User login
Adhesiolysis linked to high morbidity, higher hospitalization costs
Adhesiolysis was associated with an increased risk for a variety of morbidities during repeat abdominal surgery including inadvertent bowel defects, seromuscular injuries, and postoperative sepsis, according to the results of a prospective study.
"All physicians treating patients with disorders of the abdominal cavity that might require surgery should be aware of the adverse effects of adhesiolysis," reported Dr. Richard P.G. ten Broek and his associates in the department of surgery at Radboud University Nijmegen (the Netherlands) Medical Center. The study was published in Annals of Surgery (2013;258:98-106).
The investigators conducted the prospective cohort study to evaluate the direct effects of adhesiolysis on unintentional organ damage, morbidity, and costs during repeat operations, to address the lack of information in this area. They collected data from a total of 755 elective laparotomy or laparoscopy procedures in 715 patients performed at the medical center between June 2008 and June 2010.
The removal of adhesions was undertaken in almost 63% (475) of these procedures. Median adhesiolysis time was 20 minutes, ranging from 1 minute to almost 13 hours. Previous intra-abdominal surgery and peritonitis were among the most common causes of adhesions.
"All physicians treating patients with disorders of the abdominal cavity that might require surgery should be aware of the adverse effects of adhesiolysis,"
In the adhesiolysis group, the rates of perioperative complications were statistically significantly higher, compared with those in patients who did not require adhesiolysis, including full-thickness bowel defect (10.5% in the adhesiolysis group, versus no cases in the nonadhesiolysis group), injury to the seromuscular layer (27.6% v. 3.9%), and injuries to other organs (8.6% vs 2.5%).
Overall, the rate of surgical complications was 23.4% among those who had adhesiolysis, compared with 17.5% of those in the nonadhesiolysis group, also a statistically significant difference.
Adhesiolysis was associated with more than a fivefold increased rate of sepsis (odds ratio, 5.12), almost a fourfold increased risk of intra-abdominal complications (OR, 3.46), and more than a twofold increased risk of incisional wound infection (OR, 2.45), all statistically significant differences. The differences in mortality, urinary tract infections, pneumonia, or hemorrhage were not significantly different.
Adhesiolysis also resulted in longer surgery time (a mean of 22.5 minutes longer), recovery time (a mean of about 2 hours longer), and total hospital stay (a mean of about 3 days longer), as well as 29% greater operative blood loss. Among the cases reviewed, the mean hospital cost when adhesiolysis was performed was $18,579, vs. $14,063 when it was not performed.
This is the first study "showing adhesiolysis as a risk factor for postoperative surgical complications, longer hospital stays, more readmissions, and increased costs," the authors pointed out. These data can be helpful "when counseling patients before surgery, when physicians and health care providers make decisions on implementing antiadhesive strategies, and for the reimbursement policy of insurance companies," they added, noting that fewer than 10% of surgeons counsel patients about the risk of adhesions.
"With the projected increase in more repeat abdominal surgeries because of a longer life expectancy and newer technologies, prevention of adhesiolysis-related morbidity might be even more cost effective," they added.
The study was sponsored by Radboud University Nijmegen Medical Center, with no external funding, and the authors said they had no relevant financial conflicts.
Adhesiolysis was associated with an increased risk for a variety of morbidities during repeat abdominal surgery including inadvertent bowel defects, seromuscular injuries, and postoperative sepsis, according to the results of a prospective study.
"All physicians treating patients with disorders of the abdominal cavity that might require surgery should be aware of the adverse effects of adhesiolysis," reported Dr. Richard P.G. ten Broek and his associates in the department of surgery at Radboud University Nijmegen (the Netherlands) Medical Center. The study was published in Annals of Surgery (2013;258:98-106).
The investigators conducted the prospective cohort study to evaluate the direct effects of adhesiolysis on unintentional organ damage, morbidity, and costs during repeat operations, to address the lack of information in this area. They collected data from a total of 755 elective laparotomy or laparoscopy procedures in 715 patients performed at the medical center between June 2008 and June 2010.
The removal of adhesions was undertaken in almost 63% (475) of these procedures. Median adhesiolysis time was 20 minutes, ranging from 1 minute to almost 13 hours. Previous intra-abdominal surgery and peritonitis were among the most common causes of adhesions.
"All physicians treating patients with disorders of the abdominal cavity that might require surgery should be aware of the adverse effects of adhesiolysis,"
In the adhesiolysis group, the rates of perioperative complications were statistically significantly higher, compared with those in patients who did not require adhesiolysis, including full-thickness bowel defect (10.5% in the adhesiolysis group, versus no cases in the nonadhesiolysis group), injury to the seromuscular layer (27.6% v. 3.9%), and injuries to other organs (8.6% vs 2.5%).
Overall, the rate of surgical complications was 23.4% among those who had adhesiolysis, compared with 17.5% of those in the nonadhesiolysis group, also a statistically significant difference.
Adhesiolysis was associated with more than a fivefold increased rate of sepsis (odds ratio, 5.12), almost a fourfold increased risk of intra-abdominal complications (OR, 3.46), and more than a twofold increased risk of incisional wound infection (OR, 2.45), all statistically significant differences. The differences in mortality, urinary tract infections, pneumonia, or hemorrhage were not significantly different.
Adhesiolysis also resulted in longer surgery time (a mean of 22.5 minutes longer), recovery time (a mean of about 2 hours longer), and total hospital stay (a mean of about 3 days longer), as well as 29% greater operative blood loss. Among the cases reviewed, the mean hospital cost when adhesiolysis was performed was $18,579, vs. $14,063 when it was not performed.
This is the first study "showing adhesiolysis as a risk factor for postoperative surgical complications, longer hospital stays, more readmissions, and increased costs," the authors pointed out. These data can be helpful "when counseling patients before surgery, when physicians and health care providers make decisions on implementing antiadhesive strategies, and for the reimbursement policy of insurance companies," they added, noting that fewer than 10% of surgeons counsel patients about the risk of adhesions.
"With the projected increase in more repeat abdominal surgeries because of a longer life expectancy and newer technologies, prevention of adhesiolysis-related morbidity might be even more cost effective," they added.
The study was sponsored by Radboud University Nijmegen Medical Center, with no external funding, and the authors said they had no relevant financial conflicts.
Adhesiolysis was associated with an increased risk for a variety of morbidities during repeat abdominal surgery including inadvertent bowel defects, seromuscular injuries, and postoperative sepsis, according to the results of a prospective study.
"All physicians treating patients with disorders of the abdominal cavity that might require surgery should be aware of the adverse effects of adhesiolysis," reported Dr. Richard P.G. ten Broek and his associates in the department of surgery at Radboud University Nijmegen (the Netherlands) Medical Center. The study was published in Annals of Surgery (2013;258:98-106).
The investigators conducted the prospective cohort study to evaluate the direct effects of adhesiolysis on unintentional organ damage, morbidity, and costs during repeat operations, to address the lack of information in this area. They collected data from a total of 755 elective laparotomy or laparoscopy procedures in 715 patients performed at the medical center between June 2008 and June 2010.
The removal of adhesions was undertaken in almost 63% (475) of these procedures. Median adhesiolysis time was 20 minutes, ranging from 1 minute to almost 13 hours. Previous intra-abdominal surgery and peritonitis were among the most common causes of adhesions.
"All physicians treating patients with disorders of the abdominal cavity that might require surgery should be aware of the adverse effects of adhesiolysis,"
In the adhesiolysis group, the rates of perioperative complications were statistically significantly higher, compared with those in patients who did not require adhesiolysis, including full-thickness bowel defect (10.5% in the adhesiolysis group, versus no cases in the nonadhesiolysis group), injury to the seromuscular layer (27.6% v. 3.9%), and injuries to other organs (8.6% vs 2.5%).
Overall, the rate of surgical complications was 23.4% among those who had adhesiolysis, compared with 17.5% of those in the nonadhesiolysis group, also a statistically significant difference.
Adhesiolysis was associated with more than a fivefold increased rate of sepsis (odds ratio, 5.12), almost a fourfold increased risk of intra-abdominal complications (OR, 3.46), and more than a twofold increased risk of incisional wound infection (OR, 2.45), all statistically significant differences. The differences in mortality, urinary tract infections, pneumonia, or hemorrhage were not significantly different.
Adhesiolysis also resulted in longer surgery time (a mean of 22.5 minutes longer), recovery time (a mean of about 2 hours longer), and total hospital stay (a mean of about 3 days longer), as well as 29% greater operative blood loss. Among the cases reviewed, the mean hospital cost when adhesiolysis was performed was $18,579, vs. $14,063 when it was not performed.
This is the first study "showing adhesiolysis as a risk factor for postoperative surgical complications, longer hospital stays, more readmissions, and increased costs," the authors pointed out. These data can be helpful "when counseling patients before surgery, when physicians and health care providers make decisions on implementing antiadhesive strategies, and for the reimbursement policy of insurance companies," they added, noting that fewer than 10% of surgeons counsel patients about the risk of adhesions.
"With the projected increase in more repeat abdominal surgeries because of a longer life expectancy and newer technologies, prevention of adhesiolysis-related morbidity might be even more cost effective," they added.
The study was sponsored by Radboud University Nijmegen Medical Center, with no external funding, and the authors said they had no relevant financial conflicts.
FROM ANNALS OF SURGERY
Major finding: The adverse effects of adhesiolysis during abdominal surgery included inadvertently incurred bowel defects, as well as a fivefold greater risk of sepsis, and significantly longer hospital stays and higher hospital costs.
Data source: A prospective cohort study of 755 elective abdominal surgeries in 715 patients, evaluating perioperative and postoperative outcomes associated with those that required adhesiolysis and those that did not.
Disclosures: The study was sponsored by Radboud University Nijmegen Medical Center, with no external funding. The authors said they had no relevant financial conflicts.
Colorectal cancer risk increased with bariatric surgery
The risk of colorectal cancer was significantly increased among people who had undergone obesity surgery in a retrospective cohort study of more than 77,000 obese patients enrolled in a Swedish registry.
The increased risk for colorectal cancer was associated with all three bariatric procedures – vertical banded gastroplasty, adjustable gastric banding, and Roux-en-Y gastric bypass – and increased further over time, reported Dr. Maryam Derogar, of the Karolinska Institutet, Stockholm, and her associates. No such pattern over time was seen among the obese patients who did not have surgery.
"Our data suggest that increased colorectal cancer risk may be a long-term consequence of such surgery," they concluded. If the association is confirmed, they added, "it should stimulate research addressing colonoscopic evaluation of the incidence of colorectal adenomatous polyps after obesity surgery with a view to defining an optimum colonoscopy surveillance strategy for the increasing number of patients who undergo obesity surgery. The study was published online in the Annals of Surgery (2013 [doi:10.1097/SLA.0b013e318288463a]).
To address their "unexpected" finding in an earlier study of an apparent increase in the risk of colorectal cancer after obesity surgery, but no increase in the risk of other cancers related to obesity, they conducted a retrospective cohort study using national registry data between 1980 and 2009, of 15,095 obese patients who had undergone obesity surgery and 62,016 patients who had been diagnosed with obesity but did not undergo surgery. They calculated the colorectal cancer risk using the standardized incidence ratio (SIR), the observed number of cases divided by the number of expected cases in that group.
Over a median of 10 years, there were 70 colorectal cancers in the obesity surgery group; and over a median of 7 years, 373 among those who had no surgery. The SIR for colorectal cancer among those who had surgery was 1.60, which was statistically significant. Among those who had no surgery, there was a small, insignificant increase in risk group (a SIR of 1.26). In the surgery group, the risk increased over time in men and women, up to a twofold increased risk among those patients followed for at least 10 years, a pattern than was not observed in the obese patients who had no surgery.
The "substantial increase in colorectal cancer risk, above that associated with excess body weight alone, more than 10 years after surgery is compatible with the long natural history of colorectal carcinogenesis from normal mucosa to a malignant colorectal cancer," the authors wrote. Why the risk was increased is not clear, but one possible explanation could be that the malabsorption effects of the gastric bypass procedure results in local mucosal changes, the authors speculated. Previously, they had identified rectal mucosal hyperproliferation in patients who had undergone obesity surgery, present at least 3 years after the procedure, a finding that was "associated with increased mucosal expression of the protumorigenic cytokine macrophage migration inhibitory factor," they wrote.
The study’s strengths included the size of the sample, long follow-up, and the validity of Swedish national registry data, while the limitations included the retrospective design and the lack of data on body weight over time.
As in the United States and other countries, obesity has been increasing in Sweden, with a corresponding increase in bariatric surgery. Over the last 20 years, the prevalence of obesity in Sweden has doubled, and the annual number of obesity operations performed has increased from 1,500 in 2006 to almost 4,000 in 2009, according to the authors.
The study was supported by the Swedish Research Council. The authors had no conflicts of interest to declare.
It is well established that overweight and obese individuals have a higher incidence of certain types of cancer; such as breast, colorectal, and endometrial to name a few. The exact mechanism is not known but it is generally linked with chronic inflammation associated with adipocyte release of inflammatory cytokines, an increase in sex steroid hormones, and an increase in insulin resistance. Therefore, it would seem logical to suggest that with significant and sustained weight loss (with or without bariatric surgery) the risk of cancer development may be reduced. Unfortunately, the data on weight loss and subsequent reduction in cancer risk are not solid. This is in part attributed to the fact that significant and sustained weight loss is extremely difficult to achieve without bariatric surgery.
There are several reports that show a protective effect of bariatric surgery on future cancer risk. Christou and colleagues (Surg. Obese Relat. Dis. 2008;4:691-5) reported that obese adults who undergo bariatric surgery may reduce their risk of developing some cancers by as much as 80%. Adams and colleagues (Obesity 2009;17:796-802) compared 6,596 patients who had gastric bypass with 9,442 severely obese individuals who had not, and found a significant decrease in the incidence of cancer and cancer-related deaths after bariatric surgery.
