User login
Reduced Estimate to Fix SGR Formula Brings Hope for Change
The tiresome cycle of the sustainable growth rate (SGR) continues and, as a result, providers are facing a pay cut of approximately 25% at the end of 2013. With virtually universal agreement that something must be done to permanently repeal the SGR, the insurmountable barrier to a solution has been the cost, which is estimated at $245 billion.
However, a bright spot has emerged.
Several months ago, the Congressional Budget Office produced an anomalous, revised SGR repeal estimate of $138 billion. At nearly half the cost of previous estimates, this is a much less daunting budgetary hole to fill. Needless to say, this revised estimate has breathed new life into the potential to permanently fix the SGR this year. The only catch is that this low estimate is unlikely to persist, so a flurry of activity is expected to last throughout the summer months before the window of opportunity closes.
One of the earliest proposals to move away from fee-for-service to a payment system rooted in quality and value came from the reintroduction of legislation by U.S. Reps. Allyson Schwartz (D-Pa.) and Joe Heck (R-Nev.). SHM is actively supporting this legislation and will continue to do so, but it will give the same attention to other reasonable plans designed to move away from the SGR by incorporating the concepts of quality and value as laid out by Schwartz and Heck.
Along these lines, a joint effort by House Energy and Commerce Committee chairman
Fred Upton (R-Mich.) and House Ways and Means Committee chairman Dave Camp (R-Mich.) would repeal the SGR and replace it with a more sustainable payment system. The plan is being developed iteratively, with opportunities for specialty societies, such as SHM, to provide input along the way. Clear details have yet to emerge because the plan is still in its early stages, but broadly, it will repeal the SGR, replacing it with quality and resource use metrics coupled with value-based payment, and somehow incorporate alternative payment models, such as accountable-care organizations (ACOs). This may sound familiar
because much of it is.
The Centers for Medicare & Medicaid Services (CMS) is developing programs, guided by the Affordable Care Act (ACA), to meet many of these systemic needs in the absence of a repeal of the SGR. The Physician Quality Reporting System (PQRS) is transitioning into a mandatory program, and it’s coupling with Quality and Resource Use Reports (QRURs) brings value into the equation. Both of these programs are a part of the ACA-mandated Physician Value-Based Payment Modifier (VBPM), which implements a level of value-based payment to all physicians by 2017. Additionally, the Center for Medicare & Medicaid Innovation, along with Medicare itself, is developing and testing many alternative models, such as ACOs, bundled payments, and patient-centered medical homes, to name a few.
Upton and Camp have expressed that their goal is to not only repeal the SGR, but also to establish a system that pays for value and is less piecemeal and confusing than what is currently being implemented. For example, they are looking at ways to potentially unify the often disparate yet overlapping reporting requirements placed on physicians through such programs as PQRS, Meaningful Use, and VBPM. This is a great opportunity to take the knowledge and experience hospitalists have with these current CMS programs and advocate for aligning programs, ensuring the usefulness of quality measurement, and reducing administrative barriers and burdens.
Ultimately, the repeal of the SGR will take much thought and legislative will to accomplish. With a broad framework in place, the process has at least begun. It remains to be seen whether Congress will act now on the SGR “sale” and help the health-care system transition into something more sustainable and stable.
Josh Boswell is SHM’s senior manager of government relations
The tiresome cycle of the sustainable growth rate (SGR) continues and, as a result, providers are facing a pay cut of approximately 25% at the end of 2013. With virtually universal agreement that something must be done to permanently repeal the SGR, the insurmountable barrier to a solution has been the cost, which is estimated at $245 billion.
However, a bright spot has emerged.
Several months ago, the Congressional Budget Office produced an anomalous, revised SGR repeal estimate of $138 billion. At nearly half the cost of previous estimates, this is a much less daunting budgetary hole to fill. Needless to say, this revised estimate has breathed new life into the potential to permanently fix the SGR this year. The only catch is that this low estimate is unlikely to persist, so a flurry of activity is expected to last throughout the summer months before the window of opportunity closes.
One of the earliest proposals to move away from fee-for-service to a payment system rooted in quality and value came from the reintroduction of legislation by U.S. Reps. Allyson Schwartz (D-Pa.) and Joe Heck (R-Nev.). SHM is actively supporting this legislation and will continue to do so, but it will give the same attention to other reasonable plans designed to move away from the SGR by incorporating the concepts of quality and value as laid out by Schwartz and Heck.
Along these lines, a joint effort by House Energy and Commerce Committee chairman
Fred Upton (R-Mich.) and House Ways and Means Committee chairman Dave Camp (R-Mich.) would repeal the SGR and replace it with a more sustainable payment system. The plan is being developed iteratively, with opportunities for specialty societies, such as SHM, to provide input along the way. Clear details have yet to emerge because the plan is still in its early stages, but broadly, it will repeal the SGR, replacing it with quality and resource use metrics coupled with value-based payment, and somehow incorporate alternative payment models, such as accountable-care organizations (ACOs). This may sound familiar
because much of it is.
The Centers for Medicare & Medicaid Services (CMS) is developing programs, guided by the Affordable Care Act (ACA), to meet many of these systemic needs in the absence of a repeal of the SGR. The Physician Quality Reporting System (PQRS) is transitioning into a mandatory program, and it’s coupling with Quality and Resource Use Reports (QRURs) brings value into the equation. Both of these programs are a part of the ACA-mandated Physician Value-Based Payment Modifier (VBPM), which implements a level of value-based payment to all physicians by 2017. Additionally, the Center for Medicare & Medicaid Innovation, along with Medicare itself, is developing and testing many alternative models, such as ACOs, bundled payments, and patient-centered medical homes, to name a few.
Upton and Camp have expressed that their goal is to not only repeal the SGR, but also to establish a system that pays for value and is less piecemeal and confusing than what is currently being implemented. For example, they are looking at ways to potentially unify the often disparate yet overlapping reporting requirements placed on physicians through such programs as PQRS, Meaningful Use, and VBPM. This is a great opportunity to take the knowledge and experience hospitalists have with these current CMS programs and advocate for aligning programs, ensuring the usefulness of quality measurement, and reducing administrative barriers and burdens.
Ultimately, the repeal of the SGR will take much thought and legislative will to accomplish. With a broad framework in place, the process has at least begun. It remains to be seen whether Congress will act now on the SGR “sale” and help the health-care system transition into something more sustainable and stable.
Josh Boswell is SHM’s senior manager of government relations
The tiresome cycle of the sustainable growth rate (SGR) continues and, as a result, providers are facing a pay cut of approximately 25% at the end of 2013. With virtually universal agreement that something must be done to permanently repeal the SGR, the insurmountable barrier to a solution has been the cost, which is estimated at $245 billion.
However, a bright spot has emerged.
Several months ago, the Congressional Budget Office produced an anomalous, revised SGR repeal estimate of $138 billion. At nearly half the cost of previous estimates, this is a much less daunting budgetary hole to fill. Needless to say, this revised estimate has breathed new life into the potential to permanently fix the SGR this year. The only catch is that this low estimate is unlikely to persist, so a flurry of activity is expected to last throughout the summer months before the window of opportunity closes.
One of the earliest proposals to move away from fee-for-service to a payment system rooted in quality and value came from the reintroduction of legislation by U.S. Reps. Allyson Schwartz (D-Pa.) and Joe Heck (R-Nev.). SHM is actively supporting this legislation and will continue to do so, but it will give the same attention to other reasonable plans designed to move away from the SGR by incorporating the concepts of quality and value as laid out by Schwartz and Heck.
Along these lines, a joint effort by House Energy and Commerce Committee chairman
Fred Upton (R-Mich.) and House Ways and Means Committee chairman Dave Camp (R-Mich.) would repeal the SGR and replace it with a more sustainable payment system. The plan is being developed iteratively, with opportunities for specialty societies, such as SHM, to provide input along the way. Clear details have yet to emerge because the plan is still in its early stages, but broadly, it will repeal the SGR, replacing it with quality and resource use metrics coupled with value-based payment, and somehow incorporate alternative payment models, such as accountable-care organizations (ACOs). This may sound familiar
because much of it is.
The Centers for Medicare & Medicaid Services (CMS) is developing programs, guided by the Affordable Care Act (ACA), to meet many of these systemic needs in the absence of a repeal of the SGR. The Physician Quality Reporting System (PQRS) is transitioning into a mandatory program, and it’s coupling with Quality and Resource Use Reports (QRURs) brings value into the equation. Both of these programs are a part of the ACA-mandated Physician Value-Based Payment Modifier (VBPM), which implements a level of value-based payment to all physicians by 2017. Additionally, the Center for Medicare & Medicaid Innovation, along with Medicare itself, is developing and testing many alternative models, such as ACOs, bundled payments, and patient-centered medical homes, to name a few.
Upton and Camp have expressed that their goal is to not only repeal the SGR, but also to establish a system that pays for value and is less piecemeal and confusing than what is currently being implemented. For example, they are looking at ways to potentially unify the often disparate yet overlapping reporting requirements placed on physicians through such programs as PQRS, Meaningful Use, and VBPM. This is a great opportunity to take the knowledge and experience hospitalists have with these current CMS programs and advocate for aligning programs, ensuring the usefulness of quality measurement, and reducing administrative barriers and burdens.
Ultimately, the repeal of the SGR will take much thought and legislative will to accomplish. With a broad framework in place, the process has at least begun. It remains to be seen whether Congress will act now on the SGR “sale” and help the health-care system transition into something more sustainable and stable.
Josh Boswell is SHM’s senior manager of government relations
Quality Improvement (QI) Remains a Central Theme at HM13


Like a grinning child at a carnival, Iqbal M. Binoj, MD, steps right up and gives it a try—except instead of tossing rings, he’s gripping an intraosseous infusion drill.
A tutor shows him how the device, which looks remarkably like a glue gun, inserts into the bones of the shoulder or knee and drills down until it hits the marrow. He is guided on using a steady speed to maintain the integrity of the cavity. He’s also taught about the maneuver’s low complication rates and ability to expedite workups.
“I’ve seen it used before, but I never did it,” says Dr. Binoj, a hospitalist with Cogent HMG at Genesis Medical Center in Davenport, Iowa.
Well, he never did it before a hands-on pre-course at HM13 that focused on improving hospitalists’ proficiency at such procedures as lumbar punctures and ultrasound-guided vascular access. Quality improvement (QI) is always a focus of SHM’s annual meeting, but sometimes the science of improving care is viewed from up on high.
Not everything needs to be a national imitative, an institution-wide project, or even a unit-based intervention. Sometimes, it’s as simple as teaching a room full of hospitalists how to use an intraosseous infusion drill, says Michelle Fox, RN, BSN, senior director of clinical affairs with Vidacare, which manufactures the drill used in the demonstration.
“Hospitalists have an increasing role in doing these procedures, not only in the environment they predominantly support but in other areas of the hospital,” Fox says, adding that “the primary goal of this course is to give them the opportunity to perfect those skills.”
Hospitalist Bradley Rosen, MD, MBA, FHM, medical of the inpatient specialty program at Cedars-Sinai in Los Angeles, says the point of hands-on demonstrations is to translate QI to the bedside. Take ultrasound devices, he says. In the past few years, the technology has become less expensive, better in resolution, more common, and more portable. Hospitalists must ensure hands-on training that keeps pace with that technology.
“We actually want people to get gloves on, hands on, learn where they may have challenges in terms of their own dexterity or workflow, which hand is dominant, and how to visualize on the ultrasound machine a three-dimensional structure in 2D,” he says. “We don’t want people watching from the sidelines. ... We try to get people in it and engaged.”
And once hospitalists master procedures or diagnostic maneuvers, they invariably are sought out by other physicians to pass that knowledge on to others, Dr. Rosen says.
“In so doing, we get involved in larger quality initiatives and systemwide changes that can go top-down,” he adds, “but from our perspective, it starts with the individual practitioner. And I think SHM has always advocated and preached the importance of the individual hospitalist doing the best possible job for your patient, and the group, and the institution.”
Shared Excellence
What’s best for individual institutions moving forward is what worries SHM immediate past president Shaun Frost, MD, SFHM. He fears CMS’ Value-Based Payment Modifier (VBPM) program could have the unintended consequence of spurring some hospitals to hang on to innovative ideas in order to keep a competitive business advantage.
In health care, where quality and affordability have long been viewed as valuable for nonmonetary reasons, “the medical profession willingly shares new information” to improve patient care, Dr. Frost said in his farewell speech. But he is concerned that commodification—imbuing monetary value into something that previously had none—could change that dynamic, a situation he says is “ethically not acceptable.”
“When somebody builds a better mousetrap, it should be freely shared so that all patients have the opportunity to benefit,” Dr. Frost said. “The pursuit of economic competitive advantage should not prevent us from collaborating and sharing new ideas that hopefully make the health system better.”
Kendall Rogers, MD, FACP, SFHM, chief of the division of hospital medicine at the University of New Mexico Health Sciences Center in Albuquerque, N.M., says part of that improvement in quality and patient safety will come via hospitalists pushing for improvements to health information technology (HIT), particularly to maximize computerized physician order entry (CPOE) and order sets. He empathizes with those who complain about the operability of existing systems but urges physicians to stop complaining and take action.
“We need to stop accepting what our existing limitations are, and we need to be the innovators,” he says. “Many of us aren’t even thinking about, ‘What are the products we need?’ We’re just reacting to the products we currently have and stating how they don’t meet our needs.”
He suggests people communally report safety or troubleshooting issues, in part via Hospital Medicine Exchange (HMX), an online community SHM launched last year to discuss HM issues (www.hmxchange.org). He also wants hospitalists to push HIT vendors to provide improved functionality, and for institutions to provide necessary training.
“We just need to be vocal,” says Dr. Rogers, chair of SHM’s IT Executive Committee. “I do believe this is all leading us to a good place, but there’s a dip down before we have a swing up.”
Frustration Surge
In the long run, hospitalist Anuj Mehta, MD, medical director of the adult hospitalist program at Nyack Hospital in New York, agrees with Dr. Rogers. But as a provider seeing patients day after day, he says it’s often easier to not engage HIT than it is to slog through it.
“We try to work around the system, and sometimes it’s a much longer workaround,” he says. “So what happens is loss of productivity, greater length of stay, poor patient satisfaction, more screen time, and less bedside time.”
Dr. Mehta says frustration is building as society—outside of medicine—moves rapidly through such technology as smartphones, tablets, and other intuitive devices that make actions easier. He notes that his toddler daughter could learn how to navigate an iPad in a fraction of the time it takes him to complete an HIT training course.
“You cannot have physicians going through learning for four hours, learning a system to do step one before step two before step three,” he laments. “It should flow naturally. I don’t think the IT people have realized that as of yet.”
Richard Quinn is a freelance writer in New Jersey.
Like a grinning child at a carnival, Iqbal M. Binoj, MD, steps right up and gives it a try—except instead of tossing rings, he’s gripping an intraosseous infusion drill.
A tutor shows him how the device, which looks remarkably like a glue gun, inserts into the bones of the shoulder or knee and drills down until it hits the marrow. He is guided on using a steady speed to maintain the integrity of the cavity. He’s also taught about the maneuver’s low complication rates and ability to expedite workups.
“I’ve seen it used before, but I never did it,” says Dr. Binoj, a hospitalist with Cogent HMG at Genesis Medical Center in Davenport, Iowa.
Well, he never did it before a hands-on pre-course at HM13 that focused on improving hospitalists’ proficiency at such procedures as lumbar punctures and ultrasound-guided vascular access. Quality improvement (QI) is always a focus of SHM’s annual meeting, but sometimes the science of improving care is viewed from up on high.
