User login
As Medicare Auditors Seek to Rein in Costs, Hospital Admission Decisions Are Under Microscope
The government has made extensive efforts to combat fraud in the Medicare and Medicaid programs, recovering a record $4.2 billion in fiscal 2012 from individuals and companies trying to cheat the system. One of the largest sources of recovered monies is the Recovery Audit Contractor (RAC) program.
The RAC program was created through the Medicare Modernization Act of 2003 (MMA) to identify and recover improper Medicare payments to health-care providers under fee-for-service (FFS) Medicare plans. The goal of the RAC program is to identify improper payments made on claims of health-care services provided to Medicare beneficiaries. Improper payments could be overpayments or underpayments. Hospitals have been hit by the audits, with recoveries reaching $3.6 billion since the national program launched in 2010, according to Centers for Medicare & Medicaid Services (CMS) data.1 About $895 million was reclaimed from just six states during the RAC Demonstration Project between 2005 and 2008.1,2
CMS is more alert on the medical necessity of one-day length of stay (LOS) for inpatient admissions and is trying to detect and reduce Medicare waste, fraud, and abuse. Hospital charges represent about a third of the $718 billion spent on U.S. health care annually. Medicare reimbursement is a major source of revenue for hospitals, but some hospitals claim Medicare pays them only 93% to 97% of what it costs to provide patient care, whereas private insurers pay between 115% and 125% of those costs.3,4 These data suggest that private insurers are paying hospitals far more than they need to make up for Medicare’s “underpayment.”
So the first question is: Do hospitals overcharge for care? The next question is: What can be done? Or, in today’s economy, what is being done?
How It All Works
When an RAC determines that a provider was paid for inpatient hospital services but that the patient in question should have been treated as an outpatient, CMS takes back the entire Part A payment. Moreover, CMS takes the position that once an inpatient claim paid under Medicare Part A is later denied (usually years later), the hospital cannot receive Medicare Part B payment except for a few ancillary services. As a result, when an RAC concludes that a hospital should have provided items and services on an outpatient basis rather than an inpatient basis, the hospital ends up receiving little, if any, reimbursement for reasonable and medically necessary items and services provided.5,6
RACs function through a different model. They keep a contingency percentage—9% to 12.5%—of the entire Part A payment.5
Imagine a situation in which a physician decides that a patient needs to be admitted to the hospital for a surgical procedure, and the cost of care provided to the patient—surgery, drugs, and the like—amounts to $20,000. CMS reimburses the hospital under Part A. Two years later, an RAC employee reviewing hospital records overrules the physician’s judgment and decides the patient should have received basically the same care but on an outpatient basis. That decision, taken together with CMS’ Payment Denial Policy, means the hospital will end up receiving essentially no payment for the surgery and other care it provided. The RAC, by contrast, will receive approximately $2,000 for that one case alone.
To Admit or Not to Admit
Medicare expects attending physicians and physician reviewers to make the appropriate bedding status based on severity of signs and symptoms, comorbid and complicating conditions, and the practicality of outpatient management.
Let’s take two examples of patients presenting with acute asthma exacerbation (AAE) to differentiate observation and inpatient status. Asthma affects 20 million Americans, and 450,000 patients present to the ED annually with AAE. One third of these patients are hospitalized, which translates to more than $1 billion in costs annually.
Case 1: A 62-year-old female presents with two weeks of progressive shortness of breath and cough productive of white sputum. She has a history of asthma and hypertension. She presented to the ED with blood pressure of 140/90, heart rate of 101, respiratory rate of 20, temperature of 99.6°F, and pulse oximetry of 93% on room air, which increased to 99% on 2L of oxygen. She was given two breathing treatments with albuterol in the ED, IV methylprednisolone, and IV magnesium sulphate. Over the course of two hours, her wheezes improved, her heart rate decreased to 90 BPM, and her oxygen requirements were weaned to 1L of oxygen. Her WBC count was 9,800, with a potassium level of 4.0 and a creatinine level of 1.0. Her EKG showed sinus tachycardia, and her chest X-ray was negative for any infiltrates. The ED physician called the hospitalist for admission. What status should she be in?
Case 2: A 62-year-old female presents with a three-day history of shortness of breath and wheezing associated with vomiting. She was sent from her PCP’s office for asthma exacerbation and failure of resolution of symptoms despite one week of oral antibiotics and prednisone. Her past medical history includes asthma, diastolic congestive heart failure, hypertension, diabetes, and end-stage renal disease on hemodialysis. She presented to the ED with blood pressure of 90/63, pulse of 120, temperature of 97.7°F, respiratory rate of 24, and pulse oximetry of 89% on room air. She had bilateral wheezes on respiratory examination, and her WBC was 16,500, with a creatinine level of 3.5 and BNP level of 190. Her chest X-ray showed peribronchial thickening, and an EKG showed sinus tachycardia. She was given IV Solu-Medrol and two breathing treatments with albuterol, and the hospitalist was called for admission. What status should she be in?
Case 1 answer: Observation. The medical predictability of adverse clinical outcome from AAE is low due to hemodynamic stability, absence of fever, improvement in hypoxia, and negative chest X-ray for acute bronchopulmonary process in the setting of normal blood counts. She improved dramatically in the ED with no history of previous intubation or hospitalization or use of previous steroids. Her oxygen requirements decreased within 12 hours of first treatment. Even though FEV1 was not monitored, there is documented improvement in her vital signs as well as respiratory examination.
Case 2 answer: Inpatient. The medical predictability of adverse clinical outcome is significant due to hemodynamic instability evidenced by hypotension, tachycardia, and hypoxia; wheezes on respiratory examination with leukocytosis; and abnormal chest X-ray in the setting of comorbid diseases, such as end-stage renal disease and congestive heart failure.
The treatments given to both patients were similar; however, Case 2 had a higher predictability of adverse clinical outcome and would require medical evaluation and management that would exceed 24 hours. An inpatient level of care is justified based on her clinical presentation, comorbidities, and the risk for adverse clinical outcomes.
It is important that the patient be described appropriately in the medical record to support the status. Documentation should include clinical decision-making and rationale of the attending, objective findings, and the treatment given in the ED as well as the treatment planned during the hospitalization. It is expected that the physician will document the possibility and probability of adverse clinical outcome as well as follow evidence-based guidelines for treatment.
Financial Facts
The AHA collects data and anecdotal evidence from member hospitals regarding the RAC program and its effects. Those data show the following:
- More than 95% of the general medical-surgical hospitals that provided information to the AHA have been targeted by RACs;
- RACs have demanded more than a half-million medical records to audit;
- Many audits result in RAC determinations of “overpayment”; and
- Of those overpayment determinations, more than 60% relate to one- or two-day inpatient admissions that RACs deem medically unnecessary.
Hospitals thus have been required to give back hundreds of millions of dollars per year due to RAC determinations that services should have been provided in an outpatient, rather than inpatient, setting. In the first quarter of 2012 alone, information provided to the AHA by hospitals shows that they were forced to repay $236 million for medically necessary items and services that RACs deemed should have been provided on an outpatient, rather than inpatient, basis. And this amount does not include the millions of dollars recovered from hospitals that did not report data to the AHA.
The RAC program has been a continued financial success for CMS and the auditors: RACs collected $1.86 billion in overpayments from October 2009 through March 2012. Over that same time period, RACs identified only $245.2 million in underpayments.7
The government, no doubt, is on a mission to rein in health-care costs. All stakeholders in the system, including hospitalists and administrations, need extensive education to document appropriate patient status to ensure accurate reimbursement and prevent the fallout of future repayments.
Dr. Pahuja is founder and CEO of Aerolib Healthcare Solutions (aerolib.com). He is pursuing his MBA in health-care administration from the Isenberg School of Management at the University of Massachusetts in Amherst.
References
- PR Web. Medicare anti-fraud recovered $19 billion, how much for private self-insured plans? Fiduciary overpayment recovery programs announced from ERISAclaim.com. PR Web website. Available at: http://www.prweb.com/releases/2013/3/prweb10501376.htm. Accessed April 4, 2013.
- Viebeck E. GAO reports billions in overpayments to private Medicare plans. The Hill website. Available at: http://thehill.com/blogs/healthwatch/medicare/286041-gao-reports-billions-in-overpayments-to-private-medicare-plans#ixzz2NASaVVIK. Accessed April 4, 2013.
- Centers for Medicare & Medicare Services. Cost reports. Centers for Medicare & Medicare Services website. Available at: http://www.cms.gov/Research-Statistics-Data-and-Systems/Files-for-Order/CostReports/index.html. Accessed April 4, 2013.
- Whelan D. America’s most profitable hospitals. Forbes website. Available at: http://www.forbes.com/2010/08/30/profitable-hospitals-hca-healthcare-business-mayo-clinic.html. Accessed April 4, 2013.
- American Medical Association. Recovery Audit Contractors. American Medical Association website. Available at: http://www.ama-assn.org/ama/pub/physician-resources/solutions-managing-your-practice/coding-billing-insurance/medicare/recovery-audit-contractors.page. Accessed April 4, 2013.
- American Hospital Association, Missouri Baptist Sullivan Hospital, Munson Medical Center, Lancaster General Hospital, and Trinity Health Corporation v. Kathleen Sebelius. American Hospital Association website. Available at: http://www.aha.org/content/12/121101-aha-hhs-medicare-com.pdf. Accessed March 12, 2013.
- Centers for Medicare & Medicare Services. Medicare fee-for-service Recovery Audit Program, May 2012. Centers for Medicare & Medicare Services website. Available at: http://www.cms.gov/Research-Statistics-Data-and-Systems/Monitoring-Programs/Recovery-Audit-Program/Downloads/National-Program-Corrections-FY-2012-2nd-Qtr.pdf. Accessed April 4, 2013.
- Centers for Medicare & Medicaid Services. FY 2014 IPPS proposed rule home page items. Centers for Medicare & Medicaid Services website. Available at: http://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/AcuteInpatientPPS/FY-2014-IPPS-Proposed-Rule-Home-Page-Items/FY-2014-IPPS-Proposed-Rule-CMS-1599-P-Regulations.html. Accessed June 10, 2013.
The government has made extensive efforts to combat fraud in the Medicare and Medicaid programs, recovering a record $4.2 billion in fiscal 2012 from individuals and companies trying to cheat the system. One of the largest sources of recovered monies is the Recovery Audit Contractor (RAC) program.
The RAC program was created through the Medicare Modernization Act of 2003 (MMA) to identify and recover improper Medicare payments to health-care providers under fee-for-service (FFS) Medicare plans. The goal of the RAC program is to identify improper payments made on claims of health-care services provided to Medicare beneficiaries. Improper payments could be overpayments or underpayments. Hospitals have been hit by the audits, with recoveries reaching $3.6 billion since the national program launched in 2010, according to Centers for Medicare & Medicaid Services (CMS) data.1 About $895 million was reclaimed from just six states during the RAC Demonstration Project between 2005 and 2008.1,2
CMS is more alert on the medical necessity of one-day length of stay (LOS) for inpatient admissions and is trying to detect and reduce Medicare waste, fraud, and abuse. Hospital charges represent about a third of the $718 billion spent on U.S. health care annually. Medicare reimbursement is a major source of revenue for hospitals, but some hospitals claim Medicare pays them only 93% to 97% of what it costs to provide patient care, whereas private insurers pay between 115% and 125% of those costs.3,4 These data suggest that private insurers are paying hospitals far more than they need to make up for Medicare’s “underpayment.”
So the first question is: Do hospitals overcharge for care? The next question is: What can be done? Or, in today’s economy, what is being done?
How It All Works
When an RAC determines that a provider was paid for inpatient hospital services but that the patient in question should have been treated as an outpatient, CMS takes back the entire Part A payment. Moreover, CMS takes the position that once an inpatient claim paid under Medicare Part A is later denied (usually years later), the hospital cannot receive Medicare Part B payment except for a few ancillary services. As a result, when an RAC concludes that a hospital should have provided items and services on an outpatient basis rather than an inpatient basis, the hospital ends up receiving little, if any, reimbursement for reasonable and medically necessary items and services provided.5,6
RACs function through a different model. They keep a contingency percentage—9% to 12.5%—of the entire Part A payment.5
Imagine a situation in which a physician decides that a patient needs to be admitted to the hospital for a surgical procedure, and the cost of care provided to the patient—surgery, drugs, and the like—amounts to $20,000. CMS reimburses the hospital under Part A. Two years later, an RAC employee reviewing hospital records overrules the physician’s judgment and decides the patient should have received basically the same care but on an outpatient basis. That decision, taken together with CMS’ Payment Denial Policy, means the hospital will end up receiving essentially no payment for the surgery and other care it provided. The RAC, by contrast, will receive approximately $2,000 for that one case alone.
To Admit or Not to Admit
Medicare expects attending physicians and physician reviewers to make the appropriate bedding status based on severity of signs and symptoms, comorbid and complicating conditions, and the practicality of outpatient management.
Let’s take two examples of patients presenting with acute asthma exacerbation (AAE) to differentiate observation and inpatient status. Asthma affects 20 million Americans, and 450,000 patients present to the ED annually with AAE. One third of these patients are hospitalized, which translates to more than $1 billion in costs annually.
Case 1: A 62-year-old female presents with two weeks of progressive shortness of breath and cough productive of white sputum. She has a history of asthma and hypertension. She presented to the ED with blood pressure of 140/90, heart rate of 101, respiratory rate of 20, temperature of 99.6°F, and pulse oximetry of 93% on room air, which increased to 99% on 2L of oxygen. She was given two breathing treatments with albuterol in the ED, IV methylprednisolone, and IV magnesium sulphate. Over the course of two hours, her wheezes improved, her heart rate decreased to 90 BPM, and her oxygen requirements were weaned to 1L of oxygen. Her WBC count was 9,800, with a potassium level of 4.0 and a creatinine level of 1.0. Her EKG showed sinus tachycardia, and her chest X-ray was negative for any infiltrates. The ED physician called the hospitalist for admission. What status should she be in?
Case 2: A 62-year-old female presents with a three-day history of shortness of breath and wheezing associated with vomiting. She was sent from her PCP’s office for asthma exacerbation and failure of resolution of symptoms despite one week of oral antibiotics and prednisone. Her past medical history includes asthma, diastolic congestive heart failure, hypertension, diabetes, and end-stage renal disease on hemodialysis. She presented to the ED with blood pressure of 90/63, pulse of 120, temperature of 97.7°F, respiratory rate of 24, and pulse oximetry of 89% on room air. She had bilateral wheezes on respiratory examination, and her WBC was 16,500, with a creatinine level of 3.5 and BNP level of 190. Her chest X-ray showed peribronchial thickening, and an EKG showed sinus tachycardia. She was given IV Solu-Medrol and two breathing treatments with albuterol, and the hospitalist was called for admission. What status should she be in?
Case 1 answer: Observation. The medical predictability of adverse clinical outcome from AAE is low due to hemodynamic stability, absence of fever, improvement in hypoxia, and negative chest X-ray for acute bronchopulmonary process in the setting of normal blood counts. She improved dramatically in the ED with no history of previous intubation or hospitalization or use of previous steroids. Her oxygen requirements decreased within 12 hours of first treatment. Even though FEV1 was not monitored, there is documented improvement in her vital signs as well as respiratory examination.
Case 2 answer: Inpatient. The medical predictability of adverse clinical outcome is significant due to hemodynamic instability evidenced by hypotension, tachycardia, and hypoxia; wheezes on respiratory examination with leukocytosis; and abnormal chest X-ray in the setting of comorbid diseases, such as end-stage renal disease and congestive heart failure.
The treatments given to both patients were similar; however, Case 2 had a higher predictability of adverse clinical outcome and would require medical evaluation and management that would exceed 24 hours. An inpatient level of care is justified based on her clinical presentation, comorbidities, and the risk for adverse clinical outcomes.
It is important that the patient be described appropriately in the medical record to support the status. Documentation should include clinical decision-making and rationale of the attending, objective findings, and the treatment given in the ED as well as the treatment planned during the hospitalization. It is expected that the physician will document the possibility and probability of adverse clinical outcome as well as follow evidence-based guidelines for treatment.
Financial Facts
The AHA collects data and anecdotal evidence from member hospitals regarding the RAC program and its effects. Those data show the following:
- More than 95% of the general medical-surgical hospitals that provided information to the AHA have been targeted by RACs;
- RACs have demanded more than a half-million medical records to audit;
- Many audits result in RAC determinations of “overpayment”; and
- Of those overpayment determinations, more than 60% relate to one- or two-day inpatient admissions that RACs deem medically unnecessary.
Hospitals thus have been required to give back hundreds of millions of dollars per year due to RAC determinations that services should have been provided in an outpatient, rather than inpatient, setting. In the first quarter of 2012 alone, information provided to the AHA by hospitals shows that they were forced to repay $236 million for medically necessary items and services that RACs deemed should have been provided on an outpatient, rather than inpatient, basis. And this amount does not include the millions of dollars recovered from hospitals that did not report data to the AHA.
The RAC program has been a continued financial success for CMS and the auditors: RACs collected $1.86 billion in overpayments from October 2009 through March 2012. Over that same time period, RACs identified only $245.2 million in underpayments.7
The government, no doubt, is on a mission to rein in health-care costs. All stakeholders in the system, including hospitalists and administrations, need extensive education to document appropriate patient status to ensure accurate reimbursement and prevent the fallout of future repayments.
Dr. Pahuja is founder and CEO of Aerolib Healthcare Solutions (aerolib.com). He is pursuing his MBA in health-care administration from the Isenberg School of Management at the University of Massachusetts in Amherst.
