User login
Itchy and Pregnant? Consider Range of Skin Conditions
SAN FRANCISCO – When a pregnant woman presents with a complaint of itching, consider a range of causes, not just those triggered by pregnancy, Dr. Bethanee J. Schlosser advised.
Although some dermatoses of pregnancy are common, a pregnant woman’s itching may have nothing to do with her pregnancy and could be the result of contact dermatitis, drug eruption, scabies, folliculitis, or another cause, Dr. Schlosser said at SDEF Women’s & Pediatric Dermatology Seminar sponsored by Skin Disease Education Foundation (SDEF).

"Just because they’re pregnant doesn’t mean they only have to fit in the pregnancy dermatoses box," Dr. Schlosser of the department of dermatology, and director of the women’s skin health program, at Northwestern University in Chicago said in an interview.
With that said, the two most prominent dermatoses of pregnancy are pruritic urticarial papules and plaques of pregnancy, a condition now known under the umbrella term polymorphic eruption of pregnancy, and pemphigoid gestationis, previously called herpes gestationis.
Polymorphic eruption of pregnancy occurs in about 1 in 300 pregnancies and is generally associated with multiple gestations and increased maternal weight gain. It is also more common in women having their first child. The mean onset is at about 35 weeks, but in about 15% of cases, the onset can be post partum, according to Dr. Schlosser.
Pemphigoid gestationis is a rare acquired autoimmune blistering disease unique to pregnancy. It occurs in 1 in 50,000 pregnancies and is probably the least common dermatosis of pregnancy. The onset is usually in the second or third trimester, but in about 14% of cases, the onset can occur post partum. With pemphigoid gestationis, there is no change in maternal outcome, but there are risks to the fetus including being small for gestational age, preterm delivery, and neonatal pemphigoid disease.

Typically, patients with the polymorphic eruption present with "hivelike" or urticarial papules and plaques, but no blisters, while women with pemphigoid gestationis often have more blistering. However, the clinical presentations and the routine histopathology can be identical, Dr. Schlosser explained.
"I’ve seen patients with both entities, with both kinds of clinical features," she noted. "If it’s in your differential diagnosis and you can’t distinguish 100% clinically, then that’s where the utility of biopsy comes in."
Cutaneous biopsy is a common procedure and is low risk, she reported, even in the context of pregnancy. Routine histopathology and direct immunofluorescence are essential in terms of differentiating between pemphigoid gestationis and polymorphic eruption.
The first-line treatment for both conditions is topical corticosteroids and oral antihistamines when the condition is mild or localized and systemic corticosteroids in severe cases. Although the treatments are generally the same, the difference between the two conditions is not academic, Dr. Schlosser said, because the potential sequelae and considerations for mother and child are different.

Dr. Schlosser also recommended that dermatologists make it a priority to communicate with the referring physician, specifically to review the risks to both the mother and child that may be associated with a particular skin condition or its treatments.
For example, polymorphic eruption of pregnancy is generally nonthreatening to the mother and child. But Dr. Schlosser said she has seen patients with widespread, severe polymorphic eruptions who have needed treatment with systemic corticosteroids. That’s essential information for the ob.gyn.; if the patient has a cesarean delivery, the patient will likely require stress-dose corticosteroids. Similarly, the newborn would need to be monitored for hypoglycemia during the immediate after-birth period.
"That doesn’t mean that dermatologists shouldn’t treat pregnant women aggressively, when appropriate," Dr. Schlosser said. "But the entire multidisciplinary care team needs to be kept informed so that the risks can be managed."
Dr. Schlosser said she had no relevant financial disclosures. SDEF and this news organization are owned by Elsevier.
SAN FRANCISCO – When a pregnant woman presents with a complaint of itching, consider a range of causes, not just those triggered by pregnancy, Dr. Bethanee J. Schlosser advised.
Although some dermatoses of pregnancy are common, a pregnant woman’s itching may have nothing to do with her pregnancy and could be the result of contact dermatitis, drug eruption, scabies, folliculitis, or another cause, Dr. Schlosser said at SDEF Women’s & Pediatric Dermatology Seminar sponsored by Skin Disease Education Foundation (SDEF).
"Just because they’re pregnant doesn’t mean they only have to fit in the pregnancy dermatoses box," Dr. Schlosser of the department of dermatology, and director of the women’s skin health program, at Northwestern University in Chicago said in an interview.
With that said, the two most prominent dermatoses of pregnancy are pruritic urticarial papules and plaques of pregnancy, a condition now known under the umbrella term polymorphic eruption of pregnancy, and pemphigoid gestationis, previously called herpes gestationis.
Polymorphic eruption of pregnancy occurs in about 1 in 300 pregnancies and is generally associated with multiple gestations and increased maternal weight gain. It is also more common in women having their first child. The mean onset is at about 35 weeks, but in about 15% of cases, the onset can be post partum, according to Dr. Schlosser.
Pemphigoid gestationis is a rare acquired autoimmune blistering disease unique to pregnancy. It occurs in 1 in 50,000 pregnancies and is probably the least common dermatosis of pregnancy. The onset is usually in the second or third trimester, but in about 14% of cases, the onset can occur post partum. With pemphigoid gestationis, there is no change in maternal outcome, but there are risks to the fetus including being small for gestational age, preterm delivery, and neonatal pemphigoid disease.
Typically, patients with the polymorphic eruption present with "hivelike" or urticarial papules and plaques, but no blisters, while women with pemphigoid gestationis often have more blistering. However, the clinical presentations and the routine histopathology can be identical, Dr. Schlosser explained.
"I’ve seen patients with both entities, with both kinds of clinical features," she noted. "If it’s in your differential diagnosis and you can’t distinguish 100% clinically, then that’s where the utility of biopsy comes in."
Cutaneous biopsy is a common procedure and is low risk, she reported, even in the context of pregnancy. Routine histopathology and direct immunofluorescence are essential in terms of differentiating between pemphigoid gestationis and polymorphic eruption.
The first-line treatment for both conditions is topical corticosteroids and oral antihistamines when the condition is mild or localized and systemic corticosteroids in severe cases. Although the treatments are generally the same, the difference between the two conditions is not academic, Dr. Schlosser said, because the potential sequelae and considerations for mother and child are different.
Dr. Schlosser also recommended that dermatologists make it a priority to communicate with the referring physician, specifically to review the risks to both the mother and child that may be associated with a particular skin condition or its treatments.
For example, polymorphic eruption of pregnancy is generally nonthreatening to the mother and child. But Dr. Schlosser said she has seen patients with widespread, severe polymorphic eruptions who have needed treatment with systemic corticosteroids. That’s essential information for the ob.gyn.; if the patient has a cesarean delivery, the patient will likely require stress-dose corticosteroids. Similarly, the newborn would need to be monitored for hypoglycemia during the immediate after-birth period.
"That doesn’t mean that dermatologists shouldn’t treat pregnant women aggressively, when appropriate," Dr. Schlosser said. "But the entire multidisciplinary care team needs to be kept informed so that the risks can be managed."
Dr. Schlosser said she had no relevant financial disclosures. SDEF and this news organization are owned by Elsevier.
SAN FRANCISCO – When a pregnant woman presents with a complaint of itching, consider a range of causes, not just those triggered by pregnancy, Dr. Bethanee J. Schlosser advised.
Although some dermatoses of pregnancy are common, a pregnant woman’s itching may have nothing to do with her pregnancy and could be the result of contact dermatitis, drug eruption, scabies, folliculitis, or another cause, Dr. Schlosser said at SDEF Women’s & Pediatric Dermatology Seminar sponsored by Skin Disease Education Foundation (SDEF).
"Just because they’re pregnant doesn’t mean they only have to fit in the pregnancy dermatoses box," Dr. Schlosser of the department of dermatology, and director of the women’s skin health program, at Northwestern University in Chicago said in an interview.
With that said, the two most prominent dermatoses of pregnancy are pruritic urticarial papules and plaques of pregnancy, a condition now known under the umbrella term polymorphic eruption of pregnancy, and pemphigoid gestationis, previously called herpes gestationis.
Polymorphic eruption of pregnancy occurs in about 1 in 300 pregnancies and is generally associated with multiple gestations and increased maternal weight gain. It is also more common in women having their first child. The mean onset is at about 35 weeks, but in about 15% of cases, the onset can be post partum, according to Dr. Schlosser.
Pemphigoid gestationis is a rare acquired autoimmune blistering disease unique to pregnancy. It occurs in 1 in 50,000 pregnancies and is probably the least common dermatosis of pregnancy. The onset is usually in the second or third trimester, but in about 14% of cases, the onset can occur post partum. With pemphigoid gestationis, there is no change in maternal outcome, but there are risks to the fetus including being small for gestational age, preterm delivery, and neonatal pemphigoid disease.
Typically, patients with the polymorphic eruption present with "hivelike" or urticarial papules and plaques, but no blisters, while women with pemphigoid gestationis often have more blistering. However, the clinical presentations and the routine histopathology can be identical, Dr. Schlosser explained.
"I’ve seen patients with both entities, with both kinds of clinical features," she noted. "If it’s in your differential diagnosis and you can’t distinguish 100% clinically, then that’s where the utility of biopsy comes in."
Cutaneous biopsy is a common procedure and is low risk, she reported, even in the context of pregnancy. Routine histopathology and direct immunofluorescence are essential in terms of differentiating between pemphigoid gestationis and polymorphic eruption.
The first-line treatment for both conditions is topical corticosteroids and oral antihistamines when the condition is mild or localized and systemic corticosteroids in severe cases. Although the treatments are generally the same, the difference between the two conditions is not academic, Dr. Schlosser said, because the potential sequelae and considerations for mother and child are different.
Dr. Schlosser also recommended that dermatologists make it a priority to communicate with the referring physician, specifically to review the risks to both the mother and child that may be associated with a particular skin condition or its treatments.
For example, polymorphic eruption of pregnancy is generally nonthreatening to the mother and child. But Dr. Schlosser said she has seen patients with widespread, severe polymorphic eruptions who have needed treatment with systemic corticosteroids. That’s essential information for the ob.gyn.; if the patient has a cesarean delivery, the patient will likely require stress-dose corticosteroids. Similarly, the newborn would need to be monitored for hypoglycemia during the immediate after-birth period.
"That doesn’t mean that dermatologists shouldn’t treat pregnant women aggressively, when appropriate," Dr. Schlosser said. "But the entire multidisciplinary care team needs to be kept informed so that the risks can be managed."
