User login
Leaders: Hospitalist Urges Straight Talk with Patients
Dr. Michael J. Pistoria’s pet peeve is when physicians and nurses talk at patients instead of talking with them.
Less than a year after taking the helm as president of the medical staff at Lehigh Valley Health Network in Allentown, Pa., Dr. Pistoria has urged his colleagues to use plain language when speaking to patients about their treatment. That means avoiding technical terms that require at least a year of medical school to understand. But it also means using communication techniques like "teach-back" to make sure that patients understand what they have been told and have a plan for managing their illness outside the hospital.

He and his colleagues at Lehigh Valley have tested the teach-back concept among heart failure patients and found that it decreased readmissions. In their study, 180 heart failure patients received the teach-back intervention and had a readmission rate of about 7%, while 289 heart failure patients who didn’t receive teach-back had a readmission rate of roughly 10% during the same time period.
In an interview with Hospitalist News, Dr. Pistoria explained the key to their success.
Question: You had some encouraging results in using teach-back with heart failure patients in 2011. Why does this method work so well?
Dr. Pistoria: One factor is the engagement of the nursing staff. It’s a nurse-driven process. The other factor is the engagement of the patient or the key learner. As the teach-back process was developed, we tried to be very cognizant of how much we already ask nurses to do. The two people who spearheaded the approach were Paula Robinson, R.N., and Debra Peter, R.N. They did a great job of tapping into what the nurses were passionate about, which is teaching. This gave them the opportunity to do that in little bits each day for our heart failure patients.
For the patients, teach-back meant having a different level of accountability and involvement. We asked the heart failure patients: "After you leave the hospital, how are you going to remember to weigh yourself every day? How are you going to remember to minimize your salt intake?" I think that really empowered them.
Question: You are looking at the role of teach-back in other conditions. How is that going so far?
Dr. Pistoria: We just rolled out the stroke teach-back on May 1. We’re still working on myocardial infarction and developing teach-back around anticoagulation. We’re also working on a program for obstructive lung disease.
Question: What’s the role for the hospitalist in teach-back?
Dr. Pistoria: They should be involved. We’ve started to have some discussions around how to do that. Right now, our nurses are doing the teach-back, and they may identify particular issues that the patient may be comfortable only expressing to the nurse. The issue then becomes, how do we take those issues and apply some techniques of motivational interviewing on the physician side?
Question: Do you need to use standardized questions for teach-back?
Dr. Pistoria: It’s absolutely necessary. As the teach-back questions were developed, we made sure that everyone was using the same standard work questions and that there was standard work for the process. Then we incorporated the questions with prompters into our order entry system. There’s a pop-up screen on the system that the nurse will see so if they forget the specific question, it’s right there in front of them. They can either read it or work off of it to fit their particular style. Having the standard question and the standard work also is important because it allows us to evaluate and audit to make sure the teach-back is being done correctly.
Question: Everyone is looking for the silver bullet in reducing unnecessary readmissions. Is this it?
Dr. Pistoria: Sadly, it’s not. I think it’s a very important piece and one that we as physicians have not addressed particularly well. Too often we’re not cognizant of the message we’re giving patients and how we’re delivering that message. It’s really important for us to begin to engage patients whether it’s through teach-back or motivational interviewing or something else. This is an important element, but there are just so many other factors that impact readmissions. As much as I would love to say it’s the answer, it’s just one small piece of the puzzle.
Take us to your leader. Nominate a hospitalist whose work inspires you. E-mail suggestions to [email protected]. Read previous columns at ehospitalistnews.com.
Dr. Michael J. Pistoria’s pet peeve is when physicians and nurses talk at patients instead of talking with them.
Less than a year after taking the helm as president of the medical staff at Lehigh Valley Health Network in Allentown, Pa., Dr. Pistoria has urged his colleagues to use plain language when speaking to patients about their treatment. That means avoiding technical terms that require at least a year of medical school to understand. But it also means using communication techniques like "teach-back" to make sure that patients understand what they have been told and have a plan for managing their illness outside the hospital.
He and his colleagues at Lehigh Valley have tested the teach-back concept among heart failure patients and found that it decreased readmissions. In their study, 180 heart failure patients received the teach-back intervention and had a readmission rate of about 7%, while 289 heart failure patients who didn’t receive teach-back had a readmission rate of roughly 10% during the same time period.
In an interview with Hospitalist News, Dr. Pistoria explained the key to their success.
Question: You had some encouraging results in using teach-back with heart failure patients in 2011. Why does this method work so well?
Dr. Pistoria: One factor is the engagement of the nursing staff. It’s a nurse-driven process. The other factor is the engagement of the patient or the key learner. As the teach-back process was developed, we tried to be very cognizant of how much we already ask nurses to do. The two people who spearheaded the approach were Paula Robinson, R.N., and Debra Peter, R.N. They did a great job of tapping into what the nurses were passionate about, which is teaching. This gave them the opportunity to do that in little bits each day for our heart failure patients.
For the patients, teach-back meant having a different level of accountability and involvement. We asked the heart failure patients: "After you leave the hospital, how are you going to remember to weigh yourself every day? How are you going to remember to minimize your salt intake?" I think that really empowered them.
Question: You are looking at the role of teach-back in other conditions. How is that going so far?
Dr. Pistoria: We just rolled out the stroke teach-back on May 1. We’re still working on myocardial infarction and developing teach-back around anticoagulation. We’re also working on a program for obstructive lung disease.
Question: What’s the role for the hospitalist in teach-back?
Dr. Pistoria: They should be involved. We’ve started to have some discussions around how to do that. Right now, our nurses are doing the teach-back, and they may identify particular issues that the patient may be comfortable only expressing to the nurse. The issue then becomes, how do we take those issues and apply some techniques of motivational interviewing on the physician side?
Question: Do you need to use standardized questions for teach-back?
Dr. Pistoria: It’s absolutely necessary. As the teach-back questions were developed, we made sure that everyone was using the same standard work questions and that there was standard work for the process. Then we incorporated the questions with prompters into our order entry system. There’s a pop-up screen on the system that the nurse will see so if they forget the specific question, it’s right there in front of them. They can either read it or work off of it to fit their particular style. Having the standard question and the standard work also is important because it allows us to evaluate and audit to make sure the teach-back is being done correctly.
Question: Everyone is looking for the silver bullet in reducing unnecessary readmissions. Is this it?
Dr. Pistoria: Sadly, it’s not. I think it’s a very important piece and one that we as physicians have not addressed particularly well. Too often we’re not cognizant of the message we’re giving patients and how we’re delivering that message. It’s really important for us to begin to engage patients whether it’s through teach-back or motivational interviewing or something else. This is an important element, but there are just so many other factors that impact readmissions. As much as I would love to say it’s the answer, it’s just one small piece of the puzzle.
Take us to your leader. Nominate a hospitalist whose work inspires you. E-mail suggestions to [email protected]. Read previous columns at ehospitalistnews.com.
Dr. Michael J. Pistoria’s pet peeve is when physicians and nurses talk at patients instead of talking with them.
Less than a year after taking the helm as president of the medical staff at Lehigh Valley Health Network in Allentown, Pa., Dr. Pistoria has urged his colleagues to use plain language when speaking to patients about their treatment. That means avoiding technical terms that require at least a year of medical school to understand. But it also means using communication techniques like "teach-back" to make sure that patients understand what they have been told and have a plan for managing their illness outside the hospital.
He and his colleagues at Lehigh Valley have tested the teach-back concept among heart failure patients and found that it decreased readmissions. In their study, 180 heart failure patients received the teach-back intervention and had a readmission rate of about 7%, while 289 heart failure patients who didn’t receive teach-back had a readmission rate of roughly 10% during the same time period.
In an interview with Hospitalist News, Dr. Pistoria explained the key to their success.
Question: You had some encouraging results in using teach-back with heart failure patients in 2011. Why does this method work so well?
Dr. Pistoria: One factor is the engagement of the nursing staff. It’s a nurse-driven process. The other factor is the engagement of the patient or the key learner. As the teach-back process was developed, we tried to be very cognizant of how much we already ask nurses to do. The two people who spearheaded the approach were Paula Robinson, R.N., and Debra Peter, R.N. They did a great job of tapping into what the nurses were passionate about, which is teaching. This gave them the opportunity to do that in little bits each day for our heart failure patients.
For the patients, teach-back meant having a different level of accountability and involvement. We asked the heart failure patients: "After you leave the hospital, how are you going to remember to weigh yourself every day? How are you going to remember to minimize your salt intake?" I think that really empowered them.
Question: You are looking at the role of teach-back in other conditions. How is that going so far?
Dr. Pistoria: We just rolled out the stroke teach-back on May 1. We’re still working on myocardial infarction and developing teach-back around anticoagulation. We’re also working on a program for obstructive lung disease.
Question: What’s the role for the hospitalist in teach-back?
Dr. Pistoria: They should be involved. We’ve started to have some discussions around how to do that. Right now, our nurses are doing the teach-back, and they may identify particular issues that the patient may be comfortable only expressing to the nurse. The issue then becomes, how do we take those issues and apply some techniques of motivational interviewing on the physician side?
Question: Do you need to use standardized questions for teach-back?
Dr. Pistoria: It’s absolutely necessary. As the teach-back questions were developed, we made sure that everyone was using the same standard work questions and that there was standard work for the process. Then we incorporated the questions with prompters into our order entry system. There’s a pop-up screen on the system that the nurse will see so if they forget the specific question, it’s right there in front of them. They can either read it or work off of it to fit their particular style. Having the standard question and the standard work also is important because it allows us to evaluate and audit to make sure the teach-back is being done correctly.
Question: Everyone is looking for the silver bullet in reducing unnecessary readmissions. Is this it?
Dr. Pistoria: Sadly, it’s not. I think it’s a very important piece and one that we as physicians have not addressed particularly well. Too often we’re not cognizant of the message we’re giving patients and how we’re delivering that message. It’s really important for us to begin to engage patients whether it’s through teach-back or motivational interviewing or something else. This is an important element, but there are just so many other factors that impact readmissions. As much as I would love to say it’s the answer, it’s just one small piece of the puzzle.
Take us to your leader. Nominate a hospitalist whose work inspires you. E-mail suggestions to [email protected]. Read previous columns at ehospitalistnews.com.
ACO Rollout Expected to Vary Widely
The emergence of Accountable Care Organizations could have a significant impact on the day-to-day life of hospitalists, or then again not much at all.
It all depends on how far along hospital medicine groups are in developing systems of communication and improving transitions of care. Those groups that have invested the time and money in information technology systems, improving the discharge process, and building relationships with primary care physicians are likely to be ahead of the curve and ready to participate almost seamlessly in ACOs. The others will be playing catchup, experts agree.
Dr. Melissa Mattison, associate chief of the hospital medicine section at Beth Israel Deaconess Medical Center in Boston, currently treats patients from two different ACOs operating in the Boston area – the Beth Israel Deaconess Physician Organization and Atrius Health. She and her hospitalist colleagues were prepared for the introduction of the ACO model of care, which aims to better coordinate the management of patients by holding networks of providers financially accountable for the quality and cost of care across the inpatient and outpatient settings.
At Beth Israel, there is a robust electronic health record system that keeps primary care physicians up to date on their hospitalized patients so that communication occurs at key points of care. A postdischarge clinic provides timely follow-up care to patients who have difficulty accessing primary care services.
This proactive approach is a well-established strategy of Beth Israel’s hospital medicine program, Dr. Mattison noted. "This has been somewhat the mantra of hospital medicine: improved care for patients, improved transitions of care, and making sure we’re really creating a plan of care."
Not much has changed since the introduction of the ACO model in how she delivers care on a day-to-day basis. "Hospitalists are really trying day in and day out to do what’s right for the patient in front of them and to work with the system that they have," Dr. Mattison said.
ACOs have been a buzzword in health policy circles for about the last 5 years, and a few commercial health plans have experimented with the idea. But ACOs really got off the ground earlier this year when the Centers for Medicare and Medicaid Services (CMS) began testing the model among fee-for-service Medicare beneficiaries.
How this will impact hospitalists’ payments is still unclear. Several experts said that since hospitalist payment arrangements vary so widely already, the financial incentives associated with ACOs also are likely to be site specific.
Dr. Mattison said the ACO model provides an opportunity for hospitalists to continue the work they’ve already begun on transitions of care.
The financial incentives in the ACO environment call for keeping patients healthy and out of the hospital. For hospitalists, that means primarily preventing readmissions. That’s nothing new, said Dr. Joseph Li, chief of hospital medicine at Beth Israel Deaconess Medical Center and past president of the Society of Hospital Medicine.
"The things that hospitalists need to be thinking about should be things that we’ve really been talking about all along," he said.
But there will be some differences, too, Dr. Li said. It will likely be less important for hospitalists to focus on decreasing length of stay and doing discharges earlier in the day.
For instance, in the pre-ACO environment, a patient might be discharged to receive care at a rehabilitation facility for a few days before going home. But in the new ACO environment, the hospitalist may keep the same patient in the hospital another day and avoid the additional expense of the rehab stay.
"I think that we’re going to see that hospitalists are going to be thinking about that, and appropriately so," Dr. Li said. "That’s where it’s important for the patient, the doctor, and the hospital to be on the same page."
Dr. Li estimates that about 70% of the patients he sees are part of an ACO arrangement. But all patients that come through his hospital get the same care, he said, effectively raising the quality for everyone.
"We’re not picking and choosing which patients we don’t want readmitted," he said. "The real focus is that we want everybody not to be readmitted."
At the OSF Healthcare System – an integrated health system in Central Illinois and 1 of the 32 Pioneer ACOs selected by CMS for testing of the care model – they have the same philosophy about changing the way they provide care regardless of which patients are in an ACO.
"The goal of this is to improve the care of all of our patients, not just those in certain payment arrangements," said Dr. Stephen Hippler, vice president of quality and clinical programs for OSF Medical Group.

Most of the ACO-related preparations at OSF have occurred in the primary care setting, expanding the breadth and depth of their patient-centered medical home. But Dr. Hippler said there also is a critical role for hospitalists. The health system has developed a number of projects aimed at improving transitions of care, from risk stratification at admission to medication reconciliation to creating a more robust discharge process.
Hospitalists also will have a significant role in guiding patients to the appropriate level of care after discharge, he said. Similarly, the Pioneer ACO at Monarch Healthcare in Orange County, Calif., asks its 25 hospitalists to think about transitions of care immediately after finishing their history and physical with a new patient.
Hospitalists are in a unique position because they exist at a point of care where many inefficiencies and redundancies occur, said Dr. Michael Weiss, a pediatrician and the medical director of quality and performance improvement at Monarch Healthcare.
"Hospitalists are an absolute key to this equation," he said.
Getting the hospital piece right is critical for any ACO to be successful, since about a third of the dollars in the health care system are today spent in the acute care hospital, agreed Dr. Ron Greeno, chief medical officer for Cogent HMG and chair of the public policy committee at the Society of Hospital Medicine.
"If you don’t control those inpatient dollars, it will sink you when you start taking [financial] risk," he said.
As a result, the demand for hospitalists is only going to grow, but so will the expectations in terms of the scope of care. "The bar is going to be raised," Dr. Greeno said.
One of the biggest challenges for hospitalist leaders preparing for the ACO world is that they are still operating mainly in a fee-for-service system that pays for more care, not necessary better or more efficient care.
And many hospital medicine groups simply aren’t prepared to make the leap to the coordinated care model because they haven’t laid the groundwork in improving discharge and transitions of care, he said.
