User login
Tardive dyskinesia: How to prevent and treat a lingering nemesis
Atypical antipsychotics seldom cause tardive dyskinesia (TD), but we cannot let our guard down when prescribing them. Although they pose a much lower risk of TD than do conventional antipsychotics, atypicals can cause TD in vulnerable patients.
Less worrisome than in the past, TD’s associated problems linger, including insidious onset, tendency for persistence, and lack of reliably effective treatment. It is important, therefore, for psychiatrists to:
- identify patients at risk for developing TD
- recognize extrapyramidal symptoms (EPS) when they occur
- and manage these side effects appropriately.
A CHANGING CLINICAL PICTURE
The term “dyskinesias” covers a variety of abnormal involuntary movements (Box). The incidence and prevalence of TD have dropped markedly in the last 10 years, as:
- more and more older, chronically ill patients are switched from conventional to atypical agents
- younger psychotic patients are usually treated with atypicals as first-line therapy and are never exposed to conventional antipsychotics.
Tardive dyskinesia (TD) tends to develop in patients receiving long-term antipsychotic treatment. Its typical movements are choreiform (jerky) or athetoid (writhing), irregular, and purposeless.
TD onset is usually insidious and may occur during drug therapy or weeks after antipsychotics are discontined. Its signs are usually observed in the face or mouth, and typical orofacial dyskinetic movements are:
Lips: puckering, pouting, smacking
Jaw: chewing, biting, side-to-side movements, jaw openings
Tongue: twisting, rolling, undulations, protrusion, darting (“fly-catching”)
Face: blinking, frowning, grimacing.
The trunk and extremities are involved less often. Choreiform finger and wrist movements, flexion and rotation of the ankle, toe movements, foot tapping, and rocking or twisting of the neck, hip, and trunk may be seen. Patients are often oblivious to these movements, which may be only intermittently present and are absent during sleep. Anxiety and arousal states may aggravate TD.
TD prevalence of about 20%—as shown by earlier studies of long-term conventional agents1—is declining. Newer studies comparing atypicals with conventional antipsychotics demonstrate much lower prevalence rates.2,3
TD incidence—estimated by new cases of TD per year of drug treatment—may have declined 10-fold, from 5% with conventional antipsychotics to 0.5% with atypicals. Likewise, incidence in the elderly may have fallen from 25% to 2.5%.4
Risk factors. Despite these improvements, case reports5-7 demonstrate that TD is possible in patients treated with atypicals, even without previous exposure to a conventional antipsychotic. Besides antipsychotic use, risk factors for developing TD include:
- older age
- negative symptoms of schizophrenia
- affective disorders
- acute EPS
- and diabetes mellitus.8
RECOGNIZING TD SYMPTOMS
Recognizing TD may be complicated by the presence of other EPS, particularly drug-induced parkinsonism (DIP). DIP typically develops early and often when treating patients with conventional antipsychotics (Table 1). TD and DIP may occur simultaneously in the same patient, making accurate diagnosis even more difficult.
Other dyskinesias may complicate the diagnosis. Three common TD variants, which may be acute or tardive (occurring after long-term antipsychotic therapy), are:
- akathisia, a distressing and at times irresistible urge to move the legs or other parts of the body
- dystonia, abnormal muscle tone and posture and muscle spasms
- tics, brief muscle contractions, usually in the face, including vocal tics.
AIMS testing. Defining a “case of TD” by dyskinetic movement severity is somewhat arbitrary. A commonly accepted definition is two area scores of “mild” or one rating of “moderate” using the Abnormal Involuntary Movement Scale (AIMS).9 The AIMS has been widely used in epidemiologic and treatment studies of TD and is easy to administer in a clinical setting (see Related Resources).
A careful drug history is required before TD can be diagnosed definitively. Spontaneous dys kinesias—usually orofacial—are sometimes seen in older patients who are not taking neuroleptics.8 Antidepressants, mood stabilizers, or antihistamines may infrequently trigger neurologic side effects—including dyskinesias, akathisia, and tremor—which are almost invariably reversible after the causative agent is withdrawn.8,10
Table 1
Features that differentiate two common extrapyramidal symptoms
| Tardive dyskinesia (TD) | Drug-induced parkinsonism (DIP) | |
|---|---|---|
| Onset | Late | Early |
| Type of movement | Choreoathetoid | Tremor |
| Amount of movement | Increased | Decreased |
| Muscle tone | Decreased | Increased |
| Most common site | Orofacial | Extremities |
| Response to anticholinergics | Tends to worsen | Tends to improve |
MANAGING MILD TD
Atypical antipsychotics have radically altered the clinical outlook for patients with TD and improved our ability to manage their symptoms. The clinician treating a TD patient today rarely faces the dilemma that exists with conventional antipsychotics: discontinue treatment and risk psychotic relapse, or continue treatment and risk persistent TD.
Using atypicals. Today, patients who need antipsychotic therapy for TD are usually already taking atypicals, which may ameliorate TD and control psychotic symptoms. Case reports and some studies have shown therapeutic effects in patients with TD taking olanzapine,3 risperidone,2 quetiapine,11 ziprasidone,12 aripiprazole,13 or the substituted benzamides (such as sulpiride), which are not marketed in the United States.14
Interestingly, TD triggered by taking one atypical may respond to treatment with another. Suzuki et al15 reported that three patients who had developed early-onset TD while taking risperidone showed TD remission after risperidone was replaced by olanzapine in one patient and by quetiapine in the other two.
The atypicals are well tolerated but not without side effects. Weight gain is the most common problem and one with potentially serious health consequences.16
Using conventional agents. Even though atypicals are available, the clinician may consider continuing therapy with conventional antipsychotics in patients with TD when:
- the patient’s mental status has been satisfactory while taking conventional agents
- TD has been mild and stable over an extended time
- the patient has no side effects other than TD.
The literature supports the clinical experience that mild TD rarely worsens with continued antipsychotic therapy. Studies of 5 years or more tend to show TD stability with continued conventional antipsychotic therapy.17 It is prudent to maintain stable chronic psychotic patients with mild TD on the lowest effective dosages of conventional antipsychotics and to monitor them regularly for changes in dyskinesia and psychiatric status.
MANAGING COMPLICATED TD
Managing severe TD or patients showing dystonia, tics, marked akathisia, or DIP coexisting with TD usually calls for more-aggressive interventions (Algorithm).
Algorithm Clinical management of tardive dyskinesia (TD)

Clozapine remains the first-line treatment for difficult TD; it has a very low propensity for inducing DIP and very rarely causes TD.18 Controlled studies,18,19 case reports, and open trials demonstrate its efficacy for reducing TD of all types and severity at a usual dosage of 300 to 500 mg/d. Clozapine’s antidyskinetic effects may be attributed to the absence of rebound after withdrawal and its greater efficacy in more-severe cases.18
Long-term clozapine therapy is recommended for TD, as symptoms remit slowly. Because weight gain, sedation, and other side effects—as well as mandatory blood monitoring—make clozapine less-than-ideal in clinical practice, researchers are seeking other effective therapies for TD.
Other atypicals. The obvious place to look is the other atypicals, which are simpler than clozapine to administer long-term. To date, however, these drugs have not proven to be as reliably effective as clozapine for TD. A recent review concluded that among the atypicals only clozapine induces less EPS than low-potency conventional antipsychotics.20
Nonantipsychotic agents. Other antidyskinetic drugs have come and gone; none has stood the test of time or proven effective in controlled trials. These agents may benefit some TD patients, but improvement is usually not dramatic.
Vitamin E was found to be effective in some TD treatment studies14 but not more effective than placebo in the largest controlled trial.21 Long-term treatment with dopamine-blocking antipsychotics is thought to cause oxidative stressinduced neurotoxicity in the nigrostriatal system.22 Lipid-soluble antioxidants such as vitamin E decrease free-radical formation, and it is possible that vitamin E may yet emerge as a helpful agent in preventing TD.23
Melatonin, a stronger antioxidant than vitamin E, was found to reduce TD in a 6-week placebocontrolled study,22 but the degree of TD improvement was modest. Melatonin’s value as a therapeutic agent for TD remains dubious.23
Miscellaneous. Case reports and studies with small series of TD patients have advanced numerous compounds as possible therapeutic agents (Table 2). Other drugs that occasionally have shown benefit in TD include buspirone, propranolol, pyridoxine (vitamin B6), ondansetron, clonidine, and the neuropeptide ceruletide.
ECT and diet. Suggested nondrug treatments of TD include electroconvulsive therapy (ECT)14 and a diet of mixed branched-chain amino acids.24
Table 2
Compounds that occasionally show benefit in TD
| Class | Example |
|---|---|
| Cholinergics | Lecithin |
| Catecholamine depletors | Tetrabenazine (investigational orphan drug) |
| Calcium channel blockers | Verapamil |
| Gabaergic compounds | Baclofen |
| Benzodiazepines | Clonazepam |
MANAGING TD VARIANTS
TD variants are notoriously difficult to treat but tend to respond to clozapine.18 In addition:
- Tardive dystonia is often treated with reserpine, tetrabenazine, or high doses of anticholinergic drugs.25 Botulinum toxin A injections into affected muscles may be remarkably effective but must be repeated regularly.25
- Tardive akathisia may improve slowly with clozapine, propranolol, or benzodiazepines.25
Managing severe or atypical TD is usually beyond the expertise of the practicing psychiatrist. Obtaining consultation from a psychopharmacologist or a neurologist experienced in treating movement disorders is highly recommended.
PREVENTING TD
Conventional antipsychotics are still prescribed by psychiatrists, internists, and family physicians and are often given in emergency rooms. Avoiding these drugs whenever possible and using the lowest effective dosages will reduce the risk of TD.26
Patients at relatively high risk for TD—the elderly, those who are very sensitive to acute EPS, and those with affective disorders or diabetes mellitus—are rarely candidates for conventional neuroleptics if a suitable alternative exists. Genetic research may further identify individuals susceptible to TD.27
- Abnormal Involuntary Movement Scale (AIMS). www.dr-bob.org/tips/aims.html
- Bloom FE, Kupfer DJ (eds). Psychopharmacology: The fourth generation of progress. New York: Raven Press, 1995.
- Tandon R, Halbreich U (eds). Atypical antipsychotics: Efficacy and tolerability—achieving the optimal balance. Psychoneuroendocrinology 2003;28(suppl 1).
Drug brand names
- Aripiprazole • Abilify
- Baclofen • Lioresal
- Buspirone • BuSpar
- Clonazepam • Klonopin
- Clonidine • Catapres
- Clozapine • Clozaril
- Olanzapine • Zyprexa
- Ondansetron • Zofran
- Propranolol • Inderal
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Verapamil • Calan, others
- Ziprasidone • Geodon
Disclosure
Dr. Gardos receives research grant support from Forest Laboratories.
1. Woerner M, Kane JM, Lieberman JA, et al. The prevalence of tardive dyskinesia, J Clin Psychopharmacology 1991;11:34-42.
2. Caroff SN, Mann SC, Campbell EC, et al. Movement disorders associated with atypical antipsychotic drugs. J Clin Psychiatry 2002;63(suppl 4):12-19.
3. Tollefson GD, Beasley CM, Tran PV, et al. Olanzapine versus haloperidol in the treatment of schizophrenia and schizophreniform disorders: results of an international collaborative trial. Am J Psychiatry 1997;154:457-65.
4. Jeste DV, Lacro JP, Bailey A, et al. Lower incidence of tardive dyskinesia with risperidone compared with haloperidol in older patients. J Am Geriatr Soc 1999;47:716-19.
5. Kumet R, Freeman MP. Clozapine and tardive dyskinesia. J Clin Psychiatry 2002;63:167-8.
6. Hong KS, Cheong SS, Woo J-M, Kim E. Risperidone-induced tardive dyskinesia. Am J Psychiatry 1999;156:1290.-
7. Ghaemi SN, Ko JY. Quetiapine-related tardive dyskinesia. Am J Psychiatry 2001;158:1737.-
8. Kane JM. Tardive dyskinesia: epidemiological and clinical presentation. In: Bloom FE, Kupfer DJ (eds.) Psychopharmacology: The fourth generation of progress. New York: Raven Press, Ltd, 1995;1485-95.
9. Guy W. ECDEU assessment manual for psychopharmacology (rev. ed). Washington, DC: Department of Health, Education and Welfare, 1976.
10. Madhusoodanan S, Brenner R. Reversible choreiform dyskinesia and extrapyramidal symptoms associated with sertraline therapy. J Clin Psychopharmacology 1997;17:138-9.
11. Glazer WM, Morgenstern H, Pultz JA, et al. Incidence of tardive dyskinesia is lower with quetiapine treatment than with typical antipsychotics in patients with schizophrenia and schizo-affective disorder. Schizophrenia Res 2000;41:206-7.
12. Hirsch SR, Kissling W, Bauml J, et al. A 28-week comparison of ziprasidone and haloperidol in outpatients with stable schizophrenia. J Clin Psychiatry 2002;63:516-23.
13. Kujawa M, Sala A, Ingenito GG, et al. Aripiprazole for long-term maintenance treatment of schizophrenia (poster presentation). Montreal, Canada: Collegium Internationale Neuropsychopharmacologicum 23rd congress, June 23-27, 2002.
14. Gupta S, Mosnik D, Black DW, et al. Tardive dyskinesia: review of treatments past, present and future. Ann Clin Psychiatry 1999;11:257-66.
15. Suzuki E, Obata M, Yoshida Y, Miyaoka H. Tardive dyskinesia with risperidone and anticholinergics. Am J Psychiatry 2002;159:1948.-
16. Nasrallah HA. A review of the effect of atypical antipsychotics on weight. Psychoneuroendocrinology 2003;28(suppl 1):83-96.
17. Gardos G, Casey DE, Cole JO, et al. Ten-year outcome of tardive dyskinesia. Am J Psychiatry 1994;151:836-41.
18. Lieberman JA, Saltz BL, Johns CA, et al. The effects of clozapine on tardive dyskinesia. Br J Psychiatry 1991;158:503-10.
19. Tamminga CA, Thaker GK, Moran M, et al. Clozapine in tardive dyskinesia: observations from human and animal model studies J Clin Psychiatry 1994;55(suppl B):102-6.
20. Leucht S, Wahlbeck C, Hermann J, Kissling W. New-generation antipsychotics versus low-potency conventional antipsychotics: a systematic review and meta-analysis. Lancet 2003;361:1581-9.
21. Adler LA, Rotrosen J, Edson R, et al. Vitamin E treatment of tardive dyskinesia. Arch Gen Psychiatry 1999;56:836-41.
22. Shamir E, Barak Y, Shalman I, et al. Melatonin treatment for tardive dyskinesia. Arch Gen Psychiatry 2001;58:1046-52.
23. Glazer WM, Woods SW. Should Sisyphus have taken melatonin? Arch Gen Psychiatry 2001;58:1054-5.
24. Richardson MA, Bevans M, Read LL, et al. Efficacy of the branched-chain amino acids in the treatment of tardive dyskinesia in men. Am J Psychiatry 2003;160:1117-24.
25. Gardos G, Cole JO. The evaluation and treatment of neurolepticinduced movement disorders. Harvard Rev Psychiatry 1995;3:130-9.
26. Lohr JB, Caligiuri MP, Edson R, et al. Treatment predictors of extrapyramidal side effects in patients with tardive dyskinesia: results from Veterans Affairs Cooperative Study 394. J Clin Psychopharmacol 2002;22:196-200.
27. Casey DE. Effect of clozapine therapy in schizophrenic individuals at risk for tardive dyskinesia. J Clin Psychiatry 1998;59(suppl 3):31-7.
Atypical antipsychotics seldom cause tardive dyskinesia (TD), but we cannot let our guard down when prescribing them. Although they pose a much lower risk of TD than do conventional antipsychotics, atypicals can cause TD in vulnerable patients.
Less worrisome than in the past, TD’s associated problems linger, including insidious onset, tendency for persistence, and lack of reliably effective treatment. It is important, therefore, for psychiatrists to:
- identify patients at risk for developing TD
- recognize extrapyramidal symptoms (EPS) when they occur
- and manage these side effects appropriately.
A CHANGING CLINICAL PICTURE
The term “dyskinesias” covers a variety of abnormal involuntary movements (Box). The incidence and prevalence of TD have dropped markedly in the last 10 years, as:
- more and more older, chronically ill patients are switched from conventional to atypical agents
- younger psychotic patients are usually treated with atypicals as first-line therapy and are never exposed to conventional antipsychotics.
Tardive dyskinesia (TD) tends to develop in patients receiving long-term antipsychotic treatment. Its typical movements are choreiform (jerky) or athetoid (writhing), irregular, and purposeless.
TD onset is usually insidious and may occur during drug therapy or weeks after antipsychotics are discontined. Its signs are usually observed in the face or mouth, and typical orofacial dyskinetic movements are:
Lips: puckering, pouting, smacking
Jaw: chewing, biting, side-to-side movements, jaw openings
Tongue: twisting, rolling, undulations, protrusion, darting (“fly-catching”)
Face: blinking, frowning, grimacing.
The trunk and extremities are involved less often. Choreiform finger and wrist movements, flexion and rotation of the ankle, toe movements, foot tapping, and rocking or twisting of the neck, hip, and trunk may be seen. Patients are often oblivious to these movements, which may be only intermittently present and are absent during sleep. Anxiety and arousal states may aggravate TD.
TD prevalence of about 20%—as shown by earlier studies of long-term conventional agents1—is declining. Newer studies comparing atypicals with conventional antipsychotics demonstrate much lower prevalence rates.2,3
TD incidence—estimated by new cases of TD per year of drug treatment—may have declined 10-fold, from 5% with conventional antipsychotics to 0.5% with atypicals. Likewise, incidence in the elderly may have fallen from 25% to 2.5%.4
Risk factors. Despite these improvements, case reports5-7 demonstrate that TD is possible in patients treated with atypicals, even without previous exposure to a conventional antipsychotic. Besides antipsychotic use, risk factors for developing TD include:
- older age
- negative symptoms of schizophrenia
- affective disorders
- acute EPS
- and diabetes mellitus.8
RECOGNIZING TD SYMPTOMS
Recognizing TD may be complicated by the presence of other EPS, particularly drug-induced parkinsonism (DIP). DIP typically develops early and often when treating patients with conventional antipsychotics (Table 1). TD and DIP may occur simultaneously in the same patient, making accurate diagnosis even more difficult.
Other dyskinesias may complicate the diagnosis. Three common TD variants, which may be acute or tardive (occurring after long-term antipsychotic therapy), are:
- akathisia, a distressing and at times irresistible urge to move the legs or other parts of the body
- dystonia, abnormal muscle tone and posture and muscle spasms
- tics, brief muscle contractions, usually in the face, including vocal tics.
AIMS testing. Defining a “case of TD” by dyskinetic movement severity is somewhat arbitrary. A commonly accepted definition is two area scores of “mild” or one rating of “moderate” using the Abnormal Involuntary Movement Scale (AIMS).9 The AIMS has been widely used in epidemiologic and treatment studies of TD and is easy to administer in a clinical setting (see Related Resources).
A careful drug history is required before TD can be diagnosed definitively. Spontaneous dys kinesias—usually orofacial—are sometimes seen in older patients who are not taking neuroleptics.8 Antidepressants, mood stabilizers, or antihistamines may infrequently trigger neurologic side effects—including dyskinesias, akathisia, and tremor—which are almost invariably reversible after the causative agent is withdrawn.8,10
Table 1
Features that differentiate two common extrapyramidal symptoms
| Tardive dyskinesia (TD) | Drug-induced parkinsonism (DIP) | |
|---|---|---|
| Onset | Late | Early |
| Type of movement | Choreoathetoid | Tremor |
| Amount of movement | Increased | Decreased |
| Muscle tone | Decreased | Increased |
| Most common site | Orofacial | Extremities |
| Response to anticholinergics | Tends to worsen | Tends to improve |
MANAGING MILD TD
Atypical antipsychotics have radically altered the clinical outlook for patients with TD and improved our ability to manage their symptoms. The clinician treating a TD patient today rarely faces the dilemma that exists with conventional antipsychotics: discontinue treatment and risk psychotic relapse, or continue treatment and risk persistent TD.
Using atypicals. Today, patients who need antipsychotic therapy for TD are usually already taking atypicals, which may ameliorate TD and control psychotic symptoms. Case reports and some studies have shown therapeutic effects in patients with TD taking olanzapine,3 risperidone,2 quetiapine,11 ziprasidone,12 aripiprazole,13 or the substituted benzamides (such as sulpiride), which are not marketed in the United States.14
Interestingly, TD triggered by taking one atypical may respond to treatment with another. Suzuki et al15 reported that three patients who had developed early-onset TD while taking risperidone showed TD remission after risperidone was replaced by olanzapine in one patient and by quetiapine in the other two.
The atypicals are well tolerated but not without side effects. Weight gain is the most common problem and one with potentially serious health consequences.16
Using conventional agents. Even though atypicals are available, the clinician may consider continuing therapy with conventional antipsychotics in patients with TD when:
- the patient’s mental status has been satisfactory while taking conventional agents
- TD has been mild and stable over an extended time
- the patient has no side effects other than TD.
The literature supports the clinical experience that mild TD rarely worsens with continued antipsychotic therapy. Studies of 5 years or more tend to show TD stability with continued conventional antipsychotic therapy.17 It is prudent to maintain stable chronic psychotic patients with mild TD on the lowest effective dosages of conventional antipsychotics and to monitor them regularly for changes in dyskinesia and psychiatric status.
MANAGING COMPLICATED TD
Managing severe TD or patients showing dystonia, tics, marked akathisia, or DIP coexisting with TD usually calls for more-aggressive interventions (Algorithm).
Algorithm Clinical management of tardive dyskinesia (TD)
Clozapine remains the first-line treatment for difficult TD; it has a very low propensity for inducing DIP and very rarely causes TD.18 Controlled studies,18,19 case reports, and open trials demonstrate its efficacy for reducing TD of all types and severity at a usual dosage of 300 to 500 mg/d. Clozapine’s antidyskinetic effects may be attributed to the absence of rebound after withdrawal and its greater efficacy in more-severe cases.18
Long-term clozapine therapy is recommended for TD, as symptoms remit slowly. Because weight gain, sedation, and other side effects—as well as mandatory blood monitoring—make clozapine less-than-ideal in clinical practice, researchers are seeking other effective therapies for TD.
Other atypicals. The obvious place to look is the other atypicals, which are simpler than clozapine to administer long-term. To date, however, these drugs have not proven to be as reliably effective as clozapine for TD. A recent review concluded that among the atypicals only clozapine induces less EPS than low-potency conventional antipsychotics.20
Nonantipsychotic agents. Other antidyskinetic drugs have come and gone; none has stood the test of time or proven effective in controlled trials. These agents may benefit some TD patients, but improvement is usually not dramatic.
Vitamin E was found to be effective in some TD treatment studies14 but not more effective than placebo in the largest controlled trial.21 Long-term treatment with dopamine-blocking antipsychotics is thought to cause oxidative stressinduced neurotoxicity in the nigrostriatal system.22 Lipid-soluble antioxidants such as vitamin E decrease free-radical formation, and it is possible that vitamin E may yet emerge as a helpful agent in preventing TD.23
Melatonin, a stronger antioxidant than vitamin E, was found to reduce TD in a 6-week placebocontrolled study,22 but the degree of TD improvement was modest. Melatonin’s value as a therapeutic agent for TD remains dubious.23
Miscellaneous. Case reports and studies with small series of TD patients have advanced numerous compounds as possible therapeutic agents (Table 2). Other drugs that occasionally have shown benefit in TD include buspirone, propranolol, pyridoxine (vitamin B6), ondansetron, clonidine, and the neuropeptide ceruletide.
ECT and diet. Suggested nondrug treatments of TD include electroconvulsive therapy (ECT)14 and a diet of mixed branched-chain amino acids.24
Table 2
Compounds that occasionally show benefit in TD
| Class | Example |
|---|---|
| Cholinergics | Lecithin |
| Catecholamine depletors | Tetrabenazine (investigational orphan drug) |
| Calcium channel blockers | Verapamil |
| Gabaergic compounds | Baclofen |
| Benzodiazepines | Clonazepam |
MANAGING TD VARIANTS
TD variants are notoriously difficult to treat but tend to respond to clozapine.18 In addition:
- Tardive dystonia is often treated with reserpine, tetrabenazine, or high doses of anticholinergic drugs.25 Botulinum toxin A injections into affected muscles may be remarkably effective but must be repeated regularly.25
- Tardive akathisia may improve slowly with clozapine, propranolol, or benzodiazepines.25
Managing severe or atypical TD is usually beyond the expertise of the practicing psychiatrist. Obtaining consultation from a psychopharmacologist or a neurologist experienced in treating movement disorders is highly recommended.
PREVENTING TD
Conventional antipsychotics are still prescribed by psychiatrists, internists, and family physicians and are often given in emergency rooms. Avoiding these drugs whenever possible and using the lowest effective dosages will reduce the risk of TD.26
Patients at relatively high risk for TD—the elderly, those who are very sensitive to acute EPS, and those with affective disorders or diabetes mellitus—are rarely candidates for conventional neuroleptics if a suitable alternative exists. Genetic research may further identify individuals susceptible to TD.27
- Abnormal Involuntary Movement Scale (AIMS). www.dr-bob.org/tips/aims.html
- Bloom FE, Kupfer DJ (eds). Psychopharmacology: The fourth generation of progress. New York: Raven Press, 1995.
- Tandon R, Halbreich U (eds). Atypical antipsychotics: Efficacy and tolerability—achieving the optimal balance. Psychoneuroendocrinology 2003;28(suppl 1).
Drug brand names
- Aripiprazole • Abilify
- Baclofen • Lioresal
- Buspirone • BuSpar
- Clonazepam • Klonopin
- Clonidine • Catapres
- Clozapine • Clozaril
- Olanzapine • Zyprexa
- Ondansetron • Zofran
- Propranolol • Inderal
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Verapamil • Calan, others
- Ziprasidone • Geodon
Disclosure
Dr. Gardos receives research grant support from Forest Laboratories.
Atypical antipsychotics seldom cause tardive dyskinesia (TD), but we cannot let our guard down when prescribing them. Although they pose a much lower risk of TD than do conventional antipsychotics, atypicals can cause TD in vulnerable patients.
Less worrisome than in the past, TD’s associated problems linger, including insidious onset, tendency for persistence, and lack of reliably effective treatment. It is important, therefore, for psychiatrists to:
- identify patients at risk for developing TD
- recognize extrapyramidal symptoms (EPS) when they occur
- and manage these side effects appropriately.
A CHANGING CLINICAL PICTURE
The term “dyskinesias” covers a variety of abnormal involuntary movements (Box). The incidence and prevalence of TD have dropped markedly in the last 10 years, as:
- more and more older, chronically ill patients are switched from conventional to atypical agents
- younger psychotic patients are usually treated with atypicals as first-line therapy and are never exposed to conventional antipsychotics.
Tardive dyskinesia (TD) tends to develop in patients receiving long-term antipsychotic treatment. Its typical movements are choreiform (jerky) or athetoid (writhing), irregular, and purposeless.
TD onset is usually insidious and may occur during drug therapy or weeks after antipsychotics are discontined. Its signs are usually observed in the face or mouth, and typical orofacial dyskinetic movements are:
Lips: puckering, pouting, smacking
Jaw: chewing, biting, side-to-side movements, jaw openings
Tongue: twisting, rolling, undulations, protrusion, darting (“fly-catching”)
Face: blinking, frowning, grimacing.
The trunk and extremities are involved less often. Choreiform finger and wrist movements, flexion and rotation of the ankle, toe movements, foot tapping, and rocking or twisting of the neck, hip, and trunk may be seen. Patients are often oblivious to these movements, which may be only intermittently present and are absent during sleep. Anxiety and arousal states may aggravate TD.
TD prevalence of about 20%—as shown by earlier studies of long-term conventional agents1—is declining. Newer studies comparing atypicals with conventional antipsychotics demonstrate much lower prevalence rates.2,3
TD incidence—estimated by new cases of TD per year of drug treatment—may have declined 10-fold, from 5% with conventional antipsychotics to 0.5% with atypicals. Likewise, incidence in the elderly may have fallen from 25% to 2.5%.4
Risk factors. Despite these improvements, case reports5-7 demonstrate that TD is possible in patients treated with atypicals, even without previous exposure to a conventional antipsychotic. Besides antipsychotic use, risk factors for developing TD include:
- older age
- negative symptoms of schizophrenia
- affective disorders
- acute EPS
- and diabetes mellitus.8
RECOGNIZING TD SYMPTOMS
Recognizing TD may be complicated by the presence of other EPS, particularly drug-induced parkinsonism (DIP). DIP typically develops early and often when treating patients with conventional antipsychotics (Table 1). TD and DIP may occur simultaneously in the same patient, making accurate diagnosis even more difficult.
Other dyskinesias may complicate the diagnosis. Three common TD variants, which may be acute or tardive (occurring after long-term antipsychotic therapy), are:
- akathisia, a distressing and at times irresistible urge to move the legs or other parts of the body
- dystonia, abnormal muscle tone and posture and muscle spasms
- tics, brief muscle contractions, usually in the face, including vocal tics.
AIMS testing. Defining a “case of TD” by dyskinetic movement severity is somewhat arbitrary. A commonly accepted definition is two area scores of “mild” or one rating of “moderate” using the Abnormal Involuntary Movement Scale (AIMS).9 The AIMS has been widely used in epidemiologic and treatment studies of TD and is easy to administer in a clinical setting (see Related Resources).
A careful drug history is required before TD can be diagnosed definitively. Spontaneous dys kinesias—usually orofacial—are sometimes seen in older patients who are not taking neuroleptics.8 Antidepressants, mood stabilizers, or antihistamines may infrequently trigger neurologic side effects—including dyskinesias, akathisia, and tremor—which are almost invariably reversible after the causative agent is withdrawn.8,10
Table 1
Features that differentiate two common extrapyramidal symptoms
| Tardive dyskinesia (TD) | Drug-induced parkinsonism (DIP) | |
|---|---|---|
| Onset | Late | Early |
| Type of movement | Choreoathetoid | Tremor |
| Amount of movement | Increased | Decreased |
| Muscle tone | Decreased | Increased |
| Most common site | Orofacial | Extremities |
| Response to anticholinergics | Tends to worsen | Tends to improve |
MANAGING MILD TD
Atypical antipsychotics have radically altered the clinical outlook for patients with TD and improved our ability to manage their symptoms. The clinician treating a TD patient today rarely faces the dilemma that exists with conventional antipsychotics: discontinue treatment and risk psychotic relapse, or continue treatment and risk persistent TD.
Using atypicals. Today, patients who need antipsychotic therapy for TD are usually already taking atypicals, which may ameliorate TD and control psychotic symptoms. Case reports and some studies have shown therapeutic effects in patients with TD taking olanzapine,3 risperidone,2 quetiapine,11 ziprasidone,12 aripiprazole,13 or the substituted benzamides (such as sulpiride), which are not marketed in the United States.14
Interestingly, TD triggered by taking one atypical may respond to treatment with another. Suzuki et al15 reported that three patients who had developed early-onset TD while taking risperidone showed TD remission after risperidone was replaced by olanzapine in one patient and by quetiapine in the other two.
The atypicals are well tolerated but not without side effects. Weight gain is the most common problem and one with potentially serious health consequences.16
Using conventional agents. Even though atypicals are available, the clinician may consider continuing therapy with conventional antipsychotics in patients with TD when:
- the patient’s mental status has been satisfactory while taking conventional agents
- TD has been mild and stable over an extended time
- the patient has no side effects other than TD.
The literature supports the clinical experience that mild TD rarely worsens with continued antipsychotic therapy. Studies of 5 years or more tend to show TD stability with continued conventional antipsychotic therapy.17 It is prudent to maintain stable chronic psychotic patients with mild TD on the lowest effective dosages of conventional antipsychotics and to monitor them regularly for changes in dyskinesia and psychiatric status.
MANAGING COMPLICATED TD
Managing severe TD or patients showing dystonia, tics, marked akathisia, or DIP coexisting with TD usually calls for more-aggressive interventions (Algorithm).
Algorithm Clinical management of tardive dyskinesia (TD)
Clozapine remains the first-line treatment for difficult TD; it has a very low propensity for inducing DIP and very rarely causes TD.18 Controlled studies,18,19 case reports, and open trials demonstrate its efficacy for reducing TD of all types and severity at a usual dosage of 300 to 500 mg/d. Clozapine’s antidyskinetic effects may be attributed to the absence of rebound after withdrawal and its greater efficacy in more-severe cases.18
Long-term clozapine therapy is recommended for TD, as symptoms remit slowly. Because weight gain, sedation, and other side effects—as well as mandatory blood monitoring—make clozapine less-than-ideal in clinical practice, researchers are seeking other effective therapies for TD.
Other atypicals. The obvious place to look is the other atypicals, which are simpler than clozapine to administer long-term. To date, however, these drugs have not proven to be as reliably effective as clozapine for TD. A recent review concluded that among the atypicals only clozapine induces less EPS than low-potency conventional antipsychotics.20
Nonantipsychotic agents. Other antidyskinetic drugs have come and gone; none has stood the test of time or proven effective in controlled trials. These agents may benefit some TD patients, but improvement is usually not dramatic.
Vitamin E was found to be effective in some TD treatment studies14 but not more effective than placebo in the largest controlled trial.21 Long-term treatment with dopamine-blocking antipsychotics is thought to cause oxidative stressinduced neurotoxicity in the nigrostriatal system.22 Lipid-soluble antioxidants such as vitamin E decrease free-radical formation, and it is possible that vitamin E may yet emerge as a helpful agent in preventing TD.23
Melatonin, a stronger antioxidant than vitamin E, was found to reduce TD in a 6-week placebocontrolled study,22 but the degree of TD improvement was modest. Melatonin’s value as a therapeutic agent for TD remains dubious.23
Miscellaneous. Case reports and studies with small series of TD patients have advanced numerous compounds as possible therapeutic agents (Table 2). Other drugs that occasionally have shown benefit in TD include buspirone, propranolol, pyridoxine (vitamin B6), ondansetron, clonidine, and the neuropeptide ceruletide.
ECT and diet. Suggested nondrug treatments of TD include electroconvulsive therapy (ECT)14 and a diet of mixed branched-chain amino acids.24
Table 2
Compounds that occasionally show benefit in TD
| Class | Example |
|---|---|
| Cholinergics | Lecithin |
| Catecholamine depletors | Tetrabenazine (investigational orphan drug) |
| Calcium channel blockers | Verapamil |
| Gabaergic compounds | Baclofen |
| Benzodiazepines | Clonazepam |
MANAGING TD VARIANTS
TD variants are notoriously difficult to treat but tend to respond to clozapine.18 In addition:
- Tardive dystonia is often treated with reserpine, tetrabenazine, or high doses of anticholinergic drugs.25 Botulinum toxin A injections into affected muscles may be remarkably effective but must be repeated regularly.25
- Tardive akathisia may improve slowly with clozapine, propranolol, or benzodiazepines.25
Managing severe or atypical TD is usually beyond the expertise of the practicing psychiatrist. Obtaining consultation from a psychopharmacologist or a neurologist experienced in treating movement disorders is highly recommended.
PREVENTING TD
Conventional antipsychotics are still prescribed by psychiatrists, internists, and family physicians and are often given in emergency rooms. Avoiding these drugs whenever possible and using the lowest effective dosages will reduce the risk of TD.26
Patients at relatively high risk for TD—the elderly, those who are very sensitive to acute EPS, and those with affective disorders or diabetes mellitus—are rarely candidates for conventional neuroleptics if a suitable alternative exists. Genetic research may further identify individuals susceptible to TD.27
- Abnormal Involuntary Movement Scale (AIMS). www.dr-bob.org/tips/aims.html
- Bloom FE, Kupfer DJ (eds). Psychopharmacology: The fourth generation of progress. New York: Raven Press, 1995.
- Tandon R, Halbreich U (eds). Atypical antipsychotics: Efficacy and tolerability—achieving the optimal balance. Psychoneuroendocrinology 2003;28(suppl 1).
Drug brand names
- Aripiprazole • Abilify
- Baclofen • Lioresal
- Buspirone • BuSpar
- Clonazepam • Klonopin
- Clonidine • Catapres
- Clozapine • Clozaril
- Olanzapine • Zyprexa
- Ondansetron • Zofran
- Propranolol • Inderal
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Verapamil • Calan, others
- Ziprasidone • Geodon
Disclosure
Dr. Gardos receives research grant support from Forest Laboratories.
1. Woerner M, Kane JM, Lieberman JA, et al. The prevalence of tardive dyskinesia, J Clin Psychopharmacology 1991;11:34-42.
2. Caroff SN, Mann SC, Campbell EC, et al. Movement disorders associated with atypical antipsychotic drugs. J Clin Psychiatry 2002;63(suppl 4):12-19.
3. Tollefson GD, Beasley CM, Tran PV, et al. Olanzapine versus haloperidol in the treatment of schizophrenia and schizophreniform disorders: results of an international collaborative trial. Am J Psychiatry 1997;154:457-65.
4. Jeste DV, Lacro JP, Bailey A, et al. Lower incidence of tardive dyskinesia with risperidone compared with haloperidol in older patients. J Am Geriatr Soc 1999;47:716-19.
5. Kumet R, Freeman MP. Clozapine and tardive dyskinesia. J Clin Psychiatry 2002;63:167-8.
6. Hong KS, Cheong SS, Woo J-M, Kim E. Risperidone-induced tardive dyskinesia. Am J Psychiatry 1999;156:1290.-
7. Ghaemi SN, Ko JY. Quetiapine-related tardive dyskinesia. Am J Psychiatry 2001;158:1737.-
8. Kane JM. Tardive dyskinesia: epidemiological and clinical presentation. In: Bloom FE, Kupfer DJ (eds.) Psychopharmacology: The fourth generation of progress. New York: Raven Press, Ltd, 1995;1485-95.
9. Guy W. ECDEU assessment manual for psychopharmacology (rev. ed). Washington, DC: Department of Health, Education and Welfare, 1976.
10. Madhusoodanan S, Brenner R. Reversible choreiform dyskinesia and extrapyramidal symptoms associated with sertraline therapy. J Clin Psychopharmacology 1997;17:138-9.
11. Glazer WM, Morgenstern H, Pultz JA, et al. Incidence of tardive dyskinesia is lower with quetiapine treatment than with typical antipsychotics in patients with schizophrenia and schizo-affective disorder. Schizophrenia Res 2000;41:206-7.
12. Hirsch SR, Kissling W, Bauml J, et al. A 28-week comparison of ziprasidone and haloperidol in outpatients with stable schizophrenia. J Clin Psychiatry 2002;63:516-23.
13. Kujawa M, Sala A, Ingenito GG, et al. Aripiprazole for long-term maintenance treatment of schizophrenia (poster presentation). Montreal, Canada: Collegium Internationale Neuropsychopharmacologicum 23rd congress, June 23-27, 2002.
14. Gupta S, Mosnik D, Black DW, et al. Tardive dyskinesia: review of treatments past, present and future. Ann Clin Psychiatry 1999;11:257-66.
15. Suzuki E, Obata M, Yoshida Y, Miyaoka H. Tardive dyskinesia with risperidone and anticholinergics. Am J Psychiatry 2002;159:1948.-
16. Nasrallah HA. A review of the effect of atypical antipsychotics on weight. Psychoneuroendocrinology 2003;28(suppl 1):83-96.
17. Gardos G, Casey DE, Cole JO, et al. Ten-year outcome of tardive dyskinesia. Am J Psychiatry 1994;151:836-41.
18. Lieberman JA, Saltz BL, Johns CA, et al. The effects of clozapine on tardive dyskinesia. Br J Psychiatry 1991;158:503-10.
19. Tamminga CA, Thaker GK, Moran M, et al. Clozapine in tardive dyskinesia: observations from human and animal model studies J Clin Psychiatry 1994;55(suppl B):102-6.
20. Leucht S, Wahlbeck C, Hermann J, Kissling W. New-generation antipsychotics versus low-potency conventional antipsychotics: a systematic review and meta-analysis. Lancet 2003;361:1581-9.
21. Adler LA, Rotrosen J, Edson R, et al. Vitamin E treatment of tardive dyskinesia. Arch Gen Psychiatry 1999;56:836-41.
22. Shamir E, Barak Y, Shalman I, et al. Melatonin treatment for tardive dyskinesia. Arch Gen Psychiatry 2001;58:1046-52.
23. Glazer WM, Woods SW. Should Sisyphus have taken melatonin? Arch Gen Psychiatry 2001;58:1054-5.
24. Richardson MA, Bevans M, Read LL, et al. Efficacy of the branched-chain amino acids in the treatment of tardive dyskinesia in men. Am J Psychiatry 2003;160:1117-24.
25. Gardos G, Cole JO. The evaluation and treatment of neurolepticinduced movement disorders. Harvard Rev Psychiatry 1995;3:130-9.
26. Lohr JB, Caligiuri MP, Edson R, et al. Treatment predictors of extrapyramidal side effects in patients with tardive dyskinesia: results from Veterans Affairs Cooperative Study 394. J Clin Psychopharmacol 2002;22:196-200.
27. Casey DE. Effect of clozapine therapy in schizophrenic individuals at risk for tardive dyskinesia. J Clin Psychiatry 1998;59(suppl 3):31-7.
1. Woerner M, Kane JM, Lieberman JA, et al. The prevalence of tardive dyskinesia, J Clin Psychopharmacology 1991;11:34-42.
2. Caroff SN, Mann SC, Campbell EC, et al. Movement disorders associated with atypical antipsychotic drugs. J Clin Psychiatry 2002;63(suppl 4):12-19.
3. Tollefson GD, Beasley CM, Tran PV, et al. Olanzapine versus haloperidol in the treatment of schizophrenia and schizophreniform disorders: results of an international collaborative trial. Am J Psychiatry 1997;154:457-65.
4. Jeste DV, Lacro JP, Bailey A, et al. Lower incidence of tardive dyskinesia with risperidone compared with haloperidol in older patients. J Am Geriatr Soc 1999;47:716-19.
5. Kumet R, Freeman MP. Clozapine and tardive dyskinesia. J Clin Psychiatry 2002;63:167-8.
6. Hong KS, Cheong SS, Woo J-M, Kim E. Risperidone-induced tardive dyskinesia. Am J Psychiatry 1999;156:1290.-
7. Ghaemi SN, Ko JY. Quetiapine-related tardive dyskinesia. Am J Psychiatry 2001;158:1737.-
8. Kane JM. Tardive dyskinesia: epidemiological and clinical presentation. In: Bloom FE, Kupfer DJ (eds.) Psychopharmacology: The fourth generation of progress. New York: Raven Press, Ltd, 1995;1485-95.
9. Guy W. ECDEU assessment manual for psychopharmacology (rev. ed). Washington, DC: Department of Health, Education and Welfare, 1976.
10. Madhusoodanan S, Brenner R. Reversible choreiform dyskinesia and extrapyramidal symptoms associated with sertraline therapy. J Clin Psychopharmacology 1997;17:138-9.
11. Glazer WM, Morgenstern H, Pultz JA, et al. Incidence of tardive dyskinesia is lower with quetiapine treatment than with typical antipsychotics in patients with schizophrenia and schizo-affective disorder. Schizophrenia Res 2000;41:206-7.
12. Hirsch SR, Kissling W, Bauml J, et al. A 28-week comparison of ziprasidone and haloperidol in outpatients with stable schizophrenia. J Clin Psychiatry 2002;63:516-23.
13. Kujawa M, Sala A, Ingenito GG, et al. Aripiprazole for long-term maintenance treatment of schizophrenia (poster presentation). Montreal, Canada: Collegium Internationale Neuropsychopharmacologicum 23rd congress, June 23-27, 2002.
14. Gupta S, Mosnik D, Black DW, et al. Tardive dyskinesia: review of treatments past, present and future. Ann Clin Psychiatry 1999;11:257-66.
15. Suzuki E, Obata M, Yoshida Y, Miyaoka H. Tardive dyskinesia with risperidone and anticholinergics. Am J Psychiatry 2002;159:1948.-
16. Nasrallah HA. A review of the effect of atypical antipsychotics on weight. Psychoneuroendocrinology 2003;28(suppl 1):83-96.
17. Gardos G, Casey DE, Cole JO, et al. Ten-year outcome of tardive dyskinesia. Am J Psychiatry 1994;151:836-41.
18. Lieberman JA, Saltz BL, Johns CA, et al. The effects of clozapine on tardive dyskinesia. Br J Psychiatry 1991;158:503-10.
19. Tamminga CA, Thaker GK, Moran M, et al. Clozapine in tardive dyskinesia: observations from human and animal model studies J Clin Psychiatry 1994;55(suppl B):102-6.
20. Leucht S, Wahlbeck C, Hermann J, Kissling W. New-generation antipsychotics versus low-potency conventional antipsychotics: a systematic review and meta-analysis. Lancet 2003;361:1581-9.
21. Adler LA, Rotrosen J, Edson R, et al. Vitamin E treatment of tardive dyskinesia. Arch Gen Psychiatry 1999;56:836-41.
22. Shamir E, Barak Y, Shalman I, et al. Melatonin treatment for tardive dyskinesia. Arch Gen Psychiatry 2001;58:1046-52.
23. Glazer WM, Woods SW. Should Sisyphus have taken melatonin? Arch Gen Psychiatry 2001;58:1054-5.
24. Richardson MA, Bevans M, Read LL, et al. Efficacy of the branched-chain amino acids in the treatment of tardive dyskinesia in men. Am J Psychiatry 2003;160:1117-24.
25. Gardos G, Cole JO. The evaluation and treatment of neurolepticinduced movement disorders. Harvard Rev Psychiatry 1995;3:130-9.
26. Lohr JB, Caligiuri MP, Edson R, et al. Treatment predictors of extrapyramidal side effects in patients with tardive dyskinesia: results from Veterans Affairs Cooperative Study 394. J Clin Psychopharmacol 2002;22:196-200.
27. Casey DE. Effect of clozapine therapy in schizophrenic individuals at risk for tardive dyskinesia. J Clin Psychiatry 1998;59(suppl 3):31-7.
Reducing suicide risk in psychiatric disorders
Which psychotropics reduce the risk of suicide in patients with psychiatric disorders? Although no drugs eliminate the risk, new evidence is clarifying that some therapeutic choices can make a difference:
- Long-term lithium treatment apparently reduces suicide risk in patients with affective disorders; mood-altering anticonvulsants are less well studied but show less benefit than lithium.
- Effects of antidepressants remain inconclusive without adequate long-term studies.
- At least one atypical antipsychotic—clozapine—probably lowers suicide risk, although direct comparisons of antipsychotic agents are rare.
- Surprisingly little evidence is available on nondrug interventions, including rapid hospitalization, psychotherapy, and electroconvulsive therapy.1
Suicide is the leading cause of malpractice liability in psychiatry and of the heightened risk of death in persons with major affective and psychotic disorders (Box).1-4 Here are the latest findings to help you choose medications for at-risk patients with bipolar disorder, major depression, or chronic psychoses.
Suicide is by far the most common cause of premature death among patients with major mood and psychotic disorders.2,3 A major affective or psychotic disorder increases risk of suicide 8- to 22-fold (Table 1). A history of attempted suicide increases a person’s suicide risk 38-fold, so that the likelihood of dying by suicide becomes greater than one in four (28%).
Attempted suicide is less well-documented but may be 10 to 20 times more common than completed suicide in the general population. Persons with major affective and psychotic disorders complete suicide at an estimated rate of once in five attempts. This high rate suggests that their suicidal intent and methods are particularly lethal.4
BIPOLAR DISORDER AND MOOD STABILIZERS
Bipolar disorder is associated with the highest suicide rate among all major psychiatric illnesses, with an international incidence averaging 0.31% of patients per year.4 This rate may slightly exceed the suicide rate of patients with major depression, which averages 0.29%/year.
Risk of suicidal behavior is similar among patients with bipolar type II (depression with hypomania) and type I disorder (depression with mania), supporting the view that type II is not a milder form of bipolar illness.4-6 Indeed, one study of suicide attempts found a higher risk among bipolar II patients (24%) than in bipolar I patients (17%) as well as a higher risk in both bipolar types than in persons diagnosed with unipolar major depression (12%).4
Suicidal behavior in bipolar disorder is associated almost entirely with ongoing depression or dysphoria and is especially likely to follow severe and highly recurrent depressive episodes.5,6 Combinations of depressive-dysphoric and irritable, agitated, anxious features in “mixed states” may be particularly dangerous and can be hard to diagnose with confidence. Moreover, DSM-IV criteria for mixed states are far too narrow in requiring symptoms to simultaneously fulfill criteria for both mania and major depression. More broadly defined mixed states are very common. Underdiagnosis risks underestimation of suicidal potential, and misdiagnosis as “agitated depression” encourages potentially dangerous overuse of antidepressants.5,7
Depression or dysphoria is the most prevalent morbidity in patients with bipolar disorder. Major and minor depressive states and mixed-dysphoric phases account for nearly one-third of time in follow-up care, exceeding time in mania or hypomania by more than 4-fold.8 Ironically, however, bipolar depression is one of the least-studied forms of major depression. Suicidal bipolar patients are typically excluded from antidepressant studies because of the risks of inducing greater instability, agitation, or mania while treating them with an antidepressant but without a mood stabilizer.7
LITHIUM’S PROTECTIVE EFFECT
Decades of research and clinical use demonstrate substantially lower risks of suicide and serious suicide attempts when patients with bipolar disorder are treated long-term with lithium salts in standard clinical doses (serum concentrations typically 0.6 to 0.8 mEq/L). Lithium is highly effective in treating all phases of bipolar disorder. A recent meta-analysis of 26 long-term trials of lithium reported between 1967 and 2001 found an average 3.2-fold sparing of morbidity or relapse risk.9
Benefits in types I and II. A large European sample10 compared percent-time-ill in bipolar patients before and after they received lithium as maintenance treatment. Unexpectedly, lithium therapy reduced percent-time-ill to a greater extent among patients with type II than type I bipolar disorder. Time in mania and time in depression were reduced 2.5-fold and 2.0-fold, respectively, in type I patients, compared with nearly 5-fold for time in hypomania and 2.5-fold for time in depression among type II patients.
Because depression is associated with the highest rates of suicidal behavior in all phases of bipolar disorders, lithium’s effects in preventing depressive recurrence are especially important for reducing suicide risk.6
In a review of 22 studies11 —some including patients with bipolar or recurrent unipolar major depression—risk of death by suicide was reduced at least 5-fold, based on an informal comparison of pooled rates in treated versus untreated samples. Based on quantitative meta-analysis, the pooled risk of death by suicide was reduced nearly 9-fold (or by 89%) in patients who received lithium maintenance treatment compared with those who did not. The risk for suicide attempts fell nearly 10-fold in a compilation of 33 studies (Table 2).12 Available studies do not permit separate analysis of lithium’s effects on suicidal behavior among patients with bipolar disorder and recurrent unipolar depression, leaving the relative benefit by diagnosis uncertain.
Table 1
Suicide risks in selected psychiatric disorders*
| Condition | Relative risk | Incidence (%/year) | Lifetime risk (%) |
|---|---|---|---|
| Prior suicide attempt | 38.4 | 0.549 | 27.5 |
| Bipolar disorder | 21.7 | 0.310 | 15.5 |
| Major depression | 20.4 | 0.292 | 14.6 |
| Mixed drug abuse | 19.2 | 0.275 | 14.7 |
| Dysthymia | 12.1 | 0.173 | 8.65 |
| Obsessive-compulsive disorder | 11.5 | 0.143 | 8.15 |
| Panic disorder | 10.0 | 0.160 | 7.15 |
| Schizophrenia | 8.45 | 0.121 | 6.05 |
| Personality disorders | 7.08 | 0.101 | 5.05 |
| Alcohol abuse | 5.86 | 0.084 | 4.20 |
| Cancer | 1.80 | 0.026 | 1.30 |
| General population | 1.00 | 0.014 | 0.72 |
| * Estimated relative risks compared with the general population,2 with recently updated information about bipolar disorders.6 Annual rates are based on international general population average (14.3/100,000/year) × standardized mortality ratio; lifetime estimates are based on annual rates × 50 years as an estimate of lifetime exposure for years at major risk. | |||
Dangers of stopping lithium. In our study5 of more than 200 patients with DSM-IV bipolar I or II disorder, prophylactic lithium treatment for an average of 4 years reduced the risk of completed and attempted suicide by 6.5-fold. A subgroup of more than 100 patients discontinued lithium, usually after prolonged stability, and we excluded from analysis any cases of suspected emerging illness associated with discontinuation. Within 6 to 12 months after stopping treatment, this subgroup’s rates of suicidal behavior increased markedly—by 20-fold above treated rates.5 Thereafter, their rates returned to prelithium treatment levels.
Of particular clinical importance:
- discontinuing lithium gradually—over at least 2 weeks—was associated with a 2-fold lower suicide risk than more-abrupt discontinuation
- suicidal behavior after lithium discontinuation was almost always associated with emerging depression, which can provide an early warning of impending suicidal risk.
Table 2
Effect of lithium treatment on risk of completed and attempted suicide in patients with bipolar and recurrent depressive disorders*
| Treatment or sample | Suicides | Attempts | All acts | A/S ratio |
|---|---|---|---|---|
| With lithium | 0.16 | 0.41 | 0.57 | 2.6 |
| Without lithium | 0.88 | 4.02 | 4.90 | 4.6 |
| Off/on lithium ratio | 5.5 | 9.8 | 8.6 | — |
| General population | 0.014 | 0.21 | 0.22 | 15.3 |
| Off lithium/general population ratio | 56.4 | 19.1 | 22.3 | — |
| On lithium/general population ratio | 11.4 | 2.0 | 2.6 | — |
| A/S ratio: Attempts versus completed suicides | ||||
| * Rates (acts/year/100 persons, or %/year), based on previously reported averages derived from analyses of data from 33 studies with 55 treatment-arms,12 from a more selected analysis of 22 studies of completed suicides,11 and updated estimates for general population rates.6 | ||||
This is not the first time we have found evidence of a dramatic—but time-limited—increase in risk of recurrent bipolar illness when lithium treatment was discontinued.13 Bipolar disorder patients who discontinue long-term lithium treatment abruptly are at high risk of recurrent depression and mania.13
Incomplete protection. Lithium’s protection against suicidal risk is incomplete, as one can see by comparing lithium-treated versus untreated bipolar patients’ suicide rates with those of the general population (Table 2).6
With lithium:
- suicides plus attempts declined 8.6-fold to levels 2.6 times greater than those of the general population
- suicide attempts fell 10-fold to levels that are about twice that of the general population
- risk of completed suicides declined 5.5-fold with lithium treatment but remained 11 times higher than that of the general population.
Without lithium:
- risk of suicide in bipolar patients is approximately 22 times greater than that of the general population
- ratio of attempts to suicides among bipolar disorder patients averages 4.6, suggesting that suicide attempts by patients with bipolar disorder are relatively lethal.6
Effect of delayed lithium therapy. Many patients with bipolar disorder do not receive sustained prophylactic treatment early in the illness.
Studies typically show an average 5- to 10-year gap between illness onset and the start of sustained lithium maintenance treatment. This delay averages more than 3 years longer among women with bipolar II disorder than men with bipolar I disorder, evidently reflecting major clinical dissimilarities between these groups.6,14 In contrast, we found that nearly one-quarter of long-term risk of suicidal behavior emerges within the first year of bipolar illness.5 Clearly, patients with recurrent major affective illness require earlier intervention and more consistent clinical care.
We have also found that delayed maintenance treatment or the number of prior episodes of bipolar illness do not seem to limit therapeutic response to lithium.14,15 These findings support the conclusion that prophylactic lithium treatment can be worthwhile, even after years of illness and many recurrences. Moreover, our recent meta-analysis of treatment options for rapid-cycling bipolar illness indicates that—even though all treatments have yielded inferior results compared with nonrapidly-cycling patients—no alternative has outperformed lithium.16
Anticonvulsants. Evidence regarding the effects of other mood stabilizers on suicide risk in bipolar disorder remains limited:
- In a European collaborative study, several hundred patients with bipolar or schizoaffective disorder were randomly assigned to receive lithium or carbamazepine for nearly 2 years. Rates of suicidal acts were 2.5%/year with the anticonvulsant, but there were no suicides or attempts in patients receiving lithium.17 Direct comparisons are rare, but this difference was both striking and statistically significant.
- Computerized records of approximately 20,000 patients diagnosed with bipolar disorder at two large American HMOs were analyzed to compare suicidal behaviors associated with specific treatments. Lithium yielded 2.7-fold greater protection against suicidal behavior (mainly attempts because suicides were rare) compared with anticonvulsants (mainly divalproex).18
Treatment recommendation. These observations support lithium’s value in long-term maintenance of patients with bipolar disorder. Lithium’s apparent reduction of suicide risk is striking and may be superior to that of other mood-stabilizers. Alternate treatments and lithium’s potential value for reducing suicide risk in patients with unipolar depression require further study.
It is important to emphasize that lithium can be toxic or even fatal in acute overdose. This risk is integral to the equation when you assess risks and benefits for individual patients.
MAJOR DEPRESSION AND ANTIDEPRESSANTS
Major depression and depressive components of other disorders are major risk factors for suicide.1,2,6 Depression continues to be surprisingly underrecognized and undertreated, even though relatively safe and tolerable antidepressants are readily available.1,6,19,20 Patients with recurrent unipolar major depression often remain inconsistently or inadequately treated, even after they attempt suicide.19
Recent reviews of suicide risk during research on antidepressant treatment in major depression suggest that:
- antidepressants of various kinds may tend to reduce the risk of suicidal behavior, but any such effect is small and statistically nonsignificant (Baldessarini et al, 2003, unpublished)
- tricyclic antidepressants may yield lower rates of suicidal behavior than selective serotonin reuptake inhibitors (SSRIs). Similarly, however, such trends reflect highly variable research methods and inconsistent findings and do not hold up to quantitative analysis (Baldessarini et al, 2003, unpublished).
The suicidal events encountered during research mainly involve attempts because suicides are rare, particularly in relatively brief treatment trials that exclude acutely suicidal subjects. Analyses are further complicated by trends toward paradoxically lower suicidal risks among depressed patients randomized to a placebo in controlled antidepressant trials. This paradox is paralleled by often earlier removal of patients treated with a placebo than with an active antidepressant, perhaps in association with emerging suicidality.21
Table 3
Preventing suicide: How effective are specific treatments?
| Treatments compared | Disorder treated | Benefit/risk ratio |
|---|---|---|
| Mood stabilizers | ||
| Lithium vs. none or placebo* | Bipolar disorder | |
| Suicides | 8.8 (4.1 to 19.1)a | |
| Attempts | 9.9 (5.0 to 14.8)b | |
| Lithium vs. carbamazepine* | Bipolar disorder | ≥2.5c |
| Lithium vs. divalproex* | Bipolar disorder | 2.7 (1.2 to 6.2)d |
| Antidepressants | ||
| Antidepressants (any) vs. placebo/none | Major depressive disorder | 1.1 (0.7 to 1.6)e |
| Tricyclics vs. SSRIs | Major depressive disorder | 1.2 (0.7 to 2.1)e |
| Antipsychotics | ||
| Clozapine vs. any antipsychotic* | Schizophrenia | |
| Suicides + attempts | 3.3 (1.7 to 6.3)f | |
| Attempts | 2.9 (1.5 to 5.7)f | |
| Clozapine vs. olanzapine* | Schizophrenia | |
| Suicides + attempts | 1.3 (1.0 to 1.7)g | |
| a. Tondo et al, 200111 | ||
| b. Baldessarini et al, 20035 | ||
| c. Thies-Flechtner et al, 199517 | ||
| d. Goodwin et al, 200218 | ||
| e. Baldessarini et al, 20035 | ||
| f. Baldessarini & Hennen, 200322 | ||
| g. Meltzer et al, 200324 | ||
| * First agent is statistically more effective, based on benefit/risk ratio (95% CI). | ||
These trends toward lower suicide risk among patients receiving a placebo are somewhat reassuring, given concern that placebo randomization for scientific purposes may endanger study subjects. However, these artifacts confound interpretation of results and make it difficult to measure the effects of antidepressant treatment.
Treatment recommendation. Clinical prudence requires us to treat potentially lethal major depressive illness aggressively, even though one cannot state with confidence that any antidepressant class lowers suicide risk or that one class is significantly more effective than others (Table 3).
SCHIZOPHRENIA AND ANTIPSYCHOTICS
For schizophrenia and other primary psychotic disorders, little research exists to indicate that atypical antipsychotics reduce suicide risk. Evidence is emerging, however, that clozapine may offer this benefit,22 in addition to its well-substantiated clinical superiority in treatment-resistant psychotic illness.23
Pooled evidence from controlled trials comparing clozapine with other antipsychotics indicates a 2-fold lower risk of mortality from all causes.23 This finding was highly suggestive but not statistically significant, and the specific contribution of suicide to this risk is unknown.23 Our recent meta-analysis of the few available studies found that clozapine was associated with a statistically significant, 3.3-fold lower overall suicidal risk compared with other antipsychotic treatments.22
A well-designed, 2-year study randomly assigned 980 patients with schizophrenia or schizoaffective disorder who were at high risk for suicide to clozapine (mean 274 mg/d) or olanzapine (mean 16.6 mg/d). Clozapine showed moderately greater benefit in reducing suicide attempts and need for urgent intervention for perceived emerging suicide risk, although it did not lower suicide risk per se.24 Another study associated olanzapine with a 2.3-fold lower risk of suicidal behavior, compared with haloperidol.25
Comparing two potentially effective agents may have limited the observed difference between clozapine and olanzapine.24 Nevertheless, previous (largely uncontrolled) comparisons with other treatment options indicate substantially lower risks of both suicides and attempts with clozapine.22 In December 2002, the FDA approved a unique indication for clozapine: to reduce the risk of recurrent suicidal behavior in patients with schizophrenia or schizoaffective disorder.
Treatment recommendation. Risks of suicide and other causes of premature death are high in patients with chronic psychotic disorders, underlining the importance of appropriate longterm care. Clozapine has shown benefit in reducing risk of suicidal behaviors. When clozapine is otherwise a plausible option, this additional potential benefit can be considered when selecting therapy for individual patients.
Related resources
- American Psychiatric Association. Suicide-prevention practice guidelines. Washington, DC: American Psychiatric Press, 2003 (in press).
- American Foundation for Suicide Prevention. http://www.afsp.org
- American Association of Suicidology. www.suicidology.org
- National Institute of Mental Health (NIMH)/Suicide.
Drug brand names
- Clozapine • Clozaril
- Carbamazepine • Tegretol
- Divalproex • Depakote
- Haloperidol • Haldol
- Lithium carbonate • Eskalith, Lithobid, others
- Olanzapine • Zyprexa
Disclosure
Dr. Baldessarini has received research grants from Molecular Insight Pharmaceuticals, Eli Lilly and Co., Janssen Pharmaceutica, Protarga Inc., and Solvay Pharmaceuticals, and is a consultant to Auritec Laboratories, Molecular Insight Pharmaceuticals, Eli Lilly and Co., GlaxoSmithKline, Janssen Pharmaceutica, and Protarga Inc.
1. Goldsmith SK, Pellmar TC, Kleinman AM. Bunney WE, Jr (eds). Reducing suicide: A national imperative. Washington DC: National Academies Press, 2002.
2. Harris EC, Barraclough B. Suicide as an outcome for mental disorders: a meta-analysis. Br J Psychiatry 1997;170:205-28.
3. Angst F, Stassen HH, Clayton PJ, Angst J. Mortality of patients with mood disorders: follow-up over 34-38 years. J Affect Disord 2002;68:167-81.
4. Rihmer Z, Pestality P. Bipolar II disorder and suicidal behavior. Psychiatr Clin North Am 1999;22:667-73.
5. Baldessarini RJ, Tondo L, Hennen J. Lithium treatment and suicide risk in major affective disorders: update and new findings. J Clin Psychiatry 2003;64(suppl 5):44-52.
6. Tondo L, Isacsson G, Baldessarini RJ. Suicide in bipolar disorder: risk and prevention. CNS Drugs 2003;17:491-511.
7. Ghaemi SN, Lenox MS, Baldessarini RJ. Effectiveness and safety of long-term antidepressant treatment in bipolar disorder. J Clin Psychiatry 2001;62:565-9.
