User login
Texas-Sized Tort Reform
Advocates have written open letters to politicians describing it as “the least-expensive and best-known way to lower healthcare costs.” Detractors have blogged that it has saved almost no money and instead “gutted patient rights.” Among the recent templates for whether and how to proceed on the contentious issue of tort reform, Texas has become a prime example of either the wisdom or the folly of capping medical liability payouts, depending on your vantage point.
Tort reform is backed by most doctors and the insurance industry but opposed by lawyers and consumer advocates. The Congressional Budget Office has documented increases in both medical liability premiums and average malpractice claim payments that have significantly outpaced inflation. Congress itself has largely punted on the issue, however, leaving most of the wrangling over specifics to individual states.
Which brings us to Texas. In reaction to the perception that unsustainable medical liability costs were driving away doctors and driving up healthcare costs, state voters in 2003 approved Proposition 12. Among its provisions, the state constitutional amendment capped noneconomic medical liability payouts at $250,000 in nearly all cases.
Much of the ensuing debate over whether Texas did the right thing has focused on cost: For example, will the reduction in malpractice claims translate into significant savings within the healthcare system? Is tort reform relevant in recouping the perceived waste from “defensive medicine,” in which physicians are presumed to order unnecessary tests and procedures out of fear of lawsuits?
More centrally, however, the question boils down to this: Does tort reform improve the ability of doctors to do their jobs, and the opportunity for patients to benefit from that care? So far, statistics, reports, and anecdotal information suggest that Texas has achieved the first goal but not necessarily the latter, highlighting the extreme difficulty in striking the right balance.
Mission: Predictable
Kirk A. Calhoun, MD, who became president of the University of Texas Health Science Center at Tyler in 2002, points to two principal benefits of the state’s tort reform. First, the package of reforms led to a significant number of physicians migrating to Texas and helping to deal with the state’s chronic doctor shortage. For doctors, part of that attraction was the second big benefit, a significant decrease in liability insurance premiums.
“It has resulted in making Texas a more attractive state in which to practice medicine,” Dr. Calhoun says. “As a result of those expenses going down, we are able to better invest in our primary mission, and on patient care.”
Kenneth McDaniel, a program specialist in professional liability in the Texas Department of Insurance, says the dearth of affordable or available malpractice insurance in the state had spiraled into a crisis. “In Texas, we were staring at the brink of a chasm so deep that we virtually had to do something,” he says. “We were within probably some months or a year of having almost no malpractice insurance industry at all. It had become very dire.”
McDaniel stresses that the new liability cap is only for intangibles or pain and suffering, and it leaves intact the potential for higher economic damages. “But those can be predicted,” he says. “As soon as claims became more predictable, insurers started coming back into the field.” A summary of 17 companies’ rates supplied by McDaniel includes four new arrivals to the medical liability market and the return of a fifth.
At the very least, tort reform appears to have dramatically curbed the number and cost of claims in Texas. From 2003 to 2007, malpractice payments to patients dropped by two-thirds. Liability premiums paid by doctors also have fallen, by an average of 27.5%, and more insurers have rejoined the market. “We are now back to, I would say, a pretty healthy environment,” McDaniel says.
Physician-Friendly Environs
Hospitalist Gregory Johnson, MD, chair of the Texas Medical Association’s Young Physicians Section, moved to Texas in 2002, just before the reforms were approved. “The best part about Prop 12 passing is the fact that Texas is now seen as a very physician-friendly environment,” says Johnson, who now serves as a Houston-based regional chief medical officer for Tacoma, Wash.-based Sound Physicians. The significant drops in malpractice insurance rates and lawsuits have made it far easier for him to recruit out-of-state doctors. “That basically comes off any physician’s radar as a particular concern.”
Most Texas hospitals and healthcare systems do not employ physicians directly. Instead, they contract or affiliate with private or nonprofit physicians groups. Due to that arrangement, Dr. Johnson explains, the cost of insurance premiums “becomes a much more individually based and personal issue because it’s coming out of an individual’s pocket, or a group’s pocket.”
From his own experience, Dr. Johnson says, he believes hospitalists are more willing to go to underserved parts of the state because of tort reform. Three years ago, he helped start Amarillo Hospitalist Services, a program that began with three doctors and has since grown to eight, all affiliated with Northwest Texas Hospital.
Of course, hospitalists appear to be thriving in major metropolitan areas, too. Dr. Johnson’s new employer, Sound Physicians, now operates three HM programs within Houston’s Memorial Hermann Healthcare System and employs about two-dozen physicians in all. More are on the way. “We’re actively hiring,” he says.
Mixed Outcomes
Statistics from the Texas Medical Board and Department of State Health Services confirm the anecdotal evidence that a more doctor-friendly Texas is paying dividends. Even so, they paint a somewhat more complicated picture than some commentators have portrayed in recent editorials. Doctors have indeed flocked to the state—some 11,000 since 2002 alone, an increase of 31%. That rate has far outpaced the state’s overall population growth of 14.2%.
But not all areas of the state have benefited equally from the influx.
Starr County, the third-poorest county in the U.S. based on per capita income, is among those that have fared well since 2002. Overall, its number of doctors increased from 14 to 24, a net increase of 71%, as its population rose by a projected 17%. But the next five poorest counties in Texas, accounting for nearly 86,000 residents in 2002, lost six doctors during the same time period—a 12.5% decline, even as their collective population rose by a projected 10.2%. Contrary to some public pronouncements, tort reform alone has not solved the chronic shortage of doctors in poor rural areas.
A withering report released in December by Washington, D.C.-based Public Citizen, a nonprofit consumer advocacy group, offers a harsher assessment, concluding that Texas’ “experiment with medical liability caps has failed” (www.citizen.org/publications/release.cfm?ID=7721). The report suggests that Texas’ dead-last ranking in percentage of uninsured residents (25%) and the doctor shortage in rural areas have actually grown worse since tort reform. Meanwhile, the cost of health insurance has more than doubled, while the cost of healthcare also has increased at nearly double the national average, other metrics that led to the organization’s vote of no confidence.
The impact on quality of care has been harder to assess. But Dr. Johnson and other observers say they haven’t seen any dip within hospitals. “I think that we as physicians and we as hospitalists really want to focus on our patients, and we can help to drive down those costs if we’re given the freedom to do our job,” he says. Tort reform, he adds, has helped doctors do precisely that.
Dr. Calhoun agrees. “No one wants to be sued. Everyone wants to do a good job,” he says. The threat of a lawsuit alone is only one of many factors influencing quality, he adds. But creating a more inviting environment for doctors can make a big difference by encouraging the increased use of hospitalists. “Having a hospitalist in the hospital all the time,” he says, “is an obvious quality improvement.” TH
Bryn Nelson is a freelance medical writer based in Seattle.
IMAGE SOURCE: DRASCHWARTZ/ISTOCK.COM
Advocates have written open letters to politicians describing it as “the least-expensive and best-known way to lower healthcare costs.” Detractors have blogged that it has saved almost no money and instead “gutted patient rights.” Among the recent templates for whether and how to proceed on the contentious issue of tort reform, Texas has become a prime example of either the wisdom or the folly of capping medical liability payouts, depending on your vantage point.
Tort reform is backed by most doctors and the insurance industry but opposed by lawyers and consumer advocates. The Congressional Budget Office has documented increases in both medical liability premiums and average malpractice claim payments that have significantly outpaced inflation. Congress itself has largely punted on the issue, however, leaving most of the wrangling over specifics to individual states.
Which brings us to Texas. In reaction to the perception that unsustainable medical liability costs were driving away doctors and driving up healthcare costs, state voters in 2003 approved Proposition 12. Among its provisions, the state constitutional amendment capped noneconomic medical liability payouts at $250,000 in nearly all cases.
Much of the ensuing debate over whether Texas did the right thing has focused on cost: For example, will the reduction in malpractice claims translate into significant savings within the healthcare system? Is tort reform relevant in recouping the perceived waste from “defensive medicine,” in which physicians are presumed to order unnecessary tests and procedures out of fear of lawsuits?
More centrally, however, the question boils down to this: Does tort reform improve the ability of doctors to do their jobs, and the opportunity for patients to benefit from that care? So far, statistics, reports, and anecdotal information suggest that Texas has achieved the first goal but not necessarily the latter, highlighting the extreme difficulty in striking the right balance.
Mission: Predictable
Kirk A. Calhoun, MD, who became president of the University of Texas Health Science Center at Tyler in 2002, points to two principal benefits of the state’s tort reform. First, the package of reforms led to a significant number of physicians migrating to Texas and helping to deal with the state’s chronic doctor shortage. For doctors, part of that attraction was the second big benefit, a significant decrease in liability insurance premiums.
“It has resulted in making Texas a more attractive state in which to practice medicine,” Dr. Calhoun says. “As a result of those expenses going down, we are able to better invest in our primary mission, and on patient care.”
Kenneth McDaniel, a program specialist in professional liability in the Texas Department of Insurance, says the dearth of affordable or available malpractice insurance in the state had spiraled into a crisis. “In Texas, we were staring at the brink of a chasm so deep that we virtually had to do something,” he says. “We were within probably some months or a year of having almost no malpractice insurance industry at all. It had become very dire.”
McDaniel stresses that the new liability cap is only for intangibles or pain and suffering, and it leaves intact the potential for higher economic damages. “But those can be predicted,” he says. “As soon as claims became more predictable, insurers started coming back into the field.” A summary of 17 companies’ rates supplied by McDaniel includes four new arrivals to the medical liability market and the return of a fifth.
At the very least, tort reform appears to have dramatically curbed the number and cost of claims in Texas. From 2003 to 2007, malpractice payments to patients dropped by two-thirds. Liability premiums paid by doctors also have fallen, by an average of 27.5%, and more insurers have rejoined the market. “We are now back to, I would say, a pretty healthy environment,” McDaniel says.
Physician-Friendly Environs
Hospitalist Gregory Johnson, MD, chair of the Texas Medical Association’s Young Physicians Section, moved to Texas in 2002, just before the reforms were approved. “The best part about Prop 12 passing is the fact that Texas is now seen as a very physician-friendly environment,” says Johnson, who now serves as a Houston-based regional chief medical officer for Tacoma, Wash.-based Sound Physicians. The significant drops in malpractice insurance rates and lawsuits have made it far easier for him to recruit out-of-state doctors. “That basically comes off any physician’s radar as a particular concern.”
Most Texas hospitals and healthcare systems do not employ physicians directly. Instead, they contract or affiliate with private or nonprofit physicians groups. Due to that arrangement, Dr. Johnson explains, the cost of insurance premiums “becomes a much more individually based and personal issue because it’s coming out of an individual’s pocket, or a group’s pocket.”
From his own experience, Dr. Johnson says, he believes hospitalists are more willing to go to underserved parts of the state because of tort reform. Three years ago, he helped start Amarillo Hospitalist Services, a program that began with three doctors and has since grown to eight, all affiliated with Northwest Texas Hospital.
Of course, hospitalists appear to be thriving in major metropolitan areas, too. Dr. Johnson’s new employer, Sound Physicians, now operates three HM programs within Houston’s Memorial Hermann Healthcare System and employs about two-dozen physicians in all. More are on the way. “We’re actively hiring,” he says.
Mixed Outcomes
Statistics from the Texas Medical Board and Department of State Health Services confirm the anecdotal evidence that a more doctor-friendly Texas is paying dividends. Even so, they paint a somewhat more complicated picture than some commentators have portrayed in recent editorials. Doctors have indeed flocked to the state—some 11,000 since 2002 alone, an increase of 31%. That rate has far outpaced the state’s overall population growth of 14.2%.
But not all areas of the state have benefited equally from the influx.
Starr County, the third-poorest county in the U.S. based on per capita income, is among those that have fared well since 2002. Overall, its number of doctors increased from 14 to 24, a net increase of 71%, as its population rose by a projected 17%. But the next five poorest counties in Texas, accounting for nearly 86,000 residents in 2002, lost six doctors during the same time period—a 12.5% decline, even as their collective population rose by a projected 10.2%. Contrary to some public pronouncements, tort reform alone has not solved the chronic shortage of doctors in poor rural areas.
A withering report released in December by Washington, D.C.-based Public Citizen, a nonprofit consumer advocacy group, offers a harsher assessment, concluding that Texas’ “experiment with medical liability caps has failed” (www.citizen.org/publications/release.cfm?ID=7721). The report suggests that Texas’ dead-last ranking in percentage of uninsured residents (25%) and the doctor shortage in rural areas have actually grown worse since tort reform. Meanwhile, the cost of health insurance has more than doubled, while the cost of healthcare also has increased at nearly double the national average, other metrics that led to the organization’s vote of no confidence.
The impact on quality of care has been harder to assess. But Dr. Johnson and other observers say they haven’t seen any dip within hospitals. “I think that we as physicians and we as hospitalists really want to focus on our patients, and we can help to drive down those costs if we’re given the freedom to do our job,” he says. Tort reform, he adds, has helped doctors do precisely that.
Dr. Calhoun agrees. “No one wants to be sued. Everyone wants to do a good job,” he says. The threat of a lawsuit alone is only one of many factors influencing quality, he adds. But creating a more inviting environment for doctors can make a big difference by encouraging the increased use of hospitalists. “Having a hospitalist in the hospital all the time,” he says, “is an obvious quality improvement.” TH
Bryn Nelson is a freelance medical writer based in Seattle.
IMAGE SOURCE: DRASCHWARTZ/ISTOCK.COM
Advocates have written open letters to politicians describing it as “the least-expensive and best-known way to lower healthcare costs.” Detractors have blogged that it has saved almost no money and instead “gutted patient rights.” Among the recent templates for whether and how to proceed on the contentious issue of tort reform, Texas has become a prime example of either the wisdom or the folly of capping medical liability payouts, depending on your vantage point.
Tort reform is backed by most doctors and the insurance industry but opposed by lawyers and consumer advocates. The Congressional Budget Office has documented increases in both medical liability premiums and average malpractice claim payments that have significantly outpaced inflation. Congress itself has largely punted on the issue, however, leaving most of the wrangling over specifics to individual states.
Which brings us to Texas. In reaction to the perception that unsustainable medical liability costs were driving away doctors and driving up healthcare costs, state voters in 2003 approved Proposition 12. Among its provisions, the state constitutional amendment capped noneconomic medical liability payouts at $250,000 in nearly all cases.
Much of the ensuing debate over whether Texas did the right thing has focused on cost: For example, will the reduction in malpractice claims translate into significant savings within the healthcare system? Is tort reform relevant in recouping the perceived waste from “defensive medicine,” in which physicians are presumed to order unnecessary tests and procedures out of fear of lawsuits?
More centrally, however, the question boils down to this: Does tort reform improve the ability of doctors to do their jobs, and the opportunity for patients to benefit from that care? So far, statistics, reports, and anecdotal information suggest that Texas has achieved the first goal but not necessarily the latter, highlighting the extreme difficulty in striking the right balance.
Mission: Predictable
Kirk A. Calhoun, MD, who became president of the University of Texas Health Science Center at Tyler in 2002, points to two principal benefits of the state’s tort reform. First, the package of reforms led to a significant number of physicians migrating to Texas and helping to deal with the state’s chronic doctor shortage. For doctors, part of that attraction was the second big benefit, a significant decrease in liability insurance premiums.