Dr. Schlosser said she had no relevant financial disclosures. SDEF and this news organization are owned by Elsevier.
EXPERT ANALYSIS FROM THE SDEF WOMEN'S & PEDIATRIC DERMATOLOGY SEMINAR
Obama's Debt Plan Targets Medicare "Overpayments"
President Obama’s plan to bring down the federal deficit includes about $320 billion in cuts to Medicare, Medicaid, and other federal health programs, and gives more power to the Independent Payment Advisory Board.
In the proposal, which was sent to Congress Sept. 19, the Obama administration calls for a combination of spending cuts and tax changes that it estimates would save about $4 trillion over the next decade. The plan includes about $248 billion in Medicare cuts – but the administration said that 90% of the savings would come by reducing "overpayments" to providers and drug companies. The president’s plan would not change the eligibility age for receiving Medicare benefits.

"This plan reduces wasteful subsidies and erroneous payments while changing some incentives that often lead to excessive health care costs," President Obama said during a speech in the Rose Garden
But the president’s plan was met with immediate opposition from Republicans in Congress. The top Republican in the Senate, Sen. Mitch McConnell (R-Ky.), said the president was "punting" on entitlement reform and that the proposal would not lead to meaningful deficit reduction.
The proposal includes $32 billion in payment cuts to skilled nursing facilities, long-term care hospitals, inpatient rehabilitation facilities, and home health care from 2014 through 2021. The administration expects to save another $4 billion over the next decade by paying skilled nursing facilities and inpatient rehabilitation facilities the same price for postacute care for hip and knee replacement and hip fractures. Currently, payments are higher in inpatient rehabilitation facilities.
The plan would also tie reimbursement for skilled nursing facilities to reductions in hospital readmissions. Under the Affordable Care Act, Medicare will begin penalizing hospitals with high readmission rates. The new deficit reduction proposal would reduce skilled nursing facility payments by up to 3% beginning in 2015 for those facilities with high rates of preventable hospital readmissions. The administration estimates that the policy will save about $2 billion over 10 years.
The proposal also calls for ending add-on payments for hospitals and physicians working in low-population states, starting in 2013. That would save about $2 billion over 10 years, according to the administration’s plan. The president is also proposing 10% reductions in Indirect Medical Education add-on payments beginning in 2013, saving about $9 billion over 10 years.
In some good news for physicians, the proposal assumes that Congress will step in to stop pending cuts to Medicare physician payment rates. Without action from Congress, Medicare is scheduled to cut physician payments by nearly 30% in January 2012. However, the proposal also gives greater authority to the Independent Payment Advisory Board (IPAB), a panel that has been widely criticized by the physician community.
The panel was created under the Affordable Care Act, and charged with recommending Medicare cuts to reduce the rate of growth in the program. Under the Affordable Care Act, the IPAB would make recommendations for cuts when the projected Medicare growth rate per capita exceeds the gross domestic product plus 1%. But under the new proposal, that target rate would be lowered to gross domestic product (GDP) plus 0.5%. And the proposal calls for giving the panel new tools, such as the ability to consider "value-based benefit design" and an automatic enforcement mechanism for cuts. The president proposed that same change back in April when unveiling an earlier plan for managing the deficit.
One of the plan’s biggest targets for Medicare spending cuts is the drug industry. Under the president’s proposal, drug companies would be required to give the Medicare program the same rebates it gives to Medicaid for brand name and generic drugs provided to low-income beneficiaries. The change, which would take effect in 2013, is estimated to save about $135 billion over 10 years.
The president’s deficit reduction proposal would also reduce the amount that Medicare pays to providers to cover bad debts.
Currently, Medicare reimburses providers for 70% of nonpayment of deductibles and copayments after they have made reasonable efforts to collect the money. Under the president’s proposal, that amount would drop to 25%, which is similar to what private insurers pay. The change would be phased in over 3 years starting in 2013, and it is estimated to save about $20 billion over the next decade.
The president also plans to trim another $5 billion from the Medicare program by cutting waste, fraud, and abuse. For instance, starting in 2014 the proposal would put in place a prior-authorization requirement for the top-priced imaging services, a change that is estimated to save about $900 million over the next decade.
The plan would also make some changes that directly affect what beneficiaries pay for the program. Beginning in 2017, the administration proposes to increase income-related premiums in Medicare Part B and Part D by 15%. About 25% of beneficiaries would be subject to the higher premiums. That would save about $20 billion over 10 years.
Under the Medicaid program, the president’s proposal seeks to save about $66 billion over 10 years. The administration estimated that it would save about $26 billion by limiting the ability of states to use provider taxes as a way to boost their federal matching payments. Specifically, the administration proposes lowering the Medicaid provider tax threshold from 6% in 2014 to 3.5% in 2017.
The Obama administration is also seeking to replace the Federal Medical Assistance Percentage and enhanced FMAP formulas used by the federal government in determining state Medicaid matching rates. Starting in 2017, the federal government would use a single matching rate specific to each state that would automatically increase if a recession caused enrollment to rise. The proposal is expected to save $14.9 billion over 10 years.
The administration also plans to save about $110 million over the next decade by cracking down on waste, fraud, and abuse in the Medicaid program.
American Medical Association President Dr. Peter W. Carmel commended the administration for "recognizing that any serious plan to address the deficit must include a repeal of the Medicare sustainable growth rate formula (SGR)."
But "honest accounting of our nation’s debt should not assume $300 billion in Medicare physician cuts, which Congress has rejected repeatedly because of the significant, detrimental impact those cuts would have on patients’ access to care," Dr. Carmel cautioned in a statement. "Many bipartisan deficit reduction plans have called for repealing this flawed formula while achieving substantial deficit reduction totals."
President Obama’s plan to bring down the federal deficit includes about $320 billion in cuts to Medicare, Medicaid, and other federal health programs, and gives more power to the Independent Payment Advisory Board.
In the proposal, which was sent to Congress Sept. 19, the Obama administration calls for a combination of spending cuts and tax changes that it estimates would save about $4 trillion over the next decade. The plan includes about $248 billion in Medicare cuts – but the administration said that 90% of the savings would come by reducing "overpayments" to providers and drug companies. The president’s plan would not change the eligibility age for receiving Medicare benefits.
"This plan reduces wasteful subsidies and erroneous payments while changing some incentives that often lead to excessive health care costs," President Obama said during a speech in the Rose Garden
But the president’s plan was met with immediate opposition from Republicans in Congress. The top Republican in the Senate, Sen. Mitch McConnell (R-Ky.), said the president was "punting" on entitlement reform and that the proposal would not lead to meaningful deficit reduction.
The proposal includes $32 billion in payment cuts to skilled nursing facilities, long-term care hospitals, inpatient rehabilitation facilities, and home health care from 2014 through 2021. The administration expects to save another $4 billion over the next decade by paying skilled nursing facilities and inpatient rehabilitation facilities the same price for postacute care for hip and knee replacement and hip fractures. Currently, payments are higher in inpatient rehabilitation facilities.
The plan would also tie reimbursement for skilled nursing facilities to reductions in hospital readmissions. Under the Affordable Care Act, Medicare will begin penalizing hospitals with high readmission rates. The new deficit reduction proposal would reduce skilled nursing facility payments by up to 3% beginning in 2015 for those facilities with high rates of preventable hospital readmissions. The administration estimates that the policy will save about $2 billion over 10 years.
The proposal also calls for ending add-on payments for hospitals and physicians working in low-population states, starting in 2013. That would save about $2 billion over 10 years, according to the administration’s plan. The president is also proposing 10% reductions in Indirect Medical Education add-on payments beginning in 2013, saving about $9 billion over 10 years.
In some good news for physicians, the proposal assumes that Congress will step in to stop pending cuts to Medicare physician payment rates. Without action from Congress, Medicare is scheduled to cut physician payments by nearly 30% in January 2012. However, the proposal also gives greater authority to the Independent Payment Advisory Board (IPAB), a panel that has been widely criticized by the physician community.
The panel was created under the Affordable Care Act, and charged with recommending Medicare cuts to reduce the rate of growth in the program. Under the Affordable Care Act, the IPAB would make recommendations for cuts when the projected Medicare growth rate per capita exceeds the gross domestic product plus 1%. But under the new proposal, that target rate would be lowered to gross domestic product (GDP) plus 0.5%. And the proposal calls for giving the panel new tools, such as the ability to consider "value-based benefit design" and an automatic enforcement mechanism for cuts. The president proposed that same change back in April when unveiling an earlier plan for managing the deficit.
One of the plan’s biggest targets for Medicare spending cuts is the drug industry. Under the president’s proposal, drug companies would be required to give the Medicare program the same rebates it gives to Medicaid for brand name and generic drugs provided to low-income beneficiaries. The change, which would take effect in 2013, is estimated to save about $135 billion over 10 years.
The president’s deficit reduction proposal would also reduce the amount that Medicare pays to providers to cover bad debts.
Currently, Medicare reimburses providers for 70% of nonpayment of deductibles and copayments after they have made reasonable efforts to collect the money. Under the president’s proposal, that amount would drop to 25%, which is similar to what private insurers pay. The change would be phased in over 3 years starting in 2013, and it is estimated to save about $20 billion over the next decade.
The president also plans to trim another $5 billion from the Medicare program by cutting waste, fraud, and abuse. For instance, starting in 2014 the proposal would put in place a prior-authorization requirement for the top-priced imaging services, a change that is estimated to save about $900 million over the next decade.
The plan would also make some changes that directly affect what beneficiaries pay for the program. Beginning in 2017, the administration proposes to increase income-related premiums in Medicare Part B and Part D by 15%. About 25% of beneficiaries would be subject to the higher premiums. That would save about $20 billion over 10 years.
Under the Medicaid program, the president’s proposal seeks to save about $66 billion over 10 years. The administration estimated that it would save about $26 billion by limiting the ability of states to use provider taxes as a way to boost their federal matching payments. Specifically, the administration proposes lowering the Medicaid provider tax threshold from 6% in 2014 to 3.5% in 2017.
The Obama administration is also seeking to replace the Federal Medical Assistance Percentage and enhanced FMAP formulas used by the federal government in determining state Medicaid matching rates. Starting in 2017, the federal government would use a single matching rate specific to each state that would automatically increase if a recession caused enrollment to rise. The proposal is expected to save $14.9 billion over 10 years.
The administration also plans to save about $110 million over the next decade by cracking down on waste, fraud, and abuse in the Medicaid program.
