User login
Omega-3 supplements may impact breast cancer risk
The study was presented by Katherine Cook, PhD, during a poster session at the San Antonio Breast Cancer Symposium. Dr. Cook is a researcher at Wake Forest University, Winston-Salem, N.C.
Obesity increases risk of breast cancer, but it also alters the composition of the gut microbiome. Obesity is associated with a greater frequency of Firmicute bacteria phyla, compared with Bacteroidetes phyla, while abnormally low ratios are associated with inflammatory bowel disease.
In mice, the researchers previously showed that diet can lead to changes in the microbiome of both the gut and the breast. They conducted fecal transplants between mice who were fed normal or high-fat diets (HFD), and then used a chemical carcinogenesis model to investigate the impact on tumor outcomes. They observed changes in the microbiota populations in both the gut and the mammary glands when mice fed a normal diet received fecal transplants from HFD mice. On the other hand, when HFD mice received fecal transplants from mice with normal diets, the transplants countered the increase in serum lipopolysaccharide levels associated with HFD. In vitro models showed that microbiota from HFD mice also altered the epithelial permeability of breast tissue, and infection of breast cancer cells with HFD microbiota led to greater proliferation.
The researchers also examined breast cancer tissue from women who received omega-3 PUFA supplements or placebo before undergoing primary tumor resection, and found that there were differences in the proportional abundance of specific microbes between tumor and adjacent normal tissue, with the former having excess of Lachnospiraceae and Ruminococcus. The finding suggests that these bacteria may grow better in a tumor microenvironment, and could play a role in breast cancer cell signaling. The supplements altered the microbiota of both normal and breast cancer tissue.
In the study presented at SABCS, the researchers analyzed fecal samples from 34 obese and overweight postmenopausal women involved in a weight-loss trial, who received 3.25 g/day of omega-3 PUFA supplements or placebo combined with calorie restriction and exercise. They performed metagenomic sequencing from the fecal samples at baseline and 6 months to determine microbiome populations.
Women who experienced weight loss, with or without omega-3 PUFA supplementation, had a decline in the abundance of Firmicutes phyla – a group linked to inflammation risk – as a percentage of overall bacterial phyla. The researchers found a similar trend among women who received omega-3 PUFA, regardless of how much weight they lost. At the species level, those who received supplements had higher proportional abundance of Phocaeicola massiliensis and reduced proportions of Faecalibacterium prausnitzii, R. lactaris, Blautia obeum, and Dorea formicigenerans (P < .05).
Weight loss combined with supplementation also seemed to affect gut microbiota, with subjects who lost more than 10% of their body weight and received omega-3 PUFA supplements having elevated Bacteriodetes and reduced Firmicutes, compared with all other groups (P < .05).
At 6 months, the researchers grouped women by mean body fat composition, and found both positive and negative correlations among different bacterial species. Finally, the researchers looked at serum levels of the inflammatory cytokines interleukin-6, monocyte chemoattractant protein-1 (MCP-1), and tumor necrosis factor–alpha at 6 months. Women with elevated levels of at least two cytokines had higher levels of two species of mucin-degrading bacteria. Levels of MCP-1 alone also correlated with greater proportions of mucin-degrading bacteria (P < .05).
The authors concluded that increasing omega-3 PUFA uptake to about 2% of total daily calorie intake could push the gut microbiome in a direction that improves intestinal permeability parameters and reduces chronic inflammation. These changes could lead to a reduction in the risk for postmenopausal breast cancer.
The study was funded by the Breast Cancer Research Foundation.
The study was presented by Katherine Cook, PhD, during a poster session at the San Antonio Breast Cancer Symposium. Dr. Cook is a researcher at Wake Forest University, Winston-Salem, N.C.
Obesity increases risk of breast cancer, but it also alters the composition of the gut microbiome. Obesity is associated with a greater frequency of Firmicute bacteria phyla, compared with Bacteroidetes phyla, while abnormally low ratios are associated with inflammatory bowel disease.
In mice, the researchers previously showed that diet can lead to changes in the microbiome of both the gut and the breast. They conducted fecal transplants between mice who were fed normal or high-fat diets (HFD), and then used a chemical carcinogenesis model to investigate the impact on tumor outcomes. They observed changes in the microbiota populations in both the gut and the mammary glands when mice fed a normal diet received fecal transplants from HFD mice. On the other hand, when HFD mice received fecal transplants from mice with normal diets, the transplants countered the increase in serum lipopolysaccharide levels associated with HFD. In vitro models showed that microbiota from HFD mice also altered the epithelial permeability of breast tissue, and infection of breast cancer cells with HFD microbiota led to greater proliferation.
The researchers also examined breast cancer tissue from women who received omega-3 PUFA supplements or placebo before undergoing primary tumor resection, and found that there were differences in the proportional abundance of specific microbes between tumor and adjacent normal tissue, with the former having excess of Lachnospiraceae and Ruminococcus. The finding suggests that these bacteria may grow better in a tumor microenvironment, and could play a role in breast cancer cell signaling. The supplements altered the microbiota of both normal and breast cancer tissue.
In the study presented at SABCS, the researchers analyzed fecal samples from 34 obese and overweight postmenopausal women involved in a weight-loss trial, who received 3.25 g/day of omega-3 PUFA supplements or placebo combined with calorie restriction and exercise. They performed metagenomic sequencing from the fecal samples at baseline and 6 months to determine microbiome populations.
Women who experienced weight loss, with or without omega-3 PUFA supplementation, had a decline in the abundance of Firmicutes phyla – a group linked to inflammation risk – as a percentage of overall bacterial phyla. The researchers found a similar trend among women who received omega-3 PUFA, regardless of how much weight they lost. At the species level, those who received supplements had higher proportional abundance of Phocaeicola massiliensis and reduced proportions of Faecalibacterium prausnitzii, R. lactaris, Blautia obeum, and Dorea formicigenerans (P < .05).
Weight loss combined with supplementation also seemed to affect gut microbiota, with subjects who lost more than 10% of their body weight and received omega-3 PUFA supplements having elevated Bacteriodetes and reduced Firmicutes, compared with all other groups (P < .05).
At 6 months, the researchers grouped women by mean body fat composition, and found both positive and negative correlations among different bacterial species. Finally, the researchers looked at serum levels of the inflammatory cytokines interleukin-6, monocyte chemoattractant protein-1 (MCP-1), and tumor necrosis factor–alpha at 6 months. Women with elevated levels of at least two cytokines had higher levels of two species of mucin-degrading bacteria. Levels of MCP-1 alone also correlated with greater proportions of mucin-degrading bacteria (P < .05).
The authors concluded that increasing omega-3 PUFA uptake to about 2% of total daily calorie intake could push the gut microbiome in a direction that improves intestinal permeability parameters and reduces chronic inflammation. These changes could lead to a reduction in the risk for postmenopausal breast cancer.
The study was funded by the Breast Cancer Research Foundation.
The study was presented by Katherine Cook, PhD, during a poster session at the San Antonio Breast Cancer Symposium. Dr. Cook is a researcher at Wake Forest University, Winston-Salem, N.C.
Obesity increases risk of breast cancer, but it also alters the composition of the gut microbiome. Obesity is associated with a greater frequency of Firmicute bacteria phyla, compared with Bacteroidetes phyla, while abnormally low ratios are associated with inflammatory bowel disease.
In mice, the researchers previously showed that diet can lead to changes in the microbiome of both the gut and the breast. They conducted fecal transplants between mice who were fed normal or high-fat diets (HFD), and then used a chemical carcinogenesis model to investigate the impact on tumor outcomes. They observed changes in the microbiota populations in both the gut and the mammary glands when mice fed a normal diet received fecal transplants from HFD mice. On the other hand, when HFD mice received fecal transplants from mice with normal diets, the transplants countered the increase in serum lipopolysaccharide levels associated with HFD. In vitro models showed that microbiota from HFD mice also altered the epithelial permeability of breast tissue, and infection of breast cancer cells with HFD microbiota led to greater proliferation.
The researchers also examined breast cancer tissue from women who received omega-3 PUFA supplements or placebo before undergoing primary tumor resection, and found that there were differences in the proportional abundance of specific microbes between tumor and adjacent normal tissue, with the former having excess of Lachnospiraceae and Ruminococcus. The finding suggests that these bacteria may grow better in a tumor microenvironment, and could play a role in breast cancer cell signaling. The supplements altered the microbiota of both normal and breast cancer tissue.
In the study presented at SABCS, the researchers analyzed fecal samples from 34 obese and overweight postmenopausal women involved in a weight-loss trial, who received 3.25 g/day of omega-3 PUFA supplements or placebo combined with calorie restriction and exercise. They performed metagenomic sequencing from the fecal samples at baseline and 6 months to determine microbiome populations.
Women who experienced weight loss, with or without omega-3 PUFA supplementation, had a decline in the abundance of Firmicutes phyla – a group linked to inflammation risk – as a percentage of overall bacterial phyla. The researchers found a similar trend among women who received omega-3 PUFA, regardless of how much weight they lost. At the species level, those who received supplements had higher proportional abundance of Phocaeicola massiliensis and reduced proportions of Faecalibacterium prausnitzii, R. lactaris, Blautia obeum, and Dorea formicigenerans (P < .05).
Weight loss combined with supplementation also seemed to affect gut microbiota, with subjects who lost more than 10% of their body weight and received omega-3 PUFA supplements having elevated Bacteriodetes and reduced Firmicutes, compared with all other groups (P < .05).
At 6 months, the researchers grouped women by mean body fat composition, and found both positive and negative correlations among different bacterial species. Finally, the researchers looked at serum levels of the inflammatory cytokines interleukin-6, monocyte chemoattractant protein-1 (MCP-1), and tumor necrosis factor–alpha at 6 months. Women with elevated levels of at least two cytokines had higher levels of two species of mucin-degrading bacteria. Levels of MCP-1 alone also correlated with greater proportions of mucin-degrading bacteria (P < .05).
The authors concluded that increasing omega-3 PUFA uptake to about 2% of total daily calorie intake could push the gut microbiome in a direction that improves intestinal permeability parameters and reduces chronic inflammation. These changes could lead to a reduction in the risk for postmenopausal breast cancer.
The study was funded by the Breast Cancer Research Foundation.
FROM SABCS 2021
Women struggle with benzodiazepine addiction post chemotherapy treatment
SAN ANTONIO – shows a new study.
While benzodiazepines and nonbenzodiazepine sedative-hypnotics are effective for these indications, misuse and increased health care utilization can ensue from their prolonged use, said Jacob C. Cogan, MD, a fellow in oncology/hematology at the Herbert Irving Comprehensive Cancer Center, Columbia University, New York. Dr. Cogan recently presented the results of the study at the San Antonio Breast Cancer Symposium.
The study included patients with breast cancer who received adjuvant chemotherapy between 2008 and 2017. Prescriptions for sedatives were divided into three periods: 365 days prior to chemotherapy to the start of chemotherapy (period one); start of chemotherapy to 90 days after the end of chemotherapy (period two); and 90-365 days after chemotherapy (period three). Patients who filled at least one benzodiazepine prescription in period two and patients who filled at least two benzodiazepine in period three were classified as new persistent benzodiazepine users. The same definitions were then used for nonbenzodiazepine sedative-hypnotics.
Among 17,532 benzodiazepine-naive patients (mean age, 57 years) and 21,863 nonbenzodiazepine sedative-hypnotic drug–naive patients (mean age, 56 years) who received adjuvant chemotherapy for breast cancer, lumpectomies were performed for a small majority (56.6% benzodiazepine naive, 55.1% nonbenzodiazepine sedative-hypnotics naive) versus mastectomy, and about half of patients received less than 4 months of chemotherapy (48.0% benzodiazepine naive, 48.6% nonbenzodiazepine sedative-hypnotics naive). Among benzodiazepine-naive patients, 4,447 (25.4%) filled at least one benzodiazepine prescription during chemotherapy, and 2,160 (9.9%) filled at least one nonbenzodiazepine sedative-hypnotic prescription during chemotherapy. The rate of new persistent benzodiazepine use after initial exposure during chemotherapy was 26.8% (n = 1,192). Similarly, 33.8% (n = 730) of nonbenzodiazepine sedative-hypnotics users became new persistent users. In addition, 115 patients became new persistent users of both types of sedative-hypnotics.
New persistent benzodiazepine use was associated with several characteristics: age 50-65 (odds ratio, 1.23; P = .01) and age greater than 65 (OR, 1.38, P = .005) relative to age less than 49; as well as Medicaid insurance, relative to commercial and Medicare insurance (OR, 1.68; P < .0001). Both new persistent benzodiazepine and nonbenzodiazepine sedative-hypnotics use was associated with chemotherapy duration of less than 4 months relative to 4 or more months of chemotherapy (OR, 1.17; P = .03 for benzodiazepines; OR, 1.58; P < .0001 for nonbenzodiazepine sedative-hypnotics).
It is not clear why shorter chemotherapy duration is associated with more new persistent use, Dr. Cogan said. “It may be that, paradoxically, a shorter duration of treatment could lead to more anxiety about recurrence. These patients may need closer monitoring of mental health symptoms and earlier referral for psychological services.”
Dr. Cogan said that providers should take steps to ensure that benzodiazepines and nonbenzodiazepine sedatives are used appropriately, which includes tapering dosages and, when appropriate, encouraging nonpharmacologic strategies.
There were no funding or other conflicts of interest associated with this study.
SAN ANTONIO – shows a new study.
While benzodiazepines and nonbenzodiazepine sedative-hypnotics are effective for these indications, misuse and increased health care utilization can ensue from their prolonged use, said Jacob C. Cogan, MD, a fellow in oncology/hematology at the Herbert Irving Comprehensive Cancer Center, Columbia University, New York. Dr. Cogan recently presented the results of the study at the San Antonio Breast Cancer Symposium.
The study included patients with breast cancer who received adjuvant chemotherapy between 2008 and 2017. Prescriptions for sedatives were divided into three periods: 365 days prior to chemotherapy to the start of chemotherapy (period one); start of chemotherapy to 90 days after the end of chemotherapy (period two); and 90-365 days after chemotherapy (period three). Patients who filled at least one benzodiazepine prescription in period two and patients who filled at least two benzodiazepine in period three were classified as new persistent benzodiazepine users. The same definitions were then used for nonbenzodiazepine sedative-hypnotics.
Among 17,532 benzodiazepine-naive patients (mean age, 57 years) and 21,863 nonbenzodiazepine sedative-hypnotic drug–naive patients (mean age, 56 years) who received adjuvant chemotherapy for breast cancer, lumpectomies were performed for a small majority (56.6% benzodiazepine naive, 55.1% nonbenzodiazepine sedative-hypnotics naive) versus mastectomy, and about half of patients received less than 4 months of chemotherapy (48.0% benzodiazepine naive, 48.6% nonbenzodiazepine sedative-hypnotics naive). Among benzodiazepine-naive patients, 4,447 (25.4%) filled at least one benzodiazepine prescription during chemotherapy, and 2,160 (9.9%) filled at least one nonbenzodiazepine sedative-hypnotic prescription during chemotherapy. The rate of new persistent benzodiazepine use after initial exposure during chemotherapy was 26.8% (n = 1,192). Similarly, 33.8% (n = 730) of nonbenzodiazepine sedative-hypnotics users became new persistent users. In addition, 115 patients became new persistent users of both types of sedative-hypnotics.
New persistent benzodiazepine use was associated with several characteristics: age 50-65 (odds ratio, 1.23; P = .01) and age greater than 65 (OR, 1.38, P = .005) relative to age less than 49; as well as Medicaid insurance, relative to commercial and Medicare insurance (OR, 1.68; P < .0001). Both new persistent benzodiazepine and nonbenzodiazepine sedative-hypnotics use was associated with chemotherapy duration of less than 4 months relative to 4 or more months of chemotherapy (OR, 1.17; P = .03 for benzodiazepines; OR, 1.58; P < .0001 for nonbenzodiazepine sedative-hypnotics).
It is not clear why shorter chemotherapy duration is associated with more new persistent use, Dr. Cogan said. “It may be that, paradoxically, a shorter duration of treatment could lead to more anxiety about recurrence. These patients may need closer monitoring of mental health symptoms and earlier referral for psychological services.”
Dr. Cogan said that providers should take steps to ensure that benzodiazepines and nonbenzodiazepine sedatives are used appropriately, which includes tapering dosages and, when appropriate, encouraging nonpharmacologic strategies.
There were no funding or other conflicts of interest associated with this study.
SAN ANTONIO – shows a new study.
While benzodiazepines and nonbenzodiazepine sedative-hypnotics are effective for these indications, misuse and increased health care utilization can ensue from their prolonged use, said Jacob C. Cogan, MD, a fellow in oncology/hematology at the Herbert Irving Comprehensive Cancer Center, Columbia University, New York. Dr. Cogan recently presented the results of the study at the San Antonio Breast Cancer Symposium.
The study included patients with breast cancer who received adjuvant chemotherapy between 2008 and 2017. Prescriptions for sedatives were divided into three periods: 365 days prior to chemotherapy to the start of chemotherapy (period one); start of chemotherapy to 90 days after the end of chemotherapy (period two); and 90-365 days after chemotherapy (period three). Patients who filled at least one benzodiazepine prescription in period two and patients who filled at least two benzodiazepine in period three were classified as new persistent benzodiazepine users. The same definitions were then used for nonbenzodiazepine sedative-hypnotics.
Among 17,532 benzodiazepine-naive patients (mean age, 57 years) and 21,863 nonbenzodiazepine sedative-hypnotic drug–naive patients (mean age, 56 years) who received adjuvant chemotherapy for breast cancer, lumpectomies were performed for a small majority (56.6% benzodiazepine naive, 55.1% nonbenzodiazepine sedative-hypnotics naive) versus mastectomy, and about half of patients received less than 4 months of chemotherapy (48.0% benzodiazepine naive, 48.6% nonbenzodiazepine sedative-hypnotics naive). Among benzodiazepine-naive patients, 4,447 (25.4%) filled at least one benzodiazepine prescription during chemotherapy, and 2,160 (9.9%) filled at least one nonbenzodiazepine sedative-hypnotic prescription during chemotherapy. The rate of new persistent benzodiazepine use after initial exposure during chemotherapy was 26.8% (n = 1,192). Similarly, 33.8% (n = 730) of nonbenzodiazepine sedative-hypnotics users became new persistent users. In addition, 115 patients became new persistent users of both types of sedative-hypnotics.
New persistent benzodiazepine use was associated with several characteristics: age 50-65 (odds ratio, 1.23; P = .01) and age greater than 65 (OR, 1.38, P = .005) relative to age less than 49; as well as Medicaid insurance, relative to commercial and Medicare insurance (OR, 1.68; P < .0001). Both new persistent benzodiazepine and nonbenzodiazepine sedative-hypnotics use was associated with chemotherapy duration of less than 4 months relative to 4 or more months of chemotherapy (OR, 1.17; P = .03 for benzodiazepines; OR, 1.58; P < .0001 for nonbenzodiazepine sedative-hypnotics).
It is not clear why shorter chemotherapy duration is associated with more new persistent use, Dr. Cogan said. “It may be that, paradoxically, a shorter duration of treatment could lead to more anxiety about recurrence. These patients may need closer monitoring of mental health symptoms and earlier referral for psychological services.”
Dr. Cogan said that providers should take steps to ensure that benzodiazepines and nonbenzodiazepine sedatives are used appropriately, which includes tapering dosages and, when appropriate, encouraging nonpharmacologic strategies.
There were no funding or other conflicts of interest associated with this study.
AT SABCS 2021
‘Surprising’ lack of benefit to adding palbociclib to endocrine therapy in early HR+/HER2– breast cancer
Two years of adjuvant palbociclib added to endocrine therapy failed to improve invasive disease-free survival or any other efficacy endpoint in patients with stage II-III HR-positive, HER2-negative breast cancer.
“These definitive findings from the PALLAS trial, already indicated by an interim analysis, are surprising given the established efficacy of palbociclib and other CDK4/6i [inhibitors] in advanced breast cancer,” according to lead author Michael Gnant, MD, professor in the department of surgery, Medical University of Vienna, and colleagues.
The results from the PALLAS trial were presented Dec. 7 at the San Antonio Breast Cancer Symposium and simultaneously published in the Journal of Clinical Oncology.
At a median follow-up of 31 months and at the final protocol-defined analysis, invasive disease-free survival events occurred in 253 (8.8%) of 2,884 patients who received the cyclin-dependent kinase 4/6 (CDK4/6) inhibitor plus endocrine therapy and in 263 (9.1%) of 2,877 patients who received endocrine therapy alone. At 4 years, invasive disease-free survival rates were similar in the palbociclib group (84.2%) and standard treatment group (84.5%).
Caught by surprise
Studies have shown that combining CDK4/6 inhibitors and endocrine therapy prolongs progression-free survival (PFS) and overall survival in metastatic HR-positive, HER2-negative breast cancer, with good tolerability.
“CDK4/6 inhibitors have markedly changed outcomes in the metastatic setting and are now standard of care,” said Dr. Gnant, who presented the recent findings at SABCS. “It seem[ed] only logical to try to transfer these benefits to the curative setting of early breast cancer.”
But in 2020, palbociclib manufacturer Pfizer issued a press release noting that the PALLAS trial was unlikely to show a statistically significant improvement in the primary endpoint of invasive disease-free survival.
The results “caught many of us by surprise,” Kathy D. Miller, MD, codirector of the breast cancer program at the Melvin and Bren Simon Cancer Center at Indiana University, Indianapolis, wrote in response to this announcement.
The trial was based on strong science and incredibly positive results in the metastatic setting but did not meet its primary endpoint when incorporated into the adjuvant setting, Dr. Miller noted in a Medscape blog. “That is certainly not the result we had hoped for, and it’s not the result many of us were expecting.”
Dr. Miller emphasized that “more than anything else, this trial reminds us of the absolute necessity of putting our ideas to the test and doing appropriately powered, appropriately controlled, and well-conducted randomized trials.”
The PALLAS trial enrolled 5,796 patients from 406 centers in 21 countries worldwide over a 3-year period, with 5,761 included in the intention-to-treat population.
Participants were randomly assigned to receive 2 years of palbociclib (125 mg orally once daily, days 1-21 of a 28-day cycle) with adjuvant endocrine therapy or adjuvant endocrine therapy alone for at least 5 years.
Dr. Gnant and colleagues found that the primary endpoint – invasive disease-free survival – did not differ significantly different between the two treatment groups (hazard ratio, 0.96; P = .65). Secondary endpoints in the palbociclib versus no-palbociclib groups were also similar: 4-year survival rates for invasive breast cancer-free survival were 85.4% versus 86%, distant recurrence-free survival was 86.2% versus 87.8%, locoregional recurrence-free survival was 96.8% versus 95.4%, and overall survival was 93.8% versus 95.2%.
The main side effect of palbociclib was neutropenia, but there were no new safety signals, Dr. Gnant explained. He noted, however, that the rates of palbociclib discontinuation were monitored closely and were substantial. At 1 year, 30% of patients discontinued palbociclib and by 24 months, 45% had stopped.
Not the final word?
An interim analysis of the phase 3 monarchE trial did not align with the PALLAS trial.
The monarchE trial found that adding the CDK4/6 inhibitor abemaciclib (Verzenio) to endocrine therapy for 2 years significantly reduced the risk of early recurrence, compared with endocrine therapy alone in the same patient populations – those with early HR-positive, HER2-negative breast cancer. The researchers reported the combination was associated with a 25% relative risk reduction of invasive disease-free survival (HR, 0.75; P =.0096).
The research was presented at the ESMO Virtual Congress 2020 and simultaneously published in the Journal of Clinical Oncology.
Dr. Miller speculated how about how these two drugs that look so similar in the metastatic setting have given such different results in the adjuvant setting. One potential reason is pure chance.
“Any study, no matter how many zeros in the P value, could be simply the play of chance,” she said in an interview. “And that is true for negative and positive studies.”
The fault could also lie in the study design. “Remember, these are agents that we think of as reversing endocrine resistance and extending the benefit of hormone therapy,” she pointed out. “And yet we looked at very early results. Perhaps the study design was just wrong for palbociclib.”
Yet another possibility: The relative potency of those two CDK4/6 inhibitors could differ. “In a metastatic setting, that did not seem to affect effectiveness, but it clearly affected the toxicity profile. Perhaps in the adjuvant setting, those differences really do drive differences in efficacy,” she said.