To get ready, Dr. Greeno advised hospital medicine groups to take a series of steps that are simple in concept, but much more difficult to execute. For starters, the financial incentives have to be aligned so that hospitalists keep patients out of the hospital. Physicians also need to take a standardized approach to clinical functions and other nonclinical hospital processes. Additionally, the internal and external communications must be working well and hospitalists need to be able to track and interpret data.
Even though it’s early on in the emergence of new care delivery models such as ACOs, hospitalists must start to change their mind-set and realize that the hospital is a cost center, not a profit center, said Dr. Bradley Flansbaum, a hospitalist who blogs about health policy issues for The Hospitalist Leader.
In this new world, physicians should be doing everything they can to move patients out of the hospital efficiently. But exactly how their performance will be measured is unclear. While CMS and other payers use "rudimentary" core process measures to assess hospitalist care, there are real questions about whether these metrics are valid indicators of better care delivery, said Dr. Flansbaum, a member of the Society of Hospital Medicine’s public policy committee and the society’s representative to the American Medical Association’s House of Delegates.
"We have crude tools right now to really measure people," he said.
With those measures in flux, the best strategy for hospitalists is to focus on the areas that are sure to be important in ACOs, such as discharge planning, medication reconciliation, and communication, Dr. Flansbaum said.
Other than that, hospitalists can wait and see how the model develops and if the Pioneer ACOs are able to deliver on the promise of better quality at lower costs. The consolidation that is occurring in some ACOs could result in cost-saving economies of scale, but it also has the potential to drive prices up, he said. Another question mark is whether the model will catch on around the country. For instance, high-performing health systems with low costs, like the Mayo Clinic, may opt not to make changes.
"There’s a lot of folks who are questioning whether or not this whole ACO model is viable for every hospital and every place," Dr. Flansbaum said.
Pioneer, Shared Savings: Payment Nuts and Bolts
In January, CMS launched the Pioneer ACO Model and selected 32 organizations to test out ways to offer coordinated care that improves quality and lowers costs. The Pioneers aren’t typical health systems, but rather organizations that already have significant experience in care coordination and may already have been operating as an ACO. Both the Beth Israel Deaconess Physician Organization and Atrius Health are among the Pioneers.
Under the 3-year program, the ACOs will have 2 years to continue receiving their regular fee-for-service payments, and they will have the chance to share in either the savings or losses to the Medicare program based on the cost of the care provided. Eligibility for those bonuses also would depend on meeting quality targets. In the third year, those organizations that have saved money for the Medicare program early on will be able to switch a substantial portion of their reimbursement to a capitated payment model in which they will receive a flat, per-beneficiary, per-month payment to manage an individual’s care.
CMS officials also have selected the first 27 organizations to participate in the Shared Savings Program, an initiative designed to test the ACO concept among organizations with less experience in coordinating care across inpatient and outpatient settings.
ACOs in the Shared Savings Program will receive their fee-for-service payments and be eligible to share in any savings they generate for Medicare. Organizations can choose to share in the savings, or take on more financial risk and potentially earn higher bonus payments.
The emergence of Accountable Care Organizations could have a significant impact on the day-to-day life of hospitalists, or then again not much at all.
It all depends on how far along hospital medicine groups are in developing systems of communication and improving transitions of care. Those groups that have invested the time and money in information technology systems, improving the discharge process, and building relationships with primary care physicians are likely to be ahead of the curve and ready to participate almost seamlessly in ACOs. The others will be playing catchup, experts agree.
Dr. Melissa Mattison, associate chief of the hospital medicine section at Beth Israel Deaconess Medical Center in Boston, currently treats patients from two different ACOs operating in the Boston area – the Beth Israel Deaconess Physician Organization and Atrius Health. She and her hospitalist colleagues were prepared for the introduction of the ACO model of care, which aims to better coordinate the management of patients by holding networks of providers financially accountable for the quality and cost of care across the inpatient and outpatient settings.
At Beth Israel, there is a robust electronic health record system that keeps primary care physicians up to date on their hospitalized patients so that communication occurs at key points of care. A postdischarge clinic provides timely follow-up care to patients who have difficulty accessing primary care services.
This proactive approach is a well-established strategy of Beth Israel’s hospital medicine program, Dr. Mattison noted. "This has been somewhat the mantra of hospital medicine: improved care for patients, improved transitions of care, and making sure we’re really creating a plan of care."
Not much has changed since the introduction of the ACO model in how she delivers care on a day-to-day basis. "Hospitalists are really trying day in and day out to do what’s right for the patient in front of them and to work with the system that they have," Dr. Mattison said.
ACOs have been a buzzword in health policy circles for about the last 5 years, and a few commercial health plans have experimented with the idea. But ACOs really got off the ground earlier this year when the Centers for Medicare and Medicaid Services (CMS) began testing the model among fee-for-service Medicare beneficiaries.
How this will impact hospitalists’ payments is still unclear. Several experts said that since hospitalist payment arrangements vary so widely already, the financial incentives associated with ACOs also are likely to be site specific.
Dr. Mattison said the ACO model provides an opportunity for hospitalists to continue the work they’ve already begun on transitions of care.
The financial incentives in the ACO environment call for keeping patients healthy and out of the hospital. For hospitalists, that means primarily preventing readmissions. That’s nothing new, said Dr. Joseph Li, chief of hospital medicine at Beth Israel Deaconess Medical Center and past president of the Society of Hospital Medicine.
"The things that hospitalists need to be thinking about should be things that we’ve really been talking about all along," he said.
But there will be some differences, too, Dr. Li said. It will likely be less important for hospitalists to focus on decreasing length of stay and doing discharges earlier in the day.
For instance, in the pre-ACO environment, a patient might be discharged to receive care at a rehabilitation facility for a few days before going home. But in the new ACO environment, the hospitalist may keep the same patient in the hospital another day and avoid the additional expense of the rehab stay.
"I think that we’re going to see that hospitalists are going to be thinking about that, and appropriately so," Dr. Li said. "That’s where it’s important for the patient, the doctor, and the hospital to be on the same page."
Dr. Li estimates that about 70% of the patients he sees are part of an ACO arrangement. But all patients that come through his hospital get the same care, he said, effectively raising the quality for everyone.
"We’re not picking and choosing which patients we don’t want readmitted," he said. "The real focus is that we want everybody not to be readmitted."
At the OSF Healthcare System – an integrated health system in Central Illinois and 1 of the 32 Pioneer ACOs selected by CMS for testing of the care model – they have the same philosophy about changing the way they provide care regardless of which patients are in an ACO.
"The goal of this is to improve the care of all of our patients, not just those in certain payment arrangements," said Dr. Stephen Hippler, vice president of quality and clinical programs for OSF Medical Group.
Most of the ACO-related preparations at OSF have occurred in the primary care setting, expanding the breadth and depth of their patient-centered medical home. But Dr. Hippler said there also is a critical role for hospitalists. The health system has developed a number of projects aimed at improving transitions of care, from risk stratification at admission to medication reconciliation to creating a more robust discharge process.
Hospitalists also will have a significant role in guiding patients to the appropriate level of care after discharge, he said. Similarly, the Pioneer ACO at Monarch Healthcare in Orange County, Calif., asks its 25 hospitalists to think about transitions of care immediately after finishing their history and physical with a new patient.
Hospitalists are in a unique position because they exist at a point of care where many inefficiencies and redundancies occur, said Dr. Michael Weiss, a pediatrician and the medical director of quality and performance improvement at Monarch Healthcare.
"Hospitalists are an absolute key to this equation," he said.
Getting the hospital piece right is critical for any ACO to be successful, since about a third of the dollars in the health care system are today spent in the acute care hospital, agreed Dr. Ron Greeno, chief medical officer for Cogent HMG and chair of the public policy committee at the Society of Hospital Medicine.
"If you don’t control those inpatient dollars, it will sink you when you start taking [financial] risk," he said.
As a result, the demand for hospitalists is only going to grow, but so will the expectations in terms of the scope of care. "The bar is going to be raised," Dr. Greeno said.
One of the biggest challenges for hospitalist leaders preparing for the ACO world is that they are still operating mainly in a fee-for-service system that pays for more care, not necessary better or more efficient care.
And many hospital medicine groups simply aren’t prepared to make the leap to the coordinated care model because they haven’t laid the groundwork in improving discharge and transitions of care, he said.
To get ready, Dr. Greeno advised hospital medicine groups to take a series of steps that are simple in concept, but much more difficult to execute. For starters, the financial incentives have to be aligned so that hospitalists keep patients out of the hospital. Physicians also need to take a standardized approach to clinical functions and other nonclinical hospital processes. Additionally, the internal and external communications must be working well and hospitalists need to be able to track and interpret data.
Even though it’s early on in the emergence of new care delivery models such as ACOs, hospitalists must start to change their mind-set and realize that the hospital is a cost center, not a profit center, said Dr. Bradley Flansbaum, a hospitalist who blogs about health policy issues for The Hospitalist Leader.
In this new world, physicians should be doing everything they can to move patients out of the hospital efficiently. But exactly how their performance will be measured is unclear. While CMS and other payers use "rudimentary" core process measures to assess hospitalist care, there are real questions about whether these metrics are valid indicators of better care delivery, said Dr. Flansbaum, a member of the Society of Hospital Medicine’s public policy committee and the society’s representative to the American Medical Association’s House of Delegates.
"We have crude tools right now to really measure people," he said.
With those measures in flux, the best strategy for hospitalists is to focus on the areas that are sure to be important in ACOs, such as discharge planning, medication reconciliation, and communication, Dr. Flansbaum said.
Other than that, hospitalists can wait and see how the model develops and if the Pioneer ACOs are able to deliver on the promise of better quality at lower costs. The consolidation that is occurring in some ACOs could result in cost-saving economies of scale, but it also has the potential to drive prices up, he said. Another question mark is whether the model will catch on around the country. For instance, high-performing health systems with low costs, like the Mayo Clinic, may opt not to make changes.
"There’s a lot of folks who are questioning whether or not this whole ACO model is viable for every hospital and every place," Dr. Flansbaum said.
Pioneer, Shared Savings: Payment Nuts and Bolts
In January, CMS launched the Pioneer ACO Model and selected 32 organizations to test out ways to offer coordinated care that improves quality and lowers costs. The Pioneers aren’t typical health systems, but rather organizations that already have significant experience in care coordination and may already have been operating as an ACO. Both the Beth Israel Deaconess Physician Organization and Atrius Health are among the Pioneers.
Under the 3-year program, the ACOs will have 2 years to continue receiving their regular fee-for-service payments, and they will have the chance to share in either the savings or losses to the Medicare program based on the cost of the care provided. Eligibility for those bonuses also would depend on meeting quality targets. In the third year, those organizations that have saved money for the Medicare program early on will be able to switch a substantial portion of their reimbursement to a capitated payment model in which they will receive a flat, per-beneficiary, per-month payment to manage an individual’s care.
CMS officials also have selected the first 27 organizations to participate in the Shared Savings Program, an initiative designed to test the ACO concept among organizations with less experience in coordinating care across inpatient and outpatient settings.
ACOs in the Shared Savings Program will receive their fee-for-service payments and be eligible to share in any savings they generate for Medicare. Organizations can choose to share in the savings, or take on more financial risk and potentially earn higher bonus payments.
The emergence of Accountable Care Organizations could have a significant impact on the day-to-day life of hospitalists, or then again not much at all.
It all depends on how far along hospital medicine groups are in developing systems of communication and improving transitions of care. Those groups that have invested the time and money in information technology systems, improving the discharge process, and building relationships with primary care physicians are likely to be ahead of the curve and ready to participate almost seamlessly in ACOs. The others will be playing catchup, experts agree.
Dr. Melissa Mattison, associate chief of the hospital medicine section at Beth Israel Deaconess Medical Center in Boston, currently treats patients from two different ACOs operating in the Boston area – the Beth Israel Deaconess Physician Organization and Atrius Health. She and her hospitalist colleagues were prepared for the introduction of the ACO model of care, which aims to better coordinate the management of patients by holding networks of providers financially accountable for the quality and cost of care across the inpatient and outpatient settings.
At Beth Israel, there is a robust electronic health record system that keeps primary care physicians up to date on their hospitalized patients so that communication occurs at key points of care. A postdischarge clinic provides timely follow-up care to patients who have difficulty accessing primary care services.
This proactive approach is a well-established strategy of Beth Israel’s hospital medicine program, Dr. Mattison noted. "This has been somewhat the mantra of hospital medicine: improved care for patients, improved transitions of care, and making sure we’re really creating a plan of care."
Not much has changed since the introduction of the ACO model in how she delivers care on a day-to-day basis. "Hospitalists are really trying day in and day out to do what’s right for the patient in front of them and to work with the system that they have," Dr. Mattison said.
ACOs have been a buzzword in health policy circles for about the last 5 years, and a few commercial health plans have experimented with the idea. But ACOs really got off the ground earlier this year when the Centers for Medicare and Medicaid Services (CMS) began testing the model among fee-for-service Medicare beneficiaries.
How this will impact hospitalists’ payments is still unclear. Several experts said that since hospitalist payment arrangements vary so widely already, the financial incentives associated with ACOs also are likely to be site specific.
Dr. Mattison said the ACO model provides an opportunity for hospitalists to continue the work they’ve already begun on transitions of care.
The financial incentives in the ACO environment call for keeping patients healthy and out of the hospital. For hospitalists, that means primarily preventing readmissions. That’s nothing new, said Dr. Joseph Li, chief of hospital medicine at Beth Israel Deaconess Medical Center and past president of the Society of Hospital Medicine.
"The things that hospitalists need to be thinking about should be things that we’ve really been talking about all along," he said.
But there will be some differences, too, Dr. Li said. It will likely be less important for hospitalists to focus on decreasing length of stay and doing discharges earlier in the day.
For instance, in the pre-ACO environment, a patient might be discharged to receive care at a rehabilitation facility for a few days before going home. But in the new ACO environment, the hospitalist may keep the same patient in the hospital another day and avoid the additional expense of the rehab stay.
"I think that we’re going to see that hospitalists are going to be thinking about that, and appropriately so," Dr. Li said. "That’s where it’s important for the patient, the doctor, and the hospital to be on the same page."
Dr. Li estimates that about 70% of the patients he sees are part of an ACO arrangement. But all patients that come through his hospital get the same care, he said, effectively raising the quality for everyone.
"We’re not picking and choosing which patients we don’t want readmitted," he said. "The real focus is that we want everybody not to be readmitted."
At the OSF Healthcare System – an integrated health system in Central Illinois and 1 of the 32 Pioneer ACOs selected by CMS for testing of the care model – they have the same philosophy about changing the way they provide care regardless of which patients are in an ACO.
"The goal of this is to improve the care of all of our patients, not just those in certain payment arrangements," said Dr. Stephen Hippler, vice president of quality and clinical programs for OSF Medical Group.
Most of the ACO-related preparations at OSF have occurred in the primary care setting, expanding the breadth and depth of their patient-centered medical home. But Dr. Hippler said there also is a critical role for hospitalists. The health system has developed a number of projects aimed at improving transitions of care, from risk stratification at admission to medication reconciliation to creating a more robust discharge process.
Hospitalists also will have a significant role in guiding patients to the appropriate level of care after discharge, he said. Similarly, the Pioneer ACO at Monarch Healthcare in Orange County, Calif., asks its 25 hospitalists to think about transitions of care immediately after finishing their history and physical with a new patient.
Hospitalists are in a unique position because they exist at a point of care where many inefficiencies and redundancies occur, said Dr. Michael Weiss, a pediatrician and the medical director of quality and performance improvement at Monarch Healthcare.
"Hospitalists are an absolute key to this equation," he said.
Getting the hospital piece right is critical for any ACO to be successful, since about a third of the dollars in the health care system are today spent in the acute care hospital, agreed Dr. Ron Greeno, chief medical officer for Cogent HMG and chair of the public policy committee at the Society of Hospital Medicine.
