User login
ABIM: Majority meeting Maintenance of Certification requirements
The American Board of Internal Medicine says that "a substantial majority" of the nation’s internists have met the new Maintenance of Certification requirements as of May 1, the deadline for doctors to be listed publicly on the ABIM’s website as having met those standards.
The ABIM reported that "despite vocal concerns" from physicians, some 150,000 have enrolled in the MOC program, 50,000 since the new requirements were instituted on Jan. 1.

As part of the new MOC, every 2 years, physicians who are certified by the ABIM must earn at least some points by completing some of the educational activities approved for MOC credit. At the 5-year mark, they must earn 100 points, as well as complete patient safety and patient survey activities, to be considered up to date. Previously, physicians were given 10 years to earn 100 points. They must also pass their board exam every 10 years.
"We are listening to the feedback we have received from the community about changes to our program, but at the same time the public is seeking a way to know that their doctor is ‘keeping up in their field,’" Dr. Richard Baron, ABIM president and chief executive officer, said in a statement.
A petition to overturn most of the MOC changes begun by Dr. Paul Teirstein, chief of cardiology and director of interventional cardiology for Scripps Clinic in La Jolla, Calif., has collected more than 14,000 signatures since it was posted in late March.
According to the ABIM, since Jan. 1, physicians have claimed more than 245,000 hours of Continuing Medical Education (CME) through their MOC involvement, and nearly 20,000 physicians have already met their MOC requirements through 2015.
"MOC has clearly sparked a national conversation focused on what regular assessments are appropriate for ongoing specialty certification," Dr. Baron said. "We must look at how the MOC process meets the needs of physicians, patients, and others who rely on it as an indicator of a provider’s expertise."
The ABIM continues to say that MOC is needed because it is desired by patients and payers. "Those who choose to meet ABIM’s MOC requirements are differentiating themselves from some of their colleagues. They are saying, ‘I’m a cardiologist or oncologist, or whatever specialty they are certified in, who is meeting a standard set by my peers.’ That is a powerful statement to make to their patients, and to themselves," Dr. Clarence H. Braddock III, chair-elect of the ABIM Board of Directors, said in the ABIM statement.
The Board also said it is responding to criticism by making changes to the MOC program, including giving "credit" for activities physicians already are doing to maintain their knowledge base and improve their practices. It said it recognizes more than 270 programs created by medical societies, health systems, and others and that 32,000 ABIM diplomates already have fulfilled some requirements of MOC using those pathways.
"We recognize that the MOC program is not perfect, and we are committed to constant assessment of it," said Dr. Baron.
That may not be enough for some physicians.
Another group, Change Board Recertification, was started in 2010 with the aim of completely overhauling the MOC process.
On Twitter @aliciaault
The new MOC requirements that became effective on Jan. 1, 2014, have met with significant criticism from practicing physicians. Nevertheless, the majority of physicians with time-limited board certifications have enrolled in the program, as hospital privileges and insurance reimbursements are often linked to active certification.
Whereas it is largely agreed that some measure of ongoing knowledge and competence is vital to setting standards for the profession and protecting the interests of patients, many physicians raise significant concerns regarding the current process. These include overly burdensome costs and time commitments as well as relevance to actual practice.
Finally, there is a paucity of data demonstrating that the MOC recertification process actually translates to improved physician performance in the clinical setting. A number of recommendations have been suggested to improve the recertification process. These include decreasing the costs of recertification by the ABIM; customizing the process to dovetail with an individual physician's actual practice; testing not only rote knowledge, but also physician ability to accesses and utilize information; and further research to demonstrate efficacy in achieving and demonstrating physician competence.
The new MOC requirements that became effective on Jan. 1, 2014, have met with significant criticism from practicing physicians. Nevertheless, the majority of physicians with time-limited board certifications have enrolled in the program, as hospital privileges and insurance reimbursements are often linked to active certification.
Whereas it is largely agreed that some measure of ongoing knowledge and competence is vital to setting standards for the profession and protecting the interests of patients, many physicians raise significant concerns regarding the current process. These include overly burdensome costs and time commitments as well as relevance to actual practice.
Finally, there is a paucity of data demonstrating that the MOC recertification process actually translates to improved physician performance in the clinical setting. A number of recommendations have been suggested to improve the recertification process. These include decreasing the costs of recertification by the ABIM; customizing the process to dovetail with an individual physician's actual practice; testing not only rote knowledge, but also physician ability to accesses and utilize information; and further research to demonstrate efficacy in achieving and demonstrating physician competence.
The new MOC requirements that became effective on Jan. 1, 2014, have met with significant criticism from practicing physicians. Nevertheless, the majority of physicians with time-limited board certifications have enrolled in the program, as hospital privileges and insurance reimbursements are often linked to active certification.
Whereas it is largely agreed that some measure of ongoing knowledge and competence is vital to setting standards for the profession and protecting the interests of patients, many physicians raise significant concerns regarding the current process. These include overly burdensome costs and time commitments as well as relevance to actual practice.
Finally, there is a paucity of data demonstrating that the MOC recertification process actually translates to improved physician performance in the clinical setting. A number of recommendations have been suggested to improve the recertification process. These include decreasing the costs of recertification by the ABIM; customizing the process to dovetail with an individual physician's actual practice; testing not only rote knowledge, but also physician ability to accesses and utilize information; and further research to demonstrate efficacy in achieving and demonstrating physician competence.
The American Board of Internal Medicine says that "a substantial majority" of the nation’s internists have met the new Maintenance of Certification requirements as of May 1, the deadline for doctors to be listed publicly on the ABIM’s website as having met those standards.
The ABIM reported that "despite vocal concerns" from physicians, some 150,000 have enrolled in the MOC program, 50,000 since the new requirements were instituted on Jan. 1.
As part of the new MOC, every 2 years, physicians who are certified by the ABIM must earn at least some points by completing some of the educational activities approved for MOC credit. At the 5-year mark, they must earn 100 points, as well as complete patient safety and patient survey activities, to be considered up to date. Previously, physicians were given 10 years to earn 100 points. They must also pass their board exam every 10 years.
"We are listening to the feedback we have received from the community about changes to our program, but at the same time the public is seeking a way to know that their doctor is ‘keeping up in their field,’" Dr. Richard Baron, ABIM president and chief executive officer, said in a statement.
A petition to overturn most of the MOC changes begun by Dr. Paul Teirstein, chief of cardiology and director of interventional cardiology for Scripps Clinic in La Jolla, Calif., has collected more than 14,000 signatures since it was posted in late March.
According to the ABIM, since Jan. 1, physicians have claimed more than 245,000 hours of Continuing Medical Education (CME) through their MOC involvement, and nearly 20,000 physicians have already met their MOC requirements through 2015.
"MOC has clearly sparked a national conversation focused on what regular assessments are appropriate for ongoing specialty certification," Dr. Baron said. "We must look at how the MOC process meets the needs of physicians, patients, and others who rely on it as an indicator of a provider’s expertise."
The ABIM continues to say that MOC is needed because it is desired by patients and payers. "Those who choose to meet ABIM’s MOC requirements are differentiating themselves from some of their colleagues. They are saying, ‘I’m a cardiologist or oncologist, or whatever specialty they are certified in, who is meeting a standard set by my peers.’ That is a powerful statement to make to their patients, and to themselves," Dr. Clarence H. Braddock III, chair-elect of the ABIM Board of Directors, said in the ABIM statement.
The Board also said it is responding to criticism by making changes to the MOC program, including giving "credit" for activities physicians already are doing to maintain their knowledge base and improve their practices. It said it recognizes more than 270 programs created by medical societies, health systems, and others and that 32,000 ABIM diplomates already have fulfilled some requirements of MOC using those pathways.
"We recognize that the MOC program is not perfect, and we are committed to constant assessment of it," said Dr. Baron.
That may not be enough for some physicians.
Another group, Change Board Recertification, was started in 2010 with the aim of completely overhauling the MOC process.
On Twitter @aliciaault
The American Board of Internal Medicine says that "a substantial majority" of the nation’s internists have met the new Maintenance of Certification requirements as of May 1, the deadline for doctors to be listed publicly on the ABIM’s website as having met those standards.
The ABIM reported that "despite vocal concerns" from physicians, some 150,000 have enrolled in the MOC program, 50,000 since the new requirements were instituted on Jan. 1.
As part of the new MOC, every 2 years, physicians who are certified by the ABIM must earn at least some points by completing some of the educational activities approved for MOC credit. At the 5-year mark, they must earn 100 points, as well as complete patient safety and patient survey activities, to be considered up to date. Previously, physicians were given 10 years to earn 100 points. They must also pass their board exam every 10 years.
"We are listening to the feedback we have received from the community about changes to our program, but at the same time the public is seeking a way to know that their doctor is ‘keeping up in their field,’" Dr. Richard Baron, ABIM president and chief executive officer, said in a statement.
A petition to overturn most of the MOC changes begun by Dr. Paul Teirstein, chief of cardiology and director of interventional cardiology for Scripps Clinic in La Jolla, Calif., has collected more than 14,000 signatures since it was posted in late March.
According to the ABIM, since Jan. 1, physicians have claimed more than 245,000 hours of Continuing Medical Education (CME) through their MOC involvement, and nearly 20,000 physicians have already met their MOC requirements through 2015.
"MOC has clearly sparked a national conversation focused on what regular assessments are appropriate for ongoing specialty certification," Dr. Baron said. "We must look at how the MOC process meets the needs of physicians, patients, and others who rely on it as an indicator of a provider’s expertise."
The ABIM continues to say that MOC is needed because it is desired by patients and payers. "Those who choose to meet ABIM’s MOC requirements are differentiating themselves from some of their colleagues. They are saying, ‘I’m a cardiologist or oncologist, or whatever specialty they are certified in, who is meeting a standard set by my peers.’ That is a powerful statement to make to their patients, and to themselves," Dr. Clarence H. Braddock III, chair-elect of the ABIM Board of Directors, said in the ABIM statement.
The Board also said it is responding to criticism by making changes to the MOC program, including giving "credit" for activities physicians already are doing to maintain their knowledge base and improve their practices. It said it recognizes more than 270 programs created by medical societies, health systems, and others and that 32,000 ABIM diplomates already have fulfilled some requirements of MOC using those pathways.
"We recognize that the MOC program is not perfect, and we are committed to constant assessment of it," said Dr. Baron.
That may not be enough for some physicians.
Another group, Change Board Recertification, was started in 2010 with the aim of completely overhauling the MOC process.
On Twitter @aliciaault

Doctors’ first steps after lawsuit filing are vital, warn attorneys
Receiving notice that a patient is suing can spark a range of emotions in physicians, including fear, anger, hurt, and helplessness. But litigation experts stress that after a filing, physicians must rein in their feelings and focus on immediate next steps – crucial actions that can significantly impact the suit and its outcome.