References
- PR Web. Medicare anti-fraud recovered $19 billion, how much for private self-insured plans? Fiduciary overpayment recovery programs announced from ERISAclaim.com. PR Web website. Available at: http://www.prweb.com/releases/2013/3/prweb10501376.htm. Accessed April 4, 2013.
- Viebeck E. GAO reports billions in overpayments to private Medicare plans. The Hill website. Available at: http://thehill.com/blogs/healthwatch/medicare/286041-gao-reports-billions-in-overpayments-to-private-medicare-plans#ixzz2NASaVVIK. Accessed April 4, 2013.
- Centers for Medicare & Medicare Services. Cost reports. Centers for Medicare & Medicare Services website. Available at: http://www.cms.gov/Research-Statistics-Data-and-Systems/Files-for-Order/CostReports/index.html. Accessed April 4, 2013.
- Whelan D. America’s most profitable hospitals. Forbes website. Available at: http://www.forbes.com/2010/08/30/profitable-hospitals-hca-healthcare-business-mayo-clinic.html. Accessed April 4, 2013.
- American Medical Association. Recovery Audit Contractors. American Medical Association website. Available at: http://www.ama-assn.org/ama/pub/physician-resources/solutions-managing-your-practice/coding-billing-insurance/medicare/recovery-audit-contractors.page. Accessed April 4, 2013.
- American Hospital Association, Missouri Baptist Sullivan Hospital, Munson Medical Center, Lancaster General Hospital, and Trinity Health Corporation v. Kathleen Sebelius. American Hospital Association website. Available at: http://www.aha.org/content/12/121101-aha-hhs-medicare-com.pdf. Accessed March 12, 2013.
- Centers for Medicare & Medicare Services. Medicare fee-for-service Recovery Audit Program, May 2012. Centers for Medicare & Medicare Services website. Available at: http://www.cms.gov/Research-Statistics-Data-and-Systems/Monitoring-Programs/Recovery-Audit-Program/Downloads/National-Program-Corrections-FY-2012-2nd-Qtr.pdf. Accessed April 4, 2013.
- Centers for Medicare & Medicaid Services. FY 2014 IPPS proposed rule home page items. Centers for Medicare & Medicaid Services website. Available at: http://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/AcuteInpatientPPS/FY-2014-IPPS-Proposed-Rule-Home-Page-Items/FY-2014-IPPS-Proposed-Rule-CMS-1599-P-Regulations.html. Accessed June 10, 2013.
The government has made extensive efforts to combat fraud in the Medicare and Medicaid programs, recovering a record $4.2 billion in fiscal 2012 from individuals and companies trying to cheat the system. One of the largest sources of recovered monies is the Recovery Audit Contractor (RAC) program.
The RAC program was created through the Medicare Modernization Act of 2003 (MMA) to identify and recover improper Medicare payments to health-care providers under fee-for-service (FFS) Medicare plans. The goal of the RAC program is to identify improper payments made on claims of health-care services provided to Medicare beneficiaries. Improper payments could be overpayments or underpayments. Hospitals have been hit by the audits, with recoveries reaching $3.6 billion since the national program launched in 2010, according to Centers for Medicare & Medicaid Services (CMS) data.1 About $895 million was reclaimed from just six states during the RAC Demonstration Project between 2005 and 2008.1,2
CMS is more alert on the medical necessity of one-day length of stay (LOS) for inpatient admissions and is trying to detect and reduce Medicare waste, fraud, and abuse. Hospital charges represent about a third of the $718 billion spent on U.S. health care annually. Medicare reimbursement is a major source of revenue for hospitals, but some hospitals claim Medicare pays them only 93% to 97% of what it costs to provide patient care, whereas private insurers pay between 115% and 125% of those costs.3,4 These data suggest that private insurers are paying hospitals far more than they need to make up for Medicare’s “underpayment.”
So the first question is: Do hospitals overcharge for care? The next question is: What can be done? Or, in today’s economy, what is being done?
How It All Works
When an RAC determines that a provider was paid for inpatient hospital services but that the patient in question should have been treated as an outpatient, CMS takes back the entire Part A payment. Moreover, CMS takes the position that once an inpatient claim paid under Medicare Part A is later denied (usually years later), the hospital cannot receive Medicare Part B payment except for a few ancillary services. As a result, when an RAC concludes that a hospital should have provided items and services on an outpatient basis rather than an inpatient basis, the hospital ends up receiving little, if any, reimbursement for reasonable and medically necessary items and services provided.5,6
RACs function through a different model. They keep a contingency percentage—9% to 12.5%—of the entire Part A payment.5
Imagine a situation in which a physician decides that a patient needs to be admitted to the hospital for a surgical procedure, and the cost of care provided to the patient—surgery, drugs, and the like—amounts to $20,000. CMS reimburses the hospital under Part A. Two years later, an RAC employee reviewing hospital records overrules the physician’s judgment and decides the patient should have received basically the same care but on an outpatient basis. That decision, taken together with CMS’ Payment Denial Policy, means the hospital will end up receiving essentially no payment for the surgery and other care it provided. The RAC, by contrast, will receive approximately $2,000 for that one case alone.
To Admit or Not to Admit
Medicare expects attending physicians and physician reviewers to make the appropriate bedding status based on severity of signs and symptoms, comorbid and complicating conditions, and the practicality of outpatient management.
Let’s take two examples of patients presenting with acute asthma exacerbation (AAE) to differentiate observation and inpatient status. Asthma affects 20 million Americans, and 450,000 patients present to the ED annually with AAE. One third of these patients are hospitalized, which translates to more than $1 billion in costs annually.
Case 1: A 62-year-old female presents with two weeks of progressive shortness of breath and cough productive of white sputum. She has a history of asthma and hypertension. She presented to the ED with blood pressure of 140/90, heart rate of 101, respiratory rate of 20, temperature of 99.6°F, and pulse oximetry of 93% on room air, which increased to 99% on 2L of oxygen. She was given two breathing treatments with albuterol in the ED, IV methylprednisolone, and IV magnesium sulphate. Over the course of two hours, her wheezes improved, her heart rate decreased to 90 BPM, and her oxygen requirements were weaned to 1L of oxygen. Her WBC count was 9,800, with a potassium level of 4.0 and a creatinine level of 1.0. Her EKG showed sinus tachycardia, and her chest X-ray was negative for any infiltrates. The ED physician called the hospitalist for admission. What status should she be in?
Case 2: A 62-year-old female presents with a three-day history of shortness of breath and wheezing associated with vomiting. She was sent from her PCP’s office for asthma exacerbation and failure of resolution of symptoms despite one week of oral antibiotics and prednisone. Her past medical history includes asthma, diastolic congestive heart failure, hypertension, diabetes, and end-stage renal disease on hemodialysis. She presented to the ED with blood pressure of 90/63, pulse of 120, temperature of 97.7°F, respiratory rate of 24, and pulse oximetry of 89% on room air. She had bilateral wheezes on respiratory examination, and her WBC was 16,500, with a creatinine level of 3.5 and BNP level of 190. Her chest X-ray showed peribronchial thickening, and an EKG showed sinus tachycardia. She was given IV Solu-Medrol and two breathing treatments with albuterol, and the hospitalist was called for admission. What status should she be in?
Case 1 answer: Observation. The medical predictability of adverse clinical outcome from AAE is low due to hemodynamic stability, absence of fever, improvement in hypoxia, and negative chest X-ray for acute bronchopulmonary process in the setting of normal blood counts. She improved dramatically in the ED with no history of previous intubation or hospitalization or use of previous steroids. Her oxygen requirements decreased within 12 hours of first treatment. Even though FEV1 was not monitored, there is documented improvement in her vital signs as well as respiratory examination.
Case 2 answer: Inpatient. The medical predictability of adverse clinical outcome is significant due to hemodynamic instability evidenced by hypotension, tachycardia, and hypoxia; wheezes on respiratory examination with leukocytosis; and abnormal chest X-ray in the setting of comorbid diseases, such as end-stage renal disease and congestive heart failure.
The treatments given to both patients were similar; however, Case 2 had a higher predictability of adverse clinical outcome and would require medical evaluation and management that would exceed 24 hours. An inpatient level of care is justified based on her clinical presentation, comorbidities, and the risk for adverse clinical outcomes.
It is important that the patient be described appropriately in the medical record to support the status. Documentation should include clinical decision-making and rationale of the attending, objective findings, and the treatment given in the ED as well as the treatment planned during the hospitalization. It is expected that the physician will document the possibility and probability of adverse clinical outcome as well as follow evidence-based guidelines for treatment.
Financial Facts
The AHA collects data and anecdotal evidence from member hospitals regarding the RAC program and its effects. Those data show the following:
- More than 95% of the general medical-surgical hospitals that provided information to the AHA have been targeted by RACs;
- RACs have demanded more than a half-million medical records to audit;
- Many audits result in RAC determinations of “overpayment”; and
- Of those overpayment determinations, more than 60% relate to one- or two-day inpatient admissions that RACs deem medically unnecessary.
Hospitals thus have been required to give back hundreds of millions of dollars per year due to RAC determinations that services should have been provided in an outpatient, rather than inpatient, setting. In the first quarter of 2012 alone, information provided to the AHA by hospitals shows that they were forced to repay $236 million for medically necessary items and services that RACs deemed should have been provided on an outpatient, rather than inpatient, basis. And this amount does not include the millions of dollars recovered from hospitals that did not report data to the AHA.
The RAC program has been a continued financial success for CMS and the auditors: RACs collected $1.86 billion in overpayments from October 2009 through March 2012. Over that same time period, RACs identified only $245.2 million in underpayments.7
The government, no doubt, is on a mission to rein in health-care costs. All stakeholders in the system, including hospitalists and administrations, need extensive education to document appropriate patient status to ensure accurate reimbursement and prevent the fallout of future repayments.
Dr. Pahuja is founder and CEO of Aerolib Healthcare Solutions (aerolib.com). He is pursuing his MBA in health-care administration from the Isenberg School of Management at the University of Massachusetts in Amherst.
References
- PR Web. Medicare anti-fraud recovered $19 billion, how much for private self-insured plans? Fiduciary overpayment recovery programs announced from ERISAclaim.com. PR Web website. Available at: http://www.prweb.com/releases/2013/3/prweb10501376.htm. Accessed April 4, 2013.
- Viebeck E. GAO reports billions in overpayments to private Medicare plans. The Hill website. Available at: http://thehill.com/blogs/healthwatch/medicare/286041-gao-reports-billions-in-overpayments-to-private-medicare-plans#ixzz2NASaVVIK. Accessed April 4, 2013.
- Centers for Medicare & Medicare Services. Cost reports. Centers for Medicare & Medicare Services website. Available at: http://www.cms.gov/Research-Statistics-Data-and-Systems/Files-for-Order/CostReports/index.html. Accessed April 4, 2013.
- Whelan D. America’s most profitable hospitals. Forbes website. Available at: http://www.forbes.com/2010/08/30/profitable-hospitals-hca-healthcare-business-mayo-clinic.html. Accessed April 4, 2013.
- American Medical Association. Recovery Audit Contractors. American Medical Association website. Available at: http://www.ama-assn.org/ama/pub/physician-resources/solutions-managing-your-practice/coding-billing-insurance/medicare/recovery-audit-contractors.page. Accessed April 4, 2013.
- American Hospital Association, Missouri Baptist Sullivan Hospital, Munson Medical Center, Lancaster General Hospital, and Trinity Health Corporation v. Kathleen Sebelius. American Hospital Association website. Available at: http://www.aha.org/content/12/121101-aha-hhs-medicare-com.pdf. Accessed March 12, 2013.
- Centers for Medicare & Medicare Services. Medicare fee-for-service Recovery Audit Program, May 2012. Centers for Medicare & Medicare Services website. Available at: http://www.cms.gov/Research-Statistics-Data-and-Systems/Monitoring-Programs/Recovery-Audit-Program/Downloads/National-Program-Corrections-FY-2012-2nd-Qtr.pdf. Accessed April 4, 2013.
- Centers for Medicare & Medicaid Services. FY 2014 IPPS proposed rule home page items. Centers for Medicare & Medicaid Services website. Available at: http://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/AcuteInpatientPPS/FY-2014-IPPS-Proposed-Rule-Home-Page-Items/FY-2014-IPPS-Proposed-Rule-CMS-1599-P-Regulations.html. Accessed June 10, 2013.
Why Hospitalists Should Provide Patients with Discharge Summaries

I continue to believe that hospitalists should routinely provide patients a copy of their discharge summary. I made the case for this in a 2006 column (“Keeping Patients in the Loop,” October 2006, p. 74), but I don’t see the idea catching on. I bet this simple act would have all kinds of benefits, including at least modest reductions in overall health-care expenditures and readmissions.
The whole dynamic of this issue seems to be changing as a result of “patient portals” allowing direct access to review test results and, in some cases, physician documentation. Typically, these are integrated with or at least connected to an electronic health record (EHR) and allow a patient, and those provided access (e.g. the password) by the patient, to review records. My own PCP provides access to a portal that I’ve found very useful, but I think, like most others, it doesn’t provide access to physician notes.
So there still is a case to be made for hospitalists (and all specialties) to provide copies of the discharge summary directly to patients and perhaps other forms of documentation as well.
Timeliness
I think all discharge summaries should be completed before the patient leaves the hospital and amended as needed to capture any last-minute changes and details. The act of generating the summary often leads the discharging doctor to notice, and have a chance to address, important details that may have dropped off the daily problem list. Things like the need to recheck a lab test to ensure normalization prior to discharge, or make arrangements for outpatient colonoscopy to pursue the heme-positive stool found on admission, have sometimes slipped off the radar during the hospital stay and can be caught when preparing discharge summary.
Preparing a discharge summary the night before anticipated discharge can have many advantages, including improving early discharge times the next morning. And it means the doctor can prepare the summary late in the day after routine rounding is finished and interruptions are less likely. Although I think quality of care is enhanced by generating the summary the night before (and amending it as needed), I worked with a hospital that was cited by the Centers for Medicare & Medicaid Services (CMS) for doing this and was told they can’t be done prior to the calendar day of discharge.
Creation of the discharge summary isn’t the only relevant step. It should be transcribed on a stat basis (e.g. within two to four hours) and pushed to the PCP and other treating physicians. It isn’t enough that the document is available to the PCP via an EHR; these doctors need some sort of notice, such as an email.
To take advantage of the new “transitional-care management” codes (99495 and 99496), PCPs must make telephone contact with patients within two days of discharge and must have a face-to-face visit within one or two weeks of discharge (depending on whether the patient is high- or moderate-risk). Making the summary available to the PCP quickly can be crucial in ensuring these phone calls and visits are meaningful. (For an excellent review of the TCM codes, see Dr. Lauren Doctoroff’s article “New Codes Bridge Hospitals’ Post-Discharge Billing Gap” in the February 2013 issue of The Hospitalist.)
So I think both patients and other treating physicians should get the discharge summary on the day of discharge or no more than a day or two after. I bet this improves quality of care and readmissions, but one study found no association, and another found a trend toward reduced readmissions that did not reach statistical significance.1,2
Content
Just what information should go in a discharge summary? There are lots of opinions here, but it is worth starting with the components required by The Joint Commission. (You were aware of these, right?) The commission requires:
- Reason for hospitalization;
- Significant findings;
- Procedures and treatment provided;
- Patient’s discharge condition;
- Patient and family instructions; and
- Attending physician’s signature
To this list, I would add enumeration of tests pending at discharge.
The May/June 2005 issue of The Hospitalist has a terrific article by three thoughtful hospitalists titled “Advancing Toward the Ideal Hospital Discharge for the Elderly Patient.” It summarizes a 2005 workshop at the SHM annual meeting that produced a checklist of elements to consider including in every summary.
Brevity is a worthwhile goal but not at the expense of conveying the thought processes behind decisions. Things like how a decision was made to pursue watchful waiting versus aggressive workup now should be spelled out. Was it simply patient preference? It is common to start a trial of a medical therapy during a hospital stay, and it should be made clear that its effect should be assessed and a deliberate decision regarding continuing or stopping the therapy will be needed after discharge.
Lots of things need context and explanation for subsequent caregivers.
Format
The hospital in which I practice recently switched to a new EHR, and our hospitalist group has talked some about all of us using the same basic template for our notes. This should be valuable to all other caregivers who read a reasonable number of our notes and might improve our communication with one another around handoffs, etc. Although we haven’t reached a final decision about this, I’m an advocate for a shared template rather than each doctor using his or her own. This would be a worthwhile thing for all groups to consider.

Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is co-director for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. Write to him at [email protected].
References
I continue to believe that hospitalists should routinely provide patients a copy of their discharge summary. I made the case for this in a 2006 column (“Keeping Patients in the Loop,” October 2006, p. 74), but I don’t see the idea catching on. I bet this simple act would have all kinds of benefits, including at least modest reductions in overall health-care expenditures and readmissions.
The whole dynamic of this issue seems to be changing as a result of “patient portals” allowing direct access to review test results and, in some cases, physician documentation. Typically, these are integrated with or at least connected to an electronic health record (EHR) and allow a patient, and those provided access (e.g. the password) by the patient, to review records. My own PCP provides access to a portal that I’ve found very useful, but I think, like most others, it doesn’t provide access to physician notes.
So there still is a case to be made for hospitalists (and all specialties) to provide copies of the discharge summary directly to patients and perhaps other forms of documentation as well.
