User login
‘Intense’ end-of-life care may be common in HSCT recipients

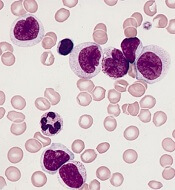
Patients who die within a year of allogeneic hematopoietic stem cell transplant (HSCT) tend to receive “medically intense” end-of-life care, an analysis suggests.
Researchers studied more than 2,000 patients who died within a year of allogeneic HSCT and found that a majority of the patients died in the hospital, and about half of them were admitted to the intensive care unit (ICU).
However, patient age, underlying diagnosis, and other factors influenced the likelihood of receiving intense end-of-life care.
For example, patients diagnosed with acute myeloid leukemia (AML) or myelodysplastic syndromes (MDS) were less likely than patients with acute lymphoblastic leukemia (ALL) to receive medically intense care.
Emily Johnston, MD, of the University of Alabama at Birmingham, and her colleagues reported these findings in the Journal of Clinical Oncology.
The researchers studied 2,135 patients in California who underwent inpatient HSCT and died within a year of the transplant (not as a result of peripartum events or trauma) between 2000 and 2013.
Fifty-three percent of the patients received some type of medically intense intervention, and 57% had at least two types of intense interventions.
Eighty-three percent of patients died in hospital, and 43% spent all of their last 30 days in the hospital.
Forty-nine percent of patients were admitted to the ICU, 45% were intubated, 22% underwent hemodialysis, and 8% received cardiopulmonary resuscitation.
Factors associated with intense care
The researchers said receipt of a medically intense intervention varied by age at death, underlying diagnosis, year of HSCT, location of care, and comorbidities. However, use of intense interventions did not vary according to sex, race/ethnicity, insurance type, or income.
Compared to patients age 60 and older, patients in the following age groups were more likely to receive medically intense interventions:
- Ages 15 to 21—odds ratio (OR)=2.6 (P<0.001)
- Ages 30 to 39—OR=1.8 (P<0.01)
- Ages 40 to 49—OR=1.4 (P<0.05).
Patients with comorbidities were more likely to receive intense interventions as well. The OR was 1.6 (P<0.01) for patients with one comorbidity and 2.5 (P<0.001) for patients with two or more comorbidities.
Patients with AML or MDS were less likely than patients with ALL to receive a medically intense intervention—OR=0.7 (P<0.05).
Patients who were transplanted between 2000 and 2004 were less likely to receive an intense intervention than patients transplanted between 2010 and 2013—OR=0.7 (P<0.01).
Patients who changed hospitals between HSCT and death were less likely to receive an intense intervention than patients who stayed at the same hospital. The OR was 0.3 if they transferred to a community hospital and 0.4 if they transferred to a specialty hospital (P<0.001 for both).
Patients living in rural areas were less likely than urban patients to receive a medically intense intervention—OR=0.6 (P<0.05).
“From our data, we understand there is a correlation with high-intensity end-of-life care in patients who die within one year after receiving a stem cell transplant, but we are still unsure if that was the care they wanted,” Dr. Johnston said.
“The findings suggest that, as oncologists, we need to start having end-of-life care conversations earlier with patients to determine if a high-intensity treatment plan is consistent with their goals or if a lower-intensity treatment plan is best. It’s not a one-size-fits-all approach in end-of-life care.”
This research was supported by Stanford University. One study author reported relationships with Corvus Pharmaceuticals, Shire Pharmaceuticals, and Adaptive Biotechnologies. All other authors reported no conflicts.
Patients who die within a year of allogeneic hematopoietic stem cell transplant (HSCT) tend to receive “medically intense” end-of-life care, an analysis suggests.
Researchers studied more than 2,000 patients who died within a year of allogeneic HSCT and found that a majority of the patients died in the hospital, and about half of them were admitted to the intensive care unit (ICU).
However, patient age, underlying diagnosis, and other factors influenced the likelihood of receiving intense end-of-life care.
For example, patients diagnosed with acute myeloid leukemia (AML) or myelodysplastic syndromes (MDS) were less likely than patients with acute lymphoblastic leukemia (ALL) to receive medically intense care.
Emily Johnston, MD, of the University of Alabama at Birmingham, and her colleagues reported these findings in the Journal of Clinical Oncology.
The researchers studied 2,135 patients in California who underwent inpatient HSCT and died within a year of the transplant (not as a result of peripartum events or trauma) between 2000 and 2013.
Fifty-three percent of the patients received some type of medically intense intervention, and 57% had at least two types of intense interventions.
Eighty-three percent of patients died in hospital, and 43% spent all of their last 30 days in the hospital.
Forty-nine percent of patients were admitted to the ICU, 45% were intubated, 22% underwent hemodialysis, and 8% received cardiopulmonary resuscitation.
Factors associated with intense care
The researchers said receipt of a medically intense intervention varied by age at death, underlying diagnosis, year of HSCT, location of care, and comorbidities. However, use of intense interventions did not vary according to sex, race/ethnicity, insurance type, or income.
Compared to patients age 60 and older, patients in the following age groups were more likely to receive medically intense interventions:
- Ages 15 to 21—odds ratio (OR)=2.6 (P<0.001)
- Ages 30 to 39—OR=1.8 (P<0.01)
- Ages 40 to 49—OR=1.4 (P<0.05).
Patients with comorbidities were more likely to receive intense interventions as well. The OR was 1.6 (P<0.01) for patients with one comorbidity and 2.5 (P<0.001) for patients with two or more comorbidities.
Patients with AML or MDS were less likely than patients with ALL to receive a medically intense intervention—OR=0.7 (P<0.05).
Patients who were transplanted between 2000 and 2004 were less likely to receive an intense intervention than patients transplanted between 2010 and 2013—OR=0.7 (P<0.01).
Patients who changed hospitals between HSCT and death were less likely to receive an intense intervention than patients who stayed at the same hospital. The OR was 0.3 if they transferred to a community hospital and 0.4 if they transferred to a specialty hospital (P<0.001 for both).
Patients living in rural areas were less likely than urban patients to receive a medically intense intervention—OR=0.6 (P<0.05).
“From our data, we understand there is a correlation with high-intensity end-of-life care in patients who die within one year after receiving a stem cell transplant, but we are still unsure if that was the care they wanted,” Dr. Johnston said.
“The findings suggest that, as oncologists, we need to start having end-of-life care conversations earlier with patients to determine if a high-intensity treatment plan is consistent with their goals or if a lower-intensity treatment plan is best. It’s not a one-size-fits-all approach in end-of-life care.”
This research was supported by Stanford University. One study author reported relationships with Corvus Pharmaceuticals, Shire Pharmaceuticals, and Adaptive Biotechnologies. All other authors reported no conflicts.
Patients who die within a year of allogeneic hematopoietic stem cell transplant (HSCT) tend to receive “medically intense” end-of-life care, an analysis suggests.
Researchers studied more than 2,000 patients who died within a year of allogeneic HSCT and found that a majority of the patients died in the hospital, and about half of them were admitted to the intensive care unit (ICU).
However, patient age, underlying diagnosis, and other factors influenced the likelihood of receiving intense end-of-life care.
For example, patients diagnosed with acute myeloid leukemia (AML) or myelodysplastic syndromes (MDS) were less likely than patients with acute lymphoblastic leukemia (ALL) to receive medically intense care.
Emily Johnston, MD, of the University of Alabama at Birmingham, and her colleagues reported these findings in the Journal of Clinical Oncology.
The researchers studied 2,135 patients in California who underwent inpatient HSCT and died within a year of the transplant (not as a result of peripartum events or trauma) between 2000 and 2013.
Fifty-three percent of the patients received some type of medically intense intervention, and 57% had at least two types of intense interventions.
Eighty-three percent of patients died in hospital, and 43% spent all of their last 30 days in the hospital.
Forty-nine percent of patients were admitted to the ICU, 45% were intubated, 22% underwent hemodialysis, and 8% received cardiopulmonary resuscitation.
Factors associated with intense care
The researchers said receipt of a medically intense intervention varied by age at death, underlying diagnosis, year of HSCT, location of care, and comorbidities. However, use of intense interventions did not vary according to sex, race/ethnicity, insurance type, or income.
Compared to patients age 60 and older, patients in the following age groups were more likely to receive medically intense interventions:
- Ages 15 to 21—odds ratio (OR)=2.6 (P<0.001)
- Ages 30 to 39—OR=1.8 (P<0.01)
- Ages 40 to 49—OR=1.4 (P<0.05).
Patients with comorbidities were more likely to receive intense interventions as well. The OR was 1.6 (P<0.01) for patients with one comorbidity and 2.5 (P<0.001) for patients with two or more comorbidities.
Patients with AML or MDS were less likely than patients with ALL to receive a medically intense intervention—OR=0.7 (P<0.05).
Patients who were transplanted between 2000 and 2004 were less likely to receive an intense intervention than patients transplanted between 2010 and 2013—OR=0.7 (P<0.01).
Patients who changed hospitals between HSCT and death were less likely to receive an intense intervention than patients who stayed at the same hospital. The OR was 0.3 if they transferred to a community hospital and 0.4 if they transferred to a specialty hospital (P<0.001 for both).
Patients living in rural areas were less likely than urban patients to receive a medically intense intervention—OR=0.6 (P<0.05).
“From our data, we understand there is a correlation with high-intensity end-of-life care in patients who die within one year after receiving a stem cell transplant, but we are still unsure if that was the care they wanted,” Dr. Johnston said.
“The findings suggest that, as oncologists, we need to start having end-of-life care conversations earlier with patients to determine if a high-intensity treatment plan is consistent with their goals or if a lower-intensity treatment plan is best. It’s not a one-size-fits-all approach in end-of-life care.”
This research was supported by Stanford University. One study author reported relationships with Corvus Pharmaceuticals, Shire Pharmaceuticals, and Adaptive Biotechnologies. All other authors reported no conflicts.
Understanding the role of HSCT in PTCL

DUBROVNIK, CROATIA—Hematopoietic stem cell transplant (HSCT) can be hit-or-miss in patients with peripheral T-cell lymphomas (PTCLs), according to a speaker at Leukemia and Lymphoma: Europe and the USA, Linking Knowledge and Practice.
Ali Bazarbachi, MD, PhD, of the American University of Beirut in Lebanon, noted that the success of HSCT varies according to the subtype of PTCL and the type of transplant.
For example, autologous (auto) HSCT given as frontline consolidation can be considered the standard of care for PTCL-not otherwise specified (NOS), angioimmunoblastic T-cell lymphoma (AITL), and certain patients with anaplastic large-cell lymphoma (ALCL), according to Dr. Bazarbachi.
On the other hand, auto-HSCT should never be used in patients with adult T-cell leukemia/lymphoma (ATLL).
