User login
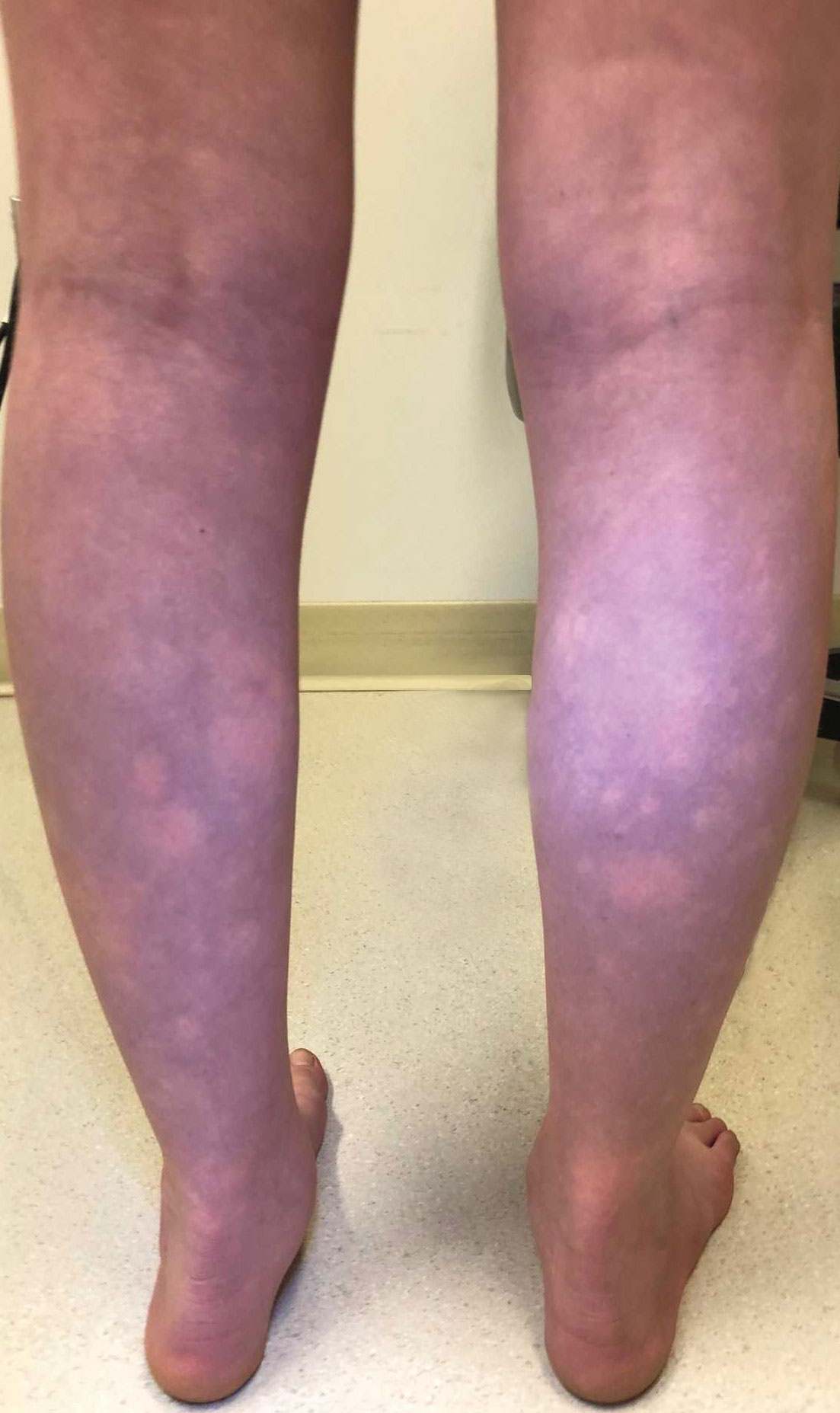
Transient Symmetric Blanching Macules on a Background of Reticulate Erythema
The Diagnosis: BASCULE Syndrome
The patient had previously been thought to have livedo reticularis by primary care. Repeat antinuclear antibody (ANA) testing was positive (1:1280 homogeneous [reflexive titers all negative]). However, upon dermatologic evaluation, the manifestation of the rash in addition to onset occurring with postural changes challenged the livedo reticularis diagnosis. Extensive research and consultation with dermatologic colleagues led to the diagnosis of the rare entity BASCULE syndrome. BASCULE (Bier anemic spots, cyanosis, and urticarialike eruption) syndrome was described by Bessis et al1 in 2016. It is a rare condition but may be underreported.2 It is a benign pediatric disorder in the vascular acrosyndrome family that is characterized by underlying vasomotor dysfunction in distal regions of the body. Raynaud phenomenon is a widely known member of this family. As seen in our patient, it typically presents on the distal legs and feet with numerous irregular hypopigmented macules on a cyanotic background. Red-orange papules may appear on the hypopigmented macules and often are pruritic. Lesions on the distal upper extremities are less common, and a case involving the trunk has been reported.3 Onset generally begins within a couple of minutes of standing or mechanical compression of the lower legs, with full reversal of symptoms occurring within minutes of laying down or walking. Commonly reported associated symptoms include tenderness, pruritus, edema, and pain; however, the cutaneous lesions may be asymptomatic. The condition tends to affect adolescents, as seen in our patient; however, there have been reports in infants as young as 3 months to adults aged 19 years.2
The pathophysiology behind BASCULE syndrome remains unclear but is believed to be centered around the role of physiologic venous stasis that occurs when standing. The hypoxia secondary to stasis is thought to induce amplified vasoconstriction of arterioles. These responses are further exaggerated due to absence of venoarteriolar reflexes in dermal ascending arterioles, leading to Bier spots.2 The role of mast cells and eosinophils remains unclear. It is a clinical diagnosis without clear histologic findings; therefore, biopsy was not pursued in our patient.
Although BASCULE syndrome is a benign entity, it is imperative that it be recognized to avoid a time consuming, expensive, and anxiety-producing diagnostic workup, as occurred in our patient. Although not a manifestation of systemic disease, BASCULE syndrome may be associated with orthostatic hypotension in up to 20% of cases.2,4 Therefore, these patients should undergo orthostatic testing, including the tilt table test. In our patient, these manifestations were not appreciated.
There are no current guidelines for effective treatment of BASCULE syndrome. Given the possible role of mast cells in the condition, H1 antihistamines are proposed as first-line treatment. Desloratadine (10 mg/d for 7 days) has been found to be associated with improvement of pruritus. However, a recent literature review found little evidence to support the use of H1 antihistamines for resolution of other symptoms.2
The differential diagnosis includes livedo reticularis, Bier spots, Sneddon syndrome, and urticarial vasculitis. Livedo reticularis presents as distinct, netlike, blue-erythematousviolaceous discoloration, which differs from the distinct orange-red macules in BASCULE syndrome.5 In addition to distinct variances in dermatologic presentation, livedo reticularis typically is associated with cold exposure as a causative agent, with cold avoidance as the treatment for this benign and often transient condition.6 This phenomenon was not appreciated in our patient. Livedo reticularis commonly occurs with antiphospholipid syndrome.5 This association in combination with our patient's positive ANA findings and her mother's history of miscarriages resulted in the misdiagnosis as livedo reticularis.