Dr. Gnant also speculated that differences in the treatment schedules for the two drugs, as abemaciclib is taken continuously without a break, could potentially explain the different efficacies in the early breast cancer setting.
He called for long-term follow up, saying it’s essential for comprehensively examining outcomes in HR-positive luminal breast cancers.
“Ongoing analyses in the Trans-PALLAS translational and clinical science program, with almost 6,000 tumor blocks and tens of thousands of blood samples, will improve understanding of CD4/6 inhibition as well as contemporary management of HR-positive, HER2-negative breast cancer,” Dr. Gnant said.
The trial was funded by Pfizer, who provided study drug and financial support. In addition, the academic organizations ABCSG and AFT supported the trial by providing human resources. Dr. Gnant reported employment at Sandoz; receiving honoraria from Amgen, Novartis, AstraZeneca, Lilly; and consulting or advisory roles at Daiichi Sankyo, Veracyte, Tolmar¸ LifeBrain, and Lilly.
A version of this article first appeared on Medscape.com.
Two years of adjuvant palbociclib added to endocrine therapy failed to improve invasive disease-free survival or any other efficacy endpoint in patients with stage II-III HR-positive, HER2-negative breast cancer.
“These definitive findings from the PALLAS trial, already indicated by an interim analysis, are surprising given the established efficacy of palbociclib and other CDK4/6i [inhibitors] in advanced breast cancer,” according to lead author Michael Gnant, MD, professor in the department of surgery, Medical University of Vienna, and colleagues.
The results from the PALLAS trial were presented Dec. 7 at the San Antonio Breast Cancer Symposium and simultaneously published in the Journal of Clinical Oncology.
At a median follow-up of 31 months and at the final protocol-defined analysis, invasive disease-free survival events occurred in 253 (8.8%) of 2,884 patients who received the cyclin-dependent kinase 4/6 (CDK4/6) inhibitor plus endocrine therapy and in 263 (9.1%) of 2,877 patients who received endocrine therapy alone. At 4 years, invasive disease-free survival rates were similar in the palbociclib group (84.2%) and standard treatment group (84.5%).
Caught by surprise
Studies have shown that combining CDK4/6 inhibitors and endocrine therapy prolongs progression-free survival (PFS) and overall survival in metastatic HR-positive, HER2-negative breast cancer, with good tolerability.
“CDK4/6 inhibitors have markedly changed outcomes in the metastatic setting and are now standard of care,” said Dr. Gnant, who presented the recent findings at SABCS. “It seem[ed] only logical to try to transfer these benefits to the curative setting of early breast cancer.”
But in 2020, palbociclib manufacturer Pfizer issued a press release noting that the PALLAS trial was unlikely to show a statistically significant improvement in the primary endpoint of invasive disease-free survival.
The results “caught many of us by surprise,” Kathy D. Miller, MD, codirector of the breast cancer program at the Melvin and Bren Simon Cancer Center at Indiana University, Indianapolis, wrote in response to this announcement.
The trial was based on strong science and incredibly positive results in the metastatic setting but did not meet its primary endpoint when incorporated into the adjuvant setting, Dr. Miller noted in a Medscape blog. “That is certainly not the result we had hoped for, and it’s not the result many of us were expecting.”
Dr. Miller emphasized that “more than anything else, this trial reminds us of the absolute necessity of putting our ideas to the test and doing appropriately powered, appropriately controlled, and well-conducted randomized trials.”
The PALLAS trial enrolled 5,796 patients from 406 centers in 21 countries worldwide over a 3-year period, with 5,761 included in the intention-to-treat population.
Participants were randomly assigned to receive 2 years of palbociclib (125 mg orally once daily, days 1-21 of a 28-day cycle) with adjuvant endocrine therapy or adjuvant endocrine therapy alone for at least 5 years.
Dr. Gnant and colleagues found that the primary endpoint – invasive disease-free survival – did not differ significantly different between the two treatment groups (hazard ratio, 0.96; P = .65). Secondary endpoints in the palbociclib versus no-palbociclib groups were also similar: 4-year survival rates for invasive breast cancer-free survival were 85.4% versus 86%, distant recurrence-free survival was 86.2% versus 87.8%, locoregional recurrence-free survival was 96.8% versus 95.4%, and overall survival was 93.8% versus 95.2%.
The main side effect of palbociclib was neutropenia, but there were no new safety signals, Dr. Gnant explained. He noted, however, that the rates of palbociclib discontinuation were monitored closely and were substantial. At 1 year, 30% of patients discontinued palbociclib and by 24 months, 45% had stopped.
Not the final word?
An interim analysis of the phase 3 monarchE trial did not align with the PALLAS trial.
The monarchE trial found that adding the CDK4/6 inhibitor abemaciclib (Verzenio) to endocrine therapy for 2 years significantly reduced the risk of early recurrence, compared with endocrine therapy alone in the same patient populations – those with early HR-positive, HER2-negative breast cancer. The researchers reported the combination was associated with a 25% relative risk reduction of invasive disease-free survival (HR, 0.75; P =.0096).
The research was presented at the ESMO Virtual Congress 2020 and simultaneously published in the Journal of Clinical Oncology.
Dr. Miller speculated how about how these two drugs that look so similar in the metastatic setting have given such different results in the adjuvant setting. One potential reason is pure chance.
“Any study, no matter how many zeros in the P value, could be simply the play of chance,” she said in an interview. “And that is true for negative and positive studies.”
The fault could also lie in the study design. “Remember, these are agents that we think of as reversing endocrine resistance and extending the benefit of hormone therapy,” she pointed out. “And yet we looked at very early results. Perhaps the study design was just wrong for palbociclib.”
Yet another possibility: The relative potency of those two CDK4/6 inhibitors could differ. “In a metastatic setting, that did not seem to affect effectiveness, but it clearly affected the toxicity profile. Perhaps in the adjuvant setting, those differences really do drive differences in efficacy,” she said.
Dr. Gnant also speculated that differences in the treatment schedules for the two drugs, as abemaciclib is taken continuously without a break, could potentially explain the different efficacies in the early breast cancer setting.
He called for long-term follow up, saying it’s essential for comprehensively examining outcomes in HR-positive luminal breast cancers.
“Ongoing analyses in the Trans-PALLAS translational and clinical science program, with almost 6,000 tumor blocks and tens of thousands of blood samples, will improve understanding of CD4/6 inhibition as well as contemporary management of HR-positive, HER2-negative breast cancer,” Dr. Gnant said.
The trial was funded by Pfizer, who provided study drug and financial support. In addition, the academic organizations ABCSG and AFT supported the trial by providing human resources. Dr. Gnant reported employment at Sandoz; receiving honoraria from Amgen, Novartis, AstraZeneca, Lilly; and consulting or advisory roles at Daiichi Sankyo, Veracyte, Tolmar¸ LifeBrain, and Lilly.
A version of this article first appeared on Medscape.com.
Two years of adjuvant palbociclib added to endocrine therapy failed to improve invasive disease-free survival or any other efficacy endpoint in patients with stage II-III HR-positive, HER2-negative breast cancer.
“These definitive findings from the PALLAS trial, already indicated by an interim analysis, are surprising given the established efficacy of palbociclib and other CDK4/6i [inhibitors] in advanced breast cancer,” according to lead author Michael Gnant, MD, professor in the department of surgery, Medical University of Vienna, and colleagues.
The results from the PALLAS trial were presented Dec. 7 at the San Antonio Breast Cancer Symposium and simultaneously published in the Journal of Clinical Oncology.
At a median follow-up of 31 months and at the final protocol-defined analysis, invasive disease-free survival events occurred in 253 (8.8%) of 2,884 patients who received the cyclin-dependent kinase 4/6 (CDK4/6) inhibitor plus endocrine therapy and in 263 (9.1%) of 2,877 patients who received endocrine therapy alone. At 4 years, invasive disease-free survival rates were similar in the palbociclib group (84.2%) and standard treatment group (84.5%).
Caught by surprise
Studies have shown that combining CDK4/6 inhibitors and endocrine therapy prolongs progression-free survival (PFS) and overall survival in metastatic HR-positive, HER2-negative breast cancer, with good tolerability.
“CDK4/6 inhibitors have markedly changed outcomes in the metastatic setting and are now standard of care,” said Dr. Gnant, who presented the recent findings at SABCS. “It seem[ed] only logical to try to transfer these benefits to the curative setting of early breast cancer.”
But in 2020, palbociclib manufacturer Pfizer issued a press release noting that the PALLAS trial was unlikely to show a statistically significant improvement in the primary endpoint of invasive disease-free survival.
The results “caught many of us by surprise,” Kathy D. Miller, MD, codirector of the breast cancer program at the Melvin and Bren Simon Cancer Center at Indiana University, Indianapolis, wrote in response to this announcement.
The trial was based on strong science and incredibly positive results in the metastatic setting but did not meet its primary endpoint when incorporated into the adjuvant setting, Dr. Miller noted in a Medscape blog. “That is certainly not the result we had hoped for, and it’s not the result many of us were expecting.”
Dr. Miller emphasized that “more than anything else, this trial reminds us of the absolute necessity of putting our ideas to the test and doing appropriately powered, appropriately controlled, and well-conducted randomized trials.”
The PALLAS trial enrolled 5,796 patients from 406 centers in 21 countries worldwide over a 3-year period, with 5,761 included in the intention-to-treat population.
Participants were randomly assigned to receive 2 years of palbociclib (125 mg orally once daily, days 1-21 of a 28-day cycle) with adjuvant endocrine therapy or adjuvant endocrine therapy alone for at least 5 years.
Dr. Gnant and colleagues found that the primary endpoint – invasive disease-free survival – did not differ significantly different between the two treatment groups (hazard ratio, 0.96; P = .65). Secondary endpoints in the palbociclib versus no-palbociclib groups were also similar: 4-year survival rates for invasive breast cancer-free survival were 85.4% versus 86%, distant recurrence-free survival was 86.2% versus 87.8%, locoregional recurrence-free survival was 96.8% versus 95.4%, and overall survival was 93.8% versus 95.2%.
The main side effect of palbociclib was neutropenia, but there were no new safety signals, Dr. Gnant explained. He noted, however, that the rates of palbociclib discontinuation were monitored closely and were substantial. At 1 year, 30% of patients discontinued palbociclib and by 24 months, 45% had stopped.
Not the final word?
An interim analysis of the phase 3 monarchE trial did not align with the PALLAS trial.
The monarchE trial found that adding the CDK4/6 inhibitor abemaciclib (Verzenio) to endocrine therapy for 2 years significantly reduced the risk of early recurrence, compared with endocrine therapy alone in the same patient populations – those with early HR-positive, HER2-negative breast cancer. The researchers reported the combination was associated with a 25% relative risk reduction of invasive disease-free survival (HR, 0.75; P =.0096).
The research was presented at the ESMO Virtual Congress 2020 and simultaneously published in the Journal of Clinical Oncology.
Dr. Miller speculated how about how these two drugs that look so similar in the metastatic setting have given such different results in the adjuvant setting. One potential reason is pure chance.
“Any study, no matter how many zeros in the P value, could be simply the play of chance,” she said in an interview. “And that is true for negative and positive studies.”
The fault could also lie in the study design. “Remember, these are agents that we think of as reversing endocrine resistance and extending the benefit of hormone therapy,” she pointed out. “And yet we looked at very early results. Perhaps the study design was just wrong for palbociclib.”
Yet another possibility: The relative potency of those two CDK4/6 inhibitors could differ. “In a metastatic setting, that did not seem to affect effectiveness, but it clearly affected the toxicity profile. Perhaps in the adjuvant setting, those differences really do drive differences in efficacy,” she said.
Dr. Gnant also speculated that differences in the treatment schedules for the two drugs, as abemaciclib is taken continuously without a break, could potentially explain the different efficacies in the early breast cancer setting.
He called for long-term follow up, saying it’s essential for comprehensively examining outcomes in HR-positive luminal breast cancers.
“Ongoing analyses in the Trans-PALLAS translational and clinical science program, with almost 6,000 tumor blocks and tens of thousands of blood samples, will improve understanding of CD4/6 inhibition as well as contemporary management of HR-positive, HER2-negative breast cancer,” Dr. Gnant said.
The trial was funded by Pfizer, who provided study drug and financial support. In addition, the academic organizations ABCSG and AFT supported the trial by providing human resources. Dr. Gnant reported employment at Sandoz; receiving honoraria from Amgen, Novartis, AstraZeneca, Lilly; and consulting or advisory roles at Daiichi Sankyo, Veracyte, Tolmar¸ LifeBrain, and Lilly.
A version of this article first appeared on Medscape.com.
FROM SABCS 2021
The evolving HER2+ metastatic breast cancer landscape: Novel agents and promising combination therapies
Recent therapeutic advances in HER2-positive metastatic breast cancer (MBC) have begun to reshape the treatment landscape for patients. Since late 2019, the U.S. Food and Drug Administration (FDA) has approved a handful of novel agents for HER2-positive MBC — most notably, the antibody-drug conjugate (ADC) trastuzumab deruxtecan in December 2019 and the tyrosine kinase inhibitors (TKIs) tucatinib and neratinib in 2020. According to the National Cancer Institute›s Surveillance, Epidemiology, and End Results (SEER) program, the 5-year survival rate for patients with advanced disease was already on the rise between 2004 and 2018, and
“I’ve been involved in the HER2 space for a long time and have watched the field evolve,” said Adam Brufsky, MD, PhD, associate chief in the division of hematology/oncology and co-director of the Comprehensive Breast Cancer Center at the University of Pittsburgh School of Medicine. “The fact that we’re now talking about fourth- and fifth-line therapies for HER2-positive MBC represents a major advance in the management of these patients.”
Oncologists are still building on this progress, focusing on designing more targeted therapies as well as studying different combinations of available agents. The main goal of treatment, experts say, is to prolong patients’ systemic response and prevent recurrences, especially in the brain. This news organization spoke to Dr. Brufksy and others about promising agents and therapeutic strategies on the horizon to treat HER2-positive MBC.
Inside emerging ADCs
Because many patients develop resistance to trastuzumab emtansine (T-DM1) — the first FDA-approved ADC in breast cancer — researchers have focused on developing the next generation of ADCs with more potent payloads, different linkers, and distinct mechanisms of action, according to Sayeh Lavasani, MD, MS, a medical oncologist at City of Hope, a comprehensive cancer center in Los Angeles County.
The second-generation ADC trastuzumab deruxtecan showed “really dramatic” results in HER2-positive MBC, demonstrating progression-free survival of 16 months, remarked Kevin Kalinsky, MD, acting associate professor in the department of hematology and medical oncology at Emory University School of Medicine in Atlanta and director of the Glenn Family Breast Center at the Winship Cancer Institute of Emory University. “These outcomes further changed how we treat patients with metastatic disease and prompted considerable excitement over the potential to develop novel ADCs to treat HER2-positive MBC.”
Most recently, two investigational ADCs — trastuzumab duocarmazine (SYD985) and ARX788 — have stood out. The FDA granted fast-track designations to trastuzumab duocarmazine in January 2018 and ARX788 in January 2021. Trastuzumab duocarmazine, the furthest along the pipeline, has shown promising results so far. In June 2021, Netherlands-based biopharmaceutical company Byondis reported preliminary phase 3 data from the TULIP trial. The open-label, randomized phase 3 study enrolled 436 patients with HER2-positive locally advanced or metastatic disease that had progressed on previous anti-HER2 regimens. The company shared early results that trastuzumab duocarmazine achieved its progression-free survival primary endpoint, marking a significant improvement over physician’s choice of chemotherapy, and promised more detailed results to come later this year.
Although only in early-phase trials, ARX788 has also shown robust anti-HER2 activity as well as low toxicity in HER2-positive tumors, according to recent data. The findings from two phase 1 studies, presented at the June 2021 virtual American Society for Clinical Oncology meeting (abstract 1038), revealed an overall response rate of 74% in the breast cancer cohort, but the investigators acknowledged it was too early to report median progression-free survival outcomes. Preclinical data also showed activity in HER2-low and T-DM1–resistant tumors.
Despite the encouraging initial findings, Dr. Kalinsky remains cautiously optimistic about long-term outcomes for both ADCs. “These data are hot off the press, but it’s too soon to know how these two ADCs and others in the pipeline will measure up to approved therapies,” he commented. As experts learn more about the efficacy of these novel ADCs, Dr. Brufsky would also like to better understand resistance mechanisms and how to integrate these agents into current treatment strategies. “The cellular biology of HER2-positive MBC is complicated, and many factors in these tumor cells affect where ADCs are released, how resistance develops, and whether or not resistance to one ADC applies to others,” Dr. Brufsky remarked. “As we gather more data, we’ll understand resistance mechanisms better and begin to figure out where to go with treatment sequencing.”
TKIs and beyond
In addition to ADCs, TKIs continue to make their mark in the targeted HER2 therapeutic space. The approvals of tucatinib and neratinib last year represented an important advance in treating HER2-positive MBC, particularly for patients with brain metastases. The HER2CLIMB trial, for instance, found that tucatinib combined with trastuzumab and capecitabine had a 4.5-month overall survival advantage compared with placebo (21.9 vs 17.4) and a median progression-free survival advantage of 5.4 months in patients with active brain metastases (9.5 vs 4.1) and 8.3 months in patients with stable metastases (13.9 vs 5.6).
Given this progress, experts are looking to add new TKIs to the armamentarium. In particular, pyrotinib — already approved in China for treating HER2-positive MBC — has demonstrated significantly longer progression-free survival compared with a standard TKI, lapatinib. The phase 3 PHOEBE trial results, published in The Lancet in early 2021, found a median progression-free survival of 12.5 months in patients randomly assigned to receive pyrotinib plus capecitabine compared with 6.8 months in those receiving lapatinib plus capecitabine. The investigators also reported “manageable toxicity”; diarrhea was the most common grade 3 adverse event, occurring in 31% of the pyrotinib group vs. 8% of the lapatinib group, and overall serious adverse events occurred in 10% of patients receiving pyrotinib vs. 8% of those receiving lapatinib.
More recent data on pyrotinib come from the phase 2 PERMEATE trial, which focused on the safety and efficacy of the agent in patients with advanced disease and brain metastases. The investigators, who presented their findings at the 2021 virtual ASCO meeting (abstract 1037), reported that radiation therapy–naive patients receiving pyrotinib plus capecitabine had an overall response rate of 74.6% in the central nervous system. Patients experiencing progression after whole-brain or stereotactic radiation therapy, however, had a comparatively lower overall response rate of 42.1%.
Similarly, median progression-free survival was much higher in the radiation therapy–naive patients (12.1 vs 5.6 months in the radiation therapy cohort). Similar to the PHOEBE trial, the most common grade 3 adverse event was diarrhea (23.1%), followed by decreased neutrophil and white blood cell counts (12.8% for both), anemia (9%), and hand-foot syndrome (7.7%). The main question for Dr. Kalinsky is how well pyrotinib will ultimately stack up to tucatinib and neratinib. “Pyrotinib — like neratinib — was shown to be superior to lapatinib plus capecitabine , but its role may be limited by its gastrointestinal toxicity,” he said. In addition to research focused on expanding the selection of novel ADCs and TKIs, researchers are also exploring new combinations of approved treatments and whether these combinations can be used earlier in treatment sequencing.
Take the CompassHER2 trials. The ongoing phase 3 trial in patients with high-risk HER2-positive breast cancer and residual disease will explore whether tucatinib plus T-DM1 compared with T-DM1 alone improves overall survival and recurrence-free survival and prevents brain metastases. Another possibility currently under investigation is pairing tucatinib and trastuzumab deruxtecan, instead of T-DM1. “Overall, it’s exciting that we are increasing the number of therapeutic options and combinations,” commented Debu Tripathy, MD, professor and chairman in the department of breast medical oncology at the University of Texas MD Anderson Cancer Center in Houston. “Having more choices allows us to tailor therapies to manage resistance and prolong patients’ responses.”
Curbing brain metastasis, according to Dr. Brufksy, is particularly important, and experts need to explore the extent to which ADCs can penetrate the blood-brain barrier. Already, a subgroup analysis of the DESTINY-Breast01 trial found that trastuzumab deruxtecan appeared to be active in patients with brain metastases. Investigators reported an overall response rate of 58.3% and a median progression-free survival of 18.1 months — results in line with those in the general study cohort — but the study population did not include patients with untreated or progressive brain metastases. A phase 2 study currently under way will examine whether patients with HER2-positive and HER2-low breast cancer who have untreated or progressive brain metastases respond to trastuzumab deruxtecan as well. Ultimately, Dr. Brufksy hopes the recent successes with preventing brain metastases in pediatric acute lymphoblastic leukemia (ALL) foreshadow what›s to come in HER2-positive MBC.
“When we figured out how to treat brain metastases prophylactically in childhood ALL, we saw a huge improvement in the cure rate, which is ultimately my vision for HER2-positive disease,” Dr. Brufsky remarked. “Are there cures for HER2-positive MBC on the horizon? We don’t know yet, but the field has really exploded in recent years.”
A version of this article first appeared on Medscape.com.
Recent therapeutic advances in HER2-positive metastatic breast cancer (MBC) have begun to reshape the treatment landscape for patients. Since late 2019, the U.S. Food and Drug Administration (FDA) has approved a handful of novel agents for HER2-positive MBC — most notably, the antibody-drug conjugate (ADC) trastuzumab deruxtecan in December 2019 and the tyrosine kinase inhibitors (TKIs) tucatinib and neratinib in 2020. According to the National Cancer Institute›s Surveillance, Epidemiology, and End Results (SEER) program, the 5-year survival rate for patients with advanced disease was already on the rise between 2004 and 2018, and
“I’ve been involved in the HER2 space for a long time and have watched the field evolve,” said Adam Brufsky, MD, PhD, associate chief in the division of hematology/oncology and co-director of the Comprehensive Breast Cancer Center at the University of Pittsburgh School of Medicine. “The fact that we’re now talking about fourth- and fifth-line therapies for HER2-positive MBC represents a major advance in the management of these patients.”
Oncologists are still building on this progress, focusing on designing more targeted therapies as well as studying different combinations of available agents. The main goal of treatment, experts say, is to prolong patients’ systemic response and prevent recurrences, especially in the brain. This news organization spoke to Dr. Brufksy and others about promising agents and therapeutic strategies on the horizon to treat HER2-positive MBC.
Inside emerging ADCs
Because many patients develop resistance to trastuzumab emtansine (T-DM1) — the first FDA-approved ADC in breast cancer — researchers have focused on developing the next generation of ADCs with more potent payloads, different linkers, and distinct mechanisms of action, according to Sayeh Lavasani, MD, MS, a medical oncologist at City of Hope, a comprehensive cancer center in Los Angeles County.
The second-generation ADC trastuzumab deruxtecan showed “really dramatic” results in HER2-positive MBC, demonstrating progression-free survival of 16 months, remarked Kevin Kalinsky, MD, acting associate professor in the department of hematology and medical oncology at Emory University School of Medicine in Atlanta and director of the Glenn Family Breast Center at the Winship Cancer Institute of Emory University. “These outcomes further changed how we treat patients with metastatic disease and prompted considerable excitement over the potential to develop novel ADCs to treat HER2-positive MBC.”
Most recently, two investigational ADCs — trastuzumab duocarmazine (SYD985) and ARX788 — have stood out. The FDA granted fast-track designations to trastuzumab duocarmazine in January 2018 and ARX788 in January 2021. Trastuzumab duocarmazine, the furthest along the pipeline, has shown promising results so far. In June 2021, Netherlands-based biopharmaceutical company Byondis reported preliminary phase 3 data from the TULIP trial. The open-label, randomized phase 3 study enrolled 436 patients with HER2-positive locally advanced or metastatic disease that had progressed on previous anti-HER2 regimens. The company shared early results that trastuzumab duocarmazine achieved its progression-free survival primary endpoint, marking a significant improvement over physician’s choice of chemotherapy, and promised more detailed results to come later this year.
Although only in early-phase trials, ARX788 has also shown robust anti-HER2 activity as well as low toxicity in HER2-positive tumors, according to recent data. The findings from two phase 1 studies, presented at the June 2021 virtual American Society for Clinical Oncology meeting (abstract 1038), revealed an overall response rate of 74% in the breast cancer cohort, but the investigators acknowledged it was too early to report median progression-free survival outcomes. Preclinical data also showed activity in HER2-low and T-DM1–resistant tumors.