Timeliness
I think all discharge summaries should be completed before the patient leaves the hospital and amended as needed to capture any last-minute changes and details. The act of generating the summary often leads the discharging doctor to notice, and have a chance to address, important details that may have dropped off the daily problem list. Things like the need to recheck a lab test to ensure normalization prior to discharge, or make arrangements for outpatient colonoscopy to pursue the heme-positive stool found on admission, have sometimes slipped off the radar during the hospital stay and can be caught when preparing discharge summary.
Preparing a discharge summary the night before anticipated discharge can have many advantages, including improving early discharge times the next morning. And it means the doctor can prepare the summary late in the day after routine rounding is finished and interruptions are less likely. Although I think quality of care is enhanced by generating the summary the night before (and amending it as needed), I worked with a hospital that was cited by the Centers for Medicare & Medicaid Services (CMS) for doing this and was told they can’t be done prior to the calendar day of discharge.
Creation of the discharge summary isn’t the only relevant step. It should be transcribed on a stat basis (e.g. within two to four hours) and pushed to the PCP and other treating physicians. It isn’t enough that the document is available to the PCP via an EHR; these doctors need some sort of notice, such as an email.
To take advantage of the new “transitional-care management” codes (99495 and 99496), PCPs must make telephone contact with patients within two days of discharge and must have a face-to-face visit within one or two weeks of discharge (depending on whether the patient is high- or moderate-risk). Making the summary available to the PCP quickly can be crucial in ensuring these phone calls and visits are meaningful. (For an excellent review of the TCM codes, see Dr. Lauren Doctoroff’s article “New Codes Bridge Hospitals’ Post-Discharge Billing Gap” in the February 2013 issue of The Hospitalist.)
So I think both patients and other treating physicians should get the discharge summary on the day of discharge or no more than a day or two after. I bet this improves quality of care and readmissions, but one study found no association, and another found a trend toward reduced readmissions that did not reach statistical significance.1,2
Content
Just what information should go in a discharge summary? There are lots of opinions here, but it is worth starting with the components required by The Joint Commission. (You were aware of these, right?) The commission requires:
- Reason for hospitalization;
- Significant findings;
- Procedures and treatment provided;
- Patient’s discharge condition;
- Patient and family instructions; and
- Attending physician’s signature
To this list, I would add enumeration of tests pending at discharge.
The May/June 2005 issue of The Hospitalist has a terrific article by three thoughtful hospitalists titled “Advancing Toward the Ideal Hospital Discharge for the Elderly Patient.” It summarizes a 2005 workshop at the SHM annual meeting that produced a checklist of elements to consider including in every summary.
Brevity is a worthwhile goal but not at the expense of conveying the thought processes behind decisions. Things like how a decision was made to pursue watchful waiting versus aggressive workup now should be spelled out. Was it simply patient preference? It is common to start a trial of a medical therapy during a hospital stay, and it should be made clear that its effect should be assessed and a deliberate decision regarding continuing or stopping the therapy will be needed after discharge.
Lots of things need context and explanation for subsequent caregivers.
Format
The hospital in which I practice recently switched to a new EHR, and our hospitalist group has talked some about all of us using the same basic template for our notes. This should be valuable to all other caregivers who read a reasonable number of our notes and might improve our communication with one another around handoffs, etc. Although we haven’t reached a final decision about this, I’m an advocate for a shared template rather than each doctor using his or her own. This would be a worthwhile thing for all groups to consider.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is co-director for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. Write to him at [email protected].
References
I continue to believe that hospitalists should routinely provide patients a copy of their discharge summary. I made the case for this in a 2006 column (“Keeping Patients in the Loop,” October 2006, p. 74), but I don’t see the idea catching on. I bet this simple act would have all kinds of benefits, including at least modest reductions in overall health-care expenditures and readmissions.
The whole dynamic of this issue seems to be changing as a result of “patient portals” allowing direct access to review test results and, in some cases, physician documentation. Typically, these are integrated with or at least connected to an electronic health record (EHR) and allow a patient, and those provided access (e.g. the password) by the patient, to review records. My own PCP provides access to a portal that I’ve found very useful, but I think, like most others, it doesn’t provide access to physician notes.
So there still is a case to be made for hospitalists (and all specialties) to provide copies of the discharge summary directly to patients and perhaps other forms of documentation as well.
Timeliness
I think all discharge summaries should be completed before the patient leaves the hospital and amended as needed to capture any last-minute changes and details. The act of generating the summary often leads the discharging doctor to notice, and have a chance to address, important details that may have dropped off the daily problem list. Things like the need to recheck a lab test to ensure normalization prior to discharge, or make arrangements for outpatient colonoscopy to pursue the heme-positive stool found on admission, have sometimes slipped off the radar during the hospital stay and can be caught when preparing discharge summary.
Preparing a discharge summary the night before anticipated discharge can have many advantages, including improving early discharge times the next morning. And it means the doctor can prepare the summary late in the day after routine rounding is finished and interruptions are less likely. Although I think quality of care is enhanced by generating the summary the night before (and amending it as needed), I worked with a hospital that was cited by the Centers for Medicare & Medicaid Services (CMS) for doing this and was told they can’t be done prior to the calendar day of discharge.
Creation of the discharge summary isn’t the only relevant step. It should be transcribed on a stat basis (e.g. within two to four hours) and pushed to the PCP and other treating physicians. It isn’t enough that the document is available to the PCP via an EHR; these doctors need some sort of notice, such as an email.
To take advantage of the new “transitional-care management” codes (99495 and 99496), PCPs must make telephone contact with patients within two days of discharge and must have a face-to-face visit within one or two weeks of discharge (depending on whether the patient is high- or moderate-risk). Making the summary available to the PCP quickly can be crucial in ensuring these phone calls and visits are meaningful. (For an excellent review of the TCM codes, see Dr. Lauren Doctoroff’s article “New Codes Bridge Hospitals’ Post-Discharge Billing Gap” in the February 2013 issue of The Hospitalist.)
So I think both patients and other treating physicians should get the discharge summary on the day of discharge or no more than a day or two after. I bet this improves quality of care and readmissions, but one study found no association, and another found a trend toward reduced readmissions that did not reach statistical significance.1,2
Content
Just what information should go in a discharge summary? There are lots of opinions here, but it is worth starting with the components required by The Joint Commission. (You were aware of these, right?) The commission requires:
- Reason for hospitalization;
- Significant findings;
- Procedures and treatment provided;
- Patient’s discharge condition;
- Patient and family instructions; and
- Attending physician’s signature
To this list, I would add enumeration of tests pending at discharge.
The May/June 2005 issue of The Hospitalist has a terrific article by three thoughtful hospitalists titled “Advancing Toward the Ideal Hospital Discharge for the Elderly Patient.” It summarizes a 2005 workshop at the SHM annual meeting that produced a checklist of elements to consider including in every summary.
Brevity is a worthwhile goal but not at the expense of conveying the thought processes behind decisions. Things like how a decision was made to pursue watchful waiting versus aggressive workup now should be spelled out. Was it simply patient preference? It is common to start a trial of a medical therapy during a hospital stay, and it should be made clear that its effect should be assessed and a deliberate decision regarding continuing or stopping the therapy will be needed after discharge.
Lots of things need context and explanation for subsequent caregivers.
Format
The hospital in which I practice recently switched to a new EHR, and our hospitalist group has talked some about all of us using the same basic template for our notes. This should be valuable to all other caregivers who read a reasonable number of our notes and might improve our communication with one another around handoffs, etc. Although we haven’t reached a final decision about this, I’m an advocate for a shared template rather than each doctor using his or her own. This would be a worthwhile thing for all groups to consider.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is co-director for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. Write to him at [email protected].
References
Prediction Model Identifies Potentially Avoidable 30-Day Readmissions
Clinical question: Can a prediction model based on administrative and clinical data identify potentially avoidable 30-day readmissions in medical patients prior to discharge?
Background: An estimated 18% of Medicare beneficiaries are readmitted to the hospital within 30 days of discharge, costing nearly $17 billion per year. Interventions to reduce readmission rates are costly and should be focused on high-risk patients. To date, using models to predict 30-day readmission has been problematic and unreliable.
Study design: Retrospective cohort.
Setting: Academic medical center in Boston.
Synopsis: Using consecutive discharges from all medical services of Brigham and Women’s Hospital occurring over one year, this study derived and internally validated a prediction model for potentially avoidable 30-day readmissions. Of 10,731 discharges, there were 2,399 (22%) 30-day readmissions, and 879 (8.5%) were deemed potentially avoidable. Seven independent predictors for readmission were identified and used to create a predictor score referred to as the HOSPITAL score. Predictors included hemoglobin and sodium levels at discharge, number of hospitalizations in the past year, and four features of the index hospitalization, including type, discharge from an oncology service, presence of procedures, and length of stay. The score was internally validated and found to predict potentially avoidable 30-day readmission in medical patients with fair discriminatory power and good calibration.
This study is unique in that none of the classic comorbidities (e.g. congestive heart failure) were associated with a higher risk of 30-day readmission. Previously unrecognized predictors, including hemoglobin, sodium, and number of procedures performed, were incorporated. This suggests that comorbidities are not as important as illness severity or clinical instability. Hospitalists should await studies that externally validate the HOSPITAL score before incorporating it into practice.
Bottom line: A unique and simple seven-item prediction model identifies potentially avoidable 30-day readmissions but needs to be externally validated before being widely utilized.
Citation: Donze J, Drahomir A, Williams D, Schnipper JL. Potentially avoidable 30-day hospital readmissions in medical patients. JAMA Intern Med. 2013;137(8):632-638.
Clinical question: Can a prediction model based on administrative and clinical data identify potentially avoidable 30-day readmissions in medical patients prior to discharge?
Background: An estimated 18% of Medicare beneficiaries are readmitted to the hospital within 30 days of discharge, costing nearly $17 billion per year. Interventions to reduce readmission rates are costly and should be focused on high-risk patients. To date, using models to predict 30-day readmission has been problematic and unreliable.
Study design: Retrospective cohort.
Setting: Academic medical center in Boston.
Synopsis: Using consecutive discharges from all medical services of Brigham and Women’s Hospital occurring over one year, this study derived and internally validated a prediction model for potentially avoidable 30-day readmissions. Of 10,731 discharges, there were 2,399 (22%) 30-day readmissions, and 879 (8.5%) were deemed potentially avoidable. Seven independent predictors for readmission were identified and used to create a predictor score referred to as the HOSPITAL score. Predictors included hemoglobin and sodium levels at discharge, number of hospitalizations in the past year, and four features of the index hospitalization, including type, discharge from an oncology service, presence of procedures, and length of stay. The score was internally validated and found to predict potentially avoidable 30-day readmission in medical patients with fair discriminatory power and good calibration.
This study is unique in that none of the classic comorbidities (e.g. congestive heart failure) were associated with a higher risk of 30-day readmission. Previously unrecognized predictors, including hemoglobin, sodium, and number of procedures performed, were incorporated. This suggests that comorbidities are not as important as illness severity or clinical instability. Hospitalists should await studies that externally validate the HOSPITAL score before incorporating it into practice.
Bottom line: A unique and simple seven-item prediction model identifies potentially avoidable 30-day readmissions but needs to be externally validated before being widely utilized.
Citation: Donze J, Drahomir A, Williams D, Schnipper JL. Potentially avoidable 30-day hospital readmissions in medical patients. JAMA Intern Med. 2013;137(8):632-638.
Clinical question: Can a prediction model based on administrative and clinical data identify potentially avoidable 30-day readmissions in medical patients prior to discharge?
Background: An estimated 18% of Medicare beneficiaries are readmitted to the hospital within 30 days of discharge, costing nearly $17 billion per year. Interventions to reduce readmission rates are costly and should be focused on high-risk patients. To date, using models to predict 30-day readmission has been problematic and unreliable.
Study design: Retrospective cohort.
Setting: Academic medical center in Boston.
Synopsis: Using consecutive discharges from all medical services of Brigham and Women’s Hospital occurring over one year, this study derived and internally validated a prediction model for potentially avoidable 30-day readmissions. Of 10,731 discharges, there were 2,399 (22%) 30-day readmissions, and 879 (8.5%) were deemed potentially avoidable. Seven independent predictors for readmission were identified and used to create a predictor score referred to as the HOSPITAL score. Predictors included hemoglobin and sodium levels at discharge, number of hospitalizations in the past year, and four features of the index hospitalization, including type, discharge from an oncology service, presence of procedures, and length of stay. The score was internally validated and found to predict potentially avoidable 30-day readmission in medical patients with fair discriminatory power and good calibration.
This study is unique in that none of the classic comorbidities (e.g. congestive heart failure) were associated with a higher risk of 30-day readmission. Previously unrecognized predictors, including hemoglobin, sodium, and number of procedures performed, were incorporated. This suggests that comorbidities are not as important as illness severity or clinical instability. Hospitalists should await studies that externally validate the HOSPITAL score before incorporating it into practice.
Bottom line: A unique and simple seven-item prediction model identifies potentially avoidable 30-day readmissions but needs to be externally validated before being widely utilized.
Citation: Donze J, Drahomir A, Williams D, Schnipper JL. Potentially avoidable 30-day hospital readmissions in medical patients. JAMA Intern Med. 2013;137(8):632-638.
Hospitalist Explains Benefits of Bundling, Other Integration Strategies
Click here to listen to excerpts of Dr. Duke's interview with The Hospitalist
Click here to listen to excerpts of Dr. Duke's interview with The Hospitalist
Click here to listen to excerpts of Dr. Duke's interview with The Hospitalist
Are Hospital Readmissions Numbers Fruit of an Imperfect Equation?
Many health-care-reform initiatives are so new that few data are available to assess whether they are working as intended. The Centers for Medicare & Medicaid Services (CMS), however, has touted the early numbers from its Hospital Readmission Reduction Program to suggest that the policy is making a difference in curbing bounce-backs. The overall impact, however, might be decidedly more nuanced and provides a telling example of the challenges that such programs can present to hospitalists and other health-care providers.
At a Senate Finance Committee Hearing in February, Jonathan Blum, deputy administrator and director for the Center of Medicare at CMS, released data suggesting that 30-day readmission rates for all causes dropped to 17.8% of hospitalizations near the end of 2012 after remaining at roughly 19% in each of the five previous years. The difference translates into 70,000 fewer readmissions annually.
During the first round of penalties, CMS dinged 2,213 hospitals for an estimated $280 million, or an average of about $126,500 per hospital, for excessive readmissions linked to heart attack, heart failure, and pneumonia care. Blum made the case that the penalties—or the threat thereof—are helping to improve rates.
Those arguing that the policy could disproportionately impact institutions caring for more vulnerable, high-risk patients also found new support in a recent New England Journal of Medicine perspective suggesting that academic medical centers and safety-net hospitals were more likely to be penalized.1 Among their suggestions, the perspective’s co-authors, from Harvard’s School of Public Health, suggested that the policy take patient socioeconomic status into account to provide a fairer basis of comparison.
A second recent study suggested that even the reduced readmission rates might not be telling the whole story. An analysis of patients released in 2010 from safety-net hospital Boston Medical Center showed that nearly 1 in 4 returned to the ED within a month of discharge.2 But more than half of those patients weren’t readmitted as inpatients, meaning that they wouldn’t show up under Medicare’s readmissions statistics.
Along with the mixed early reviews of EHR rollouts and the HCAHPS portion of the Hospital Value-Based Purchasing program, it’s another reminder that CMS metrics and incentives might not always add up as envisioned. In the near future, it seems, hospitals and health-care providers might have to contend with some imperfect numbers. TH
Bryn Nelson is a freelance medical writer in Seattle.
References
1. Joynt KE, Jha AK. Thirty-day readmissions–truth and consequences. N Engl J Med. 2012;366:1366-1369.
2. Rising KL, White LF, Fernandez WG, Boutwell, AE. Emergency department visits after hospital discharge: a missing part of the equation. Ann Emerg Med. 2013; in press.
Many health-care-reform initiatives are so new that few data are available to assess whether they are working as intended. The Centers for Medicare & Medicaid Services (CMS), however, has touted the early numbers from its Hospital Readmission Reduction Program to suggest that the policy is making a difference in curbing bounce-backs. The overall impact, however, might be decidedly more nuanced and provides a telling example of the challenges that such programs can present to hospitalists and other health-care providers.
At a Senate Finance Committee Hearing in February, Jonathan Blum, deputy administrator and director for the Center of Medicare at CMS, released data suggesting that 30-day readmission rates for all causes dropped to 17.8% of hospitalizations near the end of 2012 after remaining at roughly 19% in each of the five previous years. The difference translates into 70,000 fewer readmissions annually.
During the first round of penalties, CMS dinged 2,213 hospitals for an estimated $280 million, or an average of about $126,500 per hospital, for excessive readmissions linked to heart attack, heart failure, and pneumonia care. Blum made the case that the penalties—or the threat thereof—are helping to improve rates.
Those arguing that the policy could disproportionately impact institutions caring for more vulnerable, high-risk patients also found new support in a recent New England Journal of Medicine perspective suggesting that academic medical centers and safety-net hospitals were more likely to be penalized.1 Among their suggestions, the perspective’s co-authors, from Harvard’s School of Public Health, suggested that the policy take patient socioeconomic status into account to provide a fairer basis of comparison.
A second recent study suggested that even the reduced readmission rates might not be telling the whole story. An analysis of patients released in 2010 from safety-net hospital Boston Medical Center showed that nearly 1 in 4 returned to the ED within a month of discharge.2 But more than half of those patients weren’t readmitted as inpatients, meaning that they wouldn’t show up under Medicare’s readmissions statistics.