Bier spots manifest as white macules with surrounding erythema and typically present in young adults. When first described in the literature, it was debated if BASCULE syndrome was simply another manifestation of Bier spots or postural orthostatic intolerance,4 as there was a large consensus that postural orthostatic intolerance was associated with BASCULE syndrome, with the majority of patients not meeting criteria for the condition. Heymann4 addressed the differences in BASCULE manifestations vs typical Bier spots. The author extended the syndrome to include cyanosis, an urticarialike eruption of red-orange macules with central papules located centrally, pruritus, tenderness, and partial or diffuse edema, in addition to Bier spots.4
Sneddon syndrome is a rare progressive disorder that affects small- to medium-sized blood vessels resulting in multiple episodes of ischemia in the brain. Skin manifestations of these repeated strokes are similar to livedo reticularis, typically manifesting as livedo racemosa—irregular reticular patterns of skin mottling with reddish-blue hues.6 However, Sneddon syndrome is more generalized and widespread and differs from BASCULE syndrome in shape and histologic findings. Our patient presented with findings on the legs, which is more characteristic of livedo reticularis vs livedo racemosa. Our patient experienced resolution upon laying down and sitting, and Sneddon syndrome persists beyond postural changes. Furthermore, patients with Sneddon syndrome present with neurologic symptoms such as prodromal headaches.6
Urticarial vasculitis was ruled out in our patient because of the duration of symptoms as well as the spatial changes. Urticarial vasculitis is a rare skin condition characterized by chronic recurring urticarial lesions that may persist for more than a day. This condition typically presents in middle-aged women and rarely in children. Urticarial vasculitis is thought to be immune-complex mediated, but its cause is largely unknown. It is a common manifestation of underlying conditions such as systemic lupus erythematosus.6 Our patient had a positive ANA and possible autoimmune history from her mother; however, urticarial vasculitis does not present transiently on the legs or in the rash pattern appreciated in our patient.
- Bessis D, Jeziorski E, Rigau V, et al. Bier anaemic spots, cyanosis with urticaria-like eruption (BASCULE) syndrome: a new entity? Br J Dermatol. 2016;175:218-220. doi:10.1111/bjd.14589
- Baurens N, Briand C, Giovannini-Chami L, et al. Case report, practices survey and literature review of an under-recognized pediatric vascular disorder: the BASCULE syndrome. Front Pediatr. 2022;10:849914. doi:10.3389/fped.2022.849914
- Jiménez-Gallo D, Collantes-Rodríguez C, Ossorio-García L, et al. Bier anaemic spots, cyanosis with urticaria-like eruption (BASCULE) syndrome on trunk and upper limbs. Pediatr Dermatol. 2018;35:E313-E315. doi:10.1111/pde.13558
- Heymann WR. BASCULE syndrome: is something brewing with Bier spots? Dermatology World Insights and Inquiries. September 7, 2022. https://www.aad.org/dw/dw-insights-and-inquiries/archive/2022/bascule-syndrome
- Sajjan VV, Lunge S, Swamy MB, et al. Livedo reticularis: a review of the literature. Indian Dermatol Online J. 2015;6:315-321. doi:10.4103/2229-5178.164493
- Gu SL, Jorizzo JL. Urticarial vasculitis. Int J Womens Dermatol. 2021;7:290-297. doi:10.1016/j.ijwd.2021.01.021
The Diagnosis: BASCULE Syndrome
The patient had previously been thought to have livedo reticularis by primary care. Repeat antinuclear antibody (ANA) testing was positive (1:1280 homogeneous [reflexive titers all negative]). However, upon dermatologic evaluation, the manifestation of the rash in addition to onset occurring with postural changes challenged the livedo reticularis diagnosis. Extensive research and consultation with dermatologic colleagues led to the diagnosis of the rare entity BASCULE syndrome. BASCULE (Bier anemic spots, cyanosis, and urticarialike eruption) syndrome was described by Bessis et al1 in 2016. It is a rare condition but may be underreported.2 It is a benign pediatric disorder in the vascular acrosyndrome family that is characterized by underlying vasomotor dysfunction in distal regions of the body. Raynaud phenomenon is a widely known member of this family. As seen in our patient, it typically presents on the distal legs and feet with numerous irregular hypopigmented macules on a cyanotic background. Red-orange papules may appear on the hypopigmented macules and often are pruritic. Lesions on the distal upper extremities are less common, and a case involving the trunk has been reported.3 Onset generally begins within a couple of minutes of standing or mechanical compression of the lower legs, with full reversal of symptoms occurring within minutes of laying down or walking. Commonly reported associated symptoms include tenderness, pruritus, edema, and pain; however, the cutaneous lesions may be asymptomatic. The condition tends to affect adolescents, as seen in our patient; however, there have been reports in infants as young as 3 months to adults aged 19 years.2
The pathophysiology behind BASCULE syndrome remains unclear but is believed to be centered around the role of physiologic venous stasis that occurs when standing. The hypoxia secondary to stasis is thought to induce amplified vasoconstriction of arterioles. These responses are further exaggerated due to absence of venoarteriolar reflexes in dermal ascending arterioles, leading to Bier spots.2 The role of mast cells and eosinophils remains unclear. It is a clinical diagnosis without clear histologic findings; therefore, biopsy was not pursued in our patient.
Although BASCULE syndrome is a benign entity, it is imperative that it be recognized to avoid a time consuming, expensive, and anxiety-producing diagnostic workup, as occurred in our patient. Although not a manifestation of systemic disease, BASCULE syndrome may be associated with orthostatic hypotension in up to 20% of cases.2,4 Therefore, these patients should undergo orthostatic testing, including the tilt table test. In our patient, these manifestations were not appreciated.
There are no current guidelines for effective treatment of BASCULE syndrome. Given the possible role of mast cells in the condition, H1 antihistamines are proposed as first-line treatment. Desloratadine (10 mg/d for 7 days) has been found to be associated with improvement of pruritus. However, a recent literature review found little evidence to support the use of H1 antihistamines for resolution of other symptoms.2
The differential diagnosis includes livedo reticularis, Bier spots, Sneddon syndrome, and urticarial vasculitis. Livedo reticularis presents as distinct, netlike, blue-erythematousviolaceous discoloration, which differs from the distinct orange-red macules in BASCULE syndrome.5 In addition to distinct variances in dermatologic presentation, livedo reticularis typically is associated with cold exposure as a causative agent, with cold avoidance as the treatment for this benign and often transient condition.6 This phenomenon was not appreciated in our patient. Livedo reticularis commonly occurs with antiphospholipid syndrome.5 This association in combination with our patient's positive ANA findings and her mother's history of miscarriages resulted in the misdiagnosis as livedo reticularis.