“It has resulted in making Texas a more attractive state in which to practice medicine,” Dr. Calhoun says. “As a result of those expenses going down, we are able to better invest in our primary mission, and on patient care.”
Kenneth McDaniel, a program specialist in professional liability in the Texas Department of Insurance, says the dearth of affordable or available malpractice insurance in the state had spiraled into a crisis. “In Texas, we were staring at the brink of a chasm so deep that we virtually had to do something,” he says. “We were within probably some months or a year of having almost no malpractice insurance industry at all. It had become very dire.”
McDaniel stresses that the new liability cap is only for intangibles or pain and suffering, and it leaves intact the potential for higher economic damages. “But those can be predicted,” he says. “As soon as claims became more predictable, insurers started coming back into the field.” A summary of 17 companies’ rates supplied by McDaniel includes four new arrivals to the medical liability market and the return of a fifth.
At the very least, tort reform appears to have dramatically curbed the number and cost of claims in Texas. From 2003 to 2007, malpractice payments to patients dropped by two-thirds. Liability premiums paid by doctors also have fallen, by an average of 27.5%, and more insurers have rejoined the market. “We are now back to, I would say, a pretty healthy environment,” McDaniel says.
Physician-Friendly Environs
Hospitalist Gregory Johnson, MD, chair of the Texas Medical Association’s Young Physicians Section, moved to Texas in 2002, just before the reforms were approved. “The best part about Prop 12 passing is the fact that Texas is now seen as a very physician-friendly environment,” says Johnson, who now serves as a Houston-based regional chief medical officer for Tacoma, Wash.-based Sound Physicians. The significant drops in malpractice insurance rates and lawsuits have made it far easier for him to recruit out-of-state doctors. “That basically comes off any physician’s radar as a particular concern.”
Most Texas hospitals and healthcare systems do not employ physicians directly. Instead, they contract or affiliate with private or nonprofit physicians groups. Due to that arrangement, Dr. Johnson explains, the cost of insurance premiums “becomes a much more individually based and personal issue because it’s coming out of an individual’s pocket, or a group’s pocket.”
From his own experience, Dr. Johnson says, he believes hospitalists are more willing to go to underserved parts of the state because of tort reform. Three years ago, he helped start Amarillo Hospitalist Services, a program that began with three doctors and has since grown to eight, all affiliated with Northwest Texas Hospital.
Of course, hospitalists appear to be thriving in major metropolitan areas, too. Dr. Johnson’s new employer, Sound Physicians, now operates three HM programs within Houston’s Memorial Hermann Healthcare System and employs about two-dozen physicians in all. More are on the way. “We’re actively hiring,” he says.
Mixed Outcomes
Statistics from the Texas Medical Board and Department of State Health Services confirm the anecdotal evidence that a more doctor-friendly Texas is paying dividends. Even so, they paint a somewhat more complicated picture than some commentators have portrayed in recent editorials. Doctors have indeed flocked to the state—some 11,000 since 2002 alone, an increase of 31%. That rate has far outpaced the state’s overall population growth of 14.2%.
But not all areas of the state have benefited equally from the influx.
Starr County, the third-poorest county in the U.S. based on per capita income, is among those that have fared well since 2002. Overall, its number of doctors increased from 14 to 24, a net increase of 71%, as its population rose by a projected 17%. But the next five poorest counties in Texas, accounting for nearly 86,000 residents in 2002, lost six doctors during the same time period—a 12.5% decline, even as their collective population rose by a projected 10.2%. Contrary to some public pronouncements, tort reform alone has not solved the chronic shortage of doctors in poor rural areas.
A withering report released in December by Washington, D.C.-based Public Citizen, a nonprofit consumer advocacy group, offers a harsher assessment, concluding that Texas’ “experiment with medical liability caps has failed” (www.citizen.org/publications/release.cfm?ID=7721). The report suggests that Texas’ dead-last ranking in percentage of uninsured residents (25%) and the doctor shortage in rural areas have actually grown worse since tort reform. Meanwhile, the cost of health insurance has more than doubled, while the cost of healthcare also has increased at nearly double the national average, other metrics that led to the organization’s vote of no confidence.
The impact on quality of care has been harder to assess. But Dr. Johnson and other observers say they haven’t seen any dip within hospitals. “I think that we as physicians and we as hospitalists really want to focus on our patients, and we can help to drive down those costs if we’re given the freedom to do our job,” he says. Tort reform, he adds, has helped doctors do precisely that.
Dr. Calhoun agrees. “No one wants to be sued. Everyone wants to do a good job,” he says. The threat of a lawsuit alone is only one of many factors influencing quality, he adds. But creating a more inviting environment for doctors can make a big difference by encouraging the increased use of hospitalists. “Having a hospitalist in the hospital all the time,” he says, “is an obvious quality improvement.” TH
Bryn Nelson is a freelance medical writer based in Seattle.
IMAGE SOURCE: DRASCHWARTZ/ISTOCK.COM
Admit Documentation
In light of the recent elimination of consultation codes from the Medicare Physician Fee Schedule, physicians of all specialties are being asked to report initial hospital care services (99221-99223) for their first encounter with a patient.1 This leaves hospitalists with questions about the billing and financial implications of reporting admissions services.
Here’s a typical scenario: Dr. A admits a Medicare patient to the hospital from the ED for hyperglycemia and dehydration in the setting of uncontrolled diabetes. He performs and documents an initial hospital-care service on day one of the admission. On day two, another hospitalist, Dr. B, who works in the same HM group, sees the patient for the first time. What should each of the physicians report for their first encounter with the patient?
Each hospitalist should select the CPT code that best fits the service and their role in the case. Remember, only one physician is named “attending of record” or “admitting physician.”
When billing during the course of the hospitalization, consider all physicians of the same specialty in the same provider group as the “admitting physician/group.”
Admissions Service
On day one, Dr. A admits the patient. He performs and documents a comprehensive history, a comprehensive exam, and medical decision-making of high complexity. The documentation corresponds to the highest initial admission service, 99223. Given the recent Medicare billing changes, the attending of record is required to append modifier “AI” (principal physician of record) to the admission service (e.g., 99223-AI).
The purpose of this modifier is “to identify the physician who oversees the patient’s care from all other physicians who may be furnishing specialty care.”2 This modifier has no financial implications. It does not increase or decrease the payment associated with the reported visit level (i.e., 99223 is reimbursed at a national rate of approximately $190, with or without modifier AI).
Initial Encounter by Team Members
As previously stated, the elimination of consultation services requires physicians to report their initial hospital encounter with an initial hospital-care code (i.e., 99221-99223). However, Medicare states that “physicians in the same group practice who are in the same specialty must bill and be paid as though they were a single physician.”3 This means followup services performed on days subsequent to a group member’s initial admission service must be reported with subsequent hospital-care codes (99231-99233). Therefore, in the scenario above, Dr. B is obligated to report the appropriate subsequent hospital-care code for his patient encounter on day two.
Incomplete Documentation
Initial hospital-care services (99221-99223) require the physician to obtain, perform, and document the necessary elements of history, physical exam, and medical decision-making in support of the code reported on the claim. There are occasions when the physician’s documentation does not support the lowest code (i.e., 99221). A reasonable approach is to report the service with an unlisted E&M code (99499). “Unlisted” codes do not have a payor-recognized code description or fee. When reporting an unlisted code, the biller must manually enter a charge description (e.g., expanded problem-focused admissions service) and a fee. A payor-prompted request for documentation is likely before payment is made.
Some payors have more specific references to the situation and allow for options. Two options exist for coding services that do not meet the work and/or medical necessity requirements of 99221-99223: report an unlisted E&M service (99499); or report a subsequent hospital care code (99231-99233) that appropriately reflects physician work and medical necessity for the service, and avoids mandatory medical record submission and manual medical review.4
In fact, Medicare Administrator Contractor TrailBlazer Health’s Web site (www.trailblazerhealth.com) offers guidance to physicians who are unsure if subsequent hospital care is an appropriate choice for this dilemma: “TrailBlazer recognizes provider reluctance to miscode initial hospital care as subsequent hospital care. However, doing so is preferable in that it allows Medicare to process and pay the claims much more efficiently. For those concerned about miscoding these services, please understand that TrailBlazer will not find fault with providers who choose this option when records appropriately demonstrate the work and medical necessity of the subsequent code chosen.”4 TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She also is faculty for SHM’s inpatient coding course.
References
- CMS announces payment, policy changes for physicians services to Medicare beneficiaries in 2010. Centers for Medicare and Medicaid Services Web site. Available at: www.cms.hhs.gov/apps/media/ press/release.asp?Counter=3539&intNumPerPage=10&checkDate=&checkKey=&srchType=1&numDays=3500&srchOpt=0&srchData=&keywordType=All&chkNewsType=1%2C+2%2C+3%2C+4%2C+5&intPage=&showAll=&pYear=&year=&desc=&cboOrder=date. Accessed Nov. 12, 2009.
- Revisions to Consultation Services Payment Policy. Medicare Learning Network Web site. Available at: www.cms.hhs.gov/MLNMattersArticles/downloads/ MM6740.pdf. Accessed Jan. 16, 2010.
- Medicare Claims Processing Manual: Chapter 12, Section 30.6.5. CMS Web site. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed Jan. 16, 2010.
- Update-evaluation and management services formerly coded as consultations. Trailblazer Health Enterprises Web site. Available at: www.trailblazerhealth.com/Tools/Notices.aspx?DomainID=1. Accessed Jan. 17, 2010.
- Beebe M, Dalton J, Espronceda M, Evans D, Glenn R. Current Procedural Terminology Professional Edition. Chicago: American Medical Association Press; 2009;14-15.
In light of the recent elimination of consultation codes from the Medicare Physician Fee Schedule, physicians of all specialties are being asked to report initial hospital care services (99221-99223) for their first encounter with a patient.1 This leaves hospitalists with questions about the billing and financial implications of reporting admissions services.
Here’s a typical scenario: Dr. A admits a Medicare patient to the hospital from the ED for hyperglycemia and dehydration in the setting of uncontrolled diabetes. He performs and documents an initial hospital-care service on day one of the admission. On day two, another hospitalist, Dr. B, who works in the same HM group, sees the patient for the first time. What should each of the physicians report for their first encounter with the patient?
Each hospitalist should select the CPT code that best fits the service and their role in the case. Remember, only one physician is named “attending of record” or “admitting physician.”
When billing during the course of the hospitalization, consider all physicians of the same specialty in the same provider group as the “admitting physician/group.”
Admissions Service
On day one, Dr. A admits the patient. He performs and documents a comprehensive history, a comprehensive exam, and medical decision-making of high complexity. The documentation corresponds to the highest initial admission service, 99223. Given the recent Medicare billing changes, the attending of record is required to append modifier “AI” (principal physician of record) to the admission service (e.g., 99223-AI).
The purpose of this modifier is “to identify the physician who oversees the patient’s care from all other physicians who may be furnishing specialty care.”2 This modifier has no financial implications. It does not increase or decrease the payment associated with the reported visit level (i.e., 99223 is reimbursed at a national rate of approximately $190, with or without modifier AI).
Initial Encounter by Team Members
As previously stated, the elimination of consultation services requires physicians to report their initial hospital encounter with an initial hospital-care code (i.e., 99221-99223). However, Medicare states that “physicians in the same group practice who are in the same specialty must bill and be paid as though they were a single physician.”3 This means followup services performed on days subsequent to a group member’s initial admission service must be reported with subsequent hospital-care codes (99231-99233). Therefore, in the scenario above, Dr. B is obligated to report the appropriate subsequent hospital-care code for his patient encounter on day two.
Incomplete Documentation
Initial hospital-care services (99221-99223) require the physician to obtain, perform, and document the necessary elements of history, physical exam, and medical decision-making in support of the code reported on the claim. There are occasions when the physician’s documentation does not support the lowest code (i.e., 99221). A reasonable approach is to report the service with an unlisted E&M code (99499). “Unlisted” codes do not have a payor-recognized code description or fee. When reporting an unlisted code, the biller must manually enter a charge description (e.g., expanded problem-focused admissions service) and a fee. A payor-prompted request for documentation is likely before payment is made.
Some payors have more specific references to the situation and allow for options. Two options exist for coding services that do not meet the work and/or medical necessity requirements of 99221-99223: report an unlisted E&M service (99499); or report a subsequent hospital care code (99231-99233) that appropriately reflects physician work and medical necessity for the service, and avoids mandatory medical record submission and manual medical review.4
In fact, Medicare Administrator Contractor TrailBlazer Health’s Web site (www.trailblazerhealth.com) offers guidance to physicians who are unsure if subsequent hospital care is an appropriate choice for this dilemma: “TrailBlazer recognizes provider reluctance to miscode initial hospital care as subsequent hospital care. However, doing so is preferable in that it allows Medicare to process and pay the claims much more efficiently. For those concerned about miscoding these services, please understand that TrailBlazer will not find fault with providers who choose this option when records appropriately demonstrate the work and medical necessity of the subsequent code chosen.”4 TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She also is faculty for SHM’s inpatient coding course.
References
- CMS announces payment, policy changes for physicians services to Medicare beneficiaries in 2010. Centers for Medicare and Medicaid Services Web site. Available at: www.cms.hhs.gov/apps/media/ press/release.asp?Counter=3539&intNumPerPage=10&checkDate=&checkKey=&srchType=1&numDays=3500&srchOpt=0&srchData=&keywordType=All&chkNewsType=1%2C+2%2C+3%2C+4%2C+5&intPage=&showAll=&pYear=&year=&desc=&cboOrder=date. Accessed Nov. 12, 2009.
- Revisions to Consultation Services Payment Policy. Medicare Learning Network Web site. Available at: www.cms.hhs.gov/MLNMattersArticles/downloads/ MM6740.pdf. Accessed Jan. 16, 2010.
- Medicare Claims Processing Manual: Chapter 12, Section 30.6.5. CMS Web site. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed Jan. 16, 2010.
- Update-evaluation and management services formerly coded as consultations. Trailblazer Health Enterprises Web site. Available at: www.trailblazerhealth.com/Tools/Notices.aspx?DomainID=1. Accessed Jan. 17, 2010.
- Beebe M, Dalton J, Espronceda M, Evans D, Glenn R. Current Procedural Terminology Professional Edition. Chicago: American Medical Association Press; 2009;14-15.
In light of the recent elimination of consultation codes from the Medicare Physician Fee Schedule, physicians of all specialties are being asked to report initial hospital care services (99221-99223) for their first encounter with a patient.1 This leaves hospitalists with questions about the billing and financial implications of reporting admissions services.
Here’s a typical scenario: Dr. A admits a Medicare patient to the hospital from the ED for hyperglycemia and dehydration in the setting of uncontrolled diabetes. He performs and documents an initial hospital-care service on day one of the admission. On day two, another hospitalist, Dr. B, who works in the same HM group, sees the patient for the first time. What should each of the physicians report for their first encounter with the patient?