American Medical Association President Dr. Peter W. Carmel commended the administration for "recognizing that any serious plan to address the deficit must include a repeal of the Medicare sustainable growth rate formula (SGR)."
But "honest accounting of our nation’s debt should not assume $300 billion in Medicare physician cuts, which Congress has rejected repeatedly because of the significant, detrimental impact those cuts would have on patients’ access to care," Dr. Carmel cautioned in a statement. "Many bipartisan deficit reduction plans have called for repealing this flawed formula while achieving substantial deficit reduction totals."
President Obama’s plan to bring down the federal deficit includes about $320 billion in cuts to Medicare, Medicaid, and other federal health programs, and gives more power to the Independent Payment Advisory Board.
In the proposal, which was sent to Congress Sept. 19, the Obama administration calls for a combination of spending cuts and tax changes that it estimates would save about $4 trillion over the next decade. The plan includes about $248 billion in Medicare cuts – but the administration said that 90% of the savings would come by reducing "overpayments" to providers and drug companies. The president’s plan would not change the eligibility age for receiving Medicare benefits.
"This plan reduces wasteful subsidies and erroneous payments while changing some incentives that often lead to excessive health care costs," President Obama said during a speech in the Rose Garden
But the president’s plan was met with immediate opposition from Republicans in Congress. The top Republican in the Senate, Sen. Mitch McConnell (R-Ky.), said the president was "punting" on entitlement reform and that the proposal would not lead to meaningful deficit reduction.
The proposal includes $32 billion in payment cuts to skilled nursing facilities, long-term care hospitals, inpatient rehabilitation facilities, and home health care from 2014 through 2021. The administration expects to save another $4 billion over the next decade by paying skilled nursing facilities and inpatient rehabilitation facilities the same price for postacute care for hip and knee replacement and hip fractures. Currently, payments are higher in inpatient rehabilitation facilities.
The plan would also tie reimbursement for skilled nursing facilities to reductions in hospital readmissions. Under the Affordable Care Act, Medicare will begin penalizing hospitals with high readmission rates. The new deficit reduction proposal would reduce skilled nursing facility payments by up to 3% beginning in 2015 for those facilities with high rates of preventable hospital readmissions. The administration estimates that the policy will save about $2 billion over 10 years.
The proposal also calls for ending add-on payments for hospitals and physicians working in low-population states, starting in 2013. That would save about $2 billion over 10 years, according to the administration’s plan. The president is also proposing 10% reductions in Indirect Medical Education add-on payments beginning in 2013, saving about $9 billion over 10 years.
In some good news for physicians, the proposal assumes that Congress will step in to stop pending cuts to Medicare physician payment rates. Without action from Congress, Medicare is scheduled to cut physician payments by nearly 30% in January 2012. However, the proposal also gives greater authority to the Independent Payment Advisory Board (IPAB), a panel that has been widely criticized by the physician community.
The panel was created under the Affordable Care Act, and charged with recommending Medicare cuts to reduce the rate of growth in the program. Under the Affordable Care Act, the IPAB would make recommendations for cuts when the projected Medicare growth rate per capita exceeds the gross domestic product plus 1%. But under the new proposal, that target rate would be lowered to gross domestic product (GDP) plus 0.5%. And the proposal calls for giving the panel new tools, such as the ability to consider "value-based benefit design" and an automatic enforcement mechanism for cuts. The president proposed that same change back in April when unveiling an earlier plan for managing the deficit.
One of the plan’s biggest targets for Medicare spending cuts is the drug industry. Under the president’s proposal, drug companies would be required to give the Medicare program the same rebates it gives to Medicaid for brand name and generic drugs provided to low-income beneficiaries. The change, which would take effect in 2013, is estimated to save about $135 billion over 10 years.
The president’s deficit reduction proposal would also reduce the amount that Medicare pays to providers to cover bad debts.
Currently, Medicare reimburses providers for 70% of nonpayment of deductibles and copayments after they have made reasonable efforts to collect the money. Under the president’s proposal, that amount would drop to 25%, which is similar to what private insurers pay. The change would be phased in over 3 years starting in 2013, and it is estimated to save about $20 billion over the next decade.
The president also plans to trim another $5 billion from the Medicare program by cutting waste, fraud, and abuse. For instance, starting in 2014 the proposal would put in place a prior-authorization requirement for the top-priced imaging services, a change that is estimated to save about $900 million over the next decade.
The plan would also make some changes that directly affect what beneficiaries pay for the program. Beginning in 2017, the administration proposes to increase income-related premiums in Medicare Part B and Part D by 15%. About 25% of beneficiaries would be subject to the higher premiums. That would save about $20 billion over 10 years.
Under the Medicaid program, the president’s proposal seeks to save about $66 billion over 10 years. The administration estimated that it would save about $26 billion by limiting the ability of states to use provider taxes as a way to boost their federal matching payments. Specifically, the administration proposes lowering the Medicaid provider tax threshold from 6% in 2014 to 3.5% in 2017.
The Obama administration is also seeking to replace the Federal Medical Assistance Percentage and enhanced FMAP formulas used by the federal government in determining state Medicaid matching rates. Starting in 2017, the federal government would use a single matching rate specific to each state that would automatically increase if a recession caused enrollment to rise. The proposal is expected to save $14.9 billion over 10 years.
The administration also plans to save about $110 million over the next decade by cracking down on waste, fraud, and abuse in the Medicaid program.
American Medical Association President Dr. Peter W. Carmel commended the administration for "recognizing that any serious plan to address the deficit must include a repeal of the Medicare sustainable growth rate formula (SGR)."
But "honest accounting of our nation’s debt should not assume $300 billion in Medicare physician cuts, which Congress has rejected repeatedly because of the significant, detrimental impact those cuts would have on patients’ access to care," Dr. Carmel cautioned in a statement. "Many bipartisan deficit reduction plans have called for repealing this flawed formula while achieving substantial deficit reduction totals."
Frequent Use of CPOE Saves Lives
Current government thresholds for the "meaningful use" of computerized provider order entry in the hospital may not be high enough to actually save lives, according to a simulation conducted by researchers at the Rand Corporation.
The researchers estimated the impact on mortality in a sample of more than 2,500 hospitals used computerized provider order entry (CPOE) for 26%-50% of patients, and found that that level of use could reduce mortality for heart failure and acute myocardial infarction among hospitalized Medicare beneficiaries by 1.2% – not a statistically significant reduction.
But a second simulation found that mortality could be significantly reduced (2.1%) if CPOE were used for 51%-90% of patients hospitalized for those conditions. The findings were published Sept. 14 in the journal Health Affairs on Sept. 14 (doi: 10.1377/hlthaff.2011.0245).
The results could help influence policy makers as they set standards for the later stages of the electronic health records (EHR) incentive program, the authors noted. The program was authorized by Congress in the 2009 Health Information Technology for Economic and Clinical Health (HITECH) Act and will provide about $27 billion in payments to physicians, hospitals, and other providers by the end of 2016.
Under stage 1 of the program, hospitals are required to use CPOE on medication orders for at least 30% of their eligible patients; under initial regulations governing the program, the threshold could rise to 60% in stage 2 and 80% in stage 3 of the program.
However, even the initial requirements for CPOE have been criticized by health care providers as being too strict. And recently, the Health Information Technology Policy Committee convened by the Health and Human Services department to help implement the incentive program recommended delaying the implementation of stage 2 requirements by a year.
The Rand study results could be ammunition for policy makers seeking to make the program more robust.
"Our results do support the notion that the increased thresholds for computerized medication order entry proposed for later stages of the 'meaningful use' regulations have the potential to yield tangible benefits," Spencer S. Jones, an associate information scientist at the Rand Corp. in Boston and lead author of the study, said in an interview. "Our study should reassure policy makers at HHS and other stakeholders that high levels of use of computerized provider order entry and other health information technology have value and are likely to yield tangible health benefits for patients."
But Mr. Jones added that policy makers have a tough decision to make in this area because there is currently no research setting out the optimal pace for EHR adoption. While proceeding at a cautious pace may be an appropriate strategy, maintaining parallel paper and electronic systems could lead to unintended adverse consequences, he said.
The study, which relied on data from 2,543 privately owned general acute hospitals, also compared the impact of any use of CPOE to no use and found that hospitals that used CPOE even a small amount achieved lower mortality rates for heart failure, acute MI, and pneumonia among Medicare beneficiaries. However, when the researchers adjusted for potential confounding factors that might affect mortality, there was a statistically significant relationship between CPOE use and lower mortality only for acute MI and heart failure.
It’s unclear why pneumonia mortality was not significantly affected by CPOE use. It could be that CPOE is more helpful in reducing medication errors for such complex chronic conditions as heart failure than for acute conditions like pneumonia, the researchers wrote.
The researchers analyzed data from the 2007 American Hospital Association annual survey database and the AHA’s Information Technology Supplement from the same year. They obtained mortality data from the Centers for Medicare and Medicaid Services’ Hospital Compare database, which listed risk-standardized 30-day mortality rate for Medicare beneficiaries admitted to the hospital with acute MI, heart failure, or pneumonia.
The researchers disclosed no conflicts of interest. The study was funded by philanthropic contributions from members of the Rand Health Board of Advisors.
Current government thresholds for the "meaningful use" of computerized provider order entry in the hospital may not be high enough to actually save lives, according to a simulation conducted by researchers at the Rand Corporation.
The researchers estimated the impact on mortality in a sample of more than 2,500 hospitals used computerized provider order entry (CPOE) for 26%-50% of patients, and found that that level of use could reduce mortality for heart failure and acute myocardial infarction among hospitalized Medicare beneficiaries by 1.2% – not a statistically significant reduction.
But a second simulation found that mortality could be significantly reduced (2.1%) if CPOE were used for 51%-90% of patients hospitalized for those conditions. The findings were published Sept. 14 in the journal Health Affairs on Sept. 14 (doi: 10.1377/hlthaff.2011.0245).
The results could help influence policy makers as they set standards for the later stages of the electronic health records (EHR) incentive program, the authors noted. The program was authorized by Congress in the 2009 Health Information Technology for Economic and Clinical Health (HITECH) Act and will provide about $27 billion in payments to physicians, hospitals, and other providers by the end of 2016.
Under stage 1 of the program, hospitals are required to use CPOE on medication orders for at least 30% of their eligible patients; under initial regulations governing the program, the threshold could rise to 60% in stage 2 and 80% in stage 3 of the program.
