User login
Joint Commission Leaders Call on Physicians to Embrace Quality Improvement
In a May 12 JAMA “Viewpoint” article, Mark Chassin, MD, FACP, MPP, MPH, The Joint Commission’s president and CEO, and David Baker, MD, FACP, MPH, The Joint Commission’s vice president for healthcare quality evaluation, called on American physicians to acquire the necessary skills to take on new responsibilities to become leaders for QI and patient safety in an increasingly complex healthcare environment.1
The Joint Commission, they said, has embraced the tools, methods, and science of QI used in other industries, including Lean Six Sigma and change management, for all of its internal improvement functions and for its Center for Transforming Healthcare. They urge physicians to do the same or risk jeopardizing medicine’s long-standing self-governance status because of societal concerns about patient safety.
Drs. Chassin and Baker note that medicine has too often tolerated problematic behaviors and is viewed by some stakeholders as failing to address poor quality of care and safety, lack of access, and high costs of care.
“Physicians could make a much stronger case for continued self-government if they took a more visible and vigorous leadership role in efforts that led to major improvement in the quality and safety of patient care,” they said.
Reference
- Chassin MR, Baker DW. Aiming higher to enhance professionalism: beyond accreditation and certification. JAMA. 2015;313(18):1795-1796.
In a May 12 JAMA “Viewpoint” article, Mark Chassin, MD, FACP, MPP, MPH, The Joint Commission’s president and CEO, and David Baker, MD, FACP, MPH, The Joint Commission’s vice president for healthcare quality evaluation, called on American physicians to acquire the necessary skills to take on new responsibilities to become leaders for QI and patient safety in an increasingly complex healthcare environment.1
The Joint Commission, they said, has embraced the tools, methods, and science of QI used in other industries, including Lean Six Sigma and change management, for all of its internal improvement functions and for its Center for Transforming Healthcare. They urge physicians to do the same or risk jeopardizing medicine’s long-standing self-governance status because of societal concerns about patient safety.
Drs. Chassin and Baker note that medicine has too often tolerated problematic behaviors and is viewed by some stakeholders as failing to address poor quality of care and safety, lack of access, and high costs of care.
“Physicians could make a much stronger case for continued self-government if they took a more visible and vigorous leadership role in efforts that led to major improvement in the quality and safety of patient care,” they said.
Reference
- Chassin MR, Baker DW. Aiming higher to enhance professionalism: beyond accreditation and certification. JAMA. 2015;313(18):1795-1796.
In a May 12 JAMA “Viewpoint” article, Mark Chassin, MD, FACP, MPP, MPH, The Joint Commission’s president and CEO, and David Baker, MD, FACP, MPH, The Joint Commission’s vice president for healthcare quality evaluation, called on American physicians to acquire the necessary skills to take on new responsibilities to become leaders for QI and patient safety in an increasingly complex healthcare environment.1
The Joint Commission, they said, has embraced the tools, methods, and science of QI used in other industries, including Lean Six Sigma and change management, for all of its internal improvement functions and for its Center for Transforming Healthcare. They urge physicians to do the same or risk jeopardizing medicine’s long-standing self-governance status because of societal concerns about patient safety.
Drs. Chassin and Baker note that medicine has too often tolerated problematic behaviors and is viewed by some stakeholders as failing to address poor quality of care and safety, lack of access, and high costs of care.
“Physicians could make a much stronger case for continued self-government if they took a more visible and vigorous leadership role in efforts that led to major improvement in the quality and safety of patient care,” they said.
Reference
- Chassin MR, Baker DW. Aiming higher to enhance professionalism: beyond accreditation and certification. JAMA. 2015;313(18):1795-1796.
PHM15: New Quality Measures for Children with Medical Complexity
Pediatric Hospital Medicine 2015's keynote speaker, Rita Mangione-Smith, MD, MPH, reviewed quality measures being developed for medically complex patients by the Center of Excellence on Quality of Care Measures for Children with Complex Needs (COE4CCN). As one of the most challenging groups to not only provide care but to determine if the management provided brings value, the importance of quality measures was emphasized.
Dr. Mangione-Smith, of Seattle Children’s Hospital, reviewed the need for quality measures, as well as the process of developing these measures. Quality measures help to quantify outcomes from care practices, stated Dr. Mangione-Smith, to compare similar settings, and also to set possible benchmarks. The processes range from identifying and prioritizing measures to how they are validated as true value added outcomes. Data sources, sample size, and reliability/validity of the measures are considered important components to ensure that answers or results acquired are applicable and relevant to the population. Another important component is to clearly define a child with medical complexity.
Some reasons why medically complex patients require this focus:
- The low amount of information about their quality of care, investment, and need for coordination;
- Lack of understanding of which care practices make the biggest differences on their outcomes; and
- Their high rate of resource utilization.
The objective was to see which areas of care, such as care coordination, have the highest benefit/improvement on outcomes so as to prioritize resources more effectively. Dr. Mangione-Smith also touched on some obstacles and challenges, such as lack of insurance coverage leading to use of emergency resources as their primary care and its effect on increasing resource utilization.
Measures were determined via a multi-component methodology. Surveys using a binary and linear mean scoring tool were used. This provided multiple types of information such as assessing family’s perception of care, their understanding of medical information and care plans, and their accessibility to medical care services or information about their child.
Currently there is very little evidence on which management methods have the most significant, or any, effect on children with medical complexity. The use of quality measures to help guide which practices may have the highest positive impact on their outcomes greatly adds to the challenging care of this population and can be “used to assess quality of care coordination over time.” TH
Dr. Alvarez is a pediatric hospitalist and medical director of community hospital services at Children’s National Health System in Washington, D.C.
Pediatric Hospital Medicine 2015's keynote speaker, Rita Mangione-Smith, MD, MPH, reviewed quality measures being developed for medically complex patients by the Center of Excellence on Quality of Care Measures for Children with Complex Needs (COE4CCN). As one of the most challenging groups to not only provide care but to determine if the management provided brings value, the importance of quality measures was emphasized.
Dr. Mangione-Smith, of Seattle Children’s Hospital, reviewed the need for quality measures, as well as the process of developing these measures. Quality measures help to quantify outcomes from care practices, stated Dr. Mangione-Smith, to compare similar settings, and also to set possible benchmarks. The processes range from identifying and prioritizing measures to how they are validated as true value added outcomes. Data sources, sample size, and reliability/validity of the measures are considered important components to ensure that answers or results acquired are applicable and relevant to the population. Another important component is to clearly define a child with medical complexity.
Some reasons why medically complex patients require this focus:
- The low amount of information about their quality of care, investment, and need for coordination;
- Lack of understanding of which care practices make the biggest differences on their outcomes; and
- Their high rate of resource utilization.
The objective was to see which areas of care, such as care coordination, have the highest benefit/improvement on outcomes so as to prioritize resources more effectively. Dr. Mangione-Smith also touched on some obstacles and challenges, such as lack of insurance coverage leading to use of emergency resources as their primary care and its effect on increasing resource utilization.