This report by Derogar and colleagues, published in Annals of Surgery, is the first to suggest that bariatric surgery is associated with an increased risk of colorectal cancer over time. It is difficult to interpret the results, however, as they directly contradict other reports and our general understanding of obesity and cancer. There are clearly limitations with the retrospective design of the study and the omission of any body weight or weight loss data. In addition, certain colorectal cancer risk factors, such as family history of cancer and prior adenomatous polyps, are not controlled for between the two groups.
Furthermore, there is a notion that individuals who undergo bariatric surgery tend to be more proactive about their health and take actions to prevent cancer. The authors suggest a possible mechanism that may be related to an increase in putative mucosal biomarkers of colorectal cancer risk and mucosal proinflammatory gene expression following Roux-en-Y gastric bypass. Also, a high-protein diet can promote detrimental metabolic profiles promoting carcinogenesis in the colon and rectum.
The exact mechanism remains elusive and as in most biologic systems, the answer in the end will be complex. Further research is needed to help answer some of these questions. This paper is important because it again highlights the increased risk of cancer associated with obesity and it is important for bariatric surgery programs to implement the proper screening protocols for cancer detection and prevention. Patients who undergo bariatric surgery should be screened both pre- and postoperatively as currently recommended depending on whether they are at average or high risk for certain cancers, such as breast or colon cancer, where screening has been shown to be effective.
Dr. Alex Nagle, FACS, is director of bariatric surgery, Northwestern Memorial Hospital, and associate professor of surgery, Northwestern University Feinberg School of Medicine, Chicago. He disclosed no conflicts of interest.
It is well established that overweight and obese individuals have a higher incidence of certain types of cancer; such as breast, colorectal, and endometrial to name a few. The exact mechanism is not known but it is generally linked with chronic inflammation associated with adipocyte release of inflammatory cytokines, an increase in sex steroid hormones, and an increase in insulin resistance. Therefore, it would seem logical to suggest that with significant and sustained weight loss (with or without bariatric surgery) the risk of cancer development may be reduced. Unfortunately, the data on weight loss and subsequent reduction in cancer risk are not solid. This is in part attributed to the fact that significant and sustained weight loss is extremely difficult to achieve without bariatric surgery.
There are several reports that show a protective effect of bariatric surgery on future cancer risk. Christou and colleagues (Surg. Obese Relat. Dis. 2008;4:691-5) reported that obese adults who undergo bariatric surgery may reduce their risk of developing some cancers by as much as 80%. Adams and colleagues (Obesity 2009;17:796-802) compared 6,596 patients who had gastric bypass with 9,442 severely obese individuals who had not, and found a significant decrease in the incidence of cancer and cancer-related deaths after bariatric surgery.
This report by Derogar and colleagues, published in Annals of Surgery, is the first to suggest that bariatric surgery is associated with an increased risk of colorectal cancer over time. It is difficult to interpret the results, however, as they directly contradict other reports and our general understanding of obesity and cancer. There are clearly limitations with the retrospective design of the study and the omission of any body weight or weight loss data. In addition, certain colorectal cancer risk factors, such as family history of cancer and prior adenomatous polyps, are not controlled for between the two groups.
Furthermore, there is a notion that individuals who undergo bariatric surgery tend to be more proactive about their health and take actions to prevent cancer. The authors suggest a possible mechanism that may be related to an increase in putative mucosal biomarkers of colorectal cancer risk and mucosal proinflammatory gene expression following Roux-en-Y gastric bypass. Also, a high-protein diet can promote detrimental metabolic profiles promoting carcinogenesis in the colon and rectum.
The exact mechanism remains elusive and as in most biologic systems, the answer in the end will be complex. Further research is needed to help answer some of these questions. This paper is important because it again highlights the increased risk of cancer associated with obesity and it is important for bariatric surgery programs to implement the proper screening protocols for cancer detection and prevention. Patients who undergo bariatric surgery should be screened both pre- and postoperatively as currently recommended depending on whether they are at average or high risk for certain cancers, such as breast or colon cancer, where screening has been shown to be effective.
Dr. Alex Nagle, FACS, is director of bariatric surgery, Northwestern Memorial Hospital, and associate professor of surgery, Northwestern University Feinberg School of Medicine, Chicago. He disclosed no conflicts of interest.
It is well established that overweight and obese individuals have a higher incidence of certain types of cancer; such as breast, colorectal, and endometrial to name a few. The exact mechanism is not known but it is generally linked with chronic inflammation associated with adipocyte release of inflammatory cytokines, an increase in sex steroid hormones, and an increase in insulin resistance. Therefore, it would seem logical to suggest that with significant and sustained weight loss (with or without bariatric surgery) the risk of cancer development may be reduced. Unfortunately, the data on weight loss and subsequent reduction in cancer risk are not solid. This is in part attributed to the fact that significant and sustained weight loss is extremely difficult to achieve without bariatric surgery.
There are several reports that show a protective effect of bariatric surgery on future cancer risk. Christou and colleagues (Surg. Obese Relat. Dis. 2008;4:691-5) reported that obese adults who undergo bariatric surgery may reduce their risk of developing some cancers by as much as 80%. Adams and colleagues (Obesity 2009;17:796-802) compared 6,596 patients who had gastric bypass with 9,442 severely obese individuals who had not, and found a significant decrease in the incidence of cancer and cancer-related deaths after bariatric surgery.
This report by Derogar and colleagues, published in Annals of Surgery, is the first to suggest that bariatric surgery is associated with an increased risk of colorectal cancer over time. It is difficult to interpret the results, however, as they directly contradict other reports and our general understanding of obesity and cancer. There are clearly limitations with the retrospective design of the study and the omission of any body weight or weight loss data. In addition, certain colorectal cancer risk factors, such as family history of cancer and prior adenomatous polyps, are not controlled for between the two groups.
Furthermore, there is a notion that individuals who undergo bariatric surgery tend to be more proactive about their health and take actions to prevent cancer. The authors suggest a possible mechanism that may be related to an increase in putative mucosal biomarkers of colorectal cancer risk and mucosal proinflammatory gene expression following Roux-en-Y gastric bypass. Also, a high-protein diet can promote detrimental metabolic profiles promoting carcinogenesis in the colon and rectum.
The exact mechanism remains elusive and as in most biologic systems, the answer in the end will be complex. Further research is needed to help answer some of these questions. This paper is important because it again highlights the increased risk of cancer associated with obesity and it is important for bariatric surgery programs to implement the proper screening protocols for cancer detection and prevention. Patients who undergo bariatric surgery should be screened both pre- and postoperatively as currently recommended depending on whether they are at average or high risk for certain cancers, such as breast or colon cancer, where screening has been shown to be effective.
Dr. Alex Nagle, FACS, is director of bariatric surgery, Northwestern Memorial Hospital, and associate professor of surgery, Northwestern University Feinberg School of Medicine, Chicago. He disclosed no conflicts of interest.
The risk of colorectal cancer was significantly increased among people who had undergone obesity surgery in a retrospective cohort study of more than 77,000 obese patients enrolled in a Swedish registry.
The increased risk for colorectal cancer was associated with all three bariatric procedures – vertical banded gastroplasty, adjustable gastric banding, and Roux-en-Y gastric bypass – and increased further over time, reported Dr. Maryam Derogar, of the Karolinska Institutet, Stockholm, and her associates. No such pattern over time was seen among the obese patients who did not have surgery.
"Our data suggest that increased colorectal cancer risk may be a long-term consequence of such surgery," they concluded. If the association is confirmed, they added, "it should stimulate research addressing colonoscopic evaluation of the incidence of colorectal adenomatous polyps after obesity surgery with a view to defining an optimum colonoscopy surveillance strategy for the increasing number of patients who undergo obesity surgery. The study was published online in the Annals of Surgery (2013 [doi:10.1097/SLA.0b013e318288463a]).
To address their "unexpected" finding in an earlier study of an apparent increase in the risk of colorectal cancer after obesity surgery, but no increase in the risk of other cancers related to obesity, they conducted a retrospective cohort study using national registry data between 1980 and 2009, of 15,095 obese patients who had undergone obesity surgery and 62,016 patients who had been diagnosed with obesity but did not undergo surgery. They calculated the colorectal cancer risk using the standardized incidence ratio (SIR), the observed number of cases divided by the number of expected cases in that group.
Over a median of 10 years, there were 70 colorectal cancers in the obesity surgery group; and over a median of 7 years, 373 among those who had no surgery. The SIR for colorectal cancer among those who had surgery was 1.60, which was statistically significant. Among those who had no surgery, there was a small, insignificant increase in risk group (a SIR of 1.26). In the surgery group, the risk increased over time in men and women, up to a twofold increased risk among those patients followed for at least 10 years, a pattern than was not observed in the obese patients who had no surgery.
The "substantial increase in colorectal cancer risk, above that associated with excess body weight alone, more than 10 years after surgery is compatible with the long natural history of colorectal carcinogenesis from normal mucosa to a malignant colorectal cancer," the authors wrote. Why the risk was increased is not clear, but one possible explanation could be that the malabsorption effects of the gastric bypass procedure results in local mucosal changes, the authors speculated. Previously, they had identified rectal mucosal hyperproliferation in patients who had undergone obesity surgery, present at least 3 years after the procedure, a finding that was "associated with increased mucosal expression of the protumorigenic cytokine macrophage migration inhibitory factor," they wrote.
The study’s strengths included the size of the sample, long follow-up, and the validity of Swedish national registry data, while the limitations included the retrospective design and the lack of data on body weight over time.
As in the United States and other countries, obesity has been increasing in Sweden, with a corresponding increase in bariatric surgery. Over the last 20 years, the prevalence of obesity in Sweden has doubled, and the annual number of obesity operations performed has increased from 1,500 in 2006 to almost 4,000 in 2009, according to the authors.
The study was supported by the Swedish Research Council. The authors had no conflicts of interest to declare.
The risk of colorectal cancer was significantly increased among people who had undergone obesity surgery in a retrospective cohort study of more than 77,000 obese patients enrolled in a Swedish registry.
The increased risk for colorectal cancer was associated with all three bariatric procedures – vertical banded gastroplasty, adjustable gastric banding, and Roux-en-Y gastric bypass – and increased further over time, reported Dr. Maryam Derogar, of the Karolinska Institutet, Stockholm, and her associates. No such pattern over time was seen among the obese patients who did not have surgery.
"Our data suggest that increased colorectal cancer risk may be a long-term consequence of such surgery," they concluded. If the association is confirmed, they added, "it should stimulate research addressing colonoscopic evaluation of the incidence of colorectal adenomatous polyps after obesity surgery with a view to defining an optimum colonoscopy surveillance strategy for the increasing number of patients who undergo obesity surgery. The study was published online in the Annals of Surgery (2013 [doi:10.1097/SLA.0b013e318288463a]).
To address their "unexpected" finding in an earlier study of an apparent increase in the risk of colorectal cancer after obesity surgery, but no increase in the risk of other cancers related to obesity, they conducted a retrospective cohort study using national registry data between 1980 and 2009, of 15,095 obese patients who had undergone obesity surgery and 62,016 patients who had been diagnosed with obesity but did not undergo surgery. They calculated the colorectal cancer risk using the standardized incidence ratio (SIR), the observed number of cases divided by the number of expected cases in that group.
Over a median of 10 years, there were 70 colorectal cancers in the obesity surgery group; and over a median of 7 years, 373 among those who had no surgery. The SIR for colorectal cancer among those who had surgery was 1.60, which was statistically significant. Among those who had no surgery, there was a small, insignificant increase in risk group (a SIR of 1.26). In the surgery group, the risk increased over time in men and women, up to a twofold increased risk among those patients followed for at least 10 years, a pattern than was not observed in the obese patients who had no surgery.
The "substantial increase in colorectal cancer risk, above that associated with excess body weight alone, more than 10 years after surgery is compatible with the long natural history of colorectal carcinogenesis from normal mucosa to a malignant colorectal cancer," the authors wrote. Why the risk was increased is not clear, but one possible explanation could be that the malabsorption effects of the gastric bypass procedure results in local mucosal changes, the authors speculated. Previously, they had identified rectal mucosal hyperproliferation in patients who had undergone obesity surgery, present at least 3 years after the procedure, a finding that was "associated with increased mucosal expression of the protumorigenic cytokine macrophage migration inhibitory factor," they wrote.
The study’s strengths included the size of the sample, long follow-up, and the validity of Swedish national registry data, while the limitations included the retrospective design and the lack of data on body weight over time.
As in the United States and other countries, obesity has been increasing in Sweden, with a corresponding increase in bariatric surgery. Over the last 20 years, the prevalence of obesity in Sweden has doubled, and the annual number of obesity operations performed has increased from 1,500 in 2006 to almost 4,000 in 2009, according to the authors.
The study was supported by the Swedish Research Council. The authors had no conflicts of interest to declare.
FROM THE ANNALS OF SURGERY
Major finding: The risk of colorectal cancer increased by 60% among obese patients, a mean of 7 years after bariatric surgery but was only slightly increased among obese patients who did not undergo surgery, over the expected rate.
Data source: A retrospective cohort study using national patient registry data in Sweden compared the risk of colorectal cancer in about 15,000 obese patients who had undergone bariatric surgery and among about 62,000 obese patients who did not have surgery, compared to matched controls.
Disclosures: The study was supported by the Swedish Research Council. The authors had no conflicts of interest to declare.
FDA requires stronger peripheral neuropathy warning for quinolones
The Food and Drug Administration is requiring a stronger warning about the potential for peripheral neuropathy with fluoroquinolone antibiotics that are taken orally or by injection.
The warning does not apply to topical formulations, which have not been associated with neuropathy. Drug labels and patient medication guides must be updated, said the agency.
The potential for neuropathy was first added to the labels of all drugs in the class in 2004. The new warning was necessary because "the potential rapid onset and risk of permanence were not adequately described" in the 2004 label iteration, the FDA noted.
Before requiring new warnings, the FDA reviewed its Adverse Event Reporting System (FAERS, formerly known as AERS) database. The agency found that cases of fluoroquinolone-associated peripheral neuropathy with an outcome of "disability" had been reported to the AERS database between January 2003 and August 2012, although the FDA did not say how many cases it found. The reports indicated a rapid onset of peripheral neuropathy, often within a few days of starting the quinolone. Some cases reported neuropathy that continued for a year, even though the medication had been stopped.