"If you don’t control those inpatient dollars, it will sink you when you start taking [financial] risk," he said.
As a result, the demand for hospitalists is only going to grow, but so will the expectations in terms of the scope of care. "The bar is going to be raised," Dr. Greeno said.
One of the biggest challenges for hospitalist leaders preparing for the ACO world is that they are still operating mainly in a fee-for-service system that pays for more care, not necessary better or more efficient care.
And many hospital medicine groups simply aren’t prepared to make the leap to the coordinated care model because they haven’t laid the groundwork in improving discharge and transitions of care, he said.
To get ready, Dr. Greeno advised hospital medicine groups to take a series of steps that are simple in concept, but much more difficult to execute. For starters, the financial incentives have to be aligned so that hospitalists keep patients out of the hospital. Physicians also need to take a standardized approach to clinical functions and other nonclinical hospital processes. Additionally, the internal and external communications must be working well and hospitalists need to be able to track and interpret data.
Even though it’s early on in the emergence of new care delivery models such as ACOs, hospitalists must start to change their mind-set and realize that the hospital is a cost center, not a profit center, said Dr. Bradley Flansbaum, a hospitalist who blogs about health policy issues for The Hospitalist Leader.
In this new world, physicians should be doing everything they can to move patients out of the hospital efficiently. But exactly how their performance will be measured is unclear. While CMS and other payers use "rudimentary" core process measures to assess hospitalist care, there are real questions about whether these metrics are valid indicators of better care delivery, said Dr. Flansbaum, a member of the Society of Hospital Medicine’s public policy committee and the society’s representative to the American Medical Association’s House of Delegates.
"We have crude tools right now to really measure people," he said.
With those measures in flux, the best strategy for hospitalists is to focus on the areas that are sure to be important in ACOs, such as discharge planning, medication reconciliation, and communication, Dr. Flansbaum said.
Other than that, hospitalists can wait and see how the model develops and if the Pioneer ACOs are able to deliver on the promise of better quality at lower costs. The consolidation that is occurring in some ACOs could result in cost-saving economies of scale, but it also has the potential to drive prices up, he said. Another question mark is whether the model will catch on around the country. For instance, high-performing health systems with low costs, like the Mayo Clinic, may opt not to make changes.
"There’s a lot of folks who are questioning whether or not this whole ACO model is viable for every hospital and every place," Dr. Flansbaum said.
Pioneer, Shared Savings: Payment Nuts and Bolts
In January, CMS launched the Pioneer ACO Model and selected 32 organizations to test out ways to offer coordinated care that improves quality and lowers costs. The Pioneers aren’t typical health systems, but rather organizations that already have significant experience in care coordination and may already have been operating as an ACO. Both the Beth Israel Deaconess Physician Organization and Atrius Health are among the Pioneers.
Under the 3-year program, the ACOs will have 2 years to continue receiving their regular fee-for-service payments, and they will have the chance to share in either the savings or losses to the Medicare program based on the cost of the care provided. Eligibility for those bonuses also would depend on meeting quality targets. In the third year, those organizations that have saved money for the Medicare program early on will be able to switch a substantial portion of their reimbursement to a capitated payment model in which they will receive a flat, per-beneficiary, per-month payment to manage an individual’s care.
CMS officials also have selected the first 27 organizations to participate in the Shared Savings Program, an initiative designed to test the ACO concept among organizations with less experience in coordinating care across inpatient and outpatient settings.
ACOs in the Shared Savings Program will receive their fee-for-service payments and be eligible to share in any savings they generate for Medicare. Organizations can choose to share in the savings, or take on more financial risk and potentially earn higher bonus payments.
Awards Spotlight Hospitals' Public Reporting Efforts
Hospitals are getting another push toward public reporting.
The Leapfrog Group, along with the health care accreditation organization URAC, has created the Excellence in Hospital Website Transparency Best Practices Awards and Acknowledgement Program. The program, which was launched in April, recognizes hospitals that create the best websites for displaying their performance on quality measures to consumers.
Hospitals have until Sept. 30 to submit an application.
Applicants must meet criteria for design, credibility, literacy, connectivity, and reporting of safety and quality results. Hospitals that meet a minimum threshold will receive an Acknowledgement of Excellence in Hospital Website Transparency. Hospitals also have the option of applying for the Best Practices in Hospital Website Transparency Award. A panel of judges will review the best practice submissions and select the top three hospitals for recognition.
The Leapfrog Group and URAC will announce recipients of the Acknowledgement of Excellence in Hospital Website Transparency by the end of this year. Awards for the Best Practices in Hospital Website Transparency will be presented in March 2013.
The recognition program’s criteria are based on the guidelines on public reporting from the National Quality Forum and the Agency for Healthcare Research and Quality. The Leapfrog Survey’s former "transparency indicator" was also considered in designing the program.
Hospitals are getting another push toward public reporting.
The Leapfrog Group, along with the health care accreditation organization URAC, has created the Excellence in Hospital Website Transparency Best Practices Awards and Acknowledgement Program. The program, which was launched in April, recognizes hospitals that create the best websites for displaying their performance on quality measures to consumers.
Hospitals have until Sept. 30 to submit an application.
Applicants must meet criteria for design, credibility, literacy, connectivity, and reporting of safety and quality results. Hospitals that meet a minimum threshold will receive an Acknowledgement of Excellence in Hospital Website Transparency. Hospitals also have the option of applying for the Best Practices in Hospital Website Transparency Award. A panel of judges will review the best practice submissions and select the top three hospitals for recognition.
The Leapfrog Group and URAC will announce recipients of the Acknowledgement of Excellence in Hospital Website Transparency by the end of this year. Awards for the Best Practices in Hospital Website Transparency will be presented in March 2013.
The recognition program’s criteria are based on the guidelines on public reporting from the National Quality Forum and the Agency for Healthcare Research and Quality. The Leapfrog Survey’s former "transparency indicator" was also considered in designing the program.
Hospitals are getting another push toward public reporting.
The Leapfrog Group, along with the health care accreditation organization URAC, has created the Excellence in Hospital Website Transparency Best Practices Awards and Acknowledgement Program. The program, which was launched in April, recognizes hospitals that create the best websites for displaying their performance on quality measures to consumers.
Hospitals have until Sept. 30 to submit an application.
Applicants must meet criteria for design, credibility, literacy, connectivity, and reporting of safety and quality results. Hospitals that meet a minimum threshold will receive an Acknowledgement of Excellence in Hospital Website Transparency. Hospitals also have the option of applying for the Best Practices in Hospital Website Transparency Award. A panel of judges will review the best practice submissions and select the top three hospitals for recognition.
The Leapfrog Group and URAC will announce recipients of the Acknowledgement of Excellence in Hospital Website Transparency by the end of this year. Awards for the Best Practices in Hospital Website Transparency will be presented in March 2013.
The recognition program’s criteria are based on the guidelines on public reporting from the National Quality Forum and the Agency for Healthcare Research and Quality. The Leapfrog Survey’s former "transparency indicator" was also considered in designing the program.
Updated Measures Assess Heart Failure Care
A set of nine performance measures aimed at assessing whether adults with heart failure are receiving the best care was issued by the American College of Cardiology Foundation, the American Heart Association, and the American Medical Association’s Physician Consortium for Performance Improvement.
The measure set, which was published April 23 in the Journal of the American College of Cardiology, includes three new performance measures and six revised measures. The new measure set was drafted by a panel of physicians, pharmacists, and patient advocates (J. Am. Coll. Cardiol. April 23, 2012;doi:10.1016/j.jacc.2012.03.013). The performance measures were last revised in 2005.
The measure set includes two performance metrics for inpatient care, five that address care in the outpatient setting, and two measures that apply to care in both settings. The idea, according to the sponsors, was to stress the need to measure quality over time and across providers, not in silos.
"To be successful as quality improvement tools, the heart failure performance measures need to be integrated as routine components of patient care across various care settings, with particular attention to transitions of care from inpatient to outpatient environments," Dr. Robert O. Bonow, cochair of the work group that developed the measure set and director of the center for cardiovascular innovation at Northwestern University, Chicago, said in a statement.
Improving care transitions is likely to be a major focus for physicians in and out of the hospital as officials at the Centers for Medicare and Medicaid Services begin to test a series of alternative payment and care delivery models, from Accountable Care Organizations to bundled payments. Adding to that pressure, this October, the CMS will begin cutting Medicare payments to hospitals whose heart failure and acute myocardial infarction readmission rates are considered too high.
The updated measure set will help prepare physicians for the payment and care delivery changes, Dr. Kathleen Blake, a member of the measure work group and a senior research director at the Center for Medical Technology Policy in Baltimore, said in an interview.
Performance measures, by definition, address areas where there are gaps in care, said Dr. Blake, who is a cardiologist. So physicians can take the updated heart failure measure set and embed it in their care, like a checklist, to ensure that patients are being considered for all appropriate evidence-based treatments.
"We are inundated with medical literature these days. This basically distills it into a measure set," she said.
The work group considered the ACCF/AHA 2009 practice guidelines on heart failure as well as existing heart failure performance measures from the Joint Commission, the CMS, and the Agency for Healthcare Research and Quality in putting together the updated set of measures. Along with the new and revised measures, they retired eight performance measures from the 2005 list.
The updated measure set includes:
1. Left Ventricular Ejection Fraction (LVEF) assessment in the outpatient setting.
2. LVEF in the inpatient setting.
3. Symptom and activity assessment in the outpatient setting.
4. NEW: Symptom management in the outpatient setting (for quality improvement only).
5. Patient self-care education in the outpatient setting (for quality improvement only).
6. Beta-blocker therapy for left ventricular systolic dysfunction in the outpatient and inpatient settings.
7. ACE inhibitor for angiotensin receptor blocker therapy for left ventricular systolic dysfunction in the inpatient and outpatient setting.
8. NEW: Counseling regarding implantable cardioverter-defibrillator (ICD) implantation for patients with left ventricular systolic dysfunction combination medical therapy in the outpatient setting (for quality improvement only).
9. NEW: Postdischarge appointment for heart failure patients in the inpatient setting.
One of the significant changes in the updated measure set, according to the ACCF, is the expansion of the beta-blocker measure to the inpatient setting. In the 2005 set, the measure was only recommended for outpatient care. The panel sought to expand its use based on inpatient care information in the 2009 ACCF-AHA heart failure guidelines.
The work group also recommended that measures 6 and 7, which call for the use of beta-blockers, and ACE and ARB therapy, respectively, should be used together.
Another change in the updated measure set is the addition of a measure calling for a postdischarge appointment to be in place at the time of discharge from the hospital.
While most of the measures are considered appropriate for use in pay-for-performance programs, physician rankings, and public reporting, the writing panel recommended that the measures related to symptom management, patient self-care education, and counseling for ICD implantation be used only for internal quality improvement purposes.
Dr. Blake said these are areas where the work group wanted to give physicians time to collect data. In the case of the ICD counseling measure, they wanted to include a quality improvement measure that would serve as a reminder to physicians to discuss this option with eligible patients. "It doesn’t mean the patient should receive the device," she said. "It means that it should be a topic for discussion as part of a comprehensive review of the patient. It’s also an opportunity to discern what their goals and objectives are."
Dr. Bonow and Dr. Blake disclosed that they had no relationships with industry.
A set of nine performance measures aimed at assessing whether adults with heart failure are receiving the best care was issued by the American College of Cardiology Foundation, the American Heart Association, and the American Medical Association’s Physician Consortium for Performance Improvement.
The measure set, which was published April 23 in the Journal of the American College of Cardiology, includes three new performance measures and six revised measures. The new measure set was drafted by a panel of physicians, pharmacists, and patient advocates (J. Am. Coll. Cardiol. April 23, 2012;doi:10.1016/j.jacc.2012.03.013). The performance measures were last revised in 2005.
The measure set includes two performance metrics for inpatient care, five that address care in the outpatient setting, and two measures that apply to care in both settings. The idea, according to the sponsors, was to stress the need to measure quality over time and across providers, not in silos.
"To be successful as quality improvement tools, the heart failure performance measures need to be integrated as routine components of patient care across various care settings, with particular attention to transitions of care from inpatient to outpatient environments," Dr. Robert O. Bonow, cochair of the work group that developed the measure set and director of the center for cardiovascular innovation at Northwestern University, Chicago, said in a statement.
Improving care transitions is likely to be a major focus for physicians in and out of the hospital as officials at the Centers for Medicare and Medicaid Services begin to test a series of alternative payment and care delivery models, from Accountable Care Organizations to bundled payments. Adding to that pressure, this October, the CMS will begin cutting Medicare payments to hospitals whose heart failure and acute myocardial infarction readmission rates are considered too high.
The updated measure set will help prepare physicians for the payment and care delivery changes, Dr. Kathleen Blake, a member of the measure work group and a senior research director at the Center for Medical Technology Policy in Baltimore, said in an interview.
Performance measures, by definition, address areas where there are gaps in care, said Dr. Blake, who is a cardiologist. So physicians can take the updated heart failure measure set and embed it in their care, like a checklist, to ensure that patients are being considered for all appropriate evidence-based treatments.
"We are inundated with medical literature these days. This basically distills it into a measure set," she said.
The work group considered the ACCF/AHA 2009 practice guidelines on heart failure as well as existing heart failure performance measures from the Joint Commission, the CMS, and the Agency for Healthcare Research and Quality in putting together the updated set of measures. Along with the new and revised measures, they retired eight performance measures from the 2005 list.
The updated measure set includes:
1. Left Ventricular Ejection Fraction (LVEF) assessment in the outpatient setting.
2. LVEF in the inpatient setting.
3. Symptom and activity assessment in the outpatient setting.
4. NEW: Symptom management in the outpatient setting (for quality improvement only).
5. Patient self-care education in the outpatient setting (for quality improvement only).
6. Beta-blocker therapy for left ventricular systolic dysfunction in the outpatient and inpatient settings.
7. ACE inhibitor for angiotensin receptor blocker therapy for left ventricular systolic dysfunction in the inpatient and outpatient setting.
8. NEW: Counseling regarding implantable cardioverter-defibrillator (ICD) implantation for patients with left ventricular systolic dysfunction combination medical therapy in the outpatient setting (for quality improvement only).
9. NEW: Postdischarge appointment for heart failure patients in the inpatient setting.
One of the significant changes in the updated measure set, according to the ACCF, is the expansion of the beta-blocker measure to the inpatient setting. In the 2005 set, the measure was only recommended for outpatient care. The panel sought to expand its use based on inpatient care information in the 2009 ACCF-AHA heart failure guidelines.
The work group also recommended that measures 6 and 7, which call for the use of beta-blockers, and ACE and ARB therapy, respectively, should be used together.
Another change in the updated measure set is the addition of a measure calling for a postdischarge appointment to be in place at the time of discharge from the hospital.
While most of the measures are considered appropriate for use in pay-for-performance programs, physician rankings, and public reporting, the writing panel recommended that the measures related to symptom management, patient self-care education, and counseling for ICD implantation be used only for internal quality improvement purposes.
Dr. Blake said these are areas where the work group wanted to give physicians time to collect data. In the case of the ICD counseling measure, they wanted to include a quality improvement measure that would serve as a reminder to physicians to discuss this option with eligible patients. "It doesn’t mean the patient should receive the device," she said. "It means that it should be a topic for discussion as part of a comprehensive review of the patient. It’s also an opportunity to discern what their goals and objectives are."
Dr. Bonow and Dr. Blake disclosed that they had no relationships with industry.
A set of nine performance measures aimed at assessing whether adults with heart failure are receiving the best care was issued by the American College of Cardiology Foundation, the American Heart Association, and the American Medical Association’s Physician Consortium for Performance Improvement.