However, even the initial requirements for CPOE have been criticized by health care providers as being too strict. And recently, the Health Information Technology Policy Committee convened by the Health and Human Services department to help implement the incentive program recommended delaying the implementation of stage 2 requirements by a year.
The Rand study results could be ammunition for policy makers seeking to make the program more robust.
"Our results do support the notion that the increased thresholds for computerized medication order entry proposed for later stages of the 'meaningful use' regulations have the potential to yield tangible benefits," Spencer S. Jones, an associate information scientist at the Rand Corp. in Boston and lead author of the study, said in an interview. "Our study should reassure policy makers at HHS and other stakeholders that high levels of use of computerized provider order entry and other health information technology have value and are likely to yield tangible health benefits for patients."
But Mr. Jones added that policy makers have a tough decision to make in this area because there is currently no research setting out the optimal pace for EHR adoption. While proceeding at a cautious pace may be an appropriate strategy, maintaining parallel paper and electronic systems could lead to unintended adverse consequences, he said.
The study, which relied on data from 2,543 privately owned general acute hospitals, also compared the impact of any use of CPOE to no use and found that hospitals that used CPOE even a small amount achieved lower mortality rates for heart failure, acute MI, and pneumonia among Medicare beneficiaries. However, when the researchers adjusted for potential confounding factors that might affect mortality, there was a statistically significant relationship between CPOE use and lower mortality only for acute MI and heart failure.
It’s unclear why pneumonia mortality was not significantly affected by CPOE use. It could be that CPOE is more helpful in reducing medication errors for such complex chronic conditions as heart failure than for acute conditions like pneumonia, the researchers wrote.
The researchers analyzed data from the 2007 American Hospital Association annual survey database and the AHA’s Information Technology Supplement from the same year. They obtained mortality data from the Centers for Medicare and Medicaid Services’ Hospital Compare database, which listed risk-standardized 30-day mortality rate for Medicare beneficiaries admitted to the hospital with acute MI, heart failure, or pneumonia.
The researchers disclosed no conflicts of interest. The study was funded by philanthropic contributions from members of the Rand Health Board of Advisors.
Current government thresholds for the "meaningful use" of computerized provider order entry in the hospital may not be high enough to actually save lives, according to a simulation conducted by researchers at the Rand Corporation.
The researchers estimated the impact on mortality in a sample of more than 2,500 hospitals used computerized provider order entry (CPOE) for 26%-50% of patients, and found that that level of use could reduce mortality for heart failure and acute myocardial infarction among hospitalized Medicare beneficiaries by 1.2% – not a statistically significant reduction.
But a second simulation found that mortality could be significantly reduced (2.1%) if CPOE were used for 51%-90% of patients hospitalized for those conditions. The findings were published Sept. 14 in the journal Health Affairs on Sept. 14 (doi: 10.1377/hlthaff.2011.0245).
The results could help influence policy makers as they set standards for the later stages of the electronic health records (EHR) incentive program, the authors noted. The program was authorized by Congress in the 2009 Health Information Technology for Economic and Clinical Health (HITECH) Act and will provide about $27 billion in payments to physicians, hospitals, and other providers by the end of 2016.
Under stage 1 of the program, hospitals are required to use CPOE on medication orders for at least 30% of their eligible patients; under initial regulations governing the program, the threshold could rise to 60% in stage 2 and 80% in stage 3 of the program.
However, even the initial requirements for CPOE have been criticized by health care providers as being too strict. And recently, the Health Information Technology Policy Committee convened by the Health and Human Services department to help implement the incentive program recommended delaying the implementation of stage 2 requirements by a year.
The Rand study results could be ammunition for policy makers seeking to make the program more robust.
"Our results do support the notion that the increased thresholds for computerized medication order entry proposed for later stages of the 'meaningful use' regulations have the potential to yield tangible benefits," Spencer S. Jones, an associate information scientist at the Rand Corp. in Boston and lead author of the study, said in an interview. "Our study should reassure policy makers at HHS and other stakeholders that high levels of use of computerized provider order entry and other health information technology have value and are likely to yield tangible health benefits for patients."
But Mr. Jones added that policy makers have a tough decision to make in this area because there is currently no research setting out the optimal pace for EHR adoption. While proceeding at a cautious pace may be an appropriate strategy, maintaining parallel paper and electronic systems could lead to unintended adverse consequences, he said.
The study, which relied on data from 2,543 privately owned general acute hospitals, also compared the impact of any use of CPOE to no use and found that hospitals that used CPOE even a small amount achieved lower mortality rates for heart failure, acute MI, and pneumonia among Medicare beneficiaries. However, when the researchers adjusted for potential confounding factors that might affect mortality, there was a statistically significant relationship between CPOE use and lower mortality only for acute MI and heart failure.
It’s unclear why pneumonia mortality was not significantly affected by CPOE use. It could be that CPOE is more helpful in reducing medication errors for such complex chronic conditions as heart failure than for acute conditions like pneumonia, the researchers wrote.
The researchers analyzed data from the 2007 American Hospital Association annual survey database and the AHA’s Information Technology Supplement from the same year. They obtained mortality data from the Centers for Medicare and Medicaid Services’ Hospital Compare database, which listed risk-standardized 30-day mortality rate for Medicare beneficiaries admitted to the hospital with acute MI, heart failure, or pneumonia.
The researchers disclosed no conflicts of interest. The study was funded by philanthropic contributions from members of the Rand Health Board of Advisors.
FROM THE JOURNAL HEALTH AFFAIRS
Major Finding: Using CPOE for at least 51% of hospitalized patients can reduce mortality by 2.1% for heart failure and acute MI.
Data Source: American Hospital Association 2007 database and 2008 Hospital Compare mortality data.
Disclosures: The researchers reported no financial disclosures. The study was funded by philanthropic contributions from members of the Rand Health Board of Advisors.
Another Judge Strikes Down Individual Mandate
A federal judge in Harrisburg, Pa., ruled Sept. 13 that the Affordable Care Act’s requirement that individuals purchase health insurance is unconstitutional.
U.S. District Judge Christopher Conner struck down the so-called individual mandate, saying that the government overstepped its constitutional authority to regulate interstate commerce by requiring that individuals buy health insurance.
This is the fourth time in a month that the courts have ruled on the individual mandate.
In August, a federal appeals court in Atlanta struck down the individual mandate, saying it violated the Commerce clause.
And on Sept. 8, a three-judge panel of the Fourth Circuit Court of Appeals in Richmond, Va., dismissed two separate lawsuits challenging the Affordable Care Act’s individual mandate, both on procedural grounds. Legal experts predict that the constitutionality of the individual mandate will ultimately be decided by the Supreme Court.
The Harrisburg case was brought by Barbara Goudy-Bachman and Gregory Bachman, a married couple from Etters, Pa., who argued they would be adversely affected by the requirement to purchase insurance in 2014. The couple is self-employed and currently do not have health insurance.
In court documents, the Bachmans said that if they were required to purchase health insurance, they would not be able to afford the payments on a new car they want to purchase.
A federal judge in Harrisburg, Pa., ruled Sept. 13 that the Affordable Care Act’s requirement that individuals purchase health insurance is unconstitutional.
U.S. District Judge Christopher Conner struck down the so-called individual mandate, saying that the government overstepped its constitutional authority to regulate interstate commerce by requiring that individuals buy health insurance.
This is the fourth time in a month that the courts have ruled on the individual mandate.
In August, a federal appeals court in Atlanta struck down the individual mandate, saying it violated the Commerce clause.
And on Sept. 8, a three-judge panel of the Fourth Circuit Court of Appeals in Richmond, Va., dismissed two separate lawsuits challenging the Affordable Care Act’s individual mandate, both on procedural grounds. Legal experts predict that the constitutionality of the individual mandate will ultimately be decided by the Supreme Court.
The Harrisburg case was brought by Barbara Goudy-Bachman and Gregory Bachman, a married couple from Etters, Pa., who argued they would be adversely affected by the requirement to purchase insurance in 2014. The couple is self-employed and currently do not have health insurance.
In court documents, the Bachmans said that if they were required to purchase health insurance, they would not be able to afford the payments on a new car they want to purchase.
A federal judge in Harrisburg, Pa., ruled Sept. 13 that the Affordable Care Act’s requirement that individuals purchase health insurance is unconstitutional.
U.S. District Judge Christopher Conner struck down the so-called individual mandate, saying that the government overstepped its constitutional authority to regulate interstate commerce by requiring that individuals buy health insurance.
This is the fourth time in a month that the courts have ruled on the individual mandate.
In August, a federal appeals court in Atlanta struck down the individual mandate, saying it violated the Commerce clause.
And on Sept. 8, a three-judge panel of the Fourth Circuit Court of Appeals in Richmond, Va., dismissed two separate lawsuits challenging the Affordable Care Act’s individual mandate, both on procedural grounds. Legal experts predict that the constitutionality of the individual mandate will ultimately be decided by the Supreme Court.
The Harrisburg case was brought by Barbara Goudy-Bachman and Gregory Bachman, a married couple from Etters, Pa., who argued they would be adversely affected by the requirement to purchase insurance in 2014. The couple is self-employed and currently do not have health insurance.
In court documents, the Bachmans said that if they were required to purchase health insurance, they would not be able to afford the payments on a new car they want to purchase.
A Million More Were Uninsured in 2010
Nearly 50 million people in the United States lacked health insurance in 2010, up almost a million from the year before, according to statistics released by the Census Bureau on Sept. 13.
While the number of people without insurance rose to 49.9 million in 2010 from 49.0 million the year before, there was no statistically significant change in the uninsurance rate, which was 16.3% in 2010.
A similar trend was seen among children: 9.8% of children (7.3 million) were uninsured in 2010, a rate not significantly different from the rate of 9.7% in 2009.
Other age groups did experience significant changes. Among those aged 65 years and older, the uninsurance rate in 2010 increased to 2.0%, up from 1.7% in 2009. During a press briefing, Census Bureau officials said they could not offer an explanation for the increase in this age group, which traditionally has very low uninsurance rates because of Medicare coverage. The uninsurance rate also rose among people aged 35-64 years.
However, more young adults aged 18-24 years became insured in 2010. The uninsurance rate for that group dropped to 27.2% in 2010 from 29.3% the year before. A provision of the Affordable Care Act that allows parents to keep children on their health insurance policy up to age 26 could be a factor in the increase in coverage in this age group, Brett O’Hara, Ph.D., chief of the Health and Disability Statistics Branch at the Census Bureau, said during a press briefing.