"Doctors have two reactions to getting sued – either they’re very sad or they’re very angry," said Steven Fitzer, a medical liability defense attorney at Fitzer, Leighton & Fitzer, P.S., in Tacoma, Wash., and former chair of the Washington State Bar Association Litigation Section. "Relaxing and composing yourself are important because a lawsuit is a marathon – not a sprint."
American Medical Association data show 60% of physicians will be sued by the time they reach 55 years of age. The average span of a medical malpractice claim from start to close is generally about 2.5 years, although many suits progress longer. While most medical liability claims do not end in trial, defense attorneys say knowing how to respond to a lawsuit can raise doctors’ chances of a quicker, more ideal resolution.
First and foremost, physicians should notify their malpractice insurance carrier as soon as possible after lawsuit papers are served, said Matt Mitcham, senior vice president of claims for MagMutual Insurance Company, a medical liability insurer that operates in the Southeast. Employed physicians should immediately alert their risk management department.
"All suits have a limited time for providing a response, and there are severe consequences for not meeting these deadlines," Mr. Mitcham said. "In addition, physicians need to provide their defense team with as much time as possible to prepare a response."
Doctors should resist the desire to contact patients or their families in an attempt to work out the situation themselves, adds Mr. Fitzer, who recently shared lawsuit preparation tips in two video playlists for The Doctors Company, a national medical malpractice insurer.
"Particularly with family practice physicians, they tend to have a long and strong bond with their patients and their patients’ families, and they think, ‘If I just call and ask what’s going on, we can just fix this all right here,’ " he said. "That never works. The patient or their lawyer will take whatever you say in or out of context and use it against you."
Another action to avoid after a lawsuit filing is making additions or changes to patient records, said Mr. Mitcham.
"The original records should never be altered under any circumstance," he said. "Today’s forensic specialists are experts in identifying changes, and by altering records, a physician can potentially turn a defensible case into one that is indefensible."
Securing an attorney that doctors trust and with whom they can aptly communicate is also essential, said Michael F. Ball, a medical liability defense attorney and partner at McCormick Barstow, LLP, in Fresno, Calif. Most doctors may not realize they can typically choose from a panel of attorneys used by their insurer, he said. Physicians can also ask to view the attorney panel and conduct their own research before requesting a specific lawyer.
Mr. Ball counsels his clients to focus only on the task at hand during each stage of a lawsuit, rather than worry about future phases or a possible trial. For example, during the deposition stage, physicians should prepare by understanding the deposition’s purpose, reading through the record, and being clear on what questions may be asked. A deposition is a witness’s sworn, out-of-court testimony used to gather information as part of the discovery process.
"Some [physicians] don’t review the record as closely as they should," he said. "There’s no substitute for real preparation."
Additionally, depositions are a stage in which a physician’s emotions may come bubbling to the surface, notes Angela Dodge, Ph.D., founding partner of Dodge Consulting & Publications, LLP, a litigation consulting firm in the Seattle-Tacoma area.
"A doctor may go into a deposition feeling very angry and resentful because a patient they believe they gave good care to is now suing," said Ms. Dodge, author of the book "When Good Doctors Get Sued: A Practical Guide for Physicians Involved in Malpractice Lawsuits, and Winning at Jury Selection." "We counsel them on the importance of setting that aside because it could interfere with" their success.
Negative emotions by doctors may be interpreted by plaintiffs’ attorneys as guilt or defensiveness and used to fuel their claims, she said. Doctors should also focus only on the questions being asked during a deposition and not offer up any further or additional information. For instance, in a recent case, a doctor was asked about a specific part of his education. In response, the physician provided unnecessary information about his entire medical education, including his experience operating on pigs, how pig anatomy is relevant to human medicine, and other needless details, Ms. Dodge said.
"He was so anxious to explain how he gained his expertise; he forgot that the question was [only] where and when he gained his expertise," she said.
Litigation counselors point to strong cooperation among physicians, insurers, and defense attorneys as one of the most vital components to the successful handling of a lawsuit.
"The legal system can be a very daunting place for physicians, but when the malpractice carrier and defense attorney work together as a team, they can help the physician navigate the process and hopefully win the case," Mr. Mitcham said.
A 2011 study in the New England Journal of Medicine estimated that 75% of physicians in "low-risk" specialties and virtually 100% of physicians in "high-risk" specialties could expect to face a malpractice claim sometime in their career (N. Engl. J. Med. 2011;365:629-36). However, 60% of liability claims against doctors are dropped, withdrawn, or dismissed without payment, and physicians are found not negligent in over 90% of cases that do go to trial.
While there are no readily available national statistics on the actual number of claims filed, there is data, compiled by the federal government’s National Practitioner Data Bank (NPDB), suggesting that the number of cases filed has been dropping in the last decade.

|
|
The NPDB issues an annual report that includes the number of medical malpractice payments made each year for the preceding 10 years. For nearly every year in the past decade, the number of medical malpractice payments made on behalf of all practitioners reported to the NPDB has decreased. Between 2002 and 2011, the number of medical malpractice payments decreased nearly 40%, declining steadily from 18,696 to 11,424.
Also, in the past 10 years, the number of medical malpractice payments reported to the NPDB, attributed to physicians and dentists, has decreased steadily from 17,155 to 10,038. Between 2003 and 2011, the total amount paid out fell from $4.5 billion to less than $3.2 billion, a 29% drop. State tort-reform laws limiting noneconomic damages, growth in risk management responses to adverse events, and the growing use of apology and disclosure likely have contributed to this trend.
Dr. James A.L. Mathers, Jr., is a past president of the American College of Chest Physicians, and is recently retired with 30 years of private practice experience in pulmonary, critical care, and sleep medicine.
A 2011 study in the New England Journal of Medicine estimated that 75% of physicians in "low-risk" specialties and virtually 100% of physicians in "high-risk" specialties could expect to face a malpractice claim sometime in their career (N. Engl. J. Med. 2011;365:629-36). However, 60% of liability claims against doctors are dropped, withdrawn, or dismissed without payment, and physicians are found not negligent in over 90% of cases that do go to trial.
While there are no readily available national statistics on the actual number of claims filed, there is data, compiled by the federal government’s National Practitioner Data Bank (NPDB), suggesting that the number of cases filed has been dropping in the last decade.
|
|
|
The NPDB issues an annual report that includes the number of medical malpractice payments made each year for the preceding 10 years. For nearly every year in the past decade, the number of medical malpractice payments made on behalf of all practitioners reported to the NPDB has decreased. Between 2002 and 2011, the number of medical malpractice payments decreased nearly 40%, declining steadily from 18,696 to 11,424.
Also, in the past 10 years, the number of medical malpractice payments reported to the NPDB, attributed to physicians and dentists, has decreased steadily from 17,155 to 10,038. Between 2003 and 2011, the total amount paid out fell from $4.5 billion to less than $3.2 billion, a 29% drop. State tort-reform laws limiting noneconomic damages, growth in risk management responses to adverse events, and the growing use of apology and disclosure likely have contributed to this trend.
Dr. James A.L. Mathers, Jr., is a past president of the American College of Chest Physicians, and is recently retired with 30 years of private practice experience in pulmonary, critical care, and sleep medicine.
A 2011 study in the New England Journal of Medicine estimated that 75% of physicians in "low-risk" specialties and virtually 100% of physicians in "high-risk" specialties could expect to face a malpractice claim sometime in their career (N. Engl. J. Med. 2011;365:629-36). However, 60% of liability claims against doctors are dropped, withdrawn, or dismissed without payment, and physicians are found not negligent in over 90% of cases that do go to trial.
While there are no readily available national statistics on the actual number of claims filed, there is data, compiled by the federal government’s National Practitioner Data Bank (NPDB), suggesting that the number of cases filed has been dropping in the last decade.
|
|
|
The NPDB issues an annual report that includes the number of medical malpractice payments made each year for the preceding 10 years. For nearly every year in the past decade, the number of medical malpractice payments made on behalf of all practitioners reported to the NPDB has decreased. Between 2002 and 2011, the number of medical malpractice payments decreased nearly 40%, declining steadily from 18,696 to 11,424.
Also, in the past 10 years, the number of medical malpractice payments reported to the NPDB, attributed to physicians and dentists, has decreased steadily from 17,155 to 10,038. Between 2003 and 2011, the total amount paid out fell from $4.5 billion to less than $3.2 billion, a 29% drop. State tort-reform laws limiting noneconomic damages, growth in risk management responses to adverse events, and the growing use of apology and disclosure likely have contributed to this trend.
Dr. James A.L. Mathers, Jr., is a past president of the American College of Chest Physicians, and is recently retired with 30 years of private practice experience in pulmonary, critical care, and sleep medicine.
Receiving notice that a patient is suing can spark a range of emotions in physicians, including fear, anger, hurt, and helplessness. But litigation experts stress that after a filing, physicians must rein in their feelings and focus on immediate next steps – crucial actions that can significantly impact the suit and its outcome.
"Doctors have two reactions to getting sued – either they’re very sad or they’re very angry," said Steven Fitzer, a medical liability defense attorney at Fitzer, Leighton & Fitzer, P.S., in Tacoma, Wash., and former chair of the Washington State Bar Association Litigation Section. "Relaxing and composing yourself are important because a lawsuit is a marathon – not a sprint."
American Medical Association data show 60% of physicians will be sued by the time they reach 55 years of age. The average span of a medical malpractice claim from start to close is generally about 2.5 years, although many suits progress longer. While most medical liability claims do not end in trial, defense attorneys say knowing how to respond to a lawsuit can raise doctors’ chances of a quicker, more ideal resolution.
First and foremost, physicians should notify their malpractice insurance carrier as soon as possible after lawsuit papers are served, said Matt Mitcham, senior vice president of claims for MagMutual Insurance Company, a medical liability insurer that operates in the Southeast. Employed physicians should immediately alert their risk management department.
"All suits have a limited time for providing a response, and there are severe consequences for not meeting these deadlines," Mr. Mitcham said. "In addition, physicians need to provide their defense team with as much time as possible to prepare a response."
Doctors should resist the desire to contact patients or their families in an attempt to work out the situation themselves, adds Mr. Fitzer, who recently shared lawsuit preparation tips in two video playlists for The Doctors Company, a national medical malpractice insurer.
"Particularly with family practice physicians, they tend to have a long and strong bond with their patients and their patients’ families, and they think, ‘If I just call and ask what’s going on, we can just fix this all right here,’ " he said. "That never works. The patient or their lawyer will take whatever you say in or out of context and use it against you."
