User login
Ear Lesion Is Itchy and Sometimes Bleeds
An 84-year-old man is seeing an audiologist for hearing problems when the medical assistant notices a lesion on the patient’s right ear. When asked about it, the patient acknowledges that it has been bothering him. It itches and won't heal, no matter how much "medicine" the patient applies. Fortunately, it is not painful. But the patient is greatly annoyed that the lesion sometimes bleeds, leaving spots on his pillowcase and clothing.

The audiologist requests a consultation by the dermatology PA at her clinic.
EXAMINATION
The patient is an elderly white man in a wheelchair who is able to communicate readily. He is adamant that the lesion has only been present for about two weeks. However, his wife, who is with him, is sure it has been there for more than a year.
The lesion is a 1.6-cm ulcer with a telangiectatic, rolled pearly border. It is located between the tragus and antitragus on the outer floor of the patient’s external auditory meatus. It is seen in the context of the patient’s very fair and sun-damaged skin, which is also marked by numerous actinic keratoses on his face.
Under local anesthesia, shave biopsy is performed. A 5-mm slice is removed from the periphery of the lesion.
Continue for the outcome and discussion >>
DISCUSSION
The lesion proved to be the expected basal cell carcinoma (BCC), probably caused by sun exposure when the patient was younger. Patients are often incredulous about this connection, but the nuclei of skin cells have a long memory, often taking decades for cancers to actually develop. In a way, it doesn’t matter, since the damage is long since done even if the patient gets almost no sun at the present time.
But it does matter that this lesion is large and located in a difficult spot, one that does not lend itself to an easy fix. Primary closure would not be possible, given the complete lack of slack in the skin. A Mohs surgeon will need to remove the lesion, to ensure complete excision as well as perform the special procedures required to graft the site for closure.
Even though the lesion proved to be “just" a BCC (ie, not a melanoma), it still had to be dealt with lest it continue to spread. More than a few patients have had to have their entire external ear removed for this reason. Although it’s unusual, BCCs can metastasize to local lymph nodes and even to the brain and lung. More than a century ago, these were known as “rodent ulcers” that caused serious problems. If they could be caught in time, local cautery was the only chance at a cure.
The differential in this case included squamous cell carcinoma, which might have presented a more serious problem, given the location (near an orifice). Another diagnostic possibility was sebaceous carcinoma, a merkel cell cancer. Benign lesions, such as chondrodermatitis nodularis chronica helicis, occasionally present as ulcerated lesions on the ear.
BCCs are, far and away, the most common type of skin cancer, with more than a million new cases diagnosed each year in United States. They occur more commonly on fair-skinned patients and on prominently sun-exposed area (eg, ears, noses, and cheeks) but can also appear in areas where the sun seldom shines.
Several types of BCC have been described, but the nonhealing erosive papule (so-called noduloulcerative type) is the most common presentation. BCCs can also resemble scars or rashes. Though they are typically very slow to grow, not all BCCs are indolent. Some are quite aggressive both in terms of morphologic appearance and internal growth. And, as noted above, there is a differential for new, growing lesions in sun-exposed skin, making biopsy of such lesions mandatory.
Continue for Joe Monroe's take home learning points >>
TAKE-HOME LEARNING POINTS
• Nonhealing lesions on sun-exposed skin are considered to be skin cancers until proven otherwise by biopsy.
• Basal cell carcinomas (BCCs) are the most common skin cancer.
• BCCs typically grow very slowly.
• BCCs, if allowed to remain in place, can become extensive, invasive, destructive, and—in exceptional circumstances—can even metastasize.
• The differential for BCC includes squamous cell carcinoma, which has considerably more potential for metastasis than BCC, especially when it’s near an orifice.
• Quite frequently, it’s next to impossible to differentiate visually between BCC and SCC.
• BCCs and SCCs can take on several different morphologies, so any changing lesion needs to be biopsied to establish its identity, particularly since both are so common.
An 84-year-old man is seeing an audiologist for hearing problems when the medical assistant notices a lesion on the patient’s right ear. When asked about it, the patient acknowledges that it has been bothering him. It itches and won't heal, no matter how much "medicine" the patient applies. Fortunately, it is not painful. But the patient is greatly annoyed that the lesion sometimes bleeds, leaving spots on his pillowcase and clothing.
The audiologist requests a consultation by the dermatology PA at her clinic.
EXAMINATION
The patient is an elderly white man in a wheelchair who is able to communicate readily. He is adamant that the lesion has only been present for about two weeks. However, his wife, who is with him, is sure it has been there for more than a year.
The lesion is a 1.6-cm ulcer with a telangiectatic, rolled pearly border. It is located between the tragus and antitragus on the outer floor of the patient’s external auditory meatus. It is seen in the context of the patient’s very fair and sun-damaged skin, which is also marked by numerous actinic keratoses on his face.
Under local anesthesia, shave biopsy is performed. A 5-mm slice is removed from the periphery of the lesion.
Continue for the outcome and discussion >>
DISCUSSION
The lesion proved to be the expected basal cell carcinoma (BCC), probably caused by sun exposure when the patient was younger. Patients are often incredulous about this connection, but the nuclei of skin cells have a long memory, often taking decades for cancers to actually develop. In a way, it doesn’t matter, since the damage is long since done even if the patient gets almost no sun at the present time.
But it does matter that this lesion is large and located in a difficult spot, one that does not lend itself to an easy fix. Primary closure would not be possible, given the complete lack of slack in the skin. A Mohs surgeon will need to remove the lesion, to ensure complete excision as well as perform the special procedures required to graft the site for closure.
Even though the lesion proved to be “just" a BCC (ie, not a melanoma), it still had to be dealt with lest it continue to spread. More than a few patients have had to have their entire external ear removed for this reason. Although it’s unusual, BCCs can metastasize to local lymph nodes and even to the brain and lung. More than a century ago, these were known as “rodent ulcers” that caused serious problems. If they could be caught in time, local cautery was the only chance at a cure.
The differential in this case included squamous cell carcinoma, which might have presented a more serious problem, given the location (near an orifice). Another diagnostic possibility was sebaceous carcinoma, a merkel cell cancer. Benign lesions, such as chondrodermatitis nodularis chronica helicis, occasionally present as ulcerated lesions on the ear.
BCCs are, far and away, the most common type of skin cancer, with more than a million new cases diagnosed each year in United States. They occur more commonly on fair-skinned patients and on prominently sun-exposed area (eg, ears, noses, and cheeks) but can also appear in areas where the sun seldom shines.
Several types of BCC have been described, but the nonhealing erosive papule (so-called noduloulcerative type) is the most common presentation. BCCs can also resemble scars or rashes. Though they are typically very slow to grow, not all BCCs are indolent. Some are quite aggressive both in terms of morphologic appearance and internal growth. And, as noted above, there is a differential for new, growing lesions in sun-exposed skin, making biopsy of such lesions mandatory.
Continue for Joe Monroe's take home learning points >>
TAKE-HOME LEARNING POINTS
• Nonhealing lesions on sun-exposed skin are considered to be skin cancers until proven otherwise by biopsy.
• Basal cell carcinomas (BCCs) are the most common skin cancer.
• BCCs typically grow very slowly.
• BCCs, if allowed to remain in place, can become extensive, invasive, destructive, and—in exceptional circumstances—can even metastasize.
• The differential for BCC includes squamous cell carcinoma, which has considerably more potential for metastasis than BCC, especially when it’s near an orifice.
• Quite frequently, it’s next to impossible to differentiate visually between BCC and SCC.
• BCCs and SCCs can take on several different morphologies, so any changing lesion needs to be biopsied to establish its identity, particularly since both are so common.
An 84-year-old man is seeing an audiologist for hearing problems when the medical assistant notices a lesion on the patient’s right ear. When asked about it, the patient acknowledges that it has been bothering him. It itches and won't heal, no matter how much "medicine" the patient applies. Fortunately, it is not painful. But the patient is greatly annoyed that the lesion sometimes bleeds, leaving spots on his pillowcase and clothing.
The audiologist requests a consultation by the dermatology PA at her clinic.
EXAMINATION
The patient is an elderly white man in a wheelchair who is able to communicate readily. He is adamant that the lesion has only been present for about two weeks. However, his wife, who is with him, is sure it has been there for more than a year.
The lesion is a 1.6-cm ulcer with a telangiectatic, rolled pearly border. It is located between the tragus and antitragus on the outer floor of the patient’s external auditory meatus. It is seen in the context of the patient’s very fair and sun-damaged skin, which is also marked by numerous actinic keratoses on his face.
Under local anesthesia, shave biopsy is performed. A 5-mm slice is removed from the periphery of the lesion.
Continue for the outcome and discussion >>
DISCUSSION
The lesion proved to be the expected basal cell carcinoma (BCC), probably caused by sun exposure when the patient was younger. Patients are often incredulous about this connection, but the nuclei of skin cells have a long memory, often taking decades for cancers to actually develop. In a way, it doesn’t matter, since the damage is long since done even if the patient gets almost no sun at the present time.
But it does matter that this lesion is large and located in a difficult spot, one that does not lend itself to an easy fix. Primary closure would not be possible, given the complete lack of slack in the skin. A Mohs surgeon will need to remove the lesion, to ensure complete excision as well as perform the special procedures required to graft the site for closure.
Even though the lesion proved to be “just" a BCC (ie, not a melanoma), it still had to be dealt with lest it continue to spread. More than a few patients have had to have their entire external ear removed for this reason. Although it’s unusual, BCCs can metastasize to local lymph nodes and even to the brain and lung. More than a century ago, these were known as “rodent ulcers” that caused serious problems. If they could be caught in time, local cautery was the only chance at a cure.
The differential in this case included squamous cell carcinoma, which might have presented a more serious problem, given the location (near an orifice). Another diagnostic possibility was sebaceous carcinoma, a merkel cell cancer. Benign lesions, such as chondrodermatitis nodularis chronica helicis, occasionally present as ulcerated lesions on the ear.
BCCs are, far and away, the most common type of skin cancer, with more than a million new cases diagnosed each year in United States. They occur more commonly on fair-skinned patients and on prominently sun-exposed area (eg, ears, noses, and cheeks) but can also appear in areas where the sun seldom shines.
Several types of BCC have been described, but the nonhealing erosive papule (so-called noduloulcerative type) is the most common presentation. BCCs can also resemble scars or rashes. Though they are typically very slow to grow, not all BCCs are indolent. Some are quite aggressive both in terms of morphologic appearance and internal growth. And, as noted above, there is a differential for new, growing lesions in sun-exposed skin, making biopsy of such lesions mandatory.
Continue for Joe Monroe's take home learning points >>
TAKE-HOME LEARNING POINTS
• Nonhealing lesions on sun-exposed skin are considered to be skin cancers until proven otherwise by biopsy.
• Basal cell carcinomas (BCCs) are the most common skin cancer.
• BCCs typically grow very slowly.
• BCCs, if allowed to remain in place, can become extensive, invasive, destructive, and—in exceptional circumstances—can even metastasize.
• The differential for BCC includes squamous cell carcinoma, which has considerably more potential for metastasis than BCC, especially when it’s near an orifice.
• Quite frequently, it’s next to impossible to differentiate visually between BCC and SCC.
• BCCs and SCCs can take on several different morphologies, so any changing lesion needs to be biopsied to establish its identity, particularly since both are so common.

No Relief From Persistent Itchy Rash
It’s somewhat unusual to see a patient with an eight-year history of the same problem, but this is what happens when a 51-year-old man presents to dermatology. Specifically, the problem is a very itchy foot rash, for which the patient has tried many OTC products without success. He has also used halobetasol cream, prescribed by a dermatologist he saw several years ago.
The patient denies having a rash anywhere else. He does, however, have a markedly atopic history, significant for seasonal allergies, asthma, and very sensitive skin.
For the past several years, when the rash has been particularly unbearable, he admits to pouring rubbing alcohol on his feet. This burned terribly, but his feet felt better afterward.
Asked what else happened eight years ago, the patient recalls starting his current job as a lineman for a power company—an occupation that requires him to wear steel-toed leather boots for hours at a time.

