Project (TMAP)1-3 is a public and academic collaboration started in 1996 to develop evidence- and consensus-based medication treatment algorithms for schizophrenia, major depressive disorder, and bipolar disorder.
TMAP’s goal is to establish “best practices” to encourage uniformity of care, achieve the best possible patient outcomes, and use mental health care dollars most efficiently. The project includes four phases, in which the treatment algorithms were developed, compared with treatment-as-usual, put into practice, and will undergo periodic updates.4 The next update begins this year.
The comparison of algorithms for treating bipolar mania/hypomania and depression included 409 patients (mean age 38 to 40) with bipolar I disorder or schizoaffective disorder, bipolar type. These patients were severely and persistently mentally ill, from a diverse ethnic population, and significantly impaired in functioning.
During 12 months of treatment, psychiatric symptoms diminished more rapidly in patients in the algorithm group—as measured by the Brief Psychiatric Rating Scale (BPRS-24)—compared with those receiving usual treatment. After the first 3 months, the usual-treatment patients also showed diminished symptoms. At study’s end, symptom severity between the groups was not significantly different; both groups showed improvement.
Manic and psychotic symptoms—measured by Clinician-Administered Rating Scale subscales (CARS-M)5—improved significantly more in the algorithm group in the first 3 months, and this gap between the two groups was sustained for 12 months. Depressive symptoms declined, but no overall differences were noted between the two groups. Side effect rates and functioning were also similar.
TMAP’s treatment manual (see Related resources) describes clinicians’ preferred tactics and decision points, which we summarize here. The guidelines are an ongoing effort to apply evidence-based medicine to everyday practice and are meant to be adapted to patient needs.
Treatment goals that guided TMAP algorithm development are:
- symptomatic remission
- full return of psychosocial functioning
- prevention of relapse and recurrence.
Suggestions came from controlled clinical trials, open trials, retrospective data analyses, expert clinical consensus, and input from consumers.
Treatment selection. Initial algorithm stages recommend simple treatments (in terms of safety, tolerability, and side effects), whereas later stages recommend more-complicated regimens. A patient’s symptoms, comorbid conditions, and treatment history guide treatment selection. Patients may enter an algorithm at any stage, depending on their clinical presentation and medication history.
The clinician may consider patient preference when deciding among equivalent medications. The algorithm strongly encourages patients and families to participate, such as by keeping daily mood charts and completing symptom and side-effect checklists. When clinicians face a choice among medication brands, generics, or forms (such as immediate- versus slow-release), agents with greater tolerability are preferred.
Patient management. When patients enter the algorithm, clinic visits are frequent (such as every 2 weeks). Follow-up appointments address medication adherence, dosage adjustments, and side effects or adverse reactions.
If a patient’s symptoms show no change after two treatment stages, re-evaluate the diagnosis and consider mitigating factors such as substance abuse. Patients who complete acute treatment should receive continuation treatment.
Documentation. Clinicians are advised to document decision points and the rationale for treatment choices made outside the algorithm package.
Treating mania or hypomania
After clinical evaluation confirms the diagnosis of bipolar illness,4 the TMAP mania/hypomania algorithm (Algorithm 1) splits into three treatment pathways:
- euphoric mania/hypomania
- mixed or dysphoric mania/hypomania
- psychotic mania.
These pathways recognize the need for differing approaches to initial monotherapy and later two-drug combinations. If a patient develops persistent or severe depressive symptoms, the bipolar algorithm for a major depressive episode (Algorithm 2) is used during depressive periods with the primary mania algorithm.
Treatment recommendations. The key to using mood stabilizers is to achieve the optimum response—assuming good tolerability—before switching to another agent. Adjust medication dosages one at a time to allow adequate response and assessment.
When switching medications, use an overlap-and-taper strategy, assuming there is no medical necessity to stop a drug abruptly. Add the new medication, then gradually taper the one that is being discontinued. Monitor serum levels.
Discontinue antidepressants when appropriate in patients with hypomania/mania or rapid cycling, and continually evaluate suicide and homicide potential of patients in mixed or depressive states.
Stage 1: Monotherapy. First medication choices are lithium, divalproex, or olanzapine. For mixed or dysphoric mania, the algorithm recommends divalproex (preferred over valproic acid because of tolerability and side effects) or olanzapine.6 Data suggest dysphoric manic patients are less likely to respond to lithium.7 A Consensus Panel minority expressed concern about using olanzapine as first-line monotherapy for acute mania because of limited data on the drug’s long-term safety. Patients with partial response or residual symptoms may move to stage 2 or switch to other medication options within stage 1.
Patients with psychotic mania move directly to stage 4 for a broader range of combination therapy.
Stage 2: Combination therapy. Combination therapy has become the standard of care in treating most patients with bipolar disorder. The algorithm recommends using two agents:
- lithium or an anticonvulsant plus another anticonvulsant ([Li or AC]+AC)
- or lithium or an anticonvulsant plus an atypical antipsychotic ([Li or AC]+AAP).8
Recommended agents include lithium, divalproex, oxcarbazepine, olanzapine, or risperidone. The experts recommended oxcarbazepine as first choice because it is better tolerated and interacts with fewer drugs than carbamazepine and does not require serum level monitoring.9
A Consensus Panel minority expressed concern that few studies had examined using oxcarbazepine in bipolar disorder. Carbamazepine was also considered an option.
Stages 3 and 4: Other two-drug combinations. Other two-drug combinations are tried at these stages, drawing from the same pool of medication classes described in stage 2.
Stage 4 broadens the choice of atypical antipsychotic by adding quetiapine10 and ziprasidone11 to the recommended stage-2 agents olanzapine and risperidone. When the 2000 algorithm was developed, limited data were available on using some newer atypicals in patients with bipolar mania. Based on recent, high-quality studies of mono- and combination therapy—including quetiapine,10 ziprasidone,11 risperidone,12,13 and aripiprazole14 —the 2004 algorithm update panel will likely recommend using atypicals earlier, including at stage 1.
Algorithm 1 Treating mania/hypomania in patients with bipolar I disorder
Stage 5: Triple-drug combination. Lithium, an anticonvulsant (divalproex or oxcarbazepine), and an atypical antipsychotic (olanzapine, risperidone, quetiapine, or ziprasidone) is a recommended triple-drug combination. In the 2004 update, the choices will likely expand to include all the newer atypicals and will list carbamazepine as an option.
Stage 6: ECT or clozapine. For patients with inadequate response to triple-drug combinations, the algorithm recommends adding electroconvulsive therapy (ECT) or clozapine.
ECT15 is recommended three times a week until the patient achieves remission of manic symptoms or fails to achieve a sustained response over three to six treatment cycles. Treatment resistance is declared if no response is seen after 6 to 10 treatment cycles.
Clozapine’s16 recommendation at this stage is consistent with its use in patients who fail to respond to other atypical antipsychotics. Blood monitoring for agranulocytosis is required; other adverse effects include an increased risk of seizures, myocarditis, and orthostatic hypotension.
Stage 7: Other. Treatment options such as topiramate17,18 and lamotrigine19 are recommended at this stage. These recommendations also will be reviewed and likely revised.
Treating bipolar depression
The TMAP algorithm for treating depression in bipolar disorder (Algorithm 2) assumes that anti-depressants will be used only with optimum mood-stabilizer levels because of the risk of inducing manic symptoms. The bipolar depression algorithm is always used with the primary algorithm for mania/hypomania.
The patient’s clinical presentation guides medication selection. For the “pure” bipolar I patient with a major depressive episode but little mood lability or hypomania, starting an antide-pressant is a clear decision. On the other hand, patients with predominant depressive symptoms plus dysphoric hypomania, mood lability, and irritability need a balance of mood-stabilizing drugs and antidepressants.
Stage 1: Mood stabilizer. Initiate a mood stabilizer and optimize the dosage. Choices are the same mood stabilizers listed in the hypomania/mania treatment algorithm.
Stage 2: Antidepressant. Adding an antidepressant implies that depressive symptoms are severe enough to change treatment. Antidepressant options include a selective serotonin reuptake inhibitor (SSRI), sustained-release bupropion, or lamotrigine.20
Using SSRIs is supported by widespread clinical experience and offers the convenience of once-daily dosing. Recommended SSRIs include fluoxetine, paroxetine, fluvoxamine, sertraline, and citalopram. The SSRI escitalopram was introduced after the 2000 algorithms were published; evidence for using it and other newer medications will be reviewed for the 2004 update.
The recommendation for sustained-release bupropion is consistent with the algorithm principle to use medications in the most well-tolerated form when accessible and available.
With lamotrigine, review with patients the risk of serious rash. To minimize rash risk, start lamotrigine slowly and follow the recommended titration schedule.
Stage 3: Multiple choices. At this stage, no definitive studies, safety data, or tolerability issues are available to rank the medication choices. The algorithm suggests:
- adding lithium21 or a second antidepressant
- or switching to an alternate antidepressant such as venlafaxine or nefazodone.
If a patient moves to stage 3 because of side effects with one antidepressant class, a different class—preferably with a contrasting side-effect profile—is recommended.
Algorithm 2 Treating depression in bipolar I disorder*
Stage 4: Two antidepressants. To enhance clinical response, the algorithm recommends combining two antidepressants, preferably from different classes. Monitor patients closely for side effects.
Stage 5. Antipsychotic or MAOI. At this stage, the algorithm recommends adding an atypical antipsychotic22 or switching to a monoamine oxidase inhibitor (MAOI).
Early evidence supported the efficacy of MAOIs in bipolar depression. However, the panel ranked MAOIs lower in the algorithm because they are associated with more bothersome side effects than SSRIs and other antidepressants. When using MAOIs, provide patients with dietary restriction guidelines.
Stage 6. Other therapies. Therapies such as ECT or “other” interventions are recommended at this stage. ECT has proven efficacy in bipolar depression and is appropriate for patients with limited medication response. The panel gave ECT a low ranking because of limited availability, lack of patient acceptance, and newer options.
Medication options include experimental treatments with limited evidence, such as inositol, dopamine agonists, stimulants, thyroid supplementation, conventional antipsychotics, and tri-cyclic antidepressants.
Acute to maintenance treatment
Adjunctive treatments for agitation, insomnia, GI upset, sedation, headache, and tremor are recommended in the physician manual supporting the TMAP guidelines (see Related resources). The manual also suggests ways to manage medication side effects and modify the algorithms for inpatients.
Patient and family psychoeducation plays an important role in helping the patient:
- identify prodromal bipolar symptoms
- understand the need to take medications as prescribed.
Continuation treatment. After mania or hypomania remits, continue medication(s) at the effective acute-phase dosages for at least 3 months. Use follow-up visits to enhance patient adherence, detect early symptoms of relapse, and monitor for side effects.
During the late continuation phase, after a period of sustained stability, clinicians can try to simplify the medications. When discontinuing a medication, taper the dosage by no more than 25% per week. If symptoms recur, promptly return to acute-phase treatment. Consider restarting medications and titrating up to the dosage(s) that resulted in remission.
In a depressive episode, continue the antidepressant(s) for 1 to 3 months at the effective acutephase dosage(s). Follow up frequently, and educate patients to watch for symptom recurrence and to communicate with you to assess when medication changes are needed.
Maintenance treatment. Relatively few well-controlled studies on long-term management of bipolar patients were available for the 2000 algorithm update.23 In general, all patients need mood stabilizer(s) to prevent relapse, using the lowest dosage that maintains therapeutic efficacy. Based on new evidence for lamotrigine and atypical antipsychotics—including FDAapproval of olanzapine for bipolar maintenace therapy—we anticipate recommendations will be expanded and more delineated in the 2004 update.
Discontinuing antidepressants after 3 to 6 months of initial treatment is now recommended. However, a recent retrospective case series suggests that continuing antidepressants at least 1 year after initial successful therapy may protect against depressive relapse. During this study, continuing antidepressants more than 3 to 6 months did not appear to increase the risk of switching to mania.24
Should antidepressants be continued or discontinued after successful acute treatment of a bipolar I depressive episode? This is an active area of research and debate as to the most appropriate strategy. The 2004 algorithm update panel will consider recent evidence that supports continuing antidepressants after symptom remission.24
- Texas Medication Algorithm Project algorithms and physician manual. Texas Department of Mental Health and Mental Retardation. http://www.mhmr.state.tx.us/centraloffice/medicaldirector/TIMA.html
- American Psychiatric Association. Practice guidelines for the treatment of patients with bipolar disorder. Am J Psychiatry 2002; 159(4):suppl 2.
- Depression and Bipolar Support Alliance. www.dbsalliance.org
Drug brand names
- Bupropion • Wellbutrin SR
- Carbamazepine • Tegretol
- Citalopram • Celexa
- Clozapine • Clozaril
- Divalproex sodium • Depakote
- Escitalopram • Lexapro
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Inositol • Various
- Lamotrigine • Lamictal
- Nefazodone • Serzone
- Olanzapine • Zyprexa
- Oxcarbazepine • Trileptal
- Paroxetine • Paxil
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Sertraline • Zoloft
- Topiramate • Topamax
- Tranylcypromine • Parnate
- Valproic acid • Depakene
- Venlafaxine • Effexor
- Ziprasidone • Geodon
Disclosure
Dr. Shivakumar reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Suppes receives research support from or is a consultant to Abbott Laboratories, AstraZeneca Pharmaceuticals, Bristol-Myers Squibb, Eli Lilly and Co., GlaxoSmithKline, Janssen Pharmaceutica, Johnson & Johnson, National Institutes of Mental Health, Novartis Pharmaceuticals Corp., Pfizer Inc., Pharmaceutical Research Institute, Ortho-McNeil Pharmaceutical, Robert Wood Johnson Pharmaceutical Research Institute, The Stanley Medical Research Institute, and UCB Pharma.
1. Gilbert DA, Altshuler KZ, Rago WV, et al. Texas Medication Algorithm Project: definitions, rationale, and methods to develop medication algorithms. J Clin Psychiatry 1998;59:345-51.
2. Altshuler KZ, Rush AJ. Computerized Texas Medication Algorithm Project undergoes testing. Outcomes Accountability Alert 1999;4(1):10-11.
3. Rush AJ, Crismon ML, Kashner TM, et al. Texas Medication Algorithm Project, Phase 3 (TMAP-3): rationale and study design. J Clin Psychiatry 2003;64(4):357-69.
4. Altman E, Hedeker D, Janicak P, et al. The Clinician-Administered Rating Scale For Mania (CARS-M): development, reliability, and validity. Biol Psychiatry 1994;36:124-34.
5. Suppes T, Dennehy EB, Swann AC, et al. Report of the Texas consensus conference panel on medication treatment of bipolar disorder 2000. J Clin Psychiatry 2002;63:288-99.
6. Dennehy EB, Doyle K, Suppes T. The efficacy of olanzapine monotherapy for acute hypomania or mania in an outpatient setting. Int Clin Psychopharmacol 2003;18(3):143-5.
7. Dilsaver SC, Swann AC, Shoaib AM, et al. The manic syndrome: factors which may predict a patient’s response to lithium, carbamazepine and valproate. J Psych Neurosci 1993;18:61-6.
8. Tohen M, Chengappa KNR, Suppes T, et al. Efficacy of olanzapine in combination with valproate or lithium in the treatment of mania in patients partially nonresponsive to valproate or lithium monotherapy. Arch Gen Psychiatry 2002;59(1):62-9.
9. Emrich HM. Studies with oxcarbazepine (Trileptal) in acute mania. Int Clin Psychopharmacol 1990;190(5,suppl):83-8.
10. Vieta E, Parramon G, Padrell E, et al. Quetiapine in the treatment of rapid cycling bipolar disorder. Bipolar Disord 2002;4(5):335-40.
11. Keck PE, Versiani M, Potkin S, et al. Ziprasidone in the treatment of acute bipolar mania: a three week placebo-controlled, double-blinded randomized trial. Am J Psychiatry 2003;160(4):741-8.
12. Yatham LN, Grossman F, Augustyns I, et al. Mood stabilisers plus risperidone or placebo in the treatment of acute mania. International, double-blinded, randomised controlled trial. Br J Psychiatry 2003;182:141-7.
13. Sachs GS, Grossman F, Ghaemi SN, et al. Combination of a mood stabilizer with risperidone or haloperidol for treatment of acute mania: a double-blind, placebo-controlled comparison of efficacy and safety. Am J Psychiatry 2002;159(7):1146-54.
14. Keck PE, Jr, Marcus R, Tourkodimitris S, et al. Aripiprazole study group. A placebo-controlled, double-blind study of the efficacy and safety of aripiprazole in patients with acute bipolar mania. Am J Psychiatry 2003;160(9):1651-8.
15. Mukherjee S, Sackeim HA, Schnur DB. Electroconvulsive therapy of acute manic episode: a review of 50 years’ experience. Am J Psychiatry 1988;45:727-32.
16. Suppes T, Webb A, Paul B, et al. Clinical outcome in a randomized 1-year trail of clozapine versus treatment as usual for patients with treatment-resistant illness and a history of mania. Am J Psychiatry 1999;156(8):1164-9.
17. Guille C, Sachs G. Clinical outcome of adjunctive topiramate treatment in a sample of refractory bipolar patients with comorbid conditions. Prog Neuropsychopharmacol Biol Psychiatry 2002;26(6):1035-9.
18. Vieta E, Torrent C, Garcia-Ribas G, et al. Use of topiramate in treatment-resistant bipolar spectrum disorders. J Clin Psychopharmacol 2002;22(4):431-5.
19. Calabrese JR, Suppes T, Bowden CL, et al. A double blinded, placebo-controlled, prophylaxis study of lamotrigine in rapid-cycling bipolar disorder. J Clin Psychiatry 2000;61:841-50.
20. Calabrese JR, Bowden CL, Sachs GS, et al. A placebo-controlled 18-month trial of lamotrigine and lithium maintenance treatment in recently depressed patients with bipolar I disorder. J Clin Psychiatry 2003;64(9):1013-24.
21. Bauer M, Dopfmer S. Lithium augmentation in treatment-resistant depression: meta-analysis of placebo-controlled studies. J Clin Psychopharmacology 1999;19:427-34.
22. Shelton RC, Tollefson GD, Tohen M, et al. A novel augmentation strategy for treating resistant major depression. Am J Psychiatry 2001;158:131-4.
23. Baldessarini RJ, Tohen M, Tondo L. Maintenance treatment in bipolar disorder (comment). Arch Gen Psychiatry 2000;57:490-2.
24. Altshuler L, Suppes T, Black D, et al. Impact of antidepressant discontinuation after acute bipolar depression remission on rates of depressive relapse at 1-year follow-up. Am J Psychiatry 2003;160:1252-62.
1. Gilbert DA, Altshuler KZ, Rago WV, et al. Texas Medication Algorithm Project: definitions, rationale, and methods to develop medication algorithms. J Clin Psychiatry 1998;59:345-51.
2. Altshuler KZ, Rush AJ. Computerized Texas Medication Algorithm Project undergoes testing. Outcomes Accountability Alert 1999;4(1):10-11.
3. Rush AJ, Crismon ML, Kashner TM, et al. Texas Medication Algorithm Project, Phase 3 (TMAP-3): rationale and study design. J Clin Psychiatry 2003;64(4):357-69.
4. Altman E, Hedeker D, Janicak P, et al. The Clinician-Administered Rating Scale For Mania (CARS-M): development, reliability, and validity. Biol Psychiatry 1994;36:124-34.
5. Suppes T, Dennehy EB, Swann AC, et al. Report of the Texas consensus conference panel on medication treatment of bipolar disorder 2000. J Clin Psychiatry 2002;63:288-99.
6. Dennehy EB, Doyle K, Suppes T. The efficacy of olanzapine monotherapy for acute hypomania or mania in an outpatient setting. Int Clin Psychopharmacol 2003;18(3):143-5.
7. Dilsaver SC, Swann AC, Shoaib AM, et al. The manic syndrome: factors which may predict a patient’s response to lithium, carbamazepine and valproate. J Psych Neurosci 1993;18:61-6.
8. Tohen M, Chengappa KNR, Suppes T, et al. Efficacy of olanzapine in combination with valproate or lithium in the treatment of mania in patients partially nonresponsive to valproate or lithium monotherapy. Arch Gen Psychiatry 2002;59(1):62-9.
9. Emrich HM. Studies with oxcarbazepine (Trileptal) in acute mania. Int Clin Psychopharmacol 1990;190(5,suppl):83-8.
10. Vieta E, Parramon G, Padrell E, et al. Quetiapine in the treatment of rapid cycling bipolar disorder. Bipolar Disord 2002;4(5):335-40.
11. Keck PE, Versiani M, Potkin S, et al. Ziprasidone in the treatment of acute bipolar mania: a three week placebo-controlled, double-blinded randomized trial. Am J Psychiatry 2003;160(4):741-8.
12. Yatham LN, Grossman F, Augustyns I, et al. Mood stabilisers plus risperidone or placebo in the treatment of acute mania. International, double-blinded, randomised controlled trial. Br J Psychiatry 2003;182:141-7.
13. Sachs GS, Grossman F, Ghaemi SN, et al. Combination of a mood stabilizer with risperidone or haloperidol for treatment of acute mania: a double-blind, placebo-controlled comparison of efficacy and safety. Am J Psychiatry 2002;159(7):1146-54.
14. Keck PE, Jr, Marcus R, Tourkodimitris S, et al. Aripiprazole study group. A placebo-controlled, double-blind study of the efficacy and safety of aripiprazole in patients with acute bipolar mania. Am J Psychiatry 2003;160(9):1651-8.
15. Mukherjee S, Sackeim HA, Schnur DB. Electroconvulsive therapy of acute manic episode: a review of 50 years’ experience. Am J Psychiatry 1988;45:727-32.
16. Suppes T, Webb A, Paul B, et al. Clinical outcome in a randomized 1-year trail of clozapine versus treatment as usual for patients with treatment-resistant illness and a history of mania. Am J Psychiatry 1999;156(8):1164-9.
17. Guille C, Sachs G. Clinical outcome of adjunctive topiramate treatment in a sample of refractory bipolar patients with comorbid conditions. Prog Neuropsychopharmacol Biol Psychiatry 2002;26(6):1035-9.
18. Vieta E, Torrent C, Garcia-Ribas G, et al. Use of topiramate in treatment-resistant bipolar spectrum disorders. J Clin Psychopharmacol 2002;22(4):431-5.
19. Calabrese JR, Suppes T, Bowden CL, et al. A double blinded, placebo-controlled, prophylaxis study of lamotrigine in rapid-cycling bipolar disorder. J Clin Psychiatry 2000;61:841-50.