8. Judd LL, Akiskal HS, Schettler PJ, et al. The long-term natural history of weekly symptomatic status of bipolar I disorder. Arch Gen Psychiatry 2002;59:530-7.
9. Baldessarini RJ, Tondo L, Hennen J, Viguera AC. Is lithium still worth using? An update of selected recent research. Harvard Rev Psychiatry 2002;10:59-75.
10. Tondo L, Baldessarini RJ, Floris G. Long-term clinical effectiveness of lithium maintenance treatment in types I and II bipolar disorders. Br J Psychiatry 2001;178(suppl 41):S184-90.
11. Tondo L, Hennen J, Baldessarini RJ. Lower suicide risk with longterm lithium treatment in major affective illness: a meta-analysis. Acta Psychiatr Scand 2001;104:163-72.
12. Baldessarini RJ, Tondo L, Hennen J. Treating the suicidal patient with bipolar disorder: reducing suicide risk with lithium. Ann NY Acad Sci 2001;932:24-43.
13. Baldessarini RJ, Tondo L, Viguera AC. Discontinuing lithium maintenance treatment in bipolar disorder: risks and implications. Bipolar Disord 1999;1:17-24.
14. Baldessarini RJ, Tondo L, Hennen J. Treatment latency and previous episodes: relationships to pretreatment morbidity and response to maintenance treatment in bipolar I and II disorders. Bipolar Disord 2003;5:169-79.
15. Bratti IM, Baldessarini RJ, Baethge C, Tondo L. Pretreatment episode count and response to lithium treatment in manic-depressive illness. Harvard Rev Psychiatry (in press).
16. Tondo L, Hennen J, Baldessarini RJ. Rapid-cycling bipolar disorder: effects of long-term treatments. Acta Psychiatr Scand 2003;108:4-14.
17. Thies-Flechtner K, Miller-Oerlinghausen B, Seibert W, et al. Effect of prophylactic treatment on suicide risk in patients with major affective disorders: data from a randomized prospective trial. Pharmacopsychiatry 1996;29:103-7.
18. Goodwin FK, Fireman B, Simon G, et al. Suicide attempts in bipolar patients on lithium vs. divalproex (abstract 45; cited with permission of Dr. Goodwin). San Juan, PR: American College of Neuropsychopharmacology annual meeting, 2002.
19. Suominen KH, Isometsa ET, Henriksson MM, et al. Inadequate treatment for major depression both before and after attempted suicide. Am J Psychiatry 1998;155:1778-880.
20. Kessler RC, Berglund P, Demler O, et al. The epidemiology of major depressive disorder: results from the National Comorbidity Survey Replication (NCS-R). JAMA 2003;289:3095-105.
21. Khan A, Khan S, Kolts R, Brown WA. Suicide rates in clinical trials of SSRIs, other antidepressants, and placebo: analysis of FDA reports. Am J Psychiatry 2003;160:790-2.
22. Baldessarini RJ, Hennen J. Reduced suicidal risk during treatment with clozapine: A meta-analysis. Manuscript in review, 2003.
23. Wahlbeck K, Cheine M, Essali A, Adams C. Evidence of clozapine’s effectiveness in schizophrenia: a systematic review and meta-analysis of randomized trials. Am J Psychiatry 1999;156:990-9.
24. Meltzer HY, Alphs L, Green AI, et al. Clozapine treatment for suicidality in schizophrenia: International Suicide Prevention Trial (InterSePT). Arch Gen Psychiatry 2003;60:82-91.
25. Glazer WM. Formulary decisions and health economics. J Clin Psychiatry 1998;59(suppl 19):23-9.
Which psychotropics reduce the risk of suicide in patients with psychiatric disorders? Although no drugs eliminate the risk, new evidence is clarifying that some therapeutic choices can make a difference:
- Long-term lithium treatment apparently reduces suicide risk in patients with affective disorders; mood-altering anticonvulsants are less well studied but show less benefit than lithium.
- Effects of antidepressants remain inconclusive without adequate long-term studies.
- At least one atypical antipsychotic—clozapine—probably lowers suicide risk, although direct comparisons of antipsychotic agents are rare.
- Surprisingly little evidence is available on nondrug interventions, including rapid hospitalization, psychotherapy, and electroconvulsive therapy.1
Suicide is the leading cause of malpractice liability in psychiatry and of the heightened risk of death in persons with major affective and psychotic disorders (Box).1-4 Here are the latest findings to help you choose medications for at-risk patients with bipolar disorder, major depression, or chronic psychoses.
Suicide is by far the most common cause of premature death among patients with major mood and psychotic disorders.2,3 A major affective or psychotic disorder increases risk of suicide 8- to 22-fold (Table 1). A history of attempted suicide increases a person’s suicide risk 38-fold, so that the likelihood of dying by suicide becomes greater than one in four (28%).
Attempted suicide is less well-documented but may be 10 to 20 times more common than completed suicide in the general population. Persons with major affective and psychotic disorders complete suicide at an estimated rate of once in five attempts. This high rate suggests that their suicidal intent and methods are particularly lethal.4
BIPOLAR DISORDER AND MOOD STABILIZERS
Bipolar disorder is associated with the highest suicide rate among all major psychiatric illnesses, with an international incidence averaging 0.31% of patients per year.4 This rate may slightly exceed the suicide rate of patients with major depression, which averages 0.29%/year.
Risk of suicidal behavior is similar among patients with bipolar type II (depression with hypomania) and type I disorder (depression with mania), supporting the view that type II is not a milder form of bipolar illness.4-6 Indeed, one study of suicide attempts found a higher risk among bipolar II patients (24%) than in bipolar I patients (17%) as well as a higher risk in both bipolar types than in persons diagnosed with unipolar major depression (12%).4
Suicidal behavior in bipolar disorder is associated almost entirely with ongoing depression or dysphoria and is especially likely to follow severe and highly recurrent depressive episodes.5,6 Combinations of depressive-dysphoric and irritable, agitated, anxious features in “mixed states” may be particularly dangerous and can be hard to diagnose with confidence. Moreover, DSM-IV criteria for mixed states are far too narrow in requiring symptoms to simultaneously fulfill criteria for both mania and major depression. More broadly defined mixed states are very common. Underdiagnosis risks underestimation of suicidal potential, and misdiagnosis as “agitated depression” encourages potentially dangerous overuse of antidepressants.5,7
Depression or dysphoria is the most prevalent morbidity in patients with bipolar disorder. Major and minor depressive states and mixed-dysphoric phases account for nearly one-third of time in follow-up care, exceeding time in mania or hypomania by more than 4-fold.8 Ironically, however, bipolar depression is one of the least-studied forms of major depression. Suicidal bipolar patients are typically excluded from antidepressant studies because of the risks of inducing greater instability, agitation, or mania while treating them with an antidepressant but without a mood stabilizer.7
LITHIUM’S PROTECTIVE EFFECT
Decades of research and clinical use demonstrate substantially lower risks of suicide and serious suicide attempts when patients with bipolar disorder are treated long-term with lithium salts in standard clinical doses (serum concentrations typically 0.6 to 0.8 mEq/L). Lithium is highly effective in treating all phases of bipolar disorder. A recent meta-analysis of 26 long-term trials of lithium reported between 1967 and 2001 found an average 3.2-fold sparing of morbidity or relapse risk.9
Benefits in types I and II. A large European sample10 compared percent-time-ill in bipolar patients before and after they received lithium as maintenance treatment. Unexpectedly, lithium therapy reduced percent-time-ill to a greater extent among patients with type II than type I bipolar disorder. Time in mania and time in depression were reduced 2.5-fold and 2.0-fold, respectively, in type I patients, compared with nearly 5-fold for time in hypomania and 2.5-fold for time in depression among type II patients.
Because depression is associated with the highest rates of suicidal behavior in all phases of bipolar disorders, lithium’s effects in preventing depressive recurrence are especially important for reducing suicide risk.6
In a review of 22 studies11 —some including patients with bipolar or recurrent unipolar major depression—risk of death by suicide was reduced at least 5-fold, based on an informal comparison of pooled rates in treated versus untreated samples. Based on quantitative meta-analysis, the pooled risk of death by suicide was reduced nearly 9-fold (or by 89%) in patients who received lithium maintenance treatment compared with those who did not. The risk for suicide attempts fell nearly 10-fold in a compilation of 33 studies (Table 2).12 Available studies do not permit separate analysis of lithium’s effects on suicidal behavior among patients with bipolar disorder and recurrent unipolar depression, leaving the relative benefit by diagnosis uncertain.
Table 1
Suicide risks in selected psychiatric disorders*
| Condition | Relative risk | Incidence (%/year) | Lifetime risk (%) |
|---|---|---|---|
| Prior suicide attempt | 38.4 | 0.549 | 27.5 |
| Bipolar disorder | 21.7 | 0.310 | 15.5 |
| Major depression | 20.4 | 0.292 | 14.6 |
| Mixed drug abuse | 19.2 | 0.275 | 14.7 |
| Dysthymia | 12.1 | 0.173 | 8.65 |
| Obsessive-compulsive disorder | 11.5 | 0.143 | 8.15 |
| Panic disorder | 10.0 | 0.160 | 7.15 |
| Schizophrenia | 8.45 | 0.121 | 6.05 |
| Personality disorders | 7.08 | 0.101 | 5.05 |
| Alcohol abuse | 5.86 | 0.084 | 4.20 |
| Cancer | 1.80 | 0.026 | 1.30 |
| General population | 1.00 | 0.014 | 0.72 |
| * Estimated relative risks compared with the general population,2 with recently updated information about bipolar disorders.6 Annual rates are based on international general population average (14.3/100,000/year) × standardized mortality ratio; lifetime estimates are based on annual rates × 50 years as an estimate of lifetime exposure for years at major risk. | |||
Dangers of stopping lithium. In our study5 of more than 200 patients with DSM-IV bipolar I or II disorder, prophylactic lithium treatment for an average of 4 years reduced the risk of completed and attempted suicide by 6.5-fold. A subgroup of more than 100 patients discontinued lithium, usually after prolonged stability, and we excluded from analysis any cases of suspected emerging illness associated with discontinuation. Within 6 to 12 months after stopping treatment, this subgroup’s rates of suicidal behavior increased markedly—by 20-fold above treated rates.5 Thereafter, their rates returned to prelithium treatment levels.
Of particular clinical importance:
- discontinuing lithium gradually—over at least 2 weeks—was associated with a 2-fold lower suicide risk than more-abrupt discontinuation
- suicidal behavior after lithium discontinuation was almost always associated with emerging depression, which can provide an early warning of impending suicidal risk.
Table 2
Effect of lithium treatment on risk of completed and attempted suicide in patients with bipolar and recurrent depressive disorders*
| Treatment or sample | Suicides | Attempts | All acts | A/S ratio |
|---|---|---|---|---|
| With lithium | 0.16 | 0.41 | 0.57 | 2.6 |
| Without lithium | 0.88 | 4.02 | 4.90 | 4.6 |
| Off/on lithium ratio | 5.5 | 9.8 | 8.6 | — |
| General population | 0.014 | 0.21 | 0.22 | 15.3 |
| Off lithium/general population ratio | 56.4 | 19.1 | 22.3 | — |
| On lithium/general population ratio | 11.4 | 2.0 | 2.6 | — |
| A/S ratio: Attempts versus completed suicides | ||||
| * Rates (acts/year/100 persons, or %/year), based on previously reported averages derived from analyses of data from 33 studies with 55 treatment-arms,12 from a more selected analysis of 22 studies of completed suicides,11 and updated estimates for general population rates.6 | ||||
This is not the first time we have found evidence of a dramatic—but time-limited—increase in risk of recurrent bipolar illness when lithium treatment was discontinued.13 Bipolar disorder patients who discontinue long-term lithium treatment abruptly are at high risk of recurrent depression and mania.13
Incomplete protection. Lithium’s protection against suicidal risk is incomplete, as one can see by comparing lithium-treated versus untreated bipolar patients’ suicide rates with those of the general population (Table 2).6
With lithium:
- suicides plus attempts declined 8.6-fold to levels 2.6 times greater than those of the general population
- suicide attempts fell 10-fold to levels that are about twice that of the general population
- risk of completed suicides declined 5.5-fold with lithium treatment but remained 11 times higher than that of the general population.
Without lithium:
- risk of suicide in bipolar patients is approximately 22 times greater than that of the general population
- ratio of attempts to suicides among bipolar disorder patients averages 4.6, suggesting that suicide attempts by patients with bipolar disorder are relatively lethal.6
Effect of delayed lithium therapy. Many patients with bipolar disorder do not receive sustained prophylactic treatment early in the illness.
Studies typically show an average 5- to 10-year gap between illness onset and the start of sustained lithium maintenance treatment. This delay averages more than 3 years longer among women with bipolar II disorder than men with bipolar I disorder, evidently reflecting major clinical dissimilarities between these groups.6,14 In contrast, we found that nearly one-quarter of long-term risk of suicidal behavior emerges within the first year of bipolar illness.5 Clearly, patients with recurrent major affective illness require earlier intervention and more consistent clinical care.
We have also found that delayed maintenance treatment or the number of prior episodes of bipolar illness do not seem to limit therapeutic response to lithium.14,15 These findings support the conclusion that prophylactic lithium treatment can be worthwhile, even after years of illness and many recurrences. Moreover, our recent meta-analysis of treatment options for rapid-cycling bipolar illness indicates that—even though all treatments have yielded inferior results compared with nonrapidly-cycling patients—no alternative has outperformed lithium.16
Anticonvulsants. Evidence regarding the effects of other mood stabilizers on suicide risk in bipolar disorder remains limited:
- In a European collaborative study, several hundred patients with bipolar or schizoaffective disorder were randomly assigned to receive lithium or carbamazepine for nearly 2 years. Rates of suicidal acts were 2.5%/year with the anticonvulsant, but there were no suicides or attempts in patients receiving lithium.17 Direct comparisons are rare, but this difference was both striking and statistically significant.
- Computerized records of approximately 20,000 patients diagnosed with bipolar disorder at two large American HMOs were analyzed to compare suicidal behaviors associated with specific treatments. Lithium yielded 2.7-fold greater protection against suicidal behavior (mainly attempts because suicides were rare) compared with anticonvulsants (mainly divalproex).18
Treatment recommendation. These observations support lithium’s value in long-term maintenance of patients with bipolar disorder. Lithium’s apparent reduction of suicide risk is striking and may be superior to that of other mood-stabilizers. Alternate treatments and lithium’s potential value for reducing suicide risk in patients with unipolar depression require further study.
It is important to emphasize that lithium can be toxic or even fatal in acute overdose. This risk is integral to the equation when you assess risks and benefits for individual patients.
MAJOR DEPRESSION AND ANTIDEPRESSANTS
Major depression and depressive components of other disorders are major risk factors for suicide.1,2,6 Depression continues to be surprisingly underrecognized and undertreated, even though relatively safe and tolerable antidepressants are readily available.1,6,19,20 Patients with recurrent unipolar major depression often remain inconsistently or inadequately treated, even after they attempt suicide.19
Recent reviews of suicide risk during research on antidepressant treatment in major depression suggest that:
- antidepressants of various kinds may tend to reduce the risk of suicidal behavior, but any such effect is small and statistically nonsignificant (Baldessarini et al, 2003, unpublished)
- tricyclic antidepressants may yield lower rates of suicidal behavior than selective serotonin reuptake inhibitors (SSRIs). Similarly, however, such trends reflect highly variable research methods and inconsistent findings and do not hold up to quantitative analysis (Baldessarini et al, 2003, unpublished).
The suicidal events encountered during research mainly involve attempts because suicides are rare, particularly in relatively brief treatment trials that exclude acutely suicidal subjects. Analyses are further complicated by trends toward paradoxically lower suicidal risks among depressed patients randomized to a placebo in controlled antidepressant trials. This paradox is paralleled by often earlier removal of patients treated with a placebo than with an active antidepressant, perhaps in association with emerging suicidality.21
Table 3
Preventing suicide: How effective are specific treatments?
| Treatments compared | Disorder treated | Benefit/risk ratio |
|---|---|---|
| Mood stabilizers | ||
| Lithium vs. none or placebo* | Bipolar disorder | |
| Suicides | 8.8 (4.1 to 19.1)a | |
| Attempts | 9.9 (5.0 to 14.8)b | |
| Lithium vs. carbamazepine* | Bipolar disorder | ≥2.5c |
| Lithium vs. divalproex* | Bipolar disorder | 2.7 (1.2 to 6.2)d |
| Antidepressants | ||
| Antidepressants (any) vs. placebo/none | Major depressive disorder | 1.1 (0.7 to 1.6)e |
| Tricyclics vs. SSRIs | Major depressive disorder | 1.2 (0.7 to 2.1)e |
| Antipsychotics | ||
| Clozapine vs. any antipsychotic* | Schizophrenia | |
| Suicides + attempts | 3.3 (1.7 to 6.3)f | |
| Attempts | 2.9 (1.5 to 5.7)f | |
| Clozapine vs. olanzapine* | Schizophrenia | |
| Suicides + attempts | 1.3 (1.0 to 1.7)g | |
| a. Tondo et al, 200111 | ||
| b. Baldessarini et al, 20035 | ||
| c. Thies-Flechtner et al, 199517 | ||
| d. Goodwin et al, 200218 | ||
| e. Baldessarini et al, 20035 | ||
| f. Baldessarini & Hennen, 200322 | ||
| g. Meltzer et al, 200324 | ||
| * First agent is statistically more effective, based on benefit/risk ratio (95% CI). | ||
These trends toward lower suicide risk among patients receiving a placebo are somewhat reassuring, given concern that placebo randomization for scientific purposes may endanger study subjects. However, these artifacts confound interpretation of results and make it difficult to measure the effects of antidepressant treatment.
Treatment recommendation. Clinical prudence requires us to treat potentially lethal major depressive illness aggressively, even though one cannot state with confidence that any antidepressant class lowers suicide risk or that one class is significantly more effective than others (Table 3).
SCHIZOPHRENIA AND ANTIPSYCHOTICS
For schizophrenia and other primary psychotic disorders, little research exists to indicate that atypical antipsychotics reduce suicide risk. Evidence is emerging, however, that clozapine may offer this benefit,22 in addition to its well-substantiated clinical superiority in treatment-resistant psychotic illness.23
Pooled evidence from controlled trials comparing clozapine with other antipsychotics indicates a 2-fold lower risk of mortality from all causes.23 This finding was highly suggestive but not statistically significant, and the specific contribution of suicide to this risk is unknown.23 Our recent meta-analysis of the few available studies found that clozapine was associated with a statistically significant, 3.3-fold lower overall suicidal risk compared with other antipsychotic treatments.22
A well-designed, 2-year study randomly assigned 980 patients with schizophrenia or schizoaffective disorder who were at high risk for suicide to clozapine (mean 274 mg/d) or olanzapine (mean 16.6 mg/d). Clozapine showed moderately greater benefit in reducing suicide attempts and need for urgent intervention for perceived emerging suicide risk, although it did not lower suicide risk per se.24 Another study associated olanzapine with a 2.3-fold lower risk of suicidal behavior, compared with haloperidol.25
Comparing two potentially effective agents may have limited the observed difference between clozapine and olanzapine.24 Nevertheless, previous (largely uncontrolled) comparisons with other treatment options indicate substantially lower risks of both suicides and attempts with clozapine.22 In December 2002, the FDA approved a unique indication for clozapine: to reduce the risk of recurrent suicidal behavior in patients with schizophrenia or schizoaffective disorder.
Treatment recommendation. Risks of suicide and other causes of premature death are high in patients with chronic psychotic disorders, underlining the importance of appropriate longterm care. Clozapine has shown benefit in reducing risk of suicidal behaviors. When clozapine is otherwise a plausible option, this additional potential benefit can be considered when selecting therapy for individual patients.
Related resources
- American Psychiatric Association. Suicide-prevention practice guidelines. Washington, DC: American Psychiatric Press, 2003 (in press).
- American Foundation for Suicide Prevention. http://www.afsp.org
- American Association of Suicidology. www.suicidology.org
- National Institute of Mental Health (NIMH)/Suicide.
Drug brand names
- Clozapine • Clozaril
- Carbamazepine • Tegretol
- Divalproex • Depakote
- Haloperidol • Haldol
- Lithium carbonate • Eskalith, Lithobid, others
- Olanzapine • Zyprexa
Disclosure
Dr. Baldessarini has received research grants from Molecular Insight Pharmaceuticals, Eli Lilly and Co., Janssen Pharmaceutica, Protarga Inc., and Solvay Pharmaceuticals, and is a consultant to Auritec Laboratories, Molecular Insight Pharmaceuticals, Eli Lilly and Co., GlaxoSmithKline, Janssen Pharmaceutica, and Protarga Inc.
Which psychotropics reduce the risk of suicide in patients with psychiatric disorders? Although no drugs eliminate the risk, new evidence is clarifying that some therapeutic choices can make a difference:
- Long-term lithium treatment apparently reduces suicide risk in patients with affective disorders; mood-altering anticonvulsants are less well studied but show less benefit than lithium.
- Effects of antidepressants remain inconclusive without adequate long-term studies.
- At least one atypical antipsychotic—clozapine—probably lowers suicide risk, although direct comparisons of antipsychotic agents are rare.
- Surprisingly little evidence is available on nondrug interventions, including rapid hospitalization, psychotherapy, and electroconvulsive therapy.1
Suicide is the leading cause of malpractice liability in psychiatry and of the heightened risk of death in persons with major affective and psychotic disorders (Box).1-4 Here are the latest findings to help you choose medications for at-risk patients with bipolar disorder, major depression, or chronic psychoses.
Suicide is by far the most common cause of premature death among patients with major mood and psychotic disorders.2,3 A major affective or psychotic disorder increases risk of suicide 8- to 22-fold (Table 1). A history of attempted suicide increases a person’s suicide risk 38-fold, so that the likelihood of dying by suicide becomes greater than one in four (28%).
Attempted suicide is less well-documented but may be 10 to 20 times more common than completed suicide in the general population. Persons with major affective and psychotic disorders complete suicide at an estimated rate of once in five attempts. This high rate suggests that their suicidal intent and methods are particularly lethal.4
BIPOLAR DISORDER AND MOOD STABILIZERS
Bipolar disorder is associated with the highest suicide rate among all major psychiatric illnesses, with an international incidence averaging 0.31% of patients per year.4 This rate may slightly exceed the suicide rate of patients with major depression, which averages 0.29%/year.
Risk of suicidal behavior is similar among patients with bipolar type II (depression with hypomania) and type I disorder (depression with mania), supporting the view that type II is not a milder form of bipolar illness.4-6 Indeed, one study of suicide attempts found a higher risk among bipolar II patients (24%) than in bipolar I patients (17%) as well as a higher risk in both bipolar types than in persons diagnosed with unipolar major depression (12%).4
Suicidal behavior in bipolar disorder is associated almost entirely with ongoing depression or dysphoria and is especially likely to follow severe and highly recurrent depressive episodes.5,6 Combinations of depressive-dysphoric and irritable, agitated, anxious features in “mixed states” may be particularly dangerous and can be hard to diagnose with confidence. Moreover, DSM-IV criteria for mixed states are far too narrow in requiring symptoms to simultaneously fulfill criteria for both mania and major depression. More broadly defined mixed states are very common. Underdiagnosis risks underestimation of suicidal potential, and misdiagnosis as “agitated depression” encourages potentially dangerous overuse of antidepressants.5,7
Depression or dysphoria is the most prevalent morbidity in patients with bipolar disorder. Major and minor depressive states and mixed-dysphoric phases account for nearly one-third of time in follow-up care, exceeding time in mania or hypomania by more than 4-fold.8 Ironically, however, bipolar depression is one of the least-studied forms of major depression. Suicidal bipolar patients are typically excluded from antidepressant studies because of the risks of inducing greater instability, agitation, or mania while treating them with an antidepressant but without a mood stabilizer.7
LITHIUM’S PROTECTIVE EFFECT
Decades of research and clinical use demonstrate substantially lower risks of suicide and serious suicide attempts when patients with bipolar disorder are treated long-term with lithium salts in standard clinical doses (serum concentrations typically 0.6 to 0.8 mEq/L). Lithium is highly effective in treating all phases of bipolar disorder. A recent meta-analysis of 26 long-term trials of lithium reported between 1967 and 2001 found an average 3.2-fold sparing of morbidity or relapse risk.9
Benefits in types I and II. A large European sample10 compared percent-time-ill in bipolar patients before and after they received lithium as maintenance treatment. Unexpectedly, lithium therapy reduced percent-time-ill to a greater extent among patients with type II than type I bipolar disorder. Time in mania and time in depression were reduced 2.5-fold and 2.0-fold, respectively, in type I patients, compared with nearly 5-fold for time in hypomania and 2.5-fold for time in depression among type II patients.
Because depression is associated with the highest rates of suicidal behavior in all phases of bipolar disorders, lithium’s effects in preventing depressive recurrence are especially important for reducing suicide risk.6
In a review of 22 studies11 —some including patients with bipolar or recurrent unipolar major depression—risk of death by suicide was reduced at least 5-fold, based on an informal comparison of pooled rates in treated versus untreated samples. Based on quantitative meta-analysis, the pooled risk of death by suicide was reduced nearly 9-fold (or by 89%) in patients who received lithium maintenance treatment compared with those who did not. The risk for suicide attempts fell nearly 10-fold in a compilation of 33 studies (Table 2).12 Available studies do not permit separate analysis of lithium’s effects on suicidal behavior among patients with bipolar disorder and recurrent unipolar depression, leaving the relative benefit by diagnosis uncertain.
Table 1
Suicide risks in selected psychiatric disorders*
| Condition | Relative risk | Incidence (%/year) | Lifetime risk (%) |
|---|---|---|---|
| Prior suicide attempt | 38.4 | 0.549 | 27.5 |
| Bipolar disorder | 21.7 | 0.310 | 15.5 |
| Major depression | 20.4 | 0.292 | 14.6 |
| Mixed drug abuse | 19.2 | 0.275 | 14.7 |
| Dysthymia | 12.1 | 0.173 | 8.65 |
| Obsessive-compulsive disorder | 11.5 | 0.143 | 8.15 |
| Panic disorder | 10.0 | 0.160 | 7.15 |
| Schizophrenia | 8.45 | 0.121 | 6.05 |
| Personality disorders | 7.08 | 0.101 | 5.05 |
| Alcohol abuse | 5.86 | 0.084 | 4.20 |
| Cancer | 1.80 | 0.026 | 1.30 |
| General population | 1.00 | 0.014 | 0.72 |
| * Estimated relative risks compared with the general population,2 with recently updated information about bipolar disorders.6 Annual rates are based on international general population average (14.3/100,000/year) × standardized mortality ratio; lifetime estimates are based on annual rates × 50 years as an estimate of lifetime exposure for years at major risk. | |||
Dangers of stopping lithium. In our study5 of more than 200 patients with DSM-IV bipolar I or II disorder, prophylactic lithium treatment for an average of 4 years reduced the risk of completed and attempted suicide by 6.5-fold. A subgroup of more than 100 patients discontinued lithium, usually after prolonged stability, and we excluded from analysis any cases of suspected emerging illness associated with discontinuation. Within 6 to 12 months after stopping treatment, this subgroup’s rates of suicidal behavior increased markedly—by 20-fold above treated rates.5 Thereafter, their rates returned to prelithium treatment levels.
Of particular clinical importance:
- discontinuing lithium gradually—over at least 2 weeks—was associated with a 2-fold lower suicide risk than more-abrupt discontinuation
- suicidal behavior after lithium discontinuation was almost always associated with emerging depression, which can provide an early warning of impending suicidal risk.
Table 2
Effect of lithium treatment on risk of completed and attempted suicide in patients with bipolar and recurrent depressive disorders*
| Treatment or sample | Suicides | Attempts | All acts | A/S ratio |
|---|---|---|---|---|
| With lithium | 0.16 | 0.41 | 0.57 | 2.6 |
| Without lithium | 0.88 | 4.02 | 4.90 | 4.6 |
| Off/on lithium ratio | 5.5 | 9.8 | 8.6 | — |
| General population | 0.014 | 0.21 | 0.22 | 15.3 |
| Off lithium/general population ratio | 56.4 | 19.1 | 22.3 | — |
| On lithium/general population ratio | 11.4 | 2.0 | 2.6 | — |
| A/S ratio: Attempts versus completed suicides | ||||
| * Rates (acts/year/100 persons, or %/year), based on previously reported averages derived from analyses of data from 33 studies with 55 treatment-arms,12 from a more selected analysis of 22 studies of completed suicides,11 and updated estimates for general population rates.6 | ||||
This is not the first time we have found evidence of a dramatic—but time-limited—increase in risk of recurrent bipolar illness when lithium treatment was discontinued.13 Bipolar disorder patients who discontinue long-term lithium treatment abruptly are at high risk of recurrent depression and mania.13
Incomplete protection. Lithium’s protection against suicidal risk is incomplete, as one can see by comparing lithium-treated versus untreated bipolar patients’ suicide rates with those of the general population (Table 2).6
With lithium:
- suicides plus attempts declined 8.6-fold to levels 2.6 times greater than those of the general population
- suicide attempts fell 10-fold to levels that are about twice that of the general population
- risk of completed suicides declined 5.5-fold with lithium treatment but remained 11 times higher than that of the general population.
Without lithium:
- risk of suicide in bipolar patients is approximately 22 times greater than that of the general population
- ratio of attempts to suicides among bipolar disorder patients averages 4.6, suggesting that suicide attempts by patients with bipolar disorder are relatively lethal.6
Effect of delayed lithium therapy. Many patients with bipolar disorder do not receive sustained prophylactic treatment early in the illness.
Studies typically show an average 5- to 10-year gap between illness onset and the start of sustained lithium maintenance treatment. This delay averages more than 3 years longer among women with bipolar II disorder than men with bipolar I disorder, evidently reflecting major clinical dissimilarities between these groups.6,14 In contrast, we found that nearly one-quarter of long-term risk of suicidal behavior emerges within the first year of bipolar illness.5 Clearly, patients with recurrent major affective illness require earlier intervention and more consistent clinical care.
We have also found that delayed maintenance treatment or the number of prior episodes of bipolar illness do not seem to limit therapeutic response to lithium.14,15 These findings support the conclusion that prophylactic lithium treatment can be worthwhile, even after years of illness and many recurrences. Moreover, our recent meta-analysis of treatment options for rapid-cycling bipolar illness indicates that—even though all treatments have yielded inferior results compared with nonrapidly-cycling patients—no alternative has outperformed lithium.16
Anticonvulsants. Evidence regarding the effects of other mood stabilizers on suicide risk in bipolar disorder remains limited:
- In a European collaborative study, several hundred patients with bipolar or schizoaffective disorder were randomly assigned to receive lithium or carbamazepine for nearly 2 years. Rates of suicidal acts were 2.5%/year with the anticonvulsant, but there were no suicides or attempts in patients receiving lithium.17 Direct comparisons are rare, but this difference was both striking and statistically significant.
- Computerized records of approximately 20,000 patients diagnosed with bipolar disorder at two large American HMOs were analyzed to compare suicidal behaviors associated with specific treatments. Lithium yielded 2.7-fold greater protection against suicidal behavior (mainly attempts because suicides were rare) compared with anticonvulsants (mainly divalproex).18
Treatment recommendation. These observations support lithium’s value in long-term maintenance of patients with bipolar disorder. Lithium’s apparent reduction of suicide risk is striking and may be superior to that of other mood-stabilizers. Alternate treatments and lithium’s potential value for reducing suicide risk in patients with unipolar depression require further study.
It is important to emphasize that lithium can be toxic or even fatal in acute overdose. This risk is integral to the equation when you assess risks and benefits for individual patients.
MAJOR DEPRESSION AND ANTIDEPRESSANTS
Major depression and depressive components of other disorders are major risk factors for suicide.1,2,6 Depression continues to be surprisingly underrecognized and undertreated, even though relatively safe and tolerable antidepressants are readily available.1,6,19,20 Patients with recurrent unipolar major depression often remain inconsistently or inadequately treated, even after they attempt suicide.19
Recent reviews of suicide risk during research on antidepressant treatment in major depression suggest that:
- antidepressants of various kinds may tend to reduce the risk of suicidal behavior, but any such effect is small and statistically nonsignificant (Baldessarini et al, 2003, unpublished)
- tricyclic antidepressants may yield lower rates of suicidal behavior than selective serotonin reuptake inhibitors (SSRIs). Similarly, however, such trends reflect highly variable research methods and inconsistent findings and do not hold up to quantitative analysis (Baldessarini et al, 2003, unpublished).
The suicidal events encountered during research mainly involve attempts because suicides are rare, particularly in relatively brief treatment trials that exclude acutely suicidal subjects. Analyses are further complicated by trends toward paradoxically lower suicidal risks among depressed patients randomized to a placebo in controlled antidepressant trials. This paradox is paralleled by often earlier removal of patients treated with a placebo than with an active antidepressant, perhaps in association with emerging suicidality.21
Table 3
Preventing suicide: How effective are specific treatments?
| Treatments compared | Disorder treated | Benefit/risk ratio |
|---|---|---|
| Mood stabilizers | ||
| Lithium vs. none or placebo* | Bipolar disorder | |
| Suicides | 8.8 (4.1 to 19.1)a | |
| Attempts | 9.9 (5.0 to 14.8)b | |
| Lithium vs. carbamazepine* | Bipolar disorder | ≥2.5c |
| Lithium vs. divalproex* | Bipolar disorder | 2.7 (1.2 to 6.2)d |
| Antidepressants | ||
| Antidepressants (any) vs. placebo/none | Major depressive disorder | 1.1 (0.7 to 1.6)e |
| Tricyclics vs. SSRIs | Major depressive disorder | 1.2 (0.7 to 2.1)e |
| Antipsychotics | ||
| Clozapine vs. any antipsychotic* | Schizophrenia | |
| Suicides + attempts | 3.3 (1.7 to 6.3)f | |
| Attempts | 2.9 (1.5 to 5.7)f | |
| Clozapine vs. olanzapine* | Schizophrenia | |
| Suicides + attempts | 1.3 (1.0 to 1.7)g | |
| a. Tondo et al, 200111 | ||
| b. Baldessarini et al, 20035 | ||
| c. Thies-Flechtner et al, 199517 | ||
| d. Goodwin et al, 200218 | ||
| e. Baldessarini et al, 20035 | ||
| f. Baldessarini & Hennen, 200322 | ||
| g. Meltzer et al, 200324 | ||
| * First agent is statistically more effective, based on benefit/risk ratio (95% CI). | ||
These trends toward lower suicide risk among patients receiving a placebo are somewhat reassuring, given concern that placebo randomization for scientific purposes may endanger study subjects. However, these artifacts confound interpretation of results and make it difficult to measure the effects of antidepressant treatment.
Treatment recommendation. Clinical prudence requires us to treat potentially lethal major depressive illness aggressively, even though one cannot state with confidence that any antidepressant class lowers suicide risk or that one class is significantly more effective than others (Table 3).
SCHIZOPHRENIA AND ANTIPSYCHOTICS
For schizophrenia and other primary psychotic disorders, little research exists to indicate that atypical antipsychotics reduce suicide risk. Evidence is emerging, however, that clozapine may offer this benefit,22 in addition to its well-substantiated clinical superiority in treatment-resistant psychotic illness.23
Pooled evidence from controlled trials comparing clozapine with other antipsychotics indicates a 2-fold lower risk of mortality from all causes.23 This finding was highly suggestive but not statistically significant, and the specific contribution of suicide to this risk is unknown.23 Our recent meta-analysis of the few available studies found that clozapine was associated with a statistically significant, 3.3-fold lower overall suicidal risk compared with other antipsychotic treatments.22
A well-designed, 2-year study randomly assigned 980 patients with schizophrenia or schizoaffective disorder who were at high risk for suicide to clozapine (mean 274 mg/d) or olanzapine (mean 16.6 mg/d). Clozapine showed moderately greater benefit in reducing suicide attempts and need for urgent intervention for perceived emerging suicide risk, although it did not lower suicide risk per se.24 Another study associated olanzapine with a 2.3-fold lower risk of suicidal behavior, compared with haloperidol.25
Comparing two potentially effective agents may have limited the observed difference between clozapine and olanzapine.24 Nevertheless, previous (largely uncontrolled) comparisons with other treatment options indicate substantially lower risks of both suicides and attempts with clozapine.22 In December 2002, the FDA approved a unique indication for clozapine: to reduce the risk of recurrent suicidal behavior in patients with schizophrenia or schizoaffective disorder.
Treatment recommendation. Risks of suicide and other causes of premature death are high in patients with chronic psychotic disorders, underlining the importance of appropriate longterm care. Clozapine has shown benefit in reducing risk of suicidal behaviors. When clozapine is otherwise a plausible option, this additional potential benefit can be considered when selecting therapy for individual patients.
Related resources
- American Psychiatric Association. Suicide-prevention practice guidelines. Washington, DC: American Psychiatric Press, 2003 (in press).
- American Foundation for Suicide Prevention. http://www.afsp.org
- American Association of Suicidology. www.suicidology.org
- National Institute of Mental Health (NIMH)/Suicide.
Drug brand names
- Clozapine • Clozaril
- Carbamazepine • Tegretol
- Divalproex • Depakote
- Haloperidol • Haldol
- Lithium carbonate • Eskalith, Lithobid, others
- Olanzapine • Zyprexa
Disclosure
Dr. Baldessarini has received research grants from Molecular Insight Pharmaceuticals, Eli Lilly and Co., Janssen Pharmaceutica, Protarga Inc., and Solvay Pharmaceuticals, and is a consultant to Auritec Laboratories, Molecular Insight Pharmaceuticals, Eli Lilly and Co., GlaxoSmithKline, Janssen Pharmaceutica, and Protarga Inc.
1. Goldsmith SK, Pellmar TC, Kleinman AM. Bunney WE, Jr (eds). Reducing suicide: A national imperative. Washington DC: National Academies Press, 2002.
2. Harris EC, Barraclough B. Suicide as an outcome for mental disorders: a meta-analysis. Br J Psychiatry 1997;170:205-28.
3. Angst F, Stassen HH, Clayton PJ, Angst J. Mortality of patients with mood disorders: follow-up over 34-38 years. J Affect Disord 2002;68:167-81.
4. Rihmer Z, Pestality P. Bipolar II disorder and suicidal behavior. Psychiatr Clin North Am 1999;22:667-73.
5. Baldessarini RJ, Tondo L, Hennen J. Lithium treatment and suicide risk in major affective disorders: update and new findings. J Clin Psychiatry 2003;64(suppl 5):44-52.
6. Tondo L, Isacsson G, Baldessarini RJ. Suicide in bipolar disorder: risk and prevention. CNS Drugs 2003;17:491-511.
7. Ghaemi SN, Lenox MS, Baldessarini RJ. Effectiveness and safety of long-term antidepressant treatment in bipolar disorder. J Clin Psychiatry 2001;62:565-9.
8. Judd LL, Akiskal HS, Schettler PJ, et al. The long-term natural history of weekly symptomatic status of bipolar I disorder. Arch Gen Psychiatry 2002;59:530-7.
9. Baldessarini RJ, Tondo L, Hennen J, Viguera AC. Is lithium still worth using? An update of selected recent research. Harvard Rev Psychiatry 2002;10:59-75.
10. Tondo L, Baldessarini RJ, Floris G. Long-term clinical effectiveness of lithium maintenance treatment in types I and II bipolar disorders. Br J Psychiatry 2001;178(suppl 41):S184-90.
11. Tondo L, Hennen J, Baldessarini RJ. Lower suicide risk with longterm lithium treatment in major affective illness: a meta-analysis. Acta Psychiatr Scand 2001;104:163-72.
12. Baldessarini RJ, Tondo L, Hennen J. Treating the suicidal patient with bipolar disorder: reducing suicide risk with lithium. Ann NY Acad Sci 2001;932:24-43.
13. Baldessarini RJ, Tondo L, Viguera AC. Discontinuing lithium maintenance treatment in bipolar disorder: risks and implications. Bipolar Disord 1999;1:17-24.
14. Baldessarini RJ, Tondo L, Hennen J. Treatment latency and previous episodes: relationships to pretreatment morbidity and response to maintenance treatment in bipolar I and II disorders. Bipolar Disord 2003;5:169-79.
15. Bratti IM, Baldessarini RJ, Baethge C, Tondo L. Pretreatment episode count and response to lithium treatment in manic-depressive illness. Harvard Rev Psychiatry (in press).
16. Tondo L, Hennen J, Baldessarini RJ. Rapid-cycling bipolar disorder: effects of long-term treatments. Acta Psychiatr Scand 2003;108:4-14.
17. Thies-Flechtner K, Miller-Oerlinghausen B, Seibert W, et al. Effect of prophylactic treatment on suicide risk in patients with major affective disorders: data from a randomized prospective trial. Pharmacopsychiatry 1996;29:103-7.
18. Goodwin FK, Fireman B, Simon G, et al. Suicide attempts in bipolar patients on lithium vs. divalproex (abstract 45; cited with permission of Dr. Goodwin). San Juan, PR: American College of Neuropsychopharmacology annual meeting, 2002.
19. Suominen KH, Isometsa ET, Henriksson MM, et al. Inadequate treatment for major depression both before and after attempted suicide. Am J Psychiatry 1998;155:1778-880.
20. Kessler RC, Berglund P, Demler O, et al. The epidemiology of major depressive disorder: results from the National Comorbidity Survey Replication (NCS-R). JAMA 2003;289:3095-105.
21. Khan A, Khan S, Kolts R, Brown WA. Suicide rates in clinical trials of SSRIs, other antidepressants, and placebo: analysis of FDA reports. Am J Psychiatry 2003;160:790-2.
22. Baldessarini RJ, Hennen J. Reduced suicidal risk during treatment with clozapine: A meta-analysis. Manuscript in review, 2003.
23. Wahlbeck K, Cheine M, Essali A, Adams C. Evidence of clozapine’s effectiveness in schizophrenia: a systematic review and meta-analysis of randomized trials. Am J Psychiatry 1999;156:990-9.
24. Meltzer HY, Alphs L, Green AI, et al. Clozapine treatment for suicidality in schizophrenia: International Suicide Prevention Trial (InterSePT). Arch Gen Psychiatry 2003;60:82-91.
25. Glazer WM. Formulary decisions and health economics. J Clin Psychiatry 1998;59(suppl 19):23-9.
1. Goldsmith SK, Pellmar TC, Kleinman AM. Bunney WE, Jr (eds). Reducing suicide: A national imperative. Washington DC: National Academies Press, 2002.
2. Harris EC, Barraclough B. Suicide as an outcome for mental disorders: a meta-analysis. Br J Psychiatry 1997;170:205-28.
3. Angst F, Stassen HH, Clayton PJ, Angst J. Mortality of patients with mood disorders: follow-up over 34-38 years. J Affect Disord 2002;68:167-81.
4. Rihmer Z, Pestality P. Bipolar II disorder and suicidal behavior. Psychiatr Clin North Am 1999;22:667-73.
5. Baldessarini RJ, Tondo L, Hennen J. Lithium treatment and suicide risk in major affective disorders: update and new findings. J Clin Psychiatry 2003;64(suppl 5):44-52.
6. Tondo L, Isacsson G, Baldessarini RJ. Suicide in bipolar disorder: risk and prevention. CNS Drugs 2003;17:491-511.
7. Ghaemi SN, Lenox MS, Baldessarini RJ. Effectiveness and safety of long-term antidepressant treatment in bipolar disorder. J Clin Psychiatry 2001;62:565-9.
8. Judd LL, Akiskal HS, Schettler PJ, et al. The long-term natural history of weekly symptomatic status of bipolar I disorder. Arch Gen Psychiatry 2002;59:530-7.
9. Baldessarini RJ, Tondo L, Hennen J, Viguera AC. Is lithium still worth using? An update of selected recent research. Harvard Rev Psychiatry 2002;10:59-75.
10. Tondo L, Baldessarini RJ, Floris G. Long-term clinical effectiveness of lithium maintenance treatment in types I and II bipolar disorders. Br J Psychiatry 2001;178(suppl 41):S184-90.
11. Tondo L, Hennen J, Baldessarini RJ. Lower suicide risk with longterm lithium treatment in major affective illness: a meta-analysis. Acta Psychiatr Scand 2001;104:163-72.
12. Baldessarini RJ, Tondo L, Hennen J. Treating the suicidal patient with bipolar disorder: reducing suicide risk with lithium. Ann NY Acad Sci 2001;932:24-43.
13. Baldessarini RJ, Tondo L, Viguera AC. Discontinuing lithium maintenance treatment in bipolar disorder: risks and implications. Bipolar Disord 1999;1:17-24.
14. Baldessarini RJ, Tondo L, Hennen J. Treatment latency and previous episodes: relationships to pretreatment morbidity and response to maintenance treatment in bipolar I and II disorders. Bipolar Disord 2003;5:169-79.
15. Bratti IM, Baldessarini RJ, Baethge C, Tondo L. Pretreatment episode count and response to lithium treatment in manic-depressive illness. Harvard Rev Psychiatry (in press).
16. Tondo L, Hennen J, Baldessarini RJ. Rapid-cycling bipolar disorder: effects of long-term treatments. Acta Psychiatr Scand 2003;108:4-14.
17. Thies-Flechtner K, Miller-Oerlinghausen B, Seibert W, et al. Effect of prophylactic treatment on suicide risk in patients with major affective disorders: data from a randomized prospective trial. Pharmacopsychiatry 1996;29:103-7.
18. Goodwin FK, Fireman B, Simon G, et al. Suicide attempts in bipolar patients on lithium vs. divalproex (abstract 45; cited with permission of Dr. Goodwin). San Juan, PR: American College of Neuropsychopharmacology annual meeting, 2002.
19. Suominen KH, Isometsa ET, Henriksson MM, et al. Inadequate treatment for major depression both before and after attempted suicide. Am J Psychiatry 1998;155:1778-880.
20. Kessler RC, Berglund P, Demler O, et al. The epidemiology of major depressive disorder: results from the National Comorbidity Survey Replication (NCS-R). JAMA 2003;289:3095-105.
21. Khan A, Khan S, Kolts R, Brown WA. Suicide rates in clinical trials of SSRIs, other antidepressants, and placebo: analysis of FDA reports. Am J Psychiatry 2003;160:790-2.
22. Baldessarini RJ, Hennen J. Reduced suicidal risk during treatment with clozapine: A meta-analysis. Manuscript in review, 2003.
23. Wahlbeck K, Cheine M, Essali A, Adams C. Evidence of clozapine’s effectiveness in schizophrenia: a systematic review and meta-analysis of randomized trials. Am J Psychiatry 1999;156:990-9.
24. Meltzer HY, Alphs L, Green AI, et al. Clozapine treatment for suicidality in schizophrenia: International Suicide Prevention Trial (InterSePT). Arch Gen Psychiatry 2003;60:82-91.
25. Glazer WM. Formulary decisions and health economics. J Clin Psychiatry 1998;59(suppl 19):23-9.
5 keys to improve counseling for dual-diagnosis patients
Psychiatrists frequently encounter dual-diagnosis patients (Box) and may often wonder which to treat first—the substance abuse or the psychiatric comorbidity. Five principles can help you counsel dual-diagnosis patients more effectively. Briefly, they are to:
- appreciate this population’s heterogeneity
- adopt a longitudinal treatment approach, reassessing patients’ progress and adjusting interventions as needed over time
- be empathic rather than confrontational
- realize that treatment often proceeds in stages—not on a smooth, linear path
- recognize the importance of medication compliance.
ASSESSMENT
Different patients, different problems. All counseling of dual-diagnosis patients begins with a thorough assessment aimed at making an accurate diagnosis and understanding the relationship between the co-existing disorders. Although some people refer to “dual-diagnosis patients” as a single entity, these patients differ according to:
The National Institute of Mental Health’s Epidemiologic Catchment Area study documented high rates of substance use disorders in patients with psychiatric disorders.1 Lifetime prevalence of co-occurrence was 61% for bipolar disorder (the highest of any Axis I disorder),47% for schizophrenia, and 36% for panic disorder.
Dual-diagnosis patients face a more bleak prognosis than those with a single disorder, including higher rates of relapse, hospitalization, violence, incarceration, homelessness, and serious infections such as hepatitis and HIV.2 Unfortunately, these findings have not always led to effective treatments.
These patients represent a heterogeneous group and require individualized treatment. For example, abstinence from alcohol or drugs may worsen psychiatric symptoms in a patient with posttraumatic stress disorder and substance abuse. On the other hand, abstinence would be expected to improve the symptoms of a patient with comorbid major depressive disorder and substance abuse.
- diagnosis, with a myriad of potential combinations of substance use and psychiatric disorders
- severity of disorder, with some having a predominant psychiatric or substance use problem and others experiencing severe courses of both problems
- causes of their substance abuse and psychiatric disorders, based in part on which problem is primary and which is secondary
- level of motivation for treatment and their treatment goals.
Primary versus secondary disorders. How to distinguish “primary” from “secondary” disorders in dually diagnosed patients has prompted much research and debate.
A psychiatric disorder is typically called primary when it can be viewed as independent from the substance use disorder. The term “secondary psychiatric disorder” connotes that the substance use disorder is causing the psychiatric symptoms. For example, alcohol-dependent patients in detoxification programs often have depressive symptoms, some of which abate with abstinence. They are frequently diagnosed as having “secondary depression,” or—in DSM-IV diagnostic terms—substance-induced mood disorder.
Unfortunately, distinguishing primary from secondary disorders is sometimes difficult because of patients’ poor memory, recall bias, and inadequate periods of sobriety (“I’ve been drinking for a long time and have been depressed for a long time, so I don’t remember what I was like when I was sober”). Thus, the diagnostic assessment is generally accomplished over time, rather than in a single interview.
Our research3 and clinical experience have taught us that patients’ recall about the relationship between their substance use and psychiatric symptoms often changes over time. Determining the “primary” disorder may also have limited validity in predicting treatment response.4
Stages of Change model. The Stages of Change model5,6 is useful for assessing a dually diagnosed patient’s motivation to change, although its use in addictive disorders has been challenged.7,8 According to the transtheoretical model developed by Prochaska et al (Table 1),5 people generally make behavioral changes in stages defined by their level of willingness to make these changes.
When counseling the dually diagnosed patient, it is useful to assess readiness to change and to suggest behavioral steps the patient is able and willing to make. Thus, it would not be appropriate to discuss drug refusal methods with a patient who does not see his substance use as a problem. Rather, addressing this patient’s ambivalence would be more useful.
Table 1
5 stages of change: The transtheoretical model of behavior change
| Stage of change | Patient behavior |
|---|---|
| Precontemplation | No intention to change behavior in the foreseeable future; little or no awareness of problems |
| Contemplation | Aware that a problem exists; seriously thinking about overcoming it but no commitment to take action |
| Preparation | Intends to take action within the next month; has tried unsuccessfully to take action in the past year |
| Action | Modifies behavior, experiences, or environment to overcome problems |
| Maintenance | Works to prevent relapse and consolidate gains attained during action stage; for addictive behaviors, maintenance extends indefinitely from 6 months after the initial action |
| Source: Prochaska JO. Transtheoretical model: Stages of Change. Cancer Prevention Research Center, University of Rhode Island. http://www.uri.edu/research/cprc/TTM/StagesOfChange.htm | |
It is important to note that many patients move back and forth between stages of readiness to change. For example, a patient in the action stage (entering treatment and pursuing a goal of abstinence) may revert to contemplation and again question whether he or she has a serious substance abuse problem. We recommend that clinicians reassess patients regularly and continue to match interventions with the current level of motivation.
WHICH DISORDER IS TREATED FIRST?
Three approaches are used for treating the coexisting problems of dual-diagnosis patients—sequential, parallel, and integrated.
Sequential treatment addresses the more acute disorder first; the other disorder receives greater attention later. This model is commonly used with hospital treatment, in which comparatively little attention would be paid to substance use in a patient who is acutely psychotic.
Parallel treatment addresses each disorder contemporaneously but in different settings (such as at a substance abuse program on Monday and a mental health center on Thursday).
One limitation of the sequential and parallel models is that psychiatric and substance abuse programs typically have different orientations. A lack of comprehensive assessment may leave the substance abuse or psychiatric disorder underdiagnosed, depending on the setting. Staff members may also project negative attitudes toward patients with psychiatric or substance use disorders if they know comparatively little about the diagnosis and treatment of the other type of disorder. Treatment in two settings also can lead to communication problems and differences of opinion among the treating clinicians.
Integrated treatment, in which both disorders are treated simultaneously in the same setting, has shown favorable outcomes in several initial studies.9 11 Different integrated treatment models have been described, which vary according to the psychiatric disorders’ nature and the treatment’s theoretical orientation. Integrated treatment strategies include:
- focusing on psychiatric and substance abuse issues simultaneously or in alternating sessions
- providing intense case management
- stressing the importance of medication compliance.12
COUNSELING PRINCIPLES
As mentioned, a careful history and thorough assessment are the keys to effectively treating the dually diagnosed patient.
Assess how the patient perceives the relationship between his substance use disorder and psychiatric symptoms. For example, ask, “What do you see as the relationship between your drinking and your depression, if any?”
As part of this process, explore both the immediate and long-term relationships between the two phenomena. For example, some patients will say that drinking offers them immediate relief from their depressive symptoms but exacerbates their depression the following day. Encouraging patients to look beyond the immediate—often positive—effects of their substance use may help them understand the negative consequences of continued use.
Review previous periods of recovery and relapse. For patients who have had substantial periods of recovery, it is important to acknowledge these successes and to ask in an upbeat and admiring way, “How did you do it?” This approach may remind patients of past successes and counterbalance their frequent feelings of discouragement and hopelessness.
Table 2
4 phases in treating the dually diagnosed patient
| Phase | Therapeutic goals |
|---|---|
| Engagement | Build an alliance Attract patient to treatment program |
| Persuasion | Convince engaged patient to accept longer-term, abstinence-based treatment |
| Active treatment | Help patient develop attitudes and techniques essential to maintain sobriety |
| Relapse prevention | Help patient maintain gains made in active treatment and cope with lapses/relapses should they occur |
To help clarify the relationship between coexisting disorders, ask patients about psychiatric symptoms they have experienced during periods of substance use and recovery. Taking a relapse history can help you and the patient identify decisions and behaviors he or she must avoid (such as stopping medication, failing to attend treatment, or engaging in high-risk activities as in going to bars).
PHASES OF TREATMENT
Four phases of dual-diagnosis treatment—engagement, persuasion, active treatment, and relapse prevention—have been described, along with their therapeutic goals (Table 2).13 Consider these phases when treating this population, even though most patients do not proceed through them in an orderly, linear fashion.
Engagement. At the onset, the therapist tries to build an alliance and begins to establish trust and credibility.
Persuasion involves helping the patient comprehend the need to seriously address his or her substance use. It is important during engagement and persuasion stages to be empathic, using reflective listening and validating techniques.
Helping the patient see the discrepancy between his or her long-term goals and current behavior can create the impetus for change. Linking the substance use and psychiatric symptoms and exploring their impact on each other may help the patient understand the problem.
Ambivalence and resistance are normal reactions to this process of change, so avoid arguing with the patient. Confrontation—long a common strategy in substance abuse treatment—is losing favor and is being supplanted in many cases by a more supportive, empathic approach.14 Indeed, patients with co-occurring psychiatric illness generally respond particularly poorly to confrontation.
Active treatment focuses on techniques to achieve abstinence, including alcohol and drug refusal skills, methods to deal with craving, and ways to recognize and avoid situations that present a high risk for relapse.
Relapse prevention reinforces gains made in previous stages. Here, the patient learns how to identify and deal with risky situations and how to handle a “slip” if it occurs.
ADJUNCTIVE TREATMENTS
Self-help groups. Ask whether the patient has attended self-help groups for addiction or psychiatric illness. If so, then ask, “What did you think of the meetings? What did you like and dislike?”
Self-help groups such as Alcoholics Anonymous (AA) or the Manic-Depressive and Depressive Association (MDDA) can help enormously in the recovery process. These groups are free, readily available, and can offer patients a support network. Although many dual-diagnosis patients are reluctant to attend self-help groups, they may benefit from the support, role modeling, practical advice, and structure that these meetings offer.
Drug therapy for the dual-diagnosis patient focuses on the psychiatric disorder and is usually combined with psychosocial approaches. There is little evidence that one medication is more effective than others for these patients.
Because medication compliance is key to their effective treatment, be sure to ask patients at each visit, “Have you been taking your medication as prescribed?” Because dual-diagnosis patients have been shown to take more or less medication than prescribed,15 asking how much medication they are taking can be revealing.
Related resources
- American Academy of Addiction Psychiatry www.aaap.org
- National Institute on Drug Abuse www.nida.nih.gov
- National Institute on Alcohol Abuse and Alcoholism www.niaaa.nih.gov
Disclosure
Dr. Manwani receives research support from Abbott Laboratories.
Dr. Weiss is a speaker for Abbott Laboratories and Eli Lilly and Co.
Acknowledgment
Supported by grants K0200326, DA09400, and DA15968 from the National Institute on Drug Abuse and a grant from the Dr. Ralph and Marian C. Falk Medical Research Trust.
1. Reigier DA, Farmer ME, Rae DS, et al. Comorbidity of mental disorders with alcohol and other drug abuse: results from the Epidemiologic Catchment Area (ECA) Study. JAMA 1990;264:2511-18.
2. Drake RE, Essock SM, Shaner A, et al. Implementing dual diagnosis services for clients with severe mental illness. Psychiatr Serv 2001;52:469-76.
3. Griffin ML, Weiss RD, Mirin SM, et al. The use of the Diagnostic Interview Schedule in drug-dependent patients. Am. J Drug Alcohol Abuse 1987;13(3):281-91.
4. Mason BJ, Kocsis JH, Ritvo EC, et al. A double-blind, placebo-controlled trial of desipramine for primary alcohol dependence stratified on the presence or absence of major depression. JAMA 1996;275(10):761-7.
5. Prochaska JO, DiClemente CC, Norcross JC. In search of how people change: applications to addictive behaviors. Am Psychol 1992;47:1102-14.
6. Connors GJ, Donovan DM, DiClemente CC. Substance abuse treatment and the stages of change. New York: Guilford Press, 2001.
7. Carey KB, Purnine DM, Maisto SA, et al. Assessing readiness to change substance abuse: a critical review of instruments. Clinical Psychol 1999;6:245-66.
8. Sutton S. Back to the drawing board? A review of applications of the transtheoretical model to substance use. Addiction 2001;96:175-86.
9. Drake RE, McHugo GJ, Noordsy DL. Treatment of alcoholism among schizophrenic outpatients: 4-year outcomes. Am J Psychiatry 1993;150:328-9.
10. Hellerstein DJ, Rosenthal RN, Miner CR. A prospective study of integrated outpatient treatment for substance-abusing schizophrenic patients. Am J Addict 1995;4:33-42.
11. Drake RE, Yovetich NA, Bebout RR, et al. Integrated treatment for dually diagnosed homeless adults. J Nerv Ment Dis 1997;185:298-305.
12. Weiss RD, Najavits LM, Hennessy G. Overview of treatment modalities for dual diagnosis patients: pharmacotherapy, psychotherapy, and twelve-step programs. In: Kranzler HR, Tinsley J (eds). Dual diagnosis: substance abuse and comorbid disorders. (2nd ed). New York: Marcel Dekker. In press.
13. Osher FC, Kofoed LL. Treatment of patients with psychiatric and psychoactive substance abuse disorders. Hosp Community Psychiatry 1989;40(10):1025-30.
14. Miller WR, Rollnick S. Motivational interviewing: preparing for change (2nd ed). New York: Guilford Press, 2002.
15. Weiss RD, Greenfield SF, Najavits LM, et al. Medication compliance among patients with bipolar disorder and substance use disorder. J Clin Psychiatry 1998;59(4):172-4.
Psychiatrists frequently encounter dual-diagnosis patients (Box) and may often wonder which to treat first—the substance abuse or the psychiatric comorbidity. Five principles can help you counsel dual-diagnosis patients more effectively. Briefly, they are to:
- appreciate this population’s heterogeneity
- adopt a longitudinal treatment approach, reassessing patients’ progress and adjusting interventions as needed over time
- be empathic rather than confrontational
- realize that treatment often proceeds in stages—not on a smooth, linear path
- recognize the importance of medication compliance.
ASSESSMENT
Different patients, different problems. All counseling of dual-diagnosis patients begins with a thorough assessment aimed at making an accurate diagnosis and understanding the relationship between the co-existing disorders. Although some people refer to “dual-diagnosis patients” as a single entity, these patients differ according to:
The National Institute of Mental Health’s Epidemiologic Catchment Area study documented high rates of substance use disorders in patients with psychiatric disorders.1 Lifetime prevalence of co-occurrence was 61% for bipolar disorder (the highest of any Axis I disorder),47% for schizophrenia, and 36% for panic disorder.
Dual-diagnosis patients face a more bleak prognosis than those with a single disorder, including higher rates of relapse, hospitalization, violence, incarceration, homelessness, and serious infections such as hepatitis and HIV.2 Unfortunately, these findings have not always led to effective treatments.
These patients represent a heterogeneous group and require individualized treatment. For example, abstinence from alcohol or drugs may worsen psychiatric symptoms in a patient with posttraumatic stress disorder and substance abuse. On the other hand, abstinence would be expected to improve the symptoms of a patient with comorbid major depressive disorder and substance abuse.
- diagnosis, with a myriad of potential combinations of substance use and psychiatric disorders
- severity of disorder, with some having a predominant psychiatric or substance use problem and others experiencing severe courses of both problems
- causes of their substance abuse and psychiatric disorders, based in part on which problem is primary and which is secondary
- level of motivation for treatment and their treatment goals.
Primary versus secondary disorders. How to distinguish “primary” from “secondary” disorders in dually diagnosed patients has prompted much research and debate.
A psychiatric disorder is typically called primary when it can be viewed as independent from the substance use disorder. The term “secondary psychiatric disorder” connotes that the substance use disorder is causing the psychiatric symptoms. For example, alcohol-dependent patients in detoxification programs often have depressive symptoms, some of which abate with abstinence. They are frequently diagnosed as having “secondary depression,” or—in DSM-IV diagnostic terms—substance-induced mood disorder.
Unfortunately, distinguishing primary from secondary disorders is sometimes difficult because of patients’ poor memory, recall bias, and inadequate periods of sobriety (“I’ve been drinking for a long time and have been depressed for a long time, so I don’t remember what I was like when I was sober”). Thus, the diagnostic assessment is generally accomplished over time, rather than in a single interview.
Our research3 and clinical experience have taught us that patients’ recall about the relationship between their substance use and psychiatric symptoms often changes over time. Determining the “primary” disorder may also have limited validity in predicting treatment response.4
Stages of Change model. The Stages of Change model5,6 is useful for assessing a dually diagnosed patient’s motivation to change, although its use in addictive disorders has been challenged.7,8 According to the transtheoretical model developed by Prochaska et al (Table 1),5 people generally make behavioral changes in stages defined by their level of willingness to make these changes.
When counseling the dually diagnosed patient, it is useful to assess readiness to change and to suggest behavioral steps the patient is able and willing to make. Thus, it would not be appropriate to discuss drug refusal methods with a patient who does not see his substance use as a problem. Rather, addressing this patient’s ambivalence would be more useful.
Table 1
5 stages of change: The transtheoretical model of behavior change
| Stage of change | Patient behavior |
|---|---|
| Precontemplation | No intention to change behavior in the foreseeable future; little or no awareness of problems |
| Contemplation | Aware that a problem exists; seriously thinking about overcoming it but no commitment to take action |
| Preparation | Intends to take action within the next month; has tried unsuccessfully to take action in the past year |
| Action | Modifies behavior, experiences, or environment to overcome problems |
| Maintenance | Works to prevent relapse and consolidate gains attained during action stage; for addictive behaviors, maintenance extends indefinitely from 6 months after the initial action |
| Source: Prochaska JO. Transtheoretical model: Stages of Change. Cancer Prevention Research Center, University of Rhode Island. http://www.uri.edu/research/cprc/TTM/StagesOfChange.htm | |
It is important to note that many patients move back and forth between stages of readiness to change. For example, a patient in the action stage (entering treatment and pursuing a goal of abstinence) may revert to contemplation and again question whether he or she has a serious substance abuse problem. We recommend that clinicians reassess patients regularly and continue to match interventions with the current level of motivation.