Each hospitalist should select the CPT code that best fits the service and their role in the case. Remember, only one physician is named “attending of record” or “admitting physician.”
When billing during the course of the hospitalization, consider all physicians of the same specialty in the same provider group as the “admitting physician/group.”
Admissions Service
On day one, Dr. A admits the patient. He performs and documents a comprehensive history, a comprehensive exam, and medical decision-making of high complexity. The documentation corresponds to the highest initial admission service, 99223. Given the recent Medicare billing changes, the attending of record is required to append modifier “AI” (principal physician of record) to the admission service (e.g., 99223-AI).
The purpose of this modifier is “to identify the physician who oversees the patient’s care from all other physicians who may be furnishing specialty care.”2 This modifier has no financial implications. It does not increase or decrease the payment associated with the reported visit level (i.e., 99223 is reimbursed at a national rate of approximately $190, with or without modifier AI).
Initial Encounter by Team Members
As previously stated, the elimination of consultation services requires physicians to report their initial hospital encounter with an initial hospital-care code (i.e., 99221-99223). However, Medicare states that “physicians in the same group practice who are in the same specialty must bill and be paid as though they were a single physician.”3 This means followup services performed on days subsequent to a group member’s initial admission service must be reported with subsequent hospital-care codes (99231-99233). Therefore, in the scenario above, Dr. B is obligated to report the appropriate subsequent hospital-care code for his patient encounter on day two.
Incomplete Documentation
Initial hospital-care services (99221-99223) require the physician to obtain, perform, and document the necessary elements of history, physical exam, and medical decision-making in support of the code reported on the claim. There are occasions when the physician’s documentation does not support the lowest code (i.e., 99221). A reasonable approach is to report the service with an unlisted E&M code (99499). “Unlisted” codes do not have a payor-recognized code description or fee. When reporting an unlisted code, the biller must manually enter a charge description (e.g., expanded problem-focused admissions service) and a fee. A payor-prompted request for documentation is likely before payment is made.
Some payors have more specific references to the situation and allow for options. Two options exist for coding services that do not meet the work and/or medical necessity requirements of 99221-99223: report an unlisted E&M service (99499); or report a subsequent hospital care code (99231-99233) that appropriately reflects physician work and medical necessity for the service, and avoids mandatory medical record submission and manual medical review.4
In fact, Medicare Administrator Contractor TrailBlazer Health’s Web site (www.trailblazerhealth.com) offers guidance to physicians who are unsure if subsequent hospital care is an appropriate choice for this dilemma: “TrailBlazer recognizes provider reluctance to miscode initial hospital care as subsequent hospital care. However, doing so is preferable in that it allows Medicare to process and pay the claims much more efficiently. For those concerned about miscoding these services, please understand that TrailBlazer will not find fault with providers who choose this option when records appropriately demonstrate the work and medical necessity of the subsequent code chosen.”4 TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She also is faculty for SHM’s inpatient coding course.
References
- CMS announces payment, policy changes for physicians services to Medicare beneficiaries in 2010. Centers for Medicare and Medicaid Services Web site. Available at: www.cms.hhs.gov/apps/media/ press/release.asp?Counter=3539&intNumPerPage=10&checkDate=&checkKey=&srchType=1&numDays=3500&srchOpt=0&srchData=&keywordType=All&chkNewsType=1%2C+2%2C+3%2C+4%2C+5&intPage=&showAll=&pYear=&year=&desc=&cboOrder=date. Accessed Nov. 12, 2009.
- Revisions to Consultation Services Payment Policy. Medicare Learning Network Web site. Available at: www.cms.hhs.gov/MLNMattersArticles/downloads/ MM6740.pdf. Accessed Jan. 16, 2010.
- Medicare Claims Processing Manual: Chapter 12, Section 30.6.5. CMS Web site. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed Jan. 16, 2010.
- Update-evaluation and management services formerly coded as consultations. Trailblazer Health Enterprises Web site. Available at: www.trailblazerhealth.com/Tools/Notices.aspx?DomainID=1. Accessed Jan. 17, 2010.
- Beebe M, Dalton J, Espronceda M, Evans D, Glenn R. Current Procedural Terminology Professional Edition. Chicago: American Medical Association Press; 2009;14-15.
A Time to Be Recognized
Like so many things in HM, the story of how hospitalists first learned about the focused practice program is a modern one.
It started with a text message, which led to a blog post, which reached thousands of readers, many of them hospitalists interested in how to bolster their bona fides in a specialty known for its explosive growth in recent years.
Now, hospitalists certified in internal medicine have the opportunity to reinforce their commitment to the specialty by maintaining their certification through the Focused Practice in Hospital Medicine pathway offered by the American Board of Internal Medicine (ABIM). The Focused Practice in Hospital Medicine (FPHM) Maintenance of Certification (MOC) program enables hospitalists to distinguish their practice within the larger specialty of internal medicine.
The Evolution of FPHM
The new pathway has been years in the making, and it reflects the growing influence of HM in healthcare, according to ABIM Chief Medical Officer Eric Holmboe, MD. He sees the FPHM as the result of a combination of factors, including the fact that the specialty now has more than 30,000 hospitalists practicing nationwide. “If you look at the past years, this has been a viable and vibrant practice,” he says. “If you look at the number of people doing hospital medicine, it’s a factor.”
For Holmboe, it also is a shift in how individuals are recognized based on their practice areas. “This is an acknowledgement by ABIM and the American Board of Medical Specialties to look at Maintenance of Certification in terms of what the individual actually does,” he explains. “Hospitalists play a very important role in the hospital.”
He also credits the leadership of the HM movement—especially pioneers like Robert Wachter, MD, FHM. One of HM’s most ardent champions, Dr. Wachter, chief of the hospital medicine division, professor, and associate chair of the Department of Medicine at the University of California at San Francisco, worked with ABIM to find a way to recognize hospitalists’ specialized skill sets and their commitment to inpatient medicine. After more than a decade of advocating for a board-certified process to recognize the field, Dr. Wachter, an ABIM board member, began receiving multiple text messages from colleagues announcing that ABIM had approved the focused-practice program. He wrote a post on his blog, Wachter’s World (www.wachtersworld.com), that outlined the need for the FPHM and the significance for aspiring hospitalists.
“In any case, this is an important milestone for the field,” Dr. Wachter wrote in his Sept. 23, 2009, blog entry, “Board Certification for Hospitalists: It’s Heeeere!” “In fact, when I first began speaking to groups of hospitalists nearly 15 years ago, I often showed a slide listing the elements of a true specialty, and one by one we’ve ticked them off,” wrote Dr. Wachter, a former SHM president. “The only unchecked box was recognition of the field as a legitimate ‘specialty,’ as codified by the ABMS board certification process.”
Unchecked, that is, until now.
In early 2011, the medical world will be introduced to the first internists recognized for their focus in HM. For Holmboe, the FPHM is the beginning of an even larger movement.
“The goal is continued interest: getting people involved in quality in their hospital and encouraging people to change behaviors and be recognized by patients and credentialists as valuable,” he says. “That’s the primary mission of ABIM: using certification to improve care.”
Fellow in Hospital Medicine Spotlight
O’Neil Pyke, MD, FHM

Dr. Pyke is a clinical instructor at Commonwealth Medical College and a medical director at the Wyoming Valley Health Care System in Wilkes-Barre, Pa. He also serves as a consultant for various hospitalist programs, most actively for his own private consulting company, AMP Hospitalist Consulting, which partners with Salem, N.H.-based physician staffing company Medicus Healthcare Solutions.
Undergraduate Education: Queens College, City University of New York, Flushing, N.Y.
Medical School: Ohio State University College of Medicine and Public Health, Columbus
Notable: Dr. Pyke was born in Jamaica and moved to New York during high school. He says he owes everything to his parents. His parents, who had no education beyond high school, pushed Dr. Pyke and his siblings to achieve more than they did. His sister is an OB-GYN and his brother is pursuing a medical degree.
FYI: Dr. Pyke enjoys playing golf, cheering for his beloved Ohio State Buckeyes, and spends every Friday night with his wife and two daughters—he even admits to watching “chick flicks” on family night.
For more information about the FHM designation, visit www.hospitalmedicine.org/fellows.
Requirements and Process
Shortly after the program’s approval, ABIM, which administers the FPHM program, went to work in defining the process for the FPHM application and building infrastructure to support the tests. Holmboe expects ABIM will be ready to process pre-applications by April or May. While some details may change, the FPHM application will dovetail with ABIM’s MOC process.
Although hospitalists’ MOC must be current in order to apply for FPHM, hospitalists can begin the FPHM application process at any time. Hospitalists do not need to wait until their next MOC renewal.
Before beginning the application process, hospitalists should ensure that they are eligible. ABIM requires FPHM candidates to have:
- A current or previous ABIM certification in internal medicine;
- A valid, unrestricted medical license and confirmation of good standing in the local practice community;
- ACLS certification; and
- At least three years of hospital medicine practice experience.
Candidates who meet the requirements can then begin the enrollment process by:
- Submitting attestations. Both the hospitalist and a senior officer at the hospital must provide attestations that demonstrate the hospitalist’s experience in HM and his or her commitment to the principles of the specialty.
- Performing a self-assessment. Hospitalists must quantify their experience in HM through an MOC self-assessment. Candidates must achieve at least 100 MOC points. Successful applicants must submit a new self-assessment every three years. The self-assessment can be conducted before or after the exam.
- Taking the MOC examination in Hospital Medicine. Registration for the first HM examination will begin in May. The exam will be conducted in October, and diplomates can take the exam at any time in the process.
Passing the exam and completing the other requirements will earn ABIM diplomats recognition as “Board Certified in Internal Medicine with a Focused Practice in Hospital Medicine.” ABIM will notify successful applicants in late 2010 and ship personalized certificates in early 2011. TH
Brendon Shank is a freelance writer based in Philadelphia.
Like so many things in HM, the story of how hospitalists first learned about the focused practice program is a modern one.
It started with a text message, which led to a blog post, which reached thousands of readers, many of them hospitalists interested in how to bolster their bona fides in a specialty known for its explosive growth in recent years.
Now, hospitalists certified in internal medicine have the opportunity to reinforce their commitment to the specialty by maintaining their certification through the Focused Practice in Hospital Medicine pathway offered by the American Board of Internal Medicine (ABIM). The Focused Practice in Hospital Medicine (FPHM) Maintenance of Certification (MOC) program enables hospitalists to distinguish their practice within the larger specialty of internal medicine.
The Evolution of FPHM
The new pathway has been years in the making, and it reflects the growing influence of HM in healthcare, according to ABIM Chief Medical Officer Eric Holmboe, MD. He sees the FPHM as the result of a combination of factors, including the fact that the specialty now has more than 30,000 hospitalists practicing nationwide. “If you look at the past years, this has been a viable and vibrant practice,” he says. “If you look at the number of people doing hospital medicine, it’s a factor.”
For Holmboe, it also is a shift in how individuals are recognized based on their practice areas. “This is an acknowledgement by ABIM and the American Board of Medical Specialties to look at Maintenance of Certification in terms of what the individual actually does,” he explains. “Hospitalists play a very important role in the hospital.”
He also credits the leadership of the HM movement—especially pioneers like Robert Wachter, MD, FHM. One of HM’s most ardent champions, Dr. Wachter, chief of the hospital medicine division, professor, and associate chair of the Department of Medicine at the University of California at San Francisco, worked with ABIM to find a way to recognize hospitalists’ specialized skill sets and their commitment to inpatient medicine. After more than a decade of advocating for a board-certified process to recognize the field, Dr. Wachter, an ABIM board member, began receiving multiple text messages from colleagues announcing that ABIM had approved the focused-practice program. He wrote a post on his blog, Wachter’s World (www.wachtersworld.com), that outlined the need for the FPHM and the significance for aspiring hospitalists.
“In any case, this is an important milestone for the field,” Dr. Wachter wrote in his Sept. 23, 2009, blog entry, “Board Certification for Hospitalists: It’s Heeeere!” “In fact, when I first began speaking to groups of hospitalists nearly 15 years ago, I often showed a slide listing the elements of a true specialty, and one by one we’ve ticked them off,” wrote Dr. Wachter, a former SHM president. “The only unchecked box was recognition of the field as a legitimate ‘specialty,’ as codified by the ABMS board certification process.”
Unchecked, that is, until now.
In early 2011, the medical world will be introduced to the first internists recognized for their focus in HM. For Holmboe, the FPHM is the beginning of an even larger movement.
“The goal is continued interest: getting people involved in quality in their hospital and encouraging people to change behaviors and be recognized by patients and credentialists as valuable,” he says. “That’s the primary mission of ABIM: using certification to improve care.”
Fellow in Hospital Medicine Spotlight
O’Neil Pyke, MD, FHM
Dr. Pyke is a clinical instructor at Commonwealth Medical College and a medical director at the Wyoming Valley Health Care System in Wilkes-Barre, Pa. He also serves as a consultant for various hospitalist programs, most actively for his own private consulting company, AMP Hospitalist Consulting, which partners with Salem, N.H.-based physician staffing company Medicus Healthcare Solutions.
Undergraduate Education: Queens College, City University of New York, Flushing, N.Y.
Medical School: Ohio State University College of Medicine and Public Health, Columbus
Notable: Dr. Pyke was born in Jamaica and moved to New York during high school. He says he owes everything to his parents. His parents, who had no education beyond high school, pushed Dr. Pyke and his siblings to achieve more than they did. His sister is an OB-GYN and his brother is pursuing a medical degree.
FYI: Dr. Pyke enjoys playing golf, cheering for his beloved Ohio State Buckeyes, and spends every Friday night with his wife and two daughters—he even admits to watching “chick flicks” on family night.
For more information about the FHM designation, visit www.hospitalmedicine.org/fellows.
Requirements and Process
Shortly after the program’s approval, ABIM, which administers the FPHM program, went to work in defining the process for the FPHM application and building infrastructure to support the tests. Holmboe expects ABIM will be ready to process pre-applications by April or May. While some details may change, the FPHM application will dovetail with ABIM’s MOC process.
Although hospitalists’ MOC must be current in order to apply for FPHM, hospitalists can begin the FPHM application process at any time. Hospitalists do not need to wait until their next MOC renewal.
Before beginning the application process, hospitalists should ensure that they are eligible. ABIM requires FPHM candidates to have:
- A current or previous ABIM certification in internal medicine;
- A valid, unrestricted medical license and confirmation of good standing in the local practice community;
- ACLS certification; and
- At least three years of hospital medicine practice experience.
Candidates who meet the requirements can then begin the enrollment process by:
- Submitting attestations. Both the hospitalist and a senior officer at the hospital must provide attestations that demonstrate the hospitalist’s experience in HM and his or her commitment to the principles of the specialty.
- Performing a self-assessment. Hospitalists must quantify their experience in HM through an MOC self-assessment. Candidates must achieve at least 100 MOC points. Successful applicants must submit a new self-assessment every three years. The self-assessment can be conducted before or after the exam.
- Taking the MOC examination in Hospital Medicine. Registration for the first HM examination will begin in May. The exam will be conducted in October, and diplomates can take the exam at any time in the process.