The database was not able to show whether neuropathy was permanent, however, because it is designed to collect spontaneous reports.
The FDA said it had not been able to identify any risk factors for the development of peripheral neuropathy. But the onset of the condition seemed to have no correlation with the patient’s age or how long they took the antibiotic.
The updated warnings apply to all approved fluoroquinolones: levofloxacin (Levaquin), ciprofloxacin (Cipro), moxifloxacin (Avelox), norfloxacin (Noroxin), ofloxacin (Floxin), and gemifloxacin (Factive).
According to the FDA, 23 million outpatients were prescribed an oral quinolone in 2011. A total of 70% received ciprofloxacin; 28% were prescribed levofloxacin; and 9% were given moxifloxacin. Gemifloxacin, ofloxacin, and norfloxacin each accounted for less than 1% of those patients in 2011.
There were 3.8 million inpatients who received an injectable quinolone in 2011. The most-prescribed was levofloxacin, accounting for 63% of prescriptions, followed by ciprofloxacin (28%) and moxifloxacin (13%).
The agency recommended that patients who develop neuropathy symptoms stop taking the quinolone and be treated with a different antibiotic, unless the benefit outweighs the risk. Patients taking the medications who develop symptoms are urged to tell their physician immediately.
On Twitter @aliciaault
The Food and Drug Administration is requiring a stronger warning about the potential for peripheral neuropathy with fluoroquinolone antibiotics that are taken orally or by injection.
The warning does not apply to topical formulations, which have not been associated with neuropathy. Drug labels and patient medication guides must be updated, said the agency.
The potential for neuropathy was first added to the labels of all drugs in the class in 2004. The new warning was necessary because "the potential rapid onset and risk of permanence were not adequately described" in the 2004 label iteration, the FDA noted.
Before requiring new warnings, the FDA reviewed its Adverse Event Reporting System (FAERS, formerly known as AERS) database. The agency found that cases of fluoroquinolone-associated peripheral neuropathy with an outcome of "disability" had been reported to the AERS database between January 2003 and August 2012, although the FDA did not say how many cases it found. The reports indicated a rapid onset of peripheral neuropathy, often within a few days of starting the quinolone. Some cases reported neuropathy that continued for a year, even though the medication had been stopped.
The database was not able to show whether neuropathy was permanent, however, because it is designed to collect spontaneous reports.
The FDA said it had not been able to identify any risk factors for the development of peripheral neuropathy. But the onset of the condition seemed to have no correlation with the patient’s age or how long they took the antibiotic.
The updated warnings apply to all approved fluoroquinolones: levofloxacin (Levaquin), ciprofloxacin (Cipro), moxifloxacin (Avelox), norfloxacin (Noroxin), ofloxacin (Floxin), and gemifloxacin (Factive).
According to the FDA, 23 million outpatients were prescribed an oral quinolone in 2011. A total of 70% received ciprofloxacin; 28% were prescribed levofloxacin; and 9% were given moxifloxacin. Gemifloxacin, ofloxacin, and norfloxacin each accounted for less than 1% of those patients in 2011.
There were 3.8 million inpatients who received an injectable quinolone in 2011. The most-prescribed was levofloxacin, accounting for 63% of prescriptions, followed by ciprofloxacin (28%) and moxifloxacin (13%).
The agency recommended that patients who develop neuropathy symptoms stop taking the quinolone and be treated with a different antibiotic, unless the benefit outweighs the risk. Patients taking the medications who develop symptoms are urged to tell their physician immediately.
On Twitter @aliciaault
The Food and Drug Administration is requiring a stronger warning about the potential for peripheral neuropathy with fluoroquinolone antibiotics that are taken orally or by injection.
The warning does not apply to topical formulations, which have not been associated with neuropathy. Drug labels and patient medication guides must be updated, said the agency.
The potential for neuropathy was first added to the labels of all drugs in the class in 2004. The new warning was necessary because "the potential rapid onset and risk of permanence were not adequately described" in the 2004 label iteration, the FDA noted.
Before requiring new warnings, the FDA reviewed its Adverse Event Reporting System (FAERS, formerly known as AERS) database. The agency found that cases of fluoroquinolone-associated peripheral neuropathy with an outcome of "disability" had been reported to the AERS database between January 2003 and August 2012, although the FDA did not say how many cases it found. The reports indicated a rapid onset of peripheral neuropathy, often within a few days of starting the quinolone. Some cases reported neuropathy that continued for a year, even though the medication had been stopped.
The database was not able to show whether neuropathy was permanent, however, because it is designed to collect spontaneous reports.
The FDA said it had not been able to identify any risk factors for the development of peripheral neuropathy. But the onset of the condition seemed to have no correlation with the patient’s age or how long they took the antibiotic.
The updated warnings apply to all approved fluoroquinolones: levofloxacin (Levaquin), ciprofloxacin (Cipro), moxifloxacin (Avelox), norfloxacin (Noroxin), ofloxacin (Floxin), and gemifloxacin (Factive).
According to the FDA, 23 million outpatients were prescribed an oral quinolone in 2011. A total of 70% received ciprofloxacin; 28% were prescribed levofloxacin; and 9% were given moxifloxacin. Gemifloxacin, ofloxacin, and norfloxacin each accounted for less than 1% of those patients in 2011.
There were 3.8 million inpatients who received an injectable quinolone in 2011. The most-prescribed was levofloxacin, accounting for 63% of prescriptions, followed by ciprofloxacin (28%) and moxifloxacin (13%).
The agency recommended that patients who develop neuropathy symptoms stop taking the quinolone and be treated with a different antibiotic, unless the benefit outweighs the risk. Patients taking the medications who develop symptoms are urged to tell their physician immediately.
On Twitter @aliciaault

Collaborative quality improvement projects work, expert maintains
SAN DIEGO – In the opinion of Dr. Wayne J. English, it doesn’t take much for collaborative quality improvement projects to demonstrate a return on investment.
At the national conference of the American College of Surgeons National Surgical Quality Improvement Program (ACS NSQIP), he discussed his experience as a member of the Michigan Bariatric Surgery Collaborative (MBSC), a clinical outcomes registry and quality improvement program funded by Blue Cross Blue Shield of Michigan (BCBS) "Hospitals across the state are collecting, sharing, and analyzing data, then designing and implementing changes to improve patient care, and it’s working," said Dr. English, medical director of bariatric surgery at the Bariatric and Metabolic Institute at Marquette (Mich.) General Hospital.

In 1997, a group of five hospitals in Michigan joined with Blue Cross Blue Shield of Michigan Foundation and Blue Care Network to collaborate on the study of variation in angiography procedures and treatment. Recommendations from the group’s analysis "contributed to dramatic decreases in coronary emergency bypass surgeries and other complications," Dr. English said. "The initiative also saved an estimated $102 million in statewide health costs over 3 years." Since then, 11 more initiatives have [been] launched to address many of the most common and costly areas of surgical and medical care in Michigan. These included cardiac imaging, vascular intervention, cardiothoracic surgery, trauma, general surgery, breast cancer, surgical outcomes, hospital medicine, knee/hip replacement, radiation oncology, and bariatric surgery.
Speaking in the context of his experience with the MBSC, Dr. English said that much of the success comes from the three-part approach to each initiative. First, funding from BCBS "enables hospitals to work in collaborative environment," he said. "BCBS provides resources for data collection and analysis along with administrative oversight."
Second, a separate coordinating center serves as a data warehouse, conducts data audits, performs data analyses, and generates comparative performance reports.
Third, participating hospitals "work together by sharing data and best practices to improve patient care throughout the state of Michigan," he said.
The MBSC collects data on perioperative care and outcomes, late outcomes, structure and process of care, technical quality, subjective aspects of quality, and cost. "There are site visits that occur on a regular basis," he said. "There are usually two surgeons and two nurses that go along on a site visit. We share ideas during those visits; these are collegial events."
The primary focus is the registry data. "We look at variation in practice and determine best evidence. We meet three times a year to analyze risk- and reliability-adjusted data, develop quality improvement projects and, ultimately, best practices," Dr. English said. Currently, the collaborative comprises 39 sites, 76 surgeons, and data on more than 40,000 patients. Approximately 6,500 patients are added into the database each year.
Notable outcomes from MBSC projects to date, he said, include a 24% decrease in complication rates from 2007 to 2009, a 35% decrease in readmission rates decreased from 2007 to 2009, and a 35% decreased in ED visits from 2007 to 2010. "The decline in ED visits alone resulted in overall savings for BCBS of Michigan of $4.7 million and an overall savings for statewide plans of $14.6 million," Dr. English said.
One of the first initiatives launched by the MBSC involved a quality improvement effort to reduce the rate of pulmonary embolism, which accounts for almost half of all deaths after bariatric surgery. Standard approaches to prophylaxis include early ambulation, compression stockings/devices, and anticoagulation.
"When we surveyed surgeons in the state of Michigan, we found that there was tremendous variation in how medical chemoprophylaxis was implemented," Dr. English noted. "Many surgeons were using low-molecular-weight heparin and/or unfractionated heparin to varying degrees preoperatively, postoperatively and post discharge, while some used none at all. So the collaborative data determined statistically significant patient risk factors and developed a VTE risk calculator to stratify the baseline risk for VTE. Once surgeons started participating and utilizing risk-stratified treatment guidelines, we started to see a downward trend on the rates of thromboembolic events."
A parallel initiative evaluated the impact of placing inferior vena cava (IVC) filters during bariatric surgery. The value of IVC filters as a prophylaxis in bariatric surgery patients "is unclear, but their use has been growing rapidly since the availability of removable filters," Dr. English said. "According to data from the collaborative, there was wide variability in utilization from never to almost 40% of patients receiving IVC filters."
After analyzing outcomes data from the MBSC, it was discovered that complication rates were significantly higher in patients who had IVC filters placed during bariatric surgery, compared with those who did not. "In fact, over half of deaths and permanent disability were directly attributable to the filter itself," he said. "Once provided with the initial data feedback, many surgeons started decreasing the use of IVC filters during bariatric surgery. Now, fewer than 2% use them."
MBSC data also showed that costs were about $13,000 less per case to perform gastric bypass procedures without the use of IVC filters. "As a result of this one quality improvement project, an estimated $1.3 million was saved over the course of 1 year while all Michigan payers saved an estimated $2.6 million over the course of 1 year," Dr. English said. "That savings is more than enough to cover the cost of operating MBSC each year."
Dr. English disclosed that he serves as a consultant for ReShape Medical.
SAN DIEGO – In the opinion of Dr. Wayne J. English, it doesn’t take much for collaborative quality improvement projects to demonstrate a return on investment.
At the national conference of the American College of Surgeons National Surgical Quality Improvement Program (ACS NSQIP), he discussed his experience as a member of the Michigan Bariatric Surgery Collaborative (MBSC), a clinical outcomes registry and quality improvement program funded by Blue Cross Blue Shield of Michigan (BCBS) "Hospitals across the state are collecting, sharing, and analyzing data, then designing and implementing changes to improve patient care, and it’s working," said Dr. English, medical director of bariatric surgery at the Bariatric and Metabolic Institute at Marquette (Mich.) General Hospital.
In 1997, a group of five hospitals in Michigan joined with Blue Cross Blue Shield of Michigan Foundation and Blue Care Network to collaborate on the study of variation in angiography procedures and treatment. Recommendations from the group’s analysis "contributed to dramatic decreases in coronary emergency bypass surgeries and other complications," Dr. English said. "The initiative also saved an estimated $102 million in statewide health costs over 3 years." Since then, 11 more initiatives have [been] launched to address many of the most common and costly areas of surgical and medical care in Michigan. These included cardiac imaging, vascular intervention, cardiothoracic surgery, trauma, general surgery, breast cancer, surgical outcomes, hospital medicine, knee/hip replacement, radiation oncology, and bariatric surgery.
Speaking in the context of his experience with the MBSC, Dr. English said that much of the success comes from the three-part approach to each initiative. First, funding from BCBS "enables hospitals to work in collaborative environment," he said. "BCBS provides resources for data collection and analysis along with administrative oversight."
Second, a separate coordinating center serves as a data warehouse, conducts data audits, performs data analyses, and generates comparative performance reports.
Third, participating hospitals "work together by sharing data and best practices to improve patient care throughout the state of Michigan," he said.
The MBSC collects data on perioperative care and outcomes, late outcomes, structure and process of care, technical quality, subjective aspects of quality, and cost. "There are site visits that occur on a regular basis," he said. "There are usually two surgeons and two nurses that go along on a site visit. We share ideas during those visits; these are collegial events."
The primary focus is the registry data. "We look at variation in practice and determine best evidence. We meet three times a year to analyze risk- and reliability-adjusted data, develop quality improvement projects and, ultimately, best practices," Dr. English said. Currently, the collaborative comprises 39 sites, 76 surgeons, and data on more than 40,000 patients. Approximately 6,500 patients are added into the database each year.
Notable outcomes from MBSC projects to date, he said, include a 24% decrease in complication rates from 2007 to 2009, a 35% decrease in readmission rates decreased from 2007 to 2009, and a 35% decreased in ED visits from 2007 to 2010. "The decline in ED visits alone resulted in overall savings for BCBS of Michigan of $4.7 million and an overall savings for statewide plans of $14.6 million," Dr. English said.
One of the first initiatives launched by the MBSC involved a quality improvement effort to reduce the rate of pulmonary embolism, which accounts for almost half of all deaths after bariatric surgery. Standard approaches to prophylaxis include early ambulation, compression stockings/devices, and anticoagulation.
"When we surveyed surgeons in the state of Michigan, we found that there was tremendous variation in how medical chemoprophylaxis was implemented," Dr. English noted. "Many surgeons were using low-molecular-weight heparin and/or unfractionated heparin to varying degrees preoperatively, postoperatively and post discharge, while some used none at all. So the collaborative data determined statistically significant patient risk factors and developed a VTE risk calculator to stratify the baseline risk for VTE. Once surgeons started participating and utilizing risk-stratified treatment guidelines, we started to see a downward trend on the rates of thromboembolic events."
