User login
CORONARY Trial Fails to Show Superiority of Off-Pump CABG
CHICAGO – The CORONARY trial provides new insights into the benefits of performing coronary artery bypass grafting on a beating heart, but falls short of delivering a knockout victory for the off-pump technique.
There were no significant differences in the rate of the composite coprimary outcome of death, stroke, nonfatal myocardial infarction (MI), or new renal failure at 30 days between off-pump CABG and bypass with the induction of ischemic cardiac arrest (on-pump) (9.8% vs. 10.3%; P = .59; hazard ratio, 0.95), or in any of its individual components.
Off-pump CABG was associated with fewer transfusions, reoperations for bleeding, acute kidney injuries, and respiratory infections or failure, but more early repeat revascularizations.
"We believe that in experienced hands, both procedures are reasonable options based on short-term results," principal investigator Dr. André Lamy said in a late-breaking session at the annual meeting of the American College of Cardiology. The difference in 30-day morbidity in the CORONARY (Coronary Artery Bypass Grafting Off or On Pump Revascularization) study may or may not lead to significant differences during ongoing follow-up, he added.
Invited discussant Dr. Robert Guyton, with the adult cardiac surgery team at Emory University in Atlanta, said CORONARY is larger by a factor of two than any other prospective randomized trial comparing on-pump versus off-pump surgery and is well executed.
"However, it is a superiority trial that failed to show a superiority of off-pump surgery," he said. "Therefore the conclusion probably needs to be stated that there is no significant difference detected. You can’t claim that there’s no difference between the two in this trial."
Dr. Guyton also highlighted a Cochrane systematic review, published just days before the meeting, of 86 trials involving 10,716 patients that showed a mortality benefit with on-pump CABG. The review failed to demonstrate any significant benefit of off-pump CABG with regard to mortality, stroke, or myocardial infarction, and concluded that on-pump CABG should remain the standard surgical treatment (Cochrane Database Syst. Rev. 2012 Mar 14;3:CD007224).
Dr. Lamy said he was not well versed in the details of the review but pointed out that one of its studies reported an inordinately high mortality rate of 25% with off-pump CABG that may have shifted the review results.
A New England Journal of Medicine editorial (10.1056/NEJMe1203194) that accompanied simultaneous publication of the CORONARY study (10.1056/NEJMoa1200388) called the lack of postoperative coronary arteriography an important limitation of CORONARY, and noted that the true relative efficacy and durability of off-pump CABG will probably be determined by longer-term follow-up.
Editorialist Dr. Frederick L. Grover, chair of the department of surgery at the University of Colorado in Denver, wrote that forthcoming neurocognitive data will have a major influence on the interpretation of the primary trial results.
He observed that unlike the recent Randomized On/Off Bypass trial (N. Engl. J. Med. 2009;361:1827-37) that reported worse outcomes at 1 year with off-pump than with on-pump CABG among veterans, CORONARY was limited to surgeons with more extensive off-pump experience, and did not allow trainees to act as primary surgeons. CORONARY also included a somewhat higher-risk population of patients, who may derive a greater relative benefit from the off-pump technique. Although these differences did not significantly influence short-term outcomes between the two trials, their long-term outcome remains to be seen, said Dr. Grover, also of the cardiothoracic surgery section of the Denver Veterans Affairs Medical Center.
CORONARY randomly assigned 4,752 patients from 79 centers in 19 countries to undergo CABG either off-pump or on-pump. Patients had to be at least 70 years of age, or 60-69 years old with at least one prespecified risk factor, or 55-59 years old with at least two of the prespecified risk factors of diabetes, urgent revascularization, recent smoking history, or a left ventricular ejection fraction of no more than 35%. Only staff cardiac surgeons with more than 2 years of experience who had completed 100 cases of one or both techniques were allowed. The mean patient age was 67 years, one-third had a prior MI, and roughly 20% had a EuroSCORE (European System for Cardiac Operative Risk Evaluation) of more than 5.
Incomplete revascularization was significantly more frequent in the off-pump group, while operating time and initial ventilation were significantly higher in the on-pump group, said Dr. Lamy, with the Population Health Research Institute, Hamilton Health Sciences, McMaster University, Hamilton, Ont.
The need for any blood transfusion was significantly higher at 63.3% of the on-pump group versus 50.7% in the off-pump group (P less than .001), as was the need for antifibrinolytics (37% vs. 26%; P less than .001), and reoperation for bleeding (2.4% vs. 1.4%; P = .02).
At 30 days, there was no difference between the off-pump and on-pump groups in the coprimary outcome components of death (2.5% for both; hazard ratio, 1.02), stroke (1.0% vs 1.1%; HR, 0.89), nonfatal MI (6.7% vs. 7.2%; HR, 0.93), and new renal failure (1.2% vs. 1.1%; HR, 1.04).
Respiratory infection or failure was reported in 6% of the off-pump group and 7.5% of the on-pump group (P = .03; relative risk, 0.79), acute kidney injury stage 1 in 28% vs. 32% (P = .01; RR, 0.87) and RIFLE (risk, injury, failure, loss, and end-stage kidney disease) risk in 17% vs. 19.6% (P = .02; RR, 0.87), he said.
A subgroup analysis found no differences between the two techniques by age, cerebrovascular or peripheral arterial disease, EuroSCORE, left ventricular ejection fraction, region, or experience of the surgeon, Dr. Lamy said.
Both approaches are valid, and surgeons will need to tailor surgery for each individual patient, he said in an interview. For example, the off-pump technique may be best in a frail elderly patient to avoid transfusions and massive fluid infusion, whereas the on-pump technique may be best for a very large patient with the heart deeply placed within the chest.
Neurological outcomes and a cost-effectiveness analysis will be forthcoming. Five-year data on the coprimary end point plus repeat coronary revascularization over 5 years of follow-up are expected in 2016, Dr. Lamy said.
This study is funded by the Canadian Institutes of Health Research. Dr. Lamy reported consulting fees and honoraria from AstraZeneca.
CHICAGO – The CORONARY trial provides new insights into the benefits of performing coronary artery bypass grafting on a beating heart, but falls short of delivering a knockout victory for the off-pump technique.
There were no significant differences in the rate of the composite coprimary outcome of death, stroke, nonfatal myocardial infarction (MI), or new renal failure at 30 days between off-pump CABG and bypass with the induction of ischemic cardiac arrest (on-pump) (9.8% vs. 10.3%; P = .59; hazard ratio, 0.95), or in any of its individual components.
Off-pump CABG was associated with fewer transfusions, reoperations for bleeding, acute kidney injuries, and respiratory infections or failure, but more early repeat revascularizations.
"We believe that in experienced hands, both procedures are reasonable options based on short-term results," principal investigator Dr. André Lamy said in a late-breaking session at the annual meeting of the American College of Cardiology. The difference in 30-day morbidity in the CORONARY (Coronary Artery Bypass Grafting Off or On Pump Revascularization) study may or may not lead to significant differences during ongoing follow-up, he added.
Invited discussant Dr. Robert Guyton, with the adult cardiac surgery team at Emory University in Atlanta, said CORONARY is larger by a factor of two than any other prospective randomized trial comparing on-pump versus off-pump surgery and is well executed.
"However, it is a superiority trial that failed to show a superiority of off-pump surgery," he said. "Therefore the conclusion probably needs to be stated that there is no significant difference detected. You can’t claim that there’s no difference between the two in this trial."
Dr. Guyton also highlighted a Cochrane systematic review, published just days before the meeting, of 86 trials involving 10,716 patients that showed a mortality benefit with on-pump CABG. The review failed to demonstrate any significant benefit of off-pump CABG with regard to mortality, stroke, or myocardial infarction, and concluded that on-pump CABG should remain the standard surgical treatment (Cochrane Database Syst. Rev. 2012 Mar 14;3:CD007224).
Dr. Lamy said he was not well versed in the details of the review but pointed out that one of its studies reported an inordinately high mortality rate of 25% with off-pump CABG that may have shifted the review results.
A New England Journal of Medicine editorial (10.1056/NEJMe1203194) that accompanied simultaneous publication of the CORONARY study (10.1056/NEJMoa1200388) called the lack of postoperative coronary arteriography an important limitation of CORONARY, and noted that the true relative efficacy and durability of off-pump CABG will probably be determined by longer-term follow-up.
Editorialist Dr. Frederick L. Grover, chair of the department of surgery at the University of Colorado in Denver, wrote that forthcoming neurocognitive data will have a major influence on the interpretation of the primary trial results.
He observed that unlike the recent Randomized On/Off Bypass trial (N. Engl. J. Med. 2009;361:1827-37) that reported worse outcomes at 1 year with off-pump than with on-pump CABG among veterans, CORONARY was limited to surgeons with more extensive off-pump experience, and did not allow trainees to act as primary surgeons. CORONARY also included a somewhat higher-risk population of patients, who may derive a greater relative benefit from the off-pump technique. Although these differences did not significantly influence short-term outcomes between the two trials, their long-term outcome remains to be seen, said Dr. Grover, also of the cardiothoracic surgery section of the Denver Veterans Affairs Medical Center.
CORONARY randomly assigned 4,752 patients from 79 centers in 19 countries to undergo CABG either off-pump or on-pump. Patients had to be at least 70 years of age, or 60-69 years old with at least one prespecified risk factor, or 55-59 years old with at least two of the prespecified risk factors of diabetes, urgent revascularization, recent smoking history, or a left ventricular ejection fraction of no more than 35%. Only staff cardiac surgeons with more than 2 years of experience who had completed 100 cases of one or both techniques were allowed. The mean patient age was 67 years, one-third had a prior MI, and roughly 20% had a EuroSCORE (European System for Cardiac Operative Risk Evaluation) of more than 5.
Incomplete revascularization was significantly more frequent in the off-pump group, while operating time and initial ventilation were significantly higher in the on-pump group, said Dr. Lamy, with the Population Health Research Institute, Hamilton Health Sciences, McMaster University, Hamilton, Ont.
The need for any blood transfusion was significantly higher at 63.3% of the on-pump group versus 50.7% in the off-pump group (P less than .001), as was the need for antifibrinolytics (37% vs. 26%; P less than .001), and reoperation for bleeding (2.4% vs. 1.4%; P = .02).
At 30 days, there was no difference between the off-pump and on-pump groups in the coprimary outcome components of death (2.5% for both; hazard ratio, 1.02), stroke (1.0% vs 1.1%; HR, 0.89), nonfatal MI (6.7% vs. 7.2%; HR, 0.93), and new renal failure (1.2% vs. 1.1%; HR, 1.04).
Respiratory infection or failure was reported in 6% of the off-pump group and 7.5% of the on-pump group (P = .03; relative risk, 0.79), acute kidney injury stage 1 in 28% vs. 32% (P = .01; RR, 0.87) and RIFLE (risk, injury, failure, loss, and end-stage kidney disease) risk in 17% vs. 19.6% (P = .02; RR, 0.87), he said.
A subgroup analysis found no differences between the two techniques by age, cerebrovascular or peripheral arterial disease, EuroSCORE, left ventricular ejection fraction, region, or experience of the surgeon, Dr. Lamy said.
Both approaches are valid, and surgeons will need to tailor surgery for each individual patient, he said in an interview. For example, the off-pump technique may be best in a frail elderly patient to avoid transfusions and massive fluid infusion, whereas the on-pump technique may be best for a very large patient with the heart deeply placed within the chest.
Neurological outcomes and a cost-effectiveness analysis will be forthcoming. Five-year data on the coprimary end point plus repeat coronary revascularization over 5 years of follow-up are expected in 2016, Dr. Lamy said.
This study is funded by the Canadian Institutes of Health Research. Dr. Lamy reported consulting fees and honoraria from AstraZeneca.
CHICAGO – The CORONARY trial provides new insights into the benefits of performing coronary artery bypass grafting on a beating heart, but falls short of delivering a knockout victory for the off-pump technique.
There were no significant differences in the rate of the composite coprimary outcome of death, stroke, nonfatal myocardial infarction (MI), or new renal failure at 30 days between off-pump CABG and bypass with the induction of ischemic cardiac arrest (on-pump) (9.8% vs. 10.3%; P = .59; hazard ratio, 0.95), or in any of its individual components.
Off-pump CABG was associated with fewer transfusions, reoperations for bleeding, acute kidney injuries, and respiratory infections or failure, but more early repeat revascularizations.
"We believe that in experienced hands, both procedures are reasonable options based on short-term results," principal investigator Dr. André Lamy said in a late-breaking session at the annual meeting of the American College of Cardiology. The difference in 30-day morbidity in the CORONARY (Coronary Artery Bypass Grafting Off or On Pump Revascularization) study may or may not lead to significant differences during ongoing follow-up, he added.
Invited discussant Dr. Robert Guyton, with the adult cardiac surgery team at Emory University in Atlanta, said CORONARY is larger by a factor of two than any other prospective randomized trial comparing on-pump versus off-pump surgery and is well executed.
"However, it is a superiority trial that failed to show a superiority of off-pump surgery," he said. "Therefore the conclusion probably needs to be stated that there is no significant difference detected. You can’t claim that there’s no difference between the two in this trial."
Dr. Guyton also highlighted a Cochrane systematic review, published just days before the meeting, of 86 trials involving 10,716 patients that showed a mortality benefit with on-pump CABG. The review failed to demonstrate any significant benefit of off-pump CABG with regard to mortality, stroke, or myocardial infarction, and concluded that on-pump CABG should remain the standard surgical treatment (Cochrane Database Syst. Rev. 2012 Mar 14;3:CD007224).
Dr. Lamy said he was not well versed in the details of the review but pointed out that one of its studies reported an inordinately high mortality rate of 25% with off-pump CABG that may have shifted the review results.
A New England Journal of Medicine editorial (10.1056/NEJMe1203194) that accompanied simultaneous publication of the CORONARY study (10.1056/NEJMoa1200388) called the lack of postoperative coronary arteriography an important limitation of CORONARY, and noted that the true relative efficacy and durability of off-pump CABG will probably be determined by longer-term follow-up.
Editorialist Dr. Frederick L. Grover, chair of the department of surgery at the University of Colorado in Denver, wrote that forthcoming neurocognitive data will have a major influence on the interpretation of the primary trial results.
He observed that unlike the recent Randomized On/Off Bypass trial (N. Engl. J. Med. 2009;361:1827-37) that reported worse outcomes at 1 year with off-pump than with on-pump CABG among veterans, CORONARY was limited to surgeons with more extensive off-pump experience, and did not allow trainees to act as primary surgeons. CORONARY also included a somewhat higher-risk population of patients, who may derive a greater relative benefit from the off-pump technique. Although these differences did not significantly influence short-term outcomes between the two trials, their long-term outcome remains to be seen, said Dr. Grover, also of the cardiothoracic surgery section of the Denver Veterans Affairs Medical Center.
CORONARY randomly assigned 4,752 patients from 79 centers in 19 countries to undergo CABG either off-pump or on-pump. Patients had to be at least 70 years of age, or 60-69 years old with at least one prespecified risk factor, or 55-59 years old with at least two of the prespecified risk factors of diabetes, urgent revascularization, recent smoking history, or a left ventricular ejection fraction of no more than 35%. Only staff cardiac surgeons with more than 2 years of experience who had completed 100 cases of one or both techniques were allowed. The mean patient age was 67 years, one-third had a prior MI, and roughly 20% had a EuroSCORE (European System for Cardiac Operative Risk Evaluation) of more than 5.
Incomplete revascularization was significantly more frequent in the off-pump group, while operating time and initial ventilation were significantly higher in the on-pump group, said Dr. Lamy, with the Population Health Research Institute, Hamilton Health Sciences, McMaster University, Hamilton, Ont.
The need for any blood transfusion was significantly higher at 63.3% of the on-pump group versus 50.7% in the off-pump group (P less than .001), as was the need for antifibrinolytics (37% vs. 26%; P less than .001), and reoperation for bleeding (2.4% vs. 1.4%; P = .02).
At 30 days, there was no difference between the off-pump and on-pump groups in the coprimary outcome components of death (2.5% for both; hazard ratio, 1.02), stroke (1.0% vs 1.1%; HR, 0.89), nonfatal MI (6.7% vs. 7.2%; HR, 0.93), and new renal failure (1.2% vs. 1.1%; HR, 1.04).
Respiratory infection or failure was reported in 6% of the off-pump group and 7.5% of the on-pump group (P = .03; relative risk, 0.79), acute kidney injury stage 1 in 28% vs. 32% (P = .01; RR, 0.87) and RIFLE (risk, injury, failure, loss, and end-stage kidney disease) risk in 17% vs. 19.6% (P = .02; RR, 0.87), he said.
A subgroup analysis found no differences between the two techniques by age, cerebrovascular or peripheral arterial disease, EuroSCORE, left ventricular ejection fraction, region, or experience of the surgeon, Dr. Lamy said.
Both approaches are valid, and surgeons will need to tailor surgery for each individual patient, he said in an interview. For example, the off-pump technique may be best in a frail elderly patient to avoid transfusions and massive fluid infusion, whereas the on-pump technique may be best for a very large patient with the heart deeply placed within the chest.
Neurological outcomes and a cost-effectiveness analysis will be forthcoming. Five-year data on the coprimary end point plus repeat coronary revascularization over 5 years of follow-up are expected in 2016, Dr. Lamy said.
This study is funded by the Canadian Institutes of Health Research. Dr. Lamy reported consulting fees and honoraria from AstraZeneca.