WHICH DISORDER IS TREATED FIRST?
Three approaches are used for treating the coexisting problems of dual-diagnosis patients—sequential, parallel, and integrated.
Sequential treatment addresses the more acute disorder first; the other disorder receives greater attention later. This model is commonly used with hospital treatment, in which comparatively little attention would be paid to substance use in a patient who is acutely psychotic.
Parallel treatment addresses each disorder contemporaneously but in different settings (such as at a substance abuse program on Monday and a mental health center on Thursday).
One limitation of the sequential and parallel models is that psychiatric and substance abuse programs typically have different orientations. A lack of comprehensive assessment may leave the substance abuse or psychiatric disorder underdiagnosed, depending on the setting. Staff members may also project negative attitudes toward patients with psychiatric or substance use disorders if they know comparatively little about the diagnosis and treatment of the other type of disorder. Treatment in two settings also can lead to communication problems and differences of opinion among the treating clinicians.
Integrated treatment, in which both disorders are treated simultaneously in the same setting, has shown favorable outcomes in several initial studies.9 11 Different integrated treatment models have been described, which vary according to the psychiatric disorders’ nature and the treatment’s theoretical orientation. Integrated treatment strategies include:
- focusing on psychiatric and substance abuse issues simultaneously or in alternating sessions
- providing intense case management
- stressing the importance of medication compliance.12
COUNSELING PRINCIPLES
As mentioned, a careful history and thorough assessment are the keys to effectively treating the dually diagnosed patient.
Assess how the patient perceives the relationship between his substance use disorder and psychiatric symptoms. For example, ask, “What do you see as the relationship between your drinking and your depression, if any?”
As part of this process, explore both the immediate and long-term relationships between the two phenomena. For example, some patients will say that drinking offers them immediate relief from their depressive symptoms but exacerbates their depression the following day. Encouraging patients to look beyond the immediate—often positive—effects of their substance use may help them understand the negative consequences of continued use.
Review previous periods of recovery and relapse. For patients who have had substantial periods of recovery, it is important to acknowledge these successes and to ask in an upbeat and admiring way, “How did you do it?” This approach may remind patients of past successes and counterbalance their frequent feelings of discouragement and hopelessness.
Table 2
4 phases in treating the dually diagnosed patient
| Phase | Therapeutic goals |
|---|---|
| Engagement | Build an alliance Attract patient to treatment program |
| Persuasion | Convince engaged patient to accept longer-term, abstinence-based treatment |
| Active treatment | Help patient develop attitudes and techniques essential to maintain sobriety |
| Relapse prevention | Help patient maintain gains made in active treatment and cope with lapses/relapses should they occur |
To help clarify the relationship between coexisting disorders, ask patients about psychiatric symptoms they have experienced during periods of substance use and recovery. Taking a relapse history can help you and the patient identify decisions and behaviors he or she must avoid (such as stopping medication, failing to attend treatment, or engaging in high-risk activities as in going to bars).
PHASES OF TREATMENT
Four phases of dual-diagnosis treatment—engagement, persuasion, active treatment, and relapse prevention—have been described, along with their therapeutic goals (Table 2).13 Consider these phases when treating this population, even though most patients do not proceed through them in an orderly, linear fashion.
Engagement. At the onset, the therapist tries to build an alliance and begins to establish trust and credibility.
Persuasion involves helping the patient comprehend the need to seriously address his or her substance use. It is important during engagement and persuasion stages to be empathic, using reflective listening and validating techniques.
Helping the patient see the discrepancy between his or her long-term goals and current behavior can create the impetus for change. Linking the substance use and psychiatric symptoms and exploring their impact on each other may help the patient understand the problem.
Ambivalence and resistance are normal reactions to this process of change, so avoid arguing with the patient. Confrontation—long a common strategy in substance abuse treatment—is losing favor and is being supplanted in many cases by a more supportive, empathic approach.14 Indeed, patients with co-occurring psychiatric illness generally respond particularly poorly to confrontation.
Active treatment focuses on techniques to achieve abstinence, including alcohol and drug refusal skills, methods to deal with craving, and ways to recognize and avoid situations that present a high risk for relapse.
Relapse prevention reinforces gains made in previous stages. Here, the patient learns how to identify and deal with risky situations and how to handle a “slip” if it occurs.
ADJUNCTIVE TREATMENTS
Self-help groups. Ask whether the patient has attended self-help groups for addiction or psychiatric illness. If so, then ask, “What did you think of the meetings? What did you like and dislike?”
Self-help groups such as Alcoholics Anonymous (AA) or the Manic-Depressive and Depressive Association (MDDA) can help enormously in the recovery process. These groups are free, readily available, and can offer patients a support network. Although many dual-diagnosis patients are reluctant to attend self-help groups, they may benefit from the support, role modeling, practical advice, and structure that these meetings offer.
Drug therapy for the dual-diagnosis patient focuses on the psychiatric disorder and is usually combined with psychosocial approaches. There is little evidence that one medication is more effective than others for these patients.
Because medication compliance is key to their effective treatment, be sure to ask patients at each visit, “Have you been taking your medication as prescribed?” Because dual-diagnosis patients have been shown to take more or less medication than prescribed,15 asking how much medication they are taking can be revealing.
Related resources
- American Academy of Addiction Psychiatry www.aaap.org
- National Institute on Drug Abuse www.nida.nih.gov
- National Institute on Alcohol Abuse and Alcoholism www.niaaa.nih.gov
Disclosure
Dr. Manwani receives research support from Abbott Laboratories.
Dr. Weiss is a speaker for Abbott Laboratories and Eli Lilly and Co.
Acknowledgment
Supported by grants K0200326, DA09400, and DA15968 from the National Institute on Drug Abuse and a grant from the Dr. Ralph and Marian C. Falk Medical Research Trust.
Psychiatrists frequently encounter dual-diagnosis patients (Box) and may often wonder which to treat first—the substance abuse or the psychiatric comorbidity. Five principles can help you counsel dual-diagnosis patients more effectively. Briefly, they are to:
- appreciate this population’s heterogeneity
- adopt a longitudinal treatment approach, reassessing patients’ progress and adjusting interventions as needed over time
- be empathic rather than confrontational
- realize that treatment often proceeds in stages—not on a smooth, linear path
- recognize the importance of medication compliance.
ASSESSMENT
Different patients, different problems. All counseling of dual-diagnosis patients begins with a thorough assessment aimed at making an accurate diagnosis and understanding the relationship between the co-existing disorders. Although some people refer to “dual-diagnosis patients” as a single entity, these patients differ according to:
The National Institute of Mental Health’s Epidemiologic Catchment Area study documented high rates of substance use disorders in patients with psychiatric disorders.1 Lifetime prevalence of co-occurrence was 61% for bipolar disorder (the highest of any Axis I disorder),47% for schizophrenia, and 36% for panic disorder.
Dual-diagnosis patients face a more bleak prognosis than those with a single disorder, including higher rates of relapse, hospitalization, violence, incarceration, homelessness, and serious infections such as hepatitis and HIV.2 Unfortunately, these findings have not always led to effective treatments.
These patients represent a heterogeneous group and require individualized treatment. For example, abstinence from alcohol or drugs may worsen psychiatric symptoms in a patient with posttraumatic stress disorder and substance abuse. On the other hand, abstinence would be expected to improve the symptoms of a patient with comorbid major depressive disorder and substance abuse.
- diagnosis, with a myriad of potential combinations of substance use and psychiatric disorders
- severity of disorder, with some having a predominant psychiatric or substance use problem and others experiencing severe courses of both problems
- causes of their substance abuse and psychiatric disorders, based in part on which problem is primary and which is secondary
- level of motivation for treatment and their treatment goals.
Primary versus secondary disorders. How to distinguish “primary” from “secondary” disorders in dually diagnosed patients has prompted much research and debate.
A psychiatric disorder is typically called primary when it can be viewed as independent from the substance use disorder. The term “secondary psychiatric disorder” connotes that the substance use disorder is causing the psychiatric symptoms. For example, alcohol-dependent patients in detoxification programs often have depressive symptoms, some of which abate with abstinence. They are frequently diagnosed as having “secondary depression,” or—in DSM-IV diagnostic terms—substance-induced mood disorder.
Unfortunately, distinguishing primary from secondary disorders is sometimes difficult because of patients’ poor memory, recall bias, and inadequate periods of sobriety (“I’ve been drinking for a long time and have been depressed for a long time, so I don’t remember what I was like when I was sober”). Thus, the diagnostic assessment is generally accomplished over time, rather than in a single interview.
Our research3 and clinical experience have taught us that patients’ recall about the relationship between their substance use and psychiatric symptoms often changes over time. Determining the “primary” disorder may also have limited validity in predicting treatment response.4
Stages of Change model. The Stages of Change model5,6 is useful for assessing a dually diagnosed patient’s motivation to change, although its use in addictive disorders has been challenged.7,8 According to the transtheoretical model developed by Prochaska et al (Table 1),5 people generally make behavioral changes in stages defined by their level of willingness to make these changes.
When counseling the dually diagnosed patient, it is useful to assess readiness to change and to suggest behavioral steps the patient is able and willing to make. Thus, it would not be appropriate to discuss drug refusal methods with a patient who does not see his substance use as a problem. Rather, addressing this patient’s ambivalence would be more useful.
Table 1
5 stages of change: The transtheoretical model of behavior change
| Stage of change | Patient behavior |
|---|---|
| Precontemplation | No intention to change behavior in the foreseeable future; little or no awareness of problems |
| Contemplation | Aware that a problem exists; seriously thinking about overcoming it but no commitment to take action |
| Preparation | Intends to take action within the next month; has tried unsuccessfully to take action in the past year |
| Action | Modifies behavior, experiences, or environment to overcome problems |
| Maintenance | Works to prevent relapse and consolidate gains attained during action stage; for addictive behaviors, maintenance extends indefinitely from 6 months after the initial action |
| Source: Prochaska JO. Transtheoretical model: Stages of Change. Cancer Prevention Research Center, University of Rhode Island. http://www.uri.edu/research/cprc/TTM/StagesOfChange.htm | |
It is important to note that many patients move back and forth between stages of readiness to change. For example, a patient in the action stage (entering treatment and pursuing a goal of abstinence) may revert to contemplation and again question whether he or she has a serious substance abuse problem. We recommend that clinicians reassess patients regularly and continue to match interventions with the current level of motivation.
WHICH DISORDER IS TREATED FIRST?
Three approaches are used for treating the coexisting problems of dual-diagnosis patients—sequential, parallel, and integrated.
Sequential treatment addresses the more acute disorder first; the other disorder receives greater attention later. This model is commonly used with hospital treatment, in which comparatively little attention would be paid to substance use in a patient who is acutely psychotic.
Parallel treatment addresses each disorder contemporaneously but in different settings (such as at a substance abuse program on Monday and a mental health center on Thursday).
One limitation of the sequential and parallel models is that psychiatric and substance abuse programs typically have different orientations. A lack of comprehensive assessment may leave the substance abuse or psychiatric disorder underdiagnosed, depending on the setting. Staff members may also project negative attitudes toward patients with psychiatric or substance use disorders if they know comparatively little about the diagnosis and treatment of the other type of disorder. Treatment in two settings also can lead to communication problems and differences of opinion among the treating clinicians.
Integrated treatment, in which both disorders are treated simultaneously in the same setting, has shown favorable outcomes in several initial studies.9 11 Different integrated treatment models have been described, which vary according to the psychiatric disorders’ nature and the treatment’s theoretical orientation. Integrated treatment strategies include:
- focusing on psychiatric and substance abuse issues simultaneously or in alternating sessions
- providing intense case management
- stressing the importance of medication compliance.12
COUNSELING PRINCIPLES
As mentioned, a careful history and thorough assessment are the keys to effectively treating the dually diagnosed patient.
Assess how the patient perceives the relationship between his substance use disorder and psychiatric symptoms. For example, ask, “What do you see as the relationship between your drinking and your depression, if any?”
As part of this process, explore both the immediate and long-term relationships between the two phenomena. For example, some patients will say that drinking offers them immediate relief from their depressive symptoms but exacerbates their depression the following day. Encouraging patients to look beyond the immediate—often positive—effects of their substance use may help them understand the negative consequences of continued use.
Review previous periods of recovery and relapse. For patients who have had substantial periods of recovery, it is important to acknowledge these successes and to ask in an upbeat and admiring way, “How did you do it?” This approach may remind patients of past successes and counterbalance their frequent feelings of discouragement and hopelessness.
Table 2
4 phases in treating the dually diagnosed patient
| Phase | Therapeutic goals |
|---|---|
| Engagement | Build an alliance Attract patient to treatment program |
| Persuasion | Convince engaged patient to accept longer-term, abstinence-based treatment |
| Active treatment | Help patient develop attitudes and techniques essential to maintain sobriety |
| Relapse prevention | Help patient maintain gains made in active treatment and cope with lapses/relapses should they occur |
To help clarify the relationship between coexisting disorders, ask patients about psychiatric symptoms they have experienced during periods of substance use and recovery. Taking a relapse history can help you and the patient identify decisions and behaviors he or she must avoid (such as stopping medication, failing to attend treatment, or engaging in high-risk activities as in going to bars).
PHASES OF TREATMENT
Four phases of dual-diagnosis treatment—engagement, persuasion, active treatment, and relapse prevention—have been described, along with their therapeutic goals (Table 2).13 Consider these phases when treating this population, even though most patients do not proceed through them in an orderly, linear fashion.
Engagement. At the onset, the therapist tries to build an alliance and begins to establish trust and credibility.
Persuasion involves helping the patient comprehend the need to seriously address his or her substance use. It is important during engagement and persuasion stages to be empathic, using reflective listening and validating techniques.
Helping the patient see the discrepancy between his or her long-term goals and current behavior can create the impetus for change. Linking the substance use and psychiatric symptoms and exploring their impact on each other may help the patient understand the problem.
Ambivalence and resistance are normal reactions to this process of change, so avoid arguing with the patient. Confrontation—long a common strategy in substance abuse treatment—is losing favor and is being supplanted in many cases by a more supportive, empathic approach.14 Indeed, patients with co-occurring psychiatric illness generally respond particularly poorly to confrontation.
Active treatment focuses on techniques to achieve abstinence, including alcohol and drug refusal skills, methods to deal with craving, and ways to recognize and avoid situations that present a high risk for relapse.
Relapse prevention reinforces gains made in previous stages. Here, the patient learns how to identify and deal with risky situations and how to handle a “slip” if it occurs.
ADJUNCTIVE TREATMENTS
Self-help groups. Ask whether the patient has attended self-help groups for addiction or psychiatric illness. If so, then ask, “What did you think of the meetings? What did you like and dislike?”
Self-help groups such as Alcoholics Anonymous (AA) or the Manic-Depressive and Depressive Association (MDDA) can help enormously in the recovery process. These groups are free, readily available, and can offer patients a support network. Although many dual-diagnosis patients are reluctant to attend self-help groups, they may benefit from the support, role modeling, practical advice, and structure that these meetings offer.
Drug therapy for the dual-diagnosis patient focuses on the psychiatric disorder and is usually combined with psychosocial approaches. There is little evidence that one medication is more effective than others for these patients.
Because medication compliance is key to their effective treatment, be sure to ask patients at each visit, “Have you been taking your medication as prescribed?” Because dual-diagnosis patients have been shown to take more or less medication than prescribed,15 asking how much medication they are taking can be revealing.
Related resources
- American Academy of Addiction Psychiatry www.aaap.org
- National Institute on Drug Abuse www.nida.nih.gov
- National Institute on Alcohol Abuse and Alcoholism www.niaaa.nih.gov
Disclosure
Dr. Manwani receives research support from Abbott Laboratories.
Dr. Weiss is a speaker for Abbott Laboratories and Eli Lilly and Co.
Acknowledgment
Supported by grants K0200326, DA09400, and DA15968 from the National Institute on Drug Abuse and a grant from the Dr. Ralph and Marian C. Falk Medical Research Trust.
1. Reigier DA, Farmer ME, Rae DS, et al. Comorbidity of mental disorders with alcohol and other drug abuse: results from the Epidemiologic Catchment Area (ECA) Study. JAMA 1990;264:2511-18.
2. Drake RE, Essock SM, Shaner A, et al. Implementing dual diagnosis services for clients with severe mental illness. Psychiatr Serv 2001;52:469-76.
3. Griffin ML, Weiss RD, Mirin SM, et al. The use of the Diagnostic Interview Schedule in drug-dependent patients. Am. J Drug Alcohol Abuse 1987;13(3):281-91.
4. Mason BJ, Kocsis JH, Ritvo EC, et al. A double-blind, placebo-controlled trial of desipramine for primary alcohol dependence stratified on the presence or absence of major depression. JAMA 1996;275(10):761-7.
5. Prochaska JO, DiClemente CC, Norcross JC. In search of how people change: applications to addictive behaviors. Am Psychol 1992;47:1102-14.
6. Connors GJ, Donovan DM, DiClemente CC. Substance abuse treatment and the stages of change. New York: Guilford Press, 2001.
7. Carey KB, Purnine DM, Maisto SA, et al. Assessing readiness to change substance abuse: a critical review of instruments. Clinical Psychol 1999;6:245-66.
8. Sutton S. Back to the drawing board? A review of applications of the transtheoretical model to substance use. Addiction 2001;96:175-86.
9. Drake RE, McHugo GJ, Noordsy DL. Treatment of alcoholism among schizophrenic outpatients: 4-year outcomes. Am J Psychiatry 1993;150:328-9.
10. Hellerstein DJ, Rosenthal RN, Miner CR. A prospective study of integrated outpatient treatment for substance-abusing schizophrenic patients. Am J Addict 1995;4:33-42.
11. Drake RE, Yovetich NA, Bebout RR, et al. Integrated treatment for dually diagnosed homeless adults. J Nerv Ment Dis 1997;185:298-305.
12. Weiss RD, Najavits LM, Hennessy G. Overview of treatment modalities for dual diagnosis patients: pharmacotherapy, psychotherapy, and twelve-step programs. In: Kranzler HR, Tinsley J (eds). Dual diagnosis: substance abuse and comorbid disorders. (2nd ed). New York: Marcel Dekker. In press.
13. Osher FC, Kofoed LL. Treatment of patients with psychiatric and psychoactive substance abuse disorders. Hosp Community Psychiatry 1989;40(10):1025-30.
14. Miller WR, Rollnick S. Motivational interviewing: preparing for change (2nd ed). New York: Guilford Press, 2002.
15. Weiss RD, Greenfield SF, Najavits LM, et al. Medication compliance among patients with bipolar disorder and substance use disorder. J Clin Psychiatry 1998;59(4):172-4.
1. Reigier DA, Farmer ME, Rae DS, et al. Comorbidity of mental disorders with alcohol and other drug abuse: results from the Epidemiologic Catchment Area (ECA) Study. JAMA 1990;264:2511-18.
2. Drake RE, Essock SM, Shaner A, et al. Implementing dual diagnosis services for clients with severe mental illness. Psychiatr Serv 2001;52:469-76.
3. Griffin ML, Weiss RD, Mirin SM, et al. The use of the Diagnostic Interview Schedule in drug-dependent patients. Am. J Drug Alcohol Abuse 1987;13(3):281-91.
4. Mason BJ, Kocsis JH, Ritvo EC, et al. A double-blind, placebo-controlled trial of desipramine for primary alcohol dependence stratified on the presence or absence of major depression. JAMA 1996;275(10):761-7.
5. Prochaska JO, DiClemente CC, Norcross JC. In search of how people change: applications to addictive behaviors. Am Psychol 1992;47:1102-14.
6. Connors GJ, Donovan DM, DiClemente CC. Substance abuse treatment and the stages of change. New York: Guilford Press, 2001.
7. Carey KB, Purnine DM, Maisto SA, et al. Assessing readiness to change substance abuse: a critical review of instruments. Clinical Psychol 1999;6:245-66.
8. Sutton S. Back to the drawing board? A review of applications of the transtheoretical model to substance use. Addiction 2001;96:175-86.
9. Drake RE, McHugo GJ, Noordsy DL. Treatment of alcoholism among schizophrenic outpatients: 4-year outcomes. Am J Psychiatry 1993;150:328-9.
10. Hellerstein DJ, Rosenthal RN, Miner CR. A prospective study of integrated outpatient treatment for substance-abusing schizophrenic patients. Am J Addict 1995;4:33-42.
11. Drake RE, Yovetich NA, Bebout RR, et al. Integrated treatment for dually diagnosed homeless adults. J Nerv Ment Dis 1997;185:298-305.
12. Weiss RD, Najavits LM, Hennessy G. Overview of treatment modalities for dual diagnosis patients: pharmacotherapy, psychotherapy, and twelve-step programs. In: Kranzler HR, Tinsley J (eds). Dual diagnosis: substance abuse and comorbid disorders. (2nd ed). New York: Marcel Dekker. In press.
13. Osher FC, Kofoed LL. Treatment of patients with psychiatric and psychoactive substance abuse disorders. Hosp Community Psychiatry 1989;40(10):1025-30.
14. Miller WR, Rollnick S. Motivational interviewing: preparing for change (2nd ed). New York: Guilford Press, 2002.
15. Weiss RD, Greenfield SF, Najavits LM, et al. Medication compliance among patients with bipolar disorder and substance use disorder. J Clin Psychiatry 1998;59(4):172-4.
Domestic violence: How to detect abuse in psychiatric patients
Victims of domestic abuse/violence often present with medical and psychiatric disorders (Box 1, Table 1). Identifying abuse—and encouraging the frightened or ashamed patient to seek help—is critical to evaluating presenting complaints, improving out-come,7 and possibly saving the patient’s life.
This article will discuss ways to:
- detect signs of abuse
- determine whether a victim is in danger
- share information about crisis resources
- help those who are considering leaving an abusive partner to make a safety plan.
Domestic violence/abuse affects 1 of 4 women in the United States. Men also are victims, but the prevalence (1 of 14) and degree of injury is much lower.1 Domestic violence/abuse occurs among all socioeconomic and ethnic groups.1,2
![]()
Domestic violence/abuse impairs victims’ physical and mental health.2 Injuries and ailments more prevalent among domestic abuse victims than among the general population include:2,3
- digestive problems (diarrhea, nausea, appetite loss, spastic colon, constipation, eating disorders,
- urinary problems and infections
- vaginal infections, sexually transmitted diseases, pelvic pain, menstrual problems
- sexual dysfunction
- hypertension
- fainting
- chronic pain (headaches, pelvic, abdominal, back and neck)
- pregnancy problems (preterm labor, poor weight gain)
CASE REPORT: TWO YEARS OF HURT
Ms. W, age 26, is referred to a psychiatrist for treatment-resistant depression. Courses of fluoxetine, 20 mg/d titrated to 80 mg/d, and venlafaxine, 150 mg bid, failed to improve her symptoms. Her Beck Depression Inventory score at baseline is 18, suggesting borderline clinical depression.
Table 1
Psychiatric disorders in victims of domestic abuse/violence
| Disorder | Weighted mean prevalence among abuse victims | Lifetime prevalence among general population |
|---|---|---|
| Alcohol abuse/dependence 4 | 19% | 5 to 8% |
| Depression 4 | 48% | 10% to 21% |
| Drug abuse disorder 4 | 9% | 5% to 6% |
| Posttraumatic stress disorder 4 | 64% | 1% to 12% |
| Suicidality 4 | 18% (ideation and attempts) | Ideation 1-16% Attempts <1-4% |
| % of abused sample | % of non-abused sample | |
| Anxiety symptoms 5 | 26% | 8% |
| Generalized anxiety Disorder 6 | 10% | 4% |
| Panic disorder 6 | 13% | <1% |
She has two children—ages 2 and 4—with her husband, a habitual crack cocaine user. She does not use drugs or alcohol.
When asked about her life at home, Ms. W laments that her husband is not helpful. When asked if her husband hurts her, she replies tearfully that he constantly yells at her and insults her, calling her “ugly” and “a lousy mom.” Upon further questioning, she reveals that her husband, when high on crack, sometimes hits her.
Ms. W does not work outside the home and did not finish high school. She is afraid to leave her husband because his mother helps care for the children and provides money, housing, and food. She constantly feels tearful and trapped.
The psychiatrist increases the venlafaxine to 375 mg/d and suggests that Ms. W call a domestic violence crisis center. She does not call the center, but agrees to see the psychiatrist monthly. Across 3 months her Beck score improves to 14.
SCREENING FOR ABUSE
The American Medical Association, American College of Physicians, and other physician and nursing organizations recommend routinely screening women for domestic abuse/violence.8-10 Some patients will not disclose abuse to their physicians when asked, but most patients say they want doctors to ask them about domestic violence/abuse and to offer crisis phone numbers, pamphlets, and other resources.11
Anyone who presents with complaints of fatigue, depression, anxiety, insomnia, hypervigilance, a treatment-resistant psychiatric disorder, or a visible physical injury (such as a black eye or bruises) should be screened for domestic abuse.
Prevention and treatment guidelines for physicians9,12,13 recommend interviewing the patient—without the partner or children—in a nonjudgmental and empathic fashion.11
Written questionnaires—such as the Woman Abuse Screening Tool (WAST), WAST-short, and HITS—are another screening option.
WAST-Short has demonstrated 92% sensitivity in identifying emotional or physical abuse (Table 2).14
WAST. The longer version of WAST has demonstrated 96% sensitivity in detecting physical or emotional abuse.14 It includes the two WAST-short questions, plus five questions about whether:
- arguments with an intimate partner ever diminish the patient’s self-esteem
- such arguments ever result in kicking or hitting
- the patient ever feels frightened by the partner’s words or actions
- the patient has ever been physically or emotionally abused by his or her partner.
Because the additional questions are not scored, the longer WAST is not well suited to clinical practice. However, a patient who scores a 1 on the WAST-Short exam can provide more in-depth information on her troubled relationship by answering the extra questions.
HITS can be self-administered and its title is easy to remember, but the scoring system is cumbersome. The patient is asked: “How often does your partner:
- Hurt you physically?
- Insult you or talk down to you?
- Threaten you with harm?
- Scream or curse at you?”
Each answer is scored on a 1-to-5 scale—never, rarely, sometimes, fairly often, or frequently. A score ≥ 10.5 has demonstrated 96% sensitivity in identifying physical and verbal abuse.15
Encouraging disclosure. Ask patients about domestic abuse when inquiring about smoking, alcohol use, or household makeup as part of the patient history. Your line of questioning might proceed as follows:
- “Do you live alone?”
- “Do you have a significant other?”
- “How is your relationship going?”
- “Is your partner supportive?”
- “What happens when you and your partner disagree?”
Table 2
Woman Abuse Screening Tool-Short version
| 1. In general, how would you describe your relationship? | ||
| □ a lot of tension | □ some tension | □ no tension |
| 2. Do you and your partner work out arguments with: | ||
| □ great difficulty | □ some difficulty | □ no difficulty |
| Answers are scored on a 1-to-3 scale, with 1 meaning “a lot of tension” or “great difficulty.” A score of 1 on either question indicates possible domestic abuse/violence. | ||
| Source: Reference 14 | ||
Be empathic. Explain the association between domestic abuse/violence and mental and physical disorders. Tell the patient that domestic abuse is common and help is readily available. Share information about crisis services even if the patient does not immediately disclose suspected abuse. Victims generally feel tremendous shame from living with the abuse, so disclosure takes time and trust.
Most states do not require physicians to report domestic abuse to the police unless injuries are caused by a weapon (knife or gun). However, physicians in California, Colorado, Kentucky, and New York must report any injuries resulting from domestic abuse—even if not caused by a weapon.16 In these states, clinicians should disclose their reporting obligation at the start of the patient interview.
Assess danger to any patient who reports being a victim of domestic abuse/violence. Consider danger imminent if the patient acknowledges any one of the following:
- Homicide or suicide threats from partner
- Weapons in the home
- Excessive substance use by partner or victim
- Escalating abuse or threats
- Physical/verbal abuse of children
- Harm to pets
- Fear of the partner
Source: Reference 17
Advise a patient who reports domestic abuse/violence to pack important belongings in case she needs to immediately leave an abusive partner.
The emergency bag should contain:
- Identification for self and children (birth certificates, driver’s license)
- Important documents (school and health records, insurance cards, car title, marriage license, mortgage or rental papers, protective orders, custody papers, divorce papers)
- Medications (for victim and children)
- Keys (auto, home, safe deposit box)
- Phone numbers
- Clothing (for victim and children)
- Comfort items, such as toys and blankets for children.
Source: Reference 17
WHEN A PATIENT CONFIRMS ABUSE
Affirm the difficulty of sharing this information and reassure the patient that she is not alone. Tell her, for example, “I know this is difficult to talk about. No one deserves to be treated this way.”
Reaffirm confidentiality. Victims fear harm to themselves or their children if their abusers find out they have discussed the abuse.
Assess the danger to the patient (Box 2).17
Refer the patient to a local domestic violence crisis agency or to a therapist knowledgeable about domestic abuse. A patient who reports being threatened at gunpoint or who fears for her safety should be urged to call police.
Do not refer the victim and partner to couples counseling. Such therapy is contraindicated because of the relationship’s power imbalance and the risk that the abuser will retaliate when alone with the victim.
DEVELOPING A SAFETY PLAN
Patients who have decided to leave an abusive partner need help forming a safety plan. Assistance from a domestic violence crisis agency is invaluable, but some patients prefer to work with their physicians. Safety planning involves helping the victim identify options and needs upon leaving the relationship.
Start by asking the patient:
- “If you leave home, where will you go?
- Is there an alternative if you cannot stay where you planned?
- Do you have an emergency bag?” (Box 3) 17
Remind the patient to keep her emergency bag, purse, and keys handy in case she needs to leave quickly.
Instruct the patient to:
- Tell a neighbor about the violence and ask him or her to call police if he or she hears suspicious noises from the victim’s residence.
- Teach children to dial 911 or 0 or to make a collect call to a relative, friend, minister, or other trusted person in an emergency. Also teach children addresses of close relatives and friends.
- Learn the local domestic violence hotline number.17
IF A PATIENT DENIES ABUSE
If a suspected victim denies she is being abused, schedule regular visits and let her know you are concerned. Ask how the relationship is progressing at the next monthly visit. If you fear the patient is in danger, schedule weekly or biweekly visits.
Above all, do not tell the victim what to do. Some patients are not ready to act, while others may call the local agency from your office.
Related resources
- National Domestic Violence Hotline (24-hour). 1-800-799-SAFE (7233). Translation services available.
- National Resource Center on Domestic Violence. (800) 537-2238 or www.ndvh.org
- American Medical Association Domestic Violence Resources. www.ama-assn.org/ama/pub/article/3216-6827.html
- American Medical Women’s Association online CME course educates physicians about domestic violence. Physicians can earn two CME credits at no charge. www.dvcme.org
Drug brand names
- Fluoxetine • Prozac
- Venlafaxine • Effexor
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article, or with manufacturers of competing products.
1. Tjaden P, Thoennes N. Extent, nature, and consequences of intimate partner violence: findings from the National Violence Against Women Survey. Report for grant 93-IJ-CX-0012. Washington, DC: National Institute of Justice and the Centers for Disease Control, 2000.
2. Campbell JC. Health consequences of intimate partner violence. Lancet 2002;359:1331-6.
3. Gazmararian JA, Lazorick S, Spitz AM, et al. Prevalence of violence against pregnant women. JAMA 1996;275:1915-20.
4. Golding JM. Intimate partner violence as a risk factor for mental disorders: a meta-analysis. J Fam Violence 1999;14:99-132.
5. Carlson B, McNutt LA, Choi D. Intimate partner abuse and mental health: the role of social support and protective factors. Violence Against Women 2002;8:720-45.
6. Cascardi M, O’Leary K, Lawrence E, Schlee K. Characteristics of women physically abused by their spouses and who seek treatment regarding marital conflict. J Consult Clin Psychol 1995;63:616-23.
7. Rhodes KV, Levinson W. Interventions for intimate partner violence against women: clinical applications. JAMA 2003;289:601-5.
8. American College of Physicians. Domestic violence: Position paper of the American College of Physicians. Philadelphia: American College of Physicians, 1986
9. American Medical Association Diagnostic and treatment guidelines for domestic violence. Arch Fam Med 1992;1:39-47.
10. American College of Obstetricians and Gynecologists. Domestic Violence. Washington DC: ACOG Educational Bulletin, No. 257, December 1999.
11. Gerbert B, Abercrombie P, Caspers N, et al. How health care providers help battered women: the survivor’s perspective. Women Health 1999;29:115-35.
12. Warshaw C, Ganley A. Improving the health care response to domestic violence: a resource manual for health care providers (2nd ed). San Francisco: Family Violence Prevention Fund; 1996.
13. U.S. Preventive Services Task Force. Guide to clinical preventive services (2nd ed). Baltimore: Williams & Wilkins, 1996.
14. Brown J, Lent B, Schmidt G, Sas G. Application of the Woman Abuse Screening Tool (WAST) and WAST-short in the family practice setting. J Fam Pract 2000;49:896-903.
15. Sherin K, Sinacore J, Li X, et al. HITS: a short domestic violence screening tool for use in a family practice setting. Fam Med 1998;30:508-12.
16. National Advisory Committee of FVPF. National consensus guidelines: on identifying and responding to domestic violence victimization in the health care setting. San Francisco: Family Violence Prevention Fund, 2002.
17. Davies J, Lyon E, Monti-Cantania D. Safety planning with battered women: complex lives, difficult choices. Thousand Oaks, CA: SAGE Publications, 1998.
Victims of domestic abuse/violence often present with medical and psychiatric disorders (Box 1, Table 1). Identifying abuse—and encouraging the frightened or ashamed patient to seek help—is critical to evaluating presenting complaints, improving out-come,7 and possibly saving the patient’s life.
This article will discuss ways to:
- detect signs of abuse
- determine whether a victim is in danger
- share information about crisis resources
- help those who are considering leaving an abusive partner to make a safety plan.
Domestic violence/abuse affects 1 of 4 women in the United States. Men also are victims, but the prevalence (1 of 14) and degree of injury is much lower.1 Domestic violence/abuse occurs among all socioeconomic and ethnic groups.1,2
![]()
Domestic violence/abuse impairs victims’ physical and mental health.2 Injuries and ailments more prevalent among domestic abuse victims than among the general population include:2,3
- digestive problems (diarrhea, nausea, appetite loss, spastic colon, constipation, eating disorders,
- urinary problems and infections
- vaginal infections, sexually transmitted diseases, pelvic pain, menstrual problems
- sexual dysfunction
- hypertension
- fainting
- chronic pain (headaches, pelvic, abdominal, back and neck)
- pregnancy problems (preterm labor, poor weight gain)
CASE REPORT: TWO YEARS OF HURT
Ms. W, age 26, is referred to a psychiatrist for treatment-resistant depression. Courses of fluoxetine, 20 mg/d titrated to 80 mg/d, and venlafaxine, 150 mg bid, failed to improve her symptoms. Her Beck Depression Inventory score at baseline is 18, suggesting borderline clinical depression.
Table 1
Psychiatric disorders in victims of domestic abuse/violence
| Disorder | Weighted mean prevalence among abuse victims | Lifetime prevalence among general population |
|---|---|---|
| Alcohol abuse/dependence 4 | 19% | 5 to 8% |
| Depression 4 | 48% | 10% to 21% |
| Drug abuse disorder 4 | 9% | 5% to 6% |
| Posttraumatic stress disorder 4 | 64% | 1% to 12% |
| Suicidality 4 | 18% (ideation and attempts) | Ideation 1-16% Attempts <1-4% |
| % of abused sample | % of non-abused sample | |
| Anxiety symptoms 5 | 26% | 8% |
| Generalized anxiety Disorder 6 | 10% | 4% |
| Panic disorder 6 | 13% | <1% |
She has two children—ages 2 and 4—with her husband, a habitual crack cocaine user. She does not use drugs or alcohol.
When asked about her life at home, Ms. W laments that her husband is not helpful. When asked if her husband hurts her, she replies tearfully that he constantly yells at her and insults her, calling her “ugly” and “a lousy mom.” Upon further questioning, she reveals that her husband, when high on crack, sometimes hits her.
Ms. W does not work outside the home and did not finish high school. She is afraid to leave her husband because his mother helps care for the children and provides money, housing, and food. She constantly feels tearful and trapped.
The psychiatrist increases the venlafaxine to 375 mg/d and suggests that Ms. W call a domestic violence crisis center. She does not call the center, but agrees to see the psychiatrist monthly. Across 3 months her Beck score improves to 14.
SCREENING FOR ABUSE
The American Medical Association, American College of Physicians, and other physician and nursing organizations recommend routinely screening women for domestic abuse/violence.8-10 Some patients will not disclose abuse to their physicians when asked, but most patients say they want doctors to ask them about domestic violence/abuse and to offer crisis phone numbers, pamphlets, and other resources.11
Anyone who presents with complaints of fatigue, depression, anxiety, insomnia, hypervigilance, a treatment-resistant psychiatric disorder, or a visible physical injury (such as a black eye or bruises) should be screened for domestic abuse.
Prevention and treatment guidelines for physicians9,12,13 recommend interviewing the patient—without the partner or children—in a nonjudgmental and empathic fashion.11
Written questionnaires—such as the Woman Abuse Screening Tool (WAST), WAST-short, and HITS—are another screening option.
WAST-Short has demonstrated 92% sensitivity in identifying emotional or physical abuse (Table 2).14
WAST. The longer version of WAST has demonstrated 96% sensitivity in detecting physical or emotional abuse.14 It includes the two WAST-short questions, plus five questions about whether:
- arguments with an intimate partner ever diminish the patient’s self-esteem
- such arguments ever result in kicking or hitting
- the patient ever feels frightened by the partner’s words or actions
- the patient has ever been physically or emotionally abused by his or her partner.
Because the additional questions are not scored, the longer WAST is not well suited to clinical practice. However, a patient who scores a 1 on the WAST-Short exam can provide more in-depth information on her troubled relationship by answering the extra questions.
HITS can be self-administered and its title is easy to remember, but the scoring system is cumbersome. The patient is asked: “How often does your partner:
- Hurt you physically?
- Insult you or talk down to you?
- Threaten you with harm?
- Scream or curse at you?”
Each answer is scored on a 1-to-5 scale—never, rarely, sometimes, fairly often, or frequently. A score ≥ 10.5 has demonstrated 96% sensitivity in identifying physical and verbal abuse.15
Encouraging disclosure. Ask patients about domestic abuse when inquiring about smoking, alcohol use, or household makeup as part of the patient history. Your line of questioning might proceed as follows:
- “Do you live alone?”
- “Do you have a significant other?”
- “How is your relationship going?”
- “Is your partner supportive?”
- “What happens when you and your partner disagree?”
Table 2
Woman Abuse Screening Tool-Short version
| 1. In general, how would you describe your relationship? | ||
| □ a lot of tension | □ some tension | □ no tension |
| 2. Do you and your partner work out arguments with: | ||
| □ great difficulty | □ some difficulty | □ no difficulty |
| Answers are scored on a 1-to-3 scale, with 1 meaning “a lot of tension” or “great difficulty.” A score of 1 on either question indicates possible domestic abuse/violence. | ||
| Source: Reference 14 | ||
Be empathic. Explain the association between domestic abuse/violence and mental and physical disorders. Tell the patient that domestic abuse is common and help is readily available. Share information about crisis services even if the patient does not immediately disclose suspected abuse. Victims generally feel tremendous shame from living with the abuse, so disclosure takes time and trust.
Most states do not require physicians to report domestic abuse to the police unless injuries are caused by a weapon (knife or gun). However, physicians in California, Colorado, Kentucky, and New York must report any injuries resulting from domestic abuse—even if not caused by a weapon.16 In these states, clinicians should disclose their reporting obligation at the start of the patient interview.
Assess danger to any patient who reports being a victim of domestic abuse/violence. Consider danger imminent if the patient acknowledges any one of the following:
- Homicide or suicide threats from partner
- Weapons in the home
- Excessive substance use by partner or victim
- Escalating abuse or threats
- Physical/verbal abuse of children
- Harm to pets
- Fear of the partner
Source: Reference 17
Advise a patient who reports domestic abuse/violence to pack important belongings in case she needs to immediately leave an abusive partner.
The emergency bag should contain:
- Identification for self and children (birth certificates, driver’s license)
- Important documents (school and health records, insurance cards, car title, marriage license, mortgage or rental papers, protective orders, custody papers, divorce papers)
- Medications (for victim and children)
- Keys (auto, home, safe deposit box)
- Phone numbers
- Clothing (for victim and children)
- Comfort items, such as toys and blankets for children.
Source: Reference 17
WHEN A PATIENT CONFIRMS ABUSE
Affirm the difficulty of sharing this information and reassure the patient that she is not alone. Tell her, for example, “I know this is difficult to talk about. No one deserves to be treated this way.”
Reaffirm confidentiality. Victims fear harm to themselves or their children if their abusers find out they have discussed the abuse.
Assess the danger to the patient (Box 2).17
Refer the patient to a local domestic violence crisis agency or to a therapist knowledgeable about domestic abuse. A patient who reports being threatened at gunpoint or who fears for her safety should be urged to call police.
Do not refer the victim and partner to couples counseling. Such therapy is contraindicated because of the relationship’s power imbalance and the risk that the abuser will retaliate when alone with the victim.
DEVELOPING A SAFETY PLAN
Patients who have decided to leave an abusive partner need help forming a safety plan. Assistance from a domestic violence crisis agency is invaluable, but some patients prefer to work with their physicians. Safety planning involves helping the victim identify options and needs upon leaving the relationship.
Start by asking the patient:
- “If you leave home, where will you go?
- Is there an alternative if you cannot stay where you planned?
- Do you have an emergency bag?” (Box 3) 17
Remind the patient to keep her emergency bag, purse, and keys handy in case she needs to leave quickly.
Instruct the patient to:
- Tell a neighbor about the violence and ask him or her to call police if he or she hears suspicious noises from the victim’s residence.
- Teach children to dial 911 or 0 or to make a collect call to a relative, friend, minister, or other trusted person in an emergency. Also teach children addresses of close relatives and friends.
- Learn the local domestic violence hotline number.17
IF A PATIENT DENIES ABUSE
If a suspected victim denies she is being abused, schedule regular visits and let her know you are concerned. Ask how the relationship is progressing at the next monthly visit. If you fear the patient is in danger, schedule weekly or biweekly visits.
Above all, do not tell the victim what to do. Some patients are not ready to act, while others may call the local agency from your office.
Related resources
- National Domestic Violence Hotline (24-hour). 1-800-799-SAFE (7233). Translation services available.
- National Resource Center on Domestic Violence. (800) 537-2238 or www.ndvh.org
- American Medical Association Domestic Violence Resources. www.ama-assn.org/ama/pub/article/3216-6827.html
- American Medical Women’s Association online CME course educates physicians about domestic violence. Physicians can earn two CME credits at no charge. www.dvcme.org
Drug brand names
- Fluoxetine • Prozac
- Venlafaxine • Effexor
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article, or with manufacturers of competing products.
Victims of domestic abuse/violence often present with medical and psychiatric disorders (Box 1, Table 1). Identifying abuse—and encouraging the frightened or ashamed patient to seek help—is critical to evaluating presenting complaints, improving out-come,7 and possibly saving the patient’s life.
This article will discuss ways to:
- detect signs of abuse
- determine whether a victim is in danger
- share information about crisis resources
- help those who are considering leaving an abusive partner to make a safety plan.
Domestic violence/abuse affects 1 of 4 women in the United States. Men also are victims, but the prevalence (1 of 14) and degree of injury is much lower.1 Domestic violence/abuse occurs among all socioeconomic and ethnic groups.1,2
![]()
Domestic violence/abuse impairs victims’ physical and mental health.2 Injuries and ailments more prevalent among domestic abuse victims than among the general population include:2,3
- digestive problems (diarrhea, nausea, appetite loss, spastic colon, constipation, eating disorders,
- urinary problems and infections
- vaginal infections, sexually transmitted diseases, pelvic pain, menstrual problems
- sexual dysfunction
- hypertension
- fainting
- chronic pain (headaches, pelvic, abdominal, back and neck)
- pregnancy problems (preterm labor, poor weight gain)
CASE REPORT: TWO YEARS OF HURT
Ms. W, age 26, is referred to a psychiatrist for treatment-resistant depression. Courses of fluoxetine, 20 mg/d titrated to 80 mg/d, and venlafaxine, 150 mg bid, failed to improve her symptoms. Her Beck Depression Inventory score at baseline is 18, suggesting borderline clinical depression.
Table 1
Psychiatric disorders in victims of domestic abuse/violence
| Disorder | Weighted mean prevalence among abuse victims | Lifetime prevalence among general population |
|---|---|---|
| Alcohol abuse/dependence 4 | 19% | 5 to 8% |
| Depression 4 | 48% | 10% to 21% |
| Drug abuse disorder 4 | 9% | 5% to 6% |
| Posttraumatic stress disorder 4 | 64% | 1% to 12% |
| Suicidality 4 | 18% (ideation and attempts) | Ideation 1-16% Attempts <1-4% |
| % of abused sample | % of non-abused sample | |
| Anxiety symptoms 5 | 26% | 8% |
| Generalized anxiety Disorder 6 | 10% | 4% |
| Panic disorder 6 | 13% | <1% |
She has two children—ages 2 and 4—with her husband, a habitual crack cocaine user. She does not use drugs or alcohol.
When asked about her life at home, Ms. W laments that her husband is not helpful. When asked if her husband hurts her, she replies tearfully that he constantly yells at her and insults her, calling her “ugly” and “a lousy mom.” Upon further questioning, she reveals that her husband, when high on crack, sometimes hits her.
Ms. W does not work outside the home and did not finish high school. She is afraid to leave her husband because his mother helps care for the children and provides money, housing, and food. She constantly feels tearful and trapped.
The psychiatrist increases the venlafaxine to 375 mg/d and suggests that Ms. W call a domestic violence crisis center. She does not call the center, but agrees to see the psychiatrist monthly. Across 3 months her Beck score improves to 14.
SCREENING FOR ABUSE
The American Medical Association, American College of Physicians, and other physician and nursing organizations recommend routinely screening women for domestic abuse/violence.8-10 Some patients will not disclose abuse to their physicians when asked, but most patients say they want doctors to ask them about domestic violence/abuse and to offer crisis phone numbers, pamphlets, and other resources.11
Anyone who presents with complaints of fatigue, depression, anxiety, insomnia, hypervigilance, a treatment-resistant psychiatric disorder, or a visible physical injury (such as a black eye or bruises) should be screened for domestic abuse.
Prevention and treatment guidelines for physicians9,12,13 recommend interviewing the patient—without the partner or children—in a nonjudgmental and empathic fashion.11
Written questionnaires—such as the Woman Abuse Screening Tool (WAST), WAST-short, and HITS—are another screening option.
WAST-Short has demonstrated 92% sensitivity in identifying emotional or physical abuse (Table 2).14
WAST. The longer version of WAST has demonstrated 96% sensitivity in detecting physical or emotional abuse.14 It includes the two WAST-short questions, plus five questions about whether:
- arguments with an intimate partner ever diminish the patient’s self-esteem
- such arguments ever result in kicking or hitting
- the patient ever feels frightened by the partner’s words or actions
- the patient has ever been physically or emotionally abused by his or her partner.
Because the additional questions are not scored, the longer WAST is not well suited to clinical practice. However, a patient who scores a 1 on the WAST-Short exam can provide more in-depth information on her troubled relationship by answering the extra questions.
HITS can be self-administered and its title is easy to remember, but the scoring system is cumbersome. The patient is asked: “How often does your partner:
- Hurt you physically?
- Insult you or talk down to you?
- Threaten you with harm?
- Scream or curse at you?”
Each answer is scored on a 1-to-5 scale—never, rarely, sometimes, fairly often, or frequently. A score ≥ 10.5 has demonstrated 96% sensitivity in identifying physical and verbal abuse.15
Encouraging disclosure. Ask patients about domestic abuse when inquiring about smoking, alcohol use, or household makeup as part of the patient history. Your line of questioning might proceed as follows:
- “Do you live alone?”
- “Do you have a significant other?”
- “How is your relationship going?”
- “Is your partner supportive?”
- “What happens when you and your partner disagree?”
Table 2
Woman Abuse Screening Tool-Short version
| 1. In general, how would you describe your relationship? | ||
| □ a lot of tension | □ some tension | □ no tension |
| 2. Do you and your partner work out arguments with: | ||
| □ great difficulty | □ some difficulty | □ no difficulty |
| Answers are scored on a 1-to-3 scale, with 1 meaning “a lot of tension” or “great difficulty.” A score of 1 on either question indicates possible domestic abuse/violence. | ||
| Source: Reference 14 | ||
Be empathic. Explain the association between domestic abuse/violence and mental and physical disorders. Tell the patient that domestic abuse is common and help is readily available. Share information about crisis services even if the patient does not immediately disclose suspected abuse. Victims generally feel tremendous shame from living with the abuse, so disclosure takes time and trust.
Most states do not require physicians to report domestic abuse to the police unless injuries are caused by a weapon (knife or gun). However, physicians in California, Colorado, Kentucky, and New York must report any injuries resulting from domestic abuse—even if not caused by a weapon.16 In these states, clinicians should disclose their reporting obligation at the start of the patient interview.
Assess danger to any patient who reports being a victim of domestic abuse/violence. Consider danger imminent if the patient acknowledges any one of the following:
- Homicide or suicide threats from partner
- Weapons in the home
- Excessive substance use by partner or victim
- Escalating abuse or threats
- Physical/verbal abuse of children
- Harm to pets
- Fear of the partner
Source: Reference 17
Advise a patient who reports domestic abuse/violence to pack important belongings in case she needs to immediately leave an abusive partner.
The emergency bag should contain:
- Identification for self and children (birth certificates, driver’s license)
- Important documents (school and health records, insurance cards, car title, marriage license, mortgage or rental papers, protective orders, custody papers, divorce papers)
- Medications (for victim and children)
- Keys (auto, home, safe deposit box)
- Phone numbers
- Clothing (for victim and children)
- Comfort items, such as toys and blankets for children.
Source: Reference 17
WHEN A PATIENT CONFIRMS ABUSE
Affirm the difficulty of sharing this information and reassure the patient that she is not alone. Tell her, for example, “I know this is difficult to talk about. No one deserves to be treated this way.”
Reaffirm confidentiality. Victims fear harm to themselves or their children if their abusers find out they have discussed the abuse.
Assess the danger to the patient (Box 2).17
Refer the patient to a local domestic violence crisis agency or to a therapist knowledgeable about domestic abuse. A patient who reports being threatened at gunpoint or who fears for her safety should be urged to call police.
Do not refer the victim and partner to couples counseling. Such therapy is contraindicated because of the relationship’s power imbalance and the risk that the abuser will retaliate when alone with the victim.
DEVELOPING A SAFETY PLAN
Patients who have decided to leave an abusive partner need help forming a safety plan. Assistance from a domestic violence crisis agency is invaluable, but some patients prefer to work with their physicians. Safety planning involves helping the victim identify options and needs upon leaving the relationship.
Start by asking the patient:
- “If you leave home, where will you go?
- Is there an alternative if you cannot stay where you planned?
- Do you have an emergency bag?” (Box 3) 17
Remind the patient to keep her emergency bag, purse, and keys handy in case she needs to leave quickly.
Instruct the patient to:
- Tell a neighbor about the violence and ask him or her to call police if he or she hears suspicious noises from the victim’s residence.
- Teach children to dial 911 or 0 or to make a collect call to a relative, friend, minister, or other trusted person in an emergency. Also teach children addresses of close relatives and friends.
- Learn the local domestic violence hotline number.17
IF A PATIENT DENIES ABUSE
If a suspected victim denies she is being abused, schedule regular visits and let her know you are concerned. Ask how the relationship is progressing at the next monthly visit. If you fear the patient is in danger, schedule weekly or biweekly visits.
Above all, do not tell the victim what to do. Some patients are not ready to act, while others may call the local agency from your office.
Related resources
- National Domestic Violence Hotline (24-hour). 1-800-799-SAFE (7233). Translation services available.
- National Resource Center on Domestic Violence. (800) 537-2238 or www.ndvh.org
- American Medical Association Domestic Violence Resources. www.ama-assn.org/ama/pub/article/3216-6827.html
- American Medical Women’s Association online CME course educates physicians about domestic violence. Physicians can earn two CME credits at no charge. www.dvcme.org
Drug brand names
- Fluoxetine • Prozac
- Venlafaxine • Effexor
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article, or with manufacturers of competing products.
1. Tjaden P, Thoennes N. Extent, nature, and consequences of intimate partner violence: findings from the National Violence Against Women Survey. Report for grant 93-IJ-CX-0012. Washington, DC: National Institute of Justice and the Centers for Disease Control, 2000.
2. Campbell JC. Health consequences of intimate partner violence. Lancet 2002;359:1331-6.
3. Gazmararian JA, Lazorick S, Spitz AM, et al. Prevalence of violence against pregnant women. JAMA 1996;275:1915-20.
4. Golding JM. Intimate partner violence as a risk factor for mental disorders: a meta-analysis. J Fam Violence 1999;14:99-132.
5. Carlson B, McNutt LA, Choi D. Intimate partner abuse and mental health: the role of social support and protective factors. Violence Against Women 2002;8:720-45.
6. Cascardi M, O’Leary K, Lawrence E, Schlee K. Characteristics of women physically abused by their spouses and who seek treatment regarding marital conflict. J Consult Clin Psychol 1995;63:616-23.
7. Rhodes KV, Levinson W. Interventions for intimate partner violence against women: clinical applications. JAMA 2003;289:601-5.
8. American College of Physicians. Domestic violence: Position paper of the American College of Physicians. Philadelphia: American College of Physicians, 1986
9. American Medical Association Diagnostic and treatment guidelines for domestic violence. Arch Fam Med 1992;1:39-47.
10. American College of Obstetricians and Gynecologists. Domestic Violence. Washington DC: ACOG Educational Bulletin, No. 257, December 1999.
11. Gerbert B, Abercrombie P, Caspers N, et al. How health care providers help battered women: the survivor’s perspective. Women Health 1999;29:115-35.
12. Warshaw C, Ganley A. Improving the health care response to domestic violence: a resource manual for health care providers (2nd ed). San Francisco: Family Violence Prevention Fund; 1996.
13. U.S. Preventive Services Task Force. Guide to clinical preventive services (2nd ed). Baltimore: Williams & Wilkins, 1996.
14. Brown J, Lent B, Schmidt G, Sas G. Application of the Woman Abuse Screening Tool (WAST) and WAST-short in the family practice setting. J Fam Pract 2000;49:896-903.
15. Sherin K, Sinacore J, Li X, et al. HITS: a short domestic violence screening tool for use in a family practice setting. Fam Med 1998;30:508-12.
16. National Advisory Committee of FVPF. National consensus guidelines: on identifying and responding to domestic violence victimization in the health care setting. San Francisco: Family Violence Prevention Fund, 2002.
17. Davies J, Lyon E, Monti-Cantania D. Safety planning with battered women: complex lives, difficult choices. Thousand Oaks, CA: SAGE Publications, 1998.
1. Tjaden P, Thoennes N. Extent, nature, and consequences of intimate partner violence: findings from the National Violence Against Women Survey. Report for grant 93-IJ-CX-0012. Washington, DC: National Institute of Justice and the Centers for Disease Control, 2000.
2. Campbell JC. Health consequences of intimate partner violence. Lancet 2002;359:1331-6.
3. Gazmararian JA, Lazorick S, Spitz AM, et al. Prevalence of violence against pregnant women. JAMA 1996;275:1915-20.
4. Golding JM. Intimate partner violence as a risk factor for mental disorders: a meta-analysis. J Fam Violence 1999;14:99-132.
5. Carlson B, McNutt LA, Choi D. Intimate partner abuse and mental health: the role of social support and protective factors. Violence Against Women 2002;8:720-45.
6. Cascardi M, O’Leary K, Lawrence E, Schlee K. Characteristics of women physically abused by their spouses and who seek treatment regarding marital conflict. J Consult Clin Psychol 1995;63:616-23.
7. Rhodes KV, Levinson W. Interventions for intimate partner violence against women: clinical applications. JAMA 2003;289:601-5.
8. American College of Physicians. Domestic violence: Position paper of the American College of Physicians. Philadelphia: American College of Physicians, 1986
9. American Medical Association Diagnostic and treatment guidelines for domestic violence. Arch Fam Med 1992;1:39-47.
10. American College of Obstetricians and Gynecologists. Domestic Violence. Washington DC: ACOG Educational Bulletin, No. 257, December 1999.
11. Gerbert B, Abercrombie P, Caspers N, et al. How health care providers help battered women: the survivor’s perspective. Women Health 1999;29:115-35.
12. Warshaw C, Ganley A. Improving the health care response to domestic violence: a resource manual for health care providers (2nd ed). San Francisco: Family Violence Prevention Fund; 1996.
13. U.S. Preventive Services Task Force. Guide to clinical preventive services (2nd ed). Baltimore: Williams & Wilkins, 1996.
14. Brown J, Lent B, Schmidt G, Sas G. Application of the Woman Abuse Screening Tool (WAST) and WAST-short in the family practice setting. J Fam Pract 2000;49:896-903.
15. Sherin K, Sinacore J, Li X, et al. HITS: a short domestic violence screening tool for use in a family practice setting. Fam Med 1998;30:508-12.
16. National Advisory Committee of FVPF. National consensus guidelines: on identifying and responding to domestic violence victimization in the health care setting. San Francisco: Family Violence Prevention Fund, 2002.
17. Davies J, Lyon E, Monti-Cantania D. Safety planning with battered women: complex lives, difficult choices. Thousand Oaks, CA: SAGE Publications, 1998.
Don’t be fooled by hypochondria
A hypochondria “checklist” can help you sort through many overlapping medical and psychiatric disorders and increase your chances of making an accurate diagnosis. Then—by addressing hypochondria’s cognitive dysfunction—you can help patients achieve partial or full remission and change their distressing behaviors.
We offer a checklist that is useful in our practice and suggest behavioral therapies and medications that can help calm these patients’ excessive, unwarranted fears.
WORKING AS A TEAM
Ideal approach. Because hypochondriasis has features of medical and mental illness, working with the patient’s primary care physician is ideal. Physicians often consider these patients difficult because they demand a lot of time, support, and reassurance. Together, you can:
- offer the patient a healthy level of compassion and empathy to establish a positive therapeutic alliance
- set appropriate time limits and guidelines for the patient’s care
- dissuade patients from “doctor shopping”
- set limits on how often patients may visit their doctors and request reassurance.
Hypochondriasis: Persistent, unwarranted distress
Hypochondriasis is an excessive and persistent fear or belief that one has a serious illness, despite medical reassurance and lack of diagnostic findings that would warrant the health concern. If a medical disorder is present, the distress and preoccupation exceed what the patient’s physician considers reasonable. Illness preoccupation is intense enough to cause great distress or to interfere with daily functioning and may cause the person to miss work or cancel social engagements.1
DSM-IV criteria. A patient’s fear or conviction that he or she has a serious health threat must persist at least 6 months and may be accompanied by specific somatic symptoms, vague symptoms,1 or no symptoms.2 Hypochondriacal preoccupation may be stable over time, where one illness concern dominates, or it may shift—from fear of AIDS to fear of a heart attack.
A common disorder. Hypochondriasis occurs in 4 to 6% of the general medical population. In psychiatric or medical clinics, women are identified as having hypochondriasis three to four times more often than men. Average age of onset is in the early 20s.3
For example, you may indicate to the patient, “I will reassure you only at office visits (not by phone), the office visits will be limited to once a month, and during each visit I will reassure you no more than once.”
A doctor-patient relationship based on mutual trust and respect is vital when you treat a patient with hypochondriasis. You can help primary care physicians provide more empathic treatment by explaining that patients do not feign or desire this distressing condition.
DIAGNOSTIC FEATURES
Patients with hypochondriasis tend to be hyper-vigilant about normal physiologic fluctuations and bodily sensations, often misinterpreting them as life-threatening or serious enough to require immediate medical attention. This excessive focus on benign symptoms (such as an accelerated heart rate, sweating, or a bump on the skin) and the cognitive distortion of their significance result in increased anxiety, bodily checking, and doctor visits (Box).1-4
Presentations. Hypochondriasis has three common presentations: disease conviction, disease fear, and bodily preoccupation (Table 1).5 Psychiatrists are most likely to see disease fear, as patients with this predominant symptom tend to realize that fear plays too prominent a role in their lives. Physicians in medical practice are more likely to encounter patients with high levels of disease conviction or somatic preoccupation.
Psychiatric comorbidity. Hypochondriasis is highly comorbid with Axis I and Axis II disorders, which complicate treatment. Nearly one-half of patients with hypochondriasis also have dysthymia (45%) or major depression (43%). Other comorbidities include phobias (38%), somatization disorder (21%), panic disorder (17%), and obsessive-compulsive disorder (8%).6 Patients with hypochondriasis are three times more likely than the general population to have personality disorders;6,7 the prognosis is believed to be more promising for patients without personality disorders.
Distinguishing between primary and secondary hypochondriasis is important. Treating a primary psychiatric disorder often alleviates the symptoms of secondary hypochondriasis, particularly when hypochondriasis masks depression.
HYPOCHONDRIASIS CHECKLIST
Underlying medical disorder? Before diagnosing hypochondriasis, review the medical workup for underlying disease or illness. Medical conditions sometimes go undetected when physicians assume that complaints are an expression of longstanding hypochondriasis.
Table 1
Three common presentations of hypochondriasis
| Predominant symptom | Characterization |
|---|---|
| Disease conviction | Patient may appear delusional in believing he or she has a disease and in persistent efforts to find a doctor who will make the “accurate” diagnosis |
| Disease fear | Patient may avoid doctors because of fear associated with confirmation of a dreaded disease |
| Bodily preoccupation | Patient may complain of multiple somatic symptoms, which mask underlying fear or belief of having a serious disease |
Sometimes a patient may become anxious when mild or vague signs and symptoms do not yet meet established diagnostic criteria for a medical disorder. An effective approach is to provide ongoing support, avoid excessive diagnostic tests, and help the patient make the best use of his or her functional capacities while living with uncertainty.
Functional somatic syndrome? Fibromyalgia and chronic fatigue syndrome do not represent hypochondriasis,8 although they may be exacerbated by comorbid psychiatric disorders. Both disorders have diagnostic criteria and specified courses and have been studied to identify psychiatric comorbidity.
Transient or sustained? After it is clear that the patient is not suffering from a medical problem, determine whether hypochondriasis is transient or fully diagnostic:
- If transient, the patient may only need to be educated about how overattention may amplify symptoms; reassure him or her that a full medical workup has been negative.
- If fully diagnostic, reassurance may work for only a few days or weeks; the return of the fear or conviction helps establish the diagnosis.
Somatoform disorder? Distinguish hypochondriasis from other somatoform disorders (Table 2). In practice, the terms “hypochondriac” and “somatizer” are commonly used interchangeably, but the distinction needs to be clear. Hypochondriasis is primarily a disorder of abnormal cognition, in which symptom meaning is of greatest concern. Somatization is primarily a disorder of abnormal sensation, in which the symptoms themselves are the overwhelming focus of attention.
Anxiety disorder? Patients with generalized anxiety disorder may worry about illness, but they also worry about other life issues. Patients with panic disorder may have intense hypochondriacal concerns (such as having a heart attack), but these worries tend to be related to panic symptoms and resolve when the panic disorder is treated.
Obsessive compulsive disorder? Like obsessive-compulsive disorder (OCD), hypochondriasis is characterized by recurrent intrusive thoughts that create heightened anxiety and distress. To relieve their anxiety, patients with hypochondriasis engage in compulsions, such as:
- undergoing extensive medical tests
- seeking habitual reassurance from doctors and family
- consulting medical literature
- performing repeated body checks for perceived lumps or bumps
- avoiding activities that trigger their health-related stress.9
Table 2
How to distinguish somatoform disorders
| Disorder | Patient focuses on… |
|---|---|
| Hypochondriasis | physical symptoms’ meaning (abnormal cognition) |
| Somatization disorder | multiple unexplained physical symptoms (abnormal sensation) |
| Body dysmorphic disorder | perceived abnormal bodily appearance |
| Conversion disorder | motor or sensory function abnormalities that develop soon after life stressors or conflict |
| Pain disorder | intense pain, in which psychological factors contribute to pain onset, severity, or maintenance |
OCD and hypochondriasis also may share the diagnostic feature of pathologic doubt; patients’ uncertainty in appraising a situation leads to additional checking and reassurance-seeking behaviors. The immediate relief gained by these compulsions reinforces the patient’s urge to engage in more maladaptive behaviors and sends a stronger message to the brain that these behaviors are needed to prevent harm.