Both auto-HSCT and allogeneic (allo) HSCT are options for patients with non-localized, extranodal natural killer T-cell lymphoma (ENKTL), nasal type, but only at certain times.
State of PTCL treatment
Dr. Bazarbachi began his presentation by pointing out that patients with newly diagnosed PTCL are no longer treated like patients with B-cell lymphoma, but treatment outcomes in PTCL still leave a lot to be desired.
He noted that, with any of the chemotherapy regimens used, typically, about a third of patients are primary refractory, a third relapse, and a quarter are cured. Only two forms of PTCL are frequently curable—localized ENKTL and ALK-positive ALCL.
Current treatment strategies for PTCL do include HSCT, but recommendations vary. Dr. Bazarbachi made the following recommendations, supported by evidence from clinical trials.
HSCT in PTCL-NOS, AITL, and ALCL
For patients with PTCL-NOS, AITL, or ALK-negative, non-DUSP22 ALCL, auto-HSCT as frontline consolidation can be considered the standard of care in patients who responded to induction, Dr. Bazarbachi said.
In a study published in 20121, high-dose chemotherapy and auto-HSCT as consolidation improved 5-year overall survival—compared to previous results with CHOP2—in patients with ALK-negative ALCL, AITL, PTCL-NOS, and enteropathy-associated T-cell lymphoma.
Allo-HSCT may also be an option for frontline consolidation in patients with PTCL-NOS, AITL, or ALK-negative, non-DUSP22 ALCL, according to Dr. Bazarbachi.
“Allo-transplant is not dead in this indication,” he said. “But it should be either part of a clinical trial or [given] to some selected patients—those with persistent bone marrow involvement, very young patients, or patients with primary refractory disease.”
Results from the COMPLETE study3 showed improved survival in patients who received consolidation with auto- or allo-HSCT, as compared to patients who did not receive a transplant.
COMPLETE patients with AITL or PTCL-NOS had improvements in progression-free and overall survival with HSCT. The survival advantage was “less evident” in patients with ALCL, the researchers said, but this trial included both ALK-negative and ALK-positive patients.
Dr. Bazarbachi noted that allo- and auto-HSCT can be options after relapse in patients with PTCL-NOS, AITL, or ALK-negative, non-DUSP22 ALCL.
However, chemosensitive patients who have relapsed should only receive auto-HSCT if they did not receive it frontline. Patients who have already undergone auto-HSCT can receive allo-HSCT, Dr. Bazarbachi said.
He added that refractory patients should not undergo auto-HSCT and should receive allo-HSCT only within the context of a clinical trial.
HSCT in ATLL
Dr. Bazarbachi noted that ATLL has a dismal prognosis, but allo-HSCT as frontline consolidation is potentially curative.4,5 It is most effective in patients who have achieved a complete or partial response to induction.
However, allo-HSCT should not be given as consolidation to ATLL patients who have received prior mogamulizumab. These patients have an increased risk of morbidity and mortality if they undergo allo-HSCT.
Allo-HSCT should not be given to refractory ATLL patients, although it may be an option for relapsed patients.
Dr. Bazarbachi stressed that ATLL patients should not receive auto-HSCT at any time—as frontline consolidation, after relapse, or if they have refractory disease.
Auto-HSCT “does not work in this disease,” he said. In a study published in 20145, all four ATLL patients who underwent auto-HSCT “rapidly” died.
HSCT in ENKTL
Dr. Bazarbachi said frontline consolidation with auto-HSCT should be considered the standard of care for patients with non-localized ENKTL, nasal type.
Auto-HSCT has been shown to improve survival in these patients6, and it is most effective when patients have achieved a complete response to induction.
Allo-HSCT is also an option for frontline consolidation in patients with non-localized ENKTL, nasal type, Dr. Bazarbachi said.
He added that chemosensitive patients who have relapsed can receive allo-HSCT, but they should only receive auto-HSCT if they did not receive it in the frontline setting. Both types of transplant should take place when patients are in complete remission.
Patients with refractory, non-localized ENKTL, nasal type should not receive auto-HSCT, but allo-HSCT is an option, Dr. Bazarbachi said.
He did not declare any conflicts of interest.
1. d’Amore F et al. J Clin Oncol. 2012 Sep 1;30(25):3093-9. doi: 10.1200/JCO.2011.40.2719
2. AbouYabis AN et al. ISRN Hematol. 2011 Jun 16. doi: 10.5402/2011/623924
3. Park SI et al. Blood 2017 130:342
4. Ishida T et al. Blood 2012 Aug 23;120(8):1734-41. doi: 10.1182/blood-2012-03-414490
5. Bazarbachi A et al. Bone Marrow Transplant. 2014 Oct;49(10):1266-8. doi: 10.1038/bmt.2014.143
6. Lee J et al. Biol Blood Marrow Transplant. 2008 Dec;14(12):1356-64. doi: 10.1016/j.bbmt.2008.09.014
DUBROVNIK, CROATIA—Hematopoietic stem cell transplant (HSCT) can be hit-or-miss in patients with peripheral T-cell lymphomas (PTCLs), according to a speaker at Leukemia and Lymphoma: Europe and the USA, Linking Knowledge and Practice.
Ali Bazarbachi, MD, PhD, of the American University of Beirut in Lebanon, noted that the success of HSCT varies according to the subtype of PTCL and the type of transplant.
For example, autologous (auto) HSCT given as frontline consolidation can be considered the standard of care for PTCL-not otherwise specified (NOS), angioimmunoblastic T-cell lymphoma (AITL), and certain patients with anaplastic large-cell lymphoma (ALCL), according to Dr. Bazarbachi.
On the other hand, auto-HSCT should never be used in patients with adult T-cell leukemia/lymphoma (ATLL).
Both auto-HSCT and allogeneic (allo) HSCT are options for patients with non-localized, extranodal natural killer T-cell lymphoma (ENKTL), nasal type, but only at certain times.
State of PTCL treatment
Dr. Bazarbachi began his presentation by pointing out that patients with newly diagnosed PTCL are no longer treated like patients with B-cell lymphoma, but treatment outcomes in PTCL still leave a lot to be desired.
He noted that, with any of the chemotherapy regimens used, typically, about a third of patients are primary refractory, a third relapse, and a quarter are cured. Only two forms of PTCL are frequently curable—localized ENKTL and ALK-positive ALCL.
Current treatment strategies for PTCL do include HSCT, but recommendations vary. Dr. Bazarbachi made the following recommendations, supported by evidence from clinical trials.
HSCT in PTCL-NOS, AITL, and ALCL
For patients with PTCL-NOS, AITL, or ALK-negative, non-DUSP22 ALCL, auto-HSCT as frontline consolidation can be considered the standard of care in patients who responded to induction, Dr. Bazarbachi said.
In a study published in 20121, high-dose chemotherapy and auto-HSCT as consolidation improved 5-year overall survival—compared to previous results with CHOP2—in patients with ALK-negative ALCL, AITL, PTCL-NOS, and enteropathy-associated T-cell lymphoma.
Allo-HSCT may also be an option for frontline consolidation in patients with PTCL-NOS, AITL, or ALK-negative, non-DUSP22 ALCL, according to Dr. Bazarbachi.
“Allo-transplant is not dead in this indication,” he said. “But it should be either part of a clinical trial or [given] to some selected patients—those with persistent bone marrow involvement, very young patients, or patients with primary refractory disease.”
Results from the COMPLETE study3 showed improved survival in patients who received consolidation with auto- or allo-HSCT, as compared to patients who did not receive a transplant.
COMPLETE patients with AITL or PTCL-NOS had improvements in progression-free and overall survival with HSCT. The survival advantage was “less evident” in patients with ALCL, the researchers said, but this trial included both ALK-negative and ALK-positive patients.
Dr. Bazarbachi noted that allo- and auto-HSCT can be options after relapse in patients with PTCL-NOS, AITL, or ALK-negative, non-DUSP22 ALCL.
However, chemosensitive patients who have relapsed should only receive auto-HSCT if they did not receive it frontline. Patients who have already undergone auto-HSCT can receive allo-HSCT, Dr. Bazarbachi said.
He added that refractory patients should not undergo auto-HSCT and should receive allo-HSCT only within the context of a clinical trial.
HSCT in ATLL
Dr. Bazarbachi noted that ATLL has a dismal prognosis, but allo-HSCT as frontline consolidation is potentially curative.4,5 It is most effective in patients who have achieved a complete or partial response to induction.
However, allo-HSCT should not be given as consolidation to ATLL patients who have received prior mogamulizumab. These patients have an increased risk of morbidity and mortality if they undergo allo-HSCT.
Allo-HSCT should not be given to refractory ATLL patients, although it may be an option for relapsed patients.
Dr. Bazarbachi stressed that ATLL patients should not receive auto-HSCT at any time—as frontline consolidation, after relapse, or if they have refractory disease.
Auto-HSCT “does not work in this disease,” he said. In a study published in 20145, all four ATLL patients who underwent auto-HSCT “rapidly” died.
HSCT in ENKTL
Dr. Bazarbachi said frontline consolidation with auto-HSCT should be considered the standard of care for patients with non-localized ENKTL, nasal type.
Auto-HSCT has been shown to improve survival in these patients6, and it is most effective when patients have achieved a complete response to induction.
Allo-HSCT is also an option for frontline consolidation in patients with non-localized ENKTL, nasal type, Dr. Bazarbachi said.
He added that chemosensitive patients who have relapsed can receive allo-HSCT, but they should only receive auto-HSCT if they did not receive it in the frontline setting. Both types of transplant should take place when patients are in complete remission.
Patients with refractory, non-localized ENKTL, nasal type should not receive auto-HSCT, but allo-HSCT is an option, Dr. Bazarbachi said.
He did not declare any conflicts of interest.
1. d’Amore F et al. J Clin Oncol. 2012 Sep 1;30(25):3093-9. doi: 10.1200/JCO.2011.40.2719
2. AbouYabis AN et al. ISRN Hematol. 2011 Jun 16. doi: 10.5402/2011/623924
3. Park SI et al. Blood 2017 130:342
4. Ishida T et al. Blood 2012 Aug 23;120(8):1734-41. doi: 10.1182/blood-2012-03-414490
5. Bazarbachi A et al. Bone Marrow Transplant. 2014 Oct;49(10):1266-8. doi: 10.1038/bmt.2014.143
6. Lee J et al. Biol Blood Marrow Transplant. 2008 Dec;14(12):1356-64. doi: 10.1016/j.bbmt.2008.09.014
DUBROVNIK, CROATIA—Hematopoietic stem cell transplant (HSCT) can be hit-or-miss in patients with peripheral T-cell lymphomas (PTCLs), according to a speaker at Leukemia and Lymphoma: Europe and the USA, Linking Knowledge and Practice.