FROM A LATE-BREAKING CLINICAL TRIAL SESSION AT THE ANNUAL MEETING OF THE AMERICAN COLLEGE OF CARDIOLOGY
Four Common Comorbidities Hike Risk of Late Post-TAVI Death
CHICAGO – Frailty and three common chronic health conditions place patients at greater risk of late mortality following transcatheter aortic valve replacement, according to extended follow-up of 339 patients in the Multicenter Canadian Experience study.
The overall survival rate was 57% after a median follow-up of 3 years (interquartile range 26-44 months) following transcatheter aortic valve implantation (TAVI).
Importantly, two-thirds of deaths (67%) were of noncardiac origin, 26% were due to cardiac causes, and 7% were of unknown causes, principal investigator Dr. Josep Rodés-Cabau said at the i2 Summit, a conference sponsored by the American College of Cardiology. Nearly half of noncardiac deaths were from respiratory failure (49%).
In multivariate analysis, a history of chronic obstructive pulmonary disease (hazard ratio, 1.99), chronic kidney disease (HR, 1.62), chronic atrial fibrillation (HR 1.82), and frailty (HR, 1.76) emerged as significant independent predictors of all-cause mortality more than 30 days after TAVI.
Surprisingly, there was no difference in survival between the transfemoral and transapical approaches in the multicenter TAVI program using a balloon-expandable valve, said Dr. Rodés-Cabau of the Quebec Heart and Lung Institute, Laval University, Quebec City, Canada. At 48 months follow-up, 45% of patients were free from death and stroke, as were 47% of those treated with the transfemoral approach and 44% treated with the transapical approach.
Causes of cumulative cardiac death included cardiac failure (65.5%), sudden death (13.8%), myocardial infarction (13.8%), endocarditis (3.4%), and postmitral replacement (3.4%).
Two patients required valve explantation because of endocarditis at 7 months and 13 months following TAVI, but no cases of structural valve failure occurred during follow-up, Dr. Rodés-Cabau stressed.
At 48 months, 76% of patients were free from cardiac death, as were 78% of transfemoral patients and 75% of transapical patients.
In multivariate analysis, pulmonary hypertension (HR, 1.92) and chronic kidney disease (HR, 2.30) were significant predictors of late cardiac death.
Although the data are compelling, the patient numbers are not sufficient to use to guide patient selection for TAVI, but instead represent a first step toward TAVI risk stratification, Dr. Rodés-Cabau said. After the introduction of TAVI, the focus was on technique, and many very-sick patients underwent the procedure only to die within the first year. Now, when a patient arrives at his center with these comorbidities, they are evaluated very carefully, including involvement of specialists such as respiratory or dietary specialists.
"I have to say that, based on the results of this study and also in our own daily experience, we have been refusing more patients now than we were in the past," he told reporters at a press briefing.
When asked during the formal study presentation why late mortality was similar with the two TAVI approaches, Dr. Rodés-Cabau said there could be several factors, but that the transapical approach is very well developed in Canada.
"These data were concentrated in a few number of centers with a huge experience in transapical approach, and this could explain the absence of difference between the two approaches," he said.
The investigators also evaluated regurgitation but found no association with late mortality, Dr. Rodés-Cabau said in an interview. The rate of moderate or severe regurgitation was relatively low at 8% at discharge. Studies have found a suggestion that mild regurgitation may be related to late mortality, but the Canadian data clearly show no difference in left ventricular diameter or LV ejection fraction changes between patients with and without mild regurgitation at 3 years, he said.
Overall, valve function remained stable up to 4 years of follow-up, with only mild, nonsignificant changes in transvalvular gradient and valve area.
"Mild aortic regurgitation, mostly paravalvular, was frequent after TAVI but had no impact on left ventricular diameters and function," Dr. Rodés-Cabau said at the meeting, also sponsored by the Cardiovascular Research Foundation.
Thirty-day mortality results from the Canadian experience were previously published in 2010 (J. Am. Coll. Cardiol. 2010;55:1080-90). Overall mortality was 10.4%, with pulmonary hypertension associated with a significantly higher rate of periprocedural death. Notably, patients with either porcelain aorta or frailty had acute outcomes similar to the rest of the study population.
Dr. Rodés-Cabau stressed that data in the study was analyzed at the Echo Core Lab and that only those patients with serial echocardiographic exams were included in the analysis. In all, 158 echocardiographic exams were analyzed at 1 year follow-up, 86 at 2 years, 34 at 3 years, and 11 exams at 4 years.
The median age of the patients was 81 years, 34% had prior cardiac bypass grafting, and 91% had a New York Heart Association functional class III-IV. The majority of patients received the Edwards Sapien valve (275 patients), with 57 implanted with the Cribier-Edwards valve, and 7 with the Sapien XT valve. The transfemoral approach was performed in 162 and transapical in 177 patients.
Dr. Rodés-Cabau is a consultant for Edwards Lifesciences and St. Jude Medical.
CHICAGO – Frailty and three common chronic health conditions place patients at greater risk of late mortality following transcatheter aortic valve replacement, according to extended follow-up of 339 patients in the Multicenter Canadian Experience study.
The overall survival rate was 57% after a median follow-up of 3 years (interquartile range 26-44 months) following transcatheter aortic valve implantation (TAVI).
Importantly, two-thirds of deaths (67%) were of noncardiac origin, 26% were due to cardiac causes, and 7% were of unknown causes, principal investigator Dr. Josep Rodés-Cabau said at the i2 Summit, a conference sponsored by the American College of Cardiology. Nearly half of noncardiac deaths were from respiratory failure (49%).
In multivariate analysis, a history of chronic obstructive pulmonary disease (hazard ratio, 1.99), chronic kidney disease (HR, 1.62), chronic atrial fibrillation (HR 1.82), and frailty (HR, 1.76) emerged as significant independent predictors of all-cause mortality more than 30 days after TAVI.
Surprisingly, there was no difference in survival between the transfemoral and transapical approaches in the multicenter TAVI program using a balloon-expandable valve, said Dr. Rodés-Cabau of the Quebec Heart and Lung Institute, Laval University, Quebec City, Canada. At 48 months follow-up, 45% of patients were free from death and stroke, as were 47% of those treated with the transfemoral approach and 44% treated with the transapical approach.
Causes of cumulative cardiac death included cardiac failure (65.5%), sudden death (13.8%), myocardial infarction (13.8%), endocarditis (3.4%), and postmitral replacement (3.4%).
Two patients required valve explantation because of endocarditis at 7 months and 13 months following TAVI, but no cases of structural valve failure occurred during follow-up, Dr. Rodés-Cabau stressed.
At 48 months, 76% of patients were free from cardiac death, as were 78% of transfemoral patients and 75% of transapical patients.
In multivariate analysis, pulmonary hypertension (HR, 1.92) and chronic kidney disease (HR, 2.30) were significant predictors of late cardiac death.
Although the data are compelling, the patient numbers are not sufficient to use to guide patient selection for TAVI, but instead represent a first step toward TAVI risk stratification, Dr. Rodés-Cabau said. After the introduction of TAVI, the focus was on technique, and many very-sick patients underwent the procedure only to die within the first year. Now, when a patient arrives at his center with these comorbidities, they are evaluated very carefully, including involvement of specialists such as respiratory or dietary specialists.
"I have to say that, based on the results of this study and also in our own daily experience, we have been refusing more patients now than we were in the past," he told reporters at a press briefing.
When asked during the formal study presentation why late mortality was similar with the two TAVI approaches, Dr. Rodés-Cabau said there could be several factors, but that the transapical approach is very well developed in Canada.
"These data were concentrated in a few number of centers with a huge experience in transapical approach, and this could explain the absence of difference between the two approaches," he said.
The investigators also evaluated regurgitation but found no association with late mortality, Dr. Rodés-Cabau said in an interview. The rate of moderate or severe regurgitation was relatively low at 8% at discharge. Studies have found a suggestion that mild regurgitation may be related to late mortality, but the Canadian data clearly show no difference in left ventricular diameter or LV ejection fraction changes between patients with and without mild regurgitation at 3 years, he said.
Overall, valve function remained stable up to 4 years of follow-up, with only mild, nonsignificant changes in transvalvular gradient and valve area.
"Mild aortic regurgitation, mostly paravalvular, was frequent after TAVI but had no impact on left ventricular diameters and function," Dr. Rodés-Cabau said at the meeting, also sponsored by the Cardiovascular Research Foundation.
Thirty-day mortality results from the Canadian experience were previously published in 2010 (J. Am. Coll. Cardiol. 2010;55:1080-90). Overall mortality was 10.4%, with pulmonary hypertension associated with a significantly higher rate of periprocedural death. Notably, patients with either porcelain aorta or frailty had acute outcomes similar to the rest of the study population.
Dr. Rodés-Cabau stressed that data in the study was analyzed at the Echo Core Lab and that only those patients with serial echocardiographic exams were included in the analysis. In all, 158 echocardiographic exams were analyzed at 1 year follow-up, 86 at 2 years, 34 at 3 years, and 11 exams at 4 years.
The median age of the patients was 81 years, 34% had prior cardiac bypass grafting, and 91% had a New York Heart Association functional class III-IV. The majority of patients received the Edwards Sapien valve (275 patients), with 57 implanted with the Cribier-Edwards valve, and 7 with the Sapien XT valve. The transfemoral approach was performed in 162 and transapical in 177 patients.
Dr. Rodés-Cabau is a consultant for Edwards Lifesciences and St. Jude Medical.
CHICAGO – Frailty and three common chronic health conditions place patients at greater risk of late mortality following transcatheter aortic valve replacement, according to extended follow-up of 339 patients in the Multicenter Canadian Experience study.
The overall survival rate was 57% after a median follow-up of 3 years (interquartile range 26-44 months) following transcatheter aortic valve implantation (TAVI).
Importantly, two-thirds of deaths (67%) were of noncardiac origin, 26% were due to cardiac causes, and 7% were of unknown causes, principal investigator Dr. Josep Rodés-Cabau said at the i2 Summit, a conference sponsored by the American College of Cardiology. Nearly half of noncardiac deaths were from respiratory failure (49%).
In multivariate analysis, a history of chronic obstructive pulmonary disease (hazard ratio, 1.99), chronic kidney disease (HR, 1.62), chronic atrial fibrillation (HR 1.82), and frailty (HR, 1.76) emerged as significant independent predictors of all-cause mortality more than 30 days after TAVI.
Surprisingly, there was no difference in survival between the transfemoral and transapical approaches in the multicenter TAVI program using a balloon-expandable valve, said Dr. Rodés-Cabau of the Quebec Heart and Lung Institute, Laval University, Quebec City, Canada. At 48 months follow-up, 45% of patients were free from death and stroke, as were 47% of those treated with the transfemoral approach and 44% treated with the transapical approach.
Causes of cumulative cardiac death included cardiac failure (65.5%), sudden death (13.8%), myocardial infarction (13.8%), endocarditis (3.4%), and postmitral replacement (3.4%).
Two patients required valve explantation because of endocarditis at 7 months and 13 months following TAVI, but no cases of structural valve failure occurred during follow-up, Dr. Rodés-Cabau stressed.
At 48 months, 76% of patients were free from cardiac death, as were 78% of transfemoral patients and 75% of transapical patients.
In multivariate analysis, pulmonary hypertension (HR, 1.92) and chronic kidney disease (HR, 2.30) were significant predictors of late cardiac death.
Although the data are compelling, the patient numbers are not sufficient to use to guide patient selection for TAVI, but instead represent a first step toward TAVI risk stratification, Dr. Rodés-Cabau said. After the introduction of TAVI, the focus was on technique, and many very-sick patients underwent the procedure only to die within the first year. Now, when a patient arrives at his center with these comorbidities, they are evaluated very carefully, including involvement of specialists such as respiratory or dietary specialists.
"I have to say that, based on the results of this study and also in our own daily experience, we have been refusing more patients now than we were in the past," he told reporters at a press briefing.
When asked during the formal study presentation why late mortality was similar with the two TAVI approaches, Dr. Rodés-Cabau said there could be several factors, but that the transapical approach is very well developed in Canada.
"These data were concentrated in a few number of centers with a huge experience in transapical approach, and this could explain the absence of difference between the two approaches," he said.
The investigators also evaluated regurgitation but found no association with late mortality, Dr. Rodés-Cabau said in an interview. The rate of moderate or severe regurgitation was relatively low at 8% at discharge. Studies have found a suggestion that mild regurgitation may be related to late mortality, but the Canadian data clearly show no difference in left ventricular diameter or LV ejection fraction changes between patients with and without mild regurgitation at 3 years, he said.
Overall, valve function remained stable up to 4 years of follow-up, with only mild, nonsignificant changes in transvalvular gradient and valve area.
"Mild aortic regurgitation, mostly paravalvular, was frequent after TAVI but had no impact on left ventricular diameters and function," Dr. Rodés-Cabau said at the meeting, also sponsored by the Cardiovascular Research Foundation.
Thirty-day mortality results from the Canadian experience were previously published in 2010 (J. Am. Coll. Cardiol. 2010;55:1080-90). Overall mortality was 10.4%, with pulmonary hypertension associated with a significantly higher rate of periprocedural death. Notably, patients with either porcelain aorta or frailty had acute outcomes similar to the rest of the study population.
Dr. Rodés-Cabau stressed that data in the study was analyzed at the Echo Core Lab and that only those patients with serial echocardiographic exams were included in the analysis. In all, 158 echocardiographic exams were analyzed at 1 year follow-up, 86 at 2 years, 34 at 3 years, and 11 exams at 4 years.
The median age of the patients was 81 years, 34% had prior cardiac bypass grafting, and 91% had a New York Heart Association functional class III-IV. The majority of patients received the Edwards Sapien valve (275 patients), with 57 implanted with the Cribier-Edwards valve, and 7 with the Sapien XT valve. The transfemoral approach was performed in 162 and transapical in 177 patients.
Dr. Rodés-Cabau is a consultant for Edwards Lifesciences and St. Jude Medical.
FROM THE ANNUAL MEETING OF THE AMERICAN COLLEGE OF CARDIOLOGY
Major Finding: After a median follow-up of 3 years, 67% of deaths were of noncardiac origin, 26% were from cardiac causes, and 7% were of unknown causes.
Data Source: Data were from a long-term follow-up of the Multicenter Canadian Experience in 339 undergoing transcatheter aortic valve replacement.
Disclosures: Dr. Rodés-Cabau is a consultant for Edwards Lifesciences and St. Jude Medical.
CoreValve Excels in 'Real-World' Study
CHICAGO – Transcatheter aortic valve implantation using the CoreValve system improved hemodynamics with a very low incidence of stroke in 1,015 consecutive patients with severe aortic stenosis in the real-world ADVANCE study.
The 30-day stroke rate was 2.9% (1.2% major and 1.7% minor), and 3.4% at 6 months (1.6% major and 1.8% minor). Transient ischemic attack rates were 0.4% and 1.2%, respectively, as adjudicated by an independent neurologist.
Mean aortic valve gradient decreased from 45.6 mm Hg at baseline to 9.3 mm Hg at 30 days and to 9.5 mm Hg at 6 months, while effective orifice area increased from 0.7 cm2 at baseline to 1.7 cm2 at both 30 days and 6 months.
"The CoreValve ADVANCE study, which is the largest, multicenter, prospective, fully monitored TAVI study, shows that treatment of real-world inoperable and frail high-risk patients with the Medtronic CoreValve is safe and associated with an improvement in aortic valve function and low stroke and mortality rates at 1 month and 6 months follow-up," principal investigator Dr. Axel Linke said at the i2 Summit, a conference sponsored by the American College of Cardiology.
Medtronic’s transcatheter CoreValve System, which features a porcine pericardial tissue valve that is sutured into a self-expanding nitinol frame, is currently limited to investigational use in the United States.
The 1,015 patients, mean age 81 years, were considered inoperable or high risk and were enrolled from March 2010 to July 2011 at 44 centers in 12 countries in Western Europe, Asia, and South America. All centers had conducted at least 40 TAVI procedures prior to the study and had a heart team in place. Clinical end points were reported according to Valve Academic Research Consortium (VARC) criteria.
Among the 996 patients in whom implantation was attempted, the procedural success rate was 98%, said Dr. Linke, professor of medicine at the University of Leipzig (Germany) Heart Center.
The study’s primary end point of major adverse cardiac and cerebrovascular events occurred in 8.3%, with all-cause mortality at 4.5%, myocardial infarctions 0.2%, and emergent cardiac surgery or percutaneous reintervention 1.7%. MACE events were adjudicated by an independent clinical events committee consisting of TAVI-experienced interventional cardiologists and cardiac surgeons, Dr. Linke pointed out at the meeting, also sponsored by the Cardiovascular Research Foundation.
Additional 30-day VARC end points included cardiovascular mortality at 3.4%, major bleeding in 9.7%, life-threatening bleeding in 4%, major vascular complications in 10.7%, and acute stage III kidney injury in 0.4%.
New pacemaker implantation was required in 26.3% of patients, due largely to significant bradycardia or higher grade AV block. The timing of the implantation was left to the discretion of the surgeon, with some implantations occurring during TAVI and others at postoperative day 1 or 2. Although the pacemaker placement rate is consistent with what has been reported in European registries, Dr. Linke noted during a press briefing at the meeting that rates in the study varied widely among countries, from 8% to 30%.
Survival rates were high at both 30 days (95.5%) and 6 months (87.2%). A prespecified subgroup analysis by logistic EuroScore revealed a 6-month survival rate of 95.7% for those with a score of 0-10, 92.4% with a score of 10-20, and 88.1% with a score greater than 20.