Despite the encouraging initial findings, Dr. Kalinsky remains cautiously optimistic about long-term outcomes for both ADCs. “These data are hot off the press, but it’s too soon to know how these two ADCs and others in the pipeline will measure up to approved therapies,” he commented. As experts learn more about the efficacy of these novel ADCs, Dr. Brufsky would also like to better understand resistance mechanisms and how to integrate these agents into current treatment strategies. “The cellular biology of HER2-positive MBC is complicated, and many factors in these tumor cells affect where ADCs are released, how resistance develops, and whether or not resistance to one ADC applies to others,” Dr. Brufsky remarked. “As we gather more data, we’ll understand resistance mechanisms better and begin to figure out where to go with treatment sequencing.”
TKIs and beyond
In addition to ADCs, TKIs continue to make their mark in the targeted HER2 therapeutic space. The approvals of tucatinib and neratinib last year represented an important advance in treating HER2-positive MBC, particularly for patients with brain metastases. The HER2CLIMB trial, for instance, found that tucatinib combined with trastuzumab and capecitabine had a 4.5-month overall survival advantage compared with placebo (21.9 vs 17.4) and a median progression-free survival advantage of 5.4 months in patients with active brain metastases (9.5 vs 4.1) and 8.3 months in patients with stable metastases (13.9 vs 5.6).
Given this progress, experts are looking to add new TKIs to the armamentarium. In particular, pyrotinib — already approved in China for treating HER2-positive MBC — has demonstrated significantly longer progression-free survival compared with a standard TKI, lapatinib. The phase 3 PHOEBE trial results, published in The Lancet in early 2021, found a median progression-free survival of 12.5 months in patients randomly assigned to receive pyrotinib plus capecitabine compared with 6.8 months in those receiving lapatinib plus capecitabine. The investigators also reported “manageable toxicity”; diarrhea was the most common grade 3 adverse event, occurring in 31% of the pyrotinib group vs. 8% of the lapatinib group, and overall serious adverse events occurred in 10% of patients receiving pyrotinib vs. 8% of those receiving lapatinib.
More recent data on pyrotinib come from the phase 2 PERMEATE trial, which focused on the safety and efficacy of the agent in patients with advanced disease and brain metastases. The investigators, who presented their findings at the 2021 virtual ASCO meeting (abstract 1037), reported that radiation therapy–naive patients receiving pyrotinib plus capecitabine had an overall response rate of 74.6% in the central nervous system. Patients experiencing progression after whole-brain or stereotactic radiation therapy, however, had a comparatively lower overall response rate of 42.1%.
Similarly, median progression-free survival was much higher in the radiation therapy–naive patients (12.1 vs 5.6 months in the radiation therapy cohort). Similar to the PHOEBE trial, the most common grade 3 adverse event was diarrhea (23.1%), followed by decreased neutrophil and white blood cell counts (12.8% for both), anemia (9%), and hand-foot syndrome (7.7%). The main question for Dr. Kalinsky is how well pyrotinib will ultimately stack up to tucatinib and neratinib. “Pyrotinib — like neratinib — was shown to be superior to lapatinib plus capecitabine , but its role may be limited by its gastrointestinal toxicity,” he said. In addition to research focused on expanding the selection of novel ADCs and TKIs, researchers are also exploring new combinations of approved treatments and whether these combinations can be used earlier in treatment sequencing.
Take the CompassHER2 trials. The ongoing phase 3 trial in patients with high-risk HER2-positive breast cancer and residual disease will explore whether tucatinib plus T-DM1 compared with T-DM1 alone improves overall survival and recurrence-free survival and prevents brain metastases. Another possibility currently under investigation is pairing tucatinib and trastuzumab deruxtecan, instead of T-DM1. “Overall, it’s exciting that we are increasing the number of therapeutic options and combinations,” commented Debu Tripathy, MD, professor and chairman in the department of breast medical oncology at the University of Texas MD Anderson Cancer Center in Houston. “Having more choices allows us to tailor therapies to manage resistance and prolong patients’ responses.”
Curbing brain metastasis, according to Dr. Brufksy, is particularly important, and experts need to explore the extent to which ADCs can penetrate the blood-brain barrier. Already, a subgroup analysis of the DESTINY-Breast01 trial found that trastuzumab deruxtecan appeared to be active in patients with brain metastases. Investigators reported an overall response rate of 58.3% and a median progression-free survival of 18.1 months — results in line with those in the general study cohort — but the study population did not include patients with untreated or progressive brain metastases. A phase 2 study currently under way will examine whether patients with HER2-positive and HER2-low breast cancer who have untreated or progressive brain metastases respond to trastuzumab deruxtecan as well. Ultimately, Dr. Brufksy hopes the recent successes with preventing brain metastases in pediatric acute lymphoblastic leukemia (ALL) foreshadow what›s to come in HER2-positive MBC.
“When we figured out how to treat brain metastases prophylactically in childhood ALL, we saw a huge improvement in the cure rate, which is ultimately my vision for HER2-positive disease,” Dr. Brufsky remarked. “Are there cures for HER2-positive MBC on the horizon? We don’t know yet, but the field has really exploded in recent years.”
A version of this article first appeared on Medscape.com.
Recent therapeutic advances in HER2-positive metastatic breast cancer (MBC) have begun to reshape the treatment landscape for patients. Since late 2019, the U.S. Food and Drug Administration (FDA) has approved a handful of novel agents for HER2-positive MBC — most notably, the antibody-drug conjugate (ADC) trastuzumab deruxtecan in December 2019 and the tyrosine kinase inhibitors (TKIs) tucatinib and neratinib in 2020. According to the National Cancer Institute›s Surveillance, Epidemiology, and End Results (SEER) program, the 5-year survival rate for patients with advanced disease was already on the rise between 2004 and 2018, and
“I’ve been involved in the HER2 space for a long time and have watched the field evolve,” said Adam Brufsky, MD, PhD, associate chief in the division of hematology/oncology and co-director of the Comprehensive Breast Cancer Center at the University of Pittsburgh School of Medicine. “The fact that we’re now talking about fourth- and fifth-line therapies for HER2-positive MBC represents a major advance in the management of these patients.”
Oncologists are still building on this progress, focusing on designing more targeted therapies as well as studying different combinations of available agents. The main goal of treatment, experts say, is to prolong patients’ systemic response and prevent recurrences, especially in the brain. This news organization spoke to Dr. Brufksy and others about promising agents and therapeutic strategies on the horizon to treat HER2-positive MBC.
Inside emerging ADCs
Because many patients develop resistance to trastuzumab emtansine (T-DM1) — the first FDA-approved ADC in breast cancer — researchers have focused on developing the next generation of ADCs with more potent payloads, different linkers, and distinct mechanisms of action, according to Sayeh Lavasani, MD, MS, a medical oncologist at City of Hope, a comprehensive cancer center in Los Angeles County.
The second-generation ADC trastuzumab deruxtecan showed “really dramatic” results in HER2-positive MBC, demonstrating progression-free survival of 16 months, remarked Kevin Kalinsky, MD, acting associate professor in the department of hematology and medical oncology at Emory University School of Medicine in Atlanta and director of the Glenn Family Breast Center at the Winship Cancer Institute of Emory University. “These outcomes further changed how we treat patients with metastatic disease and prompted considerable excitement over the potential to develop novel ADCs to treat HER2-positive MBC.”
Most recently, two investigational ADCs — trastuzumab duocarmazine (SYD985) and ARX788 — have stood out. The FDA granted fast-track designations to trastuzumab duocarmazine in January 2018 and ARX788 in January 2021. Trastuzumab duocarmazine, the furthest along the pipeline, has shown promising results so far. In June 2021, Netherlands-based biopharmaceutical company Byondis reported preliminary phase 3 data from the TULIP trial. The open-label, randomized phase 3 study enrolled 436 patients with HER2-positive locally advanced or metastatic disease that had progressed on previous anti-HER2 regimens. The company shared early results that trastuzumab duocarmazine achieved its progression-free survival primary endpoint, marking a significant improvement over physician’s choice of chemotherapy, and promised more detailed results to come later this year.
Although only in early-phase trials, ARX788 has also shown robust anti-HER2 activity as well as low toxicity in HER2-positive tumors, according to recent data. The findings from two phase 1 studies, presented at the June 2021 virtual American Society for Clinical Oncology meeting (abstract 1038), revealed an overall response rate of 74% in the breast cancer cohort, but the investigators acknowledged it was too early to report median progression-free survival outcomes. Preclinical data also showed activity in HER2-low and T-DM1–resistant tumors.
Despite the encouraging initial findings, Dr. Kalinsky remains cautiously optimistic about long-term outcomes for both ADCs. “These data are hot off the press, but it’s too soon to know how these two ADCs and others in the pipeline will measure up to approved therapies,” he commented. As experts learn more about the efficacy of these novel ADCs, Dr. Brufsky would also like to better understand resistance mechanisms and how to integrate these agents into current treatment strategies. “The cellular biology of HER2-positive MBC is complicated, and many factors in these tumor cells affect where ADCs are released, how resistance develops, and whether or not resistance to one ADC applies to others,” Dr. Brufsky remarked. “As we gather more data, we’ll understand resistance mechanisms better and begin to figure out where to go with treatment sequencing.”
TKIs and beyond
In addition to ADCs, TKIs continue to make their mark in the targeted HER2 therapeutic space. The approvals of tucatinib and neratinib last year represented an important advance in treating HER2-positive MBC, particularly for patients with brain metastases. The HER2CLIMB trial, for instance, found that tucatinib combined with trastuzumab and capecitabine had a 4.5-month overall survival advantage compared with placebo (21.9 vs 17.4) and a median progression-free survival advantage of 5.4 months in patients with active brain metastases (9.5 vs 4.1) and 8.3 months in patients with stable metastases (13.9 vs 5.6).
Given this progress, experts are looking to add new TKIs to the armamentarium. In particular, pyrotinib — already approved in China for treating HER2-positive MBC — has demonstrated significantly longer progression-free survival compared with a standard TKI, lapatinib. The phase 3 PHOEBE trial results, published in The Lancet in early 2021, found a median progression-free survival of 12.5 months in patients randomly assigned to receive pyrotinib plus capecitabine compared with 6.8 months in those receiving lapatinib plus capecitabine. The investigators also reported “manageable toxicity”; diarrhea was the most common grade 3 adverse event, occurring in 31% of the pyrotinib group vs. 8% of the lapatinib group, and overall serious adverse events occurred in 10% of patients receiving pyrotinib vs. 8% of those receiving lapatinib.
More recent data on pyrotinib come from the phase 2 PERMEATE trial, which focused on the safety and efficacy of the agent in patients with advanced disease and brain metastases. The investigators, who presented their findings at the 2021 virtual ASCO meeting (abstract 1037), reported that radiation therapy–naive patients receiving pyrotinib plus capecitabine had an overall response rate of 74.6% in the central nervous system. Patients experiencing progression after whole-brain or stereotactic radiation therapy, however, had a comparatively lower overall response rate of 42.1%.
Similarly, median progression-free survival was much higher in the radiation therapy–naive patients (12.1 vs 5.6 months in the radiation therapy cohort). Similar to the PHOEBE trial, the most common grade 3 adverse event was diarrhea (23.1%), followed by decreased neutrophil and white blood cell counts (12.8% for both), anemia (9%), and hand-foot syndrome (7.7%). The main question for Dr. Kalinsky is how well pyrotinib will ultimately stack up to tucatinib and neratinib. “Pyrotinib — like neratinib — was shown to be superior to lapatinib plus capecitabine , but its role may be limited by its gastrointestinal toxicity,” he said. In addition to research focused on expanding the selection of novel ADCs and TKIs, researchers are also exploring new combinations of approved treatments and whether these combinations can be used earlier in treatment sequencing.
Take the CompassHER2 trials. The ongoing phase 3 trial in patients with high-risk HER2-positive breast cancer and residual disease will explore whether tucatinib plus T-DM1 compared with T-DM1 alone improves overall survival and recurrence-free survival and prevents brain metastases. Another possibility currently under investigation is pairing tucatinib and trastuzumab deruxtecan, instead of T-DM1. “Overall, it’s exciting that we are increasing the number of therapeutic options and combinations,” commented Debu Tripathy, MD, professor and chairman in the department of breast medical oncology at the University of Texas MD Anderson Cancer Center in Houston. “Having more choices allows us to tailor therapies to manage resistance and prolong patients’ responses.”
Curbing brain metastasis, according to Dr. Brufksy, is particularly important, and experts need to explore the extent to which ADCs can penetrate the blood-brain barrier. Already, a subgroup analysis of the DESTINY-Breast01 trial found that trastuzumab deruxtecan appeared to be active in patients with brain metastases. Investigators reported an overall response rate of 58.3% and a median progression-free survival of 18.1 months — results in line with those in the general study cohort — but the study population did not include patients with untreated or progressive brain metastases. A phase 2 study currently under way will examine whether patients with HER2-positive and HER2-low breast cancer who have untreated or progressive brain metastases respond to trastuzumab deruxtecan as well. Ultimately, Dr. Brufksy hopes the recent successes with preventing brain metastases in pediatric acute lymphoblastic leukemia (ALL) foreshadow what›s to come in HER2-positive MBC.
“When we figured out how to treat brain metastases prophylactically in childhood ALL, we saw a huge improvement in the cure rate, which is ultimately my vision for HER2-positive disease,” Dr. Brufsky remarked. “Are there cures for HER2-positive MBC on the horizon? We don’t know yet, but the field has really exploded in recent years.”
A version of this article first appeared on Medscape.com.
Ongoing HER2 breast cancer therapy may cost an additional $68,000 per patient

The current funding policy in British Columbia restricts patients to two lines of HER2-directed therapy for metastatic breast cancer, but accessing continued HER2 suppression has become more complex as novel agents have emerged, Emily Jackson, MD, and colleagues explained (in poster PD8-09) at the San Antonio Breast Cancer Symposium.
Continuing HER2 suppression has improved progression free survival (PFS) and overall survival (OS), but the financial implications of adapting funding policies to “reflect increasing lines of proven HER2 treatment” are unclear, they noted.
Drug funding is provided through the provincial government, but it can take months – and sometimes years – from when a drug is approved by Health Canada and when provincial protocols are approved and funding is made available, Dr. Jackson, co-chief resident (PGY5) at BC Cancer, Vancouver, said in an interview.
During that “lag time,” the province is negotiating drug prices with pharmaceutical companies and determining “which patients are eligible and under which circumstances,” she said.
To assess the potential costs, the investigators analyzed data from the BC Cancer outcomes unit, which collects clinical and outcome information on 85% of all patients diagnosed with breast cancer in the province. Information on therapy use was obtained from the BC Cancer pharmacy database.
Of 230 patients who received any HER2 treatment for metastatic breast cancer dispensed by BC Cancer between 2013 and 2018, 112 (49%) were eligible to continue beyond their second line of therapy.
“Of these, 86 patients accessed continued HER2-directed therapy, while 26 were eligible but unable to access continued HER2Rx,” they reported, noting that “the remaining 51% (n = 118) were not eligible for consideration of further HER2Rx due to either stable disease (n = 61) or deterioration precluding treatment (n = 57).”
At median follow-up of 42.2 months, the median number of lines of therapy in the entire study population was three. The median number of cycles in those who received HER2-directed therapy beyond second-line therapy was 33.
The median overall survival was 37.5 months for those who were eligible but did not continue HER2, compared with 57.9 months for those who did continue, they found.
The overall survival difference was not statistically significant (P = .13), but this was likely due to the small number of patients included in the initial analysis, Dr. Jackson said, noting that the finding is “hypothesis generating,” and should be further assessed.
Notably, most patients who continued HER2 therapy did so through pharmaceutical company compassionate access programs or clinical trials, she said.
The “conservative estimated cost per cycle of HER2Rx” was based on currently available trastuzumab biosimilars, and the potential financial implications were calculated based on the current cost of commonly used third-line therapies.
The findings demonstrate that most patients access continued treatment despite prohibitive funding policies, and suggest that significant increases in cost per patient can be expected if funding policies don’t evolve to meet treatment needs, they concluded, noting that “if these trends in survival continue we would expect an additional cost of $68,000 per patient over current costs.
“As the cost of novel therapies are likely to be higher than currently available biosimilars, there will be significant implications for both private payer and public payer healthcare systems,” they added.
A larger, more comprehensive analysis of the data is planned, said Dr. Jackson, who did not disclose any funding or other conflicts of interest associated with this study.
The current funding policy in British Columbia restricts patients to two lines of HER2-directed therapy for metastatic breast cancer, but accessing continued HER2 suppression has become more complex as novel agents have emerged, Emily Jackson, MD, and colleagues explained (in poster PD8-09) at the San Antonio Breast Cancer Symposium.
Continuing HER2 suppression has improved progression free survival (PFS) and overall survival (OS), but the financial implications of adapting funding policies to “reflect increasing lines of proven HER2 treatment” are unclear, they noted.
Drug funding is provided through the provincial government, but it can take months – and sometimes years – from when a drug is approved by Health Canada and when provincial protocols are approved and funding is made available, Dr. Jackson, co-chief resident (PGY5) at BC Cancer, Vancouver, said in an interview.
During that “lag time,” the province is negotiating drug prices with pharmaceutical companies and determining “which patients are eligible and under which circumstances,” she said.
To assess the potential costs, the investigators analyzed data from the BC Cancer outcomes unit, which collects clinical and outcome information on 85% of all patients diagnosed with breast cancer in the province. Information on therapy use was obtained from the BC Cancer pharmacy database.
Of 230 patients who received any HER2 treatment for metastatic breast cancer dispensed by BC Cancer between 2013 and 2018, 112 (49%) were eligible to continue beyond their second line of therapy.
“Of these, 86 patients accessed continued HER2-directed therapy, while 26 were eligible but unable to access continued HER2Rx,” they reported, noting that “the remaining 51% (n = 118) were not eligible for consideration of further HER2Rx due to either stable disease (n = 61) or deterioration precluding treatment (n = 57).”
At median follow-up of 42.2 months, the median number of lines of therapy in the entire study population was three. The median number of cycles in those who received HER2-directed therapy beyond second-line therapy was 33.
The median overall survival was 37.5 months for those who were eligible but did not continue HER2, compared with 57.9 months for those who did continue, they found.
The overall survival difference was not statistically significant (P = .13), but this was likely due to the small number of patients included in the initial analysis, Dr. Jackson said, noting that the finding is “hypothesis generating,” and should be further assessed.
Notably, most patients who continued HER2 therapy did so through pharmaceutical company compassionate access programs or clinical trials, she said.
The “conservative estimated cost per cycle of HER2Rx” was based on currently available trastuzumab biosimilars, and the potential financial implications were calculated based on the current cost of commonly used third-line therapies.
The findings demonstrate that most patients access continued treatment despite prohibitive funding policies, and suggest that significant increases in cost per patient can be expected if funding policies don’t evolve to meet treatment needs, they concluded, noting that “if these trends in survival continue we would expect an additional cost of $68,000 per patient over current costs.
“As the cost of novel therapies are likely to be higher than currently available biosimilars, there will be significant implications for both private payer and public payer healthcare systems,” they added.
A larger, more comprehensive analysis of the data is planned, said Dr. Jackson, who did not disclose any funding or other conflicts of interest associated with this study.
The current funding policy in British Columbia restricts patients to two lines of HER2-directed therapy for metastatic breast cancer, but accessing continued HER2 suppression has become more complex as novel agents have emerged, Emily Jackson, MD, and colleagues explained (in poster PD8-09) at the San Antonio Breast Cancer Symposium.
Continuing HER2 suppression has improved progression free survival (PFS) and overall survival (OS), but the financial implications of adapting funding policies to “reflect increasing lines of proven HER2 treatment” are unclear, they noted.
Drug funding is provided through the provincial government, but it can take months – and sometimes years – from when a drug is approved by Health Canada and when provincial protocols are approved and funding is made available, Dr. Jackson, co-chief resident (PGY5) at BC Cancer, Vancouver, said in an interview.
During that “lag time,” the province is negotiating drug prices with pharmaceutical companies and determining “which patients are eligible and under which circumstances,” she said.
To assess the potential costs, the investigators analyzed data from the BC Cancer outcomes unit, which collects clinical and outcome information on 85% of all patients diagnosed with breast cancer in the province. Information on therapy use was obtained from the BC Cancer pharmacy database.
Of 230 patients who received any HER2 treatment for metastatic breast cancer dispensed by BC Cancer between 2013 and 2018, 112 (49%) were eligible to continue beyond their second line of therapy.
“Of these, 86 patients accessed continued HER2-directed therapy, while 26 were eligible but unable to access continued HER2Rx,” they reported, noting that “the remaining 51% (n = 118) were not eligible for consideration of further HER2Rx due to either stable disease (n = 61) or deterioration precluding treatment (n = 57).”
At median follow-up of 42.2 months, the median number of lines of therapy in the entire study population was three. The median number of cycles in those who received HER2-directed therapy beyond second-line therapy was 33.
The median overall survival was 37.5 months for those who were eligible but did not continue HER2, compared with 57.9 months for those who did continue, they found.
The overall survival difference was not statistically significant (P = .13), but this was likely due to the small number of patients included in the initial analysis, Dr. Jackson said, noting that the finding is “hypothesis generating,” and should be further assessed.
Notably, most patients who continued HER2 therapy did so through pharmaceutical company compassionate access programs or clinical trials, she said.
The “conservative estimated cost per cycle of HER2Rx” was based on currently available trastuzumab biosimilars, and the potential financial implications were calculated based on the current cost of commonly used third-line therapies.
The findings demonstrate that most patients access continued treatment despite prohibitive funding policies, and suggest that significant increases in cost per patient can be expected if funding policies don’t evolve to meet treatment needs, they concluded, noting that “if these trends in survival continue we would expect an additional cost of $68,000 per patient over current costs.
“As the cost of novel therapies are likely to be higher than currently available biosimilars, there will be significant implications for both private payer and public payer healthcare systems,” they added.
A larger, more comprehensive analysis of the data is planned, said Dr. Jackson, who did not disclose any funding or other conflicts of interest associated with this study.
FROM SABCS 2021
Vitamin D counters bone density loss with aromatase inhibitors
Among women with breast cancer being treated with aromatase inhibitors (AI), supplementation with vitamin D and calcium protected against bone loss after 5 years, according to results from a prospective cohort study in Brazil. The study found no difference in bone mineral density outcomes at 5 years between women with hormone receptor–positive cancers treated with aromatase inhibitors (AIG) and triple negative or HER-2 positive patients who were treated with another therapy (CG).

About two-thirds of women with breast cancer have tumors that are positive for hormone receptors, and so are often treated with endocrine therapy such as selective estrogen receptor modulators or AI. However, there are concerns that AI treatment may lead to a loss of bone mineral density and impacts on quality of life. This loss is influenced by a range of factors, including body weight, physical activity, smoking, alcohol consumption, corticosteroid use, calcium in the diet, and circulating levels of vitamin D.
Vitamin D helps to regulate absorption of calcium and phosphorus, ensuring that their plasma concentrations are high enough for adequate bone health. But vitamin D deficiency is a common problem, even in tropical areas such as Brazil. “It is high in the general population and especially in postmenopausal breast cancer patients. Thus, vitamin D and calcium supplementation has an impact on these women’s lives,” said lead author Marcelo Antonini, MD, who presented the study (abstract P1-13-04) at the San Antonio Breast Cancer Symposium. He is a researcher at Hospital Servidor Publico Estadual in São Paulo, Brazil.
Although the findings are encouraging, more work needs to be done before it leads to a change in practice. “Larger studies must be carried out to prove this theory; however, in noncancer patients we have already well established the benefits of vitamin D and calcium supplementation,” Dr. Antonini said in an interview
The researchers examined women before the start of treatment, at 6 months, and at 5 years. Those with vitamin D levels below 30 ng/mL received 7,000 IU/day for 8 weeks, followed by a 1,000 IU/day maintenance dose. Subjects with osteopenia received a calcium supplement (500 mg calcium carbonate), and those with osteoporosis received 4 mg zoledronic acid (Zometa, Novartis).
There were 140 patients in both the AIG and CG groups. The average age was 65 years. Sixty-four percent of the AIG group and 71% of the CG group were vitamin D deficient at baseline. At 5 years, the frequencies were 17% and 16%, respectively. Both groups showed significant declines in bone mineral density in the femoral neck and femur at both 6 months and 5 years, but there was no significant difference between them. There was no significant difference between the two groups with respect to bone density loss in the spine.
