User login
Conclusion of 'Homeland' Proves Electrifying
The rival protagonists of Showtime’s hit series "Homeland" both suffer from exuberant Axis I psychopathology.
Ace Marine sergeant Nicholas Brody (Damien Lewis) returns from 8 years of horrific imprisonment by jihadists to a hero’s welcome. Outwardly the same stalwart patriot, he’s in fact a posttraumatic stress disorder poster boy. Ace CIA officer Carrie Mathison (Claire Danes) believes Brody also is a turncoat dispatched by his former captors to wreak havoc upon the Great Satan. Carrie herself is haunted by traumatic memories – of a bungled Iraq covert mission. She’s also covertly bipolar.

During Homeland’s first season Carrie and Brody briefly became lovers, Brody’s true-false colors were revealed, and Carrie’s mood swings grew as volatile as her conviction about Brody’s sinister intentions. In the penultimate episode, Brody took Carrie off the board by revealing her illness to the agency. Now he could proceed unhindered with the plan to suicide-bomb a hawkish vice president as the latter announced his presidential candidacy, together with top military and defense officials.
Homeland’s creators now faced a dilemma brought on precisely by the powerful, complex narrative so responsible for its popularity. Lame cliff-hangers are the traditional bane of a successful second season. With viewer expectations running so high, how to bring off a final episode that could somehow allow Brody to outlive impending martyrdom and enable disgraced, still-smitten Carrie to resume her dogged pursuit?
The series’ writers turned to electroconvulsive therapy (ECT) for a cunning, literal deus ex machina. Brody, tormented about again abandoning his wife and children – this time to their certain humiliation – opted out of martyrdom at the last moment. He chose instead to dwell in the chambers of power by running for office. Carrie, now convinced her suspicions about Brody were spinning out of paranoid despair, committed herself to a course of inpatient ECT. Hovering in anesthetized twilight on the brink of her first treatment, a memory from the affair with Brody surfaced that incontestably established his villainy. But would ECT stop her from remembering it?
The last episode’s jolting conclusion pleased viewers terrifically. Mental health professionals also praised the show for mounting a reasonable account of ECT. The treatment’s actual depiction seemed blessedly untainted by the gross shake-rattle-and-rolling so dear to the makers of mental health movies since "The Snake Pit."
However, ECT-knowledgeable psychiatrists found Homeland’s take on ECT far from balanced. They believed Carrie’s treatment was unwarranted – her depression largely reactive, symptoms not grave enough, etc. They were chiefly concerned that desperately ill patients would be frightened away from a long-established, potent, and safe remedy. Heavily emphasizing ECT’s dire threat to Carrie’s crucial recollection overrode the brief passing statement that ECT poses no danger of permanent memory loss. The stark closing shots of Carrie’s subconvulsive twitching, her jaw agonizingly clenched around a baby-blue bite plate, only served up a gentler, kinder version of Hollywood’s standard ECT epileptoid extravaganza.

Such protests ignore the central purpose of mainstream film-making, for most movie and film dramas are not crafted to educate us about anything – not ECT, or veterinary medicine, or moose stalking. They are made to garner great profits by gratifying our ancient appetite for great stories.
Not necessarily a bad thing. Should demonstrating how to stalk a moose or give ECT keep us glued to our Sixplex seats, so much the better. But if viewer pleasure commands sacrificing clinical accuracy, depend upon it, that price will be paid. Whatever its impact upon hapless Carrie’s noggin, ECT as a pure narrative device was instrumental in bringing home Homeland’s first season, leaving the viewer just unsatisfied enough to crave next season’s fix. A handsome achievement, doubtless with handsome rewards to follow.
Dr. Greenberg is clinical professor of psychiatry at the Albert Einstein College of Medicine, New York. He has written several hundred reviews and essays; two books on cinema, media, and popular culture; and numerous articles on adolescent and general psychiatry. For more information, visit http://www.doctorgreenberg.net/.
The rival protagonists of Showtime’s hit series "Homeland" both suffer from exuberant Axis I psychopathology.
Ace Marine sergeant Nicholas Brody (Damien Lewis) returns from 8 years of horrific imprisonment by jihadists to a hero’s welcome. Outwardly the same stalwart patriot, he’s in fact a posttraumatic stress disorder poster boy. Ace CIA officer Carrie Mathison (Claire Danes) believes Brody also is a turncoat dispatched by his former captors to wreak havoc upon the Great Satan. Carrie herself is haunted by traumatic memories – of a bungled Iraq covert mission. She’s also covertly bipolar.
During Homeland’s first season Carrie and Brody briefly became lovers, Brody’s true-false colors were revealed, and Carrie’s mood swings grew as volatile as her conviction about Brody’s sinister intentions. In the penultimate episode, Brody took Carrie off the board by revealing her illness to the agency. Now he could proceed unhindered with the plan to suicide-bomb a hawkish vice president as the latter announced his presidential candidacy, together with top military and defense officials.
Homeland’s creators now faced a dilemma brought on precisely by the powerful, complex narrative so responsible for its popularity. Lame cliff-hangers are the traditional bane of a successful second season. With viewer expectations running so high, how to bring off a final episode that could somehow allow Brody to outlive impending martyrdom and enable disgraced, still-smitten Carrie to resume her dogged pursuit?
The series’ writers turned to electroconvulsive therapy (ECT) for a cunning, literal deus ex machina. Brody, tormented about again abandoning his wife and children – this time to their certain humiliation – opted out of martyrdom at the last moment. He chose instead to dwell in the chambers of power by running for office. Carrie, now convinced her suspicions about Brody were spinning out of paranoid despair, committed herself to a course of inpatient ECT. Hovering in anesthetized twilight on the brink of her first treatment, a memory from the affair with Brody surfaced that incontestably established his villainy. But would ECT stop her from remembering it?
The last episode’s jolting conclusion pleased viewers terrifically. Mental health professionals also praised the show for mounting a reasonable account of ECT. The treatment’s actual depiction seemed blessedly untainted by the gross shake-rattle-and-rolling so dear to the makers of mental health movies since "The Snake Pit."
However, ECT-knowledgeable psychiatrists found Homeland’s take on ECT far from balanced. They believed Carrie’s treatment was unwarranted – her depression largely reactive, symptoms not grave enough, etc. They were chiefly concerned that desperately ill patients would be frightened away from a long-established, potent, and safe remedy. Heavily emphasizing ECT’s dire threat to Carrie’s crucial recollection overrode the brief passing statement that ECT poses no danger of permanent memory loss. The stark closing shots of Carrie’s subconvulsive twitching, her jaw agonizingly clenched around a baby-blue bite plate, only served up a gentler, kinder version of Hollywood’s standard ECT epileptoid extravaganza.
Such protests ignore the central purpose of mainstream film-making, for most movie and film dramas are not crafted to educate us about anything – not ECT, or veterinary medicine, or moose stalking. They are made to garner great profits by gratifying our ancient appetite for great stories.
Not necessarily a bad thing. Should demonstrating how to stalk a moose or give ECT keep us glued to our Sixplex seats, so much the better. But if viewer pleasure commands sacrificing clinical accuracy, depend upon it, that price will be paid. Whatever its impact upon hapless Carrie’s noggin, ECT as a pure narrative device was instrumental in bringing home Homeland’s first season, leaving the viewer just unsatisfied enough to crave next season’s fix. A handsome achievement, doubtless with handsome rewards to follow.
Dr. Greenberg is clinical professor of psychiatry at the Albert Einstein College of Medicine, New York. He has written several hundred reviews and essays; two books on cinema, media, and popular culture; and numerous articles on adolescent and general psychiatry. For more information, visit http://www.doctorgreenberg.net/.
The rival protagonists of Showtime’s hit series "Homeland" both suffer from exuberant Axis I psychopathology.
Ace Marine sergeant Nicholas Brody (Damien Lewis) returns from 8 years of horrific imprisonment by jihadists to a hero’s welcome. Outwardly the same stalwart patriot, he’s in fact a posttraumatic stress disorder poster boy. Ace CIA officer Carrie Mathison (Claire Danes) believes Brody also is a turncoat dispatched by his former captors to wreak havoc upon the Great Satan. Carrie herself is haunted by traumatic memories – of a bungled Iraq covert mission. She’s also covertly bipolar.
During Homeland’s first season Carrie and Brody briefly became lovers, Brody’s true-false colors were revealed, and Carrie’s mood swings grew as volatile as her conviction about Brody’s sinister intentions. In the penultimate episode, Brody took Carrie off the board by revealing her illness to the agency. Now he could proceed unhindered with the plan to suicide-bomb a hawkish vice president as the latter announced his presidential candidacy, together with top military and defense officials.
Homeland’s creators now faced a dilemma brought on precisely by the powerful, complex narrative so responsible for its popularity. Lame cliff-hangers are the traditional bane of a successful second season. With viewer expectations running so high, how to bring off a final episode that could somehow allow Brody to outlive impending martyrdom and enable disgraced, still-smitten Carrie to resume her dogged pursuit?
The series’ writers turned to electroconvulsive therapy (ECT) for a cunning, literal deus ex machina. Brody, tormented about again abandoning his wife and children – this time to their certain humiliation – opted out of martyrdom at the last moment. He chose instead to dwell in the chambers of power by running for office. Carrie, now convinced her suspicions about Brody were spinning out of paranoid despair, committed herself to a course of inpatient ECT. Hovering in anesthetized twilight on the brink of her first treatment, a memory from the affair with Brody surfaced that incontestably established his villainy. But would ECT stop her from remembering it?
The last episode’s jolting conclusion pleased viewers terrifically. Mental health professionals also praised the show for mounting a reasonable account of ECT. The treatment’s actual depiction seemed blessedly untainted by the gross shake-rattle-and-rolling so dear to the makers of mental health movies since "The Snake Pit."
However, ECT-knowledgeable psychiatrists found Homeland’s take on ECT far from balanced. They believed Carrie’s treatment was unwarranted – her depression largely reactive, symptoms not grave enough, etc. They were chiefly concerned that desperately ill patients would be frightened away from a long-established, potent, and safe remedy. Heavily emphasizing ECT’s dire threat to Carrie’s crucial recollection overrode the brief passing statement that ECT poses no danger of permanent memory loss. The stark closing shots of Carrie’s subconvulsive twitching, her jaw agonizingly clenched around a baby-blue bite plate, only served up a gentler, kinder version of Hollywood’s standard ECT epileptoid extravaganza.
Such protests ignore the central purpose of mainstream film-making, for most movie and film dramas are not crafted to educate us about anything – not ECT, or veterinary medicine, or moose stalking. They are made to garner great profits by gratifying our ancient appetite for great stories.
Not necessarily a bad thing. Should demonstrating how to stalk a moose or give ECT keep us glued to our Sixplex seats, so much the better. But if viewer pleasure commands sacrificing clinical accuracy, depend upon it, that price will be paid. Whatever its impact upon hapless Carrie’s noggin, ECT as a pure narrative device was instrumental in bringing home Homeland’s first season, leaving the viewer just unsatisfied enough to crave next season’s fix. A handsome achievement, doubtless with handsome rewards to follow.
Dr. Greenberg is clinical professor of psychiatry at the Albert Einstein College of Medicine, New York. He has written several hundred reviews and essays; two books on cinema, media, and popular culture; and numerous articles on adolescent and general psychiatry. For more information, visit http://www.doctorgreenberg.net/.
Meta-Analysis Outlines Lithium Toxicity Profile
Lithium is associated with an increased risk of reduced urinary concentrating ability, hypothyroidism, hyperparathyroidism, and weight gain, but, despite widespread belief to the contrary, it may not be associated with congenital malformations, alopecia, skin disorders, or clinically significant reductions in renal function, according to findings from a systematic review and meta-analysis of data from 385 studies.
The review was undertaken in part because new evidence confirming the efficacy of lithium in bipolar disorder has led to suggestions that it be used more widely. Although it is considered an effective long-term therapy for bipolar disorder, its use has declined in recent years as new, more commercially promoted – but not always equally or more effective – drugs have become available. Concerns about potential teratogenic and other adverse effects, particularly on renal function, and have also contributed to declining use, Dr. Rebecca F. McKnight of the University of Oxford (England) and her colleagues reported online in the Jan. 20 issue of the Lancet.
To provide clinicians and patients with accurate evidence of lithium’s harms and benefits, the investigators set out to provide "a clinically informative systematic toxicity profile for lithium" they said (Lancet 2012 Jan. 20 [doi: 10.1016/S0140-6736(11)61516-X]).
Based on a hierarchy of evidence from the 22 randomized controlled trials, 197 cohort studies and case-control studies, and 166 case reports included in the review and meta-analysis, the investigators found that overall, glomerular filtration was reduced by –6.22 mL/min and urinary concentrating ability was reduced by 15% of normal maximum in patients receiving lithium, compared with controls.
"Data for the most clinically important outcome, renal failure, were scarce," the investigators said, noting that the only substantial cohort study showed that only 0.5% of patients receiving lithium were treated with renal replacement therapy.
As for clinical hypothyroidism, those taking lithium were significantly more likely than those on a placebo to develop the condition (odds ratio, 5.78), and based on a meta-analysis of the case-control studies, thyroid-stimulating hormone (TSH) concentrations were also significantly greater in those taking lithium (weighted mean difference, 4.00 IU/mL). Also, based on findings from 60 studies, blood calcium and parathyroid hormone levels were increased by about 10% over normal values in those taking lithium.
Clinically significant weight gain was also more frequent among those taking lithium than in controls (OR, 1.89), the investigators noted.
The evidence indicated, however, that lithium has little effect on hair or skin, with no significant difference seen in the incidence of alopecia in 24 publications reporting on the condition, and with no significant difference found in the prevalence of skin disorders between those taking lithium and controls in a meta-analysis of 77 publications.
Of note, six case-control studies that measured the association between Ebstein’s anomaly and lithium exposure found no link between the two. Although those estimates are unstable because of the low number of events, a case-control study of nearly 10,700 infants with a major congenital abnormality and more than 21,500 healthy controls also showed no significant association between lithium and congenital abnormalities.
Though limited by the quality and quantity of the primary evidence used in this study, which involved the screening of nearly 6,000 abstracts, the findings represent a "reasonable amount of evidence that allows cautious conclusions to be drawn about the safety of lithium," according to the investigators.
"This review provides a comprehensive synthesis of the evidence of harm that should inform clinical decision and draw attention to key questions in urgent need of further clarification," they said.
Based on their findings, the investigators developed the following recommendations for monitoring of lithium in clinical practice:
Before the start of lithium therapy, the risk of major adverse events should be discussed with the patient, a serum calcium level should be added to baseline blood tests, and uncertainty about the risk of congenital malformations to women of childbearing age should be explained. The latter two of these recommendations mark a change from current U.K. guidelines, the authors noted.
Also, during lithium therapy, renal, parathyroid, and thyroid function (at least glomerular filtration rate, TSH, and calcium) should be repeated at least every 12 months – and more frequently if an abnormal result is found or if the patient has a family history of endocrine disease; blood tests should all be repeated immediately in the event of a change in mood state; the occurrence of adverse effects should be routinely recorded; and women who would like to conceive or who have become pregnant during therapy should be advised that the increased risk of congenital malformation is uncertain, and the balance of risks between harm to the baby and maternal mood instability should be discussed before making a decision to discontinue lithium. All but the recommendation regarding repeat blood tests in the setting of mood state changes mark a change from current U.K. guidelines.
This study was funded by the National Institute for Health Research Programme Grant for Applied Research. The authors had no disclosures to report.
The authors of this review should be congratulated for the systematic quantification of the potential risks associated with lithium, Dr. Gin S. Malhi and Dr. Michael Berk wrote in an editorial that accompanied the report by Dr. McKnight and her colleagues in the Lancet.
This detailed review and analysis provides meaningful and reassuring advice for clinicians and identifies areas in need of additional research in regard to the safety of lithium, said Dr. Malhi and Dr. Berk. While the available evidence is far from ideal, the study – in the context of efficacy data upgrading the ranking of lithium, and new data that "recalibrate the safety risks of alternative drugs" – provides "timely clarification of the toxicity associated with lithium therapy, and on balance, reaffirms its role as a treatment of choice for bipolar disorder," they noted (Lancet 2012 Jan. 20 [doi:10.1016/S0140-6736(11)61703-0]).
"The renal side-effects of lithium are of greatest concern to both clinicians and patients, and in this regard, the analysis is reassuring in that, even with long-term lithium use, the risk of renal toxicity, specifically end-stage renal failure, is fairly low (0.53% compared to 0.2% in the general population)," they noted.
However, since the data on dosing and its relationship with toxicity were insufficient, matters of dose-related side-effects cannot be informed by the findings.
"Instead, the study provides useful guidance for clinicians considering lithium treatment, and redirects the focus of research to dosage and safety monitoring," said Dr. Malhi and Dr. Berk.
Dr. Malhi is with the University of Sydney. Dr. Berk is with the University of Melbourne. Dr. Malhi has received research support from, and/or served as a speaker or consultant for AstraZeneca, Eli Lilly, Organon, Pfizer, Servier, Wyeth, Janssen-Cilag, Lundbeck, and Ranbaxy. Dr. Berk has received research support from, and/or served as a speaker or consultant for Medical Benefits Funds of Australia, Bristol-Myers Squibb, Eli Lilly, GlaxoSmithKline, Organon, Novartis, Mayne Pharma, Servier, Janssen-Cilag, Lundbeck, Merck, Pfizer, Sanofi-Synthelabo, Solvay, and Wyeth.
The authors of this review should be congratulated for the systematic quantification of the potential risks associated with lithium, Dr. Gin S. Malhi and Dr. Michael Berk wrote in an editorial that accompanied the report by Dr. McKnight and her colleagues in the Lancet.
This detailed review and analysis provides meaningful and reassuring advice for clinicians and identifies areas in need of additional research in regard to the safety of lithium, said Dr. Malhi and Dr. Berk. While the available evidence is far from ideal, the study – in the context of efficacy data upgrading the ranking of lithium, and new data that "recalibrate the safety risks of alternative drugs" – provides "timely clarification of the toxicity associated with lithium therapy, and on balance, reaffirms its role as a treatment of choice for bipolar disorder," they noted (Lancet 2012 Jan. 20 [doi:10.1016/S0140-6736(11)61703-0]).
"The renal side-effects of lithium are of greatest concern to both clinicians and patients, and in this regard, the analysis is reassuring in that, even with long-term lithium use, the risk of renal toxicity, specifically end-stage renal failure, is fairly low (0.53% compared to 0.2% in the general population)," they noted.
However, since the data on dosing and its relationship with toxicity were insufficient, matters of dose-related side-effects cannot be informed by the findings.
"Instead, the study provides useful guidance for clinicians considering lithium treatment, and redirects the focus of research to dosage and safety monitoring," said Dr. Malhi and Dr. Berk.
Dr. Malhi is with the University of Sydney. Dr. Berk is with the University of Melbourne. Dr. Malhi has received research support from, and/or served as a speaker or consultant for AstraZeneca, Eli Lilly, Organon, Pfizer, Servier, Wyeth, Janssen-Cilag, Lundbeck, and Ranbaxy. Dr. Berk has received research support from, and/or served as a speaker or consultant for Medical Benefits Funds of Australia, Bristol-Myers Squibb, Eli Lilly, GlaxoSmithKline, Organon, Novartis, Mayne Pharma, Servier, Janssen-Cilag, Lundbeck, Merck, Pfizer, Sanofi-Synthelabo, Solvay, and Wyeth.
The authors of this review should be congratulated for the systematic quantification of the potential risks associated with lithium, Dr. Gin S. Malhi and Dr. Michael Berk wrote in an editorial that accompanied the report by Dr. McKnight and her colleagues in the Lancet.
This detailed review and analysis provides meaningful and reassuring advice for clinicians and identifies areas in need of additional research in regard to the safety of lithium, said Dr. Malhi and Dr. Berk. While the available evidence is far from ideal, the study – in the context of efficacy data upgrading the ranking of lithium, and new data that "recalibrate the safety risks of alternative drugs" – provides "timely clarification of the toxicity associated with lithium therapy, and on balance, reaffirms its role as a treatment of choice for bipolar disorder," they noted (Lancet 2012 Jan. 20 [doi:10.1016/S0140-6736(11)61703-0]).
"The renal side-effects of lithium are of greatest concern to both clinicians and patients, and in this regard, the analysis is reassuring in that, even with long-term lithium use, the risk of renal toxicity, specifically end-stage renal failure, is fairly low (0.53% compared to 0.2% in the general population)," they noted.
However, since the data on dosing and its relationship with toxicity were insufficient, matters of dose-related side-effects cannot be informed by the findings.
"Instead, the study provides useful guidance for clinicians considering lithium treatment, and redirects the focus of research to dosage and safety monitoring," said Dr. Malhi and Dr. Berk.
Dr. Malhi is with the University of Sydney. Dr. Berk is with the University of Melbourne. Dr. Malhi has received research support from, and/or served as a speaker or consultant for AstraZeneca, Eli Lilly, Organon, Pfizer, Servier, Wyeth, Janssen-Cilag, Lundbeck, and Ranbaxy. Dr. Berk has received research support from, and/or served as a speaker or consultant for Medical Benefits Funds of Australia, Bristol-Myers Squibb, Eli Lilly, GlaxoSmithKline, Organon, Novartis, Mayne Pharma, Servier, Janssen-Cilag, Lundbeck, Merck, Pfizer, Sanofi-Synthelabo, Solvay, and Wyeth.
Lithium is associated with an increased risk of reduced urinary concentrating ability, hypothyroidism, hyperparathyroidism, and weight gain, but, despite widespread belief to the contrary, it may not be associated with congenital malformations, alopecia, skin disorders, or clinically significant reductions in renal function, according to findings from a systematic review and meta-analysis of data from 385 studies.
The review was undertaken in part because new evidence confirming the efficacy of lithium in bipolar disorder has led to suggestions that it be used more widely. Although it is considered an effective long-term therapy for bipolar disorder, its use has declined in recent years as new, more commercially promoted – but not always equally or more effective – drugs have become available. Concerns about potential teratogenic and other adverse effects, particularly on renal function, and have also contributed to declining use, Dr. Rebecca F. McKnight of the University of Oxford (England) and her colleagues reported online in the Jan. 20 issue of the Lancet.
To provide clinicians and patients with accurate evidence of lithium’s harms and benefits, the investigators set out to provide "a clinically informative systematic toxicity profile for lithium" they said (Lancet 2012 Jan. 20 [doi: 10.1016/S0140-6736(11)61516-X]).
Based on a hierarchy of evidence from the 22 randomized controlled trials, 197 cohort studies and case-control studies, and 166 case reports included in the review and meta-analysis, the investigators found that overall, glomerular filtration was reduced by –6.22 mL/min and urinary concentrating ability was reduced by 15% of normal maximum in patients receiving lithium, compared with controls.
"Data for the most clinically important outcome, renal failure, were scarce," the investigators said, noting that the only substantial cohort study showed that only 0.5% of patients receiving lithium were treated with renal replacement therapy.
As for clinical hypothyroidism, those taking lithium were significantly more likely than those on a placebo to develop the condition (odds ratio, 5.78), and based on a meta-analysis of the case-control studies, thyroid-stimulating hormone (TSH) concentrations were also significantly greater in those taking lithium (weighted mean difference, 4.00 IU/mL). Also, based on findings from 60 studies, blood calcium and parathyroid hormone levels were increased by about 10% over normal values in those taking lithium.
Clinically significant weight gain was also more frequent among those taking lithium than in controls (OR, 1.89), the investigators noted.
The evidence indicated, however, that lithium has little effect on hair or skin, with no significant difference seen in the incidence of alopecia in 24 publications reporting on the condition, and with no significant difference found in the prevalence of skin disorders between those taking lithium and controls in a meta-analysis of 77 publications.
Of note, six case-control studies that measured the association between Ebstein’s anomaly and lithium exposure found no link between the two. Although those estimates are unstable because of the low number of events, a case-control study of nearly 10,700 infants with a major congenital abnormality and more than 21,500 healthy controls also showed no significant association between lithium and congenital abnormalities.
Though limited by the quality and quantity of the primary evidence used in this study, which involved the screening of nearly 6,000 abstracts, the findings represent a "reasonable amount of evidence that allows cautious conclusions to be drawn about the safety of lithium," according to the investigators.