A parallel initiative evaluated the impact of placing inferior vena cava (IVC) filters during bariatric surgery. The value of IVC filters as a prophylaxis in bariatric surgery patients "is unclear, but their use has been growing rapidly since the availability of removable filters," Dr. English said. "According to data from the collaborative, there was wide variability in utilization from never to almost 40% of patients receiving IVC filters."
After analyzing outcomes data from the MBSC, it was discovered that complication rates were significantly higher in patients who had IVC filters placed during bariatric surgery, compared with those who did not. "In fact, over half of deaths and permanent disability were directly attributable to the filter itself," he said. "Once provided with the initial data feedback, many surgeons started decreasing the use of IVC filters during bariatric surgery. Now, fewer than 2% use them."
MBSC data also showed that costs were about $13,000 less per case to perform gastric bypass procedures without the use of IVC filters. "As a result of this one quality improvement project, an estimated $1.3 million was saved over the course of 1 year while all Michigan payers saved an estimated $2.6 million over the course of 1 year," Dr. English said. "That savings is more than enough to cover the cost of operating MBSC each year."
Dr. English disclosed that he serves as a consultant for ReShape Medical.
SAN DIEGO – In the opinion of Dr. Wayne J. English, it doesn’t take much for collaborative quality improvement projects to demonstrate a return on investment.
At the national conference of the American College of Surgeons National Surgical Quality Improvement Program (ACS NSQIP), he discussed his experience as a member of the Michigan Bariatric Surgery Collaborative (MBSC), a clinical outcomes registry and quality improvement program funded by Blue Cross Blue Shield of Michigan (BCBS) "Hospitals across the state are collecting, sharing, and analyzing data, then designing and implementing changes to improve patient care, and it’s working," said Dr. English, medical director of bariatric surgery at the Bariatric and Metabolic Institute at Marquette (Mich.) General Hospital.
In 1997, a group of five hospitals in Michigan joined with Blue Cross Blue Shield of Michigan Foundation and Blue Care Network to collaborate on the study of variation in angiography procedures and treatment. Recommendations from the group’s analysis "contributed to dramatic decreases in coronary emergency bypass surgeries and other complications," Dr. English said. "The initiative also saved an estimated $102 million in statewide health costs over 3 years." Since then, 11 more initiatives have [been] launched to address many of the most common and costly areas of surgical and medical care in Michigan. These included cardiac imaging, vascular intervention, cardiothoracic surgery, trauma, general surgery, breast cancer, surgical outcomes, hospital medicine, knee/hip replacement, radiation oncology, and bariatric surgery.
Speaking in the context of his experience with the MBSC, Dr. English said that much of the success comes from the three-part approach to each initiative. First, funding from BCBS "enables hospitals to work in collaborative environment," he said. "BCBS provides resources for data collection and analysis along with administrative oversight."
Second, a separate coordinating center serves as a data warehouse, conducts data audits, performs data analyses, and generates comparative performance reports.
Third, participating hospitals "work together by sharing data and best practices to improve patient care throughout the state of Michigan," he said.
The MBSC collects data on perioperative care and outcomes, late outcomes, structure and process of care, technical quality, subjective aspects of quality, and cost. "There are site visits that occur on a regular basis," he said. "There are usually two surgeons and two nurses that go along on a site visit. We share ideas during those visits; these are collegial events."
The primary focus is the registry data. "We look at variation in practice and determine best evidence. We meet three times a year to analyze risk- and reliability-adjusted data, develop quality improvement projects and, ultimately, best practices," Dr. English said. Currently, the collaborative comprises 39 sites, 76 surgeons, and data on more than 40,000 patients. Approximately 6,500 patients are added into the database each year.
Notable outcomes from MBSC projects to date, he said, include a 24% decrease in complication rates from 2007 to 2009, a 35% decrease in readmission rates decreased from 2007 to 2009, and a 35% decreased in ED visits from 2007 to 2010. "The decline in ED visits alone resulted in overall savings for BCBS of Michigan of $4.7 million and an overall savings for statewide plans of $14.6 million," Dr. English said.
One of the first initiatives launched by the MBSC involved a quality improvement effort to reduce the rate of pulmonary embolism, which accounts for almost half of all deaths after bariatric surgery. Standard approaches to prophylaxis include early ambulation, compression stockings/devices, and anticoagulation.
"When we surveyed surgeons in the state of Michigan, we found that there was tremendous variation in how medical chemoprophylaxis was implemented," Dr. English noted. "Many surgeons were using low-molecular-weight heparin and/or unfractionated heparin to varying degrees preoperatively, postoperatively and post discharge, while some used none at all. So the collaborative data determined statistically significant patient risk factors and developed a VTE risk calculator to stratify the baseline risk for VTE. Once surgeons started participating and utilizing risk-stratified treatment guidelines, we started to see a downward trend on the rates of thromboembolic events."
A parallel initiative evaluated the impact of placing inferior vena cava (IVC) filters during bariatric surgery. The value of IVC filters as a prophylaxis in bariatric surgery patients "is unclear, but their use has been growing rapidly since the availability of removable filters," Dr. English said. "According to data from the collaborative, there was wide variability in utilization from never to almost 40% of patients receiving IVC filters."
After analyzing outcomes data from the MBSC, it was discovered that complication rates were significantly higher in patients who had IVC filters placed during bariatric surgery, compared with those who did not. "In fact, over half of deaths and permanent disability were directly attributable to the filter itself," he said. "Once provided with the initial data feedback, many surgeons started decreasing the use of IVC filters during bariatric surgery. Now, fewer than 2% use them."
MBSC data also showed that costs were about $13,000 less per case to perform gastric bypass procedures without the use of IVC filters. "As a result of this one quality improvement project, an estimated $1.3 million was saved over the course of 1 year while all Michigan payers saved an estimated $2.6 million over the course of 1 year," Dr. English said. "That savings is more than enough to cover the cost of operating MBSC each year."
Dr. English disclosed that he serves as a consultant for ReShape Medical.
EXPERT ANALYSIS AT THE ACS NSQIP NATIONAL CONFERENCE

HIV postexposure prophylaxis guidelines revised
Revised federal guidelines for managing health care workers who are exposed to HIV recommend using at least three drugs for prophylaxis in all cases instead of assessing a person’s risk to decide on the number of drugs, among other updates to the guidelines.
Changes in the recommended drugs in preferred postexposure prophylaxis (PEP) regimens should make them easier to tolerate than earlier regimens and may increase the proportion of health care workers who are able to complete the 28-day treatment, Dr. David T. Kuhar and his associates said in the new document from the U.S. Public Health Service.
Another change is that follow-up HIV testing in health care workers on PEP can be shortened to 4 months instead of 6 months if a newer fourth-generation combination HIV p24 antigen/HIV antibody test is used, the guidelines state. The document, which updates 2005 guidelines, was published online in the journal Infection Control and Hospital Epidemiology (2013 Aug. 7 [doi: 10.1086/672271]).
The updates are based on expert opinion in a working group comprised of representatives from the Centers for Disease Control and Prevention (CDC), the National Institutes of Health, the Food and Drug Administration, and the Health Resources and Services Administration, in consultation with a panel of experts, wrote Dr. Kuhar of the CDC and his associates.
The principles of PEP remain the same: Occupational exposures to HIV in health care workers should be considered urgent medical concerns, and should be reported and managed promptly under your institution’s procedures. Determine the HIV status of the patient whose blood or other bodily fluids potentially exposed the health care worker to HIV, if possible, to guide the need for PEP. Start PEP as soon as possible (within hours) after the exposure if PEP is indicated. Expert consultation is recommended, but PEP initiation should not be delayed while waiting for a consult. Close follow-up should start within 72 hours of HIV exposure and include counseling, baseline and follow-up HIV testing, and monitoring for drug toxicity, according to the guidelines.
Clinicians can consult experts locally or can call the National Clinicians’ Post-Exposure Prophylaxis Hotline (PEPline) at 888-448-4911.
The PEPline received approximately 10,000 calls in 2012 from clinicians about potential occupational exposures to HIV, said Dr. Ronald Goldschmidt of the department of family and community medicine at the University of California, San Francisco. He is director of the university’s National HIV/AIDS Clinicians’ Consultation Center, which includes the PEPline. Dr. Goldschmidt was a member of the panel of experts that consulted on the guidelines update.
Several new antiretroviral agents have been approved since the last update to the guidelines in 2005, and more information has become available about the use and side effects of the PEP medications. Clinicians had struggled with the 2005 version’s recommendations to assess the level of risk of HIV transmission in individual exposure incidents, creating problems in deciding whether to use two or three or more drugs in PEP regiments.
The new guidelines’ preferred HIV PEP regimen is oral raltegravir (Isentress) 400 mg twice daily and once-daily Truvada (a fixed-dose combination tablet containing 300 mg of tenofovir and 200 mg of emtricitabine). "Preparation of this PEP regimen in single-dose ‘starter packets,’ which are kept on hand at sites expected to manage occupational exposures to HIV, may facilitate timely initiation of PEP," the guidelines state.
Dr. Goldschmidt cautioned that Truvada should not be used before checking for preexisting renal problems. If there’s a history of renal problems, consult an HIV expert or consider a different regimen, he said.
An appendix to the document lists recommended and contraindicated alternatives.
Although there are no new definitive data showing greater efficacy with three-drug regimens for PEP compared with two-drug regimens for occupational HIV exposures, the new recommendation to use at least three drugs rests on studies showing greater reduction of viral burden in HIV-infected patients on three antiretroviral drugs instead of two, concerns about drug resistance in source patients of occupational exposures, and better safety and tolerability with some of the newer medications. The guidelines add a caveat that two-drug PEP regimens might be considered in consultation with an expert if antiretrovirals aren’t easily available or because of adherence or toxicity issues.
None of the antiretroviral agents have been approved by the Food and Drug Administration for use as PEP.
The previous complicated recommendations to assess a health care worker’s level of risk after a potential exposure to HIV were enshrined in a 2001 version of the guidelines, Dr. Goldschmidt said. The 2005 revision updated the recommended drugs but didn’t simplify the risk assessment. The current update makes decision-making less confusing by recommending at least a three-drug regimen for all occupational PEP cases and using better-tolerated drugs.
"With the simplification at this point, they’re throwing away those old tables that required clinicians to assess risk" and decreased the likelihood that PEP would be administered appropriately and completed, he said.
Separate guidelines have been published previously for management of nonoccupational HIV exposure (sexual, pediatric, or perinatal exposures).
Dr. Kuhar reported having no financial disclosures. Some of his coauthors reported financial associations with Bristol-Myers Squibb, Janssen, and other companies. Dr. Goldschmidt reported having no financial disclosures.
Exposed health care workers and those managing their exposures will now have more PEP options to consider. This offers the benefit of being able to individualize therapy to the individual; however, for providers with less experience in managing HIV exposures, having these options may be more confusing or intimidating. For that reason, expert resources like the HIV PEPline (888-448-4911) will be increasingly important.
These regimens will be more expensive. There aren’t any data to suggest that these three-drug regimens will be more effective in PEP. Here’s why the guideline authors said they made the change:

|
|
"The recommendation for consistent use of three-drug HIV PEP regimens reflects (1) studies demonstrating superior effectiveness of three drugs in reducing viral burden in HIV-infected persons compared with two agents; (2) concerns about source patient drug resistance to agents commonly used for PEP; (3) the safety and tolerability of new HIV drugs, and (4) the potential for improved PEP regimen adherence due to newer medications that are likely to have fewer side effects. Clinicians facing challenges such as antiretroviral medication availability, potential adherence and toxicity issues, and others associated with a three-drug PEP regimen might still consider a two-drug PEP regimen in consultation with an expert."
Any time you use more drugs, there is an opportunity for side effects. While the medications recommended here are generally safe and well tolerated, careful monitoring for side effects will be important for individuals receiving PEP.
In addition their improved tolerability, I think the other rationale for recommending these exact regimens is based on these regimens being less likely to have resistance.
Dr. C. Bradley Hare is medical director of the HIV/AIDS Clinic at San Francisco General Hospital. He has been a consultant or speaker for the following companies that make HIV medications: Gilead, Bristol-Myers Squibb, Janssen Pharmaceuticals, Merck, and AbbVie Pharmaceuticals.
Exposed health care workers and those managing their exposures will now have more PEP options to consider. This offers the benefit of being able to individualize therapy to the individual; however, for providers with less experience in managing HIV exposures, having these options may be more confusing or intimidating. For that reason, expert resources like the HIV PEPline (888-448-4911) will be increasingly important.
These regimens will be more expensive. There aren’t any data to suggest that these three-drug regimens will be more effective in PEP. Here’s why the guideline authors said they made the change:
|
|
|
"The recommendation for consistent use of three-drug HIV PEP regimens reflects (1) studies demonstrating superior effectiveness of three drugs in reducing viral burden in HIV-infected persons compared with two agents; (2) concerns about source patient drug resistance to agents commonly used for PEP; (3) the safety and tolerability of new HIV drugs, and (4) the potential for improved PEP regimen adherence due to newer medications that are likely to have fewer side effects. Clinicians facing challenges such as antiretroviral medication availability, potential adherence and toxicity issues, and others associated with a three-drug PEP regimen might still consider a two-drug PEP regimen in consultation with an expert."
Any time you use more drugs, there is an opportunity for side effects. While the medications recommended here are generally safe and well tolerated, careful monitoring for side effects will be important for individuals receiving PEP.
In addition their improved tolerability, I think the other rationale for recommending these exact regimens is based on these regimens being less likely to have resistance.
Dr. C. Bradley Hare is medical director of the HIV/AIDS Clinic at San Francisco General Hospital. He has been a consultant or speaker for the following companies that make HIV medications: Gilead, Bristol-Myers Squibb, Janssen Pharmaceuticals, Merck, and AbbVie Pharmaceuticals.
