User login
Shoulder Dislocations
IN THIS ARTICLE
- Types of shoulder dislocations
- Schematics of the shoulder with three types of dislocations
- Association with seizures
CASE A 59-year-old man with a remote history of seizures is transported to the emergency department (ED) by ambulance after a witnessed tonic-clonic seizure. At the time of arrival he is postictal and confused, but his vital signs are stable. A left eyebrow laceration indicating a possible fall is observed on physical exam, as is a left shoulder displacement with no obvious signs of neurovascular compromise. The patient is not currently taking anticonvulsant medication, stating that he has been “seizure free” for five years, and therefore chose to discontinue taking phenytoin against medical advice.
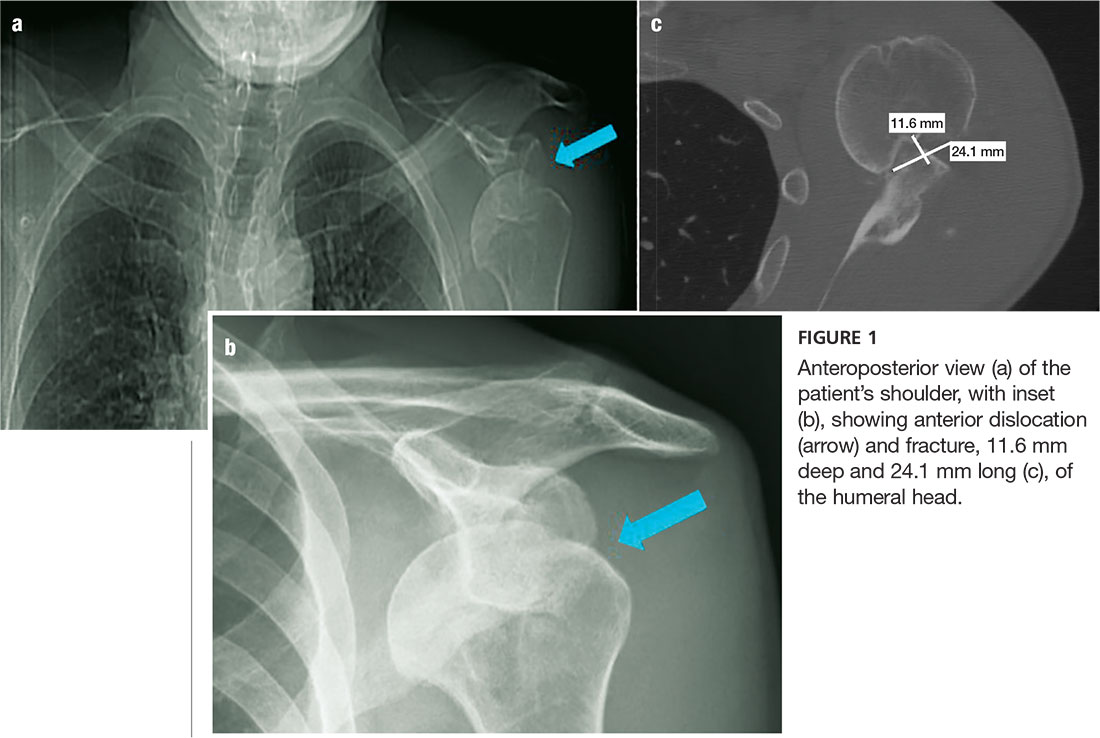
An anteroposterior (AP) bilateral shoulder x-ray is obtained in the ED (see Figures 1a and 1b). The image shows the humeral head to be anteriorly dislocated and reveals a large impaction fracture of the posterior superior humeral head. For a more detailed view of the fracture and to further assess any associated deformities, CT of the left shoulder is performed. The fracture has a depth of 11.6 mm and a length of 24.1 mm, with no additional pathology noted (see Figure 1c).
