User login
The evolution of office notes and the electronic medical record: The CAPS note
Until the advent of the electronic medical record (EMR), patient charts were filled with handwritten notes documenting visits to the office and read in linear fashion, starting with the patient’s perspective of the problem, then the objective findings of the physical examination, supporting objective data, and finally, the physician’s assessment and treatment plan.
The reliable subjective, objective, assessment, plan (SOAP) approach to notes first advocated by Lawrence Weed in the 1960s did a remarkable job of conveying the physician’s thought process, supporting data, and conclusions.1,2 The notes were brief by necessity, as the physician did not want to spend time writing extraneous information.
In the age of the EMR, large quantities of data are included in the patient notes that have no connection to or do not clearly convey the physician’s thought process. In 2013, 78% of office-based physicians were using EMRs, an increase from 18% in 2001 and an adoption rate accelerated by federal government policies.3,4 But many physicians still do not feel competent reading or writing notes in an EMR and still prefer to read succinct narrative notes.5
This problem is not unique to seasoned physicians. Medical students are also failing to learn how to appropriately document office visits in the EMR, as 52% of medical schools prohibit them from writing in patient charts.6
As a result, we believed that a reassessment of Dr. Weed’s problem-oriented approach to the medical record was required to streamline the EMR and facilitate the way information is conveyed between providers of the patient’s care. Too often, large quantities of laboratory, radiographic, and pathology results are dumped into the record, burying pertinent information about the physician’s thought process, assessment, and evaluation and treatment plan and making it difficult to quickly and efficiently determine the plan.
We recently adopted an approach to office notes that is a modification of the SOAP note. While physicians often gather subjective, objective, and laboratory information to deductively formulate a diagnosis, it is not necessary to document it in the traditional deductive format in the EMR when the information is readily accessible in other areas of the record. Furthermore, a deductive format in the modern EMR produces excessively lengthy notes that require pages of screen scrolling to find the key elements required for effective patient care. This is time-consuming and is a daily obstruction to patient care.
The format that we have been using for almost 10 years still allows the physician to adhere to the problem-oriented medical note philosophy. We call it the CAPS note, which stands for concern, assessment, plan, and supporting data. This approach allows others involved in the patient’s care to efficiently extract critical components (assessment and plan for a specifically stated problem) while still allowing the inclusion of supporting data for reference and for coding and billing.
The structure of the CAPS note is:
- Concern: The primary purpose of the patient’s visit, including the history of the present illness, as conveyed by the patient, and the current status of the concern.
- Assessment: A succinct definition of the patient’s concern along with an accompanying medical diagnosis.
- Plan: The clinician’s immediate and long-term intentions for addressing the patient’s concern or condition.
- Supporting objective and subjective information: All supporting objective data, starting with the physical examination, then the results of laboratory and radiographic tests, and any other information that contributed to the clinician’s medical reasoning. Then, subjective information is included, such as the patient’s past medical, surgical, family, and social histories; current medications; allergies; and a comprehensive review of systems.
This structure keeps the most important information at the top when the encounter is opened on the computer screen and eliminates the need for unnecessary scrolling and searching, not to mention frustration and delays in patient care. Other less pertinent information appears toward the bottom of the record.
THE APSO NOTE VS THE SOAP NOTE
Frustration over the difficulty of finding the most pertinent information in the EMR—the assessment and the plan—has led others to propose a rearrangement of the traditional SOAP note. The APSO (assessment, plan, subjective, objective) note7,8 was created for inpatient daily progress notes, a situation in which the patient’s concern is unlikely to change dramatically on a daily basis and was not intended for use in outpatient clinics.8 While the APSO format does allow colleagues rapid access to the physician’s assessment and plan, it abandons the patient-centered approach of Dr. Weed’s problem-oriented medical record in that it makes it more difficult to find why the patient initially sought care, how long the patient has had the problem, or if there were prior attempts to treat it. These critical details are buried in the bowels of the note.
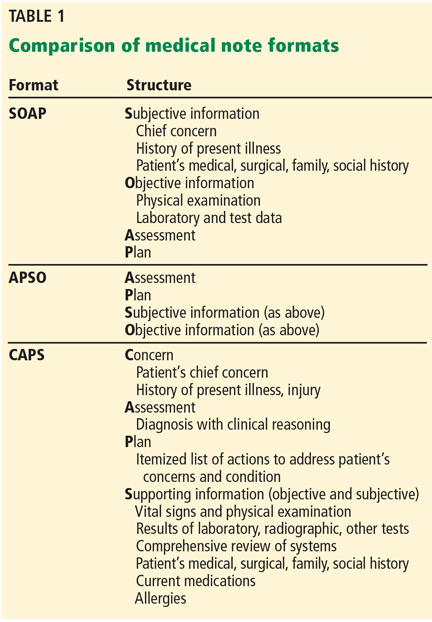
The advantage of the CAPS note (Table 1) is that it retains the patient-centered, problem-oriented spirit of the SOAP format, while moving potentially supportive yet distracting data fields to later in the note. Thus it is applicable to inpatient and outpatient settings.
In the inpatient setting, the fields remain in the same order, but the chief complaint is often the admitting diagnosis or surgical procedure, followed by a quick line on the interval history. The assessment and plan can then follow in much the same way as it would in the outpatient setting, and below that are the patient’s daily laboratory results, radiographic studies, physical examination findings, and any other relevant supporting data. This format allows rapid access to critical information needed by either consultants or cross-covering practitioners who primarily want to know why the patient was admitted, the status, and the primary team’s plan.
ANY TEMPLATE HAS LIMITATIONS
Any standardized template for progress notes in the EMR has limitations. The CAPS format would be easier for a hospital-based physician, who typically addresses one or a small number of concerns, than for an office-based general practitioner who may have to address a multitude of comorbidities in a single visit.
Also, different physicians use the EMR differently. For example, a survey of 1,088 physicians found that 60% of primary care physicians used templates (60%) vs only 34% of specialists, and that 38% of specialists relied mainly on dictation.9
The CAPS approach to the office visit note offers a blend of a template and free text, either typed or dictated, while keeping a structured format that permits others participating in the patient’s care to easily extract desired information. The template can easily be brought up in the patient’s chart, then by either typing or using voice-recognition software, the patient’s chief complaint, history of the present illness, assessment, and plan can be easily completed.