The measure set, which was published April 23 in the Journal of the American College of Cardiology, includes three new performance measures and six revised measures. The new measure set was drafted by a panel of physicians, pharmacists, and patient advocates (J. Am. Coll. Cardiol. April 23, 2012;doi:10.1016/j.jacc.2012.03.013). The performance measures were last revised in 2005.
The measure set includes two performance metrics for inpatient care, five that address care in the outpatient setting, and two measures that apply to care in both settings. The idea, according to the sponsors, was to stress the need to measure quality over time and across providers, not in silos.
"To be successful as quality improvement tools, the heart failure performance measures need to be integrated as routine components of patient care across various care settings, with particular attention to transitions of care from inpatient to outpatient environments," Dr. Robert O. Bonow, cochair of the work group that developed the measure set and director of the center for cardiovascular innovation at Northwestern University, Chicago, said in a statement.
Improving care transitions is likely to be a major focus for physicians in and out of the hospital as officials at the Centers for Medicare and Medicaid Services begin to test a series of alternative payment and care delivery models, from Accountable Care Organizations to bundled payments. Adding to that pressure, this October, the CMS will begin cutting Medicare payments to hospitals whose heart failure and acute myocardial infarction readmission rates are considered too high.
The updated measure set will help prepare physicians for the payment and care delivery changes, Dr. Kathleen Blake, a member of the measure work group and a senior research director at the Center for Medical Technology Policy in Baltimore, said in an interview.
Performance measures, by definition, address areas where there are gaps in care, said Dr. Blake, who is a cardiologist. So physicians can take the updated heart failure measure set and embed it in their care, like a checklist, to ensure that patients are being considered for all appropriate evidence-based treatments.
"We are inundated with medical literature these days. This basically distills it into a measure set," she said.
The work group considered the ACCF/AHA 2009 practice guidelines on heart failure as well as existing heart failure performance measures from the Joint Commission, the CMS, and the Agency for Healthcare Research and Quality in putting together the updated set of measures. Along with the new and revised measures, they retired eight performance measures from the 2005 list.
The updated measure set includes:
1. Left Ventricular Ejection Fraction (LVEF) assessment in the outpatient setting.
2. LVEF in the inpatient setting.
3. Symptom and activity assessment in the outpatient setting.
4. NEW: Symptom management in the outpatient setting (for quality improvement only).
5. Patient self-care education in the outpatient setting (for quality improvement only).
6. Beta-blocker therapy for left ventricular systolic dysfunction in the outpatient and inpatient settings.
7. ACE inhibitor for angiotensin receptor blocker therapy for left ventricular systolic dysfunction in the inpatient and outpatient setting.
8. NEW: Counseling regarding implantable cardioverter-defibrillator (ICD) implantation for patients with left ventricular systolic dysfunction combination medical therapy in the outpatient setting (for quality improvement only).
9. NEW: Postdischarge appointment for heart failure patients in the inpatient setting.
One of the significant changes in the updated measure set, according to the ACCF, is the expansion of the beta-blocker measure to the inpatient setting. In the 2005 set, the measure was only recommended for outpatient care. The panel sought to expand its use based on inpatient care information in the 2009 ACCF-AHA heart failure guidelines.
The work group also recommended that measures 6 and 7, which call for the use of beta-blockers, and ACE and ARB therapy, respectively, should be used together.
Another change in the updated measure set is the addition of a measure calling for a postdischarge appointment to be in place at the time of discharge from the hospital.
While most of the measures are considered appropriate for use in pay-for-performance programs, physician rankings, and public reporting, the writing panel recommended that the measures related to symptom management, patient self-care education, and counseling for ICD implantation be used only for internal quality improvement purposes.
Dr. Blake said these are areas where the work group wanted to give physicians time to collect data. In the case of the ICD counseling measure, they wanted to include a quality improvement measure that would serve as a reminder to physicians to discuss this option with eligible patients. "It doesn’t mean the patient should receive the device," she said. "It means that it should be a topic for discussion as part of a comprehensive review of the patient. It’s also an opportunity to discern what their goals and objectives are."
Dr. Bonow and Dr. Blake disclosed that they had no relationships with industry.
Hospitalists Beware: P4P Is Coming Soon
SAN DIEGO – Starting in 2017, all physicians who participate in Medicare will be paid based on the quality and cost of the care they provide.
The Physician Value-Based Payment Modifier program will compare physician performance on quality and cost and will divide physicians into quartiles, with the top performers designed as "high-quality, low-cost" providers and poor performers as "low-quality, high-cost" providers.

"This is true physician-level pay for performance," Dr. Patrick Torcson, chair of the Society of Hospital Medicine’s Performance Measurement and Reporting Committee, said during the organization’s annual meeting.
The program, which was authorized by Congress in 2008 and expanded under the Affordable Care Act, is budget neutral, meaning that physicians who provide the "high-quality, low-cost" care will earn the most, while others will earn less.
"There’s no new money coming into the system," Dr. Torcson said. "We’re going to have to compete with each other and with our other specialty colleagues to maintain our same level of reimbursement."
For example, Dr. Torcson, who is the director of hospital medicine at St. Tammany Parish Hospital in Covington, La., said that Medicare currently reimburses him and other hospitalists in his area $186.19 for a CPT code 99223 (level 3, initial admission), regardless of the quality and costliness of the care they provide. Under the new program, officials at the Centers for Medicare and Medicaid Services would use a value-based modifier to designate where physicians are on the value scale. Using one possible scenario of placing 10%-12% of reimbursement at risk, Dr. Torcson estimates that a high-quality, low-cost physician would then earn about $206.19 for that visit, whereas a low-quality, high-cost physician would earn $166.19.
"In effect, this value-based payment modifier is going to be branding physicians, and the best in class is going to be that high-quality, low-cost provider," he said.
Although CMS officials won’t be applying the value-based modifier to all physician claims until 2017, they will first test the model in 2015 on about 56,000 physicians in group practices in Iowa, Nebraska, Kansas, and Missouri. And in 2013, the CMS will begin the collecting cost and quality data that will be the basis of rating that group, Dr. Torcson said.
With the initial measurements to set the value-based modifier beginning next year, Dr. Torcson advised physicians to start preparing now. The first step, he said, is to begin participating in Medicare’s Physician Quality Reporting System. The PQRS program is currently a voluntary, pay-for-reporting system in which physicians can earn a small bonus payment on their total Medicare allowable charges if they successfully report on a certain number of performance measures. This year, for instance, physicians can earn up to a 0.5% bonus. That’s about $733 for the average hospitalist, Dr. Torcson said.
But starting in 2015, the bonus will be replaced with a penalty. Physicians who don’t participate will face a 1.5% cut to their Medicare charges. In 2016, the penalty will rise to 2%.
Dr. Torcson said he’s concerned that physicians are putting off participating in the program because of the small incentives currently available, and that they will be unprepared in 2015 when penalties begin.
Another building block in the progression to pay for performance within Medicare is the Physician Feedback Program. Dr. Torcson said this is another critical area that physicians should watch carefully. Under this program, which was established by Congress in 2008, the CMS uses claims data to provide confidential feedback reports to physicians about the cost and quality of the care they are providing. The reports, also known as Quality and Resource Use Reports (QRURs), went out to about 1,600 physicians in 2009. This year, 56,000 physicians in group practices in Iowa, Nebraska, Kansas, and Missouri will receive reports. Between 2013 and 2015, the CMS will begin sending the feedback reports to all Medicare physicians around the country.
The Physician Feedback Program is important, Dr. Torcson said, because it is the framework CMS will use for value-based purchasing.
Dr. Torcson advised physicians to get used to being measured and to develop a better understanding of quality data. But the most important thing to do to get ready for physician value-based purchasing will be to continue to focus on professionalism and taking excellent care of patients, he said.
SAN DIEGO – Starting in 2017, all physicians who participate in Medicare will be paid based on the quality and cost of the care they provide.
The Physician Value-Based Payment Modifier program will compare physician performance on quality and cost and will divide physicians into quartiles, with the top performers designed as "high-quality, low-cost" providers and poor performers as "low-quality, high-cost" providers.
"This is true physician-level pay for performance," Dr. Patrick Torcson, chair of the Society of Hospital Medicine’s Performance Measurement and Reporting Committee, said during the organization’s annual meeting.
The program, which was authorized by Congress in 2008 and expanded under the Affordable Care Act, is budget neutral, meaning that physicians who provide the "high-quality, low-cost" care will earn the most, while others will earn less.
"There’s no new money coming into the system," Dr. Torcson said. "We’re going to have to compete with each other and with our other specialty colleagues to maintain our same level of reimbursement."
For example, Dr. Torcson, who is the director of hospital medicine at St. Tammany Parish Hospital in Covington, La., said that Medicare currently reimburses him and other hospitalists in his area $186.19 for a CPT code 99223 (level 3, initial admission), regardless of the quality and costliness of the care they provide. Under the new program, officials at the Centers for Medicare and Medicaid Services would use a value-based modifier to designate where physicians are on the value scale. Using one possible scenario of placing 10%-12% of reimbursement at risk, Dr. Torcson estimates that a high-quality, low-cost physician would then earn about $206.19 for that visit, whereas a low-quality, high-cost physician would earn $166.19.
"In effect, this value-based payment modifier is going to be branding physicians, and the best in class is going to be that high-quality, low-cost provider," he said.
Although CMS officials won’t be applying the value-based modifier to all physician claims until 2017, they will first test the model in 2015 on about 56,000 physicians in group practices in Iowa, Nebraska, Kansas, and Missouri. And in 2013, the CMS will begin the collecting cost and quality data that will be the basis of rating that group, Dr. Torcson said.
With the initial measurements to set the value-based modifier beginning next year, Dr. Torcson advised physicians to start preparing now. The first step, he said, is to begin participating in Medicare’s Physician Quality Reporting System. The PQRS program is currently a voluntary, pay-for-reporting system in which physicians can earn a small bonus payment on their total Medicare allowable charges if they successfully report on a certain number of performance measures. This year, for instance, physicians can earn up to a 0.5% bonus. That’s about $733 for the average hospitalist, Dr. Torcson said.
But starting in 2015, the bonus will be replaced with a penalty. Physicians who don’t participate will face a 1.5% cut to their Medicare charges. In 2016, the penalty will rise to 2%.
Dr. Torcson said he’s concerned that physicians are putting off participating in the program because of the small incentives currently available, and that they will be unprepared in 2015 when penalties begin.
Another building block in the progression to pay for performance within Medicare is the Physician Feedback Program. Dr. Torcson said this is another critical area that physicians should watch carefully. Under this program, which was established by Congress in 2008, the CMS uses claims data to provide confidential feedback reports to physicians about the cost and quality of the care they are providing. The reports, also known as Quality and Resource Use Reports (QRURs), went out to about 1,600 physicians in 2009. This year, 56,000 physicians in group practices in Iowa, Nebraska, Kansas, and Missouri will receive reports. Between 2013 and 2015, the CMS will begin sending the feedback reports to all Medicare physicians around the country.
The Physician Feedback Program is important, Dr. Torcson said, because it is the framework CMS will use for value-based purchasing.
Dr. Torcson advised physicians to get used to being measured and to develop a better understanding of quality data. But the most important thing to do to get ready for physician value-based purchasing will be to continue to focus on professionalism and taking excellent care of patients, he said.
SAN DIEGO – Starting in 2017, all physicians who participate in Medicare will be paid based on the quality and cost of the care they provide.
The Physician Value-Based Payment Modifier program will compare physician performance on quality and cost and will divide physicians into quartiles, with the top performers designed as "high-quality, low-cost" providers and poor performers as "low-quality, high-cost" providers.
"This is true physician-level pay for performance," Dr. Patrick Torcson, chair of the Society of Hospital Medicine’s Performance Measurement and Reporting Committee, said during the organization’s annual meeting.
The program, which was authorized by Congress in 2008 and expanded under the Affordable Care Act, is budget neutral, meaning that physicians who provide the "high-quality, low-cost" care will earn the most, while others will earn less.
"There’s no new money coming into the system," Dr. Torcson said. "We’re going to have to compete with each other and with our other specialty colleagues to maintain our same level of reimbursement."
For example, Dr. Torcson, who is the director of hospital medicine at St. Tammany Parish Hospital in Covington, La., said that Medicare currently reimburses him and other hospitalists in his area $186.19 for a CPT code 99223 (level 3, initial admission), regardless of the quality and costliness of the care they provide. Under the new program, officials at the Centers for Medicare and Medicaid Services would use a value-based modifier to designate where physicians are on the value scale. Using one possible scenario of placing 10%-12% of reimbursement at risk, Dr. Torcson estimates that a high-quality, low-cost physician would then earn about $206.19 for that visit, whereas a low-quality, high-cost physician would earn $166.19.
"In effect, this value-based payment modifier is going to be branding physicians, and the best in class is going to be that high-quality, low-cost provider," he said.
Although CMS officials won’t be applying the value-based modifier to all physician claims until 2017, they will first test the model in 2015 on about 56,000 physicians in group practices in Iowa, Nebraska, Kansas, and Missouri. And in 2013, the CMS will begin the collecting cost and quality data that will be the basis of rating that group, Dr. Torcson said.
With the initial measurements to set the value-based modifier beginning next year, Dr. Torcson advised physicians to start preparing now. The first step, he said, is to begin participating in Medicare’s Physician Quality Reporting System. The PQRS program is currently a voluntary, pay-for-reporting system in which physicians can earn a small bonus payment on their total Medicare allowable charges if they successfully report on a certain number of performance measures. This year, for instance, physicians can earn up to a 0.5% bonus. That’s about $733 for the average hospitalist, Dr. Torcson said.
But starting in 2015, the bonus will be replaced with a penalty. Physicians who don’t participate will face a 1.5% cut to their Medicare charges. In 2016, the penalty will rise to 2%.
Dr. Torcson said he’s concerned that physicians are putting off participating in the program because of the small incentives currently available, and that they will be unprepared in 2015 when penalties begin.
Another building block in the progression to pay for performance within Medicare is the Physician Feedback Program. Dr. Torcson said this is another critical area that physicians should watch carefully. Under this program, which was established by Congress in 2008, the CMS uses claims data to provide confidential feedback reports to physicians about the cost and quality of the care they are providing. The reports, also known as Quality and Resource Use Reports (QRURs), went out to about 1,600 physicians in 2009. This year, 56,000 physicians in group practices in Iowa, Nebraska, Kansas, and Missouri will receive reports. Between 2013 and 2015, the CMS will begin sending the feedback reports to all Medicare physicians around the country.
The Physician Feedback Program is important, Dr. Torcson said, because it is the framework CMS will use for value-based purchasing.
Dr. Torcson advised physicians to get used to being measured and to develop a better understanding of quality data. But the most important thing to do to get ready for physician value-based purchasing will be to continue to focus on professionalism and taking excellent care of patients, he said.
EXPERT ANALYSIS FROM THE ANNUAL MEETING OF THE SOCIETY OF HOSPITAL MEDICINE
Medicare Hospital Fund Insolvent by 2024
The Medicare Hospital Insurance Trust Fund, which covers Part A hospital benefits, will remain solvent until 2024, according to a new report from the program’s trustees.
Starting in 2024, the trust fund would also be sufficient to cover about 87% of expenses, with that figure falling to 67% by 2050. These figures are similar to financial projections released in last year’s Medicare Trustees report.
The Medicare Supplemental Medical Insurance Trust Fund, which covers physician visits and prescription drugs, has adequate funding for at least the next 10 years, the trustees reported. But costs for the Part B and Part D programs are rising. Costs under Medicare Part B, which covers physician and other outpatient services, are expected to increase annually at 4.9% for the next 5 years. The Part D prescription drug program’s costs are projected to rise by 8.8% through 2021.