Measures were determined via a multi-component methodology. Surveys using a binary and linear mean scoring tool were used. This provided multiple types of information such as assessing family’s perception of care, their understanding of medical information and care plans, and their accessibility to medical care services or information about their child.
Currently there is very little evidence on which management methods have the most significant, or any, effect on children with medical complexity. The use of quality measures to help guide which practices may have the highest positive impact on their outcomes greatly adds to the challenging care of this population and can be “used to assess quality of care coordination over time.” TH
Dr. Alvarez is a pediatric hospitalist and medical director of community hospital services at Children’s National Health System in Washington, D.C.
Pediatric Hospital Medicine 2015's keynote speaker, Rita Mangione-Smith, MD, MPH, reviewed quality measures being developed for medically complex patients by the Center of Excellence on Quality of Care Measures for Children with Complex Needs (COE4CCN). As one of the most challenging groups to not only provide care but to determine if the management provided brings value, the importance of quality measures was emphasized.
Dr. Mangione-Smith, of Seattle Children’s Hospital, reviewed the need for quality measures, as well as the process of developing these measures. Quality measures help to quantify outcomes from care practices, stated Dr. Mangione-Smith, to compare similar settings, and also to set possible benchmarks. The processes range from identifying and prioritizing measures to how they are validated as true value added outcomes. Data sources, sample size, and reliability/validity of the measures are considered important components to ensure that answers or results acquired are applicable and relevant to the population. Another important component is to clearly define a child with medical complexity.
Some reasons why medically complex patients require this focus:
- The low amount of information about their quality of care, investment, and need for coordination;
- Lack of understanding of which care practices make the biggest differences on their outcomes; and
- Their high rate of resource utilization.
The objective was to see which areas of care, such as care coordination, have the highest benefit/improvement on outcomes so as to prioritize resources more effectively. Dr. Mangione-Smith also touched on some obstacles and challenges, such as lack of insurance coverage leading to use of emergency resources as their primary care and its effect on increasing resource utilization.
Measures were determined via a multi-component methodology. Surveys using a binary and linear mean scoring tool were used. This provided multiple types of information such as assessing family’s perception of care, their understanding of medical information and care plans, and their accessibility to medical care services or information about their child.
Currently there is very little evidence on which management methods have the most significant, or any, effect on children with medical complexity. The use of quality measures to help guide which practices may have the highest positive impact on their outcomes greatly adds to the challenging care of this population and can be “used to assess quality of care coordination over time.” TH
Dr. Alvarez is a pediatric hospitalist and medical director of community hospital services at Children’s National Health System in Washington, D.C.
Medicare Initiatives Improve Hospital Care, Patient Safety

As a hospitalist myself, I have seen firsthand the need for a healthcare system that provides better care, spends dollars more wisely, and keeps people healthier. I practice on weekends taking care of children, many of whom have multiple chronic conditions and fragile social support, and their families. I love patient care; however, too many times, we hospitalists see patients whose fragmented care results in poor outcomes and repeated hospitalizations.
In my current role at the Centers for Medicare and Medicaid Services (CMS), I am pleased to see that Secretary Burwell is confronting these problems head on, with concrete goals for shifting the equation in how we pay for care. Specifically, we announced the goal of moving 30% of payments by 2016 into alternative payment models such as accountable care organizations (ACOs) or bundled payments, where the provider is accountable for total cost of care and quality. We set the goal of 50% of payments in these models by 2018. In 2011, Medicare had essentially zero payments in these models, but by 2014, we have reached 20% and growing in alternative payment models. Hospitalists can play a significant role in this healthcare transformation, and several initiatives in CMS’ Innovation Center, which I lead, are relevant to our work.
Recently, a Department of Health and Human Services (HHS) report showed that an estimated 50,000 fewer patients died in hospitals, 1.3 million fewer adverse events and infections occurred, and approximately $12 billion in healthcare costs were saved as a result of a reduction in hospital-acquired conditions from 2010 to 2013. This progress toward a safer healthcare system occurred during a period of concerted attention directed by hospitals and hospitalists throughout the country at reducing adverse events. These efforts were also due in part to provisions of the Affordable Care Act such as Medicare payment incentives to improve the quality of care and the HHS Partnership for Patients initiative. The Partnership for Patients is a nationwide public-private collaboration that began in April 2011 with two main goals: Reduce preventable hospital-acquired conditions by 40% and 30-day readmissions by 20%. Since the Partnership for Patients was launched, the vast majority of U.S. hospitals and many other stakeholders have joined the collaborative effort and delivered results.
CMS is committed to making even greater progress toward keeping people as safe and healthy as possible. That is why we have launched a second round of Hospital Engagement Network (HEN) contracts to continue reducing preventable hospital-acquired conditions and readmissions. HEN funding will be available to award contracts to national, regional, or state hospital associations, large healthcare organizations, or national affinity organizations that will support hospitals in their efforts to reduce preventable hospital-acquired conditions and readmissions. In February, CMS posted a request for proposals for HEN contracts to continue the success achieved in improving patient safety.
The Partnership for Patients and HENs are just one part of an overall effort by HHS to deliver better care, spend dollars more wisely, and improve health. Initiatives like the Partnership for Patients, accountable care organizations, quality improvement organizations, and others have helped reduce hospital readmissions in Medicare by nearly 8% between January 2012 and December 2013—translating into 150,000 fewer readmissions. Hospitalists have played a major role in these improvements.
On a broader front, CMS is taking action to improve healthcare so patients and their families can get the best care possible. To this end, CMS is focused on three key areas: (1) improving the way providers and hospitals are paid, (2) improving and innovating in care delivery, and (3) sharing information more broadly with providers and hospitals, consumers, and others to support better decisions.
When it comes to improving the way providers are paid, we want to reward value and care coordination—rather than volume and care duplication. We have over 25 payment and service delivery models at the CMS Innovation Center, but I will call out three that are particularly relevant to hospitalists. First, the ACO program is demonstrating positive results. Medicare has over 400 ACOs serving almost eight million beneficiaries. The Pioneer ACO program evaluation results demonstrated over $380 million in savings and improved quality—for example, improvement in 28 out of 33 quality measures, including patient experience of care. Based on these results, this model was the first from the CMS Innovation Center to be certified by the CMS actuary, and the Secretary of Health and Human Services announced her intent to expand the model components as a permanent part of the Medicare program through rulemaking. Second, in the Bundled Payments for Care Improvement model, we have thousands of providers (e.g. hospitals, physician groups) in phase 1 determining how they might improve care and considering taking on financial risk. The model includes acute and post-acute care, such as a 90-day episode for hip and knee replacement. We have 500 providers, and more that are willing to take on two-sided financial risk will likely be added in the next quarter. Hospitalists have a large role to play in improving quality and reducing costs in this model. Finally, the State Innovation Model is driving state and local change. In this model, we are funding and partnering with states on comprehensive delivery system reform. Seventeen states are implementing interventions, and 21 states and territories are designing their plans. The state is encouraged to partner with payers, providers, employers, public health entities, and others in the state to strive within the whole state population for better care, smarter spending, and healthier people. Many states are implementing payment models such as ACOs and bundled payments in Medicaid and with private payers. Increasingly, hospital medicine groups are going to value-based in the quality and efficiency of care delivery, both within the hospital walls and for episodes of care. This will entail stronger linkages and teamwork, both within the hospital and with clinicians in the community. It will also require a much stronger focus on predicting which patients are at risk of decompensation and delivering tailored interventions, including care management and technology to monitor patients in the home and other settings.
