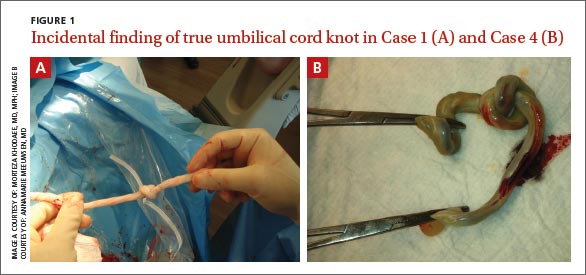
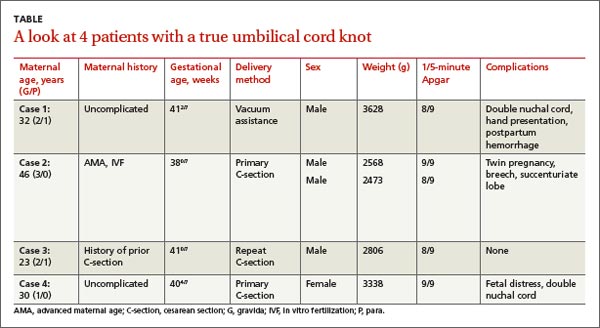
User login
4 pregnant women with an unusual finding at delivery
THE CASES
CASE 1 › A 32-year-old G2P1 with an uncomplicated prenatal course presented for induction at 41 weeks and 2 days of gestation. Fetal heart tracing showed no abnormalities. A compound presentation and a prolonged second stage of labor made vacuum assistance necessary. The infant had both a true umbilical cord knot (TUCK) (FIGURE 1A) and double nuchal cord.
CASE 2 › A 46-year-old G3P0 at 38 weeks of gestation by in vitro fertilization underwent an uncomplicated primary low transverse cesarean (C-section) delivery of dichorionic/diamniotic twins. The C-section had been necessary because baby A had been in the breech position. Fetal heart tracing showed no abnormalities. Baby A had a velamentous cord insertion, and baby B had a succenturiate lobe and a TUCK.
CASE 3 › A 23-year-old G2P1 with an uncomplicated prenatal course chose to have a repeat C-section and delivered at 41 weeks in active labor. Fetal heart monitoring showed no abnormalities. Umbilical artery pH and venous pH were normal. A TUCK was noted at time of delivery.
CASE 4 › A 30-year-old G1P0 with an uncomplicated prenatal course presented in active labor at 40 weeks and 4 days of gestation. At 7 cm cervical dilation, monitoring showed repeated deep variable fetal heart rate decelerations. The patient underwent an uncomplicated primary C-section. Umbilical artery pH and venous pH were normal. A TUCK (FIGURE 1B) and double nuchal cord were found at time of delivery.
DISCUSSION
TUCKs are thought to occur when a fetus passes through a loop in the umbilical cord. They occur in <2% of term deliveries.1,2 TUCKs differ from false knots. False knots are exaggerated loops of cord vasculature.
Risk factors that have been independently associated with TUCK include advanced maternal age (AMA; >35 years), multiparity, diabetes mellitus, gestational diabetes, polyhydramnios, and previous spontaneous abortion.1-3 In one study, 72% of women with a TUCK were multiparous.3 Hershkovitz et al2 suggested that laxity of uterine and abdominal musculature in multiparous patients may contribute to increased room for TUCK formation.
The adjusted odds ratio of having a TUCK is 2.53 in women with diabetes mellitus.3 Hyperglycemia can contribute to increased fetal movements, thereby increasing the risk of TUCK development.2 Polyhydramnios is often found in patients with diabetes mellitus and gestational diabetes.3 The incidence is higher in monoamniotic twins.4
Being a male and having a longer umbilical cord may also increase the risk of TUCK. On average, male infants have longer cords than females, which may predispose them to TUCKs.3 Räisänen et al3 found that the mean cord length in TUCK infants was 16.9 cm longer than in infants without a TUCK.
Of our 4 patients, one was of AMA, 2 were multiparous, and 3 of the 4 infants who developed TUCK were male.
TUCK is usually diagnosed at delivery
Most cases of TUCK are found incidentally at the time of delivery. Antenatal diagnosis is difficult, because loops of cord lying together are easily mistaken for knots on ultrasound.5 Sepulveda et al6 evaluated the use of 3D power Doppler in 8 cases of suspected TUCK; only 63% were confirmed at delivery. Some researchers have found improved detection of TUCK with color Doppler and 4D ultrasound, which have demonstrated a “hanging noose sign” (a transverse section of umbilical cord surrounded by a loop of cord) as well as views of the cord under pressure.7-10
Outcomes associated with TUCK vary greatly. Neonates affected by TUCK have a 4% to 10% increased risk of stillbirth, usually attributed to knot tightening.2,4,11,12
In addition, there is an increased incidence of fetal heart rate abnormalities during labor.1,3,12,13
There is no increase in the incidence of assisted vaginal or C-section delivery.12 And as for whether TUCK affects an infant’s size or weight, one study found TUCK infants had a 3.2-fold higher risk of measuring small for gestational age, potentially due to chronic umbilical cord compromise; however, mean birth weight between study and control groups did not differ significantly.3
Outcomes for our patients and their infants. All 4 cases had good outcomes (TABLE). The umbilical cord knot produced no detectable fetal compromise in cases 1 through 3. In Case 4, electronic fetal monitoring showed repeated variable fetal heart rate decelerations, presumably associated with cord compression.
THE TAKEAWAY
Pregnant women who may be at risk for experiencing a TUCK include those who are older than age 35, multiparous, carrying a boy, or have diabetes mellitus, gestational diabetes, or polyhydramnios. While it is good to be aware of these risk factors, there are no recommended changes in management based on risk or ultrasound findings unless there is additional concern for fetal compromise.
Antenatal diagnosis of TUCK is challenging, but Doppler ultrasound may be able to identify the condition. Most cases of TUCK are noted on delivery, and outcomes are generally positive, although infants in whom the TUCK tightens may have an increased risk of heart rate abnormalities or stillbirth.
1. Joura EA, Zeisler H, Sator MO. Epidemiology and clinical value of true umbilical cord knots [in German]. Wien Klin Wochenschr. 1998;110:232-235.
2. Hershkovitz R, Silberstein T, Sheiner E, et al. Risk factors associated with true knots of the umbilical cord. Eur J Obstet Gynecol Reprod Biol. 2001;98:36-39.
3. Räisänen S, Georgiadis L, Harju M, et al. True umbilical cord knot and obstetric outcome. Int J Gynaecol Obstet. 2013;122: 18-21.
4. Maher JT, Conti JA. A comparison of umbilical cord blood gas values between newborns with and without true knots. Obstet Gynecol. 1996;88:863-866.
5. Clerici G, Koutras I, Luzietti R, et al. Multiple true umbilical knots: a silent risk for intrauterine growth restriction with anomalous hemodynamic pattern. Fetal Diagn Ther. 2007;22:440-443.
6. Sepulveda W, Shennan AH, Bower S, et al. True knot of the umbilical cord: a difficult prenatal ultrasonographic diagnosis. Ultrasound Obstet Gynecol. 1995;5:106-108.
7. Hasbun J, Alcalde JL, Sepulveda W. Three-dimensional power Doppler sonography in the prenatal diagnosis of a true knot of the umbilical cord: value and limitations. J Ultrasound Med. 2007;26:1215-1220.
8. Rodriguez N, Angarita AM, Casasbuenas A, et al. Three-dimensional high-definition flow imaging in prenatal diagnosis of a true umbilical cord knot. Ultrasound Obstet Gynecol. 2012;39:245-246.
9. Scioscia M, Fornalè M, Bruni F, et al. Four-dimensional and Doppler sonography in the diagnosis and surveillance of a true cord knot. J Clin Ultrasound. 2011;39: 157-159.
10. Sherer DM, Dalloul M, Zigalo A, et al. Power Doppler and 3-dimensional sonographic diagnosis of multiple separate true knots of the umbilical cord. J Ultrasound Med. 2005;24: 1321-1323.
11. Sørnes T. Umbilical cord knots. Acta Obstet Gynecol Scand. 2000;79:157-159.
12. Airas U, Heinonen S. Clinical significance of true umbilical knots: a population-based analysis. Am J Perinatol. 2002;19:127-132.
13. Szczepanik ME, Wittich AC. True knot of the umbilical cord: a report of 13 cases. Mil Med. 2007;172:892-894.
THE CASES
CASE 1 › A 32-year-old G2P1 with an uncomplicated prenatal course presented for induction at 41 weeks and 2 days of gestation. Fetal heart tracing showed no abnormalities. A compound presentation and a prolonged second stage of labor made vacuum assistance necessary. The infant had both a true umbilical cord knot (TUCK) (FIGURE 1A) and double nuchal cord.
CASE 2 › A 46-year-old G3P0 at 38 weeks of gestation by in vitro fertilization underwent an uncomplicated primary low transverse cesarean (C-section) delivery of dichorionic/diamniotic twins. The C-section had been necessary because baby A had been in the breech position. Fetal heart tracing showed no abnormalities. Baby A had a velamentous cord insertion, and baby B had a succenturiate lobe and a TUCK.
CASE 3 › A 23-year-old G2P1 with an uncomplicated prenatal course chose to have a repeat C-section and delivered at 41 weeks in active labor. Fetal heart monitoring showed no abnormalities. Umbilical artery pH and venous pH were normal. A TUCK was noted at time of delivery.
CASE 4 › A 30-year-old G1P0 with an uncomplicated prenatal course presented in active labor at 40 weeks and 4 days of gestation. At 7 cm cervical dilation, monitoring showed repeated deep variable fetal heart rate decelerations. The patient underwent an uncomplicated primary C-section. Umbilical artery pH and venous pH were normal. A TUCK (FIGURE 1B) and double nuchal cord were found at time of delivery.
DISCUSSION
TUCKs are thought to occur when a fetus passes through a loop in the umbilical cord. They occur in <2% of term deliveries.1,2 TUCKs differ from false knots. False knots are exaggerated loops of cord vasculature.
Risk factors that have been independently associated with TUCK include advanced maternal age (AMA; >35 years), multiparity, diabetes mellitus, gestational diabetes, polyhydramnios, and previous spontaneous abortion.1-3 In one study, 72% of women with a TUCK were multiparous.3 Hershkovitz et al2 suggested that laxity of uterine and abdominal musculature in multiparous patients may contribute to increased room for TUCK formation.
The adjusted odds ratio of having a TUCK is 2.53 in women with diabetes mellitus.3 Hyperglycemia can contribute to increased fetal movements, thereby increasing the risk of TUCK development.2 Polyhydramnios is often found in patients with diabetes mellitus and gestational diabetes.3 The incidence is higher in monoamniotic twins.4
Being a male and having a longer umbilical cord may also increase the risk of TUCK. On average, male infants have longer cords than females, which may predispose them to TUCKs.3 Räisänen et al3 found that the mean cord length in TUCK infants was 16.9 cm longer than in infants without a TUCK.
