User login
Ultrasound’s arrhythmia localization surpassed ECG’s accuracy
SAN FRANCISCO – A new type of echocardiography that uses a high frame rate to track tissue motion allowed researchers to noninvasively map the source of cardiac arrhythmias in patients with significantly more precision than did standard 12-lead ECG recordings in a pilot, single-center study with 55 patients.
Electromechanical wave imaging (EWI) correctly identified the arrhythmia source in 53 of 55 (96%) patients scheduled to undergo arrhythmia ablation, whereas only 39 of the same 55 patients (71%) were correctly mapped using recordings from a standard 12-lead ECG read by several trained electrophysiologists. The findings from this pilot study suggested that EWI performed with noninvasive ultrasound can provide useful, added information to 12-lead ECG tracings to localize cardiac arrhythmias of various types prior to invasive procedures, Elaine Y. Wan, MD, said at the annual scientific sessions of the Heart Rhythm Society.
She cautioned, however, that future studies must still establish that adding EWI to standard preprocedural assessment can benefit patients by, for example, reducing their radiation dosages or shortening their procedure times.
Patients at Columbia University Medical Center in New York scheduled to undergo ablation for a cardiac arrhythmia first had noninvasive assessment with EWI and 12-lead ECG. Patients averaged 56 years old; 45% had an atrial flutter, 22% had Wolff-Parkinson-White syndrome accessory pathways, 20% had premature ventricular complexes, and 13% had an atrial tachycardia. The researchers used 3D electroanatomic arrhythmia mapping performed during ablation as the arrhythmia-localization standard against which they compared both the EWI and ECG results.
EWI can map cardiac electromechanical activity in all four heart chambers by tracking, with high temporal and spatial resolution, transient tissue deformations that occur in response to local electrical activation of cardiac myocytes, the depolarizations in cardiac muscle that produce tissue movement. The technique captures 2,000 image frames per second, creating a “video of tissue movement that lets us see where the movement started,” explained Dr. Wan, a cardiac electrophysiologist at Columbia.
Dr. Wan and associates previously reported use of EWI to successfully map accessory pathways in all 14 children with Wolff-Parkinson-White syndrome they tested versus success in 11 of these 14 patients (79%) when using expert interpretation of 12-lead ECG recordings (JACC Clin Electrophysiol. 2019 Apr;5[4]:427-37).
The new study is the first report on using EWI in adults, Dr. Wan noted. Advantages of EWI over 12-lead ECG include its lack of dependence on correct lead placement, and EWI does not share the inherent limitation of 12-lead ECG for localizing arrhythmias on the heart’s posterior wall, she said in a video interview.
SOURCE: Wan EY et al. Heart Rhythm 2019, Abstract S-LCT04-03.
SAN FRANCISCO – A new type of echocardiography that uses a high frame rate to track tissue motion allowed researchers to noninvasively map the source of cardiac arrhythmias in patients with significantly more precision than did standard 12-lead ECG recordings in a pilot, single-center study with 55 patients.
Electromechanical wave imaging (EWI) correctly identified the arrhythmia source in 53 of 55 (96%) patients scheduled to undergo arrhythmia ablation, whereas only 39 of the same 55 patients (71%) were correctly mapped using recordings from a standard 12-lead ECG read by several trained electrophysiologists. The findings from this pilot study suggested that EWI performed with noninvasive ultrasound can provide useful, added information to 12-lead ECG tracings to localize cardiac arrhythmias of various types prior to invasive procedures, Elaine Y. Wan, MD, said at the annual scientific sessions of the Heart Rhythm Society.
She cautioned, however, that future studies must still establish that adding EWI to standard preprocedural assessment can benefit patients by, for example, reducing their radiation dosages or shortening their procedure times.
Patients at Columbia University Medical Center in New York scheduled to undergo ablation for a cardiac arrhythmia first had noninvasive assessment with EWI and 12-lead ECG. Patients averaged 56 years old; 45% had an atrial flutter, 22% had Wolff-Parkinson-White syndrome accessory pathways, 20% had premature ventricular complexes, and 13% had an atrial tachycardia. The researchers used 3D electroanatomic arrhythmia mapping performed during ablation as the arrhythmia-localization standard against which they compared both the EWI and ECG results.
EWI can map cardiac electromechanical activity in all four heart chambers by tracking, with high temporal and spatial resolution, transient tissue deformations that occur in response to local electrical activation of cardiac myocytes, the depolarizations in cardiac muscle that produce tissue movement. The technique captures 2,000 image frames per second, creating a “video of tissue movement that lets us see where the movement started,” explained Dr. Wan, a cardiac electrophysiologist at Columbia.
Dr. Wan and associates previously reported use of EWI to successfully map accessory pathways in all 14 children with Wolff-Parkinson-White syndrome they tested versus success in 11 of these 14 patients (79%) when using expert interpretation of 12-lead ECG recordings (JACC Clin Electrophysiol. 2019 Apr;5[4]:427-37).
The new study is the first report on using EWI in adults, Dr. Wan noted. Advantages of EWI over 12-lead ECG include its lack of dependence on correct lead placement, and EWI does not share the inherent limitation of 12-lead ECG for localizing arrhythmias on the heart’s posterior wall, she said in a video interview.
SOURCE: Wan EY et al. Heart Rhythm 2019, Abstract S-LCT04-03.
SAN FRANCISCO – A new type of echocardiography that uses a high frame rate to track tissue motion allowed researchers to noninvasively map the source of cardiac arrhythmias in patients with significantly more precision than did standard 12-lead ECG recordings in a pilot, single-center study with 55 patients.
Electromechanical wave imaging (EWI) correctly identified the arrhythmia source in 53 of 55 (96%) patients scheduled to undergo arrhythmia ablation, whereas only 39 of the same 55 patients (71%) were correctly mapped using recordings from a standard 12-lead ECG read by several trained electrophysiologists. The findings from this pilot study suggested that EWI performed with noninvasive ultrasound can provide useful, added information to 12-lead ECG tracings to localize cardiac arrhythmias of various types prior to invasive procedures, Elaine Y. Wan, MD, said at the annual scientific sessions of the Heart Rhythm Society.
She cautioned, however, that future studies must still establish that adding EWI to standard preprocedural assessment can benefit patients by, for example, reducing their radiation dosages or shortening their procedure times.
Patients at Columbia University Medical Center in New York scheduled to undergo ablation for a cardiac arrhythmia first had noninvasive assessment with EWI and 12-lead ECG. Patients averaged 56 years old; 45% had an atrial flutter, 22% had Wolff-Parkinson-White syndrome accessory pathways, 20% had premature ventricular complexes, and 13% had an atrial tachycardia. The researchers used 3D electroanatomic arrhythmia mapping performed during ablation as the arrhythmia-localization standard against which they compared both the EWI and ECG results.
EWI can map cardiac electromechanical activity in all four heart chambers by tracking, with high temporal and spatial resolution, transient tissue deformations that occur in response to local electrical activation of cardiac myocytes, the depolarizations in cardiac muscle that produce tissue movement. The technique captures 2,000 image frames per second, creating a “video of tissue movement that lets us see where the movement started,” explained Dr. Wan, a cardiac electrophysiologist at Columbia.
Dr. Wan and associates previously reported use of EWI to successfully map accessory pathways in all 14 children with Wolff-Parkinson-White syndrome they tested versus success in 11 of these 14 patients (79%) when using expert interpretation of 12-lead ECG recordings (JACC Clin Electrophysiol. 2019 Apr;5[4]:427-37).
The new study is the first report on using EWI in adults, Dr. Wan noted. Advantages of EWI over 12-lead ECG include its lack of dependence on correct lead placement, and EWI does not share the inherent limitation of 12-lead ECG for localizing arrhythmias on the heart’s posterior wall, she said in a video interview.
SOURCE: Wan EY et al. Heart Rhythm 2019, Abstract S-LCT04-03.
REPORTING FROM HEART RHYTHM 2019

No raised risk of cardiovascular events for COPD patients on aclidinium
, compared with placebo, in a randomized trial of more than 3,000 patients.
Aclidinium, a long-acting muscarinic antagonist (LAMA), has been shown to reduce COPD exacerbation in the short term, but long-term effectiveness has not been examined, wrote Robert A. Wise, MD, of Johns Hopkins University, Baltimore, and colleagues.
ASCENT-COPD is a multicenter, double-blind, randomized, placebo-controlled, parallel-group noninferiority study conducted at 522 sites in the United States and Canada. A paper on recent data from ASCENT-COPD, published in JAMA, supports early findings reported last year at the American Thoracic Society meeting.
The researchers randomized adults with COPD to a 400-mg dose of aclidinium bromide twice daily, or placebo. The average age of the patients was 67 years; 59% were men. The median exposure time to aclidinium or placebo was 365 days during the first year of treatment, and the median exposure overall was 495 days for aclidinium patients and 478 days for placebo patients.
Of the 2,537 patients who completed the study, 69 (3.9%) in the aclidinium group and 76 (4.2%) in the placebo group experienced a major adverse cardiovascular event (MACE, defined as a composite of cardiovascular death, nonfatal myocardial infarction, and nonfatal stroke).
In addition, annual rates of moderate to severe COPD exacerbations were significantly lower in the aclidinium patients compared with placebo patients (0.44 vs. 0.57, P less than .001).
In a secondary analysis with a definition of MACE expanded to include heart failure, arrhythmias, or cerebrovascular disease, results remained similar between the groups; events occurred in 168 aclidinium patients (9.4%) and 160 placebo patients (8.9%). The rate of COPD exacerbations requiring hospitalization was significantly lower in aclidinium patients, compared with placebo patients (0.07 vs. 0.10, P = .006).
Overall, the most common treatment-emergent adverse events were similar in the aclidinium and placebo groups, respectively; pneumonia (6.1% vs. 5.8%), urinary tract infections (5.2% vs. 5.0%), and upper respiratory tract infections (4.8% vs. 5.6%). The most common serious adverse events (in at least 1% of patients) were pneumonia, atrial fibrillation, heart failure, and coronary artery disease. Dry mouth and urinary retention were rare, and occurred in less than 1% of patients in each group.
“No patient subgroup demonstrated a difference in efficacy except when analyzed by baseline COPD severity, in which the treatment benefit was observed only in patients with FEV1 [forced expiratory volume in 1 second] of 50% predicted or less,” the researchers noted. “This may be explained by the lower exacerbation rate seen in the placebo group in patients with moderate airway obstruction vs. severe or very severe obstruction,” they said.
“Outcomes of this trial add data to the long-standing controversy over the safety of LAMAs in COPD” and support the need for additional research, they said.
The study findings were limited by several factors including insufficient power to detect cause-specific mortality and the use of a LAMA with low risk of systemic effects, the researchers noted.
SOURCE: Wise R et al. JAMA. 2019. 321:1693-1701.
, compared with placebo, in a randomized trial of more than 3,000 patients.
Aclidinium, a long-acting muscarinic antagonist (LAMA), has been shown to reduce COPD exacerbation in the short term, but long-term effectiveness has not been examined, wrote Robert A. Wise, MD, of Johns Hopkins University, Baltimore, and colleagues.
ASCENT-COPD is a multicenter, double-blind, randomized, placebo-controlled, parallel-group noninferiority study conducted at 522 sites in the United States and Canada. A paper on recent data from ASCENT-COPD, published in JAMA, supports early findings reported last year at the American Thoracic Society meeting.
The researchers randomized adults with COPD to a 400-mg dose of aclidinium bromide twice daily, or placebo. The average age of the patients was 67 years; 59% were men. The median exposure time to aclidinium or placebo was 365 days during the first year of treatment, and the median exposure overall was 495 days for aclidinium patients and 478 days for placebo patients.