"This review provides a comprehensive synthesis of the evidence of harm that should inform clinical decision and draw attention to key questions in urgent need of further clarification," they said.
Based on their findings, the investigators developed the following recommendations for monitoring of lithium in clinical practice:
Before the start of lithium therapy, the risk of major adverse events should be discussed with the patient, a serum calcium level should be added to baseline blood tests, and uncertainty about the risk of congenital malformations to women of childbearing age should be explained. The latter two of these recommendations mark a change from current U.K. guidelines, the authors noted.
Also, during lithium therapy, renal, parathyroid, and thyroid function (at least glomerular filtration rate, TSH, and calcium) should be repeated at least every 12 months – and more frequently if an abnormal result is found or if the patient has a family history of endocrine disease; blood tests should all be repeated immediately in the event of a change in mood state; the occurrence of adverse effects should be routinely recorded; and women who would like to conceive or who have become pregnant during therapy should be advised that the increased risk of congenital malformation is uncertain, and the balance of risks between harm to the baby and maternal mood instability should be discussed before making a decision to discontinue lithium. All but the recommendation regarding repeat blood tests in the setting of mood state changes mark a change from current U.K. guidelines.
This study was funded by the National Institute for Health Research Programme Grant for Applied Research. The authors had no disclosures to report.
Lithium is associated with an increased risk of reduced urinary concentrating ability, hypothyroidism, hyperparathyroidism, and weight gain, but, despite widespread belief to the contrary, it may not be associated with congenital malformations, alopecia, skin disorders, or clinically significant reductions in renal function, according to findings from a systematic review and meta-analysis of data from 385 studies.
The review was undertaken in part because new evidence confirming the efficacy of lithium in bipolar disorder has led to suggestions that it be used more widely. Although it is considered an effective long-term therapy for bipolar disorder, its use has declined in recent years as new, more commercially promoted – but not always equally or more effective – drugs have become available. Concerns about potential teratogenic and other adverse effects, particularly on renal function, and have also contributed to declining use, Dr. Rebecca F. McKnight of the University of Oxford (England) and her colleagues reported online in the Jan. 20 issue of the Lancet.
To provide clinicians and patients with accurate evidence of lithium’s harms and benefits, the investigators set out to provide "a clinically informative systematic toxicity profile for lithium" they said (Lancet 2012 Jan. 20 [doi: 10.1016/S0140-6736(11)61516-X]).
Based on a hierarchy of evidence from the 22 randomized controlled trials, 197 cohort studies and case-control studies, and 166 case reports included in the review and meta-analysis, the investigators found that overall, glomerular filtration was reduced by –6.22 mL/min and urinary concentrating ability was reduced by 15% of normal maximum in patients receiving lithium, compared with controls.
"Data for the most clinically important outcome, renal failure, were scarce," the investigators said, noting that the only substantial cohort study showed that only 0.5% of patients receiving lithium were treated with renal replacement therapy.
As for clinical hypothyroidism, those taking lithium were significantly more likely than those on a placebo to develop the condition (odds ratio, 5.78), and based on a meta-analysis of the case-control studies, thyroid-stimulating hormone (TSH) concentrations were also significantly greater in those taking lithium (weighted mean difference, 4.00 IU/mL). Also, based on findings from 60 studies, blood calcium and parathyroid hormone levels were increased by about 10% over normal values in those taking lithium.
Clinically significant weight gain was also more frequent among those taking lithium than in controls (OR, 1.89), the investigators noted.
The evidence indicated, however, that lithium has little effect on hair or skin, with no significant difference seen in the incidence of alopecia in 24 publications reporting on the condition, and with no significant difference found in the prevalence of skin disorders between those taking lithium and controls in a meta-analysis of 77 publications.
Of note, six case-control studies that measured the association between Ebstein’s anomaly and lithium exposure found no link between the two. Although those estimates are unstable because of the low number of events, a case-control study of nearly 10,700 infants with a major congenital abnormality and more than 21,500 healthy controls also showed no significant association between lithium and congenital abnormalities.
Though limited by the quality and quantity of the primary evidence used in this study, which involved the screening of nearly 6,000 abstracts, the findings represent a "reasonable amount of evidence that allows cautious conclusions to be drawn about the safety of lithium," according to the investigators.
"This review provides a comprehensive synthesis of the evidence of harm that should inform clinical decision and draw attention to key questions in urgent need of further clarification," they said.
Based on their findings, the investigators developed the following recommendations for monitoring of lithium in clinical practice:
Before the start of lithium therapy, the risk of major adverse events should be discussed with the patient, a serum calcium level should be added to baseline blood tests, and uncertainty about the risk of congenital malformations to women of childbearing age should be explained. The latter two of these recommendations mark a change from current U.K. guidelines, the authors noted.
Also, during lithium therapy, renal, parathyroid, and thyroid function (at least glomerular filtration rate, TSH, and calcium) should be repeated at least every 12 months – and more frequently if an abnormal result is found or if the patient has a family history of endocrine disease; blood tests should all be repeated immediately in the event of a change in mood state; the occurrence of adverse effects should be routinely recorded; and women who would like to conceive or who have become pregnant during therapy should be advised that the increased risk of congenital malformation is uncertain, and the balance of risks between harm to the baby and maternal mood instability should be discussed before making a decision to discontinue lithium. All but the recommendation regarding repeat blood tests in the setting of mood state changes mark a change from current U.K. guidelines.
This study was funded by the National Institute for Health Research Programme Grant for Applied Research. The authors had no disclosures to report.
FROM THE LANCET
Major Finding: Lithium is associated with an increased risk of reduced urinary concentrating ability, hypothyroidism, hyperparathyroidism, and weight gain, but it may not be associated with congenital malformations, alopecia, skin disorders, or clinically significant reductions in renal function.
Data Source: A systematic review and meta-analysis of randomized controlled trials and observational studies.
Disclosures: This study was funded by the National Institute for Health Research Programme Grant for Applied Research. The authors had no disclosures to report.
Comments & Controversies
Concerns about valproate
I read Dr. Jain and Ms. Beste’s Pearl on treating alopecia developing during valproate use ("Valproate-induced hair loss: What to tell patients," Current Psychiatry, November 2011, p. 74) with some dismay.
Valproate is a valuable drug that has demonstrated efficacy in treating bipolar disorder; however, valproate use is associated with substantial side effects for women and developing fetuses.
I take no issue with any of the points made in the article, but I am concerned about the failure to mention critical side effects associated with valproate, including:
- weight gain and metabolic side effects
- for women, polycystic ovary syndrome—a serious and difficult-to-treat complication
- danger to fetuses—recent research suggests marked reductions in intelligence quotient in babies exposed to valproate in utero.1
We would be wise to remind ourselves of these issues whenever considering initiating or continuing valproate therapy.
Edward Pontius, MD, DFAPA
Private Practice
Brunswick, ME
The authors respond
The concerns expressed by Dr. Pontius regarding clinical use of valproate are genuine and worthy. The purpose of our article was to call attention to a lesser-known side effect of valproate and how to intervene. We assumed that clinicians would discuss with patients the teratogenicity of valproate, along with other common side effects—weight gain, pancreatitis, effect on liver function tests, thrombocytopenia, and polycystic ovary syndrome—before initiating the drug. Such discussion about valproate was beyond the scope of our article, but we thank Dr. Pontius for bringing these concerns to our attention.
Shailesh Jain, MD, MPH, ABDA
Regional Chair
Associate Professor
Department of Psychiatry
Beth Beste, MS
Fourth-Year Medical Student
Texas Tech University Health Sciences Center, Permian Basin
Odessa, TX
Domains of excellence
I want to thank Dr. Nasrallah, whose monthly comments I find interesting and provocative, for his first-of-its-kind description of the “ideal” psychiatrist’s role and identity (“The model psychiatrist: 7 domains of excellence,” From the Editor, Current Psychiatry, November 2011, p. 5-6). This article should be mandatory reading and discussion material for every psychiatry residency program. For this elder psychiatrist, it was a thoughtful review of where I have been and where I am going in my field.
Ronald Blank, MD
Private Practice
Easthampton, MA
Additional traits
I find Current Psychiatry to be exceedingly useful for myself and the physician assistant students I teach. I agree with the 7 domains in Dr. Nasrallah’s editorial (“The model psychiatrist: 7 domains of excellence,” From the Editor, Current Psychiatry, November 2011, p. 5-6). However, I would like to add 2 more traits:
- The role that a psychiatrist plays in his or her family, especially with their children, because ignoring one’s family in the pursuit of clinical sainthood is not a mark of greatness
- The psychiatrist today is more of a team member than team leader. Failure to recognize this role creates intolerable stresses on the treatment environment in which the psychiatrist works. This does not minimize the need for personal excellence, but it certainly helps decrease destructive narcissism.
Kim J. Masters, MD
Medical Director
Three Rivers Midlands Campus Residential Treatment Center
West Columbia, SC
Concerns about valproate
I read Dr. Jain and Ms. Beste’s Pearl on treating alopecia developing during valproate use ("Valproate-induced hair loss: What to tell patients," Current Psychiatry, November 2011, p. 74) with some dismay.
Valproate is a valuable drug that has demonstrated efficacy in treating bipolar disorder; however, valproate use is associated with substantial side effects for women and developing fetuses.
I take no issue with any of the points made in the article, but I am concerned about the failure to mention critical side effects associated with valproate, including:
- weight gain and metabolic side effects
- for women, polycystic ovary syndrome—a serious and difficult-to-treat complication
- danger to fetuses—recent research suggests marked reductions in intelligence quotient in babies exposed to valproate in utero.1
We would be wise to remind ourselves of these issues whenever considering initiating or continuing valproate therapy.
Edward Pontius, MD, DFAPA
Private Practice
Brunswick, ME
The authors respond
The concerns expressed by Dr. Pontius regarding clinical use of valproate are genuine and worthy. The purpose of our article was to call attention to a lesser-known side effect of valproate and how to intervene. We assumed that clinicians would discuss with patients the teratogenicity of valproate, along with other common side effects—weight gain, pancreatitis, effect on liver function tests, thrombocytopenia, and polycystic ovary syndrome—before initiating the drug. Such discussion about valproate was beyond the scope of our article, but we thank Dr. Pontius for bringing these concerns to our attention.
Shailesh Jain, MD, MPH, ABDA
Regional Chair
Associate Professor
Department of Psychiatry
Beth Beste, MS
Fourth-Year Medical Student
Texas Tech University Health Sciences Center, Permian Basin
Odessa, TX
Domains of excellence
I want to thank Dr. Nasrallah, whose monthly comments I find interesting and provocative, for his first-of-its-kind description of the “ideal” psychiatrist’s role and identity (“The model psychiatrist: 7 domains of excellence,” From the Editor, Current Psychiatry, November 2011, p. 5-6). This article should be mandatory reading and discussion material for every psychiatry residency program. For this elder psychiatrist, it was a thoughtful review of where I have been and where I am going in my field.
Ronald Blank, MD
Private Practice
Easthampton, MA
Additional traits
I find Current Psychiatry to be exceedingly useful for myself and the physician assistant students I teach. I agree with the 7 domains in Dr. Nasrallah’s editorial (“The model psychiatrist: 7 domains of excellence,” From the Editor, Current Psychiatry, November 2011, p. 5-6). However, I would like to add 2 more traits:
- The role that a psychiatrist plays in his or her family, especially with their children, because ignoring one’s family in the pursuit of clinical sainthood is not a mark of greatness
- The psychiatrist today is more of a team member than team leader. Failure to recognize this role creates intolerable stresses on the treatment environment in which the psychiatrist works. This does not minimize the need for personal excellence, but it certainly helps decrease destructive narcissism.
Kim J. Masters, MD
Medical Director
Three Rivers Midlands Campus Residential Treatment Center
West Columbia, SC
Concerns about valproate
I read Dr. Jain and Ms. Beste’s Pearl on treating alopecia developing during valproate use ("Valproate-induced hair loss: What to tell patients," Current Psychiatry, November 2011, p. 74) with some dismay.
Valproate is a valuable drug that has demonstrated efficacy in treating bipolar disorder; however, valproate use is associated with substantial side effects for women and developing fetuses.
I take no issue with any of the points made in the article, but I am concerned about the failure to mention critical side effects associated with valproate, including:
- weight gain and metabolic side effects
- for women, polycystic ovary syndrome—a serious and difficult-to-treat complication
- danger to fetuses—recent research suggests marked reductions in intelligence quotient in babies exposed to valproate in utero.1
We would be wise to remind ourselves of these issues whenever considering initiating or continuing valproate therapy.
Edward Pontius, MD, DFAPA
Private Practice
Brunswick, ME
The authors respond
The concerns expressed by Dr. Pontius regarding clinical use of valproate are genuine and worthy. The purpose of our article was to call attention to a lesser-known side effect of valproate and how to intervene. We assumed that clinicians would discuss with patients the teratogenicity of valproate, along with other common side effects—weight gain, pancreatitis, effect on liver function tests, thrombocytopenia, and polycystic ovary syndrome—before initiating the drug. Such discussion about valproate was beyond the scope of our article, but we thank Dr. Pontius for bringing these concerns to our attention.
Shailesh Jain, MD, MPH, ABDA
Regional Chair
Associate Professor
Department of Psychiatry
Beth Beste, MS
Fourth-Year Medical Student
Texas Tech University Health Sciences Center, Permian Basin
Odessa, TX
Domains of excellence
I want to thank Dr. Nasrallah, whose monthly comments I find interesting and provocative, for his first-of-its-kind description of the “ideal” psychiatrist’s role and identity (“The model psychiatrist: 7 domains of excellence,” From the Editor, Current Psychiatry, November 2011, p. 5-6). This article should be mandatory reading and discussion material for every psychiatry residency program. For this elder psychiatrist, it was a thoughtful review of where I have been and where I am going in my field.
Ronald Blank, MD
Private Practice
Easthampton, MA
Additional traits
I find Current Psychiatry to be exceedingly useful for myself and the physician assistant students I teach. I agree with the 7 domains in Dr. Nasrallah’s editorial (“The model psychiatrist: 7 domains of excellence,” From the Editor, Current Psychiatry, November 2011, p. 5-6). However, I would like to add 2 more traits:
- The role that a psychiatrist plays in his or her family, especially with their children, because ignoring one’s family in the pursuit of clinical sainthood is not a mark of greatness
- The psychiatrist today is more of a team member than team leader. Failure to recognize this role creates intolerable stresses on the treatment environment in which the psychiatrist works. This does not minimize the need for personal excellence, but it certainly helps decrease destructive narcissism.
Kim J. Masters, MD
Medical Director
Three Rivers Midlands Campus Residential Treatment Center
West Columbia, SC
Treating patients with suspected ultra-rapid cycling bipolar disorder
Ultra-rapid cycling bipolar disorder: A critical look
Ultra-rapid cycling (URC) entered the psychiatric lexicon in the 1990s as a proposed descriptor for manic/hypomanic, mixed, or depressed episodes of bipolar disorder (BD) that occur every few days or weeks. DSM-IV-TR incorporates rapid cycling (RC)—but not URC—as a course specifier that occurs in 10% to 15% of patients with BD who have ≥4 distinct affective episodes per year, each fulfilling duration criteria and separated by identifiable recovery periods (unless an episode directly changes polarity). Since then, the terms RC and URC have seemingly metamorphosed into imprecise, popular colloquialisms meant to loosely describe frequent mood changes rather than distinct episodes over extended time periods, with little regard for the associated signs that define manic or hypomanic episodes.
This article examines the meaning and validity of URC in BD, its relevance and differentiation from rapid mood shifts in patients without BD, and concepts relevant to treatment extrapolated from studies of RC BD.
Imprecise nomenclature
Post et al1 coined the terms “ultra-rapid cycling” and “ultra-ultra-rapid cycling” (also called “ultradian cycling”) to describe mood episodes that occur monthly (URC) or over the course of as little as 1 day (ultradian cycling). These constructs are controversial because they lack demonstrated content validity and discriminant validity relative to other disorders. (“Content validity” refers to whether the features thought to comprise an entity of interest accurately and meaningfully do so; “discriminant validity” tells researchers and clinicians whether the proposed description of a clinical entity uniquely differentiates it from other disorders—avoiding “false-positive” suspected cases.) Clinicians therefore must pay careful attention to non-bipolar psychiatric problems that can present with rapid mood changes but without the psychomotor and related signs that define bipolar mood episodes. In their looser, nontechnical meanings, “rapid cycling” or “ultra-rapid cycling” may be synonymous with affective lability. RC is neither a diagnosis in itself nor a criterion for diagnosing BD. Rather, it is a course specifier to describe episode frequency in patients with past unambiguous manic or hypomanic episodes.
In children and adolescents, whose presentations often are atypical and can be hard to differentiate from other forms of behavioral or temperamental dysregulation, severe non-episodic mood dysregulation without signs of mania or hypomania may indicate a phenomenon separate from BD.2 Geller and colleagues3 proposed using the term “episodes” to frame the duration of a DSM-IV-defined syndrome of mania/hypomania or depression, while reserving the term “cycling” to connote patterns of mood alternation within a given episode. It is not clear whether this concept of “cycling” differs qualitatively from mood lability that arises during a mood episode in children or adults, and notably, this perspective does not account for changes in psychomotor signs in conjunction with changes in mood.
Clinicians also sometimes blur the concept of “mixed episodes” with RC or URC. DSM-IV-TR defines mixed episodes within bipolar I disorder (BD I) based on criteria for a simultaneous manic and depressive episode, rather than on frequent oscillations between affective poles. These and other differential diagnostic considerations for suspected URC are summarized in Table 1.4
A further concern regarding nomenclature involves the distinction between cyclicity (ie, successive episodes regardless of pole direction) and changes in polarity (ie, switches from depression to mania/hypomania or vice versa). Some mood disorder patients may have rapid oscillations from euthymia to depression while never changing polarity to mania/hypomania and may be best described as having recurrent brief depression.
Table 1
Differential diagnosis in suspected URC
| Phenomenon | Considerations for assessment |
|---|---|
| Mixed episodes in bipolar I disorder, or mixed depressive episodes in bipolar II disorder | DSM-IV-TR mixed episodes entail the co-occurrence of manic and depressive symptoms during the same episode without an intervening period of recovery. ICD-10 includes “rapid alternation of manic, hypomanic or depressive symptoms…from day to day or even hour to hour” in its definition of a mixed episode |
| Distress responses to acute environmental adversities (eg, adjustment disorders with mixed disturbance of emotions and conduct) | One would expect an absence of corresponding sleep-wake cycle changes or speech-language and psychomotor disturbances |
| Intoxication/withdrawal from psychoactive substances or drug-induced mental status changes (eg, corticosteroids, amphetamine, cocaine); a history of substance abuse also may be associated with development of URC in BD patients4 | Substance-induced mood fluctuations caused by intoxication/withdrawal can mimic affective cycling |
| Disinhibition states and frontal lobe syndromes as seen in traumatic brain injury and other CNS disorders, such as multiple sclerosis | Assess for signs of perseveration and history of head trauma or neurologic damage from cumulative toxic-metabolic insults (eg, chronic alcoholism) |
| Autonomic hyperarousal, emotional volatility, and hyperreactivity to environmental stresses, suggestive of PTSD | Determine the presence of a trauma history and review whether DSM-IV-TR symptoms and associated features of PTSD exist, including re-experiencing/reliving and avoidance, as well as paranoid thinking, dissociation, and nightmares |
| Recurrent mood shifts related to premenstrual dysphoric disorder may mimic URC. Other endocrine dysfunctions also may present with URC (eg, thyroid or ovarian malignancies) | Affirm the independent presence of BD before inferring its manifestations solely from premenstrual mood changes |
| Trait affective instability associated with borderline personality disorder | Trait mood instability is more chronic and enduring than episodic, and would not be expected to occur in tandem with signs of psychomotor activation that define mania/hypomania |
| BD: bipolar disorder; ICD-10: International Statistical Classification of Diseases and Related Health Problems, 10th revision; PTSD: posttraumatic stress disorder; URC: ultra-rapid cycling | |
Duration criteria
Clinicians and researchers have debated the minimum duration criteria for identifying manic or hypomanic episodes, and the extent to which suspected hypomanic periods of short duration constitute distinct illness phases. Although DSM-IV-TR designates 4 days as a minimum time for classifying an episode of hypomania, empirical studies suggest that mood symptoms lasting as few as 2 days may comprise a valid and reliably distinct entity relevant to RC.5 More limited data (mainly case observations) identify “affective oscillations” and “mood shifts” occurring faster than once per 24 hours in BD patients without comorbid personality disorders.6 Phenomenologic studies that have focused on 24- to 48-hour switch cycles have described new-onset URC arising spontaneously or following closed head injuries.7 In children and younger adolescents, reports have identified long index manic episodes (mean durations as long as 80 weeks)8 that involve continual (ultradian) mood cycling in as many as 80% of cases.9
Is URC a valid construct?
A central controversy surrounding the validity and meaningfulness of URC as a BD subtype involves its sole focus on mood variation rather than the fuller constellation of associated signs and symptoms that define episodes of mania/hypomania or depression. Abrupt, sudden, drastic, or dramatic mood shifts from one moment to the next are nowhere to be found in the DSM-IV-TR definition of BD, and the construct of mood lability or affective instability is neither a cardinal nor defining element of BD. Although individuals with BD I or bipolar II disorder (BD II) may have periods of affective lability, rapid shifts in mood are neither necessary nor sufficient for a BD diagnosis, and may indicate other types of psychopathology when affective instability occurs in the absence of a history of discernible manic or hypomanic episodes.
Studies by our group10 and others11 have shown that overattention to mood variation without considering associated cognitive, speech-language, chronobiologic, and motor signs of mania/hypomania accounts for substantial overdiagnosis of BD in patients with non-specific mood disturbances, particularly in those with active substance abuse or borderline personality disorder (BPD). Whereas the construct of RC BD attempts to account for changes in energy and psychomotor function as part of recurrent syndromes of mania/hypomania, existing literature on URC does not. Assessing mood changes in <24 hours also precludes assessing associated phenomena that occur over longer periods, such as changes in the sleep-wake cycle.
A rigorous, systematic approach to differential diagnosis for patients with affective instability is essential.
Borderline personality disorder
A common diagnostic debate regarding URC involves how to differentiate it from the chronic mood instability and reactivity inherent to BPD. Although some authors have suggested that RC BD and affective instability in BPD may be the same entity,12 others object to unifying the 2 conditions without considering their phenomenologic and other clinical differences. For example, affective instability arising from borderline character organization is thought to reflect a patient’s impaired capacity to self-regulate his or her internal state and emotional responses to interpersonal and other environmental stresses, or difficulty managing impulses. By contrast, manic or depressive phases of BD tend not to be “triggered” by interpersonal conflicts or frustrations. Furthermore, reframing intense mood reactions to the environment as bipolar variants carries several pitfalls: doing so wrongly accords patients a passive role in their reactions to life events, inaccurately reinforces a sense of victimization in response to stress, and diverts inquiry away from a patient’s active role in life decisions and circumstances that may be unsatisfying, self-defeating, or volatile.
Two key considerations may be helpful in discriminating rapid mood changes in BD vs BPD. First, some longitudinal studies indicate that RC often is a transient, rather than enduring, phenomenon in BD,13 in contrast to the nonvarying, trait feature of affective instability in persons with BPD. It is unknown whether URC is more enduring than transient. Notably, whereas bipolar mood episodes constitute deviations from a baseline state, affective instability in BPD is a baseline characteristic, rather than a deviation from it. Second, by definition, a BPD diagnosis hinges on additional elements unrelated to mood disturbances, such as interpersonal styles or defense mechanisms that involve splitting, projection, and projective identification, feelings of numbness, boredom, or emptiness, identity diffusion, fears of abandonment, and proclivities toward self-mutilation or other self-injurious behaviors as a means to alleviate tension and stress. These characteristics do not overlap with the core elements of BD.
Affective lability in patients with BPD entails prominent oscillations between anger and anxiety, or depression and anxiety, but not depression and elation14; by contrast, affective instability in BD has been linked with greater oscillations between euthymia and depression, and euthymia and elation, but not euthymia and anger.15 Moreover, daily mood fluctuations in patients with BD appear to occur in a relatively random fashion,16 whereas in BPD mood fluctuations are reactions that appear intimately linked to distressing interpersonal experiences.