Bier spots manifest as white macules with surrounding erythema and typically present in young adults. When first described in the literature, it was debated if BASCULE syndrome was simply another manifestation of Bier spots or postural orthostatic intolerance,4 as there was a large consensus that postural orthostatic intolerance was associated with BASCULE syndrome, with the majority of patients not meeting criteria for the condition. Heymann4 addressed the differences in BASCULE manifestations vs typical Bier spots. The author extended the syndrome to include cyanosis, an urticarialike eruption of red-orange macules with central papules located centrally, pruritus, tenderness, and partial or diffuse edema, in addition to Bier spots.4
Sneddon syndrome is a rare progressive disorder that affects small- to medium-sized blood vessels resulting in multiple episodes of ischemia in the brain. Skin manifestations of these repeated strokes are similar to livedo reticularis, typically manifesting as livedo racemosa—irregular reticular patterns of skin mottling with reddish-blue hues.6 However, Sneddon syndrome is more generalized and widespread and differs from BASCULE syndrome in shape and histologic findings. Our patient presented with findings on the legs, which is more characteristic of livedo reticularis vs livedo racemosa. Our patient experienced resolution upon laying down and sitting, and Sneddon syndrome persists beyond postural changes. Furthermore, patients with Sneddon syndrome present with neurologic symptoms such as prodromal headaches.6
Urticarial vasculitis was ruled out in our patient because of the duration of symptoms as well as the spatial changes. Urticarial vasculitis is a rare skin condition characterized by chronic recurring urticarial lesions that may persist for more than a day. This condition typically presents in middle-aged women and rarely in children. Urticarial vasculitis is thought to be immune-complex mediated, but its cause is largely unknown. It is a common manifestation of underlying conditions such as systemic lupus erythematosus.6 Our patient had a positive ANA and possible autoimmune history from her mother; however, urticarial vasculitis does not present transiently on the legs or in the rash pattern appreciated in our patient.
The Diagnosis: BASCULE Syndrome
The patient had previously been thought to have livedo reticularis by primary care. Repeat antinuclear antibody (ANA) testing was positive (1:1280 homogeneous [reflexive titers all negative]). However, upon dermatologic evaluation, the manifestation of the rash in addition to onset occurring with postural changes challenged the livedo reticularis diagnosis. Extensive research and consultation with dermatologic colleagues led to the diagnosis of the rare entity BASCULE syndrome. BASCULE (Bier anemic spots, cyanosis, and urticarialike eruption) syndrome was described by Bessis et al1 in 2016. It is a rare condition but may be underreported.2 It is a benign pediatric disorder in the vascular acrosyndrome family that is characterized by underlying vasomotor dysfunction in distal regions of the body. Raynaud phenomenon is a widely known member of this family. As seen in our patient, it typically presents on the distal legs and feet with numerous irregular hypopigmented macules on a cyanotic background. Red-orange papules may appear on the hypopigmented macules and often are pruritic. Lesions on the distal upper extremities are less common, and a case involving the trunk has been reported.3 Onset generally begins within a couple of minutes of standing or mechanical compression of the lower legs, with full reversal of symptoms occurring within minutes of laying down or walking. Commonly reported associated symptoms include tenderness, pruritus, edema, and pain; however, the cutaneous lesions may be asymptomatic. The condition tends to affect adolescents, as seen in our patient; however, there have been reports in infants as young as 3 months to adults aged 19 years.2
The pathophysiology behind BASCULE syndrome remains unclear but is believed to be centered around the role of physiologic venous stasis that occurs when standing. The hypoxia secondary to stasis is thought to induce amplified vasoconstriction of arterioles. These responses are further exaggerated due to absence of venoarteriolar reflexes in dermal ascending arterioles, leading to Bier spots.2 The role of mast cells and eosinophils remains unclear. It is a clinical diagnosis without clear histologic findings; therefore, biopsy was not pursued in our patient.
Although BASCULE syndrome is a benign entity, it is imperative that it be recognized to avoid a time consuming, expensive, and anxiety-producing diagnostic workup, as occurred in our patient. Although not a manifestation of systemic disease, BASCULE syndrome may be associated with orthostatic hypotension in up to 20% of cases.2,4 Therefore, these patients should undergo orthostatic testing, including the tilt table test. In our patient, these manifestations were not appreciated.
There are no current guidelines for effective treatment of BASCULE syndrome. Given the possible role of mast cells in the condition, H1 antihistamines are proposed as first-line treatment. Desloratadine (10 mg/d for 7 days) has been found to be associated with improvement of pruritus. However, a recent literature review found little evidence to support the use of H1 antihistamines for resolution of other symptoms.2
The differential diagnosis includes livedo reticularis, Bier spots, Sneddon syndrome, and urticarial vasculitis. Livedo reticularis presents as distinct, netlike, blue-erythematousviolaceous discoloration, which differs from the distinct orange-red macules in BASCULE syndrome.5 In addition to distinct variances in dermatologic presentation, livedo reticularis typically is associated with cold exposure as a causative agent, with cold avoidance as the treatment for this benign and often transient condition.6 This phenomenon was not appreciated in our patient. Livedo reticularis commonly occurs with antiphospholipid syndrome.5 This association in combination with our patient's positive ANA findings and her mother's history of miscarriages resulted in the misdiagnosis as livedo reticularis.
Bier spots manifest as white macules with surrounding erythema and typically present in young adults. When first described in the literature, it was debated if BASCULE syndrome was simply another manifestation of Bier spots or postural orthostatic intolerance,4 as there was a large consensus that postural orthostatic intolerance was associated with BASCULE syndrome, with the majority of patients not meeting criteria for the condition. Heymann4 addressed the differences in BASCULE manifestations vs typical Bier spots. The author extended the syndrome to include cyanosis, an urticarialike eruption of red-orange macules with central papules located centrally, pruritus, tenderness, and partial or diffuse edema, in addition to Bier spots.4
Sneddon syndrome is a rare progressive disorder that affects small- to medium-sized blood vessels resulting in multiple episodes of ischemia in the brain. Skin manifestations of these repeated strokes are similar to livedo reticularis, typically manifesting as livedo racemosa—irregular reticular patterns of skin mottling with reddish-blue hues.6 However, Sneddon syndrome is more generalized and widespread and differs from BASCULE syndrome in shape and histologic findings. Our patient presented with findings on the legs, which is more characteristic of livedo reticularis vs livedo racemosa. Our patient experienced resolution upon laying down and sitting, and Sneddon syndrome persists beyond postural changes. Furthermore, patients with Sneddon syndrome present with neurologic symptoms such as prodromal headaches.6
Urticarial vasculitis was ruled out in our patient because of the duration of symptoms as well as the spatial changes. Urticarial vasculitis is a rare skin condition characterized by chronic recurring urticarial lesions that may persist for more than a day. This condition typically presents in middle-aged women and rarely in children. Urticarial vasculitis is thought to be immune-complex mediated, but its cause is largely unknown. It is a common manifestation of underlying conditions such as systemic lupus erythematosus.6 Our patient had a positive ANA and possible autoimmune history from her mother; however, urticarial vasculitis does not present transiently on the legs or in the rash pattern appreciated in our patient.