Of the 2,537 patients who completed the study, 69 (3.9%) in the aclidinium group and 76 (4.2%) in the placebo group experienced a major adverse cardiovascular event (MACE, defined as a composite of cardiovascular death, nonfatal myocardial infarction, and nonfatal stroke).
In addition, annual rates of moderate to severe COPD exacerbations were significantly lower in the aclidinium patients compared with placebo patients (0.44 vs. 0.57, P less than .001).
In a secondary analysis with a definition of MACE expanded to include heart failure, arrhythmias, or cerebrovascular disease, results remained similar between the groups; events occurred in 168 aclidinium patients (9.4%) and 160 placebo patients (8.9%). The rate of COPD exacerbations requiring hospitalization was significantly lower in aclidinium patients, compared with placebo patients (0.07 vs. 0.10, P = .006).
Overall, the most common treatment-emergent adverse events were similar in the aclidinium and placebo groups, respectively; pneumonia (6.1% vs. 5.8%), urinary tract infections (5.2% vs. 5.0%), and upper respiratory tract infections (4.8% vs. 5.6%). The most common serious adverse events (in at least 1% of patients) were pneumonia, atrial fibrillation, heart failure, and coronary artery disease. Dry mouth and urinary retention were rare, and occurred in less than 1% of patients in each group.
“No patient subgroup demonstrated a difference in efficacy except when analyzed by baseline COPD severity, in which the treatment benefit was observed only in patients with FEV1 [forced expiratory volume in 1 second] of 50% predicted or less,” the researchers noted. “This may be explained by the lower exacerbation rate seen in the placebo group in patients with moderate airway obstruction vs. severe or very severe obstruction,” they said.
“Outcomes of this trial add data to the long-standing controversy over the safety of LAMAs in COPD” and support the need for additional research, they said.
The study findings were limited by several factors including insufficient power to detect cause-specific mortality and the use of a LAMA with low risk of systemic effects, the researchers noted.
SOURCE: Wise R et al. JAMA. 2019. 321:1693-1701.
, compared with placebo, in a randomized trial of more than 3,000 patients.
Aclidinium, a long-acting muscarinic antagonist (LAMA), has been shown to reduce COPD exacerbation in the short term, but long-term effectiveness has not been examined, wrote Robert A. Wise, MD, of Johns Hopkins University, Baltimore, and colleagues.
ASCENT-COPD is a multicenter, double-blind, randomized, placebo-controlled, parallel-group noninferiority study conducted at 522 sites in the United States and Canada. A paper on recent data from ASCENT-COPD, published in JAMA, supports early findings reported last year at the American Thoracic Society meeting.
The researchers randomized adults with COPD to a 400-mg dose of aclidinium bromide twice daily, or placebo. The average age of the patients was 67 years; 59% were men. The median exposure time to aclidinium or placebo was 365 days during the first year of treatment, and the median exposure overall was 495 days for aclidinium patients and 478 days for placebo patients.
Of the 2,537 patients who completed the study, 69 (3.9%) in the aclidinium group and 76 (4.2%) in the placebo group experienced a major adverse cardiovascular event (MACE, defined as a composite of cardiovascular death, nonfatal myocardial infarction, and nonfatal stroke).
In addition, annual rates of moderate to severe COPD exacerbations were significantly lower in the aclidinium patients compared with placebo patients (0.44 vs. 0.57, P less than .001).
In a secondary analysis with a definition of MACE expanded to include heart failure, arrhythmias, or cerebrovascular disease, results remained similar between the groups; events occurred in 168 aclidinium patients (9.4%) and 160 placebo patients (8.9%). The rate of COPD exacerbations requiring hospitalization was significantly lower in aclidinium patients, compared with placebo patients (0.07 vs. 0.10, P = .006).
Overall, the most common treatment-emergent adverse events were similar in the aclidinium and placebo groups, respectively; pneumonia (6.1% vs. 5.8%), urinary tract infections (5.2% vs. 5.0%), and upper respiratory tract infections (4.8% vs. 5.6%). The most common serious adverse events (in at least 1% of patients) were pneumonia, atrial fibrillation, heart failure, and coronary artery disease. Dry mouth and urinary retention were rare, and occurred in less than 1% of patients in each group.
“No patient subgroup demonstrated a difference in efficacy except when analyzed by baseline COPD severity, in which the treatment benefit was observed only in patients with FEV1 [forced expiratory volume in 1 second] of 50% predicted or less,” the researchers noted. “This may be explained by the lower exacerbation rate seen in the placebo group in patients with moderate airway obstruction vs. severe or very severe obstruction,” they said.
“Outcomes of this trial add data to the long-standing controversy over the safety of LAMAs in COPD” and support the need for additional research, they said.
The study findings were limited by several factors including insufficient power to detect cause-specific mortality and the use of a LAMA with low risk of systemic effects, the researchers noted.
SOURCE: Wise R et al. JAMA. 2019. 321:1693-1701.
FROM JAMA

New risk score predicts cardiac-device infection
SAN FRANCISCO – Researchers have devised a five-item scoring formula to quantify the risk for infection in patients undergoing placement, revision, or removal of a cardiac-rhythm device based on data from nearly 20,000 patients enrolled in a recent infection-prophylaxis trial.
The risk score can help identify patients who might benefit from intensified antibiotic prophylaxis, and it can also help during shared decision making with patients to better understand the risk a patient faces from infection, compared with their predicted device benefit, David H. Birnie, MD, said at the annual scientific sessions of the Heart Rhythm Society.
The new risk score produced a concordance statistic, the area under the receiver-operator characteristic curve, of 0.704. It showed that, although it could use further validation, the score as it currently stands has substantial predictive value, said Dr. Birnie, professor of medicine at the University of Ottawa and deputy chief of cardiology at the University of Ottawa Heart Institute. “It’s certainly better than anything we have now,” he said in a video interview.
Dr. Birnie and his associates used data they collected on baseline characteristics and infection outcomes of the 19,603 patients enrolled in PADIT (Prevention of Arrhythmia Device Infection Trial) who underwent a rhythm-device procedure at 1 of 28 participating Canadian centers. The primary aim of PADIT was to assess the safety and efficacy of an intensified antibiotic-prophylaxis regimen, compared with a standard regimen of a cefazolin infusion just before the procedure. The study’s primary endpoint was the incidence of hospitalization for device infection during 1-year follow-up, and while the intensified prophylactic regimen linked with a 23% relative reduction in the hospitalization rate, compared with standard treatment, the difference was not statistically significant (J Am Coll Cardiol. 2018 Dec 18;72[24]:3098-109).
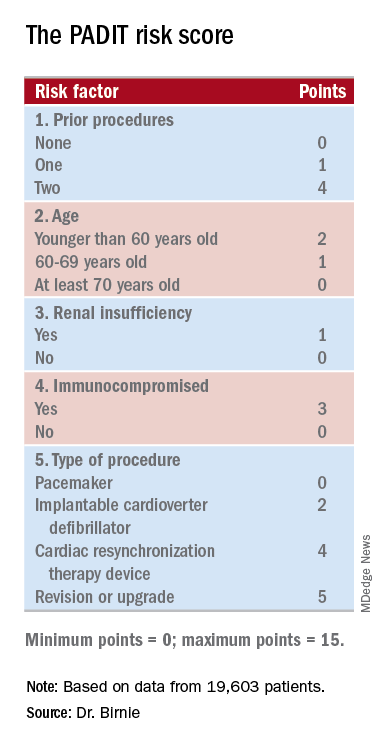
The researchers analyzed the baseline patient data and the blindly adjudicated infection outcomes and identified five factors that were independently associated with an increased infection rate. They organized the five factors and produced a formula they call the PADIT score (see chart). Those five factors are: prior procedures (the greater the number the greater the risk), age (which unexpectedly had an inverse relationship with infection incidence), depressed renal function, immuno-compromised status, and type of procedure. A patient can potentially score 0-15 points.
Among the PADIT patients a score of 0 correlated with about a 0.3% rate of hospitalization for a device-related infection during 1 year of follow-up, a score of 5 with about a 1.1% rate, a score of 6 with about a 1.8% rate, and a score of seven or more with a 3.4% infection rate over the following year. About 5% of patients had a score of 7 or more, and roughly another 5% had a score of 5 or 6, Dr. Birnie said. At his center, clinicians have begun routinely calculating scores for patients scheduled for an arrhythmia-device procedure, and they are considering routinely administering added antibiotic prophylaxis to patients with a preprocedural score of 6 or higher. They may also use the score to determine whether to use the antibacterial envelope recently reported to prevent cardiac-device infections (N Engl J Med. 2019 May 16;380[20]:1895-905).
“It’s very easy for patients to get to a PADIT score of 7 or higher,” Dr. Birnie noted. As an example, he cited a common patient, an 85-year-old with renal dysfunction who is under consideration for a second replacement of an implantable cardioverter defibrillator. The patient would score 1 point for renal insufficiency, 2 points for the type of device, and 4 points for having a prior history of two devices, and the consequent 3.4% risk for infection might counterbalance the potential benefit this elderly patient could expect from the new device. The score will be very important for targeting treatment, shared decision making, and selection of patients for future intervention trials, he concluded.

“I think this risk score will change practice by giving clinicians a better idea of a patient’s risk for infection,” commented Fred M. Kusumoto, MD, professor of medicine at the Mayo Medical School, Rochester, Minn., and director of heart rhythm services at the Mayo Clinic in Jacksonville, Fla. The PADIT score will help identify patients for whom leaving a device in place is a better option than taking it out because of their infection risk. The risk score could also help improve the cost effectiveness of preventive treatments, such as antibiotic-eluting envelopes, by targeting treatment to higher-risk patients, Dr. Kusumoto said during a press briefing.
SOURCE: Birnie DH. Heart Rhythm 2019, Absract S-LCT02-01.
I like this new infection risk score. It addresses a very clinically relevant issue. It’s important for the electrophysiology community to better understand how to best manage infections related to cardiac rhythm devices and ideally prevent them from happening.
I’m not a big fan of risk scores in general because they can sometimes detract from independent thinking about how to manage a patient. However, it is also helpful to have this type of risk-assessment information when discussing management options with a patient.
The PADIT risk score may also help identify which patients could potentially benefit the most from an antibiotic-eluting envelope when receiving an implanted cardiac-rhythm device. Recently reported results from WRAP-IT showed that routinely using envelopes cut the incidence of major infections by a relative 40%, but in absolute terms, the number needed to treat with the envelop to prevent one major infection was about 200 patients, a big number given the high cost of the envelope (N Engl J Med. 2019 May 16;380[20]:1895-905). It is therefore very interesting to think about using the PADIT risk score to better target an effective but expensive preventive measure like an antibiotic-eluting envelop to patients at the highest risk for infection.
Ulrika Birgersdotter-Green, MD , professor of medicine and director of pacemaker and ICD services at the University of California, San Diego, made these comments as a designated discussant for the report. She has been a consultant to and received honoraria from Abbott, Boston Scientific, and Medtronic.
I like this new infection risk score. It addresses a very clinically relevant issue. It’s important for the electrophysiology community to better understand how to best manage infections related to cardiac rhythm devices and ideally prevent them from happening.
I’m not a big fan of risk scores in general because they can sometimes detract from independent thinking about how to manage a patient. However, it is also helpful to have this type of risk-assessment information when discussing management options with a patient.
The PADIT risk score may also help identify which patients could potentially benefit the most from an antibiotic-eluting envelope when receiving an implanted cardiac-rhythm device. Recently reported results from WRAP-IT showed that routinely using envelopes cut the incidence of major infections by a relative 40%, but in absolute terms, the number needed to treat with the envelop to prevent one major infection was about 200 patients, a big number given the high cost of the envelope (N Engl J Med. 2019 May 16;380[20]:1895-905). It is therefore very interesting to think about using the PADIT risk score to better target an effective but expensive preventive measure like an antibiotic-eluting envelop to patients at the highest risk for infection.