Not everything needs to be a national imitative, an institution-wide project, or even a unit-based intervention. Sometimes, it’s as simple as teaching a room full of hospitalists how to use an intraosseous infusion drill, says Michelle Fox, RN, BSN, senior director of clinical affairs with Vidacare, which manufactures the drill used in the demonstration.
“Hospitalists have an increasing role in doing these procedures, not only in the environment they predominantly support but in other areas of the hospital,” Fox says, adding that “the primary goal of this course is to give them the opportunity to perfect those skills.”
Hospitalist Bradley Rosen, MD, MBA, FHM, medical of the inpatient specialty program at Cedars-Sinai in Los Angeles, says the point of hands-on demonstrations is to translate QI to the bedside. Take ultrasound devices, he says. In the past few years, the technology has become less expensive, better in resolution, more common, and more portable. Hospitalists must ensure hands-on training that keeps pace with that technology.
“We actually want people to get gloves on, hands on, learn where they may have challenges in terms of their own dexterity or workflow, which hand is dominant, and how to visualize on the ultrasound machine a three-dimensional structure in 2D,” he says. “We don’t want people watching from the sidelines. ... We try to get people in it and engaged.”
And once hospitalists master procedures or diagnostic maneuvers, they invariably are sought out by other physicians to pass that knowledge on to others, Dr. Rosen says.
“In so doing, we get involved in larger quality initiatives and systemwide changes that can go top-down,” he adds, “but from our perspective, it starts with the individual practitioner. And I think SHM has always advocated and preached the importance of the individual hospitalist doing the best possible job for your patient, and the group, and the institution.”
Shared Excellence
What’s best for individual institutions moving forward is what worries SHM immediate past president Shaun Frost, MD, SFHM. He fears CMS’ Value-Based Payment Modifier (VBPM) program could have the unintended consequence of spurring some hospitals to hang on to innovative ideas in order to keep a competitive business advantage.
In health care, where quality and affordability have long been viewed as valuable for nonmonetary reasons, “the medical profession willingly shares new information” to improve patient care, Dr. Frost said in his farewell speech. But he is concerned that commodification—imbuing monetary value into something that previously had none—could change that dynamic, a situation he says is “ethically not acceptable.”
“When somebody builds a better mousetrap, it should be freely shared so that all patients have the opportunity to benefit,” Dr. Frost said. “The pursuit of economic competitive advantage should not prevent us from collaborating and sharing new ideas that hopefully make the health system better.”
Kendall Rogers, MD, FACP, SFHM, chief of the division of hospital medicine at the University of New Mexico Health Sciences Center in Albuquerque, N.M., says part of that improvement in quality and patient safety will come via hospitalists pushing for improvements to health information technology (HIT), particularly to maximize computerized physician order entry (CPOE) and order sets. He empathizes with those who complain about the operability of existing systems but urges physicians to stop complaining and take action.
“We need to stop accepting what our existing limitations are, and we need to be the innovators,” he says. “Many of us aren’t even thinking about, ‘What are the products we need?’ We’re just reacting to the products we currently have and stating how they don’t meet our needs.”
He suggests people communally report safety or troubleshooting issues, in part via Hospital Medicine Exchange (HMX), an online community SHM launched last year to discuss HM issues (www.hmxchange.org). He also wants hospitalists to push HIT vendors to provide improved functionality, and for institutions to provide necessary training.
“We just need to be vocal,” says Dr. Rogers, chair of SHM’s IT Executive Committee. “I do believe this is all leading us to a good place, but there’s a dip down before we have a swing up.”
Frustration Surge
In the long run, hospitalist Anuj Mehta, MD, medical director of the adult hospitalist program at Nyack Hospital in New York, agrees with Dr. Rogers. But as a provider seeing patients day after day, he says it’s often easier to not engage HIT than it is to slog through it.
“We try to work around the system, and sometimes it’s a much longer workaround,” he says. “So what happens is loss of productivity, greater length of stay, poor patient satisfaction, more screen time, and less bedside time.”
Dr. Mehta says frustration is building as society—outside of medicine—moves rapidly through such technology as smartphones, tablets, and other intuitive devices that make actions easier. He notes that his toddler daughter could learn how to navigate an iPad in a fraction of the time it takes him to complete an HIT training course.
“You cannot have physicians going through learning for four hours, learning a system to do step one before step two before step three,” he laments. “It should flow naturally. I don’t think the IT people have realized that as of yet.”
Richard Quinn is a freelance writer in New Jersey.
Like a grinning child at a carnival, Iqbal M. Binoj, MD, steps right up and gives it a try—except instead of tossing rings, he’s gripping an intraosseous infusion drill.
A tutor shows him how the device, which looks remarkably like a glue gun, inserts into the bones of the shoulder or knee and drills down until it hits the marrow. He is guided on using a steady speed to maintain the integrity of the cavity. He’s also taught about the maneuver’s low complication rates and ability to expedite workups.
“I’ve seen it used before, but I never did it,” says Dr. Binoj, a hospitalist with Cogent HMG at Genesis Medical Center in Davenport, Iowa.
Well, he never did it before a hands-on pre-course at HM13 that focused on improving hospitalists’ proficiency at such procedures as lumbar punctures and ultrasound-guided vascular access. Quality improvement (QI) is always a focus of SHM’s annual meeting, but sometimes the science of improving care is viewed from up on high.
Not everything needs to be a national imitative, an institution-wide project, or even a unit-based intervention. Sometimes, it’s as simple as teaching a room full of hospitalists how to use an intraosseous infusion drill, says Michelle Fox, RN, BSN, senior director of clinical affairs with Vidacare, which manufactures the drill used in the demonstration.
“Hospitalists have an increasing role in doing these procedures, not only in the environment they predominantly support but in other areas of the hospital,” Fox says, adding that “the primary goal of this course is to give them the opportunity to perfect those skills.”
Hospitalist Bradley Rosen, MD, MBA, FHM, medical of the inpatient specialty program at Cedars-Sinai in Los Angeles, says the point of hands-on demonstrations is to translate QI to the bedside. Take ultrasound devices, he says. In the past few years, the technology has become less expensive, better in resolution, more common, and more portable. Hospitalists must ensure hands-on training that keeps pace with that technology.
“We actually want people to get gloves on, hands on, learn where they may have challenges in terms of their own dexterity or workflow, which hand is dominant, and how to visualize on the ultrasound machine a three-dimensional structure in 2D,” he says. “We don’t want people watching from the sidelines. ... We try to get people in it and engaged.”
And once hospitalists master procedures or diagnostic maneuvers, they invariably are sought out by other physicians to pass that knowledge on to others, Dr. Rosen says.
“In so doing, we get involved in larger quality initiatives and systemwide changes that can go top-down,” he adds, “but from our perspective, it starts with the individual practitioner. And I think SHM has always advocated and preached the importance of the individual hospitalist doing the best possible job for your patient, and the group, and the institution.”
Shared Excellence
What’s best for individual institutions moving forward is what worries SHM immediate past president Shaun Frost, MD, SFHM. He fears CMS’ Value-Based Payment Modifier (VBPM) program could have the unintended consequence of spurring some hospitals to hang on to innovative ideas in order to keep a competitive business advantage.
In health care, where quality and affordability have long been viewed as valuable for nonmonetary reasons, “the medical profession willingly shares new information” to improve patient care, Dr. Frost said in his farewell speech. But he is concerned that commodification—imbuing monetary value into something that previously had none—could change that dynamic, a situation he says is “ethically not acceptable.”
“When somebody builds a better mousetrap, it should be freely shared so that all patients have the opportunity to benefit,” Dr. Frost said. “The pursuit of economic competitive advantage should not prevent us from collaborating and sharing new ideas that hopefully make the health system better.”
Kendall Rogers, MD, FACP, SFHM, chief of the division of hospital medicine at the University of New Mexico Health Sciences Center in Albuquerque, N.M., says part of that improvement in quality and patient safety will come via hospitalists pushing for improvements to health information technology (HIT), particularly to maximize computerized physician order entry (CPOE) and order sets. He empathizes with those who complain about the operability of existing systems but urges physicians to stop complaining and take action.
“We need to stop accepting what our existing limitations are, and we need to be the innovators,” he says. “Many of us aren’t even thinking about, ‘What are the products we need?’ We’re just reacting to the products we currently have and stating how they don’t meet our needs.”
He suggests people communally report safety or troubleshooting issues, in part via Hospital Medicine Exchange (HMX), an online community SHM launched last year to discuss HM issues (www.hmxchange.org). He also wants hospitalists to push HIT vendors to provide improved functionality, and for institutions to provide necessary training.
“We just need to be vocal,” says Dr. Rogers, chair of SHM’s IT Executive Committee. “I do believe this is all leading us to a good place, but there’s a dip down before we have a swing up.”
Frustration Surge
In the long run, hospitalist Anuj Mehta, MD, medical director of the adult hospitalist program at Nyack Hospital in New York, agrees with Dr. Rogers. But as a provider seeing patients day after day, he says it’s often easier to not engage HIT than it is to slog through it.
“We try to work around the system, and sometimes it’s a much longer workaround,” he says. “So what happens is loss of productivity, greater length of stay, poor patient satisfaction, more screen time, and less bedside time.”
Dr. Mehta says frustration is building as society—outside of medicine—moves rapidly through such technology as smartphones, tablets, and other intuitive devices that make actions easier. He notes that his toddler daughter could learn how to navigate an iPad in a fraction of the time it takes him to complete an HIT training course.
“You cannot have physicians going through learning for four hours, learning a system to do step one before step two before step three,” he laments. “It should flow naturally. I don’t think the IT people have realized that as of yet.”
Richard Quinn is a freelance writer in New Jersey.
Fix for Sustainable Growth Rate Formula a Top Priority
The Improving Access to Medicare Coverage Act isn’t the only legislative proposal on hospitalists’ radar right now. Republican members of the U.S. House of Representatives recently revised their plan to replace the sustainable growth rate (SGR) formula used to determine physician payments. A bill has not been introduced, but Beltway buzz hints one could be forthcoming this year.
“Fixing the flawed SGR physician payment is a top priority for the Committees on Energy and Commerce and Ways and Means,” GOP legislators said in an open letter to the “provider community.”2
The letter requested feedback from physicians and other stakeholders by April 15.
Any proposed fix would look to end the series of time-stamped delays that continue to delay a pending 27% cut to physician payments under Medicare. The latest delay was approved earlier this year, meaning that the new deadline for the SGR cut to be implemented is Dec. 31.
The SGR formula was created in 1997, but the pending cuts tied to the federal sequester were included in the Budget Control Act of 2011. At the time, the massive reduction to Medicare payments was tied to political brinksmanship over the country’s debt ceiling. But the cut also was considered a Draconian penalty that was never likely to actually happen.
Richard Quinn is a freelance writer in New Jersey.
References
- SHM. Letter to Congress members. SHM website. Available at: http://www.hospitalmedicine.org/AM/Template.cfm?Section=Letters_to_Congress_and_Regulatory_Agencies&Template=/CM/ContentDisplay.cfm&ContentID=33169. Accessed May 3, 2013.
- U.S. House of Representatives' Committee on Ways and Means, Energy and Commerce Committee, Health Subcommittee. Second draft of sustainable growth rate (SGR) repeal and reform proposal—request for feedback letter. U.S. House of Representatives' Committee on Ways and Means website. Available at: http://waysandmeans.house.gov/uploadedfiles/sgr_joint_release_document.pdf. Accessed May 3, 2013.
The Improving Access to Medicare Coverage Act isn’t the only legislative proposal on hospitalists’ radar right now. Republican members of the U.S. House of Representatives recently revised their plan to replace the sustainable growth rate (SGR) formula used to determine physician payments. A bill has not been introduced, but Beltway buzz hints one could be forthcoming this year.
“Fixing the flawed SGR physician payment is a top priority for the Committees on Energy and Commerce and Ways and Means,” GOP legislators said in an open letter to the “provider community.”2
The letter requested feedback from physicians and other stakeholders by April 15.
Any proposed fix would look to end the series of time-stamped delays that continue to delay a pending 27% cut to physician payments under Medicare. The latest delay was approved earlier this year, meaning that the new deadline for the SGR cut to be implemented is Dec. 31.
The SGR formula was created in 1997, but the pending cuts tied to the federal sequester were included in the Budget Control Act of 2011. At the time, the massive reduction to Medicare payments was tied to political brinksmanship over the country’s debt ceiling. But the cut also was considered a Draconian penalty that was never likely to actually happen.
Richard Quinn is a freelance writer in New Jersey.
References
- SHM. Letter to Congress members. SHM website. Available at: http://www.hospitalmedicine.org/AM/Template.cfm?Section=Letters_to_Congress_and_Regulatory_Agencies&Template=/CM/ContentDisplay.cfm&ContentID=33169. Accessed May 3, 2013.
- U.S. House of Representatives' Committee on Ways and Means, Energy and Commerce Committee, Health Subcommittee. Second draft of sustainable growth rate (SGR) repeal and reform proposal—request for feedback letter. U.S. House of Representatives' Committee on Ways and Means website. Available at: http://waysandmeans.house.gov/uploadedfiles/sgr_joint_release_document.pdf. Accessed May 3, 2013.
The Improving Access to Medicare Coverage Act isn’t the only legislative proposal on hospitalists’ radar right now. Republican members of the U.S. House of Representatives recently revised their plan to replace the sustainable growth rate (SGR) formula used to determine physician payments. A bill has not been introduced, but Beltway buzz hints one could be forthcoming this year.
“Fixing the flawed SGR physician payment is a top priority for the Committees on Energy and Commerce and Ways and Means,” GOP legislators said in an open letter to the “provider community.”2
The letter requested feedback from physicians and other stakeholders by April 15.
Any proposed fix would look to end the series of time-stamped delays that continue to delay a pending 27% cut to physician payments under Medicare. The latest delay was approved earlier this year, meaning that the new deadline for the SGR cut to be implemented is Dec. 31.
The SGR formula was created in 1997, but the pending cuts tied to the federal sequester were included in the Budget Control Act of 2011. At the time, the massive reduction to Medicare payments was tied to political brinksmanship over the country’s debt ceiling. But the cut also was considered a Draconian penalty that was never likely to actually happen.
Richard Quinn is a freelance writer in New Jersey.
References
- SHM. Letter to Congress members. SHM website. Available at: http://www.hospitalmedicine.org/AM/Template.cfm?Section=Letters_to_Congress_and_Regulatory_Agencies&Template=/CM/ContentDisplay.cfm&ContentID=33169. Accessed May 3, 2013.
- U.S. House of Representatives' Committee on Ways and Means, Energy and Commerce Committee, Health Subcommittee. Second draft of sustainable growth rate (SGR) repeal and reform proposal—request for feedback letter. U.S. House of Representatives' Committee on Ways and Means website. Available at: http://waysandmeans.house.gov/uploadedfiles/sgr_joint_release_document.pdf. Accessed May 3, 2013.
Hospitalists Urge Congress to Reconsider Medicare’s “Observation Status” Rules


—Karim Godamunne, MD, MBA, SFHM
Hospitalists are pushing hard for a change to a Medicare rule requiring beneficiaries to accumulate at least three consecutive days of inpatient treatment at a hospital (not counting day of discharge) before it will cover care in a skilled nursing facility (SNF).
The issue was one of the talking points during last month’s Hospitalists on the Hill, SHM’s annual daylong advocacy campaign that this year coincided with the annual meeting in the nation’s capital. The issue gained attention from hospitalists and others in recent years, in part because of penalties hospitals face for readmissions—and also in part because hospitalists increasingly are providing care at SNFs and other post-acute-care facilities.
The spotlight is brighter now because a group of legislators is trying to identify Medicare beneficiaries previously given “observation status” as inpatients. The Improving Access to Medicare Coverage Act (H.R. 1179 and S. 569) also would establish a 90-day appeal period for those who have been denied the benefit.