Along with the mixed early reviews of EHR rollouts and the HCAHPS portion of the Hospital Value-Based Purchasing program, it’s another reminder that CMS metrics and incentives might not always add up as envisioned. In the near future, it seems, hospitals and health-care providers might have to contend with some imperfect numbers. TH
Bryn Nelson is a freelance medical writer in Seattle.
References
1. Joynt KE, Jha AK. Thirty-day readmissions–truth and consequences. N Engl J Med. 2012;366:1366-1369.
2. Rising KL, White LF, Fernandez WG, Boutwell, AE. Emergency department visits after hospital discharge: a missing part of the equation. Ann Emerg Med. 2013; in press.
Many health-care-reform initiatives are so new that few data are available to assess whether they are working as intended. The Centers for Medicare & Medicaid Services (CMS), however, has touted the early numbers from its Hospital Readmission Reduction Program to suggest that the policy is making a difference in curbing bounce-backs. The overall impact, however, might be decidedly more nuanced and provides a telling example of the challenges that such programs can present to hospitalists and other health-care providers.
At a Senate Finance Committee Hearing in February, Jonathan Blum, deputy administrator and director for the Center of Medicare at CMS, released data suggesting that 30-day readmission rates for all causes dropped to 17.8% of hospitalizations near the end of 2012 after remaining at roughly 19% in each of the five previous years. The difference translates into 70,000 fewer readmissions annually.
During the first round of penalties, CMS dinged 2,213 hospitals for an estimated $280 million, or an average of about $126,500 per hospital, for excessive readmissions linked to heart attack, heart failure, and pneumonia care. Blum made the case that the penalties—or the threat thereof—are helping to improve rates.
Those arguing that the policy could disproportionately impact institutions caring for more vulnerable, high-risk patients also found new support in a recent New England Journal of Medicine perspective suggesting that academic medical centers and safety-net hospitals were more likely to be penalized.1 Among their suggestions, the perspective’s co-authors, from Harvard’s School of Public Health, suggested that the policy take patient socioeconomic status into account to provide a fairer basis of comparison.
A second recent study suggested that even the reduced readmission rates might not be telling the whole story. An analysis of patients released in 2010 from safety-net hospital Boston Medical Center showed that nearly 1 in 4 returned to the ED within a month of discharge.2 But more than half of those patients weren’t readmitted as inpatients, meaning that they wouldn’t show up under Medicare’s readmissions statistics.
Along with the mixed early reviews of EHR rollouts and the HCAHPS portion of the Hospital Value-Based Purchasing program, it’s another reminder that CMS metrics and incentives might not always add up as envisioned. In the near future, it seems, hospitals and health-care providers might have to contend with some imperfect numbers. TH
Bryn Nelson is a freelance medical writer in Seattle.
References
1. Joynt KE, Jha AK. Thirty-day readmissions–truth and consequences. N Engl J Med. 2012;366:1366-1369.
2. Rising KL, White LF, Fernandez WG, Boutwell, AE. Emergency department visits after hospital discharge: a missing part of the equation. Ann Emerg Med. 2013; in press.
Hospitalist-Focused Strategies to Address Medicare's Expanded Quality, Efficiency Measures

VBP. ACO. HAC. EHR. Suddenly, Medicare-derived acronyms are everywhere, and many of them are attached to a growing set of programs aimed at boosting efficiency and quality. Some are optional; others are mandatory. Some have carrots as incentives; others have sticks. Some seem well-designed; others seemingly work at cross-purposes.
Love or hate these initiatives, the combined time, money, and resources needed to address all of them could put hospitals and hospitalists under considerable duress.
“It can either prove or dismantle the whole hospitalist movement,” says Brian Hazen, MD, medical director of the hospitalist division at Inova Fairfax Hospital in Falls Church, Va. “Hospitals expect us to be agile and adapt to the pressures to keep them alive. If we cannot adapt and provide that, then why give us a job?”
Whether or not the focus is on lowering readmission rates, decreasing the incidence of hospital-acquired conditions, or improving efficiencies, Dr. Hazen tends to lump most of the sticks and carrots together. “I throw them all into one basket because for the most part, they’re all reflective of good care,” he says.
The basket is growing, however, and the bundle of sticks could deliver a financial beating to the unwary.

—Win Whitcomb, MD, MHM, medical director of healthcare quality, Baystate Medical Center, Springfield, Mass.; SHM Performance and Measurement Reporting Committee member; co-founder and past president of SHM; author of The Hospitalist’s “On the Horizon” column
At What Cost?
For the lowest-performing hospitals, the top readmission penalties will grow to 2% of Medicare reimbursements in fiscal year 2014 and 3% in 2015. Meanwhile, CMS’ Hospital-Acquired Conditions (HAC) program will begin assessing a 1% penalty on the worst performing hospitals in 2015, and the amount withheld under the Hospital Value-Based Purchasing (VBP) program will reach 2% in 2017 (top-performing hospitals can recoup the withhold and more, depending on performance). By that year, the three programs alone could result in a 6% loss of reimbursements.
Win Whitcomb, MD, MHM, medical director of healthcare quality at Baystate Medical Center in Springfield, Mass., and a member of SHM’s Performance and Measurement Reporting Committee, estimates that by 2017, the total at-risk payments could reach about $10 million for a 650-bed academic medical center. The tally for a 90-bed community hospital, he estimates, might run a bit less than $1 million. Although the combined penalty is probably enough to get the attention of most hospitals, very few institutions are likely to be dinged for the entire amount.
Nevertheless, the cumulative loss of reimbursements could be a tipping point for hospitals already in dire straits. “It’s possible that some low-margin hospitals that are facing big penalties could actually have their solvency threatened,” Dr. Whitcomb says. “If hospitals that are a vital part of the community are threatened with insolvency because of these programs, we may need to take a second look at how we structure the penalties.”
The necessary investment in infrastructure, he says, could prove to be a far bigger concern—at least initially.
“What is more expensive is just putting out the effort to do the work to improve and perform well under these programs,” says Dr. Whitcomb, co-founder and past president of SHM and author of The Hospitalist’s “On the Horizon” column. “That’s a big unreported hidden expense of all of these programs.”
With the fairly rapid implementation of multiple measures mandated by the Accountable Care Act, Medicare may be disinclined to dramatically ramp up the programs in play until it has a better sense of what’s working well. Then again, analysts like Laurence Baker, PhD, professor of health research and policy at Stanford University, say it’s doubtful that the agency will scale back its efforts given the widely held perception that plenty of waste can yet be wrung from the system.
“If I was a hospitalist, I would expect more of this coming,” Dr. Baker says.
Of course, rolling out new incentive programs is always a difficult balancing act in which the creators must be careful not to focus too much attention on the wrong measure or create unintended disincentives.
“That’s one of the great challenges: making a program that’s going to be successful when we know that people will do what’s measured and maybe even, without thinking about it, do less of what’s not measured. So we have to be careful about that,” Dr. Baker says.

—Monty Duke, MD, chief physician executive, Lancaster General Hospital, Lancaster, Pa.
Out of Alignment
Beyond cost and infrastructure, the proliferation of new measures also presents challenges for alignment. Monty Duke, MD, chief physician executive at Lancaster General Hospital in Lancaster, Pa., says the targets are changing so rapidly that tension can arise between hospitals and hospitalists in aligning expectations about priorities and considering how much time, resources, and staffing will be required to address them.
Likewise, the impetus to install new infrastructure can sometimes have unintended consequences, as Dr. Duke has seen firsthand with his hospital’s recent implementation of electronic health records (EHRs).
“In many ways, the electronic health record has changed the dynamic of rounding between physicians and nurses, and it’s really challenging communication,” he says. How so? “Because people spend more time communicating with the computer than they do talking to one another,” he says. The discordant communication, in turn, can conspire against a clear plan of care and overall goals as well as challenge efforts that emphasize a team-based approach.
Despite federal meaningful-use incentives, a recent survey also suggested that a majority of healthcare practices still may not achieve a positive return on investment for EHRs unless they can figure out how to use the systems to increase revenue.1 A minority of providers have succeeded by seeing more patients every day or by improving their billing process so the codes are more accurate and fewer claims are rejected.
Similarly, hospitalists like Dr. Hazen contend that some patient-satisfaction measures in the HCAHPS section of the VBP program can work against good clinical care. “That one drives me crazy because we’re not waiters or waitresses in a five-star restaurant,” he says. “Health care is complicated; it’s not like sending back a bowl of cold soup the way you can in a restaurant.”
Increasing satisfaction by keeping patients in the hospital longer than warranted or leaving in a Foley catheter for patient convenience, for example, can negatively impact actual outcomes.
“Physicians and nurses get put in this catch-22 where we have to choose between patient satisfaction and by-the-book clinical care,” Dr. Hazen says. “And our job is to try to mitigate that, but you’re kind of damned if you do and damned if you don’t.”
A new study, on the other hand, suggests that HCAHPS scores reflecting lower staff responsiveness are associated with an increased risk of HACs like central line–associated bloodstream infections and that lower scores may be a symptom of hospitals “with a multitude of problems.”2
A 10-Step Program
As existing rules and metrics are revised, new ones added, and others merged or discontinued, hospitalists are likely to encounter more hiccups and headaches. So what’s the solution? Beyond establishing good personal habits like hand-washing when entering and leaving a patient’s room, hospitalist leaders and healthcare analysts point to 10 strategies that may help keep HM providers from getting squeezed by all the demands:
1) Keep everyone on the same page. Because hospitals and health systems often take a subset of CMS core measures and make them strategic priorities, Dr. Whitcomb says hospitalists must thoroughly understand their own institutions’ internal system-level quality and safety goals. He stresses the need for hospitalists to develop and maintain close working connections with their organization’s safety- and quality-improvement (QI) teams “to understand exactly what the rules of the road are.”
Dr. Whitcomb says hospitals should compensate hospitalists for time spent working with these teams on feasible solutions. Hospitalist representatives can then champion specific safety or quality issues and keep them foremost in the minds of their colleagues. “I’m a big believer in paying people to do that work,” he says.
2) Take a wider view. It’s clear that most providers wouldn’t have chosen some of the performance indicators that Medicare and other third-party payors are asking them to meet, and many physicians have been more focused on outcomes than on clinical measures. Like it or not, however, thriving in the new era of health care means accepting more benchmarks. “We’ve had to broaden our scope to say, ‘OK, these other things matter, too,’” Dr. Duke says.
3) Use visual cues. Hospitalists can’t rely on memory to keep track of the dozens of measures for which they are being held accountable. “Every hospitalist program should have a dashboard of priority measures that they’re paying attention to and that’s out in front of them on a regular basis,” Dr. Whitcomb says. “It could be presented to them at monthly meetings, or it could be in a prominent place in their office, but there needs to be a set of cues.”
4) Use bonuses for alignment. Dr. Hazen says hospitals also may find success in using bonuses as a positive reinforcement for well-aligned care. Inova Fairfax’s bonuses include a clinical component that aligns with many of CMS’s core measures, and the financial incentives ensure that discharge summaries are completed and distributed in a timely manner.
5) Emphasize a team approach. Espousing a multidisciplinary approach to care can give patients the confidence that all providers are on the same page, thereby aiding patient-satisfaction scores and easing throughput. And as Dr. Hazen points out, avoiding a silo mentality can pay dividends for improving patient safety.

6) Offer the right information. Tierza Stephan, MD, regional hospitalist medical director for Allina Health in Minneapolis and the incoming chair of SHM’s Practice Analysis Committee, says Allina has worked hard to ensure that hospitalists complete their discharge summaries within 24 hours of a patient’s release from the hospital. Beyond timeliness, the health system is emphasizing content that informs without overwhelming the patient, caregiver, or follow-up provider with unnecessary details.
The discharge summary, for example, includes a section called “Recommendations for the Outpatient Provider,” which provides a checklist of sorts so those providers don’t miss the forest for the trees. The same is true for patients. “The hospital is probably not the best place to be educating patients, so we really focus more on patient instruction at discharge and then timely follow-up,” Dr. Stephan says.
In addition to allowing better care coordination between inpatient and outpatient providers, she says, “it cuts across patient experience and readmissions, and it helps patients to be engaged because they have very clear, easy-to-read information.” Paying attention to such details may have outsized impacts: In a recent study, researchers found that patients who are actively engaged in their own health care are significantly less costly to treat, on average.3
7) Follow through after discharge. Inova Fairfax is setting up an outpatient follow-up clinic as a safety net for patients at the highest risk of being readmitted. Many of these target patients are uninsured or underinsured and battling complex medical problems like heart failure or pneumonia. Establishing a physical location for follow-ups and direct communication with primary-care providers, the hospital hopes, might reduce noncompliance among these outpatients and thereby curtail subsequent readmissions.
8) Optimize EHR. When optimized, experts say, electronic medical records can help hospitals ensure that their providers are following core measures and preventing hospital-acquired conditions while leaving channels of communication open and keeping revenue streams flowing.
“Luckily, we just switched to electronic medical records so we can monitor who has a Foley catheter in, who does or doesn’t have DVT prophylaxis, because even really good docs sometimes make these knucklehead mistakes every once in a while,” Dr. Hazen says. “So we try to use systems to back ourselves up. But for the most part, there’s just no substitute for having good docs do the right thing and documenting that.”
9) Bundle up. Although bundled payments represent yet another CMS initiative, Dr. Duke says the model has the potential to reduce waste, standardize care, and monitor outcomes. Lancaster General has been working on the approach for the past few years, with an initial focus on cardiovascular medicine, orthopedics, and neurosurgery. “We’re getting a lot of traction to get physicians to work together to improve care, where before there wasn’t an incentive to do this,” Dr. Duke says. “So we see this as a good thing, and I think it has potential to reduce expenses in high-cost areas.”
10) Connect the dots. Joane Goodroe, an independent healthcare consultant based in Atlanta, says CMS expects providers to connect the dots and combine their efforts in the separate incentive programs to maximize their resources. By providing consistent care coordination and setting patients on the right track, then, she says hospitalists might help boost savings across the board—a benefit that wouldn’t necessarily be apparent based solely on improved quality metrics in specific programs.
Even here, though, the current fee-for-service model can create awkward side effects. For example, Goodroe recommends following the path that many care groups delving into accountable care and bundled payment systems are already taking: connecting those models to efforts aimed at reducing hospital readmissions. Without the proper financial incentives, however, those efforts may be constrained due to a significant increase in expended resources and a potential decrease in overall revenues.
Some of the kinks may work themselves out of the system over time, but experts say the era of multiple metrics—and additional pressure—is just beginning. Combined, they will require providers to be much better at working as a system and coordinating care across multiple environments beyond the hospital, Dr. Stephan says.
One main question boils down to this, she says: “How do we get more efficient as a system and eliminate waste? I think the hospitalists really play a vital role, and it’s mainly through communication and transfer of information. Hospitalists have to be really well-connected with the different physicians and venues that send the patients into the hospital so that we’re not duplicating services and so that we can get right to the crux of the problem.”
Doing so, regardless of which CMS program is on tap, may be the very best way to avoid getting squeezed.
Bryn Nelson is a freelance medical writer in Seattle.
References
- Adler-Milstein J, Green CE, Bates DW. A survey analysis suggests that electronic health records will yield revenue gains for some practices and losses for many. Health Affairs. 2013;32(3):562-570.
- Saman DM, Kavanagh KT, Johnson B, Lutfiyya MN. Can inpatient hospital experiences predict central line-associated bloodstream infections? PLoS ONE. 2013;8(4):e61097.
- Hibbard JH, Greene J, Overton V. Patients with lower activation associated with higher costs; delivery systems should know their patients’ ‘scores.’ Health Affairs. 2013; 32(2):216-222.
VBP. ACO. HAC. EHR. Suddenly, Medicare-derived acronyms are everywhere, and many of them are attached to a growing set of programs aimed at boosting efficiency and quality. Some are optional; others are mandatory. Some have carrots as incentives; others have sticks. Some seem well-designed; others seemingly work at cross-purposes.
Love or hate these initiatives, the combined time, money, and resources needed to address all of them could put hospitals and hospitalists under considerable duress.
“It can either prove or dismantle the whole hospitalist movement,” says Brian Hazen, MD, medical director of the hospitalist division at Inova Fairfax Hospital in Falls Church, Va. “Hospitals expect us to be agile and adapt to the pressures to keep them alive. If we cannot adapt and provide that, then why give us a job?”
Whether or not the focus is on lowering readmission rates, decreasing the incidence of hospital-acquired conditions, or improving efficiencies, Dr. Hazen tends to lump most of the sticks and carrots together. “I throw them all into one basket because for the most part, they’re all reflective of good care,” he says.
The basket is growing, however, and the bundle of sticks could deliver a financial beating to the unwary.
—Win Whitcomb, MD, MHM, medical director of healthcare quality, Baystate Medical Center, Springfield, Mass.; SHM Performance and Measurement Reporting Committee member; co-founder and past president of SHM; author of The Hospitalist’s “On the Horizon” column
At What Cost?
For the lowest-performing hospitals, the top readmission penalties will grow to 2% of Medicare reimbursements in fiscal year 2014 and 3% in 2015. Meanwhile, CMS’ Hospital-Acquired Conditions (HAC) program will begin assessing a 1% penalty on the worst performing hospitals in 2015, and the amount withheld under the Hospital Value-Based Purchasing (VBP) program will reach 2% in 2017 (top-performing hospitals can recoup the withhold and more, depending on performance). By that year, the three programs alone could result in a 6% loss of reimbursements.
