User login
False-negative rate for sentinel nodes high after neoadjuvant chemotherapy
The false-negative rate of sentinel lymph node results was almost 13% after neoadjuvant chemotherapy, in a study of women initially presenting with biopsy-proven node-positive breast cancer, which is above the acceptable threshold, a study has shown.
Considering the threshold for a false-negative rate is 10%, "changes in approach and patient selection that result in greater sensitivity would be necessary" to support the use of sentinel lymph node (SLN) surgery "as an alternative" to axillary lymph node dissection in this population of patients with breast cancer, concluded Dr. Judy Boughey of the department of surgery, Mayo Clinic, Rochester, Minn., and her associates in the Alliance for Clinical Trials in Oncology.

The investigators also found that false-negative SLN biopsy results were significantly lower when two mapping agents were used; the false-negative rate was also significantly lower when at least three sentinel lymph nodes were sampled. The results of the study were presented at the annual clinical congress of the American Congress of Surgeons and simultaneously published online on Oct. 7, 2013, in JAMA (doi:10.1001/jama.2013.278932).
The phase II study addressed the false-negative rate of SLN biopsy after neoadjuvant chemotherapy, in women who initially presented with pathologically confirmed node-positive disease. The study enrolled 701 women from July 2009 to June 2011, at 136 institutions. The women had clinical stage T0 through T4, N1 through N2, M0 breast cancer; most (663) had cN1 disease (disease in movable axillary lymph nodes) and 38 had cN2 disease (disease in fixed or matted axillary lymph nodes). After chemotherapy was completed, the patients had surgery, involving SLN biopsy and axillary lymph node dissection.
Of the 701 women, 687 underwent both SLN biopsy and axillary lymph node dissection, 2 had only SLN biopsy, and 12 had axillary lymph node dissection only. Most of the 689 women who underwent SLN biopsy had the procedure performed with blue dye and radiolabeled colloid (79%), 116 (16.8%) had radiolabeled colloid only, and 28 (4.1%) had blue dye only.
Of the 689 women who had SLN biopsy, at least one SLN was detected in 639 (almost 93%). Among the 651 women with cN1 disease, at least one SLN was detected in 605 women (93%); and among the 38 women with cN2 disease, at least one SNL was detected in 34 (89.5%).
In 525 of the patients with cN1 disease, at least two SLNs were excised and axillary lymph node dissection was completed. There was no residual node disease found in 215 of these patients, for a nodal pathologic complete response rate of 41%.
Of the remaining 310 patients, nodal disease was found in the sentinel lymph nodes in 108 patients (20.6%), and in both axillary and sentinel nodes in 163 patients (31.1%).
Residual node disease was found in the axillary lymph nodes of only 39 (7.4%) of the patients. Therefore, the results of the SLN biopsy results were false negative in 39 of the 310 patients, for a false negative rate of 12.6%.
While the study results "suggest that surgeons cannot reliably detect all axillary lymph node metastases in patients with cN1 breast cancer following chemotherapy" with SLN procedures, "we did identify important factors influencing the likelihood of a false-negative SLN," the authors said. The false-negative rate for the SLN biopsy results was significantly decreased when both blue dye and radiolabeled colloid were used as mapping agents, and when at least three sentinel lymph nodes were biopsied.
When both blue dye and radiolabeled colloid were used, the false-negative rate was 10.8%, compared with 20.3% when only one agent was used. "Using two mapping agents with different molecule sizes and transit times is an important surgical standard that should be adhered to for SLN surgery after chemotherapy," they said, noting that after chemotherapy, "the axilla often has more fibrosis, making evaluation of lymphatic drainage and surgical dissection more challenging."
And when at least three SLNs were examined, the false negative rate was 9.1%, compared with 21.1% when two were sampled. "As the accuracy of any sampling test is dependent on the amount of material sampled, these results are not surprising," they said, noting that this has been found in other studies.
SLN is less invasive than axillary dissection and is considered a reliable way to check for axillary nodal disease in women who present with node-negative disease, but the use of SLN biopsy after neoadjuvant chemotherapy in women with cN1 disease "has been questioned," because the false-negative rate for this approach in this population has ranged from 7% to 25% in small studies, the only data available on this approach, according to the authors.
The study was supported by a grant from the National Cancer Institute to the American College of Surgeons Oncology Group (ACOSOG). The patients were in the ACOSOG Z1071 trial. Four of the authors reported having grants from the National Institutes of Health or Komen Foundation, having contracts with Galena BioPharma, or having been paid for lectures from LifeCell. The remaining 17 authors said they had no relevant financial disclosures.
"[T]he appropriateness of SLN biopsy in this setting remains uncertain," although the study provides important information, according to Dr. Monica Morrow and Dr. Chau Dang. The increasing number of targeted therapies for breast cancer has enabled physicians to "move away from the ‘one size fits all’ approach." As a result, "the prognostic information obtained from residual nodal disease after neoadjuvant therapy is likely to become increasingly important in determining the need for additional therapy." If true, "research in ways to improve the performance of the SLN biopsy after neoadjuvant therapy is needed for this approach to become a viable management strategy."
Dr. Morrow and Dr. Dang of Memorial Sloan-Kettering Cancer Center in New York made their remarks in an editorial accompanying the article (JAMA 2013 Oct. 7 [doi:10.l001/jama.2013.7844]). Dr. Dang disclosed having received grant funding from Genentech. Dr. Morrow said she had no relevant financial disclosures.
"[T]he appropriateness of SLN biopsy in this setting remains uncertain," although the study provides important information, according to Dr. Monica Morrow and Dr. Chau Dang. The increasing number of targeted therapies for breast cancer has enabled physicians to "move away from the ‘one size fits all’ approach." As a result, "the prognostic information obtained from residual nodal disease after neoadjuvant therapy is likely to become increasingly important in determining the need for additional therapy." If true, "research in ways to improve the performance of the SLN biopsy after neoadjuvant therapy is needed for this approach to become a viable management strategy."
Dr. Morrow and Dr. Dang of Memorial Sloan-Kettering Cancer Center in New York made their remarks in an editorial accompanying the article (JAMA 2013 Oct. 7 [doi:10.l001/jama.2013.7844]). Dr. Dang disclosed having received grant funding from Genentech. Dr. Morrow said she had no relevant financial disclosures.
"[T]he appropriateness of SLN biopsy in this setting remains uncertain," although the study provides important information, according to Dr. Monica Morrow and Dr. Chau Dang. The increasing number of targeted therapies for breast cancer has enabled physicians to "move away from the ‘one size fits all’ approach." As a result, "the prognostic information obtained from residual nodal disease after neoadjuvant therapy is likely to become increasingly important in determining the need for additional therapy." If true, "research in ways to improve the performance of the SLN biopsy after neoadjuvant therapy is needed for this approach to become a viable management strategy."
Dr. Morrow and Dr. Dang of Memorial Sloan-Kettering Cancer Center in New York made their remarks in an editorial accompanying the article (JAMA 2013 Oct. 7 [doi:10.l001/jama.2013.7844]). Dr. Dang disclosed having received grant funding from Genentech. Dr. Morrow said she had no relevant financial disclosures.
The false-negative rate of sentinel lymph node results was almost 13% after neoadjuvant chemotherapy, in a study of women initially presenting with biopsy-proven node-positive breast cancer, which is above the acceptable threshold, a study has shown.
Considering the threshold for a false-negative rate is 10%, "changes in approach and patient selection that result in greater sensitivity would be necessary" to support the use of sentinel lymph node (SLN) surgery "as an alternative" to axillary lymph node dissection in this population of patients with breast cancer, concluded Dr. Judy Boughey of the department of surgery, Mayo Clinic, Rochester, Minn., and her associates in the Alliance for Clinical Trials in Oncology.
The investigators also found that false-negative SLN biopsy results were significantly lower when two mapping agents were used; the false-negative rate was also significantly lower when at least three sentinel lymph nodes were sampled. The results of the study were presented at the annual clinical congress of the American Congress of Surgeons and simultaneously published online on Oct. 7, 2013, in JAMA (doi:10.1001/jama.2013.278932).
The phase II study addressed the false-negative rate of SLN biopsy after neoadjuvant chemotherapy, in women who initially presented with pathologically confirmed node-positive disease. The study enrolled 701 women from July 2009 to June 2011, at 136 institutions. The women had clinical stage T0 through T4, N1 through N2, M0 breast cancer; most (663) had cN1 disease (disease in movable axillary lymph nodes) and 38 had cN2 disease (disease in fixed or matted axillary lymph nodes). After chemotherapy was completed, the patients had surgery, involving SLN biopsy and axillary lymph node dissection.
Of the 701 women, 687 underwent both SLN biopsy and axillary lymph node dissection, 2 had only SLN biopsy, and 12 had axillary lymph node dissection only. Most of the 689 women who underwent SLN biopsy had the procedure performed with blue dye and radiolabeled colloid (79%), 116 (16.8%) had radiolabeled colloid only, and 28 (4.1%) had blue dye only.
Of the 689 women who had SLN biopsy, at least one SLN was detected in 639 (almost 93%). Among the 651 women with cN1 disease, at least one SLN was detected in 605 women (93%); and among the 38 women with cN2 disease, at least one SNL was detected in 34 (89.5%).
In 525 of the patients with cN1 disease, at least two SLNs were excised and axillary lymph node dissection was completed. There was no residual node disease found in 215 of these patients, for a nodal pathologic complete response rate of 41%.
Of the remaining 310 patients, nodal disease was found in the sentinel lymph nodes in 108 patients (20.6%), and in both axillary and sentinel nodes in 163 patients (31.1%).
Residual node disease was found in the axillary lymph nodes of only 39 (7.4%) of the patients. Therefore, the results of the SLN biopsy results were false negative in 39 of the 310 patients, for a false negative rate of 12.6%.
While the study results "suggest that surgeons cannot reliably detect all axillary lymph node metastases in patients with cN1 breast cancer following chemotherapy" with SLN procedures, "we did identify important factors influencing the likelihood of a false-negative SLN," the authors said. The false-negative rate for the SLN biopsy results was significantly decreased when both blue dye and radiolabeled colloid were used as mapping agents, and when at least three sentinel lymph nodes were biopsied.
When both blue dye and radiolabeled colloid were used, the false-negative rate was 10.8%, compared with 20.3% when only one agent was used. "Using two mapping agents with different molecule sizes and transit times is an important surgical standard that should be adhered to for SLN surgery after chemotherapy," they said, noting that after chemotherapy, "the axilla often has more fibrosis, making evaluation of lymphatic drainage and surgical dissection more challenging."
And when at least three SLNs were examined, the false negative rate was 9.1%, compared with 21.1% when two were sampled. "As the accuracy of any sampling test is dependent on the amount of material sampled, these results are not surprising," they said, noting that this has been found in other studies.
SLN is less invasive than axillary dissection and is considered a reliable way to check for axillary nodal disease in women who present with node-negative disease, but the use of SLN biopsy after neoadjuvant chemotherapy in women with cN1 disease "has been questioned," because the false-negative rate for this approach in this population has ranged from 7% to 25% in small studies, the only data available on this approach, according to the authors.
The study was supported by a grant from the National Cancer Institute to the American College of Surgeons Oncology Group (ACOSOG). The patients were in the ACOSOG Z1071 trial. Four of the authors reported having grants from the National Institutes of Health or Komen Foundation, having contracts with Galena BioPharma, or having been paid for lectures from LifeCell. The remaining 17 authors said they had no relevant financial disclosures.
The false-negative rate of sentinel lymph node results was almost 13% after neoadjuvant chemotherapy, in a study of women initially presenting with biopsy-proven node-positive breast cancer, which is above the acceptable threshold, a study has shown.
Considering the threshold for a false-negative rate is 10%, "changes in approach and patient selection that result in greater sensitivity would be necessary" to support the use of sentinel lymph node (SLN) surgery "as an alternative" to axillary lymph node dissection in this population of patients with breast cancer, concluded Dr. Judy Boughey of the department of surgery, Mayo Clinic, Rochester, Minn., and her associates in the Alliance for Clinical Trials in Oncology.
The investigators also found that false-negative SLN biopsy results were significantly lower when two mapping agents were used; the false-negative rate was also significantly lower when at least three sentinel lymph nodes were sampled. The results of the study were presented at the annual clinical congress of the American Congress of Surgeons and simultaneously published online on Oct. 7, 2013, in JAMA (doi:10.1001/jama.2013.278932).
The phase II study addressed the false-negative rate of SLN biopsy after neoadjuvant chemotherapy, in women who initially presented with pathologically confirmed node-positive disease. The study enrolled 701 women from July 2009 to June 2011, at 136 institutions. The women had clinical stage T0 through T4, N1 through N2, M0 breast cancer; most (663) had cN1 disease (disease in movable axillary lymph nodes) and 38 had cN2 disease (disease in fixed or matted axillary lymph nodes). After chemotherapy was completed, the patients had surgery, involving SLN biopsy and axillary lymph node dissection.
Of the 701 women, 687 underwent both SLN biopsy and axillary lymph node dissection, 2 had only SLN biopsy, and 12 had axillary lymph node dissection only. Most of the 689 women who underwent SLN biopsy had the procedure performed with blue dye and radiolabeled colloid (79%), 116 (16.8%) had radiolabeled colloid only, and 28 (4.1%) had blue dye only.
Of the 689 women who had SLN biopsy, at least one SLN was detected in 639 (almost 93%). Among the 651 women with cN1 disease, at least one SLN was detected in 605 women (93%); and among the 38 women with cN2 disease, at least one SNL was detected in 34 (89.5%).
In 525 of the patients with cN1 disease, at least two SLNs were excised and axillary lymph node dissection was completed. There was no residual node disease found in 215 of these patients, for a nodal pathologic complete response rate of 41%.
Of the remaining 310 patients, nodal disease was found in the sentinel lymph nodes in 108 patients (20.6%), and in both axillary and sentinel nodes in 163 patients (31.1%).
Residual node disease was found in the axillary lymph nodes of only 39 (7.4%) of the patients. Therefore, the results of the SLN biopsy results were false negative in 39 of the 310 patients, for a false negative rate of 12.6%.
While the study results "suggest that surgeons cannot reliably detect all axillary lymph node metastases in patients with cN1 breast cancer following chemotherapy" with SLN procedures, "we did identify important factors influencing the likelihood of a false-negative SLN," the authors said. The false-negative rate for the SLN biopsy results was significantly decreased when both blue dye and radiolabeled colloid were used as mapping agents, and when at least three sentinel lymph nodes were biopsied.
When both blue dye and radiolabeled colloid were used, the false-negative rate was 10.8%, compared with 20.3% when only one agent was used. "Using two mapping agents with different molecule sizes and transit times is an important surgical standard that should be adhered to for SLN surgery after chemotherapy," they said, noting that after chemotherapy, "the axilla often has more fibrosis, making evaluation of lymphatic drainage and surgical dissection more challenging."
And when at least three SLNs were examined, the false negative rate was 9.1%, compared with 21.1% when two were sampled. "As the accuracy of any sampling test is dependent on the amount of material sampled, these results are not surprising," they said, noting that this has been found in other studies.
SLN is less invasive than axillary dissection and is considered a reliable way to check for axillary nodal disease in women who present with node-negative disease, but the use of SLN biopsy after neoadjuvant chemotherapy in women with cN1 disease "has been questioned," because the false-negative rate for this approach in this population has ranged from 7% to 25% in small studies, the only data available on this approach, according to the authors.
The study was supported by a grant from the National Cancer Institute to the American College of Surgeons Oncology Group (ACOSOG). The patients were in the ACOSOG Z1071 trial. Four of the authors reported having grants from the National Institutes of Health or Komen Foundation, having contracts with Galena BioPharma, or having been paid for lectures from LifeCell. The remaining 17 authors said they had no relevant financial disclosures.
FROM THE ACS CLINICAL CONGRESS
Major finding: Sentinel lymph node findings had a false-negative rate of 12.6% among women with cN1 breast cancer, after neoadjuvant chemotherapy, above the acceptable threshold of 10%, but the false-negative rate dropped below this level when a dual mapping technique was used and when more than two sentinel nodes were biopsied.
Data source: A prospective, phase II multicenter study that evaluated the false-negative rate of sentinel lymph node surgery in more than 700 women with clinically node-positive breast cancer treated with chemotherapy before surgery.