To improve care delivery, we are supporting providers to find new ways to coordinate and integrate care. For example, discharging a patient from the hospital without clear instructions on how to take care of themselves at home, when they should take their medicines, or when to check back in with the doctor can lead to an unnecessary readmission back into the hospital. This is especially true of individuals who have complex illnesses or diseases that may be more difficult to manage. We are supporting care improvement through a variety of channels, including facilitating hospitals and community groups teaming up to share best practices, and we applaud the Society of Hospital Medicine’s BOOST program, which is focused on peer mentoring and improvement.
Finally, as we look to improve the way information is distributed, we are working to create more transparency on the cost and quality of care, to bring electronic health information to inform care, and to bring the most recent scientific evidence to the point of care so we can bolster clinical decision making. Necessary information needs to be available to the treating physician and patients across settings. We must continue to improve the interoperability and usability of electronic health records so that they can enable improvement and care delivery.
I hope that as hospitalists you will take a closer look at the HHS initiatives I’ve described here—and others—and consider becoming a participant. Hospital medicine physicians are already leading many of these initiatives and are a positive force for health system transformation. As I look back on my last four-plus years at CMS (which sometimes feel like 30 years), I am amazed by how much progress we have made in improving the quality of care (e.g. over 95% of measures in CMS quality programs have improved over the last three years), spending dollars more wisely (e.g. lowest cost growth in the last four years in over 50 years), and improving the health of the nation (e.g. decreased smoking rates). Our nation is moving rapidly toward accountable, alternative payment models, including the recent legislation to “fix the SGR,” and I have seen hospitalists lead progress towards adopting these models nationally and locally. A challenge for all of us is to accelerate the pace of positive change and relentlessly pursue improved patient outcomes and a higher performing health system. But I know hospitalists are up to this challenge.
Thank you for all the work that you do every day on behalf of your patients and a better health system.

As a hospitalist myself, I have seen firsthand the need for a healthcare system that provides better care, spends dollars more wisely, and keeps people healthier. I practice on weekends taking care of children, many of whom have multiple chronic conditions and fragile social support, and their families. I love patient care; however, too many times, we hospitalists see patients whose fragmented care results in poor outcomes and repeated hospitalizations.
In my current role at the Centers for Medicare and Medicaid Services (CMS), I am pleased to see that Secretary Burwell is confronting these problems head on, with concrete goals for shifting the equation in how we pay for care. Specifically, we announced the goal of moving 30% of payments by 2016 into alternative payment models such as accountable care organizations (ACOs) or bundled payments, where the provider is accountable for total cost of care and quality. We set the goal of 50% of payments in these models by 2018. In 2011, Medicare had essentially zero payments in these models, but by 2014, we have reached 20% and growing in alternative payment models. Hospitalists can play a significant role in this healthcare transformation, and several initiatives in CMS’ Innovation Center, which I lead, are relevant to our work.
Recently, a Department of Health and Human Services (HHS) report showed that an estimated 50,000 fewer patients died in hospitals, 1.3 million fewer adverse events and infections occurred, and approximately $12 billion in healthcare costs were saved as a result of a reduction in hospital-acquired conditions from 2010 to 2013. This progress toward a safer healthcare system occurred during a period of concerted attention directed by hospitals and hospitalists throughout the country at reducing adverse events. These efforts were also due in part to provisions of the Affordable Care Act such as Medicare payment incentives to improve the quality of care and the HHS Partnership for Patients initiative. The Partnership for Patients is a nationwide public-private collaboration that began in April 2011 with two main goals: Reduce preventable hospital-acquired conditions by 40% and 30-day readmissions by 20%. Since the Partnership for Patients was launched, the vast majority of U.S. hospitals and many other stakeholders have joined the collaborative effort and delivered results.
CMS is committed to making even greater progress toward keeping people as safe and healthy as possible. That is why we have launched a second round of Hospital Engagement Network (HEN) contracts to continue reducing preventable hospital-acquired conditions and readmissions. HEN funding will be available to award contracts to national, regional, or state hospital associations, large healthcare organizations, or national affinity organizations that will support hospitals in their efforts to reduce preventable hospital-acquired conditions and readmissions. In February, CMS posted a request for proposals for HEN contracts to continue the success achieved in improving patient safety.
The Partnership for Patients and HENs are just one part of an overall effort by HHS to deliver better care, spend dollars more wisely, and improve health. Initiatives like the Partnership for Patients, accountable care organizations, quality improvement organizations, and others have helped reduce hospital readmissions in Medicare by nearly 8% between January 2012 and December 2013—translating into 150,000 fewer readmissions. Hospitalists have played a major role in these improvements.
On a broader front, CMS is taking action to improve healthcare so patients and their families can get the best care possible. To this end, CMS is focused on three key areas: (1) improving the way providers and hospitals are paid, (2) improving and innovating in care delivery, and (3) sharing information more broadly with providers and hospitals, consumers, and others to support better decisions.
When it comes to improving the way providers are paid, we want to reward value and care coordination—rather than volume and care duplication. We have over 25 payment and service delivery models at the CMS Innovation Center, but I will call out three that are particularly relevant to hospitalists. First, the ACO program is demonstrating positive results. Medicare has over 400 ACOs serving almost eight million beneficiaries. The Pioneer ACO program evaluation results demonstrated over $380 million in savings and improved quality—for example, improvement in 28 out of 33 quality measures, including patient experience of care. Based on these results, this model was the first from the CMS Innovation Center to be certified by the CMS actuary, and the Secretary of Health and Human Services announced her intent to expand the model components as a permanent part of the Medicare program through rulemaking. Second, in the Bundled Payments for Care Improvement model, we have thousands of providers (e.g. hospitals, physician groups) in phase 1 determining how they might improve care and considering taking on financial risk. The model includes acute and post-acute care, such as a 90-day episode for hip and knee replacement. We have 500 providers, and more that are willing to take on two-sided financial risk will likely be added in the next quarter. Hospitalists have a large role to play in improving quality and reducing costs in this model. Finally, the State Innovation Model is driving state and local change. In this model, we are funding and partnering with states on comprehensive delivery system reform. Seventeen states are implementing interventions, and 21 states and territories are designing their plans. The state is encouraged to partner with payers, providers, employers, public health entities, and others in the state to strive within the whole state population for better care, smarter spending, and healthier people. Many states are implementing payment models such as ACOs and bundled payments in Medicaid and with private payers. Increasingly, hospital medicine groups are going to value-based in the quality and efficiency of care delivery, both within the hospital walls and for episodes of care. This will entail stronger linkages and teamwork, both within the hospital and with clinicians in the community. It will also require a much stronger focus on predicting which patients are at risk of decompensation and delivering tailored interventions, including care management and technology to monitor patients in the home and other settings.