Ulrika Birgersdotter-Green, MD , professor of medicine and director of pacemaker and ICD services at the University of California, San Diego, made these comments as a designated discussant for the report. She has been a consultant to and received honoraria from Abbott, Boston Scientific, and Medtronic.
I like this new infection risk score. It addresses a very clinically relevant issue. It’s important for the electrophysiology community to better understand how to best manage infections related to cardiac rhythm devices and ideally prevent them from happening.
I’m not a big fan of risk scores in general because they can sometimes detract from independent thinking about how to manage a patient. However, it is also helpful to have this type of risk-assessment information when discussing management options with a patient.
The PADIT risk score may also help identify which patients could potentially benefit the most from an antibiotic-eluting envelope when receiving an implanted cardiac-rhythm device. Recently reported results from WRAP-IT showed that routinely using envelopes cut the incidence of major infections by a relative 40%, but in absolute terms, the number needed to treat with the envelop to prevent one major infection was about 200 patients, a big number given the high cost of the envelope (N Engl J Med. 2019 May 16;380[20]:1895-905). It is therefore very interesting to think about using the PADIT risk score to better target an effective but expensive preventive measure like an antibiotic-eluting envelop to patients at the highest risk for infection.
Ulrika Birgersdotter-Green, MD , professor of medicine and director of pacemaker and ICD services at the University of California, San Diego, made these comments as a designated discussant for the report. She has been a consultant to and received honoraria from Abbott, Boston Scientific, and Medtronic.
SAN FRANCISCO – Researchers have devised a five-item scoring formula to quantify the risk for infection in patients undergoing placement, revision, or removal of a cardiac-rhythm device based on data from nearly 20,000 patients enrolled in a recent infection-prophylaxis trial.
The risk score can help identify patients who might benefit from intensified antibiotic prophylaxis, and it can also help during shared decision making with patients to better understand the risk a patient faces from infection, compared with their predicted device benefit, David H. Birnie, MD, said at the annual scientific sessions of the Heart Rhythm Society.
The new risk score produced a concordance statistic, the area under the receiver-operator characteristic curve, of 0.704. It showed that, although it could use further validation, the score as it currently stands has substantial predictive value, said Dr. Birnie, professor of medicine at the University of Ottawa and deputy chief of cardiology at the University of Ottawa Heart Institute. “It’s certainly better than anything we have now,” he said in a video interview.
Dr. Birnie and his associates used data they collected on baseline characteristics and infection outcomes of the 19,603 patients enrolled in PADIT (Prevention of Arrhythmia Device Infection Trial) who underwent a rhythm-device procedure at 1 of 28 participating Canadian centers. The primary aim of PADIT was to assess the safety and efficacy of an intensified antibiotic-prophylaxis regimen, compared with a standard regimen of a cefazolin infusion just before the procedure. The study’s primary endpoint was the incidence of hospitalization for device infection during 1-year follow-up, and while the intensified prophylactic regimen linked with a 23% relative reduction in the hospitalization rate, compared with standard treatment, the difference was not statistically significant (J Am Coll Cardiol. 2018 Dec 18;72[24]:3098-109).
The researchers analyzed the baseline patient data and the blindly adjudicated infection outcomes and identified five factors that were independently associated with an increased infection rate. They organized the five factors and produced a formula they call the PADIT score (see chart). Those five factors are: prior procedures (the greater the number the greater the risk), age (which unexpectedly had an inverse relationship with infection incidence), depressed renal function, immuno-compromised status, and type of procedure. A patient can potentially score 0-15 points.
Among the PADIT patients a score of 0 correlated with about a 0.3% rate of hospitalization for a device-related infection during 1 year of follow-up, a score of 5 with about a 1.1% rate, a score of 6 with about a 1.8% rate, and a score of seven or more with a 3.4% infection rate over the following year. About 5% of patients had a score of 7 or more, and roughly another 5% had a score of 5 or 6, Dr. Birnie said. At his center, clinicians have begun routinely calculating scores for patients scheduled for an arrhythmia-device procedure, and they are considering routinely administering added antibiotic prophylaxis to patients with a preprocedural score of 6 or higher. They may also use the score to determine whether to use the antibacterial envelope recently reported to prevent cardiac-device infections (N Engl J Med. 2019 May 16;380[20]:1895-905).
“It’s very easy for patients to get to a PADIT score of 7 or higher,” Dr. Birnie noted. As an example, he cited a common patient, an 85-year-old with renal dysfunction who is under consideration for a second replacement of an implantable cardioverter defibrillator. The patient would score 1 point for renal insufficiency, 2 points for the type of device, and 4 points for having a prior history of two devices, and the consequent 3.4% risk for infection might counterbalance the potential benefit this elderly patient could expect from the new device. The score will be very important for targeting treatment, shared decision making, and selection of patients for future intervention trials, he concluded.
“I think this risk score will change practice by giving clinicians a better idea of a patient’s risk for infection,” commented Fred M. Kusumoto, MD, professor of medicine at the Mayo Medical School, Rochester, Minn., and director of heart rhythm services at the Mayo Clinic in Jacksonville, Fla. The PADIT score will help identify patients for whom leaving a device in place is a better option than taking it out because of their infection risk. The risk score could also help improve the cost effectiveness of preventive treatments, such as antibiotic-eluting envelopes, by targeting treatment to higher-risk patients, Dr. Kusumoto said during a press briefing.
SOURCE: Birnie DH. Heart Rhythm 2019, Absract S-LCT02-01.
SAN FRANCISCO – Researchers have devised a five-item scoring formula to quantify the risk for infection in patients undergoing placement, revision, or removal of a cardiac-rhythm device based on data from nearly 20,000 patients enrolled in a recent infection-prophylaxis trial.
The risk score can help identify patients who might benefit from intensified antibiotic prophylaxis, and it can also help during shared decision making with patients to better understand the risk a patient faces from infection, compared with their predicted device benefit, David H. Birnie, MD, said at the annual scientific sessions of the Heart Rhythm Society.
The new risk score produced a concordance statistic, the area under the receiver-operator characteristic curve, of 0.704. It showed that, although it could use further validation, the score as it currently stands has substantial predictive value, said Dr. Birnie, professor of medicine at the University of Ottawa and deputy chief of cardiology at the University of Ottawa Heart Institute. “It’s certainly better than anything we have now,” he said in a video interview.
Dr. Birnie and his associates used data they collected on baseline characteristics and infection outcomes of the 19,603 patients enrolled in PADIT (Prevention of Arrhythmia Device Infection Trial) who underwent a rhythm-device procedure at 1 of 28 participating Canadian centers. The primary aim of PADIT was to assess the safety and efficacy of an intensified antibiotic-prophylaxis regimen, compared with a standard regimen of a cefazolin infusion just before the procedure. The study’s primary endpoint was the incidence of hospitalization for device infection during 1-year follow-up, and while the intensified prophylactic regimen linked with a 23% relative reduction in the hospitalization rate, compared with standard treatment, the difference was not statistically significant (J Am Coll Cardiol. 2018 Dec 18;72[24]:3098-109).
The researchers analyzed the baseline patient data and the blindly adjudicated infection outcomes and identified five factors that were independently associated with an increased infection rate. They organized the five factors and produced a formula they call the PADIT score (see chart). Those five factors are: prior procedures (the greater the number the greater the risk), age (which unexpectedly had an inverse relationship with infection incidence), depressed renal function, immuno-compromised status, and type of procedure. A patient can potentially score 0-15 points.
Among the PADIT patients a score of 0 correlated with about a 0.3% rate of hospitalization for a device-related infection during 1 year of follow-up, a score of 5 with about a 1.1% rate, a score of 6 with about a 1.8% rate, and a score of seven or more with a 3.4% infection rate over the following year. About 5% of patients had a score of 7 or more, and roughly another 5% had a score of 5 or 6, Dr. Birnie said. At his center, clinicians have begun routinely calculating scores for patients scheduled for an arrhythmia-device procedure, and they are considering routinely administering added antibiotic prophylaxis to patients with a preprocedural score of 6 or higher. They may also use the score to determine whether to use the antibacterial envelope recently reported to prevent cardiac-device infections (N Engl J Med. 2019 May 16;380[20]:1895-905).
“It’s very easy for patients to get to a PADIT score of 7 or higher,” Dr. Birnie noted. As an example, he cited a common patient, an 85-year-old with renal dysfunction who is under consideration for a second replacement of an implantable cardioverter defibrillator. The patient would score 1 point for renal insufficiency, 2 points for the type of device, and 4 points for having a prior history of two devices, and the consequent 3.4% risk for infection might counterbalance the potential benefit this elderly patient could expect from the new device. The score will be very important for targeting treatment, shared decision making, and selection of patients for future intervention trials, he concluded.
“I think this risk score will change practice by giving clinicians a better idea of a patient’s risk for infection,” commented Fred M. Kusumoto, MD, professor of medicine at the Mayo Medical School, Rochester, Minn., and director of heart rhythm services at the Mayo Clinic in Jacksonville, Fla. The PADIT score will help identify patients for whom leaving a device in place is a better option than taking it out because of their infection risk. The risk score could also help improve the cost effectiveness of preventive treatments, such as antibiotic-eluting envelopes, by targeting treatment to higher-risk patients, Dr. Kusumoto said during a press briefing.
SOURCE: Birnie DH. Heart Rhythm 2019, Absract S-LCT02-01.
REPORTING FROM HEART RHYTHM 2019
Key clinical point: Researchers have devised a five-item scoring formula to predict a patient’s risk for infection from an cardiac rhythm–device procedure.
Major finding: The risk score had an optimism-corrected concordance statistic of 0.704.
Study details: Investigators developed the risk score using data from PADIT, a multicenter, randomized trial with 19,603 patients.
Disclosures: PADIT received no commercial funding. Dr. Birnie had no relevant disclosures.
Source: Birnie DH. Heart Rhythm 2019, Absract S-LCT02-01.

AFib screening cuts hospitalizations and ED visits
NEW ORLEANS – People diagnosed with atrial fibrillation by screening with a wearable ECG patch had significantly fewer emergency department visits or hospital admissions, compared with similar people diagnosed with atrial fibrillation by usual-care surveillance in an observational study with 5,109 total participants.
People diagnosed with atrial fibrillation (AFib) through screening had a statistically significant 80% relative cut in hospitalizations and a 65% cut in emergency department visits during 12 months of follow-up, compared with controls in the study who had their AFib identified and diagnosed as part of routine practice, Steven R. Steinhubl, MD, said at the annual meeting of the American College of Cardiology.

The data also showed no difference between the screened and control patients identified with AFib in the average number of cardiologist consultations during a year of follow-up, and a trend that missed statistical significance for 16% fewer primary care physician visits in Afib patients diagnosed by screening rather than by routine surveillance.
These findings provided some insight into the potential clinical impact of AFib screening in at-risk people. Dr. Steinhubl and his associates plan to report on the incidence of strokes and MIs in the two study subgroups after 3 years of follow-up, but he noted that preliminary findings for these two outcomes after 1 year indicated that active screening for AFib also had reduced these rates, compared with waiting for the arrhythmia to become apparent by emergence of symptoms.
The data came from the mSToPS (mHealth Screening to Prevent Strokes) study, which randomized 2,659 U.S. residents enrolled in a large health plan who had risk factors for AFib to either immediate or delayed arrhythmia assessment by ECG patches. Half the participants used a patch for about 14 days immediately and then a second time 3 months later, while the other half waited 4 months and then wore an ECG patch for 2 weeks and again 3 months later. The primary endpoint, first reported at the ACC annual meeting a year before and subsequently published, was the incidence of newly diagnosed AFib during the first 4 months in the actively monitored cohort, compared with a cohort followed by usual care. The results showed that screening identified AFib in 3.9% of people, while no screening and usual-practice follow-up identified a 0.9% incidence of AFib, showing that screening worked better for AFib case identification (JAMA. 2018 Jul 10;320[2]:146-55).