SHM senior vice president Joe Miller says hospitalists used HM13 and the Hospitalists on the Hill advocacy day to discuss the issues and the proposed legislation with members of Congress, their staffs, and federal officials. He urges members to continue lobbying for changes. Although the topic might not have the resonance and impact of a fix to the sustainable growth rate (SGR), Miller says, “anybody that deals with admitting or discharging a patient will recognize the importance of this issue.”
The issue, according to Toby Edelman, a senior policy attorney for the Center for Medicare Advocacy in Washington, D.C, is that Medicare mandates that its program enrollees have at least three days of inpatient treatment before it will pay for SNF care. Medicare also covers the costs of post-acute care in other settings but does not require three days of inpatient treatment before doing so. The construct can be confusing to patients who spend time in a hospital but don’t realize that some or all of their stay is spent in “observation status,” meaning none of that time counts toward Medicare’s three-day threshold for reimbursement.
“Most people can’t believe you could be in a hospital bed for a week and then be told as you leave, ‘By the way, bring your checkbook to the nursing home because you weren’t an inpatient here and so now Medicare won’t pay for your stay in the nursing home,’” Edelman says. “This has been an issue for us for quite a while because the consequence for beneficiaries of being in observation is that people have to pay out of pocket for their nursing home care, and that cost is typically hundreds of dollars a day.”
The particular dilemma for hospitalists is managing transitions of care. Hospitalist Karim Godamunne, MD, MBA, SFHM, chief medical officer of North Fulton Hospital in Roswell, Ga., says hospitalists don’t want financial burdens to dictate care decisions, but they are caught in the middle of decisions that could saddle patients with uncovered costs.
He also worries that the issue will only grow in coming years as baby boomers put more pressure on the health-care system. “We have an aging population,” he adds. “This is not going to go away.”
That is one reason SHM is supporting the Improving Access to Medicare Coverage Act. SHM supported the bill when it was first introduced in March and it has been rapidly gaining cosponsors in recent weeks. This uptick in Congressional interest may be partly a response to the efforts of hospitalists during their time on the Hill. SHM staff and hospitalists are continuing their push now as society officials say hospitalists, who often handle both discharges from the hospital and care provided at SNFs, are in a position to lead discussions on how to sensibly fix the problem.
To that end, a recent SHM letter to the bill’s sponsors casts the issue as one of fiscal responsibility.1 Medicare not covering beneficiaries’ observation days cost patients out-of-pocket money and could cost hospitals in the long run.
“Patients who are admitted with observation status often choose to return home rather than paying out of pocket for a SNF stay,” SHM’s letter reads. “The resultant lack of appropriate post-acute SNF care can result in additional problems such as dehydration, falls, and many other avoidable complications. These complications can not only lead to otherwise preventable readmissions but also increase costs to Medicare for the treatment of conditions that were not present at the time of the original hospital stay.”
Given the debate on observation, Miller says, adopting the bill into law should be a no-brainer. The biggest sticking point likely is the perceived added cost to Medicare. Still, to streamline care and remove an added hurdle to coordinated care, Dr. Godamunne believes the bill should be embraced. He also says that many private insurers look to Medicare decisions to determine their own coverage approaches.
Basically, if Medicare changes its rules, that will carry a lot of weight in the private insurance world.
“This creates a lot of situations for the provider and the family,” Dr. Godamunne says. “You have to make a difficult decision, to try to help the family. You’re trying to provide good care, but on the other hand, there are rules and regulations and bylaws you work under. They don’t align that well, in this case.”
Richard Quinn is a freelance writer in New Jersey.
References
—Karim Godamunne, MD, MBA, SFHM
Hospitalists are pushing hard for a change to a Medicare rule requiring beneficiaries to accumulate at least three consecutive days of inpatient treatment at a hospital (not counting day of discharge) before it will cover care in a skilled nursing facility (SNF).
The issue was one of the talking points during last month’s Hospitalists on the Hill, SHM’s annual daylong advocacy campaign that this year coincided with the annual meeting in the nation’s capital. The issue gained attention from hospitalists and others in recent years, in part because of penalties hospitals face for readmissions—and also in part because hospitalists increasingly are providing care at SNFs and other post-acute-care facilities.
The spotlight is brighter now because a group of legislators is trying to identify Medicare beneficiaries previously given “observation status” as inpatients. The Improving Access to Medicare Coverage Act (H.R. 1179 and S. 569) also would establish a 90-day appeal period for those who have been denied the benefit.
SHM senior vice president Joe Miller says hospitalists used HM13 and the Hospitalists on the Hill advocacy day to discuss the issues and the proposed legislation with members of Congress, their staffs, and federal officials. He urges members to continue lobbying for changes. Although the topic might not have the resonance and impact of a fix to the sustainable growth rate (SGR), Miller says, “anybody that deals with admitting or discharging a patient will recognize the importance of this issue.”
The issue, according to Toby Edelman, a senior policy attorney for the Center for Medicare Advocacy in Washington, D.C, is that Medicare mandates that its program enrollees have at least three days of inpatient treatment before it will pay for SNF care. Medicare also covers the costs of post-acute care in other settings but does not require three days of inpatient treatment before doing so. The construct can be confusing to patients who spend time in a hospital but don’t realize that some or all of their stay is spent in “observation status,” meaning none of that time counts toward Medicare’s three-day threshold for reimbursement.
“Most people can’t believe you could be in a hospital bed for a week and then be told as you leave, ‘By the way, bring your checkbook to the nursing home because you weren’t an inpatient here and so now Medicare won’t pay for your stay in the nursing home,’” Edelman says. “This has been an issue for us for quite a while because the consequence for beneficiaries of being in observation is that people have to pay out of pocket for their nursing home care, and that cost is typically hundreds of dollars a day.”
The particular dilemma for hospitalists is managing transitions of care. Hospitalist Karim Godamunne, MD, MBA, SFHM, chief medical officer of North Fulton Hospital in Roswell, Ga., says hospitalists don’t want financial burdens to dictate care decisions, but they are caught in the middle of decisions that could saddle patients with uncovered costs.
He also worries that the issue will only grow in coming years as baby boomers put more pressure on the health-care system. “We have an aging population,” he adds. “This is not going to go away.”
That is one reason SHM is supporting the Improving Access to Medicare Coverage Act. SHM supported the bill when it was first introduced in March and it has been rapidly gaining cosponsors in recent weeks. This uptick in Congressional interest may be partly a response to the efforts of hospitalists during their time on the Hill. SHM staff and hospitalists are continuing their push now as society officials say hospitalists, who often handle both discharges from the hospital and care provided at SNFs, are in a position to lead discussions on how to sensibly fix the problem.
To that end, a recent SHM letter to the bill’s sponsors casts the issue as one of fiscal responsibility.1 Medicare not covering beneficiaries’ observation days cost patients out-of-pocket money and could cost hospitals in the long run.
“Patients who are admitted with observation status often choose to return home rather than paying out of pocket for a SNF stay,” SHM’s letter reads. “The resultant lack of appropriate post-acute SNF care can result in additional problems such as dehydration, falls, and many other avoidable complications. These complications can not only lead to otherwise preventable readmissions but also increase costs to Medicare for the treatment of conditions that were not present at the time of the original hospital stay.”
Given the debate on observation, Miller says, adopting the bill into law should be a no-brainer. The biggest sticking point likely is the perceived added cost to Medicare. Still, to streamline care and remove an added hurdle to coordinated care, Dr. Godamunne believes the bill should be embraced. He also says that many private insurers look to Medicare decisions to determine their own coverage approaches.
Basically, if Medicare changes its rules, that will carry a lot of weight in the private insurance world.
“This creates a lot of situations for the provider and the family,” Dr. Godamunne says. “You have to make a difficult decision, to try to help the family. You’re trying to provide good care, but on the other hand, there are rules and regulations and bylaws you work under. They don’t align that well, in this case.”
Richard Quinn is a freelance writer in New Jersey.
References
—Karim Godamunne, MD, MBA, SFHM
Hospitalists are pushing hard for a change to a Medicare rule requiring beneficiaries to accumulate at least three consecutive days of inpatient treatment at a hospital (not counting day of discharge) before it will cover care in a skilled nursing facility (SNF).
The issue was one of the talking points during last month’s Hospitalists on the Hill, SHM’s annual daylong advocacy campaign that this year coincided with the annual meeting in the nation’s capital. The issue gained attention from hospitalists and others in recent years, in part because of penalties hospitals face for readmissions—and also in part because hospitalists increasingly are providing care at SNFs and other post-acute-care facilities.
The spotlight is brighter now because a group of legislators is trying to identify Medicare beneficiaries previously given “observation status” as inpatients. The Improving Access to Medicare Coverage Act (H.R. 1179 and S. 569) also would establish a 90-day appeal period for those who have been denied the benefit.
SHM senior vice president Joe Miller says hospitalists used HM13 and the Hospitalists on the Hill advocacy day to discuss the issues and the proposed legislation with members of Congress, their staffs, and federal officials. He urges members to continue lobbying for changes. Although the topic might not have the resonance and impact of a fix to the sustainable growth rate (SGR), Miller says, “anybody that deals with admitting or discharging a patient will recognize the importance of this issue.”
The issue, according to Toby Edelman, a senior policy attorney for the Center for Medicare Advocacy in Washington, D.C, is that Medicare mandates that its program enrollees have at least three days of inpatient treatment before it will pay for SNF care. Medicare also covers the costs of post-acute care in other settings but does not require three days of inpatient treatment before doing so. The construct can be confusing to patients who spend time in a hospital but don’t realize that some or all of their stay is spent in “observation status,” meaning none of that time counts toward Medicare’s three-day threshold for reimbursement.
“Most people can’t believe you could be in a hospital bed for a week and then be told as you leave, ‘By the way, bring your checkbook to the nursing home because you weren’t an inpatient here and so now Medicare won’t pay for your stay in the nursing home,’” Edelman says. “This has been an issue for us for quite a while because the consequence for beneficiaries of being in observation is that people have to pay out of pocket for their nursing home care, and that cost is typically hundreds of dollars a day.”
The particular dilemma for hospitalists is managing transitions of care. Hospitalist Karim Godamunne, MD, MBA, SFHM, chief medical officer of North Fulton Hospital in Roswell, Ga., says hospitalists don’t want financial burdens to dictate care decisions, but they are caught in the middle of decisions that could saddle patients with uncovered costs.
He also worries that the issue will only grow in coming years as baby boomers put more pressure on the health-care system. “We have an aging population,” he adds. “This is not going to go away.”
That is one reason SHM is supporting the Improving Access to Medicare Coverage Act. SHM supported the bill when it was first introduced in March and it has been rapidly gaining cosponsors in recent weeks. This uptick in Congressional interest may be partly a response to the efforts of hospitalists during their time on the Hill. SHM staff and hospitalists are continuing their push now as society officials say hospitalists, who often handle both discharges from the hospital and care provided at SNFs, are in a position to lead discussions on how to sensibly fix the problem.
To that end, a recent SHM letter to the bill’s sponsors casts the issue as one of fiscal responsibility.1 Medicare not covering beneficiaries’ observation days cost patients out-of-pocket money and could cost hospitals in the long run.
“Patients who are admitted with observation status often choose to return home rather than paying out of pocket for a SNF stay,” SHM’s letter reads. “The resultant lack of appropriate post-acute SNF care can result in additional problems such as dehydration, falls, and many other avoidable complications. These complications can not only lead to otherwise preventable readmissions but also increase costs to Medicare for the treatment of conditions that were not present at the time of the original hospital stay.”
Given the debate on observation, Miller says, adopting the bill into law should be a no-brainer. The biggest sticking point likely is the perceived added cost to Medicare. Still, to streamline care and remove an added hurdle to coordinated care, Dr. Godamunne believes the bill should be embraced. He also says that many private insurers look to Medicare decisions to determine their own coverage approaches.
Basically, if Medicare changes its rules, that will carry a lot of weight in the private insurance world.
“This creates a lot of situations for the provider and the family,” Dr. Godamunne says. “You have to make a difficult decision, to try to help the family. You’re trying to provide good care, but on the other hand, there are rules and regulations and bylaws you work under. They don’t align that well, in this case.”
Richard Quinn is a freelance writer in New Jersey.
References
Speakers at HM13 Stress Overarching Reform, Day-to-Day Implementation

To some HM13 attendees, the keynote speakers might have seemed to be talking about different things.
Patrick Conway, MD, MSc, FAAP, SFHM, chief medical officer and director of the Center for Clinical Standards and Quality at the Centers for Medicare & Medicaid Services (CMS), hinted at promising results from the first accountable-care organizations (ACOs) and noted a meaningful reduction in 30-day readmission rates for the first time in years.
David Feinberg, MD, MBA, president of UCLA Health System in Los Angeles, told hospitalists that unless they’re getting patient care right every time, they’re not getting it right enough. And nothing would make him happier than seeing fewer hospitalists at SHM’s annual meeting—because that would mean fewer hospitalized patients.
HM pioneer Bob Wachter, MD, MHM, said it’s time for hospitalists to link their quality-improvement (QI) efforts and safety acumen to projects focused on cutting costs and reducing waste in the health-care system.
So while each made their points in a different way, each plenary speaker left many meeting-goers with a similar thought: Hospitalists are positioned at the nexus of big-picture reform and day-to-day implementation. So if hospitalists as a specialty continue to embrace teamwork, evidence-based practice, quality, safety, and a sense that the patient comes first, they will cement themselves as leaders in the next iteration of health-care delivery.
“There is enormous change going on in the healthcare system,” says SHM CEO Larry Wellikson. “And we are right in the middle of this. We are essential. If we are bad, we are going to sink it. And if we’re great, we are going to take it to another level.”
Needle Movement
Dr. Conway said some of that progress already is evident. He disclosed that initial findings from the first data sets coming from the first ACOs are showing promising results, though he can’t go into detail until the information is publicly released. However, he did boast that after decades of Medicare readmission rates hovering around 19%, data from late 2012 and early 2013 show that figure has dropped to below 18%.
“That is a 1.5% to 2% shift in readmissions nationally,” he said. “It is a credit to the work you and others are doing in the field. That’s hundreds of thousands of Medicare beneficiaries that are not readmitted every year, that stay home healthy. … It’s a tremendous example of moving a national needle.”
He dismissed those who attribute the initial readmission progress solely to penalties instituted on readmissions, though he acknowledged that CMS is using both carrots and sticks to push change.

“It’s a combination of interventions,” he said.
And all of those initiatives must be aimed jointly at improving the patient experience, said Dr. Feinberg, a child psychiatrist by training whose mantra is “patient-centeredness.” Dr. Feinberg’s reputation is that of a physician-administrator who puts patients first. For example, even though his health system (www.uclahealth.org) is in the 99th percentile for patient satisfaction, he is unhappy. That’s because the top ranking means roughly 85 out of every 100 patients served are pretty happy with their experience.
“It means that we’re the cream of the crap,” he said. “Of the last 100 people we took care of, 15 of them—and, by definition, those 15 people are someone’s mom, someone’s brother, someone’s coworker—would not refer us to a friend, or rate us a 9 or 10. So, I think, while we’ve really moved the needle, we’re really not done until we get it right with every patient, every time.”
He added that those who argue against difficult or time-consuming innovations and improvements that better patient care are arguing against the moral high ground of how they would want a family member to be treated in the hospital.
“The pushback I hear is, ‘Some of this stuff is unpreventable,’” Dr. Feinberg said. “Well, maybe it’s unpreventable the way we’re doing it now. But maybe we need to think differently. Maybe it is unpreventable, but if this decreases the prevalence, or makes it better, then to me, it’s important to do.”
