User login
Two key suicide risk factors identified in borderline personality disorder
Feelings of chronic emptiness and self-injury have been identified as two key risk factors for suicide attempts (SAs) in patients with borderline personality disorder (BPD), a new cross-sectional, nationally representative study suggests.

The findings also show lifetime and past-year SAs are common among patients with BPD, even when excluding self-injurious behaviors.
The results suggest that in addition to asking patients about self-harm during suicide risk screenings and assessments, clinicians should query them about “longstanding” feelings of emptiness, study investigator Carlos M. Grilo, PhD, professor of psychiatry and psychology, Yale University, New Haven, Conn., said in an interview.
Although related, chronic emptiness “is distinct and goes beyond feelings of sadness, loneliness, and hopelessness,” explained Dr. Grilo. he said.
The study was published online May 11 in JAMA Network Open.
Filling a research gap
While BPD and other psychiatric disorders are associated with suicide, the authors noted there is a “dearth of epidemiological research” examining the link between BPD and suicide.
Criteria for BPD diagnosis requires any five of the following criteria: relationships, affective instability, abandonment fear, anger, identity disturbance, emptiness, disassociation/paranoia, self-injurious behavior, and impulsivity, along with social-occupation dysfunction.
To determine SA risk with specific BPD diagnostic criteria, the investigators examined data on 36,309 individuals who participated in the third wave of the National Epidemiologic Survey on Alcohol and Related Conditions (NESARC-III), conducted from 2012 to 2013.
During computer-assisted, face-to-face interviews, study participants answered questions based on the Alcohol Use Disorder and Associated Disabilities Interview Schedule-5 (AUDADIS-5) of the National Institute on Alcohol Abuse and Alcoholism.
This structured interview assesses a range of DSM-5–defined psychiatric disorders and their criteria. In addition to BPD, the AUDADIS-5 generates diagnoses for mood disorders, anxiety disorders, posttraumatic stress disorder, substance use disorders, antisocial personality disorder, schizotypal disorder, and conduct disorder.
During the interviews, respondents were asked if they had ever attempted suicide. For those who had, interviewers recorded the total number of lifetime attempts.
Participants also answered questions about childhood maltreatment including physical neglect, emotional neglect, physical abuse, emotional abuse, and sexual abuse by parents or caregivers and other adverse events occurring before the age of 18.
Childhood trauma common
Patients with BPD frequently report a history of childhood trauma, noted Dr. Grilo, adding that such trauma is associated with self-harm and suicide attempts. Sociodemographic information, including age, sex, and ethnicity/race, education level, and income, was also gathered.
Investigators examined data on suicide attempts using relatively stringent coding that required serious dysfunction in at least five BPD criteria.
Using this definition, investigators found the lifetime SA prevalence in patients with BPD was 30.4%, and 3.2% for past-year SAs. This compared with a rate of 3.7% for lifetime SAs and 0.2% for past-year SAs in those without a BPD diagnosis.
The authors examined SA rates using diagnostic codes in the NESARC-III that required seriously impaired function in only 1 or 2 BPD criteria. Rates were higher using the 5-criteria definition.
When the researchers excluded the BPD criterion of self-injurious behavior, the prevalence was 28.1% for lifetime and 3.0% for past-year SAs among the BPD group, with corresponding rates of 3.8% and 0.2% in those without a BPD diagnosis.
It’s important to look at this, said Dr. Grilo, as some patients with BPD who engage in self-harm have suicidal intent while others don’t.
“We tested whether BPD had heightened risk for suicide attempts if we eliminated the self-injurious criterion and we found that heightened risk was still there,” he explained.
Looking at individual criteria for BPD, a model that adjusted for sociodemographic characteristics, other psychiatric disorders, age at BPD onset, and history of childhood adverse events uncovered two criteria that were significantly associated with increased odds of SAs.
One was emptiness. For lifetime suicide attempts, the adjusted odds ratio (aOR) was 1.58 (95% confidence interval, 1.16-2.14) and for past-year attempts, the aOR was 1.99 (95% CI, 1.08-3.66).
The second was self-injurious behavior. For lifetime attempts, the aOR was 24.28 (95% CI, 16.83-32.03) and for past-year attempts, the aOR was 19.32 (95% CI, 5.22-71.58).
In a model in which all BPD-specific criteria were entered while excluding self-injurious behavior, the aORs for emptiness were 1.66 (95% CI, 1.23-2.24) for lifetime suicide attempts and 2.45 (95% CI, 1.18-5.08) for past year attempts.
Unlike another recent study that included more than 700 treatment-seeking patients with BPD who were followed for 10 years, the current study did not show significant associations with SAs for two other BPD criteria – identity disturbance and frantic attempts to avoid abandonment.
Dr. Grilo explained this might be because the earlier study included treatment-seeking patients instead of community cases, or because of differences in assessment interviews or other factors.
‘Compelling evidence’
“Our epidemiological sample has much broader generalizability and fewer potential confounds than the clinical treatment-seeking sample,” said Dr. Grilo.
However, he noted that the two studies “converge strongly and provide compelling evidence that BPD is associated with substantially heightened risk for suicide attempts over the lifetime.”
The two studies “also converge in finding that the presence of symptoms such as repeated self-harm and feelings of chronic emptiness are also associated with risk for suicide attempts.”
The new findings highlight the need to ask potentially at-risk patients about feelings of emptiness as well as self-injurious behaviors. Clinicians could, for example, ask: “Have you often felt like your life had no purpose or meaning?” or “Have you often felt empty inside?”
Limitations of the study include reliance on retrospective self-reports and use of lay interviewers, although these interviewers were trained and had an average of 5 years of experience conducting health-related surveys.
Although the study included a representative sample of U.S. adults, the sample did not include groups known to have high rates of suicide and self-harm behaviors, such as institutionalized, incarcerated, or homeless individuals.
In addition, the study did not evaluate severity and duration of BPD, although the authors noted they did adjust for age at BPD onset, this did not alter the findings.
Often misdiagnosed
Commenting on the study, John M. Oldham, MD, Distinguished Emeritus Professor, Menninger Department of Psychiatry and Behavioral Sciences, Baylor College of Medicine, Houston, and past-president, American Psychiatric Association, and an expert on BPD, had high praise for the research.
BPD is often misdiagnosed, Dr. Oldham said in an interview. Many patients seek help from primary care doctors who may label the symptoms as an anxiety disorder or a mood disorder, he said.
Although medications can help treat some BPD symptoms, “the primary, core evidence-based treatment for BPD is psychotherapy,” said Dr. Oldham, who some years ago helped develop evidence-based practice guidelines for BPD.
“It’s a clear and very well-designed study, and I don’t see any major limitations or problems with it,” he said. “The authors kept their focus rigorously on their goals and they used really careful methodology.”
He noted the “huge” numbers of patients included in the data and the relatively large percentage of men (43.7%).
“There’s a general belief that it’s mostly females who have BPD, but that’s not true; it’s females who come to treatment,” said Dr. Oldham.
Requiring that all five criteria lead to seriously impaired functioning “is a much more rigorous diagnostic methodology” than requiring only one or two criteria to lead to such impairment, said Dr. Oldham. “This is really important” and makes it “a much stronger study.”
The finding that self-harm behavior was linked to suicide attempts isn’t that surprising as this association has been well documented, but the finding that chronic emptiness is also predictive of future suicide attempts “is news,” said Dr. Oldham.
“We have not paid enough attention to this criterion in the clinical world or in the research world.”
Dr. Oldham said one patient with BPD gave him an ideal metaphor for emptiness. “She said it’s like there’s just nobody home. Think of it as an empty house that may look fine on the outside but you go inside and nobody lives there; there’s no furniture; no favorite things; no photos; no possessions.”
The authors have “important messages we need to pay attention to, and the main one is to explore this sense of chronic ‘nobody home’ emptiness,” said Dr. Oldham.
Dr. Grilo has reported receiving research grants from the National Institutes of Health; serving as a consultant for Sunovion and Weight Watchers; receiving honoraria for lectures, continuing medical education activities, and presentations at scientific conferences; and receiving royalties from Guilford Press and Taylor & Francis, all outside the submitted work.
A version of this article first appeared on Medscape.com.
Feelings of chronic emptiness and self-injury have been identified as two key risk factors for suicide attempts (SAs) in patients with borderline personality disorder (BPD), a new cross-sectional, nationally representative study suggests.
The findings also show lifetime and past-year SAs are common among patients with BPD, even when excluding self-injurious behaviors.
The results suggest that in addition to asking patients about self-harm during suicide risk screenings and assessments, clinicians should query them about “longstanding” feelings of emptiness, study investigator Carlos M. Grilo, PhD, professor of psychiatry and psychology, Yale University, New Haven, Conn., said in an interview.
Although related, chronic emptiness “is distinct and goes beyond feelings of sadness, loneliness, and hopelessness,” explained Dr. Grilo. he said.
The study was published online May 11 in JAMA Network Open.
Filling a research gap
While BPD and other psychiatric disorders are associated with suicide, the authors noted there is a “dearth of epidemiological research” examining the link between BPD and suicide.
Criteria for BPD diagnosis requires any five of the following criteria: relationships, affective instability, abandonment fear, anger, identity disturbance, emptiness, disassociation/paranoia, self-injurious behavior, and impulsivity, along with social-occupation dysfunction.
To determine SA risk with specific BPD diagnostic criteria, the investigators examined data on 36,309 individuals who participated in the third wave of the National Epidemiologic Survey on Alcohol and Related Conditions (NESARC-III), conducted from 2012 to 2013.
During computer-assisted, face-to-face interviews, study participants answered questions based on the Alcohol Use Disorder and Associated Disabilities Interview Schedule-5 (AUDADIS-5) of the National Institute on Alcohol Abuse and Alcoholism.
This structured interview assesses a range of DSM-5–defined psychiatric disorders and their criteria. In addition to BPD, the AUDADIS-5 generates diagnoses for mood disorders, anxiety disorders, posttraumatic stress disorder, substance use disorders, antisocial personality disorder, schizotypal disorder, and conduct disorder.
During the interviews, respondents were asked if they had ever attempted suicide. For those who had, interviewers recorded the total number of lifetime attempts.
Participants also answered questions about childhood maltreatment including physical neglect, emotional neglect, physical abuse, emotional abuse, and sexual abuse by parents or caregivers and other adverse events occurring before the age of 18.
Childhood trauma common
Patients with BPD frequently report a history of childhood trauma, noted Dr. Grilo, adding that such trauma is associated with self-harm and suicide attempts. Sociodemographic information, including age, sex, and ethnicity/race, education level, and income, was also gathered.
Investigators examined data on suicide attempts using relatively stringent coding that required serious dysfunction in at least five BPD criteria.
Using this definition, investigators found the lifetime SA prevalence in patients with BPD was 30.4%, and 3.2% for past-year SAs. This compared with a rate of 3.7% for lifetime SAs and 0.2% for past-year SAs in those without a BPD diagnosis.
The authors examined SA rates using diagnostic codes in the NESARC-III that required seriously impaired function in only 1 or 2 BPD criteria. Rates were higher using the 5-criteria definition.
When the researchers excluded the BPD criterion of self-injurious behavior, the prevalence was 28.1% for lifetime and 3.0% for past-year SAs among the BPD group, with corresponding rates of 3.8% and 0.2% in those without a BPD diagnosis.
It’s important to look at this, said Dr. Grilo, as some patients with BPD who engage in self-harm have suicidal intent while others don’t.
“We tested whether BPD had heightened risk for suicide attempts if we eliminated the self-injurious criterion and we found that heightened risk was still there,” he explained.
Looking at individual criteria for BPD, a model that adjusted for sociodemographic characteristics, other psychiatric disorders, age at BPD onset, and history of childhood adverse events uncovered two criteria that were significantly associated with increased odds of SAs.
One was emptiness. For lifetime suicide attempts, the adjusted odds ratio (aOR) was 1.58 (95% confidence interval, 1.16-2.14) and for past-year attempts, the aOR was 1.99 (95% CI, 1.08-3.66).
The second was self-injurious behavior. For lifetime attempts, the aOR was 24.28 (95% CI, 16.83-32.03) and for past-year attempts, the aOR was 19.32 (95% CI, 5.22-71.58).
In a model in which all BPD-specific criteria were entered while excluding self-injurious behavior, the aORs for emptiness were 1.66 (95% CI, 1.23-2.24) for lifetime suicide attempts and 2.45 (95% CI, 1.18-5.08) for past year attempts.
Unlike another recent study that included more than 700 treatment-seeking patients with BPD who were followed for 10 years, the current study did not show significant associations with SAs for two other BPD criteria – identity disturbance and frantic attempts to avoid abandonment.
Dr. Grilo explained this might be because the earlier study included treatment-seeking patients instead of community cases, or because of differences in assessment interviews or other factors.
‘Compelling evidence’
“Our epidemiological sample has much broader generalizability and fewer potential confounds than the clinical treatment-seeking sample,” said Dr. Grilo.
However, he noted that the two studies “converge strongly and provide compelling evidence that BPD is associated with substantially heightened risk for suicide attempts over the lifetime.”
The two studies “also converge in finding that the presence of symptoms such as repeated self-harm and feelings of chronic emptiness are also associated with risk for suicide attempts.”
The new findings highlight the need to ask potentially at-risk patients about feelings of emptiness as well as self-injurious behaviors. Clinicians could, for example, ask: “Have you often felt like your life had no purpose or meaning?” or “Have you often felt empty inside?”
Limitations of the study include reliance on retrospective self-reports and use of lay interviewers, although these interviewers were trained and had an average of 5 years of experience conducting health-related surveys.
Although the study included a representative sample of U.S. adults, the sample did not include groups known to have high rates of suicide and self-harm behaviors, such as institutionalized, incarcerated, or homeless individuals.
In addition, the study did not evaluate severity and duration of BPD, although the authors noted they did adjust for age at BPD onset, this did not alter the findings.
Often misdiagnosed
Commenting on the study, John M. Oldham, MD, Distinguished Emeritus Professor, Menninger Department of Psychiatry and Behavioral Sciences, Baylor College of Medicine, Houston, and past-president, American Psychiatric Association, and an expert on BPD, had high praise for the research.
BPD is often misdiagnosed, Dr. Oldham said in an interview. Many patients seek help from primary care doctors who may label the symptoms as an anxiety disorder or a mood disorder, he said.
Although medications can help treat some BPD symptoms, “the primary, core evidence-based treatment for BPD is psychotherapy,” said Dr. Oldham, who some years ago helped develop evidence-based practice guidelines for BPD.
“It’s a clear and very well-designed study, and I don’t see any major limitations or problems with it,” he said. “The authors kept their focus rigorously on their goals and they used really careful methodology.”
He noted the “huge” numbers of patients included in the data and the relatively large percentage of men (43.7%).
“There’s a general belief that it’s mostly females who have BPD, but that’s not true; it’s females who come to treatment,” said Dr. Oldham.
Requiring that all five criteria lead to seriously impaired functioning “is a much more rigorous diagnostic methodology” than requiring only one or two criteria to lead to such impairment, said Dr. Oldham. “This is really important” and makes it “a much stronger study.”
The finding that self-harm behavior was linked to suicide attempts isn’t that surprising as this association has been well documented, but the finding that chronic emptiness is also predictive of future suicide attempts “is news,” said Dr. Oldham.
“We have not paid enough attention to this criterion in the clinical world or in the research world.”
Dr. Oldham said one patient with BPD gave him an ideal metaphor for emptiness. “She said it’s like there’s just nobody home. Think of it as an empty house that may look fine on the outside but you go inside and nobody lives there; there’s no furniture; no favorite things; no photos; no possessions.”
The authors have “important messages we need to pay attention to, and the main one is to explore this sense of chronic ‘nobody home’ emptiness,” said Dr. Oldham.
Dr. Grilo has reported receiving research grants from the National Institutes of Health; serving as a consultant for Sunovion and Weight Watchers; receiving honoraria for lectures, continuing medical education activities, and presentations at scientific conferences; and receiving royalties from Guilford Press and Taylor & Francis, all outside the submitted work.
A version of this article first appeared on Medscape.com.
Feelings of chronic emptiness and self-injury have been identified as two key risk factors for suicide attempts (SAs) in patients with borderline personality disorder (BPD), a new cross-sectional, nationally representative study suggests.
The findings also show lifetime and past-year SAs are common among patients with BPD, even when excluding self-injurious behaviors.
The results suggest that in addition to asking patients about self-harm during suicide risk screenings and assessments, clinicians should query them about “longstanding” feelings of emptiness, study investigator Carlos M. Grilo, PhD, professor of psychiatry and psychology, Yale University, New Haven, Conn., said in an interview.
Although related, chronic emptiness “is distinct and goes beyond feelings of sadness, loneliness, and hopelessness,” explained Dr. Grilo. he said.
The study was published online May 11 in JAMA Network Open.
Filling a research gap
While BPD and other psychiatric disorders are associated with suicide, the authors noted there is a “dearth of epidemiological research” examining the link between BPD and suicide.
Criteria for BPD diagnosis requires any five of the following criteria: relationships, affective instability, abandonment fear, anger, identity disturbance, emptiness, disassociation/paranoia, self-injurious behavior, and impulsivity, along with social-occupation dysfunction.
To determine SA risk with specific BPD diagnostic criteria, the investigators examined data on 36,309 individuals who participated in the third wave of the National Epidemiologic Survey on Alcohol and Related Conditions (NESARC-III), conducted from 2012 to 2013.
During computer-assisted, face-to-face interviews, study participants answered questions based on the Alcohol Use Disorder and Associated Disabilities Interview Schedule-5 (AUDADIS-5) of the National Institute on Alcohol Abuse and Alcoholism.
This structured interview assesses a range of DSM-5–defined psychiatric disorders and their criteria. In addition to BPD, the AUDADIS-5 generates diagnoses for mood disorders, anxiety disorders, posttraumatic stress disorder, substance use disorders, antisocial personality disorder, schizotypal disorder, and conduct disorder.
During the interviews, respondents were asked if they had ever attempted suicide. For those who had, interviewers recorded the total number of lifetime attempts.
Participants also answered questions about childhood maltreatment including physical neglect, emotional neglect, physical abuse, emotional abuse, and sexual abuse by parents or caregivers and other adverse events occurring before the age of 18.
Childhood trauma common
Patients with BPD frequently report a history of childhood trauma, noted Dr. Grilo, adding that such trauma is associated with self-harm and suicide attempts. Sociodemographic information, including age, sex, and ethnicity/race, education level, and income, was also gathered.
Investigators examined data on suicide attempts using relatively stringent coding that required serious dysfunction in at least five BPD criteria.
Using this definition, investigators found the lifetime SA prevalence in patients with BPD was 30.4%, and 3.2% for past-year SAs. This compared with a rate of 3.7% for lifetime SAs and 0.2% for past-year SAs in those without a BPD diagnosis.
The authors examined SA rates using diagnostic codes in the NESARC-III that required seriously impaired function in only 1 or 2 BPD criteria. Rates were higher using the 5-criteria definition.
