User login
Early Colonoscopy Advised in IBD and Sclerosing Cholangitis
Major Finding: In patients with primary sclerosing cholangitis and inflammatory bowel disease, the occurrence of colonic neoplasms per 100 patient-years of follow-up was 21.5 within 2 years, 20.5 at 2-4 years, 19.3 at 4-6 years, 16.8 at 6-8 years, and 20.4 at 8-10 years.
Data Source: A review of data from 54 patients seen at the Mayo Clinic, Rochester, Minn., for primary sclerosing cholangitis and inflammatory bowel disease and later diagnosed with colonic neoplasms.
Disclosures: Dr. Thackeray said that she had no financial conflicts to disclose.
SAN ANTONIO — Patients with primary sclerosing cholangitis and inflammatory bowel disease were as likely to develop colon cancer within 2 years of diagnosis as they were within 8-10 years of diagnosis, based on data from 54 patients.
Yearly colonoscopies are often recommended for patients with primary sclerosing cholangitis (PSC) and inflammatory bowel disease (IBD), but the evidence to support early screening has been limited, said Dr. Erin Thackeray of the Mayo Clinic in Rochester, Minn.
In this study, Dr. Thackeray and her colleagues reviewed medical charts from 54 adults with PSC and IBD who were seen at the Mayo Clinic between 1995 and 2005 and were later diagnosed with colonic neoplasms. Average age at the time of colon cancer diagnosis was 51 years, and 70% of the patients were male.
The occurrence of colonic neoplasms per 100 patient-years of follow-up was 21.5 within 2 years, 20.5 at 2-4 years, 19.3 at 4-6 years, 16.8 at 6-8 years, and 20.4 at 8-10 years.
Fourteen patients had colon cancer: two in the cecum, five in the ascending colon, four in the transverse colon, and three in the rectosigmoid colon. The cancers included two at stage 1, four at stage IIA, four at stage IIIB, two at stage IIIC, and two at stage IV.
Another 7 had high-grade dysplasia, 3 had dysplasia-associated lesions or a mass, and 30 had low-grade dysplasia.
The study population included 37 patients with ulcerative colitis, 6 who had Crohn's disease with colonic involvement, and 11 with indeterminate colitis. A total of 38 patients had IBD diagnosed prior to PSC by a median of 10.8 years, while 9 patients had PSC diagnosed before IBD b y a median of 4 years, and 7 patients were diagnosed simultaneously with both conditions.
The study was limited by its small size, but the results “support early and aggressive screening for colon cancer” in this patient population, Dr. Thackeray said.
Major Finding: In patients with primary sclerosing cholangitis and inflammatory bowel disease, the occurrence of colonic neoplasms per 100 patient-years of follow-up was 21.5 within 2 years, 20.5 at 2-4 years, 19.3 at 4-6 years, 16.8 at 6-8 years, and 20.4 at 8-10 years.
Data Source: A review of data from 54 patients seen at the Mayo Clinic, Rochester, Minn., for primary sclerosing cholangitis and inflammatory bowel disease and later diagnosed with colonic neoplasms.
Disclosures: Dr. Thackeray said that she had no financial conflicts to disclose.
SAN ANTONIO — Patients with primary sclerosing cholangitis and inflammatory bowel disease were as likely to develop colon cancer within 2 years of diagnosis as they were within 8-10 years of diagnosis, based on data from 54 patients.
Yearly colonoscopies are often recommended for patients with primary sclerosing cholangitis (PSC) and inflammatory bowel disease (IBD), but the evidence to support early screening has been limited, said Dr. Erin Thackeray of the Mayo Clinic in Rochester, Minn.
In this study, Dr. Thackeray and her colleagues reviewed medical charts from 54 adults with PSC and IBD who were seen at the Mayo Clinic between 1995 and 2005 and were later diagnosed with colonic neoplasms. Average age at the time of colon cancer diagnosis was 51 years, and 70% of the patients were male.
The occurrence of colonic neoplasms per 100 patient-years of follow-up was 21.5 within 2 years, 20.5 at 2-4 years, 19.3 at 4-6 years, 16.8 at 6-8 years, and 20.4 at 8-10 years.
Fourteen patients had colon cancer: two in the cecum, five in the ascending colon, four in the transverse colon, and three in the rectosigmoid colon. The cancers included two at stage 1, four at stage IIA, four at stage IIIB, two at stage IIIC, and two at stage IV.
Another 7 had high-grade dysplasia, 3 had dysplasia-associated lesions or a mass, and 30 had low-grade dysplasia.
The study population included 37 patients with ulcerative colitis, 6 who had Crohn's disease with colonic involvement, and 11 with indeterminate colitis. A total of 38 patients had IBD diagnosed prior to PSC by a median of 10.8 years, while 9 patients had PSC diagnosed before IBD b y a median of 4 years, and 7 patients were diagnosed simultaneously with both conditions.
The study was limited by its small size, but the results “support early and aggressive screening for colon cancer” in this patient population, Dr. Thackeray said.
Major Finding: In patients with primary sclerosing cholangitis and inflammatory bowel disease, the occurrence of colonic neoplasms per 100 patient-years of follow-up was 21.5 within 2 years, 20.5 at 2-4 years, 19.3 at 4-6 years, 16.8 at 6-8 years, and 20.4 at 8-10 years.
Data Source: A review of data from 54 patients seen at the Mayo Clinic, Rochester, Minn., for primary sclerosing cholangitis and inflammatory bowel disease and later diagnosed with colonic neoplasms.
Disclosures: Dr. Thackeray said that she had no financial conflicts to disclose.
SAN ANTONIO — Patients with primary sclerosing cholangitis and inflammatory bowel disease were as likely to develop colon cancer within 2 years of diagnosis as they were within 8-10 years of diagnosis, based on data from 54 patients.
Yearly colonoscopies are often recommended for patients with primary sclerosing cholangitis (PSC) and inflammatory bowel disease (IBD), but the evidence to support early screening has been limited, said Dr. Erin Thackeray of the Mayo Clinic in Rochester, Minn.
In this study, Dr. Thackeray and her colleagues reviewed medical charts from 54 adults with PSC and IBD who were seen at the Mayo Clinic between 1995 and 2005 and were later diagnosed with colonic neoplasms. Average age at the time of colon cancer diagnosis was 51 years, and 70% of the patients were male.
The occurrence of colonic neoplasms per 100 patient-years of follow-up was 21.5 within 2 years, 20.5 at 2-4 years, 19.3 at 4-6 years, 16.8 at 6-8 years, and 20.4 at 8-10 years.
Fourteen patients had colon cancer: two in the cecum, five in the ascending colon, four in the transverse colon, and three in the rectosigmoid colon. The cancers included two at stage 1, four at stage IIA, four at stage IIIB, two at stage IIIC, and two at stage IV.
Another 7 had high-grade dysplasia, 3 had dysplasia-associated lesions or a mass, and 30 had low-grade dysplasia.
The study population included 37 patients with ulcerative colitis, 6 who had Crohn's disease with colonic involvement, and 11 with indeterminate colitis. A total of 38 patients had IBD diagnosed prior to PSC by a median of 10.8 years, while 9 patients had PSC diagnosed before IBD b y a median of 4 years, and 7 patients were diagnosed simultaneously with both conditions.
The study was limited by its small size, but the results “support early and aggressive screening for colon cancer” in this patient population, Dr. Thackeray said.
Aspirin Dose, Not Duration, May Raise GI Bleeding Risk
SAN ANTONIO — Men who took more than 14 aspirin per week were more than twice as likely to report upper gastrointestinal bleeding as were men who reported no aspirin use, but increased duration of use did not appear to raise the risk of GI bleeding, said Dr. Edward Huang.
Evidence regarding the impact of aspirin use on GI bleeding is conflicting because of the limitations of previous studies, said Dr. Huang of Massachusetts General Hospital in Boston.
To examine the long-term effects of aspirin dose and duration on GI bleeding, Dr. Huang and his colleagues conducted a prospective study of 32,989 participants in the Health Professionals Follow-up Study, a longitudinal study of male health professionals in the United States. In 2006 and 2008, participants were asked to report any past episodes of GI bleeding severe enough to require hospitalization or blood transfusion.
During a mean 14-year follow-up period, 707 men had an episode of major GI bleeding. After adjustment for risk factors including use of NSAIDs, age, smoking status, exercise, and body mass index, the risk ratios for upper GI bleeding were 1.05 for men who took 0.5-1.5 standard aspirin tablets (325 mg) per week, 1.31 for those who took 2-5 tablets per week, 1.63 for those who took 6-14 tablets per week, and 2.40 for those who took more than 14 tablets per week, compared with men who reported no aspirin use.
Short-term use was defined as less than 5 years; long-term use was defined as 5 years or longer. “The dose-response relationship is significant regardless of duration of use,” Dr. Huang noted.
Longer duration of use was not significantly associated with an increased risk of upper GI bleeding, but individuals who use aspirin the longest tend to use the highest dose, he added.
The average age of the men when they enrolled in the study was 60 years, and those with a history of peptic ulcer disease were excluded.
The results suggest that both short-term and long-term aspirin users can minimize the risk of upper GI bleeding by using the lowest effective dose, Dr. Huang said.
Dr. Huang had no financial conflicts to disclose.
{kind=link}
Both short- and long-term aspirin users can minimize the risk by using the lowest effective dose.
Source DR. HUANG
SAN ANTONIO — Men who took more than 14 aspirin per week were more than twice as likely to report upper gastrointestinal bleeding as were men who reported no aspirin use, but increased duration of use did not appear to raise the risk of GI bleeding, said Dr. Edward Huang.