The CAPS format should continue to allow notes to fulfill medicolegal and billing obligations, but without cluttering true clinical reasoning. As more institutions adopt an open-notes policy, permitting patients to freely browse their own medical records, patients will benefit from a clearly structured clinical note that focuses on their problem and the practitioner’s solution. This provides patients a sense of validation and reassurance that the note starts with their concern and history, followed by the practitioner’s assessment and plan, so they can easily affirm that they were accurately heard and can identify the diagnosis given to them by the medical practitioner and the plan moving forward.
Since a return to succinct, albeit often illegible, handwritten clinic notes is impossible, our proposed method of documenting a clinic visit embraces the EMR with a concise yet comprehensive clinic note.
- Jacobs L. Interview with Lawrence Weed, MD—the father of the problem-oriented medical record looks ahead. Perm J 2009; 13:84–89.
- Cameron S, Turtle-Son I. Learning to write case notes using the SOAP format. JCD 2002; 80:286–292.
- Hsiao CJ, Hing E. Use and characteristics of electronic health record systems among office-based physician practices: United States, 2001-2013. NCHS Data Brief 2014; 143:1–8.
- Centers for Medicare & Medicaid Services (CMS). EHR incentive program. www.cms.gov/Regulations-and-Guidance/Legislation/EHRIncentivePrograms/Basics.html. Accessed April 28, 2016.
- Han H, Lopp L. Writing and reading in the electronic health record: an entirely new world. Med Educ Online 2013; 18:1–7.
- Hammoud MM, Dalrymple JL, Christner JG, et al. Medical student documentation in electronic health records: a collaborative statement from the Alliance for Clinical Education. Teach Learn Med 2012; 24:257–266.
- Shoolin J, Ozeran L, Hamann C, Bria W 2nd. Association of Medical Directors of Information Systems consensus on inpatient electronic health record documentation. Appl Clin Inform 2013; 4:293–303.
- Hahn JS, Bernstein JA, McKenzie RB, King BJ, Longhurst CA. Rapid implementation of inpatient electronic physician documentation at an academic hospital. Appl Clin Inform 2012; 3:175–185.
- Pollard SE, Neri PM, Wilcox AR, et al. How physicians document outpatient visit notes in an electronic health record. Int J Med Inform 2013; 82:39–46.
Until the advent of the electronic medical record (EMR), patient charts were filled with handwritten notes documenting visits to the office and read in linear fashion, starting with the patient’s perspective of the problem, then the objective findings of the physical examination, supporting objective data, and finally, the physician’s assessment and treatment plan.
The reliable subjective, objective, assessment, plan (SOAP) approach to notes first advocated by Lawrence Weed in the 1960s did a remarkable job of conveying the physician’s thought process, supporting data, and conclusions.1,2 The notes were brief by necessity, as the physician did not want to spend time writing extraneous information.
In the age of the EMR, large quantities of data are included in the patient notes that have no connection to or do not clearly convey the physician’s thought process. In 2013, 78% of office-based physicians were using EMRs, an increase from 18% in 2001 and an adoption rate accelerated by federal government policies.3,4 But many physicians still do not feel competent reading or writing notes in an EMR and still prefer to read succinct narrative notes.5
This problem is not unique to seasoned physicians. Medical students are also failing to learn how to appropriately document office visits in the EMR, as 52% of medical schools prohibit them from writing in patient charts.6
As a result, we believed that a reassessment of Dr. Weed’s problem-oriented approach to the medical record was required to streamline the EMR and facilitate the way information is conveyed between providers of the patient’s care. Too often, large quantities of laboratory, radiographic, and pathology results are dumped into the record, burying pertinent information about the physician’s thought process, assessment, and evaluation and treatment plan and making it difficult to quickly and efficiently determine the plan.
We recently adopted an approach to office notes that is a modification of the SOAP note. While physicians often gather subjective, objective, and laboratory information to deductively formulate a diagnosis, it is not necessary to document it in the traditional deductive format in the EMR when the information is readily accessible in other areas of the record. Furthermore, a deductive format in the modern EMR produces excessively lengthy notes that require pages of screen scrolling to find the key elements required for effective patient care. This is time-consuming and is a daily obstruction to patient care.
The format that we have been using for almost 10 years still allows the physician to adhere to the problem-oriented medical note philosophy. We call it the CAPS note, which stands for concern, assessment, plan, and supporting data. This approach allows others involved in the patient’s care to efficiently extract critical components (assessment and plan for a specifically stated problem) while still allowing the inclusion of supporting data for reference and for coding and billing.
The structure of the CAPS note is:
- Concern: The primary purpose of the patient’s visit, including the history of the present illness, as conveyed by the patient, and the current status of the concern.
- Assessment: A succinct definition of the patient’s concern along with an accompanying medical diagnosis.
- Plan: The clinician’s immediate and long-term intentions for addressing the patient’s concern or condition.
- Supporting objective and subjective information: All supporting objective data, starting with the physical examination, then the results of laboratory and radiographic tests, and any other information that contributed to the clinician’s medical reasoning. Then, subjective information is included, such as the patient’s past medical, surgical, family, and social histories; current medications; allergies; and a comprehensive review of systems.
This structure keeps the most important information at the top when the encounter is opened on the computer screen and eliminates the need for unnecessary scrolling and searching, not to mention frustration and delays in patient care. Other less pertinent information appears toward the bottom of the record.
THE APSO NOTE VS THE SOAP NOTE
Frustration over the difficulty of finding the most pertinent information in the EMR—the assessment and the plan—has led others to propose a rearrangement of the traditional SOAP note. The APSO (assessment, plan, subjective, objective) note7,8 was created for inpatient daily progress notes, a situation in which the patient’s concern is unlikely to change dramatically on a daily basis and was not intended for use in outpatient clinics.8 While the APSO format does allow colleagues rapid access to the physician’s assessment and plan, it abandons the patient-centered approach of Dr. Weed’s problem-oriented medical record in that it makes it more difficult to find why the patient initially sought care, how long the patient has had the problem, or if there were prior attempts to treat it. These critical details are buried in the bowels of the note.