The study is limited by the fact that it was conducted at a single center and had a small population size.
Another prospective observational study, published earlier this year, looked at vitamin D supplementation in 741 patients (mean age 61.9 years) being treated with aromatase inhibitors, whose baseline vitamin D levels were less 30 ng/mL. They received 16,000 IU dose of oral calcifediol every 2 weeks. At 3 months, individuals who achieved vitamin D levels of 40 ng/mL or higher were less likely to have joint pain (P < .05). At 12 months, data from 473 patients showed that for every 10-ng/mL increase in serum vitamin D at 3 months, there was a reduction in loss of bone marrow density in the lumbar spine (adjusted beta = +0.177%, P < .05), though there were no associations between vitamin D levels and BMD of the femur or total hip.
“Our results suggest that optimal levels of vitamin D are associated with a reduced risk of joint pain related to AI treatment. A target threshold (of vitamin D) levels was set at 40 ng/mL to significantly reduce the increase in joint pain. The authors noted that this threshold is well above the goal of 20 ng/mL recommended by the 2010 Institute of Medicine report.
The study did not receive external funding. Dr. Antonini has no relevant financial disclosures.
Among women with breast cancer being treated with aromatase inhibitors (AI), supplementation with vitamin D and calcium protected against bone loss after 5 years, according to results from a prospective cohort study in Brazil. The study found no difference in bone mineral density outcomes at 5 years between women with hormone receptor–positive cancers treated with aromatase inhibitors (AIG) and triple negative or HER-2 positive patients who were treated with another therapy (CG).
About two-thirds of women with breast cancer have tumors that are positive for hormone receptors, and so are often treated with endocrine therapy such as selective estrogen receptor modulators or AI. However, there are concerns that AI treatment may lead to a loss of bone mineral density and impacts on quality of life. This loss is influenced by a range of factors, including body weight, physical activity, smoking, alcohol consumption, corticosteroid use, calcium in the diet, and circulating levels of vitamin D.
Vitamin D helps to regulate absorption of calcium and phosphorus, ensuring that their plasma concentrations are high enough for adequate bone health. But vitamin D deficiency is a common problem, even in tropical areas such as Brazil. “It is high in the general population and especially in postmenopausal breast cancer patients. Thus, vitamin D and calcium supplementation has an impact on these women’s lives,” said lead author Marcelo Antonini, MD, who presented the study (abstract P1-13-04) at the San Antonio Breast Cancer Symposium. He is a researcher at Hospital Servidor Publico Estadual in São Paulo, Brazil.
Although the findings are encouraging, more work needs to be done before it leads to a change in practice. “Larger studies must be carried out to prove this theory; however, in noncancer patients we have already well established the benefits of vitamin D and calcium supplementation,” Dr. Antonini said in an interview
The researchers examined women before the start of treatment, at 6 months, and at 5 years. Those with vitamin D levels below 30 ng/mL received 7,000 IU/day for 8 weeks, followed by a 1,000 IU/day maintenance dose. Subjects with osteopenia received a calcium supplement (500 mg calcium carbonate), and those with osteoporosis received 4 mg zoledronic acid (Zometa, Novartis).
There were 140 patients in both the AIG and CG groups. The average age was 65 years. Sixty-four percent of the AIG group and 71% of the CG group were vitamin D deficient at baseline. At 5 years, the frequencies were 17% and 16%, respectively. Both groups showed significant declines in bone mineral density in the femoral neck and femur at both 6 months and 5 years, but there was no significant difference between them. There was no significant difference between the two groups with respect to bone density loss in the spine.
The study is limited by the fact that it was conducted at a single center and had a small population size.
Another prospective observational study, published earlier this year, looked at vitamin D supplementation in 741 patients (mean age 61.9 years) being treated with aromatase inhibitors, whose baseline vitamin D levels were less 30 ng/mL. They received 16,000 IU dose of oral calcifediol every 2 weeks. At 3 months, individuals who achieved vitamin D levels of 40 ng/mL or higher were less likely to have joint pain (P < .05). At 12 months, data from 473 patients showed that for every 10-ng/mL increase in serum vitamin D at 3 months, there was a reduction in loss of bone marrow density in the lumbar spine (adjusted beta = +0.177%, P < .05), though there were no associations between vitamin D levels and BMD of the femur or total hip.
“Our results suggest that optimal levels of vitamin D are associated with a reduced risk of joint pain related to AI treatment. A target threshold (of vitamin D) levels was set at 40 ng/mL to significantly reduce the increase in joint pain. The authors noted that this threshold is well above the goal of 20 ng/mL recommended by the 2010 Institute of Medicine report.
The study did not receive external funding. Dr. Antonini has no relevant financial disclosures.
Among women with breast cancer being treated with aromatase inhibitors (AI), supplementation with vitamin D and calcium protected against bone loss after 5 years, according to results from a prospective cohort study in Brazil. The study found no difference in bone mineral density outcomes at 5 years between women with hormone receptor–positive cancers treated with aromatase inhibitors (AIG) and triple negative or HER-2 positive patients who were treated with another therapy (CG).
About two-thirds of women with breast cancer have tumors that are positive for hormone receptors, and so are often treated with endocrine therapy such as selective estrogen receptor modulators or AI. However, there are concerns that AI treatment may lead to a loss of bone mineral density and impacts on quality of life. This loss is influenced by a range of factors, including body weight, physical activity, smoking, alcohol consumption, corticosteroid use, calcium in the diet, and circulating levels of vitamin D.
Vitamin D helps to regulate absorption of calcium and phosphorus, ensuring that their plasma concentrations are high enough for adequate bone health. But vitamin D deficiency is a common problem, even in tropical areas such as Brazil. “It is high in the general population and especially in postmenopausal breast cancer patients. Thus, vitamin D and calcium supplementation has an impact on these women’s lives,” said lead author Marcelo Antonini, MD, who presented the study (abstract P1-13-04) at the San Antonio Breast Cancer Symposium. He is a researcher at Hospital Servidor Publico Estadual in São Paulo, Brazil.
Although the findings are encouraging, more work needs to be done before it leads to a change in practice. “Larger studies must be carried out to prove this theory; however, in noncancer patients we have already well established the benefits of vitamin D and calcium supplementation,” Dr. Antonini said in an interview
The researchers examined women before the start of treatment, at 6 months, and at 5 years. Those with vitamin D levels below 30 ng/mL received 7,000 IU/day for 8 weeks, followed by a 1,000 IU/day maintenance dose. Subjects with osteopenia received a calcium supplement (500 mg calcium carbonate), and those with osteoporosis received 4 mg zoledronic acid (Zometa, Novartis).
There were 140 patients in both the AIG and CG groups. The average age was 65 years. Sixty-four percent of the AIG group and 71% of the CG group were vitamin D deficient at baseline. At 5 years, the frequencies were 17% and 16%, respectively. Both groups showed significant declines in bone mineral density in the femoral neck and femur at both 6 months and 5 years, but there was no significant difference between them. There was no significant difference between the two groups with respect to bone density loss in the spine.
The study is limited by the fact that it was conducted at a single center and had a small population size.
Another prospective observational study, published earlier this year, looked at vitamin D supplementation in 741 patients (mean age 61.9 years) being treated with aromatase inhibitors, whose baseline vitamin D levels were less 30 ng/mL. They received 16,000 IU dose of oral calcifediol every 2 weeks. At 3 months, individuals who achieved vitamin D levels of 40 ng/mL or higher were less likely to have joint pain (P < .05). At 12 months, data from 473 patients showed that for every 10-ng/mL increase in serum vitamin D at 3 months, there was a reduction in loss of bone marrow density in the lumbar spine (adjusted beta = +0.177%, P < .05), though there were no associations between vitamin D levels and BMD of the femur or total hip.
“Our results suggest that optimal levels of vitamin D are associated with a reduced risk of joint pain related to AI treatment. A target threshold (of vitamin D) levels was set at 40 ng/mL to significantly reduce the increase in joint pain. The authors noted that this threshold is well above the goal of 20 ng/mL recommended by the 2010 Institute of Medicine report.
The study did not receive external funding. Dr. Antonini has no relevant financial disclosures.
FROM SABCS 2021
Metformin does not improve outcomes in early breast cancer
In the primary analysis, the addition of metformin to standard therapy in moderate/high-risk hormone receptor positive or negative breast cancer did not improve invasive disease–free survival (IDFS), overall survival, or other breast outcomes, explained lead author Pamela J. Goodwin, MD, FRCPC, professor of medicine at the University of Toronto. “Metformin should not be used as breast cancer treatment in this population.”
However, an exploratory analysis suggested that metformin may have a beneficial effect in women with HER2-positive breast cancer, Dr. Goodwin noted.
In this subset, IDFS was improved in patients who received metformin (hazard ratio, 0.64; P = .03), as was overall survival (HR, 0.53; P = .04).
The findings were presented at the San Antonio Breast Cancer Symposium.
“This trial arose from the observation that obesity is associated with poor breast cancer outcomes, and insulin levels are higher in obesity and may be more strongly associated with breast cancer outcomes than obesity,” said Dr. Goodwin.
Metformin was used because of its ability to promote modest weight loss and lower insulin by about 15%-20% in nondiabetic breast cancer survivors. It has also shown anticancer effects in preclinical studies. “In some window of opportunity neoadjuvant studies, it has been shown to reduce Ki67 in breast cancer cells,” she said. “And in preclinical in vitro and in vivo research, it slows growth of breast cancer.”
In addition, emerging evidence from observational studies suggests that the use of metformin to treat diabetes in breast cancer patients may be associated with better outcomes, strengthening the rationale for the study.
The negative results in breast cancer follow recent reports of negative findings in lung cancer, when metformin was found to be ineffective when used alongside chemotherapy in locally advanced lung cancer, as reported by this news organization.
No benefit seen
Metformin was compared to placebo in the phase 3 CCTG MA.32 trial, conducted in 3,649 patients aged 18-74 years with T1-3 N0-3 M0 breast cancer. All patients were treated with standard therapy and were randomized to receive metformin 850 mg twice daily for 5 years or placebo.
In 2016, “futility was declared in ER/PR-negative patients” after a second interim analysis conducted at 29.6 months’ median follow-up, Dr. Goodwin noted. The intervention was stopped in that group, although blinding and follow-up continued.
After that, the study’s primary analysis focused on the 2,533 ER/PR-positive patients (mean age, 52.7 years; mean body mass index, 28.8; approx. 60% postmenopausal).
Just over half of these patients had T2 tumor stage, and most disease was grade 2 or 3.
In addition, 16.5% (of metformin) and 17.4% (of placebo) patients had HER2-positive disease, with the majority (97%) of all HER2 patients receiving trastuzumab.
There was no difference between the two groups in IDFS events, occurring in 18.5% of patients receiving metformin and 18.3% who received placebo, with most (75.6%) events due to breast cancer (HR, 1.01; P = .92).
There were 131 deaths in the metformin arm and 119 in the placebo arm, with most (75.8%) of the deaths related to breast cancer (HR, 1.10; P = .47).
Other breast cancer outcomes had similar results, including distant disease-free survival (HR, 0.99; P = .94) and breast cancer–free interval (HR, 0.98; P = .87), both of which showed no advantage for metformin.
Possible HER2 advantage
However, the exploratory analysis suggested there may be an advantage for patients with HER2-positive disease, but primarily those who had at least one C allele of a prespecified ATM associated rs11212617 SNP. These patients achieved a higher pathologic complete response rate with metformin than that of those without the allele.
There were 620 patients with HER2-positive disease analyzed, with 99.4% receiving chemotherapy and 96.5% receiving trastuzumab. There were 99 IDFS events, and 47 OS events.
In the entire HER2-positive cohort, patients who received metformin had fewer IDFS events (HR, 0.64; P = .026) compared with the placebo arm. Mortality was lower with metformin (HR for overall survival, 0.53; P = .038).
“Subjects with HER2-positive breast cancer, notably those with at least one C allele of the ATM-associated rs11212617 SNP, experienced improved IDFS and overall survival with metformin,” Dr. Goodwin concluded. “However, no P-value ‘spend’ was allocated to this comparison. As a result, it requires replication in a prospective trial focusing on the HER2-positive population.”
More research?
Stephanie Bernik, MD, chief of breast surgery, Mount Sinai West, and associate professor of breast surgery, Icahn School of Medicine at Mount Sinai, New York, was approached by this news organization for an independent comment.
“It has long been known that obesity, which often correlates with diabetes, increases a woman’s risk of breast cancer,” she said.
“This study tried to show that using a medication that helps control insulin levels, even in those without diabetes, might decrease one’s risk of breast cancer,” she said. “Unfortunately, using metformin had no effect on outcomes in this study, even though it has shown promise in other studies. Perhaps more research needs to be carried out to try to pinpoint which mechanisms of action, if any, might be helpful to combat cancer in those with and without diabetes.”
The study was funded by the Canadian Cancer Trials Group, Cancer Therapy Evaluation Program, Breast Cancer Researcher Foundation, Susan G. Komen for the Cure, Canadian Cancer Society, Apotex, Swiss Cancer Research, and the Canadian Breast Cancer Foundation. Dr. Goodwin has no disclosures.
A version of this article first appeared on Medscape.com.
In the primary analysis, the addition of metformin to standard therapy in moderate/high-risk hormone receptor positive or negative breast cancer did not improve invasive disease–free survival (IDFS), overall survival, or other breast outcomes, explained lead author Pamela J. Goodwin, MD, FRCPC, professor of medicine at the University of Toronto. “Metformin should not be used as breast cancer treatment in this population.”
However, an exploratory analysis suggested that metformin may have a beneficial effect in women with HER2-positive breast cancer, Dr. Goodwin noted.
In this subset, IDFS was improved in patients who received metformin (hazard ratio, 0.64; P = .03), as was overall survival (HR, 0.53; P = .04).
The findings were presented at the San Antonio Breast Cancer Symposium.
“This trial arose from the observation that obesity is associated with poor breast cancer outcomes, and insulin levels are higher in obesity and may be more strongly associated with breast cancer outcomes than obesity,” said Dr. Goodwin.
Metformin was used because of its ability to promote modest weight loss and lower insulin by about 15%-20% in nondiabetic breast cancer survivors. It has also shown anticancer effects in preclinical studies. “In some window of opportunity neoadjuvant studies, it has been shown to reduce Ki67 in breast cancer cells,” she said. “And in preclinical in vitro and in vivo research, it slows growth of breast cancer.”
In addition, emerging evidence from observational studies suggests that the use of metformin to treat diabetes in breast cancer patients may be associated with better outcomes, strengthening the rationale for the study.
The negative results in breast cancer follow recent reports of negative findings in lung cancer, when metformin was found to be ineffective when used alongside chemotherapy in locally advanced lung cancer, as reported by this news organization.
No benefit seen
Metformin was compared to placebo in the phase 3 CCTG MA.32 trial, conducted in 3,649 patients aged 18-74 years with T1-3 N0-3 M0 breast cancer. All patients were treated with standard therapy and were randomized to receive metformin 850 mg twice daily for 5 years or placebo.
In 2016, “futility was declared in ER/PR-negative patients” after a second interim analysis conducted at 29.6 months’ median follow-up, Dr. Goodwin noted. The intervention was stopped in that group, although blinding and follow-up continued.
After that, the study’s primary analysis focused on the 2,533 ER/PR-positive patients (mean age, 52.7 years; mean body mass index, 28.8; approx. 60% postmenopausal).
Just over half of these patients had T2 tumor stage, and most disease was grade 2 or 3.
In addition, 16.5% (of metformin) and 17.4% (of placebo) patients had HER2-positive disease, with the majority (97%) of all HER2 patients receiving trastuzumab.
There was no difference between the two groups in IDFS events, occurring in 18.5% of patients receiving metformin and 18.3% who received placebo, with most (75.6%) events due to breast cancer (HR, 1.01; P = .92).
There were 131 deaths in the metformin arm and 119 in the placebo arm, with most (75.8%) of the deaths related to breast cancer (HR, 1.10; P = .47).
Other breast cancer outcomes had similar results, including distant disease-free survival (HR, 0.99; P = .94) and breast cancer–free interval (HR, 0.98; P = .87), both of which showed no advantage for metformin.
Possible HER2 advantage
However, the exploratory analysis suggested there may be an advantage for patients with HER2-positive disease, but primarily those who had at least one C allele of a prespecified ATM associated rs11212617 SNP. These patients achieved a higher pathologic complete response rate with metformin than that of those without the allele.
There were 620 patients with HER2-positive disease analyzed, with 99.4% receiving chemotherapy and 96.5% receiving trastuzumab. There were 99 IDFS events, and 47 OS events.
In the entire HER2-positive cohort, patients who received metformin had fewer IDFS events (HR, 0.64; P = .026) compared with the placebo arm. Mortality was lower with metformin (HR for overall survival, 0.53; P = .038).
“Subjects with HER2-positive breast cancer, notably those with at least one C allele of the ATM-associated rs11212617 SNP, experienced improved IDFS and overall survival with metformin,” Dr. Goodwin concluded. “However, no P-value ‘spend’ was allocated to this comparison. As a result, it requires replication in a prospective trial focusing on the HER2-positive population.”
More research?
Stephanie Bernik, MD, chief of breast surgery, Mount Sinai West, and associate professor of breast surgery, Icahn School of Medicine at Mount Sinai, New York, was approached by this news organization for an independent comment.
“It has long been known that obesity, which often correlates with diabetes, increases a woman’s risk of breast cancer,” she said.
“This study tried to show that using a medication that helps control insulin levels, even in those without diabetes, might decrease one’s risk of breast cancer,” she said. “Unfortunately, using metformin had no effect on outcomes in this study, even though it has shown promise in other studies. Perhaps more research needs to be carried out to try to pinpoint which mechanisms of action, if any, might be helpful to combat cancer in those with and without diabetes.”
The study was funded by the Canadian Cancer Trials Group, Cancer Therapy Evaluation Program, Breast Cancer Researcher Foundation, Susan G. Komen for the Cure, Canadian Cancer Society, Apotex, Swiss Cancer Research, and the Canadian Breast Cancer Foundation. Dr. Goodwin has no disclosures.
A version of this article first appeared on Medscape.com.
In the primary analysis, the addition of metformin to standard therapy in moderate/high-risk hormone receptor positive or negative breast cancer did not improve invasive disease–free survival (IDFS), overall survival, or other breast outcomes, explained lead author Pamela J. Goodwin, MD, FRCPC, professor of medicine at the University of Toronto. “Metformin should not be used as breast cancer treatment in this population.”
However, an exploratory analysis suggested that metformin may have a beneficial effect in women with HER2-positive breast cancer, Dr. Goodwin noted.
In this subset, IDFS was improved in patients who received metformin (hazard ratio, 0.64; P = .03), as was overall survival (HR, 0.53; P = .04).
The findings were presented at the San Antonio Breast Cancer Symposium.
“This trial arose from the observation that obesity is associated with poor breast cancer outcomes, and insulin levels are higher in obesity and may be more strongly associated with breast cancer outcomes than obesity,” said Dr. Goodwin.
Metformin was used because of its ability to promote modest weight loss and lower insulin by about 15%-20% in nondiabetic breast cancer survivors. It has also shown anticancer effects in preclinical studies. “In some window of opportunity neoadjuvant studies, it has been shown to reduce Ki67 in breast cancer cells,” she said. “And in preclinical in vitro and in vivo research, it slows growth of breast cancer.”
In addition, emerging evidence from observational studies suggests that the use of metformin to treat diabetes in breast cancer patients may be associated with better outcomes, strengthening the rationale for the study.
The negative results in breast cancer follow recent reports of negative findings in lung cancer, when metformin was found to be ineffective when used alongside chemotherapy in locally advanced lung cancer, as reported by this news organization.
No benefit seen
Metformin was compared to placebo in the phase 3 CCTG MA.32 trial, conducted in 3,649 patients aged 18-74 years with T1-3 N0-3 M0 breast cancer. All patients were treated with standard therapy and were randomized to receive metformin 850 mg twice daily for 5 years or placebo.
In 2016, “futility was declared in ER/PR-negative patients” after a second interim analysis conducted at 29.6 months’ median follow-up, Dr. Goodwin noted. The intervention was stopped in that group, although blinding and follow-up continued.
After that, the study’s primary analysis focused on the 2,533 ER/PR-positive patients (mean age, 52.7 years; mean body mass index, 28.8; approx. 60% postmenopausal).
Just over half of these patients had T2 tumor stage, and most disease was grade 2 or 3.
In addition, 16.5% (of metformin) and 17.4% (of placebo) patients had HER2-positive disease, with the majority (97%) of all HER2 patients receiving trastuzumab.
There was no difference between the two groups in IDFS events, occurring in 18.5% of patients receiving metformin and 18.3% who received placebo, with most (75.6%) events due to breast cancer (HR, 1.01; P = .92).
There were 131 deaths in the metformin arm and 119 in the placebo arm, with most (75.8%) of the deaths related to breast cancer (HR, 1.10; P = .47).
Other breast cancer outcomes had similar results, including distant disease-free survival (HR, 0.99; P = .94) and breast cancer–free interval (HR, 0.98; P = .87), both of which showed no advantage for metformin.
Possible HER2 advantage
However, the exploratory analysis suggested there may be an advantage for patients with HER2-positive disease, but primarily those who had at least one C allele of a prespecified ATM associated rs11212617 SNP. These patients achieved a higher pathologic complete response rate with metformin than that of those without the allele.
There were 620 patients with HER2-positive disease analyzed, with 99.4% receiving chemotherapy and 96.5% receiving trastuzumab. There were 99 IDFS events, and 47 OS events.
In the entire HER2-positive cohort, patients who received metformin had fewer IDFS events (HR, 0.64; P = .026) compared with the placebo arm. Mortality was lower with metformin (HR for overall survival, 0.53; P = .038).
“Subjects with HER2-positive breast cancer, notably those with at least one C allele of the ATM-associated rs11212617 SNP, experienced improved IDFS and overall survival with metformin,” Dr. Goodwin concluded. “However, no P-value ‘spend’ was allocated to this comparison. As a result, it requires replication in a prospective trial focusing on the HER2-positive population.”
More research?
Stephanie Bernik, MD, chief of breast surgery, Mount Sinai West, and associate professor of breast surgery, Icahn School of Medicine at Mount Sinai, New York, was approached by this news organization for an independent comment.
“It has long been known that obesity, which often correlates with diabetes, increases a woman’s risk of breast cancer,” she said.
“This study tried to show that using a medication that helps control insulin levels, even in those without diabetes, might decrease one’s risk of breast cancer,” she said. “Unfortunately, using metformin had no effect on outcomes in this study, even though it has shown promise in other studies. Perhaps more research needs to be carried out to try to pinpoint which mechanisms of action, if any, might be helpful to combat cancer in those with and without diabetes.”
The study was funded by the Canadian Cancer Trials Group, Cancer Therapy Evaluation Program, Breast Cancer Researcher Foundation, Susan G. Komen for the Cure, Canadian Cancer Society, Apotex, Swiss Cancer Research, and the Canadian Breast Cancer Foundation. Dr. Goodwin has no disclosures.
A version of this article first appeared on Medscape.com.
FROM SABCS 2021
Genomic profiling can improve PFS in metastatic breast cancer
“The message is very simple,” lead study author Fabrice Andre, MD, PhD, research director, Gustave Roussy Cancer Campus, Villejuif, France, told this news organization during a virtual press briefing. “If a genomic alteration is validated, it is useful to give targeted therapy, but if the genomic alteration is not validated, we should not give a targeted therapy.”
The study, which pooled results from phase 2 randomized trials SAFIR02-BREAST and SAFIR-P13K, was presented Dec. 7 in a virtual press briefing at the San Antonio Breast Cancer Symposium (SABCS) 2021.
The new analysis explored two key questions: Is genomic testing of a cancer effective? And how should oncologists interpret a genomic report?
A total of 1,462 patients with metastatic HER2-negative breast cancer underwent next-generation sequencing. After receiving six to eight cycles of chemotherapy, 238 patients (16%) were randomized to one of nine targeted therapies matched to the genomic alteration identified on testing or to maintenance chemotherapy.
Genomic alterations in the patients’ tumors were classified using the ESMO Scale of Actionability of Molecular Targets (ESCAT). A tier I ranking indicates that the alteration-drug match is associated with improved outcomes in clinical trials, while a tier II ranking means that the alteration-drug match is associated with antitumor activity but the magnitude of benefit remains unknown.
