User login
Healthcare professionals work while sick despite risk to patients

Photo by Logan Tuttle
Results of a small survey showed that many healthcare professionals reported to work while sick, despite recognizing that this could put their patients at risk.
About 95% of survey respondents acknowledged that working while sick puts patients at risk, but 83% of respondents said they had worked while sick at least once in the past year.
About 9% of respondents reported working while sick at least 5 times.
Julia E. Szymczak, PhD, of the Children’s Hospital of Philadelphia in Pennsylvania, and her colleagues reported these results in JAMA Pediatrics alongside a related editorial.
The researchers administered an anonymous survey to attending physicians and advanced practice clinicians (APCs) at the Children’s Hospital of Philadelphia. APCs included certified registered nurse practitioners, physician assistants, clinical nurse specialists, certified registered nurse anesthetists, and certified nurse midwives.
Overall, 280 attending physicians (61%) and 256 APCs (54.5%) responded. Most respondents (504, 95.3%) said working while sick put patients at risk.
However, 446 respondents (83.1%) reported working while sick at least once in the past year, and 50 respondents (9.3%) reported working while sick at least 5 times.
Respondents reported working with symptoms that included diarrhea, fever, and the onset of significant respiratory symptoms.
The reasons physicians and APCs worked while sick included not wanting to let colleagues down (98.7%), staffing concerns (94.9%), not wanting to let patients down (92.5%), fear of being ostracized by colleagues (64%), and concerns about the continuity of care (63.8%).
An analysis of written comments about why respondents work while sick highlighted 3 areas: challenges in identifying and arranging someone to cover their work and a lack of resources to accommodate sick leave, a strong cultural norm in the hospital to report for work unless one is extremely ill, and ambiguity about what symptoms constitute being too sick to work.
Dr Szymczak and her colleagues said this study suggests complex social and logistical factors cause healthcare workers to report to work sick. But these results could inform efforts to help workers make the right choice to keep their patients and colleagues safe while caring for themselves. ![]()
Photo by Logan Tuttle
Results of a small survey showed that many healthcare professionals reported to work while sick, despite recognizing that this could put their patients at risk.
About 95% of survey respondents acknowledged that working while sick puts patients at risk, but 83% of respondents said they had worked while sick at least once in the past year.
About 9% of respondents reported working while sick at least 5 times.
Julia E. Szymczak, PhD, of the Children’s Hospital of Philadelphia in Pennsylvania, and her colleagues reported these results in JAMA Pediatrics alongside a related editorial.
The researchers administered an anonymous survey to attending physicians and advanced practice clinicians (APCs) at the Children’s Hospital of Philadelphia. APCs included certified registered nurse practitioners, physician assistants, clinical nurse specialists, certified registered nurse anesthetists, and certified nurse midwives.
Overall, 280 attending physicians (61%) and 256 APCs (54.5%) responded. Most respondents (504, 95.3%) said working while sick put patients at risk.
However, 446 respondents (83.1%) reported working while sick at least once in the past year, and 50 respondents (9.3%) reported working while sick at least 5 times.
Respondents reported working with symptoms that included diarrhea, fever, and the onset of significant respiratory symptoms.
The reasons physicians and APCs worked while sick included not wanting to let colleagues down (98.7%), staffing concerns (94.9%), not wanting to let patients down (92.5%), fear of being ostracized by colleagues (64%), and concerns about the continuity of care (63.8%).
An analysis of written comments about why respondents work while sick highlighted 3 areas: challenges in identifying and arranging someone to cover their work and a lack of resources to accommodate sick leave, a strong cultural norm in the hospital to report for work unless one is extremely ill, and ambiguity about what symptoms constitute being too sick to work.
Dr Szymczak and her colleagues said this study suggests complex social and logistical factors cause healthcare workers to report to work sick. But these results could inform efforts to help workers make the right choice to keep their patients and colleagues safe while caring for themselves. ![]()
Photo by Logan Tuttle
Results of a small survey showed that many healthcare professionals reported to work while sick, despite recognizing that this could put their patients at risk.
About 95% of survey respondents acknowledged that working while sick puts patients at risk, but 83% of respondents said they had worked while sick at least once in the past year.
About 9% of respondents reported working while sick at least 5 times.
Julia E. Szymczak, PhD, of the Children’s Hospital of Philadelphia in Pennsylvania, and her colleagues reported these results in JAMA Pediatrics alongside a related editorial.
The researchers administered an anonymous survey to attending physicians and advanced practice clinicians (APCs) at the Children’s Hospital of Philadelphia. APCs included certified registered nurse practitioners, physician assistants, clinical nurse specialists, certified registered nurse anesthetists, and certified nurse midwives.
Overall, 280 attending physicians (61%) and 256 APCs (54.5%) responded. Most respondents (504, 95.3%) said working while sick put patients at risk.
However, 446 respondents (83.1%) reported working while sick at least once in the past year, and 50 respondents (9.3%) reported working while sick at least 5 times.
Respondents reported working with symptoms that included diarrhea, fever, and the onset of significant respiratory symptoms.
The reasons physicians and APCs worked while sick included not wanting to let colleagues down (98.7%), staffing concerns (94.9%), not wanting to let patients down (92.5%), fear of being ostracized by colleagues (64%), and concerns about the continuity of care (63.8%).
An analysis of written comments about why respondents work while sick highlighted 3 areas: challenges in identifying and arranging someone to cover their work and a lack of resources to accommodate sick leave, a strong cultural norm in the hospital to report for work unless one is extremely ill, and ambiguity about what symptoms constitute being too sick to work.
Dr Szymczak and her colleagues said this study suggests complex social and logistical factors cause healthcare workers to report to work sick. But these results could inform efforts to help workers make the right choice to keep their patients and colleagues safe while caring for themselves. ![]()
NICE supports use of apixaban for VTE

Photo courtesy of the CDC
The UK’s National Institute for Health and Care Excellence (NICE) has issued a final guidance recommending the anticoagulant apixaban (Eliquis) as an option for treating and preventing venous thromboembolism (VTE) in adults.
According to NICE, data from the AMPLIFY and AMPLIFY-EXT studies suggest apixaban is clinically effective for treating and preventing VTE.
And cost analyses indicate that apixaban is a cost-effective use of National Health Service (NHS) resources.
NICE said apixaban should be available on the NHS within 3 months of the guidance release date. The guidance was made available in June.
Dosing
To treat deep vein thrombosis (DVT) or pulmonary embolism (PE), 10 mg of apixaban should be taken twice a day for the first 7 days, followed by 5 mg twice a day for at least 3 months.
To prevent recurrent VTE, patients who have completed 6 months of treatment for DVT or PE should take apixaban at 2.5 mg twice a day.
“[A]pixaban is the only oral anticoagulant for which the licensed dose is lower for secondary prevention than for initial treatment of VTE,” said Carole Longson, NICE Health Technology Evaluation Centre Director.
“This could also be of potential benefit in terms of reducing the risk of bleeding where treatment is continued and therefore increase the chance that a person would take apixaban long-term.”
Clinical effectiveness
To assess the clinical effectiveness of apixaban, a committee advising NICE evaluated data from the AMPLIFY and AMPLIFY-EXT studies.
Results of the AMPLIFY study indicated that apixaban is noninferior to standard treatment for recurrent VTE—initial parenteral enoxaparin overlapped with warfarin. Apixaban was comparable in efficacy to standard therapy and induced significantly less bleeding.
In AMPLIFY-EXT, researchers compared 12 months of treatment with apixaban at 2 doses—2.5 mg and 5 mg—to placebo in patients who had previously received anticoagulant therapy for 6 to 12 months to treat a prior VTE.
Both doses of apixaban effectively prevented VTE, VTE-related events, and death. And the incidence of bleeding events was low in all treatment arms.
The NICE committee noted that there were limited data in these trials pertaining to patients who needed less than 6 months of treatment and for patients still at high risk of recurrent VTE after 6 months of treatment.
However, the committee concluded that, despite these limitations, the AMPLIFY trials were the pivotal trials that informed the marketing authorization for apixaban. As such, they were sufficient to inform a recommendation for the whole population covered by the marketing authorization.
The committee also pointed out that there were no head-to-head trials evaluating the relative effectiveness of apixaban compared with rivaroxaban and dabigatran etexilate for treating and preventing VTE.
In addition, there were insufficient data to assess the effectiveness and safety of apixaban in patients with active cancer who had VTE, so it was not possible to make a specific recommendation for this group.
Cost-effectiveness
The cost of apixaban is £1.10 per tablet for either the 2.5 mg or 5 mg dose (excluding tax). The daily cost of apixaban is £2.20. (Costs may vary in different settings because of negotiated procurement discounts.)
Analyses suggested that the incremental cost-effectiveness ratio of apixaban was less than £20,000 per quality-adjusted life-year gained for either 6 months or life-long treatment. Therefore, NICE concluded that apixaban is a cost-effective use of NHS resources. ![]()
Photo courtesy of the CDC
The UK’s National Institute for Health and Care Excellence (NICE) has issued a final guidance recommending the anticoagulant apixaban (Eliquis) as an option for treating and preventing venous thromboembolism (VTE) in adults.
According to NICE, data from the AMPLIFY and AMPLIFY-EXT studies suggest apixaban is clinically effective for treating and preventing VTE.
And cost analyses indicate that apixaban is a cost-effective use of National Health Service (NHS) resources.
NICE said apixaban should be available on the NHS within 3 months of the guidance release date. The guidance was made available in June.
Dosing
To treat deep vein thrombosis (DVT) or pulmonary embolism (PE), 10 mg of apixaban should be taken twice a day for the first 7 days, followed by 5 mg twice a day for at least 3 months.
To prevent recurrent VTE, patients who have completed 6 months of treatment for DVT or PE should take apixaban at 2.5 mg twice a day.
“[A]pixaban is the only oral anticoagulant for which the licensed dose is lower for secondary prevention than for initial treatment of VTE,” said Carole Longson, NICE Health Technology Evaluation Centre Director.
“This could also be of potential benefit in terms of reducing the risk of bleeding where treatment is continued and therefore increase the chance that a person would take apixaban long-term.”
Clinical effectiveness
To assess the clinical effectiveness of apixaban, a committee advising NICE evaluated data from the AMPLIFY and AMPLIFY-EXT studies.
Results of the AMPLIFY study indicated that apixaban is noninferior to standard treatment for recurrent VTE—initial parenteral enoxaparin overlapped with warfarin. Apixaban was comparable in efficacy to standard therapy and induced significantly less bleeding.
In AMPLIFY-EXT, researchers compared 12 months of treatment with apixaban at 2 doses—2.5 mg and 5 mg—to placebo in patients who had previously received anticoagulant therapy for 6 to 12 months to treat a prior VTE.
Both doses of apixaban effectively prevented VTE, VTE-related events, and death. And the incidence of bleeding events was low in all treatment arms.
The NICE committee noted that there were limited data in these trials pertaining to patients who needed less than 6 months of treatment and for patients still at high risk of recurrent VTE after 6 months of treatment.
However, the committee concluded that, despite these limitations, the AMPLIFY trials were the pivotal trials that informed the marketing authorization for apixaban. As such, they were sufficient to inform a recommendation for the whole population covered by the marketing authorization.
The committee also pointed out that there were no head-to-head trials evaluating the relative effectiveness of apixaban compared with rivaroxaban and dabigatran etexilate for treating and preventing VTE.
In addition, there were insufficient data to assess the effectiveness and safety of apixaban in patients with active cancer who had VTE, so it was not possible to make a specific recommendation for this group.