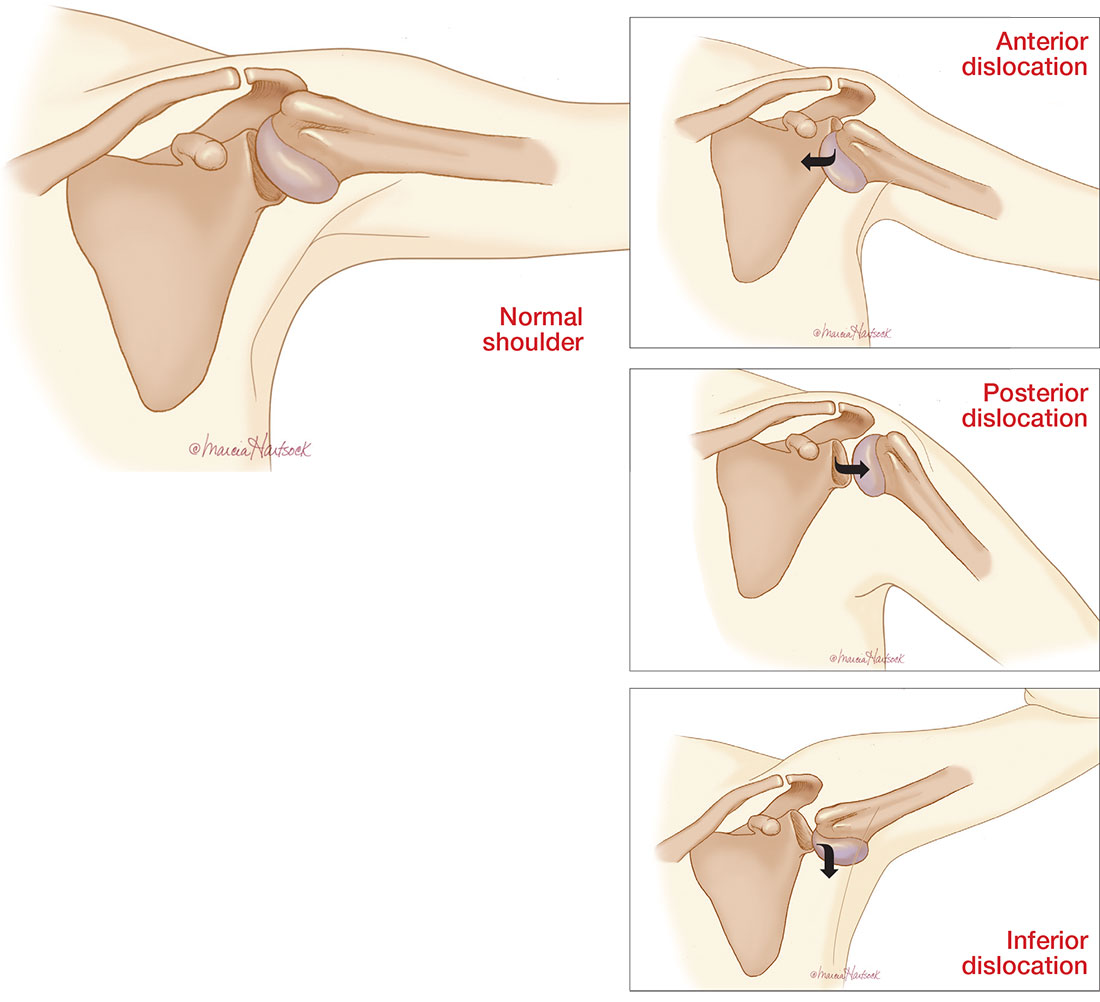
The shoulder is a large joint capable of moving in many directions and therefore is inherently unstable. The glenoid fossa is shallow, and stability of the joint is provided by both the fibrocartilaginous labrum and varying muscles of the rotator cuff. Because the shoulder joint is poorly supported, dislocations are not uncommon (see the illustrations).
The first step in evaluating a suspected shoulder dislocation is to order an AP radiographic view of the shoulder (known as the Grashey view). A transcapular view (known as the scapular “Y” view) is also sufficient.1 While diagnostic studies, such as CT or MRI arthrography, are excellent for evaluating the glenohumeral ligaments and labrum, they generally are not done in an acute setting.1 For patients who present to the ED, some would recommend taking a CT scan, especially if a posterior dislocation is suspected.2
The three types of shoulder dislocations include anterior, posterior, and inferior.
ANTERIOR
Anterior dislocations account for 95% of all presented cases of shoulder dislocation, making them the most common type.3 They may be caused by a fall on an outstretched arm, trauma to the posterior humerus, or—more frequently—trauma to the arm while it is extended, externally rotated, and abducted (eg, blocking a shot in basketball).