20. Calabrese JR, Bowden CL, Sachs GS, et al. A placebo-controlled 18-month trial of lamotrigine and lithium maintenance treatment in recently depressed patients with bipolar I disorder. J Clin Psychiatry 2003;64(9):1013-24.
21. Bauer M, Dopfmer S. Lithium augmentation in treatment-resistant depression: meta-analysis of placebo-controlled studies. J Clin Psychopharmacology 1999;19:427-34.
22. Shelton RC, Tollefson GD, Tohen M, et al. A novel augmentation strategy for treating resistant major depression. Am J Psychiatry 2001;158:131-4.
23. Baldessarini RJ, Tohen M, Tondo L. Maintenance treatment in bipolar disorder (comment). Arch Gen Psychiatry 2000;57:490-2.
24. Altshuler L, Suppes T, Black D, et al. Impact of antidepressant discontinuation after acute bipolar depression remission on rates of depressive relapse at 1-year follow-up. Am J Psychiatry 2003;160:1252-62.
Using antipsychotics in patients with dementia
Three keys can help you safely treat dementia’s difficult behavioral and psychological symptoms:
- Differentiate medical from psychiatric causes of patients’ distress.
- Use antipsychotics and other drugs as adjuncts to psychosocial treatments.
- Start low and go slow when titrating dosages.
Although no treatment reverses the pathophysiology of progressive neurodegenerative disorders, managing agitation and other behaviors can alleviate patient suffering and reduce caregiver stress. Based on the evidence and our experience, this article describes a practical approach, including a treatment algorithm and evidence of atypical antipsychotics’ efficacy and side effects in this patient population.
Algorithm Treating behavioral symptoms in patients with dementia
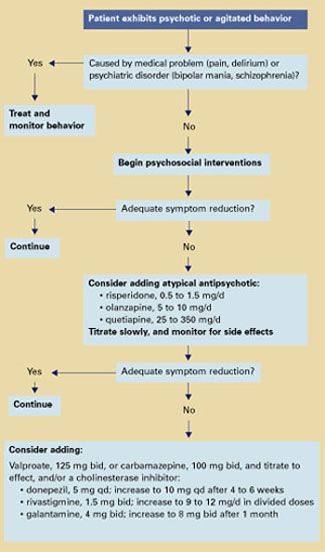
Dementia’s behavioral symptoms
An International Psychogeriatric Association consensus statement1 grouped dementia’s behavioral and psychological symptoms into two types:
- those usually assessed by interviewing patients and relatives—anxiety, depressed mood, hallucinations, and delusions
- those usually identified by observing patient behavior—aggression, screaming, restlessness, agitation, wandering, culturally inappropriate behaviors, sexual disinhibition, hoarding, cursing, and shadowing.
These behaviors in community-living patients are distressing to family members and increase the risk for caregiver burnout—the most common reason for placing older patients in long-term care. In the nursing home, dementia’s symptoms reduce patients’ quality of life; interfere with feeding, bathing, and dressing; and—when violent—may endanger staff and other patients.
Rule out a medical cause
Differential diagnosis. Behavioral symptoms in dementia tend to be unpredictable, which makes diagnosis and treatment challenging. The first step is to determine if a medical or psychiatric condition might account for the behavior. For instance:
- A patient with dementia may be agitated because of a distended bladder or arthritis but unable to communicate his or her pain in words.
- In mild dementia, a pre-existing psychiatric disorder such as schizophrenia might be causing a patient’s hallucinations or delusions.
- Pacing and restlessness may be drug side effects and might be controlled by reducing dosages or switching to less-activating agents.
Delirium is also a risk for older patients—especially those with degenerative neurologic disorders. Common triggers in older patients include acute illness such as a urinary tract infection or pneumonia, alcohol or benzodiazepine withdrawal, anticholinergic agents, medication changes, and dehydration.
Delirium is characterized by acute onset and fluctuating neuropsychiatric symptoms, including disturbed consciousness and changes in attention and cognition. Taking a careful history to learn the course of treatment and the patient’s baseline cognitive function can help you differentiate dementia from delirium. Family members, physicians, and nursing staff are valuable sources of this information.
Use antipsychotics as adjuncts
Psychosocial interventions. After medical causes have been ruled out, consensus guidelines2 recommend psychosocial interventions as first-line treatment of dementia’s behavioral symptoms (Algorithm). Suggested interventions for patients and caregivers are listed in Table 1.3
Antipsychotics. For patients who respond inadequately to psychosocial measures, the next step is to add an atypical antipsychotic. Because of side effects, conventional antipsychotics are not recommended for patients with dementia.
When prescribing atypicals, remember that older adults:
- are more sensitive to side effects than younger adults
- require lower starting and target dosages
- exhibit heterogeneity of response.
Older patients’ medical status can range from “fit” to “frail,” which influences individual response to medications. Generally, age-related changes in the way their bodies metabolize drugs account for older patients’ increased sensitivity to drug side effects (Box).4-11
Atypical antipsychotics and dosages that have been shown benefit for managing behavioral symptoms in older patients with dementia include:
- risperidone, 0.5 to 1.5 mg/d12
- olanzapine, 5 to 10 mg/d13
- quetiapine, 25 to 350 mg/d14 (Table 2).15,16
Start with low dosages, and titrate slowly. Increase once or twice a week until the lowest effective dosage is reached.
Augmenting agents. If antipsychotic monotherapy fails to achieve an adequate response or if side effects limit dosing, adjunctive agents may be added with caution. Augmenting agents that have shown benefit in some patients with dementia include:
- mood stabilizers such as divalproex17 or carbamazepine18
- cholinesterase inhibitors, such as donepezil, rivastigmine, or galantamine.19
Start divalproex at 125 mg bid or carbamazepine at 100 mg bid and titrate to effect. Concomitant carbamazepine will decrease blood levels of risperidone, olanzapine, and quetiapine because of hepatic enzyme induction.20
Start donepezil at 5 mg once daily and increase after 4 to 6 weeks to 10 mg qd. When using rivastigmine, start with 1.5 mg bid and titrate to 9 to 12 mg/d in divided doses. Start galantamine at 4 mg bid and increase after 1 month to 8 mg bid.
Table 1
Suggested psychosocial interventions for older patients with dementia
Communicate clearly
|
Minimize the impact of sensory deficits
|
Modify environment when necessary
|
Encourage consistent daily routines
|
Optimize social/physical stimulation
|
Encourage caregiver to:
|
Antipsychotic side effects
Atypical antipsychotics are more effective than conventional agents in treating negative symptoms and are associated with lower rates of extrapyramidal symptoms (EPS) and tardive dyskinesia (TD).21
Tardive dyskinesia. All antipsychotics can cause TD, although the risk is about 10 times greater with conventionals than atypicals. With conventionals, the annual cumulative TD incidence for young adults is 4 to 5%,22 and rates are much higher for middle-aged and older adults receiving chronic therapy:
- 29% after 1 year
- 50% after 2 years
- 63% after 3 years.23
In older patients, use atypical rather than conventional antipsychotics to minimize TD risk. Observe carefully; if TD symptoms occur, cautiously withdraw the antipsychotic and consider trying another agent.
Other risks. Atypical antipsychotics may cause sedation, orthostatic hypotension (with an increased risk for falls), increased serum prolactin, and weight gain (Table 2).
Weight gain from atypical antipsychotics has been associated with adverse effects on glucose metabolism and increased risk for type 2 diabetes.24 Some might argue that weight gain associated with olanzapine and other atypicals might benefit low-weight older patients. The frail elderly need to increase muscle mass, however, and the atypicals are associated with increases in fat mass.
Increased serum prolactin with risperidone theoretically could lead to loss of bone density, but evidence of this effect in older patients does not exist.
Start low, go slow
Clozapine may help control treatment-resistant psychosis in patients with schizophrenia and manage patients with severe TD.25 However, clozapine’s increased risk of agranulocytosis, neurologic side effects (seizures, sedation, confusion), and anticholinergic effects limit its use in older patients, particularly those with neurodegenerative disorders (Table 2).
Dosing. In rare cases when using clozapine in older patients, start with 6.25 to 12.5 mg/d. Increase by 6.25 to 12.5 mg once or twice a week to 50 to 100 mg/d.
Risperidone has been used to treat agitation in older patients with dementia in two small studies:
In a 9-week, open-label trial, 15 patients (mean age 78) with dementia were given risperidone, 0.5 to 3 mg/d. Agitation improved significantly, as measured by the Cohen-Mansfield Agitation Inventory (CMAI)—a 29-item questionnaire completed by caregivers.26 CMAI scores at study’s end averaged 49.5, compared with 70.5 at baseline.27
A 12-week, placebo-controlled, doubleblind study examined risperidone—0.5, 1, or 2 mg/d—in 625 institutionalized patients (mean age 83) with dementia and agitation. Ninety-six patients had Functional Assessment Staging Rating Scale scores of 6A, indicating moderate to severe dementia. In patients receiving risperidone, these behavioral measures were significantly reduced:
- Behavior Pathology in Alzheimer’s Disease Rating Scale (BEHAVE-AD) total scores, which measure behavior severity
- BEHAVE-AD psychosis subscale scores
- BEHAVE-AD aggressiveness scores
- CMAI verbal and aggression scores.
Adverse effects were reported at 82% for all three risperidone dosages and 85% for placebo. Side effects including somnolence, EPS, and peripheral edema were dose-related.12
Another trial compared risperidone or haloperidol, 0.5 to 4 mg/d, with placebo in treating 344 patients with behavioral symptoms of dementia. After 12 weeks of risperidone, mean dosage 1.1 mg/d:
- mean total BEHAVE-AD score decreased by 53%, compared with 37% in the placebo group
- CMAI score decreased by 32%, compared with 18% in the placebo group.
EPS were more severe with haloperidol than with risperidone or placebo.28
Risk of stroke. A small but significantly increased incidence of stroke and stroke-like events was recently reported in older patients with dementia when treated with risperidone. These events occurred in double-blind, placebocontrolled trials in patients (mean age 82) with Alzheimer’s, vascular, and mixed dementias.
Pharmacokinetic changes can influence concentrations of drugs in tissue compartments over time. Drug absorption declines with normal aging, but a clinically significant decrease in total absorption of psychotropics appears not to occur.13
In the liver, lipid-soluble psychotropics are metabolized into pharmacologically active or inactive metabolites. Some metabolic pathways, such as demethylation, may be influenced by age, leading to increased plasma concentrations of drugs and their metabolites.14,15 However, hydroxylation tends not to be affected by age.16
The ratio of body fat to water increases with aging,13 increasing the volume of distribution for lipid-soluble psychotropics. An age-related decrease in glomerular filtration accounts in part for increased accumulation of hydrophilic metabolites in some older patients.17,18
Pharmacodynamic changes with aging occur in neurotransmitter systems within cellular processing, such as at receptor or reuptake levels.19 These changes may exaggerate drug-drug interactions or affect complex neurotransmitter interactions.
The number of neurons in nigrostriatal pathways declines with age. Decreases are also seen in tyrosine hydroxylase activity, presynaptic dopamine D2 receptors, and dopamine levels—which may be particularly relevant to a discussion of antipsychotic medications.20
The net effect of these changes is the need to prescribe lower-than-usual starting and target dosages of many medications, including antipsychotics.
Most patients who experienced cerebrovascular events had one or more stroke risk factors, including diabetes, hypertension, atrial fibrillation, heart arrhythmia, atherosclerosis, or heart failure. They did not show a pattern of reduced blood pressure or orthostatic changes.12,29
Table 2
Antipsychotic side effects and dosages in older patients with dementia*
| Side effect | Clozapine (6.25 to 100 mg/d) | Risperidone (0.5 to 1.5 mg/d) | Olanzapine (5 to 10 mg/d) | Quetiapine (25 to 350 mg/d) |
|---|---|---|---|---|
| Orthostasis | ++++ | ++++ | +++ | ++ |
| Sedation | +++++ | ++ | +++ | ++ |
| Prolactin increase | 0 | +++ | + | 0 |
| Weight gain | ++++ | + | +++ | + |
| EPS | 0/+ | ++ | + | 0/+ |
| Tardive dyskinesia | 0 | + | + | ? |
| Anticholinergic effects | ++++ | + | + | 0 |
| Seizure risk | +++ | + | + | + |
| Hematologic effects | +++ | + | + | + |
| Source: Adapted from references 15 and 16. | ||||
| * Side-effect profiles and recommended dosages of ziprasidone and aripiprazole in older patients are not yet established. | ||||
| EPS: Extrapyramidal symptoms | ||||
| Key: | ||||
| 0 = none | ||||
| + = slight | ||||
| +++ = mild | ||||
| +++++ = marked | ||||
| 0/+ = none to slight | ||||
| ++ = very mild | ||||
| ++++ = moderate | ||||
Dosing. For older patients with dementia and psychosis, start risperidone at 0.25 to 0.5 mg/d and increase by no more than 0.25 to 0.5 mg once or twice per week. Do not exceed 3 mg/d. For agitation, a 1998 Expert Consensus Guideline Series panel2 recommended starting risperidone at 0.25 to 0.5 mg/d and increasing to an average of 0.5 to 1.5 mg/d.
Olanzapine. Two double-blind, placebo-controlled studies have examined olanzapine in treating agitation associated with dementia.
Saterlee et al30 compared olanzapine, mean 2.4 mg/d, with placebo in outpatients (mean age 79) with Alzheimer’s disease and psychosis. No significant differences were noted in hepatic transaminase levels, leukopenia, EPS, or orthostatic changes.
In a later study,13 nursing home patients (mean age 83) with Alzheimer’s disease, psychosis, and agitation were randomly assigned to receive olanzapine—5, 10, or 15 mg/d—or placebo. After 6 weeks, patients receiving olanzapine, 5 or 10 mg/d, showed significant improvement in Neuropsychiatric Inventory (NPI) total core scores. Olanzapine, 15 mg/d, was not significantly more effective than placebo.
Adverse events such as somnolence and abnormal gait occurred more often with olanzapine than placebo. The somnolence rate with olanzapine was 14% for 5 mg/d and 13% for 10 mg/d, compared with 3% for placebo. For abnormal gait, the rate with olanzapine was 11% for 5 mg/d and 7% for 10 mg/d, compared with 1% for placebo.
Dosing. Start olanzapine at 2.5 mg/d, and increase after 1 to 3 days to 5 mg/d. If symptoms are not adequately controlled, titrate by 2.5-mg increments to 10 mg/d.
Quetiapine. One open-label study14 examined using quetiapine in older patients with psychotic disorders. The study enrolled 184 patients (mean age 76) with Alzheimer’s disease, Parkinson’s disease, schizophrenia, vascular dementia, schizoaffective disorder, bipolar disorder, or major depression. Before the trial, patients were taking various conventional and atypical antipsychotics.
Brief Psychiatric Rating Scale (BPRS) and Clinical Global Impressions (CGI) scores improved significantly after 52 weeks of quetiapine, median 137.5 mg/d. BPRS scores improved 20% in 49% of patients who completed the study.
Less than one-half (48%) of enrolled patients completed the study. Reasons for withdrawal included lack of efficacy (19%), adverse events or illness (15%; adverse events alone, 11%), lost to follow-up (13%), protocol noncompliance (3%), or diminished need for treatment (2%).
EPS occurred in 13% of patients. Mean total scores on the Simpson-Angus Rating Scale for Extrapyramidal Side Effects decreased 1.8 points, indicating reduced parkinsonian symptoms.
Dosing. Start quetiapine at 25 mg once at bedtime or bid; increase in 25-mg increments until the lowest effective dosage is achieved.
Ziprasidone. Little data exist on using ziprasidone in long-term care. In one recent study,31 ziprasidone (mean 100 mg/d) was given to 62 patients ages 64 to 92 with medical illnesses plus major depression, bipolar disorder, schizoaffective disorder, Alzheimer’s disease, or multi-infarct dementia. A retrospective chart review of 10 patients showed decreased agitation, as mean NPI scores declined from 76 to 33.
Sedation was the most common side effect. QTc findings, postural hypotension, and syncope rates did not change. Despite its limitations, this study suggests that ziprasidone is safe and effective in treating psychosis associated with dementia or other disorders.
Aripiprazole. As with ziprasidone, little data exist to guide the use of aripiprazole in older patients. In a randomized preliminary trial,32 192 noninstitutionalized patients with Alzheimer’s disease and psychosis were treated for 10 weeks with aripiprazole, mean 10 mg/d, or placebo.
At 8 and 10 weeks, BPRS psychosis subscale scores improved significantly in patients taking aripiprazole, compared with placebo. EPS and akathisia improved, and somnolence was the most common side effect. Although this study enrolled noninstitutionalized patients with dementia, the results suggest that aripiprazole may help treat long-term care residents with neurodegenerative disorders and behavioral disturbances.
Related resources
- Zaraa AS. Dementia update: Pharmacologic management of agitation and psychosis in older demented patients. Geriatrics 2003;58(10):48-53.
- Mills EJ, Chow TW. Randomized controlled trials in long-term care of residents with dementia: a systematic review. J Am Med Dir Assoc 2003;4(6):302-7.
- Alzheimer’s Association. Treating agitation. www.alz.org/PhysCare/Treating/agitation.htm
Drug brand names
- Aripiprazole • Abilify
- Carbamazepine • Tegretol
- Clozapine • Clozaril
- Donepezil • Aricept
- Galantamine • Reminyl
- Haloperidol • Haldol
- Olanzapine • Zyprexa
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Rivastigmine • Exelon
- Valproate • Depakote
- Ziprasidone • Geodon
Disclosure
Dr. Kasckow receives research support from, is a consultant to, or is a speaker for Eli Lilly & Co., Forest Laboratories, Solvay Pharmaceuticals, AstraZeneca Pharmaceuticals, Organon, Janssen Pharmaceutica, and Pfizer Inc.
Dr. Mulchahey reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Mohamed receives research support form Forest Laboratories and is a speaker for Eli Lilly & Co.
1. Finkel S, Costa e Silva J, Cohen G, et al. Behavioral and psychological symptoms of dementia: a consensus statement on current knowledge and implications for research and treatment. Am J Geriatr Psychiatry 1998;6:97-100.
2. The Expert Consensus Panel for Agitation in Dementia. Treatment of agitation in older persons with dementia. Postgrad Med 1998;4(suppl):1-88.
3. Cohen-Mansfield J. Nonpharmacologic interventions for inappropriate behaviors in dementia: a review, summary, and critique. Am J Geriatr Psychiatry 2001;9(4):361-81.
4. Davidson J. Pharmacologic treatment. In: Busse E, Blazer D (eds). Textbook of geriatric psychiatry (2nd ed). Washington DC: American Psychiatric Publishing, 1996:359-79.
5. Nies A, Robinson DS, Friedman MJ, et al. Relationship between age and tricyclic antidepressant plasma levels. Am J Psychiatry 1977;134(7):790-3.
6. Greenblatt DJ, Shader RJ. Benzodiazepine kinetics in the elderly. In: Usdin E (ed). Clinical pharmacology in psychiatry. New York: Elsevier, 1981;174-81.
7. Pollock BG, Perel JM, Altieri LP, et al. Debrisoquine hydroxylation phenotyping in geriatric psychopharmacology. Psychopharmacol Bull. 1992;28(2):163-8.
8. Nelson JC, Atillasoy E, Mazure C, Jatlow PI. Hydroxydesipramine in the elderly. J Clin Psychopharmacol 1988;8(6):428-33.
9. Young RC, Alexopoulos GS, Shamoian CA, et al. Plasma 10-hydroxynortriptyline in elderly depressed patients. Clin Pharmacol Ther 1984;35(4):540-4.
10. Cantillon M, Molchan SE, Little J. Pharmacological and neuroendocrine probes in neuropsychiatric illness. In: Coffey CE, Cummings JL (eds). Textbook of geriatric neuropsychiatry. Washington, DC: American Psychiatric Publishing, 1994.
11. Young RC, Meyers BS. Psychopharmacology. In: Sadovoy J, Lazarus LW, Jarvik LF, Grossberg GT (eds). Comprehensive review of geriatric psychiatry. Washington DC: American Psychiatric Publishing, 1996;755-817.
12. Katz IR, Jeste DV, Mintzer JE, et al. Comparison of risperidone and placebo for psychosis and behavioral disturbances associated with dementia: a randomized, double-blind trial. J Clin Psychiatry 1999;60(2):107-15.
13. Street JS, Clark WS, Gannon KS, et al. Olanzapine treatment of psychotic and behavioral symptoms in patients with Alzheimer disease in nursing care facilities: a double-blind, randomized, placebo-controlled trial. The HGEU Study Group. Arch Gen Psychiatry 2000;57(10):968-76.
14. Tariot PN, Salzman C, Yeung PP, et al. Long-term use of quetiapine in elderly patients with psychotic disorders. Clin Ther 2000;22(9):1068-84.
15. Casey DE. The relationship of pharmacology to side effects. J Clin Psychiatry 1997;58(suppl):55-62.
16. Pickar D. Prospects for pharmacotherapy of schizophrenia. Lancet 1995;345:557-62.
17. Kasckow JW, McElroy SL, Cameron RL, et al. A pilot study on the use of divalproex sodium in the treatment of behavioral agitation in elderly patients with dementia: assessment with the BEHAVE-AD and CGI rating scales. Curr Ther Res 1997;58(12):981-9.
18. Tariot PN, Erb R, Podgorski CA, et al. Efficacy and tolerability of carbamazepine for agitation and aggression in dementia. Am J Psychiatry 1998;155(1):54-61.
19. Kasckow JW. Cognitive enhancers for dementia: do they work? Current Psychiatry 2002;1(3):22-8.
20. Lacy C, Armstrong L, Goldman M, Lance L. (eds) Lexicomp drug information handbook. Hudson, OH: Lexicomp, 2003-2004:1225-27, 1189-90, 1026-27.
21. Jeste DV, Lacro JP, Bailey A, et al. Lower incidence of tardive dyskinesia with risperidone compared with haloperidol in older patients. J Am Geriatr Soc 1999;47(6):716-19.
22. Kane J, Honigfeld G, Singer J, Meltzer H. Clozapine for the treatment-resistant schizophrenic. A double-blind comparison with chlorpromazine. Arch Gen Psychiatry 1988;45(9):789-96.
23. Jeste DV, Caligiuri MP, Paulsen JS, et al. Risk of tardive dyskinesia in older patients. A prospective longitudinal study of 266 outpatients. Arch Gen Psychiatry 1995;52(9):756-65.
24. Sernyak MJ, Leslie DL, Alarcon RD, et al. Association of diabetes mellitus with use of atypical neuroleptics in the treatment of schizophrenia. Am J Psychiatry 2002;159:561-6.