The projected lower spending growth for Medicare Part B is based on Congress allowing a nearly 31% cut to Medicare physician fees to occur on Jan. 1, 2013. The trustees said they doubt that lawmakers would allow that type of cut to happen.
"It’s almost certain that lawmakers will override this reduction and that Medicare Part B expenditures will therefore be higher, conceivably as much as 12% higher than is reported in these reports for 2013," said Robert D. Reischauer, one of Medicare’s public trustees and the former president of the Urban Institute.
Health and Human Services Secretary Kathleen Sebelius, who also serves as a Medicare trustee, said the Affordable Care Act has added about 8 years of solvency to the Medicare Hospital Insurance Trust Fund in part through provisions that fight health care fraud, help prevent medical errors, and cut excessive payments in the Medicare Advantage program. Without those changes, she said, the program would have become insolvent by 2016.
Whether the projections of extended solvency will turn out to be accurate depend on whether Congress moves forward with changes to the way Medicare pays physicians and hospitals, Mr. Reischauer said. He added that it will also rely on the ability of physicians to become more efficient and on private payers to join with the government to demand changes in the health care delivery system.
The Medicare Hospital Insurance Trust Fund, which covers Part A hospital benefits, will remain solvent until 2024, according to a new report from the program’s trustees.
Starting in 2024, the trust fund would also be sufficient to cover about 87% of expenses, with that figure falling to 67% by 2050. These figures are similar to financial projections released in last year’s Medicare Trustees report.
The Medicare Supplemental Medical Insurance Trust Fund, which covers physician visits and prescription drugs, has adequate funding for at least the next 10 years, the trustees reported. But costs for the Part B and Part D programs are rising. Costs under Medicare Part B, which covers physician and other outpatient services, are expected to increase annually at 4.9% for the next 5 years. The Part D prescription drug program’s costs are projected to rise by 8.8% through 2021.
The projected lower spending growth for Medicare Part B is based on Congress allowing a nearly 31% cut to Medicare physician fees to occur on Jan. 1, 2013. The trustees said they doubt that lawmakers would allow that type of cut to happen.
"It’s almost certain that lawmakers will override this reduction and that Medicare Part B expenditures will therefore be higher, conceivably as much as 12% higher than is reported in these reports for 2013," said Robert D. Reischauer, one of Medicare’s public trustees and the former president of the Urban Institute.
Health and Human Services Secretary Kathleen Sebelius, who also serves as a Medicare trustee, said the Affordable Care Act has added about 8 years of solvency to the Medicare Hospital Insurance Trust Fund in part through provisions that fight health care fraud, help prevent medical errors, and cut excessive payments in the Medicare Advantage program. Without those changes, she said, the program would have become insolvent by 2016.
Whether the projections of extended solvency will turn out to be accurate depend on whether Congress moves forward with changes to the way Medicare pays physicians and hospitals, Mr. Reischauer said. He added that it will also rely on the ability of physicians to become more efficient and on private payers to join with the government to demand changes in the health care delivery system.
The Medicare Hospital Insurance Trust Fund, which covers Part A hospital benefits, will remain solvent until 2024, according to a new report from the program’s trustees.
Starting in 2024, the trust fund would also be sufficient to cover about 87% of expenses, with that figure falling to 67% by 2050. These figures are similar to financial projections released in last year’s Medicare Trustees report.
The Medicare Supplemental Medical Insurance Trust Fund, which covers physician visits and prescription drugs, has adequate funding for at least the next 10 years, the trustees reported. But costs for the Part B and Part D programs are rising. Costs under Medicare Part B, which covers physician and other outpatient services, are expected to increase annually at 4.9% for the next 5 years. The Part D prescription drug program’s costs are projected to rise by 8.8% through 2021.
The projected lower spending growth for Medicare Part B is based on Congress allowing a nearly 31% cut to Medicare physician fees to occur on Jan. 1, 2013. The trustees said they doubt that lawmakers would allow that type of cut to happen.
"It’s almost certain that lawmakers will override this reduction and that Medicare Part B expenditures will therefore be higher, conceivably as much as 12% higher than is reported in these reports for 2013," said Robert D. Reischauer, one of Medicare’s public trustees and the former president of the Urban Institute.
Health and Human Services Secretary Kathleen Sebelius, who also serves as a Medicare trustee, said the Affordable Care Act has added about 8 years of solvency to the Medicare Hospital Insurance Trust Fund in part through provisions that fight health care fraud, help prevent medical errors, and cut excessive payments in the Medicare Advantage program. Without those changes, she said, the program would have become insolvent by 2016.
Whether the projections of extended solvency will turn out to be accurate depend on whether Congress moves forward with changes to the way Medicare pays physicians and hospitals, Mr. Reischauer said. He added that it will also rely on the ability of physicians to become more efficient and on private payers to join with the government to demand changes in the health care delivery system.
DEA Holds National Rx Collection Day
The Drug Enforcement Administration is asking everyone to clean out their medicine cabinets and dispose of unused, unwanted, and expired prescription medications.
The National Prescription Drug Take-Back Day will take place at sites around the country from 10 a.m. to 2 p.m. local time on Saturday, April 28.

The effort is aimed at preventing prescription drug abuse and diversion. Prescription medications that sit around unused in homes are vulnerable to theft or abuse. In many cases, abused prescription drugs are taken from medicine cabinets by friends and family, according to the DEA.
"Prescription drug abuse is a major epidemic across the country and DEA is committed to reducing the potential for misuse by providing a safe and secure method for Americans to clean out their medicine cabinets and properly dispose of unwanted, unneeded, or expired medications," DEA Administrator Michele M. Leonhart said in a statement.
This is the fourth Take-Back Day the DEA has sponsored since September 2010. During the last three collection days, Americans turned in nearly 500 tons of prescriptions drugs. The service is free and anonymous and takes place at locations including police and fire departments, churches, and universities.
The Drug Enforcement Administration is asking everyone to clean out their medicine cabinets and dispose of unused, unwanted, and expired prescription medications.
The National Prescription Drug Take-Back Day will take place at sites around the country from 10 a.m. to 2 p.m. local time on Saturday, April 28.
The effort is aimed at preventing prescription drug abuse and diversion. Prescription medications that sit around unused in homes are vulnerable to theft or abuse. In many cases, abused prescription drugs are taken from medicine cabinets by friends and family, according to the DEA.
"Prescription drug abuse is a major epidemic across the country and DEA is committed to reducing the potential for misuse by providing a safe and secure method for Americans to clean out their medicine cabinets and properly dispose of unwanted, unneeded, or expired medications," DEA Administrator Michele M. Leonhart said in a statement.
This is the fourth Take-Back Day the DEA has sponsored since September 2010. During the last three collection days, Americans turned in nearly 500 tons of prescriptions drugs. The service is free and anonymous and takes place at locations including police and fire departments, churches, and universities.
The Drug Enforcement Administration is asking everyone to clean out their medicine cabinets and dispose of unused, unwanted, and expired prescription medications.
The National Prescription Drug Take-Back Day will take place at sites around the country from 10 a.m. to 2 p.m. local time on Saturday, April 28.
The effort is aimed at preventing prescription drug abuse and diversion. Prescription medications that sit around unused in homes are vulnerable to theft or abuse. In many cases, abused prescription drugs are taken from medicine cabinets by friends and family, according to the DEA.
"Prescription drug abuse is a major epidemic across the country and DEA is committed to reducing the potential for misuse by providing a safe and secure method for Americans to clean out their medicine cabinets and properly dispose of unwanted, unneeded, or expired medications," DEA Administrator Michele M. Leonhart said in a statement.
This is the fourth Take-Back Day the DEA has sponsored since September 2010. During the last three collection days, Americans turned in nearly 500 tons of prescriptions drugs. The service is free and anonymous and takes place at locations including police and fire departments, churches, and universities.
Avoiding Common Hand-off Mistakes
SAN DIEGO – Hospitalists may be tempted to rely on their electronic health record systems to do all the work on patient hand-offs, but that probably won’t turn out very well, according to Dr. Vineet Arora.
Dr. Arora, an associate professor of medicine at the University of Chicago and a patient safety researcher who has investigated the barriers to proper hand-offs, said technology can be a great tool, but over-relying on it can lead to just as many errors as a traditional paper sign-out. And just because the information is in the EHR, doesn’t mean physicians can skip the verbal hand-off, he said at the annual meeting of the Society of Hospital Medicine.
"The truth is that the electronic health record doesn’t substitute for the communication, the verbal dialogue, that actually needs to happen at the time of the handoff," Dr. Arora said in an interview.
The verbal hand-off is the place where the departing physician shares their clinical judgment and reviews the "to-do" items and "if-then" items for the sickest patients.
The trick is to make sure the hand-off is focused. "Hospitalists may actually be receiving well over 50 patients, and in some cases, over a hundred." Dr. Arora said. "An electronic patient list of that size is not going to actually communicate the information that somebody might need, which is that bed two or bed three is really sick."
Information overload is a common mistake in patient hand-offs. Some physicians include so much information in the written sign-out that it becomes a "shadow chart," she said.
Beware of offering too much information in the verbal hand-off too. Dr. Arora said most people can only remember about four things from a particular conversation.
"So as opposed to having a verbal hand-over that’s an entire recitation of a patient’s history, or going through every single case in nauseating detail, what you really want to do is focus on the top things that you want somebody to remember," Dr. Arora said.
Dr. Arora offered some tips on the best ways to deliver a better verbal hand-off:
• Focus on the sickest patients first.
• Provide an update on the daily progress with the day’s baseline and updated events.
• Give directions on what needs to be done.
• Provide a rationale for any instructions and further directions on what to do with the results. Avoid ambiguous instructions such as "check CBC." Personalize the instructions for the care of the patient by giving the hemoglobin value at which blood transfusion and number of units would be needed, for example.
• Make sure the physician receiving the hand-off really understands. Encourage questions.
Hospitalists who are receiving patients in the hand-off process can also do these things to be better, and more active, listeners:
• Limit interruptions.
• Take notes.
• Ask questions.
• Use a system to keep track of to-do items.
• Read back instructions.
Dr. Arora said there are also some systems issues that can help set the stage for better hand-offs. For instance, hospitals can provide physician education on the need to curb side conversations and other interruptions during the verbal hand-off. And they can schedule shifts so that there is sufficient overlap of outgoing and incoming physicians.
Hospitalists who are looking to improve not just their own hand-offs but the overall process at their hospital, should start by describing the current situation, Dr. Arora said. From there, they can identify the areas for improvement, find physicians to champion the project, and figure out what resources will be needed to make changes.
She advised that a standard hand-off protocol should be discipline specific, so what works for neurology won’t work for hospital medicine. Both the process and the content should be standardized. And once the hospitalists have agreed on a protocol, make sure to identify problems as they arise.
Dr. Arora said she has received grants and contracts from the Agency for Healthcare Research and Quality, the Accreditation Council for Graduate Medical Education, and the National Institute on Aging.
SAN DIEGO – Hospitalists may be tempted to rely on their electronic health record systems to do all the work on patient hand-offs, but that probably won’t turn out very well, according to Dr. Vineet Arora.
Dr. Arora, an associate professor of medicine at the University of Chicago and a patient safety researcher who has investigated the barriers to proper hand-offs, said technology can be a great tool, but over-relying on it can lead to just as many errors as a traditional paper sign-out. And just because the information is in the EHR, doesn’t mean physicians can skip the verbal hand-off, he said at the annual meeting of the Society of Hospital Medicine.
"The truth is that the electronic health record doesn’t substitute for the communication, the verbal dialogue, that actually needs to happen at the time of the handoff," Dr. Arora said in an interview.
The verbal hand-off is the place where the departing physician shares their clinical judgment and reviews the "to-do" items and "if-then" items for the sickest patients.
The trick is to make sure the hand-off is focused. "Hospitalists may actually be receiving well over 50 patients, and in some cases, over a hundred." Dr. Arora said. "An electronic patient list of that size is not going to actually communicate the information that somebody might need, which is that bed two or bed three is really sick."
Information overload is a common mistake in patient hand-offs. Some physicians include so much information in the written sign-out that it becomes a "shadow chart," she said.
Beware of offering too much information in the verbal hand-off too. Dr. Arora said most people can only remember about four things from a particular conversation.
"So as opposed to having a verbal hand-over that’s an entire recitation of a patient’s history, or going through every single case in nauseating detail, what you really want to do is focus on the top things that you want somebody to remember," Dr. Arora said.
Dr. Arora offered some tips on the best ways to deliver a better verbal hand-off:
• Focus on the sickest patients first.
• Provide an update on the daily progress with the day’s baseline and updated events.
• Give directions on what needs to be done.
• Provide a rationale for any instructions and further directions on what to do with the results. Avoid ambiguous instructions such as "check CBC." Personalize the instructions for the care of the patient by giving the hemoglobin value at which blood transfusion and number of units would be needed, for example.
• Make sure the physician receiving the hand-off really understands. Encourage questions.
Hospitalists who are receiving patients in the hand-off process can also do these things to be better, and more active, listeners:
• Limit interruptions.
• Take notes.
• Ask questions.
• Use a system to keep track of to-do items.
• Read back instructions.
Dr. Arora said there are also some systems issues that can help set the stage for better hand-offs. For instance, hospitals can provide physician education on the need to curb side conversations and other interruptions during the verbal hand-off. And they can schedule shifts so that there is sufficient overlap of outgoing and incoming physicians.
Hospitalists who are looking to improve not just their own hand-offs but the overall process at their hospital, should start by describing the current situation, Dr. Arora said. From there, they can identify the areas for improvement, find physicians to champion the project, and figure out what resources will be needed to make changes.
She advised that a standard hand-off protocol should be discipline specific, so what works for neurology won’t work for hospital medicine. Both the process and the content should be standardized. And once the hospitalists have agreed on a protocol, make sure to identify problems as they arise.
Dr. Arora said she has received grants and contracts from the Agency for Healthcare Research and Quality, the Accreditation Council for Graduate Medical Education, and the National Institute on Aging.
SAN DIEGO – Hospitalists may be tempted to rely on their electronic health record systems to do all the work on patient hand-offs, but that probably won’t turn out very well, according to Dr. Vineet Arora.
Dr. Arora, an associate professor of medicine at the University of Chicago and a patient safety researcher who has investigated the barriers to proper hand-offs, said technology can be a great tool, but over-relying on it can lead to just as many errors as a traditional paper sign-out. And just because the information is in the EHR, doesn’t mean physicians can skip the verbal hand-off, he said at the annual meeting of the Society of Hospital Medicine.
"The truth is that the electronic health record doesn’t substitute for the communication, the verbal dialogue, that actually needs to happen at the time of the handoff," Dr. Arora said in an interview.
The verbal hand-off is the place where the departing physician shares their clinical judgment and reviews the "to-do" items and "if-then" items for the sickest patients.
The trick is to make sure the hand-off is focused. "Hospitalists may actually be receiving well over 50 patients, and in some cases, over a hundred." Dr. Arora said. "An electronic patient list of that size is not going to actually communicate the information that somebody might need, which is that bed two or bed three is really sick."
Information overload is a common mistake in patient hand-offs. Some physicians include so much information in the written sign-out that it becomes a "shadow chart," she said.
Beware of offering too much information in the verbal hand-off too. Dr. Arora said most people can only remember about four things from a particular conversation.
"So as opposed to having a verbal hand-over that’s an entire recitation of a patient’s history, or going through every single case in nauseating detail, what you really want to do is focus on the top things that you want somebody to remember," Dr. Arora said.