Win Whitcomb, MD, MHM, medical director of healthcare quality at Baystate Medical Center in Springfield, Mass., and a member of SHM’s Performance and Measurement Reporting Committee, estimates that by 2017, the total at-risk payments could reach about $10 million for a 650-bed academic medical center. The tally for a 90-bed community hospital, he estimates, might run a bit less than $1 million. Although the combined penalty is probably enough to get the attention of most hospitals, very few institutions are likely to be dinged for the entire amount.
Nevertheless, the cumulative loss of reimbursements could be a tipping point for hospitals already in dire straits. “It’s possible that some low-margin hospitals that are facing big penalties could actually have their solvency threatened,” Dr. Whitcomb says. “If hospitals that are a vital part of the community are threatened with insolvency because of these programs, we may need to take a second look at how we structure the penalties.”
The necessary investment in infrastructure, he says, could prove to be a far bigger concern—at least initially.
“What is more expensive is just putting out the effort to do the work to improve and perform well under these programs,” says Dr. Whitcomb, co-founder and past president of SHM and author of The Hospitalist’s “On the Horizon” column. “That’s a big unreported hidden expense of all of these programs.”
With the fairly rapid implementation of multiple measures mandated by the Accountable Care Act, Medicare may be disinclined to dramatically ramp up the programs in play until it has a better sense of what’s working well. Then again, analysts like Laurence Baker, PhD, professor of health research and policy at Stanford University, say it’s doubtful that the agency will scale back its efforts given the widely held perception that plenty of waste can yet be wrung from the system.
“If I was a hospitalist, I would expect more of this coming,” Dr. Baker says.
Of course, rolling out new incentive programs is always a difficult balancing act in which the creators must be careful not to focus too much attention on the wrong measure or create unintended disincentives.
“That’s one of the great challenges: making a program that’s going to be successful when we know that people will do what’s measured and maybe even, without thinking about it, do less of what’s not measured. So we have to be careful about that,” Dr. Baker says.
—Monty Duke, MD, chief physician executive, Lancaster General Hospital, Lancaster, Pa.
Out of Alignment
Beyond cost and infrastructure, the proliferation of new measures also presents challenges for alignment. Monty Duke, MD, chief physician executive at Lancaster General Hospital in Lancaster, Pa., says the targets are changing so rapidly that tension can arise between hospitals and hospitalists in aligning expectations about priorities and considering how much time, resources, and staffing will be required to address them.
Likewise, the impetus to install new infrastructure can sometimes have unintended consequences, as Dr. Duke has seen firsthand with his hospital’s recent implementation of electronic health records (EHRs).
“In many ways, the electronic health record has changed the dynamic of rounding between physicians and nurses, and it’s really challenging communication,” he says. How so? “Because people spend more time communicating with the computer than they do talking to one another,” he says. The discordant communication, in turn, can conspire against a clear plan of care and overall goals as well as challenge efforts that emphasize a team-based approach.
Despite federal meaningful-use incentives, a recent survey also suggested that a majority of healthcare practices still may not achieve a positive return on investment for EHRs unless they can figure out how to use the systems to increase revenue.1 A minority of providers have succeeded by seeing more patients every day or by improving their billing process so the codes are more accurate and fewer claims are rejected.
Similarly, hospitalists like Dr. Hazen contend that some patient-satisfaction measures in the HCAHPS section of the VBP program can work against good clinical care. “That one drives me crazy because we’re not waiters or waitresses in a five-star restaurant,” he says. “Health care is complicated; it’s not like sending back a bowl of cold soup the way you can in a restaurant.”
Increasing satisfaction by keeping patients in the hospital longer than warranted or leaving in a Foley catheter for patient convenience, for example, can negatively impact actual outcomes.
“Physicians and nurses get put in this catch-22 where we have to choose between patient satisfaction and by-the-book clinical care,” Dr. Hazen says. “And our job is to try to mitigate that, but you’re kind of damned if you do and damned if you don’t.”
A new study, on the other hand, suggests that HCAHPS scores reflecting lower staff responsiveness are associated with an increased risk of HACs like central line–associated bloodstream infections and that lower scores may be a symptom of hospitals “with a multitude of problems.”2
A 10-Step Program
As existing rules and metrics are revised, new ones added, and others merged or discontinued, hospitalists are likely to encounter more hiccups and headaches. So what’s the solution? Beyond establishing good personal habits like hand-washing when entering and leaving a patient’s room, hospitalist leaders and healthcare analysts point to 10 strategies that may help keep HM providers from getting squeezed by all the demands:
1) Keep everyone on the same page. Because hospitals and health systems often take a subset of CMS core measures and make them strategic priorities, Dr. Whitcomb says hospitalists must thoroughly understand their own institutions’ internal system-level quality and safety goals. He stresses the need for hospitalists to develop and maintain close working connections with their organization’s safety- and quality-improvement (QI) teams “to understand exactly what the rules of the road are.”
Dr. Whitcomb says hospitals should compensate hospitalists for time spent working with these teams on feasible solutions. Hospitalist representatives can then champion specific safety or quality issues and keep them foremost in the minds of their colleagues. “I’m a big believer in paying people to do that work,” he says.
2) Take a wider view. It’s clear that most providers wouldn’t have chosen some of the performance indicators that Medicare and other third-party payors are asking them to meet, and many physicians have been more focused on outcomes than on clinical measures. Like it or not, however, thriving in the new era of health care means accepting more benchmarks. “We’ve had to broaden our scope to say, ‘OK, these other things matter, too,’” Dr. Duke says.
3) Use visual cues. Hospitalists can’t rely on memory to keep track of the dozens of measures for which they are being held accountable. “Every hospitalist program should have a dashboard of priority measures that they’re paying attention to and that’s out in front of them on a regular basis,” Dr. Whitcomb says. “It could be presented to them at monthly meetings, or it could be in a prominent place in their office, but there needs to be a set of cues.”
4) Use bonuses for alignment. Dr. Hazen says hospitals also may find success in using bonuses as a positive reinforcement for well-aligned care. Inova Fairfax’s bonuses include a clinical component that aligns with many of CMS’s core measures, and the financial incentives ensure that discharge summaries are completed and distributed in a timely manner.
5) Emphasize a team approach. Espousing a multidisciplinary approach to care can give patients the confidence that all providers are on the same page, thereby aiding patient-satisfaction scores and easing throughput. And as Dr. Hazen points out, avoiding a silo mentality can pay dividends for improving patient safety.
6) Offer the right information. Tierza Stephan, MD, regional hospitalist medical director for Allina Health in Minneapolis and the incoming chair of SHM’s Practice Analysis Committee, says Allina has worked hard to ensure that hospitalists complete their discharge summaries within 24 hours of a patient’s release from the hospital. Beyond timeliness, the health system is emphasizing content that informs without overwhelming the patient, caregiver, or follow-up provider with unnecessary details.
The discharge summary, for example, includes a section called “Recommendations for the Outpatient Provider,” which provides a checklist of sorts so those providers don’t miss the forest for the trees. The same is true for patients. “The hospital is probably not the best place to be educating patients, so we really focus more on patient instruction at discharge and then timely follow-up,” Dr. Stephan says.
In addition to allowing better care coordination between inpatient and outpatient providers, she says, “it cuts across patient experience and readmissions, and it helps patients to be engaged because they have very clear, easy-to-read information.” Paying attention to such details may have outsized impacts: In a recent study, researchers found that patients who are actively engaged in their own health care are significantly less costly to treat, on average.3
7) Follow through after discharge. Inova Fairfax is setting up an outpatient follow-up clinic as a safety net for patients at the highest risk of being readmitted. Many of these target patients are uninsured or underinsured and battling complex medical problems like heart failure or pneumonia. Establishing a physical location for follow-ups and direct communication with primary-care providers, the hospital hopes, might reduce noncompliance among these outpatients and thereby curtail subsequent readmissions.
8) Optimize EHR. When optimized, experts say, electronic medical records can help hospitals ensure that their providers are following core measures and preventing hospital-acquired conditions while leaving channels of communication open and keeping revenue streams flowing.
“Luckily, we just switched to electronic medical records so we can monitor who has a Foley catheter in, who does or doesn’t have DVT prophylaxis, because even really good docs sometimes make these knucklehead mistakes every once in a while,” Dr. Hazen says. “So we try to use systems to back ourselves up. But for the most part, there’s just no substitute for having good docs do the right thing and documenting that.”
9) Bundle up. Although bundled payments represent yet another CMS initiative, Dr. Duke says the model has the potential to reduce waste, standardize care, and monitor outcomes. Lancaster General has been working on the approach for the past few years, with an initial focus on cardiovascular medicine, orthopedics, and neurosurgery. “We’re getting a lot of traction to get physicians to work together to improve care, where before there wasn’t an incentive to do this,” Dr. Duke says. “So we see this as a good thing, and I think it has potential to reduce expenses in high-cost areas.”
10) Connect the dots. Joane Goodroe, an independent healthcare consultant based in Atlanta, says CMS expects providers to connect the dots and combine their efforts in the separate incentive programs to maximize their resources. By providing consistent care coordination and setting patients on the right track, then, she says hospitalists might help boost savings across the board—a benefit that wouldn’t necessarily be apparent based solely on improved quality metrics in specific programs.
Even here, though, the current fee-for-service model can create awkward side effects. For example, Goodroe recommends following the path that many care groups delving into accountable care and bundled payment systems are already taking: connecting those models to efforts aimed at reducing hospital readmissions. Without the proper financial incentives, however, those efforts may be constrained due to a significant increase in expended resources and a potential decrease in overall revenues.
Some of the kinks may work themselves out of the system over time, but experts say the era of multiple metrics—and additional pressure—is just beginning. Combined, they will require providers to be much better at working as a system and coordinating care across multiple environments beyond the hospital, Dr. Stephan says.
One main question boils down to this, she says: “How do we get more efficient as a system and eliminate waste? I think the hospitalists really play a vital role, and it’s mainly through communication and transfer of information. Hospitalists have to be really well-connected with the different physicians and venues that send the patients into the hospital so that we’re not duplicating services and so that we can get right to the crux of the problem.”
Doing so, regardless of which CMS program is on tap, may be the very best way to avoid getting squeezed.
Bryn Nelson is a freelance medical writer in Seattle.
References
- Adler-Milstein J, Green CE, Bates DW. A survey analysis suggests that electronic health records will yield revenue gains for some practices and losses for many. Health Affairs. 2013;32(3):562-570.
- Saman DM, Kavanagh KT, Johnson B, Lutfiyya MN. Can inpatient hospital experiences predict central line-associated bloodstream infections? PLoS ONE. 2013;8(4):e61097.
- Hibbard JH, Greene J, Overton V. Patients with lower activation associated with higher costs; delivery systems should know their patients’ ‘scores.’ Health Affairs. 2013; 32(2):216-222.
VBP. ACO. HAC. EHR. Suddenly, Medicare-derived acronyms are everywhere, and many of them are attached to a growing set of programs aimed at boosting efficiency and quality. Some are optional; others are mandatory. Some have carrots as incentives; others have sticks. Some seem well-designed; others seemingly work at cross-purposes.
Love or hate these initiatives, the combined time, money, and resources needed to address all of them could put hospitals and hospitalists under considerable duress.
“It can either prove or dismantle the whole hospitalist movement,” says Brian Hazen, MD, medical director of the hospitalist division at Inova Fairfax Hospital in Falls Church, Va. “Hospitals expect us to be agile and adapt to the pressures to keep them alive. If we cannot adapt and provide that, then why give us a job?”
Whether or not the focus is on lowering readmission rates, decreasing the incidence of hospital-acquired conditions, or improving efficiencies, Dr. Hazen tends to lump most of the sticks and carrots together. “I throw them all into one basket because for the most part, they’re all reflective of good care,” he says.
The basket is growing, however, and the bundle of sticks could deliver a financial beating to the unwary.
—Win Whitcomb, MD, MHM, medical director of healthcare quality, Baystate Medical Center, Springfield, Mass.; SHM Performance and Measurement Reporting Committee member; co-founder and past president of SHM; author of The Hospitalist’s “On the Horizon” column
At What Cost?
For the lowest-performing hospitals, the top readmission penalties will grow to 2% of Medicare reimbursements in fiscal year 2014 and 3% in 2015. Meanwhile, CMS’ Hospital-Acquired Conditions (HAC) program will begin assessing a 1% penalty on the worst performing hospitals in 2015, and the amount withheld under the Hospital Value-Based Purchasing (VBP) program will reach 2% in 2017 (top-performing hospitals can recoup the withhold and more, depending on performance). By that year, the three programs alone could result in a 6% loss of reimbursements.
Win Whitcomb, MD, MHM, medical director of healthcare quality at Baystate Medical Center in Springfield, Mass., and a member of SHM’s Performance and Measurement Reporting Committee, estimates that by 2017, the total at-risk payments could reach about $10 million for a 650-bed academic medical center. The tally for a 90-bed community hospital, he estimates, might run a bit less than $1 million. Although the combined penalty is probably enough to get the attention of most hospitals, very few institutions are likely to be dinged for the entire amount.
Nevertheless, the cumulative loss of reimbursements could be a tipping point for hospitals already in dire straits. “It’s possible that some low-margin hospitals that are facing big penalties could actually have their solvency threatened,” Dr. Whitcomb says. “If hospitals that are a vital part of the community are threatened with insolvency because of these programs, we may need to take a second look at how we structure the penalties.”
The necessary investment in infrastructure, he says, could prove to be a far bigger concern—at least initially.
“What is more expensive is just putting out the effort to do the work to improve and perform well under these programs,” says Dr. Whitcomb, co-founder and past president of SHM and author of The Hospitalist’s “On the Horizon” column. “That’s a big unreported hidden expense of all of these programs.”
With the fairly rapid implementation of multiple measures mandated by the Accountable Care Act, Medicare may be disinclined to dramatically ramp up the programs in play until it has a better sense of what’s working well. Then again, analysts like Laurence Baker, PhD, professor of health research and policy at Stanford University, say it’s doubtful that the agency will scale back its efforts given the widely held perception that plenty of waste can yet be wrung from the system.
“If I was a hospitalist, I would expect more of this coming,” Dr. Baker says.
Of course, rolling out new incentive programs is always a difficult balancing act in which the creators must be careful not to focus too much attention on the wrong measure or create unintended disincentives.
“That’s one of the great challenges: making a program that’s going to be successful when we know that people will do what’s measured and maybe even, without thinking about it, do less of what’s not measured. So we have to be careful about that,” Dr. Baker says.
—Monty Duke, MD, chief physician executive, Lancaster General Hospital, Lancaster, Pa.
Out of Alignment
Beyond cost and infrastructure, the proliferation of new measures also presents challenges for alignment. Monty Duke, MD, chief physician executive at Lancaster General Hospital in Lancaster, Pa., says the targets are changing so rapidly that tension can arise between hospitals and hospitalists in aligning expectations about priorities and considering how much time, resources, and staffing will be required to address them.
Likewise, the impetus to install new infrastructure can sometimes have unintended consequences, as Dr. Duke has seen firsthand with his hospital’s recent implementation of electronic health records (EHRs).
“In many ways, the electronic health record has changed the dynamic of rounding between physicians and nurses, and it’s really challenging communication,” he says. How so? “Because people spend more time communicating with the computer than they do talking to one another,” he says. The discordant communication, in turn, can conspire against a clear plan of care and overall goals as well as challenge efforts that emphasize a team-based approach.
Despite federal meaningful-use incentives, a recent survey also suggested that a majority of healthcare practices still may not achieve a positive return on investment for EHRs unless they can figure out how to use the systems to increase revenue.1 A minority of providers have succeeded by seeing more patients every day or by improving their billing process so the codes are more accurate and fewer claims are rejected.
Similarly, hospitalists like Dr. Hazen contend that some patient-satisfaction measures in the HCAHPS section of the VBP program can work against good clinical care. “That one drives me crazy because we’re not waiters or waitresses in a five-star restaurant,” he says. “Health care is complicated; it’s not like sending back a bowl of cold soup the way you can in a restaurant.”
Increasing satisfaction by keeping patients in the hospital longer than warranted or leaving in a Foley catheter for patient convenience, for example, can negatively impact actual outcomes.
“Physicians and nurses get put in this catch-22 where we have to choose between patient satisfaction and by-the-book clinical care,” Dr. Hazen says. “And our job is to try to mitigate that, but you’re kind of damned if you do and damned if you don’t.”
A new study, on the other hand, suggests that HCAHPS scores reflecting lower staff responsiveness are associated with an increased risk of HACs like central line–associated bloodstream infections and that lower scores may be a symptom of hospitals “with a multitude of problems.”2
A 10-Step Program
As existing rules and metrics are revised, new ones added, and others merged or discontinued, hospitalists are likely to encounter more hiccups and headaches. So what’s the solution? Beyond establishing good personal habits like hand-washing when entering and leaving a patient’s room, hospitalist leaders and healthcare analysts point to 10 strategies that may help keep HM providers from getting squeezed by all the demands:
1) Keep everyone on the same page. Because hospitals and health systems often take a subset of CMS core measures and make them strategic priorities, Dr. Whitcomb says hospitalists must thoroughly understand their own institutions’ internal system-level quality and safety goals. He stresses the need for hospitalists to develop and maintain close working connections with their organization’s safety- and quality-improvement (QI) teams “to understand exactly what the rules of the road are.”
Dr. Whitcomb says hospitals should compensate hospitalists for time spent working with these teams on feasible solutions. Hospitalist representatives can then champion specific safety or quality issues and keep them foremost in the minds of their colleagues. “I’m a big believer in paying people to do that work,” he says.