Cost-effectiveness
The cost of apixaban is £1.10 per tablet for either the 2.5 mg or 5 mg dose (excluding tax). The daily cost of apixaban is £2.20. (Costs may vary in different settings because of negotiated procurement discounts.)
Analyses suggested that the incremental cost-effectiveness ratio of apixaban was less than £20,000 per quality-adjusted life-year gained for either 6 months or life-long treatment. Therefore, NICE concluded that apixaban is a cost-effective use of NHS resources. ![]()
Photo courtesy of the CDC
The UK’s National Institute for Health and Care Excellence (NICE) has issued a final guidance recommending the anticoagulant apixaban (Eliquis) as an option for treating and preventing venous thromboembolism (VTE) in adults.
According to NICE, data from the AMPLIFY and AMPLIFY-EXT studies suggest apixaban is clinically effective for treating and preventing VTE.
And cost analyses indicate that apixaban is a cost-effective use of National Health Service (NHS) resources.
NICE said apixaban should be available on the NHS within 3 months of the guidance release date. The guidance was made available in June.
Dosing
To treat deep vein thrombosis (DVT) or pulmonary embolism (PE), 10 mg of apixaban should be taken twice a day for the first 7 days, followed by 5 mg twice a day for at least 3 months.
To prevent recurrent VTE, patients who have completed 6 months of treatment for DVT or PE should take apixaban at 2.5 mg twice a day.
“[A]pixaban is the only oral anticoagulant for which the licensed dose is lower for secondary prevention than for initial treatment of VTE,” said Carole Longson, NICE Health Technology Evaluation Centre Director.
“This could also be of potential benefit in terms of reducing the risk of bleeding where treatment is continued and therefore increase the chance that a person would take apixaban long-term.”
Clinical effectiveness
To assess the clinical effectiveness of apixaban, a committee advising NICE evaluated data from the AMPLIFY and AMPLIFY-EXT studies.
Results of the AMPLIFY study indicated that apixaban is noninferior to standard treatment for recurrent VTE—initial parenteral enoxaparin overlapped with warfarin. Apixaban was comparable in efficacy to standard therapy and induced significantly less bleeding.
In AMPLIFY-EXT, researchers compared 12 months of treatment with apixaban at 2 doses—2.5 mg and 5 mg—to placebo in patients who had previously received anticoagulant therapy for 6 to 12 months to treat a prior VTE.
Both doses of apixaban effectively prevented VTE, VTE-related events, and death. And the incidence of bleeding events was low in all treatment arms.
The NICE committee noted that there were limited data in these trials pertaining to patients who needed less than 6 months of treatment and for patients still at high risk of recurrent VTE after 6 months of treatment.
However, the committee concluded that, despite these limitations, the AMPLIFY trials were the pivotal trials that informed the marketing authorization for apixaban. As such, they were sufficient to inform a recommendation for the whole population covered by the marketing authorization.
The committee also pointed out that there were no head-to-head trials evaluating the relative effectiveness of apixaban compared with rivaroxaban and dabigatran etexilate for treating and preventing VTE.
In addition, there were insufficient data to assess the effectiveness and safety of apixaban in patients with active cancer who had VTE, so it was not possible to make a specific recommendation for this group.
Cost-effectiveness
The cost of apixaban is £1.10 per tablet for either the 2.5 mg or 5 mg dose (excluding tax). The daily cost of apixaban is £2.20. (Costs may vary in different settings because of negotiated procurement discounts.)
Analyses suggested that the incremental cost-effectiveness ratio of apixaban was less than £20,000 per quality-adjusted life-year gained for either 6 months or life-long treatment. Therefore, NICE concluded that apixaban is a cost-effective use of NHS resources. ![]()
EAP makes drug available to MM patients

Photo by Linda Bartlett
A new expanded access program (EAP) will make daratumumab, an investigational anti-CD38 monoclonal antibody, available to patients with double-refractory multiple myeloma (MM).
The multicenter EAP is open to MM patients in the US who are 18 years of age or older.
Patients must be refractory to both a proteasome inhibitor (PI) and an immunomodulatory drug (IMiD) or have received 3 or more prior lines of therapy, including a PI and an IMiD.
In the US, EAPs are designed to make investigational medicines available for patients with serious or life-threatening illnesses who are ineligible for ongoing interventional trials and have exhausted currently available treatment options.
This EAP will make daratumumab available at up to 40 medical centers in the US while the drug’s Biologics License Application is under review by the US Food and Drug Administration (FDA).
Additional information about the EAP can be found on clinicaltrials.gov (NCT02477891). Janssen Research & Development, LLC, the company developing daratumumab, is collaborating with the Multiple Myeloma Research Foundation on this EAP.
About daratumumab
Daratumumab is a human IgG1k monoclonal antibody that binds with high affinity to the transmembrane ectoenzyme CD38 on the surface of MM cells.
Five phase 3 clinical studies with daratumumab in relapsed and frontline settings are currently ongoing. Additional studies are ongoing or planned to assess the drug’s potential in other malignant and pre-malignant diseases on which CD38 is expressed, such as smoldering myeloma and non-Hodgkin lymphoma.
On May 1, 2013, daratumumab received breakthrough designation from the FDA for the treatment of patients with MM who have received at least 3 prior lines of therapy, including a PI and an IMiD, or who are double refractory to a PI and an IMiD.
On June 5, 2015, Janssen announced it had initiated the rolling submission of its Biologics License Application for daratumumab to the FDA for the treatment of this set of MM patients. A rolling submission allows the company to submit portions of the regulatory application to the FDA as they are completed.
The regulatory submission for daratumumab will be primarily supported by data from the phase 2 MMY2002 (SIRIUS) study, the results of which were presented at the 2015 ASCO Annual Meeting.
The application will also be supported by data from 4 other studies, including the phase 1/2 GEN501 monotherapy study. ![]()
Photo by Linda Bartlett
A new expanded access program (EAP) will make daratumumab, an investigational anti-CD38 monoclonal antibody, available to patients with double-refractory multiple myeloma (MM).
The multicenter EAP is open to MM patients in the US who are 18 years of age or older.
Patients must be refractory to both a proteasome inhibitor (PI) and an immunomodulatory drug (IMiD) or have received 3 or more prior lines of therapy, including a PI and an IMiD.
In the US, EAPs are designed to make investigational medicines available for patients with serious or life-threatening illnesses who are ineligible for ongoing interventional trials and have exhausted currently available treatment options.
This EAP will make daratumumab available at up to 40 medical centers in the US while the drug’s Biologics License Application is under review by the US Food and Drug Administration (FDA).
Additional information about the EAP can be found on clinicaltrials.gov (NCT02477891). Janssen Research & Development, LLC, the company developing daratumumab, is collaborating with the Multiple Myeloma Research Foundation on this EAP.
About daratumumab
Daratumumab is a human IgG1k monoclonal antibody that binds with high affinity to the transmembrane ectoenzyme CD38 on the surface of MM cells.
Five phase 3 clinical studies with daratumumab in relapsed and frontline settings are currently ongoing. Additional studies are ongoing or planned to assess the drug’s potential in other malignant and pre-malignant diseases on which CD38 is expressed, such as smoldering myeloma and non-Hodgkin lymphoma.
On May 1, 2013, daratumumab received breakthrough designation from the FDA for the treatment of patients with MM who have received at least 3 prior lines of therapy, including a PI and an IMiD, or who are double refractory to a PI and an IMiD.
On June 5, 2015, Janssen announced it had initiated the rolling submission of its Biologics License Application for daratumumab to the FDA for the treatment of this set of MM patients. A rolling submission allows the company to submit portions of the regulatory application to the FDA as they are completed.
The regulatory submission for daratumumab will be primarily supported by data from the phase 2 MMY2002 (SIRIUS) study, the results of which were presented at the 2015 ASCO Annual Meeting.
The application will also be supported by data from 4 other studies, including the phase 1/2 GEN501 monotherapy study. ![]()
Photo by Linda Bartlett
A new expanded access program (EAP) will make daratumumab, an investigational anti-CD38 monoclonal antibody, available to patients with double-refractory multiple myeloma (MM).
The multicenter EAP is open to MM patients in the US who are 18 years of age or older.
Patients must be refractory to both a proteasome inhibitor (PI) and an immunomodulatory drug (IMiD) or have received 3 or more prior lines of therapy, including a PI and an IMiD.
In the US, EAPs are designed to make investigational medicines available for patients with serious or life-threatening illnesses who are ineligible for ongoing interventional trials and have exhausted currently available treatment options.
This EAP will make daratumumab available at up to 40 medical centers in the US while the drug’s Biologics License Application is under review by the US Food and Drug Administration (FDA).
Additional information about the EAP can be found on clinicaltrials.gov (NCT02477891). Janssen Research & Development, LLC, the company developing daratumumab, is collaborating with the Multiple Myeloma Research Foundation on this EAP.
About daratumumab
Daratumumab is a human IgG1k monoclonal antibody that binds with high affinity to the transmembrane ectoenzyme CD38 on the surface of MM cells.
Five phase 3 clinical studies with daratumumab in relapsed and frontline settings are currently ongoing. Additional studies are ongoing or planned to assess the drug’s potential in other malignant and pre-malignant diseases on which CD38 is expressed, such as smoldering myeloma and non-Hodgkin lymphoma.
On May 1, 2013, daratumumab received breakthrough designation from the FDA for the treatment of patients with MM who have received at least 3 prior lines of therapy, including a PI and an IMiD, or who are double refractory to a PI and an IMiD.
On June 5, 2015, Janssen announced it had initiated the rolling submission of its Biologics License Application for daratumumab to the FDA for the treatment of this set of MM patients. A rolling submission allows the company to submit portions of the regulatory application to the FDA as they are completed.
The regulatory submission for daratumumab will be primarily supported by data from the phase 2 MMY2002 (SIRIUS) study, the results of which were presented at the 2015 ASCO Annual Meeting.
The application will also be supported by data from 4 other studies, including the phase 1/2 GEN501 monotherapy study. ![]()
PI3K inhibitors may promote cancer spread

Photo courtesy of
The Wistar Institute
Although PI3K inhibitors have been designed to treat cancer, new research indicates these drugs may actually exacerbate the disease.
Researchers found evidence to suggest that treatment with PI3K inhibitors alone can promote more aggressive tumor cell behavior and increase the likelihood that cancer will spread.
PI3K inhibitors appeared to reprogram the mitochondria of tumor cells and move them to “strategic” positions for invasion.
However, the researchers believe that targeting mitochondrial function along with PI3K could prevent this effect.
Dario C. Altieri, MD, of The Wistar Institute in Philadelphia, Pennsylvania, and his colleagues described these findings in PNAS.
The researchers decided to investigate how mitochondria are reprogrammed when exposed to PI3K inhibition and how mitochondria might prevent targeted agents from being as effective as expected.
“Our prior studies have confirmed that tumor cells rely on energy produced by mitochondria more significantly than previously thought,” Dr Altieri said.
“What we have shown in this study is that, in somewhat of a paradox, treatment with a PI3K inhibitor causes a tumor cell’s mitochondria to produce energy in a localized manner, promoting a far more aggressive and invasive phenotype. The treatment appears to be doing the opposite of its intended effect.”
The study showed that treatment with a PI3K inhibitor causes the mitochondria to migrate to the peripheral cytoskeleton of the tumor cells.
While the mitochondria in untreated cells cluster around the cell’s nucleus, exposure of tumor cells to PI3K therapy causes the mitochondria to move to specialized regions of the cell’s membrane implicated in cell motility and invasion.
In this “strategic” position, tumor mitochondria are ideally positioned to provide a concentrated source of energy to support an increase in cell migration and invasion.
However, the researchers said the dependence of this response on mitochondrial function may offer a new therapeutic angle.