Disclosures: The study was supported by a grant from the National Cancer Institute to the American College of Surgeons Oncology Group. Four authors reported having received grants from the National Institutes of Health or the Komen Foundation, having contracts with Galena BioPharma, or having been paid for lectures by LifeCell. The remaining authors said they had no relevant financial disclosures.

Medicare drops certification requirement for bariatric surgery
Medicare is dropping its requirement that bariatric surgery facilities be certified.
In a controversial move, officials at the Centers for Medicare and Medicaid Services (CMS) announced Sept. 24 that the evidence is sufficient to conclude that certification does not improve health outcomes for Medicare beneficiaries. As a result, the agency will no longer make certification a condition of Medicare coverage.

The decision reverses the agency’s February 2006 requirements. Since then, Medicare has covered bariatric procedures only when performed at facilities that were either certified by the American College of Surgeons (ACS) as a Level 1 Bariatric Surgery Center or certified by the American Society for Metabolic and Bariatric Surgery (ASMBS) as a Bariatric Surgery Center of Excellence.
In their announcement, CMS officials said they were leaning in this direction in June when they proposed to lift the certification requirement and asked for public comments.
The response overwhelmingly supported certification. Of the 483 comments received, only 92 favored eliminating the certification requirement.
The change was opposed by physician groups including the ASMBS and the ACS, which operate the certification programs referenced in the previous CMS coverage policy. The groups warned the CMS that dropping the certification requirement would put the safety of vulnerable Medicare patients at risk.
Dr. Jaime Ponce, ASMBS President, said in a statement that he was "disappointed" in the Medicare decision but encouraged that private insurers such as Blue Cross Blue Shield, Aetna, Cigna, and Optum/United Healthcare continue to support accreditation.
The CMS agreed that there is a role for accreditation programs going forward, but said that they are not necessary to ensure safe outcomes for Medicare beneficiaries.
"The removal of a coverage requirement does not require facilities to discontinue practices which they find beneficial," according to the decision memo.
Facilities may choose to continue with certification in order to distinguish themselves from the competition, for instance.
"While CMS agrees with the value of the multidisciplinary team approach and structure, we do not believe that every valued endeavor needs to be buttressed by a Medicare mandate," the memo states. "We expect all facilities to strive to provide the proper equipment and services to meet the needs of its patient population."
CMS officials reviewed nine studies to determine if certification meaningfully improved health outcomes for Medicare beneficiaries. The results were "mixed," the agency said, but overall the evidence showed "no consistent statistical or clinically meaningful difference." Further, nothing in the literature suggested a worsening of outcomes without certification.
The factors that led to the original certification requirements – the rapid growth in bariatric procedures and concerns about higher mortality rates – have changed, the CMS wrote.
The policy switch was requested by health services researchers at the University of Michigan led by Dr. John D. Birkmeyer, professor of surgery and director of the Center for Healthcare Outcomes and Policy at the University of Michigan, Ann Arbor. The scientists asserted that certified facilities were no safer than noncertified ones and that mortality and serious complication rates for bariatric surgery had declined across the country.
The CMS coverage decision did not make changes to the bariatric procedures covered by the agency. Medicare will continue to cover open and laparoscopic Roux-en-Y gastric bypass; laparoscopic adjustable gastric banding; and open and laparoscopic biliopancreatic diversion with duodenal switch for Medicare beneficiaries with a body mass index of 35 kg/m2 or greater in those with at least one comorbidity related to obesity who previously have been unsuccessful with medical treatment for obesity.
Medicare is dropping its requirement that bariatric surgery facilities be certified.
In a controversial move, officials at the Centers for Medicare and Medicaid Services (CMS) announced Sept. 24 that the evidence is sufficient to conclude that certification does not improve health outcomes for Medicare beneficiaries. As a result, the agency will no longer make certification a condition of Medicare coverage.
The decision reverses the agency’s February 2006 requirements. Since then, Medicare has covered bariatric procedures only when performed at facilities that were either certified by the American College of Surgeons (ACS) as a Level 1 Bariatric Surgery Center or certified by the American Society for Metabolic and Bariatric Surgery (ASMBS) as a Bariatric Surgery Center of Excellence.
In their announcement, CMS officials said they were leaning in this direction in June when they proposed to lift the certification requirement and asked for public comments.
The response overwhelmingly supported certification. Of the 483 comments received, only 92 favored eliminating the certification requirement.
The change was opposed by physician groups including the ASMBS and the ACS, which operate the certification programs referenced in the previous CMS coverage policy. The groups warned the CMS that dropping the certification requirement would put the safety of vulnerable Medicare patients at risk.
Dr. Jaime Ponce, ASMBS President, said in a statement that he was "disappointed" in the Medicare decision but encouraged that private insurers such as Blue Cross Blue Shield, Aetna, Cigna, and Optum/United Healthcare continue to support accreditation.
The CMS agreed that there is a role for accreditation programs going forward, but said that they are not necessary to ensure safe outcomes for Medicare beneficiaries.
"The removal of a coverage requirement does not require facilities to discontinue practices which they find beneficial," according to the decision memo.
Facilities may choose to continue with certification in order to distinguish themselves from the competition, for instance.
"While CMS agrees with the value of the multidisciplinary team approach and structure, we do not believe that every valued endeavor needs to be buttressed by a Medicare mandate," the memo states. "We expect all facilities to strive to provide the proper equipment and services to meet the needs of its patient population."
CMS officials reviewed nine studies to determine if certification meaningfully improved health outcomes for Medicare beneficiaries. The results were "mixed," the agency said, but overall the evidence showed "no consistent statistical or clinically meaningful difference." Further, nothing in the literature suggested a worsening of outcomes without certification.
The factors that led to the original certification requirements – the rapid growth in bariatric procedures and concerns about higher mortality rates – have changed, the CMS wrote.
The policy switch was requested by health services researchers at the University of Michigan led by Dr. John D. Birkmeyer, professor of surgery and director of the Center for Healthcare Outcomes and Policy at the University of Michigan, Ann Arbor. The scientists asserted that certified facilities were no safer than noncertified ones and that mortality and serious complication rates for bariatric surgery had declined across the country.
The CMS coverage decision did not make changes to the bariatric procedures covered by the agency. Medicare will continue to cover open and laparoscopic Roux-en-Y gastric bypass; laparoscopic adjustable gastric banding; and open and laparoscopic biliopancreatic diversion with duodenal switch for Medicare beneficiaries with a body mass index of 35 kg/m2 or greater in those with at least one comorbidity related to obesity who previously have been unsuccessful with medical treatment for obesity.
Medicare is dropping its requirement that bariatric surgery facilities be certified.
In a controversial move, officials at the Centers for Medicare and Medicaid Services (CMS) announced Sept. 24 that the evidence is sufficient to conclude that certification does not improve health outcomes for Medicare beneficiaries. As a result, the agency will no longer make certification a condition of Medicare coverage.
The decision reverses the agency’s February 2006 requirements. Since then, Medicare has covered bariatric procedures only when performed at facilities that were either certified by the American College of Surgeons (ACS) as a Level 1 Bariatric Surgery Center or certified by the American Society for Metabolic and Bariatric Surgery (ASMBS) as a Bariatric Surgery Center of Excellence.
In their announcement, CMS officials said they were leaning in this direction in June when they proposed to lift the certification requirement and asked for public comments.
The response overwhelmingly supported certification. Of the 483 comments received, only 92 favored eliminating the certification requirement.
The change was opposed by physician groups including the ASMBS and the ACS, which operate the certification programs referenced in the previous CMS coverage policy. The groups warned the CMS that dropping the certification requirement would put the safety of vulnerable Medicare patients at risk.
Dr. Jaime Ponce, ASMBS President, said in a statement that he was "disappointed" in the Medicare decision but encouraged that private insurers such as Blue Cross Blue Shield, Aetna, Cigna, and Optum/United Healthcare continue to support accreditation.
The CMS agreed that there is a role for accreditation programs going forward, but said that they are not necessary to ensure safe outcomes for Medicare beneficiaries.
"The removal of a coverage requirement does not require facilities to discontinue practices which they find beneficial," according to the decision memo.
Facilities may choose to continue with certification in order to distinguish themselves from the competition, for instance.
"While CMS agrees with the value of the multidisciplinary team approach and structure, we do not believe that every valued endeavor needs to be buttressed by a Medicare mandate," the memo states. "We expect all facilities to strive to provide the proper equipment and services to meet the needs of its patient population."
CMS officials reviewed nine studies to determine if certification meaningfully improved health outcomes for Medicare beneficiaries. The results were "mixed," the agency said, but overall the evidence showed "no consistent statistical or clinically meaningful difference." Further, nothing in the literature suggested a worsening of outcomes without certification.
The factors that led to the original certification requirements – the rapid growth in bariatric procedures and concerns about higher mortality rates – have changed, the CMS wrote.
The policy switch was requested by health services researchers at the University of Michigan led by Dr. John D. Birkmeyer, professor of surgery and director of the Center for Healthcare Outcomes and Policy at the University of Michigan, Ann Arbor. The scientists asserted that certified facilities were no safer than noncertified ones and that mortality and serious complication rates for bariatric surgery had declined across the country.
The CMS coverage decision did not make changes to the bariatric procedures covered by the agency. Medicare will continue to cover open and laparoscopic Roux-en-Y gastric bypass; laparoscopic adjustable gastric banding; and open and laparoscopic biliopancreatic diversion with duodenal switch for Medicare beneficiaries with a body mass index of 35 kg/m2 or greater in those with at least one comorbidity related to obesity who previously have been unsuccessful with medical treatment for obesity.

Prophylactic beta-blockers and noncardiac surgery: It's complicated!
AMSTERDAM – Results of a new Danish national study suggest the effects of prophylactic beta-blocker therapy in patients with ischemic heart disease undergoing noncardiac surgery are considerably more heterogeneous than portrayed in current pro-prophylaxis practice guidelines or, at the opposite extreme, in a recent highly critical meta-analysis.
"This is an extraordinarily confusing area at the moment," Dr. Charlotte Andersson observed in presenting the Danish national registry findings at the annual congress of the European Society of Cardiology.
She reported on 28,263 adults with ischemic heart disease who underwent noncardiac surgery during 2004-2009. Hip or knee replacements were the most common operations, accounting for roughly one-third of the total. Patients were followed for 30 days postoperatively for the composite endpoint of acute myocardial infarction, ischemic stroke, or cardiovascular death, as well as for 30-day all-cause mortality.
In short, the effects of prophylactic beta-blocker therapy depended upon the type of background ischemic heart disease a surgical patient had.
"Our data suggest a beneficial effect of beta-blockers among patients with heart failure, perhaps a beneficial effect as well among patients with an MI within the previous 2 years, but no beneficial effect among patients with a more distant MI, and perhaps even harm associated with beta-blocker therapy among patients with neither heart failure nor a history of MI," according to Dr. Andersson of the University of Copenhagen.
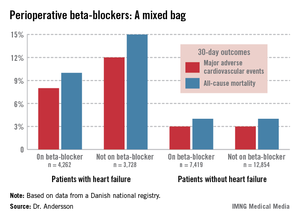
The study population included 7,990 patients with heart failure, 53% of whom were on beta-blockers when they underwent noncardiac surgery. Those on beta-blockers fared significantly better in terms of the study endpoints (see graphic).

In contrast, 30-day outcomes in the 37% of patients without heart failure were identical regardless of whether or not they were on beta-blockers at surgery.
In a multivariate analysis, the use of beta-blockers in noncardiac surgery patients with heart failure was associated with a 22% reduction in major adverse cardiovascular events (MACEs) and an 18% reduction in all-cause mortality compared with no use of beta-blockers, both of which were statistically significant advantages. The analysis was adjusted for patient demographics, acute versus elective surgery, chronic obstructive pulmonary disease, diabetes, atrial fibrillation, peripheral artery disease, cancer, anemia, smoking, alcohol consumption, cerebrovascular disease, and American Society of Anesthesiologists score.
Among the 1,664 patients with an MI within the past 2 years, being on a beta-blocker at the time of surgery was associated with an adjusted highly significant 46% reduction in MACE and a 20% decrease in all-cause mortality, compared with no use of beta-blockers.
For the 1,679 patients with an MI 2-5 years prior to surgery, being on a beta-blocker was associated with a 29% reduction in the risk of MACE and a 26% reduction in 30-day all-cause mortality.
Among the 5,018 patients with an MI more than 5 years earlier, the use of beta-blockers at surgery was associated with a 35% greater risk of MACE than in nonusers of beta-blockers as well as a 33% increase in all-cause mortality. These differences in adverse outcomes rates barely missed achieving statistical significance.
Perhaps the most striking study finding was that patients with no prior MI or heart failure who were on a beta-blocker at the time of noncardiac surgery had a 44% increased risk of 30-day MACE and a 30% higher all-cause mortality, compared with those not on a beta-blocker, with both differences being significant.
Session cochair Dr. Elmir Omerovic thanked Dr. Andersson for a presentation that "really adds important new information" and asked whether she had been surprised by the findings.
"Yes, I have to say I was surprised by the increased risk in patients without prior MI or heart failure, because the ESC [European Society of Cardiology] guidelines state as a class I recommendation that all patients with ischemic heart disease undergoing noncardiac surgery should be on a beta-blocker. Perhaps we should reevaluate beta-blockers in noncardiac surgery," Dr. Andersson replied.
Current American College of Cardiology/American Heart Association guidelines also endorse perioperative beta-blockade in patients with coronary artery disease undergoing vascular or intermediate-risk noncardiac surgery.
She noted that in drawing up the current guidelines, the ESC and ACC/AHA committees relied heavily on strongly positive randomized clinical trials whose validity has recently been called into question in a major research scandal. Indeed, the lead investigator in those studies, Dr. Don Poldermans – who also happened to be chairperson of the ESC guidelines-writing task force – has been dismissed from the faculty at Erasmus University in Rotterdam.
Dr. Omerovic, of Sahlgrenska University, Gothenburg, Sweden, asked for Dr. Andersson’s thoughts regarding a new meta-analysis by investigators at Imperial College London which excluded the suspect Dutch clinical trials. The investigators concluded that initiation of perioperative beta-blocker therapy was associated with a 27% increase in 30-day all-cause mortality, a 27% reduction in nonfatal MI, a 73% increase in stroke, and a 51% increase in hypotension.
"Patient safety being paramount, guidelines for perioperative beta-blocker initiation should be retracted without further delay," the meta-analysts argued (Heart 2013 July 31 [doi: 10.1136/heartjnl-2013-304262]).
"I read that meta-analysis with great interest," Dr. Andersson said. "I think there definitely is a heterogeneity in the effects of perioperative beta-blockers, and it depends on your baseline risk. Most of the studies in the meta-analysis included many patients at lower risk."
Dr. Andersson’s study was funded by the Danish Medical Research Foundation. She reported having no financial conflicts of interest.
Dr. Jun Chiong, FCCP, comments: There are similar studies published regarding preoperative beta-blockers. Most studies are from large databases and not randomized. The results are varied. Important factors such as severity of comorbid conditions prior to surgery (eg, uncontrolled diabetic, noncompliance), amount of blood loss, and surgical technique (not just the organ involved) are often not factored in. I applaud the authors for reporting a significant finding from such a large database. I hope this will encourage investigators to initiate a large, well-controlled, randomized study.
Dr. Jun Chiong, FCCP, comments: There are similar studies published regarding preoperative beta-blockers. Most studies are from large databases and not randomized. The results are varied. Important factors such as severity of comorbid conditions prior to surgery (eg, uncontrolled diabetic, noncompliance), amount of blood loss, and surgical technique (not just the organ involved) are often not factored in. I applaud the authors for reporting a significant finding from such a large database. I hope this will encourage investigators to initiate a large, well-controlled, randomized study.
Dr. Jun Chiong, FCCP, comments: There are similar studies published regarding preoperative beta-blockers. Most studies are from large databases and not randomized. The results are varied. Important factors such as severity of comorbid conditions prior to surgery (eg, uncontrolled diabetic, noncompliance), amount of blood loss, and surgical technique (not just the organ involved) are often not factored in. I applaud the authors for reporting a significant finding from such a large database. I hope this will encourage investigators to initiate a large, well-controlled, randomized study.