25. Chengappa KN, Baker RW, Kreinbrook SB, Adair D. Clozapine use in female geriatric patients with psychoses. JGeriatr Psychiatry Neurol 1995;8(1):12-15.
26. Cohen-Mansfield J, Marx MS, Rosenthal AS. A description of agitation in the nursing home. J Gerontol 1989;44(3):M77-84.
27. Lavretsky H, Sultzer D. A structured trial of risperidone for the treatment of agitation in dementia. Am J Geriatr Psychiatry 1998;6(2):127-35.
28. De Deyn PP, Rabheru K, Rasmussen A, et al. A randomized trial of risperidone, placebo, and haloperidol for behavioral symptoms of dementia. Neurology 1999;53(5):946-55.
29. Brodaty H, Ames D, Snowdon J, et al. A randomized placebo-controlled trial of risperidone for the treatment of aggression, agitation, and psychosis of dementia. J Clin Psychiatry 2003;64(2):134-43.
30. Satterlee W, Reams SG, Burns PR, et al. A clinical update on olanzapine treatment in schizophrenia and in elderly Alzheimer’s disease patients (abstract). Psychopharmacol Bull 1995;31:534.-
31. Berkowitz A. Ziprasidone for elderly dementia: a case series (abstract). San Francisco, CA: American Psychiatric Association annual meeting, 2003.
32. De Deyn PP, Jeste D, Auby P, Carson W. Aripiprazole in dementia of the Alzheimer’s type (abstract). Honolulu, HI: American Association for Geriatric Psychiatry annual meeting, 2003.
Three keys can help you safely treat dementia’s difficult behavioral and psychological symptoms:
- Differentiate medical from psychiatric causes of patients’ distress.
- Use antipsychotics and other drugs as adjuncts to psychosocial treatments.
- Start low and go slow when titrating dosages.
Although no treatment reverses the pathophysiology of progressive neurodegenerative disorders, managing agitation and other behaviors can alleviate patient suffering and reduce caregiver stress. Based on the evidence and our experience, this article describes a practical approach, including a treatment algorithm and evidence of atypical antipsychotics’ efficacy and side effects in this patient population.
Algorithm Treating behavioral symptoms in patients with dementia
Dementia’s behavioral symptoms
An International Psychogeriatric Association consensus statement1 grouped dementia’s behavioral and psychological symptoms into two types:
- those usually assessed by interviewing patients and relatives—anxiety, depressed mood, hallucinations, and delusions
- those usually identified by observing patient behavior—aggression, screaming, restlessness, agitation, wandering, culturally inappropriate behaviors, sexual disinhibition, hoarding, cursing, and shadowing.
These behaviors in community-living patients are distressing to family members and increase the risk for caregiver burnout—the most common reason for placing older patients in long-term care. In the nursing home, dementia’s symptoms reduce patients’ quality of life; interfere with feeding, bathing, and dressing; and—when violent—may endanger staff and other patients.
Rule out a medical cause
Differential diagnosis. Behavioral symptoms in dementia tend to be unpredictable, which makes diagnosis and treatment challenging. The first step is to determine if a medical or psychiatric condition might account for the behavior. For instance:
- A patient with dementia may be agitated because of a distended bladder or arthritis but unable to communicate his or her pain in words.
- In mild dementia, a pre-existing psychiatric disorder such as schizophrenia might be causing a patient’s hallucinations or delusions.
- Pacing and restlessness may be drug side effects and might be controlled by reducing dosages or switching to less-activating agents.
Delirium is also a risk for older patients—especially those with degenerative neurologic disorders. Common triggers in older patients include acute illness such as a urinary tract infection or pneumonia, alcohol or benzodiazepine withdrawal, anticholinergic agents, medication changes, and dehydration.
Delirium is characterized by acute onset and fluctuating neuropsychiatric symptoms, including disturbed consciousness and changes in attention and cognition. Taking a careful history to learn the course of treatment and the patient’s baseline cognitive function can help you differentiate dementia from delirium. Family members, physicians, and nursing staff are valuable sources of this information.
Use antipsychotics as adjuncts
Psychosocial interventions. After medical causes have been ruled out, consensus guidelines2 recommend psychosocial interventions as first-line treatment of dementia’s behavioral symptoms (Algorithm). Suggested interventions for patients and caregivers are listed in Table 1.3
Antipsychotics. For patients who respond inadequately to psychosocial measures, the next step is to add an atypical antipsychotic. Because of side effects, conventional antipsychotics are not recommended for patients with dementia.
When prescribing atypicals, remember that older adults:
- are more sensitive to side effects than younger adults
- require lower starting and target dosages
- exhibit heterogeneity of response.
Older patients’ medical status can range from “fit” to “frail,” which influences individual response to medications. Generally, age-related changes in the way their bodies metabolize drugs account for older patients’ increased sensitivity to drug side effects (Box).4-11
Atypical antipsychotics and dosages that have been shown benefit for managing behavioral symptoms in older patients with dementia include:
- risperidone, 0.5 to 1.5 mg/d12
- olanzapine, 5 to 10 mg/d13
- quetiapine, 25 to 350 mg/d14 (Table 2).15,16
Start with low dosages, and titrate slowly. Increase once or twice a week until the lowest effective dosage is reached.
Augmenting agents. If antipsychotic monotherapy fails to achieve an adequate response or if side effects limit dosing, adjunctive agents may be added with caution. Augmenting agents that have shown benefit in some patients with dementia include:
- mood stabilizers such as divalproex17 or carbamazepine18
- cholinesterase inhibitors, such as donepezil, rivastigmine, or galantamine.19
Start divalproex at 125 mg bid or carbamazepine at 100 mg bid and titrate to effect. Concomitant carbamazepine will decrease blood levels of risperidone, olanzapine, and quetiapine because of hepatic enzyme induction.20
Start donepezil at 5 mg once daily and increase after 4 to 6 weeks to 10 mg qd. When using rivastigmine, start with 1.5 mg bid and titrate to 9 to 12 mg/d in divided doses. Start galantamine at 4 mg bid and increase after 1 month to 8 mg bid.
Table 1
Suggested psychosocial interventions for older patients with dementia
Communicate clearly
|
Minimize the impact of sensory deficits
|
Modify environment when necessary
|
Encourage consistent daily routines
|
Optimize social/physical stimulation
|
Encourage caregiver to:
|
Antipsychotic side effects
Atypical antipsychotics are more effective than conventional agents in treating negative symptoms and are associated with lower rates of extrapyramidal symptoms (EPS) and tardive dyskinesia (TD).21
Tardive dyskinesia. All antipsychotics can cause TD, although the risk is about 10 times greater with conventionals than atypicals. With conventionals, the annual cumulative TD incidence for young adults is 4 to 5%,22 and rates are much higher for middle-aged and older adults receiving chronic therapy:
- 29% after 1 year
- 50% after 2 years
- 63% after 3 years.23
In older patients, use atypical rather than conventional antipsychotics to minimize TD risk. Observe carefully; if TD symptoms occur, cautiously withdraw the antipsychotic and consider trying another agent.
Other risks. Atypical antipsychotics may cause sedation, orthostatic hypotension (with an increased risk for falls), increased serum prolactin, and weight gain (Table 2).
Weight gain from atypical antipsychotics has been associated with adverse effects on glucose metabolism and increased risk for type 2 diabetes.24 Some might argue that weight gain associated with olanzapine and other atypicals might benefit low-weight older patients. The frail elderly need to increase muscle mass, however, and the atypicals are associated with increases in fat mass.
Increased serum prolactin with risperidone theoretically could lead to loss of bone density, but evidence of this effect in older patients does not exist.
Start low, go slow
Clozapine may help control treatment-resistant psychosis in patients with schizophrenia and manage patients with severe TD.25 However, clozapine’s increased risk of agranulocytosis, neurologic side effects (seizures, sedation, confusion), and anticholinergic effects limit its use in older patients, particularly those with neurodegenerative disorders (Table 2).
Dosing. In rare cases when using clozapine in older patients, start with 6.25 to 12.5 mg/d. Increase by 6.25 to 12.5 mg once or twice a week to 50 to 100 mg/d.
Risperidone has been used to treat agitation in older patients with dementia in two small studies:
In a 9-week, open-label trial, 15 patients (mean age 78) with dementia were given risperidone, 0.5 to 3 mg/d. Agitation improved significantly, as measured by the Cohen-Mansfield Agitation Inventory (CMAI)—a 29-item questionnaire completed by caregivers.26 CMAI scores at study’s end averaged 49.5, compared with 70.5 at baseline.27
A 12-week, placebo-controlled, doubleblind study examined risperidone—0.5, 1, or 2 mg/d—in 625 institutionalized patients (mean age 83) with dementia and agitation. Ninety-six patients had Functional Assessment Staging Rating Scale scores of 6A, indicating moderate to severe dementia. In patients receiving risperidone, these behavioral measures were significantly reduced:
- Behavior Pathology in Alzheimer’s Disease Rating Scale (BEHAVE-AD) total scores, which measure behavior severity
- BEHAVE-AD psychosis subscale scores
- BEHAVE-AD aggressiveness scores
- CMAI verbal and aggression scores.
Adverse effects were reported at 82% for all three risperidone dosages and 85% for placebo. Side effects including somnolence, EPS, and peripheral edema were dose-related.12
Another trial compared risperidone or haloperidol, 0.5 to 4 mg/d, with placebo in treating 344 patients with behavioral symptoms of dementia. After 12 weeks of risperidone, mean dosage 1.1 mg/d:
- mean total BEHAVE-AD score decreased by 53%, compared with 37% in the placebo group
- CMAI score decreased by 32%, compared with 18% in the placebo group.
EPS were more severe with haloperidol than with risperidone or placebo.28
Risk of stroke. A small but significantly increased incidence of stroke and stroke-like events was recently reported in older patients with dementia when treated with risperidone. These events occurred in double-blind, placebocontrolled trials in patients (mean age 82) with Alzheimer’s, vascular, and mixed dementias.
Pharmacokinetic changes can influence concentrations of drugs in tissue compartments over time. Drug absorption declines with normal aging, but a clinically significant decrease in total absorption of psychotropics appears not to occur.13
In the liver, lipid-soluble psychotropics are metabolized into pharmacologically active or inactive metabolites. Some metabolic pathways, such as demethylation, may be influenced by age, leading to increased plasma concentrations of drugs and their metabolites.14,15 However, hydroxylation tends not to be affected by age.16
The ratio of body fat to water increases with aging,13 increasing the volume of distribution for lipid-soluble psychotropics. An age-related decrease in glomerular filtration accounts in part for increased accumulation of hydrophilic metabolites in some older patients.17,18
Pharmacodynamic changes with aging occur in neurotransmitter systems within cellular processing, such as at receptor or reuptake levels.19 These changes may exaggerate drug-drug interactions or affect complex neurotransmitter interactions.
The number of neurons in nigrostriatal pathways declines with age. Decreases are also seen in tyrosine hydroxylase activity, presynaptic dopamine D2 receptors, and dopamine levels—which may be particularly relevant to a discussion of antipsychotic medications.20
The net effect of these changes is the need to prescribe lower-than-usual starting and target dosages of many medications, including antipsychotics.
Most patients who experienced cerebrovascular events had one or more stroke risk factors, including diabetes, hypertension, atrial fibrillation, heart arrhythmia, atherosclerosis, or heart failure. They did not show a pattern of reduced blood pressure or orthostatic changes.12,29
Table 2
Antipsychotic side effects and dosages in older patients with dementia*
| Side effect | Clozapine (6.25 to 100 mg/d) | Risperidone (0.5 to 1.5 mg/d) | Olanzapine (5 to 10 mg/d) | Quetiapine (25 to 350 mg/d) |
|---|---|---|---|---|
| Orthostasis | ++++ | ++++ | +++ | ++ |
| Sedation | +++++ | ++ | +++ | ++ |
| Prolactin increase | 0 | +++ | + | 0 |
| Weight gain | ++++ | + | +++ | + |
| EPS | 0/+ | ++ | + | 0/+ |
| Tardive dyskinesia | 0 | + | + | ? |
| Anticholinergic effects | ++++ | + | + | 0 |
| Seizure risk | +++ | + | + | + |
| Hematologic effects | +++ | + | + | + |
| Source: Adapted from references 15 and 16. | ||||
| * Side-effect profiles and recommended dosages of ziprasidone and aripiprazole in older patients are not yet established. | ||||
| EPS: Extrapyramidal symptoms | ||||
| Key: | ||||
| 0 = none | ||||
| + = slight | ||||
| +++ = mild | ||||
| +++++ = marked | ||||
| 0/+ = none to slight | ||||
| ++ = very mild | ||||
| ++++ = moderate | ||||
Dosing. For older patients with dementia and psychosis, start risperidone at 0.25 to 0.5 mg/d and increase by no more than 0.25 to 0.5 mg once or twice per week. Do not exceed 3 mg/d. For agitation, a 1998 Expert Consensus Guideline Series panel2 recommended starting risperidone at 0.25 to 0.5 mg/d and increasing to an average of 0.5 to 1.5 mg/d.
Olanzapine. Two double-blind, placebo-controlled studies have examined olanzapine in treating agitation associated with dementia.
Saterlee et al30 compared olanzapine, mean 2.4 mg/d, with placebo in outpatients (mean age 79) with Alzheimer’s disease and psychosis. No significant differences were noted in hepatic transaminase levels, leukopenia, EPS, or orthostatic changes.
In a later study,13 nursing home patients (mean age 83) with Alzheimer’s disease, psychosis, and agitation were randomly assigned to receive olanzapine—5, 10, or 15 mg/d—or placebo. After 6 weeks, patients receiving olanzapine, 5 or 10 mg/d, showed significant improvement in Neuropsychiatric Inventory (NPI) total core scores. Olanzapine, 15 mg/d, was not significantly more effective than placebo.
Adverse events such as somnolence and abnormal gait occurred more often with olanzapine than placebo. The somnolence rate with olanzapine was 14% for 5 mg/d and 13% for 10 mg/d, compared with 3% for placebo. For abnormal gait, the rate with olanzapine was 11% for 5 mg/d and 7% for 10 mg/d, compared with 1% for placebo.
Dosing. Start olanzapine at 2.5 mg/d, and increase after 1 to 3 days to 5 mg/d. If symptoms are not adequately controlled, titrate by 2.5-mg increments to 10 mg/d.
Quetiapine. One open-label study14 examined using quetiapine in older patients with psychotic disorders. The study enrolled 184 patients (mean age 76) with Alzheimer’s disease, Parkinson’s disease, schizophrenia, vascular dementia, schizoaffective disorder, bipolar disorder, or major depression. Before the trial, patients were taking various conventional and atypical antipsychotics.
Brief Psychiatric Rating Scale (BPRS) and Clinical Global Impressions (CGI) scores improved significantly after 52 weeks of quetiapine, median 137.5 mg/d. BPRS scores improved 20% in 49% of patients who completed the study.
Less than one-half (48%) of enrolled patients completed the study. Reasons for withdrawal included lack of efficacy (19%), adverse events or illness (15%; adverse events alone, 11%), lost to follow-up (13%), protocol noncompliance (3%), or diminished need for treatment (2%).
EPS occurred in 13% of patients. Mean total scores on the Simpson-Angus Rating Scale for Extrapyramidal Side Effects decreased 1.8 points, indicating reduced parkinsonian symptoms.
Dosing. Start quetiapine at 25 mg once at bedtime or bid; increase in 25-mg increments until the lowest effective dosage is achieved.
Ziprasidone. Little data exist on using ziprasidone in long-term care. In one recent study,31 ziprasidone (mean 100 mg/d) was given to 62 patients ages 64 to 92 with medical illnesses plus major depression, bipolar disorder, schizoaffective disorder, Alzheimer’s disease, or multi-infarct dementia. A retrospective chart review of 10 patients showed decreased agitation, as mean NPI scores declined from 76 to 33.
Sedation was the most common side effect. QTc findings, postural hypotension, and syncope rates did not change. Despite its limitations, this study suggests that ziprasidone is safe and effective in treating psychosis associated with dementia or other disorders.
Aripiprazole. As with ziprasidone, little data exist to guide the use of aripiprazole in older patients. In a randomized preliminary trial,32 192 noninstitutionalized patients with Alzheimer’s disease and psychosis were treated for 10 weeks with aripiprazole, mean 10 mg/d, or placebo.
At 8 and 10 weeks, BPRS psychosis subscale scores improved significantly in patients taking aripiprazole, compared with placebo. EPS and akathisia improved, and somnolence was the most common side effect. Although this study enrolled noninstitutionalized patients with dementia, the results suggest that aripiprazole may help treat long-term care residents with neurodegenerative disorders and behavioral disturbances.
Related resources
- Zaraa AS. Dementia update: Pharmacologic management of agitation and psychosis in older demented patients. Geriatrics 2003;58(10):48-53.
- Mills EJ, Chow TW. Randomized controlled trials in long-term care of residents with dementia: a systematic review. J Am Med Dir Assoc 2003;4(6):302-7.
- Alzheimer’s Association. Treating agitation. www.alz.org/PhysCare/Treating/agitation.htm
Drug brand names
- Aripiprazole • Abilify
- Carbamazepine • Tegretol
- Clozapine • Clozaril
- Donepezil • Aricept
- Galantamine • Reminyl
- Haloperidol • Haldol
- Olanzapine • Zyprexa
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Rivastigmine • Exelon
- Valproate • Depakote
- Ziprasidone • Geodon
Disclosure
Dr. Kasckow receives research support from, is a consultant to, or is a speaker for Eli Lilly & Co., Forest Laboratories, Solvay Pharmaceuticals, AstraZeneca Pharmaceuticals, Organon, Janssen Pharmaceutica, and Pfizer Inc.
Dr. Mulchahey reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Mohamed receives research support form Forest Laboratories and is a speaker for Eli Lilly & Co.
Three keys can help you safely treat dementia’s difficult behavioral and psychological symptoms:
- Differentiate medical from psychiatric causes of patients’ distress.
- Use antipsychotics and other drugs as adjuncts to psychosocial treatments.
- Start low and go slow when titrating dosages.
Although no treatment reverses the pathophysiology of progressive neurodegenerative disorders, managing agitation and other behaviors can alleviate patient suffering and reduce caregiver stress. Based on the evidence and our experience, this article describes a practical approach, including a treatment algorithm and evidence of atypical antipsychotics’ efficacy and side effects in this patient population.
Algorithm Treating behavioral symptoms in patients with dementia
Dementia’s behavioral symptoms
An International Psychogeriatric Association consensus statement1 grouped dementia’s behavioral and psychological symptoms into two types:
- those usually assessed by interviewing patients and relatives—anxiety, depressed mood, hallucinations, and delusions
- those usually identified by observing patient behavior—aggression, screaming, restlessness, agitation, wandering, culturally inappropriate behaviors, sexual disinhibition, hoarding, cursing, and shadowing.
These behaviors in community-living patients are distressing to family members and increase the risk for caregiver burnout—the most common reason for placing older patients in long-term care. In the nursing home, dementia’s symptoms reduce patients’ quality of life; interfere with feeding, bathing, and dressing; and—when violent—may endanger staff and other patients.
Rule out a medical cause
Differential diagnosis. Behavioral symptoms in dementia tend to be unpredictable, which makes diagnosis and treatment challenging. The first step is to determine if a medical or psychiatric condition might account for the behavior. For instance:
- A patient with dementia may be agitated because of a distended bladder or arthritis but unable to communicate his or her pain in words.
- In mild dementia, a pre-existing psychiatric disorder such as schizophrenia might be causing a patient’s hallucinations or delusions.
- Pacing and restlessness may be drug side effects and might be controlled by reducing dosages or switching to less-activating agents.
Delirium is also a risk for older patients—especially those with degenerative neurologic disorders. Common triggers in older patients include acute illness such as a urinary tract infection or pneumonia, alcohol or benzodiazepine withdrawal, anticholinergic agents, medication changes, and dehydration.
Delirium is characterized by acute onset and fluctuating neuropsychiatric symptoms, including disturbed consciousness and changes in attention and cognition. Taking a careful history to learn the course of treatment and the patient’s baseline cognitive function can help you differentiate dementia from delirium. Family members, physicians, and nursing staff are valuable sources of this information.
Use antipsychotics as adjuncts
Psychosocial interventions. After medical causes have been ruled out, consensus guidelines2 recommend psychosocial interventions as first-line treatment of dementia’s behavioral symptoms (Algorithm). Suggested interventions for patients and caregivers are listed in Table 1.3
Antipsychotics. For patients who respond inadequately to psychosocial measures, the next step is to add an atypical antipsychotic. Because of side effects, conventional antipsychotics are not recommended for patients with dementia.
When prescribing atypicals, remember that older adults:
- are more sensitive to side effects than younger adults
- require lower starting and target dosages
- exhibit heterogeneity of response.
Older patients’ medical status can range from “fit” to “frail,” which influences individual response to medications. Generally, age-related changes in the way their bodies metabolize drugs account for older patients’ increased sensitivity to drug side effects (Box).4-11
Atypical antipsychotics and dosages that have been shown benefit for managing behavioral symptoms in older patients with dementia include:
- risperidone, 0.5 to 1.5 mg/d12
- olanzapine, 5 to 10 mg/d13
- quetiapine, 25 to 350 mg/d14 (Table 2).15,16
Start with low dosages, and titrate slowly. Increase once or twice a week until the lowest effective dosage is reached.
Augmenting agents. If antipsychotic monotherapy fails to achieve an adequate response or if side effects limit dosing, adjunctive agents may be added with caution. Augmenting agents that have shown benefit in some patients with dementia include:
- mood stabilizers such as divalproex17 or carbamazepine18
- cholinesterase inhibitors, such as donepezil, rivastigmine, or galantamine.19
Start divalproex at 125 mg bid or carbamazepine at 100 mg bid and titrate to effect. Concomitant carbamazepine will decrease blood levels of risperidone, olanzapine, and quetiapine because of hepatic enzyme induction.20
Start donepezil at 5 mg once daily and increase after 4 to 6 weeks to 10 mg qd. When using rivastigmine, start with 1.5 mg bid and titrate to 9 to 12 mg/d in divided doses. Start galantamine at 4 mg bid and increase after 1 month to 8 mg bid.