Ali Bazarbachi, MD, PhD, of the American University of Beirut in Lebanon, noted that the success of HSCT varies according to the subtype of PTCL and the type of transplant.
For example, autologous (auto) HSCT given as frontline consolidation can be considered the standard of care for PTCL-not otherwise specified (NOS), angioimmunoblastic T-cell lymphoma (AITL), and certain patients with anaplastic large-cell lymphoma (ALCL), according to Dr. Bazarbachi.
On the other hand, auto-HSCT should never be used in patients with adult T-cell leukemia/lymphoma (ATLL).
Both auto-HSCT and allogeneic (allo) HSCT are options for patients with non-localized, extranodal natural killer T-cell lymphoma (ENKTL), nasal type, but only at certain times.
State of PTCL treatment
Dr. Bazarbachi began his presentation by pointing out that patients with newly diagnosed PTCL are no longer treated like patients with B-cell lymphoma, but treatment outcomes in PTCL still leave a lot to be desired.
He noted that, with any of the chemotherapy regimens used, typically, about a third of patients are primary refractory, a third relapse, and a quarter are cured. Only two forms of PTCL are frequently curable—localized ENKTL and ALK-positive ALCL.
Current treatment strategies for PTCL do include HSCT, but recommendations vary. Dr. Bazarbachi made the following recommendations, supported by evidence from clinical trials.
HSCT in PTCL-NOS, AITL, and ALCL
For patients with PTCL-NOS, AITL, or ALK-negative, non-DUSP22 ALCL, auto-HSCT as frontline consolidation can be considered the standard of care in patients who responded to induction, Dr. Bazarbachi said.
In a study published in 20121, high-dose chemotherapy and auto-HSCT as consolidation improved 5-year overall survival—compared to previous results with CHOP2—in patients with ALK-negative ALCL, AITL, PTCL-NOS, and enteropathy-associated T-cell lymphoma.
Allo-HSCT may also be an option for frontline consolidation in patients with PTCL-NOS, AITL, or ALK-negative, non-DUSP22 ALCL, according to Dr. Bazarbachi.
“Allo-transplant is not dead in this indication,” he said. “But it should be either part of a clinical trial or [given] to some selected patients—those with persistent bone marrow involvement, very young patients, or patients with primary refractory disease.”
Results from the COMPLETE study3 showed improved survival in patients who received consolidation with auto- or allo-HSCT, as compared to patients who did not receive a transplant.
COMPLETE patients with AITL or PTCL-NOS had improvements in progression-free and overall survival with HSCT. The survival advantage was “less evident” in patients with ALCL, the researchers said, but this trial included both ALK-negative and ALK-positive patients.
Dr. Bazarbachi noted that allo- and auto-HSCT can be options after relapse in patients with PTCL-NOS, AITL, or ALK-negative, non-DUSP22 ALCL.
However, chemosensitive patients who have relapsed should only receive auto-HSCT if they did not receive it frontline. Patients who have already undergone auto-HSCT can receive allo-HSCT, Dr. Bazarbachi said.
He added that refractory patients should not undergo auto-HSCT and should receive allo-HSCT only within the context of a clinical trial.
HSCT in ATLL
Dr. Bazarbachi noted that ATLL has a dismal prognosis, but allo-HSCT as frontline consolidation is potentially curative.4,5 It is most effective in patients who have achieved a complete or partial response to induction.
However, allo-HSCT should not be given as consolidation to ATLL patients who have received prior mogamulizumab. These patients have an increased risk of morbidity and mortality if they undergo allo-HSCT.
Allo-HSCT should not be given to refractory ATLL patients, although it may be an option for relapsed patients.
Dr. Bazarbachi stressed that ATLL patients should not receive auto-HSCT at any time—as frontline consolidation, after relapse, or if they have refractory disease.
Auto-HSCT “does not work in this disease,” he said. In a study published in 20145, all four ATLL patients who underwent auto-HSCT “rapidly” died.
HSCT in ENKTL
Dr. Bazarbachi said frontline consolidation with auto-HSCT should be considered the standard of care for patients with non-localized ENKTL, nasal type.
Auto-HSCT has been shown to improve survival in these patients6, and it is most effective when patients have achieved a complete response to induction.
Allo-HSCT is also an option for frontline consolidation in patients with non-localized ENKTL, nasal type, Dr. Bazarbachi said.
He added that chemosensitive patients who have relapsed can receive allo-HSCT, but they should only receive auto-HSCT if they did not receive it in the frontline setting. Both types of transplant should take place when patients are in complete remission.
Patients with refractory, non-localized ENKTL, nasal type should not receive auto-HSCT, but allo-HSCT is an option, Dr. Bazarbachi said.
He did not declare any conflicts of interest.
1. d’Amore F et al. J Clin Oncol. 2012 Sep 1;30(25):3093-9. doi: 10.1200/JCO.2011.40.2719
2. AbouYabis AN et al. ISRN Hematol. 2011 Jun 16. doi: 10.5402/2011/623924
3. Park SI et al. Blood 2017 130:342
4. Ishida T et al. Blood 2012 Aug 23;120(8):1734-41. doi: 10.1182/blood-2012-03-414490
5. Bazarbachi A et al. Bone Marrow Transplant. 2014 Oct;49(10):1266-8. doi: 10.1038/bmt.2014.143
6. Lee J et al. Biol Blood Marrow Transplant. 2008 Dec;14(12):1356-64. doi: 10.1016/j.bbmt.2008.09.014
Auto-FMT restores gut microbiota after HSCT

A randomized, controlled study of 25 patients has demonstrated that an autologous fecal microbiota transplant (auto-FMT) can restore beneficial gut bacteria depleted during allogeneic hematopoietic stem cell transplant (auto-HSCT), according to researchers.
Antibiotics given to prevent and treat bacterial infections during HSCT can also destroy patients’ beneficial intestinal bacteria, increasing their risk for infections and graft-versus-host disease.
The researchers reported that auto-FMT is a safe and effective way to help replenish the beneficial bacteria to near baseline levels within days.
Study patients receiving HSCT at Memorial Sloan Kettering Cancer Center (MSKCC) in New York provided fecal samples collected before transplant conditioning, which were frozen and stored before undergoing transplant.
Between 1 and 5 weeks, when physicians could confirm that patients’ stem cells had engrafted, they collected another fecal sample from patients and randomized the first 25 who lacked known beneficial bacteria to one of two groups.
Eleven control patients received standard of care without fecal transplant and 14 received auto-FMT by enema.
Researchers followed the subjects for 1 year after randomization, with fecal samples collected during this time.
Eleven of the 14 patients (79%) in the auto-FMT group recovered 75% or more of their initial good gut bacteria within days. This helped restore their digestive, immune, and other essential functions.
The beneficial microbial groups restored included Lachnospiraceae (family), Ruminococcaceae (family), and Bacteroidetes (phylum).
Patients in the standard care group took many weeks to replenish the beneficial bacteria destroyed during antibiotic treatment. Only 3 of 11 (27%) control patients had regained 75% or more of the microbiota in their initial fecal sample.
The investigators acknowledge a few study limitations, including that it was conducted at a single institution. Therefore, they say, the findings may not apply to patients undergoing allo-HSCT at other institutions.
In addition, auto-FMT patients may have been treated previously for cancer and depleted of some good bacteria as a result of prior antibiotic therapy.
Nevertheless, the investigators believe their study demonstrated the potential of auto-FMT as a clinical intervention, “thereby reversing the disruptive effects of broad-spectrum antibiotic treatment for patients undergoing allo-HSCT transplant,” they wrote.
Lead author Ying Taur, MD, MPH, of MSKCC, and colleagues published their paper in Science Translational Medicine.
The trial, supported in part by the National Institute of Allergy and Infectious Diseases (NIAID) of the National Institutes of Health, is ongoing and continues to accrue patients (NCT02269150).
“This important study suggests that clinical intervention using auto-FMT can safely reverse the disruptive effects of broad-spectrum antibiotic treatment,” said Anthony S. Fauci, MD, director of NIAID.
“If validated in larger studies, this approach may prove to be a relatively simple way to quickly restore a person’s healthy microbiome following intensive antimicrobial therapy.”
A randomized, controlled study of 25 patients has demonstrated that an autologous fecal microbiota transplant (auto-FMT) can restore beneficial gut bacteria depleted during allogeneic hematopoietic stem cell transplant (auto-HSCT), according to researchers.
Antibiotics given to prevent and treat bacterial infections during HSCT can also destroy patients’ beneficial intestinal bacteria, increasing their risk for infections and graft-versus-host disease.
The researchers reported that auto-FMT is a safe and effective way to help replenish the beneficial bacteria to near baseline levels within days.
Study patients receiving HSCT at Memorial Sloan Kettering Cancer Center (MSKCC) in New York provided fecal samples collected before transplant conditioning, which were frozen and stored before undergoing transplant.
Between 1 and 5 weeks, when physicians could confirm that patients’ stem cells had engrafted, they collected another fecal sample from patients and randomized the first 25 who lacked known beneficial bacteria to one of two groups.
Eleven control patients received standard of care without fecal transplant and 14 received auto-FMT by enema.
Researchers followed the subjects for 1 year after randomization, with fecal samples collected during this time.
Eleven of the 14 patients (79%) in the auto-FMT group recovered 75% or more of their initial good gut bacteria within days. This helped restore their digestive, immune, and other essential functions.
The beneficial microbial groups restored included Lachnospiraceae (family), Ruminococcaceae (family), and Bacteroidetes (phylum).
Patients in the standard care group took many weeks to replenish the beneficial bacteria destroyed during antibiotic treatment. Only 3 of 11 (27%) control patients had regained 75% or more of the microbiota in their initial fecal sample.
The investigators acknowledge a few study limitations, including that it was conducted at a single institution. Therefore, they say, the findings may not apply to patients undergoing allo-HSCT at other institutions.
In addition, auto-FMT patients may have been treated previously for cancer and depleted of some good bacteria as a result of prior antibiotic therapy.
Nevertheless, the investigators believe their study demonstrated the potential of auto-FMT as a clinical intervention, “thereby reversing the disruptive effects of broad-spectrum antibiotic treatment for patients undergoing allo-HSCT transplant,” they wrote.
Lead author Ying Taur, MD, MPH, of MSKCC, and colleagues published their paper in Science Translational Medicine.
The trial, supported in part by the National Institute of Allergy and Infectious Diseases (NIAID) of the National Institutes of Health, is ongoing and continues to accrue patients (NCT02269150).
“This important study suggests that clinical intervention using auto-FMT can safely reverse the disruptive effects of broad-spectrum antibiotic treatment,” said Anthony S. Fauci, MD, director of NIAID.