The advantage of the CAPS note (Table 1) is that it retains the patient-centered, problem-oriented spirit of the SOAP format, while moving potentially supportive yet distracting data fields to later in the note. Thus it is applicable to inpatient and outpatient settings.
In the inpatient setting, the fields remain in the same order, but the chief complaint is often the admitting diagnosis or surgical procedure, followed by a quick line on the interval history. The assessment and plan can then follow in much the same way as it would in the outpatient setting, and below that are the patient’s daily laboratory results, radiographic studies, physical examination findings, and any other relevant supporting data. This format allows rapid access to critical information needed by either consultants or cross-covering practitioners who primarily want to know why the patient was admitted, the status, and the primary team’s plan.
ANY TEMPLATE HAS LIMITATIONS
Any standardized template for progress notes in the EMR has limitations. The CAPS format would be easier for a hospital-based physician, who typically addresses one or a small number of concerns, than for an office-based general practitioner who may have to address a multitude of comorbidities in a single visit.
Also, different physicians use the EMR differently. For example, a survey of 1,088 physicians found that 60% of primary care physicians used templates (60%) vs only 34% of specialists, and that 38% of specialists relied mainly on dictation.9
The CAPS approach to the office visit note offers a blend of a template and free text, either typed or dictated, while keeping a structured format that permits others participating in the patient’s care to easily extract desired information. The template can easily be brought up in the patient’s chart, then by either typing or using voice-recognition software, the patient’s chief complaint, history of the present illness, assessment, and plan can be easily completed.
The CAPS format should continue to allow notes to fulfill medicolegal and billing obligations, but without cluttering true clinical reasoning. As more institutions adopt an open-notes policy, permitting patients to freely browse their own medical records, patients will benefit from a clearly structured clinical note that focuses on their problem and the practitioner’s solution. This provides patients a sense of validation and reassurance that the note starts with their concern and history, followed by the practitioner’s assessment and plan, so they can easily affirm that they were accurately heard and can identify the diagnosis given to them by the medical practitioner and the plan moving forward.
Since a return to succinct, albeit often illegible, handwritten clinic notes is impossible, our proposed method of documenting a clinic visit embraces the EMR with a concise yet comprehensive clinic note.
Until the advent of the electronic medical record (EMR), patient charts were filled with handwritten notes documenting visits to the office and read in linear fashion, starting with the patient’s perspective of the problem, then the objective findings of the physical examination, supporting objective data, and finally, the physician’s assessment and treatment plan.
The reliable subjective, objective, assessment, plan (SOAP) approach to notes first advocated by Lawrence Weed in the 1960s did a remarkable job of conveying the physician’s thought process, supporting data, and conclusions.1,2 The notes were brief by necessity, as the physician did not want to spend time writing extraneous information.
In the age of the EMR, large quantities of data are included in the patient notes that have no connection to or do not clearly convey the physician’s thought process. In 2013, 78% of office-based physicians were using EMRs, an increase from 18% in 2001 and an adoption rate accelerated by federal government policies.3,4 But many physicians still do not feel competent reading or writing notes in an EMR and still prefer to read succinct narrative notes.5
This problem is not unique to seasoned physicians. Medical students are also failing to learn how to appropriately document office visits in the EMR, as 52% of medical schools prohibit them from writing in patient charts.6
As a result, we believed that a reassessment of Dr. Weed’s problem-oriented approach to the medical record was required to streamline the EMR and facilitate the way information is conveyed between providers of the patient’s care. Too often, large quantities of laboratory, radiographic, and pathology results are dumped into the record, burying pertinent information about the physician’s thought process, assessment, and evaluation and treatment plan and making it difficult to quickly and efficiently determine the plan.
We recently adopted an approach to office notes that is a modification of the SOAP note. While physicians often gather subjective, objective, and laboratory information to deductively formulate a diagnosis, it is not necessary to document it in the traditional deductive format in the EMR when the information is readily accessible in other areas of the record. Furthermore, a deductive format in the modern EMR produces excessively lengthy notes that require pages of screen scrolling to find the key elements required for effective patient care. This is time-consuming and is a daily obstruction to patient care.
The format that we have been using for almost 10 years still allows the physician to adhere to the problem-oriented medical note philosophy. We call it the CAPS note, which stands for concern, assessment, plan, and supporting data. This approach allows others involved in the patient’s care to efficiently extract critical components (assessment and plan for a specifically stated problem) while still allowing the inclusion of supporting data for reference and for coding and billing.
The structure of the CAPS note is:
- Concern: The primary purpose of the patient’s visit, including the history of the present illness, as conveyed by the patient, and the current status of the concern.
- Assessment: A succinct definition of the patient’s concern along with an accompanying medical diagnosis.
- Plan: The clinician’s immediate and long-term intentions for addressing the patient’s concern or condition.
- Supporting objective and subjective information: All supporting objective data, starting with the physical examination, then the results of laboratory and radiographic tests, and any other information that contributed to the clinician’s medical reasoning. Then, subjective information is included, such as the patient’s past medical, surgical, family, and social histories; current medications; allergies; and a comprehensive review of systems.
This structure keeps the most important information at the top when the encounter is opened on the computer screen and eliminates the need for unnecessary scrolling and searching, not to mention frustration and delays in patient care. Other less pertinent information appears toward the bottom of the record.
THE APSO NOTE VS THE SOAP NOTE
Frustration over the difficulty of finding the most pertinent information in the EMR—the assessment and the plan—has led others to propose a rearrangement of the traditional SOAP note. The APSO (assessment, plan, subjective, objective) note7,8 was created for inpatient daily progress notes, a situation in which the patient’s concern is unlikely to change dramatically on a daily basis and was not intended for use in outpatient clinics.8 While the APSO format does allow colleagues rapid access to the physician’s assessment and plan, it abandons the patient-centered approach of Dr. Weed’s problem-oriented medical record in that it makes it more difficult to find why the patient initially sought care, how long the patient has had the problem, or if there were prior attempts to treat it. These critical details are buried in the bowels of the note.
The advantage of the CAPS note (Table 1) is that it retains the patient-centered, problem-oriented spirit of the SOAP format, while moving potentially supportive yet distracting data fields to later in the note. Thus it is applicable to inpatient and outpatient settings.