Of our 4 patients, one was of AMA, 2 were multiparous, and 3 of the 4 infants who developed TUCK were male.
TUCK is usually diagnosed at delivery
Most cases of TUCK are found incidentally at the time of delivery. Antenatal diagnosis is difficult, because loops of cord lying together are easily mistaken for knots on ultrasound.5 Sepulveda et al6 evaluated the use of 3D power Doppler in 8 cases of suspected TUCK; only 63% were confirmed at delivery. Some researchers have found improved detection of TUCK with color Doppler and 4D ultrasound, which have demonstrated a “hanging noose sign” (a transverse section of umbilical cord surrounded by a loop of cord) as well as views of the cord under pressure.7-10
Outcomes associated with TUCK vary greatly. Neonates affected by TUCK have a 4% to 10% increased risk of stillbirth, usually attributed to knot tightening.2,4,11,12
In addition, there is an increased incidence of fetal heart rate abnormalities during labor.1,3,12,13
There is no increase in the incidence of assisted vaginal or C-section delivery.12 And as for whether TUCK affects an infant’s size or weight, one study found TUCK infants had a 3.2-fold higher risk of measuring small for gestational age, potentially due to chronic umbilical cord compromise; however, mean birth weight between study and control groups did not differ significantly.3
Outcomes for our patients and their infants. All 4 cases had good outcomes (TABLE). The umbilical cord knot produced no detectable fetal compromise in cases 1 through 3. In Case 4, electronic fetal monitoring showed repeated variable fetal heart rate decelerations, presumably associated with cord compression.
THE TAKEAWAY
Pregnant women who may be at risk for experiencing a TUCK include those who are older than age 35, multiparous, carrying a boy, or have diabetes mellitus, gestational diabetes, or polyhydramnios. While it is good to be aware of these risk factors, there are no recommended changes in management based on risk or ultrasound findings unless there is additional concern for fetal compromise.
Antenatal diagnosis of TUCK is challenging, but Doppler ultrasound may be able to identify the condition. Most cases of TUCK are noted on delivery, and outcomes are generally positive, although infants in whom the TUCK tightens may have an increased risk of heart rate abnormalities or stillbirth.
THE CASES
CASE 1 › A 32-year-old G2P1 with an uncomplicated prenatal course presented for induction at 41 weeks and 2 days of gestation. Fetal heart tracing showed no abnormalities. A compound presentation and a prolonged second stage of labor made vacuum assistance necessary. The infant had both a true umbilical cord knot (TUCK) (FIGURE 1A) and double nuchal cord.
CASE 2 › A 46-year-old G3P0 at 38 weeks of gestation by in vitro fertilization underwent an uncomplicated primary low transverse cesarean (C-section) delivery of dichorionic/diamniotic twins. The C-section had been necessary because baby A had been in the breech position. Fetal heart tracing showed no abnormalities. Baby A had a velamentous cord insertion, and baby B had a succenturiate lobe and a TUCK.
CASE 3 › A 23-year-old G2P1 with an uncomplicated prenatal course chose to have a repeat C-section and delivered at 41 weeks in active labor. Fetal heart monitoring showed no abnormalities. Umbilical artery pH and venous pH were normal. A TUCK was noted at time of delivery.
CASE 4 › A 30-year-old G1P0 with an uncomplicated prenatal course presented in active labor at 40 weeks and 4 days of gestation. At 7 cm cervical dilation, monitoring showed repeated deep variable fetal heart rate decelerations. The patient underwent an uncomplicated primary C-section. Umbilical artery pH and venous pH were normal. A TUCK (FIGURE 1B) and double nuchal cord were found at time of delivery.
DISCUSSION
TUCKs are thought to occur when a fetus passes through a loop in the umbilical cord. They occur in <2% of term deliveries.1,2 TUCKs differ from false knots. False knots are exaggerated loops of cord vasculature.
Risk factors that have been independently associated with TUCK include advanced maternal age (AMA; >35 years), multiparity, diabetes mellitus, gestational diabetes, polyhydramnios, and previous spontaneous abortion.1-3 In one study, 72% of women with a TUCK were multiparous.3 Hershkovitz et al2 suggested that laxity of uterine and abdominal musculature in multiparous patients may contribute to increased room for TUCK formation.
The adjusted odds ratio of having a TUCK is 2.53 in women with diabetes mellitus.3 Hyperglycemia can contribute to increased fetal movements, thereby increasing the risk of TUCK development.2 Polyhydramnios is often found in patients with diabetes mellitus and gestational diabetes.3 The incidence is higher in monoamniotic twins.4
Being a male and having a longer umbilical cord may also increase the risk of TUCK. On average, male infants have longer cords than females, which may predispose them to TUCKs.3 Räisänen et al3 found that the mean cord length in TUCK infants was 16.9 cm longer than in infants without a TUCK.
Of our 4 patients, one was of AMA, 2 were multiparous, and 3 of the 4 infants who developed TUCK were male.
TUCK is usually diagnosed at delivery
Most cases of TUCK are found incidentally at the time of delivery. Antenatal diagnosis is difficult, because loops of cord lying together are easily mistaken for knots on ultrasound.5 Sepulveda et al6 evaluated the use of 3D power Doppler in 8 cases of suspected TUCK; only 63% were confirmed at delivery. Some researchers have found improved detection of TUCK with color Doppler and 4D ultrasound, which have demonstrated a “hanging noose sign” (a transverse section of umbilical cord surrounded by a loop of cord) as well as views of the cord under pressure.7-10
Outcomes associated with TUCK vary greatly. Neonates affected by TUCK have a 4% to 10% increased risk of stillbirth, usually attributed to knot tightening.2,4,11,12
In addition, there is an increased incidence of fetal heart rate abnormalities during labor.1,3,12,13
There is no increase in the incidence of assisted vaginal or C-section delivery.12 And as for whether TUCK affects an infant’s size or weight, one study found TUCK infants had a 3.2-fold higher risk of measuring small for gestational age, potentially due to chronic umbilical cord compromise; however, mean birth weight between study and control groups did not differ significantly.3
Outcomes for our patients and their infants. All 4 cases had good outcomes (TABLE). The umbilical cord knot produced no detectable fetal compromise in cases 1 through 3. In Case 4, electronic fetal monitoring showed repeated variable fetal heart rate decelerations, presumably associated with cord compression.
THE TAKEAWAY
Pregnant women who may be at risk for experiencing a TUCK include those who are older than age 35, multiparous, carrying a boy, or have diabetes mellitus, gestational diabetes, or polyhydramnios. While it is good to be aware of these risk factors, there are no recommended changes in management based on risk or ultrasound findings unless there is additional concern for fetal compromise.
Antenatal diagnosis of TUCK is challenging, but Doppler ultrasound may be able to identify the condition. Most cases of TUCK are noted on delivery, and outcomes are generally positive, although infants in whom the TUCK tightens may have an increased risk of heart rate abnormalities or stillbirth.
1. Joura EA, Zeisler H, Sator MO. Epidemiology and clinical value of true umbilical cord knots [in German]. Wien Klin Wochenschr. 1998;110:232-235.
2. Hershkovitz R, Silberstein T, Sheiner E, et al. Risk factors associated with true knots of the umbilical cord. Eur J Obstet Gynecol Reprod Biol. 2001;98:36-39.
3. Räisänen S, Georgiadis L, Harju M, et al. True umbilical cord knot and obstetric outcome. Int J Gynaecol Obstet. 2013;122: 18-21.
4. Maher JT, Conti JA. A comparison of umbilical cord blood gas values between newborns with and without true knots. Obstet Gynecol. 1996;88:863-866.
5. Clerici G, Koutras I, Luzietti R, et al. Multiple true umbilical knots: a silent risk for intrauterine growth restriction with anomalous hemodynamic pattern. Fetal Diagn Ther. 2007;22:440-443.
6. Sepulveda W, Shennan AH, Bower S, et al. True knot of the umbilical cord: a difficult prenatal ultrasonographic diagnosis. Ultrasound Obstet Gynecol. 1995;5:106-108.
7. Hasbun J, Alcalde JL, Sepulveda W. Three-dimensional power Doppler sonography in the prenatal diagnosis of a true knot of the umbilical cord: value and limitations. J Ultrasound Med. 2007;26:1215-1220.
8. Rodriguez N, Angarita AM, Casasbuenas A, et al. Three-dimensional high-definition flow imaging in prenatal diagnosis of a true umbilical cord knot. Ultrasound Obstet Gynecol. 2012;39:245-246.
9. Scioscia M, Fornalè M, Bruni F, et al. Four-dimensional and Doppler sonography in the diagnosis and surveillance of a true cord knot. J Clin Ultrasound. 2011;39: 157-159.
10. Sherer DM, Dalloul M, Zigalo A, et al. Power Doppler and 3-dimensional sonographic diagnosis of multiple separate true knots of the umbilical cord. J Ultrasound Med. 2005;24: 1321-1323.
11. Sørnes T. Umbilical cord knots. Acta Obstet Gynecol Scand. 2000;79:157-159.
12. Airas U, Heinonen S. Clinical significance of true umbilical knots: a population-based analysis. Am J Perinatol. 2002;19:127-132.
13. Szczepanik ME, Wittich AC. True knot of the umbilical cord: a report of 13 cases. Mil Med. 2007;172:892-894.
1. Joura EA, Zeisler H, Sator MO. Epidemiology and clinical value of true umbilical cord knots [in German]. Wien Klin Wochenschr. 1998;110:232-235.
2. Hershkovitz R, Silberstein T, Sheiner E, et al. Risk factors associated with true knots of the umbilical cord. Eur J Obstet Gynecol Reprod Biol. 2001;98:36-39.
3. Räisänen S, Georgiadis L, Harju M, et al. True umbilical cord knot and obstetric outcome. Int J Gynaecol Obstet. 2013;122: 18-21.
4. Maher JT, Conti JA. A comparison of umbilical cord blood gas values between newborns with and without true knots. Obstet Gynecol. 1996;88:863-866.
5. Clerici G, Koutras I, Luzietti R, et al. Multiple true umbilical knots: a silent risk for intrauterine growth restriction with anomalous hemodynamic pattern. Fetal Diagn Ther. 2007;22:440-443.
6. Sepulveda W, Shennan AH, Bower S, et al. True knot of the umbilical cord: a difficult prenatal ultrasonographic diagnosis. Ultrasound Obstet Gynecol. 1995;5:106-108.
7. Hasbun J, Alcalde JL, Sepulveda W. Three-dimensional power Doppler sonography in the prenatal diagnosis of a true knot of the umbilical cord: value and limitations. J Ultrasound Med. 2007;26:1215-1220.
8. Rodriguez N, Angarita AM, Casasbuenas A, et al. Three-dimensional high-definition flow imaging in prenatal diagnosis of a true umbilical cord knot. Ultrasound Obstet Gynecol. 2012;39:245-246.
9. Scioscia M, Fornalè M, Bruni F, et al. Four-dimensional and Doppler sonography in the diagnosis and surveillance of a true cord knot. J Clin Ultrasound. 2011;39: 157-159.