Session co-moderator Dr. George Dangas of the senior cardiology faculty at the Mount Sinai Medical School in New York, said the consensus is that bleeding rates with TAVI have improved over time, but remarked that "a 10% bleeding rate is still not that small."
Dr. Linke said further investigation is still needed, but that "despite the fact we have relatively high bleeding rates, they have lost their impact on mortality in the latest registries.
"I believe we still have bleeding, but we have gained so much experience to get control of the bleeding, therefore we have fewer cases of bleeding related-death."
Audience members also questioned what may have contributed to the low incidence of stroke in ADVANCE. Dr. Linke said they don’t yet have an explanation for the very low stroke rates, but that valve expansion may be at play.
One contributor may be "really aggressive oversizing with the cobalt rim that might crush the calcium and release the calcium into those bloodstream," he said. "Here, it’s a rather passive expansion and it might be that the calcium is still covered by fibrotic tissue and endothelium and not exposed to the bloodstream. This might be one reason, but we are still in the process of understanding what is going on."
At baseline, 31% of ADVANCE patients were diagnosed with diabetes, 20% had peripheral vascular disease, and 21% had undergone previous CABG. Their mean logistic EuroSCORE was 19.2. Roughly 80% were New York Heart Association class III and IV. At 6 months post-TAVI, 1% were class IV, 12% class III, 44% class II, and 43% class I.
This study was sponsored by Medtronic Bakken Research Center. Dr. Linke reported serving as a proctor for and receiving customary travel and expenses from Medtronic. Dr. Dangas serves as a consultant to AstraZeneca and Cordis.
CHICAGO – Transcatheter aortic valve implantation using the CoreValve system improved hemodynamics with a very low incidence of stroke in 1,015 consecutive patients with severe aortic stenosis in the real-world ADVANCE study.
The 30-day stroke rate was 2.9% (1.2% major and 1.7% minor), and 3.4% at 6 months (1.6% major and 1.8% minor). Transient ischemic attack rates were 0.4% and 1.2%, respectively, as adjudicated by an independent neurologist.
Mean aortic valve gradient decreased from 45.6 mm Hg at baseline to 9.3 mm Hg at 30 days and to 9.5 mm Hg at 6 months, while effective orifice area increased from 0.7 cm2 at baseline to 1.7 cm2 at both 30 days and 6 months.
"The CoreValve ADVANCE study, which is the largest, multicenter, prospective, fully monitored TAVI study, shows that treatment of real-world inoperable and frail high-risk patients with the Medtronic CoreValve is safe and associated with an improvement in aortic valve function and low stroke and mortality rates at 1 month and 6 months follow-up," principal investigator Dr. Axel Linke said at the i2 Summit, a conference sponsored by the American College of Cardiology.
Medtronic’s transcatheter CoreValve System, which features a porcine pericardial tissue valve that is sutured into a self-expanding nitinol frame, is currently limited to investigational use in the United States.
The 1,015 patients, mean age 81 years, were considered inoperable or high risk and were enrolled from March 2010 to July 2011 at 44 centers in 12 countries in Western Europe, Asia, and South America. All centers had conducted at least 40 TAVI procedures prior to the study and had a heart team in place. Clinical end points were reported according to Valve Academic Research Consortium (VARC) criteria.
Among the 996 patients in whom implantation was attempted, the procedural success rate was 98%, said Dr. Linke, professor of medicine at the University of Leipzig (Germany) Heart Center.
The study’s primary end point of major adverse cardiac and cerebrovascular events occurred in 8.3%, with all-cause mortality at 4.5%, myocardial infarctions 0.2%, and emergent cardiac surgery or percutaneous reintervention 1.7%. MACE events were adjudicated by an independent clinical events committee consisting of TAVI-experienced interventional cardiologists and cardiac surgeons, Dr. Linke pointed out at the meeting, also sponsored by the Cardiovascular Research Foundation.
Additional 30-day VARC end points included cardiovascular mortality at 3.4%, major bleeding in 9.7%, life-threatening bleeding in 4%, major vascular complications in 10.7%, and acute stage III kidney injury in 0.4%.
New pacemaker implantation was required in 26.3% of patients, due largely to significant bradycardia or higher grade AV block. The timing of the implantation was left to the discretion of the surgeon, with some implantations occurring during TAVI and others at postoperative day 1 or 2. Although the pacemaker placement rate is consistent with what has been reported in European registries, Dr. Linke noted during a press briefing at the meeting that rates in the study varied widely among countries, from 8% to 30%.
Survival rates were high at both 30 days (95.5%) and 6 months (87.2%). A prespecified subgroup analysis by logistic EuroScore revealed a 6-month survival rate of 95.7% for those with a score of 0-10, 92.4% with a score of 10-20, and 88.1% with a score greater than 20.
Session co-moderator Dr. George Dangas of the senior cardiology faculty at the Mount Sinai Medical School in New York, said the consensus is that bleeding rates with TAVI have improved over time, but remarked that "a 10% bleeding rate is still not that small."
Dr. Linke said further investigation is still needed, but that "despite the fact we have relatively high bleeding rates, they have lost their impact on mortality in the latest registries.
"I believe we still have bleeding, but we have gained so much experience to get control of the bleeding, therefore we have fewer cases of bleeding related-death."
Audience members also questioned what may have contributed to the low incidence of stroke in ADVANCE. Dr. Linke said they don’t yet have an explanation for the very low stroke rates, but that valve expansion may be at play.
One contributor may be "really aggressive oversizing with the cobalt rim that might crush the calcium and release the calcium into those bloodstream," he said. "Here, it’s a rather passive expansion and it might be that the calcium is still covered by fibrotic tissue and endothelium and not exposed to the bloodstream. This might be one reason, but we are still in the process of understanding what is going on."
At baseline, 31% of ADVANCE patients were diagnosed with diabetes, 20% had peripheral vascular disease, and 21% had undergone previous CABG. Their mean logistic EuroSCORE was 19.2. Roughly 80% were New York Heart Association class III and IV. At 6 months post-TAVI, 1% were class IV, 12% class III, 44% class II, and 43% class I.
This study was sponsored by Medtronic Bakken Research Center. Dr. Linke reported serving as a proctor for and receiving customary travel and expenses from Medtronic. Dr. Dangas serves as a consultant to AstraZeneca and Cordis.
CHICAGO – Transcatheter aortic valve implantation using the CoreValve system improved hemodynamics with a very low incidence of stroke in 1,015 consecutive patients with severe aortic stenosis in the real-world ADVANCE study.
The 30-day stroke rate was 2.9% (1.2% major and 1.7% minor), and 3.4% at 6 months (1.6% major and 1.8% minor). Transient ischemic attack rates were 0.4% and 1.2%, respectively, as adjudicated by an independent neurologist.
Mean aortic valve gradient decreased from 45.6 mm Hg at baseline to 9.3 mm Hg at 30 days and to 9.5 mm Hg at 6 months, while effective orifice area increased from 0.7 cm2 at baseline to 1.7 cm2 at both 30 days and 6 months.
"The CoreValve ADVANCE study, which is the largest, multicenter, prospective, fully monitored TAVI study, shows that treatment of real-world inoperable and frail high-risk patients with the Medtronic CoreValve is safe and associated with an improvement in aortic valve function and low stroke and mortality rates at 1 month and 6 months follow-up," principal investigator Dr. Axel Linke said at the i2 Summit, a conference sponsored by the American College of Cardiology.
Medtronic’s transcatheter CoreValve System, which features a porcine pericardial tissue valve that is sutured into a self-expanding nitinol frame, is currently limited to investigational use in the United States.
The 1,015 patients, mean age 81 years, were considered inoperable or high risk and were enrolled from March 2010 to July 2011 at 44 centers in 12 countries in Western Europe, Asia, and South America. All centers had conducted at least 40 TAVI procedures prior to the study and had a heart team in place. Clinical end points were reported according to Valve Academic Research Consortium (VARC) criteria.
Among the 996 patients in whom implantation was attempted, the procedural success rate was 98%, said Dr. Linke, professor of medicine at the University of Leipzig (Germany) Heart Center.
The study’s primary end point of major adverse cardiac and cerebrovascular events occurred in 8.3%, with all-cause mortality at 4.5%, myocardial infarctions 0.2%, and emergent cardiac surgery or percutaneous reintervention 1.7%. MACE events were adjudicated by an independent clinical events committee consisting of TAVI-experienced interventional cardiologists and cardiac surgeons, Dr. Linke pointed out at the meeting, also sponsored by the Cardiovascular Research Foundation.
Additional 30-day VARC end points included cardiovascular mortality at 3.4%, major bleeding in 9.7%, life-threatening bleeding in 4%, major vascular complications in 10.7%, and acute stage III kidney injury in 0.4%.
New pacemaker implantation was required in 26.3% of patients, due largely to significant bradycardia or higher grade AV block. The timing of the implantation was left to the discretion of the surgeon, with some implantations occurring during TAVI and others at postoperative day 1 or 2. Although the pacemaker placement rate is consistent with what has been reported in European registries, Dr. Linke noted during a press briefing at the meeting that rates in the study varied widely among countries, from 8% to 30%.
Survival rates were high at both 30 days (95.5%) and 6 months (87.2%). A prespecified subgroup analysis by logistic EuroScore revealed a 6-month survival rate of 95.7% for those with a score of 0-10, 92.4% with a score of 10-20, and 88.1% with a score greater than 20.
Session co-moderator Dr. George Dangas of the senior cardiology faculty at the Mount Sinai Medical School in New York, said the consensus is that bleeding rates with TAVI have improved over time, but remarked that "a 10% bleeding rate is still not that small."
Dr. Linke said further investigation is still needed, but that "despite the fact we have relatively high bleeding rates, they have lost their impact on mortality in the latest registries.
"I believe we still have bleeding, but we have gained so much experience to get control of the bleeding, therefore we have fewer cases of bleeding related-death."
Audience members also questioned what may have contributed to the low incidence of stroke in ADVANCE. Dr. Linke said they don’t yet have an explanation for the very low stroke rates, but that valve expansion may be at play.
One contributor may be "really aggressive oversizing with the cobalt rim that might crush the calcium and release the calcium into those bloodstream," he said. "Here, it’s a rather passive expansion and it might be that the calcium is still covered by fibrotic tissue and endothelium and not exposed to the bloodstream. This might be one reason, but we are still in the process of understanding what is going on."
At baseline, 31% of ADVANCE patients were diagnosed with diabetes, 20% had peripheral vascular disease, and 21% had undergone previous CABG. Their mean logistic EuroSCORE was 19.2. Roughly 80% were New York Heart Association class III and IV. At 6 months post-TAVI, 1% were class IV, 12% class III, 44% class II, and 43% class I.
This study was sponsored by Medtronic Bakken Research Center. Dr. Linke reported serving as a proctor for and receiving customary travel and expenses from Medtronic. Dr. Dangas serves as a consultant to AstraZeneca and Cordis.
FROM THE ANNUAL MEETING OF THE AMERICAN COLLEGE OF CARDIOLOGY
Major Finding: Major adverse cardiac and cerebrovascular events occurred in 8.3% of patients 30 days postprocedure, including a 2.9% stroke rate.
Data Source: Prospective phase IV observational cohort trial of 1,015 consecutive inoperable or high-risk patients with severe aortic valve stenosis implanted with the transcatheter CoreValve aortic valve system.
Disclosures: This study was sponsored by Medtronic Bakken Research Center. Dr. Linke reported serving as a proctor for and receiving customary travel and expenses from Medtronic.
Cardiac Surgical Transfusions Linked to Infection Risk
FT. LAUDERDALE, FLA. – Transfusion of packed red blood cells during cardiac surgery is independently associated with increased risk of major infection, researchers reported, and – in a related study – pneumonia was found to be the most common infection associated with cardiac surgery.
Cardiac procedures with transfusions were associated with a significant risk of infection, such that "with every unit of blood, you had a significant increase in the risk of infection for the patient. It appears that there might be some sort of threshold in the 2- to 4-unit range, whereafter the risk really seems to increase. But statistically, even that first drop of blood carried an additional infectious risk," Dr. Keith A. Horvath said at the annual meeting of the Society of Thoracic Surgeons.
In a related study, researchers found pneumonia to be the most common infection associated with cardiac surgery. "Pneumonia, surprisingly, was the most common infection, at 2.4%. This was much more common than other infections that we certainly worry about and get a fair amount of press and literature on, specifically sternal wound infections," said Dr. Gorav Ailawadi of the University of Virginia in Charlottesville.
Data for 5,184 adult cardiac patients were used for both studies. The patients were prospectively enrolled in a 10-center infection registry between February and September, 2010. Captured data included infection occurrence, type, and organism. Adjudication was performed by an independent panel of infectious diseases experts.
Major infections evaluated in the study included deep incisional surgical (chest), deep incisional surgical (second incisions), empyema, endocarditis, mediastinitis, myocarditis, pneumonia, bloodstream infections, Clostridium difficile colitis, and cardiac device infections. Infections were defined by a combination of clinical, laboratory, and/or radiologic evidence (according to Centers for Disease Control and Prevention surveillance definitions) for a follow-up of 65 days.
The researchers included several types of surgical interventions: isolated coronary artery bypass graft (CABG), isolated valve surgery, CABG with valve surgery, surgery for heart failure, thoracic aortic surgery, and other procedures.
The mean patient age was 64 years, mean bypass time was 115 minutes, two-thirds (67%) were men, 71% had heart failure, a quarter (27%) had diabetes, 14% had chronic obstructive pulmonary disease (COPD), and 19% had prior cardiac surgery. Mean hemoglobin was 13.2 mg/dL.
There was a significant dose-dependent association between quantity of packed red blood cells (PRBCs) and risk of infection, with the crude risk increasing by an average of 29% with each PRBC unit.
Several factors increased the risk of infection, including severe COPD (relative risk, 1.85), preoperative creatinine levels greater than 1.5 mg/dL (RR, 1.72), heart failure (RR, 1.49), mild to moderate COPD (RR, 1.36), PRBCs per unit (RR, 1.24), and surgery time per 60 minutes (RR, 1.19).
Platelet transfusion occurred in 31% of patients. However, the use of platelets was associated with a decreased risk of infection (RR, 0.71). Cell Saver use was not related to infection.
Creatinine levels greater than 1.5 mg/dL (RR, 2.40) and PRBCs per unit (RR, 1.23) significantly increased the risk of death. Many factors significantly increased the length of stay, including creatinine levels greater than 1.5 mg/dL (RR, 1.26), severe COPD (RR, 1.41), mild to moderate COPD (RR, 1.14), heart failure (RR, 1.36), PRBCs (RR, 1.12), surgery time per 60 minutes (RR, 1.11), age of 65-79 years (RR, 1.21), and age older than 80 years (RR, 1.44). The use of platelets was associated with a decreased length of stay (RR, 0.71).
All risks of transfusion must be weighed against toleration anemia, which is also associated with adverse outcomes, according to Dr. Horvath, who is the director of the Cardiothoracic Surgery Research Program for the National Heart, Lung, and Blood Institute and a member of the Cardiothoracic Surgery Trials Network.
Efforts to reduce PRBC transfusions may significantly reduce major postoperative infections. Cell salvage and ultrafiltration could be viable alternatives, he noted.
In the second study, the researchers used the same dataset. Captured data included infection occurrence, type, timing, and organisms. Infections were adjudicated by an independent panel of infectious disease experts. The risk of pneumonia, mortality, and length of stay (time to discharge) were analyzed.
Major infections included bloodstream, pneumonia, C. difficile, deep sternal incisional, mediastinitis, deep groin/leg incisional, endocarditis, and empyema.
Pneumonia was diagnosed using the 2010 surveillance criteria from the CDC/National Healthcare Safety Network, including chest x-ray with new or progressive and persistent infiltrate; fever greater than 38° C; leukopenia (defined as fewer than 4,000 leukocytes per cc); leukocytosis (at least 12,000 leukocytes per cc); or altered mental status. At least two of the following must have been present as well: purulent sputum or change; cough, dyspnea, or tachypnea; rales or bronchial breath sounds; or worsening gas exchange. Duration of follow-up was 65 days.
In all, 31% had isolated CABG, 30% had isolated valve surgery, 11% had CABG and valve surgery, 6% had thoracic aortic surgery, 2% had left ventricular assist device (LVAD) implantation/heart transplant, and 20% were categorized as other.
Overall, 2.4% of patients in the registry had pneumonia, 1.1% had blood stream infection, 1% had C. difficile colitis, and 0.5% had deep sternal infections.
The overall mean time to infection was 19 days and the median was 14 days. The mean time to infection for pneumonia was 15 days. Overall, more than 40% of infections occurred after the index hospitalization. However, 68% and 66% of pneumonias and blood stream infections, respectively, occurred during hospitalization. The three most common organisms were Pseudomonas aeruginosa (12%), Enterobacter cloacae (8%), and Klebsiella pneumoniae (7%).
Increased risk of pneumonia was associated with surgery time (RR, 1.42), a creatinine level of at least 1.5 mg/dL (RR, 1.94), mild to moderate COPD (RR, 1.78), severe COPD (RR, 4.12), and heart failure (RR, 1.76). The reference category was those without COPD.
In terms of process-of-care factors, only nasal decontamination with mupirocin was associated with reduced risk of pneumonia (RR, 0.77). Nasal decontamination with other agents (RR, 1.44); antibiotics given within 24 hours after surgery (RR, 1.26) and within 48 hours postop (RR, 2.70); ventilator use of 24-48 hours (RR, 2.31) and more than 48 hours (RR, 4.58); nasogastric tube (RR, 2.07); and use of PRBCs (RR, 1.10) were all associated with increased risk of pneumonia.
