User login
Two New Projects Embark on the Search for Parkinson's Biomarkers
Private and public sources are launching two massive efforts to identify biomarkers for Parkinson’s disease – an effort they say will speed drug research, providing more efficient ways to track disease progress and monitor therapeutic response.
In late September, the Michael J. Fox Foundation kicked off its Parkinson’s Progression Markers Initiative (PPMI) and the National Institute for Neurological Disorders and Stroke sent out a request for applications to create the Parkinson’s Disease Biomarker Identification Network (PD-BIN). The 5-year PPMI is the first large-scale clinical study to focus exclusively on identifying and validating both chemical and imaging biomarkers of the disease. The multiproject PD-BIN will be similarly devoted to identifying biological markers that contribute to an individual’s risk for Parkinson’s disease, as well as its onset and progression, with the goal of speeding disease-modifying treatments.
“We expect that the biomarkers we discover will help us better understand the disease and accelerate therapeutic trials, with the goal of assessing whether a drug can modify the progression of Parkinson’s,” PPMI primary investigator Dr. Kenneth Marek said in an interview. “In a way, this is much more complex than a clinical treatment trial. We are not testing a drug, but ideally, we will find markers that can pave the way to accomplish more effective drug testing, and speed the development of much-needed therapies for this disease.”
Speaking from the World Parkinson Congress in Glasgow, Scotland, where he unveiled the PPMI to the scientific community, Dr. Marek stressed the need for objective, measurable disease markers in diagnosis and disease progression, as well as in research studies. The diagnosis of Parkinson’s disease remains solely based on clinical signs and symptoms, with no concrete diagnostic measure. Progression, as well, can be measured only by the worsening of symptoms. And with no objective clinical measurements in hand, researchers are “shooting in the dark” when assessing response to candidate drugs, he said.
“We have been conducting these clinical trials, but we there is no way to assess when a drug is ineffective, or how to get a better sense of whether the next one will actually work,” said Dr. Marek, who also is president of the Institute for Neurodegenerative Disorders in New Haven, Conn.
Having a set of biomarkers will speed research in a way that is not now possible, said PPMI co-investigator Dr. Tanya Simuni, director of the Parkinson’s Disease and Movement Disorders Center at Northwestern University, Chicago.
“We have many ongoing clinical trials of potential disease-modifying agents, but they are slow to progress because clinical assessment is the primary efficacy measure,” Dr. Simuni said in an interview. “Because of this, these studies take a long time and need a large number of patients – and they still sometimes end up with inconclusive results. If we had an objective measure of disease progression, that would speed drug development by reducing the duration of the studies and the number of participants needed for each one.”
The discovery of a biomarker could also help clinicians identify patients in the very earliest – perhaps even prodromal – disease state, she said. “By the time symptoms of Parkinson’s appear, patients can have lost up to 70% of their dopamine-producing cells, which tells us that there is a prodromal or preclinical phase during which damage is occurring without clinical signs. Biomarkers could not only help us develop better interventions but also screening tools. It’s conceivable that in the future, we could screen for Parkinson’s in the same way that we now screen for breast cancer or other medical conditions.”
The PPMI will be conducted at 14 U.S. centers and at centers in Innsbruck, Austria; Kassel and Tubingen Germany; and Naples, Italy. It aims to recruit 200 healthy control patients and 400 patients newly diagnosed with Parkinson’s disease who are not yet receiving medication.
The absence of Parkinson’s disease medications is one key to a successful biomarker hunt, said Dr. Simuni, the principal investigator for the Midwestern region of the United States. “We want to make sure there is no over-signal of the therapy – that we are looking at the progression of disease unmasked by interventions.”
This should not be a problem with this patient population – at least initially. “For many patients with a new diagnosis, symptoms don’t interfere with their function, so it’s quite common not to start treatment at this time,” Dr. Simuni said. “At the point when the patient needs treatment, of course, it will start. They can remain in the study and count toward the follow-up. But our aim is to recruit patients early enough that we get at least 6 months of data without medication.”
Funding for the $40 million PPMI study will come from the Michael J. Fox Foundation, private contributions, Pfizer Inc., and – Dr. Marek hopes – federal grants.
In fact, he said, PPMI leaders hope to become involved in the PD-BIN.
Although the request for applications for the PD-BIN was just released, Dr. Mark Hallett, chief of NINDS’ Medical Neurology branch and its Human Motor Control Section, anticipated that the project could be up and running within 1 year.
“The deputy director of NINDS [Dr. Walter J. Koroshetz] made it clear that the goal of this project is to bring as many resources as possible to bear on advancing neuroprotective therapy for Parkinson’s,” Dr. Hallett said in an interview.
Although not officially connected, the PD-BIN and the PPMI may join forces, Dr. Marek said.
“We’ll be applying for [the federal project] and we would love for these processes to be complementary. We would be delighted to have the government, through NIH, partner with us.”
Both projects were largely inspired by the Alzheimer’s Disease Neuroimaging Initiative (ADNI), which also is a public-private collaboration. Launched in 2004, the ADNI studied the rate of change of cognition, brain structure and function, and biomarkers in healthy control patients, patients with mild cognitive impairment, and patients with Alzheimer’s disease. Discoveries made through the ADNI have shown that cerebrospinal fluid carries disease-specific biomarkers that change with disease progression, including levels of phosphorylated and unphosphorylated tau protein and amyloid-beta-42. The project also investigated new imaging compounds which allow, for the first time, visualization of amyloid plaques and tau neurofibrillary tangles in the brain and how they change during disease progression.
Like the ADNI, both the PPMI and the PD-BIN could amass an enormous bio-bank of samples, which will be available without cost to scientists with approved research projects. In fact, Dr. Marek said, PPMI data sets will be maintained by the same lab that administers ADNI data: the Laboratory of Neuroimaging at the University of California, Los Angeles.
“In addition to accessing the data, researchers will be able to apply for PPMI’s imaging and samples of CSF, blood, and urine from a biorepository we intend to maintain,” Dr. Marek said. “We want all our data to be available to researchers on an ongoing basis, and we encourage them to come up with their own research ideas based on PPMI data.”
PPMI already has specific biomarkers targeted for research. Preliminary data indicate that alpha-synuclein, urate, and expression of the Parkinson’s genetic marker DJ-1 change according to disease stage. Some data suggest that total tau, phosphorylated tau, and amyloid-beta might change as cognitive function is altered. Therefore, each of the 12 study visits will include blood, cerebrospinal fluid, urine, and DNA sampling as well as motor, neuropsychiatric, and cognitive assessments.
Single-photo emission CT with DaTSCAN (ioflupane [123I]) and MRI imaging will determine changes in brain structure and dopamine levels. Although not yet approved for clinical use in the United States, the DaTSCAN radioisotope binds to dopamine transporters in the substantia nigra, allowing researchers to study dopaminergic neurodegeneration.
Both Dr. Hallett and Dr. Marek noted that the PPMI investigation and any others that join the federal program may uncover additional biomarkers. “The constant concern about looking for things that you know is that you might overlook something that you don’t know, which could turn out to be something even better,” Dr. Hallett said.
Dr. Marek agreed. “The biomarkers we’re looking at are based on existing scientific data. But the PPMI study is a mix of what we know now and what we hope will happen – finding things we don’t yet know about.”
“Recruitment is the first, second, and third issue in a study like this,” said Dr. Marek. “We know we are asking a lot of our participants, but from what we have seen so far, a lot of patients with Parkinson’s, and their friends and families who could be controls, understand the need for this approach and are willing and excited about participating in it.”
Both Dr. Marek and his coinvestigator Dr. Simuni admitted that the repeat lumbar punctures the study calls for could intimidate potential subjects. “It’s important that they know that for most people, the possible side effects of a lumbar puncture are just about the same as for a blood draw,” she said.
The first stop for information is the PPMI Web site. From here, physicians, researchers, and participants can learn about the scope of the project, the inclusion and exclusion criteria, and even see a schedule of visits and tests that each participant will need to fulfill.
By clicking on the “For Physicians” button, doctors can download the Physician Tool Kit, which includes brochures about the study; a poster; a pocket card with the study overview; and research referral forms.
Researchers who are interested in working with biological samples from the study also can find information about submitting requests for potential projects. The site contains a wealth of information for patients and families as well.
Dr. Simuni has served as a consultant and received honorarium from GE Healthcare, which manufactures and markets DaTSCAN in Europe. She has received research support from the NIH and the Michael J. Fox Foundation.
Dr Marek is a member of the scientific advisory board for the Michael J. Fox Foundation and has been a consultant for Pfizer and GE Healthcare. He has an equity interest in Molecular NeuroImaging LLC.
Dr. Hallett has no relevant disclosures.
Private and public sources are launching two massive efforts to identify biomarkers for Parkinson’s disease – an effort they say will speed drug research, providing more efficient ways to track disease progress and monitor therapeutic response.
In late September, the Michael J. Fox Foundation kicked off its Parkinson’s Progression Markers Initiative (PPMI) and the National Institute for Neurological Disorders and Stroke sent out a request for applications to create the Parkinson’s Disease Biomarker Identification Network (PD-BIN). The 5-year PPMI is the first large-scale clinical study to focus exclusively on identifying and validating both chemical and imaging biomarkers of the disease. The multiproject PD-BIN will be similarly devoted to identifying biological markers that contribute to an individual’s risk for Parkinson’s disease, as well as its onset and progression, with the goal of speeding disease-modifying treatments.
“We expect that the biomarkers we discover will help us better understand the disease and accelerate therapeutic trials, with the goal of assessing whether a drug can modify the progression of Parkinson’s,” PPMI primary investigator Dr. Kenneth Marek said in an interview. “In a way, this is much more complex than a clinical treatment trial. We are not testing a drug, but ideally, we will find markers that can pave the way to accomplish more effective drug testing, and speed the development of much-needed therapies for this disease.”
Speaking from the World Parkinson Congress in Glasgow, Scotland, where he unveiled the PPMI to the scientific community, Dr. Marek stressed the need for objective, measurable disease markers in diagnosis and disease progression, as well as in research studies. The diagnosis of Parkinson’s disease remains solely based on clinical signs and symptoms, with no concrete diagnostic measure. Progression, as well, can be measured only by the worsening of symptoms. And with no objective clinical measurements in hand, researchers are “shooting in the dark” when assessing response to candidate drugs, he said.
“We have been conducting these clinical trials, but we there is no way to assess when a drug is ineffective, or how to get a better sense of whether the next one will actually work,” said Dr. Marek, who also is president of the Institute for Neurodegenerative Disorders in New Haven, Conn.
Having a set of biomarkers will speed research in a way that is not now possible, said PPMI co-investigator Dr. Tanya Simuni, director of the Parkinson’s Disease and Movement Disorders Center at Northwestern University, Chicago.
“We have many ongoing clinical trials of potential disease-modifying agents, but they are slow to progress because clinical assessment is the primary efficacy measure,” Dr. Simuni said in an interview. “Because of this, these studies take a long time and need a large number of patients – and they still sometimes end up with inconclusive results. If we had an objective measure of disease progression, that would speed drug development by reducing the duration of the studies and the number of participants needed for each one.”
The discovery of a biomarker could also help clinicians identify patients in the very earliest – perhaps even prodromal – disease state, she said. “By the time symptoms of Parkinson’s appear, patients can have lost up to 70% of their dopamine-producing cells, which tells us that there is a prodromal or preclinical phase during which damage is occurring without clinical signs. Biomarkers could not only help us develop better interventions but also screening tools. It’s conceivable that in the future, we could screen for Parkinson’s in the same way that we now screen for breast cancer or other medical conditions.”
The PPMI will be conducted at 14 U.S. centers and at centers in Innsbruck, Austria; Kassel and Tubingen Germany; and Naples, Italy. It aims to recruit 200 healthy control patients and 400 patients newly diagnosed with Parkinson’s disease who are not yet receiving medication.
The absence of Parkinson’s disease medications is one key to a successful biomarker hunt, said Dr. Simuni, the principal investigator for the Midwestern region of the United States. “We want to make sure there is no over-signal of the therapy – that we are looking at the progression of disease unmasked by interventions.”
This should not be a problem with this patient population – at least initially. “For many patients with a new diagnosis, symptoms don’t interfere with their function, so it’s quite common not to start treatment at this time,” Dr. Simuni said. “At the point when the patient needs treatment, of course, it will start. They can remain in the study and count toward the follow-up. But our aim is to recruit patients early enough that we get at least 6 months of data without medication.”
Funding for the $40 million PPMI study will come from the Michael J. Fox Foundation, private contributions, Pfizer Inc., and – Dr. Marek hopes – federal grants.
In fact, he said, PPMI leaders hope to become involved in the PD-BIN.
Although the request for applications for the PD-BIN was just released, Dr. Mark Hallett, chief of NINDS’ Medical Neurology branch and its Human Motor Control Section, anticipated that the project could be up and running within 1 year.
“The deputy director of NINDS [Dr. Walter J. Koroshetz] made it clear that the goal of this project is to bring as many resources as possible to bear on advancing neuroprotective therapy for Parkinson’s,” Dr. Hallett said in an interview.
Although not officially connected, the PD-BIN and the PPMI may join forces, Dr. Marek said.
“We’ll be applying for [the federal project] and we would love for these processes to be complementary. We would be delighted to have the government, through NIH, partner with us.”
Both projects were largely inspired by the Alzheimer’s Disease Neuroimaging Initiative (ADNI), which also is a public-private collaboration. Launched in 2004, the ADNI studied the rate of change of cognition, brain structure and function, and biomarkers in healthy control patients, patients with mild cognitive impairment, and patients with Alzheimer’s disease. Discoveries made through the ADNI have shown that cerebrospinal fluid carries disease-specific biomarkers that change with disease progression, including levels of phosphorylated and unphosphorylated tau protein and amyloid-beta-42. The project also investigated new imaging compounds which allow, for the first time, visualization of amyloid plaques and tau neurofibrillary tangles in the brain and how they change during disease progression.
Like the ADNI, both the PPMI and the PD-BIN could amass an enormous bio-bank of samples, which will be available without cost to scientists with approved research projects. In fact, Dr. Marek said, PPMI data sets will be maintained by the same lab that administers ADNI data: the Laboratory of Neuroimaging at the University of California, Los Angeles.
“In addition to accessing the data, researchers will be able to apply for PPMI’s imaging and samples of CSF, blood, and urine from a biorepository we intend to maintain,” Dr. Marek said. “We want all our data to be available to researchers on an ongoing basis, and we encourage them to come up with their own research ideas based on PPMI data.”
PPMI already has specific biomarkers targeted for research. Preliminary data indicate that alpha-synuclein, urate, and expression of the Parkinson’s genetic marker DJ-1 change according to disease stage. Some data suggest that total tau, phosphorylated tau, and amyloid-beta might change as cognitive function is altered. Therefore, each of the 12 study visits will include blood, cerebrospinal fluid, urine, and DNA sampling as well as motor, neuropsychiatric, and cognitive assessments.
Single-photo emission CT with DaTSCAN (ioflupane [123I]) and MRI imaging will determine changes in brain structure and dopamine levels. Although not yet approved for clinical use in the United States, the DaTSCAN radioisotope binds to dopamine transporters in the substantia nigra, allowing researchers to study dopaminergic neurodegeneration.
Both Dr. Hallett and Dr. Marek noted that the PPMI investigation and any others that join the federal program may uncover additional biomarkers. “The constant concern about looking for things that you know is that you might overlook something that you don’t know, which could turn out to be something even better,” Dr. Hallett said.
Dr. Marek agreed. “The biomarkers we’re looking at are based on existing scientific data. But the PPMI study is a mix of what we know now and what we hope will happen – finding things we don’t yet know about.”
“Recruitment is the first, second, and third issue in a study like this,” said Dr. Marek. “We know we are asking a lot of our participants, but from what we have seen so far, a lot of patients with Parkinson’s, and their friends and families who could be controls, understand the need for this approach and are willing and excited about participating in it.”
Both Dr. Marek and his coinvestigator Dr. Simuni admitted that the repeat lumbar punctures the study calls for could intimidate potential subjects. “It’s important that they know that for most people, the possible side effects of a lumbar puncture are just about the same as for a blood draw,” she said.
The first stop for information is the PPMI Web site. From here, physicians, researchers, and participants can learn about the scope of the project, the inclusion and exclusion criteria, and even see a schedule of visits and tests that each participant will need to fulfill.
By clicking on the “For Physicians” button, doctors can download the Physician Tool Kit, which includes brochures about the study; a poster; a pocket card with the study overview; and research referral forms.
Researchers who are interested in working with biological samples from the study also can find information about submitting requests for potential projects. The site contains a wealth of information for patients and families as well.
Dr. Simuni has served as a consultant and received honorarium from GE Healthcare, which manufactures and markets DaTSCAN in Europe. She has received research support from the NIH and the Michael J. Fox Foundation.
Dr Marek is a member of the scientific advisory board for the Michael J. Fox Foundation and has been a consultant for Pfizer and GE Healthcare. He has an equity interest in Molecular NeuroImaging LLC.
Dr. Hallett has no relevant disclosures.
Private and public sources are launching two massive efforts to identify biomarkers for Parkinson’s disease – an effort they say will speed drug research, providing more efficient ways to track disease progress and monitor therapeutic response.
In late September, the Michael J. Fox Foundation kicked off its Parkinson’s Progression Markers Initiative (PPMI) and the National Institute for Neurological Disorders and Stroke sent out a request for applications to create the Parkinson’s Disease Biomarker Identification Network (PD-BIN). The 5-year PPMI is the first large-scale clinical study to focus exclusively on identifying and validating both chemical and imaging biomarkers of the disease. The multiproject PD-BIN will be similarly devoted to identifying biological markers that contribute to an individual’s risk for Parkinson’s disease, as well as its onset and progression, with the goal of speeding disease-modifying treatments.
“We expect that the biomarkers we discover will help us better understand the disease and accelerate therapeutic trials, with the goal of assessing whether a drug can modify the progression of Parkinson’s,” PPMI primary investigator Dr. Kenneth Marek said in an interview. “In a way, this is much more complex than a clinical treatment trial. We are not testing a drug, but ideally, we will find markers that can pave the way to accomplish more effective drug testing, and speed the development of much-needed therapies for this disease.”
Speaking from the World Parkinson Congress in Glasgow, Scotland, where he unveiled the PPMI to the scientific community, Dr. Marek stressed the need for objective, measurable disease markers in diagnosis and disease progression, as well as in research studies. The diagnosis of Parkinson’s disease remains solely based on clinical signs and symptoms, with no concrete diagnostic measure. Progression, as well, can be measured only by the worsening of symptoms. And with no objective clinical measurements in hand, researchers are “shooting in the dark” when assessing response to candidate drugs, he said.
“We have been conducting these clinical trials, but we there is no way to assess when a drug is ineffective, or how to get a better sense of whether the next one will actually work,” said Dr. Marek, who also is president of the Institute for Neurodegenerative Disorders in New Haven, Conn.
Having a set of biomarkers will speed research in a way that is not now possible, said PPMI co-investigator Dr. Tanya Simuni, director of the Parkinson’s Disease and Movement Disorders Center at Northwestern University, Chicago.
“We have many ongoing clinical trials of potential disease-modifying agents, but they are slow to progress because clinical assessment is the primary efficacy measure,” Dr. Simuni said in an interview. “Because of this, these studies take a long time and need a large number of patients – and they still sometimes end up with inconclusive results. If we had an objective measure of disease progression, that would speed drug development by reducing the duration of the studies and the number of participants needed for each one.”
The discovery of a biomarker could also help clinicians identify patients in the very earliest – perhaps even prodromal – disease state, she said. “By the time symptoms of Parkinson’s appear, patients can have lost up to 70% of their dopamine-producing cells, which tells us that there is a prodromal or preclinical phase during which damage is occurring without clinical signs. Biomarkers could not only help us develop better interventions but also screening tools. It’s conceivable that in the future, we could screen for Parkinson’s in the same way that we now screen for breast cancer or other medical conditions.”
The PPMI will be conducted at 14 U.S. centers and at centers in Innsbruck, Austria; Kassel and Tubingen Germany; and Naples, Italy. It aims to recruit 200 healthy control patients and 400 patients newly diagnosed with Parkinson’s disease who are not yet receiving medication.