10. Sherer DM, Dalloul M, Zigalo A, et al. Power Doppler and 3-dimensional sonographic diagnosis of multiple separate true knots of the umbilical cord. J Ultrasound Med. 2005;24: 1321-1323.
11. Sørnes T. Umbilical cord knots. Acta Obstet Gynecol Scand. 2000;79:157-159.
12. Airas U, Heinonen S. Clinical significance of true umbilical knots: a population-based analysis. Am J Perinatol. 2002;19:127-132.
13. Szczepanik ME, Wittich AC. True knot of the umbilical cord: a report of 13 cases. Mil Med. 2007;172:892-894.

Advanced procedures in family medicine: The cutting edge or the lunatic fringe?
► About: “Laparoscopic cholecystectomy in a rural family practice”
On the surface, the previous article by Haynes et al1 appears to be a simple descriptive study of a well-established technology. So why publish something that is not new? Simply because the study is an incredible technical and political achievement in a JCAHO-accredited hospital by a family physician educator. All family physicians—whether they view themselves as “procedural” or not—should recognize it for its symbolic and political value.
High-touch and high-tech
If family physicians wish to provide more than “generic primary care,” they must provide clinical skills at the bedside, in addition to diagnostic and psychosocial expertise. No amount of the latter will compensate for the former at critical moments. For credibility in the community and in the life cycle of families, the provision of diagnostic and therapeutic procedures trumps prescription-writing every time.
By providing surgical or diagnostic procedures that improve access to health care in their communities, physicians such as Haynes are not regressing to a surgical mentality at the expense of psychosocial sensitivity and therapeutic listening. Our closest relations with patients and their families are established at the bedside while performing or assisting with a diagnostic or therapeutic procedure. Procedures frequently provide the ultimate “teachable moment.” As said at Keystone III: “You can pretend to know; you can pretend to care; but you can’t pretend to be there.”2
Also, procedures distinguish family physicians from the other “primary care providers” who are hired with the assumption that they will provide referrals. Patients will seek out those physicians who can simultaneously provide high-touch and high-tech.
1960s–1970s: The growth of high-tech
During the 1960s and 1970s, advances in technology were predominantly located in hospitals. The traditional office-based diagnostic and surgical skills of the general physician were gradually transferred to a more central place, namely the hospital. Many of these skills were then categorically assigned to more specialized physicians resulting in the withdrawal of the generalist physician in the participation of these skills.
Originally, family medicine educators thought the 3-year curriculum would be sufficient for procedural training, but they underestimated the political passion for control by opposing specialties with a need to maintain their training monopolies. Among 20 voting specialties, family medicine has only 1 vote. This is the democratic reality, which frames any potential turf struggle in a highly subspecialized environment. These environments include, but are not limited to, academic medical centers, most urban hospitals, and some rural hospitals.
The institutionalization of these interventions depersonalized the patient-doctor relationship, limited access, and escalated cost. Family practice as an emerging specialty willingly joined in this movement, resulting in the abandonment of many generalist-appropriate skills. During that time, studies of how tertiary-care technologies might transfer into the community were undertaken.3,4
It became increasingly evident that many diagnostic and interventional procedures (eg, diagnostic ultrasound, gastrointestinal endoscopy, and colposcopy) had multiple-specialty applications and were clearly linked with important preventive activities. 5,6 Some leaders suggested that technical skills combined with the unique biopsychosocial model of practice of family physicians was the right way to provide competent, personal care to patients. In other words, high-tech was most effective when blended with high-touch and vice-versa. 7-9
1980s–1990s: The FP curriculum expands
In 1981, the first in a series of fourth-year fellowships emphasizing this expanded curriculum for family physicians was initiated.10-12 Thereupon followed the development of CAQ experiences in Geriatric Medicine and Sports Medicine, which, while instructive, failed to create added market value to most rural and under-served communities. The American Academy of Family Physicians—through the Task Force on Obstetrics (1989–1993)13 and then the Task Force on Procedures (1993–1995)—ratified and distributed performance-based learning and competency-based testing programs. Moreover, the Advanced Life Support in Obstetrics (ALSO) program had a major impact nationally and internationally.14
By 1991, our discipline was focused on credentialing for lightning rod issues such as colonoscopy,15 esophagogastroduodenoscopy,16 colposcopy,17 obstetric ultrasound,18 and cesarean section.19 In Memphis, because of the political conflict associated with the teaching of diagnostic ultrasound, gastrointestinal endoscopy, and cesarean section, we chose not to “fan the flames” with development of office-based laparoscopy. But we were ready. We included laparoscopic tubal ligation in our FP/OB fellowship, but the resistance from specialties who felt family medicine was invading “their turf” was difficult and remains so.20-24
By 1995, the Residency Review Committee for Family Medicine had codified the rural training tracks25 and reaffirmed OB-capable faculty as part of the accreditation process. These advanced family practice curriculum needs were acknowledged, and various educational innovations with an emphasis on skills needed for success in rural or urban underserved communities began to emerge.26,27
Nebraska,28 Marshall University,29 and the University of Tennessee–Memphis 30 have summarized their experiences with the accelerated residency program and rural training tracks have done the same. These programs have recognized the need to train our future teachers and role models broadly, combating the “learned helplessness” that too often characterizes our training environments when we leave this teaching to subspecialists.
Meeting the needs of a rural practice
Some physicians with a more limited scope of practice appear threatened by proceduralists. While there is room for everyone in the big tent of family medicine, if our specialty is to survive and be credible, we must seek to meet the needs of our patients and our students. In most urban areas, family medicine has abandoned large parts of our patients’ care to the specialties of emergency medicine and obstetrics/gynecology.
From the rural perspective, it is impractical or fiscally impossible to recruit and maintain platoons of obstetricians and board-certified emergency medicine specialists to counties not located near a metropolitan area.31,32 Family physicians, if properly trained, are the ideal physicians for nonmetropolitan practice.
Moreover, the current practice management curriculum in most family practice residencies is a do-it-yourself suicide kit where few physicians understand accountability measures for billing, collections, equipment, and human resources. They may have memorized the entire amino acid sequence for the human genome, but they don’t have the time to understand billing for Medicaid or the impact of providing a full range of services to their patients. What’s wrong with this picture?
FPs must adapt to serve their patients
The net result of the production of our graduates lacking technical skills is an overstocked urban job pool and a shortage of rural physicians. There are few 9-to-5 family practice jobs available in urban areas like Nashville and Memphis for limited generalists. On the other hand, there are jobs for every family physician willing to work after 5 P.M. This includes continuing care, urgent care, and middle-of-the-night hospital care. Procedural skills and hospital service predictably require “extra effort” and extra risk. Reimbursement policies continue to favor those physicians who assume these risks and provide these services.33.34
Another result of following the path of least resistance (as reflected in nonprocedural family medicine is the decreasing student interest in family medicine.35
Responsibility also rests with unskilled faculty who will not perform a broader scope of practice within the medical specialty of family medicine. There is personal risk for “being there” at the critical moment of procedural decisions. Students do not automatically shun this risk, but family medicine may be self-selecting for those who do.
Family physicians practicing in diverse geographic, social, and political environments will naturally adopt various diagnostic and therapeutic modalities in the service of their patients. It is not up to us to judge the appropriateness of those modalities except by the ultimate yardstick of the quality of the end result.
We are not advocating the addition of laparoscopic cholecystectomy to the “required” family medicine curriculum. However, we support the right of John Haynes to practice this skill and to teach it to others to the benefit of patients. The specialty that cannot provide training and credentials for its own members has been reproductively sterilized.36,37 This is a unique market niche ideally suited for family medicine.38,39
Procedurally trained family physicians represent the cutting edge of an emerging paradigm of care that includes ambulatory surgery, maternity care, cesarean section, and laparoscopy, particularly for patients in smaller communities and developing nations. We salute John Haynes and his co-authors for taking “the road less traveled.”
Corresponding author
Wm. MacMillan Rodney, MD, 6575 Black Thorne Cove, Memphis, TN 38119. E-mail: [email protected].
1. Haynes JH, Guha SC, Taylor SG. Laparoscopic cholecystectomy by a rural family practice: the Vivian, Louisiana, experience. J Fam Pract 2004;53:3:tk-tk.
2. Green LA, Graham R, Frey JJ, Stephens GG. Keystone III. The Role of Family Medicine in a Changing Health Care Environment: A Dialogue Washington, DC: Robert Graham Center; 2001.
3. Johnson RA, Quan MA, Rodney WM. Flexible sigmoidoscopy. J Fam Pract 1982;14:757-770.
4. Morgan WC, Rodney WM, Hahn RG, Garr DA. Ultrasound for the primary care physician. Applications in family-centered obstetrics. Postgrad Med 1988;83:103-107.
5. Rodney WM, Quan MA, Johnson RA, Beaber R. Impact of flexible sigmoidoscopy in a family practice residency. J Fam Pract 1982;15:885-889.
6. Rodney WM. Doing better: Health maintenance research in family medicine. Cont Ed Fam Phys 1985;20:688-689.
7. Rodney WM. High technology is most effective when blended with high touch and vice versa: office technology in the 21st Century. Fam Pract Res J 1991;11:235-239.
8. Deutchman ME, Connor PC, Hahn RG, Rodney WM, et al. Diagnostic and therapeutic tools for the family physician’s office of the 21st century. Fam Pract Res J 1992;12:147-155.
9. Harper MB, Mayeaux EJ, Jr, Pope JB, Goel R. Procedural training in family practice residencies: current status and impact on resident recruitment. J Am Board Fam Pract 1995;8:189-194.
10. Rodney WM, Quan MA. AAFP-ACOG guidelines revisited. Female Patient 1982;97(PC):1-40.
11. Rodney WM, Felmar E. Flexible sigmoidoscopy: a “how to” guide. Your Patient and Cancer 1984;4:57-66.
12. Davies TC, Hahn RG, Rodney WM, Curry HB. The use of OB/GYN ultrasound by family physicians. Cont Ed Fam Phys 1986;21:335-338.
13. Rodney WM. A personal reflection from the AAFP Task Force on Obstetrics. Tenn Fam Physician 1990;1:4-5.
14. Dresang L, Rodney WM, Leeman L, Dees J, Koch P, Palencio M. ALSO in Ecuador: teaching the teachers. J Am Board Fam Pract[in press].
15. Carr K, Worthington JM, Rodney WM, Gentry S, Sellers A, Sizemore J. Advancing from flexible sigmoidoscopy to colonoscopy in rural family practice: a case report. Tenn Med Assoc J 1998;91:21-26.
16. Rodney WM, Weber JR, Swedberg JA, et al. Esophagogastroduodenoscopy by family physicians phase II. a national multisite study of 2,500 procedures. Fam Pract Res J 1993;13:121-131.
17. Felmar E, Cottam C, Payton CE, Rodney WM. Colposcopy: it can be part of your practice. Primary Care and Cancer 1987;7:13-20.