To improve care delivery, we are supporting providers to find new ways to coordinate and integrate care. For example, discharging a patient from the hospital without clear instructions on how to take care of themselves at home, when they should take their medicines, or when to check back in with the doctor can lead to an unnecessary readmission back into the hospital. This is especially true of individuals who have complex illnesses or diseases that may be more difficult to manage. We are supporting care improvement through a variety of channels, including facilitating hospitals and community groups teaming up to share best practices, and we applaud the Society of Hospital Medicine’s BOOST program, which is focused on peer mentoring and improvement.
Finally, as we look to improve the way information is distributed, we are working to create more transparency on the cost and quality of care, to bring electronic health information to inform care, and to bring the most recent scientific evidence to the point of care so we can bolster clinical decision making. Necessary information needs to be available to the treating physician and patients across settings. We must continue to improve the interoperability and usability of electronic health records so that they can enable improvement and care delivery.
I hope that as hospitalists you will take a closer look at the HHS initiatives I’ve described here—and others—and consider becoming a participant. Hospital medicine physicians are already leading many of these initiatives and are a positive force for health system transformation. As I look back on my last four-plus years at CMS (which sometimes feel like 30 years), I am amazed by how much progress we have made in improving the quality of care (e.g. over 95% of measures in CMS quality programs have improved over the last three years), spending dollars more wisely (e.g. lowest cost growth in the last four years in over 50 years), and improving the health of the nation (e.g. decreased smoking rates). Our nation is moving rapidly toward accountable, alternative payment models, including the recent legislation to “fix the SGR,” and I have seen hospitalists lead progress towards adopting these models nationally and locally. A challenge for all of us is to accelerate the pace of positive change and relentlessly pursue improved patient outcomes and a higher performing health system. But I know hospitalists are up to this challenge.
Thank you for all the work that you do every day on behalf of your patients and a better health system.
As a hospitalist myself, I have seen firsthand the need for a healthcare system that provides better care, spends dollars more wisely, and keeps people healthier. I practice on weekends taking care of children, many of whom have multiple chronic conditions and fragile social support, and their families. I love patient care; however, too many times, we hospitalists see patients whose fragmented care results in poor outcomes and repeated hospitalizations.
In my current role at the Centers for Medicare and Medicaid Services (CMS), I am pleased to see that Secretary Burwell is confronting these problems head on, with concrete goals for shifting the equation in how we pay for care. Specifically, we announced the goal of moving 30% of payments by 2016 into alternative payment models such as accountable care organizations (ACOs) or bundled payments, where the provider is accountable for total cost of care and quality. We set the goal of 50% of payments in these models by 2018. In 2011, Medicare had essentially zero payments in these models, but by 2014, we have reached 20% and growing in alternative payment models. Hospitalists can play a significant role in this healthcare transformation, and several initiatives in CMS’ Innovation Center, which I lead, are relevant to our work.
Recently, a Department of Health and Human Services (HHS) report showed that an estimated 50,000 fewer patients died in hospitals, 1.3 million fewer adverse events and infections occurred, and approximately $12 billion in healthcare costs were saved as a result of a reduction in hospital-acquired conditions from 2010 to 2013. This progress toward a safer healthcare system occurred during a period of concerted attention directed by hospitals and hospitalists throughout the country at reducing adverse events. These efforts were also due in part to provisions of the Affordable Care Act such as Medicare payment incentives to improve the quality of care and the HHS Partnership for Patients initiative. The Partnership for Patients is a nationwide public-private collaboration that began in April 2011 with two main goals: Reduce preventable hospital-acquired conditions by 40% and 30-day readmissions by 20%. Since the Partnership for Patients was launched, the vast majority of U.S. hospitals and many other stakeholders have joined the collaborative effort and delivered results.
CMS is committed to making even greater progress toward keeping people as safe and healthy as possible. That is why we have launched a second round of Hospital Engagement Network (HEN) contracts to continue reducing preventable hospital-acquired conditions and readmissions. HEN funding will be available to award contracts to national, regional, or state hospital associations, large healthcare organizations, or national affinity organizations that will support hospitals in their efforts to reduce preventable hospital-acquired conditions and readmissions. In February, CMS posted a request for proposals for HEN contracts to continue the success achieved in improving patient safety.
The Partnership for Patients and HENs are just one part of an overall effort by HHS to deliver better care, spend dollars more wisely, and improve health. Initiatives like the Partnership for Patients, accountable care organizations, quality improvement organizations, and others have helped reduce hospital readmissions in Medicare by nearly 8% between January 2012 and December 2013—translating into 150,000 fewer readmissions. Hospitalists have played a major role in these improvements.
On a broader front, CMS is taking action to improve healthcare so patients and their families can get the best care possible. To this end, CMS is focused on three key areas: (1) improving the way providers and hospitals are paid, (2) improving and innovating in care delivery, and (3) sharing information more broadly with providers and hospitals, consumers, and others to support better decisions.
When it comes to improving the way providers are paid, we want to reward value and care coordination—rather than volume and care duplication. We have over 25 payment and service delivery models at the CMS Innovation Center, but I will call out three that are particularly relevant to hospitalists. First, the ACO program is demonstrating positive results. Medicare has over 400 ACOs serving almost eight million beneficiaries. The Pioneer ACO program evaluation results demonstrated over $380 million in savings and improved quality—for example, improvement in 28 out of 33 quality measures, including patient experience of care. Based on these results, this model was the first from the CMS Innovation Center to be certified by the CMS actuary, and the Secretary of Health and Human Services announced her intent to expand the model components as a permanent part of the Medicare program through rulemaking. Second, in the Bundled Payments for Care Improvement model, we have thousands of providers (e.g. hospitals, physician groups) in phase 1 determining how they might improve care and considering taking on financial risk. The model includes acute and post-acute care, such as a 90-day episode for hip and knee replacement. We have 500 providers, and more that are willing to take on two-sided financial risk will likely be added in the next quarter. Hospitalists have a large role to play in improving quality and reducing costs in this model. Finally, the State Innovation Model is driving state and local change. In this model, we are funding and partnering with states on comprehensive delivery system reform. Seventeen states are implementing interventions, and 21 states and territories are designing their plans. The state is encouraged to partner with payers, providers, employers, public health entities, and others in the state to strive within the whole state population for better care, smarter spending, and healthier people. Many states are implementing payment models such as ACOs and bundled payments in Medicaid and with private payers. Increasingly, hospital medicine groups are going to value-based in the quality and efficiency of care delivery, both within the hospital walls and for episodes of care. This will entail stronger linkages and teamwork, both within the hospital and with clinicians in the community. It will also require a much stronger focus on predicting which patients are at risk of decompensation and delivering tailored interventions, including care management and technology to monitor patients in the home and other settings.