Dr. Feinberg, who took over as UCLA Health System’s president in 2011, says he still spends several hours every day talking to patients. For those who say there’s not enough time to stay connected to patients and that all the time spent making sure patients are happy takes away from other activities, he says they’re forgetting what brought them into medicine in the first place: healing. He blames the delivery system for stifling what he believes is a provider’s desire to help people.
“We haven’t allowed the culture to come out,” he said. “I think it’s there.”

Dr. Wachter has a similar faith in the hospitalist culture—although his is based in the pluripotent nature of the specialty. Hospitalists have worked hard to be viewed as “generalists, able to solve all kinds of problems,” and that means the specialty is poised to adapt and thrive.
“We will morph into what is needed,” said Dr. Wachter, a past president of SHM whose titles include chief of the division of hospital medicine at the University of California at San Francisco and chair of the American Board of Internal Medicine. “That will be all sorts of things: comanagement, dealing with the residency limits in teaching hospitals, systems improvement, cost reductions, transitions, working in skilled nursing facilities, all the specialty hospitalists.
“We will fill new niches,” he said.

What Dr. Wachter does not want to see is that the field grows “fat and happy,” as it is now firmly entrenched in the U.S. health-care delivery system. In fact, he urged hospitalists to welcome change, particularly initiatives that improve quality and safety, reduce costs and waste, and, ultimately, improve the patient experience.
But he cautioned against conceptually separating QI and cost reduction. Instead, they should be viewed as equally meaningful parts of his oft-quoted value equation, which, viewed from the health-care consumer’s point of view, is quality divided by cost.
“You can’t survive and thrive in a world with the kinds of pressures that we have to improve performance if you do business the same old way,” he added. “It’s no longer possible to achieve the things you need to achieve handling these as single projects. You need to transform the way you think about care.”
Richard Quinn is a freelance writer in New Jersey.
To some HM13 attendees, the keynote speakers might have seemed to be talking about different things.
Patrick Conway, MD, MSc, FAAP, SFHM, chief medical officer and director of the Center for Clinical Standards and Quality at the Centers for Medicare & Medicaid Services (CMS), hinted at promising results from the first accountable-care organizations (ACOs) and noted a meaningful reduction in 30-day readmission rates for the first time in years.
David Feinberg, MD, MBA, president of UCLA Health System in Los Angeles, told hospitalists that unless they’re getting patient care right every time, they’re not getting it right enough. And nothing would make him happier than seeing fewer hospitalists at SHM’s annual meeting—because that would mean fewer hospitalized patients.
HM pioneer Bob Wachter, MD, MHM, said it’s time for hospitalists to link their quality-improvement (QI) efforts and safety acumen to projects focused on cutting costs and reducing waste in the health-care system.
So while each made their points in a different way, each plenary speaker left many meeting-goers with a similar thought: Hospitalists are positioned at the nexus of big-picture reform and day-to-day implementation. So if hospitalists as a specialty continue to embrace teamwork, evidence-based practice, quality, safety, and a sense that the patient comes first, they will cement themselves as leaders in the next iteration of health-care delivery.
“There is enormous change going on in the healthcare system,” says SHM CEO Larry Wellikson. “And we are right in the middle of this. We are essential. If we are bad, we are going to sink it. And if we’re great, we are going to take it to another level.”
Needle Movement
Dr. Conway said some of that progress already is evident. He disclosed that initial findings from the first data sets coming from the first ACOs are showing promising results, though he can’t go into detail until the information is publicly released. However, he did boast that after decades of Medicare readmission rates hovering around 19%, data from late 2012 and early 2013 show that figure has dropped to below 18%.
“That is a 1.5% to 2% shift in readmissions nationally,” he said. “It is a credit to the work you and others are doing in the field. That’s hundreds of thousands of Medicare beneficiaries that are not readmitted every year, that stay home healthy. … It’s a tremendous example of moving a national needle.”
He dismissed those who attribute the initial readmission progress solely to penalties instituted on readmissions, though he acknowledged that CMS is using both carrots and sticks to push change.
“It’s a combination of interventions,” he said.
And all of those initiatives must be aimed jointly at improving the patient experience, said Dr. Feinberg, a child psychiatrist by training whose mantra is “patient-centeredness.” Dr. Feinberg’s reputation is that of a physician-administrator who puts patients first. For example, even though his health system (www.uclahealth.org) is in the 99th percentile for patient satisfaction, he is unhappy. That’s because the top ranking means roughly 85 out of every 100 patients served are pretty happy with their experience.
“It means that we’re the cream of the crap,” he said. “Of the last 100 people we took care of, 15 of them—and, by definition, those 15 people are someone’s mom, someone’s brother, someone’s coworker—would not refer us to a friend, or rate us a 9 or 10. So, I think, while we’ve really moved the needle, we’re really not done until we get it right with every patient, every time.”
He added that those who argue against difficult or time-consuming innovations and improvements that better patient care are arguing against the moral high ground of how they would want a family member to be treated in the hospital.
“The pushback I hear is, ‘Some of this stuff is unpreventable,’” Dr. Feinberg said. “Well, maybe it’s unpreventable the way we’re doing it now. But maybe we need to think differently. Maybe it is unpreventable, but if this decreases the prevalence, or makes it better, then to me, it’s important to do.”
Dr. Feinberg, who took over as UCLA Health System’s president in 2011, says he still spends several hours every day talking to patients. For those who say there’s not enough time to stay connected to patients and that all the time spent making sure patients are happy takes away from other activities, he says they’re forgetting what brought them into medicine in the first place: healing. He blames the delivery system for stifling what he believes is a provider’s desire to help people.
“We haven’t allowed the culture to come out,” he said. “I think it’s there.”
Dr. Wachter has a similar faith in the hospitalist culture—although his is based in the pluripotent nature of the specialty. Hospitalists have worked hard to be viewed as “generalists, able to solve all kinds of problems,” and that means the specialty is poised to adapt and thrive.
“We will morph into what is needed,” said Dr. Wachter, a past president of SHM whose titles include chief of the division of hospital medicine at the University of California at San Francisco and chair of the American Board of Internal Medicine. “That will be all sorts of things: comanagement, dealing with the residency limits in teaching hospitals, systems improvement, cost reductions, transitions, working in skilled nursing facilities, all the specialty hospitalists.
“We will fill new niches,” he said.
What Dr. Wachter does not want to see is that the field grows “fat and happy,” as it is now firmly entrenched in the U.S. health-care delivery system. In fact, he urged hospitalists to welcome change, particularly initiatives that improve quality and safety, reduce costs and waste, and, ultimately, improve the patient experience.
But he cautioned against conceptually separating QI and cost reduction. Instead, they should be viewed as equally meaningful parts of his oft-quoted value equation, which, viewed from the health-care consumer’s point of view, is quality divided by cost.
“You can’t survive and thrive in a world with the kinds of pressures that we have to improve performance if you do business the same old way,” he added. “It’s no longer possible to achieve the things you need to achieve handling these as single projects. You need to transform the way you think about care.”
Richard Quinn is a freelance writer in New Jersey.
To some HM13 attendees, the keynote speakers might have seemed to be talking about different things.
Patrick Conway, MD, MSc, FAAP, SFHM, chief medical officer and director of the Center for Clinical Standards and Quality at the Centers for Medicare & Medicaid Services (CMS), hinted at promising results from the first accountable-care organizations (ACOs) and noted a meaningful reduction in 30-day readmission rates for the first time in years.
David Feinberg, MD, MBA, president of UCLA Health System in Los Angeles, told hospitalists that unless they’re getting patient care right every time, they’re not getting it right enough. And nothing would make him happier than seeing fewer hospitalists at SHM’s annual meeting—because that would mean fewer hospitalized patients.
HM pioneer Bob Wachter, MD, MHM, said it’s time for hospitalists to link their quality-improvement (QI) efforts and safety acumen to projects focused on cutting costs and reducing waste in the health-care system.
So while each made their points in a different way, each plenary speaker left many meeting-goers with a similar thought: Hospitalists are positioned at the nexus of big-picture reform and day-to-day implementation. So if hospitalists as a specialty continue to embrace teamwork, evidence-based practice, quality, safety, and a sense that the patient comes first, they will cement themselves as leaders in the next iteration of health-care delivery.
“There is enormous change going on in the healthcare system,” says SHM CEO Larry Wellikson. “And we are right in the middle of this. We are essential. If we are bad, we are going to sink it. And if we’re great, we are going to take it to another level.”
Needle Movement
Dr. Conway said some of that progress already is evident. He disclosed that initial findings from the first data sets coming from the first ACOs are showing promising results, though he can’t go into detail until the information is publicly released. However, he did boast that after decades of Medicare readmission rates hovering around 19%, data from late 2012 and early 2013 show that figure has dropped to below 18%.
“That is a 1.5% to 2% shift in readmissions nationally,” he said. “It is a credit to the work you and others are doing in the field. That’s hundreds of thousands of Medicare beneficiaries that are not readmitted every year, that stay home healthy. … It’s a tremendous example of moving a national needle.”
He dismissed those who attribute the initial readmission progress solely to penalties instituted on readmissions, though he acknowledged that CMS is using both carrots and sticks to push change.
“It’s a combination of interventions,” he said.
And all of those initiatives must be aimed jointly at improving the patient experience, said Dr. Feinberg, a child psychiatrist by training whose mantra is “patient-centeredness.” Dr. Feinberg’s reputation is that of a physician-administrator who puts patients first. For example, even though his health system (www.uclahealth.org) is in the 99th percentile for patient satisfaction, he is unhappy. That’s because the top ranking means roughly 85 out of every 100 patients served are pretty happy with their experience.
“It means that we’re the cream of the crap,” he said. “Of the last 100 people we took care of, 15 of them—and, by definition, those 15 people are someone’s mom, someone’s brother, someone’s coworker—would not refer us to a friend, or rate us a 9 or 10. So, I think, while we’ve really moved the needle, we’re really not done until we get it right with every patient, every time.”
He added that those who argue against difficult or time-consuming innovations and improvements that better patient care are arguing against the moral high ground of how they would want a family member to be treated in the hospital.
“The pushback I hear is, ‘Some of this stuff is unpreventable,’” Dr. Feinberg said. “Well, maybe it’s unpreventable the way we’re doing it now. But maybe we need to think differently. Maybe it is unpreventable, but if this decreases the prevalence, or makes it better, then to me, it’s important to do.”
Dr. Feinberg, who took over as UCLA Health System’s president in 2011, says he still spends several hours every day talking to patients. For those who say there’s not enough time to stay connected to patients and that all the time spent making sure patients are happy takes away from other activities, he says they’re forgetting what brought them into medicine in the first place: healing. He blames the delivery system for stifling what he believes is a provider’s desire to help people.
“We haven’t allowed the culture to come out,” he said. “I think it’s there.”
Dr. Wachter has a similar faith in the hospitalist culture—although his is based in the pluripotent nature of the specialty. Hospitalists have worked hard to be viewed as “generalists, able to solve all kinds of problems,” and that means the specialty is poised to adapt and thrive.
“We will morph into what is needed,” said Dr. Wachter, a past president of SHM whose titles include chief of the division of hospital medicine at the University of California at San Francisco and chair of the American Board of Internal Medicine. “That will be all sorts of things: comanagement, dealing with the residency limits in teaching hospitals, systems improvement, cost reductions, transitions, working in skilled nursing facilities, all the specialty hospitalists.
“We will fill new niches,” he said.
What Dr. Wachter does not want to see is that the field grows “fat and happy,” as it is now firmly entrenched in the U.S. health-care delivery system. In fact, he urged hospitalists to welcome change, particularly initiatives that improve quality and safety, reduce costs and waste, and, ultimately, improve the patient experience.
But he cautioned against conceptually separating QI and cost reduction. Instead, they should be viewed as equally meaningful parts of his oft-quoted value equation, which, viewed from the health-care consumer’s point of view, is quality divided by cost.
“You can’t survive and thrive in a world with the kinds of pressures that we have to improve performance if you do business the same old way,” he added. “It’s no longer possible to achieve the things you need to achieve handling these as single projects. You need to transform the way you think about care.”
Richard Quinn is a freelance writer in New Jersey.
Health-Care Journalists Tackle Barriers to Hospital Safety Records

The Association of Health Care Journalists, a professional association that includes 1,400 journalists, is tackling some of the barriers consumers and advocates face when trying to access such information as hospital safety records. AHCJ’s www.HospitalInfections.org is a free, searchable news application that went live in March with detailed reports of deficiencies cited in federal inspection visits for acute- and critical-access hospitals nationwide.
Through years of advocacy, AHCJ has filed Freedom of Information Act requests and negotiated with the Centers for Medicare & Medicaid Services (CMS) to get access to hospital safety information in electronic form.
CMS’ Hospital Compare website (www.medicare.gov/hospitalcompare) and the Joint Commission’s Quality Check (www.qualitycheck.org) program both publicly report hospital quality data, but they have significant time lags and data that are difficult for the average consumer to understand, according to AHCJ. The association touts its new site as an “early attempt by an advocacy group to make hospital safety information easier to access and more consumer-driven.”
“Being able to easily review the performance of your local hospital is vital for health-care journalists and for the public,” AHCJ president Charles Ornstein, a senior reporter at ProPublica in New York, said in a statement.
Larry Beresford is a freelance writer in San Francisco
References
- Weigel C, Suen W, Gupta G. Using Lean methodology to teach quality improvement to internal medicine residents at a safety net hospital. Am J Med Qual. 2013 Feb 4 [Epub ahead of print].
- Morganti KG, Lovejoy S, Beckjord EB, Haviland AM, Haas AC, Farley DO. A retrospective evaluation of the Perfecting Patient Care University training program for health care organizations. Am J Med Qual. 2013 Apr 9 [Epub ahead of print].
- Myers JS, Tess A, Glasheen JJ, et al. The Quality and Safety Educators’ Academy: fulfilling an unmet need for faculty development. Am J Med Qual. 2013 Apr 11 [Epub ahead of print].
- Dong XQ, Simon MA. Elder abuse as a risk factor for hospitalization in older persons. JAMA Intern Med. 2013 Apr 8:1-7. doi: 10.1001/jamainternmed.2013.238 [Epub ahead of print].
- Cisco mConcierge. 90% American workers use their own smartphones for work. Cisco mConcierge website. Available at: http://www.ciscomcon.com/sw/swchannel/registration/internet/registrationcfm?SWAPPID=91&RegPageID=350200&SWTHEMEID=12949. Accessed
The Association of Health Care Journalists, a professional association that includes 1,400 journalists, is tackling some of the barriers consumers and advocates face when trying to access such information as hospital safety records. AHCJ’s www.HospitalInfections.org is a free, searchable news application that went live in March with detailed reports of deficiencies cited in federal inspection visits for acute- and critical-access hospitals nationwide.
Through years of advocacy, AHCJ has filed Freedom of Information Act requests and negotiated with the Centers for Medicare & Medicaid Services (CMS) to get access to hospital safety information in electronic form.
CMS’ Hospital Compare website (www.medicare.gov/hospitalcompare) and the Joint Commission’s Quality Check (www.qualitycheck.org) program both publicly report hospital quality data, but they have significant time lags and data that are difficult for the average consumer to understand, according to AHCJ. The association touts its new site as an “early attempt by an advocacy group to make hospital safety information easier to access and more consumer-driven.”
“Being able to easily review the performance of your local hospital is vital for health-care journalists and for the public,” AHCJ president Charles Ornstein, a senior reporter at ProPublica in New York, said in a statement.
Larry Beresford is a freelance writer in San Francisco
References
- Weigel C, Suen W, Gupta G. Using Lean methodology to teach quality improvement to internal medicine residents at a safety net hospital. Am J Med Qual. 2013 Feb 4 [Epub ahead of print].
- Morganti KG, Lovejoy S, Beckjord EB, Haviland AM, Haas AC, Farley DO. A retrospective evaluation of the Perfecting Patient Care University training program for health care organizations. Am J Med Qual. 2013 Apr 9 [Epub ahead of print].