See the table below, entitled “Rapid cycling and ultra-rapid cycling BD: A comparison,” comparing the phenomenology of RC and URC and a discussion of studies that explored genetic markers or family patterns that may be related to RC or URC.
Treatment considerations
No systematic studies exist for treating URC. Because most clinical trials of BD focus on treatment or prevention of a single episode rather than changes of mood over time, it is difficult to draw inferences about the ability of any treatment to attenuate marked, day-to-day mood variations. Some antimanic drugs, such as carbamazepine, have been suggested to offer better prophylactic efficacy compared with lithium for “non-classical” BD presentations, although the efficacy of carbamazepine has not been studied in URC.
Broadly speaking, treatment for URC, similar to RC, pragmatically involves:
- identifying and eliminating sources of mood destabilization (eg, substance abuse, erratic sleep patterns)
- treating medical comorbidities such as hypothyroidism
- optimizing treatment with mood stabilizing agents
- exercising caution when using antidepressants (see below).
Interestingly, despite frequent allusion to certain medications as “mood stabilizers,” no controlled study has examined mood instability on a day-to-day basis as a primary outcome measure in BD treatment, which limits the ability to surmise that any drug could be expected to diminish mood oscillations that occur over the course of days, or within a single day. However, a post hoc analysis by our group17 compared randomized treatment with lamotrigine or placebo over 6 months in RC BD I or BD II. Using prospective life charting, we found patients who received lamotrigine were almost twice as likely as those receiving placebo to achieve euthymia from one week to the next, which suggests the possibility that lamotrigine may offer benefit for affective instability in BD I or BD II patients, in addition to preventing discrete mood episodes.
Antidepressant controversy. Concerns that antidepressants might acutely induce mania or accelerate cycling frequency over long time periods have led to a contentious, long-standing debate within psychopharmacology. As noted in the box below, several long-term naturalistic follow-up studies have reported RC as a perceived consequence of antidepressants in most RC patients, although efforts to differentiate cycle acceleration caused by antidepressants (or other iatrogenic factors) from the natural course of illness remains exceedingly difficult without prospective randomized trials. (Antidepressants might cause more affective recurrences, but having multiple episodes may also cause more antidepressant prescriptions.) Some researchers (eg, Schneck et al18) have reported more frequent episodes among patients taking antidepressants but did not consider that patients with multiple episodes may be more likely to receive antidepressants, which fail to ameliorate acute or recurrent affective episodes. Importantly, a recent multi-site randomized trial by Ghaemi et al19 found that after a favorable acute response to antidepressants plus mood stabilizers, patients with preexisting RC who were randomized to continue antidepressants for up to 1 year had a 3-fold increased likelihood of developing a new depressive episode, which affirms suggestions that antidepressants do not help—but may exacerbate—cycling in patients with RC. No studies in BD have examined whether URC is more likely to arise as a consequence of antidepressant use.
Mood stabilizers and other biologic therapies. A small body of literature specifically addresses pharmacotherapy of URC in patients with BD (Table 2).19-26 A limitation of most existing literature is its focus on case reports, small open trials, or anecdotal observations rather than large, randomized controlled trials using systematic outcome measures. Extrapolation from reports focusing on patients with DSM-IV-TR RC is limited because it is uncertain whether URC differs fundamentally from RC and studies of DSM-IV-TR RC typically examine acute response during an index episode or time until relapse during maintenance therapy, rather than impact on mood changes over time.
Psychotherapy. A limited database on the efficacy of adjunctive cognitive-behavioral therapy (CBT) in RC BD describes improvement in depressive symptoms over short-term follow-up.27 No long-term studies of CBT or other structured psychotherapies have focused on RC or URC. Intuitively, one might expect that psychoeducation targeting sleep hygiene, substance use, stress management and coping skills, medication adherence, and prodrome recognition would be of value to patients with BD who experience frequent mood episodes, especially in those who may be unaware of or unfamiliar with basic concepts related to BD. In addition, relevant concepts from dialectical behavior therapy may be beneficial for BD patients with possible URC, such as skills to enhance emotional regulation, distress tolerance, mindfulness, and interpersonal effectiveness.
Table 2
Evidence-based treatments for ultra-rapid cycling BD
| Intervention | Strength of evidence | Comment |
|---|---|---|
| Antidepressant elimination | Cycling frequency may lengthen during antidepressant-free periods among patients with RC20; long-term (up to 1 year) antidepressant use in RC patients may increase the likelihood of depressive recurrences19 | Findings based mostly on small sample sizes; no controlled trials of antidepressant cessation as an intervention specifically for URC |
| Lithium | Single case report of ECT-induced URC resolved by lithium augmentation during continued ECT22 | No large-scale or randomized trials |
| Carbamazepine | No controlled trials or case reports | Possible anti-cycling benefits relevant for URC could be inferred from post hoc studies among patients with RC |
| Divalproex | Single case report describing resolution of a 48-hour cycle after augmentation of lithium with divalproex23 | No large-scale or randomized trials |
| Lamotrigine | Single case report of 100 mg/d lamotrigine augmentation to divalproex yielded 8 months of remission in a 25-year-old man with BD II and a long-standing pattern of 3 days of hypomania followed by 5 days of depression24 | No large-scale or randomized trials |
| Topiramate | Single case report in URC describing reduction of cycling frequency over 3 years25 | Multiple large scale placebo-controlled studies in bipolar mania have been negative |
| Second-generation antipsychotics | No controlled trials or case reports | Possible anti-cycling benefits relevant for URC could be inferred from post hoc studies in RC |
| Combinations of ≥2 mood stabilizing drugs | No controlled trials or case reports | Combining multiple anti-cycling agents is intuitively logical but largely unstudied |
| Nimodipine | 1 unipolar and 11 BD patients treated in randomized, off-on-off-on fashion (begun at 90 mg/d, increased up to 720 mg/d, mean duration of 12 weeks on active drug)26 | Response in 5 of 9 completers. Findings await replication with larger sample sizes |
| Hypermetabolic thyroid hormone (levothyroxine) | Findings from a small (N = 11) study of adjunctive high-dose levothyroxine (0.15 to 0.4 mg/d, with dosages increased by 0.05 to 0.1 mg/d every 1 to 2 weeks); an unspecified subgroup had “a very rapid cycling pattern” (reviewed by Bauer et al21) | 10 of 11 RC patients had reductions in depressive symptoms, 5 of 7 had improvement from baseline manic symptoms (observation period >60 days) |
| ECT | Case reports of improvement with ECT in refractory RC that was presumed secondary to tricyclic antidepressants | Reports of induction of URC by ECT22; whether or not ECT would more likely improve or exacerbate cyclicity for a given patient may require empirical determination |
| BD: bipolar disorder; BD II: bipolar II disorder; ECT: electroconvulsive therapy; RC: rapid cycling; URC: ultra-rapid cycling | ||
Treatment monitoring. Prospective life charting allows patients to systematically record manic/hypomanic and depressive symptoms day-to-day and week-to-week, thus creating a measure that may be particularly relevant for patients whose moods change rapidly. Simple mood charts (see Related Resources) typically take into account the severity of symptoms of either polarity with ratings of mild, moderate, or severe. Such visual records permit simple calculations over the course of a given interval (eg, week-by-week or across months) of several important parameters, including:
- number of days euthymic
- number of days with depression
- number of days with abnormal mood elevation
- number of occasions in which moods of both polarities occur on the same day.
Tracking these parameters during a treatment allows clinicians to make quantitative comparisons over time as a method of determining whether or not meaningful changes are occurring in cyclicity. See the figure below for an example of a completed mood chart and its interpretation.
Additional recommendations for assessing and managing cyclicity in BD are summarized in Table 3.
Table 3
Tips for managing suspected ultra-rapid cycling BD
| Do’s | Don’ts |
|---|---|
| Ascertain a history of ≥1 lifetime manic or hypomanic episode to diagnose BD | Diagnose BD solely on the presence of rapid mood fluctuations |
| Determine the presence of changes in sleep, energy, speech-language, and related behavior as correlates of mood to differentiate syndromes from isolated variation in mood | Ignore constellations of associated signs and symptoms of mania/hypomania |
| Obtain patient history to assess for head trauma or other medical and neurologic events that could have affective or other psychiatric manifestations | Disregard possible medical etiologies for new-onset affective dysregulation |
| Ascertain the resolution of 1 episode before counting the resurgence of symptoms as constituting a new episode; a waxing and waning course may reflect illness chronicity with incomplete recovery rather than true cyclicity | Misidentify incomplete recovery from an existing episode as the occurrence of new multiple episodes, which would inflate false-positive cases of RC or URC |
| Advise patients to refrain from alcohol or illicit substances that could destabilize mood | Assume that comorbid alcohol or illicit substance abuse will remit only after mood stabilization has been achieved, rather than the reverse |
| Monitor changes in sleep-wake cycles and the effects of erratic sleep or sleep deprivation on mood | Ignore the effects of poor sleep hygiene on mood |
| Minimize antidepressant exposure in patients with RC or URC | Continue long-term antidepressant maintenance therapy in patients with manic or mixed features or ongoing oscillations between mania/hypomania and depression |
| Assure euthyroid status and consider the potential utility of hypermetabolic levothyroxine | Assume that RC or URC will resolve solely by normalizing or optimizing thyroid function |
| Use rational, pharmacodynamically nonredundant anti-cycling drugs | Ignore the cumulative burden of adverse effects of multiple drugs |
| Consider the potential role for ECT as a strategy to arrest URC during any phase of BD | Assume ECT has value only during acute depressive phases of BD |
| Use prospective mood charting to document the evolution of mood changes over time, particularly when gauging treatment efficacy | Rely solely on impressionistic recall of mood states or polarity changes as reflecting distinct phasic changes |
| BD: bipolar disorder; ECT: electroconvulsive therapy; RC: rapid cycling; URC: ultra-rapid cycling | |
Table
Rapid cycling and ultra-rapid cycling BD: A comparison
| Construct | Rapid cycling | Ultra-rapid cycling |
|---|---|---|
| Bipolar I vs II | Predominantly BD IIa | No systematic data |
| Sex | Predominantly women | No systematic data |
| Longitudinal course | May be a transient phenomenon that can occur at any timeb or an enduring phenomenon that may persist for yearsc | Ultradian patterns may be more common across the first several episodes among pediatric BD patientsd |
| Age at onset | Associated with younger age at onsete | May be more evident in prepubescent onset mood disordersd; ultradian cycling more likely when onset occurs before age 13 than in adulthoode |
| Diurnal variation in mood | Morning-to-evening mood switches usually involve depression to mania/hypomania, with the opposite typifying evening-to-morning mood switchesf | Not reported |
| Relationship to environmental stresses | Life stresses may precede initial affective episodes but may be less important as subsequent episodes arise with increasing automaticity | No systematic data |
| Relationship to menstrual cycle | Despite case reports and self-reported links between RC and menstrual mood exacerbations, prospective data do not identify associations between RC and menstrual patternsg,h | No systematic data |
| Subclinical hypothyroidism | Bauer and Whybrow identified hypothyroidism independent of lithium use in 60% of 30 rapidly cycling BD patients, with evidence of improvement in a separate study of 11 RC patients given suprametabolic levothyroxine (reviewed by Bauer et ali) | No systematic data |
| Relationship to psychosis | Nonea | No systematic data |
| Relationship to antidepressant use | Naturalistic observations suggest RC may occur later in the illness course as a result of antidepressant use.c Small open case series data suggest shorter intermorbid intervals on antidepressants with longer intervals off antidepressants.j RC patients often receive antidepressants, but causal relationships are not well-documented.k Some case-control data dispute links between antidepressant use and RCl | No specific published cases |
| Considerations for suicide risk | RC linked with more serious suicide attemptsl | Suicide attempts may be associated with cycling within an episodem or rapid shifting in moodn |
| Time course for judging treatment efficacy | Efforts to diminish acute affective instability may be measured over the course of days to weeks | By definition, treatment of RC involves relapse prevention over the course of 1 year |
| BD: bipolar disorder; RC: rapid cycling | ||
| References a. Schneck CD, Miklowitz DJ, Calabrese JR, et al. Phenomenology of rapid-cycling bipolar disorder: data from the first 500 participants in the Systematic Treatment Enhancement Program. Am J Psychiatry. 2004;161(10):1902-1908. b. Coryell W, Endicott J, Keller M. Rapidly cycling affective disorder. Demographics, diagnosis, family history, and course. Arch Gen Psychiatry. 1992;49(2):126-131. c. Koukopoulos A, Sani G, Koukopoulos AE, et al. Duration and stability of the rapid-cycling course: a long-term personal follow-up of 109 patients. J Affect Disord. 2003;73(1-2):75-85. d. Geller B, Tillman R, Bolhofner K, et al. Child bipolar I disorder: prospective continuity with adult bipolar I disorder; characteristics of second and third episodes; predictors of 8-year outcome. Arch Gen Psychiatry. 2008;65(10):1125-1133. e. Post RM, Leverich GS, Kupka RW, et al. Early-onset bipolar disorder and treatment delay are risk factors for poor outcome in adulthood. J Clin Psychiatry. 2010;71(7):864-872. f. Feldman-Naim S, Turner EH, Leibenluft E. Diurnal variation in the direction of mood switches in patients with rapid-cycling bipolar disorder. J Clin Psychiatry. 1997;58(2):79-84. g. Leibenluft E, Ashman SB, Feldman-Naim S, et al. Lack of relationship between menstrual cycle phase and mood in a sample of women with rapid cycling bipolar disorder. Biol Psychiatry. 1999;46(4):577-580. h. Wehr TA, Sack DA, Rosenthal NE, et al. Rapid cycling affective disorder: contributing factors and treatment responses in 51 patients. Am J Psychiatry. 1988;145(2):179-184. i. Bauer M, Beaulieu S, Dunner DL, et al. Rapid cycling bipolar disorder—diagnostic concepts. Bipolar Disord. 2008;10(1 Pt 2):153-162. j. Wehr TA, Goodwin FK. Can antidepressants cause mania and worsen the course of affective illness? Am J Psychiatry. 1987;144(11):1403-1411. k. Schneck CD, Miklowitz DJ, Miyahara S, et al. The prospective course of rapid-cycling bipolar disorder: findings from the STEP-BD. Am J Psychiatry. 2008;165(3):370-377. l. Coryell W, Solomon D, Turvey C, et al. The long-term course of rapid-cycling bipolar disorder. Arch Gen Psychiatry. 2003;60(9):914-920. m. Fawcett J, Scheftner W, Clark D, et al. Clinical predictors of suicide in patients with major affective disorders: a controlled prospective study. Am J Psychiatry. 1987;144(1):35-40. n. MacKinnon DF, Potash JB, McMahon FJ, et al. Rapid mood switching and suicidality in familial bipolar disorder. Bipolar Disord. 2005;7(5):441-448. | ||
From a biologic perspective, a handful of preliminary studies have examined genetic markers or familial patterns that might be related to rapid cycling (RC) or ultra-rapid cycling (URC). These include a reported link between URC and the low activity variant of the catechol-o-methyltransferase gene polymorphism in a small group of patients with velo-cardio-facial syndrome,a although this finding was not replicated in a larger sample.a Other preliminary reports on RC have implicated both the long (l) and short (s) allelic variants of the serotonin transporter gene (SLC6A4), the val66met variant of the brain-derived neurotrophic factor gene, and the circadian cryptochrome 2 (CRY2) gene (reviewed by Bauer et alb). These candidate loci have been examined in RC but not URC.
URC has not been examined as a familial entity, although in the National Institute of Mental Health Collaborative Depression Study, DSM-IV-TR RC did not occur with elevated frequency in bipolar pedigrees.c Rapid mood switches—abrupt rather than gradual transitions from one affective pole to another—appear to be only slightly, nonsignificantly more common in first-degree bipolar relatives of BD patients who themselves have rapid rather than gradual transitions from one affective pole to the other.d
Neuroimaging studies in BD seldom focus on subpopulations with RC or URC, and have been confined mainly to case reports that have yielded limited, non-generalizable observations, such as state-dependent variations in prefrontal activity during tasks of facial recognition (reviewed by Bauer et alb).
References
a. Papolos DF, Veit S, Faedda GL, et al. Ultra-ultra rapid cycling bipolar disorder is associated with the low activity catecholamine-O-methyltransferase allele. Mol Psychiatry. 1998;3(4):346-349.
b. Bauer M, Beaulieu S, Dunner DL, et al. Rapid cycling bipolar disorder—diagnostic concepts. Bipolar Disord. 2008;10(1 Pt 2):153-162.
c. Coryell W, Endicott J, Keller M. Rapidly cycling affective disorder. Demographics, diagnosis, family history, and course. Arch Gen Psychiatry. 1992;49(2):126-131.
d. MacKinnon DF, Potash JB, McMahon FJ, et al. Rapid mood switching and suicidality in familial bipolar disorder. Bipolar Disord. 2005;7(5):441-448.
Figure: Example of prospective mood charting to document changes in manic/hypomanic and depressive symptoms across time
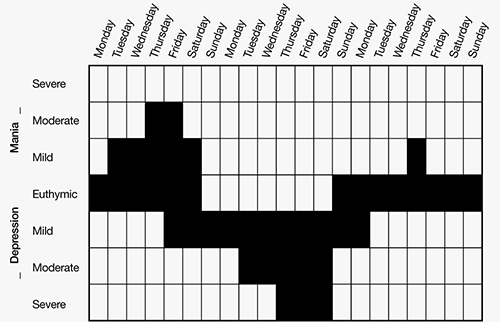
In the above example, the prevalence and severity of mood symptoms are identified over 21 days. Note the distinctly separate phases of mood elevation followed by depression, whereas euthymia was present only 6 of 21 days (29% of the time). Symptoms of at least moderate severity were more prominently depressive (5 of 21 days, or 24% of the time) than manic/hypomanic (2 of 21 days, or approximately 10% of the time). Mood charting does not capture associate DSM-IV-TR criteria for a mood episode but instead focuses solely on longitudinal changes in mood elevation or depression
Related Resources
- American Psychiatric Association practice guideline for the treatment of patients with bipolar disorder (revision). Am J Psychiatry. 2002;159(4 suppl):1-50.
- Massachusetts General Hospital Bipolar Clinic and Research Program. Sample mood chart (downloadable). www.manicdepressive.org/moodchart.html.
Drug Brand Names
- Carbamazepine • Equetro, Tegretol
- Divalproex • Depakote
- Lamotrigine • Lamictal
- Levothyroxine • Synthroid
- Lithium • Lithobid
- Nimodipine • Nimotop
- Topiramate • Topamax
Disclosures
Dr. Goldberg is on the speakers’ bureaus for AstraZeneca, Dey Pharmaceuticals, Eli Lilly and Company, Merck, and Sunovion and is a consultant for Axon Advisors, Dey Pharmaceuticals, Eli Lilly and Company, and Grünenthal Group.
Acknowledgment
The author wishes to thank David L. Dunner, MD, for his helpful comments regarding this article.
1. Kramlinger KG, Post RM. Ultra-rapid and ultradian cycling in bipolar affective illness. Br J Psychiatry. 1996;168(3):314-323.
2. Leibenluft E. Severe mood dysregulation irritability, and the diagnostic boundaries of bipolar disorder in youths. Am J Psychiatry. 2011;168(2):129-142.
3. Geller B, Tillman R, Bolhofner K. Proposed definitions of bipolar I disorder episodes and daily rapid cycling phenomena in preschoolers school-aged children, adolescents, and adults. J Child Adolesc Psychopharmacol. 2007;17(2):217-222.
4. Feinman JA, Dunner DL. The effect of alcohol and substance abuse on the course of bipolar affective disorder. J Affect Disord. 1996;37(1):43-49.
5. Maj M, Pirozzi R, Formicola AM, et al. Reliability and validity of four alternative definitions of rapid-cycling bipolar disorder. Am J Psychiatry. 1999;156(9):1421-1424.
6. Jenner FA, Gjessing LR, Cox JR, et al. A manic depressive psychotic with a persistent forty-eight hour cycle. Br J Psychiatry. 1967;113(501):895-910.
7. Zwil AS, McAllister TW, Cohen I, et al. Ultra-rapid cycling bipolar affective disorder following a closed-head injury. Brain Inj. 1993;7(2):147-152.
8. Geller B, Tillman R, Craney JL, et al. Four-year prospective outcome and natural history of mania in children with a prepubertal and early adolescent bipolar disorder phenotype. Arch Gen Psychiatry. 2004;61(5):459-467.
9. Geller B, Sun K, Zimerman B, et al. Complex and rapid-cycling in bipolar children and adolescents: a preliminary study. J Affect Disord. 1995;34(4):259-268.
10. Goldberg JF, Garno JL, Callahan AM, et al. Overdiagnosis of bipolar disorder among substance use disorder inpatients with mood instability. J Clin Psychiatry. 2008;69(11):1751-1757.
11. Zimmerman M, Ruggero CJ, Chelminski I, et al. Psychiatric diagnoses in patients previously overdiagnosed with bipolar disorder. J Clin Psychiatry. 2010;71(1):26-31.
12. MacKinnon DF, Pies R. Affective instability as rapid cycling: theoretical and clinical implications for borderline personality and bipolar spectrum disorders. Bipolar Disord. 2006;8(1):1-14.
13. Coryell W, Endicott J, Keller M. Rapidly cycling affective disorder. Demographics diagnosis, family history, and course. Arch Gen Psychiatry. 1992;49(2):126-131.
14. Koenigsberg HW, Harvey PD, Mitropoulou V, et al. Characterizing affective instability in borderline personality disorder. Am J Psychiatry. 2002;159(5):784-788.
15. Henry C, Mitropoulou V, New AS, et al. Affective instability and impulsivity in borderline personality and bipolar II disorders: similarities and differences. J Psychiatr Res. 2001;35(6):307-312.
16. Gottschalk A, Bauer MS, Whybrow PC. Evidence of chaotic mood variation in bipolar disorder. Arch Gen Psychiatry. 1995;52(11):947-959.
17. Goldberg JF, Bowden CL, Calabrese JR, et al. Six-month prospective life charting of mood symptoms with lamotrigine monotherapy versus placebo in rapid cycling bipolar disorder. Biol Psychiatry. 2008;63(1):125-130.
18. Schneck CD, Miklowitz DJ, Miyahara S, et al. The prospective course of rapid-cycling bipolar disorder: findings from the STEP-BD. Am J Psychiatry. 2008;165(3):370-377.
19. Ghaemi SN, Ostacher MM, El-Mallakh RS, et al. Antidepressant discontinuation in bipolar depression: a Systematic Treatment Enhancement Program for Bipolar Disorder (STEP-BD) randomized clinical trial of long-term effectiveness and safety. J Clin Psychiatry. 2010;71(4):372-380.
20. Wehr TA, Sack DA, Rosenthal NE, et al. Rapid cycling affective disorder: contributing factors and treatment responses in 51 patients. Am J Psychiatry. 1988;145(2):179-184.
21. Bauer M, Beaulieu S, Dunner DL, et al. Rapid cycling bipolar disorder—diagnostic concepts. Bipolar Disord. 2008;10(1 Pt 2):153-162.
22. Zavorotnyy M, Diemer J, Patzelt J, et al. Occurrence of ultra-rapid cycling during electroconvulsive therapy in bipolar depression. World J Biol Psychiatry. 2009;10(4 Pt 3):987-990.
23. Lepkifker E, Iancu I, Dannon P, et al. Valproic acid in ultra-rapid cycling: a case report. Clin Neuropharmacol. 1995;18(1):72-75.
24. Woo YS, Chae JH, Jun TY, et al. Lamotrigine added to valproate successfully treated a case of ultra-rapid cycling bipolar disorder. Psychiatry Clin Neurosci. 2007;61(1):130-131.
25. Karama S, Lal S. Adjunctive topiramate in ultradian cycling bipolar disorder: case report with 3-year follow-up. Eur Psychiatry. 2006;21(4):280-281.
26. Pazzaglia PJ, Post RM, Ketter TA, et al. Preliminary controlled trial of nimodipine in ultra-rapid cycling affective dysregulation. Psychiatry Res. 1993;49(3):257-272.