In terms of mortality, "pneumonia, among all the factors analyzed, had the greatest association with mortality, with an odds ratio greater than seven ... which was far and away greater than anything else that was examined," said Dr. Ailawadi.
Pneumonia was significantly associated with an increased risk of mortality (RR, 7.07), as were heart failure (RR, 1.87), creatinine levels of at least 1.5 mg/dL (RR, 2.97), and surgery duration (1.27). However, black race appeared to be protective, with a significantly decreased risk of pneumonia (RR, 0.43).
Pneumonia significantly increased the length of stay by a median of 13 days (19 days with pneumonia and 6 days without). A number of factors – mild to moderate COPD, severe COPD, heart failure, creatinine levels of at least 1.5 mg/dL, surgery time, age of 65-79 years, age 80 years and older, and black or Hispanic race – were significantly associated with increased risk of longer length of stay. Male sex was significantly associated with decreased length of stay (RR, 0.79).
Both Dr. Horvath and Dr. Ailawadi reported that they have no relevant financial disclosures.
Cardiac procedures with transfusions, Dr. Keith A. Horvath, the Society of Thoracic Surgeons, Dr. Gorav Ailawadi, deep incisional surgical, deep incisional surgical, empyema, endocarditis, mediastinitis, myocarditis, pneumonia, bloodstream infections, Clostridium difficile colitis, and cardiac device infections,
FT. LAUDERDALE, FLA. – Transfusion of packed red blood cells during cardiac surgery is independently associated with increased risk of major infection, researchers reported, and – in a related study – pneumonia was found to be the most common infection associated with cardiac surgery.
Cardiac procedures with transfusions were associated with a significant risk of infection, such that "with every unit of blood, you had a significant increase in the risk of infection for the patient. It appears that there might be some sort of threshold in the 2- to 4-unit range, whereafter the risk really seems to increase. But statistically, even that first drop of blood carried an additional infectious risk," Dr. Keith A. Horvath said at the annual meeting of the Society of Thoracic Surgeons.
In a related study, researchers found pneumonia to be the most common infection associated with cardiac surgery. "Pneumonia, surprisingly, was the most common infection, at 2.4%. This was much more common than other infections that we certainly worry about and get a fair amount of press and literature on, specifically sternal wound infections," said Dr. Gorav Ailawadi of the University of Virginia in Charlottesville.
Data for 5,184 adult cardiac patients were used for both studies. The patients were prospectively enrolled in a 10-center infection registry between February and September, 2010. Captured data included infection occurrence, type, and organism. Adjudication was performed by an independent panel of infectious diseases experts.
Major infections evaluated in the study included deep incisional surgical (chest), deep incisional surgical (second incisions), empyema, endocarditis, mediastinitis, myocarditis, pneumonia, bloodstream infections, Clostridium difficile colitis, and cardiac device infections. Infections were defined by a combination of clinical, laboratory, and/or radiologic evidence (according to Centers for Disease Control and Prevention surveillance definitions) for a follow-up of 65 days.
The researchers included several types of surgical interventions: isolated coronary artery bypass graft (CABG), isolated valve surgery, CABG with valve surgery, surgery for heart failure, thoracic aortic surgery, and other procedures.
The mean patient age was 64 years, mean bypass time was 115 minutes, two-thirds (67%) were men, 71% had heart failure, a quarter (27%) had diabetes, 14% had chronic obstructive pulmonary disease (COPD), and 19% had prior cardiac surgery. Mean hemoglobin was 13.2 mg/dL.
There was a significant dose-dependent association between quantity of packed red blood cells (PRBCs) and risk of infection, with the crude risk increasing by an average of 29% with each PRBC unit.
Several factors increased the risk of infection, including severe COPD (relative risk, 1.85), preoperative creatinine levels greater than 1.5 mg/dL (RR, 1.72), heart failure (RR, 1.49), mild to moderate COPD (RR, 1.36), PRBCs per unit (RR, 1.24), and surgery time per 60 minutes (RR, 1.19).
Platelet transfusion occurred in 31% of patients. However, the use of platelets was associated with a decreased risk of infection (RR, 0.71). Cell Saver use was not related to infection.
Creatinine levels greater than 1.5 mg/dL (RR, 2.40) and PRBCs per unit (RR, 1.23) significantly increased the risk of death. Many factors significantly increased the length of stay, including creatinine levels greater than 1.5 mg/dL (RR, 1.26), severe COPD (RR, 1.41), mild to moderate COPD (RR, 1.14), heart failure (RR, 1.36), PRBCs (RR, 1.12), surgery time per 60 minutes (RR, 1.11), age of 65-79 years (RR, 1.21), and age older than 80 years (RR, 1.44). The use of platelets was associated with a decreased length of stay (RR, 0.71).
All risks of transfusion must be weighed against toleration anemia, which is also associated with adverse outcomes, according to Dr. Horvath, who is the director of the Cardiothoracic Surgery Research Program for the National Heart, Lung, and Blood Institute and a member of the Cardiothoracic Surgery Trials Network.
Efforts to reduce PRBC transfusions may significantly reduce major postoperative infections. Cell salvage and ultrafiltration could be viable alternatives, he noted.
In the second study, the researchers used the same dataset. Captured data included infection occurrence, type, timing, and organisms. Infections were adjudicated by an independent panel of infectious disease experts. The risk of pneumonia, mortality, and length of stay (time to discharge) were analyzed.
Major infections included bloodstream, pneumonia, C. difficile, deep sternal incisional, mediastinitis, deep groin/leg incisional, endocarditis, and empyema.
Pneumonia was diagnosed using the 2010 surveillance criteria from the CDC/National Healthcare Safety Network, including chest x-ray with new or progressive and persistent infiltrate; fever greater than 38° C; leukopenia (defined as fewer than 4,000 leukocytes per cc); leukocytosis (at least 12,000 leukocytes per cc); or altered mental status. At least two of the following must have been present as well: purulent sputum or change; cough, dyspnea, or tachypnea; rales or bronchial breath sounds; or worsening gas exchange. Duration of follow-up was 65 days.
In all, 31% had isolated CABG, 30% had isolated valve surgery, 11% had CABG and valve surgery, 6% had thoracic aortic surgery, 2% had left ventricular assist device (LVAD) implantation/heart transplant, and 20% were categorized as other.
Overall, 2.4% of patients in the registry had pneumonia, 1.1% had blood stream infection, 1% had C. difficile colitis, and 0.5% had deep sternal infections.
The overall mean time to infection was 19 days and the median was 14 days. The mean time to infection for pneumonia was 15 days. Overall, more than 40% of infections occurred after the index hospitalization. However, 68% and 66% of pneumonias and blood stream infections, respectively, occurred during hospitalization. The three most common organisms were Pseudomonas aeruginosa (12%), Enterobacter cloacae (8%), and Klebsiella pneumoniae (7%).
Increased risk of pneumonia was associated with surgery time (RR, 1.42), a creatinine level of at least 1.5 mg/dL (RR, 1.94), mild to moderate COPD (RR, 1.78), severe COPD (RR, 4.12), and heart failure (RR, 1.76). The reference category was those without COPD.
In terms of process-of-care factors, only nasal decontamination with mupirocin was associated with reduced risk of pneumonia (RR, 0.77). Nasal decontamination with other agents (RR, 1.44); antibiotics given within 24 hours after surgery (RR, 1.26) and within 48 hours postop (RR, 2.70); ventilator use of 24-48 hours (RR, 2.31) and more than 48 hours (RR, 4.58); nasogastric tube (RR, 2.07); and use of PRBCs (RR, 1.10) were all associated with increased risk of pneumonia.
In terms of mortality, "pneumonia, among all the factors analyzed, had the greatest association with mortality, with an odds ratio greater than seven ... which was far and away greater than anything else that was examined," said Dr. Ailawadi.
Pneumonia was significantly associated with an increased risk of mortality (RR, 7.07), as were heart failure (RR, 1.87), creatinine levels of at least 1.5 mg/dL (RR, 2.97), and surgery duration (1.27). However, black race appeared to be protective, with a significantly decreased risk of pneumonia (RR, 0.43).
Pneumonia significantly increased the length of stay by a median of 13 days (19 days with pneumonia and 6 days without). A number of factors – mild to moderate COPD, severe COPD, heart failure, creatinine levels of at least 1.5 mg/dL, surgery time, age of 65-79 years, age 80 years and older, and black or Hispanic race – were significantly associated with increased risk of longer length of stay. Male sex was significantly associated with decreased length of stay (RR, 0.79).
Both Dr. Horvath and Dr. Ailawadi reported that they have no relevant financial disclosures.
FT. LAUDERDALE, FLA. – Transfusion of packed red blood cells during cardiac surgery is independently associated with increased risk of major infection, researchers reported, and – in a related study – pneumonia was found to be the most common infection associated with cardiac surgery.
Cardiac procedures with transfusions were associated with a significant risk of infection, such that "with every unit of blood, you had a significant increase in the risk of infection for the patient. It appears that there might be some sort of threshold in the 2- to 4-unit range, whereafter the risk really seems to increase. But statistically, even that first drop of blood carried an additional infectious risk," Dr. Keith A. Horvath said at the annual meeting of the Society of Thoracic Surgeons.
In a related study, researchers found pneumonia to be the most common infection associated with cardiac surgery. "Pneumonia, surprisingly, was the most common infection, at 2.4%. This was much more common than other infections that we certainly worry about and get a fair amount of press and literature on, specifically sternal wound infections," said Dr. Gorav Ailawadi of the University of Virginia in Charlottesville.
Data for 5,184 adult cardiac patients were used for both studies. The patients were prospectively enrolled in a 10-center infection registry between February and September, 2010. Captured data included infection occurrence, type, and organism. Adjudication was performed by an independent panel of infectious diseases experts.
Major infections evaluated in the study included deep incisional surgical (chest), deep incisional surgical (second incisions), empyema, endocarditis, mediastinitis, myocarditis, pneumonia, bloodstream infections, Clostridium difficile colitis, and cardiac device infections. Infections were defined by a combination of clinical, laboratory, and/or radiologic evidence (according to Centers for Disease Control and Prevention surveillance definitions) for a follow-up of 65 days.
The researchers included several types of surgical interventions: isolated coronary artery bypass graft (CABG), isolated valve surgery, CABG with valve surgery, surgery for heart failure, thoracic aortic surgery, and other procedures.
The mean patient age was 64 years, mean bypass time was 115 minutes, two-thirds (67%) were men, 71% had heart failure, a quarter (27%) had diabetes, 14% had chronic obstructive pulmonary disease (COPD), and 19% had prior cardiac surgery. Mean hemoglobin was 13.2 mg/dL.
There was a significant dose-dependent association between quantity of packed red blood cells (PRBCs) and risk of infection, with the crude risk increasing by an average of 29% with each PRBC unit.
Several factors increased the risk of infection, including severe COPD (relative risk, 1.85), preoperative creatinine levels greater than 1.5 mg/dL (RR, 1.72), heart failure (RR, 1.49), mild to moderate COPD (RR, 1.36), PRBCs per unit (RR, 1.24), and surgery time per 60 minutes (RR, 1.19).
Platelet transfusion occurred in 31% of patients. However, the use of platelets was associated with a decreased risk of infection (RR, 0.71). Cell Saver use was not related to infection.
Creatinine levels greater than 1.5 mg/dL (RR, 2.40) and PRBCs per unit (RR, 1.23) significantly increased the risk of death. Many factors significantly increased the length of stay, including creatinine levels greater than 1.5 mg/dL (RR, 1.26), severe COPD (RR, 1.41), mild to moderate COPD (RR, 1.14), heart failure (RR, 1.36), PRBCs (RR, 1.12), surgery time per 60 minutes (RR, 1.11), age of 65-79 years (RR, 1.21), and age older than 80 years (RR, 1.44). The use of platelets was associated with a decreased length of stay (RR, 0.71).
All risks of transfusion must be weighed against toleration anemia, which is also associated with adverse outcomes, according to Dr. Horvath, who is the director of the Cardiothoracic Surgery Research Program for the National Heart, Lung, and Blood Institute and a member of the Cardiothoracic Surgery Trials Network.
Efforts to reduce PRBC transfusions may significantly reduce major postoperative infections. Cell salvage and ultrafiltration could be viable alternatives, he noted.
In the second study, the researchers used the same dataset. Captured data included infection occurrence, type, timing, and organisms. Infections were adjudicated by an independent panel of infectious disease experts. The risk of pneumonia, mortality, and length of stay (time to discharge) were analyzed.
Major infections included bloodstream, pneumonia, C. difficile, deep sternal incisional, mediastinitis, deep groin/leg incisional, endocarditis, and empyema.
Pneumonia was diagnosed using the 2010 surveillance criteria from the CDC/National Healthcare Safety Network, including chest x-ray with new or progressive and persistent infiltrate; fever greater than 38° C; leukopenia (defined as fewer than 4,000 leukocytes per cc); leukocytosis (at least 12,000 leukocytes per cc); or altered mental status. At least two of the following must have been present as well: purulent sputum or change; cough, dyspnea, or tachypnea; rales or bronchial breath sounds; or worsening gas exchange. Duration of follow-up was 65 days.
In all, 31% had isolated CABG, 30% had isolated valve surgery, 11% had CABG and valve surgery, 6% had thoracic aortic surgery, 2% had left ventricular assist device (LVAD) implantation/heart transplant, and 20% were categorized as other.
Overall, 2.4% of patients in the registry had pneumonia, 1.1% had blood stream infection, 1% had C. difficile colitis, and 0.5% had deep sternal infections.
The overall mean time to infection was 19 days and the median was 14 days. The mean time to infection for pneumonia was 15 days. Overall, more than 40% of infections occurred after the index hospitalization. However, 68% and 66% of pneumonias and blood stream infections, respectively, occurred during hospitalization. The three most common organisms were Pseudomonas aeruginosa (12%), Enterobacter cloacae (8%), and Klebsiella pneumoniae (7%).
Increased risk of pneumonia was associated with surgery time (RR, 1.42), a creatinine level of at least 1.5 mg/dL (RR, 1.94), mild to moderate COPD (RR, 1.78), severe COPD (RR, 4.12), and heart failure (RR, 1.76). The reference category was those without COPD.
In terms of process-of-care factors, only nasal decontamination with mupirocin was associated with reduced risk of pneumonia (RR, 0.77). Nasal decontamination with other agents (RR, 1.44); antibiotics given within 24 hours after surgery (RR, 1.26) and within 48 hours postop (RR, 2.70); ventilator use of 24-48 hours (RR, 2.31) and more than 48 hours (RR, 4.58); nasogastric tube (RR, 2.07); and use of PRBCs (RR, 1.10) were all associated with increased risk of pneumonia.
In terms of mortality, "pneumonia, among all the factors analyzed, had the greatest association with mortality, with an odds ratio greater than seven ... which was far and away greater than anything else that was examined," said Dr. Ailawadi.
Pneumonia was significantly associated with an increased risk of mortality (RR, 7.07), as were heart failure (RR, 1.87), creatinine levels of at least 1.5 mg/dL (RR, 2.97), and surgery duration (1.27). However, black race appeared to be protective, with a significantly decreased risk of pneumonia (RR, 0.43).
Pneumonia significantly increased the length of stay by a median of 13 days (19 days with pneumonia and 6 days without). A number of factors – mild to moderate COPD, severe COPD, heart failure, creatinine levels of at least 1.5 mg/dL, surgery time, age of 65-79 years, age 80 years and older, and black or Hispanic race – were significantly associated with increased risk of longer length of stay. Male sex was significantly associated with decreased length of stay (RR, 0.79).
Both Dr. Horvath and Dr. Ailawadi reported that they have no relevant financial disclosures.
Cardiac procedures with transfusions, Dr. Keith A. Horvath, the Society of Thoracic Surgeons, Dr. Gorav Ailawadi, deep incisional surgical, deep incisional surgical, empyema, endocarditis, mediastinitis, myocarditis, pneumonia, bloodstream infections, Clostridium difficile colitis, and cardiac device infections,
Cardiac procedures with transfusions, Dr. Keith A. Horvath, the Society of Thoracic Surgeons, Dr. Gorav Ailawadi, deep incisional surgical, deep incisional surgical, empyema, endocarditis, mediastinitis, myocarditis, pneumonia, bloodstream infections, Clostridium difficile colitis, and cardiac device infections,
FROM THE ANNUAL MEETING OF THE SOCIETY OF THORACIC SURGEONS
Major Finding: There was a significant dose-dependent association between quantity of packed red blood cells (PRBCs) and risk of infection, with the crude risk increasing by an average of 29% with each PRBC unit. Pneumonia was the most common infection at 2.4%.
Data Source: A total of 5,184 adult cardiac patients were prospectively enrolled in a 10-center infection registry between February and September 2010. Captured data included infection occurrence, type, and organism. Adjudication was performed by an independent panel of infectious diseases experts.
Disclosures: Both Dr. Horvath and Dr. Ailawadi reported that they have no relevant financial disclosures.
SAPIEN Valve Makers Comment on Proposed TAVR Coverage
While commending the Centers for Medicare and Medicaid Services on its proposed coverage of the transcatheter aortic valve replacement procedure, makers of the SAPIEN artificial valve asked for more flexibility in the clinical trial limitations set by the agency, in an official comment they released on March 5.
Edwards Lifesciences, the manufacturer of the only valve approved for the TAVR procedure in the United States, posted its comment during the 60-day period, which began after CMS released its coverage proposal for TAVR in February.