“If validated in larger studies, this approach may prove to be a relatively simple way to quickly restore a person’s healthy microbiome following intensive antimicrobial therapy.”
A randomized, controlled study of 25 patients has demonstrated that an autologous fecal microbiota transplant (auto-FMT) can restore beneficial gut bacteria depleted during allogeneic hematopoietic stem cell transplant (auto-HSCT), according to researchers.
Antibiotics given to prevent and treat bacterial infections during HSCT can also destroy patients’ beneficial intestinal bacteria, increasing their risk for infections and graft-versus-host disease.
The researchers reported that auto-FMT is a safe and effective way to help replenish the beneficial bacteria to near baseline levels within days.
Study patients receiving HSCT at Memorial Sloan Kettering Cancer Center (MSKCC) in New York provided fecal samples collected before transplant conditioning, which were frozen and stored before undergoing transplant.
Between 1 and 5 weeks, when physicians could confirm that patients’ stem cells had engrafted, they collected another fecal sample from patients and randomized the first 25 who lacked known beneficial bacteria to one of two groups.
Eleven control patients received standard of care without fecal transplant and 14 received auto-FMT by enema.
Researchers followed the subjects for 1 year after randomization, with fecal samples collected during this time.
Eleven of the 14 patients (79%) in the auto-FMT group recovered 75% or more of their initial good gut bacteria within days. This helped restore their digestive, immune, and other essential functions.
The beneficial microbial groups restored included Lachnospiraceae (family), Ruminococcaceae (family), and Bacteroidetes (phylum).
Patients in the standard care group took many weeks to replenish the beneficial bacteria destroyed during antibiotic treatment. Only 3 of 11 (27%) control patients had regained 75% or more of the microbiota in their initial fecal sample.
The investigators acknowledge a few study limitations, including that it was conducted at a single institution. Therefore, they say, the findings may not apply to patients undergoing allo-HSCT at other institutions.
In addition, auto-FMT patients may have been treated previously for cancer and depleted of some good bacteria as a result of prior antibiotic therapy.
Nevertheless, the investigators believe their study demonstrated the potential of auto-FMT as a clinical intervention, “thereby reversing the disruptive effects of broad-spectrum antibiotic treatment for patients undergoing allo-HSCT transplant,” they wrote.
Lead author Ying Taur, MD, MPH, of MSKCC, and colleagues published their paper in Science Translational Medicine.
The trial, supported in part by the National Institute of Allergy and Infectious Diseases (NIAID) of the National Institutes of Health, is ongoing and continues to accrue patients (NCT02269150).
“This important study suggests that clinical intervention using auto-FMT can safely reverse the disruptive effects of broad-spectrum antibiotic treatment,” said Anthony S. Fauci, MD, director of NIAID.
“If validated in larger studies, this approach may prove to be a relatively simple way to quickly restore a person’s healthy microbiome following intensive antimicrobial therapy.”
FDA grants rezafungin QIDP and fast track designations

The U.S. Food and Drug Administration (FDA) has granted Qualified Infectious Disease Product (QIDP) and fast track designations for rezafungin, an injection for the prevention of invasive fungal infections in adults undergoing allogeneic bone marrow transplantation.
Rezafungin is a novel antifungal echinocandin being developed by Cidara Therapeutics to treat candidemia and invasive candidiasis and for prophylaxis of invasive fungal infections due to Candida, Aspergillus, and Pneumocystis.
These pathogens typically affect patients with compromised immune systems, such as patients undergoing organ, bone marrow transplants, or chemotherapy.
Rezafungin is administered as a once-weekly, high-exposure therapy. According to Cidara, no one agent is approved to prevent infections caused by these pathogens. Current prophylaxis regimens often require multiple antifungal drugs, causing safety and tolerability issues.
The QIDP designation offers incentives for the development of new antifungal and antibacterial drugs, including fast track, priority review and, if approved by the FDA, eligibility for an additional five years of marketing exclusivity.
Fast track designation enables more frequent interactions with the FDA review team to expedite drug development.
For QIDP designation, a drug candidate must treat serious or life-threatening infections, particularly those caused by bacteria and fungi resistant to treatment or by resistant pathogens identified by the FDA.
Rezafungin acetate, formerly known as CD101 IV, met its primary safety and efficacy objectives in the phase 2 STRIVE trial, providing support for the company to initiate phase 3 trials.
The phase 2 trial compared rezafungin to caspofungin in patients with candidemia and/or invasive candidiasis.
Investigators enrolled 92 patients in the microbial intent-to-treat population.
Patients were randomized to one of two dose groups of rezafungin or to the caspofungin arm.
One hundred percent of patients with invasive candidiasis responded to the rezafungin 400 mg first-week dose followed by 200 mg once weekly up to four weeks, compared to 33% of patients who responded to daily caspofungin.
The company reported no concerning adverse event trends.
Cidara is initiating phase 3 pivotal trials of rezafungin in the treatment of candidemia and invasive candidiasis and the prophylaxis of invasive fungal infections.
The U.S. Food and Drug Administration (FDA) has granted Qualified Infectious Disease Product (QIDP) and fast track designations for rezafungin, an injection for the prevention of invasive fungal infections in adults undergoing allogeneic bone marrow transplantation.
Rezafungin is a novel antifungal echinocandin being developed by Cidara Therapeutics to treat candidemia and invasive candidiasis and for prophylaxis of invasive fungal infections due to Candida, Aspergillus, and Pneumocystis.
These pathogens typically affect patients with compromised immune systems, such as patients undergoing organ, bone marrow transplants, or chemotherapy.
Rezafungin is administered as a once-weekly, high-exposure therapy. According to Cidara, no one agent is approved to prevent infections caused by these pathogens. Current prophylaxis regimens often require multiple antifungal drugs, causing safety and tolerability issues.
The QIDP designation offers incentives for the development of new antifungal and antibacterial drugs, including fast track, priority review and, if approved by the FDA, eligibility for an additional five years of marketing exclusivity.
Fast track designation enables more frequent interactions with the FDA review team to expedite drug development.
For QIDP designation, a drug candidate must treat serious or life-threatening infections, particularly those caused by bacteria and fungi resistant to treatment or by resistant pathogens identified by the FDA.
Rezafungin acetate, formerly known as CD101 IV, met its primary safety and efficacy objectives in the phase 2 STRIVE trial, providing support for the company to initiate phase 3 trials.
The phase 2 trial compared rezafungin to caspofungin in patients with candidemia and/or invasive candidiasis.
Investigators enrolled 92 patients in the microbial intent-to-treat population.
Patients were randomized to one of two dose groups of rezafungin or to the caspofungin arm.
One hundred percent of patients with invasive candidiasis responded to the rezafungin 400 mg first-week dose followed by 200 mg once weekly up to four weeks, compared to 33% of patients who responded to daily caspofungin.
The company reported no concerning adverse event trends.
Cidara is initiating phase 3 pivotal trials of rezafungin in the treatment of candidemia and invasive candidiasis and the prophylaxis of invasive fungal infections.
The U.S. Food and Drug Administration (FDA) has granted Qualified Infectious Disease Product (QIDP) and fast track designations for rezafungin, an injection for the prevention of invasive fungal infections in adults undergoing allogeneic bone marrow transplantation.
Rezafungin is a novel antifungal echinocandin being developed by Cidara Therapeutics to treat candidemia and invasive candidiasis and for prophylaxis of invasive fungal infections due to Candida, Aspergillus, and Pneumocystis.
These pathogens typically affect patients with compromised immune systems, such as patients undergoing organ, bone marrow transplants, or chemotherapy.
Rezafungin is administered as a once-weekly, high-exposure therapy. According to Cidara, no one agent is approved to prevent infections caused by these pathogens. Current prophylaxis regimens often require multiple antifungal drugs, causing safety and tolerability issues.
The QIDP designation offers incentives for the development of new antifungal and antibacterial drugs, including fast track, priority review and, if approved by the FDA, eligibility for an additional five years of marketing exclusivity.
Fast track designation enables more frequent interactions with the FDA review team to expedite drug development.
For QIDP designation, a drug candidate must treat serious or life-threatening infections, particularly those caused by bacteria and fungi resistant to treatment or by resistant pathogens identified by the FDA.
Rezafungin acetate, formerly known as CD101 IV, met its primary safety and efficacy objectives in the phase 2 STRIVE trial, providing support for the company to initiate phase 3 trials.
The phase 2 trial compared rezafungin to caspofungin in patients with candidemia and/or invasive candidiasis.
Investigators enrolled 92 patients in the microbial intent-to-treat population.
Patients were randomized to one of two dose groups of rezafungin or to the caspofungin arm.
One hundred percent of patients with invasive candidiasis responded to the rezafungin 400 mg first-week dose followed by 200 mg once weekly up to four weeks, compared to 33% of patients who responded to daily caspofungin.
The company reported no concerning adverse event trends.
Cidara is initiating phase 3 pivotal trials of rezafungin in the treatment of candidemia and invasive candidiasis and the prophylaxis of invasive fungal infections.
Placenta-derived product receives orphan designation for HSCT
The U.S. Food and Drug Administration (FDA) has granted orphan designation to PLX-R18 for the treatment of graft failure and incomplete hematopoietic recovery following hematopoietic stem cell transplant (HSCT).
PLX-R18 consists of placenta-derived, mesenchymal-like adherent stromal cells that are designed to be administered to patients without the need for tissue or genetic matching.
PLX-R18 cells release a combination of therapeutic proteins in response to a damaged or poorly functioning hematopoietic system.
PLX-R18 is currently being evaluated for the treatment of insufficient hematopoietic recovery following HSCT in an ongoing, phase 1 trial (NCT03002519).
The trial is designed to evaluate the safety of intramuscular injections of PLX-R18 cells in 24 subjects with incomplete hematopoietic recovery persisting for at least 4 months after HSCT, with a 12-month follow-up period.
The primary endpoint is safety. Exploratory endpoints include changes in platelet and hemoglobin levels, changes in transfusion frequency, a shift from transfusion dependence to transfusion independence, changes in quality of life, and changes in the serum immunological parameters.
PLX-R18 is being developed by Pluristem Therapeutics, Inc. PLX-R18 also has orphan designation for the treatment of acute radiation syndrome.
About orphan designation
The FDA grants orphan designation to products intended to treat, diagnose, or prevent diseases/disorders that affect fewer than 200,000 people in the United States.
The designation provides incentives for sponsors to develop products for rare diseases. This may include tax credits toward the cost of clinical trials, prescription drug user fee waivers, and 7 years of market exclusivity if the product is approved.
The U.S. Food and Drug Administration (FDA) has granted orphan designation to PLX-R18 for the treatment of graft failure and incomplete hematopoietic recovery following hematopoietic stem cell transplant (HSCT).