Dr. Arora offered some tips on the best ways to deliver a better verbal hand-off:
• Focus on the sickest patients first.
• Provide an update on the daily progress with the day’s baseline and updated events.
• Give directions on what needs to be done.
• Provide a rationale for any instructions and further directions on what to do with the results. Avoid ambiguous instructions such as "check CBC." Personalize the instructions for the care of the patient by giving the hemoglobin value at which blood transfusion and number of units would be needed, for example.
• Make sure the physician receiving the hand-off really understands. Encourage questions.
Hospitalists who are receiving patients in the hand-off process can also do these things to be better, and more active, listeners:
• Limit interruptions.
• Take notes.
• Ask questions.
• Use a system to keep track of to-do items.
• Read back instructions.
Dr. Arora said there are also some systems issues that can help set the stage for better hand-offs. For instance, hospitals can provide physician education on the need to curb side conversations and other interruptions during the verbal hand-off. And they can schedule shifts so that there is sufficient overlap of outgoing and incoming physicians.
Hospitalists who are looking to improve not just their own hand-offs but the overall process at their hospital, should start by describing the current situation, Dr. Arora said. From there, they can identify the areas for improvement, find physicians to champion the project, and figure out what resources will be needed to make changes.
She advised that a standard hand-off protocol should be discipline specific, so what works for neurology won’t work for hospital medicine. Both the process and the content should be standardized. And once the hospitalists have agreed on a protocol, make sure to identify problems as they arise.
Dr. Arora said she has received grants and contracts from the Agency for Healthcare Research and Quality, the Accreditation Council for Graduate Medical Education, and the National Institute on Aging.
EXPERT ANALYSIS FROM THE ANNUAL MEETING OF THE SOCIETY OF HOSPITAL MEDICINE
Why 30-Day Readmissions Are High
Once a month, a "dream team" of community and hospital physicians and nurses meets at the University of Connecticut, Farmington. Their goal: To improve the transition out of the hospital for patients with heart failure. Their progress: Since the group’s first meeting in 2008, the hospital’s 30-day, all-cause readmission rates for heart failure have fallen from 27% to less than 19%, according to figures tracked by the Connecticut Hospital Association.
"That’s a significant drop and puts the hospital below the state average of 25%. "We’re pretty proud of that," said Dr. Jason Ryan, a cardiologist and codirector of the Heart Failure Center at the university.

Dr. Ryan attributes the "dream team’s" successes to intensive patient education in the hospital, a mandatory follow-up visit with a physician at 7 days after discharge, and better communication between clinicians in the hospital and those in the community.
But possibly the biggest factor in their success has been physician commitment to keeping patients with preventable readmissions out of the hospital.
In the UConn program, the cardiologists have made a point of getting patients immediate clinic appointments to evaluate whether they are having a minor issue that can be dealt with in an outpatient setting or if they have a more serious concern that requires readmission to the hospital.
"Some of our patients call us with complaints that I could easily over the phone say, ‘Well, you need to go to the emergency room for that,’ " Dr. Ryan said. "If you’ve got a group of physicians who are not interested in this work, it’s very easy to send people to the emergency room."
The UConn program could end up being a model for other hospitals that are looking to reduce their readmission rates for heart failure and acute myocardial infarction ahead of financial penalties coming down the pike this fall from the Medicare program.
But can hospitals that serve diverse communities meaningfully enact such programs and expect similar successes?
And what will be the impact of the penalties on safety net hospitals that lack the money to undertake a major overhaul of their discharge and care coordination systems?
Even after the data are risk adjusted for their sicker patients, safety net hospitals could still end up with higher than average readmissions. If CMS penalizes them with lower reimbursements due to their excessive readmission rates, they could be left with even fewer resource to care for sicker patients.
Medicare Turns Up the Heat
Starting in October, the Centers for Medicare and Medicaid Services will begin cutting Medicare payments to hospitals whose acute MI and heart failure readmission rates are considered too high.
It’s still unclear exactly what the cutoff point will be. CMS will use readmission data from July 2008 through June 2011 to determine excessive rates and penalties for fiscal year 2013, which begins this October.
CMS is defining all-cause readmission as occurring when a patient is discharged from a hospital and then admitted to the same hospital or another acute care hospital within 30 days.
Recent, risk-adjusted data from CMS offer a glimpse of where the country is in terms of reducing readmission rates.
For acute MI, the national rate for 30-day all-cause readmissions has dropped slightly, going from 19.9% from 2006 through 2009 to 19.8% from 2007 through 2010. During the same time period, readmissions for heart failure rose slightly, creeping up from 24.5% to 24.8%.
The data show the similar trends for mortality during the two reporting periods. The acute MI rates fell from 16.2% to 15.9%, while heart failure mortality rose from 11.2% to 11.3%.
Blaming Length of Stay
A study published earlier this year paints a gloomy picture about how U.S. hospitals stack up against other countries in readmission for ST-elevation MI. The study found that 30-day readmission rates were on average 14.5% in the United States vs. 9.9% among the other countries studied (JAMA 2012;307:66-74). The study included patients in the United States, Canada, Australia, New Zealand, and 13 European countries.

At the same time, the median length of stay was shortest in the United States at 3 days. The longest median length of stay noted in the study was 8 days in Germany.
The study investigators pointed to the shorter length of stay in U.S. hospitals as a possible driver of the country’s higher rate of readmissions. But other experts say there are more complex factors at work, such as gaps in the discharge planning process and a lack of resources for patients once they leave the hospital.
There weren’t a lot of patients who were readmitted 2 days later for the same condition, which might indicate that they had been discharged too soon, Dr. Ryan said. More often, patients return to the hospital a week or several days later with a new problem. That tends to indicate that their medications may not have been adjusted correctly or that they were unable to access services in the outpatient world, he said.
There is very little evidence to support the idea that a longer initial length of stay would lead to either better use of evidence-based therapies or produce better clinical outcomes, said Dr. Gregg C. Fonarow, director of the Cardiomyopathy Center at the University of California, Los Angeles. Though there’s plenty of evidence to show that more time in the hospital increases patients’ risk for hospital-acquired infection, he added.
Over the last 2 decades, readmissions for heart failure patients have gone up as length of stay has decreased. But, Dr. Fonarow points out, during that same time the total number of days patients spent in the hospital has actually gone down, along with mortality. So from a global resource utilization perspective, patients are spending less time in the hospital and having better outcomes, he said.
"It’s important to have appropriate comparisons," he said.
Dr. Fonarow cautioned that there aren’t simple solutions to this problem. While there are many opportunities to improve readmission rates, there are also many rehospitalizations that are unavoidable or unrelated to the cardiovascular condition responsible for the initial hospitalization. Many patients hospitalized with acute MI, and to an even greater degree with heart failure, have multiple other cardiovascular and noncardiovascular comorbid conditions, he said.
"Efforts to try and reduce preventable readmissions have to go well beyond even the primary disease state that led to the hospitalization," Dr. Fonarow said. "They need to involve multiple components of care that go beyond just treating the single acute condition and focus on the multiple comorbid conditions that exist within that patient."
To make it even more complicated, patients who are hospitalized with heart failure tend to be older and to have multiple comorbid conditions. These individuals may face other challenges such as cognitive impairment, frailty, and poor socioeconomic support.
"It’s really a complex problem," he said.

Ensuring Needed Care
The looming Medicare readmission penalties have caused many hospital administrators, and in turn physicians, to look closely at the factors behind readmissions for the first time over the last few years.
"Everyone’s trying to figure this out because they do see the shift coming in the payment system," said Dr. John Rumsfeld, National Director of Cardiology at the Veterans Health Administration and Chief Science Officer for the American College of Cardiology’s National Cardiovascular Data Registry.
And the payment cuts for excessive readmissions aren’t the only way that CMS is focusing on the issue, Dr. Rumsfeld said. Readmissions are also at the heart of pilot projects Medicare is launching for Accountable Care Organizations and bundled payments.
Dr. Rumsfeld said he’s concerned that physicians are getting the message that all readmissions are bad. "This is a potentially dangerous message for clinical care," he said.
The conversation needs to shift to unnecessary or potentially preventable readmissions, he said. It’s often underappreciated, Dr. Rumsfeld said, that patients who are having recurrent chest pain or severe shortness of breath after an acute MI should be admitted to the hospital for care. "There shouldn’t be anything in the system that disincentivizes that," he said.
Dr. Clyde W. Yancy, Chief of the Division of Cardiology at Northwestern University and Associate Director of the Bluhm Cardiovascular Institute at Northwestern Memorial Hospital in Chicago, agrees.
"We’re beating the drum about this problem mostly because it’s a health care utilization problem," Dr. Yancy said. "In the process of beating the drum, we have to have enough wherewithal as clinicians and administrators to realize that there are those – and not a small number – who should in fact be readmitted because their disease is unstable, or it’s advanced, or it requires that attention."
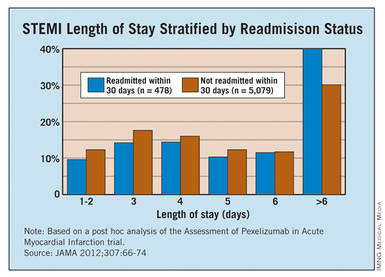
The fate of safety net hospitals is also a concern. Safety net hospitals are unlikely to have the money to undertake a major overhaul of their discharge and care coordination systems, which could leave them with higher than average readmissions, even after the data is risk adjusted for their sicker patients, Dr. Yancy said. Then, if CMS cuts their reimbursement due to their excessive readmission rates, they will be left to care for sicker patients with even fewer resources.
"There has to be a point in this whole process where reasonable people sit back and look at how the landscape is truly impacted by this focus on readmissions," he said. "We can’t allow our safety net hospitals to be further disadvantaged."
Dr. Vincent Bufalino, Senior Vice President and Senior Medical Director of Cardiology at Advocate Health Care, a 100-physician cardiology group serving 10 hospitals in the Chicago area, said he thinks the readmission rates are a bit deceptive. While the numbers are high, especially in heart failure, these are also very sick patients, he said. "I’m not so disturbed with the readmission rate, although there are obviously opportunities for us to do better," Dr. Bufalino said.
One of those opportunities is in home health. Many heart failure and acute MI patients who could benefit from home health care after discharge aren’t getting it, he said, and it’s mostly because of a paperwork burden. Physicians aren’t making the referrals for home health because the paperwork required by CMS is so daunting.
While there are plenty of areas where physicians and hospitals can do a better job at care coordination, it’s important not to set unrealistic targets that force patients to be sent home when they should be admitted, Dr. Bufalino said.
"If someone is sick and they need to be readmitted, readmit them," he said.
Lessons Learned in Heart Failure
Physicians looking to make a dent in their readmission rates for heart failure can take some cues from successful programs around the country.
While the implementation varies from place to place, programs that have been able to cut their readmissions stress the need for patients to see a physician or nurse practitioner shortly after discharge. Another essential element for success is improving the communication between providers in the hospital and those who will be caring for patients after discharge.

At the University of Connecticut Heart Failure Center, where the all-cause 30-day readmission rates for heart failure patients dropped from 27% in 2008 to under 19% in 2011, patients don’t leave the hospital without an appointment to see a physician within 7 days of discharge.
The appointment might be with a primary care physician, a cardiologist, or a physician or nurse practitioner at the university’s heart failure clinic.
"If we can’t get them in with someone else, we will always make room for them and see them," said Dr. Jason Ryan, codirector of the Heart Failure Center at the University of Connecticut, Farmington.
While patients are still in the hospital, they also meet with nurses who train them in taking their medications and monitoring for heart failure symptoms. Patients also meet with social workers who ensure they have transportation to their appointments and a way to pick up their medicines. And they spend time with a pharmacist who reviews their medications.
The other element they have employed at the University of Connecticut is community outreach. Before the push to reduce readmissions, physicians at the hospital didn’t know anyone at the nursing homes or visiting nurse organizations. Now they hold a monthly meeting with physicians and other providers who work outside the hospital. They have gone from not knowing each other’s names to exchanging cell phone numbers, Dr. Ryan said.
"So when our patients are out there we can communicate a lot more easily when problems crop up," he said.
At the University of California, San Francisco’s Medical Center, they have used similar strategies to cut their readmission rates.
The UCSF Heart Failure Readmission Reduction Program began in 2008 with a 2-year, $575,000 grant aimed at rapidly bringing down readmissions. Now in its fourth year, the nurse-run program has been a success. The 30-day all-cause readmission rates for heart failure patients age 65 and older was around 24% in 2009 but had dropped to less than 10% at the beginning of this year.
But the program couldn’t run without its two nurse coordinators, said Karen Rago, a nurse and executive director of Service Line Administration at UCSF.
"They own this population," she said. "If you don’t have a single point that owns it, there are so many things that fall through the cracks."
The nurses at the UCSF heart failure program spent the first year working with the Institute for Healthcare Improvement to learn the principles in their readmissions toolkit: teach-back, follow-up phone calls at 7 and 14 days, an appointment with a physician or heart failure nurse practitioner within 7 days, and medication reconciliation.
The nurse coordinators also serve as a bridge to providers in the outpatient setting, Ms. Rago said. During the second year of the program, they began making site visits to skilled nursing facilities and reaching out to primary care physicians, cardiologists, and home health agencies from outside of the hospital.
They created an e-mail group for each patient’s care team that includes physicians, nurses, home care, social work, and pharmacy, depending on the services the patient needed. An email goes out to the team at the time of admission and it provides a way to update everyone virtually in real-time about the care of the patient.
Having a closer relationship with the skilled nursing facilities has been a big help, Ms. Rago said. During one of the site visits, the nurses discovered that one of the facilities didn’t offer a low-salt diet. That helped explain why so many patients from that facility were being readmitted to the hospital and they were able to quickly address it, she said.
What physicians need to keep in mind is that while many of these solutions are common sense, there’s no one-size-fits-all approach to readmissions, said Dr. John Rumsfeld, National Director of Cardiology at the Veterans Health Administration and Chief Science Officer for the American College of Cardiology’s National Cardiovascular Data Registry.
"It’s different in each community, so you can’t be prescriptive," he said.
The American College of Cardiology offers resources for reducing readmissions as part of a joint effort with the Institute for Healthcare Improvement called the Hospital to Home initiative.
Unlike other areas of care, such as getting a faster angioplasty, there aren’t six key steps for physicians to implement, Dr. Rumsfeld said. Instead, Hospital to Home is a place for physicians to share best practices based on their individual experiences. So far, more than 1,100 hospitals around the country have signed up.
Once a month, a "dream team" of community and hospital physicians and nurses meets at the University of Connecticut, Farmington. Their goal: To improve the transition out of the hospital for patients with heart failure. Their progress: Since the group’s first meeting in 2008, the hospital’s 30-day, all-cause readmission rates for heart failure have fallen from 27% to less than 19%, according to figures tracked by the Connecticut Hospital Association.
"That’s a significant drop and puts the hospital below the state average of 25%. "We’re pretty proud of that," said Dr. Jason Ryan, a cardiologist and codirector of the Heart Failure Center at the university.
Dr. Ryan attributes the "dream team’s" successes to intensive patient education in the hospital, a mandatory follow-up visit with a physician at 7 days after discharge, and better communication between clinicians in the hospital and those in the community.
But possibly the biggest factor in their success has been physician commitment to keeping patients with preventable readmissions out of the hospital.
In the UConn program, the cardiologists have made a point of getting patients immediate clinic appointments to evaluate whether they are having a minor issue that can be dealt with in an outpatient setting or if they have a more serious concern that requires readmission to the hospital.
"Some of our patients call us with complaints that I could easily over the phone say, ‘Well, you need to go to the emergency room for that,’ " Dr. Ryan said. "If you’ve got a group of physicians who are not interested in this work, it’s very easy to send people to the emergency room."