Dr Altieri and his team have shown that targeting mitochondrial functions for tumor therapy is feasible and dramatically enhances the anticancer activity of PI3K inhibitors when used in combination.
“These findings continue to support the idea that the mitochondria of tumor cells are crucial to tumor survival and proliferation,” Dr Altieri said. “It’s certainly counterintuitive that a drug designed to fight cancer may in actuality help it spread, but by identifying why this is happening, we can develop better strategies that allow these drugs to treat tumors the way they should.” ![]()
Photo courtesy of
The Wistar Institute
Although PI3K inhibitors have been designed to treat cancer, new research indicates these drugs may actually exacerbate the disease.
Researchers found evidence to suggest that treatment with PI3K inhibitors alone can promote more aggressive tumor cell behavior and increase the likelihood that cancer will spread.
PI3K inhibitors appeared to reprogram the mitochondria of tumor cells and move them to “strategic” positions for invasion.
However, the researchers believe that targeting mitochondrial function along with PI3K could prevent this effect.
Dario C. Altieri, MD, of The Wistar Institute in Philadelphia, Pennsylvania, and his colleagues described these findings in PNAS.
The researchers decided to investigate how mitochondria are reprogrammed when exposed to PI3K inhibition and how mitochondria might prevent targeted agents from being as effective as expected.
“Our prior studies have confirmed that tumor cells rely on energy produced by mitochondria more significantly than previously thought,” Dr Altieri said.
“What we have shown in this study is that, in somewhat of a paradox, treatment with a PI3K inhibitor causes a tumor cell’s mitochondria to produce energy in a localized manner, promoting a far more aggressive and invasive phenotype. The treatment appears to be doing the opposite of its intended effect.”
The study showed that treatment with a PI3K inhibitor causes the mitochondria to migrate to the peripheral cytoskeleton of the tumor cells.
While the mitochondria in untreated cells cluster around the cell’s nucleus, exposure of tumor cells to PI3K therapy causes the mitochondria to move to specialized regions of the cell’s membrane implicated in cell motility and invasion.
In this “strategic” position, tumor mitochondria are ideally positioned to provide a concentrated source of energy to support an increase in cell migration and invasion.
However, the researchers said the dependence of this response on mitochondrial function may offer a new therapeutic angle.
Dr Altieri and his team have shown that targeting mitochondrial functions for tumor therapy is feasible and dramatically enhances the anticancer activity of PI3K inhibitors when used in combination.
“These findings continue to support the idea that the mitochondria of tumor cells are crucial to tumor survival and proliferation,” Dr Altieri said. “It’s certainly counterintuitive that a drug designed to fight cancer may in actuality help it spread, but by identifying why this is happening, we can develop better strategies that allow these drugs to treat tumors the way they should.” ![]()
Photo courtesy of
The Wistar Institute
Although PI3K inhibitors have been designed to treat cancer, new research indicates these drugs may actually exacerbate the disease.
Researchers found evidence to suggest that treatment with PI3K inhibitors alone can promote more aggressive tumor cell behavior and increase the likelihood that cancer will spread.
PI3K inhibitors appeared to reprogram the mitochondria of tumor cells and move them to “strategic” positions for invasion.
However, the researchers believe that targeting mitochondrial function along with PI3K could prevent this effect.
Dario C. Altieri, MD, of The Wistar Institute in Philadelphia, Pennsylvania, and his colleagues described these findings in PNAS.
The researchers decided to investigate how mitochondria are reprogrammed when exposed to PI3K inhibition and how mitochondria might prevent targeted agents from being as effective as expected.
“Our prior studies have confirmed that tumor cells rely on energy produced by mitochondria more significantly than previously thought,” Dr Altieri said.
“What we have shown in this study is that, in somewhat of a paradox, treatment with a PI3K inhibitor causes a tumor cell’s mitochondria to produce energy in a localized manner, promoting a far more aggressive and invasive phenotype. The treatment appears to be doing the opposite of its intended effect.”
The study showed that treatment with a PI3K inhibitor causes the mitochondria to migrate to the peripheral cytoskeleton of the tumor cells.
While the mitochondria in untreated cells cluster around the cell’s nucleus, exposure of tumor cells to PI3K therapy causes the mitochondria to move to specialized regions of the cell’s membrane implicated in cell motility and invasion.
In this “strategic” position, tumor mitochondria are ideally positioned to provide a concentrated source of energy to support an increase in cell migration and invasion.
However, the researchers said the dependence of this response on mitochondrial function may offer a new therapeutic angle.
Dr Altieri and his team have shown that targeting mitochondrial functions for tumor therapy is feasible and dramatically enhances the anticancer activity of PI3K inhibitors when used in combination.
“These findings continue to support the idea that the mitochondria of tumor cells are crucial to tumor survival and proliferation,” Dr Altieri said. “It’s certainly counterintuitive that a drug designed to fight cancer may in actuality help it spread, but by identifying why this is happening, we can develop better strategies that allow these drugs to treat tumors the way they should.” ![]()
Inhibitors increase burden of hemophilia care

TORONTO—When children with hemophilia develop inhibitors, their caregivers shoulder a greater burden, according to a pilot study.
Researchers surveyed 40 subjects on the burden of caring for a child with hemophilia and found that inhibitor development significantly increased the burden of care.
But other factors—such as the number of bleeds a child had experienced in the last 12 months—had no significant impact.
Sylvia von Mackensen, PhD, of the University Medical Centre Hamburg-Eppendorf in Hamburg, Germany, and her colleagues presented these findings at the ISTH 2015 Congress (abstract PO256-WED).
The study was a pilot test of the HEMOCAB questionnaire, which consists of 59 questions mapped to 13 domains. Caregivers were asked to select the response that best qualified their burden and were scored on a scale of 0 to 100, with higher values corresponding with greater burden.
Forty caregivers completed the questionnaire. All of them had children with hemophilia (n=40), with or without inhibitors, who were younger than 22 years of age.
Three-quarters of the caregivers were mothers, 17.5% were fathers, and 7.5% were grandmothers. The mean age of caregivers was 39.32 ± 8.9 years (range, 27-66), and the mean age of the hemophilia patients was 10.98 ± 5.5 years (range, 1-21).
Most of the patients had hemophilia A (95%), and most had severe disease (77.5%). Six children (15%) had inhibitors. Overall, patients had experienced an average of 4.83 ±8.9 bleeds (range, 0-52) in the previous 12 months.
Most of the patients (88.5%) were receiving prophylaxis. Caregivers said they spent 8.69 ± 7.7 hours per month on infusion and 3.84 ± 6.7 hours (range, 0-30) per month traveling to hemophilia treatment facilities.
Size of burden
Caregivers said the most burdensome aspects of care were the caregivers’ perception of the child (38%), emotional stress (36%), financial burden (34%), and the impact of care on the caregiver (31%).
For nearly all of the domains assessed—emotional stress, personal sacrifice, medical management, work situation, etc.—a caregivers’ burden was significantly higher if a child had inhibitors. The only exception was school-related burden.
When the researchers analyzed the impact of other factors on care burden, they found that only inhibitor development had a significant impact.
There was no impact for orthopedic joint score, age of the caregiver, age of the child, time for infusion, time traveling to a hemophilia treatment center, the number of bleeds in the past 12 months, the number of children with hemophilia per household, home treatment, caregiver marital status, location, or caregiver education.
Frequency of burden
The HEMOCAB questionnaire also included scales assessing the frequency of burden. Dr von Mackensen and her colleagues presented data from these scales for the caregivers’ perception of their child, emotional stress, and finances.
Sixty percent of caregivers said they sometimes, often, or always feel their child’s condition is a difficult situation. Seventy-three percent of caregivers expressed feelings of sadness about informing their child of what he can and cannot do due to his illness.
Seventy-four percent of caregivers said they sometimes, often, or always feel afraid their child might get injured when they are not around to help. Forty-six percent of caregivers reported feeling afraid their child’s condition might worsen, and 36% said they feared their child might die from his condition.
Forty-six percent of caregivers said their child’s hemophilia sometimes, often, or always causes financial problems. And 33% of caregivers said that, at least sometimes, their family does not have enough money because of their child’s hemophilia.
HEMOCAB is a trademark of Novo Nordisk Health Care AG. Dr von Mackensen received a consulting fee from Novo Nordisk for developing the HEMOCAB questionnaire. Leonard A. Valentino, MD, of Rush University Medical Center in Chicago, Illinois, was involved in developing the questionnaire as well but did not participate in the pilot study.
The other researchers involved in the study have received funding/consulting fees from—or are employees of—Novo Nordisk, Baxter, Bayer, OctaPharma, CSL Behring, OPKO Health, and Selexys. ![]()
TORONTO—When children with hemophilia develop inhibitors, their caregivers shoulder a greater burden, according to a pilot study.
Researchers surveyed 40 subjects on the burden of caring for a child with hemophilia and found that inhibitor development significantly increased the burden of care.
But other factors—such as the number of bleeds a child had experienced in the last 12 months—had no significant impact.
Sylvia von Mackensen, PhD, of the University Medical Centre Hamburg-Eppendorf in Hamburg, Germany, and her colleagues presented these findings at the ISTH 2015 Congress (abstract PO256-WED).
The study was a pilot test of the HEMOCAB questionnaire, which consists of 59 questions mapped to 13 domains. Caregivers were asked to select the response that best qualified their burden and were scored on a scale of 0 to 100, with higher values corresponding with greater burden.
Forty caregivers completed the questionnaire. All of them had children with hemophilia (n=40), with or without inhibitors, who were younger than 22 years of age.
Three-quarters of the caregivers were mothers, 17.5% were fathers, and 7.5% were grandmothers. The mean age of caregivers was 39.32 ± 8.9 years (range, 27-66), and the mean age of the hemophilia patients was 10.98 ± 5.5 years (range, 1-21).
Most of the patients had hemophilia A (95%), and most had severe disease (77.5%). Six children (15%) had inhibitors. Overall, patients had experienced an average of 4.83 ±8.9 bleeds (range, 0-52) in the previous 12 months.
Most of the patients (88.5%) were receiving prophylaxis. Caregivers said they spent 8.69 ± 7.7 hours per month on infusion and 3.84 ± 6.7 hours (range, 0-30) per month traveling to hemophilia treatment facilities.
Size of burden
Caregivers said the most burdensome aspects of care were the caregivers’ perception of the child (38%), emotional stress (36%), financial burden (34%), and the impact of care on the caregiver (31%).
For nearly all of the domains assessed—emotional stress, personal sacrifice, medical management, work situation, etc.—a caregivers’ burden was significantly higher if a child had inhibitors. The only exception was school-related burden.
When the researchers analyzed the impact of other factors on care burden, they found that only inhibitor development had a significant impact.
There was no impact for orthopedic joint score, age of the caregiver, age of the child, time for infusion, time traveling to a hemophilia treatment center, the number of bleeds in the past 12 months, the number of children with hemophilia per household, home treatment, caregiver marital status, location, or caregiver education.
Frequency of burden
The HEMOCAB questionnaire also included scales assessing the frequency of burden. Dr von Mackensen and her colleagues presented data from these scales for the caregivers’ perception of their child, emotional stress, and finances.
Sixty percent of caregivers said they sometimes, often, or always feel their child’s condition is a difficult situation. Seventy-three percent of caregivers expressed feelings of sadness about informing their child of what he can and cannot do due to his illness.
Seventy-four percent of caregivers said they sometimes, often, or always feel afraid their child might get injured when they are not around to help. Forty-six percent of caregivers reported feeling afraid their child’s condition might worsen, and 36% said they feared their child might die from his condition.