EXAMINATION
A dense, red, papulovesicular rash covers both feet in a stocking pattern. The rash stops abruptly at the same place on both lower legs, completely sparing the soles and interdigital skin. Focal areas of scaling and broken skin are seen on the tops and sides of both feet.
Continue for Joe Monroe's diagnosis and discussion >>
DISCUSSION
In the ’90s, a commercial for sneakers utilized the catchphrase, "It's the shoes!" And so it is occasionally with rashes on the feet. In this case, the patient was allergic to the leather on the inside of his work boots.
A true allergy such as this would be expected to itch and to manifest as a papulovesicular rash limited to areas touched by the leather on the upper portions of his shoes. And it would persist, despite the quantity of topical medications tried, because the patient wore the shoes for eight to 12 hours a day, five or six days per week, continually re-exposing his skin to the offending material. He had never taken any significant time off work and therefore hadn’t refrained from wearing the shoes long enough to allow the rash to abate.
Often, frustrated and uncomfortable patients take matters into their own hands, which can ultimately compound the problem. This patient didn't do his skin any favors with the rubbing alcohol and other products he'd tried (the most common offender being triple-antibiotic ointment, although this patient used it only on rare occasions). Another strategy these patients often employ is to soak their feet in watered-down bleach. Fortunately, this patient had considered this option but thought better of it. A more benign, but just as ineffective, attempt at self-treatment had been to change laundry detergents, which of course did nothing to resolve the rash. (His first clue should have been that laundry detergent would not affect the tops of his feet while sparing the rest of his body.)
The insides of leather shoes are usually tanned with potassium dichromate, a chemical known to provoke this kind of reaction. Even after the source of the rash was identified, however, getting some distance between the patient and his shoes wasn’t easy. I had to write him a note for work, requesting that he be allowed to refrain from wearing his boots for about two weeks.
During that time, he started a week-long course of cephalexin 500 mg tid and applied clobetasol foam twice a day. In dermatology, we assume that any longstanding wet rash on the feet will become secondarily infected or at least colonized with gram-positive bacteria. Of course, giving him the steroid foam meant we were utilizing a class 1 corticosteroid in a very drying vehicle.
Within a week, he was a new man, with almost totally clear foot skin. This still left him with the problem of the work boots and the job—but one problem at a time.
TAKE-HOME LEARNING POINTS
• The areas spared by a rash are often just as important as those that are affected.
• Laundry detergents, often blamed for rashes, are seldom the culprit.
• Fungal infections rarely affect the dorsum of the foot while sparing interdigital and plantar surfaces.
• The patient’s atopic state will likely render him/her more susceptible to allergens.
• The vehicle (cream, gel, ointment, solution, foam) and strength of topical steroids both matter.
• Patients can become sensitized to the preservatives or other chemicals in OTC or prescription corticosteroid creams.
It’s somewhat unusual to see a patient with an eight-year history of the same problem, but this is what happens when a 51-year-old man presents to dermatology. Specifically, the problem is a very itchy foot rash, for which the patient has tried many OTC products without success. He has also used halobetasol cream, prescribed by a dermatologist he saw several years ago.
The patient denies having a rash anywhere else. He does, however, have a markedly atopic history, significant for seasonal allergies, asthma, and very sensitive skin.
For the past several years, when the rash has been particularly unbearable, he admits to pouring rubbing alcohol on his feet. This burned terribly, but his feet felt better afterward.
Asked what else happened eight years ago, the patient recalls starting his current job as a lineman for a power company—an occupation that requires him to wear steel-toed leather boots for hours at a time.
EXAMINATION
A dense, red, papulovesicular rash covers both feet in a stocking pattern. The rash stops abruptly at the same place on both lower legs, completely sparing the soles and interdigital skin. Focal areas of scaling and broken skin are seen on the tops and sides of both feet.
Continue for Joe Monroe's diagnosis and discussion >>
DISCUSSION
In the ’90s, a commercial for sneakers utilized the catchphrase, "It's the shoes!" And so it is occasionally with rashes on the feet. In this case, the patient was allergic to the leather on the inside of his work boots.
A true allergy such as this would be expected to itch and to manifest as a papulovesicular rash limited to areas touched by the leather on the upper portions of his shoes. And it would persist, despite the quantity of topical medications tried, because the patient wore the shoes for eight to 12 hours a day, five or six days per week, continually re-exposing his skin to the offending material. He had never taken any significant time off work and therefore hadn’t refrained from wearing the shoes long enough to allow the rash to abate.
Often, frustrated and uncomfortable patients take matters into their own hands, which can ultimately compound the problem. This patient didn't do his skin any favors with the rubbing alcohol and other products he'd tried (the most common offender being triple-antibiotic ointment, although this patient used it only on rare occasions). Another strategy these patients often employ is to soak their feet in watered-down bleach. Fortunately, this patient had considered this option but thought better of it. A more benign, but just as ineffective, attempt at self-treatment had been to change laundry detergents, which of course did nothing to resolve the rash. (His first clue should have been that laundry detergent would not affect the tops of his feet while sparing the rest of his body.)
The insides of leather shoes are usually tanned with potassium dichromate, a chemical known to provoke this kind of reaction. Even after the source of the rash was identified, however, getting some distance between the patient and his shoes wasn’t easy. I had to write him a note for work, requesting that he be allowed to refrain from wearing his boots for about two weeks.
During that time, he started a week-long course of cephalexin 500 mg tid and applied clobetasol foam twice a day. In dermatology, we assume that any longstanding wet rash on the feet will become secondarily infected or at least colonized with gram-positive bacteria. Of course, giving him the steroid foam meant we were utilizing a class 1 corticosteroid in a very drying vehicle.
Within a week, he was a new man, with almost totally clear foot skin. This still left him with the problem of the work boots and the job—but one problem at a time.
TAKE-HOME LEARNING POINTS
• The areas spared by a rash are often just as important as those that are affected.
• Laundry detergents, often blamed for rashes, are seldom the culprit.
• Fungal infections rarely affect the dorsum of the foot while sparing interdigital and plantar surfaces.
• The patient’s atopic state will likely render him/her more susceptible to allergens.
• The vehicle (cream, gel, ointment, solution, foam) and strength of topical steroids both matter.
• Patients can become sensitized to the preservatives or other chemicals in OTC or prescription corticosteroid creams.
It’s somewhat unusual to see a patient with an eight-year history of the same problem, but this is what happens when a 51-year-old man presents to dermatology. Specifically, the problem is a very itchy foot rash, for which the patient has tried many OTC products without success. He has also used halobetasol cream, prescribed by a dermatologist he saw several years ago.
The patient denies having a rash anywhere else. He does, however, have a markedly atopic history, significant for seasonal allergies, asthma, and very sensitive skin.
For the past several years, when the rash has been particularly unbearable, he admits to pouring rubbing alcohol on his feet. This burned terribly, but his feet felt better afterward.
Asked what else happened eight years ago, the patient recalls starting his current job as a lineman for a power company—an occupation that requires him to wear steel-toed leather boots for hours at a time.
EXAMINATION
A dense, red, papulovesicular rash covers both feet in a stocking pattern. The rash stops abruptly at the same place on both lower legs, completely sparing the soles and interdigital skin. Focal areas of scaling and broken skin are seen on the tops and sides of both feet.
Continue for Joe Monroe's diagnosis and discussion >>
DISCUSSION
In the ’90s, a commercial for sneakers utilized the catchphrase, "It's the shoes!" And so it is occasionally with rashes on the feet. In this case, the patient was allergic to the leather on the inside of his work boots.
A true allergy such as this would be expected to itch and to manifest as a papulovesicular rash limited to areas touched by the leather on the upper portions of his shoes. And it would persist, despite the quantity of topical medications tried, because the patient wore the shoes for eight to 12 hours a day, five or six days per week, continually re-exposing his skin to the offending material. He had never taken any significant time off work and therefore hadn’t refrained from wearing the shoes long enough to allow the rash to abate.
Often, frustrated and uncomfortable patients take matters into their own hands, which can ultimately compound the problem. This patient didn't do his skin any favors with the rubbing alcohol and other products he'd tried (the most common offender being triple-antibiotic ointment, although this patient used it only on rare occasions). Another strategy these patients often employ is to soak their feet in watered-down bleach. Fortunately, this patient had considered this option but thought better of it. A more benign, but just as ineffective, attempt at self-treatment had been to change laundry detergents, which of course did nothing to resolve the rash. (His first clue should have been that laundry detergent would not affect the tops of his feet while sparing the rest of his body.)
The insides of leather shoes are usually tanned with potassium dichromate, a chemical known to provoke this kind of reaction. Even after the source of the rash was identified, however, getting some distance between the patient and his shoes wasn’t easy. I had to write him a note for work, requesting that he be allowed to refrain from wearing his boots for about two weeks.
During that time, he started a week-long course of cephalexin 500 mg tid and applied clobetasol foam twice a day. In dermatology, we assume that any longstanding wet rash on the feet will become secondarily infected or at least colonized with gram-positive bacteria. Of course, giving him the steroid foam meant we were utilizing a class 1 corticosteroid in a very drying vehicle.
Within a week, he was a new man, with almost totally clear foot skin. This still left him with the problem of the work boots and the job—but one problem at a time.
TAKE-HOME LEARNING POINTS
• The areas spared by a rash are often just as important as those that are affected.
• Laundry detergents, often blamed for rashes, are seldom the culprit.
• Fungal infections rarely affect the dorsum of the foot while sparing interdigital and plantar surfaces.
• The patient’s atopic state will likely render him/her more susceptible to allergens.
• The vehicle (cream, gel, ointment, solution, foam) and strength of topical steroids both matter.
• Patients can become sensitized to the preservatives or other chemicals in OTC or prescription corticosteroid creams.

Could "Little Thing" Cause Big Trouble?
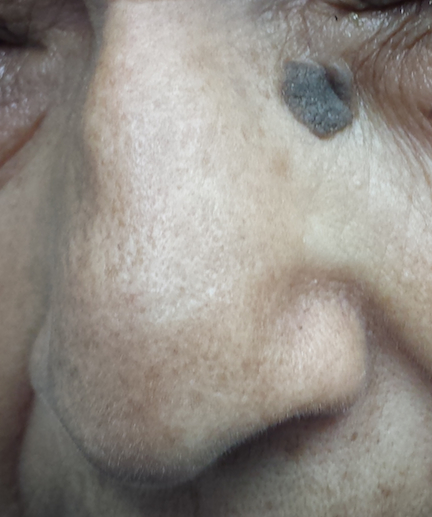
A 73-year-old woman is urgently referred to dermatology for evaluation of a facial lesion. It is unclear how long the lesion has been present, but it has caused great alarm to the patient's visiting relatives. The patient herself is not at all worried, saying that she doubts “a little thing like that could cause too much trouble.”
She denies any symptoms associated with the lesion and claims to be in good health. There is no history of weight loss, cough, or changes in mentation or gastrointestinal/genitourinary function. She admits to some sun exposure as a young adult but claims she has never been sunburned; she reports tanning easily and holding a tan well.
EXAMINATION
The lesion is a 1.4-cm round epidermal plaque with a rough, warty surface. It is located in the left lower medial epicanthal area, verging on the upper nasal sidewall. Its dark brown color is uniform, as is its surface texture. It appears in the context of the patient’s relatively dark type III skin, which is largely free of signs of sun damage.
PROCEDURE
After potential treatments are discussed with the patient, she opts to have cryosurgery. During the procedure, it is noted that the lesion remained white for several seconds after it was frozen.
Two months later, the site is rechecked. The lesion is virtually gone, except for a faint shadow of hyperpigmentation in the treated area.
Continue for Joe Monroe's discussion >>
DISCUSSION
The top three problems for which patients are seen in dermatology are acne, warts, and seborrheic keratoses (SK). The last are, hands down, the most common problem I see. With their dark color and raised surface, they epitomize what patients imagine skin cancer to look like.
Very likely, given the lesion’s size and location, it had been there for quite some time. But to the visiting relatives who hadn’t seen the patient in a while, it was new and alarming. (“Are you sure?” one of them asked when the patient shrugged off any concerns. “It looks so ugly!”)
I understand why SKs are worrisome to patients and their families. But, as a matter of fact, I was sure this lesion was safe. Why? Here are some reasons:
1. The lesion was epidermal in nature—that is, “stuck on” the surface of the skin, as opposed to being in, or part of, it. Epidermal lesions are almost always safe; intradermal ones, while not necessarily "bad," tend to require more attention.
2. Warty and rough are both good signs, dermatologically speaking.
3. Uniformity in color, texture, and borders is also usually positive; the "bad stuff" tends to be somewhat irregular in all three respects.
4. Cryo-white is our term for “stays white after treatment with liquid nitrogen." By contrast, things like skin cancer thaw almost instantly. Why? The blood supply to a cancerous lesion is far better than that to an epidermal SK, which has little if any vascularization. Warm blood dissipates the cold quickly.
5. Liquid nitrogen also highlights another diagnostic feature of SKs: pseudocysts. Peculiar to SKs, these porelike surface features are usually seen as minute follicular orifices.
6. Other diagnostic features of SKs: Most affected patients have several similar lesions. Usually, the history of SK is that it’s "been there forever,” although this case illustrates an exception. SKs are typically seen in older people, but I’ve seen them on teenagers, too.
The introduction of the liquid nitrogen gun 35 years ago made SK treatment much easier and provided a potential diagnostic tool. We often use cryotherapy as a kind of final test of whether a lesion is benign or malignant. If the lesion responds to routine cryotherapy by resolving, chances are quite good it was benign. If it doesn’t, you may need to reconsider your diagnosis.
TAKE-HOME LEARNING POINTS
• SKs are extremely common, often numerous, and favor older patients.
• SKs are usually rough, epidermal, round to oval, and tan to dark brown.
• SKs, treated with liquid nitrogen, turn white and stay that way for a few seconds at least, while the dangerous lookalikes (eg, melanoma) thaw much more quickly.
• Liquid nitrogen treatment can help with diagnosis: If the treated lesion fails to disappear as intended, it might not be an SK after all. (Note, however, that this process can take up to two weeks.)
• Liquid nitrogen also highlights surface pseudocysts, which are pathognomic for SKs.
• When cryotherapy fails to elicit the desired changes, the lesion needs to be biopsied.
A 73-year-old woman is urgently referred to dermatology for evaluation of a facial lesion. It is unclear how long the lesion has been present, but it has caused great alarm to the patient's visiting relatives. The patient herself is not at all worried, saying that she doubts “a little thing like that could cause too much trouble.”
She denies any symptoms associated with the lesion and claims to be in good health. There is no history of weight loss, cough, or changes in mentation or gastrointestinal/genitourinary function. She admits to some sun exposure as a young adult but claims she has never been sunburned; she reports tanning easily and holding a tan well.
EXAMINATION
The lesion is a 1.4-cm round epidermal plaque with a rough, warty surface. It is located in the left lower medial epicanthal area, verging on the upper nasal sidewall. Its dark brown color is uniform, as is its surface texture. It appears in the context of the patient’s relatively dark type III skin, which is largely free of signs of sun damage.
PROCEDURE
After potential treatments are discussed with the patient, she opts to have cryosurgery. During the procedure, it is noted that the lesion remained white for several seconds after it was frozen.
Two months later, the site is rechecked. The lesion is virtually gone, except for a faint shadow of hyperpigmentation in the treated area.
Continue for Joe Monroe's discussion >>
DISCUSSION
The top three problems for which patients are seen in dermatology are acne, warts, and seborrheic keratoses (SK). The last are, hands down, the most common problem I see. With their dark color and raised surface, they epitomize what patients imagine skin cancer to look like.
Very likely, given the lesion’s size and location, it had been there for quite some time. But to the visiting relatives who hadn’t seen the patient in a while, it was new and alarming. (“Are you sure?” one of them asked when the patient shrugged off any concerns. “It looks so ugly!”)
I understand why SKs are worrisome to patients and their families. But, as a matter of fact, I was sure this lesion was safe. Why? Here are some reasons:
1. The lesion was epidermal in nature—that is, “stuck on” the surface of the skin, as opposed to being in, or part of, it. Epidermal lesions are almost always safe; intradermal ones, while not necessarily "bad," tend to require more attention.
2. Warty and rough are both good signs, dermatologically speaking.
3. Uniformity in color, texture, and borders is also usually positive; the "bad stuff" tends to be somewhat irregular in all three respects.
4. Cryo-white is our term for “stays white after treatment with liquid nitrogen." By contrast, things like skin cancer thaw almost instantly. Why? The blood supply to a cancerous lesion is far better than that to an epidermal SK, which has little if any vascularization. Warm blood dissipates the cold quickly.
5. Liquid nitrogen also highlights another diagnostic feature of SKs: pseudocysts. Peculiar to SKs, these porelike surface features are usually seen as minute follicular orifices.
6. Other diagnostic features of SKs: Most affected patients have several similar lesions. Usually, the history of SK is that it’s "been there forever,” although this case illustrates an exception. SKs are typically seen in older people, but I’ve seen them on teenagers, too.
The introduction of the liquid nitrogen gun 35 years ago made SK treatment much easier and provided a potential diagnostic tool. We often use cryotherapy as a kind of final test of whether a lesion is benign or malignant. If the lesion responds to routine cryotherapy by resolving, chances are quite good it was benign. If it doesn’t, you may need to reconsider your diagnosis.
TAKE-HOME LEARNING POINTS
• SKs are extremely common, often numerous, and favor older patients.
• SKs are usually rough, epidermal, round to oval, and tan to dark brown.
• SKs, treated with liquid nitrogen, turn white and stay that way for a few seconds at least, while the dangerous lookalikes (eg, melanoma) thaw much more quickly.
• Liquid nitrogen treatment can help with diagnosis: If the treated lesion fails to disappear as intended, it might not be an SK after all. (Note, however, that this process can take up to two weeks.)
• Liquid nitrogen also highlights surface pseudocysts, which are pathognomic for SKs.
• When cryotherapy fails to elicit the desired changes, the lesion needs to be biopsied.
A 73-year-old woman is urgently referred to dermatology for evaluation of a facial lesion. It is unclear how long the lesion has been present, but it has caused great alarm to the patient's visiting relatives. The patient herself is not at all worried, saying that she doubts “a little thing like that could cause too much trouble.”
She denies any symptoms associated with the lesion and claims to be in good health. There is no history of weight loss, cough, or changes in mentation or gastrointestinal/genitourinary function. She admits to some sun exposure as a young adult but claims she has never been sunburned; she reports tanning easily and holding a tan well.
EXAMINATION
The lesion is a 1.4-cm round epidermal plaque with a rough, warty surface. It is located in the left lower medial epicanthal area, verging on the upper nasal sidewall. Its dark brown color is uniform, as is its surface texture. It appears in the context of the patient’s relatively dark type III skin, which is largely free of signs of sun damage.
PROCEDURE
After potential treatments are discussed with the patient, she opts to have cryosurgery. During the procedure, it is noted that the lesion remained white for several seconds after it was frozen.
Two months later, the site is rechecked. The lesion is virtually gone, except for a faint shadow of hyperpigmentation in the treated area.
Continue for Joe Monroe's discussion >>
DISCUSSION
The top three problems for which patients are seen in dermatology are acne, warts, and seborrheic keratoses (SK). The last are, hands down, the most common problem I see. With their dark color and raised surface, they epitomize what patients imagine skin cancer to look like.
Very likely, given the lesion’s size and location, it had been there for quite some time. But to the visiting relatives who hadn’t seen the patient in a while, it was new and alarming. (“Are you sure?” one of them asked when the patient shrugged off any concerns. “It looks so ugly!”)
I understand why SKs are worrisome to patients and their families. But, as a matter of fact, I was sure this lesion was safe. Why? Here are some reasons:
1. The lesion was epidermal in nature—that is, “stuck on” the surface of the skin, as opposed to being in, or part of, it. Epidermal lesions are almost always safe; intradermal ones, while not necessarily "bad," tend to require more attention.
2. Warty and rough are both good signs, dermatologically speaking.
3. Uniformity in color, texture, and borders is also usually positive; the "bad stuff" tends to be somewhat irregular in all three respects.
4. Cryo-white is our term for “stays white after treatment with liquid nitrogen." By contrast, things like skin cancer thaw almost instantly. Why? The blood supply to a cancerous lesion is far better than that to an epidermal SK, which has little if any vascularization. Warm blood dissipates the cold quickly.
5. Liquid nitrogen also highlights another diagnostic feature of SKs: pseudocysts. Peculiar to SKs, these porelike surface features are usually seen as minute follicular orifices.
6. Other diagnostic features of SKs: Most affected patients have several similar lesions. Usually, the history of SK is that it’s "been there forever,” although this case illustrates an exception. SKs are typically seen in older people, but I’ve seen them on teenagers, too.
The introduction of the liquid nitrogen gun 35 years ago made SK treatment much easier and provided a potential diagnostic tool. We often use cryotherapy as a kind of final test of whether a lesion is benign or malignant. If the lesion responds to routine cryotherapy by resolving, chances are quite good it was benign. If it doesn’t, you may need to reconsider your diagnosis.
TAKE-HOME LEARNING POINTS
• SKs are extremely common, often numerous, and favor older patients.
• SKs are usually rough, epidermal, round to oval, and tan to dark brown.
• SKs, treated with liquid nitrogen, turn white and stay that way for a few seconds at least, while the dangerous lookalikes (eg, melanoma) thaw much more quickly.
• Liquid nitrogen treatment can help with diagnosis: If the treated lesion fails to disappear as intended, it might not be an SK after all. (Note, however, that this process can take up to two weeks.)
• Liquid nitrogen also highlights surface pseudocysts, which are pathognomic for SKs.
• When cryotherapy fails to elicit the desired changes, the lesion needs to be biopsied.