The UConn program could end up being a model for other hospitals that are looking to reduce their readmission rates for heart failure and acute myocardial infarction ahead of financial penalties coming down the pike this fall from the Medicare program.
But can hospitals that serve diverse communities meaningfully enact such programs and expect similar successes?
And what will be the impact of the penalties on safety net hospitals that lack the money to undertake a major overhaul of their discharge and care coordination systems?
Even after the data are risk adjusted for their sicker patients, safety net hospitals could still end up with higher than average readmissions. If CMS penalizes them with lower reimbursements due to their excessive readmission rates, they could be left with even fewer resource to care for sicker patients.
Medicare Turns Up the Heat
Starting in October, the Centers for Medicare and Medicaid Services will begin cutting Medicare payments to hospitals whose acute MI and heart failure readmission rates are considered too high.
It’s still unclear exactly what the cutoff point will be. CMS will use readmission data from July 2008 through June 2011 to determine excessive rates and penalties for fiscal year 2013, which begins this October.
CMS is defining all-cause readmission as occurring when a patient is discharged from a hospital and then admitted to the same hospital or another acute care hospital within 30 days.
Recent, risk-adjusted data from CMS offer a glimpse of where the country is in terms of reducing readmission rates.
For acute MI, the national rate for 30-day all-cause readmissions has dropped slightly, going from 19.9% from 2006 through 2009 to 19.8% from 2007 through 2010. During the same time period, readmissions for heart failure rose slightly, creeping up from 24.5% to 24.8%.
The data show the similar trends for mortality during the two reporting periods. The acute MI rates fell from 16.2% to 15.9%, while heart failure mortality rose from 11.2% to 11.3%.
Blaming Length of Stay
A study published earlier this year paints a gloomy picture about how U.S. hospitals stack up against other countries in readmission for ST-elevation MI. The study found that 30-day readmission rates were on average 14.5% in the United States vs. 9.9% among the other countries studied (JAMA 2012;307:66-74). The study included patients in the United States, Canada, Australia, New Zealand, and 13 European countries.
At the same time, the median length of stay was shortest in the United States at 3 days. The longest median length of stay noted in the study was 8 days in Germany.
The study investigators pointed to the shorter length of stay in U.S. hospitals as a possible driver of the country’s higher rate of readmissions. But other experts say there are more complex factors at work, such as gaps in the discharge planning process and a lack of resources for patients once they leave the hospital.
There weren’t a lot of patients who were readmitted 2 days later for the same condition, which might indicate that they had been discharged too soon, Dr. Ryan said. More often, patients return to the hospital a week or several days later with a new problem. That tends to indicate that their medications may not have been adjusted correctly or that they were unable to access services in the outpatient world, he said.
There is very little evidence to support the idea that a longer initial length of stay would lead to either better use of evidence-based therapies or produce better clinical outcomes, said Dr. Gregg C. Fonarow, director of the Cardiomyopathy Center at the University of California, Los Angeles. Though there’s plenty of evidence to show that more time in the hospital increases patients’ risk for hospital-acquired infection, he added.
Over the last 2 decades, readmissions for heart failure patients have gone up as length of stay has decreased. But, Dr. Fonarow points out, during that same time the total number of days patients spent in the hospital has actually gone down, along with mortality. So from a global resource utilization perspective, patients are spending less time in the hospital and having better outcomes, he said.
"It’s important to have appropriate comparisons," he said.
Dr. Fonarow cautioned that there aren’t simple solutions to this problem. While there are many opportunities to improve readmission rates, there are also many rehospitalizations that are unavoidable or unrelated to the cardiovascular condition responsible for the initial hospitalization. Many patients hospitalized with acute MI, and to an even greater degree with heart failure, have multiple other cardiovascular and noncardiovascular comorbid conditions, he said.
"Efforts to try and reduce preventable readmissions have to go well beyond even the primary disease state that led to the hospitalization," Dr. Fonarow said. "They need to involve multiple components of care that go beyond just treating the single acute condition and focus on the multiple comorbid conditions that exist within that patient."
To make it even more complicated, patients who are hospitalized with heart failure tend to be older and to have multiple comorbid conditions. These individuals may face other challenges such as cognitive impairment, frailty, and poor socioeconomic support.
"It’s really a complex problem," he said.
Ensuring Needed Care
The looming Medicare readmission penalties have caused many hospital administrators, and in turn physicians, to look closely at the factors behind readmissions for the first time over the last few years.
"Everyone’s trying to figure this out because they do see the shift coming in the payment system," said Dr. John Rumsfeld, National Director of Cardiology at the Veterans Health Administration and Chief Science Officer for the American College of Cardiology’s National Cardiovascular Data Registry.
And the payment cuts for excessive readmissions aren’t the only way that CMS is focusing on the issue, Dr. Rumsfeld said. Readmissions are also at the heart of pilot projects Medicare is launching for Accountable Care Organizations and bundled payments.
Dr. Rumsfeld said he’s concerned that physicians are getting the message that all readmissions are bad. "This is a potentially dangerous message for clinical care," he said.
The conversation needs to shift to unnecessary or potentially preventable readmissions, he said. It’s often underappreciated, Dr. Rumsfeld said, that patients who are having recurrent chest pain or severe shortness of breath after an acute MI should be admitted to the hospital for care. "There shouldn’t be anything in the system that disincentivizes that," he said.
Dr. Clyde W. Yancy, Chief of the Division of Cardiology at Northwestern University and Associate Director of the Bluhm Cardiovascular Institute at Northwestern Memorial Hospital in Chicago, agrees.
"We’re beating the drum about this problem mostly because it’s a health care utilization problem," Dr. Yancy said. "In the process of beating the drum, we have to have enough wherewithal as clinicians and administrators to realize that there are those – and not a small number – who should in fact be readmitted because their disease is unstable, or it’s advanced, or it requires that attention."
The fate of safety net hospitals is also a concern. Safety net hospitals are unlikely to have the money to undertake a major overhaul of their discharge and care coordination systems, which could leave them with higher than average readmissions, even after the data is risk adjusted for their sicker patients, Dr. Yancy said. Then, if CMS cuts their reimbursement due to their excessive readmission rates, they will be left to care for sicker patients with even fewer resources.
"There has to be a point in this whole process where reasonable people sit back and look at how the landscape is truly impacted by this focus on readmissions," he said. "We can’t allow our safety net hospitals to be further disadvantaged."
Dr. Vincent Bufalino, Senior Vice President and Senior Medical Director of Cardiology at Advocate Health Care, a 100-physician cardiology group serving 10 hospitals in the Chicago area, said he thinks the readmission rates are a bit deceptive. While the numbers are high, especially in heart failure, these are also very sick patients, he said. "I’m not so disturbed with the readmission rate, although there are obviously opportunities for us to do better," Dr. Bufalino said.
One of those opportunities is in home health. Many heart failure and acute MI patients who could benefit from home health care after discharge aren’t getting it, he said, and it’s mostly because of a paperwork burden. Physicians aren’t making the referrals for home health because the paperwork required by CMS is so daunting.
While there are plenty of areas where physicians and hospitals can do a better job at care coordination, it’s important not to set unrealistic targets that force patients to be sent home when they should be admitted, Dr. Bufalino said.
"If someone is sick and they need to be readmitted, readmit them," he said.
Lessons Learned in Heart Failure
Physicians looking to make a dent in their readmission rates for heart failure can take some cues from successful programs around the country.
While the implementation varies from place to place, programs that have been able to cut their readmissions stress the need for patients to see a physician or nurse practitioner shortly after discharge. Another essential element for success is improving the communication between providers in the hospital and those who will be caring for patients after discharge.
At the University of Connecticut Heart Failure Center, where the all-cause 30-day readmission rates for heart failure patients dropped from 27% in 2008 to under 19% in 2011, patients don’t leave the hospital without an appointment to see a physician within 7 days of discharge.
The appointment might be with a primary care physician, a cardiologist, or a physician or nurse practitioner at the university’s heart failure clinic.
"If we can’t get them in with someone else, we will always make room for them and see them," said Dr. Jason Ryan, codirector of the Heart Failure Center at the University of Connecticut, Farmington.
While patients are still in the hospital, they also meet with nurses who train them in taking their medications and monitoring for heart failure symptoms. Patients also meet with social workers who ensure they have transportation to their appointments and a way to pick up their medicines. And they spend time with a pharmacist who reviews their medications.
The other element they have employed at the University of Connecticut is community outreach. Before the push to reduce readmissions, physicians at the hospital didn’t know anyone at the nursing homes or visiting nurse organizations. Now they hold a monthly meeting with physicians and other providers who work outside the hospital. They have gone from not knowing each other’s names to exchanging cell phone numbers, Dr. Ryan said.
"So when our patients are out there we can communicate a lot more easily when problems crop up," he said.
At the University of California, San Francisco’s Medical Center, they have used similar strategies to cut their readmission rates.
The UCSF Heart Failure Readmission Reduction Program began in 2008 with a 2-year, $575,000 grant aimed at rapidly bringing down readmissions. Now in its fourth year, the nurse-run program has been a success. The 30-day all-cause readmission rates for heart failure patients age 65 and older was around 24% in 2009 but had dropped to less than 10% at the beginning of this year.
But the program couldn’t run without its two nurse coordinators, said Karen Rago, a nurse and executive director of Service Line Administration at UCSF.
"They own this population," she said. "If you don’t have a single point that owns it, there are so many things that fall through the cracks."
The nurses at the UCSF heart failure program spent the first year working with the Institute for Healthcare Improvement to learn the principles in their readmissions toolkit: teach-back, follow-up phone calls at 7 and 14 days, an appointment with a physician or heart failure nurse practitioner within 7 days, and medication reconciliation.
The nurse coordinators also serve as a bridge to providers in the outpatient setting, Ms. Rago said. During the second year of the program, they began making site visits to skilled nursing facilities and reaching out to primary care physicians, cardiologists, and home health agencies from outside of the hospital.
They created an e-mail group for each patient’s care team that includes physicians, nurses, home care, social work, and pharmacy, depending on the services the patient needed. An email goes out to the team at the time of admission and it provides a way to update everyone virtually in real-time about the care of the patient.
Having a closer relationship with the skilled nursing facilities has been a big help, Ms. Rago said. During one of the site visits, the nurses discovered that one of the facilities didn’t offer a low-salt diet. That helped explain why so many patients from that facility were being readmitted to the hospital and they were able to quickly address it, she said.
What physicians need to keep in mind is that while many of these solutions are common sense, there’s no one-size-fits-all approach to readmissions, said Dr. John Rumsfeld, National Director of Cardiology at the Veterans Health Administration and Chief Science Officer for the American College of Cardiology’s National Cardiovascular Data Registry.
"It’s different in each community, so you can’t be prescriptive," he said.
The American College of Cardiology offers resources for reducing readmissions as part of a joint effort with the Institute for Healthcare Improvement called the Hospital to Home initiative.
Unlike other areas of care, such as getting a faster angioplasty, there aren’t six key steps for physicians to implement, Dr. Rumsfeld said. Instead, Hospital to Home is a place for physicians to share best practices based on their individual experiences. So far, more than 1,100 hospitals around the country have signed up.
Once a month, a "dream team" of community and hospital physicians and nurses meets at the University of Connecticut, Farmington. Their goal: To improve the transition out of the hospital for patients with heart failure. Their progress: Since the group’s first meeting in 2008, the hospital’s 30-day, all-cause readmission rates for heart failure have fallen from 27% to less than 19%, according to figures tracked by the Connecticut Hospital Association.
"That’s a significant drop and puts the hospital below the state average of 25%. "We’re pretty proud of that," said Dr. Jason Ryan, a cardiologist and codirector of the Heart Failure Center at the university.
Dr. Ryan attributes the "dream team’s" successes to intensive patient education in the hospital, a mandatory follow-up visit with a physician at 7 days after discharge, and better communication between clinicians in the hospital and those in the community.
But possibly the biggest factor in their success has been physician commitment to keeping patients with preventable readmissions out of the hospital.
In the UConn program, the cardiologists have made a point of getting patients immediate clinic appointments to evaluate whether they are having a minor issue that can be dealt with in an outpatient setting or if they have a more serious concern that requires readmission to the hospital.
"Some of our patients call us with complaints that I could easily over the phone say, ‘Well, you need to go to the emergency room for that,’ " Dr. Ryan said. "If you’ve got a group of physicians who are not interested in this work, it’s very easy to send people to the emergency room."
The UConn program could end up being a model for other hospitals that are looking to reduce their readmission rates for heart failure and acute myocardial infarction ahead of financial penalties coming down the pike this fall from the Medicare program.
But can hospitals that serve diverse communities meaningfully enact such programs and expect similar successes?
And what will be the impact of the penalties on safety net hospitals that lack the money to undertake a major overhaul of their discharge and care coordination systems?
Even after the data are risk adjusted for their sicker patients, safety net hospitals could still end up with higher than average readmissions. If CMS penalizes them with lower reimbursements due to their excessive readmission rates, they could be left with even fewer resource to care for sicker patients.
Medicare Turns Up the Heat
Starting in October, the Centers for Medicare and Medicaid Services will begin cutting Medicare payments to hospitals whose acute MI and heart failure readmission rates are considered too high.
It’s still unclear exactly what the cutoff point will be. CMS will use readmission data from July 2008 through June 2011 to determine excessive rates and penalties for fiscal year 2013, which begins this October.
CMS is defining all-cause readmission as occurring when a patient is discharged from a hospital and then admitted to the same hospital or another acute care hospital within 30 days.
Recent, risk-adjusted data from CMS offer a glimpse of where the country is in terms of reducing readmission rates.
For acute MI, the national rate for 30-day all-cause readmissions has dropped slightly, going from 19.9% from 2006 through 2009 to 19.8% from 2007 through 2010. During the same time period, readmissions for heart failure rose slightly, creeping up from 24.5% to 24.8%.
The data show the similar trends for mortality during the two reporting periods. The acute MI rates fell from 16.2% to 15.9%, while heart failure mortality rose from 11.2% to 11.3%.
Blaming Length of Stay
A study published earlier this year paints a gloomy picture about how U.S. hospitals stack up against other countries in readmission for ST-elevation MI. The study found that 30-day readmission rates were on average 14.5% in the United States vs. 9.9% among the other countries studied (JAMA 2012;307:66-74). The study included patients in the United States, Canada, Australia, New Zealand, and 13 European countries.
At the same time, the median length of stay was shortest in the United States at 3 days. The longest median length of stay noted in the study was 8 days in Germany.
The study investigators pointed to the shorter length of stay in U.S. hospitals as a possible driver of the country’s higher rate of readmissions. But other experts say there are more complex factors at work, such as gaps in the discharge planning process and a lack of resources for patients once they leave the hospital.
There weren’t a lot of patients who were readmitted 2 days later for the same condition, which might indicate that they had been discharged too soon, Dr. Ryan said. More often, patients return to the hospital a week or several days later with a new problem. That tends to indicate that their medications may not have been adjusted correctly or that they were unable to access services in the outpatient world, he said.
There is very little evidence to support the idea that a longer initial length of stay would lead to either better use of evidence-based therapies or produce better clinical outcomes, said Dr. Gregg C. Fonarow, director of the Cardiomyopathy Center at the University of California, Los Angeles. Though there’s plenty of evidence to show that more time in the hospital increases patients’ risk for hospital-acquired infection, he added.
Over the last 2 decades, readmissions for heart failure patients have gone up as length of stay has decreased. But, Dr. Fonarow points out, during that same time the total number of days patients spent in the hospital has actually gone down, along with mortality. So from a global resource utilization perspective, patients are spending less time in the hospital and having better outcomes, he said.