AMSTERDAM – Results of a new Danish national study suggest the effects of prophylactic beta-blocker therapy in patients with ischemic heart disease undergoing noncardiac surgery are considerably more heterogeneous than portrayed in current pro-prophylaxis practice guidelines or, at the opposite extreme, in a recent highly critical meta-analysis.
"This is an extraordinarily confusing area at the moment," Dr. Charlotte Andersson observed in presenting the Danish national registry findings at the annual congress of the European Society of Cardiology.
She reported on 28,263 adults with ischemic heart disease who underwent noncardiac surgery during 2004-2009. Hip or knee replacements were the most common operations, accounting for roughly one-third of the total. Patients were followed for 30 days postoperatively for the composite endpoint of acute myocardial infarction, ischemic stroke, or cardiovascular death, as well as for 30-day all-cause mortality.
In short, the effects of prophylactic beta-blocker therapy depended upon the type of background ischemic heart disease a surgical patient had.
"Our data suggest a beneficial effect of beta-blockers among patients with heart failure, perhaps a beneficial effect as well among patients with an MI within the previous 2 years, but no beneficial effect among patients with a more distant MI, and perhaps even harm associated with beta-blocker therapy among patients with neither heart failure nor a history of MI," according to Dr. Andersson of the University of Copenhagen.
The study population included 7,990 patients with heart failure, 53% of whom were on beta-blockers when they underwent noncardiac surgery. Those on beta-blockers fared significantly better in terms of the study endpoints (see graphic).
In contrast, 30-day outcomes in the 37% of patients without heart failure were identical regardless of whether or not they were on beta-blockers at surgery.
In a multivariate analysis, the use of beta-blockers in noncardiac surgery patients with heart failure was associated with a 22% reduction in major adverse cardiovascular events (MACEs) and an 18% reduction in all-cause mortality compared with no use of beta-blockers, both of which were statistically significant advantages. The analysis was adjusted for patient demographics, acute versus elective surgery, chronic obstructive pulmonary disease, diabetes, atrial fibrillation, peripheral artery disease, cancer, anemia, smoking, alcohol consumption, cerebrovascular disease, and American Society of Anesthesiologists score.
Among the 1,664 patients with an MI within the past 2 years, being on a beta-blocker at the time of surgery was associated with an adjusted highly significant 46% reduction in MACE and a 20% decrease in all-cause mortality, compared with no use of beta-blockers.
For the 1,679 patients with an MI 2-5 years prior to surgery, being on a beta-blocker was associated with a 29% reduction in the risk of MACE and a 26% reduction in 30-day all-cause mortality.
Among the 5,018 patients with an MI more than 5 years earlier, the use of beta-blockers at surgery was associated with a 35% greater risk of MACE than in nonusers of beta-blockers as well as a 33% increase in all-cause mortality. These differences in adverse outcomes rates barely missed achieving statistical significance.
Perhaps the most striking study finding was that patients with no prior MI or heart failure who were on a beta-blocker at the time of noncardiac surgery had a 44% increased risk of 30-day MACE and a 30% higher all-cause mortality, compared with those not on a beta-blocker, with both differences being significant.
Session cochair Dr. Elmir Omerovic thanked Dr. Andersson for a presentation that "really adds important new information" and asked whether she had been surprised by the findings.
"Yes, I have to say I was surprised by the increased risk in patients without prior MI or heart failure, because the ESC [European Society of Cardiology] guidelines state as a class I recommendation that all patients with ischemic heart disease undergoing noncardiac surgery should be on a beta-blocker. Perhaps we should reevaluate beta-blockers in noncardiac surgery," Dr. Andersson replied.
Current American College of Cardiology/American Heart Association guidelines also endorse perioperative beta-blockade in patients with coronary artery disease undergoing vascular or intermediate-risk noncardiac surgery.
She noted that in drawing up the current guidelines, the ESC and ACC/AHA committees relied heavily on strongly positive randomized clinical trials whose validity has recently been called into question in a major research scandal. Indeed, the lead investigator in those studies, Dr. Don Poldermans – who also happened to be chairperson of the ESC guidelines-writing task force – has been dismissed from the faculty at Erasmus University in Rotterdam.
Dr. Omerovic, of Sahlgrenska University, Gothenburg, Sweden, asked for Dr. Andersson’s thoughts regarding a new meta-analysis by investigators at Imperial College London which excluded the suspect Dutch clinical trials. The investigators concluded that initiation of perioperative beta-blocker therapy was associated with a 27% increase in 30-day all-cause mortality, a 27% reduction in nonfatal MI, a 73% increase in stroke, and a 51% increase in hypotension.
"Patient safety being paramount, guidelines for perioperative beta-blocker initiation should be retracted without further delay," the meta-analysts argued (Heart 2013 July 31 [doi: 10.1136/heartjnl-2013-304262]).
"I read that meta-analysis with great interest," Dr. Andersson said. "I think there definitely is a heterogeneity in the effects of perioperative beta-blockers, and it depends on your baseline risk. Most of the studies in the meta-analysis included many patients at lower risk."
Dr. Andersson’s study was funded by the Danish Medical Research Foundation. She reported having no financial conflicts of interest.
AMSTERDAM – Results of a new Danish national study suggest the effects of prophylactic beta-blocker therapy in patients with ischemic heart disease undergoing noncardiac surgery are considerably more heterogeneous than portrayed in current pro-prophylaxis practice guidelines or, at the opposite extreme, in a recent highly critical meta-analysis.
"This is an extraordinarily confusing area at the moment," Dr. Charlotte Andersson observed in presenting the Danish national registry findings at the annual congress of the European Society of Cardiology.
She reported on 28,263 adults with ischemic heart disease who underwent noncardiac surgery during 2004-2009. Hip or knee replacements were the most common operations, accounting for roughly one-third of the total. Patients were followed for 30 days postoperatively for the composite endpoint of acute myocardial infarction, ischemic stroke, or cardiovascular death, as well as for 30-day all-cause mortality.
In short, the effects of prophylactic beta-blocker therapy depended upon the type of background ischemic heart disease a surgical patient had.
"Our data suggest a beneficial effect of beta-blockers among patients with heart failure, perhaps a beneficial effect as well among patients with an MI within the previous 2 years, but no beneficial effect among patients with a more distant MI, and perhaps even harm associated with beta-blocker therapy among patients with neither heart failure nor a history of MI," according to Dr. Andersson of the University of Copenhagen.
The study population included 7,990 patients with heart failure, 53% of whom were on beta-blockers when they underwent noncardiac surgery. Those on beta-blockers fared significantly better in terms of the study endpoints (see graphic).
In contrast, 30-day outcomes in the 37% of patients without heart failure were identical regardless of whether or not they were on beta-blockers at surgery.
In a multivariate analysis, the use of beta-blockers in noncardiac surgery patients with heart failure was associated with a 22% reduction in major adverse cardiovascular events (MACEs) and an 18% reduction in all-cause mortality compared with no use of beta-blockers, both of which were statistically significant advantages. The analysis was adjusted for patient demographics, acute versus elective surgery, chronic obstructive pulmonary disease, diabetes, atrial fibrillation, peripheral artery disease, cancer, anemia, smoking, alcohol consumption, cerebrovascular disease, and American Society of Anesthesiologists score.
Among the 1,664 patients with an MI within the past 2 years, being on a beta-blocker at the time of surgery was associated with an adjusted highly significant 46% reduction in MACE and a 20% decrease in all-cause mortality, compared with no use of beta-blockers.
For the 1,679 patients with an MI 2-5 years prior to surgery, being on a beta-blocker was associated with a 29% reduction in the risk of MACE and a 26% reduction in 30-day all-cause mortality.
Among the 5,018 patients with an MI more than 5 years earlier, the use of beta-blockers at surgery was associated with a 35% greater risk of MACE than in nonusers of beta-blockers as well as a 33% increase in all-cause mortality. These differences in adverse outcomes rates barely missed achieving statistical significance.
Perhaps the most striking study finding was that patients with no prior MI or heart failure who were on a beta-blocker at the time of noncardiac surgery had a 44% increased risk of 30-day MACE and a 30% higher all-cause mortality, compared with those not on a beta-blocker, with both differences being significant.
Session cochair Dr. Elmir Omerovic thanked Dr. Andersson for a presentation that "really adds important new information" and asked whether she had been surprised by the findings.
"Yes, I have to say I was surprised by the increased risk in patients without prior MI or heart failure, because the ESC [European Society of Cardiology] guidelines state as a class I recommendation that all patients with ischemic heart disease undergoing noncardiac surgery should be on a beta-blocker. Perhaps we should reevaluate beta-blockers in noncardiac surgery," Dr. Andersson replied.
Current American College of Cardiology/American Heart Association guidelines also endorse perioperative beta-blockade in patients with coronary artery disease undergoing vascular or intermediate-risk noncardiac surgery.
She noted that in drawing up the current guidelines, the ESC and ACC/AHA committees relied heavily on strongly positive randomized clinical trials whose validity has recently been called into question in a major research scandal. Indeed, the lead investigator in those studies, Dr. Don Poldermans – who also happened to be chairperson of the ESC guidelines-writing task force – has been dismissed from the faculty at Erasmus University in Rotterdam.
Dr. Omerovic, of Sahlgrenska University, Gothenburg, Sweden, asked for Dr. Andersson’s thoughts regarding a new meta-analysis by investigators at Imperial College London which excluded the suspect Dutch clinical trials. The investigators concluded that initiation of perioperative beta-blocker therapy was associated with a 27% increase in 30-day all-cause mortality, a 27% reduction in nonfatal MI, a 73% increase in stroke, and a 51% increase in hypotension.
"Patient safety being paramount, guidelines for perioperative beta-blocker initiation should be retracted without further delay," the meta-analysts argued (Heart 2013 July 31 [doi: 10.1136/heartjnl-2013-304262]).
"I read that meta-analysis with great interest," Dr. Andersson said. "I think there definitely is a heterogeneity in the effects of perioperative beta-blockers, and it depends on your baseline risk. Most of the studies in the meta-analysis included many patients at lower risk."
Dr. Andersson’s study was funded by the Danish Medical Research Foundation. She reported having no financial conflicts of interest.
AT THE ESC CONGRESS 2013
Major finding: Patients with heart failure who were on beta-blocker therapy at the time of noncardiac surgery had a 22% reduction in 30-day major adverse cardiovascular events, compared with those not on a beta-blocker perioperatively. In stark contrast, patients with ischemic heart disease but no history of heart failure or MI had a 44% greater risk of such events if they were on a perioperative beta-blocker.
Data source: This was a Danish national registry study that included more than 28,000 patients with ischemic heart disease who underwent noncardiac surgery.
Disclosures: Dr. Andersson’s study was funded by the Danish Medical Research Foundation. She reported having no financial conflicts of interest.

Stats show MRSA declining, especially in hospitals
The estimated total of invasive MRSA infections across the United States fell 31% between 2005 and 2011, according to a report published online Sept. 16 in JAMA Internal Medicine.
And for the first time, the estimated number of hospital-onset invasive MRSA infections was lower than that of community-associated infections, said Dr. Raymund Dantes of the Epidemic Intelligence Service of the Centers for Disease Control and Prevention, Atlanta.

The greatest burden of disease continues to fall upon patients in the community who have recent or ongoing exposure to health care services. That includes those recently discharged from acute medical care, long-term–care residents, and patients who require repeated medical visits, such as for diabetes care or dialysis, according to Dr. Dantes and his colleagues.
Those findings, together with other results from their analysis of data in the CDC’s emerging infections surveillance system, indicate that "the U.S. is on track to meet the Department of Health and Human Services 2013 target of reducing health care–associated MRSA invasive infections by 50%," they noted (JAMA Intern. Med. 2013 Sept. 16 [doi:10.1001/jamainternmed.2013.10423]).
To better understand the national burden of invasive MRSA infections, Dr. Dantes and his colleagues analyzed data from nine states participating in the surveillance program: California, Colorado, Connecticut, Georgia, Maryland, Minnesota, New York, Oregon, and Tennessee. They focused on 2011, the most recent year for which complete data are available, and compared the information with that gathered in 2005.
Those nine sites, which represented 16,489,254 people in 2005 and 19,393,677 people in 2011, reported 4,872 cases of invasive MRSA among 4,445 patients in 2011. A total of 18% were classified as hospital-onset infections, 60% as "health-care–associated community onset" infections, and 20% as community-associated infections.
Extrapolating those results to the entire U.S. population, the investigators estimated that 80,461 invasive MRSA infections occurred nationally in 2011, of which 14,156 were hospital-onset, 48,353 were health-care–associated community onset, and 16,560 were community-associated.
"Compared with 6 years earlier, the estimated national rate of invasive MRSA has decreased by 31.2%," Dr. Dantes and his associates said. "Although this rate decrease was most precipitous among hospital-onset infections, at 54.2%, rate decreases were evident among other categories as well: health-care–associated by 27.7%, and community-associated by 5.0%," they wrote.
The 54% decline in hospital-onset cases was particularly encouraging. The exact reason for that reduction is not yet known, but it is likely that implementation of infection prevention measures contributed, especially those targeting intravascular catheter-related infections and health care transmission of multidrug-resistant organisms, they added.
"It is notable that the incidence of community-associated invasive MRSA infections, although relatively stable, has not increased over this time, despite increases in hospitalizations related to MRSA skin and soft-tissue infections documented in discharge data," the investigators said. "Progress in reducing infections among this population is likely to be most challenging due to a lack of clearly effective strategies to control endemic MRSA transmission in the community setting.
Although there is guidance on preventing community-associated MRSA transmission in institutions such as athletic facilities, correctional facilities, and schools, guidance on prevention in other community settings isn’t as well established. Changes in community settings "may be related to transmission in households, prevention of invasive disease from improved early treatment of noninvasive infections, or the natural evolution of this pathogen," they noted.
To substantially reduce the overall burden of invasive MRSA infections, significant progress must be made to prevent postdischarge and dialysis-related cases, the researchers added. In 2011, most cases of health care–associated community-onset invasive MRSA occurred among dialysis patients and patients who had been hospitalized recently.
"Invasive devices that remain placed during the postdischarge period, progression from colonization to clinical infection, and breakdowns in host defense and skin integrity during hospitalization may account for this increased risk," Dr. Dantes and his associates said.
An estimated 11,285 patients with invasive MRSA infections died of all causes during hospitalization in 2011, they added.
The Emerging Infections Program and the National Center for Emerging Zoonotic Infectious Diseases at the Centers for Disease Control and Prevention supported the study. No financial conflicts of interest were reported.
The estimated total of invasive MRSA infections across the United States fell 31% between 2005 and 2011, according to a report published online Sept. 16 in JAMA Internal Medicine.
And for the first time, the estimated number of hospital-onset invasive MRSA infections was lower than that of community-associated infections, said Dr. Raymund Dantes of the Epidemic Intelligence Service of the Centers for Disease Control and Prevention, Atlanta.
The greatest burden of disease continues to fall upon patients in the community who have recent or ongoing exposure to health care services. That includes those recently discharged from acute medical care, long-term–care residents, and patients who require repeated medical visits, such as for diabetes care or dialysis, according to Dr. Dantes and his colleagues.
Those findings, together with other results from their analysis of data in the CDC’s emerging infections surveillance system, indicate that "the U.S. is on track to meet the Department of Health and Human Services 2013 target of reducing health care–associated MRSA invasive infections by 50%," they noted (JAMA Intern. Med. 2013 Sept. 16 [doi:10.1001/jamainternmed.2013.10423]).
To better understand the national burden of invasive MRSA infections, Dr. Dantes and his colleagues analyzed data from nine states participating in the surveillance program: California, Colorado, Connecticut, Georgia, Maryland, Minnesota, New York, Oregon, and Tennessee. They focused on 2011, the most recent year for which complete data are available, and compared the information with that gathered in 2005.
Those nine sites, which represented 16,489,254 people in 2005 and 19,393,677 people in 2011, reported 4,872 cases of invasive MRSA among 4,445 patients in 2011. A total of 18% were classified as hospital-onset infections, 60% as "health-care–associated community onset" infections, and 20% as community-associated infections.