When the researchers excluded the BPD criterion of self-injurious behavior, the prevalence was 28.1% for lifetime and 3.0% for past-year SAs among the BPD group, with corresponding rates of 3.8% and 0.2% in those without a BPD diagnosis.
It’s important to look at this, said Dr. Grilo, as some patients with BPD who engage in self-harm have suicidal intent while others don’t.
“We tested whether BPD had heightened risk for suicide attempts if we eliminated the self-injurious criterion and we found that heightened risk was still there,” he explained.
Looking at individual criteria for BPD, a model that adjusted for sociodemographic characteristics, other psychiatric disorders, age at BPD onset, and history of childhood adverse events uncovered two criteria that were significantly associated with increased odds of SAs.
One was emptiness. For lifetime suicide attempts, the adjusted odds ratio (aOR) was 1.58 (95% confidence interval, 1.16-2.14) and for past-year attempts, the aOR was 1.99 (95% CI, 1.08-3.66).
The second was self-injurious behavior. For lifetime attempts, the aOR was 24.28 (95% CI, 16.83-32.03) and for past-year attempts, the aOR was 19.32 (95% CI, 5.22-71.58).
In a model in which all BPD-specific criteria were entered while excluding self-injurious behavior, the aORs for emptiness were 1.66 (95% CI, 1.23-2.24) for lifetime suicide attempts and 2.45 (95% CI, 1.18-5.08) for past year attempts.
Unlike another recent study that included more than 700 treatment-seeking patients with BPD who were followed for 10 years, the current study did not show significant associations with SAs for two other BPD criteria – identity disturbance and frantic attempts to avoid abandonment.
Dr. Grilo explained this might be because the earlier study included treatment-seeking patients instead of community cases, or because of differences in assessment interviews or other factors.
‘Compelling evidence’
“Our epidemiological sample has much broader generalizability and fewer potential confounds than the clinical treatment-seeking sample,” said Dr. Grilo.
However, he noted that the two studies “converge strongly and provide compelling evidence that BPD is associated with substantially heightened risk for suicide attempts over the lifetime.”
The two studies “also converge in finding that the presence of symptoms such as repeated self-harm and feelings of chronic emptiness are also associated with risk for suicide attempts.”
The new findings highlight the need to ask potentially at-risk patients about feelings of emptiness as well as self-injurious behaviors. Clinicians could, for example, ask: “Have you often felt like your life had no purpose or meaning?” or “Have you often felt empty inside?”
Limitations of the study include reliance on retrospective self-reports and use of lay interviewers, although these interviewers were trained and had an average of 5 years of experience conducting health-related surveys.
Although the study included a representative sample of U.S. adults, the sample did not include groups known to have high rates of suicide and self-harm behaviors, such as institutionalized, incarcerated, or homeless individuals.
In addition, the study did not evaluate severity and duration of BPD, although the authors noted they did adjust for age at BPD onset, this did not alter the findings.
Often misdiagnosed
Commenting on the study, John M. Oldham, MD, Distinguished Emeritus Professor, Menninger Department of Psychiatry and Behavioral Sciences, Baylor College of Medicine, Houston, and past-president, American Psychiatric Association, and an expert on BPD, had high praise for the research.
BPD is often misdiagnosed, Dr. Oldham said in an interview. Many patients seek help from primary care doctors who may label the symptoms as an anxiety disorder or a mood disorder, he said.
Although medications can help treat some BPD symptoms, “the primary, core evidence-based treatment for BPD is psychotherapy,” said Dr. Oldham, who some years ago helped develop evidence-based practice guidelines for BPD.
“It’s a clear and very well-designed study, and I don’t see any major limitations or problems with it,” he said. “The authors kept their focus rigorously on their goals and they used really careful methodology.”
He noted the “huge” numbers of patients included in the data and the relatively large percentage of men (43.7%).
“There’s a general belief that it’s mostly females who have BPD, but that’s not true; it’s females who come to treatment,” said Dr. Oldham.
Requiring that all five criteria lead to seriously impaired functioning “is a much more rigorous diagnostic methodology” than requiring only one or two criteria to lead to such impairment, said Dr. Oldham. “This is really important” and makes it “a much stronger study.”
The finding that self-harm behavior was linked to suicide attempts isn’t that surprising as this association has been well documented, but the finding that chronic emptiness is also predictive of future suicide attempts “is news,” said Dr. Oldham.
“We have not paid enough attention to this criterion in the clinical world or in the research world.”
Dr. Oldham said one patient with BPD gave him an ideal metaphor for emptiness. “She said it’s like there’s just nobody home. Think of it as an empty house that may look fine on the outside but you go inside and nobody lives there; there’s no furniture; no favorite things; no photos; no possessions.”
The authors have “important messages we need to pay attention to, and the main one is to explore this sense of chronic ‘nobody home’ emptiness,” said Dr. Oldham.
Dr. Grilo has reported receiving research grants from the National Institutes of Health; serving as a consultant for Sunovion and Weight Watchers; receiving honoraria for lectures, continuing medical education activities, and presentations at scientific conferences; and receiving royalties from Guilford Press and Taylor & Francis, all outside the submitted work.
A version of this article first appeared on Medscape.com.
HHS to inject billions into mental health, substance use disorders
The U.S. Department of Health and Human Services will inject billions of dollars into programs designed to address mental health and substance use disorders, including $3 billion released to states as of May 18, said federal officials.
The American Rescue Plan, a COVID-relief package signed into law in March, contained the money, which will be divided equally between the Community Mental Health Services Block Grant Program and the Substance Abuse Prevention and Treatment Block Grant Program, said Tom Coderre, Acting Assistant Secretary for Mental Health and Substance Use, in a call with reporters.
The award amounts will vary by state.
The mental health program helps states and territories provide services for children with serious emotional issues and adults with serious mental illness.
The substance use program provides money to plan, implement, and evaluate prevention, intervention, treatment, and recovery services.

, which fueled an increase in anxiety, depression, and overdose, said Assistant Secretary for Health Rachel Levine, MD, on the call.
“We know multiple stressors during the pandemic – isolation, sickness, grief, job loss, food instability, and loss of routines – have devastated many Americans and presented the unprecedented behavioral health challenges across the nation,” said Dr. Levine.
The HHS also announced that it is re-establishing a Behavioral Health Coordinating Council (BHCC). Dr. Levine and Mr. Coderre will serve as cochairs of the Council, which will coordinate action-oriented approaches to addressing the HHS’s behavioral health efforts.
However, in 2014, the U.S. Government Accountability Office criticized the BHCC for only focusing on the HHS, and noted the lack of coordination across the federal government’s various efforts to address mental health.
‘A huge step forward’
The American Psychiatric Association welcomed the new money and the return of the council.
“In the wake of the pandemic an unprecedented, and as of yet untold, number of Americans are faced with mental health and substance use disorders, particularly in communities impacted by structural racism,” said APA President Vivian Pender, MD, in a statement. “With the creation of this Council and this investment in mental health, the administration is taking a huge step forward.”

APA CEO and Medical Director Saul Levin, MD, MPA, added: “This Council has great potential to ease the challenges we face as we begin to recover from the pandemic’s impact on our society, and [the] APA looks forward to assisting in their efforts.”
HHS Secretary Xavier Becerra noted in a statement that the COVID-19 pandemic “has made clear the need to invest resources in our nation’s mental health and address the inequities that still exist around behavioral health care.” He added, “This national problem calls for department-wide coordination to address the issue.”
Dr. Levine said the Council “will assure the right prioritization and guidelines are in place to provide pathways to prevention, intervention, treatment, and recovery services.”
A version of this article first appeared on Medscape.com.
The U.S. Department of Health and Human Services will inject billions of dollars into programs designed to address mental health and substance use disorders, including $3 billion released to states as of May 18, said federal officials.
The American Rescue Plan, a COVID-relief package signed into law in March, contained the money, which will be divided equally between the Community Mental Health Services Block Grant Program and the Substance Abuse Prevention and Treatment Block Grant Program, said Tom Coderre, Acting Assistant Secretary for Mental Health and Substance Use, in a call with reporters.
The award amounts will vary by state.
The mental health program helps states and territories provide services for children with serious emotional issues and adults with serious mental illness.
The substance use program provides money to plan, implement, and evaluate prevention, intervention, treatment, and recovery services.
, which fueled an increase in anxiety, depression, and overdose, said Assistant Secretary for Health Rachel Levine, MD, on the call.
“We know multiple stressors during the pandemic – isolation, sickness, grief, job loss, food instability, and loss of routines – have devastated many Americans and presented the unprecedented behavioral health challenges across the nation,” said Dr. Levine.
The HHS also announced that it is re-establishing a Behavioral Health Coordinating Council (BHCC). Dr. Levine and Mr. Coderre will serve as cochairs of the Council, which will coordinate action-oriented approaches to addressing the HHS’s behavioral health efforts.
However, in 2014, the U.S. Government Accountability Office criticized the BHCC for only focusing on the HHS, and noted the lack of coordination across the federal government’s various efforts to address mental health.
‘A huge step forward’
The American Psychiatric Association welcomed the new money and the return of the council.
“In the wake of the pandemic an unprecedented, and as of yet untold, number of Americans are faced with mental health and substance use disorders, particularly in communities impacted by structural racism,” said APA President Vivian Pender, MD, in a statement. “With the creation of this Council and this investment in mental health, the administration is taking a huge step forward.”
APA CEO and Medical Director Saul Levin, MD, MPA, added: “This Council has great potential to ease the challenges we face as we begin to recover from the pandemic’s impact on our society, and [the] APA looks forward to assisting in their efforts.”
HHS Secretary Xavier Becerra noted in a statement that the COVID-19 pandemic “has made clear the need to invest resources in our nation’s mental health and address the inequities that still exist around behavioral health care.” He added, “This national problem calls for department-wide coordination to address the issue.”
Dr. Levine said the Council “will assure the right prioritization and guidelines are in place to provide pathways to prevention, intervention, treatment, and recovery services.”
A version of this article first appeared on Medscape.com.
The U.S. Department of Health and Human Services will inject billions of dollars into programs designed to address mental health and substance use disorders, including $3 billion released to states as of May 18, said federal officials.
The American Rescue Plan, a COVID-relief package signed into law in March, contained the money, which will be divided equally between the Community Mental Health Services Block Grant Program and the Substance Abuse Prevention and Treatment Block Grant Program, said Tom Coderre, Acting Assistant Secretary for Mental Health and Substance Use, in a call with reporters.
The award amounts will vary by state.
The mental health program helps states and territories provide services for children with serious emotional issues and adults with serious mental illness.
The substance use program provides money to plan, implement, and evaluate prevention, intervention, treatment, and recovery services.
, which fueled an increase in anxiety, depression, and overdose, said Assistant Secretary for Health Rachel Levine, MD, on the call.
“We know multiple stressors during the pandemic – isolation, sickness, grief, job loss, food instability, and loss of routines – have devastated many Americans and presented the unprecedented behavioral health challenges across the nation,” said Dr. Levine.
The HHS also announced that it is re-establishing a Behavioral Health Coordinating Council (BHCC). Dr. Levine and Mr. Coderre will serve as cochairs of the Council, which will coordinate action-oriented approaches to addressing the HHS’s behavioral health efforts.
However, in 2014, the U.S. Government Accountability Office criticized the BHCC for only focusing on the HHS, and noted the lack of coordination across the federal government’s various efforts to address mental health.
‘A huge step forward’
The American Psychiatric Association welcomed the new money and the return of the council.
“In the wake of the pandemic an unprecedented, and as of yet untold, number of Americans are faced with mental health and substance use disorders, particularly in communities impacted by structural racism,” said APA President Vivian Pender, MD, in a statement. “With the creation of this Council and this investment in mental health, the administration is taking a huge step forward.”
APA CEO and Medical Director Saul Levin, MD, MPA, added: “This Council has great potential to ease the challenges we face as we begin to recover from the pandemic’s impact on our society, and [the] APA looks forward to assisting in their efforts.”
HHS Secretary Xavier Becerra noted in a statement that the COVID-19 pandemic “has made clear the need to invest resources in our nation’s mental health and address the inequities that still exist around behavioral health care.” He added, “This national problem calls for department-wide coordination to address the issue.”
Dr. Levine said the Council “will assure the right prioritization and guidelines are in place to provide pathways to prevention, intervention, treatment, and recovery services.”
A version of this article first appeared on Medscape.com.
Acts of kindness, empathy bolster mental health
Sigmund Freud said, “Out of your vulnerabilities will come greatest strength.” What exactly did Dr. Freud mean by this?

Many aspects of mental health treatment include cognitive restructuring, behavioral changes, emotion processing, and setting boundaries. These are all critical aspects of treatment, but what about kindness and compassion?
We often forget that kindness requires us to be vulnerable and take a risk at times. Being kind to others is not always easy, and it is not always an automatic reaction. Vulnerability often involves risk, but the outcomes often outweigh fear.
Dr. Freud was highlighting that being kind, open, and honest will often result in strong character and resilience. In turn, it will help others. Psychology and psychiatry have proved time and time again that empathy, compassion, and kindness have numerous benefits for mental and physical health for both the giver and the receiver.
From a biological perspective, we know that acts of kindness signal the brain to release serotonin and dopamine, known as “feel good transmitters,” and endorphins, which in turn lessen pain, depression, and anxiety. According to Waguih W. Ishak, MD, a psychiatrist affiliated with Cedars-Sinai in Los Angeles,1 in addition to boosting oxytocin and dopamine, being kind can increase serotonin, a neurotransmitter that helps regulate mood. Kindness and compassion have been shown to release oxytocin, known as the “love hormone,” which increases self-esteem, trust, connection, and optimism. Oxytocin also reduces blood pressure and has been dubbed the “cardioprotective” hormone. According to Kelli Harding, MD, MPH, a psychiatrist affiliated with Columbia University in New York,2 kindness can extend the lifespan. Research from Emory University in Atlanta has shown that, when an individual is kind to another, the brain’s reward centers light up – resulting in a “helper’s high.” Thus, kindness is self-reinforcing.3
Kindness leads to a greater sense of connection to others and a lessening in feelings of isolation. Small acts of kindness build up compassion in oneself. Research indicates that kindness doesn’t just positively affect the giver and receiver but can also benefit onlookers. An article in Psychology Today,4 suggests that those who witness acts of kindness are also more likely to “pay it forward,” resulting in a domino effect. Along these same lines, altruistic people, specifically those who engage in charitable donations, expressed higher levels of overall happiness according to a 2010 Harvard Business School survey.5
“You can’t pour from an empty cup” is a trendy quote making its way around social media. Before we can be kind and compassionate to others, we must first be kind and compassionate to ourselves. In today’s world, productivity and pressure-filled environments consume us daily. We often find ourselves skipping meals, forgetting to connect with loved ones, missing breaks, and even neglecting our sleep. It is virtually impossible to care for others when we are depleted ourselves. Sometimes not prioritizing ourselves can result in collateral damage. We may become short-tempered, irritable, moody, and overwhelmed. At this point kindness, compassion, and empathy toward others are likely to be absent. Once we replenish ourselves, by taking time off, indulging in a nice meal, exercising, we are more likely to respond as opposed to react, ask others about themselves, and engage in overall positive interactions throughout our day. Kindness is best fostered by being kind to ourselves to sustain our own well-being and by being kind to others in order to maintain the cycle. For clinicians who have been pushed to respond to various aspects of the COVID-19 pandemic, self-care has never been more important.
COVID-19 has been difficult for everyone, particularly the elderly and vulnerable populations. However, kindness has proved to be an overwhelming response as many businesses and individuals have taken to volunteering time and resources for those in need. Even big corporations have chipped in. For example, Lyft and Uber – in a partnership with the White House – are now offering free rides to vaccine sites, and several local businesses have donated personal protective equipment to hospitals and assisted living facilities.
Kindness and empathy are ever present in the field of mental health, medicine, and substance use treatment. The very act of caring for another involves kindness. In medicine, empathy has been defined as “an emotional experience between an observer and a subject in which the observer, based on visual and auditory cues, identifies and transiently experiences the subject’s emotional state.”6
As mental health professionals, we receive empathy training early on in our schooling – increasingly so over the last decade. Research has indicated that trusting relationships between clinicians and patients result in optimal care. Evidence-based communication styles are being widely implemented. This entails using nonjudgmental language, open-ended questions, and active listening skills, for example. In addition, the mental health professionals have our conscious and unconscious judgments. If empathy training is provided, we can learn to acknowledge our biases and mitigate them. Lastly, empathy training has been proven to assist with destigmatization, increase in treatment seeking, and overall better outcomes.
Substance use treatment, which often focuses on cognition and behavior changing, boundaries, and family dynamics, also requires support and kindness. Although it is not an empirically based “treatment,” Alcoholics Anonymous (AA) has used kindness for decades.
Step 12 of AA’s 12-step program, which was developed by two people with alcohol use disorder in 1935 in Akron, Ohio, is as follows: “Having had a spiritual awakening as the result of these steps, we tried to carry this message to alcoholics, and to practice these principles in all our affairs.”
Once AA members are on solid ground with their sobriety, they are urged to help others in their recovery. This process provides many benefits. When individuals are concerned about someone else, they are less focused on themselves. This helps the individuals in recovery to decrease their rumination and “get out of themselves.” It also allows for the AA member to be kind and helpful to an individual who is suffering, thereby expressing kindness, compassion, and empathy. This act of “paying it forward” produces a domino effect that has withstood the test of time as evidenced by the ever-growing fellowship of Alcoholics Anonymous.
Several small acts of kindness can help us as clinicians and our patients:
1. Practice self-care.
2. Take a half day off from your practice.
3. Give staff a half day off.
4. Call a family member or friend and ask them how they are doing. Then engage in active listening and refrain from giving advice.
5. Donate to a homeless shelter or volunteer your time at a charity.
6. Give a stranger a compliment.
7. Surprise someone with a small gift.
8. Send a loved one a letter instead of a text.
9. Pick up litter.
10. Acknowledge family and friends who gave you extra support during the pandemic.
11. Take baked goods to your office.
12. Help a neighbor with groceries.
13. Leave a generous tip.
14. Play soft music in your office.
In conclusion, kindness, empathy, and compassion are vital concepts that are not just fluffy theories. They have vast mental, physical, and social benefits for us and our patients.
References
1. Cedars-Sinai staff. The Science of Kindness. 2019 Feb 13. Cedars-Sinai blog.
2. Harding K. The Rabbit Effect: Live Longer, Happier, and Healthier with the Groundbreaking Science of Kindness. Atria Books, 2019.
3. Ritvo E. BeKindr. Momosa Publishing, 2017.
4. Svoboda E. “Pay it Forward.” Psychology Today. Last reviewed 2016 Jun 9.
5. Aknin LB et al. “Prosocial spending and well-being: Cross-Cultural Evidence for a Psychological Universal.” Harvard Business School. Working Paper 11-038. 2010.