Evidence regarding the impact of aspirin use on GI bleeding is conflicting because of the limitations of previous studies, said Dr. Huang of Massachusetts General Hospital in Boston.
To examine the long-term effects of aspirin dose and duration on GI bleeding, Dr. Huang and his colleagues conducted a prospective study of 32,989 participants in the Health Professionals Follow-up Study, a longitudinal study of male health professionals in the United States. In 2006 and 2008, participants were asked to report any past episodes of GI bleeding severe enough to require hospitalization or blood transfusion.
During a mean 14-year follow-up period, 707 men had an episode of major GI bleeding. After adjustment for risk factors including use of NSAIDs, age, smoking status, exercise, and body mass index, the risk ratios for upper GI bleeding were 1.05 for men who took 0.5-1.5 standard aspirin tablets (325 mg) per week, 1.31 for those who took 2-5 tablets per week, 1.63 for those who took 6-14 tablets per week, and 2.40 for those who took more than 14 tablets per week, compared with men who reported no aspirin use.
Short-term use was defined as less than 5 years; long-term use was defined as 5 years or longer. “The dose-response relationship is significant regardless of duration of use,” Dr. Huang noted.
Longer duration of use was not significantly associated with an increased risk of upper GI bleeding, but individuals who use aspirin the longest tend to use the highest dose, he added.
The average age of the men when they enrolled in the study was 60 years, and those with a history of peptic ulcer disease were excluded.
The results suggest that both short-term and long-term aspirin users can minimize the risk of upper GI bleeding by using the lowest effective dose, Dr. Huang said.
Dr. Huang had no financial conflicts to disclose.
Both short- and long-term aspirin users can minimize the risk by using the lowest effective dose.
Source DR. HUANG
SAN ANTONIO — Men who took more than 14 aspirin per week were more than twice as likely to report upper gastrointestinal bleeding as were men who reported no aspirin use, but increased duration of use did not appear to raise the risk of GI bleeding, said Dr. Edward Huang.
Evidence regarding the impact of aspirin use on GI bleeding is conflicting because of the limitations of previous studies, said Dr. Huang of Massachusetts General Hospital in Boston.
To examine the long-term effects of aspirin dose and duration on GI bleeding, Dr. Huang and his colleagues conducted a prospective study of 32,989 participants in the Health Professionals Follow-up Study, a longitudinal study of male health professionals in the United States. In 2006 and 2008, participants were asked to report any past episodes of GI bleeding severe enough to require hospitalization or blood transfusion.
During a mean 14-year follow-up period, 707 men had an episode of major GI bleeding. After adjustment for risk factors including use of NSAIDs, age, smoking status, exercise, and body mass index, the risk ratios for upper GI bleeding were 1.05 for men who took 0.5-1.5 standard aspirin tablets (325 mg) per week, 1.31 for those who took 2-5 tablets per week, 1.63 for those who took 6-14 tablets per week, and 2.40 for those who took more than 14 tablets per week, compared with men who reported no aspirin use.
Short-term use was defined as less than 5 years; long-term use was defined as 5 years or longer. “The dose-response relationship is significant regardless of duration of use,” Dr. Huang noted.
Longer duration of use was not significantly associated with an increased risk of upper GI bleeding, but individuals who use aspirin the longest tend to use the highest dose, he added.
The average age of the men when they enrolled in the study was 60 years, and those with a history of peptic ulcer disease were excluded.
The results suggest that both short-term and long-term aspirin users can minimize the risk of upper GI bleeding by using the lowest effective dose, Dr. Huang said.
Dr. Huang had no financial conflicts to disclose.
Both short- and long-term aspirin users can minimize the risk by using the lowest effective dose.
Source DR. HUANG
Gentle Yoga Poses Ease Pain in Women With Fibromyalgia
Women with fibromyalgia who participated in an 8-week yoga program reported significant improvements on measures of fibromyalgia symptoms and function, based on data from a pilot study of 53 women.
The positive findings have become the basis of a grant proposal to the National Institutes of Health to fund a larger clinical trial, said lead investigator and lead study author James Carson, Ph.D.
Many fibromyalgia patients find standard medical care ineffective for reducing their symptoms, including pain and fatigue, Dr. Carson of Oregon Health and Science University in Portland said in an interview.
More effective treatments for fibromyalgia are needed, Dr. Carson said. “Exercise is often prescribed for fibromyalgia, but for many patients it is hard to find an exercise program that is tolerable for them. Yoga poses done in a gentle way may be a good option.”
Dr. Carson and colleagues randomized 53 women who met the American College of Rheumatology criteria for fibromyalgia in an 8-week Yoga Awareness program (25 women) or standard care (28 women). The program consisted of gentle yoga poses, modified as needed to accommodate conditions such as knee osteoarthritis or carpal tunnel syndrome (Pain 2010;151:530–9).
The primary outcome measure was the total score on the Fibromyalgia Impact Questionnaire Revised (FIQR). After 8 weeks, the mean FIQR total score dropped from 48.32 at baseline to 35.49 in the yoga group (a statistically significant difference), compared with a change from 49.26 at baseline to 48.69 in the control group. More than half (56%) of the yoga group had at least a 30% reduction in overall FIQR scores, which is slightly more than twice the 14% reduction that is recommended to show clinical significance, the researchers noted. In addition, 50% of patients in the yoga group had at least a 30% reduction in the pain subscale of the FIQR.
The Patient Global Impression of Change (PGIC) scale scores for overall improvement in fibromyalgia symptoms were significantly higher in the yoga group vs. the control group (5.05 vs. 3.69). The PGIC was measured only once, at the end of the study. As part of the PGIC, approximately 90% of the patients in the yoga group reported feeling “a little better,” “much better,” or “very much better,” compared with 19% of the controls.
The average age of the participants was 54 years, and 68% had been symptomatic for more than 10 years. Patients who were already engaged in a yoga practice, those who were too disabled for meaningful participation in the yoga program, and those who were scheduled for elective surgery were excluded from the study. “The most surprising finding for us was that most patients became so fully engaged in the home yoga practices they were assigned,” Dr. Carson said. On average, the patients spent 40 minutes practicing yoga at home, including about 19 minutes of postures, 13 minutes of seated meditation, and 8 minutes of breathing exercises. Those who practiced more had better results on several of the study outcomes, he noted.
“This finding suggests that yoga practices, if taught in a tailored, accessible manner, are not only well tolerated and effective; they are practiced with an unexpected degree of enthusiasm,” he said.
The results also showed that patients in the yoga group were more likely to use positive pain-management strategies such as problem solving, religion, acceptance, and relaxation, and less likely to resort to negative pain-management strategies such as self-isolation, disengagement, and catastrophizing.
Dr. Carson said he and his colleagues are preparing a grant proposal to the National Institutes of Health to fund a larger trial that will include comparison with another active treatment.
The researchers had no financial conflicts to disclose.
Women with fibromyalgia who participated in an 8-week yoga program reported significant improvements on measures of fibromyalgia symptoms and function, based on data from a pilot study of 53 women.
The positive findings have become the basis of a grant proposal to the National Institutes of Health to fund a larger clinical trial, said lead investigator and lead study author James Carson, Ph.D.
Many fibromyalgia patients find standard medical care ineffective for reducing their symptoms, including pain and fatigue, Dr. Carson of Oregon Health and Science University in Portland said in an interview.
More effective treatments for fibromyalgia are needed, Dr. Carson said. “Exercise is often prescribed for fibromyalgia, but for many patients it is hard to find an exercise program that is tolerable for them. Yoga poses done in a gentle way may be a good option.”
Dr. Carson and colleagues randomized 53 women who met the American College of Rheumatology criteria for fibromyalgia in an 8-week Yoga Awareness program (25 women) or standard care (28 women). The program consisted of gentle yoga poses, modified as needed to accommodate conditions such as knee osteoarthritis or carpal tunnel syndrome (Pain 2010;151:530–9).
The primary outcome measure was the total score on the Fibromyalgia Impact Questionnaire Revised (FIQR). After 8 weeks, the mean FIQR total score dropped from 48.32 at baseline to 35.49 in the yoga group (a statistically significant difference), compared with a change from 49.26 at baseline to 48.69 in the control group. More than half (56%) of the yoga group had at least a 30% reduction in overall FIQR scores, which is slightly more than twice the 14% reduction that is recommended to show clinical significance, the researchers noted. In addition, 50% of patients in the yoga group had at least a 30% reduction in the pain subscale of the FIQR.
The Patient Global Impression of Change (PGIC) scale scores for overall improvement in fibromyalgia symptoms were significantly higher in the yoga group vs. the control group (5.05 vs. 3.69). The PGIC was measured only once, at the end of the study. As part of the PGIC, approximately 90% of the patients in the yoga group reported feeling “a little better,” “much better,” or “very much better,” compared with 19% of the controls.
The average age of the participants was 54 years, and 68% had been symptomatic for more than 10 years. Patients who were already engaged in a yoga practice, those who were too disabled for meaningful participation in the yoga program, and those who were scheduled for elective surgery were excluded from the study. “The most surprising finding for us was that most patients became so fully engaged in the home yoga practices they were assigned,” Dr. Carson said. On average, the patients spent 40 minutes practicing yoga at home, including about 19 minutes of postures, 13 minutes of seated meditation, and 8 minutes of breathing exercises. Those who practiced more had better results on several of the study outcomes, he noted.