Ironically, the emergence of a real medical ailment—despite hypochondriacal worry—may force the patient to re-evaluate the usefulness of behaviors motivated by trying to avoid harm. A hypochondriacal patient who was diagnosed with optic neuritis and possible multiple sclerosis recently said to these authors, “I had always thought that by being vigilant I could keep illnesses away. Now I know that’s not true.”
Although hypochondriasis and OCD have similarities, certain clinical distinctions exist. Patients with hypochondriasis worry about having an illness, whereas OCD patients with somatic obsessions fear developing or transmitting an illness. A hypochondriacal patient might fear having AIDS or cancer despite reassurance from doctors, while an OCD patient more typically would fear contracting or transmitting the disease (a contamination obsession) and would engage in excessive behaviors to reduce the risk of developing the disease.
Depressive disorder? Unlike the anxious-worrying version of hypochondriasis, the depressive version is more fatalistic. Patients may be convinced they are dying of a dreaded disease, often believing it to be punishment for an indiscretion, such as marital infidelity. Or they may suddenly become hypochondriacal with mild depressive features, unaware that the actual problem is unresolved bereavement (hypochondriasis with secondary depression). The appropriate diagnosis is primary depressive disorder with secondary hypochondriacal features when depression dominates the presentation and preceded the illness fears.
Table 3
Recommended dosages for treating primary hypochondriasis
| Drug | Starting dosage | Maximum dosage |
|---|---|---|
| Fluoxetine | 10 mg/d if panic symptoms are present; 20 mg/d otherwise | 80 mg/d |
| Fluvoxamine | 50 mg at bedtime | 150 mg bid |
| Nefazodone | 100 mg bid | 300 mg bid |
| Paroxetine | 20 mg once daily | 50 mg once daily |
Delusional disorder? To distinguish hypochondriasis from delusional disorder (somatic type), consider the patient’s pattern of insight:
- Hypochondriacal patients often vacillate between poor and excellent insight, depending on their distress level.10 They may acknowledge the irrationality of their fears, then later be convinced they have a disease.
- Patients with delusional disorder are convinced they have a serious health threat, despite the absence of medical confirmation. These patients are considered to have a primary psychotic disorder that requires antipsychotic treatment.
TREATING PRIMARY SYMPTOMS
Drug therapy. When hypochondriasis is secondary—such as to depression or panic disorder—treat the primary condition first.11,12 For primary hypochondriasis, selective serotonin reuptake inhibitors (SSRIs) such as fluoxetine, paroxetine, or fluvoxamine have shown benefit, mostly in open-label studies. An uncontrolled case series suggests that nefazodone—with mixed serotonin reuptake inhibition and agonist properties—also may help patients with hypochondriasis.13 In the only published controlled study, fluoxetine was more effective than placebo for treating hypochondriasis.10
Continue drug therapy, when used, for at least 8 weeks, with each dosage maintained for at least 4 weeks. If patients do not respond to lower SSRI dosages, increase to the higher dosages reported to be more effective for OCD (Table 3).14
Except for primary illness phobia, hypochondriasis has not been shown to respond to tricyclics, benzodiazepines, or dopaminergic blockers. In our experience, electroconvulsive therapy—although inadequately studied—may help treat patients with severe, treatment-refractory hypochondriasis with marked somatization.
Psychotherapy. Cognitive-behavioral therapy (CBT)—challenging patients’ irrational fears about illness and teaching them problem-solving tools—is effective in treating hypochondriasis.15 CBT can help patients understand that distorted thoughts lead to their sad or anxious moods.
Instructing patients to keep thought diaries can help them identify irrational fears and use cognitive restructuring to correct their faulty schemas. Tailor your cognitive therapy techniques to target the patient’s level of insight at the time of therapy.
Effective behavioral techniques may include setting limits on doctor visits, checking behaviors, reassurance seeking, etc. Repeated exposure to feared stimuli such as needles, white lab coats, blood pressure cuffs, medical dialogue, or hospital wards can help the patient habituate to the anxiety.
Relaxation techniques, a healthy diet, and exercise are also useful. Relaxation exercises—such as diaphragmatic breathing, progressive muscle relaxation, and visual imagery—may help patients manage anxiety by reducing CNS and autonomic nervous system arousal.
Bottom line
Hypochondriasis’ cognitive dysfunction is treatable, once an accurate diagnosis is made. Using a checklist can help you differentiate hypochondriasis from other medical and psychiatric disorders. A trusting doctor-patient relationship enhances outcome.
Related resources
- Fallon BA., Feinstein SB. Hypochondriasis: clinical, theoretical, and therapeutic aspects. In: Oldham J (ed). Review of psychiatry (vol. 20) Washington, DC: American Psychiatric Press, 2001:27-60.
- Cantor C, Fallon BA. Phantom illness: shattering the myth of hypochondria Boston: Houghton Mifflin Company, 1996.
- Starcevic V, Lipsitt DR (eds). Hypochondriasis: modern perspectives on an ancient malady New York: Oxford University Press, 2001.
Drug brand names
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Nefazodone • Serzone
- Paroxetine • Paxil
1. Diagnostic and statistical manual of mental disorders (4th ed-text revision). Washington, DC: American Psychiatric Association, 2000.
2. Task Force on DSM-IV. DSM-IV options book. Washington DC: American Psychiatric Association, 1991.
3. Barsky AJ, Wyshak G, Klerman GL, Lathan KS. The prevalence of hypochondriasis in medical outpatients. Soc Psychiatry Psychiatr Epidemiol 1990;25(2):89-94.
4. Salkovskis PM, Clark DM. Panic and hypochondriasis. Adv Behav Res Ther 1993;15:23-48.
5. Pilowsky I. Dimensions of hypochondriasis. Br J Psychiatry 1967;113(494):89-93.
6. Barsky AJ, Wyshak G, Klerman GL. Psychiatric comorbidity in DSM-III-R hypochondriasis. Arch Gen Psychiatry 1992;49(2):101-8.
7. Kellner R. The prognosis of treated hypochondriasis: a clinical study. Acta Psychiatr Scand 1983;67(2):69-79.
8. Noyes R, Jr, Kathol RG, Fisher M, Phillips BM, et al. The validity of DSM-III-R hypochondriasis. Arch Gen Psychiatry 1993;50(12):961-70.
9. Fallon BA, Qureshi AI, Laje G, Klein B. Hypochondriasis and its relationship to obsessive-compulsive disorder. Psychiatr Clin North Am 2000;23(3):605-16.
10. Fallon BA, Schneier FR, Marshall R, Campeas R, et al. The pharmacotherapy of hypochondriasis. Psychopharmacol Bull 1996;32:607-11.
11. Kellner R, Fava GA, Lisansky J, et al. Hypochondriacal fears and beliefs in DSM-III melancholia: changes with amitriptyline. J Affect Disord 1986;10(1):21-6.
12. Noyes R, Jr, Reich J, Clancy J, O’Gorman TW. Reduction in hypochondriasis with treatment of panic disorder. Br J Psychiatry 1986;149:631-5(erratum in Br J Psychiatry 1987;150:273).
13. Kjernisted KD, Ennis MW, Lander M. An open-label clinical trial of nefazodone in hypochondriasis. Psychosomatics 2002;43:290-4.
14. Fallon BA. Pharmacologic strategies for hypochondriasis. In: Starcevic V, Lipsitt DR (eds). Hypochondriasis: modern perspectives on an ancient malady. New York: Oxford University Press, 2001;329-51.
15. Warwick HMC, Salkovskis PM. Hypochondriasis. In: Scott J, Williams JMG, Beck AT (eds). Cognitive therapy in clinical practice: an illustrative casebook. London; Routledge, 1989;78-102.
A hypochondria “checklist” can help you sort through many overlapping medical and psychiatric disorders and increase your chances of making an accurate diagnosis. Then—by addressing hypochondria’s cognitive dysfunction—you can help patients achieve partial or full remission and change their distressing behaviors.
We offer a checklist that is useful in our practice and suggest behavioral therapies and medications that can help calm these patients’ excessive, unwarranted fears.
WORKING AS A TEAM
Ideal approach. Because hypochondriasis has features of medical and mental illness, working with the patient’s primary care physician is ideal. Physicians often consider these patients difficult because they demand a lot of time, support, and reassurance. Together, you can:
- offer the patient a healthy level of compassion and empathy to establish a positive therapeutic alliance
- set appropriate time limits and guidelines for the patient’s care
- dissuade patients from “doctor shopping”
- set limits on how often patients may visit their doctors and request reassurance.
Hypochondriasis: Persistent, unwarranted distress
Hypochondriasis is an excessive and persistent fear or belief that one has a serious illness, despite medical reassurance and lack of diagnostic findings that would warrant the health concern. If a medical disorder is present, the distress and preoccupation exceed what the patient’s physician considers reasonable. Illness preoccupation is intense enough to cause great distress or to interfere with daily functioning and may cause the person to miss work or cancel social engagements.1
DSM-IV criteria. A patient’s fear or conviction that he or she has a serious health threat must persist at least 6 months and may be accompanied by specific somatic symptoms, vague symptoms,1 or no symptoms.2 Hypochondriacal preoccupation may be stable over time, where one illness concern dominates, or it may shift—from fear of AIDS to fear of a heart attack.
A common disorder. Hypochondriasis occurs in 4 to 6% of the general medical population. In psychiatric or medical clinics, women are identified as having hypochondriasis three to four times more often than men. Average age of onset is in the early 20s.3
For example, you may indicate to the patient, “I will reassure you only at office visits (not by phone), the office visits will be limited to once a month, and during each visit I will reassure you no more than once.”
A doctor-patient relationship based on mutual trust and respect is vital when you treat a patient with hypochondriasis. You can help primary care physicians provide more empathic treatment by explaining that patients do not feign or desire this distressing condition.
DIAGNOSTIC FEATURES
Patients with hypochondriasis tend to be hyper-vigilant about normal physiologic fluctuations and bodily sensations, often misinterpreting them as life-threatening or serious enough to require immediate medical attention. This excessive focus on benign symptoms (such as an accelerated heart rate, sweating, or a bump on the skin) and the cognitive distortion of their significance result in increased anxiety, bodily checking, and doctor visits (Box).1-4
Presentations. Hypochondriasis has three common presentations: disease conviction, disease fear, and bodily preoccupation (Table 1).5 Psychiatrists are most likely to see disease fear, as patients with this predominant symptom tend to realize that fear plays too prominent a role in their lives. Physicians in medical practice are more likely to encounter patients with high levels of disease conviction or somatic preoccupation.
Psychiatric comorbidity. Hypochondriasis is highly comorbid with Axis I and Axis II disorders, which complicate treatment. Nearly one-half of patients with hypochondriasis also have dysthymia (45%) or major depression (43%). Other comorbidities include phobias (38%), somatization disorder (21%), panic disorder (17%), and obsessive-compulsive disorder (8%).6 Patients with hypochondriasis are three times more likely than the general population to have personality disorders;6,7 the prognosis is believed to be more promising for patients without personality disorders.
Distinguishing between primary and secondary hypochondriasis is important. Treating a primary psychiatric disorder often alleviates the symptoms of secondary hypochondriasis, particularly when hypochondriasis masks depression.
HYPOCHONDRIASIS CHECKLIST
Underlying medical disorder? Before diagnosing hypochondriasis, review the medical workup for underlying disease or illness. Medical conditions sometimes go undetected when physicians assume that complaints are an expression of longstanding hypochondriasis.
Table 1
Three common presentations of hypochondriasis
| Predominant symptom | Characterization |
|---|---|
| Disease conviction | Patient may appear delusional in believing he or she has a disease and in persistent efforts to find a doctor who will make the “accurate” diagnosis |
| Disease fear | Patient may avoid doctors because of fear associated with confirmation of a dreaded disease |
| Bodily preoccupation | Patient may complain of multiple somatic symptoms, which mask underlying fear or belief of having a serious disease |
Sometimes a patient may become anxious when mild or vague signs and symptoms do not yet meet established diagnostic criteria for a medical disorder. An effective approach is to provide ongoing support, avoid excessive diagnostic tests, and help the patient make the best use of his or her functional capacities while living with uncertainty.
Functional somatic syndrome? Fibromyalgia and chronic fatigue syndrome do not represent hypochondriasis,8 although they may be exacerbated by comorbid psychiatric disorders. Both disorders have diagnostic criteria and specified courses and have been studied to identify psychiatric comorbidity.
Transient or sustained? After it is clear that the patient is not suffering from a medical problem, determine whether hypochondriasis is transient or fully diagnostic:
- If transient, the patient may only need to be educated about how overattention may amplify symptoms; reassure him or her that a full medical workup has been negative.
- If fully diagnostic, reassurance may work for only a few days or weeks; the return of the fear or conviction helps establish the diagnosis.
Somatoform disorder? Distinguish hypochondriasis from other somatoform disorders (Table 2). In practice, the terms “hypochondriac” and “somatizer” are commonly used interchangeably, but the distinction needs to be clear. Hypochondriasis is primarily a disorder of abnormal cognition, in which symptom meaning is of greatest concern. Somatization is primarily a disorder of abnormal sensation, in which the symptoms themselves are the overwhelming focus of attention.
Anxiety disorder? Patients with generalized anxiety disorder may worry about illness, but they also worry about other life issues. Patients with panic disorder may have intense hypochondriacal concerns (such as having a heart attack), but these worries tend to be related to panic symptoms and resolve when the panic disorder is treated.
Obsessive compulsive disorder? Like obsessive-compulsive disorder (OCD), hypochondriasis is characterized by recurrent intrusive thoughts that create heightened anxiety and distress. To relieve their anxiety, patients with hypochondriasis engage in compulsions, such as:
- undergoing extensive medical tests
- seeking habitual reassurance from doctors and family
- consulting medical literature
- performing repeated body checks for perceived lumps or bumps
- avoiding activities that trigger their health-related stress.9
Table 2
How to distinguish somatoform disorders
| Disorder | Patient focuses on… |
|---|---|
| Hypochondriasis | physical symptoms’ meaning (abnormal cognition) |
| Somatization disorder | multiple unexplained physical symptoms (abnormal sensation) |
| Body dysmorphic disorder | perceived abnormal bodily appearance |
| Conversion disorder | motor or sensory function abnormalities that develop soon after life stressors or conflict |
| Pain disorder | intense pain, in which psychological factors contribute to pain onset, severity, or maintenance |
OCD and hypochondriasis also may share the diagnostic feature of pathologic doubt; patients’ uncertainty in appraising a situation leads to additional checking and reassurance-seeking behaviors. The immediate relief gained by these compulsions reinforces the patient’s urge to engage in more maladaptive behaviors and sends a stronger message to the brain that these behaviors are needed to prevent harm.
Ironically, the emergence of a real medical ailment—despite hypochondriacal worry—may force the patient to re-evaluate the usefulness of behaviors motivated by trying to avoid harm. A hypochondriacal patient who was diagnosed with optic neuritis and possible multiple sclerosis recently said to these authors, “I had always thought that by being vigilant I could keep illnesses away. Now I know that’s not true.”
Although hypochondriasis and OCD have similarities, certain clinical distinctions exist. Patients with hypochondriasis worry about having an illness, whereas OCD patients with somatic obsessions fear developing or transmitting an illness. A hypochondriacal patient might fear having AIDS or cancer despite reassurance from doctors, while an OCD patient more typically would fear contracting or transmitting the disease (a contamination obsession) and would engage in excessive behaviors to reduce the risk of developing the disease.
Depressive disorder? Unlike the anxious-worrying version of hypochondriasis, the depressive version is more fatalistic. Patients may be convinced they are dying of a dreaded disease, often believing it to be punishment for an indiscretion, such as marital infidelity. Or they may suddenly become hypochondriacal with mild depressive features, unaware that the actual problem is unresolved bereavement (hypochondriasis with secondary depression). The appropriate diagnosis is primary depressive disorder with secondary hypochondriacal features when depression dominates the presentation and preceded the illness fears.
Table 3
Recommended dosages for treating primary hypochondriasis
| Drug | Starting dosage | Maximum dosage |
|---|---|---|
| Fluoxetine | 10 mg/d if panic symptoms are present; 20 mg/d otherwise | 80 mg/d |
| Fluvoxamine | 50 mg at bedtime | 150 mg bid |
| Nefazodone | 100 mg bid | 300 mg bid |
| Paroxetine | 20 mg once daily | 50 mg once daily |
Delusional disorder? To distinguish hypochondriasis from delusional disorder (somatic type), consider the patient’s pattern of insight:
- Hypochondriacal patients often vacillate between poor and excellent insight, depending on their distress level.10 They may acknowledge the irrationality of their fears, then later be convinced they have a disease.
- Patients with delusional disorder are convinced they have a serious health threat, despite the absence of medical confirmation. These patients are considered to have a primary psychotic disorder that requires antipsychotic treatment.
TREATING PRIMARY SYMPTOMS
Drug therapy. When hypochondriasis is secondary—such as to depression or panic disorder—treat the primary condition first.11,12 For primary hypochondriasis, selective serotonin reuptake inhibitors (SSRIs) such as fluoxetine, paroxetine, or fluvoxamine have shown benefit, mostly in open-label studies. An uncontrolled case series suggests that nefazodone—with mixed serotonin reuptake inhibition and agonist properties—also may help patients with hypochondriasis.13 In the only published controlled study, fluoxetine was more effective than placebo for treating hypochondriasis.10
Continue drug therapy, when used, for at least 8 weeks, with each dosage maintained for at least 4 weeks. If patients do not respond to lower SSRI dosages, increase to the higher dosages reported to be more effective for OCD (Table 3).14
Except for primary illness phobia, hypochondriasis has not been shown to respond to tricyclics, benzodiazepines, or dopaminergic blockers. In our experience, electroconvulsive therapy—although inadequately studied—may help treat patients with severe, treatment-refractory hypochondriasis with marked somatization.
Psychotherapy. Cognitive-behavioral therapy (CBT)—challenging patients’ irrational fears about illness and teaching them problem-solving tools—is effective in treating hypochondriasis.15 CBT can help patients understand that distorted thoughts lead to their sad or anxious moods.
Instructing patients to keep thought diaries can help them identify irrational fears and use cognitive restructuring to correct their faulty schemas. Tailor your cognitive therapy techniques to target the patient’s level of insight at the time of therapy.
Effective behavioral techniques may include setting limits on doctor visits, checking behaviors, reassurance seeking, etc. Repeated exposure to feared stimuli such as needles, white lab coats, blood pressure cuffs, medical dialogue, or hospital wards can help the patient habituate to the anxiety.
Relaxation techniques, a healthy diet, and exercise are also useful. Relaxation exercises—such as diaphragmatic breathing, progressive muscle relaxation, and visual imagery—may help patients manage anxiety by reducing CNS and autonomic nervous system arousal.
Bottom line
Hypochondriasis’ cognitive dysfunction is treatable, once an accurate diagnosis is made. Using a checklist can help you differentiate hypochondriasis from other medical and psychiatric disorders. A trusting doctor-patient relationship enhances outcome.
Related resources
- Fallon BA., Feinstein SB. Hypochondriasis: clinical, theoretical, and therapeutic aspects. In: Oldham J (ed). Review of psychiatry (vol. 20) Washington, DC: American Psychiatric Press, 2001:27-60.
- Cantor C, Fallon BA. Phantom illness: shattering the myth of hypochondria Boston: Houghton Mifflin Company, 1996.
- Starcevic V, Lipsitt DR (eds). Hypochondriasis: modern perspectives on an ancient malady New York: Oxford University Press, 2001.
Drug brand names
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Nefazodone • Serzone
- Paroxetine • Paxil
A hypochondria “checklist” can help you sort through many overlapping medical and psychiatric disorders and increase your chances of making an accurate diagnosis. Then—by addressing hypochondria’s cognitive dysfunction—you can help patients achieve partial or full remission and change their distressing behaviors.
We offer a checklist that is useful in our practice and suggest behavioral therapies and medications that can help calm these patients’ excessive, unwarranted fears.
WORKING AS A TEAM
Ideal approach. Because hypochondriasis has features of medical and mental illness, working with the patient’s primary care physician is ideal. Physicians often consider these patients difficult because they demand a lot of time, support, and reassurance. Together, you can:
- offer the patient a healthy level of compassion and empathy to establish a positive therapeutic alliance
- set appropriate time limits and guidelines for the patient’s care
- dissuade patients from “doctor shopping”
- set limits on how often patients may visit their doctors and request reassurance.
Hypochondriasis: Persistent, unwarranted distress
Hypochondriasis is an excessive and persistent fear or belief that one has a serious illness, despite medical reassurance and lack of diagnostic findings that would warrant the health concern. If a medical disorder is present, the distress and preoccupation exceed what the patient’s physician considers reasonable. Illness preoccupation is intense enough to cause great distress or to interfere with daily functioning and may cause the person to miss work or cancel social engagements.1
DSM-IV criteria. A patient’s fear or conviction that he or she has a serious health threat must persist at least 6 months and may be accompanied by specific somatic symptoms, vague symptoms,1 or no symptoms.2 Hypochondriacal preoccupation may be stable over time, where one illness concern dominates, or it may shift—from fear of AIDS to fear of a heart attack.
A common disorder. Hypochondriasis occurs in 4 to 6% of the general medical population. In psychiatric or medical clinics, women are identified as having hypochondriasis three to four times more often than men. Average age of onset is in the early 20s.3
For example, you may indicate to the patient, “I will reassure you only at office visits (not by phone), the office visits will be limited to once a month, and during each visit I will reassure you no more than once.”
A doctor-patient relationship based on mutual trust and respect is vital when you treat a patient with hypochondriasis. You can help primary care physicians provide more empathic treatment by explaining that patients do not feign or desire this distressing condition.
DIAGNOSTIC FEATURES
Patients with hypochondriasis tend to be hyper-vigilant about normal physiologic fluctuations and bodily sensations, often misinterpreting them as life-threatening or serious enough to require immediate medical attention. This excessive focus on benign symptoms (such as an accelerated heart rate, sweating, or a bump on the skin) and the cognitive distortion of their significance result in increased anxiety, bodily checking, and doctor visits (Box).1-4
Presentations. Hypochondriasis has three common presentations: disease conviction, disease fear, and bodily preoccupation (Table 1).5 Psychiatrists are most likely to see disease fear, as patients with this predominant symptom tend to realize that fear plays too prominent a role in their lives. Physicians in medical practice are more likely to encounter patients with high levels of disease conviction or somatic preoccupation.
Psychiatric comorbidity. Hypochondriasis is highly comorbid with Axis I and Axis II disorders, which complicate treatment. Nearly one-half of patients with hypochondriasis also have dysthymia (45%) or major depression (43%). Other comorbidities include phobias (38%), somatization disorder (21%), panic disorder (17%), and obsessive-compulsive disorder (8%).6 Patients with hypochondriasis are three times more likely than the general population to have personality disorders;6,7 the prognosis is believed to be more promising for patients without personality disorders.
Distinguishing between primary and secondary hypochondriasis is important. Treating a primary psychiatric disorder often alleviates the symptoms of secondary hypochondriasis, particularly when hypochondriasis masks depression.
HYPOCHONDRIASIS CHECKLIST
Underlying medical disorder? Before diagnosing hypochondriasis, review the medical workup for underlying disease or illness. Medical conditions sometimes go undetected when physicians assume that complaints are an expression of longstanding hypochondriasis.
Table 1
Three common presentations of hypochondriasis
| Predominant symptom | Characterization |
|---|---|
| Disease conviction | Patient may appear delusional in believing he or she has a disease and in persistent efforts to find a doctor who will make the “accurate” diagnosis |
| Disease fear | Patient may avoid doctors because of fear associated with confirmation of a dreaded disease |
| Bodily preoccupation | Patient may complain of multiple somatic symptoms, which mask underlying fear or belief of having a serious disease |
Sometimes a patient may become anxious when mild or vague signs and symptoms do not yet meet established diagnostic criteria for a medical disorder. An effective approach is to provide ongoing support, avoid excessive diagnostic tests, and help the patient make the best use of his or her functional capacities while living with uncertainty.
Functional somatic syndrome? Fibromyalgia and chronic fatigue syndrome do not represent hypochondriasis,8 although they may be exacerbated by comorbid psychiatric disorders. Both disorders have diagnostic criteria and specified courses and have been studied to identify psychiatric comorbidity.
Transient or sustained? After it is clear that the patient is not suffering from a medical problem, determine whether hypochondriasis is transient or fully diagnostic:
- If transient, the patient may only need to be educated about how overattention may amplify symptoms; reassure him or her that a full medical workup has been negative.
- If fully diagnostic, reassurance may work for only a few days or weeks; the return of the fear or conviction helps establish the diagnosis.
Somatoform disorder? Distinguish hypochondriasis from other somatoform disorders (Table 2). In practice, the terms “hypochondriac” and “somatizer” are commonly used interchangeably, but the distinction needs to be clear. Hypochondriasis is primarily a disorder of abnormal cognition, in which symptom meaning is of greatest concern. Somatization is primarily a disorder of abnormal sensation, in which the symptoms themselves are the overwhelming focus of attention.
Anxiety disorder? Patients with generalized anxiety disorder may worry about illness, but they also worry about other life issues. Patients with panic disorder may have intense hypochondriacal concerns (such as having a heart attack), but these worries tend to be related to panic symptoms and resolve when the panic disorder is treated.
Obsessive compulsive disorder? Like obsessive-compulsive disorder (OCD), hypochondriasis is characterized by recurrent intrusive thoughts that create heightened anxiety and distress. To relieve their anxiety, patients with hypochondriasis engage in compulsions, such as:
- undergoing extensive medical tests
- seeking habitual reassurance from doctors and family
- consulting medical literature
- performing repeated body checks for perceived lumps or bumps
- avoiding activities that trigger their health-related stress.9
Table 2
How to distinguish somatoform disorders
| Disorder | Patient focuses on… |
|---|---|
| Hypochondriasis | physical symptoms’ meaning (abnormal cognition) |
| Somatization disorder | multiple unexplained physical symptoms (abnormal sensation) |
| Body dysmorphic disorder | perceived abnormal bodily appearance |
| Conversion disorder | motor or sensory function abnormalities that develop soon after life stressors or conflict |
| Pain disorder | intense pain, in which psychological factors contribute to pain onset, severity, or maintenance |
OCD and hypochondriasis also may share the diagnostic feature of pathologic doubt; patients’ uncertainty in appraising a situation leads to additional checking and reassurance-seeking behaviors. The immediate relief gained by these compulsions reinforces the patient’s urge to engage in more maladaptive behaviors and sends a stronger message to the brain that these behaviors are needed to prevent harm.
Ironically, the emergence of a real medical ailment—despite hypochondriacal worry—may force the patient to re-evaluate the usefulness of behaviors motivated by trying to avoid harm. A hypochondriacal patient who was diagnosed with optic neuritis and possible multiple sclerosis recently said to these authors, “I had always thought that by being vigilant I could keep illnesses away. Now I know that’s not true.”
Although hypochondriasis and OCD have similarities, certain clinical distinctions exist. Patients with hypochondriasis worry about having an illness, whereas OCD patients with somatic obsessions fear developing or transmitting an illness. A hypochondriacal patient might fear having AIDS or cancer despite reassurance from doctors, while an OCD patient more typically would fear contracting or transmitting the disease (a contamination obsession) and would engage in excessive behaviors to reduce the risk of developing the disease.
Depressive disorder? Unlike the anxious-worrying version of hypochondriasis, the depressive version is more fatalistic. Patients may be convinced they are dying of a dreaded disease, often believing it to be punishment for an indiscretion, such as marital infidelity. Or they may suddenly become hypochondriacal with mild depressive features, unaware that the actual problem is unresolved bereavement (hypochondriasis with secondary depression). The appropriate diagnosis is primary depressive disorder with secondary hypochondriacal features when depression dominates the presentation and preceded the illness fears.
Table 3
Recommended dosages for treating primary hypochondriasis
| Drug | Starting dosage | Maximum dosage |
|---|---|---|
| Fluoxetine | 10 mg/d if panic symptoms are present; 20 mg/d otherwise | 80 mg/d |
| Fluvoxamine | 50 mg at bedtime | 150 mg bid |
| Nefazodone | 100 mg bid | 300 mg bid |
| Paroxetine | 20 mg once daily | 50 mg once daily |
Delusional disorder? To distinguish hypochondriasis from delusional disorder (somatic type), consider the patient’s pattern of insight:
- Hypochondriacal patients often vacillate between poor and excellent insight, depending on their distress level.10 They may acknowledge the irrationality of their fears, then later be convinced they have a disease.
- Patients with delusional disorder are convinced they have a serious health threat, despite the absence of medical confirmation. These patients are considered to have a primary psychotic disorder that requires antipsychotic treatment.
TREATING PRIMARY SYMPTOMS
Drug therapy. When hypochondriasis is secondary—such as to depression or panic disorder—treat the primary condition first.11,12 For primary hypochondriasis, selective serotonin reuptake inhibitors (SSRIs) such as fluoxetine, paroxetine, or fluvoxamine have shown benefit, mostly in open-label studies. An uncontrolled case series suggests that nefazodone—with mixed serotonin reuptake inhibition and agonist properties—also may help patients with hypochondriasis.13 In the only published controlled study, fluoxetine was more effective than placebo for treating hypochondriasis.10
Continue drug therapy, when used, for at least 8 weeks, with each dosage maintained for at least 4 weeks. If patients do not respond to lower SSRI dosages, increase to the higher dosages reported to be more effective for OCD (Table 3).14
Except for primary illness phobia, hypochondriasis has not been shown to respond to tricyclics, benzodiazepines, or dopaminergic blockers. In our experience, electroconvulsive therapy—although inadequately studied—may help treat patients with severe, treatment-refractory hypochondriasis with marked somatization.
Psychotherapy. Cognitive-behavioral therapy (CBT)—challenging patients’ irrational fears about illness and teaching them problem-solving tools—is effective in treating hypochondriasis.15 CBT can help patients understand that distorted thoughts lead to their sad or anxious moods.
Instructing patients to keep thought diaries can help them identify irrational fears and use cognitive restructuring to correct their faulty schemas. Tailor your cognitive therapy techniques to target the patient’s level of insight at the time of therapy.
Effective behavioral techniques may include setting limits on doctor visits, checking behaviors, reassurance seeking, etc. Repeated exposure to feared stimuli such as needles, white lab coats, blood pressure cuffs, medical dialogue, or hospital wards can help the patient habituate to the anxiety.
Relaxation techniques, a healthy diet, and exercise are also useful. Relaxation exercises—such as diaphragmatic breathing, progressive muscle relaxation, and visual imagery—may help patients manage anxiety by reducing CNS and autonomic nervous system arousal.
Bottom line
Hypochondriasis’ cognitive dysfunction is treatable, once an accurate diagnosis is made. Using a checklist can help you differentiate hypochondriasis from other medical and psychiatric disorders. A trusting doctor-patient relationship enhances outcome.
Related resources
- Fallon BA., Feinstein SB. Hypochondriasis: clinical, theoretical, and therapeutic aspects. In: Oldham J (ed). Review of psychiatry (vol. 20) Washington, DC: American Psychiatric Press, 2001:27-60.
- Cantor C, Fallon BA. Phantom illness: shattering the myth of hypochondria Boston: Houghton Mifflin Company, 1996.
- Starcevic V, Lipsitt DR (eds). Hypochondriasis: modern perspectives on an ancient malady New York: Oxford University Press, 2001.
Drug brand names
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Nefazodone • Serzone
- Paroxetine • Paxil
1. Diagnostic and statistical manual of mental disorders (4th ed-text revision). Washington, DC: American Psychiatric Association, 2000.
2. Task Force on DSM-IV. DSM-IV options book. Washington DC: American Psychiatric Association, 1991.
3. Barsky AJ, Wyshak G, Klerman GL, Lathan KS. The prevalence of hypochondriasis in medical outpatients. Soc Psychiatry Psychiatr Epidemiol 1990;25(2):89-94.
4. Salkovskis PM, Clark DM. Panic and hypochondriasis. Adv Behav Res Ther 1993;15:23-48.
5. Pilowsky I. Dimensions of hypochondriasis. Br J Psychiatry 1967;113(494):89-93.
6. Barsky AJ, Wyshak G, Klerman GL. Psychiatric comorbidity in DSM-III-R hypochondriasis. Arch Gen Psychiatry 1992;49(2):101-8.
7. Kellner R. The prognosis of treated hypochondriasis: a clinical study. Acta Psychiatr Scand 1983;67(2):69-79.
8. Noyes R, Jr, Kathol RG, Fisher M, Phillips BM, et al. The validity of DSM-III-R hypochondriasis. Arch Gen Psychiatry 1993;50(12):961-70.
9. Fallon BA, Qureshi AI, Laje G, Klein B. Hypochondriasis and its relationship to obsessive-compulsive disorder. Psychiatr Clin North Am 2000;23(3):605-16.
10. Fallon BA, Schneier FR, Marshall R, Campeas R, et al. The pharmacotherapy of hypochondriasis. Psychopharmacol Bull 1996;32:607-11.
11. Kellner R, Fava GA, Lisansky J, et al. Hypochondriacal fears and beliefs in DSM-III melancholia: changes with amitriptyline. J Affect Disord 1986;10(1):21-6.
12. Noyes R, Jr, Reich J, Clancy J, O’Gorman TW. Reduction in hypochondriasis with treatment of panic disorder. Br J Psychiatry 1986;149:631-5(erratum in Br J Psychiatry 1987;150:273).
13. Kjernisted KD, Ennis MW, Lander M. An open-label clinical trial of nefazodone in hypochondriasis. Psychosomatics 2002;43:290-4.
14. Fallon BA. Pharmacologic strategies for hypochondriasis. In: Starcevic V, Lipsitt DR (eds). Hypochondriasis: modern perspectives on an ancient malady. New York: Oxford University Press, 2001;329-51.
15. Warwick HMC, Salkovskis PM. Hypochondriasis. In: Scott J, Williams JMG, Beck AT (eds). Cognitive therapy in clinical practice: an illustrative casebook. London; Routledge, 1989;78-102.
1. Diagnostic and statistical manual of mental disorders (4th ed-text revision). Washington, DC: American Psychiatric Association, 2000.
2. Task Force on DSM-IV. DSM-IV options book. Washington DC: American Psychiatric Association, 1991.
3. Barsky AJ, Wyshak G, Klerman GL, Lathan KS. The prevalence of hypochondriasis in medical outpatients. Soc Psychiatry Psychiatr Epidemiol 1990;25(2):89-94.
4. Salkovskis PM, Clark DM. Panic and hypochondriasis. Adv Behav Res Ther 1993;15:23-48.
5. Pilowsky I. Dimensions of hypochondriasis. Br J Psychiatry 1967;113(494):89-93.
6. Barsky AJ, Wyshak G, Klerman GL. Psychiatric comorbidity in DSM-III-R hypochondriasis. Arch Gen Psychiatry 1992;49(2):101-8.
7. Kellner R. The prognosis of treated hypochondriasis: a clinical study. Acta Psychiatr Scand 1983;67(2):69-79.
8. Noyes R, Jr, Kathol RG, Fisher M, Phillips BM, et al. The validity of DSM-III-R hypochondriasis. Arch Gen Psychiatry 1993;50(12):961-70.
9. Fallon BA, Qureshi AI, Laje G, Klein B. Hypochondriasis and its relationship to obsessive-compulsive disorder. Psychiatr Clin North Am 2000;23(3):605-16.
10. Fallon BA, Schneier FR, Marshall R, Campeas R, et al. The pharmacotherapy of hypochondriasis. Psychopharmacol Bull 1996;32:607-11.
11. Kellner R, Fava GA, Lisansky J, et al. Hypochondriacal fears and beliefs in DSM-III melancholia: changes with amitriptyline. J Affect Disord 1986;10(1):21-6.
12. Noyes R, Jr, Reich J, Clancy J, O’Gorman TW. Reduction in hypochondriasis with treatment of panic disorder. Br J Psychiatry 1986;149:631-5(erratum in Br J Psychiatry 1987;150:273).
13. Kjernisted KD, Ennis MW, Lander M. An open-label clinical trial of nefazodone in hypochondriasis. Psychosomatics 2002;43:290-4.
14. Fallon BA. Pharmacologic strategies for hypochondriasis. In: Starcevic V, Lipsitt DR (eds). Hypochondriasis: modern perspectives on an ancient malady. New York: Oxford University Press, 2001;329-51.
15. Warwick HMC, Salkovskis PM. Hypochondriasis. In: Scott J, Williams JMG, Beck AT (eds). Cognitive therapy in clinical practice: an illustrative casebook. London; Routledge, 1989;78-102.
Preventing late-life suicide: 6 steps to detect the warning signs
CASE REPORT: I have a gun
Mr. V, age 77, appears depressed and anxious during his appointment at a mental hygiene clinic. He reports insomnia, concentration trouble, and anhedonia. He tells the psychiatrist he keeps a loaded gun at home and is not sure he can control his suicidal impulses.
The patient is Caucasian and has a history of heart failure, pulmonary disease, and type 2 diabetes. His wife died 18 months ago. He lives alone, but his sister lives nearby. He recently received a right hip replacement, which required 3 months of rehabilitation in a nursing home to recover from surgical complications. He still has trouble walking.
As in Mr. V’s case, treating older patients referred for psychiatric care often involves evaluating suicide risk. His age, race, gender, depressed mood, recent bereavement, and medical ailments place him in the population at highest risk of suicide (Box, Table 1).1-8
Approximately 20% of all suicides in the United States are committed by persons age 65 or older,1 who account for 13% of the total population. The suicide rate among persons older than 75 is three times higher than it is for the young.2 Older Caucasian men have the highest per-capita rate of completed suicide, compared with any other group of Americans.3
Psychiatric disorders. The rates of Axis I disorders among older persons who commit suicide fall within the average range for all age groups (70 to 90%). However, the types of disorders seen in the older population differ from those of younger suicides (Table 1).4-8
Affective illness has been termed “the predominant psychopathology associated with suicide in later life.”4 Among older persons who commit suicide, three-fourths (76%) have diagnosable mood disorders4 and nearly two-thirds (63%) have depression.6 Contributing risk factors include alcoholism and substance abuse,4,6,7 Axis II disorders, and dementia.6
Losses and medical illness. In later life, bereavement, loss of independence, or financial reversals may lead to depression. Older persons who take their own lives also tend to have greater physical health burdens and more functional disabilities than those who do not commit suicide.6,8
This article describes an age-based psychiatric workup of the suicidal older patient, including factors to consider when screening for depressive symptoms, prescribing drug therapy, and determining the need for hospitalization.
AGE-BASED CLINICAL WORKUP
For older patients who report suicidal ideation, an age-appropriate workup—using clinical interviews and screening instruments—is essential. The clinical interview can build rapport and gather information about the patient’s suicidal plan or intent. Based on our experience, we recommend the following 6-step screening interview, summarized in Table 2.
- Ask about a specific plan. Does the patient have the means readily available to carry out this plan? What is the timeline (imminent versus vaguely futuristic)? Does the patient report having control over this plan?
- Gather a suicide history. Has the patient attempted suicide before? By what means? Is there a family history of suicide? If yes, by what means did this family member commit suicide, and how was the patient affected?
- Assess social status. How isolated is the patient? Have there been recent changes in his or her social circle, such as loss of a spouse? Can the patient identify at least one person who would be negatively affected by the suicide?
- Assess medical health. Does the patient suffer from chronic pain? Does the patient have a recently diagnosed medical condition? Has a longstanding medical condition become more debilitating? Does the patient report feeling hopeless about impending medical difficulties? Has he or she been keeping regularly scheduled medical appointments with outpatient clinicians?
- Assess mental health. Does the patient meet DSM-IV criteria for depression or schizophrenia, which are associated with high suicide risk? Does he or she report being hopeless or helpless? Is the suicidal ideation ego dystonic?
- Ascertain clinical signs of suicidal intent. Has the patient:
Table 1
Suicide risk with mental and physical illness, by patient age
| Risk factors | Young (21 to 34 yrs) | Middle-aged (35 to 54 yrs) | Young-old (55 to 74 yrs) | Elderly (77+ yrs) |
|---|---|---|---|---|
| Psychiatric disorders | • | • | • | • |
| Mood disorders | ○ | • | • | |
| Alcohol abuse | ○ | • | ○ | |
| Primary psychoses | • | ○ | ||
| Personality disorders | ○ | |||
| Physical ailments | • | • | ||
| • Significant risk factor ○ Potential risk factor | ||||
| Source: Compiled from information in references 4-8. | ||||
CASE REPORT continued: Some telling signs
Mr. V’s laboratory screening reveals slightly elevated serum glucose and mild anemia. An ECG reveals a type I heart block, but all other lab results are unremarkable. His sister reports he recently gave away his dog, which he and his wife had owned for many years. He has also mentioned a desire to revise his will when speaking to other family members. Hospital records indicate he has missed numerous medical appointments over the past 4 months.
SCREENING INSTRUMENTS
Psychological assessments can often buttress the clinical interview findings. Several measurements are well-suited for detecting suicidal risk and concomitant depression (Table 3).
Beck SSI-C. The Beck Scale for Suicide Ideation – Current (SSI-C) assesses a patient’s preparation and motivation to commit suicide.9 This short (19-item) self-report measure asks patients to rate their wish to die, desire to attempt suicide, duration (and frequency) of suicidal thoughts, sense of control over suicide, and deterrents they face. The SSI-C helps to measure or monitor suicidality and is reliable and valid for psychiatric outpatients.9
BDI-II. The Beck Depression Inventory—recently revised in a second edition (BDI-II)10—can be useful because depression is one of the strongest risk factors for elder suicide. The 21-item BDI-II—a psychometrically sound, self-report instrument—asks about general symptoms of depression and gauges their severity. It can be applied to diverse patient populations and ages11 and is appropriate for older patients who are also being treated medically.
Beck Hopelessness Scale. Hopelessness has been recognized as a possible harbinger of suicide.12 One study showed that depression became a clinically meaningful suicide predictor only when accompanied by hopelessness.13
A score of 10 or more on the Beck Hopelessness Scale identified 91% of patients in one study who eventually committed suicide. The hopelessness patients expressed on this scale more strongly differentiated between those who did or did not commit suicide than did their scores on the BDI or SSI-C.14
Table 2
6-step clinical interview with an older suicidal patient
|
|
| Source: Adapted from the Cincinnati Veterans Affairs Medical Center general psychological suicide assessment |
HRSD-R. The revised Hamilton Rating Scale for Depression (HRSD-R) documents patients’ levels of mood disturbance and suicidality. One item in this 21-item, clinician-administered instrument specifically asks about the patient’s level of suicidality in the past week. The scale has well-documented reliability and validity and is appropriate for psychiatric populations.15
CASE REPORT continued: Alarming findings
Along with the clinical interview, Mr. V. is screened with the Beck Hopelessness Scale and Beck Depression Inventory-II. These instruments are chosen because they are easy to administer, and patients can readily comprehend the questions—even when under duress. Mr. V’s results reveal moderate depression and severe hopelessness.
INPATIENT VS. OUTPATIENT CARE
Older patients are often referred to a psychiatrist because of vague suicidal ideation, but they may also present in an acute crisis—with immediate plans for suicide and readily accessible means. The first concern for their safety is to ensure they are not left alone.
Patient interview. First, listen empathetically and ask detailed questions, especially ones that remind patients of their daily connections and responsibilities. For instance, ask, “Do you have children who would be affected by your decision?” Address patients’ immediate needs, such as hunger, thirst, or pain.16 Work on building a therapeutic alliance before asking questions that may appear trivial to agitated patients (such as tasks assessing cognitive abilities).
Avoid arguing with patients, and refrain from offering advice or sermonizing. Allow them to describe their emotions, and communicate that you understand their concerns. Discuss how they can expect to receive treatment to ease their discomfort. Inform them that mental health specialists can treat them and monitor their progress.
Hospitalization. Begin discussing treatment options and broach the notion of hospital admission if necessary. One way to foster an alliance is to frame inpatient care as a way of helping them recover from their crisis in a safe environment.
To ensure patient safety, it is best to err on the side of admission. Admitting the suicidal patient not only guarantees strict supervision but also allows time for necessary psychological assessment. Hospitalization may also allow family members to remove any weapons or hazardous conditions from the patient’s home.
Including the family in problem-solving is especially important when managing older suicidal patients. For patients who are isolated from family or friends, recovery may depend on improving their support network.
Table 3
Comparing screening instruments for suicide risk
| Measure | Description | Time (minutes) |
|---|---|---|
| Beck Depression Inventory (BDI) | 21-item, self-administered; identifies depressive symptoms in past week | 10 |
| Beck Hopelessness Scale (BHS) | 20-item, self-administered; measures hopelessness, fatalism, and pessimism in past week | 5 |
| Beck Scale for Suicide Ideation-Current (SSI-C) | 19-item, self-administered; gauges suicidal intention | 10 |
| Hamilton Rating Scale for Depression-revised (HRSD-R) | 21-item, clinician-administered; rates depressive symptoms in past week | 25 |
Outpatient care. Not all acutely suicidal older patients require hospital admission. They may be safely managed as outpatients if they:
- have strong social support
- are not isolated
- have no access to firearms or other dangerous weapons.
Safety can be enhanced by having family members take responsibility for the senior’s well-being and by asking the patient to contract for safety. A safety contract may include:
- verbal confirmation—and ideally a written statement—that the patient will not commit suicide within a specified period
- a list of people the patient will contact when feeling suicidal
- steps being taken to monitor the patient’s welfare.
Finally, schedule follow-up appointments soon after discharge to certify patients are being closely monitored. To encourage outpatient medication adherence, build strong alliances with family members and ask patients to bring in their pill bottles during follow-up appointments.
CASE REPORT continued: Observation begins
The staff is clearly concerned about Mr. V’s suicide risk and requests that he voluntarily admit himself to the VA hospital. This decision is based on his level of isolation, the lethality of his suicide plan, access to a weapon, and the depression and hopelessness revealed by his screening tests. He reluctantly agrees and is admitted to the inpatient psychiatric unit for observation and treatment by a geriatric internist and a geriatric psychiatrist.
DRUG THERAPY FOR SUICIDALITY
For patients with mild depressive symptoms, psychotherapy may be sufficient to manage depression associated with suicidality. However, those with moderate-to-severe depression require both drug treatment and psychotherapy.
Drug selection depends upon the underlying psychiatric illness. If the older patient is experiencing a depressive disorder, a selective serotonin reuptake inhibitor (SSRI) or another antidepressant could serve as first-line treatment (Table 4). These medications are safe for suicidal patients because they are not fatal in overdose.
Administration. Because age-related changes in pharmacokinetics and spharmacodynamics can slow medication clearance, reduced dosages usually achieve a therapeutic effect and minimize the risk of side effects in geriatric patients.
Antidepressants commonly used for older patients are shown in Table 4. Excepting citalopram and escitalopram, these dosages are lower than usual. We start healthy older patients on one-half the usual dosage and those who are medically ill or have neurodegenerative disorders on one-third to one-fourth the usual dosage. We also titrate more slowly to reduce the risk of side effects.
Table 4
Antidepressants commonly used to treat geriatric depression
| Medication | Recommended dosage (mg/d) |
|---|---|
| SSRIs | |
| Citalopram | 20 to 40 |
| Escitalopram | 10 to 20 |
| Fluoxetine | 10 to 40 |
| Paroxetine | 10 to 40 |
| Sertraline | 25 to 150 |
| Others | |
| Bupropion | 100 to 400 |
| Mirtazapine | 15 to 45 |
| Venlafaxine | 75 to 225 |
As in younger patients, the most common side effects of SSRIs in older patients include GI difficulties, overactivation, and sexual dysfunction. Paroxetine’s potential for anticholinergic effects may be a concern for some older patients.
Drug-drug interactions are of great concern when treating older patients, who take an average of six to nine medications per day.17 Compared with other SSRIs, fluoxetine and paroxetine, are more likely to inhibit cytochrome P-450 enzymes 2D6 and 3A4. They could thus increase blood levels of drugs taken concomitantly that are substrates of 2D6 or 3A4.
Antidepressant side effects can sometimes be used to advantage. For example, mirtazapine’s sedating property at lower dosages could help older patients with insomnia.
CASE REPORT concluded: Finding support
Mr. V is started on an SSRI antidepressant. He also receives supportive and milieu therapy and coping skills training. During his hospitalization, Mr. V contracts for safety and allows his sister to remove the handgun from his home.
Upon discharge, Mr. V is referred to a day treatment program that operates 3 to 5 days a week and offers case management, group therapy, and individual psychotherapy. The program helps him meet other older patients and allows him to discuss his life’s accomplishments and losses with others his age. His sister is an integral part of the program, and he maintains close contact with her.
Mr. V reports vague and occasional suicidal ideation, with no specific plan or intent. He and his sister note that his medical condition improved soon after his psychiatric condition stabilized.
Related resources
- Surgeon General’s Call to Action to Prevent Suicide. www.mental-health.org/suicideprevention/calltoaction.pdf
- Centers for Disease Control and Prevention. National Center for Injury Prevention and Control.
Drug brand names
- Bupropion • Wellbutrin
- Citalopram • Celexa
- Escitalopram • Lexapro
- Fluoxetine • Prozac
- Mirtazapine • Remeron
- Paroxetine • Paxil
- Sertraline • Zoloft
- Venlafaxine • Effexor
Disclosure
Drs. Montross reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Mohamed is a speaker and consultant to Forest Laboratories and Eli Lilly and Co.
Dr. Kasckow receives research support from, is a consultant to, and is a speaker for Forest Laboratories, Eli Lilly and Co., Pfizer Inc., and Janssen Pharmaceutica.
Dr. Zisook is a consultant to GlaxoSmithKline and a speaker for GlaxoSmithKline, Wyeth Pharmaceuticals, Pfizer Inc., Forest Laboratories, and Bristol-Myers Squibb Co.
1. Centers for Disease Control and Prevention. Surveillance for Injuries and Violence Among Older Adults (CDC Surveillance Summary, December 17, 1999, Chap. 3:27-50). www.cdc.gov/mmwr/PDF/SS/SS4808.pdf
2. Kaplan HI, Sadock BJ. Synopsis of psychiatry (6th ed). Baltimore: Williams & Wilkins, 1991.
3. Lyon DE, Chase LS, Farrell SP. Using an interview guide to assess suicidal ideation. Nurse Practitioner 2002;27:26-31.
4. Conwell Y, Lyness JM, Duberstein P, et al. Completed suicide among older patients in primary care practices: A controlled study. J Am Geriatr Soc 2000;48:23-9.
5. Conwell Y, Duberstein PR, Cox C, et al. Relationships of age and Axis I diagnoses in victims of completed suicide: A psychological autopsy study. Am J Psychiatry 1996;153:1001-8.
6. Harwood D, Hawton K, Hope T, Jacoby R. Psychiatric disorder and personality factors associated with suicide in older people: A descriptive and case-control study. Int J Geriatr Psychiatry 2001;16:155-65.
7. Henriksson MM, Marttunen MJ, Isometsa ET, et al. Mental disorders in elderly suicide. Int Psychogeriatr 1995;7:275-86.
8. Conwell Y, Duberstein PR, Caine ED. Risk factors for suicide in later life. Biol Psychiatry 2002;52:193-204.
9. Beck AT, Brown GK, Steer RA. Psychometric characteristics of the Scale for Suicide Ideation with psychiatric outpatients. Behav Res Ther 1997;35:1039-46.
10. Beck AT, Steer RA. Manual for the Beck Depression Inventory. San Antonio, TX: The Psychological Corporation, 1987.
11. Beck AT, Steer RA, Garbin MG. Psychometric properties of the Beck Depression Inventory: Twenty-five years later. Clin Psychol Rev 1988;8:77-100.
12. Beck AT, Weissman A, Lester D, Trexler L. The measurement of pessimism: The hopelessness scale. J Consult Clin Psychol 1974;42:861-5.
13. Drake RE, Cotton PG. Depression, hopelessness and suicide in chronic schizophrenia. Br J Psychiatry 1986;148:554-9.
14. Beck AT, Steer RA, Kovacs M, Garrison B. Hopelessness and eventual suicide: A 10-year perspective study of patients hospitalized with suicidal ideation. Am J Psychiatry 1985;142:559-63.
15. Riskind JH, Beck AT, Brown G, Steer RA. Taking the measure of anxiety and depression: Validity of the reconstructed Hamilton Scales. J Nerv Ment Dis 1987;175:474-9.
16. Lamberg L. Psychiatric emergencies call for comprehensive assessment and treatment. JAMA 2002;288:686-7.
17. Sadavoy J, Lazarus LW, Jarvik LF. Grossberg GT (eds). Comprehensive review of geriatric psychiatry (2nd ed). Washington, DC: American Psychiatric Press, 1996.
CASE REPORT: I have a gun
Mr. V, age 77, appears depressed and anxious during his appointment at a mental hygiene clinic. He reports insomnia, concentration trouble, and anhedonia. He tells the psychiatrist he keeps a loaded gun at home and is not sure he can control his suicidal impulses.
The patient is Caucasian and has a history of heart failure, pulmonary disease, and type 2 diabetes. His wife died 18 months ago. He lives alone, but his sister lives nearby. He recently received a right hip replacement, which required 3 months of rehabilitation in a nursing home to recover from surgical complications. He still has trouble walking.
As in Mr. V’s case, treating older patients referred for psychiatric care often involves evaluating suicide risk. His age, race, gender, depressed mood, recent bereavement, and medical ailments place him in the population at highest risk of suicide (Box, Table 1).1-8
Approximately 20% of all suicides in the United States are committed by persons age 65 or older,1 who account for 13% of the total population. The suicide rate among persons older than 75 is three times higher than it is for the young.2 Older Caucasian men have the highest per-capita rate of completed suicide, compared with any other group of Americans.3
Psychiatric disorders. The rates of Axis I disorders among older persons who commit suicide fall within the average range for all age groups (70 to 90%). However, the types of disorders seen in the older population differ from those of younger suicides (Table 1).4-8
Affective illness has been termed “the predominant psychopathology associated with suicide in later life.”4 Among older persons who commit suicide, three-fourths (76%) have diagnosable mood disorders4 and nearly two-thirds (63%) have depression.6 Contributing risk factors include alcoholism and substance abuse,4,6,7 Axis II disorders, and dementia.6
Losses and medical illness. In later life, bereavement, loss of independence, or financial reversals may lead to depression. Older persons who take their own lives also tend to have greater physical health burdens and more functional disabilities than those who do not commit suicide.6,8
This article describes an age-based psychiatric workup of the suicidal older patient, including factors to consider when screening for depressive symptoms, prescribing drug therapy, and determining the need for hospitalization.
AGE-BASED CLINICAL WORKUP
For older patients who report suicidal ideation, an age-appropriate workup—using clinical interviews and screening instruments—is essential. The clinical interview can build rapport and gather information about the patient’s suicidal plan or intent. Based on our experience, we recommend the following 6-step screening interview, summarized in Table 2.
- Ask about a specific plan. Does the patient have the means readily available to carry out this plan? What is the timeline (imminent versus vaguely futuristic)? Does the patient report having control over this plan?
- Gather a suicide history. Has the patient attempted suicide before? By what means? Is there a family history of suicide? If yes, by what means did this family member commit suicide, and how was the patient affected?
- Assess social status. How isolated is the patient? Have there been recent changes in his or her social circle, such as loss of a spouse? Can the patient identify at least one person who would be negatively affected by the suicide?
- Assess medical health. Does the patient suffer from chronic pain? Does the patient have a recently diagnosed medical condition? Has a longstanding medical condition become more debilitating? Does the patient report feeling hopeless about impending medical difficulties? Has he or she been keeping regularly scheduled medical appointments with outpatient clinicians?
- Assess mental health. Does the patient meet DSM-IV criteria for depression or schizophrenia, which are associated with high suicide risk? Does he or she report being hopeless or helpless? Is the suicidal ideation ego dystonic?
- Ascertain clinical signs of suicidal intent. Has the patient:
Table 1
Suicide risk with mental and physical illness, by patient age
| Risk factors | Young (21 to 34 yrs) | Middle-aged (35 to 54 yrs) | Young-old (55 to 74 yrs) | Elderly (77+ yrs) |
|---|---|---|---|---|
| Psychiatric disorders | • | • | • | • |
| Mood disorders | ○ | • | • | |
| Alcohol abuse | ○ | • | ○ | |
| Primary psychoses | • | ○ | ||
| Personality disorders | ○ | |||
| Physical ailments | • | • | ||
| • Significant risk factor ○ Potential risk factor | ||||
| Source: Compiled from information in references 4-8. | ||||
CASE REPORT continued: Some telling signs
Mr. V’s laboratory screening reveals slightly elevated serum glucose and mild anemia. An ECG reveals a type I heart block, but all other lab results are unremarkable. His sister reports he recently gave away his dog, which he and his wife had owned for many years. He has also mentioned a desire to revise his will when speaking to other family members. Hospital records indicate he has missed numerous medical appointments over the past 4 months.
SCREENING INSTRUMENTS
Psychological assessments can often buttress the clinical interview findings. Several measurements are well-suited for detecting suicidal risk and concomitant depression (Table 3).
Beck SSI-C. The Beck Scale for Suicide Ideation – Current (SSI-C) assesses a patient’s preparation and motivation to commit suicide.9 This short (19-item) self-report measure asks patients to rate their wish to die, desire to attempt suicide, duration (and frequency) of suicidal thoughts, sense of control over suicide, and deterrents they face. The SSI-C helps to measure or monitor suicidality and is reliable and valid for psychiatric outpatients.9
BDI-II. The Beck Depression Inventory—recently revised in a second edition (BDI-II)10—can be useful because depression is one of the strongest risk factors for elder suicide. The 21-item BDI-II—a psychometrically sound, self-report instrument—asks about general symptoms of depression and gauges their severity. It can be applied to diverse patient populations and ages11 and is appropriate for older patients who are also being treated medically.
Beck Hopelessness Scale. Hopelessness has been recognized as a possible harbinger of suicide.12 One study showed that depression became a clinically meaningful suicide predictor only when accompanied by hopelessness.13
A score of 10 or more on the Beck Hopelessness Scale identified 91% of patients in one study who eventually committed suicide. The hopelessness patients expressed on this scale more strongly differentiated between those who did or did not commit suicide than did their scores on the BDI or SSI-C.14
Table 2
6-step clinical interview with an older suicidal patient
|
|
| Source: Adapted from the Cincinnati Veterans Affairs Medical Center general psychological suicide assessment |
HRSD-R. The revised Hamilton Rating Scale for Depression (HRSD-R) documents patients’ levels of mood disturbance and suicidality. One item in this 21-item, clinician-administered instrument specifically asks about the patient’s level of suicidality in the past week. The scale has well-documented reliability and validity and is appropriate for psychiatric populations.15
CASE REPORT continued: Alarming findings
Along with the clinical interview, Mr. V. is screened with the Beck Hopelessness Scale and Beck Depression Inventory-II. These instruments are chosen because they are easy to administer, and patients can readily comprehend the questions—even when under duress. Mr. V’s results reveal moderate depression and severe hopelessness.
INPATIENT VS. OUTPATIENT CARE
Older patients are often referred to a psychiatrist because of vague suicidal ideation, but they may also present in an acute crisis—with immediate plans for suicide and readily accessible means. The first concern for their safety is to ensure they are not left alone.
Patient interview. First, listen empathetically and ask detailed questions, especially ones that remind patients of their daily connections and responsibilities. For instance, ask, “Do you have children who would be affected by your decision?” Address patients’ immediate needs, such as hunger, thirst, or pain.16 Work on building a therapeutic alliance before asking questions that may appear trivial to agitated patients (such as tasks assessing cognitive abilities).
Avoid arguing with patients, and refrain from offering advice or sermonizing. Allow them to describe their emotions, and communicate that you understand their concerns. Discuss how they can expect to receive treatment to ease their discomfort. Inform them that mental health specialists can treat them and monitor their progress.
Hospitalization. Begin discussing treatment options and broach the notion of hospital admission if necessary. One way to foster an alliance is to frame inpatient care as a way of helping them recover from their crisis in a safe environment.
To ensure patient safety, it is best to err on the side of admission. Admitting the suicidal patient not only guarantees strict supervision but also allows time for necessary psychological assessment. Hospitalization may also allow family members to remove any weapons or hazardous conditions from the patient’s home.
Including the family in problem-solving is especially important when managing older suicidal patients. For patients who are isolated from family or friends, recovery may depend on improving their support network.
Table 3
Comparing screening instruments for suicide risk
| Measure | Description | Time (minutes) |
|---|---|---|
| Beck Depression Inventory (BDI) | 21-item, self-administered; identifies depressive symptoms in past week | 10 |
| Beck Hopelessness Scale (BHS) | 20-item, self-administered; measures hopelessness, fatalism, and pessimism in past week | 5 |
| Beck Scale for Suicide Ideation-Current (SSI-C) | 19-item, self-administered; gauges suicidal intention | 10 |
| Hamilton Rating Scale for Depression-revised (HRSD-R) | 21-item, clinician-administered; rates depressive symptoms in past week | 25 |
Outpatient care. Not all acutely suicidal older patients require hospital admission. They may be safely managed as outpatients if they:
- have strong social support
- are not isolated
- have no access to firearms or other dangerous weapons.
Safety can be enhanced by having family members take responsibility for the senior’s well-being and by asking the patient to contract for safety. A safety contract may include:
- verbal confirmation—and ideally a written statement—that the patient will not commit suicide within a specified period
- a list of people the patient will contact when feeling suicidal
- steps being taken to monitor the patient’s welfare.
Finally, schedule follow-up appointments soon after discharge to certify patients are being closely monitored. To encourage outpatient medication adherence, build strong alliances with family members and ask patients to bring in their pill bottles during follow-up appointments.
CASE REPORT continued: Observation begins
The staff is clearly concerned about Mr. V’s suicide risk and requests that he voluntarily admit himself to the VA hospital. This decision is based on his level of isolation, the lethality of his suicide plan, access to a weapon, and the depression and hopelessness revealed by his screening tests. He reluctantly agrees and is admitted to the inpatient psychiatric unit for observation and treatment by a geriatric internist and a geriatric psychiatrist.
DRUG THERAPY FOR SUICIDALITY
For patients with mild depressive symptoms, psychotherapy may be sufficient to manage depression associated with suicidality. However, those with moderate-to-severe depression require both drug treatment and psychotherapy.
Drug selection depends upon the underlying psychiatric illness. If the older patient is experiencing a depressive disorder, a selective serotonin reuptake inhibitor (SSRI) or another antidepressant could serve as first-line treatment (Table 4). These medications are safe for suicidal patients because they are not fatal in overdose.
Administration. Because age-related changes in pharmacokinetics and spharmacodynamics can slow medication clearance, reduced dosages usually achieve a therapeutic effect and minimize the risk of side effects in geriatric patients.
Antidepressants commonly used for older patients are shown in Table 4. Excepting citalopram and escitalopram, these dosages are lower than usual. We start healthy older patients on one-half the usual dosage and those who are medically ill or have neurodegenerative disorders on one-third to one-fourth the usual dosage. We also titrate more slowly to reduce the risk of side effects.
Table 4
Antidepressants commonly used to treat geriatric depression
| Medication | Recommended dosage (mg/d) |
|---|---|
| SSRIs | |
| Citalopram | 20 to 40 |
| Escitalopram | 10 to 20 |
| Fluoxetine | 10 to 40 |
| Paroxetine | 10 to 40 |
| Sertraline | 25 to 150 |
| Others | |
| Bupropion | 100 to 400 |
| Mirtazapine | 15 to 45 |
| Venlafaxine | 75 to 225 |
As in younger patients, the most common side effects of SSRIs in older patients include GI difficulties, overactivation, and sexual dysfunction. Paroxetine’s potential for anticholinergic effects may be a concern for some older patients.