6. Hirsch EM. AMA J Ethics. Virtual Mentor. 2007;9(6):423-7.
Dr. Haji is a licensed clinical psychologist specializing in psychodiagnostic assessment, forensic assessment, dual diagnosis, serious and persistent mental illness, depression, anxiety, personality disorders, and substance abuse treatment. She practices in Miami and has no conflicts of interest.
Sigmund Freud said, “Out of your vulnerabilities will come greatest strength.” What exactly did Dr. Freud mean by this?
Many aspects of mental health treatment include cognitive restructuring, behavioral changes, emotion processing, and setting boundaries. These are all critical aspects of treatment, but what about kindness and compassion?
We often forget that kindness requires us to be vulnerable and take a risk at times. Being kind to others is not always easy, and it is not always an automatic reaction. Vulnerability often involves risk, but the outcomes often outweigh fear.
Dr. Freud was highlighting that being kind, open, and honest will often result in strong character and resilience. In turn, it will help others. Psychology and psychiatry have proved time and time again that empathy, compassion, and kindness have numerous benefits for mental and physical health for both the giver and the receiver.
From a biological perspective, we know that acts of kindness signal the brain to release serotonin and dopamine, known as “feel good transmitters,” and endorphins, which in turn lessen pain, depression, and anxiety. According to Waguih W. Ishak, MD, a psychiatrist affiliated with Cedars-Sinai in Los Angeles,1 in addition to boosting oxytocin and dopamine, being kind can increase serotonin, a neurotransmitter that helps regulate mood. Kindness and compassion have been shown to release oxytocin, known as the “love hormone,” which increases self-esteem, trust, connection, and optimism. Oxytocin also reduces blood pressure and has been dubbed the “cardioprotective” hormone. According to Kelli Harding, MD, MPH, a psychiatrist affiliated with Columbia University in New York,2 kindness can extend the lifespan. Research from Emory University in Atlanta has shown that, when an individual is kind to another, the brain’s reward centers light up – resulting in a “helper’s high.” Thus, kindness is self-reinforcing.3
Kindness leads to a greater sense of connection to others and a lessening in feelings of isolation. Small acts of kindness build up compassion in oneself. Research indicates that kindness doesn’t just positively affect the giver and receiver but can also benefit onlookers. An article in Psychology Today,4 suggests that those who witness acts of kindness are also more likely to “pay it forward,” resulting in a domino effect. Along these same lines, altruistic people, specifically those who engage in charitable donations, expressed higher levels of overall happiness according to a 2010 Harvard Business School survey.5
“You can’t pour from an empty cup” is a trendy quote making its way around social media. Before we can be kind and compassionate to others, we must first be kind and compassionate to ourselves. In today’s world, productivity and pressure-filled environments consume us daily. We often find ourselves skipping meals, forgetting to connect with loved ones, missing breaks, and even neglecting our sleep. It is virtually impossible to care for others when we are depleted ourselves. Sometimes not prioritizing ourselves can result in collateral damage. We may become short-tempered, irritable, moody, and overwhelmed. At this point kindness, compassion, and empathy toward others are likely to be absent. Once we replenish ourselves, by taking time off, indulging in a nice meal, exercising, we are more likely to respond as opposed to react, ask others about themselves, and engage in overall positive interactions throughout our day. Kindness is best fostered by being kind to ourselves to sustain our own well-being and by being kind to others in order to maintain the cycle. For clinicians who have been pushed to respond to various aspects of the COVID-19 pandemic, self-care has never been more important.
COVID-19 has been difficult for everyone, particularly the elderly and vulnerable populations. However, kindness has proved to be an overwhelming response as many businesses and individuals have taken to volunteering time and resources for those in need. Even big corporations have chipped in. For example, Lyft and Uber – in a partnership with the White House – are now offering free rides to vaccine sites, and several local businesses have donated personal protective equipment to hospitals and assisted living facilities.
Kindness and empathy are ever present in the field of mental health, medicine, and substance use treatment. The very act of caring for another involves kindness. In medicine, empathy has been defined as “an emotional experience between an observer and a subject in which the observer, based on visual and auditory cues, identifies and transiently experiences the subject’s emotional state.”6
As mental health professionals, we receive empathy training early on in our schooling – increasingly so over the last decade. Research has indicated that trusting relationships between clinicians and patients result in optimal care. Evidence-based communication styles are being widely implemented. This entails using nonjudgmental language, open-ended questions, and active listening skills, for example. In addition, the mental health professionals have our conscious and unconscious judgments. If empathy training is provided, we can learn to acknowledge our biases and mitigate them. Lastly, empathy training has been proven to assist with destigmatization, increase in treatment seeking, and overall better outcomes.
Substance use treatment, which often focuses on cognition and behavior changing, boundaries, and family dynamics, also requires support and kindness. Although it is not an empirically based “treatment,” Alcoholics Anonymous (AA) has used kindness for decades.
Step 12 of AA’s 12-step program, which was developed by two people with alcohol use disorder in 1935 in Akron, Ohio, is as follows: “Having had a spiritual awakening as the result of these steps, we tried to carry this message to alcoholics, and to practice these principles in all our affairs.”
Once AA members are on solid ground with their sobriety, they are urged to help others in their recovery. This process provides many benefits. When individuals are concerned about someone else, they are less focused on themselves. This helps the individuals in recovery to decrease their rumination and “get out of themselves.” It also allows for the AA member to be kind and helpful to an individual who is suffering, thereby expressing kindness, compassion, and empathy. This act of “paying it forward” produces a domino effect that has withstood the test of time as evidenced by the ever-growing fellowship of Alcoholics Anonymous.
Several small acts of kindness can help us as clinicians and our patients:
1. Practice self-care.
2. Take a half day off from your practice.
3. Give staff a half day off.
4. Call a family member or friend and ask them how they are doing. Then engage in active listening and refrain from giving advice.
5. Donate to a homeless shelter or volunteer your time at a charity.
6. Give a stranger a compliment.
7. Surprise someone with a small gift.
8. Send a loved one a letter instead of a text.
9. Pick up litter.
10. Acknowledge family and friends who gave you extra support during the pandemic.
11. Take baked goods to your office.
12. Help a neighbor with groceries.
13. Leave a generous tip.
14. Play soft music in your office.
In conclusion, kindness, empathy, and compassion are vital concepts that are not just fluffy theories. They have vast mental, physical, and social benefits for us and our patients.
References
1. Cedars-Sinai staff. The Science of Kindness. 2019 Feb 13. Cedars-Sinai blog.
2. Harding K. The Rabbit Effect: Live Longer, Happier, and Healthier with the Groundbreaking Science of Kindness. Atria Books, 2019.
3. Ritvo E. BeKindr. Momosa Publishing, 2017.
4. Svoboda E. “Pay it Forward.” Psychology Today. Last reviewed 2016 Jun 9.
5. Aknin LB et al. “Prosocial spending and well-being: Cross-Cultural Evidence for a Psychological Universal.” Harvard Business School. Working Paper 11-038. 2010.
6. Hirsch EM. AMA J Ethics. Virtual Mentor. 2007;9(6):423-7.
Dr. Haji is a licensed clinical psychologist specializing in psychodiagnostic assessment, forensic assessment, dual diagnosis, serious and persistent mental illness, depression, anxiety, personality disorders, and substance abuse treatment. She practices in Miami and has no conflicts of interest.
Sigmund Freud said, “Out of your vulnerabilities will come greatest strength.” What exactly did Dr. Freud mean by this?
Many aspects of mental health treatment include cognitive restructuring, behavioral changes, emotion processing, and setting boundaries. These are all critical aspects of treatment, but what about kindness and compassion?
We often forget that kindness requires us to be vulnerable and take a risk at times. Being kind to others is not always easy, and it is not always an automatic reaction. Vulnerability often involves risk, but the outcomes often outweigh fear.
Dr. Freud was highlighting that being kind, open, and honest will often result in strong character and resilience. In turn, it will help others. Psychology and psychiatry have proved time and time again that empathy, compassion, and kindness have numerous benefits for mental and physical health for both the giver and the receiver.
From a biological perspective, we know that acts of kindness signal the brain to release serotonin and dopamine, known as “feel good transmitters,” and endorphins, which in turn lessen pain, depression, and anxiety. According to Waguih W. Ishak, MD, a psychiatrist affiliated with Cedars-Sinai in Los Angeles,1 in addition to boosting oxytocin and dopamine, being kind can increase serotonin, a neurotransmitter that helps regulate mood. Kindness and compassion have been shown to release oxytocin, known as the “love hormone,” which increases self-esteem, trust, connection, and optimism. Oxytocin also reduces blood pressure and has been dubbed the “cardioprotective” hormone. According to Kelli Harding, MD, MPH, a psychiatrist affiliated with Columbia University in New York,2 kindness can extend the lifespan. Research from Emory University in Atlanta has shown that, when an individual is kind to another, the brain’s reward centers light up – resulting in a “helper’s high.” Thus, kindness is self-reinforcing.3
Kindness leads to a greater sense of connection to others and a lessening in feelings of isolation. Small acts of kindness build up compassion in oneself. Research indicates that kindness doesn’t just positively affect the giver and receiver but can also benefit onlookers. An article in Psychology Today,4 suggests that those who witness acts of kindness are also more likely to “pay it forward,” resulting in a domino effect. Along these same lines, altruistic people, specifically those who engage in charitable donations, expressed higher levels of overall happiness according to a 2010 Harvard Business School survey.5
“You can’t pour from an empty cup” is a trendy quote making its way around social media. Before we can be kind and compassionate to others, we must first be kind and compassionate to ourselves. In today’s world, productivity and pressure-filled environments consume us daily. We often find ourselves skipping meals, forgetting to connect with loved ones, missing breaks, and even neglecting our sleep. It is virtually impossible to care for others when we are depleted ourselves. Sometimes not prioritizing ourselves can result in collateral damage. We may become short-tempered, irritable, moody, and overwhelmed. At this point kindness, compassion, and empathy toward others are likely to be absent. Once we replenish ourselves, by taking time off, indulging in a nice meal, exercising, we are more likely to respond as opposed to react, ask others about themselves, and engage in overall positive interactions throughout our day. Kindness is best fostered by being kind to ourselves to sustain our own well-being and by being kind to others in order to maintain the cycle. For clinicians who have been pushed to respond to various aspects of the COVID-19 pandemic, self-care has never been more important.
COVID-19 has been difficult for everyone, particularly the elderly and vulnerable populations. However, kindness has proved to be an overwhelming response as many businesses and individuals have taken to volunteering time and resources for those in need. Even big corporations have chipped in. For example, Lyft and Uber – in a partnership with the White House – are now offering free rides to vaccine sites, and several local businesses have donated personal protective equipment to hospitals and assisted living facilities.
Kindness and empathy are ever present in the field of mental health, medicine, and substance use treatment. The very act of caring for another involves kindness. In medicine, empathy has been defined as “an emotional experience between an observer and a subject in which the observer, based on visual and auditory cues, identifies and transiently experiences the subject’s emotional state.”6
As mental health professionals, we receive empathy training early on in our schooling – increasingly so over the last decade. Research has indicated that trusting relationships between clinicians and patients result in optimal care. Evidence-based communication styles are being widely implemented. This entails using nonjudgmental language, open-ended questions, and active listening skills, for example. In addition, the mental health professionals have our conscious and unconscious judgments. If empathy training is provided, we can learn to acknowledge our biases and mitigate them. Lastly, empathy training has been proven to assist with destigmatization, increase in treatment seeking, and overall better outcomes.
Substance use treatment, which often focuses on cognition and behavior changing, boundaries, and family dynamics, also requires support and kindness. Although it is not an empirically based “treatment,” Alcoholics Anonymous (AA) has used kindness for decades.
Step 12 of AA’s 12-step program, which was developed by two people with alcohol use disorder in 1935 in Akron, Ohio, is as follows: “Having had a spiritual awakening as the result of these steps, we tried to carry this message to alcoholics, and to practice these principles in all our affairs.”
Once AA members are on solid ground with their sobriety, they are urged to help others in their recovery. This process provides many benefits. When individuals are concerned about someone else, they are less focused on themselves. This helps the individuals in recovery to decrease their rumination and “get out of themselves.” It also allows for the AA member to be kind and helpful to an individual who is suffering, thereby expressing kindness, compassion, and empathy. This act of “paying it forward” produces a domino effect that has withstood the test of time as evidenced by the ever-growing fellowship of Alcoholics Anonymous.
Several small acts of kindness can help us as clinicians and our patients:
1. Practice self-care.
2. Take a half day off from your practice.
3. Give staff a half day off.
4. Call a family member or friend and ask them how they are doing. Then engage in active listening and refrain from giving advice.
5. Donate to a homeless shelter or volunteer your time at a charity.
6. Give a stranger a compliment.
7. Surprise someone with a small gift.
8. Send a loved one a letter instead of a text.
9. Pick up litter.
10. Acknowledge family and friends who gave you extra support during the pandemic.
11. Take baked goods to your office.
12. Help a neighbor with groceries.
13. Leave a generous tip.
14. Play soft music in your office.
In conclusion, kindness, empathy, and compassion are vital concepts that are not just fluffy theories. They have vast mental, physical, and social benefits for us and our patients.
References
1. Cedars-Sinai staff. The Science of Kindness. 2019 Feb 13. Cedars-Sinai blog.
2. Harding K. The Rabbit Effect: Live Longer, Happier, and Healthier with the Groundbreaking Science of Kindness. Atria Books, 2019.
3. Ritvo E. BeKindr. Momosa Publishing, 2017.
4. Svoboda E. “Pay it Forward.” Psychology Today. Last reviewed 2016 Jun 9.
5. Aknin LB et al. “Prosocial spending and well-being: Cross-Cultural Evidence for a Psychological Universal.” Harvard Business School. Working Paper 11-038. 2010.
6. Hirsch EM. AMA J Ethics. Virtual Mentor. 2007;9(6):423-7.
Dr. Haji is a licensed clinical psychologist specializing in psychodiagnostic assessment, forensic assessment, dual diagnosis, serious and persistent mental illness, depression, anxiety, personality disorders, and substance abuse treatment. She practices in Miami and has no conflicts of interest.
COVID-19 fallout makes case for promoting the mental health czar
When the Biden administration announced who would serve on its COVID-19 task force, some asked why a mental health expert had not been included. I have a broader question: In light of the magnitude of the pandemic’s fallout, why doesn’t the administration create a mental health post parallel to the surgeon general?

I have been making the case for creation of a high-level mental health post for quite some time. In fact, in the late 1970s, toward the end of then-President Jimmy Carter’s term, I wrote and talked about the need for a special cabinet post of mental health. At the time I realized that, besides chronic mental disorders, the amount of mental distress people experienced from a myriad of life issues leading to anxiety, depression, even posttraumatic stress disorder (although not labeled as such then), needed focused and informed leadership.
Before the pandemic, the World Health Organization reported that depression was the leading cause of disability worldwide. In the prepandemic United States, mental and substance use disorders were the top cause of disability among younger people.
We’ve lost almost 600,000 people to COVID-19, and people have been unable to grieve properly. More than 2 million women have left the labor force to care for children and sick family members. As we continue to learn about the mental health–related devastation wrought by SARS-CoV-2 – particularly long-haul COVID-19 – it’s time to dust off my proposal, update it, and implement it.
Building on a good decision
Back in 2017, President Trump appointed Elinore F. McCance-Katz, MD, PhD, to a new post officially called “assistant secretary for mental health and substance use” and unofficially called the “mental health czar.” This was a groundbreaking step, because Dr. McCance-Katz, a psychiatrist, is known for developing innovative approaches to addressing the opioid crisis in her home state of Rhode Island. She resigned from her post on Jan. 7, 2021, citing her concerns about the Jan. 6 insurrection on the U.S. Capitol.
As of this writing, President Biden has nominated psychologist Miriam Delphin-Rittmon, PhD, who is commissioner of Connecticut Department of Mental Health and Addiction Services, as mental health czar. I’m glad to see that the new administration wants a new czar, but I would prefer to see a more expansive role for a mental health professional at the federal level. The reason is because
Processing the current crisis
Americans managed to recover emotionally from the ravages of death and dying from World War II; we lived through the “atomic age” of mutual destruction, sometimes calling it the age of anxiety. But nothing has come close to the overwhelming devastation that COVID-19 has brought to the world – and to this country.
A recent Government Accountability Office report shows 38% of U.S. adults reported symptoms of anxiety or depression from April 2020 through February 2021. That was up from 11% from January to June 2019, the report said, citing data from the Centers for Disease Control and Prevention. Meanwhile, the report cites data from the Substance Abuse and Mental Health Services Administration showing that opioid deaths were 25%-50% higher during the pandemic than a year earlier.
My sense is that people generally have opened up regarding their emotional problems in a freer manner, thus allowing us to speak about and accept mental health problems as part of our human reality – just as we accept physical disorders and search for treatment and care.
In terms of talk therapy, I still believe that the “thinking” therapies, that is, cognitive therapies that involved getting a new perspective on problems, are most effective in dealing with the myriad of emotional issues people experience as well as those that have arisen because of COVID-19, and the tremendous fear of severe illness and death that the virus can bring. Besides anxiety, depression, and fear, the psychological toll of a fractured lifestyle, coupled with social isolation, will lead many into a variety of PTSD-related conditions. Many of those conditions, including PTSD, might lift when COVID-19 is controlled, but the time frame for resolution is far from clear and will vary, depending on each person. National leadership, as well as therapists, need to be ready to work with the many mental health problems COVID-19 will leave in its wake.
Therapeutically, as we develop our cognitive approaches to the problems this pandemic has brought, whether affecting people with no past psychiatric history or those with a previous or ongoing problems, we are in a unique position ourselves to offer even more support based on our own experiences during the pandemic. Our patients have seen us wear masks and work remotely, and just as we know about their suffering, they know we have been affected as well. These shared experiences with patients can allow us to express even greater empathy and offer even greater support – which I believe enhances the cognitive process and adds more humanism to the therapeutic process.
The therapists I’ve talked with believe that sharing coping skills – even generally sharing anxieties – can be very therapeutic. They compared these exchanges to what is done in support or educational groups.
As a psychiatrist who has been treating patients using cognitive-behavioral therapy – the thinking therapy – for more than 40 years, I agree that sharing our experiences in this worldwide pandemic with those we are helping can be extremely beneficial. Using this approach would not distract from other cognitive work. CBT, after all, is a far cry from dynamic or psychoanalytic talking or listening.
Change is in the air. More and more Americans are getting vaccinated, and the CDC is constantly updating its guidance on COVID-19. That guidance should have a mental health component.
I urge the president to put mental health at the forefront by nominating an expert who could offer mental health solutions on a daily basis. This person should be on equal footing with the surgeon general. Taking this step would help destigmatize mental suffering and despair – and create greater awareness about how to address those conditions.
Dr. London has been a practicing psychiatrist for 4 decades and a newspaper columnist for almost as long. He has a private practice in New York and is author of “Find Freedom Fast: Short-Term Therapy That Works” (New York: Kettlehole Publishing, 2019). Dr. London has no conflicts of interest.