Forty-six percent of caregivers said their child’s hemophilia sometimes, often, or always causes financial problems. And 33% of caregivers said that, at least sometimes, their family does not have enough money because of their child’s hemophilia.
HEMOCAB is a trademark of Novo Nordisk Health Care AG. Dr von Mackensen received a consulting fee from Novo Nordisk for developing the HEMOCAB questionnaire. Leonard A. Valentino, MD, of Rush University Medical Center in Chicago, Illinois, was involved in developing the questionnaire as well but did not participate in the pilot study.
The other researchers involved in the study have received funding/consulting fees from—or are employees of—Novo Nordisk, Baxter, Bayer, OctaPharma, CSL Behring, OPKO Health, and Selexys. ![]()
TORONTO—When children with hemophilia develop inhibitors, their caregivers shoulder a greater burden, according to a pilot study.
Researchers surveyed 40 subjects on the burden of caring for a child with hemophilia and found that inhibitor development significantly increased the burden of care.
But other factors—such as the number of bleeds a child had experienced in the last 12 months—had no significant impact.
Sylvia von Mackensen, PhD, of the University Medical Centre Hamburg-Eppendorf in Hamburg, Germany, and her colleagues presented these findings at the ISTH 2015 Congress (abstract PO256-WED).
The study was a pilot test of the HEMOCAB questionnaire, which consists of 59 questions mapped to 13 domains. Caregivers were asked to select the response that best qualified their burden and were scored on a scale of 0 to 100, with higher values corresponding with greater burden.
Forty caregivers completed the questionnaire. All of them had children with hemophilia (n=40), with or without inhibitors, who were younger than 22 years of age.
Three-quarters of the caregivers were mothers, 17.5% were fathers, and 7.5% were grandmothers. The mean age of caregivers was 39.32 ± 8.9 years (range, 27-66), and the mean age of the hemophilia patients was 10.98 ± 5.5 years (range, 1-21).
Most of the patients had hemophilia A (95%), and most had severe disease (77.5%). Six children (15%) had inhibitors. Overall, patients had experienced an average of 4.83 ±8.9 bleeds (range, 0-52) in the previous 12 months.
Most of the patients (88.5%) were receiving prophylaxis. Caregivers said they spent 8.69 ± 7.7 hours per month on infusion and 3.84 ± 6.7 hours (range, 0-30) per month traveling to hemophilia treatment facilities.
Size of burden
Caregivers said the most burdensome aspects of care were the caregivers’ perception of the child (38%), emotional stress (36%), financial burden (34%), and the impact of care on the caregiver (31%).
For nearly all of the domains assessed—emotional stress, personal sacrifice, medical management, work situation, etc.—a caregivers’ burden was significantly higher if a child had inhibitors. The only exception was school-related burden.
When the researchers analyzed the impact of other factors on care burden, they found that only inhibitor development had a significant impact.
There was no impact for orthopedic joint score, age of the caregiver, age of the child, time for infusion, time traveling to a hemophilia treatment center, the number of bleeds in the past 12 months, the number of children with hemophilia per household, home treatment, caregiver marital status, location, or caregiver education.
Frequency of burden
The HEMOCAB questionnaire also included scales assessing the frequency of burden. Dr von Mackensen and her colleagues presented data from these scales for the caregivers’ perception of their child, emotional stress, and finances.
Sixty percent of caregivers said they sometimes, often, or always feel their child’s condition is a difficult situation. Seventy-three percent of caregivers expressed feelings of sadness about informing their child of what he can and cannot do due to his illness.
Seventy-four percent of caregivers said they sometimes, often, or always feel afraid their child might get injured when they are not around to help. Forty-six percent of caregivers reported feeling afraid their child’s condition might worsen, and 36% said they feared their child might die from his condition.
Forty-six percent of caregivers said their child’s hemophilia sometimes, often, or always causes financial problems. And 33% of caregivers said that, at least sometimes, their family does not have enough money because of their child’s hemophilia.
HEMOCAB is a trademark of Novo Nordisk Health Care AG. Dr von Mackensen received a consulting fee from Novo Nordisk for developing the HEMOCAB questionnaire. Leonard A. Valentino, MD, of Rush University Medical Center in Chicago, Illinois, was involved in developing the questionnaire as well but did not participate in the pilot study.
The other researchers involved in the study have received funding/consulting fees from—or are employees of—Novo Nordisk, Baxter, Bayer, OctaPharma, CSL Behring, OPKO Health, and Selexys. ![]()
Pain problems prevalent in adults with hemophilia

TORONTO—A survey of adult hemophilia patients suggests there is room for improvement in assessing and managing disease-related pain.
Roughly 85% of patients surveyed for this study, known as P-FiQ, said they had experienced acute and/or chronic pain in the past 6 months.
Although most patients had no trouble caring for themselves, the pain often had an impact on their daily lives, especially with regard to physical activity and overall mobility.
“Pain and discomfort are significant challenges for people with hemophilia,” said study investigator Michael Recht, MD, PhD, of Oregon Health Sciences University in Portland.
“These results emphasize the importance of providing comprehensive care and support beyond traditional therapy to people living with bleeding disorders.”
Dr Recht and his colleagues presented results of the P-FiQ study in 3 posters at the ISTH 2015 Congress (abstracts PO277-MON, PO297-WED, and PO298-WED).
The study included adult males with mild to severe hemophilia who had a history of joint pain or bleeding. Subjects were asked to assess pain and functional impairment using patient-reported outcome instruments.
During routine visits over the course of a year, 164 participants completed a pain history and 5 questionnaires: the EQ-5D-5L; Brief Pain Inventory Short Form, version 2; International Physical Activity Questionnaire; SF-36v2; and Hemophilia Activities List.
The patients had a median age of 34. More patients had hemophilia A (n=122) than hemophilia B (n=42), and few (n=10) had inhibitors. Sixty-one percent of patients had self-reported arthritis, bone, or joint problems.
Current patient-reported treatment regimens (n=163) were prophylaxis (42%), on-demand treatment (39%), or mostly on-demand treatment (19%). Twenty-five of the 31 patients using on-demand treatment reported using infusions ahead of activity.
Pain prevalence and management
Most participants (85.2%) said they had experienced acute and/or chronic pain over the past 6 months. Twenty-nine percent said they had experienced acute and chronic pain, 32.7% had chronic pain only, 23.5% had acute pain only, and 14.8% reported no pain.
Acute pain was most frequently described as sharp, aching, shooting, and throbbing. Chronic pain was often described as aching, nagging, throbbing, and sharp.
The most common analgesics used for acute or chronic pain were acetaminophen (69.4% and 58%, respectively), NSAIDs (40% and 52%, respectively), and hydrocodone-acetaminophen (29.4% and 33%, respectively).
The most common nonanalgesic strategies used for acute or chronic pain were ice (72.9% and 37%, respectively), rest (48.2% and 34%, respectively), factor VIII/IX or bypassing agent (48.2% and 24%, respectively), elevation (34.1% and 28%, respectively), relaxation (30.6% and 23.0%, respectively), compression (27.1% and 21%, respectively), and heat (24.7% and 15%, respectively).
Impact of pain on daily life
When completing the EQ-5D-5L questionnaire, most patients reported problems with mobility, performing usual activities, and pain or discomfort. However, most patients said they had no problems with self-care (78%) or anxiety/depression (58.5%).
A similar proportion of patients reported slight and moderate pain and discomfort (29.9% and 31.1%, respectively). Pain and discomfort was severe for 11% of patients and extreme for 1.2%, but 26.8% of patients reported no pain or discomfort.
When it came to mobility, patients reported slight (32.3%), moderate (19.5%), and severe (8.5%) problems, and 1.2% of patients said they were unable to get around. However, 38.4% of patients reported having no such problems.
About 44% of patients reported no problems performing usual activities, but 37.2% had slight problems, 14.6% had moderate problems, and 1.8% of patients each had severe problems or were unable to perform usual activities.
For the Brief Pain Inventory, pain severity and interference with daily activities were rated on a scale of 0 to 10, with 0 being no pain/no interference and 10 being pain as bad as you can imagine/pain that completely interferes with daily life.
The overall median pain severity and pain interference were 3.0 (range, 1.3-4.8) and 2.9 (range, 0.7-5.2), respectively. The median worst pain was 6.0, least pain 2.0, average pain 3.0, and current pain 2.0. Ankles were the most frequently reported site of pain.
When completing the International Physical Activity Questionnaire, 49.3% of patients (73/148) reported no activity in the prior week.
The median SF-36v2 scores were lower for physical health domains than mental health domains, and the overall median health score was 3.0 (range, 2.0-3.0).
The median score on the Hemophilia Activities List was 76.1 (range, 59.2-95.1). And patients said hemophilia had a greater impact on their lower extremities than upper extremities.
Dr Recht and his colleagues said these results substantiate the high prevalence of pain in adults with hemophilia. And the study highlights opportunities to improve the assessment and management of pain in these patients.
Study investigators have received funding/consulting fees from—or are employees/shareholders of—Novo Nordisk, Baxter, Biogen, Bayer, OctaPharma, Pfizer, CSL Behring, Kendrion, Alexion, Grifols, OPKO Health, Sanofi, Merck, and ProMeticLife Sciences. ![]()
TORONTO—A survey of adult hemophilia patients suggests there is room for improvement in assessing and managing disease-related pain.
Roughly 85% of patients surveyed for this study, known as P-FiQ, said they had experienced acute and/or chronic pain in the past 6 months.
Although most patients had no trouble caring for themselves, the pain often had an impact on their daily lives, especially with regard to physical activity and overall mobility.
“Pain and discomfort are significant challenges for people with hemophilia,” said study investigator Michael Recht, MD, PhD, of Oregon Health Sciences University in Portland.
“These results emphasize the importance of providing comprehensive care and support beyond traditional therapy to people living with bleeding disorders.”
Dr Recht and his colleagues presented results of the P-FiQ study in 3 posters at the ISTH 2015 Congress (abstracts PO277-MON, PO297-WED, and PO298-WED).
The study included adult males with mild to severe hemophilia who had a history of joint pain or bleeding. Subjects were asked to assess pain and functional impairment using patient-reported outcome instruments.
During routine visits over the course of a year, 164 participants completed a pain history and 5 questionnaires: the EQ-5D-5L; Brief Pain Inventory Short Form, version 2; International Physical Activity Questionnaire; SF-36v2; and Hemophilia Activities List.
The patients had a median age of 34. More patients had hemophilia A (n=122) than hemophilia B (n=42), and few (n=10) had inhibitors. Sixty-one percent of patients had self-reported arthritis, bone, or joint problems.
Current patient-reported treatment regimens (n=163) were prophylaxis (42%), on-demand treatment (39%), or mostly on-demand treatment (19%). Twenty-five of the 31 patients using on-demand treatment reported using infusions ahead of activity.
Pain prevalence and management
Most participants (85.2%) said they had experienced acute and/or chronic pain over the past 6 months. Twenty-nine percent said they had experienced acute and chronic pain, 32.7% had chronic pain only, 23.5% had acute pain only, and 14.8% reported no pain.
Acute pain was most frequently described as sharp, aching, shooting, and throbbing. Chronic pain was often described as aching, nagging, throbbing, and sharp.
The most common analgesics used for acute or chronic pain were acetaminophen (69.4% and 58%, respectively), NSAIDs (40% and 52%, respectively), and hydrocodone-acetaminophen (29.4% and 33%, respectively).
The most common nonanalgesic strategies used for acute or chronic pain were ice (72.9% and 37%, respectively), rest (48.2% and 34%, respectively), factor VIII/IX or bypassing agent (48.2% and 24%, respectively), elevation (34.1% and 28%, respectively), relaxation (30.6% and 23.0%, respectively), compression (27.1% and 21%, respectively), and heat (24.7% and 15%, respectively).