In the inpatient setting, the fields remain in the same order, but the chief complaint is often the admitting diagnosis or surgical procedure, followed by a quick line on the interval history. The assessment and plan can then follow in much the same way as it would in the outpatient setting, and below that are the patient’s daily laboratory results, radiographic studies, physical examination findings, and any other relevant supporting data. This format allows rapid access to critical information needed by either consultants or cross-covering practitioners who primarily want to know why the patient was admitted, the status, and the primary team’s plan.
ANY TEMPLATE HAS LIMITATIONS
Any standardized template for progress notes in the EMR has limitations. The CAPS format would be easier for a hospital-based physician, who typically addresses one or a small number of concerns, than for an office-based general practitioner who may have to address a multitude of comorbidities in a single visit.
Also, different physicians use the EMR differently. For example, a survey of 1,088 physicians found that 60% of primary care physicians used templates (60%) vs only 34% of specialists, and that 38% of specialists relied mainly on dictation.9
The CAPS approach to the office visit note offers a blend of a template and free text, either typed or dictated, while keeping a structured format that permits others participating in the patient’s care to easily extract desired information. The template can easily be brought up in the patient’s chart, then by either typing or using voice-recognition software, the patient’s chief complaint, history of the present illness, assessment, and plan can be easily completed.
The CAPS format should continue to allow notes to fulfill medicolegal and billing obligations, but without cluttering true clinical reasoning. As more institutions adopt an open-notes policy, permitting patients to freely browse their own medical records, patients will benefit from a clearly structured clinical note that focuses on their problem and the practitioner’s solution. This provides patients a sense of validation and reassurance that the note starts with their concern and history, followed by the practitioner’s assessment and plan, so they can easily affirm that they were accurately heard and can identify the diagnosis given to them by the medical practitioner and the plan moving forward.
Since a return to succinct, albeit often illegible, handwritten clinic notes is impossible, our proposed method of documenting a clinic visit embraces the EMR with a concise yet comprehensive clinic note.
- Jacobs L. Interview with Lawrence Weed, MD—the father of the problem-oriented medical record looks ahead. Perm J 2009; 13:84–89.
- Cameron S, Turtle-Son I. Learning to write case notes using the SOAP format. JCD 2002; 80:286–292.
- Hsiao CJ, Hing E. Use and characteristics of electronic health record systems among office-based physician practices: United States, 2001-2013. NCHS Data Brief 2014; 143:1–8.
- Centers for Medicare & Medicaid Services (CMS). EHR incentive program. www.cms.gov/Regulations-and-Guidance/Legislation/EHRIncentivePrograms/Basics.html. Accessed April 28, 2016.
- Han H, Lopp L. Writing and reading in the electronic health record: an entirely new world. Med Educ Online 2013; 18:1–7.
- Hammoud MM, Dalrymple JL, Christner JG, et al. Medical student documentation in electronic health records: a collaborative statement from the Alliance for Clinical Education. Teach Learn Med 2012; 24:257–266.
- Shoolin J, Ozeran L, Hamann C, Bria W 2nd. Association of Medical Directors of Information Systems consensus on inpatient electronic health record documentation. Appl Clin Inform 2013; 4:293–303.
- Hahn JS, Bernstein JA, McKenzie RB, King BJ, Longhurst CA. Rapid implementation of inpatient electronic physician documentation at an academic hospital. Appl Clin Inform 2012; 3:175–185.
- Pollard SE, Neri PM, Wilcox AR, et al. How physicians document outpatient visit notes in an electronic health record. Int J Med Inform 2013; 82:39–46.
- Jacobs L. Interview with Lawrence Weed, MD—the father of the problem-oriented medical record looks ahead. Perm J 2009; 13:84–89.
- Cameron S, Turtle-Son I. Learning to write case notes using the SOAP format. JCD 2002; 80:286–292.
- Hsiao CJ, Hing E. Use and characteristics of electronic health record systems among office-based physician practices: United States, 2001-2013. NCHS Data Brief 2014; 143:1–8.
- Centers for Medicare & Medicaid Services (CMS). EHR incentive program. www.cms.gov/Regulations-and-Guidance/Legislation/EHRIncentivePrograms/Basics.html. Accessed April 28, 2016.
- Han H, Lopp L. Writing and reading in the electronic health record: an entirely new world. Med Educ Online 2013; 18:1–7.
- Hammoud MM, Dalrymple JL, Christner JG, et al. Medical student documentation in electronic health records: a collaborative statement from the Alliance for Clinical Education. Teach Learn Med 2012; 24:257–266.
- Shoolin J, Ozeran L, Hamann C, Bria W 2nd. Association of Medical Directors of Information Systems consensus on inpatient electronic health record documentation. Appl Clin Inform 2013; 4:293–303.
- Hahn JS, Bernstein JA, McKenzie RB, King BJ, Longhurst CA. Rapid implementation of inpatient electronic physician documentation at an academic hospital. Appl Clin Inform 2012; 3:175–185.
- Pollard SE, Neri PM, Wilcox AR, et al. How physicians document outpatient visit notes in an electronic health record. Int J Med Inform 2013; 82:39–46.
KEY POINTS
- The CAPS format provides an advantage over the traditional approach by transferring potentially note-cluttering data that is available elsewhere in the EMR to the bottom of the note, allowing more efficient communication of the true purpose for the patient’s visit, the diagnosis, and the physician’s approach to resolving the patient’s concern.
- As healthcare systems allow patients to browse their electronic charts, the CAPS format shows them that their concern was heard accurately and clearly states the diagnosis and plan of care.

What is cell phone elbow, and what should we tell our patients?
With prolonged cellular telephone use, people may note the onset of aching, burning, numbness, or tingling in the ulnar forearm and hand. This constellation of symptoms, termed “cell phone elbow” by the lay press, is known medically as cubital tunnel syndrome—the second most common nerve compression syndrome in the upper extremities after carpal tunnel syndrome.
In most cases, treatment consists simply of modifying the activity and avoiding activities that aggravate the symptoms. Switching hands frequently while talking on the phone or using a hands-free headset can help. Other daily activities that produce cubital tunnel syndrome include leaning on an elbow while driving or working, and sitting at a computer workstation that requires elbow flexion greater than 90 degrees. Making ergonomic adjustments to these activities is beneficial.