PLX-R18 consists of placenta-derived, mesenchymal-like adherent stromal cells that are designed to be administered to patients without the need for tissue or genetic matching.
PLX-R18 cells release a combination of therapeutic proteins in response to a damaged or poorly functioning hematopoietic system.
PLX-R18 is currently being evaluated for the treatment of insufficient hematopoietic recovery following HSCT in an ongoing, phase 1 trial (NCT03002519).
The trial is designed to evaluate the safety of intramuscular injections of PLX-R18 cells in 24 subjects with incomplete hematopoietic recovery persisting for at least 4 months after HSCT, with a 12-month follow-up period.
The primary endpoint is safety. Exploratory endpoints include changes in platelet and hemoglobin levels, changes in transfusion frequency, a shift from transfusion dependence to transfusion independence, changes in quality of life, and changes in the serum immunological parameters.
PLX-R18 is being developed by Pluristem Therapeutics, Inc. PLX-R18 also has orphan designation for the treatment of acute radiation syndrome.
About orphan designation
The FDA grants orphan designation to products intended to treat, diagnose, or prevent diseases/disorders that affect fewer than 200,000 people in the United States.
The designation provides incentives for sponsors to develop products for rare diseases. This may include tax credits toward the cost of clinical trials, prescription drug user fee waivers, and 7 years of market exclusivity if the product is approved.
The U.S. Food and Drug Administration (FDA) has granted orphan designation to PLX-R18 for the treatment of graft failure and incomplete hematopoietic recovery following hematopoietic stem cell transplant (HSCT).
PLX-R18 consists of placenta-derived, mesenchymal-like adherent stromal cells that are designed to be administered to patients without the need for tissue or genetic matching.
PLX-R18 cells release a combination of therapeutic proteins in response to a damaged or poorly functioning hematopoietic system.
PLX-R18 is currently being evaluated for the treatment of insufficient hematopoietic recovery following HSCT in an ongoing, phase 1 trial (NCT03002519).
The trial is designed to evaluate the safety of intramuscular injections of PLX-R18 cells in 24 subjects with incomplete hematopoietic recovery persisting for at least 4 months after HSCT, with a 12-month follow-up period.
The primary endpoint is safety. Exploratory endpoints include changes in platelet and hemoglobin levels, changes in transfusion frequency, a shift from transfusion dependence to transfusion independence, changes in quality of life, and changes in the serum immunological parameters.
PLX-R18 is being developed by Pluristem Therapeutics, Inc. PLX-R18 also has orphan designation for the treatment of acute radiation syndrome.
About orphan designation
The FDA grants orphan designation to products intended to treat, diagnose, or prevent diseases/disorders that affect fewer than 200,000 people in the United States.
The designation provides incentives for sponsors to develop products for rare diseases. This may include tax credits toward the cost of clinical trials, prescription drug user fee waivers, and 7 years of market exclusivity if the product is approved.
NGS can predict AML relapse after HSCT
Next-generation sequencing (NGS) can be used to predict relapse in acute myeloid leukemia (AML) patients undergoing hematopoietic stem cell transplant (HSCT), according to research published in Blood.
Researchers found that patients with a higher variant allele frequency (VAF) 21 days after HSCT had a higher risk of relapse and death.
“We can detect mutations in patients’ bone marrow cells 3 weeks after the transplant and, based on that, predict the likelihood of their relapse,” explained study author Zhaolei Zhang, PhD, of the University of Toronto in Ontario, Canada.
Dr. Zhang and his colleagues performed NGS on 529 bone marrow samples from 104 AML patients who underwent chemotherapy and HSCT.
The samples were collected at the time of diagnosis, during the chemotherapy-induced remission, and 3 weeks after HSCT. A subset of patients also gave samples at 3 months, 6 months, and 12 months after HSCT.
The researchers identified 256 mutations that were present in 90 patients at diagnosis and looked for those same mutations at each sampling point.
Chemotherapy and HSCT eliminated most AML cells, leading to a reduction in mutation frequency. However, in some patients, mutations observed at diagnosis could still be detected after chemotherapy and at day 21 after HSCT, indicating the presence of treatment-resistant AML cells.
Allelic burdens at day 21 post-HSCT were higher in patients who ultimately relapsed, and the mutations observed at day 21 expanded at relapse.
The 3-year relapse rate was 56.2% in patients with a VAF greater than 0.2% at day 21 post-HSCT, compared to 16.0% in patients with a lower or no mutational burden (P<0.001).
The 3-year overall survival rates were 36.5% in patients with a VAF greater than 0.2% and 67.0% for patients with a lower or no mutational burden (P=0.006).
In multivariate analyses, VAF0.2% at day 21 was an independent adverse prognostic factor for relapse—hazard ratio, 4.75 (P<0.001)—and overall survival—hazard ratio, 3.07 (P=0.003).
Dr. Zhang and his colleagues said these results suggest NGS-based monitoring after HSCT “provides valuable information” that, together with a patient’s baseline mutational profile and clinical evaluation, can be used to predict outcomes of transplant.
This study was supported by research grants from the Natural Science and Engineering Council of Canada, Leukemia and Lymphoma Society of Canada, Princess Margaret Foundation, National Research Foundation of Korea, and National Natural Science Foundation of China.
Next-generation sequencing (NGS) can be used to predict relapse in acute myeloid leukemia (AML) patients undergoing hematopoietic stem cell transplant (HSCT), according to research published in Blood.
Researchers found that patients with a higher variant allele frequency (VAF) 21 days after HSCT had a higher risk of relapse and death.
“We can detect mutations in patients’ bone marrow cells 3 weeks after the transplant and, based on that, predict the likelihood of their relapse,” explained study author Zhaolei Zhang, PhD, of the University of Toronto in Ontario, Canada.
Dr. Zhang and his colleagues performed NGS on 529 bone marrow samples from 104 AML patients who underwent chemotherapy and HSCT.
The samples were collected at the time of diagnosis, during the chemotherapy-induced remission, and 3 weeks after HSCT. A subset of patients also gave samples at 3 months, 6 months, and 12 months after HSCT.
The researchers identified 256 mutations that were present in 90 patients at diagnosis and looked for those same mutations at each sampling point.
Chemotherapy and HSCT eliminated most AML cells, leading to a reduction in mutation frequency. However, in some patients, mutations observed at diagnosis could still be detected after chemotherapy and at day 21 after HSCT, indicating the presence of treatment-resistant AML cells.
Allelic burdens at day 21 post-HSCT were higher in patients who ultimately relapsed, and the mutations observed at day 21 expanded at relapse.
The 3-year relapse rate was 56.2% in patients with a VAF greater than 0.2% at day 21 post-HSCT, compared to 16.0% in patients with a lower or no mutational burden (P<0.001).
The 3-year overall survival rates were 36.5% in patients with a VAF greater than 0.2% and 67.0% for patients with a lower or no mutational burden (P=0.006).
In multivariate analyses, VAF0.2% at day 21 was an independent adverse prognostic factor for relapse—hazard ratio, 4.75 (P<0.001)—and overall survival—hazard ratio, 3.07 (P=0.003).
Dr. Zhang and his colleagues said these results suggest NGS-based monitoring after HSCT “provides valuable information” that, together with a patient’s baseline mutational profile and clinical evaluation, can be used to predict outcomes of transplant.
This study was supported by research grants from the Natural Science and Engineering Council of Canada, Leukemia and Lymphoma Society of Canada, Princess Margaret Foundation, National Research Foundation of Korea, and National Natural Science Foundation of China.
Next-generation sequencing (NGS) can be used to predict relapse in acute myeloid leukemia (AML) patients undergoing hematopoietic stem cell transplant (HSCT), according to research published in Blood.
Researchers found that patients with a higher variant allele frequency (VAF) 21 days after HSCT had a higher risk of relapse and death.
“We can detect mutations in patients’ bone marrow cells 3 weeks after the transplant and, based on that, predict the likelihood of their relapse,” explained study author Zhaolei Zhang, PhD, of the University of Toronto in Ontario, Canada.
Dr. Zhang and his colleagues performed NGS on 529 bone marrow samples from 104 AML patients who underwent chemotherapy and HSCT.
The samples were collected at the time of diagnosis, during the chemotherapy-induced remission, and 3 weeks after HSCT. A subset of patients also gave samples at 3 months, 6 months, and 12 months after HSCT.
The researchers identified 256 mutations that were present in 90 patients at diagnosis and looked for those same mutations at each sampling point.
Chemotherapy and HSCT eliminated most AML cells, leading to a reduction in mutation frequency. However, in some patients, mutations observed at diagnosis could still be detected after chemotherapy and at day 21 after HSCT, indicating the presence of treatment-resistant AML cells.
Allelic burdens at day 21 post-HSCT were higher in patients who ultimately relapsed, and the mutations observed at day 21 expanded at relapse.
The 3-year relapse rate was 56.2% in patients with a VAF greater than 0.2% at day 21 post-HSCT, compared to 16.0% in patients with a lower or no mutational burden (P<0.001).
The 3-year overall survival rates were 36.5% in patients with a VAF greater than 0.2% and 67.0% for patients with a lower or no mutational burden (P=0.006).
In multivariate analyses, VAF0.2% at day 21 was an independent adverse prognostic factor for relapse—hazard ratio, 4.75 (P<0.001)—and overall survival—hazard ratio, 3.07 (P=0.003).
Dr. Zhang and his colleagues said these results suggest NGS-based monitoring after HSCT “provides valuable information” that, together with a patient’s baseline mutational profile and clinical evaluation, can be used to predict outcomes of transplant.
This study was supported by research grants from the Natural Science and Engineering Council of Canada, Leukemia and Lymphoma Society of Canada, Princess Margaret Foundation, National Research Foundation of Korea, and National Natural Science Foundation of China.
Sequencing informs prognosis after HSCT in MDS
Gene sequencing early after transplant may provide important prognostic information in patients with myelodysplastic syndromes (MDS), according to a new study.
Patients who had disease-associated mutations in the bone marrow 30 days after hematopoietic stem cell transplant (HSCT) were significantly more likely to experience disease progression and have lower rates of progression-free survival (PFS) at 1 year.
“Using our sequencing method, we’re identifying residual tumor cells before a pathologist could see them under the microscope and before a patient develops symptoms,” said Matthew J. Walter, MD, of Washington University in St. Louis, Mo.
“At that moment, there may be time to intervene in ways that could delay the cancer from coming back or potentially prevent it completely.”
Dr. Walter and his colleagues described results with their sequencing method in The New England Journal of Medicine.
The researchers sequenced bone marrow and skin (control) samples from 90 adults with MDS who underwent allogeneic HSCT.
The team used enhanced exome sequencing to detect mutations before HSCT and evaluated mutation clearance using error-corrected sequencing to genotype mutations in bone marrow samples collected 30 days after HSCT.