The report also showed that once again, private insurance coverage in the United States is declining while public coverage is increasing. Employment-based insurance dropped to 55.3% in 2010 from 56.1% in 2009. The number of people who received their health insurance through their employer fell from 170.8 million to 169.3 million.
At the same time, the number of people covered by government-sponsored health insurance increased by nearly 2 million, bringing the total number to 95 million in 2010.
Nearly 50 million people in the United States lacked health insurance in 2010, up almost a million from the year before, according to statistics released by the Census Bureau on Sept. 13.
While the number of people without insurance rose to 49.9 million in 2010 from 49.0 million the year before, there was no statistically significant change in the uninsurance rate, which was 16.3% in 2010.
A similar trend was seen among children: 9.8% of children (7.3 million) were uninsured in 2010, a rate not significantly different from the rate of 9.7% in 2009.
Other age groups did experience significant changes. Among those aged 65 years and older, the uninsurance rate in 2010 increased to 2.0%, up from 1.7% in 2009. During a press briefing, Census Bureau officials said they could not offer an explanation for the increase in this age group, which traditionally has very low uninsurance rates because of Medicare coverage. The uninsurance rate also rose among people aged 35-64 years.
However, more young adults aged 18-24 years became insured in 2010. The uninsurance rate for that group dropped to 27.2% in 2010 from 29.3% the year before. A provision of the Affordable Care Act that allows parents to keep children on their health insurance policy up to age 26 could be a factor in the increase in coverage in this age group, Brett O’Hara, Ph.D., chief of the Health and Disability Statistics Branch at the Census Bureau, said during a press briefing.
The report also showed that once again, private insurance coverage in the United States is declining while public coverage is increasing. Employment-based insurance dropped to 55.3% in 2010 from 56.1% in 2009. The number of people who received their health insurance through their employer fell from 170.8 million to 169.3 million.
At the same time, the number of people covered by government-sponsored health insurance increased by nearly 2 million, bringing the total number to 95 million in 2010.
Nearly 50 million people in the United States lacked health insurance in 2010, up almost a million from the year before, according to statistics released by the Census Bureau on Sept. 13.
While the number of people without insurance rose to 49.9 million in 2010 from 49.0 million the year before, there was no statistically significant change in the uninsurance rate, which was 16.3% in 2010.
A similar trend was seen among children: 9.8% of children (7.3 million) were uninsured in 2010, a rate not significantly different from the rate of 9.7% in 2009.
Other age groups did experience significant changes. Among those aged 65 years and older, the uninsurance rate in 2010 increased to 2.0%, up from 1.7% in 2009. During a press briefing, Census Bureau officials said they could not offer an explanation for the increase in this age group, which traditionally has very low uninsurance rates because of Medicare coverage. The uninsurance rate also rose among people aged 35-64 years.
However, more young adults aged 18-24 years became insured in 2010. The uninsurance rate for that group dropped to 27.2% in 2010 from 29.3% the year before. A provision of the Affordable Care Act that allows parents to keep children on their health insurance policy up to age 26 could be a factor in the increase in coverage in this age group, Brett O’Hara, Ph.D., chief of the Health and Disability Statistics Branch at the Census Bureau, said during a press briefing.
The report also showed that once again, private insurance coverage in the United States is declining while public coverage is increasing. Employment-based insurance dropped to 55.3% in 2010 from 56.1% in 2009. The number of people who received their health insurance through their employer fell from 170.8 million to 169.3 million.
At the same time, the number of people covered by government-sponsored health insurance increased by nearly 2 million, bringing the total number to 95 million in 2010.
FROM THE CENSUS BUREAU REPORT ON INCOME, POVERTY, AND HEALTH INSURANCE COVERAGE, 2010
Court Tosses Out Lawsuits Challenging Health Reform
Supporters of the Affordable Care Act scored a legal victory as a federal appeals court dismissed a pair of lawsuits challenging the constitutionality of the so-called individual mandate to buy health insurance.
On Sept. 8, a three-judge panel of the Fourth Circuit Court of Appeals in Richmond, Va., tossed out a suit brought by Virginia’s Attorney General Ken Cuccinelli. They concluded that Virginia did not have the legal standing to challenge the individual mandate because it will affect individuals, not the state.
Mr. Cuccinelli argued that the individual mandate violated the "Virginia Health Care Freedom Act," a state law that says no resident can be required to obtain insurance. The panel of judges rejected that argument, writing that the Virginia law, which was signed after the Affordable Care Act was enacted, was essentially a ploy to set up a legal challenge to the health reform law. The appeals court did not address whether the individual mandate was constitutional.
In the second ruling on Sept. 8, the same three-judge panel dismissed a challenge brought by Liberty University, a Christian college in Lynchburg, Va. In that case, Liberty University charged that law’s tax penalties for individuals and employers were unconstitutional. The appeals court ruled that the university also lacked standing because it cannot challenge the provisions until they take effect in 2014.
Both cases were sent back to district court with instructions that they be dismissed.
Today’s ruling come on the heels of a federal appeals court decision in August that the individual mandate was unconstitutional and must be thrown out. There are currently more than 25 active legal challenges to the Affordable Care Act working their way through courthouses around the country. One of those cases is expected to reach the Supreme Court in the next few years.
Supporters of the Affordable Care Act scored a legal victory as a federal appeals court dismissed a pair of lawsuits challenging the constitutionality of the so-called individual mandate to buy health insurance.
On Sept. 8, a three-judge panel of the Fourth Circuit Court of Appeals in Richmond, Va., tossed out a suit brought by Virginia’s Attorney General Ken Cuccinelli. They concluded that Virginia did not have the legal standing to challenge the individual mandate because it will affect individuals, not the state.
Mr. Cuccinelli argued that the individual mandate violated the "Virginia Health Care Freedom Act," a state law that says no resident can be required to obtain insurance. The panel of judges rejected that argument, writing that the Virginia law, which was signed after the Affordable Care Act was enacted, was essentially a ploy to set up a legal challenge to the health reform law. The appeals court did not address whether the individual mandate was constitutional.
In the second ruling on Sept. 8, the same three-judge panel dismissed a challenge brought by Liberty University, a Christian college in Lynchburg, Va. In that case, Liberty University charged that law’s tax penalties for individuals and employers were unconstitutional. The appeals court ruled that the university also lacked standing because it cannot challenge the provisions until they take effect in 2014.
Both cases were sent back to district court with instructions that they be dismissed.
Today’s ruling come on the heels of a federal appeals court decision in August that the individual mandate was unconstitutional and must be thrown out. There are currently more than 25 active legal challenges to the Affordable Care Act working their way through courthouses around the country. One of those cases is expected to reach the Supreme Court in the next few years.
Supporters of the Affordable Care Act scored a legal victory as a federal appeals court dismissed a pair of lawsuits challenging the constitutionality of the so-called individual mandate to buy health insurance.
On Sept. 8, a three-judge panel of the Fourth Circuit Court of Appeals in Richmond, Va., tossed out a suit brought by Virginia’s Attorney General Ken Cuccinelli. They concluded that Virginia did not have the legal standing to challenge the individual mandate because it will affect individuals, not the state.
Mr. Cuccinelli argued that the individual mandate violated the "Virginia Health Care Freedom Act," a state law that says no resident can be required to obtain insurance. The panel of judges rejected that argument, writing that the Virginia law, which was signed after the Affordable Care Act was enacted, was essentially a ploy to set up a legal challenge to the health reform law. The appeals court did not address whether the individual mandate was constitutional.
In the second ruling on Sept. 8, the same three-judge panel dismissed a challenge brought by Liberty University, a Christian college in Lynchburg, Va. In that case, Liberty University charged that law’s tax penalties for individuals and employers were unconstitutional. The appeals court ruled that the university also lacked standing because it cannot challenge the provisions until they take effect in 2014.
Both cases were sent back to district court with instructions that they be dismissed.
Today’s ruling come on the heels of a federal appeals court decision in August that the individual mandate was unconstitutional and must be thrown out. There are currently more than 25 active legal challenges to the Affordable Care Act working their way through courthouses around the country. One of those cases is expected to reach the Supreme Court in the next few years.
HHS Plans Revamp of Human Research Rules
The federal government plans to overhaul the rules for conducting research with human subjects with the aim of bringing the regulations in line with research in the 21st century.
The Department of Health and Human Services published the advance notice of proposed rule making on human subjects research in the Federal Register on July 26. The proposal seeks public comment on a series of possible changes, from relying on a single institutional review board for multicenter studies to simplifying informed consent forms. This is the first time the regulations on human subjects’ research, known as the Common Rule, have been updated since 1991.
While the Common Rule was a landmark development in the protection of research participants, those rules were developed during a "simpler time," Dr. Howard Koh, assistant secretary for health at HHS, said during a briefing with reporters on June 22. Twenty years later, human subjects’ research includes a variety of new areas such as genomics and behavioral and social science research, as well as studies utilizing the Internet and large-scale data networks.

"These changes in the research landscape have raised questions regarding the effectiveness of the current regulatory framework," he said.
With that in mind, HHS is proposing to offer greater protection to study participants in several ways, such as:
• Giving participants the right to say whether researchers can use their biospecimens in future research.
• Helping researchers craft easier to understand informed consent forms.
• Making security and information protections uniform across studies with potentially identifiable patient information.
• Developing a more systematic approach to collecting adverse event data from ongoing studies.
Officials also aim to ease regulatory burdens in the following ways:
• Designing review requirements to match the risk posed to research subjects.
• Ensuring that any guidance issued by the federal government is consistent across departments.
• Allowing multiple sites to be overseen by a single institutional review board.
HHS also seeks to expand the reach of the regulation by extending it to all studies conducted by institutions that receive federal funding for human subjects’ research from a Common Rule agency.
Mary Woolley, president and CEO of Research!America, a not-for-profit organization that advocates for public and private funding of medical research, said the proposal benefits both patients and researchers because it streamlines the process while adding patient protections.
"We’re going to speed the conduct of research and thus speed the day when we have more and more personalized medicine based on research," she said.
Dr. Holly A. Taylor, Ph.D., of the Berman Institute of Bioethics at the Johns Hopkins University, Baltimore, praised the regulation’s focus on improving the informed consent process.
Dr. Taylor, who has conducted research on informed consent, said she agrees with HHS that, in many cases, the forms have become too long and complex for patients to understand. She urged the agency to work with investigators, who aren’t trained to write for a consumer audience.