Table 1
Suggested psychosocial interventions for older patients with dementia
Communicate clearly
|
Minimize the impact of sensory deficits
|
Modify environment when necessary
|
Encourage consistent daily routines
|
Optimize social/physical stimulation
|
Encourage caregiver to:
|
Antipsychotic side effects
Atypical antipsychotics are more effective than conventional agents in treating negative symptoms and are associated with lower rates of extrapyramidal symptoms (EPS) and tardive dyskinesia (TD).21
Tardive dyskinesia. All antipsychotics can cause TD, although the risk is about 10 times greater with conventionals than atypicals. With conventionals, the annual cumulative TD incidence for young adults is 4 to 5%,22 and rates are much higher for middle-aged and older adults receiving chronic therapy:
- 29% after 1 year
- 50% after 2 years
- 63% after 3 years.23
In older patients, use atypical rather than conventional antipsychotics to minimize TD risk. Observe carefully; if TD symptoms occur, cautiously withdraw the antipsychotic and consider trying another agent.
Other risks. Atypical antipsychotics may cause sedation, orthostatic hypotension (with an increased risk for falls), increased serum prolactin, and weight gain (Table 2).
Weight gain from atypical antipsychotics has been associated with adverse effects on glucose metabolism and increased risk for type 2 diabetes.24 Some might argue that weight gain associated with olanzapine and other atypicals might benefit low-weight older patients. The frail elderly need to increase muscle mass, however, and the atypicals are associated with increases in fat mass.
Increased serum prolactin with risperidone theoretically could lead to loss of bone density, but evidence of this effect in older patients does not exist.
Start low, go slow
Clozapine may help control treatment-resistant psychosis in patients with schizophrenia and manage patients with severe TD.25 However, clozapine’s increased risk of agranulocytosis, neurologic side effects (seizures, sedation, confusion), and anticholinergic effects limit its use in older patients, particularly those with neurodegenerative disorders (Table 2).
Dosing. In rare cases when using clozapine in older patients, start with 6.25 to 12.5 mg/d. Increase by 6.25 to 12.5 mg once or twice a week to 50 to 100 mg/d.
Risperidone has been used to treat agitation in older patients with dementia in two small studies:
In a 9-week, open-label trial, 15 patients (mean age 78) with dementia were given risperidone, 0.5 to 3 mg/d. Agitation improved significantly, as measured by the Cohen-Mansfield Agitation Inventory (CMAI)—a 29-item questionnaire completed by caregivers.26 CMAI scores at study’s end averaged 49.5, compared with 70.5 at baseline.27
A 12-week, placebo-controlled, doubleblind study examined risperidone—0.5, 1, or 2 mg/d—in 625 institutionalized patients (mean age 83) with dementia and agitation. Ninety-six patients had Functional Assessment Staging Rating Scale scores of 6A, indicating moderate to severe dementia. In patients receiving risperidone, these behavioral measures were significantly reduced:
- Behavior Pathology in Alzheimer’s Disease Rating Scale (BEHAVE-AD) total scores, which measure behavior severity
- BEHAVE-AD psychosis subscale scores
- BEHAVE-AD aggressiveness scores
- CMAI verbal and aggression scores.
Adverse effects were reported at 82% for all three risperidone dosages and 85% for placebo. Side effects including somnolence, EPS, and peripheral edema were dose-related.12
Another trial compared risperidone or haloperidol, 0.5 to 4 mg/d, with placebo in treating 344 patients with behavioral symptoms of dementia. After 12 weeks of risperidone, mean dosage 1.1 mg/d:
- mean total BEHAVE-AD score decreased by 53%, compared with 37% in the placebo group
- CMAI score decreased by 32%, compared with 18% in the placebo group.
EPS were more severe with haloperidol than with risperidone or placebo.28
Risk of stroke. A small but significantly increased incidence of stroke and stroke-like events was recently reported in older patients with dementia when treated with risperidone. These events occurred in double-blind, placebocontrolled trials in patients (mean age 82) with Alzheimer’s, vascular, and mixed dementias.
Pharmacokinetic changes can influence concentrations of drugs in tissue compartments over time. Drug absorption declines with normal aging, but a clinically significant decrease in total absorption of psychotropics appears not to occur.13
In the liver, lipid-soluble psychotropics are metabolized into pharmacologically active or inactive metabolites. Some metabolic pathways, such as demethylation, may be influenced by age, leading to increased plasma concentrations of drugs and their metabolites.14,15 However, hydroxylation tends not to be affected by age.16
The ratio of body fat to water increases with aging,13 increasing the volume of distribution for lipid-soluble psychotropics. An age-related decrease in glomerular filtration accounts in part for increased accumulation of hydrophilic metabolites in some older patients.17,18
Pharmacodynamic changes with aging occur in neurotransmitter systems within cellular processing, such as at receptor or reuptake levels.19 These changes may exaggerate drug-drug interactions or affect complex neurotransmitter interactions.
The number of neurons in nigrostriatal pathways declines with age. Decreases are also seen in tyrosine hydroxylase activity, presynaptic dopamine D2 receptors, and dopamine levels—which may be particularly relevant to a discussion of antipsychotic medications.20
The net effect of these changes is the need to prescribe lower-than-usual starting and target dosages of many medications, including antipsychotics.
Most patients who experienced cerebrovascular events had one or more stroke risk factors, including diabetes, hypertension, atrial fibrillation, heart arrhythmia, atherosclerosis, or heart failure. They did not show a pattern of reduced blood pressure or orthostatic changes.12,29
Table 2
Antipsychotic side effects and dosages in older patients with dementia*
| Side effect | Clozapine (6.25 to 100 mg/d) | Risperidone (0.5 to 1.5 mg/d) | Olanzapine (5 to 10 mg/d) | Quetiapine (25 to 350 mg/d) |
|---|---|---|---|---|
| Orthostasis | ++++ | ++++ | +++ | ++ |
| Sedation | +++++ | ++ | +++ | ++ |
| Prolactin increase | 0 | +++ | + | 0 |
| Weight gain | ++++ | + | +++ | + |
| EPS | 0/+ | ++ | + | 0/+ |
| Tardive dyskinesia | 0 | + | + | ? |
| Anticholinergic effects | ++++ | + | + | 0 |
| Seizure risk | +++ | + | + | + |
| Hematologic effects | +++ | + | + | + |
| Source: Adapted from references 15 and 16. | ||||
| * Side-effect profiles and recommended dosages of ziprasidone and aripiprazole in older patients are not yet established. | ||||
| EPS: Extrapyramidal symptoms | ||||
| Key: | ||||
| 0 = none | ||||
| + = slight | ||||
| +++ = mild | ||||
| +++++ = marked | ||||
| 0/+ = none to slight | ||||
| ++ = very mild | ||||
| ++++ = moderate | ||||
Dosing. For older patients with dementia and psychosis, start risperidone at 0.25 to 0.5 mg/d and increase by no more than 0.25 to 0.5 mg once or twice per week. Do not exceed 3 mg/d. For agitation, a 1998 Expert Consensus Guideline Series panel2 recommended starting risperidone at 0.25 to 0.5 mg/d and increasing to an average of 0.5 to 1.5 mg/d.
Olanzapine. Two double-blind, placebo-controlled studies have examined olanzapine in treating agitation associated with dementia.
Saterlee et al30 compared olanzapine, mean 2.4 mg/d, with placebo in outpatients (mean age 79) with Alzheimer’s disease and psychosis. No significant differences were noted in hepatic transaminase levels, leukopenia, EPS, or orthostatic changes.
In a later study,13 nursing home patients (mean age 83) with Alzheimer’s disease, psychosis, and agitation were randomly assigned to receive olanzapine—5, 10, or 15 mg/d—or placebo. After 6 weeks, patients receiving olanzapine, 5 or 10 mg/d, showed significant improvement in Neuropsychiatric Inventory (NPI) total core scores. Olanzapine, 15 mg/d, was not significantly more effective than placebo.
Adverse events such as somnolence and abnormal gait occurred more often with olanzapine than placebo. The somnolence rate with olanzapine was 14% for 5 mg/d and 13% for 10 mg/d, compared with 3% for placebo. For abnormal gait, the rate with olanzapine was 11% for 5 mg/d and 7% for 10 mg/d, compared with 1% for placebo.
Dosing. Start olanzapine at 2.5 mg/d, and increase after 1 to 3 days to 5 mg/d. If symptoms are not adequately controlled, titrate by 2.5-mg increments to 10 mg/d.
Quetiapine. One open-label study14 examined using quetiapine in older patients with psychotic disorders. The study enrolled 184 patients (mean age 76) with Alzheimer’s disease, Parkinson’s disease, schizophrenia, vascular dementia, schizoaffective disorder, bipolar disorder, or major depression. Before the trial, patients were taking various conventional and atypical antipsychotics.
Brief Psychiatric Rating Scale (BPRS) and Clinical Global Impressions (CGI) scores improved significantly after 52 weeks of quetiapine, median 137.5 mg/d. BPRS scores improved 20% in 49% of patients who completed the study.
Less than one-half (48%) of enrolled patients completed the study. Reasons for withdrawal included lack of efficacy (19%), adverse events or illness (15%; adverse events alone, 11%), lost to follow-up (13%), protocol noncompliance (3%), or diminished need for treatment (2%).
EPS occurred in 13% of patients. Mean total scores on the Simpson-Angus Rating Scale for Extrapyramidal Side Effects decreased 1.8 points, indicating reduced parkinsonian symptoms.
Dosing. Start quetiapine at 25 mg once at bedtime or bid; increase in 25-mg increments until the lowest effective dosage is achieved.
Ziprasidone. Little data exist on using ziprasidone in long-term care. In one recent study,31 ziprasidone (mean 100 mg/d) was given to 62 patients ages 64 to 92 with medical illnesses plus major depression, bipolar disorder, schizoaffective disorder, Alzheimer’s disease, or multi-infarct dementia. A retrospective chart review of 10 patients showed decreased agitation, as mean NPI scores declined from 76 to 33.
Sedation was the most common side effect. QTc findings, postural hypotension, and syncope rates did not change. Despite its limitations, this study suggests that ziprasidone is safe and effective in treating psychosis associated with dementia or other disorders.
Aripiprazole. As with ziprasidone, little data exist to guide the use of aripiprazole in older patients. In a randomized preliminary trial,32 192 noninstitutionalized patients with Alzheimer’s disease and psychosis were treated for 10 weeks with aripiprazole, mean 10 mg/d, or placebo.
At 8 and 10 weeks, BPRS psychosis subscale scores improved significantly in patients taking aripiprazole, compared with placebo. EPS and akathisia improved, and somnolence was the most common side effect. Although this study enrolled noninstitutionalized patients with dementia, the results suggest that aripiprazole may help treat long-term care residents with neurodegenerative disorders and behavioral disturbances.
Related resources
- Zaraa AS. Dementia update: Pharmacologic management of agitation and psychosis in older demented patients. Geriatrics 2003;58(10):48-53.
- Mills EJ, Chow TW. Randomized controlled trials in long-term care of residents with dementia: a systematic review. J Am Med Dir Assoc 2003;4(6):302-7.
- Alzheimer’s Association. Treating agitation. www.alz.org/PhysCare/Treating/agitation.htm
Drug brand names
- Aripiprazole • Abilify
- Carbamazepine • Tegretol
- Clozapine • Clozaril
- Donepezil • Aricept
- Galantamine • Reminyl
- Haloperidol • Haldol
- Olanzapine • Zyprexa
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Rivastigmine • Exelon
- Valproate • Depakote
- Ziprasidone • Geodon
Disclosure
Dr. Kasckow receives research support from, is a consultant to, or is a speaker for Eli Lilly & Co., Forest Laboratories, Solvay Pharmaceuticals, AstraZeneca Pharmaceuticals, Organon, Janssen Pharmaceutica, and Pfizer Inc.
Dr. Mulchahey reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Mohamed receives research support form Forest Laboratories and is a speaker for Eli Lilly & Co.
1. Finkel S, Costa e Silva J, Cohen G, et al. Behavioral and psychological symptoms of dementia: a consensus statement on current knowledge and implications for research and treatment. Am J Geriatr Psychiatry 1998;6:97-100.
2. The Expert Consensus Panel for Agitation in Dementia. Treatment of agitation in older persons with dementia. Postgrad Med 1998;4(suppl):1-88.
3. Cohen-Mansfield J. Nonpharmacologic interventions for inappropriate behaviors in dementia: a review, summary, and critique. Am J Geriatr Psychiatry 2001;9(4):361-81.
4. Davidson J. Pharmacologic treatment. In: Busse E, Blazer D (eds). Textbook of geriatric psychiatry (2nd ed). Washington DC: American Psychiatric Publishing, 1996:359-79.
5. Nies A, Robinson DS, Friedman MJ, et al. Relationship between age and tricyclic antidepressant plasma levels. Am J Psychiatry 1977;134(7):790-3.
6. Greenblatt DJ, Shader RJ. Benzodiazepine kinetics in the elderly. In: Usdin E (ed). Clinical pharmacology in psychiatry. New York: Elsevier, 1981;174-81.
7. Pollock BG, Perel JM, Altieri LP, et al. Debrisoquine hydroxylation phenotyping in geriatric psychopharmacology. Psychopharmacol Bull. 1992;28(2):163-8.
8. Nelson JC, Atillasoy E, Mazure C, Jatlow PI. Hydroxydesipramine in the elderly. J Clin Psychopharmacol 1988;8(6):428-33.
9. Young RC, Alexopoulos GS, Shamoian CA, et al. Plasma 10-hydroxynortriptyline in elderly depressed patients. Clin Pharmacol Ther 1984;35(4):540-4.
10. Cantillon M, Molchan SE, Little J. Pharmacological and neuroendocrine probes in neuropsychiatric illness. In: Coffey CE, Cummings JL (eds). Textbook of geriatric neuropsychiatry. Washington, DC: American Psychiatric Publishing, 1994.
11. Young RC, Meyers BS. Psychopharmacology. In: Sadovoy J, Lazarus LW, Jarvik LF, Grossberg GT (eds). Comprehensive review of geriatric psychiatry. Washington DC: American Psychiatric Publishing, 1996;755-817.
12. Katz IR, Jeste DV, Mintzer JE, et al. Comparison of risperidone and placebo for psychosis and behavioral disturbances associated with dementia: a randomized, double-blind trial. J Clin Psychiatry 1999;60(2):107-15.
13. Street JS, Clark WS, Gannon KS, et al. Olanzapine treatment of psychotic and behavioral symptoms in patients with Alzheimer disease in nursing care facilities: a double-blind, randomized, placebo-controlled trial. The HGEU Study Group. Arch Gen Psychiatry 2000;57(10):968-76.
14. Tariot PN, Salzman C, Yeung PP, et al. Long-term use of quetiapine in elderly patients with psychotic disorders. Clin Ther 2000;22(9):1068-84.
15. Casey DE. The relationship of pharmacology to side effects. J Clin Psychiatry 1997;58(suppl):55-62.
16. Pickar D. Prospects for pharmacotherapy of schizophrenia. Lancet 1995;345:557-62.
17. Kasckow JW, McElroy SL, Cameron RL, et al. A pilot study on the use of divalproex sodium in the treatment of behavioral agitation in elderly patients with dementia: assessment with the BEHAVE-AD and CGI rating scales. Curr Ther Res 1997;58(12):981-9.
18. Tariot PN, Erb R, Podgorski CA, et al. Efficacy and tolerability of carbamazepine for agitation and aggression in dementia. Am J Psychiatry 1998;155(1):54-61.
19. Kasckow JW. Cognitive enhancers for dementia: do they work? Current Psychiatry 2002;1(3):22-8.
20. Lacy C, Armstrong L, Goldman M, Lance L. (eds) Lexicomp drug information handbook. Hudson, OH: Lexicomp, 2003-2004:1225-27, 1189-90, 1026-27.
21. Jeste DV, Lacro JP, Bailey A, et al. Lower incidence of tardive dyskinesia with risperidone compared with haloperidol in older patients. J Am Geriatr Soc 1999;47(6):716-19.
22. Kane J, Honigfeld G, Singer J, Meltzer H. Clozapine for the treatment-resistant schizophrenic. A double-blind comparison with chlorpromazine. Arch Gen Psychiatry 1988;45(9):789-96.
23. Jeste DV, Caligiuri MP, Paulsen JS, et al. Risk of tardive dyskinesia in older patients. A prospective longitudinal study of 266 outpatients. Arch Gen Psychiatry 1995;52(9):756-65.
24. Sernyak MJ, Leslie DL, Alarcon RD, et al. Association of diabetes mellitus with use of atypical neuroleptics in the treatment of schizophrenia. Am J Psychiatry 2002;159:561-6.
25. Chengappa KN, Baker RW, Kreinbrook SB, Adair D. Clozapine use in female geriatric patients with psychoses. JGeriatr Psychiatry Neurol 1995;8(1):12-15.
26. Cohen-Mansfield J, Marx MS, Rosenthal AS. A description of agitation in the nursing home. J Gerontol 1989;44(3):M77-84.
27. Lavretsky H, Sultzer D. A structured trial of risperidone for the treatment of agitation in dementia. Am J Geriatr Psychiatry 1998;6(2):127-35.
28. De Deyn PP, Rabheru K, Rasmussen A, et al. A randomized trial of risperidone, placebo, and haloperidol for behavioral symptoms of dementia. Neurology 1999;53(5):946-55.
29. Brodaty H, Ames D, Snowdon J, et al. A randomized placebo-controlled trial of risperidone for the treatment of aggression, agitation, and psychosis of dementia. J Clin Psychiatry 2003;64(2):134-43.
30. Satterlee W, Reams SG, Burns PR, et al. A clinical update on olanzapine treatment in schizophrenia and in elderly Alzheimer’s disease patients (abstract). Psychopharmacol Bull 1995;31:534.-
31. Berkowitz A. Ziprasidone for elderly dementia: a case series (abstract). San Francisco, CA: American Psychiatric Association annual meeting, 2003.
32. De Deyn PP, Jeste D, Auby P, Carson W. Aripiprazole in dementia of the Alzheimer’s type (abstract). Honolulu, HI: American Association for Geriatric Psychiatry annual meeting, 2003.
1. Finkel S, Costa e Silva J, Cohen G, et al. Behavioral and psychological symptoms of dementia: a consensus statement on current knowledge and implications for research and treatment. Am J Geriatr Psychiatry 1998;6:97-100.
2. The Expert Consensus Panel for Agitation in Dementia. Treatment of agitation in older persons with dementia. Postgrad Med 1998;4(suppl):1-88.
3. Cohen-Mansfield J. Nonpharmacologic interventions for inappropriate behaviors in dementia: a review, summary, and critique. Am J Geriatr Psychiatry 2001;9(4):361-81.
4. Davidson J. Pharmacologic treatment. In: Busse E, Blazer D (eds). Textbook of geriatric psychiatry (2nd ed). Washington DC: American Psychiatric Publishing, 1996:359-79.
5. Nies A, Robinson DS, Friedman MJ, et al. Relationship between age and tricyclic antidepressant plasma levels. Am J Psychiatry 1977;134(7):790-3.
6. Greenblatt DJ, Shader RJ. Benzodiazepine kinetics in the elderly. In: Usdin E (ed). Clinical pharmacology in psychiatry. New York: Elsevier, 1981;174-81.
7. Pollock BG, Perel JM, Altieri LP, et al. Debrisoquine hydroxylation phenotyping in geriatric psychopharmacology. Psychopharmacol Bull. 1992;28(2):163-8.
8. Nelson JC, Atillasoy E, Mazure C, Jatlow PI. Hydroxydesipramine in the elderly. J Clin Psychopharmacol 1988;8(6):428-33.
9. Young RC, Alexopoulos GS, Shamoian CA, et al. Plasma 10-hydroxynortriptyline in elderly depressed patients. Clin Pharmacol Ther 1984;35(4):540-4.
10. Cantillon M, Molchan SE, Little J. Pharmacological and neuroendocrine probes in neuropsychiatric illness. In: Coffey CE, Cummings JL (eds). Textbook of geriatric neuropsychiatry. Washington, DC: American Psychiatric Publishing, 1994.
11. Young RC, Meyers BS. Psychopharmacology. In: Sadovoy J, Lazarus LW, Jarvik LF, Grossberg GT (eds). Comprehensive review of geriatric psychiatry. Washington DC: American Psychiatric Publishing, 1996;755-817.
12. Katz IR, Jeste DV, Mintzer JE, et al. Comparison of risperidone and placebo for psychosis and behavioral disturbances associated with dementia: a randomized, double-blind trial. J Clin Psychiatry 1999;60(2):107-15.
13. Street JS, Clark WS, Gannon KS, et al. Olanzapine treatment of psychotic and behavioral symptoms in patients with Alzheimer disease in nursing care facilities: a double-blind, randomized, placebo-controlled trial. The HGEU Study Group. Arch Gen Psychiatry 2000;57(10):968-76.
14. Tariot PN, Salzman C, Yeung PP, et al. Long-term use of quetiapine in elderly patients with psychotic disorders. Clin Ther 2000;22(9):1068-84.
15. Casey DE. The relationship of pharmacology to side effects. J Clin Psychiatry 1997;58(suppl):55-62.
16. Pickar D. Prospects for pharmacotherapy of schizophrenia. Lancet 1995;345:557-62.
17. Kasckow JW, McElroy SL, Cameron RL, et al. A pilot study on the use of divalproex sodium in the treatment of behavioral agitation in elderly patients with dementia: assessment with the BEHAVE-AD and CGI rating scales. Curr Ther Res 1997;58(12):981-9.
18. Tariot PN, Erb R, Podgorski CA, et al. Efficacy and tolerability of carbamazepine for agitation and aggression in dementia. Am J Psychiatry 1998;155(1):54-61.
19. Kasckow JW. Cognitive enhancers for dementia: do they work? Current Psychiatry 2002;1(3):22-8.
20. Lacy C, Armstrong L, Goldman M, Lance L. (eds) Lexicomp drug information handbook. Hudson, OH: Lexicomp, 2003-2004:1225-27, 1189-90, 1026-27.
21. Jeste DV, Lacro JP, Bailey A, et al. Lower incidence of tardive dyskinesia with risperidone compared with haloperidol in older patients. J Am Geriatr Soc 1999;47(6):716-19.
22. Kane J, Honigfeld G, Singer J, Meltzer H. Clozapine for the treatment-resistant schizophrenic. A double-blind comparison with chlorpromazine. Arch Gen Psychiatry 1988;45(9):789-96.
23. Jeste DV, Caligiuri MP, Paulsen JS, et al. Risk of tardive dyskinesia in older patients. A prospective longitudinal study of 266 outpatients. Arch Gen Psychiatry 1995;52(9):756-65.
24. Sernyak MJ, Leslie DL, Alarcon RD, et al. Association of diabetes mellitus with use of atypical neuroleptics in the treatment of schizophrenia. Am J Psychiatry 2002;159:561-6.
25. Chengappa KN, Baker RW, Kreinbrook SB, Adair D. Clozapine use in female geriatric patients with psychoses. JGeriatr Psychiatry Neurol 1995;8(1):12-15.