The researchers detected at least one validated somatic mutation in the pre-HSCT samples from 86 of 90 patients.
Of the 86 patients, 32 had at least one mutation with a maximum variant allele frequency of at least 0.5% detected 30 days after HSCT. The frequency is equivalent to 1 heterozygous mutant cell per 100 cells, the researchers explained.
Patients who experienced disease progression had mutations with a median maximum variant allele frequency of 0.9%, compared with 0% for patients who did not progress (P<0.001).
Progression occurred in 53.1% of patients who had one or more mutations with a variant allele frequency of at least 0.5% at 30 days, whereas progression occurred in 13% of patients who did not have such mutations. After adjusting for conditioning regimen, the hazard ratio (HR) for disease progression in the patients with mutations was 3.86 (P<0.001).
The 1-year PFS rate was 31.3% in patients who had one or more mutations with a variant allele frequency of at least 0.5% at 30 days and 59.3% in patients who did not have the mutations. After adjusting for conditioning, the HR for progression or death was 2.22 (P=0.005).
The researchers noted that PFS was lower in patients who had received reduced-intensity conditioning and had at least one persistent mutation with a variant allele frequency of at least 0.5% at day 30 (P≤0.001), when compared to other combinations of conditioning regimen and mutation status.
In multivariable analyses, the presence of a mutation with at least 0.5% variant allele frequency was associated with a more than four-fold risk of progression (HR, 4.48; P<0.001) and a more than two-fold risk of progression or death (HR, 2.39; P=0.002).
“Now that we have detected mutations early and shown that it predicts a higher risk of recurrence, we want to determine the best course of action for those high-risk patients,” Dr. Walter said.
He and his colleagues acknowledged that the high-coverage exome sequencing technique used for this study is not routinely available in the clinic. Therefore, the researchers also analyzed samples using a subset of genes that are usually included in gene sequencing panels for MDS and acute myeloid leukemia.
The researchers noted that this 40-gene panel revealed fewer patients (n=68; 79%) with mutations, but “the prognostic value of detection of measurable residual disease was still highly clinically significant.”
With this approach, the presence of at least one mutation with a variant allele frequency of at least 0.5% 30 days after HSCT was associated with a higher risk of disease progression at 1 year (HR, 3.39; P=0.001) and a higher risk of progression or death at 1 year (HR, 2.09; P=0.02).
This study was supported by grants from the Leukemia and Lymphoma Society and other groups.
Gene sequencing early after transplant may provide important prognostic information in patients with myelodysplastic syndromes (MDS), according to a new study.
Patients who had disease-associated mutations in the bone marrow 30 days after hematopoietic stem cell transplant (HSCT) were significantly more likely to experience disease progression and have lower rates of progression-free survival (PFS) at 1 year.
“Using our sequencing method, we’re identifying residual tumor cells before a pathologist could see them under the microscope and before a patient develops symptoms,” said Matthew J. Walter, MD, of Washington University in St. Louis, Mo.
“At that moment, there may be time to intervene in ways that could delay the cancer from coming back or potentially prevent it completely.”
Dr. Walter and his colleagues described results with their sequencing method in The New England Journal of Medicine.
The researchers sequenced bone marrow and skin (control) samples from 90 adults with MDS who underwent allogeneic HSCT.
The team used enhanced exome sequencing to detect mutations before HSCT and evaluated mutation clearance using error-corrected sequencing to genotype mutations in bone marrow samples collected 30 days after HSCT.
The researchers detected at least one validated somatic mutation in the pre-HSCT samples from 86 of 90 patients.
Of the 86 patients, 32 had at least one mutation with a maximum variant allele frequency of at least 0.5% detected 30 days after HSCT. The frequency is equivalent to 1 heterozygous mutant cell per 100 cells, the researchers explained.
Patients who experienced disease progression had mutations with a median maximum variant allele frequency of 0.9%, compared with 0% for patients who did not progress (P<0.001).
Progression occurred in 53.1% of patients who had one or more mutations with a variant allele frequency of at least 0.5% at 30 days, whereas progression occurred in 13% of patients who did not have such mutations. After adjusting for conditioning regimen, the hazard ratio (HR) for disease progression in the patients with mutations was 3.86 (P<0.001).
The 1-year PFS rate was 31.3% in patients who had one or more mutations with a variant allele frequency of at least 0.5% at 30 days and 59.3% in patients who did not have the mutations. After adjusting for conditioning, the HR for progression or death was 2.22 (P=0.005).
The researchers noted that PFS was lower in patients who had received reduced-intensity conditioning and had at least one persistent mutation with a variant allele frequency of at least 0.5% at day 30 (P≤0.001), when compared to other combinations of conditioning regimen and mutation status.
In multivariable analyses, the presence of a mutation with at least 0.5% variant allele frequency was associated with a more than four-fold risk of progression (HR, 4.48; P<0.001) and a more than two-fold risk of progression or death (HR, 2.39; P=0.002).
“Now that we have detected mutations early and shown that it predicts a higher risk of recurrence, we want to determine the best course of action for those high-risk patients,” Dr. Walter said.
He and his colleagues acknowledged that the high-coverage exome sequencing technique used for this study is not routinely available in the clinic. Therefore, the researchers also analyzed samples using a subset of genes that are usually included in gene sequencing panels for MDS and acute myeloid leukemia.
The researchers noted that this 40-gene panel revealed fewer patients (n=68; 79%) with mutations, but “the prognostic value of detection of measurable residual disease was still highly clinically significant.”
With this approach, the presence of at least one mutation with a variant allele frequency of at least 0.5% 30 days after HSCT was associated with a higher risk of disease progression at 1 year (HR, 3.39; P=0.001) and a higher risk of progression or death at 1 year (HR, 2.09; P=0.02).
This study was supported by grants from the Leukemia and Lymphoma Society and other groups.
Gene sequencing early after transplant may provide important prognostic information in patients with myelodysplastic syndromes (MDS), according to a new study.
Patients who had disease-associated mutations in the bone marrow 30 days after hematopoietic stem cell transplant (HSCT) were significantly more likely to experience disease progression and have lower rates of progression-free survival (PFS) at 1 year.
“Using our sequencing method, we’re identifying residual tumor cells before a pathologist could see them under the microscope and before a patient develops symptoms,” said Matthew J. Walter, MD, of Washington University in St. Louis, Mo.
“At that moment, there may be time to intervene in ways that could delay the cancer from coming back or potentially prevent it completely.”
Dr. Walter and his colleagues described results with their sequencing method in The New England Journal of Medicine.
The researchers sequenced bone marrow and skin (control) samples from 90 adults with MDS who underwent allogeneic HSCT.
The team used enhanced exome sequencing to detect mutations before HSCT and evaluated mutation clearance using error-corrected sequencing to genotype mutations in bone marrow samples collected 30 days after HSCT.
The researchers detected at least one validated somatic mutation in the pre-HSCT samples from 86 of 90 patients.
Of the 86 patients, 32 had at least one mutation with a maximum variant allele frequency of at least 0.5% detected 30 days after HSCT. The frequency is equivalent to 1 heterozygous mutant cell per 100 cells, the researchers explained.
Patients who experienced disease progression had mutations with a median maximum variant allele frequency of 0.9%, compared with 0% for patients who did not progress (P<0.001).
Progression occurred in 53.1% of patients who had one or more mutations with a variant allele frequency of at least 0.5% at 30 days, whereas progression occurred in 13% of patients who did not have such mutations. After adjusting for conditioning regimen, the hazard ratio (HR) for disease progression in the patients with mutations was 3.86 (P<0.001).
The 1-year PFS rate was 31.3% in patients who had one or more mutations with a variant allele frequency of at least 0.5% at 30 days and 59.3% in patients who did not have the mutations. After adjusting for conditioning, the HR for progression or death was 2.22 (P=0.005).
The researchers noted that PFS was lower in patients who had received reduced-intensity conditioning and had at least one persistent mutation with a variant allele frequency of at least 0.5% at day 30 (P≤0.001), when compared to other combinations of conditioning regimen and mutation status.
In multivariable analyses, the presence of a mutation with at least 0.5% variant allele frequency was associated with a more than four-fold risk of progression (HR, 4.48; P<0.001) and a more than two-fold risk of progression or death (HR, 2.39; P=0.002).
“Now that we have detected mutations early and shown that it predicts a higher risk of recurrence, we want to determine the best course of action for those high-risk patients,” Dr. Walter said.
He and his colleagues acknowledged that the high-coverage exome sequencing technique used for this study is not routinely available in the clinic. Therefore, the researchers also analyzed samples using a subset of genes that are usually included in gene sequencing panels for MDS and acute myeloid leukemia.
The researchers noted that this 40-gene panel revealed fewer patients (n=68; 79%) with mutations, but “the prognostic value of detection of measurable residual disease was still highly clinically significant.”
With this approach, the presence of at least one mutation with a variant allele frequency of at least 0.5% 30 days after HSCT was associated with a higher risk of disease progression at 1 year (HR, 3.39; P=0.001) and a higher risk of progression or death at 1 year (HR, 2.09; P=0.02).
This study was supported by grants from the Leukemia and Lymphoma Society and other groups.
Prophylaxis reduces bacteremia in some kids

In a phase 3 study, levofloxacin prophylaxis significantly reduced bacteremia in children with acute leukemias who received intensive chemotherapy.
However, the risk of bacteremia was not significantly reduced with levofloxacin in another cohort of children who underwent hematopoietic stem cell transplant (HSCT).
Sarah Alexander, MD, of the Hospital for Sick Children in Toronto, Ontario, Canada, and her colleagues reported these findings in JAMA.
This multicenter, randomized trial (ACCL0934) enrolled patients aged 6 months to 21 years.
There were 200 patients with acute leukemias (acute myeloid leukemia or relapsed acute lymphoblastic leukemia) who were set to receive chemotherapy and 424 patients who were to receive a myeloablative autologous or allogeneic HSCT.
The acute leukemia patients were randomized to receive no prophylaxis (n=100) or levofloxacin prophylaxis (n=100) for two consecutive cycles of chemotherapy.
The HSCT recipients were randomized to receive no prophylaxis (n=214) or levofloxacin prophylaxis (n=210) during one HSCT procedure.
Results
In the primary analysis of the acute leukemia group (n=195), the incidence of bacteremia was 21.9% for those randomized to levofloxacin and 43.4% for those who did not receive prophylaxis (P=0.001).
In the primary analysis of the HSCT group (n=418), the incidence of bacteremia was 11.0% in the levofloxacin arm and 17.3% in the control arm (P=0.06).
However, a post hoc analysis accounting for time at risk showed a significant difference in favor of prophylaxis in both the acute leukemia and HSCT groups and a similar effect size between groups.