“This finding suggests that yoga practices, if taught in a tailored, accessible manner, are not only well tolerated and effective; they are practiced with an unexpected degree of enthusiasm,” he said.
The results also showed that patients in the yoga group were more likely to use positive pain-management strategies such as problem solving, religion, acceptance, and relaxation, and less likely to resort to negative pain-management strategies such as self-isolation, disengagement, and catastrophizing.
Dr. Carson said he and his colleagues are preparing a grant proposal to the National Institutes of Health to fund a larger trial that will include comparison with another active treatment.
The researchers had no financial conflicts to disclose.
Women with fibromyalgia who participated in an 8-week yoga program reported significant improvements on measures of fibromyalgia symptoms and function, based on data from a pilot study of 53 women.
The positive findings have become the basis of a grant proposal to the National Institutes of Health to fund a larger clinical trial, said lead investigator and lead study author James Carson, Ph.D.
Many fibromyalgia patients find standard medical care ineffective for reducing their symptoms, including pain and fatigue, Dr. Carson of Oregon Health and Science University in Portland said in an interview.
More effective treatments for fibromyalgia are needed, Dr. Carson said. “Exercise is often prescribed for fibromyalgia, but for many patients it is hard to find an exercise program that is tolerable for them. Yoga poses done in a gentle way may be a good option.”
Dr. Carson and colleagues randomized 53 women who met the American College of Rheumatology criteria for fibromyalgia in an 8-week Yoga Awareness program (25 women) or standard care (28 women). The program consisted of gentle yoga poses, modified as needed to accommodate conditions such as knee osteoarthritis or carpal tunnel syndrome (Pain 2010;151:530–9).
The primary outcome measure was the total score on the Fibromyalgia Impact Questionnaire Revised (FIQR). After 8 weeks, the mean FIQR total score dropped from 48.32 at baseline to 35.49 in the yoga group (a statistically significant difference), compared with a change from 49.26 at baseline to 48.69 in the control group. More than half (56%) of the yoga group had at least a 30% reduction in overall FIQR scores, which is slightly more than twice the 14% reduction that is recommended to show clinical significance, the researchers noted. In addition, 50% of patients in the yoga group had at least a 30% reduction in the pain subscale of the FIQR.
The Patient Global Impression of Change (PGIC) scale scores for overall improvement in fibromyalgia symptoms were significantly higher in the yoga group vs. the control group (5.05 vs. 3.69). The PGIC was measured only once, at the end of the study. As part of the PGIC, approximately 90% of the patients in the yoga group reported feeling “a little better,” “much better,” or “very much better,” compared with 19% of the controls.
The average age of the participants was 54 years, and 68% had been symptomatic for more than 10 years. Patients who were already engaged in a yoga practice, those who were too disabled for meaningful participation in the yoga program, and those who were scheduled for elective surgery were excluded from the study. “The most surprising finding for us was that most patients became so fully engaged in the home yoga practices they were assigned,” Dr. Carson said. On average, the patients spent 40 minutes practicing yoga at home, including about 19 minutes of postures, 13 minutes of seated meditation, and 8 minutes of breathing exercises. Those who practiced more had better results on several of the study outcomes, he noted.
“This finding suggests that yoga practices, if taught in a tailored, accessible manner, are not only well tolerated and effective; they are practiced with an unexpected degree of enthusiasm,” he said.
The results also showed that patients in the yoga group were more likely to use positive pain-management strategies such as problem solving, religion, acceptance, and relaxation, and less likely to resort to negative pain-management strategies such as self-isolation, disengagement, and catastrophizing.
Dr. Carson said he and his colleagues are preparing a grant proposal to the National Institutes of Health to fund a larger trial that will include comparison with another active treatment.
The researchers had no financial conflicts to disclose.
Dietary Reference Intakes for Vitamin D Caution Against Excess
WASHINGTON – Daily doses of 600 international units of vitamin D and between 700 and 1,300 mg of calcium are enough for most children and adults in the United States and Canada, according to a report on new dietary reference intakes issued by the Institute of Medicine.
These new dietary reference intakes for calcium and vitamin D should provide "greater assurance that widespread vitamin D deficiency is not a public health problem," Dr. Steven Clinton, a member of the IOM committee that issued the report. Committee members spoke at a Nov. 30 press briefing.
After reviewing national databases on blood levels from the United States and Canada, the committee determined that most people in both countries are currently meeting their needs for vitamin D. Adequate vitamin D was defined as blood levels of at least 20 ng/mL as measured in the United States (50 nmol/L as measured in Canada).
Dr. Clinton, a medical oncologist at Ohio State University, Columbus, predicted that physicians will become more comfortable using recommended dietary allowances to advise patients about calcium and vitamin D intake and noted that vitamin D screening "probably should not be part of routine medical care."
Previous recommendations for vitamin D and calcium intake were defined in terms of adequate intake, which is not the same as recommended dietary allowance (RDA), noted committee member Patsy Brannon, Ph.D., a professor in the division of nutritional science at Cornell University, Ithaca, N.Y. Although the new values might not look much different, "You can't compare the two sets of numbers," she said. The evidence used to determine the new RDAs for calcium and vitamin D was much more comprehensive, especially data from studies conducted within the past 2 years, she explained.
While calcium and vitamin D are important for health, more is not necessarily better, the reviewers said.
They cautioned against excessive vitamin D supplementation beyond the RDA, but said supplements can be used in combination with diet to meet the RDAs. "The data are not sufficient to conclude that intakes higher than the recommended values would be beneficial," A. Catherine Ross, Ph.D., of Pennsylvania State University, University Park.
To reduce the risk of kidney stones, calcium supplements should be used with caution, Dr. Brannon advised.
The IOM reviewers examined approximately 1,000 published studies and scientific testimonies to determine the levels of calcium and vitamin D needed to maintain health.
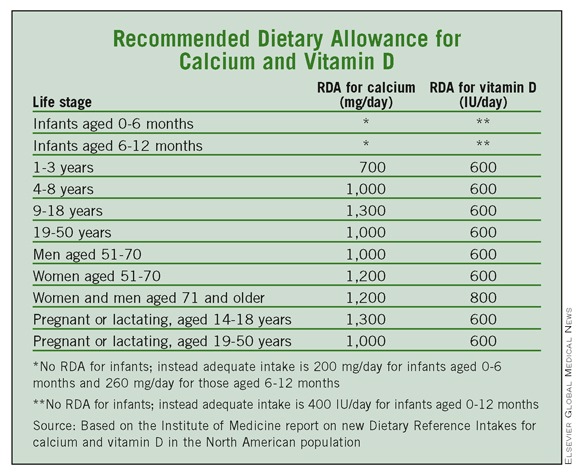
Based on their findings, 700 mg/day of calcium is enough for most children aged 1-3 years, and 1,000 mg is appropriate for most children aged 4-8 years. Older children and teens aged 9-18 years need no more than 1,300 mg/day, and most adults aged 19-50 years and men through 71 years need no more than 1,000 mg daily. For women aged 51 years and older and men aged 71 years and older, 1,200 mg of calcium per day is recommended, but more than that is unnecessary, according to the report.
As for vitamin D, the IOM report states that 600 IU/day meets the needs of almost all children and adults aged 1 year through 70 years, including pregnant and lactating women. For men and women aged 71 years and older, the RDA increases to 800 IU/day to accommodate age-related physical and behavioral changes.
The IOM review committee acknowledged the challenges of fitting sun exposure into the equation when estimating dietary reference intake values for vitamin D because of concerns about skin cancer risk. "At this time, the only solution is to proceed on the basis of the assumption of minimal sun exposure and set reference values assuming that all of the vitamin D comes from the diet," the reviewers wrote.
The report lists an upper level for daily vitamin D intake of 1,000 IU for infants up to 6 months of age and 1,500 IU for infants aged 6 months to 12 months. The upper levels for children aged 1-3 years and 4-8 years are 2,500 IU and 3,000 IU, respectively. For all other life stages, the upper level is 4,000 IU.
Upper levels for calcium for adults were based on data related to the formation of kidney stones, and the upper levels for children take adolescent growth spurts into account. The upper level for daily calcium intake for infants aged 0 to 6 months and 6-12 months are 1,000 mg and 1,500 mg, respectively. For children aged 1-8 years and 9-18 years, the upper levels are 2,500 mg and 3,000 mg, respectively, for both boys and girls. Adults aged 19-50 years have an upper level of 2,500 mg that drops to 2,000 mg after age 50 years for both men and women. The upper levels of calcium for pregnant and lactating women aged 14-18 years, 19-30 years, and 31-50 years are 3,000 mg, 2,500 mg, and 2,500 mg, respectively.
"What we have concluded may be surprising to some," Dr. Ross said. "I was surprised to find that vitamin D requirements don't vary much by age."
Dr. Ross noted that the report is not necessarily the last word on the subject, but "we are going to need to do a tremendous amount of research" before drawing any conclusions on additional benefits of vitamin D and calcium.
The study was sponsored by the federal governments of the United States and Canad
WASHINGTON – Daily doses of 600 international units of vitamin D and between 700 and 1,300 mg of calcium are enough for most children and adults in the United States and Canada, according to a report on new dietary reference intakes issued by the Institute of Medicine.
These new dietary reference intakes for calcium and vitamin D should provide "greater assurance that widespread vitamin D deficiency is not a public health problem," Dr. Steven Clinton, a member of the IOM committee that issued the report. Committee members spoke at a Nov. 30 press briefing.