A patient with an anterior dislocation will enter the ED with a slightly abducted and externally rotated arm (see illustration) and will resist any movement by the examiner. Typically, the shoulder loses its rounded appearance, and in thin individuals, the acromion may be prominent. A detailed neurovascular examination of the arm must be performed.
Dislocation of the humerus in any direction may compromise the axillary nerve, artery, or both. The axillary nerve and artery run parallel to each other, beneath and in close proximity to the humeral head. The axillary artery is located upstream from the radial artery; compression of the artery may lead to a diminution or complete absence of the radial pulse and/or coolness of the hand.4 The axillary nerve is both a sensory and motor nerve. If injured, a 2- to 3-cm area over the lateral deltoid may have complete sensory loss, which can be tested for with a light touch and pinprick.5 The patient may also have difficulty abducting the arm, but limitations of movement are difficult to measure with a new dislocation and a patient in pain.4
Any patient presenting with an anterior shoulder dislocation should also be screened for two other potential abnormalities. Hill-Sachs lesion, which occurs in up to 40% of anterior dislocations and 90% of all dislocations, is a cortical depression occurring in the humeral head. Bankart lesions, which occur in less than 5% of all dislocations, are avulsed bone fragments that occur when there is a glenoid labrum disruption.6 Both can be seen on plain films, although Bankart lesions are best seen on CT.4
The combination of an anterior dislocation and a humeral fracture, as seen in this case, is rare.7
POSTERIOR
Posterior shoulder dislocations occur far less frequently than anterior dislocations, representing 2% to 5% of all shoulder dislocations.2 They often result from blows to the anterior portion of the shoulder (ie, motor vehicle accidents or sports-related collisions) or violent muscle contractions (eg, electrocution, electroconvulsive therapy, or seizures).
Unable to externally rotate the shoulder, patients with posterior dislocations present with the arm in adduction and internal rotation, making the coracoid process prominent (see illustration).8 This position is sometimes misdiagnosed as a “frozen shoulder.”2
INFERIOR
Inferior dislocation of the shoulder is the rarest type, accounting for only 0.5% of all cases of shoulder dislocation. The mechanism of injury is forceful hyperabduction and extension of the shoulder during a fall.
Patients present with the affected arm hyperadducted, flexed at the elbow, with the hand positioned above or behind the head in fixed abduction: a “hands up” position of the affected arm (see illustration). These dislocations are best identified via the transcapular “Y” radiographs. Inferior dislocations are often associated with neurovascular compromise, and there are often related tears of the infraspinatus, supraspinatus, and teres minor muscles.9
ASSOCIATION WITH SEIZURES
Any patient who has had a seizure is subject to a variety of injuries, including lacerations, contusions, long bone and skull fractures, and dislocations. Seizures with a fall are associated with a 20% chance of injury.10
Shaw et al were the first to note that, during an active convulsion, the patient’s shoulder is in adduction, internal rotation, and flexion. This positioning predisposes to injury: With sustained contraction of the surrounding shoulder girdle muscles, the humeral head is forced superiorly and posteriorly against the acromion andmedially against the glenoid fossa. The glenoid fossa is shallow; therefore, the humeral head is forced posteriorly and dislocates.11
Researchers at the Mayo Clinic followed 247 patients who were diagnosed with seizures over nine years; 16% of the cohort experienced seizure-related injuries. Of the seizures recorded, 82% were tonic-clonic seizures. The singular predictive factor for injury was seizure frequency: Patients who had more seizures were more susceptible to injury.12
In an evaluation of outpatients with epilepsy, 25% of recorded seizures involved a fall. Among those who sustained an orthopedic injury, one injury occurred for every 178.6 generalized tonic-clonic seizures (0.6%)—a number that doubled for generalized tonic-clonic seizure associated with a fall (1.2%).10
The collective evidence from these and other studies suggests that patients who have poorly controlled tonic-clonic seizures have a higher incidence of seizures and, therefore, falls and injuries.10,12 In the absence of known trauma, a posterior shoulder dislocation is almost pathognomonic of a seizure. In high-risk populations (ie, individuals who have poorly controlled diabetes or who are experiencing alcohol or drug withdrawal), suspicion for posterior shoulder dislocation should be elevated.8
After evaluation in the ED, the patient immediately underwent a nonsurgical closed reduction of the shoulder and suturing of the laceration. He was admitted overnight for further evaluation and was started on an anticonvulsant (levetiracetam). An orthopedic consult was obtained; the dislocation/fracture was managed conservatively with a sling for immobilization. No surgical intervention was recommended, since the patient had a manageable fracture without neurovascular compromise. He was discharged home within 36 hours and scheduled for follow-up appointments with both the neurologist and orthopedic surgeon.