When the Biden administration announced who would serve on its COVID-19 task force, some asked why a mental health expert had not been included. I have a broader question: In light of the magnitude of the pandemic’s fallout, why doesn’t the administration create a mental health post parallel to the surgeon general?
I have been making the case for creation of a high-level mental health post for quite some time. In fact, in the late 1970s, toward the end of then-President Jimmy Carter’s term, I wrote and talked about the need for a special cabinet post of mental health. At the time I realized that, besides chronic mental disorders, the amount of mental distress people experienced from a myriad of life issues leading to anxiety, depression, even posttraumatic stress disorder (although not labeled as such then), needed focused and informed leadership.
Before the pandemic, the World Health Organization reported that depression was the leading cause of disability worldwide. In the prepandemic United States, mental and substance use disorders were the top cause of disability among younger people.
We’ve lost almost 600,000 people to COVID-19, and people have been unable to grieve properly. More than 2 million women have left the labor force to care for children and sick family members. As we continue to learn about the mental health–related devastation wrought by SARS-CoV-2 – particularly long-haul COVID-19 – it’s time to dust off my proposal, update it, and implement it.
Building on a good decision
Back in 2017, President Trump appointed Elinore F. McCance-Katz, MD, PhD, to a new post officially called “assistant secretary for mental health and substance use” and unofficially called the “mental health czar.” This was a groundbreaking step, because Dr. McCance-Katz, a psychiatrist, is known for developing innovative approaches to addressing the opioid crisis in her home state of Rhode Island. She resigned from her post on Jan. 7, 2021, citing her concerns about the Jan. 6 insurrection on the U.S. Capitol.
As of this writing, President Biden has nominated psychologist Miriam Delphin-Rittmon, PhD, who is commissioner of Connecticut Department of Mental Health and Addiction Services, as mental health czar. I’m glad to see that the new administration wants a new czar, but I would prefer to see a more expansive role for a mental health professional at the federal level. The reason is because
Processing the current crisis
Americans managed to recover emotionally from the ravages of death and dying from World War II; we lived through the “atomic age” of mutual destruction, sometimes calling it the age of anxiety. But nothing has come close to the overwhelming devastation that COVID-19 has brought to the world – and to this country.
A recent Government Accountability Office report shows 38% of U.S. adults reported symptoms of anxiety or depression from April 2020 through February 2021. That was up from 11% from January to June 2019, the report said, citing data from the Centers for Disease Control and Prevention. Meanwhile, the report cites data from the Substance Abuse and Mental Health Services Administration showing that opioid deaths were 25%-50% higher during the pandemic than a year earlier.
My sense is that people generally have opened up regarding their emotional problems in a freer manner, thus allowing us to speak about and accept mental health problems as part of our human reality – just as we accept physical disorders and search for treatment and care.
In terms of talk therapy, I still believe that the “thinking” therapies, that is, cognitive therapies that involved getting a new perspective on problems, are most effective in dealing with the myriad of emotional issues people experience as well as those that have arisen because of COVID-19, and the tremendous fear of severe illness and death that the virus can bring. Besides anxiety, depression, and fear, the psychological toll of a fractured lifestyle, coupled with social isolation, will lead many into a variety of PTSD-related conditions. Many of those conditions, including PTSD, might lift when COVID-19 is controlled, but the time frame for resolution is far from clear and will vary, depending on each person. National leadership, as well as therapists, need to be ready to work with the many mental health problems COVID-19 will leave in its wake.
Therapeutically, as we develop our cognitive approaches to the problems this pandemic has brought, whether affecting people with no past psychiatric history or those with a previous or ongoing problems, we are in a unique position ourselves to offer even more support based on our own experiences during the pandemic. Our patients have seen us wear masks and work remotely, and just as we know about their suffering, they know we have been affected as well. These shared experiences with patients can allow us to express even greater empathy and offer even greater support – which I believe enhances the cognitive process and adds more humanism to the therapeutic process.
The therapists I’ve talked with believe that sharing coping skills – even generally sharing anxieties – can be very therapeutic. They compared these exchanges to what is done in support or educational groups.
As a psychiatrist who has been treating patients using cognitive-behavioral therapy – the thinking therapy – for more than 40 years, I agree that sharing our experiences in this worldwide pandemic with those we are helping can be extremely beneficial. Using this approach would not distract from other cognitive work. CBT, after all, is a far cry from dynamic or psychoanalytic talking or listening.
Change is in the air. More and more Americans are getting vaccinated, and the CDC is constantly updating its guidance on COVID-19. That guidance should have a mental health component.
I urge the president to put mental health at the forefront by nominating an expert who could offer mental health solutions on a daily basis. This person should be on equal footing with the surgeon general. Taking this step would help destigmatize mental suffering and despair – and create greater awareness about how to address those conditions.
Dr. London has been a practicing psychiatrist for 4 decades and a newspaper columnist for almost as long. He has a private practice in New York and is author of “Find Freedom Fast: Short-Term Therapy That Works” (New York: Kettlehole Publishing, 2019). Dr. London has no conflicts of interest.
When the Biden administration announced who would serve on its COVID-19 task force, some asked why a mental health expert had not been included. I have a broader question: In light of the magnitude of the pandemic’s fallout, why doesn’t the administration create a mental health post parallel to the surgeon general?
I have been making the case for creation of a high-level mental health post for quite some time. In fact, in the late 1970s, toward the end of then-President Jimmy Carter’s term, I wrote and talked about the need for a special cabinet post of mental health. At the time I realized that, besides chronic mental disorders, the amount of mental distress people experienced from a myriad of life issues leading to anxiety, depression, even posttraumatic stress disorder (although not labeled as such then), needed focused and informed leadership.
Before the pandemic, the World Health Organization reported that depression was the leading cause of disability worldwide. In the prepandemic United States, mental and substance use disorders were the top cause of disability among younger people.
We’ve lost almost 600,000 people to COVID-19, and people have been unable to grieve properly. More than 2 million women have left the labor force to care for children and sick family members. As we continue to learn about the mental health–related devastation wrought by SARS-CoV-2 – particularly long-haul COVID-19 – it’s time to dust off my proposal, update it, and implement it.
Building on a good decision
Back in 2017, President Trump appointed Elinore F. McCance-Katz, MD, PhD, to a new post officially called “assistant secretary for mental health and substance use” and unofficially called the “mental health czar.” This was a groundbreaking step, because Dr. McCance-Katz, a psychiatrist, is known for developing innovative approaches to addressing the opioid crisis in her home state of Rhode Island. She resigned from her post on Jan. 7, 2021, citing her concerns about the Jan. 6 insurrection on the U.S. Capitol.
As of this writing, President Biden has nominated psychologist Miriam Delphin-Rittmon, PhD, who is commissioner of Connecticut Department of Mental Health and Addiction Services, as mental health czar. I’m glad to see that the new administration wants a new czar, but I would prefer to see a more expansive role for a mental health professional at the federal level. The reason is because
Processing the current crisis
Americans managed to recover emotionally from the ravages of death and dying from World War II; we lived through the “atomic age” of mutual destruction, sometimes calling it the age of anxiety. But nothing has come close to the overwhelming devastation that COVID-19 has brought to the world – and to this country.
A recent Government Accountability Office report shows 38% of U.S. adults reported symptoms of anxiety or depression from April 2020 through February 2021. That was up from 11% from January to June 2019, the report said, citing data from the Centers for Disease Control and Prevention. Meanwhile, the report cites data from the Substance Abuse and Mental Health Services Administration showing that opioid deaths were 25%-50% higher during the pandemic than a year earlier.
My sense is that people generally have opened up regarding their emotional problems in a freer manner, thus allowing us to speak about and accept mental health problems as part of our human reality – just as we accept physical disorders and search for treatment and care.
In terms of talk therapy, I still believe that the “thinking” therapies, that is, cognitive therapies that involved getting a new perspective on problems, are most effective in dealing with the myriad of emotional issues people experience as well as those that have arisen because of COVID-19, and the tremendous fear of severe illness and death that the virus can bring. Besides anxiety, depression, and fear, the psychological toll of a fractured lifestyle, coupled with social isolation, will lead many into a variety of PTSD-related conditions. Many of those conditions, including PTSD, might lift when COVID-19 is controlled, but the time frame for resolution is far from clear and will vary, depending on each person. National leadership, as well as therapists, need to be ready to work with the many mental health problems COVID-19 will leave in its wake.
Therapeutically, as we develop our cognitive approaches to the problems this pandemic has brought, whether affecting people with no past psychiatric history or those with a previous or ongoing problems, we are in a unique position ourselves to offer even more support based on our own experiences during the pandemic. Our patients have seen us wear masks and work remotely, and just as we know about their suffering, they know we have been affected as well. These shared experiences with patients can allow us to express even greater empathy and offer even greater support – which I believe enhances the cognitive process and adds more humanism to the therapeutic process.
The therapists I’ve talked with believe that sharing coping skills – even generally sharing anxieties – can be very therapeutic. They compared these exchanges to what is done in support or educational groups.
As a psychiatrist who has been treating patients using cognitive-behavioral therapy – the thinking therapy – for more than 40 years, I agree that sharing our experiences in this worldwide pandemic with those we are helping can be extremely beneficial. Using this approach would not distract from other cognitive work. CBT, after all, is a far cry from dynamic or psychoanalytic talking or listening.
Change is in the air. More and more Americans are getting vaccinated, and the CDC is constantly updating its guidance on COVID-19. That guidance should have a mental health component.
I urge the president to put mental health at the forefront by nominating an expert who could offer mental health solutions on a daily basis. This person should be on equal footing with the surgeon general. Taking this step would help destigmatize mental suffering and despair – and create greater awareness about how to address those conditions.
Dr. London has been a practicing psychiatrist for 4 decades and a newspaper columnist for almost as long. He has a private practice in New York and is author of “Find Freedom Fast: Short-Term Therapy That Works” (New York: Kettlehole Publishing, 2019). Dr. London has no conflicts of interest.
TMS ‘surprisingly effective’ for resistant depression
Treatment with transcranial magnetic stimulation (TMS) has a robust effect for patients with major depressive disorder (MDD), results from a large registry study show.
From patient self-reports and clinician assessments, investigators found that TMS was “surprisingly effective” and “an eye-opener” for these patients, lead investigator Harold A. Sackeim, PhD, professor of clinical psychology in psychiatry and radiology, Columbia University, New York, told this news organization.
“In a presumably treatment-resistant population, the efficacy compared favorably with virtually all pharmacologic treatments” tested in the studies, said Dr. Sackeim.
He noted that the registry from which the data were obtained “is the largest for any treatment of depression, period.” These positive results suggest TMS should be considered a first-line treatment for MDD, he added.
The study was presented at the virtual American Psychiatric Association 2021 Annual Meeting and was previously published in the Journal of Affective Disorders.
Real-world study
Results of randomized clinical trials have shown that TMS is effective for episodes of MDD. However, the investigators note that there is a need to characterize and identify patient- and treatment-related clinical outcomes.
The study included 5,010 adult patients who had received a primary diagnosis of MDD and were treated at 103 practices in the United States. Participants completed the nine-item Patient Health Questionnaire (PHQ-9) at baseline and at least one other time following a TMS treatment.
The average baseline PHQ-9 score was 19.8, indicating moderate to severe symptoms. This was also reflected in a smaller sample that included Clinical Global Impressions–Severity (CGI-S) ratings by clinicians, mostly psychiatrists.
About two-thirds of the study population were women. The average age was about 50 years. Participants typically received about 30 TMS sessions over 7 to 8 weeks.
TMS targets tissue in the dorsolateral prefrontal cortex. The standard protocol involves administering “fast” or high-frequency (10-Hz) stimulation on the left side. Sometimes, slow-frequency stimulation on the right side is added. About 57% of patients were treated on the left side, and 43% were treated on both sides. Each session involved delivery of about 3,000 pulses.
In the analysis of patient self-reports (PHQ-9), the response rate, which was defined as resolution of 50% or more of symptoms, was from 58% to 69%. The remission rate, defined as becoming asymptomatic or having minimal symptoms, ranged from 28% to 36%.
Results were about 5% higher in the “completer” sample, which included 3,814 patients who received at least 20 treatments and who completed a PHQ-9 assessment at the end the treatment course.
The number of completers in the analysis was “massive,” said Dr. Sackeim. It’s “ten times larger than in any previous TMS study; all randomized trials have a couple of hundred subjects at most, so this is whopping.”
The results provide “a full snapshot” of TMS in the “real-world” community instead of in the “highly controlled” environment of most studies, he added.
Gender differences
The analysis that included CGI-S clinician measures yielded higher outcome estimates – 79% to 83% for the response rate, and 47% to 63% for the remission rate.
Women tended to have better clinical outcomes. “It appears to me that around age 50 is where you see the difference,” said Dr. Sackeim. “Among women, it looks like the older they get, the better the outcome, whereas men are not showing that type of positive aging effect.”
This difference might be due to hormonal changes associated with menopause and the fact that older men with depression may have had a stroke or brain lesion. Dr. Sackeim said he plans to look more closely at outcomes of women in comparison with men.
This, said Dr. Sackeim, illustrates how rapidly the TMS field is evolving.
He noted that researchers are now personalizing the procedure by determining the optimal target for individual patients. Other investigators are testing different protocols.
In the current study, results tended to be better for those who received 4,000 or more pulses, said Dr. Sackeim. “There was an indication of a dose response effect in terms of how many pulses per session,” he said.
The authors note that the study’s PDQ-9 response and remission rates indicate that clinical outcomes are comparable to those of the seven antidepressants studied in Level 2 of the large Sequenced Treatment Alternatives to Relieve Depression (STAR-D) trial.
Initial data for relapse in the study population are “encouraging,” said Dr. Sackeim. “You don’t see the rapid relapse that you do when you discontinue some treatments, for example with ECT [electroconvulsive therapy].”
The “slower onset of action” over the course of several sessions “may induce longer benefit,” he added.
Expanded use warranted?
The intervention proved very safe. Side effects, including headaches, were minimal, and there were “virtually no cognitive effects,” said Dr. Sackeim.
Dr. Sackeim believes TMS, as it has evolved, “is an outstanding option for treatment-resistant depression, and it has a very bright future” and should not be reserved for patients with established treatment-resistant depression (TRD), which is the current U.S. Food and Drug Administration indication.
“Restricting it to TRD in my mind is probably a mistake. Why shouldn’t the patient who is just starting on their course of treatment for depression have this as a nonpharmacological option?” he said.
Limitations of the study included its open-label design and the fact that only patients’ age, gender, outcome scores, and TMS treatment parameters were recorded in the registry. Other clinical characteristics, including medication use, were unknown.
However, it’s presumed that most patients had TRD, because insurance reimbursement for TMS typically requires an extensive history of failed antidepressant treatment.
Commenting on the study for an interview, Mark George, MD, professor, and Layton McCurdy, endowed chair in psychiatry, the Medical University of South Carolina, Charleston, called the remission and response rates “remarkable.”
The study included a “huge sample size” of Americans suffering from depression “who have not responded to talking therapy or medications,” noted Dr. George.
“This real-world study shows how effective, safe, and important TMS is for depressed patients who do not respond to medications,” he said.
Neuronetics supported the NeuroStar Advanced Therapy System Clinical Outcomes Registry, analysis of the registry data, and the drafting of this manuscript. Dr. Sackeim serves as a scientific adviser to LivaNova PLC, MECTA Corporation, and Neuronetics. He receives honoraria and royalties from Elsevier and Oxford University Press. He is the inventor on nonremunerative U.S. patents for Focal Electrically Administered Seizure Therapy (FEAST), titration in the current domain in ECT, and the adjustment of current in ECT devices; each patent is held by the MECTA Corporation. He is also the originator of magnetic seizure therapy.
A version of this article first appeared on Medscape.com.
Treatment with transcranial magnetic stimulation (TMS) has a robust effect for patients with major depressive disorder (MDD), results from a large registry study show.
From patient self-reports and clinician assessments, investigators found that TMS was “surprisingly effective” and “an eye-opener” for these patients, lead investigator Harold A. Sackeim, PhD, professor of clinical psychology in psychiatry and radiology, Columbia University, New York, told this news organization.
“In a presumably treatment-resistant population, the efficacy compared favorably with virtually all pharmacologic treatments” tested in the studies, said Dr. Sackeim.
He noted that the registry from which the data were obtained “is the largest for any treatment of depression, period.” These positive results suggest TMS should be considered a first-line treatment for MDD, he added.
The study was presented at the virtual American Psychiatric Association 2021 Annual Meeting and was previously published in the Journal of Affective Disorders.
Real-world study
Results of randomized clinical trials have shown that TMS is effective for episodes of MDD. However, the investigators note that there is a need to characterize and identify patient- and treatment-related clinical outcomes.
The study included 5,010 adult patients who had received a primary diagnosis of MDD and were treated at 103 practices in the United States. Participants completed the nine-item Patient Health Questionnaire (PHQ-9) at baseline and at least one other time following a TMS treatment.
The average baseline PHQ-9 score was 19.8, indicating moderate to severe symptoms. This was also reflected in a smaller sample that included Clinical Global Impressions–Severity (CGI-S) ratings by clinicians, mostly psychiatrists.
About two-thirds of the study population were women. The average age was about 50 years. Participants typically received about 30 TMS sessions over 7 to 8 weeks.
TMS targets tissue in the dorsolateral prefrontal cortex. The standard protocol involves administering “fast” or high-frequency (10-Hz) stimulation on the left side. Sometimes, slow-frequency stimulation on the right side is added. About 57% of patients were treated on the left side, and 43% were treated on both sides. Each session involved delivery of about 3,000 pulses.
In the analysis of patient self-reports (PHQ-9), the response rate, which was defined as resolution of 50% or more of symptoms, was from 58% to 69%. The remission rate, defined as becoming asymptomatic or having minimal symptoms, ranged from 28% to 36%.
Results were about 5% higher in the “completer” sample, which included 3,814 patients who received at least 20 treatments and who completed a PHQ-9 assessment at the end the treatment course.
The number of completers in the analysis was “massive,” said Dr. Sackeim. It’s “ten times larger than in any previous TMS study; all randomized trials have a couple of hundred subjects at most, so this is whopping.”
The results provide “a full snapshot” of TMS in the “real-world” community instead of in the “highly controlled” environment of most studies, he added.
Gender differences
The analysis that included CGI-S clinician measures yielded higher outcome estimates – 79% to 83% for the response rate, and 47% to 63% for the remission rate.
Women tended to have better clinical outcomes. “It appears to me that around age 50 is where you see the difference,” said Dr. Sackeim. “Among women, it looks like the older they get, the better the outcome, whereas men are not showing that type of positive aging effect.”
This difference might be due to hormonal changes associated with menopause and the fact that older men with depression may have had a stroke or brain lesion. Dr. Sackeim said he plans to look more closely at outcomes of women in comparison with men.
This, said Dr. Sackeim, illustrates how rapidly the TMS field is evolving.
He noted that researchers are now personalizing the procedure by determining the optimal target for individual patients. Other investigators are testing different protocols.