Another action to avoid after a lawsuit filing is making additions or changes to patient records, said Mr. Mitcham.
"The original records should never be altered under any circumstance," he said. "Today’s forensic specialists are experts in identifying changes, and by altering records, a physician can potentially turn a defensible case into one that is indefensible."
Securing an attorney that doctors trust and with whom they can aptly communicate is also essential, said Michael F. Ball, a medical liability defense attorney and partner at McCormick Barstow, LLP, in Fresno, Calif. Most doctors may not realize they can typically choose from a panel of attorneys used by their insurer, he said. Physicians can also ask to view the attorney panel and conduct their own research before requesting a specific lawyer.
Mr. Ball counsels his clients to focus only on the task at hand during each stage of a lawsuit, rather than worry about future phases or a possible trial. For example, during the deposition stage, physicians should prepare by understanding the deposition’s purpose, reading through the record, and being clear on what questions may be asked. A deposition is a witness’s sworn, out-of-court testimony used to gather information as part of the discovery process.
"Some [physicians] don’t review the record as closely as they should," he said. "There’s no substitute for real preparation."
Additionally, depositions are a stage in which a physician’s emotions may come bubbling to the surface, notes Angela Dodge, Ph.D., founding partner of Dodge Consulting & Publications, LLP, a litigation consulting firm in the Seattle-Tacoma area.
"A doctor may go into a deposition feeling very angry and resentful because a patient they believe they gave good care to is now suing," said Ms. Dodge, author of the book "When Good Doctors Get Sued: A Practical Guide for Physicians Involved in Malpractice Lawsuits, and Winning at Jury Selection." "We counsel them on the importance of setting that aside because it could interfere with" their success.
Negative emotions by doctors may be interpreted by plaintiffs’ attorneys as guilt or defensiveness and used to fuel their claims, she said. Doctors should also focus only on the questions being asked during a deposition and not offer up any further or additional information. For instance, in a recent case, a doctor was asked about a specific part of his education. In response, the physician provided unnecessary information about his entire medical education, including his experience operating on pigs, how pig anatomy is relevant to human medicine, and other needless details, Ms. Dodge said.
"He was so anxious to explain how he gained his expertise; he forgot that the question was [only] where and when he gained his expertise," she said.
Litigation counselors point to strong cooperation among physicians, insurers, and defense attorneys as one of the most vital components to the successful handling of a lawsuit.
"The legal system can be a very daunting place for physicians, but when the malpractice carrier and defense attorney work together as a team, they can help the physician navigate the process and hopefully win the case," Mr. Mitcham said.
Receiving notice that a patient is suing can spark a range of emotions in physicians, including fear, anger, hurt, and helplessness. But litigation experts stress that after a filing, physicians must rein in their feelings and focus on immediate next steps – crucial actions that can significantly impact the suit and its outcome.
"Doctors have two reactions to getting sued – either they’re very sad or they’re very angry," said Steven Fitzer, a medical liability defense attorney at Fitzer, Leighton & Fitzer, P.S., in Tacoma, Wash., and former chair of the Washington State Bar Association Litigation Section. "Relaxing and composing yourself are important because a lawsuit is a marathon – not a sprint."
American Medical Association data show 60% of physicians will be sued by the time they reach 55 years of age. The average span of a medical malpractice claim from start to close is generally about 2.5 years, although many suits progress longer. While most medical liability claims do not end in trial, defense attorneys say knowing how to respond to a lawsuit can raise doctors’ chances of a quicker, more ideal resolution.
First and foremost, physicians should notify their malpractice insurance carrier as soon as possible after lawsuit papers are served, said Matt Mitcham, senior vice president of claims for MagMutual Insurance Company, a medical liability insurer that operates in the Southeast. Employed physicians should immediately alert their risk management department.
"All suits have a limited time for providing a response, and there are severe consequences for not meeting these deadlines," Mr. Mitcham said. "In addition, physicians need to provide their defense team with as much time as possible to prepare a response."
Doctors should resist the desire to contact patients or their families in an attempt to work out the situation themselves, adds Mr. Fitzer, who recently shared lawsuit preparation tips in two video playlists for The Doctors Company, a national medical malpractice insurer.
"Particularly with family practice physicians, they tend to have a long and strong bond with their patients and their patients’ families, and they think, ‘If I just call and ask what’s going on, we can just fix this all right here,’ " he said. "That never works. The patient or their lawyer will take whatever you say in or out of context and use it against you."
Another action to avoid after a lawsuit filing is making additions or changes to patient records, said Mr. Mitcham.
"The original records should never be altered under any circumstance," he said. "Today’s forensic specialists are experts in identifying changes, and by altering records, a physician can potentially turn a defensible case into one that is indefensible."
Securing an attorney that doctors trust and with whom they can aptly communicate is also essential, said Michael F. Ball, a medical liability defense attorney and partner at McCormick Barstow, LLP, in Fresno, Calif. Most doctors may not realize they can typically choose from a panel of attorneys used by their insurer, he said. Physicians can also ask to view the attorney panel and conduct their own research before requesting a specific lawyer.
Mr. Ball counsels his clients to focus only on the task at hand during each stage of a lawsuit, rather than worry about future phases or a possible trial. For example, during the deposition stage, physicians should prepare by understanding the deposition’s purpose, reading through the record, and being clear on what questions may be asked. A deposition is a witness’s sworn, out-of-court testimony used to gather information as part of the discovery process.
"Some [physicians] don’t review the record as closely as they should," he said. "There’s no substitute for real preparation."
Additionally, depositions are a stage in which a physician’s emotions may come bubbling to the surface, notes Angela Dodge, Ph.D., founding partner of Dodge Consulting & Publications, LLP, a litigation consulting firm in the Seattle-Tacoma area.
"A doctor may go into a deposition feeling very angry and resentful because a patient they believe they gave good care to is now suing," said Ms. Dodge, author of the book "When Good Doctors Get Sued: A Practical Guide for Physicians Involved in Malpractice Lawsuits, and Winning at Jury Selection." "We counsel them on the importance of setting that aside because it could interfere with" their success.
Negative emotions by doctors may be interpreted by plaintiffs’ attorneys as guilt or defensiveness and used to fuel their claims, she said. Doctors should also focus only on the questions being asked during a deposition and not offer up any further or additional information. For instance, in a recent case, a doctor was asked about a specific part of his education. In response, the physician provided unnecessary information about his entire medical education, including his experience operating on pigs, how pig anatomy is relevant to human medicine, and other needless details, Ms. Dodge said.
"He was so anxious to explain how he gained his expertise; he forgot that the question was [only] where and when he gained his expertise," she said.
Litigation counselors point to strong cooperation among physicians, insurers, and defense attorneys as one of the most vital components to the successful handling of a lawsuit.
"The legal system can be a very daunting place for physicians, but when the malpractice carrier and defense attorney work together as a team, they can help the physician navigate the process and hopefully win the case," Mr. Mitcham said.

Physician offices provided $10.5 billion in uncompensated care in 2013
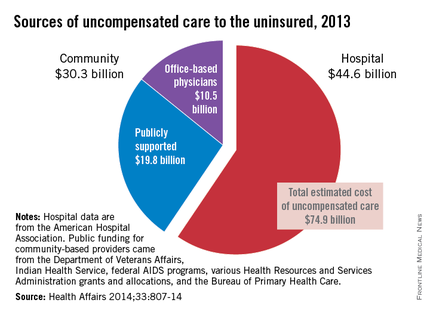
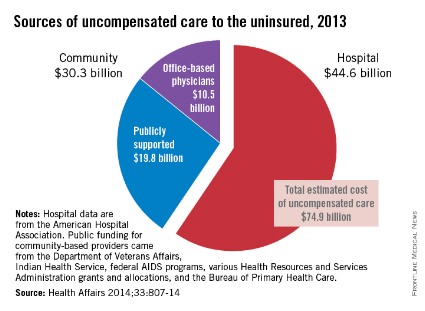
Office-based physicians provided an estimated $10.5 billion worth of in-kind services and charity care to the uninsured in 2013, according to an analysis of uncompensated care in the United States.
Total expenditures for care to the uninsured were projected by using two methods: One used data from the federal Medical Expenditure Panel Survey (MEPS), and the other "used published secondary data from health care providers and government sources," said Teresa A. Coughlin and her associates at the Urban Institute in Washington.
The MEPS data yielded a total uncompensated expenditure of $84.9 billion for 2013, while the second analysis projected a total cost of $74.9 billion. The difference reflects the exclusion of information from some sources in the second analysis, such as drugs provided at no charge by some pharmaceutical companies, and conservative assumptions made about uncompensated care provided by publicly funded sources such as the U.S. Department of Veterans Affairs and the Indian Health Service, they said (Health Aff. 2014;33:807-14).
The $10.5 billion in care provided by office-based physicians represents 14% of the $74.9 billion from the second analysis. The largest share (59.5%, or $44.6 billion) was provided by hospitals, with the other $19.8 billion (26.4%) coming from community sources funded by the VA, IHS, local and state health departments, and automobile and home-owners insurance, Ms. Coughlin and her associates reported.
The MEPS data could not be used to see how costs of uncompensated care were divided among providers and which funding sources paid for such care, so only the second analysis estimated physicians’ share, the investigators noted.
The study was part of a project for the Kaiser Commission on Medicaid and the Uninsured.
Office-based physicians provided an estimated $10.5 billion worth of in-kind services and charity care to the uninsured in 2013, according to an analysis of uncompensated care in the United States.
Total expenditures for care to the uninsured were projected by using two methods: One used data from the federal Medical Expenditure Panel Survey (MEPS), and the other "used published secondary data from health care providers and government sources," said Teresa A. Coughlin and her associates at the Urban Institute in Washington.
The MEPS data yielded a total uncompensated expenditure of $84.9 billion for 2013, while the second analysis projected a total cost of $74.9 billion. The difference reflects the exclusion of information from some sources in the second analysis, such as drugs provided at no charge by some pharmaceutical companies, and conservative assumptions made about uncompensated care provided by publicly funded sources such as the U.S. Department of Veterans Affairs and the Indian Health Service, they said (Health Aff. 2014;33:807-14).
The $10.5 billion in care provided by office-based physicians represents 14% of the $74.9 billion from the second analysis. The largest share (59.5%, or $44.6 billion) was provided by hospitals, with the other $19.8 billion (26.4%) coming from community sources funded by the VA, IHS, local and state health departments, and automobile and home-owners insurance, Ms. Coughlin and her associates reported.
The MEPS data could not be used to see how costs of uncompensated care were divided among providers and which funding sources paid for such care, so only the second analysis estimated physicians’ share, the investigators noted.
The study was part of a project for the Kaiser Commission on Medicaid and the Uninsured.