- Myers JS, Tess A, Glasheen JJ, et al. The Quality and Safety Educators’ Academy: fulfilling an unmet need for faculty development. Am J Med Qual. 2013 Apr 11 [Epub ahead of print].
- Dong XQ, Simon MA. Elder abuse as a risk factor for hospitalization in older persons. JAMA Intern Med. 2013 Apr 8:1-7. doi: 10.1001/jamainternmed.2013.238 [Epub ahead of print].
- Cisco mConcierge. 90% American workers use their own smartphones for work. Cisco mConcierge website. Available at: http://www.ciscomcon.com/sw/swchannel/registration/internet/registrationcfm?SWAPPID=91&RegPageID=350200&SWTHEMEID=12949. Accessed
The Association of Health Care Journalists, a professional association that includes 1,400 journalists, is tackling some of the barriers consumers and advocates face when trying to access such information as hospital safety records. AHCJ’s www.HospitalInfections.org is a free, searchable news application that went live in March with detailed reports of deficiencies cited in federal inspection visits for acute- and critical-access hospitals nationwide.
Through years of advocacy, AHCJ has filed Freedom of Information Act requests and negotiated with the Centers for Medicare & Medicaid Services (CMS) to get access to hospital safety information in electronic form.
CMS’ Hospital Compare website (www.medicare.gov/hospitalcompare) and the Joint Commission’s Quality Check (www.qualitycheck.org) program both publicly report hospital quality data, but they have significant time lags and data that are difficult for the average consumer to understand, according to AHCJ. The association touts its new site as an “early attempt by an advocacy group to make hospital safety information easier to access and more consumer-driven.”
“Being able to easily review the performance of your local hospital is vital for health-care journalists and for the public,” AHCJ president Charles Ornstein, a senior reporter at ProPublica in New York, said in a statement.
Larry Beresford is a freelance writer in San Francisco
References
- Weigel C, Suen W, Gupta G. Using Lean methodology to teach quality improvement to internal medicine residents at a safety net hospital. Am J Med Qual. 2013 Feb 4 [Epub ahead of print].
- Morganti KG, Lovejoy S, Beckjord EB, Haviland AM, Haas AC, Farley DO. A retrospective evaluation of the Perfecting Patient Care University training program for health care organizations. Am J Med Qual. 2013 Apr 9 [Epub ahead of print].
- Myers JS, Tess A, Glasheen JJ, et al. The Quality and Safety Educators’ Academy: fulfilling an unmet need for faculty development. Am J Med Qual. 2013 Apr 11 [Epub ahead of print].
- Dong XQ, Simon MA. Elder abuse as a risk factor for hospitalization in older persons. JAMA Intern Med. 2013 Apr 8:1-7. doi: 10.1001/jamainternmed.2013.238 [Epub ahead of print].
- Cisco mConcierge. 90% American workers use their own smartphones for work. Cisco mConcierge website. Available at: http://www.ciscomcon.com/sw/swchannel/registration/internet/registrationcfm?SWAPPID=91&RegPageID=350200&SWTHEMEID=12949. Accessed
‘Hill Trip’ Connects Legislators to Hospitalists, Health Care Issues

A veritable perfect storm of relationships brought hospitalist Jairy Hunter, MD, MBA, SFHM, to “Hospitalists on the Hill 2013,” a daylong advocacy affair that preceded HM13 last month.
First, Dr. Hunter was born and bred—and now lives—in South Carolina, a close-knit state where leaders across industries tend to run in the same circles, or at least have relatives who do. Second, Dr. Hunter’s father, Jairy Hunter Jr., is the longtime president of Charleston Southern University, where Sen. Tim Scott (R-S.C.) earned his undergraduate degree when it was still called Baptist College at Charleston. And three, Dr. Hunter is associate executive medical director of one of the state’s flagship health-care institutions, Medical University of South Carolina in Charleston.
So it was that SHM set Dr. Hunter up in meetings with the offices of Scott, Sen. Lindsey Graham (R-S.C.), and Rep. Jim Clyburn (D-S.C.), and—for the day at least—made Dr. Hunter the voice of hospital medicine.
“It was a little bit demystifying of an experience to be able to know there’s actually people you can talk to and you can develop a relationship with,” says Dr. Hunter, who also serves on Team Hospitalist. “I thought that was very rewarding.”
The connections made by Dr. Hunter are the point of the annual trek made by SHM leaders and members to lobby legislators and federal staffers “on the way policies affect your practice and your patients,” SHM says on its website (www.hospitalmedicine.org/advocacy). This year’s volunteer effort was by far the largest ever, says Public Policy Committee chair Ron Greeno, MD, FCCP, MHM. More than 150 hospitalists participated in training, 113 hospitalists visited Capitol Hill, and scores more had to be turned away. All told, hospitalists held 409 individual meetings with legislators and staff members.
“Quite frankly, if we’d have had the budget, we could have had another 100 to 150 people come,” Dr. Greeno says. “That’s how many people wanted to go.”
Dr. Greeno attributes the interest to two factors. One, having the annual meeting at the Gaylord National Resort & Convention Center, just outside Washington, D.C, makes the Hill trip a natural extension. Two, the current landscape of health-care reform has motivated many physicians to become more involved than they might otherwise be. One challenge of having so many first-timers making this year’s trip was making sure they were properly prepared. To hone the message, SHM gave the group a few hours of education by former legislative staffer Stephanie Vance of Advocacy Associates, a communications firm that helps organizations, such as medical societies, tailor their message to policymakers. Vance told hospitalists a personal visit with a constituent often becomes the most influential type of advocacy.
“That’s why it was easy to make an initial connection, because these staffers are from where I’m from, friends with people that I’m friends with,” Dr. Hunter says.

Unique Approach
SHM CEO Larry Wellikson, MD, SFHM, says the society tries to differentiate itself from other organizations through its grassroots approach to advocacy. More important, the society refrains from giving a long list of legislative requests that are self-serving.
“We’re someone they want to talk to because we’re not coming there to just say, ‘Here’s a power play for hospitalists,’” Dr. Wellikson says. “We come and try to provide solutions.”
To that end, this year’s lobbying effort was targeted to topics important both to HM and the health-care system:
- Repealing the sustainable growth rate (SGR) formula for Medicare payments, specifically via the proposed Medicare Physician Payment Innovation Act of 2013 (H.R. 574);
- Solving the quagmire of observation status time not counting toward the required three consecutive overnights as an inpatient needed to qualify for Medicare benefits at a skilled nursing facility, by supporting the Improving Access to Medicare Coverage Act of 2013 (H.R. 1179, S. 569); and
- Getting the federal government to commit to providing $434 million in funding for the Agency for Healthcare Research and Quality (AHRQ) in fiscal 2014.
“The message that we’re sending resonated with the people we met with on both sides of the aisle,” Dr. Greeno says. “The SGR, for instance, they know there needs to be a fix. We want to serve as a resource for them as they start to figure out the answer to the question: What are we going to replace it with?
“What we want to do is make everybody on the Hill understand that we can be relied upon as a resource when they’re looking for solutions,” he says.
Focused on Follow-Up
And that’s where rank-and-filers, such as Dr. Hunter, have to take charge. So for his Hill Day visits, he tried to stand out. Everyone he met with got a lapel pin in the shape of a South Carolina state flag, which has become a popular fashion statement in recent years. And Scott also got a pin from Charleston Southern University, his alma mater. The gestures were small, but they served as icebreakers and reminders that Dr. Hunter and the people he met are bound by service to the residents of the Palmetto State.
Dr. Hunter also hopes the small token will be that little extra that makes him memorable enough that the next time a Congressional staffer has an SGR question, they’ll ask him and not a doctor from another specialty.
“I’m interested to see how much feedback I get back from them,” he says. “I can feed them all day long, but I don’t want to be that crazy guy bugging them. If they respond back to me, I can hopefully make more inroads.”
He certainly would if Dr. Greeno gets his way. Moving forward, SHM hopes to be able to rely more on local advocates pushing for reform than just a once-a-year major event and formal positions drafted by SHM’s staffers or the Public Policy Committee. Dr. Greeno says the physicians who participated in this year’s Hill trip are likely to find they will be asked to be the first cohort of a grassroots initiative meant to deliver the society’s message more routinely.
“These are not easy things to change because there are not easy solutions,” Dr. Greeno adds. “If you have just one meeting on the Hill, you’ll have no impact at all. You have to follow up. You have to do it consistently. And you have to have a consistent message. And we will.”
Richard Quinn is a freelance writer in New Jersey.
A veritable perfect storm of relationships brought hospitalist Jairy Hunter, MD, MBA, SFHM, to “Hospitalists on the Hill 2013,” a daylong advocacy affair that preceded HM13 last month.
First, Dr. Hunter was born and bred—and now lives—in South Carolina, a close-knit state where leaders across industries tend to run in the same circles, or at least have relatives who do. Second, Dr. Hunter’s father, Jairy Hunter Jr., is the longtime president of Charleston Southern University, where Sen. Tim Scott (R-S.C.) earned his undergraduate degree when it was still called Baptist College at Charleston. And three, Dr. Hunter is associate executive medical director of one of the state’s flagship health-care institutions, Medical University of South Carolina in Charleston.
So it was that SHM set Dr. Hunter up in meetings with the offices of Scott, Sen. Lindsey Graham (R-S.C.), and Rep. Jim Clyburn (D-S.C.), and—for the day at least—made Dr. Hunter the voice of hospital medicine.
“It was a little bit demystifying of an experience to be able to know there’s actually people you can talk to and you can develop a relationship with,” says Dr. Hunter, who also serves on Team Hospitalist. “I thought that was very rewarding.”
The connections made by Dr. Hunter are the point of the annual trek made by SHM leaders and members to lobby legislators and federal staffers “on the way policies affect your practice and your patients,” SHM says on its website (www.hospitalmedicine.org/advocacy). This year’s volunteer effort was by far the largest ever, says Public Policy Committee chair Ron Greeno, MD, FCCP, MHM. More than 150 hospitalists participated in training, 113 hospitalists visited Capitol Hill, and scores more had to be turned away. All told, hospitalists held 409 individual meetings with legislators and staff members.
“Quite frankly, if we’d have had the budget, we could have had another 100 to 150 people come,” Dr. Greeno says. “That’s how many people wanted to go.”
Dr. Greeno attributes the interest to two factors. One, having the annual meeting at the Gaylord National Resort & Convention Center, just outside Washington, D.C, makes the Hill trip a natural extension. Two, the current landscape of health-care reform has motivated many physicians to become more involved than they might otherwise be. One challenge of having so many first-timers making this year’s trip was making sure they were properly prepared. To hone the message, SHM gave the group a few hours of education by former legislative staffer Stephanie Vance of Advocacy Associates, a communications firm that helps organizations, such as medical societies, tailor their message to policymakers. Vance told hospitalists a personal visit with a constituent often becomes the most influential type of advocacy.
“That’s why it was easy to make an initial connection, because these staffers are from where I’m from, friends with people that I’m friends with,” Dr. Hunter says.
Unique Approach
SHM CEO Larry Wellikson, MD, SFHM, says the society tries to differentiate itself from other organizations through its grassroots approach to advocacy. More important, the society refrains from giving a long list of legislative requests that are self-serving.
“We’re someone they want to talk to because we’re not coming there to just say, ‘Here’s a power play for hospitalists,’” Dr. Wellikson says. “We come and try to provide solutions.”
To that end, this year’s lobbying effort was targeted to topics important both to HM and the health-care system:
- Repealing the sustainable growth rate (SGR) formula for Medicare payments, specifically via the proposed Medicare Physician Payment Innovation Act of 2013 (H.R. 574);
- Solving the quagmire of observation status time not counting toward the required three consecutive overnights as an inpatient needed to qualify for Medicare benefits at a skilled nursing facility, by supporting the Improving Access to Medicare Coverage Act of 2013 (H.R. 1179, S. 569); and
- Getting the federal government to commit to providing $434 million in funding for the Agency for Healthcare Research and Quality (AHRQ) in fiscal 2014.
“The message that we’re sending resonated with the people we met with on both sides of the aisle,” Dr. Greeno says. “The SGR, for instance, they know there needs to be a fix. We want to serve as a resource for them as they start to figure out the answer to the question: What are we going to replace it with?
“What we want to do is make everybody on the Hill understand that we can be relied upon as a resource when they’re looking for solutions,” he says.
Focused on Follow-Up
And that’s where rank-and-filers, such as Dr. Hunter, have to take charge. So for his Hill Day visits, he tried to stand out. Everyone he met with got a lapel pin in the shape of a South Carolina state flag, which has become a popular fashion statement in recent years. And Scott also got a pin from Charleston Southern University, his alma mater. The gestures were small, but they served as icebreakers and reminders that Dr. Hunter and the people he met are bound by service to the residents of the Palmetto State.
Dr. Hunter also hopes the small token will be that little extra that makes him memorable enough that the next time a Congressional staffer has an SGR question, they’ll ask him and not a doctor from another specialty.
“I’m interested to see how much feedback I get back from them,” he says. “I can feed them all day long, but I don’t want to be that crazy guy bugging them. If they respond back to me, I can hopefully make more inroads.”
He certainly would if Dr. Greeno gets his way. Moving forward, SHM hopes to be able to rely more on local advocates pushing for reform than just a once-a-year major event and formal positions drafted by SHM’s staffers or the Public Policy Committee. Dr. Greeno says the physicians who participated in this year’s Hill trip are likely to find they will be asked to be the first cohort of a grassroots initiative meant to deliver the society’s message more routinely.
“These are not easy things to change because there are not easy solutions,” Dr. Greeno adds. “If you have just one meeting on the Hill, you’ll have no impact at all. You have to follow up. You have to do it consistently. And you have to have a consistent message. And we will.”
Richard Quinn is a freelance writer in New Jersey.
A veritable perfect storm of relationships brought hospitalist Jairy Hunter, MD, MBA, SFHM, to “Hospitalists on the Hill 2013,” a daylong advocacy affair that preceded HM13 last month.
First, Dr. Hunter was born and bred—and now lives—in South Carolina, a close-knit state where leaders across industries tend to run in the same circles, or at least have relatives who do. Second, Dr. Hunter’s father, Jairy Hunter Jr., is the longtime president of Charleston Southern University, where Sen. Tim Scott (R-S.C.) earned his undergraduate degree when it was still called Baptist College at Charleston. And three, Dr. Hunter is associate executive medical director of one of the state’s flagship health-care institutions, Medical University of South Carolina in Charleston.
So it was that SHM set Dr. Hunter up in meetings with the offices of Scott, Sen. Lindsey Graham (R-S.C.), and Rep. Jim Clyburn (D-S.C.), and—for the day at least—made Dr. Hunter the voice of hospital medicine.
“It was a little bit demystifying of an experience to be able to know there’s actually people you can talk to and you can develop a relationship with,” says Dr. Hunter, who also serves on Team Hospitalist. “I thought that was very rewarding.”
The connections made by Dr. Hunter are the point of the annual trek made by SHM leaders and members to lobby legislators and federal staffers “on the way policies affect your practice and your patients,” SHM says on its website (www.hospitalmedicine.org/advocacy). This year’s volunteer effort was by far the largest ever, says Public Policy Committee chair Ron Greeno, MD, FCCP, MHM. More than 150 hospitalists participated in training, 113 hospitalists visited Capitol Hill, and scores more had to be turned away. All told, hospitalists held 409 individual meetings with legislators and staff members.
“Quite frankly, if we’d have had the budget, we could have had another 100 to 150 people come,” Dr. Greeno says. “That’s how many people wanted to go.”