The absence of Parkinson’s disease medications is one key to a successful biomarker hunt, said Dr. Simuni, the principal investigator for the Midwestern region of the United States. “We want to make sure there is no over-signal of the therapy – that we are looking at the progression of disease unmasked by interventions.”
This should not be a problem with this patient population – at least initially. “For many patients with a new diagnosis, symptoms don’t interfere with their function, so it’s quite common not to start treatment at this time,” Dr. Simuni said. “At the point when the patient needs treatment, of course, it will start. They can remain in the study and count toward the follow-up. But our aim is to recruit patients early enough that we get at least 6 months of data without medication.”
Funding for the $40 million PPMI study will come from the Michael J. Fox Foundation, private contributions, Pfizer Inc., and – Dr. Marek hopes – federal grants.
In fact, he said, PPMI leaders hope to become involved in the PD-BIN.
Although the request for applications for the PD-BIN was just released, Dr. Mark Hallett, chief of NINDS’ Medical Neurology branch and its Human Motor Control Section, anticipated that the project could be up and running within 1 year.
“The deputy director of NINDS [Dr. Walter J. Koroshetz] made it clear that the goal of this project is to bring as many resources as possible to bear on advancing neuroprotective therapy for Parkinson’s,” Dr. Hallett said in an interview.
Although not officially connected, the PD-BIN and the PPMI may join forces, Dr. Marek said.
“We’ll be applying for [the federal project] and we would love for these processes to be complementary. We would be delighted to have the government, through NIH, partner with us.”
Both projects were largely inspired by the Alzheimer’s Disease Neuroimaging Initiative (ADNI), which also is a public-private collaboration. Launched in 2004, the ADNI studied the rate of change of cognition, brain structure and function, and biomarkers in healthy control patients, patients with mild cognitive impairment, and patients with Alzheimer’s disease. Discoveries made through the ADNI have shown that cerebrospinal fluid carries disease-specific biomarkers that change with disease progression, including levels of phosphorylated and unphosphorylated tau protein and amyloid-beta-42. The project also investigated new imaging compounds which allow, for the first time, visualization of amyloid plaques and tau neurofibrillary tangles in the brain and how they change during disease progression.
Like the ADNI, both the PPMI and the PD-BIN could amass an enormous bio-bank of samples, which will be available without cost to scientists with approved research projects. In fact, Dr. Marek said, PPMI data sets will be maintained by the same lab that administers ADNI data: the Laboratory of Neuroimaging at the University of California, Los Angeles.
“In addition to accessing the data, researchers will be able to apply for PPMI’s imaging and samples of CSF, blood, and urine from a biorepository we intend to maintain,” Dr. Marek said. “We want all our data to be available to researchers on an ongoing basis, and we encourage them to come up with their own research ideas based on PPMI data.”
PPMI already has specific biomarkers targeted for research. Preliminary data indicate that alpha-synuclein, urate, and expression of the Parkinson’s genetic marker DJ-1 change according to disease stage. Some data suggest that total tau, phosphorylated tau, and amyloid-beta might change as cognitive function is altered. Therefore, each of the 12 study visits will include blood, cerebrospinal fluid, urine, and DNA sampling as well as motor, neuropsychiatric, and cognitive assessments.
Single-photo emission CT with DaTSCAN (ioflupane [123I]) and MRI imaging will determine changes in brain structure and dopamine levels. Although not yet approved for clinical use in the United States, the DaTSCAN radioisotope binds to dopamine transporters in the substantia nigra, allowing researchers to study dopaminergic neurodegeneration.
Both Dr. Hallett and Dr. Marek noted that the PPMI investigation and any others that join the federal program may uncover additional biomarkers. “The constant concern about looking for things that you know is that you might overlook something that you don’t know, which could turn out to be something even better,” Dr. Hallett said.
Dr. Marek agreed. “The biomarkers we’re looking at are based on existing scientific data. But the PPMI study is a mix of what we know now and what we hope will happen – finding things we don’t yet know about.”
“Recruitment is the first, second, and third issue in a study like this,” said Dr. Marek. “We know we are asking a lot of our participants, but from what we have seen so far, a lot of patients with Parkinson’s, and their friends and families who could be controls, understand the need for this approach and are willing and excited about participating in it.”
Both Dr. Marek and his coinvestigator Dr. Simuni admitted that the repeat lumbar punctures the study calls for could intimidate potential subjects. “It’s important that they know that for most people, the possible side effects of a lumbar puncture are just about the same as for a blood draw,” she said.
The first stop for information is the PPMI Web site. From here, physicians, researchers, and participants can learn about the scope of the project, the inclusion and exclusion criteria, and even see a schedule of visits and tests that each participant will need to fulfill.
By clicking on the “For Physicians” button, doctors can download the Physician Tool Kit, which includes brochures about the study; a poster; a pocket card with the study overview; and research referral forms.
Researchers who are interested in working with biological samples from the study also can find information about submitting requests for potential projects. The site contains a wealth of information for patients and families as well.
Dr. Simuni has served as a consultant and received honorarium from GE Healthcare, which manufactures and markets DaTSCAN in Europe. She has received research support from the NIH and the Michael J. Fox Foundation.
Dr Marek is a member of the scientific advisory board for the Michael J. Fox Foundation and has been a consultant for Pfizer and GE Healthcare. He has an equity interest in Molecular NeuroImaging LLC.
Dr. Hallett has no relevant disclosures.
Two New Projects Embark on the Search for Parkinson's Biomarkers
Private and public sources are launching two massive efforts to identify biomarkers for Parkinson’s disease – an effort they say will speed drug research, providing more efficient ways to track disease progress and monitor therapeutic response.
In late September, the Michael J. Fox Foundation kicked off its Parkinson’s Progression Markers Initiative (PPMI) and the National Institute for Neurological Disorders and Stroke sent out a request for applications to create the Parkinson’s Disease Biomarker Identification Network (PD-BIN). The 5-year PPMI is the first large-scale clinical study to focus exclusively on identifying and validating both chemical and imaging biomarkers of the disease. The multiproject PD-BIN will be similarly devoted to identifying biological markers that contribute to an individual’s risk for Parkinson’s disease, as well as its onset and progression, with the goal of speeding disease-modifying treatments.
“We expect that the biomarkers we discover will help us better understand the disease and accelerate therapeutic trials, with the goal of assessing whether a drug can modify the progression of Parkinson’s,” PPMI primary investigator Dr. Kenneth Marek said in an interview. “In a way, this is much more complex than a clinical treatment trial. We are not testing a drug, but ideally, we will find markers that can pave the way to accomplish more effective drug testing, and speed the development of much-needed therapies for this disease.”
Speaking from the World Parkinson Congress in Glasgow, Scotland, where he unveiled the PPMI to the scientific community, Dr. Marek stressed the need for objective, measurable disease markers in diagnosis and disease progression, as well as in research studies. The diagnosis of Parkinson’s disease remains solely based on clinical signs and symptoms, with no concrete diagnostic measure. Progression, as well, can be measured only by the worsening of symptoms. And with no objective clinical measurements in hand, researchers are “shooting in the dark” when assessing response to candidate drugs, he said.
“We have been conducting these clinical trials, but we there is no way to assess when a drug is ineffective, or how to get a better sense of whether the next one will actually work,” said Dr. Marek, who also is president of the Institute for Neurodegenerative Disorders in New Haven, Conn.
Having a set of biomarkers will speed research in a way that is not now possible, said PPMI co-investigator Dr. Tanya Simuni, director of the Parkinson’s Disease and Movement Disorders Center at Northwestern University, Chicago.
“We have many ongoing clinical trials of potential disease-modifying agents, but they are slow to progress because clinical assessment is the primary efficacy measure,” Dr. Simuni said in an interview. “Because of this, these studies take a long time and need a large number of patients – and they still sometimes end up with inconclusive results. If we had an objective measure of disease progression, that would speed drug development by reducing the duration of the studies and the number of participants needed for each one.”
The discovery of a biomarker could also help clinicians identify patients in the very earliest – perhaps even prodromal – disease state, she said. “By the time symptoms of Parkinson’s appear, patients can have lost up to 70% of their dopamine-producing cells, which tells us that there is a prodromal or preclinical phase during which damage is occurring without clinical signs. Biomarkers could not only help us develop better interventions but also screening tools. It’s conceivable that in the future, we could screen for Parkinson’s in the same way that we now screen for breast cancer or other medical conditions.”
The PPMI will be conducted at 14 U.S. centers and at centers in Innsbruck, Austria; Kassel and Tubingen Germany; and Naples, Italy. It aims to recruit 200 healthy control patients and 400 patients newly diagnosed with Parkinson’s disease who are not yet receiving medication.
The absence of Parkinson’s disease medications is one key to a successful biomarker hunt, said Dr. Simuni, the principal investigator for the Midwestern region of the United States. “We want to make sure there is no over-signal of the therapy – that we are looking at the progression of disease unmasked by interventions.”
This should not be a problem with this patient population – at least initially. “For many patients with a new diagnosis, symptoms don’t interfere with their function, so it’s quite common not to start treatment at this time,” Dr. Simuni said. “At the point when the patient needs treatment, of course, it will start. They can remain in the study and count toward the follow-up. But our aim is to recruit patients early enough that we get at least 6 months of data without medication.”
Funding for the $40 million PPMI study will come from the Michael J. Fox Foundation, private contributions, Pfizer Inc., and – Dr. Marek hopes – federal grants.
In fact, he said, PPMI leaders hope to become involved in the PD-BIN.
Although the request for applications for the PD-BIN was just released, Dr. Mark Hallett, chief of NINDS’ Medical Neurology branch and its Human Motor Control Section, anticipated that the project could be up and running within 1 year.
“The deputy director of NINDS [Dr. Walter J. Koroshetz] made it clear that the goal of this project is to bring as many resources as possible to bear on advancing neuroprotective therapy for Parkinson’s,” Dr. Hallett said in an interview.
Although not officially connected, the PD-BIN and the PPMI may join forces, Dr. Marek said.
“We’ll be applying for [the federal project] and we would love for these processes to be complementary. We would be delighted to have the government, through NIH, partner with us.”
Both projects were largely inspired by the Alzheimer’s Disease Neuroimaging Initiative (ADNI), which also is a public-private collaboration. Launched in 2004, the ADNI studied the rate of change of cognition, brain structure and function, and biomarkers in healthy control patients, patients with mild cognitive impairment, and patients with Alzheimer’s disease. Discoveries made through the ADNI have shown that cerebrospinal fluid carries disease-specific biomarkers that change with disease progression, including levels of phosphorylated and unphosphorylated tau protein and amyloid-beta-42. The project also investigated new imaging compounds which allow, for the first time, visualization of amyloid plaques and tau neurofibrillary tangles in the brain and how they change during disease progression.
Like the ADNI, both the PPMI and the PD-BIN could amass an enormous bio-bank of samples, which will be available without cost to scientists with approved research projects. In fact, Dr. Marek said, PPMI data sets will be maintained by the same lab that administers ADNI data: the Laboratory of Neuroimaging at the University of California, Los Angeles.
“In addition to accessing the data, researchers will be able to apply for PPMI’s imaging and samples of CSF, blood, and urine from a biorepository we intend to maintain,” Dr. Marek said. “We want all our data to be available to researchers on an ongoing basis, and we encourage them to come up with their own research ideas based on PPMI data.”
PPMI already has specific biomarkers targeted for research. Preliminary data indicate that alpha-synuclein, urate, and expression of the Parkinson’s genetic marker DJ-1 change according to disease stage. Some data suggest that total tau, phosphorylated tau, and amyloid-beta might change as cognitive function is altered. Therefore, each of the 12 study visits will include blood, cerebrospinal fluid, urine, and DNA sampling as well as motor, neuropsychiatric, and cognitive assessments.
Single-photo emission CT with DaTSCAN (ioflupane [123I]) and MRI imaging will determine changes in brain structure and dopamine levels. Although not yet approved for clinical use in the United States, the DaTSCAN radioisotope binds to dopamine transporters in the substantia nigra, allowing researchers to study dopaminergic neurodegeneration.
Both Dr. Hallett and Dr. Marek noted that the PPMI investigation and any others that join the federal program may uncover additional biomarkers. “The constant concern about looking for things that you know is that you might overlook something that you don’t know, which could turn out to be something even better,” Dr. Hallett said.
Dr. Marek agreed. “The biomarkers we’re looking at are based on existing scientific data. But the PPMI study is a mix of what we know now and what we hope will happen – finding things we don’t yet know about.”
“Recruitment is the first, second, and third issue in a study like this,” said Dr. Marek. “We know we are asking a lot of our participants, but from what we have seen so far, a lot of patients with Parkinson’s, and their friends and families who could be controls, understand the need for this approach and are willing and excited about participating in it.”
Both Dr. Marek and his coinvestigator Dr. Simuni admitted that the repeat lumbar punctures the study calls for could intimidate potential subjects. “It’s important that they know that for most people, the possible side effects of a lumbar puncture are just about the same as for a blood draw,” she said.
The first stop for information is the PPMI Web site. From here, physicians, researchers, and participants can learn about the scope of the project, the inclusion and exclusion criteria, and even see a schedule of visits and tests that each participant will need to fulfill.
By clicking on the “For Physicians” button, doctors can download the Physician Tool Kit, which includes brochures about the study; a poster; a pocket card with the study overview; and research referral forms.
Researchers who are interested in working with biological samples from the study also can find information about submitting requests for potential projects. The site contains a wealth of information for patients and families as well.
Dr. Simuni has served as a consultant and received honorarium from GE Healthcare, which manufactures and markets DaTSCAN in Europe. She has received research support from the NIH and the Michael J. Fox Foundation.
Dr Marek is a member of the scientific advisory board for the Michael J. Fox Foundation and has been a consultant for Pfizer and GE Healthcare. He has an equity interest in Molecular NeuroImaging LLC.
Dr. Hallett has no relevant disclosures.
Private and public sources are launching two massive efforts to identify biomarkers for Parkinson’s disease – an effort they say will speed drug research, providing more efficient ways to track disease progress and monitor therapeutic response.
In late September, the Michael J. Fox Foundation kicked off its Parkinson’s Progression Markers Initiative (PPMI) and the National Institute for Neurological Disorders and Stroke sent out a request for applications to create the Parkinson’s Disease Biomarker Identification Network (PD-BIN). The 5-year PPMI is the first large-scale clinical study to focus exclusively on identifying and validating both chemical and imaging biomarkers of the disease. The multiproject PD-BIN will be similarly devoted to identifying biological markers that contribute to an individual’s risk for Parkinson’s disease, as well as its onset and progression, with the goal of speeding disease-modifying treatments.
“We expect that the biomarkers we discover will help us better understand the disease and accelerate therapeutic trials, with the goal of assessing whether a drug can modify the progression of Parkinson’s,” PPMI primary investigator Dr. Kenneth Marek said in an interview. “In a way, this is much more complex than a clinical treatment trial. We are not testing a drug, but ideally, we will find markers that can pave the way to accomplish more effective drug testing, and speed the development of much-needed therapies for this disease.”
Speaking from the World Parkinson Congress in Glasgow, Scotland, where he unveiled the PPMI to the scientific community, Dr. Marek stressed the need for objective, measurable disease markers in diagnosis and disease progression, as well as in research studies. The diagnosis of Parkinson’s disease remains solely based on clinical signs and symptoms, with no concrete diagnostic measure. Progression, as well, can be measured only by the worsening of symptoms. And with no objective clinical measurements in hand, researchers are “shooting in the dark” when assessing response to candidate drugs, he said.
“We have been conducting these clinical trials, but we there is no way to assess when a drug is ineffective, or how to get a better sense of whether the next one will actually work,” said Dr. Marek, who also is president of the Institute for Neurodegenerative Disorders in New Haven, Conn.
Having a set of biomarkers will speed research in a way that is not now possible, said PPMI co-investigator Dr. Tanya Simuni, director of the Parkinson’s Disease and Movement Disorders Center at Northwestern University, Chicago.
“We have many ongoing clinical trials of potential disease-modifying agents, but they are slow to progress because clinical assessment is the primary efficacy measure,” Dr. Simuni said in an interview. “Because of this, these studies take a long time and need a large number of patients – and they still sometimes end up with inconclusive results. If we had an objective measure of disease progression, that would speed drug development by reducing the duration of the studies and the number of participants needed for each one.”
The discovery of a biomarker could also help clinicians identify patients in the very earliest – perhaps even prodromal – disease state, she said. “By the time symptoms of Parkinson’s appear, patients can have lost up to 70% of their dopamine-producing cells, which tells us that there is a prodromal or preclinical phase during which damage is occurring without clinical signs. Biomarkers could not only help us develop better interventions but also screening tools. It’s conceivable that in the future, we could screen for Parkinson’s in the same way that we now screen for breast cancer or other medical conditions.”
The PPMI will be conducted at 14 U.S. centers and at centers in Innsbruck, Austria; Kassel and Tubingen Germany; and Naples, Italy. It aims to recruit 200 healthy control patients and 400 patients newly diagnosed with Parkinson’s disease who are not yet receiving medication.
The absence of Parkinson’s disease medications is one key to a successful biomarker hunt, said Dr. Simuni, the principal investigator for the Midwestern region of the United States. “We want to make sure there is no over-signal of the therapy – that we are looking at the progression of disease unmasked by interventions.”
This should not be a problem with this patient population – at least initially. “For many patients with a new diagnosis, symptoms don’t interfere with their function, so it’s quite common not to start treatment at this time,” Dr. Simuni said. “At the point when the patient needs treatment, of course, it will start. They can remain in the study and count toward the follow-up. But our aim is to recruit patients early enough that we get at least 6 months of data without medication.”
Funding for the $40 million PPMI study will come from the Michael J. Fox Foundation, private contributions, Pfizer Inc., and – Dr. Marek hopes – federal grants.
In fact, he said, PPMI leaders hope to become involved in the PD-BIN.
Although the request for applications for the PD-BIN was just released, Dr. Mark Hallett, chief of NINDS’ Medical Neurology branch and its Human Motor Control Section, anticipated that the project could be up and running within 1 year.
“The deputy director of NINDS [Dr. Walter J. Koroshetz] made it clear that the goal of this project is to bring as many resources as possible to bear on advancing neuroprotective therapy for Parkinson’s,” Dr. Hallett said in an interview.
Although not officially connected, the PD-BIN and the PPMI may join forces, Dr. Marek said.
“We’ll be applying for [the federal project] and we would love for these processes to be complementary. We would be delighted to have the government, through NIH, partner with us.”
Both projects were largely inspired by the Alzheimer’s Disease Neuroimaging Initiative (ADNI), which also is a public-private collaboration. Launched in 2004, the ADNI studied the rate of change of cognition, brain structure and function, and biomarkers in healthy control patients, patients with mild cognitive impairment, and patients with Alzheimer’s disease. Discoveries made through the ADNI have shown that cerebrospinal fluid carries disease-specific biomarkers that change with disease progression, including levels of phosphorylated and unphosphorylated tau protein and amyloid-beta-42. The project also investigated new imaging compounds which allow, for the first time, visualization of amyloid plaques and tau neurofibrillary tangles in the brain and how they change during disease progression.
Like the ADNI, both the PPMI and the PD-BIN could amass an enormous bio-bank of samples, which will be available without cost to scientists with approved research projects. In fact, Dr. Marek said, PPMI data sets will be maintained by the same lab that administers ADNI data: the Laboratory of Neuroimaging at the University of California, Los Angeles.
“In addition to accessing the data, researchers will be able to apply for PPMI’s imaging and samples of CSF, blood, and urine from a biorepository we intend to maintain,” Dr. Marek said. “We want all our data to be available to researchers on an ongoing basis, and we encourage them to come up with their own research ideas based on PPMI data.”
PPMI already has specific biomarkers targeted for research. Preliminary data indicate that alpha-synuclein, urate, and expression of the Parkinson’s genetic marker DJ-1 change according to disease stage. Some data suggest that total tau, phosphorylated tau, and amyloid-beta might change as cognitive function is altered. Therefore, each of the 12 study visits will include blood, cerebrospinal fluid, urine, and DNA sampling as well as motor, neuropsychiatric, and cognitive assessments.
Single-photo emission CT with DaTSCAN (ioflupane [123I]) and MRI imaging will determine changes in brain structure and dopamine levels. Although not yet approved for clinical use in the United States, the DaTSCAN radioisotope binds to dopamine transporters in the substantia nigra, allowing researchers to study dopaminergic neurodegeneration.