Passing the exam and completing the other requirements will earn ABIM diplomats recognition as “Board Certified in Internal Medicine with a Focused Practice in Hospital Medicine.” ABIM will notify successful applicants in late 2010 and ship personalized certificates in early 2011. TH
Brendon Shank is a freelance writer based in Philadelphia.
Like so many things in HM, the story of how hospitalists first learned about the focused practice program is a modern one.
It started with a text message, which led to a blog post, which reached thousands of readers, many of them hospitalists interested in how to bolster their bona fides in a specialty known for its explosive growth in recent years.
Now, hospitalists certified in internal medicine have the opportunity to reinforce their commitment to the specialty by maintaining their certification through the Focused Practice in Hospital Medicine pathway offered by the American Board of Internal Medicine (ABIM). The Focused Practice in Hospital Medicine (FPHM) Maintenance of Certification (MOC) program enables hospitalists to distinguish their practice within the larger specialty of internal medicine.
The Evolution of FPHM
The new pathway has been years in the making, and it reflects the growing influence of HM in healthcare, according to ABIM Chief Medical Officer Eric Holmboe, MD. He sees the FPHM as the result of a combination of factors, including the fact that the specialty now has more than 30,000 hospitalists practicing nationwide. “If you look at the past years, this has been a viable and vibrant practice,” he says. “If you look at the number of people doing hospital medicine, it’s a factor.”
For Holmboe, it also is a shift in how individuals are recognized based on their practice areas. “This is an acknowledgement by ABIM and the American Board of Medical Specialties to look at Maintenance of Certification in terms of what the individual actually does,” he explains. “Hospitalists play a very important role in the hospital.”
He also credits the leadership of the HM movement—especially pioneers like Robert Wachter, MD, FHM. One of HM’s most ardent champions, Dr. Wachter, chief of the hospital medicine division, professor, and associate chair of the Department of Medicine at the University of California at San Francisco, worked with ABIM to find a way to recognize hospitalists’ specialized skill sets and their commitment to inpatient medicine. After more than a decade of advocating for a board-certified process to recognize the field, Dr. Wachter, an ABIM board member, began receiving multiple text messages from colleagues announcing that ABIM had approved the focused-practice program. He wrote a post on his blog, Wachter’s World (www.wachtersworld.com), that outlined the need for the FPHM and the significance for aspiring hospitalists.
“In any case, this is an important milestone for the field,” Dr. Wachter wrote in his Sept. 23, 2009, blog entry, “Board Certification for Hospitalists: It’s Heeeere!” “In fact, when I first began speaking to groups of hospitalists nearly 15 years ago, I often showed a slide listing the elements of a true specialty, and one by one we’ve ticked them off,” wrote Dr. Wachter, a former SHM president. “The only unchecked box was recognition of the field as a legitimate ‘specialty,’ as codified by the ABMS board certification process.”
Unchecked, that is, until now.
In early 2011, the medical world will be introduced to the first internists recognized for their focus in HM. For Holmboe, the FPHM is the beginning of an even larger movement.
“The goal is continued interest: getting people involved in quality in their hospital and encouraging people to change behaviors and be recognized by patients and credentialists as valuable,” he says. “That’s the primary mission of ABIM: using certification to improve care.”
Fellow in Hospital Medicine Spotlight
O’Neil Pyke, MD, FHM
Dr. Pyke is a clinical instructor at Commonwealth Medical College and a medical director at the Wyoming Valley Health Care System in Wilkes-Barre, Pa. He also serves as a consultant for various hospitalist programs, most actively for his own private consulting company, AMP Hospitalist Consulting, which partners with Salem, N.H.-based physician staffing company Medicus Healthcare Solutions.
Undergraduate Education: Queens College, City University of New York, Flushing, N.Y.
Medical School: Ohio State University College of Medicine and Public Health, Columbus
Notable: Dr. Pyke was born in Jamaica and moved to New York during high school. He says he owes everything to his parents. His parents, who had no education beyond high school, pushed Dr. Pyke and his siblings to achieve more than they did. His sister is an OB-GYN and his brother is pursuing a medical degree.
FYI: Dr. Pyke enjoys playing golf, cheering for his beloved Ohio State Buckeyes, and spends every Friday night with his wife and two daughters—he even admits to watching “chick flicks” on family night.
For more information about the FHM designation, visit www.hospitalmedicine.org/fellows.
Requirements and Process
Shortly after the program’s approval, ABIM, which administers the FPHM program, went to work in defining the process for the FPHM application and building infrastructure to support the tests. Holmboe expects ABIM will be ready to process pre-applications by April or May. While some details may change, the FPHM application will dovetail with ABIM’s MOC process.
Although hospitalists’ MOC must be current in order to apply for FPHM, hospitalists can begin the FPHM application process at any time. Hospitalists do not need to wait until their next MOC renewal.
Before beginning the application process, hospitalists should ensure that they are eligible. ABIM requires FPHM candidates to have:
- A current or previous ABIM certification in internal medicine;
- A valid, unrestricted medical license and confirmation of good standing in the local practice community;
- ACLS certification; and
- At least three years of hospital medicine practice experience.
Candidates who meet the requirements can then begin the enrollment process by:
- Submitting attestations. Both the hospitalist and a senior officer at the hospital must provide attestations that demonstrate the hospitalist’s experience in HM and his or her commitment to the principles of the specialty.
- Performing a self-assessment. Hospitalists must quantify their experience in HM through an MOC self-assessment. Candidates must achieve at least 100 MOC points. Successful applicants must submit a new self-assessment every three years. The self-assessment can be conducted before or after the exam.
- Taking the MOC examination in Hospital Medicine. Registration for the first HM examination will begin in May. The exam will be conducted in October, and diplomates can take the exam at any time in the process.
Passing the exam and completing the other requirements will earn ABIM diplomats recognition as “Board Certified in Internal Medicine with a Focused Practice in Hospital Medicine.” ABIM will notify successful applicants in late 2010 and ship personalized certificates in early 2011. TH
Brendon Shank is a freelance writer based in Philadelphia.
Hospital-Acquired Conditions & The Hospitalist
Hospitalist Neal Axon, MD, first became aware of an important change in his hospital’s policies last year while attending to an elderly patient the morning after admission to the community hospital where he works part time.
“This new form appeared in the chart requesting a urinalysis for my patient, who’d had a Foley catheter placed,” says Dr. Axon, an assistant professor of medicine at the Medical University of South Carolina in Charleston. “I didn’t know why, so I asked. I was told that it was now necessary to document that there was no UTI present on admission.” He asked the charge nurse, “So what do I do now that the catheter has been in place for 12 hours and has colonization without a true infection?”
The next thing he heard: silence.
The new form Dr. Axon encountered was an outgrowth of the requirements of the Deficit Reduction Act (DRA) of 2005, which ordered Medicare to withhold additional hospital payments for hospital-acquired complications (HAC) developed during a hospital stay. One result of the new rule is that much of a hospital’s response to these initiatives has been placed in the hands of the hospitalist. From accurate documentation of complications already present on admission (POA), to confirming that guidelines for treatment are being followed, to taking the lead on review of staff practices and education, hospitalists are in a position to have a wide-ranging impact on patient care and the financial health of their institutions.
Congress Pushes Reforms
In order for Medicare to not provide a reimbursement, an HAC has to be high-cost and/or high-volume, result in the assignment of the case to a higher payment when present as a secondary diagnosis, and “could reasonably be prevented through the application of evidence-based guidelines,” says Barry Straube, MD, chief medical officer and director of the Office of Clinical Standards and Quality at the Centers for Medicare and Medicaid Services (CMS). “CMS was to implement a process where we would not pay the hospitals additional money for these complications.”
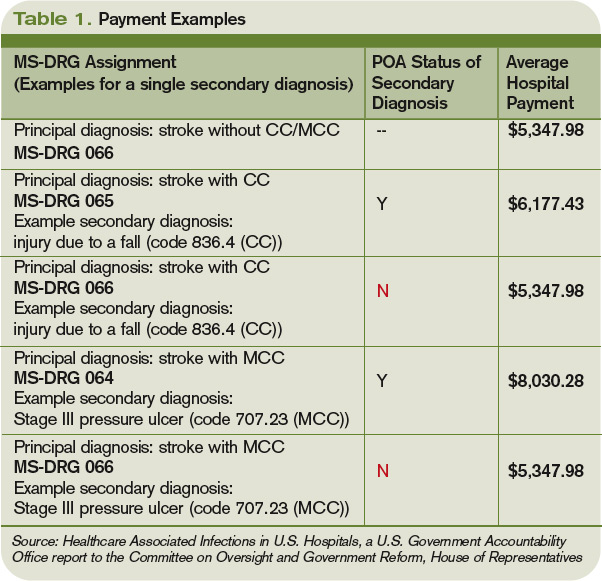
The new rules mean Medicare pays hospitals on the basis of Medicare Severity Diagnostic-Related Groups (MS-DRG), which better reflect the complexity of a patient’s illness. The biggest change was a three-tiered payment schedule: a base level for the diagnosis, a second level adding money to reflect the presence of comorbidities and complications, and a third for major complications and comorbidities (see Table 1, p. 31).
“Instituting HACs means that hospitals would no longer receive the comorbidity and complication payments if the only reason a case qualified for higher payment was the HAC,” Dr. Straube explains. “We did carve out a POA exception for those conditions that were acquired outside of the hospital. HACs only impact additional payments; the hospitals are still paid for the diagnosis that resulted in the hospital admission.”
CMS also identifies three “never events” it won’t reimburse for (see “A Brief History of Never Events,” p. 35): performing the wrong procedure, performing a procedure on the wrong body part, and performing a procedure on the wrong patient. “Neither hospitals nor physicians that are involved in such egregious situations would be paid,” Dr. Straube says.
Preventability: Subject of Controversy

The big questions surrounding HACs: Could they reasonably be prevented through the application of evidence-based guidelines? How preventable are HACs? Who decides if a complication is preventable, and therefore payment for services is withheld?
They’re concerns that are widespread among physicians, hospital administrators, and regulators alike.
“The legislation required the conditions to be ‘reasonably preventable’ using established clinical guidelines,” Dr. Straube says. “We did not have to show 100% prevention. In an imperfect world, they might still take place occasionally, but with good medical care, almost all of these are preventable in this day and age.”
For CMS, the preventable conditions are an either/or situation: Either they existed prior to admission and are subject to payment, or they did not exist at admission and additional payment for the complication will not be made. “HACs do not currently consider a patient’s individual risk for complications,” says Jennifer Meddings, MD, MSc, clinical lecturer and health researcher in the Department of Internal Medicine at the University of Michigan Health System in Ann Arbor. “We know the best strategies to prevent complications in ideal patients, and these are reflected in the HACs. In real life, many of our patients just don’t fit into the guidelines for many reasons—and you have to individualize care.”
Dr. Meddings points to DVT as a prime example. For a certain number of inpatients, the guidelines can be followed to perfection. In other patients (e.g., those with kidney conditions), previous reactions to a medication or an individual’s predisposition to clotting might interfere with treatment. However, CMS doesn’t allow appeals of nonpayment decisions for HACs based on individual circumstances.
Some experts think the rigidness of the payment policy forces physicians to treat patients exactly to guidelines. Even then, payment could be declined if an HAC develops.
“One of the points of most discussion is how preventable some of these are, particularly when choosing those you are no longer going to pay for,” Dr. Meddings says. “Many of the complications currently under review have patients that are at higher risk than others. How much our prevention strategies can alleviate or reduce the risk varies widely among patients.”
Impact on HM Practice
Many of the preventable conditions outlined by CMS do not directly affect hospitalist payment. However, hospitalists often find themselves responsible for properly documenting admission and care.
“The rule changes regarding payment for HACs are only related to hospital payments, and to date, most physicians, including hospitalists, are not directly at financial risk,” says Heidi Wald, MD, MSPH, hospitalist and assistant professor of medicine in the divisions of Health Care Policy Research and General Internal Medicine at the University of Colorado Denver School of Medicine. “Although hospitalists have no financial skin in the game, there are plenty of reasons they would take an interest in addressing HACs in their hospital. In particular, they are often seen as the ‘go-to’ group for quality improvement in their hospitals.”
For example, some HM groups have been active in working with teams of physicians, nurses, and other healthcare providers to address local policies and procedures on prevention of catheter-associated urinary tract infections (UTIs) and DVT.
“This has certainly necessitated a team approach,” says Shaun Frost, MD, FHM, an SHM board member and regional medical director for Cogent Healthcare in St. Paul, Minn. “For many of the HACs that apply to our population of patients, the hospitalist alone cannot be expected to solely execute effective quality improvements. It takes a team effort in that regard, and one that includes many different disciplines.”
The Cogent-affiliated hospitalist group at Temple University Hospital in Philadelphia formed a task force to address issues with catheter-associated UTI. One initiative focused on educating all providers involved in the proper care of the catheters and similar interventions. A secondary focus of the project was an inventory of current practices and procedures.
“It was discovered that we did not have an automatic stop order for Foley catheters, so in some situations, they were likely being left in longer than needed while nursing [staff] tried to contact a physician,” Dr. Frost explains. “We created standardized order sets that include criteria for continuing the catheter. Once the criteria are no longer applicable, nursing will be able to discontinue it.”
Although CMS has only recently turned the spotlight on HACs and never events, hospitalists have been heavily involved in the patient-safety arena for years. “It is not a new phenomenon that hospitalists work for healthcare delivery and healthcare system improvement,” Dr. Meddings says.
Hospital administration at Temple University Hospital recognized the HM group’s quality-improvement (QI) work, and has “specifically charged us with spreading the work we have done in patient safety to the entire house,” Dr. Frost says. “That speaks to the administration’s opinion of the power of the HM program to assist with institution-wide QI initiatives.”
Documentation Is Key

Beyond applying proven methods to avoid HACs, hospitalists can make a difference through documentation. If the hospitalist notes all conditions when the patient first presents to the hospital, additional comorbidity and complication payments should be made.
“The part that probably has the greatest impact on the day-to-day practice of a hospitalist is the increased importance of documentation throughout the hospital episode,” Dr. Meddings says. “If complications are occurring and they are not present in the chart, the coders may not recognize that it has occurred and will not know to include it in the bill. This can have an adverse impact on the hospital and its finances.”
Documentation issues can impact hospital payment in several ways:
- Hospitals might receive additional payment by default if certain HACs are described incorrectly or without sufficient detail (e.g., receiving overpayment because the physician did not indicate a UTI was in fact a catheter-associated UTI);
- As more attention is invested in documenting all conditions POA, hospitals might be coding more comorbidities overall than previously, which also will generate additional payment for hospitals as any POA condition is eligible for increased payment; and
- Hospitals might lose payment when admitting providers fail to adequately document the condition as POA (e.g., a pre-existing decubitus ulcer not detected until the second day of the hospital stay).
The descriptions to be used in coding are very detailed. UTIs, for example, have one code to document the POA assessment, another code to show that a UTI occurred, and a third code to indicate it was catheter-associated. Each code requires appropriate documentation in the chart (see Table 1, above).