After reviewing national databases on blood levels from the United States and Canada, the committee determined that most people in both countries are currently meeting their needs for vitamin D. Adequate vitamin D was defined as blood levels of at least 20 ng/mL as measured in the United States (50 nmol/L as measured in Canada).
Dr. Clinton, a medical oncologist at Ohio State University, Columbus, predicted that physicians will become more comfortable using recommended dietary allowances to advise patients about calcium and vitamin D intake and noted that vitamin D screening "probably should not be part of routine medical care."
Previous recommendations for vitamin D and calcium intake were defined in terms of adequate intake, which is not the same as recommended dietary allowance (RDA), noted committee member Patsy Brannon, Ph.D., a professor in the division of nutritional science at Cornell University, Ithaca, N.Y. Although the new values might not look much different, "You can't compare the two sets of numbers," she said. The evidence used to determine the new RDAs for calcium and vitamin D was much more comprehensive, especially data from studies conducted within the past 2 years, she explained.
While calcium and vitamin D are important for health, more is not necessarily better, the reviewers said.
They cautioned against excessive vitamin D supplementation beyond the RDA, but said supplements can be used in combination with diet to meet the RDAs. "The data are not sufficient to conclude that intakes higher than the recommended values would be beneficial," A. Catherine Ross, Ph.D., of Pennsylvania State University, University Park.
To reduce the risk of kidney stones, calcium supplements should be used with caution, Dr. Brannon advised.
The IOM reviewers examined approximately 1,000 published studies and scientific testimonies to determine the levels of calcium and vitamin D needed to maintain health.
Based on their findings, 700 mg/day of calcium is enough for most children aged 1-3 years, and 1,000 mg is appropriate for most children aged 4-8 years. Older children and teens aged 9-18 years need no more than 1,300 mg/day, and most adults aged 19-50 years and men through 71 years need no more than 1,000 mg daily. For women aged 51 years and older and men aged 71 years and older, 1,200 mg of calcium per day is recommended, but more than that is unnecessary, according to the report.
As for vitamin D, the IOM report states that 600 IU/day meets the needs of almost all children and adults aged 1 year through 70 years, including pregnant and lactating women. For men and women aged 71 years and older, the RDA increases to 800 IU/day to accommodate age-related physical and behavioral changes.
The IOM review committee acknowledged the challenges of fitting sun exposure into the equation when estimating dietary reference intake values for vitamin D because of concerns about skin cancer risk. "At this time, the only solution is to proceed on the basis of the assumption of minimal sun exposure and set reference values assuming that all of the vitamin D comes from the diet," the reviewers wrote.
The report lists an upper level for daily vitamin D intake of 1,000 IU for infants up to 6 months of age and 1,500 IU for infants aged 6 months to 12 months. The upper levels for children aged 1-3 years and 4-8 years are 2,500 IU and 3,000 IU, respectively. For all other life stages, the upper level is 4,000 IU.
Upper levels for calcium for adults were based on data related to the formation of kidney stones, and the upper levels for children take adolescent growth spurts into account. The upper level for daily calcium intake for infants aged 0 to 6 months and 6-12 months are 1,000 mg and 1,500 mg, respectively. For children aged 1-8 years and 9-18 years, the upper levels are 2,500 mg and 3,000 mg, respectively, for both boys and girls. Adults aged 19-50 years have an upper level of 2,500 mg that drops to 2,000 mg after age 50 years for both men and women. The upper levels of calcium for pregnant and lactating women aged 14-18 years, 19-30 years, and 31-50 years are 3,000 mg, 2,500 mg, and 2,500 mg, respectively.
"What we have concluded may be surprising to some," Dr. Ross said. "I was surprised to find that vitamin D requirements don't vary much by age."
Dr. Ross noted that the report is not necessarily the last word on the subject, but "we are going to need to do a tremendous amount of research" before drawing any conclusions on additional benefits of vitamin D and calcium.
The study was sponsored by the federal governments of the United States and Canad
WASHINGTON – Daily doses of 600 international units of vitamin D and between 700 and 1,300 mg of calcium are enough for most children and adults in the United States and Canada, according to a report on new dietary reference intakes issued by the Institute of Medicine.
These new dietary reference intakes for calcium and vitamin D should provide "greater assurance that widespread vitamin D deficiency is not a public health problem," Dr. Steven Clinton, a member of the IOM committee that issued the report. Committee members spoke at a Nov. 30 press briefing.
After reviewing national databases on blood levels from the United States and Canada, the committee determined that most people in both countries are currently meeting their needs for vitamin D. Adequate vitamin D was defined as blood levels of at least 20 ng/mL as measured in the United States (50 nmol/L as measured in Canada).
Dr. Clinton, a medical oncologist at Ohio State University, Columbus, predicted that physicians will become more comfortable using recommended dietary allowances to advise patients about calcium and vitamin D intake and noted that vitamin D screening "probably should not be part of routine medical care."
Previous recommendations for vitamin D and calcium intake were defined in terms of adequate intake, which is not the same as recommended dietary allowance (RDA), noted committee member Patsy Brannon, Ph.D., a professor in the division of nutritional science at Cornell University, Ithaca, N.Y. Although the new values might not look much different, "You can't compare the two sets of numbers," she said. The evidence used to determine the new RDAs for calcium and vitamin D was much more comprehensive, especially data from studies conducted within the past 2 years, she explained.
While calcium and vitamin D are important for health, more is not necessarily better, the reviewers said.
They cautioned against excessive vitamin D supplementation beyond the RDA, but said supplements can be used in combination with diet to meet the RDAs. "The data are not sufficient to conclude that intakes higher than the recommended values would be beneficial," A. Catherine Ross, Ph.D., of Pennsylvania State University, University Park.
To reduce the risk of kidney stones, calcium supplements should be used with caution, Dr. Brannon advised.
The IOM reviewers examined approximately 1,000 published studies and scientific testimonies to determine the levels of calcium and vitamin D needed to maintain health.
Based on their findings, 700 mg/day of calcium is enough for most children aged 1-3 years, and 1,000 mg is appropriate for most children aged 4-8 years. Older children and teens aged 9-18 years need no more than 1,300 mg/day, and most adults aged 19-50 years and men through 71 years need no more than 1,000 mg daily. For women aged 51 years and older and men aged 71 years and older, 1,200 mg of calcium per day is recommended, but more than that is unnecessary, according to the report.
As for vitamin D, the IOM report states that 600 IU/day meets the needs of almost all children and adults aged 1 year through 70 years, including pregnant and lactating women. For men and women aged 71 years and older, the RDA increases to 800 IU/day to accommodate age-related physical and behavioral changes.
The IOM review committee acknowledged the challenges of fitting sun exposure into the equation when estimating dietary reference intake values for vitamin D because of concerns about skin cancer risk. "At this time, the only solution is to proceed on the basis of the assumption of minimal sun exposure and set reference values assuming that all of the vitamin D comes from the diet," the reviewers wrote.
The report lists an upper level for daily vitamin D intake of 1,000 IU for infants up to 6 months of age and 1,500 IU for infants aged 6 months to 12 months. The upper levels for children aged 1-3 years and 4-8 years are 2,500 IU and 3,000 IU, respectively. For all other life stages, the upper level is 4,000 IU.
Upper levels for calcium for adults were based on data related to the formation of kidney stones, and the upper levels for children take adolescent growth spurts into account. The upper level for daily calcium intake for infants aged 0 to 6 months and 6-12 months are 1,000 mg and 1,500 mg, respectively. For children aged 1-8 years and 9-18 years, the upper levels are 2,500 mg and 3,000 mg, respectively, for both boys and girls. Adults aged 19-50 years have an upper level of 2,500 mg that drops to 2,000 mg after age 50 years for both men and women. The upper levels of calcium for pregnant and lactating women aged 14-18 years, 19-30 years, and 31-50 years are 3,000 mg, 2,500 mg, and 2,500 mg, respectively.
"What we have concluded may be surprising to some," Dr. Ross said. "I was surprised to find that vitamin D requirements don't vary much by age."
Dr. Ross noted that the report is not necessarily the last word on the subject, but "we are going to need to do a tremendous amount of research" before drawing any conclusions on additional benefits of vitamin D and calcium.
The study was sponsored by the federal governments of the United States and Canad
REPORT FROM THE IOM
TNF Inhibitors Protect Against Plaque Buildup in RA Patients
ATLANTA – Patients with rheumatoid arthritis showed significant arterial thickening over a 3-year period, but tumor necrosis factor inhibitor use slowed the progression, based on data from 158 patients. The findings were presented at the annual scientific meeting of the American College of Rheumatology.
"We know that many of our patients with autoimmune disease have higher risk for cardiovascular disease," said Dr. Joan M. Bathon, professor of medicine and director of the Johns Hopkins Arthritis Center at the Johns Hopkins University in Baltimore. But few studies have examined what drives the plaque buildup in these patients.
Dr. Bathon and her colleagues examined a subgroup of patients enrolled in a larger study of cardiovascular disease and RA. They used ultrasound to measure the thickness of the walls of the common carotid artery (CCA) and internal carotid artery (ICA) and compared data on each patient at two visits approximately 3 years apart. The average age of the patients was 60 years, 36% were male, and the average duration of RA at baseline was 8.5 years.
Thickening of the CCA occurred in 82% of the patients over 3 years, with a median yearly increase of 16 mcm. Thickening of the ICA occurred in 70% of the patients, with median yearly increase of 25 mcm.