Both Dr. Hallett and Dr. Marek noted that the PPMI investigation and any others that join the federal program may uncover additional biomarkers. “The constant concern about looking for things that you know is that you might overlook something that you don’t know, which could turn out to be something even better,” Dr. Hallett said.
Dr. Marek agreed. “The biomarkers we’re looking at are based on existing scientific data. But the PPMI study is a mix of what we know now and what we hope will happen – finding things we don’t yet know about.”
“Recruitment is the first, second, and third issue in a study like this,” said Dr. Marek. “We know we are asking a lot of our participants, but from what we have seen so far, a lot of patients with Parkinson’s, and their friends and families who could be controls, understand the need for this approach and are willing and excited about participating in it.”
Both Dr. Marek and his coinvestigator Dr. Simuni admitted that the repeat lumbar punctures the study calls for could intimidate potential subjects. “It’s important that they know that for most people, the possible side effects of a lumbar puncture are just about the same as for a blood draw,” she said.
The first stop for information is the PPMI Web site. From here, physicians, researchers, and participants can learn about the scope of the project, the inclusion and exclusion criteria, and even see a schedule of visits and tests that each participant will need to fulfill.
By clicking on the “For Physicians” button, doctors can download the Physician Tool Kit, which includes brochures about the study; a poster; a pocket card with the study overview; and research referral forms.
Researchers who are interested in working with biological samples from the study also can find information about submitting requests for potential projects. The site contains a wealth of information for patients and families as well.
Dr. Simuni has served as a consultant and received honorarium from GE Healthcare, which manufactures and markets DaTSCAN in Europe. She has received research support from the NIH and the Michael J. Fox Foundation.
Dr Marek is a member of the scientific advisory board for the Michael J. Fox Foundation and has been a consultant for Pfizer and GE Healthcare. He has an equity interest in Molecular NeuroImaging LLC.
Dr. Hallett has no relevant disclosures.
Private and public sources are launching two massive efforts to identify biomarkers for Parkinson’s disease – an effort they say will speed drug research, providing more efficient ways to track disease progress and monitor therapeutic response.
In late September, the Michael J. Fox Foundation kicked off its Parkinson’s Progression Markers Initiative (PPMI) and the National Institute for Neurological Disorders and Stroke sent out a request for applications to create the Parkinson’s Disease Biomarker Identification Network (PD-BIN). The 5-year PPMI is the first large-scale clinical study to focus exclusively on identifying and validating both chemical and imaging biomarkers of the disease. The multiproject PD-BIN will be similarly devoted to identifying biological markers that contribute to an individual’s risk for Parkinson’s disease, as well as its onset and progression, with the goal of speeding disease-modifying treatments.
“We expect that the biomarkers we discover will help us better understand the disease and accelerate therapeutic trials, with the goal of assessing whether a drug can modify the progression of Parkinson’s,” PPMI primary investigator Dr. Kenneth Marek said in an interview. “In a way, this is much more complex than a clinical treatment trial. We are not testing a drug, but ideally, we will find markers that can pave the way to accomplish more effective drug testing, and speed the development of much-needed therapies for this disease.”
Speaking from the World Parkinson Congress in Glasgow, Scotland, where he unveiled the PPMI to the scientific community, Dr. Marek stressed the need for objective, measurable disease markers in diagnosis and disease progression, as well as in research studies. The diagnosis of Parkinson’s disease remains solely based on clinical signs and symptoms, with no concrete diagnostic measure. Progression, as well, can be measured only by the worsening of symptoms. And with no objective clinical measurements in hand, researchers are “shooting in the dark” when assessing response to candidate drugs, he said.
“We have been conducting these clinical trials, but we there is no way to assess when a drug is ineffective, or how to get a better sense of whether the next one will actually work,” said Dr. Marek, who also is president of the Institute for Neurodegenerative Disorders in New Haven, Conn.
Having a set of biomarkers will speed research in a way that is not now possible, said PPMI co-investigator Dr. Tanya Simuni, director of the Parkinson’s Disease and Movement Disorders Center at Northwestern University, Chicago.
“We have many ongoing clinical trials of potential disease-modifying agents, but they are slow to progress because clinical assessment is the primary efficacy measure,” Dr. Simuni said in an interview. “Because of this, these studies take a long time and need a large number of patients – and they still sometimes end up with inconclusive results. If we had an objective measure of disease progression, that would speed drug development by reducing the duration of the studies and the number of participants needed for each one.”
The discovery of a biomarker could also help clinicians identify patients in the very earliest – perhaps even prodromal – disease state, she said. “By the time symptoms of Parkinson’s appear, patients can have lost up to 70% of their dopamine-producing cells, which tells us that there is a prodromal or preclinical phase during which damage is occurring without clinical signs. Biomarkers could not only help us develop better interventions but also screening tools. It’s conceivable that in the future, we could screen for Parkinson’s in the same way that we now screen for breast cancer or other medical conditions.”
The PPMI will be conducted at 14 U.S. centers and at centers in Innsbruck, Austria; Kassel and Tubingen Germany; and Naples, Italy. It aims to recruit 200 healthy control patients and 400 patients newly diagnosed with Parkinson’s disease who are not yet receiving medication.
The absence of Parkinson’s disease medications is one key to a successful biomarker hunt, said Dr. Simuni, the principal investigator for the Midwestern region of the United States. “We want to make sure there is no over-signal of the therapy – that we are looking at the progression of disease unmasked by interventions.”
This should not be a problem with this patient population – at least initially. “For many patients with a new diagnosis, symptoms don’t interfere with their function, so it’s quite common not to start treatment at this time,” Dr. Simuni said. “At the point when the patient needs treatment, of course, it will start. They can remain in the study and count toward the follow-up. But our aim is to recruit patients early enough that we get at least 6 months of data without medication.”
Funding for the $40 million PPMI study will come from the Michael J. Fox Foundation, private contributions, Pfizer Inc., and – Dr. Marek hopes – federal grants.
In fact, he said, PPMI leaders hope to become involved in the PD-BIN.
Although the request for applications for the PD-BIN was just released, Dr. Mark Hallett, chief of NINDS’ Medical Neurology branch and its Human Motor Control Section, anticipated that the project could be up and running within 1 year.
“The deputy director of NINDS [Dr. Walter J. Koroshetz] made it clear that the goal of this project is to bring as many resources as possible to bear on advancing neuroprotective therapy for Parkinson’s,” Dr. Hallett said in an interview.
Although not officially connected, the PD-BIN and the PPMI may join forces, Dr. Marek said.
“We’ll be applying for [the federal project] and we would love for these processes to be complementary. We would be delighted to have the government, through NIH, partner with us.”
Both projects were largely inspired by the Alzheimer’s Disease Neuroimaging Initiative (ADNI), which also is a public-private collaboration. Launched in 2004, the ADNI studied the rate of change of cognition, brain structure and function, and biomarkers in healthy control patients, patients with mild cognitive impairment, and patients with Alzheimer’s disease. Discoveries made through the ADNI have shown that cerebrospinal fluid carries disease-specific biomarkers that change with disease progression, including levels of phosphorylated and unphosphorylated tau protein and amyloid-beta-42. The project also investigated new imaging compounds which allow, for the first time, visualization of amyloid plaques and tau neurofibrillary tangles in the brain and how they change during disease progression.
Like the ADNI, both the PPMI and the PD-BIN could amass an enormous bio-bank of samples, which will be available without cost to scientists with approved research projects. In fact, Dr. Marek said, PPMI data sets will be maintained by the same lab that administers ADNI data: the Laboratory of Neuroimaging at the University of California, Los Angeles.
“In addition to accessing the data, researchers will be able to apply for PPMI’s imaging and samples of CSF, blood, and urine from a biorepository we intend to maintain,” Dr. Marek said. “We want all our data to be available to researchers on an ongoing basis, and we encourage them to come up with their own research ideas based on PPMI data.”
PPMI already has specific biomarkers targeted for research. Preliminary data indicate that alpha-synuclein, urate, and expression of the Parkinson’s genetic marker DJ-1 change according to disease stage. Some data suggest that total tau, phosphorylated tau, and amyloid-beta might change as cognitive function is altered. Therefore, each of the 12 study visits will include blood, cerebrospinal fluid, urine, and DNA sampling as well as motor, neuropsychiatric, and cognitive assessments.
Single-photo emission CT with DaTSCAN (ioflupane [123I]) and MRI imaging will determine changes in brain structure and dopamine levels. Although not yet approved for clinical use in the United States, the DaTSCAN radioisotope binds to dopamine transporters in the substantia nigra, allowing researchers to study dopaminergic neurodegeneration.
Both Dr. Hallett and Dr. Marek noted that the PPMI investigation and any others that join the federal program may uncover additional biomarkers. “The constant concern about looking for things that you know is that you might overlook something that you don’t know, which could turn out to be something even better,” Dr. Hallett said.
Dr. Marek agreed. “The biomarkers we’re looking at are based on existing scientific data. But the PPMI study is a mix of what we know now and what we hope will happen – finding things we don’t yet know about.”
“Recruitment is the first, second, and third issue in a study like this,” said Dr. Marek. “We know we are asking a lot of our participants, but from what we have seen so far, a lot of patients with Parkinson’s, and their friends and families who could be controls, understand the need for this approach and are willing and excited about participating in it.”
Both Dr. Marek and his coinvestigator Dr. Simuni admitted that the repeat lumbar punctures the study calls for could intimidate potential subjects. “It’s important that they know that for most people, the possible side effects of a lumbar puncture are just about the same as for a blood draw,” she said.
The first stop for information is the PPMI Web site. From here, physicians, researchers, and participants can learn about the scope of the project, the inclusion and exclusion criteria, and even see a schedule of visits and tests that each participant will need to fulfill.
By clicking on the “For Physicians” button, doctors can download the Physician Tool Kit, which includes brochures about the study; a poster; a pocket card with the study overview; and research referral forms.
Researchers who are interested in working with biological samples from the study also can find information about submitting requests for potential projects. The site contains a wealth of information for patients and families as well.
Dr. Simuni has served as a consultant and received honorarium from GE Healthcare, which manufactures and markets DaTSCAN in Europe. She has received research support from the NIH and the Michael J. Fox Foundation.
Dr Marek is a member of the scientific advisory board for the Michael J. Fox Foundation and has been a consultant for Pfizer and GE Healthcare. He has an equity interest in Molecular NeuroImaging LLC.
Dr. Hallett has no relevant disclosures.
Two New Projects Embark on the Search for Parkinson's Biomarkers
Private and public sources are launching two massive efforts to identify biomarkers for Parkinson’s disease – an effort they say will speed drug research, providing more efficient ways to track disease progress and monitor therapeutic response.
In late September, the Michael J. Fox Foundation kicked off its Parkinson’s Progression Markers Initiative (PPMI) and the National Institute for Neurological Disorders and Stroke sent out a request for applications to create the Parkinson’s Disease Biomarker Identification Network (PD-BIN). The 5-year PPMI is the first large-scale clinical study to focus exclusively on identifying and validating both chemical and imaging biomarkers of the disease. The multiproject PD-BIN will be similarly devoted to identifying biological markers that contribute to an individual’s risk for Parkinson’s disease, as well as its onset and progression, with the goal of speeding disease-modifying treatments.
“We expect that the biomarkers we discover will help us better understand the disease and accelerate therapeutic trials, with the goal of assessing whether a drug can modify the progression of Parkinson’s,” PPMI primary investigator Dr. Kenneth Marek said in an interview. “In a way, this is much more complex than a clinical treatment trial. We are not testing a drug, but ideally, we will find markers that can pave the way to accomplish more effective drug testing, and speed the development of much-needed therapies for this disease.”
Speaking from the World Parkinson Congress in Glasgow, Scotland, where he unveiled the PPMI to the scientific community, Dr. Marek stressed the need for objective, measurable disease markers in diagnosis and disease progression, as well as in research studies. The diagnosis of Parkinson’s disease remains solely based on clinical signs and symptoms, with no concrete diagnostic measure. Progression, as well, can be measured only by the worsening of symptoms. And with no objective clinical measurements in hand, researchers are “shooting in the dark” when assessing response to candidate drugs, he said.
“We have been conducting these clinical trials, but we there is no way to assess when a drug is ineffective, or how to get a better sense of whether the next one will actually work,” said Dr. Marek, who also is president of the Institute for Neurodegenerative Disorders in New Haven, Conn.
Having a set of biomarkers will speed research in a way that is not now possible, said PPMI co-investigator Dr. Tanya Simuni, director of the Parkinson’s Disease and Movement Disorders Center at Northwestern University, Chicago.
“We have many ongoing clinical trials of potential disease-modifying agents, but they are slow to progress because clinical assessment is the primary efficacy measure,” Dr. Simuni said in an interview. “Because of this, these studies take a long time and need a large number of patients – and they still sometimes end up with inconclusive results. If we had an objective measure of disease progression, that would speed drug development by reducing the duration of the studies and the number of participants needed for each one.”
The discovery of a biomarker could also help clinicians identify patients in the very earliest – perhaps even prodromal – disease state, she said. “By the time symptoms of Parkinson’s appear, patients can have lost up to 70% of their dopamine-producing cells, which tells us that there is a prodromal or preclinical phase during which damage is occurring without clinical signs. Biomarkers could not only help us develop better interventions but also screening tools. It’s conceivable that in the future, we could screen for Parkinson’s in the same way that we now screen for breast cancer or other medical conditions.”
The PPMI will be conducted at 14 U.S. centers and at centers in Innsbruck, Austria; Kassel and Tubingen Germany; and Naples, Italy. It aims to recruit 200 healthy control patients and 400 patients newly diagnosed with Parkinson’s disease who are not yet receiving medication.
The absence of Parkinson’s disease medications is one key to a successful biomarker hunt, said Dr. Simuni, the principal investigator for the Midwestern region of the United States. “We want to make sure there is no over-signal of the therapy – that we are looking at the progression of disease unmasked by interventions.”
This should not be a problem with this patient population – at least initially. “For many patients with a new diagnosis, symptoms don’t interfere with their function, so it’s quite common not to start treatment at this time,” Dr. Simuni said. “At the point when the patient needs treatment, of course, it will start. They can remain in the study and count toward the follow-up. But our aim is to recruit patients early enough that we get at least 6 months of data without medication.”
Funding for the $40 million PPMI study will come from the Michael J. Fox Foundation, private contributions, Pfizer Inc., and – Dr. Marek hopes – federal grants.
In fact, he said, PPMI leaders hope to become involved in the PD-BIN.
Although the request for applications for the PD-BIN was just released, Dr. Mark Hallett, chief of NINDS’ Medical Neurology branch and its Human Motor Control Section, anticipated that the project could be up and running within 1 year.
“The deputy director of NINDS [Dr. Walter J. Koroshetz] made it clear that the goal of this project is to bring as many resources as possible to bear on advancing neuroprotective therapy for Parkinson’s,” Dr. Hallett said in an interview.
Although not officially connected, the PD-BIN and the PPMI may join forces, Dr. Marek said.
“We’ll be applying for [the federal project] and we would love for these processes to be complementary. We would be delighted to have the government, through NIH, partner with us.”
Both projects were largely inspired by the Alzheimer’s Disease Neuroimaging Initiative (ADNI), which also is a public-private collaboration. Launched in 2004, the ADNI studied the rate of change of cognition, brain structure and function, and biomarkers in healthy control patients, patients with mild cognitive impairment, and patients with Alzheimer’s disease. Discoveries made through the ADNI have shown that cerebrospinal fluid carries disease-specific biomarkers that change with disease progression, including levels of phosphorylated and unphosphorylated tau protein and amyloid-beta-42. The project also investigated new imaging compounds which allow, for the first time, visualization of amyloid plaques and tau neurofibrillary tangles in the brain and how they change during disease progression.
Like the ADNI, both the PPMI and the PD-BIN could amass an enormous bio-bank of samples, which will be available without cost to scientists with approved research projects. In fact, Dr. Marek said, PPMI data sets will be maintained by the same lab that administers ADNI data: the Laboratory of Neuroimaging at the University of California, Los Angeles.
“In addition to accessing the data, researchers will be able to apply for PPMI’s imaging and samples of CSF, blood, and urine from a biorepository we intend to maintain,” Dr. Marek said. “We want all our data to be available to researchers on an ongoing basis, and we encourage them to come up with their own research ideas based on PPMI data.”
PPMI already has specific biomarkers targeted for research. Preliminary data indicate that alpha-synuclein, urate, and expression of the Parkinson’s genetic marker DJ-1 change according to disease stage. Some data suggest that total tau, phosphorylated tau, and amyloid-beta might change as cognitive function is altered. Therefore, each of the 12 study visits will include blood, cerebrospinal fluid, urine, and DNA sampling as well as motor, neuropsychiatric, and cognitive assessments.
Single-photo emission CT with DaTSCAN (ioflupane [123I]) and MRI imaging will determine changes in brain structure and dopamine levels. Although not yet approved for clinical use in the United States, the DaTSCAN radioisotope binds to dopamine transporters in the substantia nigra, allowing researchers to study dopaminergic neurodegeneration.
Both Dr. Hallett and Dr. Marek noted that the PPMI investigation and any others that join the federal program may uncover additional biomarkers. “The constant concern about looking for things that you know is that you might overlook something that you don’t know, which could turn out to be something even better,” Dr. Hallett said.
Dr. Marek agreed. “The biomarkers we’re looking at are based on existing scientific data. But the PPMI study is a mix of what we know now and what we hope will happen – finding things we don’t yet know about.”
“Recruitment is the first, second, and third issue in a study like this,” said Dr. Marek. “We know we are asking a lot of our participants, but from what we have seen so far, a lot of patients with Parkinson’s, and their friends and families who could be controls, understand the need for this approach and are willing and excited about participating in it.”
Both Dr. Marek and his coinvestigator Dr. Simuni admitted that the repeat lumbar punctures the study calls for could intimidate potential subjects. “It’s important that they know that for most people, the possible side effects of a lumbar puncture are just about the same as for a blood draw,” she said.
The first stop for information is the PPMI Web site. From here, physicians, researchers, and participants can learn about the scope of the project, the inclusion and exclusion criteria, and even see a schedule of visits and tests that each participant will need to fulfill.
By clicking on the “For Physicians” button, doctors can download the Physician Tool Kit, which includes brochures about the study; a poster; a pocket card with the study overview; and research referral forms.
Researchers who are interested in working with biological samples from the study also can find information about submitting requests for potential projects. The site contains a wealth of information for patients and families as well.
Dr. Simuni has served as a consultant and received honorarium from GE Healthcare, which manufactures and markets DaTSCAN in Europe. She has received research support from the NIH and the Michael J. Fox Foundation.
Dr Marek is a member of the scientific advisory board for the Michael J. Fox Foundation and has been a consultant for Pfizer and GE Healthcare. He has an equity interest in Molecular NeuroImaging LLC.
Dr. Hallett has no relevant disclosures.
Private and public sources are launching two massive efforts to identify biomarkers for Parkinson’s disease – an effort they say will speed drug research, providing more efficient ways to track disease progress and monitor therapeutic response.
In late September, the Michael J. Fox Foundation kicked off its Parkinson’s Progression Markers Initiative (PPMI) and the National Institute for Neurological Disorders and Stroke sent out a request for applications to create the Parkinson’s Disease Biomarker Identification Network (PD-BIN). The 5-year PPMI is the first large-scale clinical study to focus exclusively on identifying and validating both chemical and imaging biomarkers of the disease. The multiproject PD-BIN will be similarly devoted to identifying biological markers that contribute to an individual’s risk for Parkinson’s disease, as well as its onset and progression, with the goal of speeding disease-modifying treatments.
“We expect that the biomarkers we discover will help us better understand the disease and accelerate therapeutic trials, with the goal of assessing whether a drug can modify the progression of Parkinson’s,” PPMI primary investigator Dr. Kenneth Marek said in an interview. “In a way, this is much more complex than a clinical treatment trial. We are not testing a drug, but ideally, we will find markers that can pave the way to accomplish more effective drug testing, and speed the development of much-needed therapies for this disease.”