Subungual Lesion Hasn’t Grown Out: Benign or Malignant?
Eight months ago, this 67-year-old man first noticed a dark lesion under his second fingernail. Since then, it has not changed. It is completely asymptomatic, but it hasn’t grown out, either, which concerns the patient and his primary care provider. The latter recommends a visit to dermatology.

The patient denies any history of trauma to either the finger or the nail and says he hasn’t had any similar problems with his other fingernails. His history does include excessive sun exposure, particularly during his young adulthood. He has had several basal cell carcinomas removed over the years, mostly from his face.
EXAMINATION
The lesion in question is 4 mm, dark brown to black, and macular. It is located under the mid portion of his right index fingernail. No abnormality of the nail plate itself is felt, and all his other fingernails appear normal.
A presumptive diagnosis of subungual hematoma is challenged by the given history of at least eight months without any change or movement to the lesion. This fact is at odds with the nature of a hematoma.
Continue for the procedure and discussion >>
PROCEDURE
Since the lesion cannot simply be ignored, given the real (albeit remote) possibility of melanoma, how to proceed is thoroughly discussed with the patient. As a result, the finger is anesthetized by digital block technique, using 2% plain lidocaine. A tourniquet is then created from a small exam glove with the tip of the index finger removed. This portion of the glove is then rolled up to the base of the finger, and when the patient holds his hand above his heart, it provides a relatively bloodless field.
Then, under clean conditions, the portion of the nail plate covering the lesion is removed with iris scissors, revealing the expected subungual hematoma (characterized by clotted blood adhering to the underside of the nail plate). The nail bed now appears totally normal. After the tourniquet is released, the site is cleaned and dressed and the patient reassured as to the benignancy of the lesion.

DISCUSSION
Subungual melanoma is unusual but greatly feared because of its generally poor prognosis. This is not due to any inherent virulence but rather to delayed diagnosis. Such a delay may be caused by disbelief or denial on the part of the patient. A notable case is that of musician Bob Marley, who died in 1981 from metastatic melanoma that had started under a toenail. (Legend continues to maintain that the trauma of kicking a soccer ball caused the cancer, though this is totally anecdotal.)
Marley, who was born in Jamaica and was of mixed African and European ancestry, embodies the fact that while persons with darker skin develop melanoma far less frequently than do fair-skinned individuals, they tend to get it in locations with the least amount of pigment (eg, palms, soles, mouth, under nails). Most patients, and many unwary providers, have simply never been exposed to this very real phenomenon.
Melanoma that develops in these peripheral locations is called acral lentiginous melanoma. Hands, feet, thumbs, and halluces are the most common locations. Nearly all these melanomas begin as tan to brown macules and tend to enlarge and darken over time. They eventually transition to a vertical growth phase that allows penetration of superficial vasculature by tumor cells, leading to metastasis.
The presentation of this patient’s lesion is inconsistent with that of subungual melanoma, which usually involves the periungual margins (especially the cuticle, which eventually darkens focally, a phenomenon termed Hutchinson’s sign). In any case, whenever a subungual melanoma is suspected, a biopsy must be performed.
In all likelihood, this patient sustained trauma to this nail but forgot about it. In another two months or so, his subungual hematoma would have grown out, proving its benignancy. But in the circumstances, we had no choice but to take his given history seriously and properly evaluate the lesion.
Continue for Joe Monroe's learning points >>
TAKE-HOME LEARNING POINTS
• Acral lentiginous melanoma is associated with a generally poor prognosis, primarily due to delayed diagnosis.
• This type of melanoma is typically found on the scalp, palms, or soles, under nails, and even in the mouth. The thumb and big toe are the most common locations when hands or feet are involved.
• Patients with darker skin are far less likely to develop melanoma than their fair-skinned counterparts—but when they do, the aforementioned locations are the most common.
• For nondermatology providers, affected patients should probably be referred to dermatology for evaluation and possible biopsy.
• For any subungual or periungual lesion noted on physical examination, a history should be sought.
Eight months ago, this 67-year-old man first noticed a dark lesion under his second fingernail. Since then, it has not changed. It is completely asymptomatic, but it hasn’t grown out, either, which concerns the patient and his primary care provider. The latter recommends a visit to dermatology.
The patient denies any history of trauma to either the finger or the nail and says he hasn’t had any similar problems with his other fingernails. His history does include excessive sun exposure, particularly during his young adulthood. He has had several basal cell carcinomas removed over the years, mostly from his face.
EXAMINATION
The lesion in question is 4 mm, dark brown to black, and macular. It is located under the mid portion of his right index fingernail. No abnormality of the nail plate itself is felt, and all his other fingernails appear normal.
A presumptive diagnosis of subungual hematoma is challenged by the given history of at least eight months without any change or movement to the lesion. This fact is at odds with the nature of a hematoma.
Continue for the procedure and discussion >>
PROCEDURE
Since the lesion cannot simply be ignored, given the real (albeit remote) possibility of melanoma, how to proceed is thoroughly discussed with the patient. As a result, the finger is anesthetized by digital block technique, using 2% plain lidocaine. A tourniquet is then created from a small exam glove with the tip of the index finger removed. This portion of the glove is then rolled up to the base of the finger, and when the patient holds his hand above his heart, it provides a relatively bloodless field.
Then, under clean conditions, the portion of the nail plate covering the lesion is removed with iris scissors, revealing the expected subungual hematoma (characterized by clotted blood adhering to the underside of the nail plate). The nail bed now appears totally normal. After the tourniquet is released, the site is cleaned and dressed and the patient reassured as to the benignancy of the lesion.
DISCUSSION
Subungual melanoma is unusual but greatly feared because of its generally poor prognosis. This is not due to any inherent virulence but rather to delayed diagnosis. Such a delay may be caused by disbelief or denial on the part of the patient. A notable case is that of musician Bob Marley, who died in 1981 from metastatic melanoma that had started under a toenail. (Legend continues to maintain that the trauma of kicking a soccer ball caused the cancer, though this is totally anecdotal.)
Marley, who was born in Jamaica and was of mixed African and European ancestry, embodies the fact that while persons with darker skin develop melanoma far less frequently than do fair-skinned individuals, they tend to get it in locations with the least amount of pigment (eg, palms, soles, mouth, under nails). Most patients, and many unwary providers, have simply never been exposed to this very real phenomenon.
Melanoma that develops in these peripheral locations is called acral lentiginous melanoma. Hands, feet, thumbs, and halluces are the most common locations. Nearly all these melanomas begin as tan to brown macules and tend to enlarge and darken over time. They eventually transition to a vertical growth phase that allows penetration of superficial vasculature by tumor cells, leading to metastasis.
The presentation of this patient’s lesion is inconsistent with that of subungual melanoma, which usually involves the periungual margins (especially the cuticle, which eventually darkens focally, a phenomenon termed Hutchinson’s sign). In any case, whenever a subungual melanoma is suspected, a biopsy must be performed.
In all likelihood, this patient sustained trauma to this nail but forgot about it. In another two months or so, his subungual hematoma would have grown out, proving its benignancy. But in the circumstances, we had no choice but to take his given history seriously and properly evaluate the lesion.
Continue for Joe Monroe's learning points >>
TAKE-HOME LEARNING POINTS
• Acral lentiginous melanoma is associated with a generally poor prognosis, primarily due to delayed diagnosis.
• This type of melanoma is typically found on the scalp, palms, or soles, under nails, and even in the mouth. The thumb and big toe are the most common locations when hands or feet are involved.
• Patients with darker skin are far less likely to develop melanoma than their fair-skinned counterparts—but when they do, the aforementioned locations are the most common.
• For nondermatology providers, affected patients should probably be referred to dermatology for evaluation and possible biopsy.
• For any subungual or periungual lesion noted on physical examination, a history should be sought.
Eight months ago, this 67-year-old man first noticed a dark lesion under his second fingernail. Since then, it has not changed. It is completely asymptomatic, but it hasn’t grown out, either, which concerns the patient and his primary care provider. The latter recommends a visit to dermatology.
The patient denies any history of trauma to either the finger or the nail and says he hasn’t had any similar problems with his other fingernails. His history does include excessive sun exposure, particularly during his young adulthood. He has had several basal cell carcinomas removed over the years, mostly from his face.
EXAMINATION
The lesion in question is 4 mm, dark brown to black, and macular. It is located under the mid portion of his right index fingernail. No abnormality of the nail plate itself is felt, and all his other fingernails appear normal.
A presumptive diagnosis of subungual hematoma is challenged by the given history of at least eight months without any change or movement to the lesion. This fact is at odds with the nature of a hematoma.
Continue for the procedure and discussion >>
PROCEDURE
Since the lesion cannot simply be ignored, given the real (albeit remote) possibility of melanoma, how to proceed is thoroughly discussed with the patient. As a result, the finger is anesthetized by digital block technique, using 2% plain lidocaine. A tourniquet is then created from a small exam glove with the tip of the index finger removed. This portion of the glove is then rolled up to the base of the finger, and when the patient holds his hand above his heart, it provides a relatively bloodless field.
Then, under clean conditions, the portion of the nail plate covering the lesion is removed with iris scissors, revealing the expected subungual hematoma (characterized by clotted blood adhering to the underside of the nail plate). The nail bed now appears totally normal. After the tourniquet is released, the site is cleaned and dressed and the patient reassured as to the benignancy of the lesion.
DISCUSSION
Subungual melanoma is unusual but greatly feared because of its generally poor prognosis. This is not due to any inherent virulence but rather to delayed diagnosis. Such a delay may be caused by disbelief or denial on the part of the patient. A notable case is that of musician Bob Marley, who died in 1981 from metastatic melanoma that had started under a toenail. (Legend continues to maintain that the trauma of kicking a soccer ball caused the cancer, though this is totally anecdotal.)
Marley, who was born in Jamaica and was of mixed African and European ancestry, embodies the fact that while persons with darker skin develop melanoma far less frequently than do fair-skinned individuals, they tend to get it in locations with the least amount of pigment (eg, palms, soles, mouth, under nails). Most patients, and many unwary providers, have simply never been exposed to this very real phenomenon.
Melanoma that develops in these peripheral locations is called acral lentiginous melanoma. Hands, feet, thumbs, and halluces are the most common locations. Nearly all these melanomas begin as tan to brown macules and tend to enlarge and darken over time. They eventually transition to a vertical growth phase that allows penetration of superficial vasculature by tumor cells, leading to metastasis.
The presentation of this patient’s lesion is inconsistent with that of subungual melanoma, which usually involves the periungual margins (especially the cuticle, which eventually darkens focally, a phenomenon termed Hutchinson’s sign). In any case, whenever a subungual melanoma is suspected, a biopsy must be performed.
In all likelihood, this patient sustained trauma to this nail but forgot about it. In another two months or so, his subungual hematoma would have grown out, proving its benignancy. But in the circumstances, we had no choice but to take his given history seriously and properly evaluate the lesion.
Continue for Joe Monroe's learning points >>
TAKE-HOME LEARNING POINTS
• Acral lentiginous melanoma is associated with a generally poor prognosis, primarily due to delayed diagnosis.
• This type of melanoma is typically found on the scalp, palms, or soles, under nails, and even in the mouth. The thumb and big toe are the most common locations when hands or feet are involved.
• Patients with darker skin are far less likely to develop melanoma than their fair-skinned counterparts—but when they do, the aforementioned locations are the most common.
• For nondermatology providers, affected patients should probably be referred to dermatology for evaluation and possible biopsy.
• For any subungual or periungual lesion noted on physical examination, a history should be sought.