To examine the clinical impact of screening and an increased incidence of diagnosed AFib cases, Dr. Steinhubl and his associates focused on 1,725 of the original 2,659 patients who underwent ECG patch assessment, either immediate or delayed, and continued through 12 months of follow-up, and compared them with 3,384 matched controls who never underwent ECG patch screening but were also followed for 12 months for incident AFib identified during routine care and surveillance. This resulted in a cumulative incidence of newly diagnosed AFib of 6.3% in those who had worn two ECG patches and 2.3% among the matched controls.
During follow-up, use of various interventions was more common among the screened people than the controls. Initiation of anticoagulation treatment started in 4.0% of the entire screened group, compared with 1.9% of the controls, The screened people also had a 0.9% rate of receiving a pacemaker or defibrillator, a 0.8% rate of starting on treatment with an antiarrhythmic drug, and a 0.3% rate of undergoing catheter ablation, compared with none, 0.3%, and one of the controls, respectively, said Dr. Steinhubl, director of digital medicine at the Scripps Research Translational Institute in La Jolla, Calif.
The mSToPS study was funded by Janssen. Dr. Steinhubl has received research funding from DynoSense, EasyG, Janssen, the Qualcomm Foundation, and Striv.
SOURCE: Steinhubl SR et al. J Am Coll Cardiol. 2019 Mar 12;73(9)suppl 1:296.
NEW ORLEANS – People diagnosed with atrial fibrillation by screening with a wearable ECG patch had significantly fewer emergency department visits or hospital admissions, compared with similar people diagnosed with atrial fibrillation by usual-care surveillance in an observational study with 5,109 total participants.
People diagnosed with atrial fibrillation (AFib) through screening had a statistically significant 80% relative cut in hospitalizations and a 65% cut in emergency department visits during 12 months of follow-up, compared with controls in the study who had their AFib identified and diagnosed as part of routine practice, Steven R. Steinhubl, MD, said at the annual meeting of the American College of Cardiology.
The data also showed no difference between the screened and control patients identified with AFib in the average number of cardiologist consultations during a year of follow-up, and a trend that missed statistical significance for 16% fewer primary care physician visits in Afib patients diagnosed by screening rather than by routine surveillance.
These findings provided some insight into the potential clinical impact of AFib screening in at-risk people. Dr. Steinhubl and his associates plan to report on the incidence of strokes and MIs in the two study subgroups after 3 years of follow-up, but he noted that preliminary findings for these two outcomes after 1 year indicated that active screening for AFib also had reduced these rates, compared with waiting for the arrhythmia to become apparent by emergence of symptoms.
The data came from the mSToPS (mHealth Screening to Prevent Strokes) study, which randomized 2,659 U.S. residents enrolled in a large health plan who had risk factors for AFib to either immediate or delayed arrhythmia assessment by ECG patches. Half the participants used a patch for about 14 days immediately and then a second time 3 months later, while the other half waited 4 months and then wore an ECG patch for 2 weeks and again 3 months later. The primary endpoint, first reported at the ACC annual meeting a year before and subsequently published, was the incidence of newly diagnosed AFib during the first 4 months in the actively monitored cohort, compared with a cohort followed by usual care. The results showed that screening identified AFib in 3.9% of people, while no screening and usual-practice follow-up identified a 0.9% incidence of AFib, showing that screening worked better for AFib case identification (JAMA. 2018 Jul 10;320[2]:146-55).
To examine the clinical impact of screening and an increased incidence of diagnosed AFib cases, Dr. Steinhubl and his associates focused on 1,725 of the original 2,659 patients who underwent ECG patch assessment, either immediate or delayed, and continued through 12 months of follow-up, and compared them with 3,384 matched controls who never underwent ECG patch screening but were also followed for 12 months for incident AFib identified during routine care and surveillance. This resulted in a cumulative incidence of newly diagnosed AFib of 6.3% in those who had worn two ECG patches and 2.3% among the matched controls.
During follow-up, use of various interventions was more common among the screened people than the controls. Initiation of anticoagulation treatment started in 4.0% of the entire screened group, compared with 1.9% of the controls, The screened people also had a 0.9% rate of receiving a pacemaker or defibrillator, a 0.8% rate of starting on treatment with an antiarrhythmic drug, and a 0.3% rate of undergoing catheter ablation, compared with none, 0.3%, and one of the controls, respectively, said Dr. Steinhubl, director of digital medicine at the Scripps Research Translational Institute in La Jolla, Calif.
The mSToPS study was funded by Janssen. Dr. Steinhubl has received research funding from DynoSense, EasyG, Janssen, the Qualcomm Foundation, and Striv.
SOURCE: Steinhubl SR et al. J Am Coll Cardiol. 2019 Mar 12;73(9)suppl 1:296.
NEW ORLEANS – People diagnosed with atrial fibrillation by screening with a wearable ECG patch had significantly fewer emergency department visits or hospital admissions, compared with similar people diagnosed with atrial fibrillation by usual-care surveillance in an observational study with 5,109 total participants.
People diagnosed with atrial fibrillation (AFib) through screening had a statistically significant 80% relative cut in hospitalizations and a 65% cut in emergency department visits during 12 months of follow-up, compared with controls in the study who had their AFib identified and diagnosed as part of routine practice, Steven R. Steinhubl, MD, said at the annual meeting of the American College of Cardiology.
The data also showed no difference between the screened and control patients identified with AFib in the average number of cardiologist consultations during a year of follow-up, and a trend that missed statistical significance for 16% fewer primary care physician visits in Afib patients diagnosed by screening rather than by routine surveillance.
These findings provided some insight into the potential clinical impact of AFib screening in at-risk people. Dr. Steinhubl and his associates plan to report on the incidence of strokes and MIs in the two study subgroups after 3 years of follow-up, but he noted that preliminary findings for these two outcomes after 1 year indicated that active screening for AFib also had reduced these rates, compared with waiting for the arrhythmia to become apparent by emergence of symptoms.
The data came from the mSToPS (mHealth Screening to Prevent Strokes) study, which randomized 2,659 U.S. residents enrolled in a large health plan who had risk factors for AFib to either immediate or delayed arrhythmia assessment by ECG patches. Half the participants used a patch for about 14 days immediately and then a second time 3 months later, while the other half waited 4 months and then wore an ECG patch for 2 weeks and again 3 months later. The primary endpoint, first reported at the ACC annual meeting a year before and subsequently published, was the incidence of newly diagnosed AFib during the first 4 months in the actively monitored cohort, compared with a cohort followed by usual care. The results showed that screening identified AFib in 3.9% of people, while no screening and usual-practice follow-up identified a 0.9% incidence of AFib, showing that screening worked better for AFib case identification (JAMA. 2018 Jul 10;320[2]:146-55).
To examine the clinical impact of screening and an increased incidence of diagnosed AFib cases, Dr. Steinhubl and his associates focused on 1,725 of the original 2,659 patients who underwent ECG patch assessment, either immediate or delayed, and continued through 12 months of follow-up, and compared them with 3,384 matched controls who never underwent ECG patch screening but were also followed for 12 months for incident AFib identified during routine care and surveillance. This resulted in a cumulative incidence of newly diagnosed AFib of 6.3% in those who had worn two ECG patches and 2.3% among the matched controls.
During follow-up, use of various interventions was more common among the screened people than the controls. Initiation of anticoagulation treatment started in 4.0% of the entire screened group, compared with 1.9% of the controls, The screened people also had a 0.9% rate of receiving a pacemaker or defibrillator, a 0.8% rate of starting on treatment with an antiarrhythmic drug, and a 0.3% rate of undergoing catheter ablation, compared with none, 0.3%, and one of the controls, respectively, said Dr. Steinhubl, director of digital medicine at the Scripps Research Translational Institute in La Jolla, Calif.
The mSToPS study was funded by Janssen. Dr. Steinhubl has received research funding from DynoSense, EasyG, Janssen, the Qualcomm Foundation, and Striv.
SOURCE: Steinhubl SR et al. J Am Coll Cardiol. 2019 Mar 12;73(9)suppl 1:296.
REPORTING FROM ACC 2019
Renal denervation boosts effectiveness of AFib catheter ablation
SAN FRANCISCO – Adding renal denervation when performing catheter ablation of paroxysmal atrial fibrillation in hypertensive patients substantially reduced their arrhythmia recurrence rate during the subsequent year in a multicenter, randomized trial with 302 patients.
The findings established renal denervation (RDN) as a “reasonable” tool to increase the success of atrial fibrillation (AFib) catheter ablation, Jonathan S. Steinberg, MD, said at the annual scientific sessions of the Heart Rhythm Society.
“The RDN procedure seems remarkably safe and seems to be reliably accomplished when an electrophysiologist does it,” said Dr. Steinberg, director of the Arrhythmia Center of the Summit Medical Group in Montclair, N.J. Given the evidence he reported that performing RDN simultaneously with AFib catheter ablation by pulmonary vein isolation significantly improved freedom from arrhythmia recurrence, this approach “is ready for clinical use at institutions that could mount this kind of program,” he declared.
The rate of freedom from arrhythmia recurrence while off antiarrhythmic drugs during the year following treatment was 57% among 138 patients treated with pulmonary vein isolation only, and 72% in 145 who underwent both pulmonary vein isolation and renal denervation. That’s “a pretty big difference in outcome” with no increased risk and with about 20 added minutes of procedure time, Dr. Steinberg said in a video interview. He acknowledged that, currently, no catheter is approved for U.S. marketing that is specifically designed for renal denervation, but the operators in the study he reported all used conventional radiofrequency ablation catheters with an irrigated tip, a design with U.S. availability.
The ERADICATE-AF (Renal Artery Denervation in Addition to Catheter Ablation to Eliminate Atrial Fibrillation) study randomized 302 patients with paroxysmal AFib and hypertension uncontrolled by medication at three centers in Russia, one in Germany, and one in Poland. Enrolled patients averaged about 60 years of age, about 60% were men, and their average blood pressure was roughly 150/90 mm Hg while on treatment with a median of two antihypertensive drugs, including 100% on either an ACE inhibitor or angiotensin receptor blocker. The study operators performed RDN by placing an average of six lesions in a spiral pattern in each of the patient’s two renal arteries.
The investigators screened for arrhythmia recurrence with 7-day Holter monitoring at 3, 6, 9, and 12 months, with full 12-month follow-up available for 283 patients. After 12 months, blood pressures had declined by an average of 16/11 mm Hg among the patients who underwent RDN, with essentially no change in the patients who had pulmonary vein isolation only. Dr. Steinberg attributed the high success of the renal denervation procedures to the familiarity of the participating electrophysiologist operators with catheter-tip ablations.
“We have gone from treating patients with resistant hypertension to now treating patients with less severe hypertension,” Dr. Steinberg noted, and the next study he is planning will take this approach into patients with paroxysmal AFib but without hypertension, using RDN “solely as an anti-arrhythmic intervention,” he explained.
ERADICATE-AF did not receive commercial funding. Dr. Steinberg has been a consultant to Allergan, AtriCure, Biosense Webster, Corfigo, Medtronic, and Omron. He owns stock in AliveCor and receives salary from National Cardiac and G Medical.