In the current study, results tended to be better for those who received 4,000 or more pulses, said Dr. Sackeim. “There was an indication of a dose response effect in terms of how many pulses per session,” he said.
The authors note that the study’s PDQ-9 response and remission rates indicate that clinical outcomes are comparable to those of the seven antidepressants studied in Level 2 of the large Sequenced Treatment Alternatives to Relieve Depression (STAR-D) trial.
Initial data for relapse in the study population are “encouraging,” said Dr. Sackeim. “You don’t see the rapid relapse that you do when you discontinue some treatments, for example with ECT [electroconvulsive therapy].”
The “slower onset of action” over the course of several sessions “may induce longer benefit,” he added.
Expanded use warranted?
The intervention proved very safe. Side effects, including headaches, were minimal, and there were “virtually no cognitive effects,” said Dr. Sackeim.
Dr. Sackeim believes TMS, as it has evolved, “is an outstanding option for treatment-resistant depression, and it has a very bright future” and should not be reserved for patients with established treatment-resistant depression (TRD), which is the current U.S. Food and Drug Administration indication.
“Restricting it to TRD in my mind is probably a mistake. Why shouldn’t the patient who is just starting on their course of treatment for depression have this as a nonpharmacological option?” he said.
Limitations of the study included its open-label design and the fact that only patients’ age, gender, outcome scores, and TMS treatment parameters were recorded in the registry. Other clinical characteristics, including medication use, were unknown.
However, it’s presumed that most patients had TRD, because insurance reimbursement for TMS typically requires an extensive history of failed antidepressant treatment.
Commenting on the study for an interview, Mark George, MD, professor, and Layton McCurdy, endowed chair in psychiatry, the Medical University of South Carolina, Charleston, called the remission and response rates “remarkable.”
The study included a “huge sample size” of Americans suffering from depression “who have not responded to talking therapy or medications,” noted Dr. George.
“This real-world study shows how effective, safe, and important TMS is for depressed patients who do not respond to medications,” he said.
Neuronetics supported the NeuroStar Advanced Therapy System Clinical Outcomes Registry, analysis of the registry data, and the drafting of this manuscript. Dr. Sackeim serves as a scientific adviser to LivaNova PLC, MECTA Corporation, and Neuronetics. He receives honoraria and royalties from Elsevier and Oxford University Press. He is the inventor on nonremunerative U.S. patents for Focal Electrically Administered Seizure Therapy (FEAST), titration in the current domain in ECT, and the adjustment of current in ECT devices; each patent is held by the MECTA Corporation. He is also the originator of magnetic seizure therapy.
A version of this article first appeared on Medscape.com.
Treatment with transcranial magnetic stimulation (TMS) has a robust effect for patients with major depressive disorder (MDD), results from a large registry study show.
From patient self-reports and clinician assessments, investigators found that TMS was “surprisingly effective” and “an eye-opener” for these patients, lead investigator Harold A. Sackeim, PhD, professor of clinical psychology in psychiatry and radiology, Columbia University, New York, told this news organization.
“In a presumably treatment-resistant population, the efficacy compared favorably with virtually all pharmacologic treatments” tested in the studies, said Dr. Sackeim.
He noted that the registry from which the data were obtained “is the largest for any treatment of depression, period.” These positive results suggest TMS should be considered a first-line treatment for MDD, he added.
The study was presented at the virtual American Psychiatric Association 2021 Annual Meeting and was previously published in the Journal of Affective Disorders.
Real-world study
Results of randomized clinical trials have shown that TMS is effective for episodes of MDD. However, the investigators note that there is a need to characterize and identify patient- and treatment-related clinical outcomes.
The study included 5,010 adult patients who had received a primary diagnosis of MDD and were treated at 103 practices in the United States. Participants completed the nine-item Patient Health Questionnaire (PHQ-9) at baseline and at least one other time following a TMS treatment.
The average baseline PHQ-9 score was 19.8, indicating moderate to severe symptoms. This was also reflected in a smaller sample that included Clinical Global Impressions–Severity (CGI-S) ratings by clinicians, mostly psychiatrists.
About two-thirds of the study population were women. The average age was about 50 years. Participants typically received about 30 TMS sessions over 7 to 8 weeks.
TMS targets tissue in the dorsolateral prefrontal cortex. The standard protocol involves administering “fast” or high-frequency (10-Hz) stimulation on the left side. Sometimes, slow-frequency stimulation on the right side is added. About 57% of patients were treated on the left side, and 43% were treated on both sides. Each session involved delivery of about 3,000 pulses.
In the analysis of patient self-reports (PHQ-9), the response rate, which was defined as resolution of 50% or more of symptoms, was from 58% to 69%. The remission rate, defined as becoming asymptomatic or having minimal symptoms, ranged from 28% to 36%.
Results were about 5% higher in the “completer” sample, which included 3,814 patients who received at least 20 treatments and who completed a PHQ-9 assessment at the end the treatment course.
The number of completers in the analysis was “massive,” said Dr. Sackeim. It’s “ten times larger than in any previous TMS study; all randomized trials have a couple of hundred subjects at most, so this is whopping.”
The results provide “a full snapshot” of TMS in the “real-world” community instead of in the “highly controlled” environment of most studies, he added.
Gender differences
The analysis that included CGI-S clinician measures yielded higher outcome estimates – 79% to 83% for the response rate, and 47% to 63% for the remission rate.
Women tended to have better clinical outcomes. “It appears to me that around age 50 is where you see the difference,” said Dr. Sackeim. “Among women, it looks like the older they get, the better the outcome, whereas men are not showing that type of positive aging effect.”
This difference might be due to hormonal changes associated with menopause and the fact that older men with depression may have had a stroke or brain lesion. Dr. Sackeim said he plans to look more closely at outcomes of women in comparison with men.
This, said Dr. Sackeim, illustrates how rapidly the TMS field is evolving.
He noted that researchers are now personalizing the procedure by determining the optimal target for individual patients. Other investigators are testing different protocols.
In the current study, results tended to be better for those who received 4,000 or more pulses, said Dr. Sackeim. “There was an indication of a dose response effect in terms of how many pulses per session,” he said.
The authors note that the study’s PDQ-9 response and remission rates indicate that clinical outcomes are comparable to those of the seven antidepressants studied in Level 2 of the large Sequenced Treatment Alternatives to Relieve Depression (STAR-D) trial.
Initial data for relapse in the study population are “encouraging,” said Dr. Sackeim. “You don’t see the rapid relapse that you do when you discontinue some treatments, for example with ECT [electroconvulsive therapy].”
The “slower onset of action” over the course of several sessions “may induce longer benefit,” he added.
Expanded use warranted?
The intervention proved very safe. Side effects, including headaches, were minimal, and there were “virtually no cognitive effects,” said Dr. Sackeim.
Dr. Sackeim believes TMS, as it has evolved, “is an outstanding option for treatment-resistant depression, and it has a very bright future” and should not be reserved for patients with established treatment-resistant depression (TRD), which is the current U.S. Food and Drug Administration indication.
“Restricting it to TRD in my mind is probably a mistake. Why shouldn’t the patient who is just starting on their course of treatment for depression have this as a nonpharmacological option?” he said.
Limitations of the study included its open-label design and the fact that only patients’ age, gender, outcome scores, and TMS treatment parameters were recorded in the registry. Other clinical characteristics, including medication use, were unknown.
However, it’s presumed that most patients had TRD, because insurance reimbursement for TMS typically requires an extensive history of failed antidepressant treatment.
Commenting on the study for an interview, Mark George, MD, professor, and Layton McCurdy, endowed chair in psychiatry, the Medical University of South Carolina, Charleston, called the remission and response rates “remarkable.”
The study included a “huge sample size” of Americans suffering from depression “who have not responded to talking therapy or medications,” noted Dr. George.
“This real-world study shows how effective, safe, and important TMS is for depressed patients who do not respond to medications,” he said.
Neuronetics supported the NeuroStar Advanced Therapy System Clinical Outcomes Registry, analysis of the registry data, and the drafting of this manuscript. Dr. Sackeim serves as a scientific adviser to LivaNova PLC, MECTA Corporation, and Neuronetics. He receives honoraria and royalties from Elsevier and Oxford University Press. He is the inventor on nonremunerative U.S. patents for Focal Electrically Administered Seizure Therapy (FEAST), titration in the current domain in ECT, and the adjustment of current in ECT devices; each patent is held by the MECTA Corporation. He is also the originator of magnetic seizure therapy.
A version of this article first appeared on Medscape.com.
How to improve our response to COVID’s mental tolls
We have no way of precisely knowing how many lives might have been saved, and how much grief and loneliness spared and economic ruin contained during COVID-19 if we had risen to its myriad challenges in a timely fashion. However, I feel we can safely say that the United States deserves to be graded with an “F” for its management of the pandemic.

To render this grade, we need only to read the countless verified reports of how critically needed public health measures were not taken soon enough, or sufficiently, to substantially mitigate human and societal suffering.
This began with the failure to protect doctors, nurses, and technicians, who did not have the personal protective equipment needed to prevent infection and spare risk to their loved ones. It soon extended to the country’s failure to adequately protect all its citizens and residents. COVID-19 then rained its grievous consequences disproportionately upon people of color, those living in poverty, and those with housing and food insecurity – those already greatly foreclosed from opportunities to exit from their circumstances.
We all have heard, “Fool me once, shame on you; fool me twice, shame on me.”
Bear witness, colleagues and friends: It will be our shared shame if we too continue to fail in our response to COVID-19. But failure need not happen because protecting ourselves and our country is a solvable problem; complex and demanding for sure, but solvable.
To battle trauma, we must first define it
The sine qua non of a disaster is its psychic and social trauma. I asked Maureen Sayres Van Niel, MD, chair of the American Psychiatric Association’s Minority and Underrepresented Caucus and a former steering committee member of the U.S. Preventive Services Task Force, to define trauma. She said, “It is [the product of] a catastrophic, unexpected event over which we have little control, with grave consequences to the lives and psychological functioning of those individuals and groups affected.”
The COVID-19 pandemic is a massively amplified traumatic event because of the virulence and contagious properties of the virus and its variants; the absence of end date on the horizon; its effect as a proverbial ax that disproportionately falls on the majority of the populace experiencing racial and social inequities; and the ironic yet necessary imperative to distance ourselves from those we care about and who care about us.
Four interdependent factors drive the magnitude of the traumatic impact of a disaster: the degree of exposure to the life-threatening event; the duration and threat of recurrence; an individual’s preexisting (natural and human-made) trauma and mental and addictive disorders; and the adequacy of family and fundamental resources such as housing, food, safety, and access to health care (the social dimensions of health and mental health). These factors underline the “who,” “what,” “where,” and “how” of what should have been (and continue to be) an effective public health response to the COVID-19 pandemic.
Yet existing categories that we have used to predict risk for trauma no longer hold. The gravity, prevalence, and persistence of COVID-19’s horrors erase any differences among victims, witnesses, and bystanders. Dr Sayres Van Niel asserts that we have a “collective, national trauma.” In April, the Kaiser Family Foundation’s Vaccine Monitor reported that 24% of U.S. adults had a close friend or family member who died of COVID-19. That’s 82 million Americans! Our country has eclipsed individual victimization and trauma because we are all in its maw.
Vital lessons from the past
In a previous column, I described my role as New York City’s mental health commissioner after 9/11 and the many lessons we learned during that multiyear process. Our work served as a template for other disasters to follow, such as Hurricane Sandy. Its value to COVID-19 is equally apparent.
We learned that those most at risk of developing symptomatic, functionally impairing mental illness had prior traumatic experiences (for example, from childhood abuse or neglect, violence, war, and forced displacement from their native land) and/or a preexisting mental or substance use disorder.
Once these individuals and communities were identified, we could prioritize their treatment and care. Doing so required mobilizing both inner and external (social) resources, which can be used before disaster strikes or in its wake.
For individuals, adaptive resources include developing any of a number of mind-body activities (for example, meditation, mindfulness, slow breathing, and yoga); sufficient but not necessarily excessive levels of exercise (as has been said, if exercise were a pill, it would be the most potent of medicines); nourishing diets; sleep, nature’s restorative state; and perhaps most important, attachment and human connection to people who care about you and whom you care about and trust.
This does not necessarily mean holding or following an institutional religion or belonging to house of worship (though, of course, that melds and augments faith with community). For a great many, myself included, there is spirituality, the belief in a greater power, which need not be a God yet instills a sense of the vastness, universality, and continuity of life.
For communities, adaptive resources include safe homes and neighborhoods; diminishing housing and food insecurity; education, including pre-K; employment, with a livable wage; ridding human interactions of the endless, so-called microaggressions (which are not micro at all, because they accrue) of race, ethnic, class, and age discrimination and injustice; and ready access to quality and affordable health care, now more than ever for the rising tide of mental and substance use disorders that COVID-19 has unleashed.
Every gain we make to ablate racism, social injustice, discrimination, and widely and deeply spread resource and opportunity inequities means more cohesion among the members of our collective tribe. Greater cohesion, a love for thy neighbor, and equity (in action, not polemics) will fuel the resilience we will need to withstand more of COVID-19’s ongoing trauma; that of other, inescapable disasters and losses; and the wear and tear of everyday life. The rewards of equity are priceless and include the dignity that derives from fairness and justice – given and received.
An unprecedented disaster requires a bold response
My, what a list. But to me, the encompassing nature of what’s needed means that we can make differences anywhere, everywhere, and in countless and continuous ways.
The measure of any society is in how it cares for those who are foreclosed, through no fault of their own, from what we all want: a life safe from violence, secure in housing and food, with loving relationships and the pride that comes of making contributions, each in our own, wonderfully unique way.
Where will we all be in a year, 2, or 3 from now? Prepared, or not? Emotionally inoculated, or not? Better equipped, or not? As divided, or more cohesive?
Well, I imagine that depends on each and every one of us.
Lloyd I. Sederer, MD, is a psychiatrist, public health doctor, and writer. He is an adjunct professor at the Columbia University School of Public Health, director of Columbia Psychiatry Media, chief medical officer of Bongo Media, and chair of the advisory board of Get Help. He has been chief medical officer of McLean Hospital, a Harvard teaching hospital; mental health commissioner of New York City (in the Bloomberg administration); and chief medical officer of the New York State Office of Mental Health, the nation’s largest state mental health agency.
A version of this article first appeared on Medscape.com.
We have no way of precisely knowing how many lives might have been saved, and how much grief and loneliness spared and economic ruin contained during COVID-19 if we had risen to its myriad challenges in a timely fashion. However, I feel we can safely say that the United States deserves to be graded with an “F” for its management of the pandemic.
To render this grade, we need only to read the countless verified reports of how critically needed public health measures were not taken soon enough, or sufficiently, to substantially mitigate human and societal suffering.
This began with the failure to protect doctors, nurses, and technicians, who did not have the personal protective equipment needed to prevent infection and spare risk to their loved ones. It soon extended to the country’s failure to adequately protect all its citizens and residents. COVID-19 then rained its grievous consequences disproportionately upon people of color, those living in poverty, and those with housing and food insecurity – those already greatly foreclosed from opportunities to exit from their circumstances.
We all have heard, “Fool me once, shame on you; fool me twice, shame on me.”
Bear witness, colleagues and friends: It will be our shared shame if we too continue to fail in our response to COVID-19. But failure need not happen because protecting ourselves and our country is a solvable problem; complex and demanding for sure, but solvable.
To battle trauma, we must first define it
The sine qua non of a disaster is its psychic and social trauma. I asked Maureen Sayres Van Niel, MD, chair of the American Psychiatric Association’s Minority and Underrepresented Caucus and a former steering committee member of the U.S. Preventive Services Task Force, to define trauma. She said, “It is [the product of] a catastrophic, unexpected event over which we have little control, with grave consequences to the lives and psychological functioning of those individuals and groups affected.”
The COVID-19 pandemic is a massively amplified traumatic event because of the virulence and contagious properties of the virus and its variants; the absence of end date on the horizon; its effect as a proverbial ax that disproportionately falls on the majority of the populace experiencing racial and social inequities; and the ironic yet necessary imperative to distance ourselves from those we care about and who care about us.
Four interdependent factors drive the magnitude of the traumatic impact of a disaster: the degree of exposure to the life-threatening event; the duration and threat of recurrence; an individual’s preexisting (natural and human-made) trauma and mental and addictive disorders; and the adequacy of family and fundamental resources such as housing, food, safety, and access to health care (the social dimensions of health and mental health). These factors underline the “who,” “what,” “where,” and “how” of what should have been (and continue to be) an effective public health response to the COVID-19 pandemic.
Yet existing categories that we have used to predict risk for trauma no longer hold. The gravity, prevalence, and persistence of COVID-19’s horrors erase any differences among victims, witnesses, and bystanders. Dr Sayres Van Niel asserts that we have a “collective, national trauma.” In April, the Kaiser Family Foundation’s Vaccine Monitor reported that 24% of U.S. adults had a close friend or family member who died of COVID-19. That’s 82 million Americans! Our country has eclipsed individual victimization and trauma because we are all in its maw.
Vital lessons from the past
In a previous column, I described my role as New York City’s mental health commissioner after 9/11 and the many lessons we learned during that multiyear process. Our work served as a template for other disasters to follow, such as Hurricane Sandy. Its value to COVID-19 is equally apparent.
We learned that those most at risk of developing symptomatic, functionally impairing mental illness had prior traumatic experiences (for example, from childhood abuse or neglect, violence, war, and forced displacement from their native land) and/or a preexisting mental or substance use disorder.
Once these individuals and communities were identified, we could prioritize their treatment and care. Doing so required mobilizing both inner and external (social) resources, which can be used before disaster strikes or in its wake.
For individuals, adaptive resources include developing any of a number of mind-body activities (for example, meditation, mindfulness, slow breathing, and yoga); sufficient but not necessarily excessive levels of exercise (as has been said, if exercise were a pill, it would be the most potent of medicines); nourishing diets; sleep, nature’s restorative state; and perhaps most important, attachment and human connection to people who care about you and whom you care about and trust.
This does not necessarily mean holding or following an institutional religion or belonging to house of worship (though, of course, that melds and augments faith with community). For a great many, myself included, there is spirituality, the belief in a greater power, which need not be a God yet instills a sense of the vastness, universality, and continuity of life.
For communities, adaptive resources include safe homes and neighborhoods; diminishing housing and food insecurity; education, including pre-K; employment, with a livable wage; ridding human interactions of the endless, so-called microaggressions (which are not micro at all, because they accrue) of race, ethnic, class, and age discrimination and injustice; and ready access to quality and affordable health care, now more than ever for the rising tide of mental and substance use disorders that COVID-19 has unleashed.
Every gain we make to ablate racism, social injustice, discrimination, and widely and deeply spread resource and opportunity inequities means more cohesion among the members of our collective tribe. Greater cohesion, a love for thy neighbor, and equity (in action, not polemics) will fuel the resilience we will need to withstand more of COVID-19’s ongoing trauma; that of other, inescapable disasters and losses; and the wear and tear of everyday life. The rewards of equity are priceless and include the dignity that derives from fairness and justice – given and received.