CONCLUSION
This patient had a seizure with an associated fall; both the laceration and the anterior shoulder dislocation with a humeral fracture were associated with the fall and not with tonic-clonic activity from the seizure. Because injuries vary widely from soft tissue to joint dislocations, with possible axillary nerve and/or artery damage, clinicians must do a comprehensive examination of patients entering the ED who have had seizures. Each injury must be addressed individually.
1. Omoumi P, Teixeira P, Lecouvet F, Chung CB. Glenohumeral joint instability. J Magn Reson Imaging. 2010;33(1):2-16.
2. Rouleau DM, Hebert-Davies J. Incidence of associated injury in posterior shoulder dislocation: systematic review of the literature. J Orthop Trauma. 2012;26(4):246-251.
3. Sachit M, Shekhar A, Shekhar S, Joban SH. Acute spontaneous atraumatic bilateral anterior dislocation of the shoulder joint with Hill-Sach’s lesions: a rare case. J Orthop Case Rep. 2015;5(1):55-57.
4. Cutts S, Prempeh M, Drew S. Anterior shoulder dislocation. Ann R Coll Surg Engl. 2009;91(1):2-7.
5. Magee DJ. Orthopedic Physical Assessment. 5th ed. St. Louis, MO. Saunders Elsevier; 2008.
6. Greenspan A. Orthopedic Imaging: A Practical Approach. 5th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2011.
7. Karimi-Nasab MH, Shayesteh-Azar M, Sajjadi-Saravi M, Mehdi Daneshpoor SM. Anterior shoulder dislocation and ipsilateral humeral shaft fracture. Iran J Med Sci. 2012; 37(3):202-204.
8. Robinson CM, Aderinto J. Posterior shoulder dislocations and fracture-dislocations. J Bone Joint Surg Am. 2005; 87(3):639-650.
9. Cacioppo E, Waymack JR. Bilateral inferior shoulder dislocation. West J Emerg Med. 2015;16(1):157.
10. Tiamkao S, Shorvon SD. Seizure-related injury in an adult tertiary epilepsy clinic. Hong Kong Med J. 2006;12(4):260-263.
11. Shaw JL. Bilateral posterior fracture-dislocation of the shoulder and other trauma caused by convulsive seizures. J Bone Joint Surg Am. 1971;53(7):1437-1440.
12. Lawn ND, Bamlet WR, Radhakirshnan K, et al. Injuries due to seizures in persons with epilepsy: a population-based study. Neurology. 2004;63(9):1565-1570.
IN THIS ARTICLE
- Types of shoulder dislocations
- Schematics of the shoulder with three types of dislocations
- Association with seizures
CASE A 59-year-old man with a remote history of seizures is transported to the emergency department (ED) by ambulance after a witnessed tonic-clonic seizure. At the time of arrival he is postictal and confused, but his vital signs are stable. A left eyebrow laceration indicating a possible fall is observed on physical exam, as is a left shoulder displacement with no obvious signs of neurovascular compromise. The patient is not currently taking anticonvulsant medication, stating that he has been “seizure free” for five years, and therefore chose to discontinue taking phenytoin against medical advice.
An anteroposterior (AP) bilateral shoulder x-ray is obtained in the ED (see Figures 1a and 1b). The image shows the humeral head to be anteriorly dislocated and reveals a large impaction fracture of the posterior superior humeral head. For a more detailed view of the fracture and to further assess any associated deformities, CT of the left shoulder is performed. The fracture has a depth of 11.6 mm and a length of 24.1 mm, with no additional pathology noted (see Figure 1c).
The shoulder is a large joint capable of moving in many directions and therefore is inherently unstable. The glenoid fossa is shallow, and stability of the joint is provided by both the fibrocartilaginous labrum and varying muscles of the rotator cuff. Because the shoulder joint is poorly supported, dislocations are not uncommon (see the illustrations).