ERADICATE-AF was a well-performed, informative, and provocative study that produced exciting results. I was very impressed that, despite the added complexity of performing an extra procedure, there appeared to be virtually no added risk to patients, with essentially identical complication rates in the two arms of the study. The 15.6% absolute difference in the rate of arrhythmia recurrences means that about six patients need to have renal denervation added to their catheter ablation to prevent one arrhythmia recurrence during 12 months, a pretty remarkable number-needed-to-treat.

Despite the successful outcome, adding renal denervation is not a panacea. These patients still had a 28% rate of recurrent atrial fibrillation during follow-up, and on average they also remained above their goal blood pressure despite the pressure reduction that renal denervation produced. The 43% arrhythmia recurrence rate among the patients who underwent only pulmonary vein isolation was consistent with prior reports on the efficacy of this treatment.
The findings raise the question of whether this approach would also work in AFib patients who are not hypertensive, and we must be cautious about the longer-term safety and durability of this treatment.
Cara N. Pellegrini, MD , is director of cardiac electrophysiology at the San Francisco VA Medical Center. She had no disclosures. She made these comments as designated discussant for ERADICATE-AF.
ERADICATE-AF was a well-performed, informative, and provocative study that produced exciting results. I was very impressed that, despite the added complexity of performing an extra procedure, there appeared to be virtually no added risk to patients, with essentially identical complication rates in the two arms of the study. The 15.6% absolute difference in the rate of arrhythmia recurrences means that about six patients need to have renal denervation added to their catheter ablation to prevent one arrhythmia recurrence during 12 months, a pretty remarkable number-needed-to-treat.
Despite the successful outcome, adding renal denervation is not a panacea. These patients still had a 28% rate of recurrent atrial fibrillation during follow-up, and on average they also remained above their goal blood pressure despite the pressure reduction that renal denervation produced. The 43% arrhythmia recurrence rate among the patients who underwent only pulmonary vein isolation was consistent with prior reports on the efficacy of this treatment.
The findings raise the question of whether this approach would also work in AFib patients who are not hypertensive, and we must be cautious about the longer-term safety and durability of this treatment.
Cara N. Pellegrini, MD , is director of cardiac electrophysiology at the San Francisco VA Medical Center. She had no disclosures. She made these comments as designated discussant for ERADICATE-AF.
ERADICATE-AF was a well-performed, informative, and provocative study that produced exciting results. I was very impressed that, despite the added complexity of performing an extra procedure, there appeared to be virtually no added risk to patients, with essentially identical complication rates in the two arms of the study. The 15.6% absolute difference in the rate of arrhythmia recurrences means that about six patients need to have renal denervation added to their catheter ablation to prevent one arrhythmia recurrence during 12 months, a pretty remarkable number-needed-to-treat.
Despite the successful outcome, adding renal denervation is not a panacea. These patients still had a 28% rate of recurrent atrial fibrillation during follow-up, and on average they also remained above their goal blood pressure despite the pressure reduction that renal denervation produced. The 43% arrhythmia recurrence rate among the patients who underwent only pulmonary vein isolation was consistent with prior reports on the efficacy of this treatment.
The findings raise the question of whether this approach would also work in AFib patients who are not hypertensive, and we must be cautious about the longer-term safety and durability of this treatment.
Cara N. Pellegrini, MD , is director of cardiac electrophysiology at the San Francisco VA Medical Center. She had no disclosures. She made these comments as designated discussant for ERADICATE-AF.
SAN FRANCISCO – Adding renal denervation when performing catheter ablation of paroxysmal atrial fibrillation in hypertensive patients substantially reduced their arrhythmia recurrence rate during the subsequent year in a multicenter, randomized trial with 302 patients.
The findings established renal denervation (RDN) as a “reasonable” tool to increase the success of atrial fibrillation (AFib) catheter ablation, Jonathan S. Steinberg, MD, said at the annual scientific sessions of the Heart Rhythm Society.
“The RDN procedure seems remarkably safe and seems to be reliably accomplished when an electrophysiologist does it,” said Dr. Steinberg, director of the Arrhythmia Center of the Summit Medical Group in Montclair, N.J. Given the evidence he reported that performing RDN simultaneously with AFib catheter ablation by pulmonary vein isolation significantly improved freedom from arrhythmia recurrence, this approach “is ready for clinical use at institutions that could mount this kind of program,” he declared.
The rate of freedom from arrhythmia recurrence while off antiarrhythmic drugs during the year following treatment was 57% among 138 patients treated with pulmonary vein isolation only, and 72% in 145 who underwent both pulmonary vein isolation and renal denervation. That’s “a pretty big difference in outcome” with no increased risk and with about 20 added minutes of procedure time, Dr. Steinberg said in a video interview. He acknowledged that, currently, no catheter is approved for U.S. marketing that is specifically designed for renal denervation, but the operators in the study he reported all used conventional radiofrequency ablation catheters with an irrigated tip, a design with U.S. availability.
The ERADICATE-AF (Renal Artery Denervation in Addition to Catheter Ablation to Eliminate Atrial Fibrillation) study randomized 302 patients with paroxysmal AFib and hypertension uncontrolled by medication at three centers in Russia, one in Germany, and one in Poland. Enrolled patients averaged about 60 years of age, about 60% were men, and their average blood pressure was roughly 150/90 mm Hg while on treatment with a median of two antihypertensive drugs, including 100% on either an ACE inhibitor or angiotensin receptor blocker. The study operators performed RDN by placing an average of six lesions in a spiral pattern in each of the patient’s two renal arteries.
The investigators screened for arrhythmia recurrence with 7-day Holter monitoring at 3, 6, 9, and 12 months, with full 12-month follow-up available for 283 patients. After 12 months, blood pressures had declined by an average of 16/11 mm Hg among the patients who underwent RDN, with essentially no change in the patients who had pulmonary vein isolation only. Dr. Steinberg attributed the high success of the renal denervation procedures to the familiarity of the participating electrophysiologist operators with catheter-tip ablations.
“We have gone from treating patients with resistant hypertension to now treating patients with less severe hypertension,” Dr. Steinberg noted, and the next study he is planning will take this approach into patients with paroxysmal AFib but without hypertension, using RDN “solely as an anti-arrhythmic intervention,” he explained.
ERADICATE-AF did not receive commercial funding. Dr. Steinberg has been a consultant to Allergan, AtriCure, Biosense Webster, Corfigo, Medtronic, and Omron. He owns stock in AliveCor and receives salary from National Cardiac and G Medical.
SAN FRANCISCO – Adding renal denervation when performing catheter ablation of paroxysmal atrial fibrillation in hypertensive patients substantially reduced their arrhythmia recurrence rate during the subsequent year in a multicenter, randomized trial with 302 patients.
The findings established renal denervation (RDN) as a “reasonable” tool to increase the success of atrial fibrillation (AFib) catheter ablation, Jonathan S. Steinberg, MD, said at the annual scientific sessions of the Heart Rhythm Society.
“The RDN procedure seems remarkably safe and seems to be reliably accomplished when an electrophysiologist does it,” said Dr. Steinberg, director of the Arrhythmia Center of the Summit Medical Group in Montclair, N.J. Given the evidence he reported that performing RDN simultaneously with AFib catheter ablation by pulmonary vein isolation significantly improved freedom from arrhythmia recurrence, this approach “is ready for clinical use at institutions that could mount this kind of program,” he declared.
The rate of freedom from arrhythmia recurrence while off antiarrhythmic drugs during the year following treatment was 57% among 138 patients treated with pulmonary vein isolation only, and 72% in 145 who underwent both pulmonary vein isolation and renal denervation. That’s “a pretty big difference in outcome” with no increased risk and with about 20 added minutes of procedure time, Dr. Steinberg said in a video interview. He acknowledged that, currently, no catheter is approved for U.S. marketing that is specifically designed for renal denervation, but the operators in the study he reported all used conventional radiofrequency ablation catheters with an irrigated tip, a design with U.S. availability.
The ERADICATE-AF (Renal Artery Denervation in Addition to Catheter Ablation to Eliminate Atrial Fibrillation) study randomized 302 patients with paroxysmal AFib and hypertension uncontrolled by medication at three centers in Russia, one in Germany, and one in Poland. Enrolled patients averaged about 60 years of age, about 60% were men, and their average blood pressure was roughly 150/90 mm Hg while on treatment with a median of two antihypertensive drugs, including 100% on either an ACE inhibitor or angiotensin receptor blocker. The study operators performed RDN by placing an average of six lesions in a spiral pattern in each of the patient’s two renal arteries.
The investigators screened for arrhythmia recurrence with 7-day Holter monitoring at 3, 6, 9, and 12 months, with full 12-month follow-up available for 283 patients. After 12 months, blood pressures had declined by an average of 16/11 mm Hg among the patients who underwent RDN, with essentially no change in the patients who had pulmonary vein isolation only. Dr. Steinberg attributed the high success of the renal denervation procedures to the familiarity of the participating electrophysiologist operators with catheter-tip ablations.
“We have gone from treating patients with resistant hypertension to now treating patients with less severe hypertension,” Dr. Steinberg noted, and the next study he is planning will take this approach into patients with paroxysmal AFib but without hypertension, using RDN “solely as an anti-arrhythmic intervention,” he explained.
ERADICATE-AF did not receive commercial funding. Dr. Steinberg has been a consultant to Allergan, AtriCure, Biosense Webster, Corfigo, Medtronic, and Omron. He owns stock in AliveCor and receives salary from National Cardiac and G Medical.
REPORTING FROM HEART RHYTHM 2019
Higher AFib ablation volumes linked with better outcomes
SAN FRANCISCO – The number of atrial fibrillation (Afib) catheter ablations a hospital did a year had a substantial, independent effect on patient outcomes in a study of more than 54,000 U.S. catheter ablations performed during 2010-2014.
The results showed that the roughly one-third of studied hospitals with the lowest annual volume of catheter ablations performed, 20 or fewer, had twice the acute complication rate and twice the 30-day in-hospital mortality rate, compared with the hospitals that did 53 or more such procedures annually in patients with atrial fibrillation, Jim W. Cheung, MD, said while presenting a poster at the annual scientific sessions of the Heart Rhythm Society.
The data, taken from 1,738 U.S. hospitals during 2010-2014 and captured in the Nationwide Readmissions Database, also showed that 79% of these hospitals performed 20 or fewer catheter ablations for atrial fibrillation (AFib) annually, with 63% doing 10 or fewer cases per year during the 5 years studied.

The findings raise the question of whether U.S. guidelines for catheter ablation of AFib should specify a minimum case volume for hospital programs, and if so, how high the minimum should be. Volume thresholds are “something to think about,” or a system to designate centers of excellence, Dr. Cheung suggested in a video interview. But interest in setting volume thresholds to better insure competence is often counterbalanced by concerns about patient access, he noted.
The prevailing U.S. guidelines for catheter ablation of AFib are in a 2017 statement from the Heart Rhythm Society and several collaborating groups (J Arrhythm. 2017 Oct;33[5]:369-409). The statement focused on operator volume rather than hospital volume and said that each operator should perform “several” AFib ablation procedures each month, which is generally understood to mean at least 2 per month or at least about 25 annually, commented Hugh Calkins, MD, chair of the panel that wrote the statement and professor of medicine at Johns Hopkins Medicine in Baltimore. The major rationale for setting a suggested minimum of about 25 cases/year came largely from a 2013 report that is cited as the first study to document a volume-outcome relationship for catheter ablation of AFib (Circulation. 2013 Nov 5;128[19]:2104-12), Dr. Calkins noted. “Volume does matter,” he agreed in an interview, but no society or organization monitors hospital or operator volumes, nor takes any steps when volumes are low.