Unsightly But Not Painful
At the end of his dermatology visit for an entirely different problem, this 48-year-old man mentions that his toenails have become discolored and misshapen in recent years. Consulting a long line of providers about the problem has not produced a successful solution. Among the treatments tried were oral formulations of fluconazole, ketoconazole, and terbinafine, as well as various OTC topical products, including window-cleaning fluid, tea tree oil, and petroleum jelly.
Ten years ago, he was persuaded to have his right big toenail surgically removed, in hopes of a cure. However, when the nail grew back, it gradually reverted to its previous appearance.

He claims to be in good health otherwise and takes no prescription medications (aside from the attempts to treat his toenail problem). For many years, he has worked in construction, wearing heavy 9 in boots. For the past seven years, he has worked 12-hour days.
He denies any pain in his toes and admits that his main motivation for seeking help with this problem is that his wife is convinced she will “catch” it and end up with toenails like his.
EXAMINATION
Eight out of 10 toenails, including the first and second toes of both feet, are decidedly yellowed and thickened, displaying multiple focal areas of breakage on the ends of the nail plates. No such changes are noted on his fingernails. The surrounding skin on his feet and hands is entirely within normal limits, except for a rim of faint scaling around the periphery of both feet. The latter is KOH positive for fungal elements.
Continue for Joe Monroe's Discussion...
DISCUSSION
Onychomycosis, also known as tinea unguium, is an extremely common problem, affecting approximately 10% of adults in the US (but only 4% to 6% in Canada). Common as it is, onychomycosis is also vastly overdiagnosed and frequently mistreated, as illustrated by this particular case. This combination creates confusion among patients and clinicians alike.
Several different organisms can cause what we call onychomycosis, but the most common is Trichophyton rubrum, a dermatophytic fungus also responsible for most cases of “athlete’s foot” and “jock itch.” The changes seen in onychomycotic toenails include yellow to brown discoloration, thickening, and often, brittle ends of the nail plates. Unfortunately, other diseases—including but not limited to psoriasis and lichen planus—can cause similar changes.
In this case, the classical appearance of the patient’s toenails, along with the athlete’s foot and involvement of the big toenails, made this a relatively easy diagnosis. In other circumstances, confirmation could have been provided from a simple nail clipping. Sent for pathologic examination, it would have exhibited signs of fungal organisms.
Even with a firm diagnosis, successful treatment is problematic. This man’s employment and choice of footwear—along with a family history that was revealed through further questioning—all conspire against him. Ideal treatment would eventuate in a cure, but with these factors against him, it is unlikely.
For example, a four-month course of the best treatment (terbinafine 250 mg/d), would probably clear his nails. However, the chance of recurrence would be at least 50%, for two reasons. One: His environment and heredity would leave him no less susceptible than before. Two: Continual or repeat exposure to this ubiquitous organism is almost certain.
If his toenails cleared, he could simply continue his use of oral terbinafine (taking 250 mg once or twice a week) in hopes of maintaining that state. This would constitute an off-label use of that drug, since there have been no studies of its effectiveness or safety with ongoing use. This “prevention” strategy has been tried with some success, however.
The good news? First of all, the patient’s wife of 20 years has shown no signs of developing onychomycosis and is unlikely ever to do so. It appears that women are not as susceptible as men, either by virtue of less perspiration, circumstance of career, or choice of footwear. And furthermore, onychomycosis is not an infection in any sense that we typically use that word. It almost never causes pain or even redness, except in association with nail dystrophy so severe that the nail plate cuts into adjacent live tissue.
TAKE-HOME LEARNING POINTS
• Onychomycosis is extremely common, affecting about 10% of adults in this country.
• Heredity and environmental factors play significant roles in a person’s susceptibility to onychomycosis.
• Men are far more likely to experience onychomycosis than women.
• Surgical removal of onychomycotic toenails is completely ineffective.
• Petroleum jelly, window-cleaning fluid, and tea tree oil have not proven effective in treating onychomycosis.
• First and second toenails are usually the first to be affected by this condition, presumably as a result of trauma.
At the end of his dermatology visit for an entirely different problem, this 48-year-old man mentions that his toenails have become discolored and misshapen in recent years. Consulting a long line of providers about the problem has not produced a successful solution. Among the treatments tried were oral formulations of fluconazole, ketoconazole, and terbinafine, as well as various OTC topical products, including window-cleaning fluid, tea tree oil, and petroleum jelly.
Ten years ago, he was persuaded to have his right big toenail surgically removed, in hopes of a cure. However, when the nail grew back, it gradually reverted to its previous appearance.
He claims to be in good health otherwise and takes no prescription medications (aside from the attempts to treat his toenail problem). For many years, he has worked in construction, wearing heavy 9 in boots. For the past seven years, he has worked 12-hour days.
He denies any pain in his toes and admits that his main motivation for seeking help with this problem is that his wife is convinced she will “catch” it and end up with toenails like his.
EXAMINATION
Eight out of 10 toenails, including the first and second toes of both feet, are decidedly yellowed and thickened, displaying multiple focal areas of breakage on the ends of the nail plates. No such changes are noted on his fingernails. The surrounding skin on his feet and hands is entirely within normal limits, except for a rim of faint scaling around the periphery of both feet. The latter is KOH positive for fungal elements.
Continue for Joe Monroe's Discussion...
DISCUSSION
Onychomycosis, also known as tinea unguium, is an extremely common problem, affecting approximately 10% of adults in the US (but only 4% to 6% in Canada). Common as it is, onychomycosis is also vastly overdiagnosed and frequently mistreated, as illustrated by this particular case. This combination creates confusion among patients and clinicians alike.
Several different organisms can cause what we call onychomycosis, but the most common is Trichophyton rubrum, a dermatophytic fungus also responsible for most cases of “athlete’s foot” and “jock itch.” The changes seen in onychomycotic toenails include yellow to brown discoloration, thickening, and often, brittle ends of the nail plates. Unfortunately, other diseases—including but not limited to psoriasis and lichen planus—can cause similar changes.
In this case, the classical appearance of the patient’s toenails, along with the athlete’s foot and involvement of the big toenails, made this a relatively easy diagnosis. In other circumstances, confirmation could have been provided from a simple nail clipping. Sent for pathologic examination, it would have exhibited signs of fungal organisms.
Even with a firm diagnosis, successful treatment is problematic. This man’s employment and choice of footwear—along with a family history that was revealed through further questioning—all conspire against him. Ideal treatment would eventuate in a cure, but with these factors against him, it is unlikely.
For example, a four-month course of the best treatment (terbinafine 250 mg/d), would probably clear his nails. However, the chance of recurrence would be at least 50%, for two reasons. One: His environment and heredity would leave him no less susceptible than before. Two: Continual or repeat exposure to this ubiquitous organism is almost certain.
If his toenails cleared, he could simply continue his use of oral terbinafine (taking 250 mg once or twice a week) in hopes of maintaining that state. This would constitute an off-label use of that drug, since there have been no studies of its effectiveness or safety with ongoing use. This “prevention” strategy has been tried with some success, however.
The good news? First of all, the patient’s wife of 20 years has shown no signs of developing onychomycosis and is unlikely ever to do so. It appears that women are not as susceptible as men, either by virtue of less perspiration, circumstance of career, or choice of footwear. And furthermore, onychomycosis is not an infection in any sense that we typically use that word. It almost never causes pain or even redness, except in association with nail dystrophy so severe that the nail plate cuts into adjacent live tissue.
TAKE-HOME LEARNING POINTS
• Onychomycosis is extremely common, affecting about 10% of adults in this country.
• Heredity and environmental factors play significant roles in a person’s susceptibility to onychomycosis.
• Men are far more likely to experience onychomycosis than women.
• Surgical removal of onychomycotic toenails is completely ineffective.
• Petroleum jelly, window-cleaning fluid, and tea tree oil have not proven effective in treating onychomycosis.
• First and second toenails are usually the first to be affected by this condition, presumably as a result of trauma.
At the end of his dermatology visit for an entirely different problem, this 48-year-old man mentions that his toenails have become discolored and misshapen in recent years. Consulting a long line of providers about the problem has not produced a successful solution. Among the treatments tried were oral formulations of fluconazole, ketoconazole, and terbinafine, as well as various OTC topical products, including window-cleaning fluid, tea tree oil, and petroleum jelly.
Ten years ago, he was persuaded to have his right big toenail surgically removed, in hopes of a cure. However, when the nail grew back, it gradually reverted to its previous appearance.
He claims to be in good health otherwise and takes no prescription medications (aside from the attempts to treat his toenail problem). For many years, he has worked in construction, wearing heavy 9 in boots. For the past seven years, he has worked 12-hour days.
He denies any pain in his toes and admits that his main motivation for seeking help with this problem is that his wife is convinced she will “catch” it and end up with toenails like his.
EXAMINATION
Eight out of 10 toenails, including the first and second toes of both feet, are decidedly yellowed and thickened, displaying multiple focal areas of breakage on the ends of the nail plates. No such changes are noted on his fingernails. The surrounding skin on his feet and hands is entirely within normal limits, except for a rim of faint scaling around the periphery of both feet. The latter is KOH positive for fungal elements.
Continue for Joe Monroe's Discussion...
DISCUSSION
Onychomycosis, also known as tinea unguium, is an extremely common problem, affecting approximately 10% of adults in the US (but only 4% to 6% in Canada). Common as it is, onychomycosis is also vastly overdiagnosed and frequently mistreated, as illustrated by this particular case. This combination creates confusion among patients and clinicians alike.
Several different organisms can cause what we call onychomycosis, but the most common is Trichophyton rubrum, a dermatophytic fungus also responsible for most cases of “athlete’s foot” and “jock itch.” The changes seen in onychomycotic toenails include yellow to brown discoloration, thickening, and often, brittle ends of the nail plates. Unfortunately, other diseases—including but not limited to psoriasis and lichen planus—can cause similar changes.
In this case, the classical appearance of the patient’s toenails, along with the athlete’s foot and involvement of the big toenails, made this a relatively easy diagnosis. In other circumstances, confirmation could have been provided from a simple nail clipping. Sent for pathologic examination, it would have exhibited signs of fungal organisms.
Even with a firm diagnosis, successful treatment is problematic. This man’s employment and choice of footwear—along with a family history that was revealed through further questioning—all conspire against him. Ideal treatment would eventuate in a cure, but with these factors against him, it is unlikely.
For example, a four-month course of the best treatment (terbinafine 250 mg/d), would probably clear his nails. However, the chance of recurrence would be at least 50%, for two reasons. One: His environment and heredity would leave him no less susceptible than before. Two: Continual or repeat exposure to this ubiquitous organism is almost certain.
If his toenails cleared, he could simply continue his use of oral terbinafine (taking 250 mg once or twice a week) in hopes of maintaining that state. This would constitute an off-label use of that drug, since there have been no studies of its effectiveness or safety with ongoing use. This “prevention” strategy has been tried with some success, however.
The good news? First of all, the patient’s wife of 20 years has shown no signs of developing onychomycosis and is unlikely ever to do so. It appears that women are not as susceptible as men, either by virtue of less perspiration, circumstance of career, or choice of footwear. And furthermore, onychomycosis is not an infection in any sense that we typically use that word. It almost never causes pain or even redness, except in association with nail dystrophy so severe that the nail plate cuts into adjacent live tissue.
TAKE-HOME LEARNING POINTS
• Onychomycosis is extremely common, affecting about 10% of adults in this country.
• Heredity and environmental factors play significant roles in a person’s susceptibility to onychomycosis.
• Men are far more likely to experience onychomycosis than women.
• Surgical removal of onychomycotic toenails is completely ineffective.
• Petroleum jelly, window-cleaning fluid, and tea tree oil have not proven effective in treating onychomycosis.
• First and second toenails are usually the first to be affected by this condition, presumably as a result of trauma.