The first step in evaluating a suspected shoulder dislocation is to order an AP radiographic view of the shoulder (known as the Grashey view). A transcapular view (known as the scapular “Y” view) is also sufficient.1 While diagnostic studies, such as CT or MRI arthrography, are excellent for evaluating the glenohumeral ligaments and labrum, they generally are not done in an acute setting.1 For patients who present to the ED, some would recommend taking a CT scan, especially if a posterior dislocation is suspected.2
The three types of shoulder dislocations include anterior, posterior, and inferior.
ANTERIOR
Anterior dislocations account for 95% of all presented cases of shoulder dislocation, making them the most common type.3 They may be caused by a fall on an outstretched arm, trauma to the posterior humerus, or—more frequently—trauma to the arm while it is extended, externally rotated, and abducted (eg, blocking a shot in basketball).
A patient with an anterior dislocation will enter the ED with a slightly abducted and externally rotated arm (see illustration) and will resist any movement by the examiner. Typically, the shoulder loses its rounded appearance, and in thin individuals, the acromion may be prominent. A detailed neurovascular examination of the arm must be performed.
Dislocation of the humerus in any direction may compromise the axillary nerve, artery, or both. The axillary nerve and artery run parallel to each other, beneath and in close proximity to the humeral head. The axillary artery is located upstream from the radial artery; compression of the artery may lead to a diminution or complete absence of the radial pulse and/or coolness of the hand.4 The axillary nerve is both a sensory and motor nerve. If injured, a 2- to 3-cm area over the lateral deltoid may have complete sensory loss, which can be tested for with a light touch and pinprick.5 The patient may also have difficulty abducting the arm, but limitations of movement are difficult to measure with a new dislocation and a patient in pain.4
Any patient presenting with an anterior shoulder dislocation should also be screened for two other potential abnormalities. Hill-Sachs lesion, which occurs in up to 40% of anterior dislocations and 90% of all dislocations, is a cortical depression occurring in the humeral head. Bankart lesions, which occur in less than 5% of all dislocations, are avulsed bone fragments that occur when there is a glenoid labrum disruption.6 Both can be seen on plain films, although Bankart lesions are best seen on CT.4
The combination of an anterior dislocation and a humeral fracture, as seen in this case, is rare.7
POSTERIOR
Posterior shoulder dislocations occur far less frequently than anterior dislocations, representing 2% to 5% of all shoulder dislocations.2 They often result from blows to the anterior portion of the shoulder (ie, motor vehicle accidents or sports-related collisions) or violent muscle contractions (eg, electrocution, electroconvulsive therapy, or seizures).
Unable to externally rotate the shoulder, patients with posterior dislocations present with the arm in adduction and internal rotation, making the coracoid process prominent (see illustration).8 This position is sometimes misdiagnosed as a “frozen shoulder.”2
INFERIOR
Inferior dislocation of the shoulder is the rarest type, accounting for only 0.5% of all cases of shoulder dislocation. The mechanism of injury is forceful hyperabduction and extension of the shoulder during a fall.
Patients present with the affected arm hyperadducted, flexed at the elbow, with the hand positioned above or behind the head in fixed abduction: a “hands up” position of the affected arm (see illustration). These dislocations are best identified via the transcapular “Y” radiographs. Inferior dislocations are often associated with neurovascular compromise, and there are often related tears of the infraspinatus, supraspinatus, and teres minor muscles.9
ASSOCIATION WITH SEIZURES
Any patient who has had a seizure is subject to a variety of injuries, including lacerations, contusions, long bone and skull fractures, and dislocations. Seizures with a fall are associated with a 20% chance of injury.10
Shaw et al were the first to note that, during an active convulsion, the patient’s shoulder is in adduction, internal rotation, and flexion. This positioning predisposes to injury: With sustained contraction of the surrounding shoulder girdle muscles, the humeral head is forced superiorly and posteriorly against the acromion andmedially against the glenoid fossa. The glenoid fossa is shallow; therefore, the humeral head is forced posteriorly and dislocates.11
Researchers at the Mayo Clinic followed 247 patients who were diagnosed with seizures over nine years; 16% of the cohort experienced seizure-related injuries. Of the seizures recorded, 82% were tonic-clonic seizures. The singular predictive factor for injury was seizure frequency: Patients who had more seizures were more susceptible to injury.12
In an evaluation of outpatients with epilepsy, 25% of recorded seizures involved a fall. Among those who sustained an orthopedic injury, one injury occurred for every 178.6 generalized tonic-clonic seizures (0.6%)—a number that doubled for generalized tonic-clonic seizure associated with a fall (1.2%).10
The collective evidence from these and other studies suggests that patients who have poorly controlled tonic-clonic seizures have a higher incidence of seizures and, therefore, falls and injuries.10,12 In the absence of known trauma, a posterior shoulder dislocation is almost pathognomonic of a seizure. In high-risk populations (ie, individuals who have poorly controlled diabetes or who are experiencing alcohol or drug withdrawal), suspicion for posterior shoulder dislocation should be elevated.8
After evaluation in the ED, the patient immediately underwent a nonsurgical closed reduction of the shoulder and suturing of the laceration. He was admitted overnight for further evaluation and was started on an anticonvulsant (levetiracetam). An orthopedic consult was obtained; the dislocation/fracture was managed conservatively with a sling for immobilization. No surgical intervention was recommended, since the patient had a manageable fracture without neurovascular compromise. He was discharged home within 36 hours and scheduled for follow-up appointments with both the neurologist and orthopedic surgeon.