- Bessis D, Jeziorski E, Rigau V, et al. Bier anaemic spots, cyanosis with urticaria-like eruption (BASCULE) syndrome: a new entity? Br J Dermatol. 2016;175:218-220. doi:10.1111/bjd.14589
- Baurens N, Briand C, Giovannini-Chami L, et al. Case report, practices survey and literature review of an under-recognized pediatric vascular disorder: the BASCULE syndrome. Front Pediatr. 2022;10:849914. doi:10.3389/fped.2022.849914
- Jiménez-Gallo D, Collantes-Rodríguez C, Ossorio-García L, et al. Bier anaemic spots, cyanosis with urticaria-like eruption (BASCULE) syndrome on trunk and upper limbs. Pediatr Dermatol. 2018;35:E313-E315. doi:10.1111/pde.13558
- Heymann WR. BASCULE syndrome: is something brewing with Bier spots? Dermatology World Insights and Inquiries. September 7, 2022. https://www.aad.org/dw/dw-insights-and-inquiries/archive/2022/bascule-syndrome
- Sajjan VV, Lunge S, Swamy MB, et al. Livedo reticularis: a review of the literature. Indian Dermatol Online J. 2015;6:315-321. doi:10.4103/2229-5178.164493
- Gu SL, Jorizzo JL. Urticarial vasculitis. Int J Womens Dermatol. 2021;7:290-297. doi:10.1016/j.ijwd.2021.01.021
- Bessis D, Jeziorski E, Rigau V, et al. Bier anaemic spots, cyanosis with urticaria-like eruption (BASCULE) syndrome: a new entity? Br J Dermatol. 2016;175:218-220. doi:10.1111/bjd.14589
- Baurens N, Briand C, Giovannini-Chami L, et al. Case report, practices survey and literature review of an under-recognized pediatric vascular disorder: the BASCULE syndrome. Front Pediatr. 2022;10:849914. doi:10.3389/fped.2022.849914
- Jiménez-Gallo D, Collantes-Rodríguez C, Ossorio-García L, et al. Bier anaemic spots, cyanosis with urticaria-like eruption (BASCULE) syndrome on trunk and upper limbs. Pediatr Dermatol. 2018;35:E313-E315. doi:10.1111/pde.13558
- Heymann WR. BASCULE syndrome: is something brewing with Bier spots? Dermatology World Insights and Inquiries. September 7, 2022. https://www.aad.org/dw/dw-insights-and-inquiries/archive/2022/bascule-syndrome
- Sajjan VV, Lunge S, Swamy MB, et al. Livedo reticularis: a review of the literature. Indian Dermatol Online J. 2015;6:315-321. doi:10.4103/2229-5178.164493
- Gu SL, Jorizzo JL. Urticarial vasculitis. Int J Womens Dermatol. 2021;7:290-297. doi:10.1016/j.ijwd.2021.01.021
An 11-year-old girl was referred to the dermatology clinic for evaluation of a rash on the legs and feet of 1 year’s duration. The rash appeared every time she was standing for longer than 10 to 15 minutes and resolved when sitting or laying down. After the initial onset, the rash did not spread to other body areas but became more prominent in appearance. The patient endorsed intense pruritus associated with the rash. A review of systems was negative for fever, headaches, history of blood clots, and joint pain. She did not have any known medical conditions or take any medications. The patient’s mother reported that the patient experienced episodes of leg numbness while sitting in vehicles from 6 to 10 years of age. There was no family history of rheumatologic, hematologic, or cardiac conditions. The patient’s mother had experienced 2 miscarriages but denied any other obstetric complications. The patient had 1 sibling who was unaffected. Physical examination revealed reticulate erythema on the calves with scattered regions of blanching and evanescent pink macules as well as dermatographism.
One month prior to presenting to dermatology, the patient was evaluated by rheumatology, endocrinology, and hematology. Laboratory workup completed at age 3 years included antinuclear antibody, anticardiolipin antibody, and antithrombin III activity; factor V Leiden; cryoglobulins; quantitation (human chorionic gonadotropin); proteins S and C activity; antineutrophil cytoplasmic antibody screen; thyroid studies; prothrombin time; and partial thromboplastin time. All laboratory results were within reference range.

Diphenhydramine and Prochlorperazine Combo Not Associated With Migraine Treatment Failure
Key clinical point: The odds of treatment failure were not increased, and no extrapyramidal adverse events were reported in pediatric patients with migraine when diphenhydramine was coadministered with prochlorperazine in an emergency department (ED) setting.
Major finding: The administration of diphenhydramine plus prochlorperazine vs prochlorperazine alone was not associated with increased odds of additional migraine therapy (P = .347), hospitalization rates (P = .425), and 72-hour return visit rates (P = .271). None of the patients in the diphenhydramine plus prochlorperazine group experienced extrapyramidal adverse events, while 2.4% of patients in prochlorperazine group experienced extrapyramidal adverse events.
Study details: Findings are from a retrospective cohort study that included 1683 pediatric patients with migraine presenting to the ED who received diphenhydramine plus prochlorperazine (n = 1215) or prochlorperazine only (n = 468).
Disclosures: This study did not disclose any funding source. The authors declared no conflicts of interest.
Source: Naeem S, Lozano JM, Ruiz Castaneda AM, Lowe D. Diphenhydramine and migraine treatment failure in pediatric patients receiving prochlorperazine. Pediatr Emerg Care. 2024 (May 9). doi: 10.1097/PEC.0000000000003202 Source
Key clinical point: The odds of treatment failure were not increased, and no extrapyramidal adverse events were reported in pediatric patients with migraine when diphenhydramine was coadministered with prochlorperazine in an emergency department (ED) setting.
Major finding: The administration of diphenhydramine plus prochlorperazine vs prochlorperazine alone was not associated with increased odds of additional migraine therapy (P = .347), hospitalization rates (P = .425), and 72-hour return visit rates (P = .271). None of the patients in the diphenhydramine plus prochlorperazine group experienced extrapyramidal adverse events, while 2.4% of patients in prochlorperazine group experienced extrapyramidal adverse events.
Study details: Findings are from a retrospective cohort study that included 1683 pediatric patients with migraine presenting to the ED who received diphenhydramine plus prochlorperazine (n = 1215) or prochlorperazine only (n = 468).
Disclosures: This study did not disclose any funding source. The authors declared no conflicts of interest.
Source: Naeem S, Lozano JM, Ruiz Castaneda AM, Lowe D. Diphenhydramine and migraine treatment failure in pediatric patients receiving prochlorperazine. Pediatr Emerg Care. 2024 (May 9). doi: 10.1097/PEC.0000000000003202 Source
Key clinical point: The odds of treatment failure were not increased, and no extrapyramidal adverse events were reported in pediatric patients with migraine when diphenhydramine was coadministered with prochlorperazine in an emergency department (ED) setting.
Major finding: The administration of diphenhydramine plus prochlorperazine vs prochlorperazine alone was not associated with increased odds of additional migraine therapy (P = .347), hospitalization rates (P = .425), and 72-hour return visit rates (P = .271). None of the patients in the diphenhydramine plus prochlorperazine group experienced extrapyramidal adverse events, while 2.4% of patients in prochlorperazine group experienced extrapyramidal adverse events.