Office-based physicians provided an estimated $10.5 billion worth of in-kind services and charity care to the uninsured in 2013, according to an analysis of uncompensated care in the United States.
Total expenditures for care to the uninsured were projected by using two methods: One used data from the federal Medical Expenditure Panel Survey (MEPS), and the other "used published secondary data from health care providers and government sources," said Teresa A. Coughlin and her associates at the Urban Institute in Washington.
The MEPS data yielded a total uncompensated expenditure of $84.9 billion for 2013, while the second analysis projected a total cost of $74.9 billion. The difference reflects the exclusion of information from some sources in the second analysis, such as drugs provided at no charge by some pharmaceutical companies, and conservative assumptions made about uncompensated care provided by publicly funded sources such as the U.S. Department of Veterans Affairs and the Indian Health Service, they said (Health Aff. 2014;33:807-14).
The $10.5 billion in care provided by office-based physicians represents 14% of the $74.9 billion from the second analysis. The largest share (59.5%, or $44.6 billion) was provided by hospitals, with the other $19.8 billion (26.4%) coming from community sources funded by the VA, IHS, local and state health departments, and automobile and home-owners insurance, Ms. Coughlin and her associates reported.
The MEPS data could not be used to see how costs of uncompensated care were divided among providers and which funding sources paid for such care, so only the second analysis estimated physicians’ share, the investigators noted.
The study was part of a project for the Kaiser Commission on Medicaid and the Uninsured.
FROM HEALTH AFFAIRS
25% of lawsuits against internists end in payment
Errors in diagnosis, improper procedures, and medication errors make up the top reasons that internists are sued, according to a study published online April 28 in JAMA Internal Medicine. A quarter of claims against internists result in payment, the study found.
Researchers studied 247,073 closed cases from 1985 to 2009 collected by PIAA (Physician Insurers Association of America), a trade association that represents domestic and international medical professional liability insurers. Of the closed claims, 14% were against internists. Twenty-six percent of the lawsuits against internists involved diagnostic errors, including allegations of misdiagnosing lung cancer, acute myocardial infarction, colon cancer, and breast cancer. Another 25% of claims involved no departure from the standard of care, while 11% related to improper performance of a procedure and 9% were attributed to medication errors, wrote Dr. Sandeep S. Mangalmurti, of Bassett Medical Center, Cooperstown, N.Y., and his colleagues (JAMA Intern. Med. 2014 April 28 [doi: 10.1001/jamainternmed.2014.1116]).
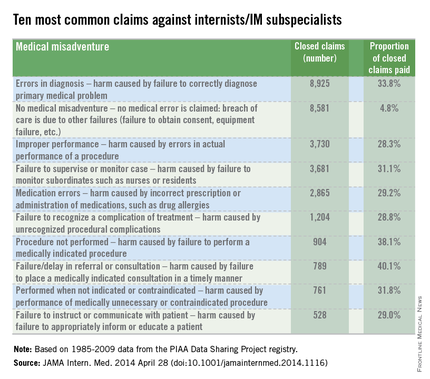
The results showed a wide variation among claims that resulted in payment against internists. For example, 40% of claims as a result of failure to refer and 38% of cases associated with failure to perform a procedure resulted in a claims payment. Cases in which no deviation from the standard of care occurred resulted in payment in 5% of suits. (In such cases, allegations such as failure to obtain consent or equipment were alleged.)
"Alleged departures from the appropriate standard of care are defined as medical misadventures," according to PIAA, the study, reported as a research letter, noted.
The findings confirm that internists are vulnerable to claims pertaining to their common practices of patient evaluation and health management, the authors noted. Insight into these claims patterns may help internists craft practice patterns and changes that will result in fewer patient injuries and fewer lawsuits, the authors said.
Errors in diagnosis, improper procedures, and medication errors make up the top reasons that internists are sued, according to a study published online April 28 in JAMA Internal Medicine. A quarter of claims against internists result in payment, the study found.
Researchers studied 247,073 closed cases from 1985 to 2009 collected by PIAA (Physician Insurers Association of America), a trade association that represents domestic and international medical professional liability insurers. Of the closed claims, 14% were against internists. Twenty-six percent of the lawsuits against internists involved diagnostic errors, including allegations of misdiagnosing lung cancer, acute myocardial infarction, colon cancer, and breast cancer. Another 25% of claims involved no departure from the standard of care, while 11% related to improper performance of a procedure and 9% were attributed to medication errors, wrote Dr. Sandeep S. Mangalmurti, of Bassett Medical Center, Cooperstown, N.Y., and his colleagues (JAMA Intern. Med. 2014 April 28 [doi: 10.1001/jamainternmed.2014.1116]).
The results showed a wide variation among claims that resulted in payment against internists. For example, 40% of claims as a result of failure to refer and 38% of cases associated with failure to perform a procedure resulted in a claims payment. Cases in which no deviation from the standard of care occurred resulted in payment in 5% of suits. (In such cases, allegations such as failure to obtain consent or equipment were alleged.)
"Alleged departures from the appropriate standard of care are defined as medical misadventures," according to PIAA, the study, reported as a research letter, noted.
The findings confirm that internists are vulnerable to claims pertaining to their common practices of patient evaluation and health management, the authors noted. Insight into these claims patterns may help internists craft practice patterns and changes that will result in fewer patient injuries and fewer lawsuits, the authors said.
Errors in diagnosis, improper procedures, and medication errors make up the top reasons that internists are sued, according to a study published online April 28 in JAMA Internal Medicine. A quarter of claims against internists result in payment, the study found.
Researchers studied 247,073 closed cases from 1985 to 2009 collected by PIAA (Physician Insurers Association of America), a trade association that represents domestic and international medical professional liability insurers. Of the closed claims, 14% were against internists. Twenty-six percent of the lawsuits against internists involved diagnostic errors, including allegations of misdiagnosing lung cancer, acute myocardial infarction, colon cancer, and breast cancer. Another 25% of claims involved no departure from the standard of care, while 11% related to improper performance of a procedure and 9% were attributed to medication errors, wrote Dr. Sandeep S. Mangalmurti, of Bassett Medical Center, Cooperstown, N.Y., and his colleagues (JAMA Intern. Med. 2014 April 28 [doi: 10.1001/jamainternmed.2014.1116]).
The results showed a wide variation among claims that resulted in payment against internists. For example, 40% of claims as a result of failure to refer and 38% of cases associated with failure to perform a procedure resulted in a claims payment. Cases in which no deviation from the standard of care occurred resulted in payment in 5% of suits. (In such cases, allegations such as failure to obtain consent or equipment were alleged.)
"Alleged departures from the appropriate standard of care are defined as medical misadventures," according to PIAA, the study, reported as a research letter, noted.
The findings confirm that internists are vulnerable to claims pertaining to their common practices of patient evaluation and health management, the authors noted. Insight into these claims patterns may help internists craft practice patterns and changes that will result in fewer patient injuries and fewer lawsuits, the authors said.
FROM JAMA INTERNAL MEDICINE
Federal legislation would provide doctors litigation safe harbor
Physician leaders are voicing support for a proposed federal law that aims to reduce litigation against doctors, lower health care costs, and establish more fairness in the analyzing of malpractice claims. The Saving Lives, Saving Costs Act, introduced in March by Rep. Dr. Ami Bera, (D-CA), would provide safe harbor protection to doctors who are sued if they followed evidence-based clinical guidelines.
"The Bera/Barr bill would accomplish two very important things," said Dr. John C. Jennings, president of the American Congress of Obstetricians and Gynecologists and professor of obstetrics and gynecology at Texas Tech University Health Sciences Center at the Permian Basin. "First, it would provide an incentive for every physician to follow the best clinical guidelines developed by his or her specialty, reducing care variations and potentially increasing patient safety and quality of care. Second, it would provide an affirmative defense for physicians who have followed their specialties’ guidelines and find themselves in the middle of a malpractice suit."

Under the bill, clinical guidelines developed by professional medical organizations would be used to determine whether a plaintiff’s lawsuit could continue against a physician defendant. If a doctor adhered to the approved guidelines during the time of the alleged malpractice event, the case would be removed from court proceedings, while a medical review panel investigated the claim. The bill would also allow for relevant cases to be moved from state to federal court if they involved federal dollars such as Medicare.The bill was referred to the Subcommittee on the Constitution and Civil Justice on March 20 for review.
Dr. Bera declined to comment for this article. In a statement, he said the measure is a practical way to decrease the skyrocketing cost of health care and to ensure the malpractice system works better for patients and physicians.
"As a doctor, I know that physicians want to do what’s best for their patients, and promoting evidence-based medicine will help us do that," he said.

The proposed safe harbor measure is a beneficial initiative that would potentially have a positive impact on multiple aspects of the health care system, adds Dr. David A. Fleming, president-elect of the American College of Physicians and chair of the department of medicine for the University of Missouri–Columbia.
"I think anything that standardized a patient-centered and evidence-based approach to care will serve only to improve clinical outcomes and decrease health care costs, as well as decrease liability costs at every level," Dr. Fleming said in an interview. "Encouraging the use of generally accepted and evidence-based clinical guidelines, as promoted by the Saving Lives, Saving Costs federal bill, is a good way to reach that."
Dr. Fleming noted an ACP position paper published in April that discusses the medical liability crisis physicians continue to face and outlines innovative solutions for a better malpractice environment. "Medical Liability Reform – Innovative Solutions for New Health Care System," also provides an update on state-based medical liability activities and summarizes traditional and newer tort reform proposals.
The paper highlights the positive effect of such state reforms as caps on noneconomic damages, injury funds, stronger expert witness rules, and alternative dispute resolution initiatives such as apology, disclosure, and compensation programs. The report provides nine approaches that should be incorporated into a multifaceted medical malpractice reform initiative, including passage of a comprehensive tort reform package, oversight of medical liability insurers, and development of effective safe harbor protections that improve quality of care, increase efficiency, and reduce costs.
As for federal reform, Dr. Fleming said legislation at the congressional level often faces successful challenges by trial attorneys and advocacy groups that argue plaintiffs’ rights would be violated. The politicization of the issue is also a problem, he said. However, federal tort reform is still possible and physicians should keep advocating significant changes by Congress, he said.
"The litigious environment in which we live continues to contribute to a sense of fear and consternation by practicing physicians that affects how they relate to patients and undoubtedly adds to health care costs," Dr. Fleming said.
Along with the Saving Lives, Saving Costs bills, doctors are closely watching several other federal malpractice reform measures under review. For instance, the Health Care Safety Net Enhancement Act would help ensure that physicians furnishing medical services, pursuant to the Emergency Medical Treatment & Active Labor Act (EMTALA), receive the same liability coverage currently extended to health professionals who provide Medicaid services at free clinics. The bill has been referred to the Subcommittee on Health.