The Nationwide Readmissions Database included 54,599 patients who underwent AFib catheter ablation during 2010-2014. Dr. Cheung and his associates divided these patients into rough tertiles based on the annual procedure volumes of the hospitals that performed these ablations. The 36% of patients treated at hospitals that did 20 or fewer procedures annually were on average older and had more comorbidities than the 31% treated at hospitals in the highest-volume tertile, which performed at least 53 ablations annually. In an analysis that adjusted for these demographic and clinical differences, patients ablated at the lower-volume hospitals had a statistically significant 2.06-fold higher rate of any complication and a 2.24-fold increased rate of in-hospital mortality, either during the index hospitalization or during a 30-day hospital readmission, reported Dr. Cheung, director of clinical electrophysiology research at Weill Cornell Medical College in New York. The increased rate of complications was driven by a fivefold increased rate of cardiac perforations, a greater than doubled periprocedural stroke rate, and a roughly 50% increased rate of vascular complications, compared with the highest-volume hospitals and after adjustment for baseline differences.
Dr. Cheung has been a consultant to Abbott and Biotronik, and has received fellowship support from Biosense Webster, Biotronik, Boston Scientific, Medtronic, and St. Jude. Dr. Calkins disclosed ties to Abbott, Altathera, AtriCure, Boehringer Ingelheim, Boston Scientific, Medtronic, St. Jude, and MRI Interventions.
SOURCE: Cheung JW. HRS 2019, Abstract S-P001-123.
SAN FRANCISCO – The number of atrial fibrillation (Afib) catheter ablations a hospital did a year had a substantial, independent effect on patient outcomes in a study of more than 54,000 U.S. catheter ablations performed during 2010-2014.
The results showed that the roughly one-third of studied hospitals with the lowest annual volume of catheter ablations performed, 20 or fewer, had twice the acute complication rate and twice the 30-day in-hospital mortality rate, compared with the hospitals that did 53 or more such procedures annually in patients with atrial fibrillation, Jim W. Cheung, MD, said while presenting a poster at the annual scientific sessions of the Heart Rhythm Society.
The data, taken from 1,738 U.S. hospitals during 2010-2014 and captured in the Nationwide Readmissions Database, also showed that 79% of these hospitals performed 20 or fewer catheter ablations for atrial fibrillation (AFib) annually, with 63% doing 10 or fewer cases per year during the 5 years studied.
The findings raise the question of whether U.S. guidelines for catheter ablation of AFib should specify a minimum case volume for hospital programs, and if so, how high the minimum should be. Volume thresholds are “something to think about,” or a system to designate centers of excellence, Dr. Cheung suggested in a video interview. But interest in setting volume thresholds to better insure competence is often counterbalanced by concerns about patient access, he noted.
The prevailing U.S. guidelines for catheter ablation of AFib are in a 2017 statement from the Heart Rhythm Society and several collaborating groups (J Arrhythm. 2017 Oct;33[5]:369-409). The statement focused on operator volume rather than hospital volume and said that each operator should perform “several” AFib ablation procedures each month, which is generally understood to mean at least 2 per month or at least about 25 annually, commented Hugh Calkins, MD, chair of the panel that wrote the statement and professor of medicine at Johns Hopkins Medicine in Baltimore. The major rationale for setting a suggested minimum of about 25 cases/year came largely from a 2013 report that is cited as the first study to document a volume-outcome relationship for catheter ablation of AFib (Circulation. 2013 Nov 5;128[19]:2104-12), Dr. Calkins noted. “Volume does matter,” he agreed in an interview, but no society or organization monitors hospital or operator volumes, nor takes any steps when volumes are low.
The Nationwide Readmissions Database included 54,599 patients who underwent AFib catheter ablation during 2010-2014. Dr. Cheung and his associates divided these patients into rough tertiles based on the annual procedure volumes of the hospitals that performed these ablations. The 36% of patients treated at hospitals that did 20 or fewer procedures annually were on average older and had more comorbidities than the 31% treated at hospitals in the highest-volume tertile, which performed at least 53 ablations annually. In an analysis that adjusted for these demographic and clinical differences, patients ablated at the lower-volume hospitals had a statistically significant 2.06-fold higher rate of any complication and a 2.24-fold increased rate of in-hospital mortality, either during the index hospitalization or during a 30-day hospital readmission, reported Dr. Cheung, director of clinical electrophysiology research at Weill Cornell Medical College in New York. The increased rate of complications was driven by a fivefold increased rate of cardiac perforations, a greater than doubled periprocedural stroke rate, and a roughly 50% increased rate of vascular complications, compared with the highest-volume hospitals and after adjustment for baseline differences.
Dr. Cheung has been a consultant to Abbott and Biotronik, and has received fellowship support from Biosense Webster, Biotronik, Boston Scientific, Medtronic, and St. Jude. Dr. Calkins disclosed ties to Abbott, Altathera, AtriCure, Boehringer Ingelheim, Boston Scientific, Medtronic, St. Jude, and MRI Interventions.
SOURCE: Cheung JW. HRS 2019, Abstract S-P001-123.
SAN FRANCISCO – The number of atrial fibrillation (Afib) catheter ablations a hospital did a year had a substantial, independent effect on patient outcomes in a study of more than 54,000 U.S. catheter ablations performed during 2010-2014.
The results showed that the roughly one-third of studied hospitals with the lowest annual volume of catheter ablations performed, 20 or fewer, had twice the acute complication rate and twice the 30-day in-hospital mortality rate, compared with the hospitals that did 53 or more such procedures annually in patients with atrial fibrillation, Jim W. Cheung, MD, said while presenting a poster at the annual scientific sessions of the Heart Rhythm Society.
The data, taken from 1,738 U.S. hospitals during 2010-2014 and captured in the Nationwide Readmissions Database, also showed that 79% of these hospitals performed 20 or fewer catheter ablations for atrial fibrillation (AFib) annually, with 63% doing 10 or fewer cases per year during the 5 years studied.
The findings raise the question of whether U.S. guidelines for catheter ablation of AFib should specify a minimum case volume for hospital programs, and if so, how high the minimum should be. Volume thresholds are “something to think about,” or a system to designate centers of excellence, Dr. Cheung suggested in a video interview. But interest in setting volume thresholds to better insure competence is often counterbalanced by concerns about patient access, he noted.
The prevailing U.S. guidelines for catheter ablation of AFib are in a 2017 statement from the Heart Rhythm Society and several collaborating groups (J Arrhythm. 2017 Oct;33[5]:369-409). The statement focused on operator volume rather than hospital volume and said that each operator should perform “several” AFib ablation procedures each month, which is generally understood to mean at least 2 per month or at least about 25 annually, commented Hugh Calkins, MD, chair of the panel that wrote the statement and professor of medicine at Johns Hopkins Medicine in Baltimore. The major rationale for setting a suggested minimum of about 25 cases/year came largely from a 2013 report that is cited as the first study to document a volume-outcome relationship for catheter ablation of AFib (Circulation. 2013 Nov 5;128[19]:2104-12), Dr. Calkins noted. “Volume does matter,” he agreed in an interview, but no society or organization monitors hospital or operator volumes, nor takes any steps when volumes are low.
The Nationwide Readmissions Database included 54,599 patients who underwent AFib catheter ablation during 2010-2014. Dr. Cheung and his associates divided these patients into rough tertiles based on the annual procedure volumes of the hospitals that performed these ablations. The 36% of patients treated at hospitals that did 20 or fewer procedures annually were on average older and had more comorbidities than the 31% treated at hospitals in the highest-volume tertile, which performed at least 53 ablations annually. In an analysis that adjusted for these demographic and clinical differences, patients ablated at the lower-volume hospitals had a statistically significant 2.06-fold higher rate of any complication and a 2.24-fold increased rate of in-hospital mortality, either during the index hospitalization or during a 30-day hospital readmission, reported Dr. Cheung, director of clinical electrophysiology research at Weill Cornell Medical College in New York. The increased rate of complications was driven by a fivefold increased rate of cardiac perforations, a greater than doubled periprocedural stroke rate, and a roughly 50% increased rate of vascular complications, compared with the highest-volume hospitals and after adjustment for baseline differences.
Dr. Cheung has been a consultant to Abbott and Biotronik, and has received fellowship support from Biosense Webster, Biotronik, Boston Scientific, Medtronic, and St. Jude. Dr. Calkins disclosed ties to Abbott, Altathera, AtriCure, Boehringer Ingelheim, Boston Scientific, Medtronic, St. Jude, and MRI Interventions.
SOURCE: Cheung JW. HRS 2019, Abstract S-P001-123.
REPORTING FROM HEART RHYTHM 2019
Key clinical point: .
Major finding: Hospitals performing 20 or fewer catheter ablations annually had twice as many acute complications as hospitals doing at least 53.
Study details: Analysis of 54,599 atrial fibrillation patients who underwent catheter ablation in the Nationwide Readmissions Database.
Disclosures: Dr. Cheung has been a consultant to Abbott and Biotronik, and has received fellowship support from Biosense Webster, Biotronik, Boston Scientific, Medtronic, and St. Jude.
Source: Cheung JW et al. Heart Rhythm 2019, Abstract S-P001-123.

FDA approves Vyndaqel, Vyndamax for amyloidosis-based heart disease

The disease is caused by the buildup of abnormal deposits of amyloid in the body’s organs and tissues, interfering with normal function, and most often occurs in the heart and nervous system. Symptoms associated with amyloid buildup in the heart include shortness of breath, fatigue, heart failure, loss of consciousness, abnormal heart rhythms, and death.
FDA approval of both drugs was based on results of a clinical trial in which 441 patients with transthyretin-mediated amyloidosis received either tafamidis meglumine or placebo. After a mean of 30 months, patients who received tafamidis meglumine had a higher survival rate and a lower number of cardiovascular-related hospitalizations than did patients in the placebo group.
No drug-associated side effects have yet been identified; however, tafamidis can cause fetal harm when administered to a pregnant woman.
“Transthyretin-mediated amyloidosis is a rare, debilitating, and often fatal disease. The treatments we’re approving today are an important advancement in the treatment of the cardiomyopathy caused by transthyretin-mediated amyloidosis,” said Norman Stockbridge, MD, PhD, director of the Division of Cardiovascular and Renal Drugs in the FDA’s Center for Drug Evaluation and Research.
Find the full press release on the FDA website.
The disease is caused by the buildup of abnormal deposits of amyloid in the body’s organs and tissues, interfering with normal function, and most often occurs in the heart and nervous system. Symptoms associated with amyloid buildup in the heart include shortness of breath, fatigue, heart failure, loss of consciousness, abnormal heart rhythms, and death.
FDA approval of both drugs was based on results of a clinical trial in which 441 patients with transthyretin-mediated amyloidosis received either tafamidis meglumine or placebo. After a mean of 30 months, patients who received tafamidis meglumine had a higher survival rate and a lower number of cardiovascular-related hospitalizations than did patients in the placebo group.
No drug-associated side effects have yet been identified; however, tafamidis can cause fetal harm when administered to a pregnant woman.
“Transthyretin-mediated amyloidosis is a rare, debilitating, and often fatal disease. The treatments we’re approving today are an important advancement in the treatment of the cardiomyopathy caused by transthyretin-mediated amyloidosis,” said Norman Stockbridge, MD, PhD, director of the Division of Cardiovascular and Renal Drugs in the FDA’s Center for Drug Evaluation and Research.
Find the full press release on the FDA website.
The disease is caused by the buildup of abnormal deposits of amyloid in the body’s organs and tissues, interfering with normal function, and most often occurs in the heart and nervous system. Symptoms associated with amyloid buildup in the heart include shortness of breath, fatigue, heart failure, loss of consciousness, abnormal heart rhythms, and death.
FDA approval of both drugs was based on results of a clinical trial in which 441 patients with transthyretin-mediated amyloidosis received either tafamidis meglumine or placebo. After a mean of 30 months, patients who received tafamidis meglumine had a higher survival rate and a lower number of cardiovascular-related hospitalizations than did patients in the placebo group.