To improve care delivery, we are supporting providers to find new ways to coordinate and integrate care. For example, discharging a patient from the hospital without clear instructions on how to take care of themselves at home, when they should take their medicines, or when to check back in with the doctor can lead to an unnecessary readmission back into the hospital. This is especially true of individuals who have complex illnesses or diseases that may be more difficult to manage. We are supporting care improvement through a variety of channels, including facilitating hospitals and community groups teaming up to share best practices, and we applaud the Society of Hospital Medicine’s BOOST program, which is focused on peer mentoring and improvement.
Finally, as we look to improve the way information is distributed, we are working to create more transparency on the cost and quality of care, to bring electronic health information to inform care, and to bring the most recent scientific evidence to the point of care so we can bolster clinical decision making. Necessary information needs to be available to the treating physician and patients across settings. We must continue to improve the interoperability and usability of electronic health records so that they can enable improvement and care delivery.
I hope that as hospitalists you will take a closer look at the HHS initiatives I’ve described here—and others—and consider becoming a participant. Hospital medicine physicians are already leading many of these initiatives and are a positive force for health system transformation. As I look back on my last four-plus years at CMS (which sometimes feel like 30 years), I am amazed by how much progress we have made in improving the quality of care (e.g. over 95% of measures in CMS quality programs have improved over the last three years), spending dollars more wisely (e.g. lowest cost growth in the last four years in over 50 years), and improving the health of the nation (e.g. decreased smoking rates). Our nation is moving rapidly toward accountable, alternative payment models, including the recent legislation to “fix the SGR,” and I have seen hospitalists lead progress towards adopting these models nationally and locally. A challenge for all of us is to accelerate the pace of positive change and relentlessly pursue improved patient outcomes and a higher performing health system. But I know hospitalists are up to this challenge.
Thank you for all the work that you do every day on behalf of your patients and a better health system.
LISTEN NOW: UCSF's Christopher Moriates, MD, discusses waste-reduction efforts in hospitals
CHRISTOPHER MORIATES, MD, assistant clinical professor in the Division of Hospital Medicine at the University of California, San Francisco, talks about the change in focus and priorities needed for medicine to make progress in waste-reduction efforts.
CHRISTOPHER MORIATES, MD, assistant clinical professor in the Division of Hospital Medicine at the University of California, San Francisco, talks about the change in focus and priorities needed for medicine to make progress in waste-reduction efforts.
CHRISTOPHER MORIATES, MD, assistant clinical professor in the Division of Hospital Medicine at the University of California, San Francisco, talks about the change in focus and priorities needed for medicine to make progress in waste-reduction efforts.
From a Near-Catastrophe, I-CARE
For Robert Fogerty, MD, MPH, it’s more than just a story. It’s a nightmare that he only narrowly avoided.
Now a hospitalist at Yale University School of Medicine in New Haven, Conn., Dr. Fogerty was an economics major in his senior year of college when he was diagnosed with metastatic testicular cancer. Early in the course of his treatment, amid multiple rounds of chemotherapy and before a major surgery, his insurance company informed him that his benefits had been exhausted. Even with family resources, the remaining bills would have been crippling. Luckily, he went to college in Massachusetts, where a state law allowed him to enroll in an individual insurance plan by exempting him from the normal pre-existing condition exclusion. Two years later, he got his life back in order and enrolled in medical school.
“What stuck with me is, yes, I was sick, and yes, I lost all my hair, and yes, I went to my final exams bald with my nausea medicine and my steroids in my pocket and all of those things,” he says. “But after that was all gone, after my hair grew back, and I had my last chemo and my surgery, and I was really starting to get my life back on track, the financial implications of that disease were still there. The financial impact of my illness outlasted the pathological impact of my illness, and the financial burdens could easily have been just as life-altering as a permanent disability.”
Although he was “unbelievably lucky” to escape with manageable medical bills, Dr. Fogerty says, other patients haven’t been as fortunate. That lesson is why he identifies so much with his patients. It’s why he posted his own story to the Costs of Care website, which stresses the importance of cost awareness in healthcare. And it’s why he has committed himself to helping other medical students and residents “remove the blinders” to understand healthcare’s often devastating financial impact.
“When I was going through my residency, I learned a lot about low sodium, and I learned a lot about bloodstream infections and what to do when someone can’t breathe and how to do a skin exam, and all of these things,” Dr. Fogerty says. “But all of these other components that were so devastating to me as a patient weren’t really a main portion of the education that we’re providing tomorrow’s doctors. I thought that was an opportunity to really change things."
By combining his clinical and economics expertise, Dr. Fogerty helped to develop a program called the Interactive Cost-Awareness Resident Exercise, or I-CARE. Launched in 2011, I-CARE seeks to make the abstract problem of healthcare costs—including unnecessary ones—more accessible to trainees. The concept is deceptively simple: Residents compete to see who can reach the correct diagnosis for a given case using the fewest possible resources.
By talking through each case, both trainees and faculty can discuss concepts like waste prevention and financial stewardship in a safe environment. Giving young doctors that “basic set of vocabulary,” Dr. Fogerty says, may help them engage in real decisions later on about a group or health system’s financial pressures and obligations.
The program has since spread to other medical centers, and what began as a cost-awareness exercise has blossomed into a broader discussion about minimizing the cost and burden to patients while maximizing safety and good medicine. TH
For Robert Fogerty, MD, MPH, it’s more than just a story. It’s a nightmare that he only narrowly avoided.
Now a hospitalist at Yale University School of Medicine in New Haven, Conn., Dr. Fogerty was an economics major in his senior year of college when he was diagnosed with metastatic testicular cancer. Early in the course of his treatment, amid multiple rounds of chemotherapy and before a major surgery, his insurance company informed him that his benefits had been exhausted. Even with family resources, the remaining bills would have been crippling. Luckily, he went to college in Massachusetts, where a state law allowed him to enroll in an individual insurance plan by exempting him from the normal pre-existing condition exclusion. Two years later, he got his life back in order and enrolled in medical school.
“What stuck with me is, yes, I was sick, and yes, I lost all my hair, and yes, I went to my final exams bald with my nausea medicine and my steroids in my pocket and all of those things,” he says. “But after that was all gone, after my hair grew back, and I had my last chemo and my surgery, and I was really starting to get my life back on track, the financial implications of that disease were still there. The financial impact of my illness outlasted the pathological impact of my illness, and the financial burdens could easily have been just as life-altering as a permanent disability.”
Although he was “unbelievably lucky” to escape with manageable medical bills, Dr. Fogerty says, other patients haven’t been as fortunate. That lesson is why he identifies so much with his patients. It’s why he posted his own story to the Costs of Care website, which stresses the importance of cost awareness in healthcare. And it’s why he has committed himself to helping other medical students and residents “remove the blinders” to understand healthcare’s often devastating financial impact.
“When I was going through my residency, I learned a lot about low sodium, and I learned a lot about bloodstream infections and what to do when someone can’t breathe and how to do a skin exam, and all of these things,” Dr. Fogerty says. “But all of these other components that were so devastating to me as a patient weren’t really a main portion of the education that we’re providing tomorrow’s doctors. I thought that was an opportunity to really change things."