Study details: Findings are from a retrospective cohort study that included 1683 pediatric patients with migraine presenting to the ED who received diphenhydramine plus prochlorperazine (n = 1215) or prochlorperazine only (n = 468).
Disclosures: This study did not disclose any funding source. The authors declared no conflicts of interest.
Source: Naeem S, Lozano JM, Ruiz Castaneda AM, Lowe D. Diphenhydramine and migraine treatment failure in pediatric patients receiving prochlorperazine. Pediatr Emerg Care. 2024 (May 9). doi: 10.1097/PEC.0000000000003202 Source
Amitriptyline May Be a Better Treatment Choice Than Cinnarizine for Pediatric Migraine
Key clinical point: Both cinnarizine and amitriptyline effectively improved migraine symptoms in children and adolescents with migraine, but amitriptyline was a more preferable treatment option since it reduced headache frequency and duration more effectively than cinnarizine.
Major finding: Amitriptyline was more effective than cinnarizine in reducing headache frequency at 4 weeks (mean difference [MD] −8.81 attacks/months; P = .004) and headache duration at 4 (MD −123.0 minutes; P = .017), 8 (MD −110.3 minutes; P = .033), and 12 (MD −123.3 minutes; P = .018) weeks. However, there were no significant differences in headache severity and migraine-related disability between the groups at 4, 8, and 12 weeks (all P > .005).
Study details: Findings are from a randomized, double-blind controlled trial including 43 children with migraine (age 4-17 years) who were randomly assigned to receive cinnarizine (n = 22) and amitriptyline (n = 21).
Disclosures: This study did not receive any funding. The authors declared no conflicts of interest.
Source: Olfat M, Hosseinpour S, Masoumi S, et al. A comparative study on prophylactic efficacy of cinnarizine and amitriptyline in childhood migraine: A randomized double-blind clinical trial. Cephalalgia. 2024 (Apr 20). doi: 10.1177/03331024241230963 Source
Key clinical point: Both cinnarizine and amitriptyline effectively improved migraine symptoms in children and adolescents with migraine, but amitriptyline was a more preferable treatment option since it reduced headache frequency and duration more effectively than cinnarizine.
Major finding: Amitriptyline was more effective than cinnarizine in reducing headache frequency at 4 weeks (mean difference [MD] −8.81 attacks/months; P = .004) and headache duration at 4 (MD −123.0 minutes; P = .017), 8 (MD −110.3 minutes; P = .033), and 12 (MD −123.3 minutes; P = .018) weeks. However, there were no significant differences in headache severity and migraine-related disability between the groups at 4, 8, and 12 weeks (all P > .005).
Study details: Findings are from a randomized, double-blind controlled trial including 43 children with migraine (age 4-17 years) who were randomly assigned to receive cinnarizine (n = 22) and amitriptyline (n = 21).
Disclosures: This study did not receive any funding. The authors declared no conflicts of interest.
Source: Olfat M, Hosseinpour S, Masoumi S, et al. A comparative study on prophylactic efficacy of cinnarizine and amitriptyline in childhood migraine: A randomized double-blind clinical trial. Cephalalgia. 2024 (Apr 20). doi: 10.1177/03331024241230963 Source
Key clinical point: Both cinnarizine and amitriptyline effectively improved migraine symptoms in children and adolescents with migraine, but amitriptyline was a more preferable treatment option since it reduced headache frequency and duration more effectively than cinnarizine.
Major finding: Amitriptyline was more effective than cinnarizine in reducing headache frequency at 4 weeks (mean difference [MD] −8.81 attacks/months; P = .004) and headache duration at 4 (MD −123.0 minutes; P = .017), 8 (MD −110.3 minutes; P = .033), and 12 (MD −123.3 minutes; P = .018) weeks. However, there were no significant differences in headache severity and migraine-related disability between the groups at 4, 8, and 12 weeks (all P > .005).
Study details: Findings are from a randomized, double-blind controlled trial including 43 children with migraine (age 4-17 years) who were randomly assigned to receive cinnarizine (n = 22) and amitriptyline (n = 21).
Disclosures: This study did not receive any funding. The authors declared no conflicts of interest.
Source: Olfat M, Hosseinpour S, Masoumi S, et al. A comparative study on prophylactic efficacy of cinnarizine and amitriptyline in childhood migraine: A randomized double-blind clinical trial. Cephalalgia. 2024 (Apr 20). doi: 10.1177/03331024241230963 Source
Severe Headache or Migraine Raises Risk for Erectile Dysfunction
Key clinical point: This cross-sectional study demonstrated a significant association between severe headache or migraine and erectile dysfunction (ED) in adult men in the US; however, the results should be interpreted carefully as it did not investigate the effects of depression and anxiety on ED.
Major finding: Presence vs absence of severe headache or migraine was associated with 51% increased risk of ED (adjusted odd ratio 1.51; P = .0036). Age of 40-60 years (P = 0.0292), body mass index < 25 kg/m2 (P = .0406) or ≥30 kg/m2 (P = .0222), metabolic disorders, such as hypertension (P = .0029), diabetes mellitus (P < .001), and hyperlipidemia (P = .0281), were significant risk factors for ED in those with severe headache or migraine.
Study details: This cross-sectional study included 3117 adult men with (n = 582) and without (n = 2535) history of ED from the US National Health and Nutrition Examination Survey (2001-2 and 2003-4), of whom 16.85% had severe headache or migraine.
Disclosures: This study was funded by National Natural Science Foundation of China. The authors declared no competing interests.
Source: Wu X, Zhang Y, Liu G, et al. Association between severe headache or migraine and erectile dysfunction in American adults: A cross-sectional of data study from the NHANES. Int J Impot Res. 2024 (Apr 12). doi: 10.1038/s41443-024-00867-w Source
Key clinical point: This cross-sectional study demonstrated a significant association between severe headache or migraine and erectile dysfunction (ED) in adult men in the US; however, the results should be interpreted carefully as it did not investigate the effects of depression and anxiety on ED.
Major finding: Presence vs absence of severe headache or migraine was associated with 51% increased risk of ED (adjusted odd ratio 1.51; P = .0036). Age of 40-60 years (P = 0.0292), body mass index < 25 kg/m2 (P = .0406) or ≥30 kg/m2 (P = .0222), metabolic disorders, such as hypertension (P = .0029), diabetes mellitus (P < .001), and hyperlipidemia (P = .0281), were significant risk factors for ED in those with severe headache or migraine.
Study details: This cross-sectional study included 3117 adult men with (n = 582) and without (n = 2535) history of ED from the US National Health and Nutrition Examination Survey (2001-2 and 2003-4), of whom 16.85% had severe headache or migraine.
Disclosures: This study was funded by National Natural Science Foundation of China. The authors declared no competing interests.