An unprecedented disaster requires a bold response
My, what a list. But to me, the encompassing nature of what’s needed means that we can make differences anywhere, everywhere, and in countless and continuous ways.
The measure of any society is in how it cares for those who are foreclosed, through no fault of their own, from what we all want: a life safe from violence, secure in housing and food, with loving relationships and the pride that comes of making contributions, each in our own, wonderfully unique way.
Where will we all be in a year, 2, or 3 from now? Prepared, or not? Emotionally inoculated, or not? Better equipped, or not? As divided, or more cohesive?
Well, I imagine that depends on each and every one of us.
Lloyd I. Sederer, MD, is a psychiatrist, public health doctor, and writer. He is an adjunct professor at the Columbia University School of Public Health, director of Columbia Psychiatry Media, chief medical officer of Bongo Media, and chair of the advisory board of Get Help. He has been chief medical officer of McLean Hospital, a Harvard teaching hospital; mental health commissioner of New York City (in the Bloomberg administration); and chief medical officer of the New York State Office of Mental Health, the nation’s largest state mental health agency.
A version of this article first appeared on Medscape.com.
We have no way of precisely knowing how many lives might have been saved, and how much grief and loneliness spared and economic ruin contained during COVID-19 if we had risen to its myriad challenges in a timely fashion. However, I feel we can safely say that the United States deserves to be graded with an “F” for its management of the pandemic.
To render this grade, we need only to read the countless verified reports of how critically needed public health measures were not taken soon enough, or sufficiently, to substantially mitigate human and societal suffering.
This began with the failure to protect doctors, nurses, and technicians, who did not have the personal protective equipment needed to prevent infection and spare risk to their loved ones. It soon extended to the country’s failure to adequately protect all its citizens and residents. COVID-19 then rained its grievous consequences disproportionately upon people of color, those living in poverty, and those with housing and food insecurity – those already greatly foreclosed from opportunities to exit from their circumstances.
We all have heard, “Fool me once, shame on you; fool me twice, shame on me.”
Bear witness, colleagues and friends: It will be our shared shame if we too continue to fail in our response to COVID-19. But failure need not happen because protecting ourselves and our country is a solvable problem; complex and demanding for sure, but solvable.
To battle trauma, we must first define it
The sine qua non of a disaster is its psychic and social trauma. I asked Maureen Sayres Van Niel, MD, chair of the American Psychiatric Association’s Minority and Underrepresented Caucus and a former steering committee member of the U.S. Preventive Services Task Force, to define trauma. She said, “It is [the product of] a catastrophic, unexpected event over which we have little control, with grave consequences to the lives and psychological functioning of those individuals and groups affected.”
The COVID-19 pandemic is a massively amplified traumatic event because of the virulence and contagious properties of the virus and its variants; the absence of end date on the horizon; its effect as a proverbial ax that disproportionately falls on the majority of the populace experiencing racial and social inequities; and the ironic yet necessary imperative to distance ourselves from those we care about and who care about us.
Four interdependent factors drive the magnitude of the traumatic impact of a disaster: the degree of exposure to the life-threatening event; the duration and threat of recurrence; an individual’s preexisting (natural and human-made) trauma and mental and addictive disorders; and the adequacy of family and fundamental resources such as housing, food, safety, and access to health care (the social dimensions of health and mental health). These factors underline the “who,” “what,” “where,” and “how” of what should have been (and continue to be) an effective public health response to the COVID-19 pandemic.
Yet existing categories that we have used to predict risk for trauma no longer hold. The gravity, prevalence, and persistence of COVID-19’s horrors erase any differences among victims, witnesses, and bystanders. Dr Sayres Van Niel asserts that we have a “collective, national trauma.” In April, the Kaiser Family Foundation’s Vaccine Monitor reported that 24% of U.S. adults had a close friend or family member who died of COVID-19. That’s 82 million Americans! Our country has eclipsed individual victimization and trauma because we are all in its maw.
Vital lessons from the past
In a previous column, I described my role as New York City’s mental health commissioner after 9/11 and the many lessons we learned during that multiyear process. Our work served as a template for other disasters to follow, such as Hurricane Sandy. Its value to COVID-19 is equally apparent.
We learned that those most at risk of developing symptomatic, functionally impairing mental illness had prior traumatic experiences (for example, from childhood abuse or neglect, violence, war, and forced displacement from their native land) and/or a preexisting mental or substance use disorder.
Once these individuals and communities were identified, we could prioritize their treatment and care. Doing so required mobilizing both inner and external (social) resources, which can be used before disaster strikes or in its wake.
For individuals, adaptive resources include developing any of a number of mind-body activities (for example, meditation, mindfulness, slow breathing, and yoga); sufficient but not necessarily excessive levels of exercise (as has been said, if exercise were a pill, it would be the most potent of medicines); nourishing diets; sleep, nature’s restorative state; and perhaps most important, attachment and human connection to people who care about you and whom you care about and trust.
This does not necessarily mean holding or following an institutional religion or belonging to house of worship (though, of course, that melds and augments faith with community). For a great many, myself included, there is spirituality, the belief in a greater power, which need not be a God yet instills a sense of the vastness, universality, and continuity of life.
For communities, adaptive resources include safe homes and neighborhoods; diminishing housing and food insecurity; education, including pre-K; employment, with a livable wage; ridding human interactions of the endless, so-called microaggressions (which are not micro at all, because they accrue) of race, ethnic, class, and age discrimination and injustice; and ready access to quality and affordable health care, now more than ever for the rising tide of mental and substance use disorders that COVID-19 has unleashed.
Every gain we make to ablate racism, social injustice, discrimination, and widely and deeply spread resource and opportunity inequities means more cohesion among the members of our collective tribe. Greater cohesion, a love for thy neighbor, and equity (in action, not polemics) will fuel the resilience we will need to withstand more of COVID-19’s ongoing trauma; that of other, inescapable disasters and losses; and the wear and tear of everyday life. The rewards of equity are priceless and include the dignity that derives from fairness and justice – given and received.
An unprecedented disaster requires a bold response
My, what a list. But to me, the encompassing nature of what’s needed means that we can make differences anywhere, everywhere, and in countless and continuous ways.
The measure of any society is in how it cares for those who are foreclosed, through no fault of their own, from what we all want: a life safe from violence, secure in housing and food, with loving relationships and the pride that comes of making contributions, each in our own, wonderfully unique way.
Where will we all be in a year, 2, or 3 from now? Prepared, or not? Emotionally inoculated, or not? Better equipped, or not? As divided, or more cohesive?
Well, I imagine that depends on each and every one of us.
Lloyd I. Sederer, MD, is a psychiatrist, public health doctor, and writer. He is an adjunct professor at the Columbia University School of Public Health, director of Columbia Psychiatry Media, chief medical officer of Bongo Media, and chair of the advisory board of Get Help. He has been chief medical officer of McLean Hospital, a Harvard teaching hospital; mental health commissioner of New York City (in the Bloomberg administration); and chief medical officer of the New York State Office of Mental Health, the nation’s largest state mental health agency.
A version of this article first appeared on Medscape.com.
Study points to best treatments for depression in primary care
according to a network meta-analysis (NMA) comparing either and both approaches with control conditions in the primary care setting.
The findings are important, since the majority of depressed patients are treated by primary care physicians, yet relatively few randomized trials of treatment have focused on this setting, noted senior study author Pim Cuijpers, PhD, from Vrije Universiteit Amsterdam, and colleagues, in the paper, which was published in Annals of Family Medicine.
“The main message is that clinicians should certainly consider psychotherapy instead of pharmacotherapy, because this is preferred by most patients, and when possible, combined treatments should be the preferred choice because the outcomes are considerably better,” he said in an interview. Either way, he emphasized that “preference of patients is very important and all three treatments are better than usual care.”
The NMA included studies comparing psychotherapy, antidepressant medication, or a combination of both, with control conditions (defined as usual care, wait list, or pill placebo) in adult primary care patients with depression.
Patients could have major depression, persistent mood disorders (dysthymia), both, or high scores on self-rating depression scales. The primary outcome of the NMA was response, defined as a 50% improvement in the Hamilton Depression Rating scores (HAM-D).
A total of 58 studies met inclusion criteria, involving 9,301 patients.
Treatment options compared
Compared with usual care, both psychotherapy alone and pharmacotherapy alone had significantly better response rates, with no significant difference between them (relative risk, 1.60 and RR, 1.65, respectively). The combination of psychotherapy and pharmacotherapy was even better (RR, 2.15), whereas the wait list was less effective (RR, 0.68).
When comparing combined therapy with psychotherapy or pharmacotherapy, the superiority of combination therapy over psychotherapy was only slightly statistically significant (RR, 1.35; 95% confidence interval, 1.00-1.81), while pharmacotherapy was only slightly inferior (RR, 1.30; 95% CI, 0.98-1.73).
“The significance level is not very high, which is related to statistical power,” said Dr. Cuijpers. “But the mean benefit is quite substantial in my opinion, with a 35% higher chance of response in the combined treatment, compared to psychotherapy alone.”
Looking at the outcome of remission, (normally defined as a score of 7 or less on the HAM-D), the outcomes were “comparable to those for response, with the exception that combined treatment was not significantly different from psychotherapy,” they wrote.
One important caveat is that several studies included in the NMA included patients with moderate to severe depression, a population that is different from the usual primary care population of depressed patients who have mild to moderate symptoms. Antidepressant medications are also assumed to work better against more severe symptoms, added the authors. “The inclusion of these studies might therefore have resulted in an overestimation of the effects of pharmacotherapy in the present NMA.”
Among other limitations, the authors noted that studies included mixed populations of patients with dysthymia and major depression; they also made no distinction between different types of antidepressants.
Psychotherapies unknown, but meta-analysis is still useful
Commenting on these findings, Neil Skolnik, MD, professor of family and community medicine at Sidney Kimmel Medical College, Philadelphia, said this is “an important study, confirming and extending the conclusions” of a systematic review published in 2016 as a Clinical Practice Guideline from the American College of Physicians.
“Unfortunately, the authors did not specify what type of psychotherapy was studied in the meta-analysis, so we have to look elsewhere if we want to advise our patients on what type of psychotherapy to seek, since there are important differences between different types of therapy,” he said.
Still, he described the study as providing “helpful information for the practicing clinician, as it gives us solid information with which to engage and advise patients in a shared decision-making process for effective treatment of depression.”
“Some patients will choose psychotherapy, some will choose medications. They can make either choice with the confidence that both approaches are effective,” Dr. Skolnik elaborated. “In addition, if psychotherapy does not seem to be sufficiently helping we are on solid ground adding an antidepressant medication to psychotherapy, with this data showing that the combined treatment works better than psychotherapy alone.”
Dr. Cuijpers receives allowances for his memberships on the board of directors of Mind, Fonds Psychische Gezondheid, and Korrelatie, and for being chair of the PACO committee of the Raad voor Civiel-militaire Zorg en Onderzoek of the Dutch Ministry of Defense. He also serves as deputy editor of Depression and Anxiety and associate editor of Psychological Bulletin, and he receives royalties for books he has authored or coauthored. He received grants from the European Union, ZonMw, and PFGV. Another study author reported receiving personal fees from Mitsubishi-Tanabe, MSD, and Shionogi and a grant from Mitsubishi-Tanabe outside the submitted work. One author has received research and consultancy fees from INCiPiT (Italian Network for Paediatric Trials), CARIPLO Foundation, and Angelini Pharmam, while another reported receiving personal fees from Boehringer Ingelheim, Kyowa Kirin, ASKA Pharmaceutical, and Toyota Motor Corporation outside the submitted work. The other authors and Dr. Skolnik reported no conflicts.
according to a network meta-analysis (NMA) comparing either and both approaches with control conditions in the primary care setting.
The findings are important, since the majority of depressed patients are treated by primary care physicians, yet relatively few randomized trials of treatment have focused on this setting, noted senior study author Pim Cuijpers, PhD, from Vrije Universiteit Amsterdam, and colleagues, in the paper, which was published in Annals of Family Medicine.
“The main message is that clinicians should certainly consider psychotherapy instead of pharmacotherapy, because this is preferred by most patients, and when possible, combined treatments should be the preferred choice because the outcomes are considerably better,” he said in an interview. Either way, he emphasized that “preference of patients is very important and all three treatments are better than usual care.”
The NMA included studies comparing psychotherapy, antidepressant medication, or a combination of both, with control conditions (defined as usual care, wait list, or pill placebo) in adult primary care patients with depression.
Patients could have major depression, persistent mood disorders (dysthymia), both, or high scores on self-rating depression scales. The primary outcome of the NMA was response, defined as a 50% improvement in the Hamilton Depression Rating scores (HAM-D).
A total of 58 studies met inclusion criteria, involving 9,301 patients.
Treatment options compared
Compared with usual care, both psychotherapy alone and pharmacotherapy alone had significantly better response rates, with no significant difference between them (relative risk, 1.60 and RR, 1.65, respectively). The combination of psychotherapy and pharmacotherapy was even better (RR, 2.15), whereas the wait list was less effective (RR, 0.68).
When comparing combined therapy with psychotherapy or pharmacotherapy, the superiority of combination therapy over psychotherapy was only slightly statistically significant (RR, 1.35; 95% confidence interval, 1.00-1.81), while pharmacotherapy was only slightly inferior (RR, 1.30; 95% CI, 0.98-1.73).
“The significance level is not very high, which is related to statistical power,” said Dr. Cuijpers. “But the mean benefit is quite substantial in my opinion, with a 35% higher chance of response in the combined treatment, compared to psychotherapy alone.”
Looking at the outcome of remission, (normally defined as a score of 7 or less on the HAM-D), the outcomes were “comparable to those for response, with the exception that combined treatment was not significantly different from psychotherapy,” they wrote.
One important caveat is that several studies included in the NMA included patients with moderate to severe depression, a population that is different from the usual primary care population of depressed patients who have mild to moderate symptoms. Antidepressant medications are also assumed to work better against more severe symptoms, added the authors. “The inclusion of these studies might therefore have resulted in an overestimation of the effects of pharmacotherapy in the present NMA.”
Among other limitations, the authors noted that studies included mixed populations of patients with dysthymia and major depression; they also made no distinction between different types of antidepressants.
Psychotherapies unknown, but meta-analysis is still useful
Commenting on these findings, Neil Skolnik, MD, professor of family and community medicine at Sidney Kimmel Medical College, Philadelphia, said this is “an important study, confirming and extending the conclusions” of a systematic review published in 2016 as a Clinical Practice Guideline from the American College of Physicians.
“Unfortunately, the authors did not specify what type of psychotherapy was studied in the meta-analysis, so we have to look elsewhere if we want to advise our patients on what type of psychotherapy to seek, since there are important differences between different types of therapy,” he said.
Still, he described the study as providing “helpful information for the practicing clinician, as it gives us solid information with which to engage and advise patients in a shared decision-making process for effective treatment of depression.”
“Some patients will choose psychotherapy, some will choose medications. They can make either choice with the confidence that both approaches are effective,” Dr. Skolnik elaborated. “In addition, if psychotherapy does not seem to be sufficiently helping we are on solid ground adding an antidepressant medication to psychotherapy, with this data showing that the combined treatment works better than psychotherapy alone.”
Dr. Cuijpers receives allowances for his memberships on the board of directors of Mind, Fonds Psychische Gezondheid, and Korrelatie, and for being chair of the PACO committee of the Raad voor Civiel-militaire Zorg en Onderzoek of the Dutch Ministry of Defense. He also serves as deputy editor of Depression and Anxiety and associate editor of Psychological Bulletin, and he receives royalties for books he has authored or coauthored. He received grants from the European Union, ZonMw, and PFGV. Another study author reported receiving personal fees from Mitsubishi-Tanabe, MSD, and Shionogi and a grant from Mitsubishi-Tanabe outside the submitted work. One author has received research and consultancy fees from INCiPiT (Italian Network for Paediatric Trials), CARIPLO Foundation, and Angelini Pharmam, while another reported receiving personal fees from Boehringer Ingelheim, Kyowa Kirin, ASKA Pharmaceutical, and Toyota Motor Corporation outside the submitted work. The other authors and Dr. Skolnik reported no conflicts.
according to a network meta-analysis (NMA) comparing either and both approaches with control conditions in the primary care setting.
The findings are important, since the majority of depressed patients are treated by primary care physicians, yet relatively few randomized trials of treatment have focused on this setting, noted senior study author Pim Cuijpers, PhD, from Vrije Universiteit Amsterdam, and colleagues, in the paper, which was published in Annals of Family Medicine.
“The main message is that clinicians should certainly consider psychotherapy instead of pharmacotherapy, because this is preferred by most patients, and when possible, combined treatments should be the preferred choice because the outcomes are considerably better,” he said in an interview. Either way, he emphasized that “preference of patients is very important and all three treatments are better than usual care.”
The NMA included studies comparing psychotherapy, antidepressant medication, or a combination of both, with control conditions (defined as usual care, wait list, or pill placebo) in adult primary care patients with depression.
Patients could have major depression, persistent mood disorders (dysthymia), both, or high scores on self-rating depression scales. The primary outcome of the NMA was response, defined as a 50% improvement in the Hamilton Depression Rating scores (HAM-D).
A total of 58 studies met inclusion criteria, involving 9,301 patients.
Treatment options compared
Compared with usual care, both psychotherapy alone and pharmacotherapy alone had significantly better response rates, with no significant difference between them (relative risk, 1.60 and RR, 1.65, respectively). The combination of psychotherapy and pharmacotherapy was even better (RR, 2.15), whereas the wait list was less effective (RR, 0.68).
When comparing combined therapy with psychotherapy or pharmacotherapy, the superiority of combination therapy over psychotherapy was only slightly statistically significant (RR, 1.35; 95% confidence interval, 1.00-1.81), while pharmacotherapy was only slightly inferior (RR, 1.30; 95% CI, 0.98-1.73).
“The significance level is not very high, which is related to statistical power,” said Dr. Cuijpers. “But the mean benefit is quite substantial in my opinion, with a 35% higher chance of response in the combined treatment, compared to psychotherapy alone.”
Looking at the outcome of remission, (normally defined as a score of 7 or less on the HAM-D), the outcomes were “comparable to those for response, with the exception that combined treatment was not significantly different from psychotherapy,” they wrote.
One important caveat is that several studies included in the NMA included patients with moderate to severe depression, a population that is different from the usual primary care population of depressed patients who have mild to moderate symptoms. Antidepressant medications are also assumed to work better against more severe symptoms, added the authors. “The inclusion of these studies might therefore have resulted in an overestimation of the effects of pharmacotherapy in the present NMA.”
Among other limitations, the authors noted that studies included mixed populations of patients with dysthymia and major depression; they also made no distinction between different types of antidepressants.
Psychotherapies unknown, but meta-analysis is still useful
Commenting on these findings, Neil Skolnik, MD, professor of family and community medicine at Sidney Kimmel Medical College, Philadelphia, said this is “an important study, confirming and extending the conclusions” of a systematic review published in 2016 as a Clinical Practice Guideline from the American College of Physicians.