Speaking from the World Parkinson Congress in Glasgow, Scotland, where he unveiled the PPMI to the scientific community, Dr. Marek stressed the need for objective, measurable disease markers in diagnosis and disease progression, as well as in research studies. The diagnosis of Parkinson’s disease remains solely based on clinical signs and symptoms, with no concrete diagnostic measure. Progression, as well, can be measured only by the worsening of symptoms. And with no objective clinical measurements in hand, researchers are “shooting in the dark” when assessing response to candidate drugs, he said.
“We have been conducting these clinical trials, but we there is no way to assess when a drug is ineffective, or how to get a better sense of whether the next one will actually work,” said Dr. Marek, who also is president of the Institute for Neurodegenerative Disorders in New Haven, Conn.
Having a set of biomarkers will speed research in a way that is not now possible, said PPMI co-investigator Dr. Tanya Simuni, director of the Parkinson’s Disease and Movement Disorders Center at Northwestern University, Chicago.
“We have many ongoing clinical trials of potential disease-modifying agents, but they are slow to progress because clinical assessment is the primary efficacy measure,” Dr. Simuni said in an interview. “Because of this, these studies take a long time and need a large number of patients – and they still sometimes end up with inconclusive results. If we had an objective measure of disease progression, that would speed drug development by reducing the duration of the studies and the number of participants needed for each one.”
The discovery of a biomarker could also help clinicians identify patients in the very earliest – perhaps even prodromal – disease state, she said. “By the time symptoms of Parkinson’s appear, patients can have lost up to 70% of their dopamine-producing cells, which tells us that there is a prodromal or preclinical phase during which damage is occurring without clinical signs. Biomarkers could not only help us develop better interventions but also screening tools. It’s conceivable that in the future, we could screen for Parkinson’s in the same way that we now screen for breast cancer or other medical conditions.”
The PPMI will be conducted at 14 U.S. centers and at centers in Innsbruck, Austria; Kassel and Tubingen Germany; and Naples, Italy. It aims to recruit 200 healthy control patients and 400 patients newly diagnosed with Parkinson’s disease who are not yet receiving medication.
The absence of Parkinson’s disease medications is one key to a successful biomarker hunt, said Dr. Simuni, the principal investigator for the Midwestern region of the United States. “We want to make sure there is no over-signal of the therapy – that we are looking at the progression of disease unmasked by interventions.”
This should not be a problem with this patient population – at least initially. “For many patients with a new diagnosis, symptoms don’t interfere with their function, so it’s quite common not to start treatment at this time,” Dr. Simuni said. “At the point when the patient needs treatment, of course, it will start. They can remain in the study and count toward the follow-up. But our aim is to recruit patients early enough that we get at least 6 months of data without medication.”
Funding for the $40 million PPMI study will come from the Michael J. Fox Foundation, private contributions, Pfizer Inc., and – Dr. Marek hopes – federal grants.
In fact, he said, PPMI leaders hope to become involved in the PD-BIN.
Although the request for applications for the PD-BIN was just released, Dr. Mark Hallett, chief of NINDS’ Medical Neurology branch and its Human Motor Control Section, anticipated that the project could be up and running within 1 year.
“The deputy director of NINDS [Dr. Walter J. Koroshetz] made it clear that the goal of this project is to bring as many resources as possible to bear on advancing neuroprotective therapy for Parkinson’s,” Dr. Hallett said in an interview.
Although not officially connected, the PD-BIN and the PPMI may join forces, Dr. Marek said.
“We’ll be applying for [the federal project] and we would love for these processes to be complementary. We would be delighted to have the government, through NIH, partner with us.”
Both projects were largely inspired by the Alzheimer’s Disease Neuroimaging Initiative (ADNI), which also is a public-private collaboration. Launched in 2004, the ADNI studied the rate of change of cognition, brain structure and function, and biomarkers in healthy control patients, patients with mild cognitive impairment, and patients with Alzheimer’s disease. Discoveries made through the ADNI have shown that cerebrospinal fluid carries disease-specific biomarkers that change with disease progression, including levels of phosphorylated and unphosphorylated tau protein and amyloid-beta-42. The project also investigated new imaging compounds which allow, for the first time, visualization of amyloid plaques and tau neurofibrillary tangles in the brain and how they change during disease progression.
Like the ADNI, both the PPMI and the PD-BIN could amass an enormous bio-bank of samples, which will be available without cost to scientists with approved research projects. In fact, Dr. Marek said, PPMI data sets will be maintained by the same lab that administers ADNI data: the Laboratory of Neuroimaging at the University of California, Los Angeles.
“In addition to accessing the data, researchers will be able to apply for PPMI’s imaging and samples of CSF, blood, and urine from a biorepository we intend to maintain,” Dr. Marek said. “We want all our data to be available to researchers on an ongoing basis, and we encourage them to come up with their own research ideas based on PPMI data.”
PPMI already has specific biomarkers targeted for research. Preliminary data indicate that alpha-synuclein, urate, and expression of the Parkinson’s genetic marker DJ-1 change according to disease stage. Some data suggest that total tau, phosphorylated tau, and amyloid-beta might change as cognitive function is altered. Therefore, each of the 12 study visits will include blood, cerebrospinal fluid, urine, and DNA sampling as well as motor, neuropsychiatric, and cognitive assessments.
Single-photo emission CT with DaTSCAN (ioflupane [123I]) and MRI imaging will determine changes in brain structure and dopamine levels. Although not yet approved for clinical use in the United States, the DaTSCAN radioisotope binds to dopamine transporters in the substantia nigra, allowing researchers to study dopaminergic neurodegeneration.
Both Dr. Hallett and Dr. Marek noted that the PPMI investigation and any others that join the federal program may uncover additional biomarkers. “The constant concern about looking for things that you know is that you might overlook something that you don’t know, which could turn out to be something even better,” Dr. Hallett said.
Dr. Marek agreed. “The biomarkers we’re looking at are based on existing scientific data. But the PPMI study is a mix of what we know now and what we hope will happen – finding things we don’t yet know about.”
“Recruitment is the first, second, and third issue in a study like this,” said Dr. Marek. “We know we are asking a lot of our participants, but from what we have seen so far, a lot of patients with Parkinson’s, and their friends and families who could be controls, understand the need for this approach and are willing and excited about participating in it.”
Both Dr. Marek and his coinvestigator Dr. Simuni admitted that the repeat lumbar punctures the study calls for could intimidate potential subjects. “It’s important that they know that for most people, the possible side effects of a lumbar puncture are just about the same as for a blood draw,” she said.
The first stop for information is the PPMI Web site. From here, physicians, researchers, and participants can learn about the scope of the project, the inclusion and exclusion criteria, and even see a schedule of visits and tests that each participant will need to fulfill.
By clicking on the “For Physicians” button, doctors can download the Physician Tool Kit, which includes brochures about the study; a poster; a pocket card with the study overview; and research referral forms.
Researchers who are interested in working with biological samples from the study also can find information about submitting requests for potential projects. The site contains a wealth of information for patients and families as well.
Dr. Simuni has served as a consultant and received honorarium from GE Healthcare, which manufactures and markets DaTSCAN in Europe. She has received research support from the NIH and the Michael J. Fox Foundation.
Dr Marek is a member of the scientific advisory board for the Michael J. Fox Foundation and has been a consultant for Pfizer and GE Healthcare. He has an equity interest in Molecular NeuroImaging LLC.
Dr. Hallett has no relevant disclosures.
Private and public sources are launching two massive efforts to identify biomarkers for Parkinson’s disease – an effort they say will speed drug research, providing more efficient ways to track disease progress and monitor therapeutic response.
In late September, the Michael J. Fox Foundation kicked off its Parkinson’s Progression Markers Initiative (PPMI) and the National Institute for Neurological Disorders and Stroke sent out a request for applications to create the Parkinson’s Disease Biomarker Identification Network (PD-BIN). The 5-year PPMI is the first large-scale clinical study to focus exclusively on identifying and validating both chemical and imaging biomarkers of the disease. The multiproject PD-BIN will be similarly devoted to identifying biological markers that contribute to an individual’s risk for Parkinson’s disease, as well as its onset and progression, with the goal of speeding disease-modifying treatments.
“We expect that the biomarkers we discover will help us better understand the disease and accelerate therapeutic trials, with the goal of assessing whether a drug can modify the progression of Parkinson’s,” PPMI primary investigator Dr. Kenneth Marek said in an interview. “In a way, this is much more complex than a clinical treatment trial. We are not testing a drug, but ideally, we will find markers that can pave the way to accomplish more effective drug testing, and speed the development of much-needed therapies for this disease.”
Speaking from the World Parkinson Congress in Glasgow, Scotland, where he unveiled the PPMI to the scientific community, Dr. Marek stressed the need for objective, measurable disease markers in diagnosis and disease progression, as well as in research studies. The diagnosis of Parkinson’s disease remains solely based on clinical signs and symptoms, with no concrete diagnostic measure. Progression, as well, can be measured only by the worsening of symptoms. And with no objective clinical measurements in hand, researchers are “shooting in the dark” when assessing response to candidate drugs, he said.
“We have been conducting these clinical trials, but we there is no way to assess when a drug is ineffective, or how to get a better sense of whether the next one will actually work,” said Dr. Marek, who also is president of the Institute for Neurodegenerative Disorders in New Haven, Conn.
Having a set of biomarkers will speed research in a way that is not now possible, said PPMI co-investigator Dr. Tanya Simuni, director of the Parkinson’s Disease and Movement Disorders Center at Northwestern University, Chicago.
“We have many ongoing clinical trials of potential disease-modifying agents, but they are slow to progress because clinical assessment is the primary efficacy measure,” Dr. Simuni said in an interview. “Because of this, these studies take a long time and need a large number of patients – and they still sometimes end up with inconclusive results. If we had an objective measure of disease progression, that would speed drug development by reducing the duration of the studies and the number of participants needed for each one.”
The discovery of a biomarker could also help clinicians identify patients in the very earliest – perhaps even prodromal – disease state, she said. “By the time symptoms of Parkinson’s appear, patients can have lost up to 70% of their dopamine-producing cells, which tells us that there is a prodromal or preclinical phase during which damage is occurring without clinical signs. Biomarkers could not only help us develop better interventions but also screening tools. It’s conceivable that in the future, we could screen for Parkinson’s in the same way that we now screen for breast cancer or other medical conditions.”
The PPMI will be conducted at 14 U.S. centers and at centers in Innsbruck, Austria; Kassel and Tubingen Germany; and Naples, Italy. It aims to recruit 200 healthy control patients and 400 patients newly diagnosed with Parkinson’s disease who are not yet receiving medication.
The absence of Parkinson’s disease medications is one key to a successful biomarker hunt, said Dr. Simuni, the principal investigator for the Midwestern region of the United States. “We want to make sure there is no over-signal of the therapy – that we are looking at the progression of disease unmasked by interventions.”
This should not be a problem with this patient population – at least initially. “For many patients with a new diagnosis, symptoms don’t interfere with their function, so it’s quite common not to start treatment at this time,” Dr. Simuni said. “At the point when the patient needs treatment, of course, it will start. They can remain in the study and count toward the follow-up. But our aim is to recruit patients early enough that we get at least 6 months of data without medication.”
Funding for the $40 million PPMI study will come from the Michael J. Fox Foundation, private contributions, Pfizer Inc., and – Dr. Marek hopes – federal grants.
In fact, he said, PPMI leaders hope to become involved in the PD-BIN.
Although the request for applications for the PD-BIN was just released, Dr. Mark Hallett, chief of NINDS’ Medical Neurology branch and its Human Motor Control Section, anticipated that the project could be up and running within 1 year.
“The deputy director of NINDS [Dr. Walter J. Koroshetz] made it clear that the goal of this project is to bring as many resources as possible to bear on advancing neuroprotective therapy for Parkinson’s,” Dr. Hallett said in an interview.
Although not officially connected, the PD-BIN and the PPMI may join forces, Dr. Marek said.
“We’ll be applying for [the federal project] and we would love for these processes to be complementary. We would be delighted to have the government, through NIH, partner with us.”
Both projects were largely inspired by the Alzheimer’s Disease Neuroimaging Initiative (ADNI), which also is a public-private collaboration. Launched in 2004, the ADNI studied the rate of change of cognition, brain structure and function, and biomarkers in healthy control patients, patients with mild cognitive impairment, and patients with Alzheimer’s disease. Discoveries made through the ADNI have shown that cerebrospinal fluid carries disease-specific biomarkers that change with disease progression, including levels of phosphorylated and unphosphorylated tau protein and amyloid-beta-42. The project also investigated new imaging compounds which allow, for the first time, visualization of amyloid plaques and tau neurofibrillary tangles in the brain and how they change during disease progression.
Like the ADNI, both the PPMI and the PD-BIN could amass an enormous bio-bank of samples, which will be available without cost to scientists with approved research projects. In fact, Dr. Marek said, PPMI data sets will be maintained by the same lab that administers ADNI data: the Laboratory of Neuroimaging at the University of California, Los Angeles.
“In addition to accessing the data, researchers will be able to apply for PPMI’s imaging and samples of CSF, blood, and urine from a biorepository we intend to maintain,” Dr. Marek said. “We want all our data to be available to researchers on an ongoing basis, and we encourage them to come up with their own research ideas based on PPMI data.”
PPMI already has specific biomarkers targeted for research. Preliminary data indicate that alpha-synuclein, urate, and expression of the Parkinson’s genetic marker DJ-1 change according to disease stage. Some data suggest that total tau, phosphorylated tau, and amyloid-beta might change as cognitive function is altered. Therefore, each of the 12 study visits will include blood, cerebrospinal fluid, urine, and DNA sampling as well as motor, neuropsychiatric, and cognitive assessments.
Single-photo emission CT with DaTSCAN (ioflupane [123I]) and MRI imaging will determine changes in brain structure and dopamine levels. Although not yet approved for clinical use in the United States, the DaTSCAN radioisotope binds to dopamine transporters in the substantia nigra, allowing researchers to study dopaminergic neurodegeneration.
Both Dr. Hallett and Dr. Marek noted that the PPMI investigation and any others that join the federal program may uncover additional biomarkers. “The constant concern about looking for things that you know is that you might overlook something that you don’t know, which could turn out to be something even better,” Dr. Hallett said.
Dr. Marek agreed. “The biomarkers we’re looking at are based on existing scientific data. But the PPMI study is a mix of what we know now and what we hope will happen – finding things we don’t yet know about.”
“Recruitment is the first, second, and third issue in a study like this,” said Dr. Marek. “We know we are asking a lot of our participants, but from what we have seen so far, a lot of patients with Parkinson’s, and their friends and families who could be controls, understand the need for this approach and are willing and excited about participating in it.”
Both Dr. Marek and his coinvestigator Dr. Simuni admitted that the repeat lumbar punctures the study calls for could intimidate potential subjects. “It’s important that they know that for most people, the possible side effects of a lumbar puncture are just about the same as for a blood draw,” she said.
The first stop for information is the PPMI Web site. From here, physicians, researchers, and participants can learn about the scope of the project, the inclusion and exclusion criteria, and even see a schedule of visits and tests that each participant will need to fulfill.
By clicking on the “For Physicians” button, doctors can download the Physician Tool Kit, which includes brochures about the study; a poster; a pocket card with the study overview; and research referral forms.
Researchers who are interested in working with biological samples from the study also can find information about submitting requests for potential projects. The site contains a wealth of information for patients and families as well.
Dr. Simuni has served as a consultant and received honorarium from GE Healthcare, which manufactures and markets DaTSCAN in Europe. She has received research support from the NIH and the Michael J. Fox Foundation.
Dr Marek is a member of the scientific advisory board for the Michael J. Fox Foundation and has been a consultant for Pfizer and GE Healthcare. He has an equity interest in Molecular NeuroImaging LLC.
Dr. Hallett has no relevant disclosures.
Infants With Large Facial Hemangiomas Demand PHACE Time
CHICAGO - Infants with large segmental facial hemangiomas should always undergo a detailed workup for PHACE syndrome.
"When we see patients with a large facial hemangioma, we have a different burden of evaluation and diagnosis than we did even a year ago," Dr. Lawrence F. Eichenfield said at the summer meeting of the American Academy of Dermatology. "A new consensus statement describing the diagnostic criteria was published last October and outlines very clearly what we should be looking for in these children."
Because the developmental syndrome can affect several systems, a diagnostic workup should include magnetic resonance imaging of the brain, an echocardiogram, ultrasound and MRI of the great vessels, and a detailed ophthalmologic exam.
"This is the standard evaluation we have now for every child who has a hemangioma of 5 cm2 or larger on the face, head or neck," said Dr. Eichenfield, chief of pediatric and adolescent dermatology at Rady Children’s Hospital, San Diego.
Hemangiomas are a fairly common finding, occurring in 4%-10% of newborns. They are more likely to appear in girls, premature or low-birthweight infants, in multiples, or in the children of older mothers.
"All of these factors can be associated with intrauterine hypoxic insult or placental insufficiency," Dr. Eichenfield said. This supports a theory that hemangiomas form from capillaries positive for the glucose transport protein type 1 (GLUT1). "It was recently found that GLUT1 is an important responder to hypoxia."
While localized, nonsegmented hemangiomas are generally of only cosmetic concern, unless they interfere with function, the larger segmented type can be dangerous, Dr. Eichenfield noted. "They are more likely to erode and become infected, interfere with vital functions, and are strongly correlated with PHACE syndrome."
The PHACE acronym refers to the abnormalities often found in the disorder: posterior fossa anomalies, hemangioma, arterial lesions, cardiac abnormalities/aortic coarctation, and abnormalities of the eye. According to the recently published Consensus Statement on Diagnostic Criteria for PHACE Syndrome, definite PHACE requires the presence of a characteristic segmental hemangioma at least 5 cm in diameter on the face or scalp plus one major or two minor structural anomalies. Possible PHACE requires the presence of a hemangioma at least 5 cm on the face or scalp plus one minor structural anomaly (Pediatrics 2009;124:1447-56).
“We now understand that the major abnormalities in PHACE are usually the cerebrovascular arteries, including the great vessels of the brain and heart,” Dr. Eichenfield said. "There may be dysplasia, stenoses, occlusions, or even a complete absence of some of these vessels. Among children with these anomalies, cerebrovascular accidents and strokes are not uncommon."
Other major abnormalities associated with PHACE are malformation of the posterior fossa and coarctation of the aorta. "In fact, coarctation of the aorta is as common in PHACE as it is in Turner syndrome," Dr. Eichenfield said.
A recent prospective study of 108 infants with large facial hemangiomas helped define the association between the lesions and the syndrome, he said. Thirty-three (31%) of the infants qualified as having PHACE. Of those, 30 had more than one extracutaneous finding. "The risk for PHACE syndrome was higher in infants with larger hemangiomas and in those with hemangiomas that encompassed more than one facial segment," wrote lead author Anita Haggstrom of Indiana University, Indianapolis. "The most common extracutaneous anomalies were of the arteries of the cerebrovasculature (91%) and cardiac anomalies (67%). Upper face (frontotemporal and frontonasal) hemangiomas were commonly observed in infants with PHACE; isolated maxillary hemangiomas were rarely associated" (Pediatrics 2010;126:e418-26).
Another recent study examined the prevalence of cervical and intracranial arterial anomalies in 70 infants with PHACE syndrome (Am. J. Neuroradiol. 2010 Aug. 12 [epub ahead of print]).
More than half (57%) had more than one arteriopathy. "Dysgenesis was the most common abnormality (56%), followed by anomalous course and/or origin (47%), narrowing (39%), and nonvisualization (20%)," wrote lead author Dr. Christopher Hess of the University of California, San Francisco.
The study also found a link between the site of the hemangioma and arterial anomalies. "Hemangiomas were ipsilateral to arteriopathy in all but one case. The frontotemporal and/or mandibular facial segments were involved in 97% of cases, but no other specific associations between arteriopathy location and hemangioma sites were detected. All cases with posterior fossa anomalies had either internal carotid anomalies or persistent embryonic carotid-basilar connections," he said.
The diagnostic consensus statement also made some observations about hemangioma location and the most likely type of associated anomaly.
"Previous reports noted that [the frontotemporal segment] is probably most predictive of cerebrovascular and ocular anomalies, whereas [the mandibular segment] seems to predict ventral developmental defects and cardiovascular abnormalities," wrote the team headed by Dr. Denise Metry of the Baylor College of Medicine, Houston. "Although the observations may offer insight into pathogenesis, they should not influence anything less than a thorough PHACE evaluation for at-risk infants, which includes MRI and magnetic resonance arteriogram brain imaging, imaging of the cardiovasculature, and an ophthalmologic examination."