No drug-associated side effects have yet been identified; however, tafamidis can cause fetal harm when administered to a pregnant woman.
“Transthyretin-mediated amyloidosis is a rare, debilitating, and often fatal disease. The treatments we’re approving today are an important advancement in the treatment of the cardiomyopathy caused by transthyretin-mediated amyloidosis,” said Norman Stockbridge, MD, PhD, director of the Division of Cardiovascular and Renal Drugs in the FDA’s Center for Drug Evaluation and Research.
Find the full press release on the FDA website.
Single-center study outlines stroke risk, DOAC type in nonvalvular AFib patients
PHILADELPHIA – A disproportionate number of breakthrough strokes were observed among patients receiving rivaroxaban for nonvalvular atrial fibrillation in a stroke unit, according to a small, single-center, retrospective study presented at the annual meeting of the American Academy of Neurology.
The researchers reviewed all patients presenting to a tertiary care stroke unit in Australia from January 2015 to June 2018.
A total of 56 patients (median age was 74 years; 61% were male) had received direct oral anticoagulant (DOAC) therapy and then had an ischemic stroke. Of those patients, 37 (66%) had strokes while receiving the treatment; 14 patients (25%) had a stroke after recently stopping a DOAC, often prior to a medical procedure; and 5 patients (9%) were not adherent to their DOAC regimen.
Of the 37 patients who had strokes during DOAC treatment, 48% were on rivaroxaban, 9% were on dabigatran, and 9% were on apixaban, Fiona Chan, MD, of The Princess Alexandra Hospital, Brisbane, Australia, and coinvestigators reported in a poster presentation.
While these findings need to be replicated in a larger study, they do “raise concern for inadequate stroke prevention within this cohort,” they said.
Moreover, the findings illustrate the importance of bridging anticoagulation prior to procedures, when appropriate, to minimize stroke risk, they added, as 25% of the strokes had occurred in patients who recently stopped the DOACs due to procedures.
To determine which DOAC was most often associated with breakthrough ischemic strokes in patients with nonvalvular atrial fibrillation, the investigators compared the proportion of DOACs prescribed in Australia to the proportion of observed strokes in their cohort.
Despite accounting for about 51% of Australian DOAC prescriptions, rivaroxaban represented nearly 73% of breakthrough strokes among the patients who had strokes while receiving the treatment (P = .001), the investigators reported.
Conversely, apixaban accounted for about 35% of prescriptions but 14% of the breakthrough strokes (P = .0007), while dabigatran accounted for 14% of prescriptions and 14% of the strokes (P = 0.99), the investigators said in their poster.
One limitation of this retrospective study is that the patient cohort came from a single specialized center, and may not reflect the true incidence of nonvalvular atrial fibrillation across Australia, the researchers noted.
Dr. Chan and coinvestigators reported that they had no relevant financial disclosures.
SOURCE: Chan F et al. AAN 2019. P1.3-001.
PHILADELPHIA – A disproportionate number of breakthrough strokes were observed among patients receiving rivaroxaban for nonvalvular atrial fibrillation in a stroke unit, according to a small, single-center, retrospective study presented at the annual meeting of the American Academy of Neurology.
The researchers reviewed all patients presenting to a tertiary care stroke unit in Australia from January 2015 to June 2018.
A total of 56 patients (median age was 74 years; 61% were male) had received direct oral anticoagulant (DOAC) therapy and then had an ischemic stroke. Of those patients, 37 (66%) had strokes while receiving the treatment; 14 patients (25%) had a stroke after recently stopping a DOAC, often prior to a medical procedure; and 5 patients (9%) were not adherent to their DOAC regimen.
Of the 37 patients who had strokes during DOAC treatment, 48% were on rivaroxaban, 9% were on dabigatran, and 9% were on apixaban, Fiona Chan, MD, of The Princess Alexandra Hospital, Brisbane, Australia, and coinvestigators reported in a poster presentation.
While these findings need to be replicated in a larger study, they do “raise concern for inadequate stroke prevention within this cohort,” they said.
Moreover, the findings illustrate the importance of bridging anticoagulation prior to procedures, when appropriate, to minimize stroke risk, they added, as 25% of the strokes had occurred in patients who recently stopped the DOACs due to procedures.
To determine which DOAC was most often associated with breakthrough ischemic strokes in patients with nonvalvular atrial fibrillation, the investigators compared the proportion of DOACs prescribed in Australia to the proportion of observed strokes in their cohort.
Despite accounting for about 51% of Australian DOAC prescriptions, rivaroxaban represented nearly 73% of breakthrough strokes among the patients who had strokes while receiving the treatment (P = .001), the investigators reported.
Conversely, apixaban accounted for about 35% of prescriptions but 14% of the breakthrough strokes (P = .0007), while dabigatran accounted for 14% of prescriptions and 14% of the strokes (P = 0.99), the investigators said in their poster.
One limitation of this retrospective study is that the patient cohort came from a single specialized center, and may not reflect the true incidence of nonvalvular atrial fibrillation across Australia, the researchers noted.
Dr. Chan and coinvestigators reported that they had no relevant financial disclosures.
SOURCE: Chan F et al. AAN 2019. P1.3-001.
PHILADELPHIA – A disproportionate number of breakthrough strokes were observed among patients receiving rivaroxaban for nonvalvular atrial fibrillation in a stroke unit, according to a small, single-center, retrospective study presented at the annual meeting of the American Academy of Neurology.
The researchers reviewed all patients presenting to a tertiary care stroke unit in Australia from January 2015 to June 2018.
A total of 56 patients (median age was 74 years; 61% were male) had received direct oral anticoagulant (DOAC) therapy and then had an ischemic stroke. Of those patients, 37 (66%) had strokes while receiving the treatment; 14 patients (25%) had a stroke after recently stopping a DOAC, often prior to a medical procedure; and 5 patients (9%) were not adherent to their DOAC regimen.
Of the 37 patients who had strokes during DOAC treatment, 48% were on rivaroxaban, 9% were on dabigatran, and 9% were on apixaban, Fiona Chan, MD, of The Princess Alexandra Hospital, Brisbane, Australia, and coinvestigators reported in a poster presentation.
While these findings need to be replicated in a larger study, they do “raise concern for inadequate stroke prevention within this cohort,” they said.
Moreover, the findings illustrate the importance of bridging anticoagulation prior to procedures, when appropriate, to minimize stroke risk, they added, as 25% of the strokes had occurred in patients who recently stopped the DOACs due to procedures.
To determine which DOAC was most often associated with breakthrough ischemic strokes in patients with nonvalvular atrial fibrillation, the investigators compared the proportion of DOACs prescribed in Australia to the proportion of observed strokes in their cohort.
Despite accounting for about 51% of Australian DOAC prescriptions, rivaroxaban represented nearly 73% of breakthrough strokes among the patients who had strokes while receiving the treatment (P = .001), the investigators reported.
Conversely, apixaban accounted for about 35% of prescriptions but 14% of the breakthrough strokes (P = .0007), while dabigatran accounted for 14% of prescriptions and 14% of the strokes (P = 0.99), the investigators said in their poster.
One limitation of this retrospective study is that the patient cohort came from a single specialized center, and may not reflect the true incidence of nonvalvular atrial fibrillation across Australia, the researchers noted.
Dr. Chan and coinvestigators reported that they had no relevant financial disclosures.
SOURCE: Chan F et al. AAN 2019. P1.3-001.
REPORTING FROM AAN 2019
Key clinical point: Rivaroxaban was associated with a disproportionate number of breakthrough strokes among patients with nonvalvular atrial fibrillation treated with direct oral anticoagulants at one stroke unit in Australia.
Major finding: Despite accounting for about 51% of Australian DOAC prescriptions, rivaroxaban represented nearly 73% of breakthrough strokes among the patients who had strokes while receiving treatment (P = .001).
Study details: Retrospective study of 56 patients with nonvalvular atrial fibrillation reporting to a tertiary care stroke unit in Australia.
Disclosures: The authors reported no financial disclosures.
Source: Chan F et al. AAN 019. Poster P1.3-001.
Some cardiac devices vulnerable to cybersecurity threats
Implantable cardiac devices made by Medtronic have cybersecurity vulnerabilities, according to a safety communication from the Food and Drug Administration. That said, so far the FDA is unaware of any reports of harm related to these vulnerabilities, and the agency still advises doctors and patients to continue using the devices as intended and in accordance with device labeling.
The Conexus wireless telemetry protocol used with Medtronic’s implantable cardioverter defibrillators and cardiac resynchronization therapy defibrillators, as well as with certain models of Medtronic’s CareLink Programmer and the MyCareLink Monitor, lacks encryption, authentication, or authorization, which leaves the devices open to exploitation. Such exploitation “could allow unauthorized individuals ... to access and potentially manipulate an implantable device, home monitor, or clinic programmer,” the agency said in its safety communication.
The FDA provides several recommendations in the safety communication, including obtaining these devices “directly from the manufacturer to ensure integrity of the system” and operating “the programmers within well-managed networks.”
Implantable cardiac devices made by Medtronic have cybersecurity vulnerabilities, according to a safety communication from the Food and Drug Administration. That said, so far the FDA is unaware of any reports of harm related to these vulnerabilities, and the agency still advises doctors and patients to continue using the devices as intended and in accordance with device labeling.
The Conexus wireless telemetry protocol used with Medtronic’s implantable cardioverter defibrillators and cardiac resynchronization therapy defibrillators, as well as with certain models of Medtronic’s CareLink Programmer and the MyCareLink Monitor, lacks encryption, authentication, or authorization, which leaves the devices open to exploitation. Such exploitation “could allow unauthorized individuals ... to access and potentially manipulate an implantable device, home monitor, or clinic programmer,” the agency said in its safety communication.
The FDA provides several recommendations in the safety communication, including obtaining these devices “directly from the manufacturer to ensure integrity of the system” and operating “the programmers within well-managed networks.”
Implantable cardiac devices made by Medtronic have cybersecurity vulnerabilities, according to a safety communication from the Food and Drug Administration. That said, so far the FDA is unaware of any reports of harm related to these vulnerabilities, and the agency still advises doctors and patients to continue using the devices as intended and in accordance with device labeling.
The Conexus wireless telemetry protocol used with Medtronic’s implantable cardioverter defibrillators and cardiac resynchronization therapy defibrillators, as well as with certain models of Medtronic’s CareLink Programmer and the MyCareLink Monitor, lacks encryption, authentication, or authorization, which leaves the devices open to exploitation. Such exploitation “could allow unauthorized individuals ... to access and potentially manipulate an implantable device, home monitor, or clinic programmer,” the agency said in its safety communication.
The FDA provides several recommendations in the safety communication, including obtaining these devices “directly from the manufacturer to ensure integrity of the system” and operating “the programmers within well-managed networks.”
Increased sudden death risk in HIV linked to cardiac fibrosis
SEATTLE – A marked increase in the risk of sudden cardiac death among people with HIV correlates with a significantly higher burden of myocardial fibrosis, according to an autopsy study presented at the Conference on Retroviruses and Opportunistic Infections.

Fibrosis is a known trigger for fatal arrhythmias, so the take home is that fibrosis should be considered as a criteria for defibrillator implantation in HIV patients, said lead investigator Zian Tseng, MD, a cardiologist, cardiac electrophysiologist, and professor of medicine at the University of California, San Francisco.
The finding also speaks to a larger issue. The main criterion right now for implantation is an ejection fraction below 35%, but “there are a lot of people who die suddenly with normal ejection fractions,” and not just people with HIV, he said.
Many of those deaths might be prevented if fibrosis is added to implantation criteria. All that’s needed for assessment is a cardiac MRI, Dr. Tseng said.