Impact of pain on daily life
When completing the EQ-5D-5L questionnaire, most patients reported problems with mobility, performing usual activities, and pain or discomfort. However, most patients said they had no problems with self-care (78%) or anxiety/depression (58.5%).
A similar proportion of patients reported slight and moderate pain and discomfort (29.9% and 31.1%, respectively). Pain and discomfort was severe for 11% of patients and extreme for 1.2%, but 26.8% of patients reported no pain or discomfort.
When it came to mobility, patients reported slight (32.3%), moderate (19.5%), and severe (8.5%) problems, and 1.2% of patients said they were unable to get around. However, 38.4% of patients reported having no such problems.
About 44% of patients reported no problems performing usual activities, but 37.2% had slight problems, 14.6% had moderate problems, and 1.8% of patients each had severe problems or were unable to perform usual activities.
For the Brief Pain Inventory, pain severity and interference with daily activities were rated on a scale of 0 to 10, with 0 being no pain/no interference and 10 being pain as bad as you can imagine/pain that completely interferes with daily life.
The overall median pain severity and pain interference were 3.0 (range, 1.3-4.8) and 2.9 (range, 0.7-5.2), respectively. The median worst pain was 6.0, least pain 2.0, average pain 3.0, and current pain 2.0. Ankles were the most frequently reported site of pain.
When completing the International Physical Activity Questionnaire, 49.3% of patients (73/148) reported no activity in the prior week.
The median SF-36v2 scores were lower for physical health domains than mental health domains, and the overall median health score was 3.0 (range, 2.0-3.0).
The median score on the Hemophilia Activities List was 76.1 (range, 59.2-95.1). And patients said hemophilia had a greater impact on their lower extremities than upper extremities.
Dr Recht and his colleagues said these results substantiate the high prevalence of pain in adults with hemophilia. And the study highlights opportunities to improve the assessment and management of pain in these patients.
Study investigators have received funding/consulting fees from—or are employees/shareholders of—Novo Nordisk, Baxter, Biogen, Bayer, OctaPharma, Pfizer, CSL Behring, Kendrion, Alexion, Grifols, OPKO Health, Sanofi, Merck, and ProMeticLife Sciences. ![]()
TORONTO—A survey of adult hemophilia patients suggests there is room for improvement in assessing and managing disease-related pain.
Roughly 85% of patients surveyed for this study, known as P-FiQ, said they had experienced acute and/or chronic pain in the past 6 months.
Although most patients had no trouble caring for themselves, the pain often had an impact on their daily lives, especially with regard to physical activity and overall mobility.
“Pain and discomfort are significant challenges for people with hemophilia,” said study investigator Michael Recht, MD, PhD, of Oregon Health Sciences University in Portland.
“These results emphasize the importance of providing comprehensive care and support beyond traditional therapy to people living with bleeding disorders.”
Dr Recht and his colleagues presented results of the P-FiQ study in 3 posters at the ISTH 2015 Congress (abstracts PO277-MON, PO297-WED, and PO298-WED).
The study included adult males with mild to severe hemophilia who had a history of joint pain or bleeding. Subjects were asked to assess pain and functional impairment using patient-reported outcome instruments.
During routine visits over the course of a year, 164 participants completed a pain history and 5 questionnaires: the EQ-5D-5L; Brief Pain Inventory Short Form, version 2; International Physical Activity Questionnaire; SF-36v2; and Hemophilia Activities List.
The patients had a median age of 34. More patients had hemophilia A (n=122) than hemophilia B (n=42), and few (n=10) had inhibitors. Sixty-one percent of patients had self-reported arthritis, bone, or joint problems.
Current patient-reported treatment regimens (n=163) were prophylaxis (42%), on-demand treatment (39%), or mostly on-demand treatment (19%). Twenty-five of the 31 patients using on-demand treatment reported using infusions ahead of activity.
Pain prevalence and management
Most participants (85.2%) said they had experienced acute and/or chronic pain over the past 6 months. Twenty-nine percent said they had experienced acute and chronic pain, 32.7% had chronic pain only, 23.5% had acute pain only, and 14.8% reported no pain.
Acute pain was most frequently described as sharp, aching, shooting, and throbbing. Chronic pain was often described as aching, nagging, throbbing, and sharp.
The most common analgesics used for acute or chronic pain were acetaminophen (69.4% and 58%, respectively), NSAIDs (40% and 52%, respectively), and hydrocodone-acetaminophen (29.4% and 33%, respectively).
The most common nonanalgesic strategies used for acute or chronic pain were ice (72.9% and 37%, respectively), rest (48.2% and 34%, respectively), factor VIII/IX or bypassing agent (48.2% and 24%, respectively), elevation (34.1% and 28%, respectively), relaxation (30.6% and 23.0%, respectively), compression (27.1% and 21%, respectively), and heat (24.7% and 15%, respectively).
Impact of pain on daily life
When completing the EQ-5D-5L questionnaire, most patients reported problems with mobility, performing usual activities, and pain or discomfort. However, most patients said they had no problems with self-care (78%) or anxiety/depression (58.5%).
A similar proportion of patients reported slight and moderate pain and discomfort (29.9% and 31.1%, respectively). Pain and discomfort was severe for 11% of patients and extreme for 1.2%, but 26.8% of patients reported no pain or discomfort.
When it came to mobility, patients reported slight (32.3%), moderate (19.5%), and severe (8.5%) problems, and 1.2% of patients said they were unable to get around. However, 38.4% of patients reported having no such problems.
About 44% of patients reported no problems performing usual activities, but 37.2% had slight problems, 14.6% had moderate problems, and 1.8% of patients each had severe problems or were unable to perform usual activities.
For the Brief Pain Inventory, pain severity and interference with daily activities were rated on a scale of 0 to 10, with 0 being no pain/no interference and 10 being pain as bad as you can imagine/pain that completely interferes with daily life.
The overall median pain severity and pain interference were 3.0 (range, 1.3-4.8) and 2.9 (range, 0.7-5.2), respectively. The median worst pain was 6.0, least pain 2.0, average pain 3.0, and current pain 2.0. Ankles were the most frequently reported site of pain.
When completing the International Physical Activity Questionnaire, 49.3% of patients (73/148) reported no activity in the prior week.
The median SF-36v2 scores were lower for physical health domains than mental health domains, and the overall median health score was 3.0 (range, 2.0-3.0).
The median score on the Hemophilia Activities List was 76.1 (range, 59.2-95.1). And patients said hemophilia had a greater impact on their lower extremities than upper extremities.
Dr Recht and his colleagues said these results substantiate the high prevalence of pain in adults with hemophilia. And the study highlights opportunities to improve the assessment and management of pain in these patients.
Study investigators have received funding/consulting fees from—or are employees/shareholders of—Novo Nordisk, Baxter, Biogen, Bayer, OctaPharma, Pfizer, CSL Behring, Kendrion, Alexion, Grifols, OPKO Health, Sanofi, Merck, and ProMeticLife Sciences. ![]()
Mutations linked to response, survival in aplastic anemia

Photo by Graham Colm
Scientists have identified genetic mutations that appear to be associated with treatment outcomes in patients with aplastic anemia.
When compared to unmutated patients, individuals with mutations in PIGA, BCOR, and BCORL1 tended to have better responses to immunosuppressive therapy and superior survival rates.
Other mutations—such as DNMT3A, ASXL1, and RUNX1—were associated with inferior response and survival rates.
Still, the investigators noted that clonal dynamics were “highly variable” in the patient samples they analyzed and might not necessarily have predicted outcomes.
Neal S. Young, MD, of the National Heart, Lung, and Blood Institute in Bethesda, Maryland, and his colleagues described this research in NEJM.
The team used next-generation DNA sequencing and array-based karyotyping to analyze 668 blood samples from 439 patients, including serial samples from 82 patients.
The investigators identified 249 somatic mutations in 156 patients (36%). The most common mutations occurred in the BCOR (9.3%), BCORL1 (9.3%), DNMT3A (8.4%), PIGA (7.5%), and ASXL1 (6.2%) genes.
Thirty-six percent of patients had multiple mutations. And some patients had multiple mutations in
the same genes, including PIGA, BCOR, DNMT3A, ASXL1, RUNX1, and ZRSR2.
The investigators identified clonal hematopoiesis in 47% of patients, most frequently as acquired mutations.
The team also found that, largely, the presence and number of mutations a patient had was positively correlated with the patient’s age. The exceptions were PIGA, BCOR, and BCORL1 mutations.
Patients with mutations in PIGA, BCOR, or BCORL1 had better responses to immunosuppressive therapy and better overall and progression-free survival than unmutated patients.
Other mutations were associated with worse outcomes. Patients with mutations in ASXL1, DNMT3A, TP53, RUNX1, JAK2, JAK3, or CSMD1 did not respond as well as unmutated patients to immunosuppressive therapy.
Mutations in ASXL1, DNMT3A, TP53, RUNX1, and CSMD1 were associated with worse overall survival, and mutations in ASXL1, DNMT3A, RUNX1, JAK2, and JAK3 were associated with worse progression-free survival.
The investigators also observed an increase in the size of clones with DNMT3A, ASXL1, RUNX1, or U2AF1 mutations. But the size of clones with PIGA, BCOR, or BCORL1 mutations remained stable or decreased with time. ![]()
Photo by Graham Colm
Scientists have identified genetic mutations that appear to be associated with treatment outcomes in patients with aplastic anemia.
When compared to unmutated patients, individuals with mutations in PIGA, BCOR, and BCORL1 tended to have better responses to immunosuppressive therapy and superior survival rates.
Other mutations—such as DNMT3A, ASXL1, and RUNX1—were associated with inferior response and survival rates.
Still, the investigators noted that clonal dynamics were “highly variable” in the patient samples they analyzed and might not necessarily have predicted outcomes.
Neal S. Young, MD, of the National Heart, Lung, and Blood Institute in Bethesda, Maryland, and his colleagues described this research in NEJM.
The team used next-generation DNA sequencing and array-based karyotyping to analyze 668 blood samples from 439 patients, including serial samples from 82 patients.
The investigators identified 249 somatic mutations in 156 patients (36%). The most common mutations occurred in the BCOR (9.3%), BCORL1 (9.3%), DNMT3A (8.4%), PIGA (7.5%), and ASXL1 (6.2%) genes.
Thirty-six percent of patients had multiple mutations. And some patients had multiple mutations in
the same genes, including PIGA, BCOR, DNMT3A, ASXL1, RUNX1, and ZRSR2.
The investigators identified clonal hematopoiesis in 47% of patients, most frequently as acquired mutations.
The team also found that, largely, the presence and number of mutations a patient had was positively correlated with the patient’s age. The exceptions were PIGA, BCOR, and BCORL1 mutations.
Patients with mutations in PIGA, BCOR, or BCORL1 had better responses to immunosuppressive therapy and better overall and progression-free survival than unmutated patients.
Other mutations were associated with worse outcomes. Patients with mutations in ASXL1, DNMT3A, TP53, RUNX1, JAK2, JAK3, or CSMD1 did not respond as well as unmutated patients to immunosuppressive therapy.
Mutations in ASXL1, DNMT3A, TP53, RUNX1, and CSMD1 were associated with worse overall survival, and mutations in ASXL1, DNMT3A, RUNX1, JAK2, and JAK3 were associated with worse progression-free survival.
The investigators also observed an increase in the size of clones with DNMT3A, ASXL1, RUNX1, or U2AF1 mutations. But the size of clones with PIGA, BCOR, or BCORL1 mutations remained stable or decreased with time. ![]()
Photo by Graham Colm
Scientists have identified genetic mutations that appear to be associated with treatment outcomes in patients with aplastic anemia.