Meanwhile, the Standard of Care Protection Act of 2013 would ensure that provisions of the Affordable Care Act and other federal laws cannot be used to create new standards of care for medical liability lawsuits. The proposed law was included in the recent Medicare Sustainable Growth Rate Formula bill, which passed out of the Energy and Commerce Committee.
"With so many changes occurring in the health care system, physicians are rightly concerned that federal rules and regulations could result in new, unwarranted, liability exposures," Dr. Jennings said. "This legislation helps safeguard physicians."
Physician leaders are voicing support for a proposed federal law that aims to reduce litigation against doctors, lower health care costs, and establish more fairness in the analyzing of malpractice claims. The Saving Lives, Saving Costs Act, introduced in March by Rep. Dr. Ami Bera, (D-CA), would provide safe harbor protection to doctors who are sued if they followed evidence-based clinical guidelines.
"The Bera/Barr bill would accomplish two very important things," said Dr. John C. Jennings, president of the American Congress of Obstetricians and Gynecologists and professor of obstetrics and gynecology at Texas Tech University Health Sciences Center at the Permian Basin. "First, it would provide an incentive for every physician to follow the best clinical guidelines developed by his or her specialty, reducing care variations and potentially increasing patient safety and quality of care. Second, it would provide an affirmative defense for physicians who have followed their specialties’ guidelines and find themselves in the middle of a malpractice suit."
Under the bill, clinical guidelines developed by professional medical organizations would be used to determine whether a plaintiff’s lawsuit could continue against a physician defendant. If a doctor adhered to the approved guidelines during the time of the alleged malpractice event, the case would be removed from court proceedings, while a medical review panel investigated the claim. The bill would also allow for relevant cases to be moved from state to federal court if they involved federal dollars such as Medicare.The bill was referred to the Subcommittee on the Constitution and Civil Justice on March 20 for review.
Dr. Bera declined to comment for this article. In a statement, he said the measure is a practical way to decrease the skyrocketing cost of health care and to ensure the malpractice system works better for patients and physicians.
"As a doctor, I know that physicians want to do what’s best for their patients, and promoting evidence-based medicine will help us do that," he said.
The proposed safe harbor measure is a beneficial initiative that would potentially have a positive impact on multiple aspects of the health care system, adds Dr. David A. Fleming, president-elect of the American College of Physicians and chair of the department of medicine for the University of Missouri–Columbia.
"I think anything that standardized a patient-centered and evidence-based approach to care will serve only to improve clinical outcomes and decrease health care costs, as well as decrease liability costs at every level," Dr. Fleming said in an interview. "Encouraging the use of generally accepted and evidence-based clinical guidelines, as promoted by the Saving Lives, Saving Costs federal bill, is a good way to reach that."
Dr. Fleming noted an ACP position paper published in April that discusses the medical liability crisis physicians continue to face and outlines innovative solutions for a better malpractice environment. "Medical Liability Reform – Innovative Solutions for New Health Care System," also provides an update on state-based medical liability activities and summarizes traditional and newer tort reform proposals.
The paper highlights the positive effect of such state reforms as caps on noneconomic damages, injury funds, stronger expert witness rules, and alternative dispute resolution initiatives such as apology, disclosure, and compensation programs. The report provides nine approaches that should be incorporated into a multifaceted medical malpractice reform initiative, including passage of a comprehensive tort reform package, oversight of medical liability insurers, and development of effective safe harbor protections that improve quality of care, increase efficiency, and reduce costs.
As for federal reform, Dr. Fleming said legislation at the congressional level often faces successful challenges by trial attorneys and advocacy groups that argue plaintiffs’ rights would be violated. The politicization of the issue is also a problem, he said. However, federal tort reform is still possible and physicians should keep advocating significant changes by Congress, he said.
"The litigious environment in which we live continues to contribute to a sense of fear and consternation by practicing physicians that affects how they relate to patients and undoubtedly adds to health care costs," Dr. Fleming said.
Along with the Saving Lives, Saving Costs bills, doctors are closely watching several other federal malpractice reform measures under review. For instance, the Health Care Safety Net Enhancement Act would help ensure that physicians furnishing medical services, pursuant to the Emergency Medical Treatment & Active Labor Act (EMTALA), receive the same liability coverage currently extended to health professionals who provide Medicaid services at free clinics. The bill has been referred to the Subcommittee on Health.
Meanwhile, the Standard of Care Protection Act of 2013 would ensure that provisions of the Affordable Care Act and other federal laws cannot be used to create new standards of care for medical liability lawsuits. The proposed law was included in the recent Medicare Sustainable Growth Rate Formula bill, which passed out of the Energy and Commerce Committee.
"With so many changes occurring in the health care system, physicians are rightly concerned that federal rules and regulations could result in new, unwarranted, liability exposures," Dr. Jennings said. "This legislation helps safeguard physicians."
Physician leaders are voicing support for a proposed federal law that aims to reduce litigation against doctors, lower health care costs, and establish more fairness in the analyzing of malpractice claims. The Saving Lives, Saving Costs Act, introduced in March by Rep. Dr. Ami Bera, (D-CA), would provide safe harbor protection to doctors who are sued if they followed evidence-based clinical guidelines.
"The Bera/Barr bill would accomplish two very important things," said Dr. John C. Jennings, president of the American Congress of Obstetricians and Gynecologists and professor of obstetrics and gynecology at Texas Tech University Health Sciences Center at the Permian Basin. "First, it would provide an incentive for every physician to follow the best clinical guidelines developed by his or her specialty, reducing care variations and potentially increasing patient safety and quality of care. Second, it would provide an affirmative defense for physicians who have followed their specialties’ guidelines and find themselves in the middle of a malpractice suit."
Under the bill, clinical guidelines developed by professional medical organizations would be used to determine whether a plaintiff’s lawsuit could continue against a physician defendant. If a doctor adhered to the approved guidelines during the time of the alleged malpractice event, the case would be removed from court proceedings, while a medical review panel investigated the claim. The bill would also allow for relevant cases to be moved from state to federal court if they involved federal dollars such as Medicare.The bill was referred to the Subcommittee on the Constitution and Civil Justice on March 20 for review.
Dr. Bera declined to comment for this article. In a statement, he said the measure is a practical way to decrease the skyrocketing cost of health care and to ensure the malpractice system works better for patients and physicians.
"As a doctor, I know that physicians want to do what’s best for their patients, and promoting evidence-based medicine will help us do that," he said.
The proposed safe harbor measure is a beneficial initiative that would potentially have a positive impact on multiple aspects of the health care system, adds Dr. David A. Fleming, president-elect of the American College of Physicians and chair of the department of medicine for the University of Missouri–Columbia.
"I think anything that standardized a patient-centered and evidence-based approach to care will serve only to improve clinical outcomes and decrease health care costs, as well as decrease liability costs at every level," Dr. Fleming said in an interview. "Encouraging the use of generally accepted and evidence-based clinical guidelines, as promoted by the Saving Lives, Saving Costs federal bill, is a good way to reach that."
Dr. Fleming noted an ACP position paper published in April that discusses the medical liability crisis physicians continue to face and outlines innovative solutions for a better malpractice environment. "Medical Liability Reform – Innovative Solutions for New Health Care System," also provides an update on state-based medical liability activities and summarizes traditional and newer tort reform proposals.
The paper highlights the positive effect of such state reforms as caps on noneconomic damages, injury funds, stronger expert witness rules, and alternative dispute resolution initiatives such as apology, disclosure, and compensation programs. The report provides nine approaches that should be incorporated into a multifaceted medical malpractice reform initiative, including passage of a comprehensive tort reform package, oversight of medical liability insurers, and development of effective safe harbor protections that improve quality of care, increase efficiency, and reduce costs.
As for federal reform, Dr. Fleming said legislation at the congressional level often faces successful challenges by trial attorneys and advocacy groups that argue plaintiffs’ rights would be violated. The politicization of the issue is also a problem, he said. However, federal tort reform is still possible and physicians should keep advocating significant changes by Congress, he said.
"The litigious environment in which we live continues to contribute to a sense of fear and consternation by practicing physicians that affects how they relate to patients and undoubtedly adds to health care costs," Dr. Fleming said.
Along with the Saving Lives, Saving Costs bills, doctors are closely watching several other federal malpractice reform measures under review. For instance, the Health Care Safety Net Enhancement Act would help ensure that physicians furnishing medical services, pursuant to the Emergency Medical Treatment & Active Labor Act (EMTALA), receive the same liability coverage currently extended to health professionals who provide Medicaid services at free clinics. The bill has been referred to the Subcommittee on Health.
Meanwhile, the Standard of Care Protection Act of 2013 would ensure that provisions of the Affordable Care Act and other federal laws cannot be used to create new standards of care for medical liability lawsuits. The proposed law was included in the recent Medicare Sustainable Growth Rate Formula bill, which passed out of the Energy and Commerce Committee.
"With so many changes occurring in the health care system, physicians are rightly concerned that federal rules and regulations could result in new, unwarranted, liability exposures," Dr. Jennings said. "This legislation helps safeguard physicians."

Insurers address ACA 90-day grace period issue
Representatives of major insurance companies assured lawmakers that they have systems in place by which physicians can check whether patients newly insured through the state and federal health exchanges were up to date on payments for their premiums and thus eligible for coverage.
The insurers – Aetna, Cigna, Health Care Service Corporation, and Wellpoint – appeared May 7 before the House Energy and Commerce Oversight and Investigations Subcommittee to answer questions about how many enrollees under the Affordable Care Act’s state and federal health insurance exchanges have paid their premiums.

Rep. Michael Burgess (R-Tex.), a physician and a subcommittee member, said that he was especially concerned about the 90-day grace period that could create a situation in which care delivered by doctors is not covered by insurance companies.
The grace period was built into the Affordable Care Act.
According to the law, patients must pay their first month’s premium to be considered enrolled and verified as insured. After that, however, they have 90 days to pay the next premium. If the patient doesn’t pay for the second month, the insurer can hold or "pend" all claims. By the third month, if the patient still has not paid, the insurer can terminate the policy. The physician is left to collect from the patient whatever is owed for all outstanding claims.
The insurance company officials who testified at the hearing said that they had systems in place that gave physicians the ability to determine if a patient was current on payments and thus eligible for coverage. They did not give much detail beyond that.
Paul Wingle, executive director of individual business and public exchange operations and strategy at Aetna, said that doctors can call Aetna for updates on a patient’s payment status.