The approach would be particularly fruitful for HIV patients, but cardiac fibrosis “isn’t just an” HIV problem, he said.
The conclusions have their roots in an investigation to determine the true incidence of sudden cardiac death (SCD) in the general public. SCD is commonly listed on death certificates, but it’s a presumed diagnosis, based on the best guesses of paramedics and clinicians. Autopsy is the only way to know for sure if a death was truly due to a sudden cardiac arrhythmia, or even related to the heart,
To clear the wheat from the chaff, Dr. Tseng and his colleagues performed autopsies on 525 out-of-hospital SCD cases among adults in San Francisco from 2011-2016; to qualify, the cases had to meet World Health Organization SCD criteria, meaning unexpected death within 1 hour of symptom onset, or, in unwitnessed cases, within 24 hours of when the person was last seen alive and well.
Cases were considered sudden arrhythmic death – and, therefore, true SCD – if no extracardiac causes of death or acute heart failure were found on autopsy. Overall, 40% of deaths attributed to SCD “were not sudden or unexpected, and nearly half of presumed SCDs were not arrhythmic.” The findings had “implications for ... mortality data, clinical trials, and cohort studies,” Dr. Tseng and his team concluded (Circulation. 2018 Jun 19;137[25]:2689-2700).
They next turned their attention to HIV. It’s known that the virus increases the risk of strokes, heart attacks, and heart failure; the researchers wanted to see if it did the same for SCD. The HIV results were presented at CROI.
Forty-seven presumed SCD cases with HIV met inclusion criteria during the study period. Based on the earlier findings and epidemiological data, people with HIV had more than an 80% higher risk of SCD and an almost 60% higher risk of confirmed arrhythmic death than did the general public. Similar to the general population, only about half of presumed SCD cases were confirmed on autopsy. About one-third of what turned out to be non-cardiac HIV deaths were due to occult overdose, versus 13.5% in the general population, which points to the increased need for drug screening and treatment in HIV.
Beyond that, though, the team found that the burden of myocardial fibrosis in HIV “was profound,” far surpassing what was found in SCD deaths in the general population. After adjustment for age, gender, and heart disease, “sudden cardiac deaths with HIV had 60% higher interstitial fibrosis by myocardial trichrome staining. Cardiac fibrosis, a known substrate for fatal arrhythmias in the general population, may underlie the mechanism by which HIV increases the risk” of sudden death in HIV, Dr. Tseng said.
It could be that the virus enters heart cells and sets off an inflammatory cardiomyopathy, or perhaps it’s related to chronic inflammation caused by the virus. Whatever the case, infection seems to have an “independent effect” on increasing fibrosis among people with HIV, he said.
Intriguingly, a large epidemiologic study in United States veterans, also presented at CROI, found a higher risk of SCD among HIV patients, but only if their infections were active over an extended period of time, as indicated by sustained high viral loads and low CD4 cell counts. Dr. Tseng was involved in that work, as well, but noted that the number of HIV SCD cases in the San Francisco study was too small to draw meaningful conclusions regarding the relationship between disease control and cardiac fibrosis.
Cardiac defibrillators can prevent arrhythmic death, so, at least for now, he said that the autopsy study findings mean that criteria for implantation should be broadened to include extensive cardiac fibrosis.
The work was funded by the National Institutes of Health. Dr. Tseng didn’t have any disclosures.
SOURCE: Tseng ZH et al. CROI 2019 abstract 32
SEATTLE – A marked increase in the risk of sudden cardiac death among people with HIV correlates with a significantly higher burden of myocardial fibrosis, according to an autopsy study presented at the Conference on Retroviruses and Opportunistic Infections.
Fibrosis is a known trigger for fatal arrhythmias, so the take home is that fibrosis should be considered as a criteria for defibrillator implantation in HIV patients, said lead investigator Zian Tseng, MD, a cardiologist, cardiac electrophysiologist, and professor of medicine at the University of California, San Francisco.
The finding also speaks to a larger issue. The main criterion right now for implantation is an ejection fraction below 35%, but “there are a lot of people who die suddenly with normal ejection fractions,” and not just people with HIV, he said.
Many of those deaths might be prevented if fibrosis is added to implantation criteria. All that’s needed for assessment is a cardiac MRI, Dr. Tseng said.
The approach would be particularly fruitful for HIV patients, but cardiac fibrosis “isn’t just an” HIV problem, he said.
The conclusions have their roots in an investigation to determine the true incidence of sudden cardiac death (SCD) in the general public. SCD is commonly listed on death certificates, but it’s a presumed diagnosis, based on the best guesses of paramedics and clinicians. Autopsy is the only way to know for sure if a death was truly due to a sudden cardiac arrhythmia, or even related to the heart,
To clear the wheat from the chaff, Dr. Tseng and his colleagues performed autopsies on 525 out-of-hospital SCD cases among adults in San Francisco from 2011-2016; to qualify, the cases had to meet World Health Organization SCD criteria, meaning unexpected death within 1 hour of symptom onset, or, in unwitnessed cases, within 24 hours of when the person was last seen alive and well.
Cases were considered sudden arrhythmic death – and, therefore, true SCD – if no extracardiac causes of death or acute heart failure were found on autopsy. Overall, 40% of deaths attributed to SCD “were not sudden or unexpected, and nearly half of presumed SCDs were not arrhythmic.” The findings had “implications for ... mortality data, clinical trials, and cohort studies,” Dr. Tseng and his team concluded (Circulation. 2018 Jun 19;137[25]:2689-2700).
They next turned their attention to HIV. It’s known that the virus increases the risk of strokes, heart attacks, and heart failure; the researchers wanted to see if it did the same for SCD. The HIV results were presented at CROI.
Forty-seven presumed SCD cases with HIV met inclusion criteria during the study period. Based on the earlier findings and epidemiological data, people with HIV had more than an 80% higher risk of SCD and an almost 60% higher risk of confirmed arrhythmic death than did the general public. Similar to the general population, only about half of presumed SCD cases were confirmed on autopsy. About one-third of what turned out to be non-cardiac HIV deaths were due to occult overdose, versus 13.5% in the general population, which points to the increased need for drug screening and treatment in HIV.
Beyond that, though, the team found that the burden of myocardial fibrosis in HIV “was profound,” far surpassing what was found in SCD deaths in the general population. After adjustment for age, gender, and heart disease, “sudden cardiac deaths with HIV had 60% higher interstitial fibrosis by myocardial trichrome staining. Cardiac fibrosis, a known substrate for fatal arrhythmias in the general population, may underlie the mechanism by which HIV increases the risk” of sudden death in HIV, Dr. Tseng said.
It could be that the virus enters heart cells and sets off an inflammatory cardiomyopathy, or perhaps it’s related to chronic inflammation caused by the virus. Whatever the case, infection seems to have an “independent effect” on increasing fibrosis among people with HIV, he said.
Intriguingly, a large epidemiologic study in United States veterans, also presented at CROI, found a higher risk of SCD among HIV patients, but only if their infections were active over an extended period of time, as indicated by sustained high viral loads and low CD4 cell counts. Dr. Tseng was involved in that work, as well, but noted that the number of HIV SCD cases in the San Francisco study was too small to draw meaningful conclusions regarding the relationship between disease control and cardiac fibrosis.
Cardiac defibrillators can prevent arrhythmic death, so, at least for now, he said that the autopsy study findings mean that criteria for implantation should be broadened to include extensive cardiac fibrosis.
The work was funded by the National Institutes of Health. Dr. Tseng didn’t have any disclosures.
SOURCE: Tseng ZH et al. CROI 2019 abstract 32
SEATTLE – A marked increase in the risk of sudden cardiac death among people with HIV correlates with a significantly higher burden of myocardial fibrosis, according to an autopsy study presented at the Conference on Retroviruses and Opportunistic Infections.
Fibrosis is a known trigger for fatal arrhythmias, so the take home is that fibrosis should be considered as a criteria for defibrillator implantation in HIV patients, said lead investigator Zian Tseng, MD, a cardiologist, cardiac electrophysiologist, and professor of medicine at the University of California, San Francisco.
The finding also speaks to a larger issue. The main criterion right now for implantation is an ejection fraction below 35%, but “there are a lot of people who die suddenly with normal ejection fractions,” and not just people with HIV, he said.
Many of those deaths might be prevented if fibrosis is added to implantation criteria. All that’s needed for assessment is a cardiac MRI, Dr. Tseng said.
The approach would be particularly fruitful for HIV patients, but cardiac fibrosis “isn’t just an” HIV problem, he said.
The conclusions have their roots in an investigation to determine the true incidence of sudden cardiac death (SCD) in the general public. SCD is commonly listed on death certificates, but it’s a presumed diagnosis, based on the best guesses of paramedics and clinicians. Autopsy is the only way to know for sure if a death was truly due to a sudden cardiac arrhythmia, or even related to the heart,
To clear the wheat from the chaff, Dr. Tseng and his colleagues performed autopsies on 525 out-of-hospital SCD cases among adults in San Francisco from 2011-2016; to qualify, the cases had to meet World Health Organization SCD criteria, meaning unexpected death within 1 hour of symptom onset, or, in unwitnessed cases, within 24 hours of when the person was last seen alive and well.
Cases were considered sudden arrhythmic death – and, therefore, true SCD – if no extracardiac causes of death or acute heart failure were found on autopsy. Overall, 40% of deaths attributed to SCD “were not sudden or unexpected, and nearly half of presumed SCDs were not arrhythmic.” The findings had “implications for ... mortality data, clinical trials, and cohort studies,” Dr. Tseng and his team concluded (Circulation. 2018 Jun 19;137[25]:2689-2700).
They next turned their attention to HIV. It’s known that the virus increases the risk of strokes, heart attacks, and heart failure; the researchers wanted to see if it did the same for SCD. The HIV results were presented at CROI.
Forty-seven presumed SCD cases with HIV met inclusion criteria during the study period. Based on the earlier findings and epidemiological data, people with HIV had more than an 80% higher risk of SCD and an almost 60% higher risk of confirmed arrhythmic death than did the general public. Similar to the general population, only about half of presumed SCD cases were confirmed on autopsy. About one-third of what turned out to be non-cardiac HIV deaths were due to occult overdose, versus 13.5% in the general population, which points to the increased need for drug screening and treatment in HIV.
Beyond that, though, the team found that the burden of myocardial fibrosis in HIV “was profound,” far surpassing what was found in SCD deaths in the general population. After adjustment for age, gender, and heart disease, “sudden cardiac deaths with HIV had 60% higher interstitial fibrosis by myocardial trichrome staining. Cardiac fibrosis, a known substrate for fatal arrhythmias in the general population, may underlie the mechanism by which HIV increases the risk” of sudden death in HIV, Dr. Tseng said.
It could be that the virus enters heart cells and sets off an inflammatory cardiomyopathy, or perhaps it’s related to chronic inflammation caused by the virus. Whatever the case, infection seems to have an “independent effect” on increasing fibrosis among people with HIV, he said.
Intriguingly, a large epidemiologic study in United States veterans, also presented at CROI, found a higher risk of SCD among HIV patients, but only if their infections were active over an extended period of time, as indicated by sustained high viral loads and low CD4 cell counts. Dr. Tseng was involved in that work, as well, but noted that the number of HIV SCD cases in the San Francisco study was too small to draw meaningful conclusions regarding the relationship between disease control and cardiac fibrosis.
Cardiac defibrillators can prevent arrhythmic death, so, at least for now, he said that the autopsy study findings mean that criteria for implantation should be broadened to include extensive cardiac fibrosis.
The work was funded by the National Institutes of Health. Dr. Tseng didn’t have any disclosures.
SOURCE: Tseng ZH et al. CROI 2019 abstract 32
REPORTING FROM CROI 2019