Comments are accepted on the proposed rule making at www.regulations.gov until 5 p.m. ET on Sept. 26.
The federal government plans to overhaul the rules for conducting research with human subjects with the aim of bringing the regulations in line with research in the 21st century.
The Department of Health and Human Services published the advance notice of proposed rule making on human subjects research in the Federal Register on July 26. The proposal seeks public comment on a series of possible changes, from relying on a single institutional review board for multicenter studies to simplifying informed consent forms. This is the first time the regulations on human subjects’ research, known as the Common Rule, have been updated since 1991.
While the Common Rule was a landmark development in the protection of research participants, those rules were developed during a "simpler time," Dr. Howard Koh, assistant secretary for health at HHS, said during a briefing with reporters on June 22. Twenty years later, human subjects’ research includes a variety of new areas such as genomics and behavioral and social science research, as well as studies utilizing the Internet and large-scale data networks.
"These changes in the research landscape have raised questions regarding the effectiveness of the current regulatory framework," he said.
With that in mind, HHS is proposing to offer greater protection to study participants in several ways, such as:
• Giving participants the right to say whether researchers can use their biospecimens in future research.
• Helping researchers craft easier to understand informed consent forms.
• Making security and information protections uniform across studies with potentially identifiable patient information.
• Developing a more systematic approach to collecting adverse event data from ongoing studies.
Officials also aim to ease regulatory burdens in the following ways:
• Designing review requirements to match the risk posed to research subjects.
• Ensuring that any guidance issued by the federal government is consistent across departments.
• Allowing multiple sites to be overseen by a single institutional review board.
HHS also seeks to expand the reach of the regulation by extending it to all studies conducted by institutions that receive federal funding for human subjects’ research from a Common Rule agency.
Mary Woolley, president and CEO of Research!America, a not-for-profit organization that advocates for public and private funding of medical research, said the proposal benefits both patients and researchers because it streamlines the process while adding patient protections.
"We’re going to speed the conduct of research and thus speed the day when we have more and more personalized medicine based on research," she said.
Dr. Holly A. Taylor, Ph.D., of the Berman Institute of Bioethics at the Johns Hopkins University, Baltimore, praised the regulation’s focus on improving the informed consent process.
Dr. Taylor, who has conducted research on informed consent, said she agrees with HHS that, in many cases, the forms have become too long and complex for patients to understand. She urged the agency to work with investigators, who aren’t trained to write for a consumer audience.
Comments are accepted on the proposed rule making at www.regulations.gov until 5 p.m. ET on Sept. 26.
The federal government plans to overhaul the rules for conducting research with human subjects with the aim of bringing the regulations in line with research in the 21st century.
The Department of Health and Human Services published the advance notice of proposed rule making on human subjects research in the Federal Register on July 26. The proposal seeks public comment on a series of possible changes, from relying on a single institutional review board for multicenter studies to simplifying informed consent forms. This is the first time the regulations on human subjects’ research, known as the Common Rule, have been updated since 1991.
While the Common Rule was a landmark development in the protection of research participants, those rules were developed during a "simpler time," Dr. Howard Koh, assistant secretary for health at HHS, said during a briefing with reporters on June 22. Twenty years later, human subjects’ research includes a variety of new areas such as genomics and behavioral and social science research, as well as studies utilizing the Internet and large-scale data networks.
"These changes in the research landscape have raised questions regarding the effectiveness of the current regulatory framework," he said.
With that in mind, HHS is proposing to offer greater protection to study participants in several ways, such as:
• Giving participants the right to say whether researchers can use their biospecimens in future research.
• Helping researchers craft easier to understand informed consent forms.
• Making security and information protections uniform across studies with potentially identifiable patient information.
• Developing a more systematic approach to collecting adverse event data from ongoing studies.
Officials also aim to ease regulatory burdens in the following ways:
• Designing review requirements to match the risk posed to research subjects.
• Ensuring that any guidance issued by the federal government is consistent across departments.
• Allowing multiple sites to be overseen by a single institutional review board.
HHS also seeks to expand the reach of the regulation by extending it to all studies conducted by institutions that receive federal funding for human subjects’ research from a Common Rule agency.
Mary Woolley, president and CEO of Research!America, a not-for-profit organization that advocates for public and private funding of medical research, said the proposal benefits both patients and researchers because it streamlines the process while adding patient protections.
"We’re going to speed the conduct of research and thus speed the day when we have more and more personalized medicine based on research," she said.
Dr. Holly A. Taylor, Ph.D., of the Berman Institute of Bioethics at the Johns Hopkins University, Baltimore, praised the regulation’s focus on improving the informed consent process.
Dr. Taylor, who has conducted research on informed consent, said she agrees with HHS that, in many cases, the forms have become too long and complex for patients to understand. She urged the agency to work with investigators, who aren’t trained to write for a consumer audience.
Comments are accepted on the proposed rule making at www.regulations.gov until 5 p.m. ET on Sept. 26.
Joint Commission Steps Up Efforts to Reduce Wrong-Site Surgery
Procedures performed on the wrong side of the body, the wrong site, and even the wrong patient continue to happen at a national rate as high as 40 times every week, according to Dr. Mark R. Chassin, president of the Joint Commission at a recent teleconference.
One example of improvements is Rhode Island Hospital in Providence. In November 2009, the hospital was facing a $150,000 fine from the state health department and an order to install video cameras in all operating rooms after reports of five wrong-site surgeries in 2 years.
Today, officials at the hospital say they have changed their ways and they have the safety record to prove it. There have been no wrong-site surgeries at the hospital in about 20 months, according to Dr. Mary Reich Cooper, chief quality officer for Lifespan Corp., which owns Rhode Island Hospital.
"We were able to show the front-line staff – as well as the surgeons and the patients coming into the hospital – that not only was safety our first priority, but we [also] were prepared to put a tremendous amount of resources into making safety our first priority," Dr. Cooper said.
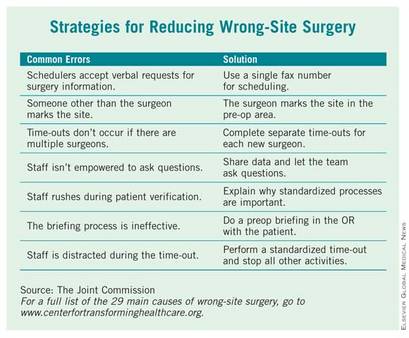
Lifespan’s Rhode Island Hospital is one of eight hospitals and ambulatory surgery centers that are working with the Joint Commission’s Center for Transforming Healthcare on a project to reduce wrong-site surgery. As a result of that project, which started at Rhode Island Hospital in 2009, the Joint Commission released a set of potential causes of wrong-site surgery and the targeted fixes that hospitals and surgery centers can use to eliminate them (see box). The plan is to begin adding those interventions to a Targeted Solutions Tool, an electronic application to allow all accredited or certified organizations to access the information and customize it.
The results of the project will give hospitals and surgery centers around the country a road map for pinpointing and measuring their risks of wrong-site surgery, said Dr. Chassin. He advised hospitals to start reviewing risks at the very beginning of the process, when an operation is scheduled. The Joint Commission’s project revealed that in 39% of cases, errors that increased the risk of wrong-site surgery were introduced during the scheduling process.
The scheduling process is ripe for errors, Dr. Chassin said, because the person supplying the patient and procedure information typically works in the surgeon’s office and often is not directly affiliated with the hospital or center where the surgery will take place. If that person is dealing with many different hospitals and surgery centers, all with different processes and requirements, it’s easy to get confused and relay incomplete or inaccurate information, he said.
And the scheduling process is just one area identified by the Joint Commission as having potential for errors that could lead to wrong-site surgery. The eight pilot organizations, some of which have never had a wrong-site surgery in their facility, found risks in all phases of their surgical processes ranging from inconsistent procedures for marking the surgical site to omissions in the "time-out" process just before surgery.
"It turns out that this is a much more complicated problem than it might seem to be at first," Dr. Chassin said. But developing specific fixes for each of those risks has helped to sharply reduce the chances of wrong-site surgeries at the eight pilot sites, he added For example, addressing documentation and verification issues in the preoperative holding areas decreased the percentage of cases with risks from a baseline of 52% to 19%.
At Rhode Island Hospital, efforts were made to improve the "time-out" before surgery. All other activities were stopped to allow operating room personnel to focus, and they used a script to ensure that all last-minute safety checks – such as asking everyone in the operating room if they could see the surgical mark – were completed, Dr. Cooper said.
The Joint Commission has been working on wrong-site surgery for a number of years, issuing Sentinel Event alerts in 1998 and 2001 and developing the Universal Protocol, a standardized approach to eliminating risks for wrong-site surgery.
Procedures performed on the wrong side of the body, the wrong site, and even the wrong patient continue to happen at a national rate as high as 40 times every week, according to Dr. Mark R. Chassin, president of the Joint Commission at a recent teleconference.
One example of improvements is Rhode Island Hospital in Providence. In November 2009, the hospital was facing a $150,000 fine from the state health department and an order to install video cameras in all operating rooms after reports of five wrong-site surgeries in 2 years.
Today, officials at the hospital say they have changed their ways and they have the safety record to prove it. There have been no wrong-site surgeries at the hospital in about 20 months, according to Dr. Mary Reich Cooper, chief quality officer for Lifespan Corp., which owns Rhode Island Hospital.
"We were able to show the front-line staff – as well as the surgeons and the patients coming into the hospital – that not only was safety our first priority, but we [also] were prepared to put a tremendous amount of resources into making safety our first priority," Dr. Cooper said.
Lifespan’s Rhode Island Hospital is one of eight hospitals and ambulatory surgery centers that are working with the Joint Commission’s Center for Transforming Healthcare on a project to reduce wrong-site surgery. As a result of that project, which started at Rhode Island Hospital in 2009, the Joint Commission released a set of potential causes of wrong-site surgery and the targeted fixes that hospitals and surgery centers can use to eliminate them (see box). The plan is to begin adding those interventions to a Targeted Solutions Tool, an electronic application to allow all accredited or certified organizations to access the information and customize it.
The results of the project will give hospitals and surgery centers around the country a road map for pinpointing and measuring their risks of wrong-site surgery, said Dr. Chassin. He advised hospitals to start reviewing risks at the very beginning of the process, when an operation is scheduled. The Joint Commission’s project revealed that in 39% of cases, errors that increased the risk of wrong-site surgery were introduced during the scheduling process.