Brian Evanko, president of the individual segment at Cigna, said that physicians and hospitals can call or check online for a patient’s current insurance eligibility. J. Darren Rodgers, a senior vice president and marketing officer at Health Care Service Corporation, and Dennis Matheis, president of exchange strategy for Wellpoint, also said that their companies offered similar services for physicians to verify eligibility.
Rep. Burgess said that he still had concerns that physicians could end up delivering uncompensated care.
The insurers also said that, so far, it appears that a majority of exchange plan enrollees are paying their premiums.
Aetna enrolled 600,000 individuals by the third week in April. Of those, 500,000 have paid, said Mr. Wingle, noting that, since many enrollees have not reached the payment due date for coverage, the figure is "dynamic."
Cigna’s Mr. Evanko did not give enrollment or payment data.
Health Care Service Corporation had 830,000 applications for coverage – 600,000 on the exchanges and 230,000 from outside the exchanges, said Mr. Rodgers. In January, February, and March, 85%-88% of exchange plan enrollees had paid.
The payment rate dropped to 83% on April 1; May figures were incomplete, he said.
Mr. Matheis of Wellpoint testified that "we are seeing strong membership growth and large percentages of our newly enrolled customers are successfully paying their premiums by the due date."
He said that, overall, 70% of premiums have been paid, but that figure includes enrollees whose payments were not yet due. For those whose premium deadline has passed, the payment rate is up to 90%, said Mr. Matheis.
Rep. Tim Murphy (R-Pa.), chairman of the oversight and investigations subcommittee, said that the data submitted to the panel by insurers in late April "paints an uneven picture about the status of enrollment and payment through April 15."
A report issued by the Energy and Commerce Committee on April 30 claimed that data from insurers showed that 67% of the enrollees in the federal exchanges had paid their first month’s premium. Rep. Murphy said that the report showed a wild variation in payment rates by state, and that more information was needed.
"We recognize that many individuals still have time to pay their first month’s premium, which is why we have asked the insurers to update this information on May 20," he said.
On Twitter @aliciaault
Representatives of major insurance companies assured lawmakers that they have systems in place by which physicians can check whether patients newly insured through the state and federal health exchanges were up to date on payments for their premiums and thus eligible for coverage.
The insurers – Aetna, Cigna, Health Care Service Corporation, and Wellpoint – appeared May 7 before the House Energy and Commerce Oversight and Investigations Subcommittee to answer questions about how many enrollees under the Affordable Care Act’s state and federal health insurance exchanges have paid their premiums.
Rep. Michael Burgess (R-Tex.), a physician and a subcommittee member, said that he was especially concerned about the 90-day grace period that could create a situation in which care delivered by doctors is not covered by insurance companies.
The grace period was built into the Affordable Care Act.
According to the law, patients must pay their first month’s premium to be considered enrolled and verified as insured. After that, however, they have 90 days to pay the next premium. If the patient doesn’t pay for the second month, the insurer can hold or "pend" all claims. By the third month, if the patient still has not paid, the insurer can terminate the policy. The physician is left to collect from the patient whatever is owed for all outstanding claims.
The insurance company officials who testified at the hearing said that they had systems in place that gave physicians the ability to determine if a patient was current on payments and thus eligible for coverage. They did not give much detail beyond that.
Paul Wingle, executive director of individual business and public exchange operations and strategy at Aetna, said that doctors can call Aetna for updates on a patient’s payment status.
Brian Evanko, president of the individual segment at Cigna, said that physicians and hospitals can call or check online for a patient’s current insurance eligibility. J. Darren Rodgers, a senior vice president and marketing officer at Health Care Service Corporation, and Dennis Matheis, president of exchange strategy for Wellpoint, also said that their companies offered similar services for physicians to verify eligibility.
Rep. Burgess said that he still had concerns that physicians could end up delivering uncompensated care.
The insurers also said that, so far, it appears that a majority of exchange plan enrollees are paying their premiums.
Aetna enrolled 600,000 individuals by the third week in April. Of those, 500,000 have paid, said Mr. Wingle, noting that, since many enrollees have not reached the payment due date for coverage, the figure is "dynamic."
Cigna’s Mr. Evanko did not give enrollment or payment data.
Health Care Service Corporation had 830,000 applications for coverage – 600,000 on the exchanges and 230,000 from outside the exchanges, said Mr. Rodgers. In January, February, and March, 85%-88% of exchange plan enrollees had paid.
The payment rate dropped to 83% on April 1; May figures were incomplete, he said.
Mr. Matheis of Wellpoint testified that "we are seeing strong membership growth and large percentages of our newly enrolled customers are successfully paying their premiums by the due date."
He said that, overall, 70% of premiums have been paid, but that figure includes enrollees whose payments were not yet due. For those whose premium deadline has passed, the payment rate is up to 90%, said Mr. Matheis.
Rep. Tim Murphy (R-Pa.), chairman of the oversight and investigations subcommittee, said that the data submitted to the panel by insurers in late April "paints an uneven picture about the status of enrollment and payment through April 15."
A report issued by the Energy and Commerce Committee on April 30 claimed that data from insurers showed that 67% of the enrollees in the federal exchanges had paid their first month’s premium. Rep. Murphy said that the report showed a wild variation in payment rates by state, and that more information was needed.
"We recognize that many individuals still have time to pay their first month’s premium, which is why we have asked the insurers to update this information on May 20," he said.
On Twitter @aliciaault
Representatives of major insurance companies assured lawmakers that they have systems in place by which physicians can check whether patients newly insured through the state and federal health exchanges were up to date on payments for their premiums and thus eligible for coverage.
The insurers – Aetna, Cigna, Health Care Service Corporation, and Wellpoint – appeared May 7 before the House Energy and Commerce Oversight and Investigations Subcommittee to answer questions about how many enrollees under the Affordable Care Act’s state and federal health insurance exchanges have paid their premiums.
Rep. Michael Burgess (R-Tex.), a physician and a subcommittee member, said that he was especially concerned about the 90-day grace period that could create a situation in which care delivered by doctors is not covered by insurance companies.
The grace period was built into the Affordable Care Act.
According to the law, patients must pay their first month’s premium to be considered enrolled and verified as insured. After that, however, they have 90 days to pay the next premium. If the patient doesn’t pay for the second month, the insurer can hold or "pend" all claims. By the third month, if the patient still has not paid, the insurer can terminate the policy. The physician is left to collect from the patient whatever is owed for all outstanding claims.
The insurance company officials who testified at the hearing said that they had systems in place that gave physicians the ability to determine if a patient was current on payments and thus eligible for coverage. They did not give much detail beyond that.
Paul Wingle, executive director of individual business and public exchange operations and strategy at Aetna, said that doctors can call Aetna for updates on a patient’s payment status.
Brian Evanko, president of the individual segment at Cigna, said that physicians and hospitals can call or check online for a patient’s current insurance eligibility. J. Darren Rodgers, a senior vice president and marketing officer at Health Care Service Corporation, and Dennis Matheis, president of exchange strategy for Wellpoint, also said that their companies offered similar services for physicians to verify eligibility.
Rep. Burgess said that he still had concerns that physicians could end up delivering uncompensated care.
The insurers also said that, so far, it appears that a majority of exchange plan enrollees are paying their premiums.
Aetna enrolled 600,000 individuals by the third week in April. Of those, 500,000 have paid, said Mr. Wingle, noting that, since many enrollees have not reached the payment due date for coverage, the figure is "dynamic."
Cigna’s Mr. Evanko did not give enrollment or payment data.
Health Care Service Corporation had 830,000 applications for coverage – 600,000 on the exchanges and 230,000 from outside the exchanges, said Mr. Rodgers. In January, February, and March, 85%-88% of exchange plan enrollees had paid.
The payment rate dropped to 83% on April 1; May figures were incomplete, he said.
Mr. Matheis of Wellpoint testified that "we are seeing strong membership growth and large percentages of our newly enrolled customers are successfully paying their premiums by the due date."
He said that, overall, 70% of premiums have been paid, but that figure includes enrollees whose payments were not yet due. For those whose premium deadline has passed, the payment rate is up to 90%, said Mr. Matheis.
Rep. Tim Murphy (R-Pa.), chairman of the oversight and investigations subcommittee, said that the data submitted to the panel by insurers in late April "paints an uneven picture about the status of enrollment and payment through April 15."
A report issued by the Energy and Commerce Committee on April 30 claimed that data from insurers showed that 67% of the enrollees in the federal exchanges had paid their first month’s premium. Rep. Murphy said that the report showed a wild variation in payment rates by state, and that more information was needed.
"We recognize that many individuals still have time to pay their first month’s premium, which is why we have asked the insurers to update this information on May 20," he said.
On Twitter @aliciaault

Analysis finds the ED a profit center; ACA may drive higher profits
The emergency department is a profit center for many hospitals – and could help drive profits even higher as the Affordable Care Act extends insurance coverage to more Americans.
Dr. Michael Wilson, an emergency physician at Brigham and Women’s Hospital, Boston, and David M. Cutler, Ph.D., an economics professor at Harvard University, Cambridge, Mass., looked at more than 11 million emergency department (ED) visits for which patient-level revenue information was available as well as 20 million observations with charge data.
Of those visits, 35% were covered by private insurance, 26% by Medicaid, 21% by Medicare, and 18% were uninsured.

They found that in 2009, hospitals generated ED revenues of about $79 billion, at a cost of $73 billion. The $6.1 billion profit translated into an almost 8% profit margin. The profits came primarily from private pay patients. Hospitals made a 40% margin on the privately insured, or about $17 billion, according to the analysis. This compensated for losses on Medicare (–6%), Medicaid (–40%), and the uninsured (–60%) (Health Affairs 2014;5792-9 [doi 10.1377/hlthaff.2013.0754]).
"One of the more surprising findings was just how dependent the emergency department is on payer mix," Dr. Wilson said, adding that EDs that do not have a large number of private pay patients may not be as profitable.
Dr. Wes Fields, *former chairman of the American College of Emergency Physicians’ Emergency Medicine Action Fund, agreed that payer mix is a key.
"For patients or policy makers trying to interpret the meaning of this study for their own community, it is important to remember that hospital profitability is like real estate valuation: ‘location, location, location,’ " Dr. Fields said.
A spokeswoman with the American Hospital Association said that it’s not just about payer mix. "It is hard to really measure the costs of ED care," said Marie Watteau, of the AHA. "Hospitals have to maintain the standby capacity of an ED 24/7 and that means having trauma teams at the ready. The costs to maintain that service is spread over all of the services provided by the hospital," she said.
Under the ACA, the number of paying patients should improve, Dr. Wilson said. He predicted that by 2023, profit margins would increase to 12%, using a scenario in which 50% of the uninsured remain uninsured, 25% gain private insurance, and 25% enroll in Medicaid. This also assumes that reimbursement for private insurance is at a rate that’s at the midpoint between employer-sponsored private insurance and Medicaid pay. Without the ACA, profit margins would continue to hover around 7%, they said.