Extrapolating those results to the entire U.S. population, the investigators estimated that 80,461 invasive MRSA infections occurred nationally in 2011, of which 14,156 were hospital-onset, 48,353 were health-care–associated community onset, and 16,560 were community-associated.
"Compared with 6 years earlier, the estimated national rate of invasive MRSA has decreased by 31.2%," Dr. Dantes and his associates said. "Although this rate decrease was most precipitous among hospital-onset infections, at 54.2%, rate decreases were evident among other categories as well: health-care–associated by 27.7%, and community-associated by 5.0%," they wrote.
The 54% decline in hospital-onset cases was particularly encouraging. The exact reason for that reduction is not yet known, but it is likely that implementation of infection prevention measures contributed, especially those targeting intravascular catheter-related infections and health care transmission of multidrug-resistant organisms, they added.
"It is notable that the incidence of community-associated invasive MRSA infections, although relatively stable, has not increased over this time, despite increases in hospitalizations related to MRSA skin and soft-tissue infections documented in discharge data," the investigators said. "Progress in reducing infections among this population is likely to be most challenging due to a lack of clearly effective strategies to control endemic MRSA transmission in the community setting.
Although there is guidance on preventing community-associated MRSA transmission in institutions such as athletic facilities, correctional facilities, and schools, guidance on prevention in other community settings isn’t as well established. Changes in community settings "may be related to transmission in households, prevention of invasive disease from improved early treatment of noninvasive infections, or the natural evolution of this pathogen," they noted.
To substantially reduce the overall burden of invasive MRSA infections, significant progress must be made to prevent postdischarge and dialysis-related cases, the researchers added. In 2011, most cases of health care–associated community-onset invasive MRSA occurred among dialysis patients and patients who had been hospitalized recently.
"Invasive devices that remain placed during the postdischarge period, progression from colonization to clinical infection, and breakdowns in host defense and skin integrity during hospitalization may account for this increased risk," Dr. Dantes and his associates said.
An estimated 11,285 patients with invasive MRSA infections died of all causes during hospitalization in 2011, they added.
The Emerging Infections Program and the National Center for Emerging Zoonotic Infectious Diseases at the Centers for Disease Control and Prevention supported the study. No financial conflicts of interest were reported.
The estimated total of invasive MRSA infections across the United States fell 31% between 2005 and 2011, according to a report published online Sept. 16 in JAMA Internal Medicine.
And for the first time, the estimated number of hospital-onset invasive MRSA infections was lower than that of community-associated infections, said Dr. Raymund Dantes of the Epidemic Intelligence Service of the Centers for Disease Control and Prevention, Atlanta.
The greatest burden of disease continues to fall upon patients in the community who have recent or ongoing exposure to health care services. That includes those recently discharged from acute medical care, long-term–care residents, and patients who require repeated medical visits, such as for diabetes care or dialysis, according to Dr. Dantes and his colleagues.
Those findings, together with other results from their analysis of data in the CDC’s emerging infections surveillance system, indicate that "the U.S. is on track to meet the Department of Health and Human Services 2013 target of reducing health care–associated MRSA invasive infections by 50%," they noted (JAMA Intern. Med. 2013 Sept. 16 [doi:10.1001/jamainternmed.2013.10423]).
To better understand the national burden of invasive MRSA infections, Dr. Dantes and his colleagues analyzed data from nine states participating in the surveillance program: California, Colorado, Connecticut, Georgia, Maryland, Minnesota, New York, Oregon, and Tennessee. They focused on 2011, the most recent year for which complete data are available, and compared the information with that gathered in 2005.
Those nine sites, which represented 16,489,254 people in 2005 and 19,393,677 people in 2011, reported 4,872 cases of invasive MRSA among 4,445 patients in 2011. A total of 18% were classified as hospital-onset infections, 60% as "health-care–associated community onset" infections, and 20% as community-associated infections.
Extrapolating those results to the entire U.S. population, the investigators estimated that 80,461 invasive MRSA infections occurred nationally in 2011, of which 14,156 were hospital-onset, 48,353 were health-care–associated community onset, and 16,560 were community-associated.
"Compared with 6 years earlier, the estimated national rate of invasive MRSA has decreased by 31.2%," Dr. Dantes and his associates said. "Although this rate decrease was most precipitous among hospital-onset infections, at 54.2%, rate decreases were evident among other categories as well: health-care–associated by 27.7%, and community-associated by 5.0%," they wrote.
The 54% decline in hospital-onset cases was particularly encouraging. The exact reason for that reduction is not yet known, but it is likely that implementation of infection prevention measures contributed, especially those targeting intravascular catheter-related infections and health care transmission of multidrug-resistant organisms, they added.
"It is notable that the incidence of community-associated invasive MRSA infections, although relatively stable, has not increased over this time, despite increases in hospitalizations related to MRSA skin and soft-tissue infections documented in discharge data," the investigators said. "Progress in reducing infections among this population is likely to be most challenging due to a lack of clearly effective strategies to control endemic MRSA transmission in the community setting.
Although there is guidance on preventing community-associated MRSA transmission in institutions such as athletic facilities, correctional facilities, and schools, guidance on prevention in other community settings isn’t as well established. Changes in community settings "may be related to transmission in households, prevention of invasive disease from improved early treatment of noninvasive infections, or the natural evolution of this pathogen," they noted.
To substantially reduce the overall burden of invasive MRSA infections, significant progress must be made to prevent postdischarge and dialysis-related cases, the researchers added. In 2011, most cases of health care–associated community-onset invasive MRSA occurred among dialysis patients and patients who had been hospitalized recently.
"Invasive devices that remain placed during the postdischarge period, progression from colonization to clinical infection, and breakdowns in host defense and skin integrity during hospitalization may account for this increased risk," Dr. Dantes and his associates said.
An estimated 11,285 patients with invasive MRSA infections died of all causes during hospitalization in 2011, they added.
The Emerging Infections Program and the National Center for Emerging Zoonotic Infectious Diseases at the Centers for Disease Control and Prevention supported the study. No financial conflicts of interest were reported.
FROM JAMA INTERNAL MEDICINE
Major Finding: The estimated national rate of invasive MRSA infections declined 31% since 2005, with hospital-onset cases dropping 54%, health care–associated cases decreasing 28%, and community-associated cases declining 5%.
Data Source: An analysis of data from a MRSA surveillance program covering more than 16 million residents of nine states in 2005 and more than 19 million residents in those states in 2011.
Disclosures: The Emerging Infections Program and the National Center for Emerging Zoonotic Infectious Diseases at the Centers for Disease Control and Prevention supported the study. No financial conflicts of interest were reported.
Patients with cirrhosis did well with laparoscopic cholecystectomy
Laparoscopic cholecystectomy is a good choice for many patients with liver cirrhosis who need the procedure.
In addition to quickly and effectively addressing the acute illness, laparoscopic cholecystectomy may offer a future advantage, Dr. Vincenzo Neri said at the minimally invasive surgery week annual meeting and endo expo.
"Some cirrhotic patients may be candidates for liver transplantation in the future," said Dr. Neri of the University of Foggia, Italy. "Laparoscopic cholecystectomy offers the chance of fewer right upper quadrant postoperative adhesions" that might complicate later transplant surgery.
He presented a retrospective analysis designed to evaluate the safety and usefulness of a laparoscopic approach in cirrhotic patients undergoing a cholecystectomy. The series comprised 65 patients with hepatic cirrhosis and symptomatic gallstone disease. Of these, six had planned open procedures and the rest laparoscopic procedures. There were 12 conversions to open surgery.
The patients were a mean of 58 years old. More than half had at least two comorbid conditions, including hypertension (14%), cardiac disease (9%), diabetes (12%), respiratory conditions (8%), cerebrovascular disease (4%), and other problems (11%).
Total bilirubin was more than 1 mg/dL in 51% of the group. Albumin was elevated in 61%, and platelets were below 160,000/mcL in 31%. More than a quarter (27%) had a prolonged prothrombin time. About 45% were a Child-Pugh class A, 20% were class B, and the rest were class C.
Cirrhosis was known preoperatively in only 24 patients. The diagnosis was made during the hospital stay in the rest of the patients.
The most common indication for admission and surgery was biliary colic (37%). Other indications included acute cholecystitis (17%), acute biliary pancreatitis (5%), gallbladder and common bile duct stones (5%), and acute cholecystitis with cholangitis (1%). Other indications were not specified.
Of the 12 conversions, 4 were due to acute cholecystitis. Other reasons for conversion were previous laparoscopy (3), acute pancreatitis (2), hypertrophic left hepatic lobe (2), and intraoperative cholangiography (1).
The investigators compared surgical outcomes to those in an unselected control group of 81 patients without cirrhosis who had undergone laparoscopic cholecystectomy.
The mean operative time in the laparoscopic cirrhotic group was 89 minutes – similar to that in the control group (85 minutes). Among the cirrhotic patients, both planned open and converted procedures lasted about the same time (141 and 149 minutes, respectively).
Length of stay was 5 days in the cirrhotic laparoscopy group and 3 in the noncirrhotic control group. Patients with open or converted surgery stayed a mean of 9 and 8 days, respectively.
The blood transfusion rate was 4% in the laparoscopic group, and 17% in both the open and converted groups. Fourteen percent of the laparoscopic group needed transfusion of blood products, compared with 17% of the open group and 33% of the converted group. Transfusions were significantly more common among patients with a Child-Pugh B score, with 26% needing plasma, 21% blood, and 21% platelets. Among Child-Pugh class A patients, 4% needed plasma, 3% blood, and 3% platelets. There were no transfusions in the Child-Pugh class C patients.
Postoperative complications were significantly more common among patients with planned open and converted procedures than total laparoscopies (27% vs. 5%). These included transient ascites (16% vs. 8%) and wound hematoma (8% vs. 4%).
The meeting was presented by the Society of Laparoendoscopic Surgeons and affiliated societies. Dr. Neri had no financial disclosures.
Laparoscopic cholecystectomy is a good choice for many patients with liver cirrhosis who need the procedure.
In addition to quickly and effectively addressing the acute illness, laparoscopic cholecystectomy may offer a future advantage, Dr. Vincenzo Neri said at the minimally invasive surgery week annual meeting and endo expo.
"Some cirrhotic patients may be candidates for liver transplantation in the future," said Dr. Neri of the University of Foggia, Italy. "Laparoscopic cholecystectomy offers the chance of fewer right upper quadrant postoperative adhesions" that might complicate later transplant surgery.
He presented a retrospective analysis designed to evaluate the safety and usefulness of a laparoscopic approach in cirrhotic patients undergoing a cholecystectomy. The series comprised 65 patients with hepatic cirrhosis and symptomatic gallstone disease. Of these, six had planned open procedures and the rest laparoscopic procedures. There were 12 conversions to open surgery.
The patients were a mean of 58 years old. More than half had at least two comorbid conditions, including hypertension (14%), cardiac disease (9%), diabetes (12%), respiratory conditions (8%), cerebrovascular disease (4%), and other problems (11%).
Total bilirubin was more than 1 mg/dL in 51% of the group. Albumin was elevated in 61%, and platelets were below 160,000/mcL in 31%. More than a quarter (27%) had a prolonged prothrombin time. About 45% were a Child-Pugh class A, 20% were class B, and the rest were class C.
Cirrhosis was known preoperatively in only 24 patients. The diagnosis was made during the hospital stay in the rest of the patients.
The most common indication for admission and surgery was biliary colic (37%). Other indications included acute cholecystitis (17%), acute biliary pancreatitis (5%), gallbladder and common bile duct stones (5%), and acute cholecystitis with cholangitis (1%). Other indications were not specified.
Of the 12 conversions, 4 were due to acute cholecystitis. Other reasons for conversion were previous laparoscopy (3), acute pancreatitis (2), hypertrophic left hepatic lobe (2), and intraoperative cholangiography (1).
The investigators compared surgical outcomes to those in an unselected control group of 81 patients without cirrhosis who had undergone laparoscopic cholecystectomy.
The mean operative time in the laparoscopic cirrhotic group was 89 minutes – similar to that in the control group (85 minutes). Among the cirrhotic patients, both planned open and converted procedures lasted about the same time (141 and 149 minutes, respectively).
Length of stay was 5 days in the cirrhotic laparoscopy group and 3 in the noncirrhotic control group. Patients with open or converted surgery stayed a mean of 9 and 8 days, respectively.
The blood transfusion rate was 4% in the laparoscopic group, and 17% in both the open and converted groups. Fourteen percent of the laparoscopic group needed transfusion of blood products, compared with 17% of the open group and 33% of the converted group. Transfusions were significantly more common among patients with a Child-Pugh B score, with 26% needing plasma, 21% blood, and 21% platelets. Among Child-Pugh class A patients, 4% needed plasma, 3% blood, and 3% platelets. There were no transfusions in the Child-Pugh class C patients.
Postoperative complications were significantly more common among patients with planned open and converted procedures than total laparoscopies (27% vs. 5%). These included transient ascites (16% vs. 8%) and wound hematoma (8% vs. 4%).
The meeting was presented by the Society of Laparoendoscopic Surgeons and affiliated societies. Dr. Neri had no financial disclosures.
Laparoscopic cholecystectomy is a good choice for many patients with liver cirrhosis who need the procedure.
In addition to quickly and effectively addressing the acute illness, laparoscopic cholecystectomy may offer a future advantage, Dr. Vincenzo Neri said at the minimally invasive surgery week annual meeting and endo expo.
"Some cirrhotic patients may be candidates for liver transplantation in the future," said Dr. Neri of the University of Foggia, Italy. "Laparoscopic cholecystectomy offers the chance of fewer right upper quadrant postoperative adhesions" that might complicate later transplant surgery.
He presented a retrospective analysis designed to evaluate the safety and usefulness of a laparoscopic approach in cirrhotic patients undergoing a cholecystectomy. The series comprised 65 patients with hepatic cirrhosis and symptomatic gallstone disease. Of these, six had planned open procedures and the rest laparoscopic procedures. There were 12 conversions to open surgery.
The patients were a mean of 58 years old. More than half had at least two comorbid conditions, including hypertension (14%), cardiac disease (9%), diabetes (12%), respiratory conditions (8%), cerebrovascular disease (4%), and other problems (11%).
Total bilirubin was more than 1 mg/dL in 51% of the group. Albumin was elevated in 61%, and platelets were below 160,000/mcL in 31%. More than a quarter (27%) had a prolonged prothrombin time. About 45% were a Child-Pugh class A, 20% were class B, and the rest were class C.
Cirrhosis was known preoperatively in only 24 patients. The diagnosis was made during the hospital stay in the rest of the patients.
The most common indication for admission and surgery was biliary colic (37%). Other indications included acute cholecystitis (17%), acute biliary pancreatitis (5%), gallbladder and common bile duct stones (5%), and acute cholecystitis with cholangitis (1%). Other indications were not specified.
Of the 12 conversions, 4 were due to acute cholecystitis. Other reasons for conversion were previous laparoscopy (3), acute pancreatitis (2), hypertrophic left hepatic lobe (2), and intraoperative cholangiography (1).
The investigators compared surgical outcomes to those in an unselected control group of 81 patients without cirrhosis who had undergone laparoscopic cholecystectomy.
The mean operative time in the laparoscopic cirrhotic group was 89 minutes – similar to that in the control group (85 minutes). Among the cirrhotic patients, both planned open and converted procedures lasted about the same time (141 and 149 minutes, respectively).
Length of stay was 5 days in the cirrhotic laparoscopy group and 3 in the noncirrhotic control group. Patients with open or converted surgery stayed a mean of 9 and 8 days, respectively.
The blood transfusion rate was 4% in the laparoscopic group, and 17% in both the open and converted groups. Fourteen percent of the laparoscopic group needed transfusion of blood products, compared with 17% of the open group and 33% of the converted group. Transfusions were significantly more common among patients with a Child-Pugh B score, with 26% needing plasma, 21% blood, and 21% platelets. Among Child-Pugh class A patients, 4% needed plasma, 3% blood, and 3% platelets. There were no transfusions in the Child-Pugh class C patients.
Postoperative complications were significantly more common among patients with planned open and converted procedures than total laparoscopies (27% vs. 5%). These included transient ascites (16% vs. 8%) and wound hematoma (8% vs. 4%).
The meeting was presented by the Society of Laparoendoscopic Surgeons and affiliated societies. Dr. Neri had no financial disclosures.