CONCLUSION
This patient had a seizure with an associated fall; both the laceration and the anterior shoulder dislocation with a humeral fracture were associated with the fall and not with tonic-clonic activity from the seizure. Because injuries vary widely from soft tissue to joint dislocations, with possible axillary nerve and/or artery damage, clinicians must do a comprehensive examination of patients entering the ED who have had seizures. Each injury must be addressed individually.
IN THIS ARTICLE
- Types of shoulder dislocations
- Schematics of the shoulder with three types of dislocations
- Association with seizures
CASE A 59-year-old man with a remote history of seizures is transported to the emergency department (ED) by ambulance after a witnessed tonic-clonic seizure. At the time of arrival he is postictal and confused, but his vital signs are stable. A left eyebrow laceration indicating a possible fall is observed on physical exam, as is a left shoulder displacement with no obvious signs of neurovascular compromise. The patient is not currently taking anticonvulsant medication, stating that he has been “seizure free” for five years, and therefore chose to discontinue taking phenytoin against medical advice.
An anteroposterior (AP) bilateral shoulder x-ray is obtained in the ED (see Figures 1a and 1b). The image shows the humeral head to be anteriorly dislocated and reveals a large impaction fracture of the posterior superior humeral head. For a more detailed view of the fracture and to further assess any associated deformities, CT of the left shoulder is performed. The fracture has a depth of 11.6 mm and a length of 24.1 mm, with no additional pathology noted (see Figure 1c).
The shoulder is a large joint capable of moving in many directions and therefore is inherently unstable. The glenoid fossa is shallow, and stability of the joint is provided by both the fibrocartilaginous labrum and varying muscles of the rotator cuff. Because the shoulder joint is poorly supported, dislocations are not uncommon (see the illustrations).
The first step in evaluating a suspected shoulder dislocation is to order an AP radiographic view of the shoulder (known as the Grashey view). A transcapular view (known as the scapular “Y” view) is also sufficient.1 While diagnostic studies, such as CT or MRI arthrography, are excellent for evaluating the glenohumeral ligaments and labrum, they generally are not done in an acute setting.1 For patients who present to the ED, some would recommend taking a CT scan, especially if a posterior dislocation is suspected.2
The three types of shoulder dislocations include anterior, posterior, and inferior.
ANTERIOR
Anterior dislocations account for 95% of all presented cases of shoulder dislocation, making them the most common type.3 They may be caused by a fall on an outstretched arm, trauma to the posterior humerus, or—more frequently—trauma to the arm while it is extended, externally rotated, and abducted (eg, blocking a shot in basketball).
A patient with an anterior dislocation will enter the ED with a slightly abducted and externally rotated arm (see illustration) and will resist any movement by the examiner. Typically, the shoulder loses its rounded appearance, and in thin individuals, the acromion may be prominent. A detailed neurovascular examination of the arm must be performed.