26. Cohen-Mansfield J, Marx MS, Rosenthal AS. A description of agitation in the nursing home. J Gerontol 1989;44(3):M77-84.
27. Lavretsky H, Sultzer D. A structured trial of risperidone for the treatment of agitation in dementia. Am J Geriatr Psychiatry 1998;6(2):127-35.
28. De Deyn PP, Rabheru K, Rasmussen A, et al. A randomized trial of risperidone, placebo, and haloperidol for behavioral symptoms of dementia. Neurology 1999;53(5):946-55.
29. Brodaty H, Ames D, Snowdon J, et al. A randomized placebo-controlled trial of risperidone for the treatment of aggression, agitation, and psychosis of dementia. J Clin Psychiatry 2003;64(2):134-43.
30. Satterlee W, Reams SG, Burns PR, et al. A clinical update on olanzapine treatment in schizophrenia and in elderly Alzheimer’s disease patients (abstract). Psychopharmacol Bull 1995;31:534.-
31. Berkowitz A. Ziprasidone for elderly dementia: a case series (abstract). San Francisco, CA: American Psychiatric Association annual meeting, 2003.
32. De Deyn PP, Jeste D, Auby P, Carson W. Aripiprazole in dementia of the Alzheimer’s type (abstract). Honolulu, HI: American Association for Geriatric Psychiatry annual meeting, 2003.
Is this patient dangerous? 5 steps to assess risk for violence
“Will this patient turn violent?” Psychiatrists face this tough question every day. Although predicting a complex behavior such as violence is nearly impossible, we can prepare for dangerous behavior and improve our safety by:
- knowing the risk factors for patient violence
- assessing individuals for violence potential before clinical encounters
- controlling situations to reduce injury risk.
In one study, more than 50% of psychiatrists and 75% of mental health nurses reported an act or threat of violence from patients within the past year.1 To help you avoid becoming a statistic, this article provides a 5-step procedure (Figure 1). to quickly assess and respond to risk of violence in a psychiatric patient.
Step 1: Seek patient history
A careful review of past events and those immediately preceding the clinical encounter is the best tool for assessing potential for violence. The more you can learn from the patient chart and other sources before you see the patient, the better (Table 1). Valuable clues can be obtained from interviews with family members, outpatient providers, police officers, and others who have had pertinent social contact with the patient.
Figure 5 steps to assess and reduce the risk of patient violence
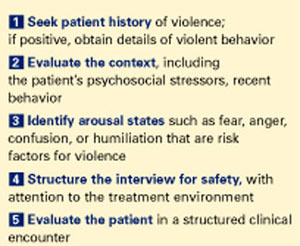
Past violence is the most powerful predictor of future violence, according to published studies. Higher frequency of aggressive episodes, greater degree of aggressive injury, and lack of apparent provocation in past episodes all increase the violence risk.3
A minority of patients account for most aggressive acts in clinical encounters. One study showed that recidivists committed 53% of all violent behaviors in a health care setting.4 A patient’s history of violence should be flagged in the chart and verbally passed on to staff to alert providers of increased risk.
However, not having a violent history does not guarantee that a patient will not become dangerous during a clinical encounter. All patients with a violent past had an initial violent episode, and that first time can occur in a practice setting.
Psychotic states by themselves appear to increase the risk of violence, although the literature is mixed.5,6 Clearly, however, psychotic states associated with arousal or agitation do predispose patients to violence, especially if the psychosis involves active paranoid delusions or hallucinations associated with negative affect (anger, sadness, anxiety).7
Increased rates of violence have also been reported in psychiatric patients with:
- acute manic states associated with arousal or agitation8
- nonspecific neurologic abnormalities such as abnormal EEGs, localizing neurologic signs, or “soft signs” (impaired face-hand test, graphesthesia, stereognosis).9
Demographic variables associated with higher violence rates include ages 15 to 24, nonwhite race, male gender, poverty, and low educational level. Other variables include history of abuse, victimization, family violence, limited employment skills, and “rootlessness,” such as poor family network and frequent moves or job changes.10
Psychiatric diagnoses associated with increased risk of violence include schizophrenia, bipolar mania, alcohol and other substance abuse, and personality disorders.11-13 In clinical practice, however, I find psychiatric diagnoses less useful in predicting violence than the patient’s arousal state and the other risk factors discussed above.
Step 2: Evaluate the context
In addition to evidence-supported risk factors (Table 2), context—or the broader situation in which a patient is embedded at the time of psychiatric evaluation—plays a prominent role in potentially violent situations. For example, if “divorce” is listed as a presenting factor:
- Is the patient recently divorced, or did it occur years ago?
- Does he hate all women or just his ex-wife?
- Was she having an affair, and did he just learn about this?
In other words, environmental stresses can be acute and destabilizing or part of the patient’s chronic life picture and serve in homeostatic functioning.
Step 3: Identify arousal states
Patients rarely commit violent acts when their anxiety and moods are well controlled. They are more likely to become aggressive in high arousal states.
Fear is probably an element of most situations where patients act out violently. Because the fearful patient may not exhibit easily interpreted danger signals, however, you may unwittingly provoke an assault by violating his or her personal space. A fearful, paranoid patient requires a greater-than-usual “intimate zone,” although this need for increased space may not be obvious.
Minimize provocation by explaining your actions and behaviors in advance (such as, “I would like to enter the room, sit down, and talk with you for about 20 minutes”). Be business-like with paranoid patients. Avoid exuding warmth, as they may view attempts at warmth as having sinister intent.
Clinicians are sometimes injured when trying to prevent a fearful, paranoid patient from fleeing. To avoid injury, don’t stand between the patient and the door. Let the patient escape from the immediate situation, and enlist security or police in further intervention attempts.
Anger is easy to recognize by signs of mounting tension. Loud voice, inappropriate staring, banging objects, clenched fists, agitated pacing, and verbal threats are common in the angry patient before a violent episode. Although this seems self-evident, it is surprising how many violent acts occur when these signs are obvious and noted by staff, yet no de-escalation measures are taken.
A patient’s verbal threats can actually help the clinician. This “red flag” alerts staff to focus on de-escalation techniques and prepare for a violent situation.
Confusion can be an underlying risk factor in patients with delirium or nonspecific organic brain syndrome. These patients may strike out unexpectedly when health care personnel are attempting to do routine procedures, and clinicians are sometimes caught off-guard when operating in a care-giving rather than defensive mode.
Table 1
Will this patient become violent? Questions to consider before a clinical encounter
Long-term behavior
|
Immediate situation
|
Clinicians can often avoid arousing confused patients by using orienting techniques and explaining their actions. For example, a nurse might say, “Hello Mr. X, I am a nurse and you are in this hospital for treatment of your illness. I will need to use this machine to check your blood pressure.”
Humiliation. Men in particular can react aggressively to loss of self-esteem and feelings of powerlessness. Take note if a man has been humiliated in front of family before being brought for evaluation; for example, was he removed by police in an emergency detention situation? This patient may need to act out violently to restore his sense of self.
Staff can lessen a patient’s potential to act on humiliation by using a therapeutic, esteem-building interview technique. For example, address the patient as “Mr.” instead of by first name, and highlight his strengths or accomplishments early in the interview.
Table 2
Risk factors for violence among psychiatric patients*
|
| * As identified in the literature. |
Step 4: Structure the interview for safety
The time you take before an interview to learn about a patient’s violence history, context, and arousal state is time well-spent and more patient-specific than past diagnoses. This information allows you to prepare for a safe intervention.
Interview environment. The physical and social environment where you interview the patient may contribute to violence potential.
- Is the patient being interviewed in a cramped room or an open hallway?
- Is the evaluation unit overcrowded?
- Are security personnel visible?
- Is the examiner of the same race or ethnic background as the patient?
Cramped and overcrowded conditions on a psychiatric ward have been associated with higher rates of patient violence.2 In one case of context-specific violence, a veteran with known institutional transference issues toward the government attacked providers in a VA hospital on several occasions but did not exhibit this behavior in other, non-VA medical settings.
Take control of the interview and treatment situation. Use the physical space and personnel as you would any other intervention tool—to increase safety and decrease potential for violent behavior. For example, some patients do better when interviewed in a small, private setting. Other interviews must be conducted in a triage area while police escorts hold the patient and handcuffs remain on.
Ideally, you and the patient should have equal access to the door if you conduct the psychiatric interview in an enclosed room. With high-risk patients, arrange your seating at a 90-degree angle—rather than face-to-face—to limit sustained, confrontational eye contact. Sit at greater than an arm swing or leg kick away from the patient, and require him or her to remain seated during the interview (or you will promptly leave).
In the outpatient practice, terminate the interview or evaluation session if a patient in a negative affective arousal state does not allow verbal redirection. Before you make any movement to exit, however, announce, “I am leaving the room now.”
Trust your intuition. I do not enter a closed, private space with a patient unless I feel safe. If I feel afraid, I take that as a valuable warning that further safety measures are necessary.
Use restraints as needed. When patients with a history of violence are brought to the hospital in high arousal states, I let them remain in restraint with security present during the initial interview. If the patient cannot have a back-and-forth conversation with me, I keep the security force present until I believe my verbal interactions have a substantial effect.
Patients must be responsive to talking interventions before restraint, security, or other environmental safety measures are removed. Some patients do not reach this point until after tranquilizing medications are given.
Step 5: Tthe clinical encounter
When discussing how to assess the likelihood of patient violence during a clinical encounter, a psychiatric colleague once commented, “Risk factors make you worry more; nothing makes you worry less.”
In other words, keep your guard up. Let clinical judgment take precedence over statistics when you are evaluating any patient. Statistics represent frequencies or averages; they may or may not apply to any one individual.
Techniques for assessing and treating violent patients are beyond the scope of this article, but at the very least:
- obtain training in safety/treatment protocols for violent patients
- ensure that your hospital/clinic has procedures in place to improve safety and to handle violent situations.
Visible, high numbers of confident-appearing—but not confrontational—staff or security may dissuade the patient from acting out. Then, most often, force will not be needed. If force is needed to control a violent patient, make sure the staff’s response is strong and overwhelming.
For every violent act requiring staff intervention, automatically schedule a debriefing session for those involved to assess the incident and allow them to express their feelings.
Related resources
- American Association for Emergency Psychiatry. www.emergencypsychiatry.org
- Volavka J. The neurobiology of violence: an update. J Neuropsychiatry Clin Neurosci 1999;11:307-14.
- McNiel DE, Eisner JP, Binder RL. The relationship between command hallucinations and violence. Psychiatric Services 2000;51:1288-92.
1. Nolan P, Dallender J, Soares J, et al. Violence in mental health care: the experiences of mental health nurses and psychiatrists. J Adv Nurs 1999;30:934-41.
2. Blomhoff S, Seim S, Friis S. Can prediction of violence among psychiatric inpatients be improved? Hosp Community Psychiatry 1990;41:771-5.
3. Convit A, Isay D, Otis D, et al. Characteristics of repeatedly assaultive psychiatric inpatients. Hosp Community Psychiatry 1990;41:1112-5.
4. Taylor P. Motives for offending among violent and psychotic men. Br J Psychiatry 1985;147:491-8.
5. Junginger J, Parks-Levy J, McGuire L. Delusions and symptom-consistent violence. Psychiatr Serv 1998;49:218-20.
6. Cheung P, Schweitzer I, Crowley K, et al. Violence in schizophrenia: role of hallucinations and delusions. Schizophr Res 1997;26:181-90.
7. Binder R, McNiel D. Effects of diagnosis and context on dangerousness. Am J Psychiatry 1988;145:728-32.
8. Convit A, Jaeger J, Pin Lin S, et al. Predicting assaultiveness in psychiatric inpatients: A pilot study. Hosp Community Psychiatry 1988;39:429-34.
9. Hyman S. The violent patient. In: Hyman S (ed). Manual of psychiatric emergencies. Boston: Little, Brown and Co., 1988;23-31.
10. Swartz M, Swanson J, Hiday V, et al. Violence and severe mental illness: the effects of substance abuse and nonadherence to medication. Am J Psychiatry 1998;155:226-31.
11. Owen C, Tarantello C, Jones M, et al. Repetitively violent patients in psychiatric units. Psychiatr Serv 1998;49:1458-61.
12. Citrome L, Volavka J. Clinical management of persistent aggressive behavior in schizophrenia, part I. Definitions, epidemiology, assessment and acute treatment. Essen Psychopharmacol 2002;5:1-16.
13. Abeyasinghe R, Jayasekera R. Violence in a general hospital psychiatry unit for men. Ceylon Med J 2003;48(2):45-7.
“Will this patient turn violent?” Psychiatrists face this tough question every day. Although predicting a complex behavior such as violence is nearly impossible, we can prepare for dangerous behavior and improve our safety by:
- knowing the risk factors for patient violence
- assessing individuals for violence potential before clinical encounters
- controlling situations to reduce injury risk.
In one study, more than 50% of psychiatrists and 75% of mental health nurses reported an act or threat of violence from patients within the past year.1 To help you avoid becoming a statistic, this article provides a 5-step procedure (Figure 1). to quickly assess and respond to risk of violence in a psychiatric patient.
Step 1: Seek patient history
A careful review of past events and those immediately preceding the clinical encounter is the best tool for assessing potential for violence. The more you can learn from the patient chart and other sources before you see the patient, the better (Table 1). Valuable clues can be obtained from interviews with family members, outpatient providers, police officers, and others who have had pertinent social contact with the patient.
Figure 5 steps to assess and reduce the risk of patient violence
Past violence is the most powerful predictor of future violence, according to published studies. Higher frequency of aggressive episodes, greater degree of aggressive injury, and lack of apparent provocation in past episodes all increase the violence risk.3
A minority of patients account for most aggressive acts in clinical encounters. One study showed that recidivists committed 53% of all violent behaviors in a health care setting.4 A patient’s history of violence should be flagged in the chart and verbally passed on to staff to alert providers of increased risk.
However, not having a violent history does not guarantee that a patient will not become dangerous during a clinical encounter. All patients with a violent past had an initial violent episode, and that first time can occur in a practice setting.
Psychotic states by themselves appear to increase the risk of violence, although the literature is mixed.5,6 Clearly, however, psychotic states associated with arousal or agitation do predispose patients to violence, especially if the psychosis involves active paranoid delusions or hallucinations associated with negative affect (anger, sadness, anxiety).7
Increased rates of violence have also been reported in psychiatric patients with:
- acute manic states associated with arousal or agitation8
- nonspecific neurologic abnormalities such as abnormal EEGs, localizing neurologic signs, or “soft signs” (impaired face-hand test, graphesthesia, stereognosis).9
Demographic variables associated with higher violence rates include ages 15 to 24, nonwhite race, male gender, poverty, and low educational level. Other variables include history of abuse, victimization, family violence, limited employment skills, and “rootlessness,” such as poor family network and frequent moves or job changes.10
Psychiatric diagnoses associated with increased risk of violence include schizophrenia, bipolar mania, alcohol and other substance abuse, and personality disorders.11-13 In clinical practice, however, I find psychiatric diagnoses less useful in predicting violence than the patient’s arousal state and the other risk factors discussed above.
Step 2: Evaluate the context
In addition to evidence-supported risk factors (Table 2), context—or the broader situation in which a patient is embedded at the time of psychiatric evaluation—plays a prominent role in potentially violent situations. For example, if “divorce” is listed as a presenting factor:
- Is the patient recently divorced, or did it occur years ago?
- Does he hate all women or just his ex-wife?
- Was she having an affair, and did he just learn about this?
In other words, environmental stresses can be acute and destabilizing or part of the patient’s chronic life picture and serve in homeostatic functioning.
Step 3: Identify arousal states
Patients rarely commit violent acts when their anxiety and moods are well controlled. They are more likely to become aggressive in high arousal states.
Fear is probably an element of most situations where patients act out violently. Because the fearful patient may not exhibit easily interpreted danger signals, however, you may unwittingly provoke an assault by violating his or her personal space. A fearful, paranoid patient requires a greater-than-usual “intimate zone,” although this need for increased space may not be obvious.
Minimize provocation by explaining your actions and behaviors in advance (such as, “I would like to enter the room, sit down, and talk with you for about 20 minutes”). Be business-like with paranoid patients. Avoid exuding warmth, as they may view attempts at warmth as having sinister intent.
Clinicians are sometimes injured when trying to prevent a fearful, paranoid patient from fleeing. To avoid injury, don’t stand between the patient and the door. Let the patient escape from the immediate situation, and enlist security or police in further intervention attempts.
Anger is easy to recognize by signs of mounting tension. Loud voice, inappropriate staring, banging objects, clenched fists, agitated pacing, and verbal threats are common in the angry patient before a violent episode. Although this seems self-evident, it is surprising how many violent acts occur when these signs are obvious and noted by staff, yet no de-escalation measures are taken.
A patient’s verbal threats can actually help the clinician. This “red flag” alerts staff to focus on de-escalation techniques and prepare for a violent situation.
Confusion can be an underlying risk factor in patients with delirium or nonspecific organic brain syndrome. These patients may strike out unexpectedly when health care personnel are attempting to do routine procedures, and clinicians are sometimes caught off-guard when operating in a care-giving rather than defensive mode.
Table 1
Will this patient become violent? Questions to consider before a clinical encounter
Long-term behavior
|
Immediate situation
|
Clinicians can often avoid arousing confused patients by using orienting techniques and explaining their actions. For example, a nurse might say, “Hello Mr. X, I am a nurse and you are in this hospital for treatment of your illness. I will need to use this machine to check your blood pressure.”
Humiliation. Men in particular can react aggressively to loss of self-esteem and feelings of powerlessness. Take note if a man has been humiliated in front of family before being brought for evaluation; for example, was he removed by police in an emergency detention situation? This patient may need to act out violently to restore his sense of self.
Staff can lessen a patient’s potential to act on humiliation by using a therapeutic, esteem-building interview technique. For example, address the patient as “Mr.” instead of by first name, and highlight his strengths or accomplishments early in the interview.
Table 2
Risk factors for violence among psychiatric patients*
|
| * As identified in the literature. |
Step 4: Structure the interview for safety
The time you take before an interview to learn about a patient’s violence history, context, and arousal state is time well-spent and more patient-specific than past diagnoses. This information allows you to prepare for a safe intervention.
Interview environment. The physical and social environment where you interview the patient may contribute to violence potential.
- Is the patient being interviewed in a cramped room or an open hallway?
- Is the evaluation unit overcrowded?
- Are security personnel visible?
- Is the examiner of the same race or ethnic background as the patient?
Cramped and overcrowded conditions on a psychiatric ward have been associated with higher rates of patient violence.2 In one case of context-specific violence, a veteran with known institutional transference issues toward the government attacked providers in a VA hospital on several occasions but did not exhibit this behavior in other, non-VA medical settings.
Take control of the interview and treatment situation. Use the physical space and personnel as you would any other intervention tool—to increase safety and decrease potential for violent behavior. For example, some patients do better when interviewed in a small, private setting. Other interviews must be conducted in a triage area while police escorts hold the patient and handcuffs remain on.
Ideally, you and the patient should have equal access to the door if you conduct the psychiatric interview in an enclosed room. With high-risk patients, arrange your seating at a 90-degree angle—rather than face-to-face—to limit sustained, confrontational eye contact. Sit at greater than an arm swing or leg kick away from the patient, and require him or her to remain seated during the interview (or you will promptly leave).
In the outpatient practice, terminate the interview or evaluation session if a patient in a negative affective arousal state does not allow verbal redirection. Before you make any movement to exit, however, announce, “I am leaving the room now.”
Trust your intuition. I do not enter a closed, private space with a patient unless I feel safe. If I feel afraid, I take that as a valuable warning that further safety measures are necessary.
Use restraints as needed. When patients with a history of violence are brought to the hospital in high arousal states, I let them remain in restraint with security present during the initial interview. If the patient cannot have a back-and-forth conversation with me, I keep the security force present until I believe my verbal interactions have a substantial effect.
Patients must be responsive to talking interventions before restraint, security, or other environmental safety measures are removed. Some patients do not reach this point until after tranquilizing medications are given.
Step 5: Tthe clinical encounter
When discussing how to assess the likelihood of patient violence during a clinical encounter, a psychiatric colleague once commented, “Risk factors make you worry more; nothing makes you worry less.”
In other words, keep your guard up. Let clinical judgment take precedence over statistics when you are evaluating any patient. Statistics represent frequencies or averages; they may or may not apply to any one individual.
Techniques for assessing and treating violent patients are beyond the scope of this article, but at the very least:
- obtain training in safety/treatment protocols for violent patients
- ensure that your hospital/clinic has procedures in place to improve safety and to handle violent situations.
Visible, high numbers of confident-appearing—but not confrontational—staff or security may dissuade the patient from acting out. Then, most often, force will not be needed. If force is needed to control a violent patient, make sure the staff’s response is strong and overwhelming.
For every violent act requiring staff intervention, automatically schedule a debriefing session for those involved to assess the incident and allow them to express their feelings.
Related resources
- American Association for Emergency Psychiatry. www.emergencypsychiatry.org
- Volavka J. The neurobiology of violence: an update. J Neuropsychiatry Clin Neurosci 1999;11:307-14.
- McNiel DE, Eisner JP, Binder RL. The relationship between command hallucinations and violence. Psychiatric Services 2000;51:1288-92.
“Will this patient turn violent?” Psychiatrists face this tough question every day. Although predicting a complex behavior such as violence is nearly impossible, we can prepare for dangerous behavior and improve our safety by:
- knowing the risk factors for patient violence
- assessing individuals for violence potential before clinical encounters
- controlling situations to reduce injury risk.
In one study, more than 50% of psychiatrists and 75% of mental health nurses reported an act or threat of violence from patients within the past year.1 To help you avoid becoming a statistic, this article provides a 5-step procedure (Figure 1). to quickly assess and respond to risk of violence in a psychiatric patient.
Step 1: Seek patient history
A careful review of past events and those immediately preceding the clinical encounter is the best tool for assessing potential for violence. The more you can learn from the patient chart and other sources before you see the patient, the better (Table 1). Valuable clues can be obtained from interviews with family members, outpatient providers, police officers, and others who have had pertinent social contact with the patient.
Figure 5 steps to assess and reduce the risk of patient violence
Past violence is the most powerful predictor of future violence, according to published studies. Higher frequency of aggressive episodes, greater degree of aggressive injury, and lack of apparent provocation in past episodes all increase the violence risk.3
A minority of patients account for most aggressive acts in clinical encounters. One study showed that recidivists committed 53% of all violent behaviors in a health care setting.4 A patient’s history of violence should be flagged in the chart and verbally passed on to staff to alert providers of increased risk.