27. Reilly-Harrington NA, Deckersbach T, Knauz R, et al. Cognitive behavioral therapy for rapid-cycling bipolar disorder: a pilot study. J Psychiatr Pract. 2007;13(5):291-297.
Ultra-rapid cycling (URC) entered the psychiatric lexicon in the 1990s as a proposed descriptor for manic/hypomanic, mixed, or depressed episodes of bipolar disorder (BD) that occur every few days or weeks. DSM-IV-TR incorporates rapid cycling (RC)—but not URC—as a course specifier that occurs in 10% to 15% of patients with BD who have ≥4 distinct affective episodes per year, each fulfilling duration criteria and separated by identifiable recovery periods (unless an episode directly changes polarity). Since then, the terms RC and URC have seemingly metamorphosed into imprecise, popular colloquialisms meant to loosely describe frequent mood changes rather than distinct episodes over extended time periods, with little regard for the associated signs that define manic or hypomanic episodes.
This article examines the meaning and validity of URC in BD, its relevance and differentiation from rapid mood shifts in patients without BD, and concepts relevant to treatment extrapolated from studies of RC BD.
Imprecise nomenclature
Post et al1 coined the terms “ultra-rapid cycling” and “ultra-ultra-rapid cycling” (also called “ultradian cycling”) to describe mood episodes that occur monthly (URC) or over the course of as little as 1 day (ultradian cycling). These constructs are controversial because they lack demonstrated content validity and discriminant validity relative to other disorders. (“Content validity” refers to whether the features thought to comprise an entity of interest accurately and meaningfully do so; “discriminant validity” tells researchers and clinicians whether the proposed description of a clinical entity uniquely differentiates it from other disorders—avoiding “false-positive” suspected cases.) Clinicians therefore must pay careful attention to non-bipolar psychiatric problems that can present with rapid mood changes but without the psychomotor and related signs that define bipolar mood episodes. In their looser, nontechnical meanings, “rapid cycling” or “ultra-rapid cycling” may be synonymous with affective lability. RC is neither a diagnosis in itself nor a criterion for diagnosing BD. Rather, it is a course specifier to describe episode frequency in patients with past unambiguous manic or hypomanic episodes.
In children and adolescents, whose presentations often are atypical and can be hard to differentiate from other forms of behavioral or temperamental dysregulation, severe non-episodic mood dysregulation without signs of mania or hypomania may indicate a phenomenon separate from BD.2 Geller and colleagues3 proposed using the term “episodes” to frame the duration of a DSM-IV-defined syndrome of mania/hypomania or depression, while reserving the term “cycling” to connote patterns of mood alternation within a given episode. It is not clear whether this concept of “cycling” differs qualitatively from mood lability that arises during a mood episode in children or adults, and notably, this perspective does not account for changes in psychomotor signs in conjunction with changes in mood.
Clinicians also sometimes blur the concept of “mixed episodes” with RC or URC. DSM-IV-TR defines mixed episodes within bipolar I disorder (BD I) based on criteria for a simultaneous manic and depressive episode, rather than on frequent oscillations between affective poles. These and other differential diagnostic considerations for suspected URC are summarized in Table 1.4
A further concern regarding nomenclature involves the distinction between cyclicity (ie, successive episodes regardless of pole direction) and changes in polarity (ie, switches from depression to mania/hypomania or vice versa). Some mood disorder patients may have rapid oscillations from euthymia to depression while never changing polarity to mania/hypomania and may be best described as having recurrent brief depression.
Table 1
Differential diagnosis in suspected URC
| Phenomenon | Considerations for assessment |
|---|---|
| Mixed episodes in bipolar I disorder, or mixed depressive episodes in bipolar II disorder | DSM-IV-TR mixed episodes entail the co-occurrence of manic and depressive symptoms during the same episode without an intervening period of recovery. ICD-10 includes “rapid alternation of manic, hypomanic or depressive symptoms…from day to day or even hour to hour” in its definition of a mixed episode |
| Distress responses to acute environmental adversities (eg, adjustment disorders with mixed disturbance of emotions and conduct) | One would expect an absence of corresponding sleep-wake cycle changes or speech-language and psychomotor disturbances |
| Intoxication/withdrawal from psychoactive substances or drug-induced mental status changes (eg, corticosteroids, amphetamine, cocaine); a history of substance abuse also may be associated with development of URC in BD patients4 | Substance-induced mood fluctuations caused by intoxication/withdrawal can mimic affective cycling |
| Disinhibition states and frontal lobe syndromes as seen in traumatic brain injury and other CNS disorders, such as multiple sclerosis | Assess for signs of perseveration and history of head trauma or neurologic damage from cumulative toxic-metabolic insults (eg, chronic alcoholism) |
| Autonomic hyperarousal, emotional volatility, and hyperreactivity to environmental stresses, suggestive of PTSD | Determine the presence of a trauma history and review whether DSM-IV-TR symptoms and associated features of PTSD exist, including re-experiencing/reliving and avoidance, as well as paranoid thinking, dissociation, and nightmares |
| Recurrent mood shifts related to premenstrual dysphoric disorder may mimic URC. Other endocrine dysfunctions also may present with URC (eg, thyroid or ovarian malignancies) | Affirm the independent presence of BD before inferring its manifestations solely from premenstrual mood changes |
| Trait affective instability associated with borderline personality disorder | Trait mood instability is more chronic and enduring than episodic, and would not be expected to occur in tandem with signs of psychomotor activation that define mania/hypomania |
| BD: bipolar disorder; ICD-10: International Statistical Classification of Diseases and Related Health Problems, 10th revision; PTSD: posttraumatic stress disorder; URC: ultra-rapid cycling | |
Duration criteria
Clinicians and researchers have debated the minimum duration criteria for identifying manic or hypomanic episodes, and the extent to which suspected hypomanic periods of short duration constitute distinct illness phases. Although DSM-IV-TR designates 4 days as a minimum time for classifying an episode of hypomania, empirical studies suggest that mood symptoms lasting as few as 2 days may comprise a valid and reliably distinct entity relevant to RC.5 More limited data (mainly case observations) identify “affective oscillations” and “mood shifts” occurring faster than once per 24 hours in BD patients without comorbid personality disorders.6 Phenomenologic studies that have focused on 24- to 48-hour switch cycles have described new-onset URC arising spontaneously or following closed head injuries.7 In children and younger adolescents, reports have identified long index manic episodes (mean durations as long as 80 weeks)8 that involve continual (ultradian) mood cycling in as many as 80% of cases.9
Is URC a valid construct?
A central controversy surrounding the validity and meaningfulness of URC as a BD subtype involves its sole focus on mood variation rather than the fuller constellation of associated signs and symptoms that define episodes of mania/hypomania or depression. Abrupt, sudden, drastic, or dramatic mood shifts from one moment to the next are nowhere to be found in the DSM-IV-TR definition of BD, and the construct of mood lability or affective instability is neither a cardinal nor defining element of BD. Although individuals with BD I or bipolar II disorder (BD II) may have periods of affective lability, rapid shifts in mood are neither necessary nor sufficient for a BD diagnosis, and may indicate other types of psychopathology when affective instability occurs in the absence of a history of discernible manic or hypomanic episodes.
Studies by our group10 and others11 have shown that overattention to mood variation without considering associated cognitive, speech-language, chronobiologic, and motor signs of mania/hypomania accounts for substantial overdiagnosis of BD in patients with non-specific mood disturbances, particularly in those with active substance abuse or borderline personality disorder (BPD). Whereas the construct of RC BD attempts to account for changes in energy and psychomotor function as part of recurrent syndromes of mania/hypomania, existing literature on URC does not. Assessing mood changes in <24 hours also precludes assessing associated phenomena that occur over longer periods, such as changes in the sleep-wake cycle.
A rigorous, systematic approach to differential diagnosis for patients with affective instability is essential.
Borderline personality disorder
A common diagnostic debate regarding URC involves how to differentiate it from the chronic mood instability and reactivity inherent to BPD. Although some authors have suggested that RC BD and affective instability in BPD may be the same entity,12 others object to unifying the 2 conditions without considering their phenomenologic and other clinical differences. For example, affective instability arising from borderline character organization is thought to reflect a patient’s impaired capacity to self-regulate his or her internal state and emotional responses to interpersonal and other environmental stresses, or difficulty managing impulses. By contrast, manic or depressive phases of BD tend not to be “triggered” by interpersonal conflicts or frustrations. Furthermore, reframing intense mood reactions to the environment as bipolar variants carries several pitfalls: doing so wrongly accords patients a passive role in their reactions to life events, inaccurately reinforces a sense of victimization in response to stress, and diverts inquiry away from a patient’s active role in life decisions and circumstances that may be unsatisfying, self-defeating, or volatile.
Two key considerations may be helpful in discriminating rapid mood changes in BD vs BPD. First, some longitudinal studies indicate that RC often is a transient, rather than enduring, phenomenon in BD,13 in contrast to the nonvarying, trait feature of affective instability in persons with BPD. It is unknown whether URC is more enduring than transient. Notably, whereas bipolar mood episodes constitute deviations from a baseline state, affective instability in BPD is a baseline characteristic, rather than a deviation from it. Second, by definition, a BPD diagnosis hinges on additional elements unrelated to mood disturbances, such as interpersonal styles or defense mechanisms that involve splitting, projection, and projective identification, feelings of numbness, boredom, or emptiness, identity diffusion, fears of abandonment, and proclivities toward self-mutilation or other self-injurious behaviors as a means to alleviate tension and stress. These characteristics do not overlap with the core elements of BD.
Affective lability in patients with BPD entails prominent oscillations between anger and anxiety, or depression and anxiety, but not depression and elation14; by contrast, affective instability in BD has been linked with greater oscillations between euthymia and depression, and euthymia and elation, but not euthymia and anger.15 Moreover, daily mood fluctuations in patients with BD appear to occur in a relatively random fashion,16 whereas in BPD mood fluctuations are reactions that appear intimately linked to distressing interpersonal experiences.
See the table below, entitled “Rapid cycling and ultra-rapid cycling BD: A comparison,” comparing the phenomenology of RC and URC and a discussion of studies that explored genetic markers or family patterns that may be related to RC or URC.
Treatment considerations
No systematic studies exist for treating URC. Because most clinical trials of BD focus on treatment or prevention of a single episode rather than changes of mood over time, it is difficult to draw inferences about the ability of any treatment to attenuate marked, day-to-day mood variations. Some antimanic drugs, such as carbamazepine, have been suggested to offer better prophylactic efficacy compared with lithium for “non-classical” BD presentations, although the efficacy of carbamazepine has not been studied in URC.
Broadly speaking, treatment for URC, similar to RC, pragmatically involves:
- identifying and eliminating sources of mood destabilization (eg, substance abuse, erratic sleep patterns)
- treating medical comorbidities such as hypothyroidism
- optimizing treatment with mood stabilizing agents
- exercising caution when using antidepressants (see below).
Interestingly, despite frequent allusion to certain medications as “mood stabilizers,” no controlled study has examined mood instability on a day-to-day basis as a primary outcome measure in BD treatment, which limits the ability to surmise that any drug could be expected to diminish mood oscillations that occur over the course of days, or within a single day. However, a post hoc analysis by our group17 compared randomized treatment with lamotrigine or placebo over 6 months in RC BD I or BD II. Using prospective life charting, we found patients who received lamotrigine were almost twice as likely as those receiving placebo to achieve euthymia from one week to the next, which suggests the possibility that lamotrigine may offer benefit for affective instability in BD I or BD II patients, in addition to preventing discrete mood episodes.
Antidepressant controversy. Concerns that antidepressants might acutely induce mania or accelerate cycling frequency over long time periods have led to a contentious, long-standing debate within psychopharmacology. As noted in the box below, several long-term naturalistic follow-up studies have reported RC as a perceived consequence of antidepressants in most RC patients, although efforts to differentiate cycle acceleration caused by antidepressants (or other iatrogenic factors) from the natural course of illness remains exceedingly difficult without prospective randomized trials. (Antidepressants might cause more affective recurrences, but having multiple episodes may also cause more antidepressant prescriptions.) Some researchers (eg, Schneck et al18) have reported more frequent episodes among patients taking antidepressants but did not consider that patients with multiple episodes may be more likely to receive antidepressants, which fail to ameliorate acute or recurrent affective episodes. Importantly, a recent multi-site randomized trial by Ghaemi et al19 found that after a favorable acute response to antidepressants plus mood stabilizers, patients with preexisting RC who were randomized to continue antidepressants for up to 1 year had a 3-fold increased likelihood of developing a new depressive episode, which affirms suggestions that antidepressants do not help—but may exacerbate—cycling in patients with RC. No studies in BD have examined whether URC is more likely to arise as a consequence of antidepressant use.
Mood stabilizers and other biologic therapies. A small body of literature specifically addresses pharmacotherapy of URC in patients with BD (Table 2).19-26 A limitation of most existing literature is its focus on case reports, small open trials, or anecdotal observations rather than large, randomized controlled trials using systematic outcome measures. Extrapolation from reports focusing on patients with DSM-IV-TR RC is limited because it is uncertain whether URC differs fundamentally from RC and studies of DSM-IV-TR RC typically examine acute response during an index episode or time until relapse during maintenance therapy, rather than impact on mood changes over time.
Psychotherapy. A limited database on the efficacy of adjunctive cognitive-behavioral therapy (CBT) in RC BD describes improvement in depressive symptoms over short-term follow-up.27 No long-term studies of CBT or other structured psychotherapies have focused on RC or URC. Intuitively, one might expect that psychoeducation targeting sleep hygiene, substance use, stress management and coping skills, medication adherence, and prodrome recognition would be of value to patients with BD who experience frequent mood episodes, especially in those who may be unaware of or unfamiliar with basic concepts related to BD. In addition, relevant concepts from dialectical behavior therapy may be beneficial for BD patients with possible URC, such as skills to enhance emotional regulation, distress tolerance, mindfulness, and interpersonal effectiveness.
Table 2
Evidence-based treatments for ultra-rapid cycling BD
| Intervention | Strength of evidence | Comment |
|---|---|---|
| Antidepressant elimination | Cycling frequency may lengthen during antidepressant-free periods among patients with RC20; long-term (up to 1 year) antidepressant use in RC patients may increase the likelihood of depressive recurrences19 | Findings based mostly on small sample sizes; no controlled trials of antidepressant cessation as an intervention specifically for URC |
| Lithium | Single case report of ECT-induced URC resolved by lithium augmentation during continued ECT22 | No large-scale or randomized trials |
| Carbamazepine | No controlled trials or case reports | Possible anti-cycling benefits relevant for URC could be inferred from post hoc studies among patients with RC |
| Divalproex | Single case report describing resolution of a 48-hour cycle after augmentation of lithium with divalproex23 | No large-scale or randomized trials |
| Lamotrigine | Single case report of 100 mg/d lamotrigine augmentation to divalproex yielded 8 months of remission in a 25-year-old man with BD II and a long-standing pattern of 3 days of hypomania followed by 5 days of depression24 | No large-scale or randomized trials |
| Topiramate | Single case report in URC describing reduction of cycling frequency over 3 years25 | Multiple large scale placebo-controlled studies in bipolar mania have been negative |
| Second-generation antipsychotics | No controlled trials or case reports | Possible anti-cycling benefits relevant for URC could be inferred from post hoc studies in RC |
| Combinations of ≥2 mood stabilizing drugs | No controlled trials or case reports | Combining multiple anti-cycling agents is intuitively logical but largely unstudied |
| Nimodipine | 1 unipolar and 11 BD patients treated in randomized, off-on-off-on fashion (begun at 90 mg/d, increased up to 720 mg/d, mean duration of 12 weeks on active drug)26 | Response in 5 of 9 completers. Findings await replication with larger sample sizes |
| Hypermetabolic thyroid hormone (levothyroxine) | Findings from a small (N = 11) study of adjunctive high-dose levothyroxine (0.15 to 0.4 mg/d, with dosages increased by 0.05 to 0.1 mg/d every 1 to 2 weeks); an unspecified subgroup had “a very rapid cycling pattern” (reviewed by Bauer et al21) | 10 of 11 RC patients had reductions in depressive symptoms, 5 of 7 had improvement from baseline manic symptoms (observation period >60 days) |
| ECT | Case reports of improvement with ECT in refractory RC that was presumed secondary to tricyclic antidepressants | Reports of induction of URC by ECT22; whether or not ECT would more likely improve or exacerbate cyclicity for a given patient may require empirical determination |
| BD: bipolar disorder; BD II: bipolar II disorder; ECT: electroconvulsive therapy; RC: rapid cycling; URC: ultra-rapid cycling | ||
Treatment monitoring. Prospective life charting allows patients to systematically record manic/hypomanic and depressive symptoms day-to-day and week-to-week, thus creating a measure that may be particularly relevant for patients whose moods change rapidly. Simple mood charts (see Related Resources) typically take into account the severity of symptoms of either polarity with ratings of mild, moderate, or severe. Such visual records permit simple calculations over the course of a given interval (eg, week-by-week or across months) of several important parameters, including:
- number of days euthymic
- number of days with depression
- number of days with abnormal mood elevation
- number of occasions in which moods of both polarities occur on the same day.
Tracking these parameters during a treatment allows clinicians to make quantitative comparisons over time as a method of determining whether or not meaningful changes are occurring in cyclicity. See the figure below for an example of a completed mood chart and its interpretation.
Additional recommendations for assessing and managing cyclicity in BD are summarized in Table 3.
Table 3
Tips for managing suspected ultra-rapid cycling BD
| Do’s | Don’ts |
|---|---|
| Ascertain a history of ≥1 lifetime manic or hypomanic episode to diagnose BD | Diagnose BD solely on the presence of rapid mood fluctuations |
| Determine the presence of changes in sleep, energy, speech-language, and related behavior as correlates of mood to differentiate syndromes from isolated variation in mood | Ignore constellations of associated signs and symptoms of mania/hypomania |
| Obtain patient history to assess for head trauma or other medical and neurologic events that could have affective or other psychiatric manifestations | Disregard possible medical etiologies for new-onset affective dysregulation |
| Ascertain the resolution of 1 episode before counting the resurgence of symptoms as constituting a new episode; a waxing and waning course may reflect illness chronicity with incomplete recovery rather than true cyclicity | Misidentify incomplete recovery from an existing episode as the occurrence of new multiple episodes, which would inflate false-positive cases of RC or URC |
| Advise patients to refrain from alcohol or illicit substances that could destabilize mood | Assume that comorbid alcohol or illicit substance abuse will remit only after mood stabilization has been achieved, rather than the reverse |
| Monitor changes in sleep-wake cycles and the effects of erratic sleep or sleep deprivation on mood | Ignore the effects of poor sleep hygiene on mood |
| Minimize antidepressant exposure in patients with RC or URC | Continue long-term antidepressant maintenance therapy in patients with manic or mixed features or ongoing oscillations between mania/hypomania and depression |
| Assure euthyroid status and consider the potential utility of hypermetabolic levothyroxine | Assume that RC or URC will resolve solely by normalizing or optimizing thyroid function |
| Use rational, pharmacodynamically nonredundant anti-cycling drugs | Ignore the cumulative burden of adverse effects of multiple drugs |
| Consider the potential role for ECT as a strategy to arrest URC during any phase of BD | Assume ECT has value only during acute depressive phases of BD |
| Use prospective mood charting to document the evolution of mood changes over time, particularly when gauging treatment efficacy | Rely solely on impressionistic recall of mood states or polarity changes as reflecting distinct phasic changes |
| BD: bipolar disorder; ECT: electroconvulsive therapy; RC: rapid cycling; URC: ultra-rapid cycling | |
Table
Rapid cycling and ultra-rapid cycling BD: A comparison
| Construct | Rapid cycling | Ultra-rapid cycling |
|---|---|---|
| Bipolar I vs II | Predominantly BD IIa | No systematic data |
| Sex | Predominantly women | No systematic data |
| Longitudinal course | May be a transient phenomenon that can occur at any timeb or an enduring phenomenon that may persist for yearsc | Ultradian patterns may be more common across the first several episodes among pediatric BD patientsd |
| Age at onset | Associated with younger age at onsete | May be more evident in prepubescent onset mood disordersd; ultradian cycling more likely when onset occurs before age 13 than in adulthoode |
| Diurnal variation in mood | Morning-to-evening mood switches usually involve depression to mania/hypomania, with the opposite typifying evening-to-morning mood switchesf | Not reported |
| Relationship to environmental stresses | Life stresses may precede initial affective episodes but may be less important as subsequent episodes arise with increasing automaticity | No systematic data |
| Relationship to menstrual cycle | Despite case reports and self-reported links between RC and menstrual mood exacerbations, prospective data do not identify associations between RC and menstrual patternsg,h | No systematic data |
| Subclinical hypothyroidism | Bauer and Whybrow identified hypothyroidism independent of lithium use in 60% of 30 rapidly cycling BD patients, with evidence of improvement in a separate study of 11 RC patients given suprametabolic levothyroxine (reviewed by Bauer et ali) | No systematic data |
| Relationship to psychosis | Nonea | No systematic data |
| Relationship to antidepressant use | Naturalistic observations suggest RC may occur later in the illness course as a result of antidepressant use.c Small open case series data suggest shorter intermorbid intervals on antidepressants with longer intervals off antidepressants.j RC patients often receive antidepressants, but causal relationships are not well-documented.k Some case-control data dispute links between antidepressant use and RCl | No specific published cases |
| Considerations for suicide risk | RC linked with more serious suicide attemptsl | Suicide attempts may be associated with cycling within an episodem or rapid shifting in moodn |
| Time course for judging treatment efficacy | Efforts to diminish acute affective instability may be measured over the course of days to weeks | By definition, treatment of RC involves relapse prevention over the course of 1 year |
| BD: bipolar disorder; RC: rapid cycling | ||
| References a. Schneck CD, Miklowitz DJ, Calabrese JR, et al. Phenomenology of rapid-cycling bipolar disorder: data from the first 500 participants in the Systematic Treatment Enhancement Program. Am J Psychiatry. 2004;161(10):1902-1908. b. Coryell W, Endicott J, Keller M. Rapidly cycling affective disorder. Demographics, diagnosis, family history, and course. Arch Gen Psychiatry. 1992;49(2):126-131. c. Koukopoulos A, Sani G, Koukopoulos AE, et al. Duration and stability of the rapid-cycling course: a long-term personal follow-up of 109 patients. J Affect Disord. 2003;73(1-2):75-85. d. Geller B, Tillman R, Bolhofner K, et al. Child bipolar I disorder: prospective continuity with adult bipolar I disorder; characteristics of second and third episodes; predictors of 8-year outcome. Arch Gen Psychiatry. 2008;65(10):1125-1133. e. Post RM, Leverich GS, Kupka RW, et al. Early-onset bipolar disorder and treatment delay are risk factors for poor outcome in adulthood. J Clin Psychiatry. 2010;71(7):864-872. f. Feldman-Naim S, Turner EH, Leibenluft E. Diurnal variation in the direction of mood switches in patients with rapid-cycling bipolar disorder. J Clin Psychiatry. 1997;58(2):79-84. g. Leibenluft E, Ashman SB, Feldman-Naim S, et al. Lack of relationship between menstrual cycle phase and mood in a sample of women with rapid cycling bipolar disorder. Biol Psychiatry. 1999;46(4):577-580. h. Wehr TA, Sack DA, Rosenthal NE, et al. Rapid cycling affective disorder: contributing factors and treatment responses in 51 patients. Am J Psychiatry. 1988;145(2):179-184. i. Bauer M, Beaulieu S, Dunner DL, et al. Rapid cycling bipolar disorder—diagnostic concepts. Bipolar Disord. 2008;10(1 Pt 2):153-162. j. Wehr TA, Goodwin FK. Can antidepressants cause mania and worsen the course of affective illness? Am J Psychiatry. 1987;144(11):1403-1411. k. Schneck CD, Miklowitz DJ, Miyahara S, et al. The prospective course of rapid-cycling bipolar disorder: findings from the STEP-BD. Am J Psychiatry. 2008;165(3):370-377. l. Coryell W, Solomon D, Turvey C, et al. The long-term course of rapid-cycling bipolar disorder. Arch Gen Psychiatry. 2003;60(9):914-920. m. Fawcett J, Scheftner W, Clark D, et al. Clinical predictors of suicide in patients with major affective disorders: a controlled prospective study. Am J Psychiatry. 1987;144(1):35-40. n. MacKinnon DF, Potash JB, McMahon FJ, et al. Rapid mood switching and suicidality in familial bipolar disorder. Bipolar Disord. 2005;7(5):441-448. | ||
From a biologic perspective, a handful of preliminary studies have examined genetic markers or familial patterns that might be related to rapid cycling (RC) or ultra-rapid cycling (URC). These include a reported link between URC and the low activity variant of the catechol-o-methyltransferase gene polymorphism in a small group of patients with velo-cardio-facial syndrome,a although this finding was not replicated in a larger sample.a Other preliminary reports on RC have implicated both the long (l) and short (s) allelic variants of the serotonin transporter gene (SLC6A4), the val66met variant of the brain-derived neurotrophic factor gene, and the circadian cryptochrome 2 (CRY2) gene (reviewed by Bauer et alb). These candidate loci have been examined in RC but not URC.