Exposed health care workers and those managing their exposures will now have more PEP options to consider. This offers the benefit of being able to individualize therapy to the individual; however, for providers with less experience in managing HIV exposures, having these options may be more confusing or intimidating. For that reason, expert resources like the HIV PEPline (888-448-4911) will be increasingly important.
These regimens will be more expensive. There aren’t any data to suggest that these three-drug regimens will be more effective in PEP. Here’s why the guideline authors said they made the change:
|
|
|
"The recommendation for consistent use of three-drug HIV PEP regimens reflects (1) studies demonstrating superior effectiveness of three drugs in reducing viral burden in HIV-infected persons compared with two agents; (2) concerns about source patient drug resistance to agents commonly used for PEP; (3) the safety and tolerability of new HIV drugs, and (4) the potential for improved PEP regimen adherence due to newer medications that are likely to have fewer side effects. Clinicians facing challenges such as antiretroviral medication availability, potential adherence and toxicity issues, and others associated with a three-drug PEP regimen might still consider a two-drug PEP regimen in consultation with an expert."
Any time you use more drugs, there is an opportunity for side effects. While the medications recommended here are generally safe and well tolerated, careful monitoring for side effects will be important for individuals receiving PEP.
In addition their improved tolerability, I think the other rationale for recommending these exact regimens is based on these regimens being less likely to have resistance.
Dr. C. Bradley Hare is medical director of the HIV/AIDS Clinic at San Francisco General Hospital. He has been a consultant or speaker for the following companies that make HIV medications: Gilead, Bristol-Myers Squibb, Janssen Pharmaceuticals, Merck, and AbbVie Pharmaceuticals.
Revised federal guidelines for managing health care workers who are exposed to HIV recommend using at least three drugs for prophylaxis in all cases instead of assessing a person’s risk to decide on the number of drugs, among other updates to the guidelines.
Changes in the recommended drugs in preferred postexposure prophylaxis (PEP) regimens should make them easier to tolerate than earlier regimens and may increase the proportion of health care workers who are able to complete the 28-day treatment, Dr. David T. Kuhar and his associates said in the new document from the U.S. Public Health Service.
Another change is that follow-up HIV testing in health care workers on PEP can be shortened to 4 months instead of 6 months if a newer fourth-generation combination HIV p24 antigen/HIV antibody test is used, the guidelines state. The document, which updates 2005 guidelines, was published online in the journal Infection Control and Hospital Epidemiology (2013 Aug. 7 [doi: 10.1086/672271]).
The updates are based on expert opinion in a working group comprised of representatives from the Centers for Disease Control and Prevention (CDC), the National Institutes of Health, the Food and Drug Administration, and the Health Resources and Services Administration, in consultation with a panel of experts, wrote Dr. Kuhar of the CDC and his associates.
The principles of PEP remain the same: Occupational exposures to HIV in health care workers should be considered urgent medical concerns, and should be reported and managed promptly under your institution’s procedures. Determine the HIV status of the patient whose blood or other bodily fluids potentially exposed the health care worker to HIV, if possible, to guide the need for PEP. Start PEP as soon as possible (within hours) after the exposure if PEP is indicated. Expert consultation is recommended, but PEP initiation should not be delayed while waiting for a consult. Close follow-up should start within 72 hours of HIV exposure and include counseling, baseline and follow-up HIV testing, and monitoring for drug toxicity, according to the guidelines.
Clinicians can consult experts locally or can call the National Clinicians’ Post-Exposure Prophylaxis Hotline (PEPline) at 888-448-4911.
The PEPline received approximately 10,000 calls in 2012 from clinicians about potential occupational exposures to HIV, said Dr. Ronald Goldschmidt of the department of family and community medicine at the University of California, San Francisco. He is director of the university’s National HIV/AIDS Clinicians’ Consultation Center, which includes the PEPline. Dr. Goldschmidt was a member of the panel of experts that consulted on the guidelines update.
Several new antiretroviral agents have been approved since the last update to the guidelines in 2005, and more information has become available about the use and side effects of the PEP medications. Clinicians had struggled with the 2005 version’s recommendations to assess the level of risk of HIV transmission in individual exposure incidents, creating problems in deciding whether to use two or three or more drugs in PEP regiments.
The new guidelines’ preferred HIV PEP regimen is oral raltegravir (Isentress) 400 mg twice daily and once-daily Truvada (a fixed-dose combination tablet containing 300 mg of tenofovir and 200 mg of emtricitabine). "Preparation of this PEP regimen in single-dose ‘starter packets,’ which are kept on hand at sites expected to manage occupational exposures to HIV, may facilitate timely initiation of PEP," the guidelines state.
Dr. Goldschmidt cautioned that Truvada should not be used before checking for preexisting renal problems. If there’s a history of renal problems, consult an HIV expert or consider a different regimen, he said.
An appendix to the document lists recommended and contraindicated alternatives.
Although there are no new definitive data showing greater efficacy with three-drug regimens for PEP compared with two-drug regimens for occupational HIV exposures, the new recommendation to use at least three drugs rests on studies showing greater reduction of viral burden in HIV-infected patients on three antiretroviral drugs instead of two, concerns about drug resistance in source patients of occupational exposures, and better safety and tolerability with some of the newer medications. The guidelines add a caveat that two-drug PEP regimens might be considered in consultation with an expert if antiretrovirals aren’t easily available or because of adherence or toxicity issues.
None of the antiretroviral agents have been approved by the Food and Drug Administration for use as PEP.
The previous complicated recommendations to assess a health care worker’s level of risk after a potential exposure to HIV were enshrined in a 2001 version of the guidelines, Dr. Goldschmidt said. The 2005 revision updated the recommended drugs but didn’t simplify the risk assessment. The current update makes decision-making less confusing by recommending at least a three-drug regimen for all occupational PEP cases and using better-tolerated drugs.
"With the simplification at this point, they’re throwing away those old tables that required clinicians to assess risk" and decreased the likelihood that PEP would be administered appropriately and completed, he said.
Separate guidelines have been published previously for management of nonoccupational HIV exposure (sexual, pediatric, or perinatal exposures).
Dr. Kuhar reported having no financial disclosures. Some of his coauthors reported financial associations with Bristol-Myers Squibb, Janssen, and other companies. Dr. Goldschmidt reported having no financial disclosures.
Revised federal guidelines for managing health care workers who are exposed to HIV recommend using at least three drugs for prophylaxis in all cases instead of assessing a person’s risk to decide on the number of drugs, among other updates to the guidelines.
Changes in the recommended drugs in preferred postexposure prophylaxis (PEP) regimens should make them easier to tolerate than earlier regimens and may increase the proportion of health care workers who are able to complete the 28-day treatment, Dr. David T. Kuhar and his associates said in the new document from the U.S. Public Health Service.
Another change is that follow-up HIV testing in health care workers on PEP can be shortened to 4 months instead of 6 months if a newer fourth-generation combination HIV p24 antigen/HIV antibody test is used, the guidelines state. The document, which updates 2005 guidelines, was published online in the journal Infection Control and Hospital Epidemiology (2013 Aug. 7 [doi: 10.1086/672271]).
The updates are based on expert opinion in a working group comprised of representatives from the Centers for Disease Control and Prevention (CDC), the National Institutes of Health, the Food and Drug Administration, and the Health Resources and Services Administration, in consultation with a panel of experts, wrote Dr. Kuhar of the CDC and his associates.
The principles of PEP remain the same: Occupational exposures to HIV in health care workers should be considered urgent medical concerns, and should be reported and managed promptly under your institution’s procedures. Determine the HIV status of the patient whose blood or other bodily fluids potentially exposed the health care worker to HIV, if possible, to guide the need for PEP. Start PEP as soon as possible (within hours) after the exposure if PEP is indicated. Expert consultation is recommended, but PEP initiation should not be delayed while waiting for a consult. Close follow-up should start within 72 hours of HIV exposure and include counseling, baseline and follow-up HIV testing, and monitoring for drug toxicity, according to the guidelines.
Clinicians can consult experts locally or can call the National Clinicians’ Post-Exposure Prophylaxis Hotline (PEPline) at 888-448-4911.
The PEPline received approximately 10,000 calls in 2012 from clinicians about potential occupational exposures to HIV, said Dr. Ronald Goldschmidt of the department of family and community medicine at the University of California, San Francisco. He is director of the university’s National HIV/AIDS Clinicians’ Consultation Center, which includes the PEPline. Dr. Goldschmidt was a member of the panel of experts that consulted on the guidelines update.
Several new antiretroviral agents have been approved since the last update to the guidelines in 2005, and more information has become available about the use and side effects of the PEP medications. Clinicians had struggled with the 2005 version’s recommendations to assess the level of risk of HIV transmission in individual exposure incidents, creating problems in deciding whether to use two or three or more drugs in PEP regiments.
The new guidelines’ preferred HIV PEP regimen is oral raltegravir (Isentress) 400 mg twice daily and once-daily Truvada (a fixed-dose combination tablet containing 300 mg of tenofovir and 200 mg of emtricitabine). "Preparation of this PEP regimen in single-dose ‘starter packets,’ which are kept on hand at sites expected to manage occupational exposures to HIV, may facilitate timely initiation of PEP," the guidelines state.
Dr. Goldschmidt cautioned that Truvada should not be used before checking for preexisting renal problems. If there’s a history of renal problems, consult an HIV expert or consider a different regimen, he said.
An appendix to the document lists recommended and contraindicated alternatives.
Although there are no new definitive data showing greater efficacy with three-drug regimens for PEP compared with two-drug regimens for occupational HIV exposures, the new recommendation to use at least three drugs rests on studies showing greater reduction of viral burden in HIV-infected patients on three antiretroviral drugs instead of two, concerns about drug resistance in source patients of occupational exposures, and better safety and tolerability with some of the newer medications. The guidelines add a caveat that two-drug PEP regimens might be considered in consultation with an expert if antiretrovirals aren’t easily available or because of adherence or toxicity issues.
None of the antiretroviral agents have been approved by the Food and Drug Administration for use as PEP.
The previous complicated recommendations to assess a health care worker’s level of risk after a potential exposure to HIV were enshrined in a 2001 version of the guidelines, Dr. Goldschmidt said. The 2005 revision updated the recommended drugs but didn’t simplify the risk assessment. The current update makes decision-making less confusing by recommending at least a three-drug regimen for all occupational PEP cases and using better-tolerated drugs.
"With the simplification at this point, they’re throwing away those old tables that required clinicians to assess risk" and decreased the likelihood that PEP would be administered appropriately and completed, he said.
Separate guidelines have been published previously for management of nonoccupational HIV exposure (sexual, pediatric, or perinatal exposures).
Dr. Kuhar reported having no financial disclosures. Some of his coauthors reported financial associations with Bristol-Myers Squibb, Janssen, and other companies. Dr. Goldschmidt reported having no financial disclosures.
FROM INFECTION CONTROL AND HOSPITAL EPIDEMIOLOGY
Major finding: All PEP regimens for health care workers should include at least three drugs from a new list of easier-to-tolerate regimens, and follow-up HIV testing can be shortened to 4 months if a newer fourth-generation combination HIV p24 antigen/HIV antibody test is used.
Data source: Updated guidelines by the U.S. Public Health Service, based on expert opinion.
Disclosures: Dr. Kuhar reported having no financial disclosures. Some of his coauthors reported financial associations with Bristol-Myers Squibb, Janssen, and other companies. Dr. Goldschmidt reported having no financial disclosures.

High BMI appears to cause gallstones
An elevated body mass index is not just associated with symptomatic gallstone disease, it appears to cause the disease, according to a report published in Hepatology (doi:10.1002/hep.26563).
Many epidemiologic and observational studies have noted a clear association between a high BMI and an increased risk for gallstones, but have not been able to pin down a causal effect. It was impossible to rule out confounding by some other factor, such as a high-fat diet, that simultaneously caused both the elevation in BMI and the elevation in risk for gallstones. Similarly, it was impossible to rule out reverse causation, such as the colicky pain of gallstone disease caused the physical inactivity that then led to a high BMI.

A new epidemiologic statistical approach known as Mendelian randomization is thought to avert both confounding and reverse causation by pinpointing the genetic variants that are linked to a high BMI (which are a constant throughout the lifespan) but that are not related to confounding factors, then determining whether they are also linked to gallstone disease. "If raised BMI truly is a causal factor in the development of gallstone disease, genetic variants that increase BMI would be expected to also increase risk of gallstone disease," said Dr. Stefan Stender of the department of clinical biochemistry, Rigshospitalet, University of Copenhagen, and his associates.
They studied 77,679 Danish adults from the general population who participated in two large prospective studies: the Copenhagen General Population Study (67,314 subjects) and the Copenhagen City Heart Study (10,365 subjects). All the participants had donated blood samples that could be used for DNA extraction and genotyping.
A total of 4,106 of these subjects developed symptomatic gallstone disease during follow-up of up to 34 years.
The researchers used genotyping to identify study subjects who carried any of the three polymorphisms that have the largest known effect sizes for association with BMI in European populations: FTO (rs9939609), MC4R (rs17782313), or TMEM18 (rs6548238). Each of these can be carried on two possible alleles, so any given subject could carry one to six affected alleles. The number of BMI-increasing alleles, from one to six, was determined for each study subject.
In an initial analysis of the data, the mean baseline BMI was 55% higher (11 kg/m2) in subjects carrying the most alleles compared with those carrying the fewest.
Increasing BMI was associated with a stepwise increase in the risk of developing symptomatic gallstone disease.
In the overall cohort, the risk of symptomatic gallstone disease was increased 7% for every 1-kg/m2 increase in BMI. In the Mendelian randomization cohort, the risk of gallstone disease increased 17% with every 1-kg/m2 increase in BMI. The concordance between these two estimates indicates that BMI itself is a causal risk factor for symptomatic gallstone disease, Dr. Stender and his associates said.
This study did not include data on gallstone composition and was not designed to examine the pathophysiologic mechanisms by which a high BMI causes gallstone formation. However, numerous other studies have proposed several possible mechanisms, they noted.