Dr. Fields said he was a little skeptical that more Medicaid coverage would increase revenues or profits. Some studies have shown that people who gain Medicaid coverage often are high utilizers of EDs, he said. More use means adding more staff, which is one of the biggest costs for hospitals.
On Twitter @aliciaault
*Correction 5/8/14: A previous version of this story misidentified Dr. Wes Fields as the chairman of the American College of Emergency Physicians’ Emergency Medicine Action Fund. This version has been corrected and updated.
The emergency department is a profit center for many hospitals – and could help drive profits even higher as the Affordable Care Act extends insurance coverage to more Americans.
Dr. Michael Wilson, an emergency physician at Brigham and Women’s Hospital, Boston, and David M. Cutler, Ph.D., an economics professor at Harvard University, Cambridge, Mass., looked at more than 11 million emergency department (ED) visits for which patient-level revenue information was available as well as 20 million observations with charge data.
Of those visits, 35% were covered by private insurance, 26% by Medicaid, 21% by Medicare, and 18% were uninsured.
They found that in 2009, hospitals generated ED revenues of about $79 billion, at a cost of $73 billion. The $6.1 billion profit translated into an almost 8% profit margin. The profits came primarily from private pay patients. Hospitals made a 40% margin on the privately insured, or about $17 billion, according to the analysis. This compensated for losses on Medicare (–6%), Medicaid (–40%), and the uninsured (–60%) (Health Affairs 2014;5792-9 [doi 10.1377/hlthaff.2013.0754]).
"One of the more surprising findings was just how dependent the emergency department is on payer mix," Dr. Wilson said, adding that EDs that do not have a large number of private pay patients may not be as profitable.
Dr. Wes Fields, *former chairman of the American College of Emergency Physicians’ Emergency Medicine Action Fund, agreed that payer mix is a key.
"For patients or policy makers trying to interpret the meaning of this study for their own community, it is important to remember that hospital profitability is like real estate valuation: ‘location, location, location,’ " Dr. Fields said.
A spokeswoman with the American Hospital Association said that it’s not just about payer mix. "It is hard to really measure the costs of ED care," said Marie Watteau, of the AHA. "Hospitals have to maintain the standby capacity of an ED 24/7 and that means having trauma teams at the ready. The costs to maintain that service is spread over all of the services provided by the hospital," she said.
Under the ACA, the number of paying patients should improve, Dr. Wilson said. He predicted that by 2023, profit margins would increase to 12%, using a scenario in which 50% of the uninsured remain uninsured, 25% gain private insurance, and 25% enroll in Medicaid. This also assumes that reimbursement for private insurance is at a rate that’s at the midpoint between employer-sponsored private insurance and Medicaid pay. Without the ACA, profit margins would continue to hover around 7%, they said.
Dr. Fields said he was a little skeptical that more Medicaid coverage would increase revenues or profits. Some studies have shown that people who gain Medicaid coverage often are high utilizers of EDs, he said. More use means adding more staff, which is one of the biggest costs for hospitals.
On Twitter @aliciaault
*Correction 5/8/14: A previous version of this story misidentified Dr. Wes Fields as the chairman of the American College of Emergency Physicians’ Emergency Medicine Action Fund. This version has been corrected and updated.
The emergency department is a profit center for many hospitals – and could help drive profits even higher as the Affordable Care Act extends insurance coverage to more Americans.
Dr. Michael Wilson, an emergency physician at Brigham and Women’s Hospital, Boston, and David M. Cutler, Ph.D., an economics professor at Harvard University, Cambridge, Mass., looked at more than 11 million emergency department (ED) visits for which patient-level revenue information was available as well as 20 million observations with charge data.
Of those visits, 35% were covered by private insurance, 26% by Medicaid, 21% by Medicare, and 18% were uninsured.
They found that in 2009, hospitals generated ED revenues of about $79 billion, at a cost of $73 billion. The $6.1 billion profit translated into an almost 8% profit margin. The profits came primarily from private pay patients. Hospitals made a 40% margin on the privately insured, or about $17 billion, according to the analysis. This compensated for losses on Medicare (–6%), Medicaid (–40%), and the uninsured (–60%) (Health Affairs 2014;5792-9 [doi 10.1377/hlthaff.2013.0754]).
"One of the more surprising findings was just how dependent the emergency department is on payer mix," Dr. Wilson said, adding that EDs that do not have a large number of private pay patients may not be as profitable.
Dr. Wes Fields, *former chairman of the American College of Emergency Physicians’ Emergency Medicine Action Fund, agreed that payer mix is a key.
"For patients or policy makers trying to interpret the meaning of this study for their own community, it is important to remember that hospital profitability is like real estate valuation: ‘location, location, location,’ " Dr. Fields said.
A spokeswoman with the American Hospital Association said that it’s not just about payer mix. "It is hard to really measure the costs of ED care," said Marie Watteau, of the AHA. "Hospitals have to maintain the standby capacity of an ED 24/7 and that means having trauma teams at the ready. The costs to maintain that service is spread over all of the services provided by the hospital," she said.
Under the ACA, the number of paying patients should improve, Dr. Wilson said. He predicted that by 2023, profit margins would increase to 12%, using a scenario in which 50% of the uninsured remain uninsured, 25% gain private insurance, and 25% enroll in Medicaid. This also assumes that reimbursement for private insurance is at a rate that’s at the midpoint between employer-sponsored private insurance and Medicaid pay. Without the ACA, profit margins would continue to hover around 7%, they said.
Dr. Fields said he was a little skeptical that more Medicaid coverage would increase revenues or profits. Some studies have shown that people who gain Medicaid coverage often are high utilizers of EDs, he said. More use means adding more staff, which is one of the biggest costs for hospitals.
On Twitter @aliciaault
*Correction 5/8/14: A previous version of this story misidentified Dr. Wes Fields as the chairman of the American College of Emergency Physicians’ Emergency Medicine Action Fund. This version has been corrected and updated.
FROM THE JOURNAL HEALTH AFFAIRS
Major finding: Hospital EDs had an 8% profit margin in 2009, which may rise to 12% with additional insurance coverage provided through the Affordable Care Act.
Data source: An analysis of Medicare, Medicaid and private insurance cost, charge, and reimbursement data for 11 million ED visits.
Disclosures: Funding provided by the National Institute on Aging. The authors reported no conflicts.

Backlash grows against MOC process
Resistance against the American Board of Internal Medicine’s maintenance of certification process is growing, with an online petition to overturn the board’s most recent changes having collected more than 13,000 signatures at press time.
The petition was organized by Dr. Paul Teirstein, chief of cardiology and director of interventional cardiology for Scripps Clinic in La Jolla, Calif.
Dr. Teirstein said that he began the drive out of his own sense of frustration with the ABIM maintenance of certification (MOC) requirements. He e-mailed some physicians he knew and encouraged them to sign. The petition went viral soon after being posted on March 20, Dr. Teirstein said.
Those who sign the petition agree that:
• ABIM has made unreasonable changes in MOC requiring more frequent participation and higher fees.
• Scientific data demonstrating the benefit of MOC is lacking.
• MOC activities are complex, of questionable value, and detract from other worthwhile pursuits, including patient care and other educational activities.
• A test administered every 10 years for recertification is a sufficient metric for MOC.

The bottom line: Petition signers want the ABIM to overhaul the process and require recertification once every 10 years.
The ABIM took the effort seriously enough to respond on its Web site.
"As medical knowledge and practices continue to change, a continuous MOC program tells the community that a physician is staying up-to-date, has met a knowledge standard established by his or her physician peers, and is engaged in ongoing assessment of his or her practice," Dr. Richard Baron, ABIM president, said in the statement.
Physicians who commented on the petition did not agree.
Dr. Jesse Naghi, a third-year fellow at the University of California, San Diego, Sulpizio Cardiovascular Center, wrote, "Asking for more money on top of our already high recertification fees seems rather greedy."
"This is an arm-twisting and money-making scam by our own board," said Dr. Garrett Sanford, of Little Rock, Ark.
"We do recognize that there is a cost – for the large majority of our physicians, the entire program costs from $200 to $400 per year," said Dr. Baron, in his statement. "Our fee structure covers the costs of developing and administering the secure, computer-based exams at test centers nationwide, as well as the ongoing development and release of all ABIM self-assessment products," he said, adding, "I encourage the petition signers to visit ABIM’s revenue and expenses [Web page] for more information."
Petition signers also claim that contrary to the board’s contention, neither patients nor payers value the MOC process nor are they demanding that physicians prove they’ve met the requirements. They also say that there is no evidence that MOC improves quality of care.
The board does not agree. "There is a good deal of research demonstrating the value of MOC. From the validity of the examination, to the importance of independent assessments – clinicians are not good at evaluating their own weaknesses," according to Dr. Baron’s statement.
Dr. Baron also promised that the ABIM would create more ways for physicians to earn credit.
The ABIM’s open letter shows that "the petition has definitely had an impact," Dr. Teirstein said.
Dr. Ron Benbassat, a cofounder of Change Board Certification, a group that wants to scale back the MOC, called Dr. Baron’s remarks a "boilerplate political statement."

The MOC "should be eliminated, given the numerous CME programs that exist that are not only cost effective, but are incredibly successful, and do not take time away from patient care," said Dr. Benbassat, a board-certified internist in Beverly Hills, Calif., who has completed MOC once already.
Dr. Benbassat and the physicians who have joined Change Board Certification, believe that MOC should not be associated with hospital privileges, insurance reimbursement, or network participation. It should not be required for maintenance of licensure either, said Dr. Benbassat, who is concerned that ABIM is discussing tying licensure to MOC.
Meanwhile, the Association of American Physicians and Surgeons has filed suit against the American Board of Medical Specialties, claiming that the MOC process is a restraint of trade because it will effectively keep doctors from practicing if they do not participate. The suit was filed in the U.S. District Court for the District of New Jersey on April 23, and seeks to stop what it calls the ABMS’s "continuing violations of antitrust law and misrepresentations about the medical skills of physicians who decline to purchase and spend time on its program."
The organization is also aiming to get a refund of fees paid by its members to ABMS and its 24 member boards.
On Twitter @aliciaault
Resistance against the American Board of Internal Medicine’s maintenance of certification process is growing, with an online petition to overturn the board’s most recent changes having collected more than 13,000 signatures at press time.
The petition was organized by Dr. Paul Teirstein, chief of cardiology and director of interventional cardiology for Scripps Clinic in La Jolla, Calif.