By combining his clinical and economics expertise, Dr. Fogerty helped to develop a program called the Interactive Cost-Awareness Resident Exercise, or I-CARE. Launched in 2011, I-CARE seeks to make the abstract problem of healthcare costs—including unnecessary ones—more accessible to trainees. The concept is deceptively simple: Residents compete to see who can reach the correct diagnosis for a given case using the fewest possible resources.
By talking through each case, both trainees and faculty can discuss concepts like waste prevention and financial stewardship in a safe environment. Giving young doctors that “basic set of vocabulary,” Dr. Fogerty says, may help them engage in real decisions later on about a group or health system’s financial pressures and obligations.
The program has since spread to other medical centers, and what began as a cost-awareness exercise has blossomed into a broader discussion about minimizing the cost and burden to patients while maximizing safety and good medicine. TH
For Robert Fogerty, MD, MPH, it’s more than just a story. It’s a nightmare that he only narrowly avoided.
Now a hospitalist at Yale University School of Medicine in New Haven, Conn., Dr. Fogerty was an economics major in his senior year of college when he was diagnosed with metastatic testicular cancer. Early in the course of his treatment, amid multiple rounds of chemotherapy and before a major surgery, his insurance company informed him that his benefits had been exhausted. Even with family resources, the remaining bills would have been crippling. Luckily, he went to college in Massachusetts, where a state law allowed him to enroll in an individual insurance plan by exempting him from the normal pre-existing condition exclusion. Two years later, he got his life back in order and enrolled in medical school.
“What stuck with me is, yes, I was sick, and yes, I lost all my hair, and yes, I went to my final exams bald with my nausea medicine and my steroids in my pocket and all of those things,” he says. “But after that was all gone, after my hair grew back, and I had my last chemo and my surgery, and I was really starting to get my life back on track, the financial implications of that disease were still there. The financial impact of my illness outlasted the pathological impact of my illness, and the financial burdens could easily have been just as life-altering as a permanent disability.”
Although he was “unbelievably lucky” to escape with manageable medical bills, Dr. Fogerty says, other patients haven’t been as fortunate. That lesson is why he identifies so much with his patients. It’s why he posted his own story to the Costs of Care website, which stresses the importance of cost awareness in healthcare. And it’s why he has committed himself to helping other medical students and residents “remove the blinders” to understand healthcare’s often devastating financial impact.
“When I was going through my residency, I learned a lot about low sodium, and I learned a lot about bloodstream infections and what to do when someone can’t breathe and how to do a skin exam, and all of these things,” Dr. Fogerty says. “But all of these other components that were so devastating to me as a patient weren’t really a main portion of the education that we’re providing tomorrow’s doctors. I thought that was an opportunity to really change things."
By combining his clinical and economics expertise, Dr. Fogerty helped to develop a program called the Interactive Cost-Awareness Resident Exercise, or I-CARE. Launched in 2011, I-CARE seeks to make the abstract problem of healthcare costs—including unnecessary ones—more accessible to trainees. The concept is deceptively simple: Residents compete to see who can reach the correct diagnosis for a given case using the fewest possible resources.
By talking through each case, both trainees and faculty can discuss concepts like waste prevention and financial stewardship in a safe environment. Giving young doctors that “basic set of vocabulary,” Dr. Fogerty says, may help them engage in real decisions later on about a group or health system’s financial pressures and obligations.
The program has since spread to other medical centers, and what began as a cost-awareness exercise has blossomed into a broader discussion about minimizing the cost and burden to patients while maximizing safety and good medicine. TH
Society of Hospital Medicine’s RIV Poster Contest Draws Best, Brightest
Implementing Physician Value-Based Purchasing in Your Practice: HM15 Session Analysis
HM15 Session: Putting Your Nickel Down: The What, Why, and How of Implementing Physician Value-Based Purchasing in Your Practice
Presenters: Stephen Besch, Simone Karp RPh, Patrick Torcson MD MMM SFHM, Gregory Seymann MD SFHM

Medicare is transforming itself from a “passive payer” to an “active purchaser” of high quality, efficient healthcare. As such- active participation by physicians, physician groups, and hospitals is required for payment eligibility.
At the physician/group level, hospitalists should be reporting PQRS measures. Incentive payments for PQRS ended in 2014, Medicare is now making “negative payment adjustments.” Penalties are equal to a percentage of all Medicare Part B FFS (Fee-for-Service) charges and there is a 2-year delay between reporting or performance failure and penalization.
Physician Value-Based Purchasing (P-VBP) affects all Eligible Providers (EPs) in 2015. P4P (Pay for Performance) assesses both quality and cost. Aim is for budget neutrality via “quality tiering” which rewards “high quality/low cost” practices with penalties from “low quality/high cost” practices. As of now (2015) ACPs and therapists can be penalized under P-VBP.
Key Points/HM Takeaways:
- Hospitalists should be reporting PQRS measures- penalty phase has begun
- Key PQRS Changes for 2015:
- 6 measures applicable to inpatient billing removed
- no useful inpatient measures added
- penalty avoidance requires 9 measures at 50% or higher rates, covering at least 3 of the 6 NQS (National Quality Strategy) domains- including 1 cross-cutting measure
- all 2015 PQRS data will be posted to Physician Compare website in 2016
- 3 Examples of hospitalist applicable “cross-cutting measures” are
- 47-advance care plan
- 130-documentation of current medications
- 317-preventative care: bp screening
- PQRS data must be reported with respect to MAV clusters (Measure Applicability Validation)- reporting only measure that have no MAV cluster is a safe strategy so long as one of the measures is “cross-cutting”
- Maximum P-VBP penalties automatically apply if group does not report enough PQRS data
- visit CMS website for more information
HM15 Session: Putting Your Nickel Down: The What, Why, and How of Implementing Physician Value-Based Purchasing in Your Practice
Presenters: Stephen Besch, Simone Karp RPh, Patrick Torcson MD MMM SFHM, Gregory Seymann MD SFHM
Medicare is transforming itself from a “passive payer” to an “active purchaser” of high quality, efficient healthcare. As such- active participation by physicians, physician groups, and hospitals is required for payment eligibility.
At the physician/group level, hospitalists should be reporting PQRS measures. Incentive payments for PQRS ended in 2014, Medicare is now making “negative payment adjustments.” Penalties are equal to a percentage of all Medicare Part B FFS (Fee-for-Service) charges and there is a 2-year delay between reporting or performance failure and penalization.
Physician Value-Based Purchasing (P-VBP) affects all Eligible Providers (EPs) in 2015. P4P (Pay for Performance) assesses both quality and cost. Aim is for budget neutrality via “quality tiering” which rewards “high quality/low cost” practices with penalties from “low quality/high cost” practices. As of now (2015) ACPs and therapists can be penalized under P-VBP.