18. Hahn RG, Davies TC, Rodney WM. Het gebruik van echografie in de huisartsenpraktijk [The potential of ultrasound for general practitioners]. Huissart Nu 1987;16:227-230 [in Dutch].
19. Deutchman M, Connor P, Gobbo R, FitzSimmons R. Outcomes of cesarean sections performed by family physicians and the training they received: A 15-year retrospective study. J Am Board Fam Pract 1995;8:81-90.
20. Rodney WM. Flexible sigmoidoscopy and the despecialization of endoscopy: an environmental impact report. Cancer 1992;70(5 suppl):1266-1271.
21. Rodney WM. Obstetrics enhanced family practice: an endangered species worth saving! Florida Fam Phys 1993;43:8-9.
22. Susman J, Rodney WM. Numbers, procedural skills and science: do the three mix? Am Fam Physician 1994;49:1591-1592.
23. Rodney WM. Will virtual reality simulators end the credentialing arms race in gastrointestinal endoscopy or the need for family physician faculty with endoscopic skills? J Am Board Fam Pract 1998;11:492-496.
24. Rodney WM. Historical observations from the RRC 1994-2000: Maternity care [OB] training in FP. J Am Board Fam Pract 2002;15:255-256.
25. Damos JR, Christman C, Gjerde CL, Beasley J, Schutz, Plane MB. A case for the development of family practice rural training tracks. J Am Board Fam Pract 1998;11:399-405.
26. Acosta D. Impact of rural training on physician workforce: the role of postresidency education. J Rural Health 2000;16:254-261.
27. Norris TE, Acosta DA. A fellowship in rural family medicine: program development and outcomes. Fam Med 1997;29:414-420.
28. Stageman JH, Bowman RC, Harrison JD. An accelerated rural training program. J Am Board Fam Pract 2003;16:124-130.
29. Petrany SM, Crespo R. The accelerated residency program: The Marshall University family practice 9-year experience. Fam Med 2002;34:669-672.
30. Delzell JE, Midtling JE, Rodney WM. The university of Tennessee’s accelerated family medicine residency program 1992-2003: An eleven year progress report. J Am Board Fam Practice [submitted].
31. Bullock K, Rodney WM, Gerard T, Hahn R. “Advanced Practice” family physicians as the foundation for rural emergency medicine services (Part I). Texas J Rur Health 2000;17:19-29.
32. Bullock K, Rodney WM, Gerard T, Hahn R. “Advanced Practice” family physicians as the foundation for rural emergency medicine services (Part II). Texas J Rur Health 2000;18:34-44.
33. Hahn RG, Rodney WM, et al. Technology transferred to family medicine: implications for clinical practice. Fourth International Meeting of Family Medicine, sponsored by the International Center of Family Medicine, May 25, 1990, Estoril, Portugal (abstract).
34. Rodney WM, Hahn RG. The impact of the limited generalist (no procedures, no hospital) on the viability of family practice training. J Am Board Fam Pract 2002;15:191-200.
35. Campos-Outcalt D. Family practice specialty selection: a research agenda. Fam Med. 1991;23:609-619.
36. Rodney WM. Foreword. Pfenninger JL, Fowler GC, eds. Procedures for Primary Care 1st ed. St Louis, Mo: Mosby; 2003;xviii.
37. Rodney WM. The dilemma of emerging technologies as required curriculum in primary care. Fam Med 1997;29:584-585.
38. Rodney WM, Crown LA, Hahn RG, Martin J. Enhancing the family medicine curriculum in deliveries and emergency medicine as a way of developing a rural teaching site. Fam Med 1998;30:712-719.
39. Deutchman ME, Hahn RG, Rodney WM. Diagnostic ultrasound imaging by physicians of first contact: extending family medicine into emergency medicine. Ann Emerg Med 1993;22:594-596.
► About: “Laparoscopic cholecystectomy in a rural family practice”
On the surface, the previous article by Haynes et al1 appears to be a simple descriptive study of a well-established technology. So why publish something that is not new? Simply because the study is an incredible technical and political achievement in a JCAHO-accredited hospital by a family physician educator. All family physicians—whether they view themselves as “procedural” or not—should recognize it for its symbolic and political value.
High-touch and high-tech
If family physicians wish to provide more than “generic primary care,” they must provide clinical skills at the bedside, in addition to diagnostic and psychosocial expertise. No amount of the latter will compensate for the former at critical moments. For credibility in the community and in the life cycle of families, the provision of diagnostic and therapeutic procedures trumps prescription-writing every time.
By providing surgical or diagnostic procedures that improve access to health care in their communities, physicians such as Haynes are not regressing to a surgical mentality at the expense of psychosocial sensitivity and therapeutic listening. Our closest relations with patients and their families are established at the bedside while performing or assisting with a diagnostic or therapeutic procedure. Procedures frequently provide the ultimate “teachable moment.” As said at Keystone III: “You can pretend to know; you can pretend to care; but you can’t pretend to be there.”2
Also, procedures distinguish family physicians from the other “primary care providers” who are hired with the assumption that they will provide referrals. Patients will seek out those physicians who can simultaneously provide high-touch and high-tech.
1960s–1970s: The growth of high-tech
During the 1960s and 1970s, advances in technology were predominantly located in hospitals. The traditional office-based diagnostic and surgical skills of the general physician were gradually transferred to a more central place, namely the hospital. Many of these skills were then categorically assigned to more specialized physicians resulting in the withdrawal of the generalist physician in the participation of these skills.
Originally, family medicine educators thought the 3-year curriculum would be sufficient for procedural training, but they underestimated the political passion for control by opposing specialties with a need to maintain their training monopolies. Among 20 voting specialties, family medicine has only 1 vote. This is the democratic reality, which frames any potential turf struggle in a highly subspecialized environment. These environments include, but are not limited to, academic medical centers, most urban hospitals, and some rural hospitals.
The institutionalization of these interventions depersonalized the patient-doctor relationship, limited access, and escalated cost. Family practice as an emerging specialty willingly joined in this movement, resulting in the abandonment of many generalist-appropriate skills. During that time, studies of how tertiary-care technologies might transfer into the community were undertaken.3,4
It became increasingly evident that many diagnostic and interventional procedures (eg, diagnostic ultrasound, gastrointestinal endoscopy, and colposcopy) had multiple-specialty applications and were clearly linked with important preventive activities. 5,6 Some leaders suggested that technical skills combined with the unique biopsychosocial model of practice of family physicians was the right way to provide competent, personal care to patients. In other words, high-tech was most effective when blended with high-touch and vice-versa. 7-9
1980s–1990s: The FP curriculum expands
In 1981, the first in a series of fourth-year fellowships emphasizing this expanded curriculum for family physicians was initiated.10-12 Thereupon followed the development of CAQ experiences in Geriatric Medicine and Sports Medicine, which, while instructive, failed to create added market value to most rural and under-served communities. The American Academy of Family Physicians—through the Task Force on Obstetrics (1989–1993)13 and then the Task Force on Procedures (1993–1995)—ratified and distributed performance-based learning and competency-based testing programs. Moreover, the Advanced Life Support in Obstetrics (ALSO) program had a major impact nationally and internationally.14
By 1991, our discipline was focused on credentialing for lightning rod issues such as colonoscopy,15 esophagogastroduodenoscopy,16 colposcopy,17 obstetric ultrasound,18 and cesarean section.19 In Memphis, because of the political conflict associated with the teaching of diagnostic ultrasound, gastrointestinal endoscopy, and cesarean section, we chose not to “fan the flames” with development of office-based laparoscopy. But we were ready. We included laparoscopic tubal ligation in our FP/OB fellowship, but the resistance from specialties who felt family medicine was invading “their turf” was difficult and remains so.20-24
By 1995, the Residency Review Committee for Family Medicine had codified the rural training tracks25 and reaffirmed OB-capable faculty as part of the accreditation process. These advanced family practice curriculum needs were acknowledged, and various educational innovations with an emphasis on skills needed for success in rural or urban underserved communities began to emerge.26,27
Nebraska,28 Marshall University,29 and the University of Tennessee–Memphis 30 have summarized their experiences with the accelerated residency program and rural training tracks have done the same. These programs have recognized the need to train our future teachers and role models broadly, combating the “learned helplessness” that too often characterizes our training environments when we leave this teaching to subspecialists.
Meeting the needs of a rural practice
Some physicians with a more limited scope of practice appear threatened by proceduralists. While there is room for everyone in the big tent of family medicine, if our specialty is to survive and be credible, we must seek to meet the needs of our patients and our students. In most urban areas, family medicine has abandoned large parts of our patients’ care to the specialties of emergency medicine and obstetrics/gynecology.
From the rural perspective, it is impractical or fiscally impossible to recruit and maintain platoons of obstetricians and board-certified emergency medicine specialists to counties not located near a metropolitan area.31,32 Family physicians, if properly trained, are the ideal physicians for nonmetropolitan practice.
Moreover, the current practice management curriculum in most family practice residencies is a do-it-yourself suicide kit where few physicians understand accountability measures for billing, collections, equipment, and human resources. They may have memorized the entire amino acid sequence for the human genome, but they don’t have the time to understand billing for Medicaid or the impact of providing a full range of services to their patients. What’s wrong with this picture?
FPs must adapt to serve their patients
The net result of the production of our graduates lacking technical skills is an overstocked urban job pool and a shortage of rural physicians. There are few 9-to-5 family practice jobs available in urban areas like Nashville and Memphis for limited generalists. On the other hand, there are jobs for every family physician willing to work after 5 P.M. This includes continuing care, urgent care, and middle-of-the-night hospital care. Procedural skills and hospital service predictably require “extra effort” and extra risk. Reimbursement policies continue to favor those physicians who assume these risks and provide these services.33.34
Another result of following the path of least resistance (as reflected in nonprocedural family medicine is the decreasing student interest in family medicine.35
Responsibility also rests with unskilled faculty who will not perform a broader scope of practice within the medical specialty of family medicine. There is personal risk for “being there” at the critical moment of procedural decisions. Students do not automatically shun this risk, but family medicine may be self-selecting for those who do.
Family physicians practicing in diverse geographic, social, and political environments will naturally adopt various diagnostic and therapeutic modalities in the service of their patients. It is not up to us to judge the appropriateness of those modalities except by the ultimate yardstick of the quality of the end result.
We are not advocating the addition of laparoscopic cholecystectomy to the “required” family medicine curriculum. However, we support the right of John Haynes to practice this skill and to teach it to others to the benefit of patients. The specialty that cannot provide training and credentials for its own members has been reproductively sterilized.36,37 This is a unique market niche ideally suited for family medicine.38,39
Procedurally trained family physicians represent the cutting edge of an emerging paradigm of care that includes ambulatory surgery, maternity care, cesarean section, and laparoscopy, particularly for patients in smaller communities and developing nations. We salute John Haynes and his co-authors for taking “the road less traveled.”
Corresponding author
Wm. MacMillan Rodney, MD, 6575 Black Thorne Cove, Memphis, TN 38119. E-mail: [email protected].