For patients who have nocturnal symptoms, a simple elbow pad worn anteriorly or a towel wrapped around the elbow to prevent flexion while sleeping can be very efficacious. Occasionally, anti-inflammatory injections can be given to quiet an inflamed ulnar nerve and reduce symptoms.1 Surgical interventions, discussed below, are available for patients with severe, persistent symptoms.
WHAT IS CUBITAL TUNNEL SYNDROME?
Cellular telephone use has increased exponentially, with 3.3 billion service contracts active worldwide—or about one for every two people on the planet. The exact incidence of cell phone elbow is not known, but anecdotal reports and our own clinical experience indicate that its incidence parallels the rise in the use of cell phones and computer workstations.
Cubital tunnel syndrome is caused by compression of the ulnar nerve as it traverses the posterior elbow, wrapping around the medial condyle of the humerus. When people hold their elbow flexed for a prolonged period, such as when speaking on the phone or sleeping at night, the ulnar nerve is placed in tension; the nerve itself can elongate 4.5 to 8 mm with elbow flexion.2 Additionally, flexion of the elbow narrows the space available for the nerve2 and can cause a sevenfold to 20-fold increase in the pressure within the cubital tunnel, depending on muscle contraction.3 This can be compounded by compression on the nerve, either from various fascial bands surrounding the nerve or from extrinsic sources of compression, such as leaning on one’s elbow while driving or talking. This increased pressure on the nerve leads to decreased blood flow and nerve ischemia; this in turn causes increased permeability of the epineurial vessels and nerve edema, enlarging the nerve and continuing the cycle. Less frequently, cubital tunnel symptoms can be caused by the ulnar nerve subluxing in and out of its groove in the posterior elbow, leading to nerve inflammation and swelling from the repetitive friction.
THE CLINICAL PRESENTATION
The clinical picture of cubital tunnel syndrome consists of numbness or paresthesias in the small and ring fingers. Dorsal ulnar hand numbness, which is not present if the ulnar nerve is compressed at Guyon’s canal, helps the clinician differentiate cubital tunnel nerve compression from distal ulnar nerve compression.
If ulnar nerve compression persists, symptoms may progress to hand fatigue and weakness, including difficulty opening bottles or jars. Chronic and severe compression may lead to permanent motor deficits, including an inability to adduct the small finger (Wartenberg sign) and severe clawing of the ring and small fingers (a hand posture of metacarpophalangeal extension and flexion of the proximal and distal interphalangeal joints due to dysfunction of the ulnar-innervated intrinsic hand musculature). Patients may be unable to grasp things in a key-pinch grip, using a fingertip grip instead (Froment sign).
THE DIAGNOSIS IS USUALLY CLINICAL
The diagnosis of cubital tunnel syndrome is first and foremost a clinical one based on a thorough history, including symptoms, duration, and aggravating activities and factors.
The physical examination should include evaluation of sensibility of the hand, including the Semmes-Weinstein monofilament test and vibratory perception test, which will be affected before the Weber two-point discrimination test. Sensibility of the entire hand should be assessed to differentiate focal ulnar deficits from more widespread peripheral neuropathies.
Motor function can be evaluated by asking the patient to hold the fingers abducted, testing key-pinch grip, or asking the patient to cross the middle finger over the index finger. This crossed-finger test is quite reliable, as it is difficult to “fake out” with other muscles.4
The examination should also evaluate the cervical spine and vascularity. Provocative maneuvers can be performed to elicit symptoms, including the Hoffman-Tinel test (tapping the ulnar nerve in its groove at the posterior medial elbow, eliciting electric shocks or tingling radiating into the small finger). The equivalent of the Phalen maneuver for carpal tunnel syndrome can be performed by having the patient sit with the elbow fully flexed for 30 seconds to see if symptoms are reproduced; this may be positive in 10% of normal individuals. 5 One can combine elbow flexion with compression over the proximal ulnar nerve; this maneuver has good sensitivity and specificity. 6 Early in the disease, these provocative maneuvers may be the only examination findings, since sensation and motor function are usually normal.
Ruling out other entities that can cause numbness in the distribution of the medial hand and forearm is also important. These entities include cervical spine conditions such as herniated disk impinging on the C8 nerve root, or a space-occupying lesion of the cervical spine such as a tumor or syrinx.
The neck should be examined for loss of motion. Also, a Spurling test of the cervical spine checks for foraminal nerve impingement: with the patient seated, the clinician extends the patient’s neck and rotates it toward the involved side, then presses down on the top of the patient’s head and asks if this reproduces or worsens the symptoms in the patient’s arm. Hyperreflexia of the upper extremities or the presence of a Hoffman sign should alert the clinician to a more central process. In unclear cases or in patients with known cervical disease, electromyography should be able to differentiate ulnar neuropathy from a C8 nerveroot impingement or confirm the presence of both conditions (a so-called “double crush” phenomenon).
Other less common entities that can present with hand tingling include an apical lung tumor compressing the lower brachial plexus, thoracic outlet syndrome, or peripheral neuropathy (diabetes, vitamin B12 deficiency, hypothyroidism, alcoholism). Other conditions that can cause medial-sided elbow pain include elbow instability or medial epicondylitis (golfer’s elbow); however, these are not associated with numbness or tingling by themselves.
DIAGNOSTIC TESTS
Advanced diagnostic studies may help in certain cases, although they are not essential if the diagnosis is obvious on clinical examination.
Imaging studies may include plain radiography to look for osteophytes or bone fragments, which may impinge on the ulnar nerve, particularly in an arthritic or previously traumatized elbow. Magnetic resonance imaging is only indicated if a space-occupying lesion is suspected. Electrodiagnostic studies may help when findings are equivocal, when the site of compression is unclear, or when coexisting conditions such as diabetes or cervical spine disease make the diagnosis unclear. Nerve conduction studies may be unreliable early in cubital tunnel syndrome, as nondiseased nerve fibers may be tested, creating a false-negative result. Performing the study with the patient’s elbow flexed may increase the sensitivity of the test. Electromyography generally does not become positive until later in the disease, when more profound changes have occurred.
TREATMENT OF CELL PHONE ELBOW
As mentioned, changing how one uses a cell phone often helps, as does avoiding activities that require the elbow to remain flexed more than 90 degrees for extended periods. But when nonoperative means fail to reduce symptoms, surgery may be warranted.