“Unfortunately, the authors did not specify what type of psychotherapy was studied in the meta-analysis, so we have to look elsewhere if we want to advise our patients on what type of psychotherapy to seek, since there are important differences between different types of therapy,” he said.
Still, he described the study as providing “helpful information for the practicing clinician, as it gives us solid information with which to engage and advise patients in a shared decision-making process for effective treatment of depression.”
“Some patients will choose psychotherapy, some will choose medications. They can make either choice with the confidence that both approaches are effective,” Dr. Skolnik elaborated. “In addition, if psychotherapy does not seem to be sufficiently helping we are on solid ground adding an antidepressant medication to psychotherapy, with this data showing that the combined treatment works better than psychotherapy alone.”
Dr. Cuijpers receives allowances for his memberships on the board of directors of Mind, Fonds Psychische Gezondheid, and Korrelatie, and for being chair of the PACO committee of the Raad voor Civiel-militaire Zorg en Onderzoek of the Dutch Ministry of Defense. He also serves as deputy editor of Depression and Anxiety and associate editor of Psychological Bulletin, and he receives royalties for books he has authored or coauthored. He received grants from the European Union, ZonMw, and PFGV. Another study author reported receiving personal fees from Mitsubishi-Tanabe, MSD, and Shionogi and a grant from Mitsubishi-Tanabe outside the submitted work. One author has received research and consultancy fees from INCiPiT (Italian Network for Paediatric Trials), CARIPLO Foundation, and Angelini Pharmam, while another reported receiving personal fees from Boehringer Ingelheim, Kyowa Kirin, ASKA Pharmaceutical, and Toyota Motor Corporation outside the submitted work. The other authors and Dr. Skolnik reported no conflicts.
FROM ANNALS OF FAMILY MEDICINE
Attending a patient’s funeral: How psychiatrists decide
Psychiatrists often develop long-term relationships with their patients, but what happens when a patient dies? Should the psychiatrist attend the patient’s funeral?

It’s a question Ashley Pettaway, MD, faced as a medical resident at the University of Alabama School of Medicine.
For 2 months, Dr. Pettaway was involved in the day-to-day care of a woman in her 40s who ultimately died. As part of that care, Dr. Pettaway had regular meetings with the patient’s husband and family members.
“The patient was about my mother’s age, so I naturally was kind of attached to her,” Dr. Pettaway told this news organization. After she died, her family invited Dr. Pettaway to the funeral.
“While I couldn’t make it to the funeral, it got me thinking. Should I go? If I go, what do I say? Who do I sit with? How do I introduce myself?” wondered Dr. Pettaway, now a resident in the department of psychiatry and neurobehavioral sciences, University of Virginia, Charlottesville.
She turned to the literature but found very little regarding psychiatrists attending their patients’ funerals. “This was surprising to me because in psychiatry, you can get so engrossed in patients’ lives,” Dr. Pettaway said.
Given the lack of rules or formal guidance on psychiatrists attending patients’ funerals, Dr. Pettaway and her mentor, Gabrielle Marzani, MD, conducted an informal survey of 12 supervising psychiatrists at the University of Virginia.
The survey results were presented at the virtual American Psychiatric Association 2021 Annual Meeting.
Ten of the 12 psychiatrists who were surveyed were caring for a patient who died while under their care. Five of those psychiatrists reported going to at least one patient’s funeral over the course of their career.
Among the psychiatrists who attended a patient’s funeral, their attendance was often based on their clinical intuition, their relationship with the family, or whether the patient was an established presence in the community. In the latter case, the psychiatrist attended as a community member.
The number of years in practice also mattered. Fewer senior faculty reported that they would be hesitant to attend and that they would not attend without a formal invitation from the family. Senior career psychiatrists were more likely to attend and felt that an invitation was not required.
None of the psychiatrists surveyed had received training or guidance on attending patients’ funerals at any point in their career.
Given the absence of formal recommendations, Dr. Pettaway believes increased conversation on this topic as part of residency training programs would help psychiatrists navigate these complex situations.
A complex issue
Commenting on the topic for an interview, Paul S. Appelbaum, MD, professor of psychiatry, medicine, and law at Columbia University, New York, said this is an “interesting and important topic that is underdiscussed.”
“I don’t think there’s a right answer that applies to every situation,” said Dr. Appelbaum, a past president of the APA.
There will be times, he said, when psychiatrists or other mental health professionals have worked closely with a patient for many years and may have interacted with the family over that period.
“When that patient passes away, they may feel, and the family may feel, that it would be comforting and appropriate for them to be at the funeral,” said Dr. Appelbaum.
However, he added,
“There are obviously a number of complexities involved. One is how the family feels about the relationship with the psychiatrist – whether they were accepting of the reality that the patient had a mental disorder and was in treatment,” he said.
There is also the question of confidentiality, said Dr. Appelbaum.
“If it’s a large funeral and the psychiatrist is just one face in the crowd, that’s not likely to be an issue. But if it’s a relatively small group of mourners, all of whom know each other, and an unknown figure pops up, that could raise questions and perhaps inadvertently reveal to family members or friends that the deceased had a psychiatric condition and was in treatment. That needs to be taken into account as well,” he added.
In cases in which the family invites the psychiatrist, confidentiality is not a concern, and attendance by the psychiatrist is something the patient would have wanted, said Dr. Appelbaum.
How the patient died may also be factor. When a patient dies by suicide, it’s an “emotionally charged situation for both sides,” said Dr. Appelbaum.
In the case of a suicide, he noted, the deceased was often an active patient, and both the psychiatrist and the family are dealing with strong emotions – the psychiatrist with regret over loss of the patient and perhaps with questions as to what could have been done differently, and the family with sorrow but “also sometimes with suspicion or anger in that the psychiatrist somehow failed to keep the patient alive,” Dr. Appelbaum noted.
“In this situation, it’s even more crucial for the psychiatrist or other mental health professionals to take the lead from the family – perhaps to initiate contact to express condolences and inquire delicately about the funeral arrangements and whether their presence would be welcomed,” he said.
The research had no specific funding. Dr. Pettaway and Dr. Appelbaum have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Psychiatrists often develop long-term relationships with their patients, but what happens when a patient dies? Should the psychiatrist attend the patient’s funeral?
It’s a question Ashley Pettaway, MD, faced as a medical resident at the University of Alabama School of Medicine.
For 2 months, Dr. Pettaway was involved in the day-to-day care of a woman in her 40s who ultimately died. As part of that care, Dr. Pettaway had regular meetings with the patient’s husband and family members.
“The patient was about my mother’s age, so I naturally was kind of attached to her,” Dr. Pettaway told this news organization. After she died, her family invited Dr. Pettaway to the funeral.
“While I couldn’t make it to the funeral, it got me thinking. Should I go? If I go, what do I say? Who do I sit with? How do I introduce myself?” wondered Dr. Pettaway, now a resident in the department of psychiatry and neurobehavioral sciences, University of Virginia, Charlottesville.
She turned to the literature but found very little regarding psychiatrists attending their patients’ funerals. “This was surprising to me because in psychiatry, you can get so engrossed in patients’ lives,” Dr. Pettaway said.
Given the lack of rules or formal guidance on psychiatrists attending patients’ funerals, Dr. Pettaway and her mentor, Gabrielle Marzani, MD, conducted an informal survey of 12 supervising psychiatrists at the University of Virginia.
The survey results were presented at the virtual American Psychiatric Association 2021 Annual Meeting.
Ten of the 12 psychiatrists who were surveyed were caring for a patient who died while under their care. Five of those psychiatrists reported going to at least one patient’s funeral over the course of their career.
Among the psychiatrists who attended a patient’s funeral, their attendance was often based on their clinical intuition, their relationship with the family, or whether the patient was an established presence in the community. In the latter case, the psychiatrist attended as a community member.
The number of years in practice also mattered. Fewer senior faculty reported that they would be hesitant to attend and that they would not attend without a formal invitation from the family. Senior career psychiatrists were more likely to attend and felt that an invitation was not required.
None of the psychiatrists surveyed had received training or guidance on attending patients’ funerals at any point in their career.
Given the absence of formal recommendations, Dr. Pettaway believes increased conversation on this topic as part of residency training programs would help psychiatrists navigate these complex situations.
A complex issue
Commenting on the topic for an interview, Paul S. Appelbaum, MD, professor of psychiatry, medicine, and law at Columbia University, New York, said this is an “interesting and important topic that is underdiscussed.”
“I don’t think there’s a right answer that applies to every situation,” said Dr. Appelbaum, a past president of the APA.
There will be times, he said, when psychiatrists or other mental health professionals have worked closely with a patient for many years and may have interacted with the family over that period.
“When that patient passes away, they may feel, and the family may feel, that it would be comforting and appropriate for them to be at the funeral,” said Dr. Appelbaum.
However, he added,
“There are obviously a number of complexities involved. One is how the family feels about the relationship with the psychiatrist – whether they were accepting of the reality that the patient had a mental disorder and was in treatment,” he said.
There is also the question of confidentiality, said Dr. Appelbaum.
“If it’s a large funeral and the psychiatrist is just one face in the crowd, that’s not likely to be an issue. But if it’s a relatively small group of mourners, all of whom know each other, and an unknown figure pops up, that could raise questions and perhaps inadvertently reveal to family members or friends that the deceased had a psychiatric condition and was in treatment. That needs to be taken into account as well,” he added.
In cases in which the family invites the psychiatrist, confidentiality is not a concern, and attendance by the psychiatrist is something the patient would have wanted, said Dr. Appelbaum.
How the patient died may also be factor. When a patient dies by suicide, it’s an “emotionally charged situation for both sides,” said Dr. Appelbaum.
In the case of a suicide, he noted, the deceased was often an active patient, and both the psychiatrist and the family are dealing with strong emotions – the psychiatrist with regret over loss of the patient and perhaps with questions as to what could have been done differently, and the family with sorrow but “also sometimes with suspicion or anger in that the psychiatrist somehow failed to keep the patient alive,” Dr. Appelbaum noted.
“In this situation, it’s even more crucial for the psychiatrist or other mental health professionals to take the lead from the family – perhaps to initiate contact to express condolences and inquire delicately about the funeral arrangements and whether their presence would be welcomed,” he said.
The research had no specific funding. Dr. Pettaway and Dr. Appelbaum have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Psychiatrists often develop long-term relationships with their patients, but what happens when a patient dies? Should the psychiatrist attend the patient’s funeral?
It’s a question Ashley Pettaway, MD, faced as a medical resident at the University of Alabama School of Medicine.
For 2 months, Dr. Pettaway was involved in the day-to-day care of a woman in her 40s who ultimately died. As part of that care, Dr. Pettaway had regular meetings with the patient’s husband and family members.
“The patient was about my mother’s age, so I naturally was kind of attached to her,” Dr. Pettaway told this news organization. After she died, her family invited Dr. Pettaway to the funeral.
“While I couldn’t make it to the funeral, it got me thinking. Should I go? If I go, what do I say? Who do I sit with? How do I introduce myself?” wondered Dr. Pettaway, now a resident in the department of psychiatry and neurobehavioral sciences, University of Virginia, Charlottesville.
She turned to the literature but found very little regarding psychiatrists attending their patients’ funerals. “This was surprising to me because in psychiatry, you can get so engrossed in patients’ lives,” Dr. Pettaway said.
Given the lack of rules or formal guidance on psychiatrists attending patients’ funerals, Dr. Pettaway and her mentor, Gabrielle Marzani, MD, conducted an informal survey of 12 supervising psychiatrists at the University of Virginia.
The survey results were presented at the virtual American Psychiatric Association 2021 Annual Meeting.
Ten of the 12 psychiatrists who were surveyed were caring for a patient who died while under their care. Five of those psychiatrists reported going to at least one patient’s funeral over the course of their career.
Among the psychiatrists who attended a patient’s funeral, their attendance was often based on their clinical intuition, their relationship with the family, or whether the patient was an established presence in the community. In the latter case, the psychiatrist attended as a community member.
The number of years in practice also mattered. Fewer senior faculty reported that they would be hesitant to attend and that they would not attend without a formal invitation from the family. Senior career psychiatrists were more likely to attend and felt that an invitation was not required.
None of the psychiatrists surveyed had received training or guidance on attending patients’ funerals at any point in their career.
Given the absence of formal recommendations, Dr. Pettaway believes increased conversation on this topic as part of residency training programs would help psychiatrists navigate these complex situations.
A complex issue
Commenting on the topic for an interview, Paul S. Appelbaum, MD, professor of psychiatry, medicine, and law at Columbia University, New York, said this is an “interesting and important topic that is underdiscussed.”
“I don’t think there’s a right answer that applies to every situation,” said Dr. Appelbaum, a past president of the APA.
There will be times, he said, when psychiatrists or other mental health professionals have worked closely with a patient for many years and may have interacted with the family over that period.
“When that patient passes away, they may feel, and the family may feel, that it would be comforting and appropriate for them to be at the funeral,” said Dr. Appelbaum.
However, he added,
“There are obviously a number of complexities involved. One is how the family feels about the relationship with the psychiatrist – whether they were accepting of the reality that the patient had a mental disorder and was in treatment,” he said.
There is also the question of confidentiality, said Dr. Appelbaum.
“If it’s a large funeral and the psychiatrist is just one face in the crowd, that’s not likely to be an issue. But if it’s a relatively small group of mourners, all of whom know each other, and an unknown figure pops up, that could raise questions and perhaps inadvertently reveal to family members or friends that the deceased had a psychiatric condition and was in treatment. That needs to be taken into account as well,” he added.
In cases in which the family invites the psychiatrist, confidentiality is not a concern, and attendance by the psychiatrist is something the patient would have wanted, said Dr. Appelbaum.
How the patient died may also be factor. When a patient dies by suicide, it’s an “emotionally charged situation for both sides,” said Dr. Appelbaum.
In the case of a suicide, he noted, the deceased was often an active patient, and both the psychiatrist and the family are dealing with strong emotions – the psychiatrist with regret over loss of the patient and perhaps with questions as to what could have been done differently, and the family with sorrow but “also sometimes with suspicion or anger in that the psychiatrist somehow failed to keep the patient alive,” Dr. Appelbaum noted.
“In this situation, it’s even more crucial for the psychiatrist or other mental health professionals to take the lead from the family – perhaps to initiate contact to express condolences and inquire delicately about the funeral arrangements and whether their presence would be welcomed,” he said.
The research had no specific funding. Dr. Pettaway and Dr. Appelbaum have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Support group for Asian Americans uses theater to cope with COVID
An online, culturally based peer support group that uses theater and other creative outlets is helping Asian Americans cope with the COVID-19 pandemic, new research shows.
The findings of the qualitative study suggest that the program could be a model to support the mental health of other minority community groups during the COVID pandemic and beyond, say investigators from the Yale University Child Study Center, New Haven, Conn.
The Yale Compassionate Home, Action Together (CHATogether) group was created to promote emotional wellness among Asian American youth, young adults, and their families.
Early in the pandemic, it expanded its purpose to serve as a COVID-19 support group. Through social media outreach, CHATogether encourages members to cope with COVID-19 by using productive and creative outlets.
“We are a community education program serving Asian American families,” said Eunice Yuen, MD, PhD, the program’s founder and director, who is with the Yale University Child Study Center.
“ such as family conflict and xenophobic attacks,” said Dr. Yuen.
She discussed the program at the annual meeting of the American Psychiatric Association, which was held as a virtual live event.
Skits, role playing
CHATogether groups consist of people with similar experiences and challenges who support each other through weekly online group meetings, she explained.
Group members work together to create family conflict scenarios and role-play dialogues on topics amplified during the COVID-19 pandemic, such as cross-cultural challenges among Asian Americans, academic expectations in home schooling, and Black Lives Matter and LGBTQ conflicts within Asian families.
Group members create skits that are based on their personal experiences and that allow them to work through their own internal conflicts and gain a sense of agency, said Dr. Yuen.
“CHATogether is really the interface of mental health, art, and theater, and we’re trying to create a vehicle that can be a lighthearted way for people to talk about mental health, especially for Asian American families,” said Dr. Yuen.
Preliminary results from a focus group with 10 CHATogether members who joined the program since the pandemic started identified four major ways in which the program has had a positive impact on the mental health and well-being of participants:
- It provides a safe and supportive environment, strengthens bonds between members, and increases the sense of belonging, thus encouraging engagement.
- It provides structural consistency/stability through regular meetings and consistent group functions. Weekly meetings provide a sense of control and hope in the midst of uncertainty during periods of sheltering in place.
- Through adapting the group to virtual platforms, group members experience the inherent strengths of a growth mindset and cognitive flexibility when facing challenges.
- It supports healthy coping skills through sublimation and altruism.
Looking ahead, Dr. Yuen said, the team plans to investigate the validity and effectiveness of this model and to expand the group to include other minorities, school educators, and medical education for trainees and medical students.
Commenting on the program, briefing moderator Jeffrey Borenstein, MD, president and CEO of the Brain and Behavior Research Foundation and editor-in-chief of Psychiatric News, described the initiative as a “great project that serves as a model that can be used not only for Asian Americans but for other groups.
“I think the key to it is that cultural sensitivity that we need to really take into account and cultural differences among people in order to best engage them and help support them. I think this program does that beautifully,” said Dr. Borenstein.
The work was supported by the APA’s Substance Abuse and Mental Health Services Administration Minority Fellowship, which provides a 1-year fellowship to psychiatry residents committed to addressing minority psychiatric mental health issues. Dr. Yuen and Dr. Borenstein disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
An online, culturally based peer support group that uses theater and other creative outlets is helping Asian Americans cope with the COVID-19 pandemic, new research shows.
The findings of the qualitative study suggest that the program could be a model to support the mental health of other minority community groups during the COVID pandemic and beyond, say investigators from the Yale University Child Study Center, New Haven, Conn.
The Yale Compassionate Home, Action Together (CHATogether) group was created to promote emotional wellness among Asian American youth, young adults, and their families.
Early in the pandemic, it expanded its purpose to serve as a COVID-19 support group. Through social media outreach, CHATogether encourages members to cope with COVID-19 by using productive and creative outlets.
“We are a community education program serving Asian American families,” said Eunice Yuen, MD, PhD, the program’s founder and director, who is with the Yale University Child Study Center.
“ such as family conflict and xenophobic attacks,” said Dr. Yuen.
She discussed the program at the annual meeting of the American Psychiatric Association, which was held as a virtual live event.
Skits, role playing
CHATogether groups consist of people with similar experiences and challenges who support each other through weekly online group meetings, she explained.
Group members work together to create family conflict scenarios and role-play dialogues on topics amplified during the COVID-19 pandemic, such as cross-cultural challenges among Asian Americans, academic expectations in home schooling, and Black Lives Matter and LGBTQ conflicts within Asian families.
Group members create skits that are based on their personal experiences and that allow them to work through their own internal conflicts and gain a sense of agency, said Dr. Yuen.
“CHATogether is really the interface of mental health, art, and theater, and we’re trying to create a vehicle that can be a lighthearted way for people to talk about mental health, especially for Asian American families,” said Dr. Yuen.