Drug-drug interactions are of great concern when treating older patients, who take an average of six to nine medications per day.17 Compared with other SSRIs, fluoxetine and paroxetine, are more likely to inhibit cytochrome P-450 enzymes 2D6 and 3A4. They could thus increase blood levels of drugs taken concomitantly that are substrates of 2D6 or 3A4.
Antidepressant side effects can sometimes be used to advantage. For example, mirtazapine’s sedating property at lower dosages could help older patients with insomnia.
CASE REPORT concluded: Finding support
Mr. V is started on an SSRI antidepressant. He also receives supportive and milieu therapy and coping skills training. During his hospitalization, Mr. V contracts for safety and allows his sister to remove the handgun from his home.
Upon discharge, Mr. V is referred to a day treatment program that operates 3 to 5 days a week and offers case management, group therapy, and individual psychotherapy. The program helps him meet other older patients and allows him to discuss his life’s accomplishments and losses with others his age. His sister is an integral part of the program, and he maintains close contact with her.
Mr. V reports vague and occasional suicidal ideation, with no specific plan or intent. He and his sister note that his medical condition improved soon after his psychiatric condition stabilized.
Related resources
- Surgeon General’s Call to Action to Prevent Suicide. www.mental-health.org/suicideprevention/calltoaction.pdf
- Centers for Disease Control and Prevention. National Center for Injury Prevention and Control.
Drug brand names
- Bupropion • Wellbutrin
- Citalopram • Celexa
- Escitalopram • Lexapro
- Fluoxetine • Prozac
- Mirtazapine • Remeron
- Paroxetine • Paxil
- Sertraline • Zoloft
- Venlafaxine • Effexor
Disclosure
Drs. Montross reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Mohamed is a speaker and consultant to Forest Laboratories and Eli Lilly and Co.
Dr. Kasckow receives research support from, is a consultant to, and is a speaker for Forest Laboratories, Eli Lilly and Co., Pfizer Inc., and Janssen Pharmaceutica.
Dr. Zisook is a consultant to GlaxoSmithKline and a speaker for GlaxoSmithKline, Wyeth Pharmaceuticals, Pfizer Inc., Forest Laboratories, and Bristol-Myers Squibb Co.
CASE REPORT: I have a gun
Mr. V, age 77, appears depressed and anxious during his appointment at a mental hygiene clinic. He reports insomnia, concentration trouble, and anhedonia. He tells the psychiatrist he keeps a loaded gun at home and is not sure he can control his suicidal impulses.
The patient is Caucasian and has a history of heart failure, pulmonary disease, and type 2 diabetes. His wife died 18 months ago. He lives alone, but his sister lives nearby. He recently received a right hip replacement, which required 3 months of rehabilitation in a nursing home to recover from surgical complications. He still has trouble walking.
As in Mr. V’s case, treating older patients referred for psychiatric care often involves evaluating suicide risk. His age, race, gender, depressed mood, recent bereavement, and medical ailments place him in the population at highest risk of suicide (Box, Table 1).1-8
Approximately 20% of all suicides in the United States are committed by persons age 65 or older,1 who account for 13% of the total population. The suicide rate among persons older than 75 is three times higher than it is for the young.2 Older Caucasian men have the highest per-capita rate of completed suicide, compared with any other group of Americans.3
Psychiatric disorders. The rates of Axis I disorders among older persons who commit suicide fall within the average range for all age groups (70 to 90%). However, the types of disorders seen in the older population differ from those of younger suicides (Table 1).4-8
Affective illness has been termed “the predominant psychopathology associated with suicide in later life.”4 Among older persons who commit suicide, three-fourths (76%) have diagnosable mood disorders4 and nearly two-thirds (63%) have depression.6 Contributing risk factors include alcoholism and substance abuse,4,6,7 Axis II disorders, and dementia.6
Losses and medical illness. In later life, bereavement, loss of independence, or financial reversals may lead to depression. Older persons who take their own lives also tend to have greater physical health burdens and more functional disabilities than those who do not commit suicide.6,8
This article describes an age-based psychiatric workup of the suicidal older patient, including factors to consider when screening for depressive symptoms, prescribing drug therapy, and determining the need for hospitalization.
AGE-BASED CLINICAL WORKUP
For older patients who report suicidal ideation, an age-appropriate workup—using clinical interviews and screening instruments—is essential. The clinical interview can build rapport and gather information about the patient’s suicidal plan or intent. Based on our experience, we recommend the following 6-step screening interview, summarized in Table 2.
- Ask about a specific plan. Does the patient have the means readily available to carry out this plan? What is the timeline (imminent versus vaguely futuristic)? Does the patient report having control over this plan?
- Gather a suicide history. Has the patient attempted suicide before? By what means? Is there a family history of suicide? If yes, by what means did this family member commit suicide, and how was the patient affected?
- Assess social status. How isolated is the patient? Have there been recent changes in his or her social circle, such as loss of a spouse? Can the patient identify at least one person who would be negatively affected by the suicide?
- Assess medical health. Does the patient suffer from chronic pain? Does the patient have a recently diagnosed medical condition? Has a longstanding medical condition become more debilitating? Does the patient report feeling hopeless about impending medical difficulties? Has he or she been keeping regularly scheduled medical appointments with outpatient clinicians?
- Assess mental health. Does the patient meet DSM-IV criteria for depression or schizophrenia, which are associated with high suicide risk? Does he or she report being hopeless or helpless? Is the suicidal ideation ego dystonic?
- Ascertain clinical signs of suicidal intent. Has the patient:
Table 1
Suicide risk with mental and physical illness, by patient age
| Risk factors | Young (21 to 34 yrs) | Middle-aged (35 to 54 yrs) | Young-old (55 to 74 yrs) | Elderly (77+ yrs) |
|---|---|---|---|---|
| Psychiatric disorders | • | • | • | • |
| Mood disorders | ○ | • | • | |
| Alcohol abuse | ○ | • | ○ | |
| Primary psychoses | • | ○ | ||
| Personality disorders | ○ | |||
| Physical ailments | • | • | ||
| • Significant risk factor ○ Potential risk factor | ||||
| Source: Compiled from information in references 4-8. | ||||
CASE REPORT continued: Some telling signs
Mr. V’s laboratory screening reveals slightly elevated serum glucose and mild anemia. An ECG reveals a type I heart block, but all other lab results are unremarkable. His sister reports he recently gave away his dog, which he and his wife had owned for many years. He has also mentioned a desire to revise his will when speaking to other family members. Hospital records indicate he has missed numerous medical appointments over the past 4 months.
SCREENING INSTRUMENTS
Psychological assessments can often buttress the clinical interview findings. Several measurements are well-suited for detecting suicidal risk and concomitant depression (Table 3).
Beck SSI-C. The Beck Scale for Suicide Ideation – Current (SSI-C) assesses a patient’s preparation and motivation to commit suicide.9 This short (19-item) self-report measure asks patients to rate their wish to die, desire to attempt suicide, duration (and frequency) of suicidal thoughts, sense of control over suicide, and deterrents they face. The SSI-C helps to measure or monitor suicidality and is reliable and valid for psychiatric outpatients.9
BDI-II. The Beck Depression Inventory—recently revised in a second edition (BDI-II)10—can be useful because depression is one of the strongest risk factors for elder suicide. The 21-item BDI-II—a psychometrically sound, self-report instrument—asks about general symptoms of depression and gauges their severity. It can be applied to diverse patient populations and ages11 and is appropriate for older patients who are also being treated medically.
Beck Hopelessness Scale. Hopelessness has been recognized as a possible harbinger of suicide.12 One study showed that depression became a clinically meaningful suicide predictor only when accompanied by hopelessness.13
A score of 10 or more on the Beck Hopelessness Scale identified 91% of patients in one study who eventually committed suicide. The hopelessness patients expressed on this scale more strongly differentiated between those who did or did not commit suicide than did their scores on the BDI or SSI-C.14
Table 2
6-step clinical interview with an older suicidal patient
|
|
| Source: Adapted from the Cincinnati Veterans Affairs Medical Center general psychological suicide assessment |
HRSD-R. The revised Hamilton Rating Scale for Depression (HRSD-R) documents patients’ levels of mood disturbance and suicidality. One item in this 21-item, clinician-administered instrument specifically asks about the patient’s level of suicidality in the past week. The scale has well-documented reliability and validity and is appropriate for psychiatric populations.15
CASE REPORT continued: Alarming findings
Along with the clinical interview, Mr. V. is screened with the Beck Hopelessness Scale and Beck Depression Inventory-II. These instruments are chosen because they are easy to administer, and patients can readily comprehend the questions—even when under duress. Mr. V’s results reveal moderate depression and severe hopelessness.
INPATIENT VS. OUTPATIENT CARE
Older patients are often referred to a psychiatrist because of vague suicidal ideation, but they may also present in an acute crisis—with immediate plans for suicide and readily accessible means. The first concern for their safety is to ensure they are not left alone.
Patient interview. First, listen empathetically and ask detailed questions, especially ones that remind patients of their daily connections and responsibilities. For instance, ask, “Do you have children who would be affected by your decision?” Address patients’ immediate needs, such as hunger, thirst, or pain.16 Work on building a therapeutic alliance before asking questions that may appear trivial to agitated patients (such as tasks assessing cognitive abilities).
Avoid arguing with patients, and refrain from offering advice or sermonizing. Allow them to describe their emotions, and communicate that you understand their concerns. Discuss how they can expect to receive treatment to ease their discomfort. Inform them that mental health specialists can treat them and monitor their progress.
Hospitalization. Begin discussing treatment options and broach the notion of hospital admission if necessary. One way to foster an alliance is to frame inpatient care as a way of helping them recover from their crisis in a safe environment.
To ensure patient safety, it is best to err on the side of admission. Admitting the suicidal patient not only guarantees strict supervision but also allows time for necessary psychological assessment. Hospitalization may also allow family members to remove any weapons or hazardous conditions from the patient’s home.
Including the family in problem-solving is especially important when managing older suicidal patients. For patients who are isolated from family or friends, recovery may depend on improving their support network.
Table 3
Comparing screening instruments for suicide risk
| Measure | Description | Time (minutes) |
|---|---|---|
| Beck Depression Inventory (BDI) | 21-item, self-administered; identifies depressive symptoms in past week | 10 |
| Beck Hopelessness Scale (BHS) | 20-item, self-administered; measures hopelessness, fatalism, and pessimism in past week | 5 |
| Beck Scale for Suicide Ideation-Current (SSI-C) | 19-item, self-administered; gauges suicidal intention | 10 |
| Hamilton Rating Scale for Depression-revised (HRSD-R) | 21-item, clinician-administered; rates depressive symptoms in past week | 25 |
Outpatient care. Not all acutely suicidal older patients require hospital admission. They may be safely managed as outpatients if they:
- have strong social support
- are not isolated
- have no access to firearms or other dangerous weapons.
Safety can be enhanced by having family members take responsibility for the senior’s well-being and by asking the patient to contract for safety. A safety contract may include:
- verbal confirmation—and ideally a written statement—that the patient will not commit suicide within a specified period
- a list of people the patient will contact when feeling suicidal
- steps being taken to monitor the patient’s welfare.
Finally, schedule follow-up appointments soon after discharge to certify patients are being closely monitored. To encourage outpatient medication adherence, build strong alliances with family members and ask patients to bring in their pill bottles during follow-up appointments.
CASE REPORT continued: Observation begins
The staff is clearly concerned about Mr. V’s suicide risk and requests that he voluntarily admit himself to the VA hospital. This decision is based on his level of isolation, the lethality of his suicide plan, access to a weapon, and the depression and hopelessness revealed by his screening tests. He reluctantly agrees and is admitted to the inpatient psychiatric unit for observation and treatment by a geriatric internist and a geriatric psychiatrist.
DRUG THERAPY FOR SUICIDALITY
For patients with mild depressive symptoms, psychotherapy may be sufficient to manage depression associated with suicidality. However, those with moderate-to-severe depression require both drug treatment and psychotherapy.
Drug selection depends upon the underlying psychiatric illness. If the older patient is experiencing a depressive disorder, a selective serotonin reuptake inhibitor (SSRI) or another antidepressant could serve as first-line treatment (Table 4). These medications are safe for suicidal patients because they are not fatal in overdose.
Administration. Because age-related changes in pharmacokinetics and spharmacodynamics can slow medication clearance, reduced dosages usually achieve a therapeutic effect and minimize the risk of side effects in geriatric patients.
Antidepressants commonly used for older patients are shown in Table 4. Excepting citalopram and escitalopram, these dosages are lower than usual. We start healthy older patients on one-half the usual dosage and those who are medically ill or have neurodegenerative disorders on one-third to one-fourth the usual dosage. We also titrate more slowly to reduce the risk of side effects.
Table 4
Antidepressants commonly used to treat geriatric depression
| Medication | Recommended dosage (mg/d) |
|---|---|
| SSRIs | |
| Citalopram | 20 to 40 |
| Escitalopram | 10 to 20 |
| Fluoxetine | 10 to 40 |
| Paroxetine | 10 to 40 |
| Sertraline | 25 to 150 |
| Others | |
| Bupropion | 100 to 400 |
| Mirtazapine | 15 to 45 |
| Venlafaxine | 75 to 225 |
As in younger patients, the most common side effects of SSRIs in older patients include GI difficulties, overactivation, and sexual dysfunction. Paroxetine’s potential for anticholinergic effects may be a concern for some older patients.
Drug-drug interactions are of great concern when treating older patients, who take an average of six to nine medications per day.17 Compared with other SSRIs, fluoxetine and paroxetine, are more likely to inhibit cytochrome P-450 enzymes 2D6 and 3A4. They could thus increase blood levels of drugs taken concomitantly that are substrates of 2D6 or 3A4.
Antidepressant side effects can sometimes be used to advantage. For example, mirtazapine’s sedating property at lower dosages could help older patients with insomnia.
CASE REPORT concluded: Finding support
Mr. V is started on an SSRI antidepressant. He also receives supportive and milieu therapy and coping skills training. During his hospitalization, Mr. V contracts for safety and allows his sister to remove the handgun from his home.
Upon discharge, Mr. V is referred to a day treatment program that operates 3 to 5 days a week and offers case management, group therapy, and individual psychotherapy. The program helps him meet other older patients and allows him to discuss his life’s accomplishments and losses with others his age. His sister is an integral part of the program, and he maintains close contact with her.
Mr. V reports vague and occasional suicidal ideation, with no specific plan or intent. He and his sister note that his medical condition improved soon after his psychiatric condition stabilized.
Related resources
- Surgeon General’s Call to Action to Prevent Suicide. www.mental-health.org/suicideprevention/calltoaction.pdf
- Centers for Disease Control and Prevention. National Center for Injury Prevention and Control.
Drug brand names
- Bupropion • Wellbutrin
- Citalopram • Celexa
- Escitalopram • Lexapro
- Fluoxetine • Prozac
- Mirtazapine • Remeron
- Paroxetine • Paxil
- Sertraline • Zoloft
- Venlafaxine • Effexor
Disclosure
Drs. Montross reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Mohamed is a speaker and consultant to Forest Laboratories and Eli Lilly and Co.
Dr. Kasckow receives research support from, is a consultant to, and is a speaker for Forest Laboratories, Eli Lilly and Co., Pfizer Inc., and Janssen Pharmaceutica.
Dr. Zisook is a consultant to GlaxoSmithKline and a speaker for GlaxoSmithKline, Wyeth Pharmaceuticals, Pfizer Inc., Forest Laboratories, and Bristol-Myers Squibb Co.
1. Centers for Disease Control and Prevention. Surveillance for Injuries and Violence Among Older Adults (CDC Surveillance Summary, December 17, 1999, Chap. 3:27-50). www.cdc.gov/mmwr/PDF/SS/SS4808.pdf
2. Kaplan HI, Sadock BJ. Synopsis of psychiatry (6th ed). Baltimore: Williams & Wilkins, 1991.
3. Lyon DE, Chase LS, Farrell SP. Using an interview guide to assess suicidal ideation. Nurse Practitioner 2002;27:26-31.
4. Conwell Y, Lyness JM, Duberstein P, et al. Completed suicide among older patients in primary care practices: A controlled study. J Am Geriatr Soc 2000;48:23-9.
5. Conwell Y, Duberstein PR, Cox C, et al. Relationships of age and Axis I diagnoses in victims of completed suicide: A psychological autopsy study. Am J Psychiatry 1996;153:1001-8.
6. Harwood D, Hawton K, Hope T, Jacoby R. Psychiatric disorder and personality factors associated with suicide in older people: A descriptive and case-control study. Int J Geriatr Psychiatry 2001;16:155-65.
7. Henriksson MM, Marttunen MJ, Isometsa ET, et al. Mental disorders in elderly suicide. Int Psychogeriatr 1995;7:275-86.
8. Conwell Y, Duberstein PR, Caine ED. Risk factors for suicide in later life. Biol Psychiatry 2002;52:193-204.
9. Beck AT, Brown GK, Steer RA. Psychometric characteristics of the Scale for Suicide Ideation with psychiatric outpatients. Behav Res Ther 1997;35:1039-46.
10. Beck AT, Steer RA. Manual for the Beck Depression Inventory. San Antonio, TX: The Psychological Corporation, 1987.
11. Beck AT, Steer RA, Garbin MG. Psychometric properties of the Beck Depression Inventory: Twenty-five years later. Clin Psychol Rev 1988;8:77-100.
12. Beck AT, Weissman A, Lester D, Trexler L. The measurement of pessimism: The hopelessness scale. J Consult Clin Psychol 1974;42:861-5.
13. Drake RE, Cotton PG. Depression, hopelessness and suicide in chronic schizophrenia. Br J Psychiatry 1986;148:554-9.
14. Beck AT, Steer RA, Kovacs M, Garrison B. Hopelessness and eventual suicide: A 10-year perspective study of patients hospitalized with suicidal ideation. Am J Psychiatry 1985;142:559-63.
15. Riskind JH, Beck AT, Brown G, Steer RA. Taking the measure of anxiety and depression: Validity of the reconstructed Hamilton Scales. J Nerv Ment Dis 1987;175:474-9.
16. Lamberg L. Psychiatric emergencies call for comprehensive assessment and treatment. JAMA 2002;288:686-7.
17. Sadavoy J, Lazarus LW, Jarvik LF. Grossberg GT (eds). Comprehensive review of geriatric psychiatry (2nd ed). Washington, DC: American Psychiatric Press, 1996.
1. Centers for Disease Control and Prevention. Surveillance for Injuries and Violence Among Older Adults (CDC Surveillance Summary, December 17, 1999, Chap. 3:27-50). www.cdc.gov/mmwr/PDF/SS/SS4808.pdf
2. Kaplan HI, Sadock BJ. Synopsis of psychiatry (6th ed). Baltimore: Williams & Wilkins, 1991.
3. Lyon DE, Chase LS, Farrell SP. Using an interview guide to assess suicidal ideation. Nurse Practitioner 2002;27:26-31.
4. Conwell Y, Lyness JM, Duberstein P, et al. Completed suicide among older patients in primary care practices: A controlled study. J Am Geriatr Soc 2000;48:23-9.
5. Conwell Y, Duberstein PR, Cox C, et al. Relationships of age and Axis I diagnoses in victims of completed suicide: A psychological autopsy study. Am J Psychiatry 1996;153:1001-8.
6. Harwood D, Hawton K, Hope T, Jacoby R. Psychiatric disorder and personality factors associated with suicide in older people: A descriptive and case-control study. Int J Geriatr Psychiatry 2001;16:155-65.
7. Henriksson MM, Marttunen MJ, Isometsa ET, et al. Mental disorders in elderly suicide. Int Psychogeriatr 1995;7:275-86.
8. Conwell Y, Duberstein PR, Caine ED. Risk factors for suicide in later life. Biol Psychiatry 2002;52:193-204.
9. Beck AT, Brown GK, Steer RA. Psychometric characteristics of the Scale for Suicide Ideation with psychiatric outpatients. Behav Res Ther 1997;35:1039-46.
10. Beck AT, Steer RA. Manual for the Beck Depression Inventory. San Antonio, TX: The Psychological Corporation, 1987.
11. Beck AT, Steer RA, Garbin MG. Psychometric properties of the Beck Depression Inventory: Twenty-five years later. Clin Psychol Rev 1988;8:77-100.
12. Beck AT, Weissman A, Lester D, Trexler L. The measurement of pessimism: The hopelessness scale. J Consult Clin Psychol 1974;42:861-5.
13. Drake RE, Cotton PG. Depression, hopelessness and suicide in chronic schizophrenia. Br J Psychiatry 1986;148:554-9.
14. Beck AT, Steer RA, Kovacs M, Garrison B. Hopelessness and eventual suicide: A 10-year perspective study of patients hospitalized with suicidal ideation. Am J Psychiatry 1985;142:559-63.
15. Riskind JH, Beck AT, Brown G, Steer RA. Taking the measure of anxiety and depression: Validity of the reconstructed Hamilton Scales. J Nerv Ment Dis 1987;175:474-9.
16. Lamberg L. Psychiatric emergencies call for comprehensive assessment and treatment. JAMA 2002;288:686-7.
17. Sadavoy J, Lazarus LW, Jarvik LF. Grossberg GT (eds). Comprehensive review of geriatric psychiatry (2nd ed). Washington, DC: American Psychiatric Press, 1996.
A low-frustration strategy for treating somatization
Mrs. M, age 34, was referred for psychiatric evaluation by her primary care physician. She reluctantly agreed to the referral and tells the psychiatrist she “really should be seeing a cardiologist.” Numerous evaluations for chest pain and palpitations—including seven emergency room visits, ECGs and cardiac catheterization—have revealed no medical pathology.
A divorced mother of two children, she says she feels anxious about her “heart condition.” Her father died of a heart attack at age 51. She experiences chest pains at home and at work, particularly when under stress. Sometimes she feels her heart racing and numbness or tingling in her arms.
Although her primary care physician has seen her frequently during the past 6 months, she says the doctor is not taking her complaints seriously. “These chest pains are real,” she says, “so don’t try to tell me they’re all in my head.”
Psychiatrists may be the last doctors patients such as Mrs. M wish to see but the ones best equipped to relieve their suffering. Our experience in treating somatizing patients and the available evidence suggest that cognitive-behavioral therapy (CBT) combined with psychoeducation, reassurance, and sometimes drug therapy is the most effective approach.
Health-related fear—or “illness worry”—is common, occurring in nearly 10% of adults who responded to a recent community survey.2 When this fear drives individuals to their physicians for evaluation, frequently no organic cause is discovered. Full evaluations are expensive and lead to increased use of health care resources, including potentially dangerous invasive testing.3,4
Defining somatization has been a source of confusion.5,6 Some authors consider somatic complaints to be expressions of suppressed psychosocial stressors. Others label them as medically unexplained complaints, although this definition fails to exclude occult medical problems. Kleinman7 defines somatization as “a somatic idiom of psychosocial distress in a setting of medical health-care seeking.” This useful definition links psychosocial problems with somatic complaints and the behavioral drive to obtain a medical evaluation.
In DSM-IV,8 the defining characteristics of somatoform disorders are somatic complaints or disease fears that are out of proportion with any identifiable somatic cause. Entities include somatization disorder, undifferentiated somatization disorder, conversion disorder, pain disorder, hypochondriasis, body dysmorphic disorder, and somatoform disorder–not otherwise specified (NOS).
Subthreshold symptoms. Unfortunately, DSM-IV’s categorization of Axis I somatoform disorders does not capture subthreshold presentations, which are common. Patients with less than the required number of somatic complaints are labeled in a wastebasket fashion with “undifferentiated somatoform disorder.”9
Mrs. M’s persistent chest pain of noncardiac origin is a familiar health anxiety, along with functional GI complaints, headaches, chronic fatigue, and lower back pain. Frustrating to their doctors and frustrated themselves, patients with medically unexplained complaints consume an inordinate amount of physicians’ time.1
Without a clear definition of somatization (Box)2-9 or useful clinical guidelines, psychiatrists must rely on the literature for guidance in managing somatization disorders. This article summarizes the evidence and describes how we apply these findings to practice. And when all else fails, we offer last-ditch advice for managing patients who resist your treatment efforts.
IDENTIFYING COMORBIDITIES
Identifying psychiatric comorbidities is the first step in successfully treating patients with somatoform complaints. In an epidemiologic study, 60% of patients with somatoform complaints also had a mood disorder and 48% had an anxiety disorder.10 In a similar study of patients with hypochondriasis, 88% also had one or more Axis I diagnosis.11
If a patient meets criteria for a comorbid psychiatric disorder and is willing to be treated for it, the somatic complaints may resolve along with the underlying disorder. In fact, the presence of an identifiable Axis I disorder order may predict a more positive prognosis.12
Personality disorders. Somatization in patients with a personality disorder poses unique challenges.13 Granted, when making a diagnosis it is difficult to tease apart somatization from personality disorders because somatization itself may be considered a chronic, maladaptive coping style. However, symptoms such as deception, impulsivity, mood lability, and self-injurious behavior introduce treatment complications that exceed the scope of this article.
Posttraumatic stress disorder (PTSD)—particularly childhood sexual and physical abuse—also predisposes some patients to somatization disorders.14,15 Patients with comorbid PTSD and somatization disorder require highly specialized treatment that is beyond the scope of this review.
COGNITIVE-BEHAVIORAL TREATMENT
Cognitive-behavioral therapy (CBT) is the best-studied and most effective treatment for somatoform disorders.16 CBT for somatization relies on both physiologic and cognitive explanations to account for the patient’s experience, without committing to an “either/or” dichotomy. It offers patients an alternate explanation of what is wrong with them—illness anxiety instead of severe physical illness.
By making patients aware of their automatic thoughts, feelings, behaviors, and underlying beliefs, CBT helps them normalize and cope with their illness anxiety. CBT techniques can be applied in a predetermined course of therapy (such as 12 sessions with a mental health clinician), in a group setting, or piecemeal by any health care provider.
Effective strategies. In a review of 30 controlled trials of CBT for somatoform disorders, Looper17 showed overall effect ranging from 0.38 to 2.5, where 0.2 was defined as a small effect, 0.5 as medium, and 0.8 as large. Hypochondriasis, somatization disorder, body dysmorphic disorder, chronic pain, chronic fatigue, and noncardiac chest pain were included in this review. The most effective strategies:
- included 6 to 16 treatment sessions
- were symptom-focused as opposed to providing general relaxation training
- included maintenance sessions after the initial series.
Four factors of health anxiety. CBT primarily targets the patient’s false beliefs that he or she is physically ill. These beliefs are based on how the patient misinterprets innocuous physical symptoms and responds to them.18 The cognitive theory of health anxiety holds that health anxiety severity is affected by four factors:
- perceived likelihood of illness
- perceived burden of illness
- perceived ability to cope with illness
- perception of the extent to which external factors will help.19
Table 1
Common dysfunctional beliefs of somatizing patients
|
The first two factors worsen and the latter two mitigate health anxiety. An individual patient’s presenting fears often suggest which factors to address. For example, Mrs. M may describe the burden of illness as the focus of her fears (“If I have a heart attack, who will care for my children?”). This information cues you to shift the focus of therapy to helping her cope with child care needs despite her recurring symptoms.
If she focuses on her likelihood of illness, then uncoupling the symptoms from the diagnosis could be more productive. When she reports palpitations, diaphoresis, and dizziness, have her do breathing exercises that induce those symptoms without producing a heart attack.
Table 2
Journaling homework: 5 questions for patients to answer about one symptom each day
|
She might describe feeling unable to cope when she feels symptoms or when cardiologists tell her nothing is wrong with her heart. In that case, focus on relaxation techniques, global stress reduction, and reducing cardiac risk factors to bolster her ability to cope with her illness.
Journaling is a critical component of CBT in treating somatization disorders. Regular journaling by the patient can reveal dysfunctional beliefs that may be driving his or her health anxieties, such as those listed in Table 1. We find it useful to assign patients to answer five questions about one symptom experience each day (Table 2). This self-monitoring provides material to work on with the patient during each session.
Cognitive restructuring. During therapy sessions, we ask patients to suggest alternate explanations for the symptoms recorded in their journals. We then ask them to determine which explanations are more feasible.
For example, if Mrs. M develops palpitations during emotionally charged arguments, we would ask her to develop explanations other than, “I was having a heart attack.” Reality testing includes rhetorical questions such as, “Would you be alive today if you were having a heart attack every time you had palpitations?” Automatic thoughts are successively identified and then tested aloud with the patient:
- “Has every unexplained symptom led to the discovery of a serious illness?”
- “Does every instance of hurt equal harm?”
Eventually, patterns of automatic thoughts emerge, and these reveal the underlying dysfunctional beliefs.
Dysfunctional beliefs are maintained when patients selectively attend to and amplify somatic sensations. Behavioral experiments during sessions can demonstrate to the patient in vivo the process by which they misattribute illness to physical symptoms. For example, overbreathing with a patient during a session may elicit light-headedness, paresthesias, or tachycardia, which can then be linked to overbreathing rather than a chronic or catastrophic illness.
Furthermore, patients can be taught to control the experience. Some patients with headaches or GI pain may be made aware of symptoms by simply asking them to focus their attention on the respective organs. Simply explaining the cycle of misattribution, autonomic activation, and further symptom development with an in vivo demonstration can be illuminating.
Response prevention. Another behavioral technique is to cut back in small increments on actions the patient takes in response to physical symptoms and automatic thoughts. For example, a patient could take medicine and seek reassurance less frequently and avoid rubbing the affected area.
PSYCHOEDUCATION
Two psychoeducation programs for somatization behavior have been formally studied.
The Personal Health Improvement Program20—led by trained facilitators—includes classroom videos, cognitive-behavioral exercises, and home study assignments. After completing the 6-week course, 171 patients with somatization disorders reported reduced physical and psychological distress and increased function. They also visited their primary care physicians less often.
Table 3
How to effectively reassure somatizing patients
| Action | Benefit |
|---|---|
| Review records in front of patients | Demonstrates that you take complaints and histories seriously |
| Acknowledge the severity of patients’ distress | Validates subjective suffering |
| Schedule follow-up visits at regular intervals | Provides access to you and continuity of care; reduces extra phone calls and emergency visits |
| Use clear and simple language | Improves communication |
| Explain that they do not have life-threatening structural disease | Opens door to cognitive restructuring |
| Assign jobs, such as journaling 15 min/day and rounding up medical records | Builds therapeutic alliance, fosters patient responsibility, and restores patients’ sense of control |
| Identify and support the patient’s strengths | Builds self-esteem |
| Use specialty referrals sparingly | Reduces risk of further medical testing and patient anxiety while awaiting results |
Coping with Illness Anxiety21 relies on mini-lectures, demonstrations, videos, and focused group discussions. After six 2-hour sessions, 33 of 43 study patients (78%) used medical services less often and reported reduced disease conviction, consequences of bodily complaints, health anxiety, and checking and avoidance behaviors. Two psychology graduate students taught the course from a manual, with 6 to 9 patients per group.
Psychoeducation in this context relies on didactic presentations, readings, role playing, and videotaped material. The goal is to teach patients to recognize thoughts, emotions, and behaviors that lead to and result from somatic preoccupation. Patients can improve when they recognize dysfunctional behavioral patterns and learn alternate coping strategies.
Somatizing patients—with their aversion to the stigma of mental illness—may find psychoeducation particularly attractive. They can be treated as students who are being educated, rather than as patients who are being treated. Classrooms in both studies cited above were located in medical outpatient offices, not in mental health facilities.
REASSURANCE
Reassurance is a common therapeutic technique in medicine, although it is poorly understood, poorly taught, and not methodically applied. Reassurance alleviates anxiety, enables patients to endure dysphoria, encourages hope, gives insight, and enhances the doctor-patient relationship.22
Table 4
How to avoid becoming frustrated with persistent somatization
| Situation | Response |
|---|---|
| Despite patients’ urgency | Watch and wait, knowing that psychological distress has been chronic |
| Despite patients’ belief that a single pill or procedure will ‘cure’ them | Persist in ‘rehabilitative’ approach |
| Despite patients’ provocations to force you to take a dichotomous approach | Persist in using both physical and psychological explanations |
| Despite your knowledge that patients are actively maintaining their illness beliefs | Try to be patient as they attribute their misfortune to ‘fate,’ ‘bad luck,’ or ‘misfortune’ |
| Despite the fact that you have agreed to treat the patient | Realize that his or her family or culture may reinforce the ‘sick role’ as the only acceptable form of distress |
| Despite patients’ desire to discuss symptoms | Reorient them to sustaining daily function (such as parenting while tolerating fatigue) |
Whereas CBT seeks to challenge patients’ underlying beliefs and restructure their thought processes,23 reassurance can help them tolerate their dysfunctional beliefs and dissuade them from believing their health is dangerously impaired. Reassurance offers a substitute explanation of patients’ dysfunction, although this explanation is not as central or detailed as it is in CBT.
How to reassure. Patients may consider reassurance offered prematurely or by a stranger to be patronizing or dismissive. Reassurance is most effective when:
- given by a trusted person who is reliable, consistent, firm, and empathic
- the patient’s condition has been established as unresponsive to conventional diagnostics or biological therapies.
Patients are most receptive to reassurance when they express distress or frustration with their unexplained symptoms. Affirming that their suffering is legitimate opens the door to further treatment.
Reassurance is least effective when a patient is expressing anger or mistrust, although this is when the physician may feel most pressured to reassure. To successfully reassure a patient, the psychiatrist needs to:
- credibly identify with the patient’s distress
- and listen empathically (such as using body language and facial expressions that convey concern and consideration to the patient).24
Starcevic suggests useful techniques for providing reassurance (Table 3).22
DRUG THERAPIES
Psychotropics are considered a first-line treatment for patients with somatization disorders when:
- the patient spontaneously identifies any discrete, vegetative, or psychological complaints that may respond to drug therapy, such as insomnia, weight loss, sadness, or preoccupation
- the patient meets diagnostic criteria for comorbid anxiety or depressive disorders
- the therapeutic alliance is strong enough to weather the inevitable struggle with side effects and incomplete response to treatment. We do not recommend medication in the first encounter, when it may threaten a nascent alliance.
A common obstacle to prescribing psychotropics to somatizing patients is their sensitivity to suggestions that their complaints are “all in their heads.” To sidestep this resistance, describe the medication as treating the stress caused. by—not causing.—their chronic physical complaints. Proposing antidepressant therapy after—rather than instead of—physical exams and other diagnostics may elicit a more positive response.
Antidepressants. In clinical trials, somatoform complaints show moderate improvement after antidepressant treatment. In a meta-analysis of 6,595 patients with unexplained symptoms treated only with antidepressants, the number needed to treat was 3 to yield a positive response.25 This report of 94 medication trials included patients with headache, fibromyalgia, functional GI syndromes, idiopathic pain, tinnitus, or chronic fatigue.
In other trials:
- Amitriptyline has reduced somatic symptoms in patients labeled as having “masked depression.”26
- Sertraline has reduced disease fear, disease conviction, and bodily preoccupation in patients with hypochondriasis and panic disorder.27
Consider side effects when choosing medication for patients with somatoform disorders. Selective serotonin reuptake inhibitors (SSRIs) in general—and sertraline, citalopram, and escitalopram specifically—have fewer side effects than tricyclics. The adage of “start low, go slow” is appropriate for somatizing patients; we usually start with one-half the dosages recommended for treating depression.
Antipsychotics. In case reports, patients with “atypical psychosis,” “monosymptomatic hypochondriacal psychosis,” or “delusional disorder, somatic type” have responded to antipsychotics. These patients’ somatic beliefs are of delusional intensity, such as the rare fear of being eaten alive by an intestinal parasite (delusional parasitosis). Reported behaviors associated with the delusion include starvation, excessive laxative abuse, ingestion of sharp objects, and self-inflicted stab wounds. Treatments described in the literature include the typical agents pimozide and haloperidol and the atypicals olanzapine and risperidone.
TREATMENT-RESISTANT PATIENTS
Some patients with somatoform disorders will not accept CBT, psychotropics, reassurance, or referrals to group psychoeducation. Despite your best efforts, they may persist in focusing on somatic complaints. If you are willing to maintain a therapeutic relationship with them, be prepared to tolerate several ongoing paradoxes (Table 4).
Behaviorally, you must “listen more and do less.” Emotionally, you must be willing to enter into a long-term relationship with an inherently frustrating patient whose pathologies make you feel therapeutically hopeless and helpless. Understand that their physical symptoms function as a metaphor for psychological distress. You are not required to explore the source, content, or meaning of the metaphor in detail but simply listen to their somatic complaints through that psychological filter.
Related resources
- Starcevic V, Lipsitt D (eds). Hypochondriasis: modern perspectives on an ancient malady. New York: Oxford University Press, 2001.
- Information and support Web site for persons with health anxiety or hypochondria. www.healthanxiety.com
- Anxiety Disorders Association of America. www.adaa.org
Drug brand names
- Amitriptyline • Elavil
- Citalopram • Celexa
- Escitalopram • Lexapro
- Haloperidol • Haldol
- Olanzapine • Zyprexa
- Pimozide • Orap
- Risperidone • Risperdal
- Sertraline • Zoloft
Disclosure
Dr. Isaac reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Wise receives grant support from Eli Lilly & Co. and is a consultant or speaker for Eli Lilly & Co., Pfizer Inc., Bristol-Myers Squibb Co., and GlaxoSmithKline.
1. Katon W, Von Korff M, Lin E, et al. Distressed high utilizers of medical care. DSM-III-R diagnoses and treatment needs. Gen Hosp Psychiatry 1990;12:355-62.
2. Noyes R, Jr, Happel RL, Yagla SJ. Correlates of hypochondriasis in a nonclinical population. Psychosomatics 1999;40:461-9.
3. Mayou R, Sprigings D, Gilbert T. Patients with palpitations referred for 24-hour ECG recording. J Psychosom Res 1999;46:491-6.
4. Mayou RA, Bass C, Hart G, et al. Can clinical assessment of chest pain be made more therapeutic? Q J Med 2000;93:805-11.
5. Lipowski ZJ. Somatization: the experience and communication of psychological distress as somatic symptoms. Psychother Psychosom 1987;47:160-7.
6. Lipowski ZJ. Somatization: medicine’s unsolved problem. Psychosomatics 1987;28(6):294-297.
7. Ware NC, Kleinman A. Culture and somatic experience: the social course of illness in neurasthenia and chronic fatigue syndrome. Psychosom Med 1992;54:546-60.
8. Diagnostic and statistical manual of mental disorders (4th ed., text revision). Washington, DC: American Psychiatric Association, 2000.
9. Bass C, Peveler R, House A. Somatoform disorders: severe psychiatric illnesses neglected by psychiatrists. Br J Psychiatry 2001;179:11-14.
10. Smith GR. The epidemiology and treatment of depression when it coexists with somatoform disorders, somatization, or pain. Gen Hosp Psychiatry 1992;14:265-72.
11. Barsky AJ, Wyshak G, Klerman GL. Psychiatric comorbidity in DSM-III-R hypochondriasis. Arch Gen Psychiatry 1992;49:101-8.
12. Starcevic V. Role of reassurance and psychopathology in hypochondriasis. Psychiatry 1990;53(4):383-95.
13. Rost KM, Akins RN, Brown FW, Smith GR. The comorbidity of DSM-III-R personality disorders in somatization disorder. Gen Hosp Psychiatry 1992;14:322-6.
14. Morrison J. Childhood sexual histories of women with somatization disorder [comment]. Am J Psychiatry 1989;146:239-41.
15. Morse DS, Suchman AL, Frankel RM. The meaning of symptoms in 10 women with somatization disorder and a history of childhood abuse. Arch Fam Med 1997;6:468-76.
16. Kroenke K, Swindle R. Cognitive-behavioral therapy for somatization and symptom syndromes: a critical review of controlled clinical trials. Psychother Psychosom 2000;69:205-15.
17. Looper KJ, Kirmayer LJ. Behavioral medicine approaches to somatoform disorders. J Consult Clin Psychol 2002;70:810-27.
18. Warwick HM, Clark DM, Cobb AM, Salkovskis PM. A controlled trial of cognitive-behavioural treatment of hypochondriasis. Br J Psychiatry 1996;169:189-95.
19. Warwick HM, Salkovskis PM. Cognitive-behavioral treatment of hypochondriasis. In: Lipsitt DR, Starcevic V (eds). Hypochondriasis: Modern perspectives on an ancient malady. New York: Oxford Press, 2001;314-28.
20. McLeod CC, Budd MA. Treatment of somatization in primary care: evaluation of the Personal Health Improvement Program. HMO Pract 1997;11:88-94.
21. Bouman TK, Visser S. Cognitive and behavioural treatment of hypochondriasis. Psychother Psychosom 1998;67:214-21.
22. Starcevic V. Reassurance in the treatment of hypochondriasis. In: Lipsitt DR, Starcevic V (eds). Hypochondriasis: Modern perspectives on an ancient malady. New York: Oxford Press, 2001;291-313.
23. Clark DM, Salkovskis PM, Hackmann A, et al. Two psychological treatments for hypochondriasis. A randomised controlled trial. Br J Psychiatry 1998;173:218-25.
24. Schwartz L. Some notes on reassurance in medical practice. Psychosomatics 1966;7:290-4.
25. O’Malley PG, Jackson JL, Santoro J, et al. Antidepressant therapy for unexplained symptoms and symptom syndromes. J Fam Pract 1999;48:980-90.
26. Kellner R, Fava GA, Lisansky J, et al. Hypochondriacal fears and beliefs in DSM-III melancholia. Changes with amitriptyline. J Affect Disord 1986;10:21-6.
27. Noyes R, Reich J, Clancy J, O’Gorman TW. Reduction in hypochondriasis with treatment of panic disorder. Br J Psychiatry 1986;149:631-5.
Mrs. M, age 34, was referred for psychiatric evaluation by her primary care physician. She reluctantly agreed to the referral and tells the psychiatrist she “really should be seeing a cardiologist.” Numerous evaluations for chest pain and palpitations—including seven emergency room visits, ECGs and cardiac catheterization—have revealed no medical pathology.
A divorced mother of two children, she says she feels anxious about her “heart condition.” Her father died of a heart attack at age 51. She experiences chest pains at home and at work, particularly when under stress. Sometimes she feels her heart racing and numbness or tingling in her arms.
Although her primary care physician has seen her frequently during the past 6 months, she says the doctor is not taking her complaints seriously. “These chest pains are real,” she says, “so don’t try to tell me they’re all in my head.”
Psychiatrists may be the last doctors patients such as Mrs. M wish to see but the ones best equipped to relieve their suffering. Our experience in treating somatizing patients and the available evidence suggest that cognitive-behavioral therapy (CBT) combined with psychoeducation, reassurance, and sometimes drug therapy is the most effective approach.
Health-related fear—or “illness worry”—is common, occurring in nearly 10% of adults who responded to a recent community survey.2 When this fear drives individuals to their physicians for evaluation, frequently no organic cause is discovered. Full evaluations are expensive and lead to increased use of health care resources, including potentially dangerous invasive testing.3,4
Defining somatization has been a source of confusion.5,6 Some authors consider somatic complaints to be expressions of suppressed psychosocial stressors. Others label them as medically unexplained complaints, although this definition fails to exclude occult medical problems. Kleinman7 defines somatization as “a somatic idiom of psychosocial distress in a setting of medical health-care seeking.” This useful definition links psychosocial problems with somatic complaints and the behavioral drive to obtain a medical evaluation.
In DSM-IV,8 the defining characteristics of somatoform disorders are somatic complaints or disease fears that are out of proportion with any identifiable somatic cause. Entities include somatization disorder, undifferentiated somatization disorder, conversion disorder, pain disorder, hypochondriasis, body dysmorphic disorder, and somatoform disorder–not otherwise specified (NOS).
Subthreshold symptoms. Unfortunately, DSM-IV’s categorization of Axis I somatoform disorders does not capture subthreshold presentations, which are common. Patients with less than the required number of somatic complaints are labeled in a wastebasket fashion with “undifferentiated somatoform disorder.”9
Mrs. M’s persistent chest pain of noncardiac origin is a familiar health anxiety, along with functional GI complaints, headaches, chronic fatigue, and lower back pain. Frustrating to their doctors and frustrated themselves, patients with medically unexplained complaints consume an inordinate amount of physicians’ time.1
Without a clear definition of somatization (Box)2-9 or useful clinical guidelines, psychiatrists must rely on the literature for guidance in managing somatization disorders. This article summarizes the evidence and describes how we apply these findings to practice. And when all else fails, we offer last-ditch advice for managing patients who resist your treatment efforts.
IDENTIFYING COMORBIDITIES
Identifying psychiatric comorbidities is the first step in successfully treating patients with somatoform complaints. In an epidemiologic study, 60% of patients with somatoform complaints also had a mood disorder and 48% had an anxiety disorder.10 In a similar study of patients with hypochondriasis, 88% also had one or more Axis I diagnosis.11
If a patient meets criteria for a comorbid psychiatric disorder and is willing to be treated for it, the somatic complaints may resolve along with the underlying disorder. In fact, the presence of an identifiable Axis I disorder order may predict a more positive prognosis.12
Personality disorders. Somatization in patients with a personality disorder poses unique challenges.13 Granted, when making a diagnosis it is difficult to tease apart somatization from personality disorders because somatization itself may be considered a chronic, maladaptive coping style. However, symptoms such as deception, impulsivity, mood lability, and self-injurious behavior introduce treatment complications that exceed the scope of this article.
Posttraumatic stress disorder (PTSD)—particularly childhood sexual and physical abuse—also predisposes some patients to somatization disorders.14,15 Patients with comorbid PTSD and somatization disorder require highly specialized treatment that is beyond the scope of this review.
COGNITIVE-BEHAVIORAL TREATMENT
Cognitive-behavioral therapy (CBT) is the best-studied and most effective treatment for somatoform disorders.16 CBT for somatization relies on both physiologic and cognitive explanations to account for the patient’s experience, without committing to an “either/or” dichotomy. It offers patients an alternate explanation of what is wrong with them—illness anxiety instead of severe physical illness.
By making patients aware of their automatic thoughts, feelings, behaviors, and underlying beliefs, CBT helps them normalize and cope with their illness anxiety. CBT techniques can be applied in a predetermined course of therapy (such as 12 sessions with a mental health clinician), in a group setting, or piecemeal by any health care provider.
Effective strategies. In a review of 30 controlled trials of CBT for somatoform disorders, Looper17 showed overall effect ranging from 0.38 to 2.5, where 0.2 was defined as a small effect, 0.5 as medium, and 0.8 as large. Hypochondriasis, somatization disorder, body dysmorphic disorder, chronic pain, chronic fatigue, and noncardiac chest pain were included in this review. The most effective strategies:
- included 6 to 16 treatment sessions
- were symptom-focused as opposed to providing general relaxation training
- included maintenance sessions after the initial series.
Four factors of health anxiety. CBT primarily targets the patient’s false beliefs that he or she is physically ill. These beliefs are based on how the patient misinterprets innocuous physical symptoms and responds to them.18 The cognitive theory of health anxiety holds that health anxiety severity is affected by four factors:
- perceived likelihood of illness
- perceived burden of illness
- perceived ability to cope with illness
- perception of the extent to which external factors will help.19
Table 1
Common dysfunctional beliefs of somatizing patients
|
The first two factors worsen and the latter two mitigate health anxiety. An individual patient’s presenting fears often suggest which factors to address. For example, Mrs. M may describe the burden of illness as the focus of her fears (“If I have a heart attack, who will care for my children?”). This information cues you to shift the focus of therapy to helping her cope with child care needs despite her recurring symptoms.
If she focuses on her likelihood of illness, then uncoupling the symptoms from the diagnosis could be more productive. When she reports palpitations, diaphoresis, and dizziness, have her do breathing exercises that induce those symptoms without producing a heart attack.
Table 2
Journaling homework: 5 questions for patients to answer about one symptom each day
|
She might describe feeling unable to cope when she feels symptoms or when cardiologists tell her nothing is wrong with her heart. In that case, focus on relaxation techniques, global stress reduction, and reducing cardiac risk factors to bolster her ability to cope with her illness.
Journaling is a critical component of CBT in treating somatization disorders. Regular journaling by the patient can reveal dysfunctional beliefs that may be driving his or her health anxieties, such as those listed in Table 1. We find it useful to assign patients to answer five questions about one symptom experience each day (Table 2). This self-monitoring provides material to work on with the patient during each session.
Cognitive restructuring. During therapy sessions, we ask patients to suggest alternate explanations for the symptoms recorded in their journals. We then ask them to determine which explanations are more feasible.
For example, if Mrs. M develops palpitations during emotionally charged arguments, we would ask her to develop explanations other than, “I was having a heart attack.” Reality testing includes rhetorical questions such as, “Would you be alive today if you were having a heart attack every time you had palpitations?” Automatic thoughts are successively identified and then tested aloud with the patient:
- “Has every unexplained symptom led to the discovery of a serious illness?”
- “Does every instance of hurt equal harm?”
Eventually, patterns of automatic thoughts emerge, and these reveal the underlying dysfunctional beliefs.
Dysfunctional beliefs are maintained when patients selectively attend to and amplify somatic sensations. Behavioral experiments during sessions can demonstrate to the patient in vivo the process by which they misattribute illness to physical symptoms. For example, overbreathing with a patient during a session may elicit light-headedness, paresthesias, or tachycardia, which can then be linked to overbreathing rather than a chronic or catastrophic illness.
Furthermore, patients can be taught to control the experience. Some patients with headaches or GI pain may be made aware of symptoms by simply asking them to focus their attention on the respective organs. Simply explaining the cycle of misattribution, autonomic activation, and further symptom development with an in vivo demonstration can be illuminating.
Response prevention. Another behavioral technique is to cut back in small increments on actions the patient takes in response to physical symptoms and automatic thoughts. For example, a patient could take medicine and seek reassurance less frequently and avoid rubbing the affected area.
PSYCHOEDUCATION
Two psychoeducation programs for somatization behavior have been formally studied.
The Personal Health Improvement Program20—led by trained facilitators—includes classroom videos, cognitive-behavioral exercises, and home study assignments. After completing the 6-week course, 171 patients with somatization disorders reported reduced physical and psychological distress and increased function. They also visited their primary care physicians less often.
Table 3
How to effectively reassure somatizing patients
| Action | Benefit |
|---|---|
| Review records in front of patients | Demonstrates that you take complaints and histories seriously |
| Acknowledge the severity of patients’ distress | Validates subjective suffering |
| Schedule follow-up visits at regular intervals | Provides access to you and continuity of care; reduces extra phone calls and emergency visits |
| Use clear and simple language | Improves communication |
| Explain that they do not have life-threatening structural disease | Opens door to cognitive restructuring |
| Assign jobs, such as journaling 15 min/day and rounding up medical records | Builds therapeutic alliance, fosters patient responsibility, and restores patients’ sense of control |
| Identify and support the patient’s strengths | Builds self-esteem |
| Use specialty referrals sparingly | Reduces risk of further medical testing and patient anxiety while awaiting results |
Coping with Illness Anxiety21 relies on mini-lectures, demonstrations, videos, and focused group discussions. After six 2-hour sessions, 33 of 43 study patients (78%) used medical services less often and reported reduced disease conviction, consequences of bodily complaints, health anxiety, and checking and avoidance behaviors. Two psychology graduate students taught the course from a manual, with 6 to 9 patients per group.
Psychoeducation in this context relies on didactic presentations, readings, role playing, and videotaped material. The goal is to teach patients to recognize thoughts, emotions, and behaviors that lead to and result from somatic preoccupation. Patients can improve when they recognize dysfunctional behavioral patterns and learn alternate coping strategies.
Somatizing patients—with their aversion to the stigma of mental illness—may find psychoeducation particularly attractive. They can be treated as students who are being educated, rather than as patients who are being treated. Classrooms in both studies cited above were located in medical outpatient offices, not in mental health facilities.
REASSURANCE
Reassurance is a common therapeutic technique in medicine, although it is poorly understood, poorly taught, and not methodically applied. Reassurance alleviates anxiety, enables patients to endure dysphoria, encourages hope, gives insight, and enhances the doctor-patient relationship.22
Table 4
How to avoid becoming frustrated with persistent somatization
| Situation | Response |
|---|---|
| Despite patients’ urgency | Watch and wait, knowing that psychological distress has been chronic |
| Despite patients’ belief that a single pill or procedure will ‘cure’ them | Persist in ‘rehabilitative’ approach |
| Despite patients’ provocations to force you to take a dichotomous approach | Persist in using both physical and psychological explanations |
| Despite your knowledge that patients are actively maintaining their illness beliefs | Try to be patient as they attribute their misfortune to ‘fate,’ ‘bad luck,’ or ‘misfortune’ |
| Despite the fact that you have agreed to treat the patient | Realize that his or her family or culture may reinforce the ‘sick role’ as the only acceptable form of distress |
| Despite patients’ desire to discuss symptoms | Reorient them to sustaining daily function (such as parenting while tolerating fatigue) |
Whereas CBT seeks to challenge patients’ underlying beliefs and restructure their thought processes,23 reassurance can help them tolerate their dysfunctional beliefs and dissuade them from believing their health is dangerously impaired. Reassurance offers a substitute explanation of patients’ dysfunction, although this explanation is not as central or detailed as it is in CBT.
How to reassure. Patients may consider reassurance offered prematurely or by a stranger to be patronizing or dismissive. Reassurance is most effective when:
- given by a trusted person who is reliable, consistent, firm, and empathic
- the patient’s condition has been established as unresponsive to conventional diagnostics or biological therapies.
Patients are most receptive to reassurance when they express distress or frustration with their unexplained symptoms. Affirming that their suffering is legitimate opens the door to further treatment.
Reassurance is least effective when a patient is expressing anger or mistrust, although this is when the physician may feel most pressured to reassure. To successfully reassure a patient, the psychiatrist needs to:
- credibly identify with the patient’s distress
- and listen empathically (such as using body language and facial expressions that convey concern and consideration to the patient).24
Starcevic suggests useful techniques for providing reassurance (Table 3).22
DRUG THERAPIES
Psychotropics are considered a first-line treatment for patients with somatization disorders when:
- the patient spontaneously identifies any discrete, vegetative, or psychological complaints that may respond to drug therapy, such as insomnia, weight loss, sadness, or preoccupation
- the patient meets diagnostic criteria for comorbid anxiety or depressive disorders
- the therapeutic alliance is strong enough to weather the inevitable struggle with side effects and incomplete response to treatment. We do not recommend medication in the first encounter, when it may threaten a nascent alliance.
A common obstacle to prescribing psychotropics to somatizing patients is their sensitivity to suggestions that their complaints are “all in their heads.” To sidestep this resistance, describe the medication as treating the stress caused. by—not causing.—their chronic physical complaints. Proposing antidepressant therapy after—rather than instead of—physical exams and other diagnostics may elicit a more positive response.
Antidepressants. In clinical trials, somatoform complaints show moderate improvement after antidepressant treatment. In a meta-analysis of 6,595 patients with unexplained symptoms treated only with antidepressants, the number needed to treat was 3 to yield a positive response.25 This report of 94 medication trials included patients with headache, fibromyalgia, functional GI syndromes, idiopathic pain, tinnitus, or chronic fatigue.
In other trials:
- Amitriptyline has reduced somatic symptoms in patients labeled as having “masked depression.”26
- Sertraline has reduced disease fear, disease conviction, and bodily preoccupation in patients with hypochondriasis and panic disorder.27
Consider side effects when choosing medication for patients with somatoform disorders. Selective serotonin reuptake inhibitors (SSRIs) in general—and sertraline, citalopram, and escitalopram specifically—have fewer side effects than tricyclics. The adage of “start low, go slow” is appropriate for somatizing patients; we usually start with one-half the dosages recommended for treating depression.
Antipsychotics. In case reports, patients with “atypical psychosis,” “monosymptomatic hypochondriacal psychosis,” or “delusional disorder, somatic type” have responded to antipsychotics. These patients’ somatic beliefs are of delusional intensity, such as the rare fear of being eaten alive by an intestinal parasite (delusional parasitosis). Reported behaviors associated with the delusion include starvation, excessive laxative abuse, ingestion of sharp objects, and self-inflicted stab wounds. Treatments described in the literature include the typical agents pimozide and haloperidol and the atypicals olanzapine and risperidone.
TREATMENT-RESISTANT PATIENTS
Some patients with somatoform disorders will not accept CBT, psychotropics, reassurance, or referrals to group psychoeducation. Despite your best efforts, they may persist in focusing on somatic complaints. If you are willing to maintain a therapeutic relationship with them, be prepared to tolerate several ongoing paradoxes (Table 4).
Behaviorally, you must “listen more and do less.” Emotionally, you must be willing to enter into a long-term relationship with an inherently frustrating patient whose pathologies make you feel therapeutically hopeless and helpless. Understand that their physical symptoms function as a metaphor for psychological distress. You are not required to explore the source, content, or meaning of the metaphor in detail but simply listen to their somatic complaints through that psychological filter.
Related resources
- Starcevic V, Lipsitt D (eds). Hypochondriasis: modern perspectives on an ancient malady. New York: Oxford University Press, 2001.
- Information and support Web site for persons with health anxiety or hypochondria. www.healthanxiety.com
- Anxiety Disorders Association of America. www.adaa.org
Drug brand names
- Amitriptyline • Elavil
- Citalopram • Celexa
- Escitalopram • Lexapro
- Haloperidol • Haldol
- Olanzapine • Zyprexa
- Pimozide • Orap
- Risperidone • Risperdal
- Sertraline • Zoloft
Disclosure
Dr. Isaac reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Wise receives grant support from Eli Lilly & Co. and is a consultant or speaker for Eli Lilly & Co., Pfizer Inc., Bristol-Myers Squibb Co., and GlaxoSmithKline.
Mrs. M, age 34, was referred for psychiatric evaluation by her primary care physician. She reluctantly agreed to the referral and tells the psychiatrist she “really should be seeing a cardiologist.” Numerous evaluations for chest pain and palpitations—including seven emergency room visits, ECGs and cardiac catheterization—have revealed no medical pathology.
A divorced mother of two children, she says she feels anxious about her “heart condition.” Her father died of a heart attack at age 51. She experiences chest pains at home and at work, particularly when under stress. Sometimes she feels her heart racing and numbness or tingling in her arms.
Although her primary care physician has seen her frequently during the past 6 months, she says the doctor is not taking her complaints seriously. “These chest pains are real,” she says, “so don’t try to tell me they’re all in my head.”
Psychiatrists may be the last doctors patients such as Mrs. M wish to see but the ones best equipped to relieve their suffering. Our experience in treating somatizing patients and the available evidence suggest that cognitive-behavioral therapy (CBT) combined with psychoeducation, reassurance, and sometimes drug therapy is the most effective approach.
Health-related fear—or “illness worry”—is common, occurring in nearly 10% of adults who responded to a recent community survey.2 When this fear drives individuals to their physicians for evaluation, frequently no organic cause is discovered. Full evaluations are expensive and lead to increased use of health care resources, including potentially dangerous invasive testing.3,4
Defining somatization has been a source of confusion.5,6 Some authors consider somatic complaints to be expressions of suppressed psychosocial stressors. Others label them as medically unexplained complaints, although this definition fails to exclude occult medical problems. Kleinman7 defines somatization as “a somatic idiom of psychosocial distress in a setting of medical health-care seeking.” This useful definition links psychosocial problems with somatic complaints and the behavioral drive to obtain a medical evaluation.
In DSM-IV,8 the defining characteristics of somatoform disorders are somatic complaints or disease fears that are out of proportion with any identifiable somatic cause. Entities include somatization disorder, undifferentiated somatization disorder, conversion disorder, pain disorder, hypochondriasis, body dysmorphic disorder, and somatoform disorder–not otherwise specified (NOS).
Subthreshold symptoms. Unfortunately, DSM-IV’s categorization of Axis I somatoform disorders does not capture subthreshold presentations, which are common. Patients with less than the required number of somatic complaints are labeled in a wastebasket fashion with “undifferentiated somatoform disorder.”9
Mrs. M’s persistent chest pain of noncardiac origin is a familiar health anxiety, along with functional GI complaints, headaches, chronic fatigue, and lower back pain. Frustrating to their doctors and frustrated themselves, patients with medically unexplained complaints consume an inordinate amount of physicians’ time.1
Without a clear definition of somatization (Box)2-9 or useful clinical guidelines, psychiatrists must rely on the literature for guidance in managing somatization disorders. This article summarizes the evidence and describes how we apply these findings to practice. And when all else fails, we offer last-ditch advice for managing patients who resist your treatment efforts.
IDENTIFYING COMORBIDITIES
Identifying psychiatric comorbidities is the first step in successfully treating patients with somatoform complaints. In an epidemiologic study, 60% of patients with somatoform complaints also had a mood disorder and 48% had an anxiety disorder.10 In a similar study of patients with hypochondriasis, 88% also had one or more Axis I diagnosis.11
If a patient meets criteria for a comorbid psychiatric disorder and is willing to be treated for it, the somatic complaints may resolve along with the underlying disorder. In fact, the presence of an identifiable Axis I disorder order may predict a more positive prognosis.12
Personality disorders. Somatization in patients with a personality disorder poses unique challenges.13 Granted, when making a diagnosis it is difficult to tease apart somatization from personality disorders because somatization itself may be considered a chronic, maladaptive coping style. However, symptoms such as deception, impulsivity, mood lability, and self-injurious behavior introduce treatment complications that exceed the scope of this article.
Posttraumatic stress disorder (PTSD)—particularly childhood sexual and physical abuse—also predisposes some patients to somatization disorders.14,15 Patients with comorbid PTSD and somatization disorder require highly specialized treatment that is beyond the scope of this review.
COGNITIVE-BEHAVIORAL TREATMENT
Cognitive-behavioral therapy (CBT) is the best-studied and most effective treatment for somatoform disorders.16 CBT for somatization relies on both physiologic and cognitive explanations to account for the patient’s experience, without committing to an “either/or” dichotomy. It offers patients an alternate explanation of what is wrong with them—illness anxiety instead of severe physical illness.
By making patients aware of their automatic thoughts, feelings, behaviors, and underlying beliefs, CBT helps them normalize and cope with their illness anxiety. CBT techniques can be applied in a predetermined course of therapy (such as 12 sessions with a mental health clinician), in a group setting, or piecemeal by any health care provider.
Effective strategies. In a review of 30 controlled trials of CBT for somatoform disorders, Looper17 showed overall effect ranging from 0.38 to 2.5, where 0.2 was defined as a small effect, 0.5 as medium, and 0.8 as large. Hypochondriasis, somatization disorder, body dysmorphic disorder, chronic pain, chronic fatigue, and noncardiac chest pain were included in this review. The most effective strategies:
- included 6 to 16 treatment sessions
- were symptom-focused as opposed to providing general relaxation training
- included maintenance sessions after the initial series.
Four factors of health anxiety. CBT primarily targets the patient’s false beliefs that he or she is physically ill. These beliefs are based on how the patient misinterprets innocuous physical symptoms and responds to them.18 The cognitive theory of health anxiety holds that health anxiety severity is affected by four factors:
- perceived likelihood of illness
- perceived burden of illness
- perceived ability to cope with illness
- perception of the extent to which external factors will help.19
Table 1
Common dysfunctional beliefs of somatizing patients
|
The first two factors worsen and the latter two mitigate health anxiety. An individual patient’s presenting fears often suggest which factors to address. For example, Mrs. M may describe the burden of illness as the focus of her fears (“If I have a heart attack, who will care for my children?”). This information cues you to shift the focus of therapy to helping her cope with child care needs despite her recurring symptoms.
If she focuses on her likelihood of illness, then uncoupling the symptoms from the diagnosis could be more productive. When she reports palpitations, diaphoresis, and dizziness, have her do breathing exercises that induce those symptoms without producing a heart attack.
Table 2
Journaling homework: 5 questions for patients to answer about one symptom each day
|
She might describe feeling unable to cope when she feels symptoms or when cardiologists tell her nothing is wrong with her heart. In that case, focus on relaxation techniques, global stress reduction, and reducing cardiac risk factors to bolster her ability to cope with her illness.
Journaling is a critical component of CBT in treating somatization disorders. Regular journaling by the patient can reveal dysfunctional beliefs that may be driving his or her health anxieties, such as those listed in Table 1. We find it useful to assign patients to answer five questions about one symptom experience each day (Table 2). This self-monitoring provides material to work on with the patient during each session.