When compared to unmutated patients, individuals with mutations in PIGA, BCOR, and BCORL1 tended to have better responses to immunosuppressive therapy and superior survival rates.
Other mutations—such as DNMT3A, ASXL1, and RUNX1—were associated with inferior response and survival rates.
Still, the investigators noted that clonal dynamics were “highly variable” in the patient samples they analyzed and might not necessarily have predicted outcomes.
Neal S. Young, MD, of the National Heart, Lung, and Blood Institute in Bethesda, Maryland, and his colleagues described this research in NEJM.
The team used next-generation DNA sequencing and array-based karyotyping to analyze 668 blood samples from 439 patients, including serial samples from 82 patients.
The investigators identified 249 somatic mutations in 156 patients (36%). The most common mutations occurred in the BCOR (9.3%), BCORL1 (9.3%), DNMT3A (8.4%), PIGA (7.5%), and ASXL1 (6.2%) genes.
Thirty-six percent of patients had multiple mutations. And some patients had multiple mutations in
the same genes, including PIGA, BCOR, DNMT3A, ASXL1, RUNX1, and ZRSR2.
The investigators identified clonal hematopoiesis in 47% of patients, most frequently as acquired mutations.
The team also found that, largely, the presence and number of mutations a patient had was positively correlated with the patient’s age. The exceptions were PIGA, BCOR, and BCORL1 mutations.
Patients with mutations in PIGA, BCOR, or BCORL1 had better responses to immunosuppressive therapy and better overall and progression-free survival than unmutated patients.
Other mutations were associated with worse outcomes. Patients with mutations in ASXL1, DNMT3A, TP53, RUNX1, JAK2, JAK3, or CSMD1 did not respond as well as unmutated patients to immunosuppressive therapy.
Mutations in ASXL1, DNMT3A, TP53, RUNX1, and CSMD1 were associated with worse overall survival, and mutations in ASXL1, DNMT3A, RUNX1, JAK2, and JAK3 were associated with worse progression-free survival.
The investigators also observed an increase in the size of clones with DNMT3A, ASXL1, RUNX1, or U2AF1 mutations. But the size of clones with PIGA, BCOR, or BCORL1 mutations remained stable or decreased with time.
Radiation increases risk of death from CML, other leukemias
![]()
power plant in Germany
Protracted exposure to ionizing radiation, even at low doses, can increase a person’s risk of dying from certain leukemias, according to research published in The Lancet Haematology.
The study showed that protracted radiation exposure was associated with an excess risk of leukemia mortality, particularly for chronic myeloid leukemia (CML).
However, there was no excess mortality risk for chronic lymphocytic leukemia (CLL).
Investigators also observed an association between ionizing radiation exposure and death from multiple myeloma or lymphoma, but they said the evidence for these associations was not strong.
“To date, this study provides the most precise evaluation of the risk of developing leukemia linked to the protracted low doses of radiation received by nuclear workers throughout their careers,” said study author Ausrele Kesminiene, MD, of the International Agency for Research on Cancer, the specialized cancer agency of the World Health Organization.
“It shows that the nuclear workers we studied have a small increase in the risk of dying from leukemia as their exposure to radiation increases.”
This study, known as INWORKS, included 308,297 workers who were monitored for exposure to radiation.
Subjects were employed for at least 1 year by the Atomic Energy Commission, AREVA Nuclear Cycle, or the National Electricity Company in France or the Departments of Energy and Defense in the US. The study also included nuclear industry employers in the National Registry for Radiation Workers in the UK.
Investigators assessed the risk of death from hematologic malignancies among these subjects. The team used Poisson regression to quantify associations between the estimated radiation dose in the red bone marrow and mortality from malignancy.
The mean follow-up was 27 years, and nearly 22% of workers died during that time. The mean cumulative radiation dose was 16 mGy, the median was 2.1 mGy, and the mean yearly dose was 1.1 mGy.
Quantifying the risk
The investigators found “strong evidence” for a positive association between exposure to ionizing radiation and the risk of death from leukemias, excluding CLL. Specifically, the excess relative risk of mortality per Gy of radiation was 2.96 (90% CI 1.17-5.21).
Even low doses of radiation posed a risk. Fifty-three percent of deaths from leukemia (excluding CLL) occurred in workers who had accrued less than 5 mGy of radiation.
However, the relative risk of death from leukemia (excluding CLL) increased with the radiation dose. The relative risk was 1.00 for 0-5 mGy, 1.01 for 5-50 mGy, 1.30 for 50-100 mGy, 1.19 for 100-200 mGy, 2.30 for 200-300 mGy, and 1.70 for more than 300 mGy.
The data also showed the risk of cancer mortality associated with radiation exposure varied according to the type of leukemia.
The excess relative risk of mortality was 10.45 for CML, 1.29 for acute myeloid leukemia, and 5.80 for acute lymphoblastic leukemia. For CLL, the excess relative risk was -1.06.
The investigators also found positive associations between radiation exposure and mortality from Hodgkin lymphoma, non-Hodgkin lymphoma, and multiple myeloma. However, the findings were “highly imprecise,” with confidence intervals that spanned 0.
![]()
power plant in Germany
Protracted exposure to ionizing radiation, even at low doses, can increase a person’s risk of dying from certain leukemias, according to research published in The Lancet Haematology.
The study showed that protracted radiation exposure was associated with an excess risk of leukemia mortality, particularly for chronic myeloid leukemia (CML).
However, there was no excess mortality risk for chronic lymphocytic leukemia (CLL).
Investigators also observed an association between ionizing radiation exposure and death from multiple myeloma or lymphoma, but they said the evidence for these associations was not strong.
“To date, this study provides the most precise evaluation of the risk of developing leukemia linked to the protracted low doses of radiation received by nuclear workers throughout their careers,” said study author Ausrele Kesminiene, MD, of the International Agency for Research on Cancer, the specialized cancer agency of the World Health Organization.
“It shows that the nuclear workers we studied have a small increase in the risk of dying from leukemia as their exposure to radiation increases.”
This study, known as INWORKS, included 308,297 workers who were monitored for exposure to radiation.
Subjects were employed for at least 1 year by the Atomic Energy Commission, AREVA Nuclear Cycle, or the National Electricity Company in France or the Departments of Energy and Defense in the US. The study also included nuclear industry employers in the National Registry for Radiation Workers in the UK.
Investigators assessed the risk of death from hematologic malignancies among these subjects. The team used Poisson regression to quantify associations between the estimated radiation dose in the red bone marrow and mortality from malignancy.
The mean follow-up was 27 years, and nearly 22% of workers died during that time. The mean cumulative radiation dose was 16 mGy, the median was 2.1 mGy, and the mean yearly dose was 1.1 mGy.
Quantifying the risk
The investigators found “strong evidence” for a positive association between exposure to ionizing radiation and the risk of death from leukemias, excluding CLL. Specifically, the excess relative risk of mortality per Gy of radiation was 2.96 (90% CI 1.17-5.21).
Even low doses of radiation posed a risk. Fifty-three percent of deaths from leukemia (excluding CLL) occurred in workers who had accrued less than 5 mGy of radiation.
However, the relative risk of death from leukemia (excluding CLL) increased with the radiation dose. The relative risk was 1.00 for 0-5 mGy, 1.01 for 5-50 mGy, 1.30 for 50-100 mGy, 1.19 for 100-200 mGy, 2.30 for 200-300 mGy, and 1.70 for more than 300 mGy.
The data also showed the risk of cancer mortality associated with radiation exposure varied according to the type of leukemia.
The excess relative risk of mortality was 10.45 for CML, 1.29 for acute myeloid leukemia, and 5.80 for acute lymphoblastic leukemia. For CLL, the excess relative risk was -1.06.
The investigators also found positive associations between radiation exposure and mortality from Hodgkin lymphoma, non-Hodgkin lymphoma, and multiple myeloma. However, the findings were “highly imprecise,” with confidence intervals that spanned 0.
![]()
power plant in Germany
Protracted exposure to ionizing radiation, even at low doses, can increase a person’s risk of dying from certain leukemias, according to research published in The Lancet Haematology.
The study showed that protracted radiation exposure was associated with an excess risk of leukemia mortality, particularly for chronic myeloid leukemia (CML).
However, there was no excess mortality risk for chronic lymphocytic leukemia (CLL).
Investigators also observed an association between ionizing radiation exposure and death from multiple myeloma or lymphoma, but they said the evidence for these associations was not strong.
“To date, this study provides the most precise evaluation of the risk of developing leukemia linked to the protracted low doses of radiation received by nuclear workers throughout their careers,” said study author Ausrele Kesminiene, MD, of the International Agency for Research on Cancer, the specialized cancer agency of the World Health Organization.
“It shows that the nuclear workers we studied have a small increase in the risk of dying from leukemia as their exposure to radiation increases.”
This study, known as INWORKS, included 308,297 workers who were monitored for exposure to radiation.
Subjects were employed for at least 1 year by the Atomic Energy Commission, AREVA Nuclear Cycle, or the National Electricity Company in France or the Departments of Energy and Defense in the US. The study also included nuclear industry employers in the National Registry for Radiation Workers in the UK.
Investigators assessed the risk of death from hematologic malignancies among these subjects. The team used Poisson regression to quantify associations between the estimated radiation dose in the red bone marrow and mortality from malignancy.
The mean follow-up was 27 years, and nearly 22% of workers died during that time. The mean cumulative radiation dose was 16 mGy, the median was 2.1 mGy, and the mean yearly dose was 1.1 mGy.
Quantifying the risk
The investigators found “strong evidence” for a positive association between exposure to ionizing radiation and the risk of death from leukemias, excluding CLL. Specifically, the excess relative risk of mortality per Gy of radiation was 2.96 (90% CI 1.17-5.21).
Even low doses of radiation posed a risk. Fifty-three percent of deaths from leukemia (excluding CLL) occurred in workers who had accrued less than 5 mGy of radiation.
However, the relative risk of death from leukemia (excluding CLL) increased with the radiation dose. The relative risk was 1.00 for 0-5 mGy, 1.01 for 5-50 mGy, 1.30 for 50-100 mGy, 1.19 for 100-200 mGy, 2.30 for 200-300 mGy, and 1.70 for more than 300 mGy.
The data also showed the risk of cancer mortality associated with radiation exposure varied according to the type of leukemia.
The excess relative risk of mortality was 10.45 for CML, 1.29 for acute myeloid leukemia, and 5.80 for acute lymphoblastic leukemia. For CLL, the excess relative risk was -1.06.
The investigators also found positive associations between radiation exposure and mortality from Hodgkin lymphoma, non-Hodgkin lymphoma, and multiple myeloma. However, the findings were “highly imprecise,” with confidence intervals that spanned 0.
Extended-interval dosing appears safe, effective

Photo courtesy of Biogen
TORONTO—Full results of a phase 3 study support extended-interval dosing with a recombinant factor IX Fc fusion protein (rFIXFc) over FIX products with a standard half-life, according to a speaker at the 2015 ISTH Congress.
Kathelijn Fischer, MD, PhD, of the University Medical Center Utrecht in The Netherlands, reported results with rFIXFc (also known as eftrenonacog alfa and Alprolix), in children with severe hemophilia B who were enrolled on the KIDS B-LONG study.
rFIXFc was successful in preventing and treating bleeding episodes in these patients. Furthermore, the patients did not develop inhibitors, and there were no serious adverse events related to treatment.