Preliminary results from a focus group with 10 CHATogether members who joined the program since the pandemic started identified four major ways in which the program has had a positive impact on the mental health and well-being of participants:
- It provides a safe and supportive environment, strengthens bonds between members, and increases the sense of belonging, thus encouraging engagement.
- It provides structural consistency/stability through regular meetings and consistent group functions. Weekly meetings provide a sense of control and hope in the midst of uncertainty during periods of sheltering in place.
- Through adapting the group to virtual platforms, group members experience the inherent strengths of a growth mindset and cognitive flexibility when facing challenges.
- It supports healthy coping skills through sublimation and altruism.
Looking ahead, Dr. Yuen said, the team plans to investigate the validity and effectiveness of this model and to expand the group to include other minorities, school educators, and medical education for trainees and medical students.
Commenting on the program, briefing moderator Jeffrey Borenstein, MD, president and CEO of the Brain and Behavior Research Foundation and editor-in-chief of Psychiatric News, described the initiative as a “great project that serves as a model that can be used not only for Asian Americans but for other groups.
“I think the key to it is that cultural sensitivity that we need to really take into account and cultural differences among people in order to best engage them and help support them. I think this program does that beautifully,” said Dr. Borenstein.
The work was supported by the APA’s Substance Abuse and Mental Health Services Administration Minority Fellowship, which provides a 1-year fellowship to psychiatry residents committed to addressing minority psychiatric mental health issues. Dr. Yuen and Dr. Borenstein disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
An online, culturally based peer support group that uses theater and other creative outlets is helping Asian Americans cope with the COVID-19 pandemic, new research shows.
The findings of the qualitative study suggest that the program could be a model to support the mental health of other minority community groups during the COVID pandemic and beyond, say investigators from the Yale University Child Study Center, New Haven, Conn.
The Yale Compassionate Home, Action Together (CHATogether) group was created to promote emotional wellness among Asian American youth, young adults, and their families.
Early in the pandemic, it expanded its purpose to serve as a COVID-19 support group. Through social media outreach, CHATogether encourages members to cope with COVID-19 by using productive and creative outlets.
“We are a community education program serving Asian American families,” said Eunice Yuen, MD, PhD, the program’s founder and director, who is with the Yale University Child Study Center.
“ such as family conflict and xenophobic attacks,” said Dr. Yuen.
She discussed the program at the annual meeting of the American Psychiatric Association, which was held as a virtual live event.
Skits, role playing
CHATogether groups consist of people with similar experiences and challenges who support each other through weekly online group meetings, she explained.
Group members work together to create family conflict scenarios and role-play dialogues on topics amplified during the COVID-19 pandemic, such as cross-cultural challenges among Asian Americans, academic expectations in home schooling, and Black Lives Matter and LGBTQ conflicts within Asian families.
Group members create skits that are based on their personal experiences and that allow them to work through their own internal conflicts and gain a sense of agency, said Dr. Yuen.
“CHATogether is really the interface of mental health, art, and theater, and we’re trying to create a vehicle that can be a lighthearted way for people to talk about mental health, especially for Asian American families,” said Dr. Yuen.
Preliminary results from a focus group with 10 CHATogether members who joined the program since the pandemic started identified four major ways in which the program has had a positive impact on the mental health and well-being of participants:
- It provides a safe and supportive environment, strengthens bonds between members, and increases the sense of belonging, thus encouraging engagement.
- It provides structural consistency/stability through regular meetings and consistent group functions. Weekly meetings provide a sense of control and hope in the midst of uncertainty during periods of sheltering in place.
- Through adapting the group to virtual platforms, group members experience the inherent strengths of a growth mindset and cognitive flexibility when facing challenges.
- It supports healthy coping skills through sublimation and altruism.
Looking ahead, Dr. Yuen said, the team plans to investigate the validity and effectiveness of this model and to expand the group to include other minorities, school educators, and medical education for trainees and medical students.
Commenting on the program, briefing moderator Jeffrey Borenstein, MD, president and CEO of the Brain and Behavior Research Foundation and editor-in-chief of Psychiatric News, described the initiative as a “great project that serves as a model that can be used not only for Asian Americans but for other groups.
“I think the key to it is that cultural sensitivity that we need to really take into account and cultural differences among people in order to best engage them and help support them. I think this program does that beautifully,” said Dr. Borenstein.
The work was supported by the APA’s Substance Abuse and Mental Health Services Administration Minority Fellowship, which provides a 1-year fellowship to psychiatry residents committed to addressing minority psychiatric mental health issues. Dr. Yuen and Dr. Borenstein disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Suicide risk prediction tools fail people of color
Current models used to predict suicide risk fall short for racialized populations including Black, Indigenous, and people of color (BIPOC), new research shows.
Investigators developed two suicide prediction models to examine whether these types of tools are accurate in their predictive abilities, or whether they are flawed.
They found both prediction models failed to identify high-risk BIPOC individuals. In the first model, nearly half of outpatient visits followed by suicide were identified in White patients versus only 7% of visits followed by suicide in BIPOC patients. The second model had a sensitivity of 41% for White patients, but just 3% for Black patients and 7% for American Indian/Alaskan Native patients.

“You don’t know whether a prediction model will be useful or harmful until it’s evaluated. The take-home message of our study is this: You have to look,” lead author Yates Coley, PhD, assistant investigator, Kaiser Permanente Washington Health Research Institute, Seattle, said in an interview.
The study was published online April 28, 2021, in JAMA Psychiatry.
Racial inequities
Suicide risk prediction models have been “developed and validated in several settings” and are now in regular use at the Veterans Health Administration, HealthPartners, and Kaiser Permanente, the authors wrote.
But the performance of suicide risk prediction models, while accurate in the overall population, “remains unexamined” in particular subpopulations, they noted.
“Health records data reflect existing racial and ethnic inequities in health care access, quality, and outcomes; and prediction models using health records data may perpetuate these disparities by presuming that past healthcare patterns accurately reflect actual needs,” Dr. Coley said.
Dr. Coley and associates “wanted to make sure that any suicide prediction model we implemented in clinical care reduced health disparities rather than exacerbated them.”
To investigate, researchers examined all outpatient mental health visits to seven large integrated health care systems by patients 13 years and older (n = 13,980,570 visits by 1,422,534 patients; 64% female, mean age, 42 years). The study spanned from Jan. 1, 2009, to Sept. 30, 2017, with follow-up through Dec. 31, 2017.
In particular, researchers looked at suicides that took place within 90 days following the outpatient visit.
Researchers used two prediction models: logistic regression with LASSO (Least Absolute Shrinkage and Selection Operator) variable selection and random forest technique, a “tree-based method that explores interactions between predictors (including those with race and ethnicity) in estimating probability of an outcome.”
The models considered prespecified interactions between predictors, including prior diagnoses, suicide attempts, and PHQ-9 [Patient Health Questionnaire–9] responses, and race and ethnicity data.
Researchers evaluated performance of the prediction models in the overall validation set and within subgroups defined by race/ethnicity.
The area under the curve measured model discrimination, and sensitivity was estimated for global and race/ethnicity-specific thresholds.
‘Unacceptable’ scenario
Within the total population, there were 768 deaths by suicide within 90 days of 3,143 visits. Suicide rates were highest for visits by patients with no recorded race/ethnicity, followed by visits by Asian, White, American Indian/Alaskan Native, Hispanic, and Black patients.
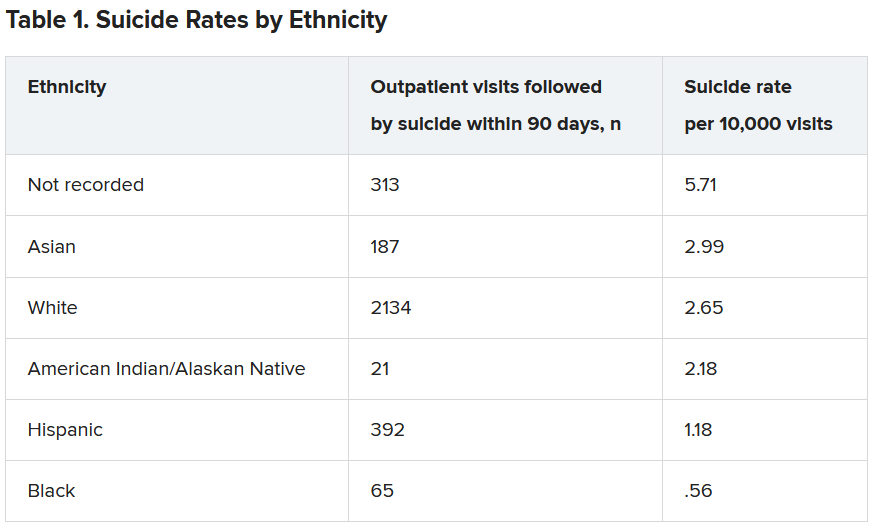
Both models showed “high” AUC sensitivity for White, Hispanic, and Asian patients but “poor” AUC sensitivity for BIPOC and patients without recorded race/ethnicity, the authors reported.
“Implementation of prediction models has to be considered in the broader context of unmet health care needs,” said Dr. Coley.
“In our specific example of suicide prediction, BIPOC populations already face substantial barriers in accessing quality mental health care and, as a result, have poorer outcomes, and using either of the suicide prediction models examined in our study will provide less benefit to already-underserved populations and widen existing care gaps,” a scenario Dr. Coley said is “unacceptable.”
“ she added.
Biased algorithms
Commenting on the study, Jonathan Singer, PhD, LCSW, associate professor at Loyola University, Chicago, described it as an “important contribution because it points to a systemic problem and also to the fact that the algorithms we create are biased, created by humans, and humans are biased.”
Although the study focused on the health care system, Dr. Singer believes the findings have implications for individual clinicians.
“If clinicians may be biased against identifying suicide risk in Black and Native American patients, they may attribute suicidal risk to something else. For example, we know that in Black Americans, expressions of intense emotions are oftentimes interpreted as aggression or being threatening, as opposed to indicators of sadness or fear,” noted Dr. Singer, who is also president of the American Academy of Suicidology and was not involved with the study,
“Clinicians who misinterpret these intense emotions are less likely to identify a Black client or patient who is suicidal,” Dr. Singer said.
The research was supported by the Mental Health Research Network from the National Institute of Mental Health. Dr. Coley has reported receiving support through a grant from the Agency for Healthcare Research and Quality. Dr. Singer reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Current models used to predict suicide risk fall short for racialized populations including Black, Indigenous, and people of color (BIPOC), new research shows.
Investigators developed two suicide prediction models to examine whether these types of tools are accurate in their predictive abilities, or whether they are flawed.
They found both prediction models failed to identify high-risk BIPOC individuals. In the first model, nearly half of outpatient visits followed by suicide were identified in White patients versus only 7% of visits followed by suicide in BIPOC patients. The second model had a sensitivity of 41% for White patients, but just 3% for Black patients and 7% for American Indian/Alaskan Native patients.
“You don’t know whether a prediction model will be useful or harmful until it’s evaluated. The take-home message of our study is this: You have to look,” lead author Yates Coley, PhD, assistant investigator, Kaiser Permanente Washington Health Research Institute, Seattle, said in an interview.
The study was published online April 28, 2021, in JAMA Psychiatry.
Racial inequities
Suicide risk prediction models have been “developed and validated in several settings” and are now in regular use at the Veterans Health Administration, HealthPartners, and Kaiser Permanente, the authors wrote.
But the performance of suicide risk prediction models, while accurate in the overall population, “remains unexamined” in particular subpopulations, they noted.
“Health records data reflect existing racial and ethnic inequities in health care access, quality, and outcomes; and prediction models using health records data may perpetuate these disparities by presuming that past healthcare patterns accurately reflect actual needs,” Dr. Coley said.
Dr. Coley and associates “wanted to make sure that any suicide prediction model we implemented in clinical care reduced health disparities rather than exacerbated them.”
To investigate, researchers examined all outpatient mental health visits to seven large integrated health care systems by patients 13 years and older (n = 13,980,570 visits by 1,422,534 patients; 64% female, mean age, 42 years). The study spanned from Jan. 1, 2009, to Sept. 30, 2017, with follow-up through Dec. 31, 2017.
In particular, researchers looked at suicides that took place within 90 days following the outpatient visit.
Researchers used two prediction models: logistic regression with LASSO (Least Absolute Shrinkage and Selection Operator) variable selection and random forest technique, a “tree-based method that explores interactions between predictors (including those with race and ethnicity) in estimating probability of an outcome.”
The models considered prespecified interactions between predictors, including prior diagnoses, suicide attempts, and PHQ-9 [Patient Health Questionnaire–9] responses, and race and ethnicity data.
Researchers evaluated performance of the prediction models in the overall validation set and within subgroups defined by race/ethnicity.
The area under the curve measured model discrimination, and sensitivity was estimated for global and race/ethnicity-specific thresholds.
‘Unacceptable’ scenario
Within the total population, there were 768 deaths by suicide within 90 days of 3,143 visits. Suicide rates were highest for visits by patients with no recorded race/ethnicity, followed by visits by Asian, White, American Indian/Alaskan Native, Hispanic, and Black patients.
Both models showed “high” AUC sensitivity for White, Hispanic, and Asian patients but “poor” AUC sensitivity for BIPOC and patients without recorded race/ethnicity, the authors reported.
“Implementation of prediction models has to be considered in the broader context of unmet health care needs,” said Dr. Coley.
“In our specific example of suicide prediction, BIPOC populations already face substantial barriers in accessing quality mental health care and, as a result, have poorer outcomes, and using either of the suicide prediction models examined in our study will provide less benefit to already-underserved populations and widen existing care gaps,” a scenario Dr. Coley said is “unacceptable.”
“ she added.
Biased algorithms
Commenting on the study, Jonathan Singer, PhD, LCSW, associate professor at Loyola University, Chicago, described it as an “important contribution because it points to a systemic problem and also to the fact that the algorithms we create are biased, created by humans, and humans are biased.”
Although the study focused on the health care system, Dr. Singer believes the findings have implications for individual clinicians.
“If clinicians may be biased against identifying suicide risk in Black and Native American patients, they may attribute suicidal risk to something else. For example, we know that in Black Americans, expressions of intense emotions are oftentimes interpreted as aggression or being threatening, as opposed to indicators of sadness or fear,” noted Dr. Singer, who is also president of the American Academy of Suicidology and was not involved with the study,
“Clinicians who misinterpret these intense emotions are less likely to identify a Black client or patient who is suicidal,” Dr. Singer said.
The research was supported by the Mental Health Research Network from the National Institute of Mental Health. Dr. Coley has reported receiving support through a grant from the Agency for Healthcare Research and Quality. Dr. Singer reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Current models used to predict suicide risk fall short for racialized populations including Black, Indigenous, and people of color (BIPOC), new research shows.
Investigators developed two suicide prediction models to examine whether these types of tools are accurate in their predictive abilities, or whether they are flawed.
They found both prediction models failed to identify high-risk BIPOC individuals. In the first model, nearly half of outpatient visits followed by suicide were identified in White patients versus only 7% of visits followed by suicide in BIPOC patients. The second model had a sensitivity of 41% for White patients, but just 3% for Black patients and 7% for American Indian/Alaskan Native patients.
“You don’t know whether a prediction model will be useful or harmful until it’s evaluated. The take-home message of our study is this: You have to look,” lead author Yates Coley, PhD, assistant investigator, Kaiser Permanente Washington Health Research Institute, Seattle, said in an interview.
The study was published online April 28, 2021, in JAMA Psychiatry.
Racial inequities
Suicide risk prediction models have been “developed and validated in several settings” and are now in regular use at the Veterans Health Administration, HealthPartners, and Kaiser Permanente, the authors wrote.
But the performance of suicide risk prediction models, while accurate in the overall population, “remains unexamined” in particular subpopulations, they noted.
“Health records data reflect existing racial and ethnic inequities in health care access, quality, and outcomes; and prediction models using health records data may perpetuate these disparities by presuming that past healthcare patterns accurately reflect actual needs,” Dr. Coley said.
Dr. Coley and associates “wanted to make sure that any suicide prediction model we implemented in clinical care reduced health disparities rather than exacerbated them.”
To investigate, researchers examined all outpatient mental health visits to seven large integrated health care systems by patients 13 years and older (n = 13,980,570 visits by 1,422,534 patients; 64% female, mean age, 42 years). The study spanned from Jan. 1, 2009, to Sept. 30, 2017, with follow-up through Dec. 31, 2017.
In particular, researchers looked at suicides that took place within 90 days following the outpatient visit.
Researchers used two prediction models: logistic regression with LASSO (Least Absolute Shrinkage and Selection Operator) variable selection and random forest technique, a “tree-based method that explores interactions between predictors (including those with race and ethnicity) in estimating probability of an outcome.”
The models considered prespecified interactions between predictors, including prior diagnoses, suicide attempts, and PHQ-9 [Patient Health Questionnaire–9] responses, and race and ethnicity data.
Researchers evaluated performance of the prediction models in the overall validation set and within subgroups defined by race/ethnicity.
The area under the curve measured model discrimination, and sensitivity was estimated for global and race/ethnicity-specific thresholds.
‘Unacceptable’ scenario
Within the total population, there were 768 deaths by suicide within 90 days of 3,143 visits. Suicide rates were highest for visits by patients with no recorded race/ethnicity, followed by visits by Asian, White, American Indian/Alaskan Native, Hispanic, and Black patients.
Both models showed “high” AUC sensitivity for White, Hispanic, and Asian patients but “poor” AUC sensitivity for BIPOC and patients without recorded race/ethnicity, the authors reported.
“Implementation of prediction models has to be considered in the broader context of unmet health care needs,” said Dr. Coley.
“In our specific example of suicide prediction, BIPOC populations already face substantial barriers in accessing quality mental health care and, as a result, have poorer outcomes, and using either of the suicide prediction models examined in our study will provide less benefit to already-underserved populations and widen existing care gaps,” a scenario Dr. Coley said is “unacceptable.”
“ she added.
Biased algorithms
Commenting on the study, Jonathan Singer, PhD, LCSW, associate professor at Loyola University, Chicago, described it as an “important contribution because it points to a systemic problem and also to the fact that the algorithms we create are biased, created by humans, and humans are biased.”
Although the study focused on the health care system, Dr. Singer believes the findings have implications for individual clinicians.
“If clinicians may be biased against identifying suicide risk in Black and Native American patients, they may attribute suicidal risk to something else. For example, we know that in Black Americans, expressions of intense emotions are oftentimes interpreted as aggression or being threatening, as opposed to indicators of sadness or fear,” noted Dr. Singer, who is also president of the American Academy of Suicidology and was not involved with the study,
“Clinicians who misinterpret these intense emotions are less likely to identify a Black client or patient who is suicidal,” Dr. Singer said.
The research was supported by the Mental Health Research Network from the National Institute of Mental Health. Dr. Coley has reported receiving support through a grant from the Agency for Healthcare Research and Quality. Dr. Singer reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.