Operative interventions include simple decompression or transposing the nerve from its usual course around the posterior elbow to a path anterior to the elbow, thus decreasing the tension on the nerve. This can be done either subcutaneously or by embedding the nerve in or under the muscles of the forearm.
In patients with coexisting medial epicondylitis or a subluxing nerve, the medial epicondyle can be excised. Techniques for minimally invasive or endoscopic ulnar nerve decompression have been recently introduced, but the long-term results with these are not yet known.
Overall, treatment for persistent paresthesias is successful even when patients present late, but those who present early have a better chance of full sensory and motor recovery.
- Pechan J, Kredba J. Treatment of cubital tunnel syndrome by means of local administration of cortisonoids. Acta Univ Carol [Med] (Praha) 1980; 26:125–133.
- Apfelberg DB, Larson SJ. Dynamic anatomy of the ulnar nerve at the elbow. Plast Reconstr Surg 1973; 51:79–81.
- Werner CO, Ohlin P, Elmqvist D. Pressures recorded in ulnar neuropathy. Acta Orthop Scand 1985; 56:404–406.
- Earle AS, Vlastou C. Crossed fingers and other tests of ulnar nerve motor function. J Hand Surg [Am] 1980; 5:560–565.
- Rayann GM, Jensen C, Duke J. Elbow flexion test in the normal population. J Hand Surg [Am] 1992; 17:86–89.
- Novak CB, Lee GW, Mackinnon SE, Lay L. Provocative testing for cubital tunnel syndrome. J Hand Surg [Am] 1994; 19:817–820.
With prolonged cellular telephone use, people may note the onset of aching, burning, numbness, or tingling in the ulnar forearm and hand. This constellation of symptoms, termed “cell phone elbow” by the lay press, is known medically as cubital tunnel syndrome—the second most common nerve compression syndrome in the upper extremities after carpal tunnel syndrome.
In most cases, treatment consists simply of modifying the activity and avoiding activities that aggravate the symptoms. Switching hands frequently while talking on the phone or using a hands-free headset can help. Other daily activities that produce cubital tunnel syndrome include leaning on an elbow while driving or working, and sitting at a computer workstation that requires elbow flexion greater than 90 degrees. Making ergonomic adjustments to these activities is beneficial.
For patients who have nocturnal symptoms, a simple elbow pad worn anteriorly or a towel wrapped around the elbow to prevent flexion while sleeping can be very efficacious. Occasionally, anti-inflammatory injections can be given to quiet an inflamed ulnar nerve and reduce symptoms.1 Surgical interventions, discussed below, are available for patients with severe, persistent symptoms.
WHAT IS CUBITAL TUNNEL SYNDROME?
Cellular telephone use has increased exponentially, with 3.3 billion service contracts active worldwide—or about one for every two people on the planet. The exact incidence of cell phone elbow is not known, but anecdotal reports and our own clinical experience indicate that its incidence parallels the rise in the use of cell phones and computer workstations.
Cubital tunnel syndrome is caused by compression of the ulnar nerve as it traverses the posterior elbow, wrapping around the medial condyle of the humerus. When people hold their elbow flexed for a prolonged period, such as when speaking on the phone or sleeping at night, the ulnar nerve is placed in tension; the nerve itself can elongate 4.5 to 8 mm with elbow flexion.2 Additionally, flexion of the elbow narrows the space available for the nerve2 and can cause a sevenfold to 20-fold increase in the pressure within the cubital tunnel, depending on muscle contraction.3 This can be compounded by compression on the nerve, either from various fascial bands surrounding the nerve or from extrinsic sources of compression, such as leaning on one’s elbow while driving or talking. This increased pressure on the nerve leads to decreased blood flow and nerve ischemia; this in turn causes increased permeability of the epineurial vessels and nerve edema, enlarging the nerve and continuing the cycle. Less frequently, cubital tunnel symptoms can be caused by the ulnar nerve subluxing in and out of its groove in the posterior elbow, leading to nerve inflammation and swelling from the repetitive friction.
THE CLINICAL PRESENTATION
The clinical picture of cubital tunnel syndrome consists of numbness or paresthesias in the small and ring fingers. Dorsal ulnar hand numbness, which is not present if the ulnar nerve is compressed at Guyon’s canal, helps the clinician differentiate cubital tunnel nerve compression from distal ulnar nerve compression.
If ulnar nerve compression persists, symptoms may progress to hand fatigue and weakness, including difficulty opening bottles or jars. Chronic and severe compression may lead to permanent motor deficits, including an inability to adduct the small finger (Wartenberg sign) and severe clawing of the ring and small fingers (a hand posture of metacarpophalangeal extension and flexion of the proximal and distal interphalangeal joints due to dysfunction of the ulnar-innervated intrinsic hand musculature). Patients may be unable to grasp things in a key-pinch grip, using a fingertip grip instead (Froment sign).
THE DIAGNOSIS IS USUALLY CLINICAL
The diagnosis of cubital tunnel syndrome is first and foremost a clinical one based on a thorough history, including symptoms, duration, and aggravating activities and factors.
The physical examination should include evaluation of sensibility of the hand, including the Semmes-Weinstein monofilament test and vibratory perception test, which will be affected before the Weber two-point discrimination test. Sensibility of the entire hand should be assessed to differentiate focal ulnar deficits from more widespread peripheral neuropathies.
Motor function can be evaluated by asking the patient to hold the fingers abducted, testing key-pinch grip, or asking the patient to cross the middle finger over the index finger. This crossed-finger test is quite reliable, as it is difficult to “fake out” with other muscles.4
The examination should also evaluate the cervical spine and vascularity. Provocative maneuvers can be performed to elicit symptoms, including the Hoffman-Tinel test (tapping the ulnar nerve in its groove at the posterior medial elbow, eliciting electric shocks or tingling radiating into the small finger). The equivalent of the Phalen maneuver for carpal tunnel syndrome can be performed by having the patient sit with the elbow fully flexed for 30 seconds to see if symptoms are reproduced; this may be positive in 10% of normal individuals. 5 One can combine elbow flexion with compression over the proximal ulnar nerve; this maneuver has good sensitivity and specificity. 6 Early in the disease, these provocative maneuvers may be the only examination findings, since sensation and motor function are usually normal.