Cognitive restructuring. During therapy sessions, we ask patients to suggest alternate explanations for the symptoms recorded in their journals. We then ask them to determine which explanations are more feasible.
For example, if Mrs. M develops palpitations during emotionally charged arguments, we would ask her to develop explanations other than, “I was having a heart attack.” Reality testing includes rhetorical questions such as, “Would you be alive today if you were having a heart attack every time you had palpitations?” Automatic thoughts are successively identified and then tested aloud with the patient:
- “Has every unexplained symptom led to the discovery of a serious illness?”
- “Does every instance of hurt equal harm?”
Eventually, patterns of automatic thoughts emerge, and these reveal the underlying dysfunctional beliefs.
Dysfunctional beliefs are maintained when patients selectively attend to and amplify somatic sensations. Behavioral experiments during sessions can demonstrate to the patient in vivo the process by which they misattribute illness to physical symptoms. For example, overbreathing with a patient during a session may elicit light-headedness, paresthesias, or tachycardia, which can then be linked to overbreathing rather than a chronic or catastrophic illness.
Furthermore, patients can be taught to control the experience. Some patients with headaches or GI pain may be made aware of symptoms by simply asking them to focus their attention on the respective organs. Simply explaining the cycle of misattribution, autonomic activation, and further symptom development with an in vivo demonstration can be illuminating.
Response prevention. Another behavioral technique is to cut back in small increments on actions the patient takes in response to physical symptoms and automatic thoughts. For example, a patient could take medicine and seek reassurance less frequently and avoid rubbing the affected area.
PSYCHOEDUCATION
Two psychoeducation programs for somatization behavior have been formally studied.
The Personal Health Improvement Program20—led by trained facilitators—includes classroom videos, cognitive-behavioral exercises, and home study assignments. After completing the 6-week course, 171 patients with somatization disorders reported reduced physical and psychological distress and increased function. They also visited their primary care physicians less often.
Table 3
How to effectively reassure somatizing patients
| Action | Benefit |
|---|---|
| Review records in front of patients | Demonstrates that you take complaints and histories seriously |
| Acknowledge the severity of patients’ distress | Validates subjective suffering |
| Schedule follow-up visits at regular intervals | Provides access to you and continuity of care; reduces extra phone calls and emergency visits |
| Use clear and simple language | Improves communication |
| Explain that they do not have life-threatening structural disease | Opens door to cognitive restructuring |
| Assign jobs, such as journaling 15 min/day and rounding up medical records | Builds therapeutic alliance, fosters patient responsibility, and restores patients’ sense of control |
| Identify and support the patient’s strengths | Builds self-esteem |
| Use specialty referrals sparingly | Reduces risk of further medical testing and patient anxiety while awaiting results |
Coping with Illness Anxiety21 relies on mini-lectures, demonstrations, videos, and focused group discussions. After six 2-hour sessions, 33 of 43 study patients (78%) used medical services less often and reported reduced disease conviction, consequences of bodily complaints, health anxiety, and checking and avoidance behaviors. Two psychology graduate students taught the course from a manual, with 6 to 9 patients per group.
Psychoeducation in this context relies on didactic presentations, readings, role playing, and videotaped material. The goal is to teach patients to recognize thoughts, emotions, and behaviors that lead to and result from somatic preoccupation. Patients can improve when they recognize dysfunctional behavioral patterns and learn alternate coping strategies.
Somatizing patients—with their aversion to the stigma of mental illness—may find psychoeducation particularly attractive. They can be treated as students who are being educated, rather than as patients who are being treated. Classrooms in both studies cited above were located in medical outpatient offices, not in mental health facilities.
REASSURANCE
Reassurance is a common therapeutic technique in medicine, although it is poorly understood, poorly taught, and not methodically applied. Reassurance alleviates anxiety, enables patients to endure dysphoria, encourages hope, gives insight, and enhances the doctor-patient relationship.22
Table 4
How to avoid becoming frustrated with persistent somatization
| Situation | Response |
|---|---|
| Despite patients’ urgency | Watch and wait, knowing that psychological distress has been chronic |
| Despite patients’ belief that a single pill or procedure will ‘cure’ them | Persist in ‘rehabilitative’ approach |
| Despite patients’ provocations to force you to take a dichotomous approach | Persist in using both physical and psychological explanations |
| Despite your knowledge that patients are actively maintaining their illness beliefs | Try to be patient as they attribute their misfortune to ‘fate,’ ‘bad luck,’ or ‘misfortune’ |
| Despite the fact that you have agreed to treat the patient | Realize that his or her family or culture may reinforce the ‘sick role’ as the only acceptable form of distress |
| Despite patients’ desire to discuss symptoms | Reorient them to sustaining daily function (such as parenting while tolerating fatigue) |
Whereas CBT seeks to challenge patients’ underlying beliefs and restructure their thought processes,23 reassurance can help them tolerate their dysfunctional beliefs and dissuade them from believing their health is dangerously impaired. Reassurance offers a substitute explanation of patients’ dysfunction, although this explanation is not as central or detailed as it is in CBT.
How to reassure. Patients may consider reassurance offered prematurely or by a stranger to be patronizing or dismissive. Reassurance is most effective when:
- given by a trusted person who is reliable, consistent, firm, and empathic
- the patient’s condition has been established as unresponsive to conventional diagnostics or biological therapies.
Patients are most receptive to reassurance when they express distress or frustration with their unexplained symptoms. Affirming that their suffering is legitimate opens the door to further treatment.
Reassurance is least effective when a patient is expressing anger or mistrust, although this is when the physician may feel most pressured to reassure. To successfully reassure a patient, the psychiatrist needs to:
- credibly identify with the patient’s distress
- and listen empathically (such as using body language and facial expressions that convey concern and consideration to the patient).24
Starcevic suggests useful techniques for providing reassurance (Table 3).22
DRUG THERAPIES
Psychotropics are considered a first-line treatment for patients with somatization disorders when:
- the patient spontaneously identifies any discrete, vegetative, or psychological complaints that may respond to drug therapy, such as insomnia, weight loss, sadness, or preoccupation
- the patient meets diagnostic criteria for comorbid anxiety or depressive disorders
- the therapeutic alliance is strong enough to weather the inevitable struggle with side effects and incomplete response to treatment. We do not recommend medication in the first encounter, when it may threaten a nascent alliance.
A common obstacle to prescribing psychotropics to somatizing patients is their sensitivity to suggestions that their complaints are “all in their heads.” To sidestep this resistance, describe the medication as treating the stress caused. by—not causing.—their chronic physical complaints. Proposing antidepressant therapy after—rather than instead of—physical exams and other diagnostics may elicit a more positive response.
Antidepressants. In clinical trials, somatoform complaints show moderate improvement after antidepressant treatment. In a meta-analysis of 6,595 patients with unexplained symptoms treated only with antidepressants, the number needed to treat was 3 to yield a positive response.25 This report of 94 medication trials included patients with headache, fibromyalgia, functional GI syndromes, idiopathic pain, tinnitus, or chronic fatigue.
In other trials:
- Amitriptyline has reduced somatic symptoms in patients labeled as having “masked depression.”26
- Sertraline has reduced disease fear, disease conviction, and bodily preoccupation in patients with hypochondriasis and panic disorder.27
Consider side effects when choosing medication for patients with somatoform disorders. Selective serotonin reuptake inhibitors (SSRIs) in general—and sertraline, citalopram, and escitalopram specifically—have fewer side effects than tricyclics. The adage of “start low, go slow” is appropriate for somatizing patients; we usually start with one-half the dosages recommended for treating depression.
Antipsychotics. In case reports, patients with “atypical psychosis,” “monosymptomatic hypochondriacal psychosis,” or “delusional disorder, somatic type” have responded to antipsychotics. These patients’ somatic beliefs are of delusional intensity, such as the rare fear of being eaten alive by an intestinal parasite (delusional parasitosis). Reported behaviors associated with the delusion include starvation, excessive laxative abuse, ingestion of sharp objects, and self-inflicted stab wounds. Treatments described in the literature include the typical agents pimozide and haloperidol and the atypicals olanzapine and risperidone.
TREATMENT-RESISTANT PATIENTS
Some patients with somatoform disorders will not accept CBT, psychotropics, reassurance, or referrals to group psychoeducation. Despite your best efforts, they may persist in focusing on somatic complaints. If you are willing to maintain a therapeutic relationship with them, be prepared to tolerate several ongoing paradoxes (Table 4).
Behaviorally, you must “listen more and do less.” Emotionally, you must be willing to enter into a long-term relationship with an inherently frustrating patient whose pathologies make you feel therapeutically hopeless and helpless. Understand that their physical symptoms function as a metaphor for psychological distress. You are not required to explore the source, content, or meaning of the metaphor in detail but simply listen to their somatic complaints through that psychological filter.
Related resources
- Starcevic V, Lipsitt D (eds). Hypochondriasis: modern perspectives on an ancient malady. New York: Oxford University Press, 2001.
- Information and support Web site for persons with health anxiety or hypochondria. www.healthanxiety.com
- Anxiety Disorders Association of America. www.adaa.org
Drug brand names
- Amitriptyline • Elavil
- Citalopram • Celexa
- Escitalopram • Lexapro
- Haloperidol • Haldol
- Olanzapine • Zyprexa
- Pimozide • Orap
- Risperidone • Risperdal
- Sertraline • Zoloft
Disclosure
Dr. Isaac reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Wise receives grant support from Eli Lilly & Co. and is a consultant or speaker for Eli Lilly & Co., Pfizer Inc., Bristol-Myers Squibb Co., and GlaxoSmithKline.
1. Katon W, Von Korff M, Lin E, et al. Distressed high utilizers of medical care. DSM-III-R diagnoses and treatment needs. Gen Hosp Psychiatry 1990;12:355-62.
2. Noyes R, Jr, Happel RL, Yagla SJ. Correlates of hypochondriasis in a nonclinical population. Psychosomatics 1999;40:461-9.
3. Mayou R, Sprigings D, Gilbert T. Patients with palpitations referred for 24-hour ECG recording. J Psychosom Res 1999;46:491-6.
4. Mayou RA, Bass C, Hart G, et al. Can clinical assessment of chest pain be made more therapeutic? Q J Med 2000;93:805-11.
5. Lipowski ZJ. Somatization: the experience and communication of psychological distress as somatic symptoms. Psychother Psychosom 1987;47:160-7.
6. Lipowski ZJ. Somatization: medicine’s unsolved problem. Psychosomatics 1987;28(6):294-297.
7. Ware NC, Kleinman A. Culture and somatic experience: the social course of illness in neurasthenia and chronic fatigue syndrome. Psychosom Med 1992;54:546-60.
8. Diagnostic and statistical manual of mental disorders (4th ed., text revision). Washington, DC: American Psychiatric Association, 2000.
9. Bass C, Peveler R, House A. Somatoform disorders: severe psychiatric illnesses neglected by psychiatrists. Br J Psychiatry 2001;179:11-14.
10. Smith GR. The epidemiology and treatment of depression when it coexists with somatoform disorders, somatization, or pain. Gen Hosp Psychiatry 1992;14:265-72.
11. Barsky AJ, Wyshak G, Klerman GL. Psychiatric comorbidity in DSM-III-R hypochondriasis. Arch Gen Psychiatry 1992;49:101-8.
12. Starcevic V. Role of reassurance and psychopathology in hypochondriasis. Psychiatry 1990;53(4):383-95.
13. Rost KM, Akins RN, Brown FW, Smith GR. The comorbidity of DSM-III-R personality disorders in somatization disorder. Gen Hosp Psychiatry 1992;14:322-6.
14. Morrison J. Childhood sexual histories of women with somatization disorder [comment]. Am J Psychiatry 1989;146:239-41.
15. Morse DS, Suchman AL, Frankel RM. The meaning of symptoms in 10 women with somatization disorder and a history of childhood abuse. Arch Fam Med 1997;6:468-76.
16. Kroenke K, Swindle R. Cognitive-behavioral therapy for somatization and symptom syndromes: a critical review of controlled clinical trials. Psychother Psychosom 2000;69:205-15.
17. Looper KJ, Kirmayer LJ. Behavioral medicine approaches to somatoform disorders. J Consult Clin Psychol 2002;70:810-27.
18. Warwick HM, Clark DM, Cobb AM, Salkovskis PM. A controlled trial of cognitive-behavioural treatment of hypochondriasis. Br J Psychiatry 1996;169:189-95.
19. Warwick HM, Salkovskis PM. Cognitive-behavioral treatment of hypochondriasis. In: Lipsitt DR, Starcevic V (eds). Hypochondriasis: Modern perspectives on an ancient malady. New York: Oxford Press, 2001;314-28.
20. McLeod CC, Budd MA. Treatment of somatization in primary care: evaluation of the Personal Health Improvement Program. HMO Pract 1997;11:88-94.
21. Bouman TK, Visser S. Cognitive and behavioural treatment of hypochondriasis. Psychother Psychosom 1998;67:214-21.
22. Starcevic V. Reassurance in the treatment of hypochondriasis. In: Lipsitt DR, Starcevic V (eds). Hypochondriasis: Modern perspectives on an ancient malady. New York: Oxford Press, 2001;291-313.
23. Clark DM, Salkovskis PM, Hackmann A, et al. Two psychological treatments for hypochondriasis. A randomised controlled trial. Br J Psychiatry 1998;173:218-25.
24. Schwartz L. Some notes on reassurance in medical practice. Psychosomatics 1966;7:290-4.
25. O’Malley PG, Jackson JL, Santoro J, et al. Antidepressant therapy for unexplained symptoms and symptom syndromes. J Fam Pract 1999;48:980-90.
26. Kellner R, Fava GA, Lisansky J, et al. Hypochondriacal fears and beliefs in DSM-III melancholia. Changes with amitriptyline. J Affect Disord 1986;10:21-6.
27. Noyes R, Reich J, Clancy J, O’Gorman TW. Reduction in hypochondriasis with treatment of panic disorder. Br J Psychiatry 1986;149:631-5.
1. Katon W, Von Korff M, Lin E, et al. Distressed high utilizers of medical care. DSM-III-R diagnoses and treatment needs. Gen Hosp Psychiatry 1990;12:355-62.
2. Noyes R, Jr, Happel RL, Yagla SJ. Correlates of hypochondriasis in a nonclinical population. Psychosomatics 1999;40:461-9.
3. Mayou R, Sprigings D, Gilbert T. Patients with palpitations referred for 24-hour ECG recording. J Psychosom Res 1999;46:491-6.
4. Mayou RA, Bass C, Hart G, et al. Can clinical assessment of chest pain be made more therapeutic? Q J Med 2000;93:805-11.
5. Lipowski ZJ. Somatization: the experience and communication of psychological distress as somatic symptoms. Psychother Psychosom 1987;47:160-7.
6. Lipowski ZJ. Somatization: medicine’s unsolved problem. Psychosomatics 1987;28(6):294-297.
7. Ware NC, Kleinman A. Culture and somatic experience: the social course of illness in neurasthenia and chronic fatigue syndrome. Psychosom Med 1992;54:546-60.
8. Diagnostic and statistical manual of mental disorders (4th ed., text revision). Washington, DC: American Psychiatric Association, 2000.
9. Bass C, Peveler R, House A. Somatoform disorders: severe psychiatric illnesses neglected by psychiatrists. Br J Psychiatry 2001;179:11-14.
10. Smith GR. The epidemiology and treatment of depression when it coexists with somatoform disorders, somatization, or pain. Gen Hosp Psychiatry 1992;14:265-72.
11. Barsky AJ, Wyshak G, Klerman GL. Psychiatric comorbidity in DSM-III-R hypochondriasis. Arch Gen Psychiatry 1992;49:101-8.
12. Starcevic V. Role of reassurance and psychopathology in hypochondriasis. Psychiatry 1990;53(4):383-95.
13. Rost KM, Akins RN, Brown FW, Smith GR. The comorbidity of DSM-III-R personality disorders in somatization disorder. Gen Hosp Psychiatry 1992;14:322-6.
14. Morrison J. Childhood sexual histories of women with somatization disorder [comment]. Am J Psychiatry 1989;146:239-41.
15. Morse DS, Suchman AL, Frankel RM. The meaning of symptoms in 10 women with somatization disorder and a history of childhood abuse. Arch Fam Med 1997;6:468-76.
16. Kroenke K, Swindle R. Cognitive-behavioral therapy for somatization and symptom syndromes: a critical review of controlled clinical trials. Psychother Psychosom 2000;69:205-15.
17. Looper KJ, Kirmayer LJ. Behavioral medicine approaches to somatoform disorders. J Consult Clin Psychol 2002;70:810-27.
18. Warwick HM, Clark DM, Cobb AM, Salkovskis PM. A controlled trial of cognitive-behavioural treatment of hypochondriasis. Br J Psychiatry 1996;169:189-95.
19. Warwick HM, Salkovskis PM. Cognitive-behavioral treatment of hypochondriasis. In: Lipsitt DR, Starcevic V (eds). Hypochondriasis: Modern perspectives on an ancient malady. New York: Oxford Press, 2001;314-28.
20. McLeod CC, Budd MA. Treatment of somatization in primary care: evaluation of the Personal Health Improvement Program. HMO Pract 1997;11:88-94.
21. Bouman TK, Visser S. Cognitive and behavioural treatment of hypochondriasis. Psychother Psychosom 1998;67:214-21.
22. Starcevic V. Reassurance in the treatment of hypochondriasis. In: Lipsitt DR, Starcevic V (eds). Hypochondriasis: Modern perspectives on an ancient malady. New York: Oxford Press, 2001;291-313.
23. Clark DM, Salkovskis PM, Hackmann A, et al. Two psychological treatments for hypochondriasis. A randomised controlled trial. Br J Psychiatry 1998;173:218-25.
24. Schwartz L. Some notes on reassurance in medical practice. Psychosomatics 1966;7:290-4.
25. O’Malley PG, Jackson JL, Santoro J, et al. Antidepressant therapy for unexplained symptoms and symptom syndromes. J Fam Pract 1999;48:980-90.
26. Kellner R, Fava GA, Lisansky J, et al. Hypochondriacal fears and beliefs in DSM-III melancholia. Changes with amitriptyline. J Affect Disord 1986;10:21-6.
27. Noyes R, Reich J, Clancy J, O’Gorman TW. Reduction in hypochondriasis with treatment of panic disorder. Br J Psychiatry 1986;149:631-5.
Switching antipsychotics: A balanced approach to ease the transition
When switching antipsychotics for patients with schizophrenia, you can ease this potentially perilous passage by choosing the right time to switch and preventing psychotic relapse. This article describes four keys to a smooth transition:
- assess response and side effects with the existing medication
- weigh the pros and cons of switching, with input from the patient or caregiver
- select a replacement with characteristics that could improve patient function
- choose a switching strategy while considering safety and efficacy data.
RISKS AND BENEFITS OF SWITCHING
The two most compelling reasons to switch antipsychotics are enhanced clinical response and improved tolerability. Others may include lower medication cost, less-frequent monitoring, fewer drug interactions, or easier administration (such as once-daily versus twice-daily dosing).
Table 1
Sample response criteria to evaluate an antipsychotic switch
Improved functioning
|
Decreased symptoms
|
Improved tolerability
|
The greatest risk in a relatively stable patient is for psychotic symptoms to re-emerge. Be very careful when switching patients who:
- might harm themselves or others if their psychosis re-emerges during the switch
- were recently stabilized after an acute psychotic episode and have been maintained for less than 6 months on the medication that controlled their symptoms
- cannot adhere to oral medications and are being maintained on long-acting depot formulations.1
Other factors to consider include:
- the need for more-frequent patient visits during the transition to monitor for adverse effects
- the patient’s willingness to switch
- influence of external stressors—such as recent bereavement—or aspects of the patient’s workplace or living environment that may interfere with adherence to a new regimen
- medication cost and coverage by third-party payers.
Establishing specific response criteria for each patient (Table 1) will help you know when to continue or terminate a switch.
INADEQUATE RESPONSE
Because antipsychotics do not eliminate all positive and negative symptoms, an adequate response is considered a reasonable therapeutic goal. Many patients with schizophrenia respond adequately to traditional or atypical antipsychotics, but approximately one-third do not.2
What is an “adequate” response? No advisory groups or consensus panels have defined this term or set standards for when to switch. Therefore, psychiatrists must evaluate a patient’s response to an antipsychotic by using clinical judgment and patient/caregiver input. To gather the information you need, it is important to:
- identify target symptoms at baseline
- regularly monitor symptom severity, frequency, and intrusion on activities of daily living and quality of life.
Quantitative measures. In research, response is measured as a percent reduction in scores on standard assessments such as the Positive and Negative Syndrome Scales (PANSS). Using the PANSS, however, is too time-consuming for clinical practice.
The Brief Psychiatric Rating Scale (BPRS) is simpler than PANSS and can be administered more quickly but is less specific for negative symptoms. Even so, using the BPRS can help quantify baseline symptoms and monitor clinical response. It is useful to complete a BPRS rating prior to a switch and at subsequent visits during the transition. A >20% reduction in the total score is considered an adequate response.
Qualitative measures. Rating scales do not measure patients’ and sfamilies’ subjective feelings. One patient may view a 50% decrease in psychotic symptoms as extremely favorable and another as unacceptable. Switching therefore may be reasonable for one patient but not for another with a similar clinical response.
Table 2
Treatment-limiting antipsychotic side effects and options for switching
| Treatment-limiting factor | Atypical antipsychotic options |
|---|---|
| Akathisia/activation | Clozapine, olanzapine, quetiapine |
| Hyperprolactinemia | Any atypical antipsychotic except risperidone |
| Insomnia | Olanzapine, quetiapine |
| Orthostatic hypotension | Ziprasidone |
| Pre-existing cardiac dysfunction | Aripiprazole, olanzapine, quetiapine, risperidone |
| Pre-existing diabetes | Aripiprazole, quetiapine, ziprasidone |
| Sedation | Aripiprazole, risperidone, ziprasidone |
| Excessive weight gain | Aripiprazole, quetiapine, risperidone, ziprasidone |
Underdosing contributes to inadequate response, so assess whether an antipsychotic has been given a sufficient trial. For example, 400 to 800 mg/d of quetiapine is considered a therapeutic dosage, assuming adequate tolerability, but some clinicians stop increasing the dosage below that range. Similarly, the usual antipsychotic trial continues at least 3 to 4 weeks at a therapeutic dosage.
TREATMENT-LIMITING EFFECTS
Antipsychotic side effects that justify switching may be treatment-limiting or simply bothersome. For example, switching is necessary for antipsychotic-induced QTc prolongation in a patient with a history of cardiac dysrhythmias and reasonable for excessive daytime sedation in a patient who is working or attending school.
Extrapyramidal symptoms (EPS) and hyperprolactinemia may limit a patient’s tolerance of an antipsychotic. Patients who are especially sensitive to EPS may not tolerate high-potency agents such an haloperidol or even low to moderate dosages of risperidone. Others may not develop EPS while receiving haloperidol or higher dosages of risperidone.
Switching to an antipsychotic with relatively less histamine or alpha-adrenergic blockade may reduce problematic side effects such as sedation and orthostatic hypotension, respectively (Table 2).
Patients vary in how well they tolerate other side effects, such as weight gain. For example, a 10-lb weight gain may be acceptable to one patient and unacceptable to another. The decision to switch may be more obvious in a patient with diabetes, for whom substantial weight gain is unacceptable.
SWITCHING STRATEGIES
No method is universally accepted for switching from one antipsychotic to another. In clinical practice and research, three common methods (Figure) are used:
- immediately discontinuing drug A while starting drug B at full dosage
- slowly tapering drug A while starting drug B at full dosage
- slowly tapering drug A while slowly increasing drug B to full dosage.
Each method has advantages and disadvantages. Gradual cross-titration and tapering may reduce the risk of relapse but increase the risk of side effects. Elaborate regimens may confuse some patients—especially those with cognitive impairment—and increase the risk for adverse events and nonadherence.
Abruptly discontinuing an agent is less confusing and more convenient than gradual tapering, but patients may experience acute withdrawal (as with clozapine). Finally, no guidelines exist on how quickly to make the transition when one or both medications are cross-titrated and tapered. For inpatients receiving intense monitoring, a transition may be completed in 3 to 7 days, whereas outpatients may require 1 to 3 weeks.
Recommendation. The evidence cited in the next section of this article suggests that any of the three methods can be used when switching antipsychotics, except clozapine. When switching from clozapine, extend the cross-taper period to help minimize or eliminate rebound psychosis and cholinergic symptoms.
SWITCHING FROM DEPOT TO ORAL AGENTS
For patients switching from depot to oral antipsychotics, a 1-month cross-titration taper has been shown to be efficient and safe.
Godleski et al3 randomized 26 patients who had received IM depot antipsychotics (haloperidol or fluphenazine decanoate) for at least 3 years to either continue the IM depot antipsychotic or switch to olanzapine. Although the study was designed to assess the safety and efficacy of the switch, it also provided data on the transition method.
Figure 3 common antipsychotic switching strategies
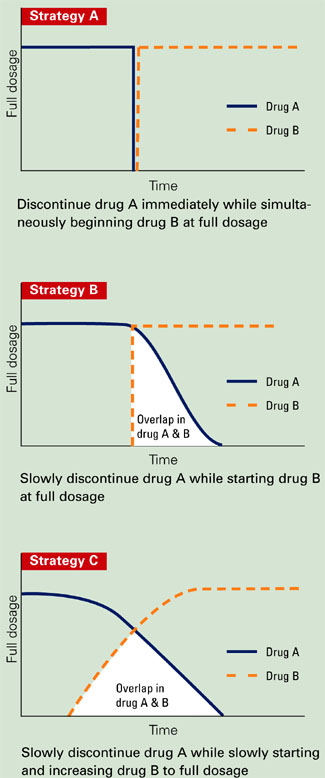
Subjects switching to olanzapine received their routine depot injection plus olanzapine, 10 mg/d for 1 month, followed by olanzapine monotherapy (5 to 20 mg/d) for 2 months. Those who continued IM depot therapy were maintained at a stable dose and dosing interval for 3 months. Safety and efficacy data were collected at baseline and monthly.
Patients receiving olanzapine improved on several efficacy measures, although the clinical relevance was minimal. For example, their mean PANSS total score decreased 3.23 points. One patient—in the control group—was hospitalized. Those who received olanzapine preferred this agent to the IM depot formulations and chose to continue daily olanzapine therapy. Adverse events did not increase significantly while patients received IM depot injections plus olanzapine.
SWITCHING ORAL AGENTS
Clozapine. When risperidone entered the U.S. market in the 1990s, a number of patients who had been treated with clozapine were abruptly switched to risperidone. Many experienced acute symptom exacerbation,4,5 including some whose rebound psychosis was more severe than their original symptoms. Other adverse effects—including nausea, diarrhea, vomiting, headache, restlessness, and sweating— have been attributed to cholinergic rebound caused by abruptly discontinuing clozapine.
To minimize the potential for rebound psychosis and cholinergic symptoms, taper clozapine across a minimum of 1 to 2 weeks. When you need to discontinue clozapine immediately—such as for patients experiencing serious hematologic effects—adding an anticholinergic such as benztropine may minimize the cholinergic rebound.
Risperidone. No studies have formally assessed methods for switching patients to risperidone.
Olanzapine. When switching to olanzapine, a direct switch or cross-titration tapering appear to be viable options.
In one multicenter, open-label study,2 108 patients were randomly assigned to olanzapine, 10 mg/d, after abruptly discontinuing a previous antipsychotic (direct switch) or by cross-titration tapering in a 1:1 fashion. Patients in the crosstitration group started olanzapine and discontinued their original antipsychotics across 2 weeks. Olanzapine dosages were adjusted as needed from 5 to 20 mg/d.
At study entry, approximately 95% of subjects in the direct-switch group and 85% in the crosstitration taper group were taking at least one typical antipsychotic—usually haloperidol. A switch was considered successful if a patient completed the 6-week trial without psychotic symptom worsening or EPS.
The 92 (85%) subjects who completed the study comprised similar percentages from both groups. Their scores on the PANSS total and subscales and Clinical Global Impression (CGI) scale also were similar.
The most common adverse events were somnolence, insomnia, and headache in the directs-witch group (all 11%), and somnolence (15%), headache (9%), insomnia (7%), and increased appetite (7%) in the cross-titration group. Differences in these percentages were not statistically significant.
EPS and akathisia improved significantly in both groups (p< 0.01) after switching to olanzapine. Thirteen (24%) patients in the direct-switch group and 17 (32%) in the cross-titration taper group required at least one dose of benztropine. Use of concomitant medications was similar.
Quetiapine can be abruptly discontinued with minimal risk of adverse events when initiating another antipsychotic.
Cutler et al6 switched 50 stable patients who had been treated with risperidone, thioridazine, haloperidol, or haloperidol plus benztropine. The original antipsychotics were abruptly discontinued, and quetiapine was initiated in a doseescalating fashion and then maintained at 300 mg/d for 12 days. After that, quetiapine was abruptly discontinued and patients were assessed for side effects, including EPS.
Most patients’ BPRS or CGI-Severity of Illness scores did not change significantly. Two patients (4%) experienced psychotic relapse during the switch. The authors speculated that these relapses might have been related to subtherapeutic quetiapine dosing. Transient nausea and vomiting were reported after quetiapine was discontinued.
Ziprasidone. When switching from another antipsychotic to ziprasidone, all three strategies appear well tolerated and maintain symptom control.
Using randomized, open-label trials, Weiden et al7 investigated strategies for switching patients to ziprasidone from olanzapine, risperidone, and traditional antipsychotics. All participants were diagnosed with schizophrenia or schizoaffective disorder and had experienced partial or inadequate response or side effects with their original antipsychotics.
Patients were assigned to one of three switching strategies:
- abruptly discontinue the initial antipsychotic
- decrease the initial antipsychotic’s dosage by 50% for 1 week, then discontinue it
- gradually taper the initial antipsychotic, so that subjects received 100% for 3 days of ziprasidone treatment, 50% for the next 4 days, and none thereafter.
For all three strategies, ziprasidone was started at 80 mg/d for 2 days, with dosing adjusted as needed to 40 to 160 mg/d.
All patients’ total score and positive and negative PANSS subscale scores improved significantly (p<0.01) across 6 weeks, although these data represent symptom changes after switching to ziprasidone. No efficacy or safety data were reported during switching. The authors concluded that patients could switch successfully to ziprasidone over a relatively short period using a variety of methods.
In another study, Stip8 switched 54 patients to ziprasidone from haloperidol. All received ziprasidone, 40 mg bid for 2 days and then 80 mg bid. Haloperidol was discontinued:
- immediately on day 1
- after the dosage was decreased by 50% for 7 days
- or after continuing the full dosage for 2 days, then taking 50% of the initial dosage for 5 days.
All patients maintained symptom control while switching, and 40 of 54 completed the trial. Among responders, BPRS and CGI scores improved significantly across 6 weeks, and EPS improved as expected.
Aripiprazole. Direct-switch and cross-titration tapering methods appear to be effective and welltolerated when switching stable patients to aripiprazole.
In an 8-week, randomized, open-label trial, Casey et al9 switched 311 outpatients with schizophrenia or schizoaffective disorder to aripiprazole. The patients—who had been taking stable dosages of haloperidol, chlorpromazine, risperidone, or olanzapine for at least 1 month—were randomly assigned to three groups:
- group 1 immediately discontinued the previous antipsychotic and started aripiprazole, 30 mg/d
- group 2 started aripiprazole, 30 mg/d, and discontinued the previous antipsychotic across 2 weeks
- group 3 started aripiprazole (10 mg/d in week 1, 20 mg/d in week 2, and 30 mg/d in week 3) and tapered the previous antipsychotic (50% less in week 1, another 50% less in week 2, then discontinued).
Investigators assessed treatment efficacy using the PANSS and CGI at baseline and weeks 4 and 8. They questioned patients about adverse events at each follow-up visit.
Nearly three-fourths (72%) of patients completed the trial. Discontinuation rates were 31% in group 1, 34% in group 2, and 19% in group 3. Efficacy, safety, tolerability, and incidence of discontinuation because of worsening psychosis were comparable across groups.
Similar percentages of patients in each group reported one or more adverse event (89%, 89%, and 81% for groups 1, 2, and 3, respectively). Most adverse events were described as mild to moderate. Insomnia was reported most frequently. Other adverse effects that occurred in >10% of subjects included nausea, akathisia, anxiety, psychosis, headache (groups 2 and 3), somnolence, lightheadedness (groups 1 and 2) vomiting (group 2 only), agitation (group 3 only), and diarrhea (group 2 only).
Seven patients were hospitalized for serious adverse events—usually worsening psychosis. Hospitalization rates were comparable among the three groups.
All groups improved slightly on the Barnes Akathisia Scale, Simpson Angus Rating Scale, and Abnormal Involuntary Movement Scale. Few patients in each group required benztropine (2%, 4%, and 7% for groups 1, 2 and 3, respectively).
Related resources
- Borison RL. Changing antipsychotic medication: guidelines on the transition to treatment with risperidone. The Consensus Study Group on Risperidone Dosing. Clin Ther 1996;18(4):592-607.
Drug brand names
- Aripiprazole • Abilify
- Benztropine • Cogentin
- Chlorpromazine • Thorazine
- Clozapine • Clozaril
- Fluphenazine • Prolixin
- Haloperidol • Haldol
- Olanzapine • Zyprexa
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Ziprasidone • Geodon
Disclosure
Dr. Winans is a consultant for Bristol-Myers Squibb Co. and is a speaker for Pfizer Inc., Abbott Laboratories, and Bristol-Myers Squibb Co.
1. Weiden PJ, Aquila R, Dalheim L, Standard JM. Switching antipsychotic medications. J Clin Psychiatry 1997;58(suppl 10):63-72.
2. Lee CT, Conde BJL, Mazlan M, et al. Switching to olanzapine from previous antipsychotics: a regional collaborative multicenter trial assessing 2 switching techniques in Asia Pacific. J Clin Psychiatry 2002;63:569-76.
3. Godleski LS, Goldsmith J, Vieweg V, et al. Switching from depot antipsychotics to olanzapine in patients with chronic schizophrenia. J Clin Psychiatry 2003;64:119-22.
4. Clinical implications of clozapine discontinuation. Reports of an NIMH workshop. Schizophr Bull 1995;21(2):333-7.
5. Shiovitz TM, Welke TL, Tigel PD, et al. Cholinergic rebound and rapid psychosis following abrupt clozapine withdrawal. Schizophr Bull 1996;22(4):591-5.
6. Cutler AJ, Goldstein JM, Tumas JA. Dosing and switching strategies for quetiapine fumarate. Clin Ther 2002;24(2):209-22.
7. Weiden PJ, Simpson G, Potkin S. Therapeutic response in stable outpatients switched to ziprasidone (poster). Stockholm, Sweden: Association of European Psychiatrists 11th Congress, May 4-8, 2002.
8. Stip E. Haloperidol to ziprasidone switching strategies in schizophrenia (abstract). Eur Neuropsychopharmacol 2001;11(suppl 3):s272.-
9. Casey DE, Carson WH, Saha AR, et al. Switching patients to aripiprazole from other antipsychotic agents: a multicenter randomized study. Psychopharmacology 2003;166(4):391-9.
When switching antipsychotics for patients with schizophrenia, you can ease this potentially perilous passage by choosing the right time to switch and preventing psychotic relapse. This article describes four keys to a smooth transition:
- assess response and side effects with the existing medication
- weigh the pros and cons of switching, with input from the patient or caregiver
- select a replacement with characteristics that could improve patient function
- choose a switching strategy while considering safety and efficacy data.
RISKS AND BENEFITS OF SWITCHING
The two most compelling reasons to switch antipsychotics are enhanced clinical response and improved tolerability. Others may include lower medication cost, less-frequent monitoring, fewer drug interactions, or easier administration (such as once-daily versus twice-daily dosing).
Table 1
Sample response criteria to evaluate an antipsychotic switch
Improved functioning
|
Decreased symptoms
|
Improved tolerability
|
The greatest risk in a relatively stable patient is for psychotic symptoms to re-emerge. Be very careful when switching patients who:
- might harm themselves or others if their psychosis re-emerges during the switch
- were recently stabilized after an acute psychotic episode and have been maintained for less than 6 months on the medication that controlled their symptoms
- cannot adhere to oral medications and are being maintained on long-acting depot formulations.1
Other factors to consider include:
- the need for more-frequent patient visits during the transition to monitor for adverse effects
- the patient’s willingness to switch
- influence of external stressors—such as recent bereavement—or aspects of the patient’s workplace or living environment that may interfere with adherence to a new regimen
- medication cost and coverage by third-party payers.
Establishing specific response criteria for each patient (Table 1) will help you know when to continue or terminate a switch.
INADEQUATE RESPONSE
Because antipsychotics do not eliminate all positive and negative symptoms, an adequate response is considered a reasonable therapeutic goal. Many patients with schizophrenia respond adequately to traditional or atypical antipsychotics, but approximately one-third do not.2
What is an “adequate” response? No advisory groups or consensus panels have defined this term or set standards for when to switch. Therefore, psychiatrists must evaluate a patient’s response to an antipsychotic by using clinical judgment and patient/caregiver input. To gather the information you need, it is important to:
- identify target symptoms at baseline
- regularly monitor symptom severity, frequency, and intrusion on activities of daily living and quality of life.
Quantitative measures. In research, response is measured as a percent reduction in scores on standard assessments such as the Positive and Negative Syndrome Scales (PANSS). Using the PANSS, however, is too time-consuming for clinical practice.
The Brief Psychiatric Rating Scale (BPRS) is simpler than PANSS and can be administered more quickly but is less specific for negative symptoms. Even so, using the BPRS can help quantify baseline symptoms and monitor clinical response. It is useful to complete a BPRS rating prior to a switch and at subsequent visits during the transition. A >20% reduction in the total score is considered an adequate response.
Qualitative measures. Rating scales do not measure patients’ and sfamilies’ subjective feelings. One patient may view a 50% decrease in psychotic symptoms as extremely favorable and another as unacceptable. Switching therefore may be reasonable for one patient but not for another with a similar clinical response.
Table 2
Treatment-limiting antipsychotic side effects and options for switching
| Treatment-limiting factor | Atypical antipsychotic options |
|---|---|
| Akathisia/activation | Clozapine, olanzapine, quetiapine |
| Hyperprolactinemia | Any atypical antipsychotic except risperidone |
| Insomnia | Olanzapine, quetiapine |
| Orthostatic hypotension | Ziprasidone |
| Pre-existing cardiac dysfunction | Aripiprazole, olanzapine, quetiapine, risperidone |
| Pre-existing diabetes | Aripiprazole, quetiapine, ziprasidone |
| Sedation | Aripiprazole, risperidone, ziprasidone |
| Excessive weight gain | Aripiprazole, quetiapine, risperidone, ziprasidone |
Underdosing contributes to inadequate response, so assess whether an antipsychotic has been given a sufficient trial. For example, 400 to 800 mg/d of quetiapine is considered a therapeutic dosage, assuming adequate tolerability, but some clinicians stop increasing the dosage below that range. Similarly, the usual antipsychotic trial continues at least 3 to 4 weeks at a therapeutic dosage.
TREATMENT-LIMITING EFFECTS
Antipsychotic side effects that justify switching may be treatment-limiting or simply bothersome. For example, switching is necessary for antipsychotic-induced QTc prolongation in a patient with a history of cardiac dysrhythmias and reasonable for excessive daytime sedation in a patient who is working or attending school.
Extrapyramidal symptoms (EPS) and hyperprolactinemia may limit a patient’s tolerance of an antipsychotic. Patients who are especially sensitive to EPS may not tolerate high-potency agents such an haloperidol or even low to moderate dosages of risperidone. Others may not develop EPS while receiving haloperidol or higher dosages of risperidone.
Switching to an antipsychotic with relatively less histamine or alpha-adrenergic blockade may reduce problematic side effects such as sedation and orthostatic hypotension, respectively (Table 2).
Patients vary in how well they tolerate other side effects, such as weight gain. For example, a 10-lb weight gain may be acceptable to one patient and unacceptable to another. The decision to switch may be more obvious in a patient with diabetes, for whom substantial weight gain is unacceptable.
SWITCHING STRATEGIES
No method is universally accepted for switching from one antipsychotic to another. In clinical practice and research, three common methods (Figure) are used:
- immediately discontinuing drug A while starting drug B at full dosage
- slowly tapering drug A while starting drug B at full dosage
- slowly tapering drug A while slowly increasing drug B to full dosage.
Each method has advantages and disadvantages. Gradual cross-titration and tapering may reduce the risk of relapse but increase the risk of side effects. Elaborate regimens may confuse some patients—especially those with cognitive impairment—and increase the risk for adverse events and nonadherence.
Abruptly discontinuing an agent is less confusing and more convenient than gradual tapering, but patients may experience acute withdrawal (as with clozapine). Finally, no guidelines exist on how quickly to make the transition when one or both medications are cross-titrated and tapered. For inpatients receiving intense monitoring, a transition may be completed in 3 to 7 days, whereas outpatients may require 1 to 3 weeks.
Recommendation. The evidence cited in the next section of this article suggests that any of the three methods can be used when switching antipsychotics, except clozapine. When switching from clozapine, extend the cross-taper period to help minimize or eliminate rebound psychosis and cholinergic symptoms.
SWITCHING FROM DEPOT TO ORAL AGENTS
For patients switching from depot to oral antipsychotics, a 1-month cross-titration taper has been shown to be efficient and safe.
Godleski et al3 randomized 26 patients who had received IM depot antipsychotics (haloperidol or fluphenazine decanoate) for at least 3 years to either continue the IM depot antipsychotic or switch to olanzapine. Although the study was designed to assess the safety and efficacy of the switch, it also provided data on the transition method.
Figure 3 common antipsychotic switching strategies
Subjects switching to olanzapine received their routine depot injection plus olanzapine, 10 mg/d for 1 month, followed by olanzapine monotherapy (5 to 20 mg/d) for 2 months. Those who continued IM depot therapy were maintained at a stable dose and dosing interval for 3 months. Safety and efficacy data were collected at baseline and monthly.
Patients receiving olanzapine improved on several efficacy measures, although the clinical relevance was minimal. For example, their mean PANSS total score decreased 3.23 points. One patient—in the control group—was hospitalized. Those who received olanzapine preferred this agent to the IM depot formulations and chose to continue daily olanzapine therapy. Adverse events did not increase significantly while patients received IM depot injections plus olanzapine.
SWITCHING ORAL AGENTS
Clozapine. When risperidone entered the U.S. market in the 1990s, a number of patients who had been treated with clozapine were abruptly switched to risperidone. Many experienced acute symptom exacerbation,4,5 including some whose rebound psychosis was more severe than their original symptoms. Other adverse effects—including nausea, diarrhea, vomiting, headache, restlessness, and sweating— have been attributed to cholinergic rebound caused by abruptly discontinuing clozapine.
To minimize the potential for rebound psychosis and cholinergic symptoms, taper clozapine across a minimum of 1 to 2 weeks. When you need to discontinue clozapine immediately—such as for patients experiencing serious hematologic effects—adding an anticholinergic such as benztropine may minimize the cholinergic rebound.
Risperidone. No studies have formally assessed methods for switching patients to risperidone.
Olanzapine. When switching to olanzapine, a direct switch or cross-titration tapering appear to be viable options.
In one multicenter, open-label study,2 108 patients were randomly assigned to olanzapine, 10 mg/d, after abruptly discontinuing a previous antipsychotic (direct switch) or by cross-titration tapering in a 1:1 fashion. Patients in the crosstitration group started olanzapine and discontinued their original antipsychotics across 2 weeks. Olanzapine dosages were adjusted as needed from 5 to 20 mg/d.
At study entry, approximately 95% of subjects in the direct-switch group and 85% in the crosstitration taper group were taking at least one typical antipsychotic—usually haloperidol. A switch was considered successful if a patient completed the 6-week trial without psychotic symptom worsening or EPS.
The 92 (85%) subjects who completed the study comprised similar percentages from both groups. Their scores on the PANSS total and subscales and Clinical Global Impression (CGI) scale also were similar.
The most common adverse events were somnolence, insomnia, and headache in the directs-witch group (all 11%), and somnolence (15%), headache (9%), insomnia (7%), and increased appetite (7%) in the cross-titration group. Differences in these percentages were not statistically significant.
EPS and akathisia improved significantly in both groups (p< 0.01) after switching to olanzapine. Thirteen (24%) patients in the direct-switch group and 17 (32%) in the cross-titration taper group required at least one dose of benztropine. Use of concomitant medications was similar.
Quetiapine can be abruptly discontinued with minimal risk of adverse events when initiating another antipsychotic.
Cutler et al6 switched 50 stable patients who had been treated with risperidone, thioridazine, haloperidol, or haloperidol plus benztropine. The original antipsychotics were abruptly discontinued, and quetiapine was initiated in a doseescalating fashion and then maintained at 300 mg/d for 12 days. After that, quetiapine was abruptly discontinued and patients were assessed for side effects, including EPS.
Most patients’ BPRS or CGI-Severity of Illness scores did not change significantly. Two patients (4%) experienced psychotic relapse during the switch. The authors speculated that these relapses might have been related to subtherapeutic quetiapine dosing. Transient nausea and vomiting were reported after quetiapine was discontinued.
Ziprasidone. When switching from another antipsychotic to ziprasidone, all three strategies appear well tolerated and maintain symptom control.
Using randomized, open-label trials, Weiden et al7 investigated strategies for switching patients to ziprasidone from olanzapine, risperidone, and traditional antipsychotics. All participants were diagnosed with schizophrenia or schizoaffective disorder and had experienced partial or inadequate response or side effects with their original antipsychotics.
Patients were assigned to one of three switching strategies:
- abruptly discontinue the initial antipsychotic
- decrease the initial antipsychotic’s dosage by 50% for 1 week, then discontinue it
- gradually taper the initial antipsychotic, so that subjects received 100% for 3 days of ziprasidone treatment, 50% for the next 4 days, and none thereafter.
For all three strategies, ziprasidone was started at 80 mg/d for 2 days, with dosing adjusted as needed to 40 to 160 mg/d.
All patients’ total score and positive and negative PANSS subscale scores improved significantly (p<0.01) across 6 weeks, although these data represent symptom changes after switching to ziprasidone. No efficacy or safety data were reported during switching. The authors concluded that patients could switch successfully to ziprasidone over a relatively short period using a variety of methods.
In another study, Stip8 switched 54 patients to ziprasidone from haloperidol. All received ziprasidone, 40 mg bid for 2 days and then 80 mg bid. Haloperidol was discontinued:
- immediately on day 1
- after the dosage was decreased by 50% for 7 days
- or after continuing the full dosage for 2 days, then taking 50% of the initial dosage for 5 days.
All patients maintained symptom control while switching, and 40 of 54 completed the trial. Among responders, BPRS and CGI scores improved significantly across 6 weeks, and EPS improved as expected.
Aripiprazole. Direct-switch and cross-titration tapering methods appear to be effective and welltolerated when switching stable patients to aripiprazole.
In an 8-week, randomized, open-label trial, Casey et al9 switched 311 outpatients with schizophrenia or schizoaffective disorder to aripiprazole. The patients—who had been taking stable dosages of haloperidol, chlorpromazine, risperidone, or olanzapine for at least 1 month—were randomly assigned to three groups:
- group 1 immediately discontinued the previous antipsychotic and started aripiprazole, 30 mg/d
- group 2 started aripiprazole, 30 mg/d, and discontinued the previous antipsychotic across 2 weeks
- group 3 started aripiprazole (10 mg/d in week 1, 20 mg/d in week 2, and 30 mg/d in week 3) and tapered the previous antipsychotic (50% less in week 1, another 50% less in week 2, then discontinued).
Investigators assessed treatment efficacy using the PANSS and CGI at baseline and weeks 4 and 8. They questioned patients about adverse events at each follow-up visit.
Nearly three-fourths (72%) of patients completed the trial. Discontinuation rates were 31% in group 1, 34% in group 2, and 19% in group 3. Efficacy, safety, tolerability, and incidence of discontinuation because of worsening psychosis were comparable across groups.
Similar percentages of patients in each group reported one or more adverse event (89%, 89%, and 81% for groups 1, 2, and 3, respectively). Most adverse events were described as mild to moderate. Insomnia was reported most frequently. Other adverse effects that occurred in >10% of subjects included nausea, akathisia, anxiety, psychosis, headache (groups 2 and 3), somnolence, lightheadedness (groups 1 and 2) vomiting (group 2 only), agitation (group 3 only), and diarrhea (group 2 only).
Seven patients were hospitalized for serious adverse events—usually worsening psychosis. Hospitalization rates were comparable among the three groups.
All groups improved slightly on the Barnes Akathisia Scale, Simpson Angus Rating Scale, and Abnormal Involuntary Movement Scale. Few patients in each group required benztropine (2%, 4%, and 7% for groups 1, 2 and 3, respectively).
Related resources
- Borison RL. Changing antipsychotic medication: guidelines on the transition to treatment with risperidone. The Consensus Study Group on Risperidone Dosing. Clin Ther 1996;18(4):592-607.
Drug brand names
- Aripiprazole • Abilify
- Benztropine • Cogentin
- Chlorpromazine • Thorazine
- Clozapine • Clozaril
- Fluphenazine • Prolixin
- Haloperidol • Haldol
- Olanzapine • Zyprexa
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Ziprasidone • Geodon
Disclosure
Dr. Winans is a consultant for Bristol-Myers Squibb Co. and is a speaker for Pfizer Inc., Abbott Laboratories, and Bristol-Myers Squibb Co.
When switching antipsychotics for patients with schizophrenia, you can ease this potentially perilous passage by choosing the right time to switch and preventing psychotic relapse. This article describes four keys to a smooth transition:
- assess response and side effects with the existing medication
- weigh the pros and cons of switching, with input from the patient or caregiver
- select a replacement with characteristics that could improve patient function
- choose a switching strategy while considering safety and efficacy data.
RISKS AND BENEFITS OF SWITCHING
The two most compelling reasons to switch antipsychotics are enhanced clinical response and improved tolerability. Others may include lower medication cost, less-frequent monitoring, fewer drug interactions, or easier administration (such as once-daily versus twice-daily dosing).
Table 1
Sample response criteria to evaluate an antipsychotic switch
Improved functioning
|
Decreased symptoms
|
Improved tolerability
|
The greatest risk in a relatively stable patient is for psychotic symptoms to re-emerge. Be very careful when switching patients who:
- might harm themselves or others if their psychosis re-emerges during the switch
- were recently stabilized after an acute psychotic episode and have been maintained for less than 6 months on the medication that controlled their symptoms
- cannot adhere to oral medications and are being maintained on long-acting depot formulations.1
Other factors to consider include:
- the need for more-frequent patient visits during the transition to monitor for adverse effects
- the patient’s willingness to switch
- influence of external stressors—such as recent bereavement—or aspects of the patient’s workplace or living environment that may interfere with adherence to a new regimen
- medication cost and coverage by third-party payers.
Establishing specific response criteria for each patient (Table 1) will help you know when to continue or terminate a switch.
INADEQUATE RESPONSE
Because antipsychotics do not eliminate all positive and negative symptoms, an adequate response is considered a reasonable therapeutic goal. Many patients with schizophrenia respond adequately to traditional or atypical antipsychotics, but approximately one-third do not.2
What is an “adequate” response? No advisory groups or consensus panels have defined this term or set standards for when to switch. Therefore, psychiatrists must evaluate a patient’s response to an antipsychotic by using clinical judgment and patient/caregiver input. To gather the information you need, it is important to:
- identify target symptoms at baseline
- regularly monitor symptom severity, frequency, and intrusion on activities of daily living and quality of life.
Quantitative measures. In research, response is measured as a percent reduction in scores on standard assessments such as the Positive and Negative Syndrome Scales (PANSS). Using the PANSS, however, is too time-consuming for clinical practice.
The Brief Psychiatric Rating Scale (BPRS) is simpler than PANSS and can be administered more quickly but is less specific for negative symptoms. Even so, using the BPRS can help quantify baseline symptoms and monitor clinical response. It is useful to complete a BPRS rating prior to a switch and at subsequent visits during the transition. A >20% reduction in the total score is considered an adequate response.
Qualitative measures. Rating scales do not measure patients’ and sfamilies’ subjective feelings. One patient may view a 50% decrease in psychotic symptoms as extremely favorable and another as unacceptable. Switching therefore may be reasonable for one patient but not for another with a similar clinical response.
Table 2
Treatment-limiting antipsychotic side effects and options for switching
| Treatment-limiting factor | Atypical antipsychotic options |
|---|---|
| Akathisia/activation | Clozapine, olanzapine, quetiapine |
| Hyperprolactinemia | Any atypical antipsychotic except risperidone |
| Insomnia | Olanzapine, quetiapine |
| Orthostatic hypotension | Ziprasidone |
| Pre-existing cardiac dysfunction | Aripiprazole, olanzapine, quetiapine, risperidone |
| Pre-existing diabetes | Aripiprazole, quetiapine, ziprasidone |
| Sedation | Aripiprazole, risperidone, ziprasidone |
| Excessive weight gain | Aripiprazole, quetiapine, risperidone, ziprasidone |
Underdosing contributes to inadequate response, so assess whether an antipsychotic has been given a sufficient trial. For example, 400 to 800 mg/d of quetiapine is considered a therapeutic dosage, assuming adequate tolerability, but some clinicians stop increasing the dosage below that range. Similarly, the usual antipsychotic trial continues at least 3 to 4 weeks at a therapeutic dosage.
TREATMENT-LIMITING EFFECTS
Antipsychotic side effects that justify switching may be treatment-limiting or simply bothersome. For example, switching is necessary for antipsychotic-induced QTc prolongation in a patient with a history of cardiac dysrhythmias and reasonable for excessive daytime sedation in a patient who is working or attending school.
Extrapyramidal symptoms (EPS) and hyperprolactinemia may limit a patient’s tolerance of an antipsychotic. Patients who are especially sensitive to EPS may not tolerate high-potency agents such an haloperidol or even low to moderate dosages of risperidone. Others may not develop EPS while receiving haloperidol or higher dosages of risperidone.
Switching to an antipsychotic with relatively less histamine or alpha-adrenergic blockade may reduce problematic side effects such as sedation and orthostatic hypotension, respectively (Table 2).
Patients vary in how well they tolerate other side effects, such as weight gain. For example, a 10-lb weight gain may be acceptable to one patient and unacceptable to another. The decision to switch may be more obvious in a patient with diabetes, for whom substantial weight gain is unacceptable.
SWITCHING STRATEGIES
No method is universally accepted for switching from one antipsychotic to another. In clinical practice and research, three common methods (Figure) are used:
- immediately discontinuing drug A while starting drug B at full dosage
- slowly tapering drug A while starting drug B at full dosage
- slowly tapering drug A while slowly increasing drug B to full dosage.
Each method has advantages and disadvantages. Gradual cross-titration and tapering may reduce the risk of relapse but increase the risk of side effects. Elaborate regimens may confuse some patients—especially those with cognitive impairment—and increase the risk for adverse events and nonadherence.
Abruptly discontinuing an agent is less confusing and more convenient than gradual tapering, but patients may experience acute withdrawal (as with clozapine). Finally, no guidelines exist on how quickly to make the transition when one or both medications are cross-titrated and tapered. For inpatients receiving intense monitoring, a transition may be completed in 3 to 7 days, whereas outpatients may require 1 to 3 weeks.
Recommendation. The evidence cited in the next section of this article suggests that any of the three methods can be used when switching antipsychotics, except clozapine. When switching from clozapine, extend the cross-taper period to help minimize or eliminate rebound psychosis and cholinergic symptoms.
SWITCHING FROM DEPOT TO ORAL AGENTS
For patients switching from depot to oral antipsychotics, a 1-month cross-titration taper has been shown to be efficient and safe.
Godleski et al3 randomized 26 patients who had received IM depot antipsychotics (haloperidol or fluphenazine decanoate) for at least 3 years to either continue the IM depot antipsychotic or switch to olanzapine. Although the study was designed to assess the safety and efficacy of the switch, it also provided data on the transition method.
Figure 3 common antipsychotic switching strategies
Subjects switching to olanzapine received their routine depot injection plus olanzapine, 10 mg/d for 1 month, followed by olanzapine monotherapy (5 to 20 mg/d) for 2 months. Those who continued IM depot therapy were maintained at a stable dose and dosing interval for 3 months. Safety and efficacy data were collected at baseline and monthly.
Patients receiving olanzapine improved on several efficacy measures, although the clinical relevance was minimal. For example, their mean PANSS total score decreased 3.23 points. One patient—in the control group—was hospitalized. Those who received olanzapine preferred this agent to the IM depot formulations and chose to continue daily olanzapine therapy. Adverse events did not increase significantly while patients received IM depot injections plus olanzapine.
SWITCHING ORAL AGENTS
Clozapine. When risperidone entered the U.S. market in the 1990s, a number of patients who had been treated with clozapine were abruptly switched to risperidone. Many experienced acute symptom exacerbation,4,5 including some whose rebound psychosis was more severe than their original symptoms. Other adverse effects—including nausea, diarrhea, vomiting, headache, restlessness, and sweating— have been attributed to cholinergic rebound caused by abruptly discontinuing clozapine.
To minimize the potential for rebound psychosis and cholinergic symptoms, taper clozapine across a minimum of 1 to 2 weeks. When you need to discontinue clozapine immediately—such as for patients experiencing serious hematologic effects—adding an anticholinergic such as benztropine may minimize the cholinergic rebound.
Risperidone. No studies have formally assessed methods for switching patients to risperidone.
Olanzapine. When switching to olanzapine, a direct switch or cross-titration tapering appear to be viable options.
In one multicenter, open-label study,2 108 patients were randomly assigned to olanzapine, 10 mg/d, after abruptly discontinuing a previous antipsychotic (direct switch) or by cross-titration tapering in a 1:1 fashion. Patients in the crosstitration group started olanzapine and discontinued their original antipsychotics across 2 weeks. Olanzapine dosages were adjusted as needed from 5 to 20 mg/d.
At study entry, approximately 95% of subjects in the direct-switch group and 85% in the crosstitration taper group were taking at least one typical antipsychotic—usually haloperidol. A switch was considered successful if a patient completed the 6-week trial without psychotic symptom worsening or EPS.
The 92 (85%) subjects who completed the study comprised similar percentages from both groups. Their scores on the PANSS total and subscales and Clinical Global Impression (CGI) scale also were similar.
The most common adverse events were somnolence, insomnia, and headache in the directs-witch group (all 11%), and somnolence (15%), headache (9%), insomnia (7%), and increased appetite (7%) in the cross-titration group. Differences in these percentages were not statistically significant.
EPS and akathisia improved significantly in both groups (p< 0.01) after switching to olanzapine. Thirteen (24%) patients in the direct-switch group and 17 (32%) in the cross-titration taper group required at least one dose of benztropine. Use of concomitant medications was similar.
Quetiapine can be abruptly discontinued with minimal risk of adverse events when initiating another antipsychotic.
Cutler et al6 switched 50 stable patients who had been treated with risperidone, thioridazine, haloperidol, or haloperidol plus benztropine. The original antipsychotics were abruptly discontinued, and quetiapine was initiated in a doseescalating fashion and then maintained at 300 mg/d for 12 days. After that, quetiapine was abruptly discontinued and patients were assessed for side effects, including EPS.
Most patients’ BPRS or CGI-Severity of Illness scores did not change significantly. Two patients (4%) experienced psychotic relapse during the switch. The authors speculated that these relapses might have been related to subtherapeutic quetiapine dosing. Transient nausea and vomiting were reported after quetiapine was discontinued.
Ziprasidone. When switching from another antipsychotic to ziprasidone, all three strategies appear well tolerated and maintain symptom control.
Using randomized, open-label trials, Weiden et al7 investigated strategies for switching patients to ziprasidone from olanzapine, risperidone, and traditional antipsychotics. All participants were diagnosed with schizophrenia or schizoaffective disorder and had experienced partial or inadequate response or side effects with their original antipsychotics.
Patients were assigned to one of three switching strategies:
- abruptly discontinue the initial antipsychotic
- decrease the initial antipsychotic’s dosage by 50% for 1 week, then discontinue it
- gradually taper the initial antipsychotic, so that subjects received 100% for 3 days of ziprasidone treatment, 50% for the next 4 days, and none thereafter.
For all three strategies, ziprasidone was started at 80 mg/d for 2 days, with dosing adjusted as needed to 40 to 160 mg/d.
All patients’ total score and positive and negative PANSS subscale scores improved significantly (p<0.01) across 6 weeks, although these data represent symptom changes after switching to ziprasidone. No efficacy or safety data were reported during switching. The authors concluded that patients could switch successfully to ziprasidone over a relatively short period using a variety of methods.
In another study, Stip8 switched 54 patients to ziprasidone from haloperidol. All received ziprasidone, 40 mg bid for 2 days and then 80 mg bid. Haloperidol was discontinued:
- immediately on day 1
- after the dosage was decreased by 50% for 7 days
- or after continuing the full dosage for 2 days, then taking 50% of the initial dosage for 5 days.
All patients maintained symptom control while switching, and 40 of 54 completed the trial. Among responders, BPRS and CGI scores improved significantly across 6 weeks, and EPS improved as expected.
Aripiprazole. Direct-switch and cross-titration tapering methods appear to be effective and welltolerated when switching stable patients to aripiprazole.
In an 8-week, randomized, open-label trial, Casey et al9 switched 311 outpatients with schizophrenia or schizoaffective disorder to aripiprazole. The patients—who had been taking stable dosages of haloperidol, chlorpromazine, risperidone, or olanzapine for at least 1 month—were randomly assigned to three groups:
- group 1 immediately discontinued the previous antipsychotic and started aripiprazole, 30 mg/d
- group 2 started aripiprazole, 30 mg/d, and discontinued the previous antipsychotic across 2 weeks
- group 3 started aripiprazole (10 mg/d in week 1, 20 mg/d in week 2, and 30 mg/d in week 3) and tapered the previous antipsychotic (50% less in week 1, another 50% less in week 2, then discontinued).
Investigators assessed treatment efficacy using the PANSS and CGI at baseline and weeks 4 and 8. They questioned patients about adverse events at each follow-up visit.
Nearly three-fourths (72%) of patients completed the trial. Discontinuation rates were 31% in group 1, 34% in group 2, and 19% in group 3. Efficacy, safety, tolerability, and incidence of discontinuation because of worsening psychosis were comparable across groups.
Similar percentages of patients in each group reported one or more adverse event (89%, 89%, and 81% for groups 1, 2, and 3, respectively). Most adverse events were described as mild to moderate. Insomnia was reported most frequently. Other adverse effects that occurred in >10% of subjects included nausea, akathisia, anxiety, psychosis, headache (groups 2 and 3), somnolence, lightheadedness (groups 1 and 2) vomiting (group 2 only), agitation (group 3 only), and diarrhea (group 2 only).
Seven patients were hospitalized for serious adverse events—usually worsening psychosis. Hospitalization rates were comparable among the three groups.
All groups improved slightly on the Barnes Akathisia Scale, Simpson Angus Rating Scale, and Abnormal Involuntary Movement Scale. Few patients in each group required benztropine (2%, 4%, and 7% for groups 1, 2 and 3, respectively).
Related resources
- Borison RL. Changing antipsychotic medication: guidelines on the transition to treatment with risperidone. The Consensus Study Group on Risperidone Dosing. Clin Ther 1996;18(4):592-607.
Drug brand names
- Aripiprazole • Abilify
- Benztropine • Cogentin
- Chlorpromazine • Thorazine
- Clozapine • Clozaril
- Fluphenazine • Prolixin
- Haloperidol • Haldol
- Olanzapine • Zyprexa
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Ziprasidone • Geodon
Disclosure
Dr. Winans is a consultant for Bristol-Myers Squibb Co. and is a speaker for Pfizer Inc., Abbott Laboratories, and Bristol-Myers Squibb Co.
1. Weiden PJ, Aquila R, Dalheim L, Standard JM. Switching antipsychotic medications. J Clin Psychiatry 1997;58(suppl 10):63-72.
2. Lee CT, Conde BJL, Mazlan M, et al. Switching to olanzapine from previous antipsychotics: a regional collaborative multicenter trial assessing 2 switching techniques in Asia Pacific. J Clin Psychiatry 2002;63:569-76.