FROM MINIMALLY INVASIVE SURGERY WEEK
Major finding: Hepatic cirrhosis patients who underwent a laparoscopic cholecystectomy had surgical outcomes similar to those of patients with normal livers, with mean operative times of 89 and 85 minutes, respectively.
Data source: Retrospective study of 65 patients with hepatic cirrhosis and 81 with normal livers.
Disclosures: The meeting was presented by the Society of Laparoendoscopic Surgeons and affiliated societies. Dr. Neri had no financial disclosures.
MammoSite has comparatively high long-term complication rate
The rate of long-term complications such as palpable masses and telangiectasias was nearly five times higher in women who had MammoSite therapy, compared with those who underwent whole breast radiation therapy, results from a retrospective study showed.
Dr. Kari Rosenkranz and her associates at Dartmouth Hitchcock Medical Center, Hanover, N.H., analyzed the data charts of all women who met criteria for brachytherapy and underwent MammoSite (n = 71) or whole breast radiation therapy (WBRT) (n = 245) at the center between 2003 and 2008.

The incidence of palpable masses at the site of the lumpectomy, telangiectasias, and local recurrence were the studied endpoints. No significant differences existed between the study groups regarding age (average was 63.5 years), mean size of tumor (average was 1.1 cm), the percentage of patients with estrogen receptor–positive tumors (92% in total), or the length of follow-up (median was 4 years).
In the MammoSite cohort with hormone receptor–positive tumors, 83% received adjuvant endocrine therapy; 94% of the WBRT group with hormone receptor–positive tumors had endocrine therapy. No significant difference was found in systemic chemotherapy rates.
The rate of long-term complications such as palpable masses, telangiectasias, or both were found to have occurred in 42% of MammoSite patients, compared with 9% in the WBRT group (J. Am. Coll. Surg. 2013;217:497-502).
During follow-up in the MammoSite group, the incidence rate of palpable mass detection at the lumpectomy site was nearly 27%; for the WBRT group, the rate was approximately 7%. MammoSite patients were three times more likely to require a core biopsy of the mass to rule out malignancy than were WBRT patients (16.9% vs. 4.9%, respectively). Telangiectasia was six times more likely to develop in MammoSite patients than in WBRT patients (24% vs. 4%).
Dr. Rosenkranz and her colleagues reported that a prospective, randomized clinical trial which began in 2005, sponsored by the National Surgical Adjuvant Breast and Bowel Project (NSABP)/Radiation Therapy Oncology Group (RTOG), is currently underway to compare WBRT with partial radiation therapies such as MammoSite. The primary endpoint of this study in women who have had surgery for ductal carcinoma in situ or stage I or stage II breast cancer, is breast tumor recurrence; secondary endpoints include toxicity. The study is expected to end in 2015, according to the researchers.
"Until this prospective, randomized trial reports, the increased rate of long-term local toxicity found in our institution’s experience with MammoSite brachytherapy should be considered when counseling women on options for adjuvant radiation therapy after breast-conserving surgery," concluded Dr. Rosenkranz and her associates.
The researchers reported no relevant disclosures.
The rate of long-term complications such as palpable masses and telangiectasias was nearly five times higher in women who had MammoSite therapy, compared with those who underwent whole breast radiation therapy, results from a retrospective study showed.
Dr. Kari Rosenkranz and her associates at Dartmouth Hitchcock Medical Center, Hanover, N.H., analyzed the data charts of all women who met criteria for brachytherapy and underwent MammoSite (n = 71) or whole breast radiation therapy (WBRT) (n = 245) at the center between 2003 and 2008.
The incidence of palpable masses at the site of the lumpectomy, telangiectasias, and local recurrence were the studied endpoints. No significant differences existed between the study groups regarding age (average was 63.5 years), mean size of tumor (average was 1.1 cm), the percentage of patients with estrogen receptor–positive tumors (92% in total), or the length of follow-up (median was 4 years).
In the MammoSite cohort with hormone receptor–positive tumors, 83% received adjuvant endocrine therapy; 94% of the WBRT group with hormone receptor–positive tumors had endocrine therapy. No significant difference was found in systemic chemotherapy rates.
The rate of long-term complications such as palpable masses, telangiectasias, or both were found to have occurred in 42% of MammoSite patients, compared with 9% in the WBRT group (J. Am. Coll. Surg. 2013;217:497-502).
During follow-up in the MammoSite group, the incidence rate of palpable mass detection at the lumpectomy site was nearly 27%; for the WBRT group, the rate was approximately 7%. MammoSite patients were three times more likely to require a core biopsy of the mass to rule out malignancy than were WBRT patients (16.9% vs. 4.9%, respectively). Telangiectasia was six times more likely to develop in MammoSite patients than in WBRT patients (24% vs. 4%).
Dr. Rosenkranz and her colleagues reported that a prospective, randomized clinical trial which began in 2005, sponsored by the National Surgical Adjuvant Breast and Bowel Project (NSABP)/Radiation Therapy Oncology Group (RTOG), is currently underway to compare WBRT with partial radiation therapies such as MammoSite. The primary endpoint of this study in women who have had surgery for ductal carcinoma in situ or stage I or stage II breast cancer, is breast tumor recurrence; secondary endpoints include toxicity. The study is expected to end in 2015, according to the researchers.
"Until this prospective, randomized trial reports, the increased rate of long-term local toxicity found in our institution’s experience with MammoSite brachytherapy should be considered when counseling women on options for adjuvant radiation therapy after breast-conserving surgery," concluded Dr. Rosenkranz and her associates.
The researchers reported no relevant disclosures.
The rate of long-term complications such as palpable masses and telangiectasias was nearly five times higher in women who had MammoSite therapy, compared with those who underwent whole breast radiation therapy, results from a retrospective study showed.
Dr. Kari Rosenkranz and her associates at Dartmouth Hitchcock Medical Center, Hanover, N.H., analyzed the data charts of all women who met criteria for brachytherapy and underwent MammoSite (n = 71) or whole breast radiation therapy (WBRT) (n = 245) at the center between 2003 and 2008.
The incidence of palpable masses at the site of the lumpectomy, telangiectasias, and local recurrence were the studied endpoints. No significant differences existed between the study groups regarding age (average was 63.5 years), mean size of tumor (average was 1.1 cm), the percentage of patients with estrogen receptor–positive tumors (92% in total), or the length of follow-up (median was 4 years).
In the MammoSite cohort with hormone receptor–positive tumors, 83% received adjuvant endocrine therapy; 94% of the WBRT group with hormone receptor–positive tumors had endocrine therapy. No significant difference was found in systemic chemotherapy rates.
The rate of long-term complications such as palpable masses, telangiectasias, or both were found to have occurred in 42% of MammoSite patients, compared with 9% in the WBRT group (J. Am. Coll. Surg. 2013;217:497-502).
During follow-up in the MammoSite group, the incidence rate of palpable mass detection at the lumpectomy site was nearly 27%; for the WBRT group, the rate was approximately 7%. MammoSite patients were three times more likely to require a core biopsy of the mass to rule out malignancy than were WBRT patients (16.9% vs. 4.9%, respectively). Telangiectasia was six times more likely to develop in MammoSite patients than in WBRT patients (24% vs. 4%).
Dr. Rosenkranz and her colleagues reported that a prospective, randomized clinical trial which began in 2005, sponsored by the National Surgical Adjuvant Breast and Bowel Project (NSABP)/Radiation Therapy Oncology Group (RTOG), is currently underway to compare WBRT with partial radiation therapies such as MammoSite. The primary endpoint of this study in women who have had surgery for ductal carcinoma in situ or stage I or stage II breast cancer, is breast tumor recurrence; secondary endpoints include toxicity. The study is expected to end in 2015, according to the researchers.
"Until this prospective, randomized trial reports, the increased rate of long-term local toxicity found in our institution’s experience with MammoSite brachytherapy should be considered when counseling women on options for adjuvant radiation therapy after breast-conserving surgery," concluded Dr. Rosenkranz and her associates.
The researchers reported no relevant disclosures.
FROM THE JOURNAL OF THE AMERICAN COLLEGE OF SURGEONS
Major finding: Forty-two percent of MammoSite patients had long-term complications, vs. 9% of those who had whole breast radiation therapy.
Data source: Retrospective study of 71 women who underwent MammoSite brachytherapy and 245 who had whole breast radiation therapy at a single academic medical center between 2003 and 2008.
Disclosures: Dr. Rosenkranz and her associates reported no relevant disclosures.

Nasogastric drainage may be unnecessary post PD
Fewer than 10% of pancreaticoduodenectomy patients required postoperative nasogastric drainage, the current postoperative standard of care for pancreaticoduodenectomy, the results of a longitudinal observational cohort study have shown.
Dr. John W. Kunstman and his colleagues in the surgery department of Yale University, New Haven, Conn., observed two consecutive cohorts of 125 pancreaticoduodenectomy (PD) patients. The first cohort had nasogastric tubes (NGTs) maintained postoperatively until clinically indicated, while the second cohort had NGTs maintained postoperatively "only in rare circumstances, such as inability to extubate the patient postoperatively," the authors said. All patients were treated by the same surgeon between July 2003 and February 2012, most commonly for pancreatic neoplasm.
There were no statistically significant differences between the two groups in patient demographics, including indications for surgery. The routine NGT group was 51% male with an average age of 63 years, while the selective NGT group was 46% male with an average age of 67 years. Bias was reduced in that both cohorts were analyzed in an intent-to-treat manner.
Pylorus-preserving pancreaticoduodenectomy (PPPD) was performed in the absence of oncologic or other disease-specific considerations; otherwise, a classic (Kausch-Whipple) PD was performed. The most common comorbidity overall was hypertension, although the routine NGT group had a higher incidence of coronary artery disease than the selective NGT group (20.8% vs. 8.8%) and a higher mean creatinine level (0.97 vs. 0.88 mg/dL) (J. Am. Coll. Surgeons 2013;217:481-8).
Primary outcomes included postoperative NGT insertion and reinsertion, delayed gastric emptying (DGE) incidence, time to dietary tolerance, and length of stay.
In the selective NGT cohort, only 9 patients required continued NGT, 5 of them for postoperative endotracheal intubation and 4 for surgical considerations.
Neither the incidence of NGT insertion and reinsertion, nor the duration of NGT replacement, differed significantly between groups. Overall complication rates were also similar, although patients in the selective NGT group were less likely to have DGE. Compared with the routine NGT cohort, the selective cohort had a shorter mean length of stay (10 vs. 7 days) and mean time to dietary tolerance.
Additionally, multivariate analysis of all outcome variables indicated that DGE, the most common adverse event associated with PD, was independently correlated with the routine use of NGT.
"This is of particular interest given the role that gastric decompression plays in treatment of DGE. However, this finding must be interpreted with care, as incidence of DGE varies from 10% to 50% of PD cases, depending on the reporting group," the authors wrote.
In terms of the study’s limitations, the higher number of PPPD and retrocolic gastroenteric anastomoses performed in the routine cohort may have been a factor in the differing DGE incidence rates, since pylorus preservation and anastomotic positioning are considered historically correlated to DGE, the authors said.
Among individually examined adverse events, routine NGT patients were more likely than selective patients to be reintubated (11.2% vs. 3.2%), require a postoperative blood transfusion (16.0% vs. 6.4%), and be diagnosed with DGE (18.4% vs. 8.0%).
There were a total of four deaths in the 30-day postoperative period, all occurring in patients over age 80. There were eight octogenarians in each cohort; three of the deaths occurred in the routine group.
Improvements in perioperative care and the surgeon’s increased skill over time may also have affected the results. However, the authors concluded, "based on these data, persistent concerns, such as fear of increased anastomotic leak or DGE, which have mandated customary nasogastric decompression after PD, can be safely reevaluated."
Dr. Kunstman and his coauthors reported no relevant disclosures.
Fewer than 10% of pancreaticoduodenectomy patients required postoperative nasogastric drainage, the current postoperative standard of care for pancreaticoduodenectomy, the results of a longitudinal observational cohort study have shown.
Dr. John W. Kunstman and his colleagues in the surgery department of Yale University, New Haven, Conn., observed two consecutive cohorts of 125 pancreaticoduodenectomy (PD) patients. The first cohort had nasogastric tubes (NGTs) maintained postoperatively until clinically indicated, while the second cohort had NGTs maintained postoperatively "only in rare circumstances, such as inability to extubate the patient postoperatively," the authors said. All patients were treated by the same surgeon between July 2003 and February 2012, most commonly for pancreatic neoplasm.
There were no statistically significant differences between the two groups in patient demographics, including indications for surgery. The routine NGT group was 51% male with an average age of 63 years, while the selective NGT group was 46% male with an average age of 67 years. Bias was reduced in that both cohorts were analyzed in an intent-to-treat manner.
Pylorus-preserving pancreaticoduodenectomy (PPPD) was performed in the absence of oncologic or other disease-specific considerations; otherwise, a classic (Kausch-Whipple) PD was performed. The most common comorbidity overall was hypertension, although the routine NGT group had a higher incidence of coronary artery disease than the selective NGT group (20.8% vs. 8.8%) and a higher mean creatinine level (0.97 vs. 0.88 mg/dL) (J. Am. Coll. Surgeons 2013;217:481-8).
Primary outcomes included postoperative NGT insertion and reinsertion, delayed gastric emptying (DGE) incidence, time to dietary tolerance, and length of stay.
In the selective NGT cohort, only 9 patients required continued NGT, 5 of them for postoperative endotracheal intubation and 4 for surgical considerations.
Neither the incidence of NGT insertion and reinsertion, nor the duration of NGT replacement, differed significantly between groups. Overall complication rates were also similar, although patients in the selective NGT group were less likely to have DGE. Compared with the routine NGT cohort, the selective cohort had a shorter mean length of stay (10 vs. 7 days) and mean time to dietary tolerance.
Additionally, multivariate analysis of all outcome variables indicated that DGE, the most common adverse event associated with PD, was independently correlated with the routine use of NGT.
"This is of particular interest given the role that gastric decompression plays in treatment of DGE. However, this finding must be interpreted with care, as incidence of DGE varies from 10% to 50% of PD cases, depending on the reporting group," the authors wrote.
In terms of the study’s limitations, the higher number of PPPD and retrocolic gastroenteric anastomoses performed in the routine cohort may have been a factor in the differing DGE incidence rates, since pylorus preservation and anastomotic positioning are considered historically correlated to DGE, the authors said.
Among individually examined adverse events, routine NGT patients were more likely than selective patients to be reintubated (11.2% vs. 3.2%), require a postoperative blood transfusion (16.0% vs. 6.4%), and be diagnosed with DGE (18.4% vs. 8.0%).
There were a total of four deaths in the 30-day postoperative period, all occurring in patients over age 80. There were eight octogenarians in each cohort; three of the deaths occurred in the routine group.
Improvements in perioperative care and the surgeon’s increased skill over time may also have affected the results. However, the authors concluded, "based on these data, persistent concerns, such as fear of increased anastomotic leak or DGE, which have mandated customary nasogastric decompression after PD, can be safely reevaluated."
Dr. Kunstman and his coauthors reported no relevant disclosures.
Fewer than 10% of pancreaticoduodenectomy patients required postoperative nasogastric drainage, the current postoperative standard of care for pancreaticoduodenectomy, the results of a longitudinal observational cohort study have shown.
Dr. John W. Kunstman and his colleagues in the surgery department of Yale University, New Haven, Conn., observed two consecutive cohorts of 125 pancreaticoduodenectomy (PD) patients. The first cohort had nasogastric tubes (NGTs) maintained postoperatively until clinically indicated, while the second cohort had NGTs maintained postoperatively "only in rare circumstances, such as inability to extubate the patient postoperatively," the authors said. All patients were treated by the same surgeon between July 2003 and February 2012, most commonly for pancreatic neoplasm.
There were no statistically significant differences between the two groups in patient demographics, including indications for surgery. The routine NGT group was 51% male with an average age of 63 years, while the selective NGT group was 46% male with an average age of 67 years. Bias was reduced in that both cohorts were analyzed in an intent-to-treat manner.