2) Take a wider view. It’s clear that most providers wouldn’t have chosen some of the performance indicators that Medicare and other third-party payors are asking them to meet, and many physicians have been more focused on outcomes than on clinical measures. Like it or not, however, thriving in the new era of health care means accepting more benchmarks. “We’ve had to broaden our scope to say, ‘OK, these other things matter, too,’” Dr. Duke says.
3) Use visual cues. Hospitalists can’t rely on memory to keep track of the dozens of measures for which they are being held accountable. “Every hospitalist program should have a dashboard of priority measures that they’re paying attention to and that’s out in front of them on a regular basis,” Dr. Whitcomb says. “It could be presented to them at monthly meetings, or it could be in a prominent place in their office, but there needs to be a set of cues.”
4) Use bonuses for alignment. Dr. Hazen says hospitals also may find success in using bonuses as a positive reinforcement for well-aligned care. Inova Fairfax’s bonuses include a clinical component that aligns with many of CMS’s core measures, and the financial incentives ensure that discharge summaries are completed and distributed in a timely manner.
5) Emphasize a team approach. Espousing a multidisciplinary approach to care can give patients the confidence that all providers are on the same page, thereby aiding patient-satisfaction scores and easing throughput. And as Dr. Hazen points out, avoiding a silo mentality can pay dividends for improving patient safety.
6) Offer the right information. Tierza Stephan, MD, regional hospitalist medical director for Allina Health in Minneapolis and the incoming chair of SHM’s Practice Analysis Committee, says Allina has worked hard to ensure that hospitalists complete their discharge summaries within 24 hours of a patient’s release from the hospital. Beyond timeliness, the health system is emphasizing content that informs without overwhelming the patient, caregiver, or follow-up provider with unnecessary details.
The discharge summary, for example, includes a section called “Recommendations for the Outpatient Provider,” which provides a checklist of sorts so those providers don’t miss the forest for the trees. The same is true for patients. “The hospital is probably not the best place to be educating patients, so we really focus more on patient instruction at discharge and then timely follow-up,” Dr. Stephan says.
In addition to allowing better care coordination between inpatient and outpatient providers, she says, “it cuts across patient experience and readmissions, and it helps patients to be engaged because they have very clear, easy-to-read information.” Paying attention to such details may have outsized impacts: In a recent study, researchers found that patients who are actively engaged in their own health care are significantly less costly to treat, on average.3
7) Follow through after discharge. Inova Fairfax is setting up an outpatient follow-up clinic as a safety net for patients at the highest risk of being readmitted. Many of these target patients are uninsured or underinsured and battling complex medical problems like heart failure or pneumonia. Establishing a physical location for follow-ups and direct communication with primary-care providers, the hospital hopes, might reduce noncompliance among these outpatients and thereby curtail subsequent readmissions.
8) Optimize EHR. When optimized, experts say, electronic medical records can help hospitals ensure that their providers are following core measures and preventing hospital-acquired conditions while leaving channels of communication open and keeping revenue streams flowing.
“Luckily, we just switched to electronic medical records so we can monitor who has a Foley catheter in, who does or doesn’t have DVT prophylaxis, because even really good docs sometimes make these knucklehead mistakes every once in a while,” Dr. Hazen says. “So we try to use systems to back ourselves up. But for the most part, there’s just no substitute for having good docs do the right thing and documenting that.”
9) Bundle up. Although bundled payments represent yet another CMS initiative, Dr. Duke says the model has the potential to reduce waste, standardize care, and monitor outcomes. Lancaster General has been working on the approach for the past few years, with an initial focus on cardiovascular medicine, orthopedics, and neurosurgery. “We’re getting a lot of traction to get physicians to work together to improve care, where before there wasn’t an incentive to do this,” Dr. Duke says. “So we see this as a good thing, and I think it has potential to reduce expenses in high-cost areas.”
10) Connect the dots. Joane Goodroe, an independent healthcare consultant based in Atlanta, says CMS expects providers to connect the dots and combine their efforts in the separate incentive programs to maximize their resources. By providing consistent care coordination and setting patients on the right track, then, she says hospitalists might help boost savings across the board—a benefit that wouldn’t necessarily be apparent based solely on improved quality metrics in specific programs.
Even here, though, the current fee-for-service model can create awkward side effects. For example, Goodroe recommends following the path that many care groups delving into accountable care and bundled payment systems are already taking: connecting those models to efforts aimed at reducing hospital readmissions. Without the proper financial incentives, however, those efforts may be constrained due to a significant increase in expended resources and a potential decrease in overall revenues.
Some of the kinks may work themselves out of the system over time, but experts say the era of multiple metrics—and additional pressure—is just beginning. Combined, they will require providers to be much better at working as a system and coordinating care across multiple environments beyond the hospital, Dr. Stephan says.
One main question boils down to this, she says: “How do we get more efficient as a system and eliminate waste? I think the hospitalists really play a vital role, and it’s mainly through communication and transfer of information. Hospitalists have to be really well-connected with the different physicians and venues that send the patients into the hospital so that we’re not duplicating services and so that we can get right to the crux of the problem.”
Doing so, regardless of which CMS program is on tap, may be the very best way to avoid getting squeezed.
Bryn Nelson is a freelance medical writer in Seattle.
References
- Adler-Milstein J, Green CE, Bates DW. A survey analysis suggests that electronic health records will yield revenue gains for some practices and losses for many. Health Affairs. 2013;32(3):562-570.
- Saman DM, Kavanagh KT, Johnson B, Lutfiyya MN. Can inpatient hospital experiences predict central line-associated bloodstream infections? PLoS ONE. 2013;8(4):e61097.
- Hibbard JH, Greene J, Overton V. Patients with lower activation associated with higher costs; delivery systems should know their patients’ ‘scores.’ Health Affairs. 2013; 32(2):216-222.
Hospitalist-Specific Data Shows Rise in Use of Some CPT Codes

Before 2011, hospitalists had only Centers for Medicare & Medicaid Services’ (CMS) specialty-specific CPT distribution data, and no hospitalist-specific data, available when looking for benchmarks against which to compare their billing practices. Thanks to recent State of Hospital Medicine surveys, however, we now have hospitalist-specific data for the distribution of commonly used CPT codes. It’s interesting to analyze how 2011 data compares to 2012, and how the use of high-level codes varies by geographic region, employment model, compensation structure, and practice size.
In 2012, the use of the higher-level inpatient (IP) discharge code (99239) increased to 52% from 48% in 2011 among HM groups serving adults only, and the use of the highest-level IP subsequent code (99233) increased to 33% from 28% in the same comparison. This increase is in keeping with national trends. According to a May 2012 report by the Department of Health and Human Services’ Office of Inspector General, from 2001 to 2010, physicians’ billing shifted from lower-level to higher-level codes. For example, the billing of the lowest-level code (99231) decreased 16%, while the billing of the two higher-level codes (99232 and 99233) increased 6% and 9%, respectively.
Possible drivers of this change include:
- Expanded use of electronic health records (EHRs);
- Increased physician education about documentation requirements; and
- A sicker hospitalized patient population due to expanded outpatient care capabilities.
Although the proportion of high-level subsequent and discharge codes reported by SHM increased in 2012, the percent of highest-level IP admission codes (99223) actually decreased to 66% from 69%. There are many possible reasons for this. First, the elimination of consult codes by CMS in 2010 increased the overall use of admission codes but might have decreased the proportion of highest-level admission codes. Additionally, there may be an increased use of higher RVU-generating critical-care codes preferentially over billing of the highest-level admission codes. Third, there is the possibility that the extra documentation required for high-level admissions is a billing deterrent. Similarly, higher-level codes may be downcoded if documentation is lacking or incomplete.
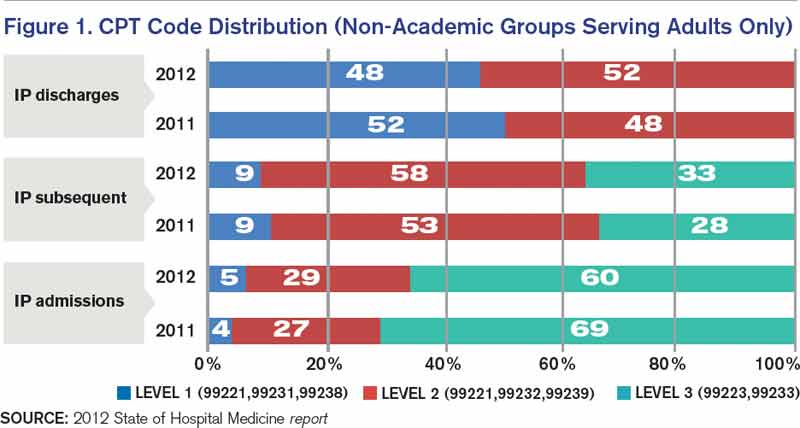
Source: 2012 State of Hospital Medicine report
Comparatively, my health system, Allina Health, showed an increase in the use of highest-level codes for all three CPT codes analyzed.
With the increasing sophistication of EHRs and coding technology tools, it will be interesting to see the future impact on coding distribution as providers adapt to new documentation processes that support health information exchange across systems.
Comparing geographic regions, the West uses the highest proportion of high-level codes for admission, follow-up, and discharge, followed by the Midwest.
Interestingly, variation in billing by group size is only correlated directly to admission codes, but not to follow-up or discharge codes—with larger services tending to bill more of the highest-level admission codes.
Admission code use correlates directly with compensation structure; groups providing 100% of total compensation in the form of salary bill the lowest percentage of high-level admission codes. As compensation trends away from straight salaries, the percentage of high-level admission codes increases. The picture is less clear for high-level follow-up and discharge codes.
Comparing academic and nonacademic HM groups shows greater use of the highest- level admission, follow-up, and discharge codes for nonacademic HM groups. This is likely because academic hospitalists can only bill for their own time and not for time spent by medical residents.
Employment model (e.g. hospital system, private hospitalist-only groups, management companies, etc.) showed no categorical effect on CPT distribution.
Dr. Stephan is regional hospitalist medical director for Allina Health in Minneapolis and the incoming chair of SHM’s Practice Analysis Committee.
Before 2011, hospitalists had only Centers for Medicare & Medicaid Services’ (CMS) specialty-specific CPT distribution data, and no hospitalist-specific data, available when looking for benchmarks against which to compare their billing practices. Thanks to recent State of Hospital Medicine surveys, however, we now have hospitalist-specific data for the distribution of commonly used CPT codes. It’s interesting to analyze how 2011 data compares to 2012, and how the use of high-level codes varies by geographic region, employment model, compensation structure, and practice size.
In 2012, the use of the higher-level inpatient (IP) discharge code (99239) increased to 52% from 48% in 2011 among HM groups serving adults only, and the use of the highest-level IP subsequent code (99233) increased to 33% from 28% in the same comparison. This increase is in keeping with national trends. According to a May 2012 report by the Department of Health and Human Services’ Office of Inspector General, from 2001 to 2010, physicians’ billing shifted from lower-level to higher-level codes. For example, the billing of the lowest-level code (99231) decreased 16%, while the billing of the two higher-level codes (99232 and 99233) increased 6% and 9%, respectively.
Possible drivers of this change include:
- Expanded use of electronic health records (EHRs);
- Increased physician education about documentation requirements; and
- A sicker hospitalized patient population due to expanded outpatient care capabilities.
Although the proportion of high-level subsequent and discharge codes reported by SHM increased in 2012, the percent of highest-level IP admission codes (99223) actually decreased to 66% from 69%. There are many possible reasons for this. First, the elimination of consult codes by CMS in 2010 increased the overall use of admission codes but might have decreased the proportion of highest-level admission codes. Additionally, there may be an increased use of higher RVU-generating critical-care codes preferentially over billing of the highest-level admission codes. Third, there is the possibility that the extra documentation required for high-level admissions is a billing deterrent. Similarly, higher-level codes may be downcoded if documentation is lacking or incomplete.
Source: 2012 State of Hospital Medicine report
Comparatively, my health system, Allina Health, showed an increase in the use of highest-level codes for all three CPT codes analyzed.
With the increasing sophistication of EHRs and coding technology tools, it will be interesting to see the future impact on coding distribution as providers adapt to new documentation processes that support health information exchange across systems.
Comparing geographic regions, the West uses the highest proportion of high-level codes for admission, follow-up, and discharge, followed by the Midwest.
Interestingly, variation in billing by group size is only correlated directly to admission codes, but not to follow-up or discharge codes—with larger services tending to bill more of the highest-level admission codes.
Admission code use correlates directly with compensation structure; groups providing 100% of total compensation in the form of salary bill the lowest percentage of high-level admission codes. As compensation trends away from straight salaries, the percentage of high-level admission codes increases. The picture is less clear for high-level follow-up and discharge codes.
Comparing academic and nonacademic HM groups shows greater use of the highest- level admission, follow-up, and discharge codes for nonacademic HM groups. This is likely because academic hospitalists can only bill for their own time and not for time spent by medical residents.
Employment model (e.g. hospital system, private hospitalist-only groups, management companies, etc.) showed no categorical effect on CPT distribution.
Dr. Stephan is regional hospitalist medical director for Allina Health in Minneapolis and the incoming chair of SHM’s Practice Analysis Committee.
Before 2011, hospitalists had only Centers for Medicare & Medicaid Services’ (CMS) specialty-specific CPT distribution data, and no hospitalist-specific data, available when looking for benchmarks against which to compare their billing practices. Thanks to recent State of Hospital Medicine surveys, however, we now have hospitalist-specific data for the distribution of commonly used CPT codes. It’s interesting to analyze how 2011 data compares to 2012, and how the use of high-level codes varies by geographic region, employment model, compensation structure, and practice size.
In 2012, the use of the higher-level inpatient (IP) discharge code (99239) increased to 52% from 48% in 2011 among HM groups serving adults only, and the use of the highest-level IP subsequent code (99233) increased to 33% from 28% in the same comparison. This increase is in keeping with national trends. According to a May 2012 report by the Department of Health and Human Services’ Office of Inspector General, from 2001 to 2010, physicians’ billing shifted from lower-level to higher-level codes. For example, the billing of the lowest-level code (99231) decreased 16%, while the billing of the two higher-level codes (99232 and 99233) increased 6% and 9%, respectively.
Possible drivers of this change include:
- Expanded use of electronic health records (EHRs);
- Increased physician education about documentation requirements; and
- A sicker hospitalized patient population due to expanded outpatient care capabilities.
Although the proportion of high-level subsequent and discharge codes reported by SHM increased in 2012, the percent of highest-level IP admission codes (99223) actually decreased to 66% from 69%. There are many possible reasons for this. First, the elimination of consult codes by CMS in 2010 increased the overall use of admission codes but might have decreased the proportion of highest-level admission codes. Additionally, there may be an increased use of higher RVU-generating critical-care codes preferentially over billing of the highest-level admission codes. Third, there is the possibility that the extra documentation required for high-level admissions is a billing deterrent. Similarly, higher-level codes may be downcoded if documentation is lacking or incomplete.
Source: 2012 State of Hospital Medicine report
Comparatively, my health system, Allina Health, showed an increase in the use of highest-level codes for all three CPT codes analyzed.
With the increasing sophistication of EHRs and coding technology tools, it will be interesting to see the future impact on coding distribution as providers adapt to new documentation processes that support health information exchange across systems.
Comparing geographic regions, the West uses the highest proportion of high-level codes for admission, follow-up, and discharge, followed by the Midwest.
Interestingly, variation in billing by group size is only correlated directly to admission codes, but not to follow-up or discharge codes—with larger services tending to bill more of the highest-level admission codes.
Admission code use correlates directly with compensation structure; groups providing 100% of total compensation in the form of salary bill the lowest percentage of high-level admission codes. As compensation trends away from straight salaries, the percentage of high-level admission codes increases. The picture is less clear for high-level follow-up and discharge codes.
Comparing academic and nonacademic HM groups shows greater use of the highest- level admission, follow-up, and discharge codes for nonacademic HM groups. This is likely because academic hospitalists can only bill for their own time and not for time spent by medical residents.
Employment model (e.g. hospital system, private hospitalist-only groups, management companies, etc.) showed no categorical effect on CPT distribution.
Dr. Stephan is regional hospitalist medical director for Allina Health in Minneapolis and the incoming chair of SHM’s Practice Analysis Committee.
Lack of Medicare CPT Codes for Hospitalist Practice Creates Dilemma

Hospitalist leaders are taking a proactive approach to the latest wrinkle of the specialty’s rock-and-a-hard-place dilemma when it comes to how clinicians code for their services. The oft-lamented issue is the Centers for Medicare & Medicaid Services’ (CMS) dearth of CPT codes designated for day-to-day hospitalist services.
But the latest twist to the story is what happens in skilled-nursing facilities (SNFs). Hospitalists increasingly are taking lead roles in SNFs, yet they must use the same care codes as nursing-home providers despite the higher acuity and longer length of stay found in SNFs compared to nursing homes. Additionally, Medicare recognizes SNFs and nursing homes as primary care for reimbursement via accountable-care organizations (ACOs).
Kerry Weiner, MD, a member of SHM’s Public Policy Committee, says SHM and others, including the American Medical Directors Association, are pushing CMS to reclassify SNF care as inpatient service, similar to acute rehabilitation facilities, inpatient psychiatric care, and long-term acute-care facilities. Dr. Weiner suggests rank-and-file practitioners do the same.