In an analysis of the overall trial population, Dr. Andre and colleagues found an improvement in progression-free survival in the targeted therapy group (median of 5.5 months) in comparison with the maintenance chemotherapy group (2.9 months), but the difference was not significant (P = .109).
In a subgroup of 115 patients presenting with I- or II-tier genomic alterations, median progression-free survival was 59% longer, at 9.1 months, among patients receiving targeted therapy, compared with 2.8 months in the maintenance chemotherapy group (hazard ratio, 0.41; P < .001).
In addition, the team carried out single-nucleotide polymorphism (SNP) array analyses on 926 patients. They identified 21 genes that were altered more frequently in the metastases compared with the primary tumors, and they observed that a high homologous recombination deficiency score in patients with BCRA 1 or 2 mutations was associated with a longer progression-free survival in patients treated with olaparib.
“We also identified a subset of patients who are resistant to CDK4/6 inhibitors who presented with CDK4 amplification, and this amplification is associated with overexpression,” Dr. Andre explained.
When asked whether most oncologists were using genomic profiling to tailor treatment for breast cancer patients, Dr. Andre said that multigene sequencing is now widely used.
“The issue is not so much whether we should use or not use genomics; the issue here is to force everyone to put the genomic alteration in the right context in terms of its level of evidence,” Dr. Andre told this news organization.
Oncologists may overinterpret the genomic activation identified and give a targeted therapy that is not validated, but “oncologists should not use genomic information when the target has not been previously validated in a therapeutic trial,” he added.
Virginia Kaklamani, MD, professor of medicine at the University of Texas Health Sciences Center in San Antonio, said in an interview that approximately 5 years ago, Dr. Andre was part of the first debate at the SABCS discussing whether oncologists should be conducting next-generation sequencing for their patients with breast cancer.
“At the time, [Dr.] Andre’s comment was that we should not be doing it,” recalled Dr. Kaklamani, who is also leader of the breast cancer program at the Mays Cancer Center at the University of Texas Health San Antonio MD Anderson. “At that point, I think it was clear that we did not have the data we needed to be able to use next-generation sequencing to change our clinical management.”
However, the evidence has evolved. “Based on this clinical trial, I think we now do have the data,” she said. “I think that [next-generation sequencing] is something we will be using more and more in practice and treating our patients based on [validated] genomic alterations.”
Dr. Andre has received grants or advisory board/speaker honoraria from Daiichi Sankyo, Roche, Pfizer, AstraZeneca, Lily, and Novartis. Dr. Kaklamani has served as a consultant for Puma, AstraZeneca, Athenex, and Immunomedics, has received research funding from Eisai, and has served as a speaker for Pfizer, Celgene, Genentech, and Genomic Health, among other companies.
A version of this article first appeared on Medscape.com.
“The message is very simple,” lead study author Fabrice Andre, MD, PhD, research director, Gustave Roussy Cancer Campus, Villejuif, France, told this news organization during a virtual press briefing. “If a genomic alteration is validated, it is useful to give targeted therapy, but if the genomic alteration is not validated, we should not give a targeted therapy.”
The study, which pooled results from phase 2 randomized trials SAFIR02-BREAST and SAFIR-P13K, was presented Dec. 7 in a virtual press briefing at the San Antonio Breast Cancer Symposium (SABCS) 2021.
The new analysis explored two key questions: Is genomic testing of a cancer effective? And how should oncologists interpret a genomic report?
A total of 1,462 patients with metastatic HER2-negative breast cancer underwent next-generation sequencing. After receiving six to eight cycles of chemotherapy, 238 patients (16%) were randomized to one of nine targeted therapies matched to the genomic alteration identified on testing or to maintenance chemotherapy.
Genomic alterations in the patients’ tumors were classified using the ESMO Scale of Actionability of Molecular Targets (ESCAT). A tier I ranking indicates that the alteration-drug match is associated with improved outcomes in clinical trials, while a tier II ranking means that the alteration-drug match is associated with antitumor activity but the magnitude of benefit remains unknown.
In an analysis of the overall trial population, Dr. Andre and colleagues found an improvement in progression-free survival in the targeted therapy group (median of 5.5 months) in comparison with the maintenance chemotherapy group (2.9 months), but the difference was not significant (P = .109).
In a subgroup of 115 patients presenting with I- or II-tier genomic alterations, median progression-free survival was 59% longer, at 9.1 months, among patients receiving targeted therapy, compared with 2.8 months in the maintenance chemotherapy group (hazard ratio, 0.41; P < .001).
In addition, the team carried out single-nucleotide polymorphism (SNP) array analyses on 926 patients. They identified 21 genes that were altered more frequently in the metastases compared with the primary tumors, and they observed that a high homologous recombination deficiency score in patients with BCRA 1 or 2 mutations was associated with a longer progression-free survival in patients treated with olaparib.
“We also identified a subset of patients who are resistant to CDK4/6 inhibitors who presented with CDK4 amplification, and this amplification is associated with overexpression,” Dr. Andre explained.
When asked whether most oncologists were using genomic profiling to tailor treatment for breast cancer patients, Dr. Andre said that multigene sequencing is now widely used.
“The issue is not so much whether we should use or not use genomics; the issue here is to force everyone to put the genomic alteration in the right context in terms of its level of evidence,” Dr. Andre told this news organization.
Oncologists may overinterpret the genomic activation identified and give a targeted therapy that is not validated, but “oncologists should not use genomic information when the target has not been previously validated in a therapeutic trial,” he added.
Virginia Kaklamani, MD, professor of medicine at the University of Texas Health Sciences Center in San Antonio, said in an interview that approximately 5 years ago, Dr. Andre was part of the first debate at the SABCS discussing whether oncologists should be conducting next-generation sequencing for their patients with breast cancer.
“At the time, [Dr.] Andre’s comment was that we should not be doing it,” recalled Dr. Kaklamani, who is also leader of the breast cancer program at the Mays Cancer Center at the University of Texas Health San Antonio MD Anderson. “At that point, I think it was clear that we did not have the data we needed to be able to use next-generation sequencing to change our clinical management.”
However, the evidence has evolved. “Based on this clinical trial, I think we now do have the data,” she said. “I think that [next-generation sequencing] is something we will be using more and more in practice and treating our patients based on [validated] genomic alterations.”
Dr. Andre has received grants or advisory board/speaker honoraria from Daiichi Sankyo, Roche, Pfizer, AstraZeneca, Lily, and Novartis. Dr. Kaklamani has served as a consultant for Puma, AstraZeneca, Athenex, and Immunomedics, has received research funding from Eisai, and has served as a speaker for Pfizer, Celgene, Genentech, and Genomic Health, among other companies.
A version of this article first appeared on Medscape.com.
“The message is very simple,” lead study author Fabrice Andre, MD, PhD, research director, Gustave Roussy Cancer Campus, Villejuif, France, told this news organization during a virtual press briefing. “If a genomic alteration is validated, it is useful to give targeted therapy, but if the genomic alteration is not validated, we should not give a targeted therapy.”
The study, which pooled results from phase 2 randomized trials SAFIR02-BREAST and SAFIR-P13K, was presented Dec. 7 in a virtual press briefing at the San Antonio Breast Cancer Symposium (SABCS) 2021.
The new analysis explored two key questions: Is genomic testing of a cancer effective? And how should oncologists interpret a genomic report?
A total of 1,462 patients with metastatic HER2-negative breast cancer underwent next-generation sequencing. After receiving six to eight cycles of chemotherapy, 238 patients (16%) were randomized to one of nine targeted therapies matched to the genomic alteration identified on testing or to maintenance chemotherapy.
Genomic alterations in the patients’ tumors were classified using the ESMO Scale of Actionability of Molecular Targets (ESCAT). A tier I ranking indicates that the alteration-drug match is associated with improved outcomes in clinical trials, while a tier II ranking means that the alteration-drug match is associated with antitumor activity but the magnitude of benefit remains unknown.
In an analysis of the overall trial population, Dr. Andre and colleagues found an improvement in progression-free survival in the targeted therapy group (median of 5.5 months) in comparison with the maintenance chemotherapy group (2.9 months), but the difference was not significant (P = .109).
In a subgroup of 115 patients presenting with I- or II-tier genomic alterations, median progression-free survival was 59% longer, at 9.1 months, among patients receiving targeted therapy, compared with 2.8 months in the maintenance chemotherapy group (hazard ratio, 0.41; P < .001).
In addition, the team carried out single-nucleotide polymorphism (SNP) array analyses on 926 patients. They identified 21 genes that were altered more frequently in the metastases compared with the primary tumors, and they observed that a high homologous recombination deficiency score in patients with BCRA 1 or 2 mutations was associated with a longer progression-free survival in patients treated with olaparib.
“We also identified a subset of patients who are resistant to CDK4/6 inhibitors who presented with CDK4 amplification, and this amplification is associated with overexpression,” Dr. Andre explained.
When asked whether most oncologists were using genomic profiling to tailor treatment for breast cancer patients, Dr. Andre said that multigene sequencing is now widely used.
“The issue is not so much whether we should use or not use genomics; the issue here is to force everyone to put the genomic alteration in the right context in terms of its level of evidence,” Dr. Andre told this news organization.
Oncologists may overinterpret the genomic activation identified and give a targeted therapy that is not validated, but “oncologists should not use genomic information when the target has not been previously validated in a therapeutic trial,” he added.
Virginia Kaklamani, MD, professor of medicine at the University of Texas Health Sciences Center in San Antonio, said in an interview that approximately 5 years ago, Dr. Andre was part of the first debate at the SABCS discussing whether oncologists should be conducting next-generation sequencing for their patients with breast cancer.
“At the time, [Dr.] Andre’s comment was that we should not be doing it,” recalled Dr. Kaklamani, who is also leader of the breast cancer program at the Mays Cancer Center at the University of Texas Health San Antonio MD Anderson. “At that point, I think it was clear that we did not have the data we needed to be able to use next-generation sequencing to change our clinical management.”
However, the evidence has evolved. “Based on this clinical trial, I think we now do have the data,” she said. “I think that [next-generation sequencing] is something we will be using more and more in practice and treating our patients based on [validated] genomic alterations.”
Dr. Andre has received grants or advisory board/speaker honoraria from Daiichi Sankyo, Roche, Pfizer, AstraZeneca, Lily, and Novartis. Dr. Kaklamani has served as a consultant for Puma, AstraZeneca, Athenex, and Immunomedics, has received research funding from Eisai, and has served as a speaker for Pfizer, Celgene, Genentech, and Genomic Health, among other companies.
A version of this article first appeared on Medscape.com.
Cancer risk-reducing strategies: Focus on chemoprevention
In her presentation at The North American Menopause Society (NAMS) 2021 annual meeting (September 22–25, 2021, in Washington, DC), Dr. Holly J. Pederson offered her expert perspectives on breast cancer prevention in at-risk women in “Chemoprevention for risk reduction: Women’s health clinicians have a role.”
Which patients would benefit from chemoprevention?
Holly J. Pederson, MD: Obviously, women with significant family history are at risk. And approximately 10% of biopsies that are done for other reasons incidentally show atypical hyperplasia (AH) or lobular carcinoma in situ (LCIS)—which are not precancers or cancers but are markers for the development of the disease—and they markedly increase risk. Atypical hyperplasia confers a 30% risk for developing breast cancer over the next 25 years, and LCIS is associated with up to a 2% per year risk. In this setting, preventive medication has been shown to cut risk by 56% to 86%; this is a targeted population that is often overlooked.
Mathematical risk models can be used to assess risk by assessing women’s risk factors. The United States Preventive Services Task Force (USPSTF) has set forth a threshold at which they believe the benefits outweigh the risks of preventive medications. That threshold is 3% or greater over the next 5 years using the Gail breast cancer risk assessment tool.1 The American Society of Clinical Oncology (ASCO) uses the Tyrer-Cuzick breast cancer risk evaluation model with a threshold of 5% over the next 10 years.2 In general, those are the situations in which chemoprevention is a no-brainer.
Certain genetic mutations also predispose to estrogen-sensitive breast cancer. While preventive medications specifically have not been studied in large groups of gene carriers, chemoprevention makes sense because these medications prevent estrogen-sensitive breast cancers that those patients are prone to. Examples would be patients with ATM and CHEK2 gene mutations, which are very common, and patients with BRCA2 and even BRCA1 variants in the postmenopausal years. Those are the big targets.
Risk assessment models
Dr. Pederson: Yes, I almost exclusively use the Tyrer-Cuzick risk model, version 8, which incorporates breast density. This model is intimidating to some practitioners initially, but once you get used to it, you can complete it very quickly.
The Gail model is very limited. It assesses only first-degree relatives, so you don’t get the paternal information at all, and you don’t use age at diagnosis, family structure, genetic testing, results of breast density, or body mass index (BMI). There are many limitations of the Gail model, but most people use it because it is so easy and they are familiar with it.
Possibly the best model is the CanRisk tool, which incorporates the Breast and Ovarian Analysis of Disease Incidence and Carrier Estimation Algorithm (BOADICEA), but it takes too much time to use in clinic; it’s too complicated. The Tyrer-Cuzick model is easy to use once you get used to it.
Dr. Pederson: Risk doesn’t always need to be formally calculated, which can be time-consuming. It’s one of those situations where most practitioners know it when they see it. Benign atypical biopsies, a strong family history, or, obviously, the presence of a genetic mutation are huge red flags.
If a practitioner has a nearby high-risk center where they can refer patients, that can be so useful, even for a one-time consultation to guide management. For example, with the virtual world now, I do a lot of consultations for patients and outline a plan, and then the referring practitioner can carry out the plan with confidence and then send the patient back periodically. There are so many more options now that previously did not exist for the busy ObGyn or primary care provider to rely on.
Continue to: Chemoprevention uptake in at-risk women...
Chemoprevention uptake in at-risk women
Dr. Pederson: We really never practice medicine using numbers. We use clinical judgment, and we use relationships with patients in terms of developing confidence and trust. I think that the uptake that we exhibit in our center probably is more based on the patients’ perception that we are confident in our recommendations. I think that many practitioners simply are not comfortable with explaining medications, explaining and managing adverse effects, and using alternative medications. While the modeling helps, I think the personal expertise really makes the difference.
Going forward, the addition of the polygenic risk score to the mathematical risk models is going to make a big difference. Right now, the mathematical risk model is simply that: it takes the traditional risk factors that a patient has and spits out a number. But adding the patient’s genomic data—that is, a weighted summation of SNPs, or single nucleotide polymorphisms, now numbering over 300 for breast cancer—can explain more about their personalized risk, which is going to be more powerful in influencing a woman to take medication or not to take medication, in my opinion. Knowing their actual genomic risk will be a big step forward in individualized risk stratification and increased medication uptake as well as vigilance with high risk screening and attention to diet, exercise, and drinking alcohol in moderation.
Dr. Pederson: The only drug that can be used in the premenopausal setting is tamoxifen (TABLE 1). Women can’t take it if they are pregnant, planning to become pregnant, or if they don’t use a reliable form of birth control because it is teratogenic. Women also cannot take tamoxifen if they have had a history of blood clots, stroke, or transient ischemic attack; if they are on warfarin or estrogen preparations; or if they have had atypical endometrial biopsies or endometrial cancer. Those are the absolute contraindications for tamoxifen use.
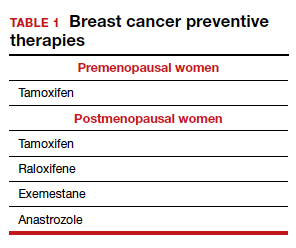
Tamoxifen is generally very well tolerated in most women; some women experience hot flashes and night sweats that often will subside (or become tolerable) over the first 90 days. In addition, some women experience vaginal discharge rather than dryness, but it is not as bothersome to patients as dryness can be.
Tamoxifen can be used in the pre- or postmenopausal setting. In healthy premenopausal women, there’s no increased risk of the serious adverse effects that are seen with tamoxifen use in postmenopausal women, such as the 1% risk of blood clots and the 1% risk of endometrial cancer.
In postmenopausal women who still have their uterus, I’ll preferentially use raloxifene over tamoxifen. If they don’t have their uterus, tamoxifen is slightly more effective than the raloxifene, and I’ll use that.
Tamoxifen and raloxifene are both selective estrogen receptor modulators, or SERMs, which means that they stimulate receptors in some tissues, like bone, keeping bones strong, and block the receptors in other tissues, like the breast, reducing risk. And so you get kind of a two-for-one in terms of breast cancer risk reduction and osteoporosis prevention.
Another class of preventive drugs is the aromatase inhibitors (AIs). They block the enzyme aromatase, which converts androgens to estrogens peripherally; that is, the androgens that are produced primarily in the adrenal gland, but in part in postmenopausal ovaries.
In general, AIs are less well tolerated. There are generally more hot flashes and night sweats, and more vaginal dryness than with the SERMs. Anastrozole use is associated with arthralgias; and with exemestane use, there can be some hair loss (TABLE 2). Relative contraindications to SERMs become more important in the postmenopausal setting because of the increased frequency of both blood clots and uterine cancer in the postmenopausal years. I won’t give it to smokers. I won’t give tamoxifen to smokers in the premenopausal period either. With obese women, care must be taken because of the risk of blood clots with the SERMS, so then I’ll resort to the AIs. In the postmenopausal setting, you have to think a lot harder about the choices you use for preventive medication. Preferentially, I’ll use the SERMS if possible as they have fewer adverse effects.
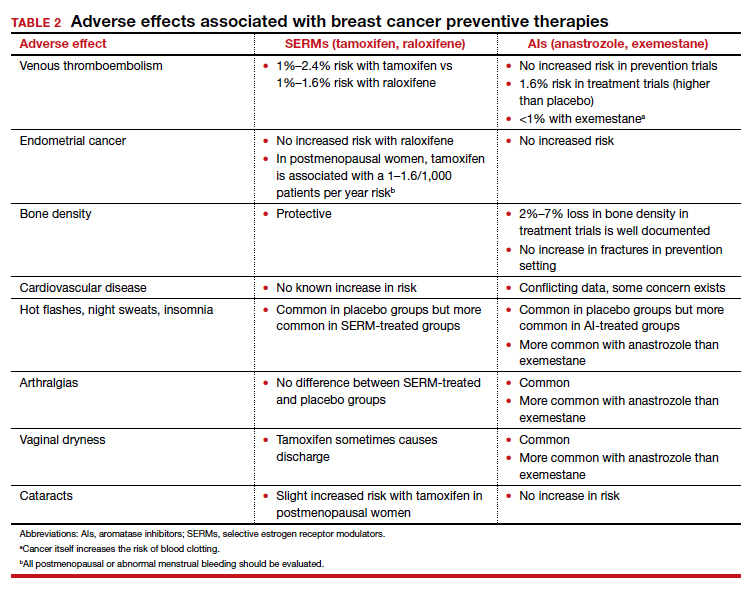
Dr. Pederson: All of them are recommended to be given for 5 years, but the MAP.3 trial, which studied exemestane compared with placebo, showed a 65% risk reduction with 3 years of therapy.3 So occasionally, we’ll use 3 years of therapy. Why the treatment recommendation is universally 5 years is unclear, given that the trial with that particular drug was done in 3 years. And with low-dose tamoxifen, the recommended duration is 3 years. That study was done in Italy with 5 mg daily for 3 years.4 In the United States we use 10 mg every other day for 3 years because the 5-mg tablet is not available here.
Continue to: Counseling points...
Counseling points
Dr. Pederson: Patients’ fears about adverse effects are often worse than the adverse effects themselves. Women will fester over, Should I take it? Should I take it possibly for years? And then they take the medication and they tell me, “I don’t even notice that I’m taking it, and I know I’m being proactive.” The majority of patients who take these medications don’t have a lot of significant adverse effects.
Severe hot flashes can be managed in a number of ways, primarily and most effectively with certain antidepressants. Oxybutynin use is another good way to manage vasomotor symptoms. Sometimes we use local vaginal estrogen if a patient has vaginal dryness. In general, however, I would say at least 80% of my patients who take preventive medications do not require management of adverse side effects, that they are tolerable.
I counsel women this way, “Don’t think of this as a 5-year course of medication. Think of it as a 90-day trial, and let’s see how you do. If you hate it, then we don’t do it.” They often are pleasantly surprised that the medication is much easier to tolerate than they thought it would be.
Dr. Pederson: It would be neat if a trial would directly compare lifestyle interventions with medications, because probably lifestyle change is as effective as medication is—but we don’t know that and probably will never have that data. We do know that alcohol consumption, every drink per day, increases risk by 10%. We know that obesity is responsible for 30% of breast cancers in this country, and that hormone replacement probably is overrated as a significant risk factor. Updated data from the Women’s Health Initiative study suggest that hormone replacement may actually reduce both breast cancer and cardiovascular risk in women in their 50s, but that’s in average-risk women and not in high-risk women, so we can’t generalize. We do recommend lifestyle measures including weight loss, exercise, and limiting alcohol consumption for all of our patients and certainly for our high-risk patients.
The only 2 things a woman can do to reduce the risk of triple negative breast cancer are to achieve and maintain ideal body weight and to breastfeed. The medications that I have mentioned don’t reduce the risk of triple negative breast cancer. Staying thin and breastfeeding do. It’s a problem in this country because at least 35% of all women and 58% of Black women are obese in America, and Black women tend to be prone to triple-negative breast cancer. That’s a real public health issue that we need to address. If we were going to focus on one thing, it would be focusing on obesity in terms of risk reduction.
Final thoughts
Dr. Pederson: I would like to direct attention to the American Heart Association scientific statement published at the end of 2020 that reported that hormone replacement in average-risk women reduced both cardiovascular events and overall mortality in women in their 50s by 30%.5 While that’s not directly related to what we are talking about, we need to weigh the pros and cons of estrogen versus estrogen blockade in women in terms of breast cancer risk management discussions. Part of shared decision making now needs to include cardiovascular risk factors and how estrogen is going to play into that.
In women with atypical hyperplasia or LCIS, they may benefit from the preventive medications we discussed. But in women with family history or in women with genetic mutations who have not had benign atypical biopsies, they may choose to consider estrogen during their 50s and perhaps take tamoxifen either beforehand or raloxifene afterward.
We need to look at patients holistically and consider all their risk factors together. We can’t look at one dimension alone.
- US Preventive Services Task Force. Medication use to reduce risk of breast cancer: US Preventive Services Task Force Recommendation Statement. JAMA. 2019;322:857-867.
- Visvanathan K, Fabian CJ, Bantug E, et al. Use of endocrine therapy for breast cancer risk reduction: ASCO clinical practice guideline update. J Clin Oncol. 2019;37:3152-3165.
- Goss PE, Ingle JN, Alex-Martinez JE, et al. Exemestane for breast-cancer prevention in postmenopausal women. N Engl J Med. 2011;364:2381-2391.
- DeCensi A, Puntoni M, Guerrieri-Gonzaga A, et al. Randomized placebo controlled trial of low-dose tamoxifen to prevent local and contralateral recurrence in breast intraepithelial neoplasia. J Clin Oncol. 2019;37:1629-1637.
- El Khoudary SR, Aggarwal B, Beckie TM, et al; American Heart Association Prevention Science Committee of the Council on Epidemiology and Prevention, and Council on Cardiovascular and Stroke Nursing. Menopause transition and cardiovascular disease risk: implications for timing of early prevention: a scientific statement from the American Heart Association. Circulation. 2020;142:e506-e532.
In her presentation at The North American Menopause Society (NAMS) 2021 annual meeting (September 22–25, 2021, in Washington, DC), Dr. Holly J. Pederson offered her expert perspectives on breast cancer prevention in at-risk women in “Chemoprevention for risk reduction: Women’s health clinicians have a role.”
Which patients would benefit from chemoprevention?
Holly J. Pederson, MD: Obviously, women with significant family history are at risk. And approximately 10% of biopsies that are done for other reasons incidentally show atypical hyperplasia (AH) or lobular carcinoma in situ (LCIS)—which are not precancers or cancers but are markers for the development of the disease—and they markedly increase risk. Atypical hyperplasia confers a 30% risk for developing breast cancer over the next 25 years, and LCIS is associated with up to a 2% per year risk. In this setting, preventive medication has been shown to cut risk by 56% to 86%; this is a targeted population that is often overlooked.
