User login
Sequential bilateral hip deformities
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
A 10-YEAR-OLD AFRICAN AMERICAN GIRL was brought to our clinic for right anterior thigh pain that she’d had for 3 weeks. She had been playing normally prior to the onset of pain and said she hadn’t experienced any trauma or injury. She was unable to run due to the pain, but continued to walk with a limp. She denied any other joint pain, fevers, rash, or other constitutional symptoms.
The patient, who was overweight and not in any distress, held her right leg in a slight external rotation. There was no asymmetry, deformity, or swelling in her right hip. She was slightly tender to palpation in the area of the right proximal anterior femur. The remainder of the right lower extremity was nontender.
The patient’s active flexion was limited to approximately 90 degrees, secondary to pain. She had marked pain with internal rotation, but none with external rotation. Her neurological exam was normal, with normal sensation throughout her right lower extremity. She had normal dorsalis pedis and posterior tibial pulses.
Plain radiographs of the right hip showed a deformity best noted on the frog leg lateral view (FIGURE 1A). The patient underwent successful in situ pinning of the right hip (FIGURE 1B), had an uncomplicated postoperative course, and returned to her prior level of activity without limitations.
Seven months later, though, the patient came back to the clinic with the same complaints—this time in her left hip—with similar x-ray findings (FIGURE 2A).
FIGURE 1
X-rays before, after pinning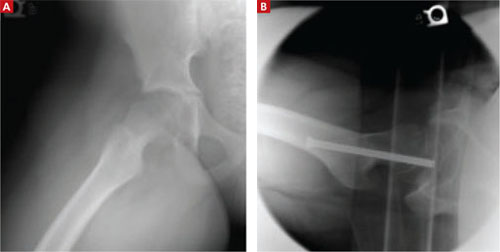
A frog leg lateral view of the patient’s right hip deformity before surgery (A). The patient underwent successful in situ pinning of the hip (B).
WHAT IS YOUR DIAGNOSIS?
Diagnosis: Bilateral slipped capital femoral epiphysis
This patient’s radiographic findings (FIGURES 1A and 2A) confirmed that she had experienced sequential bilateral slipped capital femoral epiphysis. SCFE occurs when the femoral head is displaced through the weakened physis, usually medially. Most common in the adolescent years, it is likely caused by the alteration in the plane of the physis during the adolescent growth spurt, in addition to the increased forces of weight gain. Obesity has been shown to be a significant risk factor.1 A small percentage of patients have an underlying endocrine disorder.2,3
FIGURE 2
One hip fixed, trouble in the other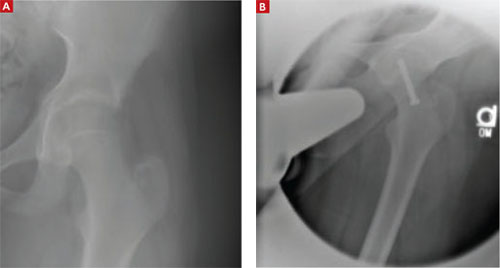
Seven months after surgery on her right hip, the patient sought treatment for her left hip (A) and underwent a second pinning procedure (B).
Differential Dx includes tumors, traumatic injuries
In adolescents who present with hip pain, the differential includes infectious etiologies (eg, septic arthritis, osteomyelitis), tumors, and traumatic injuries (eg, contusions, fractures, epiphyseal injuries). This patient’s characteristic presentation and physical exam raised my suspicion of SCFE. The classic radiographic findings confirmed my suspicion.