Ruling out other entities that can cause numbness in the distribution of the medial hand and forearm is also important. These entities include cervical spine conditions such as herniated disk impinging on the C8 nerve root, or a space-occupying lesion of the cervical spine such as a tumor or syrinx.
The neck should be examined for loss of motion. Also, a Spurling test of the cervical spine checks for foraminal nerve impingement: with the patient seated, the clinician extends the patient’s neck and rotates it toward the involved side, then presses down on the top of the patient’s head and asks if this reproduces or worsens the symptoms in the patient’s arm. Hyperreflexia of the upper extremities or the presence of a Hoffman sign should alert the clinician to a more central process. In unclear cases or in patients with known cervical disease, electromyography should be able to differentiate ulnar neuropathy from a C8 nerveroot impingement or confirm the presence of both conditions (a so-called “double crush” phenomenon).
Other less common entities that can present with hand tingling include an apical lung tumor compressing the lower brachial plexus, thoracic outlet syndrome, or peripheral neuropathy (diabetes, vitamin B12 deficiency, hypothyroidism, alcoholism). Other conditions that can cause medial-sided elbow pain include elbow instability or medial epicondylitis (golfer’s elbow); however, these are not associated with numbness or tingling by themselves.
DIAGNOSTIC TESTS
Advanced diagnostic studies may help in certain cases, although they are not essential if the diagnosis is obvious on clinical examination.
Imaging studies may include plain radiography to look for osteophytes or bone fragments, which may impinge on the ulnar nerve, particularly in an arthritic or previously traumatized elbow. Magnetic resonance imaging is only indicated if a space-occupying lesion is suspected. Electrodiagnostic studies may help when findings are equivocal, when the site of compression is unclear, or when coexisting conditions such as diabetes or cervical spine disease make the diagnosis unclear. Nerve conduction studies may be unreliable early in cubital tunnel syndrome, as nondiseased nerve fibers may be tested, creating a false-negative result. Performing the study with the patient’s elbow flexed may increase the sensitivity of the test. Electromyography generally does not become positive until later in the disease, when more profound changes have occurred.
TREATMENT OF CELL PHONE ELBOW
As mentioned, changing how one uses a cell phone often helps, as does avoiding activities that require the elbow to remain flexed more than 90 degrees for extended periods. But when nonoperative means fail to reduce symptoms, surgery may be warranted.
Operative interventions include simple decompression or transposing the nerve from its usual course around the posterior elbow to a path anterior to the elbow, thus decreasing the tension on the nerve. This can be done either subcutaneously or by embedding the nerve in or under the muscles of the forearm.
In patients with coexisting medial epicondylitis or a subluxing nerve, the medial epicondyle can be excised. Techniques for minimally invasive or endoscopic ulnar nerve decompression have been recently introduced, but the long-term results with these are not yet known.
Overall, treatment for persistent paresthesias is successful even when patients present late, but those who present early have a better chance of full sensory and motor recovery.
With prolonged cellular telephone use, people may note the onset of aching, burning, numbness, or tingling in the ulnar forearm and hand. This constellation of symptoms, termed “cell phone elbow” by the lay press, is known medically as cubital tunnel syndrome—the second most common nerve compression syndrome in the upper extremities after carpal tunnel syndrome.
In most cases, treatment consists simply of modifying the activity and avoiding activities that aggravate the symptoms. Switching hands frequently while talking on the phone or using a hands-free headset can help. Other daily activities that produce cubital tunnel syndrome include leaning on an elbow while driving or working, and sitting at a computer workstation that requires elbow flexion greater than 90 degrees. Making ergonomic adjustments to these activities is beneficial.
For patients who have nocturnal symptoms, a simple elbow pad worn anteriorly or a towel wrapped around the elbow to prevent flexion while sleeping can be very efficacious. Occasionally, anti-inflammatory injections can be given to quiet an inflamed ulnar nerve and reduce symptoms.1 Surgical interventions, discussed below, are available for patients with severe, persistent symptoms.
WHAT IS CUBITAL TUNNEL SYNDROME?
Cellular telephone use has increased exponentially, with 3.3 billion service contracts active worldwide—or about one for every two people on the planet. The exact incidence of cell phone elbow is not known, but anecdotal reports and our own clinical experience indicate that its incidence parallels the rise in the use of cell phones and computer workstations.
Cubital tunnel syndrome is caused by compression of the ulnar nerve as it traverses the posterior elbow, wrapping around the medial condyle of the humerus. When people hold their elbow flexed for a prolonged period, such as when speaking on the phone or sleeping at night, the ulnar nerve is placed in tension; the nerve itself can elongate 4.5 to 8 mm with elbow flexion.2 Additionally, flexion of the elbow narrows the space available for the nerve2 and can cause a sevenfold to 20-fold increase in the pressure within the cubital tunnel, depending on muscle contraction.3 This can be compounded by compression on the nerve, either from various fascial bands surrounding the nerve or from extrinsic sources of compression, such as leaning on one’s elbow while driving or talking. This increased pressure on the nerve leads to decreased blood flow and nerve ischemia; this in turn causes increased permeability of the epineurial vessels and nerve edema, enlarging the nerve and continuing the cycle. Less frequently, cubital tunnel symptoms can be caused by the ulnar nerve subluxing in and out of its groove in the posterior elbow, leading to nerve inflammation and swelling from the repetitive friction.
THE CLINICAL PRESENTATION
The clinical picture of cubital tunnel syndrome consists of numbness or paresthesias in the small and ring fingers. Dorsal ulnar hand numbness, which is not present if the ulnar nerve is compressed at Guyon’s canal, helps the clinician differentiate cubital tunnel nerve compression from distal ulnar nerve compression.
If ulnar nerve compression persists, symptoms may progress to hand fatigue and weakness, including difficulty opening bottles or jars. Chronic and severe compression may lead to permanent motor deficits, including an inability to adduct the small finger (Wartenberg sign) and severe clawing of the ring and small fingers (a hand posture of metacarpophalangeal extension and flexion of the proximal and distal interphalangeal joints due to dysfunction of the ulnar-innervated intrinsic hand musculature). Patients may be unable to grasp things in a key-pinch grip, using a fingertip grip instead (Froment sign).