Mathematical risk models can be used to assess risk by assessing women’s risk factors. The United States Preventive Services Task Force (USPSTF) has set forth a threshold at which they believe the benefits outweigh the risks of preventive medications. That threshold is 3% or greater over the next 5 years using the Gail breast cancer risk assessment tool.1 The American Society of Clinical Oncology (ASCO) uses the Tyrer-Cuzick breast cancer risk evaluation model with a threshold of 5% over the next 10 years.2 In general, those are the situations in which chemoprevention is a no-brainer.
Certain genetic mutations also predispose to estrogen-sensitive breast cancer. While preventive medications specifically have not been studied in large groups of gene carriers, chemoprevention makes sense because these medications prevent estrogen-sensitive breast cancers that those patients are prone to. Examples would be patients with ATM and CHEK2 gene mutations, which are very common, and patients with BRCA2 and even BRCA1 variants in the postmenopausal years. Those are the big targets.
Risk assessment models
Dr. Pederson: Yes, I almost exclusively use the Tyrer-Cuzick risk model, version 8, which incorporates breast density. This model is intimidating to some practitioners initially, but once you get used to it, you can complete it very quickly.
The Gail model is very limited. It assesses only first-degree relatives, so you don’t get the paternal information at all, and you don’t use age at diagnosis, family structure, genetic testing, results of breast density, or body mass index (BMI). There are many limitations of the Gail model, but most people use it because it is so easy and they are familiar with it.
Possibly the best model is the CanRisk tool, which incorporates the Breast and Ovarian Analysis of Disease Incidence and Carrier Estimation Algorithm (BOADICEA), but it takes too much time to use in clinic; it’s too complicated. The Tyrer-Cuzick model is easy to use once you get used to it.
Dr. Pederson: Risk doesn’t always need to be formally calculated, which can be time-consuming. It’s one of those situations where most practitioners know it when they see it. Benign atypical biopsies, a strong family history, or, obviously, the presence of a genetic mutation are huge red flags.
If a practitioner has a nearby high-risk center where they can refer patients, that can be so useful, even for a one-time consultation to guide management. For example, with the virtual world now, I do a lot of consultations for patients and outline a plan, and then the referring practitioner can carry out the plan with confidence and then send the patient back periodically. There are so many more options now that previously did not exist for the busy ObGyn or primary care provider to rely on.
Continue to: Chemoprevention uptake in at-risk women...
Chemoprevention uptake in at-risk women
Dr. Pederson: We really never practice medicine using numbers. We use clinical judgment, and we use relationships with patients in terms of developing confidence and trust. I think that the uptake that we exhibit in our center probably is more based on the patients’ perception that we are confident in our recommendations. I think that many practitioners simply are not comfortable with explaining medications, explaining and managing adverse effects, and using alternative medications. While the modeling helps, I think the personal expertise really makes the difference.
Going forward, the addition of the polygenic risk score to the mathematical risk models is going to make a big difference. Right now, the mathematical risk model is simply that: it takes the traditional risk factors that a patient has and spits out a number. But adding the patient’s genomic data—that is, a weighted summation of SNPs, or single nucleotide polymorphisms, now numbering over 300 for breast cancer—can explain more about their personalized risk, which is going to be more powerful in influencing a woman to take medication or not to take medication, in my opinion. Knowing their actual genomic risk will be a big step forward in individualized risk stratification and increased medication uptake as well as vigilance with high risk screening and attention to diet, exercise, and drinking alcohol in moderation.
Dr. Pederson: The only drug that can be used in the premenopausal setting is tamoxifen (TABLE 1). Women can’t take it if they are pregnant, planning to become pregnant, or if they don’t use a reliable form of birth control because it is teratogenic. Women also cannot take tamoxifen if they have had a history of blood clots, stroke, or transient ischemic attack; if they are on warfarin or estrogen preparations; or if they have had atypical endometrial biopsies or endometrial cancer. Those are the absolute contraindications for tamoxifen use.
Tamoxifen is generally very well tolerated in most women; some women experience hot flashes and night sweats that often will subside (or become tolerable) over the first 90 days. In addition, some women experience vaginal discharge rather than dryness, but it is not as bothersome to patients as dryness can be.
Tamoxifen can be used in the pre- or postmenopausal setting. In healthy premenopausal women, there’s no increased risk of the serious adverse effects that are seen with tamoxifen use in postmenopausal women, such as the 1% risk of blood clots and the 1% risk of endometrial cancer.
In postmenopausal women who still have their uterus, I’ll preferentially use raloxifene over tamoxifen. If they don’t have their uterus, tamoxifen is slightly more effective than the raloxifene, and I’ll use that.
Tamoxifen and raloxifene are both selective estrogen receptor modulators, or SERMs, which means that they stimulate receptors in some tissues, like bone, keeping bones strong, and block the receptors in other tissues, like the breast, reducing risk. And so you get kind of a two-for-one in terms of breast cancer risk reduction and osteoporosis prevention.
Another class of preventive drugs is the aromatase inhibitors (AIs). They block the enzyme aromatase, which converts androgens to estrogens peripherally; that is, the androgens that are produced primarily in the adrenal gland, but in part in postmenopausal ovaries.
In general, AIs are less well tolerated. There are generally more hot flashes and night sweats, and more vaginal dryness than with the SERMs. Anastrozole use is associated with arthralgias; and with exemestane use, there can be some hair loss (TABLE 2). Relative contraindications to SERMs become more important in the postmenopausal setting because of the increased frequency of both blood clots and uterine cancer in the postmenopausal years. I won’t give it to smokers. I won’t give tamoxifen to smokers in the premenopausal period either. With obese women, care must be taken because of the risk of blood clots with the SERMS, so then I’ll resort to the AIs. In the postmenopausal setting, you have to think a lot harder about the choices you use for preventive medication. Preferentially, I’ll use the SERMS if possible as they have fewer adverse effects.
Dr. Pederson: All of them are recommended to be given for 5 years, but the MAP.3 trial, which studied exemestane compared with placebo, showed a 65% risk reduction with 3 years of therapy.3 So occasionally, we’ll use 3 years of therapy. Why the treatment recommendation is universally 5 years is unclear, given that the trial with that particular drug was done in 3 years. And with low-dose tamoxifen, the recommended duration is 3 years. That study was done in Italy with 5 mg daily for 3 years.4 In the United States we use 10 mg every other day for 3 years because the 5-mg tablet is not available here.
Continue to: Counseling points...
Counseling points
Dr. Pederson: Patients’ fears about adverse effects are often worse than the adverse effects themselves. Women will fester over, Should I take it? Should I take it possibly for years? And then they take the medication and they tell me, “I don’t even notice that I’m taking it, and I know I’m being proactive.” The majority of patients who take these medications don’t have a lot of significant adverse effects.
Severe hot flashes can be managed in a number of ways, primarily and most effectively with certain antidepressants. Oxybutynin use is another good way to manage vasomotor symptoms. Sometimes we use local vaginal estrogen if a patient has vaginal dryness. In general, however, I would say at least 80% of my patients who take preventive medications do not require management of adverse side effects, that they are tolerable.
I counsel women this way, “Don’t think of this as a 5-year course of medication. Think of it as a 90-day trial, and let’s see how you do. If you hate it, then we don’t do it.” They often are pleasantly surprised that the medication is much easier to tolerate than they thought it would be.
Dr. Pederson: It would be neat if a trial would directly compare lifestyle interventions with medications, because probably lifestyle change is as effective as medication is—but we don’t know that and probably will never have that data. We do know that alcohol consumption, every drink per day, increases risk by 10%. We know that obesity is responsible for 30% of breast cancers in this country, and that hormone replacement probably is overrated as a significant risk factor. Updated data from the Women’s Health Initiative study suggest that hormone replacement may actually reduce both breast cancer and cardiovascular risk in women in their 50s, but that’s in average-risk women and not in high-risk women, so we can’t generalize. We do recommend lifestyle measures including weight loss, exercise, and limiting alcohol consumption for all of our patients and certainly for our high-risk patients.
The only 2 things a woman can do to reduce the risk of triple negative breast cancer are to achieve and maintain ideal body weight and to breastfeed. The medications that I have mentioned don’t reduce the risk of triple negative breast cancer. Staying thin and breastfeeding do. It’s a problem in this country because at least 35% of all women and 58% of Black women are obese in America, and Black women tend to be prone to triple-negative breast cancer. That’s a real public health issue that we need to address. If we were going to focus on one thing, it would be focusing on obesity in terms of risk reduction.
Final thoughts
Dr. Pederson: I would like to direct attention to the American Heart Association scientific statement published at the end of 2020 that reported that hormone replacement in average-risk women reduced both cardiovascular events and overall mortality in women in their 50s by 30%.5 While that’s not directly related to what we are talking about, we need to weigh the pros and cons of estrogen versus estrogen blockade in women in terms of breast cancer risk management discussions. Part of shared decision making now needs to include cardiovascular risk factors and how estrogen is going to play into that.
In women with atypical hyperplasia or LCIS, they may benefit from the preventive medications we discussed. But in women with family history or in women with genetic mutations who have not had benign atypical biopsies, they may choose to consider estrogen during their 50s and perhaps take tamoxifen either beforehand or raloxifene afterward.
We need to look at patients holistically and consider all their risk factors together. We can’t look at one dimension alone.
In her presentation at The North American Menopause Society (NAMS) 2021 annual meeting (September 22–25, 2021, in Washington, DC), Dr. Holly J. Pederson offered her expert perspectives on breast cancer prevention in at-risk women in “Chemoprevention for risk reduction: Women’s health clinicians have a role.”
Which patients would benefit from chemoprevention?
Holly J. Pederson, MD: Obviously, women with significant family history are at risk. And approximately 10% of biopsies that are done for other reasons incidentally show atypical hyperplasia (AH) or lobular carcinoma in situ (LCIS)—which are not precancers or cancers but are markers for the development of the disease—and they markedly increase risk. Atypical hyperplasia confers a 30% risk for developing breast cancer over the next 25 years, and LCIS is associated with up to a 2% per year risk. In this setting, preventive medication has been shown to cut risk by 56% to 86%; this is a targeted population that is often overlooked.
Mathematical risk models can be used to assess risk by assessing women’s risk factors. The United States Preventive Services Task Force (USPSTF) has set forth a threshold at which they believe the benefits outweigh the risks of preventive medications. That threshold is 3% or greater over the next 5 years using the Gail breast cancer risk assessment tool.1 The American Society of Clinical Oncology (ASCO) uses the Tyrer-Cuzick breast cancer risk evaluation model with a threshold of 5% over the next 10 years.2 In general, those are the situations in which chemoprevention is a no-brainer.
Certain genetic mutations also predispose to estrogen-sensitive breast cancer. While preventive medications specifically have not been studied in large groups of gene carriers, chemoprevention makes sense because these medications prevent estrogen-sensitive breast cancers that those patients are prone to. Examples would be patients with ATM and CHEK2 gene mutations, which are very common, and patients with BRCA2 and even BRCA1 variants in the postmenopausal years. Those are the big targets.
Risk assessment models
Dr. Pederson: Yes, I almost exclusively use the Tyrer-Cuzick risk model, version 8, which incorporates breast density. This model is intimidating to some practitioners initially, but once you get used to it, you can complete it very quickly.
The Gail model is very limited. It assesses only first-degree relatives, so you don’t get the paternal information at all, and you don’t use age at diagnosis, family structure, genetic testing, results of breast density, or body mass index (BMI). There are many limitations of the Gail model, but most people use it because it is so easy and they are familiar with it.
Possibly the best model is the CanRisk tool, which incorporates the Breast and Ovarian Analysis of Disease Incidence and Carrier Estimation Algorithm (BOADICEA), but it takes too much time to use in clinic; it’s too complicated. The Tyrer-Cuzick model is easy to use once you get used to it.
Dr. Pederson: Risk doesn’t always need to be formally calculated, which can be time-consuming. It’s one of those situations where most practitioners know it when they see it. Benign atypical biopsies, a strong family history, or, obviously, the presence of a genetic mutation are huge red flags.
If a practitioner has a nearby high-risk center where they can refer patients, that can be so useful, even for a one-time consultation to guide management. For example, with the virtual world now, I do a lot of consultations for patients and outline a plan, and then the referring practitioner can carry out the plan with confidence and then send the patient back periodically. There are so many more options now that previously did not exist for the busy ObGyn or primary care provider to rely on.
Continue to: Chemoprevention uptake in at-risk women...
Chemoprevention uptake in at-risk women
Dr. Pederson: We really never practice medicine using numbers. We use clinical judgment, and we use relationships with patients in terms of developing confidence and trust. I think that the uptake that we exhibit in our center probably is more based on the patients’ perception that we are confident in our recommendations. I think that many practitioners simply are not comfortable with explaining medications, explaining and managing adverse effects, and using alternative medications. While the modeling helps, I think the personal expertise really makes the difference.
Going forward, the addition of the polygenic risk score to the mathematical risk models is going to make a big difference. Right now, the mathematical risk model is simply that: it takes the traditional risk factors that a patient has and spits out a number. But adding the patient’s genomic data—that is, a weighted summation of SNPs, or single nucleotide polymorphisms, now numbering over 300 for breast cancer—can explain more about their personalized risk, which is going to be more powerful in influencing a woman to take medication or not to take medication, in my opinion. Knowing their actual genomic risk will be a big step forward in individualized risk stratification and increased medication uptake as well as vigilance with high risk screening and attention to diet, exercise, and drinking alcohol in moderation.
Dr. Pederson: The only drug that can be used in the premenopausal setting is tamoxifen (TABLE 1). Women can’t take it if they are pregnant, planning to become pregnant, or if they don’t use a reliable form of birth control because it is teratogenic. Women also cannot take tamoxifen if they have had a history of blood clots, stroke, or transient ischemic attack; if they are on warfarin or estrogen preparations; or if they have had atypical endometrial biopsies or endometrial cancer. Those are the absolute contraindications for tamoxifen use.
Tamoxifen is generally very well tolerated in most women; some women experience hot flashes and night sweats that often will subside (or become tolerable) over the first 90 days. In addition, some women experience vaginal discharge rather than dryness, but it is not as bothersome to patients as dryness can be.
Tamoxifen can be used in the pre- or postmenopausal setting. In healthy premenopausal women, there’s no increased risk of the serious adverse effects that are seen with tamoxifen use in postmenopausal women, such as the 1% risk of blood clots and the 1% risk of endometrial cancer.
In postmenopausal women who still have their uterus, I’ll preferentially use raloxifene over tamoxifen. If they don’t have their uterus, tamoxifen is slightly more effective than the raloxifene, and I’ll use that.
Tamoxifen and raloxifene are both selective estrogen receptor modulators, or SERMs, which means that they stimulate receptors in some tissues, like bone, keeping bones strong, and block the receptors in other tissues, like the breast, reducing risk. And so you get kind of a two-for-one in terms of breast cancer risk reduction and osteoporosis prevention.
Another class of preventive drugs is the aromatase inhibitors (AIs). They block the enzyme aromatase, which converts androgens to estrogens peripherally; that is, the androgens that are produced primarily in the adrenal gland, but in part in postmenopausal ovaries.
In general, AIs are less well tolerated. There are generally more hot flashes and night sweats, and more vaginal dryness than with the SERMs. Anastrozole use is associated with arthralgias; and with exemestane use, there can be some hair loss (TABLE 2). Relative contraindications to SERMs become more important in the postmenopausal setting because of the increased frequency of both blood clots and uterine cancer in the postmenopausal years. I won’t give it to smokers. I won’t give tamoxifen to smokers in the premenopausal period either. With obese women, care must be taken because of the risk of blood clots with the SERMS, so then I’ll resort to the AIs. In the postmenopausal setting, you have to think a lot harder about the choices you use for preventive medication. Preferentially, I’ll use the SERMS if possible as they have fewer adverse effects.
Dr. Pederson: All of them are recommended to be given for 5 years, but the MAP.3 trial, which studied exemestane compared with placebo, showed a 65% risk reduction with 3 years of therapy.3 So occasionally, we’ll use 3 years of therapy. Why the treatment recommendation is universally 5 years is unclear, given that the trial with that particular drug was done in 3 years. And with low-dose tamoxifen, the recommended duration is 3 years. That study was done in Italy with 5 mg daily for 3 years.4 In the United States we use 10 mg every other day for 3 years because the 5-mg tablet is not available here.
Continue to: Counseling points...
Counseling points
Dr. Pederson: Patients’ fears about adverse effects are often worse than the adverse effects themselves. Women will fester over, Should I take it? Should I take it possibly for years? And then they take the medication and they tell me, “I don’t even notice that I’m taking it, and I know I’m being proactive.” The majority of patients who take these medications don’t have a lot of significant adverse effects.
Severe hot flashes can be managed in a number of ways, primarily and most effectively with certain antidepressants. Oxybutynin use is another good way to manage vasomotor symptoms. Sometimes we use local vaginal estrogen if a patient has vaginal dryness. In general, however, I would say at least 80% of my patients who take preventive medications do not require management of adverse side effects, that they are tolerable.
I counsel women this way, “Don’t think of this as a 5-year course of medication. Think of it as a 90-day trial, and let’s see how you do. If you hate it, then we don’t do it.” They often are pleasantly surprised that the medication is much easier to tolerate than they thought it would be.
Dr. Pederson: It would be neat if a trial would directly compare lifestyle interventions with medications, because probably lifestyle change is as effective as medication is—but we don’t know that and probably will never have that data. We do know that alcohol consumption, every drink per day, increases risk by 10%. We know that obesity is responsible for 30% of breast cancers in this country, and that hormone replacement probably is overrated as a significant risk factor. Updated data from the Women’s Health Initiative study suggest that hormone replacement may actually reduce both breast cancer and cardiovascular risk in women in their 50s, but that’s in average-risk women and not in high-risk women, so we can’t generalize. We do recommend lifestyle measures including weight loss, exercise, and limiting alcohol consumption for all of our patients and certainly for our high-risk patients.
The only 2 things a woman can do to reduce the risk of triple negative breast cancer are to achieve and maintain ideal body weight and to breastfeed. The medications that I have mentioned don’t reduce the risk of triple negative breast cancer. Staying thin and breastfeeding do. It’s a problem in this country because at least 35% of all women and 58% of Black women are obese in America, and Black women tend to be prone to triple-negative breast cancer. That’s a real public health issue that we need to address. If we were going to focus on one thing, it would be focusing on obesity in terms of risk reduction.
Final thoughts
Dr. Pederson: I would like to direct attention to the American Heart Association scientific statement published at the end of 2020 that reported that hormone replacement in average-risk women reduced both cardiovascular events and overall mortality in women in their 50s by 30%.5 While that’s not directly related to what we are talking about, we need to weigh the pros and cons of estrogen versus estrogen blockade in women in terms of breast cancer risk management discussions. Part of shared decision making now needs to include cardiovascular risk factors and how estrogen is going to play into that.
In women with atypical hyperplasia or LCIS, they may benefit from the preventive medications we discussed. But in women with family history or in women with genetic mutations who have not had benign atypical biopsies, they may choose to consider estrogen during their 50s and perhaps take tamoxifen either beforehand or raloxifene afterward.
We need to look at patients holistically and consider all their risk factors together. We can’t look at one dimension alone.
- US Preventive Services Task Force. Medication use to reduce risk of breast cancer: US Preventive Services Task Force Recommendation Statement. JAMA. 2019;322:857-867.
- Visvanathan K, Fabian CJ, Bantug E, et al. Use of endocrine therapy for breast cancer risk reduction: ASCO clinical practice guideline update. J Clin Oncol. 2019;37:3152-3165.
- Goss PE, Ingle JN, Alex-Martinez JE, et al. Exemestane for breast-cancer prevention in postmenopausal women. N Engl J Med. 2011;364:2381-2391.
- DeCensi A, Puntoni M, Guerrieri-Gonzaga A, et al. Randomized placebo controlled trial of low-dose tamoxifen to prevent local and contralateral recurrence in breast intraepithelial neoplasia. J Clin Oncol. 2019;37:1629-1637.
- El Khoudary SR, Aggarwal B, Beckie TM, et al; American Heart Association Prevention Science Committee of the Council on Epidemiology and Prevention, and Council on Cardiovascular and Stroke Nursing. Menopause transition and cardiovascular disease risk: implications for timing of early prevention: a scientific statement from the American Heart Association. Circulation. 2020;142:e506-e532.
- US Preventive Services Task Force. Medication use to reduce risk of breast cancer: US Preventive Services Task Force Recommendation Statement. JAMA. 2019;322:857-867.
- Visvanathan K, Fabian CJ, Bantug E, et al. Use of endocrine therapy for breast cancer risk reduction: ASCO clinical practice guideline update. J Clin Oncol. 2019;37:3152-3165.
- Goss PE, Ingle JN, Alex-Martinez JE, et al. Exemestane for breast-cancer prevention in postmenopausal women. N Engl J Med. 2011;364:2381-2391.
- DeCensi A, Puntoni M, Guerrieri-Gonzaga A, et al. Randomized placebo controlled trial of low-dose tamoxifen to prevent local and contralateral recurrence in breast intraepithelial neoplasia. J Clin Oncol. 2019;37:1629-1637.
- El Khoudary SR, Aggarwal B, Beckie TM, et al; American Heart Association Prevention Science Committee of the Council on Epidemiology and Prevention, and Council on Cardiovascular and Stroke Nursing. Menopause transition and cardiovascular disease risk: implications for timing of early prevention: a scientific statement from the American Heart Association. Circulation. 2020;142:e506-e532.
Cancer prevention through cascade genetic testing: A review of the current practice guidelines, barriers to testing and proposed solutions

CASE Woman with BRCA2 mutation
An 80-year-old woman presents for evaluation of newly diagnosed metastatic pancreatic adenocarcinoma. Her medical history is notable for breast cancer. Genetic testing of pancreatic tumor tissue detected a pathogenic variant in BRCA2. Family history revealed a history of melanoma as well as bladder, prostate, breast, and colon cancer. The patient subsequently underwent germline genetic testing with an 86-gene panel and a pathogenic mutation in BRCA2 was identified.
Watch a video of this patient and her clinician, Dr. Andrea Hagemann: https://www.youtube.com/watch?
Methods of genetic testing
It is estimated that 1 in 300 to 1 in 500 women in the United States carry a deleterious mutation in BRCA1 or BRCA2. This equates to between 250,000 and 415,000 women who are at high risk for breast and ovarian cancer.1 Looking at all women with cancer, 20% with ovarian,2 10% with breast,3 2% to 3% with endometrial,4 and 5% with colon cancer5 will have a germline mutation predisposing them to cancer. Identification of germline or somatic (tumor) mutations now inform treatment for patients with cancer. An equally important goal of germline genetic testing is cancer prevention. Cancer prevention strategies include risk-based screening for breast, colon, melanoma, and pancreatic cancer and prophylactic surgeries to reduce the risk of breast and ovarian cancer based on mutation type. Evidence-based screening guidelines by mutation type and absolute risk of associated cancers can be found on the National Comprehensive Cancer Network (NCCN).6,7
Multiple strategies have been proposed to identify patients for germline genetic testing. Patients can be identified based on a detailed multigenerational family history. This strategy requires clinicians or genetic counselors to take and update family histories, to recognize when a patient requires referral for testing, and for such testing to be completed. Even then the generation of a detailed pedigree is not very sensitive or specific. Population-based screening for high-penetrance breast and ovarian cancer susceptibility genes, regardless of family history, also has been proposed.8 Such a strategy has become increasingly realistic with decreasing cost and increasing availability of genetic testing. However, it would require increased genetic counseling resources to feasibly and equitably reach the target population and to explain the results to those patients and their relatives.