For the acute leukemia group, the rate of bacteremic episodes in the post hoc analysis was 4.9 versus 9.4 per 1,000 patient-days in the prophylaxis and control arms, respectively (P=0.008).
In the HSCT group, the rate of bacteremic episodes was 5.3 versus 10.0 per 1,000 patient-days in the prophylaxis and control arms, respectively (P=0.02).
The researchers said it is possible that the effect of prophylaxis was similar between the HSCT and acute leukemia groups, but there was reduced power to detect a significant difference because of fewer events among HSCT recipients.
However, the differences between the HSCT and acute leukemia groups in the primary analysis might also be explained by differences in supportive care measures or infections with pathogens that had differential sensitivity to levofloxacin.
The researchers noted that levofloxacin-resistant pathogens, such as viridans group streptococcal isolates and several gram-negative isolates, often were detected in patients who had bacteremia events despite prophylaxis. This suggests other interventions in combination with levofloxacin prophylaxis are probably needed to further decrease risk.
Dr. Alexander and her colleagues also said further randomized studies are needed to better understand the risks of levofloxacin in relation to its benefits.
In the current study, there were 23 serious adverse events reported in 8 patients. Twelve of these events, occurring in two patients, may have been related to levofloxacin.
This research was supported by grants from the Community Clinical Oncology Program and National Cancer Institute. Dr. Alexander reported no disclosures. Coauthors reported disclosures related to Bristol-Myers Squibb, Chimerix, Jazz Pharmaceuticals, and the Children’s Oncology Group.
In a phase 3 study, levofloxacin prophylaxis significantly reduced bacteremia in children with acute leukemias who received intensive chemotherapy.
However, the risk of bacteremia was not significantly reduced with levofloxacin in another cohort of children who underwent hematopoietic stem cell transplant (HSCT).
Sarah Alexander, MD, of the Hospital for Sick Children in Toronto, Ontario, Canada, and her colleagues reported these findings in JAMA.
This multicenter, randomized trial (ACCL0934) enrolled patients aged 6 months to 21 years.
There were 200 patients with acute leukemias (acute myeloid leukemia or relapsed acute lymphoblastic leukemia) who were set to receive chemotherapy and 424 patients who were to receive a myeloablative autologous or allogeneic HSCT.
The acute leukemia patients were randomized to receive no prophylaxis (n=100) or levofloxacin prophylaxis (n=100) for two consecutive cycles of chemotherapy.
The HSCT recipients were randomized to receive no prophylaxis (n=214) or levofloxacin prophylaxis (n=210) during one HSCT procedure.
Results
In the primary analysis of the acute leukemia group (n=195), the incidence of bacteremia was 21.9% for those randomized to levofloxacin and 43.4% for those who did not receive prophylaxis (P=0.001).
In the primary analysis of the HSCT group (n=418), the incidence of bacteremia was 11.0% in the levofloxacin arm and 17.3% in the control arm (P=0.06).
However, a post hoc analysis accounting for time at risk showed a significant difference in favor of prophylaxis in both the acute leukemia and HSCT groups and a similar effect size between groups.
For the acute leukemia group, the rate of bacteremic episodes in the post hoc analysis was 4.9 versus 9.4 per 1,000 patient-days in the prophylaxis and control arms, respectively (P=0.008).
In the HSCT group, the rate of bacteremic episodes was 5.3 versus 10.0 per 1,000 patient-days in the prophylaxis and control arms, respectively (P=0.02).
The researchers said it is possible that the effect of prophylaxis was similar between the HSCT and acute leukemia groups, but there was reduced power to detect a significant difference because of fewer events among HSCT recipients.
However, the differences between the HSCT and acute leukemia groups in the primary analysis might also be explained by differences in supportive care measures or infections with pathogens that had differential sensitivity to levofloxacin.
The researchers noted that levofloxacin-resistant pathogens, such as viridans group streptococcal isolates and several gram-negative isolates, often were detected in patients who had bacteremia events despite prophylaxis. This suggests other interventions in combination with levofloxacin prophylaxis are probably needed to further decrease risk.
Dr. Alexander and her colleagues also said further randomized studies are needed to better understand the risks of levofloxacin in relation to its benefits.
In the current study, there were 23 serious adverse events reported in 8 patients. Twelve of these events, occurring in two patients, may have been related to levofloxacin.
This research was supported by grants from the Community Clinical Oncology Program and National Cancer Institute. Dr. Alexander reported no disclosures. Coauthors reported disclosures related to Bristol-Myers Squibb, Chimerix, Jazz Pharmaceuticals, and the Children’s Oncology Group.
In a phase 3 study, levofloxacin prophylaxis significantly reduced bacteremia in children with acute leukemias who received intensive chemotherapy.
However, the risk of bacteremia was not significantly reduced with levofloxacin in another cohort of children who underwent hematopoietic stem cell transplant (HSCT).
Sarah Alexander, MD, of the Hospital for Sick Children in Toronto, Ontario, Canada, and her colleagues reported these findings in JAMA.
This multicenter, randomized trial (ACCL0934) enrolled patients aged 6 months to 21 years.
There were 200 patients with acute leukemias (acute myeloid leukemia or relapsed acute lymphoblastic leukemia) who were set to receive chemotherapy and 424 patients who were to receive a myeloablative autologous or allogeneic HSCT.
The acute leukemia patients were randomized to receive no prophylaxis (n=100) or levofloxacin prophylaxis (n=100) for two consecutive cycles of chemotherapy.
The HSCT recipients were randomized to receive no prophylaxis (n=214) or levofloxacin prophylaxis (n=210) during one HSCT procedure.
Results
In the primary analysis of the acute leukemia group (n=195), the incidence of bacteremia was 21.9% for those randomized to levofloxacin and 43.4% for those who did not receive prophylaxis (P=0.001).
In the primary analysis of the HSCT group (n=418), the incidence of bacteremia was 11.0% in the levofloxacin arm and 17.3% in the control arm (P=0.06).
However, a post hoc analysis accounting for time at risk showed a significant difference in favor of prophylaxis in both the acute leukemia and HSCT groups and a similar effect size between groups.
For the acute leukemia group, the rate of bacteremic episodes in the post hoc analysis was 4.9 versus 9.4 per 1,000 patient-days in the prophylaxis and control arms, respectively (P=0.008).
In the HSCT group, the rate of bacteremic episodes was 5.3 versus 10.0 per 1,000 patient-days in the prophylaxis and control arms, respectively (P=0.02).
The researchers said it is possible that the effect of prophylaxis was similar between the HSCT and acute leukemia groups, but there was reduced power to detect a significant difference because of fewer events among HSCT recipients.
However, the differences between the HSCT and acute leukemia groups in the primary analysis might also be explained by differences in supportive care measures or infections with pathogens that had differential sensitivity to levofloxacin.
The researchers noted that levofloxacin-resistant pathogens, such as viridans group streptococcal isolates and several gram-negative isolates, often were detected in patients who had bacteremia events despite prophylaxis. This suggests other interventions in combination with levofloxacin prophylaxis are probably needed to further decrease risk.
Dr. Alexander and her colleagues also said further randomized studies are needed to better understand the risks of levofloxacin in relation to its benefits.
In the current study, there were 23 serious adverse events reported in 8 patients. Twelve of these events, occurring in two patients, may have been related to levofloxacin.
This research was supported by grants from the Community Clinical Oncology Program and National Cancer Institute. Dr. Alexander reported no disclosures. Coauthors reported disclosures related to Bristol-Myers Squibb, Chimerix, Jazz Pharmaceuticals, and the Children’s Oncology Group.
Team identifies potential immunotherapy target for AML

New research could aid the development of immunotherapies tailored to patients with acute myeloid leukemia (AML) who are undergoing stem cell transplant (SCT).
Researchers found they could use genetic sequencing and computer software to identify minor histocompatibility antigens (mHAs) known to occur in AML.
The team used this method to predict novel graft-versus-leukemia (GVL) mHAs and demonstrated that one of these mHAs could be a “potentially useful” therapeutic target.
Ben Vincent, MD, of the University of North Carolina Lineberger Comprehensive Cancer Center in Chapel Hill, and his colleagues reported these findings in Blood Advances.
In their retrospective study, the researchers tested whether their software could predict antigenic targets in 101 SCT donor-recipient pairs.
The researchers found they could correctly identify 14 of 18 mHAs known to occur in AML, but they were also able to predict 102 new GVL mHAs.
The researchers then confirmed one of these GVL mHAs, called UNC-GRK4-V, as a potential target for immunotherapy. The team observed immune responses to UNC-GRK4-V in four of nine AML patients who had undergone SCT.
Looking ahead, the researchers want to optimize their software to predict the most common AML-associated mHAs present in the U.S. population and confirm these predicted antigens as valid immunotherapy targets.
The team believes they could potentially use their predictions to engineer donor immune cells to specifically target the cancer cell antigens while preventing graft-versus-host disease.
“We’ve developed a software package that predicts leukemia-specific immune targets in any leukemia patient undergoing a stem cell transplant based on DNA and RNA sequencing and demonstrated that these data can lead to actual targets expressed on leukemia cells,” Dr. Vincent said.
“The next step of our work is to use that information for patient-specific therapies to try to improve cure rates without making graft-versus-host disease worse.”
The current research was supported by a National Cancer Institute grant, an ASCO Young Investigator Award, the North Carolina University Cancer Research Fund, and the Scott Neil Schwirck Fellowship.
New research could aid the development of immunotherapies tailored to patients with acute myeloid leukemia (AML) who are undergoing stem cell transplant (SCT).
Researchers found they could use genetic sequencing and computer software to identify minor histocompatibility antigens (mHAs) known to occur in AML.
The team used this method to predict novel graft-versus-leukemia (GVL) mHAs and demonstrated that one of these mHAs could be a “potentially useful” therapeutic target.
Ben Vincent, MD, of the University of North Carolina Lineberger Comprehensive Cancer Center in Chapel Hill, and his colleagues reported these findings in Blood Advances.
In their retrospective study, the researchers tested whether their software could predict antigenic targets in 101 SCT donor-recipient pairs.
The researchers found they could correctly identify 14 of 18 mHAs known to occur in AML, but they were also able to predict 102 new GVL mHAs.
The researchers then confirmed one of these GVL mHAs, called UNC-GRK4-V, as a potential target for immunotherapy. The team observed immune responses to UNC-GRK4-V in four of nine AML patients who had undergone SCT.
Looking ahead, the researchers want to optimize their software to predict the most common AML-associated mHAs present in the U.S. population and confirm these predicted antigens as valid immunotherapy targets.
The team believes they could potentially use their predictions to engineer donor immune cells to specifically target the cancer cell antigens while preventing graft-versus-host disease.