Dislocation of the humerus in any direction may compromise the axillary nerve, artery, or both. The axillary nerve and artery run parallel to each other, beneath and in close proximity to the humeral head. The axillary artery is located upstream from the radial artery; compression of the artery may lead to a diminution or complete absence of the radial pulse and/or coolness of the hand.4 The axillary nerve is both a sensory and motor nerve. If injured, a 2- to 3-cm area over the lateral deltoid may have complete sensory loss, which can be tested for with a light touch and pinprick.5 The patient may also have difficulty abducting the arm, but limitations of movement are difficult to measure with a new dislocation and a patient in pain.4
Any patient presenting with an anterior shoulder dislocation should also be screened for two other potential abnormalities. Hill-Sachs lesion, which occurs in up to 40% of anterior dislocations and 90% of all dislocations, is a cortical depression occurring in the humeral head. Bankart lesions, which occur in less than 5% of all dislocations, are avulsed bone fragments that occur when there is a glenoid labrum disruption.6 Both can be seen on plain films, although Bankart lesions are best seen on CT.4
The combination of an anterior dislocation and a humeral fracture, as seen in this case, is rare.7
POSTERIOR
Posterior shoulder dislocations occur far less frequently than anterior dislocations, representing 2% to 5% of all shoulder dislocations.2 They often result from blows to the anterior portion of the shoulder (ie, motor vehicle accidents or sports-related collisions) or violent muscle contractions (eg, electrocution, electroconvulsive therapy, or seizures).
Unable to externally rotate the shoulder, patients with posterior dislocations present with the arm in adduction and internal rotation, making the coracoid process prominent (see illustration).8 This position is sometimes misdiagnosed as a “frozen shoulder.”2
INFERIOR
Inferior dislocation of the shoulder is the rarest type, accounting for only 0.5% of all cases of shoulder dislocation. The mechanism of injury is forceful hyperabduction and extension of the shoulder during a fall.
Patients present with the affected arm hyperadducted, flexed at the elbow, with the hand positioned above or behind the head in fixed abduction: a “hands up” position of the affected arm (see illustration). These dislocations are best identified via the transcapular “Y” radiographs. Inferior dislocations are often associated with neurovascular compromise, and there are often related tears of the infraspinatus, supraspinatus, and teres minor muscles.9
ASSOCIATION WITH SEIZURES
Any patient who has had a seizure is subject to a variety of injuries, including lacerations, contusions, long bone and skull fractures, and dislocations. Seizures with a fall are associated with a 20% chance of injury.10
Shaw et al were the first to note that, during an active convulsion, the patient’s shoulder is in adduction, internal rotation, and flexion. This positioning predisposes to injury: With sustained contraction of the surrounding shoulder girdle muscles, the humeral head is forced superiorly and posteriorly against the acromion andmedially against the glenoid fossa. The glenoid fossa is shallow; therefore, the humeral head is forced posteriorly and dislocates.11
Researchers at the Mayo Clinic followed 247 patients who were diagnosed with seizures over nine years; 16% of the cohort experienced seizure-related injuries. Of the seizures recorded, 82% were tonic-clonic seizures. The singular predictive factor for injury was seizure frequency: Patients who had more seizures were more susceptible to injury.12
In an evaluation of outpatients with epilepsy, 25% of recorded seizures involved a fall. Among those who sustained an orthopedic injury, one injury occurred for every 178.6 generalized tonic-clonic seizures (0.6%)—a number that doubled for generalized tonic-clonic seizure associated with a fall (1.2%).10
The collective evidence from these and other studies suggests that patients who have poorly controlled tonic-clonic seizures have a higher incidence of seizures and, therefore, falls and injuries.10,12 In the absence of known trauma, a posterior shoulder dislocation is almost pathognomonic of a seizure. In high-risk populations (ie, individuals who have poorly controlled diabetes or who are experiencing alcohol or drug withdrawal), suspicion for posterior shoulder dislocation should be elevated.8
After evaluation in the ED, the patient immediately underwent a nonsurgical closed reduction of the shoulder and suturing of the laceration. He was admitted overnight for further evaluation and was started on an anticonvulsant (levetiracetam). An orthopedic consult was obtained; the dislocation/fracture was managed conservatively with a sling for immobilization. No surgical intervention was recommended, since the patient had a manageable fracture without neurovascular compromise. He was discharged home within 36 hours and scheduled for follow-up appointments with both the neurologist and orthopedic surgeon.
CONCLUSION
This patient had a seizure with an associated fall; both the laceration and the anterior shoulder dislocation with a humeral fracture were associated with the fall and not with tonic-clonic activity from the seizure. Because injuries vary widely from soft tissue to joint dislocations, with possible axillary nerve and/or artery damage, clinicians must do a comprehensive examination of patients entering the ED who have had seizures. Each injury must be addressed individually.