In its proposal, CMS restricts TAVR coverage to five criteria, including the use of an approved valve, presence of multidisciplinary teams, and enrollment in a registry.
Edwards officials wrote they were pleased that CMS had proposed "clear and flexible national coverage for TAVR," and added that "for appropriately selected Medicare beneficiaries, the evidence is more than adequate for CMS to conclude that TAVR improves health outcomes and should be considered reasonable and necessary under the Medicare statute," if provided under the CMS criteria.
The Edwards SAPIEN valve is currently approved for use in inoperable patients with severe aortic stenosis. Other use of the SAPIEN valve is limited to clinical trials. In their comments, Edwards officials asked CMS for flexibility in the trials they consider for coverage determination.
"CMS’s proposed requirement limiting coverage for unlabeled uses to ‘superiority trials’ undermines the agency’s efforts to promote continued US-based clinical investigations in Medicare beneficiaries aimed at better understanding key determinants of health and quality of life outcomes," according to the Edwards’ comments.
"Noninferiority and other clinical trial designs play an important role in the advancement of medical technology," the company added, saying that if the proposed conditions aren’t revised, important, yet relatively small, patient populations may not be able to receive treatment.
Edwards, which said its transcatheter aortic valves have been implanted in more than 25,000 patients around the world, came in strong support of multidisciplinary heart teams, one of the requirements set by CMS for TAVR coverage, and strongly encouraged by leading cardiovascular organizations.
"It is imperative that at least two engaged cardiothoracic surgeons and two interventional cardiologists at each site coordinate all clinicians to form a high-functioning multi-disciplinary heart team, a key concept integral to assuring TAVR success," Edwards officials wrote in their comment.
The company also addressed credentialing, an issue which four leading cardiovascular organizations also recently addressed in a consensus document.
"We support appropriate facility and heart team criteria -- rather than traditional individual physician-based credentialing," to achieve TAVR success.
Following the CMS proposal, the Society of Thoracic Surgeons and the American College of Cardiology issued a statement, saying that they were pleased with CMS’s comprehensive approach to the coverage of TAVR.
CMS is expected to issue a final decision on TAVR coverage by May.
While commending the Centers for Medicare and Medicaid Services on its proposed coverage of the transcatheter aortic valve replacement procedure, makers of the SAPIEN artificial valve asked for more flexibility in the clinical trial limitations set by the agency, in an official comment they released on March 5.
Edwards Lifesciences, the manufacturer of the only valve approved for the TAVR procedure in the United States, posted its comment during the 60-day period, which began after CMS released its coverage proposal for TAVR in February.
In its proposal, CMS restricts TAVR coverage to five criteria, including the use of an approved valve, presence of multidisciplinary teams, and enrollment in a registry.
Edwards officials wrote they were pleased that CMS had proposed "clear and flexible national coverage for TAVR," and added that "for appropriately selected Medicare beneficiaries, the evidence is more than adequate for CMS to conclude that TAVR improves health outcomes and should be considered reasonable and necessary under the Medicare statute," if provided under the CMS criteria.
The Edwards SAPIEN valve is currently approved for use in inoperable patients with severe aortic stenosis. Other use of the SAPIEN valve is limited to clinical trials. In their comments, Edwards officials asked CMS for flexibility in the trials they consider for coverage determination.
"CMS’s proposed requirement limiting coverage for unlabeled uses to ‘superiority trials’ undermines the agency’s efforts to promote continued US-based clinical investigations in Medicare beneficiaries aimed at better understanding key determinants of health and quality of life outcomes," according to the Edwards’ comments.
"Noninferiority and other clinical trial designs play an important role in the advancement of medical technology," the company added, saying that if the proposed conditions aren’t revised, important, yet relatively small, patient populations may not be able to receive treatment.
Edwards, which said its transcatheter aortic valves have been implanted in more than 25,000 patients around the world, came in strong support of multidisciplinary heart teams, one of the requirements set by CMS for TAVR coverage, and strongly encouraged by leading cardiovascular organizations.
"It is imperative that at least two engaged cardiothoracic surgeons and two interventional cardiologists at each site coordinate all clinicians to form a high-functioning multi-disciplinary heart team, a key concept integral to assuring TAVR success," Edwards officials wrote in their comment.
The company also addressed credentialing, an issue which four leading cardiovascular organizations also recently addressed in a consensus document.
"We support appropriate facility and heart team criteria -- rather than traditional individual physician-based credentialing," to achieve TAVR success.
Following the CMS proposal, the Society of Thoracic Surgeons and the American College of Cardiology issued a statement, saying that they were pleased with CMS’s comprehensive approach to the coverage of TAVR.
CMS is expected to issue a final decision on TAVR coverage by May.
While commending the Centers for Medicare and Medicaid Services on its proposed coverage of the transcatheter aortic valve replacement procedure, makers of the SAPIEN artificial valve asked for more flexibility in the clinical trial limitations set by the agency, in an official comment they released on March 5.
Edwards Lifesciences, the manufacturer of the only valve approved for the TAVR procedure in the United States, posted its comment during the 60-day period, which began after CMS released its coverage proposal for TAVR in February.
In its proposal, CMS restricts TAVR coverage to five criteria, including the use of an approved valve, presence of multidisciplinary teams, and enrollment in a registry.
Edwards officials wrote they were pleased that CMS had proposed "clear and flexible national coverage for TAVR," and added that "for appropriately selected Medicare beneficiaries, the evidence is more than adequate for CMS to conclude that TAVR improves health outcomes and should be considered reasonable and necessary under the Medicare statute," if provided under the CMS criteria.
The Edwards SAPIEN valve is currently approved for use in inoperable patients with severe aortic stenosis. Other use of the SAPIEN valve is limited to clinical trials. In their comments, Edwards officials asked CMS for flexibility in the trials they consider for coverage determination.
"CMS’s proposed requirement limiting coverage for unlabeled uses to ‘superiority trials’ undermines the agency’s efforts to promote continued US-based clinical investigations in Medicare beneficiaries aimed at better understanding key determinants of health and quality of life outcomes," according to the Edwards’ comments.
"Noninferiority and other clinical trial designs play an important role in the advancement of medical technology," the company added, saying that if the proposed conditions aren’t revised, important, yet relatively small, patient populations may not be able to receive treatment.
Edwards, which said its transcatheter aortic valves have been implanted in more than 25,000 patients around the world, came in strong support of multidisciplinary heart teams, one of the requirements set by CMS for TAVR coverage, and strongly encouraged by leading cardiovascular organizations.
"It is imperative that at least two engaged cardiothoracic surgeons and two interventional cardiologists at each site coordinate all clinicians to form a high-functioning multi-disciplinary heart team, a key concept integral to assuring TAVR success," Edwards officials wrote in their comment.
The company also addressed credentialing, an issue which four leading cardiovascular organizations also recently addressed in a consensus document.
"We support appropriate facility and heart team criteria -- rather than traditional individual physician-based credentialing," to achieve TAVR success.
Following the CMS proposal, the Society of Thoracic Surgeons and the American College of Cardiology issued a statement, saying that they were pleased with CMS’s comprehensive approach to the coverage of TAVR.
CMS is expected to issue a final decision on TAVR coverage by May.
Societies Release TAVR Credentialing Recommendations
Heart teams remain the cornerstone of any transcatheter aortic valve replacement procedure, new credentialing recommendations for TAVR programs emphasized.
The document, released by four leading cardiovascular organizations, serves as a starting point for programs and institutions that want to assess their potential for implementing and/or maintaining a TAVR program.
"As new technologies begin to be incorporated into cardiovascular practice, it is the responsibility of the medical societies to work together to develop standards for optimal patient care," Dr. Carl L. Tommaso, chair of the document writing committee, said in a statement. "TAVR is a complex procedure that has the potential to serve many patients, and it is up to us to deliver the highest standards of care available," added Dr. Tommaso, medical director of the cardiac catheterization lab at Skokie Hospital, NorthShore HealthSystem, Chicago.
The 48-page document, prepared jointly by the American College of Cardiology Foundation, the Society for Cardiovascular Angiography and Interventions, the American Association for Thoracic Surgery, and the Society of Thoracic Surgeons, defines operator and institutional requirements for performing the procedure, and emphasizes the presence of multidisciplinary teams, which go beyond the collaboration between interventional cardiologists and cardiac surgeons.
"A TAVR program that uses only one specialty is fundamentally deficient, and valve therapy programs should not be established without this multidisciplinary partnership," the authors write.
The document also recommends that irrespective of their specialty, physicians in TAVR programs should all have extensive knowledge of valvular heart disease, and they should be able to interpret images.
Meanwhile, facilities should contain a full range of diagnostic imaging, in addition to an active valvular heart disease surgical program and "at least two institutionally-based cardiac surgeons experienced in valvular surgery," according to the document.
The role of an invested hospital administration is also emphasized.
"There must be dedication on the part of the hospital to provide these services and support, both financially and with no time constraints on the personnel involved," the authors write.
While they lay out minimum case number requirements for surgeons and interventionalists, the authors predict that simulators are "likely to play a significant role in technical training and proficiency maintenance for these evolving procedures," and the training strategy will evolve as the procedure becomes mainstream.
TAVR, which was approved in the United States in November 2011, is still in its infancy, so due to lack of data, many of the recommendations are based on expert consensus, according to the document.
Therefore, there "is the need for this to be a dynamic document that we will revisit in the future as the technology evolves, experience grows, and data accumulate," Dr. R. Morton Bolman, cochair of the document writing committee and chief of cardiac surgery at Harvard University, said in a statement.
Dr. Tommaso and Dr. Bolman had no relevant disclosures.
Heart teams remain the cornerstone of any transcatheter aortic valve replacement procedure, new credentialing recommendations for TAVR programs emphasized.
The document, released by four leading cardiovascular organizations, serves as a starting point for programs and institutions that want to assess their potential for implementing and/or maintaining a TAVR program.
"As new technologies begin to be incorporated into cardiovascular practice, it is the responsibility of the medical societies to work together to develop standards for optimal patient care," Dr. Carl L. Tommaso, chair of the document writing committee, said in a statement. "TAVR is a complex procedure that has the potential to serve many patients, and it is up to us to deliver the highest standards of care available," added Dr. Tommaso, medical director of the cardiac catheterization lab at Skokie Hospital, NorthShore HealthSystem, Chicago.
The 48-page document, prepared jointly by the American College of Cardiology Foundation, the Society for Cardiovascular Angiography and Interventions, the American Association for Thoracic Surgery, and the Society of Thoracic Surgeons, defines operator and institutional requirements for performing the procedure, and emphasizes the presence of multidisciplinary teams, which go beyond the collaboration between interventional cardiologists and cardiac surgeons.
"A TAVR program that uses only one specialty is fundamentally deficient, and valve therapy programs should not be established without this multidisciplinary partnership," the authors write.
The document also recommends that irrespective of their specialty, physicians in TAVR programs should all have extensive knowledge of valvular heart disease, and they should be able to interpret images.
Meanwhile, facilities should contain a full range of diagnostic imaging, in addition to an active valvular heart disease surgical program and "at least two institutionally-based cardiac surgeons experienced in valvular surgery," according to the document.
The role of an invested hospital administration is also emphasized.
"There must be dedication on the part of the hospital to provide these services and support, both financially and with no time constraints on the personnel involved," the authors write.
While they lay out minimum case number requirements for surgeons and interventionalists, the authors predict that simulators are "likely to play a significant role in technical training and proficiency maintenance for these evolving procedures," and the training strategy will evolve as the procedure becomes mainstream.
TAVR, which was approved in the United States in November 2011, is still in its infancy, so due to lack of data, many of the recommendations are based on expert consensus, according to the document.
Therefore, there "is the need for this to be a dynamic document that we will revisit in the future as the technology evolves, experience grows, and data accumulate," Dr. R. Morton Bolman, cochair of the document writing committee and chief of cardiac surgery at Harvard University, said in a statement.
Dr. Tommaso and Dr. Bolman had no relevant disclosures.
Heart teams remain the cornerstone of any transcatheter aortic valve replacement procedure, new credentialing recommendations for TAVR programs emphasized.
The document, released by four leading cardiovascular organizations, serves as a starting point for programs and institutions that want to assess their potential for implementing and/or maintaining a TAVR program.
"As new technologies begin to be incorporated into cardiovascular practice, it is the responsibility of the medical societies to work together to develop standards for optimal patient care," Dr. Carl L. Tommaso, chair of the document writing committee, said in a statement. "TAVR is a complex procedure that has the potential to serve many patients, and it is up to us to deliver the highest standards of care available," added Dr. Tommaso, medical director of the cardiac catheterization lab at Skokie Hospital, NorthShore HealthSystem, Chicago.
The 48-page document, prepared jointly by the American College of Cardiology Foundation, the Society for Cardiovascular Angiography and Interventions, the American Association for Thoracic Surgery, and the Society of Thoracic Surgeons, defines operator and institutional requirements for performing the procedure, and emphasizes the presence of multidisciplinary teams, which go beyond the collaboration between interventional cardiologists and cardiac surgeons.
"A TAVR program that uses only one specialty is fundamentally deficient, and valve therapy programs should not be established without this multidisciplinary partnership," the authors write.
The document also recommends that irrespective of their specialty, physicians in TAVR programs should all have extensive knowledge of valvular heart disease, and they should be able to interpret images.
Meanwhile, facilities should contain a full range of diagnostic imaging, in addition to an active valvular heart disease surgical program and "at least two institutionally-based cardiac surgeons experienced in valvular surgery," according to the document.
The role of an invested hospital administration is also emphasized.
"There must be dedication on the part of the hospital to provide these services and support, both financially and with no time constraints on the personnel involved," the authors write.
While they lay out minimum case number requirements for surgeons and interventionalists, the authors predict that simulators are "likely to play a significant role in technical training and proficiency maintenance for these evolving procedures," and the training strategy will evolve as the procedure becomes mainstream.
TAVR, which was approved in the United States in November 2011, is still in its infancy, so due to lack of data, many of the recommendations are based on expert consensus, according to the document.
Therefore, there "is the need for this to be a dynamic document that we will revisit in the future as the technology evolves, experience grows, and data accumulate," Dr. R. Morton Bolman, cochair of the document writing committee and chief of cardiac surgery at Harvard University, said in a statement.
Dr. Tommaso and Dr. Bolman had no relevant disclosures.
Risk Factors Predict 1-Year Mortality After Elective TEVAR
SCOTTSDALE, ARIZ. – A new model for predicting 1-year survival after elective endovascular repair of degenerative thoracic aortic aneurysm suggests that the risks outweigh potential benefits of the procedure in some older patients with multiple comorbidities.
For patients aged 70 years or older who have multiple comorbidities, there is a very high risk of death in the year following thoracic endovascular aortic aneurysm repair (TEVAR), so it may be best to wait until the aneurysm is large enough that the risk from not doing TEVAR outweighs the risk of performing the procedure, according to Dr. Adam W. Beck.
Dr. Beck, of the University of Florida, Gainesville, and his associates analyzed data from a prospective registry of all 526 consecutive TEVARs performed on patients with intact degenerative, asymptomatic thoracic aneurysms at the university between 2000 and 2010. After excluding urgent or emergent cases, the researchers used data from 224 patients who underwent elective TEVAR to identify predictors of death within a year of TEVAR, and compared predictions to survival data from the Social Security Death Index.
Overall, 3% of patients died within 30 days of TEVAR, and 15% died within 1 year – rates that are comparable to those of many studies reported in the medical literature, Dr. Beck said at the annual meeting of the Southern Association for Vascular Surgery.
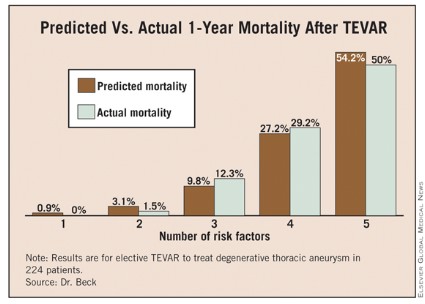
In a multivariate analysis of factors associated with mortality, being at least 70 years old conferred nearly a sixfold increase in the predicted 1-year risk of death (hazard ratio, 5.8). Patients who had an adjunctive procedure at the time of TEVAR, such as brachiocephalic/visceral stent placement or concomitant visceral debranching procedures, were 4.5 times more likely to die within a year than were patients without an adjunctive procedure.
The predicted risk of death at 1 year was 3 times higher in patients with peripheral vascular occlusive disease and 2.4 times higher in patients with coronary artery disease than in patients without those diseases. All of these associations were statistically significant. The presence of chronic obstructive pulmonary disease showed a nonsignificant trend toward a 1.9-fold higher risk of death at 1 year (P = .06).
Having a diagnosis of hyperlipidemia appeared to be protective, because it was significantly associated with a 60% decrease in the risk of death at 1 year after TEVAR. When the risk prediction model was created, the lack of a history of hyperlipidemia was considered to be a risk factor.
The risk of death at 1 year rose as the number of significant risk factors increased, and predictive risk correlated well with actual mortality data, Dr. Beck said.
In general, aneurysm diameter was larger in patients with more risk factors, and the risk of death at 1 year increased with aneurysm size and number of risk factors, he added.
The risk of rupture, as reported in the previous literature, is approximately 2% for thoracic aortic aneurysms measuring 5.5 cm in diameter, 10% for aneurysms with a diameter of 6.5 cm, 15% for those measuring 7 cm in diameter, and 45% for aneurysms with a diameter of 8 cm.
When the risk of 1-year mortality is plotted against the number of risk factors, it appears that TEVAR should be delayed in patients with three or more risk factors until their aneurysm diameter is greater than the usual 6-cm threshold commonly used to justify the risk of TEVAR, Dr. Beck said.