“We’ve developed a software package that predicts leukemia-specific immune targets in any leukemia patient undergoing a stem cell transplant based on DNA and RNA sequencing and demonstrated that these data can lead to actual targets expressed on leukemia cells,” Dr. Vincent said.
“The next step of our work is to use that information for patient-specific therapies to try to improve cure rates without making graft-versus-host disease worse.”
The current research was supported by a National Cancer Institute grant, an ASCO Young Investigator Award, the North Carolina University Cancer Research Fund, and the Scott Neil Schwirck Fellowship.
New research could aid the development of immunotherapies tailored to patients with acute myeloid leukemia (AML) who are undergoing stem cell transplant (SCT).
Researchers found they could use genetic sequencing and computer software to identify minor histocompatibility antigens (mHAs) known to occur in AML.
The team used this method to predict novel graft-versus-leukemia (GVL) mHAs and demonstrated that one of these mHAs could be a “potentially useful” therapeutic target.
Ben Vincent, MD, of the University of North Carolina Lineberger Comprehensive Cancer Center in Chapel Hill, and his colleagues reported these findings in Blood Advances.
In their retrospective study, the researchers tested whether their software could predict antigenic targets in 101 SCT donor-recipient pairs.
The researchers found they could correctly identify 14 of 18 mHAs known to occur in AML, but they were also able to predict 102 new GVL mHAs.
The researchers then confirmed one of these GVL mHAs, called UNC-GRK4-V, as a potential target for immunotherapy. The team observed immune responses to UNC-GRK4-V in four of nine AML patients who had undergone SCT.
Looking ahead, the researchers want to optimize their software to predict the most common AML-associated mHAs present in the U.S. population and confirm these predicted antigens as valid immunotherapy targets.
The team believes they could potentially use their predictions to engineer donor immune cells to specifically target the cancer cell antigens while preventing graft-versus-host disease.
“We’ve developed a software package that predicts leukemia-specific immune targets in any leukemia patient undergoing a stem cell transplant based on DNA and RNA sequencing and demonstrated that these data can lead to actual targets expressed on leukemia cells,” Dr. Vincent said.
“The next step of our work is to use that information for patient-specific therapies to try to improve cure rates without making graft-versus-host disease worse.”
The current research was supported by a National Cancer Institute grant, an ASCO Young Investigator Award, the North Carolina University Cancer Research Fund, and the Scott Neil Schwirck Fellowship.
New guidelines on antimicrobial prophylaxis

Experts have published updated guidelines on antimicrobial prophylaxis for adults with cancer-related immunosuppression.
The guidelines include antibacterial, antifungal, and antiviral prophylaxis recommendations, along with additional precautions, such as hand hygiene, that may reduce infection risk.
The guidelines were developed by the American Society of Clinical Oncology (ASCO) with the Infectious Diseases Society of America (IDSA) and published in the Journal of Clinical Oncology.
For the most part, the expert panel that created these guidelines endorsed the previous ASCO recommendations, published in 2013.
However, the panel considered six new studies and six new or updated meta-analyses to make modifications and add some new recommendations.
Recommendations
The ASCO/IDSA guidelines say health care providers should systematically assess the risk of febrile neutropenia, taking into account patient-, cancer-, and treatment-related factors.
Fluoroquinolone prophylaxis is recommended for patients at high risk of febrile neutropenia or profound, protracted neutropenia. This includes most patients with acute myeloid leukemia (AML) or myelodysplastic syndromes (MDS) and patients undergoing hematopoietic stem cell transplant (HSCT) who are treated with myeloablative conditioning regimens.
Antifungal prophylaxis with an oral triazole or parenteral echinocandin is recommended for patients at risk of profound, protracted neutropenia, which includes HSCT recipients and most patients with AML/MDS.
However, neither antifungal nor antibiotic prophylaxis are routinely recommended for patients with solid tumors.
Prophylaxis with a nucleoside analog, such as acyclovir, is recommended in patients who are herpes simplex virus–seropositive and are undergoing allogeneic HSCT or leukemia induction.
Pneumocystis jirovecii prophylaxis, such as trimethoprim-sulfamethoxazole, is recommended for patients receiving chemotherapy regimens associated with a greater than 3.5% risk for pneumonia from P jirovecii.
Treatment with a nucleoside reverse transcription inhibitor, such as entecavir or tenofovir, is recommended for patients at high risk of hepatitis B virus reactivation.
Yearly influenza vaccination with an inactivated quadrivalent vaccine is recommended for all patients undergoing chemotherapy for malignancy as well as their family members, household contacts, and health care providers.
Health care workers should follow hand hygiene and respiratory hygiene/cough etiquette to reduce the risk of pathogen transmission, according to the guidelines.
The guidelines also note that outpatients who develop neutropenia following cancer therapy should avoid prolonged contact with environments that have high concentrations of airborne fungal spores.
The guidelines do not recommend interventions such as neutropenic diet, footwear exchange, nutritional supplements, and surgical masks. “Evidence of clinical benefit is lacking” for those interventions, the expert panel said.
Members of the expert panel disclosed potential conflicts of interest related to Merck, Chimerix, GlyPharma Therapeutic, Pfizer, Cidara Therapeutics, Celgene, Astellas Pharma, Gilead Sciences, and Allergan, among other entities.
Experts have published updated guidelines on antimicrobial prophylaxis for adults with cancer-related immunosuppression.
The guidelines include antibacterial, antifungal, and antiviral prophylaxis recommendations, along with additional precautions, such as hand hygiene, that may reduce infection risk.
The guidelines were developed by the American Society of Clinical Oncology (ASCO) with the Infectious Diseases Society of America (IDSA) and published in the Journal of Clinical Oncology.
For the most part, the expert panel that created these guidelines endorsed the previous ASCO recommendations, published in 2013.
However, the panel considered six new studies and six new or updated meta-analyses to make modifications and add some new recommendations.
Recommendations
The ASCO/IDSA guidelines say health care providers should systematically assess the risk of febrile neutropenia, taking into account patient-, cancer-, and treatment-related factors.
Fluoroquinolone prophylaxis is recommended for patients at high risk of febrile neutropenia or profound, protracted neutropenia. This includes most patients with acute myeloid leukemia (AML) or myelodysplastic syndromes (MDS) and patients undergoing hematopoietic stem cell transplant (HSCT) who are treated with myeloablative conditioning regimens.
Antifungal prophylaxis with an oral triazole or parenteral echinocandin is recommended for patients at risk of profound, protracted neutropenia, which includes HSCT recipients and most patients with AML/MDS.
However, neither antifungal nor antibiotic prophylaxis are routinely recommended for patients with solid tumors.
Prophylaxis with a nucleoside analog, such as acyclovir, is recommended in patients who are herpes simplex virus–seropositive and are undergoing allogeneic HSCT or leukemia induction.
Pneumocystis jirovecii prophylaxis, such as trimethoprim-sulfamethoxazole, is recommended for patients receiving chemotherapy regimens associated with a greater than 3.5% risk for pneumonia from P jirovecii.
Treatment with a nucleoside reverse transcription inhibitor, such as entecavir or tenofovir, is recommended for patients at high risk of hepatitis B virus reactivation.
Yearly influenza vaccination with an inactivated quadrivalent vaccine is recommended for all patients undergoing chemotherapy for malignancy as well as their family members, household contacts, and health care providers.
Health care workers should follow hand hygiene and respiratory hygiene/cough etiquette to reduce the risk of pathogen transmission, according to the guidelines.
The guidelines also note that outpatients who develop neutropenia following cancer therapy should avoid prolonged contact with environments that have high concentrations of airborne fungal spores.
The guidelines do not recommend interventions such as neutropenic diet, footwear exchange, nutritional supplements, and surgical masks. “Evidence of clinical benefit is lacking” for those interventions, the expert panel said.
Members of the expert panel disclosed potential conflicts of interest related to Merck, Chimerix, GlyPharma Therapeutic, Pfizer, Cidara Therapeutics, Celgene, Astellas Pharma, Gilead Sciences, and Allergan, among other entities.
Experts have published updated guidelines on antimicrobial prophylaxis for adults with cancer-related immunosuppression.
The guidelines include antibacterial, antifungal, and antiviral prophylaxis recommendations, along with additional precautions, such as hand hygiene, that may reduce infection risk.
The guidelines were developed by the American Society of Clinical Oncology (ASCO) with the Infectious Diseases Society of America (IDSA) and published in the Journal of Clinical Oncology.
For the most part, the expert panel that created these guidelines endorsed the previous ASCO recommendations, published in 2013.
However, the panel considered six new studies and six new or updated meta-analyses to make modifications and add some new recommendations.
Recommendations
The ASCO/IDSA guidelines say health care providers should systematically assess the risk of febrile neutropenia, taking into account patient-, cancer-, and treatment-related factors.
Fluoroquinolone prophylaxis is recommended for patients at high risk of febrile neutropenia or profound, protracted neutropenia. This includes most patients with acute myeloid leukemia (AML) or myelodysplastic syndromes (MDS) and patients undergoing hematopoietic stem cell transplant (HSCT) who are treated with myeloablative conditioning regimens.
Antifungal prophylaxis with an oral triazole or parenteral echinocandin is recommended for patients at risk of profound, protracted neutropenia, which includes HSCT recipients and most patients with AML/MDS.
However, neither antifungal nor antibiotic prophylaxis are routinely recommended for patients with solid tumors.
Prophylaxis with a nucleoside analog, such as acyclovir, is recommended in patients who are herpes simplex virus–seropositive and are undergoing allogeneic HSCT or leukemia induction.
Pneumocystis jirovecii prophylaxis, such as trimethoprim-sulfamethoxazole, is recommended for patients receiving chemotherapy regimens associated with a greater than 3.5% risk for pneumonia from P jirovecii.
Treatment with a nucleoside reverse transcription inhibitor, such as entecavir or tenofovir, is recommended for patients at high risk of hepatitis B virus reactivation.
Yearly influenza vaccination with an inactivated quadrivalent vaccine is recommended for all patients undergoing chemotherapy for malignancy as well as their family members, household contacts, and health care providers.
Health care workers should follow hand hygiene and respiratory hygiene/cough etiquette to reduce the risk of pathogen transmission, according to the guidelines.
The guidelines also note that outpatients who develop neutropenia following cancer therapy should avoid prolonged contact with environments that have high concentrations of airborne fungal spores.
The guidelines do not recommend interventions such as neutropenic diet, footwear exchange, nutritional supplements, and surgical masks. “Evidence of clinical benefit is lacking” for those interventions, the expert panel said.
Members of the expert panel disclosed potential conflicts of interest related to Merck, Chimerix, GlyPharma Therapeutic, Pfizer, Cidara Therapeutics, Celgene, Astellas Pharma, Gilead Sciences, and Allergan, among other entities.