However, not having a violent history does not guarantee that a patient will not become dangerous during a clinical encounter. All patients with a violent past had an initial violent episode, and that first time can occur in a practice setting.
Psychotic states by themselves appear to increase the risk of violence, although the literature is mixed.5,6 Clearly, however, psychotic states associated with arousal or agitation do predispose patients to violence, especially if the psychosis involves active paranoid delusions or hallucinations associated with negative affect (anger, sadness, anxiety).7
Increased rates of violence have also been reported in psychiatric patients with:
- acute manic states associated with arousal or agitation8
- nonspecific neurologic abnormalities such as abnormal EEGs, localizing neurologic signs, or “soft signs” (impaired face-hand test, graphesthesia, stereognosis).9
Demographic variables associated with higher violence rates include ages 15 to 24, nonwhite race, male gender, poverty, and low educational level. Other variables include history of abuse, victimization, family violence, limited employment skills, and “rootlessness,” such as poor family network and frequent moves or job changes.10
Psychiatric diagnoses associated with increased risk of violence include schizophrenia, bipolar mania, alcohol and other substance abuse, and personality disorders.11-13 In clinical practice, however, I find psychiatric diagnoses less useful in predicting violence than the patient’s arousal state and the other risk factors discussed above.
Step 2: Evaluate the context
In addition to evidence-supported risk factors (Table 2), context—or the broader situation in which a patient is embedded at the time of psychiatric evaluation—plays a prominent role in potentially violent situations. For example, if “divorce” is listed as a presenting factor:
- Is the patient recently divorced, or did it occur years ago?
- Does he hate all women or just his ex-wife?
- Was she having an affair, and did he just learn about this?
In other words, environmental stresses can be acute and destabilizing or part of the patient’s chronic life picture and serve in homeostatic functioning.
Step 3: Identify arousal states
Patients rarely commit violent acts when their anxiety and moods are well controlled. They are more likely to become aggressive in high arousal states.
Fear is probably an element of most situations where patients act out violently. Because the fearful patient may not exhibit easily interpreted danger signals, however, you may unwittingly provoke an assault by violating his or her personal space. A fearful, paranoid patient requires a greater-than-usual “intimate zone,” although this need for increased space may not be obvious.
Minimize provocation by explaining your actions and behaviors in advance (such as, “I would like to enter the room, sit down, and talk with you for about 20 minutes”). Be business-like with paranoid patients. Avoid exuding warmth, as they may view attempts at warmth as having sinister intent.
Clinicians are sometimes injured when trying to prevent a fearful, paranoid patient from fleeing. To avoid injury, don’t stand between the patient and the door. Let the patient escape from the immediate situation, and enlist security or police in further intervention attempts.
Anger is easy to recognize by signs of mounting tension. Loud voice, inappropriate staring, banging objects, clenched fists, agitated pacing, and verbal threats are common in the angry patient before a violent episode. Although this seems self-evident, it is surprising how many violent acts occur when these signs are obvious and noted by staff, yet no de-escalation measures are taken.
A patient’s verbal threats can actually help the clinician. This “red flag” alerts staff to focus on de-escalation techniques and prepare for a violent situation.
Confusion can be an underlying risk factor in patients with delirium or nonspecific organic brain syndrome. These patients may strike out unexpectedly when health care personnel are attempting to do routine procedures, and clinicians are sometimes caught off-guard when operating in a care-giving rather than defensive mode.
Table 1
Will this patient become violent? Questions to consider before a clinical encounter
Long-term behavior
|
Immediate situation
|
Clinicians can often avoid arousing confused patients by using orienting techniques and explaining their actions. For example, a nurse might say, “Hello Mr. X, I am a nurse and you are in this hospital for treatment of your illness. I will need to use this machine to check your blood pressure.”
Humiliation. Men in particular can react aggressively to loss of self-esteem and feelings of powerlessness. Take note if a man has been humiliated in front of family before being brought for evaluation; for example, was he removed by police in an emergency detention situation? This patient may need to act out violently to restore his sense of self.
Staff can lessen a patient’s potential to act on humiliation by using a therapeutic, esteem-building interview technique. For example, address the patient as “Mr.” instead of by first name, and highlight his strengths or accomplishments early in the interview.
Table 2
Risk factors for violence among psychiatric patients*
|
| * As identified in the literature. |
Step 4: Structure the interview for safety
The time you take before an interview to learn about a patient’s violence history, context, and arousal state is time well-spent and more patient-specific than past diagnoses. This information allows you to prepare for a safe intervention.
Interview environment. The physical and social environment where you interview the patient may contribute to violence potential.
- Is the patient being interviewed in a cramped room or an open hallway?
- Is the evaluation unit overcrowded?
- Are security personnel visible?
- Is the examiner of the same race or ethnic background as the patient?
Cramped and overcrowded conditions on a psychiatric ward have been associated with higher rates of patient violence.2 In one case of context-specific violence, a veteran with known institutional transference issues toward the government attacked providers in a VA hospital on several occasions but did not exhibit this behavior in other, non-VA medical settings.
Take control of the interview and treatment situation. Use the physical space and personnel as you would any other intervention tool—to increase safety and decrease potential for violent behavior. For example, some patients do better when interviewed in a small, private setting. Other interviews must be conducted in a triage area while police escorts hold the patient and handcuffs remain on.
Ideally, you and the patient should have equal access to the door if you conduct the psychiatric interview in an enclosed room. With high-risk patients, arrange your seating at a 90-degree angle—rather than face-to-face—to limit sustained, confrontational eye contact. Sit at greater than an arm swing or leg kick away from the patient, and require him or her to remain seated during the interview (or you will promptly leave).
In the outpatient practice, terminate the interview or evaluation session if a patient in a negative affective arousal state does not allow verbal redirection. Before you make any movement to exit, however, announce, “I am leaving the room now.”
Trust your intuition. I do not enter a closed, private space with a patient unless I feel safe. If I feel afraid, I take that as a valuable warning that further safety measures are necessary.
Use restraints as needed. When patients with a history of violence are brought to the hospital in high arousal states, I let them remain in restraint with security present during the initial interview. If the patient cannot have a back-and-forth conversation with me, I keep the security force present until I believe my verbal interactions have a substantial effect.
Patients must be responsive to talking interventions before restraint, security, or other environmental safety measures are removed. Some patients do not reach this point until after tranquilizing medications are given.
Step 5: Tthe clinical encounter
When discussing how to assess the likelihood of patient violence during a clinical encounter, a psychiatric colleague once commented, “Risk factors make you worry more; nothing makes you worry less.”
In other words, keep your guard up. Let clinical judgment take precedence over statistics when you are evaluating any patient. Statistics represent frequencies or averages; they may or may not apply to any one individual.
Techniques for assessing and treating violent patients are beyond the scope of this article, but at the very least:
- obtain training in safety/treatment protocols for violent patients
- ensure that your hospital/clinic has procedures in place to improve safety and to handle violent situations.
Visible, high numbers of confident-appearing—but not confrontational—staff or security may dissuade the patient from acting out. Then, most often, force will not be needed. If force is needed to control a violent patient, make sure the staff’s response is strong and overwhelming.
For every violent act requiring staff intervention, automatically schedule a debriefing session for those involved to assess the incident and allow them to express their feelings.
Related resources
- American Association for Emergency Psychiatry. www.emergencypsychiatry.org
- Volavka J. The neurobiology of violence: an update. J Neuropsychiatry Clin Neurosci 1999;11:307-14.
- McNiel DE, Eisner JP, Binder RL. The relationship between command hallucinations and violence. Psychiatric Services 2000;51:1288-92.
1. Nolan P, Dallender J, Soares J, et al. Violence in mental health care: the experiences of mental health nurses and psychiatrists. J Adv Nurs 1999;30:934-41.
2. Blomhoff S, Seim S, Friis S. Can prediction of violence among psychiatric inpatients be improved? Hosp Community Psychiatry 1990;41:771-5.
3. Convit A, Isay D, Otis D, et al. Characteristics of repeatedly assaultive psychiatric inpatients. Hosp Community Psychiatry 1990;41:1112-5.
4. Taylor P. Motives for offending among violent and psychotic men. Br J Psychiatry 1985;147:491-8.
5. Junginger J, Parks-Levy J, McGuire L. Delusions and symptom-consistent violence. Psychiatr Serv 1998;49:218-20.
6. Cheung P, Schweitzer I, Crowley K, et al. Violence in schizophrenia: role of hallucinations and delusions. Schizophr Res 1997;26:181-90.
7. Binder R, McNiel D. Effects of diagnosis and context on dangerousness. Am J Psychiatry 1988;145:728-32.
8. Convit A, Jaeger J, Pin Lin S, et al. Predicting assaultiveness in psychiatric inpatients: A pilot study. Hosp Community Psychiatry 1988;39:429-34.
9. Hyman S. The violent patient. In: Hyman S (ed). Manual of psychiatric emergencies. Boston: Little, Brown and Co., 1988;23-31.
10. Swartz M, Swanson J, Hiday V, et al. Violence and severe mental illness: the effects of substance abuse and nonadherence to medication. Am J Psychiatry 1998;155:226-31.
11. Owen C, Tarantello C, Jones M, et al. Repetitively violent patients in psychiatric units. Psychiatr Serv 1998;49:1458-61.
12. Citrome L, Volavka J. Clinical management of persistent aggressive behavior in schizophrenia, part I. Definitions, epidemiology, assessment and acute treatment. Essen Psychopharmacol 2002;5:1-16.
13. Abeyasinghe R, Jayasekera R. Violence in a general hospital psychiatry unit for men. Ceylon Med J 2003;48(2):45-7.
1. Nolan P, Dallender J, Soares J, et al. Violence in mental health care: the experiences of mental health nurses and psychiatrists. J Adv Nurs 1999;30:934-41.
2. Blomhoff S, Seim S, Friis S. Can prediction of violence among psychiatric inpatients be improved? Hosp Community Psychiatry 1990;41:771-5.
3. Convit A, Isay D, Otis D, et al. Characteristics of repeatedly assaultive psychiatric inpatients. Hosp Community Psychiatry 1990;41:1112-5.
4. Taylor P. Motives for offending among violent and psychotic men. Br J Psychiatry 1985;147:491-8.
5. Junginger J, Parks-Levy J, McGuire L. Delusions and symptom-consistent violence. Psychiatr Serv 1998;49:218-20.
6. Cheung P, Schweitzer I, Crowley K, et al. Violence in schizophrenia: role of hallucinations and delusions. Schizophr Res 1997;26:181-90.
7. Binder R, McNiel D. Effects of diagnosis and context on dangerousness. Am J Psychiatry 1988;145:728-32.
8. Convit A, Jaeger J, Pin Lin S, et al. Predicting assaultiveness in psychiatric inpatients: A pilot study. Hosp Community Psychiatry 1988;39:429-34.
9. Hyman S. The violent patient. In: Hyman S (ed). Manual of psychiatric emergencies. Boston: Little, Brown and Co., 1988;23-31.
10. Swartz M, Swanson J, Hiday V, et al. Violence and severe mental illness: the effects of substance abuse and nonadherence to medication. Am J Psychiatry 1998;155:226-31.
11. Owen C, Tarantello C, Jones M, et al. Repetitively violent patients in psychiatric units. Psychiatr Serv 1998;49:1458-61.
12. Citrome L, Volavka J. Clinical management of persistent aggressive behavior in schizophrenia, part I. Definitions, epidemiology, assessment and acute treatment. Essen Psychopharmacol 2002;5:1-16.
13. Abeyasinghe R, Jayasekera R. Violence in a general hospital psychiatry unit for men. Ceylon Med J 2003;48(2):45-7.
Psychotic depression: State-of-the-art algorithm improves odds for remission
Psychotic depression requires a unique antidepressant approach, but how can you be sure that a patient’s major depression has psychotic features? Delusions or hallucinations—psychotic depression’s hallmarks—may not be obvious.
This article describes how to detect the distinctive diagnostic signs of psychosis in a patient with a major depressive episode. We offer a treatment algorithm for:
- choosing between electroconvulsive therapy (ECT) and medication
- safely combining antidepressant and antipsychotic agents
- addressing partial or nonresponse to ECT or medications.
Psychotic or nonpsychotic?
Similar clinical presentations make it difficult to distinguish psychotic depression from nonpsychotic depression, schizophrenia spectrum disorders, bipolar disorder, posttraumatic stress disorder (PTSD), obsessive-compulsive disorder (OCD), and body dysmorphic disorders. Comorbid substance abuse/dependency disorders can also complicate psychotic depression’s clinical manifestations and outcomes.
Because delusions and hallucinations are often subtle, researchers have sought other symptoms to differentiate psychotic from nonpsychotic depression. For example, patients with psychotic depression are more likely to exhibit paranoia1 (Table 1), which may explain their underreporting of symptoms.
Table 1
Diagnostic characteristics of psychotic depression
| DSM-IV hallmark symptoms |
| Delusions or hallucinations in the context of a depressive episode |
| More subtle symptoms may include: |
|
Using the Hamilton Rating Scale for Depression (HRSD), Frances and colleagues2 compared 64 depressed patients (34 with psychotic features and 30 without). On the scale’s paranoia item, the psychotic group’s mean score was 1.10, compared with 0.15 for those without psychosis (p = 0.01).
Family history and clinical course. Some studies suggest that first-degree relatives of patients with psychotic depression may have elevated rates of depression and the psychotic subtype.3 Patients with psychotic depression typically suffer morefrequent relapses or recurrences and therefore:
- use more psychiatric services
- are more disabled
- have a poorer clinical course.4
Suicide risk. Psychotic depression is associated with increased risk of self-harm and hospitalization compared with nonpsychotic depression. Patients hospitalized for a major depressive episode are five times more likely to commit suicide if they show evidence of delusions.5
Social impairment. Patients with psychotic depression often have “troubled” lives, with difficult marital and parental relationships, residential instability, inadequate support networks, and low economic status. These problems may be related to subtle cognitive deficits caused by hypothalamic-pituitary-adrenal (HPA) axis disturbance and elevated cortisol levels.6
Confronting similar presentations
Using the BPRS. The Brief Psychiatric Rating Scale (BPRS) is a useful tool to differentiate psychotic depression from nonpsychotic depression. It can flag symptoms such as suspiciousness, grandiosity, and somatization that even a seasoned psychiatrist might miss. The BPRS also points out:
- Any sign of psychosis is sufficient to designate major depression as “psychotic.”
- One well-developed diagnostic sign is sufficient to warrant treatment for psychotic depression.
Schizophrenia spectrum disorders. When psychosis is prominent (particularly in young adults), differentiating schizophrenic spectrum disorders from psychotic depression can be extremely challenging. Although few biological differences have been documented, patients with psychotic depression and schizophrenia differ in HPA axis activity and all-night sleep electroencephalogram readings.7
When the diagnosis is unclear, maintain a high index of suspicion for psychotic depression and its subtleties, and schedule frequent follow-up appointments.
Conversion to bipolar disorder. Adolescents diagnosed with unipolar major depression are at risk for converting to bipolar disorder, particularly if their depression includes psychotic features. In 60 hospitalized adolescents diagnosed with unipolar depression, a 20% conversion rate to bipolar disorder was predicted in part by a cluster of depressive symptoms:
- mood-congruent psychotic features (75% of converters vs. 6% of nonconverters, p< 0.001)
- psychomotor retardation
- rapid symptom onset.8
A similar study reported a 20% conversion rate to bipolar disorder in 206 adolescent outpatients diagnosed with unipolar depression.9 Psychotic depression was more common in converters (42%) than in nonconverters (15%).
Anxiety disorders—such as PTSD or OCD—can be difficult to distinguish from psychotic depression when they present with sensory disturbance.
When in doubt, explore:
- obsessions
- intrusive thoughts
- psychomotor behaviors
- fear of certain external events or people without consistent cues from reality.
PTSD and psychotic depression are not mutually exclusive; a patient may have both.10
Body dysmorphic disorder. Body image concerns correlate with poor self-esteem and depression.11 According to DSM-IV criteria, an individual with body dysmorphic disorder displays excessive concern over an imagined or slight defect, and this concern causes substantial distress or functional impairment. The concern also is not better accounted for by another mental disorder, such as psychotic depression or an eating disorder.
The body is often a focus of psychotic depression’s delusions. During depressive episodes, a patient may have a frank belief about a body part that is not consistent with reality. The history may include negative medical workups or preoccupation with having a serious illness.
Hypochondriasis is a characteristic of psychotic depression, and distinguishing body dysmorphic disorder and other somatoform-spectrum disorders from psychotic depression’s delusions may be difficult:
- Delusions in body dysmorphic disorder tend to be fixed over time.
- Delusions in psychotic depression tend to fluctuate in severity and may subside when the acute psychotic-depressive episode resolves.
ECT may be slightly more effective than medications for treating psychotic depression.13 ECT is not readily available in some regions, however, and the public has negative perceptions of “shock treatment.” Unfortunately, this stigma is often more influential than the evidence. According to some studies, less than 8% of U.S. psychiatrists offer ECT.14
Because medications are usually needed for maintenance treatment in psychotic depression, many clinicians choose medications over ECT as a first-line treatment. ECT should be considered as a first-line treatment for psychotic depression:
- in patients with a history of good response to ECT
- in patients with suicidal intent or severe inanition
- in older patients
- as second-line therapy for patients who fail to respond to or experience complications with medications.
Treatment recommendations
When a patient meets diagnostic criteria for psychotic depression, American Psychiatric Association practice guidelines12 recommend ECT or an antidepressant plus an antipsychotic. Although ECT may be slightly more effective than medications for treating psychotic depression, it is not readily available in many areas (Box).13,14
Medication has been shown to be effective in early studies that combined tricyclic antidepressants (TCAs) with conventional antipsychotics and in trials using selective serotonin reuptake inhibitors (SSRIs) and atypical antipsychotics.
Table 2
Medications reported effective for treating psychotic major depression
| Study, year of publication | Antipsychotic | Antidepressant |
|---|---|---|
| Double-blind studies | ||
| Spiker et al, 1985 | Perphenazine, 54 to 64 mg/d | Amitriptyline, 200 mg/d |
| Anton et al, 1990 | None | Amoxapine, 400 mg/d |
| Dube et al, 2002 | Olanzapine, 5 to 20 mg/d | Fluoxetine, 20 to 80 mg/d |
| Case reports and open-label studies | ||
| Quitkin et al, 1978 | Imipramine, 300 mg/d | None |
| Manberg et al, 1984 | Haloperidol, 20 mg/d | Bupropion, 300 mg/d |
| Nelson et al, 1986 | Perphenazine, 45 mg/d | Desipramine, 150 mg/d |
| Aronson et al, 1987 | Chlorpromazine, 1,000 mg/d | None |
| Howarth et al, 1989 | Imipramine, 248 mg/d | None |
| Rothschild et al, 1993 | Perphenazine, 32 mg/d | Fluoxetine, 40 mg/d |
| Banov et al, 1994 | Clozapine, 325 mg/d | None |
| Jacobsen, 1995 | Risperidone, 2.5 mg/d | None |
| Wolfersdorf et al, 1995 | Haloperidol, 2.5 to 10 mg/d | Paroxetine, 20 mg/d |
| Zarate et al, 2000 | Quetiapine (various) | ? (naturalistic chart review) |
Spiker and colleagues15 treated 58 patients with psychotic depression for 35 days, using amitriptyline, 200 mg/d; perphenazine, 64 mg/d; or the same dosages of amitriptyline plus perphenazine.15 Fourteen of 18 patients (78%) taking combination therapy achieved a >50% reduction in HRSD score, compared with 7 of 17 (41%) taking amitriptyline alone and 3 of 16 (19%) taking perphenazine alone.
In a more recent study,16 249 patients with psychotic depression were randomly assigned to:
- olanzapine, 5 to 20 mg/d, plus fluoxetine, 20 to 80 mg/d
- olanzapine, 5 to 20 mg/d, plus placebo
- or placebo.
Patients receiving olanzapine plus fluoxetine showed greater improvement in HRSD scores, compared with olanzapine monotherapy or placebo. Anecdotal reports indicate that quetiapine, risperidone, or olanzapine may be effective for patients with psychotic depression.17,18
We usually start with an SSRI plus an atypical antipsychotic (Algorithm). The atypicals have fewer side effects than conventional antipsychotics and may offer intrinsic antidepressant qualities through their effects on serotonin type-2 receptors. Table 2 lists recommended dosages.
When initial treatment fails
Consider second- and third-line options when patients fail to achieve remission with ECT or an SSRI plus an atypical antipsychotic. Document that first-line trials were of sufficient duration (8 to 12 weeks) and dosage.
We define remission as:
- HRSD score of <10 for at least 2 weeks
- score of 1 (no delusions or hallucinations) on the Schedule for Affective Disorders and Schizophrenia (SADS)
- and no longer meeting full criteria for a major depressive episode on the Structured Clinical Interview for DSM-IV.
We define partial remission as:
- HRSD score between 11 and 17
- HRSD improvement of >30% from baseline
- score of 1 on the SADS
- and no longer meeting full DSM-IV criteria for a major depressive episode.
Algorithm State-of-the-art treatment of psychotic major depression

Lithium. We suggest adding lithium when patients respond partially to an SSRI/atypical antipsychotic combination. Although limited evidence supports lithium augmentation of antidepressants for psychotic depression, this strategy is often used.
Adding lithium to an antidepressant/antipsychotic combination was examined in a retrospective chart review of patients treated for bipolar and unipolar psychotic depression.19 Lithium, 600 to 1,200 mg/d, was added when patients did not respond to desipramine, 150 mg/d, plus either perphenazine, 12 to 64 mg/d, or haloperidol, 4 to 20 mg/d. Eight of nine patients with bipolar psychotic depression achieved remission with the added lithium, compared with 3 of 12 patients with unipolar psychotic depression (p = 0.003).
To our knowledge, no data indicate how long to continue lithium augmentation. We start older adults on 300 mg/d and younger adults on 600 mg/d and increase by 300 mg per week. Target serum levels are 0.5 to 0.8 mEq/L, and maximum dosage is 1,200 mg/d for young adults and 900 mg/d for frail or elderly patients. We follow thyroid, renal, and hydration status and monitor for weight gain, tremors, cognitive slowing, and GI disturbances.
Other second-line options. Sufficient data support using the second-line drugs in our algorithm as first-line agents. However, the second-line agents pose a greater risk of adverse effects and decreased tolerability than SSRIs plus atypical antipsychotics. Second-line options include:
- SSRIs plus conventional antipsychotics
- amoxapine, a derivative of the conventional antipsychotic loxapine
- venlafaxine or TCAs plus atypical antipsychotics.