However, patients who used a tumor necrosis factor inhibitor (TNFi) agents at baseline had a 37% lower rate of CCA thickening compared to those who did not use a TNFi agent (14 mcm/year vs. 22 mcm/year), after controlling for demographic variables, cardiovascular risk factors, and baseline arterial thickening.
"We found that progression in the common carotid was much more pronounced in patients with early disease than in later disease," said Dr. Bathon. "There seems to be a particular risk when the disease first starts."
Thickening of the ICA was independently associated with prednisone use, but progression was significantly lower in patients who were taking statins at baseline, Dr. Bathon said.
A total of 68 patients showed at least some plaque development, and 14% of patients developed new plaque during the study period. Patients who developed plaque over time had higher average swollen joint counts and higher average C-reactive protein levels than those who did not show atherosclerosis progression, Dr. Bathon noted.
"The data need to be confirmed in other studies," Dr. Bathon said, "but they suggest that prednisone promotes atherosclerosis in RA, even in the tiny doses that we use." But the findings also support the protective value of statins and TNFi agents against atherosclerosis in RA patients, she said.
The study was supported in part by the American College of Rheumatology Research and Education Foundation. Dr. Bathon said she had no financial conflicts to disclose.
ATLANTA – Patients with rheumatoid arthritis showed significant arterial thickening over a 3-year period, but tumor necrosis factor inhibitor use slowed the progression, based on data from 158 patients. The findings were presented at the annual scientific meeting of the American College of Rheumatology.
"We know that many of our patients with autoimmune disease have higher risk for cardiovascular disease," said Dr. Joan M. Bathon, professor of medicine and director of the Johns Hopkins Arthritis Center at the Johns Hopkins University in Baltimore. But few studies have examined what drives the plaque buildup in these patients.
Dr. Bathon and her colleagues examined a subgroup of patients enrolled in a larger study of cardiovascular disease and RA. They used ultrasound to measure the thickness of the walls of the common carotid artery (CCA) and internal carotid artery (ICA) and compared data on each patient at two visits approximately 3 years apart. The average age of the patients was 60 years, 36% were male, and the average duration of RA at baseline was 8.5 years.
Thickening of the CCA occurred in 82% of the patients over 3 years, with a median yearly increase of 16 mcm. Thickening of the ICA occurred in 70% of the patients, with median yearly increase of 25 mcm.
However, patients who used a tumor necrosis factor inhibitor (TNFi) agents at baseline had a 37% lower rate of CCA thickening compared to those who did not use a TNFi agent (14 mcm/year vs. 22 mcm/year), after controlling for demographic variables, cardiovascular risk factors, and baseline arterial thickening.
"We found that progression in the common carotid was much more pronounced in patients with early disease than in later disease," said Dr. Bathon. "There seems to be a particular risk when the disease first starts."
Thickening of the ICA was independently associated with prednisone use, but progression was significantly lower in patients who were taking statins at baseline, Dr. Bathon said.
A total of 68 patients showed at least some plaque development, and 14% of patients developed new plaque during the study period. Patients who developed plaque over time had higher average swollen joint counts and higher average C-reactive protein levels than those who did not show atherosclerosis progression, Dr. Bathon noted.
"The data need to be confirmed in other studies," Dr. Bathon said, "but they suggest that prednisone promotes atherosclerosis in RA, even in the tiny doses that we use." But the findings also support the protective value of statins and TNFi agents against atherosclerosis in RA patients, she said.
The study was supported in part by the American College of Rheumatology Research and Education Foundation. Dr. Bathon said she had no financial conflicts to disclose.
ATLANTA – Patients with rheumatoid arthritis showed significant arterial thickening over a 3-year period, but tumor necrosis factor inhibitor use slowed the progression, based on data from 158 patients. The findings were presented at the annual scientific meeting of the American College of Rheumatology.
"We know that many of our patients with autoimmune disease have higher risk for cardiovascular disease," said Dr. Joan M. Bathon, professor of medicine and director of the Johns Hopkins Arthritis Center at the Johns Hopkins University in Baltimore. But few studies have examined what drives the plaque buildup in these patients.
Dr. Bathon and her colleagues examined a subgroup of patients enrolled in a larger study of cardiovascular disease and RA. They used ultrasound to measure the thickness of the walls of the common carotid artery (CCA) and internal carotid artery (ICA) and compared data on each patient at two visits approximately 3 years apart. The average age of the patients was 60 years, 36% were male, and the average duration of RA at baseline was 8.5 years.
Thickening of the CCA occurred in 82% of the patients over 3 years, with a median yearly increase of 16 mcm. Thickening of the ICA occurred in 70% of the patients, with median yearly increase of 25 mcm.
However, patients who used a tumor necrosis factor inhibitor (TNFi) agents at baseline had a 37% lower rate of CCA thickening compared to those who did not use a TNFi agent (14 mcm/year vs. 22 mcm/year), after controlling for demographic variables, cardiovascular risk factors, and baseline arterial thickening.
"We found that progression in the common carotid was much more pronounced in patients with early disease than in later disease," said Dr. Bathon. "There seems to be a particular risk when the disease first starts."
Thickening of the ICA was independently associated with prednisone use, but progression was significantly lower in patients who were taking statins at baseline, Dr. Bathon said.
A total of 68 patients showed at least some plaque development, and 14% of patients developed new plaque during the study period. Patients who developed plaque over time had higher average swollen joint counts and higher average C-reactive protein levels than those who did not show atherosclerosis progression, Dr. Bathon noted.
"The data need to be confirmed in other studies," Dr. Bathon said, "but they suggest that prednisone promotes atherosclerosis in RA, even in the tiny doses that we use." But the findings also support the protective value of statins and TNFi agents against atherosclerosis in RA patients, she said.
The study was supported in part by the American College of Rheumatology Research and Education Foundation. Dr. Bathon said she had no financial conflicts to disclose.
FROM THE ANNUAL MEETING OF THE AMERICAN COLLEGE OF RHEUMATOLOGY
TNF Inhibitors Protect Against Plaque Buildup in RA Patients
ATLANTA – Patients with rheumatoid arthritis showed significant arterial thickening over a 3-year period, but tumor necrosis factor inhibitor use slowed the progression, based on data from 158 patients. The findings were presented at the annual scientific meeting of the American College of Rheumatology.
"We know that many of our patients with autoimmune disease have higher risk for cardiovascular disease," said Dr. Joan M. Bathon, professor of medicine and director of the Johns Hopkins Arthritis Center at the Johns Hopkins University in Baltimore. But few studies have examined what drives the plaque buildup in these patients.
Dr. Bathon and her colleagues examined a subgroup of patients enrolled in a larger study of cardiovascular disease and RA. They used ultrasound to measure the thickness of the walls of the common carotid artery (CCA) and internal carotid artery (ICA) and compared data on each patient at two visits approximately 3 years apart. The average age of the patients was 60 years, 36% were male, and the average duration of RA at baseline was 8.5 years.
Thickening of the CCA occurred in 82% of the patients over 3 years, with a median yearly increase of 16 mcm. Thickening of the ICA occurred in 70% of the patients, with median yearly increase of 25 mcm.
However, patients who used a tumor necrosis factor inhibitor (TNFi) agents at baseline had a 37% lower rate of CCA thickening compared to those who did not use a TNFi agent (14 mcm/year vs. 22 mcm/year), after controlling for demographic variables, cardiovascular risk factors, and baseline arterial thickening.
"We found that progression in the common carotid was much more pronounced in patients with early disease than in later disease," said Dr. Bathon. "There seems to be a particular risk when the disease first starts."
Thickening of the ICA was independently associated with prednisone use, but progression was significantly lower in patients who were taking statins at baseline, Dr. Bathon said.
A total of 68 patients showed at least some plaque development, and 14% of patients developed new plaque during the study period. Patients who developed plaque over time had higher average swollen joint counts and higher average C-reactive protein levels than those who did not show atherosclerosis progression, Dr. Bathon noted.
"The data need to be confirmed in other studies," Dr. Bathon said, "but they suggest that prednisone promotes atherosclerosis in RA, even in the tiny doses that we use." But the findings also support the protective value of statins and TNFi agents against atherosclerosis in RA patients, she said.
The study was supported in part by the American College of Rheumatology Research and Education Foundation. Dr. Bathon said she had no financial conflicts to disclose.
ATLANTA – Patients with rheumatoid arthritis showed significant arterial thickening over a 3-year period, but tumor necrosis factor inhibitor use slowed the progression, based on data from 158 patients. The findings were presented at the annual scientific meeting of the American College of Rheumatology.
"We know that many of our patients with autoimmune disease have higher risk for cardiovascular disease," said Dr. Joan M. Bathon, professor of medicine and director of the Johns Hopkins Arthritis Center at the Johns Hopkins University in Baltimore. But few studies have examined what drives the plaque buildup in these patients.
Dr. Bathon and her colleagues examined a subgroup of patients enrolled in a larger study of cardiovascular disease and RA. They used ultrasound to measure the thickness of the walls of the common carotid artery (CCA) and internal carotid artery (ICA) and compared data on each patient at two visits approximately 3 years apart. The average age of the patients was 60 years, 36% were male, and the average duration of RA at baseline was 8.5 years.
Thickening of the CCA occurred in 82% of the patients over 3 years, with a median yearly increase of 16 mcm. Thickening of the ICA occurred in 70% of the patients, with median yearly increase of 25 mcm.
However, patients who used a tumor necrosis factor inhibitor (TNFi) agents at baseline had a 37% lower rate of CCA thickening compared to those who did not use a TNFi agent (14 mcm/year vs. 22 mcm/year), after controlling for demographic variables, cardiovascular risk factors, and baseline arterial thickening.