► About: “Laparoscopic cholecystectomy in a rural family practice”
On the surface, the previous article by Haynes et al1 appears to be a simple descriptive study of a well-established technology. So why publish something that is not new? Simply because the study is an incredible technical and political achievement in a JCAHO-accredited hospital by a family physician educator. All family physicians—whether they view themselves as “procedural” or not—should recognize it for its symbolic and political value.
High-touch and high-tech
If family physicians wish to provide more than “generic primary care,” they must provide clinical skills at the bedside, in addition to diagnostic and psychosocial expertise. No amount of the latter will compensate for the former at critical moments. For credibility in the community and in the life cycle of families, the provision of diagnostic and therapeutic procedures trumps prescription-writing every time.
By providing surgical or diagnostic procedures that improve access to health care in their communities, physicians such as Haynes are not regressing to a surgical mentality at the expense of psychosocial sensitivity and therapeutic listening. Our closest relations with patients and their families are established at the bedside while performing or assisting with a diagnostic or therapeutic procedure. Procedures frequently provide the ultimate “teachable moment.” As said at Keystone III: “You can pretend to know; you can pretend to care; but you can’t pretend to be there.”2
Also, procedures distinguish family physicians from the other “primary care providers” who are hired with the assumption that they will provide referrals. Patients will seek out those physicians who can simultaneously provide high-touch and high-tech.
1960s–1970s: The growth of high-tech
During the 1960s and 1970s, advances in technology were predominantly located in hospitals. The traditional office-based diagnostic and surgical skills of the general physician were gradually transferred to a more central place, namely the hospital. Many of these skills were then categorically assigned to more specialized physicians resulting in the withdrawal of the generalist physician in the participation of these skills.
Originally, family medicine educators thought the 3-year curriculum would be sufficient for procedural training, but they underestimated the political passion for control by opposing specialties with a need to maintain their training monopolies. Among 20 voting specialties, family medicine has only 1 vote. This is the democratic reality, which frames any potential turf struggle in a highly subspecialized environment. These environments include, but are not limited to, academic medical centers, most urban hospitals, and some rural hospitals.
The institutionalization of these interventions depersonalized the patient-doctor relationship, limited access, and escalated cost. Family practice as an emerging specialty willingly joined in this movement, resulting in the abandonment of many generalist-appropriate skills. During that time, studies of how tertiary-care technologies might transfer into the community were undertaken.3,4
It became increasingly evident that many diagnostic and interventional procedures (eg, diagnostic ultrasound, gastrointestinal endoscopy, and colposcopy) had multiple-specialty applications and were clearly linked with important preventive activities. 5,6 Some leaders suggested that technical skills combined with the unique biopsychosocial model of practice of family physicians was the right way to provide competent, personal care to patients. In other words, high-tech was most effective when blended with high-touch and vice-versa. 7-9
1980s–1990s: The FP curriculum expands
In 1981, the first in a series of fourth-year fellowships emphasizing this expanded curriculum for family physicians was initiated.10-12 Thereupon followed the development of CAQ experiences in Geriatric Medicine and Sports Medicine, which, while instructive, failed to create added market value to most rural and under-served communities. The American Academy of Family Physicians—through the Task Force on Obstetrics (1989–1993)13 and then the Task Force on Procedures (1993–1995)—ratified and distributed performance-based learning and competency-based testing programs. Moreover, the Advanced Life Support in Obstetrics (ALSO) program had a major impact nationally and internationally.14
By 1991, our discipline was focused on credentialing for lightning rod issues such as colonoscopy,15 esophagogastroduodenoscopy,16 colposcopy,17 obstetric ultrasound,18 and cesarean section.19 In Memphis, because of the political conflict associated with the teaching of diagnostic ultrasound, gastrointestinal endoscopy, and cesarean section, we chose not to “fan the flames” with development of office-based laparoscopy. But we were ready. We included laparoscopic tubal ligation in our FP/OB fellowship, but the resistance from specialties who felt family medicine was invading “their turf” was difficult and remains so.20-24
By 1995, the Residency Review Committee for Family Medicine had codified the rural training tracks25 and reaffirmed OB-capable faculty as part of the accreditation process. These advanced family practice curriculum needs were acknowledged, and various educational innovations with an emphasis on skills needed for success in rural or urban underserved communities began to emerge.26,27
Nebraska,28 Marshall University,29 and the University of Tennessee–Memphis 30 have summarized their experiences with the accelerated residency program and rural training tracks have done the same. These programs have recognized the need to train our future teachers and role models broadly, combating the “learned helplessness” that too often characterizes our training environments when we leave this teaching to subspecialists.
Meeting the needs of a rural practice
Some physicians with a more limited scope of practice appear threatened by proceduralists. While there is room for everyone in the big tent of family medicine, if our specialty is to survive and be credible, we must seek to meet the needs of our patients and our students. In most urban areas, family medicine has abandoned large parts of our patients’ care to the specialties of emergency medicine and obstetrics/gynecology.
From the rural perspective, it is impractical or fiscally impossible to recruit and maintain platoons of obstetricians and board-certified emergency medicine specialists to counties not located near a metropolitan area.31,32 Family physicians, if properly trained, are the ideal physicians for nonmetropolitan practice.
Moreover, the current practice management curriculum in most family practice residencies is a do-it-yourself suicide kit where few physicians understand accountability measures for billing, collections, equipment, and human resources. They may have memorized the entire amino acid sequence for the human genome, but they don’t have the time to understand billing for Medicaid or the impact of providing a full range of services to their patients. What’s wrong with this picture?
FPs must adapt to serve their patients
The net result of the production of our graduates lacking technical skills is an overstocked urban job pool and a shortage of rural physicians. There are few 9-to-5 family practice jobs available in urban areas like Nashville and Memphis for limited generalists. On the other hand, there are jobs for every family physician willing to work after 5 P.M. This includes continuing care, urgent care, and middle-of-the-night hospital care. Procedural skills and hospital service predictably require “extra effort” and extra risk. Reimbursement policies continue to favor those physicians who assume these risks and provide these services.33.34
Another result of following the path of least resistance (as reflected in nonprocedural family medicine is the decreasing student interest in family medicine.35
Responsibility also rests with unskilled faculty who will not perform a broader scope of practice within the medical specialty of family medicine. There is personal risk for “being there” at the critical moment of procedural decisions. Students do not automatically shun this risk, but family medicine may be self-selecting for those who do.
Family physicians practicing in diverse geographic, social, and political environments will naturally adopt various diagnostic and therapeutic modalities in the service of their patients. It is not up to us to judge the appropriateness of those modalities except by the ultimate yardstick of the quality of the end result.
We are not advocating the addition of laparoscopic cholecystectomy to the “required” family medicine curriculum. However, we support the right of John Haynes to practice this skill and to teach it to others to the benefit of patients. The specialty that cannot provide training and credentials for its own members has been reproductively sterilized.36,37 This is a unique market niche ideally suited for family medicine.38,39
Procedurally trained family physicians represent the cutting edge of an emerging paradigm of care that includes ambulatory surgery, maternity care, cesarean section, and laparoscopy, particularly for patients in smaller communities and developing nations. We salute John Haynes and his co-authors for taking “the road less traveled.”
Corresponding author
Wm. MacMillan Rodney, MD, 6575 Black Thorne Cove, Memphis, TN 38119. E-mail: [email protected].
1. Haynes JH, Guha SC, Taylor SG. Laparoscopic cholecystectomy by a rural family practice: the Vivian, Louisiana, experience. J Fam Pract 2004;53:3:tk-tk.
2. Green LA, Graham R, Frey JJ, Stephens GG. Keystone III. The Role of Family Medicine in a Changing Health Care Environment: A Dialogue Washington, DC: Robert Graham Center; 2001.
3. Johnson RA, Quan MA, Rodney WM. Flexible sigmoidoscopy. J Fam Pract 1982;14:757-770.
4. Morgan WC, Rodney WM, Hahn RG, Garr DA. Ultrasound for the primary care physician. Applications in family-centered obstetrics. Postgrad Med 1988;83:103-107.
5. Rodney WM, Quan MA, Johnson RA, Beaber R. Impact of flexible sigmoidoscopy in a family practice residency. J Fam Pract 1982;15:885-889.
6. Rodney WM. Doing better: Health maintenance research in family medicine. Cont Ed Fam Phys 1985;20:688-689.
7. Rodney WM. High technology is most effective when blended with high touch and vice versa: office technology in the 21st Century. Fam Pract Res J 1991;11:235-239.
8. Deutchman ME, Connor PC, Hahn RG, Rodney WM, et al. Diagnostic and therapeutic tools for the family physician’s office of the 21st century. Fam Pract Res J 1992;12:147-155.
9. Harper MB, Mayeaux EJ, Jr, Pope JB, Goel R. Procedural training in family practice residencies: current status and impact on resident recruitment. J Am Board Fam Pract 1995;8:189-194.
10. Rodney WM, Quan MA. AAFP-ACOG guidelines revisited. Female Patient 1982;97(PC):1-40.
11. Rodney WM, Felmar E. Flexible sigmoidoscopy: a “how to” guide. Your Patient and Cancer 1984;4:57-66.
12. Davies TC, Hahn RG, Rodney WM, Curry HB. The use of OB/GYN ultrasound by family physicians. Cont Ed Fam Phys 1986;21:335-338.
13. Rodney WM. A personal reflection from the AAFP Task Force on Obstetrics. Tenn Fam Physician 1990;1:4-5.
14. Dresang L, Rodney WM, Leeman L, Dees J, Koch P, Palencio M. ALSO in Ecuador: teaching the teachers. J Am Board Fam Pract[in press].
15. Carr K, Worthington JM, Rodney WM, Gentry S, Sellers A, Sizemore J. Advancing from flexible sigmoidoscopy to colonoscopy in rural family practice: a case report. Tenn Med Assoc J 1998;91:21-26.
16. Rodney WM, Weber JR, Swedberg JA, et al. Esophagogastroduodenoscopy by family physicians phase II. a national multisite study of 2,500 procedures. Fam Pract Res J 1993;13:121-131.
17. Felmar E, Cottam C, Payton CE, Rodney WM. Colposcopy: it can be part of your practice. Primary Care and Cancer 1987;7:13-20.
18. Hahn RG, Davies TC, Rodney WM. Het gebruik van echografie in de huisartsenpraktijk [The potential of ultrasound for general practitioners]. Huissart Nu 1987;16:227-230 [in Dutch].
19. Deutchman M, Connor P, Gobbo R, FitzSimmons R. Outcomes of cesarean sections performed by family physicians and the training they received: A 15-year retrospective study. J Am Board Fam Pract 1995;8:81-90.
20. Rodney WM. Flexible sigmoidoscopy and the despecialization of endoscopy: an environmental impact report. Cancer 1992;70(5 suppl):1266-1271.