URC has not been examined as a familial entity, although in the National Institute of Mental Health Collaborative Depression Study, DSM-IV-TR RC did not occur with elevated frequency in bipolar pedigrees.c Rapid mood switches—abrupt rather than gradual transitions from one affective pole to another—appear to be only slightly, nonsignificantly more common in first-degree bipolar relatives of BD patients who themselves have rapid rather than gradual transitions from one affective pole to the other.d
Neuroimaging studies in BD seldom focus on subpopulations with RC or URC, and have been confined mainly to case reports that have yielded limited, non-generalizable observations, such as state-dependent variations in prefrontal activity during tasks of facial recognition (reviewed by Bauer et alb).
References
a. Papolos DF, Veit S, Faedda GL, et al. Ultra-ultra rapid cycling bipolar disorder is associated with the low activity catecholamine-O-methyltransferase allele. Mol Psychiatry. 1998;3(4):346-349.
b. Bauer M, Beaulieu S, Dunner DL, et al. Rapid cycling bipolar disorder—diagnostic concepts. Bipolar Disord. 2008;10(1 Pt 2):153-162.
c. Coryell W, Endicott J, Keller M. Rapidly cycling affective disorder. Demographics, diagnosis, family history, and course. Arch Gen Psychiatry. 1992;49(2):126-131.
d. MacKinnon DF, Potash JB, McMahon FJ, et al. Rapid mood switching and suicidality in familial bipolar disorder. Bipolar Disord. 2005;7(5):441-448.
Figure: Example of prospective mood charting to document changes in manic/hypomanic and depressive symptoms across time
In the above example, the prevalence and severity of mood symptoms are identified over 21 days. Note the distinctly separate phases of mood elevation followed by depression, whereas euthymia was present only 6 of 21 days (29% of the time). Symptoms of at least moderate severity were more prominently depressive (5 of 21 days, or 24% of the time) than manic/hypomanic (2 of 21 days, or approximately 10% of the time). Mood charting does not capture associate DSM-IV-TR criteria for a mood episode but instead focuses solely on longitudinal changes in mood elevation or depression
Related Resources
- American Psychiatric Association practice guideline for the treatment of patients with bipolar disorder (revision). Am J Psychiatry. 2002;159(4 suppl):1-50.
- Massachusetts General Hospital Bipolar Clinic and Research Program. Sample mood chart (downloadable). www.manicdepressive.org/moodchart.html.
Drug Brand Names
- Carbamazepine • Equetro, Tegretol
- Divalproex • Depakote
- Lamotrigine • Lamictal
- Levothyroxine • Synthroid
- Lithium • Lithobid
- Nimodipine • Nimotop
- Topiramate • Topamax
Disclosures
Dr. Goldberg is on the speakers’ bureaus for AstraZeneca, Dey Pharmaceuticals, Eli Lilly and Company, Merck, and Sunovion and is a consultant for Axon Advisors, Dey Pharmaceuticals, Eli Lilly and Company, and Grünenthal Group.
Acknowledgment
The author wishes to thank David L. Dunner, MD, for his helpful comments regarding this article.
Ultra-rapid cycling (URC) entered the psychiatric lexicon in the 1990s as a proposed descriptor for manic/hypomanic, mixed, or depressed episodes of bipolar disorder (BD) that occur every few days or weeks. DSM-IV-TR incorporates rapid cycling (RC)—but not URC—as a course specifier that occurs in 10% to 15% of patients with BD who have ≥4 distinct affective episodes per year, each fulfilling duration criteria and separated by identifiable recovery periods (unless an episode directly changes polarity). Since then, the terms RC and URC have seemingly metamorphosed into imprecise, popular colloquialisms meant to loosely describe frequent mood changes rather than distinct episodes over extended time periods, with little regard for the associated signs that define manic or hypomanic episodes.
This article examines the meaning and validity of URC in BD, its relevance and differentiation from rapid mood shifts in patients without BD, and concepts relevant to treatment extrapolated from studies of RC BD.
Imprecise nomenclature
Post et al1 coined the terms “ultra-rapid cycling” and “ultra-ultra-rapid cycling” (also called “ultradian cycling”) to describe mood episodes that occur monthly (URC) or over the course of as little as 1 day (ultradian cycling). These constructs are controversial because they lack demonstrated content validity and discriminant validity relative to other disorders. (“Content validity” refers to whether the features thought to comprise an entity of interest accurately and meaningfully do so; “discriminant validity” tells researchers and clinicians whether the proposed description of a clinical entity uniquely differentiates it from other disorders—avoiding “false-positive” suspected cases.) Clinicians therefore must pay careful attention to non-bipolar psychiatric problems that can present with rapid mood changes but without the psychomotor and related signs that define bipolar mood episodes. In their looser, nontechnical meanings, “rapid cycling” or “ultra-rapid cycling” may be synonymous with affective lability. RC is neither a diagnosis in itself nor a criterion for diagnosing BD. Rather, it is a course specifier to describe episode frequency in patients with past unambiguous manic or hypomanic episodes.
In children and adolescents, whose presentations often are atypical and can be hard to differentiate from other forms of behavioral or temperamental dysregulation, severe non-episodic mood dysregulation without signs of mania or hypomania may indicate a phenomenon separate from BD.2 Geller and colleagues3 proposed using the term “episodes” to frame the duration of a DSM-IV-defined syndrome of mania/hypomania or depression, while reserving the term “cycling” to connote patterns of mood alternation within a given episode. It is not clear whether this concept of “cycling” differs qualitatively from mood lability that arises during a mood episode in children or adults, and notably, this perspective does not account for changes in psychomotor signs in conjunction with changes in mood.
Clinicians also sometimes blur the concept of “mixed episodes” with RC or URC. DSM-IV-TR defines mixed episodes within bipolar I disorder (BD I) based on criteria for a simultaneous manic and depressive episode, rather than on frequent oscillations between affective poles. These and other differential diagnostic considerations for suspected URC are summarized in Table 1.4
A further concern regarding nomenclature involves the distinction between cyclicity (ie, successive episodes regardless of pole direction) and changes in polarity (ie, switches from depression to mania/hypomania or vice versa). Some mood disorder patients may have rapid oscillations from euthymia to depression while never changing polarity to mania/hypomania and may be best described as having recurrent brief depression.
Table 1
Differential diagnosis in suspected URC
| Phenomenon | Considerations for assessment |
|---|---|
| Mixed episodes in bipolar I disorder, or mixed depressive episodes in bipolar II disorder | DSM-IV-TR mixed episodes entail the co-occurrence of manic and depressive symptoms during the same episode without an intervening period of recovery. ICD-10 includes “rapid alternation of manic, hypomanic or depressive symptoms…from day to day or even hour to hour” in its definition of a mixed episode |
| Distress responses to acute environmental adversities (eg, adjustment disorders with mixed disturbance of emotions and conduct) | One would expect an absence of corresponding sleep-wake cycle changes or speech-language and psychomotor disturbances |
| Intoxication/withdrawal from psychoactive substances or drug-induced mental status changes (eg, corticosteroids, amphetamine, cocaine); a history of substance abuse also may be associated with development of URC in BD patients4 | Substance-induced mood fluctuations caused by intoxication/withdrawal can mimic affective cycling |
| Disinhibition states and frontal lobe syndromes as seen in traumatic brain injury and other CNS disorders, such as multiple sclerosis | Assess for signs of perseveration and history of head trauma or neurologic damage from cumulative toxic-metabolic insults (eg, chronic alcoholism) |
| Autonomic hyperarousal, emotional volatility, and hyperreactivity to environmental stresses, suggestive of PTSD | Determine the presence of a trauma history and review whether DSM-IV-TR symptoms and associated features of PTSD exist, including re-experiencing/reliving and avoidance, as well as paranoid thinking, dissociation, and nightmares |
| Recurrent mood shifts related to premenstrual dysphoric disorder may mimic URC. Other endocrine dysfunctions also may present with URC (eg, thyroid or ovarian malignancies) | Affirm the independent presence of BD before inferring its manifestations solely from premenstrual mood changes |
| Trait affective instability associated with borderline personality disorder | Trait mood instability is more chronic and enduring than episodic, and would not be expected to occur in tandem with signs of psychomotor activation that define mania/hypomania |
| BD: bipolar disorder; ICD-10: International Statistical Classification of Diseases and Related Health Problems, 10th revision; PTSD: posttraumatic stress disorder; URC: ultra-rapid cycling | |
Duration criteria
Clinicians and researchers have debated the minimum duration criteria for identifying manic or hypomanic episodes, and the extent to which suspected hypomanic periods of short duration constitute distinct illness phases. Although DSM-IV-TR designates 4 days as a minimum time for classifying an episode of hypomania, empirical studies suggest that mood symptoms lasting as few as 2 days may comprise a valid and reliably distinct entity relevant to RC.5 More limited data (mainly case observations) identify “affective oscillations” and “mood shifts” occurring faster than once per 24 hours in BD patients without comorbid personality disorders.6 Phenomenologic studies that have focused on 24- to 48-hour switch cycles have described new-onset URC arising spontaneously or following closed head injuries.7 In children and younger adolescents, reports have identified long index manic episodes (mean durations as long as 80 weeks)8 that involve continual (ultradian) mood cycling in as many as 80% of cases.9
Is URC a valid construct?
A central controversy surrounding the validity and meaningfulness of URC as a BD subtype involves its sole focus on mood variation rather than the fuller constellation of associated signs and symptoms that define episodes of mania/hypomania or depression. Abrupt, sudden, drastic, or dramatic mood shifts from one moment to the next are nowhere to be found in the DSM-IV-TR definition of BD, and the construct of mood lability or affective instability is neither a cardinal nor defining element of BD. Although individuals with BD I or bipolar II disorder (BD II) may have periods of affective lability, rapid shifts in mood are neither necessary nor sufficient for a BD diagnosis, and may indicate other types of psychopathology when affective instability occurs in the absence of a history of discernible manic or hypomanic episodes.
Studies by our group10 and others11 have shown that overattention to mood variation without considering associated cognitive, speech-language, chronobiologic, and motor signs of mania/hypomania accounts for substantial overdiagnosis of BD in patients with non-specific mood disturbances, particularly in those with active substance abuse or borderline personality disorder (BPD). Whereas the construct of RC BD attempts to account for changes in energy and psychomotor function as part of recurrent syndromes of mania/hypomania, existing literature on URC does not. Assessing mood changes in <24 hours also precludes assessing associated phenomena that occur over longer periods, such as changes in the sleep-wake cycle.
A rigorous, systematic approach to differential diagnosis for patients with affective instability is essential.
Borderline personality disorder
A common diagnostic debate regarding URC involves how to differentiate it from the chronic mood instability and reactivity inherent to BPD. Although some authors have suggested that RC BD and affective instability in BPD may be the same entity,12 others object to unifying the 2 conditions without considering their phenomenologic and other clinical differences. For example, affective instability arising from borderline character organization is thought to reflect a patient’s impaired capacity to self-regulate his or her internal state and emotional responses to interpersonal and other environmental stresses, or difficulty managing impulses. By contrast, manic or depressive phases of BD tend not to be “triggered” by interpersonal conflicts or frustrations. Furthermore, reframing intense mood reactions to the environment as bipolar variants carries several pitfalls: doing so wrongly accords patients a passive role in their reactions to life events, inaccurately reinforces a sense of victimization in response to stress, and diverts inquiry away from a patient’s active role in life decisions and circumstances that may be unsatisfying, self-defeating, or volatile.
Two key considerations may be helpful in discriminating rapid mood changes in BD vs BPD. First, some longitudinal studies indicate that RC often is a transient, rather than enduring, phenomenon in BD,13 in contrast to the nonvarying, trait feature of affective instability in persons with BPD. It is unknown whether URC is more enduring than transient. Notably, whereas bipolar mood episodes constitute deviations from a baseline state, affective instability in BPD is a baseline characteristic, rather than a deviation from it. Second, by definition, a BPD diagnosis hinges on additional elements unrelated to mood disturbances, such as interpersonal styles or defense mechanisms that involve splitting, projection, and projective identification, feelings of numbness, boredom, or emptiness, identity diffusion, fears of abandonment, and proclivities toward self-mutilation or other self-injurious behaviors as a means to alleviate tension and stress. These characteristics do not overlap with the core elements of BD.
Affective lability in patients with BPD entails prominent oscillations between anger and anxiety, or depression and anxiety, but not depression and elation14; by contrast, affective instability in BD has been linked with greater oscillations between euthymia and depression, and euthymia and elation, but not euthymia and anger.15 Moreover, daily mood fluctuations in patients with BD appear to occur in a relatively random fashion,16 whereas in BPD mood fluctuations are reactions that appear intimately linked to distressing interpersonal experiences.
See the table below, entitled “Rapid cycling and ultra-rapid cycling BD: A comparison,” comparing the phenomenology of RC and URC and a discussion of studies that explored genetic markers or family patterns that may be related to RC or URC.
Treatment considerations
No systematic studies exist for treating URC. Because most clinical trials of BD focus on treatment or prevention of a single episode rather than changes of mood over time, it is difficult to draw inferences about the ability of any treatment to attenuate marked, day-to-day mood variations. Some antimanic drugs, such as carbamazepine, have been suggested to offer better prophylactic efficacy compared with lithium for “non-classical” BD presentations, although the efficacy of carbamazepine has not been studied in URC.
Broadly speaking, treatment for URC, similar to RC, pragmatically involves:
- identifying and eliminating sources of mood destabilization (eg, substance abuse, erratic sleep patterns)
- treating medical comorbidities such as hypothyroidism
- optimizing treatment with mood stabilizing agents
- exercising caution when using antidepressants (see below).
Interestingly, despite frequent allusion to certain medications as “mood stabilizers,” no controlled study has examined mood instability on a day-to-day basis as a primary outcome measure in BD treatment, which limits the ability to surmise that any drug could be expected to diminish mood oscillations that occur over the course of days, or within a single day. However, a post hoc analysis by our group17 compared randomized treatment with lamotrigine or placebo over 6 months in RC BD I or BD II. Using prospective life charting, we found patients who received lamotrigine were almost twice as likely as those receiving placebo to achieve euthymia from one week to the next, which suggests the possibility that lamotrigine may offer benefit for affective instability in BD I or BD II patients, in addition to preventing discrete mood episodes.
Antidepressant controversy. Concerns that antidepressants might acutely induce mania or accelerate cycling frequency over long time periods have led to a contentious, long-standing debate within psychopharmacology. As noted in the box below, several long-term naturalistic follow-up studies have reported RC as a perceived consequence of antidepressants in most RC patients, although efforts to differentiate cycle acceleration caused by antidepressants (or other iatrogenic factors) from the natural course of illness remains exceedingly difficult without prospective randomized trials. (Antidepressants might cause more affective recurrences, but having multiple episodes may also cause more antidepressant prescriptions.) Some researchers (eg, Schneck et al18) have reported more frequent episodes among patients taking antidepressants but did not consider that patients with multiple episodes may be more likely to receive antidepressants, which fail to ameliorate acute or recurrent affective episodes. Importantly, a recent multi-site randomized trial by Ghaemi et al19 found that after a favorable acute response to antidepressants plus mood stabilizers, patients with preexisting RC who were randomized to continue antidepressants for up to 1 year had a 3-fold increased likelihood of developing a new depressive episode, which affirms suggestions that antidepressants do not help—but may exacerbate—cycling in patients with RC. No studies in BD have examined whether URC is more likely to arise as a consequence of antidepressant use.
Mood stabilizers and other biologic therapies. A small body of literature specifically addresses pharmacotherapy of URC in patients with BD (Table 2).19-26 A limitation of most existing literature is its focus on case reports, small open trials, or anecdotal observations rather than large, randomized controlled trials using systematic outcome measures. Extrapolation from reports focusing on patients with DSM-IV-TR RC is limited because it is uncertain whether URC differs fundamentally from RC and studies of DSM-IV-TR RC typically examine acute response during an index episode or time until relapse during maintenance therapy, rather than impact on mood changes over time.
Psychotherapy. A limited database on the efficacy of adjunctive cognitive-behavioral therapy (CBT) in RC BD describes improvement in depressive symptoms over short-term follow-up.27 No long-term studies of CBT or other structured psychotherapies have focused on RC or URC. Intuitively, one might expect that psychoeducation targeting sleep hygiene, substance use, stress management and coping skills, medication adherence, and prodrome recognition would be of value to patients with BD who experience frequent mood episodes, especially in those who may be unaware of or unfamiliar with basic concepts related to BD. In addition, relevant concepts from dialectical behavior therapy may be beneficial for BD patients with possible URC, such as skills to enhance emotional regulation, distress tolerance, mindfulness, and interpersonal effectiveness.
Table 2
Evidence-based treatments for ultra-rapid cycling BD
| Intervention | Strength of evidence | Comment |
|---|---|---|
| Antidepressant elimination | Cycling frequency may lengthen during antidepressant-free periods among patients with RC20; long-term (up to 1 year) antidepressant use in RC patients may increase the likelihood of depressive recurrences19 | Findings based mostly on small sample sizes; no controlled trials of antidepressant cessation as an intervention specifically for URC |
| Lithium | Single case report of ECT-induced URC resolved by lithium augmentation during continued ECT22 | No large-scale or randomized trials |
| Carbamazepine | No controlled trials or case reports | Possible anti-cycling benefits relevant for URC could be inferred from post hoc studies among patients with RC |
| Divalproex | Single case report describing resolution of a 48-hour cycle after augmentation of lithium with divalproex23 | No large-scale or randomized trials |
| Lamotrigine | Single case report of 100 mg/d lamotrigine augmentation to divalproex yielded 8 months of remission in a 25-year-old man with BD II and a long-standing pattern of 3 days of hypomania followed by 5 days of depression24 | No large-scale or randomized trials |
| Topiramate | Single case report in URC describing reduction of cycling frequency over 3 years25 | Multiple large scale placebo-controlled studies in bipolar mania have been negative |
| Second-generation antipsychotics | No controlled trials or case reports | Possible anti-cycling benefits relevant for URC could be inferred from post hoc studies in RC |
| Combinations of ≥2 mood stabilizing drugs | No controlled trials or case reports | Combining multiple anti-cycling agents is intuitively logical but largely unstudied |
| Nimodipine | 1 unipolar and 11 BD patients treated in randomized, off-on-off-on fashion (begun at 90 mg/d, increased up to 720 mg/d, mean duration of 12 weeks on active drug)26 | Response in 5 of 9 completers. Findings await replication with larger sample sizes |
| Hypermetabolic thyroid hormone (levothyroxine) | Findings from a small (N = 11) study of adjunctive high-dose levothyroxine (0.15 to 0.4 mg/d, with dosages increased by 0.05 to 0.1 mg/d every 1 to 2 weeks); an unspecified subgroup had “a very rapid cycling pattern” (reviewed by Bauer et al21) | 10 of 11 RC patients had reductions in depressive symptoms, 5 of 7 had improvement from baseline manic symptoms (observation period >60 days) |
| ECT | Case reports of improvement with ECT in refractory RC that was presumed secondary to tricyclic antidepressants | Reports of induction of URC by ECT22; whether or not ECT would more likely improve or exacerbate cyclicity for a given patient may require empirical determination |
| BD: bipolar disorder; BD II: bipolar II disorder; ECT: electroconvulsive therapy; RC: rapid cycling; URC: ultra-rapid cycling | ||
Treatment monitoring. Prospective life charting allows patients to systematically record manic/hypomanic and depressive symptoms day-to-day and week-to-week, thus creating a measure that may be particularly relevant for patients whose moods change rapidly. Simple mood charts (see Related Resources) typically take into account the severity of symptoms of either polarity with ratings of mild, moderate, or severe. Such visual records permit simple calculations over the course of a given interval (eg, week-by-week or across months) of several important parameters, including:
- number of days euthymic
- number of days with depression
- number of days with abnormal mood elevation
- number of occasions in which moods of both polarities occur on the same day.
Tracking these parameters during a treatment allows clinicians to make quantitative comparisons over time as a method of determining whether or not meaningful changes are occurring in cyclicity. See the figure below for an example of a completed mood chart and its interpretation.
Additional recommendations for assessing and managing cyclicity in BD are summarized in Table 3.