3. Godleski LS, Goldsmith J, Vieweg V, et al. Switching from depot antipsychotics to olanzapine in patients with chronic schizophrenia. J Clin Psychiatry 2003;64:119-22.
4. Clinical implications of clozapine discontinuation. Reports of an NIMH workshop. Schizophr Bull 1995;21(2):333-7.
5. Shiovitz TM, Welke TL, Tigel PD, et al. Cholinergic rebound and rapid psychosis following abrupt clozapine withdrawal. Schizophr Bull 1996;22(4):591-5.
6. Cutler AJ, Goldstein JM, Tumas JA. Dosing and switching strategies for quetiapine fumarate. Clin Ther 2002;24(2):209-22.
7. Weiden PJ, Simpson G, Potkin S. Therapeutic response in stable outpatients switched to ziprasidone (poster). Stockholm, Sweden: Association of European Psychiatrists 11th Congress, May 4-8, 2002.
8. Stip E. Haloperidol to ziprasidone switching strategies in schizophrenia (abstract). Eur Neuropsychopharmacol 2001;11(suppl 3):s272.-
9. Casey DE, Carson WH, Saha AR, et al. Switching patients to aripiprazole from other antipsychotic agents: a multicenter randomized study. Psychopharmacology 2003;166(4):391-9.
1. Weiden PJ, Aquila R, Dalheim L, Standard JM. Switching antipsychotic medications. J Clin Psychiatry 1997;58(suppl 10):63-72.
2. Lee CT, Conde BJL, Mazlan M, et al. Switching to olanzapine from previous antipsychotics: a regional collaborative multicenter trial assessing 2 switching techniques in Asia Pacific. J Clin Psychiatry 2002;63:569-76.
3. Godleski LS, Goldsmith J, Vieweg V, et al. Switching from depot antipsychotics to olanzapine in patients with chronic schizophrenia. J Clin Psychiatry 2003;64:119-22.
4. Clinical implications of clozapine discontinuation. Reports of an NIMH workshop. Schizophr Bull 1995;21(2):333-7.
5. Shiovitz TM, Welke TL, Tigel PD, et al. Cholinergic rebound and rapid psychosis following abrupt clozapine withdrawal. Schizophr Bull 1996;22(4):591-5.
6. Cutler AJ, Goldstein JM, Tumas JA. Dosing and switching strategies for quetiapine fumarate. Clin Ther 2002;24(2):209-22.
7. Weiden PJ, Simpson G, Potkin S. Therapeutic response in stable outpatients switched to ziprasidone (poster). Stockholm, Sweden: Association of European Psychiatrists 11th Congress, May 4-8, 2002.
8. Stip E. Haloperidol to ziprasidone switching strategies in schizophrenia (abstract). Eur Neuropsychopharmacol 2001;11(suppl 3):s272.-
9. Casey DE, Carson WH, Saha AR, et al. Switching patients to aripiprazole from other antipsychotic agents: a multicenter randomized study. Psychopharmacology 2003;166(4):391-9.
Crossing the line: When does teen substance use become abuse or dependence?
Assessing an adolescent for a possible substance use disorder can be streamlined by choosing age-appropriate screening tools and asking targeted questions. Based on our experience, we offer a 4-step approach to these at-risk patients1 (Box) that focuses on:
- quantifying alcohol or drug abuse and/or dependence
- identifying and treating psychiatric comorbidity
- evaluating and addressing social influences that contribute to substance use
- assessing negative consequences associated with substance abuse.
Adolescent substance use increases the risk of motor vehicle accidents, suicide, transmission of HIV and other sexual diseases, criminal behaviors, and psychological problems. Alcohol and marijuana are the substances most commonly abused by adolescents.
In 2002, the University of Michigan Institute for Social Research’s annual “Monitoring the Future” study reported:
- drunkenness in 7% of 8th graders, 18% of 10th graders, and 30% of 12th graders at least once in the previous 30 days.
- illicit drug use by 18% of 8th graders, 35% of 10th graders, and 41% of 12th graders in the previous 12 months.
Boys used substances more frequently than girls, and boys’ use was more severe. Within the previous month, boys reported greater alcohol use, binge drinking (five or more drinks in one sitting), and heavy drinking, as well as greater illicit drug use in the past year.1
INITIAL EVALUATION
Adolescents generally do not seek substance abuse treatment but are referred because of alcohol- or drug-related legal, school, or family problems. Thus, most present for evaluation with their parents, legal guardians, or officers of the court.
We begin by finding out from parents or guardians the reasons for the evaluation, their perspectives on the adolescent’s behavior, and their expectations of treatment. Then we interview the adolescent alone, assessing for substance use and evaluating peer relationships.
Components. A typical initial evaluation takes 90 minutes to 2 hours and includes:
- psychiatric history and symptoms
- medical history
- previous hospitalizations (medical and psychiatric)
- family history
- social history.
Specifically, the assessment focuses on the reason for the evaluation, with attention to diagnostic criteria for substance use/dependence.
STEP 1: QUANTIFYING DEPENDENCE
As with adults, clinical diagnosis of substance abuse or dependence in adolescents is based on DSM-IV diagnostic criteria (Table 1). Adolescents, however, differ from adults in diagnostic presentation, risk of dependence, and patterns of substance use.
Diagnostic ‘orphans.’ DSM-IV criteria for alcohol use disorders have limitations in adolescents.2 Teens who report one or two dependence symptoms and no abuse symptoms have been described as “diagnostic orphans”3—they fall short of criteria for dependence or abuse but clearly demonstrate substance use patterns. This presentation is common; in a survey of 74,008 high school students, almost 10% of 12th graders reported one or two dependence symptoms and no abuse symptoms.4
Risk of dependence. Adolescents who begin using alcohol or drugs develop dependence more rapidly than adults do.5
Patterns of use. Adolescents are more likely than adults to binge with alcohol and drugs, which may conceal the severity of their abuse. DSM-IV diagnostic criteria for substance abuse or dependence do not consider quantity of use, such as number of drinks or percent of days drinking or using drugs.
Assessment instruments. Many assessment instruments are available to explore adolescent substance use and its associated consequences. Some are described in detail and are available on the Internet. Common screening instruments that can be used for adolescent substance use are compared in Table 2.
DUSI-A and POSIT. Two self-report instruments—Drug Use Screening Inventory-Adolescents (DUSI-A)6 and Problem Oriented Screening Instrument for Teenagers (POSIT)7—can help explore alcohol or drug use in teens who admit to substance use. Anyone who endorses at least one DSM-IV abuse or dependence criterion requires further evaluation. Either test is a good starting point, and both have a built-in “lie” scale.
T-ASI and CASI. The Teen Addiction Severity Index (T-ASI)8 and Comprehensive Adolescent Severity Inventory (CASI)9 are more labor-intensive and require training to administer. These assessments are more appropriate for adolescents with extensive alcohol or drug abuse.
A-OCDS and Deas-MOCS. Our group recently developed the Adolescent Obsessive Compulsive Drinking Scale (A-OCDS)10 and the Deas-Marijuana Obsessive Compulsive Scale (Deas-MOCS).11
These self-report instruments have been validated in treatment- and nontreatment-seeking adolescents and young adults in inpatient and outpatient populations. They are sensitive and specific in identifying problem drinkers and marijuana users, respectively, and are quick, useful screens to determine need for further assessment.
Toxicology is useful for initial assessment and to monitor substance use patterns during treatment.
Urine samples are used to assess marijuana, sedative/hypnotic, amphetamine, cocaine, opiate, and phencyclidine use. Alcohol may be detected in urine, but alcohol levels detected by blood and breath testing are more accurate.
Table 1
Diagnostic criteria for substance abuse and dependence
| Substance abuse | 1 of these 4 symptoms in a 12-month period: Role impairment Hazardous use Legal problems associated with use Social problems |
| Substance dependence | At least 3 of the following: Tolerance Withdrawal Using more or longer than intended Attempting to quit or cut down Much time spent using Activities given up to use Psychological/physical problems resulting from use Subtyped as with or without physiologic features (tolerance or withdrawal symptoms) |
| Source: DSM-IV-TR | |
Marijuana may be detected in the urine for 3 days to 4 weeks, depending on level of use. Cocaine can be detected for 2 to 4 days in urine and longer in hair analysis.
Random screening. Adolescents who use drugs usually know how long substances can be detected, so random urine drug screening is important to treatment progress. We inform adolescents at the beginning of treatment that random screening will be performed to corroborate self-report of substance use. To ensure a reliable urine sample, same-gender staff observe while the adolescent gives the sample.
Table 2
Common screening instruments for alcohol and drug use in adolescents
| Instrument | Items (#) | How administered | Administration time |
|---|---|---|---|
| Drug Use Screening Inventory (DUSI-R), Revised | 159 | Self-report | 20 to 40 minutes |
| Problem-Oriented Screening Instrument for Teenagers (POSIT) | 139 | Self-report | 20 to 30 minutes |
| Teen Addiction Severity Index (T-ASI) | 133 | Clinician | 20 to 45 minutes |
| Comprehensive Adolescent Severity Inventory (CASI) | 245 | Clinician | Varies with experience of administrator |
| Adolescent Obsessive-Compulsive Drinking Scale (A-OCDS) | 14 | Self-report | About 5 minutes |
| Deas-Marijuana Obsessive-Compulsive Scale (Deas-MOCS) | 14 | Self-report | About 5 minutes |
STEP 2: IDENTIFYING PSYCHIATRIC COMORBIDITY
In adolescents, substance use disorder frequently goes hand-in-hand with psychiatric disorders, particularly:
- mood and anxiety disorders
- disruptive disorders (attention-deficit/hyperactivity, oppositional defiant, and conduct disorders)12
- and posttraumatic stress disorder.13
Uncontrolled psychiatric disorders may sabotage substance abuse treatment. Therefore, assess any adolescent presenting with substance use for psychiatric illness.
Did psychiatric symptoms predate or postdate substance use? The answer may suggest self-medication or a substance-induced phenomenon. This assumption does not always apply, however, as many factors affect the relationship between substance use and psychiatric disorders.
Adolescents who meet DSM-IV criteria for conduct disorder—especially those who are highly aggressive—tend to initiate substance use much earlier than adolescents without conduct disorder, and they continue their use longer.
Most adolescents with comorbid psychiatric and substance use disorders develop the psychiatric disorder first. Some report using various substances to medicate their psychiatric symptoms. Early diagnosis and treatment of the psychiatric disorder may prevent or decrease the adolescent’s substance use.
STEPS 3 AND 4: EVALUATING SOCIAL INFLUENCES AND CONSEQUENCES
Social influences that contribute to adolescent alcohol and drug abuse include family dynamics and peer relationships. Consequences include educational and legal problems. We explore these areas with the adolescents and their parents/guardians. In most cases, adolescents are honest when reporting how their alcohol or drug use has affected their lives.
What is his family like? Assess the adolescent’s family, including its structure and history of substance abuse, psychiatric illness, or trauma (Table 3). Adolescents whose parents or siblings use alcohol or drugs are at increased risk for substance use.14 To what extent this association is genetic, environmental, or both is undetermined, but the genetic influence increases as adolescents age.15
Who are her friends? Adolescents who try alcohol or drugs and continue to use them tend to have peers who use these substances.16 Moreover, the severity of adolescents’ substance use is correlated with the number of substance-using peers. To explore peer relationships, ask about:
- peer group composition, including whether peers use alcohol or drugs
- peer interactions, including the adolescent’s ability to assert him- or herself in the peer group
- markers for risky sexual behaviors related to substance use, including infection with HIV and other sexually transmitted diseases.
How is she doing in school? Inquire about the teen’s academic performance, attendance, disciplinary problems, and motivation. Even a small decline in school performance or an increase in disciplinary problems that result in suspension or expulsion can indicate substance use or other at-risk behaviors.
Poor grades or attendance problems suggest but are not the only clues to substance use. Some adolescents with good school performance engage in substance use and may be impaired in other life domains.
Has he been arrested? Substance-abusing adolescents tend to engage in delinquent behaviors, including shoplifting, vandalism, curfew violations, disorderly conduct, and drunken driving. When assessing for delinquency, ask about behaviors that did or did not result in arrest. The teen who avoided arrest for illegal activities may perceive his/her behaviors as less severe than those involving arrest, and it may help to address this denial in individual or group therapy.
Table 3
Questions to assess family influence on an adolescent’s substance use
| Family structure |
|
| Parenting styles |
|
| Substance abuse |
|
| Psychiatric disorders |
|
| Trauma |
|
TREATMENT
We consider any adolescent with dependence symptoms—whether or not the presentation meets full DSM-IV diagnostic criteria—to be a candidate for further assessment and treatment. Early intervention may prevent progression to substance dependence.
Effective treatments:
- are intensive and of sufficient duration to change attitude and behaviors
- are comprehensive and target multiple domains of the adolescent’s life
- are sensitive to cultural and socioeconomic realities
- involve the family
- emphasize pro-social recreational activities, such as playing sports, attending movies, camping, having lunch or dinner with peers, etc.
Inpatient or outpatient? Managed care and insurance restrictions limit many patients’ eligibility for inpatient or residential treatment, so partial hospitalization and outpatient settings have become standard for substance abuse treatment. Partial hospitalization programs vary but may entail several hours, several days per week. Outpatient treatment may encompass individual, group, and family therapy, including after-school programs.
Inpatient treatment is usually reserved for adolescents:
- who need detoxification
- with comorbid psychiatric disorders
- or who may harm themselves or others.
PSYCHOTHERAPIES
Behavioral therapy, family-based therapy, multisystematic therapy (MST), and 12-step approaches have shown efficacy in treating adolescents with substance use disorders.
Behavioral therapy. Behavioral therapy is recommended as initial treatment because substance use plays a functional role in the adolescent’s life and is learned and reinforced in the adolescent’s environment. Homework assignments and role-play are commonly used in therapy.
Three central ingredients are:
- functional analysis (identifying internal and external triggers for starting and continuing substance use)
- skills training (targeting problems identified in the functional analysis)
- and relapse prevention.
Behavioral therapy is more effective than supportive therapy in improving family relationships and school and work attendance and in decreasing substance use, as indicated by fewer positive urine toxicology screens.17
Cognitive-behavioral therapy (CBT) approaches substance use as a maladaptive response to life problems. Its goal is to teach new skills to help the adolescent recognize and avoid high-risk situations and cope with associated problems and behaviors.
In a recent study, Kaminer et al randomly assigned 82 adolescents with psychiatric and substance use disorders to 8 weeks of CBT or psychoeducational therapy (didactic or videotaped presentations of ways to address problems associated with substance use). Substance use was reduced in both treatment groups, but:
- adolescents receiving CBT had significantly fewer positive urine toxicology tests
- adolescents with comorbid conduct disorder were least likely to complete treatment or return for follow-up
- those with depressive and anxiety disorders were most likely to complete treatment.18
Family-based therapy. Two detailed reviews19,20 demonstrate that the adolescent’s family, community, and school relationships affect his or her perceptions and behaviors. Maladaptive relationships in any of these systems may lead to high-risk behaviors. Therefore, family therapy is core to the adolescent’s treatment, regardless of what modality is chosen.
Goals of family therapy may be:
- to help the adolescent abstain from substance use
- to engage in pro-social activities
- to decrease parental denial of the adolescent’s substance use
- to decrease resistance to treatment
- treatment maintenance
- to establish or re-establish structure in the adolescent’s environment
- to improve communication in the family.
Multisystemic therapy is comprehensive and involves all systems that relate to the adolescent’s substance use, including the family, school, community, and legal system. MST requires special training and intensive supervision, so it is usually reserved for adolescents who have not benefited from other forms of treatment.21
12-step approaches. For adolescents, 12-step programs usually augment other treatments and are rarely used alone. Alcoholics Anonymous, Narcotics Anonymous, and other 12-step programs have been studied more extensively in adults than in adolescents.
Adolescents, who often feel invulnerable, may have difficulty accepting the 12-step doctrine of lack of control. A modified 12-step program and workbook for adolescents are available through the American Academy of Child and Adolescent Psychiatry.22
Referral tips. If possible, refer an adolescent to a 12-step group specifically for adolescents. Teens who attend adult groups often perceive their substance use as normal, compared with the more severe and chronic patterns of some adults. Most adolescents relate better to peers with similar problems and may benefit from reminders of the negative consequences of substance use and the benefits of abstinence.
DRUG THERAPY
Drug therapy for adolescents with substance use disorders is usually considered in the context of detoxification, treating withdrawal symptoms, and treating comorbid psychiatric disorders. The same detoxification and withdrawal treatment principles used in adults apply to adolescents.
Clinical withdrawal symptoms are less common in adolescents than adults, probably because of adolescents’ binge patterns of substance use. Even so, some adolescents do experience withdrawal and may be at risk for complications if improperly treated.
Psychiatric comorbidity. To our knowledge, only two double-blind, placebo-controlled studies of drug therapy in treating adolescent substance use disorders have been published.
Depression. Deas et al23 randomized 10 adolescents with alcohol use disorders and depression to 12 weeks of group CBT plus sertraline or placebo. Sertraline was started at 25 mg/d and titrated to a maximum of 100 mg/d. Drinks per drinking day, percent of days drinking, and Hamilton Rating Scale for Depression scores declined similarly in both groups.
Drinking decreased significantly from baseline (by an average 4.7 drinks), and adolescents in both groups no longer met DSM-IV criteria for depression at the end of treatment. CBT’s effectiveness in treating alcohol use disorders and depression might have concealed any difference in effect between sertaline and placebo.
Bipolar disorder. Geller et al24 randomly assigned 25 adolescents with bipolar disorder and substance dependence to lithium or placebo for 6 weeks. Lithium was started as an evening dose of 600 mg and titrated to achieve a lithium blood level of 0.9 to 1.3 mEq/L. Among the 21 adolescents who completed the trial, those receiving lithium had significantly fewer positive urine toxicology screens and higher clinical global assessment of function scores.
Related resources
- National Clearinghouse for Alcohol and Drug Information, Substance Abuse and Mental Health Services Administration, U.S. Department of Health and Human Services. www.health.org/govpubs/bkd306/31k.aspx
- National Institute on Alcohol Abuse and Alcoholism (assessment instruments). www.niaaa.nih.gov/publications/instable.htm
- Deas D, Thomas SE. An overview of controlled studies of adolescent substance abuse treatment. Am J Addict 2001;10:178-89.
Drug brand names
- Sertraline • Zoloft
Disclosure
Dr. Deas receives grant support from Pfizer, Inc. and the National Institute of Alcohol Abuse and Alcoholism.
Dr. Upadhyaya receives grant support from the National Institute of Drug Abuse and GlaxoSmithKline.
Acknowledgment
The authors wish to thank Alva Blair for assistance with preparing this manuscript and Natalie Johnson, MA, Kess Mughelli, BS, and Lakeleia Middleton-Robinson, MA, for technical support.
1. Johnston LD, O’Malley PM, Bachman JG. Monitoring the Future: national results on adolescent drug use. Overview of key findings, 2002. Bethesda, MD: National Institute on Drug Abuse, 2003 (in press).
2. Martin CS, Kaczynski NA, Maisto SA, et al. Patterns of DSM-IV alcohol abuse and dependence symptoms in adolescent drinkers. J Stud Alcohol 1995;56:672-80.
3. Pollock NK, Martin CS. Diagnostic orphans: adolescents with alcohol symptoms who do not qualify for DSM-IV abuse or dependence diagnoses. Am J Psychiatry 1999;156:897-901.
4. Harrison PA, Fulkerson JA, Beebe TJ. DSM-IV substance use disorder criteria for adolescents: a critical examination based on a statewide school survey. Am J Psychiatry 1998;155:486-92.
5. Grant BF, Dawson DA. Age at onset of alcohol use and its association with DSM-IV alcohol abuse/dependence: results from the National Longitudinal Alcohol Epidemiological Survey. J Subst Abuse 1997;9:103-10.
6. Tarter RE, Laird SB, Bukstein O, Kaminer Y. Validation of the adolescent drug use screening inventory: preliminary findings. Psychol Addict Behav 1992;6:322-6.
7. Rahdert E (ed). The adolescent assessment/referral system manual. DHHS pub. no. (ADM) 91-1735. Rockville, MD: U.S. Department of Health and Human Services, 1991.
8. Kaminer Y, Bukstein OG, Tarter RE. The teen addiction severity index (T-ASI): rationale and reliability. Int J Addict 1991;26:219-26.
9. Meyers K, McLellan AT, Jaeger JL, Pettinati A. The development of the Comprehensive Addiction Severity Index for Adolescents (CASI-A): an interview for assessing multiple problems of adolescents. J Subst Abuse Treat 1995;12:181-93.
10. Deas DV, Roberts JS, Randall CL, Anton RF. Adolescent Obsessive-Compulsive Drinking Scale (A-OCDS): an assessment tool for problem drinking. J Natl Med Assoc 2001;93:92-103.
11. Deas D, Randall CL, Thomas S. The utility of the Deas-Marijuana Obsessive-Compulsive Scale (Deas-MOCS) in an inpatient adolescent substance abusing sample. Drug Alcohol Depend 2002;66(June):S43.-
12. Deas-Nesmith D, Campbell S, Brady KT. Substance use disorders in an adolescent inpatient psychiatric population. JAMA 1998;90:233-8.
13. Clark DB, Lesnick L, Hegedus AM. Traumas and other adverse life events in adolescents with alcohol abuse and dependence. Am Acad Child Adolesc Psychiatry 1997;36:1744-51.
14. Kilpatrick DG, Acierno R, Saunders B, et al. Risk factors for adolescent substance abuse and dependence: data from a national sample. J Consult Clin Psychol 2000;68:19-30.
15. Rose RJ. A developmental behavioral-genetic perspective on alcoholism risk. Alcohol Health Res World 1998;22:131-43.
16. Swadi H. Individual risk factors for adolescent substance use. Drug Alcohol Depend 1999;55:209-24.
17. Azrin N, McMahon P, Donohue B, et al. Behavior therapy for drug abuse: a controlled treatment outcome study. Behav Res Ther 1994;32:857-66.
18. Kaminer Y, Burleson JA, Goldberger R. Cognitive-behavioral coping skills and psychoeducation therapies for adolescent substance abuse. J Nerv Ment Dis 2002;190:737-45.
19. Liddle H, Dakof G. Efficacy of family therapy for drug abuse: promising but not definitive. J Marital Fam Ther 1995;21:511-43.
20. Waldron HB. Adolescent substance abuse and family therapy outcome: a review of randomized trials. Adv Clin Child Psychol 1997;19:199-234.
21. Henggeler SW, Melton LA. Effects of multisystemic therapy on drug use and abuse in serious juvenile offenders: a progress report from two outcome studies. Family Dynamics of Addiction Quarterly 1991;1:40-51.
22. Jaffe S. Step workbook for adolescent chemical dependency recovery. Washington, DC: American Academy of Child and Adolescent Psychiatry, 1990.
23. Deas DV, Randall C, Roberts J, Anton R. A double-blind, placebo-controlled trial of sertraline in depressed adolescent alcoholics: a pilot study. Human Psychopharmacology Clinical and Experimental 2000;15:461-9.
24. Geller B, Cooper T, Sun K, et al. Double-blind and placebo-controlled study of lithium for adolescent bipolar disorders with secondary substance dependency. J Am Acad Child Adolesc Psychiatry 1998;37:171-8.
Assessing an adolescent for a possible substance use disorder can be streamlined by choosing age-appropriate screening tools and asking targeted questions. Based on our experience, we offer a 4-step approach to these at-risk patients1 (Box) that focuses on:
- quantifying alcohol or drug abuse and/or dependence
- identifying and treating psychiatric comorbidity
- evaluating and addressing social influences that contribute to substance use
- assessing negative consequences associated with substance abuse.
Adolescent substance use increases the risk of motor vehicle accidents, suicide, transmission of HIV and other sexual diseases, criminal behaviors, and psychological problems. Alcohol and marijuana are the substances most commonly abused by adolescents.
In 2002, the University of Michigan Institute for Social Research’s annual “Monitoring the Future” study reported:
- drunkenness in 7% of 8th graders, 18% of 10th graders, and 30% of 12th graders at least once in the previous 30 days.
- illicit drug use by 18% of 8th graders, 35% of 10th graders, and 41% of 12th graders in the previous 12 months.
Boys used substances more frequently than girls, and boys’ use was more severe. Within the previous month, boys reported greater alcohol use, binge drinking (five or more drinks in one sitting), and heavy drinking, as well as greater illicit drug use in the past year.1
INITIAL EVALUATION
Adolescents generally do not seek substance abuse treatment but are referred because of alcohol- or drug-related legal, school, or family problems. Thus, most present for evaluation with their parents, legal guardians, or officers of the court.
We begin by finding out from parents or guardians the reasons for the evaluation, their perspectives on the adolescent’s behavior, and their expectations of treatment. Then we interview the adolescent alone, assessing for substance use and evaluating peer relationships.
Components. A typical initial evaluation takes 90 minutes to 2 hours and includes:
- psychiatric history and symptoms
- medical history
- previous hospitalizations (medical and psychiatric)
- family history
- social history.
Specifically, the assessment focuses on the reason for the evaluation, with attention to diagnostic criteria for substance use/dependence.
STEP 1: QUANTIFYING DEPENDENCE
As with adults, clinical diagnosis of substance abuse or dependence in adolescents is based on DSM-IV diagnostic criteria (Table 1). Adolescents, however, differ from adults in diagnostic presentation, risk of dependence, and patterns of substance use.
Diagnostic ‘orphans.’ DSM-IV criteria for alcohol use disorders have limitations in adolescents.2 Teens who report one or two dependence symptoms and no abuse symptoms have been described as “diagnostic orphans”3—they fall short of criteria for dependence or abuse but clearly demonstrate substance use patterns. This presentation is common; in a survey of 74,008 high school students, almost 10% of 12th graders reported one or two dependence symptoms and no abuse symptoms.4
Risk of dependence. Adolescents who begin using alcohol or drugs develop dependence more rapidly than adults do.5
Patterns of use. Adolescents are more likely than adults to binge with alcohol and drugs, which may conceal the severity of their abuse. DSM-IV diagnostic criteria for substance abuse or dependence do not consider quantity of use, such as number of drinks or percent of days drinking or using drugs.
Assessment instruments. Many assessment instruments are available to explore adolescent substance use and its associated consequences. Some are described in detail and are available on the Internet. Common screening instruments that can be used for adolescent substance use are compared in Table 2.
DUSI-A and POSIT. Two self-report instruments—Drug Use Screening Inventory-Adolescents (DUSI-A)6 and Problem Oriented Screening Instrument for Teenagers (POSIT)7—can help explore alcohol or drug use in teens who admit to substance use. Anyone who endorses at least one DSM-IV abuse or dependence criterion requires further evaluation. Either test is a good starting point, and both have a built-in “lie” scale.
T-ASI and CASI. The Teen Addiction Severity Index (T-ASI)8 and Comprehensive Adolescent Severity Inventory (CASI)9 are more labor-intensive and require training to administer. These assessments are more appropriate for adolescents with extensive alcohol or drug abuse.
A-OCDS and Deas-MOCS. Our group recently developed the Adolescent Obsessive Compulsive Drinking Scale (A-OCDS)10 and the Deas-Marijuana Obsessive Compulsive Scale (Deas-MOCS).11
These self-report instruments have been validated in treatment- and nontreatment-seeking adolescents and young adults in inpatient and outpatient populations. They are sensitive and specific in identifying problem drinkers and marijuana users, respectively, and are quick, useful screens to determine need for further assessment.
Toxicology is useful for initial assessment and to monitor substance use patterns during treatment.
Urine samples are used to assess marijuana, sedative/hypnotic, amphetamine, cocaine, opiate, and phencyclidine use. Alcohol may be detected in urine, but alcohol levels detected by blood and breath testing are more accurate.
Table 1
Diagnostic criteria for substance abuse and dependence
| Substance abuse | 1 of these 4 symptoms in a 12-month period: Role impairment Hazardous use Legal problems associated with use Social problems |
| Substance dependence | At least 3 of the following: Tolerance Withdrawal Using more or longer than intended Attempting to quit or cut down Much time spent using Activities given up to use Psychological/physical problems resulting from use Subtyped as with or without physiologic features (tolerance or withdrawal symptoms) |
| Source: DSM-IV-TR | |
Marijuana may be detected in the urine for 3 days to 4 weeks, depending on level of use. Cocaine can be detected for 2 to 4 days in urine and longer in hair analysis.
Random screening. Adolescents who use drugs usually know how long substances can be detected, so random urine drug screening is important to treatment progress. We inform adolescents at the beginning of treatment that random screening will be performed to corroborate self-report of substance use. To ensure a reliable urine sample, same-gender staff observe while the adolescent gives the sample.
Table 2
Common screening instruments for alcohol and drug use in adolescents
| Instrument | Items (#) | How administered | Administration time |
|---|---|---|---|
| Drug Use Screening Inventory (DUSI-R), Revised | 159 | Self-report | 20 to 40 minutes |
| Problem-Oriented Screening Instrument for Teenagers (POSIT) | 139 | Self-report | 20 to 30 minutes |
| Teen Addiction Severity Index (T-ASI) | 133 | Clinician | 20 to 45 minutes |
| Comprehensive Adolescent Severity Inventory (CASI) | 245 | Clinician | Varies with experience of administrator |
| Adolescent Obsessive-Compulsive Drinking Scale (A-OCDS) | 14 | Self-report | About 5 minutes |
| Deas-Marijuana Obsessive-Compulsive Scale (Deas-MOCS) | 14 | Self-report | About 5 minutes |
STEP 2: IDENTIFYING PSYCHIATRIC COMORBIDITY
In adolescents, substance use disorder frequently goes hand-in-hand with psychiatric disorders, particularly:
- mood and anxiety disorders
- disruptive disorders (attention-deficit/hyperactivity, oppositional defiant, and conduct disorders)12
- and posttraumatic stress disorder.13
Uncontrolled psychiatric disorders may sabotage substance abuse treatment. Therefore, assess any adolescent presenting with substance use for psychiatric illness.
Did psychiatric symptoms predate or postdate substance use? The answer may suggest self-medication or a substance-induced phenomenon. This assumption does not always apply, however, as many factors affect the relationship between substance use and psychiatric disorders.
Adolescents who meet DSM-IV criteria for conduct disorder—especially those who are highly aggressive—tend to initiate substance use much earlier than adolescents without conduct disorder, and they continue their use longer.
Most adolescents with comorbid psychiatric and substance use disorders develop the psychiatric disorder first. Some report using various substances to medicate their psychiatric symptoms. Early diagnosis and treatment of the psychiatric disorder may prevent or decrease the adolescent’s substance use.
STEPS 3 AND 4: EVALUATING SOCIAL INFLUENCES AND CONSEQUENCES
Social influences that contribute to adolescent alcohol and drug abuse include family dynamics and peer relationships. Consequences include educational and legal problems. We explore these areas with the adolescents and their parents/guardians. In most cases, adolescents are honest when reporting how their alcohol or drug use has affected their lives.
What is his family like? Assess the adolescent’s family, including its structure and history of substance abuse, psychiatric illness, or trauma (Table 3). Adolescents whose parents or siblings use alcohol or drugs are at increased risk for substance use.14 To what extent this association is genetic, environmental, or both is undetermined, but the genetic influence increases as adolescents age.15
Who are her friends? Adolescents who try alcohol or drugs and continue to use them tend to have peers who use these substances.16 Moreover, the severity of adolescents’ substance use is correlated with the number of substance-using peers. To explore peer relationships, ask about:
- peer group composition, including whether peers use alcohol or drugs
- peer interactions, including the adolescent’s ability to assert him- or herself in the peer group
- markers for risky sexual behaviors related to substance use, including infection with HIV and other sexually transmitted diseases.
How is she doing in school? Inquire about the teen’s academic performance, attendance, disciplinary problems, and motivation. Even a small decline in school performance or an increase in disciplinary problems that result in suspension or expulsion can indicate substance use or other at-risk behaviors.
Poor grades or attendance problems suggest but are not the only clues to substance use. Some adolescents with good school performance engage in substance use and may be impaired in other life domains.
Has he been arrested? Substance-abusing adolescents tend to engage in delinquent behaviors, including shoplifting, vandalism, curfew violations, disorderly conduct, and drunken driving. When assessing for delinquency, ask about behaviors that did or did not result in arrest. The teen who avoided arrest for illegal activities may perceive his/her behaviors as less severe than those involving arrest, and it may help to address this denial in individual or group therapy.
Table 3
Questions to assess family influence on an adolescent’s substance use
| Family structure |
|
| Parenting styles |
|
| Substance abuse |
|
| Psychiatric disorders |
|
| Trauma |
|
TREATMENT
We consider any adolescent with dependence symptoms—whether or not the presentation meets full DSM-IV diagnostic criteria—to be a candidate for further assessment and treatment. Early intervention may prevent progression to substance dependence.
Effective treatments:
- are intensive and of sufficient duration to change attitude and behaviors
- are comprehensive and target multiple domains of the adolescent’s life
- are sensitive to cultural and socioeconomic realities
- involve the family
- emphasize pro-social recreational activities, such as playing sports, attending movies, camping, having lunch or dinner with peers, etc.
Inpatient or outpatient? Managed care and insurance restrictions limit many patients’ eligibility for inpatient or residential treatment, so partial hospitalization and outpatient settings have become standard for substance abuse treatment. Partial hospitalization programs vary but may entail several hours, several days per week. Outpatient treatment may encompass individual, group, and family therapy, including after-school programs.
Inpatient treatment is usually reserved for adolescents:
- who need detoxification
- with comorbid psychiatric disorders
- or who may harm themselves or others.
PSYCHOTHERAPIES
Behavioral therapy, family-based therapy, multisystematic therapy (MST), and 12-step approaches have shown efficacy in treating adolescents with substance use disorders.
Behavioral therapy. Behavioral therapy is recommended as initial treatment because substance use plays a functional role in the adolescent’s life and is learned and reinforced in the adolescent’s environment. Homework assignments and role-play are commonly used in therapy.
Three central ingredients are:
- functional analysis (identifying internal and external triggers for starting and continuing substance use)
- skills training (targeting problems identified in the functional analysis)
- and relapse prevention.
Behavioral therapy is more effective than supportive therapy in improving family relationships and school and work attendance and in decreasing substance use, as indicated by fewer positive urine toxicology screens.17
Cognitive-behavioral therapy (CBT) approaches substance use as a maladaptive response to life problems. Its goal is to teach new skills to help the adolescent recognize and avoid high-risk situations and cope with associated problems and behaviors.
In a recent study, Kaminer et al randomly assigned 82 adolescents with psychiatric and substance use disorders to 8 weeks of CBT or psychoeducational therapy (didactic or videotaped presentations of ways to address problems associated with substance use). Substance use was reduced in both treatment groups, but:
- adolescents receiving CBT had significantly fewer positive urine toxicology tests
- adolescents with comorbid conduct disorder were least likely to complete treatment or return for follow-up
- those with depressive and anxiety disorders were most likely to complete treatment.18
Family-based therapy. Two detailed reviews19,20 demonstrate that the adolescent’s family, community, and school relationships affect his or her perceptions and behaviors. Maladaptive relationships in any of these systems may lead to high-risk behaviors. Therefore, family therapy is core to the adolescent’s treatment, regardless of what modality is chosen.
Goals of family therapy may be:
- to help the adolescent abstain from substance use
- to engage in pro-social activities
- to decrease parental denial of the adolescent’s substance use
- to decrease resistance to treatment
- treatment maintenance
- to establish or re-establish structure in the adolescent’s environment
- to improve communication in the family.
Multisystemic therapy is comprehensive and involves all systems that relate to the adolescent’s substance use, including the family, school, community, and legal system. MST requires special training and intensive supervision, so it is usually reserved for adolescents who have not benefited from other forms of treatment.21
12-step approaches. For adolescents, 12-step programs usually augment other treatments and are rarely used alone. Alcoholics Anonymous, Narcotics Anonymous, and other 12-step programs have been studied more extensively in adults than in adolescents.
Adolescents, who often feel invulnerable, may have difficulty accepting the 12-step doctrine of lack of control. A modified 12-step program and workbook for adolescents are available through the American Academy of Child and Adolescent Psychiatry.22
Referral tips. If possible, refer an adolescent to a 12-step group specifically for adolescents. Teens who attend adult groups often perceive their substance use as normal, compared with the more severe and chronic patterns of some adults. Most adolescents relate better to peers with similar problems and may benefit from reminders of the negative consequences of substance use and the benefits of abstinence.
DRUG THERAPY
Drug therapy for adolescents with substance use disorders is usually considered in the context of detoxification, treating withdrawal symptoms, and treating comorbid psychiatric disorders. The same detoxification and withdrawal treatment principles used in adults apply to adolescents.
Clinical withdrawal symptoms are less common in adolescents than adults, probably because of adolescents’ binge patterns of substance use. Even so, some adolescents do experience withdrawal and may be at risk for complications if improperly treated.
Psychiatric comorbidity. To our knowledge, only two double-blind, placebo-controlled studies of drug therapy in treating adolescent substance use disorders have been published.
Depression. Deas et al23 randomized 10 adolescents with alcohol use disorders and depression to 12 weeks of group CBT plus sertraline or placebo. Sertraline was started at 25 mg/d and titrated to a maximum of 100 mg/d. Drinks per drinking day, percent of days drinking, and Hamilton Rating Scale for Depression scores declined similarly in both groups.
Drinking decreased significantly from baseline (by an average 4.7 drinks), and adolescents in both groups no longer met DSM-IV criteria for depression at the end of treatment. CBT’s effectiveness in treating alcohol use disorders and depression might have concealed any difference in effect between sertaline and placebo.
Bipolar disorder. Geller et al24 randomly assigned 25 adolescents with bipolar disorder and substance dependence to lithium or placebo for 6 weeks. Lithium was started as an evening dose of 600 mg and titrated to achieve a lithium blood level of 0.9 to 1.3 mEq/L. Among the 21 adolescents who completed the trial, those receiving lithium had significantly fewer positive urine toxicology screens and higher clinical global assessment of function scores.
Related resources
- National Clearinghouse for Alcohol and Drug Information, Substance Abuse and Mental Health Services Administration, U.S. Department of Health and Human Services. www.health.org/govpubs/bkd306/31k.aspx
- National Institute on Alcohol Abuse and Alcoholism (assessment instruments). www.niaaa.nih.gov/publications/instable.htm
- Deas D, Thomas SE. An overview of controlled studies of adolescent substance abuse treatment. Am J Addict 2001;10:178-89.
Drug brand names
- Sertraline • Zoloft
Disclosure
Dr. Deas receives grant support from Pfizer, Inc. and the National Institute of Alcohol Abuse and Alcoholism.
Dr. Upadhyaya receives grant support from the National Institute of Drug Abuse and GlaxoSmithKline.
Acknowledgment
The authors wish to thank Alva Blair for assistance with preparing this manuscript and Natalie Johnson, MA, Kess Mughelli, BS, and Lakeleia Middleton-Robinson, MA, for technical support.
Assessing an adolescent for a possible substance use disorder can be streamlined by choosing age-appropriate screening tools and asking targeted questions. Based on our experience, we offer a 4-step approach to these at-risk patients1 (Box) that focuses on:
- quantifying alcohol or drug abuse and/or dependence
- identifying and treating psychiatric comorbidity
- evaluating and addressing social influences that contribute to substance use
- assessing negative consequences associated with substance abuse.
Adolescent substance use increases the risk of motor vehicle accidents, suicide, transmission of HIV and other sexual diseases, criminal behaviors, and psychological problems. Alcohol and marijuana are the substances most commonly abused by adolescents.
In 2002, the University of Michigan Institute for Social Research’s annual “Monitoring the Future” study reported:
- drunkenness in 7% of 8th graders, 18% of 10th graders, and 30% of 12th graders at least once in the previous 30 days.
- illicit drug use by 18% of 8th graders, 35% of 10th graders, and 41% of 12th graders in the previous 12 months.
Boys used substances more frequently than girls, and boys’ use was more severe. Within the previous month, boys reported greater alcohol use, binge drinking (five or more drinks in one sitting), and heavy drinking, as well as greater illicit drug use in the past year.1
INITIAL EVALUATION
Adolescents generally do not seek substance abuse treatment but are referred because of alcohol- or drug-related legal, school, or family problems. Thus, most present for evaluation with their parents, legal guardians, or officers of the court.
We begin by finding out from parents or guardians the reasons for the evaluation, their perspectives on the adolescent’s behavior, and their expectations of treatment. Then we interview the adolescent alone, assessing for substance use and evaluating peer relationships.
Components. A typical initial evaluation takes 90 minutes to 2 hours and includes:
- psychiatric history and symptoms
- medical history
- previous hospitalizations (medical and psychiatric)
- family history
- social history.
Specifically, the assessment focuses on the reason for the evaluation, with attention to diagnostic criteria for substance use/dependence.
STEP 1: QUANTIFYING DEPENDENCE
As with adults, clinical diagnosis of substance abuse or dependence in adolescents is based on DSM-IV diagnostic criteria (Table 1). Adolescents, however, differ from adults in diagnostic presentation, risk of dependence, and patterns of substance use.
Diagnostic ‘orphans.’ DSM-IV criteria for alcohol use disorders have limitations in adolescents.2 Teens who report one or two dependence symptoms and no abuse symptoms have been described as “diagnostic orphans”3—they fall short of criteria for dependence or abuse but clearly demonstrate substance use patterns. This presentation is common; in a survey of 74,008 high school students, almost 10% of 12th graders reported one or two dependence symptoms and no abuse symptoms.4
Risk of dependence. Adolescents who begin using alcohol or drugs develop dependence more rapidly than adults do.5
Patterns of use. Adolescents are more likely than adults to binge with alcohol and drugs, which may conceal the severity of their abuse. DSM-IV diagnostic criteria for substance abuse or dependence do not consider quantity of use, such as number of drinks or percent of days drinking or using drugs.
Assessment instruments. Many assessment instruments are available to explore adolescent substance use and its associated consequences. Some are described in detail and are available on the Internet. Common screening instruments that can be used for adolescent substance use are compared in Table 2.
DUSI-A and POSIT. Two self-report instruments—Drug Use Screening Inventory-Adolescents (DUSI-A)6 and Problem Oriented Screening Instrument for Teenagers (POSIT)7—can help explore alcohol or drug use in teens who admit to substance use. Anyone who endorses at least one DSM-IV abuse or dependence criterion requires further evaluation. Either test is a good starting point, and both have a built-in “lie” scale.
T-ASI and CASI. The Teen Addiction Severity Index (T-ASI)8 and Comprehensive Adolescent Severity Inventory (CASI)9 are more labor-intensive and require training to administer. These assessments are more appropriate for adolescents with extensive alcohol or drug abuse.
A-OCDS and Deas-MOCS. Our group recently developed the Adolescent Obsessive Compulsive Drinking Scale (A-OCDS)10 and the Deas-Marijuana Obsessive Compulsive Scale (Deas-MOCS).11
These self-report instruments have been validated in treatment- and nontreatment-seeking adolescents and young adults in inpatient and outpatient populations. They are sensitive and specific in identifying problem drinkers and marijuana users, respectively, and are quick, useful screens to determine need for further assessment.
Toxicology is useful for initial assessment and to monitor substance use patterns during treatment.
Urine samples are used to assess marijuana, sedative/hypnotic, amphetamine, cocaine, opiate, and phencyclidine use. Alcohol may be detected in urine, but alcohol levels detected by blood and breath testing are more accurate.
Table 1
Diagnostic criteria for substance abuse and dependence
| Substance abuse | 1 of these 4 symptoms in a 12-month period: Role impairment Hazardous use Legal problems associated with use Social problems |
| Substance dependence | At least 3 of the following: Tolerance Withdrawal Using more or longer than intended Attempting to quit or cut down Much time spent using Activities given up to use Psychological/physical problems resulting from use Subtyped as with or without physiologic features (tolerance or withdrawal symptoms) |
| Source: DSM-IV-TR | |
Marijuana may be detected in the urine for 3 days to 4 weeks, depending on level of use. Cocaine can be detected for 2 to 4 days in urine and longer in hair analysis.
Random screening. Adolescents who use drugs usually know how long substances can be detected, so random urine drug screening is important to treatment progress. We inform adolescents at the beginning of treatment that random screening will be performed to corroborate self-report of substance use. To ensure a reliable urine sample, same-gender staff observe while the adolescent gives the sample.
Table 2
Common screening instruments for alcohol and drug use in adolescents
| Instrument | Items (#) | How administered | Administration time |
|---|---|---|---|
| Drug Use Screening Inventory (DUSI-R), Revised | 159 | Self-report | 20 to 40 minutes |
| Problem-Oriented Screening Instrument for Teenagers (POSIT) | 139 | Self-report | 20 to 30 minutes |
| Teen Addiction Severity Index (T-ASI) | 133 | Clinician | 20 to 45 minutes |
| Comprehensive Adolescent Severity Inventory (CASI) | 245 | Clinician | Varies with experience of administrator |
| Adolescent Obsessive-Compulsive Drinking Scale (A-OCDS) | 14 | Self-report | About 5 minutes |
| Deas-Marijuana Obsessive-Compulsive Scale (Deas-MOCS) | 14 | Self-report | About 5 minutes |
STEP 2: IDENTIFYING PSYCHIATRIC COMORBIDITY
In adolescents, substance use disorder frequently goes hand-in-hand with psychiatric disorders, particularly:
- mood and anxiety disorders
- disruptive disorders (attention-deficit/hyperactivity, oppositional defiant, and conduct disorders)12
- and posttraumatic stress disorder.13
Uncontrolled psychiatric disorders may sabotage substance abuse treatment. Therefore, assess any adolescent presenting with substance use for psychiatric illness.
Did psychiatric symptoms predate or postdate substance use? The answer may suggest self-medication or a substance-induced phenomenon. This assumption does not always apply, however, as many factors affect the relationship between substance use and psychiatric disorders.
Adolescents who meet DSM-IV criteria for conduct disorder—especially those who are highly aggressive—tend to initiate substance use much earlier than adolescents without conduct disorder, and they continue their use longer.
Most adolescents with comorbid psychiatric and substance use disorders develop the psychiatric disorder first. Some report using various substances to medicate their psychiatric symptoms. Early diagnosis and treatment of the psychiatric disorder may prevent or decrease the adolescent’s substance use.
STEPS 3 AND 4: EVALUATING SOCIAL INFLUENCES AND CONSEQUENCES
Social influences that contribute to adolescent alcohol and drug abuse include family dynamics and peer relationships. Consequences include educational and legal problems. We explore these areas with the adolescents and their parents/guardians. In most cases, adolescents are honest when reporting how their alcohol or drug use has affected their lives.
What is his family like? Assess the adolescent’s family, including its structure and history of substance abuse, psychiatric illness, or trauma (Table 3). Adolescents whose parents or siblings use alcohol or drugs are at increased risk for substance use.14 To what extent this association is genetic, environmental, or both is undetermined, but the genetic influence increases as adolescents age.15
Who are her friends? Adolescents who try alcohol or drugs and continue to use them tend to have peers who use these substances.16 Moreover, the severity of adolescents’ substance use is correlated with the number of substance-using peers. To explore peer relationships, ask about:
- peer group composition, including whether peers use alcohol or drugs
- peer interactions, including the adolescent’s ability to assert him- or herself in the peer group
- markers for risky sexual behaviors related to substance use, including infection with HIV and other sexually transmitted diseases.
How is she doing in school? Inquire about the teen’s academic performance, attendance, disciplinary problems, and motivation. Even a small decline in school performance or an increase in disciplinary problems that result in suspension or expulsion can indicate substance use or other at-risk behaviors.
Poor grades or attendance problems suggest but are not the only clues to substance use. Some adolescents with good school performance engage in substance use and may be impaired in other life domains.
Has he been arrested? Substance-abusing adolescents tend to engage in delinquent behaviors, including shoplifting, vandalism, curfew violations, disorderly conduct, and drunken driving. When assessing for delinquency, ask about behaviors that did or did not result in arrest. The teen who avoided arrest for illegal activities may perceive his/her behaviors as less severe than those involving arrest, and it may help to address this denial in individual or group therapy.
Table 3
Questions to assess family influence on an adolescent’s substance use
| Family structure |
|
| Parenting styles |
|
| Substance abuse |
|
| Psychiatric disorders |
|
| Trauma |
|
TREATMENT
We consider any adolescent with dependence symptoms—whether or not the presentation meets full DSM-IV diagnostic criteria—to be a candidate for further assessment and treatment. Early intervention may prevent progression to substance dependence.
Effective treatments:
- are intensive and of sufficient duration to change attitude and behaviors
- are comprehensive and target multiple domains of the adolescent’s life
- are sensitive to cultural and socioeconomic realities
- involve the family
- emphasize pro-social recreational activities, such as playing sports, attending movies, camping, having lunch or dinner with peers, etc.
Inpatient or outpatient? Managed care and insurance restrictions limit many patients’ eligibility for inpatient or residential treatment, so partial hospitalization and outpatient settings have become standard for substance abuse treatment. Partial hospitalization programs vary but may entail several hours, several days per week. Outpatient treatment may encompass individual, group, and family therapy, including after-school programs.
Inpatient treatment is usually reserved for adolescents:
- who need detoxification
- with comorbid psychiatric disorders
- or who may harm themselves or others.
PSYCHOTHERAPIES
Behavioral therapy, family-based therapy, multisystematic therapy (MST), and 12-step approaches have shown efficacy in treating adolescents with substance use disorders.
Behavioral therapy. Behavioral therapy is recommended as initial treatment because substance use plays a functional role in the adolescent’s life and is learned and reinforced in the adolescent’s environment. Homework assignments and role-play are commonly used in therapy.
Three central ingredients are:
- functional analysis (identifying internal and external triggers for starting and continuing substance use)
- skills training (targeting problems identified in the functional analysis)
- and relapse prevention.
Behavioral therapy is more effective than supportive therapy in improving family relationships and school and work attendance and in decreasing substance use, as indicated by fewer positive urine toxicology screens.17
Cognitive-behavioral therapy (CBT) approaches substance use as a maladaptive response to life problems. Its goal is to teach new skills to help the adolescent recognize and avoid high-risk situations and cope with associated problems and behaviors.
In a recent study, Kaminer et al randomly assigned 82 adolescents with psychiatric and substance use disorders to 8 weeks of CBT or psychoeducational therapy (didactic or videotaped presentations of ways to address problems associated with substance use). Substance use was reduced in both treatment groups, but:
- adolescents receiving CBT had significantly fewer positive urine toxicology tests
- adolescents with comorbid conduct disorder were least likely to complete treatment or return for follow-up
- those with depressive and anxiety disorders were most likely to complete treatment.18
Family-based therapy. Two detailed reviews19,20 demonstrate that the adolescent’s family, community, and school relationships affect his or her perceptions and behaviors. Maladaptive relationships in any of these systems may lead to high-risk behaviors. Therefore, family therapy is core to the adolescent’s treatment, regardless of what modality is chosen.
Goals of family therapy may be:
- to help the adolescent abstain from substance use
- to engage in pro-social activities
- to decrease parental denial of the adolescent’s substance use
- to decrease resistance to treatment
- treatment maintenance
- to establish or re-establish structure in the adolescent’s environment
- to improve communication in the family.
Multisystemic therapy is comprehensive and involves all systems that relate to the adolescent’s substance use, including the family, school, community, and legal system. MST requires special training and intensive supervision, so it is usually reserved for adolescents who have not benefited from other forms of treatment.21
12-step approaches. For adolescents, 12-step programs usually augment other treatments and are rarely used alone. Alcoholics Anonymous, Narcotics Anonymous, and other 12-step programs have been studied more extensively in adults than in adolescents.
Adolescents, who often feel invulnerable, may have difficulty accepting the 12-step doctrine of lack of control. A modified 12-step program and workbook for adolescents are available through the American Academy of Child and Adolescent Psychiatry.22
Referral tips. If possible, refer an adolescent to a 12-step group specifically for adolescents. Teens who attend adult groups often perceive their substance use as normal, compared with the more severe and chronic patterns of some adults. Most adolescents relate better to peers with similar problems and may benefit from reminders of the negative consequences of substance use and the benefits of abstinence.
DRUG THERAPY
Drug therapy for adolescents with substance use disorders is usually considered in the context of detoxification, treating withdrawal symptoms, and treating comorbid psychiatric disorders. The same detoxification and withdrawal treatment principles used in adults apply to adolescents.
Clinical withdrawal symptoms are less common in adolescents than adults, probably because of adolescents’ binge patterns of substance use. Even so, some adolescents do experience withdrawal and may be at risk for complications if improperly treated.
Psychiatric comorbidity. To our knowledge, only two double-blind, placebo-controlled studies of drug therapy in treating adolescent substance use disorders have been published.
Depression. Deas et al23 randomized 10 adolescents with alcohol use disorders and depression to 12 weeks of group CBT plus sertraline or placebo. Sertraline was started at 25 mg/d and titrated to a maximum of 100 mg/d. Drinks per drinking day, percent of days drinking, and Hamilton Rating Scale for Depression scores declined similarly in both groups.
Drinking decreased significantly from baseline (by an average 4.7 drinks), and adolescents in both groups no longer met DSM-IV criteria for depression at the end of treatment. CBT’s effectiveness in treating alcohol use disorders and depression might have concealed any difference in effect between sertaline and placebo.
Bipolar disorder. Geller et al24 randomly assigned 25 adolescents with bipolar disorder and substance dependence to lithium or placebo for 6 weeks. Lithium was started as an evening dose of 600 mg and titrated to achieve a lithium blood level of 0.9 to 1.3 mEq/L. Among the 21 adolescents who completed the trial, those receiving lithium had significantly fewer positive urine toxicology screens and higher clinical global assessment of function scores.
Related resources
- National Clearinghouse for Alcohol and Drug Information, Substance Abuse and Mental Health Services Administration, U.S. Department of Health and Human Services. www.health.org/govpubs/bkd306/31k.aspx
- National Institute on Alcohol Abuse and Alcoholism (assessment instruments). www.niaaa.nih.gov/publications/instable.htm
- Deas D, Thomas SE. An overview of controlled studies of adolescent substance abuse treatment. Am J Addict 2001;10:178-89.
Drug brand names
- Sertraline • Zoloft
Disclosure
Dr. Deas receives grant support from Pfizer, Inc. and the National Institute of Alcohol Abuse and Alcoholism.
Dr. Upadhyaya receives grant support from the National Institute of Drug Abuse and GlaxoSmithKline.
Acknowledgment
The authors wish to thank Alva Blair for assistance with preparing this manuscript and Natalie Johnson, MA, Kess Mughelli, BS, and Lakeleia Middleton-Robinson, MA, for technical support.
1. Johnston LD, O’Malley PM, Bachman JG. Monitoring the Future: national results on adolescent drug use. Overview of key findings, 2002. Bethesda, MD: National Institute on Drug Abuse, 2003 (in press).
2. Martin CS, Kaczynski NA, Maisto SA, et al. Patterns of DSM-IV alcohol abuse and dependence symptoms in adolescent drinkers. J Stud Alcohol 1995;56:672-80.
3. Pollock NK, Martin CS. Diagnostic orphans: adolescents with alcohol symptoms who do not qualify for DSM-IV abuse or dependence diagnoses. Am J Psychiatry 1999;156:897-901.
4. Harrison PA, Fulkerson JA, Beebe TJ. DSM-IV substance use disorder criteria for adolescents: a critical examination based on a statewide school survey. Am J Psychiatry 1998;155:486-92.
5. Grant BF, Dawson DA. Age at onset of alcohol use and its association with DSM-IV alcohol abuse/dependence: results from the National Longitudinal Alcohol Epidemiological Survey. J Subst Abuse 1997;9:103-10.
6. Tarter RE, Laird SB, Bukstein O, Kaminer Y. Validation of the adolescent drug use screening inventory: preliminary findings. Psychol Addict Behav 1992;6:322-6.
7. Rahdert E (ed). The adolescent assessment/referral system manual. DHHS pub. no. (ADM) 91-1735. Rockville, MD: U.S. Department of Health and Human Services, 1991.
8. Kaminer Y, Bukstein OG, Tarter RE. The teen addiction severity index (T-ASI): rationale and reliability. Int J Addict 1991;26:219-26.
9. Meyers K, McLellan AT, Jaeger JL, Pettinati A. The development of the Comprehensive Addiction Severity Index for Adolescents (CASI-A): an interview for assessing multiple problems of adolescents. J Subst Abuse Treat 1995;12:181-93.
10. Deas DV, Roberts JS, Randall CL, Anton RF. Adolescent Obsessive-Compulsive Drinking Scale (A-OCDS): an assessment tool for problem drinking. J Natl Med Assoc 2001;93:92-103.
11. Deas D, Randall CL, Thomas S. The utility of the Deas-Marijuana Obsessive-Compulsive Scale (Deas-MOCS) in an inpatient adolescent substance abusing sample. Drug Alcohol Depend 2002;66(June):S43.-
12. Deas-Nesmith D, Campbell S, Brady KT. Substance use disorders in an adolescent inpatient psychiatric population. JAMA 1998;90:233-8.
13. Clark DB, Lesnick L, Hegedus AM. Traumas and other adverse life events in adolescents with alcohol abuse and dependence. Am Acad Child Adolesc Psychiatry 1997;36:1744-51.
14. Kilpatrick DG, Acierno R, Saunders B, et al. Risk factors for adolescent substance abuse and dependence: data from a national sample. J Consult Clin Psychol 2000;68:19-30.
15. Rose RJ. A developmental behavioral-genetic perspective on alcoholism risk. Alcohol Health Res World 1998;22:131-43.
16. Swadi H. Individual risk factors for adolescent substance use. Drug Alcohol Depend 1999;55:209-24.
17. Azrin N, McMahon P, Donohue B, et al. Behavior therapy for drug abuse: a controlled treatment outcome study. Behav Res Ther 1994;32:857-66.
18. Kaminer Y, Burleson JA, Goldberger R. Cognitive-behavioral coping skills and psychoeducation therapies for adolescent substance abuse. J Nerv Ment Dis 2002;190:737-45.
19. Liddle H, Dakof G. Efficacy of family therapy for drug abuse: promising but not definitive. J Marital Fam Ther 1995;21:511-43.
20. Waldron HB. Adolescent substance abuse and family therapy outcome: a review of randomized trials. Adv Clin Child Psychol 1997;19:199-234.
21. Henggeler SW, Melton LA. Effects of multisystemic therapy on drug use and abuse in serious juvenile offenders: a progress report from two outcome studies. Family Dynamics of Addiction Quarterly 1991;1:40-51.
22. Jaffe S. Step workbook for adolescent chemical dependency recovery. Washington, DC: American Academy of Child and Adolescent Psychiatry, 1990.
23. Deas DV, Randall C, Roberts J, Anton R. A double-blind, placebo-controlled trial of sertraline in depressed adolescent alcoholics: a pilot study. Human Psychopharmacology Clinical and Experimental 2000;15:461-9.
24. Geller B, Cooper T, Sun K, et al. Double-blind and placebo-controlled study of lithium for adolescent bipolar disorders with secondary substance dependency. J Am Acad Child Adolesc Psychiatry 1998;37:171-8.
1. Johnston LD, O’Malley PM, Bachman JG. Monitoring the Future: national results on adolescent drug use. Overview of key findings, 2002. Bethesda, MD: National Institute on Drug Abuse, 2003 (in press).
2. Martin CS, Kaczynski NA, Maisto SA, et al. Patterns of DSM-IV alcohol abuse and dependence symptoms in adolescent drinkers. J Stud Alcohol 1995;56:672-80.
3. Pollock NK, Martin CS. Diagnostic orphans: adolescents with alcohol symptoms who do not qualify for DSM-IV abuse or dependence diagnoses. Am J Psychiatry 1999;156:897-901.
4. Harrison PA, Fulkerson JA, Beebe TJ. DSM-IV substance use disorder criteria for adolescents: a critical examination based on a statewide school survey. Am J Psychiatry 1998;155:486-92.
5. Grant BF, Dawson DA. Age at onset of alcohol use and its association with DSM-IV alcohol abuse/dependence: results from the National Longitudinal Alcohol Epidemiological Survey. J Subst Abuse 1997;9:103-10.
6. Tarter RE, Laird SB, Bukstein O, Kaminer Y. Validation of the adolescent drug use screening inventory: preliminary findings. Psychol Addict Behav 1992;6:322-6.
7. Rahdert E (ed). The adolescent assessment/referral system manual. DHHS pub. no. (ADM) 91-1735. Rockville, MD: U.S. Department of Health and Human Services, 1991.
8. Kaminer Y, Bukstein OG, Tarter RE. The teen addiction severity index (T-ASI): rationale and reliability. Int J Addict 1991;26:219-26.
9. Meyers K, McLellan AT, Jaeger JL, Pettinati A. The development of the Comprehensive Addiction Severity Index for Adolescents (CASI-A): an interview for assessing multiple problems of adolescents. J Subst Abuse Treat 1995;12:181-93.
10. Deas DV, Roberts JS, Randall CL, Anton RF. Adolescent Obsessive-Compulsive Drinking Scale (A-OCDS): an assessment tool for problem drinking. J Natl Med Assoc 2001;93:92-103.
11. Deas D, Randall CL, Thomas S. The utility of the Deas-Marijuana Obsessive-Compulsive Scale (Deas-MOCS) in an inpatient adolescent substance abusing sample. Drug Alcohol Depend 2002;66(June):S43.-
12. Deas-Nesmith D, Campbell S, Brady KT. Substance use disorders in an adolescent inpatient psychiatric population. JAMA 1998;90:233-8.
13. Clark DB, Lesnick L, Hegedus AM. Traumas and other adverse life events in adolescents with alcohol abuse and dependence. Am Acad Child Adolesc Psychiatry 1997;36:1744-51.
14. Kilpatrick DG, Acierno R, Saunders B, et al. Risk factors for adolescent substance abuse and dependence: data from a national sample. J Consult Clin Psychol 2000;68:19-30.
15. Rose RJ. A developmental behavioral-genetic perspective on alcoholism risk. Alcohol Health Res World 1998;22:131-43.
16. Swadi H. Individual risk factors for adolescent substance use. Drug Alcohol Depend 1999;55:209-24.
17. Azrin N, McMahon P, Donohue B, et al. Behavior therapy for drug abuse: a controlled treatment outcome study. Behav Res Ther 1994;32:857-66.
18. Kaminer Y, Burleson JA, Goldberger R. Cognitive-behavioral coping skills and psychoeducation therapies for adolescent substance abuse. J Nerv Ment Dis 2002;190:737-45.
19. Liddle H, Dakof G. Efficacy of family therapy for drug abuse: promising but not definitive. J Marital Fam Ther 1995;21:511-43.
20. Waldron HB. Adolescent substance abuse and family therapy outcome: a review of randomized trials. Adv Clin Child Psychol 1997;19:199-234.
21. Henggeler SW, Melton LA. Effects of multisystemic therapy on drug use and abuse in serious juvenile offenders: a progress report from two outcome studies. Family Dynamics of Addiction Quarterly 1991;1:40-51.
22. Jaffe S. Step workbook for adolescent chemical dependency recovery. Washington, DC: American Academy of Child and Adolescent Psychiatry, 1990.
23. Deas DV, Randall C, Roberts J, Anton R. A double-blind, placebo-controlled trial of sertraline in depressed adolescent alcoholics: a pilot study. Human Psychopharmacology Clinical and Experimental 2000;15:461-9.
24. Geller B, Cooper T, Sun K, et al. Double-blind and placebo-controlled study of lithium for adolescent bipolar disorders with secondary substance dependency. J Am Acad Child Adolesc Psychiatry 1998;37:171-8.
Treating bipolar disorder during pregnancy
Prescribing drug therapy for pregnant bipolar women requires psychiatrists to balance the potential for neonatal malformations against the high risk of relapse when patients discontinue their medications.1 To help you achieve this balance, we offer an evidence-based approach that includes:
- analysis of the FDA’s teratogenicity categories for psychotropics
- review of the safety profiles of drugs used in mood stabilization
- an algorithm for managing patients who are considering conception or are pregnant.
PSYCHOTROPIC RISKS TO OFFSPRING
All psychotropic medications diffuse across the placenta, which exposes the fetus to some degree. Risks include teratogenicity, obstetrical complications, perinatal syndromes, and long-term postnatal behavioral sequelae.