"We found that progression in the common carotid was much more pronounced in patients with early disease than in later disease," said Dr. Bathon. "There seems to be a particular risk when the disease first starts."
Thickening of the ICA was independently associated with prednisone use, but progression was significantly lower in patients who were taking statins at baseline, Dr. Bathon said.
A total of 68 patients showed at least some plaque development, and 14% of patients developed new plaque during the study period. Patients who developed plaque over time had higher average swollen joint counts and higher average C-reactive protein levels than those who did not show atherosclerosis progression, Dr. Bathon noted.
"The data need to be confirmed in other studies," Dr. Bathon said, "but they suggest that prednisone promotes atherosclerosis in RA, even in the tiny doses that we use." But the findings also support the protective value of statins and TNFi agents against atherosclerosis in RA patients, she said.
The study was supported in part by the American College of Rheumatology Research and Education Foundation. Dr. Bathon said she had no financial conflicts to disclose.
ATLANTA – Patients with rheumatoid arthritis showed significant arterial thickening over a 3-year period, but tumor necrosis factor inhibitor use slowed the progression, based on data from 158 patients. The findings were presented at the annual scientific meeting of the American College of Rheumatology.
"We know that many of our patients with autoimmune disease have higher risk for cardiovascular disease," said Dr. Joan M. Bathon, professor of medicine and director of the Johns Hopkins Arthritis Center at the Johns Hopkins University in Baltimore. But few studies have examined what drives the plaque buildup in these patients.
Dr. Bathon and her colleagues examined a subgroup of patients enrolled in a larger study of cardiovascular disease and RA. They used ultrasound to measure the thickness of the walls of the common carotid artery (CCA) and internal carotid artery (ICA) and compared data on each patient at two visits approximately 3 years apart. The average age of the patients was 60 years, 36% were male, and the average duration of RA at baseline was 8.5 years.
Thickening of the CCA occurred in 82% of the patients over 3 years, with a median yearly increase of 16 mcm. Thickening of the ICA occurred in 70% of the patients, with median yearly increase of 25 mcm.
However, patients who used a tumor necrosis factor inhibitor (TNFi) agents at baseline had a 37% lower rate of CCA thickening compared to those who did not use a TNFi agent (14 mcm/year vs. 22 mcm/year), after controlling for demographic variables, cardiovascular risk factors, and baseline arterial thickening.
"We found that progression in the common carotid was much more pronounced in patients with early disease than in later disease," said Dr. Bathon. "There seems to be a particular risk when the disease first starts."
Thickening of the ICA was independently associated with prednisone use, but progression was significantly lower in patients who were taking statins at baseline, Dr. Bathon said.
A total of 68 patients showed at least some plaque development, and 14% of patients developed new plaque during the study period. Patients who developed plaque over time had higher average swollen joint counts and higher average C-reactive protein levels than those who did not show atherosclerosis progression, Dr. Bathon noted.
"The data need to be confirmed in other studies," Dr. Bathon said, "but they suggest that prednisone promotes atherosclerosis in RA, even in the tiny doses that we use." But the findings also support the protective value of statins and TNFi agents against atherosclerosis in RA patients, she said.
The study was supported in part by the American College of Rheumatology Research and Education Foundation. Dr. Bathon said she had no financial conflicts to disclose.
FROM THE ANNUAL MEETING OF THE AMERICAN COLLEGE OF RHEUMATOLOGY
Major Finding: Limiting inflammation with TNFi agents reduced the progression of carotid artery atherosclerosis by 37% in rheumatoid arthritis patients.
Data Source: A prospective study of 158 adults with rheumatoid arthritis
Disclosures: The study was supported in part by the American College of Rheumatology Research and Education Foundation. Dr. Bathon said she had no financial conflicts to disclose.
Foot Deformities Are Highly Heritable
ATLANTA – Got bunions? Thank your parents. Bunions were inherited in 89% of adults younger than 60 years, according to genetic data from more than 2,000 adults that were presented at the annual scientific meeting of the American College of Rheumatology.
Bunions and other foot disorders can limit mobility and exacerbate other musculoskeletal weaknesses, but interventions are available, and they are most effective if foot deformities are identified early, said Marian Hannan, D.Sc., of Harvard Medical School, Boston.
Foot disorders occur in 20%-60% of adults, and researchers have long suspected genetic involvement, but this study is the first to examine specific associations between genes and foot deformities, Dr. Hannan said.
Dr. Hannan and her colleagues reviewed data from 959 men and 1,220 women in the Framingham Foot Study of 2002-2005. A trained examiner evaluated the study participants for any of 20 different foot disorders. In this study, Dr. Hannan reported data about the most common and least common of the disorders: hallux valgus (bunions) and pes cavus (high arches).
Overall, 675 individuals (31%) had bunions and 154 (7%) had high arches. A bunion was defined as a big toe angled at least 15 degrees toward the first metatarsal. High arches were identified by calculating weight-bearing arch width.
The researchers used statistical genetics software to determine the heritability of the two conditions. Across all ages, 39% of women and 38% of men inherited their bunions, and 68% of women and 20% of men inherited their high arches. Among individuals younger than 60 years, 99% of women and 63% of men inherited their high arches. The heritability estimates were statistically significant for both conditions.
The average age of the study participants was 66 years, and 57% were women.
"Known interventions can slow the progression of disease" for patients with foot problems, Dr. Hannan emphasized. "We are continuing with research within the Framingham Foot Study to look at the other 18 foot conditions," she added. "We are also looking at specific genetic analyses to see what specific gene might be behind what is going on."
Dr. Hannan had no financial conflicts to disclose.
ATLANTA – Got bunions? Thank your parents. Bunions were inherited in 89% of adults younger than 60 years, according to genetic data from more than 2,000 adults that were presented at the annual scientific meeting of the American College of Rheumatology.
Bunions and other foot disorders can limit mobility and exacerbate other musculoskeletal weaknesses, but interventions are available, and they are most effective if foot deformities are identified early, said Marian Hannan, D.Sc., of Harvard Medical School, Boston.
Foot disorders occur in 20%-60% of adults, and researchers have long suspected genetic involvement, but this study is the first to examine specific associations between genes and foot deformities, Dr. Hannan said.
Dr. Hannan and her colleagues reviewed data from 959 men and 1,220 women in the Framingham Foot Study of 2002-2005. A trained examiner evaluated the study participants for any of 20 different foot disorders. In this study, Dr. Hannan reported data about the most common and least common of the disorders: hallux valgus (bunions) and pes cavus (high arches).
Overall, 675 individuals (31%) had bunions and 154 (7%) had high arches. A bunion was defined as a big toe angled at least 15 degrees toward the first metatarsal. High arches were identified by calculating weight-bearing arch width.
The researchers used statistical genetics software to determine the heritability of the two conditions. Across all ages, 39% of women and 38% of men inherited their bunions, and 68% of women and 20% of men inherited their high arches. Among individuals younger than 60 years, 99% of women and 63% of men inherited their high arches. The heritability estimates were statistically significant for both conditions.
The average age of the study participants was 66 years, and 57% were women.
"Known interventions can slow the progression of disease" for patients with foot problems, Dr. Hannan emphasized. "We are continuing with research within the Framingham Foot Study to look at the other 18 foot conditions," she added. "We are also looking at specific genetic analyses to see what specific gene might be behind what is going on."
Dr. Hannan had no financial conflicts to disclose.
ATLANTA – Got bunions? Thank your parents. Bunions were inherited in 89% of adults younger than 60 years, according to genetic data from more than 2,000 adults that were presented at the annual scientific meeting of the American College of Rheumatology.
Bunions and other foot disorders can limit mobility and exacerbate other musculoskeletal weaknesses, but interventions are available, and they are most effective if foot deformities are identified early, said Marian Hannan, D.Sc., of Harvard Medical School, Boston.
Foot disorders occur in 20%-60% of adults, and researchers have long suspected genetic involvement, but this study is the first to examine specific associations between genes and foot deformities, Dr. Hannan said.
Dr. Hannan and her colleagues reviewed data from 959 men and 1,220 women in the Framingham Foot Study of 2002-2005. A trained examiner evaluated the study participants for any of 20 different foot disorders. In this study, Dr. Hannan reported data about the most common and least common of the disorders: hallux valgus (bunions) and pes cavus (high arches).
Overall, 675 individuals (31%) had bunions and 154 (7%) had high arches. A bunion was defined as a big toe angled at least 15 degrees toward the first metatarsal. High arches were identified by calculating weight-bearing arch width.
The researchers used statistical genetics software to determine the heritability of the two conditions. Across all ages, 39% of women and 38% of men inherited their bunions, and 68% of women and 20% of men inherited their high arches. Among individuals younger than 60 years, 99% of women and 63% of men inherited their high arches. The heritability estimates were statistically significant for both conditions.
The average age of the study participants was 66 years, and 57% were women.
"Known interventions can slow the progression of disease" for patients with foot problems, Dr. Hannan emphasized. "We are continuing with research within the Framingham Foot Study to look at the other 18 foot conditions," she added. "We are also looking at specific genetic analyses to see what specific gene might be behind what is going on."
Dr. Hannan had no financial conflicts to disclose.
Major Finding: Of adults younger than age 60 years who have bunions, 89% inherited the condition.
Data Source: A genetic analysis and foot examination of 2,179 adults.
Disclosures: Dr. Hannan had no financial conflicts to disclose.