Unexpected Source for Itch
A 70-year-old man is referred to dermatology for evaluation of a scalp rash that has been present for months. Complaining bitterly of the itching in his scalp, he gives a history that includes treatment attempts with a number of medications, including prescription ketoconazole shampoo, oral antibiotics (eg, minocycline), and a course of oral terbinafine (250 mg/d for three weeks)—none of which has had a positive impact on the problem.

His wife, who is with him, at first denies and then finally admits to having an itchy scalp as well. Neither has a history of prior skin problems.
The patient’s history is significant for type 2 diabetes and for well-controlled hypertension. He has been retired for many years and lives at home with his wife.
EXAMINATION
The patient appears disheveled, confused, and dirty. He is grossly oriented as to time and place, but hard of hearing and difficult to communicate with as a result.
His hair is greasy and dirty, as well as matted down in places. On closer inspection, scabs are noted in his scalp; they are widely distributed but especially heavy in the occipital and supra-auricular scalp. Many flakes of dandruff (some quite large) can also be seen.
Raising the thick hair over his nuchal scalp reveals a whitish sheen. Under 10x magnification, multiple tiny white papules are observed attached to each hair shaft, which accounts for the sheen. When examined under the microscope, the papules are clearly identified as nits. No adult lice are noted.
Significant tender adenopathy is elicited on palpation of the posterior neck area.
Continue reading for the discussion...
DISCUSSION
Clearly, the basic problem is head lice (pediculosis capitis), with everything else stemming from it. This can be quite confusing for many reasons, not least of which is that one thinks of head lice as a pediatric problem.
The related issue is bacterial infection secondary to scratching and picking, usually from coagulase-negative staph. Minocycline or trimethoprim/sulfa would have been adequate for treatment but of course would not address the main problem: the lice.
Ironically, one of the other impediments to a correct diagnosis was the severity of this patient’s case. It was, without a doubt, the worst I’ve seen in a 30-year career. The nits were so numerous as to render them almost impossible to see without magnification.
There’s little doubt that his wife had them too, adding to the potential for others (eg, grandchildren) around them to be infested as well. Furthermore, this represented a source for re-infestation despite treatment efforts.
Luckily, neither the organisms nor the nits remain viable for long off the body, which means they cannot reside and replicate on inanimate objects. Nonhumans cannot give or get human head lice. Given the organism’s need for warmth and aversion to light, there’s little chance for involvement in areas other than the scalp.
Both the patient and his wife were treated with oral and topical ivermectin. The topical form is applied once to a damp scalp, left on for 10 minutes, then rinsed out. It not only kills the adult organisms but also appears to render the nits nonviable—potentially obviating the necessity of using a nit comb.
The oral ivermectin (150 µg/kg ) was prescribed as follows: four 3-mg tablets now and another four tablets in 10 days to kill any remaining adults. Oral ivermectin is usually not necessary in the treatment of head lice and was only used in this case because of the severity.
Since their cases were so severe, I also advised them both to consider shaving their heads first to facilitate effective treatment. Again, this step is seldom necessary except in the most extreme cases. However, it also facilitated management of their secondary pyoderma, which was treated with trimethoprim/sulfa (double strength, bid for a week).
Since the itching caused by head lice is essentially an allergic reaction to the organism’s protein, that symptom may persist for some time, albeit with gradually diminishing intensity.
Continue reading for Joe Monroe's take-home learning points...
TAKE-HOME LEARNING POINTS
• Pediculosis capitis (head lice) is seen mostly in children but affects adults as well.
• Pyoderma, secondary to scratching, can mislead the diagnostician and thereby delay diagnosis of the underlying problem.
• Oral trimethoprim/sulfa is often used to treat lice-associated pyoderma but does nothing directly to kill the lice themselves.
• The itching from head lice is a delayed hypersensitivity reaction to the lice protein and can take months after infestation to develop.
• Conversely, itching will develop early on in patients who have been sensitized by having had head lice in the past.
• The use of topical ivermectin has proven to be exceptionally effective in clinical trials.
DISCLOSURE: The author discloses having spoken and written about topical ivermectin at the behest of the manufacturer, but this article was not part of that process, nor is it supported by the product’s manufacturer in any way.
A 70-year-old man is referred to dermatology for evaluation of a scalp rash that has been present for months. Complaining bitterly of the itching in his scalp, he gives a history that includes treatment attempts with a number of medications, including prescription ketoconazole shampoo, oral antibiotics (eg, minocycline), and a course of oral terbinafine (250 mg/d for three weeks)—none of which has had a positive impact on the problem.
His wife, who is with him, at first denies and then finally admits to having an itchy scalp as well. Neither has a history of prior skin problems.
The patient’s history is significant for type 2 diabetes and for well-controlled hypertension. He has been retired for many years and lives at home with his wife.
EXAMINATION
The patient appears disheveled, confused, and dirty. He is grossly oriented as to time and place, but hard of hearing and difficult to communicate with as a result.
His hair is greasy and dirty, as well as matted down in places. On closer inspection, scabs are noted in his scalp; they are widely distributed but especially heavy in the occipital and supra-auricular scalp. Many flakes of dandruff (some quite large) can also be seen.
Raising the thick hair over his nuchal scalp reveals a whitish sheen. Under 10x magnification, multiple tiny white papules are observed attached to each hair shaft, which accounts for the sheen. When examined under the microscope, the papules are clearly identified as nits. No adult lice are noted.
Significant tender adenopathy is elicited on palpation of the posterior neck area.
Continue reading for the discussion...
DISCUSSION
Clearly, the basic problem is head lice (pediculosis capitis), with everything else stemming from it. This can be quite confusing for many reasons, not least of which is that one thinks of head lice as a pediatric problem.
The related issue is bacterial infection secondary to scratching and picking, usually from coagulase-negative staph. Minocycline or trimethoprim/sulfa would have been adequate for treatment but of course would not address the main problem: the lice.
Ironically, one of the other impediments to a correct diagnosis was the severity of this patient’s case. It was, without a doubt, the worst I’ve seen in a 30-year career. The nits were so numerous as to render them almost impossible to see without magnification.
There’s little doubt that his wife had them too, adding to the potential for others (eg, grandchildren) around them to be infested as well. Furthermore, this represented a source for re-infestation despite treatment efforts.
Luckily, neither the organisms nor the nits remain viable for long off the body, which means they cannot reside and replicate on inanimate objects. Nonhumans cannot give or get human head lice. Given the organism’s need for warmth and aversion to light, there’s little chance for involvement in areas other than the scalp.
Both the patient and his wife were treated with oral and topical ivermectin. The topical form is applied once to a damp scalp, left on for 10 minutes, then rinsed out. It not only kills the adult organisms but also appears to render the nits nonviable—potentially obviating the necessity of using a nit comb.
The oral ivermectin (150 µg/kg ) was prescribed as follows: four 3-mg tablets now and another four tablets in 10 days to kill any remaining adults. Oral ivermectin is usually not necessary in the treatment of head lice and was only used in this case because of the severity.
Since their cases were so severe, I also advised them both to consider shaving their heads first to facilitate effective treatment. Again, this step is seldom necessary except in the most extreme cases. However, it also facilitated management of their secondary pyoderma, which was treated with trimethoprim/sulfa (double strength, bid for a week).
Since the itching caused by head lice is essentially an allergic reaction to the organism’s protein, that symptom may persist for some time, albeit with gradually diminishing intensity.
Continue reading for Joe Monroe's take-home learning points...
TAKE-HOME LEARNING POINTS
• Pediculosis capitis (head lice) is seen mostly in children but affects adults as well.
• Pyoderma, secondary to scratching, can mislead the diagnostician and thereby delay diagnosis of the underlying problem.
• Oral trimethoprim/sulfa is often used to treat lice-associated pyoderma but does nothing directly to kill the lice themselves.
• The itching from head lice is a delayed hypersensitivity reaction to the lice protein and can take months after infestation to develop.
• Conversely, itching will develop early on in patients who have been sensitized by having had head lice in the past.
• The use of topical ivermectin has proven to be exceptionally effective in clinical trials.
DISCLOSURE: The author discloses having spoken and written about topical ivermectin at the behest of the manufacturer, but this article was not part of that process, nor is it supported by the product’s manufacturer in any way.
A 70-year-old man is referred to dermatology for evaluation of a scalp rash that has been present for months. Complaining bitterly of the itching in his scalp, he gives a history that includes treatment attempts with a number of medications, including prescription ketoconazole shampoo, oral antibiotics (eg, minocycline), and a course of oral terbinafine (250 mg/d for three weeks)—none of which has had a positive impact on the problem.
His wife, who is with him, at first denies and then finally admits to having an itchy scalp as well. Neither has a history of prior skin problems.
The patient’s history is significant for type 2 diabetes and for well-controlled hypertension. He has been retired for many years and lives at home with his wife.
EXAMINATION
The patient appears disheveled, confused, and dirty. He is grossly oriented as to time and place, but hard of hearing and difficult to communicate with as a result.
His hair is greasy and dirty, as well as matted down in places. On closer inspection, scabs are noted in his scalp; they are widely distributed but especially heavy in the occipital and supra-auricular scalp. Many flakes of dandruff (some quite large) can also be seen.
Raising the thick hair over his nuchal scalp reveals a whitish sheen. Under 10x magnification, multiple tiny white papules are observed attached to each hair shaft, which accounts for the sheen. When examined under the microscope, the papules are clearly identified as nits. No adult lice are noted.
Significant tender adenopathy is elicited on palpation of the posterior neck area.
Continue reading for the discussion...
DISCUSSION
Clearly, the basic problem is head lice (pediculosis capitis), with everything else stemming from it. This can be quite confusing for many reasons, not least of which is that one thinks of head lice as a pediatric problem.
The related issue is bacterial infection secondary to scratching and picking, usually from coagulase-negative staph. Minocycline or trimethoprim/sulfa would have been adequate for treatment but of course would not address the main problem: the lice.
Ironically, one of the other impediments to a correct diagnosis was the severity of this patient’s case. It was, without a doubt, the worst I’ve seen in a 30-year career. The nits were so numerous as to render them almost impossible to see without magnification.
There’s little doubt that his wife had them too, adding to the potential for others (eg, grandchildren) around them to be infested as well. Furthermore, this represented a source for re-infestation despite treatment efforts.
Luckily, neither the organisms nor the nits remain viable for long off the body, which means they cannot reside and replicate on inanimate objects. Nonhumans cannot give or get human head lice. Given the organism’s need for warmth and aversion to light, there’s little chance for involvement in areas other than the scalp.
Both the patient and his wife were treated with oral and topical ivermectin. The topical form is applied once to a damp scalp, left on for 10 minutes, then rinsed out. It not only kills the adult organisms but also appears to render the nits nonviable—potentially obviating the necessity of using a nit comb.
The oral ivermectin (150 µg/kg ) was prescribed as follows: four 3-mg tablets now and another four tablets in 10 days to kill any remaining adults. Oral ivermectin is usually not necessary in the treatment of head lice and was only used in this case because of the severity.
Since their cases were so severe, I also advised them both to consider shaving their heads first to facilitate effective treatment. Again, this step is seldom necessary except in the most extreme cases. However, it also facilitated management of their secondary pyoderma, which was treated with trimethoprim/sulfa (double strength, bid for a week).
Since the itching caused by head lice is essentially an allergic reaction to the organism’s protein, that symptom may persist for some time, albeit with gradually diminishing intensity.
Continue reading for Joe Monroe's take-home learning points...
TAKE-HOME LEARNING POINTS
• Pediculosis capitis (head lice) is seen mostly in children but affects adults as well.
• Pyoderma, secondary to scratching, can mislead the diagnostician and thereby delay diagnosis of the underlying problem.
• Oral trimethoprim/sulfa is often used to treat lice-associated pyoderma but does nothing directly to kill the lice themselves.
• The itching from head lice is a delayed hypersensitivity reaction to the lice protein and can take months after infestation to develop.
• Conversely, itching will develop early on in patients who have been sensitized by having had head lice in the past.
• The use of topical ivermectin has proven to be exceptionally effective in clinical trials.
DISCLOSURE: The author discloses having spoken and written about topical ivermectin at the behest of the manufacturer, but this article was not part of that process, nor is it supported by the product’s manufacturer in any way.

It Doesn't Hurt, So It Must Not Be Serious
A 60-year-old man presents to a free clinic for evaluation of a “knot” in his left lower axilla. He first noticed it several months ago. Even though the lesion grew, the patient reasoned that it couldn’t be too serious since “it didn’t hurt.” But in the past month, the lesion has become much more firm and darkened.