Disclosures: Dr. Eichenfield said he had no relevant financial disclosures.
CHICAGO - Infants with large segmental facial hemangiomas should always undergo a detailed workup for PHACE syndrome.
"When we see patients with a large facial hemangioma, we have a different burden of evaluation and diagnosis than we did even a year ago," Dr. Lawrence F. Eichenfield said at the summer meeting of the American Academy of Dermatology. "A new consensus statement describing the diagnostic criteria was published last October and outlines very clearly what we should be looking for in these children."
Because the developmental syndrome can affect several systems, a diagnostic workup should include magnetic resonance imaging of the brain, an echocardiogram, ultrasound and MRI of the great vessels, and a detailed ophthalmologic exam.
"This is the standard evaluation we have now for every child who has a hemangioma of 5 cm2 or larger on the face, head or neck," said Dr. Eichenfield, chief of pediatric and adolescent dermatology at Rady Children’s Hospital, San Diego.
Hemangiomas are a fairly common finding, occurring in 4%-10% of newborns. They are more likely to appear in girls, premature or low-birthweight infants, in multiples, or in the children of older mothers.
"All of these factors can be associated with intrauterine hypoxic insult or placental insufficiency," Dr. Eichenfield said. This supports a theory that hemangiomas form from capillaries positive for the glucose transport protein type 1 (GLUT1). "It was recently found that GLUT1 is an important responder to hypoxia."
While localized, nonsegmented hemangiomas are generally of only cosmetic concern, unless they interfere with function, the larger segmented type can be dangerous, Dr. Eichenfield noted. "They are more likely to erode and become infected, interfere with vital functions, and are strongly correlated with PHACE syndrome."
The PHACE acronym refers to the abnormalities often found in the disorder: posterior fossa anomalies, hemangioma, arterial lesions, cardiac abnormalities/aortic coarctation, and abnormalities of the eye. According to the recently published Consensus Statement on Diagnostic Criteria for PHACE Syndrome, definite PHACE requires the presence of a characteristic segmental hemangioma at least 5 cm in diameter on the face or scalp plus one major or two minor structural anomalies. Possible PHACE requires the presence of a hemangioma at least 5 cm on the face or scalp plus one minor structural anomaly (Pediatrics 2009;124:1447-56).
“We now understand that the major abnormalities in PHACE are usually the cerebrovascular arteries, including the great vessels of the brain and heart,” Dr. Eichenfield said. "There may be dysplasia, stenoses, occlusions, or even a complete absence of some of these vessels. Among children with these anomalies, cerebrovascular accidents and strokes are not uncommon."
Other major abnormalities associated with PHACE are malformation of the posterior fossa and coarctation of the aorta. "In fact, coarctation of the aorta is as common in PHACE as it is in Turner syndrome," Dr. Eichenfield said.
A recent prospective study of 108 infants with large facial hemangiomas helped define the association between the lesions and the syndrome, he said. Thirty-three (31%) of the infants qualified as having PHACE. Of those, 30 had more than one extracutaneous finding. "The risk for PHACE syndrome was higher in infants with larger hemangiomas and in those with hemangiomas that encompassed more than one facial segment," wrote lead author Anita Haggstrom of Indiana University, Indianapolis. "The most common extracutaneous anomalies were of the arteries of the cerebrovasculature (91%) and cardiac anomalies (67%). Upper face (frontotemporal and frontonasal) hemangiomas were commonly observed in infants with PHACE; isolated maxillary hemangiomas were rarely associated" (Pediatrics 2010;126:e418-26).
Another recent study examined the prevalence of cervical and intracranial arterial anomalies in 70 infants with PHACE syndrome (Am. J. Neuroradiol. 2010 Aug. 12 [epub ahead of print]).
More than half (57%) had more than one arteriopathy. "Dysgenesis was the most common abnormality (56%), followed by anomalous course and/or origin (47%), narrowing (39%), and nonvisualization (20%)," wrote lead author Dr. Christopher Hess of the University of California, San Francisco.
The study also found a link between the site of the hemangioma and arterial anomalies. "Hemangiomas were ipsilateral to arteriopathy in all but one case. The frontotemporal and/or mandibular facial segments were involved in 97% of cases, but no other specific associations between arteriopathy location and hemangioma sites were detected. All cases with posterior fossa anomalies had either internal carotid anomalies or persistent embryonic carotid-basilar connections," he said.
The diagnostic consensus statement also made some observations about hemangioma location and the most likely type of associated anomaly.
"Previous reports noted that [the frontotemporal segment] is probably most predictive of cerebrovascular and ocular anomalies, whereas [the mandibular segment] seems to predict ventral developmental defects and cardiovascular abnormalities," wrote the team headed by Dr. Denise Metry of the Baylor College of Medicine, Houston. "Although the observations may offer insight into pathogenesis, they should not influence anything less than a thorough PHACE evaluation for at-risk infants, which includes MRI and magnetic resonance arteriogram brain imaging, imaging of the cardiovasculature, and an ophthalmologic examination."
Disclosures: Dr. Eichenfield said he had no relevant financial disclosures.
CHICAGO - Infants with large segmental facial hemangiomas should always undergo a detailed workup for PHACE syndrome.
"When we see patients with a large facial hemangioma, we have a different burden of evaluation and diagnosis than we did even a year ago," Dr. Lawrence F. Eichenfield said at the summer meeting of the American Academy of Dermatology. "A new consensus statement describing the diagnostic criteria was published last October and outlines very clearly what we should be looking for in these children."
Because the developmental syndrome can affect several systems, a diagnostic workup should include magnetic resonance imaging of the brain, an echocardiogram, ultrasound and MRI of the great vessels, and a detailed ophthalmologic exam.
"This is the standard evaluation we have now for every child who has a hemangioma of 5 cm2 or larger on the face, head or neck," said Dr. Eichenfield, chief of pediatric and adolescent dermatology at Rady Children’s Hospital, San Diego.
Hemangiomas are a fairly common finding, occurring in 4%-10% of newborns. They are more likely to appear in girls, premature or low-birthweight infants, in multiples, or in the children of older mothers.
"All of these factors can be associated with intrauterine hypoxic insult or placental insufficiency," Dr. Eichenfield said. This supports a theory that hemangiomas form from capillaries positive for the glucose transport protein type 1 (GLUT1). "It was recently found that GLUT1 is an important responder to hypoxia."
While localized, nonsegmented hemangiomas are generally of only cosmetic concern, unless they interfere with function, the larger segmented type can be dangerous, Dr. Eichenfield noted. "They are more likely to erode and become infected, interfere with vital functions, and are strongly correlated with PHACE syndrome."
The PHACE acronym refers to the abnormalities often found in the disorder: posterior fossa anomalies, hemangioma, arterial lesions, cardiac abnormalities/aortic coarctation, and abnormalities of the eye. According to the recently published Consensus Statement on Diagnostic Criteria for PHACE Syndrome, definite PHACE requires the presence of a characteristic segmental hemangioma at least 5 cm in diameter on the face or scalp plus one major or two minor structural anomalies. Possible PHACE requires the presence of a hemangioma at least 5 cm on the face or scalp plus one minor structural anomaly (Pediatrics 2009;124:1447-56).
“We now understand that the major abnormalities in PHACE are usually the cerebrovascular arteries, including the great vessels of the brain and heart,” Dr. Eichenfield said. "There may be dysplasia, stenoses, occlusions, or even a complete absence of some of these vessels. Among children with these anomalies, cerebrovascular accidents and strokes are not uncommon."
Other major abnormalities associated with PHACE are malformation of the posterior fossa and coarctation of the aorta. "In fact, coarctation of the aorta is as common in PHACE as it is in Turner syndrome," Dr. Eichenfield said.
A recent prospective study of 108 infants with large facial hemangiomas helped define the association between the lesions and the syndrome, he said. Thirty-three (31%) of the infants qualified as having PHACE. Of those, 30 had more than one extracutaneous finding. "The risk for PHACE syndrome was higher in infants with larger hemangiomas and in those with hemangiomas that encompassed more than one facial segment," wrote lead author Anita Haggstrom of Indiana University, Indianapolis. "The most common extracutaneous anomalies were of the arteries of the cerebrovasculature (91%) and cardiac anomalies (67%). Upper face (frontotemporal and frontonasal) hemangiomas were commonly observed in infants with PHACE; isolated maxillary hemangiomas were rarely associated" (Pediatrics 2010;126:e418-26).
Another recent study examined the prevalence of cervical and intracranial arterial anomalies in 70 infants with PHACE syndrome (Am. J. Neuroradiol. 2010 Aug. 12 [epub ahead of print]).
More than half (57%) had more than one arteriopathy. "Dysgenesis was the most common abnormality (56%), followed by anomalous course and/or origin (47%), narrowing (39%), and nonvisualization (20%)," wrote lead author Dr. Christopher Hess of the University of California, San Francisco.
The study also found a link between the site of the hemangioma and arterial anomalies. "Hemangiomas were ipsilateral to arteriopathy in all but one case. The frontotemporal and/or mandibular facial segments were involved in 97% of cases, but no other specific associations between arteriopathy location and hemangioma sites were detected. All cases with posterior fossa anomalies had either internal carotid anomalies or persistent embryonic carotid-basilar connections," he said.
The diagnostic consensus statement also made some observations about hemangioma location and the most likely type of associated anomaly.
"Previous reports noted that [the frontotemporal segment] is probably most predictive of cerebrovascular and ocular anomalies, whereas [the mandibular segment] seems to predict ventral developmental defects and cardiovascular abnormalities," wrote the team headed by Dr. Denise Metry of the Baylor College of Medicine, Houston. "Although the observations may offer insight into pathogenesis, they should not influence anything less than a thorough PHACE evaluation for at-risk infants, which includes MRI and magnetic resonance arteriogram brain imaging, imaging of the cardiovasculature, and an ophthalmologic examination."
Disclosures: Dr. Eichenfield said he had no relevant financial disclosures.
EXPERT ANALYSIS FROM THE SUMMER MEETING OF THE AMERICAN ACADEMY OF DERMATOLOGY
Many Children With JIA Do Not Achieve Remission, Despite Adequate Treatment
VALENCIA, Spain – Despite treatment, nearly half of children with juvenile idiopathic arthritis continue to experience active disease and many report significant physical fatigue, according to researchers at the Congress of the Pediatric Rheumatology European Society.
“Our results point out that JIA is a controllable and treatable, but not curable, disease for a majority of the children,” coauthor Dr. Marite Rygg of St. Olavs Hospital, Trondheim, Norway, said in an interview.
Her colleague, Dr. Ellen Nordal, reported 7-year follow-up data on 427 children who were enrolled in the Nordic Juvenile Idiopathic Arthritis Cohort from 1997-2000. The cohort comprised patients from 12 centers in Norway, Finland, Sweden, and Denmark. At the congress, Dr. Nordal reported complete follow-up data on 427 of the children.
Most the patients (66%) were girls. Their median age at the onset of disease was 6 years. The most common arthritis subtype in the group was oligoarthritis; this was persistent in 126 and extended in 75. Other disease subtypes included polyarthritis (n=82); psoriatic arthritis (13); enthesitis-related arthritis (49); undifferentiated arthritis (64), and systemic arthritis (18). Uveitis developed in 89 children during the follow-up period.
At baseline, almost all of the children (97%) had taken a nonsteroidal anti-inflammatory drug. About half (48%) had taken methotrexate, while 74% had received intra-articular glucocorticoids and 32% received oral glucocorticoids. More than half (58%) had used a disease-modifying anti-rheumatic drug, including an anti-TNF (anti–tumor necrosis factor) drug. Only 3% were not taking any medications at baseline.
The mean follow-up period was 98 months. By that time, 42% were in remission and off medication. However, more than half of the group (58%) were either not in remission (49%) or in remission on medication (9%) said Dr. Nordal, a pediatric rheumatologist at the University Hospital of North Norway, Troms?.
Rates of remission off medication varied by subtype, with the greatest rate occurring among those with systemic arthritis (83%). The lowest rates of remission off medication occurred in those with extended oligoarthritis (21%) and psoriatic arthritis (23%).
The highest rates of ongoing disease occurred in those children who had rheumatoid factor–positive polyarthritis (67%) and extended oligoarthritis (63%). But more than half of those children with rheumatoid factor–negative polyarthritis, psoriatic arthritis, enthesitis-related arthritis, and undifferentiated arthritis also failed to achieve remission.
Fatigue is another aspect of the disease that continues to bother young people as they grow into their teens, according to registered nurse Deborah Hilderson of the Catholic University of Leuven, Belgium. She presented the results of a small cross-sectional study of 31 adolescents with JIA, which examined the impact of fatigue on their daily lives. The patients were compared with a group of healthy controls used in a 2003 study of excess fatigue in young adult survivors of childhood cancer (Eur. J. Cancer 2003;39:204-14).
The patients had a mean age of 16 years; all had been treated at the University Hospital Leuven in Belgium. Most of the group (23) was female. Persistent or extended oligoarthritis was present in 11 patients; rheumatoid factor-negative polyarthritis in 9; systemic arthritis in 4; and enthesitis-related arthritis in 7.
They completed two quality of life measures. The Multidimensional Fatigue Inventory (MFI) scores fatigue on a 20-point scale in five domains: general fatigue, physical fatigue, mental fatigue, reduced activity, and reduced motivation. High scores indicate higher fatigue levels. The 100-point Quality of Life Linear Analog Scale rates 100 as the best quality of life imaginable, and 0 the worst.
About 13% of the patients reported a score of 15 or higher in the general fatigue domain of the MFI. There were no significant differences between the disease subtypes for any of the five fatigue domains. Compared with controls, patients reported significantly higher scores for physical fatigue and reduced activity. However, Ms. Hilderson pointed out, although the differences were statistically significant, the actual differences were “rather small.”
The median quality of life score was 74, but the range was wide (10-97). Higher quality of life scores were significantly associated with lower fatigue scores. There was a moderate association between quality of life and general and mental fatigue, Ms. Hilderson said.
“Fatigue does seem to be a problem for adolescents with JIA, and we, as health care providers, do need to pay attention to this complaint, particularly in patients with active arthritis,” Ms. Hilderson said.
Disclosures: Neither Dr. Rygg, Dr. Nordal, nor Ms. Hilderson disclosed any potential financial conflicts.

JIA Remission by Disease Subtype
VALENCIA, Spain – Despite treatment, nearly half of children with juvenile idiopathic arthritis continue to experience active disease and many report significant physical fatigue, according to researchers at the Congress of the Pediatric Rheumatology European Society.
“Our results point out that JIA is a controllable and treatable, but not curable, disease for a majority of the children,” coauthor Dr. Marite Rygg of St. Olavs Hospital, Trondheim, Norway, said in an interview.
Her colleague, Dr. Ellen Nordal, reported 7-year follow-up data on 427 children who were enrolled in the Nordic Juvenile Idiopathic Arthritis Cohort from 1997-2000. The cohort comprised patients from 12 centers in Norway, Finland, Sweden, and Denmark. At the congress, Dr. Nordal reported complete follow-up data on 427 of the children.
Most the patients (66%) were girls. Their median age at the onset of disease was 6 years. The most common arthritis subtype in the group was oligoarthritis; this was persistent in 126 and extended in 75. Other disease subtypes included polyarthritis (n=82); psoriatic arthritis (13); enthesitis-related arthritis (49); undifferentiated arthritis (64), and systemic arthritis (18). Uveitis developed in 89 children during the follow-up period.
At baseline, almost all of the children (97%) had taken a nonsteroidal anti-inflammatory drug. About half (48%) had taken methotrexate, while 74% had received intra-articular glucocorticoids and 32% received oral glucocorticoids. More than half (58%) had used a disease-modifying anti-rheumatic drug, including an anti-TNF (anti–tumor necrosis factor) drug. Only 3% were not taking any medications at baseline.
The mean follow-up period was 98 months. By that time, 42% were in remission and off medication. However, more than half of the group (58%) were either not in remission (49%) or in remission on medication (9%) said Dr. Nordal, a pediatric rheumatologist at the University Hospital of North Norway, Troms?.
Rates of remission off medication varied by subtype, with the greatest rate occurring among those with systemic arthritis (83%). The lowest rates of remission off medication occurred in those with extended oligoarthritis (21%) and psoriatic arthritis (23%).
The highest rates of ongoing disease occurred in those children who had rheumatoid factor–positive polyarthritis (67%) and extended oligoarthritis (63%). But more than half of those children with rheumatoid factor–negative polyarthritis, psoriatic arthritis, enthesitis-related arthritis, and undifferentiated arthritis also failed to achieve remission.
Fatigue is another aspect of the disease that continues to bother young people as they grow into their teens, according to registered nurse Deborah Hilderson of the Catholic University of Leuven, Belgium. She presented the results of a small cross-sectional study of 31 adolescents with JIA, which examined the impact of fatigue on their daily lives. The patients were compared with a group of healthy controls used in a 2003 study of excess fatigue in young adult survivors of childhood cancer (Eur. J. Cancer 2003;39:204-14).
The patients had a mean age of 16 years; all had been treated at the University Hospital Leuven in Belgium. Most of the group (23) was female. Persistent or extended oligoarthritis was present in 11 patients; rheumatoid factor-negative polyarthritis in 9; systemic arthritis in 4; and enthesitis-related arthritis in 7.
They completed two quality of life measures. The Multidimensional Fatigue Inventory (MFI) scores fatigue on a 20-point scale in five domains: general fatigue, physical fatigue, mental fatigue, reduced activity, and reduced motivation. High scores indicate higher fatigue levels. The 100-point Quality of Life Linear Analog Scale rates 100 as the best quality of life imaginable, and 0 the worst.
About 13% of the patients reported a score of 15 or higher in the general fatigue domain of the MFI. There were no significant differences between the disease subtypes for any of the five fatigue domains. Compared with controls, patients reported significantly higher scores for physical fatigue and reduced activity. However, Ms. Hilderson pointed out, although the differences were statistically significant, the actual differences were “rather small.”
The median quality of life score was 74, but the range was wide (10-97). Higher quality of life scores were significantly associated with lower fatigue scores. There was a moderate association between quality of life and general and mental fatigue, Ms. Hilderson said.
“Fatigue does seem to be a problem for adolescents with JIA, and we, as health care providers, do need to pay attention to this complaint, particularly in patients with active arthritis,” Ms. Hilderson said.
Disclosures: Neither Dr. Rygg, Dr. Nordal, nor Ms. Hilderson disclosed any potential financial conflicts.
JIA Remission by Disease Subtype
VALENCIA, Spain – Despite treatment, nearly half of children with juvenile idiopathic arthritis continue to experience active disease and many report significant physical fatigue, according to researchers at the Congress of the Pediatric Rheumatology European Society.
“Our results point out that JIA is a controllable and treatable, but not curable, disease for a majority of the children,” coauthor Dr. Marite Rygg of St. Olavs Hospital, Trondheim, Norway, said in an interview.
Her colleague, Dr. Ellen Nordal, reported 7-year follow-up data on 427 children who were enrolled in the Nordic Juvenile Idiopathic Arthritis Cohort from 1997-2000. The cohort comprised patients from 12 centers in Norway, Finland, Sweden, and Denmark. At the congress, Dr. Nordal reported complete follow-up data on 427 of the children.
Most the patients (66%) were girls. Their median age at the onset of disease was 6 years. The most common arthritis subtype in the group was oligoarthritis; this was persistent in 126 and extended in 75. Other disease subtypes included polyarthritis (n=82); psoriatic arthritis (13); enthesitis-related arthritis (49); undifferentiated arthritis (64), and systemic arthritis (18). Uveitis developed in 89 children during the follow-up period.
At baseline, almost all of the children (97%) had taken a nonsteroidal anti-inflammatory drug. About half (48%) had taken methotrexate, while 74% had received intra-articular glucocorticoids and 32% received oral glucocorticoids. More than half (58%) had used a disease-modifying anti-rheumatic drug, including an anti-TNF (anti–tumor necrosis factor) drug. Only 3% were not taking any medications at baseline.
The mean follow-up period was 98 months. By that time, 42% were in remission and off medication. However, more than half of the group (58%) were either not in remission (49%) or in remission on medication (9%) said Dr. Nordal, a pediatric rheumatologist at the University Hospital of North Norway, Troms?.