1. Omoumi P, Teixeira P, Lecouvet F, Chung CB. Glenohumeral joint instability. J Magn Reson Imaging. 2010;33(1):2-16.
2. Rouleau DM, Hebert-Davies J. Incidence of associated injury in posterior shoulder dislocation: systematic review of the literature. J Orthop Trauma. 2012;26(4):246-251.
3. Sachit M, Shekhar A, Shekhar S, Joban SH. Acute spontaneous atraumatic bilateral anterior dislocation of the shoulder joint with Hill-Sach’s lesions: a rare case. J Orthop Case Rep. 2015;5(1):55-57.
4. Cutts S, Prempeh M, Drew S. Anterior shoulder dislocation. Ann R Coll Surg Engl. 2009;91(1):2-7.
5. Magee DJ. Orthopedic Physical Assessment. 5th ed. St. Louis, MO. Saunders Elsevier; 2008.
6. Greenspan A. Orthopedic Imaging: A Practical Approach. 5th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2011.
7. Karimi-Nasab MH, Shayesteh-Azar M, Sajjadi-Saravi M, Mehdi Daneshpoor SM. Anterior shoulder dislocation and ipsilateral humeral shaft fracture. Iran J Med Sci. 2012; 37(3):202-204.
8. Robinson CM, Aderinto J. Posterior shoulder dislocations and fracture-dislocations. J Bone Joint Surg Am. 2005; 87(3):639-650.
9. Cacioppo E, Waymack JR. Bilateral inferior shoulder dislocation. West J Emerg Med. 2015;16(1):157.
10. Tiamkao S, Shorvon SD. Seizure-related injury in an adult tertiary epilepsy clinic. Hong Kong Med J. 2006;12(4):260-263.
11. Shaw JL. Bilateral posterior fracture-dislocation of the shoulder and other trauma caused by convulsive seizures. J Bone Joint Surg Am. 1971;53(7):1437-1440.
12. Lawn ND, Bamlet WR, Radhakirshnan K, et al. Injuries due to seizures in persons with epilepsy: a population-based study. Neurology. 2004;63(9):1565-1570.
1. Omoumi P, Teixeira P, Lecouvet F, Chung CB. Glenohumeral joint instability. J Magn Reson Imaging. 2010;33(1):2-16.
2. Rouleau DM, Hebert-Davies J. Incidence of associated injury in posterior shoulder dislocation: systematic review of the literature. J Orthop Trauma. 2012;26(4):246-251.
3. Sachit M, Shekhar A, Shekhar S, Joban SH. Acute spontaneous atraumatic bilateral anterior dislocation of the shoulder joint with Hill-Sach’s lesions: a rare case. J Orthop Case Rep. 2015;5(1):55-57.
4. Cutts S, Prempeh M, Drew S. Anterior shoulder dislocation. Ann R Coll Surg Engl. 2009;91(1):2-7.
5. Magee DJ. Orthopedic Physical Assessment. 5th ed. St. Louis, MO. Saunders Elsevier; 2008.
6. Greenspan A. Orthopedic Imaging: A Practical Approach. 5th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2011.
7. Karimi-Nasab MH, Shayesteh-Azar M, Sajjadi-Saravi M, Mehdi Daneshpoor SM. Anterior shoulder dislocation and ipsilateral humeral shaft fracture. Iran J Med Sci. 2012; 37(3):202-204.
8. Robinson CM, Aderinto J. Posterior shoulder dislocations and fracture-dislocations. J Bone Joint Surg Am. 2005; 87(3):639-650.
9. Cacioppo E, Waymack JR. Bilateral inferior shoulder dislocation. West J Emerg Med. 2015;16(1):157.
10. Tiamkao S, Shorvon SD. Seizure-related injury in an adult tertiary epilepsy clinic. Hong Kong Med J. 2006;12(4):260-263.
11. Shaw JL. Bilateral posterior fracture-dislocation of the shoulder and other trauma caused by convulsive seizures. J Bone Joint Surg Am. 1971;53(7):1437-1440.
12. Lawn ND, Bamlet WR, Radhakirshnan K, et al. Injuries due to seizures in persons with epilepsy: a population-based study. Neurology. 2004;63(9):1565-1570.