The patient denies any other health problems. He has an 80-pack-year history of smoking. He has never had health insurance and as a result has carefully avoided any interaction with the health care establishment.
Additional history-taking reveals that he has become markedly short of breath in the past few months, which he attributes to his smoking. He denies any abdominal pain or headache. As a young man, he spent 20 years working as a roofer, often going shirtless in hot weather.
EXAMINATION
The patient is in no distress. He is accompanied by his wife, who participates in the history-taking process. Both call attention to the lesion in question, a 5.5-cm dark subcutaneous mass in the left lower axilla. The overlying skin is dark as well, and on palpation, the mass is found to be fixed and firm. Palpation elsewhere in the axillae, as well as in the head and neck, fails to detect any other lesions.
The rest of the patient's type III skin (easily tanned, seldom burned) shows limited evidence of sun damage. A few minor solar lentigines are seen on the trunk, but none stand out. Then the patient's wife points out a barely discernible, depigmented, poorly defined macule on the left lateral back. It measures about 2 cm. This lesion, she reports, "used to be real black. Then it turned scabby, and then it lost all its color. It's been this way ever since."
Continue reading for the diagnostic studies...
DIAGNOSTIC STUDIES
An incisional biopsy of the residual lesion on his back is performed. Two-thirds of the macule is removed, the wound is closed with sutures, and the specimen is submitted for pathologic examination. The resulting report indicates a superficial spreading melanoma, Breslow depth (vertical thickness) of 1.6 mm, with evidence of significant regression and a brisk mitotic rate─all predictors of metastatic potential.
Accordingly, the patient is referred to the appropriate surgical specialist, who confirms the micrometastatic nature of the axillary node and refers the patient to oncology for imaging studies that will determine the extent of metastasis. The residual primary tumor is excised with 2-cm margins.
Continue reading for the discussion...
DISCUSSION
This case illustrates the phenomenon—known as regression—in which part or all of a cutaneous melanoma is rendered invisible over time by the reaction of the immune system (although not before it has a chance to spread). Not uncommonly, these patients are diagnosed with metastatic melanoma and no primary lesion is ever discovered.
A variation on this theme is the so-called amelanotic melanoma, which can present initially in a wide variety of forms—papules, nodules, or macules; in shades of pink, blue, white, or "flesh." But unlike our patient, these cases do not involve regression.
This patient and his wife assumed that because the primary lesion had essentially disappeared, it must have been safe. And of course, they failed to connect it with the new axillary nodule.
At this writing, the extent of the patient’s disease remains to be defined by imaging studies (PET and CT scans). But given the facts of the case, his prognosis at best is guarded. A more hopeful view is that he is living in a time of meaningful discovery of better treatments for advanced melanomas.
Continue reading for Joe Monroe's take home learning points...
TAKE-HOME LEARNING POINTS
• Although the classic melanoma is black and essentially flat, it can present in many other forms, including an amelanotic version, the color of which can be pink, blue, white or even skin-colored.
• Infrequently, melanoma presents initially in metastatic form, having spread from an unknown or obscure primary lesion.
• Immune response to a cutaneous melanoma can result in partial or even total destruction of the lesion, a process termed regression.
• Predictors of a relatively poor prognosis for melanoma include: the aforementioned regression, vertical thickness (Breslow depth), mitotic rate, vascular invasion, and the presence of ulceration.
• New masses in known nodal locations require examination of surrounding skin to detect or rule out suspicious lesions.
A 60-year-old man presents to a free clinic for evaluation of a “knot” in his left lower axilla. He first noticed it several months ago. Even though the lesion grew, the patient reasoned that it couldn’t be too serious since “it didn’t hurt.” But in the past month, the lesion has become much more firm and darkened.
The patient denies any other health problems. He has an 80-pack-year history of smoking. He has never had health insurance and as a result has carefully avoided any interaction with the health care establishment.
Additional history-taking reveals that he has become markedly short of breath in the past few months, which he attributes to his smoking. He denies any abdominal pain or headache. As a young man, he spent 20 years working as a roofer, often going shirtless in hot weather.
EXAMINATION
The patient is in no distress. He is accompanied by his wife, who participates in the history-taking process. Both call attention to the lesion in question, a 5.5-cm dark subcutaneous mass in the left lower axilla. The overlying skin is dark as well, and on palpation, the mass is found to be fixed and firm. Palpation elsewhere in the axillae, as well as in the head and neck, fails to detect any other lesions.
The rest of the patient's type III skin (easily tanned, seldom burned) shows limited evidence of sun damage. A few minor solar lentigines are seen on the trunk, but none stand out. Then the patient's wife points out a barely discernible, depigmented, poorly defined macule on the left lateral back. It measures about 2 cm. This lesion, she reports, "used to be real black. Then it turned scabby, and then it lost all its color. It's been this way ever since."
Continue reading for the diagnostic studies...
DIAGNOSTIC STUDIES
An incisional biopsy of the residual lesion on his back is performed. Two-thirds of the macule is removed, the wound is closed with sutures, and the specimen is submitted for pathologic examination. The resulting report indicates a superficial spreading melanoma, Breslow depth (vertical thickness) of 1.6 mm, with evidence of significant regression and a brisk mitotic rate─all predictors of metastatic potential.
Accordingly, the patient is referred to the appropriate surgical specialist, who confirms the micrometastatic nature of the axillary node and refers the patient to oncology for imaging studies that will determine the extent of metastasis. The residual primary tumor is excised with 2-cm margins.
Continue reading for the discussion...
DISCUSSION
This case illustrates the phenomenon—known as regression—in which part or all of a cutaneous melanoma is rendered invisible over time by the reaction of the immune system (although not before it has a chance to spread). Not uncommonly, these patients are diagnosed with metastatic melanoma and no primary lesion is ever discovered.
A variation on this theme is the so-called amelanotic melanoma, which can present initially in a wide variety of forms—papules, nodules, or macules; in shades of pink, blue, white, or "flesh." But unlike our patient, these cases do not involve regression.
This patient and his wife assumed that because the primary lesion had essentially disappeared, it must have been safe. And of course, they failed to connect it with the new axillary nodule.
At this writing, the extent of the patient’s disease remains to be defined by imaging studies (PET and CT scans). But given the facts of the case, his prognosis at best is guarded. A more hopeful view is that he is living in a time of meaningful discovery of better treatments for advanced melanomas.
Continue reading for Joe Monroe's take home learning points...
TAKE-HOME LEARNING POINTS
• Although the classic melanoma is black and essentially flat, it can present in many other forms, including an amelanotic version, the color of which can be pink, blue, white or even skin-colored.
• Infrequently, melanoma presents initially in metastatic form, having spread from an unknown or obscure primary lesion.
• Immune response to a cutaneous melanoma can result in partial or even total destruction of the lesion, a process termed regression.
• Predictors of a relatively poor prognosis for melanoma include: the aforementioned regression, vertical thickness (Breslow depth), mitotic rate, vascular invasion, and the presence of ulceration.
• New masses in known nodal locations require examination of surrounding skin to detect or rule out suspicious lesions.
A 60-year-old man presents to a free clinic for evaluation of a “knot” in his left lower axilla. He first noticed it several months ago. Even though the lesion grew, the patient reasoned that it couldn’t be too serious since “it didn’t hurt.” But in the past month, the lesion has become much more firm and darkened.
The patient denies any other health problems. He has an 80-pack-year history of smoking. He has never had health insurance and as a result has carefully avoided any interaction with the health care establishment.
Additional history-taking reveals that he has become markedly short of breath in the past few months, which he attributes to his smoking. He denies any abdominal pain or headache. As a young man, he spent 20 years working as a roofer, often going shirtless in hot weather.
EXAMINATION
The patient is in no distress. He is accompanied by his wife, who participates in the history-taking process. Both call attention to the lesion in question, a 5.5-cm dark subcutaneous mass in the left lower axilla. The overlying skin is dark as well, and on palpation, the mass is found to be fixed and firm. Palpation elsewhere in the axillae, as well as in the head and neck, fails to detect any other lesions.
The rest of the patient's type III skin (easily tanned, seldom burned) shows limited evidence of sun damage. A few minor solar lentigines are seen on the trunk, but none stand out. Then the patient's wife points out a barely discernible, depigmented, poorly defined macule on the left lateral back. It measures about 2 cm. This lesion, she reports, "used to be real black. Then it turned scabby, and then it lost all its color. It's been this way ever since."
Continue reading for the diagnostic studies...
DIAGNOSTIC STUDIES
An incisional biopsy of the residual lesion on his back is performed. Two-thirds of the macule is removed, the wound is closed with sutures, and the specimen is submitted for pathologic examination. The resulting report indicates a superficial spreading melanoma, Breslow depth (vertical thickness) of 1.6 mm, with evidence of significant regression and a brisk mitotic rate─all predictors of metastatic potential.
Accordingly, the patient is referred to the appropriate surgical specialist, who confirms the micrometastatic nature of the axillary node and refers the patient to oncology for imaging studies that will determine the extent of metastasis. The residual primary tumor is excised with 2-cm margins.
Continue reading for the discussion...
DISCUSSION
This case illustrates the phenomenon—known as regression—in which part or all of a cutaneous melanoma is rendered invisible over time by the reaction of the immune system (although not before it has a chance to spread). Not uncommonly, these patients are diagnosed with metastatic melanoma and no primary lesion is ever discovered.
A variation on this theme is the so-called amelanotic melanoma, which can present initially in a wide variety of forms—papules, nodules, or macules; in shades of pink, blue, white, or "flesh." But unlike our patient, these cases do not involve regression.
This patient and his wife assumed that because the primary lesion had essentially disappeared, it must have been safe. And of course, they failed to connect it with the new axillary nodule.
At this writing, the extent of the patient’s disease remains to be defined by imaging studies (PET and CT scans). But given the facts of the case, his prognosis at best is guarded. A more hopeful view is that he is living in a time of meaningful discovery of better treatments for advanced melanomas.
Continue reading for Joe Monroe's take home learning points...
TAKE-HOME LEARNING POINTS
• Although the classic melanoma is black and essentially flat, it can present in many other forms, including an amelanotic version, the color of which can be pink, blue, white or even skin-colored.
• Infrequently, melanoma presents initially in metastatic form, having spread from an unknown or obscure primary lesion.
• Immune response to a cutaneous melanoma can result in partial or even total destruction of the lesion, a process termed regression.
• Predictors of a relatively poor prognosis for melanoma include: the aforementioned regression, vertical thickness (Breslow depth), mitotic rate, vascular invasion, and the presence of ulceration.
• New masses in known nodal locations require examination of surrounding skin to detect or rule out suspicious lesions.