“We think attributing providers to be primary care versus specialty care versus acute care only on the basis of E&M codes will not really capture the nuances of primary-care practice in the country right now,” says Dr. Weiner, chief medical officer at North Hollywood, Calif.-based IPC: The Hospitalist Company. “This is an example of how just using E&M codes does not really capture the style of practice and the type of patient you’re seeing.”
The arguments for reclassification include:
- Hospitalists and other physicians practicing in SNFs need to spend most of their time there to provide optimal care, but it is difficult to financially justify maintaining that presence without an adequate patient census.
- Generating that census while practicing in one ACO is difficult because most facilities service multiple ACOs, and PCP exclusivity rules tied to many ACO contracts are a hurdle for physicians working with one just ACO (working with multiple ACOs requires multiple tax identification numbers and can be “operationally and politically difficult,” Dr. Wiener says).
- All told, ACO setup creates a fiscal hurdle for providers working in SNFs and does not recognize the clinical burden that separates the types of care provided in SNFs and nursing homes. Were care in SNFs reclassified as inpatient care, the exclusivity rule would not apply, and therefore, hospitalists in those facilities could more easily attain a patient census that justifies their continued presence. Dr. Weiner says one solution is to create a set of CPT codes just for SNFs that could be used by specialist physicians, including hospitalists.
“We are proposing a ‘work around’ by using the site of service as a determinator,” he adds.
Issues to Address
Dr. Weiner, SHM officials, and others have met with CMS to discuss the potential reclassification. Dr. Weiner says that as the Physician Quality Reporting System (PQRS) morphs into the Value-Based Payment Modifier (VBPM) program, the issue of ACO exclusivity could become even more prevalent as compensation is tied to performance.
“One of the components of physician value-based purchasing is the cost of care,” Dr. Weiner says. “If you compare a hospitalist’s cost to the pool of primary care, which includes hospitals, SNFs, etc., you’re obviously going to be higher because you have a much sicker population; A lot more things are going on, so there’s a lot higher utilization. So this concept of assigning doctors to a style of practice just based on E&M codes is just inadequate.”
Patrick Conway, MD, MSc, FAAP, SFHM, chief medical officer of CMS and director of CMS’ Center of Clinical Standards and Quality, says the agency is sympathetic to the issue. Via PQRS and VBPM, CMS is working to put in place “a robust set of measures that hospitalists can choose to report on,” he says.
“CMS has sought public comment on allowing hospitalists to align with their hospital’s quality measures for CMS quality programs,” he says. “But without this alignment option or a specialty code, we need to at least have sufficient measures to reflect hospitalists’ actual practice and what’s important to hospital medicine.”
Dr. Conway, a former hospitalist and chair of SHM’s Public Policy Committee, says he welcomes feedback from SHM and its members on suggested changes to CMS policy.
“I would certainly encourage hospital medicine to have discussions with the CMS payment and coding team that makes determinations about specialty status,” he says.
The Future?
Ironically, the potential panacea of HM-specific codes has not been fully embraced because of fears of unintended consequences. For example, in the case of hospitalists practicing in SNFs, the PCP designation is problematic in terms of lower reimbursement rates. Some hospitalists, however, will see a bump in total revenue the next two years because they will be designated PCPs and paid more via the Medicaid-to-Medicare parity regulation included in the Affordable Care Act.
“Hospital medicine will want to think about that as it goes through the process,” Dr. Conway says. “Internally with CMS, if you’re a specialty, we will specifically consider if you’re primary care or not. Whereas, if you’re in the internal-medicine bucket, by definition from the traditional CMS specialty coding perspective, you are primary care. So if you make a point to carve out your own category, then it’ll be a decision every time if you’re primary care or are you a specialty.”
Richard Quinn is a freelance writer in New Jersey.
Call for PQRS Measures

CMS’ annual call for Physician Quality Reporting System (PQRS) measures is a rite of summer. And Dr. Conway hopes that when CMS culls through this summer’s batch, hospitalists weighed in often.
“I know that the surgeons, the cardiologists, and others, every year, they say, ‘Here are the 20 new measures we’re thinking about for our specialty,’” he says. “So I just want to make clear that SHM should do the same. Identify the measures out there that are most relevant to you.”
Dr. Conway adds that the process shouldn’t be limited to the society level. Individual practitioners can reach out to CMS and weigh in as well.
Physicians “need to have sufficient measures to cover [their] specialty, and societies can play a key role in developing measures or identifying measures,” Dr. Conway says. “If there’s measures you want in the program, by all means, tell us.”
—Richard Quinn
Hospitalist leaders are taking a proactive approach to the latest wrinkle of the specialty’s rock-and-a-hard-place dilemma when it comes to how clinicians code for their services. The oft-lamented issue is the Centers for Medicare & Medicaid Services’ (CMS) dearth of CPT codes designated for day-to-day hospitalist services.
But the latest twist to the story is what happens in skilled-nursing facilities (SNFs). Hospitalists increasingly are taking lead roles in SNFs, yet they must use the same care codes as nursing-home providers despite the higher acuity and longer length of stay found in SNFs compared to nursing homes. Additionally, Medicare recognizes SNFs and nursing homes as primary care for reimbursement via accountable-care organizations (ACOs).
Kerry Weiner, MD, a member of SHM’s Public Policy Committee, says SHM and others, including the American Medical Directors Association, are pushing CMS to reclassify SNF care as inpatient service, similar to acute rehabilitation facilities, inpatient psychiatric care, and long-term acute-care facilities. Dr. Weiner suggests rank-and-file practitioners do the same.
“We think attributing providers to be primary care versus specialty care versus acute care only on the basis of E&M codes will not really capture the nuances of primary-care practice in the country right now,” says Dr. Weiner, chief medical officer at North Hollywood, Calif.-based IPC: The Hospitalist Company. “This is an example of how just using E&M codes does not really capture the style of practice and the type of patient you’re seeing.”
The arguments for reclassification include:
- Hospitalists and other physicians practicing in SNFs need to spend most of their time there to provide optimal care, but it is difficult to financially justify maintaining that presence without an adequate patient census.
- Generating that census while practicing in one ACO is difficult because most facilities service multiple ACOs, and PCP exclusivity rules tied to many ACO contracts are a hurdle for physicians working with one just ACO (working with multiple ACOs requires multiple tax identification numbers and can be “operationally and politically difficult,” Dr. Wiener says).
- All told, ACO setup creates a fiscal hurdle for providers working in SNFs and does not recognize the clinical burden that separates the types of care provided in SNFs and nursing homes. Were care in SNFs reclassified as inpatient care, the exclusivity rule would not apply, and therefore, hospitalists in those facilities could more easily attain a patient census that justifies their continued presence. Dr. Weiner says one solution is to create a set of CPT codes just for SNFs that could be used by specialist physicians, including hospitalists.
“We are proposing a ‘work around’ by using the site of service as a determinator,” he adds.
Issues to Address
Dr. Weiner, SHM officials, and others have met with CMS to discuss the potential reclassification. Dr. Weiner says that as the Physician Quality Reporting System (PQRS) morphs into the Value-Based Payment Modifier (VBPM) program, the issue of ACO exclusivity could become even more prevalent as compensation is tied to performance.
“One of the components of physician value-based purchasing is the cost of care,” Dr. Weiner says. “If you compare a hospitalist’s cost to the pool of primary care, which includes hospitals, SNFs, etc., you’re obviously going to be higher because you have a much sicker population; A lot more things are going on, so there’s a lot higher utilization. So this concept of assigning doctors to a style of practice just based on E&M codes is just inadequate.”
Patrick Conway, MD, MSc, FAAP, SFHM, chief medical officer of CMS and director of CMS’ Center of Clinical Standards and Quality, says the agency is sympathetic to the issue. Via PQRS and VBPM, CMS is working to put in place “a robust set of measures that hospitalists can choose to report on,” he says.
“CMS has sought public comment on allowing hospitalists to align with their hospital’s quality measures for CMS quality programs,” he says. “But without this alignment option or a specialty code, we need to at least have sufficient measures to reflect hospitalists’ actual practice and what’s important to hospital medicine.”
Dr. Conway, a former hospitalist and chair of SHM’s Public Policy Committee, says he welcomes feedback from SHM and its members on suggested changes to CMS policy.
“I would certainly encourage hospital medicine to have discussions with the CMS payment and coding team that makes determinations about specialty status,” he says.
The Future?
Ironically, the potential panacea of HM-specific codes has not been fully embraced because of fears of unintended consequences. For example, in the case of hospitalists practicing in SNFs, the PCP designation is problematic in terms of lower reimbursement rates. Some hospitalists, however, will see a bump in total revenue the next two years because they will be designated PCPs and paid more via the Medicaid-to-Medicare parity regulation included in the Affordable Care Act.
“Hospital medicine will want to think about that as it goes through the process,” Dr. Conway says. “Internally with CMS, if you’re a specialty, we will specifically consider if you’re primary care or not. Whereas, if you’re in the internal-medicine bucket, by definition from the traditional CMS specialty coding perspective, you are primary care. So if you make a point to carve out your own category, then it’ll be a decision every time if you’re primary care or are you a specialty.”
Richard Quinn is a freelance writer in New Jersey.
Call for PQRS Measures
CMS’ annual call for Physician Quality Reporting System (PQRS) measures is a rite of summer. And Dr. Conway hopes that when CMS culls through this summer’s batch, hospitalists weighed in often.
“I know that the surgeons, the cardiologists, and others, every year, they say, ‘Here are the 20 new measures we’re thinking about for our specialty,’” he says. “So I just want to make clear that SHM should do the same. Identify the measures out there that are most relevant to you.”
Dr. Conway adds that the process shouldn’t be limited to the society level. Individual practitioners can reach out to CMS and weigh in as well.
Physicians “need to have sufficient measures to cover [their] specialty, and societies can play a key role in developing measures or identifying measures,” Dr. Conway says. “If there’s measures you want in the program, by all means, tell us.”
—Richard Quinn
Hospitalist leaders are taking a proactive approach to the latest wrinkle of the specialty’s rock-and-a-hard-place dilemma when it comes to how clinicians code for their services. The oft-lamented issue is the Centers for Medicare & Medicaid Services’ (CMS) dearth of CPT codes designated for day-to-day hospitalist services.
But the latest twist to the story is what happens in skilled-nursing facilities (SNFs). Hospitalists increasingly are taking lead roles in SNFs, yet they must use the same care codes as nursing-home providers despite the higher acuity and longer length of stay found in SNFs compared to nursing homes. Additionally, Medicare recognizes SNFs and nursing homes as primary care for reimbursement via accountable-care organizations (ACOs).
Kerry Weiner, MD, a member of SHM’s Public Policy Committee, says SHM and others, including the American Medical Directors Association, are pushing CMS to reclassify SNF care as inpatient service, similar to acute rehabilitation facilities, inpatient psychiatric care, and long-term acute-care facilities. Dr. Weiner suggests rank-and-file practitioners do the same.
“We think attributing providers to be primary care versus specialty care versus acute care only on the basis of E&M codes will not really capture the nuances of primary-care practice in the country right now,” says Dr. Weiner, chief medical officer at North Hollywood, Calif.-based IPC: The Hospitalist Company. “This is an example of how just using E&M codes does not really capture the style of practice and the type of patient you’re seeing.”
The arguments for reclassification include:
- Hospitalists and other physicians practicing in SNFs need to spend most of their time there to provide optimal care, but it is difficult to financially justify maintaining that presence without an adequate patient census.
- Generating that census while practicing in one ACO is difficult because most facilities service multiple ACOs, and PCP exclusivity rules tied to many ACO contracts are a hurdle for physicians working with one just ACO (working with multiple ACOs requires multiple tax identification numbers and can be “operationally and politically difficult,” Dr. Wiener says).
- All told, ACO setup creates a fiscal hurdle for providers working in SNFs and does not recognize the clinical burden that separates the types of care provided in SNFs and nursing homes. Were care in SNFs reclassified as inpatient care, the exclusivity rule would not apply, and therefore, hospitalists in those facilities could more easily attain a patient census that justifies their continued presence. Dr. Weiner says one solution is to create a set of CPT codes just for SNFs that could be used by specialist physicians, including hospitalists.
“We are proposing a ‘work around’ by using the site of service as a determinator,” he adds.
Issues to Address
Dr. Weiner, SHM officials, and others have met with CMS to discuss the potential reclassification. Dr. Weiner says that as the Physician Quality Reporting System (PQRS) morphs into the Value-Based Payment Modifier (VBPM) program, the issue of ACO exclusivity could become even more prevalent as compensation is tied to performance.
“One of the components of physician value-based purchasing is the cost of care,” Dr. Weiner says. “If you compare a hospitalist’s cost to the pool of primary care, which includes hospitals, SNFs, etc., you’re obviously going to be higher because you have a much sicker population; A lot more things are going on, so there’s a lot higher utilization. So this concept of assigning doctors to a style of practice just based on E&M codes is just inadequate.”
Patrick Conway, MD, MSc, FAAP, SFHM, chief medical officer of CMS and director of CMS’ Center of Clinical Standards and Quality, says the agency is sympathetic to the issue. Via PQRS and VBPM, CMS is working to put in place “a robust set of measures that hospitalists can choose to report on,” he says.
“CMS has sought public comment on allowing hospitalists to align with their hospital’s quality measures for CMS quality programs,” he says. “But without this alignment option or a specialty code, we need to at least have sufficient measures to reflect hospitalists’ actual practice and what’s important to hospital medicine.”
Dr. Conway, a former hospitalist and chair of SHM’s Public Policy Committee, says he welcomes feedback from SHM and its members on suggested changes to CMS policy.
“I would certainly encourage hospital medicine to have discussions with the CMS payment and coding team that makes determinations about specialty status,” he says.
The Future?
Ironically, the potential panacea of HM-specific codes has not been fully embraced because of fears of unintended consequences. For example, in the case of hospitalists practicing in SNFs, the PCP designation is problematic in terms of lower reimbursement rates. Some hospitalists, however, will see a bump in total revenue the next two years because they will be designated PCPs and paid more via the Medicaid-to-Medicare parity regulation included in the Affordable Care Act.
“Hospital medicine will want to think about that as it goes through the process,” Dr. Conway says. “Internally with CMS, if you’re a specialty, we will specifically consider if you’re primary care or not. Whereas, if you’re in the internal-medicine bucket, by definition from the traditional CMS specialty coding perspective, you are primary care. So if you make a point to carve out your own category, then it’ll be a decision every time if you’re primary care or are you a specialty.”
Richard Quinn is a freelance writer in New Jersey.
Call for PQRS Measures
CMS’ annual call for Physician Quality Reporting System (PQRS) measures is a rite of summer. And Dr. Conway hopes that when CMS culls through this summer’s batch, hospitalists weighed in often.
“I know that the surgeons, the cardiologists, and others, every year, they say, ‘Here are the 20 new measures we’re thinking about for our specialty,’” he says. “So I just want to make clear that SHM should do the same. Identify the measures out there that are most relevant to you.”
Dr. Conway adds that the process shouldn’t be limited to the society level. Individual practitioners can reach out to CMS and weigh in as well.
Physicians “need to have sufficient measures to cover [their] specialty, and societies can play a key role in developing measures or identifying measures,” Dr. Conway says. “If there’s measures you want in the program, by all means, tell us.”
—Richard Quinn
Medicare Outlines Anticipated Funding Changes Under Affordable Care Act


The Centers for Medicare & Medicaid Services (CMS) recently released a few Fact Sheets on how they anticipate funding changes on a few of their programs that were implemented (or sustained) under the Affordable Care Act. As a background, CMS pays most acute-care hospitals by prospectively determining payment based on a patient’s diagnosis and the severity of illness within that diagnosis (e.g. “MS-DRG”). These payment amounts are updated annually after evaluating several factors, including the costs associated with the delivery of care.
One of the most major changes described in the Fact Sheet that will affect hospitalists is how CMS will review inpatient stays based on the number of nights in the hospital. CMS has proposed that any patient who stays in the hospital for two or more “midnights” should be appropriate for payment under Medicare Part A. For those who stay in the hospital for only one (or zero) midnights, payment under Medicare Part A will only be appropriate if:
- There is sufficient documentation at the time of admission that the anticipated length of stay is two or more nights; and.
- Further documentation that circumstances changed, and the hospital stay ended prematurely because of those changes.
Overall for hospitalists, this should substantially simplify the admitting process, whereby most inpatients being admitted with the anticipation of two or more nights should qualify for an inpatient stay. This also reduces the administrative burden of correcting the “inpatient” versus “observation” designation, which keeps many hospital staffs entirely too busy. This change also should relieve a significant burden from the patients and their families, who if kept in observation for a period of time, may have to pay substantially out of pocket to make up for the difference between the cost of the stay and the reimbursement from CMS for observation status. So this is one of the moves that CMS is making to simplify (and not complicate) an already too-complicated payment system. This should go into effect October 2013 and will be a sigh of much relief from many of us.
A few other anticipated changes that will affect hospitalists include:
Payments for Unfunded Care
Another major change that will go into affect October 2013 is the amount of monies received by hospitals that care for unfunded patients. These payments historically have been made to “Disproportionate Share Hospitals” (DSH), which are hospitals that care for a higher percentage of unfunded patients. Under the Affordable Care Act, only 25% of these payments will be distributed to DSH hospitals; the remaining 75% will be reduced based on the number of uninsured in the U.S., then redistributed to DSH hospitals based on their portion of uninsured care delivered.
Most DSH hospitals should expect a decrease in DSH payments, the amount of which will depend on their share of unfunded patients.