Key Points/HM Takeaways:
- Hospitalists should be reporting PQRS measures- penalty phase has begun
- Key PQRS Changes for 2015:
- 6 measures applicable to inpatient billing removed
- no useful inpatient measures added
- penalty avoidance requires 9 measures at 50% or higher rates, covering at least 3 of the 6 NQS (National Quality Strategy) domains- including 1 cross-cutting measure
- all 2015 PQRS data will be posted to Physician Compare website in 2016
- 3 Examples of hospitalist applicable “cross-cutting measures” are
- 47-advance care plan
- 130-documentation of current medications
- 317-preventative care: bp screening
- PQRS data must be reported with respect to MAV clusters (Measure Applicability Validation)- reporting only measure that have no MAV cluster is a safe strategy so long as one of the measures is “cross-cutting”
- Maximum P-VBP penalties automatically apply if group does not report enough PQRS data
- visit CMS website for more information
HM15 Session: Putting Your Nickel Down: The What, Why, and How of Implementing Physician Value-Based Purchasing in Your Practice
Presenters: Stephen Besch, Simone Karp RPh, Patrick Torcson MD MMM SFHM, Gregory Seymann MD SFHM
Medicare is transforming itself from a “passive payer” to an “active purchaser” of high quality, efficient healthcare. As such- active participation by physicians, physician groups, and hospitals is required for payment eligibility.
At the physician/group level, hospitalists should be reporting PQRS measures. Incentive payments for PQRS ended in 2014, Medicare is now making “negative payment adjustments.” Penalties are equal to a percentage of all Medicare Part B FFS (Fee-for-Service) charges and there is a 2-year delay between reporting or performance failure and penalization.
Physician Value-Based Purchasing (P-VBP) affects all Eligible Providers (EPs) in 2015. P4P (Pay for Performance) assesses both quality and cost. Aim is for budget neutrality via “quality tiering” which rewards “high quality/low cost” practices with penalties from “low quality/high cost” practices. As of now (2015) ACPs and therapists can be penalized under P-VBP.
Key Points/HM Takeaways:
- Hospitalists should be reporting PQRS measures- penalty phase has begun
- Key PQRS Changes for 2015:
- 6 measures applicable to inpatient billing removed
- no useful inpatient measures added
- penalty avoidance requires 9 measures at 50% or higher rates, covering at least 3 of the 6 NQS (National Quality Strategy) domains- including 1 cross-cutting measure
- all 2015 PQRS data will be posted to Physician Compare website in 2016
- 3 Examples of hospitalist applicable “cross-cutting measures” are
- 47-advance care plan
- 130-documentation of current medications
- 317-preventative care: bp screening
- PQRS data must be reported with respect to MAV clusters (Measure Applicability Validation)- reporting only measure that have no MAV cluster is a safe strategy so long as one of the measures is “cross-cutting”
- Maximum P-VBP penalties automatically apply if group does not report enough PQRS data
- visit CMS website for more information
Choosing Wisely in Hospital Medicine: Accomplishments and What the Future Holds
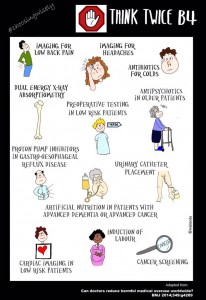
John Bulger, DO, MBA reviewed the components of the Choosing Wisely campaign and SHM’s recommendations in an era where providing high value cost-conscious care is key to optimizing the health of our patients. Choosing Wisely is an initiative of the ABIM foundation to foster communication between physicians and patients about common tests and procedures that may fail to provide value or enhance patient outcomes. It’s a partnership with 70-plus medical societies including an innovative partnership with Consumer Reports. SHM’s evidence-based recommendations are:
- Don’t leave urinary catheters in place for convenience or monitoring of output for non-critically ill patients.
- Don’t prescribe stress ulcer prophylaxis to hospitalized patients unless they are at high risk for GI complications.
- Avoid transfusion of PRBC for arbitrary hemoglobin in the absence of CAD, CHF or CVA.
- Don’t order continuous telemetry monitoring outside of the ICU without a protocol.
- Don’t perform repetitive CBC and chemistry testing in a clinically stable patient.
Dr. Bulger highlighted that the Choosing Wisely campaign is designed to encourage conversations to

Dr.Bulger concluded that while tradition is hard to change, it is of paramount importance to think differently to find innovative solutions to common problems in healthcare. Join the conversation using #ChoosingWisely or #LessIsMore on twitter.
Key Takeaways
- Choosing Wisely is an ABIM campaign developed to address and promote conversations about common tests and procedures that are of low-value.
- SHM’s recommendations were implemented in institutions with positive results as evidenced by the Choosing Wisely case competition at #HospMed15.
- Look for a summary of these efforts to be published in the spring of 2015.
- Use these guidelines to educate, provoke dialogue and achieve optimal patient outcomes in your institution.
- Join the conversation on twitter using #ChoosingWisely and #LessIsMore.
John Bulger, DO, MBA reviewed the components of the Choosing Wisely campaign and SHM’s recommendations in an era where providing high value cost-conscious care is key to optimizing the health of our patients. Choosing Wisely is an initiative of the ABIM foundation to foster communication between physicians and patients about common tests and procedures that may fail to provide value or enhance patient outcomes. It’s a partnership with 70-plus medical societies including an innovative partnership with Consumer Reports. SHM’s evidence-based recommendations are:
- Don’t leave urinary catheters in place for convenience or monitoring of output for non-critically ill patients.
- Don’t prescribe stress ulcer prophylaxis to hospitalized patients unless they are at high risk for GI complications.
- Avoid transfusion of PRBC for arbitrary hemoglobin in the absence of CAD, CHF or CVA.
- Don’t order continuous telemetry monitoring outside of the ICU without a protocol.
- Don’t perform repetitive CBC and chemistry testing in a clinically stable patient.
Dr. Bulger highlighted that the Choosing Wisely campaign is designed to encourage conversations to
Dr.Bulger concluded that while tradition is hard to change, it is of paramount importance to think differently to find innovative solutions to common problems in healthcare. Join the conversation using #ChoosingWisely or #LessIsMore on twitter.
Key Takeaways
- Choosing Wisely is an ABIM campaign developed to address and promote conversations about common tests and procedures that are of low-value.
- SHM’s recommendations were implemented in institutions with positive results as evidenced by the Choosing Wisely case competition at #HospMed15.
- Look for a summary of these efforts to be published in the spring of 2015.
- Use these guidelines to educate, provoke dialogue and achieve optimal patient outcomes in your institution.
- Join the conversation on twitter using #ChoosingWisely and #LessIsMore.
John Bulger, DO, MBA reviewed the components of the Choosing Wisely campaign and SHM’s recommendations in an era where providing high value cost-conscious care is key to optimizing the health of our patients. Choosing Wisely is an initiative of the ABIM foundation to foster communication between physicians and patients about common tests and procedures that may fail to provide value or enhance patient outcomes. It’s a partnership with 70-plus medical societies including an innovative partnership with Consumer Reports. SHM’s evidence-based recommendations are:
- Don’t leave urinary catheters in place for convenience or monitoring of output for non-critically ill patients.