The impact hospitalists have on care and payment is not the same across the HAC spectrum. For instance, documenting the presence of pressure ulcers might be easier than distinguishing colonization from infection in those admitted with in-dwelling urinary catheters. Others, such as DVT or vascular catheter-associated infections, are rarely POA unless they are part of the admitting diagnosis.
“This new focus on hospital-acquired conditions may work to the patient’s benefit,” Dr. Meddings says. “The inclusion of pressure ulcers has led to increased attention to skin exams on admission and preventive measures during hospitalizations. In the past, skin exams upon admission may have been given a lower priority, but that has changed.”
Dr. Meddings is concerned that the new rules could force the shifting of resources to areas where the hospital could lose money. If, when, and how many changes will actually take place is still up in the air. “Resource shifting is a concern whenever there is any sort of pay-for-performance attention directed toward one particular complication,” she says. “To balance this, many of the strategies hospitals used to prevent complications are not specific to just the diagnosis that is covered by the HAC.”
Dr. Meddings also hopes the new focus on preventable conditions will have a “halo effect” in the healthcare community. For instance, CMS mandating DVT prevention following orthopedic operations will, hopefully, result in a greater awareness of the problem in other susceptible patients.
POA Indicators

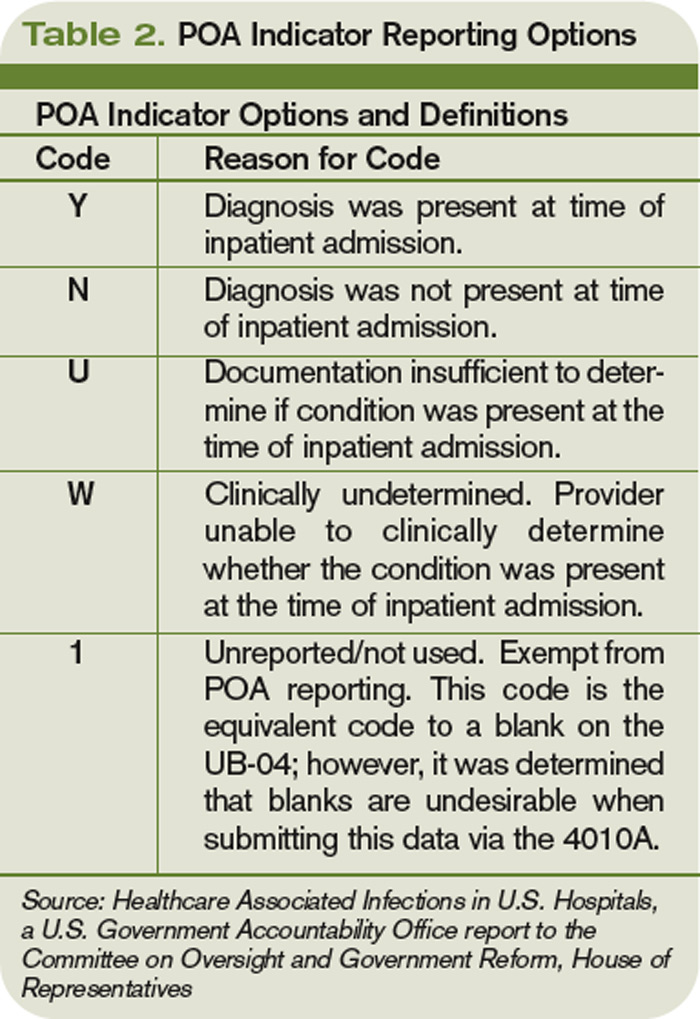
Since hospitalists often perform the initial patient history, physical, and other admission work, they are in the best position to find and document POA indicators (see Table 2, p. below). Proper notes on such things as UTIs present and the state of skin integrity are an important part of making sure the hospital is paid correctly for the care it provides.
Education on the specific definition of each potential HAC is required to help physicians avoid overtreatment of certain conditions, especially UTIs. For example, the Centers for Disease Control and Prevention (CDC) defines all UTIs as symptomatic. Therefore, the screening of all admitted patients, regardless of symptoms, is wasteful and unlikely to help the hospital’s bottom line.
“If you start screening everyone that comes through the door so you don’t miss any pre-existing UTIs, you are going to find a lot of asymptomatic colonization,” Dr. Wald says. “You are also going to spend a lot of money and time on studies and possibly treatments that may not yield many true infections. It is important that physicians know the definition of these HACs to help avoid needless interventions.”
Minimal Loss

Many hospital administrators and physicians were worried when the HAC program was first announced. Much of the stress and concern, however, seems to have dissipated. CMS estimated the HAC program would save Medicare $21 million in fiscal year 2009. Others, such as Peter McNair and colleagues writing in Health Affairs, suggest the actual impact is closer to $1.1 million.1 The CMS-projected impact of the HAC provision in fiscal-year 2009 was $21 million, out of more than $100 billion in payments.
“I think the HACs will not have a major impact because of the way payments are made,” says internist Robert Berenson, MD, a fellow at the Urban Institute in Washington, D.C., who has studied Medicare policy issues extensively, and for two years was in charge of Medicare payment policies at the Health Care Finance Administration, the precursor to CMS. “Patients who have HACs often have another comorbidity that would kick them into a higher payment category regardless of the presence of a hospital-acquired complication. In the end, it is probably more symbolic and unlikely to make a major dent in hospital income—at least at this point.”
Another limitation to CMS nonpayment for HACs is the issue of deciding which conditions are truly preventable. Dr. Berenson questions the ability of the current system to identify many additional complications for which this approach will be feasible.
“CMS has laid out its strategy, suggesting that we should be able to continue increasing the number of conditions for which providers would be paid differently based on quality,” he says. “Many observers question whether there will ever be measurement tools that are robust enough, and there will be a wide agreement on the preventability of enough conditions that this initiative will go very far.”
Although hospitalists might not face a direct financial risk, they still have their hospitals’ best interest—and their reputations—on the line. “Hospitalists care about preventing complications,” Dr. Wald says. “We are very engaged in working with our hospitals to improve care, maximize quality, and minimize cost.” TH
Kurt Ullman is a freelance medical writer based in Indiana.
Reference
- McNair PD, Luft HS, Bindman AB. Medicare’s policy not to pay for treating hospital-acquired conditions: the impact. Health Aff (Millwood). 2009;28(5):1485-1493.
TOP IMAGE SOURCE: KAREEM RIZKHALLA/ISTOCKPHOTO.COM
Hospitalist Neal Axon, MD, first became aware of an important change in his hospital’s policies last year while attending to an elderly patient the morning after admission to the community hospital where he works part time.
“This new form appeared in the chart requesting a urinalysis for my patient, who’d had a Foley catheter placed,” says Dr. Axon, an assistant professor of medicine at the Medical University of South Carolina in Charleston. “I didn’t know why, so I asked. I was told that it was now necessary to document that there was no UTI present on admission.” He asked the charge nurse, “So what do I do now that the catheter has been in place for 12 hours and has colonization without a true infection?”
The next thing he heard: silence.
The new form Dr. Axon encountered was an outgrowth of the requirements of the Deficit Reduction Act (DRA) of 2005, which ordered Medicare to withhold additional hospital payments for hospital-acquired complications (HAC) developed during a hospital stay. One result of the new rule is that much of a hospital’s response to these initiatives has been placed in the hands of the hospitalist. From accurate documentation of complications already present on admission (POA), to confirming that guidelines for treatment are being followed, to taking the lead on review of staff practices and education, hospitalists are in a position to have a wide-ranging impact on patient care and the financial health of their institutions.
Congress Pushes Reforms
In order for Medicare to not provide a reimbursement, an HAC has to be high-cost and/or high-volume, result in the assignment of the case to a higher payment when present as a secondary diagnosis, and “could reasonably be prevented through the application of evidence-based guidelines,” says Barry Straube, MD, chief medical officer and director of the Office of Clinical Standards and Quality at the Centers for Medicare and Medicaid Services (CMS). “CMS was to implement a process where we would not pay the hospitals additional money for these complications.”
The new rules mean Medicare pays hospitals on the basis of Medicare Severity Diagnostic-Related Groups (MS-DRG), which better reflect the complexity of a patient’s illness. The biggest change was a three-tiered payment schedule: a base level for the diagnosis, a second level adding money to reflect the presence of comorbidities and complications, and a third for major complications and comorbidities (see Table 1, p. 31).
“Instituting HACs means that hospitals would no longer receive the comorbidity and complication payments if the only reason a case qualified for higher payment was the HAC,” Dr. Straube explains. “We did carve out a POA exception for those conditions that were acquired outside of the hospital. HACs only impact additional payments; the hospitals are still paid for the diagnosis that resulted in the hospital admission.”
CMS also identifies three “never events” it won’t reimburse for (see “A Brief History of Never Events,” p. 35): performing the wrong procedure, performing a procedure on the wrong body part, and performing a procedure on the wrong patient. “Neither hospitals nor physicians that are involved in such egregious situations would be paid,” Dr. Straube says.
Preventability: Subject of Controversy
The big questions surrounding HACs: Could they reasonably be prevented through the application of evidence-based guidelines? How preventable are HACs? Who decides if a complication is preventable, and therefore payment for services is withheld?
They’re concerns that are widespread among physicians, hospital administrators, and regulators alike.
“The legislation required the conditions to be ‘reasonably preventable’ using established clinical guidelines,” Dr. Straube says. “We did not have to show 100% prevention. In an imperfect world, they might still take place occasionally, but with good medical care, almost all of these are preventable in this day and age.”
For CMS, the preventable conditions are an either/or situation: Either they existed prior to admission and are subject to payment, or they did not exist at admission and additional payment for the complication will not be made. “HACs do not currently consider a patient’s individual risk for complications,” says Jennifer Meddings, MD, MSc, clinical lecturer and health researcher in the Department of Internal Medicine at the University of Michigan Health System in Ann Arbor. “We know the best strategies to prevent complications in ideal patients, and these are reflected in the HACs. In real life, many of our patients just don’t fit into the guidelines for many reasons—and you have to individualize care.”
Dr. Meddings points to DVT as a prime example. For a certain number of inpatients, the guidelines can be followed to perfection. In other patients (e.g., those with kidney conditions), previous reactions to a medication or an individual’s predisposition to clotting might interfere with treatment. However, CMS doesn’t allow appeals of nonpayment decisions for HACs based on individual circumstances.
Some experts think the rigidness of the payment policy forces physicians to treat patients exactly to guidelines. Even then, payment could be declined if an HAC develops.
“One of the points of most discussion is how preventable some of these are, particularly when choosing those you are no longer going to pay for,” Dr. Meddings says. “Many of the complications currently under review have patients that are at higher risk than others. How much our prevention strategies can alleviate or reduce the risk varies widely among patients.”
Impact on HM Practice
Many of the preventable conditions outlined by CMS do not directly affect hospitalist payment. However, hospitalists often find themselves responsible for properly documenting admission and care.
“The rule changes regarding payment for HACs are only related to hospital payments, and to date, most physicians, including hospitalists, are not directly at financial risk,” says Heidi Wald, MD, MSPH, hospitalist and assistant professor of medicine in the divisions of Health Care Policy Research and General Internal Medicine at the University of Colorado Denver School of Medicine. “Although hospitalists have no financial skin in the game, there are plenty of reasons they would take an interest in addressing HACs in their hospital. In particular, they are often seen as the ‘go-to’ group for quality improvement in their hospitals.”
For example, some HM groups have been active in working with teams of physicians, nurses, and other healthcare providers to address local policies and procedures on prevention of catheter-associated urinary tract infections (UTIs) and DVT.
“This has certainly necessitated a team approach,” says Shaun Frost, MD, FHM, an SHM board member and regional medical director for Cogent Healthcare in St. Paul, Minn. “For many of the HACs that apply to our population of patients, the hospitalist alone cannot be expected to solely execute effective quality improvements. It takes a team effort in that regard, and one that includes many different disciplines.”
The Cogent-affiliated hospitalist group at Temple University Hospital in Philadelphia formed a task force to address issues with catheter-associated UTI. One initiative focused on educating all providers involved in the proper care of the catheters and similar interventions. A secondary focus of the project was an inventory of current practices and procedures.
“It was discovered that we did not have an automatic stop order for Foley catheters, so in some situations, they were likely being left in longer than needed while nursing [staff] tried to contact a physician,” Dr. Frost explains. “We created standardized order sets that include criteria for continuing the catheter. Once the criteria are no longer applicable, nursing will be able to discontinue it.”
Although CMS has only recently turned the spotlight on HACs and never events, hospitalists have been heavily involved in the patient-safety arena for years. “It is not a new phenomenon that hospitalists work for healthcare delivery and healthcare system improvement,” Dr. Meddings says.
Hospital administration at Temple University Hospital recognized the HM group’s quality-improvement (QI) work, and has “specifically charged us with spreading the work we have done in patient safety to the entire house,” Dr. Frost says. “That speaks to the administration’s opinion of the power of the HM program to assist with institution-wide QI initiatives.”
Documentation Is Key
Beyond applying proven methods to avoid HACs, hospitalists can make a difference through documentation. If the hospitalist notes all conditions when the patient first presents to the hospital, additional comorbidity and complication payments should be made.
“The part that probably has the greatest impact on the day-to-day practice of a hospitalist is the increased importance of documentation throughout the hospital episode,” Dr. Meddings says. “If complications are occurring and they are not present in the chart, the coders may not recognize that it has occurred and will not know to include it in the bill. This can have an adverse impact on the hospital and its finances.”
Documentation issues can impact hospital payment in several ways:
- Hospitals might receive additional payment by default if certain HACs are described incorrectly or without sufficient detail (e.g., receiving overpayment because the physician did not indicate a UTI was in fact a catheter-associated UTI);
- As more attention is invested in documenting all conditions POA, hospitals might be coding more comorbidities overall than previously, which also will generate additional payment for hospitals as any POA condition is eligible for increased payment; and
- Hospitals might lose payment when admitting providers fail to adequately document the condition as POA (e.g., a pre-existing decubitus ulcer not detected until the second day of the hospital stay).
The descriptions to be used in coding are very detailed. UTIs, for example, have one code to document the POA assessment, another code to show that a UTI occurred, and a third code to indicate it was catheter-associated. Each code requires appropriate documentation in the chart (see Table 1, above).
The impact hospitalists have on care and payment is not the same across the HAC spectrum. For instance, documenting the presence of pressure ulcers might be easier than distinguishing colonization from infection in those admitted with in-dwelling urinary catheters. Others, such as DVT or vascular catheter-associated infections, are rarely POA unless they are part of the admitting diagnosis.
“This new focus on hospital-acquired conditions may work to the patient’s benefit,” Dr. Meddings says. “The inclusion of pressure ulcers has led to increased attention to skin exams on admission and preventive measures during hospitalizations. In the past, skin exams upon admission may have been given a lower priority, but that has changed.”
Dr. Meddings is concerned that the new rules could force the shifting of resources to areas where the hospital could lose money. If, when, and how many changes will actually take place is still up in the air. “Resource shifting is a concern whenever there is any sort of pay-for-performance attention directed toward one particular complication,” she says. “To balance this, many of the strategies hospitals used to prevent complications are not specific to just the diagnosis that is covered by the HAC.”