Table 3
Tips for managing suspected ultra-rapid cycling BD
| Do’s | Don’ts |
|---|---|
| Ascertain a history of ≥1 lifetime manic or hypomanic episode to diagnose BD | Diagnose BD solely on the presence of rapid mood fluctuations |
| Determine the presence of changes in sleep, energy, speech-language, and related behavior as correlates of mood to differentiate syndromes from isolated variation in mood | Ignore constellations of associated signs and symptoms of mania/hypomania |
| Obtain patient history to assess for head trauma or other medical and neurologic events that could have affective or other psychiatric manifestations | Disregard possible medical etiologies for new-onset affective dysregulation |
| Ascertain the resolution of 1 episode before counting the resurgence of symptoms as constituting a new episode; a waxing and waning course may reflect illness chronicity with incomplete recovery rather than true cyclicity | Misidentify incomplete recovery from an existing episode as the occurrence of new multiple episodes, which would inflate false-positive cases of RC or URC |
| Advise patients to refrain from alcohol or illicit substances that could destabilize mood | Assume that comorbid alcohol or illicit substance abuse will remit only after mood stabilization has been achieved, rather than the reverse |
| Monitor changes in sleep-wake cycles and the effects of erratic sleep or sleep deprivation on mood | Ignore the effects of poor sleep hygiene on mood |
| Minimize antidepressant exposure in patients with RC or URC | Continue long-term antidepressant maintenance therapy in patients with manic or mixed features or ongoing oscillations between mania/hypomania and depression |
| Assure euthyroid status and consider the potential utility of hypermetabolic levothyroxine | Assume that RC or URC will resolve solely by normalizing or optimizing thyroid function |
| Use rational, pharmacodynamically nonredundant anti-cycling drugs | Ignore the cumulative burden of adverse effects of multiple drugs |
| Consider the potential role for ECT as a strategy to arrest URC during any phase of BD | Assume ECT has value only during acute depressive phases of BD |
| Use prospective mood charting to document the evolution of mood changes over time, particularly when gauging treatment efficacy | Rely solely on impressionistic recall of mood states or polarity changes as reflecting distinct phasic changes |
| BD: bipolar disorder; ECT: electroconvulsive therapy; RC: rapid cycling; URC: ultra-rapid cycling | |
Table
Rapid cycling and ultra-rapid cycling BD: A comparison
| Construct | Rapid cycling | Ultra-rapid cycling |
|---|---|---|
| Bipolar I vs II | Predominantly BD IIa | No systematic data |
| Sex | Predominantly women | No systematic data |
| Longitudinal course | May be a transient phenomenon that can occur at any timeb or an enduring phenomenon that may persist for yearsc | Ultradian patterns may be more common across the first several episodes among pediatric BD patientsd |
| Age at onset | Associated with younger age at onsete | May be more evident in prepubescent onset mood disordersd; ultradian cycling more likely when onset occurs before age 13 than in adulthoode |
| Diurnal variation in mood | Morning-to-evening mood switches usually involve depression to mania/hypomania, with the opposite typifying evening-to-morning mood switchesf | Not reported |
| Relationship to environmental stresses | Life stresses may precede initial affective episodes but may be less important as subsequent episodes arise with increasing automaticity | No systematic data |
| Relationship to menstrual cycle | Despite case reports and self-reported links between RC and menstrual mood exacerbations, prospective data do not identify associations between RC and menstrual patternsg,h | No systematic data |
| Subclinical hypothyroidism | Bauer and Whybrow identified hypothyroidism independent of lithium use in 60% of 30 rapidly cycling BD patients, with evidence of improvement in a separate study of 11 RC patients given suprametabolic levothyroxine (reviewed by Bauer et ali) | No systematic data |
| Relationship to psychosis | Nonea | No systematic data |
| Relationship to antidepressant use | Naturalistic observations suggest RC may occur later in the illness course as a result of antidepressant use.c Small open case series data suggest shorter intermorbid intervals on antidepressants with longer intervals off antidepressants.j RC patients often receive antidepressants, but causal relationships are not well-documented.k Some case-control data dispute links between antidepressant use and RCl | No specific published cases |
| Considerations for suicide risk | RC linked with more serious suicide attemptsl | Suicide attempts may be associated with cycling within an episodem or rapid shifting in moodn |
| Time course for judging treatment efficacy | Efforts to diminish acute affective instability may be measured over the course of days to weeks | By definition, treatment of RC involves relapse prevention over the course of 1 year |
| BD: bipolar disorder; RC: rapid cycling | ||
| References a. Schneck CD, Miklowitz DJ, Calabrese JR, et al. Phenomenology of rapid-cycling bipolar disorder: data from the first 500 participants in the Systematic Treatment Enhancement Program. Am J Psychiatry. 2004;161(10):1902-1908. b. Coryell W, Endicott J, Keller M. Rapidly cycling affective disorder. Demographics, diagnosis, family history, and course. Arch Gen Psychiatry. 1992;49(2):126-131. c. Koukopoulos A, Sani G, Koukopoulos AE, et al. Duration and stability of the rapid-cycling course: a long-term personal follow-up of 109 patients. J Affect Disord. 2003;73(1-2):75-85. d. Geller B, Tillman R, Bolhofner K, et al. Child bipolar I disorder: prospective continuity with adult bipolar I disorder; characteristics of second and third episodes; predictors of 8-year outcome. Arch Gen Psychiatry. 2008;65(10):1125-1133. e. Post RM, Leverich GS, Kupka RW, et al. Early-onset bipolar disorder and treatment delay are risk factors for poor outcome in adulthood. J Clin Psychiatry. 2010;71(7):864-872. f. Feldman-Naim S, Turner EH, Leibenluft E. Diurnal variation in the direction of mood switches in patients with rapid-cycling bipolar disorder. J Clin Psychiatry. 1997;58(2):79-84. g. Leibenluft E, Ashman SB, Feldman-Naim S, et al. Lack of relationship between menstrual cycle phase and mood in a sample of women with rapid cycling bipolar disorder. Biol Psychiatry. 1999;46(4):577-580. h. Wehr TA, Sack DA, Rosenthal NE, et al. Rapid cycling affective disorder: contributing factors and treatment responses in 51 patients. Am J Psychiatry. 1988;145(2):179-184. i. Bauer M, Beaulieu S, Dunner DL, et al. Rapid cycling bipolar disorder—diagnostic concepts. Bipolar Disord. 2008;10(1 Pt 2):153-162. j. Wehr TA, Goodwin FK. Can antidepressants cause mania and worsen the course of affective illness? Am J Psychiatry. 1987;144(11):1403-1411. k. Schneck CD, Miklowitz DJ, Miyahara S, et al. The prospective course of rapid-cycling bipolar disorder: findings from the STEP-BD. Am J Psychiatry. 2008;165(3):370-377. l. Coryell W, Solomon D, Turvey C, et al. The long-term course of rapid-cycling bipolar disorder. Arch Gen Psychiatry. 2003;60(9):914-920. m. Fawcett J, Scheftner W, Clark D, et al. Clinical predictors of suicide in patients with major affective disorders: a controlled prospective study. Am J Psychiatry. 1987;144(1):35-40. n. MacKinnon DF, Potash JB, McMahon FJ, et al. Rapid mood switching and suicidality in familial bipolar disorder. Bipolar Disord. 2005;7(5):441-448. | ||
From a biologic perspective, a handful of preliminary studies have examined genetic markers or familial patterns that might be related to rapid cycling (RC) or ultra-rapid cycling (URC). These include a reported link between URC and the low activity variant of the catechol-o-methyltransferase gene polymorphism in a small group of patients with velo-cardio-facial syndrome,a although this finding was not replicated in a larger sample.a Other preliminary reports on RC have implicated both the long (l) and short (s) allelic variants of the serotonin transporter gene (SLC6A4), the val66met variant of the brain-derived neurotrophic factor gene, and the circadian cryptochrome 2 (CRY2) gene (reviewed by Bauer et alb). These candidate loci have been examined in RC but not URC.
URC has not been examined as a familial entity, although in the National Institute of Mental Health Collaborative Depression Study, DSM-IV-TR RC did not occur with elevated frequency in bipolar pedigrees.c Rapid mood switches—abrupt rather than gradual transitions from one affective pole to another—appear to be only slightly, nonsignificantly more common in first-degree bipolar relatives of BD patients who themselves have rapid rather than gradual transitions from one affective pole to the other.d
Neuroimaging studies in BD seldom focus on subpopulations with RC or URC, and have been confined mainly to case reports that have yielded limited, non-generalizable observations, such as state-dependent variations in prefrontal activity during tasks of facial recognition (reviewed by Bauer et alb).
References
a. Papolos DF, Veit S, Faedda GL, et al. Ultra-ultra rapid cycling bipolar disorder is associated with the low activity catecholamine-O-methyltransferase allele. Mol Psychiatry. 1998;3(4):346-349.
b. Bauer M, Beaulieu S, Dunner DL, et al. Rapid cycling bipolar disorder—diagnostic concepts. Bipolar Disord. 2008;10(1 Pt 2):153-162.
c. Coryell W, Endicott J, Keller M. Rapidly cycling affective disorder. Demographics, diagnosis, family history, and course. Arch Gen Psychiatry. 1992;49(2):126-131.
d. MacKinnon DF, Potash JB, McMahon FJ, et al. Rapid mood switching and suicidality in familial bipolar disorder. Bipolar Disord. 2005;7(5):441-448.
Figure: Example of prospective mood charting to document changes in manic/hypomanic and depressive symptoms across time
In the above example, the prevalence and severity of mood symptoms are identified over 21 days. Note the distinctly separate phases of mood elevation followed by depression, whereas euthymia was present only 6 of 21 days (29% of the time). Symptoms of at least moderate severity were more prominently depressive (5 of 21 days, or 24% of the time) than manic/hypomanic (2 of 21 days, or approximately 10% of the time). Mood charting does not capture associate DSM-IV-TR criteria for a mood episode but instead focuses solely on longitudinal changes in mood elevation or depression
Related Resources
- American Psychiatric Association practice guideline for the treatment of patients with bipolar disorder (revision). Am J Psychiatry. 2002;159(4 suppl):1-50.
- Massachusetts General Hospital Bipolar Clinic and Research Program. Sample mood chart (downloadable). www.manicdepressive.org/moodchart.html.
Drug Brand Names
- Carbamazepine • Equetro, Tegretol
- Divalproex • Depakote
- Lamotrigine • Lamictal
- Levothyroxine • Synthroid
- Lithium • Lithobid
- Nimodipine • Nimotop
- Topiramate • Topamax
Disclosures
Dr. Goldberg is on the speakers’ bureaus for AstraZeneca, Dey Pharmaceuticals, Eli Lilly and Company, Merck, and Sunovion and is a consultant for Axon Advisors, Dey Pharmaceuticals, Eli Lilly and Company, and Grünenthal Group.
Acknowledgment
The author wishes to thank David L. Dunner, MD, for his helpful comments regarding this article.
1. Kramlinger KG, Post RM. Ultra-rapid and ultradian cycling in bipolar affective illness. Br J Psychiatry. 1996;168(3):314-323.
2. Leibenluft E. Severe mood dysregulation irritability, and the diagnostic boundaries of bipolar disorder in youths. Am J Psychiatry. 2011;168(2):129-142.
3. Geller B, Tillman R, Bolhofner K. Proposed definitions of bipolar I disorder episodes and daily rapid cycling phenomena in preschoolers school-aged children, adolescents, and adults. J Child Adolesc Psychopharmacol. 2007;17(2):217-222.
4. Feinman JA, Dunner DL. The effect of alcohol and substance abuse on the course of bipolar affective disorder. J Affect Disord. 1996;37(1):43-49.
5. Maj M, Pirozzi R, Formicola AM, et al. Reliability and validity of four alternative definitions of rapid-cycling bipolar disorder. Am J Psychiatry. 1999;156(9):1421-1424.
6. Jenner FA, Gjessing LR, Cox JR, et al. A manic depressive psychotic with a persistent forty-eight hour cycle. Br J Psychiatry. 1967;113(501):895-910.
7. Zwil AS, McAllister TW, Cohen I, et al. Ultra-rapid cycling bipolar affective disorder following a closed-head injury. Brain Inj. 1993;7(2):147-152.
8. Geller B, Tillman R, Craney JL, et al. Four-year prospective outcome and natural history of mania in children with a prepubertal and early adolescent bipolar disorder phenotype. Arch Gen Psychiatry. 2004;61(5):459-467.
9. Geller B, Sun K, Zimerman B, et al. Complex and rapid-cycling in bipolar children and adolescents: a preliminary study. J Affect Disord. 1995;34(4):259-268.
10. Goldberg JF, Garno JL, Callahan AM, et al. Overdiagnosis of bipolar disorder among substance use disorder inpatients with mood instability. J Clin Psychiatry. 2008;69(11):1751-1757.
11. Zimmerman M, Ruggero CJ, Chelminski I, et al. Psychiatric diagnoses in patients previously overdiagnosed with bipolar disorder. J Clin Psychiatry. 2010;71(1):26-31.
12. MacKinnon DF, Pies R. Affective instability as rapid cycling: theoretical and clinical implications for borderline personality and bipolar spectrum disorders. Bipolar Disord. 2006;8(1):1-14.
13. Coryell W, Endicott J, Keller M. Rapidly cycling affective disorder. Demographics diagnosis, family history, and course. Arch Gen Psychiatry. 1992;49(2):126-131.
14. Koenigsberg HW, Harvey PD, Mitropoulou V, et al. Characterizing affective instability in borderline personality disorder. Am J Psychiatry. 2002;159(5):784-788.
15. Henry C, Mitropoulou V, New AS, et al. Affective instability and impulsivity in borderline personality and bipolar II disorders: similarities and differences. J Psychiatr Res. 2001;35(6):307-312.
16. Gottschalk A, Bauer MS, Whybrow PC. Evidence of chaotic mood variation in bipolar disorder. Arch Gen Psychiatry. 1995;52(11):947-959.
17. Goldberg JF, Bowden CL, Calabrese JR, et al. Six-month prospective life charting of mood symptoms with lamotrigine monotherapy versus placebo in rapid cycling bipolar disorder. Biol Psychiatry. 2008;63(1):125-130.
18. Schneck CD, Miklowitz DJ, Miyahara S, et al. The prospective course of rapid-cycling bipolar disorder: findings from the STEP-BD. Am J Psychiatry. 2008;165(3):370-377.
19. Ghaemi SN, Ostacher MM, El-Mallakh RS, et al. Antidepressant discontinuation in bipolar depression: a Systematic Treatment Enhancement Program for Bipolar Disorder (STEP-BD) randomized clinical trial of long-term effectiveness and safety. J Clin Psychiatry. 2010;71(4):372-380.
20. Wehr TA, Sack DA, Rosenthal NE, et al. Rapid cycling affective disorder: contributing factors and treatment responses in 51 patients. Am J Psychiatry. 1988;145(2):179-184.
21. Bauer M, Beaulieu S, Dunner DL, et al. Rapid cycling bipolar disorder—diagnostic concepts. Bipolar Disord. 2008;10(1 Pt 2):153-162.
22. Zavorotnyy M, Diemer J, Patzelt J, et al. Occurrence of ultra-rapid cycling during electroconvulsive therapy in bipolar depression. World J Biol Psychiatry. 2009;10(4 Pt 3):987-990.
23. Lepkifker E, Iancu I, Dannon P, et al. Valproic acid in ultra-rapid cycling: a case report. Clin Neuropharmacol. 1995;18(1):72-75.
24. Woo YS, Chae JH, Jun TY, et al. Lamotrigine added to valproate successfully treated a case of ultra-rapid cycling bipolar disorder. Psychiatry Clin Neurosci. 2007;61(1):130-131.
25. Karama S, Lal S. Adjunctive topiramate in ultradian cycling bipolar disorder: case report with 3-year follow-up. Eur Psychiatry. 2006;21(4):280-281.
26. Pazzaglia PJ, Post RM, Ketter TA, et al. Preliminary controlled trial of nimodipine in ultra-rapid cycling affective dysregulation. Psychiatry Res. 1993;49(3):257-272.
27. Reilly-Harrington NA, Deckersbach T, Knauz R, et al. Cognitive behavioral therapy for rapid-cycling bipolar disorder: a pilot study. J Psychiatr Pract. 2007;13(5):291-297.
1. Kramlinger KG, Post RM. Ultra-rapid and ultradian cycling in bipolar affective illness. Br J Psychiatry. 1996;168(3):314-323.
2. Leibenluft E. Severe mood dysregulation irritability, and the diagnostic boundaries of bipolar disorder in youths. Am J Psychiatry. 2011;168(2):129-142.
3. Geller B, Tillman R, Bolhofner K. Proposed definitions of bipolar I disorder episodes and daily rapid cycling phenomena in preschoolers school-aged children, adolescents, and adults. J Child Adolesc Psychopharmacol. 2007;17(2):217-222.
4. Feinman JA, Dunner DL. The effect of alcohol and substance abuse on the course of bipolar affective disorder. J Affect Disord. 1996;37(1):43-49.
5. Maj M, Pirozzi R, Formicola AM, et al. Reliability and validity of four alternative definitions of rapid-cycling bipolar disorder. Am J Psychiatry. 1999;156(9):1421-1424.
6. Jenner FA, Gjessing LR, Cox JR, et al. A manic depressive psychotic with a persistent forty-eight hour cycle. Br J Psychiatry. 1967;113(501):895-910.
7. Zwil AS, McAllister TW, Cohen I, et al. Ultra-rapid cycling bipolar affective disorder following a closed-head injury. Brain Inj. 1993;7(2):147-152.
8. Geller B, Tillman R, Craney JL, et al. Four-year prospective outcome and natural history of mania in children with a prepubertal and early adolescent bipolar disorder phenotype. Arch Gen Psychiatry. 2004;61(5):459-467.
9. Geller B, Sun K, Zimerman B, et al. Complex and rapid-cycling in bipolar children and adolescents: a preliminary study. J Affect Disord. 1995;34(4):259-268.
10. Goldberg JF, Garno JL, Callahan AM, et al. Overdiagnosis of bipolar disorder among substance use disorder inpatients with mood instability. J Clin Psychiatry. 2008;69(11):1751-1757.
11. Zimmerman M, Ruggero CJ, Chelminski I, et al. Psychiatric diagnoses in patients previously overdiagnosed with bipolar disorder. J Clin Psychiatry. 2010;71(1):26-31.
12. MacKinnon DF, Pies R. Affective instability as rapid cycling: theoretical and clinical implications for borderline personality and bipolar spectrum disorders. Bipolar Disord. 2006;8(1):1-14.
13. Coryell W, Endicott J, Keller M. Rapidly cycling affective disorder. Demographics diagnosis, family history, and course. Arch Gen Psychiatry. 1992;49(2):126-131.
14. Koenigsberg HW, Harvey PD, Mitropoulou V, et al. Characterizing affective instability in borderline personality disorder. Am J Psychiatry. 2002;159(5):784-788.
15. Henry C, Mitropoulou V, New AS, et al. Affective instability and impulsivity in borderline personality and bipolar II disorders: similarities and differences. J Psychiatr Res. 2001;35(6):307-312.
16. Gottschalk A, Bauer MS, Whybrow PC. Evidence of chaotic mood variation in bipolar disorder. Arch Gen Psychiatry. 1995;52(11):947-959.
17. Goldberg JF, Bowden CL, Calabrese JR, et al. Six-month prospective life charting of mood symptoms with lamotrigine monotherapy versus placebo in rapid cycling bipolar disorder. Biol Psychiatry. 2008;63(1):125-130.
18. Schneck CD, Miklowitz DJ, Miyahara S, et al. The prospective course of rapid-cycling bipolar disorder: findings from the STEP-BD. Am J Psychiatry. 2008;165(3):370-377.
19. Ghaemi SN, Ostacher MM, El-Mallakh RS, et al. Antidepressant discontinuation in bipolar depression: a Systematic Treatment Enhancement Program for Bipolar Disorder (STEP-BD) randomized clinical trial of long-term effectiveness and safety. J Clin Psychiatry. 2010;71(4):372-380.
20. Wehr TA, Sack DA, Rosenthal NE, et al. Rapid cycling affective disorder: contributing factors and treatment responses in 51 patients. Am J Psychiatry. 1988;145(2):179-184.
21. Bauer M, Beaulieu S, Dunner DL, et al. Rapid cycling bipolar disorder—diagnostic concepts. Bipolar Disord. 2008;10(1 Pt 2):153-162.
22. Zavorotnyy M, Diemer J, Patzelt J, et al. Occurrence of ultra-rapid cycling during electroconvulsive therapy in bipolar depression. World J Biol Psychiatry. 2009;10(4 Pt 3):987-990.
23. Lepkifker E, Iancu I, Dannon P, et al. Valproic acid in ultra-rapid cycling: a case report. Clin Neuropharmacol. 1995;18(1):72-75.
24. Woo YS, Chae JH, Jun TY, et al. Lamotrigine added to valproate successfully treated a case of ultra-rapid cycling bipolar disorder. Psychiatry Clin Neurosci. 2007;61(1):130-131.
25. Karama S, Lal S. Adjunctive topiramate in ultradian cycling bipolar disorder: case report with 3-year follow-up. Eur Psychiatry. 2006;21(4):280-281.
26. Pazzaglia PJ, Post RM, Ketter TA, et al. Preliminary controlled trial of nimodipine in ultra-rapid cycling affective dysregulation. Psychiatry Res. 1993;49(3):257-272.
27. Reilly-Harrington NA, Deckersbach T, Knauz R, et al. Cognitive behavioral therapy for rapid-cycling bipolar disorder: a pilot study. J Psychiatr Pract. 2007;13(5):291-297.
Severe Mental Disorders Highly Prevalent in Jails, Prisons
BOSTON – U.S. correctional institutions are estimated to be housing 1 million men and women with serious mental illnesses such as schizophrenia or a major affective disorder, investigators reported at the annual meeting of the American Academy of Psychiatry and the Law.
The estimated prevalence of serious mental disorders among U.S. inmates ranges from 7% to 16%. Men with mental illness are four times more likely to be incarcerated than the general population, and women with mental illness have an eightfold higher risk, reported Georgia Stathopoulou, Ph.D., and her colleagues from Massachusetts General Hospital and Harvard Medical School, both in Boston.
"The prevalence of serious mental health issues is higher among incarcerated individuals than in the general population, and is associated with specific sociodemographic characteristics like male gender, younger age, and non-white race. Severe psychopathology is also associated with higher recidivism and more serious criminal offenses," wrote Dr. Stathopoulou and colleagues Dr. Fabian Saleh and Kristen Czarnecki in a poster presentation.
The investigators reviewed the medical literature and U.S. Department of Justice statistics to get a handle on the size of the problem.
They found that about 804,000 people with severe mental disorders are jailed annually, and that 72% of both men and women with serious mental illness who are in jail had a co-occurring substance use disorder.
The high rates of substance use and abuse is one of the primary factors contributing to the high incarceration rate of the mentally ill, they said. Other factors, they said, are:
"The prevalence of serious mental health issues is higher among incarcerated individuals than in the general population."
• Insufficient community resources.
• A national drug policy that emphasizes interdiction over treatment.
• Delays in release from prisons and jails to the community.
• Insufficient inmate access to evidence-based mental health therapies.
• Insufficient planning for reentry of mental health inmates into the community.
Jail inmates with mental health disorders are twice as likely as inmates without mental illness to have been homeless in the year before their arrest (13% vs. 6%), 3 times more likely to report a history of sexual or physical abuse (24% vs. 8%), and twice as likely to have lived in a foster home or institution when they were growing up, the authors found.
Specific criminal actions associated with mental disorder diagnoses include higher rates of assault among inmates with bipolar disorder, and higher assault, homicide, and drug possession rates among those with schizophrenia or nonschizophrenic psychosis.
High Recidivism Rates
The investigators cited a retrospective study of more than 79,000 Texas inmates, which found that inmates with bipolar disorder were more than 3 times more likely than inmates without psychiatric disorders to be incarcerated 4 or more times during a 6-year period (Am. J. Psychiatry 2009;166:103-9).
Inmates with major depressive disorder, schizophrenia, and nonschizophrenic psychotic disorders also were significantly more likely to be imprisoned repeatedly, compared with the general prison population.
In all, 89% of the state public and private adult correctional facilities provide some type of mental health services to inmates. Of this group, 51% provide around-the-clock services, 71% offer therapy or counseling from trained mental health professional, and 73% dispense psychotropic drugs.
"We need new treatments, and these treatments have to be evidence based. These treatments have to address both public safety and the clinical needs of inmates," Dr. Stathopoulou said in an interview.
The authors did not disclose a funding source for the study. Dr. Stathopoulou reported that she had no relevant conflicts of interest.
BOSTON – U.S. correctional institutions are estimated to be housing 1 million men and women with serious mental illnesses such as schizophrenia or a major affective disorder, investigators reported at the annual meeting of the American Academy of Psychiatry and the Law.
The estimated prevalence of serious mental disorders among U.S. inmates ranges from 7% to 16%. Men with mental illness are four times more likely to be incarcerated than the general population, and women with mental illness have an eightfold higher risk, reported Georgia Stathopoulou, Ph.D., and her colleagues from Massachusetts General Hospital and Harvard Medical School, both in Boston.
"The prevalence of serious mental health issues is higher among incarcerated individuals than in the general population, and is associated with specific sociodemographic characteristics like male gender, younger age, and non-white race. Severe psychopathology is also associated with higher recidivism and more serious criminal offenses," wrote Dr. Stathopoulou and colleagues Dr. Fabian Saleh and Kristen Czarnecki in a poster presentation.
The investigators reviewed the medical literature and U.S. Department of Justice statistics to get a handle on the size of the problem.
They found that about 804,000 people with severe mental disorders are jailed annually, and that 72% of both men and women with serious mental illness who are in jail had a co-occurring substance use disorder.
The high rates of substance use and abuse is one of the primary factors contributing to the high incarceration rate of the mentally ill, they said. Other factors, they said, are:
"The prevalence of serious mental health issues is higher among incarcerated individuals than in the general population."
• Insufficient community resources.
• A national drug policy that emphasizes interdiction over treatment.
• Delays in release from prisons and jails to the community.
• Insufficient inmate access to evidence-based mental health therapies.
• Insufficient planning for reentry of mental health inmates into the community.
Jail inmates with mental health disorders are twice as likely as inmates without mental illness to have been homeless in the year before their arrest (13% vs. 6%), 3 times more likely to report a history of sexual or physical abuse (24% vs. 8%), and twice as likely to have lived in a foster home or institution when they were growing up, the authors found.
Specific criminal actions associated with mental disorder diagnoses include higher rates of assault among inmates with bipolar disorder, and higher assault, homicide, and drug possession rates among those with schizophrenia or nonschizophrenic psychosis.
High Recidivism Rates
The investigators cited a retrospective study of more than 79,000 Texas inmates, which found that inmates with bipolar disorder were more than 3 times more likely than inmates without psychiatric disorders to be incarcerated 4 or more times during a 6-year period (Am. J. Psychiatry 2009;166:103-9).
Inmates with major depressive disorder, schizophrenia, and nonschizophrenic psychotic disorders also were significantly more likely to be imprisoned repeatedly, compared with the general prison population.