Source: Wu X, Zhang Y, Liu G, et al. Association between severe headache or migraine and erectile dysfunction in American adults: A cross-sectional of data study from the NHANES. Int J Impot Res. 2024 (Apr 12). doi: 10.1038/s41443-024-00867-w Source
Key clinical point: This cross-sectional study demonstrated a significant association between severe headache or migraine and erectile dysfunction (ED) in adult men in the US; however, the results should be interpreted carefully as it did not investigate the effects of depression and anxiety on ED.
Major finding: Presence vs absence of severe headache or migraine was associated with 51% increased risk of ED (adjusted odd ratio 1.51; P = .0036). Age of 40-60 years (P = 0.0292), body mass index < 25 kg/m2 (P = .0406) or ≥30 kg/m2 (P = .0222), metabolic disorders, such as hypertension (P = .0029), diabetes mellitus (P < .001), and hyperlipidemia (P = .0281), were significant risk factors for ED in those with severe headache or migraine.
Study details: This cross-sectional study included 3117 adult men with (n = 582) and without (n = 2535) history of ED from the US National Health and Nutrition Examination Survey (2001-2 and 2003-4), of whom 16.85% had severe headache or migraine.
Disclosures: This study was funded by National Natural Science Foundation of China. The authors declared no competing interests.
Source: Wu X, Zhang Y, Liu G, et al. Association between severe headache or migraine and erectile dysfunction in American adults: A cross-sectional of data study from the NHANES. Int J Impot Res. 2024 (Apr 12). doi: 10.1038/s41443-024-00867-w Source
Study Shows Reciprocal Causal Association Between Migraine and Venous Thromboembolism
Key clinical point: Presence of migraine poses a strong risk for incident venous thromboembolism (VTE), whereas VTE is modest risk factor for the onset of migraine.
Major finding: The risk of developing VTE was significantly higher in patients with vs without migraine (odds ratio [OR] 96.155; P = .004). Conversely, the risk for migraine was modestly higher in patients with vs without VTE (OR 1.002; P = .016).
Study details: This two-sample bidirectional Mendelian randomization study evaluated the causal association between migraine and VTE using single-nucleotide polymorphisms as instrumental variables obtained from large-scale Genome-Wide Association Studies public databases (IEU Open GWAS project, FinnGen).
Disclosures: The study did not disclose any funding. The authors declared no conflicts of interest.
Source: Wang Y, Hu X, Wang X, et al. Exploring the two-way link between migraines and venous thromboembolism: A bidirectional two-sample Mendelian randomization study. Thromb Haemost. 2024 (Apr 24). doi: 10.1055/a-2313-0311 Source
Key clinical point: Presence of migraine poses a strong risk for incident venous thromboembolism (VTE), whereas VTE is modest risk factor for the onset of migraine.
Major finding: The risk of developing VTE was significantly higher in patients with vs without migraine (odds ratio [OR] 96.155; P = .004). Conversely, the risk for migraine was modestly higher in patients with vs without VTE (OR 1.002; P = .016).
Study details: This two-sample bidirectional Mendelian randomization study evaluated the causal association between migraine and VTE using single-nucleotide polymorphisms as instrumental variables obtained from large-scale Genome-Wide Association Studies public databases (IEU Open GWAS project, FinnGen).
Disclosures: The study did not disclose any funding. The authors declared no conflicts of interest.
Source: Wang Y, Hu X, Wang X, et al. Exploring the two-way link between migraines and venous thromboembolism: A bidirectional two-sample Mendelian randomization study. Thromb Haemost. 2024 (Apr 24). doi: 10.1055/a-2313-0311 Source
Key clinical point: Presence of migraine poses a strong risk for incident venous thromboembolism (VTE), whereas VTE is modest risk factor for the onset of migraine.
Major finding: The risk of developing VTE was significantly higher in patients with vs without migraine (odds ratio [OR] 96.155; P = .004). Conversely, the risk for migraine was modestly higher in patients with vs without VTE (OR 1.002; P = .016).
Study details: This two-sample bidirectional Mendelian randomization study evaluated the causal association between migraine and VTE using single-nucleotide polymorphisms as instrumental variables obtained from large-scale Genome-Wide Association Studies public databases (IEU Open GWAS project, FinnGen).
Disclosures: The study did not disclose any funding. The authors declared no conflicts of interest.
Source: Wang Y, Hu X, Wang X, et al. Exploring the two-way link between migraines and venous thromboembolism: A bidirectional two-sample Mendelian randomization study. Thromb Haemost. 2024 (Apr 24). doi: 10.1055/a-2313-0311 Source
Meta-analysis Shows Inverse Correlation Between PACAP and Migraine Duration
Key clinical point: Very low-quality evidence showed that serum pituitary adenylates cyclase–activating polypeptide (PACAP) levels were lower in adults with a longer history of migraine.
Major finding: Serum levels of PACAP were inversely associated with history of migraine duration in adults with migraine (summary r −0.35; P < .01). It was also seen that serum PACAP levels were higher during the ictal vs interictal period in both adults and children with migraine (standardized mean difference 0.41; 95% CI 0.17-0.66).
Study details: Findings are from a meta-analysis of eight observational studies including 674 patients with migraine and 371 control individuals without migraine.
Disclosures: This study did not receive any funding. The authors declared no conflicts of interest.
Source: Zhu G, Wang M, Kong F. Blood serum levels of PACAP and migraine onset: A systematic review and meta-analysis of observational studies. Headache. 2024 (Apr 24). doi: 10.1111/head.14711 Source
Key clinical point: Very low-quality evidence showed that serum pituitary adenylates cyclase–activating polypeptide (PACAP) levels were lower in adults with a longer history of migraine.
Major finding: Serum levels of PACAP were inversely associated with history of migraine duration in adults with migraine (summary r −0.35; P < .01). It was also seen that serum PACAP levels were higher during the ictal vs interictal period in both adults and children with migraine (standardized mean difference 0.41; 95% CI 0.17-0.66).
Study details: Findings are from a meta-analysis of eight observational studies including 674 patients with migraine and 371 control individuals without migraine.
Disclosures: This study did not receive any funding. The authors declared no conflicts of interest.
Source: Zhu G, Wang M, Kong F. Blood serum levels of PACAP and migraine onset: A systematic review and meta-analysis of observational studies. Headache. 2024 (Apr 24). doi: 10.1111/head.14711 Source
Key clinical point: Very low-quality evidence showed that serum pituitary adenylates cyclase–activating polypeptide (PACAP) levels were lower in adults with a longer history of migraine.
Major finding: Serum levels of PACAP were inversely associated with history of migraine duration in adults with migraine (summary r −0.35; P < .01). It was also seen that serum PACAP levels were higher during the ictal vs interictal period in both adults and children with migraine (standardized mean difference 0.41; 95% CI 0.17-0.66).
Study details: Findings are from a meta-analysis of eight observational studies including 674 patients with migraine and 371 control individuals without migraine.
Disclosures: This study did not receive any funding. The authors declared no conflicts of interest.
Source: Zhu G, Wang M, Kong F. Blood serum levels of PACAP and migraine onset: A systematic review and meta-analysis of observational studies. Headache. 2024 (Apr 24). doi: 10.1111/head.14711 Source
Rimegepant Effective and Well Tolerated for Acute Migraine
Key clinical point: Rimegepant orally disintegrating tablet (ODT) offers pain relief within 2 hours of treatment in adults with migraine, with a tolerable safety profile.