Rates of remission off medication varied by subtype, with the greatest rate occurring among those with systemic arthritis (83%). The lowest rates of remission off medication occurred in those with extended oligoarthritis (21%) and psoriatic arthritis (23%).
The highest rates of ongoing disease occurred in those children who had rheumatoid factor–positive polyarthritis (67%) and extended oligoarthritis (63%). But more than half of those children with rheumatoid factor–negative polyarthritis, psoriatic arthritis, enthesitis-related arthritis, and undifferentiated arthritis also failed to achieve remission.
Fatigue is another aspect of the disease that continues to bother young people as they grow into their teens, according to registered nurse Deborah Hilderson of the Catholic University of Leuven, Belgium. She presented the results of a small cross-sectional study of 31 adolescents with JIA, which examined the impact of fatigue on their daily lives. The patients were compared with a group of healthy controls used in a 2003 study of excess fatigue in young adult survivors of childhood cancer (Eur. J. Cancer 2003;39:204-14).
The patients had a mean age of 16 years; all had been treated at the University Hospital Leuven in Belgium. Most of the group (23) was female. Persistent or extended oligoarthritis was present in 11 patients; rheumatoid factor-negative polyarthritis in 9; systemic arthritis in 4; and enthesitis-related arthritis in 7.
They completed two quality of life measures. The Multidimensional Fatigue Inventory (MFI) scores fatigue on a 20-point scale in five domains: general fatigue, physical fatigue, mental fatigue, reduced activity, and reduced motivation. High scores indicate higher fatigue levels. The 100-point Quality of Life Linear Analog Scale rates 100 as the best quality of life imaginable, and 0 the worst.
About 13% of the patients reported a score of 15 or higher in the general fatigue domain of the MFI. There were no significant differences between the disease subtypes for any of the five fatigue domains. Compared with controls, patients reported significantly higher scores for physical fatigue and reduced activity. However, Ms. Hilderson pointed out, although the differences were statistically significant, the actual differences were “rather small.”
The median quality of life score was 74, but the range was wide (10-97). Higher quality of life scores were significantly associated with lower fatigue scores. There was a moderate association between quality of life and general and mental fatigue, Ms. Hilderson said.
“Fatigue does seem to be a problem for adolescents with JIA, and we, as health care providers, do need to pay attention to this complaint, particularly in patients with active arthritis,” Ms. Hilderson said.
Disclosures: Neither Dr. Rygg, Dr. Nordal, nor Ms. Hilderson disclosed any potential financial conflicts.
JIA Remission by Disease Subtype
Many Children With JIA Do Not Achieve Remission, Despite Adequate Treatment
VALENCIA, Spain - Despite treatment, nearly half of children with juvenile idiopathic arthritis continue to experience active disease and many report significant physical fatigue, according to researchers at the Congress of the Pediatric Rheumatology European Society.
“Our results point out that JIA is a controllable and treatable, but not curable, disease for a majority of the children,” coauthor Dr. Marite Rygg of St. Olavs Hospital, Trondheim, Norway, said in an interview.
Her colleague, Dr. Ellen Nordal, reported 7-year follow-up data on 427 children who were enrolled in the Nordic Juvenile Idiopathic Arthritis Cohort from 1997-2000. The cohort comprised patients from 12 centers in Norway, Finland, Sweden, and Denmark. At the congress, Dr. Nordal reported complete follow-up data on 427 of the children.
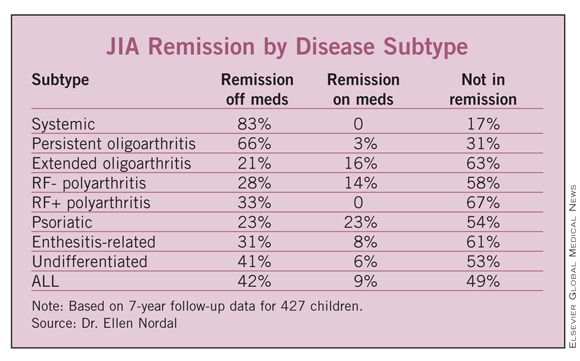
Most the patients (66%) were girls. Their median age at the onset of disease was 6 years. The most common arthritis subtype in the group was oligoarthritis; this was persistent in 126 and extended in 75. Other disease subtypes included polyarthritis (n=82); psoriatic arthritis (13); enthesitis-related arthritis (49); undifferentiated arthritis (64), and systemic arthritis (18). Uveitis developed in 89 children during the follow-up period.
At baseline, almost all of the children (97%) had taken a nonsteroidal anti-inflammatory drug. About half (48%) had taken methotrexate, while 74% had received intra-articular glucocorticoids and 32% received oral glucocorticoids. More than half (58%) had used a disease-modifying anti-rheumatic drug, including an anti-TNF (anti–tumor necrosis factor) drug. Only 3% were not taking any medications at baseline.
The mean follow-up period was 98 months. By that time, 42% were in remission and off medication. However, more than half of the group (58%) were either not in remission (49%) or in remission on medication (9%) said Dr. Nordal, a pediatric rheumatologist at the University Hospital of North Norway, Troms?.
Rates of remission off medication varied by subtype, with the greatest rate occurring among those with systemic arthritis (83%). The lowest rates of remission off medication occurred in those with extended oligoarthritis (21%) and psoriatic arthritis (23%).
The highest rates of ongoing disease occurred in those children who had rheumatoid factor–positive polyarthritis (67%) and extended oligoarthritis (63%). But more than half of those children with rheumatoid factor–negative polyarthritis, psoriatic arthritis, enthesitis-related arthritis, and undifferentiated arthritis also failed to achieve remission.
Fatigue is another aspect of the disease that continues to bother young people as they grow into their teens, according to registered nurse Deborah Hilderson of the Catholic University of Leuven, Belgium. She presented the results of a small cross-sectional study of 31 adolescents with JIA, which examined the impact of fatigue on their daily lives. The patients were compared with a group of healthy controls used in a 2003 study of excess fatigue in young adult survivors of childhood cancer (Eur. J. Cancer 2003;39:204-14).
The patients had a mean age of 16 years; all had been treated at the University Hospital Leuven in Belgium. Most of the group (23) was female. Persistent or extended oligoarthritis was present in 11 patients; rheumatoid factor-negative polyarthritis in 9; systemic arthritis in 4; and enthesitis-related arthritis in 7.
They completed two quality of life measures. The Multidimensional Fatigue Inventory (MFI) scores fatigue on a 20-point scale in five domains: general fatigue, physical fatigue, mental fatigue, reduced activity, and reduced motivation. High scores indicate higher fatigue levels. The 100-point Quality of Life Linear Analog Scale rates 100 as the best quality of life imaginable, and 0 the worst.
About 13% of the patients reported a score of 15 or higher in the general fatigue domain of the MFI. There were no significant differences between the disease subtypes for any of the five fatigue domains. Compared with controls, patients reported significantly higher scores for physical fatigue and reduced activity. However, Ms. Hilderson pointed out, although the differences were statistically significant, the actual differences were “rather small.”
The median quality of life score was 74, but the range was wide (10-97). Higher quality of life scores were significantly associated with lower fatigue scores. There was a moderate association between quality of life and general and mental fatigue, Ms. Hilderson said.
“Fatigue does seem to be a problem for adolescents with JIA, and we, as health care providers, do need to pay attention to this complaint, particularly in patients with active arthritis,” Ms. Hilderson said.
VALENCIA, Spain - Despite treatment, nearly half of children with juvenile idiopathic arthritis continue to experience active disease and many report significant physical fatigue, according to researchers at the Congress of the Pediatric Rheumatology European Society.
“Our results point out that JIA is a controllable and treatable, but not curable, disease for a majority of the children,” coauthor Dr. Marite Rygg of St. Olavs Hospital, Trondheim, Norway, said in an interview.
Her colleague, Dr. Ellen Nordal, reported 7-year follow-up data on 427 children who were enrolled in the Nordic Juvenile Idiopathic Arthritis Cohort from 1997-2000. The cohort comprised patients from 12 centers in Norway, Finland, Sweden, and Denmark. At the congress, Dr. Nordal reported complete follow-up data on 427 of the children.
Most the patients (66%) were girls. Their median age at the onset of disease was 6 years. The most common arthritis subtype in the group was oligoarthritis; this was persistent in 126 and extended in 75. Other disease subtypes included polyarthritis (n=82); psoriatic arthritis (13); enthesitis-related arthritis (49); undifferentiated arthritis (64), and systemic arthritis (18). Uveitis developed in 89 children during the follow-up period.
At baseline, almost all of the children (97%) had taken a nonsteroidal anti-inflammatory drug. About half (48%) had taken methotrexate, while 74% had received intra-articular glucocorticoids and 32% received oral glucocorticoids. More than half (58%) had used a disease-modifying anti-rheumatic drug, including an anti-TNF (anti–tumor necrosis factor) drug. Only 3% were not taking any medications at baseline.
The mean follow-up period was 98 months. By that time, 42% were in remission and off medication. However, more than half of the group (58%) were either not in remission (49%) or in remission on medication (9%) said Dr. Nordal, a pediatric rheumatologist at the University Hospital of North Norway, Troms?.
Rates of remission off medication varied by subtype, with the greatest rate occurring among those with systemic arthritis (83%). The lowest rates of remission off medication occurred in those with extended oligoarthritis (21%) and psoriatic arthritis (23%).
The highest rates of ongoing disease occurred in those children who had rheumatoid factor–positive polyarthritis (67%) and extended oligoarthritis (63%). But more than half of those children with rheumatoid factor–negative polyarthritis, psoriatic arthritis, enthesitis-related arthritis, and undifferentiated arthritis also failed to achieve remission.
Fatigue is another aspect of the disease that continues to bother young people as they grow into their teens, according to registered nurse Deborah Hilderson of the Catholic University of Leuven, Belgium. She presented the results of a small cross-sectional study of 31 adolescents with JIA, which examined the impact of fatigue on their daily lives. The patients were compared with a group of healthy controls used in a 2003 study of excess fatigue in young adult survivors of childhood cancer (Eur. J. Cancer 2003;39:204-14).
The patients had a mean age of 16 years; all had been treated at the University Hospital Leuven in Belgium. Most of the group (23) was female. Persistent or extended oligoarthritis was present in 11 patients; rheumatoid factor-negative polyarthritis in 9; systemic arthritis in 4; and enthesitis-related arthritis in 7.
They completed two quality of life measures. The Multidimensional Fatigue Inventory (MFI) scores fatigue on a 20-point scale in five domains: general fatigue, physical fatigue, mental fatigue, reduced activity, and reduced motivation. High scores indicate higher fatigue levels. The 100-point Quality of Life Linear Analog Scale rates 100 as the best quality of life imaginable, and 0 the worst.
About 13% of the patients reported a score of 15 or higher in the general fatigue domain of the MFI. There were no significant differences between the disease subtypes for any of the five fatigue domains. Compared with controls, patients reported significantly higher scores for physical fatigue and reduced activity. However, Ms. Hilderson pointed out, although the differences were statistically significant, the actual differences were “rather small.”
The median quality of life score was 74, but the range was wide (10-97). Higher quality of life scores were significantly associated with lower fatigue scores. There was a moderate association between quality of life and general and mental fatigue, Ms. Hilderson said.
“Fatigue does seem to be a problem for adolescents with JIA, and we, as health care providers, do need to pay attention to this complaint, particularly in patients with active arthritis,” Ms. Hilderson said.
VALENCIA, Spain - Despite treatment, nearly half of children with juvenile idiopathic arthritis continue to experience active disease and many report significant physical fatigue, according to researchers at the Congress of the Pediatric Rheumatology European Society.
“Our results point out that JIA is a controllable and treatable, but not curable, disease for a majority of the children,” coauthor Dr. Marite Rygg of St. Olavs Hospital, Trondheim, Norway, said in an interview.
Her colleague, Dr. Ellen Nordal, reported 7-year follow-up data on 427 children who were enrolled in the Nordic Juvenile Idiopathic Arthritis Cohort from 1997-2000. The cohort comprised patients from 12 centers in Norway, Finland, Sweden, and Denmark. At the congress, Dr. Nordal reported complete follow-up data on 427 of the children.
Most the patients (66%) were girls. Their median age at the onset of disease was 6 years. The most common arthritis subtype in the group was oligoarthritis; this was persistent in 126 and extended in 75. Other disease subtypes included polyarthritis (n=82); psoriatic arthritis (13); enthesitis-related arthritis (49); undifferentiated arthritis (64), and systemic arthritis (18). Uveitis developed in 89 children during the follow-up period.
At baseline, almost all of the children (97%) had taken a nonsteroidal anti-inflammatory drug. About half (48%) had taken methotrexate, while 74% had received intra-articular glucocorticoids and 32% received oral glucocorticoids. More than half (58%) had used a disease-modifying anti-rheumatic drug, including an anti-TNF (anti–tumor necrosis factor) drug. Only 3% were not taking any medications at baseline.
The mean follow-up period was 98 months. By that time, 42% were in remission and off medication. However, more than half of the group (58%) were either not in remission (49%) or in remission on medication (9%) said Dr. Nordal, a pediatric rheumatologist at the University Hospital of North Norway, Troms?.
Rates of remission off medication varied by subtype, with the greatest rate occurring among those with systemic arthritis (83%). The lowest rates of remission off medication occurred in those with extended oligoarthritis (21%) and psoriatic arthritis (23%).
The highest rates of ongoing disease occurred in those children who had rheumatoid factor–positive polyarthritis (67%) and extended oligoarthritis (63%). But more than half of those children with rheumatoid factor–negative polyarthritis, psoriatic arthritis, enthesitis-related arthritis, and undifferentiated arthritis also failed to achieve remission.
Fatigue is another aspect of the disease that continues to bother young people as they grow into their teens, according to registered nurse Deborah Hilderson of the Catholic University of Leuven, Belgium. She presented the results of a small cross-sectional study of 31 adolescents with JIA, which examined the impact of fatigue on their daily lives. The patients were compared with a group of healthy controls used in a 2003 study of excess fatigue in young adult survivors of childhood cancer (Eur. J. Cancer 2003;39:204-14).
The patients had a mean age of 16 years; all had been treated at the University Hospital Leuven in Belgium. Most of the group (23) was female. Persistent or extended oligoarthritis was present in 11 patients; rheumatoid factor-negative polyarthritis in 9; systemic arthritis in 4; and enthesitis-related arthritis in 7.
They completed two quality of life measures. The Multidimensional Fatigue Inventory (MFI) scores fatigue on a 20-point scale in five domains: general fatigue, physical fatigue, mental fatigue, reduced activity, and reduced motivation. High scores indicate higher fatigue levels. The 100-point Quality of Life Linear Analog Scale rates 100 as the best quality of life imaginable, and 0 the worst.
About 13% of the patients reported a score of 15 or higher in the general fatigue domain of the MFI. There were no significant differences between the disease subtypes for any of the five fatigue domains. Compared with controls, patients reported significantly higher scores for physical fatigue and reduced activity. However, Ms. Hilderson pointed out, although the differences were statistically significant, the actual differences were “rather small.”
The median quality of life score was 74, but the range was wide (10-97). Higher quality of life scores were significantly associated with lower fatigue scores. There was a moderate association between quality of life and general and mental fatigue, Ms. Hilderson said.
“Fatigue does seem to be a problem for adolescents with JIA, and we, as health care providers, do need to pay attention to this complaint, particularly in patients with active arthritis,” Ms. Hilderson said.
FROM THE CONGRESS OF THE PEDIATRIC RHEUMATOLOGY EUROPEAN SOCIETY
Major Finding: More than half of 427 children with juvenile idiopathic arthritis were not in remission or were in remission but still taking medications, after 98 months of follow-up.
Data Source: A report of 7-year follow-up data on 427 children enrolled in the Nordic Juvenile Idiopathic Arthritis Cohort from 1997-2000.
Disclosures: Neither Dr. Rygg, Dr. Nordal, nor Ms. Hilderson disclosed any potential financial conflicts.
Lack of New Antibiotics Helps Superbugs Flourish
CHICAGO — By all measures, methicillin-resistant Staphylococcus aureus cases and related deaths are steadily increasing around the globe, according to Dr. Theodore Rosen. But MRSA isn't the only bug that's ramping up its antibiotic smarts these days.
"We are being bombarded every year by increasingly resistant bacteria," Dr. Rosen said in an interview. "Some of these are relatively trivial, some are really bad – like MRSA – and some are wreaking havoc. I'm talking about Klebsiella causing horrendous, frequently fatal drug-resistant pneumonia; multidrug resistant forms of the plague (the same plague that wiped out a third of Europe); and drug-resistant tuberculosis, a disease we thought we'd cornered years ago."
"The number of new antibiotics approved over the past few years has been steadily decreasing, and in the last 2 or 3 years, only one new antibiotic has been approved," despite promising data, said Dr. Rosen, professor of dermatology at Baylor College of Medicine, Houston.
Stung by recent problems with already approved drugs, the Food and Drug Administration has become increasingly stringent about the approval of new medications, including antibiotics, he noted.
Pharmaceutical companies also play a role. "You stand to make a lot more money developing a drug for a chronic disease than one only given for 14 days, like an antibiotic," said Dr. Rosen.
He discussed several antibiotics that showed promise but never found their way to the federal finish line. Two – oritavancin and dalbavancin – are molecularly related to telavancin, which was approved in 2009. "Oritavancin was rejected [by the FDA] because it did not show noninferiority to vancomycin," he said.
Dalbavancin did well in phase III trials for uncomplicated skin and soft tissue infections. "You can give it once a week, and it's incredibly potent, doing better by far in vitro than anything else available," Dr. Rosen said. The drug received an FDA approvable letter, but never went further. According to the FDA "the studies were not well done and questioned some of the methodology, so Pfizer sold the rights to the drug, fearing it would not be the blockbuster they had hoped," he said. The drug is now in developmental limbo.
Iclaprim, a trimethoprim-related drug, is also languishing. "It's a good drug, with a 99.9% kill rate in vitro. It works in trimethoprim resistance and can be given orally or intravenously. It looked great in its phase II and III trials," said Dr. Rosen. However, the FDA rejected the drug. Iclaprim met its initial requirement of no more than a 12.5% efficacy difference with its comparator, linezolid. However, the FDA upped the ante to no more than a 10% difference, at which time Roche sold the drug to another company, which merged with another and sold iclaprim again. "No one knows this drug's future," Dr. Rosen said.
Monoclonal antibodies that bind to the staphylococcal clumping factor are also in the works. "This is a very clever way of treating staph bacteria, by keeping them from grabbing hold of fibrinogen so they can't get into tissue," Dr. Rosen said. Early studies have shown that patients who received the antibody plus an antibiotic did better than those who only received the antibiotic, and that the combination was able to clear MRSA carriage.
"Unfortunately, the company developing this ran out of money, so this antibody is sitting on the shelf somewhere until the company finds a new financial partner," he added.
FDA's insistence on noninferiority trials for antibiotics hinders approval, Dr. Rosen opined. "It's difficult to figure out how noninferior the new drug has to be. Several have shown noninferiority – there were failures, but the failure rate was relatively low. The FDA has said the rate must be lower, because otherwise, a certain number of patients would have done better on the comparator drug, even though each drug has its own positive and negative attributes. The FDA has had conference after conference with infectious disease experts. We have made little progress in negotiation and have no new antibiotics at a time when resistance is rising, and it's critical that we develop more."
Time may be running out. Before the advent of penicillin in 1928, infection was the leading cause of death worldwide; in 2000, it was still the fourth-leading cause of death. "If our antibiotics stop working, we will rapidly go back to those pre–World War II days when all we had to treat infections were arsenic and sulfa…. It's not inconceivable that we could once again live in a time when infections reign supreme," said Dr. Rosen, who reported having no relevant financial disclosures.
The development of new antibacterial drugs is an important public health issue and one that the Food and Drug Administration is working with academia and industry to address. FDA plays an important role in providing recommendations to companies on the types of trial designs to use to study a new drug.
Antimicrobial resistance is a problem. We need new therapeutic options to treat resistant bacteria, and we will continue to need new therapeutic options in the future to treat patients with infections.
There are scientific, economic, and regulatory challenges that affect the development of new antibacterial drugs. Based on our current understanding of a number of infectious diseases, antibacterial drug effects, and clinical trial design, it is clear that some clinical trial designs used in the past were not an informative means to evaluate drug effectiveness.