"This is an important contribution to our literature," said Dr. Hazim J. Safi, a discussant at the meeting. "Most of us implicitly, when we decide how to manage these patients, would categorize the patient by presumed risk," said Dr. Safi, professor and chair of cardiovascular and thoracic surgery at the University of Texas, Houston. "I congratulate the authors for quantifying the relationship between the risk factors and mortality rate."
Usually, surgeons discuss the annual risk of thoracic aneurysm rupture and compare this with the 30-day operative mortality risk when advising patients who are considering TEVAR, Dr. Beck said. To adequately assess the success of aneurysm repair, however, longer survival should be considered, he said.

"It’s important to note that only 21% of deaths within 1 year of repair occurred within 30 days after the procedure, underscoring the importance of looking beyond the first 30 days to determine the benefit of therapy," Dr. Beck said. Even for the groups with multiple risk factors who are at very high risk, the majority of deaths occurred outside the 30-day window.
The risk prediction model should help clinicians select patients who would benefit most from early TEVAR, and delay TEVAR in patients who might be better managed nonoperatively.
To evaluate whether surgeons at his institution were accounting for higher-risk patients, Dr. Beck and his associates performed a secondary analysis. As the number of risk factors for death within 1 year of TEVAR increased, so did the aneurysm diameter at which patients underwent repair. This suggests that surgeons were taking into account risk factors, at least to some extent, in deciding when to operate on these patients.
Patients in the study had a mean age of 61 years, and 63% were male. The average aneurysm diameter was 6.25 cm. At the time of treatment, 38% of patients had coronary artery disease, 28% had chronic obstructive pulmonary disease, and 12% had peripheral vascular occlusive disease. Nine percent of patients underwent an intraoperative adjunctive procedure.
Among other comorbidities, 85% had hypertension, 51% had dyslipidemia, 14% had diabetes, 11% had chronic renal insufficiency, and 7% had heart failure.
Eighty percent of patients were taking antiplatelet medications, 55% were on statins, and 67% were considered to be in American Society of Anesthesiologists classification 4.
Dr. Beck reported having no financial disclosures.
SCOTTSDALE, ARIZ. – A new model for predicting 1-year survival after elective endovascular repair of degenerative thoracic aortic aneurysm suggests that the risks outweigh potential benefits of the procedure in some older patients with multiple comorbidities.
For patients aged 70 years or older who have multiple comorbidities, there is a very high risk of death in the year following thoracic endovascular aortic aneurysm repair (TEVAR), so it may be best to wait until the aneurysm is large enough that the risk from not doing TEVAR outweighs the risk of performing the procedure, according to Dr. Adam W. Beck.
Dr. Beck, of the University of Florida, Gainesville, and his associates analyzed data from a prospective registry of all 526 consecutive TEVARs performed on patients with intact degenerative, asymptomatic thoracic aneurysms at the university between 2000 and 2010. After excluding urgent or emergent cases, the researchers used data from 224 patients who underwent elective TEVAR to identify predictors of death within a year of TEVAR, and compared predictions to survival data from the Social Security Death Index.
Overall, 3% of patients died within 30 days of TEVAR, and 15% died within 1 year – rates that are comparable to those of many studies reported in the medical literature, Dr. Beck said at the annual meeting of the Southern Association for Vascular Surgery.
In a multivariate analysis of factors associated with mortality, being at least 70 years old conferred nearly a sixfold increase in the predicted 1-year risk of death (hazard ratio, 5.8). Patients who had an adjunctive procedure at the time of TEVAR, such as brachiocephalic/visceral stent placement or concomitant visceral debranching procedures, were 4.5 times more likely to die within a year than were patients without an adjunctive procedure.
The predicted risk of death at 1 year was 3 times higher in patients with peripheral vascular occlusive disease and 2.4 times higher in patients with coronary artery disease than in patients without those diseases. All of these associations were statistically significant. The presence of chronic obstructive pulmonary disease showed a nonsignificant trend toward a 1.9-fold higher risk of death at 1 year (P = .06).
Having a diagnosis of hyperlipidemia appeared to be protective, because it was significantly associated with a 60% decrease in the risk of death at 1 year after TEVAR. When the risk prediction model was created, the lack of a history of hyperlipidemia was considered to be a risk factor.
The risk of death at 1 year rose as the number of significant risk factors increased, and predictive risk correlated well with actual mortality data, Dr. Beck said.
In general, aneurysm diameter was larger in patients with more risk factors, and the risk of death at 1 year increased with aneurysm size and number of risk factors, he added.
The risk of rupture, as reported in the previous literature, is approximately 2% for thoracic aortic aneurysms measuring 5.5 cm in diameter, 10% for aneurysms with a diameter of 6.5 cm, 15% for those measuring 7 cm in diameter, and 45% for aneurysms with a diameter of 8 cm.
When the risk of 1-year mortality is plotted against the number of risk factors, it appears that TEVAR should be delayed in patients with three or more risk factors until their aneurysm diameter is greater than the usual 6-cm threshold commonly used to justify the risk of TEVAR, Dr. Beck said.
"This is an important contribution to our literature," said Dr. Hazim J. Safi, a discussant at the meeting. "Most of us implicitly, when we decide how to manage these patients, would categorize the patient by presumed risk," said Dr. Safi, professor and chair of cardiovascular and thoracic surgery at the University of Texas, Houston. "I congratulate the authors for quantifying the relationship between the risk factors and mortality rate."
Usually, surgeons discuss the annual risk of thoracic aneurysm rupture and compare this with the 30-day operative mortality risk when advising patients who are considering TEVAR, Dr. Beck said. To adequately assess the success of aneurysm repair, however, longer survival should be considered, he said.
"It’s important to note that only 21% of deaths within 1 year of repair occurred within 30 days after the procedure, underscoring the importance of looking beyond the first 30 days to determine the benefit of therapy," Dr. Beck said. Even for the groups with multiple risk factors who are at very high risk, the majority of deaths occurred outside the 30-day window.
The risk prediction model should help clinicians select patients who would benefit most from early TEVAR, and delay TEVAR in patients who might be better managed nonoperatively.
To evaluate whether surgeons at his institution were accounting for higher-risk patients, Dr. Beck and his associates performed a secondary analysis. As the number of risk factors for death within 1 year of TEVAR increased, so did the aneurysm diameter at which patients underwent repair. This suggests that surgeons were taking into account risk factors, at least to some extent, in deciding when to operate on these patients.
Patients in the study had a mean age of 61 years, and 63% were male. The average aneurysm diameter was 6.25 cm. At the time of treatment, 38% of patients had coronary artery disease, 28% had chronic obstructive pulmonary disease, and 12% had peripheral vascular occlusive disease. Nine percent of patients underwent an intraoperative adjunctive procedure.
Among other comorbidities, 85% had hypertension, 51% had dyslipidemia, 14% had diabetes, 11% had chronic renal insufficiency, and 7% had heart failure.
Eighty percent of patients were taking antiplatelet medications, 55% were on statins, and 67% were considered to be in American Society of Anesthesiologists classification 4.
Dr. Beck reported having no financial disclosures.
SCOTTSDALE, ARIZ. – A new model for predicting 1-year survival after elective endovascular repair of degenerative thoracic aortic aneurysm suggests that the risks outweigh potential benefits of the procedure in some older patients with multiple comorbidities.
For patients aged 70 years or older who have multiple comorbidities, there is a very high risk of death in the year following thoracic endovascular aortic aneurysm repair (TEVAR), so it may be best to wait until the aneurysm is large enough that the risk from not doing TEVAR outweighs the risk of performing the procedure, according to Dr. Adam W. Beck.
Dr. Beck, of the University of Florida, Gainesville, and his associates analyzed data from a prospective registry of all 526 consecutive TEVARs performed on patients with intact degenerative, asymptomatic thoracic aneurysms at the university between 2000 and 2010. After excluding urgent or emergent cases, the researchers used data from 224 patients who underwent elective TEVAR to identify predictors of death within a year of TEVAR, and compared predictions to survival data from the Social Security Death Index.
Overall, 3% of patients died within 30 days of TEVAR, and 15% died within 1 year – rates that are comparable to those of many studies reported in the medical literature, Dr. Beck said at the annual meeting of the Southern Association for Vascular Surgery.
In a multivariate analysis of factors associated with mortality, being at least 70 years old conferred nearly a sixfold increase in the predicted 1-year risk of death (hazard ratio, 5.8). Patients who had an adjunctive procedure at the time of TEVAR, such as brachiocephalic/visceral stent placement or concomitant visceral debranching procedures, were 4.5 times more likely to die within a year than were patients without an adjunctive procedure.
The predicted risk of death at 1 year was 3 times higher in patients with peripheral vascular occlusive disease and 2.4 times higher in patients with coronary artery disease than in patients without those diseases. All of these associations were statistically significant. The presence of chronic obstructive pulmonary disease showed a nonsignificant trend toward a 1.9-fold higher risk of death at 1 year (P = .06).
Having a diagnosis of hyperlipidemia appeared to be protective, because it was significantly associated with a 60% decrease in the risk of death at 1 year after TEVAR. When the risk prediction model was created, the lack of a history of hyperlipidemia was considered to be a risk factor.
The risk of death at 1 year rose as the number of significant risk factors increased, and predictive risk correlated well with actual mortality data, Dr. Beck said.
In general, aneurysm diameter was larger in patients with more risk factors, and the risk of death at 1 year increased with aneurysm size and number of risk factors, he added.
The risk of rupture, as reported in the previous literature, is approximately 2% for thoracic aortic aneurysms measuring 5.5 cm in diameter, 10% for aneurysms with a diameter of 6.5 cm, 15% for those measuring 7 cm in diameter, and 45% for aneurysms with a diameter of 8 cm.
When the risk of 1-year mortality is plotted against the number of risk factors, it appears that TEVAR should be delayed in patients with three or more risk factors until their aneurysm diameter is greater than the usual 6-cm threshold commonly used to justify the risk of TEVAR, Dr. Beck said.
"This is an important contribution to our literature," said Dr. Hazim J. Safi, a discussant at the meeting. "Most of us implicitly, when we decide how to manage these patients, would categorize the patient by presumed risk," said Dr. Safi, professor and chair of cardiovascular and thoracic surgery at the University of Texas, Houston. "I congratulate the authors for quantifying the relationship between the risk factors and mortality rate."
Usually, surgeons discuss the annual risk of thoracic aneurysm rupture and compare this with the 30-day operative mortality risk when advising patients who are considering TEVAR, Dr. Beck said. To adequately assess the success of aneurysm repair, however, longer survival should be considered, he said.
"It’s important to note that only 21% of deaths within 1 year of repair occurred within 30 days after the procedure, underscoring the importance of looking beyond the first 30 days to determine the benefit of therapy," Dr. Beck said. Even for the groups with multiple risk factors who are at very high risk, the majority of deaths occurred outside the 30-day window.
The risk prediction model should help clinicians select patients who would benefit most from early TEVAR, and delay TEVAR in patients who might be better managed nonoperatively.
To evaluate whether surgeons at his institution were accounting for higher-risk patients, Dr. Beck and his associates performed a secondary analysis. As the number of risk factors for death within 1 year of TEVAR increased, so did the aneurysm diameter at which patients underwent repair. This suggests that surgeons were taking into account risk factors, at least to some extent, in deciding when to operate on these patients.
Patients in the study had a mean age of 61 years, and 63% were male. The average aneurysm diameter was 6.25 cm. At the time of treatment, 38% of patients had coronary artery disease, 28% had chronic obstructive pulmonary disease, and 12% had peripheral vascular occlusive disease. Nine percent of patients underwent an intraoperative adjunctive procedure.
Among other comorbidities, 85% had hypertension, 51% had dyslipidemia, 14% had diabetes, 11% had chronic renal insufficiency, and 7% had heart failure.
Eighty percent of patients were taking antiplatelet medications, 55% were on statins, and 67% were considered to be in American Society of Anesthesiologists classification 4.
Dr. Beck reported having no financial disclosures.
FROM THE ANNUAL MEETING OF THE SOUTHERN ASSOCIATION FOR VASCULAR SURGERY
Race and Sex Skew Congenital Heart Surgery Outcomes
FT. LAUDERDALE, FLA. – Sex and race appear to play a role in outcomes following congenital heart surgery in children and adolescents, according to a new analysis of data from almost 21,000 patients.
Black patients had significantly greater rates of mortality and complications and a significantly longer length of postoperative stay than other races, while female patients had a significantly shorter length of stay than males, Dr. Daniel J. DiBardino reported at the annual meeting of the Society of Thoracic Surgeons.
"The analysis of demographic and clinical data from nearly 21,000 patients in the congenital heart surgery database revealed important associations between gender, race, and outcome," said Dr. DiBardino, who is a cardiac surgeon at the Blair E. Batson Children’s Hospital in Jackson, Miss. Dr. DiBardino’s study was chosen as a 2011 Richard E. Clark Paper by the Society of Thoracic Surgeons.
The researchers used data from the Society of Thoracic Surgeons Congenital Heart Surgery Database (STS-CHSD). Patients were included in the analysis if they were less than 18 years of age and had undergone cardiac surgery between 2007 and 2009. Exclusion criteria included centers with more than 15% of data missing for key variables and centers with very small samples (fewer than five cases).
Data collection included demographics (age, sex, weight, and race) and preoperative data (noncardiac/genetic abnormalities and STS-defined risk factors). Race was classified as white, black, Hispanic, and other. Operations were classified by STAT Mortality category, which is "a complexity stratification tool based on empiric data from 80,000 cases in STS and EACTS (European Association for Cardio-Thoracic Surgery) databases," said Dr. DiBardino.
The researchers looked at hospital mortality, postoperative length of stay, and complications. Multivariable analyses included dichotomous variables (mortality, complications) and a continuous variable (postoperative length of stay). Models were adjusted for age, weight, noncardiac/genetic abnormalities, any other STS preoperative risk factor, and STAT Mortality category.
In all, 20,399 patients were included from 49 centers. Of these, 54% were male. In terms of race, 55% were white, 17% were black, 16% were Hispanic, and 12% were other.
Based on unadjusted outcomes, there were no differences between the sexes for in-hospital mortality or complications. However, females had significantly shorter postoperative stays. In terms of race, white patients had significantly lower mortality, shorter length of stay, and fewer complications than any of the other racial groups.
In the adjusted multivariate analysis, there was no difference for mortality between the sexes. However, black patients had a significantly greater mortality risk with an odds ratio of 1.67.
Females did have a significantly shorter mean length of stay – 0.8 fewer days. In terms of race, black patients had a significantly longer mean length of stay by 2.4 hospital days, compared with white patients. Hispanic patients also had a significantly longer mean length of stay by almost 1 hospital day.
There was no difference between the sexes in terms of the occurrence of complications. In terms of race, "black patients experienced significantly more complications than other races with an odds ratio of 1.15," said Dr. DiBardino.
The study is unique with the respect to the use of multivariable models. The researchers measured the association of sex and race with outcomes within each center and then combined the results, in order to mitigate the potential center effects. "Our results cannot be explained by the possibility that patients of certain races might be disproportionately treated at centers with poorer outcomes in general."
The evaluation of complex relationships between clinical variables and socioeconomic and other factors affecting health care remains a significant challenge. Since some pertinent socioeconomic data are not collected in the STS-CHSD, an analysis of a linked data set, which capitalizes on the strengths of both the CHSD and those of an administrative claims data set may be the next logical step, said Dr. DiBardino.
Dr. DiBardino and his coinvestigators reported that they have no relevant disclosures.
FT. LAUDERDALE, FLA. – Sex and race appear to play a role in outcomes following congenital heart surgery in children and adolescents, according to a new analysis of data from almost 21,000 patients.
Black patients had significantly greater rates of mortality and complications and a significantly longer length of postoperative stay than other races, while female patients had a significantly shorter length of stay than males, Dr. Daniel J. DiBardino reported at the annual meeting of the Society of Thoracic Surgeons.
"The analysis of demographic and clinical data from nearly 21,000 patients in the congenital heart surgery database revealed important associations between gender, race, and outcome," said Dr. DiBardino, who is a cardiac surgeon at the Blair E. Batson Children’s Hospital in Jackson, Miss. Dr. DiBardino’s study was chosen as a 2011 Richard E. Clark Paper by the Society of Thoracic Surgeons.
The researchers used data from the Society of Thoracic Surgeons Congenital Heart Surgery Database (STS-CHSD). Patients were included in the analysis if they were less than 18 years of age and had undergone cardiac surgery between 2007 and 2009. Exclusion criteria included centers with more than 15% of data missing for key variables and centers with very small samples (fewer than five cases).
Data collection included demographics (age, sex, weight, and race) and preoperative data (noncardiac/genetic abnormalities and STS-defined risk factors). Race was classified as white, black, Hispanic, and other. Operations were classified by STAT Mortality category, which is "a complexity stratification tool based on empiric data from 80,000 cases in STS and EACTS (European Association for Cardio-Thoracic Surgery) databases," said Dr. DiBardino.
The researchers looked at hospital mortality, postoperative length of stay, and complications. Multivariable analyses included dichotomous variables (mortality, complications) and a continuous variable (postoperative length of stay). Models were adjusted for age, weight, noncardiac/genetic abnormalities, any other STS preoperative risk factor, and STAT Mortality category.
In all, 20,399 patients were included from 49 centers. Of these, 54% were male. In terms of race, 55% were white, 17% were black, 16% were Hispanic, and 12% were other.