Treatment can’t wait
Untreated or delayed treatment of SCFE is associated with significant morbidity, including osteonecrosis, chondrolysis, and chronic pain and deformity. Among patients who experience an initial SCFE, an estimated 30% to 60% will experience a future contralateral slip.4,5
The management of the contralateral hip is controversial. Several studies have explored which patient factors are most predictive of future contralateral slips, and which patients would benefit from prophylactic contralateral pinning. Younger age at presentation—<12 years for girls and <14 years for boys—has been shown to be the most predictive factor of future contralateral slips.6 Other factors, such as race, sex, and skeletal maturity, have not been statistically significant predictors of future slips.6 Older age, in contrast, has been associated with increased slip severity.7
Two studies compared outcomes of observation vs prophylactic in situ pinning after an initial SCFE.8,9 The first showed benefit in the pinning of the contralateral hip,8 while the second study showed optimal benefit in the observation group, except among higher risk patients or patients in whom follow-up was problematic.9
Because of the heightened likelihood of future contralateral SCFE and the significant morbidity associated with delayed treatment, prophylactic pinning of the contralateral hip should be considered in patients after an initial SCFE—especially in certain high-risk groups8,9(strength of recommendation: B). Future large, randomized trials with patient-oriented outcomes would be useful.
Clearly, final treatment decisions will involve patient preferences and patient-specific factors including age and comorbidities.
Back on track after 2 surgeries
My patient did well after recovering from her second surgery (FIGURE 2B). I encouraged her to lose weight by eating well and exercising regularly.
The patient followed standard postoperative instructions of nonweight bearing for 6 weeks after each surgery. She returned to her prior functional status and continues to do well.
CORRESPONDENCE: Mark A. McElhannon, MD, Atlanta Medical Center Family Practice Residency, 1000 Corporate Center Drive, Suite 200, Morrow, GA 30260; [email protected]
1. Loder RT. The demographics of slipped capital femoral epiphysis. An international multicenter study. Clin Orthop Relat Res. 1996;322:8-27.
2. Wells D, King JD, Roe TF. Review of slipped capital femoral epiphysis associated with endocrine disease. J Pediatr Orthop. 1993;13:610-614.
3. Burrow SR, Alman B, Wright JG. Short stature as a screening test for endocrinopathy in slipped capital femoral epiphysis. J Bone Joint Surg Br. 2001;83:263-268.
4. Loder RT, Aronson DD, Greenfield ML. The epidemiology of bilateral slipped capital femoral epiphysis. A study of children in Michigan. J Bone Joint Surg Am. 1993;75:1141-1147.
5. Hagglund G, Hansson LI, Ordeberg G, et al. Bilaterality in slipped upper femoral epiphysis. J Bone Joint Surg Br. 1988;70:179-181.
6. Riad J, Bajelidze G, Gabos PG. Bilateral slipped capital epiphysis: predictive factors for contralateral slip. J Pediatr Orthop. 2007;27:411-414.
7. Loder RT, Starnes T, Dikos G, et al. Demographic predictors of severity of stable slipped capital femoral epiphysis. J Bone Joint Surg Am. 2006;88:97-105
8. Schultz WR, Weinstein JN, Weinstein SL, et al. Prophylactic pinning of the contralateral hip in slipped capital femoral epiphysis; evaluation of long term outcome for the contralateral hip with use of decision analysis. J Bone Joint Surg Am. 2002;84-A:1305-1314.
9. Kocher MS, Bishop JA, Hresko MT, et al. Prophylactic pinning of the contralateral hip after unilateral slipped capital femoral epiphysis. J Bone Joint Surg Am. 2004;86-A:2658-2665.
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
A 10-YEAR-OLD AFRICAN AMERICAN GIRL was brought to our clinic for right anterior thigh pain that she’d had for 3 weeks. She had been playing normally prior to the onset of pain and said she hadn’t experienced any trauma or injury. She was unable to run due to the pain, but continued to walk with a limp. She denied any other joint pain, fevers, rash, or other constitutional symptoms.
The patient, who was overweight and not in any distress, held her right leg in a slight external rotation. There was no asymmetry, deformity, or swelling in her right hip. She was slightly tender to palpation in the area of the right proximal anterior femur. The remainder of the right lower extremity was nontender.