Dr. Greeno attributes the interest to two factors. One, having the annual meeting at the Gaylord National Resort & Convention Center, just outside Washington, D.C, makes the Hill trip a natural extension. Two, the current landscape of health-care reform has motivated many physicians to become more involved than they might otherwise be. One challenge of having so many first-timers making this year’s trip was making sure they were properly prepared. To hone the message, SHM gave the group a few hours of education by former legislative staffer Stephanie Vance of Advocacy Associates, a communications firm that helps organizations, such as medical societies, tailor their message to policymakers. Vance told hospitalists a personal visit with a constituent often becomes the most influential type of advocacy.
“That’s why it was easy to make an initial connection, because these staffers are from where I’m from, friends with people that I’m friends with,” Dr. Hunter says.
Unique Approach
SHM CEO Larry Wellikson, MD, SFHM, says the society tries to differentiate itself from other organizations through its grassroots approach to advocacy. More important, the society refrains from giving a long list of legislative requests that are self-serving.
“We’re someone they want to talk to because we’re not coming there to just say, ‘Here’s a power play for hospitalists,’” Dr. Wellikson says. “We come and try to provide solutions.”
To that end, this year’s lobbying effort was targeted to topics important both to HM and the health-care system:
- Repealing the sustainable growth rate (SGR) formula for Medicare payments, specifically via the proposed Medicare Physician Payment Innovation Act of 2013 (H.R. 574);
- Solving the quagmire of observation status time not counting toward the required three consecutive overnights as an inpatient needed to qualify for Medicare benefits at a skilled nursing facility, by supporting the Improving Access to Medicare Coverage Act of 2013 (H.R. 1179, S. 569); and
- Getting the federal government to commit to providing $434 million in funding for the Agency for Healthcare Research and Quality (AHRQ) in fiscal 2014.
“The message that we’re sending resonated with the people we met with on both sides of the aisle,” Dr. Greeno says. “The SGR, for instance, they know there needs to be a fix. We want to serve as a resource for them as they start to figure out the answer to the question: What are we going to replace it with?
“What we want to do is make everybody on the Hill understand that we can be relied upon as a resource when they’re looking for solutions,” he says.
Focused on Follow-Up
And that’s where rank-and-filers, such as Dr. Hunter, have to take charge. So for his Hill Day visits, he tried to stand out. Everyone he met with got a lapel pin in the shape of a South Carolina state flag, which has become a popular fashion statement in recent years. And Scott also got a pin from Charleston Southern University, his alma mater. The gestures were small, but they served as icebreakers and reminders that Dr. Hunter and the people he met are bound by service to the residents of the Palmetto State.
Dr. Hunter also hopes the small token will be that little extra that makes him memorable enough that the next time a Congressional staffer has an SGR question, they’ll ask him and not a doctor from another specialty.
“I’m interested to see how much feedback I get back from them,” he says. “I can feed them all day long, but I don’t want to be that crazy guy bugging them. If they respond back to me, I can hopefully make more inroads.”
He certainly would if Dr. Greeno gets his way. Moving forward, SHM hopes to be able to rely more on local advocates pushing for reform than just a once-a-year major event and formal positions drafted by SHM’s staffers or the Public Policy Committee. Dr. Greeno says the physicians who participated in this year’s Hill trip are likely to find they will be asked to be the first cohort of a grassroots initiative meant to deliver the society’s message more routinely.
“These are not easy things to change because there are not easy solutions,” Dr. Greeno adds. “If you have just one meeting on the Hill, you’ll have no impact at all. You have to follow up. You have to do it consistently. And you have to have a consistent message. And we will.”
Richard Quinn is a freelance writer in New Jersey.
Hospitalists Can Address Causes of Skyrocketing Health Care Costs


Alarms about our nation’s health-care costs have been sounding for well over a decade. According to the Centers for Medicare & Medicaid Services (CMS), spending on U.S. health care doubled between 1999 and 2011, climbing to $2.7 trillion from $1.3 trillion, and now represents 17.9% of the United States’ GDP.1
“The medical care system is bankrupting the country,” Paul B. Ginsburg, PhD, president of the Center for Studying Health System Change (HSC), based in Washington, D.C., says bluntly. A four-decade-long upward spending trend is “unsustainable,” he wrote in the New England Journal of Medicine with Chapin White, PhD, a senior health researcher at HSC.2
Recent reports suggest that rising premiums and out-of-pocket costs are rendering the price of health care untenable for the average consumer. A 2011 RAND Corp. study found that, for the average American family, the rate of increased costs for health care had outpaced growth in earnings from 1999 to 2009.3 And last year, for the first time, the cost of health care for a typical American family of four surpassed $20,000, the annual Milliman Medical Index reported.4
Should hospitalists be concerned, professionally and personally, about these trends? Absolutely, say hospitalist leaders who spoke with The Hospitalist. HM clinicians have much to contribute at both the macro level (addressing systemic causes of overutilization through quality improvement and other initiatives) and at the micro level, by understanding their personal contributions and by engaging patients and their families in shared decision-making.
But getting at and addressing the root causes of rising health-care costs, according to health-care policy analysts and veteran hospitalists, will require major shifts in thinking and processes.
Contributors to Rising Costs
It’s difficult to pinpoint the root causes of the recent surge in health-care costs. Victor Fuchs, emeritus professor of economics and health research and policy at Stanford University, points to the U.S.’ high administrative costs and complicated billing systems.5 A fragmented, nontransparent system for negotiating fees between insurers and providers also plays a role, as demonstrated in a Consumer Reports investigation into geographic variations in costs for common tests and procedures. A complete blood count might be as low as $15 or as high as $105; a colonoscopy ranges from $800 to $3,160.6
Bradley Flansbaum, DO, MPH, SFHM, an SHM Public Policy Committee member and AMA delegate, says rising costs are a provider-specific issue. He challenges colleagues to take an honest look at their own practice patterns to assess whether they’re contributing to overuse of resources (see “A Lesson in Change,”).
“The culture of practice has developed so that this is not going to change overnight,” says Dr. Flansbaum, director of hospitalist services at Lenox Hill Hospital in New York City. That’s because many physicians fail to view their own decisions as a problem. For example, says Dr. Flansbaum, “an oncologist may not identify a third round of chemotherapy as an embodiment of the problem, or a gastroenterologist might not embody the colonoscopy at Year Four instead of Year Five as the problem. We must come to grips with the usual mindset, look in the mirror, and admit, ‘Maybe we are part of the problem.’”

—Bradley Flansbaum, DO, MPH, SFHM
Potential Solutions
Hospitalists, intensivists, and ED clinicians are tasked with finding a balance between being prudent stewards of resources and staying within a comfort zone that promotes patient safety. SHM supports the goals of the ABIM Foundation’s Choosing Wisely campaign, which aims to reduce waste by curtailing duplicative and unnecessary care (see “Better Choices, Better Care,” March 2013). Also included in the campaign (www.ChoosingWisely.org) are the American College of Physicians’ recommendations against low-value testing (e.g. obtaining imaging studies in patients with nonspecific low back pain).
“Those recommendations are not going to solve our health spending problem,” says White, “but they are part of a broader move to give permission to clinicians, based on evidence, to follow more conservative practice patterns.”
Still, counters David I. Auerbach, PhD, a health economist at RAND in Boston and author of the RAND study, “there’s another value to these tests that the cost-effectiveness equations do not always consider, which is, they can bring peace of mind. We’re trying to nudge patients down the pathway that we think is best for them without rationing care. That’s a delicate balance.”
Dr. Flansbaum says SHM’s Public Policy Committee has discussed a variety of issues related to rising costs, although the group has not directly tackled advice in the form of a white paper. He suggests some ways that hospitalists can address cost savings:
- Involve patients in shared decision-making, and discuss the evidence against unnecessary testing;
- Utilize generic medications on discharge, when available, especially if patients are uninsured or have limited drug coverage with their insurance plans;
- Use palliative care whenever appropriate; and
- Adhere to transitional-care standards.
On the macro level, HM has “always been the specialty invited to champion the important discussion relating to resource utilization, and the evidence-based medicine driving that resource utilization,” says Christopher Frost, MD, FHM, medical director of hospital medicine at the Hospital Corporation of America (HCA) in Nashville, Tenn. He points to SHM’s leadership with Project BOOST (www.hospitalmedicine.org/boost) as one example of addressing the utilization of resources in caring for older adults (see “Resources for Improving Transitions in Care,”).
What else can hospitalists do? Going forward, says Dan Fuller, president and co-founder of IN Compass Health in Alpharetta, Ga., it might be a good idea for the SHM Practice Analysis Committee, of which he’s a member, to look at its possible role in the issue.

—Dr. Frederickson
Embrace Reality
Whatever the downstream developments around the Affordable Care Act, Dr. Ginsburg is “confident” that Medicare policies will continue in a direction of reduced reimbursements. Thomas Frederickson, MD, FACP, FHM, MBA, medical director of the hospital medicine service at Alegent Health in Omaha, Neb., agrees with such an assessment. He also believes that hospitalists are in a prime position to improve care delivery at less cost. To do so, though, requires deliberate partnership-building with outpatient providers to better bridge the transitions of care.
At his institution, Dr. Frederickson says, hospitalists invite themselves to primary-care physicians’ (PCP) meetings. This facilitates rapport so that calls to PCPs at discharge not only communicate essential clinical information, but also build confidence in the hospitalists’ care of their patients. As hospitalists demonstrate value, they must intentionally put metrics in place so that administrators appreciate the need to keep the census at a certain level, Dr. Frederickson says.
“We need the time to make these calls, to sit down with families,” he says. “This adds value to our health system and to society at large.”
SHM does a good job, says Dr. Frost, of being part of the conversation as the hospital C-suite focuses more on episodes of care.
“The intensity of that discussion is getting dialed up and will be driven more by government and the payors,” he adds. The challenge going forward will be to bridge those arenas just outside the acute episode of care, where hospitalists have ownership of processes, to those where they do not have as much control. If payors apply broader definitions to the episode of care, Dr. Frost says, hospitalists might be “invited to play an increasing role, that of ‘transitionist.’”
And in that context, he says, hospitalists need to look at length of stay with a new lens.
Partnership-building will become more important as the definition of “episode of care” expands beyond the hospital stay to the post-acute setting.
“Including post-acute care in the episode of care is a core aspect of the whole” value-based purchasing approach, Dr. Ginsburg says. “Hospitals [and hospitalists] will be wise to opt for the model with the greatest potential to reduce costs, particularly costs incurred by other providers.”
Gretchen Henkel is a freelance writer in California.
References
- Centers for Medicare & Medicaid Services. National health expenditures 2011 highlights. Centers for Medicare & Medicaid Services website. Available at: http://www.cms.gov/Research-Statistics-Data-and-Systems/Statistics-Trends-and-Reports/NationalHealthExpendData/Downloads/highlights.pdf. Accessed May 6, 2013. costs how much? Consumer Reports website. Available at: http://www.consumerreports.org/cro/magazine/ 2012/07/that-ct-scan-costs-how-much/index.htm. Accessed Aug. 2, 2012.
- White C, Ginsburg PB. Slower growth in Medicare spending—is this the new normal? N Engl J Med. 2012;366(12):1073-1075.
- Auerbach DI, Kellermann AL. A decade of health care cost growth has wiped out real income gains for an average US family. Health Aff (Millwood). 2011;30(9):1630-1636.
- Milliman Inc. 2012 Milliman Medical Index. Milliman Inc. website. Available at: http://publications.milliman.com/periodicals/mmi/pdfs/milliman-medical-index-2012.pdf. Accessed Aug. 1, 2012.
- Kolata G. Knotty challenges in health care costs. The New York Times website. Available at: http://www.nytimes.com/2012/03/06/health/policy/an-interview-with-victor-fuchs-on-health-care-costs.html. Accessed March 8, 2012.
- Consumer Reports. That CT scan costs how much? Consumer Reports website. Available at: http://www.consumerreports.org/cro/magazine/ 2012/07/that-ct-scan-costs-how-much/index.htm.
Alarms about our nation’s health-care costs have been sounding for well over a decade. According to the Centers for Medicare & Medicaid Services (CMS), spending on U.S. health care doubled between 1999 and 2011, climbing to $2.7 trillion from $1.3 trillion, and now represents 17.9% of the United States’ GDP.1
“The medical care system is bankrupting the country,” Paul B. Ginsburg, PhD, president of the Center for Studying Health System Change (HSC), based in Washington, D.C., says bluntly. A four-decade-long upward spending trend is “unsustainable,” he wrote in the New England Journal of Medicine with Chapin White, PhD, a senior health researcher at HSC.2
Recent reports suggest that rising premiums and out-of-pocket costs are rendering the price of health care untenable for the average consumer. A 2011 RAND Corp. study found that, for the average American family, the rate of increased costs for health care had outpaced growth in earnings from 1999 to 2009.3 And last year, for the first time, the cost of health care for a typical American family of four surpassed $20,000, the annual Milliman Medical Index reported.4
Should hospitalists be concerned, professionally and personally, about these trends? Absolutely, say hospitalist leaders who spoke with The Hospitalist. HM clinicians have much to contribute at both the macro level (addressing systemic causes of overutilization through quality improvement and other initiatives) and at the micro level, by understanding their personal contributions and by engaging patients and their families in shared decision-making.
But getting at and addressing the root causes of rising health-care costs, according to health-care policy analysts and veteran hospitalists, will require major shifts in thinking and processes.
Contributors to Rising Costs
It’s difficult to pinpoint the root causes of the recent surge in health-care costs. Victor Fuchs, emeritus professor of economics and health research and policy at Stanford University, points to the U.S.’ high administrative costs and complicated billing systems.5 A fragmented, nontransparent system for negotiating fees between insurers and providers also plays a role, as demonstrated in a Consumer Reports investigation into geographic variations in costs for common tests and procedures. A complete blood count might be as low as $15 or as high as $105; a colonoscopy ranges from $800 to $3,160.6
Bradley Flansbaum, DO, MPH, SFHM, an SHM Public Policy Committee member and AMA delegate, says rising costs are a provider-specific issue. He challenges colleagues to take an honest look at their own practice patterns to assess whether they’re contributing to overuse of resources (see “A Lesson in Change,”).
“The culture of practice has developed so that this is not going to change overnight,” says Dr. Flansbaum, director of hospitalist services at Lenox Hill Hospital in New York City. That’s because many physicians fail to view their own decisions as a problem. For example, says Dr. Flansbaum, “an oncologist may not identify a third round of chemotherapy as an embodiment of the problem, or a gastroenterologist might not embody the colonoscopy at Year Four instead of Year Five as the problem. We must come to grips with the usual mindset, look in the mirror, and admit, ‘Maybe we are part of the problem.’”
—Bradley Flansbaum, DO, MPH, SFHM
Potential Solutions
Hospitalists, intensivists, and ED clinicians are tasked with finding a balance between being prudent stewards of resources and staying within a comfort zone that promotes patient safety. SHM supports the goals of the ABIM Foundation’s Choosing Wisely campaign, which aims to reduce waste by curtailing duplicative and unnecessary care (see “Better Choices, Better Care,” March 2013). Also included in the campaign (www.ChoosingWisely.org) are the American College of Physicians’ recommendations against low-value testing (e.g. obtaining imaging studies in patients with nonspecific low back pain).
“Those recommendations are not going to solve our health spending problem,” says White, “but they are part of a broader move to give permission to clinicians, based on evidence, to follow more conservative practice patterns.”
Still, counters David I. Auerbach, PhD, a health economist at RAND in Boston and author of the RAND study, “there’s another value to these tests that the cost-effectiveness equations do not always consider, which is, they can bring peace of mind. We’re trying to nudge patients down the pathway that we think is best for them without rationing care. That’s a delicate balance.”