Major finding: At 2 hours post dose, rimegepant was more effective than placebo in providing freedom from pain (risk difference 7.6; P = .0004) and the most bothersome symptom (risk difference 16.2; P < .0001). The overall rates of treatment-emergent adverse events were comparable between the rimegepant and placebo groups (15.2% and 16.4%, respectively).
Study details: This subgroup analysis of a double-blind, randomized, placebo-controlled phase 3 clinical trial included 1075 patients with acute migraine with or without aura (age ≥ 18 years) who were randomly assigned to receive either 75 mg rimegepant ODT (n = 538) or placebo (n = 537).
Disclosures: This study was funded by BioShin, a wholly owned subsidiary of Biohaven Pharmaceuticals, which was acquired by Pfizer. Pfizer provided writing support. Five authors declared being employees or stock owners of Biohaven, BioShin, or Pfizer. The remaining authors declared no conflicts of interest.
Source: Yu S, Guo A, Wang Z, et al. Rimegepant orally disintegrating tablet 75 mg for acute treatment of migraine in adults from China: A subgroup analysis of a double-blind, randomized, placebo-controlled, phase 3 clinical trial. J Headache Pain. 2024;25:57 (Apr 16). Source
Key clinical point: Rimegepant orally disintegrating tablet (ODT) offers pain relief within 2 hours of treatment in adults with migraine, with a tolerable safety profile.
Major finding: At 2 hours post dose, rimegepant was more effective than placebo in providing freedom from pain (risk difference 7.6; P = .0004) and the most bothersome symptom (risk difference 16.2; P < .0001). The overall rates of treatment-emergent adverse events were comparable between the rimegepant and placebo groups (15.2% and 16.4%, respectively).
Study details: This subgroup analysis of a double-blind, randomized, placebo-controlled phase 3 clinical trial included 1075 patients with acute migraine with or without aura (age ≥ 18 years) who were randomly assigned to receive either 75 mg rimegepant ODT (n = 538) or placebo (n = 537).
Disclosures: This study was funded by BioShin, a wholly owned subsidiary of Biohaven Pharmaceuticals, which was acquired by Pfizer. Pfizer provided writing support. Five authors declared being employees or stock owners of Biohaven, BioShin, or Pfizer. The remaining authors declared no conflicts of interest.
Source: Yu S, Guo A, Wang Z, et al. Rimegepant orally disintegrating tablet 75 mg for acute treatment of migraine in adults from China: A subgroup analysis of a double-blind, randomized, placebo-controlled, phase 3 clinical trial. J Headache Pain. 2024;25:57 (Apr 16). Source
Key clinical point: Rimegepant orally disintegrating tablet (ODT) offers pain relief within 2 hours of treatment in adults with migraine, with a tolerable safety profile.
Major finding: At 2 hours post dose, rimegepant was more effective than placebo in providing freedom from pain (risk difference 7.6; P = .0004) and the most bothersome symptom (risk difference 16.2; P < .0001). The overall rates of treatment-emergent adverse events were comparable between the rimegepant and placebo groups (15.2% and 16.4%, respectively).
Study details: This subgroup analysis of a double-blind, randomized, placebo-controlled phase 3 clinical trial included 1075 patients with acute migraine with or without aura (age ≥ 18 years) who were randomly assigned to receive either 75 mg rimegepant ODT (n = 538) or placebo (n = 537).
Disclosures: This study was funded by BioShin, a wholly owned subsidiary of Biohaven Pharmaceuticals, which was acquired by Pfizer. Pfizer provided writing support. Five authors declared being employees or stock owners of Biohaven, BioShin, or Pfizer. The remaining authors declared no conflicts of interest.
Source: Yu S, Guo A, Wang Z, et al. Rimegepant orally disintegrating tablet 75 mg for acute treatment of migraine in adults from China: A subgroup analysis of a double-blind, randomized, placebo-controlled, phase 3 clinical trial. J Headache Pain. 2024;25:57 (Apr 16). Source
Meta-analysis Compares Effectiveness of Parenteral Agents for Migraine Pain in ED
Key clinical point: Combination therapy with two parenteral agents or monotherapy with either neuroleptics or metoclopramide can be considered as a first-line treatment option for the management of acute migraine pain in the emergency department (ED) settings.
Major finding: Combination therapy of two parenteral agents vs placebo was an effective treatment option in reducing pain intensity scores (mean difference −3.36; 95% CI −4.64 to −2.08) and increasing the rate of achievement of pain relief (risk ratio 2.83; 95% CI 1.74-4.61). Monotherapy with neuroleptics and metoclopramide also provided pain relief and helped patients achieve pain-free status prior to discharge from the ED but increased the risk for adverse events, especially akathisia.
Study details: This meta-analysis of 97 randomized controlled trials evaluated the effectiveness of various parenteral agents for pain relief in patients with acute migraine presenting to the ED.
Disclosures: This study was funded by the Emergency Medicine Research Group, Canada. The authors declared no conflicts of interest.
Source: Kirkland SW, Visser L, Meyer J, et al. The effectiveness of parenteral agents for pain reduction in patients with migraine presenting to emergency settings: A systematic review and network analysis. Headache. 2024;64(4):424-447. doi: 10.1111/head.14704 Source
Key clinical point: Combination therapy with two parenteral agents or monotherapy with either neuroleptics or metoclopramide can be considered as a first-line treatment option for the management of acute migraine pain in the emergency department (ED) settings.
Major finding: Combination therapy of two parenteral agents vs placebo was an effective treatment option in reducing pain intensity scores (mean difference −3.36; 95% CI −4.64 to −2.08) and increasing the rate of achievement of pain relief (risk ratio 2.83; 95% CI 1.74-4.61). Monotherapy with neuroleptics and metoclopramide also provided pain relief and helped patients achieve pain-free status prior to discharge from the ED but increased the risk for adverse events, especially akathisia.
Study details: This meta-analysis of 97 randomized controlled trials evaluated the effectiveness of various parenteral agents for pain relief in patients with acute migraine presenting to the ED.
Disclosures: This study was funded by the Emergency Medicine Research Group, Canada. The authors declared no conflicts of interest.
Source: Kirkland SW, Visser L, Meyer J, et al. The effectiveness of parenteral agents for pain reduction in patients with migraine presenting to emergency settings: A systematic review and network analysis. Headache. 2024;64(4):424-447. doi: 10.1111/head.14704 Source
Key clinical point: Combination therapy with two parenteral agents or monotherapy with either neuroleptics or metoclopramide can be considered as a first-line treatment option for the management of acute migraine pain in the emergency department (ED) settings.
Major finding: Combination therapy of two parenteral agents vs placebo was an effective treatment option in reducing pain intensity scores (mean difference −3.36; 95% CI −4.64 to −2.08) and increasing the rate of achievement of pain relief (risk ratio 2.83; 95% CI 1.74-4.61). Monotherapy with neuroleptics and metoclopramide also provided pain relief and helped patients achieve pain-free status prior to discharge from the ED but increased the risk for adverse events, especially akathisia.