An alternative is to test the enriched population of family members of a patient with cancer who has been found to carry a pathogenic variant in a clinically relevant cancer susceptibility gene. This type of testing is termed cascade genetic testing. Cascade testing in first-degree family members carries a 50% probability of detecting the same pathogenic mutation. A related testing model is traceback testing where genetic testing is performed on pathology or tumor registry specimens from deceased patients with cancer.9 This genetic testing information is then provided to the family. Traceback models of genetic testing are an active area of research but can introduce ethical dilemmas. The more widely accepted cascade testing starts with the testing of a living patient affected with cancer. A recent article demonstrated the feasibility of a cascade testing model. Using a multiple linear regression model, the authors determined that all carriers of pathogenic mutations in 18 clinically relevant cancer susceptibility genes in the United States could be identified in 9.9 years if there was a 70% cascade testing rate of first-, second- and third-degree relatives, compared to 59.5 years with no cascade testing.10
Gaps in practice
Identification of mutation carriers, either through screening triggered by family history or through testing of patients affected with cancer, represents a gap between guidelines and clinical practice. Current NCCN guidelines outline genetic testing criteria for hereditary breast and ovarian cancer syndrome and for hereditary colorectal cancer. Despite well-established criteria, a survey in the United States revealed that only 19% of primary care providers were able to accurately assess family history for BRCA1 and 2 testing.11 Looking at patients who meet criteria for testing for Lynch syndrome, only 1 in 4 individuals have undergone genetic testing.12 Among patients diagnosed with breast and ovarian cancer, current NCCN guidelines recommend germline genetic testing for all patients with epithelial ovarian cancer; emerging evidence suggests all patients with breast cancer should be offered germline genetic testing.7,13 Large population-based studies have repeatedly demonstrated that testing rates fall short of this goal, with only 10% to 30% of patients undergoing genetic testing.9,14
Among families with a known hereditary mutation, rates of cascade genetic testing are also low, ranging from 17% to 50%.15-18 Evidence-based management guidelines, for both hereditary breast and ovarian cancer as well as Lynch syndrome, have been shown to reduce mortality.19,20 Failure to identify patients who carry these genetic mutations equates to increased mortality for our patients.
Barriers to cascade genetic testing
Cascade genetic testing ideally would be performed on entire families. Actual practice is far from ideal, and barriers to cascade testing exist. Barriers encompass resistance on the part of the family and provider as well as environmental or system factors.
Family factors
Because of privacy laws, the responsibility of disclosure of genetic testing results to family members falls primarily to the patient. Proband education is critical to ensure disclosure amongst family members. Family dynamics and geographic distribution of family members can further complicate disclosure. Following disclosure, family member gender, education, and demographics as well as personal views, attitudes, and emotions affect whether a family member decides to undergo testing.21 Furthermore, insurance status and awareness of and access to specialty-specific care for the proband’s family members may influence cascade genetic testing rates.
Provider factors
Provider factors that affect cascade genetic testing include awareness of testing guidelines, interpretation of genetic testing results, and education and knowledge of specific mutations. For instance, providers must recognize that cascade testing is not appropriate for variants of uncertain significance. This can lead to unnecessary surveillance testing and prophylactic surgeries. Providers, however, must continue to follow patients and periodically update testing results as variants may be reclassified over time. Additionally, providers must be knowledgeable about the complex and nuanced nature of the screening guidelines for each mutation. The NCCN provides detailed recommendations by mutation.7 Patients may benefit from care with cancer specialists who are aware of the guidelines, particularly for moderate-penetrance genes like BRIP1 and PALB2, as discussions about the timing of risk-reducing surgery are more nuanced in this population. Finally, which providers are responsible for facilitating cascade testing may be unclear; oncologists and genetic counselors not primarily treating probands’ relatives may assume the proper information has been passed along to family members without a practical means to follow up, and primary care providers may assume it is being taken care of by the oncology provider.
Continue to: Environmental or system factors...
Environmental or system factors
Accessibility of genetic counseling and testing is a common barrier to cascade testing. Family members may be geographically remote and connecting them to counseling and testing can be challenging. Working with local genetic counselors can facilitate this process. Insurance coverage of testing is a common perceived barrier; however, many testing companies now provide cascade testing free of charge if within a certain window from the initial test. Despite this, patients often site cost as a barrier to undergoing testing. Concerns about insurance coverage are common after a positive result. The Genetic Information Nondiscrimination Act of 2008 prohibits discrimination against employees or insurance applicants because of genetic information. Life insurance or long-term care policies, however, can incorporate genetic testing information into policy rates, so patients should be recommended to consider purchasing life insurance prior to undergoing genetic testing. This is especially important if the person considering testing has not yet been diagnosed with cancer.
Implications of a positive result
Family members who receive a positive test result should be referred for genetic counseling and to the appropriate specialists for evidence-based screening and discussion for risk-reducing surgery (FIGURE).7 For mutations associated with hereditary breast and ovarian cancer, referral to breast and gynecologic surgeons with expertise in risk reducing surgery is critical as the risk of diagnosing an occult malignancy is approximately 1%.22 Surgical technique with a 2-cm margin on the
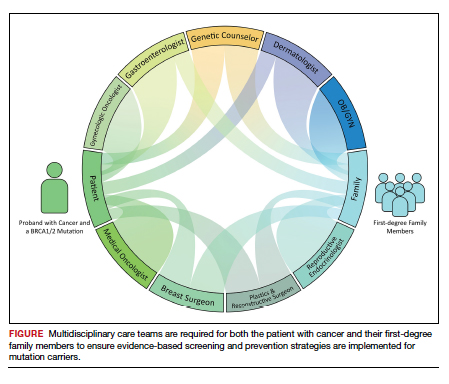
Patient resources: decision aids, websites
As genetic testing becomes more accessible and people are tested at younger ages, studies examining the balance of risk reduction and quality of life (QOL) are increasingly important. Fertility concerns, effects of early menopause, and the interrelatedness between decisions for breast and gynecologic risk reduction should all be considered in the counseling for surgical risk reduction. Patient decision aids can help mutation carriers navigate the complex information and decisions.25 Websites specifically designed by advocacy groups can be useful adjuncts to in-office counseling (Facing Our Risk Empowered, FORCE; Facingourrisk.org).
Family letters
The American College of Obstetricians and Gynecologists recommends an ObGyn have a letter or documentation stating that the patient’s relative has a specific mutation before initiating cascade testing for an at-risk family member. The indicated test (such as BRCA1) should be ordered only after the patient has been counseled about potential outcomes and has expressly decided to be tested.26 Letters, such as the example given in the American College of Obstetricians and Gynecologists practice bulletin,26 are a key component of communication between oncology providers, probands, family members, and their primary care providers. ObGyn providers should work together with genetic counselors and gynecologic oncologists to determine the most efficient strategies in their communities.
Technology
Access to genetic testing and genetic counseling has been improved with the rise in telemedicine. Geographically remote patients can now access genetic counseling through medical center–based counselors as well as company-provided genetic counseling over the phone. Patients also can submit samples remotely without needing to be tested in a doctor’s office.
Databases from cancer centers that detail cascade genetic testing rates. As the preventive impact of cascade genetic testing becomes clearer, strategies to have recurrent discussions with cancer patients regarding their family members’ risk should be implemented. It is still unclear which providers—genetic counselors, gynecologic oncologists, medical oncologists, breast surgeons, ObGyns, to name a few—are primarily responsible for remembering to have these follow-up discussions, and despite advances, the burden still rests on the cancer patient themselves. Databases with automated follow-up surveys done every 6 to 12 months could provide some aid to busy providers in this regard.
Emerging research
If gynecologic risk-reducing surgery is chosen, clinical trial involvement should be encouraged. The Women Choosing Surgical Prevention (NCT02760849) in the United States and the TUBA study (NCT02321228) in the Netherlands were designed to compare menopause-related QOL between standard risk-reducing salpingo-oophorectomy (RRSO) and the innovative risk-reducing salpingectomy with delayed oophorectomy for mutation carriers. Results from the nonrandomized controlled TUBA trial suggest that patients have better menopause-related QOL after risk-reducing salpingectomy than after RRSO, regardless of hormone replacement therapy.27 International collaboration is continuing to better understand oncologic safety. In the United States, the SOROCk trial (NCT04251052) is a noninferiority surgical choice study underway for BRCA1 mutation carriers aged 35 to 50, powered to determine oncologic outcome differences in addition to QOL outcomes between RRSO and delayed oophorectomy arms.
Returning to the case
The patient and her family underwent genetic counseling. The patient’s 2 daughters, each in their 50s, underwent cascade genetic testing and were found to carry the same pathogenic mutation in BRCA2. After counseling from both breast and gynecologic surgeons, they both elected to undergo risk reducing bilateral salpingo-oophorectomy with hysterectomy. Both now complete regular screening for breast cancer and melanoma with plans to start screening for pancreatic cancer. Both are currently cancer free.
Summary
Cascade genetic testing is an efficient strategy to identify mutation carriers for hereditary breast and ovarian cancer syndrome. Implementation of the best patient-centric care will require continued collaboration and communication across and within disciplines. ●
Cascade, or targeted, genetic testing within families known to carry a hereditary mutation in a cancer susceptibility gene should be performed on all living first-degree family members over the age of 18. All mutation carriers should be connected to a multidisciplinary care team (FIGURE) to ensure implementation of evidence-based screening and risk-reducing surgery for cancer prevention. If gynecologic risk-reducing surgery is chosen, clinical trial involvement should be encouraged.
- Gabai-Kapara E, Lahad A, Kaufman B, et al. Population-based screening for breast and ovarian cancer risk due to BRCA1 and BRCA2. Proc Natl Acad Sci U S A. 2014;111:14205-14210.
- Norquist BM, Harrell MI, Brady MF, et al. Inherited mutations in women with ovarian carcinoma. JAMA Oncol. 2016;2:482-490.
- Yamauchi H, Takei J. Management of hereditary breast and ovarian cancer. Int J Clin Oncol. 2018;23:45-51.
- Kahn RM, Gordhandas S, Maddy BP, et al. Universal endometrial cancer tumor typing: how much has immunohistochemistry, microsatellite instability, and MLH1 methylation improved the diagnosis of Lynch syndrome across the population? Cancer. 2019;125:3172-3183.
- Jasperson KW, Tuohy TM, Neklason DW, et al. Hereditary and familial colon cancer. Gastroenterology. 2010;138:2044-2058.
- Gupta S, Provenzale D, Llor X, et al. NCCN guidelines insights: genetic/familial high-risk assessment: colorectal, version 2.2019. J Natl Compr Canc Netw. 2019;17:1032-1041.
- Daly MB, Pal T, Berry MP, et al. Genetic/familial high-risk assessment: breast, ovarian, and pancreatic, version 2.2021, NCCN clinical practice guidelines in oncology. J Natl Compr Canc Netw. 2021;19:77-102.
- King MC, Levy-Lahad E, Lahad A. Population-based screening for BRCA1 and BRCA2: 2014 Lasker Award. JAMA. 2014;312:1091-1092.
- Samimi G, et al. Traceback: a proposed framework to increase identification and genetic counseling of BRCA1 and BRCA2 mutation carriers through family-based outreach. J Clin Oncol. 2017;35:2329-2337.
- Offit K, Tkachuk KA, Stadler ZK, et al. Cascading after peridiagnostic cancer genetic testing: an alternative to population-based screening. J Clin Oncol. 2020;38:1398-1408.
- Bellcross CA, Kolor K, Goddard KAB, et al. Awareness and utilization of BRCA1/2 testing among U.S. primary care physicians. Am J Prev Med. 2011;40:61-66.
- Cross DS, Rahm AK, Kauffman TL, et al. Underutilization of Lynch syndrome screening in a multisite study of patients with colorectal cancer. Genet Med. 2013;15:933-940.
- Beitsch PD, Whitworth PW, Hughes K, et al. Underdiagnosis of hereditary breast cancer: are genetic testing guidelines a tool or an obstacle? J Clin Oncol. 2019;37:453-460.
- Childers CP, Childers KK, Maggard-Gibbons M, et al. National estimates of genetic testing in women with a history of breast or ovarian cancer. J Clin Oncol. 2017;35:3800-3806.
- Samadder NJ, Riegert-Johnson D, Boardman L, et al. Comparison of universal genetic testing vs guideline-directed targeted testing for patients with hereditary cancer syndrome. JAMA Oncol. 2021;7:230-237.
- Sharaf RN, Myer P, Stave CD, et al. Uptake of genetic testing by relatives of Lynch syndrome probands: a systematic review. Clin Gastroenterol Hepatol. 2013;11:1093-1100.
- Menko FH, Ter Stege JA, van der Kolk LE, et al. The uptake of presymptomatic genetic testing in hereditary breast-ovarian cancer and Lynch syndrome: a systematic review of the literature and implications for clinical practice. Fam Cancer. 2019;18:127-135.
- Griffin NE, Buchanan TR, Smith SH, et al. Low rates of cascade genetic testing among families with hereditary gynecologic cancer: an opportunity to improve cancer prevention. Gynecol Oncol. 2020;156:140-146.
- Roberts MC, Dotson WD, DeVore CS, et al. Delivery of cascade screening for hereditary conditions: a scoping review of the literature. Health Aff (Millwood). 2018;37:801-808.
- Finch AP, Lubinski J, Møller P, et al. Impact of oophorectomy on cancer incidence and mortality in women with a BRCA1 or BRCA2 mutation. J Clin Oncol. 2014;32:1547-1553.
- Srinivasan S, Won NY, Dotson WD, et al. Barriers and facilitators for cascade testing in genetic conditions: a systematic review. Eur J Hum Genet. 2020;28:1631-1644.
- Piedimonte S, Frank C, Laprise C, et al. Occult tubal carcinoma after risk-reducing salpingo-oophorectomy: a systematic review. Obstet Gynecol. 2020;135:498-508.
- Shu CA, Pike MC, Jotwani AR, et al. Uterine cancer after risk-reducing salpingo-oophorectomy without hysterectomy in women with BRCA mutations. JAMA Oncol. 2016;2:1434-1440.
- Gordhandas S, Norquist BM, Pennington KP, et al. Hormone replacement therapy after risk reducing salpingo-oophorectomy in patients with BRCA1 or BRCA2 mutations; a systematic review of risks and benefits. Gynecol Oncol. 2019;153:192-200.
- Steenbeek MP, van Bommel MHD, Harmsen MG, et al. Evaluation of a patient decision aid for BRCA1/2 pathogenic variant carriers choosing an ovarian cancer prevention strategy. Gynecol Oncol. 2021;163:371-377.
- Committee on Gynecologic Practice. ACOG committee opinion No. 727: Cascade testing: testing women for known hereditary genetic mutations associated with cancer. Obstet Gynecol. 2018;131:E31-E34.
- Steenbeek MP, Harmsen MG, Hoogerbrugge N, et al. Association of salpingectomy with delayed oophorectomy versus salpingo-oophorectomy with quality of life in BRCA1/2 pathogenic variant carriers: a nonrandomized controlled trial. JAMA Oncol. 2021;7:1203-1212.
Dr. Stock is a Fellow in the Division of Gynecologic Oncology, Washington University School of Medicine, St. Louis, Missouri.

Dr. Mutch is Ira C. and Judith Gall Professor and Vice Chair of Obstetrics and Gynecology in the Department of ObGyn, Division of Gynecologic Oncology, Washington University School of Medicine.

Dr. Hagemann is Associate Professor of Obstetrics and Gynecology, and Director of Hereditary Genetics Clinic in the Division of Gynecologic Oncology, Washington University School of Medicine.
The authors report no financial relationships relevant to this article.
Dr. Stock is a Fellow in the Division of Gynecologic Oncology, Washington University School of Medicine, St. Louis, Missouri.
Dr. Mutch is Ira C. and Judith Gall Professor and Vice Chair of Obstetrics and Gynecology in the Department of ObGyn, Division of Gynecologic Oncology, Washington University School of Medicine.
Dr. Hagemann is Associate Professor of Obstetrics and Gynecology, and Director of Hereditary Genetics Clinic in the Division of Gynecologic Oncology, Washington University School of Medicine.
The authors report no financial relationships relevant to this article.
Dr. Stock is a Fellow in the Division of Gynecologic Oncology, Washington University School of Medicine, St. Louis, Missouri.
Dr. Mutch is Ira C. and Judith Gall Professor and Vice Chair of Obstetrics and Gynecology in the Department of ObGyn, Division of Gynecologic Oncology, Washington University School of Medicine.
Dr. Hagemann is Associate Professor of Obstetrics and Gynecology, and Director of Hereditary Genetics Clinic in the Division of Gynecologic Oncology, Washington University School of Medicine.
The authors report no financial relationships relevant to this article.
CASE Woman with BRCA2 mutation
An 80-year-old woman presents for evaluation of newly diagnosed metastatic pancreatic adenocarcinoma. Her medical history is notable for breast cancer. Genetic testing of pancreatic tumor tissue detected a pathogenic variant in BRCA2. Family history revealed a history of melanoma as well as bladder, prostate, breast, and colon cancer. The patient subsequently underwent germline genetic testing with an 86-gene panel and a pathogenic mutation in BRCA2 was identified.
Watch a video of this patient and her clinician, Dr. Andrea Hagemann: https://www.youtube.com/watch?
Methods of genetic testing
It is estimated that 1 in 300 to 1 in 500 women in the United States carry a deleterious mutation in BRCA1 or BRCA2. This equates to between 250,000 and 415,000 women who are at high risk for breast and ovarian cancer.1 Looking at all women with cancer, 20% with ovarian,2 10% with breast,3 2% to 3% with endometrial,4 and 5% with colon cancer5 will have a germline mutation predisposing them to cancer. Identification of germline or somatic (tumor) mutations now inform treatment for patients with cancer. An equally important goal of germline genetic testing is cancer prevention. Cancer prevention strategies include risk-based screening for breast, colon, melanoma, and pancreatic cancer and prophylactic surgeries to reduce the risk of breast and ovarian cancer based on mutation type. Evidence-based screening guidelines by mutation type and absolute risk of associated cancers can be found on the National Comprehensive Cancer Network (NCCN).6,7
Multiple strategies have been proposed to identify patients for germline genetic testing. Patients can be identified based on a detailed multigenerational family history. This strategy requires clinicians or genetic counselors to take and update family histories, to recognize when a patient requires referral for testing, and for such testing to be completed. Even then the generation of a detailed pedigree is not very sensitive or specific. Population-based screening for high-penetrance breast and ovarian cancer susceptibility genes, regardless of family history, also has been proposed.8 Such a strategy has become increasingly realistic with decreasing cost and increasing availability of genetic testing. However, it would require increased genetic counseling resources to feasibly and equitably reach the target population and to explain the results to those patients and their relatives.
An alternative is to test the enriched population of family members of a patient with cancer who has been found to carry a pathogenic variant in a clinically relevant cancer susceptibility gene. This type of testing is termed cascade genetic testing. Cascade testing in first-degree family members carries a 50% probability of detecting the same pathogenic mutation. A related testing model is traceback testing where genetic testing is performed on pathology or tumor registry specimens from deceased patients with cancer.9 This genetic testing information is then provided to the family. Traceback models of genetic testing are an active area of research but can introduce ethical dilemmas. The more widely accepted cascade testing starts with the testing of a living patient affected with cancer. A recent article demonstrated the feasibility of a cascade testing model. Using a multiple linear regression model, the authors determined that all carriers of pathogenic mutations in 18 clinically relevant cancer susceptibility genes in the United States could be identified in 9.9 years if there was a 70% cascade testing rate of first-, second- and third-degree relatives, compared to 59.5 years with no cascade testing.10
Gaps in practice
Identification of mutation carriers, either through screening triggered by family history or through testing of patients affected with cancer, represents a gap between guidelines and clinical practice. Current NCCN guidelines outline genetic testing criteria for hereditary breast and ovarian cancer syndrome and for hereditary colorectal cancer. Despite well-established criteria, a survey in the United States revealed that only 19% of primary care providers were able to accurately assess family history for BRCA1 and 2 testing.11 Looking at patients who meet criteria for testing for Lynch syndrome, only 1 in 4 individuals have undergone genetic testing.12 Among patients diagnosed with breast and ovarian cancer, current NCCN guidelines recommend germline genetic testing for all patients with epithelial ovarian cancer; emerging evidence suggests all patients with breast cancer should be offered germline genetic testing.7,13 Large population-based studies have repeatedly demonstrated that testing rates fall short of this goal, with only 10% to 30% of patients undergoing genetic testing.9,14
Among families with a known hereditary mutation, rates of cascade genetic testing are also low, ranging from 17% to 50%.15-18 Evidence-based management guidelines, for both hereditary breast and ovarian cancer as well as Lynch syndrome, have been shown to reduce mortality.19,20 Failure to identify patients who carry these genetic mutations equates to increased mortality for our patients.
Barriers to cascade genetic testing
Cascade genetic testing ideally would be performed on entire families. Actual practice is far from ideal, and barriers to cascade testing exist. Barriers encompass resistance on the part of the family and provider as well as environmental or system factors.
Family factors
Because of privacy laws, the responsibility of disclosure of genetic testing results to family members falls primarily to the patient. Proband education is critical to ensure disclosure amongst family members. Family dynamics and geographic distribution of family members can further complicate disclosure. Following disclosure, family member gender, education, and demographics as well as personal views, attitudes, and emotions affect whether a family member decides to undergo testing.21 Furthermore, insurance status and awareness of and access to specialty-specific care for the proband’s family members may influence cascade genetic testing rates.
Provider factors
Provider factors that affect cascade genetic testing include awareness of testing guidelines, interpretation of genetic testing results, and education and knowledge of specific mutations. For instance, providers must recognize that cascade testing is not appropriate for variants of uncertain significance. This can lead to unnecessary surveillance testing and prophylactic surgeries. Providers, however, must continue to follow patients and periodically update testing results as variants may be reclassified over time. Additionally, providers must be knowledgeable about the complex and nuanced nature of the screening guidelines for each mutation. The NCCN provides detailed recommendations by mutation.7 Patients may benefit from care with cancer specialists who are aware of the guidelines, particularly for moderate-penetrance genes like BRIP1 and PALB2, as discussions about the timing of risk-reducing surgery are more nuanced in this population. Finally, which providers are responsible for facilitating cascade testing may be unclear; oncologists and genetic counselors not primarily treating probands’ relatives may assume the proper information has been passed along to family members without a practical means to follow up, and primary care providers may assume it is being taken care of by the oncology provider.
Continue to: Environmental or system factors...
Environmental or system factors
Accessibility of genetic counseling and testing is a common barrier to cascade testing. Family members may be geographically remote and connecting them to counseling and testing can be challenging. Working with local genetic counselors can facilitate this process. Insurance coverage of testing is a common perceived barrier; however, many testing companies now provide cascade testing free of charge if within a certain window from the initial test. Despite this, patients often site cost as a barrier to undergoing testing. Concerns about insurance coverage are common after a positive result. The Genetic Information Nondiscrimination Act of 2008 prohibits discrimination against employees or insurance applicants because of genetic information. Life insurance or long-term care policies, however, can incorporate genetic testing information into policy rates, so patients should be recommended to consider purchasing life insurance prior to undergoing genetic testing. This is especially important if the person considering testing has not yet been diagnosed with cancer.
Implications of a positive result
Family members who receive a positive test result should be referred for genetic counseling and to the appropriate specialists for evidence-based screening and discussion for risk-reducing surgery (FIGURE).7 For mutations associated with hereditary breast and ovarian cancer, referral to breast and gynecologic surgeons with expertise in risk reducing surgery is critical as the risk of diagnosing an occult malignancy is approximately 1%.22 Surgical technique with a 2-cm margin on the
Patient resources: decision aids, websites
As genetic testing becomes more accessible and people are tested at younger ages, studies examining the balance of risk reduction and quality of life (QOL) are increasingly important. Fertility concerns, effects of early menopause, and the interrelatedness between decisions for breast and gynecologic risk reduction should all be considered in the counseling for surgical risk reduction. Patient decision aids can help mutation carriers navigate the complex information and decisions.25 Websites specifically designed by advocacy groups can be useful adjuncts to in-office counseling (Facing Our Risk Empowered, FORCE; Facingourrisk.org).
Family letters
The American College of Obstetricians and Gynecologists recommends an ObGyn have a letter or documentation stating that the patient’s relative has a specific mutation before initiating cascade testing for an at-risk family member. The indicated test (such as BRCA1) should be ordered only after the patient has been counseled about potential outcomes and has expressly decided to be tested.26 Letters, such as the example given in the American College of Obstetricians and Gynecologists practice bulletin,26 are a key component of communication between oncology providers, probands, family members, and their primary care providers. ObGyn providers should work together with genetic counselors and gynecologic oncologists to determine the most efficient strategies in their communities.
Technology
Access to genetic testing and genetic counseling has been improved with the rise in telemedicine. Geographically remote patients can now access genetic counseling through medical center–based counselors as well as company-provided genetic counseling over the phone. Patients also can submit samples remotely without needing to be tested in a doctor’s office.