Dr. Flansbaum says SHM’s Public Policy Committee has discussed a variety of issues related to rising costs, although the group has not directly tackled advice in the form of a white paper. He suggests some ways that hospitalists can address cost savings:
- Involve patients in shared decision-making, and discuss the evidence against unnecessary testing;
- Utilize generic medications on discharge, when available, especially if patients are uninsured or have limited drug coverage with their insurance plans;
- Use palliative care whenever appropriate; and
- Adhere to transitional-care standards.
On the macro level, HM has “always been the specialty invited to champion the important discussion relating to resource utilization, and the evidence-based medicine driving that resource utilization,” says Christopher Frost, MD, FHM, medical director of hospital medicine at the Hospital Corporation of America (HCA) in Nashville, Tenn. He points to SHM’s leadership with Project BOOST (www.hospitalmedicine.org/boost) as one example of addressing the utilization of resources in caring for older adults (see “Resources for Improving Transitions in Care,”).
What else can hospitalists do? Going forward, says Dan Fuller, president and co-founder of IN Compass Health in Alpharetta, Ga., it might be a good idea for the SHM Practice Analysis Committee, of which he’s a member, to look at its possible role in the issue.
—Dr. Frederickson
Embrace Reality
Whatever the downstream developments around the Affordable Care Act, Dr. Ginsburg is “confident” that Medicare policies will continue in a direction of reduced reimbursements. Thomas Frederickson, MD, FACP, FHM, MBA, medical director of the hospital medicine service at Alegent Health in Omaha, Neb., agrees with such an assessment. He also believes that hospitalists are in a prime position to improve care delivery at less cost. To do so, though, requires deliberate partnership-building with outpatient providers to better bridge the transitions of care.
At his institution, Dr. Frederickson says, hospitalists invite themselves to primary-care physicians’ (PCP) meetings. This facilitates rapport so that calls to PCPs at discharge not only communicate essential clinical information, but also build confidence in the hospitalists’ care of their patients. As hospitalists demonstrate value, they must intentionally put metrics in place so that administrators appreciate the need to keep the census at a certain level, Dr. Frederickson says.
“We need the time to make these calls, to sit down with families,” he says. “This adds value to our health system and to society at large.”
SHM does a good job, says Dr. Frost, of being part of the conversation as the hospital C-suite focuses more on episodes of care.
“The intensity of that discussion is getting dialed up and will be driven more by government and the payors,” he adds. The challenge going forward will be to bridge those arenas just outside the acute episode of care, where hospitalists have ownership of processes, to those where they do not have as much control. If payors apply broader definitions to the episode of care, Dr. Frost says, hospitalists might be “invited to play an increasing role, that of ‘transitionist.’”
And in that context, he says, hospitalists need to look at length of stay with a new lens.
Partnership-building will become more important as the definition of “episode of care” expands beyond the hospital stay to the post-acute setting.
“Including post-acute care in the episode of care is a core aspect of the whole” value-based purchasing approach, Dr. Ginsburg says. “Hospitals [and hospitalists] will be wise to opt for the model with the greatest potential to reduce costs, particularly costs incurred by other providers.”
Gretchen Henkel is a freelance writer in California.
References
- Centers for Medicare & Medicaid Services. National health expenditures 2011 highlights. Centers for Medicare & Medicaid Services website. Available at: http://www.cms.gov/Research-Statistics-Data-and-Systems/Statistics-Trends-and-Reports/NationalHealthExpendData/Downloads/highlights.pdf. Accessed May 6, 2013. costs how much? Consumer Reports website. Available at: http://www.consumerreports.org/cro/magazine/ 2012/07/that-ct-scan-costs-how-much/index.htm. Accessed Aug. 2, 2012.
- White C, Ginsburg PB. Slower growth in Medicare spending—is this the new normal? N Engl J Med. 2012;366(12):1073-1075.
- Auerbach DI, Kellermann AL. A decade of health care cost growth has wiped out real income gains for an average US family. Health Aff (Millwood). 2011;30(9):1630-1636.
- Milliman Inc. 2012 Milliman Medical Index. Milliman Inc. website. Available at: http://publications.milliman.com/periodicals/mmi/pdfs/milliman-medical-index-2012.pdf. Accessed Aug. 1, 2012.
- Kolata G. Knotty challenges in health care costs. The New York Times website. Available at: http://www.nytimes.com/2012/03/06/health/policy/an-interview-with-victor-fuchs-on-health-care-costs.html. Accessed March 8, 2012.
- Consumer Reports. That CT scan costs how much? Consumer Reports website. Available at: http://www.consumerreports.org/cro/magazine/ 2012/07/that-ct-scan-costs-how-much/index.htm.
Alarms about our nation’s health-care costs have been sounding for well over a decade. According to the Centers for Medicare & Medicaid Services (CMS), spending on U.S. health care doubled between 1999 and 2011, climbing to $2.7 trillion from $1.3 trillion, and now represents 17.9% of the United States’ GDP.1
“The medical care system is bankrupting the country,” Paul B. Ginsburg, PhD, president of the Center for Studying Health System Change (HSC), based in Washington, D.C., says bluntly. A four-decade-long upward spending trend is “unsustainable,” he wrote in the New England Journal of Medicine with Chapin White, PhD, a senior health researcher at HSC.2
Recent reports suggest that rising premiums and out-of-pocket costs are rendering the price of health care untenable for the average consumer. A 2011 RAND Corp. study found that, for the average American family, the rate of increased costs for health care had outpaced growth in earnings from 1999 to 2009.3 And last year, for the first time, the cost of health care for a typical American family of four surpassed $20,000, the annual Milliman Medical Index reported.4
Should hospitalists be concerned, professionally and personally, about these trends? Absolutely, say hospitalist leaders who spoke with The Hospitalist. HM clinicians have much to contribute at both the macro level (addressing systemic causes of overutilization through quality improvement and other initiatives) and at the micro level, by understanding their personal contributions and by engaging patients and their families in shared decision-making.
But getting at and addressing the root causes of rising health-care costs, according to health-care policy analysts and veteran hospitalists, will require major shifts in thinking and processes.
Contributors to Rising Costs
It’s difficult to pinpoint the root causes of the recent surge in health-care costs. Victor Fuchs, emeritus professor of economics and health research and policy at Stanford University, points to the U.S.’ high administrative costs and complicated billing systems.5 A fragmented, nontransparent system for negotiating fees between insurers and providers also plays a role, as demonstrated in a Consumer Reports investigation into geographic variations in costs for common tests and procedures. A complete blood count might be as low as $15 or as high as $105; a colonoscopy ranges from $800 to $3,160.6
Bradley Flansbaum, DO, MPH, SFHM, an SHM Public Policy Committee member and AMA delegate, says rising costs are a provider-specific issue. He challenges colleagues to take an honest look at their own practice patterns to assess whether they’re contributing to overuse of resources (see “A Lesson in Change,”).
“The culture of practice has developed so that this is not going to change overnight,” says Dr. Flansbaum, director of hospitalist services at Lenox Hill Hospital in New York City. That’s because many physicians fail to view their own decisions as a problem. For example, says Dr. Flansbaum, “an oncologist may not identify a third round of chemotherapy as an embodiment of the problem, or a gastroenterologist might not embody the colonoscopy at Year Four instead of Year Five as the problem. We must come to grips with the usual mindset, look in the mirror, and admit, ‘Maybe we are part of the problem.’”
—Bradley Flansbaum, DO, MPH, SFHM
Potential Solutions
Hospitalists, intensivists, and ED clinicians are tasked with finding a balance between being prudent stewards of resources and staying within a comfort zone that promotes patient safety. SHM supports the goals of the ABIM Foundation’s Choosing Wisely campaign, which aims to reduce waste by curtailing duplicative and unnecessary care (see “Better Choices, Better Care,” March 2013). Also included in the campaign (www.ChoosingWisely.org) are the American College of Physicians’ recommendations against low-value testing (e.g. obtaining imaging studies in patients with nonspecific low back pain).
“Those recommendations are not going to solve our health spending problem,” says White, “but they are part of a broader move to give permission to clinicians, based on evidence, to follow more conservative practice patterns.”
Still, counters David I. Auerbach, PhD, a health economist at RAND in Boston and author of the RAND study, “there’s another value to these tests that the cost-effectiveness equations do not always consider, which is, they can bring peace of mind. We’re trying to nudge patients down the pathway that we think is best for them without rationing care. That’s a delicate balance.”
Dr. Flansbaum says SHM’s Public Policy Committee has discussed a variety of issues related to rising costs, although the group has not directly tackled advice in the form of a white paper. He suggests some ways that hospitalists can address cost savings:
- Involve patients in shared decision-making, and discuss the evidence against unnecessary testing;
- Utilize generic medications on discharge, when available, especially if patients are uninsured or have limited drug coverage with their insurance plans;
- Use palliative care whenever appropriate; and
- Adhere to transitional-care standards.
On the macro level, HM has “always been the specialty invited to champion the important discussion relating to resource utilization, and the evidence-based medicine driving that resource utilization,” says Christopher Frost, MD, FHM, medical director of hospital medicine at the Hospital Corporation of America (HCA) in Nashville, Tenn. He points to SHM’s leadership with Project BOOST (www.hospitalmedicine.org/boost) as one example of addressing the utilization of resources in caring for older adults (see “Resources for Improving Transitions in Care,”).
What else can hospitalists do? Going forward, says Dan Fuller, president and co-founder of IN Compass Health in Alpharetta, Ga., it might be a good idea for the SHM Practice Analysis Committee, of which he’s a member, to look at its possible role in the issue.
—Dr. Frederickson
Embrace Reality
Whatever the downstream developments around the Affordable Care Act, Dr. Ginsburg is “confident” that Medicare policies will continue in a direction of reduced reimbursements. Thomas Frederickson, MD, FACP, FHM, MBA, medical director of the hospital medicine service at Alegent Health in Omaha, Neb., agrees with such an assessment. He also believes that hospitalists are in a prime position to improve care delivery at less cost. To do so, though, requires deliberate partnership-building with outpatient providers to better bridge the transitions of care.
At his institution, Dr. Frederickson says, hospitalists invite themselves to primary-care physicians’ (PCP) meetings. This facilitates rapport so that calls to PCPs at discharge not only communicate essential clinical information, but also build confidence in the hospitalists’ care of their patients. As hospitalists demonstrate value, they must intentionally put metrics in place so that administrators appreciate the need to keep the census at a certain level, Dr. Frederickson says.
“We need the time to make these calls, to sit down with families,” he says. “This adds value to our health system and to society at large.”
SHM does a good job, says Dr. Frost, of being part of the conversation as the hospital C-suite focuses more on episodes of care.
“The intensity of that discussion is getting dialed up and will be driven more by government and the payors,” he adds. The challenge going forward will be to bridge those arenas just outside the acute episode of care, where hospitalists have ownership of processes, to those where they do not have as much control. If payors apply broader definitions to the episode of care, Dr. Frost says, hospitalists might be “invited to play an increasing role, that of ‘transitionist.’”
And in that context, he says, hospitalists need to look at length of stay with a new lens.
Partnership-building will become more important as the definition of “episode of care” expands beyond the hospital stay to the post-acute setting.
“Including post-acute care in the episode of care is a core aspect of the whole” value-based purchasing approach, Dr. Ginsburg says. “Hospitals [and hospitalists] will be wise to opt for the model with the greatest potential to reduce costs, particularly costs incurred by other providers.”
Gretchen Henkel is a freelance writer in California.
References
- Centers for Medicare & Medicaid Services. National health expenditures 2011 highlights. Centers for Medicare & Medicaid Services website. Available at: http://www.cms.gov/Research-Statistics-Data-and-Systems/Statistics-Trends-and-Reports/NationalHealthExpendData/Downloads/highlights.pdf. Accessed May 6, 2013. costs how much? Consumer Reports website. Available at: http://www.consumerreports.org/cro/magazine/ 2012/07/that-ct-scan-costs-how-much/index.htm. Accessed Aug. 2, 2012.
- White C, Ginsburg PB. Slower growth in Medicare spending—is this the new normal? N Engl J Med. 2012;366(12):1073-1075.
- Auerbach DI, Kellermann AL. A decade of health care cost growth has wiped out real income gains for an average US family. Health Aff (Millwood). 2011;30(9):1630-1636.
- Milliman Inc. 2012 Milliman Medical Index. Milliman Inc. website. Available at: http://publications.milliman.com/periodicals/mmi/pdfs/milliman-medical-index-2012.pdf. Accessed Aug. 1, 2012.
- Kolata G. Knotty challenges in health care costs. The New York Times website. Available at: http://www.nytimes.com/2012/03/06/health/policy/an-interview-with-victor-fuchs-on-health-care-costs.html. Accessed March 8, 2012.
- Consumer Reports. That CT scan costs how much? Consumer Reports website. Available at: http://www.consumerreports.org/cro/magazine/ 2012/07/that-ct-scan-costs-how-much/index.htm.
Letters: Medicare Official Says 'Physician Compare' Website Does Not Provide Performance Data on Individual Doctors
I read the article “Call for Transparency in Health-Care Performance Results to Impact Hospitalists” (January 2013, p. 47) by Shaun Frost, MD, SFHM, president of the Society of Hospital Medicine, with interest. I’d like to clarify a key point about Physician Compare. In the article, the statement that the Physician Compare website (www.medicare.gov/find-a-doctor) provides performance information on individual doctors is inaccurate.
The Affordable Care Act (ACA) states that the Centers for Medicare & Medicaid Services (CMS) must have a plan in place by Jan. 1, 2013, to include quality-of-care information on the site. To meet that requirement, CMS has established a plan that initiates a phased approach to public reporting. The 2012 Physician Fee Schedule (PFS) Final Rule was the first step in that phased approach. This rule established that the first measures to be reported on the site would be group-level measures for data collected no sooner than program year 2012. A second critical step is the 2013 PFS Proposed Rule, which outlines a longer-term public reporting plan. According to this plan, we expect the first set of group-level quality measure data to be included on the site in calendar year 2014. We are targeting publishing individual-level quality measures no sooner than 2015 reflecting data collected in program year 2014, if technically feasible.
As you may be aware, Physician Compare is undergoing a redesign to significantly improve the underlying database and thus the information on Physician Compare, as well as the ease of use and functionality of the site. We’ll be unveiling the redesigned site soon. We welcome your feedback and look forward to maintaining a dialogue with you as Physician Compare continues to evolve.
Rashaan Byers, MPH, social science research analyst, Centers forMedicare & Medicaid Services, Center for Clinical Standards & Quality, Quality Measurement & Health Assessment Group
Dr. Frost responds:
I thank Mr. Byers for his clarification regarding the current content on the CMS Physician Compare website, and agree that at the present time the website does not report individual physician clinical performance data.
Physician Compare, however, does currently report if an individual physician participated in the CMS Physician Quality Reporting System (PQRS) by stating “this professional chose to take part in Medicare’s PQRS, and reported quality information satisfactorily for the year 2010.” For those physicians who did not participate in PQRS, their personal website pages do not make reference to the PQRS program.
As the intent of transparency is to educate consumers to make informed choices about where to seek health care, care providers should know that their participation in PQRS is currently publically reported. It is, therefore, possible that patient decisions about whom to seek care from may be influenced by this.
As acknowledged in my January 2013 column in The Hospitalist, Physician Compare currently reports very little information. We should expect this to change, however, as Medicare moves forward with developing a plan to publically report valid and reliable individual physician performance metrics. CMS’ clarification of the timeline by which we can expect to see more detailed information is thus greatly appreciated.
The take-home message for hospitalists is that public reporting of care provider performance will become increasingly comprehensive and transparent in the future. As pointed out, CMS’ present plan targets the publication of individual, physician-level quality measures as soon as 2015, which will reflect actual performance during program year 2014. The measurement period is thus less than one year away, so it behooves us all to focus ever more intently on delivering high-value healthcare.