The patient’s active flexion was limited to approximately 90 degrees, secondary to pain. She had marked pain with internal rotation, but none with external rotation. Her neurological exam was normal, with normal sensation throughout her right lower extremity. She had normal dorsalis pedis and posterior tibial pulses.
Plain radiographs of the right hip showed a deformity best noted on the frog leg lateral view (FIGURE 1A). The patient underwent successful in situ pinning of the right hip (FIGURE 1B), had an uncomplicated postoperative course, and returned to her prior level of activity without limitations.
Seven months later, though, the patient came back to the clinic with the same complaints—this time in her left hip—with similar x-ray findings (FIGURE 2A).
FIGURE 1
X-rays before, after pinning
A frog leg lateral view of the patient’s right hip deformity before surgery (A). The patient underwent successful in situ pinning of the hip (B).
WHAT IS YOUR DIAGNOSIS?
Diagnosis: Bilateral slipped capital femoral epiphysis
This patient’s radiographic findings (FIGURES 1A and 2A) confirmed that she had experienced sequential bilateral slipped capital femoral epiphysis. SCFE occurs when the femoral head is displaced through the weakened physis, usually medially. Most common in the adolescent years, it is likely caused by the alteration in the plane of the physis during the adolescent growth spurt, in addition to the increased forces of weight gain. Obesity has been shown to be a significant risk factor.1 A small percentage of patients have an underlying endocrine disorder.2,3
FIGURE 2
One hip fixed, trouble in the other
Seven months after surgery on her right hip, the patient sought treatment for her left hip (A) and underwent a second pinning procedure (B).
Differential Dx includes tumors, traumatic injuries
In adolescents who present with hip pain, the differential includes infectious etiologies (eg, septic arthritis, osteomyelitis), tumors, and traumatic injuries (eg, contusions, fractures, epiphyseal injuries). This patient’s characteristic presentation and physical exam raised my suspicion of SCFE. The classic radiographic findings confirmed my suspicion.
Treatment can’t wait
Untreated or delayed treatment of SCFE is associated with significant morbidity, including osteonecrosis, chondrolysis, and chronic pain and deformity. Among patients who experience an initial SCFE, an estimated 30% to 60% will experience a future contralateral slip.4,5
The management of the contralateral hip is controversial. Several studies have explored which patient factors are most predictive of future contralateral slips, and which patients would benefit from prophylactic contralateral pinning. Younger age at presentation—<12 years for girls and <14 years for boys—has been shown to be the most predictive factor of future contralateral slips.6 Other factors, such as race, sex, and skeletal maturity, have not been statistically significant predictors of future slips.6 Older age, in contrast, has been associated with increased slip severity.7
Two studies compared outcomes of observation vs prophylactic in situ pinning after an initial SCFE.8,9 The first showed benefit in the pinning of the contralateral hip,8 while the second study showed optimal benefit in the observation group, except among higher risk patients or patients in whom follow-up was problematic.9
Because of the heightened likelihood of future contralateral SCFE and the significant morbidity associated with delayed treatment, prophylactic pinning of the contralateral hip should be considered in patients after an initial SCFE—especially in certain high-risk groups8,9(strength of recommendation: B). Future large, randomized trials with patient-oriented outcomes would be useful.
Clearly, final treatment decisions will involve patient preferences and patient-specific factors including age and comorbidities.
Back on track after 2 surgeries
My patient did well after recovering from her second surgery (FIGURE 2B). I encouraged her to lose weight by eating well and exercising regularly.
The patient followed standard postoperative instructions of nonweight bearing for 6 weeks after each surgery. She returned to her prior functional status and continues to do well.
CORRESPONDENCE: Mark A. McElhannon, MD, Atlanta Medical Center Family Practice Residency, 1000 Corporate Center Drive, Suite 200, Morrow, GA 30260; [email protected]
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
A 10-YEAR-OLD AFRICAN AMERICAN GIRL was brought to our clinic for right anterior thigh pain that she’d had for 3 weeks. She had been playing normally prior to the onset of pain and said she hadn’t experienced any trauma or injury. She was unable to run due to the pain, but continued to walk with a limp. She denied any other joint pain, fevers, rash, or other constitutional symptoms.