Based on unadjusted outcomes, there were no differences between the sexes for in-hospital mortality or complications. However, females had significantly shorter postoperative stays. In terms of race, white patients had significantly lower mortality, shorter length of stay, and fewer complications than any of the other racial groups.
In the adjusted multivariate analysis, there was no difference for mortality between the sexes. However, black patients had a significantly greater mortality risk with an odds ratio of 1.67.
Females did have a significantly shorter mean length of stay – 0.8 fewer days. In terms of race, black patients had a significantly longer mean length of stay by 2.4 hospital days, compared with white patients. Hispanic patients also had a significantly longer mean length of stay by almost 1 hospital day.
There was no difference between the sexes in terms of the occurrence of complications. In terms of race, "black patients experienced significantly more complications than other races with an odds ratio of 1.15," said Dr. DiBardino.
The study is unique with the respect to the use of multivariable models. The researchers measured the association of sex and race with outcomes within each center and then combined the results, in order to mitigate the potential center effects. "Our results cannot be explained by the possibility that patients of certain races might be disproportionately treated at centers with poorer outcomes in general."
The evaluation of complex relationships between clinical variables and socioeconomic and other factors affecting health care remains a significant challenge. Since some pertinent socioeconomic data are not collected in the STS-CHSD, an analysis of a linked data set, which capitalizes on the strengths of both the CHSD and those of an administrative claims data set may be the next logical step, said Dr. DiBardino.
Dr. DiBardino and his coinvestigators reported that they have no relevant disclosures.
FT. LAUDERDALE, FLA. – Sex and race appear to play a role in outcomes following congenital heart surgery in children and adolescents, according to a new analysis of data from almost 21,000 patients.
Black patients had significantly greater rates of mortality and complications and a significantly longer length of postoperative stay than other races, while female patients had a significantly shorter length of stay than males, Dr. Daniel J. DiBardino reported at the annual meeting of the Society of Thoracic Surgeons.
"The analysis of demographic and clinical data from nearly 21,000 patients in the congenital heart surgery database revealed important associations between gender, race, and outcome," said Dr. DiBardino, who is a cardiac surgeon at the Blair E. Batson Children’s Hospital in Jackson, Miss. Dr. DiBardino’s study was chosen as a 2011 Richard E. Clark Paper by the Society of Thoracic Surgeons.
The researchers used data from the Society of Thoracic Surgeons Congenital Heart Surgery Database (STS-CHSD). Patients were included in the analysis if they were less than 18 years of age and had undergone cardiac surgery between 2007 and 2009. Exclusion criteria included centers with more than 15% of data missing for key variables and centers with very small samples (fewer than five cases).
Data collection included demographics (age, sex, weight, and race) and preoperative data (noncardiac/genetic abnormalities and STS-defined risk factors). Race was classified as white, black, Hispanic, and other. Operations were classified by STAT Mortality category, which is "a complexity stratification tool based on empiric data from 80,000 cases in STS and EACTS (European Association for Cardio-Thoracic Surgery) databases," said Dr. DiBardino.
The researchers looked at hospital mortality, postoperative length of stay, and complications. Multivariable analyses included dichotomous variables (mortality, complications) and a continuous variable (postoperative length of stay). Models were adjusted for age, weight, noncardiac/genetic abnormalities, any other STS preoperative risk factor, and STAT Mortality category.
In all, 20,399 patients were included from 49 centers. Of these, 54% were male. In terms of race, 55% were white, 17% were black, 16% were Hispanic, and 12% were other.
Based on unadjusted outcomes, there were no differences between the sexes for in-hospital mortality or complications. However, females had significantly shorter postoperative stays. In terms of race, white patients had significantly lower mortality, shorter length of stay, and fewer complications than any of the other racial groups.
In the adjusted multivariate analysis, there was no difference for mortality between the sexes. However, black patients had a significantly greater mortality risk with an odds ratio of 1.67.
Females did have a significantly shorter mean length of stay – 0.8 fewer days. In terms of race, black patients had a significantly longer mean length of stay by 2.4 hospital days, compared with white patients. Hispanic patients also had a significantly longer mean length of stay by almost 1 hospital day.
There was no difference between the sexes in terms of the occurrence of complications. In terms of race, "black patients experienced significantly more complications than other races with an odds ratio of 1.15," said Dr. DiBardino.
The study is unique with the respect to the use of multivariable models. The researchers measured the association of sex and race with outcomes within each center and then combined the results, in order to mitigate the potential center effects. "Our results cannot be explained by the possibility that patients of certain races might be disproportionately treated at centers with poorer outcomes in general."
The evaluation of complex relationships between clinical variables and socioeconomic and other factors affecting health care remains a significant challenge. Since some pertinent socioeconomic data are not collected in the STS-CHSD, an analysis of a linked data set, which capitalizes on the strengths of both the CHSD and those of an administrative claims data set may be the next logical step, said Dr. DiBardino.
Dr. DiBardino and his coinvestigators reported that they have no relevant disclosures.
FROM THE ANNUAL MEETING OF THE SOCIETY OF THORACIC SURGEONS
Major Finding: In adjusted multivariate analyses, black patients had a significantly greater mortality risk (67%), a significantly longer mean length of stay by 2.4 hospital days, and a significantly greater risk of complications (15%). Female patients had a significantly shorter mean length of stay – 0.8 fewer days.
Data Source: The retrospective review included 20,399 patients younger than 18 years from 49 centers, collected in the Society of Thoracic Surgeons Congenital Heart Surgery Database.
Disclosures: Dr. DiBardino and his coinvestigators reported that they have no relevant disclosures.
CABG Beats Stents for Long-Term Outcomes in High-Risk Patients
FT. LAUDERDALE, FLA. – Coronary artery bypass graft surgery shows a clear long-term survival advantage in certain high-risk groups over percutaneous coronary intervention, based on results of the largest study of real-world data so far.
The survival advantage for a composite high-risk group – including patients aged 75 years and older, patients with diabetes, those with ejection fractions (EF) less than 50%, and those with a glomerular filtration rate (GFR) less than 60 mL/min per 1.73 m2 – was 28% at 4 years, Dr. Fred H. Edwards reported at the annual meeting of the Society of Thoracic Surgeons.
The findings come from the ASCERT (The American College of Cardiology Foundation – The Society of Thoracic Surgeons Collaboration on the Comparative Effectiveness of Revascularization Strategies) study, in which researchers compared catheter- and surgery-based procedures using the existing ACC and STS databases, as well as the Centers for Medicare and Medicaid Services 100% denominator file data. The study was designed to identify specific patient characteristics that favor one mode of treatment over the other. The study is also supported by the National Heart, Lung, and Blood Institute.
The ACC and the STS both have large registries containing detailed clinical information on millions of procedures. However, the information in these databases extends to only 1 month after the procedure. The researchers linked this short-term clinical information with the administrative data registry from the CMS to provide long-term mortality, rehospitalization, and resource utilization outcomes. The 3- to 5-year outcomes after coronary artery bypass graft (CABG) surgery are being compared with those after percutaneous coronary intervention (PCI) – primarily using drug-eluting coronary stents, from the STS and ACC databases, respectively. In addition to survival, researchers are assessing the need for additional procedures and hospitalizations, new cardiac disease conditions, and the medications being taken at various points in time after the coronary artery procedure.
Patients in this CMS population were aged at least 65 years with two- to three-vessel disease. Patients with either single-vessel disease or left-main disease were excluded. Emergent procedures were also excluded.
"So what’s different about this [study]? Well, the N [number] is huge. We’ve got a population that is actually 10 times greater than the sum total of all patients ever having been enrolled in randomized [revascularization] trials," said Dr. Edwards, who is a professor of surgery and medical director of cardiothoracic surgery at the University of Florida/Shands Jacksonville, as well as chairman of the STS National Database. In addition to the size of this observational study, the focus is on real-world experience with a true national scope.
For the head-to-head comparison, data from both the STS and ACC databases were linked to data from the CMS. A propensity score – the probability of having CABG – was calculated for each patient, and clinically important subgroups were identified before the files were linked. The propensity scores and inverse weighting were used to calculate adjusted survival curves. "Then we compared the survival for coronary bypass and percutaneous intervention for groups having very similar characteristics," said Dr. Edwards.
High- and Low-Risk Groups Identified
This analysis included a total of 189,793 patients, of which 103,549 received PCI. Dr. Edwards presented the survival results for high-risk subgroups; the overall results will be presented at the ACC’s Annual Scientific Session in March, he said.
High-risk subgroups include patients who were aged 75 years and older, had diabetes, had EFs less than 50%, and had a GFR less than 60 mL/min per 1.73 m2.
For those aged 75 years and older, the mortality risk ratio at 4 years was 0.78 favoring surgery. Correspondingly, the survival advantage in this group for surgery was 22%. For patients with three-vessel disease, the survival advantage at 4 years was 25%. Patients with insulin-dependent diabetes had a 28% survival advantage at 4 years with CABG, compared with PCI. For patients with EFs less than 50%, the survival advantage with surgery was 30% at 4 years.
However, there appears to be a survival advantage with PCI in these groups at up to 1 year of follow-up. "We should keep in mind that in many of these subgroups, the survival with percutaneous intervention is better than surgery in that first 6-10 months after the procedure. The reason for that, of course, is the procedural mortality," Dr. Edwards said.
They also defined a low-risk population (about 20% of the total population). They looked at survival advantages at years 1-4. "I think this is important because it illustrates that surgery really does start to declare its advantage in year 1 to year 2. Then it looks like it begins to plateau off a little bit," he said. "Still, at 4 years for both high-risk and low-risk patients, you’ve got more than a 25% survival advantage for surgery."
He noted that "this is a Medicare population that I’ve presented, so we would be on shaky ground if we tried to extrapolate these results to a global population."
He concluded by saying that "the results should improve the quality of care for patients with coronary disease, and it should clarify the indications for intervention in the subgroups that we’ve presented here. Ideally, it would minimize overuse and underuse, so that we could really provide optimal care for patients with coronary disease."
Prediction Models Gleaned From Data
During the same presentation, Dr. David M. Shahian reported on long-term prediction models of death and nonfatal events for both CABG and PCI. "Longer term outcomes are clearly going to be necessary if we’re really going to determine the true comparative effectiveness of these various strategies," he said.
In this analysis, the researchers looked at all isolated CABG patients at STS-participating hospitals who were discharged between the beginning of 2002 and the end of 2007. STS procedural records were linked to CMS claims and denominator files.
The final study cohort included 348,341 CABG patients at 917 sites. Follow-up was carried through 2008 (median follow-up, 4 years). Long-term variables were based on those from short-term CABG models and clinical experience. Separate hazard ratios were estimated for each of these variables for four time intervals: 0-30 days, 31-80 days, 181-730 days, and more than 2 years. The researchers focused on main effects for this model.
Kaplan-Meier estimated mortality rates for CABG were 3% at 30 days, 6% at 180 days, 8% at 1 year, 11% at 2 years, and 23% at 3 years. Predicted mortality rates were superimposable with observed mortality rates, said Dr. Shahian, who is a cardiothoracic surgeon at Harvard Medical School in Boston. Dr. Shahian is also the chair of the STS Adult Cardiac Surgery Database and the STS Quality Measurement Task Force.
"We did observe the obesity paradox here. It’s the frail, almost cachectic individuals, who do the worst, while the more obese individuals tend to do better over time," he said. In addition, EF appears to be protective, with the greater the EF, the lower the long-term mortality.
However, smoking increases risk over time, as does diabetes. Immunosuppresive therapy has a stable and substantial negative effect over time.
The impact of some predictors changed over time. For example, patients with an acute MI have an increased initial mortality risk, which becomes generally insignificant over 1-2 years. In addition, early reoperation, shock, and emergency status have high up-front risks that decrease over time. However, preoperative atrial fibrillation progressively increases risk over time, he said.
"Among hospital survivors, higher ejection fraction and higher [body mass index] are protective at all time periods. A past history of stroke ... [and] chronic lung-disease immunosuppression have a persistent and negative impact on survival. Smoking, diabetes, dialysis-dependent renal failure – their negative impact increases over time. ... Some early important risk factors, like shock, emergency status, and reoperation are not predictors of late outcomes."
Dr. Edwards, who is the principal investigator of the ASCERT trial, reported that he is a consultant and/or on the advisory board for Humana. Dr. Shahian reported that he has no relevant financial relationships. However, several of their collaborators reported financial ties to several pharmaceutical or device manufacturers, including Boston Scientific and Medtronic Inc.
FT. LAUDERDALE, FLA. – Coronary artery bypass graft surgery shows a clear long-term survival advantage in certain high-risk groups over percutaneous coronary intervention, based on results of the largest study of real-world data so far.
The survival advantage for a composite high-risk group – including patients aged 75 years and older, patients with diabetes, those with ejection fractions (EF) less than 50%, and those with a glomerular filtration rate (GFR) less than 60 mL/min per 1.73 m2 – was 28% at 4 years, Dr. Fred H. Edwards reported at the annual meeting of the Society of Thoracic Surgeons.
The findings come from the ASCERT (The American College of Cardiology Foundation – The Society of Thoracic Surgeons Collaboration on the Comparative Effectiveness of Revascularization Strategies) study, in which researchers compared catheter- and surgery-based procedures using the existing ACC and STS databases, as well as the Centers for Medicare and Medicaid Services 100% denominator file data. The study was designed to identify specific patient characteristics that favor one mode of treatment over the other. The study is also supported by the National Heart, Lung, and Blood Institute.
The ACC and the STS both have large registries containing detailed clinical information on millions of procedures. However, the information in these databases extends to only 1 month after the procedure. The researchers linked this short-term clinical information with the administrative data registry from the CMS to provide long-term mortality, rehospitalization, and resource utilization outcomes. The 3- to 5-year outcomes after coronary artery bypass graft (CABG) surgery are being compared with those after percutaneous coronary intervention (PCI) – primarily using drug-eluting coronary stents, from the STS and ACC databases, respectively. In addition to survival, researchers are assessing the need for additional procedures and hospitalizations, new cardiac disease conditions, and the medications being taken at various points in time after the coronary artery procedure.
Patients in this CMS population were aged at least 65 years with two- to three-vessel disease. Patients with either single-vessel disease or left-main disease were excluded. Emergent procedures were also excluded.
"So what’s different about this [study]? Well, the N [number] is huge. We’ve got a population that is actually 10 times greater than the sum total of all patients ever having been enrolled in randomized [revascularization] trials," said Dr. Edwards, who is a professor of surgery and medical director of cardiothoracic surgery at the University of Florida/Shands Jacksonville, as well as chairman of the STS National Database. In addition to the size of this observational study, the focus is on real-world experience with a true national scope.
For the head-to-head comparison, data from both the STS and ACC databases were linked to data from the CMS. A propensity score – the probability of having CABG – was calculated for each patient, and clinically important subgroups were identified before the files were linked. The propensity scores and inverse weighting were used to calculate adjusted survival curves. "Then we compared the survival for coronary bypass and percutaneous intervention for groups having very similar characteristics," said Dr. Edwards.
High- and Low-Risk Groups Identified
This analysis included a total of 189,793 patients, of which 103,549 received PCI. Dr. Edwards presented the survival results for high-risk subgroups; the overall results will be presented at the ACC’s Annual Scientific Session in March, he said.
High-risk subgroups include patients who were aged 75 years and older, had diabetes, had EFs less than 50%, and had a GFR less than 60 mL/min per 1.73 m2.
For those aged 75 years and older, the mortality risk ratio at 4 years was 0.78 favoring surgery. Correspondingly, the survival advantage in this group for surgery was 22%. For patients with three-vessel disease, the survival advantage at 4 years was 25%. Patients with insulin-dependent diabetes had a 28% survival advantage at 4 years with CABG, compared with PCI. For patients with EFs less than 50%, the survival advantage with surgery was 30% at 4 years.
However, there appears to be a survival advantage with PCI in these groups at up to 1 year of follow-up. "We should keep in mind that in many of these subgroups, the survival with percutaneous intervention is better than surgery in that first 6-10 months after the procedure. The reason for that, of course, is the procedural mortality," Dr. Edwards said.
They also defined a low-risk population (about 20% of the total population). They looked at survival advantages at years 1-4. "I think this is important because it illustrates that surgery really does start to declare its advantage in year 1 to year 2. Then it looks like it begins to plateau off a little bit," he said. "Still, at 4 years for both high-risk and low-risk patients, you’ve got more than a 25% survival advantage for surgery."
He noted that "this is a Medicare population that I’ve presented, so we would be on shaky ground if we tried to extrapolate these results to a global population."
He concluded by saying that "the results should improve the quality of care for patients with coronary disease, and it should clarify the indications for intervention in the subgroups that we’ve presented here. Ideally, it would minimize overuse and underuse, so that we could really provide optimal care for patients with coronary disease."
Prediction Models Gleaned From Data
During the same presentation, Dr. David M. Shahian reported on long-term prediction models of death and nonfatal events for both CABG and PCI. "Longer term outcomes are clearly going to be necessary if we’re really going to determine the true comparative effectiveness of these various strategies," he said.
In this analysis, the researchers looked at all isolated CABG patients at STS-participating hospitals who were discharged between the beginning of 2002 and the end of 2007. STS procedural records were linked to CMS claims and denominator files.
The final study cohort included 348,341 CABG patients at 917 sites. Follow-up was carried through 2008 (median follow-up, 4 years). Long-term variables were based on those from short-term CABG models and clinical experience. Separate hazard ratios were estimated for each of these variables for four time intervals: 0-30 days, 31-80 days, 181-730 days, and more than 2 years. The researchers focused on main effects for this model.