Dr. Meddings also hopes the new focus on preventable conditions will have a “halo effect” in the healthcare community. For instance, CMS mandating DVT prevention following orthopedic operations will, hopefully, result in a greater awareness of the problem in other susceptible patients.
POA Indicators
Since hospitalists often perform the initial patient history, physical, and other admission work, they are in the best position to find and document POA indicators (see Table 2, p. below). Proper notes on such things as UTIs present and the state of skin integrity are an important part of making sure the hospital is paid correctly for the care it provides.
Education on the specific definition of each potential HAC is required to help physicians avoid overtreatment of certain conditions, especially UTIs. For example, the Centers for Disease Control and Prevention (CDC) defines all UTIs as symptomatic. Therefore, the screening of all admitted patients, regardless of symptoms, is wasteful and unlikely to help the hospital’s bottom line.
“If you start screening everyone that comes through the door so you don’t miss any pre-existing UTIs, you are going to find a lot of asymptomatic colonization,” Dr. Wald says. “You are also going to spend a lot of money and time on studies and possibly treatments that may not yield many true infections. It is important that physicians know the definition of these HACs to help avoid needless interventions.”
Minimal Loss
Many hospital administrators and physicians were worried when the HAC program was first announced. Much of the stress and concern, however, seems to have dissipated. CMS estimated the HAC program would save Medicare $21 million in fiscal year 2009. Others, such as Peter McNair and colleagues writing in Health Affairs, suggest the actual impact is closer to $1.1 million.1 The CMS-projected impact of the HAC provision in fiscal-year 2009 was $21 million, out of more than $100 billion in payments.
“I think the HACs will not have a major impact because of the way payments are made,” says internist Robert Berenson, MD, a fellow at the Urban Institute in Washington, D.C., who has studied Medicare policy issues extensively, and for two years was in charge of Medicare payment policies at the Health Care Finance Administration, the precursor to CMS. “Patients who have HACs often have another comorbidity that would kick them into a higher payment category regardless of the presence of a hospital-acquired complication. In the end, it is probably more symbolic and unlikely to make a major dent in hospital income—at least at this point.”
Another limitation to CMS nonpayment for HACs is the issue of deciding which conditions are truly preventable. Dr. Berenson questions the ability of the current system to identify many additional complications for which this approach will be feasible.
“CMS has laid out its strategy, suggesting that we should be able to continue increasing the number of conditions for which providers would be paid differently based on quality,” he says. “Many observers question whether there will ever be measurement tools that are robust enough, and there will be a wide agreement on the preventability of enough conditions that this initiative will go very far.”
Although hospitalists might not face a direct financial risk, they still have their hospitals’ best interest—and their reputations—on the line. “Hospitalists care about preventing complications,” Dr. Wald says. “We are very engaged in working with our hospitals to improve care, maximize quality, and minimize cost.” TH
Kurt Ullman is a freelance medical writer based in Indiana.
Reference
- McNair PD, Luft HS, Bindman AB. Medicare’s policy not to pay for treating hospital-acquired conditions: the impact. Health Aff (Millwood). 2009;28(5):1485-1493.
TOP IMAGE SOURCE: KAREEM RIZKHALLA/ISTOCKPHOTO.COM
Hospitalist Neal Axon, MD, first became aware of an important change in his hospital’s policies last year while attending to an elderly patient the morning after admission to the community hospital where he works part time.
“This new form appeared in the chart requesting a urinalysis for my patient, who’d had a Foley catheter placed,” says Dr. Axon, an assistant professor of medicine at the Medical University of South Carolina in Charleston. “I didn’t know why, so I asked. I was told that it was now necessary to document that there was no UTI present on admission.” He asked the charge nurse, “So what do I do now that the catheter has been in place for 12 hours and has colonization without a true infection?”
The next thing he heard: silence.
The new form Dr. Axon encountered was an outgrowth of the requirements of the Deficit Reduction Act (DRA) of 2005, which ordered Medicare to withhold additional hospital payments for hospital-acquired complications (HAC) developed during a hospital stay. One result of the new rule is that much of a hospital’s response to these initiatives has been placed in the hands of the hospitalist. From accurate documentation of complications already present on admission (POA), to confirming that guidelines for treatment are being followed, to taking the lead on review of staff practices and education, hospitalists are in a position to have a wide-ranging impact on patient care and the financial health of their institutions.
Congress Pushes Reforms
In order for Medicare to not provide a reimbursement, an HAC has to be high-cost and/or high-volume, result in the assignment of the case to a higher payment when present as a secondary diagnosis, and “could reasonably be prevented through the application of evidence-based guidelines,” says Barry Straube, MD, chief medical officer and director of the Office of Clinical Standards and Quality at the Centers for Medicare and Medicaid Services (CMS). “CMS was to implement a process where we would not pay the hospitals additional money for these complications.”
The new rules mean Medicare pays hospitals on the basis of Medicare Severity Diagnostic-Related Groups (MS-DRG), which better reflect the complexity of a patient’s illness. The biggest change was a three-tiered payment schedule: a base level for the diagnosis, a second level adding money to reflect the presence of comorbidities and complications, and a third for major complications and comorbidities (see Table 1, p. 31).
“Instituting HACs means that hospitals would no longer receive the comorbidity and complication payments if the only reason a case qualified for higher payment was the HAC,” Dr. Straube explains. “We did carve out a POA exception for those conditions that were acquired outside of the hospital. HACs only impact additional payments; the hospitals are still paid for the diagnosis that resulted in the hospital admission.”
CMS also identifies three “never events” it won’t reimburse for (see “A Brief History of Never Events,” p. 35): performing the wrong procedure, performing a procedure on the wrong body part, and performing a procedure on the wrong patient. “Neither hospitals nor physicians that are involved in such egregious situations would be paid,” Dr. Straube says.
Preventability: Subject of Controversy
The big questions surrounding HACs: Could they reasonably be prevented through the application of evidence-based guidelines? How preventable are HACs? Who decides if a complication is preventable, and therefore payment for services is withheld?
They’re concerns that are widespread among physicians, hospital administrators, and regulators alike.
“The legislation required the conditions to be ‘reasonably preventable’ using established clinical guidelines,” Dr. Straube says. “We did not have to show 100% prevention. In an imperfect world, they might still take place occasionally, but with good medical care, almost all of these are preventable in this day and age.”
For CMS, the preventable conditions are an either/or situation: Either they existed prior to admission and are subject to payment, or they did not exist at admission and additional payment for the complication will not be made. “HACs do not currently consider a patient’s individual risk for complications,” says Jennifer Meddings, MD, MSc, clinical lecturer and health researcher in the Department of Internal Medicine at the University of Michigan Health System in Ann Arbor. “We know the best strategies to prevent complications in ideal patients, and these are reflected in the HACs. In real life, many of our patients just don’t fit into the guidelines for many reasons—and you have to individualize care.”
Dr. Meddings points to DVT as a prime example. For a certain number of inpatients, the guidelines can be followed to perfection. In other patients (e.g., those with kidney conditions), previous reactions to a medication or an individual’s predisposition to clotting might interfere with treatment. However, CMS doesn’t allow appeals of nonpayment decisions for HACs based on individual circumstances.
Some experts think the rigidness of the payment policy forces physicians to treat patients exactly to guidelines. Even then, payment could be declined if an HAC develops.
“One of the points of most discussion is how preventable some of these are, particularly when choosing those you are no longer going to pay for,” Dr. Meddings says. “Many of the complications currently under review have patients that are at higher risk than others. How much our prevention strategies can alleviate or reduce the risk varies widely among patients.”
Impact on HM Practice
Many of the preventable conditions outlined by CMS do not directly affect hospitalist payment. However, hospitalists often find themselves responsible for properly documenting admission and care.
“The rule changes regarding payment for HACs are only related to hospital payments, and to date, most physicians, including hospitalists, are not directly at financial risk,” says Heidi Wald, MD, MSPH, hospitalist and assistant professor of medicine in the divisions of Health Care Policy Research and General Internal Medicine at the University of Colorado Denver School of Medicine. “Although hospitalists have no financial skin in the game, there are plenty of reasons they would take an interest in addressing HACs in their hospital. In particular, they are often seen as the ‘go-to’ group for quality improvement in their hospitals.”
For example, some HM groups have been active in working with teams of physicians, nurses, and other healthcare providers to address local policies and procedures on prevention of catheter-associated urinary tract infections (UTIs) and DVT.
“This has certainly necessitated a team approach,” says Shaun Frost, MD, FHM, an SHM board member and regional medical director for Cogent Healthcare in St. Paul, Minn. “For many of the HACs that apply to our population of patients, the hospitalist alone cannot be expected to solely execute effective quality improvements. It takes a team effort in that regard, and one that includes many different disciplines.”
The Cogent-affiliated hospitalist group at Temple University Hospital in Philadelphia formed a task force to address issues with catheter-associated UTI. One initiative focused on educating all providers involved in the proper care of the catheters and similar interventions. A secondary focus of the project was an inventory of current practices and procedures.
“It was discovered that we did not have an automatic stop order for Foley catheters, so in some situations, they were likely being left in longer than needed while nursing [staff] tried to contact a physician,” Dr. Frost explains. “We created standardized order sets that include criteria for continuing the catheter. Once the criteria are no longer applicable, nursing will be able to discontinue it.”
Although CMS has only recently turned the spotlight on HACs and never events, hospitalists have been heavily involved in the patient-safety arena for years. “It is not a new phenomenon that hospitalists work for healthcare delivery and healthcare system improvement,” Dr. Meddings says.
Hospital administration at Temple University Hospital recognized the HM group’s quality-improvement (QI) work, and has “specifically charged us with spreading the work we have done in patient safety to the entire house,” Dr. Frost says. “That speaks to the administration’s opinion of the power of the HM program to assist with institution-wide QI initiatives.”
Documentation Is Key
Beyond applying proven methods to avoid HACs, hospitalists can make a difference through documentation. If the hospitalist notes all conditions when the patient first presents to the hospital, additional comorbidity and complication payments should be made.
“The part that probably has the greatest impact on the day-to-day practice of a hospitalist is the increased importance of documentation throughout the hospital episode,” Dr. Meddings says. “If complications are occurring and they are not present in the chart, the coders may not recognize that it has occurred and will not know to include it in the bill. This can have an adverse impact on the hospital and its finances.”
Documentation issues can impact hospital payment in several ways:
- Hospitals might receive additional payment by default if certain HACs are described incorrectly or without sufficient detail (e.g., receiving overpayment because the physician did not indicate a UTI was in fact a catheter-associated UTI);
- As more attention is invested in documenting all conditions POA, hospitals might be coding more comorbidities overall than previously, which also will generate additional payment for hospitals as any POA condition is eligible for increased payment; and
- Hospitals might lose payment when admitting providers fail to adequately document the condition as POA (e.g., a pre-existing decubitus ulcer not detected until the second day of the hospital stay).
The descriptions to be used in coding are very detailed. UTIs, for example, have one code to document the POA assessment, another code to show that a UTI occurred, and a third code to indicate it was catheter-associated. Each code requires appropriate documentation in the chart (see Table 1, above).
The impact hospitalists have on care and payment is not the same across the HAC spectrum. For instance, documenting the presence of pressure ulcers might be easier than distinguishing colonization from infection in those admitted with in-dwelling urinary catheters. Others, such as DVT or vascular catheter-associated infections, are rarely POA unless they are part of the admitting diagnosis.
“This new focus on hospital-acquired conditions may work to the patient’s benefit,” Dr. Meddings says. “The inclusion of pressure ulcers has led to increased attention to skin exams on admission and preventive measures during hospitalizations. In the past, skin exams upon admission may have been given a lower priority, but that has changed.”
Dr. Meddings is concerned that the new rules could force the shifting of resources to areas where the hospital could lose money. If, when, and how many changes will actually take place is still up in the air. “Resource shifting is a concern whenever there is any sort of pay-for-performance attention directed toward one particular complication,” she says. “To balance this, many of the strategies hospitals used to prevent complications are not specific to just the diagnosis that is covered by the HAC.”
Dr. Meddings also hopes the new focus on preventable conditions will have a “halo effect” in the healthcare community. For instance, CMS mandating DVT prevention following orthopedic operations will, hopefully, result in a greater awareness of the problem in other susceptible patients.
POA Indicators
Since hospitalists often perform the initial patient history, physical, and other admission work, they are in the best position to find and document POA indicators (see Table 2, p. below). Proper notes on such things as UTIs present and the state of skin integrity are an important part of making sure the hospital is paid correctly for the care it provides.
Education on the specific definition of each potential HAC is required to help physicians avoid overtreatment of certain conditions, especially UTIs. For example, the Centers for Disease Control and Prevention (CDC) defines all UTIs as symptomatic. Therefore, the screening of all admitted patients, regardless of symptoms, is wasteful and unlikely to help the hospital’s bottom line.
“If you start screening everyone that comes through the door so you don’t miss any pre-existing UTIs, you are going to find a lot of asymptomatic colonization,” Dr. Wald says. “You are also going to spend a lot of money and time on studies and possibly treatments that may not yield many true infections. It is important that physicians know the definition of these HACs to help avoid needless interventions.”
Minimal Loss
Many hospital administrators and physicians were worried when the HAC program was first announced. Much of the stress and concern, however, seems to have dissipated. CMS estimated the HAC program would save Medicare $21 million in fiscal year 2009. Others, such as Peter McNair and colleagues writing in Health Affairs, suggest the actual impact is closer to $1.1 million.1 The CMS-projected impact of the HAC provision in fiscal-year 2009 was $21 million, out of more than $100 billion in payments.
“I think the HACs will not have a major impact because of the way payments are made,” says internist Robert Berenson, MD, a fellow at the Urban Institute in Washington, D.C., who has studied Medicare policy issues extensively, and for two years was in charge of Medicare payment policies at the Health Care Finance Administration, the precursor to CMS. “Patients who have HACs often have another comorbidity that would kick them into a higher payment category regardless of the presence of a hospital-acquired complication. In the end, it is probably more symbolic and unlikely to make a major dent in hospital income—at least at this point.”
Another limitation to CMS nonpayment for HACs is the issue of deciding which conditions are truly preventable. Dr. Berenson questions the ability of the current system to identify many additional complications for which this approach will be feasible.
“CMS has laid out its strategy, suggesting that we should be able to continue increasing the number of conditions for which providers would be paid differently based on quality,” he says. “Many observers question whether there will ever be measurement tools that are robust enough, and there will be a wide agreement on the preventability of enough conditions that this initiative will go very far.”
Although hospitalists might not face a direct financial risk, they still have their hospitals’ best interest—and their reputations—on the line. “Hospitalists care about preventing complications,” Dr. Wald says. “We are very engaged in working with our hospitals to improve care, maximize quality, and minimize cost.” TH
Kurt Ullman is a freelance medical writer based in Indiana.
Reference
- McNair PD, Luft HS, Bindman AB. Medicare’s policy not to pay for treating hospital-acquired conditions: the impact. Health Aff (Millwood). 2009;28(5):1485-1493.