The scheduling process is ripe for errors, Dr. Chassin said, because the person supplying the patient and procedure information typically works in the surgeon’s office and often is not directly affiliated with the hospital or center where the surgery will take place. If that person is dealing with many different hospitals and surgery centers, all with different processes and requirements, it’s easy to get confused and relay incomplete or inaccurate information, he said.
And the scheduling process is just one area identified by the Joint Commission as having potential for errors that could lead to wrong-site surgery. The eight pilot organizations, some of which have never had a wrong-site surgery in their facility, found risks in all phases of their surgical processes ranging from inconsistent procedures for marking the surgical site to omissions in the "time-out" process just before surgery.
"It turns out that this is a much more complicated problem than it might seem to be at first," Dr. Chassin said. But developing specific fixes for each of those risks has helped to sharply reduce the chances of wrong-site surgeries at the eight pilot sites, he added For example, addressing documentation and verification issues in the preoperative holding areas decreased the percentage of cases with risks from a baseline of 52% to 19%.
At Rhode Island Hospital, efforts were made to improve the "time-out" before surgery. All other activities were stopped to allow operating room personnel to focus, and they used a script to ensure that all last-minute safety checks – such as asking everyone in the operating room if they could see the surgical mark – were completed, Dr. Cooper said.
The Joint Commission has been working on wrong-site surgery for a number of years, issuing Sentinel Event alerts in 1998 and 2001 and developing the Universal Protocol, a standardized approach to eliminating risks for wrong-site surgery.
Procedures performed on the wrong side of the body, the wrong site, and even the wrong patient continue to happen at a national rate as high as 40 times every week, according to Dr. Mark R. Chassin, president of the Joint Commission at a recent teleconference.
One example of improvements is Rhode Island Hospital in Providence. In November 2009, the hospital was facing a $150,000 fine from the state health department and an order to install video cameras in all operating rooms after reports of five wrong-site surgeries in 2 years.
Today, officials at the hospital say they have changed their ways and they have the safety record to prove it. There have been no wrong-site surgeries at the hospital in about 20 months, according to Dr. Mary Reich Cooper, chief quality officer for Lifespan Corp., which owns Rhode Island Hospital.
"We were able to show the front-line staff – as well as the surgeons and the patients coming into the hospital – that not only was safety our first priority, but we [also] were prepared to put a tremendous amount of resources into making safety our first priority," Dr. Cooper said.
Lifespan’s Rhode Island Hospital is one of eight hospitals and ambulatory surgery centers that are working with the Joint Commission’s Center for Transforming Healthcare on a project to reduce wrong-site surgery. As a result of that project, which started at Rhode Island Hospital in 2009, the Joint Commission released a set of potential causes of wrong-site surgery and the targeted fixes that hospitals and surgery centers can use to eliminate them (see box). The plan is to begin adding those interventions to a Targeted Solutions Tool, an electronic application to allow all accredited or certified organizations to access the information and customize it.
The results of the project will give hospitals and surgery centers around the country a road map for pinpointing and measuring their risks of wrong-site surgery, said Dr. Chassin. He advised hospitals to start reviewing risks at the very beginning of the process, when an operation is scheduled. The Joint Commission’s project revealed that in 39% of cases, errors that increased the risk of wrong-site surgery were introduced during the scheduling process.
The scheduling process is ripe for errors, Dr. Chassin said, because the person supplying the patient and procedure information typically works in the surgeon’s office and often is not directly affiliated with the hospital or center where the surgery will take place. If that person is dealing with many different hospitals and surgery centers, all with different processes and requirements, it’s easy to get confused and relay incomplete or inaccurate information, he said.
And the scheduling process is just one area identified by the Joint Commission as having potential for errors that could lead to wrong-site surgery. The eight pilot organizations, some of which have never had a wrong-site surgery in their facility, found risks in all phases of their surgical processes ranging from inconsistent procedures for marking the surgical site to omissions in the "time-out" process just before surgery.
"It turns out that this is a much more complicated problem than it might seem to be at first," Dr. Chassin said. But developing specific fixes for each of those risks has helped to sharply reduce the chances of wrong-site surgeries at the eight pilot sites, he added For example, addressing documentation and verification issues in the preoperative holding areas decreased the percentage of cases with risks from a baseline of 52% to 19%.
At Rhode Island Hospital, efforts were made to improve the "time-out" before surgery. All other activities were stopped to allow operating room personnel to focus, and they used a script to ensure that all last-minute safety checks – such as asking everyone in the operating room if they could see the surgical mark – were completed, Dr. Cooper said.
The Joint Commission has been working on wrong-site surgery for a number of years, issuing Sentinel Event alerts in 1998 and 2001 and developing the Universal Protocol, a standardized approach to eliminating risks for wrong-site surgery.
Leaders: Neurohospitalist Helps Define New Specialty Niche
Dr. David Likosky is helping to shape the future for neurologists who practice primarily in the hospital.
Dr. Likosky, director of the stroke program at Evergreen Hospital Medical Center in Kirkland, Wash., was the founding chair of the neurohospitalist section of the American Academy of Neurology and cofounder of the Neurohospitalist Society. As a leader in these organizations, he is helping to define the role of the "neurohospitalist."

In an interview with Hospitalist News, Dr. Likosky shared his thoughts on the growing field and how neurohospitalists can help their medicine hospitalist colleagues.
Hospitalist News: Who is the typical neurohospitalist and how does he or she get into the field?
Dr. Likosky: The field is still young so the typical neurohospitalist remains to be defined. I’d say overall, neurohospitalists skew younger. They are people who are more likely to be new in practice or just out of residency, and are more familiar with the internal medicine hospitalist model and comfortable with that model of care. A number of neurohospitalists are trained in vascular neurology as well, and there’s a lot of overlap between neurohospitalists and vascular neurologists.
HN: What attracted you to hospital medicine?
Dr. Likosky: I’ve never practiced in an office. I’ve always enjoyed the inpatient population. Some people see neurohospitalist work as an escape from having to run a practice. In some ways, that’s true. But, at the same time, you still have to manage your practice, there’s just a different set of issues, politics, and dynamics. For me, it was mostly about having a chance to practice internal medicine and neurology in the hospital with patients who are sick or very sick. The other great thing about working in the hospital is the opportunity to work on systems of care and quality metrics in a more controlled environment.
HN: Are more hospitals paying for so-called stroke call, and how does call compensation help or harm the development of the neurohospitalist field?
Dr. Likosky: More hospitals are paying for stroke call. Much of that is due to the pressure for hospitals to become certified as stroke centers by the Joint Commission. Some of it is as a result of medicine hospitalists pressuring hospitals to make sure that they have neurology backup. But no matter what the pressures are, it does seem to be an increasing trend overall. One of the things that paying for a stroke call does is to foster an environment in which the hospital administration is willing to pay for a neurohospitalist program or to subsidize a neurohospitalist program.
HN: You teach neurology courses to internal medicine–trained hospitalists, what’s their comfort level with neurology, and how can neurohospitalists assist them?
Dr. Likosky: Internal medicine hospitalists, when they leave residency and go into practice, are frequently uncomfortable with the amount of neurology that they’re seeing and feel inadequately prepared. They look for help from their neurologist colleagues. But even with a neurologist working in a nearby clinic, a hospitalist may not always feel comfortable interrupting them or asking for assistance. A neurohospitalist, who is in the hospital and dedicated to inpatient care, is available and is a great help to your average medicine hospitalist. It’s a great partnership.
HN: What has been the reaction of your community-based neurology colleagues to the emergence of neurohospitalists?
Dr. Likosky: Most are very happy to have a neurohospitalist in the community. It lightens up the call schedule, particularly during the day. So when their office is busy, there’s less of a need to reschedule patients or cancel parts of the day. Few see it as competition and, if set up well, a program can benefit all. By and large, your average community-based neurologist is very happy to have a neurohospitalist program around whether as a part of their practice or not. It’s a good source of referrals for them and may remove the type of work with which they are either uncomfortable, unhappy, or just don’t have the time to do.
Take us to your leader. Nominate a hospitalist whose work inspires you. E-mail suggestions to [email protected] and read previous columns at ehospitalistnews.com.
Dr. David Likosky is helping to shape the future for neurologists who practice primarily in the hospital.
Dr. Likosky, director of the stroke program at Evergreen Hospital Medical Center in Kirkland, Wash., was the founding chair of the neurohospitalist section of the American Academy of Neurology and cofounder of the Neurohospitalist Society. As a leader in these organizations, he is helping to define the role of the "neurohospitalist."
In an interview with Hospitalist News, Dr. Likosky shared his thoughts on the growing field and how neurohospitalists can help their medicine hospitalist colleagues.
Hospitalist News: Who is the typical neurohospitalist and how does he or she get into the field?
Dr. Likosky: The field is still young so the typical neurohospitalist remains to be defined. I’d say overall, neurohospitalists skew younger. They are people who are more likely to be new in practice or just out of residency, and are more familiar with the internal medicine hospitalist model and comfortable with that model of care. A number of neurohospitalists are trained in vascular neurology as well, and there’s a lot of overlap between neurohospitalists and vascular neurologists.
HN: What attracted you to hospital medicine?
Dr. Likosky: I’ve never practiced in an office. I’ve always enjoyed the inpatient population. Some people see neurohospitalist work as an escape from having to run a practice. In some ways, that’s true. But, at the same time, you still have to manage your practice, there’s just a different set of issues, politics, and dynamics. For me, it was mostly about having a chance to practice internal medicine and neurology in the hospital with patients who are sick or very sick. The other great thing about working in the hospital is the opportunity to work on systems of care and quality metrics in a more controlled environment.
HN: Are more hospitals paying for so-called stroke call, and how does call compensation help or harm the development of the neurohospitalist field?
Dr. Likosky: More hospitals are paying for stroke call. Much of that is due to the pressure for hospitals to become certified as stroke centers by the Joint Commission. Some of it is as a result of medicine hospitalists pressuring hospitals to make sure that they have neurology backup. But no matter what the pressures are, it does seem to be an increasing trend overall. One of the things that paying for a stroke call does is to foster an environment in which the hospital administration is willing to pay for a neurohospitalist program or to subsidize a neurohospitalist program.
HN: You teach neurology courses to internal medicine–trained hospitalists, what’s their comfort level with neurology, and how can neurohospitalists assist them?