"It’s important to have appropriate comparisons," he said.
Dr. Fonarow cautioned that there aren’t simple solutions to this problem. While there are many opportunities to improve readmission rates, there are also many rehospitalizations that are unavoidable or unrelated to the cardiovascular condition responsible for the initial hospitalization. Many patients hospitalized with acute MI, and to an even greater degree with heart failure, have multiple other cardiovascular and noncardiovascular comorbid conditions, he said.
"Efforts to try and reduce preventable readmissions have to go well beyond even the primary disease state that led to the hospitalization," Dr. Fonarow said. "They need to involve multiple components of care that go beyond just treating the single acute condition and focus on the multiple comorbid conditions that exist within that patient."
To make it even more complicated, patients who are hospitalized with heart failure tend to be older and to have multiple comorbid conditions. These individuals may face other challenges such as cognitive impairment, frailty, and poor socioeconomic support.
"It’s really a complex problem," he said.
Ensuring Needed Care
The looming Medicare readmission penalties have caused many hospital administrators, and in turn physicians, to look closely at the factors behind readmissions for the first time over the last few years.
"Everyone’s trying to figure this out because they do see the shift coming in the payment system," said Dr. John Rumsfeld, National Director of Cardiology at the Veterans Health Administration and Chief Science Officer for the American College of Cardiology’s National Cardiovascular Data Registry.
And the payment cuts for excessive readmissions aren’t the only way that CMS is focusing on the issue, Dr. Rumsfeld said. Readmissions are also at the heart of pilot projects Medicare is launching for Accountable Care Organizations and bundled payments.
Dr. Rumsfeld said he’s concerned that physicians are getting the message that all readmissions are bad. "This is a potentially dangerous message for clinical care," he said.
The conversation needs to shift to unnecessary or potentially preventable readmissions, he said. It’s often underappreciated, Dr. Rumsfeld said, that patients who are having recurrent chest pain or severe shortness of breath after an acute MI should be admitted to the hospital for care. "There shouldn’t be anything in the system that disincentivizes that," he said.
Dr. Clyde W. Yancy, Chief of the Division of Cardiology at Northwestern University and Associate Director of the Bluhm Cardiovascular Institute at Northwestern Memorial Hospital in Chicago, agrees.
"We’re beating the drum about this problem mostly because it’s a health care utilization problem," Dr. Yancy said. "In the process of beating the drum, we have to have enough wherewithal as clinicians and administrators to realize that there are those – and not a small number – who should in fact be readmitted because their disease is unstable, or it’s advanced, or it requires that attention."
The fate of safety net hospitals is also a concern. Safety net hospitals are unlikely to have the money to undertake a major overhaul of their discharge and care coordination systems, which could leave them with higher than average readmissions, even after the data is risk adjusted for their sicker patients, Dr. Yancy said. Then, if CMS cuts their reimbursement due to their excessive readmission rates, they will be left to care for sicker patients with even fewer resources.
"There has to be a point in this whole process where reasonable people sit back and look at how the landscape is truly impacted by this focus on readmissions," he said. "We can’t allow our safety net hospitals to be further disadvantaged."
Dr. Vincent Bufalino, Senior Vice President and Senior Medical Director of Cardiology at Advocate Health Care, a 100-physician cardiology group serving 10 hospitals in the Chicago area, said he thinks the readmission rates are a bit deceptive. While the numbers are high, especially in heart failure, these are also very sick patients, he said. "I’m not so disturbed with the readmission rate, although there are obviously opportunities for us to do better," Dr. Bufalino said.
One of those opportunities is in home health. Many heart failure and acute MI patients who could benefit from home health care after discharge aren’t getting it, he said, and it’s mostly because of a paperwork burden. Physicians aren’t making the referrals for home health because the paperwork required by CMS is so daunting.
While there are plenty of areas where physicians and hospitals can do a better job at care coordination, it’s important not to set unrealistic targets that force patients to be sent home when they should be admitted, Dr. Bufalino said.
"If someone is sick and they need to be readmitted, readmit them," he said.
Lessons Learned in Heart Failure
Physicians looking to make a dent in their readmission rates for heart failure can take some cues from successful programs around the country.
While the implementation varies from place to place, programs that have been able to cut their readmissions stress the need for patients to see a physician or nurse practitioner shortly after discharge. Another essential element for success is improving the communication between providers in the hospital and those who will be caring for patients after discharge.
At the University of Connecticut Heart Failure Center, where the all-cause 30-day readmission rates for heart failure patients dropped from 27% in 2008 to under 19% in 2011, patients don’t leave the hospital without an appointment to see a physician within 7 days of discharge.
The appointment might be with a primary care physician, a cardiologist, or a physician or nurse practitioner at the university’s heart failure clinic.
"If we can’t get them in with someone else, we will always make room for them and see them," said Dr. Jason Ryan, codirector of the Heart Failure Center at the University of Connecticut, Farmington.
While patients are still in the hospital, they also meet with nurses who train them in taking their medications and monitoring for heart failure symptoms. Patients also meet with social workers who ensure they have transportation to their appointments and a way to pick up their medicines. And they spend time with a pharmacist who reviews their medications.
The other element they have employed at the University of Connecticut is community outreach. Before the push to reduce readmissions, physicians at the hospital didn’t know anyone at the nursing homes or visiting nurse organizations. Now they hold a monthly meeting with physicians and other providers who work outside the hospital. They have gone from not knowing each other’s names to exchanging cell phone numbers, Dr. Ryan said.
"So when our patients are out there we can communicate a lot more easily when problems crop up," he said.
At the University of California, San Francisco’s Medical Center, they have used similar strategies to cut their readmission rates.
The UCSF Heart Failure Readmission Reduction Program began in 2008 with a 2-year, $575,000 grant aimed at rapidly bringing down readmissions. Now in its fourth year, the nurse-run program has been a success. The 30-day all-cause readmission rates for heart failure patients age 65 and older was around 24% in 2009 but had dropped to less than 10% at the beginning of this year.
But the program couldn’t run without its two nurse coordinators, said Karen Rago, a nurse and executive director of Service Line Administration at UCSF.
"They own this population," she said. "If you don’t have a single point that owns it, there are so many things that fall through the cracks."
The nurses at the UCSF heart failure program spent the first year working with the Institute for Healthcare Improvement to learn the principles in their readmissions toolkit: teach-back, follow-up phone calls at 7 and 14 days, an appointment with a physician or heart failure nurse practitioner within 7 days, and medication reconciliation.
The nurse coordinators also serve as a bridge to providers in the outpatient setting, Ms. Rago said. During the second year of the program, they began making site visits to skilled nursing facilities and reaching out to primary care physicians, cardiologists, and home health agencies from outside of the hospital.
They created an e-mail group for each patient’s care team that includes physicians, nurses, home care, social work, and pharmacy, depending on the services the patient needed. An email goes out to the team at the time of admission and it provides a way to update everyone virtually in real-time about the care of the patient.
Having a closer relationship with the skilled nursing facilities has been a big help, Ms. Rago said. During one of the site visits, the nurses discovered that one of the facilities didn’t offer a low-salt diet. That helped explain why so many patients from that facility were being readmitted to the hospital and they were able to quickly address it, she said.
What physicians need to keep in mind is that while many of these solutions are common sense, there’s no one-size-fits-all approach to readmissions, said Dr. John Rumsfeld, National Director of Cardiology at the Veterans Health Administration and Chief Science Officer for the American College of Cardiology’s National Cardiovascular Data Registry.
"It’s different in each community, so you can’t be prescriptive," he said.
The American College of Cardiology offers resources for reducing readmissions as part of a joint effort with the Institute for Healthcare Improvement called the Hospital to Home initiative.
Unlike other areas of care, such as getting a faster angioplasty, there aren’t six key steps for physicians to implement, Dr. Rumsfeld said. Instead, Hospital to Home is a place for physicians to share best practices based on their individual experiences. So far, more than 1,100 hospitals around the country have signed up.
Beyond Cash: Using Rewards to Motivate Physicians
SAN DIEGO – Cash is king, but it’s probably not the best way to make physicians feel appreciated. A flat-screen TV, a vacation, or a chance to take a professional development course, on the other hand, are all good ways for practices to recognize high-quality work and motivate physicians, according to Dr. John Nelson.
Dr. Nelson, a principal at Nelson Flores Hospital Medicine Consultants and a past president of the Society of Hospital Medicine, said it’s important to compensate hospitalists well. But just adding on cash bonuses doesn’t do much to energize employees and convince them to stay with a group," he said at the annual meeting of the Society of Hospital Medicine.
"Cash compensation is generally seen as an entitlement, so in most cases it doesn’t wind up being much of a motivator," he said in an interview. "It might help encourage someone to take a position in your practice, but it probably won’t do a lot to change their performance."
Base salary, health benefits, vacation time, seniority-based pay, and cost of living adjustments are all standard compensation that physicians expect to receive.
Practice leaders should instead consider offering nonmonetary incentives to their physicians, Dr. Nelson said. While cash bonuses can be viewed as cold or unemotional, nonmonetary awards have the potential to be memorable and special for employees. And while $100 is always just $100, a nonmonetary award can often have a higher perceived value.
Here are some nonmonetary incentive options:
• Write a note of thanks for doing a good job.
• Award a trophy for work in improving quality of care.
• Offer a promotion or a new title.
• Pay for attendance at a professional-development course.
• Provide a chance to contribute ideas to the group or hospital through one-on-one meeting with leadership or by leading special projects.
• Offer gifts such as vacations, televisions, or gift cards.
There are a number of different ways that these types of awards can be structured, said Dr. Nelson, who is also director of the hospitalist practice at Overlake Hospital Medical Center in Bellevue, Wash. They can be offered as recognition to teams or individuals. They can also be set up to celebrate milestones or to honor important achievements.
When designing a plan, Dr. Nelson said it’s important not to set up a reward system that creates a feeling of unfairness and produces strife within the group. Group leaders also need to keep in mind that nonmonetary awards, such as trips or gift cards, still count as compensation under the Stark Law and anti-kickback regulations. This is especially important for physicians who contract with, but are not directly employed by a hospital.
These types of awards do carry some cost for employers, but not nearly as much as a cost of living raise, for example. Exactly how much to spend will vary, Dr. Nelson said, but it should be a small percentage of the physicians’ overall salary, as low as 1%.
"If structured in the form of a nonmonetary reward, such as recognition, promotion, [or] professional development, that might be enough to inspire and encourage good performance on the part of the hospitalist," Dr. Nelson said.
SAN DIEGO – Cash is king, but it’s probably not the best way to make physicians feel appreciated. A flat-screen TV, a vacation, or a chance to take a professional development course, on the other hand, are all good ways for practices to recognize high-quality work and motivate physicians, according to Dr. John Nelson.
Dr. Nelson, a principal at Nelson Flores Hospital Medicine Consultants and a past president of the Society of Hospital Medicine, said it’s important to compensate hospitalists well. But just adding on cash bonuses doesn’t do much to energize employees and convince them to stay with a group," he said at the annual meeting of the Society of Hospital Medicine.
"Cash compensation is generally seen as an entitlement, so in most cases it doesn’t wind up being much of a motivator," he said in an interview. "It might help encourage someone to take a position in your practice, but it probably won’t do a lot to change their performance."
Base salary, health benefits, vacation time, seniority-based pay, and cost of living adjustments are all standard compensation that physicians expect to receive.
Practice leaders should instead consider offering nonmonetary incentives to their physicians, Dr. Nelson said. While cash bonuses can be viewed as cold or unemotional, nonmonetary awards have the potential to be memorable and special for employees. And while $100 is always just $100, a nonmonetary award can often have a higher perceived value.
Here are some nonmonetary incentive options:
• Write a note of thanks for doing a good job.
• Award a trophy for work in improving quality of care.
• Offer a promotion or a new title.
• Pay for attendance at a professional-development course.
• Provide a chance to contribute ideas to the group or hospital through one-on-one meeting with leadership or by leading special projects.
• Offer gifts such as vacations, televisions, or gift cards.
There are a number of different ways that these types of awards can be structured, said Dr. Nelson, who is also director of the hospitalist practice at Overlake Hospital Medical Center in Bellevue, Wash. They can be offered as recognition to teams or individuals. They can also be set up to celebrate milestones or to honor important achievements.
When designing a plan, Dr. Nelson said it’s important not to set up a reward system that creates a feeling of unfairness and produces strife within the group. Group leaders also need to keep in mind that nonmonetary awards, such as trips or gift cards, still count as compensation under the Stark Law and anti-kickback regulations. This is especially important for physicians who contract with, but are not directly employed by a hospital.
These types of awards do carry some cost for employers, but not nearly as much as a cost of living raise, for example. Exactly how much to spend will vary, Dr. Nelson said, but it should be a small percentage of the physicians’ overall salary, as low as 1%.
"If structured in the form of a nonmonetary reward, such as recognition, promotion, [or] professional development, that might be enough to inspire and encourage good performance on the part of the hospitalist," Dr. Nelson said.
SAN DIEGO – Cash is king, but it’s probably not the best way to make physicians feel appreciated. A flat-screen TV, a vacation, or a chance to take a professional development course, on the other hand, are all good ways for practices to recognize high-quality work and motivate physicians, according to Dr. John Nelson.
Dr. Nelson, a principal at Nelson Flores Hospital Medicine Consultants and a past president of the Society of Hospital Medicine, said it’s important to compensate hospitalists well. But just adding on cash bonuses doesn’t do much to energize employees and convince them to stay with a group," he said at the annual meeting of the Society of Hospital Medicine.
"Cash compensation is generally seen as an entitlement, so in most cases it doesn’t wind up being much of a motivator," he said in an interview. "It might help encourage someone to take a position in your practice, but it probably won’t do a lot to change their performance."
Base salary, health benefits, vacation time, seniority-based pay, and cost of living adjustments are all standard compensation that physicians expect to receive.
Practice leaders should instead consider offering nonmonetary incentives to their physicians, Dr. Nelson said. While cash bonuses can be viewed as cold or unemotional, nonmonetary awards have the potential to be memorable and special for employees. And while $100 is always just $100, a nonmonetary award can often have a higher perceived value.
Here are some nonmonetary incentive options:
• Write a note of thanks for doing a good job.
• Award a trophy for work in improving quality of care.
• Offer a promotion or a new title.
• Pay for attendance at a professional-development course.
• Provide a chance to contribute ideas to the group or hospital through one-on-one meeting with leadership or by leading special projects.
• Offer gifts such as vacations, televisions, or gift cards.
There are a number of different ways that these types of awards can be structured, said Dr. Nelson, who is also director of the hospitalist practice at Overlake Hospital Medical Center in Bellevue, Wash. They can be offered as recognition to teams or individuals. They can also be set up to celebrate milestones or to honor important achievements.
When designing a plan, Dr. Nelson said it’s important not to set up a reward system that creates a feeling of unfairness and produces strife within the group. Group leaders also need to keep in mind that nonmonetary awards, such as trips or gift cards, still count as compensation under the Stark Law and anti-kickback regulations. This is especially important for physicians who contract with, but are not directly employed by a hospital.
These types of awards do carry some cost for employers, but not nearly as much as a cost of living raise, for example. Exactly how much to spend will vary, Dr. Nelson said, but it should be a small percentage of the physicians’ overall salary, as low as 1%.
"If structured in the form of a nonmonetary reward, such as recognition, promotion, [or] professional development, that might be enough to inspire and encourage good performance on the part of the hospitalist," Dr. Nelson said.
EXPERT ANALYSIS FROM THE ANNUAL MEETING OF THE SOCIETY OF HOSPITAL MEDICINE