The patient, who was overweight and not in any distress, held her right leg in a slight external rotation. There was no asymmetry, deformity, or swelling in her right hip. She was slightly tender to palpation in the area of the right proximal anterior femur. The remainder of the right lower extremity was nontender.
The patient’s active flexion was limited to approximately 90 degrees, secondary to pain. She had marked pain with internal rotation, but none with external rotation. Her neurological exam was normal, with normal sensation throughout her right lower extremity. She had normal dorsalis pedis and posterior tibial pulses.
Plain radiographs of the right hip showed a deformity best noted on the frog leg lateral view (FIGURE 1A). The patient underwent successful in situ pinning of the right hip (FIGURE 1B), had an uncomplicated postoperative course, and returned to her prior level of activity without limitations.
Seven months later, though, the patient came back to the clinic with the same complaints—this time in her left hip—with similar x-ray findings (FIGURE 2A).
FIGURE 1
X-rays before, after pinning
A frog leg lateral view of the patient’s right hip deformity before surgery (A). The patient underwent successful in situ pinning of the hip (B).
WHAT IS YOUR DIAGNOSIS?
Diagnosis: Bilateral slipped capital femoral epiphysis
This patient’s radiographic findings (FIGURES 1A and 2A) confirmed that she had experienced sequential bilateral slipped capital femoral epiphysis. SCFE occurs when the femoral head is displaced through the weakened physis, usually medially. Most common in the adolescent years, it is likely caused by the alteration in the plane of the physis during the adolescent growth spurt, in addition to the increased forces of weight gain. Obesity has been shown to be a significant risk factor.1 A small percentage of patients have an underlying endocrine disorder.2,3
FIGURE 2
One hip fixed, trouble in the other
Seven months after surgery on her right hip, the patient sought treatment for her left hip (A) and underwent a second pinning procedure (B).
Differential Dx includes tumors, traumatic injuries
In adolescents who present with hip pain, the differential includes infectious etiologies (eg, septic arthritis, osteomyelitis), tumors, and traumatic injuries (eg, contusions, fractures, epiphyseal injuries). This patient’s characteristic presentation and physical exam raised my suspicion of SCFE. The classic radiographic findings confirmed my suspicion.
Treatment can’t wait
Untreated or delayed treatment of SCFE is associated with significant morbidity, including osteonecrosis, chondrolysis, and chronic pain and deformity. Among patients who experience an initial SCFE, an estimated 30% to 60% will experience a future contralateral slip.4,5
The management of the contralateral hip is controversial. Several studies have explored which patient factors are most predictive of future contralateral slips, and which patients would benefit from prophylactic contralateral pinning. Younger age at presentation—<12 years for girls and <14 years for boys—has been shown to be the most predictive factor of future contralateral slips.6 Other factors, such as race, sex, and skeletal maturity, have not been statistically significant predictors of future slips.6 Older age, in contrast, has been associated with increased slip severity.7
Two studies compared outcomes of observation vs prophylactic in situ pinning after an initial SCFE.8,9 The first showed benefit in the pinning of the contralateral hip,8 while the second study showed optimal benefit in the observation group, except among higher risk patients or patients in whom follow-up was problematic.9
Because of the heightened likelihood of future contralateral SCFE and the significant morbidity associated with delayed treatment, prophylactic pinning of the contralateral hip should be considered in patients after an initial SCFE—especially in certain high-risk groups8,9(strength of recommendation: B). Future large, randomized trials with patient-oriented outcomes would be useful.
Clearly, final treatment decisions will involve patient preferences and patient-specific factors including age and comorbidities.
Back on track after 2 surgeries
My patient did well after recovering from her second surgery (FIGURE 2B). I encouraged her to lose weight by eating well and exercising regularly.