Obesity may raise cholesterol synthesis and hepatobiliary cholesterol efflux, "a key event in the development of cholesterol gallstones." High abdominal fat mass may induce gallbladder hypomotility and bile stasis, "another risk factor for gallstone formation."
In addition, substances secreted by or metabolized by adipocytes could influence gallstone formation. For example, estrogen is produced by adipocytes and may promote gallstone formation by raising the rate of hepatobiliary cholesterol efflux. And leptin, which is also secreted by adipocytes, may have lithogenic effects.
Adinopectin, another hormone secreted by adipocytes, has been linked to gallstones in both animal and human studies. And obesity-associated hyperinsulinemia may induce gallstone formation by causing the secretion of more lithogenic bile.
This study was limited in that it included only white people of Danish descent. "Because ethnic differences in gallstone prevalence are well known, the results reported here may not necessarily translate to other ethnicities," Dr. Stender and his colleagues said.
This study was supported by the Danish Medical Research Council, the Rigshospitalet at Copenhagen University, and the Odd Fellow Order. No financial conflicts of interest were reported.
An elevated body mass index is not just associated with symptomatic gallstone disease, it appears to cause the disease, according to a report published in Hepatology (doi:10.1002/hep.26563).
Many epidemiologic and observational studies have noted a clear association between a high BMI and an increased risk for gallstones, but have not been able to pin down a causal effect. It was impossible to rule out confounding by some other factor, such as a high-fat diet, that simultaneously caused both the elevation in BMI and the elevation in risk for gallstones. Similarly, it was impossible to rule out reverse causation, such as the colicky pain of gallstone disease caused the physical inactivity that then led to a high BMI.
A new epidemiologic statistical approach known as Mendelian randomization is thought to avert both confounding and reverse causation by pinpointing the genetic variants that are linked to a high BMI (which are a constant throughout the lifespan) but that are not related to confounding factors, then determining whether they are also linked to gallstone disease. "If raised BMI truly is a causal factor in the development of gallstone disease, genetic variants that increase BMI would be expected to also increase risk of gallstone disease," said Dr. Stefan Stender of the department of clinical biochemistry, Rigshospitalet, University of Copenhagen, and his associates.
They studied 77,679 Danish adults from the general population who participated in two large prospective studies: the Copenhagen General Population Study (67,314 subjects) and the Copenhagen City Heart Study (10,365 subjects). All the participants had donated blood samples that could be used for DNA extraction and genotyping.
A total of 4,106 of these subjects developed symptomatic gallstone disease during follow-up of up to 34 years.
The researchers used genotyping to identify study subjects who carried any of the three polymorphisms that have the largest known effect sizes for association with BMI in European populations: FTO (rs9939609), MC4R (rs17782313), or TMEM18 (rs6548238). Each of these can be carried on two possible alleles, so any given subject could carry one to six affected alleles. The number of BMI-increasing alleles, from one to six, was determined for each study subject.
In an initial analysis of the data, the mean baseline BMI was 55% higher (11 kg/m2) in subjects carrying the most alleles compared with those carrying the fewest.
Increasing BMI was associated with a stepwise increase in the risk of developing symptomatic gallstone disease.
In the overall cohort, the risk of symptomatic gallstone disease was increased 7% for every 1-kg/m2 increase in BMI. In the Mendelian randomization cohort, the risk of gallstone disease increased 17% with every 1-kg/m2 increase in BMI. The concordance between these two estimates indicates that BMI itself is a causal risk factor for symptomatic gallstone disease, Dr. Stender and his associates said.
This study did not include data on gallstone composition and was not designed to examine the pathophysiologic mechanisms by which a high BMI causes gallstone formation. However, numerous other studies have proposed several possible mechanisms, they noted.
Obesity may raise cholesterol synthesis and hepatobiliary cholesterol efflux, "a key event in the development of cholesterol gallstones." High abdominal fat mass may induce gallbladder hypomotility and bile stasis, "another risk factor for gallstone formation."
In addition, substances secreted by or metabolized by adipocytes could influence gallstone formation. For example, estrogen is produced by adipocytes and may promote gallstone formation by raising the rate of hepatobiliary cholesterol efflux. And leptin, which is also secreted by adipocytes, may have lithogenic effects.
Adinopectin, another hormone secreted by adipocytes, has been linked to gallstones in both animal and human studies. And obesity-associated hyperinsulinemia may induce gallstone formation by causing the secretion of more lithogenic bile.
This study was limited in that it included only white people of Danish descent. "Because ethnic differences in gallstone prevalence are well known, the results reported here may not necessarily translate to other ethnicities," Dr. Stender and his colleagues said.
This study was supported by the Danish Medical Research Council, the Rigshospitalet at Copenhagen University, and the Odd Fellow Order. No financial conflicts of interest were reported.
An elevated body mass index is not just associated with symptomatic gallstone disease, it appears to cause the disease, according to a report published in Hepatology (doi:10.1002/hep.26563).
Many epidemiologic and observational studies have noted a clear association between a high BMI and an increased risk for gallstones, but have not been able to pin down a causal effect. It was impossible to rule out confounding by some other factor, such as a high-fat diet, that simultaneously caused both the elevation in BMI and the elevation in risk for gallstones. Similarly, it was impossible to rule out reverse causation, such as the colicky pain of gallstone disease caused the physical inactivity that then led to a high BMI.
A new epidemiologic statistical approach known as Mendelian randomization is thought to avert both confounding and reverse causation by pinpointing the genetic variants that are linked to a high BMI (which are a constant throughout the lifespan) but that are not related to confounding factors, then determining whether they are also linked to gallstone disease. "If raised BMI truly is a causal factor in the development of gallstone disease, genetic variants that increase BMI would be expected to also increase risk of gallstone disease," said Dr. Stefan Stender of the department of clinical biochemistry, Rigshospitalet, University of Copenhagen, and his associates.
They studied 77,679 Danish adults from the general population who participated in two large prospective studies: the Copenhagen General Population Study (67,314 subjects) and the Copenhagen City Heart Study (10,365 subjects). All the participants had donated blood samples that could be used for DNA extraction and genotyping.
A total of 4,106 of these subjects developed symptomatic gallstone disease during follow-up of up to 34 years.
The researchers used genotyping to identify study subjects who carried any of the three polymorphisms that have the largest known effect sizes for association with BMI in European populations: FTO (rs9939609), MC4R (rs17782313), or TMEM18 (rs6548238). Each of these can be carried on two possible alleles, so any given subject could carry one to six affected alleles. The number of BMI-increasing alleles, from one to six, was determined for each study subject.
In an initial analysis of the data, the mean baseline BMI was 55% higher (11 kg/m2) in subjects carrying the most alleles compared with those carrying the fewest.
Increasing BMI was associated with a stepwise increase in the risk of developing symptomatic gallstone disease.
In the overall cohort, the risk of symptomatic gallstone disease was increased 7% for every 1-kg/m2 increase in BMI. In the Mendelian randomization cohort, the risk of gallstone disease increased 17% with every 1-kg/m2 increase in BMI. The concordance between these two estimates indicates that BMI itself is a causal risk factor for symptomatic gallstone disease, Dr. Stender and his associates said.
This study did not include data on gallstone composition and was not designed to examine the pathophysiologic mechanisms by which a high BMI causes gallstone formation. However, numerous other studies have proposed several possible mechanisms, they noted.
Obesity may raise cholesterol synthesis and hepatobiliary cholesterol efflux, "a key event in the development of cholesterol gallstones." High abdominal fat mass may induce gallbladder hypomotility and bile stasis, "another risk factor for gallstone formation."
In addition, substances secreted by or metabolized by adipocytes could influence gallstone formation. For example, estrogen is produced by adipocytes and may promote gallstone formation by raising the rate of hepatobiliary cholesterol efflux. And leptin, which is also secreted by adipocytes, may have lithogenic effects.
Adinopectin, another hormone secreted by adipocytes, has been linked to gallstones in both animal and human studies. And obesity-associated hyperinsulinemia may induce gallstone formation by causing the secretion of more lithogenic bile.
This study was limited in that it included only white people of Danish descent. "Because ethnic differences in gallstone prevalence are well known, the results reported here may not necessarily translate to other ethnicities," Dr. Stender and his colleagues said.
This study was supported by the Danish Medical Research Council, the Rigshospitalet at Copenhagen University, and the Odd Fellow Order. No financial conflicts of interest were reported.
FROM HEPATOLOGY
Major finding: In the overall cohort, the risk of symptomatic gallstone disease was increased 7% for every 1-kg/m2 increase in BMI, and in the Mendelian randomization cohort, the risk of gallstone disease increased 17% with every 1-kg/m2 increase in BMI.
Data source: A Mendelian randomization study involving 77,679 adults from the Danish general population who were genotyped to identify carriers of three BMI-increasing polymorphisms and who were followed for up to 34 years for the development of symptomatic gallstone disease.
Disclosures: This study was supported by the Danish Medical Research Council, the Rigshospitalet at Copenhagen University, and the Odd Fellow Order. No financial conflicts of interest were reported.

Low-dose perioperative steroids effective in IBD patients
Postoperative postural hypotension or adrenal insufficiency in patients with inflammatory bowel disease can be effectively prevented with low-dose rather than high-dose steroids, according to data published in the June 14 online issue of Annals of Surgery [doi: 10.1097/SLA.b013e318297adca].
"Corticosteroid-treated patients undergoing major colorectal surgery are commonly prescribed high-dose steroids to prevent perioperative adrenal insufficiency and cardiovascular collapse," wrote Dr. Karen Zaghiyan and her colleagues from Cedars-Sinai Medical Center, Los Angeles. "There is little evidence to support this practice."
A randomized, single-blinded noninferiority trial in 92 steroid-treated inflammatory bowel disease (IBD) patients undergoing major colorectal surgery showed that 96% of patients randomized to low-dose steroids and 95% of patients randomized to high-dose steroids did not exhibit postural hypotension on the first day after surgery (noninferiority 95% confidence interval, –0.08 to 0.09; P = .007).
"Because reports of postoperative adrenal insufficiency and hemodynamic collapse have implicated the first 24 hours after surgery as the most susceptible, and postural hypotension is likely to be a more reliable indicator of hemodynamic instability than supine hypotension, our primary endpoint was clinically meaningful," the researchers reported.
Patients were randomized to receive either 100 mg of IV hydrocortisone at the time of incision and three times daily for the first postoperative day, then tapered, or to low-dose IV hydrocortisone equivalent to presurgical oral dosing, followed by taper.
The primary outcome was the absence of postural hypotension on postoperative day 1, defined as a decrease in systolic blood pressure by 20 mm Hg after sitting from a supine position.
"We found no significant difference in perioperative factors, including operative time, intraoperative blood loss, volume of intravenous fluids administered, number of patients requiring intravenous fluid boluses, or blood transfusions between our two patient groups," the researchers reported.
The investigators also found no significant differences in other outcomes such as surgical or medical complications, length of postoperative stay, fatigue, nausea, and pain, although there was an insignificant trend toward more infectious complications in the high-dose steroid group.
The practice of administering high doses of corticosteroids perioperatively was sparked in the 1950s by two incidences of postoperative cardiovascular collapse and death in patients whose preoperative corticosteroids were discontinued before surgery, the authors said.
"However, high-dose corticosteroids are not without consequence and have been associated with various postoperative complications, including wound infection and anastomotic dehiscence," the authors reported.
Some studies had already suggested that steroid-treated patients undergoing surgery could remain on their baseline corticosteroid dose perioperatively; however, these studies were mostly focused on organ transplant recipients or included patients taking low maintenance doses of corticosteroids undergoing minor or moderate surgical procedures.
"Patients with IBD represent a unique study cohort because they are frequently taking high doses of steroids for a prolonged period of time, and surgery in these patients often involves major stress," the researchers reported.
"Although we recently published our retrospective data to suggest safety of low-dose steroids in steroid-treated IBD patients undergoing major colorectal surgery, this is the first prospective study to evaluate the role of stress-dose steroids in patients undergoing major abdominal and pelvic surgery," the investigators wrote.
There were no conflicts of interest declared.
Postoperative postural hypotension or adrenal insufficiency in patients with inflammatory bowel disease can be effectively prevented with low-dose rather than high-dose steroids, according to data published in the June 14 online issue of Annals of Surgery [doi: 10.1097/SLA.b013e318297adca].
"Corticosteroid-treated patients undergoing major colorectal surgery are commonly prescribed high-dose steroids to prevent perioperative adrenal insufficiency and cardiovascular collapse," wrote Dr. Karen Zaghiyan and her colleagues from Cedars-Sinai Medical Center, Los Angeles. "There is little evidence to support this practice."
A randomized, single-blinded noninferiority trial in 92 steroid-treated inflammatory bowel disease (IBD) patients undergoing major colorectal surgery showed that 96% of patients randomized to low-dose steroids and 95% of patients randomized to high-dose steroids did not exhibit postural hypotension on the first day after surgery (noninferiority 95% confidence interval, –0.08 to 0.09; P = .007).
"Because reports of postoperative adrenal insufficiency and hemodynamic collapse have implicated the first 24 hours after surgery as the most susceptible, and postural hypotension is likely to be a more reliable indicator of hemodynamic instability than supine hypotension, our primary endpoint was clinically meaningful," the researchers reported.
Patients were randomized to receive either 100 mg of IV hydrocortisone at the time of incision and three times daily for the first postoperative day, then tapered, or to low-dose IV hydrocortisone equivalent to presurgical oral dosing, followed by taper.
The primary outcome was the absence of postural hypotension on postoperative day 1, defined as a decrease in systolic blood pressure by 20 mm Hg after sitting from a supine position.
"We found no significant difference in perioperative factors, including operative time, intraoperative blood loss, volume of intravenous fluids administered, number of patients requiring intravenous fluid boluses, or blood transfusions between our two patient groups," the researchers reported.
The investigators also found no significant differences in other outcomes such as surgical or medical complications, length of postoperative stay, fatigue, nausea, and pain, although there was an insignificant trend toward more infectious complications in the high-dose steroid group.