Study details: This meta-analysis of 97 randomized controlled trials evaluated the effectiveness of various parenteral agents for pain relief in patients with acute migraine presenting to the ED.
Disclosures: This study was funded by the Emergency Medicine Research Group, Canada. The authors declared no conflicts of interest.
Source: Kirkland SW, Visser L, Meyer J, et al. The effectiveness of parenteral agents for pain reduction in patients with migraine presenting to emergency settings: A systematic review and network analysis. Headache. 2024;64(4):424-447. doi: 10.1111/head.14704 Source
Migraine Diagnosis Shortens Exclusive Breastfeeding Period in Women
Key clinical point: Women with migraine tend to exclusively breastfeed their infants for a shorter duration than those without migraine.
Major finding: There was no significant difference between the proportions of women with and without migraine who did not breastfeed their infants (adjusted odds ratio [aOR] 1.03; 95% CI 0.74-1.27), but the odds of exclusively breastfeeding infants for 6 months and more were 16% lower in women with vs without migraine (aOR 0.84; 95% CI 0.71-0.99; P = .033).
Study details: Findings are from a cross-sectional study including 5282 women (age 20-49 years) who had given birth in the last 5 years, of whom 862 (16.3%) had migraine.
Disclosures: The study did not receive any specific funding. Christine Lay declared receiving research support from and serving on ad boards for various sources. The other authors declared no conflicts of interest.
Source: Vyas MV, Lee N, Lay C. Association between migraine and exclusive breastfeeding: A cross-sectional study. Headache. 2024 (Apr 21). doi: 10.1111/head.14713 Source
Key clinical point: Women with migraine tend to exclusively breastfeed their infants for a shorter duration than those without migraine.
Major finding: There was no significant difference between the proportions of women with and without migraine who did not breastfeed their infants (adjusted odds ratio [aOR] 1.03; 95% CI 0.74-1.27), but the odds of exclusively breastfeeding infants for 6 months and more were 16% lower in women with vs without migraine (aOR 0.84; 95% CI 0.71-0.99; P = .033).
Study details: Findings are from a cross-sectional study including 5282 women (age 20-49 years) who had given birth in the last 5 years, of whom 862 (16.3%) had migraine.
Disclosures: The study did not receive any specific funding. Christine Lay declared receiving research support from and serving on ad boards for various sources. The other authors declared no conflicts of interest.
Source: Vyas MV, Lee N, Lay C. Association between migraine and exclusive breastfeeding: A cross-sectional study. Headache. 2024 (Apr 21). doi: 10.1111/head.14713 Source
Key clinical point: Women with migraine tend to exclusively breastfeed their infants for a shorter duration than those without migraine.
Major finding: There was no significant difference between the proportions of women with and without migraine who did not breastfeed their infants (adjusted odds ratio [aOR] 1.03; 95% CI 0.74-1.27), but the odds of exclusively breastfeeding infants for 6 months and more were 16% lower in women with vs without migraine (aOR 0.84; 95% CI 0.71-0.99; P = .033).
Study details: Findings are from a cross-sectional study including 5282 women (age 20-49 years) who had given birth in the last 5 years, of whom 862 (16.3%) had migraine.
Disclosures: The study did not receive any specific funding. Christine Lay declared receiving research support from and serving on ad boards for various sources. The other authors declared no conflicts of interest.
Source: Vyas MV, Lee N, Lay C. Association between migraine and exclusive breastfeeding: A cross-sectional study. Headache. 2024 (Apr 21). doi: 10.1111/head.14713 Source
Photophobia Impairs Sleep Quality in Migraine
Key clinical point: In patients with migraine, greater severity of photophobia is significantly associated with worse sleep-related outcomes, such as sleep quality (SQ), sleep disturbance (SDi), sleep onset latency (SOL), sleep-related impairment (SRI), and insomnia.
Major finding: Compared with patients with migraine and without photophobia, those with migraine and photophobia presented significantly poorer SQ (β 0.15; P < .001), longer SOL (β 0.10; P = .011), higher levels of SDi (β 0.12; P < .001) and SRI (β 0.08; P = .020), and a higher prevalence of insomnia (β 0.11; P = .005).
Study details: This cross-sectional observational study evaluated the association between photophobia and sleep-related outcomes in 852 patients with migraine using data from the American Registry for Migraine Research.
Disclosures: This study did not receive any specific funding. Some authors declared receiving compensation for consulting from, serving as consultants for, or having other ties with various sources.
Source: Sharp N, Burish MJ, Digre KB, et al. Photophobia is associated with lower sleep quality in individuals with migraine: Results from the American Registry for Migraine Research (ARMR). J Headache Pain. 2024;25:55. doi: 10.1186/s10194-024-01756-9 Source
Key clinical point: In patients with migraine, greater severity of photophobia is significantly associated with worse sleep-related outcomes, such as sleep quality (SQ), sleep disturbance (SDi), sleep onset latency (SOL), sleep-related impairment (SRI), and insomnia.
Major finding: Compared with patients with migraine and without photophobia, those with migraine and photophobia presented significantly poorer SQ (β 0.15; P < .001), longer SOL (β 0.10; P = .011), higher levels of SDi (β 0.12; P < .001) and SRI (β 0.08; P = .020), and a higher prevalence of insomnia (β 0.11; P = .005).
Study details: This cross-sectional observational study evaluated the association between photophobia and sleep-related outcomes in 852 patients with migraine using data from the American Registry for Migraine Research.
Disclosures: This study did not receive any specific funding. Some authors declared receiving compensation for consulting from, serving as consultants for, or having other ties with various sources.
Source: Sharp N, Burish MJ, Digre KB, et al. Photophobia is associated with lower sleep quality in individuals with migraine: Results from the American Registry for Migraine Research (ARMR). J Headache Pain. 2024;25:55. doi: 10.1186/s10194-024-01756-9 Source
Key clinical point: In patients with migraine, greater severity of photophobia is significantly associated with worse sleep-related outcomes, such as sleep quality (SQ), sleep disturbance (SDi), sleep onset latency (SOL), sleep-related impairment (SRI), and insomnia.
Major finding: Compared with patients with migraine and without photophobia, those with migraine and photophobia presented significantly poorer SQ (β 0.15; P < .001), longer SOL (β 0.10; P = .011), higher levels of SDi (β 0.12; P < .001) and SRI (β 0.08; P = .020), and a higher prevalence of insomnia (β 0.11; P = .005).
Study details: This cross-sectional observational study evaluated the association between photophobia and sleep-related outcomes in 852 patients with migraine using data from the American Registry for Migraine Research.
Disclosures: This study did not receive any specific funding. Some authors declared receiving compensation for consulting from, serving as consultants for, or having other ties with various sources.
Source: Sharp N, Burish MJ, Digre KB, et al. Photophobia is associated with lower sleep quality in individuals with migraine: Results from the American Registry for Migraine Research (ARMR). J Headache Pain. 2024;25:55. doi: 10.1186/s10194-024-01756-9 Source