Pylorus-preserving pancreaticoduodenectomy (PPPD) was performed in the absence of oncologic or other disease-specific considerations; otherwise, a classic (Kausch-Whipple) PD was performed. The most common comorbidity overall was hypertension, although the routine NGT group had a higher incidence of coronary artery disease than the selective NGT group (20.8% vs. 8.8%) and a higher mean creatinine level (0.97 vs. 0.88 mg/dL) (J. Am. Coll. Surgeons 2013;217:481-8).
Primary outcomes included postoperative NGT insertion and reinsertion, delayed gastric emptying (DGE) incidence, time to dietary tolerance, and length of stay.
In the selective NGT cohort, only 9 patients required continued NGT, 5 of them for postoperative endotracheal intubation and 4 for surgical considerations.
Neither the incidence of NGT insertion and reinsertion, nor the duration of NGT replacement, differed significantly between groups. Overall complication rates were also similar, although patients in the selective NGT group were less likely to have DGE. Compared with the routine NGT cohort, the selective cohort had a shorter mean length of stay (10 vs. 7 days) and mean time to dietary tolerance.
Additionally, multivariate analysis of all outcome variables indicated that DGE, the most common adverse event associated with PD, was independently correlated with the routine use of NGT.
"This is of particular interest given the role that gastric decompression plays in treatment of DGE. However, this finding must be interpreted with care, as incidence of DGE varies from 10% to 50% of PD cases, depending on the reporting group," the authors wrote.
In terms of the study’s limitations, the higher number of PPPD and retrocolic gastroenteric anastomoses performed in the routine cohort may have been a factor in the differing DGE incidence rates, since pylorus preservation and anastomotic positioning are considered historically correlated to DGE, the authors said.
Among individually examined adverse events, routine NGT patients were more likely than selective patients to be reintubated (11.2% vs. 3.2%), require a postoperative blood transfusion (16.0% vs. 6.4%), and be diagnosed with DGE (18.4% vs. 8.0%).
There were a total of four deaths in the 30-day postoperative period, all occurring in patients over age 80. There were eight octogenarians in each cohort; three of the deaths occurred in the routine group.
Improvements in perioperative care and the surgeon’s increased skill over time may also have affected the results. However, the authors concluded, "based on these data, persistent concerns, such as fear of increased anastomotic leak or DGE, which have mandated customary nasogastric decompression after PD, can be safely reevaluated."
Dr. Kunstman and his coauthors reported no relevant disclosures.
FROM THE JOURNAL OF THE AMERICAN COLLEGE OF SURGEONS
Major finding: Selective use of nasogastric decompression is shown to be an effective treatment strategy post pancreaticoduodenectomy.
Data source: An observational cohort study of 250 PD patients, via a retrospective study of prospectively collected data.
Disclosures: Dr. Kunstman and his coauthors reported no relevant disclosures.
Bariatric surgery doesn’t cut health care costs
Bariatric surgery doesn’t reduce long-term health care costs, according to a report in the June issue of JAMA Surgery.
In a 6-year follow-up study comparing nearly 30,000 patients who underwent bariatric surgery against the same number of well-matched patients who did not have the surgery, the surgery group showed decreases in costs for office visits and prescriptions, but these were offset by their significant increases in inpatient costs, said Jonathan P. Weiner, Dr.P.H., of the department of health policy and management, Johns Hopkins Bloomberg School of Public Health, Baltimore, and his associates.
Health care costs for the bariatric surgery patients did fall off somewhat during the fourth, fifth, and sixth years following the operation, but not enough to outweigh the expenses incurred during the first 3 postoperative years, the investigators said.
Taken together with the results of two other recent studies of the total health care costs related to bariatric surgery, these findings indicate that "to assess the value of bariatric surgery, future studies should focus on the potential benefit of improved health and well-being of persons undergoing the procedure rather than on cost savings," they noted.
It seems intuitive that bariatric surgery, which produces considerable weight loss and alleviates or eliminates many obesity-related disorders such as hypertension and diabetes, would of course save future health care costs, at least in the long term. But studies of the impact of the procedure on such costs have shown mixed results.
"Many uncertainties remain about whether and when a return on investment can be expected, which type of bariatric surgical procedure produces the greatest cost reduction, and whether cost reductions are sustained over time," Dr. Weiner and his colleagues said.
To clarify the issue, they analyzed health care costs in a large cohort of privately insured people covered by seven Blue Cross Blue Shield plans in seven states, of which 29,820 underwent a variety of bariatric procedures during a 6-year period. Each of these subjects was matched for age, sex, area of residence, and 33 markers of obesity with a control subject who did not have bariatric surgery.
Surgical trends shifted during the course of the study. At the beginning, 72% of the procedures were open gastric bypass operations; by the end, laparoscopic procedures were predominant.
Although laparoscopic operations were associated with lower costs in the short term than other procedures, this advantage lasted only for a brief period. So overall, health care costs were not significantly different by type of bariatric surgery.
In an unadjusted analysis of the data, the surgical group showed an approximately 30% decrease in pharmacy costs during the first 3 years after the procedure. The control group showed no such drop.
However, the surgical group had significantly more hospital admissions for GI-related diagnoses than the control group during all 6 years of follow-up, which were concentrated during the second and third years following the procedure. Most of these admissions likely were for surgery-related complications, the investigators said.
In an analysis that adjusted for multiple possible confounders, inpatient costs remained higher for the surgical group than the control group throughout follow-up, but particularly during year 2 and year 3 following the procedure. Pharmacy and office visit costs were significantly lower for the surgery group but did not offset the excess in inpatient costs, Dr. Weiner and his associates reported (JAMA Surg. 2013;148:555-61).
This study "adds substantially to the existing literature on cost of bariatric surgery" because the study population was the largest to date and was representative of a broad cross section of the commercially insured U.S. population. The study also boasts one of the longest follow-ups of bariatric surgery outcomes in the United States, since previous studies generally had follow-ups of only 6 months to 2 years, the researchers said.
In a Clinical Review & Education piece accompanying this report (JAMA Surg. 2013;310:742-3), Matthew L. Maciejewski, Ph.D., and Dr. David E. Arterburn said that bariatric surgery may still be cost-effective even if it is not cost-saving.
"Does bariatric surgery need to be cost-effective (i.e., more effective but more costly than usual care), or does it need to achieve the higher standard of cost savings (i.e., more effective and less costly than usual care) to justify broader insurance coverage?" they asked.
The procedures are so expensive that they are unlikely to meet the threshold of "cost saving" for most patients. Even if a patient’s total health care costs are cut by half after the surgery, "it may take up to 20 years to achieve cost neutrality," said Dr. Maciejewski of the Center for Health Services Research in Primary Care, Durham (N.C.) VA Medical Center, and Dr. Arterburn of the Group Health Research Institute, Seattle.
This lack of cost savings shouldn’t be surprising, given that Roux-en-Y gastric bypass and laparoscopic adjustable gastric banding are invasive procedures that carry high early complication rates. It is possible that newer procedures such as sleeve gastrectomy might eventually yield cost savings because of relatively low complication rates, but these operations haven’t yet undergone long-term economic evaluation, they added.
This study was supported in part by Ethicon Endo-Surgery (a division of Johnson & Johnson), Pfizer, and GlaxoSmithKline, as well as by the National BlueCross BlueShield Association and the seven local plans that participated. No other financial conflicts of interest were reported.
"Bariatric surgery has dramatic short-term results, but on a population level its outcomes are far less impressive," said Dr. Edward H. Livingston.
The study by Weiner et al. adds to "the accumulating evidence" that weight-loss surgery carries no particular economic benefit. "Coupled with findings that bariatric surgery confers little to no long-term survival benefit, these observations show that bariatric surgery does not provide an overall societal benefit," he noted.
"In other words, the indications for bariatric surgery should be viewed in terms of individual patient benefit without anticipating that there will be cost savings to a health care system offering this treatment," Dr. Livingston said.
Dr. Edward H. Livingston is with the JAMA Network in Chicago. He is deputy editor of JAMA. These remarks were taken from his Invited Critique accompanying Dr. Weiner’s report (JAMA Surg. 2013;148:561).
"Bariatric surgery has dramatic short-term results, but on a population level its outcomes are far less impressive," said Dr. Edward H. Livingston.
The study by Weiner et al. adds to "the accumulating evidence" that weight-loss surgery carries no particular economic benefit. "Coupled with findings that bariatric surgery confers little to no long-term survival benefit, these observations show that bariatric surgery does not provide an overall societal benefit," he noted.
"In other words, the indications for bariatric surgery should be viewed in terms of individual patient benefit without anticipating that there will be cost savings to a health care system offering this treatment," Dr. Livingston said.
Dr. Edward H. Livingston is with the JAMA Network in Chicago. He is deputy editor of JAMA. These remarks were taken from his Invited Critique accompanying Dr. Weiner’s report (JAMA Surg. 2013;148:561).
"Bariatric surgery has dramatic short-term results, but on a population level its outcomes are far less impressive," said Dr. Edward H. Livingston.
The study by Weiner et al. adds to "the accumulating evidence" that weight-loss surgery carries no particular economic benefit. "Coupled with findings that bariatric surgery confers little to no long-term survival benefit, these observations show that bariatric surgery does not provide an overall societal benefit," he noted.
"In other words, the indications for bariatric surgery should be viewed in terms of individual patient benefit without anticipating that there will be cost savings to a health care system offering this treatment," Dr. Livingston said.
Dr. Edward H. Livingston is with the JAMA Network in Chicago. He is deputy editor of JAMA. These remarks were taken from his Invited Critique accompanying Dr. Weiner’s report (JAMA Surg. 2013;148:561).
Bariatric surgery doesn’t reduce long-term health care costs, according to a report in the June issue of JAMA Surgery.
In a 6-year follow-up study comparing nearly 30,000 patients who underwent bariatric surgery against the same number of well-matched patients who did not have the surgery, the surgery group showed decreases in costs for office visits and prescriptions, but these were offset by their significant increases in inpatient costs, said Jonathan P. Weiner, Dr.P.H., of the department of health policy and management, Johns Hopkins Bloomberg School of Public Health, Baltimore, and his associates.
Health care costs for the bariatric surgery patients did fall off somewhat during the fourth, fifth, and sixth years following the operation, but not enough to outweigh the expenses incurred during the first 3 postoperative years, the investigators said.
Taken together with the results of two other recent studies of the total health care costs related to bariatric surgery, these findings indicate that "to assess the value of bariatric surgery, future studies should focus on the potential benefit of improved health and well-being of persons undergoing the procedure rather than on cost savings," they noted.
It seems intuitive that bariatric surgery, which produces considerable weight loss and alleviates or eliminates many obesity-related disorders such as hypertension and diabetes, would of course save future health care costs, at least in the long term. But studies of the impact of the procedure on such costs have shown mixed results.
"Many uncertainties remain about whether and when a return on investment can be expected, which type of bariatric surgical procedure produces the greatest cost reduction, and whether cost reductions are sustained over time," Dr. Weiner and his colleagues said.
To clarify the issue, they analyzed health care costs in a large cohort of privately insured people covered by seven Blue Cross Blue Shield plans in seven states, of which 29,820 underwent a variety of bariatric procedures during a 6-year period. Each of these subjects was matched for age, sex, area of residence, and 33 markers of obesity with a control subject who did not have bariatric surgery.
Surgical trends shifted during the course of the study. At the beginning, 72% of the procedures were open gastric bypass operations; by the end, laparoscopic procedures were predominant.
Although laparoscopic operations were associated with lower costs in the short term than other procedures, this advantage lasted only for a brief period. So overall, health care costs were not significantly different by type of bariatric surgery.
In an unadjusted analysis of the data, the surgical group showed an approximately 30% decrease in pharmacy costs during the first 3 years after the procedure. The control group showed no such drop.
However, the surgical group had significantly more hospital admissions for GI-related diagnoses than the control group during all 6 years of follow-up, which were concentrated during the second and third years following the procedure. Most of these admissions likely were for surgery-related complications, the investigators said.
In an analysis that adjusted for multiple possible confounders, inpatient costs remained higher for the surgical group than the control group throughout follow-up, but particularly during year 2 and year 3 following the procedure. Pharmacy and office visit costs were significantly lower for the surgery group but did not offset the excess in inpatient costs, Dr. Weiner and his associates reported (JAMA Surg. 2013;148:555-61).
This study "adds substantially to the existing literature on cost of bariatric surgery" because the study population was the largest to date and was representative of a broad cross section of the commercially insured U.S. population. The study also boasts one of the longest follow-ups of bariatric surgery outcomes in the United States, since previous studies generally had follow-ups of only 6 months to 2 years, the researchers said.
In a Clinical Review & Education piece accompanying this report (JAMA Surg. 2013;310:742-3), Matthew L. Maciejewski, Ph.D., and Dr. David E. Arterburn said that bariatric surgery may still be cost-effective even if it is not cost-saving.
"Does bariatric surgery need to be cost-effective (i.e., more effective but more costly than usual care), or does it need to achieve the higher standard of cost savings (i.e., more effective and less costly than usual care) to justify broader insurance coverage?" they asked.
The procedures are so expensive that they are unlikely to meet the threshold of "cost saving" for most patients. Even if a patient’s total health care costs are cut by half after the surgery, "it may take up to 20 years to achieve cost neutrality," said Dr. Maciejewski of the Center for Health Services Research in Primary Care, Durham (N.C.) VA Medical Center, and Dr. Arterburn of the Group Health Research Institute, Seattle.
This lack of cost savings shouldn’t be surprising, given that Roux-en-Y gastric bypass and laparoscopic adjustable gastric banding are invasive procedures that carry high early complication rates. It is possible that newer procedures such as sleeve gastrectomy might eventually yield cost savings because of relatively low complication rates, but these operations haven’t yet undergone long-term economic evaluation, they added.
This study was supported in part by Ethicon Endo-Surgery (a division of Johnson & Johnson), Pfizer, and GlaxoSmithKline, as well as by the National BlueCross BlueShield Association and the seven local plans that participated. No other financial conflicts of interest were reported.
Bariatric surgery doesn’t reduce long-term health care costs, according to a report in the June issue of JAMA Surgery.
In a 6-year follow-up study comparing nearly 30,000 patients who underwent bariatric surgery against the same number of well-matched patients who did not have the surgery, the surgery group showed decreases in costs for office visits and prescriptions, but these were offset by their significant increases in inpatient costs, said Jonathan P. Weiner, Dr.P.H., of the department of health policy and management, Johns Hopkins Bloomberg School of Public Health, Baltimore, and his associates.
Health care costs for the bariatric surgery patients did fall off somewhat during the fourth, fifth, and sixth years following the operation, but not enough to outweigh the expenses incurred during the first 3 postoperative years, the investigators said.
Taken together with the results of two other recent studies of the total health care costs related to bariatric surgery, these findings indicate that "to assess the value of bariatric surgery, future studies should focus on the potential benefit of improved health and well-being of persons undergoing the procedure rather than on cost savings," they noted.
It seems intuitive that bariatric surgery, which produces considerable weight loss and alleviates or eliminates many obesity-related disorders such as hypertension and diabetes, would of course save future health care costs, at least in the long term. But studies of the impact of the procedure on such costs have shown mixed results.
"Many uncertainties remain about whether and when a return on investment can be expected, which type of bariatric surgical procedure produces the greatest cost reduction, and whether cost reductions are sustained over time," Dr. Weiner and his colleagues said.
To clarify the issue, they analyzed health care costs in a large cohort of privately insured people covered by seven Blue Cross Blue Shield plans in seven states, of which 29,820 underwent a variety of bariatric procedures during a 6-year period. Each of these subjects was matched for age, sex, area of residence, and 33 markers of obesity with a control subject who did not have bariatric surgery.
Surgical trends shifted during the course of the study. At the beginning, 72% of the procedures were open gastric bypass operations; by the end, laparoscopic procedures were predominant.
Although laparoscopic operations were associated with lower costs in the short term than other procedures, this advantage lasted only for a brief period. So overall, health care costs were not significantly different by type of bariatric surgery.
In an unadjusted analysis of the data, the surgical group showed an approximately 30% decrease in pharmacy costs during the first 3 years after the procedure. The control group showed no such drop.
However, the surgical group had significantly more hospital admissions for GI-related diagnoses than the control group during all 6 years of follow-up, which were concentrated during the second and third years following the procedure. Most of these admissions likely were for surgery-related complications, the investigators said.