The patient followed standard postoperative instructions of nonweight bearing for 6 weeks after each surgery. She returned to her prior functional status and continues to do well.
CORRESPONDENCE: Mark A. McElhannon, MD, Atlanta Medical Center Family Practice Residency, 1000 Corporate Center Drive, Suite 200, Morrow, GA 30260; [email protected]
1. Loder RT. The demographics of slipped capital femoral epiphysis. An international multicenter study. Clin Orthop Relat Res. 1996;322:8-27.
2. Wells D, King JD, Roe TF. Review of slipped capital femoral epiphysis associated with endocrine disease. J Pediatr Orthop. 1993;13:610-614.
3. Burrow SR, Alman B, Wright JG. Short stature as a screening test for endocrinopathy in slipped capital femoral epiphysis. J Bone Joint Surg Br. 2001;83:263-268.
4. Loder RT, Aronson DD, Greenfield ML. The epidemiology of bilateral slipped capital femoral epiphysis. A study of children in Michigan. J Bone Joint Surg Am. 1993;75:1141-1147.
5. Hagglund G, Hansson LI, Ordeberg G, et al. Bilaterality in slipped upper femoral epiphysis. J Bone Joint Surg Br. 1988;70:179-181.
6. Riad J, Bajelidze G, Gabos PG. Bilateral slipped capital epiphysis: predictive factors for contralateral slip. J Pediatr Orthop. 2007;27:411-414.
7. Loder RT, Starnes T, Dikos G, et al. Demographic predictors of severity of stable slipped capital femoral epiphysis. J Bone Joint Surg Am. 2006;88:97-105
8. Schultz WR, Weinstein JN, Weinstein SL, et al. Prophylactic pinning of the contralateral hip in slipped capital femoral epiphysis; evaluation of long term outcome for the contralateral hip with use of decision analysis. J Bone Joint Surg Am. 2002;84-A:1305-1314.
9. Kocher MS, Bishop JA, Hresko MT, et al. Prophylactic pinning of the contralateral hip after unilateral slipped capital femoral epiphysis. J Bone Joint Surg Am. 2004;86-A:2658-2665.
1. Loder RT. The demographics of slipped capital femoral epiphysis. An international multicenter study. Clin Orthop Relat Res. 1996;322:8-27.
2. Wells D, King JD, Roe TF. Review of slipped capital femoral epiphysis associated with endocrine disease. J Pediatr Orthop. 1993;13:610-614.
3. Burrow SR, Alman B, Wright JG. Short stature as a screening test for endocrinopathy in slipped capital femoral epiphysis. J Bone Joint Surg Br. 2001;83:263-268.
4. Loder RT, Aronson DD, Greenfield ML. The epidemiology of bilateral slipped capital femoral epiphysis. A study of children in Michigan. J Bone Joint Surg Am. 1993;75:1141-1147.
5. Hagglund G, Hansson LI, Ordeberg G, et al. Bilaterality in slipped upper femoral epiphysis. J Bone Joint Surg Br. 1988;70:179-181.
6. Riad J, Bajelidze G, Gabos PG. Bilateral slipped capital epiphysis: predictive factors for contralateral slip. J Pediatr Orthop. 2007;27:411-414.
7. Loder RT, Starnes T, Dikos G, et al. Demographic predictors of severity of stable slipped capital femoral epiphysis. J Bone Joint Surg Am. 2006;88:97-105
8. Schultz WR, Weinstein JN, Weinstein SL, et al. Prophylactic pinning of the contralateral hip in slipped capital femoral epiphysis; evaluation of long term outcome for the contralateral hip with use of decision analysis. J Bone Joint Surg Am. 2002;84-A:1305-1314.
9. Kocher MS, Bishop JA, Hresko MT, et al. Prophylactic pinning of the contralateral hip after unilateral slipped capital femoral epiphysis. J Bone Joint Surg Am. 2004;86-A:2658-2665.