21. Rodney WM. Obstetrics enhanced family practice: an endangered species worth saving! Florida Fam Phys 1993;43:8-9.
22. Susman J, Rodney WM. Numbers, procedural skills and science: do the three mix? Am Fam Physician 1994;49:1591-1592.
23. Rodney WM. Will virtual reality simulators end the credentialing arms race in gastrointestinal endoscopy or the need for family physician faculty with endoscopic skills? J Am Board Fam Pract 1998;11:492-496.
24. Rodney WM. Historical observations from the RRC 1994-2000: Maternity care [OB] training in FP. J Am Board Fam Pract 2002;15:255-256.
25. Damos JR, Christman C, Gjerde CL, Beasley J, Schutz, Plane MB. A case for the development of family practice rural training tracks. J Am Board Fam Pract 1998;11:399-405.
26. Acosta D. Impact of rural training on physician workforce: the role of postresidency education. J Rural Health 2000;16:254-261.
27. Norris TE, Acosta DA. A fellowship in rural family medicine: program development and outcomes. Fam Med 1997;29:414-420.
28. Stageman JH, Bowman RC, Harrison JD. An accelerated rural training program. J Am Board Fam Pract 2003;16:124-130.
29. Petrany SM, Crespo R. The accelerated residency program: The Marshall University family practice 9-year experience. Fam Med 2002;34:669-672.
30. Delzell JE, Midtling JE, Rodney WM. The university of Tennessee’s accelerated family medicine residency program 1992-2003: An eleven year progress report. J Am Board Fam Practice [submitted].
31. Bullock K, Rodney WM, Gerard T, Hahn R. “Advanced Practice” family physicians as the foundation for rural emergency medicine services (Part I). Texas J Rur Health 2000;17:19-29.
32. Bullock K, Rodney WM, Gerard T, Hahn R. “Advanced Practice” family physicians as the foundation for rural emergency medicine services (Part II). Texas J Rur Health 2000;18:34-44.
33. Hahn RG, Rodney WM, et al. Technology transferred to family medicine: implications for clinical practice. Fourth International Meeting of Family Medicine, sponsored by the International Center of Family Medicine, May 25, 1990, Estoril, Portugal (abstract).
34. Rodney WM, Hahn RG. The impact of the limited generalist (no procedures, no hospital) on the viability of family practice training. J Am Board Fam Pract 2002;15:191-200.
35. Campos-Outcalt D. Family practice specialty selection: a research agenda. Fam Med. 1991;23:609-619.
36. Rodney WM. Foreword. Pfenninger JL, Fowler GC, eds. Procedures for Primary Care 1st ed. St Louis, Mo: Mosby; 2003;xviii.
37. Rodney WM. The dilemma of emerging technologies as required curriculum in primary care. Fam Med 1997;29:584-585.
38. Rodney WM, Crown LA, Hahn RG, Martin J. Enhancing the family medicine curriculum in deliveries and emergency medicine as a way of developing a rural teaching site. Fam Med 1998;30:712-719.
39. Deutchman ME, Hahn RG, Rodney WM. Diagnostic ultrasound imaging by physicians of first contact: extending family medicine into emergency medicine. Ann Emerg Med 1993;22:594-596.
1. Haynes JH, Guha SC, Taylor SG. Laparoscopic cholecystectomy by a rural family practice: the Vivian, Louisiana, experience. J Fam Pract 2004;53:3:tk-tk.
2. Green LA, Graham R, Frey JJ, Stephens GG. Keystone III. The Role of Family Medicine in a Changing Health Care Environment: A Dialogue Washington, DC: Robert Graham Center; 2001.
3. Johnson RA, Quan MA, Rodney WM. Flexible sigmoidoscopy. J Fam Pract 1982;14:757-770.
4. Morgan WC, Rodney WM, Hahn RG, Garr DA. Ultrasound for the primary care physician. Applications in family-centered obstetrics. Postgrad Med 1988;83:103-107.
5. Rodney WM, Quan MA, Johnson RA, Beaber R. Impact of flexible sigmoidoscopy in a family practice residency. J Fam Pract 1982;15:885-889.
6. Rodney WM. Doing better: Health maintenance research in family medicine. Cont Ed Fam Phys 1985;20:688-689.
7. Rodney WM. High technology is most effective when blended with high touch and vice versa: office technology in the 21st Century. Fam Pract Res J 1991;11:235-239.
8. Deutchman ME, Connor PC, Hahn RG, Rodney WM, et al. Diagnostic and therapeutic tools for the family physician’s office of the 21st century. Fam Pract Res J 1992;12:147-155.
9. Harper MB, Mayeaux EJ, Jr, Pope JB, Goel R. Procedural training in family practice residencies: current status and impact on resident recruitment. J Am Board Fam Pract 1995;8:189-194.
10. Rodney WM, Quan MA. AAFP-ACOG guidelines revisited. Female Patient 1982;97(PC):1-40.
11. Rodney WM, Felmar E. Flexible sigmoidoscopy: a “how to” guide. Your Patient and Cancer 1984;4:57-66.
12. Davies TC, Hahn RG, Rodney WM, Curry HB. The use of OB/GYN ultrasound by family physicians. Cont Ed Fam Phys 1986;21:335-338.
13. Rodney WM. A personal reflection from the AAFP Task Force on Obstetrics. Tenn Fam Physician 1990;1:4-5.
14. Dresang L, Rodney WM, Leeman L, Dees J, Koch P, Palencio M. ALSO in Ecuador: teaching the teachers. J Am Board Fam Pract[in press].
15. Carr K, Worthington JM, Rodney WM, Gentry S, Sellers A, Sizemore J. Advancing from flexible sigmoidoscopy to colonoscopy in rural family practice: a case report. Tenn Med Assoc J 1998;91:21-26.
16. Rodney WM, Weber JR, Swedberg JA, et al. Esophagogastroduodenoscopy by family physicians phase II. a national multisite study of 2,500 procedures. Fam Pract Res J 1993;13:121-131.
17. Felmar E, Cottam C, Payton CE, Rodney WM. Colposcopy: it can be part of your practice. Primary Care and Cancer 1987;7:13-20.
18. Hahn RG, Davies TC, Rodney WM. Het gebruik van echografie in de huisartsenpraktijk [The potential of ultrasound for general practitioners]. Huissart Nu 1987;16:227-230 [in Dutch].
19. Deutchman M, Connor P, Gobbo R, FitzSimmons R. Outcomes of cesarean sections performed by family physicians and the training they received: A 15-year retrospective study. J Am Board Fam Pract 1995;8:81-90.
20. Rodney WM. Flexible sigmoidoscopy and the despecialization of endoscopy: an environmental impact report. Cancer 1992;70(5 suppl):1266-1271.
21. Rodney WM. Obstetrics enhanced family practice: an endangered species worth saving! Florida Fam Phys 1993;43:8-9.
22. Susman J, Rodney WM. Numbers, procedural skills and science: do the three mix? Am Fam Physician 1994;49:1591-1592.
23. Rodney WM. Will virtual reality simulators end the credentialing arms race in gastrointestinal endoscopy or the need for family physician faculty with endoscopic skills? J Am Board Fam Pract 1998;11:492-496.
24. Rodney WM. Historical observations from the RRC 1994-2000: Maternity care [OB] training in FP. J Am Board Fam Pract 2002;15:255-256.
25. Damos JR, Christman C, Gjerde CL, Beasley J, Schutz, Plane MB. A case for the development of family practice rural training tracks. J Am Board Fam Pract 1998;11:399-405.
26. Acosta D. Impact of rural training on physician workforce: the role of postresidency education. J Rural Health 2000;16:254-261.
27. Norris TE, Acosta DA. A fellowship in rural family medicine: program development and outcomes. Fam Med 1997;29:414-420.
28. Stageman JH, Bowman RC, Harrison JD. An accelerated rural training program. J Am Board Fam Pract 2003;16:124-130.
29. Petrany SM, Crespo R. The accelerated residency program: The Marshall University family practice 9-year experience. Fam Med 2002;34:669-672.
30. Delzell JE, Midtling JE, Rodney WM. The university of Tennessee’s accelerated family medicine residency program 1992-2003: An eleven year progress report. J Am Board Fam Practice [submitted].
31. Bullock K, Rodney WM, Gerard T, Hahn R. “Advanced Practice” family physicians as the foundation for rural emergency medicine services (Part I). Texas J Rur Health 2000;17:19-29.
32. Bullock K, Rodney WM, Gerard T, Hahn R. “Advanced Practice” family physicians as the foundation for rural emergency medicine services (Part II). Texas J Rur Health 2000;18:34-44.
33. Hahn RG, Rodney WM, et al. Technology transferred to family medicine: implications for clinical practice. Fourth International Meeting of Family Medicine, sponsored by the International Center of Family Medicine, May 25, 1990, Estoril, Portugal (abstract).
34. Rodney WM, Hahn RG. The impact of the limited generalist (no procedures, no hospital) on the viability of family practice training. J Am Board Fam Pract 2002;15:191-200.
35. Campos-Outcalt D. Family practice specialty selection: a research agenda. Fam Med. 1991;23:609-619.
36. Rodney WM. Foreword. Pfenninger JL, Fowler GC, eds. Procedures for Primary Care 1st ed. St Louis, Mo: Mosby; 2003;xviii.
37. Rodney WM. The dilemma of emerging technologies as required curriculum in primary care. Fam Med 1997;29:584-585.
38. Rodney WM, Crown LA, Hahn RG, Martin J. Enhancing the family medicine curriculum in deliveries and emergency medicine as a way of developing a rural teaching site. Fam Med 1998;30:712-719.
39. Deutchman ME, Hahn RG, Rodney WM. Diagnostic ultrasound imaging by physicians of first contact: extending family medicine into emergency medicine. Ann Emerg Med 1993;22:594-596.
Cesarean Delivery and Hospitals: Size Matters
In this issue of JFP, Janssen and colleagues1 document that low-risk women delivering at a tertiary-care maternity hospital had 3.4 times the likelihood of cesarean delivery of similar low-risk women delivering at a nearby community hospital (95% confidence interval, 2.1-5.4). Differing rates of epidural analgesia appeared to be the most significant association with cesarean delivery.
This study adds to the data suggesting that epidurals increase the cesarean delivery rate, but the controversy about the cause-and-effect role of epidurals in cesarean delivery is extensive, complicated, sometimes heated, and destined to continue. The consideration of factors that might account for the differing cesarean delivery rates arouses 2 more interesting and complex questions. First, how do my attitudes and behaviors as a physician interact with those prevalent in my practice setting to determine the fate of my patient? Second, can patients use information about differing institutional and physician cesarean rates to make choices about whom they select for a maternity care provider and where delivery takes place?