Shaun Frost, MD, SFHM, past president, SHM
I read the article “Call for Transparency in Health-Care Performance Results to Impact Hospitalists” (January 2013, p. 47) by Shaun Frost, MD, SFHM, president of the Society of Hospital Medicine, with interest. I’d like to clarify a key point about Physician Compare. In the article, the statement that the Physician Compare website (www.medicare.gov/find-a-doctor) provides performance information on individual doctors is inaccurate.
The Affordable Care Act (ACA) states that the Centers for Medicare & Medicaid Services (CMS) must have a plan in place by Jan. 1, 2013, to include quality-of-care information on the site. To meet that requirement, CMS has established a plan that initiates a phased approach to public reporting. The 2012 Physician Fee Schedule (PFS) Final Rule was the first step in that phased approach. This rule established that the first measures to be reported on the site would be group-level measures for data collected no sooner than program year 2012. A second critical step is the 2013 PFS Proposed Rule, which outlines a longer-term public reporting plan. According to this plan, we expect the first set of group-level quality measure data to be included on the site in calendar year 2014. We are targeting publishing individual-level quality measures no sooner than 2015 reflecting data collected in program year 2014, if technically feasible.
As you may be aware, Physician Compare is undergoing a redesign to significantly improve the underlying database and thus the information on Physician Compare, as well as the ease of use and functionality of the site. We’ll be unveiling the redesigned site soon. We welcome your feedback and look forward to maintaining a dialogue with you as Physician Compare continues to evolve.
Rashaan Byers, MPH, social science research analyst, Centers forMedicare & Medicaid Services, Center for Clinical Standards & Quality, Quality Measurement & Health Assessment Group
Dr. Frost responds:
I thank Mr. Byers for his clarification regarding the current content on the CMS Physician Compare website, and agree that at the present time the website does not report individual physician clinical performance data.
Physician Compare, however, does currently report if an individual physician participated in the CMS Physician Quality Reporting System (PQRS) by stating “this professional chose to take part in Medicare’s PQRS, and reported quality information satisfactorily for the year 2010.” For those physicians who did not participate in PQRS, their personal website pages do not make reference to the PQRS program.
As the intent of transparency is to educate consumers to make informed choices about where to seek health care, care providers should know that their participation in PQRS is currently publically reported. It is, therefore, possible that patient decisions about whom to seek care from may be influenced by this.
As acknowledged in my January 2013 column in The Hospitalist, Physician Compare currently reports very little information. We should expect this to change, however, as Medicare moves forward with developing a plan to publically report valid and reliable individual physician performance metrics. CMS’ clarification of the timeline by which we can expect to see more detailed information is thus greatly appreciated.
The take-home message for hospitalists is that public reporting of care provider performance will become increasingly comprehensive and transparent in the future. As pointed out, CMS’ present plan targets the publication of individual, physician-level quality measures as soon as 2015, which will reflect actual performance during program year 2014. The measurement period is thus less than one year away, so it behooves us all to focus ever more intently on delivering high-value healthcare.
Shaun Frost, MD, SFHM, past president, SHM
I read the article “Call for Transparency in Health-Care Performance Results to Impact Hospitalists” (January 2013, p. 47) by Shaun Frost, MD, SFHM, president of the Society of Hospital Medicine, with interest. I’d like to clarify a key point about Physician Compare. In the article, the statement that the Physician Compare website (www.medicare.gov/find-a-doctor) provides performance information on individual doctors is inaccurate.
The Affordable Care Act (ACA) states that the Centers for Medicare & Medicaid Services (CMS) must have a plan in place by Jan. 1, 2013, to include quality-of-care information on the site. To meet that requirement, CMS has established a plan that initiates a phased approach to public reporting. The 2012 Physician Fee Schedule (PFS) Final Rule was the first step in that phased approach. This rule established that the first measures to be reported on the site would be group-level measures for data collected no sooner than program year 2012. A second critical step is the 2013 PFS Proposed Rule, which outlines a longer-term public reporting plan. According to this plan, we expect the first set of group-level quality measure data to be included on the site in calendar year 2014. We are targeting publishing individual-level quality measures no sooner than 2015 reflecting data collected in program year 2014, if technically feasible.
As you may be aware, Physician Compare is undergoing a redesign to significantly improve the underlying database and thus the information on Physician Compare, as well as the ease of use and functionality of the site. We’ll be unveiling the redesigned site soon. We welcome your feedback and look forward to maintaining a dialogue with you as Physician Compare continues to evolve.
Rashaan Byers, MPH, social science research analyst, Centers forMedicare & Medicaid Services, Center for Clinical Standards & Quality, Quality Measurement & Health Assessment Group
Dr. Frost responds:
I thank Mr. Byers for his clarification regarding the current content on the CMS Physician Compare website, and agree that at the present time the website does not report individual physician clinical performance data.
Physician Compare, however, does currently report if an individual physician participated in the CMS Physician Quality Reporting System (PQRS) by stating “this professional chose to take part in Medicare’s PQRS, and reported quality information satisfactorily for the year 2010.” For those physicians who did not participate in PQRS, their personal website pages do not make reference to the PQRS program.
As the intent of transparency is to educate consumers to make informed choices about where to seek health care, care providers should know that their participation in PQRS is currently publically reported. It is, therefore, possible that patient decisions about whom to seek care from may be influenced by this.
As acknowledged in my January 2013 column in The Hospitalist, Physician Compare currently reports very little information. We should expect this to change, however, as Medicare moves forward with developing a plan to publically report valid and reliable individual physician performance metrics. CMS’ clarification of the timeline by which we can expect to see more detailed information is thus greatly appreciated.
The take-home message for hospitalists is that public reporting of care provider performance will become increasingly comprehensive and transparent in the future. As pointed out, CMS’ present plan targets the publication of individual, physician-level quality measures as soon as 2015, which will reflect actual performance during program year 2014. The measurement period is thus less than one year away, so it behooves us all to focus ever more intently on delivering high-value healthcare.
Shaun Frost, MD, SFHM, past president, SHM
Effective Clinical Documentation Can Influence Medicare Reimbursement

Back in the 1980s, I would go by medical records every day or two and find, on the front of the charts of my recently discharged patients, a form listing the diagnoses the hospital was billing to Medicare. Before the hospital could submit a patient’s bill, the attending physician was required to review the form and, by signing it, indicate agreement.
The requirement for this signature by the physician went away a long time ago and in my memory is one of the very few examples of reducing a doctor’s paperwork.
For my first few months in practice, I regularly would seek out the people who completed the form and explain they had misunderstood the patient’s clinical situation. “The main issue was a urinary tract infection,” I would say, “but you listed diabetes as the principal diagnosis.”
I don’t ever remember them changing anything based on my feedback. Instead, they explained to me that, for billing purposes, it was legitimate to list diabetes as the principal diagnosis because it had the additional benefit of resulting in a higher payment to the hospital than having “urinary tract infection” listed first.
Such was my introduction to the world of documentation and coding for hospital billing purposes and how it can sometimes differ significantly from the way a doctor sees the clinical picture. Things have evolved a lot since then, but the way doctors document medical conditions still has a huge influence on hospital reimbursement.
Hospital CDI Programs
About 80% of hospitals have formal clinical documentation improvement (CDI) programs to help ensure all clinical conditions are captured and described in the medical record in ways that are valuable for billing and other recordkeeping purposes. These programs might lead to you receive queries about your documentation. For example, you might be asked to clarify whether your patient’s pneumonia might be on the basis of aspiration.
Within SHM’s Code-H program, Dr. Richard Pinson, a former ED physician who now works with Houston-based HCQ Consulting, has a good presentation explaining these documentation issues. In it, he makes the point that, in addition to influencing how hospitals are paid, the way various conditions are documented also influences quality ratings.
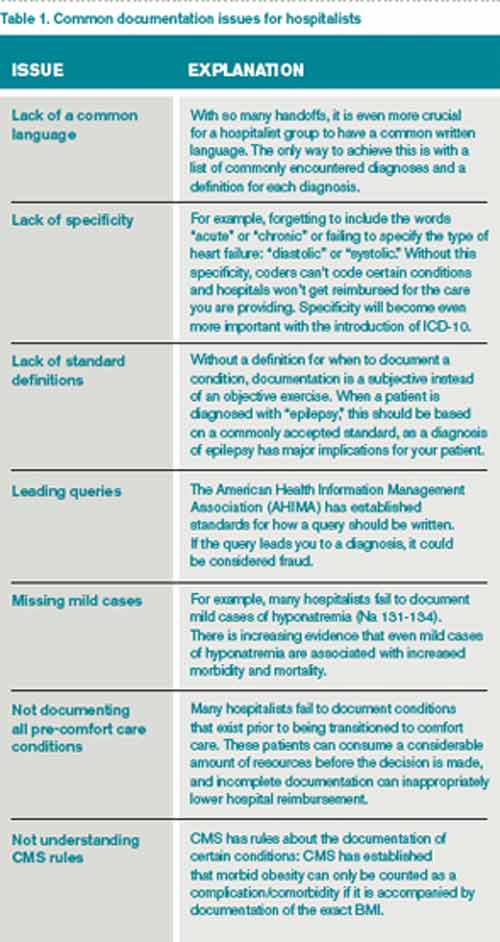
Novel Approach
The most common approach to engaging hospitalists in CDI initiatives is to have them attend a presentation on the topic, then put in place documentation specialists who generate queries asking the doctor to clarify diagnoses when it might influence payment, severity of illness determination, etc. Dr. Kenji Asakura, a Seattle hospitalist, and Erik Ordal, MBA, have a company called ClinIntell that analyzes each hospitalist (or other specialty) group’s historical patient mix and trains them on the documentation issues that they see most often. The idea of this focused approach is to make “documentation queries” unnecessary, or at least much less necessary. The benefits of this approach are many, including reducing or eliminating the risk of “leading queries”—that is, queries that seem to encourage the doctor to document a diagnosis because it is an advantage to the hospital rather than a well-considered medical opinion. Leading queries can be regarded as fraudulent and can get a lot of people in trouble.
I asked Kenji and Erik if they could provide me with a list of common documentation issues that most hospitalists need to know more about. Table 1 is what they came up with. I hope it helps you and your practice.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is co-director for SHM's "Best Practices in Managing a Hospital Medicine Program" course. Write to him at [email protected].
Back in the 1980s, I would go by medical records every day or two and find, on the front of the charts of my recently discharged patients, a form listing the diagnoses the hospital was billing to Medicare. Before the hospital could submit a patient’s bill, the attending physician was required to review the form and, by signing it, indicate agreement.
The requirement for this signature by the physician went away a long time ago and in my memory is one of the very few examples of reducing a doctor’s paperwork.
For my first few months in practice, I regularly would seek out the people who completed the form and explain they had misunderstood the patient’s clinical situation. “The main issue was a urinary tract infection,” I would say, “but you listed diabetes as the principal diagnosis.”
I don’t ever remember them changing anything based on my feedback. Instead, they explained to me that, for billing purposes, it was legitimate to list diabetes as the principal diagnosis because it had the additional benefit of resulting in a higher payment to the hospital than having “urinary tract infection” listed first.
Such was my introduction to the world of documentation and coding for hospital billing purposes and how it can sometimes differ significantly from the way a doctor sees the clinical picture. Things have evolved a lot since then, but the way doctors document medical conditions still has a huge influence on hospital reimbursement.
Hospital CDI Programs
About 80% of hospitals have formal clinical documentation improvement (CDI) programs to help ensure all clinical conditions are captured and described in the medical record in ways that are valuable for billing and other recordkeeping purposes. These programs might lead to you receive queries about your documentation. For example, you might be asked to clarify whether your patient’s pneumonia might be on the basis of aspiration.
Within SHM’s Code-H program, Dr. Richard Pinson, a former ED physician who now works with Houston-based HCQ Consulting, has a good presentation explaining these documentation issues. In it, he makes the point that, in addition to influencing how hospitals are paid, the way various conditions are documented also influences quality ratings.
Novel Approach
The most common approach to engaging hospitalists in CDI initiatives is to have them attend a presentation on the topic, then put in place documentation specialists who generate queries asking the doctor to clarify diagnoses when it might influence payment, severity of illness determination, etc. Dr. Kenji Asakura, a Seattle hospitalist, and Erik Ordal, MBA, have a company called ClinIntell that analyzes each hospitalist (or other specialty) group’s historical patient mix and trains them on the documentation issues that they see most often. The idea of this focused approach is to make “documentation queries” unnecessary, or at least much less necessary. The benefits of this approach are many, including reducing or eliminating the risk of “leading queries”—that is, queries that seem to encourage the doctor to document a diagnosis because it is an advantage to the hospital rather than a well-considered medical opinion. Leading queries can be regarded as fraudulent and can get a lot of people in trouble.
I asked Kenji and Erik if they could provide me with a list of common documentation issues that most hospitalists need to know more about. Table 1 is what they came up with. I hope it helps you and your practice.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is co-director for SHM's "Best Practices in Managing a Hospital Medicine Program" course. Write to him at [email protected].
Back in the 1980s, I would go by medical records every day or two and find, on the front of the charts of my recently discharged patients, a form listing the diagnoses the hospital was billing to Medicare. Before the hospital could submit a patient’s bill, the attending physician was required to review the form and, by signing it, indicate agreement.
The requirement for this signature by the physician went away a long time ago and in my memory is one of the very few examples of reducing a doctor’s paperwork.
For my first few months in practice, I regularly would seek out the people who completed the form and explain they had misunderstood the patient’s clinical situation. “The main issue was a urinary tract infection,” I would say, “but you listed diabetes as the principal diagnosis.”
I don’t ever remember them changing anything based on my feedback. Instead, they explained to me that, for billing purposes, it was legitimate to list diabetes as the principal diagnosis because it had the additional benefit of resulting in a higher payment to the hospital than having “urinary tract infection” listed first.
Such was my introduction to the world of documentation and coding for hospital billing purposes and how it can sometimes differ significantly from the way a doctor sees the clinical picture. Things have evolved a lot since then, but the way doctors document medical conditions still has a huge influence on hospital reimbursement.
Hospital CDI Programs
About 80% of hospitals have formal clinical documentation improvement (CDI) programs to help ensure all clinical conditions are captured and described in the medical record in ways that are valuable for billing and other recordkeeping purposes. These programs might lead to you receive queries about your documentation. For example, you might be asked to clarify whether your patient’s pneumonia might be on the basis of aspiration.
Within SHM’s Code-H program, Dr. Richard Pinson, a former ED physician who now works with Houston-based HCQ Consulting, has a good presentation explaining these documentation issues. In it, he makes the point that, in addition to influencing how hospitals are paid, the way various conditions are documented also influences quality ratings.
Novel Approach
The most common approach to engaging hospitalists in CDI initiatives is to have them attend a presentation on the topic, then put in place documentation specialists who generate queries asking the doctor to clarify diagnoses when it might influence payment, severity of illness determination, etc. Dr. Kenji Asakura, a Seattle hospitalist, and Erik Ordal, MBA, have a company called ClinIntell that analyzes each hospitalist (or other specialty) group’s historical patient mix and trains them on the documentation issues that they see most often. The idea of this focused approach is to make “documentation queries” unnecessary, or at least much less necessary. The benefits of this approach are many, including reducing or eliminating the risk of “leading queries”—that is, queries that seem to encourage the doctor to document a diagnosis because it is an advantage to the hospital rather than a well-considered medical opinion. Leading queries can be regarded as fraudulent and can get a lot of people in trouble.
I asked Kenji and Erik if they could provide me with a list of common documentation issues that most hospitalists need to know more about. Table 1 is what they came up with. I hope it helps you and your practice.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is co-director for SHM's "Best Practices in Managing a Hospital Medicine Program" course. Write to him at [email protected].