In an analysis that adjusted for multiple possible confounders, inpatient costs remained higher for the surgical group than the control group throughout follow-up, but particularly during year 2 and year 3 following the procedure. Pharmacy and office visit costs were significantly lower for the surgery group but did not offset the excess in inpatient costs, Dr. Weiner and his associates reported (JAMA Surg. 2013;148:555-61).
This study "adds substantially to the existing literature on cost of bariatric surgery" because the study population was the largest to date and was representative of a broad cross section of the commercially insured U.S. population. The study also boasts one of the longest follow-ups of bariatric surgery outcomes in the United States, since previous studies generally had follow-ups of only 6 months to 2 years, the researchers said.
In a Clinical Review & Education piece accompanying this report (JAMA Surg. 2013;310:742-3), Matthew L. Maciejewski, Ph.D., and Dr. David E. Arterburn said that bariatric surgery may still be cost-effective even if it is not cost-saving.
"Does bariatric surgery need to be cost-effective (i.e., more effective but more costly than usual care), or does it need to achieve the higher standard of cost savings (i.e., more effective and less costly than usual care) to justify broader insurance coverage?" they asked.
The procedures are so expensive that they are unlikely to meet the threshold of "cost saving" for most patients. Even if a patient’s total health care costs are cut by half after the surgery, "it may take up to 20 years to achieve cost neutrality," said Dr. Maciejewski of the Center for Health Services Research in Primary Care, Durham (N.C.) VA Medical Center, and Dr. Arterburn of the Group Health Research Institute, Seattle.
This lack of cost savings shouldn’t be surprising, given that Roux-en-Y gastric bypass and laparoscopic adjustable gastric banding are invasive procedures that carry high early complication rates. It is possible that newer procedures such as sleeve gastrectomy might eventually yield cost savings because of relatively low complication rates, but these operations haven’t yet undergone long-term economic evaluation, they added.
This study was supported in part by Ethicon Endo-Surgery (a division of Johnson & Johnson), Pfizer, and GlaxoSmithKline, as well as by the National BlueCross BlueShield Association and the seven local plans that participated. No other financial conflicts of interest were reported.
FROM JAMA SURGERY
Major finding: Inpatient costs were significantly higher for the surgical group than the control group, particularly during year 2 and year 3 following the procedure; pharmacy and office visit costs were significantly lower for the surgery group but did not offset the excess in inpatient costs.
Data source: A 6-year longitudinal analysis of private insurance claims data for 29,820 patients who underwent bariatric surgery and 29,820 matched nonsurgical control subjects.
Disclosures: This study was supported in part by Ethicon Endo-Surgery (a division of Johnson & Johnson), Pfizer, and GlaxoSmithKline, as well as by the National BlueCross BlueShield Association and the seven local plans that participated. No other financial conflicts of interest were reported.
Five top hospital-acquired infections cost billions
An estimated 440,000 adult inpatients acquire one of the top five nosocomial infections in the United States every year, according to a report published online Sept. 2 in JAMA Internal Medicine.
The annual cost of these hospital-acquired infections is an estimated $9.8 billion. One-third of these costs are attributable to surgical site infections. One-fourth are due to ventilator-associated pneumonia, and another fourth are due to catheter-associated urinary tract infections, said Dr. Eyal Zimlichman of the Center for Patient Safety Research and Practice, Brigham and Women’s Hospital and Harvard Medical School, Boston.

Other studies have estimated that 55%-75% of hospital-acquired infections are preventable with currently available evidence-based interventions. If hospitals nationwide were to implement these existing interventions, an estimated $5.0-$5.5 billion would be saved annually, and the hospitals themselves would be able to tap into those savings.
"Thus, implementation of readily available strategies has the potential to produce significant bottom-line savings to hospitals," the investigators noted.
Dr. Zimlichman and his colleagues analyzed data from the Centers for Disease Control and Prevention’s National Healthcare Safety Network and from a systematic review of the medical literature to estimate the impact of hospital-acquired infections on the U.S. health care system. They focused on a single year (2009) and the five most common, most costly, most preventable, and most well-monitored infections among adult inpatients: surgical site infection, central line–associated bloodstream infection, catheter-associated urinary tract infection, ventilator-associated pneumonia, and Clostridium difficile infection.
These infections occurred against a background of approximately 34.7 million adults receiving inpatient care in U.S. hospitals, for a total of 165.1 million patient-days. These patients underwent approximately 8 million surgical procedures and were treated with invasive medical devices for approximately 96.2 million days of care, which placed them at risk for hospital-acquired infections.
"On an annual basis, surgical site infections (158,639) and Clostridium difficile infections (133,657) were estimated to be the most frequent hospital-acquired infections nationwide," accounting for 36% and 30% of the total number. Catheter-associated UTIs accounted for another 17%, central line–associated bloodstream infection accounted for 9%, and ventilator-associated pneumonia accounted for 7%, Dr. Zimlichman and his associates wrote (JAMA Intern. Med. 2013 Sept. 2 [doi:10.1001/jamainternmed.2013.9763]).
Surgical site infections contributed the greatest portion (34%) to the $9.8 billion estimated total. Catheter-associated UTIs, while frequent, contributed less than 1% to the total expenditure. Ventilator-associated pneumonia contributed 32%, central line–associated bloodstream infection contributed 19%, and C. difficile contributed 15%.
"Since surgical site infections constitute the largest portion of hospital-acquired infection–related costs nationally, and since less progress has been made in preventing these infections than in other areas of care, research and quality improvement efforts are clearly needed in this area," noted Dr. Zimlichman and his associates.
Even though central line–associated bloodstream infections were relatively infrequent, accounting for less than 10% of the total number, these were the most costly infections on a case-by-case basis. Each case of this infection was estimated to cost $45,814. The subgroup of central line–associated bloodstream infections caused by methicillin-resistant Staphylococcus aureus was even more expensive, at $58,614 per case.
The study findings indicate that although much progress has been made in preventing hospital-acquired infections, "much more remains to be done."
"Our study provides updated, robust, and applicable estimates for resources attributable to the major hospital-acquired infections that continue to plague modern health care systems and create considerable harm to patients," they noted.
The investigators added that their findings underestimate the true health care costs of hospital-acquired infection because this study excluded "not only neonatal and pediatric patients but also patients in non–acute care facilities such as long-term care and dialysis centers."
This study was sponsored by the Texas Medical Institute of Technology in Austin. No financial conflicts of interest were reported.
An estimated 440,000 adult inpatients acquire one of the top five nosocomial infections in the United States every year, according to a report published online Sept. 2 in JAMA Internal Medicine.
The annual cost of these hospital-acquired infections is an estimated $9.8 billion. One-third of these costs are attributable to surgical site infections. One-fourth are due to ventilator-associated pneumonia, and another fourth are due to catheter-associated urinary tract infections, said Dr. Eyal Zimlichman of the Center for Patient Safety Research and Practice, Brigham and Women’s Hospital and Harvard Medical School, Boston.
Other studies have estimated that 55%-75% of hospital-acquired infections are preventable with currently available evidence-based interventions. If hospitals nationwide were to implement these existing interventions, an estimated $5.0-$5.5 billion would be saved annually, and the hospitals themselves would be able to tap into those savings.
"Thus, implementation of readily available strategies has the potential to produce significant bottom-line savings to hospitals," the investigators noted.
Dr. Zimlichman and his colleagues analyzed data from the Centers for Disease Control and Prevention’s National Healthcare Safety Network and from a systematic review of the medical literature to estimate the impact of hospital-acquired infections on the U.S. health care system. They focused on a single year (2009) and the five most common, most costly, most preventable, and most well-monitored infections among adult inpatients: surgical site infection, central line–associated bloodstream infection, catheter-associated urinary tract infection, ventilator-associated pneumonia, and Clostridium difficile infection.
These infections occurred against a background of approximately 34.7 million adults receiving inpatient care in U.S. hospitals, for a total of 165.1 million patient-days. These patients underwent approximately 8 million surgical procedures and were treated with invasive medical devices for approximately 96.2 million days of care, which placed them at risk for hospital-acquired infections.
"On an annual basis, surgical site infections (158,639) and Clostridium difficile infections (133,657) were estimated to be the most frequent hospital-acquired infections nationwide," accounting for 36% and 30% of the total number. Catheter-associated UTIs accounted for another 17%, central line–associated bloodstream infection accounted for 9%, and ventilator-associated pneumonia accounted for 7%, Dr. Zimlichman and his associates wrote (JAMA Intern. Med. 2013 Sept. 2 [doi:10.1001/jamainternmed.2013.9763]).
Surgical site infections contributed the greatest portion (34%) to the $9.8 billion estimated total. Catheter-associated UTIs, while frequent, contributed less than 1% to the total expenditure. Ventilator-associated pneumonia contributed 32%, central line–associated bloodstream infection contributed 19%, and C. difficile contributed 15%.
"Since surgical site infections constitute the largest portion of hospital-acquired infection–related costs nationally, and since less progress has been made in preventing these infections than in other areas of care, research and quality improvement efforts are clearly needed in this area," noted Dr. Zimlichman and his associates.
Even though central line–associated bloodstream infections were relatively infrequent, accounting for less than 10% of the total number, these were the most costly infections on a case-by-case basis. Each case of this infection was estimated to cost $45,814. The subgroup of central line–associated bloodstream infections caused by methicillin-resistant Staphylococcus aureus was even more expensive, at $58,614 per case.
The study findings indicate that although much progress has been made in preventing hospital-acquired infections, "much more remains to be done."
"Our study provides updated, robust, and applicable estimates for resources attributable to the major hospital-acquired infections that continue to plague modern health care systems and create considerable harm to patients," they noted.
The investigators added that their findings underestimate the true health care costs of hospital-acquired infection because this study excluded "not only neonatal and pediatric patients but also patients in non–acute care facilities such as long-term care and dialysis centers."
This study was sponsored by the Texas Medical Institute of Technology in Austin. No financial conflicts of interest were reported.
An estimated 440,000 adult inpatients acquire one of the top five nosocomial infections in the United States every year, according to a report published online Sept. 2 in JAMA Internal Medicine.
The annual cost of these hospital-acquired infections is an estimated $9.8 billion. One-third of these costs are attributable to surgical site infections. One-fourth are due to ventilator-associated pneumonia, and another fourth are due to catheter-associated urinary tract infections, said Dr. Eyal Zimlichman of the Center for Patient Safety Research and Practice, Brigham and Women’s Hospital and Harvard Medical School, Boston.
Other studies have estimated that 55%-75% of hospital-acquired infections are preventable with currently available evidence-based interventions. If hospitals nationwide were to implement these existing interventions, an estimated $5.0-$5.5 billion would be saved annually, and the hospitals themselves would be able to tap into those savings.
"Thus, implementation of readily available strategies has the potential to produce significant bottom-line savings to hospitals," the investigators noted.
Dr. Zimlichman and his colleagues analyzed data from the Centers for Disease Control and Prevention’s National Healthcare Safety Network and from a systematic review of the medical literature to estimate the impact of hospital-acquired infections on the U.S. health care system. They focused on a single year (2009) and the five most common, most costly, most preventable, and most well-monitored infections among adult inpatients: surgical site infection, central line–associated bloodstream infection, catheter-associated urinary tract infection, ventilator-associated pneumonia, and Clostridium difficile infection.
These infections occurred against a background of approximately 34.7 million adults receiving inpatient care in U.S. hospitals, for a total of 165.1 million patient-days. These patients underwent approximately 8 million surgical procedures and were treated with invasive medical devices for approximately 96.2 million days of care, which placed them at risk for hospital-acquired infections.
"On an annual basis, surgical site infections (158,639) and Clostridium difficile infections (133,657) were estimated to be the most frequent hospital-acquired infections nationwide," accounting for 36% and 30% of the total number. Catheter-associated UTIs accounted for another 17%, central line–associated bloodstream infection accounted for 9%, and ventilator-associated pneumonia accounted for 7%, Dr. Zimlichman and his associates wrote (JAMA Intern. Med. 2013 Sept. 2 [doi:10.1001/jamainternmed.2013.9763]).
Surgical site infections contributed the greatest portion (34%) to the $9.8 billion estimated total. Catheter-associated UTIs, while frequent, contributed less than 1% to the total expenditure. Ventilator-associated pneumonia contributed 32%, central line–associated bloodstream infection contributed 19%, and C. difficile contributed 15%.
"Since surgical site infections constitute the largest portion of hospital-acquired infection–related costs nationally, and since less progress has been made in preventing these infections than in other areas of care, research and quality improvement efforts are clearly needed in this area," noted Dr. Zimlichman and his associates.
Even though central line–associated bloodstream infections were relatively infrequent, accounting for less than 10% of the total number, these were the most costly infections on a case-by-case basis. Each case of this infection was estimated to cost $45,814. The subgroup of central line–associated bloodstream infections caused by methicillin-resistant Staphylococcus aureus was even more expensive, at $58,614 per case.
The study findings indicate that although much progress has been made in preventing hospital-acquired infections, "much more remains to be done."
"Our study provides updated, robust, and applicable estimates for resources attributable to the major hospital-acquired infections that continue to plague modern health care systems and create considerable harm to patients," they noted.
The investigators added that their findings underestimate the true health care costs of hospital-acquired infection because this study excluded "not only neonatal and pediatric patients but also patients in non–acute care facilities such as long-term care and dialysis centers."
This study was sponsored by the Texas Medical Institute of Technology in Austin. No financial conflicts of interest were reported.
FROM JAMA INTERNAL MEDICINE
Major finding: There were an estimated 440,000 hospital-acquired infections among adult inpatients in 2009, and total health care costs directly associated with these infections were estimated to be $9.8 billion.
Data source: An analysis of data from the CDC’s National Healthcare Safety Network in 2009 and from a review of the literature published in 1986 through 2013 regarding hospital-acquired infections in the United States.
Disclosures: This study was sponsored by the Texas Medical Institute of Technology in Austin. No financial conflicts of interest were reported.
Endoscopy, surgery for pancreatic pseudocysts show equal efficacy
Endoscopic cystogastrostomy was as effective as surgical cystogastrostomy for pancreatic pseudocyst drainage in a randomized trial comparing the two approaches.
None of the 20 patients randomized to undergo endoscopic treatment, and 1 of 20 patients randomized to undergo surgery, experienced pseudocyst recurrence within 24 months of follow-up, Dr. Shyam Varadarajulu of the University of Alabama at Birmingham and his colleagues reported online May 31, ahead of print in Gastroenterology.
Source: American Gastroenterological Association
Moreover, those in the endoscopy group had a shorter hospital length of stay than did the patients in the surgery group (median of 2 vs. 6 days) and a lower mean cost of care ($7,011 vs. $15,052), the investigators reported (Gastroenterology 2013 May 31 [doi: 10.1053/j.gastro.2013.05.046]).
Patients included in the study were adults with intrapancreatic or extrapancreatic pseudocysts who were enrolled between Jan. 20 and Dec. 28, 2009, following evaluation by a gastroenterologist or surgeon in an outpatient clinic or inpatient setting.
The 20 patients in the endoscopy group underwent cystogastrostomy using endoscopic ultrasound guidance and fluoroscopy while they were under conscious sedation.
"Once the pseudocyst was identified, it was accessed using a 19-gauge needle, and the gastric wall was dilated up to 15 mm using a wire-guided balloon. Two plastic stents then were deployed to facilitate the drainage of pseudocyst contents into the stomach," the investigators explained, noting that endoscopy patients were discharged following the procedure.
No procedural complications occurred in any of the 20 patients. However, one patient presented to the hospital 13 days later with persistent abdominal pain; a computed tomography scan showed a residual 7-cm pseudocyst, which was successfully treated by deployment of additional stents. At 8-week follow-up, abdominal CT scans showed pseudocyst resolution in all 20 patients.
Endoscopic retrograde cholangiopancreatography (ERCP), which was performed in all of the endoscopy patients to assess and treat any pancreatic duct leaks, was successful in 18 of the 20 patients. Magnetic resonance cholangiopancreatography (MRCP), performed in those two patients, showed a normal pancreatic duct in one and a disconnected duct in the other, the investigators said.
The 20 patients in the surgery group were all treated by the same pancreatic surgeon, who used an endovascular stapler to create at least a 6-cm cystogastrostomy after obtaining entry to the pseudocyst.