Factors affecting maternity care
Physician specialty, institutional practices, and geographic location are known to affect the use of tests, therapies, procedures, and patient outcomes in a wide range of conditions, including maternity care. Even within a specialty such as obstetrics, different institutions, different geographic areas, and individual care givers within a given institution produce widely differing rates of cesarean delivery for similar patients.2-4 Some physicians may consciously or unconsciously consider every patient to be on the verge of disaster and in need of interventions until proven otherwise: “There is no low-risk obstetrics patient, only high-risk and unknown risk.” Others view pregnancy and birth as natural processes that will most often proceed normally if left alone except for support and encouragement. Although it is a generalization that does not hold true for all individuals, obstetricians are generally found to practice a more interventional style, while family physicians and midwives increasingly tend to be less interventional.5-7
Maternity care practices and outcomes are also subject to strong influence by the institutional environment and culture. This may be particularly important in understanding the differences in cesarean delivery rates between some tertiary-care centers and community hospitals as demonstrated in the study by Janssen and colleagues. It is the nature and mission of a tertiary-care center to attract patients with complications. These centers house systems to care for complicated cases and keep those systems and necessary personnel at the ready. Trainees eager to intervene may also be present. This may create an environment in which interventions designed for patients with complications spill over to patients without complications.
This tertiary-care institution effect can be powerful. In these environments the care provided by family physicians and the resulting outcomes, including cesarean delivery rates, tend to resemble those of the dominant culture.8 In the study by Janssen and coworkers, family physicians were more numerous than obstetricians in both hospitals (3:1 at the tertiary-care center and 12:1 in the community hospital). Although we can assume that family physicians delivered the majority of babies in the community hospital, the data in the study do not reveal what percentage of babies were delivered by family physicians in the tertiary-care center. Although more prevalent numerically, the family physicians may not have been (and probably were not) the dominant culture in the tertiary-care center.
Another recognized component of the institutional effect is nursing care style, with the likelihood of whether any given patient is delivered vaginally or by cesarean being directly related to the individual nurse caring for her. Some features of nursing care that may relate to patient outcome include the following: time spent with the patient, technique of fetal monitoring, nursing expectations, and the type and timing of analgesia offered.9
Patient demographics and expectations were examined in the study by Janssen and colleagues, and no differences were found. However, we do not know if patient expectations may have affected her choice of a care provider or her choice of a place of delivery. It makes sense that patients motivated to have less intervention and not wanting epidural analgesia would seek out the community hospital if the hospital’s usual practices were known to them.
Other questions to consider
Thus as Janssen and coworkers suggest, epidural analgesia may represent a proxy for a large conglomeration of other small parameters that do not themselves reach statistical significance. Most of these small parameters appear to be under human control, and it is in regard to them that we need to examine our attitudes and actions on behalf of our patients. Instead of examining our cesarean rates or our epidural rates, it may be more important to ask ourselves 2 questions: First, do we view labor and birth as natural processes? Second, do we base interventions on evidence that they will do more good than harm? We may never have the answer to “What is the right number of cesarean deliveries?”10 However, we are more likely to approach the right number by making sure we can answer the first 2 questions affirmatively than by agonizing over the statistics related to various parts of the patient’s care.
What about the babies? There was no statistically significant difference in the current study between APGAR scores at the 2 hospitals, indicating that the increased cesarean delivery rate at the tertiary-care center did not produce improved short-term infant outcomes for the low-risk patients as assessed by this one parameter. This is an often-repeated story. Other studies that have examined other parameters have shown that term, normal birthweight infants can have better outcomes at community hospitals than at tertiary-care centers, possibly related to the effect of the previously mentioned physician and institutional factors on their mother’s intrapartum care.11-13
Conclusions
Janssen and colleagues make us think about our role as family physicians who provide maternity care and about what our patients should know. Although family physicians do have important maternity care roles in tertiary care centers as care providers, teachers, and role models, most of us provide care in community hospital settings. Although family physicians deliver approximately 20% of the babies in the United States, we deliver a much larger portion in smaller communities and are the main maternity care providers in rural areas. Providing this access is very important, since we know that pregnancy outcomes are poorer when maternity care is not available locally and women must travel for that care.14,15 Modern medicine has fostered a “bigger is better” mentality, but this study and others like it provide evidence that where hospitals are concerned size matters in an unexpected way: Low-risk women and their babies may be better off in community hospitals than in tertiary-care centers.
1. Janssen PA, Klein MC, Soolsma JH. Differences in institutional cesarean section rates: the role of pain management. J Fam Pract 2001;50:217-223.
2. Lagrew DC, Adashek JA. Lowering the cesarean section rate in a private hospital: comparison of individual physicians’ rates, risk factors and outcomes. Am J Obstet Gynecol 1998;178:1207-14.
3. Ventura SJ, Martin JA, Curtin SC, Mathews TJ. Births: final data for 1997. Natl Vital Stat Rep 1999;47:1-84.
4. DeMott RK, Sandmire HF. The Green Bay cesarean section study. II. The physician factor as a determinant of cesarean birth rates for failed labor. Am J Obstet Gynecol 1992;166:1799-810.
5. Deutchman ME, Sills D, Connor PD. Perinatal outcomes: a comparison between family physicians and obstetricians. J Am Board Fam Pract 1995;8:81-90.
6. Hueston WJ, Applegate JA, Mansfield CJ, King DE, McClaflin RR. Practice variations between family physicians and obstetricians in the management of low-risk pregnancies. J Fam Pract 1995;40:345-51.
7. Rosenblatt RA, Dobie SA, Hart LG, et al. Interspecialty differences in the obstetric care of low-risk women. Am J Publ Health 1997;87:344-51.
8. Carroll JC, Reid AJ, Ruderman J, Murray MA. The influence of the high-risk environment on the practice of low risk obstetrics. Fam Med 1991;23:184-88.
9. Radin T, Harmon J, Hanson M. Nurses’ care during labor: its effect on the cesarean birth rate of healthy, nulliparous women. Birth 1993;20:14-21.
10. What is the right number of cesarean sections? The Lancet 1997;349:815.-
11. LeFevre M, Sanner L, Anderson S, Tsutakawa R. The relationship between neonatal mortality and hospital level. J Fam Pract 1992;35:259-64.
12. Mayfield J, Rosenblatt R, Baldwin L, Chu J, Logerfo J. The relation of obstetrical volume and nursery level to perinatal mortality. Am J Publ Health 1990;80:819-23.
13. Rosenblatt RA, Reinken J, Shoemack P. Is obstetrics safe in a small hospital? Evidence from New Zealand’s regionalised perinatal system. The Lancet 1985;24:429-32.
14. Nesbitt TS, Connell FA, Hart LG, Rosenblatt RA. Access to obstetric care in rural areas: effect on birth outcomes. Am J Publ Health 1990;80:814-18.
15. Larimore WL, Davis A. Relation of infant mortality to the availability of maternity care in rural Florida. J Am Board Fam Pract 1995;8:392.-
In this issue of JFP, Janssen and colleagues1 document that low-risk women delivering at a tertiary-care maternity hospital had 3.4 times the likelihood of cesarean delivery of similar low-risk women delivering at a nearby community hospital (95% confidence interval, 2.1-5.4). Differing rates of epidural analgesia appeared to be the most significant association with cesarean delivery.
This study adds to the data suggesting that epidurals increase the cesarean delivery rate, but the controversy about the cause-and-effect role of epidurals in cesarean delivery is extensive, complicated, sometimes heated, and destined to continue. The consideration of factors that might account for the differing cesarean delivery rates arouses 2 more interesting and complex questions. First, how do my attitudes and behaviors as a physician interact with those prevalent in my practice setting to determine the fate of my patient? Second, can patients use information about differing institutional and physician cesarean rates to make choices about whom they select for a maternity care provider and where delivery takes place?
Factors affecting maternity care
Physician specialty, institutional practices, and geographic location are known to affect the use of tests, therapies, procedures, and patient outcomes in a wide range of conditions, including maternity care. Even within a specialty such as obstetrics, different institutions, different geographic areas, and individual care givers within a given institution produce widely differing rates of cesarean delivery for similar patients.2-4 Some physicians may consciously or unconsciously consider every patient to be on the verge of disaster and in need of interventions until proven otherwise: “There is no low-risk obstetrics patient, only high-risk and unknown risk.” Others view pregnancy and birth as natural processes that will most often proceed normally if left alone except for support and encouragement. Although it is a generalization that does not hold true for all individuals, obstetricians are generally found to practice a more interventional style, while family physicians and midwives increasingly tend to be less interventional.5-7
Maternity care practices and outcomes are also subject to strong influence by the institutional environment and culture. This may be particularly important in understanding the differences in cesarean delivery rates between some tertiary-care centers and community hospitals as demonstrated in the study by Janssen and colleagues. It is the nature and mission of a tertiary-care center to attract patients with complications. These centers house systems to care for complicated cases and keep those systems and necessary personnel at the ready. Trainees eager to intervene may also be present. This may create an environment in which interventions designed for patients with complications spill over to patients without complications.
This tertiary-care institution effect can be powerful. In these environments the care provided by family physicians and the resulting outcomes, including cesarean delivery rates, tend to resemble those of the dominant culture.8 In the study by Janssen and coworkers, family physicians were more numerous than obstetricians in both hospitals (3:1 at the tertiary-care center and 12:1 in the community hospital). Although we can assume that family physicians delivered the majority of babies in the community hospital, the data in the study do not reveal what percentage of babies were delivered by family physicians in the tertiary-care center. Although more prevalent numerically, the family physicians may not have been (and probably were not) the dominant culture in the tertiary-care center.
Another recognized component of the institutional effect is nursing care style, with the likelihood of whether any given patient is delivered vaginally or by cesarean being directly related to the individual nurse caring for her. Some features of nursing care that may relate to patient outcome include the following: time spent with the patient, technique of fetal monitoring, nursing expectations, and the type and timing of analgesia offered.9
Patient demographics and expectations were examined in the study by Janssen and colleagues, and no differences were found. However, we do not know if patient expectations may have affected her choice of a care provider or her choice of a place of delivery. It makes sense that patients motivated to have less intervention and not wanting epidural analgesia would seek out the community hospital if the hospital’s usual practices were known to them.
Other questions to consider
Thus as Janssen and coworkers suggest, epidural analgesia may represent a proxy for a large conglomeration of other small parameters that do not themselves reach statistical significance. Most of these small parameters appear to be under human control, and it is in regard to them that we need to examine our attitudes and actions on behalf of our patients. Instead of examining our cesarean rates or our epidural rates, it may be more important to ask ourselves 2 questions: First, do we view labor and birth as natural processes? Second, do we base interventions on evidence that they will do more good than harm? We may never have the answer to “What is the right number of cesarean deliveries?”10 However, we are more likely to approach the right number by making sure we can answer the first 2 questions affirmatively than by agonizing over the statistics related to various parts of the patient’s care.