In all, 89% of the state public and private adult correctional facilities provide some type of mental health services to inmates. Of this group, 51% provide around-the-clock services, 71% offer therapy or counseling from trained mental health professional, and 73% dispense psychotropic drugs.
"We need new treatments, and these treatments have to be evidence based. These treatments have to address both public safety and the clinical needs of inmates," Dr. Stathopoulou said in an interview.
The authors did not disclose a funding source for the study. Dr. Stathopoulou reported that she had no relevant conflicts of interest.
BOSTON – U.S. correctional institutions are estimated to be housing 1 million men and women with serious mental illnesses such as schizophrenia or a major affective disorder, investigators reported at the annual meeting of the American Academy of Psychiatry and the Law.
The estimated prevalence of serious mental disorders among U.S. inmates ranges from 7% to 16%. Men with mental illness are four times more likely to be incarcerated than the general population, and women with mental illness have an eightfold higher risk, reported Georgia Stathopoulou, Ph.D., and her colleagues from Massachusetts General Hospital and Harvard Medical School, both in Boston.
"The prevalence of serious mental health issues is higher among incarcerated individuals than in the general population, and is associated with specific sociodemographic characteristics like male gender, younger age, and non-white race. Severe psychopathology is also associated with higher recidivism and more serious criminal offenses," wrote Dr. Stathopoulou and colleagues Dr. Fabian Saleh and Kristen Czarnecki in a poster presentation.
The investigators reviewed the medical literature and U.S. Department of Justice statistics to get a handle on the size of the problem.
They found that about 804,000 people with severe mental disorders are jailed annually, and that 72% of both men and women with serious mental illness who are in jail had a co-occurring substance use disorder.
The high rates of substance use and abuse is one of the primary factors contributing to the high incarceration rate of the mentally ill, they said. Other factors, they said, are:
"The prevalence of serious mental health issues is higher among incarcerated individuals than in the general population."
• Insufficient community resources.
• A national drug policy that emphasizes interdiction over treatment.
• Delays in release from prisons and jails to the community.
• Insufficient inmate access to evidence-based mental health therapies.
• Insufficient planning for reentry of mental health inmates into the community.
Jail inmates with mental health disorders are twice as likely as inmates without mental illness to have been homeless in the year before their arrest (13% vs. 6%), 3 times more likely to report a history of sexual or physical abuse (24% vs. 8%), and twice as likely to have lived in a foster home or institution when they were growing up, the authors found.
Specific criminal actions associated with mental disorder diagnoses include higher rates of assault among inmates with bipolar disorder, and higher assault, homicide, and drug possession rates among those with schizophrenia or nonschizophrenic psychosis.
High Recidivism Rates
The investigators cited a retrospective study of more than 79,000 Texas inmates, which found that inmates with bipolar disorder were more than 3 times more likely than inmates without psychiatric disorders to be incarcerated 4 or more times during a 6-year period (Am. J. Psychiatry 2009;166:103-9).
Inmates with major depressive disorder, schizophrenia, and nonschizophrenic psychotic disorders also were significantly more likely to be imprisoned repeatedly, compared with the general prison population.
In all, 89% of the state public and private adult correctional facilities provide some type of mental health services to inmates. Of this group, 51% provide around-the-clock services, 71% offer therapy or counseling from trained mental health professional, and 73% dispense psychotropic drugs.
"We need new treatments, and these treatments have to be evidence based. These treatments have to address both public safety and the clinical needs of inmates," Dr. Stathopoulou said in an interview.
The authors did not disclose a funding source for the study. Dr. Stathopoulou reported that she had no relevant conflicts of interest.
FROM THE ANNUAL MEETING OF THE AMERICAN ACADEMY OF PSYCHIATRY AND THE LAW
Major Finding: The estimated prevalence of serious mental disorders among U.S. inmates ranges from 7% to 16%.
Data Source: Review of medical literature and Department of Justice statistics.
Disclosures: The authors did not disclose a funding source for the study. Dr. Stathopoulou reported that she had no relevant conflicts of interest.
Caffeine Linked to Psychosis in Case Series
BOSTON – Most people just get a mild buzz from their morning coffee, but an unfortunate few have reactions to caffeine ranging from severe agitation to paranoid delusions and psychosis, forensic psychiatrists reported in a poster presented at the annual meeting of the American Academy of Psychiatry in the Law.

Caffeine is known to act as an antagonist of the adenosine A2a receptor, thereby causing an increase in dopaminergic neurotransmission, especially in areas of the brain rich in D2 receptors. "This mechanism may cause or exacerbate psychotic symptoms, and is also triggered by modulation of transmission in the mesolimbic dopaminergic pathways," wrote Dr. Christopher M. Davidson of the University of South Dakota Sanford School of Medicine, Sioux Falls, and his associates.
Caffeine is metabolized by the cytochrome P450 1A2 enzyme. Polymorphisms in the enzyme might affect how individuals metabolize and respond to caffeine, the authors said.
They reported on a forensic case and two corrections cases of caffeine-induced mental and behavioral problems.
In the forensics case, a 24-year old man with no history of mental illness assaulted an emergency room nurse after he had driven all night and ingested the caffeine equivalent of about three cups of coffee, said coauthor Dr. James B. Reynolds of the Northwest Missouri Psychiatric Rehabilitation Center, St. Joseph, in an interview.
The patient had been brought to the emergency department by police whom he had sought out when he began experiencing confusion and paranoia. At one point, without apparent provocation, he jumped out of bed, grabbed the nurse, and shouted: "Why do you do that to me, why do you do that to me?" and cut her neck with a box cutter in his possession.
He was charged with first-degree assault, but was found to have no apparent motive for the assault, no criminal or mental health history, and no evidence of drug or alcohol abuse. He did, however, have a box of caffeine pills in his possession, leading to the conclusion that he was likely suffering from pathologic intoxication.
Dr. Reynolds said that if intoxication occurs because of unforeseeable circumstances, it might qualify as a valid defense against a criminal charge.
Given the circumstances, the prosecutor agreed with the defense, and the man was found not guilty by reason of insanity.
"He came into my hospital, and for nearly 3 years this man was under our observation, and never had one symptom of mental illness and no repeat episode," Dr. Reynolds said.
In the first of the two corrections cases, a 22-year-old man who had been diagnosed with schizophrenia of the catatonic type was living in a section for mentally ill prisoners. He developed new symptoms of activation, irritability, confrontation, restlessness, and high energy with little need for sleep. The episodes occurred at intervals of 1-2 weeks and lasted for 1-3 days.
The mental health staff suspected he had rapid-cycling bipolar-type schizoaffective disorder, and tried treating him with higher doses of olanzapine, augmented with fluphenazine, aripiprazole, and valproic acid, none of which seemed to work.
Through careful observation and documentation, staff noticed that the episodes corresponded to the prisoner’s visits to the commissary, where he bought caffeinated beverages. After he was forbidden to buy coffee or tea, the patient’s maniclike episodes vanished.
In the second case, prison staff saw that a 24-year-old man who had been diagnosed with schizophrenia, undifferentiated type, became agitated and spent most of the night pacing and yelling after he had visited the unit commissary.
"In the months following careful monitoring and restriction of caffeine use in the patient’s housing unit, he had such significant resolution of his symptoms that his doses of trifluophenazine and benzotropine were halved, and he was able to transition to the general population," the authors wrote.
They noted that caffeine is not necessary for the health and functioning of patients in correctional settings, and recommended that institutions either monitor and limit caffeine use, or eliminate it in some correctional settings. They also called for further investigation of highly variable responses to caffeine.
The authors did not disclose a funding source. Dr. Davidson, Dr. Reynolds, and their coauthors reported that they had no relevant financial disclosures.
BOSTON – Most people just get a mild buzz from their morning coffee, but an unfortunate few have reactions to caffeine ranging from severe agitation to paranoid delusions and psychosis, forensic psychiatrists reported in a poster presented at the annual meeting of the American Academy of Psychiatry in the Law.
Caffeine is known to act as an antagonist of the adenosine A2a receptor, thereby causing an increase in dopaminergic neurotransmission, especially in areas of the brain rich in D2 receptors. "This mechanism may cause or exacerbate psychotic symptoms, and is also triggered by modulation of transmission in the mesolimbic dopaminergic pathways," wrote Dr. Christopher M. Davidson of the University of South Dakota Sanford School of Medicine, Sioux Falls, and his associates.
Caffeine is metabolized by the cytochrome P450 1A2 enzyme. Polymorphisms in the enzyme might affect how individuals metabolize and respond to caffeine, the authors said.
They reported on a forensic case and two corrections cases of caffeine-induced mental and behavioral problems.
In the forensics case, a 24-year old man with no history of mental illness assaulted an emergency room nurse after he had driven all night and ingested the caffeine equivalent of about three cups of coffee, said coauthor Dr. James B. Reynolds of the Northwest Missouri Psychiatric Rehabilitation Center, St. Joseph, in an interview.
The patient had been brought to the emergency department by police whom he had sought out when he began experiencing confusion and paranoia. At one point, without apparent provocation, he jumped out of bed, grabbed the nurse, and shouted: "Why do you do that to me, why do you do that to me?" and cut her neck with a box cutter in his possession.
He was charged with first-degree assault, but was found to have no apparent motive for the assault, no criminal or mental health history, and no evidence of drug or alcohol abuse. He did, however, have a box of caffeine pills in his possession, leading to the conclusion that he was likely suffering from pathologic intoxication.
Dr. Reynolds said that if intoxication occurs because of unforeseeable circumstances, it might qualify as a valid defense against a criminal charge.
Given the circumstances, the prosecutor agreed with the defense, and the man was found not guilty by reason of insanity.
"He came into my hospital, and for nearly 3 years this man was under our observation, and never had one symptom of mental illness and no repeat episode," Dr. Reynolds said.
In the first of the two corrections cases, a 22-year-old man who had been diagnosed with schizophrenia of the catatonic type was living in a section for mentally ill prisoners. He developed new symptoms of activation, irritability, confrontation, restlessness, and high energy with little need for sleep. The episodes occurred at intervals of 1-2 weeks and lasted for 1-3 days.
The mental health staff suspected he had rapid-cycling bipolar-type schizoaffective disorder, and tried treating him with higher doses of olanzapine, augmented with fluphenazine, aripiprazole, and valproic acid, none of which seemed to work.
Through careful observation and documentation, staff noticed that the episodes corresponded to the prisoner’s visits to the commissary, where he bought caffeinated beverages. After he was forbidden to buy coffee or tea, the patient’s maniclike episodes vanished.
In the second case, prison staff saw that a 24-year-old man who had been diagnosed with schizophrenia, undifferentiated type, became agitated and spent most of the night pacing and yelling after he had visited the unit commissary.
"In the months following careful monitoring and restriction of caffeine use in the patient’s housing unit, he had such significant resolution of his symptoms that his doses of trifluophenazine and benzotropine were halved, and he was able to transition to the general population," the authors wrote.
They noted that caffeine is not necessary for the health and functioning of patients in correctional settings, and recommended that institutions either monitor and limit caffeine use, or eliminate it in some correctional settings. They also called for further investigation of highly variable responses to caffeine.
The authors did not disclose a funding source. Dr. Davidson, Dr. Reynolds, and their coauthors reported that they had no relevant financial disclosures.
BOSTON – Most people just get a mild buzz from their morning coffee, but an unfortunate few have reactions to caffeine ranging from severe agitation to paranoid delusions and psychosis, forensic psychiatrists reported in a poster presented at the annual meeting of the American Academy of Psychiatry in the Law.
Caffeine is known to act as an antagonist of the adenosine A2a receptor, thereby causing an increase in dopaminergic neurotransmission, especially in areas of the brain rich in D2 receptors. "This mechanism may cause or exacerbate psychotic symptoms, and is also triggered by modulation of transmission in the mesolimbic dopaminergic pathways," wrote Dr. Christopher M. Davidson of the University of South Dakota Sanford School of Medicine, Sioux Falls, and his associates.
Caffeine is metabolized by the cytochrome P450 1A2 enzyme. Polymorphisms in the enzyme might affect how individuals metabolize and respond to caffeine, the authors said.
They reported on a forensic case and two corrections cases of caffeine-induced mental and behavioral problems.
In the forensics case, a 24-year old man with no history of mental illness assaulted an emergency room nurse after he had driven all night and ingested the caffeine equivalent of about three cups of coffee, said coauthor Dr. James B. Reynolds of the Northwest Missouri Psychiatric Rehabilitation Center, St. Joseph, in an interview.
The patient had been brought to the emergency department by police whom he had sought out when he began experiencing confusion and paranoia. At one point, without apparent provocation, he jumped out of bed, grabbed the nurse, and shouted: "Why do you do that to me, why do you do that to me?" and cut her neck with a box cutter in his possession.
He was charged with first-degree assault, but was found to have no apparent motive for the assault, no criminal or mental health history, and no evidence of drug or alcohol abuse. He did, however, have a box of caffeine pills in his possession, leading to the conclusion that he was likely suffering from pathologic intoxication.
Dr. Reynolds said that if intoxication occurs because of unforeseeable circumstances, it might qualify as a valid defense against a criminal charge.
Given the circumstances, the prosecutor agreed with the defense, and the man was found not guilty by reason of insanity.
"He came into my hospital, and for nearly 3 years this man was under our observation, and never had one symptom of mental illness and no repeat episode," Dr. Reynolds said.
In the first of the two corrections cases, a 22-year-old man who had been diagnosed with schizophrenia of the catatonic type was living in a section for mentally ill prisoners. He developed new symptoms of activation, irritability, confrontation, restlessness, and high energy with little need for sleep. The episodes occurred at intervals of 1-2 weeks and lasted for 1-3 days.
The mental health staff suspected he had rapid-cycling bipolar-type schizoaffective disorder, and tried treating him with higher doses of olanzapine, augmented with fluphenazine, aripiprazole, and valproic acid, none of which seemed to work.
Through careful observation and documentation, staff noticed that the episodes corresponded to the prisoner’s visits to the commissary, where he bought caffeinated beverages. After he was forbidden to buy coffee or tea, the patient’s maniclike episodes vanished.
In the second case, prison staff saw that a 24-year-old man who had been diagnosed with schizophrenia, undifferentiated type, became agitated and spent most of the night pacing and yelling after he had visited the unit commissary.
"In the months following careful monitoring and restriction of caffeine use in the patient’s housing unit, he had such significant resolution of his symptoms that his doses of trifluophenazine and benzotropine were halved, and he was able to transition to the general population," the authors wrote.
They noted that caffeine is not necessary for the health and functioning of patients in correctional settings, and recommended that institutions either monitor and limit caffeine use, or eliminate it in some correctional settings. They also called for further investigation of highly variable responses to caffeine.
The authors did not disclose a funding source. Dr. Davidson, Dr. Reynolds, and their coauthors reported that they had no relevant financial disclosures.
FROM THE ANNUAL MEETING OF THE AMERICAN ACADEMY OF PSYCHIATRY AND THE LAW
Major Finding: Caffeine-induced psychosis may lead to misdiagnosis, unnecessary treatment, or incarceration of susceptible individuals.
Data Source: Case series of patients in correctional and forensic settings.
Disclosures: The authors did not disclose a funding source. Dr. Davidson, Dr. Reynolds, and their coauthors reported that they had no relevant financial disclosures.
Topiramate Plus Quetiapine Cut Cannabis Use in Bipolar Teens
TORONTO – Topiramate in combination with quetiapine was well tolerated in adolescents who had bipolar disorder and reported frequent cannabis use, based on a 75-patient study presented at the annual meeting of the American Academy of Child and Adolescent Psychiatry.
Concurrent substance use is a barrier to treating adolescents with bipolar disorder, said Dr. Melissa DelBello of the University of Cincinnati. Topiramate is approved by the Food and Drug Administration as an antiepileptic drug for children as young as age 2 years. Topiramate has been shown to reduce drug cravings, but is not approved for that indication, she added.

©ron hilton/iStockphoto.com
|
The researchers recruited adolescents, aged 12-21 years, who met criteria for bipolar disorder, had a Young Mania Rating Scale (YMRS) score of at least 20, and were using cannabis an average of at least twice a week for the 28 days before entering the study. In a previous study, Dr. DelBello and her colleagues found that topiramate was effective for reducing mania symptoms in adolescents (J. Am. Acad. Child Adolesc. Psychiatry 2005; 44:539-47).
The 75 teens were randomized to a maximum of 800 mg of quetiapine and placebo or to quetiapine and a minimum dose of 75 mg of topiramate twice daily that was increased gradually to 150 mg twice daily by day 21 of treatment.
At baseline, the average number of joints smoked per week was 14 in the quetiapine and placebo group and 11 in the quetiapine and topiramate group.
After 16 weeks of treatment, the average weekly use dropped to four joints in the quetiapine and placebo group and to 0.4 joints in the quetiapine and topiramate group. The difference was statistically significant.
On average, teens in the quetiapine and topiramate group used cannabis 1 day per week, and teens in the quetiapine and placebo group used cannabis 2 days per week, Dr. DelBello said.
Over the 16-week study, scores on the YMRS improved significantly from baseline, with an average drop of –14 with quetiapine and topiramate and –16 with quetiapine and placebo. Scores on the Childhood Rating Depression Scale-Revised (CRDS-R) also improved significantly from baseline to 16 weeks in both groups.
The presence of conduct disorder and ADHD were significant predictors of reduction in cannabis use while taking topiramate, said Dr. DelBello. Teens given topiramate showed significant improvement in general scores on the Marijuana Craving Questionnaire, compared with teens given placebo.
The groups did not differ in laboratory measures or vital signs, but excitement and pallor occurred in 26% of the topiramate group and in 16% of the placebo group.
Eleven serious events occurred during the study; five occurred in the topiramate group (two cases of suicidal ideation with intent and three cases of mania) and six occurred in the placebo group (four cases of mania, one suicide attempt, and one pregnancy).
The study was limited by a lack of data on cognition, Dr. DelBello noted. The neurobiological effects of topiramate and its effects when combined with other medications and used in different mood states need further study.
Dr. DelBello has received research support and/or served as a consultant, advisory board member, or speakers’ bureau member for multiple companies including Schering-Plough, Merck, Bristol-Myers Squibb Somerset, Lilly, and Pfizer.
TORONTO – Topiramate in combination with quetiapine was well tolerated in adolescents who had bipolar disorder and reported frequent cannabis use, based on a 75-patient study presented at the annual meeting of the American Academy of Child and Adolescent Psychiatry.
Concurrent substance use is a barrier to treating adolescents with bipolar disorder, said Dr. Melissa DelBello of the University of Cincinnati. Topiramate is approved by the Food and Drug Administration as an antiepileptic drug for children as young as age 2 years. Topiramate has been shown to reduce drug cravings, but is not approved for that indication, she added.
©ron hilton/iStockphoto.com
|
The researchers recruited adolescents, aged 12-21 years, who met criteria for bipolar disorder, had a Young Mania Rating Scale (YMRS) score of at least 20, and were using cannabis an average of at least twice a week for the 28 days before entering the study. In a previous study, Dr. DelBello and her colleagues found that topiramate was effective for reducing mania symptoms in adolescents (J. Am. Acad. Child Adolesc. Psychiatry 2005; 44:539-47).
The 75 teens were randomized to a maximum of 800 mg of quetiapine and placebo or to quetiapine and a minimum dose of 75 mg of topiramate twice daily that was increased gradually to 150 mg twice daily by day 21 of treatment.
At baseline, the average number of joints smoked per week was 14 in the quetiapine and placebo group and 11 in the quetiapine and topiramate group.
After 16 weeks of treatment, the average weekly use dropped to four joints in the quetiapine and placebo group and to 0.4 joints in the quetiapine and topiramate group. The difference was statistically significant.
On average, teens in the quetiapine and topiramate group used cannabis 1 day per week, and teens in the quetiapine and placebo group used cannabis 2 days per week, Dr. DelBello said.
Over the 16-week study, scores on the YMRS improved significantly from baseline, with an average drop of –14 with quetiapine and topiramate and –16 with quetiapine and placebo. Scores on the Childhood Rating Depression Scale-Revised (CRDS-R) also improved significantly from baseline to 16 weeks in both groups.
The presence of conduct disorder and ADHD were significant predictors of reduction in cannabis use while taking topiramate, said Dr. DelBello. Teens given topiramate showed significant improvement in general scores on the Marijuana Craving Questionnaire, compared with teens given placebo.
The groups did not differ in laboratory measures or vital signs, but excitement and pallor occurred in 26% of the topiramate group and in 16% of the placebo group.
Eleven serious events occurred during the study; five occurred in the topiramate group (two cases of suicidal ideation with intent and three cases of mania) and six occurred in the placebo group (four cases of mania, one suicide attempt, and one pregnancy).
The study was limited by a lack of data on cognition, Dr. DelBello noted. The neurobiological effects of topiramate and its effects when combined with other medications and used in different mood states need further study.
Dr. DelBello has received research support and/or served as a consultant, advisory board member, or speakers’ bureau member for multiple companies including Schering-Plough, Merck, Bristol-Myers Squibb Somerset, Lilly, and Pfizer.
TORONTO – Topiramate in combination with quetiapine was well tolerated in adolescents who had bipolar disorder and reported frequent cannabis use, based on a 75-patient study presented at the annual meeting of the American Academy of Child and Adolescent Psychiatry.
Concurrent substance use is a barrier to treating adolescents with bipolar disorder, said Dr. Melissa DelBello of the University of Cincinnati. Topiramate is approved by the Food and Drug Administration as an antiepileptic drug for children as young as age 2 years. Topiramate has been shown to reduce drug cravings, but is not approved for that indication, she added.
©ron hilton/iStockphoto.com
|
The researchers recruited adolescents, aged 12-21 years, who met criteria for bipolar disorder, had a Young Mania Rating Scale (YMRS) score of at least 20, and were using cannabis an average of at least twice a week for the 28 days before entering the study. In a previous study, Dr. DelBello and her colleagues found that topiramate was effective for reducing mania symptoms in adolescents (J. Am. Acad. Child Adolesc. Psychiatry 2005; 44:539-47).
The 75 teens were randomized to a maximum of 800 mg of quetiapine and placebo or to quetiapine and a minimum dose of 75 mg of topiramate twice daily that was increased gradually to 150 mg twice daily by day 21 of treatment.
At baseline, the average number of joints smoked per week was 14 in the quetiapine and placebo group and 11 in the quetiapine and topiramate group.
After 16 weeks of treatment, the average weekly use dropped to four joints in the quetiapine and placebo group and to 0.4 joints in the quetiapine and topiramate group. The difference was statistically significant.
On average, teens in the quetiapine and topiramate group used cannabis 1 day per week, and teens in the quetiapine and placebo group used cannabis 2 days per week, Dr. DelBello said.
Over the 16-week study, scores on the YMRS improved significantly from baseline, with an average drop of –14 with quetiapine and topiramate and –16 with quetiapine and placebo. Scores on the Childhood Rating Depression Scale-Revised (CRDS-R) also improved significantly from baseline to 16 weeks in both groups.
The presence of conduct disorder and ADHD were significant predictors of reduction in cannabis use while taking topiramate, said Dr. DelBello. Teens given topiramate showed significant improvement in general scores on the Marijuana Craving Questionnaire, compared with teens given placebo.
The groups did not differ in laboratory measures or vital signs, but excitement and pallor occurred in 26% of the topiramate group and in 16% of the placebo group.
Eleven serious events occurred during the study; five occurred in the topiramate group (two cases of suicidal ideation with intent and three cases of mania) and six occurred in the placebo group (four cases of mania, one suicide attempt, and one pregnancy).
The study was limited by a lack of data on cognition, Dr. DelBello noted. The neurobiological effects of topiramate and its effects when combined with other medications and used in different mood states need further study.
Dr. DelBello has received research support and/or served as a consultant, advisory board member, or speakers’ bureau member for multiple companies including Schering-Plough, Merck, Bristol-Myers Squibb Somerset, Lilly, and Pfizer.
FROM THE ANNUAL MEETING OF THE AMERICAN ACADEMY OF CHILD AND ADOLESCENT PSYCHIATRY
Major Finding: After 16 weeks of treatment, the average weekly use of cannabis dropped from 14 to 4 joints in the quetiapine and placebo group and from 11 to 0.4 joints in the quetiapine and topiramate group.