As with first-line therapy, 8 to 12 weeks is an adequate trial for second-line medications. ECT may be considered for patients who fail to respond to medications or experience complications.
SSRI/conventional antipsychotic. Our group used fluoxetine, 20 to 40 mg/d, plus perphenazine, 32 mg/d, in the first study of combined SSRI/conventional antipsychotic therapy for patients with psychotic depression.20 After 5 weeks, 22 of 30 patients’ HRSD and BPRS scores were reduced by >50%.
Amoxapine monotherapy. Anton and Burch21 compared amoxapine, 400 mg/d, with amitriptyline, 200 mg/d, plus perphenazine, 32 mg/d. Response rates (>50% reduction on the HRSD) were 71% and 81% for the two groups, respectively. Extrapyramidal symptoms (EPS) were more frequent with the combination therapy.
Venlafaxine’s mechanism of action is thought to be similar to that of TCAs, and we know from the Spiker study15 that TCAs are effective in treating psychotic depression. To our knowledge, venlafaxine dosages for psychotic depression have not been studied; 75 to 375 mg/d is recommended for nonpsychotic depression. Potential side effects include insomnia, nervousness, nausea, headache, dry mouth, fatigue, and elevations of supine diastolic blood pressure.
Third-line therapy. Clozapine may be considered when second-line options do not achieve adequate results.22 When making this choice, consider the need for biweekly blood monitoring and the risk of serious side effects such as agranulocytosis and seizures.
Maintenance therapy
Psychotic depression has a higher relapse rate than nonpsychotic depression. Relapse rates are 50 to 92% in patients with psychotic depression, and recurrence often develops within 2 to 14 months after recovery from the index episode.23 With little data on which to base a maintenance regimen, we recommend that you continue antipsychotics for 4 months after the acute episode resolves.
Recently our group reported that after a taper of perphenazine—following 4 months of treatment with fluoxetine and perphenazine—22 of 30 patients (73%) showed no signs of relapse over the next 11 months.24 We usually maintain patients on antidepressants indefinitely.
Related resources
- DeBattista C, Rothschild AJ, Schatzberg AF. A dynamic algorithm for the treatment of psychotic major depression. Psychiatric Ann 2002;32:681-91.
- Rothschild AJ. Challenges in the treatment of depression with psychotic features. Biol Psychiatry 2003;53:680-90.
- National Institutes of Health. http://www.clinicaltrials.gov. Enter “Medication treatment for psychotic depression” in “Search clinical trials” field, then click on appropriate link.
Drug brand names
- Amitriptyline • Elavil
- Amoxapine • Asendin
- Bupropion • Wellbutrin
- Chlorpromazine • Thorazine
- Clozapine • Clozaril
- Desipramine • Norpramin
- Fluoxetine • Prozac
- Imipramine • Tofranil
- Loxapine • Loxitane
- Olanzapine • Zyprexa
- Paroxetine • Paxil
- Perphenazine • Trilafon
- Risperidone • Risperdal
- Quetiapine • Seroquel
- Venlafaxine • Effexor
Disclosure
Dr. Bell reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Rothschild receives research support from Bristol-Myers Squibb, Eli Lilly and Co., Merck & Co., Wyeth Pharmaceuticals, and the National Institute of Mental Health. He is a consultant to and/or speaker for Forest Pharmaceuticals, Eli Lilly and Co., Abbott Laboratories, Bristol-Myers Squibb, and Pfizer Inc. In the past, he has been a consultant to and received research grants from Corcept Therapeutics.
1. Lykouras E, Malliaras D, Christodoulou GN, et al. Delusional depression: phenomenology and response to treatment, a prospective study. Acta Psychiatry Scand 1986;73:324-9.
2. Frances A, Brown RP, Kocsis JG, Mann JJ. Psychotic depression: a separate entity? Am J Psychiatry 1981;138:831-3.
3. Leckman JF, Weissman MM, Prusoff BA, et al. Subtypes of depression: family study perspective. Arch Gen Psychiatry 1984;41:833-9.
4. Coryell W, Leon A, Winokur G, et al. The importance of psychotic features to long-term course in depressive disorders. Am J Psychiatry 1996;153:483-9.
5. Roose SP, Glassman AH, Walsh BT, et al. Depression, delusions, and suicide. Am J Psychiatry 1983;140:1159-62.
6. Rothschild AJ, Samson JA, Bond TC, et al. Hypothalamic-pituitary-adrenal axis activity and one-year outcome in depression. Biol Psychiatry 1993;34:392-400.
7. Rothschild AJ, Schatzberg AF. Diagnosis and treatment of psychotic (delusional) depression. In: Grunhaus L, Greden JF (eds). Severe depressive disorder. Washington, DC: American Psychiatric Press, 1994;195-207.
8. Strober M, Carlson G. Bipolar illness in adolescents with major depression: Clinical, genetic, and psychopharmacologic predictors in a three to four year prospective follow-up investigation. Arch Gen Psychiatry 1982;39:549-55.
9. Akiskal HS, Walker P, Puzantian VR, et al. Bipolar outcome in the course of depressive illness: Phenomenological, familial, and pharmacologic predictors. J Affect Disord 1983;5:115-28.
10. Zimmerman M, Mattia JI. Psychotic subtyping of major depressive disorder and posttraumatic stress disorder. J Clin Psychiatry 1999;60(5):311-4.
11. Buhne A, Keuthen N. Prevalence of symptoms of body dysmorphic disorder and its correlates: a cross-cultural comparison. Psychosomatics 2002;43:486-90.
12. American Psychiatric Association Practice guidelines for the treatment of major depressive disorder (revision). Am J Psychiatry 200;157:(suppl 4).
13. Parker G, Roy K, Hadzi-Pavlovic D, Pedic F. Psychotic (delusional) depression: A meta-analysis of physical treatments. J Affect Disord 1992;24:17-24.
14. Thompson JW, Weiner RD, Myers CP. Use of ECT in the United States in 1975, 1980 and 1986. Am J Psychiatry 1994;151:1657-61.
15. Spiker DG, Weiss JC, Dealy RS, et al. The pharmacological treatment of delusional depression. Am J Psychiatry 1985;142:430-6.
16. Dube S, Rothschild A, Andersen SE, et al. Olanzapine-fluoxetine combination for psychotic depression (presentation). Barcelona, Spain: European College of Neuropsychopharmacology, 2002.
17. Hillert A, Maier W, Wetzel H, Benkert O. Risperidone in the treatment of disorders with a combined psychotic and depressive syndrome: a functional approach. Pharmacopsychiatry 1992;25:213-17.
18. Zarate CA, Jr, Rothschild AJ, Fletcher KE, et al. Clinical predictors of acute response with quetiapine in psychotic mood disorder. J Clin Psychiatry 2000;61:185-9.
19. Nelson JC, Mazure CM. Lithium augmentation in psychotic depression refractory to combined drug treatment. Am J Psychiatry 1986;143:363-6.
20. Rothschild AJ, Samson JA, Bessette MP, Carter-Campbell JT. Efficacy of combination fluoxetine and perphenazine in the treatment of psychotic depression. J Clin Psychiatry 1993;54:338-42.
21. Anton RF, Jr, Burch EA, Jr. Amoxapine versus amitriptyline combined with perphenazine in the treatment of psychotic depression. Am J Psychiatry 1990;147:1203-8.
22. Banov MD, Zarate CA, Jr, Tohen M, et al. Clozapine therapy in refractory affective disorder: polarity predicts response in long-term follow-up. J Clin Psychiatry 1994;55:295-300.
23. Aronson TA, Shukla S, Gujavarty K, et al. Relapse in delusional depression: a retrospective study of the course of treatment. Comp Psychiatry 1988;29:12-21.
24. Rothschild AJ, Duval SE. How long should patients with psychotic depression stay on the antipsychotic medication. J Clin Psychiatry 2003;64:390-6.
Psychotic depression requires a unique antidepressant approach, but how can you be sure that a patient’s major depression has psychotic features? Delusions or hallucinations—psychotic depression’s hallmarks—may not be obvious.
This article describes how to detect the distinctive diagnostic signs of psychosis in a patient with a major depressive episode. We offer a treatment algorithm for:
- choosing between electroconvulsive therapy (ECT) and medication
- safely combining antidepressant and antipsychotic agents
- addressing partial or nonresponse to ECT or medications.
Psychotic or nonpsychotic?
Similar clinical presentations make it difficult to distinguish psychotic depression from nonpsychotic depression, schizophrenia spectrum disorders, bipolar disorder, posttraumatic stress disorder (PTSD), obsessive-compulsive disorder (OCD), and body dysmorphic disorders. Comorbid substance abuse/dependency disorders can also complicate psychotic depression’s clinical manifestations and outcomes.
Because delusions and hallucinations are often subtle, researchers have sought other symptoms to differentiate psychotic from nonpsychotic depression. For example, patients with psychotic depression are more likely to exhibit paranoia1 (Table 1), which may explain their underreporting of symptoms.
Table 1
Diagnostic characteristics of psychotic depression
| DSM-IV hallmark symptoms |
| Delusions or hallucinations in the context of a depressive episode |
| More subtle symptoms may include: |
|
Using the Hamilton Rating Scale for Depression (HRSD), Frances and colleagues2 compared 64 depressed patients (34 with psychotic features and 30 without). On the scale’s paranoia item, the psychotic group’s mean score was 1.10, compared with 0.15 for those without psychosis (p = 0.01).
Family history and clinical course. Some studies suggest that first-degree relatives of patients with psychotic depression may have elevated rates of depression and the psychotic subtype.3 Patients with psychotic depression typically suffer morefrequent relapses or recurrences and therefore:
- use more psychiatric services
- are more disabled
- have a poorer clinical course.4
Suicide risk. Psychotic depression is associated with increased risk of self-harm and hospitalization compared with nonpsychotic depression. Patients hospitalized for a major depressive episode are five times more likely to commit suicide if they show evidence of delusions.5
Social impairment. Patients with psychotic depression often have “troubled” lives, with difficult marital and parental relationships, residential instability, inadequate support networks, and low economic status. These problems may be related to subtle cognitive deficits caused by hypothalamic-pituitary-adrenal (HPA) axis disturbance and elevated cortisol levels.6
Confronting similar presentations
Using the BPRS. The Brief Psychiatric Rating Scale (BPRS) is a useful tool to differentiate psychotic depression from nonpsychotic depression. It can flag symptoms such as suspiciousness, grandiosity, and somatization that even a seasoned psychiatrist might miss. The BPRS also points out:
- Any sign of psychosis is sufficient to designate major depression as “psychotic.”
- One well-developed diagnostic sign is sufficient to warrant treatment for psychotic depression.
Schizophrenia spectrum disorders. When psychosis is prominent (particularly in young adults), differentiating schizophrenic spectrum disorders from psychotic depression can be extremely challenging. Although few biological differences have been documented, patients with psychotic depression and schizophrenia differ in HPA axis activity and all-night sleep electroencephalogram readings.7
When the diagnosis is unclear, maintain a high index of suspicion for psychotic depression and its subtleties, and schedule frequent follow-up appointments.
Conversion to bipolar disorder. Adolescents diagnosed with unipolar major depression are at risk for converting to bipolar disorder, particularly if their depression includes psychotic features. In 60 hospitalized adolescents diagnosed with unipolar depression, a 20% conversion rate to bipolar disorder was predicted in part by a cluster of depressive symptoms:
- mood-congruent psychotic features (75% of converters vs. 6% of nonconverters, p< 0.001)
- psychomotor retardation
- rapid symptom onset.8
A similar study reported a 20% conversion rate to bipolar disorder in 206 adolescent outpatients diagnosed with unipolar depression.9 Psychotic depression was more common in converters (42%) than in nonconverters (15%).
Anxiety disorders—such as PTSD or OCD—can be difficult to distinguish from psychotic depression when they present with sensory disturbance.
When in doubt, explore:
- obsessions
- intrusive thoughts
- psychomotor behaviors
- fear of certain external events or people without consistent cues from reality.
PTSD and psychotic depression are not mutually exclusive; a patient may have both.10
Body dysmorphic disorder. Body image concerns correlate with poor self-esteem and depression.11 According to DSM-IV criteria, an individual with body dysmorphic disorder displays excessive concern over an imagined or slight defect, and this concern causes substantial distress or functional impairment. The concern also is not better accounted for by another mental disorder, such as psychotic depression or an eating disorder.
The body is often a focus of psychotic depression’s delusions. During depressive episodes, a patient may have a frank belief about a body part that is not consistent with reality. The history may include negative medical workups or preoccupation with having a serious illness.
Hypochondriasis is a characteristic of psychotic depression, and distinguishing body dysmorphic disorder and other somatoform-spectrum disorders from psychotic depression’s delusions may be difficult:
- Delusions in body dysmorphic disorder tend to be fixed over time.
- Delusions in psychotic depression tend to fluctuate in severity and may subside when the acute psychotic-depressive episode resolves.
ECT may be slightly more effective than medications for treating psychotic depression.13 ECT is not readily available in some regions, however, and the public has negative perceptions of “shock treatment.” Unfortunately, this stigma is often more influential than the evidence. According to some studies, less than 8% of U.S. psychiatrists offer ECT.14
Because medications are usually needed for maintenance treatment in psychotic depression, many clinicians choose medications over ECT as a first-line treatment. ECT should be considered as a first-line treatment for psychotic depression:
- in patients with a history of good response to ECT
- in patients with suicidal intent or severe inanition
- in older patients
- as second-line therapy for patients who fail to respond to or experience complications with medications.
Treatment recommendations
When a patient meets diagnostic criteria for psychotic depression, American Psychiatric Association practice guidelines12 recommend ECT or an antidepressant plus an antipsychotic. Although ECT may be slightly more effective than medications for treating psychotic depression, it is not readily available in many areas (Box).13,14
Medication has been shown to be effective in early studies that combined tricyclic antidepressants (TCAs) with conventional antipsychotics and in trials using selective serotonin reuptake inhibitors (SSRIs) and atypical antipsychotics.
Table 2
Medications reported effective for treating psychotic major depression
| Study, year of publication | Antipsychotic | Antidepressant |
|---|---|---|
| Double-blind studies | ||
| Spiker et al, 1985 | Perphenazine, 54 to 64 mg/d | Amitriptyline, 200 mg/d |
| Anton et al, 1990 | None | Amoxapine, 400 mg/d |
| Dube et al, 2002 | Olanzapine, 5 to 20 mg/d | Fluoxetine, 20 to 80 mg/d |
| Case reports and open-label studies | ||
| Quitkin et al, 1978 | Imipramine, 300 mg/d | None |
| Manberg et al, 1984 | Haloperidol, 20 mg/d | Bupropion, 300 mg/d |
| Nelson et al, 1986 | Perphenazine, 45 mg/d | Desipramine, 150 mg/d |
| Aronson et al, 1987 | Chlorpromazine, 1,000 mg/d | None |
| Howarth et al, 1989 | Imipramine, 248 mg/d | None |
| Rothschild et al, 1993 | Perphenazine, 32 mg/d | Fluoxetine, 40 mg/d |
| Banov et al, 1994 | Clozapine, 325 mg/d | None |
| Jacobsen, 1995 | Risperidone, 2.5 mg/d | None |
| Wolfersdorf et al, 1995 | Haloperidol, 2.5 to 10 mg/d | Paroxetine, 20 mg/d |
| Zarate et al, 2000 | Quetiapine (various) | ? (naturalistic chart review) |
Spiker and colleagues15 treated 58 patients with psychotic depression for 35 days, using amitriptyline, 200 mg/d; perphenazine, 64 mg/d; or the same dosages of amitriptyline plus perphenazine.15 Fourteen of 18 patients (78%) taking combination therapy achieved a >50% reduction in HRSD score, compared with 7 of 17 (41%) taking amitriptyline alone and 3 of 16 (19%) taking perphenazine alone.
In a more recent study,16 249 patients with psychotic depression were randomly assigned to:
- olanzapine, 5 to 20 mg/d, plus fluoxetine, 20 to 80 mg/d
- olanzapine, 5 to 20 mg/d, plus placebo
- or placebo.
Patients receiving olanzapine plus fluoxetine showed greater improvement in HRSD scores, compared with olanzapine monotherapy or placebo. Anecdotal reports indicate that quetiapine, risperidone, or olanzapine may be effective for patients with psychotic depression.17,18
We usually start with an SSRI plus an atypical antipsychotic (Algorithm). The atypicals have fewer side effects than conventional antipsychotics and may offer intrinsic antidepressant qualities through their effects on serotonin type-2 receptors. Table 2 lists recommended dosages.
When initial treatment fails
Consider second- and third-line options when patients fail to achieve remission with ECT or an SSRI plus an atypical antipsychotic. Document that first-line trials were of sufficient duration (8 to 12 weeks) and dosage.
We define remission as:
- HRSD score of <10 for at least 2 weeks
- score of 1 (no delusions or hallucinations) on the Schedule for Affective Disorders and Schizophrenia (SADS)
- and no longer meeting full criteria for a major depressive episode on the Structured Clinical Interview for DSM-IV.
We define partial remission as:
- HRSD score between 11 and 17
- HRSD improvement of >30% from baseline
- score of 1 on the SADS
- and no longer meeting full DSM-IV criteria for a major depressive episode.
Algorithm State-of-the-art treatment of psychotic major depression
Lithium. We suggest adding lithium when patients respond partially to an SSRI/atypical antipsychotic combination. Although limited evidence supports lithium augmentation of antidepressants for psychotic depression, this strategy is often used.
Adding lithium to an antidepressant/antipsychotic combination was examined in a retrospective chart review of patients treated for bipolar and unipolar psychotic depression.19 Lithium, 600 to 1,200 mg/d, was added when patients did not respond to desipramine, 150 mg/d, plus either perphenazine, 12 to 64 mg/d, or haloperidol, 4 to 20 mg/d. Eight of nine patients with bipolar psychotic depression achieved remission with the added lithium, compared with 3 of 12 patients with unipolar psychotic depression (p = 0.003).
To our knowledge, no data indicate how long to continue lithium augmentation. We start older adults on 300 mg/d and younger adults on 600 mg/d and increase by 300 mg per week. Target serum levels are 0.5 to 0.8 mEq/L, and maximum dosage is 1,200 mg/d for young adults and 900 mg/d for frail or elderly patients. We follow thyroid, renal, and hydration status and monitor for weight gain, tremors, cognitive slowing, and GI disturbances.
Other second-line options. Sufficient data support using the second-line drugs in our algorithm as first-line agents. However, the second-line agents pose a greater risk of adverse effects and decreased tolerability than SSRIs plus atypical antipsychotics. Second-line options include:
- SSRIs plus conventional antipsychotics
- amoxapine, a derivative of the conventional antipsychotic loxapine
- venlafaxine or TCAs plus atypical antipsychotics.
As with first-line therapy, 8 to 12 weeks is an adequate trial for second-line medications. ECT may be considered for patients who fail to respond to medications or experience complications.
SSRI/conventional antipsychotic. Our group used fluoxetine, 20 to 40 mg/d, plus perphenazine, 32 mg/d, in the first study of combined SSRI/conventional antipsychotic therapy for patients with psychotic depression.20 After 5 weeks, 22 of 30 patients’ HRSD and BPRS scores were reduced by >50%.
Amoxapine monotherapy. Anton and Burch21 compared amoxapine, 400 mg/d, with amitriptyline, 200 mg/d, plus perphenazine, 32 mg/d. Response rates (>50% reduction on the HRSD) were 71% and 81% for the two groups, respectively. Extrapyramidal symptoms (EPS) were more frequent with the combination therapy.
Venlafaxine’s mechanism of action is thought to be similar to that of TCAs, and we know from the Spiker study15 that TCAs are effective in treating psychotic depression. To our knowledge, venlafaxine dosages for psychotic depression have not been studied; 75 to 375 mg/d is recommended for nonpsychotic depression. Potential side effects include insomnia, nervousness, nausea, headache, dry mouth, fatigue, and elevations of supine diastolic blood pressure.
Third-line therapy. Clozapine may be considered when second-line options do not achieve adequate results.22 When making this choice, consider the need for biweekly blood monitoring and the risk of serious side effects such as agranulocytosis and seizures.
Maintenance therapy
Psychotic depression has a higher relapse rate than nonpsychotic depression. Relapse rates are 50 to 92% in patients with psychotic depression, and recurrence often develops within 2 to 14 months after recovery from the index episode.23 With little data on which to base a maintenance regimen, we recommend that you continue antipsychotics for 4 months after the acute episode resolves.
Recently our group reported that after a taper of perphenazine—following 4 months of treatment with fluoxetine and perphenazine—22 of 30 patients (73%) showed no signs of relapse over the next 11 months.24 We usually maintain patients on antidepressants indefinitely.
Related resources
- DeBattista C, Rothschild AJ, Schatzberg AF. A dynamic algorithm for the treatment of psychotic major depression. Psychiatric Ann 2002;32:681-91.
- Rothschild AJ. Challenges in the treatment of depression with psychotic features. Biol Psychiatry 2003;53:680-90.
- National Institutes of Health. http://www.clinicaltrials.gov. Enter “Medication treatment for psychotic depression” in “Search clinical trials” field, then click on appropriate link.
Drug brand names
- Amitriptyline • Elavil
- Amoxapine • Asendin
- Bupropion • Wellbutrin
- Chlorpromazine • Thorazine
- Clozapine • Clozaril
- Desipramine • Norpramin
- Fluoxetine • Prozac
- Imipramine • Tofranil
- Loxapine • Loxitane
- Olanzapine • Zyprexa
- Paroxetine • Paxil
- Perphenazine • Trilafon
- Risperidone • Risperdal
- Quetiapine • Seroquel
- Venlafaxine • Effexor
Disclosure
Dr. Bell reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Rothschild receives research support from Bristol-Myers Squibb, Eli Lilly and Co., Merck & Co., Wyeth Pharmaceuticals, and the National Institute of Mental Health. He is a consultant to and/or speaker for Forest Pharmaceuticals, Eli Lilly and Co., Abbott Laboratories, Bristol-Myers Squibb, and Pfizer Inc. In the past, he has been a consultant to and received research grants from Corcept Therapeutics.
Psychotic depression requires a unique antidepressant approach, but how can you be sure that a patient’s major depression has psychotic features? Delusions or hallucinations—psychotic depression’s hallmarks—may not be obvious.
This article describes how to detect the distinctive diagnostic signs of psychosis in a patient with a major depressive episode. We offer a treatment algorithm for:
- choosing between electroconvulsive therapy (ECT) and medication
- safely combining antidepressant and antipsychotic agents
- addressing partial or nonresponse to ECT or medications.