Dr Fischer presented these results as abstract LB009. Interim results of this study helped support the US approval of rFIXFc for use in children. The trial was sponsored by Sobi and Biogen, the companies developing rFIXFc.
KIDS B-LONG included 30 boys younger than 12 who had severe hemophilia B. The patients had at least 50 prior exposure days to FIX therapies and no history of inhibitors.
At baseline, all patients were receiving FIX prophylaxis. Seventy-seven percent of patients were receiving 2 or more doses a week.
On day 1 of the study, patients received rFIXFc at 50 IU/kg. They then received weekly prophylaxis at an initial dose of 50 IU/kg to 60 IU/kg. Doses were adjusted throughout the study, but the maximum was 100 IU/kg. The minimum dosing frequency was once a week, and the maximum was twice a week.
Twenty-seven patients (90%) completed the study. The median time spent on study was 49.4 weeks, and 24 patients (80%) received rFIXFc injections on at least 50 separate days.
Safety
None of the patients developed inhibitors or non-neutralizing anti-rFIXFc antibodies. There were no anaphylactic reactions, hypersensitivity reactions, thrombotic events, or deaths.
Adverse events occurred in 86.7% of patients. The most frequent were nanopharyngitis (23.3%) and falls (20%). Eleven serious adverse events occurred in 4 patients. None were considered related to treatment, and none led to study discontinuation.
One adverse event was considered related to rFIXFc. A 3-year-old child experienced decreased appetite.
Efficacy
The median annualized bleeding rate (ABR) was 2.0 overall, 1.1 in children under 6, and 2.1 in children ages 6 to 11.
For spontaneous bleeds, the median ABR was 0, both overall and in the 2 age groups. For joint bleeds, the median ABR was 0 overall and in the younger age group, but it was 1.1 for the older children.
Thirty-three percent of patients had no bleeding episodes while on study, and 63% had no joint bleeds.
Ninety-seven percent of patients receiving rFIXFc prophylaxis had no change in their dosing interval.
For patients under 6, the median prophylactic dose was 59.4 IU/kg/week (range, 53.0-64.8). For patients ages 6 to 11, the median dose was 57.8 IU/kg/week (range, 51.7-65.0)
When patients received rFIXFc to treat bleeding, 75% of bleeds were controlled with 1 infusion, and 91.7% were controlled with 1 or 2 infusions. The median dose per infusion was 63.5 IU/kg (range, 48.9-99.4).
Pharmacokinetics
The terminal half-life of rFIXFc was 66.5 hours for children under 6 and 70.3 hours for children ages 6 to 11. The clearance was 4.4 mL/hour/kg and 3.5 mL/hour/kg, respectively. The incremental recovery (IR) was 0.59 IU/dL per IU/kg and 0.72 IU/dL per IU/kg, respectively.
Compared to pre-study treatment with BeneFIX (recombinant FIX) at 50 IU/kg, rFIXFc at 50 IU/kg had a significantly longer half-life. In children younger than 6, the half-life was 66.5 hours for rFIXFc and 18.2 hours for BeneFIX (P<0.001). In children ages 6 to 11, the half-lives were 71.1 and 19.2 hours, respectively (P<0.001).
There was no significant difference between the treatments with regard to IR for children under 6. IR was 0.59 with rFIXFc and 0.52 with BeneFIX (P=0.109). However, there was a significant difference in IR for children ages 6 to 11—0.70 for rFIXFc and 0.54 for BeneFIX (P=0.003).
Photo courtesy of Biogen
TORONTO—Full results of a phase 3 study support extended-interval dosing with a recombinant factor IX Fc fusion protein (rFIXFc) over FIX products with a standard half-life, according to a speaker at the 2015 ISTH Congress.
Kathelijn Fischer, MD, PhD, of the University Medical Center Utrecht in The Netherlands, reported results with rFIXFc (also known as eftrenonacog alfa and Alprolix), in children with severe hemophilia B who were enrolled on the KIDS B-LONG study.
rFIXFc was successful in preventing and treating bleeding episodes in these patients. Furthermore, the patients did not develop inhibitors, and there were no serious adverse events related to treatment.
Dr Fischer presented these results as abstract LB009. Interim results of this study helped support the US approval of rFIXFc for use in children. The trial was sponsored by Sobi and Biogen, the companies developing rFIXFc.
KIDS B-LONG included 30 boys younger than 12 who had severe hemophilia B. The patients had at least 50 prior exposure days to FIX therapies and no history of inhibitors.
At baseline, all patients were receiving FIX prophylaxis. Seventy-seven percent of patients were receiving 2 or more doses a week.
On day 1 of the study, patients received rFIXFc at 50 IU/kg. They then received weekly prophylaxis at an initial dose of 50 IU/kg to 60 IU/kg. Doses were adjusted throughout the study, but the maximum was 100 IU/kg. The minimum dosing frequency was once a week, and the maximum was twice a week.
Twenty-seven patients (90%) completed the study. The median time spent on study was 49.4 weeks, and 24 patients (80%) received rFIXFc injections on at least 50 separate days.
Safety
None of the patients developed inhibitors or non-neutralizing anti-rFIXFc antibodies. There were no anaphylactic reactions, hypersensitivity reactions, thrombotic events, or deaths.
Adverse events occurred in 86.7% of patients. The most frequent were nanopharyngitis (23.3%) and falls (20%). Eleven serious adverse events occurred in 4 patients. None were considered related to treatment, and none led to study discontinuation.
One adverse event was considered related to rFIXFc. A 3-year-old child experienced decreased appetite.
Efficacy
The median annualized bleeding rate (ABR) was 2.0 overall, 1.1 in children under 6, and 2.1 in children ages 6 to 11.
For spontaneous bleeds, the median ABR was 0, both overall and in the 2 age groups. For joint bleeds, the median ABR was 0 overall and in the younger age group, but it was 1.1 for the older children.
Thirty-three percent of patients had no bleeding episodes while on study, and 63% had no joint bleeds.
Ninety-seven percent of patients receiving rFIXFc prophylaxis had no change in their dosing interval.
For patients under 6, the median prophylactic dose was 59.4 IU/kg/week (range, 53.0-64.8). For patients ages 6 to 11, the median dose was 57.8 IU/kg/week (range, 51.7-65.0)
When patients received rFIXFc to treat bleeding, 75% of bleeds were controlled with 1 infusion, and 91.7% were controlled with 1 or 2 infusions. The median dose per infusion was 63.5 IU/kg (range, 48.9-99.4).
Pharmacokinetics
The terminal half-life of rFIXFc was 66.5 hours for children under 6 and 70.3 hours for children ages 6 to 11. The clearance was 4.4 mL/hour/kg and 3.5 mL/hour/kg, respectively. The incremental recovery (IR) was 0.59 IU/dL per IU/kg and 0.72 IU/dL per IU/kg, respectively.
Compared to pre-study treatment with BeneFIX (recombinant FIX) at 50 IU/kg, rFIXFc at 50 IU/kg had a significantly longer half-life. In children younger than 6, the half-life was 66.5 hours for rFIXFc and 18.2 hours for BeneFIX (P<0.001). In children ages 6 to 11, the half-lives were 71.1 and 19.2 hours, respectively (P<0.001).
There was no significant difference between the treatments with regard to IR for children under 6. IR was 0.59 with rFIXFc and 0.52 with BeneFIX (P=0.109). However, there was a significant difference in IR for children ages 6 to 11—0.70 for rFIXFc and 0.54 for BeneFIX (P=0.003).
Photo courtesy of Biogen
TORONTO—Full results of a phase 3 study support extended-interval dosing with a recombinant factor IX Fc fusion protein (rFIXFc) over FIX products with a standard half-life, according to a speaker at the 2015 ISTH Congress.
Kathelijn Fischer, MD, PhD, of the University Medical Center Utrecht in The Netherlands, reported results with rFIXFc (also known as eftrenonacog alfa and Alprolix), in children with severe hemophilia B who were enrolled on the KIDS B-LONG study.
rFIXFc was successful in preventing and treating bleeding episodes in these patients. Furthermore, the patients did not develop inhibitors, and there were no serious adverse events related to treatment.
Dr Fischer presented these results as abstract LB009. Interim results of this study helped support the US approval of rFIXFc for use in children. The trial was sponsored by Sobi and Biogen, the companies developing rFIXFc.
KIDS B-LONG included 30 boys younger than 12 who had severe hemophilia B. The patients had at least 50 prior exposure days to FIX therapies and no history of inhibitors.
At baseline, all patients were receiving FIX prophylaxis. Seventy-seven percent of patients were receiving 2 or more doses a week.
On day 1 of the study, patients received rFIXFc at 50 IU/kg. They then received weekly prophylaxis at an initial dose of 50 IU/kg to 60 IU/kg. Doses were adjusted throughout the study, but the maximum was 100 IU/kg. The minimum dosing frequency was once a week, and the maximum was twice a week.
Twenty-seven patients (90%) completed the study. The median time spent on study was 49.4 weeks, and 24 patients (80%) received rFIXFc injections on at least 50 separate days.
Safety
None of the patients developed inhibitors or non-neutralizing anti-rFIXFc antibodies. There were no anaphylactic reactions, hypersensitivity reactions, thrombotic events, or deaths.
Adverse events occurred in 86.7% of patients. The most frequent were nanopharyngitis (23.3%) and falls (20%). Eleven serious adverse events occurred in 4 patients. None were considered related to treatment, and none led to study discontinuation.
One adverse event was considered related to rFIXFc. A 3-year-old child experienced decreased appetite.
Efficacy
The median annualized bleeding rate (ABR) was 2.0 overall, 1.1 in children under 6, and 2.1 in children ages 6 to 11.
For spontaneous bleeds, the median ABR was 0, both overall and in the 2 age groups. For joint bleeds, the median ABR was 0 overall and in the younger age group, but it was 1.1 for the older children.
Thirty-three percent of patients had no bleeding episodes while on study, and 63% had no joint bleeds.
Ninety-seven percent of patients receiving rFIXFc prophylaxis had no change in their dosing interval.
For patients under 6, the median prophylactic dose was 59.4 IU/kg/week (range, 53.0-64.8). For patients ages 6 to 11, the median dose was 57.8 IU/kg/week (range, 51.7-65.0)
When patients received rFIXFc to treat bleeding, 75% of bleeds were controlled with 1 infusion, and 91.7% were controlled with 1 or 2 infusions. The median dose per infusion was 63.5 IU/kg (range, 48.9-99.4).
Pharmacokinetics
The terminal half-life of rFIXFc was 66.5 hours for children under 6 and 70.3 hours for children ages 6 to 11. The clearance was 4.4 mL/hour/kg and 3.5 mL/hour/kg, respectively. The incremental recovery (IR) was 0.59 IU/dL per IU/kg and 0.72 IU/dL per IU/kg, respectively.
Compared to pre-study treatment with BeneFIX (recombinant FIX) at 50 IU/kg, rFIXFc at 50 IU/kg had a significantly longer half-life. In children younger than 6, the half-life was 66.5 hours for rFIXFc and 18.2 hours for BeneFIX (P<0.001). In children ages 6 to 11, the half-lives were 71.1 and 19.2 hours, respectively (P<0.001).
There was no significant difference between the treatments with regard to IR for children under 6. IR was 0.59 with rFIXFc and 0.52 with BeneFIX (P=0.109). However, there was a significant difference in IR for children ages 6 to 11—0.70 for rFIXFc and 0.54 for BeneFIX (P=0.003).
Drug can produce durable responses in rel/ref PTCL
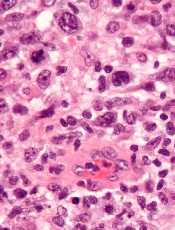
anaplastic large cell lymphoma
The histone deacetylase inhibitor belinostat can produce durable responses in patients with relapsed/refractory peripheral T-cell lymphoma (PTCL), results of the BELIEF study suggest.