Dr. Teirstein said that he began the drive out of his own sense of frustration with the ABIM maintenance of certification (MOC) requirements. He e-mailed some physicians he knew and encouraged them to sign. The petition went viral soon after being posted on March 20, Dr. Teirstein said.
Those who sign the petition agree that:
• ABIM has made unreasonable changes in MOC requiring more frequent participation and higher fees.
• Scientific data demonstrating the benefit of MOC is lacking.
• MOC activities are complex, of questionable value, and detract from other worthwhile pursuits, including patient care and other educational activities.
• A test administered every 10 years for recertification is a sufficient metric for MOC.
The bottom line: Petition signers want the ABIM to overhaul the process and require recertification once every 10 years.
The ABIM took the effort seriously enough to respond on its Web site.
"As medical knowledge and practices continue to change, a continuous MOC program tells the community that a physician is staying up-to-date, has met a knowledge standard established by his or her physician peers, and is engaged in ongoing assessment of his or her practice," Dr. Richard Baron, ABIM president, said in the statement.
Physicians who commented on the petition did not agree.
Dr. Jesse Naghi, a third-year fellow at the University of California, San Diego, Sulpizio Cardiovascular Center, wrote, "Asking for more money on top of our already high recertification fees seems rather greedy."
"This is an arm-twisting and money-making scam by our own board," said Dr. Garrett Sanford, of Little Rock, Ark.
"We do recognize that there is a cost – for the large majority of our physicians, the entire program costs from $200 to $400 per year," said Dr. Baron, in his statement. "Our fee structure covers the costs of developing and administering the secure, computer-based exams at test centers nationwide, as well as the ongoing development and release of all ABIM self-assessment products," he said, adding, "I encourage the petition signers to visit ABIM’s revenue and expenses [Web page] for more information."
Petition signers also claim that contrary to the board’s contention, neither patients nor payers value the MOC process nor are they demanding that physicians prove they’ve met the requirements. They also say that there is no evidence that MOC improves quality of care.
The board does not agree. "There is a good deal of research demonstrating the value of MOC. From the validity of the examination, to the importance of independent assessments – clinicians are not good at evaluating their own weaknesses," according to Dr. Baron’s statement.
Dr. Baron also promised that the ABIM would create more ways for physicians to earn credit.
The ABIM’s open letter shows that "the petition has definitely had an impact," Dr. Teirstein said.
Dr. Ron Benbassat, a cofounder of Change Board Certification, a group that wants to scale back the MOC, called Dr. Baron’s remarks a "boilerplate political statement."
The MOC "should be eliminated, given the numerous CME programs that exist that are not only cost effective, but are incredibly successful, and do not take time away from patient care," said Dr. Benbassat, a board-certified internist in Beverly Hills, Calif., who has completed MOC once already.
Dr. Benbassat and the physicians who have joined Change Board Certification, believe that MOC should not be associated with hospital privileges, insurance reimbursement, or network participation. It should not be required for maintenance of licensure either, said Dr. Benbassat, who is concerned that ABIM is discussing tying licensure to MOC.
Meanwhile, the Association of American Physicians and Surgeons has filed suit against the American Board of Medical Specialties, claiming that the MOC process is a restraint of trade because it will effectively keep doctors from practicing if they do not participate. The suit was filed in the U.S. District Court for the District of New Jersey on April 23, and seeks to stop what it calls the ABMS’s "continuing violations of antitrust law and misrepresentations about the medical skills of physicians who decline to purchase and spend time on its program."
The organization is also aiming to get a refund of fees paid by its members to ABMS and its 24 member boards.
On Twitter @aliciaault
Resistance against the American Board of Internal Medicine’s maintenance of certification process is growing, with an online petition to overturn the board’s most recent changes having collected more than 13,000 signatures at press time.
The petition was organized by Dr. Paul Teirstein, chief of cardiology and director of interventional cardiology for Scripps Clinic in La Jolla, Calif.
Dr. Teirstein said that he began the drive out of his own sense of frustration with the ABIM maintenance of certification (MOC) requirements. He e-mailed some physicians he knew and encouraged them to sign. The petition went viral soon after being posted on March 20, Dr. Teirstein said.
Those who sign the petition agree that:
• ABIM has made unreasonable changes in MOC requiring more frequent participation and higher fees.
• Scientific data demonstrating the benefit of MOC is lacking.
• MOC activities are complex, of questionable value, and detract from other worthwhile pursuits, including patient care and other educational activities.
• A test administered every 10 years for recertification is a sufficient metric for MOC.
The bottom line: Petition signers want the ABIM to overhaul the process and require recertification once every 10 years.
The ABIM took the effort seriously enough to respond on its Web site.
"As medical knowledge and practices continue to change, a continuous MOC program tells the community that a physician is staying up-to-date, has met a knowledge standard established by his or her physician peers, and is engaged in ongoing assessment of his or her practice," Dr. Richard Baron, ABIM president, said in the statement.
Physicians who commented on the petition did not agree.
Dr. Jesse Naghi, a third-year fellow at the University of California, San Diego, Sulpizio Cardiovascular Center, wrote, "Asking for more money on top of our already high recertification fees seems rather greedy."
"This is an arm-twisting and money-making scam by our own board," said Dr. Garrett Sanford, of Little Rock, Ark.
"We do recognize that there is a cost – for the large majority of our physicians, the entire program costs from $200 to $400 per year," said Dr. Baron, in his statement. "Our fee structure covers the costs of developing and administering the secure, computer-based exams at test centers nationwide, as well as the ongoing development and release of all ABIM self-assessment products," he said, adding, "I encourage the petition signers to visit ABIM’s revenue and expenses [Web page] for more information."
Petition signers also claim that contrary to the board’s contention, neither patients nor payers value the MOC process nor are they demanding that physicians prove they’ve met the requirements. They also say that there is no evidence that MOC improves quality of care.
The board does not agree. "There is a good deal of research demonstrating the value of MOC. From the validity of the examination, to the importance of independent assessments – clinicians are not good at evaluating their own weaknesses," according to Dr. Baron’s statement.
Dr. Baron also promised that the ABIM would create more ways for physicians to earn credit.
The ABIM’s open letter shows that "the petition has definitely had an impact," Dr. Teirstein said.
Dr. Ron Benbassat, a cofounder of Change Board Certification, a group that wants to scale back the MOC, called Dr. Baron’s remarks a "boilerplate political statement."
The MOC "should be eliminated, given the numerous CME programs that exist that are not only cost effective, but are incredibly successful, and do not take time away from patient care," said Dr. Benbassat, a board-certified internist in Beverly Hills, Calif., who has completed MOC once already.
Dr. Benbassat and the physicians who have joined Change Board Certification, believe that MOC should not be associated with hospital privileges, insurance reimbursement, or network participation. It should not be required for maintenance of licensure either, said Dr. Benbassat, who is concerned that ABIM is discussing tying licensure to MOC.
Meanwhile, the Association of American Physicians and Surgeons has filed suit against the American Board of Medical Specialties, claiming that the MOC process is a restraint of trade because it will effectively keep doctors from practicing if they do not participate. The suit was filed in the U.S. District Court for the District of New Jersey on April 23, and seeks to stop what it calls the ABMS’s "continuing violations of antitrust law and misrepresentations about the medical skills of physicians who decline to purchase and spend time on its program."
The organization is also aiming to get a refund of fees paid by its members to ABMS and its 24 member boards.
On Twitter @aliciaault

Black children more likely to visit ED with injuries
African American children and teenagers had higher rates of injury-related emergency department visits than did whites or Hispanics during 2009-2010, the National Center for Health Statistics said in a report released May 6.
Rates of such visits for non-Hispanic blacks were higher in all three age groups examined, with statistically significant differences seen between black children (232 visits per 1,000 persons) and Hispanic children (145 per 1,000) aged 0-4 years. The difference between blacks and whites aged 0-4 years (180 per 1,000) did not reach significance, according to the NCHS.
In the other two age groups, 5-12 years and 13-18 years, the visit rates between all three groups were statistically significant. For those aged 5-12 years, rates were 181 per 1,000 black children, 138 per 1,000 whites, and 90 per 1,000 Hispanics. Among 13- to 18-year-olds, ED visit rates for injuries were 241 for black teens, 176 for whites, and 135 for Hispanics, the NCHS said.
The researchers used data from the 2009-2010 National Hospital Ambulatory Medical Care Survey, which involved approximately 480 nonfederal, general, and short-stay hospitals and 35,000 ED visits each year.
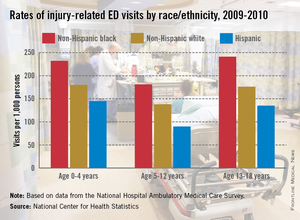
African American children and teenagers had higher rates of injury-related emergency department visits than did whites or Hispanics during 2009-2010, the National Center for Health Statistics said in a report released May 6.
Rates of such visits for non-Hispanic blacks were higher in all three age groups examined, with statistically significant differences seen between black children (232 visits per 1,000 persons) and Hispanic children (145 per 1,000) aged 0-4 years. The difference between blacks and whites aged 0-4 years (180 per 1,000) did not reach significance, according to the NCHS.
In the other two age groups, 5-12 years and 13-18 years, the visit rates between all three groups were statistically significant. For those aged 5-12 years, rates were 181 per 1,000 black children, 138 per 1,000 whites, and 90 per 1,000 Hispanics. Among 13- to 18-year-olds, ED visit rates for injuries were 241 for black teens, 176 for whites, and 135 for Hispanics, the NCHS said.
The researchers used data from the 2009-2010 National Hospital Ambulatory Medical Care Survey, which involved approximately 480 nonfederal, general, and short-stay hospitals and 35,000 ED visits each year.
African American children and teenagers had higher rates of injury-related emergency department visits than did whites or Hispanics during 2009-2010, the National Center for Health Statistics said in a report released May 6.
Rates of such visits for non-Hispanic blacks were higher in all three age groups examined, with statistically significant differences seen between black children (232 visits per 1,000 persons) and Hispanic children (145 per 1,000) aged 0-4 years. The difference between blacks and whites aged 0-4 years (180 per 1,000) did not reach significance, according to the NCHS.
In the other two age groups, 5-12 years and 13-18 years, the visit rates between all three groups were statistically significant. For those aged 5-12 years, rates were 181 per 1,000 black children, 138 per 1,000 whites, and 90 per 1,000 Hispanics. Among 13- to 18-year-olds, ED visit rates for injuries were 241 for black teens, 176 for whites, and 135 for Hispanics, the NCHS said.
The researchers used data from the 2009-2010 National Hospital Ambulatory Medical Care Survey, which involved approximately 480 nonfederal, general, and short-stay hospitals and 35,000 ED visits each year.