"A nasogastric tube then was left in the stomach and passed into the pseudocyst cavity to allow for intermittent irrigation until postoperative day 1 ... the nasogastric tube was removed on postoperative day 1 and clear liquids were started on day 2," they said.
Patients were discharged once a soft diet was tolerated and pain adequately controlled.
One patient with ongoing alcohol consumption developed pseudocyst recurrence at 4 months and was managed by endoscopic cystogastrostomy.
Two surgery patients experienced complications, including a wound infection treated by local debridement and antibiotics in one patient, and a case of hematemesis in one patient who was on anticoagulation and who was readmitted 9 days after discharge. "At endoscopy, a visible clot was noted at the site of surgical anastomosis, and hemostasis was achieved by application of electrocautery," the investigators said.
Two other patients were not able to tolerate oral intake postoperatively; one of them was managed conservatively, and one required surgical placement of a temporary enteral feeding tube. In addition, one patient presented at 6 months with abdominal pain and was found on ERCP to have a stricture in the pancreatic tail that required management by distal pancreatectomy.
Overall, there were no differences in the rates of treatment success, treatment failure, complications, or reinterventions between the endoscopy and surgery groups.
However, in addition to the shorter hospital stay and lower costs in the endoscopy group, patients in that group had significantly greater improvement over time in physical and mental health component scores on the Medical Outcomes Study 36-Item Short-Form General Survey. Although the scores improved for both cohorts, they were 4.48 points and 4.41 points lower, respectively, in the surgery group than the endoscopy group, the investigators said.
The findings are of note because although endoscopic drainage of pancreatic pseudocysts is increasingly performed, surgical cystogastrostomy is still considered the gold standard for treatment, as randomized trials comparing the two approaches had not previously been performed.
"The clinical relevance of this study is substantial because it shows that endoscopically managed patients can be discharged home earlier with a better health-related quality of life, and treatment can be delivered at a lower cost," the investigators said.
The authors reported having no disclosures.
There has been marked evolution in the understanding and management of acute and chronic pancreatitis over the last decade. Walled-off necroses and pseudocysts are consequences of pancreatitis that may be intrapancreatic, extrapancreatic, or both. These two entities are often confused. Fortunately, a recent international consensus has clarified that pseudocysts are liquid-filled, are almost always extrapancreatic, and rarely occur as the consequence of severe pancreatitis or involve "disconnected duct" (Gut 2013;62:102-11).

|
| Dr. Martin L. Freeman |
Dr. Varadarajulu and his colleagues are to be congratulated for performing a landmark study comparing surgery and endoscopy for internal drainage of pseudocysts (Gastroenterology 2013 May 31 [doi: 10.1053/j.gastro.2013.05.046]). They covered all the bases for an outstanding efficacy trial, including performance by experts at a tertiary center, and careful definitions of endpoints. Although the title of the paper is "Equal efficacy … [of the two approaches]," based on the primary endpoint of recurrence at 24 months, they addressed cost, hospital stay, and quality of life measures, all increasingly important in the current health care environment. In the latter regard, endoscopic ultrasound-guided cystgastrostomy emerged to be clearly superior to open surgery. If patients with more comorbidity such as portal hypertension were included, the differences would likely have been even more striking.
Thus, for pseudocysts, as for walled-off necroses, the picture is becoming increasingly clear: Minimally invasive and in particular endoscopic techniques are superior to open surgical approaches. This represents a paradigm shift in clinical practice. However, to be effective and safe in widespread applicability, it is incumbent that endoscopists attempting to manage these conditions have highly specialized expertise in pancreatic diseases and techniques, and manage these complex patients in close collaboration with their colleagues in surgery and interventional radiology.
Dr. Martin L. Freeman, FACG, FASGE, is professor of medicine at the University of Minnesota, Minneapolis. He disclosed receiving speaking honoraria from Boston Scientific and Cook, and consulting for Boston Scientific.
There has been marked evolution in the understanding and management of acute and chronic pancreatitis over the last decade. Walled-off necroses and pseudocysts are consequences of pancreatitis that may be intrapancreatic, extrapancreatic, or both. These two entities are often confused. Fortunately, a recent international consensus has clarified that pseudocysts are liquid-filled, are almost always extrapancreatic, and rarely occur as the consequence of severe pancreatitis or involve "disconnected duct" (Gut 2013;62:102-11).
|
|
| Dr. Martin L. Freeman |
Dr. Varadarajulu and his colleagues are to be congratulated for performing a landmark study comparing surgery and endoscopy for internal drainage of pseudocysts (Gastroenterology 2013 May 31 [doi: 10.1053/j.gastro.2013.05.046]). They covered all the bases for an outstanding efficacy trial, including performance by experts at a tertiary center, and careful definitions of endpoints. Although the title of the paper is "Equal efficacy … [of the two approaches]," based on the primary endpoint of recurrence at 24 months, they addressed cost, hospital stay, and quality of life measures, all increasingly important in the current health care environment. In the latter regard, endoscopic ultrasound-guided cystgastrostomy emerged to be clearly superior to open surgery. If patients with more comorbidity such as portal hypertension were included, the differences would likely have been even more striking.
Thus, for pseudocysts, as for walled-off necroses, the picture is becoming increasingly clear: Minimally invasive and in particular endoscopic techniques are superior to open surgical approaches. This represents a paradigm shift in clinical practice. However, to be effective and safe in widespread applicability, it is incumbent that endoscopists attempting to manage these conditions have highly specialized expertise in pancreatic diseases and techniques, and manage these complex patients in close collaboration with their colleagues in surgery and interventional radiology.
Dr. Martin L. Freeman, FACG, FASGE, is professor of medicine at the University of Minnesota, Minneapolis. He disclosed receiving speaking honoraria from Boston Scientific and Cook, and consulting for Boston Scientific.
There has been marked evolution in the understanding and management of acute and chronic pancreatitis over the last decade. Walled-off necroses and pseudocysts are consequences of pancreatitis that may be intrapancreatic, extrapancreatic, or both. These two entities are often confused. Fortunately, a recent international consensus has clarified that pseudocysts are liquid-filled, are almost always extrapancreatic, and rarely occur as the consequence of severe pancreatitis or involve "disconnected duct" (Gut 2013;62:102-11).
|
|
| Dr. Martin L. Freeman |
Dr. Varadarajulu and his colleagues are to be congratulated for performing a landmark study comparing surgery and endoscopy for internal drainage of pseudocysts (Gastroenterology 2013 May 31 [doi: 10.1053/j.gastro.2013.05.046]). They covered all the bases for an outstanding efficacy trial, including performance by experts at a tertiary center, and careful definitions of endpoints. Although the title of the paper is "Equal efficacy … [of the two approaches]," based on the primary endpoint of recurrence at 24 months, they addressed cost, hospital stay, and quality of life measures, all increasingly important in the current health care environment. In the latter regard, endoscopic ultrasound-guided cystgastrostomy emerged to be clearly superior to open surgery. If patients with more comorbidity such as portal hypertension were included, the differences would likely have been even more striking.
Thus, for pseudocysts, as for walled-off necroses, the picture is becoming increasingly clear: Minimally invasive and in particular endoscopic techniques are superior to open surgical approaches. This represents a paradigm shift in clinical practice. However, to be effective and safe in widespread applicability, it is incumbent that endoscopists attempting to manage these conditions have highly specialized expertise in pancreatic diseases and techniques, and manage these complex patients in close collaboration with their colleagues in surgery and interventional radiology.
Dr. Martin L. Freeman, FACG, FASGE, is professor of medicine at the University of Minnesota, Minneapolis. He disclosed receiving speaking honoraria from Boston Scientific and Cook, and consulting for Boston Scientific.
Endoscopic cystogastrostomy was as effective as surgical cystogastrostomy for pancreatic pseudocyst drainage in a randomized trial comparing the two approaches.
None of the 20 patients randomized to undergo endoscopic treatment, and 1 of 20 patients randomized to undergo surgery, experienced pseudocyst recurrence within 24 months of follow-up, Dr. Shyam Varadarajulu of the University of Alabama at Birmingham and his colleagues reported online May 31, ahead of print in Gastroenterology.
Source: American Gastroenterological Association
Moreover, those in the endoscopy group had a shorter hospital length of stay than did the patients in the surgery group (median of 2 vs. 6 days) and a lower mean cost of care ($7,011 vs. $15,052), the investigators reported (Gastroenterology 2013 May 31 [doi: 10.1053/j.gastro.2013.05.046]).
Patients included in the study were adults with intrapancreatic or extrapancreatic pseudocysts who were enrolled between Jan. 20 and Dec. 28, 2009, following evaluation by a gastroenterologist or surgeon in an outpatient clinic or inpatient setting.
The 20 patients in the endoscopy group underwent cystogastrostomy using endoscopic ultrasound guidance and fluoroscopy while they were under conscious sedation.
"Once the pseudocyst was identified, it was accessed using a 19-gauge needle, and the gastric wall was dilated up to 15 mm using a wire-guided balloon. Two plastic stents then were deployed to facilitate the drainage of pseudocyst contents into the stomach," the investigators explained, noting that endoscopy patients were discharged following the procedure.
No procedural complications occurred in any of the 20 patients. However, one patient presented to the hospital 13 days later with persistent abdominal pain; a computed tomography scan showed a residual 7-cm pseudocyst, which was successfully treated by deployment of additional stents. At 8-week follow-up, abdominal CT scans showed pseudocyst resolution in all 20 patients.
Endoscopic retrograde cholangiopancreatography (ERCP), which was performed in all of the endoscopy patients to assess and treat any pancreatic duct leaks, was successful in 18 of the 20 patients. Magnetic resonance cholangiopancreatography (MRCP), performed in those two patients, showed a normal pancreatic duct in one and a disconnected duct in the other, the investigators said.
The 20 patients in the surgery group were all treated by the same pancreatic surgeon, who used an endovascular stapler to create at least a 6-cm cystogastrostomy after obtaining entry to the pseudocyst.
"A nasogastric tube then was left in the stomach and passed into the pseudocyst cavity to allow for intermittent irrigation until postoperative day 1 ... the nasogastric tube was removed on postoperative day 1 and clear liquids were started on day 2," they said.
Patients were discharged once a soft diet was tolerated and pain adequately controlled.
One patient with ongoing alcohol consumption developed pseudocyst recurrence at 4 months and was managed by endoscopic cystogastrostomy.
Two surgery patients experienced complications, including a wound infection treated by local debridement and antibiotics in one patient, and a case of hematemesis in one patient who was on anticoagulation and who was readmitted 9 days after discharge. "At endoscopy, a visible clot was noted at the site of surgical anastomosis, and hemostasis was achieved by application of electrocautery," the investigators said.
Two other patients were not able to tolerate oral intake postoperatively; one of them was managed conservatively, and one required surgical placement of a temporary enteral feeding tube. In addition, one patient presented at 6 months with abdominal pain and was found on ERCP to have a stricture in the pancreatic tail that required management by distal pancreatectomy.
Overall, there were no differences in the rates of treatment success, treatment failure, complications, or reinterventions between the endoscopy and surgery groups.
However, in addition to the shorter hospital stay and lower costs in the endoscopy group, patients in that group had significantly greater improvement over time in physical and mental health component scores on the Medical Outcomes Study 36-Item Short-Form General Survey. Although the scores improved for both cohorts, they were 4.48 points and 4.41 points lower, respectively, in the surgery group than the endoscopy group, the investigators said.
The findings are of note because although endoscopic drainage of pancreatic pseudocysts is increasingly performed, surgical cystogastrostomy is still considered the gold standard for treatment, as randomized trials comparing the two approaches had not previously been performed.
"The clinical relevance of this study is substantial because it shows that endoscopically managed patients can be discharged home earlier with a better health-related quality of life, and treatment can be delivered at a lower cost," the investigators said.
The authors reported having no disclosures.
Endoscopic cystogastrostomy was as effective as surgical cystogastrostomy for pancreatic pseudocyst drainage in a randomized trial comparing the two approaches.
None of the 20 patients randomized to undergo endoscopic treatment, and 1 of 20 patients randomized to undergo surgery, experienced pseudocyst recurrence within 24 months of follow-up, Dr. Shyam Varadarajulu of the University of Alabama at Birmingham and his colleagues reported online May 31, ahead of print in Gastroenterology.
Source: American Gastroenterological Association
Moreover, those in the endoscopy group had a shorter hospital length of stay than did the patients in the surgery group (median of 2 vs. 6 days) and a lower mean cost of care ($7,011 vs. $15,052), the investigators reported (Gastroenterology 2013 May 31 [doi: 10.1053/j.gastro.2013.05.046]).
Patients included in the study were adults with intrapancreatic or extrapancreatic pseudocysts who were enrolled between Jan. 20 and Dec. 28, 2009, following evaluation by a gastroenterologist or surgeon in an outpatient clinic or inpatient setting.
The 20 patients in the endoscopy group underwent cystogastrostomy using endoscopic ultrasound guidance and fluoroscopy while they were under conscious sedation.
"Once the pseudocyst was identified, it was accessed using a 19-gauge needle, and the gastric wall was dilated up to 15 mm using a wire-guided balloon. Two plastic stents then were deployed to facilitate the drainage of pseudocyst contents into the stomach," the investigators explained, noting that endoscopy patients were discharged following the procedure.
No procedural complications occurred in any of the 20 patients. However, one patient presented to the hospital 13 days later with persistent abdominal pain; a computed tomography scan showed a residual 7-cm pseudocyst, which was successfully treated by deployment of additional stents. At 8-week follow-up, abdominal CT scans showed pseudocyst resolution in all 20 patients.
Endoscopic retrograde cholangiopancreatography (ERCP), which was performed in all of the endoscopy patients to assess and treat any pancreatic duct leaks, was successful in 18 of the 20 patients. Magnetic resonance cholangiopancreatography (MRCP), performed in those two patients, showed a normal pancreatic duct in one and a disconnected duct in the other, the investigators said.
The 20 patients in the surgery group were all treated by the same pancreatic surgeon, who used an endovascular stapler to create at least a 6-cm cystogastrostomy after obtaining entry to the pseudocyst.
"A nasogastric tube then was left in the stomach and passed into the pseudocyst cavity to allow for intermittent irrigation until postoperative day 1 ... the nasogastric tube was removed on postoperative day 1 and clear liquids were started on day 2," they said.
Patients were discharged once a soft diet was tolerated and pain adequately controlled.
One patient with ongoing alcohol consumption developed pseudocyst recurrence at 4 months and was managed by endoscopic cystogastrostomy.
Two surgery patients experienced complications, including a wound infection treated by local debridement and antibiotics in one patient, and a case of hematemesis in one patient who was on anticoagulation and who was readmitted 9 days after discharge. "At endoscopy, a visible clot was noted at the site of surgical anastomosis, and hemostasis was achieved by application of electrocautery," the investigators said.
Two other patients were not able to tolerate oral intake postoperatively; one of them was managed conservatively, and one required surgical placement of a temporary enteral feeding tube. In addition, one patient presented at 6 months with abdominal pain and was found on ERCP to have a stricture in the pancreatic tail that required management by distal pancreatectomy.
Overall, there were no differences in the rates of treatment success, treatment failure, complications, or reinterventions between the endoscopy and surgery groups.
However, in addition to the shorter hospital stay and lower costs in the endoscopy group, patients in that group had significantly greater improvement over time in physical and mental health component scores on the Medical Outcomes Study 36-Item Short-Form General Survey. Although the scores improved for both cohorts, they were 4.48 points and 4.41 points lower, respectively, in the surgery group than the endoscopy group, the investigators said.
The findings are of note because although endoscopic drainage of pancreatic pseudocysts is increasingly performed, surgical cystogastrostomy is still considered the gold standard for treatment, as randomized trials comparing the two approaches had not previously been performed.
"The clinical relevance of this study is substantial because it shows that endoscopically managed patients can be discharged home earlier with a better health-related quality of life, and treatment can be delivered at a lower cost," the investigators said.
The authors reported having no disclosures.
FROM GASTROENTEROLOGY
Major finding: Pseudocysts recurred in 0 of 20 endoscopy patients, and 1 of 20 surgery patients.
Data source: An open-label randomized trial involving 40 patients.
Disclosures: The authors reported having no disclosures.