FDA Committee Considers Gardasil for Anal Cancer Prevention
SILVER SPRING, Md. – The human papillomavirus vaccine Gardasil moved closer to an indication for anal cancer prevention after a meeting of the Food and Drug Administration’s Vaccines and Related Biological Products Advisory Committee on Nov. 17.
The vaccine, manufactured by Merck & Co. Inc., is approved for the prevention of cervical, vulvar, and vaginal cancers and precancerous lesions in females aged 9-26 years, and for the prevention of genital warts in males and females aged 9-26 years. The company is seeking an indication for the prevention of anal cancer in males and females aged 9-26 years.
Previous studies have shown that anal cancer and cervical cancer are biologically similar, and both are associated with HPV infections, Dr. Joel Palefsky, professor of medicine at the University of California, San Francisco, said at the meeting.
The primary data supporting an anal cancer indication for Gardasil came from a randomized, controlled trial of 602 men who have sex with men (MSM), who were part of the larger study that led to the indication for preventing genital warts in boys and men. The participants received three doses of vaccine or a placebo.
The vaccine showed 78% effectiveness, compared with placebo in preventing anal intraepithelial neoplasms related to human papillomavirus types 6, 11, 16, and 18. These lesions are considered precursors to anal cancer, Dr. Palefsky said.
Although MSM are at increased risk for HPV-associated anal cancer, they are not the only population at risk. Data from the National Cancer Institute presented at the meeting showed that anal cancer incidence in the United States is increasing by a rate of approximately 2% per year, and that approximately 60% of cases and deaths occur in women.
A majority of the committee members expressed opinions in favor of the indication, but no formal vote was taken. The FDA will consider the committee’s recommendations. If the indication is approved before the February 2011 meeting of the Centers for Disease Control and Prevention’s Advisory Committee on Immunization Practices, the ACIP might revisit its previous recommendation against routine HPV vaccination for boys and men for genital wart prevention. ACIP has given a permissive recommendation for HPV vaccination for boys and men aged 9-26 years at the discretion of the physician.
Dr. Palefsky has served as a consultant and clinical investigator for Merck & Co. Inc.
SILVER SPRING, Md. – The human papillomavirus vaccine Gardasil moved closer to an indication for anal cancer prevention after a meeting of the Food and Drug Administration’s Vaccines and Related Biological Products Advisory Committee on Nov. 17.
The vaccine, manufactured by Merck & Co. Inc., is approved for the prevention of cervical, vulvar, and vaginal cancers and precancerous lesions in females aged 9-26 years, and for the prevention of genital warts in males and females aged 9-26 years. The company is seeking an indication for the prevention of anal cancer in males and females aged 9-26 years.
Previous studies have shown that anal cancer and cervical cancer are biologically similar, and both are associated with HPV infections, Dr. Joel Palefsky, professor of medicine at the University of California, San Francisco, said at the meeting.
The primary data supporting an anal cancer indication for Gardasil came from a randomized, controlled trial of 602 men who have sex with men (MSM), who were part of the larger study that led to the indication for preventing genital warts in boys and men. The participants received three doses of vaccine or a placebo.
The vaccine showed 78% effectiveness, compared with placebo in preventing anal intraepithelial neoplasms related to human papillomavirus types 6, 11, 16, and 18. These lesions are considered precursors to anal cancer, Dr. Palefsky said.
Although MSM are at increased risk for HPV-associated anal cancer, they are not the only population at risk. Data from the National Cancer Institute presented at the meeting showed that anal cancer incidence in the United States is increasing by a rate of approximately 2% per year, and that approximately 60% of cases and deaths occur in women.
A majority of the committee members expressed opinions in favor of the indication, but no formal vote was taken. The FDA will consider the committee’s recommendations. If the indication is approved before the February 2011 meeting of the Centers for Disease Control and Prevention’s Advisory Committee on Immunization Practices, the ACIP might revisit its previous recommendation against routine HPV vaccination for boys and men for genital wart prevention. ACIP has given a permissive recommendation for HPV vaccination for boys and men aged 9-26 years at the discretion of the physician.
Dr. Palefsky has served as a consultant and clinical investigator for Merck & Co. Inc.
SILVER SPRING, Md. – The human papillomavirus vaccine Gardasil moved closer to an indication for anal cancer prevention after a meeting of the Food and Drug Administration’s Vaccines and Related Biological Products Advisory Committee on Nov. 17.
The vaccine, manufactured by Merck & Co. Inc., is approved for the prevention of cervical, vulvar, and vaginal cancers and precancerous lesions in females aged 9-26 years, and for the prevention of genital warts in males and females aged 9-26 years. The company is seeking an indication for the prevention of anal cancer in males and females aged 9-26 years.
Previous studies have shown that anal cancer and cervical cancer are biologically similar, and both are associated with HPV infections, Dr. Joel Palefsky, professor of medicine at the University of California, San Francisco, said at the meeting.
The primary data supporting an anal cancer indication for Gardasil came from a randomized, controlled trial of 602 men who have sex with men (MSM), who were part of the larger study that led to the indication for preventing genital warts in boys and men. The participants received three doses of vaccine or a placebo.
The vaccine showed 78% effectiveness, compared with placebo in preventing anal intraepithelial neoplasms related to human papillomavirus types 6, 11, 16, and 18. These lesions are considered precursors to anal cancer, Dr. Palefsky said.
Although MSM are at increased risk for HPV-associated anal cancer, they are not the only population at risk. Data from the National Cancer Institute presented at the meeting showed that anal cancer incidence in the United States is increasing by a rate of approximately 2% per year, and that approximately 60% of cases and deaths occur in women.
A majority of the committee members expressed opinions in favor of the indication, but no formal vote was taken. The FDA will consider the committee’s recommendations. If the indication is approved before the February 2011 meeting of the Centers for Disease Control and Prevention’s Advisory Committee on Immunization Practices, the ACIP might revisit its previous recommendation against routine HPV vaccination for boys and men for genital wart prevention. ACIP has given a permissive recommendation for HPV vaccination for boys and men aged 9-26 years at the discretion of the physician.
Dr. Palefsky has served as a consultant and clinical investigator for Merck & Co. Inc.
FROM A MEETING OF THE FOOD AND DRUG ADMINISTRATION’S VACCINE AND RELATED BIOLOGICAL PRODUCTS ADVISORY COMMITTEE
FDA Committee Considers Gardasil for Anal Cancer Prevention
SILVER SPRING, Md. – The human papillomavirus vaccine Gardasil moved closer to an indication for anal cancer prevention after a meeting of the Food and Drug Administration’s Vaccines and Related Biological Products Advisory Committee on Nov. 17.
The vaccine, manufactured by Merck & Co. Inc., is approved for the prevention of cervical, vulvar, and vaginal cancers and precancerous lesions in females aged 9-26 years, and for the prevention of genital warts in males and females aged 9-26 years. The company is seeking an indication for the prevention of anal cancer in males and females aged 9-26 years.
Previous studies have shown that anal cancer and cervical cancer are biologically similar, and both are associated with HPV infections, Dr. Joel Palefsky, professor of medicine at the University of California, San Francisco, said at the meeting.
The primary data supporting an anal cancer indication for Gardasil came from a randomized, controlled trial of 602 men who have sex with men (MSM), who were part of the larger study that led to the indication for preventing genital warts in boys and men. The participants received three doses of vaccine or a placebo.
The vaccine showed 78% effectiveness, compared with placebo in preventing anal intraepithelial neoplasms related to human papillomavirus types 6, 11, 16, and 18. These lesions are considered precursors to anal cancer, Dr. Palefsky said.
Although MSM are at increased risk for HPV-associated anal cancer, they are not the only population at risk. Data from the National Cancer Institute presented at the meeting showed that anal cancer incidence in the United States is increasing by a rate of approximately 2% per year, and that approximately 60% of cases and deaths occur in women.
A majority of the committee members expressed opinions in favor of the indication, but no formal vote was taken. The FDA will consider the committee’s recommendations. If the indication is approved before the February 2011 meeting of the Centers for Disease Control and Prevention’s Advisory Committee on Immunization Practices, the ACIP might revisit its previous recommendation against routine HPV vaccination for boys and men for genital wart prevention. ACIP has given a permissive recommendation for HPV vaccination for boys and men aged 9-26 years at the discretion of the physician.
Dr. Palefsky has served as a consultant and clinical investigator for Merck & Co. Inc.
SILVER SPRING, Md. – The human papillomavirus vaccine Gardasil moved closer to an indication for anal cancer prevention after a meeting of the Food and Drug Administration’s Vaccines and Related Biological Products Advisory Committee on Nov. 17.
The vaccine, manufactured by Merck & Co. Inc., is approved for the prevention of cervical, vulvar, and vaginal cancers and precancerous lesions in females aged 9-26 years, and for the prevention of genital warts in males and females aged 9-26 years. The company is seeking an indication for the prevention of anal cancer in males and females aged 9-26 years.
Previous studies have shown that anal cancer and cervical cancer are biologically similar, and both are associated with HPV infections, Dr. Joel Palefsky, professor of medicine at the University of California, San Francisco, said at the meeting.
The primary data supporting an anal cancer indication for Gardasil came from a randomized, controlled trial of 602 men who have sex with men (MSM), who were part of the larger study that led to the indication for preventing genital warts in boys and men. The participants received three doses of vaccine or a placebo.
The vaccine showed 78% effectiveness, compared with placebo in preventing anal intraepithelial neoplasms related to human papillomavirus types 6, 11, 16, and 18. These lesions are considered precursors to anal cancer, Dr. Palefsky said.