Kaplan-Meier estimated mortality rates for CABG were 3% at 30 days, 6% at 180 days, 8% at 1 year, 11% at 2 years, and 23% at 3 years. Predicted mortality rates were superimposable with observed mortality rates, said Dr. Shahian, who is a cardiothoracic surgeon at Harvard Medical School in Boston. Dr. Shahian is also the chair of the STS Adult Cardiac Surgery Database and the STS Quality Measurement Task Force.
"We did observe the obesity paradox here. It’s the frail, almost cachectic individuals, who do the worst, while the more obese individuals tend to do better over time," he said. In addition, EF appears to be protective, with the greater the EF, the lower the long-term mortality.
However, smoking increases risk over time, as does diabetes. Immunosuppresive therapy has a stable and substantial negative effect over time.
The impact of some predictors changed over time. For example, patients with an acute MI have an increased initial mortality risk, which becomes generally insignificant over 1-2 years. In addition, early reoperation, shock, and emergency status have high up-front risks that decrease over time. However, preoperative atrial fibrillation progressively increases risk over time, he said.
"Among hospital survivors, higher ejection fraction and higher [body mass index] are protective at all time periods. A past history of stroke ... [and] chronic lung-disease immunosuppression have a persistent and negative impact on survival. Smoking, diabetes, dialysis-dependent renal failure – their negative impact increases over time. ... Some early important risk factors, like shock, emergency status, and reoperation are not predictors of late outcomes."
Dr. Edwards, who is the principal investigator of the ASCERT trial, reported that he is a consultant and/or on the advisory board for Humana. Dr. Shahian reported that he has no relevant financial relationships. However, several of their collaborators reported financial ties to several pharmaceutical or device manufacturers, including Boston Scientific and Medtronic Inc.
FT. LAUDERDALE, FLA. – Coronary artery bypass graft surgery shows a clear long-term survival advantage in certain high-risk groups over percutaneous coronary intervention, based on results of the largest study of real-world data so far.
The survival advantage for a composite high-risk group – including patients aged 75 years and older, patients with diabetes, those with ejection fractions (EF) less than 50%, and those with a glomerular filtration rate (GFR) less than 60 mL/min per 1.73 m2 – was 28% at 4 years, Dr. Fred H. Edwards reported at the annual meeting of the Society of Thoracic Surgeons.
The findings come from the ASCERT (The American College of Cardiology Foundation – The Society of Thoracic Surgeons Collaboration on the Comparative Effectiveness of Revascularization Strategies) study, in which researchers compared catheter- and surgery-based procedures using the existing ACC and STS databases, as well as the Centers for Medicare and Medicaid Services 100% denominator file data. The study was designed to identify specific patient characteristics that favor one mode of treatment over the other. The study is also supported by the National Heart, Lung, and Blood Institute.
The ACC and the STS both have large registries containing detailed clinical information on millions of procedures. However, the information in these databases extends to only 1 month after the procedure. The researchers linked this short-term clinical information with the administrative data registry from the CMS to provide long-term mortality, rehospitalization, and resource utilization outcomes. The 3- to 5-year outcomes after coronary artery bypass graft (CABG) surgery are being compared with those after percutaneous coronary intervention (PCI) – primarily using drug-eluting coronary stents, from the STS and ACC databases, respectively. In addition to survival, researchers are assessing the need for additional procedures and hospitalizations, new cardiac disease conditions, and the medications being taken at various points in time after the coronary artery procedure.
Patients in this CMS population were aged at least 65 years with two- to three-vessel disease. Patients with either single-vessel disease or left-main disease were excluded. Emergent procedures were also excluded.
"So what’s different about this [study]? Well, the N [number] is huge. We’ve got a population that is actually 10 times greater than the sum total of all patients ever having been enrolled in randomized [revascularization] trials," said Dr. Edwards, who is a professor of surgery and medical director of cardiothoracic surgery at the University of Florida/Shands Jacksonville, as well as chairman of the STS National Database. In addition to the size of this observational study, the focus is on real-world experience with a true national scope.
For the head-to-head comparison, data from both the STS and ACC databases were linked to data from the CMS. A propensity score – the probability of having CABG – was calculated for each patient, and clinically important subgroups were identified before the files were linked. The propensity scores and inverse weighting were used to calculate adjusted survival curves. "Then we compared the survival for coronary bypass and percutaneous intervention for groups having very similar characteristics," said Dr. Edwards.
High- and Low-Risk Groups Identified
This analysis included a total of 189,793 patients, of which 103,549 received PCI. Dr. Edwards presented the survival results for high-risk subgroups; the overall results will be presented at the ACC’s Annual Scientific Session in March, he said.
High-risk subgroups include patients who were aged 75 years and older, had diabetes, had EFs less than 50%, and had a GFR less than 60 mL/min per 1.73 m2.
For those aged 75 years and older, the mortality risk ratio at 4 years was 0.78 favoring surgery. Correspondingly, the survival advantage in this group for surgery was 22%. For patients with three-vessel disease, the survival advantage at 4 years was 25%. Patients with insulin-dependent diabetes had a 28% survival advantage at 4 years with CABG, compared with PCI. For patients with EFs less than 50%, the survival advantage with surgery was 30% at 4 years.
However, there appears to be a survival advantage with PCI in these groups at up to 1 year of follow-up. "We should keep in mind that in many of these subgroups, the survival with percutaneous intervention is better than surgery in that first 6-10 months after the procedure. The reason for that, of course, is the procedural mortality," Dr. Edwards said.
They also defined a low-risk population (about 20% of the total population). They looked at survival advantages at years 1-4. "I think this is important because it illustrates that surgery really does start to declare its advantage in year 1 to year 2. Then it looks like it begins to plateau off a little bit," he said. "Still, at 4 years for both high-risk and low-risk patients, you’ve got more than a 25% survival advantage for surgery."
He noted that "this is a Medicare population that I’ve presented, so we would be on shaky ground if we tried to extrapolate these results to a global population."
He concluded by saying that "the results should improve the quality of care for patients with coronary disease, and it should clarify the indications for intervention in the subgroups that we’ve presented here. Ideally, it would minimize overuse and underuse, so that we could really provide optimal care for patients with coronary disease."
Prediction Models Gleaned From Data
During the same presentation, Dr. David M. Shahian reported on long-term prediction models of death and nonfatal events for both CABG and PCI. "Longer term outcomes are clearly going to be necessary if we’re really going to determine the true comparative effectiveness of these various strategies," he said.
In this analysis, the researchers looked at all isolated CABG patients at STS-participating hospitals who were discharged between the beginning of 2002 and the end of 2007. STS procedural records were linked to CMS claims and denominator files.
The final study cohort included 348,341 CABG patients at 917 sites. Follow-up was carried through 2008 (median follow-up, 4 years). Long-term variables were based on those from short-term CABG models and clinical experience. Separate hazard ratios were estimated for each of these variables for four time intervals: 0-30 days, 31-80 days, 181-730 days, and more than 2 years. The researchers focused on main effects for this model.
Kaplan-Meier estimated mortality rates for CABG were 3% at 30 days, 6% at 180 days, 8% at 1 year, 11% at 2 years, and 23% at 3 years. Predicted mortality rates were superimposable with observed mortality rates, said Dr. Shahian, who is a cardiothoracic surgeon at Harvard Medical School in Boston. Dr. Shahian is also the chair of the STS Adult Cardiac Surgery Database and the STS Quality Measurement Task Force.
"We did observe the obesity paradox here. It’s the frail, almost cachectic individuals, who do the worst, while the more obese individuals tend to do better over time," he said. In addition, EF appears to be protective, with the greater the EF, the lower the long-term mortality.
However, smoking increases risk over time, as does diabetes. Immunosuppresive therapy has a stable and substantial negative effect over time.
The impact of some predictors changed over time. For example, patients with an acute MI have an increased initial mortality risk, which becomes generally insignificant over 1-2 years. In addition, early reoperation, shock, and emergency status have high up-front risks that decrease over time. However, preoperative atrial fibrillation progressively increases risk over time, he said.
"Among hospital survivors, higher ejection fraction and higher [body mass index] are protective at all time periods. A past history of stroke ... [and] chronic lung-disease immunosuppression have a persistent and negative impact on survival. Smoking, diabetes, dialysis-dependent renal failure – their negative impact increases over time. ... Some early important risk factors, like shock, emergency status, and reoperation are not predictors of late outcomes."
Dr. Edwards, who is the principal investigator of the ASCERT trial, reported that he is a consultant and/or on the advisory board for Humana. Dr. Shahian reported that he has no relevant financial relationships. However, several of their collaborators reported financial ties to several pharmaceutical or device manufacturers, including Boston Scientific and Medtronic Inc.
FROM THE ANNUAL MEETING OF THE SOCIETY OF THORACIC SURGEONS
Major Finding: The survival advantage of CABG over PCI for a composite high-risk group (patients aged 75 years and older, patients with diabetes, those with EFs less than 50%, and those with a GFR less than 60 mL/min per 1.73 m2) was 28% at 4 years.
Data Source: Almost 190,000 patients in the ASCERT study, in which researchers compared catheter- andsurgery-based procedures using the existing ACC and STS databases,as well as the Centers for Medicare and Medicaid Services 100%denominator file data.
Disclosures: The study was sponsored by the National Heart, Lung, and Blood Institute. Dr. Edwards reported that he is a consultant and/or on the advisory board for Humana. Dr. Shahian reported that he has no relevant financial relationships. Several of their collaborators reported financial ties to several pharmaceutical or device manufacturers, including Boston Scientific and Medtronic.
Neurologic Improvements Possible in Neonatal ASO
FT. LAUDERDALE, FLA. – The use of full-flow cardiopulmonary bypass, coupled with neurological monitoring, improved cognitive and motor outcomes in a prospective neurologic outcome study of 97 neonates with transposition of the great arteries (both single- and two-ventricle lesions) who underwent an arterial switch operation.
The cohort study, conducted by Dr. Dean B. Andropoulos and his colleagues at the Texas Children’s Hospital in Houston, examined early MRI changes and longer-term neurodevelopmental outcomes after the arterial switch operation (ASO) was performed using a cardiopulmonary bypass (CPB) protocol that avoided deep hypothermic circulatory arrest (DHCA) and low-flow CPB.

The ASO was performed by using CPB with 150-mL/kg per min flows with no low-flow CPB or DHCA; pH stat management; hematocrit 30% or higher; and hypothermia to 24° -28° C. Regional oxygen saturation greater than 50% was maintained by using near infrared spectroscopic monitoring.
Neurologic assessment was performed using brain MRI performed immediately before the operation and 7 days postoperatively. The Bayley Scales of Infant and Toddler Development, Third Edition were used at 12 and 36 months (mean score of 100).
Dextrotransposition of the great arteries was present in 31 of the 97 enrolled patients. Ten of these 31 (32%) had preoperative MRI change, and 19 of 31 (61%) showed new postoperative MRI change, with 75% showing minimal new white matter injury, he said at the annual meeting of the Society of Thoracic Surgeons.
At 2 months, Bayley Scales were performed on 17 of the patients. Their mean cognitive score was 106.5, mean motor score was 90.4, and mean language score was 89.4. Twelve patients had Bayley III testing at 36 months, with a cognitive score of 106.5, motor score of 107.4, and language score of 98.2.
"Our series demonstrates a significant incidence of pre-existing MRI changes, and 61% have new postoperative changes, but all changes in this series were mild," said Dr. Andropoulos.
"At 12 months, the cognitive score of these children was above the population mean, but their motor and language performance was lower. By 36 months, language and motor scores had improved significantly. Thus, full-flow CPB coupled to cerebral monitoring may improve neurological outcomes."
Because of these results, "future studies of ASO patients should include short- and long-term neurodevelopmental studies," he said.
With greatly improved 30-day neonatal arterial switch operation mortality rates (for example, at the Texas Children’s Hospital in Houston there were no 30-day hospital mortalities for 175 ASOs since 2000), there are increasing expectations for better neurologic outcomes, according to Dr. Andropoulos, and such considerations are increasingly important.
Dr. Andropoulos reported having no financial conflicts.
FT. LAUDERDALE, FLA. – The use of full-flow cardiopulmonary bypass, coupled with neurological monitoring, improved cognitive and motor outcomes in a prospective neurologic outcome study of 97 neonates with transposition of the great arteries (both single- and two-ventricle lesions) who underwent an arterial switch operation.
The cohort study, conducted by Dr. Dean B. Andropoulos and his colleagues at the Texas Children’s Hospital in Houston, examined early MRI changes and longer-term neurodevelopmental outcomes after the arterial switch operation (ASO) was performed using a cardiopulmonary bypass (CPB) protocol that avoided deep hypothermic circulatory arrest (DHCA) and low-flow CPB.
The ASO was performed by using CPB with 150-mL/kg per min flows with no low-flow CPB or DHCA; pH stat management; hematocrit 30% or higher; and hypothermia to 24° -28° C. Regional oxygen saturation greater than 50% was maintained by using near infrared spectroscopic monitoring.
Neurologic assessment was performed using brain MRI performed immediately before the operation and 7 days postoperatively. The Bayley Scales of Infant and Toddler Development, Third Edition were used at 12 and 36 months (mean score of 100).
Dextrotransposition of the great arteries was present in 31 of the 97 enrolled patients. Ten of these 31 (32%) had preoperative MRI change, and 19 of 31 (61%) showed new postoperative MRI change, with 75% showing minimal new white matter injury, he said at the annual meeting of the Society of Thoracic Surgeons.
At 2 months, Bayley Scales were performed on 17 of the patients. Their mean cognitive score was 106.5, mean motor score was 90.4, and mean language score was 89.4. Twelve patients had Bayley III testing at 36 months, with a cognitive score of 106.5, motor score of 107.4, and language score of 98.2.
"Our series demonstrates a significant incidence of pre-existing MRI changes, and 61% have new postoperative changes, but all changes in this series were mild," said Dr. Andropoulos.
"At 12 months, the cognitive score of these children was above the population mean, but their motor and language performance was lower. By 36 months, language and motor scores had improved significantly. Thus, full-flow CPB coupled to cerebral monitoring may improve neurological outcomes."
Because of these results, "future studies of ASO patients should include short- and long-term neurodevelopmental studies," he said.
With greatly improved 30-day neonatal arterial switch operation mortality rates (for example, at the Texas Children’s Hospital in Houston there were no 30-day hospital mortalities for 175 ASOs since 2000), there are increasing expectations for better neurologic outcomes, according to Dr. Andropoulos, and such considerations are increasingly important.
Dr. Andropoulos reported having no financial conflicts.
FT. LAUDERDALE, FLA. – The use of full-flow cardiopulmonary bypass, coupled with neurological monitoring, improved cognitive and motor outcomes in a prospective neurologic outcome study of 97 neonates with transposition of the great arteries (both single- and two-ventricle lesions) who underwent an arterial switch operation.
The cohort study, conducted by Dr. Dean B. Andropoulos and his colleagues at the Texas Children’s Hospital in Houston, examined early MRI changes and longer-term neurodevelopmental outcomes after the arterial switch operation (ASO) was performed using a cardiopulmonary bypass (CPB) protocol that avoided deep hypothermic circulatory arrest (DHCA) and low-flow CPB.
The ASO was performed by using CPB with 150-mL/kg per min flows with no low-flow CPB or DHCA; pH stat management; hematocrit 30% or higher; and hypothermia to 24° -28° C. Regional oxygen saturation greater than 50% was maintained by using near infrared spectroscopic monitoring.
Neurologic assessment was performed using brain MRI performed immediately before the operation and 7 days postoperatively. The Bayley Scales of Infant and Toddler Development, Third Edition were used at 12 and 36 months (mean score of 100).
Dextrotransposition of the great arteries was present in 31 of the 97 enrolled patients. Ten of these 31 (32%) had preoperative MRI change, and 19 of 31 (61%) showed new postoperative MRI change, with 75% showing minimal new white matter injury, he said at the annual meeting of the Society of Thoracic Surgeons.
At 2 months, Bayley Scales were performed on 17 of the patients. Their mean cognitive score was 106.5, mean motor score was 90.4, and mean language score was 89.4. Twelve patients had Bayley III testing at 36 months, with a cognitive score of 106.5, motor score of 107.4, and language score of 98.2.
"Our series demonstrates a significant incidence of pre-existing MRI changes, and 61% have new postoperative changes, but all changes in this series were mild," said Dr. Andropoulos.
"At 12 months, the cognitive score of these children was above the population mean, but their motor and language performance was lower. By 36 months, language and motor scores had improved significantly. Thus, full-flow CPB coupled to cerebral monitoring may improve neurological outcomes."
Because of these results, "future studies of ASO patients should include short- and long-term neurodevelopmental studies," he said.
With greatly improved 30-day neonatal arterial switch operation mortality rates (for example, at the Texas Children’s Hospital in Houston there were no 30-day hospital mortalities for 175 ASOs since 2000), there are increasing expectations for better neurologic outcomes, according to Dr. Andropoulos, and such considerations are increasingly important.
Dr. Andropoulos reported having no financial conflicts.
FROM THE ANNUAL MEETING OF THE SOCIETY OF THORACIC SURGEONS
Major Finding: The series demonstrated a significant incidence of preexisting MRI changes, and 61% had new postoperative changes, but all changes in the series were deemed mild.
Data Source: A prospective cohort study was performed examining early MRI changes and longer-term neurodevelopmental outcomes in 97 neonates with transposition of the great arteries.
Disclosures: Dr. Andropoulos reported having no financial disclosures.