- Don’t prescribe stress ulcer prophylaxis to hospitalized patients unless they are at high risk for GI complications.
- Avoid transfusion of PRBC for arbitrary hemoglobin in the absence of CAD, CHF or CVA.
- Don’t order continuous telemetry monitoring outside of the ICU without a protocol.
- Don’t perform repetitive CBC and chemistry testing in a clinically stable patient.
Dr. Bulger highlighted that the Choosing Wisely campaign is designed to encourage conversations to
Dr.Bulger concluded that while tradition is hard to change, it is of paramount importance to think differently to find innovative solutions to common problems in healthcare. Join the conversation using #ChoosingWisely or #LessIsMore on twitter.
Key Takeaways
- Choosing Wisely is an ABIM campaign developed to address and promote conversations about common tests and procedures that are of low-value.
- SHM’s recommendations were implemented in institutions with positive results as evidenced by the Choosing Wisely case competition at #HospMed15.
- Look for a summary of these efforts to be published in the spring of 2015.
- Use these guidelines to educate, provoke dialogue and achieve optimal patient outcomes in your institution.
- Join the conversation on twitter using #ChoosingWisely and #LessIsMore.
Educational Opportunities for Hospitalists Beyond HM15
Whether you’re packing your bags for HM15 or following from afar, there are plenty of other opportunities to get the most up to date clinical, management, and quality improvement information in the specialty:
- Leadership Academy 2015
October 19-22
Austin, Texas
Get the managerial confidence you need to take your hospital medicine career to the next level. All three Leadership Academy courses will be offered in what’s now called the “Live Music Capital of the World.” www.hospitalmedicine.org/leadership
- Quality and Safety Educators Academy
May 7-9
Tempe, Ariz.
Medical students and residents are turning to hospitalists to learn about quality improvement and patient safety. The Quality and Safety Educators Academy (QSEA) is a great way to stay up to speed on the latest knowledge and tools to teach quality improvement. www.hospitalmedicine.org/qsea
- Project BOOST
Ongoing Applications
Have you thought about enrolling your hospital in SHM’s award-winning Project BOOST only to find that you missed the enrollment deadline? SHM has now made Project BOOST’s application process more flexible by accepting rolling applications throughout the year. www.hospitalmedicine.org/boost
- ABIM Maintenance of Certification
Deadline is August 1
Now is the time to start planning to enroll in the Focused Practice in Hospital Medicine Maintenance of Certification program. The enrollment deadline for the Fall 2015 exam is August 1, but don’t wait until the end of July to get started! http://www.hospitalmedicine.org/moc
Whether you’re packing your bags for HM15 or following from afar, there are plenty of other opportunities to get the most up to date clinical, management, and quality improvement information in the specialty:
- Leadership Academy 2015
October 19-22
Austin, Texas
Get the managerial confidence you need to take your hospital medicine career to the next level. All three Leadership Academy courses will be offered in what’s now called the “Live Music Capital of the World.” www.hospitalmedicine.org/leadership
- Quality and Safety Educators Academy
May 7-9
Tempe, Ariz.
Medical students and residents are turning to hospitalists to learn about quality improvement and patient safety. The Quality and Safety Educators Academy (QSEA) is a great way to stay up to speed on the latest knowledge and tools to teach quality improvement. www.hospitalmedicine.org/qsea
- Project BOOST
Ongoing Applications
Have you thought about enrolling your hospital in SHM’s award-winning Project BOOST only to find that you missed the enrollment deadline? SHM has now made Project BOOST’s application process more flexible by accepting rolling applications throughout the year. www.hospitalmedicine.org/boost
- ABIM Maintenance of Certification
Deadline is August 1
Now is the time to start planning to enroll in the Focused Practice in Hospital Medicine Maintenance of Certification program. The enrollment deadline for the Fall 2015 exam is August 1, but don’t wait until the end of July to get started! http://www.hospitalmedicine.org/moc
Whether you’re packing your bags for HM15 or following from afar, there are plenty of other opportunities to get the most up to date clinical, management, and quality improvement information in the specialty:
- Leadership Academy 2015
October 19-22
Austin, Texas
Get the managerial confidence you need to take your hospital medicine career to the next level. All three Leadership Academy courses will be offered in what’s now called the “Live Music Capital of the World.” www.hospitalmedicine.org/leadership
- Quality and Safety Educators Academy
May 7-9
Tempe, Ariz.
Medical students and residents are turning to hospitalists to learn about quality improvement and patient safety. The Quality and Safety Educators Academy (QSEA) is a great way to stay up to speed on the latest knowledge and tools to teach quality improvement. www.hospitalmedicine.org/qsea
- Project BOOST
Ongoing Applications
Have you thought about enrolling your hospital in SHM’s award-winning Project BOOST only to find that you missed the enrollment deadline? SHM has now made Project BOOST’s application process more flexible by accepting rolling applications throughout the year. www.hospitalmedicine.org/boost
- ABIM Maintenance of Certification
Deadline is August 1
Now is the time to start planning to enroll in the Focused Practice in Hospital Medicine Maintenance of Certification program. The enrollment deadline for the Fall 2015 exam is August 1, but don’t wait until the end of July to get started! http://www.hospitalmedicine.org/moc
Society of Hospital Medicine's Quality Improvement Module Approved for ABIM Maintenance of Certification
If you’re among the many physicians enrolled in the American Board of Internal Medicine’s (ABIM) Maintenance of Certification (MOC) program, you have to earn a combined 100 points in medical knowledge and practice improvement throughout your 10-year certificate period. SHM wants to help you with this process.
SHM is pleased to announce that the ABIM has approved SHM’s Hospital Quality Improvement and Patient Safety Medical Knowledge Module for credit in the ABIM MOC program.
Take the QI and Patient Safety Medical Knowledge Module and many other online courses—free for members—at www.shmlearningportal.org.
If you’re among the many physicians enrolled in the American Board of Internal Medicine’s (ABIM) Maintenance of Certification (MOC) program, you have to earn a combined 100 points in medical knowledge and practice improvement throughout your 10-year certificate period. SHM wants to help you with this process.
SHM is pleased to announce that the ABIM has approved SHM’s Hospital Quality Improvement and Patient Safety Medical Knowledge Module for credit in the ABIM MOC program.
Take the QI and Patient Safety Medical Knowledge Module and many other online courses—free for members—at www.shmlearningportal.org.
If you’re among the many physicians enrolled in the American Board of Internal Medicine’s (ABIM) Maintenance of Certification (MOC) program, you have to earn a combined 100 points in medical knowledge and practice improvement throughout your 10-year certificate period. SHM wants to help you with this process.
SHM is pleased to announce that the ABIM has approved SHM’s Hospital Quality Improvement and Patient Safety Medical Knowledge Module for credit in the ABIM MOC program.
Take the QI and Patient Safety Medical Knowledge Module and many other online courses—free for members—at www.shmlearningportal.org.