How to Manage a Keloid

A 39-year-old African-American man has had a keloid on his right earlobe for several years. It was triggered by ear-piercing and has grown slowly to its current size. The patient denies any symptoms with the lesion.
EXAMINATION
The 5 x 2-cm lobulated mass is consistent in every way with a keloid: firm and pedunculated, with no epidermal changes. It hangs from his right earlobe. The patient has type IV skin, of African-American ancestry. After an extended discussion regarding treatment options, the patient decides to have the lesion excised.
PROCEDURE
Under sterile conditions and with local anesthesia (1% lidocaine with epinephrine), the entire keloid is removed. The wound edges are shaped to enhance the final appearance, and the wound is closed in one layer.
Since the risk for reformation is all too real, at one week post-op, the wound edges are injected with 3 mg/cc of triamcinolone, with a total of 1.5 cc used. The injections continue for three months as the wound heals. The outcome is totally acceptable to the patient, representing a huge improvement from his pre-operative appearance.
Continue reading for Joe Monroe's discussion...
DISCUSSION
Although the exact cause is still unknown, there appears to be an inheritable tendency to develop keloids. They are far more common, and grow to larger size, in patients with darker skin. Certain anatomical locations are especially at risk, such as the sternum, earlobes, shoulders (especially the deltoid areas), neck, and trunk. Keloids of the central face are almost unknown.
Keloids lie at the extreme end of the scarring continuum, with normal scars at the other end and so-called hypertrophic scars in the middle. The latter often resolve spontaneously within months of their initial formation, while true keloids never do.
Keloids are irregularly shaped, fibrous hyperpigmented (red to brown) excresences covered by thin, shiny skin. They often send out clawlike projections that ultimately obscure the original causative trauma. These tendencies help to distinguish them from mere hypertrophic scars. Biopsy, when necessary, can also help, as well as eliminate other items in the differential, including cancer (eg, dermatofibrosarcoma protuberans or metastatic cancer).
Early on, keloids are often red and uncomfortably tender. As they mature, they become less red and stabilize in size. They can become huge, especially on the chest, arms, and earlobes.
A case for surgical excision can be made, since large keloids are so cosmetically disfiguring and obvious. This patient was willing to accept the attendant risk for an even bigger postoperative keloid. With excision, primary closure, good wound care, and periodic injection of the wound edges with steroid suspension, however, he has an excellent chance to avoid this outcome.
Prior to his surgery, we reviewed alternate treatment choices, which include postexcision radiation treatment of the site, injection of the wound edges with 5-fluorouracil, or treatment of the keloid with flashlamp pulsed dye laser.
As with virtually everything we remove surgically, the keloid was sent for pathologic examination. It revealed the expected dense collection of myofibroblasts arranged in a whorled pattern, as well as a notable lack of elastic tissue.
Continue reading for Joe Monroe's take home learning points...
TAKE-HOME LEARNING POINTS
• The size and shape of keloids obscure the original triggering insult, a fact that serves to distinguish them from normal and hypertrophic scars.
• Keloids never resolve spontaneously, whereas hypertrophic scars can and do.
• Areas most prone to keloid formation include the sternum, deltoids, shoulders, earlobes, and trunk; they are almost unknown on the central face.
• In general, the darker the patient’s skin, the higher the risk for keloid formation.
• Elective surgery (eg, cyst removal) on high-risk areas and in keloid-prone patients should be avoided.
• Keloids can be injected intralesionally with glucocorticoid solutions, such as triamcinolone, or can be excised with proper postop follow-up.
A 39-year-old African-American man has had a keloid on his right earlobe for several years. It was triggered by ear-piercing and has grown slowly to its current size. The patient denies any symptoms with the lesion.
EXAMINATION
The 5 x 2-cm lobulated mass is consistent in every way with a keloid: firm and pedunculated, with no epidermal changes. It hangs from his right earlobe. The patient has type IV skin, of African-American ancestry. After an extended discussion regarding treatment options, the patient decides to have the lesion excised.
PROCEDURE
Under sterile conditions and with local anesthesia (1% lidocaine with epinephrine), the entire keloid is removed. The wound edges are shaped to enhance the final appearance, and the wound is closed in one layer.
Since the risk for reformation is all too real, at one week post-op, the wound edges are injected with 3 mg/cc of triamcinolone, with a total of 1.5 cc used. The injections continue for three months as the wound heals. The outcome is totally acceptable to the patient, representing a huge improvement from his pre-operative appearance.
Continue reading for Joe Monroe's discussion...
DISCUSSION
Although the exact cause is still unknown, there appears to be an inheritable tendency to develop keloids. They are far more common, and grow to larger size, in patients with darker skin. Certain anatomical locations are especially at risk, such as the sternum, earlobes, shoulders (especially the deltoid areas), neck, and trunk. Keloids of the central face are almost unknown.
Keloids lie at the extreme end of the scarring continuum, with normal scars at the other end and so-called hypertrophic scars in the middle. The latter often resolve spontaneously within months of their initial formation, while true keloids never do.
Keloids are irregularly shaped, fibrous hyperpigmented (red to brown) excresences covered by thin, shiny skin. They often send out clawlike projections that ultimately obscure the original causative trauma. These tendencies help to distinguish them from mere hypertrophic scars. Biopsy, when necessary, can also help, as well as eliminate other items in the differential, including cancer (eg, dermatofibrosarcoma protuberans or metastatic cancer).
Early on, keloids are often red and uncomfortably tender. As they mature, they become less red and stabilize in size. They can become huge, especially on the chest, arms, and earlobes.
A case for surgical excision can be made, since large keloids are so cosmetically disfiguring and obvious. This patient was willing to accept the attendant risk for an even bigger postoperative keloid. With excision, primary closure, good wound care, and periodic injection of the wound edges with steroid suspension, however, he has an excellent chance to avoid this outcome.
Prior to his surgery, we reviewed alternate treatment choices, which include postexcision radiation treatment of the site, injection of the wound edges with 5-fluorouracil, or treatment of the keloid with flashlamp pulsed dye laser.
As with virtually everything we remove surgically, the keloid was sent for pathologic examination. It revealed the expected dense collection of myofibroblasts arranged in a whorled pattern, as well as a notable lack of elastic tissue.
Continue reading for Joe Monroe's take home learning points...
TAKE-HOME LEARNING POINTS
• The size and shape of keloids obscure the original triggering insult, a fact that serves to distinguish them from normal and hypertrophic scars.
• Keloids never resolve spontaneously, whereas hypertrophic scars can and do.
• Areas most prone to keloid formation include the sternum, deltoids, shoulders, earlobes, and trunk; they are almost unknown on the central face.
• In general, the darker the patient’s skin, the higher the risk for keloid formation.
• Elective surgery (eg, cyst removal) on high-risk areas and in keloid-prone patients should be avoided.
• Keloids can be injected intralesionally with glucocorticoid solutions, such as triamcinolone, or can be excised with proper postop follow-up.
A 39-year-old African-American man has had a keloid on his right earlobe for several years. It was triggered by ear-piercing and has grown slowly to its current size. The patient denies any symptoms with the lesion.
EXAMINATION
The 5 x 2-cm lobulated mass is consistent in every way with a keloid: firm and pedunculated, with no epidermal changes. It hangs from his right earlobe. The patient has type IV skin, of African-American ancestry. After an extended discussion regarding treatment options, the patient decides to have the lesion excised.
PROCEDURE
Under sterile conditions and with local anesthesia (1% lidocaine with epinephrine), the entire keloid is removed. The wound edges are shaped to enhance the final appearance, and the wound is closed in one layer.
Since the risk for reformation is all too real, at one week post-op, the wound edges are injected with 3 mg/cc of triamcinolone, with a total of 1.5 cc used. The injections continue for three months as the wound heals. The outcome is totally acceptable to the patient, representing a huge improvement from his pre-operative appearance.
Continue reading for Joe Monroe's discussion...
DISCUSSION
Although the exact cause is still unknown, there appears to be an inheritable tendency to develop keloids. They are far more common, and grow to larger size, in patients with darker skin. Certain anatomical locations are especially at risk, such as the sternum, earlobes, shoulders (especially the deltoid areas), neck, and trunk. Keloids of the central face are almost unknown.
Keloids lie at the extreme end of the scarring continuum, with normal scars at the other end and so-called hypertrophic scars in the middle. The latter often resolve spontaneously within months of their initial formation, while true keloids never do.
Keloids are irregularly shaped, fibrous hyperpigmented (red to brown) excresences covered by thin, shiny skin. They often send out clawlike projections that ultimately obscure the original causative trauma. These tendencies help to distinguish them from mere hypertrophic scars. Biopsy, when necessary, can also help, as well as eliminate other items in the differential, including cancer (eg, dermatofibrosarcoma protuberans or metastatic cancer).
Early on, keloids are often red and uncomfortably tender. As they mature, they become less red and stabilize in size. They can become huge, especially on the chest, arms, and earlobes.
A case for surgical excision can be made, since large keloids are so cosmetically disfiguring and obvious. This patient was willing to accept the attendant risk for an even bigger postoperative keloid. With excision, primary closure, good wound care, and periodic injection of the wound edges with steroid suspension, however, he has an excellent chance to avoid this outcome.
Prior to his surgery, we reviewed alternate treatment choices, which include postexcision radiation treatment of the site, injection of the wound edges with 5-fluorouracil, or treatment of the keloid with flashlamp pulsed dye laser.
As with virtually everything we remove surgically, the keloid was sent for pathologic examination. It revealed the expected dense collection of myofibroblasts arranged in a whorled pattern, as well as a notable lack of elastic tissue.
Continue reading for Joe Monroe's take home learning points...
TAKE-HOME LEARNING POINTS
• The size and shape of keloids obscure the original triggering insult, a fact that serves to distinguish them from normal and hypertrophic scars.
• Keloids never resolve spontaneously, whereas hypertrophic scars can and do.
• Areas most prone to keloid formation include the sternum, deltoids, shoulders, earlobes, and trunk; they are almost unknown on the central face.
• In general, the darker the patient’s skin, the higher the risk for keloid formation.
• Elective surgery (eg, cyst removal) on high-risk areas and in keloid-prone patients should be avoided.
• Keloids can be injected intralesionally with glucocorticoid solutions, such as triamcinolone, or can be excised with proper postop follow-up.

If Not Fungal Infection, Then What?
A month’s worth of terbinafine 250 mg/d did not improve the appearance of this 47-year-old woman's fifth fingernail and surrounding skin, so she was referred to dermatology. Affecting only this finger, the condition manifested slowly, several months ago, for no apparent reason. Fortunately, few if any symptoms have accompanied the changes—but the patient is quite upset nonetheless.

She denies any antecedent trauma to the finger and says it has not been excessively exposed to wetting and drying. She is otherwise in excellent health. Her only complaint about her health is mild seasonal allergies, along with sensitive skin (which manifested as eczema when she was a child).
EXAMINATION
The skin around the patient's right fifth fingernail is quite dry and scaly. It appears a bit inflamed, and there is visible separation between the cuticle and the adjacent nail plate. The nail itself is abnormal, with a rumpled, dystrophic surface on which transverse ridges are seen. No tenderness is elicited on palpation, nor can any pus be expressed from the subungual area. The rest of her fingernails and her toenails are unaffected.
Continue reading for Joe Monroe's discussion...
DISCUSSION
This problem—chronic paronychia (also known as chronic candidal paronychia)—is not well known outside derm circles. It's even a bit of a mystery within the specialty, although we see it often enough to become comfortable with its diagnosis and treatment.
Here is what we know about it: Separation of the cuticle from the underlying nail plate appears to be the initial insult, with bacteria (candida) and food particles subsequently becoming trapped in the space and provoking an inflammatory response. There is often a history of excessive wetting and drying of the hands. The condition is rarely painful, but initially it can make the area sensitive to touch. The women who present with it—we virtually never see it in men—are usually middle-aged.
Primary care providers confronted with chronic paronychia often prescribe terbinafine for "fungal infection," but this never works because fungi are not involved. Some consider candida to be a type of fungus; however, for practical purposes, it is quite different. It causes completely different disease, is grown on totally different media in the lab, and requires special treatment. Terbinafine, an allylamine, has little if any activity against candida.
It should be noted that in many cases, the infectious component of chronic paronychia is minimal to absent. Therefore, the thrust of treatment is aimed at healing the damaged cuticle and helping it to reattach to the nail plate. This eventually resolves the problem, as the dystrophic nail will grow out and be replaced by healthy, normal-looking nail. Adding an imidazole cream to the treatment regimen will eliminate any suspected organism.
For this patient, I prescribed a month-long course of betamethasone/clotrimazole ointment to be applied twice daily. At follow-up, reconnection of the cuticle to the nail plate was noted, along with complete resolution of the modest redness. The nail was still dystrophic distally but clearing proximally. It should be clear within four to five months.
Continue reading for the take-home learning points...
TAKE-HOME LEARNING POINTS
• Fungal infection is approximately 18 times less likely to occur in fingernails than in toenails, so skepticism is warranted in such cases.
• Atopy probably plays a role in the genesis of chronic paronychia, given the sensitivity of atopic skin to wetting and drying.
• The primary goal of treatment in these cases is to encourage reattachment of the cuticle to the nail plate.
• Oral terbinafine is ineffective against candida and should only be used in cases of proven or strongly suspected fungal infection.
• Chronic candidal paronychia can affect one or more fingernails but is almost never seen in toenails.
A month’s worth of terbinafine 250 mg/d did not improve the appearance of this 47-year-old woman's fifth fingernail and surrounding skin, so she was referred to dermatology. Affecting only this finger, the condition manifested slowly, several months ago, for no apparent reason. Fortunately, few if any symptoms have accompanied the changes—but the patient is quite upset nonetheless.
She denies any antecedent trauma to the finger and says it has not been excessively exposed to wetting and drying. She is otherwise in excellent health. Her only complaint about her health is mild seasonal allergies, along with sensitive skin (which manifested as eczema when she was a child).
EXAMINATION
The skin around the patient's right fifth fingernail is quite dry and scaly. It appears a bit inflamed, and there is visible separation between the cuticle and the adjacent nail plate. The nail itself is abnormal, with a rumpled, dystrophic surface on which transverse ridges are seen. No tenderness is elicited on palpation, nor can any pus be expressed from the subungual area. The rest of her fingernails and her toenails are unaffected.
Continue reading for Joe Monroe's discussion...
DISCUSSION
This problem—chronic paronychia (also known as chronic candidal paronychia)—is not well known outside derm circles. It's even a bit of a mystery within the specialty, although we see it often enough to become comfortable with its diagnosis and treatment.
Here is what we know about it: Separation of the cuticle from the underlying nail plate appears to be the initial insult, with bacteria (candida) and food particles subsequently becoming trapped in the space and provoking an inflammatory response. There is often a history of excessive wetting and drying of the hands. The condition is rarely painful, but initially it can make the area sensitive to touch. The women who present with it—we virtually never see it in men—are usually middle-aged.
Primary care providers confronted with chronic paronychia often prescribe terbinafine for "fungal infection," but this never works because fungi are not involved. Some consider candida to be a type of fungus; however, for practical purposes, it is quite different. It causes completely different disease, is grown on totally different media in the lab, and requires special treatment. Terbinafine, an allylamine, has little if any activity against candida.
It should be noted that in many cases, the infectious component of chronic paronychia is minimal to absent. Therefore, the thrust of treatment is aimed at healing the damaged cuticle and helping it to reattach to the nail plate. This eventually resolves the problem, as the dystrophic nail will grow out and be replaced by healthy, normal-looking nail. Adding an imidazole cream to the treatment regimen will eliminate any suspected organism.
For this patient, I prescribed a month-long course of betamethasone/clotrimazole ointment to be applied twice daily. At follow-up, reconnection of the cuticle to the nail plate was noted, along with complete resolution of the modest redness. The nail was still dystrophic distally but clearing proximally. It should be clear within four to five months.
Continue reading for the take-home learning points...
TAKE-HOME LEARNING POINTS
• Fungal infection is approximately 18 times less likely to occur in fingernails than in toenails, so skepticism is warranted in such cases.
• Atopy probably plays a role in the genesis of chronic paronychia, given the sensitivity of atopic skin to wetting and drying.
• The primary goal of treatment in these cases is to encourage reattachment of the cuticle to the nail plate.
• Oral terbinafine is ineffective against candida and should only be used in cases of proven or strongly suspected fungal infection.
• Chronic candidal paronychia can affect one or more fingernails but is almost never seen in toenails.
A month’s worth of terbinafine 250 mg/d did not improve the appearance of this 47-year-old woman's fifth fingernail and surrounding skin, so she was referred to dermatology. Affecting only this finger, the condition manifested slowly, several months ago, for no apparent reason. Fortunately, few if any symptoms have accompanied the changes—but the patient is quite upset nonetheless.
She denies any antecedent trauma to the finger and says it has not been excessively exposed to wetting and drying. She is otherwise in excellent health. Her only complaint about her health is mild seasonal allergies, along with sensitive skin (which manifested as eczema when she was a child).
EXAMINATION
The skin around the patient's right fifth fingernail is quite dry and scaly. It appears a bit inflamed, and there is visible separation between the cuticle and the adjacent nail plate. The nail itself is abnormal, with a rumpled, dystrophic surface on which transverse ridges are seen. No tenderness is elicited on palpation, nor can any pus be expressed from the subungual area. The rest of her fingernails and her toenails are unaffected.
Continue reading for Joe Monroe's discussion...
DISCUSSION
This problem—chronic paronychia (also known as chronic candidal paronychia)—is not well known outside derm circles. It's even a bit of a mystery within the specialty, although we see it often enough to become comfortable with its diagnosis and treatment.
Here is what we know about it: Separation of the cuticle from the underlying nail plate appears to be the initial insult, with bacteria (candida) and food particles subsequently becoming trapped in the space and provoking an inflammatory response. There is often a history of excessive wetting and drying of the hands. The condition is rarely painful, but initially it can make the area sensitive to touch. The women who present with it—we virtually never see it in men—are usually middle-aged.
Primary care providers confronted with chronic paronychia often prescribe terbinafine for "fungal infection," but this never works because fungi are not involved. Some consider candida to be a type of fungus; however, for practical purposes, it is quite different. It causes completely different disease, is grown on totally different media in the lab, and requires special treatment. Terbinafine, an allylamine, has little if any activity against candida.
It should be noted that in many cases, the infectious component of chronic paronychia is minimal to absent. Therefore, the thrust of treatment is aimed at healing the damaged cuticle and helping it to reattach to the nail plate. This eventually resolves the problem, as the dystrophic nail will grow out and be replaced by healthy, normal-looking nail. Adding an imidazole cream to the treatment regimen will eliminate any suspected organism.
For this patient, I prescribed a month-long course of betamethasone/clotrimazole ointment to be applied twice daily. At follow-up, reconnection of the cuticle to the nail plate was noted, along with complete resolution of the modest redness. The nail was still dystrophic distally but clearing proximally. It should be clear within four to five months.
Continue reading for the take-home learning points...
TAKE-HOME LEARNING POINTS
• Fungal infection is approximately 18 times less likely to occur in fingernails than in toenails, so skepticism is warranted in such cases.
• Atopy probably plays a role in the genesis of chronic paronychia, given the sensitivity of atopic skin to wetting and drying.
• The primary goal of treatment in these cases is to encourage reattachment of the cuticle to the nail plate.
• Oral terbinafine is ineffective against candida and should only be used in cases of proven or strongly suspected fungal infection.
• Chronic candidal paronychia can affect one or more fingernails but is almost never seen in toenails.