What about the babies? There was no statistically significant difference in the current study between APGAR scores at the 2 hospitals, indicating that the increased cesarean delivery rate at the tertiary-care center did not produce improved short-term infant outcomes for the low-risk patients as assessed by this one parameter. This is an often-repeated story. Other studies that have examined other parameters have shown that term, normal birthweight infants can have better outcomes at community hospitals than at tertiary-care centers, possibly related to the effect of the previously mentioned physician and institutional factors on their mother’s intrapartum care.11-13
Conclusions
Janssen and colleagues make us think about our role as family physicians who provide maternity care and about what our patients should know. Although family physicians do have important maternity care roles in tertiary care centers as care providers, teachers, and role models, most of us provide care in community hospital settings. Although family physicians deliver approximately 20% of the babies in the United States, we deliver a much larger portion in smaller communities and are the main maternity care providers in rural areas. Providing this access is very important, since we know that pregnancy outcomes are poorer when maternity care is not available locally and women must travel for that care.14,15 Modern medicine has fostered a “bigger is better” mentality, but this study and others like it provide evidence that where hospitals are concerned size matters in an unexpected way: Low-risk women and their babies may be better off in community hospitals than in tertiary-care centers.
In this issue of JFP, Janssen and colleagues1 document that low-risk women delivering at a tertiary-care maternity hospital had 3.4 times the likelihood of cesarean delivery of similar low-risk women delivering at a nearby community hospital (95% confidence interval, 2.1-5.4). Differing rates of epidural analgesia appeared to be the most significant association with cesarean delivery.
This study adds to the data suggesting that epidurals increase the cesarean delivery rate, but the controversy about the cause-and-effect role of epidurals in cesarean delivery is extensive, complicated, sometimes heated, and destined to continue. The consideration of factors that might account for the differing cesarean delivery rates arouses 2 more interesting and complex questions. First, how do my attitudes and behaviors as a physician interact with those prevalent in my practice setting to determine the fate of my patient? Second, can patients use information about differing institutional and physician cesarean rates to make choices about whom they select for a maternity care provider and where delivery takes place?
Factors affecting maternity care
Physician specialty, institutional practices, and geographic location are known to affect the use of tests, therapies, procedures, and patient outcomes in a wide range of conditions, including maternity care. Even within a specialty such as obstetrics, different institutions, different geographic areas, and individual care givers within a given institution produce widely differing rates of cesarean delivery for similar patients.2-4 Some physicians may consciously or unconsciously consider every patient to be on the verge of disaster and in need of interventions until proven otherwise: “There is no low-risk obstetrics patient, only high-risk and unknown risk.” Others view pregnancy and birth as natural processes that will most often proceed normally if left alone except for support and encouragement. Although it is a generalization that does not hold true for all individuals, obstetricians are generally found to practice a more interventional style, while family physicians and midwives increasingly tend to be less interventional.5-7
Maternity care practices and outcomes are also subject to strong influence by the institutional environment and culture. This may be particularly important in understanding the differences in cesarean delivery rates between some tertiary-care centers and community hospitals as demonstrated in the study by Janssen and colleagues. It is the nature and mission of a tertiary-care center to attract patients with complications. These centers house systems to care for complicated cases and keep those systems and necessary personnel at the ready. Trainees eager to intervene may also be present. This may create an environment in which interventions designed for patients with complications spill over to patients without complications.
This tertiary-care institution effect can be powerful. In these environments the care provided by family physicians and the resulting outcomes, including cesarean delivery rates, tend to resemble those of the dominant culture.8 In the study by Janssen and coworkers, family physicians were more numerous than obstetricians in both hospitals (3:1 at the tertiary-care center and 12:1 in the community hospital). Although we can assume that family physicians delivered the majority of babies in the community hospital, the data in the study do not reveal what percentage of babies were delivered by family physicians in the tertiary-care center. Although more prevalent numerically, the family physicians may not have been (and probably were not) the dominant culture in the tertiary-care center.
Another recognized component of the institutional effect is nursing care style, with the likelihood of whether any given patient is delivered vaginally or by cesarean being directly related to the individual nurse caring for her. Some features of nursing care that may relate to patient outcome include the following: time spent with the patient, technique of fetal monitoring, nursing expectations, and the type and timing of analgesia offered.9
Patient demographics and expectations were examined in the study by Janssen and colleagues, and no differences were found. However, we do not know if patient expectations may have affected her choice of a care provider or her choice of a place of delivery. It makes sense that patients motivated to have less intervention and not wanting epidural analgesia would seek out the community hospital if the hospital’s usual practices were known to them.
Other questions to consider
Thus as Janssen and coworkers suggest, epidural analgesia may represent a proxy for a large conglomeration of other small parameters that do not themselves reach statistical significance. Most of these small parameters appear to be under human control, and it is in regard to them that we need to examine our attitudes and actions on behalf of our patients. Instead of examining our cesarean rates or our epidural rates, it may be more important to ask ourselves 2 questions: First, do we view labor and birth as natural processes? Second, do we base interventions on evidence that they will do more good than harm? We may never have the answer to “What is the right number of cesarean deliveries?”10 However, we are more likely to approach the right number by making sure we can answer the first 2 questions affirmatively than by agonizing over the statistics related to various parts of the patient’s care.
What about the babies? There was no statistically significant difference in the current study between APGAR scores at the 2 hospitals, indicating that the increased cesarean delivery rate at the tertiary-care center did not produce improved short-term infant outcomes for the low-risk patients as assessed by this one parameter. This is an often-repeated story. Other studies that have examined other parameters have shown that term, normal birthweight infants can have better outcomes at community hospitals than at tertiary-care centers, possibly related to the effect of the previously mentioned physician and institutional factors on their mother’s intrapartum care.11-13
Conclusions
Janssen and colleagues make us think about our role as family physicians who provide maternity care and about what our patients should know. Although family physicians do have important maternity care roles in tertiary care centers as care providers, teachers, and role models, most of us provide care in community hospital settings. Although family physicians deliver approximately 20% of the babies in the United States, we deliver a much larger portion in smaller communities and are the main maternity care providers in rural areas. Providing this access is very important, since we know that pregnancy outcomes are poorer when maternity care is not available locally and women must travel for that care.14,15 Modern medicine has fostered a “bigger is better” mentality, but this study and others like it provide evidence that where hospitals are concerned size matters in an unexpected way: Low-risk women and their babies may be better off in community hospitals than in tertiary-care centers.
1. Janssen PA, Klein MC, Soolsma JH. Differences in institutional cesarean section rates: the role of pain management. J Fam Pract 2001;50:217-223.
2. Lagrew DC, Adashek JA. Lowering the cesarean section rate in a private hospital: comparison of individual physicians’ rates, risk factors and outcomes. Am J Obstet Gynecol 1998;178:1207-14.
3. Ventura SJ, Martin JA, Curtin SC, Mathews TJ. Births: final data for 1997. Natl Vital Stat Rep 1999;47:1-84.
4. DeMott RK, Sandmire HF. The Green Bay cesarean section study. II. The physician factor as a determinant of cesarean birth rates for failed labor. Am J Obstet Gynecol 1992;166:1799-810.
5. Deutchman ME, Sills D, Connor PD. Perinatal outcomes: a comparison between family physicians and obstetricians. J Am Board Fam Pract 1995;8:81-90.
6. Hueston WJ, Applegate JA, Mansfield CJ, King DE, McClaflin RR. Practice variations between family physicians and obstetricians in the management of low-risk pregnancies. J Fam Pract 1995;40:345-51.
7. Rosenblatt RA, Dobie SA, Hart LG, et al. Interspecialty differences in the obstetric care of low-risk women. Am J Publ Health 1997;87:344-51.
8. Carroll JC, Reid AJ, Ruderman J, Murray MA. The influence of the high-risk environment on the practice of low risk obstetrics. Fam Med 1991;23:184-88.
9. Radin T, Harmon J, Hanson M. Nurses’ care during labor: its effect on the cesarean birth rate of healthy, nulliparous women. Birth 1993;20:14-21.
10. What is the right number of cesarean sections? The Lancet 1997;349:815.-
11. LeFevre M, Sanner L, Anderson S, Tsutakawa R. The relationship between neonatal mortality and hospital level. J Fam Pract 1992;35:259-64.
12. Mayfield J, Rosenblatt R, Baldwin L, Chu J, Logerfo J. The relation of obstetrical volume and nursery level to perinatal mortality. Am J Publ Health 1990;80:819-23.
13. Rosenblatt RA, Reinken J, Shoemack P. Is obstetrics safe in a small hospital? Evidence from New Zealand’s regionalised perinatal system. The Lancet 1985;24:429-32.
14. Nesbitt TS, Connell FA, Hart LG, Rosenblatt RA. Access to obstetric care in rural areas: effect on birth outcomes. Am J Publ Health 1990;80:814-18.
15. Larimore WL, Davis A. Relation of infant mortality to the availability of maternity care in rural Florida. J Am Board Fam Pract 1995;8:392.-
1. Janssen PA, Klein MC, Soolsma JH. Differences in institutional cesarean section rates: the role of pain management. J Fam Pract 2001;50:217-223.
2. Lagrew DC, Adashek JA. Lowering the cesarean section rate in a private hospital: comparison of individual physicians’ rates, risk factors and outcomes. Am J Obstet Gynecol 1998;178:1207-14.
3. Ventura SJ, Martin JA, Curtin SC, Mathews TJ. Births: final data for 1997. Natl Vital Stat Rep 1999;47:1-84.
4. DeMott RK, Sandmire HF. The Green Bay cesarean section study. II. The physician factor as a determinant of cesarean birth rates for failed labor. Am J Obstet Gynecol 1992;166:1799-810.
5. Deutchman ME, Sills D, Connor PD. Perinatal outcomes: a comparison between family physicians and obstetricians. J Am Board Fam Pract 1995;8:81-90.
6. Hueston WJ, Applegate JA, Mansfield CJ, King DE, McClaflin RR. Practice variations between family physicians and obstetricians in the management of low-risk pregnancies. J Fam Pract 1995;40:345-51.
7. Rosenblatt RA, Dobie SA, Hart LG, et al. Interspecialty differences in the obstetric care of low-risk women. Am J Publ Health 1997;87:344-51.
8. Carroll JC, Reid AJ, Ruderman J, Murray MA. The influence of the high-risk environment on the practice of low risk obstetrics. Fam Med 1991;23:184-88.
9. Radin T, Harmon J, Hanson M. Nurses’ care during labor: its effect on the cesarean birth rate of healthy, nulliparous women. Birth 1993;20:14-21.
10. What is the right number of cesarean sections? The Lancet 1997;349:815.-
11. LeFevre M, Sanner L, Anderson S, Tsutakawa R. The relationship between neonatal mortality and hospital level. J Fam Pract 1992;35:259-64.
12. Mayfield J, Rosenblatt R, Baldwin L, Chu J, Logerfo J. The relation of obstetrical volume and nursery level to perinatal mortality. Am J Publ Health 1990;80:819-23.
13. Rosenblatt RA, Reinken J, Shoemack P. Is obstetrics safe in a small hospital? Evidence from New Zealand’s regionalised perinatal system. The Lancet 1985;24:429-32.
14. Nesbitt TS, Connell FA, Hart LG, Rosenblatt RA. Access to obstetric care in rural areas: effect on birth outcomes. Am J Publ Health 1990;80:814-18.
15. Larimore WL, Davis A. Relation of infant mortality to the availability of maternity care in rural Florida. J Am Board Fam Pract 1995;8:392.-