Any reduction in the “bottom line” to the hospital can affect hospitalists, especially those who are directly employed by the hospital.
Hospital-Acquired Conditions
CMS has long had the Hospital-Acquired Condition (HAC) program in effect, which has the ability to reduce the amount of payment for inpatients who acquire a HAC during their hospital stay. Starting in October 2014, CMS will impose additional financial penalties for hospitals with high HAC rates.
Specifically, those hospitals in the highest 25th percentile of HAC rates will be penalized 1% of their overall CMS payments. Another proposed change is that the following be included in the HAC reduction plan (two “domains” of measures):
- Domain No. 1: Six of the AHRQ Patient Safety Indicators (PSIs), including pressure ulcers, foreign bodies left in after surgery, iatrogenic pneumothorax, postoperative physiologic or metabolic derangements, postoperative VTE, and accidental puncture/laceration.
- Domain No. 2: Central-line-associated bloodstream infections (CLABSI) and catheter-associated urinary tract infections (CAUTIs).
The domains will be weighted equally, and an average score will determine the total score. There will be some methodology for risk adjustment, and hospitals will be given a review and comment period to validate their own scores.
Most hospitalists have at least indirect control over many of these HACs,and all need to pay very close attention to their hospital’s rates of these now and in the future.
Readmissions
As we all know, the Hospital Readmission Reduction program went into effect October 2012; it placed 1% of CMS payments at risk. This will increase to 2% of payments as of October 2013. CMS will continue to use AMI, CHF, and pneumonia as the three conditions under which the readmissions are measured but will put in some methodology to account for planned readmissions.
In addition, in October 2014, they plan to add readmission rates for COPD and for hip/knee arthroplasty.
Hospitalists will continue to need to progress their transitions of care programs, at least for these five patients conditions but more likely (and more effectively) for all hospital discharges.
Quality Measures
Currently more than 99% of acute-care hospitals participate in the pay-for-reporting quality program through CMS, the results of which have been displayed on the Hospital Compare website (www.hospitalcompare.hhs.gov) for years. The program started in 2004 with 10 quality metrics and now includes 57 metrics. These include process and outcome measures for AMI, CHF, and pneumonia, as well as process measures for surgical care, HACs, and patient-satisfaction surveys, among others.
This program will continue to expand over time, including hospital-acquired MRSA and Clostridium difficile rates. The few hospitals not participating will have their CMS annual payments reduced by 2%.
EHR Incentives
CMS is evaluating ways to reduce the burden of reporting by aligning EHR incentives with the Inpatient Quality Reporting program.
Summary
After an open commentary period, the Final Rule will be published Aug. 1, and will become effective for discharges on or after Oct. 1. Although CMS will continue to expand the total number of measures that need to be reported, and the penalties for non-reporting or low performance will continue to escalate, CMS is at least attempting to reduce the overall burden of reporting by combining measures and programs over time and using EHRs to facilitate the bulk of reporting over time.
The global message to hospitalists is: Continue to focus on reducing the burden of HACs, enhance throughput, and carefully and thoughtfully transition patients to the next provider after their hospital discharge. All in all, although at times this can feel overwhelming, these changes represent the right direction to move for high-quality and safe patient care.
Dr. Scheurer is a hospitalist and chief quality officer at the Medical University of South Carolina in Charleston. She is physician editor of The Hospitalist. Email her at [email protected].
Reference
The Centers for Medicare & Medicaid Services (CMS) recently released a few Fact Sheets on how they anticipate funding changes on a few of their programs that were implemented (or sustained) under the Affordable Care Act. As a background, CMS pays most acute-care hospitals by prospectively determining payment based on a patient’s diagnosis and the severity of illness within that diagnosis (e.g. “MS-DRG”). These payment amounts are updated annually after evaluating several factors, including the costs associated with the delivery of care.
One of the most major changes described in the Fact Sheet that will affect hospitalists is how CMS will review inpatient stays based on the number of nights in the hospital. CMS has proposed that any patient who stays in the hospital for two or more “midnights” should be appropriate for payment under Medicare Part A. For those who stay in the hospital for only one (or zero) midnights, payment under Medicare Part A will only be appropriate if:
- There is sufficient documentation at the time of admission that the anticipated length of stay is two or more nights; and.
- Further documentation that circumstances changed, and the hospital stay ended prematurely because of those changes.
Overall for hospitalists, this should substantially simplify the admitting process, whereby most inpatients being admitted with the anticipation of two or more nights should qualify for an inpatient stay. This also reduces the administrative burden of correcting the “inpatient” versus “observation” designation, which keeps many hospital staffs entirely too busy. This change also should relieve a significant burden from the patients and their families, who if kept in observation for a period of time, may have to pay substantially out of pocket to make up for the difference between the cost of the stay and the reimbursement from CMS for observation status. So this is one of the moves that CMS is making to simplify (and not complicate) an already too-complicated payment system. This should go into effect October 2013 and will be a sigh of much relief from many of us.
A few other anticipated changes that will affect hospitalists include:
Payments for Unfunded Care
Another major change that will go into affect October 2013 is the amount of monies received by hospitals that care for unfunded patients. These payments historically have been made to “Disproportionate Share Hospitals” (DSH), which are hospitals that care for a higher percentage of unfunded patients. Under the Affordable Care Act, only 25% of these payments will be distributed to DSH hospitals; the remaining 75% will be reduced based on the number of uninsured in the U.S., then redistributed to DSH hospitals based on their portion of uninsured care delivered.
Most DSH hospitals should expect a decrease in DSH payments, the amount of which will depend on their share of unfunded patients.
Any reduction in the “bottom line” to the hospital can affect hospitalists, especially those who are directly employed by the hospital.
Hospital-Acquired Conditions
CMS has long had the Hospital-Acquired Condition (HAC) program in effect, which has the ability to reduce the amount of payment for inpatients who acquire a HAC during their hospital stay. Starting in October 2014, CMS will impose additional financial penalties for hospitals with high HAC rates.
Specifically, those hospitals in the highest 25th percentile of HAC rates will be penalized 1% of their overall CMS payments. Another proposed change is that the following be included in the HAC reduction plan (two “domains” of measures):
- Domain No. 1: Six of the AHRQ Patient Safety Indicators (PSIs), including pressure ulcers, foreign bodies left in after surgery, iatrogenic pneumothorax, postoperative physiologic or metabolic derangements, postoperative VTE, and accidental puncture/laceration.
- Domain No. 2: Central-line-associated bloodstream infections (CLABSI) and catheter-associated urinary tract infections (CAUTIs).
The domains will be weighted equally, and an average score will determine the total score. There will be some methodology for risk adjustment, and hospitals will be given a review and comment period to validate their own scores.
Most hospitalists have at least indirect control over many of these HACs,and all need to pay very close attention to their hospital’s rates of these now and in the future.
Readmissions
As we all know, the Hospital Readmission Reduction program went into effect October 2012; it placed 1% of CMS payments at risk. This will increase to 2% of payments as of October 2013. CMS will continue to use AMI, CHF, and pneumonia as the three conditions under which the readmissions are measured but will put in some methodology to account for planned readmissions.
In addition, in October 2014, they plan to add readmission rates for COPD and for hip/knee arthroplasty.
Hospitalists will continue to need to progress their transitions of care programs, at least for these five patients conditions but more likely (and more effectively) for all hospital discharges.
Quality Measures
Currently more than 99% of acute-care hospitals participate in the pay-for-reporting quality program through CMS, the results of which have been displayed on the Hospital Compare website (www.hospitalcompare.hhs.gov) for years. The program started in 2004 with 10 quality metrics and now includes 57 metrics. These include process and outcome measures for AMI, CHF, and pneumonia, as well as process measures for surgical care, HACs, and patient-satisfaction surveys, among others.
This program will continue to expand over time, including hospital-acquired MRSA and Clostridium difficile rates. The few hospitals not participating will have their CMS annual payments reduced by 2%.
EHR Incentives
CMS is evaluating ways to reduce the burden of reporting by aligning EHR incentives with the Inpatient Quality Reporting program.
Summary
After an open commentary period, the Final Rule will be published Aug. 1, and will become effective for discharges on or after Oct. 1. Although CMS will continue to expand the total number of measures that need to be reported, and the penalties for non-reporting or low performance will continue to escalate, CMS is at least attempting to reduce the overall burden of reporting by combining measures and programs over time and using EHRs to facilitate the bulk of reporting over time.
The global message to hospitalists is: Continue to focus on reducing the burden of HACs, enhance throughput, and carefully and thoughtfully transition patients to the next provider after their hospital discharge. All in all, although at times this can feel overwhelming, these changes represent the right direction to move for high-quality and safe patient care.
Dr. Scheurer is a hospitalist and chief quality officer at the Medical University of South Carolina in Charleston. She is physician editor of The Hospitalist. Email her at [email protected].
Reference
The Centers for Medicare & Medicaid Services (CMS) recently released a few Fact Sheets on how they anticipate funding changes on a few of their programs that were implemented (or sustained) under the Affordable Care Act. As a background, CMS pays most acute-care hospitals by prospectively determining payment based on a patient’s diagnosis and the severity of illness within that diagnosis (e.g. “MS-DRG”). These payment amounts are updated annually after evaluating several factors, including the costs associated with the delivery of care.
One of the most major changes described in the Fact Sheet that will affect hospitalists is how CMS will review inpatient stays based on the number of nights in the hospital. CMS has proposed that any patient who stays in the hospital for two or more “midnights” should be appropriate for payment under Medicare Part A. For those who stay in the hospital for only one (or zero) midnights, payment under Medicare Part A will only be appropriate if:
- There is sufficient documentation at the time of admission that the anticipated length of stay is two or more nights; and.
- Further documentation that circumstances changed, and the hospital stay ended prematurely because of those changes.
Overall for hospitalists, this should substantially simplify the admitting process, whereby most inpatients being admitted with the anticipation of two or more nights should qualify for an inpatient stay. This also reduces the administrative burden of correcting the “inpatient” versus “observation” designation, which keeps many hospital staffs entirely too busy. This change also should relieve a significant burden from the patients and their families, who if kept in observation for a period of time, may have to pay substantially out of pocket to make up for the difference between the cost of the stay and the reimbursement from CMS for observation status. So this is one of the moves that CMS is making to simplify (and not complicate) an already too-complicated payment system. This should go into effect October 2013 and will be a sigh of much relief from many of us.
A few other anticipated changes that will affect hospitalists include:
Payments for Unfunded Care
Another major change that will go into affect October 2013 is the amount of monies received by hospitals that care for unfunded patients. These payments historically have been made to “Disproportionate Share Hospitals” (DSH), which are hospitals that care for a higher percentage of unfunded patients. Under the Affordable Care Act, only 25% of these payments will be distributed to DSH hospitals; the remaining 75% will be reduced based on the number of uninsured in the U.S., then redistributed to DSH hospitals based on their portion of uninsured care delivered.
Most DSH hospitals should expect a decrease in DSH payments, the amount of which will depend on their share of unfunded patients.
Any reduction in the “bottom line” to the hospital can affect hospitalists, especially those who are directly employed by the hospital.
Hospital-Acquired Conditions
CMS has long had the Hospital-Acquired Condition (HAC) program in effect, which has the ability to reduce the amount of payment for inpatients who acquire a HAC during their hospital stay. Starting in October 2014, CMS will impose additional financial penalties for hospitals with high HAC rates.
Specifically, those hospitals in the highest 25th percentile of HAC rates will be penalized 1% of their overall CMS payments. Another proposed change is that the following be included in the HAC reduction plan (two “domains” of measures):
- Domain No. 1: Six of the AHRQ Patient Safety Indicators (PSIs), including pressure ulcers, foreign bodies left in after surgery, iatrogenic pneumothorax, postoperative physiologic or metabolic derangements, postoperative VTE, and accidental puncture/laceration.
- Domain No. 2: Central-line-associated bloodstream infections (CLABSI) and catheter-associated urinary tract infections (CAUTIs).
The domains will be weighted equally, and an average score will determine the total score. There will be some methodology for risk adjustment, and hospitals will be given a review and comment period to validate their own scores.
Most hospitalists have at least indirect control over many of these HACs,and all need to pay very close attention to their hospital’s rates of these now and in the future.
Readmissions
As we all know, the Hospital Readmission Reduction program went into effect October 2012; it placed 1% of CMS payments at risk. This will increase to 2% of payments as of October 2013. CMS will continue to use AMI, CHF, and pneumonia as the three conditions under which the readmissions are measured but will put in some methodology to account for planned readmissions.
In addition, in October 2014, they plan to add readmission rates for COPD and for hip/knee arthroplasty.
Hospitalists will continue to need to progress their transitions of care programs, at least for these five patients conditions but more likely (and more effectively) for all hospital discharges.
Quality Measures
Currently more than 99% of acute-care hospitals participate in the pay-for-reporting quality program through CMS, the results of which have been displayed on the Hospital Compare website (www.hospitalcompare.hhs.gov) for years. The program started in 2004 with 10 quality metrics and now includes 57 metrics. These include process and outcome measures for AMI, CHF, and pneumonia, as well as process measures for surgical care, HACs, and patient-satisfaction surveys, among others.
This program will continue to expand over time, including hospital-acquired MRSA and Clostridium difficile rates. The few hospitals not participating will have their CMS annual payments reduced by 2%.
EHR Incentives
CMS is evaluating ways to reduce the burden of reporting by aligning EHR incentives with the Inpatient Quality Reporting program.
Summary
After an open commentary period, the Final Rule will be published Aug. 1, and will become effective for discharges on or after Oct. 1. Although CMS will continue to expand the total number of measures that need to be reported, and the penalties for non-reporting or low performance will continue to escalate, CMS is at least attempting to reduce the overall burden of reporting by combining measures and programs over time and using EHRs to facilitate the bulk of reporting over time.
The global message to hospitalists is: Continue to focus on reducing the burden of HACs, enhance throughput, and carefully and thoughtfully transition patients to the next provider after their hospital discharge. All in all, although at times this can feel overwhelming, these changes represent the right direction to move for high-quality and safe patient care.
Dr. Scheurer is a hospitalist and chief quality officer at the Medical University of South Carolina in Charleston. She is physician editor of The Hospitalist. Email her at [email protected].
Reference
Should Skyrocketing Health Care Costs Concern Hospitalists?
Median hospitalist compensation has grown steadily over the past decade, but physicians aren’t immune to the sting of accelerated premiums, copays, and contributions imposed by health insurers.
According to the Hay Group’s 2011 Physician Compensation Survey, the number of physicians who contributing to health insurance premiums increased to 68% in 2011 from 58% in 2010. The survey showed only 9% of physicians did not pay anything for medical coverage, down from 19% in 2010.
Moreover, the expected physician contribution was between 1% and 25% of the premium.
Dan Fuller, president and cofounder of Alpharetta, Ga.-based IN Compass Health, has noticed an uptick in candidates’ interest in their health-care benefits. “Especially for physicians who have families, health benefits have become one of the top issues in recruiting,” the SHM Practice Analysis Committee (PAC) member says.
Christopher Frost, MD, FHM, medical director of hospital medicine at the Hospital Corporation of America in Nashville, Tenn., reports that he is seeing an upward trend in employees’ contributions to premiums and out-of-pocket costs. He’s also observed colleagues becoming more selective when choosing their own health-care plans and how they use those plans.
Gretchen Henkel is a freelance writer in California.
Median hospitalist compensation has grown steadily over the past decade, but physicians aren’t immune to the sting of accelerated premiums, copays, and contributions imposed by health insurers.
According to the Hay Group’s 2011 Physician Compensation Survey, the number of physicians who contributing to health insurance premiums increased to 68% in 2011 from 58% in 2010. The survey showed only 9% of physicians did not pay anything for medical coverage, down from 19% in 2010.
Moreover, the expected physician contribution was between 1% and 25% of the premium.
Dan Fuller, president and cofounder of Alpharetta, Ga.-based IN Compass Health, has noticed an uptick in candidates’ interest in their health-care benefits. “Especially for physicians who have families, health benefits have become one of the top issues in recruiting,” the SHM Practice Analysis Committee (PAC) member says.
Christopher Frost, MD, FHM, medical director of hospital medicine at the Hospital Corporation of America in Nashville, Tenn., reports that he is seeing an upward trend in employees’ contributions to premiums and out-of-pocket costs. He’s also observed colleagues becoming more selective when choosing their own health-care plans and how they use those plans.
Gretchen Henkel is a freelance writer in California.
Median hospitalist compensation has grown steadily over the past decade, but physicians aren’t immune to the sting of accelerated premiums, copays, and contributions imposed by health insurers.
According to the Hay Group’s 2011 Physician Compensation Survey, the number of physicians who contributing to health insurance premiums increased to 68% in 2011 from 58% in 2010. The survey showed only 9% of physicians did not pay anything for medical coverage, down from 19% in 2010.
Moreover, the expected physician contribution was between 1% and 25% of the premium.
Dan Fuller, president and cofounder of Alpharetta, Ga.-based IN Compass Health, has noticed an uptick in candidates’ interest in their health-care benefits. “Especially for physicians who have families, health benefits have become one of the top issues in recruiting,” the SHM Practice Analysis Committee (PAC) member says.
Christopher Frost, MD, FHM, medical director of hospital medicine at the Hospital Corporation of America in Nashville, Tenn., reports that he is seeing an upward trend in employees’ contributions to premiums and out-of-pocket costs. He’s also observed colleagues becoming more selective when choosing their own health-care plans and how they use those plans.
Gretchen Henkel is a freelance writer in California.