Databases from cancer centers that detail cascade genetic testing rates. As the preventive impact of cascade genetic testing becomes clearer, strategies to have recurrent discussions with cancer patients regarding their family members’ risk should be implemented. It is still unclear which providers—genetic counselors, gynecologic oncologists, medical oncologists, breast surgeons, ObGyns, to name a few—are primarily responsible for remembering to have these follow-up discussions, and despite advances, the burden still rests on the cancer patient themselves. Databases with automated follow-up surveys done every 6 to 12 months could provide some aid to busy providers in this regard.
Emerging research
If gynecologic risk-reducing surgery is chosen, clinical trial involvement should be encouraged. The Women Choosing Surgical Prevention (NCT02760849) in the United States and the TUBA study (NCT02321228) in the Netherlands were designed to compare menopause-related QOL between standard risk-reducing salpingo-oophorectomy (RRSO) and the innovative risk-reducing salpingectomy with delayed oophorectomy for mutation carriers. Results from the nonrandomized controlled TUBA trial suggest that patients have better menopause-related QOL after risk-reducing salpingectomy than after RRSO, regardless of hormone replacement therapy.27 International collaboration is continuing to better understand oncologic safety. In the United States, the SOROCk trial (NCT04251052) is a noninferiority surgical choice study underway for BRCA1 mutation carriers aged 35 to 50, powered to determine oncologic outcome differences in addition to QOL outcomes between RRSO and delayed oophorectomy arms.
Returning to the case
The patient and her family underwent genetic counseling. The patient’s 2 daughters, each in their 50s, underwent cascade genetic testing and were found to carry the same pathogenic mutation in BRCA2. After counseling from both breast and gynecologic surgeons, they both elected to undergo risk reducing bilateral salpingo-oophorectomy with hysterectomy. Both now complete regular screening for breast cancer and melanoma with plans to start screening for pancreatic cancer. Both are currently cancer free.
Summary
Cascade genetic testing is an efficient strategy to identify mutation carriers for hereditary breast and ovarian cancer syndrome. Implementation of the best patient-centric care will require continued collaboration and communication across and within disciplines. ●
Cascade, or targeted, genetic testing within families known to carry a hereditary mutation in a cancer susceptibility gene should be performed on all living first-degree family members over the age of 18. All mutation carriers should be connected to a multidisciplinary care team (FIGURE) to ensure implementation of evidence-based screening and risk-reducing surgery for cancer prevention. If gynecologic risk-reducing surgery is chosen, clinical trial involvement should be encouraged.
CASE Woman with BRCA2 mutation
An 80-year-old woman presents for evaluation of newly diagnosed metastatic pancreatic adenocarcinoma. Her medical history is notable for breast cancer. Genetic testing of pancreatic tumor tissue detected a pathogenic variant in BRCA2. Family history revealed a history of melanoma as well as bladder, prostate, breast, and colon cancer. The patient subsequently underwent germline genetic testing with an 86-gene panel and a pathogenic mutation in BRCA2 was identified.
Watch a video of this patient and her clinician, Dr. Andrea Hagemann: https://www.youtube.com/watch?
Methods of genetic testing
It is estimated that 1 in 300 to 1 in 500 women in the United States carry a deleterious mutation in BRCA1 or BRCA2. This equates to between 250,000 and 415,000 women who are at high risk for breast and ovarian cancer.1 Looking at all women with cancer, 20% with ovarian,2 10% with breast,3 2% to 3% with endometrial,4 and 5% with colon cancer5 will have a germline mutation predisposing them to cancer. Identification of germline or somatic (tumor) mutations now inform treatment for patients with cancer. An equally important goal of germline genetic testing is cancer prevention. Cancer prevention strategies include risk-based screening for breast, colon, melanoma, and pancreatic cancer and prophylactic surgeries to reduce the risk of breast and ovarian cancer based on mutation type. Evidence-based screening guidelines by mutation type and absolute risk of associated cancers can be found on the National Comprehensive Cancer Network (NCCN).6,7
Multiple strategies have been proposed to identify patients for germline genetic testing. Patients can be identified based on a detailed multigenerational family history. This strategy requires clinicians or genetic counselors to take and update family histories, to recognize when a patient requires referral for testing, and for such testing to be completed. Even then the generation of a detailed pedigree is not very sensitive or specific. Population-based screening for high-penetrance breast and ovarian cancer susceptibility genes, regardless of family history, also has been proposed.8 Such a strategy has become increasingly realistic with decreasing cost and increasing availability of genetic testing. However, it would require increased genetic counseling resources to feasibly and equitably reach the target population and to explain the results to those patients and their relatives.
An alternative is to test the enriched population of family members of a patient with cancer who has been found to carry a pathogenic variant in a clinically relevant cancer susceptibility gene. This type of testing is termed cascade genetic testing. Cascade testing in first-degree family members carries a 50% probability of detecting the same pathogenic mutation. A related testing model is traceback testing where genetic testing is performed on pathology or tumor registry specimens from deceased patients with cancer.9 This genetic testing information is then provided to the family. Traceback models of genetic testing are an active area of research but can introduce ethical dilemmas. The more widely accepted cascade testing starts with the testing of a living patient affected with cancer. A recent article demonstrated the feasibility of a cascade testing model. Using a multiple linear regression model, the authors determined that all carriers of pathogenic mutations in 18 clinically relevant cancer susceptibility genes in the United States could be identified in 9.9 years if there was a 70% cascade testing rate of first-, second- and third-degree relatives, compared to 59.5 years with no cascade testing.10
Gaps in practice
Identification of mutation carriers, either through screening triggered by family history or through testing of patients affected with cancer, represents a gap between guidelines and clinical practice. Current NCCN guidelines outline genetic testing criteria for hereditary breast and ovarian cancer syndrome and for hereditary colorectal cancer. Despite well-established criteria, a survey in the United States revealed that only 19% of primary care providers were able to accurately assess family history for BRCA1 and 2 testing.11 Looking at patients who meet criteria for testing for Lynch syndrome, only 1 in 4 individuals have undergone genetic testing.12 Among patients diagnosed with breast and ovarian cancer, current NCCN guidelines recommend germline genetic testing for all patients with epithelial ovarian cancer; emerging evidence suggests all patients with breast cancer should be offered germline genetic testing.7,13 Large population-based studies have repeatedly demonstrated that testing rates fall short of this goal, with only 10% to 30% of patients undergoing genetic testing.9,14
Among families with a known hereditary mutation, rates of cascade genetic testing are also low, ranging from 17% to 50%.15-18 Evidence-based management guidelines, for both hereditary breast and ovarian cancer as well as Lynch syndrome, have been shown to reduce mortality.19,20 Failure to identify patients who carry these genetic mutations equates to increased mortality for our patients.
Barriers to cascade genetic testing
Cascade genetic testing ideally would be performed on entire families. Actual practice is far from ideal, and barriers to cascade testing exist. Barriers encompass resistance on the part of the family and provider as well as environmental or system factors.
Family factors
Because of privacy laws, the responsibility of disclosure of genetic testing results to family members falls primarily to the patient. Proband education is critical to ensure disclosure amongst family members. Family dynamics and geographic distribution of family members can further complicate disclosure. Following disclosure, family member gender, education, and demographics as well as personal views, attitudes, and emotions affect whether a family member decides to undergo testing.21 Furthermore, insurance status and awareness of and access to specialty-specific care for the proband’s family members may influence cascade genetic testing rates.
Provider factors
Provider factors that affect cascade genetic testing include awareness of testing guidelines, interpretation of genetic testing results, and education and knowledge of specific mutations. For instance, providers must recognize that cascade testing is not appropriate for variants of uncertain significance. This can lead to unnecessary surveillance testing and prophylactic surgeries. Providers, however, must continue to follow patients and periodically update testing results as variants may be reclassified over time. Additionally, providers must be knowledgeable about the complex and nuanced nature of the screening guidelines for each mutation. The NCCN provides detailed recommendations by mutation.7 Patients may benefit from care with cancer specialists who are aware of the guidelines, particularly for moderate-penetrance genes like BRIP1 and PALB2, as discussions about the timing of risk-reducing surgery are more nuanced in this population. Finally, which providers are responsible for facilitating cascade testing may be unclear; oncologists and genetic counselors not primarily treating probands’ relatives may assume the proper information has been passed along to family members without a practical means to follow up, and primary care providers may assume it is being taken care of by the oncology provider.
Continue to: Environmental or system factors...
Environmental or system factors
Accessibility of genetic counseling and testing is a common barrier to cascade testing. Family members may be geographically remote and connecting them to counseling and testing can be challenging. Working with local genetic counselors can facilitate this process. Insurance coverage of testing is a common perceived barrier; however, many testing companies now provide cascade testing free of charge if within a certain window from the initial test. Despite this, patients often site cost as a barrier to undergoing testing. Concerns about insurance coverage are common after a positive result. The Genetic Information Nondiscrimination Act of 2008 prohibits discrimination against employees or insurance applicants because of genetic information. Life insurance or long-term care policies, however, can incorporate genetic testing information into policy rates, so patients should be recommended to consider purchasing life insurance prior to undergoing genetic testing. This is especially important if the person considering testing has not yet been diagnosed with cancer.
Implications of a positive result
Family members who receive a positive test result should be referred for genetic counseling and to the appropriate specialists for evidence-based screening and discussion for risk-reducing surgery (FIGURE).7 For mutations associated with hereditary breast and ovarian cancer, referral to breast and gynecologic surgeons with expertise in risk reducing surgery is critical as the risk of diagnosing an occult malignancy is approximately 1%.22 Surgical technique with a 2-cm margin on the
Patient resources: decision aids, websites
As genetic testing becomes more accessible and people are tested at younger ages, studies examining the balance of risk reduction and quality of life (QOL) are increasingly important. Fertility concerns, effects of early menopause, and the interrelatedness between decisions for breast and gynecologic risk reduction should all be considered in the counseling for surgical risk reduction. Patient decision aids can help mutation carriers navigate the complex information and decisions.25 Websites specifically designed by advocacy groups can be useful adjuncts to in-office counseling (Facing Our Risk Empowered, FORCE; Facingourrisk.org).
Family letters
The American College of Obstetricians and Gynecologists recommends an ObGyn have a letter or documentation stating that the patient’s relative has a specific mutation before initiating cascade testing for an at-risk family member. The indicated test (such as BRCA1) should be ordered only after the patient has been counseled about potential outcomes and has expressly decided to be tested.26 Letters, such as the example given in the American College of Obstetricians and Gynecologists practice bulletin,26 are a key component of communication between oncology providers, probands, family members, and their primary care providers. ObGyn providers should work together with genetic counselors and gynecologic oncologists to determine the most efficient strategies in their communities.
Technology
Access to genetic testing and genetic counseling has been improved with the rise in telemedicine. Geographically remote patients can now access genetic counseling through medical center–based counselors as well as company-provided genetic counseling over the phone. Patients also can submit samples remotely without needing to be tested in a doctor’s office.
Databases from cancer centers that detail cascade genetic testing rates. As the preventive impact of cascade genetic testing becomes clearer, strategies to have recurrent discussions with cancer patients regarding their family members’ risk should be implemented. It is still unclear which providers—genetic counselors, gynecologic oncologists, medical oncologists, breast surgeons, ObGyns, to name a few—are primarily responsible for remembering to have these follow-up discussions, and despite advances, the burden still rests on the cancer patient themselves. Databases with automated follow-up surveys done every 6 to 12 months could provide some aid to busy providers in this regard.
Emerging research
If gynecologic risk-reducing surgery is chosen, clinical trial involvement should be encouraged. The Women Choosing Surgical Prevention (NCT02760849) in the United States and the TUBA study (NCT02321228) in the Netherlands were designed to compare menopause-related QOL between standard risk-reducing salpingo-oophorectomy (RRSO) and the innovative risk-reducing salpingectomy with delayed oophorectomy for mutation carriers. Results from the nonrandomized controlled TUBA trial suggest that patients have better menopause-related QOL after risk-reducing salpingectomy than after RRSO, regardless of hormone replacement therapy.27 International collaboration is continuing to better understand oncologic safety. In the United States, the SOROCk trial (NCT04251052) is a noninferiority surgical choice study underway for BRCA1 mutation carriers aged 35 to 50, powered to determine oncologic outcome differences in addition to QOL outcomes between RRSO and delayed oophorectomy arms.
Returning to the case
The patient and her family underwent genetic counseling. The patient’s 2 daughters, each in their 50s, underwent cascade genetic testing and were found to carry the same pathogenic mutation in BRCA2. After counseling from both breast and gynecologic surgeons, they both elected to undergo risk reducing bilateral salpingo-oophorectomy with hysterectomy. Both now complete regular screening for breast cancer and melanoma with plans to start screening for pancreatic cancer. Both are currently cancer free.
Summary
Cascade genetic testing is an efficient strategy to identify mutation carriers for hereditary breast and ovarian cancer syndrome. Implementation of the best patient-centric care will require continued collaboration and communication across and within disciplines. ●
Cascade, or targeted, genetic testing within families known to carry a hereditary mutation in a cancer susceptibility gene should be performed on all living first-degree family members over the age of 18. All mutation carriers should be connected to a multidisciplinary care team (FIGURE) to ensure implementation of evidence-based screening and risk-reducing surgery for cancer prevention. If gynecologic risk-reducing surgery is chosen, clinical trial involvement should be encouraged.
- Gabai-Kapara E, Lahad A, Kaufman B, et al. Population-based screening for breast and ovarian cancer risk due to BRCA1 and BRCA2. Proc Natl Acad Sci U S A. 2014;111:14205-14210.
- Norquist BM, Harrell MI, Brady MF, et al. Inherited mutations in women with ovarian carcinoma. JAMA Oncol. 2016;2:482-490.
- Yamauchi H, Takei J. Management of hereditary breast and ovarian cancer. Int J Clin Oncol. 2018;23:45-51.
- Kahn RM, Gordhandas S, Maddy BP, et al. Universal endometrial cancer tumor typing: how much has immunohistochemistry, microsatellite instability, and MLH1 methylation improved the diagnosis of Lynch syndrome across the population? Cancer. 2019;125:3172-3183.
- Jasperson KW, Tuohy TM, Neklason DW, et al. Hereditary and familial colon cancer. Gastroenterology. 2010;138:2044-2058.
- Gupta S, Provenzale D, Llor X, et al. NCCN guidelines insights: genetic/familial high-risk assessment: colorectal, version 2.2019. J Natl Compr Canc Netw. 2019;17:1032-1041.
- Daly MB, Pal T, Berry MP, et al. Genetic/familial high-risk assessment: breast, ovarian, and pancreatic, version 2.2021, NCCN clinical practice guidelines in oncology. J Natl Compr Canc Netw. 2021;19:77-102.
- King MC, Levy-Lahad E, Lahad A. Population-based screening for BRCA1 and BRCA2: 2014 Lasker Award. JAMA. 2014;312:1091-1092.
- Samimi G, et al. Traceback: a proposed framework to increase identification and genetic counseling of BRCA1 and BRCA2 mutation carriers through family-based outreach. J Clin Oncol. 2017;35:2329-2337.
- Offit K, Tkachuk KA, Stadler ZK, et al. Cascading after peridiagnostic cancer genetic testing: an alternative to population-based screening. J Clin Oncol. 2020;38:1398-1408.
- Bellcross CA, Kolor K, Goddard KAB, et al. Awareness and utilization of BRCA1/2 testing among U.S. primary care physicians. Am J Prev Med. 2011;40:61-66.
- Cross DS, Rahm AK, Kauffman TL, et al. Underutilization of Lynch syndrome screening in a multisite study of patients with colorectal cancer. Genet Med. 2013;15:933-940.
- Beitsch PD, Whitworth PW, Hughes K, et al. Underdiagnosis of hereditary breast cancer: are genetic testing guidelines a tool or an obstacle? J Clin Oncol. 2019;37:453-460.
- Childers CP, Childers KK, Maggard-Gibbons M, et al. National estimates of genetic testing in women with a history of breast or ovarian cancer. J Clin Oncol. 2017;35:3800-3806.
- Samadder NJ, Riegert-Johnson D, Boardman L, et al. Comparison of universal genetic testing vs guideline-directed targeted testing for patients with hereditary cancer syndrome. JAMA Oncol. 2021;7:230-237.
- Sharaf RN, Myer P, Stave CD, et al. Uptake of genetic testing by relatives of Lynch syndrome probands: a systematic review. Clin Gastroenterol Hepatol. 2013;11:1093-1100.
- Menko FH, Ter Stege JA, van der Kolk LE, et al. The uptake of presymptomatic genetic testing in hereditary breast-ovarian cancer and Lynch syndrome: a systematic review of the literature and implications for clinical practice. Fam Cancer. 2019;18:127-135.
- Griffin NE, Buchanan TR, Smith SH, et al. Low rates of cascade genetic testing among families with hereditary gynecologic cancer: an opportunity to improve cancer prevention. Gynecol Oncol. 2020;156:140-146.
- Roberts MC, Dotson WD, DeVore CS, et al. Delivery of cascade screening for hereditary conditions: a scoping review of the literature. Health Aff (Millwood). 2018;37:801-808.
- Finch AP, Lubinski J, Møller P, et al. Impact of oophorectomy on cancer incidence and mortality in women with a BRCA1 or BRCA2 mutation. J Clin Oncol. 2014;32:1547-1553.
- Srinivasan S, Won NY, Dotson WD, et al. Barriers and facilitators for cascade testing in genetic conditions: a systematic review. Eur J Hum Genet. 2020;28:1631-1644.
- Piedimonte S, Frank C, Laprise C, et al. Occult tubal carcinoma after risk-reducing salpingo-oophorectomy: a systematic review. Obstet Gynecol. 2020;135:498-508.
- Shu CA, Pike MC, Jotwani AR, et al. Uterine cancer after risk-reducing salpingo-oophorectomy without hysterectomy in women with BRCA mutations. JAMA Oncol. 2016;2:1434-1440.
- Gordhandas S, Norquist BM, Pennington KP, et al. Hormone replacement therapy after risk reducing salpingo-oophorectomy in patients with BRCA1 or BRCA2 mutations; a systematic review of risks and benefits. Gynecol Oncol. 2019;153:192-200.
- Steenbeek MP, van Bommel MHD, Harmsen MG, et al. Evaluation of a patient decision aid for BRCA1/2 pathogenic variant carriers choosing an ovarian cancer prevention strategy. Gynecol Oncol. 2021;163:371-377.
- Committee on Gynecologic Practice. ACOG committee opinion No. 727: Cascade testing: testing women for known hereditary genetic mutations associated with cancer. Obstet Gynecol. 2018;131:E31-E34.
- Steenbeek MP, Harmsen MG, Hoogerbrugge N, et al. Association of salpingectomy with delayed oophorectomy versus salpingo-oophorectomy with quality of life in BRCA1/2 pathogenic variant carriers: a nonrandomized controlled trial. JAMA Oncol. 2021;7:1203-1212.
- Gabai-Kapara E, Lahad A, Kaufman B, et al. Population-based screening for breast and ovarian cancer risk due to BRCA1 and BRCA2. Proc Natl Acad Sci U S A. 2014;111:14205-14210.
- Norquist BM, Harrell MI, Brady MF, et al. Inherited mutations in women with ovarian carcinoma. JAMA Oncol. 2016;2:482-490.
- Yamauchi H, Takei J. Management of hereditary breast and ovarian cancer. Int J Clin Oncol. 2018;23:45-51.
- Kahn RM, Gordhandas S, Maddy BP, et al. Universal endometrial cancer tumor typing: how much has immunohistochemistry, microsatellite instability, and MLH1 methylation improved the diagnosis of Lynch syndrome across the population? Cancer. 2019;125:3172-3183.
- Jasperson KW, Tuohy TM, Neklason DW, et al. Hereditary and familial colon cancer. Gastroenterology. 2010;138:2044-2058.
- Gupta S, Provenzale D, Llor X, et al. NCCN guidelines insights: genetic/familial high-risk assessment: colorectal, version 2.2019. J Natl Compr Canc Netw. 2019;17:1032-1041.
- Daly MB, Pal T, Berry MP, et al. Genetic/familial high-risk assessment: breast, ovarian, and pancreatic, version 2.2021, NCCN clinical practice guidelines in oncology. J Natl Compr Canc Netw. 2021;19:77-102.
- King MC, Levy-Lahad E, Lahad A. Population-based screening for BRCA1 and BRCA2: 2014 Lasker Award. JAMA. 2014;312:1091-1092.
- Samimi G, et al. Traceback: a proposed framework to increase identification and genetic counseling of BRCA1 and BRCA2 mutation carriers through family-based outreach. J Clin Oncol. 2017;35:2329-2337.
- Offit K, Tkachuk KA, Stadler ZK, et al. Cascading after peridiagnostic cancer genetic testing: an alternative to population-based screening. J Clin Oncol. 2020;38:1398-1408.
- Bellcross CA, Kolor K, Goddard KAB, et al. Awareness and utilization of BRCA1/2 testing among U.S. primary care physicians. Am J Prev Med. 2011;40:61-66.
- Cross DS, Rahm AK, Kauffman TL, et al. Underutilization of Lynch syndrome screening in a multisite study of patients with colorectal cancer. Genet Med. 2013;15:933-940.
- Beitsch PD, Whitworth PW, Hughes K, et al. Underdiagnosis of hereditary breast cancer: are genetic testing guidelines a tool or an obstacle? J Clin Oncol. 2019;37:453-460.
- Childers CP, Childers KK, Maggard-Gibbons M, et al. National estimates of genetic testing in women with a history of breast or ovarian cancer. J Clin Oncol. 2017;35:3800-3806.
- Samadder NJ, Riegert-Johnson D, Boardman L, et al. Comparison of universal genetic testing vs guideline-directed targeted testing for patients with hereditary cancer syndrome. JAMA Oncol. 2021;7:230-237.
- Sharaf RN, Myer P, Stave CD, et al. Uptake of genetic testing by relatives of Lynch syndrome probands: a systematic review. Clin Gastroenterol Hepatol. 2013;11:1093-1100.
- Menko FH, Ter Stege JA, van der Kolk LE, et al. The uptake of presymptomatic genetic testing in hereditary breast-ovarian cancer and Lynch syndrome: a systematic review of the literature and implications for clinical practice. Fam Cancer. 2019;18:127-135.
- Griffin NE, Buchanan TR, Smith SH, et al. Low rates of cascade genetic testing among families with hereditary gynecologic cancer: an opportunity to improve cancer prevention. Gynecol Oncol. 2020;156:140-146.
- Roberts MC, Dotson WD, DeVore CS, et al. Delivery of cascade screening for hereditary conditions: a scoping review of the literature. Health Aff (Millwood). 2018;37:801-808.
- Finch AP, Lubinski J, Møller P, et al. Impact of oophorectomy on cancer incidence and mortality in women with a BRCA1 or BRCA2 mutation. J Clin Oncol. 2014;32:1547-1553.
- Srinivasan S, Won NY, Dotson WD, et al. Barriers and facilitators for cascade testing in genetic conditions: a systematic review. Eur J Hum Genet. 2020;28:1631-1644.
- Piedimonte S, Frank C, Laprise C, et al. Occult tubal carcinoma after risk-reducing salpingo-oophorectomy: a systematic review. Obstet Gynecol. 2020;135:498-508.
- Shu CA, Pike MC, Jotwani AR, et al. Uterine cancer after risk-reducing salpingo-oophorectomy without hysterectomy in women with BRCA mutations. JAMA Oncol. 2016;2:1434-1440.
- Gordhandas S, Norquist BM, Pennington KP, et al. Hormone replacement therapy after risk reducing salpingo-oophorectomy in patients with BRCA1 or BRCA2 mutations; a systematic review of risks and benefits. Gynecol Oncol. 2019;153:192-200.
- Steenbeek MP, van Bommel MHD, Harmsen MG, et al. Evaluation of a patient decision aid for BRCA1/2 pathogenic variant carriers choosing an ovarian cancer prevention strategy. Gynecol Oncol. 2021;163:371-377.
- Committee on Gynecologic Practice. ACOG committee opinion No. 727: Cascade testing: testing women for known hereditary genetic mutations associated with cancer. Obstet Gynecol. 2018;131:E31-E34.
- Steenbeek MP, Harmsen MG, Hoogerbrugge N, et al. Association of salpingectomy with delayed oophorectomy versus salpingo-oophorectomy with quality of life in BRCA1/2 pathogenic variant carriers: a nonrandomized controlled trial. JAMA Oncol. 2021;7:1203-1212.