The FDA is working to update guidance and meets with companies developing antibacterial drugs to provide advice on their development programs so that they will be designed to meet the efficacy standards established by law. As part of these efforts, the FDA recognizes the need for approval pathways which are feasible.
The challenges we are facing in antibacterial drug development are largely scientific, and the path forward must be supported by sound science. To that end, the FDA has engaged scientific experts, including members of the Infectious Disease Society of America, in a series of recent public workshops and advisory committee meetings.
Draft guidance documents have been issued for acute bacterial otitis media, acute bacterial exacerbations of chronic bronchitis, acute bacterial sinusitis, community-acquired bacterial pneumonia, noninferiority clinical trial design, and acute bacterial skin and skin structure infections. And a draft guidance document for hospital-acquired bacterial pneumonia/ventilator-associated bacterial pneumonia will be issued in the coming months.
In addition to publishing guidance documents, the FDA meets with companies developing new antibacterial drugs and provides advice throughout drug development. The Agency looks forward to continuing to work with scientific experts to address the challenges of new antibacterial drug development.
The development of new antibacterial drugs is an important public health issue and one that the Food and Drug Administration is working with academia and industry to address. FDA plays an important role in providing recommendations to companies on the types of trial designs to use to study a new drug.
Antimicrobial resistance is a problem. We need new therapeutic options to treat resistant bacteria, and we will continue to need new therapeutic options in the future to treat patients with infections.
There are scientific, economic, and regulatory challenges that affect the development of new antibacterial drugs. Based on our current understanding of a number of infectious diseases, antibacterial drug effects, and clinical trial design, it is clear that some clinical trial designs used in the past were not an informative means to evaluate drug effectiveness.
The FDA is working to update guidance and meets with companies developing antibacterial drugs to provide advice on their development programs so that they will be designed to meet the efficacy standards established by law. As part of these efforts, the FDA recognizes the need for approval pathways which are feasible.
The challenges we are facing in antibacterial drug development are largely scientific, and the path forward must be supported by sound science. To that end, the FDA has engaged scientific experts, including members of the Infectious Disease Society of America, in a series of recent public workshops and advisory committee meetings.
Draft guidance documents have been issued for acute bacterial otitis media, acute bacterial exacerbations of chronic bronchitis, acute bacterial sinusitis, community-acquired bacterial pneumonia, noninferiority clinical trial design, and acute bacterial skin and skin structure infections. And a draft guidance document for hospital-acquired bacterial pneumonia/ventilator-associated bacterial pneumonia will be issued in the coming months.
In addition to publishing guidance documents, the FDA meets with companies developing new antibacterial drugs and provides advice throughout drug development. The Agency looks forward to continuing to work with scientific experts to address the challenges of new antibacterial drug development.
The development of new antibacterial drugs is an important public health issue and one that the Food and Drug Administration is working with academia and industry to address. FDA plays an important role in providing recommendations to companies on the types of trial designs to use to study a new drug.
Antimicrobial resistance is a problem. We need new therapeutic options to treat resistant bacteria, and we will continue to need new therapeutic options in the future to treat patients with infections.
There are scientific, economic, and regulatory challenges that affect the development of new antibacterial drugs. Based on our current understanding of a number of infectious diseases, antibacterial drug effects, and clinical trial design, it is clear that some clinical trial designs used in the past were not an informative means to evaluate drug effectiveness.
The FDA is working to update guidance and meets with companies developing antibacterial drugs to provide advice on their development programs so that they will be designed to meet the efficacy standards established by law. As part of these efforts, the FDA recognizes the need for approval pathways which are feasible.
The challenges we are facing in antibacterial drug development are largely scientific, and the path forward must be supported by sound science. To that end, the FDA has engaged scientific experts, including members of the Infectious Disease Society of America, in a series of recent public workshops and advisory committee meetings.
Draft guidance documents have been issued for acute bacterial otitis media, acute bacterial exacerbations of chronic bronchitis, acute bacterial sinusitis, community-acquired bacterial pneumonia, noninferiority clinical trial design, and acute bacterial skin and skin structure infections. And a draft guidance document for hospital-acquired bacterial pneumonia/ventilator-associated bacterial pneumonia will be issued in the coming months.
In addition to publishing guidance documents, the FDA meets with companies developing new antibacterial drugs and provides advice throughout drug development. The Agency looks forward to continuing to work with scientific experts to address the challenges of new antibacterial drug development.
CHICAGO — By all measures, methicillin-resistant Staphylococcus aureus cases and related deaths are steadily increasing around the globe, according to Dr. Theodore Rosen. But MRSA isn't the only bug that's ramping up its antibiotic smarts these days.
"We are being bombarded every year by increasingly resistant bacteria," Dr. Rosen said in an interview. "Some of these are relatively trivial, some are really bad – like MRSA – and some are wreaking havoc. I'm talking about Klebsiella causing horrendous, frequently fatal drug-resistant pneumonia; multidrug resistant forms of the plague (the same plague that wiped out a third of Europe); and drug-resistant tuberculosis, a disease we thought we'd cornered years ago."
"The number of new antibiotics approved over the past few years has been steadily decreasing, and in the last 2 or 3 years, only one new antibiotic has been approved," despite promising data, said Dr. Rosen, professor of dermatology at Baylor College of Medicine, Houston.
Stung by recent problems with already approved drugs, the Food and Drug Administration has become increasingly stringent about the approval of new medications, including antibiotics, he noted.
Pharmaceutical companies also play a role. "You stand to make a lot more money developing a drug for a chronic disease than one only given for 14 days, like an antibiotic," said Dr. Rosen.
He discussed several antibiotics that showed promise but never found their way to the federal finish line. Two – oritavancin and dalbavancin – are molecularly related to telavancin, which was approved in 2009. "Oritavancin was rejected [by the FDA] because it did not show noninferiority to vancomycin," he said.
Dalbavancin did well in phase III trials for uncomplicated skin and soft tissue infections. "You can give it once a week, and it's incredibly potent, doing better by far in vitro than anything else available," Dr. Rosen said. The drug received an FDA approvable letter, but never went further. According to the FDA "the studies were not well done and questioned some of the methodology, so Pfizer sold the rights to the drug, fearing it would not be the blockbuster they had hoped," he said. The drug is now in developmental limbo.
Iclaprim, a trimethoprim-related drug, is also languishing. "It's a good drug, with a 99.9% kill rate in vitro. It works in trimethoprim resistance and can be given orally or intravenously. It looked great in its phase II and III trials," said Dr. Rosen. However, the FDA rejected the drug. Iclaprim met its initial requirement of no more than a 12.5% efficacy difference with its comparator, linezolid. However, the FDA upped the ante to no more than a 10% difference, at which time Roche sold the drug to another company, which merged with another and sold iclaprim again. "No one knows this drug's future," Dr. Rosen said.
Monoclonal antibodies that bind to the staphylococcal clumping factor are also in the works. "This is a very clever way of treating staph bacteria, by keeping them from grabbing hold of fibrinogen so they can't get into tissue," Dr. Rosen said. Early studies have shown that patients who received the antibody plus an antibiotic did better than those who only received the antibiotic, and that the combination was able to clear MRSA carriage.
"Unfortunately, the company developing this ran out of money, so this antibody is sitting on the shelf somewhere until the company finds a new financial partner," he added.
FDA's insistence on noninferiority trials for antibiotics hinders approval, Dr. Rosen opined. "It's difficult to figure out how noninferior the new drug has to be. Several have shown noninferiority – there were failures, but the failure rate was relatively low. The FDA has said the rate must be lower, because otherwise, a certain number of patients would have done better on the comparator drug, even though each drug has its own positive and negative attributes. The FDA has had conference after conference with infectious disease experts. We have made little progress in negotiation and have no new antibiotics at a time when resistance is rising, and it's critical that we develop more."
Time may be running out. Before the advent of penicillin in 1928, infection was the leading cause of death worldwide; in 2000, it was still the fourth-leading cause of death. "If our antibiotics stop working, we will rapidly go back to those pre–World War II days when all we had to treat infections were arsenic and sulfa…. It's not inconceivable that we could once again live in a time when infections reign supreme," said Dr. Rosen, who reported having no relevant financial disclosures.
CHICAGO — By all measures, methicillin-resistant Staphylococcus aureus cases and related deaths are steadily increasing around the globe, according to Dr. Theodore Rosen. But MRSA isn't the only bug that's ramping up its antibiotic smarts these days.
"We are being bombarded every year by increasingly resistant bacteria," Dr. Rosen said in an interview. "Some of these are relatively trivial, some are really bad – like MRSA – and some are wreaking havoc. I'm talking about Klebsiella causing horrendous, frequently fatal drug-resistant pneumonia; multidrug resistant forms of the plague (the same plague that wiped out a third of Europe); and drug-resistant tuberculosis, a disease we thought we'd cornered years ago."
"The number of new antibiotics approved over the past few years has been steadily decreasing, and in the last 2 or 3 years, only one new antibiotic has been approved," despite promising data, said Dr. Rosen, professor of dermatology at Baylor College of Medicine, Houston.
Stung by recent problems with already approved drugs, the Food and Drug Administration has become increasingly stringent about the approval of new medications, including antibiotics, he noted.
Pharmaceutical companies also play a role. "You stand to make a lot more money developing a drug for a chronic disease than one only given for 14 days, like an antibiotic," said Dr. Rosen.
He discussed several antibiotics that showed promise but never found their way to the federal finish line. Two – oritavancin and dalbavancin – are molecularly related to telavancin, which was approved in 2009. "Oritavancin was rejected [by the FDA] because it did not show noninferiority to vancomycin," he said.
Dalbavancin did well in phase III trials for uncomplicated skin and soft tissue infections. "You can give it once a week, and it's incredibly potent, doing better by far in vitro than anything else available," Dr. Rosen said. The drug received an FDA approvable letter, but never went further. According to the FDA "the studies were not well done and questioned some of the methodology, so Pfizer sold the rights to the drug, fearing it would not be the blockbuster they had hoped," he said. The drug is now in developmental limbo.
Iclaprim, a trimethoprim-related drug, is also languishing. "It's a good drug, with a 99.9% kill rate in vitro. It works in trimethoprim resistance and can be given orally or intravenously. It looked great in its phase II and III trials," said Dr. Rosen. However, the FDA rejected the drug. Iclaprim met its initial requirement of no more than a 12.5% efficacy difference with its comparator, linezolid. However, the FDA upped the ante to no more than a 10% difference, at which time Roche sold the drug to another company, which merged with another and sold iclaprim again. "No one knows this drug's future," Dr. Rosen said.
Monoclonal antibodies that bind to the staphylococcal clumping factor are also in the works. "This is a very clever way of treating staph bacteria, by keeping them from grabbing hold of fibrinogen so they can't get into tissue," Dr. Rosen said. Early studies have shown that patients who received the antibody plus an antibiotic did better than those who only received the antibiotic, and that the combination was able to clear MRSA carriage.
"Unfortunately, the company developing this ran out of money, so this antibody is sitting on the shelf somewhere until the company finds a new financial partner," he added.
FDA's insistence on noninferiority trials for antibiotics hinders approval, Dr. Rosen opined. "It's difficult to figure out how noninferior the new drug has to be. Several have shown noninferiority – there were failures, but the failure rate was relatively low. The FDA has said the rate must be lower, because otherwise, a certain number of patients would have done better on the comparator drug, even though each drug has its own positive and negative attributes. The FDA has had conference after conference with infectious disease experts. We have made little progress in negotiation and have no new antibiotics at a time when resistance is rising, and it's critical that we develop more."
Time may be running out. Before the advent of penicillin in 1928, infection was the leading cause of death worldwide; in 2000, it was still the fourth-leading cause of death. "If our antibiotics stop working, we will rapidly go back to those pre–World War II days when all we had to treat infections were arsenic and sulfa…. It's not inconceivable that we could once again live in a time when infections reign supreme," said Dr. Rosen, who reported having no relevant financial disclosures.
Hypothyroid Tx in Early Pregnancy Evaluated
Major Finding: Generalized screening and treatment of pregnant women for hypothyroidism does not improve intellectual outcomes for their offspring.
Data Source: CATS randomized almost 22,000 pregnant women to screening and treatment for hypothyroidism or no screening. At age 3, the children of treated women were intellectually comparable to those of nontreated women.
Disclosures: The trial was funded by the U.K. Wellcome Trust. Dr. Lazarus had no financial conflicts to declare.
PARIS — Screening pregnant women for hypothyroidism and treating them early in pregnancy doesn't seem to improve their children's intellectual development.
The preliminary results of the CATS (Controlled Antenatal Thyroid Screening) trial, presented at the congress, found no differences in the intellectual development of 3-year-olds whose hypothyroid mothers took levothyroxine during pregnancy and those who did not take the hormone, said primary investigator Dr. John Lazarus.
“At the moment, I think we have data that argues against population-based screening and treatment for these women,” he said in an interview. “This leaves the decision of whether to screen and treat up to the individual physician. The Endocrine Society guidelines, so far, say that testing should only be done in early pregnancy if there is some significant risk factor. But other studies show that if you adopt this method, you miss a significant number of women who should be treated.”
CATS is the first large-scale randomized controlled trial to tackle the issue. An earlier study (N. Engl. J. Med. 1999; 341:549–55) was retrospective, so it could not draw any direct conclusion about causation, said Dr. Lazarus, professor of clinical endocrinology at the University Hospital Wales and Cardiff University.
He presented preliminary data on the CATS study population comprising nearly 22,000 women with singleton pregnancies whose blood was tested for free thyroxine (T4) and thyroid stimulating hormone before 16 weeks' gestation. Before being tested, the sera were randomized to either screening (10,923) or control (10,198). Women in the screening group with low T4 and/or high TSH were given 150 mcg/day levothyroxine, and those in the control group with these results were given the drug after delivery.
Among the screening group, 4.7% were found to be hypothyroid and received treatment. Among the control group, 3.6% were found to be hypothyroid, a statistically nonsignificant difference.
When the children of these women were aged 38–40 months, they underwent intellectual testing. Dr. Lazarus presented data on 404 children in the control group and 390 in the screening group.
In the intention-to-treat analysis, the investigators found no difference in the mean IQ scores of children randomized to screening or no screening (100 vs. 99). Nor was there a significant between-group difference in the percentage of children with an IQ of less than 85 (11.5% in the screening group vs. 15.6% in the control group).
A subgroup analysis found a different result, however. The investigators examined results only among women whose consecutive blood levels showed that they were compliant with their medication. In this analysis, the mean IQ was still similar (100 vs. 100), but the percentage of those with an IQ below 85 became significantly different (9.5% screening group vs. 15.6% control group).
Dr. Lazarus cautioned against using this finding as a case for population screening, however. “By looking at it that way, we are no longer looking at a randomized group, so this is why these are very preliminary data,” he said.
Major Finding: Generalized screening and treatment of pregnant women for hypothyroidism does not improve intellectual outcomes for their offspring.
Data Source: CATS randomized almost 22,000 pregnant women to screening and treatment for hypothyroidism or no screening. At age 3, the children of treated women were intellectually comparable to those of nontreated women.
Disclosures: The trial was funded by the U.K. Wellcome Trust. Dr. Lazarus had no financial conflicts to declare.
PARIS — Screening pregnant women for hypothyroidism and treating them early in pregnancy doesn't seem to improve their children's intellectual development.
The preliminary results of the CATS (Controlled Antenatal Thyroid Screening) trial, presented at the congress, found no differences in the intellectual development of 3-year-olds whose hypothyroid mothers took levothyroxine during pregnancy and those who did not take the hormone, said primary investigator Dr. John Lazarus.
“At the moment, I think we have data that argues against population-based screening and treatment for these women,” he said in an interview. “This leaves the decision of whether to screen and treat up to the individual physician. The Endocrine Society guidelines, so far, say that testing should only be done in early pregnancy if there is some significant risk factor. But other studies show that if you adopt this method, you miss a significant number of women who should be treated.”
CATS is the first large-scale randomized controlled trial to tackle the issue. An earlier study (N. Engl. J. Med. 1999; 341:549–55) was retrospective, so it could not draw any direct conclusion about causation, said Dr. Lazarus, professor of clinical endocrinology at the University Hospital Wales and Cardiff University.
He presented preliminary data on the CATS study population comprising nearly 22,000 women with singleton pregnancies whose blood was tested for free thyroxine (T4) and thyroid stimulating hormone before 16 weeks' gestation. Before being tested, the sera were randomized to either screening (10,923) or control (10,198). Women in the screening group with low T4 and/or high TSH were given 150 mcg/day levothyroxine, and those in the control group with these results were given the drug after delivery.
Among the screening group, 4.7% were found to be hypothyroid and received treatment. Among the control group, 3.6% were found to be hypothyroid, a statistically nonsignificant difference.
When the children of these women were aged 38–40 months, they underwent intellectual testing. Dr. Lazarus presented data on 404 children in the control group and 390 in the screening group.
In the intention-to-treat analysis, the investigators found no difference in the mean IQ scores of children randomized to screening or no screening (100 vs. 99). Nor was there a significant between-group difference in the percentage of children with an IQ of less than 85 (11.5% in the screening group vs. 15.6% in the control group).
A subgroup analysis found a different result, however. The investigators examined results only among women whose consecutive blood levels showed that they were compliant with their medication. In this analysis, the mean IQ was still similar (100 vs. 100), but the percentage of those with an IQ below 85 became significantly different (9.5% screening group vs. 15.6% control group).
Dr. Lazarus cautioned against using this finding as a case for population screening, however. “By looking at it that way, we are no longer looking at a randomized group, so this is why these are very preliminary data,” he said.
Major Finding: Generalized screening and treatment of pregnant women for hypothyroidism does not improve intellectual outcomes for their offspring.
Data Source: CATS randomized almost 22,000 pregnant women to screening and treatment for hypothyroidism or no screening. At age 3, the children of treated women were intellectually comparable to those of nontreated women.
Disclosures: The trial was funded by the U.K. Wellcome Trust. Dr. Lazarus had no financial conflicts to declare.
PARIS — Screening pregnant women for hypothyroidism and treating them early in pregnancy doesn't seem to improve their children's intellectual development.
The preliminary results of the CATS (Controlled Antenatal Thyroid Screening) trial, presented at the congress, found no differences in the intellectual development of 3-year-olds whose hypothyroid mothers took levothyroxine during pregnancy and those who did not take the hormone, said primary investigator Dr. John Lazarus.
“At the moment, I think we have data that argues against population-based screening and treatment for these women,” he said in an interview. “This leaves the decision of whether to screen and treat up to the individual physician. The Endocrine Society guidelines, so far, say that testing should only be done in early pregnancy if there is some significant risk factor. But other studies show that if you adopt this method, you miss a significant number of women who should be treated.”
CATS is the first large-scale randomized controlled trial to tackle the issue. An earlier study (N. Engl. J. Med. 1999; 341:549–55) was retrospective, so it could not draw any direct conclusion about causation, said Dr. Lazarus, professor of clinical endocrinology at the University Hospital Wales and Cardiff University.
He presented preliminary data on the CATS study population comprising nearly 22,000 women with singleton pregnancies whose blood was tested for free thyroxine (T4) and thyroid stimulating hormone before 16 weeks' gestation. Before being tested, the sera were randomized to either screening (10,923) or control (10,198). Women in the screening group with low T4 and/or high TSH were given 150 mcg/day levothyroxine, and those in the control group with these results were given the drug after delivery.
Among the screening group, 4.7% were found to be hypothyroid and received treatment. Among the control group, 3.6% were found to be hypothyroid, a statistically nonsignificant difference.
When the children of these women were aged 38–40 months, they underwent intellectual testing. Dr. Lazarus presented data on 404 children in the control group and 390 in the screening group.
In the intention-to-treat analysis, the investigators found no difference in the mean IQ scores of children randomized to screening or no screening (100 vs. 99). Nor was there a significant between-group difference in the percentage of children with an IQ of less than 85 (11.5% in the screening group vs. 15.6% in the control group).
A subgroup analysis found a different result, however. The investigators examined results only among women whose consecutive blood levels showed that they were compliant with their medication. In this analysis, the mean IQ was still similar (100 vs. 100), but the percentage of those with an IQ below 85 became significantly different (9.5% screening group vs. 15.6% control group).