The practice of administering high doses of corticosteroids perioperatively was sparked in the 1950s by two incidences of postoperative cardiovascular collapse and death in patients whose preoperative corticosteroids were discontinued before surgery, the authors said.
"However, high-dose corticosteroids are not without consequence and have been associated with various postoperative complications, including wound infection and anastomotic dehiscence," the authors reported.
Some studies had already suggested that steroid-treated patients undergoing surgery could remain on their baseline corticosteroid dose perioperatively; however, these studies were mostly focused on organ transplant recipients or included patients taking low maintenance doses of corticosteroids undergoing minor or moderate surgical procedures.
"Patients with IBD represent a unique study cohort because they are frequently taking high doses of steroids for a prolonged period of time, and surgery in these patients often involves major stress," the researchers reported.
"Although we recently published our retrospective data to suggest safety of low-dose steroids in steroid-treated IBD patients undergoing major colorectal surgery, this is the first prospective study to evaluate the role of stress-dose steroids in patients undergoing major abdominal and pelvic surgery," the investigators wrote.
There were no conflicts of interest declared.
Postoperative postural hypotension or adrenal insufficiency in patients with inflammatory bowel disease can be effectively prevented with low-dose rather than high-dose steroids, according to data published in the June 14 online issue of Annals of Surgery [doi: 10.1097/SLA.b013e318297adca].
"Corticosteroid-treated patients undergoing major colorectal surgery are commonly prescribed high-dose steroids to prevent perioperative adrenal insufficiency and cardiovascular collapse," wrote Dr. Karen Zaghiyan and her colleagues from Cedars-Sinai Medical Center, Los Angeles. "There is little evidence to support this practice."
A randomized, single-blinded noninferiority trial in 92 steroid-treated inflammatory bowel disease (IBD) patients undergoing major colorectal surgery showed that 96% of patients randomized to low-dose steroids and 95% of patients randomized to high-dose steroids did not exhibit postural hypotension on the first day after surgery (noninferiority 95% confidence interval, –0.08 to 0.09; P = .007).
"Because reports of postoperative adrenal insufficiency and hemodynamic collapse have implicated the first 24 hours after surgery as the most susceptible, and postural hypotension is likely to be a more reliable indicator of hemodynamic instability than supine hypotension, our primary endpoint was clinically meaningful," the researchers reported.
Patients were randomized to receive either 100 mg of IV hydrocortisone at the time of incision and three times daily for the first postoperative day, then tapered, or to low-dose IV hydrocortisone equivalent to presurgical oral dosing, followed by taper.
The primary outcome was the absence of postural hypotension on postoperative day 1, defined as a decrease in systolic blood pressure by 20 mm Hg after sitting from a supine position.
"We found no significant difference in perioperative factors, including operative time, intraoperative blood loss, volume of intravenous fluids administered, number of patients requiring intravenous fluid boluses, or blood transfusions between our two patient groups," the researchers reported.
The investigators also found no significant differences in other outcomes such as surgical or medical complications, length of postoperative stay, fatigue, nausea, and pain, although there was an insignificant trend toward more infectious complications in the high-dose steroid group.
The practice of administering high doses of corticosteroids perioperatively was sparked in the 1950s by two incidences of postoperative cardiovascular collapse and death in patients whose preoperative corticosteroids were discontinued before surgery, the authors said.
"However, high-dose corticosteroids are not without consequence and have been associated with various postoperative complications, including wound infection and anastomotic dehiscence," the authors reported.
Some studies had already suggested that steroid-treated patients undergoing surgery could remain on their baseline corticosteroid dose perioperatively; however, these studies were mostly focused on organ transplant recipients or included patients taking low maintenance doses of corticosteroids undergoing minor or moderate surgical procedures.
"Patients with IBD represent a unique study cohort because they are frequently taking high doses of steroids for a prolonged period of time, and surgery in these patients often involves major stress," the researchers reported.
"Although we recently published our retrospective data to suggest safety of low-dose steroids in steroid-treated IBD patients undergoing major colorectal surgery, this is the first prospective study to evaluate the role of stress-dose steroids in patients undergoing major abdominal and pelvic surgery," the investigators wrote.
There were no conflicts of interest declared.
FROM ANNALS OF SURGERY
Major finding: Low-dose corticosteroids are as effective as high dose in preventing postoperative postural hypotension or adrenal insufficiency in patients with inflammatory bowel disease.
Data source: Randomized, single-blinded noninferiority trial in 92 patients.
Disclosures: No conflicts of interest were declared.
More hospitals providing palliative care
The prevalence of palliative care programs in U.S. hospitals is expected to reach 84% by 2014, according to an analysis from the Center to Advance Palliative Care.
From 2000 to 2011, the number of hospitals with 50 or more beds that had a palliative care program went from 658 to 1,692, an increase of 157%. If that trend continues, there should be 2,023 hospitals – approximately 84% – providing palliative care in the United States by 2014, the CAPC reported.
The CAPC analysis, conducted in January 2013, involved data from the American Hospital Association and the center’s own National Palliative Care Registry.
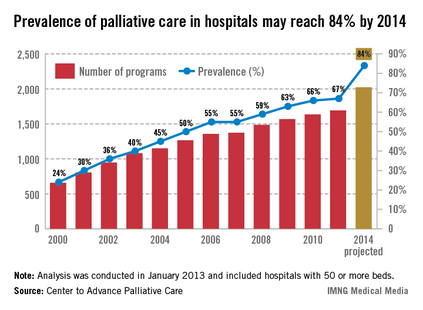
The prevalence of palliative care programs in U.S. hospitals is expected to reach 84% by 2014, according to an analysis from the Center to Advance Palliative Care.
From 2000 to 2011, the number of hospitals with 50 or more beds that had a palliative care program went from 658 to 1,692, an increase of 157%. If that trend continues, there should be 2,023 hospitals – approximately 84% – providing palliative care in the United States by 2014, the CAPC reported.
The CAPC analysis, conducted in January 2013, involved data from the American Hospital Association and the center’s own National Palliative Care Registry.
The prevalence of palliative care programs in U.S. hospitals is expected to reach 84% by 2014, according to an analysis from the Center to Advance Palliative Care.
From 2000 to 2011, the number of hospitals with 50 or more beds that had a palliative care program went from 658 to 1,692, an increase of 157%. If that trend continues, there should be 2,023 hospitals – approximately 84% – providing palliative care in the United States by 2014, the CAPC reported.
The CAPC analysis, conducted in January 2013, involved data from the American Hospital Association and the center’s own National Palliative Care Registry.
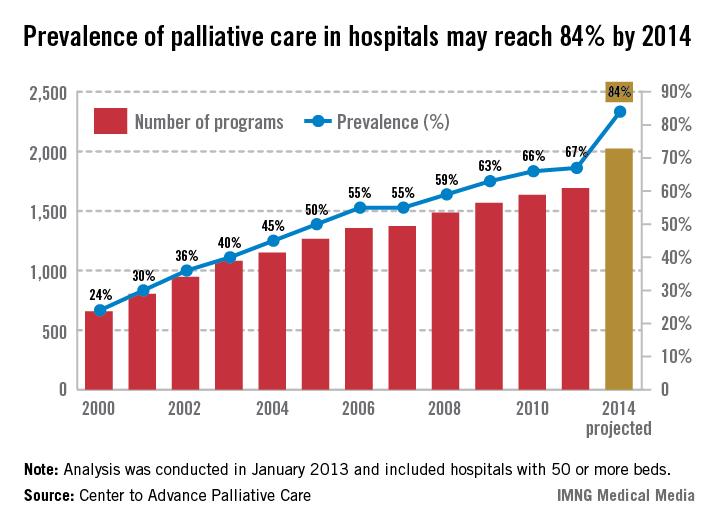
Postop pneumonia risk strong for subset of thoracic surgery patients
SAN DIEGO – For thoracic surgery patients, being on neoadjuvant chemotherapy, having chronic obstructive pulmonary disease, and a weight loss of greater than 10% were all associated with the development of postoperative pneumonia, results from a single-center study showed.
At the national conference of the American College of Surgeons/National Surgical Quality Improvement Program, Dr. Elisabeth Dexter noted that after the first ACS/NSQIP data harvest at the Roswell Park Cancer Institute in Buffalo, N.Y., the risk of postoperative pneumonia was found to be 4.4%, compared with a rate of 1.1% in all other NSQIP hospitals.
"Of particular note, the thoracic surgery service had a high incidence of 13.2%," said Dr. Dexter, an attending surgeon in the department of thoracic surgery at the Institute. "The high incidence of our postoperative pneumonia was likely [affected] by our thoracic surgery service because our thoracic surgery service had an increased percentage of the abstracted NSQIP data in our cohort, from 12% to 14%, compared with other NSQIP hospitals of similar academic size abstracting 2%. When we found this high postoperative pneumonia rate, we decided to query our NSQIP data and our tumor registry between July 1, 2011, and Oct. 8, 2012, to ask the question: Is there an increased incidence of postoperative pneumonia in thoracic surgery patients who received neoadjuvant chemotherapy compared with those who did not?"

Dr. Dexter and her associates cross-referenced ACS/NSQIP data on 1,723 patients at the cancer center with the tumor registry. Of the 1,723 patients, 1,645 had no postoperative pneumonia while 78 did. Compared with the non-pneumonia patients, those who had pneumonia tended to be older (a mean of 67 vs. 60 years, respectively; odds ratio, 1.05; P less than .001), more likely to be male (59% vs. 37%; OR, 2.48; P less than .001), have chronic obstructive pulmonary disease (35% vs. 9%; OR, 5.08; P less than .001), be a smoker (36% vs. 24%; OR, 1.75; P = .021), and had lost more than 10% of body weight (10% vs. 2.5%; OR, 4.47; P less than .001).
On univariate analysis, postoperative pneumonia was associated with being on neoadjuvant chemotherapy (4.2% vs. 14%; OR, 3.75; P less than .001).
In addition, certain surgical subspecialties at the Institute had a high incidence of postoperative pneumonia, including thoracic surgery (46%), GI surgery (21%), and gynecology (12%).
When the researchers included the entire cohort of patients, those who were on neoadjuvant therapy had an increased incidence of postoperative pneumonia, compared with those who were not on neoadjuvant chemotherapy (P = .001). When thoracic surgery patients were excluded from the analysis, non-thoracic surgery patients who were on neoadjuvant chemotherapy had no increased incidence of postoperative pneumonia, compared with the patients who were not on neoadjuvant chemotherapy (P = .681). On multivariate analysis, significant variables associated with postoperative pneumonia were being on neoadjuvant chemotherapy (P= .001), having chronic obstructive pulmonary disease (P less than .0001), and having weight loss of greater than 10% (P = .004).
"Institutions with disproportionately busy complex thoracic surgery programs may have rates of postoperative pneumonia skewed higher than predicted by NSQIP models," Dr. Dexter concluded. "Optimization of nutritional status and COPD treatment in neoadjuvant chemotherapy patients may reduce postoperative pneumonia risk and incidence. Balance of oncologic benefit of neoadjuvant chemotherapy versus risk and morbidity of postoperative chemotherapy warrants future study in thoracic surgery patients."
Dr. Dexter said that she had no relevant financial conflicts to make.
SAN DIEGO – For thoracic surgery patients, being on neoadjuvant chemotherapy, having chronic obstructive pulmonary disease, and a weight loss of greater than 10% were all associated with the development of postoperative pneumonia, results from a single-center study showed.
At the national conference of the American College of Surgeons/National Surgical Quality Improvement Program, Dr. Elisabeth Dexter noted that after the first ACS/NSQIP data harvest at the Roswell Park Cancer Institute in Buffalo, N.Y., the risk of postoperative pneumonia was found to be 4.4%, compared with a rate of 1.1% in all other NSQIP hospitals.
"Of particular note, the thoracic surgery service had a high incidence of 13.2%," said Dr. Dexter, an attending surgeon in the department of thoracic surgery at the Institute. "The high incidence of our postoperative pneumonia was likely [affected] by our thoracic surgery service because our thoracic surgery service had an increased percentage of the abstracted NSQIP data in our cohort, from 12% to 14%, compared with other NSQIP hospitals of similar academic size abstracting 2%. When we found this high postoperative pneumonia rate, we decided to query our NSQIP data and our tumor registry between July 1, 2011, and Oct. 8, 2012, to ask the question: Is there an increased incidence of postoperative pneumonia in thoracic surgery patients who received neoadjuvant chemotherapy compared with those who did not?"
Dr. Dexter and her associates cross-referenced ACS/NSQIP data on 1,723 patients at the cancer center with the tumor registry. Of the 1,723 patients, 1,645 had no postoperative pneumonia while 78 did. Compared with the non-pneumonia patients, those who had pneumonia tended to be older (a mean of 67 vs. 60 years, respectively; odds ratio, 1.05; P less than .001), more likely to be male (59% vs. 37%; OR, 2.48; P less than .001), have chronic obstructive pulmonary disease (35% vs. 9%; OR, 5.08; P less than .001), be a smoker (36% vs. 24%; OR, 1.75; P = .021), and had lost more than 10% of body weight (10% vs. 2.5%; OR, 4.47; P less than .001).
On univariate analysis, postoperative pneumonia was associated with being on neoadjuvant chemotherapy (4.2% vs. 14%; OR, 3.75; P less than .001).
In addition, certain surgical subspecialties at the Institute had a high incidence of postoperative pneumonia, including thoracic surgery (46%), GI surgery (21%), and gynecology (12%).
When the researchers included the entire cohort of patients, those who were on neoadjuvant therapy had an increased incidence of postoperative pneumonia, compared with those who were not on neoadjuvant chemotherapy (P = .001). When thoracic surgery patients were excluded from the analysis, non-thoracic surgery patients who were on neoadjuvant chemotherapy had no increased incidence of postoperative pneumonia, compared with the patients who were not on neoadjuvant chemotherapy (P = .681). On multivariate analysis, significant variables associated with postoperative pneumonia were being on neoadjuvant chemotherapy (P= .001), having chronic obstructive pulmonary disease (P less than .0001), and having weight loss of greater than 10% (P = .004).