A 10-Year Wait for Diagnosis
An 84-year-old woman has had a lesion on her face for 10 years. During that time, it has slowly changed, becoming darker and larger. For the past few months, it has developed a new, raised area in its center.
Several providers, including a dermatologist, have seen the lesion over the years; none has ever ordered a biopsy. The lesion is asymptomatic and only began to change noticeably a few years ago.
The patient mentions having multiple sunburns as a young woman. But she says she never tried to tan, because she could only do so with difficulty.
Her medical history is significant for breast cancer, for which she is receiving chemotherapy. She was told she did not need surgery and has little chance of metastasis.
EXAMINATION
The patient is alert and cooperative. A large, black, 3.5-cm lesion is obvious on the right jawline. In the center of the lesion is a 2-cm, faintly eroded nodule. No tenderness can be elicited on palpation of the lesion or the area, and there are no palable nodes in the adjacent head and neck. The patient has type 2 skin, blue eyes, and modest evidence of sun damage elsewhere on her face.
DISCUSSION
Of course, the next logical step was to biopsy the lesion. The rule of thumb for biopsy of a possible melanoma is this: Removal of the entire lesion, down to adipose tissue, is the gold standard, because it is certain to provide both an accurate diagnosis and an assessment of the lesion’s vertical thickness—a key predictor of prognosis.
The drawback to complete excision of lesions this size is that the defect can be huge (about 10 cm in this case) and almost certainly disfiguring. If the lesion turns out to be benign, this outcome might well be seen as unacceptable. Therefore, an alternative to complete excision is incisional biopsy, in which a significant but modest portion of the lesion is removed, purposely obtaining the darkest, most irregular part. In this case, such a biopsy would include either all or a significant part of the nodular portion of the lesion, along with a generous section of the discolored macular area.
Shave biopsy of a suspected melanoma is acceptable with small, shallow lesions, as long as it effectively removes the lesion with deep margins. Shave biopsy in this case would be unacceptable for several reasons. Among them is the cosmetic outcome and the possibility of transecting the lesion, thereby making an accurate vertical assessment difficult. The latter is important, since it is the single most accurate prognostic indicator, in effect dictating the margins of re-excision as well as the extent of subsequent workup (imaging, bloodwork, lymph node dissection, and possible chemotherapeutic regimen).
Punch biopsy of suspected melanoma is generally unacceptable, unless the punch effectively removes most or all of the lesion. Referral to dermatology is almost never the wrong thing to do, but it often requires provider-to-provider communication to expedite.
Providers who don’t perform these biopsies often tend to quote the misinformed attending physicians who taught them that “cutting through a melanoma will make it spread.” This is a totally unfounded fear, long since disproven in large studies that showed no difference in mortality or morbidity between patients whose melanomas were incised versus those whose cancers were removed without incision.
DIAGNOSIS AND TREATMENT
Incisional biopsy was performed on this lesion, with about one-third removed by wedge incision. Essentially, the center of the lesion was removed. This was, of course, done under local and sterile conditions, with closure by simple interrupted sutures.
Within 48 hours, the report was issued. It showed a nodular melanoma with 3.7-mm Breslow thickness, definite signs of focal ulceration, and an increased mitotic rate of 6 to 8 per high-powered field—all of which predict a less-than-favorable prognosis.
The patient was scheduled for Mohs surgery, which will likely involve wide excision of the lesion and surrounding skin. She will also have the option of lymph node dissection, done for prognostic value only (as it will add nothing to her potential for survival).
TAKE-HOME LEARNING POINTS
• Biopsy of melanoma (or other skin cancers) cannot cause it to spread.
• The object of biopsying a potential melanoma is to obtain a specimen that, on pathologic examination, not only conveys the correct diagnosis but also allows for accurate staging.
• Successful biopsy entails going deep and wide enough, but without causing unnecessary scarring or deformation.
• The diagnosis and staging then determine the extent of any re-excision and the need for ancillary studies (eg, lymph node dissection, imaging, referral to oncology).
• This particular case also shows that melanoma growth can be unbelievably slow, allowing plenty of opportunity for discovery.
• Unfortunately, given enough time, many melanomas will reach a point at which they will begin to grow vertically, becoming more dangerous and invasive.
An 84-year-old woman has had a lesion on her face for 10 years. During that time, it has slowly changed, becoming darker and larger. For the past few months, it has developed a new, raised area in its center.
Several providers, including a dermatologist, have seen the lesion over the years; none has ever ordered a biopsy. The lesion is asymptomatic and only began to change noticeably a few years ago.
The patient mentions having multiple sunburns as a young woman. But she says she never tried to tan, because she could only do so with difficulty.
Her medical history is significant for breast cancer, for which she is receiving chemotherapy. She was told she did not need surgery and has little chance of metastasis.
EXAMINATION
The patient is alert and cooperative. A large, black, 3.5-cm lesion is obvious on the right jawline. In the center of the lesion is a 2-cm, faintly eroded nodule. No tenderness can be elicited on palpation of the lesion or the area, and there are no palable nodes in the adjacent head and neck. The patient has type 2 skin, blue eyes, and modest evidence of sun damage elsewhere on her face.
DISCUSSION
Of course, the next logical step was to biopsy the lesion. The rule of thumb for biopsy of a possible melanoma is this: Removal of the entire lesion, down to adipose tissue, is the gold standard, because it is certain to provide both an accurate diagnosis and an assessment of the lesion’s vertical thickness—a key predictor of prognosis.
The drawback to complete excision of lesions this size is that the defect can be huge (about 10 cm in this case) and almost certainly disfiguring. If the lesion turns out to be benign, this outcome might well be seen as unacceptable. Therefore, an alternative to complete excision is incisional biopsy, in which a significant but modest portion of the lesion is removed, purposely obtaining the darkest, most irregular part. In this case, such a biopsy would include either all or a significant part of the nodular portion of the lesion, along with a generous section of the discolored macular area.
Shave biopsy of a suspected melanoma is acceptable with small, shallow lesions, as long as it effectively removes the lesion with deep margins. Shave biopsy in this case would be unacceptable for several reasons. Among them is the cosmetic outcome and the possibility of transecting the lesion, thereby making an accurate vertical assessment difficult. The latter is important, since it is the single most accurate prognostic indicator, in effect dictating the margins of re-excision as well as the extent of subsequent workup (imaging, bloodwork, lymph node dissection, and possible chemotherapeutic regimen).
Punch biopsy of suspected melanoma is generally unacceptable, unless the punch effectively removes most or all of the lesion. Referral to dermatology is almost never the wrong thing to do, but it often requires provider-to-provider communication to expedite.
Providers who don’t perform these biopsies often tend to quote the misinformed attending physicians who taught them that “cutting through a melanoma will make it spread.” This is a totally unfounded fear, long since disproven in large studies that showed no difference in mortality or morbidity between patients whose melanomas were incised versus those whose cancers were removed without incision.
DIAGNOSIS AND TREATMENT
Incisional biopsy was performed on this lesion, with about one-third removed by wedge incision. Essentially, the center of the lesion was removed. This was, of course, done under local and sterile conditions, with closure by simple interrupted sutures.
Within 48 hours, the report was issued. It showed a nodular melanoma with 3.7-mm Breslow thickness, definite signs of focal ulceration, and an increased mitotic rate of 6 to 8 per high-powered field—all of which predict a less-than-favorable prognosis.
The patient was scheduled for Mohs surgery, which will likely involve wide excision of the lesion and surrounding skin. She will also have the option of lymph node dissection, done for prognostic value only (as it will add nothing to her potential for survival).
TAKE-HOME LEARNING POINTS
• Biopsy of melanoma (or other skin cancers) cannot cause it to spread.
• The object of biopsying a potential melanoma is to obtain a specimen that, on pathologic examination, not only conveys the correct diagnosis but also allows for accurate staging.
• Successful biopsy entails going deep and wide enough, but without causing unnecessary scarring or deformation.
• The diagnosis and staging then determine the extent of any re-excision and the need for ancillary studies (eg, lymph node dissection, imaging, referral to oncology).
• This particular case also shows that melanoma growth can be unbelievably slow, allowing plenty of opportunity for discovery.
• Unfortunately, given enough time, many melanomas will reach a point at which they will begin to grow vertically, becoming more dangerous and invasive.
An 84-year-old woman has had a lesion on her face for 10 years. During that time, it has slowly changed, becoming darker and larger. For the past few months, it has developed a new, raised area in its center.
Several providers, including a dermatologist, have seen the lesion over the years; none has ever ordered a biopsy. The lesion is asymptomatic and only began to change noticeably a few years ago.
The patient mentions having multiple sunburns as a young woman. But she says she never tried to tan, because she could only do so with difficulty.
Her medical history is significant for breast cancer, for which she is receiving chemotherapy. She was told she did not need surgery and has little chance of metastasis.
EXAMINATION
The patient is alert and cooperative. A large, black, 3.5-cm lesion is obvious on the right jawline. In the center of the lesion is a 2-cm, faintly eroded nodule. No tenderness can be elicited on palpation of the lesion or the area, and there are no palable nodes in the adjacent head and neck. The patient has type 2 skin, blue eyes, and modest evidence of sun damage elsewhere on her face.
DISCUSSION
Of course, the next logical step was to biopsy the lesion. The rule of thumb for biopsy of a possible melanoma is this: Removal of the entire lesion, down to adipose tissue, is the gold standard, because it is certain to provide both an accurate diagnosis and an assessment of the lesion’s vertical thickness—a key predictor of prognosis.
The drawback to complete excision of lesions this size is that the defect can be huge (about 10 cm in this case) and almost certainly disfiguring. If the lesion turns out to be benign, this outcome might well be seen as unacceptable. Therefore, an alternative to complete excision is incisional biopsy, in which a significant but modest portion of the lesion is removed, purposely obtaining the darkest, most irregular part. In this case, such a biopsy would include either all or a significant part of the nodular portion of the lesion, along with a generous section of the discolored macular area.
Shave biopsy of a suspected melanoma is acceptable with small, shallow lesions, as long as it effectively removes the lesion with deep margins. Shave biopsy in this case would be unacceptable for several reasons. Among them is the cosmetic outcome and the possibility of transecting the lesion, thereby making an accurate vertical assessment difficult. The latter is important, since it is the single most accurate prognostic indicator, in effect dictating the margins of re-excision as well as the extent of subsequent workup (imaging, bloodwork, lymph node dissection, and possible chemotherapeutic regimen).
Punch biopsy of suspected melanoma is generally unacceptable, unless the punch effectively removes most or all of the lesion. Referral to dermatology is almost never the wrong thing to do, but it often requires provider-to-provider communication to expedite.
Providers who don’t perform these biopsies often tend to quote the misinformed attending physicians who taught them that “cutting through a melanoma will make it spread.” This is a totally unfounded fear, long since disproven in large studies that showed no difference in mortality or morbidity between patients whose melanomas were incised versus those whose cancers were removed without incision.
DIAGNOSIS AND TREATMENT
Incisional biopsy was performed on this lesion, with about one-third removed by wedge incision. Essentially, the center of the lesion was removed. This was, of course, done under local and sterile conditions, with closure by simple interrupted sutures.
Within 48 hours, the report was issued. It showed a nodular melanoma with 3.7-mm Breslow thickness, definite signs of focal ulceration, and an increased mitotic rate of 6 to 8 per high-powered field—all of which predict a less-than-favorable prognosis.
The patient was scheduled for Mohs surgery, which will likely involve wide excision of the lesion and surrounding skin. She will also have the option of lymph node dissection, done for prognostic value only (as it will add nothing to her potential for survival).
TAKE-HOME LEARNING POINTS
• Biopsy of melanoma (or other skin cancers) cannot cause it to spread.
• The object of biopsying a potential melanoma is to obtain a specimen that, on pathologic examination, not only conveys the correct diagnosis but also allows for accurate staging.
• Successful biopsy entails going deep and wide enough, but without causing unnecessary scarring or deformation.
• The diagnosis and staging then determine the extent of any re-excision and the need for ancillary studies (eg, lymph node dissection, imaging, referral to oncology).
• This particular case also shows that melanoma growth can be unbelievably slow, allowing plenty of opportunity for discovery.
• Unfortunately, given enough time, many melanomas will reach a point at which they will begin to grow vertically, becoming more dangerous and invasive.