TOP IMAGE SOURCE: KAREEM RIZKHALLA/ISTOCKPHOTO.COM
Obama Releases 2011 Budget Requests for Federal Health
Petzel Sworn In as VA Under Secretary for Health
The Year Ahead
Rising pressure to contain healthcare costs, increasing demands for safety and quality improvement, more focus on institutional accountability: In 2010, healthcare experts expect several dominant themes to continue converging and moving hospitalists even more to the center of key policy debates.
Peter Pronovost, MD, PhD, medical director of the Center for Innovation in Quality Patient Care and director of the Quality and Safety Research Group at Johns Hopkins University in Baltimore, sees three big themes moving to the fore. One is a greater focus on outcome measurements and accountability for performance, and he expects both carrots and sticks to be wielded. “So, both payment reform and social humiliation, or making things public,” Dr. Pronovost says. “Two, I see a lot more focus on measures that are population-based rather than hospital-based, so looking more at episodes of care.” The shift will force hospitalists to expand their purview beyond the hospital and, he says, partner more with community physicians to develop and monitor performance in such areas as transitions of care and general benchmarks of care.
Dr. Pronovost also expects “significant pressure on both the provider organization and individual clinician being paid less for what they do.” Finding ways to minimize costs will be a priority as payors increase scrutiny on expenses like unnecessary hospital readmissions. But hospitalists, he says, are better positioned than many other physicians to play a key role in the drive toward efficiency while also improving healthcare quality and safety. “I think hospitalists’ roles are going to go up dramatically,” Dr. Pronovost adds, “and I hope the field responds by making sure they put out people who have the skills to lead.”
End-of-Life Issues
Nancy Berlinger, PhD, deputy director and research scholar at The Hastings Center in Garrison, N.Y., cites end-of-life care as another theme likely to gain traction in 2010. As project director of the center’s revised ethical guidelines for end-of-life care, Dr. Berlinger notes how often clinicians in her working group have invoked the hospitalist profession. It’s no accident. “Hospitalists are increasingly associated with the care of patients on Medicare,” she says, adding Medicare beneficiaries are far more likely to be nearing the end of life.
Demographics suggest that connection will continue to grow in 2010 and beyond. Dr. Berlinger points to a 2009 New England Journal of Medicine study showing that the odds of a hospitalized Medicare patient receiving care from a hospitalist increased at a brisk 29.2% annual clip from 1997 through 2006.1 And while the U.S. faces a shortage of geriatricians, HM is growing rapidly as a medical profession. “By default, whether or not hospitalists self-identify as caring for older Americans,” Dr. Berlinger says, “this is their area of practical specialization.”
With that specialization comes added responsibility to assist with advanced-care planning and helping patients to document their wishes. Similarly, she says, it means acknowledging that these patients are more likely to have comorbid conditions and identify with goals of care. “I don’t think there’s any way around this,” she says. “Medicare and hospitalists, whether by accident or design, are increasingly joined at the hip. That is something that hospitalists, as a profession, will always need to keep their eye on.”
A parallel trend is that other doctors increasingly view hospitalists as hospital specialists. “The hospitalist’s responsibilities are not just in terms of the patients they care for, but also in terms of the institution itself,” Dr. Berlinger says. Non-staff physicians, for example, expect hospitalists to know how a hospital’s in-patient care system works. Practically speaking, as electronic medical records (EMR) become more commonplace, hospitalists will be increasingly relied upon to understand a hospital’s information technology.
—Peter Pronovost, MD, PhD, medical director, Center for Innovation in Quality Patient Care, Johns Hopkins University, Baltimore
New Economy, New Hospital Landscape
Douglas Wood, MD, chair of the Division of Health Care Policy and Research at the Mayo Clinic in Rochester, Minn., points to language in the federal healthcare reform legislation as evidence that hospitals and hospitalists will need to be in sync in other ways to avoid future penalties. One provision, for example, would increase the penalties for hospital-acquired infections. Other language seeks to reduce unnecessary readmissions.
Likewise, Dr. Wood says, addressing geographical variations in healthcare payments driven largely by unnecessary overutilization—including excessive use of ICU care, in-patient care, imaging, and specialist services—might mean asking hospitalists to take on more aspects of patient care.
Meanwhile, increased interest in demonstration projects that might achieve savings (e.g., accountable care organizations and bundled payments) suggests that proactive hospitals should again look to hospitalists. The flurry of new proposals won’t fundamentally change hospitalists’ responsibilities to provide effective and efficient care, “but it will put more emphasis on what they’re doing,” Dr. Wood says, “to the degree that hospitalists could take a lead in demonstrating how you can provide better outcomes at a lower overall utilization of resources.”
Regardless of how slowly or quickly these initiatives proceed at the national level, he says, hospitalists should be mindful that several states are well ahead of the curve and are likely to be more aggressive in instituting policy changes.
The Bottom Line
If there’s a single, overriding theme for 2010, Bradley Flansbaum, DO, MPH, FACP, FHM, director of hospitalist services at Lenox Hill Hospital in New York City and a member of SHM’s Public Policy Committee, says it might be that of dealing with the unknown. Squeezing healthcare costs and more tightly regulating inflation will have a greater effect on a hospital’s bottom line and thus impact what’s required of hospitalists. Even so, the profession will have to wait and see whether and how various proposals are codified and implemented. “We don’t know exactly what things are going to look like,” he says.
Nor is there a good sense of how new standards for transparency, quality, and accountability might be measured. “While people want more measurement and they want more report-card-type information, the data that we can acquire right now and how we analyze that data are still fairly primitive,” Dr. Flansbaum says. Even current benchmarks are lacking in how to determine who’s doing a good job and who isn’t, he says.
One big question that must be answered, then: Are we even looking at the right measurements? “Or, do the right measurements exist, or do we have the databases, the registries, the sources, to make the decisions we need to make?” he says.
Any new proposals will require another round of such questions and filling-in of blanks to add workable details to vague and potentially confusing language.
“I think we know that change is afoot, and most smart hospitalists know that the system needs to run leaner,” Dr. Flansbaum says. “But how each one of us is going to function in our hospital, and the kinds of demands that will be placed on us, and what we’re going to need to do with the doctors in the community and the other nonphysician colleagues that we work with, is all really unknown.” TH
Bryn Nelson is a freelance medical writer based in Seattle.
Reference
- Kuo YF, Sharma G, Freeman JL, Goodwin JS. Growth in the care of older patients by hospitalists in the United States. N Engl J Med. 2009;360(11): 1102-1112.
Image Source: PAGADESIGN, OVERSNAP/ISTOCKPHOTO.COM
Rising pressure to contain healthcare costs, increasing demands for safety and quality improvement, more focus on institutional accountability: In 2010, healthcare experts expect several dominant themes to continue converging and moving hospitalists even more to the center of key policy debates.
Peter Pronovost, MD, PhD, medical director of the Center for Innovation in Quality Patient Care and director of the Quality and Safety Research Group at Johns Hopkins University in Baltimore, sees three big themes moving to the fore. One is a greater focus on outcome measurements and accountability for performance, and he expects both carrots and sticks to be wielded. “So, both payment reform and social humiliation, or making things public,” Dr. Pronovost says. “Two, I see a lot more focus on measures that are population-based rather than hospital-based, so looking more at episodes of care.” The shift will force hospitalists to expand their purview beyond the hospital and, he says, partner more with community physicians to develop and monitor performance in such areas as transitions of care and general benchmarks of care.
Dr. Pronovost also expects “significant pressure on both the provider organization and individual clinician being paid less for what they do.” Finding ways to minimize costs will be a priority as payors increase scrutiny on expenses like unnecessary hospital readmissions. But hospitalists, he says, are better positioned than many other physicians to play a key role in the drive toward efficiency while also improving healthcare quality and safety. “I think hospitalists’ roles are going to go up dramatically,” Dr. Pronovost adds, “and I hope the field responds by making sure they put out people who have the skills to lead.”
End-of-Life Issues
Nancy Berlinger, PhD, deputy director and research scholar at The Hastings Center in Garrison, N.Y., cites end-of-life care as another theme likely to gain traction in 2010. As project director of the center’s revised ethical guidelines for end-of-life care, Dr. Berlinger notes how often clinicians in her working group have invoked the hospitalist profession. It’s no accident. “Hospitalists are increasingly associated with the care of patients on Medicare,” she says, adding Medicare beneficiaries are far more likely to be nearing the end of life.
Demographics suggest that connection will continue to grow in 2010 and beyond. Dr. Berlinger points to a 2009 New England Journal of Medicine study showing that the odds of a hospitalized Medicare patient receiving care from a hospitalist increased at a brisk 29.2% annual clip from 1997 through 2006.1 And while the U.S. faces a shortage of geriatricians, HM is growing rapidly as a medical profession. “By default, whether or not hospitalists self-identify as caring for older Americans,” Dr. Berlinger says, “this is their area of practical specialization.”
With that specialization comes added responsibility to assist with advanced-care planning and helping patients to document their wishes. Similarly, she says, it means acknowledging that these patients are more likely to have comorbid conditions and identify with goals of care. “I don’t think there’s any way around this,” she says. “Medicare and hospitalists, whether by accident or design, are increasingly joined at the hip. That is something that hospitalists, as a profession, will always need to keep their eye on.”
A parallel trend is that other doctors increasingly view hospitalists as hospital specialists. “The hospitalist’s responsibilities are not just in terms of the patients they care for, but also in terms of the institution itself,” Dr. Berlinger says. Non-staff physicians, for example, expect hospitalists to know how a hospital’s in-patient care system works. Practically speaking, as electronic medical records (EMR) become more commonplace, hospitalists will be increasingly relied upon to understand a hospital’s information technology.
—Peter Pronovost, MD, PhD, medical director, Center for Innovation in Quality Patient Care, Johns Hopkins University, Baltimore
New Economy, New Hospital Landscape
Douglas Wood, MD, chair of the Division of Health Care Policy and Research at the Mayo Clinic in Rochester, Minn., points to language in the federal healthcare reform legislation as evidence that hospitals and hospitalists will need to be in sync in other ways to avoid future penalties. One provision, for example, would increase the penalties for hospital-acquired infections. Other language seeks to reduce unnecessary readmissions.
Likewise, Dr. Wood says, addressing geographical variations in healthcare payments driven largely by unnecessary overutilization—including excessive use of ICU care, in-patient care, imaging, and specialist services—might mean asking hospitalists to take on more aspects of patient care.
Meanwhile, increased interest in demonstration projects that might achieve savings (e.g., accountable care organizations and bundled payments) suggests that proactive hospitals should again look to hospitalists. The flurry of new proposals won’t fundamentally change hospitalists’ responsibilities to provide effective and efficient care, “but it will put more emphasis on what they’re doing,” Dr. Wood says, “to the degree that hospitalists could take a lead in demonstrating how you can provide better outcomes at a lower overall utilization of resources.”
Regardless of how slowly or quickly these initiatives proceed at the national level, he says, hospitalists should be mindful that several states are well ahead of the curve and are likely to be more aggressive in instituting policy changes.
The Bottom Line
If there’s a single, overriding theme for 2010, Bradley Flansbaum, DO, MPH, FACP, FHM, director of hospitalist services at Lenox Hill Hospital in New York City and a member of SHM’s Public Policy Committee, says it might be that of dealing with the unknown. Squeezing healthcare costs and more tightly regulating inflation will have a greater effect on a hospital’s bottom line and thus impact what’s required of hospitalists. Even so, the profession will have to wait and see whether and how various proposals are codified and implemented. “We don’t know exactly what things are going to look like,” he says.
Nor is there a good sense of how new standards for transparency, quality, and accountability might be measured. “While people want more measurement and they want more report-card-type information, the data that we can acquire right now and how we analyze that data are still fairly primitive,” Dr. Flansbaum says. Even current benchmarks are lacking in how to determine who’s doing a good job and who isn’t, he says.
One big question that must be answered, then: Are we even looking at the right measurements? “Or, do the right measurements exist, or do we have the databases, the registries, the sources, to make the decisions we need to make?” he says.
Any new proposals will require another round of such questions and filling-in of blanks to add workable details to vague and potentially confusing language.
“I think we know that change is afoot, and most smart hospitalists know that the system needs to run leaner,” Dr. Flansbaum says. “But how each one of us is going to function in our hospital, and the kinds of demands that will be placed on us, and what we’re going to need to do with the doctors in the community and the other nonphysician colleagues that we work with, is all really unknown.” TH
Bryn Nelson is a freelance medical writer based in Seattle.
Reference
- Kuo YF, Sharma G, Freeman JL, Goodwin JS. Growth in the care of older patients by hospitalists in the United States. N Engl J Med. 2009;360(11): 1102-1112.
Image Source: PAGADESIGN, OVERSNAP/ISTOCKPHOTO.COM
Rising pressure to contain healthcare costs, increasing demands for safety and quality improvement, more focus on institutional accountability: In 2010, healthcare experts expect several dominant themes to continue converging and moving hospitalists even more to the center of key policy debates.
Peter Pronovost, MD, PhD, medical director of the Center for Innovation in Quality Patient Care and director of the Quality and Safety Research Group at Johns Hopkins University in Baltimore, sees three big themes moving to the fore. One is a greater focus on outcome measurements and accountability for performance, and he expects both carrots and sticks to be wielded. “So, both payment reform and social humiliation, or making things public,” Dr. Pronovost says. “Two, I see a lot more focus on measures that are population-based rather than hospital-based, so looking more at episodes of care.” The shift will force hospitalists to expand their purview beyond the hospital and, he says, partner more with community physicians to develop and monitor performance in such areas as transitions of care and general benchmarks of care.
Dr. Pronovost also expects “significant pressure on both the provider organization and individual clinician being paid less for what they do.” Finding ways to minimize costs will be a priority as payors increase scrutiny on expenses like unnecessary hospital readmissions. But hospitalists, he says, are better positioned than many other physicians to play a key role in the drive toward efficiency while also improving healthcare quality and safety. “I think hospitalists’ roles are going to go up dramatically,” Dr. Pronovost adds, “and I hope the field responds by making sure they put out people who have the skills to lead.”
End-of-Life Issues
Nancy Berlinger, PhD, deputy director and research scholar at The Hastings Center in Garrison, N.Y., cites end-of-life care as another theme likely to gain traction in 2010. As project director of the center’s revised ethical guidelines for end-of-life care, Dr. Berlinger notes how often clinicians in her working group have invoked the hospitalist profession. It’s no accident. “Hospitalists are increasingly associated with the care of patients on Medicare,” she says, adding Medicare beneficiaries are far more likely to be nearing the end of life.
Demographics suggest that connection will continue to grow in 2010 and beyond. Dr. Berlinger points to a 2009 New England Journal of Medicine study showing that the odds of a hospitalized Medicare patient receiving care from a hospitalist increased at a brisk 29.2% annual clip from 1997 through 2006.1 And while the U.S. faces a shortage of geriatricians, HM is growing rapidly as a medical profession. “By default, whether or not hospitalists self-identify as caring for older Americans,” Dr. Berlinger says, “this is their area of practical specialization.”