"Institutions with disproportionately busy complex thoracic surgery programs may have rates of postoperative pneumonia skewed higher than predicted by NSQIP models," Dr. Dexter concluded. "Optimization of nutritional status and COPD treatment in neoadjuvant chemotherapy patients may reduce postoperative pneumonia risk and incidence. Balance of oncologic benefit of neoadjuvant chemotherapy versus risk and morbidity of postoperative chemotherapy warrants future study in thoracic surgery patients."
Dr. Dexter said that she had no relevant financial conflicts to make.
SAN DIEGO – For thoracic surgery patients, being on neoadjuvant chemotherapy, having chronic obstructive pulmonary disease, and a weight loss of greater than 10% were all associated with the development of postoperative pneumonia, results from a single-center study showed.
At the national conference of the American College of Surgeons/National Surgical Quality Improvement Program, Dr. Elisabeth Dexter noted that after the first ACS/NSQIP data harvest at the Roswell Park Cancer Institute in Buffalo, N.Y., the risk of postoperative pneumonia was found to be 4.4%, compared with a rate of 1.1% in all other NSQIP hospitals.
"Of particular note, the thoracic surgery service had a high incidence of 13.2%," said Dr. Dexter, an attending surgeon in the department of thoracic surgery at the Institute. "The high incidence of our postoperative pneumonia was likely [affected] by our thoracic surgery service because our thoracic surgery service had an increased percentage of the abstracted NSQIP data in our cohort, from 12% to 14%, compared with other NSQIP hospitals of similar academic size abstracting 2%. When we found this high postoperative pneumonia rate, we decided to query our NSQIP data and our tumor registry between July 1, 2011, and Oct. 8, 2012, to ask the question: Is there an increased incidence of postoperative pneumonia in thoracic surgery patients who received neoadjuvant chemotherapy compared with those who did not?"
Dr. Dexter and her associates cross-referenced ACS/NSQIP data on 1,723 patients at the cancer center with the tumor registry. Of the 1,723 patients, 1,645 had no postoperative pneumonia while 78 did. Compared with the non-pneumonia patients, those who had pneumonia tended to be older (a mean of 67 vs. 60 years, respectively; odds ratio, 1.05; P less than .001), more likely to be male (59% vs. 37%; OR, 2.48; P less than .001), have chronic obstructive pulmonary disease (35% vs. 9%; OR, 5.08; P less than .001), be a smoker (36% vs. 24%; OR, 1.75; P = .021), and had lost more than 10% of body weight (10% vs. 2.5%; OR, 4.47; P less than .001).
On univariate analysis, postoperative pneumonia was associated with being on neoadjuvant chemotherapy (4.2% vs. 14%; OR, 3.75; P less than .001).
In addition, certain surgical subspecialties at the Institute had a high incidence of postoperative pneumonia, including thoracic surgery (46%), GI surgery (21%), and gynecology (12%).
When the researchers included the entire cohort of patients, those who were on neoadjuvant therapy had an increased incidence of postoperative pneumonia, compared with those who were not on neoadjuvant chemotherapy (P = .001). When thoracic surgery patients were excluded from the analysis, non-thoracic surgery patients who were on neoadjuvant chemotherapy had no increased incidence of postoperative pneumonia, compared with the patients who were not on neoadjuvant chemotherapy (P = .681). On multivariate analysis, significant variables associated with postoperative pneumonia were being on neoadjuvant chemotherapy (P= .001), having chronic obstructive pulmonary disease (P less than .0001), and having weight loss of greater than 10% (P = .004).
"Institutions with disproportionately busy complex thoracic surgery programs may have rates of postoperative pneumonia skewed higher than predicted by NSQIP models," Dr. Dexter concluded. "Optimization of nutritional status and COPD treatment in neoadjuvant chemotherapy patients may reduce postoperative pneumonia risk and incidence. Balance of oncologic benefit of neoadjuvant chemotherapy versus risk and morbidity of postoperative chemotherapy warrants future study in thoracic surgery patients."
Dr. Dexter said that she had no relevant financial conflicts to make.
AT THE ACS NSQIP NATIONAL CONFERENCE
Major finding: On multivariate analysis, significant variables associated with postoperative pneumonia were being on neoadjuvant chemotherapy (P = .001), having COPD (P less than .0001), and having weight loss of greater than 10% (P = .004).
Data source: A study of 1,723 patients who underwent surgery at Roswell Park Cancer Institute in Buffalo, N.Y. Of the postoperative pneumonia cases that developed, 46% were from the thoracic surgery service.
Disclosures: Dr. Dexter said that she had no relevant financial disclosures to make.

Preoperative screening program helped reduce 30-day mortality
SAN DIEGO – The implementation of an intensive preoperative screening and intervention process led to a significant decrease in 30-day mortality for general surgery and vascular procedures, results from a single-center study demonstrated.
In 2007, Carilion Roanoke (Va.) Memorial Hospital became a member of the American College of Surgeons/National Surgical Quality Improvement Program (ACS/NSQIP). "After receiving our first report, it became evident that surgical mortality at our institution was significantly higher than expected and significantly higher than the national average," Dr. Agathoklis Konstantinidis said at the ACS/NSQIP National Conference. "After further evaluation of this data, it became obvious that we were operating on people with several undiagnosed, untreated medical diseases such as diabetes, obstructive sleep apnea, hypertension, lung disease, and renal disease that all constituted significant preoperative risk factors."

In an effort to improve surgical mortality at the hospital, Dr. Konstantinidis and his associates implemented a strict preoperative screening and intervention program that began in January 2010. Since that time, every patient scheduled for surgery is required to undergo a preoperative screening appointment with a registered nurse who performs an extensive computer-based checklist of risk factors for heart disease, renal disease, abnormal EKG, sleep apnea, and pulmonary disease.
"If a problem is identified, the surgery is postponed until the issue is addressed, either by the primary care physician or by the surgeon who is directly involved in the care of the patient, and in close communication with other specialists, such as those in internal medicine, family practice, and endocrinology," explained Dr. Konstantinidis, who is a surgeon at the hospital.
Between July 2007 and December 2009 – prior to initiation of the preoperative screening and intervention program – the odds ratios for 30-day mortality in all cases were 1.40, 1.43, 1.58, and 1.56 in successive reporting periods. Beginning with the first report after implementation of the preoperative screening and intervention program, 30-day mortality in all cases progressively decreased in successive reporting periods (OR, 1.26, 1.19, 1.14, and 0.86, respectively), with similar reductions in both general surgery (OR, 0.92) and vascular surgery (OR, 0.92) for the last year.
"After the implementation of our new preoperative screening and intervention process, overall 30-day surgical mortality at our institution decreased from 3.5% to 1.9%, which is clinically and also statistically significant based on the P value (P = .007)," Dr. Konstantinidis said.
He went on to report that out of 5,866 patients who underwent screening in 2012 alone, 3,691 had undiagnosed obstructive sleep apnea, 2,361 had an abnormal preoperative EKG, 437 had undiagnosed diabetes, 192 had undiagnosed hypertension, and 167 had undiagnosed shortness of breath. "As a result of the screening intervention, surgery was canceled in 218 patients, and 147 were referred to cardiology specialists for further evaluation," he said.
Dr. Konstantinidis said that he had no relevant financial conflicts to disclose.
Carilion Roanoke (Va.) Memorial Hospital, American College of Surgeons/National Surgical Quality Improvement Program (ACS/NSQIP), Dr. Agathoklis Konstantinidis, ACS/NSQIP National Conference, diabetes, obstructive sleep apnea, hypertension, lung disease, renal disease, preoperative risk factors, improve surgical mortality,
SAN DIEGO – The implementation of an intensive preoperative screening and intervention process led to a significant decrease in 30-day mortality for general surgery and vascular procedures, results from a single-center study demonstrated.
In 2007, Carilion Roanoke (Va.) Memorial Hospital became a member of the American College of Surgeons/National Surgical Quality Improvement Program (ACS/NSQIP). "After receiving our first report, it became evident that surgical mortality at our institution was significantly higher than expected and significantly higher than the national average," Dr. Agathoklis Konstantinidis said at the ACS/NSQIP National Conference. "After further evaluation of this data, it became obvious that we were operating on people with several undiagnosed, untreated medical diseases such as diabetes, obstructive sleep apnea, hypertension, lung disease, and renal disease that all constituted significant preoperative risk factors."
In an effort to improve surgical mortality at the hospital, Dr. Konstantinidis and his associates implemented a strict preoperative screening and intervention program that began in January 2010. Since that time, every patient scheduled for surgery is required to undergo a preoperative screening appointment with a registered nurse who performs an extensive computer-based checklist of risk factors for heart disease, renal disease, abnormal EKG, sleep apnea, and pulmonary disease.
"If a problem is identified, the surgery is postponed until the issue is addressed, either by the primary care physician or by the surgeon who is directly involved in the care of the patient, and in close communication with other specialists, such as those in internal medicine, family practice, and endocrinology," explained Dr. Konstantinidis, who is a surgeon at the hospital.
Between July 2007 and December 2009 – prior to initiation of the preoperative screening and intervention program – the odds ratios for 30-day mortality in all cases were 1.40, 1.43, 1.58, and 1.56 in successive reporting periods. Beginning with the first report after implementation of the preoperative screening and intervention program, 30-day mortality in all cases progressively decreased in successive reporting periods (OR, 1.26, 1.19, 1.14, and 0.86, respectively), with similar reductions in both general surgery (OR, 0.92) and vascular surgery (OR, 0.92) for the last year.
"After the implementation of our new preoperative screening and intervention process, overall 30-day surgical mortality at our institution decreased from 3.5% to 1.9%, which is clinically and also statistically significant based on the P value (P = .007)," Dr. Konstantinidis said.
He went on to report that out of 5,866 patients who underwent screening in 2012 alone, 3,691 had undiagnosed obstructive sleep apnea, 2,361 had an abnormal preoperative EKG, 437 had undiagnosed diabetes, 192 had undiagnosed hypertension, and 167 had undiagnosed shortness of breath. "As a result of the screening intervention, surgery was canceled in 218 patients, and 147 were referred to cardiology specialists for further evaluation," he said.
Dr. Konstantinidis said that he had no relevant financial conflicts to disclose.
SAN DIEGO – The implementation of an intensive preoperative screening and intervention process led to a significant decrease in 30-day mortality for general surgery and vascular procedures, results from a single-center study demonstrated.
In 2007, Carilion Roanoke (Va.) Memorial Hospital became a member of the American College of Surgeons/National Surgical Quality Improvement Program (ACS/NSQIP). "After receiving our first report, it became evident that surgical mortality at our institution was significantly higher than expected and significantly higher than the national average," Dr. Agathoklis Konstantinidis said at the ACS/NSQIP National Conference. "After further evaluation of this data, it became obvious that we were operating on people with several undiagnosed, untreated medical diseases such as diabetes, obstructive sleep apnea, hypertension, lung disease, and renal disease that all constituted significant preoperative risk factors."
In an effort to improve surgical mortality at the hospital, Dr. Konstantinidis and his associates implemented a strict preoperative screening and intervention program that began in January 2010. Since that time, every patient scheduled for surgery is required to undergo a preoperative screening appointment with a registered nurse who performs an extensive computer-based checklist of risk factors for heart disease, renal disease, abnormal EKG, sleep apnea, and pulmonary disease.
"If a problem is identified, the surgery is postponed until the issue is addressed, either by the primary care physician or by the surgeon who is directly involved in the care of the patient, and in close communication with other specialists, such as those in internal medicine, family practice, and endocrinology," explained Dr. Konstantinidis, who is a surgeon at the hospital.
Between July 2007 and December 2009 – prior to initiation of the preoperative screening and intervention program – the odds ratios for 30-day mortality in all cases were 1.40, 1.43, 1.58, and 1.56 in successive reporting periods. Beginning with the first report after implementation of the preoperative screening and intervention program, 30-day mortality in all cases progressively decreased in successive reporting periods (OR, 1.26, 1.19, 1.14, and 0.86, respectively), with similar reductions in both general surgery (OR, 0.92) and vascular surgery (OR, 0.92) for the last year.
"After the implementation of our new preoperative screening and intervention process, overall 30-day surgical mortality at our institution decreased from 3.5% to 1.9%, which is clinically and also statistically significant based on the P value (P = .007)," Dr. Konstantinidis said.
He went on to report that out of 5,866 patients who underwent screening in 2012 alone, 3,691 had undiagnosed obstructive sleep apnea, 2,361 had an abnormal preoperative EKG, 437 had undiagnosed diabetes, 192 had undiagnosed hypertension, and 167 had undiagnosed shortness of breath. "As a result of the screening intervention, surgery was canceled in 218 patients, and 147 were referred to cardiology specialists for further evaluation," he said.
Dr. Konstantinidis said that he had no relevant financial conflicts to disclose.
Carilion Roanoke (Va.) Memorial Hospital, American College of Surgeons/National Surgical Quality Improvement Program (ACS/NSQIP), Dr. Agathoklis Konstantinidis, ACS/NSQIP National Conference, diabetes, obstructive sleep apnea, hypertension, lung disease, renal disease, preoperative risk factors, improve surgical mortality,
Carilion Roanoke (Va.) Memorial Hospital, American College of Surgeons/National Surgical Quality Improvement Program (ACS/NSQIP), Dr. Agathoklis Konstantinidis, ACS/NSQIP National Conference, diabetes, obstructive sleep apnea, hypertension, lung disease, renal disease, preoperative risk factors, improve surgical mortality,
AT THE ACS NSQIP NATIONAL CONFERENCE
Major finding: After implementation of a new preoperative screening and intervention process, overall 30-day surgical mortality decreased from 3.5% to 1.9%, which reached clinical and statistical significance (P = .007).
Data source: A single-center study of patients who underwent general surgery and vascular surgery procedures between 2007 and 2011 at Carilion Roanoke (Va.) Memorial Hospital.
Disclosures: Dr. Konstantinidis said that he had no relevant financial conflicts to disclose.