The overall response rate (ORR) was low in this heavily pretreated population, at about 26%.
But responses occurred across PTCL subtypes and irrespective of a patient’s prior treatment, and the median duration of response was 13.6 months.
The researchers said toxicity was manageable, and the rate of grade 3/4 thrombocytopenia was low.
“This is a very exciting time in the treatment of patients with PTCL,” said Owen O’Connor, MD, PhD, of Columbia University Medical Center in New York, New York.
“At long last, we finally have tools in the therapeutic armamentarium to help our patients. Belinostat represents the latest drug approved for patients with [relapsed/refractory] PTCL that has relatively few side effects and produces long durations of benefit, even in patients who have received multiple conventional treatments in the past.”
Dr O’Connor and his colleagues reported results with belinostat in the Journal of Clinical Oncology. The research was sponsored by Spectrum Pharmaceuticals, Inc., the company developing belinostat (as Beleodaq).
BELIEF was a single-arm, phase 2 trial that enrolled 129 patients with relapsed/refractory PTCL. One hundred and twenty patients were evaluable. They had a median age of 64 (range, 29-81), and roughly half of patients were female.
PTCL subtypes included PTCL-not otherwise specified (n=77), angioimmunoblastic T-cell lymphoma (n=22), ALK-negative anaplastic large cell lymphoma (n=13), ALK-positive anaplastic large cell lymphoma (n=2), enteropathy-associated T-cell lymphoma (n=2), nasal type extranodal natural killer T-cell lymphoma (n=2), and hepatosplenic T-cell lymphoma (n=2).
The patients had received a median of 2 prior therapies (range, 1-8), including multi-agent and single-agent regimens, as well as transplant.
For this study, the patients received belinostat (1000 mg/m2) as daily, 30-minute infusions on days 1-5 every 21 days until disease progression or unacceptable toxicity.
Response and survival
The study’s primary endpoint was ORR, as assessed by an independent review committee using the International Working Group criteria. The ORR was 25.8% (n=31), including 13 complete responses (10.8%) and 18 partial responses (15%).
The median time to response was 5.6 weeks, and the median duration of response was 13.6 months by International Working Group criteria. The median duration of response based on the date of first response to progressive disease or death was 8.4 months.
Among patients who achieved a complete response, the median duration of response was not reached and exceeded 29 months. The longest ongoing patient response is more than 36 months.
The median progression-free survival was 1.6 months, and the median overall survival was 7.9 months.
Forty-six patients were censored for overall survival because they were alive at the data cutoff point. Seven of these patients continued to receive belinostat. Five were in complete response, 1 had a partial response, and 1 had stable disease.
Twelve patients underwent stem cell transplant after belinostat, and 10 of these patients were still alive at the data cutoff. Their overall survival ranged from 9.4 months to 22.9 months.
Adverse events
Treatment-emergent adverse events (AEs) occurred in 96.9% of patients, and treatment-related AEs occurred in 83.7%. The most common treatment-related AEs were nausea (38.0%), fatigue (28.7%), and vomiting (24.0%). Serious AEs occurred in 47.3% of patients.
Grade 3/4 related AEs were reported in 61.2% of patients, and the most common were anemia (10.9%), thrombocytopenia (7.0%), dyspnea (6.2%), neutropenia (6.2%), fatigue (5.4%), and pneumonia (5.4%).
About 12% of patients underwent a dose reduction due to AEs, 19.4% discontinued treatment due to AEs, and 10.9% of these AEs were considered treatment-related.
Twenty-two patients (17.1%) died, 12 (9.3%) of progressive disease and 10 (7.8%) of AEs. One death was considered related to belinostat. This patient had tolerated 9 cycles of the drug without complications but had elevated liver function tests at the start of cycle 10 that subsequently led to death from toxic liver failure.
anaplastic large cell lymphoma
The histone deacetylase inhibitor belinostat can produce durable responses in patients with relapsed/refractory peripheral T-cell lymphoma (PTCL), results of the BELIEF study suggest.
The overall response rate (ORR) was low in this heavily pretreated population, at about 26%.
But responses occurred across PTCL subtypes and irrespective of a patient’s prior treatment, and the median duration of response was 13.6 months.
The researchers said toxicity was manageable, and the rate of grade 3/4 thrombocytopenia was low.
“This is a very exciting time in the treatment of patients with PTCL,” said Owen O’Connor, MD, PhD, of Columbia University Medical Center in New York, New York.
“At long last, we finally have tools in the therapeutic armamentarium to help our patients. Belinostat represents the latest drug approved for patients with [relapsed/refractory] PTCL that has relatively few side effects and produces long durations of benefit, even in patients who have received multiple conventional treatments in the past.”
Dr O’Connor and his colleagues reported results with belinostat in the Journal of Clinical Oncology. The research was sponsored by Spectrum Pharmaceuticals, Inc., the company developing belinostat (as Beleodaq).
BELIEF was a single-arm, phase 2 trial that enrolled 129 patients with relapsed/refractory PTCL. One hundred and twenty patients were evaluable. They had a median age of 64 (range, 29-81), and roughly half of patients were female.
PTCL subtypes included PTCL-not otherwise specified (n=77), angioimmunoblastic T-cell lymphoma (n=22), ALK-negative anaplastic large cell lymphoma (n=13), ALK-positive anaplastic large cell lymphoma (n=2), enteropathy-associated T-cell lymphoma (n=2), nasal type extranodal natural killer T-cell lymphoma (n=2), and hepatosplenic T-cell lymphoma (n=2).
The patients had received a median of 2 prior therapies (range, 1-8), including multi-agent and single-agent regimens, as well as transplant.
For this study, the patients received belinostat (1000 mg/m2) as daily, 30-minute infusions on days 1-5 every 21 days until disease progression or unacceptable toxicity.
Response and survival
The study’s primary endpoint was ORR, as assessed by an independent review committee using the International Working Group criteria. The ORR was 25.8% (n=31), including 13 complete responses (10.8%) and 18 partial responses (15%).
The median time to response was 5.6 weeks, and the median duration of response was 13.6 months by International Working Group criteria. The median duration of response based on the date of first response to progressive disease or death was 8.4 months.
Among patients who achieved a complete response, the median duration of response was not reached and exceeded 29 months. The longest ongoing patient response is more than 36 months.
The median progression-free survival was 1.6 months, and the median overall survival was 7.9 months.
Forty-six patients were censored for overall survival because they were alive at the data cutoff point. Seven of these patients continued to receive belinostat. Five were in complete response, 1 had a partial response, and 1 had stable disease.
Twelve patients underwent stem cell transplant after belinostat, and 10 of these patients were still alive at the data cutoff. Their overall survival ranged from 9.4 months to 22.9 months.
Adverse events
Treatment-emergent adverse events (AEs) occurred in 96.9% of patients, and treatment-related AEs occurred in 83.7%. The most common treatment-related AEs were nausea (38.0%), fatigue (28.7%), and vomiting (24.0%). Serious AEs occurred in 47.3% of patients.
Grade 3/4 related AEs were reported in 61.2% of patients, and the most common were anemia (10.9%), thrombocytopenia (7.0%), dyspnea (6.2%), neutropenia (6.2%), fatigue (5.4%), and pneumonia (5.4%).
About 12% of patients underwent a dose reduction due to AEs, 19.4% discontinued treatment due to AEs, and 10.9% of these AEs were considered treatment-related.
Twenty-two patients (17.1%) died, 12 (9.3%) of progressive disease and 10 (7.8%) of AEs. One death was considered related to belinostat. This patient had tolerated 9 cycles of the drug without complications but had elevated liver function tests at the start of cycle 10 that subsequently led to death from toxic liver failure.
anaplastic large cell lymphoma
The histone deacetylase inhibitor belinostat can produce durable responses in patients with relapsed/refractory peripheral T-cell lymphoma (PTCL), results of the BELIEF study suggest.
The overall response rate (ORR) was low in this heavily pretreated population, at about 26%.
But responses occurred across PTCL subtypes and irrespective of a patient’s prior treatment, and the median duration of response was 13.6 months.
The researchers said toxicity was manageable, and the rate of grade 3/4 thrombocytopenia was low.
“This is a very exciting time in the treatment of patients with PTCL,” said Owen O’Connor, MD, PhD, of Columbia University Medical Center in New York, New York.
“At long last, we finally have tools in the therapeutic armamentarium to help our patients. Belinostat represents the latest drug approved for patients with [relapsed/refractory] PTCL that has relatively few side effects and produces long durations of benefit, even in patients who have received multiple conventional treatments in the past.”
Dr O’Connor and his colleagues reported results with belinostat in the Journal of Clinical Oncology. The research was sponsored by Spectrum Pharmaceuticals, Inc., the company developing belinostat (as Beleodaq).
BELIEF was a single-arm, phase 2 trial that enrolled 129 patients with relapsed/refractory PTCL. One hundred and twenty patients were evaluable. They had a median age of 64 (range, 29-81), and roughly half of patients were female.
PTCL subtypes included PTCL-not otherwise specified (n=77), angioimmunoblastic T-cell lymphoma (n=22), ALK-negative anaplastic large cell lymphoma (n=13), ALK-positive anaplastic large cell lymphoma (n=2), enteropathy-associated T-cell lymphoma (n=2), nasal type extranodal natural killer T-cell lymphoma (n=2), and hepatosplenic T-cell lymphoma (n=2).
The patients had received a median of 2 prior therapies (range, 1-8), including multi-agent and single-agent regimens, as well as transplant.
For this study, the patients received belinostat (1000 mg/m2) as daily, 30-minute infusions on days 1-5 every 21 days until disease progression or unacceptable toxicity.
Response and survival
The study’s primary endpoint was ORR, as assessed by an independent review committee using the International Working Group criteria. The ORR was 25.8% (n=31), including 13 complete responses (10.8%) and 18 partial responses (15%).
The median time to response was 5.6 weeks, and the median duration of response was 13.6 months by International Working Group criteria. The median duration of response based on the date of first response to progressive disease or death was 8.4 months.
Among patients who achieved a complete response, the median duration of response was not reached and exceeded 29 months. The longest ongoing patient response is more than 36 months.
The median progression-free survival was 1.6 months, and the median overall survival was 7.9 months.
Forty-six patients were censored for overall survival because they were alive at the data cutoff point. Seven of these patients continued to receive belinostat. Five were in complete response, 1 had a partial response, and 1 had stable disease.
Twelve patients underwent stem cell transplant after belinostat, and 10 of these patients were still alive at the data cutoff. Their overall survival ranged from 9.4 months to 22.9 months.
Adverse events
Treatment-emergent adverse events (AEs) occurred in 96.9% of patients, and treatment-related AEs occurred in 83.7%. The most common treatment-related AEs were nausea (38.0%), fatigue (28.7%), and vomiting (24.0%). Serious AEs occurred in 47.3% of patients.
Grade 3/4 related AEs were reported in 61.2% of patients, and the most common were anemia (10.9%), thrombocytopenia (7.0%), dyspnea (6.2%), neutropenia (6.2%), fatigue (5.4%), and pneumonia (5.4%).
About 12% of patients underwent a dose reduction due to AEs, 19.4% discontinued treatment due to AEs, and 10.9% of these AEs were considered treatment-related.
Twenty-two patients (17.1%) died, 12 (9.3%) of progressive disease and 10 (7.8%) of AEs. One death was considered related to belinostat. This patient had tolerated 9 cycles of the drug without complications but had elevated liver function tests at the start of cycle 10 that subsequently led to death from toxic liver failure.