Data Source: 75 patients, aged 12 to 21 years, who met criteria for bipolar disorder, had a Young Mania Rating Scale (YMRS) score of at least 20, and were using cannabis an average of at least twice a week during the 28 days before entering the study.
Disclosures: Dr. DelBello has received research support and/or served as a consultant, advisory board member, or speakers’ bureau member for multiple companies including Schering-Plough, Merck, Bristol-Myers Squibb Somerset, Lilly, and Pfizer.
Valproate-induced hair loss: What to tell patients
Ms. B, age 29, has bipolar disorder that is stabilized by valproate, 1,250 mg/d. After 1 month of treatment, she shows scalp hair loss. She takes no other medications and is distressed because she had never experienced such copious hair loss. Ms. B’s blood valproate level is at a therapeutic level. She wants to know if the hair loss will be permanent and what she can do to stop it.
Up to 28% of patients who take valproate suffer temporary alopecia.1,2 In most cases, hair loss is associated with long-term valproate pharmacotherapy. Hair loss appears to be dose-related2 and may be more common in women than in men. Usually patients will report gradual but steady hair loss, commonly beginning 2 to 6 months after initiating treatment.3 Complete hair loss is rare and new hair growth typically begins approximately 2 to 3 months after alopecia onset.
Valproate can cause telogen effluvium, a non-scarring form of alopecia that occurs by precipitating the follicles into a premature rest phase. Other medications that may cause this type of hair loss include desipramine, imipramine, selective serotonin reuptake inhibitors, dopaminergics, anticoagulants, beta blockers, angiotensin-converting enzyme inhibitors, and cimetidine, as well as withdrawal from minoxidil, oral contraceptives, sulfasalazine, and antithyroid medicines.3
Advising patients
In addition to reducing a patient’s valproate dosage when clinically feasible, you can suggest pharmacologic and lifestyle changes to help patients minimize hair loss:
1. Recommend a biotin supplement. Valproate can cause biotin deficiency and may lead to low serum and liver tissue biotinidase enzyme4; a major clinical manifestation of biotin deficiency is alopecia.
2. Tell patients to avoid taking valproate during meals to prevent its chelating effect on food. The chelating effect of valproate makes metals that facilitate hair growth, such as zinc and selenium, unavailable for absorption.5
3. Recommend zinc and selenium supplements, which can help stop further hair loss and regenerate hair.5
4. Suggest practical advice for hair care, including using soft brushes and mild shampoos and avoiding dyes, heated curlers, and hair dryers.
5. Consider minoxidil therapy. However, this is an expensive option and there are no cases documenting its use for alopecia caused by mood stabilizers.
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Castro-Gago M, Gómez-Lado C, Eirís-Puñal J, et al. Serum biotinidase activity in children treated with valproic acid and carbamazepine. J Child Neurol. 2010;25(1):32-35.
2. Patrizi A, Savoia F, Negosanti F, et al. Telogen effluvium caused by magnesium valproate and lamotrigine. Acta Derm Venereol. 2005;85(1):77-78.
3. Mercke Y, Sheng H, Khan T, et al. Hair loss in psychopharmacology. Ann Clin Psychiatry. 2000;12(1):35-42.
4. Yilmaz Y, Tasdemir HA, Paksu MS. The influence of valproic acid treatment on hair and serum zinc levels and serum biotinidase activity. Eur J Paediatr Neurol. 2009;13(5):439-443.
4. Fatemi SH, Calabrese JR. Treatment of valproate-induced alopecia. Ann Pharmacother. 1995;29(12):1302.-
Ms. B, age 29, has bipolar disorder that is stabilized by valproate, 1,250 mg/d. After 1 month of treatment, she shows scalp hair loss. She takes no other medications and is distressed because she had never experienced such copious hair loss. Ms. B’s blood valproate level is at a therapeutic level. She wants to know if the hair loss will be permanent and what she can do to stop it.
Up to 28% of patients who take valproate suffer temporary alopecia.1,2 In most cases, hair loss is associated with long-term valproate pharmacotherapy. Hair loss appears to be dose-related2 and may be more common in women than in men. Usually patients will report gradual but steady hair loss, commonly beginning 2 to 6 months after initiating treatment.3 Complete hair loss is rare and new hair growth typically begins approximately 2 to 3 months after alopecia onset.
Valproate can cause telogen effluvium, a non-scarring form of alopecia that occurs by precipitating the follicles into a premature rest phase. Other medications that may cause this type of hair loss include desipramine, imipramine, selective serotonin reuptake inhibitors, dopaminergics, anticoagulants, beta blockers, angiotensin-converting enzyme inhibitors, and cimetidine, as well as withdrawal from minoxidil, oral contraceptives, sulfasalazine, and antithyroid medicines.3
Advising patients
In addition to reducing a patient’s valproate dosage when clinically feasible, you can suggest pharmacologic and lifestyle changes to help patients minimize hair loss:
1. Recommend a biotin supplement. Valproate can cause biotin deficiency and may lead to low serum and liver tissue biotinidase enzyme4; a major clinical manifestation of biotin deficiency is alopecia.
2. Tell patients to avoid taking valproate during meals to prevent its chelating effect on food. The chelating effect of valproate makes metals that facilitate hair growth, such as zinc and selenium, unavailable for absorption.5
3. Recommend zinc and selenium supplements, which can help stop further hair loss and regenerate hair.5
4. Suggest practical advice for hair care, including using soft brushes and mild shampoos and avoiding dyes, heated curlers, and hair dryers.
5. Consider minoxidil therapy. However, this is an expensive option and there are no cases documenting its use for alopecia caused by mood stabilizers.
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Ms. B, age 29, has bipolar disorder that is stabilized by valproate, 1,250 mg/d. After 1 month of treatment, she shows scalp hair loss. She takes no other medications and is distressed because she had never experienced such copious hair loss. Ms. B’s blood valproate level is at a therapeutic level. She wants to know if the hair loss will be permanent and what she can do to stop it.
Up to 28% of patients who take valproate suffer temporary alopecia.1,2 In most cases, hair loss is associated with long-term valproate pharmacotherapy. Hair loss appears to be dose-related2 and may be more common in women than in men. Usually patients will report gradual but steady hair loss, commonly beginning 2 to 6 months after initiating treatment.3 Complete hair loss is rare and new hair growth typically begins approximately 2 to 3 months after alopecia onset.
Valproate can cause telogen effluvium, a non-scarring form of alopecia that occurs by precipitating the follicles into a premature rest phase. Other medications that may cause this type of hair loss include desipramine, imipramine, selective serotonin reuptake inhibitors, dopaminergics, anticoagulants, beta blockers, angiotensin-converting enzyme inhibitors, and cimetidine, as well as withdrawal from minoxidil, oral contraceptives, sulfasalazine, and antithyroid medicines.3
Advising patients
In addition to reducing a patient’s valproate dosage when clinically feasible, you can suggest pharmacologic and lifestyle changes to help patients minimize hair loss:
1. Recommend a biotin supplement. Valproate can cause biotin deficiency and may lead to low serum and liver tissue biotinidase enzyme4; a major clinical manifestation of biotin deficiency is alopecia.
2. Tell patients to avoid taking valproate during meals to prevent its chelating effect on food. The chelating effect of valproate makes metals that facilitate hair growth, such as zinc and selenium, unavailable for absorption.5
3. Recommend zinc and selenium supplements, which can help stop further hair loss and regenerate hair.5
4. Suggest practical advice for hair care, including using soft brushes and mild shampoos and avoiding dyes, heated curlers, and hair dryers.
5. Consider minoxidil therapy. However, this is an expensive option and there are no cases documenting its use for alopecia caused by mood stabilizers.
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Castro-Gago M, Gómez-Lado C, Eirís-Puñal J, et al. Serum biotinidase activity in children treated with valproic acid and carbamazepine. J Child Neurol. 2010;25(1):32-35.
2. Patrizi A, Savoia F, Negosanti F, et al. Telogen effluvium caused by magnesium valproate and lamotrigine. Acta Derm Venereol. 2005;85(1):77-78.
3. Mercke Y, Sheng H, Khan T, et al. Hair loss in psychopharmacology. Ann Clin Psychiatry. 2000;12(1):35-42.
4. Yilmaz Y, Tasdemir HA, Paksu MS. The influence of valproic acid treatment on hair and serum zinc levels and serum biotinidase activity. Eur J Paediatr Neurol. 2009;13(5):439-443.
4. Fatemi SH, Calabrese JR. Treatment of valproate-induced alopecia. Ann Pharmacother. 1995;29(12):1302.-
1. Castro-Gago M, Gómez-Lado C, Eirís-Puñal J, et al. Serum biotinidase activity in children treated with valproic acid and carbamazepine. J Child Neurol. 2010;25(1):32-35.
2. Patrizi A, Savoia F, Negosanti F, et al. Telogen effluvium caused by magnesium valproate and lamotrigine. Acta Derm Venereol. 2005;85(1):77-78.
3. Mercke Y, Sheng H, Khan T, et al. Hair loss in psychopharmacology. Ann Clin Psychiatry. 2000;12(1):35-42.
4. Yilmaz Y, Tasdemir HA, Paksu MS. The influence of valproic acid treatment on hair and serum zinc levels and serum biotinidase activity. Eur J Paediatr Neurol. 2009;13(5):439-443.
4. Fatemi SH, Calabrese JR. Treatment of valproate-induced alopecia. Ann Pharmacother. 1995;29(12):1302.-
Treating Bipolar Depression Depends on Evidence, Judgment
PARIS – Existing evidence on the best ways to treat bipolar depression is limited, and must balance against what works in the real world based on empirical experience. When treating bipolar depression "we are in the land of the uncertain, where [psychiatrists] must improvise and do their best with what’s available," Dr. Andrew A. Nierenberg said at the annual congress of the European College of Neuropsychopharmacology.
The trials that get drugs approved by the Food and Drug Administration often do not inform routine care. Patients in trials often differ from "real" patients, generally have milder disease, and are less susceptible to the worst outcomes. The published evidence base for treating bipolar depression should not be viewed as synonymous with best practice. Treatment is not a cookbook, and evidence-based medicine is very difficult to actually implement, said Dr. Nierenberg, medical director of the bipolar clinic and research program at Massachusetts General Hospital, and professor of psychiatry at Harvard Medical School, both in Boston.

Treatment of patients with bipolar disorder in actual practice requires personalization, including prescribing agents that work and expecting patients to continue to take them despite possible adverse effects. Published evidence leaves it unclear how best to treat any specific patient, he said. That requires not only evidence but also clinical experience and knowledge of the results obtained by others, followed by feedback and outcomes assessment to guide future changes in treatment.
Perhaps the biggest question in the treatment of bipolar depression today is whether antidepressants work. A 2004 meta-analysis said they did (Am. J. Psychiatry 2004;161:1537-47), but this was "a terrible" meta-analysis because the overall numbers of patients were small, and the results from a single study heavily influenced the overall meta-analysis results, Dr. Nierenberg said. In addition, results from the STEP-BD (Systematic Treatment Enhancement Program for Bipolar Disorder) trial showed that adding an antidepressant to the mood stabilizer lithium gave no significant added benefit (N. Engl. J. Med. 2007;356:1711-22).
Taken together, the literature provides insufficient evidence to document a beneficial role for antidepressants in the treatment of bipolar depression, along with some evidence against any efficacy, yet Dr. Nierenberg said he prescribes an antidepressant as monotherapy or as an add-on treatment to many patients, as do many other psychiatrists. Psychiatrists generally feel that the data against adding an antidepressant are unconvincing, because they have seen antidepressants work on many prior patients. "The data are inconsistent with their clinical experience," he noted.
The roles of several other drugs or drug combinations also feature conflicts between the evidence base and their use in everyday practice.
The combination of olanzapine and fluoxetine showed efficacy in a highly influential 2003 study (Arch. Gen. Psychiatry 2003;60:1079-88). But the olanzapine and fluoxetine pairing is seldom used today because of concerns that it causes weight gain and tends to trigger metabolic syndrome. It’s ironic that olanzapine and fluoxetine is an FDA-approved combination that few patients actually receive, he said. Patients don’t like to gain weight, and when they do, they often stop taking the drugs.
Lamotrigine showed efficacy for treating bipolar depression in a 1999 study (J. Clin. Psychiatry 1999;60:79-88), but failed to show substantial efficacy in five other studies. In addition, lamotrigine failed to receive FDA approval for treating acute depression. Despite that, U.S. physicians appear to have embraced lamotrigine for treating depression in patients with bipolar disorder, "a discrepancy between what the literature says and what people actually do," Dr. Nierenberg noted. Results from a 2009 study showed that adding lamotrigine to lithium led to an improved decrease in depression, compared with lithium plus placebo (J. Clin. Psychiatry 2009;70:223-31), but physicians also prescribe lamotrigine monotherapy, even though published findings do not support that approach.
Perhaps the drug with the best clinical performance on paper is quetiapine, which has produced the largest effect size seen in depression (Am. J. Psychiatry 2005;162:1351-60), both monopolar and bipolar, and has had efficacy for mania, anxiety, insomnia, and psychosis. Based on this evidence, Dr. Nierenberg said that he would expect the extensive prescribing of quetiapine, but in reality, few patients receive it. Again, it’s a drug with significant side effects, including sedation and weight gain.
Other approaches to treating bipolar depression that are often used as first-line therapy, despite a poor evidence base, include optimization of a regimen of lithium, valproate, or carbamazepine that the patient might already take. Psychotherapy also can help, but less so once a patient has had 10-20 depressive or manic episodes. And electroconvulsive therapy is an important option for treatment-refractory bipolar depression. But the right treatment in many other clinical situations might involve unclear options, such as how to handle patients who are already on antimania treatment, and how to continue an antidepressant that produced partial improvement. Common complications of bipolar depression that can influence treatment decisions include attention-deficit/hyperactivity disorder, substance abuse, a chaotic life, and poor drug compliance. These and other factors make it impossible to rely just on evidence when choosing a patient’s treatment, Dr. Nierenberg said.
Dr. Nierenberg said he has a patent pending on combined treatment of mood disorders with buspirone, bupropion, and melatonin, and he co-owns a copyright on a structured clinical interview for the Montgomery-Åsberg Depression Rating Scale. He said he has received honoraria from Eli Lilly, AstraZeneca, Forest, and Janssen, and that he has received research grants from Pam Labs, Pfizer, and Shire.
PARIS – Existing evidence on the best ways to treat bipolar depression is limited, and must balance against what works in the real world based on empirical experience. When treating bipolar depression "we are in the land of the uncertain, where [psychiatrists] must improvise and do their best with what’s available," Dr. Andrew A. Nierenberg said at the annual congress of the European College of Neuropsychopharmacology.
The trials that get drugs approved by the Food and Drug Administration often do not inform routine care. Patients in trials often differ from "real" patients, generally have milder disease, and are less susceptible to the worst outcomes. The published evidence base for treating bipolar depression should not be viewed as synonymous with best practice. Treatment is not a cookbook, and evidence-based medicine is very difficult to actually implement, said Dr. Nierenberg, medical director of the bipolar clinic and research program at Massachusetts General Hospital, and professor of psychiatry at Harvard Medical School, both in Boston.
Treatment of patients with bipolar disorder in actual practice requires personalization, including prescribing agents that work and expecting patients to continue to take them despite possible adverse effects. Published evidence leaves it unclear how best to treat any specific patient, he said. That requires not only evidence but also clinical experience and knowledge of the results obtained by others, followed by feedback and outcomes assessment to guide future changes in treatment.
Perhaps the biggest question in the treatment of bipolar depression today is whether antidepressants work. A 2004 meta-analysis said they did (Am. J. Psychiatry 2004;161:1537-47), but this was "a terrible" meta-analysis because the overall numbers of patients were small, and the results from a single study heavily influenced the overall meta-analysis results, Dr. Nierenberg said. In addition, results from the STEP-BD (Systematic Treatment Enhancement Program for Bipolar Disorder) trial showed that adding an antidepressant to the mood stabilizer lithium gave no significant added benefit (N. Engl. J. Med. 2007;356:1711-22).
Taken together, the literature provides insufficient evidence to document a beneficial role for antidepressants in the treatment of bipolar depression, along with some evidence against any efficacy, yet Dr. Nierenberg said he prescribes an antidepressant as monotherapy or as an add-on treatment to many patients, as do many other psychiatrists. Psychiatrists generally feel that the data against adding an antidepressant are unconvincing, because they have seen antidepressants work on many prior patients. "The data are inconsistent with their clinical experience," he noted.
The roles of several other drugs or drug combinations also feature conflicts between the evidence base and their use in everyday practice.
The combination of olanzapine and fluoxetine showed efficacy in a highly influential 2003 study (Arch. Gen. Psychiatry 2003;60:1079-88). But the olanzapine and fluoxetine pairing is seldom used today because of concerns that it causes weight gain and tends to trigger metabolic syndrome. It’s ironic that olanzapine and fluoxetine is an FDA-approved combination that few patients actually receive, he said. Patients don’t like to gain weight, and when they do, they often stop taking the drugs.
Lamotrigine showed efficacy for treating bipolar depression in a 1999 study (J. Clin. Psychiatry 1999;60:79-88), but failed to show substantial efficacy in five other studies. In addition, lamotrigine failed to receive FDA approval for treating acute depression. Despite that, U.S. physicians appear to have embraced lamotrigine for treating depression in patients with bipolar disorder, "a discrepancy between what the literature says and what people actually do," Dr. Nierenberg noted. Results from a 2009 study showed that adding lamotrigine to lithium led to an improved decrease in depression, compared with lithium plus placebo (J. Clin. Psychiatry 2009;70:223-31), but physicians also prescribe lamotrigine monotherapy, even though published findings do not support that approach.
Perhaps the drug with the best clinical performance on paper is quetiapine, which has produced the largest effect size seen in depression (Am. J. Psychiatry 2005;162:1351-60), both monopolar and bipolar, and has had efficacy for mania, anxiety, insomnia, and psychosis. Based on this evidence, Dr. Nierenberg said that he would expect the extensive prescribing of quetiapine, but in reality, few patients receive it. Again, it’s a drug with significant side effects, including sedation and weight gain.
Other approaches to treating bipolar depression that are often used as first-line therapy, despite a poor evidence base, include optimization of a regimen of lithium, valproate, or carbamazepine that the patient might already take. Psychotherapy also can help, but less so once a patient has had 10-20 depressive or manic episodes. And electroconvulsive therapy is an important option for treatment-refractory bipolar depression. But the right treatment in many other clinical situations might involve unclear options, such as how to handle patients who are already on antimania treatment, and how to continue an antidepressant that produced partial improvement. Common complications of bipolar depression that can influence treatment decisions include attention-deficit/hyperactivity disorder, substance abuse, a chaotic life, and poor drug compliance. These and other factors make it impossible to rely just on evidence when choosing a patient’s treatment, Dr. Nierenberg said.
Dr. Nierenberg said he has a patent pending on combined treatment of mood disorders with buspirone, bupropion, and melatonin, and he co-owns a copyright on a structured clinical interview for the Montgomery-Åsberg Depression Rating Scale. He said he has received honoraria from Eli Lilly, AstraZeneca, Forest, and Janssen, and that he has received research grants from Pam Labs, Pfizer, and Shire.
PARIS – Existing evidence on the best ways to treat bipolar depression is limited, and must balance against what works in the real world based on empirical experience. When treating bipolar depression "we are in the land of the uncertain, where [psychiatrists] must improvise and do their best with what’s available," Dr. Andrew A. Nierenberg said at the annual congress of the European College of Neuropsychopharmacology.
The trials that get drugs approved by the Food and Drug Administration often do not inform routine care. Patients in trials often differ from "real" patients, generally have milder disease, and are less susceptible to the worst outcomes. The published evidence base for treating bipolar depression should not be viewed as synonymous with best practice. Treatment is not a cookbook, and evidence-based medicine is very difficult to actually implement, said Dr. Nierenberg, medical director of the bipolar clinic and research program at Massachusetts General Hospital, and professor of psychiatry at Harvard Medical School, both in Boston.
Treatment of patients with bipolar disorder in actual practice requires personalization, including prescribing agents that work and expecting patients to continue to take them despite possible adverse effects. Published evidence leaves it unclear how best to treat any specific patient, he said. That requires not only evidence but also clinical experience and knowledge of the results obtained by others, followed by feedback and outcomes assessment to guide future changes in treatment.
Perhaps the biggest question in the treatment of bipolar depression today is whether antidepressants work. A 2004 meta-analysis said they did (Am. J. Psychiatry 2004;161:1537-47), but this was "a terrible" meta-analysis because the overall numbers of patients were small, and the results from a single study heavily influenced the overall meta-analysis results, Dr. Nierenberg said. In addition, results from the STEP-BD (Systematic Treatment Enhancement Program for Bipolar Disorder) trial showed that adding an antidepressant to the mood stabilizer lithium gave no significant added benefit (N. Engl. J. Med. 2007;356:1711-22).
Taken together, the literature provides insufficient evidence to document a beneficial role for antidepressants in the treatment of bipolar depression, along with some evidence against any efficacy, yet Dr. Nierenberg said he prescribes an antidepressant as monotherapy or as an add-on treatment to many patients, as do many other psychiatrists. Psychiatrists generally feel that the data against adding an antidepressant are unconvincing, because they have seen antidepressants work on many prior patients. "The data are inconsistent with their clinical experience," he noted.
The roles of several other drugs or drug combinations also feature conflicts between the evidence base and their use in everyday practice.
The combination of olanzapine and fluoxetine showed efficacy in a highly influential 2003 study (Arch. Gen. Psychiatry 2003;60:1079-88). But the olanzapine and fluoxetine pairing is seldom used today because of concerns that it causes weight gain and tends to trigger metabolic syndrome. It’s ironic that olanzapine and fluoxetine is an FDA-approved combination that few patients actually receive, he said. Patients don’t like to gain weight, and when they do, they often stop taking the drugs.
Lamotrigine showed efficacy for treating bipolar depression in a 1999 study (J. Clin. Psychiatry 1999;60:79-88), but failed to show substantial efficacy in five other studies. In addition, lamotrigine failed to receive FDA approval for treating acute depression. Despite that, U.S. physicians appear to have embraced lamotrigine for treating depression in patients with bipolar disorder, "a discrepancy between what the literature says and what people actually do," Dr. Nierenberg noted. Results from a 2009 study showed that adding lamotrigine to lithium led to an improved decrease in depression, compared with lithium plus placebo (J. Clin. Psychiatry 2009;70:223-31), but physicians also prescribe lamotrigine monotherapy, even though published findings do not support that approach.
Perhaps the drug with the best clinical performance on paper is quetiapine, which has produced the largest effect size seen in depression (Am. J. Psychiatry 2005;162:1351-60), both monopolar and bipolar, and has had efficacy for mania, anxiety, insomnia, and psychosis. Based on this evidence, Dr. Nierenberg said that he would expect the extensive prescribing of quetiapine, but in reality, few patients receive it. Again, it’s a drug with significant side effects, including sedation and weight gain.
Other approaches to treating bipolar depression that are often used as first-line therapy, despite a poor evidence base, include optimization of a regimen of lithium, valproate, or carbamazepine that the patient might already take. Psychotherapy also can help, but less so once a patient has had 10-20 depressive or manic episodes. And electroconvulsive therapy is an important option for treatment-refractory bipolar depression. But the right treatment in many other clinical situations might involve unclear options, such as how to handle patients who are already on antimania treatment, and how to continue an antidepressant that produced partial improvement. Common complications of bipolar depression that can influence treatment decisions include attention-deficit/hyperactivity disorder, substance abuse, a chaotic life, and poor drug compliance. These and other factors make it impossible to rely just on evidence when choosing a patient’s treatment, Dr. Nierenberg said.
Dr. Nierenberg said he has a patent pending on combined treatment of mood disorders with buspirone, bupropion, and melatonin, and he co-owns a copyright on a structured clinical interview for the Montgomery-Åsberg Depression Rating Scale. He said he has received honoraria from Eli Lilly, AstraZeneca, Forest, and Janssen, and that he has received research grants from Pam Labs, Pfizer, and Shire.
EXPERT ANALYSIS FROM THE ANNUAL CONGRESS OF THE EUROPEAN COLLEGE OF NEURO-
PSYCHOPHARMACOLOGY