Teratogenicity. A medication is considered teratogenic when prenatal exposure significantly increases the risk of congenital deformities over the baseline risk, which is 2% in the United States.2 The cause of most congenital malformations is unknown. Risk for teratogenicity occurs in the first 12 weeks of gestation, as organs are formed.
Table 1
FDA Use-in-Pregnancy ratings for medications The FDA system weighs the degree to which research findings have ruled out risk to the fetus
| Category | Interpretation |
|---|---|
| A | Controlled studies show no risk |
| B | No evidence of risk in humans |
| C | Risk cannot be ruled out |
| D | Positive evidence of risk |
| X | Contraindicated in pregnancy |
| Source: Physicians’ Desk Reference. Montvale, NJ: Medical Economics Co., 2003. | |
Obstetrical complications include preterm delivery, low birth weight, and delivery complications such as low Apgar scores or behavioral effects requiring intensive care.
Perinatal syndromes include physical and behavioral symptoms noticed shortly after birth (such as jitteriness). These consequences are putatively related to drug use at or near birth and have limited duration.
Postnatal behavioral sequelae include long-term neurobehavioral abnormalities in children who were exposed to psychotropics in utero.
BALANCING RISKS
Risks with medication. The FDA’s “use in pregnancy” rating system (Table 1) uses available data to assess the degree of teratogenic risk. These guidelines can be confusing and are one of many tools to use when considering a possible drug treatment.
Most psychotropics are category “C” or “D,” which imply a chance of harm to the exposed fetus. Category “B” drugs would appear safer, but this rating could simply indicate a lack of adequate human data or that no data have shown harm in animals.
Moreover, a category “D” drug may be chosen more often during pregnancy than a category “C” drug. This may occur when more human data exist on using the category “D” drug in patients with a particular disorder (such as using lithium versus valproate or olanzapine in pregnant bipolar women).
No psychotropics are classified as “A,” meaning either some risks are associated with every psychotropic or the risk of some agents has not been adequately explored. Furthermore, no psychotropics are FDA-approved for use during pregnancy.
Risks without medication. Teratogenicity notwithstanding, psychotropic intervention is the most effective treatment for women with bipolar disorder. Patients who discontinue mood-stabilizing medication after conception increase their risk of relapse into depression or mania,3 either of which could lead to complications and untoward effects on the fetus.
Depression during pregnancy has been linked to low birth weight and preterm delivery.4,5 These effects may be mediated by the illness itself or by other factors that indirectly affect birth outcomes. For example, depression during pregnancy is associated with decreased appetite, substance use and abuse, and lower use of prenatal care.6
Untreated mania may also be associated with perinatal risks, as a pregnant patient in a manic state may engage in impulsive, high-risk behaviors that endanger her and the fetus.7
MOOD STABILIZERS
The FDA categorizes as “D” the three most commonly used mood stabilizers: lithium, valproate, and carbamazepine (Table 2). This rating implies that studies have demonstrated fetal risk but the drug’s potential benefit may still outweigh the risk.
Lithium. The International Registry of Lithium reported increased rates of cardiovascular malformations— such as Ebstein’s anomaly—in children whose mothers took lithium during pregnancy.
Relative risk for Ebstein’s anomaly in children with fetal exposure to lithium may be 20 times higher than the risk in unexposed children, although the absolute risk with lithium exposure remains low (1 in 1,000 births).1,8
No significant neurobehavioral teratogenicity has been reported in infants exposed in utero to lithium, although few cases have been studied. One study reported that 22 lithium-exposed infants attained developmental milestones at a pace comparable to that of unexposed controls.9
“Floppy baby” syndrome, in which infants experience hypotonicity and cyanosis, is the most recognized adverse effect in infants exposed to lithium in utero.10 Its frequency is unknown, but rare. Neonatal hypothyroidism and nephrogenic diabetes insipidus have also been documented.
Anticonvulsants. To date, no studies have examined the outcomes of children whose mothers took anticonvulsants for bipolar disorder during pregnancy, though the research concerning epileptic mothers is extensive.
Neural tube defects. Data associate anticonvulsant exposure with a significantly greater risk for malformations than in the general population. Specifically, anticonvulsants may cause neural tube defects such as spina bifida, ancephaly, and encephaly in 2 to 5% of those exposed, as well as craniofacial anomalies, microcephaly, growth retardation, and heart defects.11-14
Table 2
FDA’s teratogenicity ratings of mood stabilizers and other antimanic agents
| Category | Medication | Teratogenicity |
|---|---|---|
| Mood stabilizers | Lithium Carbamazepine Valproate | Category D Category D Category D |
| Anticonvulsants | Gabapentin Lamotrigine Topiramate | Category C Category C Category C |
| Antipsychotics | Olanzapine Risperidone Chlorpromazine Haloperidol Trifluoperazine | Category C Category C Safety in pregnancy not known Category C Safety in pregnancy not known |
| Source: Physicians’ Desk Reference. Montvale, NJ: Medical Economics Co., 2003. | ||
More minor malformations—such as rotated ears, depressed nasal bridge, short nose, elongated upper lip, and fingernail hypoplasia—have been reported in infants exposed to anticonvulsants in utero.14 These malformations disappear with age.13 Teratogenicity increases with the use of multiple anticonvulsants and possibly with higher maternal plasma levels and toxic metabolites.15
Conclusion. The three most commonly used mood stabilizers are all teratogenic. The least risk may occur with lithium (0.1%) versus valproate (2 to 5%) or carbamazepine (1 to 3%). These risks must be weighed against the up to 50% chance of relapse with medication discontinuation.3
ANTIPSYCHOTICS
Antipsychotics are often used to treat mania because of their rapid effects and sedative properties. Most antipsychotics—specifically, haloperidol, olanzapine, and risperidone—are labeled “C,” specifying that fetal risk cannot be ruled out.
Table 3
FDA’s teratogenicity ratings of common antidepressants
| Category | Medication | Teratogenicity |
|---|---|---|
| Tricyclics | Amitriptyline Clomipramine Desipramine Imipramine Nortriptyline | Category C Category C Safety in pregnancy not known Safety in pregnancy not known Safety in pregnancy not known |
| Selective serotonin reuptake inhibitors | Citalopram Fluoxetine Fluvoxamine Paroxetine Sertraline | Category C Category C Category C Category C Category C |
| Other antidepressants | Bupropion Phenelzine Tranylcypromine | Category B Safety in pregnancy and nursing not known Safety in pregnancy and nursing not known |
| Source: Physicians’ Desk Reference. Montvale, NJ: Medical Economics Co., 2003. | ||
Chlorpromazine and haloperidol have been most studied during pregnancy but in relation to treating hyperemesis gravidarum and psychosis, not bipolar disorder. Results regarding antipsychotics’ teratogenic and behavioral risks are mixed,16-21 probably because the various compounds have different effects on the fetus.
The underlying illness—rather than the medications—may increase the rate of anomalies seen with exposure to antipsychotics:
- Rieder et al22 reported an increased rate of perinatal death in infants of schizophrenic mothers but no significant association between the mothers’ use of antipsychotics and perinatal death.
- Sobel23 compared psychotic women with and without histories of chlorpromazine exposure during pregnancy. Rates of fetal damage were similar and approximately twice that of the general population.
A meta-analysis of 74,337 live births revealed that first-trimester exposure to low-potency antipsychotics increases the relative risk of fetal anomalies in nonpsychotic women. Phenothiazines may increase the 2% baseline incidence of malformations to 2.4%.1 No specific organ malformation following fetal exposure to phenothiazines has been consistently identified.
Olanzapine was recently approved for treating mania. Very little data exist regarding its impact on fetal development when used during pregnancy, although studies on small numbers of women have not revealed teratogenicity.24,25
Conclusion. Psychotic illness itself may increase the risk of poor fetal outcome to a greater extent than does antipsychotic use. Prenatal exposure to low-potency phenothiazines may further increase this risk, although only slightly. The effect of prenatal exposure to atypical antipsychotics requires further study.
BENZODIAZEPINES
Benzodiazepines are rarely a primary treatment for mania or depression. Thus, a comprehensive review of their effect on fetal outcome is beyond the scope of this review. A meta-analysis of exposure in the first trimester suggests a very small but significant increase in risk for cleft palate.1 The absolute risk is <1 in 1,000 cases.
ANTIDEPRESSANTS
Whereas treatment of acute mania is considered a medical emergency, women with bipolar disorder may also relapse into depression during pregnancy. An antidepressant should not be used without a mood stabilizer when treating bipolar I disorder, although a mood stabilizer alone may be inadequate to treat depression. Using tricyclics and selective serotonin reuptake inhibitors (SSRIs) during pregnancy has not been associated with teratogenicity (Table 3),26 although perinatal effects have been reported.1
Tricyclics. In case-control studies involving more than 300,000 live births, 414 incidences of first-trimester exposure to tricyclics were followed. Information from these patients found no significant association between fetal exposure to tricyclics and increased rates of congenital malformations.1 The few studies that have been performed suggest no long-term effects from in utero exposure.26 Although these results suggest that prenatal exposure to tricyclics is relatively safe, more research is needed.
SSRIs. To date, no significant teratogenic effects of SSRIs have been identified in offspring of treated women.
The manufacturer’s register for fluoxetine contains approximately 2,000 cases of treated patients, with no excess cases of congenital anomalies or malformations following prenatal exposure. Citalopram has the next largest database of in utero exposure (n=365), again with no increased risk for teratogenicity. Several smaller systematic reports are available on in utero exposure to sertraline, paroxetine, or escitalopram.26
Most studies of pregnant women taking fluoxetine in the first trimester have found no increased risk of obstetrical complications—including spontaneous pregnancy loss, preterm labor, or low birth weight—compared with women not taking fluoxetine. Taking fluoxetine during the third trimester may increase the risk for perinatal complications,27 although this has been inconsistently reported and requires further study. Effects of other SSRIs in the third trimester have not been systematically explored.
Case reports and one controlled study have addressed possible neonatal perinatal symptoms from in utero exposure to SSRIs.28,29 Preliminary data show no adverse neurobehavioral function in exposed neonates.26
Electroconvulsive therapy (ECT) has been proven effective for acute mania and depression, demonstrating few deleterious effects on neonates. ECT has few side effects and may be safer than drug therapy in this population. Two reviews support the efficacy and relative safety of ECT treatment during pregnancy, although more evidence is needed.30,31
RECOMMENDATIONS
Discuss pregnancy and medication risks with all bipolar women, regardless of proximal plans for pregnancy. If psychotropic medication is used, prescribe carefully during the first trimester, using the minimum number of drugs and the lowest dosages needed to restore or maintain well-being.32
Pros and cons of switching. Some clinicians may encourage a patient to taper a medication during the first trimester because of its unknown or high teratogenicity. Depending on the patient’s illness severity, this might not be the optimal decision. A more conservative option would be to switch to a lower-risk drug during pregnancy.
Lithium has both antidepressant and antimanic properties and is less teratogenic compared with first-trimester exposure to an anticonvulsant. However, if lithium has not been successful for the woman’s mania prophylaxis in the past and she has demonstrated antimanic response to an anticonvulsant, switching to lithium or another anticonvulsant is not recommended.
Algorithm Suggested approach to the bipolar patient who wishes to conceive or is pregnant
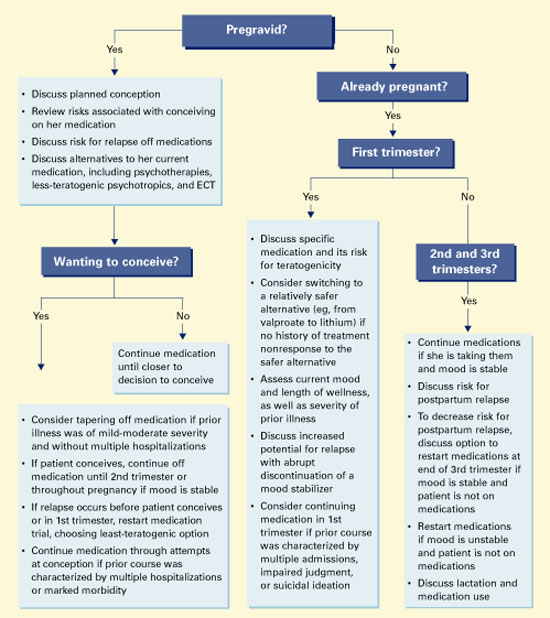
Folate and neural tube defects. As first-trimester exposure to carbamazepine or valproate increases the risk for neural tube defects, using the lowest available dosage may decrease the risk for spina bifida, at least with valproate.
Low maternal folate levels are often associated with neural tube defects from any cause.33 Valproate lowers folate levels by inhibiting one of the enzymes necessary for its formation, which may be a mechanism for the increased risk of spina bifida.34
Folate supplementation. To date, no study has demonstrated that giving folate supplements to women taking anticonvulsants during pregnancy reduces the risk of neural tube defects.35 Nonetheless, we recommend that women who continue to take valproate or carbamazepine during pregnancy receive folate, 3 to 4 mg/d, as a precaution.
Treating manic relapse. Data show high rates of relapse in patients who stop taking lithium, particularly if done abruptly.3 Counsel women taking lithium to plan their pregnancies to allow enough time to taper off the medication prior to conception, if they want to try this. Lithium should be decreased slowly—approximately 50% every 2 weeks—to avoid relapse.
Treat aggressively if relapse occurs during pregnancy. Consider:
- psychiatric hospitalization in case of suicidality or psychosis
- reinstituting drug therapy with a less-teratogenic agent
- ECT for a manic or depressive episode.
As the pregnancy advances and the mother’s volume of distribution increases, dosage increases may be needed to maintain therapeutic drug levels.
Treating depressive relapse. Should depression occur in pregnancy, SSRIs or tricyclics added to mood stabilizer therapy have been shown to be effective, with few teratogenic effects.
Cognitive-behavioral and interpersonal psychotherapies also have shown efficacy in pregnant women with major depressive disorder36 and may be effective for women with bipolar disorder in pregnancy. Cognitive psychotherapies, when used with medication, have been reported effective in preventing relapse in nongravid bipolar patients.36-37
Related resources
Psychiatric disorders during pregnancy. Massachusetts General Hospital Center for Women’s Health. Perinatal Resource Center. www.womensmentalhealth.org/topics/pregnancy_lib.html
Drug brand names
- Amitriptyline • Elavil
- Bupropion • Wellbutrin
- Carbamazepine • Tegretol
- Chlorpromazine • Thorazine
- Citalopram • Celexa
- Clomipramine • Anafranil
- Desipramine • Norpramin
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Gabapentin • Neurontin
- Haloperidol • Haldol
- Imipramine • Tofranil
- Lamotrigine • Lamictal
- Lithium • Lithobid et al
- Methylphenidate • Ritalin et al
- Nortriptyline • Pamelor
- Olanzapine • Zyprexa
- Paroxetine • Paxil
- Phenelzine • Nardil
- Risperidone • Risperdal
- Sertraline • Zoloft
- Topiramate • Topamax
- Tranylcypromine • Parnate
- Trifluoperazine • Stelazine
- Valproate • Depakote et al
Disclosure
Dr. Altshuler receives research support from Abbott Laboratories, is a consultant to Abbott Laboratories, Forest Laboratories, and Eli Lilly & Co., and is a speaker for GlaxoSmithKline and Janssen Pharmaceutica.
Ms. Richards reports no financial relationship with any company whose products are mentioned in this article, or with manufacturers of competing products.
Dr. Yonkers receives research support from GlaxoSmithKline and Berlex Laboratories, is a consultant to GlaxoSmithKline, and is a speaker for Eli Lilly and Co., Pfizer Inc., GlaxoSmithKline, and Wyeth Pharmaceuticals.
1. Altshuler L, Cohen L, Szuba, et al. Pharmacologic management of psychiatric illness during pregnancy: dilemmas and guidelines. Am J Psychiatry 1996;153:592-606.
2. Nelson K, Holmes LB. Malformations due to presumed spontaneous mutations in newborn infants. N Engl J Med 1989;320:19-23.
3. Viguera AC, Nonacs R, Cohen LS, et al. Risk of recurrence of bipolar disorder in pregnant and nonpregnant women after discontinuing lithium maintenance. Am J Psychiatry 2000;157:179-84.
4. Steer RA, Scholl TO, Hediger ML, Fischer RL. Self-reported depression and negative pregnancy outcomes. J Clin Epidemiol 1992;45(10):1093-9.
5. Orr ST, Miller CA. Maternal depressive symptoms and the risk of poor pregnancy outcome. Review of the literature and preliminary findings. Epidemiol Rev 1995;17(1):165-71.
6. Zuckerman B, Amaro H, Bauchner H, Cabral H. Depressive symptoms during pregnancy: relationship to poor health behaviors. Am J Obstet Gynecol 1989;160:1107-11.
7. Miller LJ. Psychotic denial of pregnancy: phenomenology and clinical management. Hosp Community Psychiatry 1990;41:1233-7.
8. Cohen LS, Friedman JM, Jefferson JW, et al. A reevaluation of risk of in utero exposure to lithium. JAMA 1994;271(2):146-50correction JAMA 1994;271(19):1485.
9. Schou M. What happened later to the lithium babies? A follow-up study of children born without malformations. Acta Psychiatr Scand 1976;54(3):193-7.
10. Woody JN, London WL, Wilbanks GD. Lithium toxicity in a newborn. Pediatrics 1971;47:94-6.
11. Jones K, Lacro R, Johnson K, Adams J. Patterns of malformations in the children of women treated with carbamazepine during pregnancy. N Engl J Med 1989;320:1661-6.
12. Rosa F. Spina bifida in infants of women treated with carbamazepine during pregnancy. N Engl J Med 1991;324(10):674-7.
13. Koch S, Losche G, Jager-Roman E, et al. Major and minor birth malformations and antiepileptic drugs. Neurology 1992;42:83-8.
14. Jager-Roman E, Deichl A, Jakob S, et al. Fetal growth, major malformations, and minor anomalies in infants born to women receiving valproic acid. J Pediatr 1986;108:997-1004.
15. Nakane Y, Okuma T, Takahashi R, et al. Multi-institutional study on the teratogenicity and fetal toxicity of antiepileptic drugs: a report of a collaborative study group in Japan. Epilepsia 1980;21:663-80.
16. Edlund MJ, Craig TJ. Antipsychotic drug use and birth defects: an epidemiologic reassessment. Compr Psychiatry 1984;25:32-8.
17. Kris EB. Children of mothers maintained on pharmacotherapy during pregnancy and postpartum. Curr Ther Res 1965;7:785-9.
18. Clark CVH, Gorman D, Vernadakis A. Effects of prenatal administration of psychotropic drugs on behavior of developing rats. Dev Psychobiol 1970;3:225-35.
19. Golub M, Kornetsky C. Seizure susceptibility and avoidance conditioning in adult rats treated prenatally with chlorpromazine. Dev Psychobiol 1974;7:79-88.
20. Spear LP, Shalaby IA, Brick J. Chronic administration of haloperidol during development: behavioral and psychopharmacological effects. Psychopharmacology (Berl) 1980;70:47-58.
21. Cagiano R, Barfield RJ, White NR, et al. Subtle behavioral changes produced in rat pups exposed in utero to haloperidol. Eur J Pharmacol 1988;157:45-50.
22. Rieder RO, Rosenthal D, Wender P, Blumenthal H. The offspring of schizophrenics: fetal and neonatal deaths. Arch Gen Psychiatry 1975;32:200-11.
23. Sobel DE. Fetal damage due to ECT, insulin coma, chlorpromazine, or reserpine. Arch Gen Psychiatry 1960;2:606-11.
24. Dickson R. Olanzapine and pregnancy. Can J Psychiatry 1998;43:196-7.
25. Goldstein DJ, Corbin LA, Fung MC. Olanzapine-exposed pregnancies and lactation; early experience. J Clin Psychopharmacol 2000;24(4):399-403.
26. Altshuler LL, Cohen LS, Moline ML, et al. The expert consensus guideline series: treatment of depression in women. Postgrad Med 2001 Mar;(Spec No):1-22.
27. Chambers CD, Johnson KA, Dick LM, et al. Birth outcomes in pregnant women taking fluoxetine. N Engl J Med 1996;335:1010-15.
28. Spencer MJ. Fluoxetine hydrochloride (Prozac) toxicity in the neonate. Pediatrics 1993;92:721-2.
29. Cabrera FM, Battaglia G. Delayed decreases in brain 5-HT 2a and 2c receptor density and function in male rat progeny following prenatal fluoxetine. J Pharmacol Exp Ther 1994;269:637-45.
30. Miller LJ. Use of electroconvulsive therapy during pregnancy. Hosp Community Psychiatry 1994;45:444-50.
31. Ferrill MJ, Kehoe WA, Jacisin JJ. ECT during pregnancy: physiologic and pharmacologic considerations. Convuls Ther 1992;8:186-200.
32. Yonkers K, Wisner K, Cohen L, et al. Management of bipolar disorder during pregnancy and the postpartum period. Bipolar Consensus Statement. Submitted for publication.
33. Dansky L, Rosenblatt D, Andermann E. Mechanisms of teratogenesis: folic acid and antiepileptic therapy. Neurology 1992;42(suppl 5):32-42.
34. Wegner C, Nau H. Alteration of embryonic folate metabolism by valproic acid during organogenesis: implications for mechanism of teratogenesis. Neurology 1992;42(suppl 5):17-24.
35. MRC Vitamin Study Research Group. Prevention of neural tube defects: results of the Medical Research Council Vitamin Study. Lancet 1991;338:131-7.
36. Spinelli MG, Endicott J. Controlled clinical trial of interpersonal psychotherapy versus parenting education program for depressed pregnant women. Am J Psychiatry 2003;160:555-62.
37. Lam DH, Watkins ER, Hayward P, et al. A randomized controlled study of cognitive therapy for relapse prevention for bipolar affective disorder: outcome in the first year. Arch Gen Psychiatry 2003;60(2):145-52.
Prescribing drug therapy for pregnant bipolar women requires psychiatrists to balance the potential for neonatal malformations against the high risk of relapse when patients discontinue their medications.1 To help you achieve this balance, we offer an evidence-based approach that includes:
- analysis of the FDA’s teratogenicity categories for psychotropics
- review of the safety profiles of drugs used in mood stabilization
- an algorithm for managing patients who are considering conception or are pregnant.
PSYCHOTROPIC RISKS TO OFFSPRING
All psychotropic medications diffuse across the placenta, which exposes the fetus to some degree. Risks include teratogenicity, obstetrical complications, perinatal syndromes, and long-term postnatal behavioral sequelae.
Teratogenicity. A medication is considered teratogenic when prenatal exposure significantly increases the risk of congenital deformities over the baseline risk, which is 2% in the United States.2 The cause of most congenital malformations is unknown. Risk for teratogenicity occurs in the first 12 weeks of gestation, as organs are formed.
Table 1
FDA Use-in-Pregnancy ratings for medications The FDA system weighs the degree to which research findings have ruled out risk to the fetus
| Category | Interpretation |
|---|---|
| A | Controlled studies show no risk |
| B | No evidence of risk in humans |
| C | Risk cannot be ruled out |
| D | Positive evidence of risk |
| X | Contraindicated in pregnancy |
| Source: Physicians’ Desk Reference. Montvale, NJ: Medical Economics Co., 2003. | |
Obstetrical complications include preterm delivery, low birth weight, and delivery complications such as low Apgar scores or behavioral effects requiring intensive care.
Perinatal syndromes include physical and behavioral symptoms noticed shortly after birth (such as jitteriness). These consequences are putatively related to drug use at or near birth and have limited duration.
Postnatal behavioral sequelae include long-term neurobehavioral abnormalities in children who were exposed to psychotropics in utero.
BALANCING RISKS
Risks with medication. The FDA’s “use in pregnancy” rating system (Table 1) uses available data to assess the degree of teratogenic risk. These guidelines can be confusing and are one of many tools to use when considering a possible drug treatment.
Most psychotropics are category “C” or “D,” which imply a chance of harm to the exposed fetus. Category “B” drugs would appear safer, but this rating could simply indicate a lack of adequate human data or that no data have shown harm in animals.
Moreover, a category “D” drug may be chosen more often during pregnancy than a category “C” drug. This may occur when more human data exist on using the category “D” drug in patients with a particular disorder (such as using lithium versus valproate or olanzapine in pregnant bipolar women).
No psychotropics are classified as “A,” meaning either some risks are associated with every psychotropic or the risk of some agents has not been adequately explored. Furthermore, no psychotropics are FDA-approved for use during pregnancy.
Risks without medication. Teratogenicity notwithstanding, psychotropic intervention is the most effective treatment for women with bipolar disorder. Patients who discontinue mood-stabilizing medication after conception increase their risk of relapse into depression or mania,3 either of which could lead to complications and untoward effects on the fetus.
Depression during pregnancy has been linked to low birth weight and preterm delivery.4,5 These effects may be mediated by the illness itself or by other factors that indirectly affect birth outcomes. For example, depression during pregnancy is associated with decreased appetite, substance use and abuse, and lower use of prenatal care.6
Untreated mania may also be associated with perinatal risks, as a pregnant patient in a manic state may engage in impulsive, high-risk behaviors that endanger her and the fetus.7
MOOD STABILIZERS
The FDA categorizes as “D” the three most commonly used mood stabilizers: lithium, valproate, and carbamazepine (Table 2). This rating implies that studies have demonstrated fetal risk but the drug’s potential benefit may still outweigh the risk.
Lithium. The International Registry of Lithium reported increased rates of cardiovascular malformations— such as Ebstein’s anomaly—in children whose mothers took lithium during pregnancy.
Relative risk for Ebstein’s anomaly in children with fetal exposure to lithium may be 20 times higher than the risk in unexposed children, although the absolute risk with lithium exposure remains low (1 in 1,000 births).1,8
No significant neurobehavioral teratogenicity has been reported in infants exposed in utero to lithium, although few cases have been studied. One study reported that 22 lithium-exposed infants attained developmental milestones at a pace comparable to that of unexposed controls.9
“Floppy baby” syndrome, in which infants experience hypotonicity and cyanosis, is the most recognized adverse effect in infants exposed to lithium in utero.10 Its frequency is unknown, but rare. Neonatal hypothyroidism and nephrogenic diabetes insipidus have also been documented.
Anticonvulsants. To date, no studies have examined the outcomes of children whose mothers took anticonvulsants for bipolar disorder during pregnancy, though the research concerning epileptic mothers is extensive.
Neural tube defects. Data associate anticonvulsant exposure with a significantly greater risk for malformations than in the general population. Specifically, anticonvulsants may cause neural tube defects such as spina bifida, ancephaly, and encephaly in 2 to 5% of those exposed, as well as craniofacial anomalies, microcephaly, growth retardation, and heart defects.11-14
Table 2
FDA’s teratogenicity ratings of mood stabilizers and other antimanic agents
| Category | Medication | Teratogenicity |
|---|---|---|
| Mood stabilizers | Lithium Carbamazepine Valproate | Category D Category D Category D |
| Anticonvulsants | Gabapentin Lamotrigine Topiramate | Category C Category C Category C |
| Antipsychotics | Olanzapine Risperidone Chlorpromazine Haloperidol Trifluoperazine | Category C Category C Safety in pregnancy not known Category C Safety in pregnancy not known |
| Source: Physicians’ Desk Reference. Montvale, NJ: Medical Economics Co., 2003. | ||
More minor malformations—such as rotated ears, depressed nasal bridge, short nose, elongated upper lip, and fingernail hypoplasia—have been reported in infants exposed to anticonvulsants in utero.14 These malformations disappear with age.13 Teratogenicity increases with the use of multiple anticonvulsants and possibly with higher maternal plasma levels and toxic metabolites.15
Conclusion. The three most commonly used mood stabilizers are all teratogenic. The least risk may occur with lithium (0.1%) versus valproate (2 to 5%) or carbamazepine (1 to 3%). These risks must be weighed against the up to 50% chance of relapse with medication discontinuation.3
ANTIPSYCHOTICS
Antipsychotics are often used to treat mania because of their rapid effects and sedative properties. Most antipsychotics—specifically, haloperidol, olanzapine, and risperidone—are labeled “C,” specifying that fetal risk cannot be ruled out.
Table 3
FDA’s teratogenicity ratings of common antidepressants
| Category | Medication | Teratogenicity |
|---|---|---|
| Tricyclics | Amitriptyline Clomipramine Desipramine Imipramine Nortriptyline | Category C Category C Safety in pregnancy not known Safety in pregnancy not known Safety in pregnancy not known |
| Selective serotonin reuptake inhibitors | Citalopram Fluoxetine Fluvoxamine Paroxetine Sertraline | Category C Category C Category C Category C Category C |
| Other antidepressants | Bupropion Phenelzine Tranylcypromine | Category B Safety in pregnancy and nursing not known Safety in pregnancy and nursing not known |
| Source: Physicians’ Desk Reference. Montvale, NJ: Medical Economics Co., 2003. | ||
Chlorpromazine and haloperidol have been most studied during pregnancy but in relation to treating hyperemesis gravidarum and psychosis, not bipolar disorder. Results regarding antipsychotics’ teratogenic and behavioral risks are mixed,16-21 probably because the various compounds have different effects on the fetus.
The underlying illness—rather than the medications—may increase the rate of anomalies seen with exposure to antipsychotics:
- Rieder et al22 reported an increased rate of perinatal death in infants of schizophrenic mothers but no significant association between the mothers’ use of antipsychotics and perinatal death.
- Sobel23 compared psychotic women with and without histories of chlorpromazine exposure during pregnancy. Rates of fetal damage were similar and approximately twice that of the general population.
A meta-analysis of 74,337 live births revealed that first-trimester exposure to low-potency antipsychotics increases the relative risk of fetal anomalies in nonpsychotic women. Phenothiazines may increase the 2% baseline incidence of malformations to 2.4%.1 No specific organ malformation following fetal exposure to phenothiazines has been consistently identified.
Olanzapine was recently approved for treating mania. Very little data exist regarding its impact on fetal development when used during pregnancy, although studies on small numbers of women have not revealed teratogenicity.24,25
Conclusion. Psychotic illness itself may increase the risk of poor fetal outcome to a greater extent than does antipsychotic use. Prenatal exposure to low-potency phenothiazines may further increase this risk, although only slightly. The effect of prenatal exposure to atypical antipsychotics requires further study.
BENZODIAZEPINES
Benzodiazepines are rarely a primary treatment for mania or depression. Thus, a comprehensive review of their effect on fetal outcome is beyond the scope of this review. A meta-analysis of exposure in the first trimester suggests a very small but significant increase in risk for cleft palate.1 The absolute risk is <1 in 1,000 cases.
ANTIDEPRESSANTS
Whereas treatment of acute mania is considered a medical emergency, women with bipolar disorder may also relapse into depression during pregnancy. An antidepressant should not be used without a mood stabilizer when treating bipolar I disorder, although a mood stabilizer alone may be inadequate to treat depression. Using tricyclics and selective serotonin reuptake inhibitors (SSRIs) during pregnancy has not been associated with teratogenicity (Table 3),26 although perinatal effects have been reported.1
Tricyclics. In case-control studies involving more than 300,000 live births, 414 incidences of first-trimester exposure to tricyclics were followed. Information from these patients found no significant association between fetal exposure to tricyclics and increased rates of congenital malformations.1 The few studies that have been performed suggest no long-term effects from in utero exposure.26 Although these results suggest that prenatal exposure to tricyclics is relatively safe, more research is needed.
SSRIs. To date, no significant teratogenic effects of SSRIs have been identified in offspring of treated women.
The manufacturer’s register for fluoxetine contains approximately 2,000 cases of treated patients, with no excess cases of congenital anomalies or malformations following prenatal exposure. Citalopram has the next largest database of in utero exposure (n=365), again with no increased risk for teratogenicity. Several smaller systematic reports are available on in utero exposure to sertraline, paroxetine, or escitalopram.26
Most studies of pregnant women taking fluoxetine in the first trimester have found no increased risk of obstetrical complications—including spontaneous pregnancy loss, preterm labor, or low birth weight—compared with women not taking fluoxetine. Taking fluoxetine during the third trimester may increase the risk for perinatal complications,27 although this has been inconsistently reported and requires further study. Effects of other SSRIs in the third trimester have not been systematically explored.
Case reports and one controlled study have addressed possible neonatal perinatal symptoms from in utero exposure to SSRIs.28,29 Preliminary data show no adverse neurobehavioral function in exposed neonates.26
Electroconvulsive therapy (ECT) has been proven effective for acute mania and depression, demonstrating few deleterious effects on neonates. ECT has few side effects and may be safer than drug therapy in this population. Two reviews support the efficacy and relative safety of ECT treatment during pregnancy, although more evidence is needed.30,31
RECOMMENDATIONS
Discuss pregnancy and medication risks with all bipolar women, regardless of proximal plans for pregnancy. If psychotropic medication is used, prescribe carefully during the first trimester, using the minimum number of drugs and the lowest dosages needed to restore or maintain well-being.32
Pros and cons of switching. Some clinicians may encourage a patient to taper a medication during the first trimester because of its unknown or high teratogenicity. Depending on the patient’s illness severity, this might not be the optimal decision. A more conservative option would be to switch to a lower-risk drug during pregnancy.
Lithium has both antidepressant and antimanic properties and is less teratogenic compared with first-trimester exposure to an anticonvulsant. However, if lithium has not been successful for the woman’s mania prophylaxis in the past and she has demonstrated antimanic response to an anticonvulsant, switching to lithium or another anticonvulsant is not recommended.
Algorithm Suggested approach to the bipolar patient who wishes to conceive or is pregnant
Folate and neural tube defects. As first-trimester exposure to carbamazepine or valproate increases the risk for neural tube defects, using the lowest available dosage may decrease the risk for spina bifida, at least with valproate.
Low maternal folate levels are often associated with neural tube defects from any cause.33 Valproate lowers folate levels by inhibiting one of the enzymes necessary for its formation, which may be a mechanism for the increased risk of spina bifida.34
Folate supplementation. To date, no study has demonstrated that giving folate supplements to women taking anticonvulsants during pregnancy reduces the risk of neural tube defects.35 Nonetheless, we recommend that women who continue to take valproate or carbamazepine during pregnancy receive folate, 3 to 4 mg/d, as a precaution.
Treating manic relapse. Data show high rates of relapse in patients who stop taking lithium, particularly if done abruptly.3 Counsel women taking lithium to plan their pregnancies to allow enough time to taper off the medication prior to conception, if they want to try this. Lithium should be decreased slowly—approximately 50% every 2 weeks—to avoid relapse.
Treat aggressively if relapse occurs during pregnancy. Consider:
- psychiatric hospitalization in case of suicidality or psychosis
- reinstituting drug therapy with a less-teratogenic agent
- ECT for a manic or depressive episode.
As the pregnancy advances and the mother’s volume of distribution increases, dosage increases may be needed to maintain therapeutic drug levels.
Treating depressive relapse. Should depression occur in pregnancy, SSRIs or tricyclics added to mood stabilizer therapy have been shown to be effective, with few teratogenic effects.
Cognitive-behavioral and interpersonal psychotherapies also have shown efficacy in pregnant women with major depressive disorder36 and may be effective for women with bipolar disorder in pregnancy. Cognitive psychotherapies, when used with medication, have been reported effective in preventing relapse in nongravid bipolar patients.36-37
Related resources
Psychiatric disorders during pregnancy. Massachusetts General Hospital Center for Women’s Health. Perinatal Resource Center. www.womensmentalhealth.org/topics/pregnancy_lib.html
Drug brand names
- Amitriptyline • Elavil
- Bupropion • Wellbutrin
- Carbamazepine • Tegretol
- Chlorpromazine • Thorazine
- Citalopram • Celexa
- Clomipramine • Anafranil
- Desipramine • Norpramin
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Gabapentin • Neurontin
- Haloperidol • Haldol
- Imipramine • Tofranil
- Lamotrigine • Lamictal
- Lithium • Lithobid et al
- Methylphenidate • Ritalin et al
- Nortriptyline • Pamelor
- Olanzapine • Zyprexa
- Paroxetine • Paxil
- Phenelzine • Nardil
- Risperidone • Risperdal
- Sertraline • Zoloft
- Topiramate • Topamax
- Tranylcypromine • Parnate
- Trifluoperazine • Stelazine
- Valproate • Depakote et al
Disclosure
Dr. Altshuler receives research support from Abbott Laboratories, is a consultant to Abbott Laboratories, Forest Laboratories, and Eli Lilly & Co., and is a speaker for GlaxoSmithKline and Janssen Pharmaceutica.
Ms. Richards reports no financial relationship with any company whose products are mentioned in this article, or with manufacturers of competing products.
Dr. Yonkers receives research support from GlaxoSmithKline and Berlex Laboratories, is a consultant to GlaxoSmithKline, and is a speaker for Eli Lilly and Co., Pfizer Inc., GlaxoSmithKline, and Wyeth Pharmaceuticals.
Prescribing drug therapy for pregnant bipolar women requires psychiatrists to balance the potential for neonatal malformations against the high risk of relapse when patients discontinue their medications.1 To help you achieve this balance, we offer an evidence-based approach that includes:
- analysis of the FDA’s teratogenicity categories for psychotropics
- review of the safety profiles of drugs used in mood stabilization
- an algorithm for managing patients who are considering conception or are pregnant.
PSYCHOTROPIC RISKS TO OFFSPRING
All psychotropic medications diffuse across the placenta, which exposes the fetus to some degree. Risks include teratogenicity, obstetrical complications, perinatal syndromes, and long-term postnatal behavioral sequelae.
Teratogenicity. A medication is considered teratogenic when prenatal exposure significantly increases the risk of congenital deformities over the baseline risk, which is 2% in the United States.2 The cause of most congenital malformations is unknown. Risk for teratogenicity occurs in the first 12 weeks of gestation, as organs are formed.
Table 1
FDA Use-in-Pregnancy ratings for medications The FDA system weighs the degree to which research findings have ruled out risk to the fetus
| Category | Interpretation |
|---|---|
| A | Controlled studies show no risk |
| B | No evidence of risk in humans |
| C | Risk cannot be ruled out |
| D | Positive evidence of risk |
| X | Contraindicated in pregnancy |
| Source: Physicians’ Desk Reference. Montvale, NJ: Medical Economics Co., 2003. | |
Obstetrical complications include preterm delivery, low birth weight, and delivery complications such as low Apgar scores or behavioral effects requiring intensive care.
Perinatal syndromes include physical and behavioral symptoms noticed shortly after birth (such as jitteriness). These consequences are putatively related to drug use at or near birth and have limited duration.
Postnatal behavioral sequelae include long-term neurobehavioral abnormalities in children who were exposed to psychotropics in utero.
BALANCING RISKS
Risks with medication. The FDA’s “use in pregnancy” rating system (Table 1) uses available data to assess the degree of teratogenic risk. These guidelines can be confusing and are one of many tools to use when considering a possible drug treatment.
Most psychotropics are category “C” or “D,” which imply a chance of harm to the exposed fetus. Category “B” drugs would appear safer, but this rating could simply indicate a lack of adequate human data or that no data have shown harm in animals.
Moreover, a category “D” drug may be chosen more often during pregnancy than a category “C” drug. This may occur when more human data exist on using the category “D” drug in patients with a particular disorder (such as using lithium versus valproate or olanzapine in pregnant bipolar women).
No psychotropics are classified as “A,” meaning either some risks are associated with every psychotropic or the risk of some agents has not been adequately explored. Furthermore, no psychotropics are FDA-approved for use during pregnancy.
Risks without medication. Teratogenicity notwithstanding, psychotropic intervention is the most effective treatment for women with bipolar disorder. Patients who discontinue mood-stabilizing medication after conception increase their risk of relapse into depression or mania,3 either of which could lead to complications and untoward effects on the fetus.
Depression during pregnancy has been linked to low birth weight and preterm delivery.4,5 These effects may be mediated by the illness itself or by other factors that indirectly affect birth outcomes. For example, depression during pregnancy is associated with decreased appetite, substance use and abuse, and lower use of prenatal care.6
Untreated mania may also be associated with perinatal risks, as a pregnant patient in a manic state may engage in impulsive, high-risk behaviors that endanger her and the fetus.7
MOOD STABILIZERS
The FDA categorizes as “D” the three most commonly used mood stabilizers: lithium, valproate, and carbamazepine (Table 2). This rating implies that studies have demonstrated fetal risk but the drug’s potential benefit may still outweigh the risk.
Lithium. The International Registry of Lithium reported increased rates of cardiovascular malformations— such as Ebstein’s anomaly—in children whose mothers took lithium during pregnancy.
Relative risk for Ebstein’s anomaly in children with fetal exposure to lithium may be 20 times higher than the risk in unexposed children, although the absolute risk with lithium exposure remains low (1 in 1,000 births).1,8
No significant neurobehavioral teratogenicity has been reported in infants exposed in utero to lithium, although few cases have been studied. One study reported that 22 lithium-exposed infants attained developmental milestones at a pace comparable to that of unexposed controls.9
“Floppy baby” syndrome, in which infants experience hypotonicity and cyanosis, is the most recognized adverse effect in infants exposed to lithium in utero.10 Its frequency is unknown, but rare. Neonatal hypothyroidism and nephrogenic diabetes insipidus have also been documented.
Anticonvulsants. To date, no studies have examined the outcomes of children whose mothers took anticonvulsants for bipolar disorder during pregnancy, though the research concerning epileptic mothers is extensive.
Neural tube defects. Data associate anticonvulsant exposure with a significantly greater risk for malformations than in the general population. Specifically, anticonvulsants may cause neural tube defects such as spina bifida, ancephaly, and encephaly in 2 to 5% of those exposed, as well as craniofacial anomalies, microcephaly, growth retardation, and heart defects.11-14
Table 2
FDA’s teratogenicity ratings of mood stabilizers and other antimanic agents
| Category | Medication | Teratogenicity |
|---|---|---|
| Mood stabilizers | Lithium Carbamazepine Valproate | Category D Category D Category D |
| Anticonvulsants | Gabapentin Lamotrigine Topiramate | Category C Category C Category C |
| Antipsychotics | Olanzapine Risperidone Chlorpromazine Haloperidol Trifluoperazine | Category C Category C Safety in pregnancy not known Category C Safety in pregnancy not known |
| Source: Physicians’ Desk Reference. Montvale, NJ: Medical Economics Co., 2003. | ||
More minor malformations—such as rotated ears, depressed nasal bridge, short nose, elongated upper lip, and fingernail hypoplasia—have been reported in infants exposed to anticonvulsants in utero.14 These malformations disappear with age.13 Teratogenicity increases with the use of multiple anticonvulsants and possibly with higher maternal plasma levels and toxic metabolites.15
Conclusion. The three most commonly used mood stabilizers are all teratogenic. The least risk may occur with lithium (0.1%) versus valproate (2 to 5%) or carbamazepine (1 to 3%). These risks must be weighed against the up to 50% chance of relapse with medication discontinuation.3
ANTIPSYCHOTICS
Antipsychotics are often used to treat mania because of their rapid effects and sedative properties. Most antipsychotics—specifically, haloperidol, olanzapine, and risperidone—are labeled “C,” specifying that fetal risk cannot be ruled out.
Table 3
FDA’s teratogenicity ratings of common antidepressants
| Category | Medication | Teratogenicity |
|---|---|---|
| Tricyclics | Amitriptyline Clomipramine Desipramine Imipramine Nortriptyline | Category C Category C Safety in pregnancy not known Safety in pregnancy not known Safety in pregnancy not known |
| Selective serotonin reuptake inhibitors | Citalopram Fluoxetine Fluvoxamine Paroxetine Sertraline | Category C Category C Category C Category C Category C |
| Other antidepressants | Bupropion Phenelzine Tranylcypromine | Category B Safety in pregnancy and nursing not known Safety in pregnancy and nursing not known |
| Source: Physicians’ Desk Reference. Montvale, NJ: Medical Economics Co., 2003. | ||
Chlorpromazine and haloperidol have been most studied during pregnancy but in relation to treating hyperemesis gravidarum and psychosis, not bipolar disorder. Results regarding antipsychotics’ teratogenic and behavioral risks are mixed,16-21 probably because the various compounds have different effects on the fetus.
The underlying illness—rather than the medications—may increase the rate of anomalies seen with exposure to antipsychotics:
- Rieder et al22 reported an increased rate of perinatal death in infants of schizophrenic mothers but no significant association between the mothers’ use of antipsychotics and perinatal death.
- Sobel23 compared psychotic women with and without histories of chlorpromazine exposure during pregnancy. Rates of fetal damage were similar and approximately twice that of the general population.
A meta-analysis of 74,337 live births revealed that first-trimester exposure to low-potency antipsychotics increases the relative risk of fetal anomalies in nonpsychotic women. Phenothiazines may increase the 2% baseline incidence of malformations to 2.4%.1 No specific organ malformation following fetal exposure to phenothiazines has been consistently identified.
Olanzapine was recently approved for treating mania. Very little data exist regarding its impact on fetal development when used during pregnancy, although studies on small numbers of women have not revealed teratogenicity.24,25
Conclusion. Psychotic illness itself may increase the risk of poor fetal outcome to a greater extent than does antipsychotic use. Prenatal exposure to low-potency phenothiazines may further increase this risk, although only slightly. The effect of prenatal exposure to atypical antipsychotics requires further study.
BENZODIAZEPINES
Benzodiazepines are rarely a primary treatment for mania or depression. Thus, a comprehensive review of their effect on fetal outcome is beyond the scope of this review. A meta-analysis of exposure in the first trimester suggests a very small but significant increase in risk for cleft palate.1 The absolute risk is <1 in 1,000 cases.
ANTIDEPRESSANTS
Whereas treatment of acute mania is considered a medical emergency, women with bipolar disorder may also relapse into depression during pregnancy. An antidepressant should not be used without a mood stabilizer when treating bipolar I disorder, although a mood stabilizer alone may be inadequate to treat depression. Using tricyclics and selective serotonin reuptake inhibitors (SSRIs) during pregnancy has not been associated with teratogenicity (Table 3),26 although perinatal effects have been reported.1
Tricyclics. In case-control studies involving more than 300,000 live births, 414 incidences of first-trimester exposure to tricyclics were followed. Information from these patients found no significant association between fetal exposure to tricyclics and increased rates of congenital malformations.1 The few studies that have been performed suggest no long-term effects from in utero exposure.26 Although these results suggest that prenatal exposure to tricyclics is relatively safe, more research is needed.
SSRIs. To date, no significant teratogenic effects of SSRIs have been identified in offspring of treated women.
The manufacturer’s register for fluoxetine contains approximately 2,000 cases of treated patients, with no excess cases of congenital anomalies or malformations following prenatal exposure. Citalopram has the next largest database of in utero exposure (n=365), again with no increased risk for teratogenicity. Several smaller systematic reports are available on in utero exposure to sertraline, paroxetine, or escitalopram.26
Most studies of pregnant women taking fluoxetine in the first trimester have found no increased risk of obstetrical complications—including spontaneous pregnancy loss, preterm labor, or low birth weight—compared with women not taking fluoxetine. Taking fluoxetine during the third trimester may increase the risk for perinatal complications,27 although this has been inconsistently reported and requires further study. Effects of other SSRIs in the third trimester have not been systematically explored.
Case reports and one controlled study have addressed possible neonatal perinatal symptoms from in utero exposure to SSRIs.28,29 Preliminary data show no adverse neurobehavioral function in exposed neonates.26
Electroconvulsive therapy (ECT) has been proven effective for acute mania and depression, demonstrating few deleterious effects on neonates. ECT has few side effects and may be safer than drug therapy in this population. Two reviews support the efficacy and relative safety of ECT treatment during pregnancy, although more evidence is needed.30,31
RECOMMENDATIONS
Discuss pregnancy and medication risks with all bipolar women, regardless of proximal plans for pregnancy. If psychotropic medication is used, prescribe carefully during the first trimester, using the minimum number of drugs and the lowest dosages needed to restore or maintain well-being.32
Pros and cons of switching. Some clinicians may encourage a patient to taper a medication during the first trimester because of its unknown or high teratogenicity. Depending on the patient’s illness severity, this might not be the optimal decision. A more conservative option would be to switch to a lower-risk drug during pregnancy.
Lithium has both antidepressant and antimanic properties and is less teratogenic compared with first-trimester exposure to an anticonvulsant. However, if lithium has not been successful for the woman’s mania prophylaxis in the past and she has demonstrated antimanic response to an anticonvulsant, switching to lithium or another anticonvulsant is not recommended.
Algorithm Suggested approach to the bipolar patient who wishes to conceive or is pregnant
Folate and neural tube defects. As first-trimester exposure to carbamazepine or valproate increases the risk for neural tube defects, using the lowest available dosage may decrease the risk for spina bifida, at least with valproate.
Low maternal folate levels are often associated with neural tube defects from any cause.33 Valproate lowers folate levels by inhibiting one of the enzymes necessary for its formation, which may be a mechanism for the increased risk of spina bifida.34
Folate supplementation. To date, no study has demonstrated that giving folate supplements to women taking anticonvulsants during pregnancy reduces the risk of neural tube defects.35 Nonetheless, we recommend that women who continue to take valproate or carbamazepine during pregnancy receive folate, 3 to 4 mg/d, as a precaution.
Treating manic relapse. Data show high rates of relapse in patients who stop taking lithium, particularly if done abruptly.3 Counsel women taking lithium to plan their pregnancies to allow enough time to taper off the medication prior to conception, if they want to try this. Lithium should be decreased slowly—approximately 50% every 2 weeks—to avoid relapse.
Treat aggressively if relapse occurs during pregnancy. Consider:
- psychiatric hospitalization in case of suicidality or psychosis
- reinstituting drug therapy with a less-teratogenic agent
- ECT for a manic or depressive episode.
As the pregnancy advances and the mother’s volume of distribution increases, dosage increases may be needed to maintain therapeutic drug levels.
Treating depressive relapse. Should depression occur in pregnancy, SSRIs or tricyclics added to mood stabilizer therapy have been shown to be effective, with few teratogenic effects.
Cognitive-behavioral and interpersonal psychotherapies also have shown efficacy in pregnant women with major depressive disorder36 and may be effective for women with bipolar disorder in pregnancy. Cognitive psychotherapies, when used with medication, have been reported effective in preventing relapse in nongravid bipolar patients.36-37
Related resources
Psychiatric disorders during pregnancy. Massachusetts General Hospital Center for Women’s Health. Perinatal Resource Center. www.womensmentalhealth.org/topics/pregnancy_lib.html
Drug brand names
- Amitriptyline • Elavil
- Bupropion • Wellbutrin
- Carbamazepine • Tegretol
- Chlorpromazine • Thorazine
- Citalopram • Celexa
- Clomipramine • Anafranil
- Desipramine • Norpramin
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Gabapentin • Neurontin
- Haloperidol • Haldol
- Imipramine • Tofranil
- Lamotrigine • Lamictal
- Lithium • Lithobid et al
- Methylphenidate • Ritalin et al
- Nortriptyline • Pamelor
- Olanzapine • Zyprexa
- Paroxetine • Paxil
- Phenelzine • Nardil
- Risperidone • Risperdal
- Sertraline • Zoloft
- Topiramate • Topamax
- Tranylcypromine • Parnate
- Trifluoperazine • Stelazine
- Valproate • Depakote et al
Disclosure
Dr. Altshuler receives research support from Abbott Laboratories, is a consultant to Abbott Laboratories, Forest Laboratories, and Eli Lilly & Co., and is a speaker for GlaxoSmithKline and Janssen Pharmaceutica.
Ms. Richards reports no financial relationship with any company whose products are mentioned in this article, or with manufacturers of competing products.
Dr. Yonkers receives research support from GlaxoSmithKline and Berlex Laboratories, is a consultant to GlaxoSmithKline, and is a speaker for Eli Lilly and Co., Pfizer Inc., GlaxoSmithKline, and Wyeth Pharmaceuticals.
1. Altshuler L, Cohen L, Szuba, et al. Pharmacologic management of psychiatric illness during pregnancy: dilemmas and guidelines. Am J Psychiatry 1996;153:592-606.
2. Nelson K, Holmes LB. Malformations due to presumed spontaneous mutations in newborn infants. N Engl J Med 1989;320:19-23.
3. Viguera AC, Nonacs R, Cohen LS, et al. Risk of recurrence of bipolar disorder in pregnant and nonpregnant women after discontinuing lithium maintenance. Am J Psychiatry 2000;157:179-84.
4. Steer RA, Scholl TO, Hediger ML, Fischer RL. Self-reported depression and negative pregnancy outcomes. J Clin Epidemiol 1992;45(10):1093-9.
5. Orr ST, Miller CA. Maternal depressive symptoms and the risk of poor pregnancy outcome. Review of the literature and preliminary findings. Epidemiol Rev 1995;17(1):165-71.
6. Zuckerman B, Amaro H, Bauchner H, Cabral H. Depressive symptoms during pregnancy: relationship to poor health behaviors. Am J Obstet Gynecol 1989;160:1107-11.
7. Miller LJ. Psychotic denial of pregnancy: phenomenology and clinical management. Hosp Community Psychiatry 1990;41:1233-7.
8. Cohen LS, Friedman JM, Jefferson JW, et al. A reevaluation of risk of in utero exposure to lithium. JAMA 1994;271(2):146-50correction JAMA 1994;271(19):1485.
9. Schou M. What happened later to the lithium babies? A follow-up study of children born without malformations. Acta Psychiatr Scand 1976;54(3):193-7.
10. Woody JN, London WL, Wilbanks GD. Lithium toxicity in a newborn. Pediatrics 1971;47:94-6.
11. Jones K, Lacro R, Johnson K, Adams J. Patterns of malformations in the children of women treated with carbamazepine during pregnancy. N Engl J Med 1989;320:1661-6.
12. Rosa F. Spina bifida in infants of women treated with carbamazepine during pregnancy. N Engl J Med 1991;324(10):674-7.
13. Koch S, Losche G, Jager-Roman E, et al. Major and minor birth malformations and antiepileptic drugs. Neurology 1992;42:83-8.
14. Jager-Roman E, Deichl A, Jakob S, et al. Fetal growth, major malformations, and minor anomalies in infants born to women receiving valproic acid. J Pediatr 1986;108:997-1004.
15. Nakane Y, Okuma T, Takahashi R, et al. Multi-institutional study on the teratogenicity and fetal toxicity of antiepileptic drugs: a report of a collaborative study group in Japan. Epilepsia 1980;21:663-80.
16. Edlund MJ, Craig TJ. Antipsychotic drug use and birth defects: an epidemiologic reassessment. Compr Psychiatry 1984;25:32-8.
17. Kris EB. Children of mothers maintained on pharmacotherapy during pregnancy and postpartum. Curr Ther Res 1965;7:785-9.
18. Clark CVH, Gorman D, Vernadakis A. Effects of prenatal administration of psychotropic drugs on behavior of developing rats. Dev Psychobiol 1970;3:225-35.
19. Golub M, Kornetsky C. Seizure susceptibility and avoidance conditioning in adult rats treated prenatally with chlorpromazine. Dev Psychobiol 1974;7:79-88.
20. Spear LP, Shalaby IA, Brick J. Chronic administration of haloperidol during development: behavioral and psychopharmacological effects. Psychopharmacology (Berl) 1980;70:47-58.
21. Cagiano R, Barfield RJ, White NR, et al. Subtle behavioral changes produced in rat pups exposed in utero to haloperidol. Eur J Pharmacol 1988;157:45-50.
22. Rieder RO, Rosenthal D, Wender P, Blumenthal H. The offspring of schizophrenics: fetal and neonatal deaths. Arch Gen Psychiatry 1975;32:200-11.
23. Sobel DE. Fetal damage due to ECT, insulin coma, chlorpromazine, or reserpine. Arch Gen Psychiatry 1960;2:606-11.
24. Dickson R. Olanzapine and pregnancy. Can J Psychiatry 1998;43:196-7.
25. Goldstein DJ, Corbin LA, Fung MC. Olanzapine-exposed pregnancies and lactation; early experience. J Clin Psychopharmacol 2000;24(4):399-403.
26. Altshuler LL, Cohen LS, Moline ML, et al. The expert consensus guideline series: treatment of depression in women. Postgrad Med 2001 Mar;(Spec No):1-22.
27. Chambers CD, Johnson KA, Dick LM, et al. Birth outcomes in pregnant women taking fluoxetine. N Engl J Med 1996;335:1010-15.
28. Spencer MJ. Fluoxetine hydrochloride (Prozac) toxicity in the neonate. Pediatrics 1993;92:721-2.
29. Cabrera FM, Battaglia G. Delayed decreases in brain 5-HT 2a and 2c receptor density and function in male rat progeny following prenatal fluoxetine. J Pharmacol Exp Ther 1994;269:637-45.
30. Miller LJ. Use of electroconvulsive therapy during pregnancy. Hosp Community Psychiatry 1994;45:444-50.
31. Ferrill MJ, Kehoe WA, Jacisin JJ. ECT during pregnancy: physiologic and pharmacologic considerations. Convuls Ther 1992;8:186-200.
32. Yonkers K, Wisner K, Cohen L, et al. Management of bipolar disorder during pregnancy and the postpartum period. Bipolar Consensus Statement. Submitted for publication.
33. Dansky L, Rosenblatt D, Andermann E. Mechanisms of teratogenesis: folic acid and antiepileptic therapy. Neurology 1992;42(suppl 5):32-42.
34. Wegner C, Nau H. Alteration of embryonic folate metabolism by valproic acid during organogenesis: implications for mechanism of teratogenesis. Neurology 1992;42(suppl 5):17-24.
35. MRC Vitamin Study Research Group. Prevention of neural tube defects: results of the Medical Research Council Vitamin Study. Lancet 1991;338:131-7.
36. Spinelli MG, Endicott J. Controlled clinical trial of interpersonal psychotherapy versus parenting education program for depressed pregnant women. Am J Psychiatry 2003;160:555-62.
37. Lam DH, Watkins ER, Hayward P, et al. A randomized controlled study of cognitive therapy for relapse prevention for bipolar affective disorder: outcome in the first year. Arch Gen Psychiatry 2003;60(2):145-52.
1. Altshuler L, Cohen L, Szuba, et al. Pharmacologic management of psychiatric illness during pregnancy: dilemmas and guidelines. Am J Psychiatry 1996;153:592-606.
2. Nelson K, Holmes LB. Malformations due to presumed spontaneous mutations in newborn infants. N Engl J Med 1989;320:19-23.
3. Viguera AC, Nonacs R, Cohen LS, et al. Risk of recurrence of bipolar disorder in pregnant and nonpregnant women after discontinuing lithium maintenance. Am J Psychiatry 2000;157:179-84.
4. Steer RA, Scholl TO, Hediger ML, Fischer RL. Self-reported depression and negative pregnancy outcomes. J Clin Epidemiol 1992;45(10):1093-9.
5. Orr ST, Miller CA. Maternal depressive symptoms and the risk of poor pregnancy outcome. Review of the literature and preliminary findings. Epidemiol Rev 1995;17(1):165-71.
6. Zuckerman B, Amaro H, Bauchner H, Cabral H. Depressive symptoms during pregnancy: relationship to poor health behaviors. Am J Obstet Gynecol 1989;160:1107-11.
7. Miller LJ. Psychotic denial of pregnancy: phenomenology and clinical management. Hosp Community Psychiatry 1990;41:1233-7.
8. Cohen LS, Friedman JM, Jefferson JW, et al. A reevaluation of risk of in utero exposure to lithium. JAMA 1994;271(2):146-50correction JAMA 1994;271(19):1485.
9. Schou M. What happened later to the lithium babies? A follow-up study of children born without malformations. Acta Psychiatr Scand 1976;54(3):193-7.
10. Woody JN, London WL, Wilbanks GD. Lithium toxicity in a newborn. Pediatrics 1971;47:94-6.
11. Jones K, Lacro R, Johnson K, Adams J. Patterns of malformations in the children of women treated with carbamazepine during pregnancy. N Engl J Med 1989;320:1661-6.
12. Rosa F. Spina bifida in infants of women treated with carbamazepine during pregnancy. N Engl J Med 1991;324(10):674-7.
13. Koch S, Losche G, Jager-Roman E, et al. Major and minor birth malformations and antiepileptic drugs. Neurology 1992;42:83-8.
14. Jager-Roman E, Deichl A, Jakob S, et al. Fetal growth, major malformations, and minor anomalies in infants born to women receiving valproic acid. J Pediatr 1986;108:997-1004.
15. Nakane Y, Okuma T, Takahashi R, et al. Multi-institutional study on the teratogenicity and fetal toxicity of antiepileptic drugs: a report of a collaborative study group in Japan. Epilepsia 1980;21:663-80.
16. Edlund MJ, Craig TJ. Antipsychotic drug use and birth defects: an epidemiologic reassessment. Compr Psychiatry 1984;25:32-8.
17. Kris EB. Children of mothers maintained on pharmacotherapy during pregnancy and postpartum. Curr Ther Res 1965;7:785-9.
18. Clark CVH, Gorman D, Vernadakis A. Effects of prenatal administration of psychotropic drugs on behavior of developing rats. Dev Psychobiol 1970;3:225-35.
19. Golub M, Kornetsky C. Seizure susceptibility and avoidance conditioning in adult rats treated prenatally with chlorpromazine. Dev Psychobiol 1974;7:79-88.
20. Spear LP, Shalaby IA, Brick J. Chronic administration of haloperidol during development: behavioral and psychopharmacological effects. Psychopharmacology (Berl) 1980;70:47-58.
21. Cagiano R, Barfield RJ, White NR, et al. Subtle behavioral changes produced in rat pups exposed in utero to haloperidol. Eur J Pharmacol 1988;157:45-50.
22. Rieder RO, Rosenthal D, Wender P, Blumenthal H. The offspring of schizophrenics: fetal and neonatal deaths. Arch Gen Psychiatry 1975;32:200-11.
23. Sobel DE. Fetal damage due to ECT, insulin coma, chlorpromazine, or reserpine. Arch Gen Psychiatry 1960;2:606-11.
24. Dickson R. Olanzapine and pregnancy. Can J Psychiatry 1998;43:196-7.
25. Goldstein DJ, Corbin LA, Fung MC. Olanzapine-exposed pregnancies and lactation; early experience. J Clin Psychopharmacol 2000;24(4):399-403.
26. Altshuler LL, Cohen LS, Moline ML, et al. The expert consensus guideline series: treatment of depression in women. Postgrad Med 2001 Mar;(Spec No):1-22.
27. Chambers CD, Johnson KA, Dick LM, et al. Birth outcomes in pregnant women taking fluoxetine. N Engl J Med 1996;335:1010-15.
28. Spencer MJ. Fluoxetine hydrochloride (Prozac) toxicity in the neonate. Pediatrics 1993;92:721-2.
29. Cabrera FM, Battaglia G. Delayed decreases in brain 5-HT 2a and 2c receptor density and function in male rat progeny following prenatal fluoxetine. J Pharmacol Exp Ther 1994;269:637-45.
30. Miller LJ. Use of electroconvulsive therapy during pregnancy. Hosp Community Psychiatry 1994;45:444-50.
31. Ferrill MJ, Kehoe WA, Jacisin JJ. ECT during pregnancy: physiologic and pharmacologic considerations. Convuls Ther 1992;8:186-200.
32. Yonkers K, Wisner K, Cohen L, et al. Management of bipolar disorder during pregnancy and the postpartum period. Bipolar Consensus Statement. Submitted for publication.
33. Dansky L, Rosenblatt D, Andermann E. Mechanisms of teratogenesis: folic acid and antiepileptic therapy. Neurology 1992;42(suppl 5):32-42.
34. Wegner C, Nau H. Alteration of embryonic folate metabolism by valproic acid during organogenesis: implications for mechanism of teratogenesis. Neurology 1992;42(suppl 5):17-24.
35. MRC Vitamin Study Research Group. Prevention of neural tube defects: results of the Medical Research Council Vitamin Study. Lancet 1991;338:131-7.
36. Spinelli MG, Endicott J. Controlled clinical trial of interpersonal psychotherapy versus parenting education program for depressed pregnant women. Am J Psychiatry 2003;160:555-62.
37. Lam DH, Watkins ER, Hayward P, et al. A randomized controlled study of cognitive therapy for relapse prevention for bipolar affective disorder: outcome in the first year. Arch Gen Psychiatry 2003;60(2):145-52.