Psychotic or nonpsychotic?
Similar clinical presentations make it difficult to distinguish psychotic depression from nonpsychotic depression, schizophrenia spectrum disorders, bipolar disorder, posttraumatic stress disorder (PTSD), obsessive-compulsive disorder (OCD), and body dysmorphic disorders. Comorbid substance abuse/dependency disorders can also complicate psychotic depression’s clinical manifestations and outcomes.
Because delusions and hallucinations are often subtle, researchers have sought other symptoms to differentiate psychotic from nonpsychotic depression. For example, patients with psychotic depression are more likely to exhibit paranoia1 (Table 1), which may explain their underreporting of symptoms.
Table 1
Diagnostic characteristics of psychotic depression
| DSM-IV hallmark symptoms |
| Delusions or hallucinations in the context of a depressive episode |
| More subtle symptoms may include: |
|
Using the Hamilton Rating Scale for Depression (HRSD), Frances and colleagues2 compared 64 depressed patients (34 with psychotic features and 30 without). On the scale’s paranoia item, the psychotic group’s mean score was 1.10, compared with 0.15 for those without psychosis (p = 0.01).
Family history and clinical course. Some studies suggest that first-degree relatives of patients with psychotic depression may have elevated rates of depression and the psychotic subtype.3 Patients with psychotic depression typically suffer morefrequent relapses or recurrences and therefore:
- use more psychiatric services
- are more disabled
- have a poorer clinical course.4
Suicide risk. Psychotic depression is associated with increased risk of self-harm and hospitalization compared with nonpsychotic depression. Patients hospitalized for a major depressive episode are five times more likely to commit suicide if they show evidence of delusions.5
Social impairment. Patients with psychotic depression often have “troubled” lives, with difficult marital and parental relationships, residential instability, inadequate support networks, and low economic status. These problems may be related to subtle cognitive deficits caused by hypothalamic-pituitary-adrenal (HPA) axis disturbance and elevated cortisol levels.6
Confronting similar presentations
Using the BPRS. The Brief Psychiatric Rating Scale (BPRS) is a useful tool to differentiate psychotic depression from nonpsychotic depression. It can flag symptoms such as suspiciousness, grandiosity, and somatization that even a seasoned psychiatrist might miss. The BPRS also points out:
- Any sign of psychosis is sufficient to designate major depression as “psychotic.”
- One well-developed diagnostic sign is sufficient to warrant treatment for psychotic depression.
Schizophrenia spectrum disorders. When psychosis is prominent (particularly in young adults), differentiating schizophrenic spectrum disorders from psychotic depression can be extremely challenging. Although few biological differences have been documented, patients with psychotic depression and schizophrenia differ in HPA axis activity and all-night sleep electroencephalogram readings.7
When the diagnosis is unclear, maintain a high index of suspicion for psychotic depression and its subtleties, and schedule frequent follow-up appointments.
Conversion to bipolar disorder. Adolescents diagnosed with unipolar major depression are at risk for converting to bipolar disorder, particularly if their depression includes psychotic features. In 60 hospitalized adolescents diagnosed with unipolar depression, a 20% conversion rate to bipolar disorder was predicted in part by a cluster of depressive symptoms:
- mood-congruent psychotic features (75% of converters vs. 6% of nonconverters, p< 0.001)
- psychomotor retardation
- rapid symptom onset.8
A similar study reported a 20% conversion rate to bipolar disorder in 206 adolescent outpatients diagnosed with unipolar depression.9 Psychotic depression was more common in converters (42%) than in nonconverters (15%).
Anxiety disorders—such as PTSD or OCD—can be difficult to distinguish from psychotic depression when they present with sensory disturbance.
When in doubt, explore:
- obsessions
- intrusive thoughts
- psychomotor behaviors
- fear of certain external events or people without consistent cues from reality.
PTSD and psychotic depression are not mutually exclusive; a patient may have both.10
Body dysmorphic disorder. Body image concerns correlate with poor self-esteem and depression.11 According to DSM-IV criteria, an individual with body dysmorphic disorder displays excessive concern over an imagined or slight defect, and this concern causes substantial distress or functional impairment. The concern also is not better accounted for by another mental disorder, such as psychotic depression or an eating disorder.
The body is often a focus of psychotic depression’s delusions. During depressive episodes, a patient may have a frank belief about a body part that is not consistent with reality. The history may include negative medical workups or preoccupation with having a serious illness.
Hypochondriasis is a characteristic of psychotic depression, and distinguishing body dysmorphic disorder and other somatoform-spectrum disorders from psychotic depression’s delusions may be difficult:
- Delusions in body dysmorphic disorder tend to be fixed over time.
- Delusions in psychotic depression tend to fluctuate in severity and may subside when the acute psychotic-depressive episode resolves.
ECT may be slightly more effective than medications for treating psychotic depression.13 ECT is not readily available in some regions, however, and the public has negative perceptions of “shock treatment.” Unfortunately, this stigma is often more influential than the evidence. According to some studies, less than 8% of U.S. psychiatrists offer ECT.14
Because medications are usually needed for maintenance treatment in psychotic depression, many clinicians choose medications over ECT as a first-line treatment. ECT should be considered as a first-line treatment for psychotic depression:
- in patients with a history of good response to ECT
- in patients with suicidal intent or severe inanition
- in older patients
- as second-line therapy for patients who fail to respond to or experience complications with medications.
Treatment recommendations
When a patient meets diagnostic criteria for psychotic depression, American Psychiatric Association practice guidelines12 recommend ECT or an antidepressant plus an antipsychotic. Although ECT may be slightly more effective than medications for treating psychotic depression, it is not readily available in many areas (Box).13,14
Medication has been shown to be effective in early studies that combined tricyclic antidepressants (TCAs) with conventional antipsychotics and in trials using selective serotonin reuptake inhibitors (SSRIs) and atypical antipsychotics.
Table 2
Medications reported effective for treating psychotic major depression
| Study, year of publication | Antipsychotic | Antidepressant |
|---|---|---|
| Double-blind studies | ||
| Spiker et al, 1985 | Perphenazine, 54 to 64 mg/d | Amitriptyline, 200 mg/d |
| Anton et al, 1990 | None | Amoxapine, 400 mg/d |
| Dube et al, 2002 | Olanzapine, 5 to 20 mg/d | Fluoxetine, 20 to 80 mg/d |
| Case reports and open-label studies | ||
| Quitkin et al, 1978 | Imipramine, 300 mg/d | None |
| Manberg et al, 1984 | Haloperidol, 20 mg/d | Bupropion, 300 mg/d |
| Nelson et al, 1986 | Perphenazine, 45 mg/d | Desipramine, 150 mg/d |
| Aronson et al, 1987 | Chlorpromazine, 1,000 mg/d | None |
| Howarth et al, 1989 | Imipramine, 248 mg/d | None |
| Rothschild et al, 1993 | Perphenazine, 32 mg/d | Fluoxetine, 40 mg/d |
| Banov et al, 1994 | Clozapine, 325 mg/d | None |
| Jacobsen, 1995 | Risperidone, 2.5 mg/d | None |
| Wolfersdorf et al, 1995 | Haloperidol, 2.5 to 10 mg/d | Paroxetine, 20 mg/d |
| Zarate et al, 2000 | Quetiapine (various) | ? (naturalistic chart review) |
Spiker and colleagues15 treated 58 patients with psychotic depression for 35 days, using amitriptyline, 200 mg/d; perphenazine, 64 mg/d; or the same dosages of amitriptyline plus perphenazine.15 Fourteen of 18 patients (78%) taking combination therapy achieved a >50% reduction in HRSD score, compared with 7 of 17 (41%) taking amitriptyline alone and 3 of 16 (19%) taking perphenazine alone.
In a more recent study,16 249 patients with psychotic depression were randomly assigned to:
- olanzapine, 5 to 20 mg/d, plus fluoxetine, 20 to 80 mg/d
- olanzapine, 5 to 20 mg/d, plus placebo
- or placebo.
Patients receiving olanzapine plus fluoxetine showed greater improvement in HRSD scores, compared with olanzapine monotherapy or placebo. Anecdotal reports indicate that quetiapine, risperidone, or olanzapine may be effective for patients with psychotic depression.17,18
We usually start with an SSRI plus an atypical antipsychotic (Algorithm). The atypicals have fewer side effects than conventional antipsychotics and may offer intrinsic antidepressant qualities through their effects on serotonin type-2 receptors. Table 2 lists recommended dosages.
When initial treatment fails
Consider second- and third-line options when patients fail to achieve remission with ECT or an SSRI plus an atypical antipsychotic. Document that first-line trials were of sufficient duration (8 to 12 weeks) and dosage.
We define remission as:
- HRSD score of <10 for at least 2 weeks
- score of 1 (no delusions or hallucinations) on the Schedule for Affective Disorders and Schizophrenia (SADS)
- and no longer meeting full criteria for a major depressive episode on the Structured Clinical Interview for DSM-IV.
We define partial remission as:
- HRSD score between 11 and 17
- HRSD improvement of >30% from baseline
- score of 1 on the SADS
- and no longer meeting full DSM-IV criteria for a major depressive episode.
Algorithm State-of-the-art treatment of psychotic major depression
Lithium. We suggest adding lithium when patients respond partially to an SSRI/atypical antipsychotic combination. Although limited evidence supports lithium augmentation of antidepressants for psychotic depression, this strategy is often used.
Adding lithium to an antidepressant/antipsychotic combination was examined in a retrospective chart review of patients treated for bipolar and unipolar psychotic depression.19 Lithium, 600 to 1,200 mg/d, was added when patients did not respond to desipramine, 150 mg/d, plus either perphenazine, 12 to 64 mg/d, or haloperidol, 4 to 20 mg/d. Eight of nine patients with bipolar psychotic depression achieved remission with the added lithium, compared with 3 of 12 patients with unipolar psychotic depression (p = 0.003).
To our knowledge, no data indicate how long to continue lithium augmentation. We start older adults on 300 mg/d and younger adults on 600 mg/d and increase by 300 mg per week. Target serum levels are 0.5 to 0.8 mEq/L, and maximum dosage is 1,200 mg/d for young adults and 900 mg/d for frail or elderly patients. We follow thyroid, renal, and hydration status and monitor for weight gain, tremors, cognitive slowing, and GI disturbances.
Other second-line options. Sufficient data support using the second-line drugs in our algorithm as first-line agents. However, the second-line agents pose a greater risk of adverse effects and decreased tolerability than SSRIs plus atypical antipsychotics. Second-line options include:
- SSRIs plus conventional antipsychotics
- amoxapine, a derivative of the conventional antipsychotic loxapine
- venlafaxine or TCAs plus atypical antipsychotics.
As with first-line therapy, 8 to 12 weeks is an adequate trial for second-line medications. ECT may be considered for patients who fail to respond to medications or experience complications.
SSRI/conventional antipsychotic. Our group used fluoxetine, 20 to 40 mg/d, plus perphenazine, 32 mg/d, in the first study of combined SSRI/conventional antipsychotic therapy for patients with psychotic depression.20 After 5 weeks, 22 of 30 patients’ HRSD and BPRS scores were reduced by >50%.
Amoxapine monotherapy. Anton and Burch21 compared amoxapine, 400 mg/d, with amitriptyline, 200 mg/d, plus perphenazine, 32 mg/d. Response rates (>50% reduction on the HRSD) were 71% and 81% for the two groups, respectively. Extrapyramidal symptoms (EPS) were more frequent with the combination therapy.
Venlafaxine’s mechanism of action is thought to be similar to that of TCAs, and we know from the Spiker study15 that TCAs are effective in treating psychotic depression. To our knowledge, venlafaxine dosages for psychotic depression have not been studied; 75 to 375 mg/d is recommended for nonpsychotic depression. Potential side effects include insomnia, nervousness, nausea, headache, dry mouth, fatigue, and elevations of supine diastolic blood pressure.
Third-line therapy. Clozapine may be considered when second-line options do not achieve adequate results.22 When making this choice, consider the need for biweekly blood monitoring and the risk of serious side effects such as agranulocytosis and seizures.
Maintenance therapy
Psychotic depression has a higher relapse rate than nonpsychotic depression. Relapse rates are 50 to 92% in patients with psychotic depression, and recurrence often develops within 2 to 14 months after recovery from the index episode.23 With little data on which to base a maintenance regimen, we recommend that you continue antipsychotics for 4 months after the acute episode resolves.
Recently our group reported that after a taper of perphenazine—following 4 months of treatment with fluoxetine and perphenazine—22 of 30 patients (73%) showed no signs of relapse over the next 11 months.24 We usually maintain patients on antidepressants indefinitely.
Related resources
- DeBattista C, Rothschild AJ, Schatzberg AF. A dynamic algorithm for the treatment of psychotic major depression. Psychiatric Ann 2002;32:681-91.
- Rothschild AJ. Challenges in the treatment of depression with psychotic features. Biol Psychiatry 2003;53:680-90.
- National Institutes of Health. http://www.clinicaltrials.gov. Enter “Medication treatment for psychotic depression” in “Search clinical trials” field, then click on appropriate link.
Drug brand names
- Amitriptyline • Elavil
- Amoxapine • Asendin
- Bupropion • Wellbutrin
- Chlorpromazine • Thorazine
- Clozapine • Clozaril
- Desipramine • Norpramin
- Fluoxetine • Prozac
- Imipramine • Tofranil
- Loxapine • Loxitane
- Olanzapine • Zyprexa
- Paroxetine • Paxil
- Perphenazine • Trilafon
- Risperidone • Risperdal
- Quetiapine • Seroquel
- Venlafaxine • Effexor
Disclosure
Dr. Bell reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Rothschild receives research support from Bristol-Myers Squibb, Eli Lilly and Co., Merck & Co., Wyeth Pharmaceuticals, and the National Institute of Mental Health. He is a consultant to and/or speaker for Forest Pharmaceuticals, Eli Lilly and Co., Abbott Laboratories, Bristol-Myers Squibb, and Pfizer Inc. In the past, he has been a consultant to and received research grants from Corcept Therapeutics.
1. Lykouras E, Malliaras D, Christodoulou GN, et al. Delusional depression: phenomenology and response to treatment, a prospective study. Acta Psychiatry Scand 1986;73:324-9.
2. Frances A, Brown RP, Kocsis JG, Mann JJ. Psychotic depression: a separate entity? Am J Psychiatry 1981;138:831-3.
3. Leckman JF, Weissman MM, Prusoff BA, et al. Subtypes of depression: family study perspective. Arch Gen Psychiatry 1984;41:833-9.
4. Coryell W, Leon A, Winokur G, et al. The importance of psychotic features to long-term course in depressive disorders. Am J Psychiatry 1996;153:483-9.
5. Roose SP, Glassman AH, Walsh BT, et al. Depression, delusions, and suicide. Am J Psychiatry 1983;140:1159-62.
6. Rothschild AJ, Samson JA, Bond TC, et al. Hypothalamic-pituitary-adrenal axis activity and one-year outcome in depression. Biol Psychiatry 1993;34:392-400.
7. Rothschild AJ, Schatzberg AF. Diagnosis and treatment of psychotic (delusional) depression. In: Grunhaus L, Greden JF (eds). Severe depressive disorder. Washington, DC: American Psychiatric Press, 1994;195-207.
8. Strober M, Carlson G. Bipolar illness in adolescents with major depression: Clinical, genetic, and psychopharmacologic predictors in a three to four year prospective follow-up investigation. Arch Gen Psychiatry 1982;39:549-55.
9. Akiskal HS, Walker P, Puzantian VR, et al. Bipolar outcome in the course of depressive illness: Phenomenological, familial, and pharmacologic predictors. J Affect Disord 1983;5:115-28.
10. Zimmerman M, Mattia JI. Psychotic subtyping of major depressive disorder and posttraumatic stress disorder. J Clin Psychiatry 1999;60(5):311-4.
11. Buhne A, Keuthen N. Prevalence of symptoms of body dysmorphic disorder and its correlates: a cross-cultural comparison. Psychosomatics 2002;43:486-90.
12. American Psychiatric Association Practice guidelines for the treatment of major depressive disorder (revision). Am J Psychiatry 200;157:(suppl 4).
13. Parker G, Roy K, Hadzi-Pavlovic D, Pedic F. Psychotic (delusional) depression: A meta-analysis of physical treatments. J Affect Disord 1992;24:17-24.
14. Thompson JW, Weiner RD, Myers CP. Use of ECT in the United States in 1975, 1980 and 1986. Am J Psychiatry 1994;151:1657-61.
15. Spiker DG, Weiss JC, Dealy RS, et al. The pharmacological treatment of delusional depression. Am J Psychiatry 1985;142:430-6.
16. Dube S, Rothschild A, Andersen SE, et al. Olanzapine-fluoxetine combination for psychotic depression (presentation). Barcelona, Spain: European College of Neuropsychopharmacology, 2002.
17. Hillert A, Maier W, Wetzel H, Benkert O. Risperidone in the treatment of disorders with a combined psychotic and depressive syndrome: a functional approach. Pharmacopsychiatry 1992;25:213-17.
18. Zarate CA, Jr, Rothschild AJ, Fletcher KE, et al. Clinical predictors of acute response with quetiapine in psychotic mood disorder. J Clin Psychiatry 2000;61:185-9.
19. Nelson JC, Mazure CM. Lithium augmentation in psychotic depression refractory to combined drug treatment. Am J Psychiatry 1986;143:363-6.
20. Rothschild AJ, Samson JA, Bessette MP, Carter-Campbell JT. Efficacy of combination fluoxetine and perphenazine in the treatment of psychotic depression. J Clin Psychiatry 1993;54:338-42.
21. Anton RF, Jr, Burch EA, Jr. Amoxapine versus amitriptyline combined with perphenazine in the treatment of psychotic depression. Am J Psychiatry 1990;147:1203-8.
22. Banov MD, Zarate CA, Jr, Tohen M, et al. Clozapine therapy in refractory affective disorder: polarity predicts response in long-term follow-up. J Clin Psychiatry 1994;55:295-300.
23. Aronson TA, Shukla S, Gujavarty K, et al. Relapse in delusional depression: a retrospective study of the course of treatment. Comp Psychiatry 1988;29:12-21.
24. Rothschild AJ, Duval SE. How long should patients with psychotic depression stay on the antipsychotic medication. J Clin Psychiatry 2003;64:390-6.
1. Lykouras E, Malliaras D, Christodoulou GN, et al. Delusional depression: phenomenology and response to treatment, a prospective study. Acta Psychiatry Scand 1986;73:324-9.
2. Frances A, Brown RP, Kocsis JG, Mann JJ. Psychotic depression: a separate entity? Am J Psychiatry 1981;138:831-3.
3. Leckman JF, Weissman MM, Prusoff BA, et al. Subtypes of depression: family study perspective. Arch Gen Psychiatry 1984;41:833-9.
4. Coryell W, Leon A, Winokur G, et al. The importance of psychotic features to long-term course in depressive disorders. Am J Psychiatry 1996;153:483-9.
5. Roose SP, Glassman AH, Walsh BT, et al. Depression, delusions, and suicide. Am J Psychiatry 1983;140:1159-62.
6. Rothschild AJ, Samson JA, Bond TC, et al. Hypothalamic-pituitary-adrenal axis activity and one-year outcome in depression. Biol Psychiatry 1993;34:392-400.
7. Rothschild AJ, Schatzberg AF. Diagnosis and treatment of psychotic (delusional) depression. In: Grunhaus L, Greden JF (eds). Severe depressive disorder. Washington, DC: American Psychiatric Press, 1994;195-207.
8. Strober M, Carlson G. Bipolar illness in adolescents with major depression: Clinical, genetic, and psychopharmacologic predictors in a three to four year prospective follow-up investigation. Arch Gen Psychiatry 1982;39:549-55.
9. Akiskal HS, Walker P, Puzantian VR, et al. Bipolar outcome in the course of depressive illness: Phenomenological, familial, and pharmacologic predictors. J Affect Disord 1983;5:115-28.
10. Zimmerman M, Mattia JI. Psychotic subtyping of major depressive disorder and posttraumatic stress disorder. J Clin Psychiatry 1999;60(5):311-4.
11. Buhne A, Keuthen N. Prevalence of symptoms of body dysmorphic disorder and its correlates: a cross-cultural comparison. Psychosomatics 2002;43:486-90.
12. American Psychiatric Association Practice guidelines for the treatment of major depressive disorder (revision). Am J Psychiatry 200;157:(suppl 4).
13. Parker G, Roy K, Hadzi-Pavlovic D, Pedic F. Psychotic (delusional) depression: A meta-analysis of physical treatments. J Affect Disord 1992;24:17-24.
14. Thompson JW, Weiner RD, Myers CP. Use of ECT in the United States in 1975, 1980 and 1986. Am J Psychiatry 1994;151:1657-61.
15. Spiker DG, Weiss JC, Dealy RS, et al. The pharmacological treatment of delusional depression. Am J Psychiatry 1985;142:430-6.
16. Dube S, Rothschild A, Andersen SE, et al. Olanzapine-fluoxetine combination for psychotic depression (presentation). Barcelona, Spain: European College of Neuropsychopharmacology, 2002.
17. Hillert A, Maier W, Wetzel H, Benkert O. Risperidone in the treatment of disorders with a combined psychotic and depressive syndrome: a functional approach. Pharmacopsychiatry 1992;25:213-17.
18. Zarate CA, Jr, Rothschild AJ, Fletcher KE, et al. Clinical predictors of acute response with quetiapine in psychotic mood disorder. J Clin Psychiatry 2000;61:185-9.
19. Nelson JC, Mazure CM. Lithium augmentation in psychotic depression refractory to combined drug treatment. Am J Psychiatry 1986;143:363-6.
20. Rothschild AJ, Samson JA, Bessette MP, Carter-Campbell JT. Efficacy of combination fluoxetine and perphenazine in the treatment of psychotic depression. J Clin Psychiatry 1993;54:338-42.
21. Anton RF, Jr, Burch EA, Jr. Amoxapine versus amitriptyline combined with perphenazine in the treatment of psychotic depression. Am J Psychiatry 1990;147:1203-8.
22. Banov MD, Zarate CA, Jr, Tohen M, et al. Clozapine therapy in refractory affective disorder: polarity predicts response in long-term follow-up. J Clin Psychiatry 1994;55:295-300.
23. Aronson TA, Shukla S, Gujavarty K, et al. Relapse in delusional depression: a retrospective study of the course of treatment. Comp Psychiatry 1988;29:12-21.
24. Rothschild AJ, Duval SE. How long should patients with psychotic depression stay on the antipsychotic medication. J Clin Psychiatry 2003;64:390-6.