THE DIAGNOSIS IS USUALLY CLINICAL
The diagnosis of cubital tunnel syndrome is first and foremost a clinical one based on a thorough history, including symptoms, duration, and aggravating activities and factors.
The physical examination should include evaluation of sensibility of the hand, including the Semmes-Weinstein monofilament test and vibratory perception test, which will be affected before the Weber two-point discrimination test. Sensibility of the entire hand should be assessed to differentiate focal ulnar deficits from more widespread peripheral neuropathies.
Motor function can be evaluated by asking the patient to hold the fingers abducted, testing key-pinch grip, or asking the patient to cross the middle finger over the index finger. This crossed-finger test is quite reliable, as it is difficult to “fake out” with other muscles.4
The examination should also evaluate the cervical spine and vascularity. Provocative maneuvers can be performed to elicit symptoms, including the Hoffman-Tinel test (tapping the ulnar nerve in its groove at the posterior medial elbow, eliciting electric shocks or tingling radiating into the small finger). The equivalent of the Phalen maneuver for carpal tunnel syndrome can be performed by having the patient sit with the elbow fully flexed for 30 seconds to see if symptoms are reproduced; this may be positive in 10% of normal individuals. 5 One can combine elbow flexion with compression over the proximal ulnar nerve; this maneuver has good sensitivity and specificity. 6 Early in the disease, these provocative maneuvers may be the only examination findings, since sensation and motor function are usually normal.
Ruling out other entities that can cause numbness in the distribution of the medial hand and forearm is also important. These entities include cervical spine conditions such as herniated disk impinging on the C8 nerve root, or a space-occupying lesion of the cervical spine such as a tumor or syrinx.
The neck should be examined for loss of motion. Also, a Spurling test of the cervical spine checks for foraminal nerve impingement: with the patient seated, the clinician extends the patient’s neck and rotates it toward the involved side, then presses down on the top of the patient’s head and asks if this reproduces or worsens the symptoms in the patient’s arm. Hyperreflexia of the upper extremities or the presence of a Hoffman sign should alert the clinician to a more central process. In unclear cases or in patients with known cervical disease, electromyography should be able to differentiate ulnar neuropathy from a C8 nerveroot impingement or confirm the presence of both conditions (a so-called “double crush” phenomenon).
Other less common entities that can present with hand tingling include an apical lung tumor compressing the lower brachial plexus, thoracic outlet syndrome, or peripheral neuropathy (diabetes, vitamin B12 deficiency, hypothyroidism, alcoholism). Other conditions that can cause medial-sided elbow pain include elbow instability or medial epicondylitis (golfer’s elbow); however, these are not associated with numbness or tingling by themselves.
DIAGNOSTIC TESTS
Advanced diagnostic studies may help in certain cases, although they are not essential if the diagnosis is obvious on clinical examination.
Imaging studies may include plain radiography to look for osteophytes or bone fragments, which may impinge on the ulnar nerve, particularly in an arthritic or previously traumatized elbow. Magnetic resonance imaging is only indicated if a space-occupying lesion is suspected. Electrodiagnostic studies may help when findings are equivocal, when the site of compression is unclear, or when coexisting conditions such as diabetes or cervical spine disease make the diagnosis unclear. Nerve conduction studies may be unreliable early in cubital tunnel syndrome, as nondiseased nerve fibers may be tested, creating a false-negative result. Performing the study with the patient’s elbow flexed may increase the sensitivity of the test. Electromyography generally does not become positive until later in the disease, when more profound changes have occurred.
TREATMENT OF CELL PHONE ELBOW
As mentioned, changing how one uses a cell phone often helps, as does avoiding activities that require the elbow to remain flexed more than 90 degrees for extended periods. But when nonoperative means fail to reduce symptoms, surgery may be warranted.
Operative interventions include simple decompression or transposing the nerve from its usual course around the posterior elbow to a path anterior to the elbow, thus decreasing the tension on the nerve. This can be done either subcutaneously or by embedding the nerve in or under the muscles of the forearm.
In patients with coexisting medial epicondylitis or a subluxing nerve, the medial epicondyle can be excised. Techniques for minimally invasive or endoscopic ulnar nerve decompression have been recently introduced, but the long-term results with these are not yet known.
Overall, treatment for persistent paresthesias is successful even when patients present late, but those who present early have a better chance of full sensory and motor recovery.
- Pechan J, Kredba J. Treatment of cubital tunnel syndrome by means of local administration of cortisonoids. Acta Univ Carol [Med] (Praha) 1980; 26:125–133.
- Apfelberg DB, Larson SJ. Dynamic anatomy of the ulnar nerve at the elbow. Plast Reconstr Surg 1973; 51:79–81.
- Werner CO, Ohlin P, Elmqvist D. Pressures recorded in ulnar neuropathy. Acta Orthop Scand 1985; 56:404–406.
- Earle AS, Vlastou C. Crossed fingers and other tests of ulnar nerve motor function. J Hand Surg [Am] 1980; 5:560–565.
- Rayann GM, Jensen C, Duke J. Elbow flexion test in the normal population. J Hand Surg [Am] 1992; 17:86–89.
- Novak CB, Lee GW, Mackinnon SE, Lay L. Provocative testing for cubital tunnel syndrome. J Hand Surg [Am] 1994; 19:817–820.
- Pechan J, Kredba J. Treatment of cubital tunnel syndrome by means of local administration of cortisonoids. Acta Univ Carol [Med] (Praha) 1980; 26:125–133.
- Apfelberg DB, Larson SJ. Dynamic anatomy of the ulnar nerve at the elbow. Plast Reconstr Surg 1973; 51:79–81.
- Werner CO, Ohlin P, Elmqvist D. Pressures recorded in ulnar neuropathy. Acta Orthop Scand 1985; 56:404–406.
- Earle AS, Vlastou C. Crossed fingers and other tests of ulnar nerve motor function. J Hand Surg [Am] 1980; 5:560–565.
- Rayann GM, Jensen C, Duke J. Elbow flexion test in the normal population. J Hand Surg [Am] 1992; 17:86–89.
- Novak CB, Lee GW, Mackinnon SE, Lay L. Provocative testing for cubital tunnel syndrome. J Hand Surg [Am] 1994; 19:817–820.