Dr. Likosky: Internal medicine hospitalists, when they leave residency and go into practice, are frequently uncomfortable with the amount of neurology that they’re seeing and feel inadequately prepared. They look for help from their neurologist colleagues. But even with a neurologist working in a nearby clinic, a hospitalist may not always feel comfortable interrupting them or asking for assistance. A neurohospitalist, who is in the hospital and dedicated to inpatient care, is available and is a great help to your average medicine hospitalist. It’s a great partnership.
HN: What has been the reaction of your community-based neurology colleagues to the emergence of neurohospitalists?
Dr. Likosky: Most are very happy to have a neurohospitalist in the community. It lightens up the call schedule, particularly during the day. So when their office is busy, there’s less of a need to reschedule patients or cancel parts of the day. Few see it as competition and, if set up well, a program can benefit all. By and large, your average community-based neurologist is very happy to have a neurohospitalist program around whether as a part of their practice or not. It’s a good source of referrals for them and may remove the type of work with which they are either uncomfortable, unhappy, or just don’t have the time to do.
Take us to your leader. Nominate a hospitalist whose work inspires you. E-mail suggestions to [email protected] and read previous columns at ehospitalistnews.com.
Dr. David Likosky is helping to shape the future for neurologists who practice primarily in the hospital.
Dr. Likosky, director of the stroke program at Evergreen Hospital Medical Center in Kirkland, Wash., was the founding chair of the neurohospitalist section of the American Academy of Neurology and cofounder of the Neurohospitalist Society. As a leader in these organizations, he is helping to define the role of the "neurohospitalist."
In an interview with Hospitalist News, Dr. Likosky shared his thoughts on the growing field and how neurohospitalists can help their medicine hospitalist colleagues.
Hospitalist News: Who is the typical neurohospitalist and how does he or she get into the field?
Dr. Likosky: The field is still young so the typical neurohospitalist remains to be defined. I’d say overall, neurohospitalists skew younger. They are people who are more likely to be new in practice or just out of residency, and are more familiar with the internal medicine hospitalist model and comfortable with that model of care. A number of neurohospitalists are trained in vascular neurology as well, and there’s a lot of overlap between neurohospitalists and vascular neurologists.
HN: What attracted you to hospital medicine?
Dr. Likosky: I’ve never practiced in an office. I’ve always enjoyed the inpatient population. Some people see neurohospitalist work as an escape from having to run a practice. In some ways, that’s true. But, at the same time, you still have to manage your practice, there’s just a different set of issues, politics, and dynamics. For me, it was mostly about having a chance to practice internal medicine and neurology in the hospital with patients who are sick or very sick. The other great thing about working in the hospital is the opportunity to work on systems of care and quality metrics in a more controlled environment.
HN: Are more hospitals paying for so-called stroke call, and how does call compensation help or harm the development of the neurohospitalist field?
Dr. Likosky: More hospitals are paying for stroke call. Much of that is due to the pressure for hospitals to become certified as stroke centers by the Joint Commission. Some of it is as a result of medicine hospitalists pressuring hospitals to make sure that they have neurology backup. But no matter what the pressures are, it does seem to be an increasing trend overall. One of the things that paying for a stroke call does is to foster an environment in which the hospital administration is willing to pay for a neurohospitalist program or to subsidize a neurohospitalist program.
HN: You teach neurology courses to internal medicine–trained hospitalists, what’s their comfort level with neurology, and how can neurohospitalists assist them?
Dr. Likosky: Internal medicine hospitalists, when they leave residency and go into practice, are frequently uncomfortable with the amount of neurology that they’re seeing and feel inadequately prepared. They look for help from their neurologist colleagues. But even with a neurologist working in a nearby clinic, a hospitalist may not always feel comfortable interrupting them or asking for assistance. A neurohospitalist, who is in the hospital and dedicated to inpatient care, is available and is a great help to your average medicine hospitalist. It’s a great partnership.
HN: What has been the reaction of your community-based neurology colleagues to the emergence of neurohospitalists?
Dr. Likosky: Most are very happy to have a neurohospitalist in the community. It lightens up the call schedule, particularly during the day. So when their office is busy, there’s less of a need to reschedule patients or cancel parts of the day. Few see it as competition and, if set up well, a program can benefit all. By and large, your average community-based neurologist is very happy to have a neurohospitalist program around whether as a part of their practice or not. It’s a good source of referrals for them and may remove the type of work with which they are either uncomfortable, unhappy, or just don’t have the time to do.
Take us to your leader. Nominate a hospitalist whose work inspires you. E-mail suggestions to [email protected] and read previous columns at ehospitalistnews.com.
Hospital-Employed Physicians May Raise Costs
Hospital employment of physicians continues to rise rapidly around the country, but the trend could drive up costs at least in the short term, according to a report released this month.
Physicians who are employed by hospitals are often paid based on their productivity, which offers them an incentive to increase the volume of services. And in some cases, physicians are under pressure from their hospitals to order more expensive tests, according to the report.
The researchers from the Center for Studying Health System Change based their analysis on interviews with nearly 550 physicians, hospital executives, health plan officials, and others, in 12 nationally representative metropolitan communities (Findings From HSC 2011 August [Issue Brief No. 13]).
The communities are Boston; Cleveland; Greenville, S.C.; Indianapolis; Lansing, Mich.; Little Rock, Ark.; Miami; northern New Jersey, Orange County, Calif.; Phoenix; Seattle; and Syracuse, N.Y.
In one area, at least two cardiologists said they declined job offers from a local hospital because they believed the pressure to drive up volume would be stronger there than in their independent cardiology practice, according to the report.
“The acceleration in hospital employment of physicians risks raising costs and not improving quality of care unless payment reforms shift provider incentives away from volume toward higher quality and efficiency,” said Dr. Ann S. O'Malley, who is a senior health researcher at the Center for Studying Health System Change and a coauthor of the study.
The trend toward hospitals' employing more physicians can also drive up costs for the health system because hospitals are able to charge hospital facility fees for office visits and procedures, even when those services are administered in a physician's office. That means that Medicare – and in some cases private insurers – are paying significantly more for the same services simply because the physician is employed by the hospital.
Employment of physicians by hospitals does have the potential to improve quality through better integration of care and communication between physicians. The problem, the researchers noted, is that integration and communication can be slow to improve just because the physicians get their paychecks from the hospital.
Interview respondents from the 12 communities said that the hospital employment model is generally helpful in coordinating care for a single diagnosis, such as heart failure. But integration across all of a patient's medical needs requires more time and effort, they told the researchers.
The research was funded by the Robert Wood Johnson Foundation and the National Institute for Health Care Reform.
Hospital employment of physicians continues to rise rapidly around the country, but the trend could drive up costs at least in the short term, according to a report released this month.
Physicians who are employed by hospitals are often paid based on their productivity, which offers them an incentive to increase the volume of services. And in some cases, physicians are under pressure from their hospitals to order more expensive tests, according to the report.
The researchers from the Center for Studying Health System Change based their analysis on interviews with nearly 550 physicians, hospital executives, health plan officials, and others, in 12 nationally representative metropolitan communities (Findings From HSC 2011 August [Issue Brief No. 13]).
The communities are Boston; Cleveland; Greenville, S.C.; Indianapolis; Lansing, Mich.; Little Rock, Ark.; Miami; northern New Jersey, Orange County, Calif.; Phoenix; Seattle; and Syracuse, N.Y.
In one area, at least two cardiologists said they declined job offers from a local hospital because they believed the pressure to drive up volume would be stronger there than in their independent cardiology practice, according to the report.
“The acceleration in hospital employment of physicians risks raising costs and not improving quality of care unless payment reforms shift provider incentives away from volume toward higher quality and efficiency,” said Dr. Ann S. O'Malley, who is a senior health researcher at the Center for Studying Health System Change and a coauthor of the study.
The trend toward hospitals' employing more physicians can also drive up costs for the health system because hospitals are able to charge hospital facility fees for office visits and procedures, even when those services are administered in a physician's office. That means that Medicare – and in some cases private insurers – are paying significantly more for the same services simply because the physician is employed by the hospital.
Employment of physicians by hospitals does have the potential to improve quality through better integration of care and communication between physicians. The problem, the researchers noted, is that integration and communication can be slow to improve just because the physicians get their paychecks from the hospital.
Interview respondents from the 12 communities said that the hospital employment model is generally helpful in coordinating care for a single diagnosis, such as heart failure. But integration across all of a patient's medical needs requires more time and effort, they told the researchers.
The research was funded by the Robert Wood Johnson Foundation and the National Institute for Health Care Reform.
Hospital employment of physicians continues to rise rapidly around the country, but the trend could drive up costs at least in the short term, according to a report released this month.
Physicians who are employed by hospitals are often paid based on their productivity, which offers them an incentive to increase the volume of services. And in some cases, physicians are under pressure from their hospitals to order more expensive tests, according to the report.
The researchers from the Center for Studying Health System Change based their analysis on interviews with nearly 550 physicians, hospital executives, health plan officials, and others, in 12 nationally representative metropolitan communities (Findings From HSC 2011 August [Issue Brief No. 13]).
The communities are Boston; Cleveland; Greenville, S.C.; Indianapolis; Lansing, Mich.; Little Rock, Ark.; Miami; northern New Jersey, Orange County, Calif.; Phoenix; Seattle; and Syracuse, N.Y.
In one area, at least two cardiologists said they declined job offers from a local hospital because they believed the pressure to drive up volume would be stronger there than in their independent cardiology practice, according to the report.
“The acceleration in hospital employment of physicians risks raising costs and not improving quality of care unless payment reforms shift provider incentives away from volume toward higher quality and efficiency,” said Dr. Ann S. O'Malley, who is a senior health researcher at the Center for Studying Health System Change and a coauthor of the study.
The trend toward hospitals' employing more physicians can also drive up costs for the health system because hospitals are able to charge hospital facility fees for office visits and procedures, even when those services are administered in a physician's office. That means that Medicare – and in some cases private insurers – are paying significantly more for the same services simply because the physician is employed by the hospital.
Employment of physicians by hospitals does have the potential to improve quality through better integration of care and communication between physicians. The problem, the researchers noted, is that integration and communication can be slow to improve just because the physicians get their paychecks from the hospital.
Interview respondents from the 12 communities said that the hospital employment model is generally helpful in coordinating care for a single diagnosis, such as heart failure. But integration across all of a patient's medical needs requires more time and effort, they told the researchers.
The research was funded by the Robert Wood Johnson Foundation and the National Institute for Health Care Reform.
An Analysis from the Center for Studying Health System Change