Dr. Lazarus cautioned against using this finding as a case for population screening, however. “By looking at it that way, we are no longer looking at a randomized group, so this is why these are very preliminary data,” he said.
Most Tanning-Bed Users Know About Devices' Cancer Risks
Major Finding: 94% of clinic patients knew the cancer risk associated with tanning beds; one-third of patients surveyed used the devices.
Data Source: Survey of 102 patients in a university dermatology clinic.
Disclosures: Dr. Ninan had no financialconflicts.
CANCUN, MEXICO — Knowledge doesn't necessarily mean power when it comes to tanning beds.
The results of a small British survey show that the majority of patients in a dermatology clinic who used tanning beds for purely cosmetic reasons were well acquainted with the risks.
Ninety-four percent of the patients surveyed were aware of the link between tanning bed use and skin cancer, and even volunteered that they knew other risks, Dr. Tina Ninan said.
“Knowing the risks does not deter patients from engaging in this risky behavior,” said Dr. Ninan, a general practice physician in Newcastle upon Tyne, England.
She distributed some simple surveys to 102 patients waiting in a dermatology clinic at the University Hospital of North Durham. Most of the respondents (65%) were women, and most (60%) were older than 40 years.
Thirty-four patients admitted to using tanning beds. Most of these (27) were women, meaning that 42% of the women surveyed admitted to using the devices. But they weren't alone: 18% of the men surveyed also said they used tanning beds.
Most of the users (88%) said that they had started visiting tanning salons before they turned 35 years old—a period considered crucial in developing an increased risk of skin cancers. “More disturbingly, 58% said they began tanning at age 17–25, and 18% of the users started at younger than 16 years,” Dr. Ninan said.
Although most reported occasional use, 38% of the tanners said they visited a tanning bed weekly. Most used tanning beds at their local beauty salon, but 9% said they had the devices at home. “Six percent also said they tanned at their gym. Having [tanning] beds at gyms and other health centers really sends a mixed message,” Dr. Ninan said.
Coin-operated tanning beds were also popular among the group, with 16% reporting use. This trend is particularly disturbing, Dr. Ninan said, because it circumvents what little control there may be over exposure.
And although the United Kingdom recently passed a law forbidding teens to use tanning beds, no one can prevent them from accessing the coin-operated types, she added.
Major Finding: 94% of clinic patients knew the cancer risk associated with tanning beds; one-third of patients surveyed used the devices.
Data Source: Survey of 102 patients in a university dermatology clinic.
Disclosures: Dr. Ninan had no financialconflicts.
CANCUN, MEXICO — Knowledge doesn't necessarily mean power when it comes to tanning beds.
The results of a small British survey show that the majority of patients in a dermatology clinic who used tanning beds for purely cosmetic reasons were well acquainted with the risks.
Ninety-four percent of the patients surveyed were aware of the link between tanning bed use and skin cancer, and even volunteered that they knew other risks, Dr. Tina Ninan said.
“Knowing the risks does not deter patients from engaging in this risky behavior,” said Dr. Ninan, a general practice physician in Newcastle upon Tyne, England.
She distributed some simple surveys to 102 patients waiting in a dermatology clinic at the University Hospital of North Durham. Most of the respondents (65%) were women, and most (60%) were older than 40 years.
Thirty-four patients admitted to using tanning beds. Most of these (27) were women, meaning that 42% of the women surveyed admitted to using the devices. But they weren't alone: 18% of the men surveyed also said they used tanning beds.
Most of the users (88%) said that they had started visiting tanning salons before they turned 35 years old—a period considered crucial in developing an increased risk of skin cancers. “More disturbingly, 58% said they began tanning at age 17–25, and 18% of the users started at younger than 16 years,” Dr. Ninan said.
Although most reported occasional use, 38% of the tanners said they visited a tanning bed weekly. Most used tanning beds at their local beauty salon, but 9% said they had the devices at home. “Six percent also said they tanned at their gym. Having [tanning] beds at gyms and other health centers really sends a mixed message,” Dr. Ninan said.
Coin-operated tanning beds were also popular among the group, with 16% reporting use. This trend is particularly disturbing, Dr. Ninan said, because it circumvents what little control there may be over exposure.
And although the United Kingdom recently passed a law forbidding teens to use tanning beds, no one can prevent them from accessing the coin-operated types, she added.
Major Finding: 94% of clinic patients knew the cancer risk associated with tanning beds; one-third of patients surveyed used the devices.
Data Source: Survey of 102 patients in a university dermatology clinic.
Disclosures: Dr. Ninan had no financialconflicts.
CANCUN, MEXICO — Knowledge doesn't necessarily mean power when it comes to tanning beds.
The results of a small British survey show that the majority of patients in a dermatology clinic who used tanning beds for purely cosmetic reasons were well acquainted with the risks.
Ninety-four percent of the patients surveyed were aware of the link between tanning bed use and skin cancer, and even volunteered that they knew other risks, Dr. Tina Ninan said.
“Knowing the risks does not deter patients from engaging in this risky behavior,” said Dr. Ninan, a general practice physician in Newcastle upon Tyne, England.
She distributed some simple surveys to 102 patients waiting in a dermatology clinic at the University Hospital of North Durham. Most of the respondents (65%) were women, and most (60%) were older than 40 years.
Thirty-four patients admitted to using tanning beds. Most of these (27) were women, meaning that 42% of the women surveyed admitted to using the devices. But they weren't alone: 18% of the men surveyed also said they used tanning beds.
Most of the users (88%) said that they had started visiting tanning salons before they turned 35 years old—a period considered crucial in developing an increased risk of skin cancers. “More disturbingly, 58% said they began tanning at age 17–25, and 18% of the users started at younger than 16 years,” Dr. Ninan said.
Although most reported occasional use, 38% of the tanners said they visited a tanning bed weekly. Most used tanning beds at their local beauty salon, but 9% said they had the devices at home. “Six percent also said they tanned at their gym. Having [tanning] beds at gyms and other health centers really sends a mixed message,” Dr. Ninan said.
Coin-operated tanning beds were also popular among the group, with 16% reporting use. This trend is particularly disturbing, Dr. Ninan said, because it circumvents what little control there may be over exposure.
And although the United Kingdom recently passed a law forbidding teens to use tanning beds, no one can prevent them from accessing the coin-operated types, she added.
Shortage of New Antibiotics May Help Superbugs Flourish
CHICAGO — By all measures, methicillin-resistant Staphylococcus aureus cases and related deaths are steadily increasing around the globe, according to Dr. Theodore Rosen.
But MRSA isn't the only bug that's ramping up its antibiotic smarts these days.
“We are being bombarded every year by increasingly resistant bacteria,” Dr. Rosen said in an interview. “Some of these are relatively trivial, some are really bad — like MRSA — and some are wreaking havoc. I'm talking about Klebsiella causing horrendous, frequently fatal drug-resistant pneumonia; multidrug resistant forms of the plague (the same plague that wiped out a third of Europe); and drug-resistant tuberculosis, a disease we thought we'd cornered years ago.”
The surge in resistance is a predictable evolutionary response to the widespread use — and overuse — of antibiotics, said Dr. Rosen, professor of dermatology at Baylor College of Medicine, Houston. Unfortunately, science, industry, and federal administrators are not adapting to the new environment nearly as quickly as their microscopic enemies.
“The number of new antibiotics approved over the past few years has been steadily decreasing, and in the last 2 or 3 years, only one new antibiotic has been approved,” despite promising data, said Dr. Rosen.
Stung by recent problems with already approved drugs, the Food and Drug Administration has become increasingly stringent about the approval of new medications, including antibiotics, he noted.
Pharmaceutical companies also play a role. “You stand to make a lot more money developing a drug for a chronic disease than one only given for 14 days, like an antibiotic,” said Dr. Rosen.
He discussed several antibiotics that showed promise but never found their way to the federal finish line. Two — oritavancin and dalbavancin — are molecularly related to telavancin, which was approved in 2009. “Oritavancin was rejected [by the FDA] because it did not show noninferiority to vancomycin,” he said.
Dalbavancin did well in phase III trials for uncomplicated skin and soft tissue infections. “You can give it once a week, and it's incredibly potent, doing better by far in vitro than anything else available,” Dr. Rosen said. The drug received an FDA approvable letter, but never went further. According to the FDA “the studies were not well done and questioned some of the methodology, so Pfizer sold the rights to the drug, fearing it would not be the blockbuster they had hoped,” he said. The drug is now in developmental limbo.
Iclaprim, a trimethoprim-related drug, is also languishing. “It's a good drug, with a 99.9% kill rate in vitro. It works in trimethoprim resistance and can be given orally or intravenously. It looked great in its phase II and III trials,” said Dr. Rosen.
However, the FDA rejected the drug. Iclaprim met its initial requirement of no more than a 12.5% efficacy difference with its comparator, linezolid. The FDA upped the ante to no more than a 10% difference, at which time Roche sold the drug to another company, which merged with another and sold iclaprim again. “No one knows this drug's future,” Dr. Rosen said.
Several linezolid-like drugs have completed phase II trials “and look good,” Dr. Rosen said.
“They have greater potency, can be taken orally once daily, and have solved some of the problems associated with linezolid — no hypertension, better gastrointestinal absorption, and less risk of myelosuppression.”
Monoclonal antibodies that bind to the staphylococcal clumping factor are also in the works. “This is a very clever way of treating staph bacteria, by keeping them from grabbing hold of fibrinogen so they can't get into tissue,” Dr. Rosen said. Early studies have shown that patients who received the antibody plus an antibiotic did better than those who only received the antibiotic, and that the combination was able to clear MRSA carriage.
“Unfortunately, the company developing this ran out of money, so this antibody is sitting on the shelf somewhere until the company finds a new financial partner,” he added.
The FDA's insistence on noninferiority trials for antibiotics hinders approval, Dr. Rosen opined.
“It's difficult to figure out how noninferior the new drug has to be. Several have shown noninferiority — there were failures, but the failure rate was relatively low. The FDA, however, has said the rate must be lower, because otherwise, a certain number of patients would have done better on the comparator drug, even though each drug has its own positive and negative attributes.”
Placebo-controlled studies “are unconscionable” in patients with infection, and the only other method to determine effectiveness is a superiority study, “which is not really feasible with antibiotics, because so many work so well,” Dr. Rosen said.
Both paths to approval have flaws. “The FDA has had conference after conference with infectious disease experts. We have made little progress in negotiation and have no new antibiotics at a time when resistance is rising, and it's critical that we develop more,” he said.
Time may be running out. Before the advent of penicillin in 1928, infection was the leading cause of death worldwide; in 2000, it was still the fourth-leading cause of death.
“If our antibiotics stop working, we will rapidly go back to those pre-World War II days when all we had to treat infections were arsenic and sulfa. Yes, that's a doomsday scenario, but it's not inconceivable that we could once again live in a time when infections reign supreme,” he concluded.
Dr. Rosen reported having no relevant financial disclosures.
{kind=link}
'You stand to make a lot more money developing a drug for a chronic disease than one only given for 14 days.'
Source DR. ROSEN
CHICAGO — By all measures, methicillin-resistant Staphylococcus aureus cases and related deaths are steadily increasing around the globe, according to Dr. Theodore Rosen.
But MRSA isn't the only bug that's ramping up its antibiotic smarts these days.
“We are being bombarded every year by increasingly resistant bacteria,” Dr. Rosen said in an interview. “Some of these are relatively trivial, some are really bad — like MRSA — and some are wreaking havoc. I'm talking about Klebsiella causing horrendous, frequently fatal drug-resistant pneumonia; multidrug resistant forms of the plague (the same plague that wiped out a third of Europe); and drug-resistant tuberculosis, a disease we thought we'd cornered years ago.”
The surge in resistance is a predictable evolutionary response to the widespread use — and overuse — of antibiotics, said Dr. Rosen, professor of dermatology at Baylor College of Medicine, Houston. Unfortunately, science, industry, and federal administrators are not adapting to the new environment nearly as quickly as their microscopic enemies.
“The number of new antibiotics approved over the past few years has been steadily decreasing, and in the last 2 or 3 years, only one new antibiotic has been approved,” despite promising data, said Dr. Rosen.
Stung by recent problems with already approved drugs, the Food and Drug Administration has become increasingly stringent about the approval of new medications, including antibiotics, he noted.
Pharmaceutical companies also play a role. “You stand to make a lot more money developing a drug for a chronic disease than one only given for 14 days, like an antibiotic,” said Dr. Rosen.
He discussed several antibiotics that showed promise but never found their way to the federal finish line. Two — oritavancin and dalbavancin — are molecularly related to telavancin, which was approved in 2009. “Oritavancin was rejected [by the FDA] because it did not show noninferiority to vancomycin,” he said.
Dalbavancin did well in phase III trials for uncomplicated skin and soft tissue infections. “You can give it once a week, and it's incredibly potent, doing better by far in vitro than anything else available,” Dr. Rosen said. The drug received an FDA approvable letter, but never went further. According to the FDA “the studies were not well done and questioned some of the methodology, so Pfizer sold the rights to the drug, fearing it would not be the blockbuster they had hoped,” he said. The drug is now in developmental limbo.
Iclaprim, a trimethoprim-related drug, is also languishing. “It's a good drug, with a 99.9% kill rate in vitro. It works in trimethoprim resistance and can be given orally or intravenously. It looked great in its phase II and III trials,” said Dr. Rosen.
However, the FDA rejected the drug. Iclaprim met its initial requirement of no more than a 12.5% efficacy difference with its comparator, linezolid. The FDA upped the ante to no more than a 10% difference, at which time Roche sold the drug to another company, which merged with another and sold iclaprim again. “No one knows this drug's future,” Dr. Rosen said.
Several linezolid-like drugs have completed phase II trials “and look good,” Dr. Rosen said.
“They have greater potency, can be taken orally once daily, and have solved some of the problems associated with linezolid — no hypertension, better gastrointestinal absorption, and less risk of myelosuppression.”
Monoclonal antibodies that bind to the staphylococcal clumping factor are also in the works. “This is a very clever way of treating staph bacteria, by keeping them from grabbing hold of fibrinogen so they can't get into tissue,” Dr. Rosen said. Early studies have shown that patients who received the antibody plus an antibiotic did better than those who only received the antibiotic, and that the combination was able to clear MRSA carriage.
“Unfortunately, the company developing this ran out of money, so this antibody is sitting on the shelf somewhere until the company finds a new financial partner,” he added.
The FDA's insistence on noninferiority trials for antibiotics hinders approval, Dr. Rosen opined.
“It's difficult to figure out how noninferior the new drug has to be. Several have shown noninferiority — there were failures, but the failure rate was relatively low. The FDA, however, has said the rate must be lower, because otherwise, a certain number of patients would have done better on the comparator drug, even though each drug has its own positive and negative attributes.”
Placebo-controlled studies “are unconscionable” in patients with infection, and the only other method to determine effectiveness is a superiority study, “which is not really feasible with antibiotics, because so many work so well,” Dr. Rosen said.
Both paths to approval have flaws. “The FDA has had conference after conference with infectious disease experts. We have made little progress in negotiation and have no new antibiotics at a time when resistance is rising, and it's critical that we develop more,” he said.
Time may be running out. Before the advent of penicillin in 1928, infection was the leading cause of death worldwide; in 2000, it was still the fourth-leading cause of death.
“If our antibiotics stop working, we will rapidly go back to those pre-World War II days when all we had to treat infections were arsenic and sulfa. Yes, that's a doomsday scenario, but it's not inconceivable that we could once again live in a time when infections reign supreme,” he concluded.
Dr. Rosen reported having no relevant financial disclosures.
'You stand to make a lot more money developing a drug for a chronic disease than one only given for 14 days.'
Source DR. ROSEN
CHICAGO — By all measures, methicillin-resistant Staphylococcus aureus cases and related deaths are steadily increasing around the globe, according to Dr. Theodore Rosen.
But MRSA isn't the only bug that's ramping up its antibiotic smarts these days.
“We are being bombarded every year by increasingly resistant bacteria,” Dr. Rosen said in an interview. “Some of these are relatively trivial, some are really bad — like MRSA — and some are wreaking havoc. I'm talking about Klebsiella causing horrendous, frequently fatal drug-resistant pneumonia; multidrug resistant forms of the plague (the same plague that wiped out a third of Europe); and drug-resistant tuberculosis, a disease we thought we'd cornered years ago.”
The surge in resistance is a predictable evolutionary response to the widespread use — and overuse — of antibiotics, said Dr. Rosen, professor of dermatology at Baylor College of Medicine, Houston. Unfortunately, science, industry, and federal administrators are not adapting to the new environment nearly as quickly as their microscopic enemies.
“The number of new antibiotics approved over the past few years has been steadily decreasing, and in the last 2 or 3 years, only one new antibiotic has been approved,” despite promising data, said Dr. Rosen.
Stung by recent problems with already approved drugs, the Food and Drug Administration has become increasingly stringent about the approval of new medications, including antibiotics, he noted.
Pharmaceutical companies also play a role. “You stand to make a lot more money developing a drug for a chronic disease than one only given for 14 days, like an antibiotic,” said Dr. Rosen.
He discussed several antibiotics that showed promise but never found their way to the federal finish line. Two — oritavancin and dalbavancin — are molecularly related to telavancin, which was approved in 2009. “Oritavancin was rejected [by the FDA] because it did not show noninferiority to vancomycin,” he said.
Dalbavancin did well in phase III trials for uncomplicated skin and soft tissue infections. “You can give it once a week, and it's incredibly potent, doing better by far in vitro than anything else available,” Dr. Rosen said. The drug received an FDA approvable letter, but never went further. According to the FDA “the studies were not well done and questioned some of the methodology, so Pfizer sold the rights to the drug, fearing it would not be the blockbuster they had hoped,” he said. The drug is now in developmental limbo.
Iclaprim, a trimethoprim-related drug, is also languishing. “It's a good drug, with a 99.9% kill rate in vitro. It works in trimethoprim resistance and can be given orally or intravenously. It looked great in its phase II and III trials,” said Dr. Rosen.
However, the FDA rejected the drug. Iclaprim met its initial requirement of no more than a 12.5% efficacy difference with its comparator, linezolid. The FDA upped the ante to no more than a 10% difference, at which time Roche sold the drug to another company, which merged with another and sold iclaprim again. “No one knows this drug's future,” Dr. Rosen said.
Several linezolid-like drugs have completed phase II trials “and look good,” Dr. Rosen said.
“They have greater potency, can be taken orally once daily, and have solved some of the problems associated with linezolid — no hypertension, better gastrointestinal absorption, and less risk of myelosuppression.”
Monoclonal antibodies that bind to the staphylococcal clumping factor are also in the works. “This is a very clever way of treating staph bacteria, by keeping them from grabbing hold of fibrinogen so they can't get into tissue,” Dr. Rosen said. Early studies have shown that patients who received the antibody plus an antibiotic did better than those who only received the antibiotic, and that the combination was able to clear MRSA carriage.
“Unfortunately, the company developing this ran out of money, so this antibody is sitting on the shelf somewhere until the company finds a new financial partner,” he added.
The FDA's insistence on noninferiority trials for antibiotics hinders approval, Dr. Rosen opined.
“It's difficult to figure out how noninferior the new drug has to be. Several have shown noninferiority — there were failures, but the failure rate was relatively low. The FDA, however, has said the rate must be lower, because otherwise, a certain number of patients would have done better on the comparator drug, even though each drug has its own positive and negative attributes.”
Placebo-controlled studies “are unconscionable” in patients with infection, and the only other method to determine effectiveness is a superiority study, “which is not really feasible with antibiotics, because so many work so well,” Dr. Rosen said.
Both paths to approval have flaws. “The FDA has had conference after conference with infectious disease experts. We have made little progress in negotiation and have no new antibiotics at a time when resistance is rising, and it's critical that we develop more,” he said.
Time may be running out. Before the advent of penicillin in 1928, infection was the leading cause of death worldwide; in 2000, it was still the fourth-leading cause of death.
“If our antibiotics stop working, we will rapidly go back to those pre-World War II days when all we had to treat infections were arsenic and sulfa. Yes, that's a doomsday scenario, but it's not inconceivable that we could once again live in a time when infections reign supreme,” he concluded.
Dr. Rosen reported having no relevant financial disclosures.
'You stand to make a lot more money developing a drug for a chronic disease than one only given for 14 days.'
Source DR. ROSEN