With that specialization comes added responsibility to assist with advanced-care planning and helping patients to document their wishes. Similarly, she says, it means acknowledging that these patients are more likely to have comorbid conditions and identify with goals of care. “I don’t think there’s any way around this,” she says. “Medicare and hospitalists, whether by accident or design, are increasingly joined at the hip. That is something that hospitalists, as a profession, will always need to keep their eye on.”
A parallel trend is that other doctors increasingly view hospitalists as hospital specialists. “The hospitalist’s responsibilities are not just in terms of the patients they care for, but also in terms of the institution itself,” Dr. Berlinger says. Non-staff physicians, for example, expect hospitalists to know how a hospital’s in-patient care system works. Practically speaking, as electronic medical records (EMR) become more commonplace, hospitalists will be increasingly relied upon to understand a hospital’s information technology.
—Peter Pronovost, MD, PhD, medical director, Center for Innovation in Quality Patient Care, Johns Hopkins University, Baltimore
New Economy, New Hospital Landscape
Douglas Wood, MD, chair of the Division of Health Care Policy and Research at the Mayo Clinic in Rochester, Minn., points to language in the federal healthcare reform legislation as evidence that hospitals and hospitalists will need to be in sync in other ways to avoid future penalties. One provision, for example, would increase the penalties for hospital-acquired infections. Other language seeks to reduce unnecessary readmissions.
Likewise, Dr. Wood says, addressing geographical variations in healthcare payments driven largely by unnecessary overutilization—including excessive use of ICU care, in-patient care, imaging, and specialist services—might mean asking hospitalists to take on more aspects of patient care.
Meanwhile, increased interest in demonstration projects that might achieve savings (e.g., accountable care organizations and bundled payments) suggests that proactive hospitals should again look to hospitalists. The flurry of new proposals won’t fundamentally change hospitalists’ responsibilities to provide effective and efficient care, “but it will put more emphasis on what they’re doing,” Dr. Wood says, “to the degree that hospitalists could take a lead in demonstrating how you can provide better outcomes at a lower overall utilization of resources.”
Regardless of how slowly or quickly these initiatives proceed at the national level, he says, hospitalists should be mindful that several states are well ahead of the curve and are likely to be more aggressive in instituting policy changes.
The Bottom Line
If there’s a single, overriding theme for 2010, Bradley Flansbaum, DO, MPH, FACP, FHM, director of hospitalist services at Lenox Hill Hospital in New York City and a member of SHM’s Public Policy Committee, says it might be that of dealing with the unknown. Squeezing healthcare costs and more tightly regulating inflation will have a greater effect on a hospital’s bottom line and thus impact what’s required of hospitalists. Even so, the profession will have to wait and see whether and how various proposals are codified and implemented. “We don’t know exactly what things are going to look like,” he says.
Nor is there a good sense of how new standards for transparency, quality, and accountability might be measured. “While people want more measurement and they want more report-card-type information, the data that we can acquire right now and how we analyze that data are still fairly primitive,” Dr. Flansbaum says. Even current benchmarks are lacking in how to determine who’s doing a good job and who isn’t, he says.
One big question that must be answered, then: Are we even looking at the right measurements? “Or, do the right measurements exist, or do we have the databases, the registries, the sources, to make the decisions we need to make?” he says.
Any new proposals will require another round of such questions and filling-in of blanks to add workable details to vague and potentially confusing language.
“I think we know that change is afoot, and most smart hospitalists know that the system needs to run leaner,” Dr. Flansbaum says. “But how each one of us is going to function in our hospital, and the kinds of demands that will be placed on us, and what we’re going to need to do with the doctors in the community and the other nonphysician colleagues that we work with, is all really unknown.” TH
Bryn Nelson is a freelance medical writer based in Seattle.
Reference
- Kuo YF, Sharma G, Freeman JL, Goodwin JS. Growth in the care of older patients by hospitalists in the United States. N Engl J Med. 2009;360(11): 1102-1112.
Image Source: PAGADESIGN, OVERSNAP/ISTOCKPHOTO.COM
DoD Releases Data on Sexual Assault and Harassment at Military Academies
VA and Kaiser Permanente Launch Medical Data Exchange Program
Necessary Evil: Change

The amount and complexity of medical knowledge we need to keep up with is changing and growing at a remarkable rate. I was trained in an era in which it was taken as a given that congestive heart failure patients should not receive beta-blockers; now it is a big mistake if we don’t prescribe them in most cases. But even before starting medical school, most of us realize that things will change a lot, and many of us see that as a good thing. It keeps our work interesting. Just recently, our hospital had a guest speaker who talked about potential medical applications of nanotechnology. It was way over my head, but it sounded pretty cool.
While I was prepared for ongoing changes in medical knowledge, I failed to anticipate how quickly the business of medicine would change during my career. I think the need to keep up with ever-increasing financial and regulatory issues siphons a lot of time and energy that could be used to keep up with the medical knowledge base. I wasn’t prepared for this when I started my career.
Because it is the start of a new year, I thought I would highlight one issue related to CPT coding: Medicare stopped recognizing consult codes as of Jan. 1 (see “Consultation Elimination,” p. 31).
What It Means for Hospitalists
The good news is that we can just use initial hospital visit codes, inpatient or observation, for all new visits. For example, it won’t matter anymore whether I’m admitting and serving as attending for a patient, or whether a surgeon admitted the patient and asked me to consult for preoperative medical evaluation (“clearance”). I should use the same CPT code in either situation, simply appending a modifier if I’m the admitting physician. And for billing purposes, we won’t have to worry about documenting which doctor requested that we see the patient, though it is a good idea to document it as part of the clinical record anyway.
But it gets a little more complicated. The codes aren’t going away or being removed from the CPT “bible” published by the American Medical Association (AMA). Instead, Medicare simply won’t recognize them anymore. Other payors probably will follow suit within a few months, but that isn’t certain. So it is possible that when asked by a surgeon to provide a preoperative evaluation, you will need to bill an initial hospital (or office or nursing facility) care visit if the patient is on Medicare but bill a consult code if the patient has other insurance. You should check with your billers to ensure you’re doing this correctly.
Medicare-paid consults are at a slightly higher rate than the equivalent service billed as initial hospital care (e.g., when the hospitalist is attending). So a higher reimbursing code has been replaced with one that pays a little less. For example, a 99253 consultation code requires a detailed history, detailed examination, and medical decision-making of low complexity; last year, 99253 was reimbursed by Medicare at an average rate of $114.69. The equivalent admission code for a detailed history, detailed examination, and low-complexity medical decision-making is a 99221 code, for which Medicare pays about $99.90. This represents a difference of about 14%.
However, the net financial impact of this change probably will be positive for most HM groups because you probably bill very few initial consult codes, and instead were stuck billing a follow-up visit code when seeing co-management “consults” (i.e., a patient admitted by a surgeon who asks you to follow and manage diabetes and other medical issues). Now, at least in the case of Medicare, it is appropriate for us to bill an initial hospital visit code, which provides significantly higher reimbursement than follow-up codes.
In addition, there is a modest (about 0.3%) proposed increase in work relative value units attached to the initial hospital visit codes, which will benefit us not only when we’re consulting, but also when we admit and serve as a patient’s attending.
Some specialists may be less interested in consulting on our patients because the initial visit codes will reimburse a little less than similar consultation codes. I don’t anticipate this will be a significant problem for most of us, particularly since many specialists bill the highest level of consultation code (99255), which pays about the same as the equivalent admission code (99223).
Although I think elimination of the use of consultation codes seems like a reasonable step toward simplifying how hospitalists bill for our services, keeping up with these frequent coding changes requires a high level of diligence on our part, and on the part of our administrative and clerical staffs. And it consumes time and resources that I—and my team—could better spend keeping up with changes in clinical practice.
Perhaps when all the dust settles around the healthcare reform debate, we will begin to move toward new, more creative payment models that will allow us to focus on what we do best. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is cofounder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is also course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
The amount and complexity of medical knowledge we need to keep up with is changing and growing at a remarkable rate. I was trained in an era in which it was taken as a given that congestive heart failure patients should not receive beta-blockers; now it is a big mistake if we don’t prescribe them in most cases. But even before starting medical school, most of us realize that things will change a lot, and many of us see that as a good thing. It keeps our work interesting. Just recently, our hospital had a guest speaker who talked about potential medical applications of nanotechnology. It was way over my head, but it sounded pretty cool.
While I was prepared for ongoing changes in medical knowledge, I failed to anticipate how quickly the business of medicine would change during my career. I think the need to keep up with ever-increasing financial and regulatory issues siphons a lot of time and energy that could be used to keep up with the medical knowledge base. I wasn’t prepared for this when I started my career.
Because it is the start of a new year, I thought I would highlight one issue related to CPT coding: Medicare stopped recognizing consult codes as of Jan. 1 (see “Consultation Elimination,” p. 31).
What It Means for Hospitalists
The good news is that we can just use initial hospital visit codes, inpatient or observation, for all new visits. For example, it won’t matter anymore whether I’m admitting and serving as attending for a patient, or whether a surgeon admitted the patient and asked me to consult for preoperative medical evaluation (“clearance”). I should use the same CPT code in either situation, simply appending a modifier if I’m the admitting physician. And for billing purposes, we won’t have to worry about documenting which doctor requested that we see the patient, though it is a good idea to document it as part of the clinical record anyway.
But it gets a little more complicated. The codes aren’t going away or being removed from the CPT “bible” published by the American Medical Association (AMA). Instead, Medicare simply won’t recognize them anymore. Other payors probably will follow suit within a few months, but that isn’t certain. So it is possible that when asked by a surgeon to provide a preoperative evaluation, you will need to bill an initial hospital (or office or nursing facility) care visit if the patient is on Medicare but bill a consult code if the patient has other insurance. You should check with your billers to ensure you’re doing this correctly.
Medicare-paid consults are at a slightly higher rate than the equivalent service billed as initial hospital care (e.g., when the hospitalist is attending). So a higher reimbursing code has been replaced with one that pays a little less. For example, a 99253 consultation code requires a detailed history, detailed examination, and medical decision-making of low complexity; last year, 99253 was reimbursed by Medicare at an average rate of $114.69. The equivalent admission code for a detailed history, detailed examination, and low-complexity medical decision-making is a 99221 code, for which Medicare pays about $99.90. This represents a difference of about 14%.
However, the net financial impact of this change probably will be positive for most HM groups because you probably bill very few initial consult codes, and instead were stuck billing a follow-up visit code when seeing co-management “consults” (i.e., a patient admitted by a surgeon who asks you to follow and manage diabetes and other medical issues). Now, at least in the case of Medicare, it is appropriate for us to bill an initial hospital visit code, which provides significantly higher reimbursement than follow-up codes.
In addition, there is a modest (about 0.3%) proposed increase in work relative value units attached to the initial hospital visit codes, which will benefit us not only when we’re consulting, but also when we admit and serve as a patient’s attending.
Some specialists may be less interested in consulting on our patients because the initial visit codes will reimburse a little less than similar consultation codes. I don’t anticipate this will be a significant problem for most of us, particularly since many specialists bill the highest level of consultation code (99255), which pays about the same as the equivalent admission code (99223).
Although I think elimination of the use of consultation codes seems like a reasonable step toward simplifying how hospitalists bill for our services, keeping up with these frequent coding changes requires a high level of diligence on our part, and on the part of our administrative and clerical staffs. And it consumes time and resources that I—and my team—could better spend keeping up with changes in clinical practice.
Perhaps when all the dust settles around the healthcare reform debate, we will begin to move toward new, more creative payment models that will allow us to focus on what we do best. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is cofounder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is also course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
The amount and complexity of medical knowledge we need to keep up with is changing and growing at a remarkable rate. I was trained in an era in which it was taken as a given that congestive heart failure patients should not receive beta-blockers; now it is a big mistake if we don’t prescribe them in most cases. But even before starting medical school, most of us realize that things will change a lot, and many of us see that as a good thing. It keeps our work interesting. Just recently, our hospital had a guest speaker who talked about potential medical applications of nanotechnology. It was way over my head, but it sounded pretty cool.
While I was prepared for ongoing changes in medical knowledge, I failed to anticipate how quickly the business of medicine would change during my career. I think the need to keep up with ever-increasing financial and regulatory issues siphons a lot of time and energy that could be used to keep up with the medical knowledge base. I wasn’t prepared for this when I started my career.
Because it is the start of a new year, I thought I would highlight one issue related to CPT coding: Medicare stopped recognizing consult codes as of Jan. 1 (see “Consultation Elimination,” p. 31).
What It Means for Hospitalists
The good news is that we can just use initial hospital visit codes, inpatient or observation, for all new visits. For example, it won’t matter anymore whether I’m admitting and serving as attending for a patient, or whether a surgeon admitted the patient and asked me to consult for preoperative medical evaluation (“clearance”). I should use the same CPT code in either situation, simply appending a modifier if I’m the admitting physician. And for billing purposes, we won’t have to worry about documenting which doctor requested that we see the patient, though it is a good idea to document it as part of the clinical record anyway.
But it gets a little more complicated. The codes aren’t going away or being removed from the CPT “bible” published by the American Medical Association (AMA). Instead, Medicare simply won’t recognize them anymore. Other payors probably will follow suit within a few months, but that isn’t certain. So it is possible that when asked by a surgeon to provide a preoperative evaluation, you will need to bill an initial hospital (or office or nursing facility) care visit if the patient is on Medicare but bill a consult code if the patient has other insurance. You should check with your billers to ensure you’re doing this correctly.
Medicare-paid consults are at a slightly higher rate than the equivalent service billed as initial hospital care (e.g., when the hospitalist is attending). So a higher reimbursing code has been replaced with one that pays a little less. For example, a 99253 consultation code requires a detailed history, detailed examination, and medical decision-making of low complexity; last year, 99253 was reimbursed by Medicare at an average rate of $114.69. The equivalent admission code for a detailed history, detailed examination, and low-complexity medical decision-making is a 99221 code, for which Medicare pays about $99.90. This represents a difference of about 14%.
However, the net financial impact of this change probably will be positive for most HM groups because you probably bill very few initial consult codes, and instead were stuck billing a follow-up visit code when seeing co-management “consults” (i.e., a patient admitted by a surgeon who asks you to follow and manage diabetes and other medical issues). Now, at least in the case of Medicare, it is appropriate for us to bill an initial hospital visit code, which provides significantly higher reimbursement than follow-up codes.
In addition, there is a modest (about 0.3%) proposed increase in work relative value units attached to the initial hospital visit codes, which will benefit us not only when we’re consulting, but also when we admit and serve as a patient’s attending.
Some specialists may be less interested in consulting on our patients because the initial visit codes will reimburse a little less than similar consultation codes. I don’t anticipate this will be a significant problem for most of us, particularly since many specialists bill the highest level of consultation code (99255), which pays about the same as the equivalent admission code (99223).
Although I think elimination of the use of consultation codes seems like a reasonable step toward simplifying how hospitalists bill for our services, keeping up with these frequent coding changes requires a high level of diligence on our part, and on the part of our administrative and clerical staffs. And it consumes time and resources that I—and my team—could better spend keeping up with changes in clinical practice.
Perhaps when all the dust settles around the healthcare reform debate, we will begin to move toward new, more creative payment models that will allow us to focus on what we do best. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is cofounder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is also course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.