Although MSM are at increased risk for HPV-associated anal cancer, they are not the only population at risk. Data from the National Cancer Institute presented at the meeting showed that anal cancer incidence in the United States is increasing by a rate of approximately 2% per year, and that approximately 60% of cases and deaths occur in women.
A majority of the committee members expressed opinions in favor of the indication, but no formal vote was taken. The FDA will consider the committee’s recommendations. If the indication is approved before the February 2011 meeting of the Centers for Disease Control and Prevention’s Advisory Committee on Immunization Practices, the ACIP might revisit its previous recommendation against routine HPV vaccination for boys and men for genital wart prevention. ACIP has given a permissive recommendation for HPV vaccination for boys and men aged 9-26 years at the discretion of the physician.
Dr. Palefsky has served as a consultant and clinical investigator for Merck & Co. Inc.
SILVER SPRING, Md. – The human papillomavirus vaccine Gardasil moved closer to an indication for anal cancer prevention after a meeting of the Food and Drug Administration’s Vaccines and Related Biological Products Advisory Committee on Nov. 17.
The vaccine, manufactured by Merck & Co. Inc., is approved for the prevention of cervical, vulvar, and vaginal cancers and precancerous lesions in females aged 9-26 years, and for the prevention of genital warts in males and females aged 9-26 years. The company is seeking an indication for the prevention of anal cancer in males and females aged 9-26 years.
Previous studies have shown that anal cancer and cervical cancer are biologically similar, and both are associated with HPV infections, Dr. Joel Palefsky, professor of medicine at the University of California, San Francisco, said at the meeting.
The primary data supporting an anal cancer indication for Gardasil came from a randomized, controlled trial of 602 men who have sex with men (MSM), who were part of the larger study that led to the indication for preventing genital warts in boys and men. The participants received three doses of vaccine or a placebo.
The vaccine showed 78% effectiveness, compared with placebo in preventing anal intraepithelial neoplasms related to human papillomavirus types 6, 11, 16, and 18. These lesions are considered precursors to anal cancer, Dr. Palefsky said.
Although MSM are at increased risk for HPV-associated anal cancer, they are not the only population at risk. Data from the National Cancer Institute presented at the meeting showed that anal cancer incidence in the United States is increasing by a rate of approximately 2% per year, and that approximately 60% of cases and deaths occur in women.
A majority of the committee members expressed opinions in favor of the indication, but no formal vote was taken. The FDA will consider the committee’s recommendations. If the indication is approved before the February 2011 meeting of the Centers for Disease Control and Prevention’s Advisory Committee on Immunization Practices, the ACIP might revisit its previous recommendation against routine HPV vaccination for boys and men for genital wart prevention. ACIP has given a permissive recommendation for HPV vaccination for boys and men aged 9-26 years at the discretion of the physician.
Dr. Palefsky has served as a consultant and clinical investigator for Merck & Co. Inc.
FROM A MEETING OF THE FOOD AND DRUG ADMINISTRATION’S VACCINE AND RELATED BIOLOGICAL PRODUCTS ADVISORY COMMITTEE
FDA Committee Considers Gardasil for Anal Cancer Prevention
SILVER SPRING, Md. - The human papillomavirus vaccine Gardasil moved closer to an indication for anal cancer prevention after a meeting of the Food and Drug Administration’s Vaccines and Related Biological Products Advisory Committee on Nov. 17.
The vaccine, manufactured by Merck & Co. Inc., is approved for the prevention of cervical, vulvar, and vaginal cancers and precancerous lesions in females aged 9-26 years, and for the prevention of genital warts in males and females aged 9-26 years. The company is seeking an indication for the prevention of anal cancer in males and females aged 9-26 years.
Previous studies have shown that anal cancer and cervical cancer are biologically similar, and both are associated with HPV infections, Dr. Joel Palefsky, professor of medicine at the University of California, San Francisco, said at the meeting.
The primary data supporting an anal cancer indication for Gardasil came from a randomized, controlled trial of 602 men who have sex with men (MSM), who were part of the larger study that led to the indication for preventing genital warts in boys and men. The participants received three doses of vaccine or a placebo.
The vaccine showed 78% effectiveness, compared with placebo in preventing anal intraepithelial neoplasms related to human papillomavirus types 6, 11, 16, and 18. These lesions are considered precursors to anal cancer, Dr. Palefsky said.
Although MSM are at increased risk for HPV-associated anal cancer, they are not the only population at risk. Data from the National Cancer Institute presented at the meeting showed that anal cancer incidence in the United States is increasing by a rate of approximately 2% per year, and that approximately 60% of cases and deaths occur in women.
A majority of the committee members expressed opinions in favor of the indication, but no formal vote was taken. The FDA will consider the committee’s recommendations. If the indication is approved before the February 2011 meeting of the Centers for Disease Control and Prevention’s Advisory Committee on Immunization Practices, the ACIP might revisit its previous recommendation against routine HPV vaccination for boys and men for genital wart prevention. ACIP has given a permissive recommendation for HPV vaccination for boys and men aged 9-26 years at the discretion of the physician.
Dr. Palefsky has served as a consultant and clinical investigator for Merck & Co. Inc.
Body text goes here
Doctor’s Bio
Body text goes here
Doctor’s Bio
Body text goes here
Doctor’s Bio
SILVER SPRING, Md. - The human papillomavirus vaccine Gardasil moved closer to an indication for anal cancer prevention after a meeting of the Food and Drug Administration’s Vaccines and Related Biological Products Advisory Committee on Nov. 17.
The vaccine, manufactured by Merck & Co. Inc., is approved for the prevention of cervical, vulvar, and vaginal cancers and precancerous lesions in females aged 9-26 years, and for the prevention of genital warts in males and females aged 9-26 years. The company is seeking an indication for the prevention of anal cancer in males and females aged 9-26 years.
Previous studies have shown that anal cancer and cervical cancer are biologically similar, and both are associated with HPV infections, Dr. Joel Palefsky, professor of medicine at the University of California, San Francisco, said at the meeting.
The primary data supporting an anal cancer indication for Gardasil came from a randomized, controlled trial of 602 men who have sex with men (MSM), who were part of the larger study that led to the indication for preventing genital warts in boys and men. The participants received three doses of vaccine or a placebo.
The vaccine showed 78% effectiveness, compared with placebo in preventing anal intraepithelial neoplasms related to human papillomavirus types 6, 11, 16, and 18. These lesions are considered precursors to anal cancer, Dr. Palefsky said.
Although MSM are at increased risk for HPV-associated anal cancer, they are not the only population at risk. Data from the National Cancer Institute presented at the meeting showed that anal cancer incidence in the United States is increasing by a rate of approximately 2% per year, and that approximately 60% of cases and deaths occur in women.
A majority of the committee members expressed opinions in favor of the indication, but no formal vote was taken. The FDA will consider the committee’s recommendations. If the indication is approved before the February 2011 meeting of the Centers for Disease Control and Prevention’s Advisory Committee on Immunization Practices, the ACIP might revisit its previous recommendation against routine HPV vaccination for boys and men for genital wart prevention. ACIP has given a permissive recommendation for HPV vaccination for boys and men aged 9-26 years at the discretion of the physician.
Dr. Palefsky has served as a consultant and clinical investigator for Merck & Co. Inc.
SILVER SPRING, Md. - The human papillomavirus vaccine Gardasil moved closer to an indication for anal cancer prevention after a meeting of the Food and Drug Administration’s Vaccines and Related Biological Products Advisory Committee on Nov. 17.
The vaccine, manufactured by Merck & Co. Inc., is approved for the prevention of cervical, vulvar, and vaginal cancers and precancerous lesions in females aged 9-26 years, and for the prevention of genital warts in males and females aged 9-26 years. The company is seeking an indication for the prevention of anal cancer in males and females aged 9-26 years.
Previous studies have shown that anal cancer and cervical cancer are biologically similar, and both are associated with HPV infections, Dr. Joel Palefsky, professor of medicine at the University of California, San Francisco, said at the meeting.
The primary data supporting an anal cancer indication for Gardasil came from a randomized, controlled trial of 602 men who have sex with men (MSM), who were part of the larger study that led to the indication for preventing genital warts in boys and men. The participants received three doses of vaccine or a placebo.
The vaccine showed 78% effectiveness, compared with placebo in preventing anal intraepithelial neoplasms related to human papillomavirus types 6, 11, 16, and 18. These lesions are considered precursors to anal cancer, Dr. Palefsky said.
Although MSM are at increased risk for HPV-associated anal cancer, they are not the only population at risk. Data from the National Cancer Institute presented at the meeting showed that anal cancer incidence in the United States is increasing by a rate of approximately 2% per year, and that approximately 60% of cases and deaths occur in women.
A majority of the committee members expressed opinions in favor of the indication, but no formal vote was taken. The FDA will consider the committee’s recommendations. If the indication is approved before the February 2011 meeting of the Centers for Disease Control and Prevention’s Advisory Committee on Immunization Practices, the ACIP might revisit its previous recommendation against routine HPV vaccination for boys and men for genital wart prevention. ACIP has given a permissive recommendation for HPV vaccination for boys and men aged 9-26 years at the discretion of the physician.
Dr. Palefsky has served as a consultant and clinical investigator for Merck & Co. Inc.
FROM A MEETING OF THE FOOD AND DRUG ADMINISTRATION’S VACCINE AND RELATED BIOLOGICAL PRODUCTS ADVISORY COMMITTEE